steps rating description translation ++ back-translation
TRANSCRIPT
Autism 1 –16© The Author(s) 2014Reprints and permissions: sagepub.co.uk/journalsPermissions.navDOI: 10.1177/1362361314541012aut.sagepub.com
Prevalence estimates of Autism Spectrum Disorder (ASD) have increased over the last decade; however, epidemio-logical studies report variation in these estimates across geographical areas and ethnic and racial groups (Elsabbagh et al., 2012). Rather than differences in actual prevalence, these findings may instead reflect a lack of awareness of autism, effects of stigma, differing methods used to inves-tigate prevalence rates, identify cases, and evaluate cases, and different samples across studies. Inadequate psycho-metric properties as well as lack of appropriate cultural adaptations of screening and diagnostic tools may further contribute to varying prevalence estimates.
Screening is frequently proposed as a key step to iden-tifying children at risk for ASD and to expedite early behavioral and educational interventions to improve out-comes (National Research Council (US) Committee on Educational Interventions for Children with Autism, 2001; Szatmari et al., 2003), although some question a popula-tion-wide strategy (e.g. Al-Qabandi et al., 2011; Le Couteur, 2003). As currently defined, an autism screening tool is a formalized brief questionnaire completed by a parent or provider before an in-depth diagnostic evaluation to identify a child at risk of autism (Filipek et al., 2000;
Plauché Johnson et al., 2007). Administration of the tool may take place before a concern is identified, as in the case with whole-population-based screening, or after a parent or provider raises a concern. Current guidance from the American Academy of Pediatrics (Plauché Johnson et al., 2007) and others (Filipek et al., 2000) recommend formal screening in pediatric primary care beginning at 18 months. While significant improvements have been made in the development, validation, and implementation of autism screening tools in several countries (Ehlers et al., 1999; Kamp-Becker et al., 2005; Nordenbæk et al., 2011; Song et al., 2009; Swinkels et al., 2006), most tools have been developed in the United States or United Kingdom and are
A review of cultural adaptations of screening tools for autism spectrum disorders
Sandra Soto1, Keri Linas2, Diane Jacobstein2, Matthew Biel3, Talia Migdal2 and Bruno J Anthony2
AbstractScreening children to determine risk for Autism Spectrum Disorders has become more common, although some question the advisability of such a strategy. The purpose of this systematic review is to identify autism screening tools that have been adapted for use in cultures different from that in which they were developed, evaluate the cultural adaptation process, report on the psychometric properties of the adapted instruments, and describe the implications for further research and clinical practice. A total of 21 articles met criteria for inclusion, reporting on the cultural adaptation of autism screening in 18 countries and in nine languages. The cultural adaptation process was not always clearly outlined and often did not include the recommended guidelines. Cultural/linguistic modifications to the translated tools tended to increase with the rigor of the adaptation process. Differences between the psychometric properties of the original and adapted versions were common, indicating the need to obtain normative data on populations to increase the utility of the translated tool.
Keywordsautism, cultural adaptation, screening tools
1San Diego State University/University of California, USA2Georgetown Center for Child and Human Development, USA3School of Medicine, Georgetown University, USA
Corresponding author:Sandra Soto, San Diego State University/University of California, San Diego Joint Doctoral Program in Public Health (Health Behavior), 9245 Sky Park Court, Suite 221 San Diego, CA 92123-4311, USA. Email: [email protected]
541012 AUT0010.1177/1362361314541012AutismSoto et al.research-article2014
Review Article
2 Autism
increasingly being used in cultures other than those in which they were created (Dixon et al., 2011).
Appropriate use of existing tools in other cultural and linguistic environments goes beyond translation to include a thorough process of identifying potential incongruities in language and concepts and then modifying the tool so that it is understood by the target population. The goal of cul-tural adaptation is to establish functional equivalence with the original version (Banville et al., 2000; Beaton et al., 2000). Moreover, one cannot assume that psychometric properties are retained within the new version of a screen-ing tool simply because language and concept equivalence have been established, and therefore psychometric analy-sis of the adapted tool is also recommended (Beaton et al., 2000).
The purpose of this systematic review is to (1) identify ASD screening tools that have been culturally adapted across cultures and countries, (2) evaluate the extent to which the adaptation process adhered to recommended cultural adaptation guidelines, (3) report on the psycho-metric properties of the adapted tools, and (4) describe the implications of these findings for further research and practice.
Method
Search strategy
Based on the predetermined scope of the review, a medical research librarian conducted searches of applicable data-bases, including MEDLINE, CINAHL, PsycINFO, Web of Science, ERIC, Embase, OVID, Mental Measurements of Tests in Print, PubMED, HaPI, World Health Organization (WHO), and Google Scholar. Search terms were grouped into six categories: all variants of ASD (e.g. autism, ASD, pervasive developmental disorder (PDD)), screening tools, cultural adaptation, language considera-tions, child, and psychometrics. The search included stud-ies published in languages other than English.
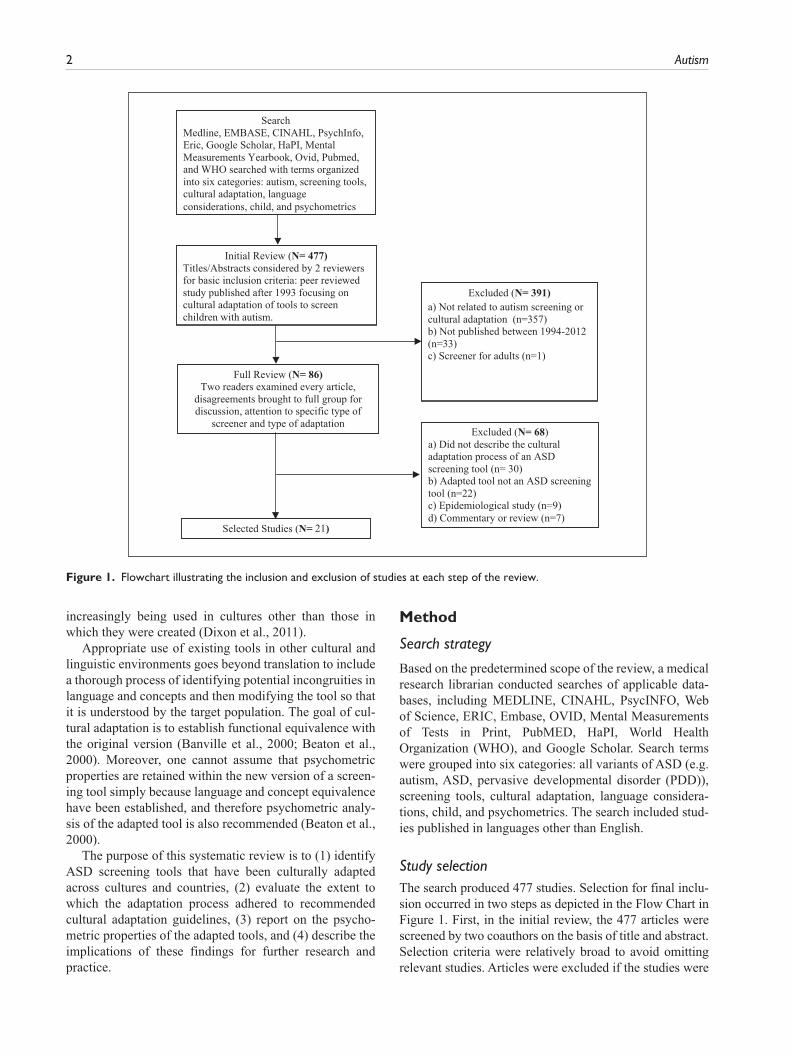
Study selectionThe search produced 477 studies. Selection for final inclu-sion occurred in two steps as depicted in the Flow Chart in Figure 1. First, in the initial review, the 477 articles were screened by two coauthors on the basis of title and abstract. Selection criteria were relatively broad to avoid omitting relevant studies. Articles were excluded if the studies were
Full Review (N= 86) Two readers examined every article,
disagreements brought to full group for discussion, attention to specific type of
screener and type of adaptation
Selected Studies (N= 21)
SearchMedline, EMBASE, CINAHL, PsychInfo, Eric, Google Scholar, HaPI, Mental Measurements Yearbook, Ovid, Pubmed,and WHO searched with terms organized into six categories: autism, screening tools, cultural adaptation, languageconsiderations, child, and psychometrics
Initial Review (N= 477) Titles/Abstracts considered by 2 reviewers for basic inclusion criteria: peer reviewed study published after 1993 focusing on cultural adaptation of tools to screen children with autism.
Excluded (N= 391) a) Not related to autism screening or cultural adaptation (n=357) b) Not published between 1994-2012 (n=33) c) Screener for adults (n=1)
Excluded (N= 68) a) Did not describe the cultural adaptation process of an ASD screening tool (n= 30) b) Adapted tool not an ASD screening tool (n=22) c) Epidemiological study (n=9) d) Commentary or review (n=7)
Figure 1. Flowchart illustrating the inclusion and exclusion of studies at each step of the review.
Soto et al. 3
unrelated to ASD screening or cultural adaptation, con-ducted prior to the publication of Diagnostic and Statistical Manual of Mental Disorders–Fourth Edition (DSM-IV), or focused on adult populations. From this initial review, 86 articles were selected for full review, using criteria designed to capture only those studies involving adaptation of a screener to a different culture/language than that in which it was developed. These articles were read by at least two coauthors; disagreement or uncertainty regarding selection between the readers was brought to the full group for dis-cussion. An article was excluded if the study (1) did not involve cultural adaptation of an autism screening tool, (2) examined a diagnostic rather than a screening instrument, (3) was solely an investigation of ASD prevalence, or (4) was a commentary or a review. Based on these criteria, 68 articles were eliminated, leaving 21 articles for inclusion. A final search was conducted to identify additional studies through reference lists, however, no new studies were identified.
Assessment of cultural adaptations and reporting of psychometric properties
At least two reviewers independently rated the rigor of the adaptation process for each study based on established guidelines for achieving linguistic and cultural
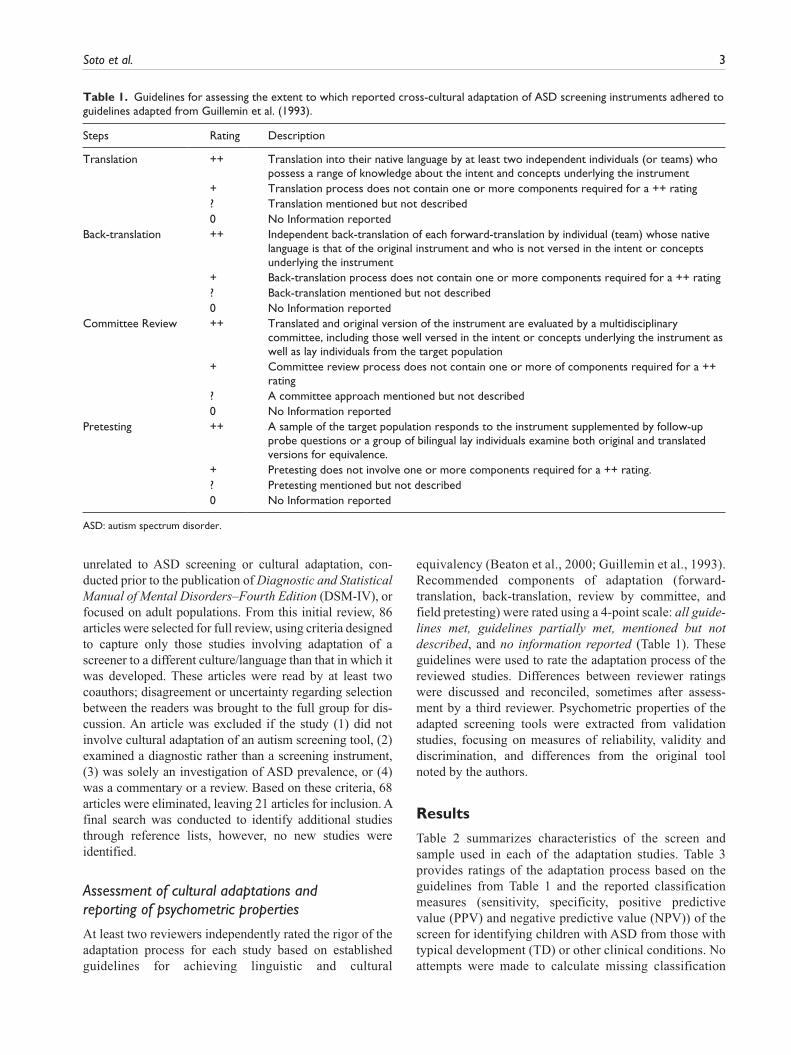
equivalency (Beaton et al., 2000; Guillemin et al., 1993). Recommended components of adaptation (forward- translation, back-translation, review by committee, and field pretesting) were rated using a 4-point scale: all guide-lines met, guidelines partially met, mentioned but not described, and no information reported (Table 1). These guidelines were used to rate the adaptation process of the reviewed studies. Differences between reviewer ratings were discussed and reconciled, sometimes after assess-ment by a third reviewer. Psychometric properties of the adapted screening tools were extracted from validation studies, focusing on measures of reliability, validity and discrimination, and differences from the original tool noted by the authors.
Results
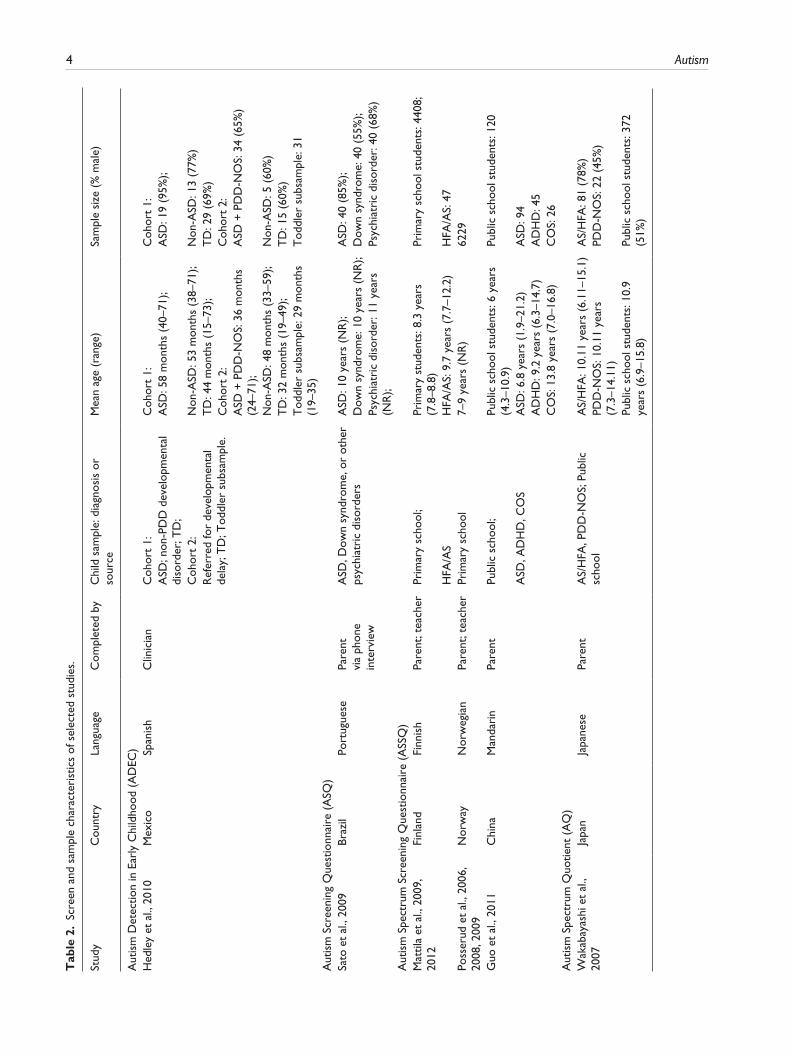
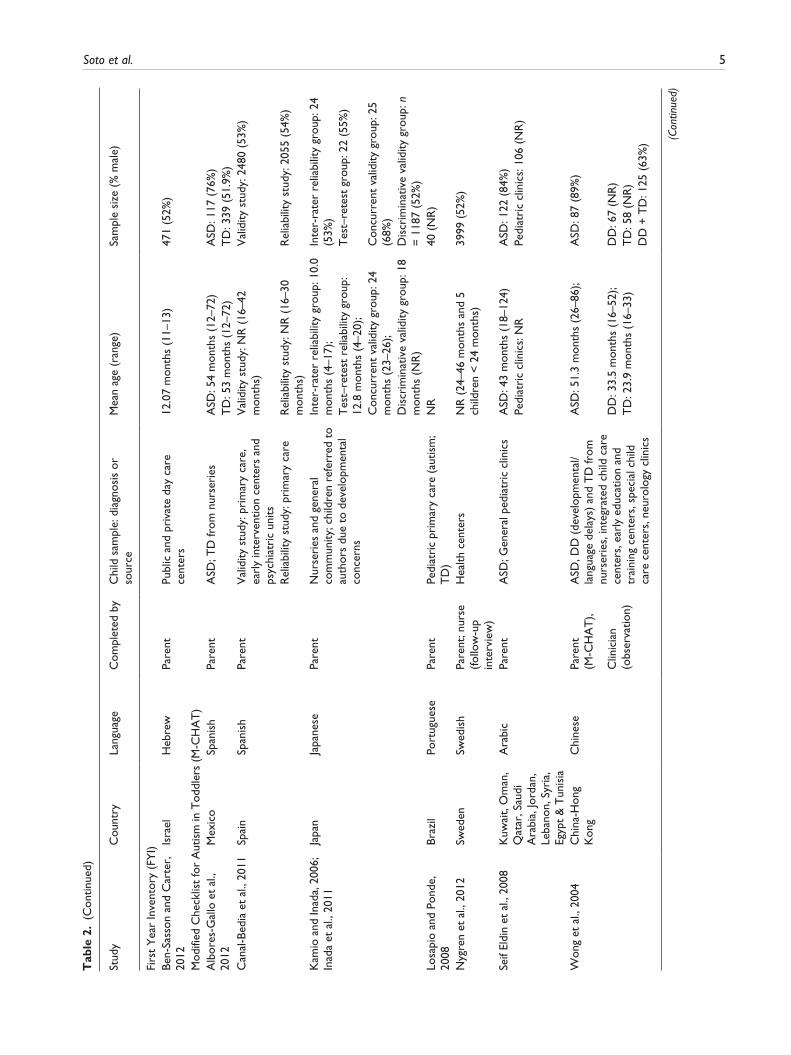
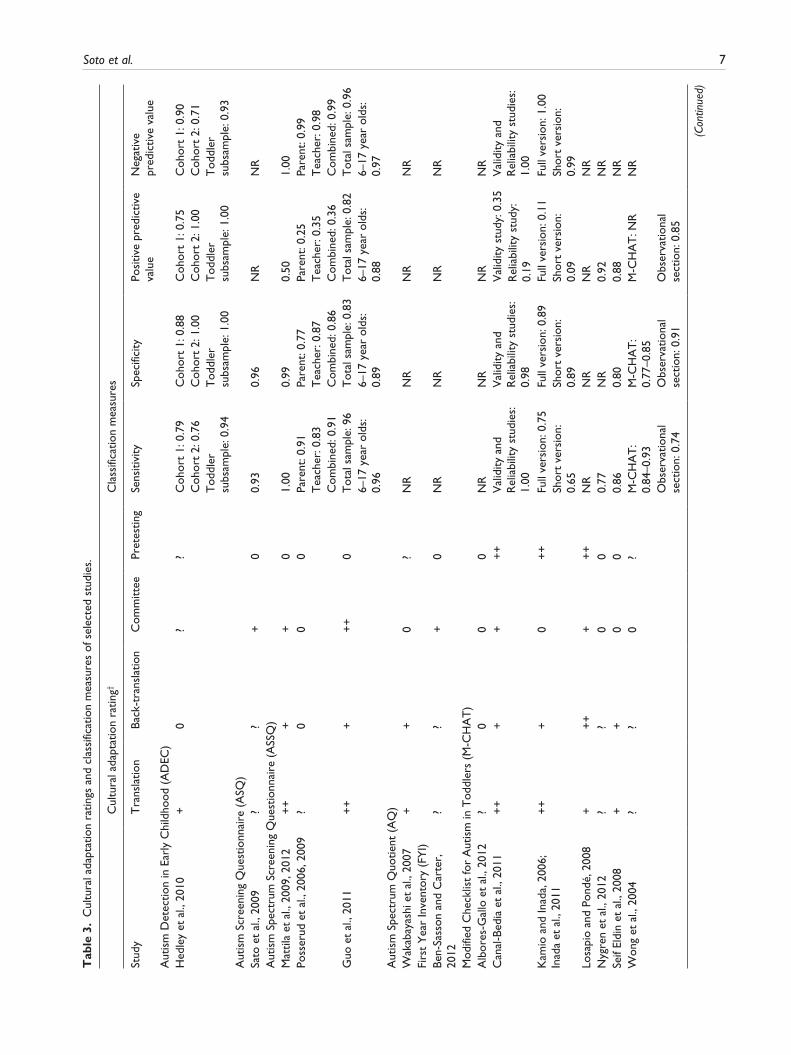
Table 2 summarizes characteristics of the screen and sample used in each of the adaptation studies. Table 3 provides ratings of the adaptation process based on the guidelines from Table 1 and the reported classification measures (sensitivity, specificity, positive predictive value (PPV) and negative predictive value (NPV)) of the screen for identifying children with ASD from those with typical development (TD) or other clinical conditions. No attempts were made to calculate missing classification
Table 1. Guidelines for assessing the extent to which reported cross-cultural adaptation of ASD screening instruments adhered to guidelines adapted from Guillemin et al. (1993).
Steps Rating Description
Translation ++ Translation into their native language by at least two independent individuals (or teams) who possess a range of knowledge about the intent and concepts underlying the instrument
+ Translation process does not contain one or more components required for a ++ rating? Translation mentioned but not described0 No Information reported
Back-translation ++ Independent back-translation of each forward-translation by individual (team) whose native language is that of the original instrument and who is not versed in the intent or concepts underlying the instrument
+ Back-translation process does not contain one or more components required for a ++ rating? Back-translation mentioned but not described0 No Information reported
Committee Review ++ Translated and original version of the instrument are evaluated by a multidisciplinary committee, including those well versed in the intent or concepts underlying the instrument as well as lay individuals from the target population
+ Committee review process does not contain one or more of components required for a ++ rating
? A committee approach mentioned but not described0 No Information reported
Pretesting ++ A sample of the target population responds to the instrument supplemented by follow-up probe questions or a group of bilingual lay individuals examine both original and translated versions for equivalence.
+ Pretesting does not involve one or more components required for a ++ rating.? Pretesting mentioned but not described0 No Information reported
ASD: autism spectrum disorder.
4 Autism T
able
2.
Scre
en a
nd s
ampl
e ch
arac
teri
stic
s of
sel
ecte
d st
udie
s.
Stud
yC
ount
ryLa
ngua
geC
ompl
eted
by
Chi
ld s
ampl
e: d
iagn
osis
or
sour
ceM
ean
age
(ran
ge)
Sam
ple
size
(%
mal
e)
Aut
ism
Det
ectio
n in
Ear
ly C
hild
hood
(A
DEC
)H
edle
y et
al.,
201
0M
exic
oSp
anis
hC
linic
ian
Coh
ort
1:C
ohor
t 1:
Coh
ort
1:A
SD; n
on-P
DD
dev
elop
men
tal
diso
rder
; TD
;A
SD: 5
8 m
onth
s (4
0–71
);A
SD: 1
9 (9
5%);
Coh
ort
2:N
on-A
SD: 5
3 m
onth
s (3
8–71
);N
on-A
SD: 1
3 (7
7%)
Ref
erre
d fo
r de
velo
pmen
tal
dela
y; T
D; T
oddl
er s
ubsa
mpl
e.T
D: 4
4 m
onth
s (1
5–73
);T
D: 2
9 (6
9%)
Coh
ort
2:C
ohor
t 2:
ASD
+ P
DD
-NO
S: 3
6 m
onth
s (2
4–71
);A
SD +
PD
D-N
OS:
34
(65%
)
Non
-ASD
: 48
mon
ths
(33–
59);
Non
-ASD
: 5 (
60%
)T
D: 3
2 m
onth
s (1
9–49
);T
D: 1
5 (6
0%)
Tod
dler
sub
sam
ple:
29
mon
ths
(19–
35)
Tod
dler
sub
sam
ple:
31
Aut
ism
Scr
eeni
ng Q
uest
ionn
aire
(A
SQ)
Sato
et
al.,
2009
Braz
ilPo
rtug
uese
Pare
nt
via
phon
e in
terv
iew
ASD
, Dow
n sy
ndro
me,
or
othe
r ps
ychi
atri
c di
sord
ers
ASD
: 10
year
s (N
R);
ASD
: 40
(85%
);D
own
synd
rom
e: 1
0 ye
ars
(NR
);D
own
synd
rom
e: 4
0 (5
5%);
Psyc
hiat
ric
diso
rder
: 11
year
s (N
R);
Psyc
hiat
ric
diso
rder
: 40
(68%
)
Aut
ism
Spe
ctru
m S
cree
ning
Que
stio
nnai
re (
ASS
Q)
Mat
tila
et a
l., 2
009,
20
12Fi
nlan
dFi
nnis
hPa
rent
; tea
cher
Prim
ary
scho
ol;
Prim
ary
stud
ents
: 8.3
yea
rs
(7.8
–8.8
)Pr
imar
y sc
hool
stu
dent
s: 4
408;
HFA
/AS
HFA
/AS:
9.7
yea
rs (
7.7–
12.2
)H
FA/A
S: 4
7Po
sser
ud e
t al
., 20
06,
2008
, 200
9N
orw
ayN
orw
egia
nPa
rent
; tea
cher
Prim
ary
scho
ol7–
9 ye
ars
(NR
)62
29
Guo
et
al.,
2011
Chi
naM
anda
rin
Pare
ntPu
blic
sch
ool;
Publ
ic s
choo
l stu
dent
s: 6
yea
rs
(4.3
–10.
9)Pu
blic
sch
ool s
tude
nts:
120
ASD
, AD
HD
, CO
SA
SD: 6
.8 y
ears
(1.
9–21
.2)
ASD
: 94
AD
HD
: 9.2
yea
rs (
6.3–
14.7
)A
DH
D: 4
5C
OS:
13.
8 ye
ars
(7.0
–16.
8)C
OS:
26
Aut
ism
Spe
ctru
m Q
uotie
nt (
AQ
)W
akab
ayas
hi e
t al
., 20
07Ja
pan
Japa
nese
Pare
ntA
S/H
FA, P
DD
-NO
S; P
ublic
sc
hool
AS/
HFA
: 10.
11 y
ears
(6.
11–1
5.1)
AS/
HFA
: 81
(78%
)PD
D-N
OS:
10.
11 y
ears
(7
.3–1
4.11
)PD
D-N
OS:
22
(45%
)
Publ
ic s
choo
l stu
dent
s: 1
0.9
year
s (6
.9–1
5.8)
Publ
ic s
choo
l stu
dent
s: 3
72
(51%
)
Soto et al. 5
Stud
yC
ount
ryLa
ngua
geC
ompl
eted
by
Chi
ld s
ampl
e: d
iagn
osis
or
sour
ceM
ean
age
(ran
ge)
Sam
ple
size
(%
mal
e)
Firs
t Y
ear
Inve
ntor
y (F
YI)
Ben-
Sass
on a
nd C
arte
r,
2012
Isra
elH
ebre
wPa
rent
Publ
ic a
nd p
riva
te d
ay c
are
cent
ers
12.0
7 m
onth
s (1
1–13
)47
1 (5
2%)
Mod
ified
Che
cklis
t fo
r A
utis
m in
Tod
dler
s (M
-CH
AT
)A
lbor
es-G
allo
et
al.,
2012
Mex
ico
Span
ish
Pare
ntA
SD; T
D fr
om n
urse
ries
ASD
: 54
mon
ths
(12–
72)
ASD
: 117
(76
%)
TD
: 53
mon
ths
(12–
72)
TD
: 339
(51
.9%
)C
anal
-Bed
ia e
t al
., 20
11Sp
ain
Span
ish
Pare
ntV
alid
ity s
tudy
: pri
mar
y ca
re,
earl
y in
terv
entio
n ce
nter
s an
d ps
ychi
atri
c un
its
Val
idity
stu
dy: N
R (
16–4
2 m
onth
s)V
alid
ity s
tudy
: 248
0 (5
3%)
Rel
iabi
lity
stud
y: p
rim
ary
care
Rel
iabi
lity
stud
y: N
R (
16–3
0 m
onth
s)R
elia
bilit
y st
udy:
205
5 (5
4%)
Kam
io a
nd In
ada,
200
6;
Inad
a et
al.,
201
1Ja
pan
Japa
nese
Pare
ntN
urse
ries
and
gen
eral
co
mm
unity
; chi
ldre
n re
ferr
ed t
o au
thor
s du
e to
dev
elop
men
tal
conc
erns
Inte
r-ra
ter
relia
bilit
y gr
oup:
10.
0 m
onth
s (4
–17)
;In
ter-
rate
r re
liabi
lity
grou
p: 2
4 (5
3%)
Tes
t–re
test
rel
iabi
lity
grou
p:
12.8
mon
ths
(4–2
0);
Tes
t–re
test
gro
up: 2
2 (5
5%)
Con
curr
ent
valid
ity g
roup
: 24
mon
ths
(23–
26);
Con
curr
ent
valid
ity g
roup
: 25
(68%
)D
iscr
imin
ativ
e va
lidity
gro
up: 1
8 m
onth
s (N
R)
Dis
crim
inat
ive
valid
ity g
roup
: n
= 1
187
(52%
)Lo
sapi
o an
d Po
nde,
20
08Br
azil
Port
ugue
sePa
rent
Pedi
atri
c pr
imar
y ca
re (
autis
m;
TD
)N
R40
(N
R)
Nyg
ren
et a
l., 2
012
Swed
enSw
edis
hPa
rent
; nur
se
(follo
w-u
p in
terv
iew
)
Hea
lth c
ente
rsN
R (
24–4
6 m
onth
s an
d 5
child
ren
< 2
4 m
onth
s)39
99 (
52%
)
Seif
Eldi
n et
al.,
200
8K
uwai
t, O
man
, Q
atar
, Sau
di
Ara
bia,
Jord
an,
Leba
non,
Syr
ia,
Egyp
t &
Tun
isia
Ara
bic
Pare
ntA
SD; G
ener
al p
edia
tric
clin
ics
ASD
: 43
mon
ths
(18–
124)
ASD
: 122
(84
%)
Pedi
atri
c cl
inic
s: N
RPe
diat
ric
clin
ics:
106
(N
R)
Won
g et
al.,
200
4C
hina
-Hon
g K
ong
Chi
nese
Pare
nt
(M-C
HA
T),
ASD
, DD
(de
velo
pmen
tal/
lang
uage
del
ays)
and
TD
from
nu
rser
ies,
inte
grat
ed c
hild
car
e ce
nter
s, e
arly
edu
catio
n an
d tr
aini
ng c
ente
rs, s
peci
al c
hild
ca
re c
ente
rs, n
euro
logy
clin
ics
ASD
: 51.
3 m
onth
s (2
6–86
);A
SD: 8
7 (8
9%)
Clin
icia
n (o
bser
vatio
n)D
D: 3
3.5
mon
ths
(16–
52);
DD
: 67
(NR
)T
D: 2
3.9
mon
ths
(16–
33)
TD
: 58
(NR
)D
D +
TD
: 125
(63
%)
(Con
tinue
d)
Tab
le 2
. (C
ontin
ued)

6 Autism
Stud
yC
ount
ryLa
ngua
geC
ompl
eted
by
Chi
ld s
ampl
e: d
iagn
osis
or
sour
ceM
ean
age
(ran
ge)
Sam
ple
size
(%
mal
e)
Soci
al a
nd C
omm
unic
atio
n D
isor
ders
Che
cklis
t (S
CD
C)
Bölte
et
al.,
2011
Ger
man
yG
erm
anPa
rent
ASD
, Oth
er p
sych
iatr
ic
diag
nose
s, T
D fr
om c
hild
&
adol
esce
nt p
sych
iatr
ic c
linic
s,
pres
choo
ls, p
rim
ary,
and
se
cond
ary
scho
ols,
and
per
sona
l co
ntac
ts
ASD
: 11.
2 ye
ars
(4–1
8)A
SD: 1
48 (
82%
)O
ther
psy
chia
tric
dia
gnos
es: 9
.9
year
s (4
–18
year
s)O
ther
psy
chia
tric
dia
gnos
es:
255
(73%
)T
D: 9
.3 y
ears
(N
R)
TD
: 77
(53%
)
Soci
al C
omm
unic
atio
n Q
uest
ionn
aire
(SC
Q)
Gau
et
al.,
2011
Tai
wan
Chi
nese
Pare
ntA
SD fr
om h
ospi
tals
and
sib
lings
ASD
: 2–1
8 ye
ars
ASD
: 682
(82
%)
Sibl
ings
: 4–1
8 ye
ars
Sibl
ings
: 240
(N
R)
Soci
al R
espo
nsiv
enes
s Sc
ale
(SR
S)Bö
lte e
t al
., 20
08 (
SRS)
Ger
man
yG
erm
anPa
rent
ASD
, Oth
er p
sych
iatr
ic
diag
nose
s fr
om h
ospi
tals
;A
SD: 9
.2 y
ears
ASD
: 160
(81
%)
TD
from
pre
scho
ols,
pri
mar
y,
and
seco
ndar
y sc
hool
sO
ther
psy
chia
tric
dia
gnos
is: 1
0.4
year
sO
ther
psy
chia
tric
dia
gnos
es:
367
(69%
)T
D: 9
.9 y
ears
TD
: 838
(53
%)
AD
HD
: Att
entio
n D
efic
it H
yper
activ
ity D
isor
der,
AS:
Asp
erge
r’s
synd
rom
e, A
SD: a
utis
m s
pect
rum
dis
orde
r, C
OS:
Chi
ldho
od O
nset
Sch
izop
hren
ia, D
D: D
evel
opm
enta
l Del
ay, H
FA: h
igh
func
tioni
ng
autis
m, N
R: N
ot R
epor
ted,
PD
D: P
erva
sive
Dev
elop
men
tal D
isor
der,
PD
D-N
OS:
PD
D n
ot o
ther
wis
e sp
ecifi
ed, T
D: T
ypic
ally
Dev
elop
ing.
Tab
le 2
. (C
ontin
ued)
Soto et al. 7
Tab
le 3
. C
ultu
ral a
dapt
atio
n ra
tings
and
cla
ssifi
catio
n m
easu
res
of s
elec
ted
stud
ies.
Cul
tura
l ada
ptat
ion
ratin
g†C
lass
ifica
tion
mea
sure
s
Stud
yT
rans
latio
nBa
ck-t
rans
latio
nC
omm
ittee
Pret
estin
gSe
nsiti
vity
Spec
ifici
tyPo
sitiv
e pr
edic
tive
valu
eN
egat
ive
pred
ictiv
e va
lue
Aut
ism
Det
ectio
n in
Ear
ly C
hild
hood
(A
DEC
)H
edle
y et
al.,
201
0+
0?
?C
ohor
t 1:
0.7
9C
ohor
t 1:
0.8
8C
ohor
t 1:
0.7
5C
ohor
t 1:
0.9
0C
ohor
t 2:
0.7
6C
ohor
t 2:
1.0
0C
ohor
t 2:
1.0
0C
ohor
t 2:
0.7
1T
oddl
er
subs
ampl
e: 0
.94
Tod
dler
su
bsam
ple:
1.0
0T
oddl
er
subs
ampl
e: 1
.00
Tod
dler
su
bsam
ple:
0.9
3A
utis
m S
cree
ning
Que
stio
nnai
re (
ASQ
)Sa
to e
t al
., 20
09?
?+
00.
930.
96N
RN
RA
utis
m S
pect
rum
Scr
eeni
ng Q
uest
ionn
aire
(A
SSQ
)M
attil
a et
al.,
200
9, 2
012
++
++
01.
000.
990.
501.
00Po
sser
ud e
t al
., 20
06, 2
009
?0
00
Pare
nt: 0
.91
Pare
nt: 0
.77
Pare
nt: 0
.25
Pare
nt: 0
.99
Tea
cher
: 0.8
3T
each
er: 0
.87
Tea
cher
: 0.3
5T
each
er: 0
.98
Com
bine
d: 0
.91
Com
bine
d: 0
.86
Com
bine
d: 0
.36
Com
bine
d: 0
.99
Guo
et
al.,
2011
++
++
+0
Tot
al s
ampl
e: 9
6T
otal
sam
ple:
0.8
3T
otal
sam
ple:
0.8
2T
otal
sam
ple:
0.9
66–
17 y
ear
olds
: 0.
966–
17 y
ear
olds
: 0.
896–
17 y
ear
olds
: 0.
886–
17 y
ear
olds
: 0.
97A
utis
m S
pect
rum
Quo
tient
(A
Q)
Wak
abay
ashi
et
al.,
2007
++
0?
NR
NR
NR
NR
Firs
t Y
ear
Inve
ntor
y (F
YI)
Ben-
Sass
on a
nd C
arte
r,
2012
??
+0
NR
NR
NR
NR
Mod
ified
Che
cklis
t fo
r A
utis
m in
Tod
dler
s (M
-CH
AT
)A
lbor
es-G
allo
et
al.,
2012
?0
00
NR
NR
NR
NR
Can
al-B
edia
et
al.,
2011
++
++
++
Val
idity
and
R
elia
bilit
y st
udie
s:
1.00
Val
idity
and
R
elia
bilit
y st
udie
s:
0.98
Val
idity
stu
dy: 0
.35
Val
idity
and
R
elia
bilit
y st
udie
s:
1.00
Rel
iabi
lity
stud
y:
0.19
Kam
io a
nd In
ada,
200
6;
Inad
a et
al.,
201
1+
++
0+
+Fu
ll ve
rsio
n: 0
.75
Full
vers
ion:
0.8
9Fu
ll ve
rsio
n: 0
.11
Full
vers
ion:
1.0
0Sh
ort
vers
ion:
0.
65Sh
ort
vers
ion:
0.
89Sh
ort
vers
ion:
0.
09Sh
ort
vers
ion:
0.
99Lo
sapi
o an
d Po
ndé,
200
8+
++
++
+N
RN
RN
RN
RN
ygre
n et
al.,
201
2?
?0
00.
77N
R0.
92N
RSe
if El
din
et a
l., 2
008
++
00
0.86
0.80
0.88
NR
Won
g et
al.,
200
4?
?0
?M
-CH
AT
: 0.
84–0
.93
M-C
HA
T:
0.77
–0.8
5M
-CH
AT
: NR
NR
Obs
erva
tiona
l se
ctio
n: 0
.74
Obs
erva
tiona
l se
ctio
n: 0
.91
Obs
erva
tiona
l se
ctio
n: 0
.85
(Con
tinue
d)
8 Autism
Cul
tura
l ada
ptat
ion
ratin
g†C
lass
ifica
tion
mea
sure
s
Soci
al a
nd C
omm
unic
atio
n D
isor
ders
Che
cklis
t (S
CD
C)
Bölte
et
al.,
2011
??
0?
ASD
/TD
: 0.
87–0
.90
ASD
/TD
: 0.
75–0
.82
NR
NR
ASD
/Oth
er
clin
ical
dia
gnos
is:
0.90
–0.8
5
ASD
/Oth
er
clin
ical
dia
gnos
is:
0.28
–0.4
4So
cial
Com
mun
icat
ion
Que
stio
nnai
re (
SCQ
)G
au e
t al
., 20
11+
+0
0N
RN
RN
RN
RSo
cial
Res
pons
iven
ess
Scal
e (S
RS)
Bölte
et
al.,
2008
, 201
1?
?0
00.
73–0
.90
(dep
endi
ng o
n sa
mpl
e an
d cu
t-of
f)
0.56
–1.0
0 (d
epen
ding
on
sam
ple
and
cut-
off)
NR
NR
ASD
: Aut
ism
Spe
ctru
m D
isor
der;
TD
: Typ
ical
ly D
evel
opin
g; N
R =
Not
Rep
orte
d.†
See
Tab
le 1
for
key.
Tab
le 3
. (C
ontin
ued)
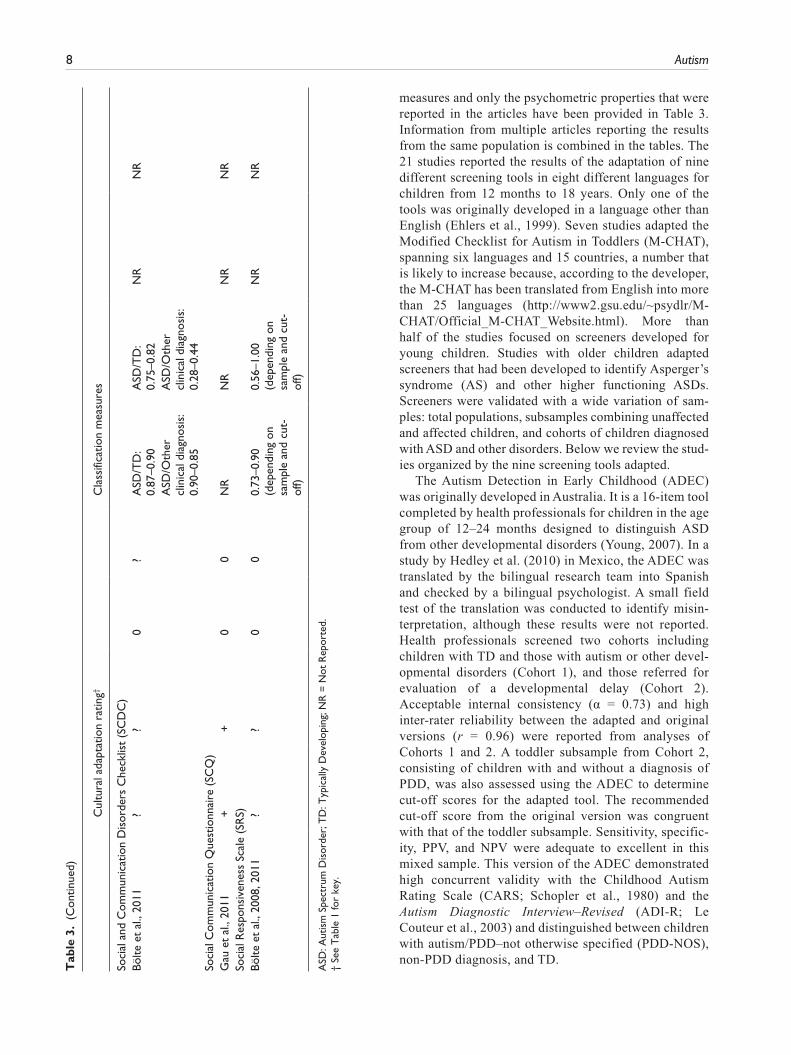
measures and only the psychometric properties that were reported in the articles have been provided in Table 3. Information from multiple articles reporting the results from the same population is combined in the tables. The 21 studies reported the results of the adaptation of nine different screening tools in eight different languages for children from 12 months to 18 years. Only one of the tools was originally developed in a language other than English (Ehlers et al., 1999). Seven studies adapted the Modified Checklist for Autism in Toddlers (M-CHAT), spanning six languages and 15 countries, a number that is likely to increase because, according to the developer, the M-CHAT has been translated from English into more than 25 languages (http://www2.gsu.edu/~psydlr/M-CHAT/Official_M-CHAT_Website.html). More than half of the studies focused on screeners developed for young children. Studies with older children adapted screeners that had been developed to identify Asperger’s syndrome (AS) and other higher functioning ASDs. Screeners were validated with a wide variation of sam-ples: total populations, subsamples combining unaffected and affected children, and cohorts of children diagnosed with ASD and other disorders. Below we review the stud-ies organized by the nine screening tools adapted.
The Autism Detection in Early Childhood (ADEC) was originally developed in Australia. It is a 16-item tool completed by health professionals for children in the age group of 12–24 months designed to distinguish ASD from other developmental disorders (Young, 2007). In a study by Hedley et al. (2010) in Mexico, the ADEC was translated by the bilingual research team into Spanish and checked by a bilingual psychologist. A small field test of the translation was conducted to identify misin-terpretation, although these results were not reported. Health professionals screened two cohorts including children with TD and those with autism or other devel-opmental disorders (Cohort 1), and those referred for evaluation of a developmental delay (Cohort 2). Acceptable internal consistency (α = 0.73) and high inter-rater reliability between the adapted and original versions (r = 0.96) were reported from analyses of Cohorts 1 and 2. A toddler subsample from Cohort 2, consisting of children with and without a diagnosis of PDD, was also assessed using the ADEC to determine cut-off scores for the adapted tool. The recommended cut-off score from the original version was congruent with that of the toddler subsample. Sensitivity, specific-ity, PPV, and NPV were adequate to excellent in this mixed sample. This version of the ADEC demonstrated high concurrent validity with the Childhood Autism Rating Scale (CARS; Schopler et al., 1980) and the Autism Diagnostic Interview–Revised (ADI-R; Le Couteur et al., 2003) and distinguished between children with autism/PDD–not otherwise specified (PDD-NOS), non-PDD diagnosis, and TD.

Soto et al. 9
The Autism Screening Questionnaire (Berument et al., 1999), an earlier version of the Social Communication Questionnaire (SCQ; Rutter et al., 2003), is a 40-question yes/no, caregiver completed screening tool developed in the United Kingdom with versions for children below and above the age of 6 years. Sato et al. (2009) created the Brazilian version through translation into Portuguese and back-translation. Review of these versions by a multidisci-plinary committee resulted in only minor semantic changes to two items. Researchers completed the questionnaire via telephone with parents of children previously diagnosed with ASD, Down syndrome, and other psychiatric disor-ders. Internal consistency (α = 0.90) and test–retest relia-bility were high. Using the same cut-off score as the original version of the tool, sensitivity and specificity were also high.
The Autism Spectrum Screening Questionnaire (ASSQ: Ehlers and Gillberg, 1993; Ehlers et al., 1999) is a 27-item, 3-point questionnaire developed in Sweden and intended to screen for AS and other higher functioning ASDs in children in the age group of 7–16 months. Items assess social problems, communication problems, repetitive and restrictive behavior, motor clumsiness, and tics. The ASSQ has been translated into English (Ehlers and Gillberg, 1993), Lithuanian (Lesinskiene, 2000), Norwegian (Posserud et al., 2006), Finnish (Mattila et al., 2009), and Mandarin Chinese (Guo et al., 2011). Validation studies have been published for the latter three versions.
Finnish studies (Mattila et al., 2009, 2012) described an adaptation of the ASSQ consisting of translation by two psychologists, back-translation by an official Swedish translator, and comparison of the two versions (translation vs back-translation) by a panel of pediatric neurologists. The wording of the highest alternative on the scale was changed from “fits definitely” to “fits” because clinical experience suggested that Finnish parents would be reluc-tant to select the former alternative. Screening comprised ASSQ ratings by teachers and parents of all 8-year-old children, mainly of Finnish descent, living in the catch-ment area of one hospital area in one county and attending 304 schools. All children in the screened sample who met criteria for ASD through diagnostic evaluation with the Autism Diagnostic Observation Schedule (ADOS; Lord et al., 1999) and ADI-R or hospital records were identified. Parent and teacher ASSQ scores showed a low correlation, but the means and medians of both ratings were signifi-cantly higher in 7–12-year-old children with high func-tioning autism (HFA)/AS in outpatient treatment than in the total sample. On summation, parent and teacher scores showed the best discrimination between children with and without an ASD diagnosis in the analysis of the total sam-ple; sensitivity, specificity, and NPV were extremely high (Mattila et al., 2012). Mattila et al. (2009) also evaluated cut-offs in the same sample; however, sensitivity and spec-ificity values were slightly different for the same optimal
cut-off because all subjects with ASD had not yet been identified. Of note, the cut-off score recommendations dif-fered from those reported in the original Swedish and Mandarin Chinese studies (see below).
The ASSQ was also translated into Norwegian (Posserud et al., 2006) for the Norwegian Bergen Child Study (Heiervang et al., 2007). In a large sample of 7–9-year-olds, the adapted instrument was found to have good internal consistency (0.86 for teachers and 0.89 for parents) and a stable three-factor structure (Posserud et al., 2008). All children who screened positive and a sample of those who screened negative participated in a full diagnos-tic evaluation. Receiver Operating Characteristic (ROC) analyses, assessing the ability of the ASSQ to distinguish ASD from non-ASD cases, revealed excellent discrimi-nant ability for parent and teacher ratings with even more optimal screening properties for the score combining rat-ings from both respondents (Posserud et al., 2009).
Guo et al. (2011) evaluated the validity of a Mandarin Chinese translation of the ASSQ (CH-ASSQ). The ASSQ was translated by two of the native-speaking authors and further refined through back-translation. After review by four native-speaking experts and two English-speaking authors, minor changes were made to make the translation more culturally appropriate, while maintaining the clinical meaning of the items. The CH-ASSQ was completed by parents of 165 children recruited from the Institute of Mental Health, Peking University, who had diagnoses of ASD, Attention Deficit Hyperactivity Disorder (ADHD), or Childhood Onset Schizophrenia, and by parents of 120 unaffected children recruited from the public school sys-tem. Analyses were performed on the entire sample as well as a subsample of those children between the ages of 6 and 17 years (66% of the ASD group and 59% of the unaf-fected group), the same age range used in the validation of the original Swedish ASSQ. An ROC analysis of children with ASD versus unaffected children revealed excellent discrimination using an empirically determined cut-off score, somewhat lower than that determined in the Swedish version, with an overall diagnostic accuracy of 88.3% for the total sample and 92.6% for 6–17-year-olds. A similar analysis comparing children with ASD with the other clin-ical groups determined a higher optimal cut-off score with slightly reduced but still strong discrimination.
The Autism Spectrum Quotient–Child Form (AQ-Child Form) is a 50-item parent-report questionnaire for children in the age group of 4–11 years developed in the United Kingdom (Auyeung et al., 2008). Wakabayashi et al. (2007) adapted the AQ-Child Form for use in Japan and included forward-translation by one of the Japanese authors, comparison of the two versions by a bilingual psychologist, and backward translation by native English speakers. Pilot testing revealed parental confusion over items tapping imagination (e.g. “When s/he is reading a story, s/he can easily imagine what the characters might

10 Autism
look like?”); therefore a “Don’t Know” response option was included. The study used a sample of 475 children with normal intelligence, consisting of those with AS, HFA, or PDD-NOS, as well as unaffected students recruited from primary and secondary schools. The adapted tool demonstrated good internal consistency across domains (α = 0.84) but somewhat weaker reliability within subdomains (α = 0.69–0.84). Group comparisons showed that the Japanese AQ significantly discriminated youth diagnosed with HFA and AS from children with TD. The best- discriminating cut-off score and overall scores were lower than in the original sample, a difference, the authors sug-gested, that may have resulted from the addition of the “Don’t Know” option or from a reduced recognition of social problems. Other psychometric properties were not reported.
The First Year Inventory (FYI) is a 63-item parent ques-tionnaire developed in the United States for 12-month-olds to assess behaviors in two domains that indicate a risk for ASD: social-communication and sensory–regulatory (Baranek et al., 2003; Reznick et al., 2007). Ben-Sasson and Carter (2012) produced an Israeli version with back-translation. A linguistic and cultural review by a bilingual, interdisciplinary panel of experts was conducted, although no description of the results was provided. Parents of 12-month-old children drawn from private and publicly subsidized day care centers completed the FYI. Internal reliability within the social subdomain (α = 0.68) and sen-sory subdomain (α = 0.53) was questionable to poor. Construct validity was demonstrated with the Autism Observation Scale for Infants (AOSI; Bryson et al., 2008) and with the Early Learning Composite scores of the Mullen Scales of Early Learning (MSEL; Mullen, 1995). In this sample, lower socioeconomic status (SES) was cor-related with higher FYI risk scores. Additionally, the Israeli sample presented with higher scores on the sen-sory–regulatory domain than the original study. The authors suggested that this may reflect increased rates of dysregulation problems and sensory symptoms found in other studies of Israeli children (Neuman et al., 2004; Tirosh et al., 2003) but note that methodological differ-ences prevent direct cross-country comparison. Sensitivity, specificity, PPV, and NPV were not reported.
The M-CHAT, created in the United States, is a 23-item yes/no parent-report checklist designed for universal screening for ASD in toddlers in the age group of 16–30 months (Kleinman et al., 2008; Robins et al., 2001). Development of a Mexican Spanish language version of the M-CHAT (MM-CHAT) included translation into Spanish with cultural adjustments of some items (Albores-Gallo et al., 2012). For example, because Mexican mothers reportedly had no specific name for the game of “peek-a-boo,” a description was provided. Nevertheless, parents had difficulty understanding some of the translated items. Psychometric properties were investigated with a case
control study that included 456 children in the age group of 18–72 months, either with TD or an ASD diagnosis. Reliability was acceptable (α = 0.76) for the total score and for six critical items (α = 0.70). Concurrent validity esti-mates were in the moderate range using the Child Behavior Checklist (CBCL; Achenbach and Rescorla, 2000) but showed more mixed results with the ADI-R. The MM-CHAT scores were significantly greater in children with ASD than those with TD; however, the critical items distinguishing the two groups were not the same as in the original validation sample. The authors suggested that var-iation in the endorsed critical items might reflect cultural differences in parenting and social behavioral styles. Other psychometric properties were not reported.
The M-CHAT was adapted for use in Spain with parents of 4535 toddlers in two population-based validation studies (Canal-Bedia et al., 2011). All components of the recom-mended cultural adaptation process were included, although some were not described fully. Two translations by bilingual individuals with child development expertise were carried out and a back-translation by a native English speaker included a comparison with the original version by the authors and the developers. Following pretesting with 622 children, six items were modified to clarify their meaning. For instance, examples were added to items that referred to the use of specific toys. The adapted M-CHAT discrimi-nated children with ASD from those with TD but not from those with a developmental disorder other than ASD. Sensitivity, specificity, and NPV were high. However, PPVs were low in both studies conducted for this adaptation, a finding attributed to low prevalence rates in the samples.
Kamio and Inada (2006) constructed a Japanese version of the M-CHAT (M-CHAT-JV) through translation by the research team and back-translation by a bilingual, profes-sional translator. A pilot study with the parents of 659, 18-month-old children at well-child, pediatric visits showed adequate discrimination with critical items similar to those of the original instrument but prompted the addi-tion of illustrations to four items to enhance caregiver rec-ognition of delayed typical development (i.e. negative symptoms). Inada et al. (2011) reported psychometric properties of the M-CHAT-JV administered to volunteer parents of children from local day care centers and of tod-dlers referred to the authors for developmental concerns. The adapted screening tool had strong inter-rater (mothers and fathers) and test–retest reliability and was highly cor-related (r = 0.58) with the CARS-Tokyo Version (Kurita et al., 1989). Ratings of 18-month-old children participat-ing in well-child visits differed significantly between chil-dren diagnosed with autism or PDD-NOS at 3 years of age and those without a diagnosis. Sensitivity, specificity, and NPV were moderate to high, though PPV was low. Of note, a proposed short version with nine items demon-strated comparable validity, specificity, PPV, and NPV to the full version.

Soto et al. 11
In the full version of the M-CHAT-JV, sensitivity and specificity were improved by using a cut-off of two posi-tive responses (rather than three as originally recom-mended) because children who were later diagnosed with ASD passed the screen at a higher rate than children in the original US sample. The authors suggested that this differ-ence could have resulted from sampling differences or a culturally based reluctance to endorse “yes” in the yes/no format of the M-CHAT. In addition, a critical item from the original M-CHAT (“interest in other children”) was not useful, as all toddlers later diagnosed with ASD received passing scores on this item. The investigators suggested that Japanese parents might have interpreted their chil-dren’s behavior as shyness or modesty.
Losapio and Pondé (2008) adapted the M-CHAT with a Brazilian sample of 40 parents of children from pediat-ric outpatient clinics. All of the recommended cultural adaptation steps were reported. A Brazilian psychiatrist translated the M-CHAT to Portuguese and a native English-speaking professional translator without prior knowledge of the instrument back-translated the screen-ing tool. A bilingual rater evaluated the equivalence of the original and back-translated versions. Pretesting involved interviews and follow-up probe questions with the parents of two groups of 20 toddlers seen in pediatric clinics: those with autism and those without a diagnosis. Two autism experts evaluated the results and a variety of semantic and grammatical changes were made to items to maintain referential and conceptual meaning. Psychometric analyses were not reported.
Nygren et al. (2012) assessed the psychometric proper-ties of a Swedish version of the M-CHAT through popula-tion-based screening over 12 months in Swedish health centers (N = 3999). A few minor, unspecified adjustments of the Swedish language version were made following translation and back-translation to ensure the integrity of the instrument. Little detail was provided about the trans-lation process, and pretesting was not reported. Reliability and validity were not reported but sensitivity and PPV were moderate to high. Only three of the six critical items from the original M-CHAT overlapped with those show-ing the strongest prediction of ASD diagnosis. One of the original six critical items, “Does your child respond to his/her name when you call?” had the lowest endorsement by parents whose children were later confirmed to have ASD.
Seif Eldin et al. (2008) translated the M-CHAT for use in nine countries in the Gulf and eastern Mediterranean regions. In each country, small numbers of children from child development centers and general pediatric clinics, including a subsample of children with ASD, were recruited for assessment of diagnostic accuracy. Members of the Eastern Mediterranean Association of Child and Adolescent Psychiatry from five countries carried out for-ward- and back-translation and compared the two
versions. Changes resulting from this process were not reported. To address the unique language needs of each country, the authors altered classical Arabic with country-specific dialects for some words. Reliability and validity data were not provided, but the translated version yielded strong sensitivity, specificity, and PPV.
Wong et al. (2004) translated the M-CHAT into Chinese and combined it with the professional-completed observa-tional section B from the original Checklist for Autism in Toddlers (Baron-Cohen et al., 2000) to develop the CHAT-23. Reported cultural and linguistic adaptation procedures included forward- and back-translation, although no description of the process was provided. In pretesting, par-ents reported difficulty with the forced choice “yes/no” format, preferring qualitative words to describe children’s symptoms. Thus, a graded score was employed: never, sel-dom, usually, and often. The mixed sample in the valida-tion study included children with AS, non-ASD with developmental delay, and TD. The CHAT-23 successfully discriminated Chinese toddlers between 18 and 24 months, with diagnosed autism from toddlers with and without global developmental or language delays. ROC analysis revealed moderate to high sensitivity and specificity using three cut-off criteria: (1) failing 2 of 7 critical questions, (2) failing any 6 of the 23 questions, or (3) failing any 2 of the 4 items in the part B observational section. The inter-rater reliability for scoring section B was high (r = 0.95).
The Social Communication Disorders Checklist (SCDC) is a 12-item screening tool developed in the United Kingdom and completed by parents of children in the age group of 5–17 years (Skuse et al., 1997, 2005). Bölte et al. (2011) validated an adapted German version of the SCDC with a mixed sample composed of children with ASD, a clinical (behavioral or psychiatric) diagnosis, or TD. The tool was translated, back-translated, and adjusted by a native English speaker. The adapted version was pre-tested for understandability, although details or resulting alterations were not reported. Cronbach’s alphas for chil-dren with ASD, other psychiatric diagnoses, and TD were 0.78, 0.91, and 0.80, respectively. ROC analysis yielded excellent discrimination between children with ASD and TD but less so between children with ASD and other clini-cal diagnoses. Sensitivity for detecting ASD in popula-tions including TD and clinical children were quite high but specificity values varied widely, with low values dis-tinguishing ASD and clinical groups. Convergent validity demonstrated significant correlations with the ADI-R and the ADOS, as well as the SCQ-21. However, correlations were modest with the ADOS.
The SCQ is a 40-item, yes/no parent-report question-naire for children over the age of 4 developed in the United Kingdom (Eaves et al., 2006; Rutter et al., 2003). Gau et al. (2011) collaborated with child psychiatrists and psy-chologists to create a Chinese version and validated it with children with ASD and non-affected siblings (N = 922).

12 Autism
Translation and back-translation were conducted but no details were provided. Culture-relevant colloquial expres-sions were substituted, although the nature of these changes was not reported. Similar to the English language version, exploratory and confirmatory factor analyses yielded a 3-factor structure (social interaction, repetitive behaviors, and communication). However, differences with the UK version were evident in the specific items that cross-loaded on each factor. For example, some items that loaded on the communication subscale in the English ver-sion either loaded on the social interaction subscale or cross-loaded on to the communication and social interac-tion subscales in the Chinese version. The authors suggest that Taiwanese parents may consider gesturing (e.g. nod-ding, head shaking, pointing, imitation) and conversing behaviors (chit-chat) to be socially interactive rather than communicative. Additionally, since repetition and same-ness are stressed in Chinese language, the verbal ritual item may have been interpreted as communicative rather than as a repetitive and stereotyped behavior. Test–retest correlations were moderate (ICC = 0.77–0.78) and internal consistency was acceptable to excellent (α = 0.73–0.91) for all three subscales. Concurrent validity between the subscales of the SCQ and the ADI-R demonstrated corre-lations ranging from slight to high (r = 0.11–0.65). The SCQ discriminated between children with and without ASD but not between autism and AS.
The Social Responsiveness Scale (SRS) is a measure of autistic traits in social reciprocal behavior developed in the United States, employing a 65-item parent or teacher rat-ing scale for children in the age group of 4–18 months (Constantino and Gruber, 2002; Constantino et al., 2003). Bölte et al. (2008) assessed a German version of the SRS but offered little description of the adaptation procedures. Screening was applied to a large population of German youth who were typically developing or referred from clin-ics with ASD or other psychiatric diagnoses. Overall SRS scores for the entire normative sample and for children with ASD were lower in the normative German sample than in comparable US samples. Reliability of ratings for typically developing and clinic-referred children was greater than 0.91, and correlations between the SRS and different components of the ADOS, ADI-R, and SCQ indi-cated moderate to good convergent validity, ranging from 0.35 to 0.58. The authors also collected SRS data on sib-lings of youth with autism and found increased SRS scores in male siblings, providing what they described as the first cross-cultural validation of familial aggregation of autistic traits as measured by the SRS. ROC analyses of the total sample revealed steep declines in sensitivity and steep increases in specificity as the cut-off-score increased (from 56 to 100). The clinical and TD samples in the Bölte et al. (2011) study of the SCDC (see above) also completed the SRS. In analyses of only the ASD and TD groups, cut-offs of 75 and 85 yielded sensitivities of 0.80 and 0.74,
respectively, and specificities were 1.0. For ASD versus the group diagnosed with other psychiatric disorders, cut-offs of 75 and 85 yielded sensitivities of 0.80 and 0.74, respectively, and specificities of 0.69 and 0.79, respectively.
Discussion
The goal of screening for autism is to identify children at risk, facilitate conversations between providers and par-ents, and further evaluation, leading to earlier identifica-tion and improved outcomes. Although there are advantages favoring the use of screening tools developed in the specific culture and language in which they will be implemented, the construction of such measures requires extensive resources and effort. As a result, the adaptation and use of tools created in other cultural/language contexts is increasing. In this systematic review of adaptations of autism screening tools, all of the studies reviewed were published since 2004, with the majority appearing between 2009 and 2012. The results revealed a wide variation in the rigor of the reported adaptation across studies, although the details of the methods were rarely reported. More com-prehensive cultural adaptation procedures tended to result in more extensive modifications.
Forward-translation procedures meeting full guidelines were reported in only four of the 21 studies and almost half failed to provide information on this process at all. Three studies failed to include back-translation in their adapta-tion process, six indicated that it was done but provided no description, and only one study followed full guidelines. Review of the translation and/or back-translation and com-parison with the original source was mentioned in 10 of the 21 articles, although, in four of these adaptations, only one person carried out the review. All six of the studies employing a committee review involved experts but the composition of the group was multidisciplinary in only two cases. Involvement of individuals from the general population was never mentioned. Pretesting was reported in only seven studies, although details (e.g. sample, recruit-ment, and analytic procedures) were provided in only two instances.
In 12 studies, adaptation led to changes in the tool, var-ying from minor alterations of a few items to more wide-spread adjustments to improve clarity and comprehension, retain conceptual equivalence, and conform to the lan-guage and culture. In general, the more rigorous/well-described the adaption process, the more likely that modifications were made to the tools. No modifications were reported for five studies and in these studies, for-ward-translation was never described, back-translation either did not occur or was not described, committee review was not discussed, and pretesting was only men-tioned once, though the process was not described. In six of the 21 studies, minor modifications of the screening tool

Soto et al. 13
were made, such as substituting equivalents for hard-to-translate idiomatic and colloquial expressions or providing culturally relevant examples. These studies were more likely to report recommended components of adaptation; the forward-translation process was described (four stud-ies), back-translation was mentioned (five studies) and described (three studies), and four studies submitted the translations for review. Major adaptations or changes in format were made in six studies and, except for one, trans-lation or back-translation met recommended guidelines. Review was carried out in four cases and pretesting occurred in five cases. Besides changes in wording, these more extensive cultural adaptations revealed the need to construct items in a way that could be understood or deemed appropriate by the respondents, such as altering response alternatives or adding illustrations. However, even with such adaptations, we have found it necessary to use a trained bicultural/bilingual individual to administer the Spanish M-CHAT to produce adequate understanding (Linas et al., 2013). This is an issue that will need to be addressed in future studies involving culturally or linguis-tically distinct subgroups, or persons with lower or no literacy.
The studies reviewed varied greatly in the extent of psychometric analyses described. Nine studies reported indices of internal consistency, and few reported assess-ments of test–retest reliability and factor structure, where appropriate. Evidence for convergent or concurrent valid-ity of the adapted tool was provided in only seven cases. Ten studies included comparisons of children and youth screening positive or diagnosed with ASD with unaffected individuals, with all reporting higher scores for the diag-nosed or at-risk children. A small number of studies com-pared ASD samples to other conditions (e.g. other developmental disorders, behavioral health problems) or within the ASD spectrum (e.g. autism vs AS). In general, the tools differentiated among these conditions less well.
A total of eleven studies provided analysis of the diag-nostic accuracy of the adapted instruments, although the samples differed markedly. Only four studies from Scandinavia and Spain examined the accuracy of adapted tools (ASSQ and M-CHAT) with population-based sam-ples. In most cases, sensitivity and specificity of the instru-ments were determined in populations that included a mixture of clinical and population-based samples; how-ever, such estimates may be unstable (Camp, 2006). In general, estimates of sensitivity and specificity, when pro-vided, were sufficient to discriminate ASD children from typically developing children. The PPV value was often lower than the sensitivity estimate; however, a low PPV is to be expected in a screening instrument that assesses a disorder with low prevalence, such as ASD. Sensitivity and specificity are not dependent on the prevalence of a disorder because sensitivity is calculated using affected individuals and specificity is calculated using unaffected
individuals. If a sample includes a higher proportion of people with autism (e.g. Hedley et al., 2010; Seif Eldin et al., 2008; Wong et al., 2004), then the PPV tends to be higher than studies using samples with a lower proportion of people with autism.
Most of the studies reporting psychometric characteris-tics noted differences between the adapted and original versions. The nature of the differences depended on the analytic strategies used. A handful of studies reported dif-ferences in mean scores (Bölte et al., 2011; Wakabayashi et al., 2007) and factor loadings (Gau et al., 2011). In six cases, the optimal cut-off score for identifying children with ASD varied from that suggested in the original tool. For instance, there was broad variation of ASSQ cut-off scores across Swedish, Finnish, Norwegian, and Chinese versions. Five adaptations reported differences from the original in the frequency with which particular items were endorsed, mostly in terms of lack of overlap of critical items on the M-CHAT with those identified in the US sam-ple. Various reasons were proposed to account for the dif-ferences in psychometric properties of the adapted and original tools, including shared community experience or cultural differences in the meaning and perceived norms of certain behaviors, particularly social interactions, linguis-tic factors, and in parenting attitudes. However, evidence was not provided to confirm these possible explanations.
Although screening for ASDs is promoted by different organizations (mostly in the United States) and the adapta-tion of screening tools is increasing, there are concerns over the psychometric properties of autism screening tools (e.g. the possibility of missing cases and low “hit rates” in population-based studies). In addition, within-culture fac-tors may limit the validity of a tool, such as variations in education levels, SES, literacy, knowledge of ASD, and experience of stigma, as suggested by some of the studies covered in this review. As a result, some argue that justifi-cation for the use of ASD screening tools for whole popu-lation-based screening is lacking (Le Couteur, 2003; Williams and Brayne, 2006). While there has been an increase in the number of published autism screening tools, there have not been equal efforts to validate the tools (Dixon et al., 2011). Rather than whole-population screen-ing for autism, some suggest regular opportunities for “surveillance” by professionals to detect and respond rap-idly to any developmental concerns at pre-school and school age. Given this approach, some suggest that autism scales should be geared to identify children with autism from an at-risk population, rather than the total population (Matson et al., 2011).
Ten studies used a diagnostic tool (e.g. ADOS, ADI-, R) to validate the adapted screening tool (Albores-Gallo et al., 2012; Bölte et al., 2008, 2011; Canal-Bedia et al., 2011; Gau et al., 2011; Mattila et al., 2009, 2012; Nygren et al., 2012; Posserud et al., 2009; Wong et al., 2004). Of these, six studies mentioned the use of a translated

14 Autism
diagnostic tool (Bölte et al., 2008, 2011; Canal-Bedia et al., 2011; Gau et al., 2011; Mattila et al., 2009, 2012). The rationale for developing culturally appropriate screening tools extends to the development of culturally appropriate diagnostic tools. The use of culturally adapted diagnostic tools is necessary for reducing false positive and false nega-tive diagnoses. Diagnostic tools that have been culturally adapted are also necessary to the process of validating screening tools to avoid conclusions based on circular rea-soning—if the diagnostic tool used to validate a screening tool is not culturally valid, the cultural validity of the screen-ing tool is also compromised.
The major limitation of this review is that evaluation of the cultural adaptation process depended on information provided in the published articles. Our review suggested that the more the adaptation process employed recom-mended procedures, the more likely that changes related to cultural/linguistic differences were made. However, it is possible that components or details of the cultural adapta-tion were conducted but not reported. Second, our focus in this systematic review was to identify studies where the adaptation of the screening tool occurred from one country to another. We did not review articles that reported adapta-tion of a screening tool for different groups (e.g. ethnic/racial, dominant language, SES) within a country.
Conclusion
This review points to the importance of a reasonable adaptation process of a tool in a new cultural and linguis-tic setting. Failure to adapt the existing screening tool could result in the unintended consequence of over- or under-identification of children at risk of autism. Working with culturally and linguistically diverse populations requires efforts beyond translation. The adaptations reviewed modified screening tools in the following ways: (1) added specific culturally relevant indicators of ASD, thus reducing the possibility that socially appropriate and reinforced behaviors within a particular culture could be misinterpreted as risk factors for ASD; (2) changed word-ing to avoid misinterpretation because of cultural norms related to non-verbal and social communication; (3) added examples to avoid confusion over item meaning; and (4) altered the format of the tools to align with response styles of respondents. A pretest or cognitive interview process almost always led to important changes in the translated measure, suggesting that these compo-nents of adaptation may be necessary to increase the validity of the tool. Many of the studies also reported dif-ferences in the psychometric properties between the orig-inal and translated tool. These results suggest that screening tools used in research, clinical, and educational settings should be adapted to the specific culture and lan-guage of the population screened.
Funding
This work was supported by the U.S. Department of Health and Human Services, Health Resources and Services Administration, Maternal and Child Health Research Program (R40 MC 20171).
References
Achenbach TM and Rescorla LA (2000) Manual for the ASEBA Preschool Forms and Profiles. Burlington, VT: Research Center for Children, Youth and Families, University of Vermont.
Albores-Gallo L, Roldan-Ceballos O, Villarreal-Valdes G, et al. (2012) M-CHAT Mexican version validity and reli-ability and some cultural considerations. ISRN Neurology. Available at: http://dx.doi.org/10.5402/2012/408694
Al-Qabandi M, Gorter JW and Rosenbaum P (2011) Early autism detection: are we ready for routine screening? Pediatrics 128(1): e211–e217.
Auyeung B, Baron-Cohen S, Wheelwright S, et al. (2008) The Autism Spectrum Quotient: children’s version (AQ-Child). Journal of Autism and Developmental Disorders 38(7): 1230–1240.
Banville D, Desrosiers P and Genet-Volet Y (2000) Research note. Translating questionnaires and inventories using a cross-cultural translation technique. Journal of Teaching in Physical Education 19(3): 374–387.
Baranek G, Watson L, Crais E, et al. (2003) First Year Inventory (FYI) 2.0. Chapel Hill, NC: University of North Carolina at Chapel Hill.
Baron-Cohen S, Wheelwright S, Cox A, et al. (2000) Early iden-tification of autism by the Checklist for Autism in Toddlers (CHAT). Journal of the Royal Society of Medicine 93(10): 521–525.
Beaton DE, Bombardier C, Guillemin F, et al. (2000) Guidelines for the process of cross-cultural adaptation of self-report measures. Spine 25(24): 3186–3191.
Ben-Sasson A and Carter AS (2012) The application of the first year inventory for ASD screening in Israel. Journal of Autism and Developmental Disorders 42(9): 1906–1916.
Berument SK, Rutter M, Lord C, et al. (1999) Autism screen-ing questionnaire: diagnostic validity. The British Journal of Psychiatry 175: 444–451.
Bölte S, Poustka F and Constantino JN (2008) Assessing autistic traits: cross-cultural validation of the Social Responsiveness Scale (SRS). Autism Research: Official Journal of the International Society for Autism Research 1(6): 354–363.
Bölte S, Westerwald E, Holtmann M, et al. (2011) Autistic traits and autism spectrum disorders: the clinical validity of two measures presuming a continuum of social communication skills. Journal of Autism and Developmental Disorders 41(1): 66–72.
Bryson SE, Zwaigenbaum L, McDermott C, et al. (2008) The Autism Observation Scale for Infants: scale development and reliability data. Journal of Autism and Developmental Disorders 38(4): 731–738.
Camp BW (2006) What the clinician really wants to know: ques-tioning the clinical usefulness of sensitivity and specificity in studies of screening tests. Journal of Developmental and Behavioral Pediatrics 27: 226–230.
Soto et al. 15
Canal-Bedia R, Garcia-Primo P, Martin-Cilleros MV, et al. (2011) Modified checklist for autism in toddlers: cross-cultural adaptation and validation in Spain. Journal of Autism and Developmental Disorders 41(10): 1342–1351.
Constantino JN and Gruber CP (2002) The Social Responsiveness Scale. Los Angeles, CA: Western Psychological Services.
Constantino JN, Davis SA, Todd RD, et al. (2003) Validation of a brief quantitative measure of autistic traits: comparison of the social responsiveness scale with the autism diagnostic interview-revised. Journal of Autism and Developmental Disorders 33(4): 427–433.
Dixon DR, Granpeesheh D, Tarbox J, et al. (2011) Early detection of autism spectrum disorders. In: Matson JL and Sturmey P (eds) International Handbook of Autism and Pervasive Developmental Disorders. New York: Springer Science and Business Media, pp. 197–214.
Eaves LC, Wingert HD, Ho HH, et al. (2006) Screening for autism spectrum disorders with the social communication questionnaire. Journal of Developmental and Behavioral Pediatrics 27(Suppl. 2): S95–S103.
Ehlers S and Gillberg C (1993) The epidemiology of Asperger syndrome: A total population study. Journal of Child Psychology and Psychiatry 34(8): 1327–1350.
Ehlers S, Gilberg C and Wing L (1999) A screening question-naire for Asperger Syndrome and other high functioning autism spectrum disorders in school age children. Journal of Autism and Developmental Disorders 29(2): 129–141.
Elsabbagh M, Divan G, Koh YJ, et al. (2012) Global preva-lence of autism and other pervasive developmental disor-ders. Autism Research: Official Journal of the International Society for Autism Research 5(3): 160–179.
Filipek P, Accardo P, Ashwal S, et al. (2000) Practice param-eter: screening and diagnosis of autism report of the Quality Standards Subcommittee of the American Academy of Neurology and the Child Neurology Society. Neurology 55(4): 468–479.
Gau SS-F, Lee C-M, Lai M-C, et al. (2011) Psychometric prop-erties of the Chinese version of the Social Communication Questionnaire. Research in Autism Spectrum Disorders 5(2): 809–818.
Guillemin F, Bombardier C and Beaton D (1993) Cross-cultural adaptation of health-related quality of life measures: litera-ture review and proposed guidelines. Journal of Clinical Epidemiology 46(12): 1417–1432.
Guo Y-Q, Tang Y, Rice C, et al. (2011) Validation of the Autism Spectrum Screening Questionnaire, Mandarin Chinese ver-sion (CH-ASSQ) in Beijing, China. Autism 15(6): 713–727.
Hedley D, Young R, Angelica M, et al. (2010) Cross-cultural evaluation of the Autism Detection in Early Childhood (ADEC) in Mexico. Autism 14(2): 93–112.
Heiervang E, Stormark K, Lundervold AJ, et al. (2007) Psychiatric disorders in Norwegian 8- to 10-year-olds: an epidemiological survey of prevalence, risk factors, and ser-vice use. Journal of the American Academy of Child and Adolescent Psychiatry 46(4): 438–447.
Inada N, Koyama T, Inouchi E, et al. (2011) Reliability and validity of the Japanese version of the Modified Checklist for Autism in Toddlers (M-CHAT). Research in Autism Spectrum Disorders 5(1): 330–336.
Kamio Y and Inada N (2006) A preliminary study on the early detection of pervasive developmental disorders at 18-month check-up. Clinical Psychiatry 48(9): 981–990.
Kamp-Becker I, Mattejat F, Wolf-Ostermann K, et al. (2005) The Marburg Rating Scale for Aspergers Syndrome (MBAS) - a screening instrument for high functioning autistic disor-ders. Zeitschrift Fur-Kinder-und Jugendpsychiatrie und Psychotherapie 33(1): 15–26.
Kleinman JM, Robins DL, Ventola PE, et al. (2008) The modi-fied checklist for autism in toddlers: a follow-up study investigating the early detection of autism spectrum dis-orders. Journal of Autism and Developmental Disorders 38(5): 827–839.
Kurita H, Miyake Y and Katsuno K (1989) Reliability and validity of the Childhood Autism Rating Scale-Tokyo ver-sion (CARS-TV). Journal of Autism and Developmental Disorders 19: 389–396.
Le Couteur AL (2003) National Initiative for Autism, Screening, and Assessment: National Autism Plan for Children (NAPC): Plan for the Identification, Assessment, Diagnosis and Access to Early Interventions for Pre-school and Primary School Aged Children with Autism Spectrum Disorders (ASD). London: National Autistic Society.
Le Couteur A, Lord C and Rutter M (2003) Autism Diagnostic Interview–Revised. Los Angeles, CA: Western Psychological Services.
Lesinskiene S (2000) Child autism in Vilnius. PhD Thesis, Vilnius University, Vilnius.
Linas K, Dos Santos S, Mendez R, et al. (2013) Exploring the dis-parities in rates of disparities in autism in young Latino chil-dren. Poster presented the Biennial meeting for the Society for Research in Child Development, Seattle, WA, 18–20 April 2013.
Lord C, Rutter M, DiLavore PC, et al. (1999) Autism Diagnostic Observation Schedule-WPS (ADOS-WPS). Los Angeles, CA: Western Psychological Services.
Losapio MF and Pondé MP (2008) Translation into Portuguese of the M-CHAT scale for early screening of autism. Revista De Psiquiatria do Rio Grande do Sul 30(3): 221–229.
Matson JL, Rieske RD and Tureck K (2011) Additional con-siderations for the early detection and diagnosis of autism: review of available instruments. Research in Autism Spectrum Disorders 5(4): 1319–1326.
Mattila M-L, Jussila K, Kuusikko S, et al. (2009) When does the Autism Spectrum Screening Questionnaire (ASSQ) predict autism spectrum disorders in primary school-aged children? European Child & Adolescent Psychiatry 18(8): 499–509.
Mattila M-L, Jussila K, Linna S-L, et al. (2012) Validation of the Finnish Autism Spectrum Screening Questionnaire (ASSQ) for clinical settings and total population screening. Journal of Autism and Developmental Disorders 42: 2162–2180.
Mullen EM (1995) Mullen Scales of Early Learning. Circle Pines, MN: American Guidance Service.
National Research Council (US) Committee on Educational Interventions for Children with Autism (2001) Educating Children with Autism. Washington, DC: National Academies Press.
Neuman A, Greenberg DF, Labovitz DR, et al. (2004) Cross-cultural adaptation of the sensory profile: establishing
16 Autism
linguistic equivalency of the Hebrew version. Occupational Therapy International 11(2): 112–130.
Nordenbæk C, Kyvik KO, Skytthe A, et al. (2011) Efficiency of a small size screening instrument in identifying children with autism spectrum disorders in a large population of twins. Epidemiology Research International 2011: 412150.
Nygren G, Sandberg E, Gillstedt F, et al. (2012) A new screening programme for autism in a general population of Swedish tod-dlers. Research in Developmental Disabilities 33: 1200–1210.
Plauché Johnson C, Myers S and the Council on Children with Disabilities (2007) Identification and evaluation of children with autism spectrum disorders. Pediatrics 120: 1183–1215.
Posserud M-B, Lundervold AJ and Gillberg C (2006) Autistic fea-tures in a total population of 7–9-year-old children assessed by the ASSQ (Autism Spectrum Screening Questionnaire). Journal of Child Psychology and Psychiatry 47: 167–175.
Posserud M-B, Lundervold AJ and Gillberg C (2009) Validation of the autism spectrum screening questionnaire in a total population sample. Journal of Autism and Developmental Disorders 39: 126–134.
Posserud M-B, Lundervold AJ, Steijenen MC, et al. (2008) Factor analysis of the autism spectrum screening question-naire. Autism 12(1): 99–112.
Reznick JS, Baranek GT, Reavis S, et al. (2007) A parent-report instrument for identifying one-year-olds at risk for an even-tual diagnosis of autism: the first year inventory. Journal of Autism and Developmental Disorders 37(9): 1691–1710.
Robins DL, Fein D, Barton ML, et al. (2001) The Modified Checklist for Autism in Toddlers: an initial study investi-gating the early detection of autism and pervasive devel-opmental disorders. Journal of Autism and Developmental Disorders 31(2): 131–144.
Rutter M, Bailey A and Lord C (2003) Social Communication Questionnaire-WPS (SCQ-WPS). Los Angeles, CA: Western Psychological Services.
Sato FP, Silvestre P, Lowenthal R, et al. (2009) Instrument to screen cases of pervasive developmental disorder: a prelimi-nary indication of validity. Revista Brasileira de Psiquiatria 31(1): 30–33.
Schopler E, Reichler RJ, DeVellis RF, et al. (1980) Toward objective classification of childhood autism: childhood
Autism Rating Scale (CARS). Journal of Autism and Developmental Disorders 10(1): 91–103.
Seif Eldin A, Habib D, Noufal A, et al. (2008) Use of M-CHAT for a multinational screening of young children with autism in the Arab countries. International Review of Psychiatry 20(3): 281–289.
Skuse DH, James RS, Bishop DV, et al. (1997) Evidence from Turner’s syndrome of an imprinted X-linked locus affecting cognitive function. Nature 387(6634): 705–708.
Skuse DH, Mandy WP and Scourfield J (2005) Measuring autis-tic traits: heritability, reliability and validity of the social and communication disorders checklist. British Journal of Psychiatry 187: 568–572.
Song YJ, Juan F and Lining S (2009) A new, high precision behavior-based questionnaire for screening and pre- diagnosing autism in children: implications for clinical appli-cations and large population investigations. Psychological Science 32(6): 1504–1507.
Swinkels SH, Dietz C, van Daalen E, et al. (2006) Screening for autistic spectrum in children aged 14 to 15 months. I: the development of the Early Screening of Autistic Traits Questionnaire (ESAT). Journal of Autism and Developmental Disorders 36(6): 723–732.
Szatmari P, Bryson SE, Boyle MH, et al. (2003) Predictors of outcome among high functioning children with autism and Asperger syndrome. Journal of Child Psychology and Psychiatry and Allied Disciplines 44(4): 520–528.
Tirosh E, Bettesh-Bendrian S, Golan G, et al. (2003) Regulatory disorders in Israeli infants: epidemiologic perspective. Journal of Child Neurology 18: 748–754.
Wakabayashi A, Baron-Cohen S, Uchiyama T, et al. (2007) The Autism-Spectrum Quotient (AQ) children’s version in Japan: a cross-cultural comparison. Journal of Autism and Developmental Disorders 37(3): 491–500.
Williams J and Brayne C (2006) Screening for autism spectrum disorders: what is the evidence? Autism 10(1): 11–35.
Wong V, Hui LS, Lee W, et al. (2004) A modified screening tool for autism (Checklist for Autism in Toddlers (CHAT-23)) for Chinese children. Pediatrics 114(2): e166–e176.
Young R (2007) Autism Detection in Early Childhood. Camberwell, VIC, Australia: ACER Press.