scar revision - hindawi.com
TRANSCRIPT
Scar RevisionGuest Editors: Hayes B. Gladstone, Daniel Berg, and Michel McDonald
Dermatology Research and Practice
Scar Revision
Dermatology Research and Practice
Scar Revision
Guest Editors: Hayes B. Gladstone, Daniel Berg,and Michel McDonald

Copyright © 2010 Hindawi Publishing Corporation. All rights reserved.
This is a special issue published in volume 2010 of “Dermatology Research and Practice.” All articles are open access articles dis-tributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in anymedium, provided the original work is properly cited.
Dermatology Research and Practice
Editorial Board
Dietrich Abeck, GermanyChristoph Abels, GermanyGiuseppe Argenziano, ItalyJorge Arrese, BelgiumKhusru Asadullah, GermanyRobert Baran, FranceW. F. Bergfeld, USABruno A. Bernard, FranceJag Bhawan, USACraig G. Burkhart, USAAndrea Cavani, ItalyEung-Ho Choi, Republic of KoreaEnno Christophers, GermanyClay Cockerell, USAI. Kelman Cohen, USAPhilip J. Cooper, UKJonathan L. Curry, USAVincent J. Falanga, USAMasutaka Furue, JapanThilo Gambichler, GermanyAziz Ghahary, Canada
D. M. Ghazarian, CanadaSalvador Gonzalez, USAJane Grant-Kels, USAJoan Guitart, USATakashi Hashimoto, JapanJana Hercogova, Czech RepublicH. Hoenigsmann, AustriaDrazen Jukic, USAJean C. Kanitakis, FranceD. V. Kazakov, Czech RepublicLajos Kemeny, HungaryElizabeth Helen Kemp, UKKaoru Kiguchi, USAYasuo Kitajima, JapanRossitza Lazova, USAPhilip E. LeBoit, USAJan A. Marcusson, NorwayAshfaq A. Marghoob, USAM. Michal, Czech RepublicLuigi Naldi, ItalyJohannes Norgauer, Germany
H. Peter Soyer, AustraliaJean Revuz, FranceJ. Ring, GermanyGavin P. Robertson, USAFranco Rongioletti, ItalyStefano Rosso, ItalyToshiaki Saida, JapanMario Santinami, ItalyTadamichi Shimizu, JapanGiuseppe Stinco, ItalyM. Stucker, GermanyD. J. Tobin, UKFranz Trautinger, AustriaUwe Trefzer, GermanyHelgi Valdimarsson, IcelandVladimir Vincek, USAJanine Wechsler, FranceXiaowei Xu, USAK. Yamanishi, JapanIris Zalaudek, AustriaBernhard W. H. Zelger, Austria

Contents
Scar Revision, Hayes B. Gladstone, Daniel Berg, and Michel McDonaldVolume 2010, Article ID 545796, 2 pages
Cellular and Molecular Characteristics of Scarless versus Fibrotic Wound Healing, Latha Satish andSandeep KathjuVolume 2010, Article ID 790234, 11 pages
Therapeutic Improvement of Scarring: Mechanisms of Scarless and Scar-Forming Healing andApproaches to the Discovery of New Treatments, Nick L. Occleston, Anthony D. Metcalfe, Adam Boanas,Nicholas J. Burgoyne, Kerry Nield, Sharon O’Kane, and Mark W. J. FergusonVolume 2010, Article ID 405262, 10 pages
Therapies with Emerging Evidence of Efficacy: Avotermin for the Improvement of Scarring, Jim Bush,Karen So, Tracey Mason, Nick L. Occleston, Sharon O’Kane, and Mark W. J. FergusonVolume 2010, Article ID 690613, 6 pages
Z-Plasty Made Simple, Sumaira Z. AasiVolume 2010, Article ID 982623, 5 pages
Long-Term Followup of Dermal Substitution with Acellular Dermal Implant in Burns and PostburnScar Corrections, I. Juhasz, B. Kiss, L. Lukacs, I. Erdei, Z. Peter, and E. RemenyikVolume 2010, Article ID 210150, 7 pages
Acne Scars: Pathogenesis, Classification and Treatment, Gabriella Fabbrocini, M. C. Annunziata,V. D’Arco, V. De Vita, G. Lodi, M. C. Mauriello, F. Pastore, and G. MonfrecolaVolume 2010, Article ID 893080, 13 pages

Hindawi Publishing CorporationDermatology Research and PracticeVolume 2010, Article ID 545796, 2 pagesdoi:10.1155/2010/545796
Editorial
Scar Revision
Hayes B. Gladstone,1 Daniel Berg,2 and Michel McDonald3
1 Division of Dermatologic Surgery, Stanford University, Stanford, CA 94305, USA2 Division of Dermatologic Surgery, University of Washington, 4225 Roosevelt Way NE, 4th Floor Dermatology, Box 354697 Seattle,WA 98195, USA
3 Division of Cosmetic Dermatology, Vanderbilt University Medical Center, 719 Thompson Lane Suite 26300, NashvilleTN 37204, USA
Correspondence should be addressed to Hayes B. Gladstone, [email protected]
Received 31 December 2010; Accepted 31 December 2010
Copyright © 2010 Hayes B. Gladstone et al. This is an open access article distributed under the Creative Commons AttributionLicense, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properlycited.
1. Introduction
Scarring is the body’s natural response to a wound. Yet,this healing process can create significant functional andcosmetic problems. It impacts daily life and can createissues in self-esteem. Traditionally, the treatment of scarshas been surgical. Despite meticulous surgical technique,scars still form. Revision may be in the form of excisingthe scar to create a “thinner” line, or the surgeon mayperform a geometric broken line to create an illusion ofnatural creases. Lasers or mechanical dermabrasion can alsobe performed to minimize the scar. Lasers including thepulse dye laser has also been used intraoperatively and inthe acute postoperative period to suppress scar formation.Topical treatments such as silicone may also help soften ascar. Yet the cicatrix still exists.
Other types of scars such as those from inflammatoryprocesses including acne create a skin topography thatfeatures alternating depressions and papules. There is nosingle satisfactory treatment for acne scars. Because of thecomplexity of this scarring process, a combined approachmust be undertaken.
Historically, dermabrasion has been performed. ForFitzpatrick Skin I, II, and III, conventional ablative laserresurfacing has been used. Despite many case series, it is notclear if the carbon dioxide laser or the erbium laser alone pro-vides a long-term significant improvement. More recently,fractionated resurfacing both nonablative and ablative havebeen shown to have some effect on subsets of acne scars.Subscision which manually breaks apart the acne scars isoften combined with the laser treatment. Subscision can be
performed with Nokor needles through small puncture sites,or more recently using a roller device that percutaneouslydisrupts the scar. Other techniques including punch graftingand excision may ameliorate acne scars.
On the other end of the spectrum of acne and smallsurgical scars are those from burns. Because of the severetrauma of a burn, large deforming contractures can occur,or large areas of denuded skin. An artificial or natural skinsubstitute may need to be used foremost for coverage andprotection from the environment, but also to minimize scars.
Perhaps the reason that clinicians have difficulty ineradicating scars is because we do not quite understandthe mechanism from a cellular and molecular basis. Break-throughs have been made in the past 20 years, particularlyfrom fetal surgery and the discovery that fetal skin does notscar after wounding. The treatment implications of this typeof research has still not been fully realized. Yet, it is no doubtthat in the future, the prevention and treatment of scars willbe in the form of targeted molecular therapies including theuse of stem cells.
2. Mechanisms
It is this contrast between healing in the womb and healingafter birth that the authors Satish and Kathju discuss intheir article entitled Cellular and Molecular Characteristicsof Scarless versus Fibrotic Wound Healing. They reviewthe biology of fetal wound healing including the role ofgrowth factors, keratinocytes, and reepithelialization andgene expression. This article is an excellent primer for those

2 Dermatology Research and Practice
interested in fetal wound healing. Occleston et al. build uponthe understanding of the mechanisms of scarring in theircomprehensive article entitled Therapeutic Improvement ofScarring: Mechanisms of Scarless and Scar-Forming Healingand Approaches to the Discovery of New Treatments. Theseauthors point out that scar-free to scar-forming healing reallyis a continuous spectrum. They discuss preclinical examplesof wound healing and how this translates to humans. Froma treatment standpoint, they elucidate the mechanisms of aprophylactic scar treatment.
2.1. Molecular Treatment of Scars. It is has long been under-stood that TGF B plays an important role in wound healingand scarring in human beings. In their fine manuscript enti-tled Therapies with Emerging Evidence of Efficacy: Avoterminfor the Improvement of Scarring, Bush et al. evaluate therole of TGF B3 as a potential therapeutic agent. Echoing,the previous paper, these authors emphasize the importanceof prophylactic treatment after surgery in order to reducesubsequent scarring. They describe the successful Phase I/IItrials of this biologic agent. However, the Phase III trials (notpublished here) have been disappointing, so the march goeson for the optimal prophylactic biologic agent. Nevertheless,the success of the company’s early trials may shed additionallight on TGF-B and could lead to future discoveries by otherresearch groups.
2.2. Surgical Treatment. Despite meticulous technique, sur-gical scars can still distort mobile anatomic regions suchas the nasal ala, the lip, and the eyelid. The conventionalmethod to lengthen a scar and change its orientation is bytransposing its limbs. In Z-plasty Made Simple, Aasi demon-strates her technique for demystifying Z plasties which canbe conceptually complex particularly for trainees. She offersfoolproof methods with excellent results to optimize scarsthat need revision after Mohs Micrographic Surgery. Thistechnique needs to be in the armamentarium of everysurgeon performing skin and soft tissue surgery.
2.2.1. Surgical Treatment: Special Considerations. The reduc-tion of scarring and skin coverage in burn patients is one ofthe most difficult challenges facing reconstructive surgeons.Prompt replacement of the charred skin with a functionalalternative is fundamental in minimizing contractures as wellas eventual cosmesis. In Long-Term Followup of Dermal Sub-stitution with Acellular Dermal Implant in Burns and PostburnScar Corrections, Juhasz et al. describe their experience inusing Alloderm in 18 patients as well as reviewing the variouscoverage options. In their study, they used the VancouverScar Scale with a 50-month followup. They demonstratedvery favorable results when combined with a split thicknessskin graft compared to more complicated flaps.
Finally, Fabbrocini et al. provide a comprehensive reviewof acne scars in their paper entitled Acne Scars: Pathogenesis,Classification and Treatment. In a very straightforwardapproach, the authors explain the current theory on whyacne scars occur, how to classify them into atrophic,boxcar or icepick, and then how to choose the appropriate
treatment(s). The authors nicely summarize the varioustherapeutic options including the increasingly popular tech-nique of needling using a roller device. They tackle thistopic well and astutely point out that there are no universalguidelines for treating acne scars and that randomizedcontrolled studies are needed as well as evaluating the all-important psychological impact of this scarring on thispatient population.
As editors, we can only hope that these articles stimulatefurther discussion and spur new research to minimizescarring and allow these patients to live healthy and activelives without disfigurement.
Hayes B. GladstoneDaniel Berg
Michel McDonald
Hindawi Publishing CorporationDermatology Research and PracticeVolume 2010, Article ID 790234, 11 pagesdoi:10.1155/2010/790234
Review Article
Cellular and Molecular Characteristics of Scarless versus FibroticWound Healing
Latha Satish1 and Sandeep Kathju1, 2
1 Center for Genomic Sciences, Allegheny-Singer Research Institute, Allegheny General Hospital, 320 East North Avenue,Pittsburgh, PA 15212, USA
2 Department of Microbiology and Immunology, Drexel University College of Medicine, Allegheny Campus,Pittsburgh, PA 15212, USA
Correspondence should be addressed to Latha Satish, [email protected]
Received 27 March 2010; Accepted 24 November 2010
Academic Editor: Hayes B. Gladstone
Copyright © 2010 L. Satish and S. Kathju. This is an open access article distributed under the Creative Commons AttributionLicense, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properlycited.
The purpose of this paper is to compare and contrast the discrete biology differentiating fetal wound repair from its adultcounterpart. Integumentary wound healing in mammalian fetuses is essentially different from wound healing in adult skin. Adult(postnatal) skin wound healing is a complex and well-orchestrated process spurred by attendant inflammation that leads to woundclosure with scar formation. In contrast, fetal wound repair occurs with minimal inflammation, faster re-epithelialization, andwithout the accumulation of scar. Although research into scarless healing began decades ago, the critical molecular mechanismsdriving the process of regenerative fetal healing remain uncertain. Understanding the molecular and cellular events duringregenerative healing may provide clues that one day enable us to modulate adult wound healing and consequently reduce scarring.
1. Introduction
In adult (postnatal) mammalian organisms, injury to cuta-neous tissue with disruption of normal skin architectureis repaired by means of an inflammatory and fibroticresponse that leads to accumulation of scar [1]. Althoughscar formation allows for the rapid sealing of an injured area,it can frequently prove the source of persistent pathologyin the organism. For example, scar formation after ten-don repair will limit their gliding ability, restricting handfunction; intra-abdominal scar/adhesions frequently lead tosmall bowel obstruction, necessitating surgical intervention;cirrhosis of the liver and pulmonary fibrosis are also forms ofexcessive scarring.
Nowhere, however, is scar more evident or problematicthan in the skin. Cicatrix in the extremities and digits cancause contracture and restrict motion, resulting in significantdisability. Scar in the genitalia can interfere with sexualfunction and even urination. Scar formation in the facialskin of the head and neck is particularly problematic, withmultiple vital functions at risk. Scar in the external ear
can cause substantial hearing loss, and constriction of thenasal apertures can interfere with respiration, smell, andderivatively, taste. Scar contractures following burn injuryare well known to progress to microstomia, nasal stenosis,lip or eyelid ectropion if severe enough. They can leadto restriction of neck movement and permanent mouthopening [2–4]. If left untreated in a growing child, suchsevere contractures can even lead to secondary facial skeletalabnormalities, compounding the problem [5]. In additionto the functional deficits facial scar can inflict, there isalso the obvious social opprobrium of visible disfigurement.Scar, then, represents a significant source of morbidity, andcan frequently require aggressive measures to deal with itssequelae [6].
In contrast to adults, fetal integumentary wounds inhumans and other mammals heal rapidly without associatedscarring until late in gestation [7–9]. Investigation into thephenomenon of fetal wound healing started in the early1950s with the study of animal models, which showedthat fetal skin wounds could heal rapidly but without anyapparent “dedifferentiation” of cellular components such

2 Dermatology Research and Practice
as occurred in regenerating amphibians [10]. Later, exam-ination by Rowlatt [11] of healing limbs after intrauterineamputation by amniotic constriction bands in a 20-weekold human fetus showed that human skin at this stageof development healed without apparent inflammation.Subsequent work has confirmed that fetal wounds healdifferently depending on the gestational age of the fetus,including even in the pouch young of a marsupial [12].In general, the scarless character of fetal wound repairpersists until roughly the middle of the third trimester ofintrauterine gestation, at which point a transition to theadult, scar-forming pattern of wound repair occurs [13–15]. This scarless healing is a property intrinsic to fetaltissues, and not a conferred benefit of the protected uterineenvironment: fetal skin placed subcutaneously into athymicmice and then wounded still heals without scar, in spite ofoccurring in an environment free of amniotic fluid [16].Conversely, adult skin grafted onto immunoprivileged fetalhosts in utero and then wounded still heals with scar [17].
Because early- to mid-gestational fetal wound healingoccurs with evident restoration of normal skin architectureand no significant scar deposition, it has been termed“regenerative,” and has been taken as a model by whichwe may attempt to engineer the same process in adults. Ittherefore becomes important to understand at the cellularand molecular level the distinctions between these twophysiologies, in the hopes that an understanding of fetalbiology may one day enable its recapitulation in the adult.
2. The Biology of Adult Wound Healing
2.1. Inflammatory Phase. The process of skin wound repairin adult mammalian organisms is an intricate and highlycoordinated process that generally can be divided into fouroverlapping phases: hemostasis, inflammation, proliferation,and remodeling [18]. Any injury that severs blood vessels willtrigger events that try to effect immediate hemostasis. Thisprocess includes vasoconstriction, platelet aggregation, andplatelet α-degranulation of vesicles containing both clottingand growth factors. Platelets are also believed to play anadditional role in the wound healing cascade, not only asinitiators of coagulation but also through the release of amultitude of growth factors and cytokines that modulatefibroblast activity, such as transforming growth factor β1(TGF-β1) and platelet-derived growth factor (PDGF) [19].These growth factors provide a chemotactic stimulus forneutrophils, fibroblasts, and monocytes and ultimately affectthe dynamics of extracellular matrix (ECM) synthesis [20,21]. Neutrophils are early responders to these chemotacticagents and begin to infiltrate to the site of injury well beforethe activation and/or arrival of fibroblasts and monocytes.They accomplish phagocytosis of bacteria and functionaldebridement of injured tissue while themselves secretingadditional proinflammatory cytokines. In the presence offoreign body or infection, a persistent neutrophil-richinflammatory response results which can lead to poor woundhealing and excess fibrosis [22].
Monocytes are also attracted to the wound site inresponse to a variety of chemoattractants derived from intra-
and extravascular sources. Monocytes become macrophages,which are considered the principle coordinators of adultwound healing [23]. Macrophages act as avid phagocytes,ingesting debris in the wound field (including even spentneutrophils), and they also produce numerous cytokinesand growth factors crucial for fibroblast recruitment andangiogenesis. Monocytes and activated macrophages areknown to bind to the ECM through cell surface integrinreceptors; this adherence to the ECM induces ECM phago-cytosis, promoting wound debridement. Attachment to theECM also alters the gene expression profile of macrophages,leading to increased expression and subsequent secretion ofcolony stimulating factor 1 (CSF-1, required for macrophagesurvival), tumor necrosis factor (TNF-α, inflammatorycytokine), and PDGF (chemotactic agent for fibroblasts)[24, 25]. As in the case of an extended neutrophilic infiltrate,a persistent macrophage response may also lead to excess scarformation, itself an unwanted outcome [26].
Another key leukocyte lineage, the mast cell (MC),derived from circulating basophils, is postulated to con-tribute to the healing of skin wounds, and MC’s have beenimplicated in multiple phases of wound healing [27, 28].Egozi et al. [29] showed using MC-deficient KitW /KitW−v
mice that neutrophil infiltration was reduced at early timepoints (inflammatory phase) but that the absence of mastcells had no effect on the proliferative aspects of wound heal-ing. Weller et al. [30] showed using the same MC-deficientKitW /KitW−v mice that MC activation and histamine releaseare required for proper recruitment of neutrophils and alsofor the normal closure of wounds. Ultimately, fibroblastsenter the wound site and replace the initial wound fibrinmatrix by depositing glycosaminoglycans, proteoglycans,and other ECM proteins such as fibronectin and tenascin.This last is another example of the complicated interplayof multiple factors in cutaneous wound healing and scarformation, since fibronectin promotes cellular adhesionto the underlying substratum, whereas tenascin actuallyfacilitates fibroblast migration by antagonizing fibronectin[31, 32].
Interestingly, although inflammatory cells are intimatelyinvolved in the regulation and progression of normal adultwound healing, several lines of evidence suggest that deple-tion of one or more of the inflammatory cell types can actu-ally have a positive outcome on the closure of wounds. Exper-iments conducted by Szpaderska et al. [33] demonstrate that,as long as bleeding is adequately controlled, mice dosed withantiplatelet antisera to induce thrombocytopenia show nodeficit in the proliferative aspects of repair, including woundclosure, angiogenesis, and collagen synthesis, all of whichwere unaffected compared to controls. This data suggeststhat platelets are not absolutely essential for normal adultwound healing to occur. Similar experiments in neutrophil-depleted mice [34] showed that wound closure was actuallymore rapid in the mice with induced neutropenia than incontrol animals, suggesting that neutrophils, while perhapshighly utile in combating infection, may in other respectsactually be inhibitory to wound healing. Neonatal PU.1-knockout mice (which lack macrophages and functioningneutrophils) healed wounds with minimal scarring, with an

Dermatology Research and Practice 3
altered growth factor and cytokine profile at the wound site,reduced cell death, and with phagocytic fibroblasts standingin for more conventional inflammatory cells [35]. It thereforeappears that macrophages too are not absolutely required fornormal adult wound repair, and their absence may actuallyallow a more scarless mode of healing.
2.2. Proliferative Phase. The formation of granulation tissue,a well-vascularized connective tissue containing macro-phages and fibroblasts that replaces fibrin clot, is a notablefeature of the proliferative phase of adult wound healing.This granulation tissue has been considered to be a con-tractile organ, responsible for the active wound contractionseen in the proliferative phase of adult wound healing, acontraction affected chiefly by fibroblasts and their derivativesubtypes, myofibroblasts (see below). The rate of granulationtissue formation appears to be dependent on interaction ofthe fibroblast integrin receptor with fibronectin [36]. Theinitial fibrin clot functions as a chemokine to stimulatemacrophages and fibroblasts to migrate into the woundspace; in the case of the latter, this migration itself isthought to apply traction to the wound periphery, assistingin its contraction and ultimate closure. Within the woundbed macrophages provide a continuing source of growthfactors necessary for angiogenesis [37], and fibroblasts laydown a provisional matrix mainly composed of collagen andproteoglycans.
Multiple studies have pointed to a particularly importantrole for transforming growth factor- beta in this phaseof wound healing. Expression of the TGF-β1 and TGF-β2isoforms (in comparison to TGF-β3) is increased in adultwounds, and studies show that exogenous administration ofTGF-β1 and TGF-β2 to healing wounds results in increasedcollagen, protein, and inflammatory cell accumulation [38].In contrast, Ferguson et al. (2009) [39] assessed scar qualityafter treatment with avotermin (recombinant human TGF-β3) in Phase II clinical trials in humans, and showed thatavotermin has the potential to provide an improvement inthe appearance of scars. As repair progresses, fibroblasts alsodisplay increased expression levels of adhesion molecules andassume a contractile myofibroblast phenotype with increasedalpha-smooth muscle actin (α-SMA) expression, known tobe stimulated by TGF-β1 and TGF-β2 as well as by PDGF[40, 41]. Wound fibroblasts and myofibroblasts work inconcert to draw the wound closed and also contribute to thesynthesis and alignment of collagen fibers [42].
The formation of granulation tissue in an open woundalso allows the process of re-epithelialization to begin, asepithelial cells migrate across the new tissue to form abarrier between the wound and the environment. Intracel-lular actin microfilaments are formed, and alterations inintermediate filament gene and protein regulation have alsobeen observed, [43] enabling the epidermal cells to creepacross the wound surface. Multiple growth factors, includingepidermal growth factor (EGF), keratinocyte growth factor(KGF), transforming growth factor-alpha (TGF-α), andepiregulin are thought to act synergistically to stimulate re-epithelialization [44–46].
2.3. Remodeling Phase. In the remodeling phase, which canlast for up to a year after injury, there is ongoing synthesis,degradation, cross-linking, and reorientation of collagen toform the mature scar. The healing and remodeling tissue willmanifest increasing tensile strength, however, the resultantscar will never attain physical properties equal to that of theuninjured tissue [47]. Remodeling allows for some removalof accumulated connective tissue and is made possible bymatrix metalloproteinases (MMPs) under the control of acytokine network [48]. The coordinated regulation of theseenzymes and their inhibitors ensures tight control of localproteolytic activity.
Over time the quantity of fibroblasts and myofibroblastswithin the maturing wound bed are reduced by apoptosis,which may be precipitated by the withdrawal of cytokinesas the wound heals, although the precise mechanismsgoverning this response remain unclear [49]. With continuedremodeling the outgrowth of capillaries is halted, blood flowto the area is reduced and metabolic activity in the areadeclines with the maturation of a relatively hypocellular andhypovascular scar.
3. Disorders of Excessive Cutaneous Fibrosis
While the above summarizes many of the important featuresof normal adult wound healing, there also exist conditionsmarked by an abnormal pathological response to cutaneouswound healing resulting in excessive fibrosis, the two mainexamples of which are hypertrophic scars and keloids.Hypertrophic scars typically take the form of a reddish raisedlump on the skin; they remain within the boundaries ofthe original zone of injury and often naturally improve inappearance after some years [50, 51]. They are frequentlyamenable to surgical revision, with the expectation that therevision will obtain a more favorable result. In contrastkeloidal scars will typically progress into large, tumorous(although benign) masses that clearly exceed the originalzone of injury. Keloids are not known to regress spon-taneously and their recurrence rate is high after surgicalexcision [51], even with the use of such adjunctive measuresas local corticosteroid injection or pressure appliances. Bothhypertrophic scars and keloids represent a type of abnormalfibroproliferative wound repair, and it appears that severalstages of wound healing, from the inflammatory phase to theremodeling phase, are significantly altered [52, 53].
Gene profiling studies have identified previously unsus-pected genes of potential relevance to the pathogenesis ofhypertrophic scars and keloids. cDNA microarray examina-tion of tissue mRNA obtained from burn hypertrophic scars(compared to normal skin) revealed that genes displayingaltered expression included proto-oncogenes, genes involvedwith apoptosis, immune regulatory genes, cytoskeletal ele-ments, and transcription factors, signifying that multiplepathways are involved in hypertrophic scar formation andcontraction [54]. Similar microarray studies examiningaltered gene expression in keloids and in fibroblasts derivedfrom keloid lesions identified genes which have previouslybeen noted by biochemical studies, but interestingly also

4 Dermatology Research and Practice
identified multiple genes not previously suspected to play arole in keloid formation. Naitoh et al. [55] observed strongerectopic expression (in keloids) of chondrocyte/osteoblastmarker genes, namely, periostin, OB-cadherin, lumican, andmimecan as well as increased expression of transcriptionfactors SOX9 and CBFA1, known to be involved in regulationof the above-mentioned gene products. The same study alsomarked upregulation of two tumorigenesis- related genes,p311 and fibroblast activation protein alpha (FAP-α). Satishet al. [56] also showed the upregulation of tumor-relatedgenes in keloid fibroblasts, namely, TCTP (tumor proteintranslationally controlled 1), MORF-related gene 15 (MRF15), annexin 2, and ribosomal proteins RPS 18, 10, and L23A.This interesting increase in genes related to tumorigenesis iscongruent with the behavior of keloidal fibroblasts, whichproliferate in a rapid and unregulated manner and invadenormal skin tissues, beyond the boundaries of the initialregion of injury.
4. Characteristics of Fetal Skin
In order to understand the basis of regenerative fetal skinhealing, and to contrast it to the adult tissue repair describedabove, it is helpful to first recognize the pattern of devel-opment of fetal skin. In humans, prior to the 24th week ofgestation, fetal skin tissue is less differentiated than adultskin [15]. The human fetal integument begins with twocell layers, the basal cell layer and the periderm, at about 4weeks gestation. The periderm is the outermost single-celllayer of the fetal skin; although the function of the peridermhas not been determined, a secretory or absorptive processhas been hypothesized [14]. As development continues, anintermediate epidermal cell layer develops. Keratinizationbegins at 9 to 10 weeks gestation, and during this period hairfollicles and sebaceous glands become apparent. By 24 weeksgestation, that is, toward the end of the second trimester,at which time fetal skin wounds continue to demonstratescarless healing, the epidermis has completely keratinizedand stratified into adult morphologic layers [57].
Fetal skin contains fibroblasts and fetal extracellularmatrix (ECM) that are distinct from adult fibroblasts andadult ECM. Fetal dermis thickens by increasing collagencontent and replacing nonsulfated glycosaminoglycans withsulfated glycosaminoglycans. Fetal ECM contains higherproportions of type III collagen, chondroitin sulfate, pro-teoglycan, and hyaluronic acid than does adult ECM [15].Coolen et al. [58] have recently examined multiple dermaland epidermal components of human fetal and adult skin,finding that most differences between these tissue typesreside at the level of dermal ECM molecular expression. Forexample, elastin was present in adult dermis, but was notdetected in fetal dermis. Conversely, chondroitin sulfate andfibronectin both were expressed at substantially higher levelsin fetal dermis compared to adult. The expression patternsof basement membrane proteins, keratin isoforms (e.g.,K10, K14, K16) and epidermal Ki-67 were not significantlydifferent between fetal skin and adult skin biopsies.
MMPs and tissue inhibitors of the proteolytic activity ofMMPs (TIMPs), molecules that regulate ECM turnover, are
also shown to be differentially regulated as fetal skin devel-ops. Dang et al. [59] found that baseline expression of MMPs1, 2, and 14 all increased with the transition to a scarring phe-notype in fetal rat skin, with MMP2 message levels increasingby 50-fold. Nonetheless, they determined that E16 (scarlesslyhealing) wounds had a higher MMP to TIMP expressionratio than E19 scarring wounds. Other ECM moleculesdifferentially expressed in developing fetal skin and woundsinclude decorin, a proteoglycan implicated in regulation ofTGF-β bioactivity, which has been shown to increase duringthe ontogenic transition from scarless fetal healing to adultwound healing, but which is actually decreased by woundingduring the scarless healing period [60]. In contrast, fibro-modulin, another small interstitial proteoglycan which canbind to and modulate TGF-β activity, has been shown todecrease with advancing gestational age, and decreases aswell when adult skin is wounded, but is actually increased inscarlessly healing fetal wounds relative to control [61]. Theseobservations give some indication of the complicated andmixed functions ECM molecules may play in determiningthe scarless nature of early fetal wound repair.
5. The Biology of Fetal Wound Healing
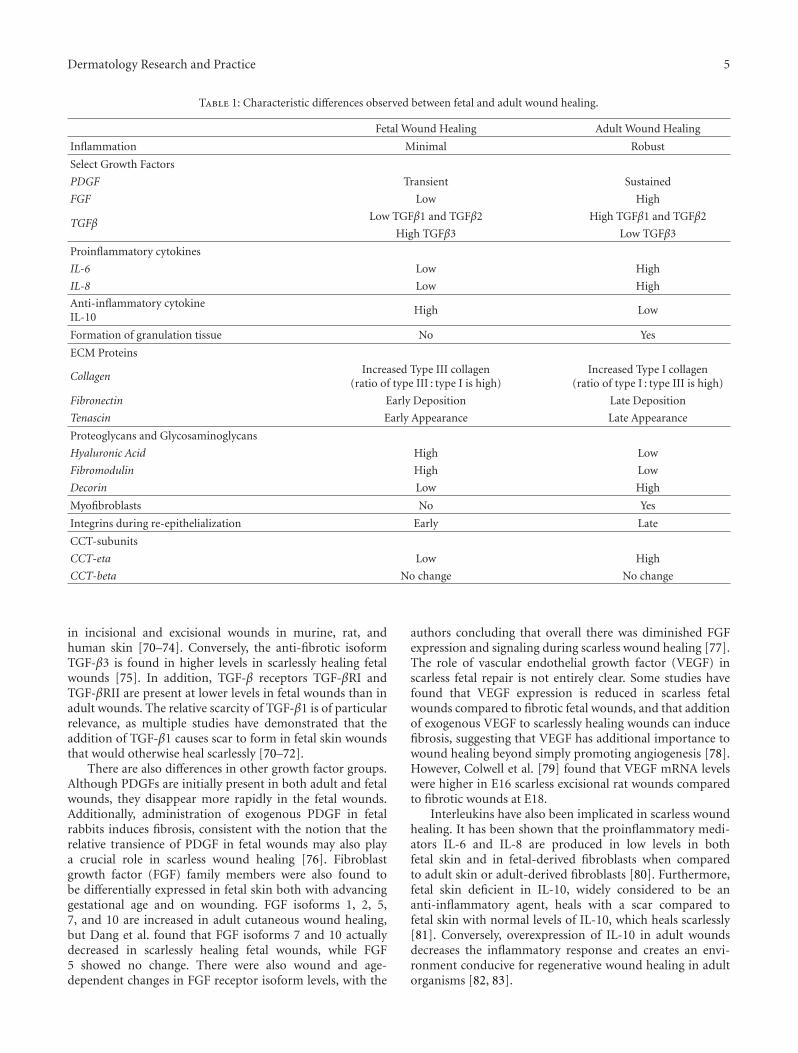
Healing cutaneous wounds in mammalian fetuses showsmultiple important differences from adult healing; many ofthese are enumerated in Table 1. Perhaps the most significantcharacteristic feature of scarless fetal wound healing thatstands in contradistinction to adult is a significantly reducedinflammatory response [62]. A markedly diminished orminimal inflammatory response in fetal wounds has beendemonstrated in multiple fetal animal models [62–65]. Theabsence of an acute inflammatory infiltrate in fetal woundsmay partly be explained by decreased platelet aggregationand degranulation in fetal tissues; fetal platelets are alsothought to release lower levels of cytokines, thereby alsopotentially reducing the recruitment of inflammatory cells tofetal wounds [66]. Hopkinson-Woolley et al. [67], examiningembryonic and fetal mice, have found that macrophagesare not normally recruited to fetal wound sites beforedevelopmental stage E14.5, but that after this transition stagethere was a significant recruitment of macrophages within 12hours of injury. Furthermore, few neutrophils are present inthe fetal wound, and an age-dependent defect in the abilityof fetal neutrophils to phagocytose pathogenic bacteria hasbeen demonstrated in fetal sheep, signifying that early fetalneutrophils are physiologically distinct from those presentat the end of gestation or postnatal cells [68]. Thus, thereare multiple facets to the much diminished inflammatoryresponse seen in scarlessly healing fetal wounds.
5.1. Growth Factor Profiles During Fetal Wound Healing.The cytokine and growth factor profile of fetal healingdiffers significantly from adult wound healing. Many studieshave focused on TGF-β family members as these proteinshave been shown to have a major role in fibrosis [69]. Inparticular, the profibrotic isoform TGF-β1 has been noted tobe reduced in early fetal wounds, and this has been confirmed
Dermatology Research and Practice 5
Table 1: Characteristic differences observed between fetal and adult wound healing.
Fetal Wound Healing Adult Wound Healing
Inflammation Minimal Robust
Select Growth Factors
PDGF Transient Sustained
FGF Low High
TGFβLow TGFβ1 and TGFβ2 High TGFβ1 and TGFβ2
High TGFβ3 Low TGFβ3
Proinflammatory cytokines
IL-6 Low High
IL-8 Low High
Anti-inflammatory cytokineIL-10
High Low
Formation of granulation tissue No Yes
ECM Proteins
CollagenIncreased Type III collagen
(ratio of type III : type I is high)Increased Type I collagen
(ratio of type I : type III is high)
Fibronectin Early Deposition Late Deposition
Tenascin Early Appearance Late Appearance
Proteoglycans and Glycosaminoglycans
Hyaluronic Acid High Low
Fibromodulin High Low
Decorin Low High
Myofibroblasts No Yes
Integrins during re-epithelialization Early Late
CCT-subunits
CCT-eta Low High
CCT-beta No change No change
in incisional and excisional wounds in murine, rat, andhuman skin [70–74]. Conversely, the anti-fibrotic isoformTGF-β3 is found in higher levels in scarlessly healing fetalwounds [75]. In addition, TGF-β receptors TGF-βRI andTGF-βRII are present at lower levels in fetal wounds than inadult wounds. The relative scarcity of TGF-β1 is of particularrelevance, as multiple studies have demonstrated that theaddition of TGF-β1 causes scar to form in fetal skin woundsthat would otherwise heal scarlessly [70–72].
There are also differences in other growth factor groups.Although PDGFs are initially present in both adult and fetalwounds, they disappear more rapidly in the fetal wounds.Additionally, administration of exogenous PDGF in fetalrabbits induces fibrosis, consistent with the notion that therelative transience of PDGF in fetal wounds may also playa crucial role in scarless wound healing [76]. Fibroblastgrowth factor (FGF) family members were also found tobe differentially expressed in fetal skin both with advancinggestational age and on wounding. FGF isoforms 1, 2, 5,7, and 10 are increased in adult cutaneous wound healing,but Dang et al. found that FGF isoforms 7 and 10 actuallydecreased in scarlessly healing fetal wounds, while FGF5 showed no change. There were also wound and age-dependent changes in FGF receptor isoform levels, with the
authors concluding that overall there was diminished FGFexpression and signaling during scarless wound healing [77].The role of vascular endothelial growth factor (VEGF) inscarless fetal repair is not entirely clear. Some studies havefound that VEGF expression is reduced in scarless fetalwounds compared to fibrotic fetal wounds, and that additionof exogenous VEGF to scarlessly healing wounds can inducefibrosis, suggesting that VEGF has additional importance towound healing beyond simply promoting angiogenesis [78].However, Colwell et al. [79] found that VEGF mRNA levelswere higher in E16 scarless excisional rat wounds comparedto fibrotic wounds at E18.
Interleukins have also been implicated in scarless woundhealing. It has been shown that the proinflammatory medi-ators IL-6 and IL-8 are produced in low levels in bothfetal skin and in fetal-derived fibroblasts when comparedto adult skin or adult-derived fibroblasts [80]. Furthermore,fetal skin deficient in IL-10, widely considered to be ananti-inflammatory agent, heals with a scar compared tofetal skin with normal levels of IL-10, which heals scarlessly[81]. Conversely, overexpression of IL-10 in adult woundsdecreases the inflammatory response and creates an envi-ronment conducive for regenerative wound healing in adultorganisms [82, 83].
6 Dermatology Research and Practice
Table 2: Observed differences between fetal and adult fibroblasts.
Fetal Fibroblast Adult Fibroblast
alpha-SMA(serum containing cultures)
Low High
In-vitro collagencontraction
Less More
Hyaluronic acid(HA)
Increased HAsynthesisirrespective of celldensity
Decreased HAsynthesisas cell densityincreases
Hyaluronic acidreceptor
High Low
Proinflammatorycytokines
IL-6 Low High
IL-8 Low High
CCT-subunits
CCT-eta Low High
CCT-beta No change No change
As noted above, many growth factors and cytokinesappear to vary in their expression in fetal and adult wounds.While each may be important, their overall significancemay be obscured by the complexity of the cytokine mileu,including other unknown or unexamined factors acting infetal and adult wound healing.
6. Fibroblasts and Myofibroblasts in FetalWound Healing
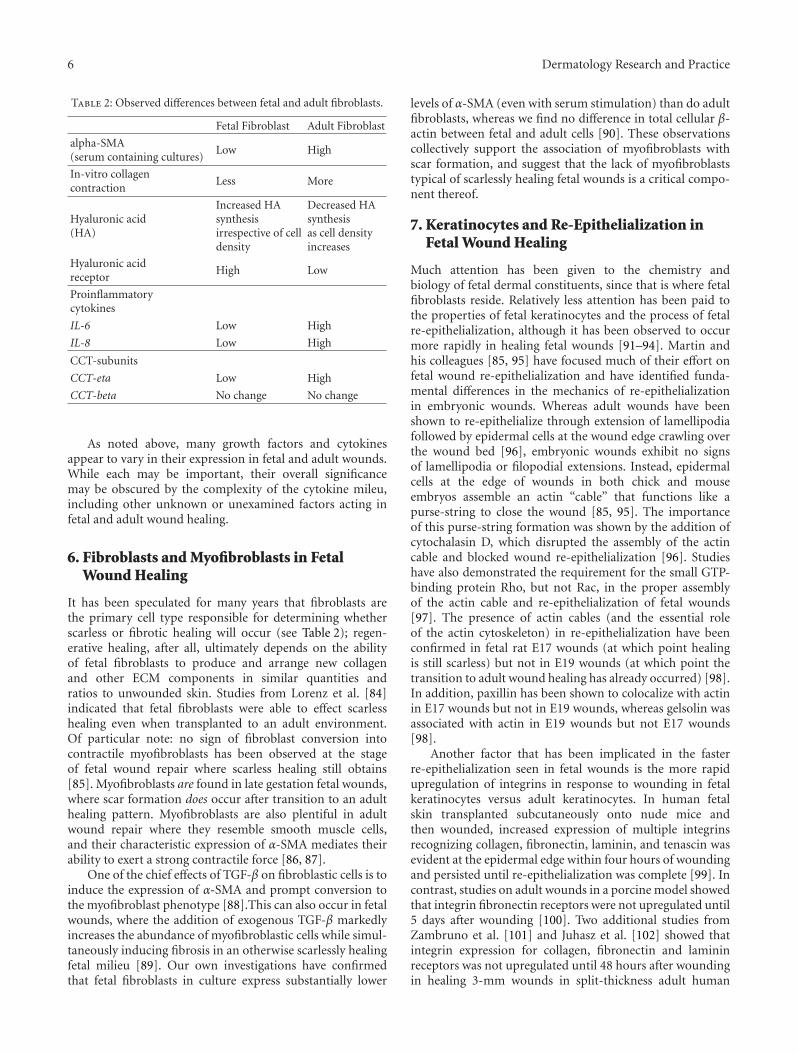
It has been speculated for many years that fibroblasts arethe primary cell type responsible for determining whetherscarless or fibrotic healing will occur (see Table 2); regen-erative healing, after all, ultimately depends on the abilityof fetal fibroblasts to produce and arrange new collagenand other ECM components in similar quantities andratios to unwounded skin. Studies from Lorenz et al. [84]indicated that fetal fibroblasts were able to effect scarlesshealing even when transplanted to an adult environment.Of particular note: no sign of fibroblast conversion intocontractile myofibroblasts has been observed at the stageof fetal wound repair where scarless healing still obtains[85]. Myofibroblasts are found in late gestation fetal wounds,where scar formation does occur after transition to an adulthealing pattern. Myofibroblasts are also plentiful in adultwound repair where they resemble smooth muscle cells,and their characteristic expression of α-SMA mediates theirability to exert a strong contractile force [86, 87].
One of the chief effects of TGF-β on fibroblastic cells is toinduce the expression of α-SMA and prompt conversion tothe myofibroblast phenotype [88].This can also occur in fetalwounds, where the addition of exogenous TGF-β markedlyincreases the abundance of myofibroblastic cells while simul-taneously inducing fibrosis in an otherwise scarlessly healingfetal milieu [89]. Our own investigations have confirmedthat fetal fibroblasts in culture express substantially lower
levels of α-SMA (even with serum stimulation) than do adultfibroblasts, whereas we find no difference in total cellular β-actin between fetal and adult cells [90]. These observationscollectively support the association of myofibroblasts withscar formation, and suggest that the lack of myofibroblaststypical of scarlessly healing fetal wounds is a critical compo-nent thereof.
7. Keratinocytes and Re-Epithelialization inFetal Wound Healing
Much attention has been given to the chemistry andbiology of fetal dermal constituents, since that is where fetalfibroblasts reside. Relatively less attention has been paid tothe properties of fetal keratinocytes and the process of fetalre-epithelialization, although it has been observed to occurmore rapidly in healing fetal wounds [91–94]. Martin andhis colleagues [85, 95] have focused much of their effort onfetal wound re-epithelialization and have identified funda-mental differences in the mechanics of re-epithelializationin embryonic wounds. Whereas adult wounds have beenshown to re-epithelialize through extension of lamellipodiafollowed by epidermal cells at the wound edge crawling overthe wound bed [96], embryonic wounds exhibit no signsof lamellipodia or filopodial extensions. Instead, epidermalcells at the edge of wounds in both chick and mouseembryos assemble an actin “cable” that functions like apurse-string to close the wound [85, 95]. The importanceof this purse-string formation was shown by the addition ofcytochalasin D, which disrupted the assembly of the actincable and blocked wound re-epithelialization [96]. Studieshave also demonstrated the requirement for the small GTP-binding protein Rho, but not Rac, in the proper assemblyof the actin cable and re-epithelialization of fetal wounds[97]. The presence of actin cables (and the essential roleof the actin cytoskeleton) in re-epithelialization have beenconfirmed in fetal rat E17 wounds (at which point healingis still scarless) but not in E19 wounds (at which point thetransition to adult wound healing has already occurred) [98].In addition, paxillin has been shown to colocalize with actinin E17 wounds but not in E19 wounds, whereas gelsolin wasassociated with actin in E19 wounds but not E17 wounds[98].
Another factor that has been implicated in the fasterre-epithelialization seen in fetal wounds is the more rapidupregulation of integrins in response to wounding in fetalkeratinocytes versus adult keratinocytes. In human fetalskin transplanted subcutaneously onto nude mice andthen wounded, increased expression of multiple integrinsrecognizing collagen, fibronectin, laminin, and tenascin wasevident at the epidermal edge within four hours of woundingand persisted until re-epithelialization was complete [99]. Incontrast, studies on adult wounds in a porcine model showedthat integrin fibronectin receptors were not upregulated until5 days after wounding [100]. Two additional studies fromZambruno et al. [101] and Juhasz et al. [102] showed thatintegrin expression for collagen, fibronectin and lamininreceptors was not upregulated until 48 hours after woundingin healing 3-mm wounds in split-thickness adult human

Dermatology Research and Practice 7
skin grafts transplanted onto nude mice. Thus, it appearsthat similar integrins are stimulated in both fetal and adultwounds but the timing at which they appear varies greatly.Reports have also identified differences in the expressionpatterns of the transcription factor c-fos and AP-1 inepidermis during fetal wound healing [103]. These multipleobservations collectively show that the process of woundre-epithelialization and the physiology of fetal keratinocytesdiffer substantially from adult wound healing biology.
8. Expressomic Evaluation of Scarlessversus Scarring Wounds
In the above sections we have reviewed many of the geneproducts found to display differential expression in fetal andadult wound healing, focusing mostly on growth factors andECM constituents. However, multiple other genes have beenimplicated in fetal skin development and scarless woundhealing. Colwell et al. [104] determined that mRNA levels oflysyl oxidase, an enzyme that cross-links collagen and elastin,were significantly greater in E19 late-gestation wounds (thatheal with a scar) in comparison to E17 early-gestationscarless wounds in mouse. The homeobox genes Msx-1,Msx-2, and Mox-1 display altered expression with increasinggestational age, with Mox-1 becoming undetectable in adultskin tissues [105].
Recognizing that there remained thousands of geneproducts that had not been directly assayed in healing fetalwounds, investigators have begun applying more compre-hensive transcriptomic techniques to the study of scarlesswound healing. Several laboratories have used microarrayas a tool to identify expressomic differences during scarlessrepair. Chen et al. [106] used a 5,705 oligonucleotide array toexamine early gestational (scarless) rat skin versus late gesta-tional (scarring) skin. They found 53 differentially expressedgenes, and directly confirmed by RT-PCR and Western blotthat FGF8 and follistatin had stronger expression in early ges-tational skin compared to late, whereas lymphoid enhancerbinding factor-1 and beta-catenin showed weaker expression.Colwell et al. [107] showed that the scarlessly healing fetalskin wound transcriptome has rapid upregulation of manygenes from 1 to 24 hrs, but that by 24 hrs many fetal wound-elevated gene expression levels had already begun to reverseto baseline. They suggest that numerous gene products areinvolved in coordinating the regenerative pattern of healingfound in early fetal wounds. Recent studies by Antony et al.[108] show rapid upregulation of neurodevelopmental genesduring scarless repair on after injury days 1–3. The authorsspeculate that these factors may promote the survival andregeneration of peripheral neurons, which may promote ascarless pattern of repair in response to injury.
Our own laboratory has used multiple expressomictechniques to examine the transcriptome of scarlessly healingfetal wounds, including differential display [109], PCR sup-pression subtraction hybridization (PCR-SSH) [110], andfetal wound-specific microarrays. Each of these techniquesallows an interrogation of the fetal wound expressomewithout any preconceptions as to which gene products maybe important. Using PCR-SSH we have identified multiple
candidate genes and expressed sequence tags (ESTs) to bedifferentially expressed in healing fetal wounds, and alsofragments of genes with no clear match in the GenBankdatabase, suggesting that the relevant gene set to scar-less fetal wound healing may be larger than anticipated[110]. Using rabbit fetal wound-specific microarrays thatwe ourselves constructed from a cDNA library, we foundthat some 20% of the recovered cDNA sequence fragmentsdemonstrated either no homology to GenBank sequences orhad such limited homology that we could not confidentlyidentify a known cognate gene (Kathju et al., manuscript inpreparation). While some of these putative unknown geneproducts may well turn out to be species-specific variationsof actual known genes, we have also obtained full lengthclones of several previously uncharacterized sequences, againsuggesting that the determinative fetal wound gene setincludes novel factors.
Assay of the scarless wound transcriptome by differentialdisplay in our lab identified the eta subunit of the chaperonincontaining T-complex polypeptide (CCT-eta) as a geneproduct specifically downregulated in fetal wound healing.We have subsequently shown that this pattern of expressionis not shared by any other CCT subunit (of which there areeight), and that CCT-eta is less abundant in fetal fibroblaststhan in adult cells [90, 111] We have also demonstratedthat CCT-eta is a specific regulator of fibroblast motility andcontractility, with siRNA-mediated reduction of CCT-etainhibiting the ability of adult fibroblasts to respond to migra-tory and contractile stimuli, rendering them more “fetal-like” in their behavior, possibly by secondary inhibition of α-SMA protein expression. This observation suggests that geneproducts that control fibroblast motility and contractilitymay be especially relevant to distinguishing scarless fromfibrotic wound healing [90].
9. Future Perspectives
Through the past 50 years, studies have been directedtowards explicating the remarkable ability of mammalianfetuses to heal cutaneous wounds by regeneration, but weare still far from a complete understanding of the criticalmolecular determinants of this phenomenon. Althoughmuch has been learned, there remain numerous unexploredquestions about the relative biology of fetal wounds versustheir scirrhous adult counterparts. The role of nitric oxide,increasingly thought to be important to adult wound healing,is still largely a mystery in fetal wounds. The role ofmicroRNAs, now also emerging as important players inadult wound healing [112] similarly remains unexplored.Ultimately, a fuller appreciation of the most importantfactors governing the scarless pattern of fetal wound repairwill hopefully allow for intervention in the adult woundhealing milieu to mitigate scar formation and improve theclinical outcome of those afflicted with the morbidity of scar.
Acknowledgments
Work in our laboratory has been supported by Grantsfrom the Pittsburgh Tissue Engineering Initiative (SK),

8 Dermatology Research and Practice
3M Wound Healing Fellowship (LS), NIH DE014780 (SK),AFIRM (SK) and support from Allegheny-Singer ResearchInstitute and Allegheny General Hospital.
References
[1] R. A. F. Clark, “Wound repair: overview and general con-siderations,” in The Molecular and Cellular Biology of WoundRepair, R. A. F. Clark, Ed., pp. 3–50, Plenum Press, New York,NY, USA, 2nd edition, 1996.
[2] G. M. Maragakis and M. Garcia-Tempone, “Microstomiafollowing facial burns,” Journal of Clinical Pediatric Dentistry,vol. 23, no. 1, pp. 69–74, 1998.
[3] G. S. La Trenta, R. T. Grant, R. D. Haworth, M. Madden,and L. A. Hoffman, “Functional reconstruction for severepostburn microstomia,” Annals of Plastic Surgery, vol. 29, no.2, pp. 178–181, 1992.
[4] M. Staley, R. Richard, D. Billmire, and G. Warden,“Head/face/neck burns: therapist considerations for thepediatric patient,” Journal of Burn Care and Rehabilitation,vol. 18, no. 2, pp. 164–171, 1997.
[5] N. B. Fricke, M. L. Omnell, K. D. Dutcher, L. G. Hollender,and L. H. Engrav, “Skeletal and dental disturbances afterfacial burns and pressure garments,” Journal of Burn Care andRehabilitation, vol. 17, no. 4, pp. 338–345, 1996.
[6] I. Tower, L. A. Lasko, and S. Kathju, “Secondary surgery forcicatricial complications of facial injury,” Journal of Oral andMaxillofacial Surgery, vol. 68, no. 4, pp. 751–755, 2010.
[7] A. S. Colwell, M. T. Longaker, and H. P. Lorenz, “Mammalianfetal organ regeneration,” Advances in Biochemical Engineer-ing/Biotechnology, vol. 93, pp. 83–100, 2005.
[8] T. A. Wilgus, “Continuing education information: regenera-tive healing in fetal skin: a review of the literature,” OstomyWound Management, vol. 53, no. 6, pp. 16–31, 2007.
[9] B. M. Hantash, L. Zhao, J. A. Knowles, and H. P. Lorenz,“Adult and fetal wound healing,” Frontiers in Bioscience, vol.13, no. 1, pp. 51–61, 2008.
[10] A. Hess, “Reactions of mammalian fetal tissues to injury. II.Skin,” The Anatomical Record, vol. 119, no. 1, pp. 435–447,1954.
[11] U. Rowlatt, “Intrauterine wound healing in a 20 week humanfetus,” Virchows Archiv Abteilung A Pathologische Anatomie,vol. 381, no. 3, pp. 353–361, 1979.
[12] J. R. Armstrong and M. W. J. Ferguson, “Ontogeny of theskin and the transition from scar-free to scarring phenotypeduring wound healing in the pouch young of a marsupial,Monodelphis domestica,” Developmental Biology, vol. 169,no. 1, pp. 242–260, 1995.
[13] S. Ihara, Y. Motobayashi, E. Nagao, and A. Kistler, “Onto-genetic transition of wound healing pattern in rat skinoccurring at the fetal stage,” Development, vol. 110, no. 3, pp.671–680, 1990.
[14] M. T. Longaker, D. J. Whitby, N. S. Adzick et al., “Studies infetal wound healing, VI. Second and early third trimester fetalwounds demonstrate rapid collagen deposition without scarformation,” Journal of Pediatric Surgery, vol. 25, no. 1, pp. 63–69, 1990.
[15] H. P. Lorenz and N. S. Adzick, “Scarless skin wound repairin the fetus,” Western Journal of Medicine, vol. 159, no. 3, pp.350–355, 1993.
[16] M. T. Longaker, D. J. Whitby, M. W. J. Ferguson, H. P. Lorenz,M. R. Harrison, and N. S. Adzick, “Adult skin wounds inthe fetal environment heal with scar formation,” Annals ofSurgery, vol. 219, no. 1, pp. 65–72, 1994.
[17] M. T. Longaker, D. J. Whitby, M. W. J. Ferguson, H. P. Lorenz,M. R. Harrison, and N. S. Adzick, “Adult skin wounds inthe fetal environment heal with scar formation,” Annals ofSurgery, vol. 219, no. 1, pp. 65–72, 1994.
[18] B. A. Mast, “The skin,” in Wound Healing: Biochemical andClinical Aspects, K. Cohen, R. F. Diegelmann, and W. J.Lindblad, Eds., pp. 344–355, WB Saunders, Philadelphia, Pa,USA, 1992.
[19] V. Moulin, F. Lawny, D. Barritault, and J. P. Caruelle, “Plateletreleasate treatment improves skin healing in diabetic ratsthrough endogenous growth factor secretion,” Cellular andMolecular Biology, vol. 44, no. 6, pp. 961–971, 1998.
[20] R. Ross, E. W. Raines, and D. F. Bowen-Pope, “The biology ofplatelet-derived growth factor,” Cell, vol. 46, no. 2, pp. 155–169, 1986.
[21] M. B. Sporn and A. B. Roberts, “Transforming growth factor-β: recent progress and new challenges,” Journal of Cell Biology,vol. 119, no. 5, pp. 1017–1022, 1992.
[22] H. Muller-Eberhard, “Complement: chemistry and path-ways,” in Inflammation Basic Principles and Clinical Corre-lates, Raven Press, New York, NY, USA, 1992.
[23] R. F. Diegelmann, I. K. Cohen, and A. M. Kaplan, “Therole of macrophages in wound repair: a review,” Plastic andReconstructive Surgery, vol. 68, no. 1, pp. 107–113, 1981.
[24] R. J. Shaw, D. E. Doherty, A. G. Ritter, S. H. Benedict, andR. A. F. Clark, “Adherence-dependent increase in humanmonocyte PDGF(B) mRNA is associated with increases in c-fos, c-jun, and EGR2 mRNA,” Journal of Cell Biology, vol. 111,no. 5, pp. 2139–2148, 1990.
[25] R. L. Juliano and S. Haskill, “Signal transduction from theextracellular matrix,” Journal of Cell Biology, vol. 120, no. 3,pp. 577–585, 1993.
[26] M. C. Robson, R. A. Barnett, I. O. W. Leitch, and P. G.Hayward, “Prevention and treatment of postburn scars andcontracture,” World Journal of Surgery, vol. 16, no. 1, pp. 87–96, 1992.
[27] E. Trabucchi, E. Radaelli, M. Marazzi et al., “The role ofmast cells in wound healing,” International Journal of TissueReactions, vol. 10, no. 6, pp. 367–372, 1988.
[28] C. Noli and A. Miolo, “The mast cell in wound healing,”Veterinary Dermatology, vol. 12, no. 6, pp. 303–313, 2001.
[29] E. I. Egozi, A. M. Ferreira, A. L. Burns, R. L. Gamelli, and L.A. DiPietro, “Mast cells modulate the inflammatory but notthe proliferative response in healing wounds,” Wound Repairand Regeneration, vol. 11, no. 1, pp. 46–54, 2003.
[30] K. Weller, K. Foitzik, R. Paus, W. Syska, and M. Maurer, “Mastcells are required for normal healing of skin wounds in mice,”FASEB Journal, vol. 20, no. 13, pp. E1628–E1635, 2006.
[31] F. Grinnell, “Fibronectin and wound healing,” Journal ofCellular Biochemistry, vol. 26, no. 2, pp. 107–116, 1984.
[32] R. Chiquet-Ehrismann, P. Kalla, C. A. Pearson, K. Beck, andM. Chiquet, “Tenascin interferes with fibronectin action,”Cell, vol. 53, no. 3, pp. 383–390, 1988.
[33] A. M. Szpaderska, E. I. Egozi, R. L. Gamelli, and L. A.DiPietro, “The effect of thrombocytopenia on dermal woundhealing,” Journal of Investigative Dermatology, vol. 120, no. 6,pp. 1130–1137, 2003.
[34] J. V. Dovi, L. K. He, and L. A. DiPietro, “Accelerated woundclosure in neutrophil-depleted mice,” Journal of LeukocyteBiology, vol. 73, no. 4, pp. 448–455, 2003.
[35] P. Martin, D. D’Souza, J. Martin et al., “Wound healing inthe PU.1 null mouse—tissue repair is not dependent oninflammatory cells,” Current Biology, vol. 13, no. 13, pp.1122–1128, 2003.
Dermatology Research and Practice 9
[36] J. Xu and R. A. F. Clark, “Extracellular matrix alters PDGFregulation of fibroblast integrins,” Journal of Cell Biology, vol.132, no. 1-2, pp. 239–249, 1996.
[37] T. K. Hunt, Wound Healing and Wound Infection: Theory andSurgical Practice, Appleton-Century-Crofts, New York, NY,USA, 1980.
[38] A. B. Roberts and M. B. Sporn, “Transforming growth factor-β,” in The Molecular Basis of Wound Repair, RAF Clark, NewYork, NY, USA, 1996.
[39] M. W. Ferguson, J. Duncan, J. Bond et al., “Prophylac-tic administration of avotermin for improvement of skinscarring: three double-blind, placebo-controlled, phase I/IIstudies,” The Lancet, vol. 373, no. 9671, pp. 1264–1274, 2009.
[40] A. Desmouliere and G. Gabbiani, “The role of the myofibrob-last in wound healing and fibrocontractive diseases,” in TheMolecular Basis of Wound Repair, Clark RAF, New York, NY,USA, 1996.
[41] R. Montesano and L. Orci, “Transforming growth factorbeta stimulates collagen-matrix contraction by fibroblasts:implications for wound healing,” Proceedings of the NationalAcademy of Sciences of the United States of America, vol. 85,no. 13, pp. 4894–4897, 1988.
[42] B. Hinz, “Formation and function of the myofibroblastduring tissue repair,” Journal of Investigative Dermatology,vol. 127, no. 3, pp. 526–537, 2007.
[43] P. Wong and P. A. Coulombe, “Loss of keratin 6 (K6) proteinsreveals a function for intermediate filaments during woundrepair,” Journal of Cell Biology, vol. 163, no. 2, pp. 327–337,2003.
[44] L. B. Nanney and L. King Jr., “Epidermal growth factor andtransforming growth factor-α,” in The Molecular and CellularBasis of Wound Repair, R. A. F. Clark, Ed., Plenum Press, NewYork, NY, USA, 1996.
[45] S. Werner, H. Smola, X. Liao et al., “The function of KGFin morphogenesis of epithelium and reepithelialization ofwounds,” Science, vol. 266, no. 5186, pp. 819–822, 1994.
[46] B. K. Draper, T. Komurasaki, M. K. Davidson, and L. B.Nanney, “Epiregulin is more potent than EGF or TGFαin promoting in vitro wound closure due to enhancedERK/MAPK activation,” Journal of Cellular Biochemistry, vol.89, no. 6, pp. 1126–1137, 2003.
[47] B. A. Mast, “The skin,” in Wound Healing: Biochemical andChemical Aspects, K. Cohen, R. F. Diegelmann, and W. J.Lindblad, Eds., pp. 344–355, WB Saunders, Philadelphia, Pa,USA, 1992.
[48] W. C. Parks, “Matrix metalloproteinases in repair,” WoundRepair and Regeneration, vol. 7, no. 6, pp. 423–432, 1999.
[49] A. Desmouliere, M. Redard, I. Darby, and G. Gabbiani,“Apoptosis mediates the decrease in cellularity during thetransition between granulation tissue and scar,” AmericanJournal of Pathology, vol. 146, no. 1, pp. 56–66, 1995.
[50] E. E. Peacock, J. W. Madden, and W. C. Trier, “Biologic basisfor the treatment of keloids and hypertrophic scars,” SouthernMedical Journal, vol. 63, no. 7, pp. 755–760, 1970.
[51] B. D. Haverstock, “Hypertrophic scars and keloids,” Clinicsin Podiatric Medicine and Surgery, vol. 18, no. 1, pp. 147–159,2001.
[52] W. M. van der Veer, M. C. T. Bloemen, M. M. W. Ulrich et al.,“Potential cellular and molecular causes of hypertrophic scarformation,” Burns, vol. 35, no. 1, pp. 15–29, 2009.
[53] B. Shih and A. Bayat, “Genetics of keloid scarring,” Archivesof Dermatological Research, vol. 302, no. 5, pp. 319–339, 2010.
[54] J. Wu, B. Ma, S. Yi et al., “Gene expression of early hyper-trophic scar tissue screened by means of cDNA microarrays,”Journal of Trauma, vol. 57, no. 6, pp. 1276–1286, 2004.
[55] M. Naitoh, H. Kubota, M. Ikeda et al., “Gene expression inhuman keloids is altered from dermal to chondrocytic andosteogenic lineage,” Genes to Cells, vol. 10, no. 11, pp. 1081–1091, 2005.
[56] L. Satish, J. Lyons-Weiler, P. A. Hebda, and A. Wells, “Geneexpression patterns in isolated keloid fibroblasts,” WoundRepair and Regeneration, vol. 14, no. 4, pp. 463–470, 2006.
[57] A. T. Lane, “Human fetal skin development,” PediatricDermatology, vol. 3, no. 6, pp. 487–491, 1986.
[58] N. A. Coolen, K. C. W. M. Schouten, E. Middelkoop, and M.M. W. Ulrich, “Comparison between human fetal and adultskin,” Archives of Dermatological Research, vol. 302, no. 1, pp.47–55, 2010.
[59] C. M. Dang, S. R. Beanes, H. Lee, X. Zhang, C. Soo, and K.Ting, “Scarless fetal wounds are associated with an increasedmatrix metalloproteinase-to-tissue-derived inhibitor of met-alloproteinase ratio,” Plastic and Reconstructive Surgery, vol.111, no. 7, pp. 2273–2285, 2003.
[60] S. R. Beanes, C. Dang, C. Soo et al., “Down-regulationof decorin, a transforming growth factor-beta modulator,is associated with scarless fetal wound healing,” Journal ofPediatric Surgery, vol. 36, no. 11, pp. 1666–1671, 2001.
[61] C. Soo, F.-Y. Hu, X. Zhang et al., “Differential expression offibromodulin, a transforming growth factor-β modulator, infetal skin development and scarless repair,” American Journalof Pathology, vol. 157, no. 2, pp. 423–433, 2000.
[62] T. M. Krummel, J. M. Nelson, and R. F. Diegelmann, “Fetalresponse to injury in the rabbit,” Journal of Pediatric Surgery,vol. 22, no. 7, pp. 640–644, 1987.
[63] A. J. Cowin, M. P. Brosnan, T. M. Holmes, and M. W.J.Ferguson, “Endogenous inflammatory response to dermalwound healing in the fetal and adult mouse,” DevelopmentalDynamics, vol. 212, no. 3, pp. 385–393, 1998.
[64] E. J. Stelnicki, K. M. Bullard, M. R. Harrison, D. L. Cass, andN. Scott Adzick, “A new in vivo model for the study of fetalwound healing,” Annals of Plastic Surgery, vol. 39, no. 4, pp.374–380, 1997.
[65] T. A. Wilgus, V. K. Bergdall, K. L. Tober et al., “The impactof cyclooxygenase-2 mediated inflammation on scarless fetalwound healing,” American Journal of Pathology, vol. 165, no.3, pp. 753–761, 2004.
[66] O. O. Olutoye, D. R. Yager, I. K. Cohen, and R. F. Diegelmann,“Lower cytokine release by fetal porcine platelets: a possibleexplanation for reduced inflammation after fetal wounding,”Journal of Pediatric Surgery, vol. 31, no. 1, pp. 91–95, 1996.
[67] J. Hopkinson-Woolley, D. Hughes, S. Gordon, and P. Martin,“Macrophage recruitment during limb development andwound healing in the embryonic and foetal mouse,” Journalof Cell Science, vol. 107, no. 5, pp. 1159–1167, 1994.
[68] R. W. Jennings, N. S. Adzick, M. T. Longaker, B. W.Duncan, H. Scheuenstuhl, and T. K. Hunt, “Ontogeny of fetalsheep polymorphonuclear leukocyte phagocytosis,” Journalof Pediatric Surgery, vol. 26, no. 7, pp. 853–855, 1991.
[69] A. B. Roberts, M. B. Sporn, R. K. Assoian et al., “Trans-forming growth factor type β: rapid induction of fibrosis andangiogenesis in vivo and stimulation of collagen formation invitro,” Proceedings of the National Academy of Sciences of theUnited States of America, vol. 83, no. 12, pp. 4167–4171, 1986.
[70] T. M. Krummel, B. A. Michna, B. L. Thomas et al.,“Transforming growth factor beta (TGF-β) induces fibrosis
10 Dermatology Research and Practice
in a fetal wound model,” Journal of Pediatric Surgery, vol. 23,no. 7, pp. 647–652, 1988.
[71] K. M. Sullivan, H. P. Lorenz, M. Meuli et al., “A model ofscarless human fetal wound repair is deficient in transform-ing growth factor beta,” Journal of Pediatric Surgery, vol. 30,no. 2, pp. 198–203, 1995.
[72] R. Y. Lin, K. M. Sullivan, P. A. Argenta, M. Meuli, H. P.Lorenz, and N. S. Adzick, “Exogenous transforming growthfactor-beta amplifies its own expression and induces scarformation in a model of human fetal skin repair,” Annals ofSurgery, vol. 222, no. 2, pp. 146–154, 1995.
[73] A. J. Cowin, T. M. Holmes, P. Brosnan, and M. W. J. Ferguson,“Expression of TGF-β and its receptors in murine fetal andadult dermal wounds,” European Journal of Dermatology, vol.11, no. 5, pp. 424–431, 2001.
[74] R. K. Nath, M. LaRegina, H. Markham, G. A. Ksander, andP. M. Weeks, “The expression of transforming growth factortype beta in fetal and adult rabbit skin wounds,” Journal ofPediatric Surgery, vol. 29, no. 3, pp. 416–421, 1994.
[75] M. Shah, D. M. Foreman, and M. W. J. Ferguson, “Neutral-isation of TGF-β and TGF-β or exogenous addition of TGF-β to cutaneous rat wounds reduces scarring,” Journal of CellScience, vol. 108, no. 3, pp. 985–1002, 1995.
[76] J. H. Haynes, D. E. Johnson, B. A. Mast et al., “Platelet-derived growth factor induces fetal wound fibrosis,” Journalof Pediatric Surgery, vol. 29, no. 11, pp. 1405–1408, 1994.
[77] C. M. Dang, S. R. Beanes, C. Soo et al., “Decreased expressionof fibroblast and keratinocyte growth factor isoforms andreceptors during scarless repair,” Plastic and ReconstructiveSurgery, vol. 111, no. 6, pp. 1969–1979, 2003.
[78] T. A. Wilgus, A. M. Ferreira, T. M. Oberyszyn, V. K. Bergdall,and L. A. DiPietro, “Regulation of scar formation by vascularendothelial growth factor,” Laboratory Investigation, vol. 88,no. 6, pp. 579–590, 2008.
[79] A. S. Colwell, S. R. Beanes, C. Soo et al., “Increased angio-genesis and expression of vascular endothelial growth factorduring scarless repair,” Plastic and Reconstructive Surgery, vol.115, no. 1, pp. 204–212, 2005.
[80] K. W. Liechty, N. S. Adzick, and T. M. Crombleholme,“Diminished interleukin 6 (IL-6) production during scarlesshuman fetal wound repair,” Cytokine, vol. 12, no. 6, pp. 671–676, 2000.
[81] K. W. Liechty, H. B. Kim, N. S. Adzick, and T. M.Crombleholme, “Fetal wound repair results in scar formationin interleukin-10-deficient mice in a syngeneic murine modelof scarless fetal wound repair,” Journal of Pediatric Surgery,vol. 35, no. 6, pp. 866–873, 2000.
[82] W. H. Peranteau, L. Zhang, N. Muvarak et al., “IL-10 over-expression decreases inflammatory mediators and promotesregenerative healing in an adult model of scar formation,”Journal of Investigative Dermatology, vol. 128, no. 7, pp. 1852–1860, 2008.
[83] A. Gordon, E. D. Kozin, S. G. Keswani et al., “Permissiveenvironment in postnatal wounds induced by adenoviral-mediated overexpression of the anti-inflammatory cytokineinterleukin-10 prevents scar formation,” Wound Repair andRegeneration, vol. 16, no. 1, pp. 70–79, 2008.
[84] H. P. Lorenz, R. Y. Lin, M. T. Longaker, D. J. Whitby, and N. S.Adzick, “The fetal fibroblast: the effector cell of scarless fetalskin repair,” Plastic and Reconstructive Surgery, vol. 96, no. 6,pp. 1251–1259, 1995.
[85] J. McCluskey and P. Martin, “Analysis of the tissue move-ments of embryonic wound healing—DiI studies in the limb
bud stage mouse embryo,” Developmental Biology, vol. 170,no. 1, pp. 102–114, 1995.
[86] O. Skalli and G. Gabbiani, “The biology of the myofibroblast.Relationship to wound contraction and fibrocontractivediseases,” in The Molecular and Cellular Biology of WoundRepair, R. A. F. Clark and P. M. Henson, Eds., Plenum, NewYork, NY, USA, 1988.
[87] J. Chen, H. Li, N. SundarRaj, and J. H. C. Wang, “Alpha-smooth muscle actin expression enhances cell traction force,”Cell Motility and the Cytoskeleton, vol. 64, no. 4, pp. 248–257,2007.
[88] A. Desmouliere, A. Geinoz, F. Gabbiani, and G. Gabbiani,“Transforming growth factor-β1 induces α-smooth muscleactin expression in granulation tissue myofibroblasts and inquiescent and growing cultured fibroblasts,” Journal of CellBiology, vol. 122, no. 1, pp. 103–111, 1993.
[89] D. A. Lanning, R. F. Diegelmann, D. R. Yager, M. L. Wallace,C. E. Bagwell, and J. H. Haynes, “Myofibroblast inductionwith transforming growth factor-β and -β in cutaneous fetalexcisional wounds,” Journal of Pediatric Surgery, vol. 35, no.2, pp. 183–188, 2000.
[90] L. Satish, S. Johnson, J. H.-C. Wang, J. C. Post, G. D.Ehrlich, and S. Kathju, “Chaperonin containing T-complexpolypeptide subunit eta (CCT-eta) is a specific regulator offibroblast motility and contractility,” PLoS One, vol. 5, no. 4,Article ID e10063, 2010.
[91] M. Stern, T. B. Dodson, M. T. Longaker et al., “Fetal cleftlip repair in lambs: histologic characteristics of the healingwound,” International Journal of Oral and MaxillofacialSurgery, vol. 22, no. 6, pp. 371–374, 1993.
[92] D. J. Whitby and M. W. J. Ferguson, “The extracellularmatrix of lip wounds in fetal, neonatal and adult mice,”Development, vol. 112, no. 2, pp. 651–668, 1991.
[93] D. J. Whitby, M. T. Longaker, M. R. Harrison, N. S. Adzick,and M. W. J. Ferguson, “Rapid epithelialisation of fetalwounds is associated with the early deposition of tenascin,”Journal of Cell Science, vol. 99, no. 3, pp. 583–586, 1991.
[94] J. McCluskey, J. Hopkinson-Woolley, B. Luke, and P. Martin,“A study of wound healing in the E11.5 mouse embryo bylight and electron microscopy,” Tissue and Cell, vol. 25, no. 2,pp. 173–181, 1993.
[95] P. Martin and J. Lewis, “Actin cables and epidermal move-ment in embryonic wound healing,” Nature, vol. 360, no.6400, pp. 179–183, 1992.
[96] R. C. Buck, “Cell migration in repair of mouse cornealepithelium,” Investigative Ophthalmology and Visual Science,vol. 18, no. 8, pp. 767–784, 1979.
[97] J. Brock, K. Midwinter, J. Lewis, and P. Martin, “Healingof incisional wounds in the embryonic chick wing bud:characterization of the actin purse-string and demonstrationof a requirement for Rho activation,” Journal of Cell Biology,vol. 135, no. 4, pp. 1097–1107, 1996.
[98] A. J. Cowin, N. Hatzirodos, J. T. Teusner, and D. A. Belford,“Differential effect of wounding on actin and its associatedproteins, paxillin and gelsolin, in fetal skin explants,” Journalof Investigative Dermatology, vol. 120, no. 6, pp. 1118–1129,2003.
[99] D. L. Cass, K. M. Bullard, K. G. Sylvester et al., “Epidermalintegrin expression is upregulated rapidly in human fetalwound repair,” Journal of Pediatric Surgery, vol. 33, no. 2, pp.312–316, 1998.
[100] R. A. F. Clark, “Fibronectin matrix deposition andfibronectin receptor expression in healing and normal skin,”

Dermatology Research and Practice 11
Journal of Investigative Dermatology, vol. 94, no. 6, pp. 128S–134S, 1990.
[101] G. Zambruno, A. Cavani, V. Manca et al., “Integrin expres-sion during wound healing in human skin transplanted ontonude mice,” Journal of Investigative Dermatology, vol. 96,article 1015, 1991.
[102] I. Juhasz, G. F. Murphy, H. C. Yan, M. Herlyn, and S. M.Albelda, “Regulation of extracellular matrix proteins andintegrin cell substratum adhesion receptors on epitheliumduring cutaneous human wound healing in vivo,” AmericanJournal of Pathology, vol. 143, no. 5, pp. 1458–1469, 1993.
[103] P. Martin and C. D. Nobes, “An early molecular componentof the wound healing response in rat embryos—inductionof c-fos protein in cell at the epidermal wound margin,”Mechanisms of Development, vol. 38, no. 3, pp. 209–216, 1992.
[104] A. S. Colwell, T. M. Krummel, M. T. Longaker, and H. P.Lorenz, “Early-gestation fetal scarless wounds have less lysyloxidase expression,” Plastic and Reconstructive Surgery, vol.118, no. 5, pp. 1125–1129, 2006.
[105] E. J. Stelnicki, L. G. Komuves, D. Holmes et al., “Thehuman homeobox genes MSX-1, MSX-2, and MOX-1 aredifferentially expressed in the dermis and epidermis in fetaland adult skin,” Differentiation, vol. 62, no. 1, pp. 33–41,1997.
[106] W. Chen, X. Fu, S. Ge et al., “Profiling of genes differentiallyexpressed in a rat of early and later gestational ages withhigh-density oligonucleotide DNA array,” Wound Repair andRegeneration, vol. 15, no. 1, pp. 147–155, 2007.
[107] A. S. Colwell, M. T. Longaker, and H. P. Lorenz, “Identifica-tion of differentially regulated genes in fetal wounds duringregenerative repair,” Wound Repair and Regeneration, vol. 16,no. 3, pp. 450–459, 2008.
[108] A. K. Antony, W. Kong, and H. P. Lorenz, “Upregulation ofneurodevelopmental genes during scarless healing,” Annals ofPlastic Surgery, vol. 64, no. 2, pp. 247–250, 2010.
[109] D. L. Darden, F. Z. Hu, M. D. Ehrlich et al., “RNAdifferential display of scarless wound healing in fetal rabbitindicates downregulation of a CCT chaperonin subunit andupregulation of a glycophorin-like gene transcript,” Journalof Pediatric Surgery, vol. 35, no. 3, pp. 406–419, 2000.
[110] S. Kathju, L. Satish, C. Rabik et al., “Identification ofdifferentially expressed genes in scarless wound healingutilizing polymerase chain reaction-suppression subtractivehybridization,” Wound Repair and Regeneration, vol. 14, no.4, pp. 413–420, 2006.
[111] L. Satish, A. Abdulally, D. Oswald et al., “Differentialexpression of chaperonin containing T-complex polypeptide(CCT) subunits during fetal and adult skin wound healing,”Cell Stress and Chaperones, vol. 13, no. 4, pp. 527–533, 2008.
[112] S. Shilo, S. Roy, S. Khanna, and C. K. Sen, “MicroRNA incutaneous wound healing: a new paradigm,” DNA and CellBiology, vol. 26, no. 4, pp. 227–237, 2007.

Hindawi Publishing CorporationDermatology Research and PracticeVolume 2010, Article ID 405262, 10 pagesdoi:10.1155/2010/405262
Review Article
Therapeutic Improvement of Scarring: Mechanisms ofScarless and Scar-Forming Healing and Approaches tothe Discovery of New Treatments
Nick L. Occleston, Anthony D. Metcalfe, Adam Boanas, Nicholas J. Burgoyne, Kerry Nield,Sharon O’Kane, and Mark W. J. Ferguson
Renovo Group plc, Core Technology Facility, 48 Grafton Street, Manchester M13 9XX, UK
Correspondence should be addressed to Anthony D. Metcalfe, [email protected]
Received 15 March 2010; Accepted 17 June 2010
Academic Editor: Hayes B. Gladstone
Copyright © 2010 Nick L. Occleston et al. This is an open access article distributed under the Creative Commons AttributionLicense, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properlycited.
Scarring in the skin after trauma, surgery, burn or sports injury is a major medical problem, often resulting in loss of function,restriction of tissue movement and adverse psychological effects. Whilst various studies have utilised a range of model systems thathave increased our understanding of the pathways and processes underlying scar formation, they have typically not translated tothe development of effective therapeutic approaches for scar management. Existing treatments are unreliable and unpredictableand there are no prescription drugs for the prevention or treatment of dermal scarring. As a consequence, scar improvement stillremains an area of clear medical need. Here we describe the basic science of scar-free and scar-forming healing, the utility of pre-clinical model systems, their translation to humans, and our pioneering approach to the discovery and development of therapeuticapproaches for the prophylactic improvement of scarring in man
1. Introduction
Anything greater than a superficial injury to the skin ofchildren and adults results in scar formation. Scarring is amajor cause of physical and psychological morbidity [1–8].Whilst various studies have utilised a range of model systemsthat have increased our understanding of the pathways andprocesses underlying scar formation, they have not been typ-ically translated to the development of effective therapeuticapproaches for scar management. This is evidenced by thefact that despite a number of potential treatment regimens,no single therapy is accepted universally as the standard ofcare [9–11]. As such, scar improvement still remains an areaof clear medical need. Herein, we describe the basic scienceunderlying scar-free and scar-forming healing, the utility andtranslation of preclinical model systems to humans, and ourpioneering approach to the discovery and development oftherapeutic approaches for the prophylactic improvement ofscarring in man.
2. Scar-Free and Scar-Forming Healing
Scarring and wound healing occur within a spectrumranging from the ability to completely regenerate tissuein amphibians, through scar-free healing in embryos ofdifferent mammalian species, to scar-forming healing inchildren and adults. From an evolutionary perspective, thescarring response results in rapid replacement of missingtissue and, although suboptimal in terms of appearance andfunction, results in a reduction in the likelihood of infectionand an increased likelihood of organism survival followinginjury. The ability of organisms to heal wounds withoutscar formation has nevertheless been demonstrated in theearly embryos of a range of mammalian species includingmice, rats, rabbits, sheep, pigs, marsupials, and monkeys[12]. Comparison of the architecture of regenerated skinin embryos with that of adults demonstrates that it is theorganisation of collagen that is largely responsible for scarformation. Whereas the dermis of embryonic skin is restored

2 Dermatology Research and Practice
to the normal “basket weave” architecture of collagen, inadult scars the collagen is abnormally organised in parallelbundles of fine fibres that are distinct from the normal skin(Figure 1). It is of particular note that there appear to beno major differences between the composition of the dermaltissue of scar-free and scar-forming healing. This indicatesthat scarring is primarily a failure of the regeneration of thenormal skin structure rather than a biochemical problemrelated to an abnormal composition of the scar tissue [13].
The mechanisms underlying scar-free and scar-forminghealing have been studied at the molecular, biochemical, andcellular level. Whilst there are a number of differences thathave been identified between healing in the embryo and theadult, many of these are not mechanistically causative. Inillustration, the mammalian embryo is surrounded by thesterile aqueous environment of the amniotic fluid, whereasadult wounds are exposed to air and a range of potentiallycontaminating agents including bacteria and foreign bodies.Originally, it was thought that the sterile aqueous environ-ment provided by the amniotic fluid was important in scar-free healing. However, studies on marsupials such as theopossum, which complete development in their mother’spouch, proved otherwise [14]. In this model, incisionalwounds were made in young pouch opossums and at anequivalent embryonic time to mouse embryos in an amnioticenvironment. Pouch opossums, like embryonic mammals,were found to heal without scarring despite developingoutside of a sterile amniotic environment. Following injuryto the embryo, the inflammatory response (by virtue of aless than mature immune system) is less marked and differsin terms of the types and number of inflammatory cellsthat enter the wound [15]. Finally, whilst the profiles andquantities of growth factors and cytokines associated withscar-free healing are often different to those in adult scar-forming healing [16–19], there are only a few of these factorsthat present themselves as potential therapeutic targets [12,13, 20].
Data from our studies and those in the literature demon-strate that the scarring response represents a continuousspectrum of phenotypes in organisms ranging from scar-free through to scar-forming healing (Figure 2). Both scar-free and scar-forming healing can occur in the same animal,for example, an axolotl can regenerate an amputated limbbut heals an incisional wound on the flank with a scar; ifpart of the liver is removed in mammals by hepatectomy,the liver regenerates, whilst stab wounds made to the liverheal with scarring; MRL and other strains of adult miceincluding athymic nude-nu mice regenerate ear wounds,where the absence of T-lymphocytes in wounded earsprovides a microenvironment conducive to regeneration ofmesenchymal tissues, which is in contrast to wounds madeon the dorsum of MRL mice that heal with a scar; penetratingwounds to the cheek of humans heal with scarring of theexternal cutaneous surface but the oral mucosal surface healswith no discernable scar [13, 21–26]. The likelihood is thattissue repair and regeneration are not that dissimilar and, infact, share many common mechanisms that differ very subtly.Furthermore, the fact that all mammalian embryos exhibit aregenerative capacity demonstrates that even adult mammals
contain the genetic program for regeneration. The aboveobservations are critically important as they demonstratethat organisms retain the ability to heal via a regenerative aswell as a scar-forming process, which gives a biological basisfor therapeutic modulation of the healing response in adultsto reduce scar formation.
3. In Vitro and In Vivo Models toInvestigate the Mechanisms of Scarring andEvaluate Potential Treatments
A number of in vitro and in vivo models have been usedto investigate the mechanisms underlying the healing andscarring response. The range of model systems, their uses andlimitations are summarised below.
The healing and scarring response consists of a robustseries of complex, dynamic and interacting cellular, andmolecular processes including haemostasis, the inflamma-tory response, granulation tissue formation, and remod-elling. The functions of the cell types involved in theseprocesses are also regulated by a wide range of extra-cellular stimuli including growth factors/cytokines as wellas interaction with the extracellular matrix [27], whichelicit effects by cell surface receptors and a range ofintracellular signalling cascades that result in changes ingene and protein expression. Taken together, these eventscontribute to complex dynamic microenvironments withinthe injured tissue during healing and scar maturation withwhich resident and infiltrating cells interact. A numberof in vitro models have been utilised to investigate thevarious aspects of the healing and scarring response at themolecular and cellular level and include different cell types(e.g., neutrophils, macrophages, lymphocytes, keratinocytes,melanocytes, fibroblasts, and endothelial cells) and differentmolecular and cellular processes (e.g., signal transduction,gene expression, proliferation, migration, growth factor pro-duction, extracellular matrix production, and remodelling)[28–32]. Whilst in vitro models represent applicable systemsto study individual components, these systems do not alwaysaccurately model the vastly more complex and interactivein vivo situation. Typically, we employ in vitro systems tofurther evaluate and refine findings generated from in vivomodels.
A number of species including mice, rats, and pigs havebeen used as potential models of scarring in preclinicalstudies (Table 1). These studies include the use of excisionaland incisional wounds in rodents and pigs, typically withmacroscopic and/or microscopic endpoints for scarring,as well as the use of transgenic mice and more recentlythe Red Duroc pig, which exhibits some of the featuresof hypertrophic scarring seen in humans [54–56]. Moststudies have not systematically compared the molecular,cellular, and tissue responses in these models to those inman. More importantly, most studies have not investigatedthe translation of therapeutic modulation in preclinicalmodels to that in man. Addressing these issues is key tonot only discovering and developing potential therapeuticsfor humans, but also investigating and understanding their
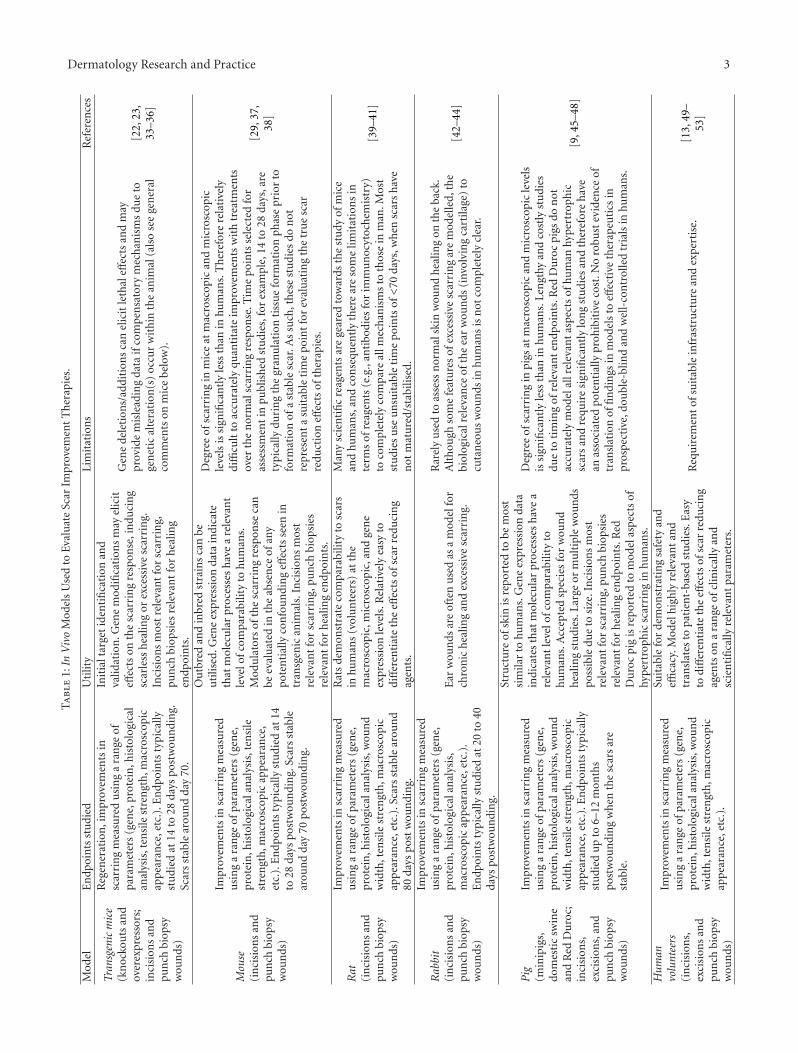
Dermatology Research and Practice 3T
abl
e1:
InV
ivo
Mod
els
Use
dto
Eval
uat
eSc
arIm
prov
emen
tT
her
apie
s.
Mod
elE
ndp
oin
tsst
udi
edU
tilit
yLi
mit
atio
ns
Ref
eren
ces
Tran
sgen
icm
ice
(kn
ocko
uts
and
over
expr
esso
rs;
inci
sion
san
dpu
nch
biop
syw
oun
ds)
Reg
ener
atio
n,i
mpr
ovem
ents
insc
arri
ng
mea
sure
du
sin
ga
ran
geof
para
met
ers
(gen
e,pr
otei
n,h
isto
logi
cal
anal
ysis
,ten
sile
stre
ngt
h,m
acro
scop
icap
pear
ance
,etc
.).E
ndp
oin
tsty
pica
llyst
udi
edat
14to
28da
yspo
stw
oun
din
g.Sc
ars
stab
lear
oun
dda
y70
.
Init
ialt
arge
tid
enti
fica
tion
and
valid
atio
n.G
ene
mod
ifica
tion
sm
ayel
icit
effec
tson
the
scar
rin
gre
spon
se,i
ndu
cin
gsc
arle
ssh
ealin
gor
exce
ssiv
esc
arri
ng.
Inci
sion
sm
ost
rele
van
tfo
rsc
arri
ng,
pun
chbi
opsi
esre
leva
nt
for
hea
ling
endp
oin
ts.
Gen
ede
leti
ons/
addi
tion
sca
nel
icit
leth
aleff
ects
and
may
prov
ide
mis
lead
ing
data
ifco
mpe
nsa
tory
mec
han
ism
sdu
eto
gen
etic
alte
rati
on(s
)oc
cur
wit
hin
the
anim
al(a
lso
see
gen
eral
com
men
tson
mic
ebe
low
).
[22,
23,
33–3
6]
Mou
se(i
nci
sion
san
dpu
nch
biop
syw
oun
ds)
Impr
ovem
ents
insc
arri
ng
mea
sure
du
sin
ga
ran
geof
para
met
ers
(gen
e,pr
otei
n,h
isto
logi
cala
nal
ysis
,ten
sile
stre
ngt
h,m
acro
scop
icap
pea
ran
ce,
etc.
).E
ndp
oin
tsty
pica
llyst
udi
edat
14to
28da
yspo
stw
oun
din
g.Sc
ars
stab
lear
oun
dda
y70
post
wou
ndi
ng.
Ou
tbre
dan
din
bred
stra
ins
can
beu
tilis
ed.G
ene
expr
essi
onda
tain
dica
teth
atm
olec
ula
rpr
oces
ses
hav
ea
rele
van
tle
velo
fcom
para
bilit
yto
hum
ans.
Mod
ula
tors
ofth
esc
arri
ng
resp
onse
can
beev
alu
ated
inth
eab
sen
ceof
any
pote
nti
ally
con
fou
ndi
ng
effec
tsse
enin
tran
sgen
ican
imal
s.In
cisi
ons
mos
tre
leva
nt
for
scar
rin
g,pu
nch
biop
sies
rele
van
tfo
rh
ealin
gen
dpoi
nts
.
Deg
ree
ofsc
arri
ng
inm
ice
atm
acro
scop
ican
dm
icro
scop
icle
vels
issi
gnifi
can
tly
less
than
inhu
man
s.T
her
efor
ere
lati
vely
diffi
cult
toac
cura
tely
quan
tita
teim
prov
emen
tsw
ith
trea
tmen
tsov
erth
en
orm
alsc
arri
ng
resp
onse
.Tim
ep
oin
tsse
lect
edfo
ras
sess
men
tin
publ
ish
edst
udi
es,f
orex
ampl
e,14
to28
days
,are
typi
cally
duri
ng
the
gran
ula
tion
tiss
ue
form
atio
nph
ase
prio
rto
form
atio
nof
ast
able
scar
.As
such
,th
ese
stu
dies
don
otre
pres
ent
asu
itab
leti
me
poin
tfo
rev
alu
atin
gth
etr
ue
scar
redu
ctio
neff
ects
ofth
erap
ies.
[29,
37,
38]
Rat
(in
cisi
ons
and
pun
chbi
opsy
wou
nds
)
Impr
ovem
ents
insc
arri
ng
mea
sure
du
sin
ga
ran
geof
para
met
ers
(gen
e,pr
otei
n,h
isto
logi
cala
nal
ysis
,wou
nd
wid
th,t
ensi
lest
ren
gth
,mac
rosc
opic
app
eara
nce
,etc
.).S
cars
stab
lear
oun
d80
days
post
wou
ndi
ng.
Rat
sde
mon
stra
teco
mpa
rabi
lity
tosc
ars
inhu
man
s(v
olu
nte
ers)
atth
em
acro
scop
ic,m
icro
scop
ic,a
nd
gen
eex
pres
sion
leve
ls.R
elat
ivel
yea
syto
diff
eren
tiat
eth
eeff
ects
ofsc
arre
duci
ng
agen
ts.
Man
ysc
ien
tifi
cre
agen
tsar
ege
ared
tow
ards
the
stu
dyof
mic
ean
dhu
man
s,an
dco
nse
quen
tly
ther
ear
eso
me
limit
atio
ns
inte
rms
ofre
agen
ts(e
.g.,
anti
bodi
esfo
rim
mu
noc
ytoc
hem
istr
y)to
com
plet
ely
com
pare
allm
ech
anis
ms
toth
ose
inm
an.M
ost
stu
dies
use
un
suit
able
tim
epo
ints
of<
70da
ys,w
hen
scar
sh
ave
not
mat
ure
d/st
abili
sed.
[39–
41]
Rab
bit
(in
cisi
ons
and
pun
chbi
opsy
wou
nds
)
Impr
ovem
ents
insc
arri
ng
mea
sure
du
sin
ga
ran
geof
para
met
ers
(gen
e,pr
otei
n,h
isto
logi
cala
nal
ysis
,m
acro
scop
icap
pea
ran
ce,e
tc.)
.E
ndp
oin
tsty
pica
llyst
udi
edat
20to
40da
yspo
stw
oun
din
g.
Ear
wou
nds
are
ofte
nu
sed
asa
mod
elfo
rch
ron
ich
ealin
gan
dex
cess
ive
scar
rin
g.
Rar
ely
use
dto
asse
ssn
orm
alsk
inw
oun
dh
ealin
gon
the
back
.A
lth
ough
som
efe
atu
res
ofex
cess
ive
scar
rin
gar
em
odel
led,
the
biol
ogic
alre
leva
nce
ofth
eea
rw
oun
ds(i
nvol
vin
gca
rtila
ge)
tocu
tan
eou
sw
oun
dsin
hum
ans
isn
otco
mpl
etel
ycl
ear.
[42–
44]
Pig
(min
ipig
s,do
mes
tic
swin
ean
dR
edD
uro
c;in
cisi
ons,
exci
sion
s,an
dpu
nch
biop
syw
oun
ds)
Impr
ovem
ents
insc
arri
ng
mea
sure
du
sin
ga
ran
geof
para
met
ers
(gen
e,pr
otei
n,h
isto
logi
cala
nal
ysis
,wou
nd
wid
th,t
ensi
lest
ren
gth
,mac
rosc
opic
appe
aran
ce,e
tc.)
.En
dpoi
nts
typi
cally
stu
died
up
to6–
12m
onth
spo
stw
oun
din
gw
hen
the
scar
sar
est
able
.
Stru
ctu
reof
skin
isre
port
edto
bem
ost
sim
ilar
tohu
man
s.G
ene
expr
essi
onda
tain
dica
tes
that
mol
ecu
lar
proc
esse
sh
ave
are
leva
nt
leve
lofc
ompa
rabi
lity
tohu
man
s.A
ccep
ted
spec
ies
for
wou
nd
hea
ling
stu
dies
.Lar
geor
mu
ltip
lew
oun
dspo
ssib
ledu
eto
size
.In
cisi
ons
mos
tre
leva
nt
for
scar
rin
g,pu
nch
biop
sies
rele
van
tfo
rh
ealin
gen
dpoi
nts
.Red
Du
roc
pig
isre
port
edto
mod
elas
pect
sof
hype
rtro
phic
scar
rin
gin
hum
ans.
Deg
ree
ofsc
arri
ng
inpi
gsat
mac
rosc
opic
and
mic
rosc
opic
leve
lsis
sign
ifica
ntl
yle
ssth
anin
hum
ans.
Len
gthy
and
cost
lyst
udi
esdu
eto
tim
ing
ofre
leva
nt
endp
oin
ts.R
edD
uro
cpi
gsdo
not
accu
rate
lym
odel
allr
elev
ant
aspe
cts
ofhu
man
hype
rtro
phic
scar
san
dre
quir
esi
gnifi
can
tly
lon
gst
udi
esan
dth
eref
ore
hav
ean
asso
ciat
edpo
ten
tial
lypr
ohib
itiv
eco
st.N
oro
bust
evid
ence
oftr
ansl
atio
nof
fin
din
gsin
mod
els
toeff
ecti
veth
erap
euti
csin
pros
pect
ive,
dou
ble-
blin
dan
dw
ell-
con
trol
led
tria
lsin
hum
ans.
[9,4
5–48
]
Hum
anvo
lunt
eers
(in
cisi
ons,
exci
sion
san
dpu
nch
biop
syw
oun
ds)
Impr
ovem
ents
insc
arri
ng
mea
sure
du
sin
ga
ran
geof
para
met
ers
(gen
e,pr
otei
n,h
isto
logi
cala
nal
ysis
,wou
nd
wid
th,t
ensi
lest
ren
gth
,mac
rosc
opic
app
eara
nce
,etc
.).
Suit
able
for
dem
onst
rati
ng
safe
tyan
deffi
cacy
.Mod
elh
igh
lyre
leva
nt
and
tran
slat
esto
pati
ent-
base
dst
udi
es.E
asy
todi
ffer
enti
ate
the
effec
tsof
scar
redu
cin
gag
ents
ona
ran
geof
clin
ical
lyan
dsc
ien
tifi
cally
rele
van
tpa
ram
eter
s.
Req
uir
emen
tof
suit
able
infr
astr
uct
ure
and
expe
rtis
e.[1
3,49
–53
]

4 Dermatology Research and Practice
Scar
Normal skin
(a)
ScarNormal skin
err
(b)
ScarNormal skin
err
(c)
Figure 1: Scarring results from an abnormal deposition and organisation of collagen cutaneous scar in a noncaucasian subject at 12 monthsfollowing a 1 cm full thickness incision to the inner aspect of the upper arm (a). Histological staining of the excised scar with Van Gieson’sstain demonstrating collagen (blue/green) and elastin (purple) staining in the normal skin compared to scar tissue and a normal undulatingepidermis with rete ridges in the normal skin compared to a flattened epidermis overlying the scar (b). Picrosirius red staining of the samescar viewed using polarised light (c), illustrating the normal “basket-weave” organisation of collagen in the normal skin resulting in organisedlight scattering (birefringence) compared to the abnormal organisation of collagen fibres within the scar resulting in a lack of birefringence.Arrowheads indicate the border of normal skin and scar tissue. Scale bars in (b) and (c) are 500 mm. In (b) and (c), rr = rete ridges; e =epithelium.
Species
Axolotl
Mouse(MRL and
other strains)
Mouse, rat, pig, sheep,
marsupial, andmonkey
Human
Mouse, rat pig, and human
Axolotl
Mouse Mouse (MRL strain)
Human (children andadults)
Exemplar model/body site
Limbs
Ear
Embryo
Liver, gums, oral mucosa, andsmall cutaneous wounds
(all adult)
Prophylactic cutaneous scar reduction therapeutics (in adult)
e.g., TGFβ3
Incision (on flank)
Embryo (TGFβ3 knockout)Incision (on dorsum)
Cutaneous wounds Hypertrophic scars
Keloids
Regenerative healing
Scar-free healing
Scar-forminghealing
Figure 2: Scar-free to Scar-forming healing in vertebrates represents a continuous spectrum of responses.
mechanisms of action. We have addressed these issues ina series of extensive longitudinal studies utilising a rangeof endpoints and technologies both in pre-clinical modelsand humans. Our studies in mice, rats, and pigs havedemonstrated that scars are stable and mature at ≥ 70days postwounding in mice/rats and ≥6 months in pigs
compared to 6 to 12 months in man. Comparison ofthe macroscopic appearance of these scars and the abilityto assess a scar reduction effect within these pre-clinicalmodels demonstrates that next to man, rats scar the worstand represent the most appropriate model (Figure 3). Wehave also compared the gene expression profiles during the

Dermatology Research and Practice 5
(a) (b) (c) (d)
(e) (f) (g) (h)
Figure 3: Comparison of Scarring at the Macroscopic and Microscopic Levels between experimental incisional wound models in pre-clinicalspecies and humans. Scarring response in mice 70 days following a 1 cm full thickness incisional wound on the dorsum at the macroscopic((a) arrowheads indicate ends of original wound) and microscopic ((b) arrowheads indicate scar) levels. Scarring response in rats 84 daysfollowing a 1 cm full thickness incisional wound on the dorsum at the macroscopic ((c) arrowheads indicate ends of original wound) andmicroscopic ((d) arrowheads indicate scar) levels. Scarring response in pigs 168 days following a 1 cm full thickness incisional wound on thedorsum at the macroscopic ((e) arrowheads indicate ends of original wound) and microscopic ((f) arrowheads indicate scar) levels. Scarringresponse in humans 365 days following a 1 cm full thickness incisional wound on the inner aspect of the upper arm at the macroscopic ((g)arrowheads indicate ends of original wound) and microscopic ((h) arrowheads indicate scar) levels.
healing and scarring process in these pre-clinical species(up to 30,000 genes per sample per time point; >300samples; 11 time points) and compared these to profilesin man (Caucasians and Noncaucasians; 30,000 genes persample per time point; >250 samples; 9 time points).Analyses of the expression of genes involved in all the majorphases of healing and scarring have clearly demonstratedmolecular comparability, particularly between rat and man,indicating that the major difference between the healing andscarring in these models is time, with humans exhibitingan extended scar maturation phase [50, 51] (Figure 4).In addition, a number of genes/gene pathways have beenidentified from these studies in rats and man as furtherpotential novel targets for the reduction of scarring in theskin.
4. Translation from Pre-Clinical Studies toClinical Efficacy
As noted above, we have demonstrated that there is signifi-cant molecular and cellular comparability between the heal-ing and scarring process in relevant pre-clinical models andin man. Unlike other therapeutic/chronic disease indications,it is important to note that healing and scarring represent anacute biological response that is conserved across species, andthe progression of which is somewhat predictable. However,whilst a number of studies have reported therapeutic scarreduction in a variety of pre-clinical models, very few, if any,have demonstrated a translation of these findings to man insuitably designed, controlled, prospective, and randomisedclinical trials [9–11].

6 Dermatology Research and Practice
Time post-wounding
Rat
Infl
amm
atio
nG
ran
ula
tion
Rem
odel
ling/
mat
ura
tion
Low expression High expression
1h
our
6h
our
12h
our
1da
y
3da
ys
5da
ys
7da
ys
14da
ys
28da
ys
84da
ys
Nor
mal
skin
(a)
Time post-wounding
Human
Infl
amm
atio
nG
ran
ula
tion
Rem
odel
ling/
mat
ura
tion
Low expression High expression
30da
ys
180
days
365
days
3da
ys
5da
ys
7da
ys
14da
ys
Nor
mal
skin
1da
y
(b)
Figure 4: Gene expression in models of incisional wounds and scars in rat and man demonstrate molecular comparability heatmaps ofsamples of normal skin, wounds, and scars following 1 cm incisional wounds analysed for gene expression using Affymetrix Microarrayscomparing the levels and timings of expression of genes involved in the inflammatory, granulation, remodelling, and maturation phases ofhealing and scarring (examples shown consist of comparison of ∼300 genes for each phase).
Our approach for the development of therapies hasfocused on agents for the prophylactic reduction of scarringin man. This involves local administration of these agents tothe margins of a wound at the time of surgery that leadsto long-term improvements in scarring. The use of pro-phylactic, regenerative medicines is a novel pharmaceuticalapproach to scar improvement, and there are a number ofchallenges associated with this including: designing clinicaltrials in what is considered a pioneering therapeutic area,developing and validating suitable endpoints for evaluat-ing the effectiveness of a prophylactic drug, where thereis no established baseline against which improvementsin scarring could be determined (since baseline wouldotherwise be normal skin before surgery or injury), andpatients vary markedly in their propensity for scarring[57, 58]. Our novel approach has been to utilise a within-subject, placebo-controlled, human volunteer model, priorto starting patient studies, not only to establish local drugsafety and tolerability but also to investigate a number ofother key parameters including: optimal dose(s) and dosingfrequency of the drug, evaluation of a variety of relevantendpoints, effects of the drug in subjects with differentdemographics, for example, sex, race, and age, effects ofthe drug in different wound types, for example, incisionsand excisions. Studies to date have demonstrated that theseprospective, double-blind, within-subject designs allow fora relevant and well-controlled approach for determining
the proof-of-concept for potential therapies. Since thereare no registered pharmaceuticals for the prophylacticreduction of scarring, we have had to pioneer this areain terms of clinical trial design and so have explored avariety of potential surgical models in patient populationsto define their appropriateness for demonstration of drugeffects.
We have successfully demonstrated a translation of scarreduction approaches from pre-clinical models to clinicalstudies, showing clear and robust effects with both ilodecakin(recombinant human interleukin-10, IL-10, Prevascar) ina Phase II clinical trial and with avotermin (recombinanthuman transforming growth factor beta 3, TGFβ3, Juvista)in extensive Phase II volunteer- and patient-based studies[49, 52, 59]. For example, in three double-blind, placebo-controlled studies, intradermal avotermin (concentrationsranging from 0.25 to 500 ng/100 μL per linear cm woundmargin) was administered to both margins of 1 cm, full-thickness skin incisions, before wounding and 24 h later,in healthy men and women [59]. Treatments (avoterminand placebo or standard wound care) were randomlyassigned to wound sites by a computer-generated randomi-sation scheme, and within-participant controls comparedavotermin versus placebo or standard wound care alone.Primary endpoints consisted of visual assessment of scarformation at 6 months and 12 months after wounding intwo studies, and from week 6 to month 7 after wounding
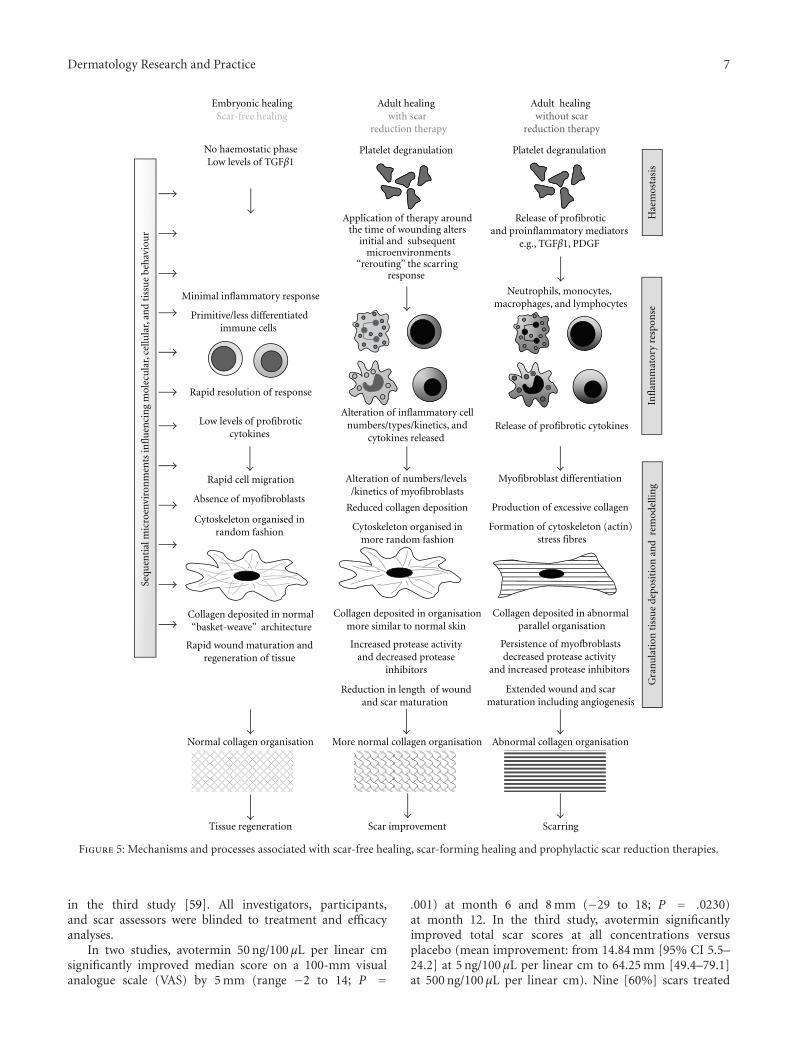
Dermatology Research and Practice 7
Tissue regeneration ScarringScar improvement
More normal collagen organisation
Alteration of numbers/levels /kinetics of myofibroblasts
Reduced collagen deposition
Cytoskeleton organised in more random fashion
Collagen deposited in organisationmore similar to normal skin
Increased protease activity and decreased protease
inhibitors
Reduction in length of wound and scar maturation
Sequ
enti
al m
icro
envi
ron
men
ts in
flu
enci
ng
mol
ecu
lar,
cellu
lar,
and
tiss
ue
beh
avio
ur
Hae
mos
tasi
sIn
flam
mat
ory
resp
onse
Gra
nu
lati
on t
issu
e de
posi
tion
an
d r
emod
ellin
g
Myofibroblast differentiation
Production of excessive collagen
Formation of cytoskeleton (actin) stress fibres
Collagen deposited in abnormal parallel organisation
Persistence of myofbroblastsdecreased protease activity
and increased protease inhibitors
Extended wound and scar maturation including angiogenesis
Release of profibroticand proinflammatory mediators
e.g., TGFβ1, PDGF
Release of profibrotic cytokines
Adult healing without scar
reduction therapy
Neutrophils, monocytes, macrophages, and lymphocytes
Abnormal collagen organisation
Alteration of inflammatory cell numbers/types/kinetics, and
cytokines released
Adult healing with scar
reduction therapy
Platelet degranulation Platelet degranulation
Application of therapy around the time of wounding alters
initial and subsequent microenvironments
‘‘rerouting’’ the scarring response
Rapid cell migration
Absence of myofibroblasts
Cytoskeleton organised in random fashion
Collagen deposited in normal ‘‘basket-weave’’ architecture
Rapid wound maturation and regeneration of tissue
Embryonic healingScar-free healing
Normal collagen organisation
No haemostatic phaseLow levels of TGFβ1
Minimal inflammatory response
Primitive/less differentiated immune cells
Rapid resolution of response
Low levels of profibroticcytokines
Figure 5: Mechanisms and processes associated with scar-free healing, scar-forming healing and prophylactic scar reduction therapies.
in the third study [59]. All investigators, participants,and scar assessors were blinded to treatment and efficacyanalyses.
In two studies, avotermin 50 ng/100 μL per linear cmsignificantly improved median score on a 100-mm visualanalogue scale (VAS) by 5 mm (range −2 to 14; P =
.001) at month 6 and 8 mm (−29 to 18; P = .0230)at month 12. In the third study, avotermin significantlyimproved total scar scores at all concentrations versusplacebo (mean improvement: from 14.84 mm [95% CI 5.5–24.2] at 5 ng/100 μL per linear cm to 64.25 mm [49.4–79.1]at 500 ng/100 μL per linear cm). Nine [60%] scars treated

8 Dermatology Research and Practice
with avotermin at 50 ng/100 μL per linear cm showed 25% orless abnormal orientation of collagen fibres in the reticulardermis versus five [33%] placebo scars. After only 6 weeksfrom wounding, avotermin at 500 ng/100 μL per linear cmimproved VAS score by 16.12 mm (95% CI 10.61–21.63).
Similarly, in another Phase II clinical study, intradermaladministration of ilodecakin was well tolerated, and atconcentrations of 5 ng/100 μL and 25 ng/100 μL per linear cmwound margin, resulted in statistically significant improve-ments (P < .05) in scar appearance with multiple endpointscompared with controls at 12 months postwounding.
Taken together, the results of these clinical studieshave demonstrated that acute, local applications of bothavotermin and ilodecakin have the potential to providean accelerated and permanent improvement in scarring inhumans.
5. Understanding the Mechanisms of Action ofProphylactic Scar Improvement Therapies
Following cutaneous injury, numerous interacting anddynamic molecular and cellular events are initiated. Theseinclude a series of cascades involved in amplification,induction, repression, feed-forward, and feed-back processesthat result in a series of sequential and temporal microen-vironments within the wound, with which resident cellsand those infiltrating the wound interact (Figure 5). Themolecular and cellular behaviour of the wound is dependenton the composition of the tissue microenvironment atany one time. Therefore, any alteration of the molecu-lar or functional behaviour of cells (e.g., by appropriatetherapeutic modulation) results in changes to subsequentwound microenvironments and ultimately affects the tissueresponse. In wound healing and scarring, like embryonicdevelopment, the system contains a number of pathwaysexhibiting multiple redundancy which gives robustness tothe system. If minor pathways are therapeutically modulated,whilst subsequent microenvironments may be rerouted,they nevertheless result in a scarring phenotype. However,modulation of a major pathway that alters multiple microen-vironments synergistically, results in significant alterationsand a major “rerouting” of the healing response, leadingto the propagation and amplification of a phenotype ofimproved scar appearance (Figure 5). From our studies ina range of pre-clinical species, we have identified a numberof key pathways that are central to generating a scarringresponse. Our use of human volunteers, in an experimentalmedicine context, has also rapidly allowed us to confirmwhich of these identified pathways are relevant in man andhence identify and progress new therapeutics into the clinicalarena.
6. Summary
The reduction of scarring represents a clear medical need.Currently, there are no registered pharmaceuticals for theprophylactic improvement of scarring, and no single therapyis accepted universally as the standard of care. The spectrum
of healing following wounding ranges from the ability tocompletely regenerate tissue through to the formation ofhypertrophic and keloid scars. Importantly, a number ofstudies have demonstrated that all mammalian organismsretain the ability to heal via both regenerative and scar-forming processes. This is the key in terms of being able totherapeutically modulate the healing response in adults andreduce the severity of subsequent scarring.
Our approach to the development of therapies hasfocused on agents for the prophylactic reduction of scarring.This has been significantly aided by our extensive studies,comparing and understanding the molecular processes andscarring phenotypes in pre-clinical models, as well as ourpioneering use of human volunteers both in longitudinalscarring studies and in an experimental medicine contextwhich has rapidly allowed us to confirm which of theidentified pathways are relevant in man. The translationof findings in the rat pre-clinical model to man has beenshown in suitably designed and controlled prospective andrandomised clinical trials.
In terms of the mechanisms of action, the prophylacticadministration of scar improvement therapeutics results insignificant alterations and a major “rerouting” of the healingresponse, resulting in the propagation and amplification ofa phenotype of improved scar appearance, by virtue of achange in the architecture of the deposited collagen.
The understanding of the scientific basis of scar-free andscar-forming healing and our pioneering approach to thedevelopment of therapies have allowed the identification andprogression of new treatments. We have demonstrated thatthe development of pharmaceuticals for prophylactic scarimprovement, that are additive to good surgical technique, isachievable, resulting in new therapies with a sound scientificbasis and clear evidence of effectiveness in robust clinicaltrials.
References
[1] D. A. McGrouther, “Facial disfigurement,” British MedicalJournal, vol. 314, no. 7086, p. 991, 1997.
[2] R. Robert, W. Meyer, S. Bishop, L. Rosenberg, L. Murphy,and P. Blakeney, “Disfiguring burn scars and adolescent self-esteem,” Burns, vol. 25, no. 7, pp. 581–585, 1999.
[3] R. Newell, “Psychological difficulties amongst plastic surgeryex-patients following surgery to the face: a survey,” BritishJournal of Plastic Surgery, vol. 53, no. 5, pp. 386–392, 2000.
[4] A. M. Layton, “Optimal management of acne to preventscarring and psychological sequelae,” American Journal ofClinical Dermatology, vol. 2, no. 3, pp. 135–141, 2001.
[5] N. Rumsey, A. Clarke, and P. White, “Exploring the psy-chosocial concerns of outpatients with disfiguring conditions,”Journal of Wound Care, vol. 12, no. 7, pp. 247–252, 2003.
[6] J. W. Lawrence, J. A. Fauerbach, L. Heinberg, and M. Doctor,“Visible vs hidden scars and their relation to body esteem,”Journal of Burn Care and Rehabilitation, vol. 25, no. 1, pp. 25–32, 2004.
[7] S. M. Valente, “Visual disfigurement and depression,” PlasticSurgical Nursing, vol. 24, no. 4, pp. 140–146, 2004.
[8] A. Bayat and D. A. McGrouther, “Clinical management of skinscarring,” Skinmed, vol. 4, no. 3, pp. 165–173, 2005.
Dermatology Research and Practice 9
[9] K. Meier and L. B. Nanney, “Emerging new drugs for scarreduction,” Expert Opinion on Emerging Drugs, vol. 11, no. 1,pp. 39–47, 2006.
[10] R. G. Reish and E. Eriksson, “Scars: a review of emergingand currently available therapies,” Plastic and ReconstructiveSurgery, vol. 122, no. 4, pp. 1068–1078, 2008.
[11] R. G. Reish and E. Eriksson, “Scar treatments: preclinical andclinical studies,” Journal of the American College of Surgeons,vol. 206, no. 4, pp. 719–730, 2008.
[12] R. L. McCallion and M. W. J. Ferguson, “Fetal wound healingand the development of antiscarring therapies for adultwound healing,” in The Molecular and Cellular Biology ofWound Repair, R. A. F. Clark, Ed., pp. 561–600, Plenum Press,New York, NY, USA, 1996.
[13] M. W. J. Ferguson and S. O’Kane, “Scar-free healing: fromembryonic mechanism to adult therapeutic intervention,”Philosophical Transactions of the Royal Society B, vol. 359, no.1445, pp. 839–850, 2004.
[14] J. R. Armstrong and M. W. J. Ferguson, “Ontogeny of theskin and the transition from scar-free to scarring phenotypeduring wound healing in the pouch young of a marsupial,Monodelphis domestica,” Developmental Biology, vol. 169, no.1, pp. 242–260, 1995.
[15] A. J. Cowin, M. P. Brosnan, T. M. Holmes, and M. W. J.Ferguson, “Endogenous inflammatory response to dermalwound healing in the fetal and adult mouse,” DevelopmentalDynamics, vol. 212, no. 3, pp. 385–393, 1998.
[16] D. J. Whitby and M. W. J. Ferguson, “Immunohistochemicallocalization of growth factors in fetal wound healing,” Devel-opmental Biology, vol. 147, no. 1, pp. 207–215, 1991.
[17] S. O’Kane and M. W. J. Ferguson, “Transforming growth factorβs and wound healing,” International Journal of Biochemistryand Cell Biology, vol. 29, no. 1, pp. 63–78, 1997.
[18] M. Shah, P. Rorison, and M. W. J. Ferguson, “The role oftransforming growth factors beta in cutaneous scarring,” inScarless Wound Healing, H. G. Garg and M. T. Longaker, Eds.,pp. 213–226, Marcel Dekker, New York, NY, USA, 2000.
[19] A. J. Cowin, T. M. Holmes, P. Brosnan, and M. W. J. Ferguson,“Expression of TGF-β and its receptors in murine fetal andadult dermal wounds,” European Journal of Dermatology, vol.11, no. 5, pp. 424–431, 2001.
[20] M. W. J. Ferguson, D. J. Whitby, M. Shah, J. Armstrong,J. W. Siebert, and M. T. Longaker, “Scar formation: thespectral nature of fetal and adult wound repair,” Plastic andReconstructive Surgery, vol. 97, no. 4, pp. 854–860, 1996.
[21] B. Gawronska-Kozak, “Regeneration in the ears of immunod-eficient mice: identification and lineage analysis of mesenchy-mal stem cells,” Tissue Engineering, vol. 10, no. 7-8, pp. 1251–1265, 2004.
[22] B. Gawronska-Kozak, M. Bogacki, J.-S. Rim, W. T. Monroe,and J. A. Manuel, “Scarless skin repair in immunodeficientmice,” Wound Repair and Regeneration, vol. 14, no. 3, pp. 265–276, 2006.
[23] A. H. M. Beare, A. D. Metcalfe, and M. W. J. Ferguson,“Location of injury influences the mechanisms of bothregeneration and repair within the MRL/MpJ mouse,” Journalof Anatomy, vol. 209, no. 4, pp. 547–559, 2006.
[24] A. S. Colwell, T. M. Krummel, M. T. Longaker, and H. P.Lorenz, “An in vivo mouse excisional wound model of scarlesshealing,” Plastic and Reconstructive Surgery, vol. 117, no. 7, pp.2292–2296, 2006.
[25] M. E. Schrementi, A. M. Ferreira, C. Zender, and L. A.DiPietro, “Site-specific production of TGF-β in oral mucosal
and cutaneous wounds,” Wound Repair and Regeneration, vol.16, no. 1, pp. 80–86, 2008.
[26] A. D. Metcalfe, H. Willis, A. Beare, and M. W. J. Ferguson,“Characterizing regeneration in the mammalian external ear,”Journal of Anatomy, vol. 209, no. 4, pp. 439–446, 2006.
[27] A. J. Singer and R. A. F. Clark, “Cutaneous wound healing,”New England Journal of Medicine, vol. 341, no. 10, pp. 738–746, 1999.
[28] S.-C. Su, E. A. Mendoza, H.-I. Kwak, and K. J. Bayless, “Molec-ular profile of endothelial invasion of three-dimensionalcollagen matrices: insights into angiogenic sprout inductionin wound healing,” American Journal of Physiology, vol. 295,no. 5, pp. C1215–C1229, 2008.
[29] R. Mori, T. J. Shaw, and P. Martin, “Molecular mechanismslinking wound inflammation and fibrosis: knockdown ofosteopontin leads to rapid repair and reduced scarring,”Journal of Experimental Medicine, vol. 205, no. 1, pp. 43–51,2008.
[30] C. J. Kirkpatrick, S. Fuchs, M. Iris Hermanns, K. Peters, and R.E. Unger, “Cell culture models of higher complexity in tissueengineering and regenerative medicine,” Biomaterials, vol. 28,no. 34, pp. 5193–5198, 2007.
[31] J. C. Dallon and H. P. Ehrlich, “A review of fibroblast-populated collagen lattices,” Wound Repair and Regeneration,vol. 16, no. 4, pp. 472–479, 2008.
[32] A. A. Ucuzian and H. P. Greisler, “In vitro models ofangiogenesis,” World Journal of Surgery, vol. 31, no. 4, pp. 654–663, 2007.
[33] G. Proetzel, S. A. Pawlowski, M. V. Wiles et al., “Transforminggrowth factor-β3 is required for secondary palate fusion,”Nature Genetics, vol. 11, no. 4, pp. 409–414, 1995.
[34] M. Isoda, S. Ueda, S. Imayama, and K. Tsukahara, “Newformulation of chemical peeling agent: histological evaluationin sun-damaged skin model in hairless mice,” Journal ofDermatological Science, supplement 1, pp. S60–S67, 2001.
[35] K. C. Flanders, C. D. Major, A. Arabshahi et al., “Interferencewith transforming growth factor-β/Smad3 signaling results inaccelerated healing of wounds in previously irradiated skin,”American Journal of Pathology, vol. 163, no. 6, pp. 2247–2257,2003.
[36] S. B. Cho, C. O. Park, W. G. Chung, K. H. Lee, J. B. Lee,and K. Y. Chung, “Histometric and histochemical analysis ofthe effect of trichloroacetic acid concentration in the chemicalreconstruction of skin scars method,” Dermatologic Surgery,vol. 32, no. 10, pp. 1231–1236, 2006.
[37] S. Aarabi, K. A. Bhatt, Y. Shi et al., “Mechanical load initiateshypertrophic scar formation through decreased cellular apop-tosis,” FASEB Journal, vol. 21, no. 12, pp. 3250–3261, 2007.
[38] C. Qiu, P. Coutinho, S. Frank et al., “Targeting connexin43expression accelerates the rate of wound repair,” CurrentBiology, vol. 13, no. 19, pp. 1697–1703, 2003.
[39] C. M. Dang, S. R. Beanes, H. Lee, X. Zhang, C. Soo, and K.Ting, “Scarless fetal wounds are associated with an increasedmatrix metalloproteinase-to-tissue-derived inhibitor of met-alloproteinase ratio,” Plastic and Reconstructive Surgery, vol.111, no. 7, pp. 2273–2285, 2003.
[40] M. Birch, A. Tomlinson, and M. W. Ferguson, “Animal modelsfor adult dermal wound healing,” Methods in MolecularMedicine, vol. 117, pp. 223–235, 2005.
[41] A. S. Colwell, S. R. Beanes, C. Soo et al., “Increased angiogene-sis and expression of vascular endothelial growth factor duringscarless repair,” Plastic and Reconstructive Surgery, vol. 115, no.1, pp. 204–212, 2005.
10 Dermatology Research and Practice
[42] O. Kloeters, A. Tandara, and T. A. Mustoe, “Hypertrophic scarmodel in the rabbit ear: a reproducible model for studying scartissue behavior with new observations on silicone gel sheetingfor scar reduction,” Wound Repair and Regeneration, vol. 15,supplement 1, pp. S40–S45, 2007.
[43] Z. B. Kryger, M. Sisco, N. K. Roy, L. Lu, D. Rosenberg, and T.A. Mustoe, “Temporal expression of the transforming growthfactor-beta pathway in the rabbit ear model of wound healingand scarring,” Journal of the American College of Surgeons, vol.205, no. 1, pp. 78–88, 2007.
[44] I. Kim, J. E. Mogford, C. Witschi, M. Nafissi, and T. A. Mustoe,“Inhibition of prolyl 4-hydroxylase reduces scar hypertrophyin a rabbit model of cutaneous scarring,” Wound Repair andRegeneration, vol. 11, no. 5, pp. 368–372, 2003.
[45] L. S. Moy, S. Peace, and R. L. Moy, “Comparison of theeffect of various chemical peeling agents in a mini-pig model,”Dermatologic Surgery, vol. 22, no. 5, pp. 429–432, 1996.
[46] M. M. W. Ulrich, M. Verkerk, L. Reijnen, M. Vlig, A. J.Van Den Bogaerdt, and E. Middelkoop, “Expression profileof proteins involved in scar formation in the healing processof full-thickness excisional wounds in the porcine model,”Wound Repair and Regeneration, vol. 15, no. 4, pp. 482–490,2007.
[47] C. L. Gallant, M. E. Olson, and D. A. Hart, “Molecular,histologic, and gross phenotype of skin wound healing inred Duroc pigs reveals an abnormal healing phenotype ofhypercontracted, hyperpigmented scarring,” Wound Repairand Regeneration, vol. 12, no. 3, pp. 305–319, 2004.
[48] K. Q. Zhu, G. J. Carrougher, O. P. Couture, C. K. Tuggle, N.S. Gibran, and L. H. Engrav, “Expression of collagen genesin the cones of skin in the Duroc/Yorkshire porcine model offibroproliferative scarring,” Journal of Burn Care and Research,vol. 29, no. 5, pp. 815–827, 2008.
[49] N. L. Occleston, S. O’Kane, N. Goldspink, and M. W. J.Ferguson, “New therapeutics for the prevention and reductionof scarring,” Drug Discovery Today, vol. 13, no. 21-22, pp. 973–981, 2008.
[50] J. S. Bond, J. A. L. Duncan, A. Sattar et al., “The maturationof the human scar: an observational study,” Plastic andReconstructive Surgery, vol. 121, no. 5, pp. 1650–1658, 2008.
[51] J. S. Bond, J. A.L. Duncan, T. Mason et al., “Scar redness inhumans: how long does it persist after incisional and excisionalwounding?” Plastic and Reconstructive Surgery, vol. 121, no. 2,pp. 487–496, 2008.
[52] N. L. Occleston, H. G. Laverty, S. O’Kane, and M. W. J.Ferguson, “Prevention and reduction of scarring in the skin bytransforming growth factor beta 3 (TGFβ3): from laboratorydiscovery to clinical pharmaceutical,” Journal of BiomaterialsScience, Polymer Edition, vol. 19, no. 8, pp. 1047–1063, 2008.
[53] J. S. Bond, J. A. L. Duncan, T. Mason et al., “Scar redness inhumans: how long does it persist after incisional and excisionalwounding?” Plastic and Reconstructive Surgery, vol. 121, no. 2,pp. 487–496, 2008.
[54] N. Harunari, K. Q. Zhu, R. T. Armendariz et al., “Histology ofthe thick scar on the female, red Duroc pig: final similarities tohuman hypertrophic scar,” Burns, vol. 32, no. 6, pp. 669–677,2006.
[55] K. Q. Zhu, G. J. Carrougher, N. S. Gibran, F. F. Isik, andL. H. Engrav, “Review of the female Duroc/Yorkshire pigmodel of human fibroproliferative scarring,” Wound Repairand Regeneration, vol. 15, supplement 1, pp. S32–S39, 2007.
[56] Y. Xie, K. Q. Zhu, H. Deubner et al., “The microvasculature incutaneous wound healing in the female red duroc pig is similarto that in human hypertrophic scars and different from that in
the female yorkshire pig,” Journal of Burn Care and Research,vol. 28, no. 3, pp. 500–506, 2007.
[57] T. A. Mustoe, R. D. Cooter, M. H. Gold et al., “Internationalclinical recommendations on scar management,” Plastic andReconstructive Surgery, vol. 110, no. 2, pp. 560–571, 2002.
[58] A. Bayat, D. A. McGrouther, and M. W. J. Ferguson, “Skinscarring,” British Medical Journal, vol. 326, no. 7380, pp. 88–92, 2003.
[59] M. W. Ferguson, J. Duncan, J. Bond et al., “Prophylac-tic administration of avotermin for improvement of skinscarring: three double-blind, placebo-controlled, phase I/IIstudies,” The Lancet, vol. 373, no. 9671, pp. 1264–1274, 2009.
Hindawi Publishing CorporationDermatology Research and PracticeVolume 2010, Article ID 690613, 6 pagesdoi:10.1155/2010/690613
Review Article
Therapies with Emerging Evidence of Efficacy:Avotermin for the Improvement of Scarring
Jim Bush, Karen So, Tracey Mason, Nick L. Occleston, Sharon O’Kane,and Mark W. J. Ferguson
Renovo, Core Technology Facility, 48 Grafton Street, Manchester M13 9XX, UK
Correspondence should be addressed to Jim Bush, [email protected] andMark W. J. Ferguson, [email protected]
Received 15 March 2010; Accepted 3 July 2010
Academic Editor: Hayes B. Gladstone
Copyright © 2010 Jim Bush et al. This is an open access article distributed under the Creative Commons Attribution License,which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Many patients are dissatisfied with scars on both visible and non-visible body sites and would value any opportunity to improveor minimise scarring following surgery. Approximately 44 million procedures in the US and 42 million procedures in the EUper annum could benefit from scar reduction therapy. A wide range of non-invasive and invasive techniques have been used inan attempt to improve scarring although robust, prospective clinical trials to support the efficacy of these therapies are lacking.Differences in wound healing and scar outcome between early fetal and adult wounds led to interest in the role of the TGFβ familyof cytokines in scar formation and the identification of TGFβ3 (avotermin) as a potential therapeutic agent for the improvementof scar appearance. Extensive pre-clinical and human Phase I and II clinical trial programmes have confirmed the scar improvingefficacy of avotermin which produces macroscopic and histological improvements in scar architecture, with improved restitutionof the epidermis and an organisation of dermal extracellular matrix that more closely resembles normal skin. Avotermin is safeand well tolerated and is currently in Phase III of clinical development, with the first study, in patients undergoing scar revisionsurgery, fully recruited.
1. There Is a Medical Need for Therapies ThatReduce Scarring following Surgery
A recent survey performed in the USA confirmed that manypatients are disappointed with their scar resulting from asurgical procedure, irrespective of gender, age or ethnicity[1]. Understandably, patients are very conscious about visiblescars. However, the survey showed that it is not only visiblescars that cause dissatisfaction, with many patients reportingscars on nonvisible body sites that they wished were lessnoticeable [1]. A patient’s perception of the severity of theirscar can be influenced not only by the objective appearanceof the scar, but also by other factors including the surgicaltechnique used and the patient’s sensitivity to the resultingscar [1, 2]. Many patients would value any opportunityto improve or minimise scarring following surgery [1].Indeed it was estimated that there are approximately 44million procedures performed in the US (Independentresearch: Mattson Jack Group) and approximately 42 million
procedures performed in the EU per annum (Independentresearch for Renovo: MedTech Insights and TforG) thatcould benefit from scar reduction therapy.
2. Current Treatments for Scar ManagementAre Unsatisfactory
The optimal outcome of wound repair following trauma,injury or surgery is complete restoration of normal skin.However, adult wound healing has evolved to rapidly replacemissing tissue with repaired tissue, consisting predominantlyof fibronectin and collagen types I and III. The repaired tissueprovides an immediate barrier to foreign bodies and infec-tious agents, irrespective of optimal function or appearance[3]. However, in the context of modern surgery, which isperformed under sterile conditions, this immediate barrieris unnecessary and therefore scarring can be considered aninappropriate response. Furthermore, dermal scarring can

2 Dermatology Research and Practice
Table 1: Commonly used approaches to manage scarring postsurgery.
Approaches currently used to manage scarring post-surgery
Non-invasive Invasive
Silicone gel sheeting Steroid injections
Pressure garments Lasers
Hydrating creams/ointments Dermabrasion
Scar-revision surgery
have significant adverse consequences including restrictionof movement and psychological trauma.
A number of different approaches have been used inan effort to manage scarring post surgery ranging fromnoninvasive (silicone gel sheeting, pressure garments,hydrating creams, and ointments) to invasive (steroidinjections, lasers, dermabrasion, and surgery) techniques[4–9] (Table 1). Unfortunately, many of these approaches areuncomfortable or burdensome for the patients, and manyrequire a high level of patient compliance. Furthermore,prospective, robust clinical trials to demonstrate the efficacyof scar therapies are lacking, with the majority of publishedstudies providing only level 4 evidence [10]. Withoutclear definitions of criteria for scar improvement, coupledwith the heterogenous nature of scars themselves, it isdifficult to interpret and compare data from these studies.Consequently, no single treatment or regimen has beenuniversally adopted as the standard of care to managescarring post surgery. The high level of dissatisfactionwith scar therapies among patients is reflected by the highnumber of patients who undergo scar revision surgery,estimated to be over 150,000 per annum in the USA(http://www.yourplasticsurgeryguide.com/trends/asps-2007.htm). Indeed many more patients are believed to requestscar revision surgery but are refused as the clinician believesimprovement is unlikely with surgery alone.
3. New Biological Approaches Are inDevelopment for the ProphylacticImprovement of Scarring
An increase in our understanding of the processes involved inscarring at the molecular, cellular, and tissue levels has facil-itated the development of new pharmaceutical approachesto prevent or treat scarring. While the majority of theseapproaches are still being investigated in the laboratory, a fewhave progressed to human clinical trials (Table 2) [9]. To datethere is no approved pharmaceutical product in the US or theEU indicated for the reduction, improvement, or preventionof dermal scarring.
3.1. The TGFβ Isoforms Play a Key Role in Scar Formation.Scarring in adult skin is a macroscopic disturbance of thenormal structure and function of the skin architecture thatresults from a healed wound [11], although the severityof the resulting scars differs between people and bodylocations. By contrast, skin wounds on early mammalian
embryos have been shown to heal perfectly with no signsof scarring. The transition between scar-free healing (e.g.,in early embryonic wounds), to scar-forming healing, (e.g.,in adults) is characterised by a change in the organisationof the dermal extracellular matrix from a normal basketweave orientation to the deposition of parallel bundles of finecollagen fibres that form a scar [11].
There are a large number of differences between earlyfetal and adult wounds, the majority of which appear to beirrelevant to healing and scar formation. However, mucheffort has gone into identifying factors that play a causativerole in the scar-free healing phenotype [12].
In particular, the Transforming Growth Factor beta(TGFβ) isoforms have been shown to play a key role indetermining the scarring outcome. The high ratio of TGFβ3to TGFβ1 and β2 in embryonic wounds that heal withouta scar compared with adult wounds that scar [13], ledto interest in the role of this family of cytokines in scarformation. More recently, a significantly higher ratio ofTGFβ3 to the other TGFβ isoforms has been shown inthe adult oral mucosa, also known to heal with minimalscarring, compared with dermal wounds [14]. Conversely,TGFβ1 and β2 are elevated in adult wounds that heal witha scar compared with embryonic wounds that heal withouta scar [15]. The addition of TGFβ1 to a rat fetal wound thatwould normally heal without a scar results in scar formation[16], whereas in adult rats, scarring can be reduced bythe inhibition of TGFβ1 or TGFβ2 using antibodies or theaddition of TGFβ3[17, 18]. Furthermore, mice embryos thatare genetically null for TGFβ3 heal with a scar in comparisonwith wild-type littermates (with two normal copies of theTGFβ3 genes), which exhibit scar-free healing [19].
Collectively, data from these experimental manipulationssuggest that TGFβ3 plays an important role in scar-free heal-ing and that the application of this cytokine to adult woundsmay reduce the magnitude and accelerate the resolution ofthe scarring response, resulting in a phenotype that moreclosely resembles that of normal skin [3] (Figure 1).
3.2. Preclinical Studies Have Demonstrated the Efficacy andSafety of Avotermin (TGFβ3) for the Improvement of ScarAppearance. An extensive, preclinical programme has inves-tigated the feasibility of therapeutically manipulating thescarring response using human recombinant TGFβ3, avoter-min (Juvista�: Renovo, UK) to improve the appearance ofscars [20]. This preclinical programme was facilitated bythe high level of amino acid homology between humansand animals for TGFβ3 and the surface receptors throughwhich it exerts its biological effects (TGFβ receptors typeI and type II). A standardised rat model was used toinvestigate the efficacy of avotermin for the improvementof scarring. Intradermal injection of avotermin (50 and100 ng/100 μL/linear cm) to cutaneous incisional woundssignificantly reduced scarring compared with controls inadult rats [18]. The macroscopic improvements in scarringachieved with avotermin were accompanied by histolog-ical improvements in the architecture of the neodermis,including a more normal basket weave arrangement of
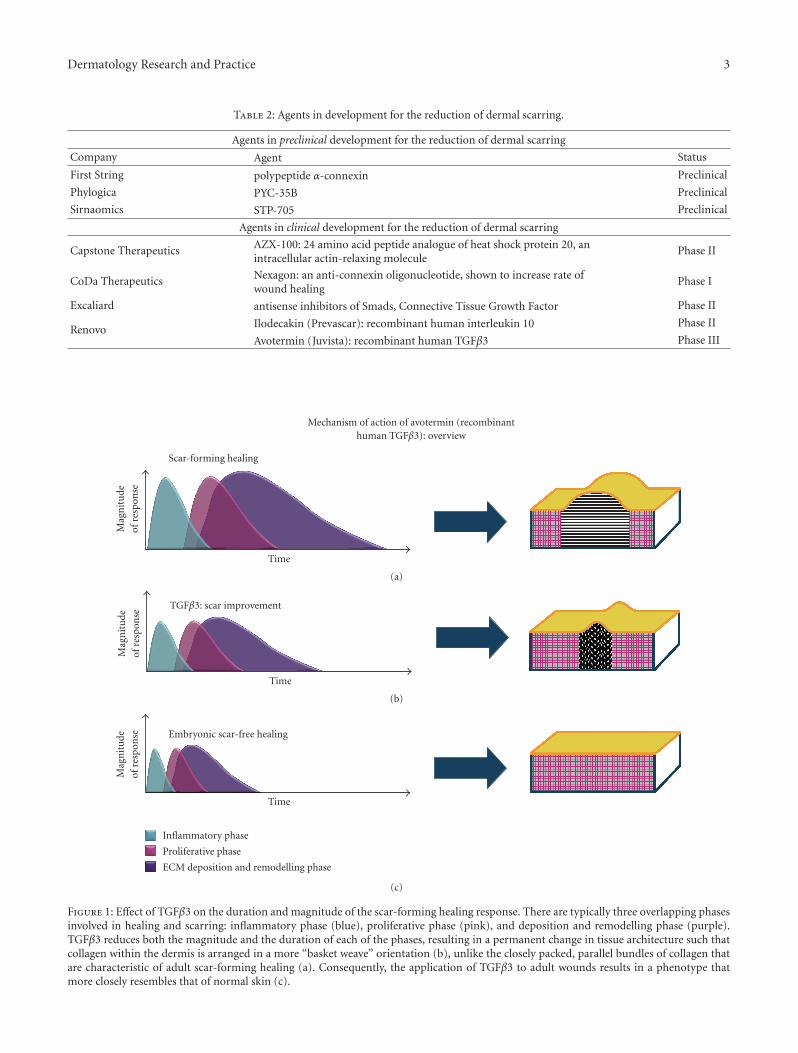
Dermatology Research and Practice 3
Table 2: Agents in development for the reduction of dermal scarring.
Agents in preclinical development for the reduction of dermal scarring
Company Agent Status
First String polypeptide α-connexin Preclinical
Phylogica PYC-35B Preclinical
Sirnaomics STP-705 Preclinical
Agents in clinical development for the reduction of dermal scarring
Capstone Therapeutics AZX-100: 24 amino acid peptide analogue of heat shock protein 20, anintracellular actin-relaxing molecule
Phase II
CoDa Therapeutics Nexagon: an anti-connexin oligonucleotide, shown to increase rate ofwound healing
Phase I
Excaliard antisense inhibitors of Smads, Connective Tissue Growth Factor Phase II
Renovo Ilodecakin (Prevascar): recombinant human interleukin 10 Phase II
Avotermin (Juvista): recombinant human TGFβ3 Phase III
Mechanism of action of avotermin (recombinanthuman TGFβ3): overview
Scar-forming healing
Time
Mag
nit
ude
ofre
spon
se
(a)
TGFβ3: scar improvement
Time
Mag
nit
ude
ofre
spon
se
(b)
Embryonic scar-free healing
Time
Mag
nit
ude
ofre
spon
se
Inflammatory phase
Proliferative phase
ECM deposition and remodelling phase
(c)
Figure 1: Effect of TGFβ3 on the duration and magnitude of the scar-forming healing response. There are typically three overlapping phasesinvolved in healing and scarring: inflammatory phase (blue), proliferative phase (pink), and deposition and remodelling phase (purple).TGFβ3 reduces both the magnitude and the duration of each of the phases, resulting in a permanent change in tissue architecture such thatcollagen within the dermis is arranged in a more “basket weave” orientation (b), unlike the closely packed, parallel bundles of collagen thatare characteristic of adult scar-forming healing (a). Consequently, the application of TGFβ3 to adult wounds results in a phenotype thatmore closely resembles that of normal skin (c).

4 Dermatology Research and Practice
collagen [2, 18, 19]. The rat model was also used tooptimise the dose, frequency, and formulation of avotermin,demonstrating that two injections of avotermin (50 and100 ng/100 μL/linear cm) administered at the time of wound-ing and 24 hours later, resulted in the greatest improve-ments in scarring compared with controls. A comprehensivepreclinical safety program to support the developmentof avotermin was also completed. Specific safety studiesin a clinically relevant pig model also demonstrated thatintradermal administration of avotermin, at concentrations>12 times higher than those shown to be efficacious inpeople, is well tolerated, does not adversely affect woundhealing or wound tensile strength, has low systemic bioavail-ability and is rapidly cleared with no systemic toxicity[21].
3.3. Avotermin is the First in a New Class of ProphylacticMedicines in Clinical Development to Improve Scar Appear-ance. Following encouraging efficacy and safety data fromthe preclinical studies, an extensive phase I/II clinical trialprogramme was executed to evaluate the safety and optimiseboth the administration of avotermin and the design ofclinical studies to assess its scar improving effects.
The phase I/II trial programme included a series ofprospective, double-blind, within-subject placebo-control-led, randomised clinical trials in human volunteers andpatients. A number of parameters that can influence theappearance of scars (e.g. age, race, sex, anatomical location,etc.) have been identified. To overcome scar variability dueto these parameters, a within-subject trial design, whichallowed the effect of the drug to be compared with placeboacross anatomically matched pairs of scars, was used inthe phase I/II clinical programme. This within-subjectdesign controlled for genetic and environmental factorsaffecting wound healing and scarring between individuals.By exploring a number of ways of assessing scars thatresult from experimental wounds, robust endpoints for theassessment of scarring have been developed and validated.In addition to assessing standard, objective endpoints forexample, scar redness, pigmentation, width, height, volume,surface area [22, 23], more holistic assessments of scars havebeen developed. A visual analogue scale was used alongwith scar ranking to assess scars either on the patients(assessed by either the investigator or the patient themselves)or using standardised digital images (assessed by panels ofclinicians/lay people). The visual analogue scale and scarranking assessments have been shown to be robust andsensitive methods for accurately assessing dermal scarring[24]. During the phase I/II programme, an improved scarassessment tool was developed, the Global Scar ComparisonScale (GSCS) specifically for use in within-subject controlledtrials. The GSCS incorporates the well-established principlesof a visual analogue scale, with the benefits of scar ranking toprovide a more accurate and sensitive measure of treatmenteffect with clinical relevance. The scale allows assessors toindicate which of two scars on the same subject is betterand by how much, and is effectively a double VAS scale,symmetrical around a zero point, with one end of the scaleused to indicate that one scar is better and the other end
of the scale used to indicate that the other scar is better.The midpoint of the scale is used to indicate that there isno difference between the two scars and scores further awayfrom the midpoint indicate a greater difference between twoscars. The GSCS is also a holistic assessment tool; assessorsare asked to take all scar features into consideration includingscar width, height, contour, and colour. Both the within-patient design and use of the GSCS, which has now beenvalidated in a number of phase II studies, received favourablefeedback from the European Medicines Agency (EMEA)and will be used to assess avotermin further in phase IIIstudies.
In all clinical studies, avotermin was administeredaround the time of surgery as an intradermal injection eitheralong the planned line of incision or down both margins of aclosed wound, to direct delivery and ensure accurate dosing.The data collected from more than 1,100 subjects who havebeen exposed to avotermin during the extensive phase I/IIprogramme demonstrate that avotermin is well toleratedwith a favourable safety profile. Furthermore, no adverseeffects on normal healing have been reported. To date, sevendouble-blind, placebo-controlled, prospective trials havemet their primary endpoint, demonstrating a statisticallysignificant improvement in scarring with avotermin. (Thesetrials are registered with ClinicalTrials.gov: NCT00847925,NCT00847795, NCT00432211, NCT00629811,NCT00627536, NCT00594581, and NCT00430326.)
Intradermal avotermin has a broad efficacious doserange with doses of 50 to 500 ng/100μL per linear cm ofwound margin, administered around the time of surgery,significantly improving scar appearance [25] (Figure 2).Although effective following a single application, optimalefficacy is achieved using a twice dosing regimen, the firstdose given at the time of wounding and the second dose24 hours later. The rationale for dosing at the time ofwounding is to influence the initial cascade of molecular andcellular processes involved in wound healing and scarringthat are triggered immediately after wounding. A subsequentadministration, 24 hours later, has been shown to providefurther improvements in scarring compared with placebo,which are apparent after only 6 weeks and are maintainedbeyond one year [25]. Dosing schedules involving more thantwo administrations have been assessed and found to be sub-optimal due to potential injury caused by repeated injectionsat the wound site and inconvenient due to multiple clinicvisits.
Although the majority of the phase II studies investigat-ing the safety and efficacy of avotermin have been conductedin volunteers, two recent studies performed in patientsdemonstrate that the improvements in scarring translateto a clinical setting. Two double-blind, placebo-controlled,randomised, phase II trials in patients demonstrated thescar-improving efficacy and safety of intradermal avoterminadministered at a dose of 500 ng/100 μL per linear cm ofwound margin on a single occasion following bilateral vari-cose vein surgery, or administered at a dose of 200 ng/100 μLper linear cm of wound margin on two occasions (imme-diately after wound closure and 24 hours later) in patientsundergoing scar revision surgery (Figure 3). The mechanism
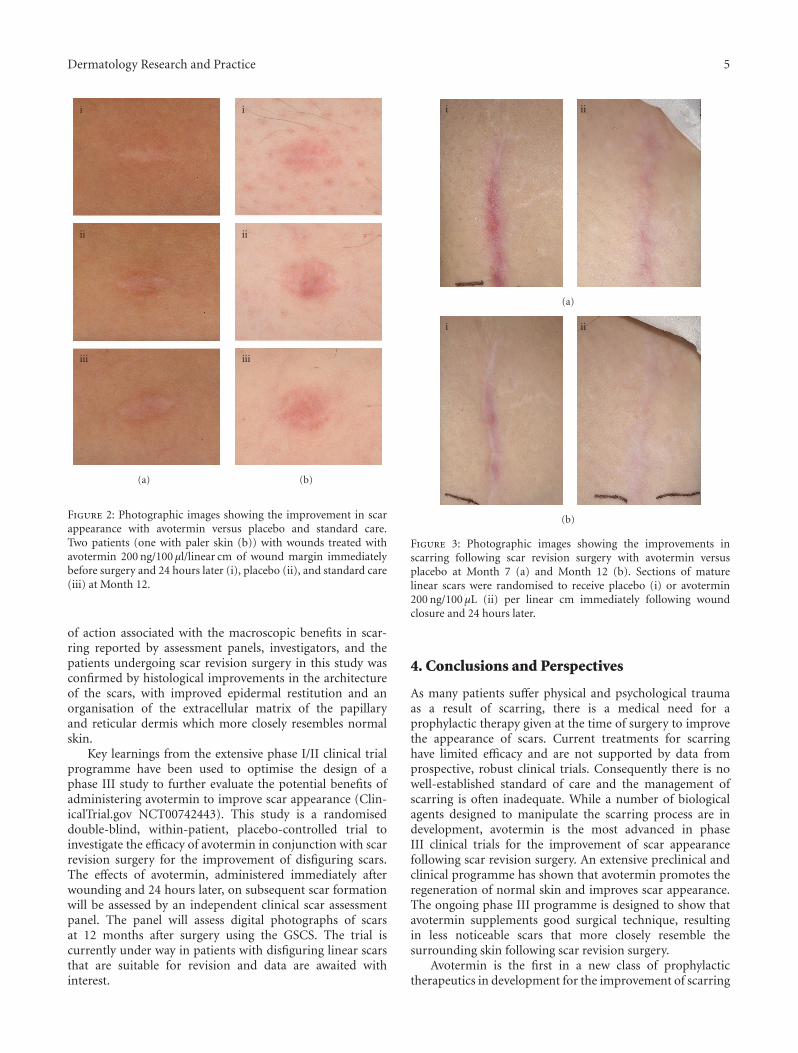
Dermatology Research and Practice 5
i
ii
iii
(a)
i
ii
iii
(b)
Figure 2: Photographic images showing the improvement in scarappearance with avotermin versus placebo and standard care.Two patients (one with paler skin (b)) with wounds treated withavotermin 200 ng/100 μl/linear cm of wound margin immediatelybefore surgery and 24 hours later (i), placebo (ii), and standard care(iii) at Month 12.
of action associated with the macroscopic benefits in scar-ring reported by assessment panels, investigators, and thepatients undergoing scar revision surgery in this study wasconfirmed by histological improvements in the architectureof the scars, with improved epidermal restitution and anorganisation of the extracellular matrix of the papillaryand reticular dermis which more closely resembles normalskin.
Key learnings from the extensive phase I/II clinical trialprogramme have been used to optimise the design of aphase III study to further evaluate the potential benefits ofadministering avotermin to improve scar appearance (Clin-icalTrial.gov NCT00742443). This study is a randomiseddouble-blind, within-patient, placebo-controlled trial toinvestigate the efficacy of avotermin in conjunction with scarrevision surgery for the improvement of disfiguring scars.The effects of avotermin, administered immediately afterwounding and 24 hours later, on subsequent scar formationwill be assessed by an independent clinical scar assessmentpanel. The panel will assess digital photographs of scarsat 12 months after surgery using the GSCS. The trial iscurrently under way in patients with disfiguring linear scarsthat are suitable for revision and data are awaited withinterest.
i ii
(a)
i ii
(b)
Figure 3: Photographic images showing the improvements inscarring following scar revision surgery with avotermin versusplacebo at Month 7 (a) and Month 12 (b). Sections of maturelinear scars were randomised to receive placebo (i) or avotermin200 ng/100 μL (ii) per linear cm immediately following woundclosure and 24 hours later.
4. Conclusions and Perspectives
As many patients suffer physical and psychological traumaas a result of scarring, there is a medical need for aprophylactic therapy given at the time of surgery to improvethe appearance of scars. Current treatments for scarringhave limited efficacy and are not supported by data fromprospective, robust clinical trials. Consequently there is nowell-established standard of care and the management ofscarring is often inadequate. While a number of biologicalagents designed to manipulate the scarring process are indevelopment, avotermin is the most advanced in phaseIII clinical trials for the improvement of scar appearancefollowing scar revision surgery. An extensive preclinical andclinical programme has shown that avotermin promotes theregeneration of normal skin and improves scar appearance.The ongoing phase III programme is designed to show thatavotermin supplements good surgical technique, resultingin less noticeable scars that more closely resemble thesurrounding skin following scar revision surgery.
Avotermin is the first in a new class of prophylactictherapeutics in development for the improvement of scarring
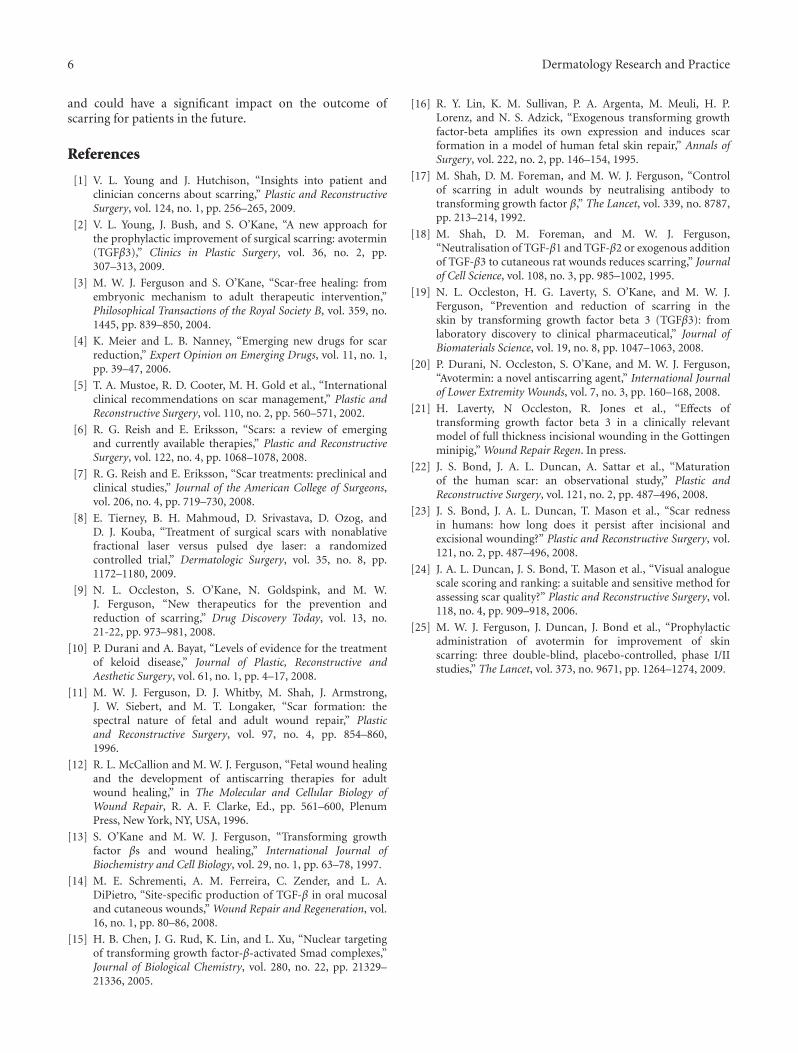
6 Dermatology Research and Practice
and could have a significant impact on the outcome ofscarring for patients in the future.
References
[1] V. L. Young and J. Hutchison, “Insights into patient andclinician concerns about scarring,” Plastic and ReconstructiveSurgery, vol. 124, no. 1, pp. 256–265, 2009.
[2] V. L. Young, J. Bush, and S. O’Kane, “A new approach forthe prophylactic improvement of surgical scarring: avotermin(TGFβ3),” Clinics in Plastic Surgery, vol. 36, no. 2, pp.307–313, 2009.
[3] M. W. J. Ferguson and S. O’Kane, “Scar-free healing: fromembryonic mechanism to adult therapeutic intervention,”Philosophical Transactions of the Royal Society B, vol. 359, no.1445, pp. 839–850, 2004.
[4] K. Meier and L. B. Nanney, “Emerging new drugs for scarreduction,” Expert Opinion on Emerging Drugs, vol. 11, no. 1,pp. 39–47, 2006.
[5] T. A. Mustoe, R. D. Cooter, M. H. Gold et al., “Internationalclinical recommendations on scar management,” Plastic andReconstructive Surgery, vol. 110, no. 2, pp. 560–571, 2002.
[6] R. G. Reish and E. Eriksson, “Scars: a review of emergingand currently available therapies,” Plastic and ReconstructiveSurgery, vol. 122, no. 4, pp. 1068–1078, 2008.
[7] R. G. Reish and E. Eriksson, “Scar treatments: preclinical andclinical studies,” Journal of the American College of Surgeons,vol. 206, no. 4, pp. 719–730, 2008.
[8] E. Tierney, B. H. Mahmoud, D. Srivastava, D. Ozog, andD. J. Kouba, “Treatment of surgical scars with nonablativefractional laser versus pulsed dye laser: a randomizedcontrolled trial,” Dermatologic Surgery, vol. 35, no. 8, pp.1172–1180, 2009.
[9] N. L. Occleston, S. O’Kane, N. Goldspink, and M. W.J. Ferguson, “New therapeutics for the prevention andreduction of scarring,” Drug Discovery Today, vol. 13, no.21-22, pp. 973–981, 2008.
[10] P. Durani and A. Bayat, “Levels of evidence for the treatmentof keloid disease,” Journal of Plastic, Reconstructive andAesthetic Surgery, vol. 61, no. 1, pp. 4–17, 2008.
[11] M. W. J. Ferguson, D. J. Whitby, M. Shah, J. Armstrong,J. W. Siebert, and M. T. Longaker, “Scar formation: thespectral nature of fetal and adult wound repair,” Plasticand Reconstructive Surgery, vol. 97, no. 4, pp. 854–860,1996.
[12] R. L. McCallion and M. W. J. Ferguson, “Fetal wound healingand the development of antiscarring therapies for adultwound healing,” in The Molecular and Cellular Biology ofWound Repair, R. A. F. Clarke, Ed., pp. 561–600, PlenumPress, New York, NY, USA, 1996.
[13] S. O’Kane and M. W. J. Ferguson, “Transforming growthfactor βs and wound healing,” International Journal ofBiochemistry and Cell Biology, vol. 29, no. 1, pp. 63–78, 1997.
[14] M. E. Schrementi, A. M. Ferreira, C. Zender, and L. A.DiPietro, “Site-specific production of TGF-β in oral mucosaland cutaneous wounds,” Wound Repair and Regeneration, vol.16, no. 1, pp. 80–86, 2008.
[15] H. B. Chen, J. G. Rud, K. Lin, and L. Xu, “Nuclear targetingof transforming growth factor-β-activated Smad complexes,”Journal of Biological Chemistry, vol. 280, no. 22, pp. 21329–21336, 2005.
[16] R. Y. Lin, K. M. Sullivan, P. A. Argenta, M. Meuli, H. P.Lorenz, and N. S. Adzick, “Exogenous transforming growthfactor-beta amplifies its own expression and induces scarformation in a model of human fetal skin repair,” Annals ofSurgery, vol. 222, no. 2, pp. 146–154, 1995.
[17] M. Shah, D. M. Foreman, and M. W. J. Ferguson, “Controlof scarring in adult wounds by neutralising antibody totransforming growth factor β,” The Lancet, vol. 339, no. 8787,pp. 213–214, 1992.
[18] M. Shah, D. M. Foreman, and M. W. J. Ferguson,“Neutralisation of TGF-β1 and TGF-β2 or exogenous additionof TGF-β3 to cutaneous rat wounds reduces scarring,” Journalof Cell Science, vol. 108, no. 3, pp. 985–1002, 1995.
[19] N. L. Occleston, H. G. Laverty, S. O’Kane, and M. W. J.Ferguson, “Prevention and reduction of scarring in theskin by transforming growth factor beta 3 (TGFβ3): fromlaboratory discovery to clinical pharmaceutical,” Journal ofBiomaterials Science, vol. 19, no. 8, pp. 1047–1063, 2008.
[20] P. Durani, N. Occleston, S. O’Kane, and M. W. J. Ferguson,“Avotermin: a novel antiscarring agent,” International Journalof Lower Extremity Wounds, vol. 7, no. 3, pp. 160–168, 2008.
[21] H. Laverty, N Occleston, R. Jones et al., “Effects oftransforming growth factor beta 3 in a clinically relevantmodel of full thickness incisional wounding in the Gottingenminipig,” Wound Repair Regen. In press.
[22] J. S. Bond, J. A. L. Duncan, A. Sattar et al., “Maturationof the human scar: an observational study,” Plastic andReconstructive Surgery, vol. 121, no. 2, pp. 487–496, 2008.
[23] J. S. Bond, J. A. L. Duncan, T. Mason et al., “Scar rednessin humans: how long does it persist after incisional andexcisional wounding?” Plastic and Reconstructive Surgery, vol.121, no. 2, pp. 487–496, 2008.
[24] J. A. L. Duncan, J. S. Bond, T. Mason et al., “Visual analoguescale scoring and ranking: a suitable and sensitive method forassessing scar quality?” Plastic and Reconstructive Surgery, vol.118, no. 4, pp. 909–918, 2006.
[25] M. W. J. Ferguson, J. Duncan, J. Bond et al., “Prophylacticadministration of avotermin for improvement of skinscarring: three double-blind, placebo-controlled, phase I/IIstudies,” The Lancet, vol. 373, no. 9671, pp. 1264–1274, 2009.

Hindawi Publishing CorporationDermatology Research and PracticeVolume 2010, Article ID 982623, 5 pagesdoi:10.1155/2010/982623
Review Article
Z-Plasty Made Simple
Sumaira Z. Aasi
Section of Dermatologic Surgery and Cutaneous Oncology, Department of Dermatology,Yale University School of Medicine, New Haven, CT 06510, USA
Correspondence should be addressed to Sumaira Z. Aasi, [email protected]
Received 1 November 2010; Accepted 31 December 2010
Academic Editor: Daniel Berg
Copyright © 2010 Sumaira Z. Aasi. This is an open access article distributed under the Creative Commons Attribution License,which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
A Z-plasty is a critical and reliable technique that is useful for scar revisions and correction of free margin distortion. A Z-plastycan help lengthen a contracted scar, change the direction of a scar so that it is better aligned with the relaxed skin tension lines, orinterrupt and break a scar for better camouflage. This article will review the technique of a basic Z-plasty as well as provide caseexamples of its use in free margin distortion and scar revision.
1. Introduction
In order to achieve optimal aesthetic and functional results,there is no substitute for careful planning and meticuloussurgical technique. Yet even in the most competent hands,surgical complications are an inevitable fact of life. Inparticular, areas of the face that border free margins, suchas the eyes, nose, and lips, present a special challenge tothe dermatologic surgeon. These areas offer little resistanceto any tension created by surgical movement of nearbytissue and are not very forgiving. Any abnormality in thenatural contours of these visually critical structures focusesthe attention to the disruption or distortion itself. Often thedistortion not only leads to an unacceptable cosmetic resultbut may also have functional consequences.
A Z-plasty [1] is a critical and reliable technique for thedermatologic surgeon when performing revisions or correct-ing free margin distortion. There are three main objectiveswhen performing a Z-plasty: to lengthen a contracted scar,to change the direction of a scar so that it is better alignedwith the relaxed skin tension lines, or to interrupt and breaka scar for better camouflage. When it comes to free margins,a Z-plasty is particularly useful because it does not requireexcising more tissue which is often at a premium near freemargins.
2. Design and Execution
As with all surgical reconstruction, it is essential to carefullyplan, measure, and draw out the Z-plasty. Ideally this is
done before any local anesthesia is injected to prevent tissuedistortion. The fundamental unit of a Z-plasty is a triangulardouble transposition flap. However, as with most lifting flaps,there are also elements of rotation and advancement. In aclassic Z-plasty three incisions of equal length create twoequilateral triangular flaps (see Figures 1(b) and 1(c)). Thereis a central limb which is either the scar itself that needs tobe redirected or an incision parallel to this scar. There arealso two arms that originate from this central limb at variousangles. Ideally, the angles may be measured using a protractoror they can be estimated free hand. That is, one can drawa 90-degree limb that comes off the central limb and theneither bisect it to create a 45-degree angles or trisect it tocreate a 30- and, the more commonly used, 60-degree angles.Precise, confident incisions and delicate tissue handling arecritical because the triangular flaps that are being excised andtransposed are often rather small.
Undermining as in any transposition flap is also a keyso that the flap can be transposed without tension. Whentrying to free a contracture or redirect a scar, it is especiallyimportant to undermine widely below any fibrosis thatconstrains the scar. If one only undermines above this plane,the flaps will transpose but the scar tissue below the flaps willprevent release of the contracture and will not significantlyredirect or lengthen the original scar. In addition, for thenovice, it may be helpful to place an indelible dot of ink onone of the flap tips. It is easy to sew the flaps back into theiroriginal position and not actually transpose them once theyhave been undermined and freed (since suturing the flapswith or without transposing will create a z or mirror image

2 Dermatology Research and Practice
(a) (b)
(c) (d)
(e) (f)
Figure 1: (a) Complication of eclabium secondary to herpetic infection of an advancement flap of the upper lip. (b) A 45-degree Z-plastyis planned and drawn. (c) The flaps are widely undermined and transposed. Note the use of skin hooks to minimize trauma to the tenuoustips. (d) Flaps sutured in place. Transposition of the triangular flaps brings about the following changes: the central limb is rotated (from avertical to a horizontal direction), the distance between the original vertical scar (or limb) is increased, and the final scar is “broken” froma straight line to a nonlinear Z configuration. (e) Patient at suture removal. Note the immediate correction of the eclabium. (f) Results atseveral months. The scar lines have become more subtle.
25% gain 50% gain 75% gain
30-angle 45-angle 60-angle
Figure 2: The degree of scar directional change and lengthening is affected by the angles of the flap. In the 30-degree Z-plasty, the directionof the change is approximately 45 degrees from the initial position of the central limb and there is a 25% gain in scar length. With a 45-degreeZ-plasty, the resultant limb lies in a more oblique position, approximately 60 degrees from the initial position and there is a 50% gain in scarlength. A 60-degree Z-plasty will yield a 75% increase in scar length and a 90-degree change in scar direction (the broken line represents theoriginal scar).

Dermatology Research and Practice 3
Figure 3: A multiple Z-plasty.
(a) (b)
(c) (d)
Figure 4: For a scar that crosses the melolabial fold (black line) in an undesirable perpendicular fashion, there are two ways that the Z-plastycould be performed to change the scar direction (represented by the green and red inks in Figures 4(a) and 4(c)). Although both optionswill change the scar direction to match the melolabial fold, only one of the designs (green ink Figure 4(b)) allows for the limbs of the Z-plasty to align with the RSTLs of the cheek and lip. Conversely, in Figure 4(d) even though the mirror image also realigns the central limbappropriately, the resultant lateral limbs cross the RSTL of the lip and cheek in an undesirable perpendicular fashion.
of a z). After undermining, one triangular flap is transposedabout its pivotal point in a clockwise direction and the otherin a counterclockwise direction to create the Z-plasty. Inmost cases, one does not need a lot of buried interruptedsutures and must be fairly gentle with the tips of the Z-plastyto avoid vascular compromise of these small flaps [2].
3. Limitations and Considerations
The degree of scar directional change and lengthening isdetermined by the angles of the flap: the larger the angle,the greater the lengthening and the greater the change in
direction of the original scar, the smaller the angle, the lessthe lengthening and change in the direction of the originalscar (Figure 2). Although angles between 30 and 90 degreesare possible, the 60-degree Z-plasty is most common. A 60-degree Z-plasty will yield a 75% increase in scar length and a90-degree change in scar direction. In the 45-degree Z-plasty,the resultant central limb lies in a more oblique position,approximately 60 degrees from the initial position. In the30-degree Z-plasty, the direction of the change is even less,approximately 45 degrees from the initial position of thecentral limb. Z-plasties with angles less than 30 degrees willgreatly increase the risk of tip necrosis. Z-plasties created by

4 Dermatology Research and Practice
(a) (b) (c) (d) (e)
(f) (g) (h) (i)
(j) (k)
Figure 5: (a) Alar retraction secondary to multiple tumor extirpations resulting in an ecnasion. (b) A Z-plasty is planned. One relativelysimple way to estimate the angles is to draw out the peripheral arms at 90 angles to the central limb and then divide this in 1/2 to get 45-degree angles or trisect it to obtain 30- or 60-degree angles as shown. (c) Z-plasty sutured in place. ((d) and (e)) Frontal and lateral viewsdemonstrating that alar retraction has improved but not completely resolved (cf. Figure 5(a)). (f) Another, more inferior Z-plasty is plannedat a later date. (g) A strip of cartilage is used underneath the flap to provide structural support to the alar rim. (h) Z-plasty sutured in place.(i) Patient at suture removal. (j-k) Frontal and lateral views demonstrating resolution of the ecnasion.
(a) (b) (c) (d)
Figure 6: (a) Scar creating webbing in the retroauricular sulcus. (b) Z-plasty designed. (c) A Z-plasty is performed to release the contracture.(d) Patient at suture removal.

Dermatology Research and Practice 5
angles greater than 60 degrees will make it more difficult totranspose the two flaps without tension and also producestanding cutaneous deformities or “dog ears.” It is importantto bear in mind that these mathematical predictions donot bear out precisely in practice when dealing with livetissue because of factors such as pliability and tensile forcesthat place constraints on skin. Thus, the gain in scarlengthening or directional change is almost always less thancalculated.
The limb lengths of the Z-plasty also influence the lengthgained: the longer the limbs, the greater the gain in scarlength. Yet these limbs of the Z-plasty have some practicallimitations in terms of their length. Although the brokenline scar created by a Z-plasty allows for an overall lessperceptible scar, this advantage diminishes with longer limbsas they will eventually create more obvious scar lines (andan unnatural appearance of a Z-shaped scar). Usually 6 to10 millimeters is as long as any segment of the Z-plastyshould be designed, particularly if the segment does not liein a favorable direction or at the junction of two cosmeticunits. In order to decrease the formation of a noticeable Z-shaped scar and overcome the practical limb lengths, a longerscar can be broken up by using multiple Z-plasties (Figure 3).Finally, mechanical dermabrasion or laser resurfacing can beperformed afterwards to camouflage and make the Z-shapedscar more subtle.
Finally one should also consider the relaxed skin tensionlines of the face when planning the Z-plasty such that theamount of directional change (and hence final scar lines) canbe most similar to the RSTLs. For each particular scar orcentral limb, there are always two choices for the alignmentof the peripheral arms, these being mirror images of oneanother (Figure 4). Both options should be considered sinceboth designs will change the scar direction; however, oneof these options will usually be a better choice for scarcamouflage due to placement of the lateral limbs such thatthey more correctly mimic the RSTL.
Like other transposition flaps, a Z-plasties can createtrapdoor or pincushion effect. Wide undermining to createan even scar contraction plate may help decrease this risk.Post-operative intralesional steroids may also help diminishsuch an effect should it occur.
Case Examples.
Case 1. Figure 5 represents an example of Case 1.
Case 2. Figure 6 represents an example of Case 2.
References
[1] C. R. Hove, E. F. Williams III, and B. J. Rodgers, “Z-plasty: aconcise review,” Facial Plastic Surgery, vol. 17, no. 4, pp. 289–293, 2001.
[2] J. L. Frodel and T. D. Wang, “Z-plasty,” in Local Flaps in FacialReconstruction, S. R. Baker and N. A. Swanson, Eds., pp. 131–149, Mosby, St. Louis, Mo, USA, 1995.

Hindawi Publishing CorporationDermatology Research and PracticeVolume 2010, Article ID 210150, 7 pagesdoi:10.1155/2010/210150
Clinical Study
Long-Term Followup of Dermal Substitution with AcellularDermal Implant in Burns and Postburn Scar Corrections
I. Juhasz,1, 2 B. Kiss,1 L. Lukacs,2 I. Erdei,1, 3 Z. Peter,1 and E. Remenyik1
1 Department of Dermatology, Burn and Dermatosurgery Unit, University of Debrecen Medical and Health Science Center,4032 Debrecen, Hungary
2 Faculty of Dentistry, University of Debrecen Medical and Health Science Center, 4032 Debrecen, Hungary3 Department of Anesthesiology and Intensive Care, University of Debrecen Medical and Health Science Center,4032 Debrecen, Hungary
Correspondence should be addressed to I. Juhasz, [email protected]
Received 14 June 2010; Accepted 24 November 2010
Academic Editor: Hayes B. Gladstone
Copyright © 2010 I. Juhasz et al. This is an open access article distributed under the Creative Commons Attribution License, whichpermits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Full-thickness burn and other types of deep skin loss will result in scar formation. For at least partial replacement of the lost dermallayer, there are several options to use biotechnologically derived extracellular matrix components or tissue scaffolds of cadaver skinorigin. In a survey, we have collected data on 18 pts who have previously received acellular dermal implant Alloderm. The age ofthese patients at the injury varied between 16 months and 84 years. The average area of the implants was 185 cm2. Among those,15 implant sites of 14 patients were assessed at an average of 50 months after surgery. The scar function was assessed by using themodified Vancouver Scar Scale. We have found that the overall scar quality and function was significantly better over the implantedareas than over the surrounding skin. Also these areas received a better score for scar height and pliability. Our findings suggest thatacellular dermal implants are especially useful tools in the treatment of full-thickness burns as well as postburn scar contractures.
1. Introduction
Once the dermis of the injured skin is lost due to full-thickness burn, it will either be replaced by scar thatoriginates from granulation tissue and epithelized from thewound edges, or skin grafting will close the wound. Neitherthe scar tissue, nor the patchy dermal residual islands ofdermal papillae provided by the split-thickness skin graft(STSG) will result in a continuous healthy dermal layer to thewound site. The quality and function of dermal connectivetissue and the amount and orientation of dermal elastic fibershave great impact on postinjury skin quality. The typicalscar tissue is characterized by sparse elastic fibers and newlyformed collagen bundles in random orientation. There areseveral methods available that are designed to improve thequalities of the dermal wound bed, while some of thesemethods aim to provide dermal tissue for replacement.Harvesting thicker grafts will enormously increase donor sitemorbidity; full-thickness skin grafting has a strict limitationof a mere few square cms. Donor site is often limited
and when applying the gold standard of wound closure,autologous stsg, it has to be expanded to a ratio wheredisfiguring scarring is inevitable. A widely used alternative isto restore barrier function until definitive closure by applyingtemporary coverage, preferably with biological dressings.A large variety of methods are available ranging fromxenograft (frog’s membrane to porcine skin) to allogenictissue (e.g., placenta, frozen-, cryopreserved- or glycerolpreserved human skin). Risk of transmission of infectiousdiseases is a theoretical drawback of these materials; despiteimplementing tissue banking guidelines, this risk is relativelow. There is a range of bioengineered skin substitutesavailable for the purpose of improving the quality of skinin the area of dermal loss. These can either be appliedduring tissue repair or after scar formation, as tools forreconstructive surgery.
Due to the diversity of the commercially availablebiotechnologically produced materials, it is rather difficult tocompare their real value and usefulness, and there remainssome uncertainty regarding their effectiveness. Some of

2 Dermatology Research and Practice
these materials contain cells, some only cellular products,characteristically in a rather complex manner. Clinically,as it seems, the simple delivery of macromolecules, suchas collagen, in an unstructured manner (powder, cream,gel, etc.) may not fulfill the many requirements of theproliferative phase of wound healing. It is likely, that a 3-dimensional structure is mandatory, effectively provided byan acellular natural dermal scaffold or a tissue-engineerednewly formed biological matrix. There remains a questionwhether the more complex cellular products could deliver theextra clinical advantage, that justifies the higher cost associ-ated with their production. Besides the high price, challengesin obtaining reimbursement, together with complicatedregulations and approval regarding the use of allogeneic cellsmake the future of these products uncertain [1]. The nameand origin of some of the most typical and important tissue-engineered materials are summarized in Table 1 in the orderof their complexity and appearance on the market.
2. Acellular Preparations
MB-Collagen or Collagen-Klee (Medical Biomaterial Prod-ucts GmbH Neustadt-Glewe, BRD), a resorbable, 5 mm thickcollagen membrane made of porcine origin is an example ofthe many collagen delivery devices on the market to promoteconnective tissue proliferation during wound repair [2].
BGC Matrix (Brennen Medical Inc, St. Paul MN, USA)consists of beta-Glucan, a complex carbohydrate isolatedfrom the cell wall of oats and a porcine collagen hydrocolloidmatrix combined in a multifilament mesh [3].
Promogran (Systagenix Wound Management Ltd., Gar-grave, UK), in addition to its bovine collagen content,also contains regenerated oxidized cellulose as an additionalsource of substrate for binding to matrix metalloproteasespresent in the chronic wounds. Substrate substitution aimsat the inactivation of ECM degrading enzymes and theprotection of naturally occurring growth factors. It is con-cluded that protease-modulation by substrate substitutionacts synergistically with autologous growth factors in diabeticfoot ulcers [4].
Biostep/Biostep Ag Collagen Matrix Dressing (Smith &Nephew Inc. St. Petersburg, FL USA) provides its porcinecollagen content considerable antimicrobial activity with thecombination of Silver ions (company information).
Matriderm (Dr. Suwelack Skin & Health Care AG,Billerbeck, BRD) is a three-dimensional matrix consistingof collagen and elastin, comparable to the structure ofhuman dermis. The sheets are used in a one-step procedure,applied dry, possess unique hemostyptical characteristics,and rehydrate “in loco” after grafting. When full-thicknessacute burn wounds are treated with STSG alone, and with theuse of Matriderm, the use of the device results in improvedscar (skin) formation [5].
Alloderm regenerative tissue matrix (LifeCell Co., TheWoodlands, TX USA) is a freeze-dried extracellular matrix(ECM) tissue derived from cadaver skin, through a processresulting in removal of all cellular components and residues.The ECM has high hyaluronan and proteoglycan content,while the scaffold retains its collagen and elastic fiber content
and structure, with an intact basement membrane. Thematerial is made from tissue bank skin and has a 2-year shelflife. The acellular dermal implant Alloderm is available alsoin a meshed version and has been advocated and approvedsince 1995 for the management of acute burns in whichthe dermis is severely damaged [6]. It allows the utilizationof ultra thin autograft skin, (0,1-0,2 mm instead of 0,35–0,5 mm), strongly reducing donor site morbidity and soonallowing for reharvesting the donor area. The product in facthas received its FDA approval, as “banked human tissue” andnot as a “medical device” if used in an orthotopic way, thatis, as skin replacement. Probably it is the most widely usedproduct for dermal regeneration as of now.
The European version of Alloderm is called Glyadermacellular dermal collagen-elastin matrix. It is a dermalsubstitute produced by the Euro Skin Bank (Beverwijk,NL) and is based on the glycerol-preservation technique,developed for producing allogenic temporary skin grafts forburn treatment [7].
SureDerm (Hans Biomed Corp., Seoul, Korea) is anothersimilar product to Alloderm. It is made according toAATB (American Association of Tissue Banks) guidelines inSouth Korea, requiring less rehydration time (10 minutesversus 20–40 minutes). Only limited scientific informationis available [8], but this relatively newcomer product hasboth FDA and CE approval, allowing to gain its share of themarket.
Integra (Integra LifeSciences Co., Plainsboro, NJ USA)dermal regeneration template consists of two layers; a porouschondroitin 6 sulphate glucosaminoglycane (GAG) andbovine collagen-based dermal analogue, which integrateswith the patient’s own cells and a supporting epidermalsilicone sheet. The product besides promoting and regulatingdermal development also provides a massive temporarycover of the wound area; the protective layer, later as thewound heals, gets peeled off. A very thin autograft is thengrafted onto the neo-dermis. Integra is primarily indicatedfor the postexcisional treatment of full-thickness or deeppartial-thickness burns and similar tissue defects. A relativelyhigh incidence rate of infectious complications follows itsapplication, but its frequency can be reduced by more carefultiming, that is, earlier application [9].
3. Cell-Containing Devices
TransCyte, formerly Dermagraft TC (Advanced BioHeal-ing Inc, Westport, CT USA) is a temporary, biosyntheticcovering material composed of a semipermeable siliconemembrane and human fibroblast cells of newborn foreskinorigin cultured on a porcine collagen coated nylon mesh.During the 17 days manufacturing cycle in a so-called“bioreactor” the cellular products, fibronectin, tenascin, gly-cosaminoglycans, growth factors reach high concentration.The device is then frozen and stored at −70◦C until it isused. Human application is possible, because the fibroblastsreaching the wound surface are metabolically already inactiveand do not provoke immunological rejection [10]. It hasbeen indicated for use as a temporary covering for excisedburns prior to autografting. Another indication is to use it

Dermatology Research and Practice 3
Table 1: Biotechnologically derived products designed to improve dermal wound repair.
Biotechnological device
Name Composition ManufacturerCellularcontent
Ref. no
MB-Collagen/Collagen-Klee
Porcine collagenMedical Biomaterial Products GmbHNeustadt-Glewe, BRD
no [2]
BGC Matrix Porcine collagen and beta-GlucanBrennen Medical Inc, St. Paul MN,USA
no [3]
PromogranBovine collagen, regenerated oxidizedcellulose
Systagenix Wound Management Ltd.,Gargrave, UK
no [4]
Biostep/Biostep AgCollagen Matrix Dressing
Porcine collagenSmith & Nephew Inc. St. Petersburg,FL USA
no —
Matriderm Bovine collagen and elastin matrixDr. Suwelack Skin & Health Care AG,Billerbeck, BRD
no [5]
Alloderm regenerativetissue matrix
Freeze-dried ECM from cadaver skin LifeCell Co., The Woodlands, TX USA no [6]
Glyaderm dermalreplacement material
Dermal collagen-elastin matrix Euro Skin Bank, Beverwijk, NL no [7]
SureDerm Freeze-dried ECM from cadaver skin Hans Biomed Corp., Seoul, Korea no [8]
Integra dermalregeneration template
Bovine collagen and GAG, with asupporting epidermal silicone sheet
Integra LifeSciences Co., Plainsboro,NJ USA
no [9]
TransCyte/Dermagraft TCtemporary, biosyntheticwound cover
Porcine collagen coated nylon meshwith human fibroblast and siliconemembrane
Advanced BioHealing Inc, Westport,CT USA
yes [11]
DermagraftBiodegradable polyglactin mesh withhuman fibroblast
Advanced BioHealing Inc, Westport,CT USA
yes [12]
Apligraf/Graftskin livingskin equivalent
Bilayered structure bovine collagenwith human fibroblasts and humankeratinocytes
Organogenesis Inc., Canton, MA USAand Novartis AG Basel, CH
yes [13]
OrCel cryopreservedbilayered matrix
Bilayered structure bovine collagenwith human fibroblasts and humankeratinocytes
Forticell BioScience Inc., New York,NY USA
yes [16]
StrataGraft Pathogen-freehuman temporary allograft
Bilayered structure: non-bovinecollagen with human fibroblasts andimmortalized human keratinocytes
Stratatech Corporation, Madison, WIUSA
yes [17]
on donor sites or burns that do not require autografting, thatis, as a biological dressing material [11].
Dermagraft (Advanced BioHealing Inc, Westport, CTUSA) is similar to the previous device, but the scaffold isa biodegradable polyglactin mesh seeded with allogeneicneonatal fibroblasts. The fibroblasts proliferate and pro-duce dermal collagen, growth factors, glycosaminoglycans(GAGs), and fibronectin to restore the dermal bed, whilethe mesh material is gradually absorbed. It is intended tobe used as a temporary covering to promote wound healingvia multiple applications of the device. The result of thistype of approach is second intention healing, one reason whyDermagraft is primarily intended for diabetic foot ulcer [12].
Apligraf formerly Graftskin (Organogenesis Inc., Can-ton, MA, USA and Novartis AG Basel, CH) is a bilayeredliving skin equivalent composed of allogeneic fibroblasts andtype I bovine collagen as dermis and allogeneic neonatalforeskin-derived keratinocytes as epidermis. It has a shortshelf-life of 5 days, so needs to be applied while “fresh”. Itis on the market since 1998 and is currently approved foraccelerating the closure of chronic wounds, diabetic foot,
and venous leg ulcer. Experimental application in exciseddeep burn wounds combined with autografting was reportedby Waymack et al. [13]. Apligraf ’s DNA persisted in aminority of patients only at 4 weeks after grafting in acutepartial-thickness wounds [14]. Its success in speeding thehealing of acute wounds appears to be related to otherfactors than the persistence of donor DNA or basementmembrane restoration. For the treatment of deep chronicwounds, the same manufacturer developed a monolayerproduct, with live human fibroblasts in a collagen matrix,without a keratinocyte layer [15], which is currently notavailable. A further developed version of Apligraf aimingto omit the use of xenogenic collagen and utilizing humancollagen produced de novo by the human fibroblasts is inlate-stage development (VCT01, company information).
OrCel (Forticell BioScience Inc., New York, NY USA)is a cryopreserved bilayered matrix with fibroblasts andkeratinocytes cultured on type I. collagen 3D matrix. ItsFDA approval was obtained in 2001 for treatment of acutesurgical excisions, such as contracture release sites and donorsites in epidermolysis bullosa (EB) patients undergoing hand
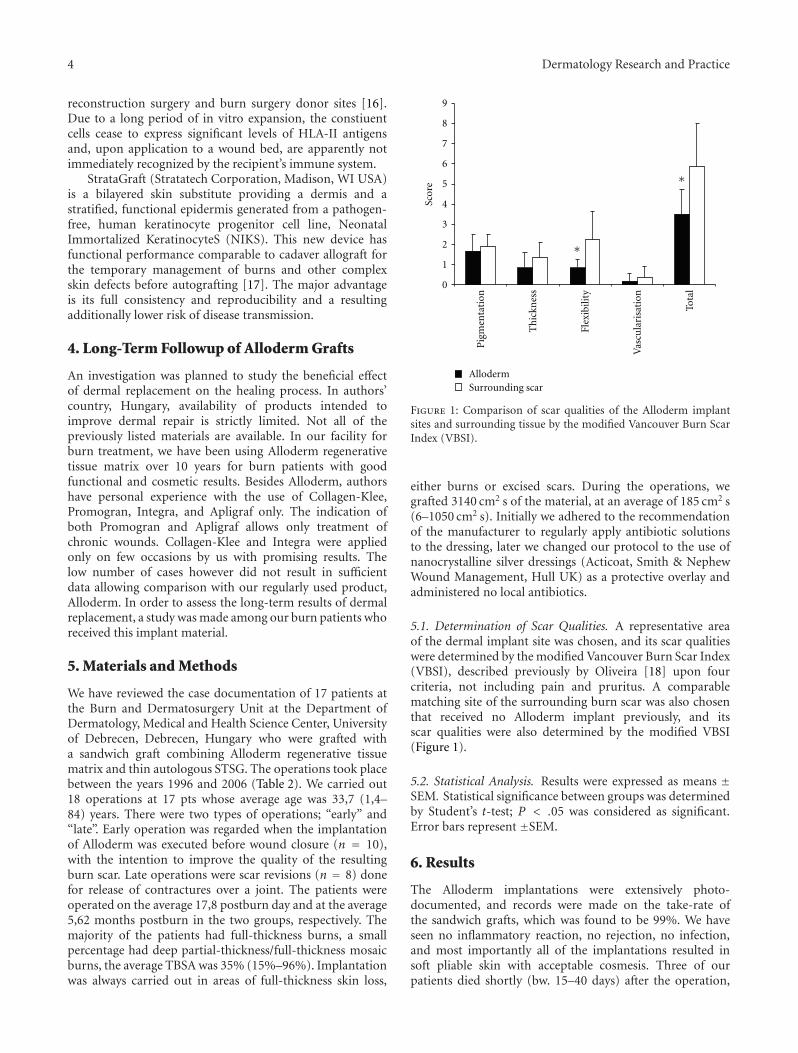
4 Dermatology Research and Practice
reconstruction surgery and burn surgery donor sites [16].Due to a long period of in vitro expansion, the constiuentcells cease to express significant levels of HLA-II antigensand, upon application to a wound bed, are apparently notimmediately recognized by the recipient’s immune system.
StrataGraft (Stratatech Corporation, Madison, WI USA)is a bilayered skin substitute providing a dermis and astratified, functional epidermis generated from a pathogen-free, human keratinocyte progenitor cell line, NeonatalImmortalized KeratinocyteS (NIKS). This new device hasfunctional performance comparable to cadaver allograft forthe temporary management of burns and other complexskin defects before autografting [17]. The major advantageis its full consistency and reproducibility and a resultingadditionally lower risk of disease transmission.
4. Long-Term Followup of Alloderm Grafts
An investigation was planned to study the beneficial effectof dermal replacement on the healing process. In authors’country, Hungary, availability of products intended toimprove dermal repair is strictly limited. Not all of thepreviously listed materials are available. In our facility forburn treatment, we have been using Alloderm regenerativetissue matrix over 10 years for burn patients with goodfunctional and cosmetic results. Besides Alloderm, authorshave personal experience with the use of Collagen-Klee,Promogran, Integra, and Apligraf only. The indication ofboth Promogran and Apligraf allows only treatment ofchronic wounds. Collagen-Klee and Integra were appliedonly on few occasions by us with promising results. Thelow number of cases however did not result in sufficientdata allowing comparison with our regularly used product,Alloderm. In order to assess the long-term results of dermalreplacement, a study was made among our burn patients whoreceived this implant material.
5. Materials and Methods
We have reviewed the case documentation of 17 patients atthe Burn and Dermatosurgery Unit at the Department ofDermatology, Medical and Health Science Center, Universityof Debrecen, Debrecen, Hungary who were grafted witha sandwich graft combining Alloderm regenerative tissuematrix and thin autologous STSG. The operations took placebetween the years 1996 and 2006 (Table 2). We carried out18 operations at 17 pts whose average age was 33,7 (1,4–84) years. There were two types of operations; “early” and“late”. Early operation was regarded when the implantationof Alloderm was executed before wound closure (n = 10),with the intention to improve the quality of the resultingburn scar. Late operations were scar revisions (n = 8) donefor release of contractures over a joint. The patients wereoperated on the average 17,8 postburn day and at the average5,62 months postburn in the two groups, respectively. Themajority of the patients had full-thickness burns, a smallpercentage had deep partial-thickness/full-thickness mosaicburns, the average TBSA was 35% (15%–96%). Implantationwas always carried out in areas of full-thickness skin loss,
0
1
2
3
4
5
6
7
8
9
AllodermSurrounding scar
∗
∗
Pig
men
tati
on
Th
ickn
ess
Flex
ibili
ty
Vas
cula
risa
tion
Tota
l
S co r
e
Figure 1: Comparison of scar qualities of the Alloderm implantsites and surrounding tissue by the modified Vancouver Burn ScarIndex (VBSI).
either burns or excised scars. During the operations, wegrafted 3140 cm2 s of the material, at an average of 185 cm2 s(6–1050 cm2 s). Initially we adhered to the recommendationof the manufacturer to regularly apply antibiotic solutionsto the dressing, later we changed our protocol to the use ofnanocrystalline silver dressings (Acticoat, Smith & NephewWound Management, Hull UK) as a protective overlay andadministered no local antibiotics.
5.1. Determination of Scar Qualities. A representative areaof the dermal implant site was chosen, and its scar qualitieswere determined by the modified Vancouver Burn Scar Index(VBSI), described previously by Oliveira [18] upon fourcriteria, not including pain and pruritus. A comparablematching site of the surrounding burn scar was also chosenthat received no Alloderm implant previously, and itsscar qualities were also determined by the modified VBSI(Figure 1).
5.2. Statistical Analysis. Results were expressed as means ±SEM. Statistical significance between groups was determinedby Student’s t-test; P < .05 was considered as significant.Error bars represent ±SEM.
6. Results
The Alloderm implantations were extensively photo-documented, and records were made on the take-rate ofthe sandwich grafts, which was found to be 99%. We haveseen no inflammatory reaction, no rejection, no infection,and most importantly all of the implantations resulted insoft pliable skin with acceptable cosmesis. Three of ourpatients died shortly (bw. 15–40 days) after the operation,
Dermatology Research and Practice 5
Table 2: List of patients grafted with a sandwich graft combining Alloderm regenerative tissue matrix and thin autologous split thicknessskin graft.
Age of pt. atburn
Dermal replacementDepth of burn TBSA %
Burnmechanism
Age of scar atcontrol (mo)
Graft area(cm2)
TypeDays after
burnMonths
after burn
(1) 6 early 30 (III) degree 96 flame exit 32
(2) 35 late 2 (III) degree, scar 25 scald 48 180
(3) 8 late 4 (III) degree, scar 20 contact 86 104
(4) 40 late 6 (III) degree, scar 15 scald 46 110
(5) 42 early 14 (III) degree 20 contact 14 200
(6) 42 early 3 (IIb-III) degree 25 contact 36 44
(7) 14 late 3 (III) degree, scar 65 electr + contact 85 130
(8) 28 early 4 (III) degree 18 contact 19 720
(9)16
early 10 (III) degree75
electr + contact 122 850
(10) late 4 (III) degree, scar electr + contact 118 200
(11) 1,8 late 22 (III) degree, scar 20 scald 34 30
(12) 1,4 early 16 (IIb-III) degree 15 scald 70 6
(13) 43 late 2 (III) degree, scar 19 scald 13 90
(14) 84 late 2 (III) degree, scar 35 flame exit 40
(15) 47 early 27 (III) degree 55 flame exit 110
(16) 49 early 25 (III) degree 25 contact 18 220
(17) 72 early 28 (III) degree 32 flame 36 45
(18) 43 early 21 (III) degree 39 contact 1430
3140
Avg. 33.66 17,8 5,62 35 50,6 185
Table 3: Determination of scar qualities of the Alloderm implant sites and surrounding tissue by the modified Vancouver Burn Scar Index(VBSI).
PIGM HEIGHT FLX VASC SUM PIGM HEIGHT FLX VASC SUM
(1) 1 1 1 0 3 1 2 1 0 4
(2) 1 1 1 0 3 1 2 1 0 4
(3) 2 0 1 0 3 2 2 3 0 7
(4) 2 0 0 0 2 2 1 1 0 4
(5) 1 1 1 0 3 2 1 4 0 7
(6) 1 0 0 0 1 2 1 1 0 4
(7) 0 0 1 0 1 2 2 4 0 8
(8) 2 1 1 0 4 2 2 4 2 10
(9) 1 0 0 0 1 2 1 1 0 4
(10) 3 1 1 0 5 3 2 3 0 8
(11) 1 2 1 1 5 1 1 1 1 4
(12) 1 0 0 0 1 1 1 1 0 3
(13) 1 0 0 0 1 1 1 1 0 3
(14) 2 0 1 1 4 3 0 2 1 6
(15) 2 0 1 1 4 3 0 2 1 6
Dermal replacement area Surrounding scarred skin
Abbreviations: PIGM: pigmentation, FLX: flexibility, VASC: vascularization, SUM: summary.
their grafts were also problem free. In order to determine thelong-term results of the interventions, we called the patientsto control in 2007. During the control, 14 patients with 15operation sites were investigated. The average age of scarat investigation was 50,6 months (14–122 months). Scar
qualities were determined by VBSI, both of a representativearea of the dermal implant site, and that of a chosencomparable matching site of the surrounding burn scar,that received no Alloderm implant previously. The VBSImeasurements of the sites are collected in Table 3.

6 Dermatology Research and Practice
(a)
(b) (c) (d) (e)
Figure 2: Patient no. 3, 8-years-old male suffered 4 months earlier from full-thickness burn on 20% body surface area and had conservativetreatment (at another institution). (a) Upon admission: spontaneous rupture of scar that was causing severe axillary contracture. (b)Intraoperative photograph after removal of scar tissue. Full axillary function following sandwich grafting with Alloderm and thin autologousskin at (c) 3 months and (d) 7 years postoperatively. (e) No visible trace of previous harvesting of autograft skin can be seen at the donor siteon right thigh (picture taken at 7 years post-op.).
The examinations revealed uniformly better VBSI valuesin the Alloderm implant group than in the control group.The differences in color, thickness, and vascularization ofthe skin at the dermal replacement site were not significantwhen compared to control. Flexibility and overall scar qualityhowever were significantly better at the Alloderm implantsite than at the control area. In addition to the favorablequality of scar (skin) at the site of dermal replacement, thefunctional results were also excellent; all of the patients withno exception, who were operated due to scar contracture,regained their full joint movement.
7. Discussion
In an elegant series of nude mouse transplantation experi-ments, Truong et al. [19] compared effects of dermal substi-tutes on wound healing. They experienced that human skin-derived products, Alloderm and their similarly processedown acellular dermal matrix produced the least contractionand the thickest neodermis in the healed wounds, whencompared to control or synthetic dermal substitutes. Theapplication of processed acellular cadaver dermis has provenextremely useful in the fields of burns and reconstructivesurgery and is gaining acceptance elsewhere, for variousoff-label indications for example, in neurosurgery [20],ophthalmic surgery [21], head and neck surgery [22, 23],and in hernia repair [24]. Its application in extensive burnsprovides the grafted area with functionally and estheticallyoutstanding skin as a result. Despite being an additional layerbetween the wound bed and epithelial cover, it does not hin-der graft take. Possibly due to its intact ECM structure, therepopulation by recipient cells, fibroblasts, endothelial cells,and so forth, is extremely rapid. Clinically the STSG overlayacts no differently than a simple skin graft, their color andother vitality signs are identical. There is the added advantageof the possibility of harvesting ultra thin (0,1-0,2 mm thick)skin for autografting, which dramatically reduces the trauma
of the donor area. The resulting neodermis is soft, pliableresembling normal skin. In two early cases the Allodermcontaining sandwich graft was applied to the decorticatedbone of the scapula (unpublished case) and of the proximalthird of the tibia [25]. In both cases, a vital neodermiswas the result, that could be easily wrinkled and providedprotective support to the overlaying epidermis. Histologicalexamination revealed an inflammation-free neodermis, withample vascularization and abundant loose collagen fibrilsplus oligocellular elastic connective tissue. The epidermishad normal structure and keratinisation, with apparentcell proliferation (indicated by Ki67 mAb expression). TheAlloderm implant converted into a compact, functionallyand morphologically live neodermis as an interconnectionbetween the epidermal layer of the skin and the underlyingbony tissue [25]. In the opinion of the authors, the easy, one-step procedure of Alloderm grafting with a simultaneous thinSTSG overlay is an ideal, minimally invasive procedure incase of joint contractures, delivering in most cases superioror comparable results to complicated skin or fasciocutaneousflaps without the associated donor site morbidity.
Hereby, we present cases in which we have used thisimplant during the surgery of acute burns as well as in thetreatment of postburn scar contractures. In our survey, wehave collected data on our patients with full-thickness burnsand scar contractures and assessed scar qualities compared tothat of their neighboring similarly treated but nonimplantedburn scars. A total of 15 dermal replacement sites and 15control sites were evaluated and compared. The applied VBSIresults confirmed our hypothesis, namely, the implantationof acellular dermal implant makes a considerable impact onthe quality of the resulting scar, by making it softer andmore elastic than the surrounding tissue receiving no dermalimplant.
A major advantage of the technique is the reduction ofdonor-site morbidity (Figure 2) due to the application ofvery thin autologous skin required.
Dermatology Research and Practice 7
Acknowledgment
The authors wish to Acknowledge the research supportfor the following grant: Hungarian Science and TechnologyFoundation (FR-26/2009) IKUT TAMOP (4.2.2-08/1-2008-0019 Derminova).
References
[1] M. Ehrenreich and Z. Ruszczak, “Update on dermal substi-tutes,” Acta Dermatovenerologica Croatica, vol. 14, no. 3, pp.172–187, 2006.
[2] A. Neumann-Scholz, M. Lessee, and B. Winkler, “Weiter-entwicklung zum Kollagen- Hamostyptikum-Vlies,” Medica-mentum Berlin, vol. 29, pp. 64–65, 1988.
[3] S. J. Delatte, J. Evans, A. Hebra, W. Adamson, H. B. Othersen,and E. P. Tagge, “Effectiveness of beta-glucan collagen fortreatment of partial-thickness burns in children,” Journal ofPediatric Surgery, vol. 36, no. 1, pp. 113–118, 2001.
[4] D. D. Kakagia, K. J. Kazakos, K. C. Xarchas et al., “Synergisticaction of protease-modulating matrix and autologous growthfactors in healing of diabetic foot ulcers. A prospectiverandomized trial,” Journal of Diabetes and its Complications,vol. 21, no. 6, pp. 387–391, 2007.
[5] H. Ryssel, E. Gazyakan, G. Germann, and M. Ohlbauer,“The use of MatriDerm in early excision and simultaneousautologous skin grafting in burns-A pilot study,” Burns, vol.34, no. 1, pp. 93–97, 2008.
[6] H. Yim, Y. S. Cho, C. H. Seo et al., “The use of AlloDermon major burn patients: AlloDerm prevents post-burn jointcontracture,” Burns, vol. 36, no. 3, pp. 322–328, 2010.
[7] C. D. Richters, A. Pirayesh, H. Hoeksema et al., “Developmentof a dermal matrix from glycerol preserved allogeneic skin,”Cell and Tissue Banking, vol. 9, no. 4, pp. 309–315, 2008.
[8] K. C. Lee, NO. H. Lee, J. H. Ban, and S. M. Jin, “Surgicaltreatment using an allograft dermal matrix for nasal septalperforation,” Yonsei Medical Journal, vol. 49, no. 2, pp. 244–248, 2008.
[9] L. Bargues, S. Boyer, T. Leclerc, P. Duhamel, and E. Bey,“Incidence and microbiology of infectious complications withthe use of artificial skin Integra in burns,” Annales de ChirurgiePlastique et Esthetique, vol. 54, no. 6, pp. 533–539, 2009.
[10] S. E. Sher, B. E. Hull, and S. Rosen, “Acceptance of allogeneicfibroblasts in skin equivalent transplants,” Transplantation,vol. 36, no. 5, pp. 552–557, 1983.
[11] R. J. Kumar, R. M. Kimble, R. Boots, and S. P. Pegg, “Treatmentof partial-thickness burns: a prospective, randomized trial
using transcyteTM
,” ANZ Journal of Surgery, vol. 74, no. 8, pp.622–626, 2004.
[12] W. A. Marston, “Dermagraft�, a bioengineered humandermal equivalent for the treatment of chronic nonhealingdiabetic foot ulcer,” Expert Review of Medical Devices, vol. 1,no. 1, pp. 21–31, 2004.
[13] P. Waymack, R. G. Duff, and M. Sabolinski, “The effect of atissue engineered bilayered living skin analog, over meshedsplit-thickness autografts on the healing of excised burnwounds,” Burns, vol. 26, no. 7, pp. 609–619, 2000.
[14] S. Hu, R. S. Kirsner, V. Falanga, T. Phillips, and W. H.Eaglstein, “Evaluation of Apligraf� persistence and basementmembrane restoration in donor site wounds: a pilot study,”Wound Repair and Regeneration, vol. 14, no. 4, pp. 427–433,2006.
[15] M. Lımova, “New therapeutic options for chronic wounds,”Dermatologic Clinics, vol. 20, no. 2, pp. 357–363, 2002.
[16] J. Still, P. Glat, P. Silverstein, J. Griswold, and D. Mozingo, “Theuse of a collagen sponge/living cell composite material to treatdonor sites in burn patients,” Burns, vol. 29, no. 8, pp. 837–841, 2003.
[17] M. J. Schurr, K. N. Foster, J. M. Centanni et al., “Phase I/IIclinical evaluation of StrataGraft: a consistent, pathogen-freehuman skin substitute,” The Journal of Trauma, vol. 66, no. 3,pp. 866–874, 2009.
[18] G. V. Oliveira, D. Chinkes, C. Mitchell, G. Oliveras, H.K. Hawkins, and D. N. Herndon, “Objective assessment ofburn scar vascularity, erythema, pliability, thickness, andplanimetry,” Dermatologic Surgery, vol. 31, no. 1, pp. 48–58,2005.
[19] A.-T. N. Truong, A. Kowal-Vern, B. A. Latenser, D. E. Wiley,and R. J. Walter, “Comparison of dermal substitutes in woundhealing utilizing a nude mouse model,” Journal of Burns andWounds, vol. 4, article e4, 2005.
[20] W. L. Warren, M. B. Medary, C. D. Dureza et al., “Duralrepair using acellular human dermis: experience with 200cases: technique assessment,” Neurosurgery, vol. 46, no. 6, pp.1391–1396, 2000.
[21] P. A. D. Rubin, A. M. Fay, H. D. Remulla, and M. Maus, “Oph-thalmic plastic applications of acellular dermal allografts,”Ophthalmology, vol. 106, no. 11, pp. 2091–2097, 1999.
[22] R. W. H. Kridel, H. Foda, and K. C. Lunde, “Septal perforationrepair with acellular human dermal allograft,” Archives ofOtolaryngology. Head and Neck Surgery, vol. 124, no. 1, pp. 73–78, 1998.
[23] J. N. Fayad, T. Baino, and S. C. Parisier, “Preliminaryresults with the use of AlloDerm in chronic otitis media,”Laryngoscope, vol. 113, no. 7, pp. 1228–1230, 2003.
[24] B. Buinewicz and B. Rosen, “Acellular cadaveric dermis(AlloDerm): a new alternative for abdominal hernia repair,”Annals of Plastic Surgery, vol. 52, no. 2, pp. 188–194, 2004.
[25] K. Gaspar, I. Erdei, Z. Peter, B. Dezso, J. Hunyadi, and I.Juhasz, “Role of acellular dermal matrix allograft in minimalinvasive coverage of deep burn wound with bone exposed—case report and histological evaluation,” International WoundJournal, vol. 3, no. 1, pp. 51–58, 2006.

Hindawi Publishing CorporationDermatology Research and PracticeVolume 2010, Article ID 893080, 13 pagesdoi:10.1155/2010/893080
Review Article
Acne Scars: Pathogenesis, Classification and Treatment
Gabriella Fabbrocini, M. C. Annunziata, V. D’Arco, V. De Vita, G. Lodi,M. C. Mauriello, F. Pastore, and G. Monfrecola
Division of Clinical Dermatology, Department of Systematic Pathology, University of Naples Federico II,Via Sergio Pansini 5, 80133 Napoli, Italy
Correspondence should be addressed to Gabriella Fabbrocini, [email protected]
Received 17 March 2010; Revised 7 September 2010; Accepted 28 September 2010
Academic Editor: Daniel Berg
Copyright © 2010 Gabriella Fabbrocini et al. This is an open access article distributed under the Creative Commons AttributionLicense, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properlycited.
Acne has a prevalence of over 90% among adolescents and persists into adulthood in approximately 12%–14% of cases withpsychological and social implications. Possible outcomes of the inflammatory acne lesions are acne scars which, although they canbe treated in a number of ways, may have a negative psychological impact on social life and relationships. The main types of acnescars are atrophic and hypertrophic scars. The pathogenesis of acne scarring is still not fully understood, but several hypotheseshave been proposed. There are numerous treatments: chemical peels, dermabrasion/microdermabrasion, laser treatment, punchtechniques, dermal grafting, needling and combined therapies for atrophic scars: silicone gels, intralesional steroid therapy,cryotherapy, and surgery for hypertrophic and keloidal lesions. This paper summarizes acne scar pathogenesis, classification andtreatment options.
1. Introduction
Acne has a prevalence of over 90% among adolescents [1]and persists into adulthood in approximately 12%–14%of cases with psychological and social implications of highgravity [2, 3].
All body areas with high concentrations of pilosebaceousglands are involved, but in particular the face, back and chest.Inflammatory acne lesions can result in permanent scars,the severity of which may depend on delays in treating acnepatients. The prevalence and severity of acne scarring in thepopulation has not been well studied, although the availableliterature is usually correlated to the severity of acne [4].2133 volunteers aged 18 to 70 from the general populationshowed that nearly 1% of people had acne scars, althoughonly 1 in 7 of these were considered to have “disfiguringscars” [5]. Severe scarring caused by acne is associated withsubstantial physical and psychological distress, particularly inadolescents.
2. Pathogenesis
The pathogenesis of acne is currently attributed to multiplefactors, such as increased sebum production, alteration of
the quality of sebum lipids, androgen activity, proliferationof Propionibacterium acnes (P. acnes) within the follicle andfollicular hyperkeratinization [6]. Increased sebum excretioncontributes to the development of acne. Neutral and polarlipids produced by sebaceous glands serve a variety of roles insignal transduction and are involved in biological pathways[7]. Additionally, fatty acids act as ligands of nuclearreceptors such as PPARs. Sebaceous gland lipids exhibitdirect pro- and anti-inflammatory properties, whereas theinduction of 5-lipoxygenase and cyclooxygenase-2 pathwaysin sebocytes leads to the production of proinflammatorylipids [8]. Furthermore, hormones like androgens controlsebaceous gland size and sebum secretion. In cell culture,androgens only promote sebocyte proliferation, whereasPPAR ligands are required for the induction of differentiationand lipogenic activity [9]. On the other hand, keratinocytesand sebocytes may be activated by P. acnes via TLR, CD14,and CD1 molecules [10]. Pilosebaceous follicles in acnelesions are surrounded by macrophages expressing TLR2on their surface. TLR2 activation leads to a triggering ofthe transcription nuclear factor and thus the production ofcytokines/chemokines, phenomena observed in acne lesions.Furthermore, P. acnes induces IL-8 and IL-12 release fromTLR2 positive monocytes [11].
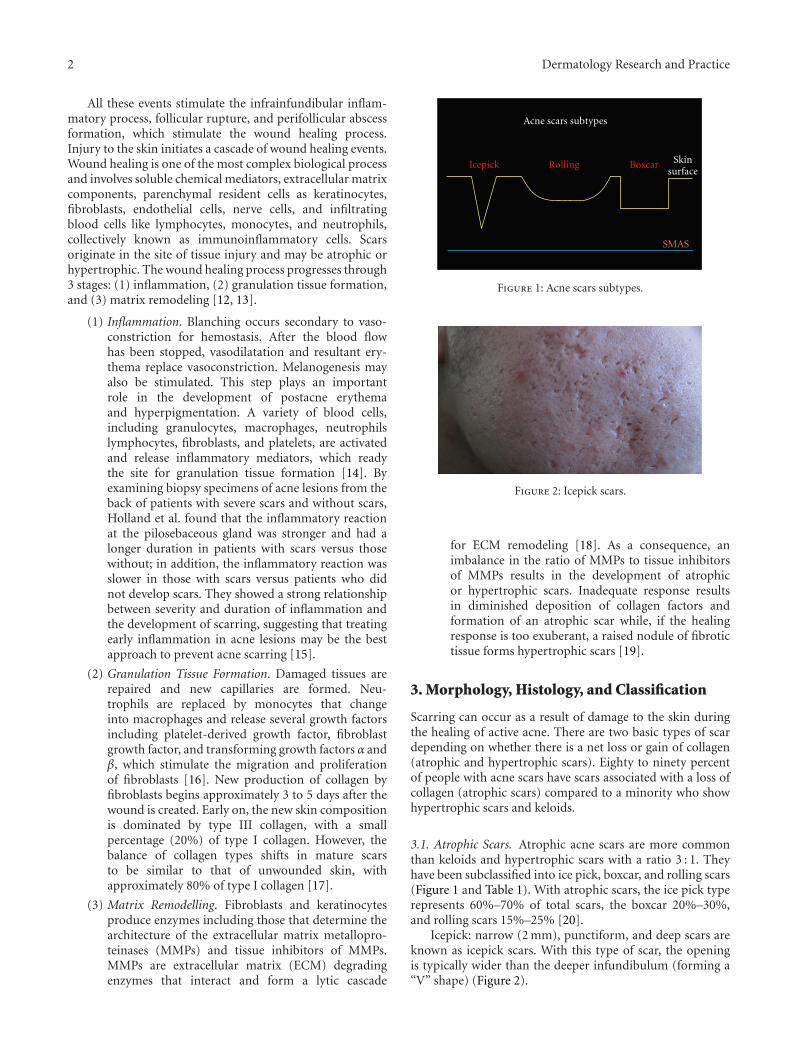
2 Dermatology Research and Practice
All these events stimulate the infrainfundibular inflam-matory process, follicular rupture, and perifollicular abscessformation, which stimulate the wound healing process.Injury to the skin initiates a cascade of wound healing events.Wound healing is one of the most complex biological processand involves soluble chemical mediators, extracellular matrixcomponents, parenchymal resident cells as keratinocytes,fibroblasts, endothelial cells, nerve cells, and infiltratingblood cells like lymphocytes, monocytes, and neutrophils,collectively known as immunoinflammatory cells. Scarsoriginate in the site of tissue injury and may be atrophic orhypertrophic. The wound healing process progresses through3 stages: (1) inflammation, (2) granulation tissue formation,and (3) matrix remodeling [12, 13].
(1) Inflammation. Blanching occurs secondary to vaso-constriction for hemostasis. After the blood flowhas been stopped, vasodilatation and resultant ery-thema replace vasoconstriction. Melanogenesis mayalso be stimulated. This step plays an importantrole in the development of postacne erythemaand hyperpigmentation. A variety of blood cells,including granulocytes, macrophages, neutrophilslymphocytes, fibroblasts, and platelets, are activatedand release inflammatory mediators, which readythe site for granulation tissue formation [14]. Byexamining biopsy specimens of acne lesions from theback of patients with severe scars and without scars,Holland et al. found that the inflammatory reactionat the pilosebaceous gland was stronger and had alonger duration in patients with scars versus thosewithout; in addition, the inflammatory reaction wasslower in those with scars versus patients who didnot develop scars. They showed a strong relationshipbetween severity and duration of inflammation andthe development of scarring, suggesting that treatingearly inflammation in acne lesions may be the bestapproach to prevent acne scarring [15].
(2) Granulation Tissue Formation. Damaged tissues arerepaired and new capillaries are formed. Neu-trophils are replaced by monocytes that changeinto macrophages and release several growth factorsincluding platelet-derived growth factor, fibroblastgrowth factor, and transforming growth factors α andβ, which stimulate the migration and proliferationof fibroblasts [16]. New production of collagen byfibroblasts begins approximately 3 to 5 days after thewound is created. Early on, the new skin compositionis dominated by type III collagen, with a smallpercentage (20%) of type I collagen. However, thebalance of collagen types shifts in mature scarsto be similar to that of unwounded skin, withapproximately 80% of type I collagen [17].
(3) Matrix Remodelling. Fibroblasts and keratinocytesproduce enzymes including those that determine thearchitecture of the extracellular matrix metallopro-teinases (MMPs) and tissue inhibitors of MMPs.MMPs are extracellular matrix (ECM) degradingenzymes that interact and form a lytic cascade
Acne scars subtypes
Icepick Rolling Boxcar Skinsurface
SMAS
Figure 1: Acne scars subtypes.
Figure 2: Icepick scars.
for ECM remodeling [18]. As a consequence, animbalance in the ratio of MMPs to tissue inhibitorsof MMPs results in the development of atrophicor hypertrophic scars. Inadequate response resultsin diminished deposition of collagen factors andformation of an atrophic scar while, if the healingresponse is too exuberant, a raised nodule of fibrotictissue forms hypertrophic scars [19].
3. Morphology, Histology, and Classification
Scarring can occur as a result of damage to the skin duringthe healing of active acne. There are two basic types of scardepending on whether there is a net loss or gain of collagen(atrophic and hypertrophic scars). Eighty to ninety percentof people with acne scars have scars associated with a loss ofcollagen (atrophic scars) compared to a minority who showhypertrophic scars and keloids.
3.1. Atrophic Scars. Atrophic acne scars are more commonthan keloids and hypertrophic scars with a ratio 3 : 1. Theyhave been subclassified into ice pick, boxcar, and rolling scars(Figure 1 and Table 1). With atrophic scars, the ice pick typerepresents 60%–70% of total scars, the boxcar 20%–30%,and rolling scars 15%–25% [20].
Icepick: narrow (2 mm), punctiform, and deep scars areknown as icepick scars. With this type of scar, the openingis typically wider than the deeper infundibulum (forming a“V” shape) (Figure 2).
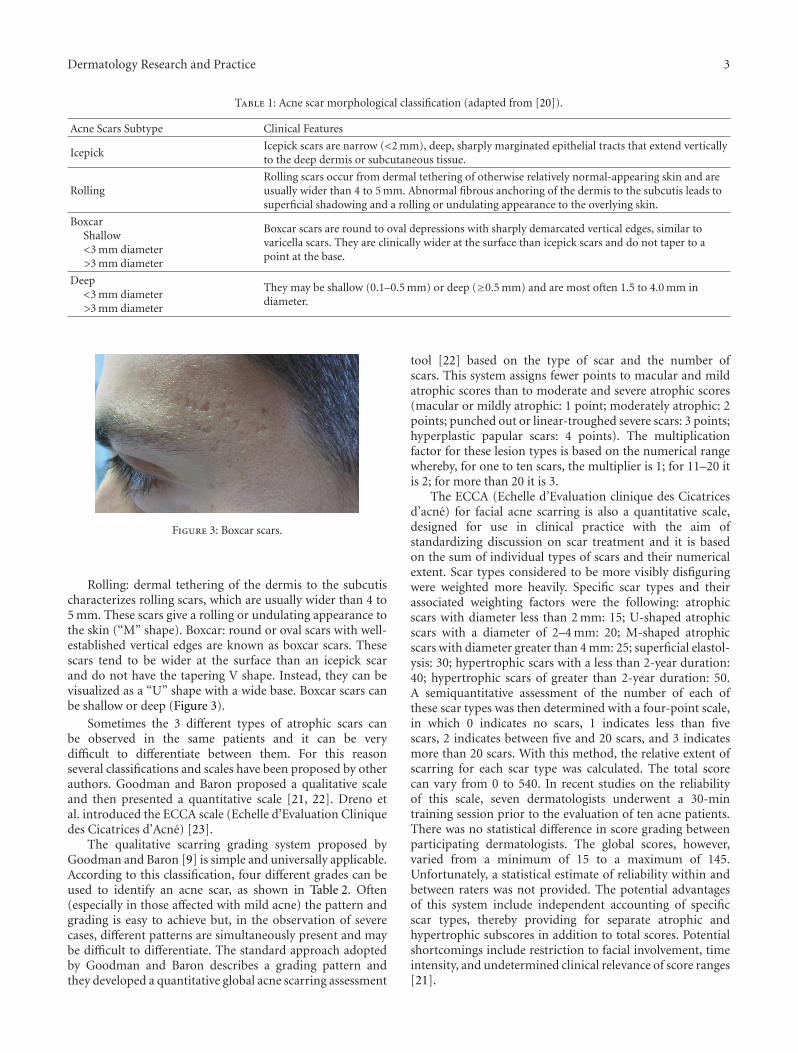
Dermatology Research and Practice 3
Table 1: Acne scar morphological classification (adapted from [20]).
Acne Scars Subtype Clinical Features
IcepickIcepick scars are narrow (<2 mm), deep, sharply marginated epithelial tracts that extend verticallyto the deep dermis or subcutaneous tissue.
RollingRolling scars occur from dermal tethering of otherwise relatively normal-appearing skin and areusually wider than 4 to 5 mm. Abnormal fibrous anchoring of the dermis to the subcutis leads tosuperficial shadowing and a rolling or undulating appearance to the overlying skin.
BoxcarShallow<3 mm diameter>3 mm diameter
Boxcar scars are round to oval depressions with sharply demarcated vertical edges, similar tovaricella scars. They are clinically wider at the surface than icepick scars and do not taper to apoint at the base.
Deep<3 mm diameter>3 mm diameter
They may be shallow (0.1–0.5 mm) or deep (≥0.5 mm) and are most often 1.5 to 4.0 mm indiameter.
Figure 3: Boxcar scars.
Rolling: dermal tethering of the dermis to the subcutischaracterizes rolling scars, which are usually wider than 4 to5 mm. These scars give a rolling or undulating appearance tothe skin (“M” shape). Boxcar: round or oval scars with well-established vertical edges are known as boxcar scars. Thesescars tend to be wider at the surface than an icepick scarand do not have the tapering V shape. Instead, they can bevisualized as a “U” shape with a wide base. Boxcar scars canbe shallow or deep (Figure 3).
Sometimes the 3 different types of atrophic scars canbe observed in the same patients and it can be verydifficult to differentiate between them. For this reasonseveral classifications and scales have been proposed by otherauthors. Goodman and Baron proposed a qualitative scaleand then presented a quantitative scale [21, 22]. Dreno etal. introduced the ECCA scale (Echelle d’Evaluation Cliniquedes Cicatrices d’Acne) [23].
The qualitative scarring grading system proposed byGoodman and Baron [9] is simple and universally applicable.According to this classification, four different grades can beused to identify an acne scar, as shown in Table 2. Often(especially in those affected with mild acne) the pattern andgrading is easy to achieve but, in the observation of severecases, different patterns are simultaneously present and maybe difficult to differentiate. The standard approach adoptedby Goodman and Baron describes a grading pattern andthey developed a quantitative global acne scarring assessment
tool [22] based on the type of scar and the number ofscars. This system assigns fewer points to macular and mildatrophic scores than to moderate and severe atrophic scores(macular or mildly atrophic: 1 point; moderately atrophic: 2points; punched out or linear-troughed severe scars: 3 points;hyperplastic papular scars: 4 points). The multiplicationfactor for these lesion types is based on the numerical rangewhereby, for one to ten scars, the multiplier is 1; for 11–20 itis 2; for more than 20 it is 3.
The ECCA (Echelle d’Evaluation clinique des Cicatricesd’acne) for facial acne scarring is also a quantitative scale,designed for use in clinical practice with the aim ofstandardizing discussion on scar treatment and it is basedon the sum of individual types of scars and their numericalextent. Scar types considered to be more visibly disfiguringwere weighted more heavily. Specific scar types and theirassociated weighting factors were the following: atrophicscars with diameter less than 2 mm: 15; U-shaped atrophicscars with a diameter of 2–4 mm: 20; M-shaped atrophicscars with diameter greater than 4 mm: 25; superficial elastol-ysis: 30; hypertrophic scars with a less than 2-year duration:40; hypertrophic scars of greater than 2-year duration: 50.A semiquantitative assessment of the number of each ofthese scar types was then determined with a four-point scale,in which 0 indicates no scars, 1 indicates less than fivescars, 2 indicates between five and 20 scars, and 3 indicatesmore than 20 scars. With this method, the relative extent ofscarring for each scar type was calculated. The total scorecan vary from 0 to 540. In recent studies on the reliabilityof this scale, seven dermatologists underwent a 30-mintraining session prior to the evaluation of ten acne patients.There was no statistical difference in score grading betweenparticipating dermatologists. The global scores, however,varied from a minimum of 15 to a maximum of 145.Unfortunately, a statistical estimate of reliability within andbetween raters was not provided. The potential advantagesof this system include independent accounting of specificscar types, thereby providing for separate atrophic andhypertrophic subscores in addition to total scores. Potentialshortcomings include restriction to facial involvement, timeintensity, and undetermined clinical relevance of score ranges[21].

4 Dermatology Research and Practice
Table 2: Qualitative scarring grading system (adapted from [21]).
Grades of PostAcne Scarring
Level of disease Clinical features
1 MacularThese scars can be erythematous, hyper- or hypopigmented flat marks.They do not represent a problem of contour like other scar grades but ofcolor.
2 Mild
Mild atrophy or hypertrophy scars that may not be obvious at socialdistances of 50 cm or greater and may be covered adequately by makeup orthe normal shadow of shaved beard hair in men or normal body hair ifextrafacial.
3 Moderate
Moderate atrophic or hypertrophic scarring that is obvious at socialdistances of 50 cm or greater and is not covered easily by makeup or thenormal shadow of shaved beard hair in men or body hair if extrafacial, butis still able to be flattened by manual stretching of the skin (if atrophic).
4 Severe
Severe atrophic or hypertrophic scarring that is evident at social distancesgreater than 50 cm and is not covered easily by makeup or the normalshadow of shaved beard hair in men or body hair if extrafacial and is notable to be flattened by manual stretching of the skin.
3.2. Hypertrophic and Keloidal Scars. Hypertrophic andkeloidal scars are associated with excess collagen deposi-tion and decreased collagenase activity. Hypertrophic scarsare typically pink, raised, and firm, with thick hyalinizedcollagen bundles that remain within the borders of theoriginal site of injury. The histology of hypertrophic scarsis similar to that of other dermal scars. In contrast, keloidsform as reddish-purple papules and nodules that proliferatebeyond the borders of the original wound; histologically,they are characterized by thick bundles of hyalinized acellularcollagen arranged in whorls. Hypertrophic and keloidal scarsare more common in darker-skinned individuals and occurpredominantly on the trunk.
4. Treatment
New acquisitions by the literature have showed that preven-tion is the main step in avoiding the appearance of post-acnescars. Genetic factors and the capacity to respond to traumaare the main factors influencing scar formation [24]. Anumber of treatments are available to reduce the appearanceof scars. First, it is important to reduce as far as possible theduration and intensity of the inflammation, thus stressingthe importance of the acne treatment. The use of topicalretinoids is useful in the prevention of acne scars but morethan any other measure, the use of silicone gel has a provenefficacy in the prevention of scars, especially for hypertrophicscars and keloids.
4.1. Atrophic Scars
4.1.1. Chemical Peels. By chemical peeling we mean theprocess of applying chemicals to the skin to destroy the outerdamaged layers and accelerate the repair process [25].
Chemical peeling is used for the reversal of signs of skinaging and for the treatment of skin lesions as well as scars,particularly acne scars. Dyschromias, wrinkles, and acne
scars are the major clinical indications for facial chemicalpeeling [26, 27].
As regards acne scars, the best results are achieved inmacular scars. Icepick and rolling scars cannot disappearcompletely and need sequential peelings together with home-care treatment with topical retinoids and alpha hydroxy acids[28, 29]. The level of improvement expected is extremelyvariable in different diseases and patients. For example, icepick acne scars in a patient with hyperkeratotic skin are onlymildly improved even if skin texture is remodeled. On theother hand, a patient with isolated box scars can obtain asignificant improvement by application of TCA at 50%–90%on the single scars.
Several hydroxy acids can be used.
(A) Glycolic Acid. Glycolic acid is an alpha-hydroxy acid,soluble in alcohol, derived from fruit and milk sugars. Gly-colic acid acts by thinning the stratum corneum, promotingepidermolysis and dispersing basal layer melanin. It increasesdermal hyaluronic acid and collagen gene expression byincreasing secretion of IL-6 [30]. The procedure is well tol-erated and patient compliance is excellent, but glycolic acidpeels are contraindicated in contact dermatitis, pregnancy,and in patients with glycolate hypersensitivity. Side effects,such as temporary hyperpigmentation or irritation, are notvery significant [31]. Some studies showed that the level ofskin damage with glycolic acid peel increases in a dose- andtime-dependent manner. The acid at the higher concentra-tion (70%) created more tissue damage than the acid at thelower concentration (50%) compared to solutions with freeacid. An increase in the transmembrane permeability coeffi-cient is observed with a decrease in pH, providing a possibleexplanation for the effectiveness of glycolic acid in skin treat-ment [32]. The best results achieved for acne scars regard fivesequential sessions of 70% glycolic acid every 2 weeks.
(B) Jessner’s Solution. Formulated by Dr. Max Jessner, thiscombination of salicylic acid, resorcinol, and lactic acid

Dermatology Research and Practice 5
in 95% ethanol is an excellent superficial peeling agent.Resorcinol is structurally and chemically similar to phenol. Itdisrupts the weak hydrogen bonds of keratin and enhances-penetration of other agents [33]. Lactic acid is an alphahydroxy acid which causes corneocyte detachment andsubsequent desquamation of the stratum corneum [34].As with other superficial peeling agents, Jessner’s peelsare well tolerated. General contraindications include activeinflammation, dermatitis or infection of the area to betreated, isotretinoin therapy within 6 months of peelingand delayed or abnormal wound healing. Allergic contactdermatitis and systemic allergic reactions to resorcinol arerare and need to be considered as absolute contraindications[35, 36].
(C) Pyruvic Acid. Pyruvic acid is an alpha-ketoacid andan effective peeling agent [37]. It presents keratolytic,antimicrobial and sebostatic properties as well as the abilityto stimulate new collagen production and the formation ofelastic fibers [38]. The use of 40%–70% pyruvic acid hasbeen proposed for the treatment of moderate acne scars[39, 40]. Side effects include desquamation, crusting in areasof thinner skin, intense stinging, and a burning sensationduring treatment. Pyruvic acid has stinging and irritatingvapors for the upper respiratory mucosa, and it is advisableto ensure adequate ventilation during application.
(D) Salicylic Acid. Salicylic acid is one of the best peelingagents for the treatment of acne scars [41]. It is a beta hydroxyacid agent which removes intercellular lipids that are cova-lently linked to the cornified envelope surrounding cornifiedepithelioid cells. The most efficacious concentration for acnescars is 30% in multiple sessions, 3–5 times, every 3-4 weeks[42–44]. The side effects of salicylic acid peeling are mild andtransient. These include erythema and dryness. Persistentpostinflammatory hyperpigmentation or scarring are veryrare and for this reason it is used to treat dark skin [45].Rapid breathing, tinnitus, hearing loss, dizziness, abdominalcramps, and central nervous system symptoms characterizesalicylism or salicylic acid toxicity. This has been observedwith 20% salicylic acid applied to 50% of the body surface[46]. Grimes has peeled more than 1,000 patients with thecurrent 20 and 30% marketed ethanol formulations and hasobserved no cases of salicylism [47].
(E) Trichloroacetic Acid. The use of trichloroacetic acid(TCA) as a peeling agent was first described by P.G. Unna, aGerman dermatologist, in 1882. TCA application to the skincauses protein denaturation, the so-called keratocoagulation,resulting in a readily observed white frost [48]. For thepurposes of chemical peeling, it is mixed with 100 mLof distilled water to create the desired concentration. Thedegree of tissue penetration and injury by a TCA solutionis dependent on several factors, including percentage ofTCA used, anatomic site, and skin preparation. Selectionof appropriate TCA-concentrated solutions is critical whenperforming a peel. TCA in a percentage of 10%–20% resultsin a very light superficial peel with no penetration below thestratum granulosum; a concentration of 25%–35% produces
a light superficial peel with diffusion encompassing the fullthickness of the epidermis; 40%–50% can produce injury tothe papillary dermis; and finally, greater than 50% resultsin injury extending to the reticular dermis. Unfortunatelythe use of TCA concentrations above 35% TCA can produceunpredictable results such as scarring. Consequently, themedium depth chemical peel should only be obtained withthe combination of 35% TCA. The use of TCA in con-centrations greater than 35%, should be avoided. It can bepreferred in some cases of isolated lesions or for treatment ofisolated icepick scars (TCA CROSS) [49]. When performedproperly, peeling with TCA can be one of the most satisfyingprocedures in acne scar treatment but it is not indicatedfor dark skin because of the high risk of hyperpigmentation[50].
(F) TCA Cross. In our experience the TCA CROSS techniquehas shown high efficacy in the case of few isolated scarson healthy skin. CROSS stands for chemical reconstructionof skin scars method and involves local serial applicationof high concentration TCA to skin scars with woodenapplicators sized via a number 10 blade to a dull point toapproximate the shape of the scar. No local anesthesia orsedation is needed to perform this technique [51]. Unlikethe reports found in the literature, in which 90% TCA issuggested, our experiences have shown that a lower TCAconcentration (50%) has similar results and much lessadverse reactions [52]. TCA is applied for a few secondsuntil the scar displays a white frosting. Emollients then needsto be prescribed for the following 7 days and high photo-protection is required. The procedure should be repeated at4-week intervals, and each patient receives a total of threetreatments. Our experiences have shown that, comparedwith other procedures, this technique can avoid scarringand reduce the risk of hypopigmentation by sparing theadjacent normal skin and adnexal structures [53] (Figures 4and 5).
4.1.2. Dermabrasion/Microdermabrasion. Dermabrasionand microdermabrasion are facial resurfacing techniquesthat mechanically ablate damaged skin in order to promotereepithelialisation. Although the act of physical abrasion ofthe skin is common to both procedures, dermabrasion, andmicrodermabrasion employ different instruments with adifferent technical execution [54]. Dermabrasion completelyremoves the epidermis and penetrates to the level of thepapillary or reticular dermis, inducing remodeling of theskin’s structural proteins. Microdermabrasion, a moresuperficial variation of dermabrasion, only removes theouter layer of the epidermis, accelerating the natural processof exfoliation [55, 56]. Both techniques are particularlyeffective in the treatment of scars and produce clinicallysignificant improvements in skin appearance. Dermabrasionis performed under local or general anaesthesia. A motorizedhand piece rotates a wire brush or a diamond fraise. Severaldecades ago, the hand piece was made of aluminum oxide orsodium bicarbonate crystals, whereas now diamond tips havereplaced these hand pieces to increase accuracy and decreaseirritation. There is often a small pinpoint bleeding of the raw
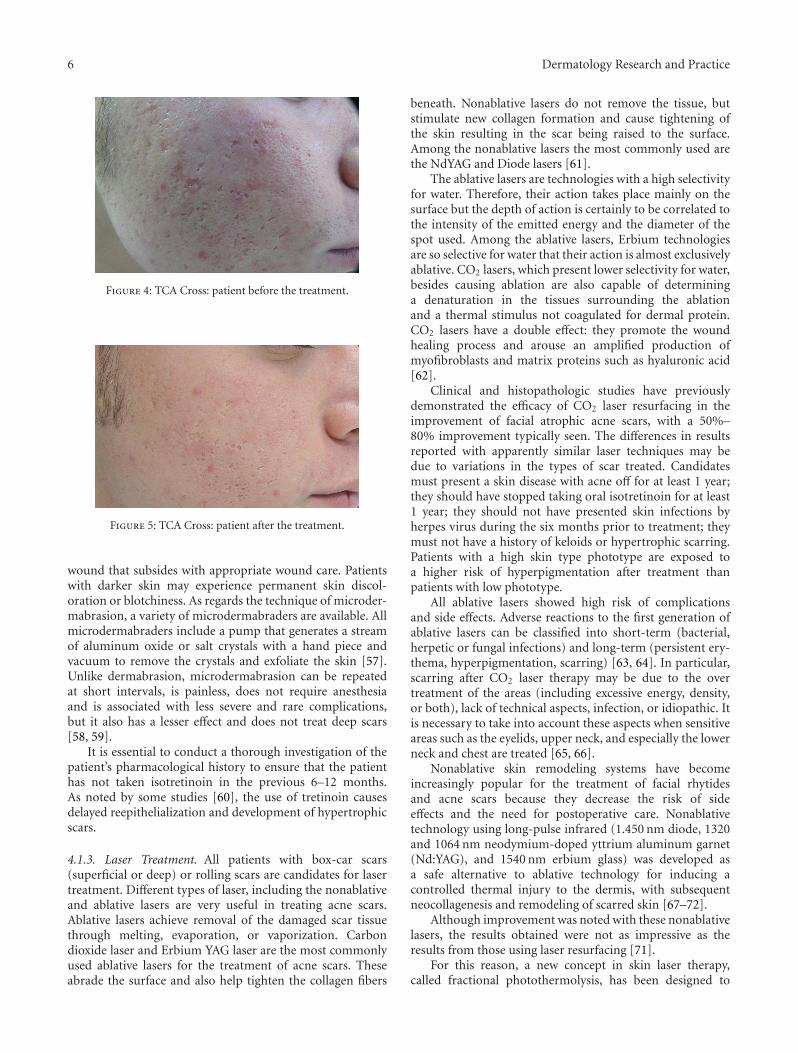
6 Dermatology Research and Practice
Figure 4: TCA Cross: patient before the treatment.
Figure 5: TCA Cross: patient after the treatment.
wound that subsides with appropriate wound care. Patientswith darker skin may experience permanent skin discol-oration or blotchiness. As regards the technique of microder-mabrasion, a variety of microdermabraders are available. Allmicrodermabraders include a pump that generates a streamof aluminum oxide or salt crystals with a hand piece andvacuum to remove the crystals and exfoliate the skin [57].Unlike dermabrasion, microdermabrasion can be repeatedat short intervals, is painless, does not require anesthesiaand is associated with less severe and rare complications,but it also has a lesser effect and does not treat deep scars[58, 59].
It is essential to conduct a thorough investigation of thepatient’s pharmacological history to ensure that the patienthas not taken isotretinoin in the previous 6–12 months.As noted by some studies [60], the use of tretinoin causesdelayed reepithelialization and development of hypertrophicscars.
4.1.3. Laser Treatment. All patients with box-car scars(superficial or deep) or rolling scars are candidates for lasertreatment. Different types of laser, including the nonablativeand ablative lasers are very useful in treating acne scars.Ablative lasers achieve removal of the damaged scar tissuethrough melting, evaporation, or vaporization. Carbondioxide laser and Erbium YAG laser are the most commonlyused ablative lasers for the treatment of acne scars. Theseabrade the surface and also help tighten the collagen fibers
beneath. Nonablative lasers do not remove the tissue, butstimulate new collagen formation and cause tightening ofthe skin resulting in the scar being raised to the surface.Among the nonablative lasers the most commonly used arethe NdYAG and Diode lasers [61].
The ablative lasers are technologies with a high selectivityfor water. Therefore, their action takes place mainly on thesurface but the depth of action is certainly to be correlated tothe intensity of the emitted energy and the diameter of thespot used. Among the ablative lasers, Erbium technologiesare so selective for water that their action is almost exclusivelyablative. CO2 lasers, which present lower selectivity for water,besides causing ablation are also capable of determininga denaturation in the tissues surrounding the ablationand a thermal stimulus not coagulated for dermal protein.CO2 lasers have a double effect: they promote the woundhealing process and arouse an amplified production ofmyofibroblasts and matrix proteins such as hyaluronic acid[62].
Clinical and histopathologic studies have previouslydemonstrated the efficacy of CO2 laser resurfacing in theimprovement of facial atrophic acne scars, with a 50%–80% improvement typically seen. The differences in resultsreported with apparently similar laser techniques may bedue to variations in the types of scar treated. Candidatesmust present a skin disease with acne off for at least 1 year;they should have stopped taking oral isotretinoin for at least1 year; they should not have presented skin infections byherpes virus during the six months prior to treatment; theymust not have a history of keloids or hypertrophic scarring.Patients with a high skin type phototype are exposed toa higher risk of hyperpigmentation after treatment thanpatients with low phototype.
All ablative lasers showed high risk of complicationsand side effects. Adverse reactions to the first generation ofablative lasers can be classified into short-term (bacterial,herpetic or fungal infections) and long-term (persistent ery-thema, hyperpigmentation, scarring) [63, 64]. In particular,scarring after CO2 laser therapy may be due to the overtreatment of the areas (including excessive energy, density,or both), lack of technical aspects, infection, or idiopathic. Itis necessary to take into account these aspects when sensitiveareas such as the eyelids, upper neck, and especially the lowerneck and chest are treated [65, 66].
Nonablative skin remodeling systems have becomeincreasingly popular for the treatment of facial rhytidesand acne scars because they decrease the risk of sideeffects and the need for postoperative care. Nonablativetechnology using long-pulse infrared (1.450 nm diode, 1320and 1064 nm neodymium-doped yttrium aluminum garnet(Nd:YAG), and 1540 nm erbium glass) was developed asa safe alternative to ablative technology for inducing acontrolled thermal injury to the dermis, with subsequentneocollagenesis and remodeling of scarred skin [67–72].
Although improvement was noted with these nonablativelasers, the results obtained were not as impressive as theresults from those using laser resurfacing [71].
For this reason, a new concept in skin laser therapy,called fractional photothermolysis, has been designed to

Dermatology Research and Practice 7
create microscopic thermal wounds to achieve homogeneousthermal damage at a particular depth within the skin,a method that differs from chemical peeling and laserresurfacing. Prior studies using fractional photothermolysishave demonstrated its effectiveness in the treatment of acnescars [73] with particular attention for dark skin to avoidpostinflammatory hyperpigmentation [74].
Newer modalities using the principles of fractionalphotothermolysis devices (FP) to create patterns of tinymicroscopic wounds surrounded by undamaged tissues arenew devices that are preferred for these treatments. Thesedevices produce more modest results in many cases thantraditional carbon dioxide lasers but have few side effectsand short recovery periods [75]. Many fractional lasersare available with different types of source. A great dealof experience with nonablative 1550 nm erbium dopedfractional photothermolysis has shown that the system canbe widely used for clinical purposes.
An ablative 30 W CO2 laser device uses ablative fractionalresurfacing (AFR) and combines CO2 ablation with an FPsystem. By depositing a pixilated pattern of microscopicablative wounds surrounded by healthy tissue in a mannersimilar to that of FP [76], AFR combines the increasedefficacy of ablative techniques with the safety and reduceddowntime associated with FP.
Topographic analysis performed by some authors hasshown that the depth of acneiform scars has quantifiableobjective improvement ranging from 43% to 80% witha mean level of 66.8% [77]. The different experiencesof numerous authors in this field have shown that, bycombining ablative technology with FP, AFR treatments con-stitute a safe and effective treatment modality for acneiformscarring. Compared to conventional ablative CO2 devicesthe side effects profile is greatly improved and, as withFP, rapid reepithelization from surrounding undamagedtissue is believed to be responsible for the comparativelyrapid recovery and reduced downtime noted with AFR[78–80].
Pigmentation abnormalities following laser treatment isalways a concern. Alster and West reported 36% incidenceof hyperpigmentation when using conventional CO2 resur-facing compared to a minority of patients treated with AFRtreatments, probably linked to shortened period of recoveryand posttreatment erythema [81]. The treatment strategyis linked to establishing the optimal energy, the intervalbetween sessions, and a longer follow-up period to optimizetreatment parameters.
4.1.4. Punch Techniques. Atrophic scarring is the morecommon type of scarring encountered after acne. Autologousand nonautologous tissue augmentation, and the use ofpunch replacement techniques has added more precision andefficacy to the treatment of these scars [82].
The laser punch-out method is better than even depthresurfacing for improving deep acne scars and can be com-bined with the shoulder technique or even depth resurfacingaccording to the type of acne scar [83].
Laser skin resurfacing with the concurrent use of punchexcision improves facial acne scarring [84].
4.1.5. Dermal Grafting. Acne scars may be treated surgicallyusing procedures such as dermabrasion and/or simple scarexcision, scar punch elevation, or punch grafting [85].
The useful modalities available are dermal punch graft-ing, excision, and facelifting. The selection of these tech-niques is dependent on the above classification and thepatient’s desire for improvement [86].
Split-thickness or full-thickness grafts “take” on a bed ofscar tissue or dermis following the removal of the epidermis.The technique is useful in repairing unstable scars fromchronic leg ulcers or X-ray scars. It can also camouflage acnescars, extensive nevi pigmentosus, and tattoos [87, 88]. It isprepackaged dermal graft material that is easy to use, safe,and effective [89].
4.1.6. Tissue Augmenting Agents. Fat transplantation. Fat iseasily available and it has low incidence of side effects [90].The technique consists of two phases: procurement of thegraft and placement of the graft. The injection phase withsmall parcels of fat implanted in multiple tunnels allows thefat graft maximal access to its available bloody supply. The fatinjected will normalize the contour excepted where residualscar attachments impede this.
4.1.7. Other Tissue Augmenting Agents. There are manynew and older autologous, nonautologous biologic, andnonbiologic tissue augmentation agents that have been usedin the past for atrophic scars, such as autologous collagen,bovine collagen, isolagen, alloderm, hyaluronic acid, fibrel,artecoll, and silicon, but nowadays, because of the highincidence of side effects, the recommended material to useis hyaluronic acid [91].
4.1.8. Needling. Skin needling is a recently proposed tech-nique that involves using a sterile roller comprised of aseries of fine, sharp needles to puncture the skin. At first,facial skin must be disinfected, then a topical anesthetic isapplied, left for 60 minutes. The skin needling procedure isachieved by rolling a performed tool on the cutaneous areasaffected by acne scars (Figure 6), backward and forward withsome pressure in various directions. The needles penetrateabout 1.5 to 2 mm into the dermis. As expected, the skinbleeds for a short time, but that soon stops. The skindevelops multiple microbruises in the dermis that initiatethe complex cascade of growth factors that finally resultsin collagen production. Histology shows thickening of skinand a dramatic increase in new collagen and elastin fibers.Results generally start to be seen after about 6 weeks butthe full effects can take at least three months to occur and,as the deposition of new collagen takes place slowly, theskin texture will continue to improve over a 12 monthperiod. Clinical results vary between patients, but all patientsachieve some improvements (Figures 7 and 8). The numberof treatments required varies depending on the individualcollagen response, on the condition of the tissue and on thedesired results. Most patients require around 3 treatmentsapproximately 4 weeks apart. Skin needling can be safelyperformed on all skin colours and types: there is a lower
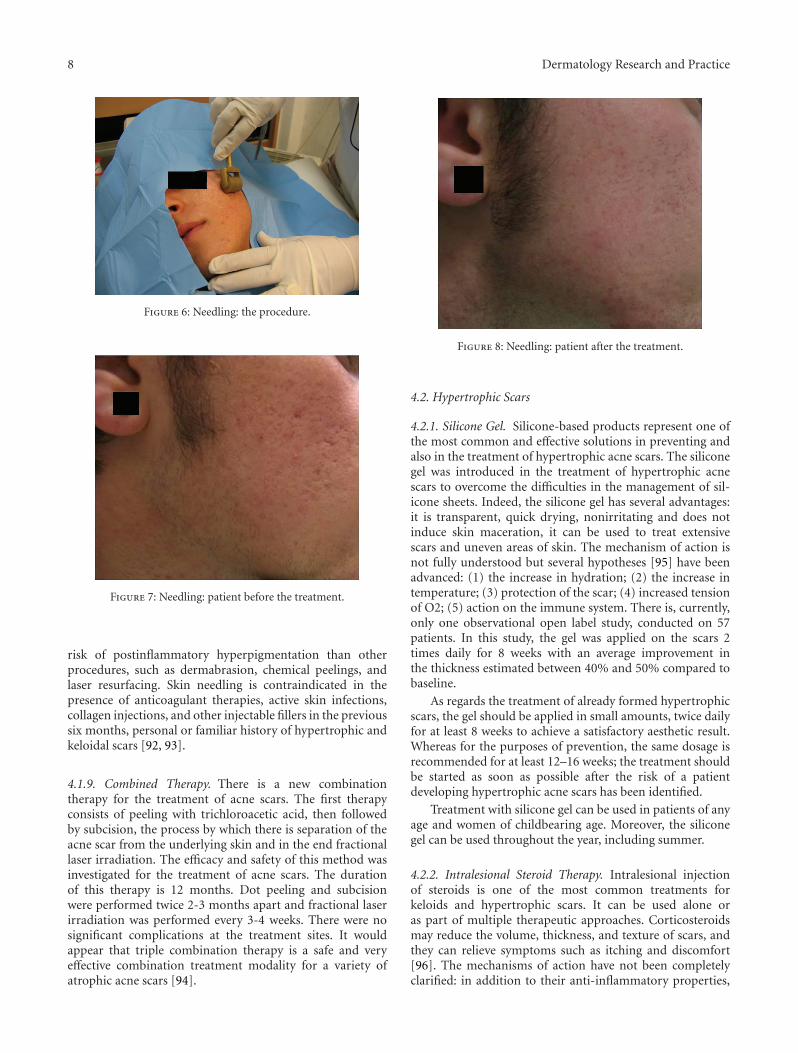
8 Dermatology Research and Practice
Figure 6: Needling: the procedure.
Figure 7: Needling: patient before the treatment.
risk of postinflammatory hyperpigmentation than otherprocedures, such as dermabrasion, chemical peelings, andlaser resurfacing. Skin needling is contraindicated in thepresence of anticoagulant therapies, active skin infections,collagen injections, and other injectable fillers in the previoussix months, personal or familiar history of hypertrophic andkeloidal scars [92, 93].
4.1.9. Combined Therapy. There is a new combinationtherapy for the treatment of acne scars. The first therapyconsists of peeling with trichloroacetic acid, then followedby subcision, the process by which there is separation of theacne scar from the underlying skin and in the end fractionallaser irradiation. The efficacy and safety of this method wasinvestigated for the treatment of acne scars. The durationof this therapy is 12 months. Dot peeling and subcisionwere performed twice 2-3 months apart and fractional laserirradiation was performed every 3-4 weeks. There were nosignificant complications at the treatment sites. It wouldappear that triple combination therapy is a safe and veryeffective combination treatment modality for a variety ofatrophic acne scars [94].
Figure 8: Needling: patient after the treatment.
4.2. Hypertrophic Scars
4.2.1. Silicone Gel. Silicone-based products represent one ofthe most common and effective solutions in preventing andalso in the treatment of hypertrophic acne scars. The siliconegel was introduced in the treatment of hypertrophic acnescars to overcome the difficulties in the management of sil-icone sheets. Indeed, the silicone gel has several advantages:it is transparent, quick drying, nonirritating and does notinduce skin maceration, it can be used to treat extensivescars and uneven areas of skin. The mechanism of action isnot fully understood but several hypotheses [95] have beenadvanced: (1) the increase in hydration; (2) the increase intemperature; (3) protection of the scar; (4) increased tensionof O2; (5) action on the immune system. There is, currently,only one observational open label study, conducted on 57patients. In this study, the gel was applied on the scars 2times daily for 8 weeks with an average improvement inthe thickness estimated between 40% and 50% compared tobaseline.
As regards the treatment of already formed hypertrophicscars, the gel should be applied in small amounts, twice dailyfor at least 8 weeks to achieve a satisfactory aesthetic result.Whereas for the purposes of prevention, the same dosage isrecommended for at least 12–16 weeks; the treatment shouldbe started as soon as possible after the risk of a patientdeveloping hypertrophic acne scars has been identified.
Treatment with silicone gel can be used in patients of anyage and women of childbearing age. Moreover, the siliconegel can be used throughout the year, including summer.
4.2.2. Intralesional Steroid Therapy. Intralesional injectionof steroids is one of the most common treatments forkeloids and hypertrophic scars. It can be used alone oras part of multiple therapeutic approaches. Corticosteroidsmay reduce the volume, thickness, and texture of scars, andthey can relieve symptoms such as itching and discomfort[96]. The mechanisms of action have not been completelyclarified: in addition to their anti-inflammatory properties,

Dermatology Research and Practice 9
it has been suggested that steroids exert a vasoconstrictorand an antimitotic activity. It is believed that steroidsarrest pathological collagen production through two distinctmechanisms: the reduction of oxygen and nutrients to thescar with inhibition of the proliferation of keratinocytesand fibroblasts [96]; the stimulation of digestion of collagendeposition through block of a collagenase-inhibitor, thealpha-2-microglobulin [97]. During the injection the syringeneedle should be kept upright [24]. It is always preferable forthe injections to be preceded by the application of anestheticcreams or be associated with injections of lidocaine [97].
Intralesional steroid therapy may be preceded by a lightcryotherapy with liquid nitrogen, 10–15 minutes beforeinjection, to improve the dispersion of the drug in scartissue and minimize the deposition in the subcutaneous andperilesional tissue [98]. The steroid that is currently mostfrequently used in the treatment of hypertrophic scars andkeloids is triamcinolone acetonide (10–40 mg/mL) [99]. Themost common adverse reactions are hypopigmentation, skinatrophy, telangiectasia, and infections [100]. As for injuriesto the face, the use of intralesional steroids is recommendedfor the treatment of individual elements which areparticularly bulky and refractory to previous less invasivemethods.
4.2.3. Cryotherapy. Cryotherapy with liquid nitrogen cansignificantly improve the clinical appearance of hypertrophicscars and keloids and also determine their complete regres-sion.
The low temperatures reached during cryotherapy ses-sions cause a slowing of blood flow and cause the formationof intraluminal thrombus hesitant to anoxia and tissuenecrosis [101]. Age and size of the scar are important factorsconditioning the outcome of this technique: younger andsmaller scars are most responsive to cryotherapy [102].Compared with intralesional injections of corticosteroids,cryosurgery is significantly more effective than alternativemethods for richly vascularized injuries 12 months younger[103]. During each session of cryotherapy the patient isusually subjected to 2-3 cycles, each lasting less than 25seconds. Cryotherapy can also be used before each cycleof intralesional injections of steroids to reduce the pain ofinjection therapy and to facilitate the injection of cortisone,generating a small area of edema at the level of the scar tissueto be treated [98]. Possible adverse reactions are representedby hypo- and hyperpigmentation, skin atrophy, and pain[102]. With regard to localized lesions to the face, thepossible outcomes of freezing restrict the use of cryotherapyin these areas, especially in cases where the scars arenumerous or for dark phenotypes. Therefore, cryotherapycan be taken into consideration especially for scars locatedon the trunk or for particularly bulky scars on the face.
4.2.4. Pulsed Dye Laser. The use of lasers for hypertrophicscars and keloids was first proposed by Apfelberg et al.[104] and Castro et al. [105] in the 1980s, and since thenmore lasers with various wavelengths have been introduced.Unfortunately, laser therapy for hypertrophic scars has
had only variable success in the past due to the minimalimprovement in a high percent of patients [106–108].
On the contrary, the use of pulsed dye laser (PDL) hasprovided encouraging results in the treatment of hyper-trophic/keloidal scars over the past 10 years. Several studieshave been conducted to investigate how the PDL works onhypertrophic/keloidal scars. They have revealed that PDLdecreases the number and proliferation of fibroblasts andcollagen fibers appear looser and less coarse [109]. Moreover,PDL also produces an increase in MMP-I3 (collagenese-3) activity and a decrease in collagen type III deposition[110]. As a consequence, PDL flattens and decreases thevolume of hypertrophic scars [111, 112], improves texture[113], and increases elasticity [114], usually after two to threetreatments [115]. Additionally, pruritis and pain within thescars are significantly improved [116]. Besides, no recurrenceor worsening of PDL-treated scars occurs during the 4-year followup after cessation of treatment [116]. The mostcommon side effect of the PDL is purpura which can lastas long as 7–10 days. Blistering can also occur as well ashypo- and hyperpigmentation which is more likely in darkerskinned individuals [117]. Therefore, the ideal candidatesfor PDL are patients with lighter skin types (FitzpatrickTypes I–III) because less melanin is present to compete withhemoglobin laser energy absorption [118, 119].
4.2.5. Surgery. For the correction of large facial scars, W-plasty seems to be optimal [12]. This therapeutic procedurecauses a disruption of the scar which makes the lesionless conspicuous. Especially in facial surgery, autologousskin transplants, namely, full thickness skin transplant orcomposite fat-skin graft, are another valuable alternativefor achieving wound closure with minimal tension. Thepreferred donor sites for skin graft used for facial defects arethe retro- and preauricular sites as well as the neck [120].
4.2.6. Other Approaches. Other treatment options for hyper-trophic acne scars and keloids that can be taken intoaccount include elastic compression, intralesional injectionof 5-fluorouracil, imiquimod, interferon, radiotherapy, andbleomycin. All these approaches, however, are more effectivefor the treatment of hypertrophic scars not caused by acneand their use is not recommended due to their impracticality(elastic compression), the lack of clinical experience in theliterature (5 FU, interferon, radiotherapy, bleomycin) thelack of efficacy (imiquimod), and the high costs (interferon).
5. Conclusion
There are no general guidelines available to optimize acnescar treatment. There are several multiple managementoptions, both medical and surgical, and laser devices are use-ful in obtaining significant improvement. Further primaryresearch such as randomized controlled trials is needed inorder to quantify the benefits and to establish the durationof the effects, the cost-effective ratio of different treatments,and the evaluation of the psychological improvement and thequality of life of these patients.
10 Dermatology Research and Practice
References
[1] S. Z. Ghodsi, H. Orawa, and C. C. Zouboulis, “Prevalence,severity, and severity risk factors of acne in high schoolpupils: a community-based study,” Journal of InvestigativeDermatology, vol. 129, no. 9, pp. 2136–2141, 2009.
[2] C. Williams and A. M. Layton, “Persistent acne in women:implications for the patient and for therapy,” American Jour-nal of Clinical Dermatology, vol. 7, no. 5, pp. 281–290, 2006.
[3] B. Capitanio, J. L. Sinagra, V. Bordignon, P. C. Fei, M.Picardo, and C. C. Zouboulis, “Underestimated clinicalfeatures of postadolescent acne,” Journal of the AmericanAcademy of Dermatology, vol. 63, no. 5, pp. 782–788, 2010.
[4] A. M. Layton, C. A. Henderson, and W. J. Cunliffe, “A clinicalevaluation of acne scarring and its incidence,” Clinical andExperimental Dermatology, vol. 19, no. 4, pp. 303–308, 1994.
[5] W. J. Cunliffe and D. J. Gould, “Prevalence of facial acnevulgaris in late adolescence and in adults,” British MedicalJournal, vol. 1, no. 6171, pp. 1109–1110, 1979.
[6] I. Kurokawa, F. W. Danby, Q. Ju et al., “New developmentsin our understanding of acne pathogenesis and treatment,”Experimental Dermatology, vol. 18, no. 10, pp. 821–832, 2009.
[7] C. C. Zouboulis, “Acne and sebaceous gland function,”Clinics in Dermatology, vol. 22, no. 5, pp. 360–366, 2004.
[8] T. Alestas, R. Ganceviciene, S. Fimmel, K. Muller-Decker,and C. C. Zouboulis, “Enzymes involved in the biosynthesisof leukotriene B4 and prostaglandin E2 are active insebaceous glands,” Journal of Molecular Medicine, vol. 84, no.1, pp. 75–87, 2006.
[9] E. Makrantonaki and C. C. Zouboulis, “Testosteronemetabolism to 5α-dihydrotestosterone and synthesis ofsebaceous lipids is regulated by the peroxisome proliferator-activated receptor ligand linoleic acid in human sebocytes,”British Journal of Dermatology, vol. 156, no. 3, pp. 428–432,2007.
[10] I. Nagy, A. Pivarcsi, K. Kis et al., “Propionibacteriumacnes and lipopolysaccharide induce the expression ofantimicrobial peptides and proinflammatory cytokines/chemokines in human sebocytes,” Microbes and Infection,vol. 8, no. 8, pp. 2195–2205, 2006.
[11] J. Kim, M.-T. Ochoa, S. R. Krutzik et al., “Activation oftoll-like receptor 2 in acne triggers inflammatory cytokineresponses,” Journal of Immunology, vol. 169, no. 3, pp.1535–1541, 2002.
[12] D. Wolfram, A. Tzankov, P. Pulzl, and H. Piza-Katzer,“Hypertrophic scars and keloids—a review of theirpathophysiology, risk factors, and therapeutic management,”Dermatologic Surgery, vol. 35, no. 2, pp. 171–181, 2009.
[13] A. J. Cowin, M. P. Brosnan, T. M. Holmes, and M. W. J.Ferguson, “Endogenous inflammatory response to dermalwound healing in the fetal and adult mouse,” DevelopmentalDynamics, vol. 212, no. 3, pp. 385–393, 1998.
[14] P. Martin and S. J. Leibovich, “Inflammatory cells duringwound repair: the good, the bad and the ugly,” Trends in CellBiology, vol. 15, no. 11, pp. 599–607, 2005.
[15] D. B. Holland, A. H. T. Jeremy, S. G. Roberts, D. C. Seukeran,A. M. Layton, and W. J. Cunliffe, “Inflammation in acnescarring: a comparison of the responses in lesions frompatients prone and not prone to scar,” British Journal ofDermatology, vol. 150, no. 1, pp. 72–81, 2004.
[16] W. K. Stadelmann, A. G. Digenis, and G. R. Tobin,“Physiology and healing dynamics of chronic cutaneouswounds,” American Journal of Surgery, vol. 176, no. 2A, pp.26S–38S, 1998.
[17] C. L. Baum and C. J. Arpey, “Normal cutaneous wound heal-ing: clinical correlation with cellular and molecular events,”Dermatologic Surgery, vol. 31, no. 6, pp. 674–686, 2005.
[18] K. S. Midwood, L. V. Williams, and J. E. Schwarzbauer,“Tissue repair and the dynamics of the extracellular matrix,”International Journal of Biochemistry and Cell Biology, vol.36, no. 6, pp. 1031–1037, 2004.
[19] M. Chivot, H. Pawin, C. Beylot et al., “Acne scars: epide-miology, physiopathology, clinical features and treatment,”Annales de Dermatologie et de Venereologie, vol. 133, no. 10,pp. 813–824, 2006.
[20] C. I. Jacob, J. S. Dover, and M. S. Kaminer, “Acne scarring:a classification system and review of treatment options,”Journal of the American Academy of Dermatology, vol. 45, no.1, pp. 109–117, 2001.
[21] G. J. Goodman and J. A. Baron, “Postacne scarring: aqualitative global scarring grading system,” DermatologicSurgery, vol. 32, no. 12, pp. 1458–1466, 2006.
[22] G. J. Goodman and J. A. Baron, “Postacne scarring—aquantitative global scarring grading system,” Journal ofCosmetic Dermatology, vol. 5, no. 1, pp. 48–52, 2006.
[23] B. Dreno, A. Khammari, N. Orain et al., “ECCA gradingscale: an original validated acne scar grading scale for clinicalpractice in dermatology,” Dermatology, vol. 214, no. 1, pp.46–51, 2006.
[24] R. S. English and P. D. Shenefelt, “Keloids and hypertrophicscars,” Dermatologic Surgery, vol. 25, no. 8, pp. 631–638,1999.
[25] I. Ghersetich, B. Brazzini, and T. Lotti, “Chemical peeling,”in European Handbook of Dermatological Treatments, T. M.Lotti and A. D. Katsambas, Eds., Springer, Berlin, Germany,2nd edition, 2003.
[26] I. Ghersetich, P. Teofoll, M. Gantcheva, M. Ribuffo, and P.Puddu, “Chemical peeling: how, when, why?” Journal of theEuropean Academy of Dermatology and Venereology, vol. 8,no. 1, pp. 1–11, 1997.
[27] M. Landau, “Chemical peels,” Clinics in Dermatology, vol.26, no. 2, pp. 200–208, 2008.
[28] G. J. Goodman, “Management of post-acne scarring: whatare the options for treatment?” American Journal of ClinicalDermatology, vol. 1, no. 1, pp. 3–17, 2000.
[29] G. J. Goodman, “Postacne scarring: a review of itspathophysiology and treatment,” Dermatologic Surgery,vol. 26, no. 9, pp. 857–871, 2000.
[30] E. F. Bernstein, J. Lee, D. B. Brown, R. Yu, and E. Van Scott,“Glycolic acid treatment increases type I collagen mRNAand hyaluronic acid content of human skin,” DermatologicSurgery, vol. 27, no. 5, pp. 429–433, 2001.
[31] S. M. Javaheri, S. Handa, I. Kaur, and B. Kumar, “Safety andefficacy of glycolic acid facial peel in Indian women withmelasma,” International Journal of Dermatology, vol. 40, no.5, pp. 354–357, 2001.
[32] F. F. Becker, F. P. J. Langford, M. G. Rubin, and P. Speelman,“A histological comparison of 50% and 70% glycolic acidpeels using solutions with various pHs,” DermatologicSurgery, vol. 22, no. 5, pp. 463–465, 1996.
[33] A. Rook, D. S. Wilkinson, and F. J. G. Ebling, Textbook ofDermatology, Blackwell Scientific, Oxford, UK, 1972.
[34] E. J. Van Scott and R. J. Yu, “Hyperkeratinization, corneocytecohesion and alpha hydroxy acids,” Journal of the AmericanAcademy of Dermatology, vol. 11, no. 5, pp. 867–879, 1984.
Dermatology Research and Practice 11
[35] B. S. Lynch, E. S. Delzell, and D. H. Bechtel, “Toxicologyreview and risk assessment of resorcinol: thyroid effects,”Regulatory Toxicology and Pharmacology, vol. 36, no. 2, pp.198–210, 2002.
[36] A. Barbaud, P. Modiano, M. Cocciale, S. Reichert, and J.-L.Schmutz, “The topical application of resorcinol can provokea systemic allergic reaction,” British Journal of Dermatology,vol. 135, no. 6, pp. 1014–1015, 1996.
[37] T. D. Griffin, E. J. Van Scott, and S. Maddin, “The useof pyruvic acid as a chemical peeling agent,” Journal ofDermatologic Surgery & Oncology, vol. 15, p. 1316, 1989.
[38] G. D. Monheit, “Medium-depth combination peels,”Dermatologic Therapy, vol. 13, no. 2, pp. 183–191, 2000.
[39] E. J. Van Scott and R. J. Yu, “Alpha hydroxy acids: therapeuticpotentials,” Canadian Journal of Dermatology, vol. 1, no. 5,pp. 108–112, 1989.
[40] E. Berardesca, N. Cameli, G. Primavera, and M. Carrera,“Clinical and instrumental evaluation of skin improvementafter treatment with a new 50% pyruvic acid peel,”Dermatologic Surgery, vol. 32, no. 4, pp. 526–531, 2006.
[41] P. G. Unna, “Therapeutiques generales des maladies de lapeau,” 1882.
[42] N. D. Lazo, J. G. Meine, and D. T. Downing, “Lipidsare covalently attached to rigid corneocyte proteinenvelopes existing predominantly as β-sheets: a solid-statenuclear magnetic resonance study,” Journal of InvestigativeDermatology, vol. 105, no. 2, pp. 296–300, 1995.
[43] J. M. Swinehart, “Salicylic acid ointment peeling of the handsand forearms: effective nonsurgical removal of pigmentedlesions and actinic damage,” Journal of Dermatologic Surgeryand Oncology, vol. 18, no. 6, pp. 495–498, 1992.
[44] S. Imayama, S. Ueda, and M. Isoda, “Histologic changes inthe skin of hairless mice following peeling with salicylic acid,”Archives of Dermatology, vol. 136, no. 11, pp. 1390–1395,2000.
[45] P. E. Grimes, “The safety and efficacy of salicylic acidchemical peels in darker racial-ethnic groups,” DermatologicSurgery, vol. 25, no. 1, pp. 18–22, 1999.
[46] J. M. Swinehart, “Salicylic acid ointment peeling of the handsand forearms: effective nonsurgical removal of pigmentedlesions and actinic damage,” Journal of Dermatologic Surgeryand Oncology, vol. 18, no. 6, pp. 495–498, 1992.
[47] G. Fabbrocini, M. P. De Padova, and A. Tosti, “Chemicalpeels: what’s new and what isn’t new but still works well,”Facial Plastic Surgery, vol. 25, no. 5, pp. 329–336, 2009.
[48] M. I. Dinner and J. S. Artz, “The art of the trichloroaceticacid chemical peel,” Clinics in Plastic Surgery, vol. 25, no. 1,pp. 53–62, 1998.
[49] J. W. Slavin, “Trichloroacetic acid peels,” Aesthetic SurgeryJournal, vol. 24, no. 5, pp. 469–470, 2004.
[50] M. M. Al-Waiz and A. I. Al-Sharqi, “Medium-depth chemicalpeels in the treatment of acne scars in dark-skinned individ-uals,” Dermatologic Surgery, vol. 28, no. 5, pp. 383–387, 2002.
[51] J. B. Lee, W. G. Chung, H. Kwahck, K. H. Lee, and G.Monheit, “Focal treatment of acne scars with trichloroaceticacid: Chemical reconstruction of skin scars method,”Dermatologic Surgery, vol. 28, no. 11, pp. 1017–1021, 2002.
[52] G. Fabbrocini, S. Cacciapuoti, N. Fardella, F. Pastore, and G.Monfrecola, “CROSS technique: chemical reconstruction ofskin scars method,” Dermatologic Therapy, vol. 21, no. 3, pp.S29–S32, 2008.
[53] A. Yug, J. E. Lane, M. S. Howard, and D. E. Kent, “Histologicstudy of depressed acne scars treated with serial high-concentration (95%) trichloroacetic acid,” DermatologicSurgery, vol. 32, no. 8, pp. 985–990, 2006.
[54] L. Alkhawam and M. Alam, “Dermabrasion and micro-dermabrasion,” Facial Plastic Surgery, vol. 25, no. 5, pp.301–310, 2009.
[55] E. K. Shim, D. Barnette, K. Hughes, and H. T. Greenway,“Microdermabrasion: a clinical and histopathologic study,”Dermatologic Surgery, vol. 27, no. 6, pp. 524–530, 2001.
[56] B. M. Freedman, E. Rueda-Pedraza, and S. P. Waddell,“The epidermal and dermal changes associated withmicrodermabrasion,” Dermatologic Surgery, vol. 27, no. 12,pp. 1031–1034, 2001.
[57] R. Shpall, F. C. Beddingfield III, D. Watson, and G. P. Lask,“Microdermabrasion: a review,” Facial Plastic Surgery, vol.20, no. 1, pp. 47–50, 2004.
[58] R.-Y. Tsai, C.-N. Wang, and H.-L. Chan, “Aluminum oxidecrystal microdermabrasion: a new technique for treatingfacial scarring,” Dermatologic Surgery, vol. 21, no. 6, pp.539–542, 1995.
[59] J. R. Lloyd, “The use of microdermabrasion for acne: a pilotstudy,” Dermatologic Surgery, vol. 27, no. 4, pp. 329–331,2001.
[60] S. H. Mandy, “Tretinoin in the preoperative and postopera-tive management of dermabrasion,” Journal of the AmericanAcademy of Dermatology, vol. 15, no. 4, pp. 888–889, 1986.
[61] S. Nelson, “An introduction to laser and laser-tissueinteractions in dermatology,” in Principles and Practices inCutaneous Laser Surgery, A. N. B. Kauvar, Ed., p. 70, Taylorand Francis Group, Boca Raton, Fla, USA, 2005.
[62] K. J. Smith, H. G. Skelton, J. S. Graham, C. G. Hurst, and B.E. Hackley Jr., “Increased smooth muscle actin, factor XIIIa,and vimentin-positive cells in the papillary dermis of carbondioxide laser-debrided porcine skin,” Dermatologic Surgery,vol. 23, no. 10, pp. 891–895, 1997.
[63] E. M. Graber, E. L. Tanzi, and T. S. Alster, “Side effectsand complications of fractional laser photothermolysis:experience with 961 treatments,” Dermatologic Surgery, vol.34, no. 3, pp. 301–305, 2008.
[64] H. H. L. Chan, D. Manstein, C. S. Yu, S. Shek, T. Kono,and W. I. Wei, “The prevalence and risk factors of post-inflammatory hyperpigmentation after fractional resurfacingin Asians,” Lasers in Surgery and Medicine, vol. 39, no. 5, pp.381–385, 2007.
[65] D. J. Fife, R. E. Fitzpatrick, and C. B. Zachary, “Complicationsof fractional CO2 laser resurfacing: four cases,” Lasers inSurgery and Medicine, vol. 41, no. 3, pp. 179–184, 2009.
[66] M. M. Avram, W. D. Tope, T. Yu, E. Szachowicz, and J.S. Nelson, “Hypertrophic scarring of the neck followingablative fractional carbon dioxide laser resurfacing,” Lasersin Surgery and Medicine, vol. 41, no. 3, pp. 185–188,2009.
[67] N. Fournier and S. Mordon, “Nonablative remodeling witha 1,540 nm erbium:glass laser,” Dermatologic Surgery, vol. 31,no. 9, pp. 1227–1235, 2005.
[68] P. M. Friedman, M. H. Jih, G. R. Skover, G. S. Payonk, A.Kimyai-Asadi, and R. G. Geronemus, “Treatment of atrophicfacial acne scars with the 1064-nm Q-switched Nd:YAGlaser: six-month follow-up study,” Archives of Dermatology,vol. 140, no. 11, pp. 1337–1341, 2004.
[69] G. M. Lipper and M. Perez, “Nonablative acne scar reductionafter a series of treatments with a short-pulsed 1,064-nmNeodymium:YAG laser,” Dermatologic Surgery, vol. 32, no. 8,pp. 998–1006, 2006.
12 Dermatology Research and Practice
[70] A. C. Bhatia, J. S. Dover, K. A. Arndt, B. Stewart, andM. Alam, “Patient satisfaction and reported long-termtherapeutic efficacy associated with 1,320 nm Nd:YAG lasertreatment of acne scarring and photoaging,” DermatologicSurgery, vol. 32, no. 3, pp. 346–352, 2006.
[71] E. L. Tanzi and T. S. Alster, “Comparison of a 1450-nmdiode laser and a 1320-nm Nd:YAG laser in the treatmentof atrophic facial scars: a prospective clinical and histologicstudy,” Dermatologic Surgery, vol. 30, no. 2, pp. 152–157,2004.
[72] T. S. Alster and J. R. Lupton, “Are all infrared lasers equallyeffective in skin rejuvenation,” Seminars in CutaneousMedicine and Surgery, vol. 21, no. 4, pp. 274–279, 2002.
[73] T. Hasegawa, T. Matsukura, Y. Mizuno, Y. Suga, H.Ogawa, and S. Ikeda, “Clinical trial of a laser device calledfractional photothermolysis system for acne scars,” Journalof Dermatology, vol. 33, no. 9, pp. 623–627, 2006.
[74] E. M. Graber, E. L. Tanzi, and T. S. Alster, “Side effectsand complications of fractional laser photothermolysis:experience with 961 treatments,” Dermatologic Surgery, vol.34, no. 3, pp. 301–305, 2008.
[75] T. S. Alster, E. L. Tanzi, and M. Lazarus, “The use of fractionallaser photothermolysis for the treatment of atrophic scars,”Dermatologic Surgery, vol. 33, no. 3, pp. 295–299, 2007.
[76] B. M. Hantash, V. P. Bedi, B. Kapadia et al., “In vivohistological evaluation of a novel ablative fractionalresurfacing device,” Lasers in Surgery and Medicine, vol. 39,no. 2, pp. 96–107, 2007.
[77] A. M. Chapas, L. Brightman, S. Sukal et al., “Successfultreatment of acneiform scarring with CO2 ablative fractionalresurfacing,” Lasers in Surgery and Medicine, vol. 40, no. 6,pp. 381–386, 2008.
[78] J. Waibel, K. Beer, V. Narurkar, and T. Alster, “Preliminaryobservations on fractional ablative resurfacing devices:clinical impressions,” Journal of Drugs in Dermatology, vol. 8,no. 5, pp. 481–485, 2009.
[79] B. M. Hantash, V. P. Bedi, K. F. Chan, and C. B. Zachary,“Ex vivo histological characterization of a novel ablativefractional resurfacing device,” Lasers in Surgery and Medicine,vol. 39, no. 2, pp. 87–95, 2007.
[80] B. M. Hantash, V. P. Bedi, B. Kapadia et al., “In vivohistological evaluation of a novel ablative fractionalresurfacing device,” Lasers in Surgery and Medicine, vol. 39,no. 2, pp. 96–107, 2007.
[81] T. S. Alster and T. B. West, “Resurfacing of atrophic facialacne scars with a high-energy, pulsed carbon dioxide laser,”Dermatologic Surgery, vol. 22, no. 2, pp. 151–155, 1996.
[82] G. J. Goodman, “Postacne scarring: a review of itspathophysiology and treatment,” Dermatologic Surgery,vol. 26, no. 9, pp. 857–871, 2000.
[83] S. H. Koo, E. S. Yoon, D. S. Ahn, and S. H. Park, “Laserpunch-out for acne scars,” Aesthetic Plastic Surgery, vol. 25,no. 1, pp. 46–51, 2001.
[84] J. M. Grevelink and V. R. White, “Concurrent use of laserskin resurfacing and punch excision in the treatment offacial acne scarring,” Dermatologic Surgery, vol. 24, no. 5, pp.527–530, 1998.
[85] L. Y. Matsuoka, “Acne and related disorders,” Clinics inPlastic Surgery, vol. 20, no. 1, pp. 35–41, 1993.
[86] D. A. Ellis and M. J. Michell, “Surgical treatment of acnescarring: non-linear scar revision,” Journal of Otolaryngology,vol. 16, no. 2, pp. 116–119, 1987.
[87] J. R. Trimble, “Dermal overgrafting in dermatology,” Journalof Dermatologic Surgery and Oncology, vol. 9, no. 12, pp.987–993, 1983.
[88] S. A. Burres, “Recollagenation of acne scars,” DermatologicSurgery, vol. 22, no. 4, pp. 364–367, 1996.
[89] B. Besecker and C. G. Hart, “A new treatment option for acnescars: allograft dermis,” Dermatology nursing / DermatologyNurses” Association, vol. 11, no. 2, pp. 111–114, 1999.
[90] R. Ellenbogen, “Invited comment on autologous fatinjection,” Annals of Plastic Surgery, vol. 24, p. 297, 1990.
[91] G. J. Goodman, “Postacne scarring: a review of its patho-physiology and treatment,” Dermatologic Surgery, vol. 26, no.9, pp. 857–871, 2000.
[92] D. Fernandes, “Minimally invasive percutaneous collageninduction,” Oral and Maxillofacial Surgery Clinics of NorthAmerica, vol. 17, no. 1, pp. 51–63, 2005.
[93] G. Fabbrocini, N. Fardella, A. Monfrecola, I. Proietti, and D.Innocenzi, “Acne scarring treatment using skin needling,”Clinical and Experimental Dermatology, vol. 34, no. 8, pp.874–879, 2009.
[94] W. H. Kang, Y. J. Kim, W. S. Pyo, S. J. Park, and J. H. Kim,“Atrophic acne scar treatment using triple combination ther-apy: dot peeling, subcision and fractional laser,” Journal ofCosmetic and Laser Therapy, vol. 11, no. 4, pp. 212–215, 2009.
[95] B. Berman, O. A. Perez, S. Konda et al., “A review of thebiologic effects, clinical efficacy, and safety of silicone elasto-mer sheeting for hypertrophic and keloid scar treatmentand management,” Dermatologic Surgery, vol. 33, no. 11, pp.1291–1302, 2007.
[96] T. A. Mustoe, R. D. Cooter, M. H. Gold et al., “Internationalclinical recommendations on scar management,” Plastic andReconstructive Surgery, vol. 110, no. 2, pp. 560–571, 2002.
[97] A. P. Kelly, “Medical and surgical therapies for keloids,”Dermatologic Therapy, vol. 17, no. 2, pp. 212–218, 2004.
[98] A. J. Nemeth, “Keloids and hypertrophic scars,” Journalof Dermatologic Surgery and Oncology, vol. 19, no. 8, pp.738–746, 1993.
[99] B. S. Atiyeh, “Nonsurgical management of hypertrophicscars: evidence-based therapies, standard practices, andemerging methods,” Aesthetic Plastic Surgery, vol. 31, no. 5,pp. 468–492, 2007.
[100] W. Manuskiatti and R. E. Fitzpatrick, “Treatment responseof keloidal and hypertrophic sternotomy scars: comparisonamong intralesional corticosteroid, 5-fluorouracil, and585-nm flashlamp-pumped pulsed-dye laser treatments,”Archives of Dermatology, vol. 138, no. 9, pp. 1149–1155, 2002.
[101] F. Boutli-Kasapidou, A. Tsakiri, E. Anagnostou, and O.Mourellou, “Hypertrophic and keloidal scars: an approachto polytherapy,” International Journal of Dermatology, vol.44, no. 4, pp. 324–327, 2005.
[102] L. Rusciani, G. Rossi, and R. Bono, “Use of cryotherapy inthe treatment of keloids,” Journal of Dermatologic Surgeryand Oncology, vol. 19, no. 6, pp. 529–534, 1993.
[103] A. M. Layton, J. Yip, and W. J. Cunliffe, “A comparison ofintralesional triamcinolone and cryosurgery in the treatmentof acne keloids,” British Journal of Dermatology, vol. 130, no.4, pp. 498–501, 1994.
[104] D. B. Apfelberg, M. R. Maser, and H. Lash, “Preliminaryresults of argon and carbon dioxide laser treatment of keloidscars,” Lasers in Surgery and Medicine, vol. 4, no. 3, pp.283–290, 1984.
Dermatology Research and Practice 13
[105] D. J. Castro, R. P. Abergel, and C. Meeker, “Effects of theNd:YAG laser on DNA synthesis and collagen productionin human skin fibroblast cultures,” Annals of Plastic Surgery,vol. 11, no. 3, pp. 214–222, 1983.
[106] J. E. C. Norris, “The effect of carbon dioxide laser surgery onthe recurrence of keloids,” Plastic and Reconstructive Surgery,vol. 87, no. 1, pp. 44–53, 1991.
[107] W. T. Lawrence, “In search of the optimal treatment ofkeloids: report of a series and a review of the literature,”Annals of Plastic Surgery, vol. 27, no. 2, pp. 164–178, 1991.
[108] R. Sherman and H. Rosenfeld, “Experience with the Nd:YAGlaser in the treatment of keloid scars,” Annals of PlasticSurgery, vol. 21, no. 3, pp. 231–235, 1988.
[109] Y.-R. Kuo, W.-S. Wu, S.-F. Jeng et al., “Activation of ERKand p38 kinase mediated keloid fibroblast apoptosis afterflashlamp pulsed-dye laser treatment,” Lasers in Surgery andMedicine, vol. 36, no. 1, pp. 31–37, 2005.
[110] Y.-R. Kuo, W.-S. Wu, S.-F. Jeng et al., “Suppressed TGF-β1 expression is correlated with up-regulation of matrixmetalloproteinase-13 in keloid regression after flashlamppulsed-dye laser treatment,” Lasers in Surgery and Medicine,vol. 36, no. 1, pp. 38–42, 2005.
[111] T. S. Alster and C. M. Williams, “Treatment of keloidsternotomy scars with 585 nm flashlamp-pumped pulsed-dye laser,” Lancet, vol. 345, no. 8959, pp. 1198–1200, 1995.
[112] T. Alster, “Laser scar revision: Comparison study of 585-nmpulsed dye laser with and without intralesional corticos-teroids,” Dermatologic Surgery, vol. 29, no. 1, pp. 25–29, 2003.
[113] T. S. Alster and C. A. Nanni, “Pulsed dye laser treatment ofhypertrophic burn scars,” Plastic and Reconstructive Surgery,vol. 102, no. 6, pp. 2190–2195, 1998.
[114] T. Alster and L. Zaulyanov-Scanlon, “Laser scar revision: areview,” Dermatologic Surgery, vol. 33, no. 2, pp. 131–140,2007.
[115] W. Manuskiatti, R. Wanitphakdeedecha, and R. E.Fitzpatrick, “Effect of pulse width of a 595-nm flashlamp-pumped pulsed dye laser on the treatment response ofkeloidal and hypertrophic sternotomy scars,” DermatologicSurgery, vol. 33, no. 2, pp. 152–161, 2007.
[116] C. Dierickx, M. P. Goldman, R. E. Fitzpatrick, and T. S.Alster, “Laser treatment of erythematous/hypertrophic andpigmented scars in 26 patients,” Plastic and ReconstructiveSurgery, vol. 95, no. 1, pp. 84–92, 1995.
[117] L. E. Bowes, K. Nouri, B. Berman et al., “Treatment ofpigmented hypertrophic scars with the 585 nm pulsed dyelaser and the 532 nm frequency-doubled Nd:YAG laser in theQ-switched and variable pulse modes: a comparative study,”Dermatologic Surgery, vol. 28, no. 8, pp. 714–719, 2002.
[118] W. Manuskiatti, R. Wanitphakdeedecha, and R. E.Fitzpatrick, “Effect of pulse width of a 595-nm flashlamp-pumped pulsed dye laser on the treatment response ofkeloidal and hypertrophic sternotomy scars,” DermatologicSurgery, vol. 33, no. 2, pp. 152–161, 2007.
[119] M. P. Goldman and R. E. Fitzpatrick, “Laser treatment ofscars,” Dermatologic Surgery, vol. 21, no. 8, pp. 685–687,1995.
[120] F. Riedel and K. Hormann, “Plastic surgery of skin defects inthe face. Principles and prospective,” HNO, vol. 53, no. 12,pp. 1020–1036, 2005.