sleep onset abnormalities in depressed adolescents
TRANSCRIPT
Sleep Onset Abnormalities in Depressed Adolescents
Ronald E. Dahl, Neal D. Ryan, Mary K. Matty, Boris Birmaher,
Mayadah A1-Shabbout, Douglas E. Williamson, and David J. Kupfer
Sleep measures were obtained in 16 depressed and 21 control adolescents following 1 week of adherence to a uniformly imposed and strictly enforced sleep~wake schedule. Three nights of baseline electroencephalographic (EEG) sleep on the same 10:00 PM to 7:00 AM schedule revealed prolonged sleep latency and reduced rapid eye movement (REM) latency in the depressed adolescents. Following baseline measures, sleep was restricted for 2 nights (10:00 PM-4:00 AM) and measures of recovery sleep were obtained showing further sleep latency differences. There was no evidence for delta sleep changes or sleep continuity differences in depressed adolescents. These results suggest that control over sleep/wake schedules is an important methodological issue in adolescent sleep studies. Furthermore, the findings are consistent with a larger body of evidence indicating that dysregulation near sleep onset represents a primary psychobiological change in early-onset depression.
Key Words: EEG sleep, sleep onset, depression, adolescents.
B~OL PSYCHIATRY 1996;39:400--410
Introduction
Over the past decade, a large body of research has provided evidence for continuities in affective disorders across the life span from child, to adolescent, and adult depression. This evidence includes longitudinal follow-up studies (Harrington et al 1991; Kovacs et al 1984a,b; Flemming et al 1993; Rao et al 1993), similarity in syndromic picture (Ryan et al 1987), and family/genetic studies (Weissman et al 1987; Puig-Antich et al 1989; Orvaschel 1990; Williamson et al, in press). Psychobio- logical studies of growth hormone and serotonergic regu- lation have also reported close parallels between early-
From the Department of Psychiatry, University of Pittsburgh Medical Center, Pittsburgh, Pennsylvania.
These results were presented in part at the Annual Meeting of the American Sleep Disorders Association in Boston, Massachusetts, June of 1994.
Address reprint requests to Ronald E. Dahl, M.D., Western Psychiatric Institute and Clinic, 3811 O'Hara Street Room E733, Pittsburgh, PA 15213.
Received November 14, 1994; revised March 7, 1995.
onset depression and adult studies (Puig-Antich et al 1984; Ryan et al 1988, 1992b, 1994; Ryan and Dahl 1994). However, maturational variations from child and adoles- cent to adult depression have also been highlighted, including differences in pharmacological responses (Ryac 1992; Ambrosini et al, 1993), cortisol regulation (Dahl et al 1991b, 1992a) and, the focus of this paper: variations in the expression of sleep abnormalities. Electroencephalo- graphic (EEG) sleep changes associated with adult major depressive disorder (MDD) are among the best-replicated findings in biological psychiatry (Reynolds and Kupfer 1987). Controlled studies in early-onset depression, how- ever, have yielded infrequent evidence of the same abnor- malities. Among four studies of prepubertal MDD sub- jects with normal controls (Puig-Antich et al 1982; Young et al 1982; Emslie et al 1990; Dahl et al 1991a), three reported no significant group differences in any sleep variables. One prepubertal study (Emslie et al 1990) found decreased rapid eye movement (REM) latency and in-
© 1996 Society of Biological Psychiatry 0006-3223/96/$15.00 SSDI 0006-3223(95)00190-R

Sleep in Depressed Adolescents BIOL PSYCHIATRY 401 1996;39:400-410
creased sleep latency in a sample of inpatient MDD children; however, paradoxically, the depressed children had better sleep efficiency than control children. Puig- Antich et al (1983) reported evidence of reduced REM latency and improved sleep efficiency in depressed sub- jects restudied after recovery from depression. Also, Dahl et al (1994) found reduced REM latency in MDD children following infusion of arecoline (a cholinergic agonist), suggesting that sleep dysregulation may be subthreshold among some prepubertal MDD subjects. Among published adolescent studies with normal control subjects (Lab- meyer et al 1983; Appleboon-Fondu et al 1988; Goetz et al 1987; Dahl et al 1990a; Kahn and Todd 1990; Kutcher et al 1992; Emslie et al 1994), four of seven reported increased sleep latency, three studies found reduced REM latency, two reported decreased sleep efficiency, and none found delta sleep changes in the MDD subjects.
Taken together, these results suggest that the adult pattern of sleep abnormalities in depression is infrequently expressed or partially masked in early-onset depression. Two meta-analyses further support this interpretation. Knowles and MacLean (1990) reported that age and depression appear to interact with respect to sleep dys- regulation, with the smallest differences (or no differ- ences) at early ages and increasingly larger differences across the lifespan. Benca et al (1992) found that sleep latency emerged as the only variable differentiating de- pressed from control subjects among studies with samples younger than 20 years. Maturational influences on sleep and/or depression appear to be the most likely factors contributing to these findings. A variety of clinical factors have also been considered as sources of discrepancies. One study suggested that suicidality may be a critical factor in the early emergence of sleep dysregulation (Dahl et al 1990a). Another found that REM latency was reduced in the subgroup of depressed adolescents with psychotic features (Naylor et al 1990). Severity of MDD has been suggested as a potential factor, and in the Dahl et al (1991a) study, there was a subgroup (8 of 36 depressed children) with adult pattern sleep findings and more severe depression. However, most studies have not found that severity of depression correlates with sleep findings (Puig- Antich et al 1982; Goetz et al 1987; Emslie et al 1990, 1994; Dahl et al 1990a).
The potential influence of hospitalization on adolescent sleep findings has also been considered. Reduced REM latency has been found primarily in samples studying inpatient depressed subjects (Dahl et al 1990a Emslie et al 1990; Kutcher et al 1992) and in one outpatient study using uniform control over sleep times (Lahmeyer et al 1983). This pattern was also seen in a study of young adults with MDD (Goetz et al 1991). This association with inpatient status and EEG sleep abnormalities raised a set
of methodological questions. (1) Since inpatients follow an imposed rigid schedule in the hospital while many outpatient adolescents have erratic schedules at home, what is the role of sleep/wake schedules? (2) What is the role of adaptational effects that may be different in outpatients who are coming to the laboratory from their home environment compared to inpatients who are already acclimated to sleeping in an unfamiliar environment? (3) What are the possible effects of covert access to caffeine, alcohol, nicotine, and other substances among outpatient adolescents?
These methodological questions formed the basis for the study described in this paper. The specific aims of this study were to (1) control as rigidly as possible the sleep/wake schedules (with objective validation) across inpatients, outpatients, and normal controls; (2) to verify avoidance of caffeine, nicotine, alcohol, medications, and other substances before and during the study in all groups; and (3) to challenge the sleep system with a sleep restriction protocol and measure recovery sleep to exam- ine further the possibility of uncovering "subthreshold" abnormalities in sleep regulation.
Methods
Subjects
Adolescents were recruited through inpatient and outpa- tient programs at Western Psychiatric Institute and Clinic. If depression was suspected on screening, a diagnostic protocol was performed, including structured interviews with the Schedule for Affective Disorders and Schizophre- nia (K-SADS-P) (Puig-Antich et al 1986) and K-SADS-E (Orvaschel and Puig-Antich 1987), as well as pediatric examination and Tanner staging for pubertal development. All symptom ratings were made by first interviewing the parents alone, then interviewing the adolescent alone.
Criteria for Inclusion
1. Diagnostic and Statistical Manual of Mental Disor- ders, 3rd ed., revised, (DSM-III-R) criteria for MDD at least probable at two separate K-SADS-P evalu- ations
2. Age 12-18 and Tanner stage 3, 4, or 5 of sexual development
Criteria for Exclusion
1. Any medications within 2 weeks of the protocol or any history of fluoxetine (no patient in this study had received any treatment with an Selective Sero- tonin uptake inhibitor agent)
2. Any significant medical or neurological illness 3. Obesity as defined by weight/height ratio greater

402 BIOL PSYCHIATRY R.E. Dalai et al 1996;39:400 -410
than 95th percentile on the National Center for Health Statistics curve
4. Significant growth failure (weight or height under the 3rd percentile)
5. I.Q. lower than 70 6. DSM-III-R criteria for anorexia nervosa, autism, or
schizophrenia
Normal control adolescents were recruited by newspa- per advertising, personal contacts, and friends and family members of controls from previous studies. Normal con- trol adolescents were evaluated with K-SADS-E and had no history of any DSM-III-R axis I disorder, no medical problems, and no history of medications. Each adolescent was age 12-18, Tanner stage 3, 4, or 5 of sexual devel- opment, and had normal growth and development. In addition, normal control adolescents had no first-degree relative with a history of major affective disorders as assessed by family history-research diagnostic criteria.
For all subjects, informed consent was obtained from the parent or legal guardian and the subjects were paid for their participation in the study.
Protocol
IMPOSED SLEEP/WAKE SCHEDULE. The first step of the protocol was to ensure that all adolescents aligned their sleep/wake to the following structure: 10:00 PM bedtime, 7:00 AM wake-up time, and avoiding any naps, medica- tions, caffeine, alcohol, or other substances. In cases in which the adolescents' bedtime or wake-up time habitu- ally deviated 3 hours or more from this schedule, the changes were made gradually over 1 week to realign the sleep/wake schedule to the imposed structure by working closely with the adolescent and family. Once the adoles- cent was aligned to the 10:00 PM-7:00 AM sleep schedule, 1 week of documented compliance with the protocol was carded out, including continuous wrist actigraphy, sleep/ wake log, telephone verification (on weekends and school vacations adolescents called the laboratory to verify they were awake on time), and urine tests for substances/ medication. Adolescents were shown that the wrist actig- raphy could identify periods of sleep, and were instructed not to remove the wrist-worn actigraph for more than 5 min for bathing or other activities. Adolescents understood that payment for participation in the laboratory component of the study was contingent on successfully demonstrating that they were following the protocol precisely.
BASELINE LABORATORY MEASURES. Following 1 week of data collection on the imposed schedule in the home environment (inpatients followed the same schedule in- cluding actigraphy on the inpatient unit), all subjects came
to the sleep laboratory for 3 nights of baseline EEG sleep recording carried out on the same 10:00 PM-7:00 AM sleep schedule. Standard polysomnographic methods were used as described previously (Dahl et al 1991a). Subjects continued to wear wrist actigraphs; perform ratings of mood, tiredness, sleepiness; and avoid substances, medi- cations, and naps.
SLEEP RESTRICTION PROTOCOL. Following the 3 nights of baseline recordings in the laboratory, the outpa- tient depressed adolescents and the normal control adoles- cents remained in the sleep laboratory for 4 additional days and nights to undergo a sleep restriction protocol. Inpatient depressed adolescents were ineligible to partici- pate in the sleep restriction component of the study because of limits as to how long they could be off the inpatient unit. The sleep restriction protocol consisted of 2 nights of restricted sleep (10:00 PM bedtime with a 4:00 AM wake-up) with no daytime naps, followed by 2 nights of recovery sleep (10:00 PM to 7:00 AM sleep schedule on the first night, 10:00 PM bedtime to ad lib morning awakening as the final night).
Data Management and Analyses
Sleep records were scored visually in 30 s epochs by trained technicians using standard methods (Rechtschaffen and Kales, 1968). Interrater reliabilities were assessed bimonthly with high reliability (kappa values of 0.85 or above) for all major sleep variables. Data from each sleep epoch were entered into a computer program that gener- ated summary sleep variables as follows: sleep onset (the first minute of 10 consecutive minutes of stage 2 or deeper sleep with less than 1 min of intervening wakefulness); sleep latency (the time from "lights out" to sleep onset); REM latency (the time from sleep onset to the first 30 s epoch of REM sleep); minutes of each sleep stage (stages 1, 2, 3, 4, and REM); REM density (a semiquantitative scale to assess the rate of eye movements within each epoch of REM sleep [Taska and Kupfer 1987]), sleep efficiency (percentage of total recording period spent asleep); awake time (number of minutes after sleep onset spent awake); and total time spent asleep.
Statistical Analysis
Prior to applying parametric statistical methods, all data were examined for normality using the Shapiro and Wilks' W statistic. Nonnormal data were normalized using either a square root (Stage 1 and Arousal) or logarithmic (Sleep Latency, Awake Time, Stage 3, and REM Density) trans- formation. When the variances were not homogeneous
Sleep in Depressed Adolescents BIOL PSYCHIATRY 403 1996;39:400-410
Table 1. Demographic Variables
MDD Normal Variable (n = 16) (n = 21) Test Statistic p Value
Age (years) 16.1 ± 1.6 15.3 ± 1.6 t3s = 1.48 NS Gender (male/female) 9/7 10/11 ×2 (df = 1) = 0.27 NS Race (white/black) 14/2 19/2 F.E.T NS
MDD, major depressive disorder. F.E.T, Fisher's exact test.
(REM Latency), a Box-Cox diagnostic plot was used to find the appropriate transformation that resulted in greater variance homogeneity by plotting the logarithm of the standard deviations against the logarithm of the means. Based on the slope of this relationship, 131 , the variable was transformed by raising it to the power ( 1 - [31) (Box and Cox 1964). Analysis of variance (ANOVA) with repeated measures was used to test for the effects of diagnosis, night, and their interaction (diagnosis by night). Analysis of variance and covariance (ANCOVA) with repeated measures were used to examine the effects of age, gender, and their interaction by including their effect as a constant effect over time. All reported p values are two-sided with et = 0.05. All untransformed sleep vari- ables are presented as mean _+ standard deviation.
Within the MDD group, the following clinical charac- teristics were examined: inpatients vs. outpatients, suicidal vs. nonsuicidal subjects, depression severity (as estimated by the K-SADS), and duration of episode.
Subsequent analyses compared depressed and control adolescents during sleep restriction and recovery sleep. These analyses focused on night 6, the first night of recovery sleep, examining both group effects and night effects, compared to night 3 on the baseline measure (Night 3 was chosen as the "cleanest" night of baseline sleep since it was the farthest from any adaptational influences on night 1, prior to the sleep restriction.) Exploratory analyses were also performed on mood and sleepiness ratings during the sleep restriction and recovery protocol.
Results
Sample
Twenty-two MDD subjects and 21 normal control subjects were enrolled in this study. All normal control subjects successfully completed all phases of the study. Among the MDD sample, however, six outpatient MDD subjects were unable successfully to realign their sleep/wake schedules to the imposed time frame. These failures occurred despite extensive efforts by staff and clinicians to assist the adolescent and family to realign their sleep times gradu- ally, including telephone call reminders in the morning, problem-solving strategies concerning behaviors that in-
terfered with going to bed, and general sleep/wake hygiene advice and counseling. Despite these extensive efforts, these six depressed subjects were unable to follow the imposed schedule, primarily because of oversleeping in the morning. Two failures in the same week (greater than 30 min deviation from imposed schedule) resulted in the participants being dropped from the study because of inability to follow the schedule. There were no subjects in either the normal control or the MDD group dropped because of the detection of substances or medications in the urine screen.
The laboratory sample, therefore, consisted of 21 nor- mal control adolescents and 16 MDD adolescents. Demo- graphic and clinical variables are shown in Table 1. There were no significant group differences in age, gender, or race.
Within the MDD sample, there were 10 outpatients and six inpatients. Six subjects were suicidal (ideation with a definite plan and/or an actual attempt; five of the six suicidal subjects were inpatients). The mean nine-item depression score from the K-SADS was 27.0 _+ 5.4 (the mean score per item was 3.0 --- 0.6). The mean extracted (17-item) Hamilton score (Williamson et al 1992) was 21.3 _+ 4.6. Three of the MDD adolescents had comorbid anxiety disorders. There were no other comorbid psychi- atric disorders.
Baseline Night Sleep Results
During the first 3 nights in the laboratory, the adolescents followed the same imposed 10:00 PM-7:00 AM schedule as had been followed at home. Results, including diagnosis effects, night effects, and interactions are shown in Table 2. A significant effect of diagnosis was observed for longer sleep latency in the depressed group (p = 0.006) and reduced REM latency in the depressed group (p = 0.04). Significant night effects were seen in awake time after sleep onset (p = 0.0002), stage REM minutes (p = 0.0007), REM latency (p = 0.01), and total minutes of sleep (p = 0.02). There were no significant diagnoses by night interactions. Significant age effects were observed for sleep latency, sleep efficiency, awake time, REM time, and stage 4 sleep, but there were no significant age by
4 0 4 BIOL PSYCHIATRY R.E. Dahl et al 1996;39:400-410
Table 2. Baseline Night Sleep Variables
Night 1 Night 2 Night 3
Sleep Variables Mean _+ SD Mean ___ SD Mean -+ SD Diagnosis Effect Night Effect Diagnosis by Night Effect
Sleep latency (min) MDDs c, 30.1 _+ 15.0 32.2 _+ 17.6 33.7 _+ 20.3 Fi,35 = 8.68
Normals ~ 21.7 _+ 14.1 19.9 + 10.4 23.0 + 12.0 p = 0.0057
Sleep efficiency (%) MDDs 87.9 + 7.7 91.3 _+ 4.7 89.8 -+ 9.2 NS
Normals 92.2 _+ 4.0 92.3 _+ 5.7 92.6 _+ 4.7
Awake time (min) MDDs 34.0 _+ 32.7 13.3 +_ 11.7 21.3 -+ 33.4 NS
Normals 19.3 _+ 15.1 21.2 + 27.1 16.3 +_ 17.1
Arousal (number) MDDs 12.6 +_ 4.4 11.4 +_ 5.6 11.6 -+ 4.8 NS
Normals 13.0 -+ 5.9 12.5 +- 6.4 12.1 -+ 6.0
Stage 1 (rain) MDDs 21.7 _+ 9.8 20.7 _+ 10.3 19.8 +- 10.2 NS
Normals 18.1 +_ 10.0 19.7 +_ 14.5 19.0 -+ 10.4
Stage 2 (min) MDDs 229.9 _+ 38.6 228.3 _+ 37.6 235.1 -+ 44.7 NS
Normals 242.6 _+ 40.5 237.8 _+ 32.4 239.0 -+ 37.1
Stage 3 (min) MDDs 39.0 _+ 14.6 39.3 + 13.1 41.0 _+ 16.0 NS
Normals 44.8 + 21.4 42.8 _+ 18.4 40.7 _+ 12.0
Stage 4 (min) MDDs 81.2 + 25.9 85.1 _+ 27.2 84.8 + 21.8 NS
Normals 81.0 _+ 25.5 81.5 _+ 24.4 84.8 +- 22.9
Stage REM (min) MDDs 92.8 +_ 22.0 110.4 _+ 20.1 103.3 _+ 23.3 NS
Normals 96.0 -+ 16.0 105.5 +- 22.2 110.8 -+ 21.9
REM latency (rain) MDDs 106.8 -4- 41.1 72.6 _+ 31.7 82.8 -+ 33.5 F~,35 = 4.35
Normals 114.9 + 42.4 104.9 +_ 42.2 97.3 +_ 42.6 p = 0.044
REM density (units) MDDs 2.0 -4- 0.4 1.8 -+ 0.5 1.9 - 0.5 NS
Normals 1.6 -+ 0.3 1.7 -+ 0.4 1.7 + 0.
Total min of sleep MDDs 464.8 +_ 41.5 484.0 _+ 35.2 484.0 -+ 49.3 NS
Normals 482.5 -4- 23.5 487.3 _+ 28.9 494.3 + 27.0
NS
NS
NS
F2,7o = 9.58 p = 0.0002
NS
NS
NS
NS
NS
F:z,7o = 8. l 1
p - 0.0007
F2,7o = 4.59 p = 0.013
NS
Fz,7o = 3.96 p = 0.024
NS
NS
F2,7o = 2.51
p = 0.09
NS
NS
NS
NS
NS
NS
NS
NS
NS
" Number of subjects in the MDD group and the normal group are n = 16 and n = 21. NS, nonsignificant at p -< 0.05 level.
diagnoses interactions. There were no significant gender effects in the summary sleep variables.
Subgroup Analyses
Analyses were performed within the MDD subjects com- paring inpatients to outpatients. With identical sleep/wake schedules prior to and during the study, there were no group differences between inpatients and outpatients for any of the major sleep variables. The mean sleep latency across the three nights for the inpatients was 31.3 min vs. 32.4 min in the outpatients, the average REM latency for the inpatients was 81.1 rain and 91.1 rain in the outpa- tients. Mean REM density in the inpatients was 1.82 vs. 1.88 in the outpatients. Suicidal subjects were also com- pared to nonsuicidal depressed subjects, again with no significant group differences and very similar patterns of results. Analyses of severity of symptoms estimated from the K-SADS, and duration of depressive episode showed no significant effects or sleep variables.
Sleep Restriction Protocol
On nights 4 and 5, subjects went to bed at the usual 10:00 PM time but were awakened at 4:00 AM and remained awake throughout the day. On night 6, the subjects returned to the usual 10:00 PM-7:00 AM sleep schedule. On
night 7 they slept from 10:00 PM to spontaneous awaken- ing in the morning. The primary analyses focused on night 6, the first recovery night, examining diagnostic effects, night effects, and interactions, to evaluate the effects of the sleep restriction intervention. For the night effects and interaction analyses, night 3 was chosen prospectively as the comparison night.
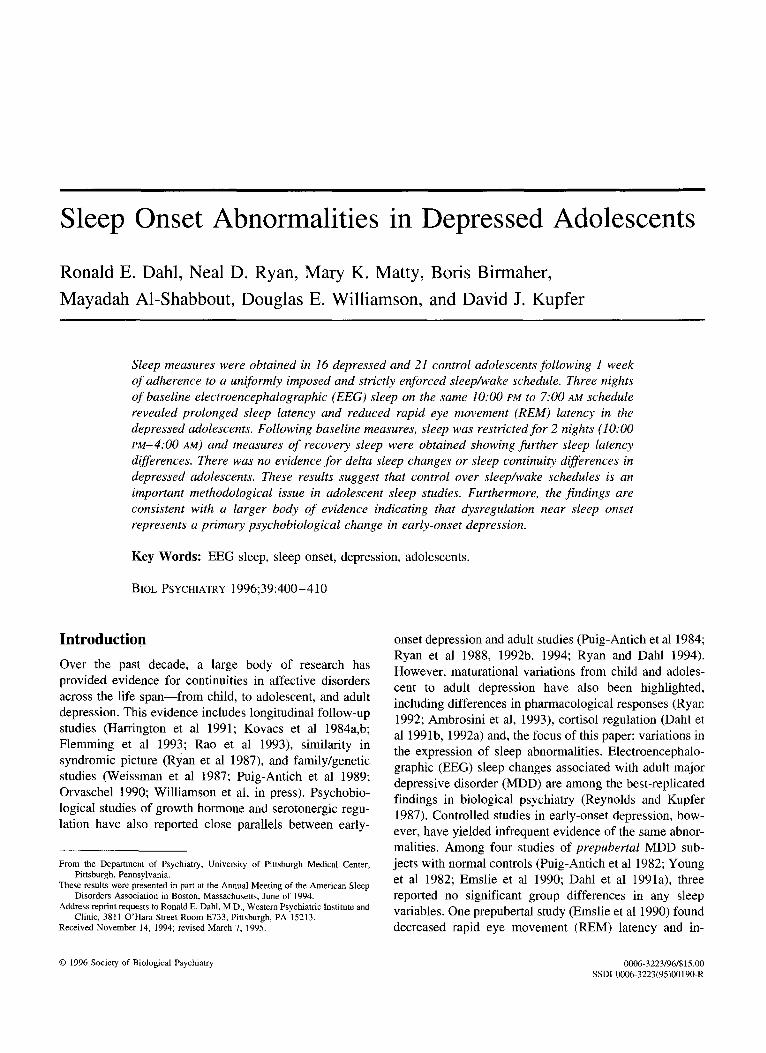
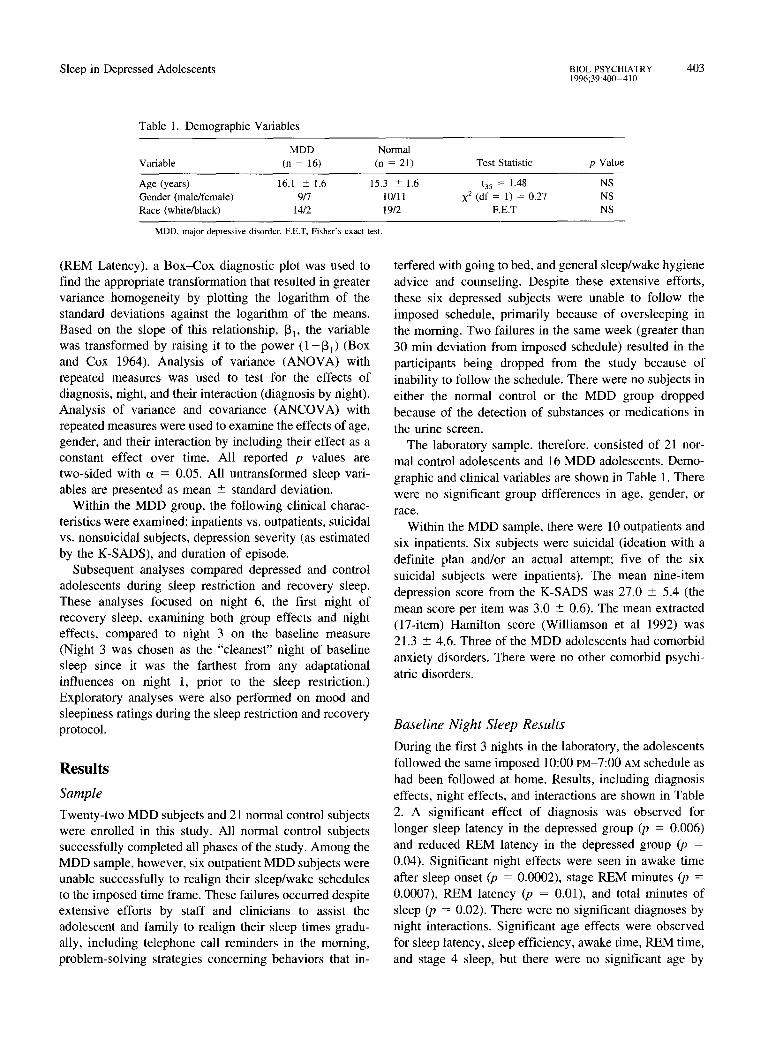
These results are shown in Table 3. Sleep latency showed a significant diagnostic effect and diagnosis by night interaction (p = 0.006 and 0.0006, respectively). Within the normal control group, there was a rapid sleep onset (mean 9.5 rain with a small standard deviation of 4.1 min). The MDD group, however, continued to show difficulties falling asleep, with a mean sleep latency of 25.2 + 25.0 rain. There were no other significant diag- nostic effects or diagnosis by night interactions. REM latency was 68.0 + 14.1 min in the MDD group following sleep restriction and was 83.3 4- 37.2 min in the normal controls (p = 0.19). (It is noteworthy that the variation in REM latency was much smaller in the MDD group, but variation in sleep latency was much smaller in the con- trols). REM latency and sleep latency across nights are shown graphically in Figures 1 and 2.
As can be seen on Table 3, the mild sleep restriction resulted in significant effects on most sleep variables in the expected directions (more deep sleep, more REM, with
Sleep in Depressed Adolescents BIOL PSYCHIATRY 405 1996;39:400-410
Table 3. Summary Sleep Variables on Night 6 (Recovery Sleep Following Sleep Restriction)
MDDs Norrnals Diagnosis Diagnosis by (n = 10) (n = 21) Effect Night Effect" Night Effect
Sleep latency (min) 25.2 ± 25.0 9.5 ± 4.1 FI,29 = 8 . 8 2 F1,29 = 4 8 . 3 6 Fi.29 = 14.99 p = 0.006 p = 0.0001 p = 0.0006
Sleep efficiency (%) 93.3 + 5.2 96.4 ± 1.8 NS F~.29 = 14.75 NS p = 0.0006
Awake time (min) 11.2 _+ 10.0 10.0 +_ 8.4 NS FI,29 = 7.18 NS p = 0.012
Arousal (number) 10.8 ± 5.9 10.6 ± 5.8 NS FI,29 = 3.63 NS p = 0.07
Stage 1 (min) 14.9 ± 10.3 17.1 ± 11.3 NS F1,29 = 9.61 NS p < 0.0043
Stage 2 (min) 226.9 ± 54.6 233.2 ± 34.3 NS NS NS Stage 3 (min) 39.4 - 15.2 41.6 -+ 16.3 NS NS NS Stage 4 (min) 96.4 ± 26.5 95.8 ± 26.5 NS F~.29 = 9.55 NS
p = 0.0044 Stage REM (rain) 129.5 ± 17.5 131.4 -+ 17.5 NS F1,29 =25.4 NS
p = 0.00001 REM latency (rain) 68.0 ± 14.2 83.3 ± 37.2 NS Fi ,29 = 4.55 NS
p = 0.042 REM density (units) 1.85 ± 0.45 1.68 ± 0.35 NS NS NS Total min of sleep 507.1 _+ 36.2 519.2 ± 12.8 NS FL29 = 16.13 NS
p = 0.0004
a Comparing night 6 with night 3 within the MDD outpatients and the normals. NS, nonsignificant at p <: 0.05 level.
less a w a k e t ime and less l ight s leep); howeve r , the effects
we re in genera l , qui te s imi la r in b o t h groups .
O n n igh t 7 ( the s econd r ecove ry night) , there were no
s ign i f ican t g roup d i f fe rences , bu t a nons i gn i f i c an t t rend
for p r o l o n g e d s leep la tency in the M D D group (27.4 _
15.8 min vs. 19.5 + 13.1 m i n in the n o r m a l con t ro l g roup
(p = 0.10) and a t r end towards r educed R E M la tency (70.2
ra in + 22.3 in the M D D group vs. 90 .4 _+ 39.0 in the
n o r m a l con t ro l g roup (p = 0.10). T h e r e were no g roup
d i f fe rences in the l eng th o f s leep pe r iod or the a m o u n t o f
" s l eep ing in" on the ad lib s chedu le for the f inal morn ing .
Total sleep on night 7 in the MDD group was 618.1 - 111.0 min and in the control adolescents 633.6 --+ 96.3 min.
Subjective Measures: Measures of Sleepiness and Tiredness Two measures of sleepiness were used during the baseline, sleep restriction, and recovery sleep periods: The Stanford Sleepiness Scale (a six point self-rating scale for sleepi- ness) (Hoddes et al 1973) and The Matty/Nelson scale (a staff rating of appearance of tiredness o b s e r v e d in the
100-
r., '~ 80-
60-
E 40-
20-
night I night 2 night 3 sleep night 6 night 7 restriction
Figure ]. REM latency values on baseline (nights 1, 2, and 3) and following sleep restriction (nights 6 and 7) in MDD (closed box) and normals (open box).
4o
~, 30
lO-
J
night I night 2 night 3 sleep night 6 night 7 restriction
Figure 2. Sleep latency values on baseline (nights 1, 2, and 3) and following sleep restriction (nights 6 and 7) in MDD (closed box) and normals (open box).
406 BIOL PSYCHIATRY R.E. Dahl et al 1996;39:400-410
Figure 3.
Day 4 3.5.
x 1 i
0.5-
2.5"
r- "~. 2" 0)
1.s-
Night 4
Day 5
Night 5 Night 6
, ~ ~ D a y 6 • , Day7
" t ~ . . . . e f - ' "
lOa 2p u i ' ~3 1 i i i i i i i i
1 4p 8p 6p 8a 12p 4p 8p lOa 2p 6p 10a 2p 6p 8a 12p 4p 8p lOa 2p 6p 8a 12p 4p 8p
Time of Day ** Group Differences P < .01 "Group Differences P < .05 ~ MDD Outpatients --rq-- Normals
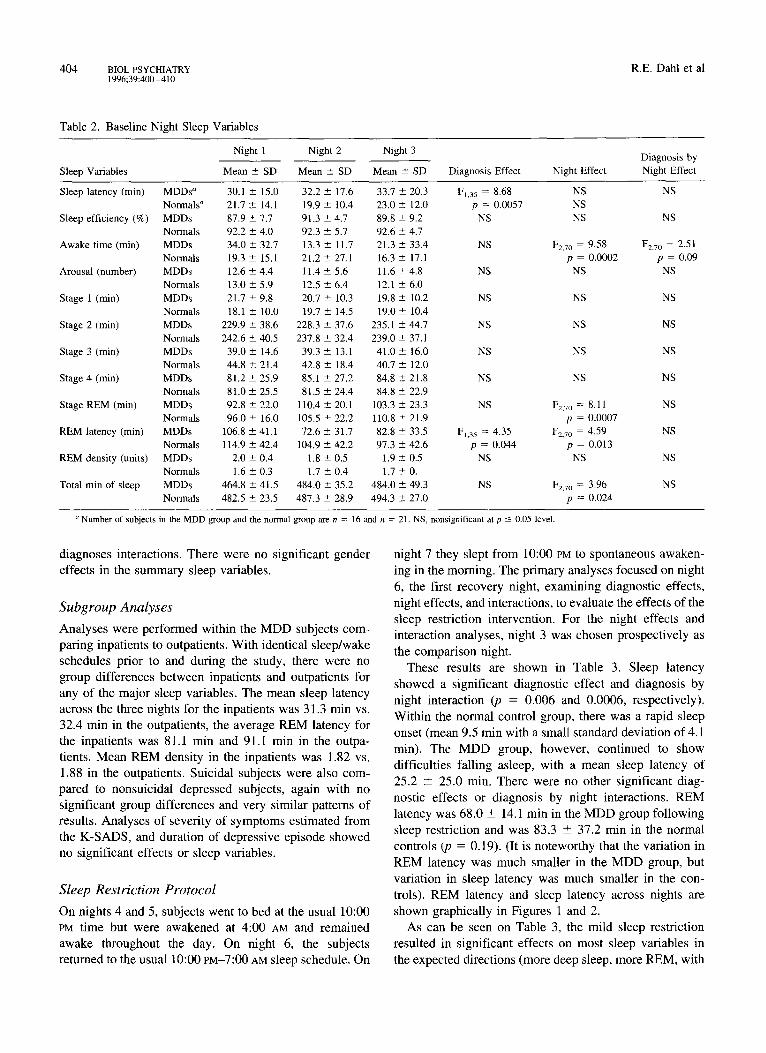
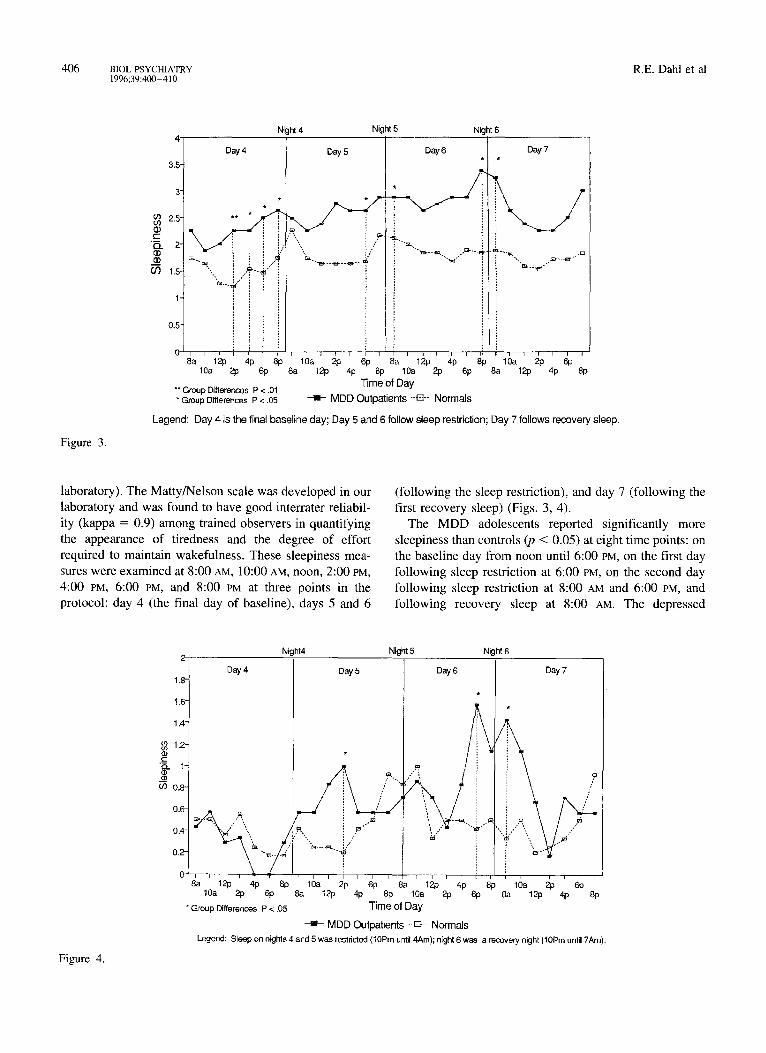
Legend: Day 4 is the final baseline day; Day 5 and 6 follow sleep restriction; Day 7 follows recovery sleep.
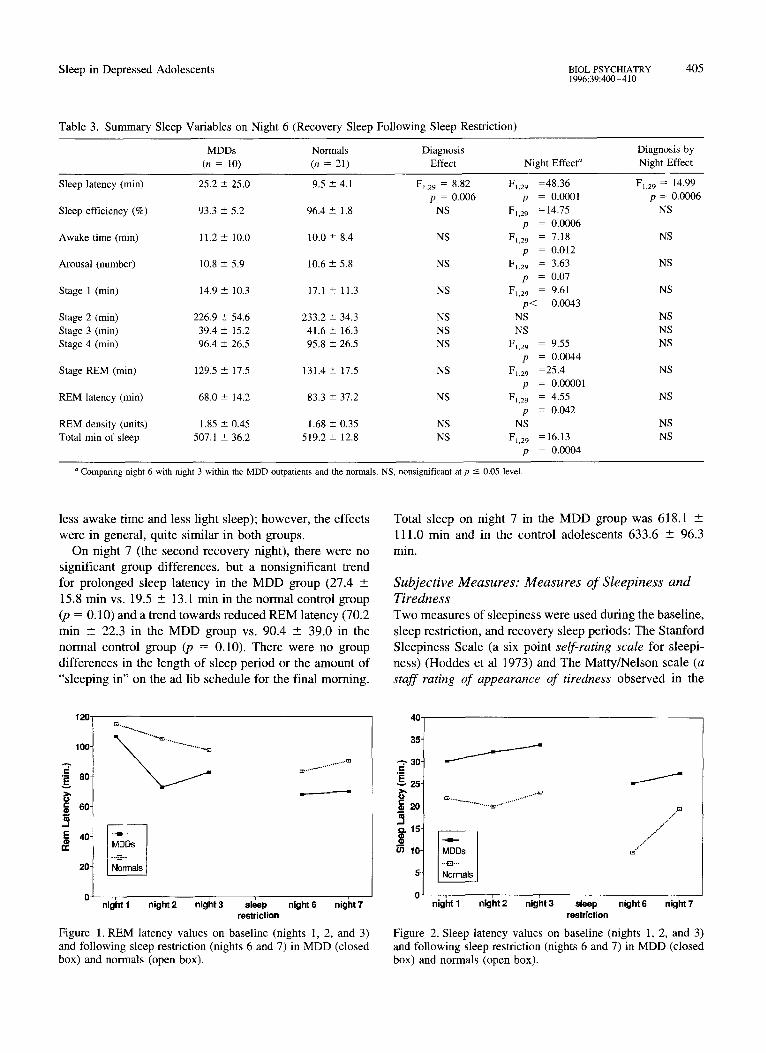
laboratory). The Matty/Nelson scale was developed in our laboratory and was found to have good interrater reliabil- ity (kappa = 0.9) among trained observers in quantifying the appearance of tiredness and the degree of effort required to maintain wakefulness. These sleepiness mea- sures were examined at 8:00 AM, 10:00 AM, noon, 2:00 PM, 4:00 PM, 6:00 PM, and 8:00 PM at three points in the protocol: day 4 (the final day of baseline), days 5 and 6
(following the sleep restriction), and day 7 (following the first recovery sleep) (Figs. 3, 4).
The MDD adolescents reported significantly more sleepiness than controls (p < 0.05) at eight time points: on the baseline day from noon until 6:00 PM, on the first day following sleep restriction at 6:00 PM, on the second day following sleep restriction at 8:00 AM and 6:00 PM, and following recovery sleep at 8:00 AM. The depressed
Figure 4.
1.8-
1.6-
1,4-
1.2- {D c '~.. l- _m of) 0.8-
Day 4
Night4 Ni ht5 Night 6
0.~ Q. , , " ,
0 . 4 - , ~ " ",,
0.2- "'-
8a 1 2p 4p 8p 10a 2p 613
* Group Differences P < .05
Day5 Day 6
&[
1 0a 2p 6p 8a 1243 4p 8p 8a 12p 4p 8p 10a 2p 6p
Time of Day
Day 7
1 a 2p 6p 8a 12p 4p 8p
- i - MDD Outpatients -E3- Normals Legend: Sleep on nights 4 ard 5 was restricted (10Pro until 4Am); n[ghl 6 was a recovery night (10Pm until 7Am).

Sleep in Depressed Adolescents B1OL PSYCHIATRY 407 1996;39:400-410
adolescents were also rated as significantly more tired in appearance and behavior at three time points: 2:00 PM of day 5, 6:00 PM of day 6, and at 8:00 AM of day 7. Thus, on the evening following sleep restriction, the MDD adoles- cents reported more sleepiness and appeared more tired than the normal control adolescents; however, that evening (night 6), difficulty falling asleep was most apparent compared to controls. Mood was assessed at the same time points as the sleepiness measures using 100 mm visual analog scales. There was no significant change in either group in mood measures following the mild degree of sleep restriction.
Measures in the Home Environment
Sleep diaries and actigraphy data from the home schedule in the week prior to the laboratory protocol were also examined. There were no significant group differences in reported bedtimes or wake-up times between depressed and control adolescents. Sleep diary estimates of time to fall asleep (in minutes) showed a trend for longer subjec- tive sleep latency in the depressed adolescents compared to controls on all nights, and this reached statistical significance on two of the nights.
Discussion
With precise and uniform control over the amount and timing of sleep, depressed adolescents had significantly increased sleep latency and reduced REM latency, but no differences or trends in delta or slow wave sleep, com- pared to controls. Challenging the sleep system with mild sleep restriction further amplified the group differences in sleep latency. The depressed adolescents had consistent difficulty falling asleep across conditions: at home, in the laboratory, when well-rested, and following restricted sleep. This pattern was observed despite evidence that the depressed adolescents were following the identical sched- ule as the controls, and were sleepier (subjectively) and appeared more tired in staff ratings than control adoles- cents.
These results are consistent with a number of other findings focusing attention on the importance of the sleep onset transition. The meta analysis by Benca et al (1992) indicated that among sleep variables only sleep latency discriminated depressed subjects less than 20 years of age from controls. (One important caveat in interpreting the literature, however, is that the number of children and adolescents studied with nonaffective psychopathology has been very small, precluding any definitive interpreta- tion regarding the specificity of these changes regarding depression).
There is a larger body of data pointing toward the
importance of scrutinizing the transition from wakefulness into sleep as critical to understanding dysregulation rele- vant to affective disorders. Studies of depressed adoles- cents have shown neuroendocrine dysregulation at or near sleep onset (Dahl et al 1991 a, b; 1992). Adult sleep studies also indicate that the period of time around sleep onset is a critical window of regulation relevant to depres- sion. Depressed adults have less growth hormone (GH) secretion just after sleep onset, both during an episode and after recovery (Jarrett et al 1990, 1994). Furthermore, GH dysregulation near sleep onset predicted clinical course in depressed adults (Franz et al in press). Circadian temper- ature measures show a blunted temperature drop in early sleep in some depressed patients (Avery et al 1986). Furthermore, antidepressants have complementary (or "normalizing") effects on these variables: clomipramine increases GH secretion after sleep onset; fluoxetine and imipramine enhance temperature drop during early sleep; and imipramine, clomipramine, and nortriptyline have been shown to shift delta EEG activity in the first NREM period to a more normal pattern (Kupfer et al 1990, 1994, and in press). Other investigators have reported epidemi- ological evidence suggesting that impaired sleep onset may predict the onset of depression in adult longitudinal studies (Ford and Kammerow 1989). Taken together, these results suggest that abnormalities in the gating of sleep onset represent a primary element of dysregulation asso- ciated with early-onset depression.
These results are also consistent with the hypothesis that control over sleep/wake and social schedules may be a crucial methodological issue in adolescent sleep and neu- roendocrine studies. Previous adolescent studies by our group and others had emphasized the role of inpatient status or suicidality. Suicidal patients tend to be inpatients, and inpatients are placed on uniform schedules. In this study with precise control over schedules, significant group differences in REM latency were observed, but there was no significant effect of inpatient status or suicidality. These results are also consistent with the findings of Lahmeyer et al, who reported reduced REM latency in outpatient depressed adolescents when they were studied on an imposed, uniform schedule (Lahmeyer et al 1983). However, these results also raise questions about interpreting sleep results in studies when all de- pressed subjects are inpatients (on an imposed schedule) while all normal controls are coming to the laboratory from home environments and schedules. Adolescent com- pliance with instructions simply to follow a regular sched- ule may not be simply assumed, given the extensive efforts required to get many normal and depressed adolescents to follow such a schedule consistently.
It is worth reemphasizing that the depressed adolescents were significantly more difficult to align to the imposed

408 BIOL PSYCHIATRY R.E. Dalai et al 1996;39:400-410
schedules (eg, six of 22 MDD subjects were dropped from the study because of the inability to follow the imposed schedule, vs. 0 of 21 controls, Fisher exact test p = 0.02). One interpretation of these results is that depression may contribute directly to symptoms of difficulty falling asleep as well as erratic sleep/wake schedules. The extreme difficulty of many depressed adolescents in following the imposed schedules suggests that this not only has meth- odological relevance to adolescent sleep studies but may also have clinical implications. It is also interesting to note that in contrast to older depressed adults, no depressed adolescents in this study were found to have early morning awakening. Further studies to address these issues are needed.
It is also important to consider the absence of any group differences or trends in delta sleep variables in this study. Delta sleep comparisons have been consistently negative across studies in this age group. This is in sharp contrast to findings of robust delta sleep changes in adult depression (Kupfer et al 1990). In previous and continuing studies by our research group, we have also examined automated techniques for quantifying delta sleep, including period- amplitude analyses and spectral analyses, which have failed to find evidence for delta sleep changes in young depressed subjects (Dahl et al 1990 b; and unpublished data). These observations raise questions as to the devel-
opmental sequence of changes in sleep regulation associ- ated with depression, or the role of other maturational influences on sleep/wake regulation. From a maturational perspective, it would appear that changes in sleep onset represent the first robust sleep abnormality associated with depression.
One central question emerging from these results, how- ever, is what specifically is abnormal about the sleep onset processes? Sleep onset is a remarkable transition involving an ensemble of changes at cortical and subcortical levels. One possibility is that there is some persistent elevation in "physiological" arousal (such as decreased parasympa- thetic tone, increased core body temperature, or other psychophysiological change) that inhibits the process of going to sleep. The observation that hypothalamic-pitu- itary axis (HPA) changes occur on both sides of sleep onset (Dahl e t a l 1991b; Jarrett et al 1983; Young et al 1994) and growth hormone changes are seen near sleep onset (Dahl et al 1992b; Jarrett et al 1994; Dahl et al unpublished data) would appear to support this concept of a physiological component contributing to the difficulties with sleep in depressed subjects.
On the other hand, the cognitive component must also be considered. At the cognitive level, the onset of sleep is ostensibly a sudden diminishment of awareness and re- sponsiveness to the immediate environment. It is intrigu- ing to consider the evolutionary biology underlying this transition. That is, the evolutionary refinement of neural mechanisms regulating this nocturnal loss of vigilance took place in an ancestral environment with a preponder- ance of nocturnal predators and a minimum of safe sleeping sites (Ellis 1991). It appears that inhibiting sleep onset in a context of cognitive appraisals of danger may have been highly adaptive as a means to restrict sleep to relatively "safe" places. Such cognitive appraisals of safety tend to be highly influenced by social context and emotional state. The integration of social cues, emotional arousal, and cognitive appraisal of safety/threat are also likely to show maturational changes across adolescence. A more comprehensive discussion of these issues has been presented elsewhere (Dahl and Ryan in press a).
From a clinical perspective, it is clear that negative or distressing thoughts and images at or near bedtime can result in emotional arousal interfering with sleep onset. Intrusive thoughts or negative ruminations at bedtime may lead to an altered pattern of arousal over time that could result in changes in neuroendocrine regulation, as well as difficulty going to sleep. Along these lines, investigators have suggested that intrusive thoughts and negative rumi- nations may have relevance to the development of depres- sion (Nolen-Hoeksema et al 1994) and may mediate the chronic effects of some acute stressors (Baum et al 1993). Our research group recently performed a retrospective analysis of the impact of adverse life events in the year prior to adolescent sleep studies and found significant effects on REM latency, but no effect on sleep latency (Williamson et al in press). Prospective studies incorpo- rating other physiological measures of arousal, measures of stressful life experiences, and related cognitive pro- cesses near sleep onset will be necessary to address these issues.
The authors gratefully acknowledge Beverly Nelson, B.S.N., Laura Trubnick, RPSGT., Dorothy Adams, RPSGT., Sherri Kahle, RPSGT, and Gregg Roby, PSGT for their assistance in conducting the laboratory protocol. The authors would also like to acknowledge Deborah Small for her administrative assistance with manuscript preparation. This work was supported by NIMH Grant #R29-MH46510 to Dr. Dahl.
References
Ambrosini PJ, Bianchi MD, Rabinovich H, Elia J (1993): Antidepressant treatments in children and adolescents. I
Affective disorders. J Am Acad Child Adolesc Psychiatry 32:1-6.

Sleep in Depressed Adolescents BIOL PSYCHIATRY 409 1996;39:400-410
Appleboom-Fondu J, Kerkhofs M, Mendlewicz J (1988): De- pression in adolescents and young adults--polysomnographic and neuroendocrine aspects. J Affect Disord 14:35-40.
Avery DH, Wildschiodtz G, Smallwood G, Martin D, Rafaelsen OJ (1986): REM latency and core temperature relationships in primary depression. Acta Psychiatr Scand 74:269- 280.
Baum A, Cohen L, Hall M (1993): Control and intrusive memories as possible determinants of chronic stress. Psycho- sore Med 55:274-286.
Benca RM, Obermeyer WH, Thisted RA, Gillin JC (1992): Sleep and psychiatric disorders: A meta-analysis Arch Gen Psychi- atry 49:651-668.
Box GEP, Cox DR (1964): Analysis of transformations. J R Stat Soc B 26:211-252.
Dahl RE, Puig-Antich J, Ryan NE, Cunningham S, Nelson B, Klepper T (1990a): EEG sleep in adolescents with major depression: The role of suicidality and inpatient status. J Affect Disord 19:63-75.
Dahl RE, Neidig MH, Ryan ND, Puig-Antich J (1990b): Auto- mated delta counts in childhood depression. Sleep Res 19: 365.
Dahl RE, Ryan ND, Birmaher B, A1-Shabbout M, Williamson DE, Neidig M, Nelson B, Puig-Antich J (1991a): EEG sleep measures in prepubertal depression. Psychiatry Res 38:201- 214.
Dahl RE, Ryan ND, Puig-Antich J, Nguyen NA, A1-Shabbout M, Meyer VA, Perel J (1991b): 24-Hour cortisol measures in adolescents with major depressive disorder: A controlled study. Biol Psychiatry 30:25-36.
Dahl RE, Ryan ND, Williamson DE, Ambrosini PJ, Rabinovich H, Novacenko H, Nelson B, Puig-Antich J (1992b): The regulation of sleep and growth hormone in adolescent depres- sion. J Am Acad Child Adolesc Psychiatry 31(4):615-621.
Dahl RE, Kaufman J, Ryan ND, Perel J, A1-Shabbout M, Birmaher B, Nelson B, and Puig-Antich J (1992a): The dexamethasone suppression test in children and adolescents: A Review and a controlled study. Biol Psychiatry 32:109- 126.
Dahl RE, Ryan ND, Perel J, Birmaher B, A1-Shabbout M, Nelson B, and Puig-Antich J (1994): Cholinergic REM induction test with arecoline in depressed children. Psychiatry Res. 5 1:269- 282.
Dahl RE, Ryan ND (in press a): The psychobiology of adolescent depression. In Cicchetti D. Toth S.L. (eds), Rochester Sym- posium on Developmental Psychopathology, Volume VII: Adolescence: Opportunities and Challenges. Rochester, NY: University of Rochester Press.
Dahl RE, Ryan ND (in press b): Sleep and neuroendocrine measures. In Shaffer D, Richters J (eds), Assessment in Child Psychopathology. New York: Guildford Press.
Ellis EM (1991): Watchers in the night: An anthropological look at sleep disorders. Am J Psychother 45(2):211-220.
Emslie GJ, Rush AJ, Weinberg WA, Rintelmann JW, Roffwarg HP (1990): Children with major depression show reduced rapid eye movement latencies. Arch Gen Psychiatry 47:119- 124.
Emslie GJ, Rush A J, Weinberg WA, Rintelmann JW, Roffwarg HP (1994): Sleep EEG features of adolescents with major depression. Biol Psychiatry 36:573-581.
Flemming JE, Boyle MH, Offord DR (1993): The outcome of adolescent depression in the Ontario child health study follow-up. J Am Acad Child Adolesc Psychiatry 32(1):28- 33.
Ford DE, Kamerow DB (1989): Epidemiological studies of sleep disturbances and psychiatric disorders: An opportunity for prevention? J JAMA 262( 11 ): 1479-1484.
Franz B, Kupfer D J, Miewald JM, Jarrett DB, Grochocinski VJ (in press): Growth hormone secretion timing in depression: Clinical outcome comparisons. Biol Psychiatry
Goetz R, Puig-Antich J, Ryan N, Rabinovich H, Ambrosini PJ, Nelson B, Krawiec V (1987): Electroencephalographic sleep of adolescents with major depression and normal controls. Arch Gen Psychiatry 44:61-68.
Goetz R, Puig-Antich J, Dahl RE, Ryan ND, Asnis G, Rabinov- ich H, Nelson B (1991): EEG sleep of young adults with major depression: A controlled study J Affect Disord 22:91- 100.
Harrington R, Fudge H, Rutter M, Pickles A, Hill J (1991): Adult outcomes of childhood and adolescent depression: II. Links with antisocial disorders. J Am Acad Child Adolesc Psychia- try 30:434-439.
Hoddes E, Zarcone V, Smythe H, Phillips R, Dement WC (1973): Quantification of sleepiness: A new approach Psy- chophysiology 10(4):431-436.
Hoeksema SN, Parker LE, Larson J (1994): Ruminative coping with depressed mood following loss. J Personality and Social Psychology 67(1):92-104.
Jarrett DB, Coble PA, Kupfer DJ (1983): Reduced cortisol latency in depressive illness Arch Gen Psychiatry 40:506- 510.
Jarrett DB, Miewald JM, Kupfer DJ (1990): Recurrent depres- sion is associated with a persistent reduction in sleep-related growth hormone secretion. Arch Gen Psychiatry 47:113-118.
Jarrett DB, Kupfer DJ, Miewald JM, Grochocinski VJ, Franz B (1994): Sleep-related growth hormone secretion is persis- tently suppressed in women with recurrent depression: a preliminary longitudinal analysis. J Psychiatr Res 28:211- 223.
Kahn AU, Todd S (1990): Polysomnographic findings in ado- lescents with major depression. Psychiatry Res 33:313-320.
Knowles JB, MacLean AW (1990): Age-related changes in sleep in depressed and healthy subjects. NeuropsychopharmacoI- ogy 3(4):251-259.
Kovacs M, Feinberg TL, Crouse-Novak MA, Panlauskas S, Finkelstein R (1984a): Depressive disorders in childhood. I. A longitudinal prospective study of characteristics and recov- ery. Arch Gen Psychiatry 41:219-239.
Kovacs M, Feinberg TL, Crouse-Novak MA, Panlauskas S, Pollock M, Finkelstein R (1984b): Depressive disorders in childhood. II. A longitudinal study of the risk for a subse- quent major depression. Arch Gen Psychiatry 41:643-649.
Kupfer DJ, Frank E, McEachran AB, Grochocinski VJ (1990): Delta sleep ratio: A biological correlate of early recurrence in unipolar affective disorder. Arch Gen Psychiatry. 47:100- 1105.
Kupfer D J, Ehlers CL, Frank E, Grochocinski V J, McEachran AB, Buhari A (1994): Persistent effects of antidepressants: EEG sleep studies in depressed patients during maintenance treatment Biol Psychiatry 35:781-793.

410 BIOL PSYCHIATRY R.E. Dahl et al 1996;39:400 -410
Kupfer D J, Pollock BG, Perel JM, Miewald JM, Grochocinski VJ, Ehlers CL (1994): Effect of pulse loading with clomipra- mine on EEG sleep. Psychiatry Res 54:161-175.
Kutcher S, Williamson P, Szalai J, Marton P (1992): REM latency in endogenously depressed adolescents Br J Psychi- atry 161:399-402.
Lahmeyer HW, Poznanski EO, Bellur SN (1983): EEG sleep in depressed adolescents. Am J Psychiatry 140:9:1150-1153.
Naylor MW, Shain BN, Shipley JE (1990): REM latency in psychotically depressed adolescents. Biol Psychiatry 28:161- 164.
Nolen-Hoeksema S, Parker LE, Larson J (1994): Ruminative coping with depressed mood following loss J Pers Soc Psychol 67(1):92-104.
Orvaschel H, Puig-Antich J (1987): Schedule for affective disorder and schizophrenia for school-age children, epidemi- ologic version, K-SADS-E, fourth version, 1987.
Orvaschel H (1990): Early onset psychiatric disorder in high risk children and increased familial morbidity. J Am Acad Child Adolesc Psychiatry 29(2): 184-188.
Puig-Antich J, Chambers WJ (1986): Schedule for affective disorders and schizophrenia for school-age children (6-18), K-SADS-P, fourth working draft.
Puig-Antich J, Novacenko H, Davies M, Chambers WJ, Tabrizi MA, Krawiec V, Ambrosini PJ, Sachar EJ (1984): Growth hormone secretion in prepubertal major depressive children. I, Response to insulin induced hypoglycemia. Final report. Arch Gen Psychiatry 41(5):455-460.
Puig-Antich J, Goetz R, Hanlon C, Tabrizi MA, Davies M, Weitzman E (1983): Sleep architecture and REM sleep measures in prepubertal major depressives: Studies during recovery from a major depressive episode in a drug free state. Arch Gen Psychiatry 40:187-192.
Puig-Antich J, Dahl R, Ryan N, Novacenko H, Goetz D, Twomey J, Klepper T (1989): Cortisol secretion in prepuber- tal children with major depressive disorder: Episode and recovery. Arch Gen Psychiatry 46:801-809.
Puig-Antich J, Goetz R, Hanlon C, Tabrizi MA, Davies M, Weitzman E (1982): Sleep architecture and REM sleep measures in prepubertal major depressives during an episode. Arch Gen Psychiatry 39:932-939.
Rao U, Weissman MM, Martin JA, Hammond RW (1993): Childhood depression and risk of suicide: A preliminary report of a longitudinal study. J Am Acad Child Adolesc Psychiatry 32(1):21-27.
Rechtschaffen A, Kales A (eds) (1968): A Manual of Standard- ized Terminology, Techniques and Scoring System for Sleep Stages of Human Subjects. Los Angeles: Brain Information Service/Brain Research Institute, University of California.
Reynolds CF, Kupfer DJ (1987): Sleep research in affective
illness: State of the art circa 1987 (state-of-the-art review). Sleep 10:199-215.
Ryan ND, Puig-Antich J, Rabinovich H, Ambrosini P, Robinson D, Nelson B, Novacenko H (1988): Growth hor- mone response to desmethylimipramine in depressed and suicidal adolescents. J Am Acad Child Adolesc Psychiatry 27:755-758.
Ryan ND (1992): The pharmacologic treatment of child and adolescent depression In Shaffer D (ed), Psychiatric Clinics of North America: Pediatric Psychopharmacology. Philadel- phia: WB Saunders, pp 29-40.
Ryan ND, Dahl RE (1993): The biology of depression in children and adolescents. In Mann JJ, Kupfer DJ (eds): The Biology of Depressive Disorders. New York: Plenum Press.
Ryan ND, Dahl RE, Birmaher B, Williamson DE, Iyengar S, Nelson B, Puig-Antich J, Perel JM (1994): Stimulatory tests of growth hormone secretion in prepubertal major depression: Depressed versus normal children. J Am Acad Child Adolesc Psychiatry. 33:824-833.
Ryan ND, Williamson DE, Iyengar S, Orvaschal H, Reich T, Dahl RE, Puig-Antich J (1992a): A secular increase in child and adolescent onset affective disorder. J Am Acad Child Adolesc Psychiatry 31 (4):600-605.
Ryan ND, Puig-Antich J, Rabinovich H, Robinson D, Ambrosini PJ, Nelson B, Iyengar S (1987): The clinical picture of major depression in children and adolescents. Arch Gen Psychiatry 44: 854- 861.
Ryan ND, Birmaher B, Perel J, Dahl RE, Meyer VA, A1- Shabbout M, Iyengar S, Puig-Antich J (1992b): Neuroendo- crine response to L-5-hydroxytryptophan challenge in prepu- bertal major depression: Depressed versus normal children. Arch Gen Psychiatry 49:843-852.
Taska LS, Kupfer DJ (1987): Sleep Scoring Manual. Weissman MM, Gammon GD, John K, Merikangas KR, Warner
V, Prusoff BA, Sholomskas D (1987): Children of depressed parents: Increased psychopathology and early onset of major depression. Arch Gen Psychiatry 44:847-853.
Williamson DE, Ryan ND, Dahl RE, Jeannette L (1992): Hamilton depression scores can be extracted from the K- SADS-P in adolescents. J Child Adolesc Psychopharmacol 2:175-181; 1992.
Williamson DE, Dahl RE, Birmaher B, Goetz RR, Ryan ND: Stressful life events and EEG sleep in depressed and normal control adolescents. Biol Psychiatry (in press).
Young W, Knowles JB, MacLean AW, Boag L, McConville BJ (1982): The sleep of childhood depressives: comparison with age-matched controls. Biol Psychiatry 17:1163-1169.
Young EA, Haskett RF, Grunhaus L, Pande A, Weinberg VM, Watson S J, Akil H (1994): Increased evening activation of the hypothalamic-pituitary-adrenal axis in depressed patients. Arch Gen Psychiatry 51:701-707.