results of supraceliac aortic clamping in the difficult elective resection of infrarenal abdominal...
TRANSCRIPT

Results of supraceliac aortic clamping in difficult elective resection of inffarenal abdominal aortic aneurysm Richard M. Green, MD, John J. Ricot ta , MD, Kenne th Ouriel , MD, and James A. DeWeese, MD, Rochester, N.Y.
the
We have used clamping of the aorta above the celiac axis (SC) in 30 of 431 elective resections of infrainguinal abdominal aortic aneurysms (AAA) during the past five years as an alternative to a difficult aortic cuff dissection. The results of SC clamping in these 30 patients are compared with the results of 379 routine aneurysm resections with in- frarenal (IR) clamping and 22 additional aneurysm resections where the clamp was placed immediately above the renal arteries. These difficult cuff dissections occurred in 12 pa- tients with inflanmmtory AAA, in 11 patients with juxtarenal AAA, and in seven patients with recurrent or noninfected false AAA of the proximal cuff. Patients with ruptured or suprarenal aneurysms and those undergoing combined operation for a visceral ischemic syndrome and an aneurysm were excluded from this study. Patients with SC clamping had similar operative mortality rates, comparable renal function, and frequency of cardiac events as patients with IR damping. Blood loss was slightly higher in the SC group (p = 0.07) and serum aspartate amino transferase (AST) levels were three times higher than in the IR group; however, this was of no clinical significance. In contrast, those 22 patients whose aortas were damped immediately above the renal arteries (AR) had higher perioperative mortafity rates (2% IR, 3% SC vs 32% AR) and a higher incidence of kidney failure requiring dialysis (1% IR, 3% SC vs 23% AR). The mean values of serum creatinine and blood urea nitrogen were also significantly higher in the AR group when compared with both the IR and the SC groups (IR: 25 and 1.5 mg/dl, respectively; SC: 27 and 1.8 mg/dl; AR: 41 and 3.5 mg/dl). The single most important risk factor accounting for the differences between clamping above the celiac artery and clamping above the renal arteries was the presence of atherosclerotic debris in the non- aneurysmal, juxtarenal aortic segment. Clamping the aorta with juxtarenal atherosclerosis caused either atheroembolization to kidneys, legs, and intestine or injury to the aorta, renal arteries, or both; it was the cause of morbidity in all five cases of kidney failure requiring dialysis and accounted for all seven of the deaths in the AR group. SC clamping does not add risk to the patient undergoing resection of an infrarenal AAA and is the preferred method of achieving proximal control of the infrarenal aorta when a hazardous cuff dissection is likely. (J VAs¢ SuRG 1989;9:125-34.)
The elective treatment o f aneurysms involving the infrarenal abdominal aorta is performed in centers all over the world with an operative mortality rate o f 2% to 6%. ~-s This low perioperative mortality rate is due in part to improved preoperative evaluation and treatment o f associated medical conditions, im- proved anesthetic management, and postoperative
From the Department of Surgery, University of Rochester Medical Center.
Presented at the Thirty-sixth Annual Meeting of the Society for Vascular Surgery, Chicago, Ill., June 13-14, 1988.
Reprint requests: Richard M. Green, MD, Dept. of Surgery, Uni- versity of Rochester Medical Center, 601 Elmwood Ave., Roch- ester, NY 14642.
I24
care. Despite these improvements, conditions found at operation may increase the technical difficulty o f repair and adversely affect these low mortality rates. Proximal dissection in these so-called difficult an- eurysms (i.e., inflammatory aneurysms, juxtarenal an- eurysms, aneurysms with juxtarenal atherosclerosis, false aneurysms at the proximal anastomosis, and an- eurysms o f the residual infrarenal cuff) may result in injury to the duodenum, renal arteries, or the cuff itself or may dislodge atheromatous debris with se- vere end-organ damage.
We have reviewed our experience during the past five years with operations on infrarenal abdominal aortic aneurysms. During this period we recognized
Volume 9 Number 1 January. 1989 Results of supraceliac aortic clamping 125
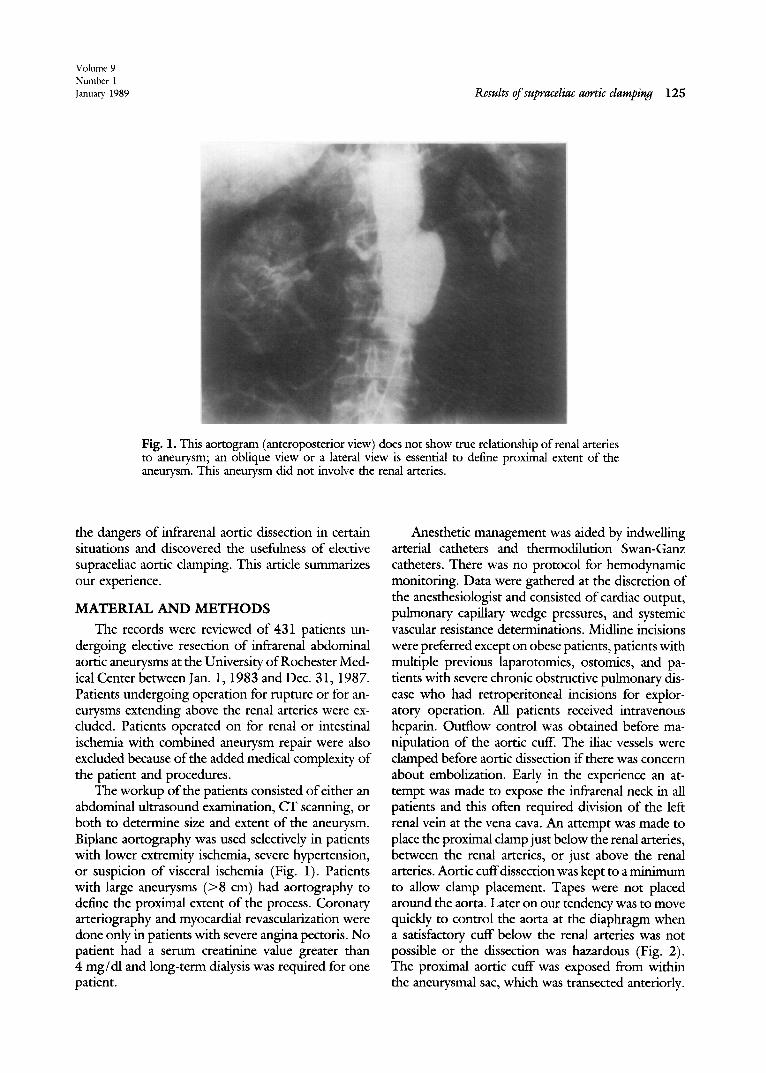
Fig. 1. This aortogram (anteroposterior view) does not show true relationship of renal arteries to aneurysm; an oblique view or a lateral view is essential to define proximal extent of the aneurysm. This aneurysm did not involve the renal arteries.
the dangers of infrarenal aortic dissection in certain situations and discovered the usefulness of elective supraceliac aortic clamping. This article summarizes our experience.
MATERIAL AND M E T H O D S
The records were reviewed of 431 patients un- dergoing elective resection of infrarenal abdominal aortic aneurysms at the University of Rochester Med- ical Center between Jan. 1, 1983 and Dec. 31, 1987. Patients undergoing operation for rupture or for an- eurysms extending above the renal arteries were ex- cluded. Patients operated on for renal or intestinal ischemia with combined aneurysm repair were also excluded because of the added medical complexity of the patient and procedures.
The workup of the patients consisted of either an abdominal ultrasound examination, CT scanning, or both to determine size and extent of the aneurysm. Biplane aortography was used selectively in patients with lower extremity ischemia, severe hypertension, or suspicion of visceral ischemia (Fig. 1). Patients with large aneurysms (>8 cm) had aortography to define the proximal extent of the process. Coronary arteriography and myocardial revascularization were done only in patients with severe angina pectoris. No patient had a serum creatinine value greater than 4 mg/dl and long-term dialysis was required for one patient.
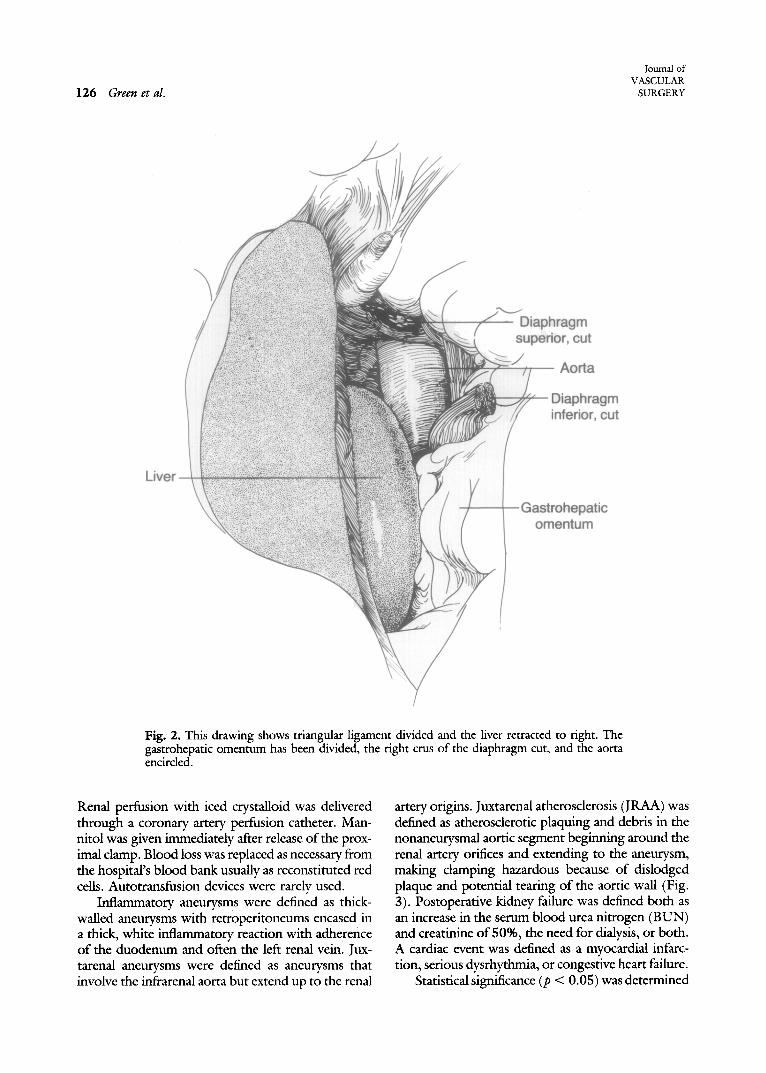
Anesthetic management was aided by indwelling arterial catheters and thermodilution Swan-Ganz catheters. There was no protocol for hemodynamic monitoring. Data were gathered at the discretion of the anesthesiologist and consisted of cardiac output, pulmonary capillary wedge pressures, and systemic vascular resistance determinations. Midline incisions were preferred except on obese patients, patients with multiple previous laparotomies, ostomies, and pa- tients with severe chronic obstructive pulmonary dis- ease who had retroperitoneal incisions for explor- atory operation. All patients received intravenous heparin. Outflow control was obtained before ma- nipulation of the aortic cuff. The iliac vessels were clamped before aortic dissection if there was concern about embolization. Early in the experience an at- tempt was made to expose the infrarenal neck in all patients and this often required division of the left renal vein at the vena cava. An attempt was made to place the proximal clamp just below the renal arteries, between the renal arteries, or just above the renal arteries. Aortic cuffdissection was kept to a minimum to allow clamp placement. Tapes were not placed around the aorta. Later on our tendency was to move quickly to control the aorta at the diaphragm when a satisfactory cuff below the renal arteries was not possible or the dissection was hazardous (Fig. 2). The proximal aortic cuff was exposed from within the aneurysmal sac, which was transected anteriorly.
126 Green et al.
Journal of VASCULAR
SURGERY
m ut
Fig. 2. This drawing shows triangular ligament divided and the liver retracted to right. The gastrohepatic omentum has been divided, the right crus of the diaphragm cut, and the aorta encircled.
Renal perfusion with iced crystalloid was delivered through a coronary artery perfusion catheter. Man- nitol was given immediately after release of the prox- imal clamp. Blood loss was replaced as necessary from the hospital's blood bank usually as reconstituted red cells. Autotransfusion devices were rarely used.
Inflammatory aneurysms were defined as thick- walled aneurysms with retroperitoneums encased in a thick, white inflammatory reaction with adherence of the duodenum and often the left renal vein. Jux- tarenal aneurysms were defined as aneurysms that involve the infrarenal aorta but extend up to the renal
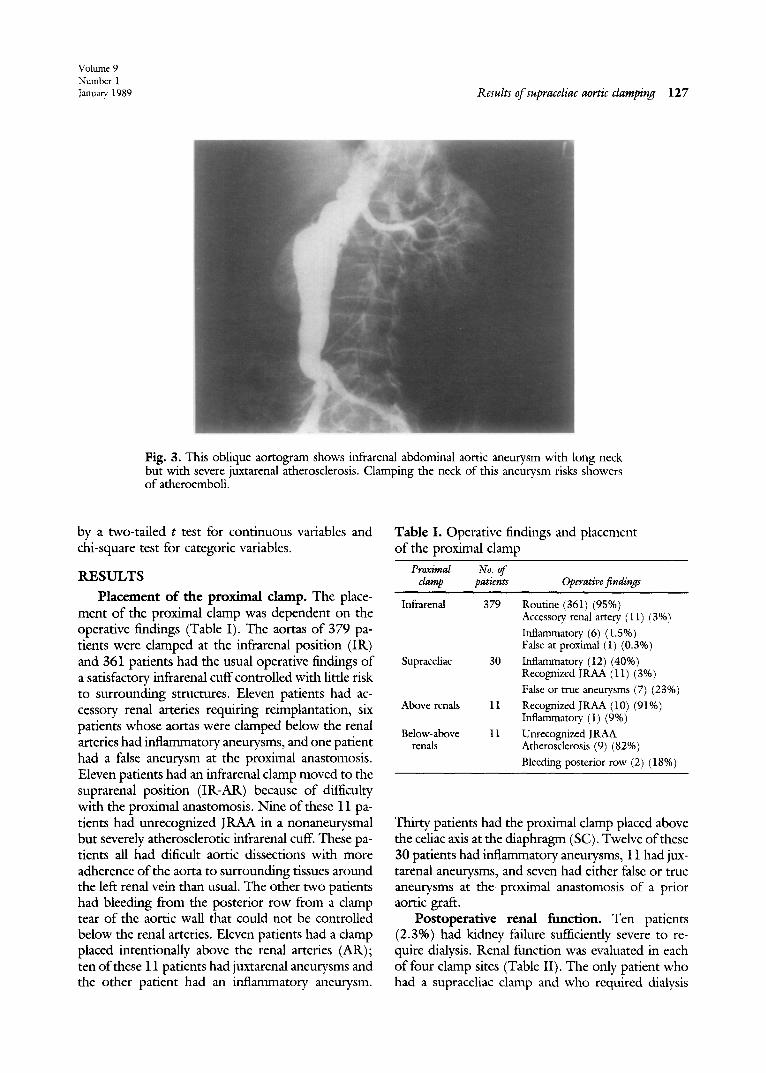
artery origins. Juxtarenal atherosclerosis (JRAA) was defined as atherosclerotic plaquing and debris in the nonaneurysmal aortic segment beginning around the renal artery orifices and extending to the aneurysm, making clamping hazardous because of dislodged plaque and potential tearing of the aortic wall (Fig. 3). Postoperative kidney failure was defined both as an increase in the serum blood urea nitrogen (BUN) and creatinine of 50%, the need for dialysis, or both. A cardiac event was defined as a myocardial infarc- tion, serious dysrhythmia, or congestive heart failure.
Statistical significance (p < 0.05) was determined
Volume 9 Ntunber 1 January 1989 Results of supraceliac aortic clamping 127
Fig. 3. This oblique aortogram shows infrarenal abdominal aortic aneurysm with long neck but with severe juxtarenal atherosclerosis. Clamping the neck of this aneurysm risks showers of atheroemboli.
by a two-tailed t test for continuous variables and chi-square test for categoric variables.
RESULTS
Placement of the proximal clamp. The place- ment of the proximal clamp was dependent on the operative findings (Table I). The aortas of 379 pa- tients were clamped at the infrarenal position (IR) and 361 patients had the usual operative findings of a satisfactory infrarenal cuff controlled with little risk to surrounding structures. Eleven patients had ac- cessory renal arteries requiring reimplantation, six patients whose aortas were clamped below the renal arteries had inflammatory aneurysms, and one patient had a false aneurysm at the proximal anastomosis. Eleven patients had an infrarenal clamp moved to the suprarenal position (IR-AR) because of difficulty with the proximal anastomosis. Nine of these 11 pa- tients had unrecognized JRAA in a nonaneurysmal but severely atherosclerotic infrarenal cuff. These pa- tients all had dificult aortic dissections with more adherence of the aorta to surrounding tissues around the left renal vein than usual. The other two patients had bleeding from the posterior row from a clamp tear of the aortic wall that could not be controlled below the renal arteries. Eleven patients had a clamp placed intentionally above the renal arteries (AR); ten of these 11 patients had juxtarenal aneurysms and the other patient had an inflammatory aneurysm.
Table I. Operative findings and placement of the proximal clamp
Proximal No. of clamp patients Operative findings
Infrarenal 379 Routine (361) (95%) Accessory, renal artery. (11) (3%) Inflammatory (6) (1.5%) False at proximal (1) (0.3%)
30 Inflammatory (12) (40%) Recognized JRAA (11) (3%) False or true aneurysms (7) (23%)
11 Recognized JRAA (10) (91%) Inflammatory (1) (9%)
11 Unrecognized JRAA Atherosclerosis (9) (82%) Bleeding posterior row (2) (18%)
Supraceliac
Above renals
Below-above renals
Thirty patients had the proximal clamp placed above the celiac axis at the diaphragm (SC). Twelve of these 30 patients had inflammatory aneurysms, 11 had jux- tarenal aneurysms, and seven had either false or true aneurysms at the proximal anastomosis of a prior aortic graft.
Postoperative renal function. Ten patients (2.3%) had kidney failure sufficiently severe to re- quire dialysis. Renal function was evaluated in each of four clamp sites (Table II). The only patient who had a supraceliac clamp and who required dialysis
128 Green et al.
Journal of VASCULAR
SURGERY
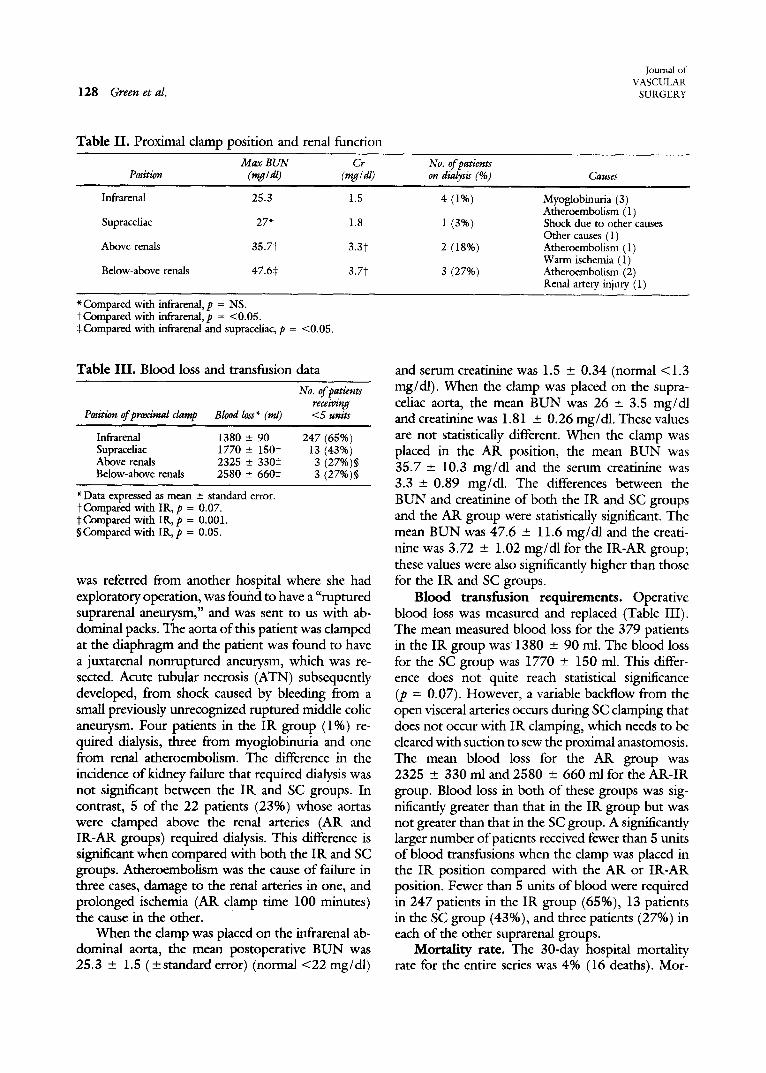
Table II. Proximal clamp position and renal function
Max BUN Cr No. of patients Position (rag / dl) (rag / dl) on dialysis (%) Causes
Infrarenal 25.3 1.5 4 (1%) Myoglobinuria (3) Atheroembolism (1)
Supraceliac 27* 1.8 1 (3%) Shock due to other causes Other causes (1)
Above renals 35.7t 3.3t 2 (18%) Atheroembolism (1) Warm ischemia (1)
Below-above renals 47.6~: 3.7t 3 (27%) Atheroembolism (2) Renal artery injury (1)
* Compared with infrarenal, p = NS. tCompared with infrarenal, p = <0.05. 0;Compared with infrarenal and supraceliac, p = <0.05.
Table III. Blood loss and transfusion data
Posiaon of prarimal clamp Blood loss* (ml)
No. of pazienu receiving <5 units
Infrarenal 1380 _+ 90 247 (65%) Supraceliac 1770 _+ 150t 13 (43%) Above renals 2325 _+ 330:~ 3 (27%)§ Below-above renals 2580 + 660~ 3 (27%)§
*Data expressed as mean + standard error. tCompared with IR, p = 0.07. :~Compared with IR, p = 0.001. §Compared with IR, p = 0.05.
was referred from another hospital where she had exploratory operation, was found to have a "ruptured suprarenal aneurysm," and was sent to us with ab- dominal packs. The aorta of this patient was clamped at the diaphragm and the patient was found to have a juxtarenal nonruptured aneurysm, which was re- sected. Acute tubular necrosis (ATN) subsequently developed, from shock caused by bleeding from a small previously unrecognized ruptured middle colic aneurysm. Four patients in the IR group (1%) re- quired dialysis, three from myoglobinuria and one from renal atheroembolism. The difference in the incidence of kidney failure that required dialysis was not significant between the IR and SC groups. In contrast, 5 of the 22 patients (23%) whose aortas were clamped above the renal arteries (AR and IR-AR groups) required dialysis. This difference is significant when compared with both the IR and SC groups. Atheroembolism was the cause of failure in three cases, damage to the renal arteries in one, and prolonged ischemia (AR clam p time 100 minutes) the cause in the other.
When the clamp was placed on the infrarenal ab- dominal aorta, the mean postoperative BUN was 25.3 _-4- 1.5 (_+standard error) (normal <22 mg/dl)
and serum creatinine was 1.5 _+ 0.34 (normal <1.3 mg/dl). When the clamp was placed on the supra- celiac aorta, the mean BUN was 26 +_ 3.5 mg/dl and creatinine was 1.81 + 0.26 mg/dl. These values are not statistically different. When the clamp was placed in the AR position, the mean BUN was 35.7 + 10.3 mg/dl and the serum creatinine was 3.3 _+ 0.89 mg/dl. The differences between the BUN and creatinine of both the IR and SC groups and the AR group were statistically significant. The mean BUN was 47.6 _+ 11.6 mg/dl and the creati- nine was 3.72 -+ 1.02 mg/dl for the IR-AR group; these values were also significantly higher than those for the IR and SC groups.
Blood transfusion requirements. Operative blood loss was measured and replaced (Table III). The mean measured blood loss for the 379 patients in the IR group was 1380 _+ 90 ml. The blood loss for the SC group was 1770 +- 150 ml. This differ- ence does not quite reach statistical significance (p = 0.07). However, a variable backflow from the open visceral arteries occurs during SC clamping that does not occur with IR clamping, which needs to be cleared with suction to sew the proximal anastomosis. The mean blood loss for the AR group was 2325 _+ 330 ml and 2580 -+ 660 ml for the AR-IR group. Blood loss in both of these groups was sig- nificantly greater than that in the IR group but was not greater than that in the SC group. A significantly larger number of patients received fewer than 5 units of blood transfusions when the clamp was placed in the IR position compared with the AR or IR-AR position. Fewer than 5 units of blood were required in 247 patients in the IR group (65%), 13 patients in the SC group (43%), and three patients (27%) in each of the other suprarenal groups.
Mortality rate. The 30-day hospital mortality rate for the entire series was 4% (16 deaths). Mor-
Volume 9 Number 1 Janua~ 1989 Results of supraceliac aortic clamping 129
Table IV. Proximal clamp site and mortality rates
No. of Site deaths Causes
Infrarenal 8 (2%) MI (2), bowel ischemia (2), leg ischemia (2), aspiration (1), ruptured pulmonary artery (1)
Supraceliac 1 (3%) lhalmonary embolus (1) Above renals 2 (18%) Atheroemboli (2) Below-above 5 (45%)* Atheroemboli (4), damaged renal
renals artery (1)
*p = 0.01 when compared with IR and SC.
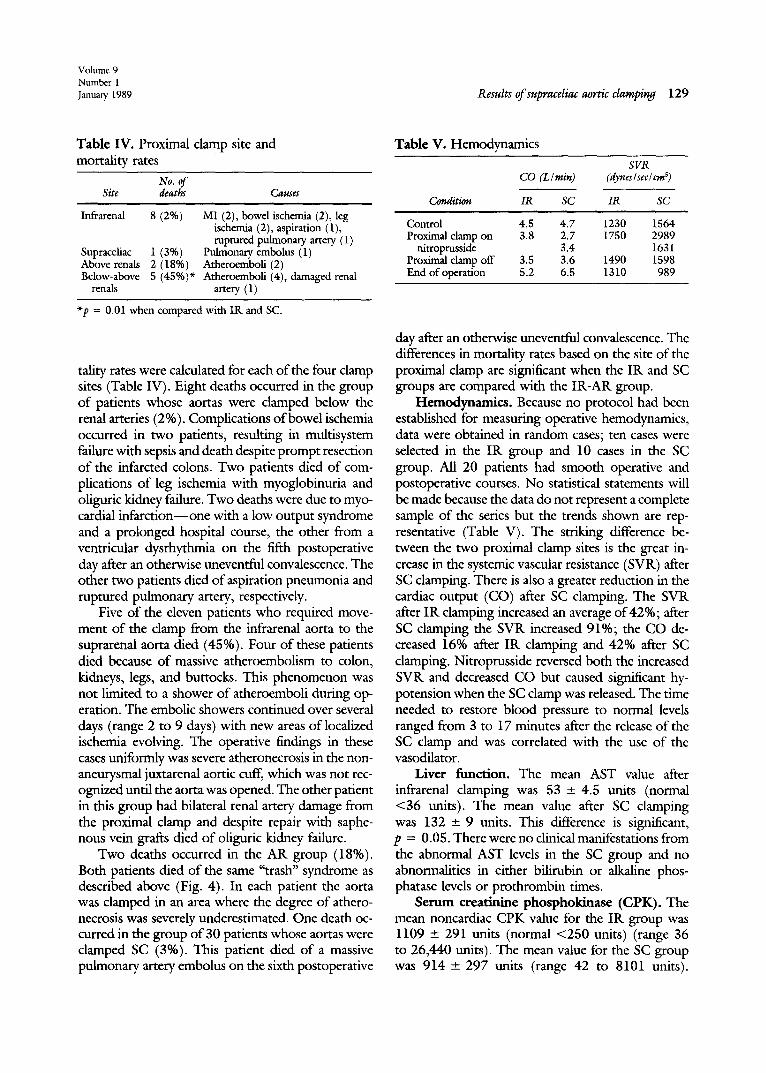
tality rates were calculated for each of the four clamp sites (Table IV). Eight deaths occurred in the group of patients whose aortas were clamped below the renal arteries ( 2 %). Complications of bowel ischemia occurred in two patients, resulting in multisystem failure with sepsis and death despite prompt resection of the infarcted colons. Two patients died of com- plications of leg ischemia with myoglobinuria and oliguric kidney failure. Two deaths were due to myo- cardial infarction--one with a low output syndrome and a prolonged hospital course, the other from a ventricular dysrhythmia on the fifth postoperative day after an otherwise uneventful convalescence. The other two patients died of aspiration pneumonia and ruptured pulmonary artery, respectively.
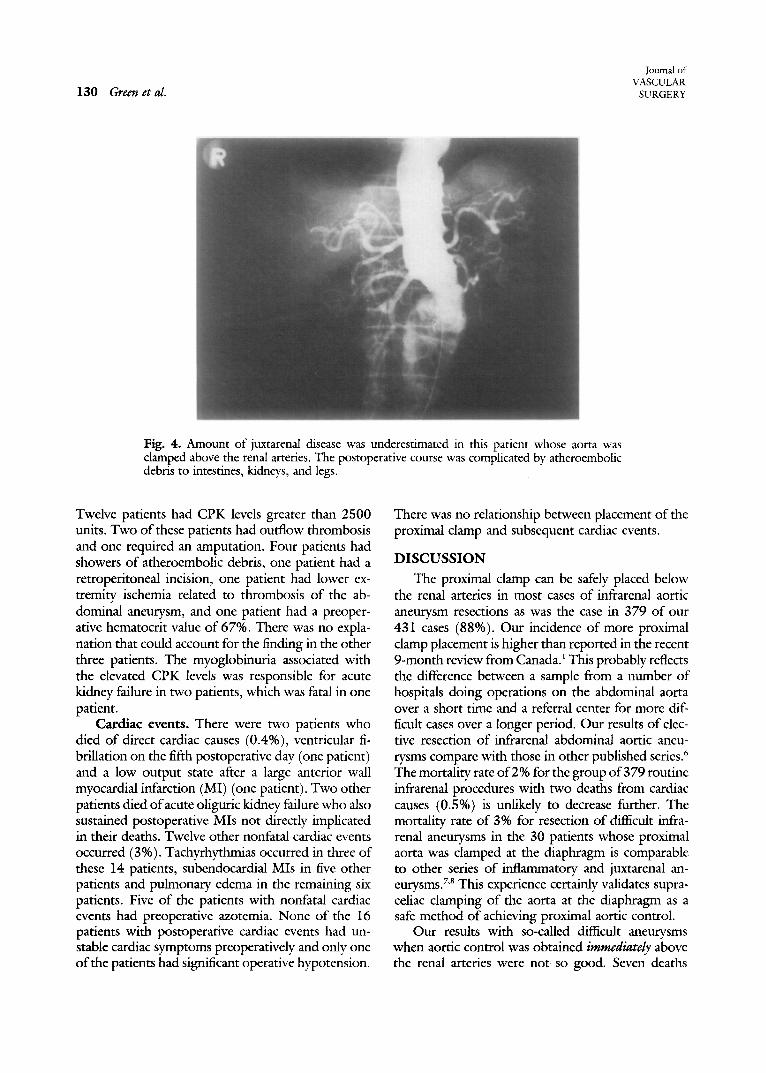
Five of the eleven patients who required move- ment of the clamp from the infrarenal aorta to the suprarenal aorta died (45%). Four of these patients died because of massive atheroembolism to colon, kidneys, legs, and buttocks. This phenomenon was not limited to a shower of atheroemboli during op- eration. The embolic showers continued over several days (range 2 to 9 days) with new areas of localized ischemia evolving. The operative findings in these cases uniformly was severe atheronecrosis in the non- aneurysmal juxtarenal aortic cuff, which was not rec- ognized until the aorta was opened. The other patient in this group had bilateral renal artery damage from the proximal clamp and despite repair with saphe- nous vein grafts died of oliguric kidney failure.
Two deaths occurred in the AR group (18%). Both patients died of the same "trash" syndrome as described above (Fig. 4). In each patient the aorta was damped in an area where the degree of athero- necrosis was severely underestimated. One death oc- curred in the group of 30 patients whose aortas were clamped SC (3%). This patient died of a massive pulmonary artery embolus on the sixth postoperative
Table V. Hemodynamics
SVR CO (Llmin) (dyneslsec/on s)
Condition IR SC IR SC
Control 4.5 4.7 1230 1564 Proximal clamp on 3.8 2.7 1750 2989
nitroprusside 3.4 1631 Proximal clamp off 3.5 3.6 1490 1598 End of operation 5.2 6.5 1310 989
day after an otherwise uneventful convalescence. The differences in mortality rates based on the site of the proximal clamp are significant when the IR and SC groups are compared with the IR-AR group.
Hemodynamics. Because no protocol had been established for measuring operative hemodynamics, data were obtained in random cases; ten cases were selected in the IR group and 10 cases in the SC group. All 20 patients had smooth operative and postoperative courses. No statistical statements will be made because the data do not represent a complete sample of the series but the trends shown are rep- resentative (Table V). The striking difference be- tween the two proximal clamp sites is the great in- crease in the systemic vascular resistance (SVR) after SC clamping. There is also a greater reduction in the cardiac output (CO) after SC clamping. The SVR after IR clamping increased an average of 42%; after SC clamping the SVR increased 91%; the CO de- creased 16% after IR clamping and 42% after SC damping. Nitroprusside reversed both the increased SVR and decreased CO but caused significant hy- potension when the SC clamp was released. The time needed to restore blood pressure to normal levels ranged from 3 to 17 minutes after the release of the SC clamp and was correlated with the use of the vasodilator.
Liver function. The mean AST value after infrarenal clamping was 53 _+ 4.5 units (normal <36 units). The mean value after SC clamping was 132 _+ 9 units. This difference is significant, p = 0.05. There were no clinical manifestations from the abnormal AST levels in the SC group and no abnormalities in either bilirubin or alkaline phos- phatase levels or prothrombin times.
Serum ereatinine phosphokinase (CPK). The mean noncardiac CPK value for the IR group was 1109 -+ 291 units (normal <250 units) (range 36 to 26,440 units). The mean value for the SC group was 9 1 4 _ 297 units (range 42 to 8101 units).
130 Green et al.
Journal of VASCULAR
SURGERY
Fig. 4. Amount of juxtarenal disease was underestimated in this patient whose aorta was clamped above the renal arteries. The postoperative course was complicated by atheroembolic debris to intestines, kidneys, and legs.
Twelve patients had CPK levels greater than 2500 units. Two of these patients had outflow thrombosis and one required an amputation. Four patients had showers of atheroembolic debris, one patient had a retroperitoneal incision, one patient had lower ex- tremity ischemia related to thrombosis of the ab- dominal aneurysm, and one patient had a preoper- ative hematocrit value of 67%. There was no expla- nation that could account for the finding in the other three patients. The myoglobinuria associated with the elevated CPK levels was responsible for acute kidney failure in two patients, which was fatal in one patient.
Cardiac events. There were two patients who died of direct cardiac causes (0.4%), ventricular fi- brillation on the fifth postoperative day (one patient) and a low output state after a large anterior wall myocardial infarction (MI) (one patient). Two other patients died of acute oliguric kidney failure who also sustained postoperative MIs not directly implicated in their deaths. Twelve other nonfatal cardiac events occurred (3%). Tachyrhythmias occurred in three of these 14 patients, subendocardial MIs in five other patients and pulmonary edema in the remaining six patients. Five of the patients with nonfatal cardiac events had preoperative azotemia. None of the 16 patients with postoperative cardiac events had un- stable cardiac symptoms preoperatively and only one of the patients had significant operative hypotension.
There was no relationship between placement of the proximal clamp and subsequent cardiac events.
DISCUSSION
The proximal clamp can be safely placed below the renal arteries in most cases of infrarenal aortic aneurysm resections as was the case in 379 of our 431 cases (88%). Our incidence of more proximal clamp placement is higher than reported in the recent 9-month review from Canada.1 This probably reflects the difference between a sample from a number of hospitals doing operations on the abdominal aorta over a short time and a referral center for more dif- ficult cases over a longer period. Our results of elec- tive resection of infrarenal abdominal aortic aneu- rysms compare with those in other published series. 6 The mortality rate of 2% for the group of 379 routine infrarenal procedures with two deaths from cardiac causes (0.5%) is unlikely to decrease further. The mortality rate of 3% for resection of difficult infra- renal aneurysms in the 30 patients whose proximal aorta was clamped at the diaphragm is comparable to other series of inflammatory and juxtarenal an- eurysms. 7'8 This experience certainly validates supra- celiac clamping of the aorta at the diaphragm as a safe method of achieving proximal aortic control.
Our results with so-caUed difficult aneurysms when aortic control was obtained immediately above the renal arteries were not so good. Seven deaths
Volume 9 Number 1 January 1989 Results of supraceliac aortic clamping 131
occurred in the suprarenal clamp groups (AR and IR-AR), all caused by either dislodging of athero- sclerotic debris or damage to the aorta and renal arteries. When AR clamping was performed, our mortality rate was 18%. When an infrarenal clamp had to be moved to the suprarenal aorta because a satisfactory infrarenal cuff could not be obtained be- cause of aortic damage or JRAA, the mortality rate in our series was 45%. The latter two mortality rates do not compare favorably with the reported results of supraceliac clamping or other reports of aortic control above the renal arteries 7 and are not ac- ceptable.
The outstanding results with with 77 pararenal aneurysms (mortality rate of 1%) reported by Qvar- fordt et al.9 with clamping above the renal arteries (58%), above the superior mesenteric artery (22%), and at the diaphragm (20%) and showing no dif- ference among the three sites make us reflect on our own poor results with clamping immediately above the renal arteries. Fifty-four of their patients had jux- tarenal aneurysms comparable to the ones described in our series but a significant percentage of these patients underwent combined renal artery repair not because of aneurysmal involvement but because of atherosclerotic renal artery disease. One can only as- sume that the philosophy of Qvarfordt et al. to look for and aggressively treat the JRAA and attendant renal artery lesions most often by transaortic end- arterectomy is critical in avoiding the atheroembolic debris to the kidneys, intestine, and legs that was the single most important cause of morbidity and mor- tality in our series and others. If one chooses to clamp immediately above the renal arteries, one must be prepared to repair them, as was done in 70% of the patients of Qvarfordt et al. 9 Failure to treat the JRAA as well as the aneurysm itself will lead to poor results. Placement of the proximal clamp above the celiac artery avoids the risk of damaging the aorta with JRAA just as it avoids the duodenum in the inflam- matory aneurysm and the redo aorta. This is the ap- proach we have adopted and is the standard approach described in the series reported by Crawford et al.10 of 101 patients with juxtarenal aneurysms.
Supraceliac aortic clamping did not adversely ef- fect renal function after operation. There was no dif- ference in either the level of BUN, creatinine, or the incidence of kidney failure requiring dialysis between the IR and the SC groups. However, a difference was noted in comparing renal function and the need for dialysis in the IR and the SC group with both suprarenal groups (AR and IR-AR). The Canadian
series reported that the clamping "above the renals" did increase the likelihood of kidney failure. Five of their six cases of azotemia and both patients who required dialysis were clamped above the renal ar- teries but not at the diaphragm. Like us, they believe that the clamp placed above the renal arteries may damage an atherosclerotic aorta with resultant em- bolization into the kidneys. This view is also sup- ported by Cohen et al.ll from the Peter Bent Brigham Hospital who reported that the prime mechanism responsible for postoperative kidney failure consists of embolic "showers" to the kidneys from dislodge- ment of atherosclerotic material just proximal to the proximal clamp.
Our hemodynamic data are not complete but ap- pear to reflect the experience of others during in- frarenal aortic clamping. 12,x3 Usually a 15% to 21% decrease in CO and an increase in SVR of 36% to 41% are noted after infrarenal clamping. These changes can be managed by preload reduction with nitroglycerin or afterload reduction with nitroprus- side. The changes after supraceliac clamping are more pronounced. A greater decrease in CO and a greater increase in the SVR are noted but they too can be managed pharmacologically. The only caution is that release of the supraceliac clamp particularly after va- sodilators have been given must be done with great caution to avoid serious hypotension.
The hepatocellular abnormalities as manifested in the higher AST after supraceliac clamping were not associated with any clinical problems and probably reflect hepatic ischemia during the cross-clamp pe- riod. The value of noncardiac CPK was elevated in all clamp groups. The very high levels (>2500 units) were usually associated with clinically significant lower extremity ischemia. The remaining patients with abnormal values of noncardiac CPK did not have clinically apparent lower extremity ischemia. The elevated skeletal muscle degradation product must reflect a degree of subclinical ischemia that we were not aware of and deserves future evaluation. It has been shown in dogs and rats that partial skeletal muscle ischemia can cause progressive deterioration in muscle cell membrane electrical potentials.14 There is evidence that these changes persist in the reper- fusion period and that the damage is due to oxygen- derived free radicals. It is not known whether the free radical scavengers such as superoxide dismutase and mannitol will reduce this muscle injury. Al- though mannitol was given to our patients to protect renal function after supraceliac and suprarenal clamp- ing, we could not demonstrate a difference in CPK
132 Green et al.
Journal of VASCULAR
SURGERY
between those patients damped above and below the renal arteries.
The spectrum of mortality rates from operations on infrarenal aortic aneurysms has changed dramat- icaUy during the past 20 years. More complicated anatomic problems are taken on now that medical risk factors can be better handled in the operative and perioperative periods. We now believe that in the coming decade the biggest risk factor will be handling of the juxtarenal aortic segment and avoid- ing compromise when deciding where to place to aortic clamp. Therefore it is essential that the surgeon know as much about this segment as possible before operation. Although ultrasonography and CT scan- ning are helpful and often diagnostic of inflamma- tory, recurrent, and false aneurysms, they fall short in evaluating the juxtarenal segment for atheroscle- rosis and renal artery involvement in the aneurysmal process. A lateral aortogram becomes essential for defining this segment. An anteroposterior view often suggests renal artery involvement because the supe- rior aspect of the aneurysm overlays the renal artery orifice. If the aortic segment from which the superior mesenteric artery and celiac axis arise is normal, the aneurysm is juxtarenal and can be handled with clamping above the celiac artery as described. The issue of whether preoperative angiography is essen- tial for all cases of abdominal aortic aneurysms has been debated in the past. In the Canadian series preoperative angiograms were available in 44% of patients but did not seem to affect the outcome of operation. 1 Bunt and Cropper is showed that pre- operative aortography gave "decisive" information in 18% of their patients and "helpful" information in another 14%. Our failure to perform aortography in all patients resulted in our missing some patients with JRAA that became an operative and perioperative problem. However, aortograms were obtained for some patients with JRAA and we underestimated it. We do not believe that aortograms are necessary for every patient undergoing evaluation for aneurysm resection. However, we do believe that biplane aor- tography is essential if one is suspicious of the in- frarenal aortic cuff or renal artery orifices.
Dissection around the aorta in the presence of JRAA is dangerous and should be avoided just as one would avoid the infrarenal cuff when operating on an inflammatory aneurysm with an adherent du- odenum. There are clues at operation such as adher- ence of the aorta to surrounding tissues in the area of the left renal vein which should lead one away from the juxtarenal segment before damage has oc- curred. If it is necessary to treat concomitant renal
artery occlusive disease, one must be sure that the clamp is placed sufficiently high and that all the ath- erosclerotic debris is removed from the aorta. When renal artery repair is not necessary, it is easier and safer to approach the aorta at the diaphragm and to work inside the cuff to remove debris and sew the proximal anastomosis. Supraceliac aortic clamping does not increase the risk to the patient and using this technique may significantly reduce the risk in the patient with the so-caUed "difficult" infrarenal ab- dominal aortic aneurysm.
REFERENCES
1. Johnston KW, Scobie TK. Multicenter prospective study of nonruptured abdominal aortic aneurysms. Population and operative management. J VASC SURG 1988;7:69-81.
2. Crawford ES, Saleh SA, Babb JW III, Glaeser DH, Vaccaro PS, Silvers A. Infrarenal abdominal aortic aneurysm. Factors influencing survival after operation performed.over a 25-year period. Ann Surg 1981;193:699-709.
3. Hertzer NR, AveLIone JC, FarreU CJ, et al. The risk of vascular surgery in a metropolitan community. With observations on surgeon experience and hospital size. I VASC SURG 1984; 1:13-21.
4. Darling RC, Brewster DC. Elective treatment of abdominal aortic aneurysm. World J Surg 1980;4:661-7.
5. Reigel MM, Hollier LH, Kazmier FJ, et al. Late survival in abdominal aortic aneurysm patients: the role of selective myo- cardial revascularization on the basis of clinical symptoms. J VASC SURG 1987;2:222-7.
6. Hertzer NR. Basic data concerning associated coronary dis- ease in peripheral vascular patients. Ann Vase Surg 1988; 1:616-20.
7. Stoney RJ, Skioldebrand CG, Qvarfordt PG, Reilly LM, Eh- renfeld WK. Juxtarenal aortic atherosclerosis. Ann Surg 1984;200:345-54.
8. Crawford JL, Stowe CL, Sail HJ, Hallman CH, Crawford ES. Inflammatory aneurysm of the abdominal aorta. J VAsc SURG 1985;2:113-24.
9. Qvarfordt PG, Stoney RJ, Reilly LM, Skioldebrand CG, Goldstone J, Ehrenfeld WK. Management of pararenal an- eurysms of the abdominal aorta. J VAsc SURG 1986;3:84- 93.
10. Crawford ES, Beckett WC, Greer MS. Juxtarenal infrarenal abdominal aortic aneurysm. Ann Surg 1986;203:661-70.
11. Cohen JR, Mannick JA, Couch NP, Whittemore AD. Ab- dominal aortic aneurysm repair in patients with preoperative renal failure. J VASC SURG 1986;3:867-70.
12. Hudson JC, Wurm WH, O'Donnell TF, et al. Hemodynamics and prostacyclin release in the early phases of aortic sur- gery: comparison of transabdominal and retroperitoneal ap- proaches. J VAsc SURG 1988;7:190-8.
13. Huval WV, Lelcuk S, Allen PD, Mannick JA, Shepro D, Hechtman HB. Determinants of cardiovascular stability dur- ing abdominal aortic aneurysmectomy. Ann Surg 1984;199: 216-22.
14. Perry MO, Fantini G. Ischemia: profile of an enemy. I VASC SURG 1987;3:231-4.
15. Bunt TJ, Cropper L. Routine angiography for abdominal aortic aneurysm: the case for informed operative selection. J Cardiovasc Surg 1986;27:725-7.

Volume 9 Number 1 Januaq~ 1989 Results of supraceliac aortic clamping 133
DISCUSSION
Dr. William K. Ehrenfeld (San Francisco, Calif.). Dr. Green and his coauthors have identified important features regarding appropriate placement of the proximal occluding aortic clamp and, in particular, the usefulness ofsupraceliac aortic clamping. They have delineated most of the selected indications for this maneuver in the treatment of difficult or potentially difficult infrarenal abdominal aortic aneu- rysms.
I will discuss our mutual experience with supraceliac aortic clamping emphasizing appropriate indications and technical maneuvers for safe use of this valuable technique. Several issues should be considered. These include the role of preoperative aortography, anesthetic management, in- traoperative pathologic findings, and surgical technique. With time and experience the ultimate findings and con- clusions of both groups have been largely although not completely similar.
Increasingly, many vascular surgeons have come to re- alize the value of preoperative biplane aortography in pa- tients with abdominal aortic aneurysms. Commonly un- anticipated findings may profoundly influence operative management. Aortography of an apparent "routine" ab- dominal aortic aneurysm should then prepare the surgeon for an anticipated need for suprarenal or supraceliac aortic clamping. Preoperative aortography is now routinely per- formed on almost all of our patients with aneurysms.
Because of the marked hemodynamic changes involved with suprarenal infrarenal aortic clamping, there should be a planned anesthetic regimen. Supraceliac aortic occlusion usually causes systemic hypertension and may precipitate myocardial ischemia and left ventricular dysfunction.
Pathologic aortic changes noted at surgery often influ- ence the leve of aortic cross-clamping. The surgeon should be alert to the hazards of a degenerated aorta at or near the aneurysm neck.
Identification of significant atherosclerotic lesions at the level o f or above the renal arteries is important in minimizing serious atheroembolic complications. Widen- ing of the infrarenal aorta to the level of the renal arteries should alert the surgeon to the need to clamp the aorta at a higher level. This will eliminate the need for operative clamp switching and should allow safe graft anastomosis to the level of the renal arteries.
In addition, the infrarenal aortic cuff may be tailored to allow repair of contiguous pararenal aneurysmal com- ponents. If the aneurysm extends above the renal arteries, then thoracoabdominal aortic techniques best described by Dr. Stanley Crawford should be employed.
Dr. Green identifies factors that allowed our group to obtain a 1% mortality rate with clamping above the renals, superior mesenteric artery, or at the supraceliac level.
We carefully evaluate the juxtarenal aortic segment and take great care both before and during operation to identify safe clamping levels. I f renal artery lesions are also present,
these are repaired, most commonly by transaortic endar- terectomy.
I believe this report to be a most valuable addition to further defining risk factors and therapeutic recommen- dations towards reducing operative morbidity and mor- tality in the most challenging and difficult infrarenal aortic aneurysm. Dr. Green correctly points out that the juxta- renal segment is the most threatening area towards gaining successul operative results.
Regarding your recommendations for biplane aortog- raphy, we no longer believe that selective aortography is appropriate. A good case for routine aortography has been made by the authors.
Dr. John A. Mannick (Boston, Mass.). I want to offer some words of corroboration. We too have used increas- ingly the supraceliac clamping maneuver to get us out of trouble with the so-called difficult aneurysm, in particular the juxtarenal aneurysm and the inflammatory aneurysm, and we have found that this is a safe and kidney-saving rather than kidney-injuring maneuver. However, I have one warning; sometimes juxtarenal shaggy atheromatous disease proceeds all the way to the heart and clamping such an aorta at the diaphragm has hazards similar to trying to clamp it at the renal arteries.
We have had a couple of instances over the past decade of atheroembolization to the gut from diaphragmatic clamping in such patients. I think under those circum- stances the only satisfactory maneuver is to clean out the entire atheromatous abdominal aorta from the diaphragm down and avoid this problem. That, of course, is probably greatly facilitated by the retroperitoneal approach.
Dr. Green, my question is the same as Dr. Ehrenfeld's. In view of these hazards, do you think it is time to rec- ommend routine preoperative biplane angiography for all patients with abdominal aortic aneurysms?
Dr. Green (closing). I thank Drs. Ehrenfeld and Man- nick for their kind remarks. Both have written on this subject and deserve credit for already saying many of the same things as we have shown today. Dr. Ehrenfeld and his colleagues have drawn our attention to the dangers of the pararenal aneurysm and juxtarenal atherosclerosis. We had not listened carefully enough to what they and Dr. Crawford said about dissecting around and clamping the aortic cuff. Dr. Mannick has pointed out that the most common cause of kidney failure after resection of an ab- dominal aortic aneurysm is not clamping above the renal arteries but rather atheroemboli from the juxtarenal seg- ment. I think that our study corroborates and emphasizes what both have said in their writings.
Our policy towards preoperative aortography is un- dergoing a change from rarely obtaining the test to con- sidering it in every patient. We find ourselves using it more often especially when the CT scan suggests involvement of the juxtarenal aorta or the patient has some physiologic
134 Green et al.
Journal of VASCULAR
SURGERY
sign of renal artery involvement. Although some may be- lieve that we have made a case for its use, we remain skep- tical about routinely recommending it. Several of our pa- tients who had atheroembolic complications had preop- erative aortograms. Likewise, the recent Canadian Vascular Society review failed to show a difference in morbidity and
mortality related to the use of this test. The ability to handle the juxtarenal aorta when it is diseased is more important than the aortogram. Therefore we believe that avoidance of the problem by clamping at the diaphragm, a strategy that does not increase the risk to the patient, is the safest way to deal with the situation.
T H E E. J. WYLIE T R A V E L I N G F E L L O W S H I P OF T H E E D U C A T I O N A L F O U N D A T I O N OF THE SOCIETY FOR VASCULAR SURGERY
The Educational Foundation of the Society for Vascular Surgery (with financial assistance from W. L. Gore & Associates, Inc.) has established an E. J. Wylie Traveling Fellowship.
The purpose of the Fellowship is to enable young surgeons to visit centers of excellence in vascular surgery in the United States and abroad. The benefits of educational travel for the maintenance and enhancement of excellence in the practice of vascular surgery are obvious.
To be considered for selection a candidate must: 1. Be younger than 40 years of age at the time the traveling fellowship is awarded 2. Have completed a postgraduate vascular training program or have considerable experience
in vascular surgery supplemental to general surgical training 3. Be committed to an academic career in vascular surgery and have obtained an academic
appointment in a medical school or freestanding clinic devoted to excellence in medical education
4. Have a demonstrated record of success in pursuing clinical or basic science research sufficient to achieve academic excellence in his or her pursuit of a career in vascular surgery
Selection will be made without regard to the candidate's geographic location. A candidate submitting documentation for consideration for selection must furnish an up-
to-date curriculum vitae and a list of publications, research projects, current research support, and a list of the centers that he or she wishes to visit. Three letters of recommendation are required, including one from the Division Head and another from the Chairman of the De- partment of Surgery of the institution in which the candidate holds a faculty appointment. A 500-word essay describing the objectives of the candidate's travel plans and linking these to his or her career goals must be appended.
The first Selection Committee has been appointed and consists of John Bergan, Chairman, and members Henry Bahnson, Ben Eiseman, Robert Hobson, Ronald Stoney, and James Yao. The incumbent Recorder of the Society for Vascular Surgery will serve as an ex officio member of the Committee. The length of service of each of the members of the Committee and future members of the Committee will be determined by members of the Council of the Society for Vascular Surgery.
The Travel Fellowship Award is $10,000, granted to one person for use during a time limit and for an itinerary to be arranged by agreement between the awardee and the Committee.
Application for the Fellowship award shall be made in a letter containing the information and documents as detailed. The deadline for receiving applications is March 1, 1989. Letter of nomination or intent should be directed to:
Konald J. Stoney, M.D., F.A.C.S. Chairman, E. J. Wylie Traveling Fellowship Committee Division of Vascular Surgery University of California Medical Center 505 Parnassus Ave., M-488 San Francisco, CA 94143