role of the paclitaxel-eluting stent and tirofiban in patients with st-elevation myocardial...
TRANSCRIPT

ISSN: 1941-7632 Copyright © 2010 American Heart Association. All rights reserved. Print ISSN: 1941-7640. Online
Greenville Avenue, Dallas, TX 72514Circulation: Cardiovascular Interventions is published by the American Heart Association. 7272
DOI: 10.1161/CIRCINTERVENTIONS.109.920868 2010;3;297-307 Circ Cardiovasc Interv
Román and Francisco Fernández-Avilés Juan López-Messa, Armando Pérez de Prado, Joaquin J. Alonso, J. Alberto San
Alonso-Briales, Francisco Bosa, Ignacio Santos, Juan Sanchis, Armando Bethencourt, Pedro L. Sánchez, Federico Gimeno, Pablo Ancillo, Juan J. Sanz, Juan H.
Randomized Clinical TrialMyocardial Infarction Undergoing Postfibrinolysis Angioplasty: The GRACIA-3 Role of the Paclitaxel-Eluting Stent and Tirofiban in Patients With ST-Elevation
http://circinterventions.ahajournals.org/cgi/content/full/3/4/297located on the World Wide Web at:
The online version of this article, along with updated information and services, is
http://www.lww.com/reprintsReprints: Information about reprints can be found online at
[email protected]. E-mail:
Fax:Kluwer Health, 351 West Camden Street, Baltimore, MD 21202-2436. Phone: 410-528-4050. Permissions: Permissions & Rights Desk, Lippincott Williams & Wilkins, a division of Wolters
http://circinterventions.ahajournals.org/subscriptions/at Subscriptions: Information about subscribing to Circulation: Cardiovascular Interventions is online
by guest on August 18, 2010 circinterventions.ahajournals.orgDownloaded from

Original Articles
Role of the Paclitaxel-Eluting Stent and Tirofiban inPatients With ST-Elevation Myocardial Infarction
Undergoing Postfibrinolysis AngioplastyThe GRACIA-3 Randomized Clinical Trial
Pedro L. Sanchez, MD, PhD; Federico Gimeno, MD, PhD; Pablo Ancillo, MD, PhD;Juan J. Sanz, MD, PhD; Juan H. Alonso-Briales, MD, PhD; Francisco Bosa, MD, PhD;Ignacio Santos, MD, PhD; Juan Sanchis, MD, PhD; Armando Bethencourt, MD, PhD;
Juan Lopez-Messa, MD, PhD; Armando Perez de Prado, MD, PhD; Joaquin J. Alonso, MD, PhD;J. Alberto San Roman, MD, PhD; Francisco Fernandez-Aviles, MD, PhD
Background—A catheter-based approach after fibrinolysis is recommended if fibrinolysis is likely to be successful inpatients with acute ST-elevation myocardial infarction. We designed a 2�2 randomized, open-label, multicenter trial toevaluate the efficacy and safety of the paclitaxel-eluting stent and tirofiban administered after fibrinolysis but beforecatheterization to optimize the results of this reperfusion strategy.
Methods and Results—We randomly assigned 436 patients with acute ST-elevation myocardial infarction to (1) bare-metalstent without tirofiban, (2) bare-metal stent with tirofiban, (3) paclitaxel-eluting stent without tirofiban, and (4)paclitaxel-eluting stent with tirofiban. All patients were initially treated with tenecteplase and enoxaparin. Tirofiban wasstarted 120 minutes after tenecteplase in those patients randomly assigned to tirofiban. Cardiac catheterization wasperformed within the first 3 to 12 hours after inclusion, and stenting (randomized paclitaxel or bare stent) was appliedto the culprit artery. The primary objectives were the rate of in-segment binary restenosis of paclitaxel-eluting stentcompared with that of bare-metal stent and the effect of tirofiban on epicardial and myocardial flow before and aftermechanical revascularization. At 12 months, in-segment binary restenosis was similar between paclitaxel-eluting stentand bare-metal stent (10.1% versus 11.3%; relative risk, 1.06; 95% confidence interval, 0.74 to 1.52; P�0.89).However, late lumen loss (0.04�0.055 mm versus 0.27�0.057 mm, P�0.003) was reduced in the paclitaxel-elutingstent group. No evidence was found of any association between the use of tirofiban and any improvement in theepicardial and myocardial perfusion. Major bleeding was observed in 6.1% of patients receiving tirofiban and in 2.7%of patients not receiving it (relative risk, 2.22; 95% confidence interval, 0.86 to 5.73; P�0.14).
Conclusions—This trial does not provide evidence to support the use of tirofiban after fibrinolysis to improve epicardialand myocardial perfusion. Compared with bare-metal stent, paclitaxel-eluting stent significantly reduced late loss butappeared not to reduce in-segment binary restenosis.
Clinical Trial Registration—URL: http://clinicaltrials.gov. Unique identifier: NCT00306228.(Circ Cardiovasc Interv. 2010;3:297-307.)
Key Words: acute myocardial infarction � fibrinolysis � postfibrinolysis angioplasty � tirofiban � IIb/IIIa inhibitors� paclitaxel � drug-eluting stents
The preferred reperfusion therapy in patients with acuteST-elevation myocardial infarction (STEMI) is primary
percutaneous coronary intervention (PCI).1 However, manyhospitals, even in the United States and Europe, lack PCI
facilities, and few provide around-the-clock staffing for theseprocedures.2 Thus, fibrinolysis is administered to eligiblepatients if primary PCI cannot be performed in a timelyfashion. Recent studies have demonstrated that routine ad-
Received November 3, 2009; accepted June 10, 2010.From the Hospital General Universitario Gregorio Maranon (P.L.S., F.F.-A.), Madrid, Spain; Hospital Clínico de Valladolid (F.G., J.A.S.R.), Spain;
Hospital General de Segovia (P.A.), Spain; Hospital Rio Hortega (J.J.S.), Valladolid, Spain; Hospital Virgen de la Victoria (J.H.A.-B.), Malaga, Spain;Hospital Universitario de Canarias (F.B.), Santa Cruz de Tenerife, Spain; Hospital Universitario de Salamanca (I.S.), Spain; Hospital Clínico Universitario(J.S.), Valencia, Spain; Hospital Son Dureta (A.B.), Palma de Mallorca, Spain; Hospital Rio Carrion (J.L.-M.), Palencia, Spain; Complejo Hospitalariode Leon (A.P.), Spain; and Hospital de Fuenlabrada (J.J.A.), Madrid, Spain.
The GRACIA-3 (Grupo de Analisis de la Cardiopatía Isquemica Aguda) Investigators and centers are listed in the Appendix.The online-only Data Supplement is available at http://circinterventions.ahajournals.org/cgi/content/full/CIRCINTERVENTIONS.109.920868/DC1.Correspondence to Francisco Fernandez-Aviles, MD, Servicio de Cardiología, Hospital General Universitario Gregorio Maranon, C/Doctor Esquerdo
46, 28007, Madrid, Spain. E-mail [email protected]© 2010 American Heart Association, Inc.
Circ Cardiovasc Interv is available at http://circinterventions.ahajournals.org DOI: 10.1161/CIRCINTERVENTIONS.109.920868
297 by guest on August 18, 2010 circinterventions.ahajournals.orgDownloaded from

junctive or early postfibrinolytic angiography and, if appro-priate, PCI may improve outcome.3–11 This approach com-bines the advantages of the rapid and simple use offibrinolysis for myocardial salvage with those of stenting inachieving a normal stable flow and is a reasonably usefulstrategy in most patients even in the absence of ischemia atrest or after stress, arrhythmias, left ventricular dysfunction,or heart failure.12,13 However, the most effective dose andtiming of antiplatelet therapy remains unresolved, as does thesafety and efficacy of drug elution.
Editorial see p 294Clinical Perspective on p 307
We performed an open-label, 2�2, controlled, randomizedtrial in STEMI patients receiving fibrinolysis, enoxaparin,and aspirin followed by early cardiac catheterization andcoronary stenting to compare the efficacy of the paclitaxel-eluting stent with that of the conventional bare-metal stent inrestenosis. We also determined the effect of tirofiban admin-istered 120 minutes after fibrinolysis but before PCI onepicardial and myocardial flow both before and after mechan-ical revascularization.
MethodsPatient PopulationFrom October 2004 to August 2006, patients were enrolled from 20Spanish hospitals, 13 of which had interventional facilities. Theinclusion criteria were as follows: age 18 years or older; symptomonset within 12 hours before random assignment; chest pain lastingmore than 30 minutes; ST-segment elevation of at least 0.1 mV in atleast 2 limb leads, ST-segment elevation of at least 0.2 mV in 2 ormore contiguous precordial leads, or left bundle-branch block orpaced rhythm; and no severe heart failure (Killip class �3). Theexclusion criteria were as follows: cardiogenic shock, defined as asystolic blood pressure �90 mm Hg with no response to fluidadministration or �100 mm Hg in patients with supportive treatmentand no bradycardia; suspected mechanical complications of acutemyocardial infarction; previous coronary artery bypass graft; non-cardiac disease that is likely to jeopardize the planned termination ofthe study; women of childbearing potential unless they had anegative pregnancy test result; active bleeding and recent surgery(within 2 weeks) that contraindicate the use of heparin, tirofiban, orplatelet aggregation inhibitors; contraindications for thrombolysis(previous hemorrhagic stroke at any time, history of nonhemorrhagiccerebrovascular accident within the previous 12 months, intracere-bral neoplasm, active internal bleeding, suspected aortic dissection,uncontrolled hypertension �180/110 in several measurements, anyother known intracerebral condition not covered in contraindications,current use of anticoagulants or heparin use within 8 hours, knownbleeding diathesis, recent trauma [�4 weeks] including head traumaor traumatic or prolonged [�10 minutes] cardiopulmonary resusci-tation or recent major surgery or biopsy [�8 weeks], noncompress-ible vascular punctures, recent [�4 weeks] internal bleeding, preg-nancy, and active peptic ulcer); history of hypersensitivity to aspirin,ticlopidine, clopidogrel, heparin, tirofiban, or stainless steel; knownrenal failure, creatinine �2.5 mg/dL; known impaired hepaticfunction that contraindicates the use of clopidogrel; known throm-bocytopenia (�100 000); participation in other trials; known mul-tivessel disease identified as not suitable for revascularization; andknown peripheral vascular disease that makes cardiac catheterizationdifficult.
Approval was obtained from the relevant ethics committees atboth national and institutional level. An informational brochure wasprovided to each patient who met the inclusion criteria, and informedwritten consent was obtained. All patients were then randomlyassigned using a central telephone system, and the doctors who
informed the patient rang for the allocation. Blocking was used togenerate the random allocation sequence and to ensure a closebalance of the numbers in each group at any time during the trial.The block lengths were 4, 8, and successive 4 size blocks. Patientsadmitted to noninterventional hospitals were transported to thenearest interventional hospital and returned to the original hospitalafter angiography and revascularization.
Study Protocol and InterventionsAfter providing informed consent, patients who satisfied the inclu-sion and exclusion criteria were randomly assigned to 1 of 4treatment groups: (1) bare-metal stent without tirofiban, (2) bare-metal stent with tirofiban, (3) paclitaxel-eluting stent without tirofi-ban, and (4) paclitaxel-eluting stent with tirofiban. All patientsreceived fibrinolysis and aspirin, and the use of tirofiban orpaclitaxel-eluting stent was evaluated on this background therapy.
Patients randomly assigned to tirofiban received 150 mg to 325mg of nonenteric coated aspirin orally (chewed) or 500 mg iv as soonas STEMI was identified. Immediate thrombolysis with tenecteplasewas administered according to the instructions in the Summary ofProduct Characteristics for the treatment of STEMI (30 mg if bodyweight was less than 60 kg, 35 mg if it was 60 to 69 kg, 40 mg if itwas 70 to 79 kg, 45 mg if it was 80 to 89 kg, and 50 mg if it was 90kg or more). No enoxaparin bolus was given to these patients;enoxaparin was administered as a subcutaneous injection at 0.75mg/kg. This subcutaneous dose was the only dose administered if thecoronary intervention was successfully performed within 8 hours ofrandomization. Tirofiban was started 2 hours after tenecteplase witha fixed 25-�g/kg intravenous bolus followed by 0.15 �g/kg/min inintravenous infusion for 24 hours. The infusion was reduced by 50%if severe renal failure (creatinine clearance �30 mL/h or creatinine�2 mg/dL) was observed. The rationale for withholding tirofiban for2 hours after fibrinolytic treatment was based on the pharmacoki-netics and pharmacodynamics of tenecteplase. In a previous studywith 103 patients,14 tenecteplase exhibited biphasic elimination fromthe plasma with a mean initial half-life of 22 minutes and a meanterminal half-life of 115 minutes. This mean terminal half-life of 115minutes motivated the rationale for withholding tirofiban for 2 hoursin order to avoid bleeding complications.
Patients randomly assigned to no tirofiban received 150 mg to 325mg of non–enteric-coated aspirin orally (chewed) or 500 mg iv assoon as STEMI was identified. Immediate thrombolysis with tenect-eplase was administered, with the doses and mode of administrationdescribed above. An enoxaparin bolus of 30 mg followed by asubcutaneous dose of 1 mg/kg was administered in patients �75years old. Patients over 75 did not receive the enoxaparin bolus andthe subcutaneous injection was reduced to 0.75 mg/kg. This subcu-taneous dose was also the only dose administered if coronaryintervention was successfully performed within 8 hours of randomassignment.
Patients underwent catheterization within 3 to 12 hours of randomassignment. The infarct-related artery was dilated if there was totalocclusion, the stenosis was greater than 50%, or the TIMI flow gradewas less than 3. Stenting of culprit lesions was performed when theywere morphologically suitable for stenting and when the procedurewas expected to achieve an adequate result. To avoid thrombuscompression and embolization, direct stenting was attempted whenpossible. The stenting procedure was carried out using Express stents(Boston Scientific, Natick, Mass) or TAXUS stents (Boston Scien-tific), for patients randomly assigned to the bare-metal stent orpaclitaxel-eluting stent, respectively. When a large amount of myo-cardium was threatened by severe stenosis (�90% reduction inlumen diameter by visual estimation in a coronary segment with areference diameter larger than 2.75 mm), stenting of nonculpritlesions was also performed.
No additional low-molecular-weight heparin was administered ifrevascularization was successful. In the group randomly assigned tono tirofiban, investigators were encouraged not to use glycoproteinIIb/IIIa inhibitors during the revascularization procedure. If theinvestigator decided that a glycoprotein IIb/IIIa inhibitor was re-quired during the procedure, tirofiban was suggested as a bail-out.
298 Circ Cardiovasc Interv August 2010
by guest on August 18, 2010 circinterventions.ahajournals.orgDownloaded from

Immediate rescue angioplasty was undertaken when both chest painand ST-segment elevation persisted at 3 hours after administration oftenecteplase.
Immediately after stenting, patients received a loading dose of 300mg of clopidogrel and 75 mg daily for 1 year. Maintenance aspirintherapy was administered indefinitely at 80 to 325 mg once daily(coated or uncoated), unless contraindicated. The tirofiban infusionwas stopped 24 hours after initiation. Finally, �-blockers, angioten-sin-converting enzyme inhibitors, statins, and any additional postin-farction therapy were administered, as outlined in internationalguidelines.13,15
Study End Points and DefinitionsThe primary objectives of the study were, first, to compare theefficacy of the paclitaxel-eluting stent with that of the conventionalbare-metal stent, and, second, to determine the effect of tirofibanadministered 120 minutes after fibrinolysis but before PCI onepicardial and myocardial reperfusion in patients with STEMItreated with routine early postfibrinolysis PCI.
For the first objective, the primary efficacy end point was the rateof binary restenosis after 12 months of angiographic follow-up, asdetermined by independent quantitative angiographic analysis. Bi-nary angiographic restenosis was defined as a �50% narrowing ofthe lumen diameter in the target segment (defined as all portions ofthe vessel that received treatment within the stent zone, including theproximal and distal 5-mm margins).
For the second objective, the primary efficacy end point was thedegree of epicardial and myocardial flow before and after mechan-ical revascularization. This was measured angiographically using theangiographic perfusion score (APS). The APS combines grades ofepicardial and myocardial perfusion before and after PCI to arrive ata single angiographic variable that is associated with infarct size andclinical outcomes.16 The APS is calculated by summing the epicar-dial and myocardial flow grades before and after PCI (total possiblegrade, 0 to 12). Full perfusion is defined as an APS of 10 to 12,partial perfusion as an APS of 4 to 9, and failed perfusion as an APSof 0 to 3.
Prespecified secondary endpoints included the safety of thepaclitaxel-eluting stent in terms of rate of stent thrombosis, determi-nation of the interaction between the paclitaxel-eluting stent and thecomplicated myocardial infarction lesion in terms of reduction inintimal proliferation as evaluated by quantitative coronary angiog-raphy, and determination of the clinical efficacy and safety offull-dose fibrinolysis plus delayed tirofiban compared with fibrino-lysis alone, both in the whole cohort of patients and in differentsubgroups. The clinical definitions provided were identical to thoseused in the previous GRACIA 1 and 2 trials4,10; as for example majorbleeding was defined as any bleeding complication causing death,need for surgery or transfusion, or extended time in hospital. Wefollowed the Academic Research Consortium (ARC) criteria forclassifying stent-related thrombosis events in an attempt to establishuniformity.17
Data Collection and Core Laboratory AnalysisData were entered using a double entry system, and the accuracy ofcollected data were validated against medical records by an inde-pendent clinical research organization (Chiltern International, SpainS.A.). Data were then submitted to the data coordinating center(Hospital General Universitario Gregorio Maranon, Madrid). Clini-cal outcome was adjudicated by an independent clinical eventscommittee blinded to study group assignment. A separate data andsafety monitoring board not affiliated with the study investigatorsreviewed data periodically throughout the trial to identify potentialsafety issues and monitor study conduct.
Coronary angiography was performed at baseline, at the comple-tion of the procedure, and after 12 months of follow-up. Allangiograms were analyzed at an independent angiographic corelaboratory (ICICOR, Valladolid, Spain) with a quantitativecomputer-based system (Medis, Leesburg, Va). The epicardial andmyocardial flow grades were assessed by an experienced reader whowas blinded to treatment assignment and clinical outcome.
Additional assessment of myocardial perfusion was performedusing ST-segment analysis. The amount of ST-segment elevationwas measured manually 20 ms after the J point. The sum ofST-segment elevation was measured from leads I, aVL, and V1 to V6for anterior myocardial infarction and leads II, III, aVF, V5, and V6for inferior myocardial infarction. We divided patients into 3 groupsaccording to the resolution of ST-segment deviation (complete,�70% resolution; partial, �30% but �70% resolution; and noresolution, �30% resolution).
Statistical AnalysisThe number of patients included in the study was based on anestimate of the sample size needed to identify a statistically signif-icant difference in the 2 principal endpoints. Thus, for the samplesize calculation, we used 2 different variables: binary restenosis(categorical variable) and the APS (categorical variable).
For binary restenosis, we assumed that the restenosis rate in thebare-metal stent group would be 22% and that this rate would beclinically significant if it was reduced by 50% (from 22% to 11%) inthe paclitaxel-eluting stent group. The predicted restenosis rate withthe bare-metal stent and the assumed benefit with the paclitaxel-eluting stent were determined using data from the CADILLAC18 andthe TAXUS IV19 studies. Based on the assumed restenosis rate, tohave at least 80% power at the overall 5% significance level(2-tailed), the trial had to enroll a total of 436 patients. We expecteda 20% loss to follow-up (a 12-month angiographic follow-up isrequired for this assumption).
For the APS, the sample size calculation was based on theassumption that full APS is present in approximately 50% of patientswith STEMI who had received fibrinolytics16 and that this rate wouldbe clinically significant if it increased by 25% (from 50% to 62.5%)in the tirofiban group. On the basis of this assumption, with 80%power at the overall 5% significance level (2-tailed), the trial shouldenroll a total of 408 patients to show the superiority of treatment withtirofiban. We expected a 5% loss to follow-up (pre- and post-PCIangiography is required for this assumption).
All the analyses were performed according to the intention-to-treatprinciple. We analyzed the primary and secondary efficacy andsafety end points using the �2 test or Student t test. Additionally, weused the �2 test for trend to analyze categorical variables or theANOVA test to analyze quantitative variables, in each of the 4groups. The data are presented as the mean and the standard error,medians and interquartile range, or proportions. A 2-tailed probabil-ity value of �0.05 indicated statistical significance.
ResultsPatient CharacteristicsFigure 1 shows the trial profile: 110 patients were initiallyrandomly assigned to receive no tirofiban and a bare-metalstent, 107 to receive tirofiban and a bare-metal stent, 110 toreceive no tirofiban and a placlitaxel-eluting stent, and 109 toreceive tirofiban and a paclitaxel-eluting stent. Three patients(1 in each of the last 3 groups) were excluded from theanalysis because they did not meet the inclusion criteria. Ofthe 433 patients, 147 (34%) were included and randomlyassigned to hospitals with no PCI facilities; they weresubsequently transferred to a hospital with PCI facilities,where the remaining 286 of 433 (66%) patients were alsoincluded and randomly assigned. Eleven (7.5%) patients hadcardiac complications during the transfer: 8 of 147 (5.4%)had cardiac arrhythmias, 1 of 147 (0.7%) had heart failure,and 2 of 147 (1.4%) had ischemic pain. These were allsuccessfully resolved during transport. Overall, the baselinecharacteristics of the study population were similar betweengroups and similar to those of the populations of previoustrials on primary angioplasty or fibrinolysis (Table 1). All
Sanchez et al The GRACIA-3 Trial 299
by guest on August 18, 2010 circinterventions.ahajournals.orgDownloaded from
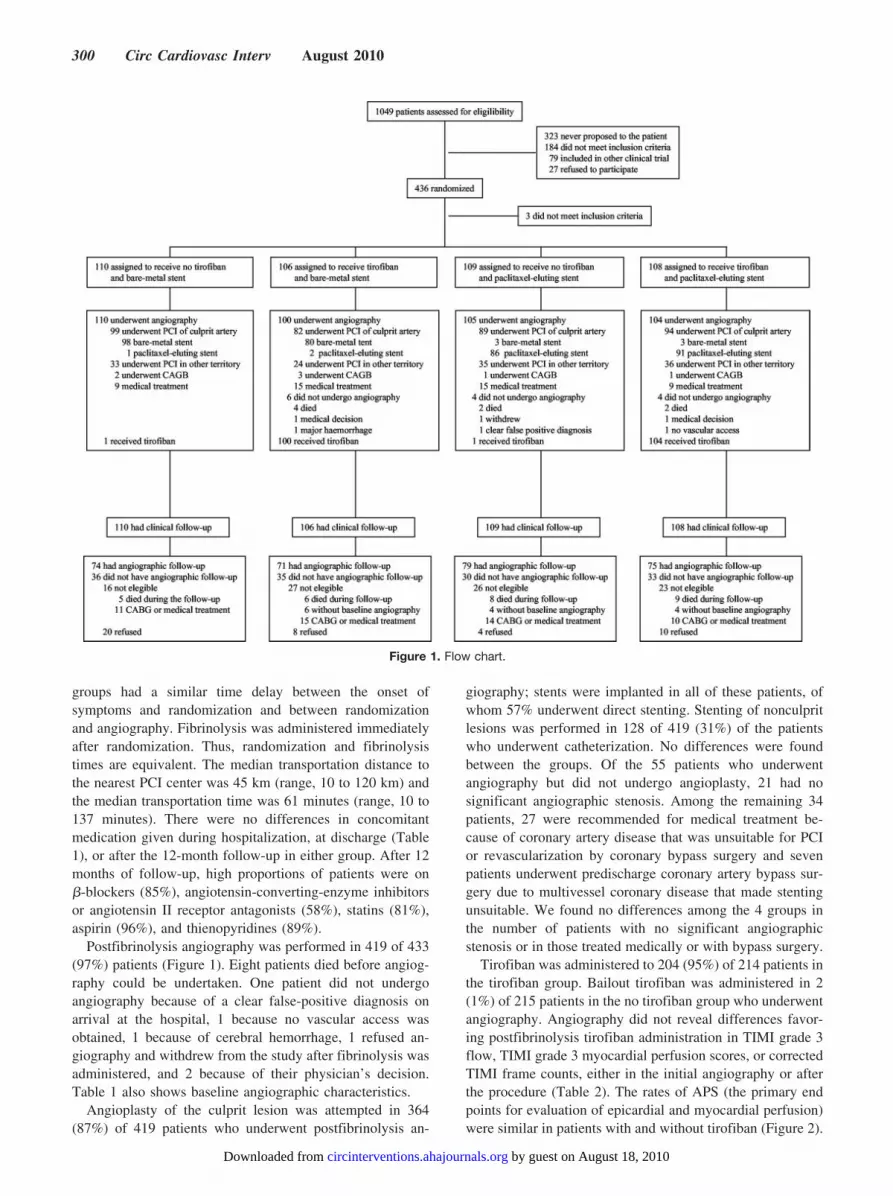
groups had a similar time delay between the onset ofsymptoms and randomization and between randomizationand angiography. Fibrinolysis was administered immediatelyafter randomization. Thus, randomization and fibrinolysistimes are equivalent. The median transportation distance tothe nearest PCI center was 45 km (range, 10 to 120 km) andthe median transportation time was 61 minutes (range, 10 to137 minutes). There were no differences in concomitantmedication given during hospitalization, at discharge (Table1), or after the 12-month follow-up in either group. After 12months of follow-up, high proportions of patients were on�-blockers (85%), angiotensin-converting-enzyme inhibitorsor angiotensin II receptor antagonists (58%), statins (81%),aspirin (96%), and thienopyridines (89%).
Postfibrinolysis angiography was performed in 419 of 433(97%) patients (Figure 1). Eight patients died before angiog-raphy could be undertaken. One patient did not undergoangiography because of a clear false-positive diagnosis onarrival at the hospital, 1 because no vascular access wasobtained, 1 because of cerebral hemorrhage, 1 refused an-giography and withdrew from the study after fibrinolysis wasadministered, and 2 because of their physician’s decision.Table 1 also shows baseline angiographic characteristics.
Angioplasty of the culprit lesion was attempted in 364(87%) of 419 patients who underwent postfibrinolysis an-
giography; stents were implanted in all of these patients, ofwhom 57% underwent direct stenting. Stenting of nonculpritlesions was performed in 128 of 419 (31%) of the patientswho underwent catheterization. No differences were foundbetween the groups. Of the 55 patients who underwentangiography but did not undergo angioplasty, 21 had nosignificant angiographic stenosis. Among the remaining 34patients, 27 were recommended for medical treatment be-cause of coronary artery disease that was unsuitable for PCIor revascularization by coronary bypass surgery and sevenpatients underwent predischarge coronary artery bypass sur-gery due to multivessel coronary disease that made stentingunsuitable. We found no differences among the 4 groups inthe number of patients with no significant angiographicstenosis or in those treated medically or with bypass surgery.
Tirofiban was administered to 204 (95%) of 214 patients inthe tirofiban group. Bailout tirofiban was administered in 2(1%) of 215 patients in the no tirofiban group who underwentangiography. Angiography did not reveal differences favor-ing postfibrinolysis tirofiban administration in TIMI grade 3flow, TIMI grade 3 myocardial perfusion scores, or correctedTIMI frame counts, either in the initial angiography or afterthe procedure (Table 2). The rates of APS (the primary endpoints for evaluation of epicardial and myocardial perfusion)were similar in patients with and without tirofiban (Figure 2).
Figure 1. Flow chart.
300 Circ Cardiovasc Interv August 2010
by guest on August 18, 2010 circinterventions.ahajournals.orgDownloaded from

Table 1. Baseline and Angiographic Characteristics
No Tirofiban�Bare-Metal Stent(n�110)
Tirofiban�Bare-Metal Stent(n�106)
No Tirofiban�Paclitaxel Stent(n�109)
Tirofiban�Paclitaxel Stent(n�108)
Baseline characteristic
Age, y 61.2�1.28 60.6�1.26 61.4�1.19 60.8�1.27
Median 63 61 62 61
Interquartile range 59�64 58�63 59�64 58�63
Male sex 93 (84.5) 92 (86.8) 87 (79.8) 86 (79.6)
Hypertension 46 (41.8) 47 (44.3) 44 (40.8) 51 (47.2)
Diabetes 21 (19.1) 15 (14.1) 23 (21.1) 21 (19.4)
Current smoking 56 (50.9) 55 (51.9) 51 (46.8) 48 (44.4)
Cholesterol �5.5 mmol/L 47 (42.7) 42 (39.6) 45 (41.3) 52 (48.1)
Family history 20 (18.2) 18 (17.0) 20 (18.3) 24 (22.2)
Previous myocardial infarction 8 (7.3) 4 (3.8) 4 (3.7) 9 (8.3)
Previous angina 13 (11.8) 16 (15.1) 10 (9.2) 22 (20.4)
Previous angioplasty 4 (3.6) 5 (4.7) 0 (0) 4 (3.7)
Heart rate, beats/min 71.4�1.49 76.1�1.58 74.4�1.51 75.4�1.37
Systolic blood pressure, mm Hg 133�2.49 136�2.13 135�2.09 134�2.24
Medical treatment at inclusion*
Aspirin 99 (90.0) 94 (88.7) 95 (87.2) 96 (88.9)
�-blockers 10 (9.1) 12 (11.3) 11 (10.1) 17 (15.9)
ACE inhibitors 9 (8.2) 5 (4.7) 10 (9.2) 11 (10.3)
ARA II inhibitors 4 (3.6) 2 (1.9) 4 (3.7) 9 (8.4)
Calcium antagonists 2 (1.8) 3 (2.8) 3 (2.7) 5 (4.7)
Time, h
Symptoms to fibrinolysis 3.43�0.20 3.75�0.21 3.57�0.19 3.62�0.21
Median 3.00 3.25 3.17 3.00
Interquartile range 3.04�3.83 3.33�4.17 3.19�3.94 3.21�4.03
Fibrinolysis to angiography 6.07�0.33 6.56�0.32 5.78�0.32 6.07�0.32
Median 5.08 5.83 4.62 5.08
Interquartile range 5.41�6.73 5.92�7.20 5.15�6.40 5.43�6.71
Angiographic features n�110 n�100 n�105 n�104
Infarct-related artery location
Left anterior descending 44 (40.4) 43 (43.0) 52 (49.5) 51 (49.0)
Left circumflex 15 (13.7) 17 (17.0) 12 (11.4) 10 (9.6)
Right coronary artery 50 (45.9) 40 (40.0) 41 (39.1) 43 (41.4)
Unclassified 1 0 0 0
No. of vessel disease
Nonstenotic vessels 3 (2.7) 5 (5.0) 7 (6.7) 6 (5.8)
Single-vessel disease 61 (55.4) 60 (60.0) 51 (48.6) 58 (55.8)
Double-vessel disease 33 (30.0) 23 (23.0) 31 (29.5) 25 (24.0)
Triple-vessel disease 13 (11.8) 12 (12.0) 14 (13.3) 12 (11.5)
Medical treatment at discharge n�104 n�98 n�100 n�99
Aspirin 99 (95.2) 96 (98.0) 93 (93.0) 97 (98.0)
Clopidogrel 93 (89.4) 83 (84.7) 89 (89.0) 91 (91.9)
�-blockers 85 (81.7) 84 (85.7) 86 (86.0) 85 (85.9)
ACE inhibitors 56 (53.9) 43 (43.9) 46 (46.0) 68 (68.7)
ARA II inhibitors 4 (3.8) 3 (3.1) 2 (2.0) 5 (5.1)
Calcium antagonists 3 (2.9) 3 (3.1) 2 (2.0) 5 (5.1)
Statins 81 (77.9) 79 (80.6) 83 (83.0) 81 (81.2)
Data are presented as n (%) or mean�standard error.*Medical treatment at inclusion represents medical treatment received by the patient before random assignment. The use of aspirin was high because patients
received it at the onset of STEMI by the Emergency Services, primary care doctors, or emergency at referral hospitals.
Sanchez et al The GRACIA-3 Trial 301
by guest on August 18, 2010 circinterventions.ahajournals.orgDownloaded from

Furthermore, ST-segment resolution was also similar inpatients with or without tirofiban (Figure 3).
Angiographic follow-up at 12 months was completed in299 of 346 (86%) eligible patients (Figure 1) at a median of382 days, and data were analyzed at the core angiographiclaboratory (Table 3). The rate of the major primary end point,analysis-segment binary restenosis (which includes measure-ments within the stent and 5 mm proximal and distal to thestent), was similar for both the bare-metal and paclitaxel-eluting stent: 11.3% (16/142) for the bare-metal stent and10.1% (15/149) for the paclitaxel-eluting stent (relative risk,[RR], 1.06; 95% confidence interval [CI], 0.74 to 1.52;P�0.89). In-segment late lumen loss was significantly lowerfor the paclitaxel-eluting stent than for the bare-metal stent(0.04�0.055 mm versus 0.27�0.057 mm, difference, �0.23[95% CI, �0.39 to �0.07] P�0.003).
The 12-month clinical follow-up was complete for almostall patients (Figure 1). Table 4 shows the clinical outcomesand safety parameters. The combined rates of death, recurrentmyocardial infarction, revascularization, and/or rehospitaliza-tion were similar for all 4 groups: 21.0% in patients randomlyassigned to tirofiban compared with 15.5% in patients ran-
domly assigned to no tirofiban (relative risk with tirofiban,1.19; 95% CI, 0.96 to 1.49; P�0.174) and 21.2% in patientsrandomly assigned to the paclitaxel-eluting stent as comparedwith in 15.3% patients randomly assigned to bare-metal stents(RR with paclitaxel-eluting stent; 1.20; 95% CI, 0.97 to 1.49;P�0.141). The individual rates of death, reinfarction, revas-cularization, rehospitalization, and stent thrombosis were alsosimilar in all 4 groups in the comparison between tirofibanand no tirofiban and in the comparison between thepaclitaxel-eluting stent and the bare-metal stent after 12months of follow-up (Table 4).
Table 2. Angiographic Characteristics of Both Epicardial andMyocardial Perfusion
VariableNo Tirofiban
(n�215)Tirofiban(n�204) P
At baseline
Infarct-related artery TIMI grade n�214 n�204 0.102
0 34 (15.89) 18 (8.82)
1 10 (4.67) 9 (4.41)
2 18 (8.41) 26 (12.75)
3 152 (71.03) 151 (74.02)
TIMI myocardial perfusion grade n�196 n�196 0.884
0 61 (31.12) 54 (28.57)
1 11 (5.61) 13 (6.88)
2 26 (13.27) 23 (12.17)
3 98 (50.00) 99 (52.38)
cTFC 40.33�1.93 36.63�1.68 0.461
cTFC post 26.60�1.42 28.24�1.38 0.300
After the procedure
Infarct-related artery TIMI grade n�191 n�178 0.670
0 4 (2.09) 1 (0.56)
1 3 (1.57) 2 (1.12)
2 8 (4.19) 9 (5.06)
3 176 (92.15) 166 (93.26)
TIMI myocardial perfusion grade n�173 n�162 0.518
0 23 (13.29) 17 (10.49)
1 21 (12.14) 16 (9.88)
2 34 (19.65) 27 (16.67)
3 95 (54.91) 102 (62.96)
cTFC 26.70�1.24 25.36�0.99 0.992
cTFC post 20.08�0.83 20.19�0.84 0.958
cTFC indicates corrected TIMI frame count.Data are presented as n (%) or mean�standard error.
Figure 2. Epicardial and myocardial perfusion data for angiogra-phy, according to tirofiban treatment. The percentages ofpatients are shown according to the degree of the angiographicperfusion score (APS). The APS is calculated summing the epi-cardial and myocardial flow grades before and after PCI (totalpossible grade, 0 to 12). Full perfusion is defined as an APS of10 to 12, partial perfusion as an APS of 4 to 9, and failed perfu-sion as an APS of 0 to 3.
Figure 3. Myocardial reperfusion data for ECG, according totirofiban treatment. Percentage of patients with complete(�70% resolution) or partial (�30% but �70% resolution)ST-segment resolution on the ECG at 90 minutes, 3 hours, 6hours, 12 hours, and 24 hours. No significant differences wereobserved between patients treated with or without tirofiban.
302 Circ Cardiovasc Interv August 2010
by guest on August 18, 2010 circinterventions.ahajournals.orgDownloaded from
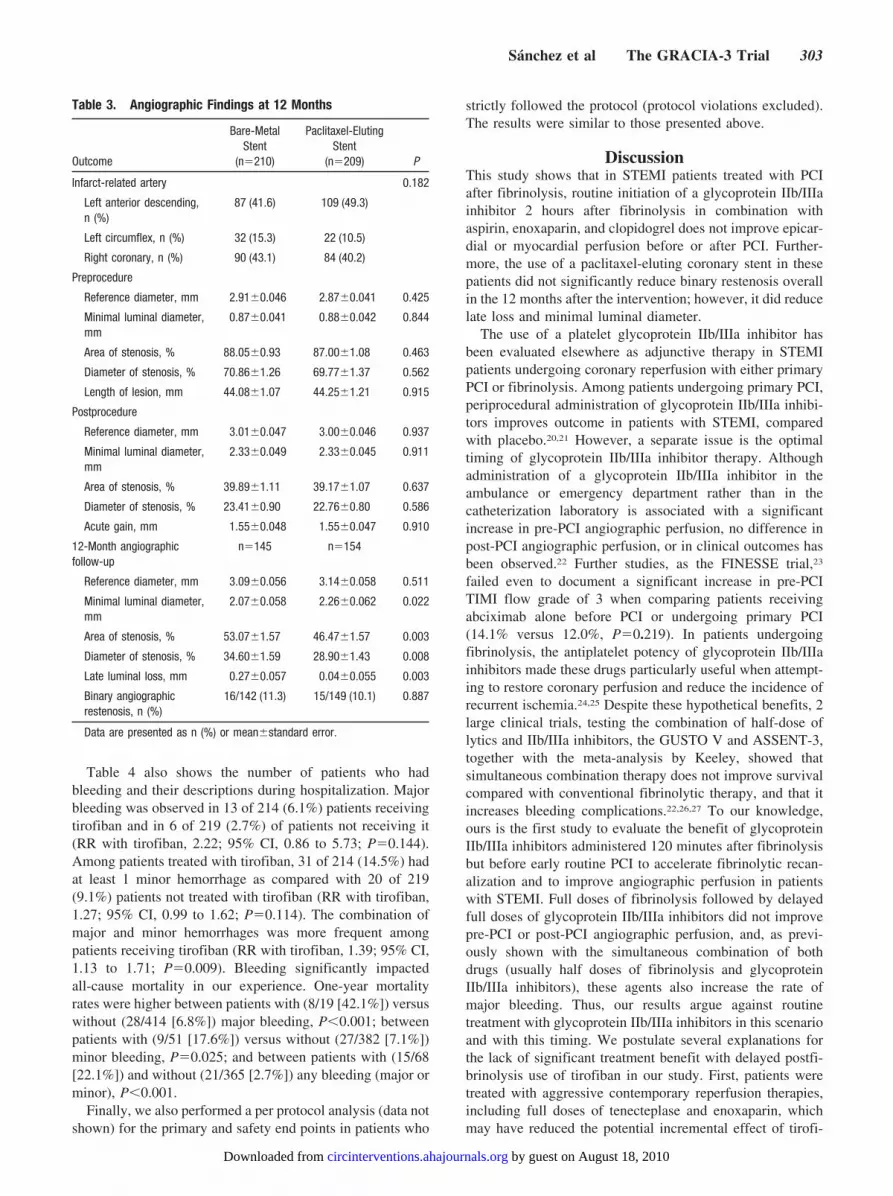
Table 4 also shows the number of patients who hadbleeding and their descriptions during hospitalization. Majorbleeding was observed in 13 of 214 (6.1%) patients receivingtirofiban and in 6 of 219 (2.7%) of patients not receiving it(RR with tirofiban, 2.22; 95% CI, 0.86 to 5.73; P�0.144).Among patients treated with tirofiban, 31 of 214 (14.5%) hadat least 1 minor hemorrhage as compared with 20 of 219(9.1%) patients not treated with tirofiban (RR with tirofiban,1.27; 95% CI, 0.99 to 1.62; P�0.114). The combination ofmajor and minor hemorrhages was more frequent amongpatients receiving tirofiban (RR with tirofiban, 1.39; 95% CI,1.13 to 1.71; P�0.009). Bleeding significantly impactedall-cause mortality in our experience. One-year mortalityrates were higher between patients with (8/19 [42.1%]) versuswithout (28/414 [6.8%]) major bleeding, P�0.001; betweenpatients with (9/51 [17.6%]) versus without (27/382 [7.1%])minor bleeding, P�0.025; and between patients with (15/68[22.1%]) and without (21/365 [2.7%]) any bleeding (major orminor), P�0.001.
Finally, we also performed a per protocol analysis (data notshown) for the primary and safety end points in patients who
strictly followed the protocol (protocol violations excluded).The results were similar to those presented above.
DiscussionThis study shows that in STEMI patients treated with PCIafter fibrinolysis, routine initiation of a glycoprotein IIb/IIIainhibitor 2 hours after fibrinolysis in combination withaspirin, enoxaparin, and clopidogrel does not improve epicar-dial or myocardial perfusion before or after PCI. Further-more, the use of a paclitaxel-eluting coronary stent in thesepatients did not significantly reduce binary restenosis overallin the 12 months after the intervention; however, it did reducelate loss and minimal luminal diameter.
The use of a platelet glycoprotein IIb/IIIa inhibitor hasbeen evaluated elsewhere as adjunctive therapy in STEMIpatients undergoing coronary reperfusion with either primaryPCI or fibrinolysis. Among patients undergoing primary PCI,periprocedural administration of glycoprotein IIb/IIIa inhibi-tors improves outcome in patients with STEMI, comparedwith placebo.20,21 However, a separate issue is the optimaltiming of glycoprotein IIb/IIIa inhibitor therapy. Althoughadministration of a glycoprotein IIb/IIIa inhibitor in theambulance or emergency department rather than in thecatheterization laboratory is associated with a significantincrease in pre-PCI angiographic perfusion, no difference inpost-PCI angiographic perfusion, or in clinical outcomes hasbeen observed.22 Further studies, as the FINESSE trial,23
failed even to document a significant increase in pre-PCITIMI flow grade of 3 when comparing patients receivingabciximab alone before PCI or undergoing primary PCI(14.1% versus 12.0%, P�0.219). In patients undergoingfibrinolysis, the antiplatelet potency of glycoprotein IIb/IIIainhibitors made these drugs particularly useful when attempt-ing to restore coronary perfusion and reduce the incidence ofrecurrent ischemia.24,25 Despite these hypothetical benefits, 2large clinical trials, testing the combination of half-dose oflytics and IIb/IIIa inhibitors, the GUSTO V and ASSENT-3,together with the meta-analysis by Keeley, showed thatsimultaneous combination therapy does not improve survivalcompared with conventional fibrinolytic therapy, and that itincreases bleeding complications.22,26,27 To our knowledge,ours is the first study to evaluate the benefit of glycoproteinIIb/IIIa inhibitors administered 120 minutes after fibrinolysisbut before early routine PCI to accelerate fibrinolytic recan-alization and to improve angiographic perfusion in patientswith STEMI. Full doses of fibrinolysis followed by delayedfull doses of glycoprotein IIb/IIIa inhibitors did not improvepre-PCI or post-PCI angiographic perfusion, and, as previ-ously shown with the simultaneous combination of bothdrugs (usually half doses of fibrinolysis and glycoproteinIIb/IIIa inhibitors), these agents also increase the rate ofmajor bleeding. Thus, our results argue against routinetreatment with glycoprotein IIb/IIIa inhibitors in this scenarioand with this timing. We postulate several explanations forthe lack of significant treatment benefit with delayed postfi-brinolysis use of tirofiban in our study. First, patients weretreated with aggressive contemporary reperfusion therapies,including full doses of tenecteplase and enoxaparin, whichmay have reduced the potential incremental effect of tirofi-
Table 3. Angiographic Findings at 12 Months
Outcome
Bare-MetalStent
(n�210)
Paclitaxel-ElutingStent
(n�209) P
Infarct-related artery 0.182
Left anterior descending,n (%)
87 (41.6) 109 (49.3)
Left circumflex, n (%) 32 (15.3) 22 (10.5)
Right coronary, n (%) 90 (43.1) 84 (40.2)
Preprocedure
Reference diameter, mm 2.91�0.046 2.87�0.041 0.425
Minimal luminal diameter,mm
0.87�0.041 0.88�0.042 0.844
Area of stenosis, % 88.05�0.93 87.00�1.08 0.463
Diameter of stenosis, % 70.86�1.26 69.77�1.37 0.562
Length of lesion, mm 44.08�1.07 44.25�1.21 0.915
Postprocedure
Reference diameter, mm 3.01�0.047 3.00�0.046 0.937
Minimal luminal diameter,mm
2.33�0.049 2.33�0.045 0.911
Area of stenosis, % 39.89�1.11 39.17�1.07 0.637
Diameter of stenosis, % 23.41�0.90 22.76�0.80 0.586
Acute gain, mm 1.55�0.048 1.55�0.047 0.910
12-Month angiographicfollow-up
n�145 n�154
Reference diameter, mm 3.09�0.056 3.14�0.058 0.511
Minimal luminal diameter,mm
2.07�0.058 2.26�0.062 0.022
Area of stenosis, % 53.07�1.57 46.47�1.57 0.003
Diameter of stenosis, % 34.60�1.59 28.90�1.43 0.008
Late luminal loss, mm 0.27�0.057 0.04�0.055 0.003
Binary angiographicrestenosis, n (%)
16/142 (11.3) 15/149 (10.1) 0.887
Data are presented as n (%) or mean�standard error.
Sanchez et al The GRACIA-3 Trial 303
by guest on August 18, 2010 circinterventions.ahajournals.orgDownloaded from

ban. Furthermore, such a benefit may have been attenuated bythe shorter time between initiation of symptoms and fibrino-lysis (median, 2.92 hours) or between fibrinolysis and PCI(median, 5.16 hours). Thus, considering that tirofiban wasadministered at least 2 hours after fibrinolysis, the time gainfor tirofiban was short in most patients.
A separate issue is the optimal timing between fibrinolysis andPCI, as trials show some overlap in the timing of PCI3–11,22,23,28–31
and this leads to different, somewhat arbitrary definitions.Facilitated PCI involves pharmacological therapy beforeplanned primary PCI for STEMI to achieve an open infarct-related artery before arrival at the catheterization laboratory.Trials have been conducted using fibrinolytic agents, glyco-protein IIb/IIIa inhibitors, and combinations of both. Incontrast, adjunctive or early elective PCI is used in patientswho are initially successfully reperfused with fibrinolysis andin whom early catheterization and, if appropriate, PCI isperformed. Our trial would be better placed in the seconddefinition, although the distinction between facilitated andadjunctive/early angioplasty is somewhat arbitrary.
There are few data on the use of drug-eluting stents inSTEMI.32–39 Information is restricted to drug-eluting stentsused during primary PCI, when they appear to be associatedwith a marked and sustained reduction in the rate of restenosisand the attendant risks of repeat revascularization after PCI.Concerns exist, however, over the safety of these stents,particularly in terms of the risk of stent thrombosis. To thebest of our knowledge, no randomized trial has specificallyexamined the efficacy and safety of drug-eluting stents in thesetting of postfibrinolysis adjunctive routine PCI for STEMI.Our results demonstrate that implantation of a paclitaxel-eluting stent during adjunctive routine postfibrinolysis PCIwas safe but did not result in overall decreased angiographicin-segment binary restenosis. On the other hand, the use of apaclitaxel-eluting stent did lead to a decrease in the extent oflate lumen loss, as compared with the use of a bare-metalstent, thus suggesting a reduced risk of restenosis. Wepostulate several explanations for the lack of significantlyreduced binary restenosis (primary end point) with the use ofthe paclitaxel-eluting stent in our study. First, we underesti-
Table 4. Clinical Outcome at 12 Months
VariableBare-Metal Stent
(n�216)Paclitaxel-Eluting Stent
(n�217) PNo Tirofiban
(n�219)Tirofiban(n�214) P
Cardiovascular event
Death 15 (6.9) 21 (9.7) 0.392 15 (6.9) 21 (9.8) 0.346
Nonfatal myocardial infarction 3 (1.4) 5 (2.3) 0.724 3 (1.4) 5 (2.3) 0.499
Ischemia-driven revascularization 10 (4.6) 9 (4.2) 0.992 11 (5.0) 8 (3.7) 0.676
PCI 10 (4.6) 8 (3.7) 0.802 10 (4.6) 8 (3.7) 0.849
CABG 0 (0) 1 (0.5) 1.000 1 (0.5) 0 (0) 1.000
Stent thrombosis 5 (2.3) 4 (1.8) 0.751 4 (1.8) 5 (2.3) 0.749
Definite 3 (1.4) 2 (0.9) 0.685 2 (0.9) 3 (1.4) 0.682
Probable 2 (0.9) 2 (0.9) 1.000 2 (0.9) 2 (0.9) 1.000
Any of the previous cardiovascularevents
33 (15.3) 46 (21.2) 0.141 34 (15.5) 45 (21.0) 0.174
Bleeding complications duringhospitalization
Major bleeding 11 (5.9) 8 (3.7) 0.632 6 (2.7) 13 (6.1) 0.145
Intracranial 4 (1.8) 5 (2.3) 1.000 2 (0.9) 7 (3.3) 0.102
Nonintracranial requiring transfusion 6(2.8) 3 (1.4) 0.338 4 (1.8) 5 (2.3) 0.749
Nonintracranial requiring additionalsurgery
1 (0.5) 0 (0) 0.499 0 (0) 1 (0.5) 0.494
Minor bleeding 24 (11.2) 27 (12.4) 0.779 20 (9.1) 31 (14.5) 0.114
Access site 15 (6.9) 9 (4.2) 0.288 9 (4.1) 15 (7.0) 0.268
Gastrointestinal 3 (1.4) 7 (3.2) 0.338 4 (1.8) 6 (2.8) 0.540
Gingival 5 (2.3) 5 (2.3) 1.000 4 (1.8) 6 (2.8) 0.540
Hematuria 4 (1.8) 4 (1.8) 1.000 1 (0.5) 7 (3.3) 0.035
Epistaxis 1 (0.5) 3 (1.4) 0.623 2 (0.9) 2 (0.9) 1.000
Other 2 (5.9) 2 (3.7) 1.000 2 (0.9) 2 (0.9) 1.000
Any bleeding 35 (16.2) 33 (15.2) 0.878 24 (11.0) 44 (20.6) 0.009
Death, reinfarction, revascularization,or major bleeding
40 (18.5) 48 (22.1) 0.417 35 (16.0) 53 (24.8) 0.031
Readmission 19 (8.8) 27 (12.4) 0.282 20 (9.1) 26 (12.1) 0.388
Index hospitalization, d 8.2�0.37 8.0�0.41 0.864 7.8�0.40 8.4�0.37 0.051
PCI indicates percutaneous coronary intervention; CABG, coronary artery bypass graft.
304 Circ Cardiovasc Interv August 2010
by guest on August 18, 2010 circinterventions.ahajournals.orgDownloaded from

mated the power of the effect of bare-metal stent implantationon the rate of follow-up binary restenosis (11% and not22%).18,36,37,39 Our strategy of postfibrinolysis PCI representsa different approach to mural thrombus in damaged plaquefrom that of primary PCI, and, consequently, reduced neoin-timal proliferation must be confirmed in future studies.Second, studies carried out since the initiation of our trial haveshown that late loss is more reliable than restenosis rates atdetermining neointimal proliferation between drug-eluting andbare-metal stents, particularly in early efficacy studies.40,41 Themean late lumen loss was significantly lower (0.04�0.055versus 0.27�0.057 mm, P�0.003) in the paclitaxel-elutinggroup than in the bare-metal group in our study, as we failed todefine binary restenosis, instead of late lumen loss, as ourprimary end point.
Some important limitations must be admitted regarding theinterpretation of our results. First, we use surrogate endpointsto compare four strategies of postfibrinolysis PCI rather thanrely on clinical outcomes. However, the mechanistic endpoints chosen are validated, and core laboratory–blindedinterpretation of the data were performed. Second, it is notunthinkable that earlier administration of tirofiban might haveled to different results, although the bleeding rates might beincreased by the concomitant administration of fibrinolytictreatment and tirofiban. Third, and very importantly, this trialdid not properly address the issue of rescue angioplasty forfailed fibrinolysis, as it was designed before recent findingsdocumenting the importance of early resolution of ST-segment elevation as an independent guide for the indicationrescue angioplasty.42 Fourth, the use of an angiographic endpoint to assess restenosis implied that repeat angiographycould strongly affect the repeat revascularization rates, whichtend to be largely increased compared with those that occur inthe setting of clinically driven repeat angiography. In ourexperience, 11 of 299 (3.7%) patients with 12-months angio-graphic follow-up underwent repeat revascularization underthis condition. Finally, as stated, the study was undersized(bare metal stent restenosis was 11%, not 22%), and clopi-dogrel was not given on admission, as is now recommendedby the guidelines.
Despite these limitations, our results have important impli-cations for the use of tirofiban and paclitaxel-eluting stents inpatients with STEMI undergoing early routine postfibrinoly-sis angioplasty. First, the routine use of tirofiban at least 120minutes after fibrinolysis but before PCI was not superior tofibrinolysis alone for improvement of epicardial and myocar-dial perfusion. Furthermore, patients in the tirofiban grouphad a 1.1- to 1.7-fold increased risk of major and minorbleeding that significantly impacted 1-year all-cause mortal-ity in our experience. Second, compared with bare-metalstents, paclitaxel-eluting stents significantly reduced late lossbut appeared not to reduce in-segment binary restenosis.
AcknowledgmentsWe thank Javier Botas and Rafael Gabriel (methodological advice)and Igor Martín and Itziar Gomez (database management andstatistical help). We also thank the investigators and the coordinatorsof the GRACIA-3 trial and all the medical and nursing staff in therecruitment and intervention centers who made the trial possible.Most of all, we thank all the patients who participated in the trial.
Sources of FundingThis study is an academic clinical trial. The sponsors of the studyhave no role in the study design, data collection, data analysis, datainterpretation, or writing of the report. The corresponding author hadfull access to all the data in the study and was responsible for thedecision to submit for publication. Unrestricted grants to fund thestudy were obtained from Red Tematica de Enfermedades Cardio-vasculares (RECAVA) of the Instituto de Salud Carlos III (SpanishMinistry of Science and Innovation), from the Fondo de Investiga-cion Sanitaria (FIS: PI040308, PI040235, PI040361, PI042035,PI042686, PI040166, PI040276, PI 040306, PI040309, PI040350,PI040478, and PI0402037) of the Instituto de Salud Carlos III(Spanish Ministry of Science and Innovation), and from the Junta deCastilla y Leon.
DisclosuresNone.
References1. Keeley EC, Boura JA, Grines CL. Primary angioplasty versus intravenous
thrombolytic therapy for acute myocardial infarction: a quantitativereview of 23 randomised trials. Lancet. 2003;361:13–20.
2. Nallamothu BK, Bradley EH, Krumholz HM. Time to treatment inprimary percutaneous coronary intervention. N Engl J Med. 2007;357:1631–1638.
3. Scheller B, Hennen B, Hammer B, Walle J, Hofer C, Hilpert V, WinterH, Nickenig G, Bohm M. Beneficial effects of immediate stenting afterthrombolysis in acute myocardial infarction. J Am Coll Cardiol. 2003;42:634–641.
4. Fernandez-Aviles F, Alonso JJ, Castro-Beiras A, Vazquez N, Blanco J,Alonso-Briales J, Lopez-Mesa J, Fernandez-Vazquez F, Calvo I,Martinez-Elbal L, San Roman JA, Ramos B. Routine invasive strategywithin 24 hours of thrombolysis versus ischaemia-guided conservativeapproach for acute myocardial infarction with ST-segment elevation(GRACIA-1): a randomised controlled trial. Lancet. 2004;364:1045–1053.
5. Le May MR, Wells GA, Labinaz M, Davies RF, Turek M, Leddy D,Maloney J, McKibbin T, Quinn B, Beanlands RS, Glover C, Marquis JF,O’Brien ER, Williams WL, Higginson LA. Combined angioplasty andpharmacological intervention versus thrombolysis alone in acute myo-cardial infarction (CAPITAL AMI study). J Am Coll Cardiol. 2005;46:417–424.
6. Thiele H, Engelmann L, Elsner K, Kappl MJ, Storch WH, Rahimi K,Hartmann A, Pfeiffer D, Kneissl GD, Schneider D, Moller T, HeberlingHJ, Weise I, Schuler G. Comparison of pre-hospital combination-fibri-nolysis plus conventional care with pre-hospital combination-fibrinolysisplus facilitated percutaneous coronary intervention in acute myocardialinfarction. Eur Heart J. 2005;26:1956–1963.
7. Armstrong PW. A comparison of pharmacologic therapy with/withouttimely coronary intervention vs primary percutaneous intervention earlyafter ST-elevation myocardial infarction: the WEST (Which Early S.T-elevation myocardial infarction Therapy) study. Eur Heart J. 2006;27:1530–1538.
8. Di Mario C, Dudek D, Piscione F, Mielecki W, Savonitto S, Murena E,Dimopoulos K, Manari A, Gaspardone A, Ochala A, Zmudka K,Bolognese L, Steg PG, Flather M. Immediate angioplasty versus standardtherapy with rescue angioplasty after thrombolysis in the CombinedAbciximab REteplase Stent Study in Acute Myocardial Infarction(CARESS-in-AMI): an open, prospective, randomised, multicentre trial.Lancet. 2008;371:559–568.
9. Cantor WJ, Fitchett D, Borgundvaag B, Heffernan M, Cohen EA,Morrison LJ, Ducas J, Langer A, Mehta S, Lazzam C, Schwartz B,Dzavik V, Goodman SG. Rationale and design of the Trial of RoutineANgioplasty and Stenting After Fibrinolysis to Enhance Reperfusion inAcute Myocardial Infarction (TRANSFER-AMI). Am Heart J. 2008;155:19–25.
10. Fernandez-Aviles F, Alonso JJ, Pena G, Blanco J, Alonso-Briales J,Lopez-Mesa J, Fernandez-Vazquez F, Moreu J, Hernandez RA, Castro-Beiras A, Gabriel R, Gibson CM, Sanchez PL. Primary angioplasty vsearly routine post-fibrinolysis angioplasty for acute myocardial infarctionwith ST-segment elevation: the GRACIA-2 non-inferiority, randomized,controlled trial. Eur Heart J. 2007;28:949–960.
Sanchez et al The GRACIA-3 Trial 305
by guest on August 18, 2010 circinterventions.ahajournals.orgDownloaded from

11. Danchin N, Coste P, Ferrieres J, Steg PG, Cottin Y, Blanchard D, BelleL, Ritz B, Kirkorian G, Angioi M, Sans P, Charbonnier B, EltchaninoffH, Gueret P, Khalife K, Asseman P, Puel J, Goldstein P, Cambou JP,Simon T. Comparison of thrombolysis followed by broad use of percu-taneous coronary intervention with primary percutaneous coronary inter-vention for ST-segment-elevation acute myocardial infarction: data fromthe French registry on acute ST-elevation myocardial infarction(FAST-MI). Circulation. 2008;118:268–276.
12. Silber S, Albertsson P, Aviles FF, Camici PG, Colombo A, Hamm C,Jorgensen E, Marco J, Nordrehaug JE, Ruzyllo W, Urban P, Stone GW,Wijns W. Guidelines for percutaneous coronary interventions. The TaskForce for Percutaneous Coronary Interventions of the European Societyof Cardiology. Eur Heart J. 2005;26:804–847.
13. Van de Werf F, Bax J, Betriu A, Blomstrom-Lundqvist C, Crea F, FalkV, Filippatos G, Fox K, Huber K, Kastrati A, Rosengren A, Steg PG,Tubaro M, Verheugt F, Weidinger F, Weis M, Vahanian A, Camm J, DeCaterina R, Dean V, Dickstein K, Filippatos G, Funck-Brentano C,Hellemans I, Kristensen SD, McGregor K, Sechtem U, Silber S, TenderaM, Widimsky P, Zamorano JL, Silber S, Aguirre FV, Al-Attar N, AlegriaE, Andreotti F, Benzer W, Breithardt O, Danchin N, Di Mario C, DudekD, Gulba D, Halvorsen S, Kaufmann P, Kornowski R, Lip GY, Rutten F.Management of acute myocardial infarction in patients presenting withpersistent ST-segment elevation: the Task Force on the Management ofST-Segment Elevation Acute Myocardial Infarction of the EuropeanSociety of Cardiology. Eur Heart J. 2008;29:2909–2945.
14. Modi NB, Fox NL, Clow FW, Tanswell P, Cannon CP, Van de Werf F,Braunwald E. Pharmacokinetics and pharmacodynamics of tenecteplase:results from a phase II study in patients with acute myocardial infarction.J Clin Pharmacol. 2000;40:508–515.
15. Antman EM, Hand M, Armstrong PW, Bates ER, Green LA,Halasyamani LK, Hochman JS, Krumholz HM, Lamas GA, Mullany CJ,Pearle DL, Sloan MA, Smith SC Jr, Anbe DT, Kushner FG, Ornato JP,Jacobs AK, Adams CD, Anderson JL, Buller CE, Creager MA, EttingerSM, Halperin JL, Hunt SA, Lytle BW, Nishimura R, Page RL, Riegel B,Tarkington LG, Yancy CW. 2007 Focused Update of the ACC/AHA2004 Guidelines for the Management of Patients With ST-ElevationMyocardial Infarction: a report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines:developed in collaboration With the Canadian Cardiovascular Societyendorsed by the American Academy of Family Physicians: 2007 WritingGroup to Review New Evidence and Update the ACC/AHA 2004Guidelines for the Management of Patients With ST-Elevation Myo-cardial Infarction, Writing on Behalf of the 2004 Writing Committee.Circulation. 2008;117:296–329.
16. Gibson CM, Murphy SA, Morrow DA, Aroesty JM, Gibbons RJ, GourlaySG, Barron HV, Giugliano RP, Antman EM, Braunwald E. Angiographicperfusion score: an angiographic variable that integrates both epicardialand tissue level perfusion before and after facilitated percutaneouscoronary intervention in acute myocardial infarction. Am Heart J. 2004;148:336–340.
17. Cutlip DE, Windecker S, Mehran R, Boam A, Cohen DJ, van Es GA, StegPG, Morel MA, Mauri L, Vranckx P, McFadden E, Lansky A, Hamon M,Krucoff MW, Serruys PW. Clinical end points in coronary stent trials: acase for standardized definitions. Circulation. 2007;115:2344–2351.
18. Stone GW, Grines CL, Cox DA, Garcia E, Tcheng JE, Griffin JJ, Gua-gliumi G, Stuckey T, Turco M, Carroll JD, Rutherford BD, LanskyAJ. Comparison of angioplasty with stenting, with or without abciximab,in acute myocardial infarction. N Engl J Med. 2002;346:957–966.
19. Stone GW, Ellis SG, Cox DA, Hermiller J, O’Shaughnessy C, Mann JT,Turco M, Caputo R, Bergin P, Greenberg J, Popma JJ, Russell ME. Apolymer-based, paclitaxel-eluting stent in patients with coronary arterydisease. N Engl J Med. 2004;350:221–231.
20. De Luca G, Suryapranata H, Stone GW, Antoniucci D, Tcheng JE,Neumann FJ, Van de Werf F, Antman EM, Topol EJ. Abciximab asadjunctive therapy to reperfusion in acute ST-segment elevation myo-cardial infarction: a meta-analysis of randomized trials. JAMA. 2005;293:1759–1765.
21. Van’t Hof AW, Ten Berg J, Heestermans T, Dill T, Funck RC, vanWerkum W, Dambrink JH, Suryapranata H, van Houwelingen G, Otter-vanger JP, Stella P, Giannitsis E, Hamm C. Prehospital initiation oftirofiban in patients with ST-elevation myocardial infarction undergoingprimary angioplasty (On-TIME 2): a multicentre, double-blind, ran-domised controlled trial. Lancet. 2008;372:537–546.
22. Keeley EC, Boura JA, Grines CL. Comparison of primary and facilitatedpercutaneous coronary interventions for ST-elevation myocardial
infarction: quantitative review of randomised trials. Lancet. 2006;367:579–588.
23. Ellis SG, Tendera M, de Belder MA, van Boven AJ, Widimsky P,Janssens L, Andersen HR, Betriu A, Savonitto S, Adamus J, PerugaJZ, Kosmider M, Katz O, Neunteufl T, Jorgova J, Dorobantu M,Grinfeld L, Armstrong P, Brodie BR, Herrmann HC, Montalescot G,Neumann FJ, Effron MB, Barnathan ES, Topol EJ. Facilitated PCI inpatients with ST-elevation myocardial infarction. N Engl J Med.2008;358:2205–2217.
24. Antman EM, Giugliano RP, Gibson CM, McCabe CH, Coussement P,Kleiman NS, Vahanian A, Adgey AA, Menown I, Rupprecht HJ, Van derWieken R, Ducas J, Scherer J, Anderson K, Van de Werf F, BraunwaldE. Abciximab facilitates the rate and extent of thrombolysis: results of thethrombolysis in myocardial infarction (TIMI) 14 trial. The TIMI 14Investigators. Circulation. 1999;99:2720–2732.
25. Trial of abciximab with and without low-dose reteplase for acute myo-cardial infarction. Strategies for Patency Enhancement in the EmergencyDepartment (SPEED) Group. Circulation. 2000;101:2788–2794.
26. Topol EJ. Reperfusion therapy for acute myocardial infarction withfibrinolytic therapy or combination reduced fibrinolytic therapy andplatelet glycoprotein IIb/IIIa inhibition: the GUSTO V randomised trial.Lancet. 2001;357:1905–1914.
27. Efficacy and safety of tenecteplase in combination with enoxaparin,abciximab, or unfractionated heparin: the ASSENT-3 randomised trial inacute myocardial infarction. Lancet. 2001;358:605–613.
28. Ross AM, Coyne KS, Reiner JS, Greenhouse SW, Fink C, Frey A,Moreyra E, Traboulsi M, Racine N, Riba AL, Thompson MA, RohrbeckS, Lundergan CF. A randomized trial comparing primary angioplastywith a strategy of short-acting thrombolysis and immediate plannedrescue angioplasty in acute myocardial infarction: the PACT trial. PACTinvestigators: Plasminogen-activator Angioplasty Compatibility Trial.J Am Coll Cardiol. 1999;34:1954–1962.
29. Primary versus tenecteplase-facilitated percutaneous coronary inter-vention in patients with ST-segment elevation acute myocardial infarction(ASSENT-4 PCI): randomised trial. Lancet. 2006;367:569–578.
30. Kastrati A, Mehilli J, Schlotterbeck K, Dotzer F, Dirschinger J, SchmittC, Nekolla SG, Seyfarth M, Martinoff S, Markwardt C, Clermont G,Gerbig HW, Leiss J, Schwaiger M, Schomig A. Early administration ofreteplase plus abciximab vs abciximab alone in patients with acute myo-cardial infarction referred for percutaneous coronary intervention: a ran-domized controlled trial. JAMA. 2004;291:947–954.
31. Cantor WJ, Fitchett D, Borgundvaag B, Ducas J, Heffernan M, CohenEA, Morrison LJ, Langer A, Dzavik V, Mehta SR, Lazzam C,Schwartz B, Casanova A, Goodman SG. Routine early angioplastyafter fibrinolysis for acute myocardial infarction. N Engl J Med.2009;360:2705–2718.
32. Kastrati A, Dibra A, Spaulding C, Laarman GJ, Menichelli M, ValgimigliM, Di Lorenzo E, Kaiser C, Tierala I, Mehilli J, Seyfarth M, Varenne O,Dirksen MT, Percoco G, Varricchio A, Pittl U, Syvanne M, Suttorp MJ,Violini R, Schomig A. Meta-analysis of randomized trials on drug-elutingstents vs. bare-metal stents in patients with acute myocardial infarction.Eur Heart J. 2007;28:2706–2713.
33. Laarman GJ, Suttorp MJ, Dirksen MT, van Heerebeek L, Kiemeneij F,Slagboom T, van der Wieken LR, Tijssen JG, Rensing BJ, Patterson M.Paclitaxel-eluting versus uncoated stents in primary percutaneouscoronary intervention. N Engl J Med. 2006;355:1105–1113.
34. Menichelli M, Parma A, Pucci E, Fiorilli R, De Felice F, Nazzaro M,Giulivi A, Alborino D, Azzellino A, Violini R. Randomized trial ofSirolimus-Eluting Stent Versus Bare-Metal Stent in Acute MyocardialInfarction (SESAMI). J Am Coll Cardiol. 2007;49:1924–1930.
35. Spaulding C, Henry P, Teiger E, Beatt K, Bramucci E, Carrie D, SlamaMS, Merkely B, Erglis A, Margheri M, Varenne O, Cebrian A, Stoll HP,Snead DB, Bode C. Sirolimus-eluting versus uncoated stents in acutemyocardial infarction. N Engl J Med. 2006;355:1093–1104.
36. Valgimigli M, Percoco G, Malagutti P, Campo G, Ferrari F, Barbieri D,Cicchitelli G, McFadden EP, Merlini F, Ansani L, Guardigli G, Bettini A,Parrinello G, Boersma E, Ferrari R. Tirofiban and sirolimus-eluting stentvs abciximab and bare-metal stent for acute myocardial infarction: arandomized trial. JAMA. 2005;293:2109–2117.
37. van der Hoeven BL, Liem SS, Jukema JW, Suraphakdee N, Putter H,Dijkstra J, Atsma DE, Bootsma M, Zeppenfeld K, Oemrawsingh PV, vander Wall EE, Schalij MJ. Sirolimus-eluting stents versus bare-metal stentsin patients with ST-segment elevation myocardial infarction: 9-monthangiographic and intravascular ultrasound results and 12-month clinical
306 Circ Cardiovasc Interv August 2010
by guest on August 18, 2010 circinterventions.ahajournals.orgDownloaded from

outcome results from the MISSION! Intervention Study. J Am CollCardiol. 2008;51:618–626.
38. Steg PG, Fox KA, Eagle KA, Furman M, Van de Werf F, Montalescot G,Goodman SG, Avezum A, Huang W, Gore JM. Mortality followingplacement of drug-eluting and bare-metal stents for ST-segment elevationacute myocardial infarction in the Global Registry of Acute CoronaryEvents. Eur Heart J. 2009;30:321–329.
39. Stone GW, Lansky AJ, Pocock SJ, Gersh BJ, Dangas G, Wong SC,Witzenbichler B, Guagliumi G, Peruga JZ, Brodie BR, Dudek D, MockelM, Ochala A, Kellock A, Parise H, Mehran R. Paclitaxel-eluting stentsversus bare-metal stents in acute myocardial infarction. N Engl J Med.2009;360:1946–1959.
40. Mauri L, Orav EJ, Kuntz RE. Late loss in lumen diameter and binaryrestenosis for drug-eluting stent comparison. Circulation. 2005;111:3435–3442.
41. Mauri L, Orav EJ, Candia SC, Cutlip DE, Kuntz RE. Robustness oflate lumen loss in discriminating drug-eluting stents across variableobservational and randomized trials. Circulation. 2005;112:2833–2839.
42. Gershlick AH, Stephens-Lloyd A, Hughes S, Abrams KR, Stevens SE,Uren NG, de Belder A, Davis J, Pitt M, Banning A, Baumbach A, ShiuMF, Schofield P, Dawkins KD, Henderson RA, Oldroyd KG, Wilcox R.Rescue angioplasty after failed thrombolytic therapy for acute myocardialinfarction. N Engl J Med. 2005;353:2758–2768.
CLINICAL PERSPECTIVEFibrinolysis is still administered in a high percentage of patients with acute ST-elevation myocardial infarction in whomprimary percutaneous coronary intervention (PCI) cannot be performed in a timely fashion. Routine adjunctive or earlypostfibrinolytic angiography is often done in these patients to improve outcome. This study was performed to explore theusefulness of administering a IIb/IIIa glycoprotein inhibitor (tirofiban) in patients with acute ST-elevation myocardialinfarction treated with postfibrinolytic angioplasty. In this study, tirofiban did not improve any perfusion parameter andwas associated with an increase in overall bleeding. Thus, after full-dose tenecteplase, enoxaparin and aspirin are a goodantithrombotic combination for a postfibrinolysis PCI reperfusion strategy. In our study, clopidogrel was given after PCIand not on admission, as currently recommended. We further explored the efficacy of the paclitaxel-eluting stent with thisregimen. The use of paclitaxel-eluting stents was not associated with an increase in stent thrombosis. Compared withbare-metal stents, paclitaxel-eluting stents significantly reduced late loss but appeared not to reduce in-segment binaryrestenosis as the rate of binary restenosis with bare-metal stents (11% and not 22%) was unexpectedly low. Implantationof bare-metal stents in postfibrinolysis-PCI patients appeared to be a cost-effective approach compared with paclitaxel-eluting stents.
Sanchez et al The GRACIA-3 Trial 307
by guest on August 18, 2010 circinterventions.ahajournals.orgDownloaded from