statutory health insurance competition in europe: a four-country comparison
TRANSCRIPT

R
Sc
SWa
b
c
d
e
a
ARRA
KHCCE
1h
s
rv(
0h
Health Policy 109 (2013) 209– 225
Contents lists available at SciVerse ScienceDirect
Health Policy
j ourna l ho me pag e: ww w.elsev ier .com/ locate /hea l thpol
eview
tatutory health insurance competition in Europe: A four-countryomparison
arah Thomsona,∗, Reinhard Busseb, Luca Crivelli c,ynand van de Vend, Carine Van de Voordee
LSE Health and European Observatory on Health Systems and Policies, LSE Health (COW3.01), Houghton Street, London WC2A 2AE, United KingdomBerlin University of Technology, Department of Health Care Management, Strasse des 17. Juni 135, 10623 Berlin, GermanyUniversità della Svizzera italiana, Faculty of Economics, Via Buffi 13, 6900 Lugano, SwitzerlandErasmus University Rotterdam, Burgemeester Oudlaan 50, 3000 DR Rotterdam, The NetherlandsCatholic University Leuven, Naamsestraat 69, 3000 Leuven, Belgium
r t i c l e i n f o
rticle history:eceived 8 September 2011eceived in revised form 8 January 2013ccepted 9 January 2013
eywords:ealth insurancehoiceompetitionurope
a b s t r a c t
This paper explores the goals and implementation of reforms introducing choice of andcompetition among insurers providing statutory health coverage in Belgium, Germany, theNetherlands and Switzerland. In theory, health insurance competition can enhance effi-ciency in health care administration and delivery only if people have free choice of insurer(consumer mobility), if insurers do not have incentives to select risks, and if insurers areable to influence health service quality and costs. In practice, reforms in the four countrieshave not always prioritised efficiency and implementation has varied. Differences in pol-icy goals explain some but not all of the differences in implementation. Despite significantinvestment in risk adjustment, incentives for risk selection remain and consumer mobilityis not evenly distributed across the population. Better risk adjustment might make it easierfor older and less healthy people to change insurer. Policy makers could also do more to pre-vent insurers from linking the sale of statutory and voluntary health insurance, particularlywhere take-up of voluntary coverage is widespread. Collective negotiation between insur-ers and providers in Belgium, Germany and Switzerland curbs insurers’ ability to influencehealth care quality and costs. Nevertheless, while insurers in the Netherlands have good
access to efficiency-enhancing tools, data and capacity constraints and resistance fromstakeholders limit the extent to which tools are used. The experience of these countriesoffers an important lesson to other countries: it is not straightforward to put in place theconditions under which health insurance competition can enhance efficiency. Policy makersre, und
should not, therefo. The rationale for competition among statutoryealth insurers
Choice of and competition among insurers offeringtatutory (mandatory) health coverage has become more
∗ Corresponding author. Tel.: +44 20 7955 6474; fax: +44 20 7955 6803.E-mail addresses: [email protected] (S. Thomson),
[email protected] (R. Busse), [email protected] (L. Crivelli),[email protected] (W. van de Ven), [email protected]. Van de Voorde).
168-8510/$ – see front matter © 2013 Elsevier Ireland Ltd. All rights reserved.ttp://dx.doi.org/10.1016/j.healthpol.2013.01.005
erestimate the challenges involved.© 2013 Elsevier Ireland Ltd. All rights reserved.
prominent in Europe in the last 15 years and is now an inte-gral feature of health financing policy in Belgium, the CzechRepublic, Georgia, Germany, the Netherlands, the Rus-sian Federation, Switzerland and Slovakia [1,2]. Althoughthis form of competition is not widespread in practice,the idea that third-party payers should compete for pub-licly financed clients is debated in countries as diverse as
England and Estonia [3,4].In theory, competition between insurers is intended toenhance allocative and productive efficiency in health careadministration and delivery through two mechanisms:

lth Polic
210 S. Thomson et al. / Heamaking insurers bear financial risk and giving people freechoice of insurer [5]. Having a fixed and prospectivelydetermined budget within which to meet enrolee healthcare costs may encourage insurers to use resources judi-ciously; if they cannot stay within budget they will haveto charge higher premiums and risk losing enrolees. Thethreat of consumer exit may also encourage insurers tobe more responsive to public preferences; if people aresensitive to price and quality, insurers will try to main-tain or improve quality while minimising costs using arange of tools, including cutting overheads and engaging inmore ‘strategic’ purchasing of health services [6]. At leastthree other conditions must be met for insurer competi-tion to achieve efficiency objectives.1 First, people shouldbe able to choose and switch insurer with ease and with-out incurring significant transaction costs. This implies thatindividuals are able to make an informed choice of insurerand do not face barriers to switching. Second, insurer com-petition should be based on price and quality, rather thanrisk selection [7]. Third, insurers should have access to toolsthat allow them to influence health care quality and costs,and be willing to use them.
In practice, European countries have introduced choiceof insurer in response to a range of problems with existingstatutory health insurance arrangements. Some countrieshave explicitly pursued efficiency goals. Others have beendriven more by concerns for equity, access and expenditurecontrol. Even where efficiency has not been a stated or pri-mary rationale, however, those in favour of insurer choicemay have expected competition to result in efficiency gainsand, ultimately, to improve health system performance. Inaddition to differences in goals, there are also differencesin key aspects of health insurance market reform in Euro-pean health systems – for example, Dutch insurers haveaccess to many more efficiency-enhancing tools than dotheir counterparts in other countries (see below).
Cross-national variation in policy goals and implemen-tation prompts three observations. First, differences inimplementation may be linked to differences in goals. Sec-ond, there is little evidence to suggest that health insurancecompetition has had the desired effect on efficiency, evenwhere efficiency has been an explicit goal [8]. For exam-ple, recent evaluations of the 2006 health insurance marketreform in the Netherlands report mixed results: waitingtimes for inpatient treatment and pharmaceutical priceshave fallen [9], but so far only some aspects of healthinsurer performance have improved (the transparency ofuser charges requirements and health plan information)[10]. Third, expectations about efficiency gains may con-flict with other stated objectives such as expenditure caps
or expenditure control.This paper explores differences in the goals and imple-mentation of statutory health insurance competition in
1 Bevan and van de Ven (2010) have set out a larger number of condi-tions that must be fulfilled if insurer competition is to achieve its goals.We have condensed some of these conditions so that they fall under thethree conditions listed here. We also take some of the conditions in Bevanand van de Ven’s list, such as regulation, as a given since (for example)universal freedom to switch could probably only be achieved throughregulation.
y 109 (2013) 209– 225
Europe. To do so it compares the experience of four westernEuropean countries (Belgium, Germany, the Netherlandsand Switzerland), focusing on these countries because oftheir similar health system characteristics and economicand political context. The paper’s analysis is structuredas follows. The next section outlines the policy goalsunderpinning statutory health insurance reforms in eachcountry. Subsequent sections review the implementationand development of policies to ensure consumer mobility,remove incentives for risk selection and give insurers toolsto enhance efficiency. A further section discusses implica-tions for policy.
The paper adds to the literature by applying a uniformset of criteria to enable a systematic comparison of choiceand competition in statutory health insurance across thefour countries and by providing a comprehensive and upto date cross-national overview of health insurance cov-erage, regulation and market structure. A comparison offour countries cannot hope to explore the complexities ofreform implementation in great depth; a detailed anal-ysis of the policy context in each country is thereforebeyond the scope of the paper. An evaluation of the out-comes of insurer competition is also beyond the paper’sscope; robust evaluation poses challenges due to lack ofdata, noise from other reforms and absence of knowledgeabout the counterfactual, and comparative evaluation isfurther complicated by cross-national differences in goalsand implementation. Finally, the paper does not aim totest the validity of the three conditions (that is, the extentto which they are necessary for insurer competition to‘work’); rather, it uses the conditions to structure discus-sion about differences across countries and to highlightareas requiring policy attention.
2. Policy history, development and goals
This section outlines the history and development ofpolicies to facilitate insurer choice and competition in thefour countries in chronological order. It reviews the pol-icy goals underpinning more recent reforms. Awareness ofthe goals specific to each country, and the context in whichthey have been formulated, is important for the analysisof implementation and discussion of policy implicationsin subsequent sections. Tables 1–3 depict key features ofcurrent health insurance coverage, regulation and marketstructure.
2.1. Switzerland
Choice of health insurer in Switzerland dates to 1911,when the first federal law on Sickness and AccidentInsurance came into force. At that time the health insur-ance system was mainly managed by small-scale, private,non-profit institutions. State subsidies were required toencourage people to enrol from an early age and to makepremiums more affordable. In order to qualify for subsidies,insurers had to offer open enrolment to people under the
age of 55, provide portable benefits and limit any differencein premiums for men and women to no more than 25%. By1945, about half of the population was covered, expandingto near-universal coverage between 1985 and 1990.
S. Thomson et al. / Health Policy 109 (2013) 209– 225 211
Table 1Health insurance coverage, 2012.
Belgium Germany Netherlands Switzerland
Statutory coveragebreadth(universality)
Coverage compulsoryfor all residents since2008 (salariedworkers: 1944;inpatient care for selfemployed: 1964;outpatient care forself-employed: 2008).
Coverage compulsoryunder SHI since 2007;coverage compulsoryfor all residents since2009. Around 85%covered by SHI, 10%through PHI, 4%through othergovernment schemes.
Coverage compulsoryfor all legal residentssince 2006.
Coverage compulsory for allresidents since 1996.
What % of thepopulation is notcovered?
Less than 1.0% of thepopulation (a high of1.4% in 2007).
Probably less than 0.5%of the population (in2007, before theintroduction ofcompulsory insurance).
About 0.2% of thepopulation in 2012(plus a further 1.0%who are illegallyresident) [53].
About 1.9% in 2010. Newregulations introduced in 2012should have significantlyreduced this percentage (butno official data available yet).
What are thecharacteristics of theuninsured?
Not known (a mixtureof people unable andunwilling to pay healthinsurance premiums).
Before 2007/09:Self-employed,formerly voluntary SHImembers, people aged55 + no longer eligiblefor SHI, divorcedwomen formerlycovered as dependantsand illegal immigrants.
Low-incomeindividuals, both legaland illegal immigrants(illegal immigrants arenot allowed topurchase subsidisedhealth insurance).
Not known (there was a bigdebate about whether theuninsured were unable orunwilling to pay healthinsurance premiums). Morelikely to be aged 20–59,foreigners, divorced or single,below or just above thethreshold for social assistance,users of mental health services[54].
What is the main roleof voluntary healthinsurance?
Supplementary(mainly for superioraccommodation in ahospital, not toincrease choice or forfaster access) andcomplementarycovering eye anddental care.
Substitutive, coveringcivil servants,self-employed andhigh-earningemployees who chooseprivate insurance (intotal, around 10% of thepopulation);complementary,covering user chargesand some uncoveredservices (around 20% ofthe population).
Complementary,offering mainly dentalcare and physiotherapybenefits (about 90% ofthe population).
Supplementary cover (offeringfree choice of hospital acrossall cantons, free choice ofphysician in public hospitals,higher standards of hotelcomfort in private andsemi-private wards, daily cashbenefits) and complementarycover of excluded or partiallycovered services (e.g. dentalcare and home care). In 200559% of the population hadhospital cover, 37% had cashbenefit cover, 11% had dentalcover and 52% had cover forother excluded services [55].
Coverage scope(benefits)
Broad coverage. Broad coverage. Broad coverage. Broad coverage.
What health servicesare typically notcovered?
Eyeglasses and contactlenses, hearing aids,orthodontic care,cosmetic plasticsurgery, less necessarydrugs (e.g.over-the-counter drugsand some prescribeddrugs such asbenzodiazepines) andalternative medicine.
Eyeglasses, contactlenses andover-the-counter and‘lifestyle’ drugs.
Eyeglasses and contactlenses, dental care foradults, orthodonticcare, cosmetic plasticsurgery and alternativemedicine.
For eyeglasses and contactlenses only a lump sum is paid.Inpatient care provided at ahospital not on a specificcantonal list, psychotherapy(covered subject to certainconditions), drugs not listed inthe ‘catalogue ofpharmaceutical specialities’,alternative medicine, dentalcare, and cosmetic plasticsurgery.
Who defines thestatutory benefitspackage?
Federal governmentbased on proposalsnegotiated betweensickness funds andproviders. The Minsterof Social Affairs definesentitlement to drugsbased on advice fromthe DrugReimbursementCommittee.
In general terms,federallegislature/parliament;details by Federal JointCommitteerepresenting payers,providers and patients.
Central governmentbased on advice fromthe independent DutchHealth Care InsuranceBoard (CVZ).
Central government based onadvice from the FederalCommission on HealthInsurance Benefits and GeneralQuestions representing payers,providers, patients andscientific advisors.

212 S. Thomson et al. / Health Policy 109 (2013) 209– 225
Table 1 (Continued)
Belgium Germany Netherlands Switzerland
Coverage depth (usercharges)
Co-insurance orco-payments appliedto most health services,with an annualout-of-pocketmaximum.
Co-payments for adultsapplied to most healthservices, with anannual out-of-pocketmaximum.
Annual deductible ofD220 (in 2012) peradult (18+) applied fornon-primary careservices.
Minimum annual deductible ofCHF 300 (D248) plusco-insurance or co-paymentsapplied to most healthservices, with an annualout-of-pocket maximum. Themaximum optional deductiblefor adults is CHF 2500 (D2068).
Who defines usercharges policy?
Federal legislation. Federallegislature/parliament.Sickness funds canwaive some charges(e.g. for enrolment inDMPs).
Central government.Insurers can waive orincrease some chargesfor use ofpreferred/non-preferred providers.The insured can chooseto pay a higher annualdeductible.
Central government. Insurersmay waive or increase somecharges. The insured canchoose to pay a higher annualdeductible.
ww.oa
health care costs. Free choice of fund was intended toimprove efficiency and responsiveness to consumer prefer-ences. By the end of 2005, the sickness funds bore financial
2 Compulsory additional benefits refer to items not included in thestatutory benefits package, which does not vary across insurers. Addi-tional benefits are offered at the discretion of individual insurers (andmight include things like orthodontics, alternative medicine or homecare services); they must be purchased by all those who enrol with aparticular insurer. The local sickness funds have traditionally offered a
Source: Authors’ research.Note: Currency converted using 1 October 2012 exchange rates from winsurance; SHI = statutory health insurance.
Under the 1911 legislation, switching was not easy orcostless for everyone. Weak regulation, premiums basedon age at enrolment, and the entry of new insurers ledto a degree of unfair competition based on risk selection.During the early 1990s, many sickness funds collapsed ormerged with others to avoid bankruptcy. Concerns aboutunequal access to health insurance, combined with con-cerns about solidarity, rising health expenditure and gapsin coverage, gave rise to a new Federal Health InsuranceAct (FHIA) in 1996. To address access concerns and toencourage fair competition based on price and quality, thenew law made health insurance universally compulsory,extended open enrolment and introduced a standard ben-efits package, risk equalisation and minimum user charges.The law maintained collective contracting of providersbut, to enhance efficiency by encouraging better purchas-ing, it gave insurers leeway to develop and sell so-calledmanaged-care plans to those willing to accept limitedchoice of provider in return for lower premiums. Managed-care plans can involve referral to specialists, selectivecontracting and capitation-based provider payment. TheSwiss reform therefore aimed to enhance equity of accessto health care, to strengthen solidarity and, at the sametime, to create incentives for organisational innovation andexpenditure control [11].
2.2. Belgium
Compulsory health insurance for employees was estab-lished in Belgium in 1944 and is currently managed by fivenon-governmental, non-profit sickness fund associationscomprising 54 local sickness funds, a special fund for rail-road employees and a public insurer of last resort [12]. In1964 the government extended compulsory coverage ofinpatient care to self-employed people and in 2008 cover-age for the self-employed was further extended to include
outpatient care.Although Belgian residents have enjoyed free choice ofsickness fund since 1944, this choice has not been regardedas a means of stimulating insurer competition. Rather,
nda.com. DMP = disease management programme; PHI = private health
funds were associated with different political or religiousgroups and choice simply allowed people to express theirpreference for a ‘Christian’ or ‘Socialist’ insurer. In 1995the government introduced partial prospective funding ofsickness funds, accompanied by risk equalisation, to makethem take on some financial risk. Even so, the underly-ing policy intention was not to foster competition amongsickness funds but to place them on an equal footing andencourage them to control health care expenditure [13].The sickness funds were not given new tools to influencehealth service quality and costs [14].
Belgium is the only one of the four countries to havea public insurer of last resort. Unlike the sickness funds,the public fund has no historical affiliation to political orreligious groups, nor does it offer compulsory additionalbenefits2 (as the local sickness funds do). As a result, itssmall share of the market (1%) is made up of people whodo not wish to pay for additional benefits or who prefer a‘neutral’ fund.
2.3. The Netherlands
In 1991 the Dutch government introduced free choice ofnon-profit sickness fund for the two-thirds of the popula-tion eligible for statutory health care coverage and sicknessfunds began to take on financial risk for their enrolees’
mixture of compulsory additional benefits and voluntary supplementaryand complementary health insurance. In 2010 a change in the law sepa-rated compulsory and voluntary activity. From 2012 voluntary additionalbenefits have been sold by new non-profit societies of mutual assistance,which are part of the national sickness fund associations.

S. Thomson et al. / Health Policy 109 (2013) 209– 225 213
Table 2Regulation of statutory health insurance, 2012.
Belgium Germany Netherlands Switzerland
Who sets andcollectscontributions?
Federalgovernment setsand collects auniformincome-relatedcontribution.Sickness funds setand collectadditionalcommunity-ratedpremiums.
Since 2011 a nationalcontribution rate has beendefined in legislation. In2009/10 the federalgovernment (the cabinet)set a uniformincome-relatedcontribution rate. Prior tothis the sickness fundsdetermined their owncontribution rate.Contributions are collectedby sickness funds buttransferred to a centralhealth fund. Sickness fundsset and collect additionalcommunity-ratedpremiums.
Central government sets andcollects a uniformincome-related contribution.Insurers set and collectadditional community-ratedpremiums.
Insurers set and collect their owncommunity-rated premiums.
How are statutoryhealth insurancerevenues pooledand(re)allocated?
Income-relatedcontributions andgeneral taxrevenue pooled bya central fund andallocated tosickness fundsbased on arisk-adjustedformula and actualcosts.
Income-relatedcontributions and generaltax revenue pooled by acentral fund (see note) andallocated to sickness fundsbased on a risk-adjustedformula.
Income-related contributionsand general tax revenue tocover children pooled by acentral fund and allocated toinsurers based on arisk-adjusted formula.
Premiums pooled by insurers andredistributed at cantonal levelbased on a risk-adjusted formulamanaged by a foundation ownedby the insurers. General taxrevenue is pooled by Cantons andused to pay for about half of allinpatient care costs.
Who sets theformula for(re)allocatingresources?
Federalgovernment.
Parliament defines theprinciples in law. TheFederal Ministry of Healthdefines the details throughordinance.
Central government. Parliament defines the principleson which risk adjustment shouldbe based. The Federal Council isresponsible for applying them insetting the formula.
Who monitorsinsurercompetition?
A governmentagency (ControlOffice of theSickness Funds)and the BelgianCentral Bank (NBB).
SHI: the Federal InsuranceAuthority; PHI: the FederalFinancial SupervisoryAuthority
Semi-public supervisoryauthorities at arm’s length:the Dutch HealthcareAuthority (NZa) managescompetition among theproviders and insurers; theDutch Competition Authority(NMa) covers all sectors(monitoring the health sectornow accounts for about onethird of its time); the DutchCentral Bank (DNB)supervises financial solvency.
Under the FHIA, the Federal Officeof Public Health controls SHIactivity; VHI activity falling underthe private Law on InsuranceContracts (VVG) is supervised byFINMA, the Swiss FinancialMarkets Supervisory Authority,which replaced the Federal Officeof Private Insurance in 2009. Thegovernment has recently proposeda new law to strengthen controland regulation of health insurers[56].
Source: Authors’ research.N al fund
i nce.
riotcivla
dgo
ote: Farmers’ sickness funds in Germany do not participate in the centrnsurance; SHI = statutory health insurance; VHI = voluntary health insura
isk for 53% of their revenue. However, there was grow-ng dissatisfaction among policy makers with the absencef other incentives for efficiency and innovation withinhe prevailing regulatory framework, coupled with con-erns about long waiting times for specialist care. Thencreasingly heavy regulation required to ensure access to
oluntary health insurance (VHI) for the third of the popu-ation excluded from statutory health care coverage3 waslso seen as unsatisfactory.3 Before 2006 people with incomes above a certain level and theirependants – around one third of the population in total – were not eli-ible for statutory coverage of health care costs. These individuals reliedn voluntary health insurance sold by competing private insurers.
and are not subject to the risk equalisation scheme. PHI = private health
The 2006 Health Insurance Act extended statutorycoverage to the whole population under a new systemmanaged by private insurers (some of whom were formerlysickness funds; others had been active in the market forVHI). Insurers now have stronger incentives to be prudentpurchasers of health services, including increased financialrisk (92% of revenue), and tools to stimulate competitionamong providers. It was expected that over time consumerchoice of insurer would reduce the emphasis on govern-ment regulation of health care supply and increase the use
of strategic purchasing to enhance efficiency. This in turnwould make health care more affordable, more responsiveto patient needs and more effective, bringing about a betterbalance between costs and benefits [8].
214 S. Thomson et al. / Health Policy 109 (2013) 209– 225
Table 3Market structure of statutory health insurance, 2012.
Belgium Germany Netherlands Switzerland
What is the legal/profitstatus of insurers?
Sickness funds arenon-governmentalnon-profitorganisations underpublic law. The marketis closed to newentrants.
Sickness funds arenon-governmental,non-profitorganisations underpublic law.
Insurers are private entitiesallowed to share profitswith their shareholders.
Insurers are privateentities and cannot shareprofits on SHI business.
If profit status varies,what is the balancebetween non-profitand for-profit?
Not relevant. Not relevant. Most insurers arenon-profit mutualassociations.
About 60% have non-profitlegal status (foundations orassociations) and 40% arestock companies owned bynon-profit institutions.
If profits are allowed,are there anycontrols on profitmargins?
Not relevant. No. No. Profits not allowed for SHIbusiness (see note).
How many insurers arethere?
Five sickness fundassociations (dividedinto 54 local funds), apublic insurer of lastresort and a scheme forrailroad workers.
146 sickness funds. 11 health insuranceholding companies in2010, 28 different healthinsurers in total. Thelargest holding companycontains 7 insurers.
68 insurers involved in SHIin 2012 (8 of which onlyoffer voluntary daily cashinsurance).
What is the marketshare of the largestthree insurers?
About 90%. About 32%. 74% for holding companies. Nationally: 45% (holdings);28% (individual insurers).Cantonal markets are muchmore concentrated.
Can insurers who sellSHI also sellvoluntary cover?
Yes, but in 2010 localsickness fundcompulsory healthinsurance activity wasseparated from VHIactivity. From 2012 thelatter will be offered bynon-profit societies ofmutual assistance (partof the national sicknessfund associations).
Sickness funds canbroker VHI sold byprivate insurers; inpractice the line isbecoming blurred asSHI policies for‘integrated care’include somesupplementarybenefits (e.g. smallerwards in hospital).
Yes. The Dutch HealthInsurance Act prohibits thetermination of VHIcontracts when enroleesswitch to another insurerfor SHI cover.
Yes. Legislation prohibitstied sales of VHI and SHI.
Source: Authors’ research.Note: In Germany PHI falls under private law. Of the 43 private insurers, 19 are non-profit and 24 are for-profit (2011) and the market share of the largestthree insurers is around 42%. A survey of 65 Swiss funds found that only one had distributed part of its VHI profits to the holding company. This suggestsprofits on VHI business are generally kept within companies to increase reserves, reduce premiums or invest in marketing campaigns [57]. PHI = private
insuran
health insurance; SHI = statutory health insurance; VHI = voluntary health2.4. Germany
Historically, statutory health insurance (SHI) inGermany was compulsory for all blue-collar employeesand for white-collar employees with earnings below athreshold. Employees were assigned to a non-profit, quasi-public sickness fund based on geographical or occupationalcriteria. Only white-collar employees with earnings abovethe threshold were allowed to choose between voluntaryenrolment in the SHI system, buying substitutive VHIfrom private insurers or not being covered at all. If theychose SHI, they had free choice of sickness fund and theoption of switching fund at regular intervals (unlike otheremployees) [15]. Assigned membership among blue-collarand lower-earning white collar employees led to largevariation in income-related contribution rates – of up to
8 percentage points in the early 1990s – because sicknessfunds covered people with very different income levelsand risk profiles [16]. Over time, variation in contributionrates and differences in the rights of white- and blue-collarce.
employees came to be regarded as inequitable, particu-larly since blue-collar employees often experienced highercontribution rates than white-collar employees.
In 1992 the German legislature extended free choice ofsickness fund to almost all those covered by SHI, with effectfrom 1996. This was primarily intended to tackle equityconcerns about varying contribution rates by permittinganyone to choose a sickness fund with a lower contribu-tion rate. It was expected that free choice would lead to aconvergence in contribution rates. Since the national andinternational ideological climate at that time favoured theintroduction of market mechanisms in health care, it wasalso hoped that fostering competition within the SHI sys-tem would lead to health care expenditure control andenhance efficiency. Choice of sickness fund was precededby the introduction (in 1994–1995) of risk equalisation to
prevent risk selection and ensure contribution rates wouldsignal a sickness fund’s ability to operate efficiently. It wasclear from the outset that the risk-adjustment formulawas crude, but the government did not have the tools and
lth Polic
dBa
pedpag1pLvVsc
3
twcl(nipia–meaett
3
ttldofigptTc
o
(a
S. Thomson et al. / Hea
ata necessary to implement a more sophisticated scheme.ecause the sickness funds bore significant financial risk,ny risk adjustment was seen as better than none.
The change in legislation made health insurance com-ulsory for all permanent residents in 2009. SHI coversmployees (with the exception of civil servants) and theirependants (non-earning spouses and children), the unem-loyed, pensioners, students, farmers and (since 2007)nyone not covered by substitutive VHI. Employees whoseross wages exceed D50,850 a year (in 2012) – less than5% of the population – can choose between statutory andrivate cover, but they must have some form of insurance.ess than a third of this high-earning group opts for pri-ate cover. SHI covers about 85% of the population, privateHI covers around 10% (more than half of whom are civilervants and the self-employed) and government schemesover about 4%.
. Ensuring consumer mobility
If people cannot move (switch) freely from one insurero another, the threat of exit may be muted for insurers,hich would undermine a major pre-requisite for insurer
ompetition. In the absence of a single metric to estab-ish the degree of consumer mobility in insurance marketsthere is no optimal rate of switching), a range of factorseeds to be considered. These include financial and admin-
strative barriers to joining a new insurer, the reasonseople give for switching or staying put and the character-
stics of those who do and do not switch. If non-switchersre mainly people with predictably high health care costs
a situation termed ‘adverse retention’ [17] – the instru-ental effect of exit might be severely weakened or even
liminated, particularly if risk adjustment (see below) isbsent or of poor quality. Insurers who assume that thesenrolees have no real alternative may not have much incen-ive to respond to their preferences [18] and might attempto erode service quality or encourage them to switch.
.1. Strategies to facilitate switching
All four countries employ multiple strategies to ensurehat the whole population is able to switch from one insurero another (for statutory benefits) with relative ease and atow cost: open enrolment,4 coverage of pre-existing con-itions, premiums that are not linked to individual riskf ill health, fully portable benefits, a standardised bene-ts package to enable straightforward price comparisons,ood comparative information available through newspa-
5
ers, web sites and intermediaries, and risk adjustmento compensate insurers for covering high-risk individuals.hese universally applied strategies mean that the finan-ial and administrative costs of switching are likely to be4 In Belgium since 2007 only, replacing a system of guaranteed renewalf contract.5 Government-sponsored web sites in the Netherlands
www.kiesbeter.nl) and (since 2012) in Switzerland (www.priminfo.ch)nd private initiatives in all four countries.
y 109 (2013) 209– 225 215
low. Other transaction costs may be high, however, as wediscuss below.
3.2. Switcher characteristics
Switching rates vary across the four countries, with thelowest rates in Belgium and the highest rates in Switzerland(Table 4). People who switch are more likely to be youngerin Germany, the Netherlands and Switzerland (no data areavailable for Belgium) and are more likely to be health-ier in Germany and the Netherlands. In Switzerland peoplewho switch are more likely to be healthier (reporting theirhealth to be ‘very good’ rather than ‘good’ or ‘poor’) if theyhave VHI.
3.3. Reasons for switching and for staying put
Reasons for switching differ in importance across thefour countries, with price playing no role in Belgium anda significant role in the Netherlands, Switzerland andGermany. Consumer perceptions of differences in qualityseem to play some role in all four countries (Table 5). TheNetherlands and Switzerland have the largest differences inprice across insurers. In the Netherlands the gap betweenthe cheapest and most expensive community-rated pre-miums is not as large as in Switzerland and has narrowedsince 2006, while the average community-rated premiumremains below the break-even threshold calculated by theMinistry of Health in 2006 [8].
In contrast, premiums have grown rapidly inSwitzerland in recent years, prompting the much higherthan usual rates of switching seen in 2008/2009 and2009/2010 (Table 4), and premium variation is substantial.By selecting the highest deductible and enrolling in amanaged-care network, policy holders in Switzerland canlower their premiums by up to 50%; in Zurich canton, forexample, 5% of people paid an annual premium of less thanCHF 3500 (D2895) in 2010, while 5% paid over CHF 4900(D4053), a difference of more than CHF 1400 (D1158) [19].Unlike the Netherlands, there is no evidence of premiumvariation within cantons narrowing over time [20], whichmay be an indication of insufficient consumer mobility.
In Germany in 2010 only 13 of the (then) more than 150sickness funds charged additional community-rated pre-miums and these are low in comparison to the Netherlandsand Switzerland. Nevertheless, people appear to be verysensitive to price. In the first half of 2010 sickness fundsthat introduced an additional community-rated premiumof D8 per month lost up to 20% of their enrolees [21]. In2011 the cap on additional premiums was lifted, which mayintensify price competition in future.
Survey data from the Netherlands and Switzerland sug-gest many people feel no need to switch because they aresatisfied with their current insurer (45% in the Netherlandsand 79% in Switzerland) [22,23]. There is also evidence ofpeople preferring to maintain the status quo [24] or usingsubjective measures of quality to determine insurer choice.
Forty per cent of people surveyed in Switzerland chose aninsurer based on parents’ and friends’ choices and ‘tradi-tion’, while 13.5% said they stayed with their insurer out ofhabit; those who had been with an insurer for longer were
216 S. Thomson et al. / Health Policy 109 (2013) 209– 225
Table 4Switching rates among enrolees for statutory benefits and characteristics of switchers.
Country Switching rates Characteristics of switchers
Belgium Early 2000s: around 1% [14]. No data available.Germany 1997–2007: varied from 4.0% to 5.8% [58]. 1995–2001: switchers more likely to be younger and healthier
[25,28,59,60]; 2010: switchers more likely to be younger, higherincome, better educated and not chronically ill [61].
Netherlands Before 2000: around 1% [62]; 2005: around 3%[8]; 2006: 18%; 2007: 4.4%; 2008: 3.6%; 2009:3.5% [26]; 2010: 5.5% [63]; 6.0% in 2011 [64].
Prior to 2006: switchers more likely to be younger and better educated[25,65]; 2006–2009: switchers have better self-reported health [26].
Switzerland Switching rates fell from 4.8% in 1997 to 2.1%in 2000 [23] and rose from 12% in 2008/9 to15.4% in 2009/10 (25% among those choosingthe largest annual deductible) [66].
1996–2005: switching more likely among people choosing higherdeductibles, less likely with age and less likely among people with VHIwhose self-reported health is ‘poor’ or ‘good’ (as opposed to ‘verygood’) [20]; 2000: switching less likely among people with VHI [23].
Source: Authors’ research.Note: VHI = voluntary health insurance.
less likely to express an intention to switch [23]. About 25%said they did not try to choose the insurer with the lowestpremiums. Prior to the 2006 reform in the Netherlands, themost frequently mentioned reason for being enrolled witha particular insurer was having joined the fund in earlyadulthood [25], a status quo bias that was perhaps rein-forced by the relatively small difference between insurersat that time. In spite of the growth in premium and productdifferentiation since then, the proportion of Dutch respon-dents who believe they do not stand to benefit much byswitching has risen from 68% in 2006 to 74% in 2008 and18% of all respondents said it was too much trouble toswitch [22]. In 2009 7% said they did not switch becausethey felt they would not be able to obtain a new VHI pol-icy if they changed to a new insurer for statutory cover, upfrom 4% in 2006 [26].
3.4. Barriers to consumer mobility
Research indicates that many people in the fourcountries have legitimate reasons (from a policy perspec-tive) for not switching. However, the links between age,health and switching in Germany and the Netherlands, and
Table 5Price and quality differences between insurers.
Country Is price a reason for switching?
Belgium No. Price differences are negligible. In 2010 additionalcommunity-rated premiums did not exceed D20 per enrolee
year. Price elasticity < 1 [62].Germany Yes. In the late 1990s substantial differences in contribution r
across insurers and the role of employers in financing coverato high price elasticity [60,62]. Since 2009, with the introductthe nationally uniform contribution rate, price signals havegenerally been weak, but people are very sensitive to price wsignals exist.
Netherlands Yes. Negligible price differences before 2006. Since 2006 insudifferentiate themselves through premium discounts for highdeductibles or group coverage.
Switzerland Yes. Substantial variation in premiums; insurers differentiatethemselves through discounts for children under 18, student19–25, enrolees who opt for higher deductibles (up to 70% ofdifference between the minimum and the chosen deductiblemanaged-care contracts (up to 20%).
Source: Authors’ research.Note: VHI = voluntary health insurance.
between age, health, VHI and switching in Switzerland sug-gest that older and less healthy people may face barriersto switching. In the following paragraphs we discuss threereasons why this might be the case.
First, evidence from research in the United States showsthat switching costs tend to be higher for older and lesshealthy people [27], who risk having to change provider,having to interrupt current treatment and losing valu-able knowledge about how things work with their currentinsurer [27,28]. In general, switching costs are proba-bly much lower in the European countries than in theUnited States, although they are far from absent, as the18% of Dutch people reporting it was too much trouble toswitch demonstrates [22]. However, if selective contractingbecomes more common in these European health systems(see below), the costs of switching could grow. Selectivecontracting is intended to enhance productive efficiency,but it has the potential to undermine continuity of careand equity of access to services [29].
Second, the availability of complementary or supple-mentary VHI may reduce consumer mobility among olderand less healthy people if sales of voluntary and statu-tory cover are linked, creating a lock-in effect [30,31]. In
Is quality a reason for switching?
perYes. People switch to be with the same insurer as apartner, for better customer service or to obtain a differentset of VHI benefits (the main reason).
atesge ledion of
here
Yes. The reasons given for switching include betterbenefits, better service, better image and change ofemployer or industry [59]. In 2010 additional care offerswere also mentioned [61].
rerser
Yes. Little product differentiation before 2006. Greaterdifferentiation since 2006 in terms of the range ofprescription drugs reimbursed within a given therapeuticcategory, modes of customer service and VHI products.
s aged
) or
Yes. People can opt for managed-care contracts involvinggatekeeping and preferred provider networks.

lth Polic
Btrcaticobii[lfufbmiloh[
r[tbpalnsohtttftd
bttwvrrt
rvi
cava
S. Thomson et al. / Hea
elgium, the Netherlands and Switzerland VHI is sold byhe entities that provide statutory cover (Table 3). Untilecently, Belgian households were actually required to pur-hase voluntary and statutory cover from the same entitynd VHI was the main way in which insurers differentiatedhemselves. Legislation in Switzerland explicitly preventsnsurers from linking the sale of voluntary and statutoryover [20,26], but there are close ties between the two typesf cover; 93% of those with voluntary policies (purchasedy 75% of the population) obtain VHI and SHI from the same
nsurer, partly because reimbursement is much simpler forndividuals to manage when it comes from one company20]. In the Netherlands VHI covers about 90% of the popu-ation and most people buy voluntary and statutory coverrom the same insurer [8]. Although the termination of vol-ntary contracts when enrolees switch to another insureror statutory cover is prohibited by law, insurers frequentlyreach the law [26].6 Dutch insurers can raise VHI pre-iums when people switch for statutory cover (and many
nsurers do) and there are other ways in which they canink the sale of voluntary and statutory cover.7 In 2009 97%f insurers adopted at least one linking strategy, a muchigher proportion than in 2006 (at least 44% of insurers)26].
There is no clear evidence of insurers using VHI to selectisks in the statutory market in any of the four countries20,26,31]. Nevertheless, consumer beliefs about risk selec-ion by insurers in the VHI market seem to be a powerfularrier to switching in the statutory market for less healthyeople. In Switzerland switching was found to be less likelymong people with VHI whose self-reported health wasess than ‘very good’. In the Netherlands the proportion ofon-switching survey respondents who said they did notwitch because they believed they would not be able tobtain a new voluntary policy at all due to their age orealth status (that is, they believed insurers would rejectheir application for voluntary cover) rose from 4% in 2006o 7% in 2009 [26]. The proportion of respondents who gavehis as the most important reason for not switching roserom 1.5% in 2006 to 3.4% in 2009. Similar figures appliedo respondents who did not switch but seriously consideredoing so.
Third, choice ‘overload’ may reduce consumer mobilityy lowering transparency, which increases the transac-ion costs of switching [32,33]. Swiss research shows howhe probability of switching is significantly lower in areasith larger numbers of insurers, even where premium
ariation is significant [23]. Furthermore, among survey
espondents who were very dissatisfied with their cur-ent insurer, 34% intended to switch in areas with fewerhan 50 statutory health insurers versus 22% in areas with6 Recent research found that, when queried, the customer services rep-esentatives of half of all insurers in the Netherlands specified that aoluntary contract would be terminated if the enrolee switched to anothernsurer for statutory cover [26].
7 Only offering voluntary contracts in combination with statutoryover; charging higher premiums when people apply for voluntary coverlone; applying more stringent acceptance criteria when people want onlyoluntary cover; and offering free voluntary cover for children if parentsnd children obtain statutory cover from the same insurer [26].
y 109 (2013) 209– 225 217
more than 50 insurers. Growing product differentiationcan also contribute to choice overload. With the excep-tion of Belgium, insurers have many more ways now thanin the past of modifying the standard statutory product:they can offer choice of cash or in-kind benefits, higherdeductibles in return for lower premiums or contributions,no-claims bonuses and reduced user charges for accept-ing gatekeeping, disease management and use of preferredproviders (Table 6). These options may benefit some indi-viduals but there is likely to be a trade-off in terms oftransparency and ease of price comparison [34,35]. Theymay also restrict choice in other areas. In Germany peoplewho opt for a contract involving gatekeeping, integratedcare or cost reimbursement lose the right to switch fora three-year period. In Switzerland parliament had pro-posed to offer people choosing managed care the optionof a three-year contract (instead of an annual one), but theproposal was rejected in a referendum held in 2012.
4. Incentives for risk selection
Insurer competition should be based on price andquality rather than on risk selection (encouraging enrol-ment among people with lower-than-average risk anddiscouraging or deterring enrolment among those withhigher-than-average risk). If insurers are able to generatea surplus (at least in the short term) through risk selec-tion, they may not be sufficiently motivated to focus onoperating efficiently – that is, obtaining most output fromleast input. Risk selection is also undesirable because itmay threaten equitable, affordable access to health insur-ance and quality of care [7]. Incentives to select risks willbe stronger if insurers bear financial risk and if the moneythey have to spend per enrolee does not reflect the enrolee’srisk of ill health [36]. The degree of risk selection that takesplace in a given situation may also depend on the extent towhich insurers have access to selective tools – for example,the ability to link the sale of statutory and voluntary healthinsurance. The primary mechanism for reducing incentivesto select risks is risk adjustment (also known as risk equal-isation).
4.1. Financial risk
Prior to the introduction of insurer competition, insur-ers in Belgium and the Netherlands did not bear anyfinancial risk. They were little more than financial con-duits, channelling centrally raised resources to providersor raising their own revenue but with leeway to increasecontribution rates and accumulate deficits. The degreeof financial risk borne by insurers has increased inall four countries and is particularly high in Germany,Switzerland and the Netherlands, but remains low inBelgium.
4.2. Risk equalisation
Each country has focused on developing a risk-adjustment formula to allocate resources to healthinsurers, although there are differences across countriesin the design of the formula and in the degree of insurer

218 S. Thomson et al. / Health Policy 109 (2013) 209– 225
Table 6Choice for users, 2012.
Choice regarding: Belgium Germany Netherlands Switzerland
Insurance status (to beinsured or not)
No. No. No. No.
Insurers Yes. After 12 months ofenrolment, people canswitch quarterly.
Yes. People can switchafter 18 months orwithin 2 months if theinsurer introduces orraises acommunity-ratedpremium.
Yes. People can switchonce a year.
Yes. People can switchtwice a year givingthree months’ notice.
Level of pre-paidcontribution
Yes, forcommunity-ratedpremiums, but theamounts are negligible.
Yes, for thecommunity-ratedpremiums (but this iscurrently very small).
Yes, forcommunity-ratedpremiums.
Yes.
Range of benefits No. No, except for a veryfew benefits defined byindividual sicknessfunds.
No. No.
Benefit modality (cashvs in kind)
No. Yes. Yes. No.
Extent of user charges Only in conjunctionwith other conditions(e.g. use of genericdrugs, use of regularGP, gatekeeping). Samefor all sickness funds.
Only in conjunctionwith other conditions(e.g. gatekeeping,enrolment in DMP).Varies by sickness fund.
Yes. Yes.
to ensure that they provided quality customer services,
Providers Yes. Yes.
Source: Authors’ research.Note: GP = general practitioner; DMP = disease management programme.
revenue subject to the formula (Table 7). The extent towhich risk equalisation succeeds in lowering incentives toselect risks largely depends on the sophistication of theformula,8 but also on the presence of risk-sharing arrange-ments such as ex-post compensation based on actual healthcare costs incurred. Risk sharing lessens the degree of finan-cial risk insurers bear and therefore lowers incentives forrisk selection, but it also dampens incentives to operateefficiently [36]. All four countries have strengthened theirrisk equalisation schemes in the last ten years and Belgium,Germany and the Netherlands now have relatively sophis-ticated formulas that include health-based risk adjusters[37–39].
Incentives for risk selection are low in Belgium becauseof the low level of financial risk the sickness funds bear:only 30% of sickness fund revenue is subject to risk adjust-ment and insurers are only financially responsible for 25%of any difference between allocated revenue and actualhealth care expenditure. Risk selection does not seem to bea policy concern, even though the link between statutoryand voluntary cover provides insurers with an effectiveselection tool [13,14]. At the same time as the currentarrangements in Belgium limit incentives for risk selec-tion, they are probably not sufficient to motivate insurersto operate more efficiently. Insurers in both Germany andthe Netherlands have incentives to select risks beyond the
criteria included in the risk adjustment formula. However,German insurers may have less opportunity to do so, sincethe market for complementary VHI is small in Germany (in8 The formula need not be perfect, but it must be sufficiently sophisti-cated to make risk selection more costly to the insurer than it is worth.
Yes. Yes.
terms of population coverage) compared to VHI markets inBelgium and the Netherlands [31].
Insurers in Switzerland probably face the strongestincentives to select risks because they bear full financialrisk for outpatient care (although they are much less atrisk for inpatient costs, which they share with the can-tons) [40,41] and, perhaps more importantly, the Swiss riskequalisation scheme was weak for over 20 years, adjustingfor age and gender only. The need for better risk adjust-ment was recognised in Switzerland for many years, butattempts to improve the formula were blocked or sloweddown by lobbying on the part of some insurers who werehighly influential politically [41]. In 2012 the Swiss formulawas substantially improved by the introduction of a newfactor, hospitalisation in the previous year; other factorsmay be introduced in the near future [42].9
5. The availability and use of tools to enhanceefficiency through strategic purchasing
The final dimension of interest is the extent to whichindividual insurers are able to influence health care qual-ity and costs – that is, to engage in strategic purchasing.If insurers were not able to do this, the main reasons forencouraging them to compete with each other would be
kept administrative costs to a minimum and passed on anycost savings to enrolees in the form of lower premiums.
9 Strengthening the risk adjustment formula was the only part of thereform rejected in a 2012 referendum that had the support of a largemajority of the population.

S. Thomson et al. / Health Policy 109 (2013) 209– 225 219
Table 7Strength of insurer incentives to select risks, 2012.
Belgium Germany Netherlands Switzerland
Prospective resource allocationsubject to risk equalisation(%)
30% 100% 100% 100%
Risk equalisation scheme Yes. Yes. Yes. Yes.Risk adjustment includes
health-based criteriaYes. Yes. Yes. Partially (hospitalisation of at least 3
days in the previous year); plans toinclude additional health-basedcriteria.
Risk sharing Insurers pay 25% of anyrevenue-expenditure gap.
No. No. No (see note).
Hig
SN sts of inp
Tfseoth
5
rmfwphpen
aoticacmcnTtapclbtIi2oi
Incentive to select risks Low.
ource: Authors’ research.ote: Swiss insurers bear full financial risk for outpatient care, but the co
hese would be satisfactory outcomes, but the rationaleor insurer competition goes beyond notions of customerervice and administrative efficiency. At least in theory, itncompasses the notion of enhancing efficiency at the levelf the health system through stronger purchasing leadingo better delivery of health care and, ultimately, to betterealth outcomes.
.1. The range of tools available
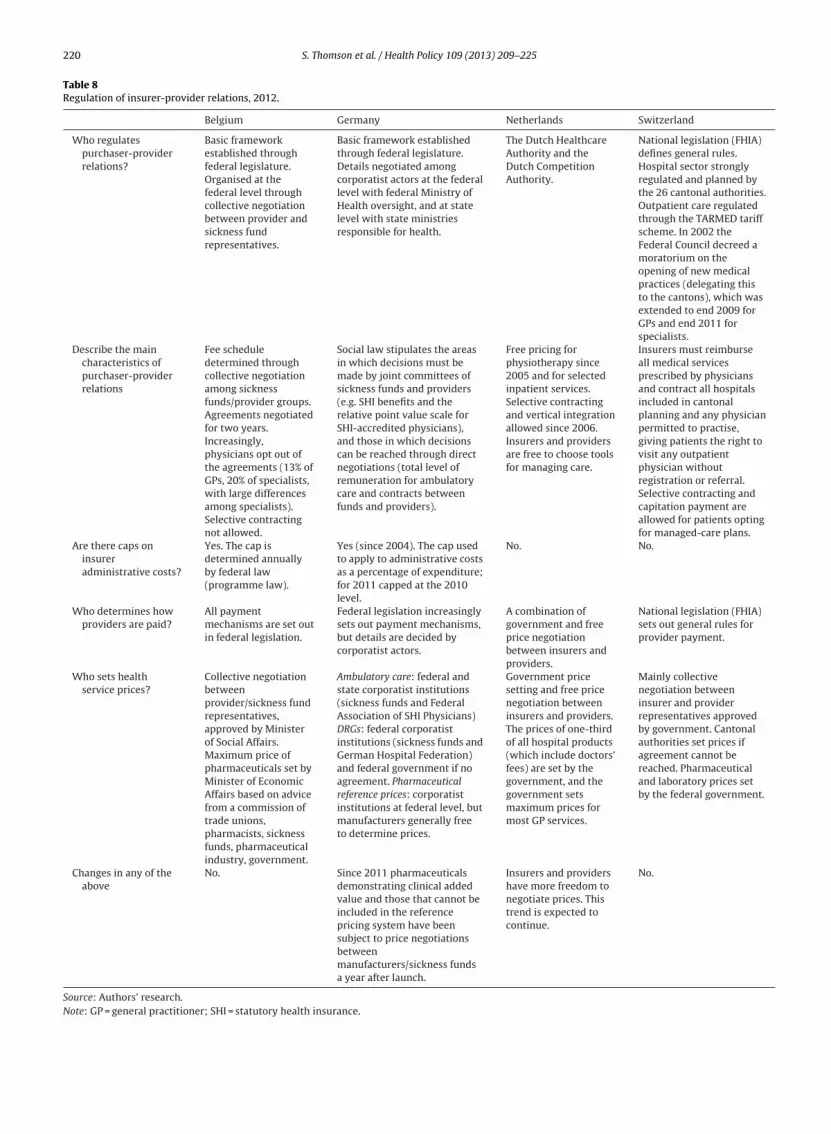
Tables 8 and 9 show how insurer-provider relations areegulated and the availability and take-up of tools insurersight use to engage in strategic purchasing. The tools range
rom allowing insurers to integrate with providers, whichould strengthen incentives for expenditure control, toermitting them to selectively contract providers, chooseow best to reward or penalise good or poor providererformance and influence the types of services to whichnrolees have access. The list of tools included in Table 9 isot exhaustive.
In Belgium, Germany and Switzerland collective negoti-tion between insurers and providers is the default methodf setting prices and concluding contracts, which limitshe ability of individual insurers to influence the qual-ty and cost of most health services, but preserves freehoice of provider for service users (Table 8). In Germanynd Switzerland insurers have a degree of leeway in theontracting process. Policies offering a GP gatekeepingodel of care allow German sickness funds to selectively
ontract GPs (in addition to the collective contract) andegotiate prices and other conditions on a bilateral basis.he same applies if providers sign integrated-care con-racts with sickness funds. Similarly, Swiss insurers arellowed to engage in selective contracting, negotiate lowerrices and use capitation to pay providers when peoplehoose managed-care plans [43]. However, because col-ectively negotiated prices and contracts are the norm inoth countries, insurers need to offer particularly attrac-ive terms to convince doctors to sign alternative contracts.nsurers in the Netherlands have more freedom in contract-
ng than their counterparts in the other countries. Since006, selective contracting has been permitted for all formsf care and, while the government continues to set max-mum prices for GP services and prices for one-third ofh. High. Very high.
atient care are shared between insurers and cantons.
hospital services, the aim is to move towards greater priceliberalisation.
5.2. Take-up of purchasing tools
There are clear differences between Belgium and theother countries in the range of tools available to enablestrategic purchasing by insurers. The more limited recourseto purchasing tools in Belgium reflects the absence ofnational policy emphasis on competition as a mechanismfor stronger purchasing and a preference for sickness fundsto operate collectively. Although this suggests Belgianinsurers are at a disadvantage when it comes to purchas-ing, insurers in the other countries do not make full useof purchasing tools for a range of reasons including legalrestrictions, concerns about restricting consumer choice,technical challenges and lack of information.
Legal restrictions preclude widespread take-up of sometools in Germany and Switzerland. German sickness fundscan only engage in selective contracting or develop theirown clinical guidelines and prescription drug formulariesif funds, GP associations and patients opt for gatekeep-ing contracts or if funds, providers and patients opt forintegrated-care contracts. A proposal by the federal gov-ernment in the early 2000s to extend selective contractingto elective inpatient treatment was blocked by the states onthe grounds that it would threaten their ability to plan hos-pital capacity. For Swiss insurers, many purchasing toolsare limited to managed-care plans, primarily to preservefree choice of provider for those who value it. In 2010 46.9%of enrolees opted for a managed-care contract [44], but onlya few of these chose the capitation model involving selec-tive contracting; most chose a less restrictive family doctoror call centre model [45]. Recent legislation passed by theSwiss parliament in 2011 aimed to boost the developmentof integrated care networks, to strengthen financial incen-tives to enrol in a capitation-based managed care plan (byincreasing user charges, for those who do not enrol, from10% to 15% of care costs) and to ban vertical integration ofinsurers and providers [42], but was rejected in a referen-dum held in 2012.
A different form of legal restriction occurs whennational authorities block the use of permitted tools onthe grounds (for example) that they are anti-competitive.In 2009 a dominant regional insurer and a group of local
220 S. Thomson et al. / Health Policy 109 (2013) 209– 225
Table 8Regulation of insurer-provider relations, 2012.
Belgium Germany Netherlands Switzerland
Who regulatespurchaser-providerrelations?
Basic frameworkestablished throughfederal legislature.Organised at thefederal level throughcollective negotiationbetween provider andsickness fundrepresentatives.
Basic framework establishedthrough federal legislature.Details negotiated amongcorporatist actors at the federallevel with federal Ministry ofHealth oversight, and at statelevel with state ministriesresponsible for health.
The Dutch HealthcareAuthority and theDutch CompetitionAuthority.
National legislation (FHIA)defines general rules.Hospital sector stronglyregulated and planned bythe 26 cantonal authorities.Outpatient care regulatedthrough the TARMED tariffscheme. In 2002 theFederal Council decreed amoratorium on theopening of new medicalpractices (delegating thisto the cantons), which wasextended to end 2009 forGPs and end 2011 forspecialists.
Describe the maincharacteristics ofpurchaser-providerrelations
Fee scheduledetermined throughcollective negotiationamong sicknessfunds/provider groups.Agreements negotiatedfor two years.Increasingly,physicians opt out ofthe agreements (13% ofGPs, 20% of specialists,with large differencesamong specialists).Selective contractingnot allowed.
Social law stipulates the areasin which decisions must bemade by joint committees ofsickness funds and providers(e.g. SHI benefits and therelative point value scale forSHI-accredited physicians),and those in which decisionscan be reached through directnegotiations (total level ofremuneration for ambulatorycare and contracts betweenfunds and providers).
Free pricing forphysiotherapy since2005 and for selectedinpatient services.Selective contractingand vertical integrationallowed since 2006.Insurers and providersare free to choose toolsfor managing care.
Insurers must reimburseall medical servicesprescribed by physiciansand contract all hospitalsincluded in cantonalplanning and any physicianpermitted to practise,giving patients the right tovisit any outpatientphysician withoutregistration or referral.Selective contracting andcapitation payment areallowed for patients optingfor managed-care plans.
Are there caps oninsureradministrative costs?
Yes. The cap isdetermined annuallyby federal law(programme law).
Yes (since 2004). The cap usedto apply to administrative costsas a percentage of expenditure;for 2011 capped at the 2010level.
No. No.
Who determines howproviders are paid?
All paymentmechanisms are set outin federal legislation.
Federal legislation increasinglysets out payment mechanisms,but details are decided bycorporatist actors.
A combination ofgovernment and freeprice negotiationbetween insurers andproviders.
National legislation (FHIA)sets out general rules forprovider payment.
Who sets healthservice prices?
Collective negotiationbetweenprovider/sickness fundrepresentatives,approved by Ministerof Social Affairs.Maximum price ofpharmaceuticals set byMinister of EconomicAffairs based on advicefrom a commission oftrade unions,pharmacists, sicknessfunds, pharmaceuticalindustry, government.
Ambulatory care: federal andstate corporatist institutions(sickness funds and FederalAssociation of SHI Physicians)DRGs: federal corporatistinstitutions (sickness funds andGerman Hospital Federation)and federal government if noagreement. Pharmaceuticalreference prices: corporatistinstitutions at federal level, butmanufacturers generally freeto determine prices.
Government pricesetting and free pricenegotiation betweeninsurers and providers.The prices of one-thirdof all hospital products(which include doctors’fees) are set by thegovernment, and thegovernment setsmaximum prices formost GP services.
Mainly collectivenegotiation betweeninsurer and providerrepresentatives approvedby government. Cantonalauthorities set prices ifagreement cannot bereached. Pharmaceuticaland laboratory prices setby the federal government.
Changes in any of theabove
No. Since 2011 pharmaceuticalsdemonstrating clinical addedvalue and those that cannot beincluded in the referencepricing system have beensubject to price negotiationsbetweenmanufacturers/sickness fundsa year after launch.
Insurers and providershave more freedom tonegotiate prices. Thistrend is expected tocontinue.
No.
Source: Authors’ research.Note: GP = general practitioner; SHI = statutory health insurance.

S. Thomson et al. / Health Policy 109 (2013) 209– 225 221
Table 9Availability and take-up of purchasing tools by insurers offering statutory benefits, 2012.
Tools Belgium Germany Netherlands Switzerland
Vertical insurer-providerintegration
Yes; take-up very low. No, with rare historicalexceptions; otherwiseonly permitted forrehabilitation.
Yes; take-up low butgrowing.
Yes, but take-up low; an attemptto ban vertical integration ofinsurer and providers wasrejected by popular ballot, alongwith a proposal for integratedcare networks, in 2012.
Selective contracting No. Yes, but only in thecontext of integratedcare contracts,therefore low take-up.
Yes; take-up low butgrowing strongly.
Yes, but only for enrolees optingfor managed-care contracts (46%of the population in 2010);however, only part of thesecontracts are genuinely based onselective contracting.
Financial incentives forpatients to use preferredproviders
No. Yes; moderate take-up(GP contracts lesspopular thanexpected).
Yes; take-up low butgrowing strongly.
A 15% co-insurance rate forordinary coverage and a 10% ratefor plans with preferredproviders and integrated carenetworks was approved byparliament but cancelledfollowing the referendum held inJune 2012.
Clinicalguidelines/protocols
Yes, collectively. Yes, possible within GPcontracts andintegrated carecontracts; low take-up.
Yes; moderate to hightake-up.
Not explicitly. It is up to thephysicians to use these tools todeal with e.g. capitation paymentwithin managed-care contracts.
Formularies for medicines Yes, collectively. Yes, possible within GPcontracts andintegrated carecontracts; low take-up.
Yes; moderate take-up. No. Pharmaceuticals included inthe benefits package cannot berestricted through managed-carearrangements.
Incentives for rationalprescribing/dispensing ofmedicines
Yes, collectively. Directed at physicians:prescription limits;directed towardspharmacists: genericsubstitution unlessruled out; directed atpatients: lowerco-payments for drugspriced at least 30%below reference price.
Financial incentives topharmacists toencourage genericsubstitution.
A higher co-insurance rate (20%rather than 10%) for brand drugsif a generic alternative isavailable.
Disease managementprogrammes
Yes, collectively. Yes; high take-up(about 9% of SHIenrolees in 2011).
Yes; take-up low butgrowing.
Not explicitly.
Utilisation review Yes, collectively, butonly for very expensiveservices.
Yes, collectively androutinely; individuallyonly in integrated carecontracts, low take-up.
Yes; moderate take-up. Yes, within managed-carearrangements.
Waiting list management Not relevant. Not relevant. Yes; high take-up andsuccessful.
Not relevant.
Price negotiation No. Yes, partial (e.g.GP-based gatekeepingor integrated carecontracts); currentlymainly withpharmaceuticalmanufacturers, hightake-up (about 60% ofdrugs distributedunder rebatecontracts).
Yes, partial; high take-up. Yes, but only for enrolees optingfor managed-care contracts.
Performance-basedpayment of providers
No Yes, but used onlywithin integrated carecontracts; low take-up.
Yes, partial; take-upgrowing.
Yes, within managed-carearrangements.
Public disclosure ofperformance indicators
Yes, collectively,mainly forsupplementaryhospital costs
Yes; mandatory forcertain hospitalindicators (but not veryrelevant forpurchasing).
Yes; moderate take-upbut growing.
Yes, in the hospital sector;modest results.
Source: Authors’ research.Note: GP = general practitioner; SHI = statutory health insurance.

lth Polic
222 S. Thomson et al. / Heahealth care providers, including GPs, tried to take over afailing Dutch hospital [46]. Some members of parliamentpressured the Minister of Health to prevent the takeoveron the grounds that all parties involved would have afinancial incentive to direct patients towards the hospitalin question, which would restrict consumer choice. Con-versely, residents expressed a desire for their local hospitalto remain open since closure would also have limited theiroptions [46]. Something similar can be seen in Germany,where ownership of ambulatory care centres by hospitalsis disputed. The government had proposed to prohibit thisbut did not introduce the necessary legislation.
Concerns about restricting consumer choice of providermay prevent insurers from using selective contracting. InGermany and the Netherlands insurers reveal a strong pref-erence for offering enrolees financial incentives (lower usercharges or lower premiums) to choose preferred providernetworks or GP gatekeeping. It is argued that Dutch insur-ers are reluctant to de-select hospitals because they believeconsumers will regard them as being motivated by finan-cial rather than quality considerations [46,47]. Some ofthese concerns may be justified, since consumers gener-ally reveal a preference for wider choice of provider: theGP gatekeeping option has not been as popular amongpatients and sickness funds as expected in Germany (partlybecause evaluations do not show savings); take-up of pre-ferred provider networks in the Netherlands is low; andmost Swiss enrolees who opt for managed-care plans donot opt for plans involving selective contracting [45]. Selec-tive contracting has also been resisted by regulators andproviders. In 2010 a large Dutch insurer published hospitalrankings for quality of breast cancer care on its websiteand announced it would no longer send enrolees withbreast cancer to hospitals that did not reach minimumvolume thresholds for breast cancer treatment, a movesupported by patient groups [48]. The Dutch HealthcareInspectorate initially stated that all breast cancer treat-ment in the Netherlands met its standards for responsiblecare, while the Dutch Association of Surgeons suggested theinsurer had used inappropriate standards [48]. The decisionwas upheld by the courts, however, and other insurers soonfollowed suit.
Some purchasing tools present technical challengesunder certain circumstances, particularly selective con-tracting and price negotiation. As a result, insurers maylack the capacity to use them effectively or the transac-tion costs involved may be high. In Germany selectivecontracting is unattractive partly due to the complexityof having to re-calculate global payments to office-basedphysicians (Table 8) when some patients are treated underseparate contracts, and partly because hospitals cannotbe de-selected on a service-by-service basis (as in theNetherlands). Switzerland has seen mergers among pri-vate clinics to strengthen provider bargaining power andincrease their ability to negotiate higher prices with insur-ers. Since 2006, price negotiation has been promoted as akey purchasing tool in the Netherlands, where individual
insurers are encouraged to negotiate prices with individualhospitals for pre-defined services covering 4000 Diagnos-tic Treatment Combinations (DTCs, case-based paymentsper episode of illness) equal to 70% of hospital revenue (upy 109 (2013) 209– 225
from one third of hospital revenue in 2010). To help insur-ers cope with the magnitude of the task, the Dutch Insurers’Association publishes an annual purchasing guide focusingon 200 of the most frequently used DTCs [49].
The lack of information on health care quality andcosts, particularly at the level of individual providers, isa major obstacle to the effective use of some purchas-ing tools, notably selective contracting, price negotiationand performance-based provider payment. Without goodinformation it is not possible to carry out systematic bench-marking, which in turn precludes fully informed decisionmaking by insurers and enrolees. There is some public dis-closure of information about provider performance (mainlyhospitals) in all four countries and government-led effortsto improve data collection and disclosure in Germany [50]and the Netherlands [8]. However, public disclosure issometimes controversial (as in the Dutch case) and the lackof informative indicators based on reliable data may repre-sent a significant barrier to improved purchasing for sometime to come.
6. Policy implications
This paper has reviewed the policy goals underlying theintroduction of insurer choice and competition for statu-tory health coverage in Belgium, Germany, the Netherlandsand Switzerland. It has examined policy implementation inthree areas: consumer mobility, incentives for risk selec-tion, and the availability and use of tools to enhanceefficiency. In this section we discuss important similari-ties and differences across the four countries, consider theextent to which the conditions underpinning the theoreti-cal rationale for insurer competition – to enhance allocativeand productive efficiency, mainly through stronger pur-chasing – have been met in practice, and highlight someimplications for policy.
The range of policy goals underlying insurer choice andcompetition varies across the four countries, but thereis common ground. Germany and Switzerland introducedreforms primarily to address access and equity concerns.Belgium is the only one of the four countries in which pub-lic policy has not emphasised competition among insurers.We included it in the analysis because the shifting of somefinancial risk to sickness funds in 1995 aimed to stim-ulate greater expenditure control; from 1995 onwards,consumer choice of insurer became an integral part of theincentive structure facing sickness funds, even though itwas not originally intended to have that effect. Expenditurecontrol has also been one of the goals of insurer com-petition in Germany and Switzerland. Germany and theNetherlands expected consumer choice of insurer, com-bined with greater financial risk for insurers, to enhanceefficiency and quality in health care administration anddelivery. Efficiency was not explicitly stated as a goal inSwitzerland, but it has been used in public debate to justifymaintaining the status quo – in other words, alternatives toinsurer competition are portrayed as being likely to lower
efficiency.Risk adjustment has been a priority for policy mak-ers – for good reason, since risk selection erodes insurers’incentives to operate efficiently and may threaten equity

lth Polic
aiiamwitmablitcaaahsfo
tmcbbi–Tfhc
mopoiftsscwaw–
wg(a
Gstt
b
S. Thomson et al. / Hea
nd quality of care. However, while all four countries haventroduced and improved risk adjustment formulas, theres variation across countries in the quality of the formuland in the pace at which it has been strengthened. Policyakers in Germany accepted that their original formulaas relatively crude because they lacked the necessary
nformation for a more effective formula; once they hadhe information, however, they were able to refine the for-
ula. The weakness of Switzerland’s formula was widelycknowledged nationally, but action to strengthen it waslocked for many years not by lack of data but by industry
obbying. In spite of the energy devoted to strengthen-ng formulas, no country has fully eliminated incentiveso select risks [38]. Circumstantial evidence for all of theountries indicates there is risk selection through targeteddvertising, through the use of reminders and discountsnd through product differentiation in VHI10 [8,20,38,51],nd anecdotal evidence suggests insurers in some countriesave tried to deter high risks from enrolling.11 Furthertrengthening of the formula continues to be a priorityor Switzerland, but there is scope for improvement in thether countries too.
Consumer mobility has not received as much atten-ion as risk adjustment. Extensive regulation to facilitate
obility (much of it predating the introduction of insurerompetition) may mean that switching costs are negligi-le for most people in all four countries. However, a smallut growing body of evidence suggests consumer mobil-
ty is limited among older and less healthy individuals those likely to use health services on a regular basis.his ought to be a cause for concern because if insurerseel these enrolees are unlikely to switch, they may notave sufficient incentive to provide them with high-qualityare.
Research identifies two potential barriers to consumerobility: first, increasingly close links between the sale
f statutory health insurance and complementary or sup-lementary VHI and second, choice overload. Tied salesf statutory and voluntary health insurance are prohib-ted in the Netherlands and Switzerland, but insurers haveound ways of linking the two types of cover. While a mix-ure of regulation, risk adjustment and accepted normseems to have prevented most insurers from using VHI toelect risks for statutory health insurance, it has not allayedonsumer fears about obtaining adequate voluntary coverhen switching to a new insurer for statutory cover. This is
particular problem in the Netherlands and Switzerland,here VHI coverage is widespread. The Belgian solution
greater regulation of VHI12 – may not be attractive to
10 Swiss insurers use holding companies to direct enrolees to a planith an ‘appropriate’ premium, while in the Netherlands the growth of
roup contracts has allowed insurers to offer discounts to some groupsemployers, self-employed people, sports clubs) but not others (patientssociations) [38].11 In 2011 several hundred members of an insolvent sickness fund inermany were put off joining other sickness funds through statementsuch as “we cannot guarantee that your insurance card will be ready inime” etc.; the Federal Insurance Authority had to intervene and remindedhe sickness funds to obey legal requirements.12 In Belgium open enrolment is guaranteed for compulsory additionalenefits. In 2007 legislation extended open enrolment requirements to the
y 109 (2013) 209– 225 223
policy makers elsewhere, in part due to concerns aboutinfringing EU internal market rules [52]. Nevertheless, theimportance of VHI as an obstacle to consumer mobilityamong older and less healthy people requires some formof policy action. Better risk adjustment might help, along-side better information for consumers and closer scrutinyof the sales process. Policy attention should also focus onthe potential for choice overload, particularly in the contextof a trend towards allowing insurers to offer differentiatedbenefits to suit individual preferences – for example, dif-ferent levels of user charges or additional services. It iswell established that product differentiation, even at themargin, lowers transparency [35]. This in turn increasestransaction costs for consumers and can therefore under-mine competition.
Making sure insurers have and use tools to influencehealth care quality and costs is essential if competition isto enhance efficiency through stronger purchasing. Indi-vidual insurers in Belgium do not have many of thesetools, insurers in Germany and Switzerland have access tosome tools, and insurers in the Netherlands have accessto a wider range of tools but do not always use them.Differences in policy goals across countries – the lack ofpolicy emphasis on competition in Belgium and the pol-icy emphasis on access and equity goals in Germany andSwitzerland – may explain some of this variation; but theexperience of the four countries under review suggests thatdifferences may arise for other reasons, including lack ofrelevant data and stakeholder resistance to the use of sometools.
In all four countries commentators have emphasised theneed for better information about health care quality andcosts. The importance of good information and informa-tion systems cannot be overstated, particularly in enablingrobust risk adjustment, facilitating selective contracting,setting prices, developing priorities, fostering best practiceand linking provider payment to performance. However,good information is not the only pre-requisite for strate-gic purchasing. Policy also needs to ensure that insurershave incentives to operate efficiently, that there is suffi-cient capacity to make use of tools, and that incentives arealigned across the health system.
Resistance seems inevitable given that some purchas-ing tools have the potential to restrict enrolee choice (ofboth insurer and provider, in the case of selective con-tracting), many of them will affect provider autonomy andincome, and most require information that is not readilyavailable. Cross-country variation may therefore reflect dif-ferences in the extent to which policy makers and insurersare willing and able to curb enrolee choice and challengeproviders. This in turn may reflect uncertainty on the partof policy makers about the appropriate place for compe-tition – among insurers or among providers? – and aboutwho is best placed to influence provider behaviour – gov-
ernment, insurers collectively, individual insurers or healthcare users?sale of VHI and prohibited premium differentiation based on pre-existingmedical conditions (except for people aged 65 years and above who didnot already hold a similar policy with their former insurer).

lth Polic
[
[
[
[
[
[
[
[
[
[
[
[
[
[
224 S. Thomson et al. / Hea
7. Conclusions
Reforms introducing insurer choice and competitionhave had diverse goals in European health systems. Theyhave not always aimed to enhance efficiency, but wherethey have, expectations about efficiency gains may con-flict with other stated goals such as expenditure control.Reforms have also been implemented in different ways andin different timeframes. Differences in policy goals explainsome but not all of the differences in policy design anddevelopment across countries. Not surprisingly, politicalfactors have an explanatory role.
Each country has put in place some measures to meetthe three conditions highlighted in this paper as beingnecessary for insurer competition to enhance efficiency,including extensive regulation to secure consumer mobil-ity, reduce incentives for risk selection and provide insurerswith tools for strategic purchasing. However, there areimportant variations in the implementation of these meas-ures. The pace with which risk adjustment has beenstrengthened has been much slower in Switzerland than inthe other countries and, in spite of significant investment inrisk adjustment, incentives for risk selection remain in allfour countries. Consumer mobility is not evenly distributedacross the population in the three countries for whichdata are available. Better risk adjustment may enhancemobility among older and less healthy people and policymakers should do more to prevent insurers from linkingthe sale of statutory and voluntary health insurance, par-ticularly in the Netherlands and Switzerland. In Belgium,Germany and Switzerland collective negotiation betweeninsurers and providers curbs the ability of individual insur-ers to influence the quality and costs of many healthservices. Insurers in the Netherlands have good access toefficiency-enhancing tools; nevertheless, data and capacityconstraints and resistance from enrolees, providers, regula-tors and politicians limit the extent to which tools are used.
The experience of the four countries reviewed in thispaper offers an important lesson to countries thinking ofintroducing competition in statutory health insurance: it isnot straightforward to put in place the conditions underwhich health insurance competition can enhance effi-ciency. Policy makers should not, therefore, underestimatethe challenges involved. Effective risk adjustment requiresextensive data and sophisticated information systems andmay be obstructed by insurers. Consumer mobility needsto be underpinned by substantial regulation and may bethreatened where the same insurers sell statutory and vol-untary benefits, the take-up of VHI is widespread and thereis reluctance to regulate the VHI market. Finally, the avail-ability and use of tools to enhance efficiency is likely to beopposed by a range of stakeholders.
Acknowledgements
The authors are grateful to two anonymous referees
for their comments on an earlier draft and the Common-wealth Fund for financial support. The views presented inthe paper are those of the authors and not necessarily thoseof the Commonwealth Fund, its directors, officers or staff.[
[
y 109 (2013) 209– 225
References
[1] Thomson S, Foubister T, Mossialos E. Financing health care in theEuropean Union: challenges and policy responses. Copenhagen:World Health Organization on behalf of the European Observatoryon Health Systems and Policies; 2009.
[2] Schneider P. Health insurance and competition. Washington DC: TheWorld Bank; 2009.
[3] Thomson S, Võrk A, Habicht T, Rooväli L, Evetovits T, Habicht J.Responding to the challenge of financial sustainability in Estonia’shealth system. Copenhagen: World Health Organization RegionalOffice for Europe; 2010.
[4] Bevan G, van de Ven WPMM. Choice of providers and mutualhealthcare purchasers: can the English National Health Servicelearn from the Dutch reforms? Health Economics. Policy and Law2010;5(3):343–63.
[5] Enthoven AC. Managed competition: an agenda for action. HealthAffairs 1988;7(3):25–47.
[6] Figueras J, Robinson R, Jakubowski E, editors. Purchasing to improvehealth systems performance. Buckingham: Open University Press;2005.
[7] van de Ven WPMM, Ellis RP. Risk adjustment in competitive healthplan markets. In: Newhouse JP, Culyer AJ, editors. Handbook of healtheconomics. Amsterdam: Elsevier; 1999. p. 755–845.
[8] Westert GP, van den Berg M, Zwakhals SLN, de Jong JD, Verkleij H,editors. Dutch health care performance report 2010. Bilthoven: RIVM(National Institute for Public Health and the Environment; 2010.
[9] Schut E, van de Ven WPMM. Effects of purchaser competition in theDutch health system: is the glass half full or half empty? HealthEconomics, Policy and Law 2011;6(1):109–23.
10] Hendriks M, Spreeuwenberg P, Rademakers J, Delnoij D. Dutchhealthcare reform: did it result in performance improvementof health plans? A comparison of consumer experiences overtime. BMC Health Services Research 2009;9(167). Available from:http://www.biomedcentral.com/1472-6963/9/167
11] Crivelli L. Consumer-driven health insurance in Switzerland, wherepolitics is governed by federalism and direct democracy. In: ThomsonS, Mossialos E, editors. Private health insurance and medical sav-ings accounts: history, politics, performance. Cambridge: CambridgeUniversity Press; in press.
12] Gerkens S, Merkur S. Belgium: health system review. Health Systemsin Transition 2010;12(5):1–266.
13] Schokkaert E, Van de Voorde C. Risk adjustment and the fear ofmarkets: the case of Belgium. Health Care Management Science2000;3:121–30.
14] Schokkaert E, Van de Voorde C. Belgium: risk adjustment andfinancial responsibility in a centralised system. Health Policy2003;65(1):5–19.
15] Busse R, Bluemel M, Ognyanova D. Germany: health system review.Health Systems in Transition 2013;15, in press.
16] Gaskins M, Busse R. Morbidity-based risk adjustment in Germany– long in coming, but worth the wait? Eurohealth 2009;15(3):28–32.
17] Altman D, Cutler DM, Zeckhauser RJ. Adverse selection and adverseretention. American Economic Review 1998;88(2):122–6.
18] Strombom BA, Buchmueller TC, Feldstein PJ. Switching costs, pricesensitivity and health plan choice. Journal of Health Economics2002;21(1):89–116.
19] Federal Office of Public Health. Statistik der obligatorischen Kranken-versicherung 2008. Bern: Federal Office of Public Health, 2008.
20] Dormont B, Geoffard P-Y, Lamiraud K. The influence of supplemen-tary health insurance on switching behaviour: evidence from Swissdata. Health Economics 2009;18(11):1339–56.
21] Mihm A. Versicherte fliehen vor Zusatzbeiträgen. FAZ.net, 27.7.2010[cited 1 October 2012]. Available from: http://www.faz.net/s/Rub0E9EEF84AC1E4A389A8DC6C23161FE44/Doc∼E3DD42423BB964609BD540E7D977D5ED3∼ATpl∼Ecommon∼Scontent.html
22] Vos L, De Jong JD. Percentage overstappers van zorgverzekeraar 3%.Ouderen wisselen nauwelijks van zorgverzekeraar. Utrecht: NIVEL;2009.
23] Frank R, Lamiraud K. Choice, price competition and complexity inmarkets for health insurance. Journal of Economic Behavior andOrganization 2009;71(2):550–62.
24] Samuelson W, Zeckhauser R. Status quo bias in decision making.Journal of Risk and Uncertainty 1988;1(1):7–59.
25] Gresz S, Groenewegen P, Kerssens J, Braun B, Wasem J. Free choiceof sickness fund in regulated competition: evidence from Germanyand the Netherlands. Health Policy 2002;60(3):235–54.

lth Polic
[
[
[
[
[
[
[
[
[
[
[
[
[
[
[
[
[
[
[
[
[
[
[
[
[
[
[
[
[
[
[
[
[
[
[
[
[
[
[
[
ance. International Journal of Health Care Finance and Economics
S. Thomson et al. / Hea
26] Roos A-F, Schut FT. Spillover effects of supplementary on basichealth insurance: evidence from the Netherlands. European Journalof Health Economics 2012;13(1):52–61.
27] Buchmueller TC, Feldstein PJ. The effect of price on switching amonghealth plans. Journal of Health Economics 1997;16(2):231–47.
28] Knaus T, Nuscheler R. Risk selection in the German public healthinsurance system. Health Economics 2005;14(12):1253–71.
29] Mobley LR. Effects of selective contracting on hospital efficiency,costs and accessibility. Health Economics 1998;7(3):247–61.
30] Mossialos E, Thomson S. Voluntary health insurance in the Euro-pean Union: report prepared for the European Commission. London:London School of Economics and Political Science; 2002.
31] Paolucci F, Schut E, Beck K, Greß S, Van de Voorde C, Zmora I. Supple-mentary health insurance as a tool for risk selection in mandatorybasic health insurance markets: a five country comparison. HealthEconomics, Policy and Law 2007;2(2):173–92.
32] Schwartz B. The tyranny of choice. Scientific American2004;290(4):70–5.
33] Rice T. Should consumer choice be encouraged in health care? In:Davis JB, editor. The social economics of health care. London: Rout-ledge; 2001.
34] Office of Fair Trading. Health insurance: a report by the Officeof Fair Trading. London: Office of Fair Trading; 1996 [cited 7January 2013]. Available from: http://www.oft.gov.uk/shared oft/reports/financial products/oft168.pdf
35] Office of Fair Trading. Consumer detriment under conditions ofimperfect information. London: Office of Fair Trading; 1997 [cited7 January 2013]. Available from: http://www.oft.gov.uk/sharedoft/reports/consumer protection/oft194.pdf
36] van de Ven WPMM. Risk adjustment and risk equalization:what needs to be done? Health Economics, Policy and Law2011;6(1):147–56.
37] van de Ven WP, Beck K, Buchner F, Chernichovsky D, Gardiol L,Holly A, et al. Risk adjustment and risk selection on the sicknessfund insurance market in five European countries. Health Policy2003;65(1):75–98.
38] van de Ven WPMM, Beck K, Van de Voorde C, Wasem J, Zmora I. Riskadjustment and risk selection in Europe: six years later. Health Policy2007;83(2/3):162–79.
39] Buchner F, Goepffarth D, Wasem J. The new risk adjustment formulain Germany: implementation and first experiences. Health Policy2013;109(3):253–62.
40] Minder A, Schoenholzer H, Amiet M. Health care systems in tran-sition: Switzerland. Copenhagen: European Observatory on HealthCare Systems; 2000.
41] Trottmann M. Reforming health insurance in a direct democracy –lags, inconsistencies, and some important steps forward. In: Paperpresented at the European Conference on Health Economics, Zurich,18–21 July. 2012.
42] Federal Authorities of the Swiss Confederation. Bundesgesetzüber die Krankenversicherung (Managed Care) Änderung vom30 September 2011 [cited 7 September 2012]. Available from:http://www.admin.ch/ch/d/ff/2011/7441.pdf
43] Lehmann HJ, Zweifel P. Innovation and risk selection in reg-ulated social health insurance. Journal of Health Economics2004;23(12):997–1012.
44] Federal Office of Public Health. Statistik der obligatorischenKrankenversicherung 2010 (Table 11.07d) [cited 7 September2012]. Available from: http://www.bag.admin.ch/themen/krankenversicherung/01156/index.html?lang=de
45] Reich O, Rapold R, Thöni M. An empirical investigation of the effi-ciency effects of integrated care models in Switzerland. InternationalJournal of Integrated Care. 2012; 12(January-March). Available from:http://www.ijic.org/index.php/ijic/article/view/685
46] Maarse H, Paulus A. The politics of health care reform inthe Netherlands since 2006. Health Economics, Policy and Law2011;6(1):125–34.
47] Boonen LHHM, Schut FT. Preferred providers and the credible com-mitment problem in health insurance: first experiences with the
[
y 109 (2013) 209– 225 225
implementation of managed competition in the Dutch health caresystem. Health Economics, Policy and Law 2011;6(2):219–35.
48] Sheldon T. Dutch health insurer ranks hospitals on breastcancer surgery. British Medical Journal 2010;341(6853),http://dx.doi.org/10.1136/bmj.c6853.
49] Bal R, Zuiderent-Jerak T. The practice of markets in Dutch health care:are we drinking from the same glass? Health Economics, Policy andLaw 2011;6(1):139–45.
50] Busse R, Nimptsch U, Mansky T. Measuring, monitoring,and managing quality in Germany’s hospitals. Health Affairs2009;28(2):w294–304.
51] Nuscheler R, Knaus T. Risk selection in the German public healthinsurance system. Health Economics 2005;14(12):1253–71.
52] Thomson S, Mossialos E. Private health insurance and the internalmarket. In: Mossialos E, Permanand G, Baeten R, Hervey T, editors.Health systems governance in Europe: the role of EU law and policy.Cambridge: Cambridge University Press; 2010. p. 419–60.
53] Ministerie van Volksgezondheid WeS. VWS-Verzekerdenmonitor 2012. Den Haag: Ministerie vanVolksgezondheid, Welzijn en Sport; 2012 [cited 1October 2012]. Available from: http://www.rijksoverheid.nl/ministeries/vws/documenten-en-publicaties?page=1
54] Egloff M. Studio sul fenomeno degli assicurati morosi. Mandatodel Consiglio di Stato 2009 [cited 7 September 2012]. Available from:www.ti.ch/CAN/SegGC/comunicazioni/GC/odg-mes/allegati/M6275-Allegato.pdf
55] Kocher G, Oggier W, editors. Gesundheitswesen Schweiz 2007-2009.Bern: Hans Huber; 2007.
56] Federal Council. Botschaft zum Bundesgesetz betreffend die Aufsichtüber die soziale Krankenversicherung; 2012 [cited 7 September2012]. Available from: http://www.bag.admin.ch/themen/krankenversicherung/06368/index.html?lang=de
57] Hefti C, Frey M. Die Entwicklung der Versicherungslandschaftin der Krankenversicherung 1996-2006: Schlussbericht. Neuchâ-tel: Schweizerisches Gesundheitsobservatoriums; 2008 [cited 8January 2013]. Available from: www.obsan.admin.ch/bfs/obsan/de/index/05/publikationsdatenbank.Document.113391.pdf
58] Potratz A, Zerres M. Kundenmanagement in Krankenversicherun-gen. In: Busse R, Schreyögg J, Tiemann O, editors. Management imGesundheitswesen. Berlin: Springer-Verlag; 2010. p. 155–62.
59] Zok K. Anforderungen an die Gesetzliche Krankenversicherung: Ein-schatzungen und Erwartungen aus Sicht der Versicherten [Demandson statutory health insurance: assessments and expectations ofinsurees]. WIdO Monitor 2009;2009(1):1–8.
60] Schut F, Gresz S, Wasem J. Consumer price sensitivity and socialhealth insurer choice in Germany and the Netherlands. Interna-tional Journal of Health Care Finance and Economics 2003;3(2):117–39.
61] Zok K. Reaktionen auf Zusatzbeiträgein der GKV - Ergebnisse einerRepräsentativ-Umfrage. WIdO Monitor 2011;2011(1):1–8.
62] Laske-Aldershof T, Schut FT, Beck K, Gres S, Shmueli A, Van de VoordeC. Consumer mobility in social health insurance markets: a five-country comparison. Applied Health Economics and Health Policy2004;3(4):229–41.
63] Vektis. Zorgthermometer: Verzekerden in beweging 2011. Zeist:Vektis; 2011 [cited 20 July 2011]. Available from: http://www.vektis.nl/./downloads/Publicaties/2011/Zorgthermometer%20nr1%202011.pdf
64] Vektis. Zorgthermometer: Verzekerden in beweging 2012. Zeist:Vektis; 2012 [cited 3 October 2012]. Available from: http://www.vektis.nl/index.php/publicaties/publicatie-zorgthermometer
65] van Dijk M, Pomp M, Douven R, Laske-Aldershof T, Schut E, deBoer W, et al. Consumer price sensitivity in Dutch health insur-
2008;8(4):225–44.66] Comparis.ch. Krankenkassen vergleichen und sparen. Zurich: Com-
paris.ch; 2011 [cited 8 January 2013]. Available from: http://www.comparis.ch/krankenkassen/default.aspx