retinal manifestations of ophthalmic artery hypoperfusion
TRANSCRIPT

Clinical and Experimental Ophthalmology (2002) 30, 284–291
Photographic Essay ________________________________
Photographic Essay
Retinal manifestations of ophthalmic artery hypoperfusionTerrence J Ong MBBS, Mark Paine FRACP and Justin O’Day FRANZCODepartment of Neuro-Ophthalmology, The Royal Victorian Eye and Ear Hospital, Melbourne, Victoria, Australia
ABSTRACT
Ophthalmic artery hypoperfusion is a relatively uncommonclinical entity. This study illustrates the posterior segmentfindings of ophthalmic artery hypoperfusion in a series of ninepatients. Colour photographs and relevant fluorescein angi-ograms highlighting the findings are shown. The retinal mani-festations of ophthalmic artery hypoperfusion in this series ofpatients include midperipheral haemorrhages, dilated retinalveins, optic disk collaterals, optic disk neovascularization,cotton wool spots, grey intraretinal lesions, fundus pallor,optic disk swelling and choroidal infarcts. Recognition of theophthalmic changes in this condition may lead to detection ofcarotid artery disease, the surgical and medical treatment ofwhich has important bearing on patient management.
Key words: giant cell arteritis, ocular ischaemic syndrome,ophthalmic artery hypoperfusion, venous stasis retinopathy.
INTRODUCTION
Rubeosis iridis is the classical sign of ophthalmic arteryhypoperfusion (OAH). Less commonly discussed are theposterior segment features. These may occur in conjunctionwith the anterior segment changes or in isolation. Recogni-tion of the varying patterns of retinal changes will enablediagnosis and appropriate clinical management to be under-taken.
The ophthalmic artery, which is a branch of the internalcarotid artery (ICA), is the major blood supply of the eye.Complete occlusion of the ICA system, if it occurs gradu-ally, does not commonly cause blindness owing to thecollateral blood supply to the ophthalmic artery from thebranches of the external carotid artery (ECA).1–3
The site of vascular occlusion can be from the commoncarotid artery to the ophthalmic artery and its branches.The most common cause is carotid artery atheroma.2,4 Lesscommon causes are arteritis (e.g. giant cell arteritis), caro-ticocavernous fistula and carotid dissection.5
The perfusion may be insufficient for normal ocular func-tion. This results in a variety of features, both in the anteriorand posterior segments. This report analyzes the posterior
segment changes that are due to a combination of choroidaland retinal ischaemia.
RETINAL FEATURES OF OPHTHALMIC ARTERY HYPOPERFUSION
Midperipheral haemorrhages
Chronic hypoperfusion of the retina from a reduction inboth the choroidal and retinal circulations may cause ischae-mia of the retinal tissue. The capillary bed within this areaof ischaemia may become incompetent, leading to thedevelopment of microaneurysms and scattered haemor-rhages.6 These changes together with venous dilatationwere described by Kearns and Hollenhorst as venous stasisretinopathy.7
Case 1
An 81-year-old woman presented with multiple episodes ofcollapse in association with seeing transient ‘grey curtains’across her left visual field lasting less than a minute. Thevision was count fingers in her right eye and 6/9 the left.There was a disciform scar on the right and midperipheralhaemorrhages in the left fundus (Fig. 1). A fluoresceinangiogram (FA) showed a delayed choroidal filling time of12 s. A carotid angiogram showed an obstructed leftcommon carotid artery with a patent ICA filling by collater-als. The right ICA had a 95% stenosis. A left subclavian tocommon carotid bypass graft was performed. Three monthspostoperatively, she noticed a definite improvement in herleft central acuity, measured to be 6/6. She had no recur-rence of visual blurring. A postoperative FA was not per-formed, but carotid Doppler ultrasound showed good flowin the ICA.
Dilated retinal veins
When the ocular circulation is reduced leading to retinalischaemia of a significant area, then the veins passingthrough this area may dilate.
� Correspondence: Associate Professor Justin O’Day, 55 Victoria Parade, Fitzroy, Vic. 3065, Australia. Email: [email protected]

Ophthalmic artery hypoperfusion 285
Case 2
A 65-year-old man presented with a 4-day history of blurredvision and pain in the right eye due to neovascular glau-coma. The vision in the right eye was count fingers. Therewere slightly dilated retinal veins (Fig. 2a) and arteriolarpulsations on minimal extrinsic pressure on both eyes. A FArevealed feathery leaking from the retinal vessels and a slowtransit time in the right eye (Fig. 2b). Both ICA wereoccluded. He later developed a dense cataract in this eye,postulated to be a result of ocular ischaemia.
Optic disc collaterals
If there is chronic incomplete retinal ischaemia of slowonset, then collateral vessels may form at the optic disc.
Case 3
A 47-year-old man developed two episodes of transientvisual blurring (like looking at things under water) lastingabout 90 min each. These episodes were associated with lossof coordination of the lower limbs and dysarthria. His visualacuity was 6/6 bilaterally, and his intraocular pressures(IOP) and colour vision were normal. Fundoscopy revealedcilioretinal shunt vessels on both optic discs (Fig. 3a), con-firmed on FA (Fig. 3b). He was found to have a 90% stenosison the right ICA, which was surgically treated. The arterycompletely occluded 5 months later and he continued toexperience transient blurring of vision. The collateral vesselspersisted over a 5-year period of observation.
Optic disc neovascularization
Another response to prolonged retinal ischaemia is thedevelopment of optic disc neovascularization, particularly ifthere is another cofactor such as diabetes or radiationretinopathy.
Case 4
A 69-year-old diabetic man with bilateral advanced carotidartery disease had bilateral superficial temporal artery tomiddle cerebral artery anastomoses (STAMCA). He pre-sented a year later for routine ophthalmic review and wasfound to have visual acuities of 6/9 and 6/6 in his right andleft eyes, respectively. His left eye had rubeosis and opticdisk neovascularization (Fig. 4a). The FA showed prolongedcirculation time and disk hyperfluorescence (Fig. 4b). It wasunlikely that his disc neovascularization was due solely tohis diabetes, as there were no other signs of diabetic retino-pathy in that eye. He did, however, have evidence of OAHon his FA which could account for his disc neovasculariza-tion. Despite receiving panretinal photocoagulation (PRP),he had persistent neovascularization (Fig. 4c).
Cotton wool spots
Retinal ischaemia may lead to axoplasmic stasis and thedevelopment of cotton wool spots.
Figure 1. Case 1. Midperipheral haemorrhages (→).
Figure 2. Case 2. (a) Normal fundus except slight venous dilata-tion inferiorly. (b) Feathery leak from retinal vessels especiallyinferiorly (→).

286 Ong et al.
Case 5
A 69-year-old man with a history of vascular disease pre-sented with a 1-week history of inferior field loss in the lefteye. His vision was 6/6 in both eyes. In the left eye there wasa relative afferent pupillary defect and decreased colourvision. Fundoscopy revealed a pale swollen disk especiallysuperiorly, associated with cotton wool spots and moderatelyengorged veins (Fig. 5a). His erythrocyte sedimentation rate(ESR), C-reactive protein, vasculitic screen and temporalartery biopsy were normal. The FA showed delayed choroidalfilling (Fig. 5b). There was no carotid artery lesion; however,a stenosis of the proximal ophthalmic artery was found oncomputed tomography (CT) angiography. In the followingmonths, his colour vision improved and his field stabilized.The cotton wool spots disappeared (Fig. 5c) and choroidalfilling time returned to normal (Fig. 5d).
Grey intraretinal lesions
Combined retinal and choroidal hypoperfusion may lead toretinal ischaemia deep to the axons, involving the outerretinal layers and possibly the retinal pigment epithelium.
Case 6
Cherney et al. reported a case of a 49-year-old woman whodeveloped a right carotico cavernous fistula after minor headtrauma.8 Her visual acuities were 6/9 and 6/9 in the right andleft, respectively. Fundus examination was normal at thattime. Owing to her progressive chemosis, proptosis andophthalmoplegia, she had an attempted balloon occlusion
Figure 3. Case 3. (a) Cilioretinal shunt vessels at optic disc (→).(b) Delayed choroidal perfusion around the disc after completeretinal arteriolar filling and presence of collaterals at 3 and 7 o’clock(→).
Figure 4. Case 4. (a) Neovascularization of the optic disc (→).(b) Delayed and patchy choroidal filling (→) even after completefilling of arterioles. (c) Leakage from optic disk neovascularization(→). Photograph taken at 63 s.

Ophthalmic artery hypoperfusion 287
of the fistula. This failed to occlude the fistula but causedthrombosis of the right ICA proximal to the ophthalmicartery. Consequently, there was ‘arterial steal’ created byretrograde flow in the ophthalmic artery, resulting in ocularhypoperfusion. Within 24 h, the vision in the right eyedeteriorated to hand movements. Fundoscopy revealedcotton wool spots and grey intraretinal lesions in the poste-rior pole (Fig. 6a). The FA confirmed delayed choroidalperfusion (Fig. 6b). The grey intraretinal lesions, unlikecotton wool spots, were located at a level deep to the retinalvessels when viewed stereoscopically. It was postulated thatthey may represent an area of watershed ischaemia betweenthe choroidal and retinal circulations within the retina. Thisis different from cotton wool spots, which are thought torepresent areas of interrupted axoplasmic flow in the retinalnerve fibre layer.
Pallor of fundus
If there is profound slow loss of choroidal and retinal circu-lation then the vascular colour on fundoscopic examinationmay be markedly attenuated.
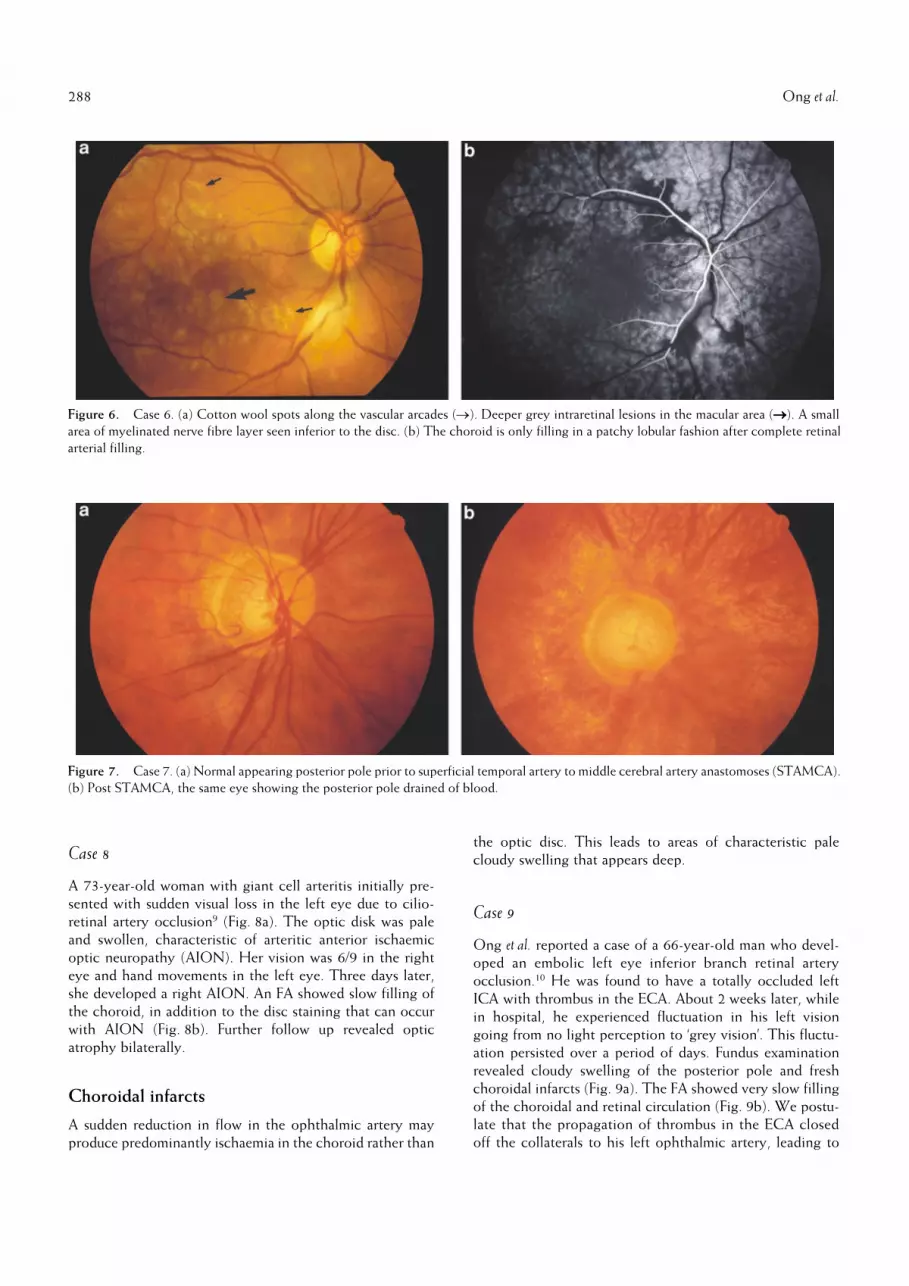
Case 7
A 55-year-old man presented with a painful right eye due torubeotic glaucoma. The vision was count fingers and 6/6 inthe right and left, respectively. His right ICA was found tobe occluded and he subsequently had a right STAMCA. Therubeosis and IOP were reduced. His posterior pole postoperatively appeared drained of blood (Fig. 7b) comparedto preoperatively (Fig. 7a). This was most likely due to anarterial steal phenomenon caused by the STAMCA, as theblood involved in ocular perfusion by the branches of theexternal carotid artery is shunted into the middle cerebralartery. His right visual acuity was no light perception at1 year follow up.
Optic disc swelling
A sudden reduction in the circulation to the optic disc (viathe short posterior ciliary arteries) may lead to interrup-tion of axoplasmic flow and subsequent optic disc swell-ing. The classic disease producing this change is giant cellarteritis.
Figure 5. Case 5. (a) Pale swollen disc with surrounding cotton wool spots. (b) Delayed choroidal filling nasal to the disc (→). Photographtaken at 65 s after fluorescein injection. (c) Disappearance of cotton wool spots. (d) Normalization of choroidal filling at 34.37 s.
288 Ong et al.
Case 8
A 73-year-old woman with giant cell arteritis initially pre-sented with sudden visual loss in the left eye due to cilio-retinal artery occlusion9 (Fig. 8a). The optic disk was paleand swollen, characteristic of arteritic anterior ischaemicoptic neuropathy (AION). Her vision was 6/9 in the righteye and hand movements in the left eye. Three days later,she developed a right AION. An FA showed slow filling ofthe choroid, in addition to the disc staining that can occurwith AION (Fig. 8b). Further follow up revealed opticatrophy bilaterally.
Choroidal infarcts
A sudden reduction in flow in the ophthalmic artery mayproduce predominantly ischaemia in the choroid rather than
the optic disc. This leads to areas of characteristic palecloudy swelling that appears deep.
Case 9
Ong et al. reported a case of a 66-year-old man who devel-oped an embolic left eye inferior branch retinal arteryocclusion.10 He was found to have a totally occluded leftICA with thrombus in the ECA. About 2 weeks later, whilein hospital, he experienced fluctuation in his left visiongoing from no light perception to ‘grey vision’. This fluctu-ation persisted over a period of days. Fundus examinationrevealed cloudy swelling of the posterior pole and freshchoroidal infarcts (Fig. 9a). The FA showed very slow fillingof the choroidal and retinal circulation (Fig. 9b). We postu-late that the propagation of thrombus in the ECA closedoff the collaterals to his left ophthalmic artery, leading to
Figure 6. Case 6. (a) Cotton wool spots along the vascular arcades (→). Deeper grey intraretinal lesions in the macular area (→→→→). A smallarea of myelinated nerve fibre layer seen inferior to the disc. (b) The choroid is only filling in a patchy lobular fashion after complete retinalarterial filling.
Figure 7. Case 7. (a) Normal appearing posterior pole prior to superficial temporal artery to middle cerebral artery anastomoses (STAMCA).(b) Post STAMCA, the same eye showing the posterior pole drained of blood.

Ophthalmic artery hypoperfusion 289
hypoperfusion of the eye. He had an ECA endarterectomyand thrombectomy. Postoperatively, his vision stabilized tocount fingers, and his FA showed normalization of retinal
and choroidal filling times (Fig. 9c,d). This patient demon-strates the importance of the external carotid circulation inthe maintenance of ocular perfusion.
Figure 8. Case 8. (a) Cilioretinal artery occlusion and pale swollen disk typical of giant cell arteritis. (b) Delayed and patchy filling of thechoroid (→) at 51 s after fluorescein injection.
Figure 9. Case 9. (a) Cloudy swelling of the posterior pole with choroidal infarcts (→). (b) Very delayed choroidal filling at 232 s afterfluorescein injection. (c) Residual choroidal scarring (→). (d) Normalization of choroidal filling post external carotid endarterectomy at 41 s.

290 Ong et al.
DISCUSSION
Ophthalmic artery hypoperfusion refers to inadequateblood flow in the ophthalmic artery. It can occur as a resultof stenosis of the arterial system, the site ranging from thecommon carotid artery to the branches of the ophthalmicartery itself. Ophthalmic artery hypoperfusion is a relativelyrare entity because the eye can still remain perfused by thebranches of the ECA in the advent of occlusion of the ICAsystem owing to the numerous anastomotic channelsbetween the two circulations.1–3 However, when the crucialperfusion by the ECA system is compromised, either bythrombus or arterial steal as illustrated in several of thecases, the eye becomes ischaemic.
The retinal changes seen in OAH are determined byseveral interrelated factors. One of the main factors is oph-thalmic artery blood flow, which is difficult to estimate invivo.11 The other, which is impossible to measure, is theindividual’s susceptibility to developing these changes.
Amaurosis fugax is the classical symptom of OAH. Thisis frequently associated with the signs of OAH previouslydescribed. It is important to recognize these signs and havea high index of suspicion of OAH, as the detection hasimportant consequences, not only for the eye. It can alert usto the presence of carotid artery disease, the surgical andmedical treatment of which may have important bearing onpatient management.12 Slow choroidal circulation may becaused by giant cell arteritis, which must be excluded as apotentially preventable cause of further visual loss in theunaffected eye.9
It is commonly accepted that blindness due to a vascularcause is usually irreversible.13,14 However, in rare cases, forexample case 9, some recovery of visual function is possibledespite prolonged vascular compromise of both choroidaland retinal circulations. We postulate that in these cases,especially where there has been a slower rather than abruptreduction of blood flow, the reduced perfusion is adequatefor some anatomical viability but insufficient for normalvisual function. Reduced choroidal perfusion may lead tothe retina ceasing to transmit visual information and there-fore lead to visual loss, even though the retina may still beanatomically viable. Choroidal reperfusion may then lead torecovery of visual function.
Neovascularization following OAH differs in its pathol-ogy from neovascularization secondary to retinal vasculardisease (for example diabetic retinopathy and retinal veinocclusions). In OAH, there is global reduction in bothchoroidal and retinal circulations, which may be reversiblefollowing carotid endarterectomy. In retinal vascular dis-ease, the ischaemia is focal and generally irreversible. How-ever, the final common pathway, the generation ofneovascular factors such as vascular endothelial growthfactor from ischaemic tissue, is the same in both situations.
The use of PRP to reduce the ischaemic drive has beenextensively studied and proven to be beneficial in focalretinal vascular disease (Diabetic Retinopathy Study,15
Central Vein Occlusion Study16 and Branch Vein Occlusion
Study17). Some clinicians suggest the use of PRP to preventrubeosis and neovascularization, prior to carotid endarterec-tomy in patients with OAH due to carotid stenosis. This iscontroversial, and has not been fully investigated in clinicaltrials. In our anecdotal experience, the course of neovasculardisease is highly variable after reperfusion surgery. We donot routinely apply PRP to patients with OAH and noneovascularization. If the patient has pre-existing neovascu-larization and is having ipsilateral carotid endarterectomy,the neovascularization may regress postoperatively.
Ophthalmic artery hypoperfusion therefore has quite avariable clinical picture, which if recognized may lead toimproved visual outcome. Fluorescein angiography is animportant investigation to confirm and monitor ophthalmicartery perfusion.
REFERENCES
1. Burnbaum MD, Selhorst JB, Harbison JW, Brush JJ. Amaurosisfugax from disease of the external carotid artery. Arch. Neurol.1977; 34: 532–5.
2. Walker PJ, May J, Harris JP, White GH, Hallinan J. Externalcarotid endarterectomy for amaurosis fugax in the presence ofinternal carotid artery occlusion. Aust. N.Z. J. Surg. 1994; 64:48–52.
3. Lasjuanais P, Vingaud J, Hasso AN. Maxillary artery supply tothe orbit. Normal and pathological aspects. Neuroradiology1975; 9: 87–97.
4. Kahn BS, Green WR, Knox DL, Muller NR. Ocular features ofcarotid occlusive disease. Retina 1986; 6: 239–51.
5. Duker JS, Belmont JB. Ocular ischemic syndrome secondary tocarotid artery dissection. Am. J. Ophthalmol. 1998; 106: 750–52.
6. Mizener JB, Podhajsky P, Hayreh SS. Ocular ischemic syn-drome. Ophthalmology 1997; 104: 859–64.
7. Kearns TP, Hollenhorst RW. Venous stasis retinopathy ofocclusive disease of the carotid artery. Staff Proc. Mayo Clin.1963; 38: 304–12.
8. Cherney M, O’Day J, Currie J. Intraretinal grey lesions as asign of reversible visual loss following prolonged ophthalmicartery hypoperfusion. J. Clin. Neuro-Ophthalmol. 1991; 11:228–32.
9. Mack HG, O’Day J, Currie J. Delayed choroidal perfusion ingiant cell arteritis. J. Clin. Neuro-Ophthalmol. 1991; 11: 221–7.
10. Ong TJ, Harper CA, O’Day J. Restoration of ocular circulationand some visual function following external carotid endarter-ectomy. Clin. Experiment. Ophthalmol. 2000; 28: 329–31.
11. Costa VP, Kuzniec S, Molnar LZ, Cerri GG, Puech-Leao P,Carvalho CA. Clinical findings and hemodynamic changesassociated with severe occlusive carotid artery disease. Oph-thalmology 1997; 104: 1994–2002.
12. North American Symptomatic Carotid Endarterectomy Trial(NASCET). Methods, patient characteristics and progress.Stroke 1991; 22: 711–20.
13. Duker JS, Brown GC. Recovery following acute obstruction ofretinal and choroidal circulations. Retina 1988; 8: 257–60.
14. Hayreh SS, Weingeist TA. Experimental occlusion of thecentral artery of the retina. Br. J. Ophthalmol. 1980; 64:896–912.

Ophthalmic artery hypoperfusion 291
15. The Diabetic Retinopathy Study Research Group. Indicationsfor photocoagulation treatment for diabetic retinopathy: Dia-betic Retinopathy Study Report no. 14. Int. Ophthalmol. Clin.1987; 27: 239–53.
16. Magargal LE, Brown GC, Augsburger JJ, Donoso LA. Efficacyof panretinal photocoagulation in preventing neovascularglaucoma following ischemic central retinal vein obstruction.Ophthalmology 1982; 89: 780–84.
17. Branch Vein Occlusion Study Group. Argon laser scatterphotocoagulation for prevention of neovascularization andvitreous hemorrhage in branch vein occlusion. A randomisedclinical trial. Arch. Ophthalmol. 1986; 104: 34–41.