researching violence against women - request rejected
TRANSCRIPT

Researching Violence Against Women
A P R A C T I C A L G U I D E F O R R E S E A R C H E R S A N D A C T I V I S T S

Researching Violence Against Women
A P R A C T I C A L G U I D E F O R R E S E A R C H E R S A N D A C T I V I S T S
M a r y E l l s b e r g ■ L o r i H e i s e

WHO Library Cataloguing-in-Publication Data
Ellsberg, Mary Carroll, Heise, Lori.Researching Violence Against Women: A Practical Guide for Researchers and Activists/Mary Ellsberg, Lori Heise.
Suggested citation: Ellsberg M, and Heise L. Researching Violence Against Women: APractical Guide for Researchers and Activists. Washington DC, United States: World HealthOrganization, PATH; 2005.
1. Domestic violence 2. Spouse abuse 3. Women 4. Research design 5. ManualsI. Title
ISBN 92 4 154647 6 (LC/NLM classification: HV 6556)
© World Health Organization and Program for Appropriate Technology in Health (PATH)2005. All rights reserved. Publications of the World Health Organization can be obtainedfrom WHO Press, World Health Organization, 20 Avenue Appia, 1211 Geneva 27,Switzerland (tel: +41 22 791 3264; fax: +41 22 791 4857; email: [email protected]).Requests for permission to reproduce or translate WHO publications – whether for sale orfor noncommercial distribution – should be addressed to Publications, at the above address(fax: +41 22 791 4806; email: [email protected]). Publications of PATH can be obtainedfrom [email protected].
The designations employed and the presentation of the material in this publication do not imply the expression of any opinion whatsoever on the part of the World HealthOrganization or PATH concerning the legal status of any country, territory, city, or area or ofits authorities, or concerning the delimitation of its frontiers or boundaries. Dotted lines onmaps represent approximate border lines for which there may not yet be full agreement.
The mention of specific companies or of certain manufacturers’ products does not implythat they are endorsed or recommended by the World Health Organization or PATH inpreference to others of a similar nature that are not mentioned. Errors and omissionsexcepted, the names of proprietary products are distinguished by initial capital letters.
Neither the World Health Organization nor PATH warrants that the information contained inthis publication is complete and correct and neither shall be liable for any damagesincurred as a result of its use.
The named authors alone are responsible for the views expressed in this publication.
Printed in the United States.
PATH creates sustainable, culturally relevant solutions that enable communities worldwide tobreak longstanding cycles of poor health. By collaborating with diverse public- and private-sector partners, we help provide appropriate health technologies and vital strategies thatchange the way people think and act. Our work improves global health and well-being.
For more information, please visit www.who.int/gender/en or www.path.org.

Table of Contents
ACKNOWLEDGEMENTS . . . . . . . . . . . . . . . . . . . . . . . . . . . 1
INTRODUCTION . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 5
CHAPTER ONE: VIOLENCE AGAINST WOMEN AS A HEALTH AND DEVELOPMENT ISSUE . . . . . . . . . . . . . . . 8Definitions of violence against womenPrevalence of intimate partner violenceThe patterning of intimate partner violencePrevalence and characteristics of sexual coercion and abuseThe effects of violence on women’s healthExplaining gender-based violenceHow do women respond to abuse?Challenges for international research on gender-based violence
CHAPTER TWO: ETHICAL CONSIDERATIONS FOR RESEARCHING VIOLENCE AGAINST WOMEN . . . . . . . . . . . . 34Respect for persons at all stages of the research processMinimizing harm to respondents and research staff Maximizing benefits to participants and communities (beneficence)Justice: Balancing risks and benefits of research on violence against women
CHAPTER THREE: DEVELOPING A RESEARCH STRATEGY . . . . . 48Different types of researchThe research processChoosing a research topic and objectivesFormulating your research questionsChoosing a research designQuantitative or qualitative methods?Population- or service-based researchCollaboration between researchers and activistsDrafting the protocol
CHAPTER FOUR: QUANTITATIVE APPROACHES TO RESEARCH . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 62Cross-sectional surveysCohort studiesCase control studies

CHAPTER F IVE : QUALITAT IVE APPROACHES TO RESEARCH . . . 72Rapid Assessments In-depth qualitative studies
CHAPTER S IX: THE CHALLENGE OF DEF INING AND MEASURING VIOLENCE IN QUANTITATIVE RESEARCH . . . . . . 84Estimating the prevalence of violence The study population: Choosing interview subjectsDefinitions of violence Enhancing disclosure of violence Common tools for measuring violence
CHAPTER SEVEN: DEVELOPING A SAMPLING STRATEGY . . . 104 Sampling considerations in qualitative studiesSampling issues in quantitative research surveys
CHAPTER E IGHT: TOOLS FOR COLLECT ING QUANTITATIVE DATA . . . . . . . . . . . . . . . . . . . . . . . . . . 116Developing the conceptual framework Operationalizing the main variablesFormulating your questionsFormatting your questionnaireTranslating the instrumentPre-testing the instrument
CHAPTER NINE: TOOLS FOR COLLECT ING QUALITAT IVE DATA . . . . . . . . . . . . . . . . . . . . . . . . . . . 128Personal interviewsFocus group discussionsObservationFree listingRankingPair-wise rankingTimelines and seasonal calendarsCausal flow analysis Open-ended storiesGenogramsCircular or Venn diagramsCommunity mappingRole playingBody mappingPhoto voice

CHAPTER TEN: BUILDING YOUR RESEARCH TEAM . . . . . . . . 154What is special about research on gender-based violence?Building the research field teamTraining fieldworkersRemuneration of interviewers
CHAPTER ELEVEN: IN THE F IELD . . . . . . . . . . . . . . . . . . . 168 Organizing the fieldworkNegotiating community accessProtecting the safety and well-being of respondents and fieldworkersFinalizing the procedures and instrumentsManaging nonresponseData quality controlData entry
CHAPTER TWELVE: ANALYZING QUANTITATIVE DATA . . . . . 186Basic analysis of survey data on violence against womenLooking at associations between violence and other variablesAssessing the validity of survey results Interpreting the results
CHAPTER THIRTEEN: ANALYZING QUALITAT IVE DATA . . . . . 202 Approaches to qualitative analysisData codingUsing a computer for coding and categorizingData reduction and data displaysEnsuring rigor in qualitative research
CHAPTER FOURTEEN: FROM RESEARCH TO ACTION . . . . . . 216Outreach to key constituenciesMatching your message to your audienceSharing findings with the community Reaching beyond your borders
APPENDIX 1: THE WHO VIOLENCE AGAINST WOMEN INSTRUMENT . . . . . . . . . . . . . . . . . . . . . . . . . . 230
APPENDIX 2: TRAINING EXERCISES FOR INTERVIEWERS . . . 240
APPENDIX 3: SUGGESTED RESOURCES . . . . . . . . . . . . . . . 244
s
m
Y
z
o
1

A Practical Guide for Researchers and Activists 1
This manual was truly a collectiveeffort, as can be seen by the extensive listof contributors. The authors would like tothank the many individuals who gener-ously contributed their time and energy toenrich this manual over the course ofnearly a decade.
We are especially indebted to ElizabethShrader, who drafted an early version ofthis manual as a consultant to the Centerfor Health and Gender Equity (CHANGE).Her pioneering research on violence inMexico, and later in the Ruta Crítica Study,inspired a generation of researchers, andhelped inform the early work of theInternational Research Network onViolence Against Women (IRNVAW).
This project was initiated by CHANGE.We are therefore indebted to CHANGEand the current Executive Director, JodiJacobson, for support of the manual dur-ing its initial stages.
We also wish to acknowledge the indi-vidual participants of IRNVAW whoseefforts and critical reflections form the basisof many of the recommendations con-tained herein.
Participants in IRNVAW meetings whosework and reflections contributed to thismanual include:
Naeema Abrahams, South Africa; AnnAdair, USA; Zeinab Abdi Ahmed, Kenya;Cherub Antwi-Nsiah, Ghana; Lilian Artz,South Africa; Jill Astbury, Australia; SafiaAzim, Bangladesh; Suzanna Stout Banwell,
USA; Srilatha Batliwala, India; DeviBhuyan, India; Rebecca Calder, Lesotho;Jacquelyn C. Campbell, USA; Cheng Yimin,China; Desiree Daniels, South Africa; NishaDhawan, India; Joy Dladla, South Africa;Nata Duvvury, India; Gillian Fawcett,Mexico; Rezina Ferdous, Bangladesh;Fariyal Fikree, Pakistan; Liz Frank, Namibia;Soledad Gonzalez Montes, Mexico; MaryGoodwin, USA; Lorelei Goodyear, USA;Nicole Haberland, USA; Muhammad Haj-Yahia, Israel; Penn Handwerker, USA;Pamela Hartigan, USA; Zanele Hlatswayo,South Africa; Dianne Hubbard, Namibia;Wanda M. Hunter, USA; Susan Igras, USA;Surinder K.P. Jaswal, India; Carol Jenkins,Bangladesh/USA; Peggy Jennings, USA;Rachel Jewkes, South Africa; HollyJohnson, Canada; Pumzile Kedama, SouthAfrica; Barbara Kenyon, South Africa;Mpefe Ketihapile, South Africa; Julia Kim,South Africa; Sunita Kishor, USA; MaryKoss, USA; Shubhada Maitra, India;Suzanne Maman, USA; Lorna Martin, SouthAfrica; Sandra Martin, USA; BongiweMasilela, Swaziland; Raymond Matsi, SouthAfrica; Donna McCarraher, USA; LoriMichau, Tanzania/USA; Claudia GarciaMoreno, Mexico/Switzerland; AndrewMorrison, USA; Caroline Moser, USA;Oswaldo Montoya, Nicaragua; KhosiMthethwa, Swaziland; Bernadette Muthien;Shenaaz Nair, South Africa; DorothyNairne, South Africa; Mavis Ndlovu,Zimbabwe; Mzikazi Nduna, South Africa;
Acknowledgements

2 Researching Violence Against Women
Sydia Nduna, Tanzania; Erin Nelson, USA;Nguyen Thi Hoai Duc, Vietnam; TaraNutley, USA; Kwadzanai Nyanyungo,Zimbabwe; Maria Beatriz Orlando, USA;Loveday Penn-Kekana, South Africa; JasjitPurewal, India; Hnin Hnin Pyne, USA;Regan Ralph, USA; Juan Carlos RamirezRodriguez, Mexico; Laurie Ramiro,Philippines; Koketso Rantona, Botswana;Matsie Ratsaka, South Africa; HeatherRobinson, USA; Louise Robinson, Lesotho;Mariana Romero, Argentina; StephanieRosseti, Botswana; Laura Sadowski, USA;Irma Saucedo Gonzalez, Mexico; LynnShort, USA; Patrick Sikana, Zambia; SaweraSingh, South Africa; Pinky Singh Rana,Nepal; Paige Hall Smith, USA; ShobhaSrinivasan, India/USA; Shana Swiss, USA;Imani Tafari-Ama, Jamaica; Kathryn Tolbert,Mexico; Tran Anh Vinh, Vietnam; IanTweedie, USA; Sandi Tyler, USA; LisaVetten, South Africa; Penny Ward, SouthAfrica; Carole Warshaw, USA; CharlotteWatts, Zimbabwe/UK; Linda Williams, USA;Kate Wood, UK; Pamela Wyville-Staples,South Africa; Mieko Yoshihama,Japan/USA; Cathy Zimmerman,Cambodia/USA.
We have also drawn heavily on experi-ences and insights emerging from our par-ticipation in research collaborations withcolleagues from the Department ofEpidemiology and Public Health, UmeåUniversity, Sweden, particularly Lars ÅkePersson, Stig Wall, Lars Dalgren, AnnaWinkvist, Maria Emmelin, Jerker Liljestrand,Gunnar Kullgren and Ulf Högberg, as wellas colleagues from Addis Ababa University,Ethiopia: Yemane Berhane, NegussieDeyessa, Yegomawork Gossaye, and AtalayAlem; from Gadjah Mada University andRifka Annisa Women’s Crisis Center inYogyakarta, Indonesia: MohammadHakimi and Elli Nur Hayati; and from theAutonomous Nicaraguan University at León(UNAN-León): Rodolfo Peña, AndrésHerrera, and Eliette Valladares. We are par-
ticularly indebted to Lars Åke Persson andStig Wall for graciously allowing us to drawheavily from their book on epidemiologyand field methods, as well as to LarsDalgren, Anna Winkvist, and MariaEmmelin for the inspiration we receivedfrom their book on qualitative researchmethods.
Likewise, many of the examples used inthis manual have come from the WHOMulti-country Study on Women’s Healthand Domestic Violence. In particular,Claudia García Moreno, coordinator of thestudy, has supported this project from itsinception and has provided invaluablefinancial, technical, and moral supportthroughout. We are also grateful to HenricaJansen for permission to use her beautifulphotographs from the WHO study. Wewould also like to acknowledge the ableguidance of the steering committee of theWHO multi-country study, and the valu-able contributions of all the researchersinvolved in this study:
Core Research Team Claudia Garcia-Moreno, World Health
Organization, Geneva, Switzerland(Study Coordinator),
Charlotte Watts, London School of Hygieneand Tropical Medicine, London, UK,
Lori Heise, PATH, Washington, DC, USA, Mary Ellsberg, PATH, Washington DC, USA,Henrica A.F.M. Jansen, World Health
Organization, Geneva, Switzerland
Country ResearchersBangladesh: Ruchira Tabassum Naved,ICCDR,B, Dhaka; Safia Azim, Naripokkho,Dhaka; Abbas Bhuiya, ICCDR,B, Dhaka; Lars-Åke Persson, Uppsala University, Sweden.
Brazil: Lilia Blima Schraiber, University ofSao Paulo – Faculty of Medicine, SaoPaulo; Ana Flavia Lucas D’Oliveira,University of Sao Paulo – Faculty ofMedicine, Sao Paulo; Ivan Franca-Junior,

A Practical Guide for Researchers and Activists 3
University of Sao Paulo – School of PublicHealth, Sao Paulo; Carmen Simone GriloDiniz, Feminist Collective for Health andSexuality, Sao Paulo; Ana Paula Portella,SOS Corpo, Genero e Cidadania, Recife,Pernambuco; Ana Bernarda Ludermir,Federal University of Pernambuco, Recife.
Ethiopia: Yemane Berhane, Addis AbabaUniversity, Addis Ababa; Ulf Högberg,Umeå University, Umeå, Sweden; GunnarKullgren, Umeå University, Umeå, Sweden;Negussie Deyessa, Addis Ababa University,Addis Ababa; Maria Emmelin, UmeåUniversity, Umeå, Sweden; YegomaworkGossaye, Addis Ababa University, AddisAbaba; Mary Ellsberg, PATH, Washington,DC, USA; Atalay Alem, Addis AbabaUniversity, Addis Ababa; Derege Kebede,Addis Ababa University, Addis Ababa;Alemayehu Negash, Addis AbabaUniversity, Addis Ababa.
Japan: Mieko Yoshihama, University ofMichigan, Ann Arbor, USA; Saori Kamano,National Institute of Population and SocialSecurity Research, Tokyo; Tamie Kaino,Ochanomizu University, Tokyo; FumiHayashi, Toyo Eiwa Women’s University,Tokyo; Hiroko Akiyama, University ofTokyo, Tokyo; Tomoko Yunomae, JapanAccountability Caucus.
Namibia: Eveline January, Ministry ofHealth and Social Services, Windhoek;Hetty Rose-Junius, Ministry of Health andSocial Services, Windhoek; Johan Van Wyk,Ministry of Health and Social Services,Windhoek; Alves Weerasinghe, NationalPlanning Commission, Windhoek.
Peru: Ana Güezmes Garcia, Centro de laMujer Peruana Flora Tristan, Lima; NancyPalomino Ramirez, Universidad PeruanaCayetano Heredia, Lima; Miguel RamosPadilla, Universidad Peruana CayetanoHeredia, Lima.
Samoa: Tina Tauasosi-Posiulai, Tima Levai-Peteru, Dorothy Counts and ChrisMcMurray, Secretariat of the PacificCommunity.
Serbia and Montenegro: StanislavaOtasevic, Autonomous Women’s Center,Belgrade; Silvia Koso, AutonomousWomen’s Center, Belgrade; KatarinaBogavac, Autonomous Women’s Center,Belgrade; Dragisa Bjeloglav, StrategicMarketing, Belgrade; Viktorija Cucic,University of Belgrade, Belgrade.
Thailand: Churnrurtai Kanchanachitra,Mahidol University, Bangkok; KritayaArchavanitkul, Mahidol University,Bangkok; Wassana Im-em, MahidolUniversity, Bangkok; Usa Lerdsrisanthat,Foundation for Women, Bangkok.
United Republic of Tanzania: JessieMbwambo, Muhimbili University College ofHealth Sciences, Dar es Salaam; GideonKwesigabo, Muhimbili University Collegeof Health Sciences, Dar es Salaam; JoeLugalla, University of New Hampshire,Durham, USA; Sherbanu Kassim, Universityof Dar es Salaam, Dar es Salaam.
WHO Steering Committee Members:Jacquelyn Campbell, Johns HopkinsUniversity (Co-Chair), Baltimore, USA;Lucienne Gillioz, Bureau d’Egalite, Geneva,Switzerland; Irma Saucedo Gonzalez, ElColegio de Mexico, Mexico City, Mexico;Rachel Jewkes, Medical Research Council,Pretoria, South Africa; Ivy Josiah, Women’sAID Organisation, Selangor, Malaysia; OlavMeirik, Instituto Chileno de MedicinaReproductiva (ICMER) (Co-Chair), Santiago,Chile; Laura Rodrigues, London School ofHygiene and Tropical Medicine, London,UK; Berit Schei, Norwegian University ofScience and Technology, Trondheim,Norway; Stig Wall, Umeå University, Umeå,Sweden.

4 Researching Violence Against Women
We are deeply grateful to all those indi-viduals who reviewed the manuscript atdifferent stages of preparation and inmany cases provided extensive comments,research examples, and field experiencesthat greatly enriched the manual. We are particularly grateful to the followingindividuals:
Elizabeth Shrader, Sara Bott, LoriMichau, Claudia Garcia Moreno, ChristineBradley, Jacquelyn Campbell, Victoria Frye,Henrica Jansen, Alessandra Guedes,Shireen Jeejeebhoy, Erica Keogh, MaryKoss, Linda Morison, Elaine Murphy,Monica O’Connor, Vijayendra Rao, StigWall, Rachel Jewkes, Naeema Abrahams,Charlotte Watts, Michelle Folsom, MiekoYoshihama, Anna Winkvist.
We also gratefully acknowledge the serv-ices of the following individuals and theirsupport in the production of the book:
Editing by Cheryl Silver.Graphic Design by Gretchen Maxwell of
GLM Design.Support in production and editing pro-
vided by Rani Boehlke, Rebeca Quiroga,and Tricia Klosky at PATH.
Proofreading by Janet Saulsbury at PATHand Lenore Jackson.
Cover graphic by Liliana Gutierrez Lopezof Lapiz y Papel, Quito, Ecuador
This manual was produced with thegenerous financial support of WHO, theFord Foundation, The Moriah Fund,CHANGE, and The Swedish Agency forInternational Development Cooperation(Sida).

A Practical Guide for Researchers and Activists 5
Twenty years ago, violence againstwomen was not considered an issue wor-thy of international attention or concern.Victims of violence suffered in silence,with little public recognition of theirplight. This began to change in the 1980sas women’s groups organized locally andinternationally to demand attention to thephysical, psychological, and economicabuse of women. Gradually, violenceagainst women has come to be recognizedas a legitimate human rights issue and as asignificant threat to women’s health andwell-being.
Now that international attention isfocused on gender-based violence,methodologically rigorous research isneeded to guide the formulation andimplementation of effective interventions,policies, and prevention strategies. Untilfairly recently, the majority of research onviolence consisted of anecdotal accounts orexploratory studies performed on nonrep-resentative samples of women, such asthose attending services for batteredwomen. While this research has played acritical role in bringing to light the issuesof wife abuse, rape, trafficking, incest, andother manifestations of gender-based vio-lence, it is less useful for understanding thedimensions or characteristics of abuseamong the broader population.
This manual has been developed inresponse to the growing need to improvethe quality, quantity, and comparability of
international data on physical and sexualabuse. It outlines some of the method-ological and ethical challenges of conduct-ing research on violence against womenand describes a range of innovative tech-niques that have been used to addressthese challenges. We hope that the man-ual will be useful for those interested inpursuing research on violence, especiallyin developing countries and otherresource-poor settings.
The manual draws on the collectiveexperiences and insights of many individu-als, most notably the members of theInternational Research Network onViolence Against Women (IRNVAW), an adhoc group of researchers and activists thatmeets periodically to share experiencesregarding research on violence. TheNetwork arose out of a two-day meetingon methodology and research ethics organ-ized in June 1995 by the Center for Healthand Gender Equity. To date the IRNVAWhas sponsored four international meetingsand several members have collaboratedwith the World Health Organization(WHO) in the design and implementationof a multi-country study on women’shealth and domestic violence. Many of theexamples and insights included in thismanual come from the pioneering work ofIRNVAW members, as well as the WHOMulti-country Study on Women’s Healthand Domestic Violence, a household sur-vey of women that has been conducted in
Introduction

6 Researching Violence Against Women
at least ten countries to date. We have alsodrawn extensively from our own researchexperiences, primarily in Nicaragua,Indonesia, and Ethiopia.
ReadershipThis manual is written for anyone inter-ested in the application of social scienceand public health research methods to thestudy of gender-based violence. The man-ual assumes a certain level of familiaritywith the logic of research and is not a sub-stitute for training in research or researchmethodologies.
It is designed for researchers whowant to know more about adapting tradi-tional research techniques to the specialcase of investigating physical and sexualabuse. And it is designed for activists,community workers, and serviceproviders who want to become conver-sant in methodological issues. One of thegoals of this manual is to facilitate collabo-rations between researchers and commu-nity-based workers and activists byproviding practitioners with an introductionto the tools and language of research, andby giving researchers greater insight intothe specific issues that accompany researchon violence.
Focus of the manualFor the sake of brevity, this manualfocuses primarily on the issue of violenceagainst women by their intimate part-ners. Gender-based violence assumesmany forms, including rape, sexual assaultand coercion, stalking, incest, sexualharassment, female genital mutilation, andtrafficking in women. Although many ofthe insights presented herein will apply tothese other types of violence, no singlemanual could exhaustively address allforms of abuse. Additionally, we concen-trate on applied research, as opposed toresearch designed to advance theory or toaddress questions of primarily academicrelevance.
The manual is directed particularly tothose researchers interested in the intersec-tion of violence and health in develop-ing countries, given the clear impact thatgender violence has on women’s healthstatus. However, much of the informationpresented in the manual is applicable toviolence research as it relates to otherissues, such as human rights, the well-being of families and children, and eco-nomic development. Similarly, the lessonsfor developing countries may be relevantto some violence research undertaken inindustrialized countries, particularly amongeconomically marginalized and/or politi-cally disenfranchised populations.
Finally, the manual advances an ethic ofresearch that is action-oriented, account-able to the antiviolence movement, andresponsive to the needs of women livingwith violence. It strongly encourages col-laboration between researchers and thoseworking directly on violence as activistsand/or practitioners. Recent experiences incountries as diverse as Canada, Zimbabwe,Indonesia, South Africa, Nicaragua, andCambodia have shown that powerful syn-ergies can be achieved from partnershipsbetween researchers and advocates.Whereas researchers help to ensure thatthe endeavor is grounded in the principlesof scientific inquiry, the involvement ofadvocates and service providers helpsensure that the right questions are asked inthe right way, and that the knowledge gen-erated is used for social change.

A Practical Guide for Researchers and Activists 7
This document was based on the contributions of thousands of women from around the
world who shared their stories and personal experiences in the hopes that their voices
would contribute to diminishing the suffering of future generations of women from
violence. The publication is dedicated to them.

1 PHO
TO B
Y H
AFM
JAN
SEN

A Practical Guide for Researchers and Activists 9
society in the world legitimize, obscure, anddeny abuse. The same acts that would bepunished if directed at an employer, a neigh-bor, or an acquaintance often go unchal-lenged when men direct them at women,especially within the family.
For over three decades, women’s advo-cacy groups around the world have beenworking to draw more attention to thephysical, psychological, and sexual abuseof women and to stimulate action. Theyhave provided abused women with shelter,lobbied for legal reforms, and challengedthe widespread attitudes and beliefs thatsupport violence against women.2
Increasingly, these efforts are having
Violence against women is the most per-vasive yet underrecognized human rights vio-lation in the world. It is also a profoundhealth problem that saps women’s energy,compromises their physical and mentalhealth, and erodes their self-esteem. In addi-tion to causing injury, violence increaseswomen’s long-term risk of a number of otherhealth problems, including chronic pain,physical disability, drug and alcohol abuse,and depression.1, 2 Women with a history ofphysical or sexual abuse are also at increasedrisk for unintended pregnancy, sexuallytransmitted infections, and miscarriages.3-5
Despite the high costs of violence againstwomen, social institutions in almost every
C H A P T E R O N E
Violence Against Women as aHealth and Development Issue*
Topics covered in this chapter:
Definitions of violence against women Prevalence of intimate partner violenceThe patterning of intimate partner violencePrevalence and characteristics of sexual coercion and abuseThe effects of violence on women’s healthExplaining gender-based violenceHow do women respond to abuse?Challenges for international research on gender-based violence
* Parts of this chapter are reprinted from Heise, Ellsberg and Gottemoeller, 19992 (available online athttp://www.infoforhealth.org/pr/l11edsum.shtml).

10 Researching Violence Against Women
C H A P T E R O N E
results. Today, international institutions arespeaking out against gender-based vio-lence. Surveys and studies are collectingmore information about the prevalence andnature of abuse. More organizations, serv-ice providers, and policy makers are recog-nizing that violence against women hasserious adverse consequences for women’shealth and for society.
This chapter provides a brief overviewof the issue of violence against women,including definitions, international preva-lence, the documented health conse-quences of abuse, and evidence regardingcausation and women’s experiences ofabuse. We include this information here forindividuals who may be new to the topicand/or for those who are writing researchproposals and may not have easy access tothe international literature.
DEFINIT IONS OF VIOLENCEAGAINST WOMEN
Although both men and women can bevictims as well as perpetrators of violence,
the characteristics of violence most com-monly committed against women differ incritical respects from violence commonlycommitted against men. Men are morelikely to be killed or injured in wars oryouth- and gang-related violence thanwomen, and they are more likely to bephysically assaulted or killed on the streetby a stranger. Men are also more likely tobe the perpetrators of violence, regardlessof the sex of the victim.1 In contrast,women are more likely to be physicallyassaulted or murdered by someone theyknow, often a family member or intimatepartner.2 They are also at greater risk ofbeing sexually assaulted or exploited,either in childhood, adolescence, or asadults. Women are vulnerable to differenttypes of violence at different moments intheir lives (see Figure 1.1).
There is still no universally agreed-uponterminology for referring to violence againstwomen. Many of the most commonly usedterms have different meanings in differentregions, and are derived from diverse theo-retical perspectives and disciplines.
FIGURE 1.1 THE LIFE CYCLE OF VIOLENCE AGAINST WOMEN
(Adapted from Watts and Zimmerman, 20026 and Shane and Ellsberg, 2002.7)
Pre-birth
Infancy
Childhood
Elderly
Adolescence
Reproductive Age
Sex-selective abortion Elder/widow abuse
Female infanticideNeglect (health care,nutrition)
Child abuseMalnutritionFGM
Forced prostitutionTraffickingForced early marriagePsychological abuseRape
Honor killingDowry killingIntimate partner violenceSexual assault by non-partnerHomicide/FemicideSex traffickingSexual harassment

A Practical Guide for Researchers and Activists 11
One frequently used model for under-standing intimate partner abuse and sexualabuse of girls is the “family violence”framework, which has been developed pri-marily from the fields of sociology andpsychology.8, 9 “Family violence” refers toall forms of abuse within the family regard-less of the age or sex of the victim or theperpetrator. Although women are fre-quently victimized by a spouse, parent, orother family member, the concept of “fam-ily violence” does not encompass the manytypes of violence to which women areexposed outside the home, such as sexualassault and harassment in the workplace.Moreover, feminist researchers find theassumption of gender neutrality in the term“family violence” problematic because itfails to highlight that violence in the familyis mostly perpetrated by men againstwomen and children.
There is increasing international consen-sus that the abuse of women and girls,regardless of where it occurs, should beconsidered as “gender-based violence,” as itlargely stems from women’s subordinate sta-tus in society with regard to men (Figure1.2). The official United Nations definitionof gender-based violence was first presentedin 1993 when the General Assembly passedthe Declaration on the Elimination ofViolence against Women.10 According to thisdefinition, gender-based violence includes ahost of harmful behaviors directed atwomen and girls because of their sex,including wife abuse, sexual assault, dowry-related murder, marital rape, selective mal-nourishment of female children, forcedprostitution, female genital mutilation, andsexual abuse of female children (see Box1.1 for the complete definition).10
Even when the abuse of women bymale partners is conceptualized as gender-based violence, the terms used to describethis type of violence are not consistent. Inmany parts of the world, the term “domes-tic violence” refers to the abuse of women
by current or former male intimate part-ners.11, 12 However, in some regions, includ-ing Latin America, “domestic violence”refers to any violence that takes place inthe home, including violence against chil-dren and the elderly.13, 14 The term “bat-tered women” emerged in the 1970s and iswidely used in the United States andEurope to describe women who experi-ence a pattern of systematic dominationand physical assault by their male part-ners.15 The terms “spouse abuse,” “sexual-ized violence,” “intimate partner violence,”and “wife abuse” or “wife assault” are gen-erally used interchangeably, although eachterm has weaknesses. “Spouse abuse” and“intimate partner violence” do not makeexplicit that the victims are generallywomen, whereas “wife abuse” and “wifeassault” can be read to exclude common-law unions and dating violence.
For the purposes of this manual, we usethe terms “violence against women” (VAW)and “gender-based violence” (GBV) inter-changeably to refer to the full range ofabuses recognized by the UN Declarationand other international agreements. We use
V I O L E N C E A G A I N S T W O M E N A S A H E A L T H A N D D E V E L O P M E N T I S S U E
The term “violence against women” means any act of gender-based violence thatresults in, or is likely to result in, physical, sexual or psychological harm or suffer-ing to women, including threats of such acts, coercion or arbitrary deprivation ofliberty, whether occurring in public or private life. Accordingly, violence againstwomen encompasses but is not limited to the following:
a) Physical, sexual and psychological violence occurring in the family, includingbattering, sexual abuse of female children in the household, dowry-related vio-lence, marital rape, female genital mutilation and other traditional practicesharmful to women, non-spousal violence and violence related to exploitation;
b) Physical, sexual and psychological violence occurring within the general com-munity, including rape, sexual abuse, sexual harassment and intimidation atwork, in educational institutions and elsewhere, trafficking in women and forcedprostitution;
c) Physical, sexual and psychological violence perpetrated or condoned by theState, wherever it occurs.
Acts of violence against women also include forced sterilization and forcedabortion, coercive/forced use of contraceptives, female infanticide and prenatalsex selection.
BOX 1.1 UNITED NATIONS DEFINITION OF VIOLENCE AGAINST WOMEN
(From United Nations, 1993.10)

12 Researching Violence Against Women
the terms “intimate partner violence,” “wifeabuse” and “domestic violence” inter-changeably to refer to the range of sexu-ally, psychologically, and physicallycoercive acts used against adult and ado-lescent women by current or former maleintimate partners.
PREVALENCE OF INT IMATEPARTNER VIOLENCE
International research consistently demon-strates that a woman is more likely to beassaulted, injured, raped, or killed by a cur-rent or former partner than by any otherperson. Table 1.1 presents findings fromnearly 80 population-based studies carriedout in more than 50 countries. These studiesindicate that between 10 percent and 60 per-cent of women who have ever been marriedor partnered have experienced at least oneincident of physical violence from a currentor former intimate partner. Most studies esti-mate a lifetime prevalence of partner vio-lence between 20 percent and 50 percent.Although women can also be violent, andabuse exists in some same-sex relationships,the vast majority of partner abuse is perpe-trated by men against their female partners.
Researchers find considerable variationin the prevalence of partner violence fromcountry to country, and among studieswithin a country. Unfortunately, lack ofconsistency in study methods, studydesign, and presentation of results makes itdifficult to explore the causes and conse-quences of violence. As a result, it is oftendifficult to compare results even betweenstudies performed in the same country.
Partly to address this shortcoming, theWorld Health Organization worked withcollaborating institutions in 15 sites in tencountries between 1998 and 2004 to imple-ment a multi-country study of domesticviolence and women’s health. The WHOMulti-country Study on Women’s Healthand Domestic Violence Against Women—also referred to here as the WHO VAWStudy—was the first ever to produce trulycomparable data on physical and sexualabuse across settings.16 This research proj-ect sought to minimize differences relatedto methods by employing standardizedquestionnaires and procedures, as well as acommon approach to interviewer training.
We will return to the WHO VAW Studymany times throughout the manual tohighlight some of the challenges posed bythis project and how they were resolved.
THE PATTERNING OFINTIMATE PARTNERVIOLENCE
The WHO VAW Study also provided a rareopportunity to examine the “patterning” ofviolence across settings. Does physical vio-lence occur together with other types ofviolence? Do violent acts tend to escalateover time? Are women most at risk frompartners or from others in their lives?
The WHO VAW Study findings confirmthat most women who suffer physical orsexual abuse by a partner generally experi-ence multiple acts over time. Likewise, phys-ical and sexual abuse tend to co-occur in
C H A P T E R O N E
FIGURE 1.2 THE OVERLAP BETWEEN GENDER-BASED VIOLENCE ANDFAMILY/DOMESTIC VIOLENCE
Gender-basedviolence
For example:■ Rape by strangers■ Female genital
mutilation■ Sexual harassament
in the workplace■ Selective malnutrition
of girls
Intimatepartnerviolence
Sexual abuseof womenand girlsin the family
For example:■ Child abuse■ Elder abuse
Family violence

A Practical Guide for Researchers and Activists 13
V I O L E N C E A G A I N S T W O M E N A S A H E A L T H A N D D E V E L O P M E N T I S S U E
Proportion of womenphysically assaulted
Year of Sample Study* by a partner (%) Country Ref study Coverage size population* Age (years) last 12 mo Ever
AfricaEthiopia ◆
17 2002 Meskanena Woreda 2261 III 15–49 29 49
Kenya 18 1984–87 Kisii District 612 V >15 42d
■19 2003 National 3856 III 15–49 24 40
Namibia ◆20 2002 Winhoek 1367 III 15–49 16 31
South Africa 21 1998 Eastern Cape 396 III 18–49 11 27
1998 Mpumalanga 419 III 18–49 12 28
1998 Northern Province 464 III 18–49 5 19
■22 1998 National 10,190 II 15–49 6 13
Tanzania ◆20 2002 Dar es Salaam 1442 III 15–49 15 33
◆20 2002 Mbeya 1256 III 15–49 19 47
Uganda 23 1995–1996 Lira & Masaka 1660 II 20–44 41d
Zambia ■24 2001–2002 National 3792 III 15–49 27 49
Zimbabwe 25 1996 Midlands Province 966 I >18 17b
Latin America and the CaribbeanBarbados 26 1990 National 264 I 20–45 30a,c
Brazil ◆20 2001 Sao Paulo 940 III 15–49 8 27
◆20 2001 Pernambuco 1188 III 15–49 13 34
Chile 27 1993 Santiago Province 1000 II 22–55 26d
28 1997 Santiago 310 II 15–49 23
●29 2004p Santa Rosa 422 IV 15–49 4 25
Colombia ■30 1995 National 6097 II 15–49 19d
■31 2000 National 7602 III 15–49 3 44
Dominican Republic ■24 2002 National 6807 III 15–49 11 22
Ecuador ▲32 1995 National 11,657 II 15–49 12
El Salvador ▲33 2002 National 10,689 III 15–49 6 20d
Guatemala ▲34 2002 National 6595f VI 15–49 9
Honduras ▲35 2001 National 6827 VI 15–49 6 10
Haiti ■24 2000 National 2347 III 15–49 21 29
Mexico 36 1996 Guadalajara 650 III >15 2737 1996p Monterrey 1064 III >15 1738 2003 National 34,184 II >15 9
Nicaragua 39 1995 Leon 360 III 15–49 27 5240 1997 Managua 378 III 15–49 33 69
■41 1998 National 8507 III 15–49 13 30
Paraguay ▲42 1995–1996 National 5940 III 15–49 10
▲43 2004 National 5070 III 15–44 7 19
Peru ■24 2000 National 17,369 III 15–49 2 42
TABLE 1.1 PHYSICAL ASSAULTS ON WOMEN BY AN INTIMATE MALE PARTNER, SELECTED POPULATION-BASED STUDIES, 1982–2004

14 Researching Violence Against Women
C H A P T E R O N E
Proportion of womenphysically assaulted
Year of Sample Study* by a partner (%) Country Ref study Coverage size population* Age (years) last 12 mo Ever
Latin America and the Caribbean (continued)Peru (continued) ◆
20 2001 Lima 1019 III 15–49 17 50
◆20 2001 Cusco 1497 III 15–49 25 62
Puerto Rico ▲44 1995–1996 National 4755 III 15–49 13e
Uruguay 45 1997 National 545 IIk 22–55 10c
North AmericaCanada 46 1993 National 12,300 I >18 3b,c 29b,c
47 1999 National 8356 III >15 3 8g
United States 48 1995–1996 National 8000 I >18 1a 22a
Asia and Western PacificAustralia * 49 1996 National 6300 I 3b 8b,d
50 2002–2003 National 6438 III 18–69 3 31
Bangladesh 51 1992 National (villages) 1225 II <50 19 4752 1993 Two rural regions 10,368 II 15–49 42d
◆20 2003 Dhaka 1373 III 15–49 19 40
◆20 2003 Matlab 1329 III 15–49 16 42
Cambodia 53 1996 Six regions 1374 III 15–49 16
■24 2000 National 2403 III 15–49 15 18
China 54 1999–2000 National 1665 II 20–64 15
India ■24 1998–1999 National 90,303 III 15–49 10 1953 1999 Six states 9938 III 15–49 14 40
●29 2004p Lucknow 506 IV 15–49 25 35
●29 2004p Trivandrum 700 IV 15–49 20 43
●29 2004p Vellore 716 IV 15–49 16 31
Indonesia 55 2000 Central Java 765 IV 15–49 2 11
Japan ◆20 2001 Yokohama 1276 III 18–49 3 13
New Zealand ◆56 2002 Auckland 1309 III 18–64 5 30
◆56 2002 North Waikato 1360 III 18–64 34
Papua New Guinea 57 1982 National, rural villages 628 IIIk 67
Philippines ■58 1993 National 8481 IV 15–49 1059 1998 Cagayan de Oro 1660 II 15–49 26
City & Bukidnon
●29 2004p Paco 1000 IV 15–49 6 21
Republic of Korea 60 1989 National 707 II >20 38
Samoa ◆20 2000 National 1204 III 15–49 18 41
Thailand ◆20 2002 Bangkok 1048 III 15–49 8 2320 2002 Nakonsawan 1024 III 15–49 13 34
Vietnam 61 2004 Ha Tay province 1090 III 15–60 14 25
TABLE 1.1 PHYSICAL ASSAULTS ON WOMEN BY AN INTIMATE MALE PARTNER, SELECTED POPULATION-BASED STUDIES, 1982–2004

A Practical Guide for Researchers and Activists 15
V I O L E N C E A G A I N S T W O M E N A S A H E A L T H A N D D E V E L O P M E N T I S S U E
Proportion of womenphysically assaulted
Year of Sample Study* by a partner (%) Country Ref study Coverage size population* Age (years) last 12 mo Ever
EuropeAlbania ▲
62 2002 National 4049 III 15–44 5 8
Azerbaijan ▲63 2001 National 5533 III 15–44 8 20
Finland * 64 1997 National 4955 I 18–74 30
France * 65 2002 National 5908 II >18 3 9i
Georgia ▲66 1999 National 5694 III 15–44 2 5
Germany * 67 2003 National 10,264 III 16–85 23b
Lithuania * 68 1999 National 1010 II 18–74 42b,d,h
Netherlands 69 1986 National 989 I 20–60 21a
Norway 70 1989 Trondheim 111 III 20–49 18
* 71 2003 National 2143 III 20–56 6 27
Republic of Moldova ▲72 1997 National 4790 III 15–44 8 15
Romania ▲73 1999 National 5322 III 15–44 10 29
Russia ▲74 2000 Three provinces 5482 III 15–44 7 22
Serbia/Montenegro ◆20 2003 Belgrade 1189 III 15–49 3 23
Sweden * 75 2000 National 5868 III 18–64 4e 18e
Switzerland 76 1994–1996 National 1500 II 20–60 6c 21c
* 77 2003 National 1882 III >18 10
Turkey 78 1998 E & SE Anatolia 599 I 14–75 58a
Ukraine ▲79 1999 National 5596 III 15–44 7 19
United Kingdom 80 1993p North London 430 I >16 12a 30a
81 2001 National 12,226 I 16–59 3 19j
Eastern MediterraneanEgypt ■
82 1995–1996 National 7123 III 15–49 13 34
●29 2004p El–Sheik Zayed 631 IV 15–49 11 11
Israel 83 1997 Arab population 1826 II 19–67 32
West Bank andGaza Strip 84 1994 Palestinian population 2410 II 17–65 52
Key ■ DHS survey data24● INCLEN data85
▲ CDC study ◆ WHO study20 * International Violence Against Women (IVAWS) Study
TABLE 1.1 PHYSICAL ASSAULTS ON WOMEN BY AN INTIMATE MALE PARTNER, SELECTED POPULATION-BASED STUDIES, 1982–2004
* Study population: I = all women;II = currently married/partnered women;III = ever–married/partnered women;IV = women with a pregnancy outcome;V = married women – half with pregnancyoutcome, half without; VI women who had apartner within the last 12 months.a Sample group included women who hadnever been in a relationship and thereforewere not in exposed group.
b Although sample included all women, rate ofabuse is shown for ever–married/partneredwomen (number not given).c Physical or sexual assault.d During current relationship.e Rate of partner abuse among ever–married/partnered women recalculated from authors’ data.f Weighted for national representativity.
g Within the last five years.h Includes threats.i Since the age of 18.j Since the age of 16.k Nonrandom sampling methods used.p Publication date (field work dates notreported).
(Updated from Heise et al, 1999.2)

16 Researching Violence Against Women
many relationships. Figure 1.3 summarizesthe proportion of women who have experi-enced violence by an intimate partneramong ever-partnered women aged 15 to 49in the various sites included in the study.The first bar portrays the percentage ofwomen in each setting who have experi-enced physical violence by a partner; thesecond bar portrays sexual violence by apartner; and the third bar represents the per-centage of ever-partnered women who haveexperienced either physical and/or sexualviolence by a partner in their lifetime.
Until recently, it was believed that fewwomen exclusively experienced sexual vio-lence by an intimate partner. Available stud-ies from North and Central America hadindicated that sexual violence was generallyaccompanied by physical abuse and by emo-tional violence and controlling behaviors.2
The findings from the WHO VAW Study
suggest that, although this pattern is main-tained in many countries, a few sitesdemonstrate a significant departure. Inboth the capital and province of Thailand,a substantial portion of women who expe-rience partner violence, experience sexualviolence only (Figure 1.4). In Bangkok, 44percent of all cases of lifetime partner vio-lence have experienced only sexual vio-lence. The corresponding statistic in theThai province is 29 percent of cases. Asimilarly high percentage of cases of vio-lence in Bangladesh province (32 percent)and Ethiopia province (31 percent) involvesexual violence only.
These results speak to the importance ofdeveloping a broader international researchbase on violence against women. Insightsderived exclusively from the NorthAmerican literature may not reflect the real-ity of women’s experiences in other settings.
C H A P T E R O N E
FIGURE 1.3 PREVALENCE OF PHYSICAL VIOLENCE AND/OR SEXUAL PARTNER VIOLENCE IN TEN COUNTRIES
(From WHO, 2005.20)
80 -
70 -
60 -
50 -
40 -
30 -
20 -
10 -
0 -
■ % women who have ever experienced physical violence by a partner
■ % women who have ever experienced sexual violence by a partner
■ % women who have ever experienced physical and/or sexual violence by a partner
Bang
lades
h Ci
tyBa
nglad
esh
Provin
ceBr
azil C
ityBr
azil P
rovin
ceEth
iopia
Pro
vince
Japan
City
Nam
ibia
City
Peru
City
Peru
Provin
ceTh
ailan
d Ci
tyTh
ailan
d Pro
vince
Tanz
ania
City
Tanz
ania
Pro
vince
Serb
ia
Samo
a
Percent
4037
53
42
50
10
62
27 29
14
3437
49
59
71
13
6
15
31
17
36
23
50 5247
62
23
3034
29
23
33
41
47
41
31
47
69
56
6
23 2420
4146

A Practical Guide for Researchers and Activists 17
PREVALENCE ANDCHARACTERIST ICSOF SEXUAL COERCIONAND ABUSE
For many women and girls, sexual coercionand abuse are defining features of theirlives. Forced sexual contact can take placeat any time in a woman’s life and includesa range of behaviors, from forcible rape tononphysical forms of pressure that compelgirls and women to engage in sex againsttheir will. The touchstone of coercion isthat a woman lacks choice and faces severephysical, social, or economic consequencesif she resists sexual advances.
Studies indicate that the majority of non-consensual sex takes place among individu-als who know each other—spouses, familymembers, dating partners, or acquain-tances.86, 87 In fact, much nonconsensual sextakes place within consensual unions andincludes a woman being compelled to havesex when she does not want it, or toengage in types of sexual activity that shefinds degrading or humiliating.1, 88, 89
Much sexual coercion also takes placeagainst children and adolescents in bothindustrial and developing countries.Between one-third and two-thirds ofknown sexual assault victims are age 15 oryounger, according to justice system statis-tics and information from rape crisis cen-ters in Chile, Peru, Malaysia, Mexico,Panama, Papua New Guinea, and theUnited States.2
Sexual exploitation of children is wide-spread in virtually all societies. Child sex-ual abuse refers to any sexual act thatoccurs between an adult or older adoles-cent and a child, and any nonconsensualsexual contact between a child and a peer.Laws generally consider the issue of con-sent to be irrelevant in cases of sexualcontact by an adult with a child, definedvariously as someone under 13, 14, 15, or16 years of age.
Because of the taboo nature of thetopic, it is difficult to collect reliable figureson the prevalence of sexual abuse in child-hood. Nonetheless, the few representativesample surveys provide cause for concern.
V I O L E N C E A G A I N S T W O M E N A S A H E A L T H A N D D E V E L O P M E N T I S S U E
FIGURE 1.4 INTIMATE PARTNER VIOLENCE ACCORDING TO TYPES OFVIOLENCE (AMONG EVER-ABUSED WOMEN)
100 -
80 -
60 -
40 -
20 -
0 -
Bang
lades
h Ci
tyBa
nglad
esh
Provin
ceBr
azil C
ityBr
azil P
rovin
ceEth
iopia
Pro
vince
Japan
City
Nam
ibia
City
Peru
City
Peru
Provin
ceTh
ailan
d Ci
tyTh
ailan
d Pro
vince
Tanz
ania
City
Tanz
ania
Pro
vince
Serb
ia
Samo
a
■ sexual violence only ■ physical violence only ■ sexual and physical violence
(From WHO, 2005.20)
Percent
44
30
26
48
19
32
29
65
6
30
61
8
51
17
31
25
62
13
32
54
14
39
56
57
32
11
28
28
44
32
39
29
35
45
21
39
45
17
23
73
4
30
58
124

18 Researching Violence Against Women
A review of 25 studies worldwide indicatesthat 0 to 32 percent of women report thatthey experienced sexual abuse in child-hood (see Table 1.2). Although both girlsand boys can be victims of sexual abuse,most studies report that the prevalence ofabuse among girls is at least 1.5 to 3 timeshigher than among boys.90 Abuse amongboys may be underreported compared withabuse among girls, however.
Further data reveal that coercion may bean element in many young girls’ initiationinto sexual life. An increasing number ofstudies have begun to document that asubstantial number of young women’s first sexual experiences are forced orunwanted, especially among younger ado-lescents. Table 1.3 summarizes data from anumber of population-based surveys onthe prevalence of forced first sex, includingdata emerging from the WHO VAW Study.A plethora of studies now confirm that theyounger a girl is when she first has sex,the more likely she is to report her sexualdebut as forced.91
Trafficking in women and girls forforced labor and sexual exploitation isanother type of gender-based violence thathas grown rapidly during the past decade,largely as a result of war, displacement,and economic and social inequitiesbetween and within countries. Althoughreliable statistics on the number of womenand children who are trafficked are lack-ing, rough estimates suggest that from700,000 to 2 million women and girls aretrafficked across international borders everyyear.6, 92, 93 These women face many risks,including physical violence and rape, bothin their work and when trying to negotiatesafer-sex practices.
Another aspect of gender-based violencethat has been largely overlooked untilrecently is violence against women in situ-ations of armed conflict. Recent reportshave documented systematic rape in manyconflicts, including the former Yugoslavia,
Rwanda, Liberia, Sierra Leone, andUganda.94-96 These reports have highlightedthe extent to which rape has been used asa deliberate strategy to “destabilize popula-tion, advance ethnic cleansing, expresshatred for the enemy or supply combatantswith sexual services.”96 In 2002, theInternational Criminal Tribunal in TheHague recognized the seriousness of sex-ual offences in war as a crime againsthumanity. International relief agencies arealso calling attention to the precarious situ-ation of women in refugee settings whererape, child sexual abuse, intimate partnerviolence, and other forms of sexualexploitation are widespread.
THE EFFECTS OF VIOLENCEON WOMEN’S HEALTH
Gender-based violence is associated withserious health problems affecting bothwomen and children, including injuries,gynecological disorders, mental health dis-orders, adverse pregnancy outcomes, andsexually transmitted infections (STIs)(Figure 1.5). Violence can have direct con-sequences for women’s health, and it canincrease women’s risk of future ill health.Therefore, victimization, like tobacco oralcohol use, can best be conceptualized asa risk factor for a variety of diseases andconditions, rather than primarily as a healthproblem in and of itself.2, 4
Both population-based research andstudies of emergency room visits in theUnited States indicate that physical abuse isan important cause of injury amongwomen.97 Documented injuries sustainedfrom such physical abuse include contu-sions, concussions, lacerations, fractures,and gunshot wounds. Population-basedstudies indicate that 40 to 75 percent ofwomen who are physically abused by apartner report injuries due to violence atsome point in their life.2
Nevertheless, injury is not the most
C H A P T E R O N E

A Practical Guide for Researchers and Activists 19
V I O L E N C E A G A I N S T W O M E N A S A H E A L T H A N D D E V E L O P M E N T I S S U E
Country & Year (Ref. No.)
Australia 1997 98
Bangladesh 2002 20
Barbados 1993 99
Brazil 2002 20
Canada 1990 100
Costa Rica 1992 101
Ethiopia 2002 20
Germany 1992 102
Japan 2002 20
Malaysia 1996 103
Namibia 2002 20
New Zealand 1997 104
Nicaragua 1997 105
Norway (Oslo) 1996 106
Study Method & Sample
■ Retrospective study of 710women
■ Population-based survey ofwomen ages 15–49 (Dhaka1602, Matlab 1527)
■ National random sample of264 women
■ Population-based survey ofwomen ages 15–49 (SaoPaulo 1172, Pernambuco1473)
■ Population survey of 9953men and women age 15+
■ Retrospective survey ofuniversity students
■ Population-based survey of3014 women ages 15–49
■ Multiple-screen questionnaireanswered by 2,151 studentsin Würzburg and Leipzig
■ Population-based survey of1361 women ages 15–49
■ Retrospective self-administeredquestionnaire answered by616 paramedical students
■ Population-based survey of1492 women ages 15–49
■ Birth cohort of 520 girls,studied from birth to age 18
■ Anonymous self-administeredquestionnaire answered by134 men and 202 womenages 25–44 drawn frompopulation-based sample
■ Population-based sample of465 adolescents, ages13–19, followed for 6 years
Definition of ChildSexual Abuse
■ Sexual contact before the ageof 12 with perpetrator 5+years older; or unwanted sex-ual activity at ages 12-16
■ Unwanted sexual activity, con-tact and noncontact before theage of 15
■ Sexual contact that isunwanted or with a biologicalrelative; or before the age of16 with perpetrator 5+ yearsolder
■ Unwanted sexual activity, con-tact and noncontact before theage of 15
■ Unwanted sexual activity, con-tact and noncontact, whilegrowing up
■ Unwanted sexual activity, con-tact and noncontact; no agesspecified
■ Unwanted sexual activity, con-tact and noncontact before theage of 15
■ Distressing sexual activity, con-tact and noncontact, beforethe age of 14; or with perpe-trator 5+ years older
■ Unwanted sexual activity, con-tact and noncontact before theage of 15
■ Vaginal or anal penetration, orunsolicited sexual contact, orwitnessing exhibitionism beforethe age of 18
■ Unwanted sexual activity, con-tact and noncontact before theage of 15
■ Unwanted sexual activity, con-tact and noncontact, beforethe age of 16
■ Sexual contact, includingattempted penetration, beforethe age of 13 with perpetrator5+ years older; or nonconsen-sual activity over the age of 12
■ Sexual contact, including"intercourse after pressure,"occurring between a childbefore the age of 13 and anadult over the age of 17; orinvolving force
Prevalence
■ 20% of women report abuse
■ In Dhaka 7% of women; inMatlab 1% of women reportabuse
■ 30% of women report abuse
■ In Sao Paulo 8% of women; inPernambuco 6% of womenreport abuse
■ 13% of women, 4% of menreport abuse
■ 32% of women, 13% of menreport abuse
■ 0.2% of women report abuse
■ In Würzburg 16% of girls, 6%boys; in Leipzig 10% of girls,6% of boys report abuse
■ 10% of women report abuse
■ 8% of women, 2% of menreport abuse
■ 5% of women report abuse
■ 14% of girls report contactabuse; 17% report any abuse
■ 26% of women, 20% of menreport abuse
■ 17% of girls, 1% of boysreport abuse
TABLE 1.2 PREVALENCE OF CHILD SEXUAL ABUSE: SELECTED STUDIES, 1990–2003

20 Researching Violence Against Women
C H A P T E R O N E
Country & Year (Ref. No.)
Peru 2002 20
Samoa 2000 20
Serbia & Montenegro 2003 20
Spain 1995 107
Switzerland (Geneva) 1996 108
Switzerland (National) 1998 109
Thailand 2002 20
Tanzania 2002 20
United States 1997 110
United States (Midwest) 1997 111
United States (Washington State)1997 112
Study Method & Sample
■ Population-based survey ofwomen ages 15–49 (Lima1414, Cusco 1837)
■ Population-based survey of1640 women ages 15–49
■ Population-based survey of1453 women ages 15–49
■ Face-to-face interviews andself-administered question-naires answered by 895adults ages 18–60
■ Self-administered questionnaireanswered by 1193 9th gradestudents
■ National survey of 3993 girls,ages 15–20, enrolled inschools or professional trainingprograms
■ Population-based survey ofwomen ages 15–49(Bangkok 1534,Nakhonsawan 1280)
■ Population-based survey ofwomen ages 15–49 (Dar esSalaam 1816, Mbeya 1443)
■ National 10-year longitudinalstudy of women's drinking thatincluded questions about sex-ual abuse, answered by1099 women
■ Self-administered questionnaireanswered by 42,568 studentsin grades 7–12
■ Multiple-choice survey of3128 girls in grades 8,10and 12
Definition of ChildSexual Abuse
■ Unwanted sexual activity, con-tact and noncontact before theage of 15.
■ Unwanted sexual activity, con-tact and noncontact before theage of 15.
■ Unwanted sexual activity, con-tact and noncontact before theage of 15.
■ Unwanted sexual activity, con-tact and noncontact before theage of 17.
■ Unwanted sexual activity, con-tact and noncontact.
■ “Sexual victimization,” definedas “when someone in yourfamily, or someone else,touches you in a place youdidn’t want to be touched, ordoes something to you sexu-ally which they shouldn't havedone.”
■ Unwanted sexual activity, con-tact and noncontact before theage of 15.
■ Unwanted sexual activity, con-tact and noncontact before theage of 15.
■ Unwanted sexual activity, con-tact and noncontact, beforethe age of 18; or before theage of 13 with perpetrator 5+years older.
■ “Sexual abuse,” defined as“when someone in your familyor another person does sexualthings to you or makes you dosexual things to them that youdon’t want to do.”
■ “Sexual abuse,” defined as“when someone in your familyor someone else touches youin a sexual way in a placeyou didn’t want to betouched, or does something toyou sexually which theyshouldn’t have done.”
Prevalence
■ In Lima 20% of women; inCusco 8% of women reportabuse
■ 2% of women report abuse
■ 2% of women report abuse
■ 22% of women and 15% ofmen report abuse
■ 20% of girls, 3% of boysreport contact abuse; 34% ofgirls, 11% of boys report anyabuse
■ 19% of girls report abuse
■ In Bangkok 7.6% of women;in Nakhonsawan 4.7% ofwomen report abuse
■ In Dar es Salaam 4% ofwomen; in Mbeya 4% ofwomen report abuse
■ 21% of women report abuse
■ 12% of girls, 4% of boysreport abuse
■ 23% of all girls; 18% of 8thgraders, 24% of 10thgraders, 28% of 12thgraders report abuse
TABLE 1.2 PREVALENCE OF CHILD SEXUAL ABUSE: SELECTED STUDIES, 1990–2003
(Updated and adapted from Heise et al, 19992 and WHO, 2002.1)

A Practical Guide for Researchers and Activists 21
common physical health outcome of gen-der-based abuse. More common are “func-tional disorders”—ailments that frequentlyhave no identifiable cause, such as irritablebowel syndrome; gastrointestinal disorders;and various chronic pain syndromes,including chronic pelvic pain. Studies con-sistently link such disorders with a historyof physical or sexual abuse. Women whohave been abused also tend to experiencepoorer physical functioning, more physicalsymptoms, and more days in bed than do
V I O L E N C E A G A I N S T W O M E N A S A H E A L T H A N D D E V E L O P M E N T I S S U E
Percentage reporting Age first sexual intercourse
Country or Study Sample Group as forcedArea Population Year Size (years) Females Males
Bangladesh Dhaka 2002 1369 15–49 24
Bangladesh Matlab 2002 1326 15–49 30
Brazil Sao Paulo 2002 1051 15–49 3
Brazil Pernambuco 2002 1234 15–49 4
Cameroon Bamenda 1995 646 12–25 37 30
Caribbean Nine countries 1997–1998 15,695 10–18 48 32
Ethiopia Gurage 2002 2238 15–49 17
Ghana Three urban towns 1996 750 12–24 21 5
Japan Yokohama 2002 1116 15–49 0
Mozambique Maputo 1999 1659 13–18 19 7
Namibia Windhoek 2002 1357 15–49 2
New Zealand Dunedin 1993–1994 935 Birth cohort 7 0
Peru Lima 1995 611 16–17 40 11
Peru Lima 2002 1103 15–49 7
Peru Cusco 2002 1557 15–49 24
Samoa National 2002 1317 15–49 8
Serbia & Montenegro Belgrade 2002 1310 15–49 1
South Africa Transkei 1994–1995 1975 15–18 28 6
Tanzania Dar es Salaam 2002 1556 15–49 14
Tanzania Mbeya 2002 1287 15–49 17
Tanzania Mwanza 1996 892 12–19 29 7
Thailand Bangkok 2002 1051 15–49 4
Thailand Nakhonsawan 2002 1028 15–49 5
United States National 1995 2042 15–24 9 —
TABLE 1.3 PERCENTAGE OF MEN AND WOMEN REPORTING FORCED SEXUAL INITIATION:SELECTED POPULATION-BASED SURVEYS, 1993—2003
(From World Health Organization, 20021, 2005.20)
women who have not been abused.113-116
For many women, the psychologicalconsequences of abuse are even more seri-ous than its physical effects. The experi-ence of abuse often erodes women’sself-esteem and puts them at greater risk ofa variety of mental health problems,including depression, anxiety, phobias,post-traumatic stress disorder, and alcoholand drug abuse.2
Violence and sexual abuse also liebehind some of the most intractable

22 Researching Violence Against Women
reproductive health issues of our times—unwanted pregnancies, HIV and otherSTIs, and complications of pregnancy.Physical violence and sexual abuse canput women at risk of infection andunwanted pregnancies directly, if womenare forced to have sex, for example, or ifthey fear using contraception or condomsbecause of their partner’s reaction. A his-tory of sexual abuse in childhood also canlead to unwanted pregnancies and STIsindirectly by increasing sexual risk-takingin adolescence and adulthood. There is agrowing body of research indicating thatviolence may increase women’s suscepti-bility to HIV infection.117-120 Studies carriedout in Tanzania and South Africa foundthat seropositive women were more likelythan their seronegative peers to reportphysical partner abuse. The results indi-cate that women with violent or control-ling male partners are at increased risk ofHIV infection. There is little informationas yet to indicate how violence increaseswomen’s risk for HIV. Dunkle and col-leagues suggest that abusive men aremore likely to have HIV and imposerisky sexual practices on their partners.There are also indications that disclosureof HIV status may put women at risk forviolence.118
Violence can also be a risk factor duringpregnancy. Studies from around the worlddemonstrate that violence during preg-nancy is not a rare phenomenon. Withinthe United States, for example, between 1percent and 20 percent of currently preg-nant women report physical violence, withthe majority of findings between 4 percentand 8 percent.5 The differences are duepartly to differences in the way womenwere asked about violence.3, 5, 121, 122 A recentreview found that the prevalence of abuseduring pregnancy is 3 to 11 percent inindustrialized countries outside of NorthAmerica and between 4 and 32 percent indeveloping countries, including studies
from China, Egypt, Ethiopia, Mexico, India,Nicaragua, Pakistan, Saudi Arabia, andSouth Africa.3
Violence during pregnancy can haveserious health consequences for womenand their children.2 Documented effectsinclude delayed prenatal care, inadequateweight gain, increased smoking and sub-stance abuse, STIs, vaginal and cervicalinfections, kidney infections, miscarriagesand abortions, premature labor, fetal dis-tress, and bleeding during pregnancy.4
Recent research has focused on the rela-tionship between violence in pregnancyand low birth weight, a leading cause ofinfant deaths in the developing world.Although research is still emerging, find-ings of six different studies performed inthe United States, Mexico, and Nicaraguasuggest that violence during pregnancycontributes to low birth weight, pre-termdelivery, and to fetal growth retardation, atleast in some settings.121, 123 A recent metaanalysis of existing studies confirms thatintimate partner violence during pregnancyis indeed associated with a significant,albeit small, reduction in birth weight.124
In its most extreme form, violence killswomen. Worldwide, an estimated 40 tomore than 70 percent of homicides ofwomen are perpetrated by intimate part-ners, frequently in the context of an abu-sive relationship.125 By contrast, only a smallpercentage of men who are murdered arekilled by their female partners, and in manysuch cases, the women are defendingthemselves or retaliating against abusivemen.126 A study of female homicide inSouth Africa found that intimate femicide(female murder by an intimate partner)accounted for 41 percent of all femalehomicides. This study estimated that awoman is killed by her intimate partner inSouth Africa every six hours.127 Violence isalso a significant risk factor for suicide.Studies in numerous countries have foundthat women who have suffered domestic
C H A P T E R O N E

A Practical Guide for Researchers and Activists 23
V I O L E N C E A G A I N S T W O M E N A S A H E A L T H A N D D E V E L O P M E N T I S S U E
Gender-Based VictimizationChild sexual abuse
Sexual assaultPhysical abuse
Nonfatal Outcomes Fatal Outcomes
Direct & Indirect
Physical Health Mental Health
■ Injury ■ Post traumatic stress ■ Femicide
■ Functional impairment ■ Depression ■ Suicide
■ Physical symptoms ■ Anxiety ■ Maternal mortality
■ Poor subjective health ■ Phobias/panic disorders ■ AIDS-related
■ Permanent disability ■ Eating disorders
■ Sexual dysfunction
Injurious Health Behaviors ■ Low self-esteem
■ Smoking ■ Mental distress
■ Alcohol and drug use ■ Substance abuse disorders
■ Sexual risk-taking
■ Physical inactivity
■ Overeating
Functional Disorders
■ Chronic pain syndromes
■ Irritable bowel syndrome
■ Gastrointestinal disorders
■ Somatic complaints
■ Fibromyalgia
Reproductive Health
■ Unwanted pregnancy
■ STIs/HIV
■ Gynecological disorders
■ Unsafe abortion
■ Pregnancy complications
■ Miscarriage/low birth weight
■ Pelvic inflammatory disease
FIGURE 1.5 HEALTH OUTCOMES OF VIOLENCE AGAINST WOMEN
(From Heise et al, 1999.2)

24 Researching Violence Against Women
violence or sexual assault are much morelikely to have had suicidal thoughts, or tohave attempted to kill themselves.19
EXPLAINING GENDER-BASED VIOLENCE
Violence against women is widespread, butit is not universal. Anthropologists havedocumented small-scale societies—such asthe Wape of Papua New Guinea—wheredomestic violence is virtually absent.128, 129
This reality stands as testament to the factthat social relations can be organized tominimize abuse.
Why is violence more widespread insome places than in others? Increasingly,researchers are using an “ecological frame-work” to understand the interplay of per-sonal, situational, and socio-cultural factorsthat combine to cause abuse.21, 130-133 In thisframework, violence against women resultsfrom the interaction of factors at differentlevels of the social environment (Figure 1.6).
The framework can best be visualized asfour concentric circles. The innermost cir-cle represents the biological and personalhistory that each individual brings to his orher behavior in relationships. The secondcircle represents the immediate context inwhich abuse takes place: frequently thefamily or other intimate or acquaintancerelationship. The third circle represents theinstitutions and social structures, both for-mal and informal, in which relationshipsare embedded, such as neighborhoods, theworkplace, social networks, and peergroups. The fourth, outermost circle is theeconomic and social environment, includ-ing cultural norms.
A wide range of studies shows that several factors at each of these levelsincrease the likelihood that a man willabuse his partner:
■ At the individual level, the male wasabused as a child or witnessed marital
violence in the home, had an absent orrejecting father, or frequently uses alco-hol. A recent review of nationally repre-sentative surveys in nine countriesfound that for women, low educationalattainment, being under 25 years of age,having witnessed her father’s violenceagainst her mother, living in an urbanarea, and low socio-economic statuswere consistently associated with anincreased risk of abuse.24
■ At the level of the family and rela-tionship, the male controls wealth anddecision making within the family andmarital conflict is frequent.
■ At the community level, women areisolated with reduced mobility and lackof social support. Male peer groupscondone and legitimize men’s violence.
■ At the societal level, gender roles arerigidly defined and enforced and theconcept of masculinity is linked totoughness, male honor, or dominance.The prevailing culture tolerates physicalpunishment of women and children,accepts violence as a means to settleinterpersonal disputes, and perpetuatesthe notion that men “own” women.
The ecological framework combinesindividual level risk factors with family,community, and society level factors identi-fied through cross cultural studies, andhelps explain why some societies andsome individuals are more violent thanothers, and why women, especially wives,are so much more likely to be the victimsof violence within the family. Other factorscombine to protect some women. Forexample, women who have authority andpower outside the family tend to experi-ence lower levels of abuse in intimate part-nerships. Likewise, when family membersand friends intervene promptly, they
C H A P T E R O N E

A Practical Guide for Researchers and Activists 25
appear to reduce the likelihood of domes-tic violence. In contrast, wives are morefrequently abused in cultures where familyaffairs are considered “private” and outsidepublic scrutiny.
Justifications for violence frequentlyevolve from gender norms, that is, socialnorms about the proper roles and respon-sibilities of men and women. Many cul-tures hold that a man has the right tocontrol his wife’s behavior and that womenwho challenge that right—even by askingfor household money or by expressing theneeds of the children—may be punished.In countries as different as Bangladesh,Cambodia, India, Mexico, Nigeria, Pakistan,Papua New Guinea, Nicaragua, Tanzania,and Zimbabwe, studies find that violence isfrequently viewed as physical chastise-ment—the husband’s right to “correct” anerring wife.2 As one husband said in afocus group discussion in Tamil Nadu,India, “If it is a great mistake, then the hus-band is justified in beating his wife. Whynot? A cow will not be obedient withoutbeatings.”134
Worldwide, studies identify a consistentlist of events that are said to “trigger” vio-lence.130 These include: not obeying thehusband, talking back, not having foodready on time, failing to care adequatelyfor the children or home, questioning himabout money or girlfriends, going some-where without his permission, refusing himsex, or expressing suspicions of infidelity.All of these represent transgressions ofdominant gender norms in many societies.
Although the ecological framework hasgained broad acceptance for conceptualiz-ing violence, there have been few attemptsto explore how individual and communitylevel risk factors relate to each other andultimately influence women’s vulnerabilityto violence. One study performed in theUnited States found that the socio-eco-nomic status of the neighborhood had agreater impact on the risk of violence than
individual household income levels.135 Astudy in Bangladesh found that someaspects of women’s status could eitherincrease or decrease a woman’s risk ofbeing beaten, depending on the socio-cul-tural conditions of the community she livesin. In one site, characterized by more con-servative norms regarding women’s rolesand status, women with greater personalautonomy and those who participated for ashort time in savings and credit groupsexperienced more violence than womenwith less autonomy. Community-levelmeasures of women’s status had no effecton the risk of violence.
The opposite was true in the less conser-vative setting where women had betteroverall status. In this site, individual meas-ures of autonomy and participation in creditschemes had no impact on the risk of vio-lence, whereas living in a community wheremore women participated in credit groupsand where women had a higher status over-all had a protective effect. These findingssuggest that the same condition (mobility orparticipating in a credit group) may havecompletely different effects on a woman’srisk of violence, according to whether theactivity is seen as acceptable by communitynorms. These findings underscore the com-plexity of these issues and the dangers inapplying knowledge gained from one site toanother without understanding of thebroader cultural context.136
HOW DO WOMENRESPOND TO ABUSE?
Most abused women are not passive vic-tims, but use active strategies to maximizetheir safety and that of their children.Some women resist, others flee, and stillothers attempt to keep the peace by capit-ulating to their husband’s demands. Whatmay seem to an observer to be lack ofresponse to living with violence may infact be a woman’s strategic assessment of
V I O L E N C E A G A I N S T W O M E N A S A H E A L T H A N D D E V E L O P M E N T I S S U E

26 Researching Violence Against Women
what it takes to survive and to protect her-self and her children.
A woman’s response to abuse is oftenlimited by the options available to her.Women consistently cite similar reasons forremaining in abusive relationships: fear ofretribution, lack of other means of eco-nomic support, concern for the children,emotional dependence, lack of supportfrom family and friends, and an abidinghope that “he will change.” In some coun-tries, women say that the social unaccept-ability of being single or divorced poses anadditional barrier that keeps them fromleaving destructive marriages.2
At the same time, denial and fear ofsocial stigma often prevent women fromreaching out for help. In numerous sur-veys, for example, from 22 to almost 70percent of abused women say that untilthe interview they never told anyone abouttheir abuse. Those who reach out do soprimarily to family members and friends.Few have ever contacted the police.1, 20
Despite the obstacles, many womeneventually do leave violent partners—evenif after many years. In a study in León,Nicaragua, for example, 70 percent ofabused women eventually left theirabusers. The median time that womenspent in a violent relationship was sixyears. Younger women were likely to leavesooner than older women.137
Studies suggest a consistent set of factorsthat propel a woman to leave an abusiverelationship: The violence gets more severeand triggers a realization that her partner isnot going to change, or the violencebegins to take a toll on the children.Women also cite emotional and logisticalsupport from family or friends as pivotal intheir decision to leave.2
Leaving an abusive relationship is a multi-stage process. The process often includesperiods of denial, self-blame, and endurancebefore women recognize the abuse as apattern and identify with other women inthe same situation, thereby beginning to
C H A P T E R O N E
FIGURE 1.6. AN ECOLOGICAL FRAMEWORK FOR EXPLAINING GENDER-BASED VIOLENCE
■ Norms and lawsgranting men controlover female behavior
■ Violence accepted forresolving conflict
■ Masculinity linked todominance, honor oragression
■ Isolation ofwomen andfamily
■ Delinquent peergroups
■ Low socio -economic status
■ Marital conflict■ Male control of
wealth anddecision makingin the family
■ Poverty■ Unemployment
■ Being male■ Witnessing marital
conflict as a child■ Absent or rejecting
father■ Being abused as
a child■ Alcohol use
Societal Community Family Individual
(From Heise, 1998.130)

A Practical Guide for Researchers and Activists 27
disengage and recover. Most women leaveand return several times before they finallyleave once and for all.138 Leaving does notnecessarily guarantee a woman’s safety,however, because violence may continueeven after a woman leaves. In fact, awoman’s risk of being murdered by herabuser is often greatest immediately afterseparation.139
CHALLENGES FORINTERNATIONAL RESEARCH ON GENDER-BASED VIOLENCE
Nearly 30 years of groundbreakingresearch in the field of gender-based vio-lence has greatly expanded internationalawareness of the dimensions and dynamicsof violence. However, there are still manygaps in our current state of knowledge.Researchers interested in gender-based vio-lence from a public health perspective facea number of important challenges.
■ The scarcity of population-baseddata limits our understanding ofhow violence affects differentgroups of women. Until very recently,the majority of research was been car-ried out with nonrepresentative samplesof women, often those who haveattended shelters or other services forvictims. Although these studies are use-ful for understanding the dynamics ofabuse, they do not tell us how manywomen overall are affected, nor provideinformation about individuals who donot seek services. According to mostestimates, these women greatly outnum-ber those who seek help.
■ Most international prevalence figureson violence are not comparable. Thisis due mainly to inconsistencies in theway that violence is conceptualized andmeasured. Researchers need to develop
consensus around violence researchmethods that allow us to make mean-ingful comparisons between studies.Methodological consistency refers notonly to defining violence using similarcriteria, but also the use of measures tominimize underreporting of violence,such as ensuring privacy during theinterview and providing interviewerswith special training on violence.139
■ Research on violence may putwomen at risk. Many researchers pointout that research on violence involves anumber of inherent risks to both respon-dents and interviewers.140 The WorldHealth Organization has developed a setof guidelines to minimize the risk ofharm to researchers and participants.141
However, these guidelines are just nowbeing incorporated more widely intointernational research practice.
■ More public health research isneeded to understand how violenceaffects the health of women andchildren in different settings. Studiesof battered women consistently demon-strate the negative impact of abuse onwomen’s psychological status and repro-ductive health, and emerging epidemio-logical studies indicate that violencetowards mothers may even affect infantbirth weight and survival. However,more research is needed to determinewhat proportion of women’s overallmental and physical health problems isassociated with violence and to investi-gate the mechanisms through whichviolence affects health.
■ More cross-cultural research isneeded to reveal how societal normsand institutions promote or discour-age violent behavior. Most researchersagree that cultural norms can greatlyaffect the extent and characteristics of
V I O L E N C E A G A I N S T W O M E N A S A H E A L T H A N D D E V E L O P M E N T I S S U E

28 Researching Violence Against Women
violence, as well as the way that spe-cific acts are interpreted in differentsocieties. Nonetheless, there have beenfew systematic attempts to comparethese issues in different settings. Mosttheories about the dynamics of abusehave been based on the experiences ofUS and European women, and it isunclear how relevant these are towomen from other cultures.
■ Research evaluating differentapproaches to violence prevention isscarce. Although there has been anenormous increase in both communityand clinic-based programs to preventviolence and to support abused womenand girls, few programs have been sys-tematically documented or evaluated.For example, many activists and profes-sional associations in the United Statescurrently encourage health providers toask each woman at every visit whethershe has been abused. However, there islittle information about what happens towomen after disclosing violence, orwhether asking women is an effectivetool for enhancing women’s safety. Inparticular, we need to develop criteriafor assessing whether practices that areeffective in one setting are likely to berelevant or feasible in another, very dif-ferent setting.
The greatest challenge facingresearchers in the field of violence is tolearn from past mistakes, to identify “bestpractices,” and to find out what makesthem successful so that we can channelresources and efforts where they are mostlikely to make a difference.
1. World Health Organization. World Report onViolence and Health. Geneva, Switzerland:World Health Organization; 2002.
2. Heise L, Ellsberg M, Gottemoeller M. EndingViolence Against Women. Baltimore: John’sHopkins University School of Public Health;Population Information Program; 1999. ReportNo.: Series L, No. 11.
3. Campbell J, Garcia-Moreno C, Sharps P. Abuseduring pregnancy in industrialized and devel-oping countries. Violence against Women.2004;10(7):770-789.
4. Campbell JC. Health consequences of inti-mate partner violence. Lancet.2002;359(9314):1331-1336.
5. Gazmararian JA, Lazorick S, Spitz AM, et al.Prevalence of violence against pregnantwomen. Journal of the American MedicalAssociation. 1996;275(24):1915-1920.
6. Watts C, Zimmerman C. Violence againstwomen: Global scope and magnitude. Lancet.2002;359(9313):1232-1237.
7. Shane B, Ellsberg M. Violence Against Women:Effects on Reproductive Health. Seattle,Washington: PATH, UNFPA; 2002. Report No.:20 (1).
8. Denzin NK. Toward a phenomenology ofdomestic family violence. American Journal ofSociology. 1984;90:483-513.
9. Straus MA, Gelles RJ. Societal change andchange in family violence from 1975 to 1985 asrevealed by two national surveys. Journal ofMarriage and the Family. 1986;48:465-480.
10. United Nations General Assembly. Declarationon the Elimination of Violence Against Women.In: 85th Plenary Meeting. December 20, 1993.Geneva, Switzerland; 1993.
11. Fischbach RL, Herbert B. Domestic violenceand mental health: Correlates and conundrumswithin and across cultures. Social Science andMedicine. 1997;45(8):1161-1176.
12. Johnson J, Sacco V. Researching violenceagainst women: Statistics Canada’s nationalsurvey. Canadian Journal of Criminology.1995;37:281-304.
13. Kornblit AL. Domestic violence: An emerginghealth issue. Social Science and Medicine.1994;39:1181-1188.
14. Claramunt MC. Casitas Quebradas: El Problemade la Violencia Doméstica en Costa Rica. SanJosé: Editorial Universidad Estatal a Distancia;1997.
15. Walker L. The Battered Woman. New York:Harper and Row; 1979.
C H A P T E R O N E

A Practical Guide for Researchers and Activists 29
16. Garcia Moreno C, Watts C, Jansen H, EllsbergM, Heise L. Responding to violence againstwomen: WHO’s Multi-country Study onWomen’s Health and Domestic Violence.Health and Human Rights. 2003;6(2):112-127.
17. Gossaye Y, Deyessa N, Berhane Y, et al.Women’s health and life events study in ruralEthiopia. Ethiopian Journal of HealthDevelopment. 2003;17(Second Special Issue):1-49.
18. Raikes A. Pregnancy, Birthing and FamilyPlanning in Kenya: Changing Patterns ofBehaviour: A Health Service Utilization Study inKisii District. Copenhagen, Denmark: Centre forDevelopment Research; 1990.
19. Central Bureau of Statistics (CBS) [Kenya],Ministry of Health [Kenya], ORC Macro. KenyaDemographic and Health Survey 2003.Calverton, Maryland: CBS, MOH, and ORCMacro; 2004.
20. World Health Organization. WHO Multi-countryStudy on Women’s Health and DomesticViolence Against Women: Report on the FirstResults. Geneva, Switzerland: WHO; 2005.
21. Jewkes R, Levin J, Penn-Kekana L. Risk factorsfor domestic violence: Findings from a SouthAfrican cross-sectional study. Social Scienceand Medicine. 2002;55(9):1603.-1617.
22. Macro International, South Africa Departmentof Health. South Africa Demographic andHealth Survey 1998: Preliminary Report. DHSsurvey. Calverton, Maryland: MacroInternational; 1998.
23. Blanc AK, Wolff B, Gage AJ, et al. NegotiatingReproductive Outcomes in Uganda. DHSSurvey: Institute of Statistics and AppliedEconomics and Macro International Inc; 1996.
24. Kishor S, Johnson K. Domestic Violence in NineDeveloping Countries: A Comparative Study.Calverton, Maryland: Macro International; 2004.
25. Watts C, Ndlovu M, Keogh E, Kwaramb R.Withholding of sex and forced sex: Dimensionsof violence against Zimbabwean women.Reproductive Health Matters. 1998;6:57-65.
26. Handwerker WP. Power and gender: Violenceand affection experienced by children inBarbados, West Indies. Med Anthropol.1996;17(2):101-128.
27. Larrain SH. Violencia Puertas Adentro: LaMujer Golpeada. Santiago, Chile: EditorialUniversitaria; 1994.
28. Morrison AR, Orlando MB. Social andEconomic Costs of Domestic Violence: Chileand Nicaragua. In: Morrison AR, Biehl ML, edi-tors. Too Close to Home: Domestic Violence inthe Americas. Washington, DC: Inter-AmericanDevelopment Bank; 1999. 51-80.
29. Hassan F, Sadowski L, Shrikant B, et al.Physical intimate partner violence in Chile,Egypt, India and the Philippines. Injury Controland Safety Promotion. 2004;2:111-116.
30. PROFAMILIA. Encuesta Nacional deDemografia y Salud 1995. Bogotá, Colombia:PROFAMILIA and Macro International; 1995.
31. PROFAMILIA. Salud Sexual y Reproductiva:Resultados Encuesta Nacional de Demografía ySalud 2000. Bogotá: Asociación Probienestarde la Familia Colombiana; 2000.
32. CEPAR C. ENDEMAIN-94: EncuestaDemográfica y de Salud Materna e Infantil:Informe General. Quito, Ecuador: Centers forDisease Control, Centro de Estudios dePoblación y Desarrollo Social; 1995.
33. Asociación Demográfica Salvadoreña. EncuestaNacional de Salud Familiar de 2002-2003. SanSalvador, El Salvador: ADS, Centers for DiseaseControl; 2002.
34. Ministerio de Salud Publica y Asistencia Social,Centers for Disease Control and Prevention.Guatemala, Encuesta Nacional de SaludMaterno Infantil 2002. Guatemala City,Guatemala: MSPAS, CDC; 2003.
35. Secretaría de Salud Honduras. EncuestaNacional de Epidemiología y Salud Familiar,Encuesta Nacional de Salud Masculina, 2001.Atlanta, Georgia: Centers for Disease Control;2002.
36. Ramirez J, et al. Mujeres de Guadalajara y vio-lencia doméstica: Resultados de un estudiopiloto. Cadernos de Saude Pública.1996;12(3):405-409.
37. Granados M. Salud Reproductiva y ViolenciaContra la Mujer: Un Análisis Desde laPerspectiva de Género. Nuevo León, Mexico:Asociación Mexicana de Población (AMEP),Consejo Estatal de Población, Nuevo León(COESPO), El Colegio de México; 1996.
38. Instituto Nacional de Estadística Geografía eInformática. Encuesta Nacional sobre laDinámica de las Relaciones en los Hogares2003 (ENDIREH). Distrito Federal, México:Instituto Nacional de Estadística, Geografía eInformática, Instituto Nacional de las Mujeres,Fondo de Población de Naciones Unidas; 2004.
39. Ellsberg MC, Peña R, Herrera A, Liljestrand J,Winkvist A. Wife abuse among women ofchildbearing age in Nicaragua. AmericanJournal of Public Health. 1999;89(2):241-244.
40. Ellsberg M, Heise L, Peña R, Agurto S, WinkvistA. Researching domestic violence against women:Methodological and ethical considerations. Studiesin Family Planning. 2001;32(1):1-16.
V I O L E N C E A G A I N S T W O M E N A S A H E A L T H A N D D E V E L O P M E N T I S S U E

30 Researching Violence Against Women
41. Rosales J, Loaiza E, Primante D, et al. EncuestaNicaraguense de Demografia y Salud, 1998.Managua, Nicaragua: Instituto Nacional deEstadisticas y Censos (INEC); 1999.
42. CEPEP. Encuesta Nacional de Demografia ySalud Reproductiva, 1995-1996. Asunción,Paraguay: Centro Paraguayo de Estudios dePoblación, Centers for Disease Control andPrevention, USAID; 1997.
43. CEPEP. Encuesta Nacional de Demografía ySalud Sexual y Reproductiva 2004: ENDSSR2004. Informe Resumido. Asunción, Paraguay:Centro Paraguayo de Estudios de Población,Centers for Disease Control and Prevention,USAID; 2004.
44. Dávila AL, Ramos G, Mattei H. Encuesta deSalud Reproductiva: Puerto Rico, 1995-96. SanJuan, Puerto Rico: CDC; 1998.
45. Traverso MT. Violencia en la Pareja: La CaraOculta de la Relación. Washington, DC: IDB;1999.
46. Johnson H. Dangerous Domains: ViolenceAgainst Women in Canada. Ontario, Canada:International Thomson Publishing; 1996.
47. Statistics Canada. Family Violence in Canada: AStatistical Profile 2000. Ottawa, Canada:Statistics Canada; 2000.
48. Tjaden P, Thoennes N. Extent, Nature andConsequences of Intimate Partner Violence:Findings from the National Violence AgainstWomen Survey. Washington, DC: NationalInstitute of Justice, Centers for Disease Controland Prevention; 2000.
49. Australian Statistics Bureau (ASB). Women’sSafety: Australia. Belconnen, Australia: ASB;1996.
50. Mouzos J, Makkai T. Women’s Experience ofMale Violence: Findings from the AustralianComponent of the International Violence AgainstWomen Survey (IVAWS). Canberra, Australia:Australian Institute of Criminology; 2004.
51. Schuler SR, Hashemi SM, Riley AP, Akhter S.Credit programs, patriarchy and men’s violenceagainst women in rural Bangladesh. SocialScience and Medicine. 1996;43(12):1729-1742.
52. Steele F, Amin S, Naved RT. Savings/creditgroup formation and change in contraception.Demography. 2001;38(2):267-282.
53. Nelson E, Zimmerman C. Household Survey onDomestic Violence in Cambodia. Phnom Penh,Cambodia: Ministry of Women’s Affairs, ProjectAgainst Domestic Violence (PADV); 1996.
54. Parish W, Wang T, Laumann E, Pan S, Luo Y.Intimate partner violence in China: Nationalprevalence, risk factors and associated healthproblems. International Family PlanningPerspectives. 2004;30(4):174-181.
55. Hakimi M, Nur Hayati E, Ellsberg M, WinkvistA. Silence for the Sake of Harmony: DomesticViolence and Health in Central Java, Indonesia.Yogyakarta, Indonesia: Gadjah Mada University,PATH, Rifka Annisa, Umeå Univeristy; 2002.
56. Fanslow J, Robinson EM. Violence againstwomen in New Zealand: Prevalence and healthconsequences. The New Zealand MedicalJournal. 2004;117(1206):1173-1184.
57. Toft S, Bonnell S. Marriage and DomesticViolence in Rural Papua New Guinea,Occasional Paper No. 18, 1985. Boroko, PapuaNew Guinea: Law Reform Commission; 1985.
58. Macro International, National Statistics Office ofPhilippines. National Safe Motherhood Survey,1993. Manila, Philippines: National StatisticsOffice, Macro International; 1994.
59. Cabaraban M, Morales B. Social and EconomicConsequences for Family Planning Use inSouthern Philippines. Cagayan de Oro City,Philippines: Research Institute for MindanaoCulture; 1998.
60. Kim K-I, Cho Y-G. Epidemiological Survey ofSpousal Abuse in Korea. In: Viano EC, ed.Intimate Violence: Interdisciplinary Perspectives.Washington, DC: Hemisphere Publishing Corp.;1992. p. 277-282.
61. Krantz G. Domestic violence against women: Apopulation-based study in Vietnam. Stockholm;2003.
62. Herold J, Seither R, Ylli A, et al. AlbaniaReproductive Health Survey 2002: PreliminaryReport. Tirana, Albania: Institute of PublicHealth, Albania Ministry of Health, Institute ofStatistics, CDC-Altanta; 2003.
63. Serbanescu F, Morris L, Rahimova S, Stupp P.Reproductive Health Survey, Azerbaijan, 2001.Final Report. Atlanta, Georgia: AzerbaijanMinistry of Health and Centers for DiseaseControl and Prevention; 2003.
64. Heiskanen M, Piisspa M. Faith, Hope,Battering: A survey of men’s violence againstwomen in Finland. Helsinki, Finland: StatisticsFinland, Council for Equality; 1998.
65. Jaspard M, Brown E, Condon S, et al. LesViolences enver les Femmes en France: UneEnquete Nationale. Paris, France: Idup, Ined,CNRS, Universite de Paris Dauphine; 2001.
C H A P T E R O N E

A Practical Guide for Researchers and Activists 31
66. Serbanescu F, Morris L, Nutsubidze N, ImnadzeP, Shaknazarova M. Reproductive Health SurveyGeorgia, 1999-2000. Final Report. Atlanta,Georgia: Georgian National Center for DiseaseControl, Centers for Disease Control andPrevention; 2001.
67. Federal Ministry for Family Affairs, SeniorCitizens, Women and Youth (BMFSFJ). Health,Well-being and Personal Safety of Women inGermany: A Representative Study of Women inGermany. Bonn, Germany: BMFSFJ; 2004.
68. Women’s Issues Information Centre (WHC),United Nations Development Fund for Women(UNIFEM). Violence against Women in Lithuania.Vilnius, Lithuania: WHC, UNIFEM; 1999.
69. Römkens R. Prevalence of wife abuse in theNetherlands: Combining quantitative and quali-tative methods in survey research. Journal ofInterpersonal Violence. 1997;12:99-125.
70. Schei B, Bakketeig LS. Gynaecological impactof sexual and physical abuse by spouse. Astudy of a random sample of Norwegianwomen. British Journal of Obstetrics andGynaecology. 1989;96(12):1379-1383.
71. Schei B. Report from the First NationalNorwegian Study on Violence against Women.Oslo, Norway: Statistics Norway; forthcoming.
72. Serbanescu F, Morris L, Stratila M, Bivol O.Reproductive Health Survey, Moldova, 1997.Atlanta, Georgia: Institute for Mother and ChildHealth Care and Centers for Disease Controland Prevention; 1998.
73. Serbanescu F, Morris L, Marin M. ReproductiveHealth Survey, Romania, 1999. Final Report.Atlanta, Georgia: Romanian Association ofPublic Health and Management and Centers forDisease Control and Prevention; 2001.
74. Russian Center for Public Opinion and MarketResearch, Centers for Disease Control andPrevention. 1999 Russian Women’s ReproductiveHealth Survey: A Follow-up of Three Sites. FinalReport. Atlanta, Georgia: Centers for DiseaseControl and Prevention; 2000.
75. Lundgren E, Heimer G, Westerstand J,Kalliokoski A-M. Captured Queen: Men’sViolence Against Women in “Equal” Sweden: APrevalence Study. Umeå, Sweden: FritzesOffentliga Publikationer; 2001.
76. Gillioz L, De Puy J, Ducret V. Domination etViolence Envers la Femme dans le Couple.Geneva, Switzerland: Editions Payot Lausanne;1997.
77. Killias M, Simonin M, De Puy J. ViolenceExperienced by Women in Switzerland overtheir Lifespan. Results of the InternationalViolence against Women Survey (IVAWS). Berne,Switzerland: Staempfli Publishers Ltd; 2005.
78. Ilkkaracan P. Exploring the context of women’ssexuality in eastern Turkey. ReproductiveHealth Matters. 1998;6(12).
79. KIIS, CDC, USAID. 1999 Ukraine ReproductiveHealth Survey. Kiev, Ukraine: Kiev InternationalInstitute of Sociology, Centers for DiseaseControl and Prevention, U.S.Agency forInternational Development; 2001.
80. Mooney J. The Hidden Figure: DomesticViolence in North London. London, UK:Middlesex University; 1993.
81. Walby S, Allen J. Domestic Violence, SexualAssault and Stalking: Findings from the BritishCrime Survey. London, U.K.: Home OfficeResearch, Development and StatisticsDirectorate; 2004.
82. El-Zanaty F, Hussein EM, Shawky GA, Way AA,Kishor S. Egypt Demographic and HealthSurvey 1995. Calverton, Maryland: MacroInternational; 1996.
83. Haj-Yahia MM. The First National Survey ofAbuse and Battering Against Arab Women fromIsrael: Preliminary Results: Unpublished; 1997.
84. Haj-Yahia MM. The Incidence of Wife Abuseand Battering and Some Socio-demographicCorrelates as Revealed in Two National Surveysin Palestinian Society. Ramallah, ThePalestinian Authority: Besir Center for Researchand Development; 1998.
85. Sadowski L, Hunter W, Bangdiwala S, Munoz S.The world studies of abuse in the family envi-ronment (WorldSAFE): A model of a multi-national study of family violence. InjuryControl and Safety Promotion. 2004;11(2):81-90.
86. Heise L, Moore K, Toubia N. Sexual Coercionand Women’s Reproductive Health: A Focus onResearch. New York, New York: PopulationCouncil; 1995.
87. World Health Organization. Violence AgainstWomen: A Priority Health Issue. Fact sheets.Geneva, Switzerland: World HealthOrganization; 1997.
88. Jewkes R, Levin J, Mbananga N, Bradshaw D.Rape of girls in South Africa. Lancet.2002;359(9303):319-320.
89. Jewkes R, Abrahams N. The epidemiology ofrape and sexual coercion in South Africa: Anoverview. Social Science and Medicine.2002;55(7):1231-1244.
V I O L E N C E A G A I N S T W O M E N A S A H E A L T H A N D D E V E L O P M E N T I S S U E

32 Researching Violence Against Women
90. Finkelhor D. The international epidemiology ofchild sexual abuse. Child Abuse and Neglect.1994;18(5):409-417.
91. Jejeebhoy S, Bott S. Non-consensual SexualExperiences of Young People: A Review of theEvidence from Developing Countries. South andEast Asia Regional Working Papers. New Delhi,India: Population Council; 2003. Report No.: 16.
92. Zimmerman C, Yun K, Shvab I, et al. TheHealth Risks and Consequences of Traffickingin Women and Adolescents: Findings from aEuropean Study. London, United Kingdom:London School of Hygiene and TropicalMedicine (LSHTM); 2003.
93. Orhant M, Murphy E. Trafficking in Persons. In:Murphy E, Ringheim K, editors. ReproductiveHealth and Rights: Reaching the HardlyReached. Washington, DC: PATH; 2002.
94. Swiss S, Jennings PJ, Aryee GV, et al. Violenceagainst women during the Liberian civil con-flict. Journal of the American MedicalAssociation. 1998;279:625-629.
95. Ward J. If Not Now, When? Addressing Gender-based Violence in Refugee, Internally Displacedand Post-conflict Settings: A Global Overview.New York, New York: Reproductive HealthResponse in Conflict Consortium; 2002.
96. Ward J, Vann B. Gender-based violence inrefugee settings. Lancet. 2002;360 Suppl:s13-14.
97. Kyriacou DN, Anglin D, Taliaferro E, et al. Riskfactors for injury to women from domestic vio-lence against women. New England Journal ofMedicine. 1999;341(25):1892-1898.
98. Fleming JM. Prevalence of childhood sexualabuse in a community sample of Australianwomen. Medical Journal of Australia.1997;166(2):65-68.
99. Handwerker WP. Gender power differencesbetween parents and high-risk sexual behaviorby their children: AIDS/STD risk factors extendto a prior generation. Journal of Women’sHealth. 1993;2(3):301-316.
100. MacMillan HL, Fleming JE, Trocme N, et al.Prevalence of child physical and sexual abusein the community. Results from the OntarioHealth Supplement. Journal of the AmericanMedical Association. 1997;278(2):131-135.
101. Krugman S, Mata L, Krugman R. Sexual abuseand corporal punishment during childhood: Apilot retrospective survey of university studentsin Costa Rica. Pediatrics. 1992;90(1 Pt 2):157-161.
102. Schotensack K, Elliger T, Gross A, Nissen G.Prevalence of sexual abuse of children inGermany. Acta Paedopsychiatrica.1992;55(4):211-216.
103. Singh HS, Yiing WW, Nurani HN. Prevalence ofchildhood sexual abuse among Malaysian para-medical students. Child Abuse and Neglect.1996;20(6):487-492.
104. Fergusson DM, Horwood LJ, Lynskey MT.Childhood sexual abuse, adolescent sexualbehaviors and sexual revictimization. ChildAbuse and Neglect. 1997;21(8):789-803.
105. Olsson A, Ellsberg M, Berglund S, et al. Sexualabuse during childhood and adolescenceamong Nicaraguan men and women: A popula-tion-based anonymous survey. Child Abuseand Neglect. 2000;24(12):1579-1589.
106. Pedersen W, Skrondal A. Alcohol and sexualvictimization: A longitudinal study ofNorwegian girls. Addiction. 1996;91(4):565-581.
107. López F, Carpintero E, Hernandez A, Martin MJ,Fuertes A. Prevalence and sequelae of child-hood sexual abuse in Spain. Child Abuse andNeglect. 1995;19(9):1039-1050.
108. Halperin DS, Bouvier P, Jaffe PD, et al.Prevalence of child sexual abuse among ado-lescents in Geneva: Results of a cross sectionalstudy. British Medical Journal.1996;312(7042):1326-1329.
109. Tschumper A, Narring F, Meier C, Michaud PA.Sexual victimization in adolescent girls (age 15-20 years) enrolled in post-mandatory schools orprofessional training programmes in Switzerland.Acta Paediatrica. 1998;87(2):212-217.
110. Wilsnack SC, Vogeltanz ND, Klassen AD, HarrisTR. Childhood sexual abuse and women’s sub-stance abuse: National survey findings. J StudAlcohol. 1997;58(3):264-271.
111. Luster T, Small SA. Sexual abuse history andproblems in adolescence: Exploring the effectsof moderating variables. Journal of Marriageand the Family. 1997;59:131-142.
112. Stock JL, Bell MA, Boyer DK, Connell FA.Adolescent pregnancy and sexual risk-takingamong sexually abused girls. Family PlanningPerspectives. 1997;29(5):200-203, 227.
113. Golding J. Sexual assault history and women’sreproductive and sexual health. Psychology ofWomen Quarterly. 1996;20:101-121.
114. Walker EA, Katon WJ, Roy-Byrne PP, JemelkaRP, Russo J. Histories of sexual victimization inpatients with irritable bowel syndrome orinflammatory bowel disease. American Journalof Psychiatry. 1993;150(10):1502-1506.
115. Golding JM. Sexual assault history and limita-tions in physical functioning in two generalpopulation samples. Research in Nursing andHealth. 1996;19(1):33-44.
C H A P T E R O N E

A Practical Guide for Researchers and Activists 33
116. Campbell J, Jones AS, Dienemann J, et al.Intimate partner violence and physical healthconsequences. Archives of Internal Medicine.2002;162(10):1157-1163.
117. Garcia-Moreno C, Watts C. Violence againstwomen: Its importance for HIV/AIDS. AIDS.2000;14(Suppl 3):S253-265.
118. Maman S, Campbell J, Sweat MD, Gielen AC.The intersections of HIV and violence:Directions for future research and interventions.Social Science and Medicine. 2000;50(4):459-478.
119. Maman S, Mbwambo JK, Hogan NM, et al. HIV-positive women report more lifetime partnerviolence: Findings from a voluntary counselingand testing clinic in Dar es Salaam, Tanzania.American Journal of Public Health.2002;92(8):1331-1337.
120. Dunkle KL, Jewkes RK, Brown HC, et al.Gender-based violence, relationship power, andrisk of HIV infection in women attending ante-natal clinics in South Africa. Lancet.2004;363(9419):1415-1421.
121. Petersen R, Gazmararian JA, Spitz AM, et al.Violence and adverse pregnancy outcomes: Areview of the literature and directions for futureresearch. American Journal of PreventiveMedicine. 1997;13(5):366-373.
122. Nasir K. Violence against pregnant women indeveloping countries. European Journal ofPublic Health. 2003;13(2):105-107.
123. Valladares E, Ellsberg M, Peña R, Högberg U,Persson L-Å. Physical partner abuse duringpregnancy: A risk factor for low birth weight inNicaragua. Obstetrics and Gynecology.2002;100(4):100-105.
124. Murphy D, Schei B, Myhr T, Du Mont J. Abuse:A risk factor for low birth weight? A systematicreview and meta-analysis. 2001;164:1567-1572.
125. Bailey JE, Kellermann AL, Somes GW, et al. Riskfactors for violent death of women in thehome. Archives of Internal Medicine.1997;157(7):777-782.
126. Smith PH, Moracco KE, Butts JD. Partner homi-cide in context: A population-based perspec-tive. Homicide Studies. 1998;2(4):400-421.
127. Mathews S, Abrahams N, Martin L, et al. EverySix Hours a Woman is Killed by her IntimatePartner: A National Study of Female Homicidein South Africa. Pretoria, South Africa: Genderand Health Research Group, Medical ResearchCouncil, South Africa; 2004.
128. Counts D, Brown JK, Campbell JC. To Haveand To Hit. 2nd ed. Chicago, Illinois: Universityof Chicago Press; 1999.
129. Levinson D. Violence in Cross-culturalPerspective. Newbury Park, California: SagePublishers; 1989.
130. Heise L. Violence against women: An integrated,ecological framework. Violence against Women.1998;4(3):262-290.
131. Jewkes R. Intimate partner violence: Causes andprevention. Lancet. 2002;359(9315):1423-1429.
132. Koenig MA, Lutalo T, Zhao F, et al. Coercivesex in rural Uganda: Prevalence and associatedrisk factors. Social Science and Medicine.2004;58:787-798.
133. Koenig M, Lutalo T, Zhao F, et al. Domestic vio-lence in rural Uganda: Evidence from a com-munity-based study. Bulletin of the WorldHealth Organization. 2003;81:53-60.
134. Jejeebhoy SJ. Wife-beating in rural India: A hus-band’s right? Economic and Political Weekly(India). 1998;23(15):855-862.
135. O’Campo P, Gielen AC, Faden RR, et al.Violence by male partners against women dur-ing the childbearing year: A contextual analysis.American Journal of Public Health.1995;85(8):1092-1097.
136. Koenig MA, Ahmed S, Hossain MB, KhorshedAlam Mozumder AB. Women’s status anddomestic violence in rural Bangladesh: individ-ual- and community-level effects. Demography.2003;40(2):269-288.
137. Ellsberg MC, Winkvist A, Peña R, Stenlund H.Women’s strategic responses to violence inNicaragua. Journal of Epidemiology andCommunity Health. 2001;55(8):547-555.
138. Landenburger K. A process of entrapment inand recovery from an abusive relationship.Issues in Mental Health Nursing. 1989;10(3-4):209-227.
139. Campbell J. Assessing Dangerousness: Violenceby Sexual Offenders, Batterers, and ChildAbusers. Thousand Oaks, California: SagePublications; 1995.
140. Ellsberg M, Heise L. Bearing witness: Ethics indomestic violence research. Lancet.2002;359(9317):1599-1604.
141. World Health Organization. Putting Women’sSafety First: Ethical and SafetyRecommendations for Research on DomesticViolence Against Women. Geneva, Switzerland:Global Programme on Evidence for HealthPolicy, World Health Organization; 1999. ReportNo.: WHO/EIP/GPE/99.2.
V I O L E N C E A G A I N S T W O M E N A S A H E A L T H A N D D E V E L O P M E N T I S S U E

2PHO
TO B
Y H
AFM
JAN
SEN

[The experience] that most affected me was with a girl my age, maybe 22 years old...She toldme all about how her husband beat her while she was washing clothes in the back patio.Her mother-in-law would spy on her and tell her son things so that he would punish her. Shewas very afraid, and her voice trembled as she spoke, but she really wanted to tell me abouther tragedy. She kept looking over to where her mother-in-law was watching us. She askedme for help and I told her about the Women’s Police Station. When her mother-in-law got upto go to the latrine, I quickly gave her a copy of the pamphlet and she hid it. She thanked mewhen I left and I ended up crying in the street because I couldn’t stand to see such a younggirl being so mistreated… Nicaraguan interviewer. (Ellsberg et al, 2001.19)
A Practical Guide for Researchers and Activists 35
that transcend those in other areas becauseof the potentially threatening and traumaticnature of the subject matter. In the case ofviolence, the safety and even the lives ofwomen respondents and interviewers maybe at risk.1
In 1991, the Council for InternationalOrganization of Medical Sciences (CIOMS)
In many ways, researching violenceagainst women is similar to researchingother sensitive topics. There are issues ofconfidentiality, problems of disclosure, andthe need to ensure adequate and informedconsent. As the previous quote from aninterviewer illustrates, however, there areaspects of gender-based violence research
C H A P T E R T W O
Ethical Considerations for Researching ViolenceAgainst Women*
Topics covered in this chapter:
Respect for persons at all stages of the research processMinimizing harm to respondents and research staffMaximizing benefits to participants and communities (beneficence)Justice: Balancing risks and benefits of research on violence against women
* This chapter was adapted from Ellsberg and Heise, 2002.1

36 Researching Violence Against Women
C H A P T E R T W O
presented a set of International Guidelinesfor Ethical Review of EpidemiologicalStudies.3 These guidelines apply the basicethical principles of biomedical researchinvolving human subjects to the field ofepidemiology: respect for persons, non-maleficence (minimizing harm), benefi-cence (maximizing benefits), and justice.In 1999, the World Health Organization(WHO) published guidelines for address-ing ethical and safety issues in gender-based violence research.4 The guidelineswere based on the experiences of theInternational Research Network on ViolenceAgainst Women (IRNVAW) and weredesigned to inform the WHO Multi-countryStudy on Women’s Health and DomesticViolence Against Women. (See Box 2.1 for adescription of the main points.) The authorsargue that these ethical guidelines are criti-cal, not only to protecting the safety ofrespondents and researchers, but also toensuring data quality.
This chapter examines each of thebasic principles mentioned in the CIOMS
guidelines in turn and explores the chal-lenges of applying them to the specialcase of conducting research on domesticand sexual violence.
RESPECT FOR PERSONS AT ALL STAGES OF THERESEARCH PROCESS
Informed consent for respondents The principle of respect for persons incor-porates two fundamental ethical principles:respect for autonomy and protection ofvulnerable persons. These are commonlyaddressed by individual informed consentprocedures that ensure that respondentsunderstand the purpose of the researchand that their participation is voluntary.
There is still no consensus on whetherthe informed consent process for VAW stud-ies should explicitly acknowledge that thestudy will include questions on violence orwhether it is sufficient to warn participantsthat sensitive topics will be raised. TheWHO VAW study used an oral consentprocess that referred to the survey as astudy on women’s health and life experi-ences.5 Women were advised that, “Some ofthe topics discussed may be personal anddifficult to talk about, but many womenhave found it useful to have the opportunityto talk.” Women were told that they couldend the interview at any time or skip anyquestion they did not want to answer. (SeeBox 2.3 for an example of the informedconsent form used in the WHO VAW study.)A more detailed explanation of the natureof the questions on violence was provideddirectly before the violence questions, andrespondents were asked whether theywanted to continue and were againreminded of their option not to answer. It isa good idea to prepare a list of responsesfor questions that a woman might ask aboutthe study, such as how she was selected forthe study, what will the study be used for,and how her responses will be kept secret.
■ The safety of respondents and the research team is paramount and should infuseall project decisions.
■ Prevalence studies need to be methodologically sound and to build upon currentresearch experience about how to minimize the underreporting of abuse.
■ Protecting confidentiality is essential to ensure both women’s safety and dataquality.
■ All research team members should be carefully selected and receive specializedtraining and ongoing support.
■ The study design must include a number of actions aimed at reducing anypossible distress caused to the participants by the research.
■ Fieldworkers should be trained to refer women requesting assistance to availablesources of support. Where few resources exist, it may be necessary for the studyto create short-term support mechanisms.
■ Researchers and donors have an ethical obligation to help ensure that theirfindings are properly interpreted and used to advance policy and interventiondevelopment.
■ Violence questions should be incorporated into surveys designed for other purposes only when ethical and methodological requirements can be met.
(From WHO, 1999.4)
BOX 2.1 ETHICAL AND SAFETY RECOMMENDATIONS FOR DOMEST IC V IOLENCE RESEARCH

A Practical Guide for Researchers and Activists 37
because children are generally consideredmore vulnerable and less able to act ontheir own behalf. The dilemma is particu-larly acute in settings where there are noeffective services to assist troubled families,or where reporting is likely to trigger a cas-cade of events that might put the child ateven greater risk (such as being removedfrom his/her home and placed in an institu-tion). The WHO VAW study specificallyexcluded questions about child abuse, butrequired teams to develop local protocols
E T H I C A L C O N S I D E R AT I O N S F O R R E S E A R C H I N G V I O L E N C E A G A I N S T W O M E N
Mandatory reporting of abuse Some countries have laws that require cer-tain kinds of professionals to report casesof suspected abuse to authorities or socialservice agencies. Such laws raise difficultissues for researchers because they throwinto conflict several key ethical principles:respect for confidentiality, the need to pro-tect vulnerable populations, and respect forautonomy. In the case of adult women,there is consensus among most researchersthat the principles of autonomy and confi-dentiality should prevail and thatresearchers should do everything withintheir power to avoid usurping a woman’sright to make autonomous decisions abouther life. (Of course if a woman seeks sup-port in reporting her abuse, researchersshould oblige.)
The dilemma of whether to comply withlegal reporting requirements is particularlyproblematic when dealing with child abuse.There is no consensus internationally abouthow to handle cases of child abuse
Researchers involved in the WHO Multi-country Studyon Women’s Health and Domestic Violence AgainstWomen debated at length the value of mentioningviolence directly in the initial consent process versusadding a second-order consent process immediatelybefore the questions on abuse. Some researchersargued that it was important to alert women up frontas to the true nature of the questions whereas othersfelt it was preferable to postpone introducing thenotion of violence until immediately prior to the actualabuse-related questions. This would allow some rap-port to develop, but still give a woman an opportu-nity to opt out of the violence-related questions.
The consent process was well received by respon-dents in all countries except Japan. During pilot test-ing, several Japanese respondents expressed asense of betrayal because they had not beeninformed that the interview contained questionsabout violence.6 As a result, the Japan team modi-fied its consent language to explicitly acknowledgeviolence up front. This is an excellent example ofhow ethical principles and actual experience cancombine to guide practice.
BOX 2.2 ADAPTING ETHICAL GUIDEL INES TO LOCAL SETT INGS
Used in the WHO Multi-country Study on Women’s Health and Domestic ViolenceAgainst Women
Hello, my name is [*]. I work for [*]. We are conducting a survey in [study loca-tion] to learn about women’s health and life experiences. You have been chosen bychance (as in a lottery/raffle) to participate in the study.
I want to assure you that all of your answers will be kept strictly secret. I will notkeep a record of your name or address. You have the right to stop the interview atany time, or to skip any questions that you don’t want to answer. There are no rightor wrong answers. Some of the topics may be difficult to discuss, but many womenhave found it useful to have the opportunity to talk.
Your participation is completely voluntary but your experiences could be very helpfulto other women in [country].
Do you have any questions?
(The interview takes approximately [*] minutes to complete). Do you agree to beinterviewed?
NOTE WHETHER RESPONDENT AGREES TO INTERVIEW.
[ ] DOES NOT AGREE TO BE INTERVIEWED
THANK PARTICIPANT FOR HER TIME AND END INTERACTION.
[ ] AGREES TO BE INTERVIEWED.Is now a good time to talk?It’s very important that we talk in private. Is this a good place to hold the inter-view, or is there somewhere else that you would like to go?
TO BE COMPLETED BY INTERVIEWER
I CERTIFY THAT I HAVE READ THE ABOVE CONSENT PROCEDURE TO THEPARTICIPANT.
SIGNED: ____________________________________________________________
(From WHO, 2004.5)
BOX 2.3 INDIVIDUAL CONSENT FORM

38 Researching Violence Against Women
for handling cases of child abuse that inter-viewers might nonetheless come to knowabout. The guiding principle of these proto-cols was to act in “the best interests of thechild,” a standard that each team opera-tionalized locally, based on advice from keyagencies about prevailing conditions.
Community agreement In many countries, it is also important toobtain community support for research, aswell as individual consent. (Communityconsent, however, should never replaceindividual consent.) This is often sought bymeeting with community leaders to explainthe overall objectives of the research. Forsafety reasons, when obtaining communitysupport for VAW research, it is important toframe the study in general terms—such asa study on women’s health or life experi-ences rather than mention violence orabuse directly. If it becomes well known inthe community that women are beingquestioned about violence, men may pro-hibit their partners from participating ormay retaliate against them for their partici-pation. In addition to potentially jeopardiz-ing the safety of respondents, this couldalso undermine the study objectives anddata accuracy.
MINIMIZING HARM TORESPONDENTS ANDRESEARCH STAFF
Ensuring participant safety The primary ethical concern related toresearching VAW is the potential for inflict-ing harm to respondents through their par-ticipation in the study. A respondent maysuffer physical harm if a partner finds outthat she has been talking to others abouther relationship with him. Because manyviolent partners control the actions of theirspouses closely, even the act of speakingto another person without his permissionmay trigger a beating.
No systematic studies have been per-formed to determine how often womensuffer negative consequences from partici-pating in research on violence. However,several VAW researchers have recordedchilling examples of experiences wherewomen have been placed at risk as a resultof inadequate attention to safety issues.8
For example, researchers from Chiapas,Mexico, describe how, when they firstbegan researching domestic violence, theywere not fully aware of the risks involved.They included a small set of questions ondomestic violence within a larger study onreproductive health without taking anyspecial precautions regarding safety ofrespondents. They were shocked to learnlater that three respondents were beaten bytheir partners because they had partici-pated in the survey.9
The WHO guidelines provide a numberof suggestions about how to minimize risksto respondents, including:
■ Interviewing only one woman per house-hold (to avoid alerting other women whomay communicate the nature of the studyback to potential abusers).
■ Not informing the wider community thatthe survey includes questions on violence.
■ Not conducting any research on violencewith men in the same clusters wherewomen have been interviewed.4
Protecting privacy and confidentialityHis mother and sisters kept passing by, andwould peek in the doorway to see what wewere talking about, so we would have tospeak really softly…and the girl said to me,“Ay, don’t ask me anything in front ofthem.” (Nicaraguan interviewer) 2
Protecting privacy is important in itsown right and is also an essential elementin ensuring women’s safety. In addition to
C H A P T E R T W O

A Practical Guide for Researchers and Activists 39
supervisors and even drivers can also playa role in distracting household memberswho are intent on listening to the inter-view. In one instance in Zimbabwe, field-workers entered into lengthy negotiationsto purchase a chicken from the husband ofa respondent so that she could be inter-viewed in private.10 Other researchers havecarried candy and coloring books to keepchildren busy during interviews.
Indeed, the Japanese team for theWHO VAW study found it so difficultto achieve privacy in Japan’scrowded apartments that they had todepart from the protocol and useself-response booklets for especiallysensitive questions. In this highly lit-erate population, women were ableto read and record their answerswithout the questions having to beread aloud.6
Ensuring privacy may be evenmore problematic in telephone sur-veys. Interviewers for the VAW sur-vey in Canada were trained to detectwhether anyone else was in theroom or listening on another line,and to ask whether they should callback at another time. They providedrespondents with a toll free numberto call back if they wanted to verify
E T H I C A L C O N S I D E R AT I O N S F O R R E S E A R C H I N G V I O L E N C E A G A I N S T W O M E N
interviewing only one woman per house-hold, the WHO recommendations adviseresearchers to conduct violence-relatedinterviews in complete privacy, with theexception of children under the age oftwo. In cases where privacy cannot beensured, interviewers should be encour-aged to reschedule the interview for a dif-ferent time or place. Achieving this level ofprivacy is difficult and may require moreresources than might be needed forresearch on less sensitive topics.
Researchers have developed a variety ofcreative methods for ensuring privacy.Interviewers in Zimbabwe and Nicaraguaoften held interviews outside or accompa-nied women to the river as they washedclothes. Many studies have successfullyused “dummy” questionnaires, containingunthreatening questions on issues such asbreastfeeding or reproductive health.Respondents are forewarned that if some-one enters the room, the interviewer willchange the topic of conversation byswitching to a dummy questionnaire. Othermembers of the research team such as
■ Interview only one woman per household.
■ Don’t inform the wider community that the survey includes questions on violence.
■ Don’t interview men about violence in the same households or clusters wherewomen have been asked about violence.
■ Interviews should be conducted in complete privacy.
■ Dummy questionnaires may be used if others enter the room during the interview.
■ Candy and games may be used to distract children during interviews.
■ Use of self-response questionnaires for some portions of the interview may beuseful for literate populations.
■ Train interviewers to recognize and deal with a respondent’s distress during theinterview.
■ End the interview on a positive note that emphasizes a woman’s strengths.
BOX 2.4 SUGGEST IONS FOR MINIMIZ ING HARM TO WOMEN PART IC IPAT ING IN RESEARCH
Interview in Thailand
PHO
TO B
Y H
AFM
JAN
SEN

40 Researching Violence Against Women
that the interview was legitimate, or in casethey needed to hang up quickly. About1,000 out of a sample of 12,000 womencalled back, and 15 percent of the callswere to finish interrupted interviews.11
Minimizing participant distressInterviews on sensitive topics can provokepowerful emotional responses in some par-ticipants. The interview may cause awoman to relive painful and frighteningevents, and this in itself can be distressingif she does not have a supportive socialenvironment.12 Interviewers therefore needto be trained to be aware of the effects thatthe questions may have on informants andhow best to respond, based on a woman’slevel of distress.
Most women who become emotionalduring an interview actively choose to pro-ceed, after being given a moment to collectthemselves. Interviewer training shouldinclude practice sessions on how to iden-tify and respond appropriately to symp-toms of distress as well as how toterminate an interview if the impact of thequestions becomes too negative.
Interviewer training should also includeexplicit exercises to help field staff exam-
ine their own attitudes and beliefs aroundrape and other forms of violence.Interviewers frequently share many of thesame stereotypes and biases about victimsthat are dominant in the society at large.Left unchallenged, these beliefs can lead tovictim-blaming and other destructive atti-tudes that can undermine both the respon-dent’s self esteem and the interviewer’sability to obtain quality data.
Referrals for care and supportAt a minimum, the WHO guidelines sug-gest that researchers have an ethical obliga-tion to provide a respondent withinformation or services that can help hersituation. In areas where specific violence-related services are available, researchteams have developed detailed directoriesthat interviewers can use to make referrals.In Canada’s VAW survey, for example, thecomputer program used by telephoneinterviewers had a pop-up screen thatlisted resources near the respondent, basedon her mail code. In Zimbabwe, Brazil,Peru, and South Africa, researchers devel-oped small pamphlets for respondents thatlisted resources for victims along with ahost of other health and social serviceagencies.10 All women were offered thepamphlet after being asked if it would besafe for them to receive it (cases have beenreported where women have been beatenwhen a partner found informational mate-rial addressing violence). In Zimbabwe,interviewers carried a referral directory andwrote out addresses on physician referralpads so that the referral would not attractsuspicion if discovered. Ideally, contactshould be made in advance with the serv-ices so that they are prepared to receivereferrals from the study.
In settings where resources are scarce ornonexistent, researchers have developedinterim support measures. For example, astudy on violence against women per-formed in rural Indonesia brought in a
C H A P T E R T W O
Respondent inTanzania tells childrento go play beforestarting her interview
PHO
TO B
Y H
AFM
JAN
SEN

A Practical Guide for Researchers and Activists 41
counselor to the field once a week to meetwith respondents.13 In Ethiopia, the studyhired mental health nurses to work in theclosest health center for the duration of thefieldwork.14 The number of women whoactually make use of such services is oftenquite low, but subsequent interviews withwomen indicate that they appreciate know-ing that services are available if needed.11
In Peru and in Bangladesh, the WHO VAWteam has used the study as an opportunityto train local health promoters in basiccounseling and support skills. In this way,the team will leave behind a permanentresource for the community.
Bearing witness to violence The image of these stories affects you, to seehow these women suffer, and especially thefeeling that no one supports them. These areexperiences that you never forget…(Nicaraguan interviewer)2
Although preventing harm to respon-dents is of primary importance, researchersalso have an ethical obligation to minimizepossible risks to field staff and researchers.Sources of risk include threats to physicalsafety either as a result of having to travelin dangerous neighborhoods or fromunplanned encounters with abusive indi-viduals who object to the study. Some
strategies to reduce the first source of riskinclude removing extremely dangerousneighborhoods from the sampling framebefore drawing the sample (for examplethose controlled by narco-traffickers); out-fitting teams with cell phones; and havingmale drivers accompany female interview-ers into dangerous areas.
Abusive partners have also been knownto threaten interviewers with physical harm.In a South African study, for example, aman came home from a bar in the middleof his partner’s interview and pulled a gunon the fieldworker, demanding to see thequestionnaire. Because of prior training, theinterviewer had the presence of mind togive the man an English version of thequestionnaire, which he was unable toread.10 “Dummy” questionnaires would alsohave been helpful in this situation.
The most common risk for fieldwork-ers, however, is the emotional toll of listen-ing to women’s repeated stories of despair,physical pain, and degradation. It is hardto overestimate the emotional impact thatresearch on violence may have on field-
E T H I C A L C O N S I D E R AT I O N S F O R R E S E A R C H I N G V I O L E N C E A G A I N S T W O M E N
Researchers in a study performed in Cambodia found a young woman who washeld prisoner in her own home by her husband. When the research team arrivedto interview her, they found the woman locked in her house, with only a peepholewhere a chain was threaded through a crudely cut hole in the door. The womanconducted the interview through the peephole. During the interview, the husbandappeared and was suspicious about their activity. The team gave him a falseexplanation for their visit and then left the home.
The next day, the team sought help from the Ministry of Women’s Affairs, which co-sponsored the study. Secretariat staff informed the researchers that the woman’s hus-band had stormed into their office the preceding afternoon, dragging his wife bythe arm. He demanded to know who had been at his door. He told the Secretariatpersonnel that if they couldn’t confirm her explanation, then his wife would suffer.They readily confirmed her story. She was safe for the moment, but the researchersrealized that it would be too dangerous to ever approach this woman again.
The team made several overtures with different government officials and the policeto help get the woman freed, but everyone was afraid to intervene because thewoman’s husband had an important position. Researchers described the frustrationthat the team felt at not being able to free the woman and the guilt they felt at having put the woman in greater danger.
(From Zimmerman, 1995.8)
BOX 2.5 PROTECT ING RESPONDENT SAFETY IN CAMBODIA
Interview in Bangladesh
PHO
TO B
Y H
AFM
JAN
SEN

42 Researching Violence Against Women
workers and researchers. As the narrativefrom a Nicaraguan fieldworker presented atthe beginning of this chapter illustrates, astudy on violence often becomes anintensely personal and emotional journeyfor which many researchers are not pre-pared. Particularly when field staff havehad personal experiences of abuse, theexperience can be overwhelming. JudithHerman, in her work on psychologicaltrauma in survivors of political and domes-tic violence, describes this as a commonexperience for those who study violence:
To study psychological trauma is to comeface to face both with human vulnerabilityin the natural world and with the capacityfor evil in human nature. To study psycho-logical trauma means bearing witness tohorrible events.15
Including discussions of violence ininterviewer training is crucial for reducingdistress during fieldwork. During fieldwork,another important measure is to provideinterviewers and research staff with regularopportunities for emotional debriefing, orwhen necessary, individual counseling.Researchers have used a variety of creativestrategies for protecting the emotionalhealth of their staff. In Peru, for example,the WHO multi-country team employed aprofessional counselor to lead weekly sup-port sessions that incorporated guidedimagery and relaxation techniques.Experience has repeatedly demonstratedthat emotional support for fieldworkers isessential. Not only does it help interview-ers withstand the demands of the field-work, but it also improves their ability togather quality data.
Transcripts of debriefing sessions withinterviewers who participated in studieswithout adequate support illustrate thispoint:
…When I heard stories about womenbeing beaten and tied up, I would leavethere feeling desperate… I would be awreck, and my supervisor would tell me
“get a hold of yourself, you cry for every lit-tle thing.” But how could I control myself? Icouldn’t stand it… I would try, but some-times it was impossible, and I would burstinto tears during the next interview…(Nicaraguan interviewer) 2
Other interviewers commented that theyfelt extremely drained and distracted by theinterviews where women reported vio-lence. One woman reported that she hadstopped working for the study because shecould not bear to listen to women’s storiesof abuse. 2
Experience has shown that trauma-related stress is not confined to field staffwho are directly involved with respon-dents. Field supervisors, transcribers, driv-ers, and even data entry personnel may beaffected. In one study in Belize, a tran-scriber broke down after hours of listeningto in-depth qualitative interviews with sur-vivors of abuse.16
It is particularly important to provideopportunities during training for inter-viewers to address their own experiencesof abuse. Given the high prevalence ofgender-based violence globally, it is likelythat a substantial proportion of interview-ers will have experienced gender-basedviolence themselves at some point. Theseexperiences need to be taken into consid-eration. Most people learn to cope withpainful past experiences, and usually donot dwell on them in their everyday lives.However, when trainees are confrontedwith the subject matter the informationmay awaken disturbing images and oremotions. For many trainees, simplyacknowledging the fact that these reac-tions are normal and providing timelyopportunities to discuss them will be suffi-cient to help them complete the trainingand participate successfully in fieldwork.In those rare cases where feelings becometoo overwhelming, trainees should besupported in their decision to withdrawfrom the study.
C H A P T E R T W O

A Practical Guide for Researchers and Activists 43
MAXIMIZING BENEFITS TO PARTIC IPANTS AND COMMUNIT IES(BENEF ICENCE)
The principle of beneficence refers to theethical obligation to maximize possiblebenefits to study participants and thegroup of individuals to which they belong.This principle gives rise to norms requiringthat the risks of research be reasonable inlight of the expected benefits, that theresearch design be sound, and that theinvestigators be competent both to conductthe research and to ensure the well-beingof participants.
The interview as an interventionAsking women to reveal stories of traumacan be a transforming experience for bothresearchers and respondents. Indeed, thereis ample evidence that most women wel-come the opportunity to tell their stories if they are asked in a sympathetic, non-judgmental way. In our experience,women rarely refuse to answer questionson violence.
Many women who disclose violence insurveys have never told anyone abouttheir situations.17 Many studies find thatparticipants find the experience to be sohelpful that they ask fieldworkers to “inter-view” a friend or relative who has a storyto tell. As Herman notes, “rememberingand telling the truth about terrible eventsare prerequisites both for the restoration ofthe social order and for the healing ofindividual victims.”15
Even the act of telling her story canoffer a woman some small way of trans-forming her personal ordeal into a way tohelp others. Indeed, researchers sensitiveto this issue encourage interviewers andfield staff to take hope and satisfactionfrom their participation in the process ofgiving a voice to women’s suffering.
A qualitative study of survivors of
abuse who had visited a women’s crisiscenter in Nicaragua found that a centralpart of women’s process of recovery andpersonal as well as collective empower-ment came not only from increasedknowledge of their rights, but also fromthe opportunity to share their experiencesand to help other women in similar situa-tions.18 In this sense, asking women aboutexperiences of violence may be seen asan intervention in itself. At the very least,asking conveys the message that violenceis a topic worthy of study, and not ashameful or unimportant issue.
In this same vein, many fieldworkers inthe León, Nicaragua, research describedthe experience of listening to women’s sto-ries, as well as the opportunity to tell theirown stories in the debriefing sessions, as aprofoundly healing experience. One inter-viewer who had never before discussedher experiences said,
[when I joined this study] I felt that I hadfinally found someone I couldtell everything to, someone withwhom I could share my bur-den, because it’s horrible to feelso alone. Now I feel that aweight has been taken offme…I feel relieved…19
The interview is also anopportunity to provide womenwith information on gender-based violence.Many studies have issued small cards thatcan be easily hidden in a shoe or inside ablouse with information about localresources for abused women and messagessuch as, “If you are being abused, thereare ways out” or “Violence is never justi-fied.” Such messages may enable womento see experiences in a new light or toidentify violence in others close to them.
Researchers also stress the importance ofending the interview on a note thatemphasizes women’s strengths and tries tominimize distress, particularly as a respon-dent may have revealed information that
E T H I C A L C O N S I D E R AT I O N S F O R R E S E A R C H I N G V I O L E N C E A G A I N S T W O M E N
Remembering and telling the truth about terrible eventsare prerequisites both for the restoration of the socialorder and for the healing of individual victims. (Herman,
1992.15)

44 Researching Violence Against Women
made her feel vulnerable.20 A number ofstudies have carefully scripted such end-ings to ensure that the interview finisheswith clear statements that explicitlyacknowledge the abuse, highlight theunacceptability of the violence, andemphasise the respondent’s strengths inenduring and/or ending the violence. TheWHO study ends each interview with thewords, “From what you have told me, I cantell that you have had some very difficulttimes in your life. No one has the right totreat someone else in that way. However,from what you have told me I can also seethat you are strong and have survivedthrough some difficult circumstances.”7
One indication of how women haveviewed the interview process can beobtained by assessing respondents’ satisfac-tion with the interview. At the end of theWHO interview, respondents were askedthe following question: “I have askedabout many difficult things. How has talk-ing about these things made you feel?” Theanswers were written down verbatim andcoded by the interviewer into the followingthree categories: good/better, bad/worse,and same/no difference. The majority(between 60 and 95 percent in seven sites)of women who had experienced physicalor sexual partner violence reported that
they felt good/better at the end of theinterview. In most countries, the range wassimilar between women who had or hadnot experienced partner violence. Very fewwomen reported feeling worse after beinginterviewed. Between 0.5 and 8.4 percentof women reporting partner violence ever(highest in Peru) and between zero and 3.2percent of women with no history of part-ner violence felt worse.17
Assuring scientific soundnessThe CIOMS guidelines note: “A study thatis scientifically unsound is unethical in thatit exposes subjects to risk or inconveniencewhile achieving no benefit in knowledge.”3
This principle is particularly important inthe area of gender-based violence wherewomen are asked to disclose difficult andpainful experiences and where the act ofresearch itself may put women at furtherrisk of abuse. Thus the WHO guidelinesnote that violence researchers have an ethi-cal responsibility to ensure the soundnessof their work by selecting a large enoughsample size to permit conclusions to bedrawn, and by building upon currentknowledge about how to minimize under-reporting of violence. (See Chapter 7 formore discussion of sampling techniques.)Underreporting of violence will dilute asso-ciations between potential risk factors andhealth outcomes, leading to falsely nega-tive results. Underestimating the dimen-sions of violence may also preventviolence intervention programs fromreceiving the priority they deserve in theallocation of resources.
Research demonstrates that disclosurerates of violence are highly influenced bythe design and wording of questions, thetraining of interviewers, and the imple-mentation of the study.2 In Chapter 6, wediscuss this issue in much greater depthand outline the variety of measures thathave been developed to enhance disclo-sure of violence.
C H A P T E R T W O
Looking for householdsin Samoa
PHO
TO B
Y H
AFM
JAN
SEN

A Practical Guide for Researchers and Activists 45
Using study results for social changeIt is important to feed research findingsinto ongoing advocacy, policy making,and intervention activities. Too often criti-cal research findings never reach the atten-tion of the policy makers and advocatesbest positioned to use them. The enor-mous personal, social, and health-relatedcosts of violence against women place amoral obligation on researchers anddonors to try to ensure that study findingsare applied in the real world. It is alsoimportant that the study communityreceives early feedback on the results ofthe research in which it has participated.Chapter 14 addresses this issue in moredetail and describes several successfulexamples of how research findings havebeen used to contribute to changing lawsand policies on domestic violence.
One way to improve the relevance ofresearch projects is, from the outset, toinvolve organizations that carry out advo-cacy and direct support for survivors ofviolence, either as full partners in theresearch or as members of an advisorycommittee. Such committees can play animportant role in helping guide the studydesign, advise on the wording of ques-tions, assist with interviewer training, andgive guidance on possible forms of analy-sis and the interpretation of results. Thesegroups also have a central role to play inpublicizing and applying the project’sfindings.
JUST ICE : BALANCINGRISKS AND BENEFITS OFRESEARCH ON VIOLENCEAGAINST WOMEN
Research, like any endeavor that touchespeople’s lives, involves inherent risks. Theprinciple of distributive justice demandsthat the class of individuals bearing theburden of research should receive anappropriate benefit, and those who stand
E T H I C A L C O N S I D E R AT I O N S F O R R E S E A R C H I N G V I O L E N C E A G A I N S T W O M E N
to benefit most should bear a fair propor-tion of the risks and burdens of the study.
In the case of gender-based violenceresearch, the risks are potentially large, butso too are the risks of ignorance, silence,and inaction. Researchers and ethicalreview boards must constantly balance thisreality. Lisa Fontes cites the case of a col-league from India who wanted to studywives who were hospitalized after havingbeen burned by their husbands in disputesover dowry. She ultimatelydecided not to conduct theresearch for fear that theresearch would put women atfurther risk. As Fontesobserves, “Her decision elimi-nated the research-related riskto the participants, but alsoeliminated the potential benefitof reducing the terrible isola-tion and vulnerability of thesevictims.”21
It is possible to conductresearch on violence with full respect forethical and safety considerations if propercare and resources are devoted to this end.We must remember that women living withviolence are already at risk. Researcherscannot eliminate this reality, just as theycannot fully eliminate the possibility thatfurther harm will be caused by their study.The obligation of researchers is to carefullyweigh the risks and benefits of any studyand to take every measure possible to limitpossible harm and to maximize possiblebenefit. At the very least, we must ensurethat when women take risks to share theirstories, we honor that risk by using thefindings for social change.
Women would ask me whatthis survey was for, and howit would help them. I wouldtell them that we won’t seethe solution tomorrow or thenext year. Our daughtersand granddaughters will seethe fruits of this work, maybethings will be better by then.Nicaraguan fieldworker. (From
Ellsberg, et al, 2000.19)

46 Researching Violence Against Women
C H A P T E R T W O
1. Ellsberg M, Heise L. Bearing witness: Ethics indomestic violence research. Lancet.2002;359(9317):1599-1604.
2. Ellsberg M, Heise L, Peña R, Agurto S, Winkvist A.Researching domestic violence against women:Methodological and ethical considerations. Studiesin Family Planning. 2001;32(1):1-16.
3. Council for International Organizations of MedicalSciences. International Guidelines for EthicalReview of Epidemiological Studies. Geneva:CIOMS; 1991.
4. World Health Organization. Putting Women’sSafety First: Ethical and Safety Recommendationsfor Research on Domestic Violence AgainstWomen. Geneva: Global Programme on Evidencefor Health Policy, World Health Organization;1999. Report No.: WHO/EIP/GPE/99.2.
5. World Health Organization. WHO Multi-countryStudy on Women’s Health and Domestic ViolenceAgainst Women: Study Protocol. Geneva: WorldHealth Organization; 2004.
6. Yoshihama M. Personal Communication. AnnArbor, Michigan. Washington, DC. 2004.
7. World Health Organization. WHO Multi-countryStudy on Women’s Health and Domestic ViolenceAgainst Women: Study Questionnaire V10.Geneva: World Health Organization; 2004.
8. Zimmerman K. Plates in a Basket Will Rattle:Domestic Violence in Cambodia, a Summary.Phnom Penh, Cambodia: Project AgainstDomestic Violence; 1995.
9. Health and Development Policy Project.Measuring Violence Against Women Cross-cultur-ally: Notes from a Meeting. Takoma Park,Maryland: Health and Development PolicyProject; 1995.
10.Jewkes R, Watts C, Abrahams N, Penn-Kekana L,Garcia-Moreno C. Ethical and methodologicalissues in conducting research on gender-basedviolence in Southern Africa. Reproductive HealthMatters. 2000;8(15):93-103.
11.Johnson H. Dangerous Domains: ViolenceAgainst Women in Canada. Ontario, Canada:International Thomson Publishing; 1996.
12.Finkelhor D, Hotaling GT, Yllo K. Special EthicalConcerns in Family Violence Research. In:Finkelhor D, Hotaling GT, Yllo K, editors.Stopping Family Violence: Research Priorities forthe Coming Decade. London: Sage; 1988.
13.Hakimi M, Nur Hayati E, Ellsberg M, Winkvist A.Silence for the Sake of Harmony: DomesticViolence and Health in Central Java, Indonesia.Yogyakarta, Indonesia: Gadjah MadaUniversity;PATH, Rifka Annisa, Umeå University;2002.
14.Gossaye Y, Deyessa N, Berhane Y, et al. Women’shealth and life events study in rural Ethiopia.Ethiopian Journal of Health Development.2003;17(Second Special Issue):1-49.
15.Herman J. Trauma and Recovery: The Aftermathof Violence: From Domestic Abuse to PoliticalTerror. New York: Basic Books; 1992.
16.Shrader E. Personal Communication. Washington,DC; 2000.
17.Jansen HAFM, Watts C, Ellsberg M, Heise L,Garcia-Moreno C. Interviewer training in theWHO Multi-country Study on Women’s Healthand Domestic Violence Against Women. Violenceagainst Women. 2004;10(7):831-849.
18.Wessel L, Campbell J. Providing sanctuary for bat-tered women: Nicaragua’s Casas de la Mujer.Issues in Mental Health Nursing. 1997;18:455-476.
19.Ellsberg M. Candies in Hell: Research and Actionon Domestic Violence in Nicaragua [DoctoralDissertation]. Umeå, Sweden: Umeå University;2000.
20.Parker B, Ulrich Y. A protocol of safety: Researchon abuse of women. Nursing Research.1990;38:248-250.
21.Fontes LA. Ethics in family violence research:Cross-cultural issues. Family Relations.1998;47:53-61.

3PH
OTO
BY
HAF
M JA
NSE
N

A Practical Guide for Researchers and Activists 49
question and objectives—and gives exam-ples that show how these concepts can beapplied to issues of violence.
Next it describes some of the more com-mon research designs used in social sci-ence and public health research anddiscusses the advantages and disadvantagesof each. Box 3.1 provides a study checklistof the tasks that researchers need toaddress throughout the research process.Asterisks denote elements most relevant forresearchers using a quantitative approach(e.g., a community survey).
DIFFERENT TYPES OF RESEARCH
There are many different types of researchand the language of research can be daunt-ing. For the purposes of this manual, we
Developing a research strategy maybe the most crucial task in any researchproject. The entire project can be derailedby errors in this phase. Common errorsinclude research questions that are not wellconceptualized or articulated, a researchdesign that is not well suited to the task, ormethods that do not match the needs ofthe project or the skills and resources athand. With proper planning, however,these pitfalls can be avoided.
Which elements are most critical todeveloping an effective research pro-posal protocol? This chapter begins witha brief overview of the different types ofresearch and the roles they can play instrengthening the global response to vio-lence against women. It continues with adiscussion of the early steps in the researchprocess—namely, formulating the research
C H A P T E R T H R E E
Developing a Research Strategy
Topics covered in this chapter:
Different types of researchThe research processChoosing a research topic and objectivesFormulating your research questionsChoosing a research designQuantitative or qualitative methods?Population- or service-based research?Collaboration between researchers and activistsDrafting the protocol

50 Researching Violence Against Women
C H A P T E R T H R E E
have adopted the following typology todescribe the many different types ofresearch (see Table 3.1).
Basic research is dedicated to advanc-ing theory and may not necessarily answerquestions that have obvious program or pol-icy implications. Applied research usesmany of the same techniques but concen-trates on asking questions of more immedi-ate, practical relevance. Formative orexploratory research tends to be less in-depth and is geared toward generating thebackground insights and knowledge neces-sary to pursue further research or to designan actual intervention. Operations
research concentrates on improving theprocess of ongoing interventions.Evaluation research helps evaluate theimpact or success of interventions.
This manual concentrates primarily onthe logic and tools of formative andapplied research. All types of research areimportant and can make substantial contri-butions to knowledge in the field of gen-der violence. Theory building, evaluation,and operations research are complex fieldsin their own right, however, and arebeyond the scope of this book.
THE RESEARCH PROCESS
Four basic steps are common to virtuallyall research projects:
■ Identify a problem to study■ Collect data■ Analyze the data■ Report the results
Box 3.1 presents a more detailed list ofthe steps that are commonly taken toachieve the goals of the study. The orderin which these steps are performed andthe techniques used to achieve them mayvary widely from study to study dependingon the researcher’s theoretical frame-work—the underlying assumptions abouthow knowledge is produced.
The two main traditions withinresearch—positivistic and naturalisticinquiry—approach the enterprise in dis-tinctly different ways. Positivistic inquiry,also known as science-based or deductiveinquiry, generally starts with a hypothesisand proceeds to test it in a systematic andlinear way (see Figure 3.1). In contrast, nat-uralistic inquiry (also known as interpre-tive inquiry) concentrates on studying thenatural environment without manipulationor predetermined constraints on the out-come. The research process in naturalisticinquiry tends to follow a circular path. A
Qualitative CircularQuantitative Linear
Collectdata
Identifyproblem
Analyzedata
Develop“working hypothesis”
Report
Identify problem
State hypothesis
Collect data
Analyze data
Report
F IGURE 3.1 THE RESEARCH PROCESS IN QUANTITAT IVE AND QUALITAT IVE RESEARCH
TABLE 3.1 DIFFERENT KINDS OF RESEARCH
Type of Research PurposeBasic To increase knowledge and advance theory as an end
in itselfApplied To understand the magnitude, nature and/or origins of
social problems in order to identify solutionsFormative To facilitate the development of an intervention (e.g., a
program or policy) or help develop quantitative instrumentsOperations To monitor and improve ongoing interventionsEvaluation To evaluate the impact/effectiveness of completed
interventions
Naturalistic InquiryPositivistic Inquiry
(From Dahlgren et al, 2003.1)

D E V E L O P I N G A R E S E A R C H S T R AT E G Y
general theme may be identified for study,and the research question becomes morefocused as additional data are collected andanalyzed. This is referred to as an emer-gent design because the actual focus ofthe study and even the methods used fordata collection and analysis may emerge asthe study progresses. Naturalistic studiestend to use qualitative research methodsand positivistic studies tend to use quantita-tive methods. Both traditions can be eitherdescriptive or analytic and both can play animportant role in the study of violenceagainst women. This manual presentsexamples from both approaches.
CHOOSING A RESEARCHTOPIC AND OBJECT IVES
The first step in any research endeavor isto identify a problem or area that couldbenefit from further investigation. In thefield of violence there are hundreds of top-ics worthy of further study. One simplyneeds to determine what kind of informa-tion is most needed in a specific context.
The next step in the process is to narrowthe focus of inquiry to a topic amenable toinvestigation. Guiding questions here are:What do you want to know and what isworth knowing? Researchers generallybegin to narrow their topic by gatheringand reading all the relevant articles andbooks on the subject (also known as a “lit-erature review”). It is very important toidentify what is already known about anissue before deciding on a research topic.Otherwise, you risk either “reinventing thewheel” or investigating questions that donot contribute to advancing knowledge orimproving people’s quality of life.
When the research impulse emerges fromthe need of a service provider, an NGO, oran activist group, it may be relatively easy todefine a research objective. For example,you may be a family planning provider whowants to know the degree to which coercion
Following are some of the most important steps that will need to be taken in thecourse of most studies. There may be some differences according to whether theresearch is based primarily on quantitative or qualitative methods.
Problem formulation ■ Explore the research problem through contacts with community representatives,
health workers, local women’s groups, and through a review of the published andunpublished literature.
■ Formulate the research problem; discuss within the research team and with others concerned to get suggestions and identify a conceptual framework.
■ Formulate and decide on research objectives, study design, study area, studypopulation, and study methods.
■ Operationalize the variables under study.*■ Design an appropriate sampling plan or strategy. ■ Prepare draft questionnaire.*■ Plan for initial data analysis. ■ Translate materials, questionnaires, forms.■ Plan for study personnel, equipment to be used, transport, accommodation,
finance, and other logistics.■ Write a preliminary study protocol.
Organization■ Obtain consent from the participating communities (individually or via
representatives).■ Obtain consent from other local, district, or national authorities concerned.■ Obtain financial support.■ Obtain ethical clearance from ethical review committee.■ Develop manual or instructions for fieldworkers.■ Organize support network for women participants and fieldworkers.■ Obtain educational materials on violence for use by study participants.■ Recruit fieldworkers.■ Train fieldworkers.■ Pilot study of organization, questionnaire, equipment, standardize measurement
procedures.*■ Revise questionnaire, instructions to fieldworkers, study protocol.*
Fieldwork■ Supervise fieldwork.■ Edit interviews to identify errors.*■ Maintain contact with the local community to ensure a good participation in and
support for the study.■ Hold “debriefing” sessions with fieldworkers to avoid “burnout.”
Analysis and reporting■ Control data entry to minimize errors.*■ Discuss quality of data, difficulties with certain questions, and routines with
fieldworkers.*■ Inspect the data matrix together, collaborate with fieldworkers in the control and
clearing of data.*■ Perform preliminary analysis, discuss with the research team and with community
representatives and relevant authorities.■ Complete final analysis and interpretation.■ Report back to community, health authorities, and political authorities. Discuss
consequences and possible actions.■ Present results in reports and publications both for local and broader audiences,
where relevant.■ Plan for intervention and evaluation.
* These steps are particularly relevant for quantitative studies.(Adapted from Persson and Wall, 2003.2)
BOX 3.1 STUDY CHECKL IST
A Practical Guide for Researchers and Activists 51

52 Researching Violence Against Women
and abuse affects your clients’ interest inand ability to use different methods of con-traception. Or you may be the director of awomen’s shelter who wants to know what
happens to women once theyleave your care. Even here it isimportant to investigate whatmay already be known aboutthe topic, either in the researchliterature or by others in thecommunity.
When the motivation for research comesfrom outside the local community, perhapsfrom a university or government agency, it isespecially important to to involve others—preferably service providers and activists—inthe process of refining your research topic.One way to do this is to consult with localstakeholders or individuals who, by virtueof their work and/or life experience, mayhave insights into questions that need to beasked, and answered. This can take the formof consultation with a local advisory board,or individual meetings with women’s groups
and others who may haveopinions on what researchwould be useful to pursue.Consulting with potential stake-holders early in the processcan help ensure that the
research is both relevant and doable, and itcan help build trust and alliances with thevery groups that will probably be in a posi-tion to use and disseminate the findings. Toooften researchers only seek out localwomen’s groups or other nongovernmentalorganizations when they want access to aresearch population (e.g., approaching alocal shelter in order to find “abusedwomen” to interview). Not surprisingly, thiscan breed resentment and distrust.
FORMULATING YOURRESEARCH QUEST IONS
The next task is to express your researchinterests in simply worded, direct questions,
preferably one question for each topic.The research questions should supportyour research objectives. Table 3.2 givesseveral examples of how you might goabout developing research questions. Youmay start out with many more questionsthan can be resolved in a single study. Ifyou do, trim the list to a manageablenumber. This can be a sensitive process,particularly if you are balancing the needsof different actors. For example, the kindof information that a governmentalwomen’s institute would like to collect onviolence may be quite different from thedata that women activists need for advo-cacy purposes, or what a researcher mightconsider important from a theoretical per-spective. Although reaching a consensusregarding the research questions can betime-consuming, including the perspec-tives of stakeholders at this stage is likelyto greatly increase the potential impact ofthe study results.
Remember that as a rule, research ques-tions in qualitative research can be initiallymore general, because they will be refinedas data are collected and analyzed.However, in quantitative research, whenconducting surveys, for example, you needto determine the research questions beforedata collection begins because they formthe basis for establishing the hypotheses tobe tested. (See Table 3.2.)
CHOOSINGA RESEARCH DESIGN
Many organizations interested in usingresearch to improve the quality of theirprograms or services make the same mis-take: They choose a study design beforeclarifying exactly what information isneeded. We recommend that you carefullyconsider alternative study designs, andchoose one that best addresses theresearch objectives and is most likely toanswer the research questions you have
C H A P T E R T H R E E
The best way to build trust and long-term allies is to include
individuals and organizations in the process of establishing
research topics and questions.
Decide on a researchdesign or on data collection
methods after you decidewhat you want to know.

A Practical Guide for Researchers and Activists 53
carried out with a sample size that is toosmall to yield significant results mayunderestimate the prevalence of violenceor its impact on a given population,which could in turn negatively affect poli-cies or program funding.
While there is a wide range of differentresearch designs available to address differ-ent research questions, this manual will
D E V E L O P I N G A R E S E A R C H S T R AT E G Y
developed. This decision must, of course,take into account what is feasible given aproject’s material and human resources. Ifyou cannot implement the most appropri-ate design for a given research question, itis better to change the focus of theresearch or to modify the design. A poorlydesigned study may actually do moreharm than good. For example, a survey
Research Objective
A Cambodian woman’s advocacy organization wanted to determine how widespread violence was in Cambodia and how women responded to domesticviolence. They also wanted understand how communitymembers viewed victims and perpetrators of abuse. Thepurpose of the research was to bolster lobbying effortsand to produce a public awareness campaign.4, 5
An international organization working with Somalirefugees in Kenya was interested in finding out moreabout sexual violence in the refugee camps. Aid workershad heard rumors that a number of women in the campwere raped when they left the camp to get firewood and feared that some pregnancies may have been theproduct of forced sex by guards or bandits.6, 7
The International Planned Parenthood Federation,Western Hemisphere Division (IPPF/WHD) initiated a program to integrate screening and care for survivors of gender-based violence within reproductive health programs in Venezuela, Peru, and the DominicanRepublic. The program managers wanted to evaluatehow the program had succeeded in changing the atti-tudes and practices of health providers and whetherwomen felt satisfied with the care they were receiving.8
A Voluntary Testing and Counseling (VCT) clinic inTanzania was interested in finding out whether the threatof violence after disclosure of HIV status was an obstaclefor women to come in for testing. The program man-agers also wanted to know whether violence was a riskfactor for women contracting HIV.9
Research Question
How common is abuse by an intimate partner inCambodia? How common is forced sex? Who are the perpetrators? Where does the violence take place?In the home? On the street? At work? Other places? To whom do women turn after they have been victim-ized? What services do they think are important? How commonly do community members subscribe tocommon rape myths?
Do women in the camps feel at risk of rape? What arethe most common circumstances of forced sex? Who arethe perpetrators? What do women and men think couldbe done to improve women’s safety?
What did the health promoters know about domestic vio-lence prior to the training? What did they learn duringthe training course about the identification, assessment,and referral of abused women and children? Was therea positive change in providers’ attitudes towards victimsof violence? How many women attending family plan-ning and sexually transmitted infection clinics were askedabout violence? How many were appropriately referredaccording to the protocols developed? How satisfiedwere women with the care they received at the clinics?
What percentage of women attending voluntary clinicaltreatment services have been physically or sexuallyabused by their partners? Did the violence take placebefore the testing or afterwards? Was fear of violencean important issue in women’s ability to protect them-selves from HIV? Was fear of violence a reason that women might be reluctant to go for VCT?
Possible Study Design
Population-based survey of men and women
Focus group discussions with community leaders
In-depth interviews with survivors of violence
Survey of women in the camp
In-depth interviews
Participatory appraisal
Before and after surveys of providers’ attitudes and knowledge
Review of service data
Focus groups with providers and clients
Exit interviews with clients
Survey of clients
In-depth interviews
Focus groups with community men and women
TABLE 3.2 SELECT ING A RESEARCH DESIGN
Examples of different methods that might be used for different research questions. Descriptions of the specific methods are provided in later chapters.
(Adapted from Shrader, 2000.3)

54 Researching Violence Against Women
focus on five broad types of designs thatare often used in public health research.
Quantitative approaches
■ Cross-sectional surveys■ Cohort studies■ Case-control studies
Qualitative approaches
■ Rapid assessment techniques ■ In-depth qualitative studies
These study designs will be described ingreater depth in Chapters 4 and 5.
QUANTITATIVE ORQUALITAT IVE METHODS?
Quantitative research methods produceinformation that can be presented and ana-lyzed with numbers, such as the percentageof women who have been raped or whoattend shelters for battered women. These
methods are drawn largelyfrom the fields of epidemiol-ogy, sociology, economics,and psychology. In contrast,qualitative methods gatherinformation that is presentedprimarily in text form throughnarratives, verbatim quotes,
descriptions, lists, and case studies.Qualitative methods are primarily borrowedfrom the disciplines of anthropology, soci-ology, nursing, and psychology. As wementioned earlier, although research meth-ods are not necessarily tied to a specifictheoretical tradition, quantitative methods
tend to be used in researchusing a positivistic or post-positivistic framework,whereas qualitative methodsare more associated with thenaturalistic or interpretiveframework.
The two approaches represent differentresearch paradigms, or views about thenature of reality and how knowledge isproduced. The positivistic paradigmassumes that there is only one true versionof reality and that it can be uncoveredthrough scientific research. In contrast, thenaturalistic paradigm assumes that reality issubjective rather than objective—it exists inthe views, feelings, and interpretations ofindividuals, including the researcher.According to this perspective, many differ-ent and equally valid versions of realitymay exist at the same time, and some ofthese versions may actually be createdthrough the interaction of researchers andsubjects. Positivistic researchers try toreduce outside influences or bias to a min-imum, whereas naturalistic researchersbelieve that research is inherently biased.They try to be aware of different sourcesof subjective bias, for example, by keepingreflexive journals of their own reactionsand thoughts throughout the researchprocess.
A third paradigm has emerged in recentyears, known as a critical or “emancipatory”paradigm.10-12 According to Ford-Gilboe andcolleagues, “The aim of research within thecritical paradigm is the development ofapproaches that have the potential toexpose hidden power imbalances and toempower those involved to understand, aswell as to transform, the world.”12 Criticaltheory is embraced by most feminist andparticipatory researchers, and because itemphasizes uncovering power relationsbased on class, gender, and ethnicity, it isparticularly well suited for research on vio-lence against women.13 As Ulin and col-leagues point out, “An important premise offeminist theory is that social life and behav-ior are constrained in various ways by whatis considered acceptable behavior based ongender. Feminist research focuses on thepolitical dimension inherent in understand-ing these constraints from the standpoints of
C H A P T E R T H R E E
Quantitative methods usuallyproduce findings that can be
summarized in numbers.Qualitative methods produce
results that are commonly summarized in words or pictures.
Quantitative methods tendto provide less in-depth
information about many people,while qualitative methods
give more detailed informationabout relatively few people.

A Practical Guide for Researchers and Activists 55
people in different power and gender posi-tions.”14 Because the underlying goal is tocontribute to social change, criticalresearchers tend to be more pragmatic inthe use of methods, and often use a combi-nation of qualitative and quantitative datadepending on what is likely to be most per-suasive to policy makers and to the public.12
Quantitative methods are useful fordrawing conclusions that are valid for thebroader population under study. They areparticularly appropriate for measuring thefrequency of a problem or condition andits distribution in a population (for exam-ple, how many women in a communityhave experienced violence and which agegroups are most affected). Surveys areoften used to obtain information aboutpeople’s opinions and behavior, for exam-ple through Knowledge, Attitudes, andPractices (KAP) surveys. When quantitativedata are collected about a group of peoplethat is chosen using special methodsknown as “random sampling techniques,” itis possible to carry out statistical analysisand to generalize the results of the study toa larger population. (For more informationabout sampling techniques, see Chapter 7.)If the target group of the program is notvery large—for example, if it is limited to asingle community—then it may be possibleto survey all homes or individuals in thestudy population (i.e., conduct a census).
The main disadvantage of surveys is thatthey often provide fairly superficial infor-mation, and may not contribute much tounderstanding complex processes or theircauses. For example, a survey may indicatehow many women are experiencing vio-lence or how many have heard an educa-tional message, but it provides lessinformation about how women experienceviolence, or how well they understood theeducational message. Qualitative methodsare more appropriate when the aim is togain understanding about a process, orwhen an issue is being studied for the first
time in a particular setting. Qualitativeresults allow you to understand thenuances and details of complex social phe-nomena from the respondents’ point ofview. Although you cannot say your find-ings are true for everyone, you can revealmultiple layers of meaning for a particulargroup of people. This level of understand-ing is particularly important when studyinghuman behavior and trying to discern howit interacts with people’s beliefs, attitudes,and perceptions.
As an example, the National Committeefor the Abandonment of Harmful TraditionalPractices in Mali, a network of organizationsthat work to discourage female genital muti-lation (FGM), wanted to learn why someapproaches had been more successful thanothers in motivating villages to abandonFGM. Instead of carrying out a population-based survey to measure individual behav-iors and attitudes towards FGM, theydecided to carry out a qualitative study inthree villages where the practice of FGMhad been abandoned. Although this studydid not give information about the numberof villages that had taken this step, it pro-vided very rich information about the differ-ent issues and considerations that helpedvillage leaders and community membersmake their decision. For the purpose ofimproving community-levelinterventions, this study wasmuch more useful than a sur-vey would have been.15
Most research objectives arebest achieved through a com-bination of qualitative andquantitative methodologies. Weencourage researchers to use avariety of methods to look atthe same issue, or triangulation, toenhance the validity and utility of theirresearch. Because triangulation allows you toview your subject from different perspectivesand to look for potential inconsistencies, itincreases the validity and trustworthiness of
D E V E L O P I N G A R E S E A R C H S T R AT E G Y
Triangulation refers to the use of more than one method to lookat the same issue. It can alsoinvolve the use of one method on different study populations.Triangulation helps to ensure that your findings are trustworthy,or convincing to others.

56 Researching Violence Against Women
your findings. For example, the results ofsurvey research may be complemented andenriched by in-depth interviews with a sub-sample of women who were interviewed.Their words, thoughts, and observationslend depth and meaning to the numbersgenerated to describe the essentially painfulreality of physical and sexual abuse.Similarly, one can strengthen qualitative datadisplays and narrative with references topopulation-based data, thereby giving anapproximation of how widespread certaintypes of violent behavior are.
In Nicaragua, researchers combined theresults of a survey of 488 women on expe-riences of violence with narratives of threewomen’s experiences obtained through in-depth interviews.16 The narratives coveredmany of the same themes as the survey,and often provided moving illustrations ofhow women felt about the violence.Figure 3.2 illustrates how survey resultsand narratives may be used to provide
different perspectives on how children areaffected by domestic violence. Althoughthe feelings expressed by the youngwoman cannot be generalized to all bat-tered women, her story provides a win-dow into the devastating impact that abusecan have on women and their children.This type of insight is difficult to obtainfrom numbers.
Likewise, a research project in Tanzaniaused qualitative and quantitative methodsto examine how violence affectedwomen’s decisions to seek VCT forHIV/AIDS.9 Through in-depth interviewswith men and women, the researcherslearned about how testing and disclosureof HIV status could lead to violence. Twowomen described the aftermath of disclos-ing their seropositive status with the fol-lowing words:
“It took two weeks to tell him. He told me,‘You know who has brought it?’ I told him,‘If you are blaming me then blame me, butyou are the one who has brought it.’”
“When I informed him of the resultsthere was endless violence in the house.”
In a second stage, the researchers inter-viewed 245 women who attended theclinic, and asked them standardized ques-tions about experiences of violence. Theyfound that HIV positive women were twiceas likely to have been beaten by a partnerthan were HIV negative women, andamong young women, HIV positivewomen were ten times more likely to havebeen beaten than HIV negative women.The researchers concluded that violence isa risk factor for HIV/AIDS because it limitswomen’s ability to protect themselves.Moreover, HIV positive women are atgreater risk of physical abuse if they dis-close their serostatus. It was difficult todetermine from survey data alone whenthe violence took place in relation to dis-closure of serostatus. Thus, the qualitativeinformation provided insights useful ininterpreting the survey results.
C H A P T E R T H R E E
F IGURE 3.2 AN EXAMPLE OF COMBINING QUALITAT IVE AND QUANTITAT IVE DATA
“Mommy, you look l ike a mons ter”
“When he would beat me, my daughters would get involved in the fight. Then he would throw them around in his fury, and this hurt me more than when he beatme. …and once, I was recovering after he had beaten me, and my daughtercame up to me and said “Mommy, you look like a monster.” And she began tocry, and what really hurt me wasn’t so much the blows, it was her sobbing and the bitterness that she was feeling… Survivor of violence from Nicaragua
Wife’s friends
Husband’s friends
Husband’s family
Children
% of women who report witnesses to violence against them
Type
s of
witn
esse
s to
vio
lenc
e
0 10 20 30 40 50 60
(From Ellsberg et al, 2000.16)

A Practical Guide for Researchers and Activists 57
POPULATION- OR SERVICE-BASED RESEARCH?
A key decision regarding design is whetherto draw one’s sample from the communityat large (this is often referred to as a “popu-lation-based study”) or from a serviceprovider, for example, a women’s crisis cen-ter or a community health center. The deci-sion should be based on the goals andobjectives of your research. If the goal ofthe research is to evaluate a service (e.g.,how well the women’s police station meetsvictims’ needs) or determine what propor-tion of emergency room clients suffer abuse,then it makes sense to focus your researchon women attending these services. If, how-ever, your goal is to be able to say some-thing that applies to abuse victims moregenerally, then it is important to recruit yoursample from the community at large. Toooften, researchers rely on service-based data(police statistics, hospital records, or inter-views with women attending crisis services)to draw conclusions about patterns of phys-ical or sexual abuse in a larger population.In reality, these data apply only to womenwho seek formal services—a group that dif-fers substantially from the full universe ofabused women and children. Women thatmake their way into police or hospitalrecords have frequently suffered moresevere abuse and are more likely to havebeen abused by a stranger than women thatdo not report abuse.
An example of this can be seen in thecomparison of results from two studies car-ried out in Nicaragua on sexual abuse ofchildren. One study was based on policerecords, and included only cases of abusethat were reported to the police. This studyconcluded that in 95 percent of child sexualabuse cases girls were the victims of abuse.17
In contrast, a study carried out in León,Nicaragua, asked men and women whowere randomly selected from the communityto respond to an anonymous questionnaire
about their experiences of sexual abuse inchildhood. This study found that 30 percentof the total number of incidents of child sex-ual abuse were reported by men.18 Thesefindings indicate that either boys are lesslikely than girls to disclose abuse when ithappens, perhaps because of shame or fearof being stigmatized, or that parents are lesslikely to report cases of abuse of boys to thepolice. This comparison shows that theinformation obtained from service-basedsamples can differ greatly from resultsobtained from a community-based survey.
Record reviews can nonetheless yieldimportant information, especially about thequality of services that women receive fromhealth and justice system professionals. Acase in point is a study conducted by theSouth African NGO ADAPT that reviewedthe charts of 398 women presenting with ahistory of assault to the CasualtyDepartment of Alexandra Health Clinic dur-ing October and November in 1991.(Alexandra Township is a rapidly urbanizingcommunity near the heart of Johannesburg.)This study found that providers failed torecord the identity of the perpetrator in 78percent of cases. The charts included onlydisembodied descriptions of the violencesuch as “chopped with an axe” or “stabbedwith a knife.” Organizers used these data toemphasize to clinic administrators the needto sensitize providers to issues of violenceand to encourage more complete and accu-rate documentation.19
In another example, the IPPF carried outa study before initiating a program to trainproviders to screen for abuse in three LatinAmerican countries (Peru, Venezuela, andDominican Republic). They reviewedrecords to see how many women werebeing asked about violence in reproductivehealth clinics, and carried out a surveyamong providers to measure their knowl-edge and attitudes towards survivors ofviolence. By carrying out periodic follow-up surveys and record reviews, program
D E V E L O P I N G A R E S E A R C H S T R AT E G Y

58 Researching Violence Against Women
managers were able to measure changes inattitudes as a result of training, andincreases in screening and care for survivorsof violence.8
COLLABORATION BETWEEN RESEARCHERSAND ACTIVISTS
Throughout this manual, we emphasize theimportance of creating partnershipsbetween researchers and those who are ina position to use the research effectively,such as service providers, governmentagencies, women’s health advocates, orNGOs. We believe that this is the best wayto ensure that research objectives aregrounded in local needs and perspectives,and that the results will be used for pro-moting social change. Those who work
with victims of abuse alsobring knowledge and skillsthat will surely enrich theresearch process and improveits quality.
We recognize, however,that successful partnershipsbetween researchers and prac-titioners are not always easyto forge, as each group bringsa different set of expectations,needs, and skills to theendeavor. Practitioners fre-quently worry that the
research process could compromise theirprimary mission or undermine services.Researchers, for their part, often fear thatnonresearchers may not appreciate theimportance of scientific rigor.
There is also a legacy of past experi-ences that any potential collaboration mustovercome. Researchers are sometimes sur-prised when their overtures to activists orservice providers are met with suspicion.They don’t realize that many activists havehad negative experiences with researchers.
At a 1993 symposium on research
around sexual coercion, a panel of serviceproviders and activists explored the originsof the historical tension betweenresearchers and community-based organi-zations. As panel members explained,many NGOs had experiences with researchin the past that left them distrustful ofrequests to “collaborate” on research.Frequently, they noted, researchers appearmore concerned with their own profes-sional advancement than with the well-being of the respondents. The powerimbalance between researcher and respon-dent becomes especially problematic whennorthern researchers conduct research insouthern countries. Panelists could allrelate instances in which research resultsfrom developing countries were widelyreported at international conferences, butremained unavailable and unknown in thehost country.
At the same time, all panelists could giveexamples of research collaborations thatwere highly positive. In these examples,the researchers involved the serviceproviders or community group in the for-mulation of the research questions. Theinvestigators treated the NGO as a truepartner, as opposed to a site for research.They also recognized the practical expert-ise that comes from years of living with orworking on an issue. Most importantly, thestudy generated knowledge that was use-ful, not only for advancing the field of vio-lence research, but also for improving thework of the service providers.
Past experiences have highlighted thefollowing points as key to facilitating suc-cessful collaboration:20-22
■ Flexibility■ Shared goals■ Clear sense of responsibilities and roles■ Benefits on both sides■ Mutual respect and recognition of each
other’s strengths■ Equal access to funding and credit
C H A P T E R T H R E E
“Collaboration works best when there is mutual learning
on both sides,” notes GitaMisra of SAKHI, a community-
based group that works withSouth Asian battered women
in New York City. SAKHIencourages anyone undertakingresearch on abuse in the SouthAsian community to participatein its 20-hour intensive training
course for community volunteers.

A Practical Guide for Researchers and Activists 59
The last point is particularly important.The organization that controls the budgetin any collaboration often wields the great-est power. Collaborating partners, there-fore, should develop written agreements inadvance about how to allocate availableresources and/or how practitioners andtheir agencies will be compensated fortheir time and expertise.
The WHO VAW study has developedan effective model for research based onthe partnership between researchers, poli-cymakers and women’s organizations thatwork on violence against women. Thegoals of the study explicitly includedstrengthening national capacity to addressviolence against women by raising aware-ness and fostering collaboration betweenlocal actors. To achieve this, eachnational research team includedresearchers with the technical skillsneeded to carry out the research, as wellas representatives from organizationsinvolved in work on violence againstwomen. In addition, consultative groupswere formed in each country to bringtogether policy makers, researchers, andactivists to oversee the implementation ofthe study. This process has helped estab-lish long-term working relationshipsbetween these groups that in some caseshave continued beyond the study. Boththe researchers and activists agree thatthis model of collaboration has beenimportant, both by increasing the qualityof the data and the interpretation of thefindings, and by ensuring that the resultsare used to inform policy changes.23
DRAFT ING THE PROTOCOL
Once all the basic issues regarding studydesign have been resolved, it is time todraft the study protocol. The protocol sum-marizes the decisions that have been madethus far regarding the study objectives,study population, and sampling strategy,
D E V E L O P I N G A R E S E A R C H S T R AT E G Y
Title: As short as possible, but covering and indicating the research problem formulated.
Researchers: List of researchers, their titles, and professional affiliations.
Background: Explain why this study should be done. What is already knownabout the problem through other studies? What experience do you have in thisresearch area? What is your theoretical or conceptual framework? A well-refer-enced literature review is essential.
Research objectives: State the general objectives of the study and specify eachof the specific research questions. The objectives should correspond to studydesign and methods used.
Study area: Specify the geographical area for the study. What is known aboutthe social, economic, and epidemiological context?
Study design: Will the design involve a population-based survey, a case-controlstudy, participatory action research, in-depth interviews, focus groups, or some combination of the above?
Study population: This specifies who makes up the study population, includingage, sex, other characteristics, and follow-up period.
Sampling design and procedures: What is the sample size and the rationalefor the sample size calculation? What are the eligibility requirements for partici-pation? How will respondents be located, recruited, and selected? Will thesample be selected using randomization procedures? If so, provide the details.
Study methods: Describe in detail or refer to standard descriptions of methodsused. Attach any research instrument to be used (e.g., survey questionnaire,interview guide).
Description of main variables: Include a detailed description of how you willdefine and measure them.
Data management and analysis plans: How will the data be processed and analyzed?
Organization of fieldwork: All steps in the fieldwork should be described.What should be done, when, how, and by whom? What obstacles are antici-pated? How will they be dealt with?
Ethical considerations: Ethical issues should be identified and assessed by theresearchers as well as by an ethical review committee.
Timetable: When will stages such as preparations, piloting, study start, studyend, analysis, writing, and reporting take place?
Budget: Costs should be specified and should correspond to the time plan andthe general description in a realistic way.
Potential policy and program implications: What are the potential policy and program implications of this research? What changes, interventions, or otherconsequences could you expect as a result of your research?
References: Back up statements with references to other studies and methoddescriptions.
Appendices: Often the research instrument, such as an interview guide or question-naire is attached, as well as a curriculum vitae for each researcher and maybesome more specific details and instructions for some parts of the study performance.
(From Persson and Wall, 2003.2)
BOX 3.2 SUGGESTED OUTL INE OF STUDY PROTOCOL

60 Researching Violence Against Women
and will serve as a guide throughout theresearch process. It will be essential forobtaining funding and ethical clearance,for training research personnel, and forproviding information to the advisoryboard and others interested in the study.The protocol will evolve over the courseof the project, so that the final version,while the same in terms of content,reflects the refinements and details addedalong the way. Box 3.2 presents a sug-gested structure for the research protocol.It is a recommendation for the kinds ofinformation a research protocol shouldhave. You probably will want to add otherinformation or rearrange the contents tobetter reflect your research project.
1. Dahlgren L, Emmelin M, Winqvist A. QualitativeApproaches for International Public Health.Umeå, Sweden: Umeå University; 2003.
2. Persson LÅ, Wall S. Epidemiology for PublicHealth. Umeå, Sweden: Umeå InternationalSchool of Public Health; 2003.
3. Shrader E. Personal Communication. Washington,DC; 2000.
4. Nelson E, Zimmerman C. Household Survey onDomestic Violence in Cambodia. Phnom Penh,Cambodia: Ministry of Women’s Affairs andProject Against Domestic Violence; 1996.
5. Zimmerman K. Plates in a Basket Will Rattle:Domestic Violence in Cambodia, a Summary.Phnom Penh, Cambodia: Project AgainstDomestic Violence; 1995.
6. Igras S, Monahan B, Syphrines O. Issues andResponses to Sexual Violence: Assessment Report ofthe Dadaab Refugee Camps, Kenya. Nairobi,Kenya: CARE International; 1998.
7. Reproductive Health Response in ConflictConsortium. Gender-based Violence Tools Manualfor Assessment and Program Design, Monitoring,and Evaluation in Conflict-affected Settings. NewYork, New York: Reproductive Health Responsein Conflict Consortium; 2004.
8. Guedes A, Bott S, Cuca Y. Integrating systematicscreening for gender-based violence into sexualand reproductive health services: Results of abaseline study by the International PlannedParenthood Federation, Western HemisphereRegion. International Journal of Gynecology andObstetrics. 2002;78:557-563.
9. Maman S, Mbwambo JK, Hogan NM, et al. HIV-positive women report more lifetime partner vio-lence: Findings from a voluntary counseling andtesting clinic in Dar es Salaam, Tanzania.American Journal of Public Health.2002;92(8):1331-1337.
10.Guba E, Lincoln Y. Competing paradigms in qual-itative research. In: Denzin N, Lincoln Y, editors.Handbook of Qualitative Research. ThousandOaks: Sage; 1994.
11.Berman H, Ford-Gilboe M, Campbell JC.Combining stories and numbers: A methodologicapproach for a critical nursing science. Advancesin Nursing Science. 1998;21(1):1-15.
12.Ford-Gilboe M, Campbell J, Berman H. Storiesand numbers: Coexistence without compromise.Advances in Nursing Science. 1995;18(1):14-26.
13.Olesen V. Feminisms and Models of QualitativeResearch. In: Denzin N, Lincoln Y, editors.Handbook of Qualitative Research. ThousandOaks: Sage; 1994.
C H A P T E R T H R E E

A Practical Guide for Researchers and Activists 61
14.Ulin P, Robinson E, Tolley E, McNeill E.Qualitative Methods: A Field Guide for AppliedResearch in Sexual and Reproductive Health.Research Triangle Park: Family HealthInternational; 2002.
15.Boussen C. Give the Spirit Time to Ripen: Efforts toAbandon Female Genital Cutting in Mali.Washington, DC: PATH; 2004.
16.Ellsberg M, Peña R, Herrera A, Liljestrand J,Winkvist A. Candies in hell: Women’s experiencesof violence in Nicaragua. Social Science andMedicine. 2000;51(11):1595-1610.
17.Policía Nacional. Violencia Física y Sexual Contrala Mujer. Managua, Nicaragua: Policía Nacional;1997.
18.Olsson A, Ellsberg M, Berglund S, et al. Sexualabuse during childhood and adolescence amongNicaraguan men and women: A population-basedanonymous survey. Child Abuse and Neglect.2000;24(12):1579-1589.
19.Motsei M, The Centre for Health Policy. Detectionof Women Battering in Health Care Settings: TheCase of Alexandra Health Clinic. Cape Town,South Africa: Galvin & Sales; 1993.
20.Edleson JL, Bible AL. Forced Bonding orCommunity Collaboration? Partnerships BetweenScience and Practice in Research on WomanBattering. Paper presented at: National Instituteof Justice Annual Conference on Criminal JusticeResearch and Evaluation: Viewing Crime andJustice from a Collaborative Perspective.Washington, DC; 1998.
21.Campbell J, Dienemann JC, Kub J, Wurmser T,Loy E. Collaboration as a partnership. Violenceagainst Women. 1999;5(10):1140-1157.
22.Michau L, Naker D. Mobilising Communities toPrevent Domestic Violence. Kampala, Uganda:Raising Voices; 2003.
23.Garcia Moreno C, Watts C, Jansen H, Ellsberg M,Heise L. Responding to violence against women:WHO’s Multi-country Study on Women’s Healthand Domestic Violence. Health and HumanRights. 2003;6(2):112-127.
D E V E L O P I N G A R E S E A R C H S T R AT E G Y

4PHO
TO B
Y H
AFM
JAN
SEN

A Practical Guide for Researchers and Activists 63
■ Gender relations (e.g., decision makingand control of resources within thefamily).
Until recently, violence against womenhas been virtually invisible in most coun-tries, either because women are ashamed
CROSS-SECT IONALSURVEYS: EXPLORING THEMAGNITUDE OF VIOLENCE
Cross-sectional surveys provide an image ofa situation at a specific time. When appliedto the study of violence, cross-sectional sur-veys are useful for providing informationabout the proportion of women in a com-munity who have experienced or are cur-rently experiencing abuse. In the languageof epidemiology, this figure is known as aprevalence estimate. (See Box 6.1 inChapter 6 for a description of how preva-lence estimates are calculated.)
Cross-sectional surveys can also givevaluable insights into elements that definethe context in which violence occurs:
■ Characteristics and dynamics of abuse.■ How effectively women are being
reached by existing services.■ The attitudes of men and women with
regard to violence.
C H A P T E R F O U R
Quantitative Approachesto Research
Topics covered in this chapter:
Cross-sectional surveysCohort studiesCase-control studies
Interview in Ethiopia
PHO
TO B
Y M
. ELLS
BERG

64 Researching Violence Against Women
C H A P T E R F O U R
Cross-sectional surveys
The WHO Multi-country Study on Women’s Health and Domestic Violence Against Women was initiated in 1997 with the aim of obtaining reliable and comparable data within and across culturally diverse countries on:
■ The prevalence and frequency of different forms of physical, sexual, and emotional violence against women, particularly that inflicted by intimate partners.
■ The association of violence by intimate partners with a range of health outcomes.■ Factors that may protect or put women at risk for intimate-partner violence.■ Strategies and services that women use to deal with the violence they experience.
It had, in addition to these, a number of process-oriented objectives:
■ To develop and test new instruments for measuring violence cross-culturally.■ To increase national capacity amongst researchers and women’s organizations working on violence.■ To increase sensitivity to violence among researchers, policy makers and health providers.■ To promote a new model of research on domestic violence, involving women’s organizations with expertise on violence against women and
fully addressing safety issues and safeguarding women’s well-being.
Participating countries
The study involves collaboration between WHO, international research organizations (London School of Hygiene and Tropical Medicine andPATH, an expert steering committee of international content experts (researchers and advocates), and country research teams involving researchinstitutions and women’s health and rights organizations. The countries that participated in the first stage of the WHO multi-country study were:Bangladesh, Brazil, Thailand, Peru, Japan, Tanzania, and Namibia. Studies have also been performed in several other countries using theWHO methodology, including Samoa, Chile, Indonesia, Ethiopia, New Zealand, Serbia and Montenegro, and China.
Study methodology
The collection of rigorously sound and internationally comparable quantitative data on intimate partner violence has been a major focus of theWHO study. Qualitative data were also collected to inform the development and country adaptations of the questionnaire, as well as the inter-pretation of results. In most participating countries, the quantitative component of the study consisted of a cross-sectional population-based house-hold survey conducted in two sites: the capital (or other large city) and one province with rural and urban populations. In each of these sites arepresentative sample of around 1,500 women aged 15 to 49 was selected to participate in face-to-face interviews. Women were asked aboutexperiences of violence from intimate partners as well as nonpartners. Mechanisms to ensure comparability across countries included: a uniformcore questionnaire, detailed documentation of the local adaptations to the core questionnaire (which were kept to a minimum), a standard module for interviewer training, the involvement of the core research team in all interviewer and data-processing training and in piloting activities,and the use of standardized procedures for data processing and analysis.
Questionnaire
A uniform core questionnaire with structured questions was used as the basis for all country questionnaires, with country modifications related toeither adding country-specific issues or ensuring appropriate response categories. The questionnaire consisted of 12 sections; early sections col-lected information on less sensitive issues, whilst more sensitive issues, including the nature and extent of partner and nonpartner violence, areintroduced in later sections, after rapport has been established between interviewers and respondents. As in many other surveys of partner vio-lence, estimates of the prevalence of different forms of VAW were obtained by asking female respondents direct questions about their experienceof specific acts of physical and sexual violence from any partner. Follow-up questions were asked regarding the timing and frequency of violence.Women were also asked about experiences of emotionally abusive acts and controlling behaviors by their partners, and violence duringpregnancy. Questions about women’s experience of physical and sexual violence by nonpartners since the age of 15, and of sexual abuse bynonpartners before the age of 15, were also included in the study.
Results
The range of lifetime physical partner violence found among the sites was 13 to 61 percent of ever-partnered women. The range of reported sex-ual violence was even greater, from 6 to 58 percent, whereas the range of women reporting either sexual and/or physical violence by a partnerwas 16 to 69 percent. In all of the sites, women who experienced physical and/or sexual violence consistently reported more emotional distressand recent physical problems such as pain, trouble walking, and dizziness.
BOX 4.1 THE WHO MULTI-COUNTRY STUDY ON WOMEN’S HEALTH AND DOMESTIC VIOLENCE AGAINST WOMEN1
(From WHO, 2005.1)

A Practical Guide for Researchers and Activists 65
It is often common for cross-sectional surveys to collectsome retrospective information(e.g., “when did the violencebegin?”). However, to deter-mine causality with greater pre-cision, it is preferable to study individuals over time,or longitudinally.Longitudinal studies may beeither prospective (forwards)or retrospective (historical). The mostcommon public health research designs forcollecting longitudinal data, cohort studiesor case-control studies, will be describedin the next section.
COHORT STUDIES:EXPLORING THECONSEQUENCES OFVIOLENCECohort studies, also called follow-up orincidence studies, begin with a group ofpeople (a cohort) that has not experi-enced a problem or condition. The peopleare classifiedaccording towhether they havebeen “exposed” to apotential cause (orrisk factor) of acondition or dis-ease. The wholecohort is then fol-lowed over time tosee whether thoseindividuals with thesuspected risk factorare more likely todevelop the condi-tion or disease thanthe group withoutprior exposure. (SeeFigure 4.1 for anexample of how acohort study couldbe applied to a
Q U A N T I TAT I V E A P P R O A C H E S T O R E S E A R C H
to discuss it, because no one has thoughtto ask them about it, or because it is considered as a natural part of culture.Therefore, prevalence data are oftenneeded to convince policy makers of boththe pervasiveness of violence and its seri-ous implications for women’s health. Evensurveys carried out in a single region haveproven very useful in many countries indrawing attention to the dimensions of violence. Women’s rights activists inCambodia, (described in Box 4.2)Zimbabwe, and Nicaragua used surveyresults with great success to create publicawareness around domestic violence, andto effect changes in national policy as wellas legislation.
A cross-sectional survey may not be themost appropriate method to use if the goalis to determine the causes of violence orthe impact of violence on women’s physi-cal or emotional well-being. Cross-sectionalstudies provide a snapshot of a conditionand its suspected causal agents (referred toas “exposures” or “risk factors” in epi-demiology), where both are measured atthe same time.
It is usually difficult to assess accuratelywhich came first, exposure to the sus-pected risk factor or the condition. Forexample, many community surveys havefound that women who have been bat-tered tend to have more children than non-battered women. However, these studiesoften do not collect information on whenin the marriage the violence began. Norcan one tell from this kind of data whetherhaving many children increases women’srisk of being abused, or whether it is actu-ally a consequence of abuse and resultsfrom coerced sex or the control many abu-sive partners exert over their partner’s useof contraception. It is sometimes possibleto assume that one event occurs beforeanother. (For example, “injuries due to vio-lence” by definition must have taken placeafter the violence, not before.)
Longitudinal studies follow agroup of individuals overtime. Longitudinal studies maybe either:• Prospective, meaning that
changes are followed start-ing at the present time andinto the future, or
• Retrospective, or looking atindividuals’ past history.
Cross-sectional surveys
• Provide a snapshot of a population’scharacteristics.
• Can be carried out on a population orcommunity level, or in a service context.
• Require special sampling techniques toensure that the findings are representa-tive of the general population fromwhich the sample was selected.
• Are relatively easy and inexpensive todesign and implement, compared withcohort and case-control studies.
• Can provide retrospective (historical)information.
• Make it more difficult to determine whenevents took place, compared with a lon-gitudinal study. Therefore it is importantto be careful in concluding whether onecondition or event causes or leads toanother (also referred to as causality).

66 Researching Violence Against Women
study of violence during pregnancy andlow birth weight.)
Well-known examples of this type ofresearch design include long-term studiesto determine whether smoking causes lungcancer, or whether exercise reduces therisk of heart disease. The likelihood that anindividual who has been exposed to a cer-tain risk factor will contract the disease orcondition can be calculated as the relativerisk, which compares the rates or risks ofa specified outcome between groups thathave different exposures to the risk factorunder study. For example, relative risks areused to estimate the probability that awoman who is beaten during pregnancywill have a baby with low birth weightcompared to a woman who has not expe-rienced abuse during pregnancy
Cohort studies provide the best informa-tion about the causes of health and socialproblems and the most direct measurementof the risk of developing a certain condi-tion or disease. They also permit aresearcher to study several outcomes withregard to a single exposure. For example,it would be possible to determine theeffect of violence during pregnancy oninfant birth weight as well as on women’sphysical and mental health.
A cohort study design might also beused is to evaluate the effectiveness of anintervention over time. For example, the
C H A P T E R F O U R
Background and methods
In 1995, Cambodia became the first Asian country to undertake a representa-tive sample survey of domestic violence. This study, initiated as a joint projectbetween the Ministry of Women's Affairs (MoWA) and a Cambodian NGO,The Project Against Domestic Violence (PADV), surveyed 2,764 Cambodianhouseholds in six provinces and in Phnom Penh, the capital of Cambodia. Theaim of the study was to determine the prevalence and nature of violence inCambodian families, as well as awareness of violence. The survey grew out ofan earlier qualitative study entitled Plates in a Basket Will Rattle (see Box 5.5 inChapter 5). This study revealed the devastating impact of violence on the lives ofCambodian women, but raised questions about how widespread domestic vio-lence actually was and whether men were also victims of partner abuse.
In all, 1,374 women and 1,286 men were interviewed (the men were not thepartners of the women, but were sampled from nearby villages). The quantitativestudy used a modified version of the Conflict Tactics Scale (CTS) as a basis formeasuring abusive behavior (the CTS is described in Chapter 6). In this survey, theCTS was modified to include behaviors that the Khmer staff of MoWA and PADVidentified as common in Cambodia. Questionnaires were first written in Khmer,then translated and back-translated several times to ensure that the English andKhmer versions were clear, consistent, and meaningful. The survey used two ques-tionnaires per household. The first instrument was a brief questionnaire that servedto gather basic demographic information on all of the residents of the household.The second instrument was an individual-level questionnaire that was used to collectinformation on the respondent's perceptions of violence and on their individualexperiences of specific abusive acts. Prior to the field work, all members of theresearch team underwent a three-week training course on domestic violence issues,interviewing techniques, and the logistics of random selection of households.
Findings
Sixteen percent of women reported having been physically abused by a spouse,and 8 percent, or one-half of all women reporting abuse, sustained injuries. Morethan 50 percent of reported injuries were head injuries. In contrast, 3 percent ofmen reported abuse by a spouse and less than 1 percent reported injuries due toabuse. Women living with their natal kin were less vulnerable to spousal abuse,suffering half as much abuse (8.3 percent) as the overall population of women.Thirty-four percent of abused women said they had not sought help from anyone.
(From Nelson and Zimmerman, 1996.2)
BOX 4.2 DOMESTIC VIOLENCE IN CAMBODIA: A CROSS-SECTIONAL STUDY
FIGURE 4.1 DIAGRAM OF COHORT STUDIES (USING A STUDY OF LOW BIRTH WEIGHT AS AN EXAMPLE)
Population
People w/othe condition(i.e., pregnant
women)
Exposed (i.e., violencein pregnancy)
Problem develops (LBW)
Problem does not develop (no LBW)
Problem develops (LBW)
Problem does not develop (no LBW)
Not exposed (i.e., noviolence in pregnancy)
(Adapted from Persson and Wall, 2003.3)

A Practical Guide for Researchers and Activists 67
nancy on birthweight. This studywould be fairly easyto replicate in othersettings becausewomen are recruitedto the cohortthrough their atten-dance at prenatalservices, andbecause the follow-up period is rela-tively short. Thisdesign would workwell in settingswhere a majority ofwomen attend pre-natal care, becausethe women in thecohort would belikely to be fairly similar to women in thepopulation in general. However, it is lesssuited to a setting where few womenattend prenatal care, because the womenin the cohort would likely be quite differ-ent from other pregnant women in thecommunity. Also, if women do not givebirth close to where they received prenatalcare, or if most women deliver at home, itmay be difficult to obtain accurate birthweight information. In this case, a case-control design, suchas the one describedin Box 4.5, may bemore suitable.
CASE-CONTROLSTUDIES
Case-control stud-ies—also known ascase referent stud-ies—are relativelysimple and econom-ical to carry out.They include people
Q U A N T I TAT I V E A P P R O A C H E S T O R E S E A R C H
Nicaraguan NGO Puntos de Encuentro iscurrently carrying out a cohort study of4,500 young people in three sites to findout whether their mass media program hasbeen successful in changing the attitudesand behavior of youth with regard to high-risk sexual practices, use of violence, andstigmatizing attitudes toward persons livingwith HIV/AIDS. The same individuals willbe interviewed at the beginning, middle,and end of a television series, developedby Puntos, called Sexto Sentido (SixthSense). The study will compare changes inattitudes and behavior between individualswho watched the program regularly, andthose who never watched the program.4
The main drawback to cohort studies isthat, despite being conceptually simple,they require more resources and time thanother research designs. This is particularlytrue when studying relatively rare condi-tions, such as infant or maternal deaths, orwhere the outcome of interest occurs along time after exposure to the risk factor,as in the effect of smoking on cancer inci-dence. These kinds of studies tend toinvolve very large samples and many yearsof follow-up before results are obtained.
Box 4.3 presents an example of a rela-tively simple cohort study by Parker andcolleagues carried out in the United Statesto look at the impact of violence in preg-
Cohort Studies
• Follow a group of individuals over time. • Allow researchers to determine whether
individuals who have been exposed toa suspected risk factor for disease aremore likely to develop the condition ordisease than the group without priorexposure.
• May study several outcomes in relationto single (or multiple) exposures.
• May be prospective or retrospective(although prospective cohort studies aremore common).
• Are considered the best way to determinethe causes of a disease or condition.
• May be costly to perform, as cohortstudies often require very large samplesand follow-up over long periods.
Case-control studies
• Include people with a disease or othercondition and a suitable control or reference group of people not affectedby the condition or problem.
• Collect retrospective data on the individ-uals’ exposure to potential risk factors.
• Study only one outcome at a time.• Permit the identification of risk factors
for disease.• Usually require much smaller sample
sizes than cohort studies.• Are relatively simple and economical to
carry out.
Interview in EthiopiaPH
OTO
BY
M. E
LLSBE
RG

68 Researching Violence Against Women
with a disease or other condition (such asexperiencing violence or depression) and asuitable control or reference group of peo-ple not affected by the condition or prob-lem. The “cases” should represent allindividuals from the specified populationhaving the condition or disease being stud-ied. The controls are then selected ran-domly from the same population,excluding those who already have theproblem (see Figure 4.2).
Retrospective information is collectedfrom both groups, with particular attentionto the time before the onset of the condi-tion. The frequency and distribution ofsuspected risk factors is then comparedbetween cases and controls, and infer-ences may be made regarding the causalfactors that increase the risk that a particu-lar outcome will occur. The results areexpressed as an odds ratio, which com-municates the odds that a person with thedisease or condition was exposed to therisk factor, compared to someone withoutthe condition. See Box 4.4 for an explana-tion of the differences between odds ratiosand relative risk.
In the study of violence, case-controlstudies may be useful for exploring factorsthat increase women’s risk for abuse, or forexamining the effects of violence on otherhealth outcomes. They are particularly use-ful for studying events or diseases thatoccur infrequently in a given population,such as infant mortality, because the over-all sample size needed is much smallerthan in cohort studies. When cases andcontrols are matched according to knownconfounding factors such as age and sex,the design is even more powerful in itsability to predict the outcome.
One constraint of case-control studies isthat although multiple causes of a condi-tion may be examined, only one outcomecan be studied at a time. For example, tostudy the effects of violence on both birthweight and infant mortality, it would be
C H A P T E R F O U R
Background and methods
The purpose of this study was to determine the incidence of physical and sexualabuse in a cohort of adult and teen pregnant women and to determine the effectof abuse on the birth weight of their babies. Using three simple screening questionsfor abuse, 1,203 African American, Hispanic, and white urban women in theUnited States were interviewed on their first prenatal visit and in the second andthird trimesters. Infant birth weight was obtained by record review.
Findings
Abuse during pregnancy was reported by 20.6 percent of teens and 14.2 percent of adult women. Both abused teens and adults were significantly morelikely than nonabused women to enter prenatal care during the third trimester (21.9vs. 7.5 percent for teens; 15.8 vs. 8.7 percent for adults). Among the total sam-ple of 1,203 women, women who were abused during pregnancy were signifi-cantly more likely to deliver infants with low birth weight, and to experience lowmaternal weight gain, infections, and anemia. They were also more likely to smokeand to use alcohol or drugs.
BOX 4.3 ABUSE DURING PREGNANCY: A COHORT STUDY
The association between risk factors and outcomes is expressed somewhat differ-ently in case-control studies and cohort studies. Cohort studies use relative risk andcase-control studies use odds ratios.
Both can be translated into lay terms by referring to the relative likelihood of an out-come occurring in the case of cohort studies (e.g., low birth weight), or the relativelikelihood of being exposed to a risk factor (e.g., violence during pregnancy) in thecase of case-control studies. Although this distinction may appear small, it is usefulto keep in mind when interpreting research results. For example:
■ A relative risk of 3.0 in a cohort study of violence during pregnancy and lowbirth weight indicates that women who are beaten during pregnancy are threetimes more likely to have low birth weight infants than their nonabused peers.
■ An odds ratio of 2.0 in a case-control study on the causes of low birth weightindicates that infants with a low birth weight are twice as likely to have motherswho were beaten during pregnancy.
When an odds ratio or relative risk equals 1.0, it means that there is no associa-tion between two variables, and a value greater than 1.0 indicates risk. A valueless than 1.0 indicates that the exposure has a “protective” or preventive effect withregard to the outcome. Both odds ratios and relative risk figures are usually accom-panied by 95 percent confidence intervals (95 percent CI), indicating the likelyrange for the true ratio. A statistically significant range is one that does not include1.0. Sometimes a statistical test is performed resulting in a p-value. This gives theprobability that the observed association is simply due to chance. If the p-value isvery small (< 0.05), then we can say there is evidence that the association is real,and not merely due to chance.
BOX 4.4 THE DIFFERENCE BETWEEN ODDS RATIO AND RELATIVE RISK
(From Parker et al, 1994.5)

A Practical Guide for Researchers and Activists 69
necessary to design two different studies,one where the “cases” were infants withlow birth weight, and another where thecases were defined as children who diedunder a certain age.
Boxes 4.5 and 4.6 describe two exam-ples of case-control studies—a low birthweight study that was carried out in ahospital setting, and a study of child mor-tality risk that was nested as a substudywithin a larger household survey onreproductive and child health. The childmortality study in particular demonstratesthe potential benefits of integratingresearch on violence into other researchprojects. Although violence was not theprimary focus of the child mortality study,the integration of a set of questionsregarding mothers’ experiences of vio-lence complemented other research effortson violence in the same region. They pro-vided unique insight into violence as acontributing cause of child mortality,which would otherwise have been quitedifficult and costly to obtain.
Q U A N T I TAT I V E A P P R O A C H E S T O R E S E A R C H
FIGURE 4.2 DIAGRAM OF CASE-CONTROL STUDIES
Population
Cases (i.e., low birthweight infants)
Controls (normalweight infants)
Have the exposure(mother abused in
pregnancy)
Do not have the exposure(mother not abused in
pregnancy)
Have the exposure(mother abused in
pregnancy)
Do not have the exposure(mother not abused in
pregnancy)
Background and methodsThis study was performed in León, Nicaragua, in 1996. It differs from the childmortality study (Box 4.6) in that it was carried out in a hospital setting. This designwas chosen because of the difficulties in obtaining reliable birth weight informa-tion from women interviewed in a household survey.
During a two-month period, all births in the León Teaching Hospital were moni-tored and 101 infants weighing less than 2,500 grams were selected as cases.Two controls were randomly selected for each case among infants weighing2,500 grams or more. Mothers were interviewed in a special private roombefore leaving the hospital, usually within 24 hours of delivery. Women’s obstetri-cal histories were taken and compared whenever possible with hospital and pre-natal records. Women were also asked about other relevant risk factors for lowbirth weight (LBW), such as smoking and alcohol use, and experiences of vio-lence ever and during pregnancy, using the Abuse Assessment Screen.
Main findingsIn this study, the following factors among mothers were found to be associatedwith having a LBW infant: mother’s young age, pre-eclampsia and bleeding, lackof or inadequate prenatal care, smoking, mother’s stress during pregnancy,poverty, and violence during pregnancy. Physical abuse during pregnancy wasfound in 22 percent of mothers of LBW infants (cases) compared with 5 percentamong controls. This association was significant even after adjusting for socio-economic and medical risk factors. The study concluded that after poverty, vio-lence was the second major cause of low birth weight in León, accounting forabout 16 percent of LBW. This placed violence ahead of smoking, pre-eclamp-sia, or bleeding, all of which are recognized risk factors for LBW.
BOX 4.5 DOMESTIC VIOLENCE AND LOW BIRTH WEIGHT:A CASE-CONTROL STUDY
(From Valladares et al, 2002.6)
(Adapted from Persson and Wall, 2003.3)

70 Researching Violence Against Women
1. World Health Organization. WHO Multi-countryStudy on Women’s Health and Domestic ViolenceAgainst Women: Report on the First Results.Geneva, Switzerland: WHO; 2005.
2. Nelson E, Zimmerman C. Household Survey onDomestic Violence in Cambodia. Phnom Penh,Cambodia: Ministry of Women’s Affairs andProject Against Domestic Violence; 1996.
3. Persson LÅ, Wall S. Epidemiology for PublicHealth. Umeå, Sweden: Umeå InternationalSchool of Public Health; 2003.
4. Solorzano I, Peña R, Montoya O, et al. Informede los Primeros Resultados de la Evaluación delPrograma Juvenil, Somos Diferentes, SomosIguales. Managua, Nicaragua: Fundación Puntosde Encuentro, Centro de Investigación yDesarrollo en Salud, HORIZONS, PATH; 2005.
5. Parker B, McFarlane J, Soeken K. Abuse duringpregnancy: Effects on maternal complications andbirth weight in adult and teenage women.Obstetrics and Gynecology. 1994;84(3):323-328.
6. Valladares E, Ellsberg M, Peña R, Högberg U,Persson L-Å. Physical partner abuse during preg-nancy: A risk factor for low birth weight inNicaragua. Obstetrics and Gynecology.2002;100(4):100-105.
7. Åsling-Monemi K, Peña R, Ellsberg M, Persson L.Violence against women increases the risk ofinfant and child mortality: A case-referent study inNicaragua. The Bulletin of the World HealthOrganization. 2003;81:10-18.
C H A P T E R F O U R
Background and methods This study was carried out in León, Nicaragua, in 1996 by researchers from theNational University at León and Umeå University, Sweden. The purpose of thestudy was to determine the impact of physical and sexual violence against womenon both infant and under-five mortality risks.
The study was obtained from an ongoing demographic surveillance system inLeón. A household survey was conducted of 9,500 homes, in which 12,000women ages 15-49 years were asked about their reproductive histories, includinginformation about any children who were born, or who had died in the last twoyears. Through this process, 132 children were identified who had died within theprevious two years before the age of five. These children were classified as thecases. For each case, two controls, matched by sex and age at the time of death,were randomly selected from the same population. Specially trained interviewersreturned to the homes of the cases and controls and administered a new question-naire to the mothers. The questionnaire focused on the circumstances leading up tothe death of the child (for cases) or the 12 months prior to the interview (for con-trols), including her experiences of physical and sexual abuse. Because it was notpossible to trace all the mothers, a final total of 110 mothers of cases and 203mothers of controls were interviewed.
FindingsThe study found that 61 percent of mothers of deceased children and 39 percentof those of controls had lifetime experience of physical or sexual abuse. Physicalabuse by a partner during pregnancy was twice as frequent among mothers ofchildren who had died (23 percent vs.13 percent). The risk of under-five mortality,adjusted for relevant socio-economic factors, was two times greater among childrenwhose mothers had experience of either physical or sexual partner abuse. The riskof under-five mortality for a child whose mother had experienced both physical andsexual partner abuse was six times greater than children whose mothers had neverexperienced violence. The study concluded, after adjusting for other risk factors,that violence against mothers could be responsible for as much as one third ofchild deaths in León.
BOX 4.6 THE IMPACT OF VIOLENCE AGAINST WOMEN ON CHILD MORTALITY: A CASE-CONTROL STUDY
(From Åsling-Monemi et al, 2003.7)

5PH
OTO
BY
HAF
M JA
NSE
N

A Practical Guide for Researchers and Activists 73
process of doing research can initiate apublic discussion of violence and open adialogue with key institutional actors.
Likewise, if the goal is to better under-stand the mindset and attitudes of abusivemen, it will be more productive to usequalitative techniques to probe how menview their partners, how they justify andinterpret their behavior, and the incidentsor “transgressions” that set them off.Qualitative techniques will foster muchmore nuanced understanding of theseissues than will quantitative surveys.
For the purposes of this manual, wedivide qualitative research into two maintypes of research designs: rapid assess-ments and in-depth qualitativestudies. Individuals new to the field ofqualitative research will want to seekguidance from someone familiar withthese techniques before pursuing a quali-tative research project. In addition, read-ers are encouraged to consult some ofthe excellent resources on qualitativedata collection and analysis listed inAppendix III.
Qualitative research methods areextremely useful to researchers andadvocates interested in violence.Qualitative methods—especially rapidassessment techniques—are helpful forassessing community needs, designingprevention campaigns, planning andevaluating interventions, and engagingcommunity actors via participatoryresearch. They are also useful in design-ing and field-testing questionnaires, andin interpreting quantitative research find-ings. Qualitative methods provide greaterinsight into motivation, meanings, anddynamics of violent relationships.
In many cases, a qualitative approachwill suit a specific study aim better thanquantitative methods. For example, if theprimary purpose of research is to helpplan an intervention, it may be more con-structive to use available resources tounderstand community attitudes towardviolence and the responses and attitudesof institutional actors—such as the police,health care providers, and the clergy—toward victims. In such cases, the very
C H A P T E R F I V E
Qualitative Approachesto Research
Topics covered in this chapter:
Rapid assessmentsIn-depth qualitative studies

74 Researching Violence Against Women
C H A P T E R F I V E
RAPID ASSESSMENTS
A rapid assessment is an exploratory studydone as a prelude to designing an inter-vention or as a means of supplementingand/or refining quantitative research (forexample, helping to identify local termsused for different diseases in order todesign a questionnaire). A rapid assess-ment responds over a relatively shortperiod to a few specific questions withconcrete applications; for example, Whatkinds of services do rape victims want?What words do women use to describeabuse? How do community leaders regardthe use of advocates to accompany womenwhen they report violence to the police?
A rapid assessment does not pretend toprovide a full, detailed account of allaspects of abuse. Its purpose is to guidethe development of research instruments(e.g., survey questionnaires), to assess localneeds, or to evaluate interventions.Participatory research designs are particu-larly appropriate when the aim is to stimu-late discussion and reflection within acommunity about an issue, and to promotecommunity-based actions.
In the last 20 years, rapid assessmenttechniques have become very popular as ameans to aid project and instrument
design, and to evaluate inter-ventions. The field of publichealth research—once domi-nated by Knowledge,Attitudes, and Practices (KAP)surveys and epidemiologicalresearch—has now incorpo-rated a broad array of qualita-tive methods borrowed fromthe fields of marketing, popu-lar education, agriculture, andsocial anthropology. Rapid
assessments can draw on any number oftechniques including focus groups, partici-pant observation, in-depth interviews, ormore participatory techniques such as
mapping, pile sorts, community mapping,and seasonal calendars.
Within the larger category of rapidassessments are a variety of research tradi-tions, including Rapid Rural Appraisal,Participatory Rural Appraisal, ParticipatoryAction Research, and situation analysis.The diversity of names and methods usedfor these approaches reflects their differenthistorical roots as well as some key con-ceptual differences. One major distinctionis the degree to which the investigator ver-sus the community guides and implementsthe research process. In recent decades,various forms of participatory researchhave evolved as an alternative to investiga-tor-led initiatives. Participatory researchtends to blur the distinction betweenresearch and intervention and can be anexcellent way to raise consciousness aboutviolence and to initiate community workon sensitive topics like violence. The fol-lowing is a brief summary of the mostcommonly used approaches to rapidassessment.
Participatory appraisals In the 1970s, researchers in the field ofagricultural development and naturalresource management developed a set ofrapid assessment techniques that provideda quick and reliable alternative to tradi-tional methods for conducting agriculturalresearch. Collectively known as RapidRural Appraisal (RRA), these methodsincluded such techniques as seasonal cal-endars to determine patterns of rainfall,crop production, and disease; “transectwalks” to document soil and vegetationpatterns; and community mapping. Themethods of RRA were primarily adaptedfrom social anthropology and quicklybecame popular among researchersbecause they produced reliable results,often as good as or better than thoseobtained by much more costly and time-consuming quantitative studies.
Participatory RuralAppraisal is a growingfamily of approaches and
methods designed to enablelocal (rural or urban) peopleto express, enhance, share,
and analyze their knowl-edge of life and conditions,
to plan and to act.(Chambers, 1994.1)

A Practical Guide for Researchers and Activists 75
In the 1980s, RRA was increasingly criti-cized because of its emphasis on extract-ing information from communities for theuse of outsiders. The critiques of RRA ledto the development of a new researchtrend called Participatory Rural Appraisal(PRA). PRA emphasized participation ofthe local community in the developmentof the appraisal, the use of diverse meth-ods, and the knowledge generated by thecommunity. In recent years, the methodsof PRA have been used in many otherfields, including urban development.Although the methodology did not origi-nally incorporate a systematic gender per-spective, many of the techniques havebeen modified to give greater visibility togender gaps in access and control ofresources.
In contrast to PRA, which developed outof the experience of northern-basedresearchers, Participatory ActionResearch (PAR) is rooted in the populareducation movements of the south, particu-larly those of Latin America. Popular edu-cation, initially conceptualized by PauloFreire in Brazil and later developed bysocial movements in many countries duringthe 1980s, considers research within a par-ticipatory framework of learning andaction, and takes the knowledge and expe-rience of community members as a pointof reference. The educational techniquesused in PAR are designed to stimulategroup reflection on an issue and to moti-vate participants to act collectively toaddress the problem.
The PAR process follows a circular logicof research and action; empowerment ofindividuals and the community is achievedprimarily through collective endeavor.Therefore PAR, as well as popular educa-tion, is a much more political process thanPRA, in that individual and collectiveempowerment of participants is an explicitgoal. In fact, the “success” of a PAR projectis measured by the social transformations
it catalyzes rather than by the informationit generates. PAR is an excellent choice ifthe main goal is social change and thetransfer of skills. If accuracy of the data is
Q U A L I TAT I V E A P P R O A C H E S T O R E S E A R C H
Background and methods
Sexual violence against women in the Dadaab refugee camps, located inNortheast Kenya, has been an issue since refugees began arriving from Somalia in1991. The number of reported rapes (106 in a population of 106,000) in the firstnine months of 1998 was higher than the number for all of 1997. CARE and theGerman technical cooperation agency GTZ conducted an assessment of sexualviolence in the Dadaab refugee camps as part of a wider initiative by CARE toreview women’s issues in the camps.
The assessment was designed to collect information to answer several critical ques-tions to guide future programming, including:
■ Determining the extent of the problem. ■ Determining areas of security concern regarding sexual violence. ■ Identifying what services and programs exist. ■ Obtaining information and perceptions of those most affected by the issue. ■ Obtaining information and perceptions of potential service providers. ■ Analyzing the collected information with agencies and community representa-
tives to develop proposal ideas.
The assessment was refugee-driven, in the sense that it focused on substantive dis-cussions with many refugee groups to define the problem and causes and to sug-gest solutions to reduce sexual violence. Participatory Learning and Actionmethodologies, including free listing, community mapping, causal flow diagrams,and pairwise ranking, were used to structure discussion sessions with refugees(examples of how these methods were used in the Dadaab appraisal are pre-sented in Chapter 9). The team also interviewed main agencies involved in protec-tion services and prevention activities. Additionally, a record review was conductedof reported cases of sexual violence in the past three months. The following wereamong the findings that were discussed with the communities and involved agen-cies to improve security for women at the camps.
Areas of vulnerability
Groups identified several areas within the camps, including in and around boreholes and water tap stands and places where the living thorn fences that surroundthe camp had been destroyed. Vulnerability was also linked to time: People statedthat they were afraid to leave their homes after dark. Women reported that they feltvulnerable when they left their homes to line up predawn at the hospital to beassured an entry ticket for health services that day.
Firewood collection
The record review of sexual violence cases showed that over 90 percent of thereported rapes and attempted rapes occurred when women left the camps to col-lect firewood. The firewood issue is the most problematic, because inexpensiveoptions to replace firewood as a fuel are limited for a camp population estimatedat about 106,000 people. Many women are now traveling in large groups to col-lect firewood. Sudanese and Ethiopian males collect or purchase firewood toreduce the need to go to the bush in search of fuel.
(From Igras et al, 1998.2)
BOX 5.1 SEXUAL VIOLENCE IN KENYAN REFUGEE CAMPS:A PARTICIPATORY APPRAISAL

76 Researching Violence Against Women
critical, a more traditional approach maybe a better choice.
The main tenets of participatory researchare that:
■ It involves a flexible, iterative processof exploration that stimulates creativity,improvisation, and flexibility in the useof methods to facilitate learning.
■ Community members direct theprocess, in the sense that knowledge isproduced on the basis of their ownexperiences. By the same token, com-munity members define the priorities ofthe appraisal, as well as the collection,analysis, and interpretation of data.
■ The role of outsiders is to facilitaterather than direct the learning processand the production of knowledge.
■ Participants, not just the researchersor external agents, own the methodsand the results. The socialization ofknowledge and techniques in participa-tory research is greatly encouraged.
■ Diversity is enhanced rather thanaveraged out. Participatory researchattempts to reveal differences betweensituations, attitudes, and practicesaccording to social class, gender, andethnicity and tries to learn from casesthat apparently do not conform to theexpected.
■ Triangulation is used to validateresults. This refers to the use of differ-ent methods for studying the same phe-nomena, or using the same method withgroups that represent diversity, forinstance by gender and class, to seewhether results are valid for each group.
■ The entire process, not just theresults, is designed to enhance
C H A P T E R F I V E
Background and methods
In 1996, Jijenge!, which means to ”build yourself” in Kiswahili, was established inMwanza, Tanzania, in an effort to address the physical and social determinants ofwomen's poor sexual health by promoting sexual health. The programs at Jijenge!include a reproductive health clinic, sexual health and HIV counseling and testingservices, advocacy, community awareness, and training, and all work to empowerwomen to proactively claim their rights. In 1997, Jijenge! staff and volunteersdecided to undertake a participatory rapid assessment on violence againstwomen. The goals of the project were to initiate public discussion of the topic andto lay the groundwork for a more extensive intervention.
The rapid assessment consisted of focus group discussions (FGDs), a baseline sur-vey, and in-depth interviews. Most of the research, conducted by Jijenge!’sCommunity Awareness Coordinator and the volunteers, was done in the commu-nity, except for a few in-depth interviews and one women's FGD which were heldat Jijenge! for safety reasons.
Focus group discussions. Seventy-seven people—37 women and 40 men—wereinvolved in the FGDs: two female groups, two male groups, two mixed groupswith general community members, and one mixed group with community leaders.The single sex FGDs were extremely useful; participants shared experiences andopinions honestly and the women were particularly supportive of one another. Thetwo mixed groups with general community members were somewhat less fruitfulbecause some women were noticeably inhibited in the company of men.Participation of both women and men in these mixed groups was clearly influencedby perceptions of status and power, and the roles they needed to maintain inmixed company.
In-depth interviews. Eighteen in-depth interviews were held with ten women andeight men. The interviews provided rich contextual information that deepenedunderstanding about the complexity of beliefs perpetuating violence and the subse-quent effects on women and men's lives.
Selected findings
Community members commonly referred to violence as a necessary form of disci-pline. A man, as the head of the household, is believed to have the responsibilityto discipline all family members. In the study, violence—physical, verbal, or emo-tional—emerged as an acceptable way to teach lessons to women and children.Family violence is a common tactic for asserting authority and power over women.
Although violence occurs at an alarming rate in this community, it is also believedthat violence between a husband and wife is a ”domestic matter” that should notbe raised by an outsider. Some women experiencing violence did not confide infamily or friends because they felt that this would label them as a “bad wife ormother.” Women accepted responsibility for men's violence, blaming their ownbehavior instead of their partner’s inability to manage his emotions appropriately.This shame and stigma keeps violence underground and prevents community mem-bers from supporting the women experiencing violence or confronting violent men.
The findings from this study helped organizers better understand local attitudestoward abuse before designing a program of intervention.
(From Michau, 2002.3)
BOX 5.2 JIJENGE! A PARTICIPATORY ACTION RESEARCHPROJECT IN TANZANIA

A Practical Guide for Researchers and Activists 77
Q U A L I TAT I V E A P P R O A C H E S T O R E S E A R C H
empowerment of individuals and com-munities, thereby stimulating socialchange.
Examples of participatory research stud-ies are presented in Box 5.1 and 5.2.
Situation analysisSituation analysis first became popularwithin family planning research in develop-ing countries. In the 1990s, violenceresearchers appropriated the term, whichthey used to refer to a set of rapid assess-ment techniques designed to evaluateexisting community attitudes and practicesregarding victims of abuse. Situation analy-ses were first used in violence research inseveral Mexican cities; New Delhi, India;and Harare, Zimbabwe. Situation analysesare a useful way to enter a community andbegin working on violence.
Situation analyses rely on a combinationof focus groups, semistructured interviews,and observation, directed at establishingboth community attitudes and beliefsregarding violence and the attitudes andpractices of key institutional actors, such aspolice, judges, social workers, clergy, andhealth professionals. Generally, situationanalyses include focus groups with key sub-groups in the population (young women,old women, young men, older men, abusedwomen, rape victims, and so on) and inter-views with a quota sample of differentproviders. Questions are geared towardassessing the adequacy of current institu-tional responses to victims of violence andthe degree of support and/or victim-blamingextended to abused women. An example ofa situation analysis performed in Kenya toimprove postexposure HIV prophylaxis torape survivors is described in Box 5.3.
Situation analyses can serve as a sort ofcommunity “diagnostic” that providesinsights into needed areas of reform. Thedata they provide can also help convincecommunity leaders that reforms are indeed
Background
Violence is an important risk factor contributing towards vulnerability to HIV andAIDS. Discussions of opportunities and challenges around postexposure prophy-laxis to reduce HIV transmission following sexual violence is growing. Gender-based sexual violence in Kenya is almost invisible, though reportedly moreprevalent than officially acknowledged. Health care workers at primary healthcenters and voluntary counseling and testing sites are reporting increasing num-bers of rape clients. There is increasing demand for VCT services and VCT scale-up as a key Kenyan strategy to fight HIV and provide infrastructure, capacity,and political support for provision of comprehensive postrape services.
Objectives
A qualitative situation analysis was undertaken to develop a strategy for the provi-sion of comprehensive postrape services in the VCT context. A review of literatureand international experience on sexual violence and service provision includingthe use of postexposure prophylaxis was undertaken. The study had two mainobjectives:
■ To establish perceptions of gender-based sexual violence in Kenya.■ To document and analyze service provision for gender-based sexual violence
within Kenya.
Methodology
The study focused on three districts. Nairobi, Thika, and Malindi were selectedbecause of availability of VCT services and to capture geographical, social, and religious diversities. Assessment was done in 10 VCT sites, 16 hospitals,and 8 legal and advocacy support programs. Forty key informants were inter-viewed and 20 FGDs were undertaken. Analysis involved comparing and con-trasting key themes emerging from different participants such as counselors andcommunity members. Different research sites and research methodologies such as focus groups and interviews were triangulated.
Findings
Sexual violence was seen as shameful, with diverse views on whether rapehappens in relationships. Greater participation in discussions on rape from malegroups in comparison to female groups may suggest less social barriers to pub-lic discussions of sexuality for men. Generally, views presented by male groupsseem to edge towards justification and tolerance for rape, in contrast towomen’s groups that felt the need for concerted efforts to address rape. Mostpeople were unaware of what to do or where to go in the event of sexual vio-lence. Provision of services by the police and at hospitals was seen to be lack-ing and rape survivors were often humiliated and retraumatized. Further, there isno documentation for rape and a weak chain of custody for investigation.Counseling services are nonexistent in public health institutions except in placeswhere VCT services are available.
Conclusions
The implementation of postrape services within the VCT framework in Kenya mustinclude:
■ Multidisciplinary approaches to developing a regulatory framework. ■ Integration of both counseling and clinical management in health care services. ■ Building capacities for services provision. ■ Development of referral systems.
(From Kilonzo et al, 2003.4)
BOX 5.3 POSTRAPE SERVICES IN KENYA: A SITUATION ANALYSIS

78 Researching Violence Against Women
C H A P T E R F I V E
In 1995, PAHO began the implementation of a ten-country diagnostic study to document what happens when awoman affected by family violence decides to break the silence and seek assistance in ending the abuse. InSpanish, this process was called the “ruta crítica” or the “way out.” In effect, the study asked, what happens whena woman decides to seek help? To whom does she turn for help? What factors motivate her to act or inhibit herfrom acting? What kinds of attitudes and responses does she encounter from institutional actors?
Altogether, researchers conducted over 500 in-depth interviews with battered women, interviewed more than1,000 service providers, and completed approximately 50 focus group sessions.
Results show many factors—both internal and external—influence a woman’s decision to act to stop the violence.In some cases, it takes many years and several attempts at seeking help from several sources. Rarely is there a sin-gle event that precipitates action. Findings suggest that many battered women are resourceful in seeking help andfinding ways of mitigating the violence.
Battered women identified several factors that act as catalysts for action. An increase in the severity or frequency ofthe violence may trigger a recognition that the abuser is not going to change. An event may make it clear to herthat she cannot modify the situation with her own internal resources. A primary motivating factor is the realizationthat lives—hers or her children’s—are in danger.
“He mistreated the children badly. He only knew how to shout orders. There was a period when he wouldbeat them. The children, particularly my oldest son, had become very disobedient, rebellious and had lostall motivation to study. He didn’t go to school…”
“I finally decided to leave when he burned all my clothes and also burned me.”
“The moment came when I said to myself that I had to find someone to help me because it was not possi-ble to keep going on in this way. I had become hysterical, problematic, unhappy, mainly because I couldsee my beaten face every week in the mirror.”
What factors inhibit the process of seeking help?
As with the precipitating factors, the obstacles for seeking help are multiple and intertwined.
“One learns to live with the person even though he is an abuser. I don’t know, for me he was my compan-ion because I felt alone, without the support of a family. He was my family…”
“I used to excuse him for that and I believed that through the love I had for him he was going to get better,and that this was not going to keep on.”
However, economic factors appear to weigh more heavily than do emotional considerations:
“The children were very young and I didn’t think I could support them on my own. And I didn’t want toburden my mother.”
These barriers are reinforced by battered women’s feelings of guilt, self-blame, or abnormality.
“I tried to reflect on my own actions. What did I do to provoke him? I considered my personality…”
“My mother would tell me that I was crazy and that is why I was seeing a psychologist and my brothersand sisters said the same thing.”
“There came a moment in which I really thought ‘Am I crazy?’ Then I sought help to make sure that whatwas happening to me was true.”
Women who sought help rarely began with formal health or police services. They initially relied instead on supportfrom other women in the community, including female family members, neighbors, and health promoters. Manywomen related instances of being ridiculed or treated with indifference by health providers and local authorities.
“I finally told a friend that I trusted. I went to tell her because she is an older lady and she told me that hewas wrong, that he was a sadist. She told me that I should get out of the house.”
“…Almost every time he abused me I would go to my friend’s house and she would give me a place tosleep. I would even sleep on the floor, because she was poor. She was the one who finally said, ‘This istoo much. I am going to help you find help because that man is abusing you too much!’”
(From Sagot, 2000.6)
BOX 5.4 “LA RUTA CRÍTICA”—INSTITUTIONAL RESPONSES TO DOMESTIC VIOLENCE: A MULTI-COUNTRY QUALITATIVE STUDY

A Practical Guide for Researchers and Activists 79
needed. Situation analyses can be particu-larly productive when local communitymembers assist in doing the interviews. Inthe Pan American Health Organization(PAHO) project, members of the localwomen’s organization that provides serv-ices for victims of abuse frequently con-ducted interviews. Because of thedemands of assisting victims, many advo-cates had never taken the time toapproach the local forensic doctor, the vil-lage priest, or the chief of police. The
research provided a structured environ-ment through which to analyze institu-tional responses and to initiate dialoguewith key institutional actors. (See Box 5.4)
IN-DEPTH QUALITAT IVESTUDIES
Rapid assessments and in-depth qualita-tive studies differ mainly in the scope ofresearch and methods of analysis. An in-depth qualitative study requires a more
Q U A L I TAT I V E A P P R O A C H E S T O R E S E A R C H
A common Cambodian proverb—”plates in a basket will rattle”—is used to explain family problems.
“If people live in the same house there will inevitably be some collisions. It's normal—it can't be helped.But, from time to time, plates break. So do women.”
Background and Methods
The study, Plates in a Basket will Rattle—Domestic Violence in Cambodia, is based on in-depth interviews with 50 victims of domestic violence and one interview with the mother of awoman who was killed by her husband. Additional information was gathered from interviewswith individuals that an abused woman is likely to encounter in her search for assistance,including judges and court personnel, police officers, district chiefs, village heads, medicalworkers and midwives, and staff from NGOs.
The subjects for the study were located primarily by word-of-mouth with the help of local com-munity organizations. The main researcher (a North American) worked with two Cambodiancolleagues to conduct the interviews. Before the research began, they had first to create wordsin high and low Khmer to refer to "domestic violence," since no words previously existed.Interviews took an average of half a day, and women were compensated for the income theycould have made during this time by trading in the market. (This generally amounted tobetween 7,500 and 10,000 riels, or between $3 and $5 per woman.)
Prior to beginning the interviews, the team made contingency plans in case there was awoman who might be in immediate danger and request assistance. To this end, they con-tacted three local NGOs that offered to provide temporary shelter for victims.
Interview information was collected in the form of handwritten notes in Khmer, which were tran-scribed and translated into English immediately after each encounter.
Findings
The study highlighted the difficult plight of women who were severely beaten by their husbands. It showed howcultural norms, shame, and the lack of viable alternatives kept women in abusive relationships. Many of thewomen interviewed suffered physical abuse in pregnancy as well as sexual abuse and degrading treatment fromtheir partners. Virtually no public institutions, including the police and health sector, were trained or sensitive to theneeds of battered women.
The most important outcome of the study was that domestic violence became a public issue in Cambodia. Theresearch helped catalyze a conference on violence, sponsored by UNICEF, and it played a role in the develop-ment of an antiviolence organization called the Project Against Domestic Violence. Many of the findings from thequalitative study proved critical in helping to lay the foundation for the quantitative study carried out subsequently(described in Box 4.2).
(From Zimmerman, 1995.7)
BOX 5.5 “PLATES IN A BASKET WILL RATTLE”:IN-DEPTH QUALITATIVE STUDY ON DOMESTIC VIOLENCE IN CAMBODIA

80 Researching Violence Against Women
detailed and more time-consumingresearch design. It involves extensive datacollection, processing, and analysis. Whilein-depth studies often use many of thesame techniques as rapid assessmentsfor collecting data (e.g., focus groups,observation, and interviews), they are gen-erally conducted over longer periods, usemore respondents, and entail more sys-tematic data analysis. (Chapter 13describes in greater detail some of thebasic techniques for qualitative data analy-sis.) In general, one conducts an in-depthstudy for the following reasons:
■ To advance theoretical understanding ofan issue and/or to gain a more completeunderstanding of a phenomenon thancan be gained during a shorter study.
■ To understand cultural norms, beliefs,and behaviors or to capture and analyzecomplex motivations. Such studies frequently rely on detailed
interviews that require enormous amountsof time and energy to transcribe, code,and analyze. Many researchers underesti-mate the challenge of coding and inter-preting reams of qualitative data.Performing an in-depth qualitative study is
C H A P T E R F I V E
Background
In 1998, the Nicaraguan NGO Puntos de Encuentro embarked on a study designed to gain information useful fordesigning a public education campaign that called on men to renounce violence in their intimate relationships. Thestudy used qualitative research techniques to generate hypotheses about the type of antiviolence messages that menwould accept and find appropriate to their needs and expectations.
Methodology
The research included three phases:
■ Compilation and content analysis of the workshop transcripts and reports from meetings about men and mas-culinity in Nicaragua, including:
1. Men’s views about what it means to be a man in Nicaragua.2. Images and attitudes men hold about women.3. The advantages and disadvantages of “being a man.”4. Men’s memories of how they were raised to become adults (socialization).
■ In-depth interviews with a sample of 12 nonviolent men. Researchers chose to interview nonviolent men basedon the rationale that, rather than looking for "causes" of men’s violence (and then offer a "medicine" with the cam-paign), it would be more productive to study what creates “health”—that is, how do we understand men who,in spite of growing up in a violent socio-cultural context, do not become violent themselves? To be considered“nonviolent,” men had to be identified by their peers and pass a series of behavioral screens. Men exposed tofeminist discourse were explicitly excluded.
■ In-depth interviews with “ordinary” men.
Selected results
The research revealed that large differences exist between nonviolent and "ordinary” men. For example, ordinarymen say that their relationships are best when their partner does not complain, or when she does what she is told.On the other hand, nonviolent men held very different expectations for relationships. For them, a “good relationship”is one where there is mutuality, reciprocity, and mutual support.
Nonviolent men perceived both benefits and costs to this behavior. Among the benefits identified were greater tran-quility and harmony at home; a “good reputation” in the community, feeling good about oneself, health and well-being of one’s children, and a household that runs more smoothly day to day. Among the costs of "swimmingupstream" against a machista culture were ridicule and ostracism by other men.
Nonviolent men either grew up in very loving homes where they were taught to respect women or in very violenthomes, where their own mothers were beaten and they vowed never to be like their fathers.
(From Montoya, 1998.8)
BOX 5.6 SWIMMING UPSTREAM: VIOLENCE AND MASCULINITY AMONG NICARAGUAN MEN

A Practical Guide for Researchers and Activists 81
as complex and time-consuming as con-ducting a community survey.
In-depth qualitative studies are not allthe same, however. In fact, this termrefers to a broad category with many dif-ferent traditions. Creswell identifies thefive most commonly used traditions inqualitative research as: biography, phe-nomenology, grounded theory, ethnogra-phy, and case studies.5 Although themethods for data collection are similar,the theoretical underpinnings and theapproaches to data analysis and interpre-tation differ greatly. Table 5.1 presents abrief description of these traditions.
Because an in-depth description ofeach tradition is beyond the scope of thismanual, we recommend that readers con-sult the resources mentioned in Appendix
III for more information about qualitativeresearch.
Further examples of qualitative researchon gender-based violence are provided inBoxes 5.4-6. Box 5.4 presents an ambitiousmulti-country study carried out by PAHOas a point of entry for developing coordi-nated community interventions againstdomestic violence in 25 pilot communitiesthroughout Latin America.
Box 5.5 describes one in-depth qualita-tive study on domestic violence derivedfrom interviews with abused women inCambodia as well as with communityleaders and service providers. This study,entitled Plates in a Basket Will Rattle, wasthe first of its kind in Cambodia, and pro-vided extremely rich information aboutpartner abuse in a society that has long
Q U A L I TAT I V E A P P R O A C H E S T O R E S E A R C H
Dimension
Focus
Discipline origin
Data collection
Data analysis
Narrative form
Biography
Explaining the life ofan individual
Anthropology, litera-ture, history, psychol-ogy, sociology
Primarily interviewsand documents
Stories, epiphanies,historical content
Detailed picture ofan individual’s life
Phenomenology
Understanding theessence of experi-ences about aphenomenon
Philosophy, sociol-ogy, psychology
Long interviews withup to ten people
StatementsMeaningsMeaning themesGeneral descriptionof the experience
Description of the“essence” of theexperience
Grounded Theory
Developing a theorygrounded in datafrom the field
Sociology
Interviews with 20-30 individuals to“saturate” categoriesand detail a theory
Open codingAxial codingSelective codingConditional matrix
Theory or theoreticalmodel
Ethnography
Describing and inter-preting a culturaland social group
Cultural anthropol-ogy, sociology
Primarily observa-tions and interviewswith additionalartifacts duringextended time inthe field (e.g., sixmonths to a year)
DescriptionAnalysisInterpretation
Description of thecultural behaviorof a group or anindividual
Case Study
Developing anin-depth analysis ofa single case ormultiple cases
Political science,sociology, evalua-tion, urban studies,other social sciences
Multiple sources,documents, archivalrecords, interviews,observations, physi-cal artifacts
DescriptionThemesAssertions
In-depth study of a“case” or “cases”
TABLE 5.1 D IFFERENT TRADIT IONS IN QUALITAT IVE RESEARCH
(From Creswell, 1998.5)

82 Researching Violence Against Women
been ravaged by war. Finally, Box 5.6presents a qualitative study done inNicaragua to examine the roots of maleviolence against women. This study wasperformed to provide information for thedevelopment of a campaign directedtowards men on violence prevention.
1. Chambers R. Participatory Rural Appraisal (PRA):Analysis of experience. World Development.1994;22:1253-1268.
2. Igras S, Monahan B, Syphrines O. Issues andResponses to Sexual Violence: Assessment Report ofthe Dadaab Refugee Camps, Kenya. Nairobi:CARE International in Kenya; 1998.
3. Michau L. Mobilizing Communities to EndViolence Against Women in Tanzania. In:Haberland N, Measham D, eds. Responding toCario: Case Studies of Changing Practice inReproductive Health and Family Planning. NewYork: Population Council; 2002.
4. Kilonzo N, Theobald S, Molyneux S, Kibaru J,Taegtmeyer M. Post Rape Services in Kenya: ASituation Analysis. Nairobi: Liverpool VCT; 2003.
5. Creswell JW. Qualitative Inquiry and ResearchDesign: Choosing Among Five Traditions.Thousand Oaks: Sage Publications; 1998.
6. Sagot M. La Ruta Crítica de las Mujeres Afectadaspor la Violencia Intrafamiliar en América Latina:Estudio de Caso en Diez Países [The Critical RouteFollowed by Women Affected by Violence: A CaseStudy of 10 Countries]. Washington, DC: OPS/OMS Programa Mujer, Salud y Desarrollo; 2000.
7. Zimmerman K. Plates in a Basket Will Rattle:Domestic Violence in Cambodia, a Summary.Phnom Penh, Cambodia: Project AgainstDomestic Violence; 1995.
8. Montoya O. Nadando contra Corriente:Buscando Pistas para Prevenir la ViolenciaMasculina en las Relaciones de Pareja. Managua,Nicaragua: Fundación Puntos de Encuentro; 1998.
C H A P T E R F I V E

6PH
OTO
BY
HAF
M JA
NSE
N

A Practical Guide for Researchers and Activists 85
that underlie different approaches to meas-uring violence against women and reviewsand critiques some of the most commoninstruments used internationally.
EST IMATING THEPREVALENCE OF VIOLENCE
It is difficult to compare most interna-tional prevalence data on violencebecause different methods were used toobtain them. Prevalence is defined as theproportion of women who are abused ina given study population. (See Box 6.1 fora more detailed description of how preva-lence figures are calculated.) Therefore,researchers face two major challenges inobtaining accurate prevalence data: howto define “abuse” and how to determinethe study population. Researchers haveaddressed these methodological issues in
How does one decide what criteriato use to define and measure gender-basedviolence? Operationalizing main variables isa key issue in all cross-cultural studies, andespecially in the study of violence. In quali-tative research, it is not usually necessary tofinalize these decisions before initiating datacollection. In fact, a main goal of a qualita-tive study may be to understand what kindsof acts are considered violent by a particu-lar woman or group of women. However,in most quantitative studies, particularlywhen the aim is to estimate the magnitudeof violence in different settings, researchersneed to develop clear definitions that canbe compared across settings.
This chapter explores the challenge ofmeasuring violence and emphasizes esti-mating the prevalence of different forms ofabuse across a wide range of settings. Itdescribes some major conceptual issues
C H A P T E R S I X
The Challenge of Definingand Measuring Violence inQuantitative Research
Topics covered in this chapter:
Estimating the prevalence of violenceThe study population: Choosing interview subjectsDefinitions of violenceEnhancing disclosure of violenceCommon tools for measuring violence

86 Researching Violence Against Women
C H A P T E R S I X
many different ways, and there is little con-sensus as to the most appropriate method.A further complication is that surveys donot measure the actual number of womenwho have been abused, but rather, thenumber of women who are willing to dis-close abuse. It is always possible thatresults are biased by either overreporting orunderreporting.
In reality, researchers around theworld have found no evidence that abuse
is overreported.1 To be identified as a vic-tim of abuse in most societies is soshameful that few women report abusewhen it has not actually occurred. Womenare far more likely to deny or minimizeexperiences of violence due to shame,fear of reprisals, feelings of self-blame, orloyalty to the abuser. Box 6.2 outlinessome of the most critical issues that canaffect how prevalence data are calculatedand interpreted.
THE STUDY POPULATION:CHOOSING INTERVIEWSUBJECTS
Study populations used for gender vio-lence research vary greatly. Many studiesinclude all women within a specific agerange (frequently 15-49 or over 18), whileother studies classify women according tomarital status, and interview only womenwho have been married at some point intheir lives, or women who are currentlymarried. The logic underlying differencesin the range of women included rests inthe way researchers define the populationat risk of abuse. Table 6.1 gives anoverview of approaches used in past stud-ies of partner violence.
Sometimes, researchers decide not tointerview women below a certain agebecause of specific legal requirementsregarding the participation of minors asresearch informants. In some countries, thisdecision depends on the average age ofmarriage. Because many prevalence studiesare embedded in larger studies that focuson women’s reproductive health—such asthe Demographic and Health Surveys(DHS)—only women of reproductive ageare included, thereby excluding the experi-ences of older women.2
Relationship statusSome studies further refine the study popu-lation according to the relationship status
Prevalence is defined as the number of persons having a specific characteristicor problem, divided by the number of persons in the study population who areconsidered to be at risk of having the problem, usually expressed as a percent-age. Incidence refers to the number of new cases of a problem divided by thestudy population over a specific period. For example, the incidence rate of dia-betes refers to the number (usually expressed as x out of 1000, etc.) of peoplewho are newly diagnosed with diabetes each year in a community, whereas theprevalence is the total proportion of people with diabetes in the community,regardless of how long ago they were diagnosed. The prevalence of violenceagainst women refers to the number of women who have experienced violencedivided by the number of at-risk women in the study population. (In the case ofsome kinds of violence, such as sexual assault, all girls and women may be con-sidered at risk, but in other cases, such as intimate partner violence, only womenwho have ever had an intimate partner would be considered as at risk.) Thiscan be measured as:
Period prevalence
Women abused during a certain period (usually the last year) X 100
Women at risk in the study population
or
Lifetime prevalence
Women abused at any time in their life X 100
Women at risk in the study population
The incidence rate of partner abuse refers to the number of violent events womenexperience during a specific period, such as one year. In crime studies, inci-dence of violence is generally measured as the number of assaults per inhabi-tant, rather than the number of women being assaulted, so that each beatingthat a woman receives is counted separately. Thus, the incidence rate can tellyou what happened over the last year, but it may not tell you how many peoplewere affected.
Although some kinds of violence might be measured as discrete incidents (e.g.,a sexual assault by a stranger), many forms of gender-based violence, such aschild sexual abuse and partner violence, may be ongoing processes and noteasily captured as discrete events. Furthermore, the effects of a single assaultmay be long-lived. For this reason it is less practical or useful to measure violencein terms of incidence rates, and the magnitude of gender-based violence is mostcommonly presented in terms of prevalence.
BOX 6.1 DEFINING PREVALENCE AND INCIDENCE

A Practical Guide for Researchers and Activists 87
of respondents. For example, studies onpartner violence often include only womenwho are currently married because experi-ence shows that these women are at great-est risk of current partner abuse. In somecases, researchers exclude from studieswomen in common-law relationships, orthose who have been married for less thanone or two years (see Table 6.1). We rec-ommend using the broadest criteria possi-ble for defining the study population. Inthe case of wife abuse, this would includeinterviewing all women in a specified agerange, or at least all those who have everhad an intimate partner. Restricting thestudy population further may bias resultsfor the following reasons:
■ The risk of partner abuse is not con-fined to women who are currentlyin formal marriages. Some studiesindicate that women in common-lawrelationships suffer a greater risk for vio-lence than do married women.3
Unmarried women may also be abusedby their boyfriends. Many studies findthat women who are currently separatedare more likely to have been abused atsome point in their lives by a partner,indicating that violence may be animportant reason for women to separatefrom or divorce their partners.2 In somecountries, women are at greatest risk ofabuse and even homicide immediatelyafter separating from their partners.Therefore, excluding these women fromthe study population means that valu-able information may be lost, and thestudy results will not reveal a true pic-ture of how violence is affectingwomen’s lives.
■ The risk of partner abuse is not con-fined to women who have been in arelationship for a certain length oftime. Some research indicates that wifeabuse starts early in a relationship. In
the Nicaragua survey, for example, 50percent of abused women reported thatthe violence began in the first twoyears of the relationship, and 80 per-cent reported that the violence beganwithin four years.4 This indicates thatwomen are at risk of partner violence
T H E C H A L L E N G E O F D E F I N I N G A N D M E A S U R I N G V I O L E N C E I N Q U A N T I TAT I V E R E S E A R C H
How is the study population identified?
■ Are there cut-off ages?■ Is marital status considered for eligibility? ■ What geographic area is included in the study?
How is violence defined and measured?
■ Who defines abuse—the researcher or the respondent?■ Over what period of time is violence being measured? ■ Does the study distinguish between different types of abusers in terms of their
relationship to the victim? ■ Is frequency of violence measured?■ What types of violence are included (e.g., physical, sexual, emotional, eco-
nomic, etc.)?■ Does the study gather information regarding the severity of violence?
Is the interview carried out in such a way that women are likely to discloseexperiences of violence?
■ How are questions on violence worded?■ What questions precede them?■ How are the questions introduced?■ How many opportunities do the respondents have to disclose?■ What is the context of the interview (privacy, length, skill of interviewer)?
BOX 6.2 ISSUES THAT AFFECT THE MEASUREMENT OF GENDER-BASED VIOLENCE
Country Study Population
Cambodia Ever-married women and men
Canada All women aged 18 or older
Chile Women aged 22–55 married or in a common-lawrelationship for more than two years
Colombia Currently married women aged 15–49
Egypt Ever married women aged 15–49
Nicaragua All women aged 15–49
Philippines All women aged 15–49 with a pregnancy outcome
Uganda All women 20–44
Zimbabwe All women 18 years or older
* References for the studies are listed in Table 1.1.
TABLE 6.1 VARIATION AMONG STUDY POPULATIONS FROMRECENT POPULATION-BASED SURVEYS ON PARTNER VIOLENCE*
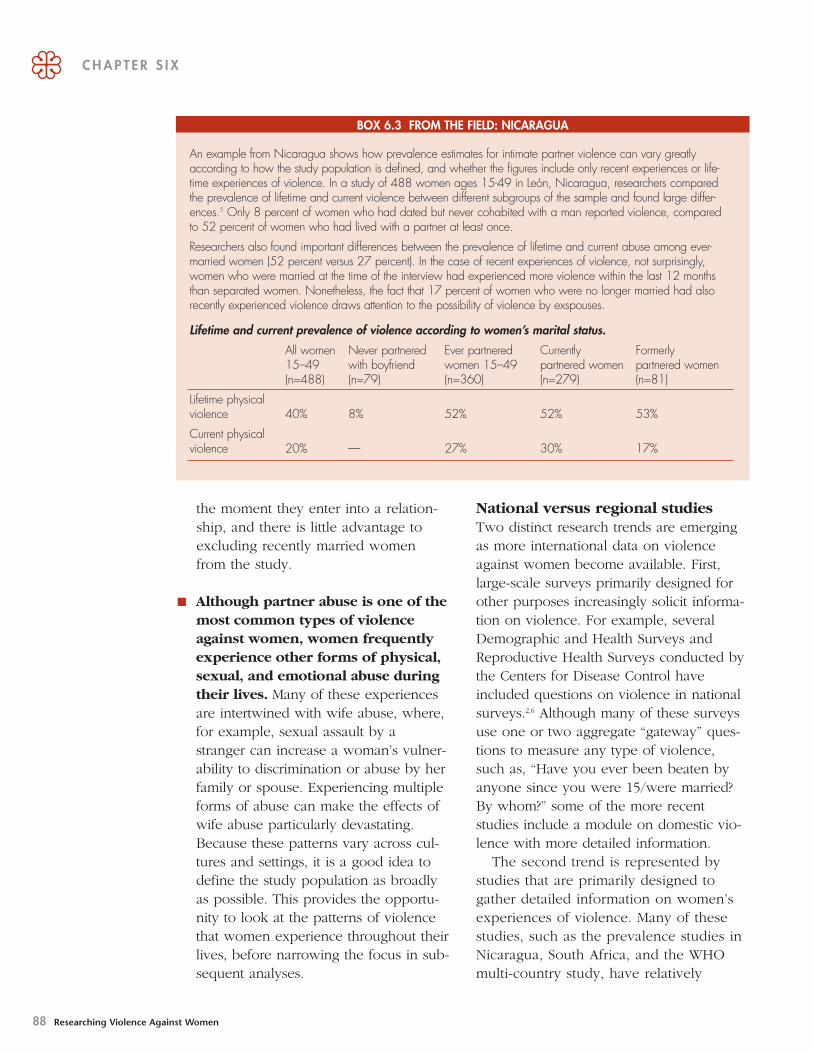
88 Researching Violence Against Women
the moment they enter into a relation-ship, and there is little advantage toexcluding recently married womenfrom the study.
■ Although partner abuse is one of themost common types of violenceagainst women, women frequentlyexperience other forms of physical,sexual, and emotional abuse duringtheir lives. Many of these experiencesare intertwined with wife abuse, where,for example, sexual assault by astranger can increase a woman’s vulner-ability to discrimination or abuse by herfamily or spouse. Experiencing multipleforms of abuse can make the effects ofwife abuse particularly devastating.Because these patterns vary across cul-tures and settings, it is a good idea todefine the study population as broadlyas possible. This provides the opportu-nity to look at the patterns of violencethat women experience throughout theirlives, before narrowing the focus in sub-sequent analyses.
National versus regional studiesTwo distinct research trends are emergingas more international data on violenceagainst women become available. First,large-scale surveys primarily designed forother purposes increasingly solicit informa-tion on violence. For example, severalDemographic and Health Surveys andReproductive Health Surveys conducted bythe Centers for Disease Control haveincluded questions on violence in nationalsurveys.2,6 Although many of these surveysuse one or two aggregate “gateway” ques-tions to measure any type of violence,such as, “Have you ever been beaten byanyone since you were 15/were married?By whom?” some of the more recentstudies include a module on domestic vio-lence with more detailed information.
The second trend is represented bystudies that are primarily designed togather detailed information on women’sexperiences of violence. Many of thesestudies, such as the prevalence studies inNicaragua, South Africa, and the WHOmulti-country study, have relatively
C H A P T E R S I X
An example from Nicaragua shows how prevalence estimates for intimate partner violence can vary greatlyaccording to how the study population is defined, and whether the figures include only recent experiences or life-time experiences of violence. In a study of 488 women ages 15-49 in León, Nicaragua, researchers comparedthe prevalence of lifetime and current violence between different subgroups of the sample and found large differ-ences.5 Only 8 percent of women who had dated but never cohabited with a man reported violence, comparedto 52 percent of women who had lived with a partner at least once.
Researchers also found important differences between the prevalence of lifetime and current abuse among ever-married women (52 percent versus 27 percent). In the case of recent experiences of violence, not surprisingly,women who were married at the time of the interview had experienced more violence within the last 12 monthsthan separated women. Nonetheless, the fact that 17 percent of women who were no longer married had alsorecently experienced violence draws attention to the possibility of violence by exspouses.
Lifetime and current prevalence of violence according to women’s marital status.
All women Never partnered Ever partnered Currently Formerly15–49 with boyfriend women 15–49 partnered women partnered women(n=488) (n=79) (n=360) (n=279) (n=81)
Lifetime physicalviolence 40% 8% 52% 52% 53%
Current physicalviolence 20% — 27% 30% 17%
BOX 6.3 FROM THE FIELD: NICARAGUA

A Practical Guide for Researchers and Activists 89
Thus, one tradeoff of using multipur-pose surveys to produce prevalence esti-mates on violence is the risk thatviolence will be significantly under-reported. Such underreporting can diluteassociations between potential risk fac-tors and health outcomes, leading toresults that are falsely negative.Underestimating the dimensions of vio-lence could also prevent violence inter-vention programs from receiving thepriority they deserve in the allocation ofresources.
■ Finally, because many of these studieshave not systematically addressed safetyconcerns, women who participate inthem may face increased risk of retalia-tion or other harm.
Researchers and advocates should con-sider carefully whether they need national-level data in order to achieve their policyobjectives. In many countries, advocateshave successfully used the results of repre-sentative sample surveys of asingle region, province, or sig-nificant city to raise publicawareness of violence and toguide policy decisions. It isusually more important to havehigh-quality data that are notvulnerable to criticism onmethodological or ethicalgrounds. Rather than expend-ing extra effort to make a study “national,”researchers might do well to explore vio-lence in depth among a smaller, more con-densed sample of individuals.
When conducting a regional study, it isimportant to select a study populationdiverse enough to allow comparisonsbetween women of different socio-eco-nomic groups. The study population shouldalso share important characteristics withother parts of the country. The results of aprevalence study carried out in a single
T H E C H A L L E N G E O F D E F I N I N G A N D M E A S U R I N G V I O L E N C E I N Q U A N T I TAT I V E R E S E A R C H
smaller sample sizes and cover a limitedgeographical region, although there areimportant exceptions, such as theNational Surveys on Violence AgainstWomen in Canada (1993),7 the UnitedStates (1997),8 Sweden,9 and Finland(1997).10 These studies tend to gathermuch more information about differenttypes of violence and perpetrators, aswell as information on circumstances andwomen’s responses to violence. They alsotend to devote more attention to theinteraction between interviewers andrespondents and issues of safety.
There are potential advantages to includ-ing violence questions in national surveysdesigned primarily for other purposes. Forexample:
■ In many cases, national statisticsbureaus conduct the studies, and theresults assume the legitimacy of “officialstatistics.” This can be very useful forpurposes of advocacy.
■ Nationally representative data are usefulfor local program planning, and alsopermit in-depth analysis of variationbetween regions.
■ The large data sets generated by thesestudies, including many other reproduc-tive and child health outcomes, can beused to deepen understanding of risk fac-tors and health consequences of violence.
There are also drawbacks to this strategy:
■ In general, prevalence estimates havebeen higher in the more focused studiesthan in the national surveys designedprimarily for other purposes.11 Oneexplanation may be that because thefocused studies emphasize the use ofmethods for enhancing disclosure, theyare able to produce more accurateprevalence estimates.12
The study populationshould be as broadly definedas possible, and, if possible,should be diverse with respectto ethnicity and socio-economicbackground, so that the resultswill be meaningful to a largersegment of the population.

90 Researching Violence Against Women
neighborhood of poor urban dwellers or ina small village composed only of members
of an ethnic minority may becritically important for design-ing local interventions.However, because such a studydoes not include large sectorsof the population, such as rural
or middle class women or women of dif-ferent religious or ethnic backgrounds, it isless useful for understanding how differentwomen experience violence. Moreover,such studies are often dismissed as beingtoo narrow, and have little effect on policy.
DEFINIT IONS OF VIOLENCE
Who defines abuse?The way in which violence is defined hasan enormous impact on the final results.Thus, it is crucial to establish from thebeginning how violence will be defined andwho will be considered a “case of abuse,”to borrow a term from epidemiology.
The following are examples of criteriathat have been used in studies of intimatepartner violence:
■ Any kind of physical, sexual, or emo-tional violence by any perpetrator atany time.
■ One or more acts of physical violenceby a partner at any time.
■ Only physical violence of a certain levelof severity, or which has been repeateda certain number of times.
■ Only acts of partner violence occurringin the last year.
■ Economic, as well as physical, sexual,or emotional violence.
■ Any behavior that women themselvesidentify as abusive by virtue of its intent
or effect (this may include such diverseacts as infidelity, verbal aggression orhumiliating acts, coerced sex, or refus-ing to pay for household expenses).
How does one decide whether to usedefinitions developed according to criteriaestablished by researchers, or to focus onacts which women themselves view asmost harmful? The danger in relying exclu-sively on women’s own definitions ofabuse, referred to in social science as an“emic” approach, is that these may vary sogreatly from one woman to the next, andbetween cultures, that it may not be possi-ble to draw meaningful conclusions fromthe results. For example, the question,“Have you ever been abused by your part-ner?” is likely to underestimate the trueoccurrence of violence. Many women mayexperience severe physical violence andyet not identify this behavior as abusive,either because they are used to it orbecause such behavior is considered nor-mal in their culture. Other women mayanswer positively, citing verbal offenses orhumiliations as evidence of abuse. Thisinformation may help the researcherunderstand how different women perceiveviolence, but it is less useful in planninginterventions or making cross-culturalcomparisons.
One advantage of using externallyderived definitions—an “etic” approach—isthat this enables the researcher to makecomparisons across different groups ofwomen. The most common method is toask women whether they have experi-enced a series of behaviorally specific actsof physical, sexual, or emotional violence,such as hitting, slapping, kicking, or forcedsex. Women who disclose violence arethen asked to specify their relationship tothe perpetrator and the frequency orperiod in which it took place. The draw-back of this approach is that you cannotknow whether these acts have the same
C H A P T E R S I X
Prevalence studies need tohave clearly defined criteria
for determining what acts areconsidered as violence.

A Practical Guide for Researchers and Activists 91
meaning in different cultures or to differentwomen. For example, punching a womanwith a fist and kicking her may appearfrom the outside to be roughly equivalent,if “risk of injury” is used as the main crite-ria for severity. However, in some cultures,it is particularly demeaning to kick awoman because it implies that she is nobetter than an animal. In another country,an outsider might assume that a partner’srefusal to speak to a woman is less seriousthan physical abuse. Nonetheless, thewoman enduring the abuse might experi-ence the same emotional pain and humilia-tion that she would from a physical blow.
Many researchers address this dilemmaby combining approaches that ask aboutspecific behaviors and ask women to inter-pret them. A researcher may ask womenabout specific acts, frequency, and perpetra-tors, followed by open-ended questions ask-ing her to describe “the worst incident” orany other behavior or experience that sheconsiders abusive. This approach can gener-ate information on violence that researcherscan compare to other settings and to otherwomen’s perceptions of their experience.
Types of violencePartner violence. The range of violentacts that women may experience is quitevaried, and so is the impact of specific actson their lives. For this reason, it is impor-tant not to define partner violence too nar-rowly. For example, if you ask only aboutexperiences of being hit or beaten, womenmay not mention that they have beenraped, kicked, or burned. Althoughresearchers initially focused primarily onphysical violence, today their work alsoconsiders emotional and sexual abuse.Many studies also include other kinds ofabusive or controlling behavior, such aslimiting decision making power or mobil-ity, or economic violence.
While it may be useful to identify womenwho have experienced abuse, it is important
to present separately the prevalence of eachtype of violence. For cross-cultural compar-isons, aggregating emotional, sexual, andphysical abuse in a single domestic violencefigure is likely to lead to confusion, for thefollowing reasons:
■ Definitions of emotionally abusive actsvary across cultures, which makes it dif-ficult to find a valid definition.
■ Combining these categories may reducethe credibility of the findings, as manypolicy makers consider emotional abuseto be less severe than the other types ofviolence.
■ Different types of violence affectwomen’s physical and psychologicalhealth in different ways. Therefore,grouping them together may obscurecertain consequences of violence.
You should design your questionnaireso that different types of violence can beappropriately disaggregated. Althoughgrouping some behaviors together canhelp avoid overly long or tedious lists ofquestions, these acts should be similar inseverity or type of violence. Answers tobroad questions such as “Have you everbeen insulted, beaten, or raped by yourhusband?” or questions that combine actsof different severity such as “Has yourhusband ever hit you on the head orpulled your hair?” will be difficult to interpret.
The list of abusive behaviors need notbe exhaustive. Their purpose is not todescribe every possible act that a womanmay have experienced. Rather, the aim is tomaximize disclosure and to allow for gen-eral characterizations regarding the mostcommon types and severity of violence.
Some countries may have specific typesof violence that are not common else-where, such as dowry-related abuse, abuse
T H E C H A L L E N G E O F D E F I N I N G A N D M E A S U R I N G V I O L E N C E I N Q U A N T I TAT I V E R E S E A R C H

92 Researching Violence Against Women
by in-laws, and acid throwing in SouthAsia or group rape in Papua New Guineaand Cambodia. Formative research carriedout before developing the questionnairemay help you identify forms of violencethat are specific to the country setting andthat the survey needs to address. Box 6.4presents the definitions used by WHO fordifferent kinds of violence.
Rape and sexual coercion. Researchon rape also raises important definitionalissues. Definitions of rape and coercionvariously focus on the type of sexual con-tact, the abuse of a trusting relationship,the force or tactic employed, the powerdifferential, or the imposition of will uponanother person, and whether the abuser isan intimate partner. At a minimum, defini-tions of rape used in research shouldinclude notions of force, nonconsent, pen-etration, and the age boundary betweenrape and child sexual abuse.
Internationally, traditional legal definitionsof rape tend to be limited to penile-vaginalpenetration by force or threat of force. Rapereform initiatives in many countries havewidened this definition to include all formsof nonconsensual sexual penetration (vagi-nal, oral, or anal) obtained by physical forceor by threat of bodily harm. Some jurisdic-tions, including most of the United States,also recognize penetration obtained whenthe victim is incapable of giving consent byvirtue of mental illness, mental retardation,or intoxication. In many settings, penetra-tion by anything other than the penis isclassified as sexual assault rather than rape.
Other researchers have operationalizedrape differently, relying on notions of“coercion” defined variously as:
■ Using physical force or threat of physi-cal force.
■ Using verbal or psychological pressure,including trickery or deceit.
■ Against a woman’s will (unwanted asdefined by the woman).
■ Ignoring a woman’s refusal.
Childhood sexual abuse. As with rape,definitional issues complicate research intothe prevalence of childhood sexual abuse.Definitions of child sexual abuse in theNorth American literature have variedalong several dimensions: whether non-contact abuse (e.g., exhibitionism) isincluded together with sexual touching, themaximum age of the victim, the minimumage of the perpetrator, a minimum age dif-ference between victim and perpetrator(generally five years), and whether onlyincidents experienced as unpleasant orabusive are considered.13 The upper limiton childhood, for example, varies in stud-ies from age 12 to age 18. Some definitionsrequire that the incident be experienced bythe victim as abusive; others define all sex-ual contact between a child and someonesignificantly older as inherently abusive.
Research has shown that differences indefinition can greatly affect estimates ofprevalence. This effect is demonstratedclearly in the work of Haugaard and Emerywho constructed three definitions of abuse:a broad definition that included all forms ofcontact and noncontact abuse; a narrowdefinition that excluded exhibitionism andany incident that was experienced as posi-tive; and a very narrow definition thatincluded only oral, anal, or vaginal penetra-tion.13 Among the middle class collegewomen in their sample, the prevalence ofchild sexual abuse was 11.9 percent usingthe broadest definition; 9.6 percent usingthe narrow definition; and 1.8 percent usingthe “intercourse only” definition. The levelof impact of abuse on the women’s healthand lives increased as the definitionbecame more restrictive, although some sig-nificant relationships emerged even whenusing the broadest definition of abuse.
C H A P T E R S I X

A Practical Guide for Researchers and Activists 93
T H E C H A L L E N G E O F D E F I N I N G A N D M E A S U R I N G V I O L E N C E I N Q U A N T I TAT I V E R E S E A R C H
Violence against women and girls is defined in the Declaration on the Elimination of Violence Against Women as occurring in three domains: thefamily, the community, and perpetrated or condoned by the state. The focus of the WHO VAW study is on intimate partner violence and sexualviolence against women.
For the purposes of the study, a series of separate definitions were adopted for the different forms of violence included in the survey:
Domestic violence against women
Any act or omission by a family member (most often a current or former husband or partner), regardless of the physical location where the acttakes place, which negatively effects the well being, physical or psychological integrity, freedom, or right to full development of a woman.
Intimate partner violence
Any act or omission by a current or former intimate partner which negatively effects the well-being, physical or psychological integrity, freedom, orright to full development of a woman.
Physical violence
The intentional use of physical force with the potential for causing death, injury, or harm. Physical violence includes, but is not limited to, scratching,pushing, shoving, throwing, grabbing, biting, choking, shaking, poking, hair pulling, slapping, punching, hitting, burning, the use of restraints orone’s body size or strength against another person, and the use, or threat to use, a weapon (gun, knife, or object).
Severe physical violence
Physical violence that is likely to lead to external or internal injuries.
Abusive sexual contact
Any act in which one person in a power relationship uses force, coercion, or psychological intimidation to force another to carry out a sexual actagainst her or his will or participate in unwanted sexual relations from which the offender obtains gratification. Abusive sexual contact occurs in avariety of situations, including within marriage, on dates, at work and school, and in families (i.e., incest). Other manifestations include undesiredtouching; oral, anal or vaginal penetration with the penis or objects; and obligatory exposure to pornographic material.
Forced sex
Where one person has used force, coercion, or psychological intimidation to force another to engage in a sex act against her or his will,whether or not the act is completed.
Sex act
Contact between the penis and vulva, or the penis and the anus, involving penetration, however slight; contact between the mouth and the penis,vulva, or anus; or penetration of the anal or genital opening of another person by a hand, finger, or other object.
Psychological abuse
Any act or omission that damages the self-esteem, identity, or development of the individual. It includes, but is not limited to, humiliation, threaten-ing loss of custody of children, forced isolation from family or friends, threatening to harm the individual or someone they care about, repeatedyelling or degradation, inducing fear through intimidating words or gestures, controlling behavior, and the destruction of possessions.*
Child sexual abuse
The use of a child (defined as any person under the legal age of consent) by an adult for sexual purposes, whether or not consent is alleged tohave been given. It includes, acts of exposure; sexual touching; oral, anal, or vaginal penetration; and the exposing of a child to, or involving achild in, pornography or prostitution. Any form of direct or indirect sexual contact between a child and an adult is abusive since it is motivatedpurely by adult needs and involves a child who, by virtue of her/his age and position in life, is unable to give consent. Sexual activity betweenchildren constitutes sexual abuse when it is between siblings or when it is clear, by difference in developmental levels, coercion and/or lack ofmutuality, that one child is taking advantage of another.
* Some of the acts that are perceived as being psychologically abusive may vary between countries. WHO recognizes that there is no accepted definition of psy-chological abuse, and that there are also many other forms of severe psychological abuse, e.g., having children taken away from you, being evicted from yourhome, and having your wages taken away from you, that were not included in the questions used in the study.
(From WHO, 2004.14)
BOX 6.4 WORKING DEFINITIONS OF VIOLENCE USED BY WHO MULTI-COUNTRY STUDY ONWOMEN’S HEALTH AND DOMESTIC VIOLENCE AGAINST WOMEN

94 Researching Violence Against Women
The challenges of deriving appropriatedefinitions for child sexual abuse are evenmore difficult when contemplating cross-cultural research, in which even definitionsof childhood can be points of contentionand debate. The WHO VAW study choseage 15 as a cutoff point between child-hood and adulthood and asked respon-dents whether before the age of 15 hadanyone ever touched them sexually orforced them to do something sexual thatthey did not want to do.
PerpetratorsJust as it is crucial to be able to distinguishbetween different types of abuse,researchers also need specific informationabout the number of perpetrators and theirrelationship to the victim. Some researchindicates that women who are victimizedin childhood are more likely to be victim-ized as adults and that women who arevictimized more than once are at greaterrisk for mental and reproductive healthproblems. Watch out for a fairly commonmistake: asking women about the violencethey have experienced and the perpetra-tors, without linking each perpetrator tothe specific form of abuse. This can lead toconfusing results. For example, in the
León, Nicaragua, study, one woman, whowas abused by both her mother and herhusband, said she was beaten, raped, andemotionally abused. However, because ofthe way that the questionnaire was struc-tured, it was not possible to determinefrom the data who did what.
Some researchers suggest that providingspecific cues about context may be moreeffective than a single general question inhelping a woman remember violentevents.15 Therefore, interviewers may betrained to probe about specific situations inwhich women might have experienced vio-lence, such as the workplace or school, orviolence by family members.
Time frame and frequencyTo fully understand patterns of abuse,researchers need a time frame by whichthe abuse can be measured. For example,many studies on partner abuse only meas-ure whether women have experienced vio-lence in the last year, or since the start ofthe current relationship, thereby excludingviolence inflicted by former partners, orprior to the last year. This decision maystem from the belief that women are likelyto remember recent events more accuratelythan events in the more distant past. Othertimes, interventions focus on current vic-tims of abuse.
Using such a narrow time frameobscures the true impact of partner vio-lence, especially because a history of abusemay be the underlying cause of currentproblems. For example, the Nicaraguastudy found that women who experiencedabuse years before the interview tookplace were much more likely than non-abused women to be experiencing emo-tional distress at the time of the interview.16
Although women may be less likely torecall single incidents of moderate abuse,research indicates that experiences ofsevere, frequent, or particularly traumaticviolence are not easily forgotten, no matter
C H A P T E R S I X
FIGURE 6.1 DRAWING USED IN WHO VAW STUDY TO ASK WOMENANONYMOUSLY ABOUT SEXUAL ABUSE

A Practical Guide for Researchers and Activists 95
when they took place.* If no one asksabout former experiences of violence,many women with problems related toabuse will be improperly classified as“nonabused.” This error will weaken theassociations found between violence andspecific health or social outcomes.
To determine how many women haveexperienced partner abuse, it is generallysufficient to obtain information pertainingto the last year and to lifetime experiencesof abuse. However, where the purpose isto link the “exposure” to violence to spe-cific health outcomes, for example, incohort and case-referent studies, moredetailed information is particularly useful.Such information might include, for exam-ple, when the abuse began, how fre-quently it occurred, how long it lasted, and
whether it took place during a specific rel-evant period such as pregnancy or beforethe onset of a health condition.
When the aim of the study is to examineexperiences of physical or sexual abuse inchildhood, it is important to ask therespondent’s age when the abuse started,as well as the age of the perpetrator. Did ithappen one time? A few or many times?How many years did the abuse last?
ENHANCING DISCLOSUREOF VIOLENCE
Experience shows that in most settingswomen are willing to talk about theirexperiences of violence, although, as wementioned earlier, most prevalence figuresare probably too low. Experience from
T H E C H A L L E N G E O F D E F I N I N G A N D M E A S U R I N G V I O L E N C E I N Q U A N T I TAT I V E R E S E A R C H
FIGURE 6.2 COMPARISON OF DISCLOSURE OF CHILD SEXUAL ABUSE USING TWO DIFFERENT METHODS (D IRECT QUEST IONS
IN A FACE-TO-FACE INTERVIEW AND ANONYMOUS REPORTING)
25
20
15
10
5
0
■ Direct report ■ Anonymous reportTa
nzan
ia pr
ovinc
e
Tanz
ania
city
Thail
and p
rovin
ce
Thail
and c
ity
Peru
prov
ince
Peru
city
Namibi
a city
Japa
n city
Ethiop
ia pr
ovinc
e
Braz
il pro
vince
Braz
il city
8
12
6
9
0
7
10
14
5
2120
19
8
18
8 9
5 54
11
4
9
* An exception to this observation may be sexual abuse, where women and men have been known to repressmemories of particularly traumatic events experienced in childhood
(From WHO, 2005.3)
Perc
enta
ge o
f wom
en w
ho r
epor
t sex
ual a
buse
bef
ore
the
age
of 1
5

96 Researching Violence Against Women
international research nonetheless indi-cates that some methods are more effec-tive than others in encouraging women totalk about violence. The following series
of issues may affect women’swillingness to discuss experi-ences of violence.
How are women askedabout violence? The methods used to askwomen about violence mayinfluence how comfortablethey are disclosing abuse.Studies in industrialized coun-tries have found that for thepurpose of identifying intimatepartner abuse, either face-to-face interviews or interviewsby telephone give better resultsthan self-administered ques-tionnaires.17, 18 On the other
hand, anonymous techniques frequentlyencourage greater disclosure of childhoodsexual abuse. The WHO multi-countrystudy tested the use of different methodsfor eliciting disclosure of child sexualabuse. Women were asked during a face-to-face interview whether they had everbeen touched sexually or made to dosomething sexual against their will beforethe age of 15. At the end of the interview,women were asked to mark on a separatepiece of paper whether they had been sex-ually abused as a child by placing a checknext to either a happy or sad face, regard-
less of what they had chosen to reveal dur-ing the face-to-face interview (Figure 6.1).Women were assured that since their namewas not on the paper, no one would everbe able to trace their answer back to them.Then, to preserve the anonymity of therespondents these papers were placedtogether in a large plastic bag. In mostcountries, considerably more women dis-closed violence using this method thanthey did in personal interviews (Figure6.2).
Who is asking? As in all research on sensitive topics, dis-closure rates are affected by the skill of theinterviewer, and her or his ability to estab-lish rapport with the informant. Women aremore likely to be willing to share intimateand potentially painful or embarrassingaspects of their lives when they perceivethe interviewer as empathetic, nonjudg-mental, and genuinely interested in theirsituation. It is generally believed thatfemale interviewers are more successful ineliciting personal information from women,although this has rarely been tested. Insome settings, difficulties have beenencountered when using young or unmar-ried women as interviewers, or when usinginterviewers who lack experience dis-cussing sensitive issues. This highlights theimportance of using carefully selected andappropriately trained female interviewers.
Although it is often helpful to have field-workers who share some cultural back-ground with informants, it may bepreferable if they do not belong to thesame village or neighborhood, so that therespondent may feel more confident thatthe information she shares will not getback to others.
How many times should you ask awoman about violence? It may seem strange at first, and even a lit-tle insulting, to ask women more than once
C H A P T E R S I X
“Many women told me thatthey never talked about this
with anyone, not even with theneighbors, friends, or relatives,‘because if I tell her, she mighttell her husband or her mother,and word will get around and
might reach my husband,which would be terrible. If he
found out he would kill me.’So many of them would keep
all their suffering inside, forfear that their husbands would
mistreat them more…”Nicaraguan interviewer(Ellsberg, et al, 2001.12)
A DHS carried out in Nicaragua used two sets of questions to identify partnerabuse. One question asked in general, “Have you ever been physically beaten ormistreated by anyone?” Women who responded affirmatively were questionedabout the perpetrator. The next set of questions referred to specific acts such aspushing, slapping, choking, beating, and forced sex. For each act, women wereasked whether their partner had carried out the act within the last year, or at anytime during their marriage. While 14 percent of women reported partner abuseusing the first set of more general questions, 29 percent of women reported acts ofphysical or sexual partner abuse in the more specific set of questions.12
BOX 6.5 FROM THE FIELD: NICARAGUA

A Practical Guide for Researchers and Activists 97
whether they have experienced violence, asif we did not believe her the first timeround. However, numerous studies haveshown the importance of giving womenmore than one opportunity to disclose vio-lence during an interview. Women may notfeel comfortable talking about something sointimate the first time it is mentioned, orthey may not recall incidents that tookplace long ago. This is why studies thatinclude only one or two questions on vio-lence are likely to result in substantialunderreporting of abuse. Researchers havefound that many women initially deny hav-ing experienced violence, but over thecourse of the interview, overcome theirreluctance to talk. For this reason, it is alsowise to avoid using “gateway” or “filter”questions, where women who reply nega-tively to the first violence question are notasked the more specific questions in thesurvey. Box 6.5 gives an example of howprevalence estimates for violence weredoubled by adding a set of specific ques-tions after an initial general question.
The context of the interview The overall framework of the survey andthe items immediately preceding questionson abuse can profoundly affect howwomen interpret and respond to violence-related questions. For example, embeddingquestions on physical assault immediatelyfollowing items on relationships will cuerespondents to the issue of partner abuse,whereas asking a similarly worded ques-tion after items on crime victimization willtend to cue respondents toward assaultsperpetrated by strangers.
The issue of context is particularly rele-vant in large-scale surveys in which abuse-related questions are integrated intoquestionnaires designed for other pur-poses. When questions on violence imme-diately follow lengthy discussions onunrelated topics such as family planning,nutrition, or childhood illness, a woman
may be disconcerted and less likely to disclose experiences of violence. In thiscase, it is particularly important to give therespondent a chance to“switch gears.” An introductoryparagraph can make it clearthat the interview is shifting toa completely different subject.
Questions on violence maythemselves be framed in a vari-ety of ways that convey differ-ent messages to the womenbeing interviewed. For exam-ple, one well-known instru-ment, the Conflict TacticsScale, presents the use of violence as away of resolving conflict and includes aseries of questions about nonviolent waysto resolve conflicts, such as “discussing theissue calmly” or “sulking.” This lead-incould be problematic in a country wherephysical assault is not understood as a wayto resolve conflict, but rather as a form ofpunishment or discipline. Other instru-ments describe acts that the partner “doeswhen he is mad.”
Some researchers have usedlead-in questions that allowwomen to describe positiveaspects of the relationship, asa way of showing women thatthey are not interested in onlythe bad things a partner does.The rationale for this approachis that women may be morewilling to disclose abuse ifgiven an opportunity toacknowledge that their rela-tionship is complex, with bothgood and bad parts.
Even the timing of the violence ques-tions within the overview interview mayaffect how women respond, particularlywhen the questions are part of a muchlarger study. Asking about violence tooearly may not provide interviewers enoughtime to build rapport with the informant.
T H E C H A L L E N G E O F D E F I N I N G A N D M E A S U R I N G V I O L E N C E I N Q U A N T I TAT I V E R E S E A R C H
“…In the first question, theywould say that he didn’t beatthem, but when we got to theother questions, then theywould say ‘Yes, sometimes hebeats me and kicks me or usesa gun,’ or whatever.”Nicaraguan interviewer(Ellsberg, et al, 2001.12)
“…They would say that theyhad never told anyone beforetheir situation. But then we gotto be so close during the inter-view that she would ask me‘What do you think I shoulddo?’ Sometimes we couldn’tget off the subject…” Nicaraguan interviewer(Ellsberg, et al, 2001.12)

98 Researching Violence Against Women
On the other hand, if questions are placedat the end of a long interview, both theinterviewers and the respondents maybe tired or anxious to finish the interviewand therefore less likely to probe into
experiences of violence.One important way to ensure confiden-
tiality is to interview only one woman perhousehold. When the study is exclusivelyfocused on violence, this is relatively easyto achieve. Chapter 9 describes a few waysto randomly select the woman to be inter-viewed. The situation is more complexwhen other members of the household areto be interviewed on other topics, such asreproductive health. When incorporating amodule on violence in the NicaraguanDHS, researchers selected only one womanper household to answer the violence por-tion of the survey, presented as a sectionon “Household Relations.” Interviewerswere instructed to inform her that she wasselected by chance to be asked these ques-tions, and that no one else in the house-hold would know she was being asked.
By the same token, both ethical andmethodological principles suggest that it isbetter to avoid interviewing women andmen from the same household on violence.It is true that questioning both partners of acouple would enable comparisons betweenwives and husbands, as well as direct infor-mation about life events preceding abusivebehavior by men. However, this methodmay place a woman at risk if her abusivehusband suspects that she has been talkingabout his behavior. In anticipation of hisreaction, she may be reluctant to discloseviolence. Therefore, we recommend thatsurveys not include women and men fromthe same household. If it is necessary tointerview husbands for some other reason,do not ask about violence, and let thewoman know that she is the only onebeing asked about abuse.
COMMON TOOLS FORMEASURING VIOLENCE
Intimate Partner ViolenceThe Conflict Tactics Scale (CTS) is one ofthe best known tools for measuring intimate
C H A P T E R S I X
One of the greatest challenges of a multi-country study is ensuring that cross-coun-try comparability is maintained, and that the same core issues and concepts arebeing explored and analyzed in the same way in each participating country. Atthe time the study was carried out, there were still many gaps in knowledge aboutthe prevalence, causes, and consequences of domestic violence against women.The WHO VAW study and future research using the study methodology have thepotential to substantially advance current understanding. For this reason, maintain-ing cross-country comparability is a high priority for WHO. For the first phase ofthe study, to ensure that a high level of teamwork, coordination, and communica-tion was maintained, WHO committed resources to establishing a core researchteam, which regularly met with each country team. They also brought together thedifferent country team members at important points in the study, to ensure that thekey developments were finalized together.
Several steps were also taken to ensure that there was central coordination ofeach phase of the study and to maintain cross-country comparability:
■ Careful selection and standardized training of interviewers and supervisorsoccurred at the country level.
■ Core research team members made country visits during the interviewer train-ing and piloting phases of the study.
■ The core questionnaire and study procedures were finalized at a central levelwith a question-by-question description of the questionnaire, as well as detailedtraining manuals for facilitators, supervisors, interviewers, and data processors.
■ Sampling strategies were carefully reviewed, discussed, adapted, and docu-mented by a member of the core research team.
■ Adaptations to questionnaires were carefully reviewed and documented by amember of the core research team.
■ One data entry system and the same database structure was used in all coun-tries with interactive error checking and compulsory double entry and data vali-dations. Adaptation of the data entry program, as well as training of dataentry and data processing procedures, was done on site by one of the mem-bers of the core research team.
■ During field implementation, standard quality control measures were imple-mented in all countries, such as questionnaire checking on site, regular debrief-ings, and support to the interviewers.
■ Data cleaning was done with support of one member of the core researchteam to ensure similar procedures were followed in all countries.
■ A standard list of preliminary analyses was identified and conducted in eachcountry.
■ Annual meetings were held with the country research teams to share lessonslearned.
BOX 6.6 ENSURING THE COMPARABILITY OF DATA IN THEWHO MULTI-COUNTRY STUDY ON WOMEN’S HEALTH AND
DOMESTIC VIOLENCE AGAINST WOMEN
(From WHO, 2004.15)

A Practical Guide for Researchers and Activists 99
partner violence, particularly in the UnitedStates. The original CTS has several sub-scales that measure acts used in the courseof conflict, including negotiating tactics, andverbal and physical aggression. The physicalaggression subscale of the CTS measuresthe frequency and severity of specific acts ofphysical violence within the family, includ-ing husband-to-wife, wife-to-husband, andparent to child violence.19, 20 The revised ver-sion, called the CTS2, also includes ques-tions on sexual violence and injuries.21 TheCTS approach is particularly useful for inter-national comparisons because it is behav-iorally specific. Therefore it is likely todetect women who have experienced actsof violence but do not necessarily identifythemselves as battered or abused. Althoughit was designed to measure all kinds of vio-lence between husbands and wives, thesubscales can be used independently.
Used alone, however, many researchersobserve that the CTS has some drawbacks.It provides limited information about thecontext and consequences of abuse, aswell some of the more complex issues ofcontrol and psychological degradation thatmany researchers consider central featuresof wife abuse.18
A further problem with the CTS is thatit frames the occurrence of violencewithin the context of conflict resolution,and includes a subscale of negotiatingtactics for resolving conflict. Feministresearchers question the assumption ofgender neutrality behind the CTS becausethey view male violence as a coercivetactic for maintaining power and domina-tion within a relationship. In an interna-tional setting, the assumption that equalpartners come together to “negotiate”conflict is even more problematic, sincemany cultures define women as perpet-ual minors, both socially and legally.Men are granted the right to physicallycorrect or punish their wives much asparents in other cultures are granted
this right over children.22
Because the focus of the CTS is on theacts themselves, it does not provide infor-mation about the context, or the intentionbehind the use of violence. For example, itdoes not distinguish between violenceused for self-defense and violence used forthe purpose of control or punishment.Therefore, when used to measure bothhusband-to-wife and wife-to-husband vio-lence, the CTS has led to what manyresearchers consider to be misleading con-clusions about the supposed symmetry ofmarital violence.23 Most internationalresearch, however, consistently shows thatviolence used by males and females isboth quantitatively and qualitatively differ-ent.24, 25 Whereas female violence is morelikely to take place in the context of self-defense, male violence is more likely tolead to injury.
Other well-known instruments for meas-uring wife abuse include the Index ofSpouse Abuse, which is a 30-item self-report scale designed to measure the sever-ity or magnitude of physical (ISA-P) andnonphysical abuse (ISA-NP).26 More conciseinstruments such as the Abuse AssessmentScreen have been used successfully in
T H E C H A L L E N G E O F D E F I N I N G A N D M E A S U R I N G V I O L E N C E I N Q U A N T I TAT I V E R E S E A R C H
■ Use broad criteria in defining the study population. For studies thataddress multiple forms of violence, all women from a specific age groupshould be included. For studies of intimate partner violence, considerincluding all women who have ever been married or who are in a com-mon-law relationship.
■ Provide multiple opportunities to disclose. Do not use “gateway” or “filter” questions.
■ Use behaviorally specific acts to ask about violence. Use at least two orthree questions per type of violence.
■ Be specific about time frames—include at least one recent (last year) andone long-term time frame (since you were 18; since you were married).
■ Ask about specific perpetrators and specific contexts to cue the respondent’smemory.
■ In order to ensure confidentiality and increase disclosure, interview only onewoman per household. Do not interview men and women from the samehouseholds about violence.
BOX 6.7 RECOMMENDATIONS FOR MEASURING VIOLENCE

100 Researching Violence Against Women
screening for abuse, particularly withinhealth services.27 The Abuse AssessmentScreen, which has only five questions, isan effective tool for measuring physicaland sexual abuse in the last year and dur-ing pregnancy.
Another recently developed instrument,the Women’s Experience with BatteringFramework (WEB), is unique because itmeasures battering based on the subjectiveexperience of the woman, rather than ondiscrete incidences of physical violence.28, 29
The WEB scale has ten items, based onqualitative research with U.S. batteredwomen, which describe different dimen-sions of the experience of battering, suchas shame and diminished autonomy.Examples of questions are “I feel ashamedof the things he does to me,” and “He hasa look which terrifies me even when hedoesn’t touch me.” However, the WEBFramework has not yet been validatedinternationally to determine whether theexperiences provide a meaningful measureof battering in a cross-cultural context.
Two more recently developed instru-ments for international surveys are theDomestic Violence Module of theDemographic and Health Surveys,2 andWHO’s instrument for the VAW study. TheDHS module is designed to be included ina larger survey on women’s reproductivehealth and can be obtained fromhttp://macroint.com. The WHO question-naire is designed primarily as a stand-alone questionnaire for violence research.This questionnaire, which has beenenriched by the experiences of previousinternational research, collects detailedinformation about acts of physical, sexual,and emotional violence committed bypartners and nonpartners. It includesinformation about the frequency andduration of violence, violence duringpregnancy, health consequences forwomen and their children, women’sresponses to abuse, and access to
services for battered women. The studyalso explores such related issues as com-munity norms regarding violence, deci-sion making within the family, women’sfinancial autonomy, and physical mobil-ity. The full questionnaire is availablefrom the WHO by writing to: [email protected].
A subset version of the WHO question-naire, called the Violence AgainstWomen Instrument, includes a basic setof questions that may be included in othersurveys for the purpose of measuring vio-lence. In a relatively concise manner, thisinstrument measures experiences of violentacts carried out by a partner, includingemotional abuse, moderate and severephysical violence, and sexual coercion withand without the use of physical force. Itfurther measures the frequency of eachtype of violence during the last year and atany time. This instrument, together withnotes on the use of the instrument, is pre-sented in Appendix I.
Sexual coercion/rape Instruments to measure sexual coercionand/or forced sex are less well developedcross culturally than those to measure part-ner violence. Due to the shame associatedwith sexual violation in many settings, it iseven harder for women to speak freelyabout forced sex than it is to admit tobeing beaten.
There is general agreement that meas-ures of sexual coercion should include ref-erence to the type of sexual act, the typeof tactic or force used, the relationshipwith the perpetrator, the number of perpe-trators, and whether the acts wereattempted or were in fact completed. Inaddition, researchers should preferablyrefer to specific acts, rather than vagueterms such as “sexual abuse” or “assault.”
In the United States, the most commonlyused instrument for measuring sexualaggression is the Sexual Experiences
C H A P T E R S I X

A Practical Guide for Researchers and Activists 101
Survey (SES) first developed by Koss.1, 14, 30-32
The revised SES uses ten items to assessdifferent forms and degrees of sexual coer-cion. An example of a question describinga relatively mild level of sexual coercion is“Have you ever given in to sex play(fondling, kissing or petting, but not inter-course) when you didn’t want to becauseyou were overwhelmed by your partner’scontinual arguments and ‘pressure’?” Asample question that refers to more severeaggression asks “Have you ever had sexualintercourse when you didn’t want tobecause you were threatened or becausesomeone used some degree of physicalforce (twisting your arm, holding youdown) to make you?” Within each item,sexual aggression is treated dichotomously(yes, no), although some investigators havemodified the SES to assess the frequency ofdifferent experiences.
Child sexual abuse Individuals researching child sexual abusehave used instruments specific to sexualabuse as well as broader instrumentsdesigned to capture different forms of mal-treatment in childhood. An increasinglypopular instrument known as theChildhood Trauma Questionnaire(CTQ) investigates a variety of forms oftrauma that children can experience grow-ing up, and yields separate estimates ofemotional abuse, physical abuse, sexualabuse, emotional neglect, and physicalneglect.33
In contrast to instruments that inquireabout specific acts, the CTQ presentsrespondents with a series of statementsabout childhood experiences that areranked on a five-point scale, withresponse options ranging from “nevertrue” to “very often true.” Most items arephrased in objective terms (e.g., “When Iwas growing up, someone touched me in
a sexual way or made me touch them.”),whereas others call for more subjectiveevaluation (“When I was growing up, Ibelieve I was sexually abused.”) The ques-tionnaire is introduced with the statement“In this section, we would like to knowabout experiences you may have hadbefore you were 18 years of age.”
Other instruments inquire about a seriesof specific sexual acts, followed by clarify-ing questions regarding when and withwhom it happened, how it made therespondent feel, and the degree of persua-sion or force used.
Violence against women in conflictsituationsIn recent years, researchers have addressedthe specific challenges of documenting vio-lence suffered by women in conflict situa-tions.34, 35 A group of organizations involvedin the Reproductive Health Response inConflict Consortium has developed a seriesof excellent tools for monitoring and evalu-ating violence against women in conflictsituations. One of these tools is a surveyinstrument that measures different kinds ofviolence against women, including physicaland sexual violence by partners and byothers, including soldiers or paramilitaryforces, and aid workers.36 More informationcan be found about these instruments athttp://www.rhrc.org/.
T H E C H A L L E N G E O F D E F I N I N G A N D M E A S U R I N G V I O L E N C E I N Q U A N T I TAT I V E R E S E A R C H

102 Researching Violence Against Women
1. Koss MP. Detecting the scope of rape: A reviewof prevalence research methods. Journal ofInterpersonal Violence. 1993;8(2):198-222.
2. Kishor S, Johnson K. Domestic Violence in NineDeveloping Countries: A Comparative Study.Calverton, Maryland: Macro International; 2004.
3. World Health Organization. WHO Multi-countryStudy on Women’s Health and Domestic ViolenceAgainst Women: Report on the First Results.Geneva, Switzerland: WHO; 2005.
4. Ellsberg M, Peña R, Herrera A, Liljestrand J,Winkvist A. Candies in hell: Women’s experiencesof violence in Nicaragua. Social Science andMedicine. 2000;51(11):1595-1610.
5. Ellsberg MC, Peña R, Herrera A, Liljestrand J,Winkvist A. Wife abuse among women of child-bearing age in Nicaragua. American Journal ofPublic Health. 1999;89(2):241-244.
6. Serbanescu F, Morris L, Rahimova S, Stupp P.Reproductive Health Survey, Azerbaijan, 2001.Final Report. Atlanta, Georgia: Azerbaijan Ministryof Health and Centers for Disease Control andPrevention; 2003.
7. Johnson H. Dangerous Domains: ViolenceAgainst Women in Canada. Ontario, Canada:International Thomson Publishing; 1996.
8. Tjaden P, Thoennes N. Extent, Nature andConsequences of Intimate Partner Violence:Findings from the National Violence AgainstWomen Survey. Washington, DC: NationalInstitute of Justice, Centers for Disease Controland Prevention; 2000.
9. Lundgren E, Heimer G, Westerstand J,Kalliokoski A-M. Captured Queen: Men’sViolence Against Women in “Equal” Sweden: APrevalence Study. Umeå, Sweden: FritzesOffentliga Publikationer; 2001.
10.Heiskanen M, Piisspa M. Faith, Hope, Battering: Asurvey of men’s violence against women inFinland. Helsinki: Statistics Finland, Council forEquality; 1998.
11.Heise L, Ellsberg M, Gottemoeller M. EndingViolence Against Women. Population Reports,Series L, No.11. Baltimore: John’s HopkinsUniversity School of Public Health; PopulationInformation Program; December,1999.
12.Ellsberg M, Heise L, Peña R, Agurto S, Winkvist A.Researching domestic violence against women:Methodological and ethical considerations. Studiesin Family Planning. 2001;32(1):1-16.
13.Hauggard JJ, Emery RE. Methodological issues inchild sexual abuse research. Child Abuse &Neglect. 1989;13:89-100.
14.World Health Organization. WHO Multi-CountryStudy on Women’s Health and Domestic Violence:Study Protocol. Geneva, Switzerland: WorldHealth Organization; 2004.
15.Koss M. The underdetection of rape:Methodological choices influence incidence esti-mates. Journal of Social Issues. 1992;48:61-75.
16.Ellsberg M, Caldera T, Herrera A, Winkvist A,Kullgren G. Domestic violence and emotional dis-tress among Nicaraguan women: Results from apopulation-based study. American Psychologist.1999;54(1):30-36.
17. Johnson J, Sacco V. Researching violence againstwomen: Statistics Canada’s national survey.Canadian Journal of Criminology. 1995;37:281-304.
18.Smith MD. Enhancing the quality of survey dataon violence against women: A feminist approach.Gender and Society. 1994;8(1):109-127.
19.Straus MA, Gelles RJ. Societal change and changein family violence from 1975 to 1985 as revealedby two national surveys. Journal of Marriage andthe Family. 1986;48:465-480.
20.Straus MA, Gelles RJ. Measuring intrafamily con-flict and violence: The Conflict Tactics (CT) Scale.Journal of Marriage and the Family. 1979;41:75-88.
21.Straus MA, Hamby SL, Boney-McCoy S, SugarmanDB. The Revised Conflict Tactics Scales (CTS2).Journal of Family Issues. 1996;17(3):283-316.
22.Heise L. Violence against women: An integrated,ecological framework. Violence Against Women.1998;4(3):262-290.
23.Steinmetz SK. The battered husband syndrome.Victimology. 1978;2:499-509.
24.Dobash R, Dobash R, Wilson M, Daly M. Themyth of sexual symmetry in marital violence.Social Problems. 1992;39(1):71-91.
25.Morse B. Beyond the Conflict Tactics Scale:Assessing gender differences in partner violence.Violence and Victims. 1995;10(4):251-272.
26.Hudson WW, McIntosh SR. The assessment ofspouse abuse: Two quantifiable dimensions.Journal of Marriage and Family. 1981;43:873-885.
27.McFarlane J, Parker B, Soeken K, Bullock L.Assessing for abuse during pregnancy. Severityand frequency of injuries and associated entryinto prenatal care. Journal of the AmericanMedical Association. 1992;267(23):3176-3178.
28.Smith PH, Earp JA, DeVellis R. Measuring batter-ing: Development of the Women’s Experiencewith Battering (WEB) Scale. Women’s Health.1995;1(4):273-288.
C H A P T E R S I X

A Practical Guide for Researchers and Activists 103
29.Smith PH, Smith J, Earp JA. Beyond the measure-ment trap: A reconstructed conceptualization andmeasurement of women battering. Psychology ofWomen Quarterly. 1999;23:177-193.
30.Koss M, Oros C. Sexual Experiences Survey: Aresearch instrument investigating sexual aggres-sion and victimization. Journal of Consulting andClinical Psychology. 1982;50:455-457.
31.Koss M, Gidycz C, Wisniewski N. The scope ofrape: Incidence and prevalence of sexual aggres-sion and victimization in a national sample ofhigher education students. Journal of Consultingand Clinical Psychology. 1987;55:162-170.
32.Alksnis C, Desmarais S, Senn C, Hunter N.Methodologic concerns regarding estimates ofphysical violence in sexual coercion:Overstatement or understatement? Archives ofSexual Behavior. 2000;29(4):323-334.
33.Bernstein D, Fink L, Handelsman L, et al. Initialreliability and validity of a new retrospectivemeasure of child abuse and neglect. AmericanJournal of Psychiatry. 1994;151(8):1132-1136.
34.Vann B. Gender-Based Violence: Emerging Issuesin Programs Serving Displaced Populations.Arlington: Reproductive Health Response inConflict Consortium; 2002.
35.Ward J. If Not Now, When? Addressing Gender-based Violence in Refugee, Internally Displacedand Post-Conflict Settings: A Global Overview.New York: Reproductive Health Response inConflict Consortium; 2002.
36.Reproductive Health Response in ConflictConsortium. Gender-based Violence Tools Manualfor Assessment and Program Design, Monitoring,and Evaluation in Conflict-affected Settings. NewYork, New York: Reproductive Health Responsein Conflict Consortium; 2004.
T H E C H A L L E N G E O F D E F I N I N G A N D M E A S U R I N G V I O L E N C E I N Q U A N T I TAT I V E R E S E A R C H

7PHO
TO B
Y H
AFM
JAN
SEN

A Practical Guide for Researchers and Activists 105
designing a sample for qualitative or quan-titative research. It also gives examples ofhow different strategies have been used tofit the specific needs and circumstances ofresearch projects.
SAMPLINGCONSIDERATIONS INQUALITAT IVE STUDIES
There are no hard and fast rules for samplesizes in qualitative research. As Hudelsonpoints out, “The sample size will dependon the purpose of the research, the specificresearch questions to be addressed, whatwill be useful, what will have credibility,and what can be done with available timeand resources.”2
In qualitative sampling, the selection ofrespondents usually continues until thepoint of redundancy (saturation). Thismeans that when new interviews nolonger yield new information and allpotential sources of variation have beenadequately explored, sampling may stop.For most qualitative studies, 10 to 30 inter-views and/or 4 to 8 focus groups will suf-fice. Table 7.1 summarizes a number of
One cannot overemphasize theimportance of developing an appropriatesample for the type of research designselected. Although qualitative and quantita-tive research use different approaches forselecting the individuals or groups to bestudied, in all studies it is crucial to planthe sampling strategy carefully. Particularlyin the case of population-based surveys, apoorly selected sample may harm the cred-ibility of a study, even if the rest of thestudy is well executed.
Qualitative studies generally focus indepth on a relatively small number ofcases selected purposefully. By contrast,quantitative methods typically depend onlarger samples selected randomly. Thesetendencies evolve from the underlying pur-pose of sampling in the two traditions ofinquiry. In quantitative research, the goalof sampling is to maximize how represen-tative the sample is so as to be able togeneralize findings from the sample to alarger population. In qualitative inquiry, thegoal is to select for information richness soas to illuminate the questions under study.1
This chapter discusses the major issuesthat should be taken into account when
C H A P T E R S E V E N
Developing a Sampling Strategy
Topics covered in this chapter:
Sampling considerations in qualitative studiesSampling considerations in quantitative research surveys

106 Researching Violence Against Women
C H A P T E R S E V E N
different approaches to qualitative sampling. In qualitative research, the sampling
strategy should be selected to help eluci-date the question at hand. For example,researchers with the Nicaraguan organiza-tion Puntos de Encuentro embarked on aproject to collect information useful fordesigning a national media campaign thatcalled on men to renounce violence in
their intimate relationships. They wantedto understand the beliefs and attitudes thatexisted in Nicaraguan culture that sup-ported violent behavior toward women.More importantly, they wanted to know ifthere were any “benefits” of nonviolencethat could be promoted to encourage mento reconsider their behavior (Box 5.6).
Rather than concentrating on collecting
Type of Sampling
Intensity sampling
Deviant case sampling
Stratified purposeful sampling
Snowball or chain sampling (Locateone or two key individuals, andthen ask them to name other likelyinformants.)
Maximum variation sampling(Purposely select a wide range ofvariation on dimensions of interest.)
Convenience sampling (Select who-ever is easiest, closest, etc.)
Criterion sampling
Purpose
To provide rich information from afew select cases that manifest thephenomenon intensely (but are notextreme cases).
To learn from highly unusual mani-festations of the phenomenon inquestion.
To illustrate characteristics of particu-lar subgroups of interest; to facilitatecomparisons.
To facilitate the identification ofhard-to-find cases.
To document diverse variations; canhelp to identify common patternsthat cut across variations.
To save time, money, and effort.Information collected generally hasvery low credibility.
To investigate in depth a particular“type” of case; identify all sourcesof variation.
Example
Interviewing survivors of date rapeto learn more about how coercedsex affects women’s sexuality.
Interviewing men who do not beattheir wives in a culture where wifeabuse is culturally accepted.
Interviewing different types of serv-ice providers (police, social work-ers, doctors, clergy) to comparetheir attitudes toward and treatmentof abuse victims.
Finding commercial sex workers tointerview about experiences ofchildhood sexual abuse by gettingcases referred through friendshipnetworks.
Researching variations in normsabout the acceptability of wife beat-ing by conducting focus groupsamong different sub groups: youngurban women, old urban women,young rural men, old rural men,women who have been abused,women who have not experiencedabuse.
Forming focus groups based onwho is available that day at thelocal community center, rather thanaccording to clear criteria.
Specifically interviewing onlyabused women who have left theirpartners within the last year in orderto better understand the variety offactors that spur women to leave.
TABLE 7.1 TYPES OF SAMPLING STRATEGIES FOR QUALITATIVE STUDIES
(From Patton, 1990.3)

A Practical Guide for Researchers and Activists 107
information on the norms and attitudes of“typical” Nicaraguan men, the researchersdecided to use “deviant case” sampling andconcentrate on interviewing men who hadalready had a reputation for being nonvio-lent and renouncing machismo.4 They wereinterested in finding out from these menwhat benefits, if any, they perceived fromthis choice, and what life-course events,influences, or individuals pushed them inthis direction. The goal was to investigatewhat aspirations and life experiences helpcreate “healthy” intimate partnerships. Thefindings were used to design an informa-tion campaign aimed at recruiting moremen to a nonviolent lifestyle.
SAMPLINGCONSIDERATIONS IN QUANTITATIVERESEARCH SURVEYS
In contrast to qualitative research, whichgenerally uses nonprobability or “purpo-sive” sampling, quantitative research relieson random sampling of informants. Aprobability or “representative” sample is agroup of informants selected from the pop-ulation in such a way that the results maybe generalized to the whole population.
When a sample is referred to as ran-dom, it means that specific techniqueshave been used to ensure that every indi-vidual who meets certain eligibility criteriahas an equal probability of being includedin the study. Failure to adhere to thesetechniques can introduce error or biasinto the sample, which may lessen thevalidity of the study. For example, if ahousehold survey on violence only con-ducted interviews during the day, then therespondents most likely to be included inthe study would be women who work athome, and women who worked outsidethe home would be less likely to be inter-viewed. Since women working outside thehome may have different experiences with
violence, the study resultswould be biased towardswomen who work at home.One way to reduce this partic-ular bias would be to return tohomes at night or on week-ends to increase the likelihoodof reaching all women.
The way in which the sample is chosenaffects its generalizability, or the extent towhich the situation found among a particu-lar sample at a particular time can beapplied more generally. There are manytechniques for sampling, each with its owntradeoffs in terms of cost,effort, and potential to gener-ate statistically significantresults. Some strategies, suchas simple random sampling,may not be feasible wherethere is little information avail-able on the population understudy. The following is a brief
D E V E L O P I N G A S A M P L I N G S T R AT E G Y
A probability or representativesample is a group of informants selected from thepopulation in such a way thatthe results may be generalizedto the whole population.
When a sample is referred to as random, it means thatspecific statistical techniqueshave been used to ensure thatevery individual who meetscertain eligibility criteria hasan equal probability of beingincluded in the study.
PHO
TO B
Y H
AFM
JAN
SEN

108 Researching Violence Against Women
description of the more common samplingtechniques used.
Many people underestimate the chal-lenge of obtaining a well-designed sample.Mistakes are often made due to confusionover the meaning of the term randomselection. A random selection does notmean that participants are simply selectedin no particular order. In fact, the tech-niques for obtaining a truly random sampleare quite complex, and inexperiencedresearchers should consult an expert insampling before proceeding. A wellthought-out and tested questionnaire usedon a poorly designed sample will still ren-der meaningless results.
Random samples are often confusedwith convenience or quota samples. Aconvenience sample is when informantsare selected according to who is available,in no particular order. In a quota samplea fixed number of informants of a certaintype are selected. Neither strategy willresult in a random sample appropriate forsurvey research.
Simple random samplingThis sampling technique involves selectionat random from a list of the population,known as the sampling frame. If properlyconducted, it ensures that each person hasan equal and independent chance ofbeing included in the sample.Independence in this case means that the
selection of any one individual in no wayinfluences the selection of any other. Theword “simple” does not mean that thismethod is any easier, but rather that stepsare taken to ensure that only chance influ-ences the selection of respondents.Random selection can be achieved using alottery method, random number tables(found in many statistical books), or acomputer program such as Epi Info. Toavoid bias, it is very important to includein the sampling frame only individuals whoare eligible to be interviewed by criteriasuch as age, sex, or residence. By the sametoken, if certain individuals are left off theoriginal list due to an outdated census thatdoes not include individuals who haverecently moved into the population area,then these omissions could bias the results,particularly if migration is the result ofcrises such as war, natural disasters, or eco-nomic collapse. In these cases, you willneed to update the sampling list.
Systematic samplingIn random sampling, each individual orhousehold is chosen randomly. In contrast,systematic sampling starts at a randompoint in the sampling frame, and every nthperson is chosen. For example, if youwant a sample of 100 women from a sam-pling frame of 5,000 women, then youwould randomly select a number betweenone and 50 to start off the sequence, andthen select every fiftieth woman thereafter.Both random and systematic samplingrequire a full list of the population inorder to make a selection. It is also impor-tant to know how the list itself was made,and whether individuals are placed ran-domly or in some kind of order. If individ-uals from the same household or withcertain characteristics are groupedtogether, this may result in a biased sam-ple in which individuals with these charac-teristics are either overrepresented orunderrepresented.
C H A P T E R S E V E N
PHO
TO B
Y H
AFM
JAN
SEN

A Practical Guide for Researchers and Activists 109
clusters (such as villages or neighbor-hoods). Then a random sample of theseclusters is drawn for the survey. This is thefirst stage of sampling. The second stagemay involve either selecting all of the sam-pling units (respondents, households) inthe selected clusters, or selecting a groupof sampling units from within the clusters.Sometimes more than two stages arerequired. Thus, one might randomlychoose districts within a province, andthen randomly select villages from theselected districts as the second stage.Individual respondents would be selectedfrom the clusters as a third stage. At eachstage, simple random, systematic, or strati-fied techniques might be used. It is advis-able to consult a statistician if you areconsidering a multistage sampling scheme.
The advantage of multistage sampling isthat a sampling frame (e.g., a list of house-holds) is only needed for the selected clus-ters (villages) rather than for the wholestudy population. Also, the logistics will beeasier because the sample is restricted tothe selected clusters and need not coverthe whole study area. An example of amultistage sampling strategy in Peru isdescribed in Box 7.3.
The disadvantages of multistage sam-pling are that the sample size needs to besubstantially larger than if the sample was
D E V E L O P I N G A S A M P L I N G S T R AT E G Y
Stratified samplingStratified sampling may be used togetherwith either simple random sampling or sys-tematic sampling. This ensures that thesample is as close as possible to the studypopulation with regard to certain character-istics, such as age, sex, ethnicity, or socio-economic status. In this case, the studypopulation is classified into strata, or sub-groups, and then individuals are randomlyselected from each stratum. Because strati-fication involves additional effort, it onlymakes sense if the characteristic beingstratified is related to the outcome understudy. For the purpose of analysis it is eas-ier if the number of individuals selectedfrom each stratum is proportional to theiractual distribution in the population. (SeeBox 7.1 on self-weighting samples.) Forexample, in a sample stratified according tourban/rural residence, the proportion ofrural women in the sample would be thesame as the proportion of rural women inthe study population.
A weighted stratified sample may bepreferable when there are some groupswhich are proportionately small in thepopulation, but which are relevant for thepurpose of the study, such as individualsfrom a certain geographical region or eth-nic group. Ensuring that these groups areadequately represented might require aninordinately large sample size using simplerandom sampling techniques. In this case,it may be appropriate to oversample, or toselect a disproportionately large number ofrespondents from this stratum. This resultsin a weighted sample that will have to betaken into account in the analysis process.
Multistage and cluster sampling Multistage sampling is often used fordrawing samples from very large popula-tions covering a large geographical area. Itinvolves selecting the sample in stages, ortaking samples from samples. The popula-tion is first divided into naturally occurring
A street map used forlocating households inthe Japan WHO study.
PHO
TO B
Y H
AFM
JAN
SEN

110 Researching Violence Against Women
selected by simple random sampling. Also,it can be more complicated to get a self-weighting sample. Another difficulty withmultistage sampling can be defining clus-ters if the study area is, for example, alarge urban area. Sometimes these havealready been defined for previous censusesor surveys, but otherwise they have to becreated from a map or based on someother criteria such as school or health cen-ter catchment areas.
How large a sample do you need? The ideal sample size for a survey dependson several factors:
■ How sure do you want to be of yourconclusions? Larger sample size gener-ally increases the precision of the results,or the confidence with which one cansay that they represent a reliable meas-ure of the phenomena under study.
■ What are the characteristics of thestudy population? The more variabilitythere is in the population, the larger thesample size needed.
■ How common is the phenomenonunder study? If any of the conditionsyou want to measure in your study arevery rare, for example, infant mortalityor maternal mortality, then you willneed a very large sample size.
■ What is the purpose of the research?The sample size calculation will alsodepend on whether you simply want tomeasure the prevalence of a conditionin a population or whether you want tomeasure an expected differencebetween two groups. Programs such asEpi Info contain two different formulasfor these two different approaches.
■ What kind of statistical analysis willyou use? This underscores the need toconsider how you are going to analyzeyour data from the very beginning. Thesample size must be large enough toprovide for desired levels of accuracy inestimates of prevalence, and to test forthe significance of differences betweendifferent variables.
■ What kind of sampling strategy willbe used? Commonly used sample sizeformulae and computer packagesassume you are using simple randomsampling. If you plan to use multistageor cluster sampling, you may need toincrease your sample size to achieve theprecision you require. Consider asking a
C H A P T E R S E V E N
The way in which the sample is chosen greatly influences the usefulness of theresulting estimates. Suppose that there is a district with only two villages:
■ Village A has 4,000 women, of which 800 (20 percent) have been abused.
■ Village B has 800 women, of which 40 (5 percent) have been abused.
The true prevalence of abuse in this district would be calculated as follows:
Total cases of violence = (800 + 40) X 100 = 17.5 percent
Total number of women (4000 + 800)
However, if we decided to determine the prevalence of abuse in this districtbased on a random sample of 100 women from each village, we would findthe following:
■ 20 out of 100 women in Village A reporting abuse.
■ 5 out of 100 women in Village B reporting abuse.
Combining these two figures we would find that 25 out of the 200 women inter-viewed were abused, which would give us a prevalence of 12.5 percent.
What has happened here?
Our sampling procedure led us to an underestimated prevalence because the num-ber of informants selected from each village was not in proportion to the relativesize of each village. Assuming that we knew the relative sizes of the villages, wecould perform a weighted analysis where the results from Village A would countfive times as much as those from Village B. However, it is usually preferable toobtain a self-weighting sample. One way to do this would be to select five timesmore respondents from Village A than Village B. Another approach is to select thevillages with probability proportional to size. This means that if you have a list of vil-lages, a large village like Village A would be five times more likely to be selectedfor the sample than a village the size of Village B. After the villages were selected,you could then to select an equal number of respondents from each village. (For anexample of how a self-weighting sample was obtained in Peru, see Box 7.3.)
BOX 7.1 SELF-WEIGHTING IN CLUSTER SAMPLES
(From Morison, 2000.5)

A Practical Guide for Researchers and Activists 111
statistician for help in deciding by howmuch the sample size needs to beincreased.
It is better to collect excellent data fromfewer respondents than to collect data ofdubious validity and reliability from manyrespondents. Statistical computer packagesor mathematical formulas can be used todetermine sample size for a study. Box 7.2presents a table produced by Epi Info’sSTATCALC program for ideal sample sizecalculations. This program is availableonline at http://www.cdc.gov/epiinfo.
If your proposed analysis calls for study-ing particular subgroups of your sample,the sample size will need to be expandedaccordingly. For example, to determine theprevalence of violence, you may need asample of only 300 women. But if youwant to know whether the prevalence ofviolence varies by age, education, or socio-economic group, then you will need asample size sufficiently large to allow forcomparisons among these groups.
The initial calculation was made basedon a simple random sample from a studypopulation of 100,000 women, where itwas assumed that approximately 30 per-cent of women have experienced violenceand that a 10 percent margin of errorwould be acceptable (5 percent above and5 percent below). If these assumptions areactually true, the table indicates that with asample size of 322 women, one wouldobtain a 95 percent confidence interval forthe true prevalence of 25 percent and 35percent. Note, however, that if the esti-mates used for sample size calculations arevery inaccurate then the required precisionmay not be obtained.
The table also shows that differences inthe size of the study population do notgreatly influence sample size, whereaschanges in the expected frequency andparticularly the level of precision that isneeded can have an enormous effect on
sample size calcula-tions. It should also be noted that thesample size willneed to be increasedif a multistage sam-ple is being used.Because these calcu-lations can be quitecomplex, inexperi-enced researchersare urged to consultwith someone whois knowledgeable insurvey samplingtechniques.
To explore thehealth consequencesof violence withgreater precision, andto compare the occurrence of violence indifferent sites within each country, theWHO VAW study uses a multistage sam-pling strategy aiming for 3,000 interviewsin two sites; 1,500 in the capital city and1,500 in a province. However, to end upwith 1,500 completed interviews, it is usu-ally necessary to increase the estimatedsample size by 10-20 percent to account
D E V E L O P I N G A S A M P L I N G S T R AT E G Y
Population Size 100,000 10,000 10,000 10,000Expected Frequency 30% 30% 20% 30%Worst AcceptableFrequency 25% 25% 15% 28%
Confidence Sample Sample Sample SampleLevel Size Size Size Size
80% 138 136 104 794
90% 227 222 170 1,244
95% 322 313 270 1,678
99% 554 528 407 2,583
99.9% 901 834 648 3,624
99.99% 1,256 1,128 883 4,428
BOX 7.2 POPULATION SURVEY USING RANDOM SAMPLING(STATCALC SAMPLE SIZE AND POWER)
How large a sample?
This is one of the most common ques-tions asked of statisticians. A frequentbut erroneous answer is “as large aspossible” when it instead should be “assmall as possible.” It is also important to emphasize that theamount of information that can begained from a sample depends on itsabsolute size, not upon the samplingfraction, or its size as a proportion ofthe population size. It is actually truethat 99 out of one million tells you asmuch about the 1 million as 99 out ofone thousand tells you about the onethousand.
(From Persson and Wall, 2003.6)

112 Researching Violence Against Women
C H A P T E R S E V E N
Lima
1. The team obtained from the National Institute of Statistics andInformation (INEI) a list of selected clusters. INEI had divided Limainto 12,000 clusters with about 50 to 150 houses in each cluster.The team randomly selected 166 clusters, using probability propor-tional to size (assigning a weighted value to the larger clusters togive them a greater likelihood of being selected). INEI provided theteam with maps that showed where the clusters were in relation toeach other, and a map of each selected cluster indicating buildingssuch as houses, shops, and warehouses.
2. Because the maps had been made a few years earlier, the Peruteam had to update them to take migration into account. A team ofenumerators was sent to each cluster a few weeks before fieldworkbegan and went to each building to verify how many householdslived there. They also obtained information regarding the number ofeligible women in each household. A total of 21,322 householdswere enumerated in this process.
3. Based on this information, the team estimated that they would needa sample size of 2,000 in order to end up with 1,500 completedinterviews after accounting for refusals and households without eligi-ble women. Therefore, 12 households were selected in each of the166 clusters. The sampling interval varied according to the size ofthe cluster. In a cluster with 120 households, every tenth householdwas chosen, in a cluster with 72 households every sixth house waschosen, and so forth. In the clusters with less than 48 households, adifferent strategy was used. To avoid interviewing women living veryclose to each other (this might undermine confidentiality), a minimuminterval of four houses between selected households was estab-lished. This meant that in a cluster with 36 households, only ninewomen would be interviewed, instead of 12.
4. To choose the households, the team supervisor chose a house ineach cluster at random using the same technique to start off the num-bering (for example the northernmost house in a block). Interviewers
then followed the sam-pling interval to select thehouses where womenwould be interviewed.No replacements wereallowed in the case ofhouseholds without eligi-ble women.
Cusco
A multistage samplingstrategy was used in
Cusco, where there are a few rural towns, and the rest of the popula-tion is dispersed throughout the mountains. The region has 12provinces, and includes the regional capital, Cusco, where a largepart of the population lives. The other provinces are mostly rural.
1. Four provinces were selected randomly. These included the town ofCusco plus three rural provinces.
2. INEI selected 46 clusters for the town of Cusco and 66 for the threeprovinces. Each cluster was selected with probability proportional tosize. INEI had maps only for the town, and these were updated inthe same fashion as in Lima. In Cusco, 12,558 buildings were enu-merated with 5,619 households. Twenty-three households wereselected to be visited in each cluster.
3. For the rural clusters, only general maps were available indicatingwhere larger towns were located. In the larger towns, the teammade a quick inventory of households and sketched a map. Thetotal number of households was divided by 23 to obtain the sam-pling interval. The first household was selected randomly, then therest were selected systematically.
4. In the rural area, no information was available. To generate detailedmaps, the team held meetings with the leaders of rural communitiesand local women’s clubs. The leaders were informed about the gen-eral goals of the study and the approximate dates that fieldworkwould be performed in their communities. The leaders preparedmaps of each village, with all houses and landmarks indicated, andthen together mapped out the routes that fieldworkers would followto reach the villages.
5. With the help of the maps, one household was randomly selected,and from this starting point all households were visited following aspiral direction, until 23 households with eligible women were vis-ited. Because households were very dispersed, it was not necessaryto have a minimum sampling interval. If one village did not have 23households in it, then the closest village was visited, following thesame procedure until the 23 interviews were completed.
BOX 7.3 SAMPLING IN PERU
The WHO VAW Study was carried out in two sites in Peru: Lima, the capital, and Cusco, a mountainous region with a mostly Quechua-speakingpopulation. The research team used two very different sampling strategies for the study.
Community leaders mapping out villagesin Cusco, Peru
Community map with schools, roads marked.(From Guezmes et al, 2002.7)

A Practical Guide for Researchers and Activists 113
for missing households, where there is noeligible woman, or where the selectedrespondent is unavailable or refuses to par-ticipate in the study.
Obtaining a sampling frameAs pointed out earlier, to select a randomsample, it is necessary to have a list ormap of all households or individuals(depending on the sampling unit) in thestudy population. Wherever possible, pre-viously developed sampling framesshould be used, for example:
■ Official census data.■ Voter registration records.■ Census carried out by the Health
Ministry for immunization or malariacampaigns.
■ Sampling frames developed by otherlarge-scale studies carried out in thecountry (such as Demographic andHealth Surveys or Living StandardsMeasurement Surveys).
Each of these options will have to bereviewed carefully to assess the quality ofthe information. In some kinds of officialdata, certain individuals may be left out (forexample, resident foreigners or domesticservants). Moreover, unless the data werecollected quite recently, it will probably benecessary to update the records. Even so,this will be much less time-consuming andcostly than developing your own samplingframe. If there is nothing already availablethen you will have to develop your ownsampling frame. This is often done by enu-merating (listing and mapping) house-holds and/or eligible respondents in theselected clusters. An example of some otherapproaches used in Liberia in a conflict sit-uation is shown in Box 7.4.
Who is eligible to be interviewed?Other sections addressed the importance,for safety reasons, of interviewing only one
woman per household. However, eachresearch team will have to consider care-fully what criteria to use for eligibility. Inother words, which women within thehousehold can be considered as a possibleinformant? For example, will domestic ser-vants be included? What about visitingfriends or relatives, or lodgers such as stu-dents who are renting a room in the house?
Researchers have resolved these issuesin different ways, and each solution has itsown advantages and tradeoffs. For exam-ple, if whether a woman slept in thehousehold the night before is used as abasic criterion, then domestic servants maybe included in their place of work.However, in this case, much of the eco-nomic status information collected aboutthe household will not reflect this woman’s
D E V E L O P I N G A S A M P L I N G S T R AT E G Y
A study in Liberia on violence against women during the civil war used several dif-ferent survey sites to maximize the breadth of representation, including marketplaces, high schools, urban communities, and displaced persons camps. Each siterequired a different sampling strategy. Although each strategy yielded a goodapproximation of the situation of women from the specific target group sampled, itshould be noted that one cannot combine the three groups to obtain a prevalenceestimate for Liberian women as a whole.
■ Sampling older women: In the market places, the sampling unit was a marketstall. Surveyors drew a detailed map of the number and location of tables, fromwhich the computed sampling interval and specific tables were randomlyselected. Because lotteries were common in Liberia, the team made colorful“lucky tickets” for the tables that had been randomly selected. After introducingherself to a market woman, the interviewer placed the ticket on the table, say-ing “lucky ticket” and invited the woman to participate in the survey.
■ Sampling young girls: The team derived a sampling plan for the high schoolsby obtaining from the teachers the number of girls in attendance that day ingrades nine through twelve. After the sampling interval was computed, the girlsin each class counted off starting from “one” to the sampling interval. If the sam-pling interval was four, for example, every girl who counted off “four” wasinvited to participate in the survey. The sampling was done publicly so thateveryone knew that the girls had not been selected because of any particularexperience, thereby preventing any stigma that might be attached to beingselected to participate in a survey about sexual violence.
■ Sampling refugees: The availability of food distribution census data made iteasier to sample in the communities and in the displaced persons camps. Aftercalculating the sampling interval, households were systematically chosen byselecting a starting household at random using the last two digits of the serialnumber on a Liberian $5 bill chosen at random.
BOX 7.4 CREATIVE SAMPLING IN LIBERIA
(From Swiss et al, 1998.8)

114 Researching Violence Against Women
true status. On the other hand, if domesticservants are not considered eligible intheir place of work, then it is important tomake sure that they may have an oppor-tunity to be included in their permanenthouseholds. This places an additional bur-den on interviewers because to avoid hav-ing a high nonresponse rate, it will benecessary to return in some cases on spe-cific days or evenings when the womanwill be home. The key to not introducingbias into the sample is to remember thateligibility criteria must be determined insuch a way that all eligible women withinthe cluster have an equal opportunity tobe chosen as informants, whether at theirhomes, place of work, or school.
The WHO VAW study decided to con-sider permanent lodgers and domestic ser-vants who spend fewer than two nightsper week away from the household as eli-gible informants. Women who worked inthe household as domestic servants butspent at least two nights a week awaywould not be included. These womencould potentially be selected to be inter-viewed in their own homes on their daysoff work.
To avoid biasing the sample, it isimportant that interviewers select thewoman to be interviewed using randommethods, and not simply the first womanto answer the door, or the oldest, or theone who seems most available. In theWHO VAW study, this was achieved bychoosing women’s names out of a paperbag. In Nicaragua, a random number chartwas used to select the women to inter-view. Box 7.5 describes how to use thesemethods. If you are using a list ofwomen’s names generated from a sam-pling frame of individuals, and it is possi-ble to determine whether two women areliving in the same household, then youcan select one woman from each pair byalternating between the older andyounger woman.
C H A P T E R S E V E N
Lottery
Make a list of all the women in the household who are eligible to participate in thestudy according to the study criteria (such as over 15, ever been partnered). Besure to include women even if they are not in the house at the time of the visit.Write the name of each woman on a separate piece of paper and place thepapers in a paper bag. Ask someone in the household (perhaps the oldest person)to select a paper from the bag. Advantages of this method are the simplicity ofadministration and that it makes clear to everyone in the household that the personhas been selected by chance, not because of any special characteristics. The dis-advantage of this method is that it is difficult to monitor whether interviewers areusing the system correctly.
Randomized chart
A randomized chart may be helpful for selecting a woman to interview once youhave a complete list of all members of the household. This method makes it fairlyeasy to monitor whether fieldworkers are using the procedure correctly, but it is lesstransparent to household members.
Check the last digit on the number of the questionnaire. This indicates the row touse. Then, check on the list of household members the total number of womenbetween 15 and 49 who have ever been married or partnered. This indicates thecolumn to use. The number that appears in the intersection of the row and columnindicates the number of the woman who should be interviewed.
Last digit on thequestionnaire Number of eligible women in the household
1 2 3 4 5 6 7 8
0 1 2 2 4 3 6 5 41 1 1 3 1 4 1 6 52 1 2 1 2 5 2 7 63 1 1 2 3 1 3 1 74 1 2 3 4 2 4 2 85 1 1 1 1 3 5 3 16 1 2 2 2 4 6 4 27 1 1 3 3 5 1 5 38 1 2 1 4 1 2 6 49 1 1 2 1 2 3 7 5
BOX 7.5 TWO METHODS FOR SELECTING INFORMANTS
PHO
TO B
Y H
AFM
JAN
SEN

A Practical Guide for Researchers and Activists 115
1. Crabtree B, Miller W. Doing Qualitative Research.Newbury Park: Sage; 1992.
2. Hudelson P. Qualitative Research for HealthPrograms. Geneva: Division of Mental Health,World Health Organization; 1994.
3. Patton M. Qualitative Evaluation and ResearchMethods. 2nd ed. Newbury Park: SagePublications; 1990.
4. Montoya O. Nadando contra Corriente:Buscando Pistas para Prevenir la ViolenciaMasculina en las Relaciones de Pareja. Managua,Nicaragua: Fundación Puntos de Encuentro; 1998.
5. Morison L. Self-weighting in Cluster Samples.Personal Communication. London; 2002.
6. Persson LÅ, Wall S. Epidemiology for PublicHealth. Umeå, Sweden: Umeå InternationalSchool of Public Health; 2003.
7. Guezmes A, Palomino N, Ramos M. ViolenciaSexual y Física contra las Mujeres en el Perú.Lima: Flora Tristan, Organización Munidial de laSalud, Universidad Peruana Cayetano Heredia;2002.
8. Swiss S, Jennings PJ, Aryee GV, et al. Violenceagainst women during the Liberian civil conflict.Journal of the American Medical Association.1998;279:625-629.
D E V E L O P I N G A S A M P L I N G S T R AT E G Y

8PHOTO B
Y M
. ELLS
BERG

A Practical Guide for Researchers and Activists 117
respondents’ willingness to disclose per-sonal information.
Finally, decide whether you understandthe topic and setting well enough to designa questionnaire. If not, you may want toconduct some formative research to iden-tify areas of inquiry and to refine issues oflanguage. Chapter 9 presents a number ofqualitative techniques for gathering infor-mation before you design a more struc-tured questionnaire.
DEVELOPING THECONCEPTUAL FRAMEWORK
Before developing your questionnaire it isessential to decide exactly what informa-tion you will need and how you will meas-ure it. One way to do this is to map outvisually all the information in your researchquestions and organize it according to howyou think the variables are related to each
Quantitative data are generally col-lected using a standardized questionnaire,which may be administered in a face-to-face interview or as a self-administeredquestionnaire. The process of developing awell-conceptualized and user-friendlyinstrument for collecting quantitative datais complex and time-consuming, but cru-cial for successful research.
Before starting, clarify what you want toknow, according to the goals of yourstudy. Next, consider whether you canobtain all of the answers you seek byquestioning respondents, or if you willneed to use additional techniques such asobservation or analysis of records. Howwill you administer your questionnaire—by phone, in person, by mail, or by com-puter? In making this decision, considerboth the literacy levels of likely respon-dents and the positive or negative influ-ence each option may have on the
C H A P T E R E I G H T
Tools for CollectingQuantitative Data
Topics covered in this chapter:
Developing the conceptual frameworkOperationalizing the main variablesFormulating your questions Formatting your questionnaireTranslating the instrumentPre-testing the instrument

118 Researching Violence Against Women
C H A P T E R E I G H T
other. This exercise will be informed bythe review you have carried out of relevantliterature and the “brainstorming” sessionsthat you have carried out with the researchteam and knowledgeable members of thecommunity. Start out by including as broada range of factors as possible.
Figure 8.1 shows how individual char-acteristics of women and their partners,
combined with community level characteris-tics such as norms around violence and theexistence of services for abused women,might increase or decrease a woman’s riskof being abused by her partner. The charac-teristics of the abuse, whether sexual, physi-cal, or emotional, and its severity andfrequency, are likely to determine whethershe will suffer either physical or emotional
FIGURE 8.1 EXAMPLE OF A CONCEPTUAL FRAMEWORK FOR UNDERSTANDING RISKS ANDIMPACT OF INTIMATE PARTNER VIOLENCE
Women’scharacteristics
■ Age (younger than partner)■ Urban residence■ Number of children■ Works outside home■ Low education■ Witnessed violence as
a child
Partner’scharacteristics
■ Age discrepancy(higher than respondent)
■ Low education■ Employment■ Witnessed violence as
a child■ Uses drugs or alcohol
Women’s responses
■ Seeks formal help(police, judges)
■ Seeks informal help(friends, family)
■ Defends self physically■ Leaves relationship tem-
porarily or permanently
Violence against womenby intimate partners
■ Type■ Severity■ Frequency
Health consequences
■ Injuries■ Emotional distress■ Miscarriages■ Abortions■ Physical symptoms
Communitycharacteristics
■ Community norms favorviolence against women
■ Belief that violence is a“private family problem” andothers should not interfere
■ No support services forabused women

A Practical Guide for Researchers and Activists 119
health effects from the violence. Finally, thecharacteristics of the violence, the healtheffects, and community attitudes and theavailability of support services determine theoptions she has for protecting herself.
If you are looking at a specific outcomefor which there are already known risk fac-tors, these risk factors should be includedin the map. For example, if you want toexamine the relationship between lowbirth weight and violence, it is important tocollect information about a woman's repro-ductive history—such as number of preg-nancies and use of alcohol or tobaccoduring her pregnancy.
Each concept included in the map willbe translated into one or more variables.These are the components of the researchquestion, conceptually isolated and unam-biguously defined. The variables that repre-sent specific outcomes under study areknown as the outcome or dependentvariables, while those variables that helpexplain the causes of these outcomes areknown as explanatory or independentvariables. Some variables, such as “vio-lence,” can be considered as both, depend-ing on whether one is looking at thecauses or consequences of violence.
Once you map out all the possible vari-ables, it is time to narrow the focus of thestudy according to what is feasible andmost relevant to the study’s objectives.Some of the variables may be outside thescope of the survey. These variablesshould be discarded; there is no point incollecting data that will not yield meaning-ful results.
OPERATIONALIZING THE MAIN VARIABLES
Once you determine which specific out-comes and background variables toinclude in the questionnaire, it is necessaryto decide how each will be defined andmeasured. In Chapter 6, we discussed how
different types of violence might be moreprecisely measured. As an example, Table8.1 presents how the WHO VAW Studyaddressed different issues regarding riskand protective factors and consequencesof violence.
FORMULATING YOUR QUEST IONS
Once you identify your study variables, itis time to turn them into clearly wordedquestions. Survey questionnaires commonlyuse two types of questions:
■ Closed questions. Respondents areasked to choose from one or more fixedalternatives. These can be yes/no ques-tions (“Has your husband ever hit youduring pregnancy?”) or ordinal cate-gories (“Would you say thatlast year your husband hityou once, several times, ormany times?”). Another typeof closed question, thescale item, asks for aresponse in the form ofdegree of agreement or dis-agreement, or level of inten-sity, (“How do you feelabout the following statement: Womenshould put up with abuse in order tokeep the family together? Stronglyagree, Agree, Don’t know, Disagree,Strongly disagree.”)
■ Open questions. These do not restrictthe content or manner of the replyother than the subject area (“Whom didyou tell about your situation?” or “Whowas present the last time you werebeaten?”)
The majority of questions in the surveyquestionnaire will probably be in theform of closed questions. Open-endedquestions are flexible and allow the
T O O L S F O R C O L L E C T I N G Q U A N T I TAT I V E D ATA
A dependent variable refersto the specific outcome or condi-tion under study (e.g., violence).
An independent orexplanatory variable is onethat helps explain the causes ofthe dependent variable.

120 Researching Violence Against Women
interviewer to probe a subject in greaterdepth, but they are also more time-con-suming to administer and analyze. Wetherefore recommend that you limit theuse of open-ended questions when con-ducting large-scale surveys. Piloting andformative research may facilitate the useof open-ended questions by providingsuggestions for standard responses thatcan be precoded and included in thequestionnaire.
Use of international instruments For many concepts, such as emotional dis-tress, socio-economic status, or reproduc-tive health outcomes, internationalquestionnaires already exist, and mayalready be adapted and even validated for
use in your country. Using instruments thathave already been validated makes it easierto compare the findings in your study withother national and international studies. Asthe example from South Africa in Box 8.1shows, it’s still important to pre-test theinstruments to be sure that the conceptsare clear and meaningful in your setting.Box 8.2 describes the process of develop-ing the WHO VAW instrument.
FORMATTING YOURQUEST IONNAIRE
The way the questionnaire is organizedand formatted can make a big difference inhow smoothly the interviews go. The mainissues are:
C H A P T E R E I G H T
Prevalence and characteristics of violence
■ Prevalence during last year■ Prevalence ever■ Severity of abuse■ Type of abuse (physical, sexual, emotional)■ Frequency during last year■ Frequency of previous violence■ Relationship to offender■ Violence during pregnancy■ Initiation and duration of violence
Background socio-economic information
Details of respondent Details of current or most recent partner
■ Age ■ Age■ Education ■ Education and training■ Marital status/marital history ■ Marital status■ Household composition ■ Current or most recent employment■ Socio-economic status of household■ Current or most recent employment/sources of income
Risk and protective factors for violence against women in families
About woman Details of current or most recent partner
■ Female access to and control of resources ■ Expectations, communication, and decision making in relationship■ History of previous victimization ■ Extent of participation in looking after family and home■ Indicators of empowerment ■ Use of alcohol and drugs■ Resistance to violence ■ Employment status■ Whether witnessed violence between parents as a child ■ Whether witnessed violence between parents as a child■ Whether can access support outside the household from friends ■ Whether physically aggressive towards other men■ Whether belongs to any group/association■ Use of alcohol or drug
TABLE 8.1 TOPICS INCLUDED IN THE WHO MULTI-COUNTRY STUDY ON WOMEN’S HEALTH AND DOMESTIC VIOLENCE AGAINST WOMEN
(From WHO, 2004.1)

A Practical Guide for Researchers and Activists 121
to continue the survey. In telephone orpersonal interviews, they help build rap-port with the interviewer. Groupingtogether questions on the same topic alsomakes the questionnaire easier to answer.
Whenever possible, place difficult orsensitive questions towards the end of thesurvey. Any rapport that has been built upwill make it more likely people will answerthese questions. If people quit at that pointanyway, at least they will have answeredmost of your questions.
If conducting research in a culture that isnot your own, don’t assume you can pre-dict what will be considered sensitive. In
T O O L S F O R C O L L E C T I N G Q U A N T I TAT I V E D ATA
■ The sequence of questions■ Appropriate answer scales■ Appropriate skip patterns
The sequence of questionsKeep two broad issues in mind when con-sidering the order of your questions. Oneis how the order can encourage or discour-age people from completing the survey.The other is how the order of questions orthe order of answer choices could affectyour results.
Ideally, the early questions in a surveyshould be easy and pleasant to answer.These kinds of questions encourage people
Health outcomes
■ Reproductive history including pregnancies, live births, miscarriages, and still births■ Whether she wanted pregnancy with last child ■ Details of last child and use of prenatal services■ Use of family planning■ Smoking and alcohol consumption in last month■ Indicators of physical health problems in last month■ Indicators of reduced mobility or functioning in last month■ Indicators of psychological distress in last month■ Suicidal thoughts and attempted suicides■ Health care utilization in last month■ Use of medication in last month■ Hospitalization and operations in last year■ Injuries resulting from physical violence■ Use of health services as a result of injuries
Other consequences of violence
Impact on women’s lives Impact on children’s lives
■ Perception of whether affected physical or mental health ■ Reported birth weight for last child under 5■ Prevented from working ■ Child aged 5–12 had to repeat year at school■ Disruption of work/ability to earn money ■ Child aged 5–12 ran away from home■ Ability to attend community meetings ■ Child has emotional problems (thumb-sucking, bed-wetting)
■ Extent to which children witness physical or sexual violence
Women’s responses to violence
Sources of help and response Actions to prevent or reduce violence
■ Who knows about situation ■ Did she ever defend herself physically■ Who intervened or tried to stop violence ■ Whether she ever hit first■ Use of formal and informal services ■ Whether she ever left/frequency left■ Who got help from/forms of help provided ■ Satisfaction with response■ Who she would have liked to get more help from
TABLE 8.1 TOPICS INCLUDED IN THE WHO MULTI-COUNTRY STUDY ON WOMEN’S HEALTH AND DOMESTIC VIOLENCE AGAINST WOMEN
(From WHO, 2004.1)

122 Researching Violence Against Women
the WHO VAW study, for example, thequestions considered most sensitive varieddramatically by country. In Bangladesh, itwas considered routine to ask womenabout family planning and this was seen asa good rapport-building topic. In Japan,questions about birth control were per-ceived as highly sensitive. The Japan teamurged leaving these questions until later inthe questionnaire.
Another strategy for increasing responserates on highly sensitive questions, or in sit-uations where privacy is difficult to achieve,is to allow individuals to respond by point-ing out the appropriate answer on responsecards rather than saying an answer outloud. Keep in mind that this strategy onlyworks with literate populations.
C H A P T E R E I G H T
The questionnaire used in the study was the product of a long process of discussion and consultation. This hasinvolved reviewing existing literature and numerous instruments, and incorporating input from technical experts inspecific areas (including violence against women, reproductive health, mental health, and drug and alcohol use)from members of the expert steering committee, and from experts in the field of conducting large population-basedsurveys (e.g., the DHS). Moreover, to ensure maximum comparability across studies, discussions were also heldwith groups such as the International Network of Clinical Epidemiologists (INCLEN) that were conducting researchin related areas. For practical reasons, the questionnaire consists primarily of structured questions with closedresponses.
In the development phase, the questionnaire was first translated and pre-tested in a limited number of countries on aconvenience sample of women. This process was used to explore a range of issues associated with the content ofthe different sections of the questionnaire. At this stage, respondents were not only asked to answer questions fromthe questionnaire, but also were requested to provide feedback on the clarity and acceptability of the questionsasked, and the way in which the questionnaire was being delivered. At the end of this first pre-test, all interviewersmet with the country research team to review the questionnaire, to determine where problems were arising, and toexplore possible solutions. This feedback was used to revise different modules within the questionnaire.
Subsequent drafts were informed by qualitative research in the culturally diverse countries and were field-testedagain in a second pre-test in the remaining participating countries. This experience resulted in extensive revisions toimprove accuracy and cross-cultural comparability, and in the final content and structure. The final revisions to thequestionnaire were made following the fourth research team meeting. The revised questionnaire was then sent toeach country research team for a final pre-test. This resulted in version 9.9, which was used in the first eight coun-tries of the multi-country study.
Each country could add only a limited number of relevant country specific questions, and adapted certain responsecodes to reflect local circumstances.
Between 1999 and 2002, the final questionnaire was used in 13 languages during the implementation of theWHO multi-country study in Bangladesh, Brazil, Japan, Namibia, Peru, Samoa, Tanzania, and Thailand.Additional studies in Chile, China, Serbia, New Zealand, Ethiopia, and Indonesia have also usedthis questionnaire. The questionnaire and a manual with the question-by-question description of the questionnaire isavailable from WHO at genderandhealth@ who.int. A shortened version of the instrument can be found inAppendix I of this guide.
BOX 8.2 DEVELOPING THE CORE QUESTIONNAIRE FOR THE WHO MULTI-COUNTRY STUDY ON WOMEN’S HEALTH AND DOMESTIC VIOLENCE AGAINST WOMEN
BOX 8.1 QUESTIONNAIRE DEVELOPMENT IN SOUTH AFRICA
In 1998, the South African Medical Research Council conducted a survey on vio-lence against women. The survey was applied to a random sample of 750 house-holds per province in three (of nine) rural provinces with women aged 18-49. Thequestionnaire for the women’s survey was developed using instruments from othercountries and two South African focus groups. It was tested and refined over a three-month period with abused women, other women, and NGO staff. The final revi-sions were made after a pilot training session for fieldworkers.
Mental health questions were particularly difficult. At the outset, researchers consid-ered using a 20-item self-reporting questionnaire that had been tested and calibratedto similar African settings. During testing, however, informants and fieldworkers hadenormous difficulty understanding the questions, and the instrument’s length wasproblematic in an already long questionnaire. In addition, scores seemed to beimprobably high.
This prompted an investigation of indigenous and lay expressions of mental illhealth—a process that yielded several expressions of distress shared among allAfrican linguistic groups in South Africa. Idioms used to describe mental distressinclude ”the spirit is low” and, if more severe, ”the spirit/heart is painful.” Theseexpressions were incorporated into the questionnaire.
(From Jewkes et al, 1999.2)
(From WHO, 2004.1)

A Practical Guide for Researchers and Activists 123
The other way question order canaffect results is habituation. This problemapplies to a series of questions that allhave the same answer choices. Afterbeing asked a series of similar questionspeople may give the same answer with-out really considering it. One way toavoid this is by asking some questions so
that positive attitudes or beliefs aresometimes scored with a yes answer or ahigh number on a scale and on otherquestions with a no answer or a lownumber.
Box 8.3 presents an example of ques-tions asked in the WHO VAW study aboutwomen’s attitudes toward gender roles.
T O O L S F O R C O L L E C T I N G Q U A N T I TAT I V E D ATA
In this community and elsewhere, people have different ideas about families and what is acceptable behavior formen and women in the home. I am going to read you a list of statements, and I would like you to tell me whetheryou generally agree or disagree with the statement. There are no right or wrong answers.
A good wife obeys her husband even if she disagrees. Agree __________
Disagree __________
Don’t Know __________
Refused/No Answer __________
Family problems should only be discussed with people in the family. Agree __________
Disagree __________
Don’t Know __________
Refused/No Answer __________
It is important for a man to show his wife/partner who is the boss. Agree __________
Disagree __________
Don’t Know __________
Refused/No Answer __________
A woman should be able to choose her own friends even if her Agree __________
husband disapproves. Disagree __________
Don’t Know __________
Refused/No Answer __________
It’s a wife’s obligation to have sex with her husband even if she doesn’t Agree __________
feel like it. Disagree __________
Don’t Know __________
Refused/No Answer __________
If a man mistreats his wife, others outside of the family should intervene Agree __________
Disagree __________
Don’t Know __________
Refused/No Answer __________
BOX 8.3 QUESTIONS FROM THE WHO VAW STUDY ON GENDER ROLES
(From WHO, 2004.1)

124 Researching Violence Against Women
In some cases, such as a woman choos-ing her own friends, a respondent whoagrees with the statement would beexpressing views in favor of women’sautonomy, whereas in the question aboutthe importance of a man showing his wifewho is the boss, agreement would indicateacceptance of traditional values.
Appropriate answer scalesQuestions related to attitudes, frequency ofevents, or opinions usually require partici-pants to answer based on some form ofscaled response. In the developed world,such scales usually allow for at least fivedistinct answers. Such complex scales,however, can be difficult for some popula-tions to understand and interpret. Moreover,certain cultural patterns and expectationscan influence how individuals reply to dif-ferent response options. For example,researchers in Nicaragua found when usinga five-point scale to measure perceptions ofchildhood experiences that respondentsalmost invariably answered that they“strongly agreed” or “strongly disagreed.”Almost no responses indicated that they“somewhat” agreed or disagreed. In con-trast, in other countries, particularly in Asia,researchers have found that respondentsare reluctant to express a very strong opin-ion, for fear of seeming rude. Therefore,responses tend to be more neutral.3
Appropriate skip patternsThe skip patterns in a questionnairedetermine the order of specific questionsthat will be asked according to answers thatare previously given. They help make theinterview flow smoothly and avoid annoy-ing mistakes, such as asking a woman theage of her children when she has alreadyindicated that she has no children, or ask-ing women who have never had sexualrelations whether they use birth control.Special care should be taken to ensure thatthe skip patterns are correctly placed and
that women are not inadvertently excludedfrom being asked important questions.
As an example of how important infor-mation may be lost through errors in skippatterns, the León, Nicaragua, survey onlyasked questions about problems in preg-nancy to women who had suffered abuse.This made it impossible to compare therates of miscarriages and abortions amongabused and nonabused women. A similarproblem occurred when questions aboutphysical injuries as a result of abuse wereasked of women who had only sufferedemotional and not physical violence.
TRANSLATING THEINSTRUMENT
Now that you’ve developed your testinstrument, how do you translate it into thelocal language? You need an accurate andprecise translation, but professional transla-tors may not be familiar with the termswomen use to talk about violence and inti-mate relationships.
Several steps can enhance your transla-tion efforts. First, involve activists or serviceproviders in translating the test instrument.You may find that formative research helpsyou identify the appropriate terms andexpressions to describe the issues understudy. Researchers often use a techniquecalled back-translation (having someoneunfamiliar with the study translate the ques-tionnaire back into English) to ensure thatthe instrument has been properly translated.However, researchers in South Africa andZimbabwe found that back-translationswere not a reliable way to check the accu-racy of questions on violence and its conse-quences. They achieved better results whensomeone who understood the purpose ofthe study and who could compare theEnglish version with its translation checkedthe translated questionnaire.2 Box 8.4describes the steps that were taken in trans-lating the WHO VAW questionnaire.
C H A P T E R E I G H T

A Practical Guide for Researchers and Activists 125
PRE-TEST ING THEINSTRUMENT
Before beginning the fieldwork, it is essen-tial to pre-test the questionnaire thor-oughly. The many errors or unforeseensituations you will find are fairly easy tocorrect at this stage, but would be quitecostly to repair later. To pre-test, try thequestionnaire on women who do not livein the research area, but who are similar tothe women you are planning to study (thisdoes not have to be a random sample).This step enables you to detect any prob-lems in terms of the content or wording ofquestions as well as interview length. Trythe test on women of different ages andbackgrounds, including women who areknown to be experiencing different formsof abuse. The women’s organizations par-ticipating in your advisory group may behelpful in identifying women who are will-ing to be interviewed about their experi-ences of violence.
If the questionnaire is to be translatedinto different languages, pre-test the trans-lated versions too. In addition, askingrespondents to answer questions from thequestionnaire, invite them to provide feed-back: “Are the questions asked clear andacceptable? How do you feel about howthe interview was conducted?” At the endof the pre-test, all interviewers should meetwith the research team to review the ques-tionnaire, to pinpoint problems with thequestions and coding categories, and toexplore possible solutions. Box 8.5 givessome examples of the kinds of questionsyou might ask in the pre-testing stage.
T O O L S F O R C O L L E C T I N G Q U A N T I TAT I V E D ATA
BOX 8.4 TRANSLATING THE WHO QUESTIONNAIRE
The working language for the development of the core questionnaire was English.Before pre-testing, each country questionnaire was professionally translated intoeach of the local languages used by the study population. The formative researchwas used to guide the forms of language and expressions used, with the focusbeing on using words and expressions that are widely understood in the studysites. In settings where there are a number of languages in use, it was necessaryto develop questionnaires in each language.
The translated questionnaire was first checked by local researchers involved in thestudy who could compare the English version with its translation. Lengthy oral back-translation sessions with step-by-step discussion of each question were conductedwith people not familiar with the questionnaire but fluent in the language and withpeople who understood the questionnaire and violence issues. The main purposewas to identify differences in translations that could alter the meaning and to estab-lish cognitive understanding of the items in the questionnaire. Adjustments weremade where needed. Once the translated questionnaire had been finalized duringthe interviewer training, questions were discussed using the manual with explana-tions for each question. Having interviewers from various cultural backgroundsaided in ascertaining whether wording used was culturally acceptable. During thetraining itself, further revisions to the translation of the questionnaire were made.Finally, usually during the field pilot in the third week of the interviewer training,final modifications to fine tune the translated questionnaire were made.
Pitfalls in Translation
In a Zimbabwe study, a series of questions were used to define the time frameduring which women had attended health services. In English the question was,“In the last year (1995), have you attended a clinic or hospital because youwere sick?”
In Shona, the question was translated as, “In 1995, did you attend…” Since thesurvey was conducted in May 1996, this question only obtained informationabout the previous calendar year.
In Nbele, the question was translated as, “In the last year (12 months) have youattended…”
Therefore, the information obtained from the two translated versions referred todifferent periods.
(From Watts, 1997.4)

126 Researching Violence Against Women
C H A P T E R E I G H T
1. During the interview, the interviewer should jot down observations about any questions that seem to beproblematic.
2. After the interview, take another 15-30 minutes to ask the respondents their own views about the interview:
■ What do you consider the main topics of the survey?
■ Are there any questions you feel are inappropriate, too personal, or that people would not be likely toanswer truthfully?
■ Do you feel comfortable with the informed consent process (i.e., were you adequately informed about thenature of the study)?
■ Were there any questions that you did not understand or that you thought were confusing?
■ Is the length of the interview acceptable or too long? (You may want to ask how long they thought the inter-view lasted and compare this to the actual duration.)
3. After each interview, take detailed notes of both your own and your respondent’s observations.
4. After each researcher/interviewer has performed several interviews, it is useful to sit down and analyze theresponses to the questionnaire. The following issues might be explored in this discussion:
■ Are there any questions that are particularly sensitive, or that women seem reluctant to answer?In the Nicaragua survey, a question about the last time a couple had intercourse caused a lot of discomfortamong respondents, and women often asked why we wanted to know this.
■ Are there questions women seem to answer almost automatically? Are they telling us what they think we wantto hear, rather than drawing from their own experiences?Researchers in some Asian countries have found that women are unlikely to report violence between theirparents and in-laws, as it is considered disloyal to speak ill of relatives.
■ Are there questions for which the women give unusual answers, or seem not to understand the purpose of thequestion? For example, does the interviewer need to explain it several times, or use different language sothat the women understand the question? What wording would be easier to understand?
■ Are there questions for which it is difficult to code the response, or where it seems that the questionnaire ismissing important data?In one pre-testing exercise, it became clear that many women have been abused by a spouse prior to theircurrent partner. Therefore it was necessary to collect some basic information about former spouses.
■ Do the skip patterns seem to flow smoothly, so that no women are left out of questions they should be asked?Conversely, are women made to repeat the same answers? Are they asked inapplicable questions?
■ Is there a fairly broad range of responses to most of the questions?Too much uniformity may indicate that women are answering in a way that they believe is expected, or thatthey don’t really understand the question, or that it is simply not a useful or relevant question.
■ If we ask hypothetical questions such as, “Do you think a woman should accept being beaten in orderto keep her family intact?” do women seem to understand that we are asking about opinions and notexperiences? Women who are not used to this kind of question may find it difficult to respond, and may giveanswers such as, “I can’t speak for anyone else.”
■ Are there questions where similarly coded answers might mean two very different things? Do we need to addadditional responses or improve the wording of the question to enhance clarity?
■ Do the initial sections allow the interviewer to develop sufficient rapport before asking about violence?Would the questions on violence fit better at an earlier point? Does the order of the questions seem to flowlogically and smoothly?
■ Is the questionnaire too long? Do women seem tired or restless by the end of the survey? Does the averageduration of the interview correspond to what you have told respondents in the consent form? Consent formsusually give the respondent an estimate of how long the questionnaire will take to complete. If the averageinterview during the pre-test is substantially longer than what the consent form suggests, then you may have torevise either the estimate or the questionnaire.
■ Is it difficult to achieve privacy? Do the procedures for ensuring confidentiality work?
■ Are there differences in the way that women responded in the versions that are translated into other lan-guages? Are there specific problems with the wording or translations?
BOX 8.5 SUGGESTIONS FOR PRE-TESTING THE QUESTIONNAIRE

A Practical Guide for Researchers and Activists 127
T O O L S F O R C O L L E C T I N G Q U A N T I TAT I V E D ATA
1. World Health Organization. WHO Multi-countryStudy on Women’s Health and Domestic Violence:Study Protocol. Geneva, Switzerland: WorldHealth Organization; 2004.
2. Jewkes R, Penn-Kekana L, Levin J, Ratsaka M,Schrieber M. He Must Give Me Money, He Mustn’tBeat Me: Violence Against Women in Three SouthAfrican Provinces. Pretoria, South Africa: MedicalResearch Council; 1999.
3. Yoshihama M. Personal Communication. AnnArbor, Michigan; 2004.
4. Watts C. Violence in Zimbabwe. PersonalCommunication. London, UK;1997.

9PH
OTO
BY
HAF
M JA
NSE
N

A Practical Guide for Researchers and Activists 129
tative data. Talking face to face withrespondents on highly sensitive mattersrequires sensitivity, skill, and the ability tointerpret and respond to both verbal andnonverbal cues. Interview styles vary fromhighly structured or semistructured for-mats to highly fluid and flexibleexchanges. In addition to recording thecontent of the interview, interviewers maywish to keep a field log, where theykeep track of their own observations,reflections, feelings, and interpretations.Because the skills required for gatheringqualitative data are quite different than
Researchers employ a wide range oftechniques when collecting qualitative data.In fact, most studies rely on a combinationof methods. This section describes some ofthe most frequently used qualitative datacollection tools, with examples describinghow they have been used by researchersto get individuals to speak openly andhonestly about violence.
PERSONAL INTERVIEWS
The personal interview is one of themost common means for collecting quali-
C H A P T E R N I N E
Tools for CollectingQualitative Data
Topics covered in this chapter:
Personal interviewsFocus group discussionsObservationFree listingRankingPair-wise rankingTimelines and seasonal calendarsCausal flow analysisOpen-ended storiesGenogramsCircular or Venn diagramsCommunity mapping Role playingBody mappingPhoto voice

130 Researching Violence Against Women
C H A P T E R N I N E
those needed for survey interviews, prepa-ration of field staff also needs to be quitedifferent.
Structured interviewsUse structured interviews when it isimportant to collect the same informationfrom every informant. Structured interviewsrely on a standardized interview guide thatpermits easy aggregation of responsesacross respondents. Because the structuredinterview guides allow less latitude, inter-viewers need not be as skilled as thosewho conduct unstructured interviews.
In structured interviews, the wording andorder of interview questions are determinedahead of time. Interviewers are instructedto cover every question included in theguide. For an example of a structured
interview guide, see Box 9.1. This excerptfrom an interview guide shows how thePan American Health Organization (PAHO)“Critical Path” study collected informationon how different institutions view andrespond to survivors of violence.1
Semistructured interviewsSemistructured interviews use an openframework that allows focused yet conver-sational communication. They are usefulfor collecting information about historicalevents, opinions, interpretations, andmeanings.
Unlike a survey questionnaire, in whichdetailed questions are formulated aheadof time, semistructured interviews startwith more general questions or topics.Relevant topics such as violence or
(As the interviewer, introduce yourself, explain the objectives of the study, and request the respondent's consent to be interviewed.Note the respondent's name, position, and job title; describe his or her duties; and enter the institution's name and location and thedate of the interview.)
Work performed by the respondent
■ What does your work as ________consist of?
■ What percentage of the patients you see are women? What are the most frequent reasons women give for coming to the office/emergency room?
■ Are cases of family violence seen? What are the most common cases?
■ Do you (or your colleagues) routinely ask questions to determine whether the patient might be a victim of family violence?
■ What tests or examinations do you routinely perform when a woman indicates that she has been the victim of violence? How do you decidewhich tests to perform?
■ What is the procedure for obtaining an official report from the medical examiner?
■ How many people with this type of problem does your institution serve per month? Do you have a way of keeping records on cases? Is therea form and procedure for recording them? Can you explain it to me?(Request a copy of the record form, referral slips, and any other documents that may exist.)
■ Do you (or your colleagues) provide follow-up care to women who have been victims of family violence? Are there mechanisms for referringthem to other institutions? Do you think the record-keeping system is adequate to identify women affected by family violence, refer them to theappropriate services, and provide timely follow-up services?
Experience with women affected by violence
■ Have you ever come into contact with cases of family violence among your clients?
■ Can you tell me how these experiences originated, what you did, and what the client did?
■ Do you know of other organizations or persons in this community that work on family violence issues? Who are they? What is your relationshipwith them? Is there coordination with other institutions to address the needs of abused women?
■ What changes in legislation, policy, or staffing would facilitate your work?
■ What changes in the behaviors or attitudes of the personnel with whom you work would facilitate your work?
BOX 9.1 STRUCTURED INTERVIEW: GUIDE FOR SERVICE PROVIDERS IN THE HEALTH SECTOR

A Practical Guide for Researchers and Activists 131
women’s participation on the communitycouncil are initially identified and organ-ized into an interview guide or matrix.(See Box 9.2 for an example of an inter-view guide used in formative research inthe WHO VAW study.)
Not all questions are designed andphrased ahead of time. Most questionsarise naturally during the interview, allow-ing both the interviewer and the personbeing interviewed some flexibility to probefor details or to discuss issues that werenot included in the interview guide.
Semistructured interviews require skillon the part of the interviewer, so it is agood idea to carry out some practice inter-views to become familiar with the subjectand the questions.
If possible, tape all interviews and theneither transcribe them later or developdetailed notes of the conversation basedon the tapes. If you cannot tape the inter-views, take brief notes during the interviewand complete and expand the notes imme-diately after the interview. It is best to ana-lyze the information at the end of each dayof interviewing. This can be done with theinterview team or group.
Unstructured interviewsUnstructured interviews allow the inter-viewer and respondent the most flexibility.Questions are open-ended, and the inter-viewer lets the respondent lead the conver-sation. The interviewer asks additionalquestions to gain as much useful informa-tion as possible.
Unstructured interviews are based on aloosely organized interview plan that laysout the purpose of the interview andincludes a list of topics to be explored. Theflow of the conversation—not what is writ-ten in the guide—determines the timingand sequence of topics. One type of quali-tative inquiry called “narrative analysis”particularly relies on unstructured inter-views. In this case, the interviewer attempts
to obtain a detailed story from a respon-dent about a specific event or aspect ofhis/her life. This is a story with a begin-ning, middle, and an end, although itmight not be presented in that order dur-ing the interview.
Because unstructured interviews allow alot of freedom, they require especiallyskilled interviewers. You need to be espe-cially alert for inconsistencies, pieces of thestory that seem to be missing, and newangles that might provide additional infor-mation, and then probe accordingly. Whenconducting in-depth interviews with sur-vivors of violence, beware of the temptationto slip from “interview” mode to “counsel-ing” mode. Because of their conversationalstyle, in-depth interviews tend to encourageemotional disclosure and intimacy. Thisincreases the need for interviewers to staytrue to their role, monitor their boundaries,and be attentive to levels of distress of therespondent. (See Box 10.4 for a thoroughdiscussion of the role of the interviewer.)
T O O L S F O R C O L L E C T I N G Q U A L I TAT I V E D ATA
1. Can you please tell me a little about yourself? Did you go to school?Where do you live now? Do you have children?How do you normally spend your days?What things do you like to do?
2. Tell me about your husband. How did you first meet?When did you get married?What does he do?
3. When did your problems with your husband start?How long has this continued?Are there times when this has improved, or gotten worse?
4. Has it had a great effect on your physical well-being? In what ways?How has it affected your feelings about yourself?Do you think that it is having an effect on your children? In what ways?Has it affected your ability to provide for the family or go to work?Has it made it difficult for you to meet friends or relatives? How?
5. Have you ever discussed your problems with others? How did they respond?Was there more that you would have liked them to do?What sort of things would have helped?
6. Looking back at your situation, what advice would you give another womanwho has just started to have these sorts of problems with her husband?
BOX 9.2 SEMISTRUCTURED INTERVIEW GUIDE
(From WHO, 2004.2)

132 Researching Violence Against Women
One advantage of unstructured inter-views is that they can yield very rich andnuanced information. The downside is thatdata analysis may be more complex andtime-consuming than in the case of struc-tured interviews.
FOCUS GROUPDISCUSSIONS
Focus group discussions are a powerfulmethod for collecting information relativelyquickly. They are better suited for explor-ing norms, beliefs, practices, and languagethan for seeking information on actualbehaviors or details of individual lives. Thefocus group is a special type of group interms of its purpose, size, composition,and procedures. A focus group is usuallycomposed of six to ten individuals whohave been selected because they share cer-tain characteristics that are relevant to thetopic to be discussed. In some cases, theparticipants are selected specifically so thatthey do not know each other, but in manycases that is not possible, particularly whenparticipants belong to the same communityor organization. The discussion is carefullyplanned, and is designed to obtain infor-mation on participants’ beliefs about and
perceptions of a defined area of interest.3-5
Focus groups differ in several importantways from informal discussion groups:
■ Specific, predetermined criteria are usedfor recruiting focus group participants.
■ The topics to be discussed are decidedbeforehand, and the moderator usuallyuses a predetermined list of open-endedquestions that are arranged in a naturaland logical sequence.
■ Focus group discussions may also becarried out using participatory tech-niques such as ranking, story comple-tion, or Venn diagrams (thesetechniques are all described in thischapter). This may be particularly use-ful when working with groups with lit-tle formal education or when talkingabout very sensitive issues. (In theNicaraguan study on a new domesticviolence law, described in the followingpages, however, participatory tech-niques were used successfully in focusgroup discussions with judges andmental health professionals as well aswith rural men and women.)
■ Unlike individual interviews, focusgroup discussions rely on the interac-tions among participants about the top-ics presented. Group members mayinfluence each other by responding toideas and comments that arise duringthe discussion, but there is no pressureon the moderator to have the groupreach consensus.
Focus groups have been used success-fully to assess needs, develop interven-tions, test new ideas or programs, improveexisting programs, and generate a range ofideas on a particular subject as back-ground information for constructing morestructured questionnaires. However, they
C H A P T E R N I N E
Purpose: To explore the impact of sexual harassment on individualwomen’s lives.
Definition/understanding of sexual harassment.
■ Behaviors included?■ Contexts included?
Personal experiences of harassment.
■ How did it make her feel?■ What did she do?■ How did others react?
Changes in cultural attitudes toward harassment in her lifetime.
■ Opinion on whether men can be sexually harassed by women.
Knowledge of others who have been harassed.
BOX 9.3 UNSTRUCTURED INTERVIEW GUIDE
(From WHO, 2004.2)

A Practical Guide for Researchers and Activists 133
■ Analyze the data by group. Data analy-sis consists of several steps. First, writesummaries for each group discussion.Next, write a summary for each “type”of group (e.g., a summary of all dis-cussions conducted with young moth-ers). Finally, compare results fromdifferent “types” of groups (e.g.,results from groups of young versusolder mothers).
■ The discussions may be taped for tran-scription later, but this substantiallyincreases the time and cost of analysis.One alternative is to take careful notesduring the discussion and to refer to theaudiotapes for specific areas wherethere are doubts.
Focus groups give information aboutgroups of people rather than individuals.They do not provide any informationabout the frequency or the distribution ofbeliefs or behavior in the population.When interpreting the data, it is importantto remember that focus groups aredesigned to gather information that reflectswhat is considered normative in that cul-ture. In other words, if wife abuse is cul-turally accepted, then it should not bedifficult to get participants to speak franklyabout it. However, some topics are verysensitive because they imply actions or ori-entations that are either culturally taboo orstigmatizing.
For the same reason, focus grouprespondents should not be asked to revealthe details of their individual, personallives in a focus group setting, especiallywhen the subject matter of the focusgroup deals with sensitive issues such asdomestic violence and sexual abuse. If aresearcher wants information on women’sindividual experiences, then that shouldbe done in private individual interviews.
T O O L S F O R C O L L E C T I N G Q U A L I TAT I V E D ATA
are not easy to conduct. They requirethorough planning and training of groupmoderators.
When planning a focus group, considerthe following recommendations:*
■ Focus groups require trained moderators.You will need three types of people:recruiters, who locate and invite partici-pants; moderators, who conduct thegroup discussions; and note-takers, wholist topics discussed, record reactions ofthe group participants, and tape-recordthe entire discussion (if all participantsgive consent). Note-takers also help tran-scribe the taped discussions.
■ Focus groups are usually composed ofhomogeneous members of the targetpopulation. It is often a good idea toform groups of respondents that aresimilar in terms of social class, age, levelof knowledge, cultural/ethnic character-istics, and sex. This will help to createan environment in which participantsare comfortable with each other andfeel free to express their opinions. Italso helps to distinguish opinions thatmight be attributed to these differentcharacteristics among groups.
■ If possible, experienced focus groupleaders suggest conducting at least twogroups for each “type” of respondent tobe interviewed.
■ The optimal size group consists of sixto ten respondents. This helps ensurethat all individuals participate and thateach participant has enough time tospeak. However, sometimes, it is notpossible to regulate the size of a group,and successful focus group discussionshave been carried out with many moreparticipants.
* (Adapted from Hudelson, 1994.3)

134 Researching Violence Against Women
In many cases, facilitators ask respondentsto think about the perspectives andbehavior of their peers, for example,which allows them to draw on their expe-riences in general terms but does not askthem to reveal the details of their ownbehavior or experiences in a group set-ting. The following example describeshow focus groups were used in Nicaraguain advocacy for a new domestic violencelaw. Box 9.4 presents a sample discussionguide for a focus group discussion onsexual violence performed with membersof a refugee camp.
Example of focus group discussion:Evaluating a domestic violence lawin Nicaragua The Nicaraguan Network of Womenagainst Violence used focus group discus-sions in the consultation process for a newdomestic violence law that was presentedbefore the National Assembly. Because thenew law was controversial (it criminalizedinflicting emotional injuries, and estab-lished restraining orders for abusive hus-bands), the purpose of the study was toassess both the political and technical via-bility of the new law.
The research team conducted 19 focusgroups with over 150 individuals represent-ing different sectors of the population,such as urban and rural men and women,youth, police officers, survivors of violence,judges, mental health experts, and medicalexaminers.
The main questions asked by the studywere, What kinds of acts were consideredviolent? What kinds of legal measureswere considered to be most effective forpreventing violence? The researchers usedranking, Venn diagrams, and free listingexercises to initiate discussions. A team ofmen and women from member groups ofthe Network were trained as focus groupmoderators, and two team members ledeach group. Focus groups sessions were
audio-taped and researchers presentedtyped notes and diagrams from each ses-sion. The team did the analysis as agroup, and participants’ responses wereorganized according to themes. The studyrevealed a broad consensus on severalissues, the most significant of which werethe gravity of psychological injury and theimportance of protective measures forbattered women. It was widely agreedthat the psychological consequences ofabuse were often much more serious andlong-lasting than physical injuries and thatthe legal definition of injury should takethis into account. One rural woman notedthat harsh and demeaning words canmake you ”feel like an old shoe.” A judgenoted that “bruises and cuts will healeventually but psychological damage lastsforever.” The results of the study werepresented in testimony to the JusticeCommission of the National Assembly,which subsequently ruled unanimously infavor of the law.6
OBSERVATION
Observation, a time-honored form of qual-itative data collection, has its roots in cul-tural anthropology. Researchers mayeither actively participate in the phenome-non being observed (known as partici-pant observation) or they may observeas “on-lookers.”
Observation may be either “structured” or“unstructured.” Even the most unstructuredobservations must have a system for captur-ing information as clearly and faithfully aspossible. Wherever possible, it is best torecord observations on the spot, during theevent. This can take the form of abbreviatednotes that you elaborate on later as youwrite more detailed notes. Records shoulddenote who was present; any unusualdetails of the scene; verbatim comments;and incongruities (it may help to ask your-self questions—“Why did he do that?”).
C H A P T E R N I N E

A Practical Guide for Researchers and Activists 135
Shortly after leaving the field, reviewthese notes and add detail and substance.Getting the full record straight may take aslong as the original observation did. As arule, always prepare the detailed notes of
the observation within 24 hours of the fieldsession, and never embark on a secondsession until you have fully developedyour notes from the first. (Adapted fromPatton, 1990.8)
T O O L S F O R C O L L E C T I N G Q U A L I TAT I V E D ATA
[Note: This guide served as the basis for most refugee group discussions, although in later groups, certain topical areas wereprioritized to obtain more in-depth information than in more general interviews.]
Name of group interviewed: ______________Date:_________Camp:_________
Time discussion started:______Time ended:_________Team no:___________
Participant summary: ______ Women __________Men _________ Children
Introduction
1. Introduce facilitators.
2. Introduce community members.
3. Explain why we are here: ”We want help in understanding the health and security problems of women and girls in Dadaab. We will bedoing similar interviews in all camps this week.”
4. Explain how all answers will be treated confidentially. “We are all from organizations working in the camps and will treat answers withrespect and will not share them except as general answers combined from all people who talk to us. We will not give names of individuals,to make you feel comfortable in talking freely with us. Participation in the discussion is completely voluntary and you do not have to answerany questions that you do not want to answer.” Ask community members whether they are willing to participate in the group interviews.
Discussion Guide
1. What problems have women and girls experienced in health and security in your community? (PROBE on violence, not on health.)
2. Can you give examples of sexual violence in the camps?
3. When and where does sexual violence occur?
4. Who are the perpetrators? (PROBE: outside/inside of camp, people you know/don’t know.) What happens to the perpetrators?
5. What are the problems that women face after an attack? (PROBE: physical, psychological, social problems.)
6. How do survivors of sexual violence cope after the attack?
7. What are community responses when sexual violence occurs? What is done to prevent violence? What is done to help survivors? Howcould these efforts be improved? Do women’s support networks exist to help survivors?
8. What social and legal services exist to help address these problems? (PROBE: health, police, legal counseling, social counseling.) Whoprovides these services? How could these efforts be improved?
9. Has the problem of sexual violence gotten worse, better, or stayed the same since you arrived in Dadaab?
10. EXTRA QUESTIONS TO ADD FOR SPECIAL GROUPS:
RELIGIOUS LEADERS: 1. What does Islam teach on sexual violence, both for preventing violence and sanctioning those that are violentagainst women? 2. Is there anything that religious leaders can do to prevent sexual violence?
DISABLED: Do the existing services prevent or help those assaulted address you as well, as a special group with special needs?
WOMEN LEADERS: Is there anything women leaders can do to prevent sexual violence?
Closing
1. Thank people for their time and ideas, and express how helpful it has been to facilitators.
2. Explain next steps: “We will look at all information and will make a presentation of findings to representatives of the community and agen-cies working in camps. Representatives can give you information after this meeting.”
BOX 9.4 FOCUS GROUP INTERVIEW GUIDE: DADAAB REFUGEE CAMP, KENYA
(From Igras et al, 1998.7)

136 Researching Violence Against Women
Many women’s groups have successfullyused observation to assess whether serv-ices for abuse victims are adequate and todocument bias and/or victim-blaming atti-tudes by the police, justice system, healthprofessionals, or counselors.
Example of observation: Justice forrape survivors in Bangladesh The Bangladeshi women’s groupNarippokko used semistructured observa-tions to document how the courts inDhaka treat abuse victims and rape sur-vivors. Advocates sat for days in opencourt recording the behavior, words, anddemeanor of Bangladeshi judges. Theyrecorded verbatim comments of judgesindicating their bias against rape victimsand noted instances of humiliating anddegrading treatment of women by courtofficials. These data were useful for raisingawareness of the biases inherent in thetreatment of female victims of violence inBangladesh by the courts.9
Example of observation: Readinessof reproductive health clinics toaddress violence in Latin AmericaThe International Planned ParenthoodFederation, Western Hemisphere Region,
used an observation guide to assess thereadiness of local affiliate centers to inte-grate gender-based violence into reproduc-tive health programs (Box 9.5). Theobservation guide was used at the begin-ning of the project, as part of a situationanalysis, and later on as part of the moni-toring and evaluation program (the fullguide is available in Spanish atwww.ippfwhr.org.)
FREE L IST ING
Free listing is a particularly useful tool forexploring a subject about which theresearcher has little previous knowledge,or when the researcher wants to have asbroad a discussion as possible.
The researcher asks participants to gen-erate a list of items that correspond to aparticular topic and then writes them onthe blackboard or chart. Or, the researchermay hand out cards so that participantscan write down their answers and thenstick them up on the wall.
Free listing can be an interesting way tocompare attitudes or experiences amongdifferent groups of individuals. For exam-ple, in one study, participants in a focusgroup were asked to name as many
C H A P T E R N I N E
Time observation is initiated:_________________________
Characteristics of the clinic:
1. Is there a space dedicated to ob-gyn consultations?
2. Can conversations within the examining room be heard outside the room?
3. Can the client be seen from outside the examining room?
4. Are there interruptions during the consultations?
5. Is there any separation (e.g., a screen) between the desk and the examining table?
6. Is there a place where children can be watched while the mother is in the consultation?
7. Are there educational materials (e.g., posters, videos, pamphlets) regarding domestic violence inside theexamining rooms or waiting rooms? What kind of materials? What subjects are covered in the materials?
Time observation is completed: _________________________
BOX 9.5 OBSERVATION GUIDE TO ASSESS READINESS FOR INTEGRATION OF GENDER-BASEDVIOLENCE INTO REPRODUCTIVE HEALTH CLINICS

A Practical Guide for Researchers and Activists 137
different forms of violence as they could. Agroup of women came up with a list ofmore than 30 types of violence, whereas agroup of men was only able to mentionfive different types.
Another advantage of free listing is that itmay enable the researcher to detect issues(for example, a type of violence) that hadnot previously been considered, but whichare important for community members.Free listing can be also used as a startingpoint for a subsequent ranking exercise todetermine which acts are considered, forinstance, more severe or more important.
Example of free listing: Causes of sexual violence in Kenyanrefugee campsFree listing was used as part of a participa-tory assessment of sexual violence in theDadaab refugee camps in Kenya7 as a wayto identify individuals assessments of thedifferent causes of violence (see Box 9.6).Organizers asked groups of refugees to listall the reasons why women get raped. Thenthey synthesized the answers according tohow many groups listed each problem.
The responses indicated that refugeesclearly associated sexual violence with inse-curity, both inside and outside the camps.Lack of adequate cooking fuel emerged asa significant source of women’s vulnerabil-ity because women routinely have to travellong distances outside the camp to collectfirewood. When researchers reviewedrecords of sexual violence cases reported inthe preceding year, they found that 90 per-cent of assaults occurred while womenwere searching for wood, reinforcing theinsights gleaned from the participatoryassessment. This combination of data fromdifferent sources is also an excellent exam-ple of triangulation.
Example of free listing: Supportgroups for survivors in El SalvadorIn a review of Central American gender-
based violence programs, health workerswere asked to list the symptoms that awoman might have that lead them to sus-pect that she was living with violence. In
T O O L S F O R C O L L E C T I N G Q U A L I TAT I V E D ATA
Number of groups that notedProblem as cause (n=16 groups)
Insecurity inside and outside the camps 11Lack of firewood 9Lack of fencing 6Unemployment 5Poverty 4Clanism 3Being a refugee 2Proximity to border 2Bandits in camp 2No police patrol at night 2More men than women 2Single women living alone 2Economic problems 2
BOX 9.6 FREE LISTING FREQUENTLY CITED CAUSES OF SEXUAL VIOLENCE:DADAAB REFUGEE CAMPS, KENYA
■ To be independent■ To value ourselves■ To be more responsible with our children■ To make responsible decisions for oneself■ To recognize our qualities■ Not to be violent■ To esteem ourselves■ To put our abilities into practice■ To say, “I am competent, I can do it.”■ To empower ourselves■ To have our rights respected and not be abused ■ To love ourselves■ To forgive■ To liberate ourselves■ To respect■ To love■ To have solidarity within the group
BOX 9.7 FREE L IST ING: WHAT WE LEARNED:SUPPORT GROUP FOR SURVIVORS OF VIOLENCE,
BARRIO LOURDES, EL SALVADOR
(From Igras et al, 1998.7)
(From Velzeboer et al, 2003.10)

138 Researching Violence Against Women
the same study, researchers used free list-ing to ask women in a self-help groupwhat they had learned from the process(Box 9.7).
RANKING
Ranking is a useful technique to help par-ticipants prioritize problems and solutions.The researcher gives participants a series ofcategories or problems (they may be theones that resulted from the process of freelisting) and asks participants to rank themin order of priority, urgency, or severity.This activity may be carried out with differ-ent sectors of the community (such asmen, women, or children) to obtain infor-mation about differences of opinion. It isalso possible to do this activity at thebeginning of a program and at later inter-vals to detect changes in attitudes.
Example of ranking: “What is severeviolence?” in NicaraguaIn the participatory study carried out bythe Nicaraguan Network of Women againstViolence, a ranking exercise was used toidentify perceptions regarding the severityof different kinds of violence (physical,economic, sexual, and emotional). In thisexercise, the researchers gave each partici-pant a packet of cards with the names ofdifferent acts written on them. Participantswere asked to classify the acts in fivegroups according to severity. Afterwards,they were asked to stick the cards on thewall under the signs “not violence,” “minorviolence,” “moderate violence,” “seriousviolence,” and “very serious violence.”
Then the moderator led a discussionabout why some acts are considered moresevere than others, and what criteria areused to establish severity. She initiated thediscussion around acts that most partici-pants considered serious. The moderatorencouraged group members whoexpressed different opinions to explain
their views. A list of the acts mentioned onthe cards included:
■ Yelling at or humiliating in public■ Throwing things■ Having affairs outside of marriage ■ Demanding sex from your partner when
she doesn’t want it■ Threatening to hit ■ Threatening to withdraw financial support ■ Destroying objects that belong to the
partner (such as clothes, dishes, radio) ■ Not paying for household expenses■ Pushing or shoving■ Slapping■ Blows with the fist, on any part of the
body except the head, that don’t leave ascar
■ Beating up with bruises or swelling■ Saying constantly that your partner is
stupid or worthless■ Controlling your partner’s activities
(work, visits, friends) ■ Beating up with wounds or fractures ■ Blows with a fist to the head■ Blows during pregnancy ■ Threats with a gun or knife
The ranking exercise has the advantageof allowing comparisons between differ-ent groups around the same acts. Forpurposes of comparison, one can assessthe average severity assigned to an act ona scale of 0 to 4. In the Nicaraguan study,there was a great diversity of opinion asto whether having sex outside of mar-riage was a form of violence. Whereasmiddle class women felt that adultery wasnot violence, rural women considered itto be very severe violence because itoften led to men becoming economicallyirresponsible at home. There was alsogreat divergence between men andwomen with regard to forced sex inmarriage. While men in general felt thatforcing a wife to have sex should notbe considered violence, most women
C H A P T E R N I N E

A Practical Guide for Researchers and Activists 139
considered forced sex to be severeviolence. In the words of one woman,“If he forces me, I make up excuses, myfeelings change, and I come to hate whatI once loved.”6
PAIR-WISE RANKING*
Pair-wise ranking allows communitymembers to determine collectively theirmost significant problem or issue. Theybegin by listing problems/issues, and thenthey compare them systematically by pairs.Community members can compare andcontrast the issues they have identified.Each item is successively compared againstthe others and the winning issue or prob-lem is chosen. Once the matrix is com-plete community members can score andthen rank issues/problems from mostimportant to least important. Pair-wiseranking is a powerful tool to help commu-nity members see how different percep-tions of significant reproductive healthproblems can be within a single-sex groupand between women and men. In theDadaab assessment, pair-wise ranking wasused to prioritize issues related to sexualviolence, such as most important causes ofviolence, most important solutions, andbest coping mechanisms.
The procedure should be as follows:1. Once rapport has been established
with a group of community members,
introduce the pair-wise ranking exercise.First, use free-listing techniques to listpreferences or problems in response tospecific well-phrased questions. Forexample, what are the types of violenceor abuse that women and girls experi-ence in this community? If people iden-tify multiple forms of violence that canbe grouped under the same heading(e.g., a husband calling his wife names,telling her she is stupid, or criticizing herfeelings), encourage them to identify ageneral category that captures thesemultiple forms of violence (i.e., emo-tional violence by husbands).
2. Draw a matrix (see Figure 9.1). As peo-ple identify different types of violenceand abuse, write those types in the hori-zontal column at the top of the matrix.After the participants are satisfied thatthey have listed as many forms of vio-lence as they can, stop and write thesame list in the vertical column, startingthe vertical list with the last categorylisted in the horizontal column. Put an Xin the boxes where the pairs arerepeated. For example, looking at thematrix in Figure 9.1, A, B, and C eachrepresent a type of violence identifiedby community members. The X’s repre-sent boxes where no ranking is needed,since other boxes already make thesame comparison of A with C, A with B,
T O O L S F O R C O L L E C T I N G Q U A L I TAT I V E D ATA
A. Emotional abuse B. Physical abuse C. Sexual harassment ofby husbands of wives by husbands of wives women or girls on the street
C. Sexual harassment ofwomen or girls on the street X
B. Physical abuse byhusbands of wives X X
A. Emotional abuse byhusbands of wives X X X
FIGURE 9.1 MATRIX FOR PAIR-WISE RANKING EXERCISE
* (Adapted from Igras, 19987 and RHRCC, 2004.11)

140 Researching Violence Against Women
and B with C. Remember that you donot need to prioritize in terms of worsttypes of violence. At this point, youonly need to list different types of vio-lence affecting women and girls in thecommunity.
3. Starting in the upper left-hand corner,ask participants to do the following:“Compare the problem or issue identi-fied in the first row with the problem orissue identified in the first column.Which is the more important of thetwo?” Let the group discuss and recordone answer in the cell.
4. Continue comparing problems listed inthe rows with the problems listed in thefirst column. Be sure to give the groupplenty of time for discussion. Throughthis discussion, individual ranking crite-ria will emerge and people will begin tounderstand why another person holdsan opinion different from their own.
5. Move on to pair-wise comparisons withthe problem in the second column ofthe problems listed in the row.
6. Continue the process of pair-wise rank-ing comparisons until all cells in thematrix have been filled.
7. Tally the result, recording a numericalscore (count) in the appropriate column.Then prioritize the problems. First prior-ity goes to the problem that received thehighest score, second priority to thenext, and so on.
8. Discuss the resulting priorities withparticipants. Most importantly, giventhe discussion and process, ask if par-ticipants feel that the ranking reflectsreality. If a community group is goingto move ahead with a sexual violenceprevention program, will the people
support it? Will they participate? Doesit speak to their needs?”
Remember to record the visual output(charts, etc.), identifying place, dates,names of participants, if possible. Provide anarrative description of the process and thedata. Note: Pair-wise ranking can also beused to rank other issues, such as whatkinds of interventions the community feelsare most important to reduce violenceagainst women and girls. In this case, sam-ple lead questions might be: What do youthink are the most effective methods forreducing sexual violence against women inthis community? What do you think are themost effective methods for reducingdomestic violence against women in thiscommunity?
T IMEL INES AND SEASONALCALENDARS
Timelines or seasonal calendars are usefulfor exploring trends over time, and impor-tant events leading up to certain changes.They can be used to measure experiencesat a national level (for example, theevents leading up to specific changes indomestic violence legislation). They arealso useful for diagramming change in acommunity (e.g., when social violencebecame a serious problem) or personalexperiences in the life of an individual(for example, when a woman first startedbeing abused by her husband, and whatactions she subsequently took to over-come the violence).
In a timeline, events or trends arecharted according to years, months, ordays. Events may be plotted along a line,or a line may be plotted along a verticalaxis to indicate increases in the frequencyor severity of a specific problem.
A common method in participatoryresearch is to have community membersdiagram or “draw” the timeline or calendar
C H A P T E R N I N E

A Practical Guide for Researchers and Activists 141
on the ground using sticks and other natu-ral items (such as leaves, rocks, or flow-ers) to mark key events.
Example of seasonal calendars:Sexual violence in Kenyan refugee campsIn the Dadaab refugee camp assessmentdescribed above, the organizers used sea-sonal calendars to monitor periods whenwomen are most vulnerable to rape. Theyasked community participants to reflect onwhether there are periods or events thatsignal increased or decreased sexual vio-lence. A timeline reproduced the commu-nity members’ observations aboutincidence of rape between January 1997and September 1998. The patterns identi-fied through the seasonal calendar closelytrack the ups and downs of rapes reportedto camp authorities.7
Example of timelines: “The RoadTraveled” in Central America In the participatory review of gender-basedviolence programs in Central America (seeBox 9.7), researchers used an exercisecalled “The Road Traveled.” The facilitatorgave the following introduction:
If we imagine that every process ofchange is a road that we follow from oneplace to another, we can see that the road isnot usually a straight line. Sometimes thereare curves and bumps. Sometimes there arestreams to cross and stones to climb over.Sometimes we end up someplace far awayfrom where we imagined we would be, andsometimes we take a long journey and endup practically at home again. Sometimes,however, we manage to cross long dis-tances, and find many beautiful thingsalong the way—flowers, and trees to give usfruits and shade.
Let’s imagine that the work of yourgroup is like a journey. At one end is theplace where you started and the other endis where we are now. Let’s recreate thesteps we took along the way to get to wherewe are.
When (what year) and how did the jour-ney begin for this group? What were themajor steps that helped you grow, or chal-lenged you?
Dates and descriptions are placed alongthe timeline. Above the line are events thatwere helpful (the “flowers”). Below theline are placed the negative events or cir-cumstances (“the stones”). Figure 9.2
T O O L S F O R C O L L E C T I N G Q U A L I TAT I V E D ATA
FIGURE 9.2 TIMELINE CONSTRUCTED BY COMMUNITY ACTIVISTS IN ESTELI, NICARAGUA.
1995Inaugurationof theWomen’sPoliceStation
1996The violenceprevention networkexpands coverage-and carries out extensive training,dissemination, andcoordination activities
1997Networkcreated inCondegamunicipality.
1998Children’srightsnetworkcreated.
1999Workshops inmasculinity aregiven to police,youth, ruralcommunities.
2000TravelexchangebetweennetworksNicaragua/Bolivia.
2001 New projectof Women’s PoliceStation starts.
“At first it was hard tojoin forces.”
1999–2000The funding of the Women’s Police Stationproject was discontinued for 18 months.During this period there were fewer meetings,and no extra projects. The social worker waslaid off.
(From Velzeboer et al, 2003.10)

142 Researching Violence Against Women
shows the timeline constructed by a groupof community activists in Estelí, Nicaragua.
CAUSAL FLOW ANALYSIS*
A causal flow analysis (also known asweb analysis) shows the relationshipbetween causes and effects of a selected
issue, problem, or desired state. This toolcan be extremely useful in gaining anunderstanding of the underlying causes ofsensitive issues. It is especially good forinvolving community members in settingpriorities and in planning interventions.
For a causal flow analysis, the procedureshould be along the following lines:
1. Once rapport has been established with acommunity group of participants, suggesta topic for analysis and try to link it backto comments that group members madeduring the exercise. For example, “Youmentioned that lack of security was acause of sexual violence. Let’s talk aboutthat. Why does sexual violence occur?”
2. On a flipchart, draw a circle and indicatethe topic for discussion, which in thisexample is sexual violence. Ensure thatall of the participants understand thetopic so that they can participate fully.
3. The facilitator then asks participants to listthe causes of the problem or situation.
4. Causes are written on the left-hand sideof the topic, with arrows drawn into thecenter (i.e., from left to right, or ➯).Write clearly and recheck the directionof the arrows.
C H A P T E R N I N E
FIGURE 9.3 EXAMPLE OF CAUSAL FLOW DIAGRAM
Issue
FIGURE 9.4 CAUSAL FLOW ANALYSIS OF UNEMPLOYMENT, PREPARED BY A GROUP OF WOMEN IN PARK TOWN, JAMAICA
UNEMPLOYMENT
ABUSE
Domestic violence
Dependencyon males STDs
Sketel
Free mentality
Morepregnancy
Family feud
Death
Family involvementResolving
the problem
Fatherless children
Bun
Independence
Free money
Police harassment
Pregnancy
Note: “free mentality” refers to too much free time. “Sketel” is a “loose woman.”
(From Moser and Holland, 1997.12)
* (Adapted from Igras, 19987 and RHRCC, 2004.11)

A Practical Guide for Researchers and Activists 143
5. Once the list of causes has beenexhausted, ask participants to list theeffects of the problem. Again, let thegroup discuss as much as necessarybefore beginning to record effects onthe right-hand side of the topic. Thetopic is linked to effects by arrowsdrawn out from the center, (again left toright or ➯). Recheck the direction of thearrows. This is one of the most commonerrors in drawing causal flow diagrams.
6. Now “interview” the diagram by askingopen-ended questions about each causeand each effect. The diagrams canbecome quite elaborate and will allowthe facilitator to delve even more deeplyinto an issue. Think about this exercisein terms of unpeeling the outer layers ofan onion to get to the inner core.
7. Try limiting the number of causes andeffects to 20 or so. Simpler diagramstend to be easier to follow.
8. Record the visual output as shown inFigure 9.3, identifying it as necessary byplace, dates, names of participants, andso on. Include a narrative description ofthe process.
Researchers from the World Bank and theUniversity of the West Indies explored theimpact of violence on poor communities inJamaica in a Rapid Urban Appraisal. In oneexercise, young women were asked to ana-lyze the impact that unemployment amongwomen had on young women in their com-munity. They said unemployment leads tostronger dependency on males for money—either through higher rates of teenage
T O O L S F O R C O L L E C T I N G Q U A L I TAT I V E D ATA
FIGURE 9.5 EXAMPLE OF CAUSAL FLOW ANALYSIS ON CAUSES AND EFFECTS OF SEXUAL VIOLENCE IN DADAAB REFUGEE CAMPS
Sexual violenceMen coming at night to
be with youYoung boys with young girls
Forced cohabitation(when husband is away or
by “choice”)
War anddestruction
Peoplehave the right to abuse the
childBad
communityfeelings
Childis abused
Motherfeels guilty over
child
Insufficientincome
Bastardchildren
Minoritymen cannot have
relations with Somaliwomen
Unwantedpregnancy
Womennot respected
by men
Menput pressure on“easy” women
for sex
Nomedicines at
the hospital forsickness
Toomany men,
too fewwomen
Lotsto think about,
sadness
Youngboys with no
ecomonic base,cannot marry
Sickness,fear of infection,
AIDS
TribalismMinorityand majority clansdon’t understand
each other
Majorityclans think theyare better thanminority clans
Insufficientincomes to buy
food, fuel
Lossof husband, divorce,unmarried women
Husbandssay divorce
Parentsworry
Noone wants tomarry you
Badimpression ofthe community
Motherfights for
child
(From Igras et al, 1998.7)

144 Researching Violence Against Women
pregnancy or through a shift from self-reliance to a reliance on “free money” pro-vided by men. This dependency in turn givesrise to an increase in abuse and domesticviolence. Subsequent family involvementmight either resolve the problem or lead to afamily feud and deaths through reprisals.
Figure 9.4 illustrates the web analysisthat emerged from this exercise.Significantly, young women in this commu-nity clearly articulated the associationbetween community violence and intimatepartner abuse, a link that is frequently leftout when outsiders analyze communityviolence.12 Figure 9.5 shows the results of acausal flow exercise carried out in theDadaab refugee camps to explore thecauses and effects of sexual violence.
OPEN-ENDED STORIES
Open-ended stories are useful for explor-ing people’s beliefs and opinions, and foridentifying problems or solutions whiledeveloping a program. The method isespecially appropriate for use with peoplewith less formal education, and helps stim-ulate participation in discussions.
In an open-ended story, the beginning,middle, or ending of a relevant story ispurposely left out. The audience discusseswhat might happen in the part of the storythat is missing. Usually, the beginning tellsa story about a problem, the middle tells astory about a solution, and the end tells astory of an outcome.
To use this technique, consider the following:
■ It is important to design the whole storyin advance, so that the part that is leftout “fits” the complete story. You willneed a storyteller with good communi-cation skills. Depending on the amountof group discussion, telling the storyand filling in the missing part may takeas long as two hours.
■ The storyteller must be able to tell thestory, listen, and respond to the com-munity analysis. Using two facilitatorscan help—one to tell the story and oneto help the community fill in the “gaps.”
The story and the response need to becaptured. Tape recording can be helpful inthis instance.
Example of open-ended stories:Forced sex among adolescents in GhanaIn Ghana, investigators used a version ofthe open-ended story technique to dis-cover ways in which adolescents say “no”to sex if they do not want to participateand what would happen if the adolescentstried to use condoms.13 By learning howyoung people react in such situations, theteam hoped to refine its health promotionmaterials to support healthy sexual behav-ior better.
In this adaptation, investigators used astoryline approach in which participantsact out a story based on a scene describedby the facilitator. At appropriate moments,the facilitator cut into the story to elicit dis-cussion and to introduce a new element or“twist” that might change people’s reac-tions. The storyline technique created arelaxed and entertaining atmosphere foryoung people to act out and discuss issuesof sexuality and abuse in a nonthreateningatmosphere.
The stories allowed participants to dis-cuss an issue without necessarily implicat-ing themselves in the situation. To helpanimate the characters in the minds of par-ticipants, the facilitators solicited input fromthe group about the names, traits, and per-sonality of the characters. Following is anexample of one of the stories used to dis-cuss forced early marriage:
Alhaji married Kande with her parents’blessing. Kande (meaning the only girlamong three boys) is 14 years old and
C H A P T E R N I N E
A Practical Guide for Researchers and Activists 145
Alhaji is 50 years old. Alhaji has threewives already but none of them gave birthto a son. So one day he calls Kande anddiscusses his problem and his wish of get-ting a son from her. He also tells her thatsince she is a virgin, she will by all meansgive birth to a boy. Kande gets frightenedand tells him that she is too young to givebirth now. She also assures him that if hecan wait for two more years, she will givehim a son. Alhaji replies, “I married you.You can’t tell me what to do. Whetheryou like it or not, you are sleeping withme tonight.”
After the drama sketch was played out,the facilitator asked the group if theythought the story was realistic and if similarsituations happened in their area. Afteranalyzing their data, the authors noted,“These stories seemed to show that, atleast among these participants, coercion,trickery, deceit, force, and financial needare well known and all too common ele-ments of sexuality for youth in Ghana.”
Example of open-ended stories:Rosita’s story, MexicoMexican researchers used a similarapproach to explore community attitudestoward women living with abusive part-ners.14 As part of a research and demon-stration project in Ixtacalco, Mexico, theyconducted a series of focus group ses-sions during which they presented partic-ipants with a series of questions basedon the lives of a fictional couple, Victorand Rosita. In this case, the facilitatorread the scenario. Then researchershanded each subgroup of participants acard with a question on it to spur discus-sion (Box 9.8).
Example of open-ended stories:Rosita goes to the health clinicIn the PAHO review of gender-based vio-lence services in Central America, the storyof Rosita was adapted to talk to health
workers about how women living with vio-lence are treated in the health center.10
The story ends when Rosita goes to thehealth center for a routine visit and thenurse asks her whether she has ever beenmistreated by her husband. The group isasked to imagine how the story endsthrough a discussion of the followingquestions:
■ What will Rosita tell the nurse when sheasks about violence?
T O O L S F O R C O L L E C T I N G Q U A L I TAT I V E D ATA
BOX 9.8 ROSITA’S STORY
Rosita lives with her husband Victor and hertwo children, a three-year-old son and a five-year old daughter. She finished fifth gradeand is a housewife, but for some time nowshe has wanted to leave Victor. He does notgive her enough housekeeping money, anddoes not let her work because he gets jeal-ous. When he comes home drunk, he insultsher and sometimes he forces her to have sexeven though she doesn't want to. Rosita hastried talking to him, but it's like talking to awall. She has put up with this situation for
the last four years and hasn't told anybody. She doesn't know what to do…
The facilitator divides the group into four subgroups, and gives a different card toeach. Each card describes an alternative that Rosita has and contains a series ofquestions that the participants are asked to answer to complete the story.
Group One Group Three
Rosita decides to ask for help: Rosita decides to leave Victor:
1. Where does she go to ask for help? 1. What is going to be the most
2. What do they say to her? difficult challenge for her?
3. What does she decide to do? 2. How will it affect her children?
3. What does Rosita need to succeed
on her own?
Group Two Group Four
Rosita asks someone to talk to Victor: Rosita decides to leave Victor but two
1. Who would Victor listen to? weeks later returns to him:
What should this person say? 1. What makes Rosita return to Victor?
2. What would Victor’s reaction be if 2. How do her family/friends react?
other people try to intervene? 3. Do you think this is best for her and
3. What reasons does Victor give for her children?
treating Rosita this way?
(From Fawcett et al, 1999.14)

146 Researching Violence Against Women
■ How will Rosita feel when she is askedabout violence?
■ How does the nurse feel about askingRosita about her family life?
■ What will happen to Rosita if she admitswhat is happening to her at home?
■ What type of help would be most use-ful to her?
■ Do you think she will receive this helpat the health center?
■ Is Rosita’s situation common for womenin this community?
■ What happens when women come tothis health center asking for help withdomestic violence situations?
These questions were used to introducea more focused discussion on the type ofservices offered to women in Rosita’s situa-tion in the participants’ health center. Thestory stimulated a very rich discussion ofhow providers detected violence in theirclients, and how they treated them.Examples of providers’ comments follow:
■ I used to treat women with musclespasms all the time and I never askedthem any questions. Then I started torealize that many of these cases weredue to violence.
■ Women are waiting for someone toknock on their door, some of them havebeen waiting for many years…They aregrateful for the opportunity to unloadtheir burden.
■ Sometimes taking a Pap smear, I’ll seeolder women with injuries, dryness, andbruises from forced sex.
GENOGRAMS
The genogram is a diagramming techniqueoften used in counseling to record generalinformation about families and/or house-holds (such as names, dates of birth, anddeaths). It is also used to capture more com-plex information, such as relationshipsamong members or patterns of violence.Counselors use the genogram to examinepatterns of abuse within families to explorepossible sources of support. The technique
C H A P T E R N I N E
BOX 9.9 COMMONLY USED GENOGRAM SYMBOLS
Encircle members ofcurrent household
Respondent
Death, Age, Cause
Woman
Man
HouseholdHead
HH
Year married
Children,listed byage
Divorced,year
Divorced,man hascustody ofson
1945
53
FIGURE 9.6 EXAMPLE OF A GENGRAM, ZIMBABWE
Neighbors
Saw V170
b. 1942 HH
m. 1956b. 1938
7 months 8 years 14 years 7 years 2 years 3 years
Exp172
V170V172V175
Help170172
(From Watts et al, 1998.16)
Exp 170Exp 175

A Practical Guide for Researchers and Activists 147
can be adapted to the research setting tocapture complex patterns of violence, includ-ing who participates, who intervenes, andwho has witnessed violent incidents. Thegenogram can aid interpretation because itvisually summarizes complex data.15
The genogram is drawn in a mannersimilar to a family tree. Box 9.9 includessome symbols used to represent differentinformation in the genogram. Thegenogram can be used during an interviewto document complicated family and house-hold structures. Such visual representations
of households are especially helpful in situ-ations in which there are multiple mar-riages, in which children from variouspartnerships live under one roof, and incultures where local kinship terms (such assister or auntie) are not specific and canrefer to individuals with various relation-ships to the respondent.
Example of genograms: Domesticviolence in ZimbabweIn Zimbabwe, the Musasa Project used thegenogram to capture data on patterns of
T O O L S F O R C O L L E C T I N G Q U A L I TAT I V E D ATA
FIGURE 9.7 OPINIONS OF RURAL NICARAGUAN WOMEN ON SERVICES FORBATTERED WOMEN USING A VENN DIAGRAM
“It’s important butdifficult for someto get to.”
The Woman’sHouse
“Sometimes yourfamily supports you.You feel relievedwhen you can relyon family for help.”
TheFamily
“This is someoneyou can reallytrust.” Good
Friends
“The church is important. Theministers give advice, they visitus; if a man kicks his wife outthey will give her shelter andfood until she resolves thesituation.”
TheChristian
Community
“The police told me, ‘If youkeep nagging, I am goingto throw both you and yourhusband in jail.”
The Police
“The judge told me,‘I’m sorry, but I neverget involved in familyfights. That man couldhave me killed.’”
The Judge
“Sometimes theyhelp. Other timesthey fan the flames.”
Neighbors
Maria is all alone ina world of abuse
“They can giveyou medicine butnothing else.
The HealthCenter

148 Researching Violence Against Women
violence within households.16 BecauseZimbabweans are accustomed to thinking interms of “family trees,” it was relatively easyfor most respondents to relate to thegenogram. The interviewer began the inter-view by drawing the genogram, noting datesof birth, death, relationships, lodgers, andother key data. At the section of the ques-tionnaire where the respondent was askedabout her experiences of violence, the inter-viewer returned to the genogram and identi-fied who perpetrated different forms ofviolence, and whether there were otherswho also experienced, witnessed, or sup-ported acts of violence by other perpetrators.
For example, if a woman reported beinghit by her husband (Q74), the interviewerwould write V74 (for violence on Question74) next to the husband’s square on thegenogram. If he hit her on several occa-sions, the interviewer would add more thanonce. If he had also hit the respondent’sson, and the mother-in-law witnessed theincident, the interviewer would noteexpV74 next to the son’s symbol, andsawV74 next to the mother-in-law’s symbol.
In Figure 9.6, an example taken fromthe survey, the respondent is married andlives with her husband who is the head ofthe household, their three living children,and her brother-in-law. She had two chil-dren who died—a boy at seven months,and a girl at age 14. Her husband has asecond wife and a three-year-old boy whodo not live with them. He has been violenttoward the respondent, punching her andkicking her. Her father-in-law supportedthe violence. Neighbors saw the respon-dent being humiliated, but did not witnessthe physical assaults.
CIRCULAR OR VENNDIAGRAMS
Venn diagrams, also known as circularor “chapati” diagrams, are useful for analyzing social distance, organizational
structures, or institutional relationships.The facilitator draws circles of different
sizes to represent individuals or organiza-tions that are linked to the problem orcommunity under study. The circles canalso be cut out of colored paper and tapedto a flip chart. The size of the circles indi-cates the item’s importance. The item’slocation on the sheet represents howaccessible this person or institution is. Thetechnique may be used in small or largegroups.
Another method is to make two dia-grams per group—one that indicates thereal situation, and another that representsthe ideal situation. Through these dia-grams, one can compare how differentgroups perceive a subject.
Rural Nicaraguan women in a participa-tory study carried out by the NicaraguanNetwork of Women against Violence pro-duced a Venn diagram to assess the pub-lic’s view of the proposed domesticviolence law (Figure 9.7). The diagramindicates the individuals or institutions thatmight be able to help “Maria,” a womanwhose husband beats her. The circles indi-cate by size and proximity to Maria howhelpful and accessible each individual orinstitution is perceived to be to her. Thetext accompanying the circles illustrates theviews expressed by women in the group.6
COMMUNITY MAPPING
A community map is an excellent tool forcollecting qualitative data, especially in cul-tures that have a strong visual tradition. Aswith many other participatory techniques,maps can be created on paper with col-ored pens or constructed in the dirt, usingnatural materials such as sticks and peb-bles. Mapping can be used to identify orhighlight many aspects of a community,including geographic, demographic, his-toric, cultural, and economic factors.Following are suggestions for conducting a
C H A P T E R N I N E

A Practical Guide for Researchers and Activists 149
mapping exercise by the CARE team’sreport on the Dadaab refugee camp.7
Visit the community and ask communitymembers to participate:
1. Introduce the purpose of your visit,assess people’s interest and availability.
2. Request that someone draw a map ofthe desired area.
3. Some people will naturally reach for astick and begin drawing on the ground.Others will look around for paper andpencils. Have materials ready to offer, ifit is appropriate.
4. As the map is beginning to take shape,other community members will becomeinvolved. Give people plenty of timeand space. Do not hurry the process.
5. Wait until people are completely fin-ished before you start asking questions.Then interview the visual output. Phrasequestions so that they are open-endedand nonjudgmental. Probe often, showinterest, let people talk.
6. If there is additional information thatwould be useful, you may ask focusedquestions once conversation about themap has finished.
7. Record any visual output, whether it wasdrawn on the ground or sketched onpaper. Be accurate and include identify-ing information (place, date, and partici-pant’s names if possible).
Example of community mapping:Sexual violence in Kenyan refugee campsThe team from CARE used communitymapping as part of its rapid assessment ofsexual violence in the Dadaab refugeecamps on the border between Kenya and
Somalia.7 Participants were asked to makea map of the camp community and toidentify areas of heightened risk forwomen. The women identified several keyareas where they did not feel safe: (1) thebushes around the community well, whereattackers lie in wait for women; (2) thecamp’s western border, where bandits caneasily enter through weakened sections ofthe live thorn fences; and (3) the hospital,where women line up before dawn to col-lect coupons guaranteeing them access tothe health center later in the day. Thisexercise allowed NGO organizers to iden-tify ways to improve women’s safety.
Example of community mapping:Sexual violence in schools in South AfricaResearchers in Cape Town, South Africa,asked high school girls to draw a map ofplaces where they felt unsafe.17 The map
T O O L S F O R C O L L E C T I N G Q U A L I TAT I V E D ATA
FIGURE 9.8 SCHOOL MAP
A map of their school drawn by female high school students to indicate placeswhere they feel unsafe. The main “unsafe” zones are the girls’ toilets (upper lefthand corner), the outer entrance, and the male staff room (lower right hand corner),where male teachers harass girls. The picture next to the staff room shows a mantaking a girl by the hand with the caption “girl is crying.”17
(From Abrahams, 2003.17)

150 Researching Violence Against Women
(Figure 9.8) shows that the girls consideredthe most unsafe places to be:
■ The gates of the school, where formerstudents would come to sell drugs andharass students.
■ The toilets, which, in addition to beingfilthy, were places where girls could beharassed by gangs.
■ The male teachers’ staff room, whereteachers would collude to send girls forerrands so that other teachers could sex-ually harass or rape them during theirfree hours. The girls were so afraid togo near the staff room that theyarranged always to do errands in pairsso as to be able to protect each other.
ROLE PLAYING
Using role-playing can be an effective wayto stimulate group discussion, in much thesame way as incomplete stories do.
Example: Role playing used in theStepping Stones program for HIVprevention in South Africa The South African Medical ResearchCouncil adapted the well-known SteppingStones methodology for HIV prevention toinclude activities around domestic violence.One of the exercises used role playing,and was an effective tool for understandingcommunity members’ views on domesticviolence.18 The exercise is described below.
Different ways that men and womenmistreat each other
Divide the group into subgroups of fouror five people and ask them to develop avery short role-play showing ways in whichmen and women mistreat each other.
Present these role-plays to the wholegroup. After the role-play has finished, askthe characters to stay in role for a few min-utes while you invite the rest of the groupto ask the characters questions. The char-acters should answer these in role. Thesorts of questions that they might ask are:
■ How does she feel when he does this?What does she fear?
■ Why does he do this? How does he feel?
■ Who else is there? Who witnesses it?
C H A P T E R N I N E
FIGURE 9.9 DRAWINGS MADE BY CHILDREN AGED 13–16 YEARSHELD IN A HOME FOR ABANDONED CHILDREN AND THOSE WHOSE
PARENTS COULD NO LONGER CARE FOR THEM
Picture one: “This girl, her enemy rapedher. They were going out first and he said‘If you love me you will have sex with me.’She said ‘No.’ She doesn’t have a T-shirtnow. He tore off her T-shirt, you see she isonly wearing a bra. He took off her shirtand raped her. He slapped her and shescratched him on the neck and he is smil-ing. He is saying, ‘Yes I raped her.’ So shegoes to the doctor and asks the doctor todo some tests. The doctor says she has HIVand AIDS…Her virginity is broken.”
Picture two: “Mine is a boy who drinksalcohol and he is peeing. He just pees allover and he does not care about people.If he gets drunk he can rape you.”
Picture three: “This is me and my ownbrother has raped me. Here I cry and Idon’t want to tell my mother.”

A Practical Guide for Researchers and Activists 151
Who is involved in it?
■ How do they feel?
■ What does the woman do? Why doesshe respond in this way?
■ What do the other people do? Why dothey act in these ways?
■ What can a person do to help him/her-self when he or she experiences suchproblems?
Replay the role-play showing some ofthese strategies.
It is important to de-role after thisexercise. Go around the group and askparticipants in turn to say their name andmake a statement about themselves fromreal life, e.g., “I am Matsie and I am notabused by my husband” or “I am Zolileand I hit a girlfriend once but do not doit anymore.”
BODY MAPPING
Body mapping is used frequently in stud-ies of sexuality and reproductive health togain an understanding of how participantsview their bodies, or what information theyhave about how their bodies function. It isparticularly useful for children who mayhave difficulty expressing their experiencesin words, and for discussing sensitiveand/or traumatic experiences.
Example of body mapping: Sexualviolence against children in SouthAfrica and NamibiaResearchers in South Africa and Namibiaconducting interviews with children whohad been sexually abused asked the chil-dren to draw pictures and tell storiesabout them. Examples of the drawingsmade by the children are shown in Figure 9.9.19
PHOTO VOICE
The photo voice technique, also knownas Shoot Back,20 is an excellent method forparticipatory research. Wang, who usedphoto voice with Chinese peasant womento engage them in discussions about theirhealth, notes that “Photo voice enablespeople to identify, represent, and enhancetheir community through a specific photo-graphic technique. It provides people withcameras to photograph their perceivedhealth and work realities. Photo voice hasthree main goals: to enable people (1) torecord and reflect their personal and com-munity strengths and concerns, (2) to pro-mote critical dialogue and knowledgeabout personal and community issuesthrough group discussions of photographs,and (3) to reach policy makers.”
The steps of photo voice, as presentedby Wang, are the following:
■ Conceptualize the problem.■ Define broader goals and objectives. ■ Recruit policy makers as the audience
for photo voice findings. ■ Train the trainers. ■ Conduct photo voice training. ■ Devise the initial theme/s for taking
pictures.■ Take pictures. ■ Facilitate group discussion. ■ Allow for critical reflection and dialogue.■ Select photographs for discussion.■ Contextualize and storytell.■ Codify issues, themes, and theories. ■ Document the stories. ■ Conduct the formative evaluation. ■ Reach policymakers, donors, media,
researchers, and others who may bemobilized to create change.
■ Conduct participatory evaluation of pol-icy and program implementation.
More information is available on thismethod at www.photovoice.com.
T O O L S F O R C O L L E C T I N G Q U A L I TAT I V E D ATA

152 Researching Violence Against Women
Example of photo voice: Sexual violence in South African schools In the study on sexual violence in schoolsin South Africa, researchers gave femalestudents disposable cameras and askedthen to take pictures of places where theyfelt unsafe. The film was developed thesame day, and the following day, the pho-tos were used to initiate discussion aroundproblems at the school. The photos werealso used subsequently to convince schoolauthorities to improve the sanitary condi-tions of the school.17
1. Shrader E, Sagot M. Domestic Violence: Women’sWay Out. Washington, DC: Pan American HealthOrganization; 2000.
2. World Health Organization. WHO Multi-countryStudy on Women’s Health and Domestic Violence:Study Protocol. Geneva, Switzerland: WorldHealth Organization; 2004.
3. Hudelson P. Qualitative Research for HealthPrograms. Geneva: Division of Mental Health,World Health Organization; 1994.
4. Barbour R, Kitzinger J, eds. Developing FocusGroup Research: Politics, Theory and Practice.London: Sage Publications; 1995.
5. Barbour R. Using focus groups in general practiceresearch. Family Practice. 1995;12(3):328-334.
6. Ellsberg M, Liljestrand J, Winkvist A. TheNicaraguan Network of Women Against Violence:Using research and action for change.Reproductive Health Matters. 1997;10:82-92.
7. Igras S, Monahan B, Syphrines O. Issues andResponses to Sexual Violence: Assessment Report ofthe Dadaab Refugee Camps, Kenya. Nairobi,Kenya: CARE International; 1998.
8. Patton M. Qualitative Evaluation and ResearchMethods. 2nd ed. Newbury Park: SagePublications; 1990.
9. Azim S. Personal Communication. Washington,DC; 2002.
10.Velzeboer M, Ellsberg M, Clavel C, Garcia-MorenoC. Violence against Women: The Health SectorResponds. Washington, DC: Pan American HealthOrganization, PATH; 2003.
11.Reproductive Health Response in ConflictConsortium. Gender-based Violence Tools Manualfor Assessment and Program Design, Monitoring,and Evaluation in Conflict-affected Settings. NewYork, New York: Reproductive Health Responsein Conflict Consortium; 2004.
12.Moser C, Holland J. Urban Poverty and Violencein Jamaica. Washington, DC: World Bank; 1997.
13.Tweedie I. Content and context of condom andabstinence nagotiation among youth in Ghana. In:Third Annual Meeting of the InternationalResearch Network on Violence against Women.Takoma Park, Maryland: Center for Health andGender Equity; 1998. p. 21-26.
14.Fawcett GM, Heise L, Isita-Espejel L, Pick S.Changing community responses to wife abuse: Aresearch and demonstration project Ixtacalco,Mexico. American Psychologist. 1999;54(1):41-49.
15.Watts C, Shrader E. The genogram: A new researchtool to document patterns of decision-making, con-flict and vulnerability within households. HealthPolicy and Planning. 1998;13(4):459-464.
C H A P T E R N I N E
FIGURE 9.10 TWO BOYS ATTACKING A GIRL AND TAKING AWAY HER FOOD
When this photo was discussed the girls told researchers that boys oftengrabbed their breasts and genitals in order to extort food or money.

A Practical Guide for Researchers and Activists 153
16.Watts C, Ndlovu M, Keogh E, Kwaramb R.Withholding of sex and forced sex: Dimensionsof violence against Zimbabwean women.Reproductive Health Matters. 1998;6:57-65.
17.Abrahams N. School-based Sexual Violence:Understanding the Risks of Using School ToiletsAmong School-going Girls. Cape Town, SouthAfrica: South African Medical Research Council;2003.
18.Welbourn A, Rachel J, Nduna M, Jama N.Stepping Stones: A Training Manual for Sexualand Reproductive Health Communication andRelationship Skills. 2nd ed. Pretoria, South Africa:South African Medical Research Council; 2002.
19.Jewkes R, Penn-Kekana L, Rose-Junius H. “If theyrape me, I can’t blame them”: Reflections on thesocial context of child sexual abuse in SouthAfrica and Namibia. Submitted.
20.Wang C. Photo Voice: A participatory actionresearch strategy applied to women’s health.Journal of Women’s Health. 1999;8(2):185-192.
T O O L S F O R C O L L E C T I N G Q U A L I TAT I V E D ATA

s
10PH
OTO
BY
HAF
M JA
NSE
N

A Practical Guide for Researchers and Activists 155
s
ects and the challenges unique to gender-based violence research.
WHAT IS SPECIAL ABOUTRESEARCH ON GENDER-BASED VIOLENCE?
Just as violence research raises specialissues around respondent safety, the emo-tional sensitivity of the topic raises specialissues for building and sustaining yourfield team. Working on a violence projectcan be extremely taxing, and it is impor-tant—both for ethical reasons and toensure the quality of the data—thatresearchers take active steps to protect theemotional well-being of team members.This means that research plans and budg-ets need to include specific measures foraddressing the emotional consequences ofdoing gender-based violence research.Chapter 11 describes in much greater detailthe kinds of issues that need to beaddressed to protect the safety and well-being of both respondents and interviewersduring fieldwork.
Building and training your researchteam is particularly important whenresearching violence against women. Thevalue of good fieldworkers, interviewers,transcribers, and data processors that havebeen sensitized to the issues cannot be over-stated. Experiences worldwide consistentlyindicate that a key to getting reliable, valid,timely data is making sure that field person-nel are appropriately selected and trained.1
In many ways, the process of selectingand training interviewers for gender-basedviolence research is similar to that for otherresearch projects. Training workshops aredesigned to improve interviewing skills,explain the research protocol, detail thesampling procedures, and practice applyingthe research instruments. Nevertheless,there are several issues that set violenceresearch apart, most notably the need todeal explicitly with violence and genderduring the interviewer-training programand the need to provide emotional supportto project staff throughout the researchprocess. This chapter will deal with boththe issues common to most research proj-
C H A P T E R T E N
Building Your Research Team
Topics covered in this chapter:
What is special about research on gender-based violence?Building the research field teamTraining fieldworkersRemuneration of interviewers

156 Researching Violence Against Women
C H A P T E R T E Ns
Another reality that all projects on vio-lence must confront is the fact that manymembers of the research team themselvesmay have unresolved issues around abuse.The worldwide prevalence of gender-basedabuse means that, almost without excep-tion, any research team will have one ormore members who have been a direct tar-get of violence or come from a familywhere violence was common. Someresearchers have argued that this personalhistory will bias the quality of data. Theytherefore conclude that screening questionsfor hiring should include past history ofabuse. However, several internationalexperiences suggest that these issues,
when appropriately addressed, do notadversely affect data quality.1, 2
The reality of researchers’ own historyof abuse has several implications for gen-der-based violence research. First, it rein-forces the importance of providingemotional support to team membersthroughout the study. Second, it has impli-cations for the training of interviewers.Many researchers have found that it isextremely helpful to raise this issue explic-itly during interviewer training and to pro-vide an opportunity for women toacknowledge their own experiences ofabuse. Most people learn ways of copingwith painful past experiences, and usuallydo not dwell on them in their everydaylives. However, discussion of violence dur-ing training sessions may awaken disturb-ing images and/or emotions. For manytrainees, simply acknowledging that thesereactions are normal, and providing timelyopportunities to discuss them, will be suf-ficient to help them complete the trainingand participate successfully in fieldwork.In those rare cases where feelings becomeoverwhelming, trainees will have anopportunity to withdraw from the project.
Whereas personal experience with abusemay prove problematic for some women,for others it will improve their skill andempathy as interviewers. In fact, womenwho have experienced violence themselvesoften make very good interviewers.Women frequently find that participating ina research project on violence can beempowering and an important route tohealing. An interviewer from the Leónstudy in Nicaragua described her experi-ence this way:
…What helped me the most [in my ownlife] was working on this study. It helped meto be who I am today because I have beenable to help others. I felt that I could helpthem because I had lived through it myself,and I didn’t like it, and I wouldn’t like foranyone, anyone to live through what I have
■ Don’t skimp on field workers. Look for skills you can’t teach: intelligence, reliabil-ity, imagination, curiosity, and sensitivity.
■ Hire people who have a personal and intellectual interest in your study subject:Don't hire people if they are not committed to the issue of violence prevention.
■ Look for field workers everywhere. Don’t assume that people who make their liv-ing doing interviews can perform well, or even adequately. Conversely, don’tassume that people with little or no experience will not perform well.
■ Do not ask any field worker to conduct more than 100 standardized interviews(including pilot interviews). Interview quality deteriorates rapidly after 100.
■ Anticipate a significant trainee dropout rate. Begin training sessions with manymore field workers than you want to hire.
■ Building a research team should be the goal of your field worker training, notjust imparting information or skills. Explain the project and its goals as “our” proj-ect and goals; actively solicit the views of team members and use their insights.Include team-building exercises and group dynamics in the training session.
■ Pay your field workers well. Pay them more than they usually receive for equiva-lent work.
■ Distinguish pay during the training period, which merely compensates for theirtime, from pay for carrying out interviews. Pay for specific work produced.Allow for incentive payments for exceptional work.
■ Make sure that field workers know when they perform well; when they don’t,don’t accept their work. But don’t blame people when they make a mistake.Solve problems in ways that teach new skills.
■ Do everything you can to show your field workers how valuable they are. Haveteam dinners. Celebrate birthdays or research milestones.
■ When field workers begin collecting data, spend a day or half day with each.See the problems that your field workers encounter from their perspective, andsolve them.
■ Tell your field workers your findings. Ask for their critique. Pursue leads that theysuggest.
(Adapted from Handwerker, 2001.3)
BOX 10.1 BUILDING A RESEARCH TEAM

A Practical Guide for Researchers and Activists 157
lived through in my life ever. And when awoman told these things, I could under-stand what she was going through…WhenI was carrying out the interviews, I livedthrough each experience as if it were myown, and I could say to them, “Yes, I livedthrough this also, I know what this is.” 2
BUILDING THE F IELD TEAM
Building a good field team involves findingthe right people, preparing them well, andsustaining them throughout the researchprocess. This means building personal aswell as professional relationships with fieldstaff. A committed and loyal research teamis the surest insurance for a successfulresearch project. See Box 10.1 for someteam-building tips by a seasoned researcher.
Size and composition of the field teamThe number of fieldworkers needed willdepend on several factors, such as howmany and what type of interviews areplanned, how spread out geographicallythe study region is, how many differentlanguages are needed, and whether thefieldwork needs to be completed during acertain period (for example before therainy season begins).
Generally, studies relying on qualitativeresearch methods utilize fewer interviewersthan surveys. For a population-based sur-vey, you will probably need at least two tothree field teams with four to six interview-ers per team, as well as a supervisor.Depending on the length and complexityof the questionnaire, it may also be neces-sary to hire a field editor to check ques-tionnaires for errors as they are completed.In many settings, particularly in rural areaswhere transportation is not readily avail-able, each team will also need a driver.The drivers may also escort female inter-viewers in unsafe areas. Depending onhow emotional follow-up for respondents
and interviewers will be addressed, it maymake sense to add a psychologist and/orwomen’s advocate to the overall team.Box 10.2 gives an example of the composi-tion of the research team for a survey per-formed in Brazil.
Selecting interviewersThere are few “rules” that can be applied tothe selection of interviewers, except thatgenerally speaking, women should inter-view women and men should interviewmen. An exception to this rule is whenwomen’s mobility is so socially constrainedthat it is not feasible for female interviewersto be out in public. It might also be neces-sary to use men to interview women whenthe research requires bilingual interviewers,and few women from the research area arebilingual. This situation occurs frequentlyamong indigenous populations wherewomen are less likely to have receivededucation in the dominant language.
If the characteristics of your study popu-lation require using men to interviewwomen, you will need to plan for additional
B U I L D I N G Y O U R R E S E A R C H T E A M s
BOX 10.2 THE ORGANIZATION OF FIELDWORK IN BRAZIL
The São Paulo research team for the WHO VAW study hired 34 staff members to perform and supervise fieldwork and data entry for a survey of 1500 women.
In addition to the three principal investigators, the research team included the following members:
Central team1 general field coordinator 3 office editors3 counselors
Data entry team1 data entry coordinator2 typists for the first entry (double entry was used) 1 typist for the second entry
Fieldwork4 teams were created, each consisting of 7 members:1 supervisor1 editor5 interviewers

158 Researching Violence Against Women
training and extra time for them to absorbinformation and acquire appropriate inter-view techniques. If, due to budget or timeconstraints, additional training is not possi-ble, you should seriously reconsider con-ducting the research in this particularpopulation. Other criteria—such aswhether respondents would be more trust-ing of individuals from the community orfrom outside of it—are best explored dur-ing formative research.
Interviewers for violence research havegenerally been drawn from four groups:professional interviewers, communitywomen, health workers, and women’sadvocates. Each group has strengths anddrawbacks that should be assessed prior toconducting the workshop. If possible, anideal team would consist of individuals
C H A P T E R T E Ns
Type of Experience Advantages Disadvantages
Professional interviewers ■ Prior experience in conducting ■ May not be available to workinterviews and use of in remote areasquestionnaires ■ May require higher pay
■ Skill in gaining confidence of ■ May be resistant to specialrespondents procedures for violence
research or collaboration with community groups
Community women ■ Familiarity with local community ■ Respondents may be reluctant customs and language to talk to someone from the
■ May help in gaining access to community for fear of gossipthe community ■ May not have necessary
literacy or interviewing skills
Health workers ■ Skills in gaining confidence and ■ May have a hard time (nurses, psychologists, asking questions; comfortable with managing the differencesocial workers) sensitive issues between counseling and
■ Knowledge of health issues research(an asset if this is included in the ■ May have a less skills in study aims) coding interviews
■ Used to confidentiality concerns■ May be more respected by
respondents■ May have knowledge of the
local community
Women’s advocates ■ Experience and knowledge on ■ May have less skill in violence issues interviewing and coding
■ Good rapport with respondents ■ May have a hard time manag-■ May have good ties with community ing the difference between
counseling and research
TABLE 10.1 WHO ARE THE BEST INTERVIEWERS FOR SURVEY RESEARCH?Research training inNamibia
PHO
TO B
Y H
AFM
JAN
SEN

A Practical Guide for Researchers and Activists 159
group work, and part crisis interventiontraining. It is a good idea to invite localwomen’s organizations to present or facili-tate these sessions.
Begin with the basics. Define the topicand discuss why it is important andinclude exercises that help reveal the cul-tural biases and attitudes commonly heldabout victims of rape or domestic assault.Discuss the physical, psychological, andsocietal ramifications of abusive relation-ships, as well as underlying causes. Talkabout the myths surrounding victimizationand the reasons why women might bereluctant to talk or seek assistance. Theuse of participatory exercises encourages
B U I L D I N G Y O U R R E S E A R C H T E A M
with varied backgrounds so that they canexchange experiences, learn from oneanother, and complement one another’sabilities.
Table 10.1 discusses some of theadvantages and disadvantages of inter-viewers according to past experiencesthat may affect the selection process andfieldwork. In Box 10.3 we describe howfieldworkers were selected in the WHOstudy in Peru.
TRAINING F IELDWORKERS
There are at least three important goals toaccomplish in the fieldworker trainingsessions:
■ To sensitize your team to issues of gen-der and violence.
■ To instruct them in the use of theresearch protocol and interviewingtechniques.
■ To build a team spirit that motivatesfield staff.
At minimum, consider including the fol-lowing six topics in the training sessions:gender-based violence, stress management,review of the research protocol, employ-ment expectations, interviewing tech-niques, and ethics in gender-basedviolence research.
In this section we outline what shouldbe covered in each topic. A summary ofthe program and exercises used in theWHO training workshops is included inAppendix II of this manual.
Orientation to gender and violenceToward the beginning of the training, youwill need to devote a significant amount oftime to sensitizing the research team togender-based violence issues. These exer-cises are part public education, part support
s
Interviewers for the WHO VAW study in Peru were selected in two stages. Out ofover 100 women who applied for the job, 27 women were chosen to participatein the training program. The criteria and points used for the initial selection were:
■ Relevant academic training (0–3 pts)
■ Age (between 25–50) (0–3 pts)
■ Experience as an interviewer (0–3 pts)
■ Experience in women's health (0–3 pts)
■ Experience with gender-based violence (0–3 pts)
■ Gender training/experience (0–3 pts)
■ Interview (0–10 pts)
During the two-week training program, participants were scored on their perform-ance on tests and practice interviews, as well as other skills. All participants wereasked to nominate three people they felt would make good supervisors, and theirpreferences were also taken into account. In the end, 18 women were selectedas interviewers and six as supervisors/field editors. The criteria for the final selec-tion were the following:
■ Communication skills (0–4 pts)
■ Nonverbal communication (0–4 pts)
■ Appearance (0–4 pts)
■ Drives (0–2 pts)
■ Works well under pressure (0–2 pts)
■ Works well in teams (0–3 pts)
■ Views on violence (0–3 pts)
■ Speaks Quechua
■ Score on CV (0–10 pts)
■ Interview (0–10 pts)
BOX 10.3 SELECTION OF FIELDWORKERS IN PERU

160 Researching Violence Against Women
participants to examine their own experi-ences and attitudes about violence,although the open sharing of this informa-tion should never be required. Mentionthat virtually all people involved in vio-lence research have had some experiencewith abuse, regardless of nationality, eth-nicity, or background. Interviewers needto be aware of how their personal histo-ries and potential reactions may affecttheir work.
Finally, you will want to conduct a brieftraining in crisis intervention techniques.These skills may be used with respondentsas well as members of the research staff.Prior to the workshop, it is wise to developa protocol for dealing with crises, includinga list of community resources, structured
meetings for staff, and what to do in case awoman is in immediate danger. Emphasizethat the interviewers are part of a researchteam, not a counseling team, but thatnonetheless they have an ethical obligationto provide assistance when it is called for.You will want to role-play potential situa-tions and conduct group discussions ana-lyzing the dynamics of abuse.
Employment expectationsEarly on in the recruitment of interviewers(and other research team members), candi-dates should be given a job description thatoutlines the responsibilities and remunera-tion of field staff. The job description shouldalso include a description of the evaluationcriteria that will be used to select final can-didates and to evaluate performance.
Trainees should understand that partici-pating in the training does not ensureemployment with the project. Only the best,most competent interviewers will be hiredafter the training. All trainees, however,should be compensated for their time dur-ing training, even if they are not hired forthe project. Interviewers hired at the end oftraining should have employment contractsor terms of reference. Sample job descrip-tions for survey interviewers, supervisors,and field editors are provided in Box 10.4.
Review the research protocol and instrumentA principal training objective is to familiar-ize the participants with the key elementsof the research protocol. When they finish
C H A P T E R T E Ns
Interviewer training inBangladesh andThailand
Interviewers in Ethiopia
PHO
TO B
Y M
. ELLS
BERG
PHO
TO B
Y H
AFM
JAN
SEN
PHO
TO B
Y H
AFM
JAN
SEN

A Practical Guide for Researchers and Activists 161
B U I L D I N G Y O U R R E S E A R C H T E A M s
BOX 10.4 THE ROLES OF FIELD STAFF IN THE WHO MULTI-COUNTRY STUDY ONWOMEN’S HEALTH AND DOMESTIC VIOLENCE AGAINST WOMEN
THE INTERVIEWER
The interviewer plays a central role in the study since she is the onewho collects information from respondents. Therefore, the success of thestudy depends on the quality of each interviewer's work.
In general, the responsibilities of the interviewer include:
1. Locating the households in the sample that are assigned to her andcompleting the Household Selection Form and HouseholdQuestionnaire.
2. Identifying all eligible women in those households.
3. Randomly selecting one eligible woman for interview.
4. Interviewing one eligible woman in the household in private, usingthe Individual Questionnaire.
5. Checking completed interviews to be sure that all questions wereasked and the responses are neatly and legibly recorded.
6. Returning to households to interview women that could not be con-tacted during her initial visits.
THE FIELD SUPERVISOR
The supervisor is the senior member of the field team. She is responsi-ble for the well-being and safety of team members, as well as the com-pletion of the assigned workload and the maintenance of data quality.The supervisor receives her assignments from and reports to the fieldcoordinator. The specific responsibilities of the field supervisor are tomake the necessary preparations for the fieldwork, to organize anddirect the fieldwork, and to spot-check the data collected using thequestionnaire.
Preparation for fieldworkPreparing for fieldwork requires that the field supervisor:
1. Obtain sample household lists and/or maps for each area inwhich her team will be working and discuss any special problemswith the field coordinator.
2. Become familiar with the area where the team will be working anddetermine the best arrangements for travel and accommodations.
3. Contact local authorities to inform them about the survey and togain their support and cooperation.
4. Obtain all monetary advances, supplies, and equipment necessaryfor the team to complete its assigned interviews.
Careful preparation by the supervisor is important for facilitating thework of the team in the field, for maintaining interviewer morale, andfor ensuring contact with the central office throughout the fieldwork.
Organization of fieldworkOrganizing fieldwork requires that the field supervisor:
1. Assign work to interviewers, taking into account the linguistic com-petence of individual interviewers and ensuring that there is anequitable distribution of the workload.
2. Maintain fieldwork control sheets and make sure that assignmentsare carried out.
3. Maintain a fieldwork diary, keeping a record of the main eventsand issues arising.
4. Regularly send completed questionnaires and progress reports tothe field coordinator and keep headquarters informed of the team'slocation.
5. Communicate any problems to the field coordinator/project director.
6. Take charge of the team vehicle, ensuring that it is kept in goodrepair and that it is used only for project work.
7. Be responsible for coordinating the referral and/or support ofrespondents identified as requiring support during the survey.
8. Manage the finances provided to cover fieldwork expenses, includ-ing keeping receipts for all expenditures.
9. Support the interviewers as they carry out their work, includingholding a daily team meeting with interviewers.
10. Make an effort to develop a positive team spirit. A congenial workatmosphere, along with careful planning of field activities, con-tributes to the overall quality of the survey.
THE FIELD EDITOR
The specific duties of the field editor are to monitor interviewer perform-ance. Close supervision of interviewers and editing of completed inter-views is essential to ensure that accurate and complete data arecollected. As the collection of high quality data is crucial to the successof the survey, the study will seek to recruit mature responsible women toact as field editors. It is important that those who are selected executetheir duties with care and precision. This is especially important duringthe initial phases of fieldwork when it is possible to address interviewermistakes before they become habit.
Monitoring interviewer performance requires that the field editor:
1. Observe the first part of several interviews every day.
2. Edit all completed questionnaires in the field. Editing must be com-pleted prior to leaving the sample area. As far as possible, thefield supervisor should assist the editor in performing this task sothat all interviews are field-edited while still in the sample area.
3. Conduct regular review sessions with interviewers and advise themof any problems found in their questionnaires.
4. Arrange the completed questionnaires and monitoring forms from a sample area (cluster) in order, and pack them to be sent to thecentral office.
The following job descriptions were used by the WHO Multi-country Study on Women’s Health and Domestic Violence Against Women in thetraining of interviewers, supervisors, and field editors:
(From WHO, 2004.4)

162 Researching Violence Against Women
the training, participants should be conver-sant in the protocol’s contents and be ableto use it as a reference tool throughout thefieldwork.
In reviewing the protocol, it is importantto emphasize the importance of accuracyand rigor in identifying and randomizingrespondents and collecting data. You willalso need to review strategies for glitchesin fieldwork. For example, the team willhave to develop strategies about what todo in household sampling when no one ishome or if there are no eligible respon-dents. Other important topics are how to
approach the household and how toobtain informed consent. (Examples ofexercises for establishing contact with thehousehold are presented in Box 10.5.)
Depending on the degree of flexibility inthe research timetable and the level ofexpertise of your trainees, you may wantto use the training workshop as a chanceto “pilot test” the protocol instrument. Youcan solicit suggestions and recommenda-tions for improving the questionnaire fromthe trainees, thereby creating a researchproduct from a group effort.
Practice interviewsThe qualities of a good interviewer includethe ability to:
■ Establish rapport with the interview sub-ject in a short period.
■ Communicate complex ideas effectively,directly, and simply.
■ Apply the research instrument in such away that it sounds like a conversation.
■ Listen to the respondent without beingjudgmental.
■ Guide the respondent in the interviewprocess without pushing her unnaturallyor being rude by cutting her off orignoring her answers.
Interviewing is more of an art than a sci-ence, requiring skill and, to a certainextent, innate talent and empathy. Theobjective of the training workshop is toenhance natural skills and talents, throughrole-plays and pilot testing of instruments.Box 10.6 presents some guidelines forinterviewing that were used in a qualitativestudy on violence in Sri Lanka.
After you have reviewed the researchprotocol, you will want to practice theapplication of the research instruments
C H A P T E R T E Ns
Interviewer training inBangladesh andTanzania
PHO
TO B
Y H
AFM
JAN
SEN
PHO
TO B
Y H
AFM
JAN
SEN

A Practical Guide for Researchers and Activists 163
using different techniques. Assigningtrainees to the roles of interviewer andrespondent is a useful exercise. Therespondent may improvise her answers, oryou can provide her with an outline“script” to follow. You may also want toassign roles of other members of thehousehold or allow other trainees toobserve the exercise. Be sure to allowenough time for an interview from start tofinish, as well as time for all participants toevaluate the exercise through verbal feed-back. When survey instruments are beingused, another good exercise is to have oneperson interview a “respondent” while asecond person observes the interview andalso records responses to the questions.Afterwards the sets of answers arereviewed by the team together.
As trainees become more comfortablewith the instrument itself, it may be usefulto practice with people outside theresearch team, for example, with familymembers or friends. It is particularly help-ful to include interviews with women whohave experienced violence. Often,
women’s centers can identify women whohave attended their centers and who arewilling to be interviewed.
Trainees may also pilot test the instru-ments under more realistic conditions byvisiting a community with characteristicssimilar to those of the research communityand applying the questionnaire or otherinterview schedule, using the same criteriafor sampling and respondent selection aswill be used in the study protocol.
B U I L D I N G Y O U R R E S E A R C H T E A M s
Gaining access to a household in order to talk to the respondent can be very challenging. In this exercise, traineesare divided into small groups and each is given a situation that might be encountered by a fieldworker. They shoulddiscuss how they would handle this situation and then present their conclusions to the plenary group for discussion.
Case 1: Maria arrives at a large apartment building where she is supposed to conduct an interview. There is nodoorman so she uses the intercom to talk to someone in the household. The person who answers says they do notwant to be interviewed and refuses to open the door.
Case 2. Elli needs to interview a respondent living in a compound where the watchman informs her that he is notauthorized to let her enter and cannot give her any information about the household.
Case 3. Wassana goes to a small house in a poor neighborhood. A woman answers the door accompanied byseveral small children. She looks at Wassana suspiciously and as soon as Wassana starts to explain why she isthere, the woman interrupts her and says she has no time to talk.
Case 4. Mieko knocks on the door of a house and a man opens the door. As she begins to explain the purpose ofher visit, he interrupts and starts to interrogate her with the following questions:
■ What are you here for?
■ What is this study about?
■ Who sent you?
■ What do you want to know?
■ What are you going to do with the results?
BOX 10.5 TRAINING EXERCISES FOR GAINING ACCESS TO A HOUSEHOLD
Practice interviews inBangladesh
PHO
TO B
Y H
AFM
JAN
SEN

164 Researching Violence Against Women
C H A P T E R T E Ns
BOX 10.6 INTERVIEWING TECHNIQUES FOR QUALITATIVE RESEARCH ON VIOLENCE AGAINST WOMEN
(Notes for interviewers taken from a qualitative study carried out inSri Lanka)In this research, we are asking women to talk about a subject that isembarrassing and painful to them. Your job is to:■ Create a relaxed and supportive atmosphere.■ Collect the information in an unbiased way.■ Make the experience as empowering for the woman as possible.Create a relaxed and supportive atmosphere.To help the woman relax, you must be relaxed and confident yourself:■ Check your preparations: interview checklist, notepad and pen,
working tape recorder with extra tapes and batteries (and anextension cord if there is a power source), a watch for keepingtrack of time.
■ Calm yourself by deep breathing, if necessary.■ Spend a few moments remembering the purpose of the research
and your own personal motivations. Arranging the space:■ Choose a place where you will have privacy and will not be inter-
rupted.■ Sit facing the woman, on the same level. ■ Put the tape recorder between you and the respondent where you
can see it, but to one side, if possible, so she does not need to lookdirectly at it. (ALWAYS DO A TEST TO MAKE SURE IT IS CLOSEENOUGH TO RECORD HER VOICE CLEARLY.)
Your behavior and appearance:■ Dress in a way that conforms as closely as possible to local conser-
vative standards. Consider also your hairstyle, jewelry, and makeup. Avoid fashionable or expensive items, or anything transparent.
■ Act respectfully: She is the expert on the subject for discussion.Avoid acting as if you are an authority figure, even if she seemsto expect that.
■ Smile when you meet her for the first time.■ Do not rush into the interview. Take your time explaining the purpose
of the research, why her experiences and views are important, whatwill happen in the interview, and what confidentiality means.
■ Answer any questions she may have. (BE CAREFUL NOT TO IMPLYTHAT SHE WILL RECEIVE DIRECT PERSONAL HELP IN HER OWN CASEBECAUSE OF DOING THE INTERVIEW.)
■ Ask if she is willing to participate in the study.■ Ask her permission to begin.Your manner of speaking and questioning:■ Speak calmly and gently, in a pleasant tone of voice.■ Appear interested in everything she has to say; keep your eyes and
attention focused on her while she is speaking.■ Use words that are easily understood.■ Don’t fiddle with your pen, tap your foot, or exhibit other nervous
mannerisms.■ Use active listening:
1. Encourage her to keep talking by giving verbal and visual cues(e.g., nodding, saying “hmmm,” mirroring her facial expressions).
2. Show you have understood both the content and her feelingsabout it by rephrasing what she said (“So you felt...because...”).
3. Watch her facial expressions and body language for cluesabout how she is feeling.
Collect the information in an unbiased way.■ Be thoroughly familiar with the checklists, and use them systematically.■ Use open-ended questions that encourage the woman to talk, not
closed-ended questions that can be answered with one word.■ Be prepared to reword the question if necessary.■ Don’t use “leading questions” that imply a certain answer.■ Avoid using questions beginning with “why.” These tend to make peo-
ple feel defensive.■ Be patient; don’t be afraid of silences.■ Avoid showing by your tone or facial expression that you are
shocked by, or don’t approve of, something she says.■ Never interrupt while she is speaking. If there is piece of information
you need to check and think you might forget, jot it on your pad asshe speaks and ask her when she has finished.
■ If the woman strays off the subject, wait for a pause, then ask aquestion from the checklist.
■ Don’t finish her sentences, or put words in her mouth.■ Don’t attempt to do any “consciousness raising” during the informa-
tion-gathering part of the interview. Even remarks intended to encour-age her, such as “you didn’t deserve that treatment,” can bias herresponses to later questions.
Make the experience as empowering for the woman as possible.■ Encourage the woman to tell her story in her own way, even if it
involves a lot of repetition. Often the process of telling her own storyto a sympathetic listener brings relief.
■ Avoid the temptation to give advice, even if she asks you to. Butyou can “brainstorm” with her to help her come up with her ownsolutions, if she really wants some input from you.
■ Make sure you are able to answer any of her requests for informa-tion (as opposed to advice) in a way that is locally relevant.
■ If she starts to cry during the interview, don’t try to stop her. Cryingmay provide her with some relief. Acknowledge her distress, andexpress sympathy for her feelings. There is no need to end the inter-view unless she requests it.
■ After the interview, thank her and remind her that by sharing herviews and experiences, she is helping to prevent other women fromhaving to suffer as she did/does.
What to do after the interview?■ Review the session in your mind, and make a written list of:
1. Problems that arose, or items missed.2. New insights.3. Matters you need to follow up.
■ Spend a few moments getting in touch with your own feelings. Ifyou are feeling upset, don’t brush it off. Make sure you discuss itwith your colleagues and supervisor.
■ PAT YOURSELF ON THE BACK!!! Your efforts are helping to makeyour community a safer place for women.
(From Bradley,1999.5)

A Practical Guide for Researchers and Activists 165
When trainees become more skilled withthe interview scenario, it is time to focuson specific challenges that may arise dur-ing the fieldwork. For example, you mighthave role-playing exercises where there arefrequent interruptions or where the respon-dent wants to discontinue the interviewbecause she is crying. It is important tostress the importance of leaving enoughtime during the interview to meet respon-dent’s needs while maintaining rigor in theresearch methodology.
Ethics in gender-based violence researchBecause ethical issues arise throughoutevery stage of the research project, theymerit a specific section in the trainingworkshop. It is important to highlight theirsignificance, not only for data collectionbut also for fieldwork preparation, analysis,and dissemination.
The research protocol should include asection on the ethics of gender-based vio-lence research, outlining the specific waysthat these issues will be addressed by thestudy. During the training workshop, youwill need to reiterate the importance ofinformed consent and confidentiality, aswell as protocols for dealing with crisesduring interviews with informants, proto-cols for dealing with safety/security issuesfor fieldworkers, and other pertinent ethicalconsiderations.
Stress managementIt is important to address stress-relatedsymptoms among fieldworkers and discusscoping mechanisms for research staff.
As you plan your training workshop,keep in mind the varying strengths andtraining needs of different members of theresearch team. Your team may includeinterviewers; transcribers (in qualitativestudies); field supervisors; and administra-tive and support personnel such as drivers,translators, interpreters, or representatives
from collaborating institutions. Each posi-tion entails different responsibilities, skills,and training needs. The training workshopshould be a team-building effort in whicheveryone is aware of the role he or sheplays and its importance to the study.
It may seem that some personnel, suchas data processors or transcribers, do notneed training or sensitization in gender-based violence issues. However, experi-ence has shown that even members one ortwo steps removed from direct contactwith respondents may be deeply affectedby the subject matter (see Box 10.7). Stress
B U I L D I N G Y O U R R E S E A R C H T E A M s
A qualitative study of battered women in Belize generated hours of taped interviewsfrom 24 in-depth interviews and three focus groups. A transcriber was hired to pro-duce transcripts of interviews conducted in the study’s three languages of Creole,Spanish, and English.
During the first few weeks of fieldwork, the transcriber’s turnaround time was excel-lent, and the categorization and analysis of the data went smoothly. However, bythe third week the transcriber began to make excuses as to why she wasn’t finishingthe tapes. She complained of feeling under the weather and occasionally would notreturn phone calls from the supervisor. Eventually, the delayed transcriptions beganto hinder progress in the research, and the supervisor confronted the transcriber withthis problem. She revealed that the taped interviews were affecting her deeply, par-ticularly listening to the women’s voices describe the horrors of their married life.Weeping uncontrollably, many times she had to stop transcribing and each day shefound it increasingly difficult to turn on the tape recorder. From this experience, theresearchers realized the importance of including all team members, not only in thetraining on violence, but also in stress management activities.
(From Shrader, 2000.6)
BOX 10.7 IN THE FIELD: BELIZE
Practice interviews inEthiopia
PHO
TO B
Y M
. ELLS
BERG

166 Researching Violence Against Women
may show up in a number of ways, includ-ing headaches, malaise, reluctance to work,conflictive relationships at home, and soforth. As with fieldworkers, supervisorsneed to be aware of the signs of stressamong research staff and intervene accord-ingly. If resources allow, the ideal work-shop would train all members of theresearch team, at least in the basics of vio-lence against women, stress management,and the contributions of action research toviolence prevention.
REMUNERATION OFINTERVIEWERS
The system for paying field staff can haveimportant implications, not only for theresearch budget, but also for data quality.
The most commonly used approaches arepayment per completed interview and pay-ment for time.
Per completed interview With this system, interviewers are paid afixed amount for each questionnaire or setof notes that they complete. This approachtends to maximize the number of question-naires turned in and creates an incentivefor reducing the duration of fieldwork.However, it can also create an incentive toturn in incomplete or poor quality ques-tionnaires. Of greater concern is that it maylead unscrupulous employees to falsifyinterview data. Because women who havebeen abused usually take longer to inter-view, a per-interview approach risks creat-ing a situation where interviewersconsciously or unconsciously discouragedisclosure.
Daily or weekly rate of payThis strategy involves remunerating inter-viewers by time worked rather than byproduct delivered. Because there is nobuilt-in incentive to work quickly, inter-viewers are encouraged to take the timethat they need to do quality interviews.This is especially important in studies thatcollect data on sensitive topics. The pri-mary disadvantage of this system is that thelikelihood of running over budget andovertime is greater. One way to offset thisrisk is to offer individual or group incen-tives to meet project timelines and thatreward good work.
Based on our field experiences, we rec-ommend that interviewers be paid on adaily or weekly basis, with monetaryincentives for quality work. Additionally,you should consider creating mechanismsfor public recognition of work well doneto ensure that interviewers feel valued.
C H A P T E R T E Ns
Ethiopian fieldworkersorganized a traditionalcoffee ceremony to celebrate the end ofthe training workshop.
Trainees in Tanzaniavisited the local shelterfor abused women tolearn about violence intheir community.
PHO
TO B
Y M
. ELLS
BERG
PHO
TO B
Y H
AFM
JAN
SEN

A Practical Guide for Researchers and Activists 167
1. Jansen HAFM, Watts C, Ellsberg M, Heise L,Garcia-Moreno C. Interviewer training in theWHO Multi-country Study on Women’s Healthand Domestic Violence. Violence against Women.2004;10(7):831-849.
2. Ellsberg M, Heise L, Peña R, Agurto S, Winkvist A.Researching domestic violence against women:Methodological and ethical considerations. Studiesin Family Planning. 2001;32(1):1-16.
3. Handwerker WP. Quick Ethnography: A Guide toRapid Multi-Method Research. Lanham, MD:Altamira Press; 2001.
4. World Health Organization. WHO Multi-countryStudy on Women’s Health and Domestic Violence:Study Protocol. Geneva, Switzerland: WorldHealth Organization; 2004.
5. Bradley C. Interviewing Techniques forQualitative Research on Violence against Women.Personal Communication. Washington, DC; 1999.
6. Shrader E. Personal Communication. Washington,DC; 2000.
B U I L D I N G Y O U R R E S E A R C H T E A M s

m
11PH
OTO
BY
M. E
LLSBE
RG

A Practical Guide for Researchers and Activists 169
m
respondent is crucial to the validity of thedata. A great many practical issues need tobe resolved before initiating fieldworksuch as:
■ Preparation of a detailed budget. Thisincludes training, equipment, salaries offieldworkers, transportation, and contin-gencies.
■ The timing of the fieldwork. Doesfieldwork coincide with periods duringwhich access to communities will bemore difficult, such as rainy season,elections, or when people are likely tobe away from their homes for harvest-ing crops, seasonal labor, or religious orcultural festivals?
■ Transportation. Arrangements mayvary among different regions andbetween urban and rural areas. It isimportant to determine where public
The process of data collection is themost critical link in the research chain.Mistakes made during this period are themost likely to have repercussions forwomen’s safety, as well as for determiningthe usefulness of data. No amount of care-ful analysis can make up for flaws in dataquality. This chapter will outline some ofthe main steps for carrying out fieldworkwith attention both to the safety of womenparticipating in the study and to the qualityof data.
ORGANIZING THEF IELDWORK
Before beginning data collection, it is criti-cal to make a detailed plan for how basicorganizational and logistical issues will beaddressed. This is particularly important insurvey research, where the numbers ofinterviews are usually much greater, andwhere precision in selecting the right
C H A P T E R E L E V E N
In the Field
Topics covered in this chapter:
Organizing the fieldworkNegotiating community accessProtecting the safety and well-being of respondents and fieldworkersFinalizing the procedures and instrumentsManaging nonresponseData quality controlData entry

170 Researching Violence Against Women
C H A P T E R E L E V E Nm
transportation may be available, andwhen it will be necessary to hire vehi-cles, horses, boats, or other modes oftransportation.
■ Food and lodging. Basic necessities forfieldworkers may be difficult to arrangein some areas, whereas in other areasfieldworkers may be able to purchasefood or rent rooms. In many rural areas,fieldworkers may need to carry provi-sions with them and prepare their ownfood or hire someone to cook.
■ Printing of questionnaires, manuals,pamphlets, and other materials.These include supervisor forms, referralsheets, and directories for local servicesfor women.
In addition to the basic materials needed for performing interviews, there are manyother items that research teams have found useful to take into the field with them,such as:
■ Packets of tissues for interviewers to offer respondents if they cry.■ Coloring books, balls, and other distractions to keep children busy during
interviews.■ A first aid kit with plenty of aspirin. ■ A petty cash fund to be used to subsidize women’s transport to sources of
follow-up support.■ Cash reserves for emergencies.■ Educational materials about violence.■ Malaria prophylaxis for interviewers, where necessary.■ Small gifts for respondents such as posters, calendars, pens, canvas book bags.■ Phone cards or cellular phones (where appropriate).
BOX 11.1 AND DON’T FORGET . . .
Transportation conditions may vary a great dealbetween sites (examples from Japan, Bangladeshand Tanzania
PHO
TO B
Y H
AFM
JAN
SEN
PHO
TO B
Y H
AFM
JAN
SEN
PHO
TO B
Y H
AFM
JAN
SEN

A Practical Guide for Researchers and Activists 171
■ Computers and equipment for dataprocessing. In survey research, severalcomputers and printers will probably beneeded in order to enter the data at thesame time as the data collection isbeing performed.
■ Field office. It may be necessary toborrow or rent a space for the period ofthe fieldwork to provide a meetingplace for field staff storage for com-pleted questionnaires and others materi-als, and space to perform data entry.This is especially important due to theneed to maintain the confidentiality ofthe information collected.
■ Payment. You need to plan in advanceprocedures for making sure that fieldworkers receive their payment while inthe field. If supervisors will be carryinglarge sums of cash, how will the moneybe protected? Breakdowns in financialsystems can be demoralizing to staff andlead to serious disruptions in fieldwork.
■ Communication. It is important toorganize a system for maintaining contactbetween fieldworkers and mainresearchers during data collection. Insome areas, telephones may be available,whereas in others, it will be necessary tolook for alternative sources of communi-cation, such as radios or cellular phones.
■ Purchasing and preparation of sup-plies. Large amounts of materials needto be prepared in advance for inter-viewers and supervisors such as:
■ Backpacks for carrying materials■ Identification cards■ Special vests or T-shirts for
interviewers, where appropriate■ Blank paper■ Colored pens and pencils■ Clipboards■ Tape, clips, staplers
■ Management and transportation ofcompleted questionnaires. A system
I N T H E F I E L D m
Preparingquestionnaires inBangladesh
PHO
TO B
Y H
AFM
JAN
SEN

172 Researching Violence Against Women
must be developed for ensuring thatcompleted questionnaires arrive intact tothe field office as soon as possible andare stored in a secure location.
Keeping track of all these details is anenormous job, and most survey researchersfind that it is helpful to hire a full-time staffperson to coordinate logistics. This shouldinclude sending out advance teams toupdate maps, to find out what arrange-ments are needed regarding food, trans-portation, and lodging, and to identify anypossible obstacles to fieldwork. Investingresources in finding a person who is expe-rienced in conducting community surveyswill save enormous amounts of time andeffort later on, and will ensure that thedata collection proceeds smoothly.
NEGOTIAT INGCOMMUNITY ACCESS
In addition to discussing plans with theadvisory board and obtaining ethical clear-ance, it is important to obtain clearancefrom local authorities in each community.The research should be framed in generalterms, for example, as a study on women’s
health or family relations, to avoid havingthe content of the study become widelyknown beforehand. The same explanationcan be used to describe the survey toother members of the community and inthe households where women will beinterviewed. In some areas, local groupsprovide services for victims of violence.These groups should also be contactedbefore initiating the study to explore thepossibility of referring women with vio-lence-related problems to these services,or coordinating in some other way. In theWHO study in Peru, rural community lead-ers were invited to an informational meet-ing where they helped the research teamto construct community maps for samplingand to plan the route to follow betweencommunities (see Chapter 7). In Thailand,village health workers were recruited toaccompany the interviewers to each housein order to introduce them to the head ofthe household, and to help secure cooper-ation for the study.
PROTECT ING THE SAFETYAND WELL-BE ING OFRESPONDENTS ANDFIELDWORKERS
The risk of harm to both respondents andfieldworkers has already been addressed atlength in Chapter 2. This section will addressmore specifically the measures that will helpto ensure the health and safety of respon-dents and interviewers while in the field.
Maintaining confidentiality Much of the information provided byrespondents will be extremely personal. Asexperiences in Ethiopia and South Africaillustrate (Box 11.1), the act of revealingdetails of abuse to someone outside thefamily can expose respondents to furtherrisk. For these reasons, it is critical to main-tain the confidentiality of information col-lected during a survey or from qualitative
C H A P T E R E L E V E Nm
Sampling householdsin Thailand
PHO
TO B
Y H
AFM
JAN
SEN

A Practical Guide for Researchers and Activists 173
assist with this. The interviewer canforewarn the respondent that she willturn to the alternative questionnaire ifthe interview is interrupted.
■ The logistics of safety. Logistics plan-ning should include consideration ofrespondent and interviewer safety. Thiswill require that sufficient time is bud-geted to accommodate the possibleneed to reschedule interviews. It mayalso be necessary to identify additionallocations (such as a health center)where interviews can be conductedsafely and privately. It is a good ideafor female interviewers to travel in pairswith a male escort in areas known to beunsafe for women alone. This is particu-larly true in circumstances where thereis some likelihood that an interviewmay be interrupted, or where interview-ers may have to conduct interviews inthe evenings.
■ Secure storage of data sources.Where tapes are made of in depthinterviews with survivors of violence,these should be kept in a locked fileand erased following transcription.
I N T H E F I E L D
research with survivors of violence. A num-ber of mechanisms should be used to pro-tect the confidentiality of the informationcollected, including:
■ Interviewer emphasis on confiden-tiality. All interviewers should receivestrict instructions about the importanceof maintaining confidentiality. No inter-viewers should conduct interviews intheir own community.
■ Do not write the respondent’s nameon the questionnaire. Unique codesshould be used to distinguish question-naires. Where identifiers are needed tolink a questionnaire with the householdlocation or respondent, they should bekept separately from the questionnaires.Upon completion of the research, theyshould be destroyed, or, if consent wasobtained for follow-up visits, should bekept safely and destroyed after anagreed upon period. In all further analy-sis, the codes should be used to distin-guish questionnaires.
■ Privacy of interviews. Interviewsshould only be conducted in a privatesetting. The participant should be freeto reschedule (or relocate) the interviewto a time (or place) that may be moresafe or convenient for her. Other fieldstaff (drivers, supervisors) may beenlisted to help distract spouses andother family members if it is difficult toachieve privacy.
■ Training on how to handle inter-ruptions. Interviewers should betrained to terminate or change the sub-ject of discussion if an interview isinterrupted by anyone. A short alterna-tive questionnaire on a less sensitivetopic concerning women’s health (suchas menstruation, family planning, orchild spacing) can be developed to
m
Interviews in Ethiopia
PHO
TO B
Y M
. ELLS
BERG

174 Researching Violence Against Women
Again, no record of the names of thewomen interviewed should be kept.
■ One interview per household. Whenthe sampling unit for the survey is thehousehold, only one woman per house-hold should be interviewed about herexperiences of violence. This is done toprotect the confidentiality of the inter-view. In households with more thanone eligible woman, the WHO EthicalGuidelines for Researching ViolenceAgainst Women recommend that a sin-gle respondent should be selected ran-domly for interview. Any interviewsconducted with other household mem-
bers (either male or female)should not include questionsdirectly exploring their use ofviolence, as this may result inthem concluding that the keyrespondent was also askedabout violence.*
Support for respondentsAlthough most women inter-viewed will not require anyspecial help after participatingin the interview, some womenmay be particularly distressed,
or may ask the interviewer for help in over-coming their situation. It is important tohave resources set up in advance to dealwith these situations. The research teamshould identify existing resources wherewomen may be referred in each site, forexample, a women’s center or shelter, orcommunity clinic where personnel havesome training in helping abused women. Aninterviewer can then provide a woman witha leaflet with the address of the center and
times when she can be attended to there.Some researchers have found it helpful toput a number of other addresses on thesame piece of paper so that it is not obviousthat these are services for abused women, incase someone else reads the paper.
Where few resources exist, it may benecessary either to arrange for the inter-viewers themselves to receive training incrisis intervention or to train other localindividuals to provide such support. In par-ticularly remote areas, it may be easier tohave a trained counselor or women’s advo-cate accompany the interview teams andprovide support on an as-needed basis.This may take the form of alerting all par-ticipants that a staff person trained in fam-ily issues will be available to meet withanyone who wishes at a set time andplace. Preferably, this location should be ahealth center, church, or local organizationwhere women can easily go without arous-ing suspicion. In Indonesia, during field-work in a rural area, a psychologist fromthe women’s crisis center in the city cameon a weekly basis to visit the field site. Inthe morning, she would meet with any ofthe respondents who had been referred forcounseling by the fieldworkers. In theafternoon, she would hold a group debrief-ing session for fieldworkers, as well asindividual sessions if needed.1
Finally, educational leaflets may be pro-vided to women, giving additional informa-tion about violence and suggestions forhow to protect themselves and where togo for help if they or someone they knowis being abused. The leaflets should besmall enough to be easily hidden, and careshould be taken to ask women whether itis safe for them to receive the leaflet.
C H A P T E R E L E V E Nm
“Sometimes when I offered themthe pamphlet the woman wouldsay to me, ‘No no, please don’tgive me the pamphlet, write theaddress down where I can go
and put it on a separate paper,because if my husband found
this paper he would kill me.’ SoI would write the address in my
notebook for her…”Nicaraguan interviewer
(Ellsberg et al, 2001.4)
* This procedure can lead to a biased sample, as women in households with many eligible women will have alesser chance of being selected to be interviewed. However, we believe that the risks of interviewing morethan one woman per household outweigh the benefits obtained by a more complete sample. It is possible toadjust for this potential bias in the analysis stage. Experiences in Nicaragua and in the WHO multi-countrystudy indicate that the prevalence estimates of violence were not significantly affected by this measure.

A Practical Guide for Researchers and Activists 175
Emotional support for field staffListening day in and day out to stories ofabuse can have emotional and personalconsequences for interviewers. A commonoccurrence recounted by researchers onviolence is that feelings evoked during theresearch begin to invade other areas ofstaff members’ lives. For example, it is notunusual for team members involved ingender-based violence research to begin tohave problems in their own relationships,either because they start to recognizeaspects of their own relationships as abu-sive, or because the anger they feeltowards male perpetrators begins to gener-alize to the men in their own life. Thisoccurs so frequently in violence researchthat many researchers openly discuss itduring interviewer training and encourageteam members not to make any major lifedecisions during the course of the project.
Emotional support for team members isessential. Not only does it help interview-ers withstand the physical and emotionaldemands of intense fieldwork, but it alsocontributes to the quality of the data col-lection process. A focus group conductedwith interviewers after completing a large-scale health survey that included a moduleon violence illustrates how disturbing anddraining this work can be when appropri-ate support is not provided.4 One womanacknowledged that she had lived throughsimilar experiences herself, and found itparticularly hard to listen to the stories ofabuse. Another interviewer admitted thatshe had dropped out of the study becauseshe was unable to withstand the pressureof listening to women’s stories. Sheexplained:
…When we got to the part about vio-lence, [the respondent] started to tell methat she had been raped first by herbrother and her stepfather, but her mothernever believed her, and mistreatedher…She broke down crying, and I was somoved that I didn’t know what to do,
because as a human being you can’t listento a story like this and not be moved. Itried to calm her down and give her someencouraging words, but the image of thesestories affects you, to see how these womensuffer, and especially the feeling that no
I N T H E F I E L D m
In the WHO VAW study in rural Ethiopia, researchers visited a village for the pur-pose of piloting the questionnaire.2 In this village, women were very reluctant tospeak to interviewers alone, and when the subject of violence was brought up,many of them refused to continue the interview. Almost no woman who completedthe interview acknowledged having ever been beaten by her husband (in starkcontrast with the study findings that more than half of Ethiopian women in this regionhad been physically abused by a partner). One woman told an interviewer, “Doyou think I am a fool, that I would talk to you about such things? My husbandwould kill me if I did.” Eventually, the team learned that a group of people fromthe city had come to talk about domestic violence with the women. They askedwomen to describe their experiences in a public meeting, and one woman toldhow her husband had beaten her. Later in the day, the husband found out andbeat her savagely. Everyone heard her cries but no one came to her rescue. Manywomen thought she had brought the abuse on herself by discussing personal mat-ters in public and shaming her husband.
In another study carried out among female high school students in Cape Town,South Africa, the students revealed in the focus group discussions that they hadbeen sexually harassed by male teachers in the school.3 According to theresearchers,
The learners were grateful to have a sympathetic listener and spent a lot of timediscussing these incidents. The girls were clearly victimized and feared theseeducators and did not want to identify them and neither did they want to beidentified as being part of the research group. Plans had to be devised to keeptheir participation in the research secret from these men. During one incident, amale educator spoke to the researchers enquiring about the research, just out-side the room in which the discussions took place. He appeared more than nor-mally interested and asked to see the room. He was very forceful and openedthe door, clearly wanting to see more than the room. It is suspected that he hadsome idea of what the research was about and he wanted to see which learn-ers were involved. Luckily, none of the learners had arrived yet.
BOX 11.2 PROTECTING THE SAFETY OF RESPONDENTS IN GROUPDISCUSSIONS: EXPERIENCES FROM ETHIOPIA AND SOUTH AFRICA.
BOX 11.3 HOW TO PREVENT INTERVIEWER BURNOUT
1. Include as part of the research team a part-time psychologist or someone withcounseling skills who can provide timely counseling for research staff.
2. Schedule weekly debriefing sessions for research staff to specifically discuss theways in which the fieldwork is affecting their personal lives and physical andmental health.
3. Rotate job responsibilities among field staff to reduce the intensity of informationgathering.
4. Schedule frequent team-building activities such as celebrations of achievementsand birthdays to help team members feel comfortable asking for support whenthey need it.

176 Researching Violence Against Women
one supports them, these are experiencesthat you never forget…
…We spent days thinking about thatpoor girl and how we left her, without beingable to help her. All we did was give her thepamphlet and leave, and the interviewerswere very upset, because they would thinkabout their daughters, and that tomorrowsomething could happen to them and therewould be no one to help them...4
Even in situations where support isavailable, researchers may be surprised bythe intensity of the emotions that areawoken. One of us (Ellsberg) described anearly experience with violence researchthis way:
Although I was not involved in the dailyinteraction with abused women, evensupervising the fieldwork and analyzing thedata turned out to be more painful than Icould possibly have imagined…I foundmyself in tears as I added up the numbersof women who had been kicked in thestomach during pregnancy, or scrollingdown the pages of responses to the question“How were you affected by the violence?”where the same words were repeated overand over, “I cry a lot,” “I am very nervous,”“I am always afraid.”
…What sustained us through this periodwas the sense that women had entrusted uswith their stories and it was our job to
C H A P T E R E L E V E Nm
It is important toorganize regularactivities to help field staff relax
and “decompress”from the stress of
interviews (examplesfrom Samoa,
Bangladesh and Peru).
PHO
TO B
Y H
AFM
JAN
SEN
PHO
TO B
Y H
AFM
JAN
SEN
PHO
TO B
Y H
AFM
JAN
SEN

A Practical Guide for Researchers and Activists 177
ensure they were used to help other women.We reminded ourselves that our main con-tribution was to bear witness to women’sexperiences, and that women were alsograteful for the chance to be able to telltheir stories… 5
There are many ways that researcherscan provide needed support to teammembers. One strategy is to retain a part-time psychologist or someone with coun-seling skills, trained in gender-basedviolence issues, who can provide timelycounseling to interviewers and otherresearch staff. The counselor can partici-pate in the training workshop as well,assisting in discussions of post-traumaticstress disorder, crisis intervention, andother relevant topics.
A second preventive strategy is to sched-ule periodic “decompression sessions” ordebriefings for field staff to discuss howthe emotional impact of the research expe-rience is affecting them. These meetings,similar to a “self-help group,” should beseparate from meetings for reviewing tech-nical aspects of the research. In these ses-sions, maintaining the confidentiality ofboth respondents and field staff is a pri-mary consideration. The purpose of thedebriefing sessions is to create an opportu-nity for the interviewers to discuss the con-tent of the interviews and their feelingsabout the work. The goal is to reduce thestress of the fieldwork and prevent anynegative consequences. Scheduling weeklysessions should meet the needs of mostresearch teams. This strategy has the addedadvantage of being relatively cost-effective,as opposed to hiring a team psychologistor social worker for crisis intervention orcounseling sessions.
A third strategy is to rotate job responsi-bilities, so interviewers have a break fromlistening to heart-wrenching stories.Research team members could temporarilyshift from field interviews to quality con-trol, driving, data entry, clerical and/or
administrative tasks. This strategy alsoallows fieldworkers to participate in andunderstand various stages in the processof data collection and preparation. It isimportant to be on the lookout for signsof “burn out” among field staff and to takeimmediate steps to reduce their exposureto potentially upsetting situations (Box11.3). A single day’s rest can often beenough to allow team members to recu-perate from stress.
I N T H E F I E L D m
“Have faith, women:Protect your health!”was the message ofthese canvas totebags given to respon-dents in the PeruWHO study.
Thai researchersprepare gifts forrespondentsPH
OTO
BY
HAF
M JA
NSE
N

178 Researching Violence Against Women
Compensation for respondents The decision to compensate respondentsfor their participation is a sensitive one,and should be discussed carefully withthe local advisory group to ensure that thestudy is in line with what is consideredappropriate locally. In many settings, it isfelt that offering money to respondentsprovides an incentive for participation thatviolates the ethical principle of voluntaryparticipation. On the other hand, it isimportant to recognize that respondentshave sacrificed valuable time and effort tocooperate with the study. Many researchteams have found ways of compensatingrespondents that do not involve money,such as key chains, canvas bags, calen-dars, and wall clocks with messagesrelated to women's rights. In Japan,respondents were given gift certificates for bookstores.
It is important that the messages do notmention violence, as this could put womenat risk. In Peru, canvas bags were printedwith the message “Have faith, women, pro-tect your health!” In Brazil, calendars mark-ing important dates for human rights andwomen’s issues were distributed.
F INALIZ ING THEPROCEDURES ANDINSTRUMENTS
After the questionnaire has been pre-testedand the necessary adjustments have beenmade, the next step is to perform a finalpilot test before actual data collectionbegins. By this time, the questionnaireshould not require substantial revisions.The pilot testing is used mainly to refinethe overall data collection procedures.Usually this phase is carried out as part ofthe process of training field staff.
After the interviewers have studied thequestionnaire and practiced on each other,they can be sent to perform interviews in aneighborhood that is similar to, but notincluded in, the actual study sample. Thisprocess gives interviewers and supervisorsthe opportunity to practice selecting eligi-ble households and informants, to makesure that questionnaires are being filled outproperly, and to detect any other surveyprocedures that need to be streamlined oradapted. The questionnaires should also beentered by the data entry personnel, andused to test the data entry screens and dataquality tables for errors.
MANAGING NONRESPONSE
Nonresponse occurs when the selectedwoman is unavailable because she hasmoved away and cannot be located,because she is temporarily away, orbecause she refuses to participate in allor part of the study. A high nonre-sponse rate reduces the validity of thefindings because we cannot tell whetherwomen who have experienced violencehave participated to a greater or lesserextent than nonabused women. As aresult, findings may underestimate oroverestimate the prevalence of violence.For example, a survey on violence inLeón, Nicaragua, found that several
C H A P T E R E L E V E Nm
The Tanzania researchteam making the final
adjustments in thequestionnaire
PHO
TO B
Y H
AFM
JAN
SEN

A Practical Guide for Researchers and Activists 179
women had left their homes since thetime when the sampling frame was devel-oped. Efforts were made to track thewomen down in other cities and to talkto family members regarding the reasonfor the migration. It was found that manyof the women had left their homesbecause of domestic violence, and in afew cases, women were currently hidingfrom their abusive spouses. This indicatedthat abuse might be even more commonamong nonrespondents than among theoverall sample of women.
Nonresponse may be a great problem incertain areas, such as cities where mostwomen work outside the home or live inapartment buildings.
Nonresponse may be classified in differ-ent groups, for example:
■ Household refusal (no one in thehousehold will give information aboutits members).
■ No eligible woman is found in thehousehold.
■ The eligible woman is selected but sheis not available to be interviewed.
■ The eligible respondent refuses to par-ticipate in part or all of the survey.
In all surveys, it is important to minimizethe degree of nonresponse. Box 11.4 givesexamples of measures that research teamsin the WHO multi-country study took toreduce refusals. It is a good idea to moni-tor the details of nonresponse by cluster,with follow-up procedures implemented inlocations with high levels of nonresponse.It is important to obtain as much informa-tion as possible about nonresponses, toidentify whenever possible why the persondid not participate in the survey, and toassess whether there may be any degree ofbias (such as lower prevalence of abuse)resulting from the incomplete data.
I N T H E F I E L D m
N % IRR*
Eligible woman refused/absent/didn't complete interview 184 5 5
Individual interviews completed 3255 83 95
Total households with an eligible woman 3439 87 100
No eligible women in household/ household empty/destroyed 502 13
Total households selected 3941 100
* Individual response rate (IRR) is calculated as: number of completed interviews/number households with eligiblewomen x 100.
TABLE 11.1 CALCULATING RESPONSE RATES
Gaining access to ahousehold in Brazil
PHO
TO B
Y H
AFM
JAN
SEN

180 Researching Violence Against Women
Further, nonresponses should be care-fully documented. Table 11.1 illustrateshow the response rate may be calculatedand presented. In this case, interviewswere completed in 83 percent of the 3,941households selected. However, in 13 per-cent of the households, there were no eli-gible women or the house on the map wasempty or had been destroyed. Because theresponse rate only measures the percent-age of completed interviews out of house-holds with an eligible woman, theindividual response rate is 95 percentrather than 83 percent.
DATA QUALITY CONTROL
Maintaining control over the quality of dataas it is being collected and entered into thecomputer will avoid many problems lateron. Following are some suggestions forimproving data quality.
Standardized training manuals
■ Training manuals for interviewersand supervisors. The instruction man-ual helps ensure that all procedureswith regard to carrying out the inter-views are performed in a uniform way,thereby reducing the possibility of sys-tematic bias in the study. The manualshould outline the roles and responsibil-ities of each member of the field staff,how to select and approach house-holds, and how to deal with unex-pected situations.
■ Question-by-question coding manual.This may be included with the inter-viewer manual if the questionnaire isnot too long. It provides additionalinformation about the purpose of eachquestion and how it should be asked,as well as how to code the answers.
SupervisionThe role of supervisors is to ensure thatinterviewers are following the guidelinesof the study, for example in the waythey are asking questions and maintain-ing privacy. Supervisors may observeinterviews occasionally to monitor thequality of the interviews. Either thesupervisors or an editor will review eachquestionnaire before leaving the field tomake sure that it is filled out properly,that the skip patterns are followed, noinformation is missing, and the informa-tion obtained makes sense. This shouldbe done as soon as possible after theinterview is completed. Any mistakes
C H A P T E R E L E V E Nm
These are some of the measures that were used in the WHO study in Peru, Brazil,and Japan to reduce refusals:
■ Sending letters in advance on official stationary asking for permission to visit,and calling by phone to set up appointments.
■ Sending letters to building managers asking permission for interviewers to enterthe building.
■ Meeting with community leaders beforehand to encourage community participa-tion.
■ Visiting households several times if necessary to find the respondent at home,including at night and on weekends.
■ Asking community leaders or village health workers to accompany fieldworkerson the initial visit to a household.
BOX 11.4 TECHNIQUES FOR MINIMIZING REFUSALS
Checking questionnairein Thailand
PHO
TO B
Y H
AFM
JAN
SEN

A Practical Guide for Researchers and Activists 181
found at this stage should be correctedimmediately. Interviewers may need toreturn to a household to obtain missinginformation (unless the respondent didnot want to provide that information).
Random repeat interviews Supervisors may randomly repeat parts ofinterviews to make sure that the informa-tion in both the interviews is the same.This is particularly important in the studyof violence, where an interviewer’s ownattitudes or behavior may influencewhether a woman will disclose experi-ences of violence. Therefore, the “inter-viewer effect” is particularly important tocontrol as much as possible. If supervi-sors will be revisiting households, it isimportant to mention this in the informed
I N T H E F I E L D m
Fieldworkers editingquestionnaires inSamoa
BOX 11.5 ENSURING DATA QUALITY IN THE WHO MULTI-COUNTRY STUDY ON WOMEN’S HEALTH AND DOMESTIC VIOLENCE AGAINST WOMEN
Within each country, a range of mechanisms was used to ensure and monitor the quality of the survey implemen-tation in different settings. This included:
■ The use of a standardized and detailed training package.
■ Clearly explaining the requirements and conditions of employment to each interviewer and supervisor, andmaintaining the option to fire staff who were not performing adequately, or who had negative attitudestowards the topic of study.
■ Compiling details of eligible members of each household during the survey. Possible sampling biases couldthen be explored by comparing the sample interviewed with the distribution of eligible respondents.
■ Close supervision of interviewers during fieldwork, including having the beginning of the interview observedby the supervisor for a proportion of interviews.
■ Conducting random re-checks of some households, without warning. Several respondents were reinterviewedby the supervisor using a brief questionnaire. This visit was used to assess how the respondent was selectedand to assess the respondent’s perceptions about the interview (at the time of the original interview respon-dents were asked for permission for the supervisor to return).
■ Continuous monitoring for each interviewer and each team of a number of performance indicators such asthe response rate, number of completed interviews, and rate of disclosure of physical violence.
■ Having a questionnaire editor in each team, who reviewed each of the questionnaires once they were com-pleted, identifying inconsistencies and skipped questions. Within any cluster, this enabled any gaps or errorsto be identified and corrected before the team moved on to another cluster.
■ A second level of questionnaire editing was done upon arrival in the central office by “office editors.”
■ Extensive validity, consistency, and range checking was conducted at the time of data entry by the check pro-gram that is part of the data entry system.
■ All the survey data were double entered, and inconsistencies were identified and addressed through a com-parison of the two data sets.
(From WHO, 2000.6)
PHO
TO B
Y H
AFM
JAN
SEN

182 Researching Violence Against Women
consent procedure and to ask for permis-sion to revisit the respondent.
Technical debriefingIn addition to the emotional debriefingmeetings already referred to in ChapterTen, regular meetings with interviewersduring the fieldwork are important foridentifying and correcting problems in thedata collection. Such problems includeambiguities in questions that are beinginterpreted differently by various interview-ers or questions where large discrepanciesare found.
Interviewer observationsWhenever possible, interviewers shouldbe encouraged to write detailed observa-tions at the end of the interview. Theseobservations can include information
about the interview itself, such aswhether anyone interrupted and whetherthe informant seemed nervous or credi-ble. The observations can also provideadditional information about thewoman’s history that may help to clearup apparent inconsistencies, or con-tribute valuable insights into the problemunder study.
Final debriefingA final debriefing should be carried outwith fieldworkers and supervisors after thedata collection is completed. The purposeis to gather information about the fieldprocess in general, problems that wereencountered that might influence the qual-ity of the data, and the general views ofstaff regarding the veracity of the informa-tion provided by respondents. For exam-ple, it would be useful to hear whetherwomen seemed reluctant to answer thequestions on violence, and whether therewere problems achieving complete privacy.Did it appear that respondents were tellingthe truth about their experiences? In onesuch debriefing, a fieldworker commentedthat “some women said no with theirmouths [about being abused] but yes withtheir eyes.”4 These comments will beextremely valuable later on in helping tointerpret the findings.
DATA ENTRY
Data entry and analysis is greatly facilitatedby using a computer package designedspecifically for the entry and statisticalanalysis of survey data. We recommend theuse of Epi Info, an epidemiological pack-age developed by the Centers for DiseaseControl (available in DOS or Windows for-mat at http://www.cdc.gov/epiinfo/). Theadvantages of Epi Info are many:
■ It is free, easy to obtain, and has beentranslated into several languages.
C H A P T E R E L E V E Nm
All WHO VAW studysites used standard-
ized data entryscreens that were
modified in each siteto include any addi-
tional questions(example from
Bangladesh).
This woman was raped by her brother, and then beaten and sexually abused byher husband. She finally left him, after 10 years of abuse, but he continued to fol-low her, to threaten her with a machete, and once dragged her by the hair downthe street. She went to the police for help, but they said there was nothing theycould do. She is still frightened that he will come back to kill her, and she brokedown crying during the interview. I gave her a booklet about violence and Ireferred her to the university mental health clinic. Nicaraguan interviewer
(From Ellsberg, 2000.5)
BOX 11.6 EXAMPLE OF A F IELDWORKER’S OBSERVATIONS
PHO
TO B
Y H
AFM
JAN
SEN

A Practical Guide for Researchers and Activists 183
■ It is easy to use, and many researchersand data analysts are already familiarwith it.
■ It allows for data entry screens with log-ical checks, and basic statistical analysis.The Windows version also does moreadvanced statistical analysis, such aslogistic regression and life table analysis.
■ Data entered in Epi Info can easily beexported to other statistical programsfor more advanced analysis, such asSPSS or Stata.
No matter what data entry system youuse, it is important to ensure that the dataare entered correctly. Sloppy data entry canlead to enormous problems later on, thattake months to detect and clean. Wheneverpossible, data entry should be carried out atthe same time as data collection. This willmake it much easier to identify and correctproblems in the data collection before it istoo late. Following are some of the mostcommon methods for controlling the qualityof data entry.
■ Logical controls. Many data processingsoftware packages (including Epi Info)
allow you to program logical checksinto the data entry program. Thesechecks can reduce errors by specifyingthe values that can be entered in a spe-cific field (for example, if it is a yes/noquestion, then only the two values rep-resenting yes and no will be accepted).They can also carry out automaticchecks to maintain the internal consis-tency of the data. For example, the pro-gram will check to make sure that awoman’s reported age coincides withher birth date, or if she has already
I N T H E F I E L D m
A data entry system was developed in Epi Info 6.0 with standardized data entry screens and extensive error checkprograms. In each country, all information collected on the administration sheet, household selection forms, house-hold questionnaire, and female questionnaire needed to be entered in this system. The system was developed cen-trally. A member of the Core Research Team installed the program in each country, assisted in customizing theprogram to accommodate country adaptations of the questionnaire, and trained data entry staff and the data entrysupervisor during one week in use of the program and in all other aspects of data processing. Although some of thequestions and/or answer options differed between countries, a standardized approach to coding was adopted andevery deviation of the original question was carefully documented in a central codebook. These procedures helpedensure that the data in each country were essentially entered in the same way, and that decisions about codingwere implemented universally. All data were double entered and double entry errors were identified using the valida-tion module Epi Data.
Open-ended questions were initially entered verbatim, and then coded, based on a uniform coding system that wasdeveloped after reviewing the responses obtained in each country. Each country team was responsible for the entry,cleaning, and preliminary analysis of the data for their own country. Assistance from the central technical supportteam was provided where necessary.
(From WHO, 2000.6)
BOX 11.7 DATA ENTRY AND PROCESSING IN THE WHO MULTI-COUNTRY STUDY ONWOMEN’S HEALTH AND DOMESTIC VIOLENCE
Data entry in Tanzania
PHO
TO B
Y H
AFM
JAN
SEN

184 Researching Violence Against Women
indicated that she has no children, theprogram will automatically skip anyquestions regarding children.
■ Double entry of data. This is the mostreliable way to ensure the quality ofdata entry. It involves entering eachquestionnaire twice by different people,and then comparing the data for dis-crepancies. While this is a very reliablemethod, it does increase costs.Therefore, some researchers prefer touse double entry at the beginning ofdata entry, to identify and correct com-mon mistakes. Then, as errors arereduced, data can either be enteredonce, or double entry of data can beperformed randomly on a smaller pro-portion of questionnaires.
■ Data quality tables. Data quality tablesare useful for determining refusal ratesand comparing results on specific vari-ables for which information alreadyexists. They can reveal problems occur-ring in specific field teams or with indi-vidual interviewers. In prevalencestudies, it is a good idea to keep trackof the percentage of women disclosingviolence per interviewer, and to performadditional supervision of interviewerswith particularly high or low rates ofdisclosure.
1. Hakimi M, Nur Hayati E, Ellsberg M, Winkvist A.Silence for the Sake of Harmony: DomesticViolence and Health in Central Java, Indonesia.Yogyakarta, Indonesia: Gadjah Mada University,Rifka Annisa, PATH, Umeå University; 2002.
2. Gossaye Y, Deyessa N, Berhane Y, et al. Women'shealth and life events study in rural Ethiopia.Ethiopian Journal of Health Development.2003;17(Second Special Issue):1-49.
3. Abrahams N. School-based Sexual Violence:Understanding the Risks of Using School ToiletsAmong School-going Girls. Cape Town, South Africa:South African Medical Research Council; 2003.
4. Ellsberg M, Heise L, Peña R, Agurto S, Winkvist A.Researching domestic violence against women:Methodological and ethical considerations. Studiesin Family Planning. 2001;32(1):1-16.
5. Ellsberg M. Candies in Hell: Research andAction on Domestic Violence in Nicaragua[Doctoral Dissertation]. Umeå, Sweden: UmeåUniversity; 2000.
6. World Health Organization. WHO multi-CountryStudy on Women's Health and Domestic ViolenceAgainst Women: Study Protocol. Geneva,Switzerland: World Health Organization; 2004.
C H A P T E R E L E V E Nm

Y
12PH
OTO
BY
HAF
M JA
NSE
N

A Practical Guide for Researchers and Activists 187
Y
BASIC ANALYSIS OFSURVEY DATA ON VIOLENCEAGAINST WOMEN
Look at the data matrixBefore initiating data analysis, it isimportant to make sure that the data areentered properly and that there are noobvious mistakes. There are several ways
Once the fieldwork has been com-pleted, the next task, and arguably the mostrewarding part of the research process, is tounravel the mysteries hidden within the data.This involves transforming endless pages ofwords, numbers, and codes into meaningfulresults to inform theory building or action.
One of the common limitations of sur-vey research on violence is the tendency topresent results mostly in the form ofdescriptive statistics, for example, percent-ages of women who are abused and char-acteristics of abuse. While these types offigures are certainly necessary, there is abroad range of statistical techniques fordata analysis that allows researchers toexplore the relationships between violenceand other variables with greater depth andprecision. In this chapter, we show how avariety of statistical techniques may becombined to enrich data analysis.Providing detailed guidance for advancedstatistical analysis is beyond the scope ofthis manual, and we urge researchersneeding further assistance to consult anexperienced statistician during this stage.
C H A P T E R T W E LV E
Analyzing Quantitative Data
Topics covered in this chapter:
Basic analysis of survey data on violence against womenLooking at associations between violence and other variablesAssessing the validity of survey resultsInterpreting the results
■ Inspect and clean the data matrix.
■ Display frequencies of the variables.
■ Make cross tabulations to check for inconsistencies.
■ Check graphic distributions of relevant variables.
■ Review basic hypothesis.
■ Plan initial tables.
■ Write down expected results.
■ Carry out additional analysis.
■ Illustrate results in tables and graphs.
■ Interpret results and assess critically.
■ Synthesize results in writing.
(Adapted from Persson and Wall, 2003.1)
BOX 12.1 STEPS FOR ANALYZING AND INTERPRETING THE DATA

188 Researching Violence Against Women
C H A P T E R T W E LV EY
to do this. One way to check data entryis to look over the data matrix frame byframe and make sure that nothing ismissing.
Another method is to make frequenciesof the basic variables. Look for variablesthat seem to have been miscoded, andcheck for missing values on key variablessuch as age and education.
Finally, do cross-tabulations to look forobvious inconsistencies. For example,make sure that all the women who haveanswered questions about the characteris-tics of violence are also coded as havingbeen abused, and that none of the womencoded as not having children haveanswered the questions about children’sage and schooling.
Whenever you find inconsistencies ormissing data, you will probably need toconsult the original questionnaire to findthe correct answer. Be sure to keep a logof any corrections made to the data file. Assoon as you have a fully updated andcleaned version of the data set, make sev-eral copies and keep them in a safe place!
This is certainly the most tedious part ofdata analysis. Doing it carefully can, how-ever, save you time and anguish later on.Table 12.1 presents an example of what adata matrix looks like. Each row representsa different informant, and the columns rep-resent different variables.
Prepare for data analysisIn preparing for the data analysis, youshould return to your hypothesis and
review the relationships you are expectingto test. These can be presented in the formof empty tables that serve as your initialanalysis plan. First, look at the frequenciesof variables such as age and education tosee how they are distributed. One way tolook at distribution graphically is by meansof a histogram (Figure 12.1), which meas-ures the frequencies of observations ineach category. This will be helpful later onin finding meaningful ways to recode thedata into smaller categories, such as agegroup and educational attainment.
Different ways to describe theoccurrence of violenceOne of the most important findings of aprevalence survey on violence is the per-centage of women who have been abused.However, there are many different ways toquantify and describe the frequency of vio-lence, and you will need to analyze yourdata from several different angles to findthe most meaningful way to describe yourresults. Following are some examples ofthe different ways that data on violencemay be presented.
As we mentioned in Chapter 6, theprevalence of violence can be expressed asthe percentage of women interviewed whohave experienced violence during a spe-cific period of time (for example, the last12 months), or as the percentage ofwomen who have ever experienced vio-lence in their lives.
It is also useful to break down these fig-ures according to the type of violence
TABLE 12.1 EXAMPLE OF A DATA MATRIX
Record Code Abused Age Numchild Educ Poverty Urban1 MY132 1 15 1 4 1 1
2 KJ423 1 29 3 2 0 2
3 MC341 2 31 2 2 1 2
4 KJ153 2 46 5 3 2 1
5 MI253 1 24 3 1 1 1
6 KU124 2 19 2 3 0 2

A Practical Guide for Researchers and Activists 189
(physical, sexual, emotional, or economic)and the perpetrator (in other words, abuseby partner should be presented separatelyfrom abuse by other individuals).
It is further useful to look at the over-laps between different types of violence,
for example, how many women haveexperienced both partner and nonpartnerabuse, or how many women have experi-enced both sexual and physical violence.These can be illustrated using Venn dia-grams. The diagram in Figure 12.2 was
A N A LY Z I N G Q U A N T I TAT I V E D ATA Y
FIGURE 12.1 HISTOGRAM INDICATING THE AGE DISTRIBUTION OFEVER-MARRIED WOMEN 15–35 YEARS OF AGE
Numberof women
Age of women
18–
16–
14–
12–
10–
8–
6–
4–
2–
0–15 16 17 18 19 20 21 22 23 24 25 26 27 28 29 30 31 32 33 34 35
FIGURE 12.2 OVERLAP BETWEEN SEXUAL, PHYSICAL, AND EMOTIONAL VIOLENCEEXPERIENCED BY 613 WOMEN IN JAPAN
Emotional (85.3%)
Physical (77.2%) Sexual (76.2%)
8.4%
57.4%
12.4%
2.9%
8.3% 3.4%
7.0%
(From Yoshihama and Sorenson, 1994.2)

190 Researching Violence Against Women
produced by Yoshihama and Sorenson,and presents the types of abuse that werereported by women in Japan.2 The percent-ages within parentheses represent the pro-portion of abused women who experienceeach type of abuse, whereas the numberswithout parentheses represent the propor-tion of abused women who experiencedspecific combinations of violence. In thisexample, 57 percent of abused women
experienced all three types of abuse.Most women who suffer abuse experi-
ence several different acts of violence, aswell as repeated incidents of violence. Toenable readers to visualize the range ofabusive behaviors, it may be helpful todescribe the percentage of abused womenwho have experienced specific acts of vio-lence. These may be presented as lifetimeexperiences, or as in Figure 12.3, from the
C H A P T E R T W E LV EY
FIGURE 12.3 DESCRIPTION OF THE SPECIFIC ACTS OF VIOLENCE EXPERIENCED BY NICARAGUAN WOMENDURING THE LAST 12 MONTHS AND PRIOR TO THE LAST 12 MONTHS
Forced to have sex using threats
Forced to have sex using physical violence
Choked or burned
Kicked or dragged
Hit with fist or instrument
Slapped or threw something
Pushed or shoved
0 10 20 30 40 50 60 70 80 90
% of abused women who have experienced violence
■ Current (last 12 months) ■ Former
10.4
9.7
9
10.9
25.3
22.4
33.7
19.9
21.1
15.4
21
42.3
37.1
44.3
FIGURE 12.4 WOMEN’S EXPERIENCES OF PARTNER VIOLENCE IN LEÓN, NICARAGUA,ACCORDING TO SEVERITY AND TIME FRAME
360 ever-married women
188 ever abused 172 never abused
97 current abuse 91 former abuse
68 severe 29 moderate 64 severe 27 moderate
Acts of Violence
(From Rosales et al, 1999.3)
(From Ellsberg et al, 1999.4)

A Practical Guide for Researchers and Activists 191
be critically important later on for lookingat the relationship between violence andspecific health outcomes. (For an examplesee the association between violence andemotional distress shown in Figure 12.11.)
LOOKING AT ASSOCIATIONSBETWEEN VIOLENCE ANDOTHER VARIABLES
After completing the descriptive analysis,the next step is to perform cross-tabula-tions to look for associations between
A N A LY Z I N G Q U A N T I TAT I V E D ATA
1998 Nicaraguan Demographic and HealthSurvey, broken down by recent and formeracts of violence experienced.
Figure 12.4 and Table 12.2 presentother examples of how to present descrip-tive information on violence. Figure 12.4shows that about half of the womenreporting violence were abused during thelast 12 months, and that 70 percent ofboth current and former violence wasclassified as severe. Table 12.2 shows that60 percent of the women experiencingviolence during the last year sufferedmore than one incident, and that 22 per-cent of women were severely abusedmore than five times in the last year. Aftercompleting this descriptive analysis, werecommend developing a scale thatenables you to group women accordingto their experience of violence, for exam-ple: never abused, former moderateabuse, former severe abuse, current mod-erate abuse, and current severe abuse.This kind of detailed information aboutwhat kind of violence women suffer will
Y
Moderate SevereViolence Violence Total
Frequency % (N) % (N) % (N)Once 18 (17) 22 (21) 40 (38)
Occasional (3–5 times) 10 (10) 28 (27) 38 (37)
Frequent (6–20 times) 2 (2) 9 (9) 11 (11)
Very frequent (more than 20 times) 0 11 (11) 11 (11)
Total 30 (29) 70 (68) 100 (97)
TABLE 12.2 FREQUENCY OF VIOLENCE IN LEÓN, NICARAGUA,DURING THE LAST 12 MONTHS ACCORDING TO SEVERITY (N=97)
FIGURE 12.5 THE PREVALENCE OF VIOLENCE AMONG 360 EVER-MARRIED WOMEN IN LEÓN, NICARAGUA,ACCORDING TO SOCIO-ECONOMIC STATUS, URBAN/RURAL RESIDENCE, AND NUMBER OF CHILDREN
Percentwomenabusedphysically
70–
60–
50–
40–
30–
20–
10–
0–Not PoorPoor
Rural Urban 0–1 2–4 >4Children
3942
48
65
55 54
40
(From Ellsberg et al, 1999.4)
(From Ellsberg et al, 1999.4)

192 Researching Violence Against Women
violence and possible risk or protectivefactors or specific health outcomes. Simplystated, this involves comparing differentgroups of women to find out whetherthere is more violence among women withcertain characteristics, or whether womenwho have experienced violence have agreater frequency of certain kinds of prob-lems. Figures 12.5 and 12.6 show howthese differences might be presented bymeans of a bar graph. You will certainlywant to look at the associations betweenexperience of violence and such back-ground factors as age, urban rural resi-dence, socio-economic status, education,and number of live children. You shouldalso look at how each of these variables isrelated to the others. It may be helpful tomap the associations out visually, as shownin Figure 12.7.
In order to determine whether the preva-lence of violence actually varies accordingto different characteristics such as age oreducation, you will need to perform testsfor statistical significance. When used byresearchers, the word significance refers not
to the importance or size of the difference,but to the likelihood that the associationsare real and not simply due to chance. Twoof the most common tests for statistical sig-nificance are chi-square (X2) and theStudent’s T test, and most computer pack-ages can perform them automatically. Eachtest is appropriate for different kinds ofdata. Therefore, you should consult a statis-tician to determine the most appropriatestatistical tests for your data.
For example, initial analysis of surveydata in León, Nicaragua, found that lifetimeexperience of physical violence was signifi-cantly associated with poverty, living in theurban area, and having a mother ormother-in-law who was also abused. Noassociations were found between violenceand a woman’s age or education. However,both age and low education were associ-ated with a high number of children, andlow education was associated with povertyand living in the rural area (Figure 12.7). InFigures 12.8 and 12.9, bar graphs showfindings from a study in Central Java,Indonesia. Figure 12.8 shows that
C H A P T E R T W E LV EY
FIGURE 12.6 THE PERCENTAGE OF EVER-MARRIED NICARAGUAN WOMEN WHO REPORT THAT THEY HAVECONSIDERED OR ATTEMPTED SUICIDE RELATED TO EXPERIENCES OF VIOLENCE (N=8507)
25–
20–
15–
10–
5–
0–Thought of commiting suicide Tried to commit suicide
■ All women ■ Women with violence ■ Women without violence
8.4
4.8
9.8
17.1
4.52.4
(From Rosales et al, 1999.3)
Percent

A Practical Guide for Researchers and Activists 193
A N A LY Z I N G Q U A N T I TAT I V E D ATA Y
FIGURE 12.7 VISUAL MAPPING EXERCISE TO SHOW ASSOCIATIONS FOUND BETWEENBACKGROUND VARIABLES AND THE RISK OF WIFE ABUSE IN LEÓN, NICARAGUA
Lines with arrows between variables indicate significant associations.
Mother-in-lawabused
Urban/ruralresidence
Motherabused
Number ofchildren
Poverty
Woman’seducation
Woman’sage
Lifetime experiencesof violence
FIGURE 12.8 PHYSICAL SYMPTOMS AMONG WOMEN ACCORDING TO EXPERIENCES OFSEXUAL AND PHYSICAL PARTNER VIOLENCE IN CENTRAL JAVA, INDONESIA
Ulcers
Vaginal discharge
Dizziness
Aches and pains
Intestinal problems
Lower abdominal pain
0 10 20 30 40 50 60 70
* p<.05 **p<.001
■ No violence ■ Violence
10*15
2018
42**60
30**43
8**17
7**15
Percentages are given for women who had experienced each symptom in the previous four weeksaccording to whether they had ever been physically or sexually abused by an intimate partner.Asterisks indicate that associations are statistically significant.
(From Ellsberg et al, 1999.4)
% of women
Symptom
(From Hakimi et al, 2002.5)

194 Researching Violence Against Women
Indonesian women who had ever experi-enced partner violence reported morerecent symptoms of ill health such as pain,dizziness, ulcers, and intestinal problems.Figure 12.9 shows that Indonesian menwho have been violent towards their wivesare also more likely to have used alcohol,and to have had extra-marital relationships.They are more likely to have beeninvolved in fights with other men, to prefersons over daughters, and to have little orno education.
ASSESSING THE VALIDITYOF SURVEY RESULTS
Once you have found what seem to be themost important results from your data, andyou have performed basic statistical testsbetween variables (for example, violenceand ill health), you need to assess theirvalidity. This means you need to deter-mine to what degree the study measuredwhat it was supposed to, and whether thefindings mean what they are supposed to.Internal validity refers to the extent to
which variations in a specific outcome (forexample, the risk of violence) may beattributed to variations in an independentvariable (for example women’s age or edu-cation). External validity refers to thedegree to which results from a given studymay be used to draw conclusions about alarger population. If a study is performedon a randomly selected population, itshould be possible to generalize the resultsof the study to the general population fromwhich the sample was drawn.
Another important question is Are thefindings consistent? That is, do they makesense, according to what is known aboutthe subject locally and internationally? Ifthey differ greatly from previous findings,are there any additional data to support thenew results? Are there any aspects of datacollection, sampling, design, or analysisthat might have altered the results by intro-ducing bias? Has the analysis taken intoaccount possible sources of confounding?The following pages present different waysto address these issues.
The effects of confounding in data analysisIn studying the association between riskfactors and a specific problem, confound-ing can occur when another characteristicexists in the study population and is asso-ciated with both the problem and the riskfactor under study.
Confounding can have a very impor-tant effect on study results, and can cre-ate the appearance of a cause-effectrelationship that in reality does not exist.Age and social class are often con-founders in epidemiological studies. Inthe study of risk factors for violence, con-founding variables can give misleadingimpressions about what risk factors influ-ence the occurrence of violence.Stratified analysis and multivariateanalysis are two ways to control for theeffects of confounding variables.
C H A P T E R T W E LV EY
FIGURE 12.9 HUSBAND’S CHARACTERISTICS ACCORDING TO USE OF VIOLENCE(AS REPORTED BY WIFE) IN CENTRAL JAVA, INDONESIA
Alcohol use
Son preference
Low education
Fights with men
Has other women
0 10 20 30 40 50 60
** p<.001 N=765 men
■ Not violent ■ Violent
3**13
20**30
42**49
2**6
2**13
Percentages are given for the proportion of men with each characteristic,according to whether or not they have ever used physical or sexual violenceagainst their wives.5
Husband characteristics
Percent of men
(From Hakimi et al, 2002.5)

A Practical Guide for Researchers and Activists 195
Stratification involves analyzing dataseparately using defined categories of theconfounding factor, such as age groups.For example, some studies using bivari-ate analysis (analysis using only twovariables) have found that pregnantwomen were more likely to be abusedthan non-pregnant women. However,after analyzing the same data stratified byage groups, it turned out that this associa-tion was confounded by age. It turnedout that being young was the real riskfactor for violence rather than pregnancy.It just happened that younger womenwere more likely to be pregnant thanolder women. This explained theincreased prevalence of violence amongpregnant women.
Violence can also be analyzed as a con-founding variable for other risk factors, asshown in the following example of a studyon mental distress. Preliminary resultsfound that women who had been marriedat least once in their lives had twice asmuch emotional distress as women whohad never been married (Table 12.3). Thiswould imply that marriage is an importantrisk factor for mental distress.
However, when the prevalence of mentaldistress among ever-married women wasanalyzed separately according to whetherwomen had experienced wife abuse, alarge difference was found between thetwo groups. Thirty-one percent of abusedwomen suffered mental distress, comparedto only seven percent of women who hadnever been abused, which is even less thanthe prevalence of distress among never-married women (Table 12.4).
Since wife abuse is associated with mar-riage (by definition only ever-partneredwomen can experience wife abuse) and itis also associated with mental distress, ithas a confounding effect on the associationbetween marriage and mental distress(Figure 12.10). Therefore, after stratifiedanalysis it becomes evident that it is wife
abuse and not marriage itself that accountsfor the increase in mental distress amongmarried women.
This analysis is further strengthened bycomparing women’s current mental dis-tress according to the severity of violencethey experienced and when it took place,as shown in Figure 12.11. Breaking downthe analysis this way demonstrates thatwomen who were severely abused in thelast 12 months were over ten times morelikely to be distressed than women whohad never been abused. Further, itrevealed that the severity of abusewas more important than when it tookplace, since women experiencing severe
A N A LY Z I N G Q U A N T I TAT I V E D ATA Y
Selection of women Percentage of emotional distress
All women 15–49 (n=488) 17%
Ever-married women (n=360) 20%
Never-married women (n=128) 10%
TABLE 12.3 PREVALENCE OF EMOTIONAL DISTRESS ACCORDING TOMARITAL STATUS AMONG NICARAGUAN WOMEN
Experience of wife abuse Prevalence of emotional distress
Never abused (n=172) 7%
Ever abused (n=188) 31%
TABLE 12.4 PREVALENCE OF EMOTIONAL DISTRESS AMONG EVER-MARRIEDNICARAGUAN WOMEN ACCORDING TO EXPERIENCES OF WIFE ABUSE
FIGURE 12.10 THE CONFOUNDING EFFECT OF VIOLENCE ON THEASSOCIATION BETWEEN MARRIAGE AND MENTAL DISTRESS
Marriage
Violence
Mental Distress
(From Ellsberg et al, 1999.6)
(From Ellsberg et al, 1999.6)

196 Researching Violence Against Women
violence formerly were still more likely tobe currently distressed than women whohad suffered only minor abuse, eventhough it took place more recently.
The use of multivariate analysis toadjust for confounding factorsWhen it appears that there are severalvariables confounding an association, thenit is no longer practical to use stratifiedanalysis, as it would be excessively com-plex to perform. For example, in Figure12.7, we saw that in the León study therewere several variables, such as poverty,living in the urban area, and number ofchildren, which were associated with therisk of violence. It was further shown thatthese three variables are associated witheach other as well as with women’s levelof education. Could it be that poverty isthe true underlying factor influencingwomen’s risk of violence, and therefore
that urban women and women with manychildren are found to have greater levelsof violence, simply because they are morelikely to be poor? How can we unravelthe complex relationships between thesevariables?
Multivariate analysis techniques, suchas logistic regression modeling, areuseful for examining the relationshipsbetween several explanatory factors and aspecific outcome variable. Logisticregression helps to uncover the degreeto which several explanatory variables arerelated and to control for confoundingvariables. In Table 12.5 (next page), thesame relationships presented in Figure12.7 are examined using crude or unad-justed odds ratios as well as multivariateor adjusted odds ratios. The 95 percentconfidence intervals are used to assessthe statistical significance of the associa-tion by indicating that there is a 95
C H A P T E R T W E LV EY
FIGURE 12.11 PREVALENCE OF EMOTIONAL DISTRESS ACCORDING TOEXPERIENCES OF VIOLENCE AMONG NICARAGUAN WOMEN
Percentages are given for the proportion of ever-married women who experienced emotional distress inthe four weeks prior to the survey, according to whether they had experienced physical partner violence.Violence was classified by severity and by whether it took place within the 12 months previous to thestudy, or earlier. In the right hand columns, crude (unadjusted) odds ratios and their corresponding confi-dence intervals are given. Intervals where the lower and upper figures do not include 1.0 are consideredstatistically significant. (In this case, all types of violence except for former moderate violence are signifi-cantly associated with emotional distress.)
No violence
Former moderate
Current moderate
Former severe
Current severe
7%
15%
21%
27%
44%
Emotional Distress %
10 20 30 40 50 Crude Odds Ratios 95% Confidence Interval
1.0
2.3
3.6
4.8
10.3
.7–7.8
1.0 –12.0
2.2–10.8
4.9–21.6
Experiences ofViolence

A Practical Guide for Researchers and Activists 197
percent probability that the true figurelies between this range. If the rangebetween the lower and upper figure inthe confidence interval does not includeone, then it can be said that there is a 95percent probability that the association isnot due to chance.
When comparing the crude and multi-variate odds ratios for each variable, onecan see that they do not vary much inmost of the cases. The associationbetween violence and poverty, havingmore than four children, and a history offamily violence in the husband’s familyare all maintained. Living in the urbanarea, which had a confidence intervalslightly below one in the crude analysis,becomes significant in the multivariatemodel, while a history of family violencein the wife’s family becomes insignificant.After performing the multivariate analy-sis, it is possible to say that althoughpoverty, urban/rural residence, and highparity are all related, their effect onwomen’s risk of violence is independentand should not be interpreted as theresult of confounding.
Using advanced statistical analysis creativelyIn earlier sections of this chapter, we pre-sented the most commonly used tech-niques for statistical analysis of survey data
A N A LY Z I N G Q U A N T I TAT I V E D ATA Y
Crude AdjustedVariable Categories OR (95% CI) OR (95% CI)Poverty Nonpoor 1.0 1.0
Poor 1.91 (1.12-–3.23) 1.82 (1.03–3.23)
Zone Rural 1.0 1.0Urban 1.62 (.94-–2.78) 2.07 (1.12–3.82)
Number of 0–1 1.0 1.0children 2–3 1.40 (.82-–2.39) 1.34 (.74–-2.43)
4 or more 2.77 (1.59-–4.82) 2.23 (1.21–-4.15)
Family No historyhistory in wife’s family 1.0 1.0of abuse Wife’s mother
abused 1.8 (1.24-–2.90) 1.28 (.79-–2.09)
No history inhusband’s family 1.0 1.0Husband’s motherabused 3.13 (2.00-–4.96) 2.98 (1.86–4.73)
Crude and adjusted odds ratios are given (together with 95 percent confi-dence intervals) for having experienced violence at least once in their lives.
TABLE 12.5 ASSOCIATIONS BETWEEN BACKGROUND FACTORSAND PREVALENCE OF VIOLENCE AMONG 360 EVER-MARRIED
NICARAGUAN WOMEN AGES 15–49
FIGURE 12.12 TIME FROM THE START OF A RELATIONSHIP TO THE ONSET OF VIOLENCE
Number of years from start of marriage to onset of violence
100–
80–
60–
40–
20–
0–0 2 4 6 8 10 12 14 16 18 20 22
Percentageof women
The figure shows the cumulative incidence of domestic violence over time among 188 women who reportedhaving experienced marital violence at least once in their lives, using Kaplan Meier Life Table Analysis.8
(From Ellsberg et al, 1999.4)
(From Ellsberg et al, 2000.8)

198 Researching Violence Against Women
on violence. However, additional insightmay be revealed by the creative use ofmore advanced statistical techniques.
For example, life table or survivalanalysis was used to gain a deeperunderstanding of the relationship betweenviolence and high parity in Nicaragua.Many international studies have found asimilar association.7 One interpretation forthis is that having many children placesadditional stress on a marriage andincreases a woman’s likelihood of beingbeaten by her husband.
However, using life table analysis, astatistical technique which measures theprobability of events occurring over time,it was possible to determine that violencebegan early on in relationships, in manycases well before women had startedbearing children. Figure 12.12 shows that50 percent of violence begins within twoyears of marriage, while 80 percent ofabuse starts within four years. This
implies that high parity, instead of beinga risk factor for abuse, is more likely tobe a result of violence, because batteredwomen are less likely to be able to con-trol the timing of sex or the use of birthcontrol.
The same techniques were applied tothe likelihood of a woman leaving anabusive relationship, and it was foundthat 70 percent of women eventually didleave their abusers, although somewomen stayed as long as 25 years ormore before separating. Stratifying thisanalysis according to age groups showsthat younger women are more likely tohave left an abusive relationship withinfour years, compared to womenbetween 35-49 years (Figure 12.13). Thisindicates that younger women are lesslikely to tolerate abuse than olderwomen. In order to use survival analysistechniques, it is necessary to collectdetailed data regarding each of a
C H A P T E R T W E LV EY
FIGURE 12.13 THE PROBABILITY OF LEAVING AN ABUSIVE RELATIONSHIP OVER TIME,BASED ON A WOMAN’S CURRENT AGE GROUP
Number of years from onset of violence to leaving
100–90–80–70–60–50–40–30–20–10–0–
0 2 4 6 8 10 12 14 16 18 20 22 24 26
Percentage ofwomen leaving
This figure shows that 50% of young women (ages 15–25) leave a relationship within four years ofviolence starting, whereas 20 years was the median time of older women.
15–24 25–34 35–49p<.01
(From Ellsberg, 2000.10)

A Practical Guide for Researchers and Activists 199
woman’s relationships: when did it start,how long did it last, was there violence,and if so, when did the first and lastincidents of violence take place. Thesetypes of analyses are somewhat compli-cated to perform and interpret, so it isimportant to consult with an experi-enced statistician.
INTERPRET INGTHE RESULTS
The process of data analysis will oftentake longer than you initially expect.However, you can plan data analysis instages, so that initial findings, such asprevalence and descriptive characteristics,can be made available as soon as possibleto the communities and local institutionsthat have been supporting the research,and that will be anxiously awaiting results.Further analysis can be performed over alonger period to explore some of the moreinteresting findings in greater depth. Box12.2 presents guidelines for writing upresearch results for publication in scientificjournals. Chapter 14 will discuss in detailhow research results may be tailored to fitthe needs of different groups.
When interpreting and writing up theresults of data analysis, it is important tobe cautious. Each research design yieldsdifferent kinds of data, with their respec-tive limitations. Be careful not to drawconclusions that are not supported by thedata, as overstating your results can seri-ously undermine the credibility of theresearch. People are more likely to listento your findings when you are openabout whatever limitations the study hadin terms of design, data collection, oranalysis. Some examples of common pit-falls are the following:
■ Inferring causal relationships fromcross-sectional data. Cross-sectional sur-veys can highlight associations between
two variables, but unless you havegood information about when differentconditions or events occurred it is diffi-cult to know with certainty what camefirst. A good example of how causalrelationships can be misinterpreted isthe relationship between parity and vio-lence presented in the last section. It isa good idea when presenting resultsfrom cross-sectional surveys to talkabout “associations” rather than causes.The discussion section can assesswhich variables are most likely to becauses or outcomes, based on yourconceptual framework and other stud-ies on the subject.
■ Inferring causal relationships from bi-variate analysis. As we showed in the
A N A LY Z I N G Q U A N T I TAT I V E D ATA Y
AbstractApproximately 100 words.
BackgroundLiterature, national context, objectives.
MethodsDescribe the study population, how the sample was selected, what instruments wereused, how the fieldwork was conducted, how data were analyzed, how ethicalclearance was obtained, and any special measures, such as safety procedures.
ResultsThis section should describe all the major results of data analysis, including relevanttables and figures, and measures of statistical significance.
DiscussionThe purpose of this section is to interpret the meaning of data, assessing the validityand generalizability, possible sources of bias, how the findings relate to interna-tional and national studies on the same subject, and possible explanations for themost important findings.
ConclusionsThese are sometimes included in the discussion section. How might these findingsbe used for improving interventions and policy? What are areas that might benefitfrom future research?
ReferencesMake sure to include citations from the most relevant literature in the field of study.
(From Persson and Wall, 2003.1)
BOX 12.2 SUGGESTED GUIDELINES FOR WRITING A SCIENTIFIC PAPER

200 Researching Violence Against Women
example on marriage and emotionaldistress, other variables may confounda relationship between two variables. Ifyou have not performed stratified ormultivariate analysis, it is wise to becautious in interpreting your results.
■ Generalizing conclusions for differentpopulations than the study population.Results that are representative for oneregion are not necessarily true forother regions in the country, or for thecountry as a whole. This does notmean that regional studies cannot pro-vide important insights that are rele-vant for a much broader context. Thereare many examples of regional studiesthat made critical contributions forguiding national policies and programs.However, it is still important to becareful in stating clearly what the limi-tations of the sample are, both in termsof its power to capture important asso-ciations and its generalizability.
1. Persson LÅ, Wall S. Epidemiology for PublicHealth. Umeå, Sweden: Umeå InternationalSchool of Public Health; 2003.
2. Yoshihama M, Sorenson SB. Physical, sexual, andemotional abuse by male intimates: Experiencesof women in Japan. Violence and Victims.1994;9(1):63-77.
3. Rosales J, Loaiza E, Primante D, et al. EncuestaNicaraguense de Demografia y Salud, 1998.Managua, Nicaragua: Instituto Nacional deEstadisticas y Censos, INEC; 1999.
4. Ellsberg MC, Peña R, Herrera A, Liljestrand J,Winkvist A. Wife abuse among women of child-bearing age in Nicaragua. American Journal ofPublic Health. 1999;89(2):241-244.
5. Hakimi M, Nur Hayati E, Ellsberg M, Winkvist A.Silence for the Sake of Harmony: DomesticViolence and Health in Central Java, Indonesia.Yogyakarta, Indonesia: Gadjah Mada University;2002.
6. Ellsberg M, Caldera T, Herrera A, Winkvist A,Kullgren G. Domestic violence and emotionaldistress among Nicaraguan women: Results froma population-based study. American Psychologist.1999;54(1):30-36.
7. Kishor S, Johnson K. Domestic Violence in NineDeveloping Countries: A Comparative Study.Calverton, MD: Macro International; 2004.
8. Ellsberg M, Peña R, Herrera A, Liljestrand J,Winkvist A. Candies in hell: Women's experiencesof violence in Nicaragua. Social Science andMedicine. 2000;51(11):1595-1610.
9. Ellsberg MC, Winkvist A, Peña R, Stenlund H.Women's strategic responses to violence inNicaragua. Journal of Epidemiology andCommunity Health. 2001;55(8):547-555.
10.Ellsberg M. Candies in Hell: Research andAction on Domestic Violence in Nicaragua[Doctoral Dissertation]. Umeå, Sweden: UmeåUniversity; 2000.
C H A P T E R T W E LV EY

13PH
OTO
BY
HAF
M JA
NSE
N

A Practical Guide for Researchers and Activists 203
z
meant to acquaint the reader with theprocess and to direct interested parties touseful texts in the field. Generally, projectsinvolving qualitative data analysis shouldproceed under the direction of someonetrained in qualitative research.
We have found the framework ofresearchers Miles and Huberman helpfulin understanding qualitative analysis.1
Analysis, according to them, consists of“three concurrent flows of activity: datareduction, data display, and conclusiondrawing or verification.” Ulin and col-leagues offer a slightly revised version of the Miles and Huberman frameworkthat identifies four separate flows of activ-ity—data reading, coding, reducing, anddisplaying—all informing a constantprocess of interpretation.2 As emphasizedin Figure 13.1, this constant interplay ofactivity is an iterative process that begins inthe field and continues at your desk onceall the data are collected.
Below we describe each of theseprocesses briefly before exploring data
In this chapter, we concentrate on mak-ing sense of textual data in the form ofexpanded field notes, transcripts ofrecorded interviews, or naturally occurringtexts such as newspaper accounts, popularliterature, or policy documents.
APPROACHES TOQUALITAT IVE ANALYSIS
There are as many different ways to ana-lyze qualitative data as there are means tocollect it. Generally, however, all forms ofanalysis involve organizing the data accord-ing to specific criteria, reducing it to amore manageable form, displaying it in aform to aid analysis, and interpreting it.
Analyzing reams of written text is ascomplex and time-consuming as analyzingquantitative data—if not more so. Goodqualitative analysis is part art and part sci-ence, and hundreds of books have beenwritten on the topic. This chapter is notintended to substitute for these texts or to“teach” qualitative data analysis. Rather it is
C H A P T E R T H I R T E E N
Analyzing Qualitative Data
Topics covered in this chapter:
Approaches to qualitative analysisData codingUsing a computer for coding and categorizingData reduction and data displaysEnsuring rigor in qualitative research

204 Researching Violence Against Women
C H A P T E R T H I R T E E Nz
coding and interpretation in greater depth.Data immersion is the process of read-
ing and rereading each set of notes or tran-scripts until you are intimately familiar withthe content. Early readings of the data canhelp guide future data collection. Are yougetting the kinds of data that youexpected? Does your reading suggest newavenues of inquiry? Repeated readings arealso the first step toward identifying emerg-ing themes, possible relationships amongthemes or categories, and unusual or con-tradictory responses.
Data coding means attaching labels orcodes to different segments of text thatare associated with different issues. Codingis a way to help separate information intocategories or themes so that informationfrom different sources can be easily sortedand compared. With key themes coded inthis way, you can later search and retrieveinteresting segments and look at them asseparate files. Data can either be coded byhand (by writing codes into the margins ofthe text) or with the aid of a computer.Computers have helped revolutionizequalitative data analysis by greatly easing
the task of sorting text segments by the-matic code.
Data display is defined as an organ-ized assembly of information that allowsconclusions to be drawn and actions to betaken.1 Most frequently qualitative data isdisplayed as narrative text, which tends tooverload people’s information-processingcapabilities. Matrices, graphs, networks,and charts can present information inmore compact form that make the datamore accessible. Many of these techniquesare presented later in this chapter.
Data reduction involves selecting,focusing, simplifying, abstracting, andtransforming the “raw” data of field notesor transcriptions into typed summariesorganized around themes or patterns basedon the original objectives of the research.Data reduction continues until the finalreport is written.
Interpretation/conclusion drawingrefers to the process of deciding whatthings mean, noting themes, regularities,patterns, and explanations. The researchermay begin to draw conclusions in draftform throughout the entire data collection
FIGURE 13.1 THE PROCESS OF QUALITATIVE DATA ANALYSIS
Reading
Interpreting
Coding
Reducing Displaying
In the field
In the field
(From Miles & Huberman, 19941 and Ulin, et.al, 2002.2)

A Practical Guide for Researchers and Activists 205
exercise, but eventually these becomemore explicit and firm at the point whenthe “final report” is written. Conclusionsmust also be verified as analysis proceeds.As researchers try to explain what the datamean, they should continually examinetheir explanations for plausibility and valid-ity—do their explanations make sensewithin the context of the study? It is oftenpossible to test the validity of conclusionsby presenting preliminary findings andinterpretations back to project stakeholdersand/or members of the population beingresearched. Researchers can then incorpo-rate this feedback into the final version oftheir written report.
DATA CODING
Although most qualitative research usessome process of coding to organize data,there are no standard rules about how todo so. As Ulin and colleagues observe:
Researchers differ on how to derivecodes, when to start and stop coding, andthe level of detail they want. Someresearchers develop codes that closely matchthe ideas or language found in the textualdata. They want to avoid imposing wordsor concepts that might prevent them fromseeing their data in a new way. Others bor-row terms from the social science literaturethat represent more abstract concepts
A N A LY Z I N G Q U A L I TAT I V E D ATA z
Transcribe and organize the information into files—one for each interview, focus group, or observation session.
Immerse yourself in the data. Get a sense of the whole. Read through all of the transcripts several times. Perhaps jotdown some ideas as they come to mind.
Pick one transcript or document—the most interesting, the shortest, the one on the top of the pile. Go through it, ask-ing yourself: What is this about? Read both for content and to identify emergent themes and insights into underlyingmeaning. Write thoughts in the margin or in your field notebook.
When you have completed this task for several documents, make a list of all the topics you encountered. Follow thetrail of issues, intuitions, and ideas that arise from reading the data. Cluster together similar topics. Form these topicsinto columns that might be arrayed as major topics, unique topics, and leftovers.
1. Develop preliminary coding categories. Start by listing all the issues, perceptions, attitudes, beliefs, andother important aspects identified during the preceding stage. Once the principal coding categories havebeen identified, review the list and see if any categories overlap or are repeated. Then assign a codeand, if so desired, code by color.
2. Now take this list and go back to your data. Write the codes next to the appropriate segments of the text.Try out this preliminary organizing scheme on several transcripts to see whether new categories and codesemerge.
3. Make a final decision on the abbreviation for each category and alphabetize these codes.
4. In the margin of each transcript, write the code assigned to each category found in the text (or use a com-puter to assign codes to particular segments of text).
5. Assemble the data belonging to each category in one place and perform a preliminary analysis.
6. Look for the most important relationships between the data. Also look for relationships between differentanalysis categories. In other words, look for the most important relationships between people, events,ideas, perceptions, behavior patterns, and other aspects of the data.
7. Discovering what is significant should lead to a search for similarities and differences. Look for the mostcommon and recurrent norms and patterns in behavior, ideas, perceptions, attitudes, and expressions.Also look for the most salient differences.
8. Consider using one or more data display techniques to help make sense of your data—for example,matrices, decision trees, or flow charts.
(Adapted from Creswell,19943 and Shrader and Sagot, 2000.4)
BOX 13.1 WHERE TO START: AN APPROACH TO QUALITATIVE DATA ANALYSIS

206 Researching Violence Against Women
C H A P T E R T H I R T E E Nz
The following is an example of data coding and organization using the software OpenCode developed by Umeå University, Sweden.OpenCode allows the researcher to apply an unlimited number of codes to specific pieces of text, which may then be reorganized accordingto specific themes, or sets of codes. In this example, we used two interviews from Nicaraguan women, Ana Cristina and Maria, both of whomhad been abused by their former husbands. In the interviews, both women described the characteristics of the violence, its effect on them andtheir families, different strategies they had used for coping with the violence, different sources of family and social support (or lack thereof), andfinally how they made the decision to separate from their abusive partners.
BOX 13.2 AN EXAMPLE OF DATA CODING USING OPENCODE
Each interview was coded separately, and more than 100 different codes were generated at this stage. Some of the codes were related to specific language or feelings that the respondents used (e.g., “bitterness,” “sadness”) whereas others were thematic categories such as “effectson children” or “disengagement.” After both interviews were coded, we organized the data into common themes, using the program’s “search”option.
The second figure shows a piece of text where Ana Cristina describes how her children were affected by her husband’s violence, as well ashow their suffering influenced her own views towards the marriage. It appeared that the desire to protect her children was a significant factor inAna Cristina’s decision to leave her husband. To see whether similar themes might also be relevant for Maria, we conducted a search of bothinterviews using the criteria “effect_on_children” AND “separation.”
The text that appears in the next figure shows that both women felt that their children’s suffering was a major influence on their decision to leave.
In further analysis, we looked for commonalities and differences in other types of motivations mentioned for leaving (for example, the existence orlack of family support, economic resources, self-esteem) The same results could certainly have been accomplished by cutting and pasting text, butthe use of the computer software was particularly useful for looking at a single piece of text from different perspectives, and in different combina-tions of codes.

A Practical Guide for Researchers and Activists 207
relationships among codes. Because thisapproach allows conceptual categories toemerge from the text rather than from themind of the researcher, it is especially wellsuited for theory building.5
For more applied research projects, it ispossible to code segments using cate-gories that correspond to well-recognizedphenomena or concepts. For example,when coding an interview from a womanliving with abuse, it is easy to imaginecodes emerging that correspond to differ-ent feelings, coping strategies, responsesto abuse, and reactions of others. Evenwhen working with more categorical
A N A LY Z I N G Q U A L I TAT I V E D ATA
important to their field. These have theadvantage of being understood by a wideraudience. Whether borrowed or emergent,labels allow you to assemble under oneconcept many seemingly disparate pieces oftext and to search for connections.2
In part, these different approaches tocoding evolve from the theoretical under-pinnings of different types of qualitativeresearch. Grounded theory, an approachto qualitative research pioneered in thelate 1960s by Glaser and Straus, empha-sizes coding that sticks close to the textand then constructs increasingly abstractcategories and domains by analyzing the
z
BOX 13.2 AN EXAMPLE OF DATA CODING USING OPENCODE
Using computer software (OpenCode) to organize text by common themes.

208 Researching Violence Against Women
labels, one’s coding system will necessar-ily evolve over time as new insights andways to organize the data emerge.
Figure 13.1 describes one approach totackling qualitative analysis, following theconceptual approach outlined by Milesand Huberman and Ulin and colleagues.It begins with data immersion andincludes developing and applying morecategorical labels to segments of text. For
very simple projects, it may be possibleto organize segments of text according tothe various research questions of interestand then begin to look for similarities,differences, themes, and relationships. Byits very nature, one’s approach to qualita-tive analysis will vary based on complex-ity of the research question being askedand the resources and time available foranalysis.
C H A P T E R T H I R T E E Nz
Forms of Violence
Physical
Psychological
Sexual
Economic
Motivating FactorsInternal
■ Fear that herdaughter will betaken away.
■ Search forprotection, she isbeaten becauseof anotherwoman.
■ Depression;takes drugs tofeel better.
■ Seeks supportbecause ofstress; wants tovent her feelings;wants to beheard.
■ Wants someoneto talk with herhusband.
■ Fear of dying ofan infectionbecause hedoes not gettreated.
■ Loss of libido.
■ She thinks heshould supportand help her.
■ She doesn’t thinkher status shouldbe reducedunfairly.
External
■ Beatings, biting,miscarriages.
■ Loss of teeth.■ Referred by a
service provider;taken by herfamily.
■ He leaves thehome.
■ He refuses tomarry her.
■ The childrenhave problemsat school.
■ Sexual rejectionfrom him.
■ She has beentold that thisis sexualaggression.
■ He won’t giveher money.
■ Her mother-in-law stays sheshould turnhim in to theauthorities.
Inhibiting FactorsInternal
■ He is the fatherof her children.
■ She does notbelieve in the system, fearsmore abuse.
■ She doesn’t thinkthis a matter tobe handled bythe authorities.
■ She thinks it isher fault.
■ She thinks hewill change.
■ She thinks thather jealousycauses hisinfidelity.
■ She is ashamedto have othersfind out abouther problem.
■ She thinks noone will believeher.
■ Fear.■ She thinks she
does not needmoney or prefersnot to insist on itin order to keepthe peace.
External
■ The abuser isreleased fromjail.
■ He threatens tokill her.
■ Her mother tellsher she shouldput up with it.
■ The church tellsher to forgivehim.
■ He asksforgiveness.
■ He leaves theother woman.
■ She thinks it isher duty toaccept herrelationship withher husband.
■ The authoritiesdo not force himto pay.
■ They do notmonitor hissupportpayments.
TABLE 13.1 SAMPLE MATRIX: FACTORS THAT MOTIVATE AN ABUSED WOMANTO SEEK HELP OR INHIBIT HER FROM SEEKING HELP
(From Shrader & Sagot, 2000.4)

A Practical Guide for Researchers and Activists 209
USING A COMPUTER FOR CODING ANDCATEGORIZING
Sometimes a more complex classificationscheme is necessary than can be managedand interpreted by hand. Here is wherecomputers can come in handy. Whenusing a computer for text-based analysis,the investigator still must “code” the data—that is associate a code word with piecesof the text that represent a certain theme.But the computer allows the investigator tosearch and organize large volumes of dataaccording to predefined codes and combi-nations of codes.
Many computer programs are availablefor use in coding and analyzing data, andall are different. Examples of some of themore common programs used for qualita-tive data analysis include HyperQual,NUDIST, Ethnograph, and QUALPRO.Generally these programs allow the investi-gator to attach one or more codes to differ-ent text segments. Data can then be sortedand resorted according to different themesand coding categories. A number of popu-lar qualitative software programs are avail-able commercially through Scolari Softwareat: http://12.22.103.11/.
We especially recommend consideringone of three free “share-ware” programsthat have been explicitly developed toassist researchers in the field of publichealth. The first, known as OpenCode, is aversatile, but highly accessible, programthat can be downloaded from the web siteof Umeå University, Sweden, athttp://www.umu.se/phmed/epidemi/forskning/open_code.html. The second is CDCEZ Text, a simple program designed by theCenters for Disease Control and Prevention(CDC) to facilitate analysis of open-endedresponses to structured questionnaires.CDC has also developed a third program,
called AnSWR, which is designed for morecomplex qualitative projects. Both CDCprograms can be downloaded fromhttp://www.cdc.gov/hiv/software.
There are also potential drawbacks tousing computers, and the time and costof using computers must be weighedagainst the potential benefits. For exam-ple, it is time-consuming to set up andcode data by computer and the investiga-tor must invest time, money, and energyinto acquiring and learning a new software program. Clearly, for manysmall projects, it is best to conduct theanalysis manually using highlighters and colored pens.
DATA REDUCTION ANDDATA DISPLAYS*
Data reduction means distilling the infor-mation to make visible the most essentialconcepts and relationships. The reductionprocess usually begins after all the datahave been collected, coded, and theresearcher is thoroughly familiar with thematerial. The goal of data reduction is to getthe bigger picture from the data and beginto discern distinctions between primary andsecondary themes.2 While coding helpsbreak down the data into smaller parts, datareduction is the process of abstracting backout from the particular to the conceptual.
To get a wider perspective on thedata, it is often helpful to use one ormore visual devices known as data dis-plays. Data display is a nonnarrative wayof analyzing and presenting qualitativedata. The analysis may be intra-case (thatis, analysis of the data related to a singlerespondent) or inter-case (comparativeanalysis of the data from two or morerespondents). As with any other aspect of qualitative analysis, it is necessary todocument the processes followed, the
A N A LY Z I N G Q U A L I TAT I V E D ATA z
* Information in this section is reprinted with permission from Shrader and Sagot, 2000.4

210 Researching Violence Against Women
conclusions generated, and the way inwhich the analysis influenced the subse-quent stages of the fieldwork.
Matrices, decision trees, and tax-onomies are examples of different datadisplay tools that can be useful for aidinganalysis as well as in presenting results.Following is a presentation of these three
methods using examples from the “RutaCrítica” study, a multi-country study quali-tative study on women’s responses to vio-lence performed by the Pan AmericanHealth Organization in ten Latin Americancountries. (See Box 5.4 for a descriptionof the study.) Keep in mind that it is notnecessary to display data in every way
C H A P T E R T H I R T E E Nz
FIGURE 13.2 SAMPLE DECISION TREE: MAKING THE DECISION TO SEEK HELP
Is my life indanger?
Are my children’s livesendangered?
Engages in the critical path(seeks support)
Yes No
Can I keep changing my behavior andthus avoid conflicts with him?
Engages in the critical path(seeks support)
Yes No
Engages in the critical path(seeks support)
Yes No
Will hechange?
Engages in the critical path(seeks support)
Stay in the situation; does notengage in the critical path
Yes No
(From Shrader & Sagot, 2000.4)

A Practical Guide for Researchers and Activists 211
suggested, only in those that can elucidatesome aspect of the analysis.
MatricesA matrix is a table that displays the intersec-tion of two or more concepts. It consists ofcells, which may be filled with summarytext, graphs, or other explanatory informa-tion. The matrix is very useful for summariz-ing a great deal of information or presentingcomparative information on a single sheet.Table 13.1, for example, represents a datamatrix used to summarize the factors thatemerged as critical to either motivating awoman affected by violence to seek outsidehelp or inhibiting her from seeking help.This particular matrix is taken from thePanama country report of the Ruta Críticastudy. It illustrates the complexity and detailthat can be included in a single table.
Decision treesA decision tree is a graphic representationthat depicts the sequence of decisions thatleads to an action. In general, the decisionsare formulated as a dichotomous question,i.e., one that is answered with “yes” or“no.” Arrows indicate the consequent ques-tion, depending on the answer given. Asimple decision tree shows the sequenceof decisions made by a person; a complexdecision tree shows the combined deci-sions of one or more persons.
Figure 13.2 illustrates a simple decisiontree derived from Ecuador data of PAHO’sRuta Crítica study. The figure illustratesthe thinking and decisions characteristicof an abused woman’s process of decid-ing whether to seek outside help for theviolence.
Flow chartsAlso known as an explanatory network,flow charts show the relationship betweentwo or more elements, emphasizing direc-tionality, causality, or temporary associa-tion. Geometric figures and arrows usually
are used to indicate temporary or causalrelationships between the concepts. Figure13.3 presents a sample flow chart showingthe path followed by a woman who seeksto escape from a violent relationship. Thechart includes an analysis of the timeelapsed between one violent incident andthe next one, as well as the time it takes tocarry out the trial. It reveals that thisrespondent was the victim of three seriousincidents of violence before finally obtain-ing the desired result—for him to stopdrinking and beating her.
TaxonomiesA taxonomy attempts to summarize con-cepts in a hierarchy that goes from thegreatest level of generalization to the great-est level of specificity. Taxonomies are use-ful for showing the relationship betweenmany separate concepts, joining conceptsthat share one or more characteristics incumulative stages.
Figure 13.4 presents an example of ataxonomy developed by the U.S. Centersfor Disease Control to describe severalforms of interpersonal violence.
ENSURING RIGOR INQUALITAT IVE RESEARCH
Ensuring rigor, while equally important inqualitative as in quantitative research, isaddressed somewhat differently by the twotraditions. Lincoln and Guba suggest thatthe four issues that must be addressed inany systematic enquiry into humans andhuman behavior are truth value, applica-bility, consistency, and neutrality.6 (SeeTable 13.2.) Whereas quantitative researchtends to use such criteria as external andinternal validity, reliability, and objectivityto assess whether research has been car-ried out and interpreted using acceptedscientific standards of rigor, qualitativeresearch tends to assess the trustworthi-ness of research in terms of credibility,
A N A LY Z I N G Q U A L I TAT I V E D ATA z

212 Researching Violence Against Women
transferability, dependability, and con-firmability. The naturalistic research tradi-tion does not assume that there is a singletruth that may be revealed by inquiry.Instead it affirms that many truths mayexist at the same time, and these may bediscovered by research, and at the sametime modified by the research endeavor
itself. Different standards are thereforeneeded to assess the rigor of qualitativeresearch. Table 13.2 presents a comparisonof how different aspects of rigor areaddressed in the different traditions.
Lincoln and Guba also propose alterna-tive criteria and techniques for establish-ing trustworthiness within a naturalistic
C H A P T E R T H I R T E E Nz
FIGURE 13.3 SAMPLE FLOW CHART: ITINERARY OF A WOMAN LIVING WITH VIOLENCE
Violent incident
Justice of the Peace (3 times)
Violent incident
Health unit (nurse)
Public prosecutor
Family court
Temporary asylum
Hearing/sentencing
Violent incident Family court
3–4 weeks
3 weeks
Escorting
Financial support
Psychological support
3 weeks without beatingher or drinking
From data presented in the final report of the critical path study in El Salvador.
5 m
onth
s be
twee
n se
rious
viole
nt in
cide
nts
5 m
onth
s be
twee
n se
rious
viole
nt in
cide
nts
Results
(From Shrader & Sagot, 2000.4)

A Practical Guide for Researchers and Activists 213
framework. In place of validity, credibilityis suggested as a criterion for determiningthe truth value of a qualitative study.According to Sandelowski,
A qualitative study is credible when itpresents such faithful descriptions or inter-pretations of a human experience that thepeople having that experience would imme-diately recognize it from those descriptionsor interpretations as their own. A study isalso credible when other people (otherresearchers or readers) can recognize theexperience when confronted with it afterhaving only read about it in a study.8
There are a variety of techniques that mayenhance credibility of a study. For example:
Prolonged engagement in the field.The researcher should be involved in acommunity or study site long enough to be
thoroughly oriented to the cultural and his-torical context, and to be able to detectand take into account possible distortionsdue to misinformation or his or her ownsubjective responses to the data.
Triangulation. The use of multiplesources, methods, and investigators toexplore the same topic can increase credi-bility. For example, if the goal of a study isto assess the quality of care given to sur-vivors of abuse in a community clinic, itmight be useful to compare the views ofhealth care providers with women whohave used the services. The use of multiplesources might reveal important differences,not only as to the overall level of client sat-isfaction, but also in the way that clientsand providers define quality of care. A mixof methods, for example, combining an
A N A LY Z I N G Q U A L I TAT I V E D ATA z
FIGURE 13.4 SAMPLE TAXONOMY: PUBLIC HEALTH PERSPECTIVES TOWARD VIOLENCE
This taxonomy was adapted from a typology used by Rosenberg et al. of the United States Centers for DiseaseControl and Prevention (CDC), Center for Injury Prevention and Control, Atlanta, Georgia. (Cited in Shrader andSagot, 2000.4)
Intentionalinjuries
Interpersonalviolence
Self-inflictedviolence
Familyviolence
Youthviolence
Groupviolence
Sexualassault
Economicviolence
Childabuse
Spousalabuse
Abuse ofthe elderly
Hatecrimes War Abduction Theft
Gangviolence Delinquency Rape Rape of
a minorSexual
harassment
Suicide Attemptedsuicide
Bulimia/Anorexia Alcoholism Tobacco
useDrug
addiction

214 Researching Violence Against Women
exit survey of clients with in-depth inter-views, focus groups, or reviews of medicalcharts, might provide additional insight.Having two different researchers codeinterview transcripts and compare resultsafterwards is another form of triangulationthat may increase the credibility of thefindings.
Negative case analysis. This refers toseeking cases actively that appear to beexceptions to the general pattern, as a wayof testing and refining hypotheses. Themethod relies on the analysis of “outliers”to improve the credibility of the findings.
Member checking. Member checkingrefers to the process by which data, conclu-sions, and interpretations are presented tomembers of the groups from which thedata were collected. It is a powerful tech-nique for establishing credibility. Memberchecking may be performed throughout theresearch process, through both formal andinformal sessions. It allows stakeholders the
opportunity to react to the data and to cor-rect errors in the collection and interpreta-tion of data. Most importantly, it helps toestablish the meaningfulness of the findingsand interpretations. In a review of CentralAmerican health programs addressing gen-der-based violence, the preliminary resultswere presented to representatives from thedifferent countries that participated in theoriginal focus group discussions. The pur-pose of the session was to correct factualerrors, as well as to hear reactions to theoverall conclusions of the study. Not onlydid the discussion strengthen the interpreta-tion of the findings, but it also createdownership of the findings among the partic-ipants. The study results were disseminatedand discussed widely among the programs,and many of the recommendations wereimplemented.
Qualitative research refers to the trans-ferability of findings instead of externalvalidity or generalizability. In surveyresearch, the ability to generalize findingsto a broader population depends largelyon how representative the sample is withregard to demographic characteristics andother key variables. Since qualitativeresearch relies on purposive rather thanrandom sampling, there is no expectationthat findings from one small group ofstudy participants can be statistically repre-sentative of a larger population. Theorygenerated from qualitative research maywell be generalizable to a broader popula-tion. As Dahlgren and colleagues argue,qualitative researchers aim for analyticalgeneralizations, taking into account that,
Each subject has been selected to con-tribute to the theory that is being developed,and the knowledge gained from this theoryshould fit all scenarios that may be identi-fied in a larger population. Hence the theoryis applicable also beyond the study sample toall similar situations, questions and prob-lems, regardless of demographic characteris-tics. In this way, qualitative researchers are
C H A P T E R T H I R T E E Nz
AspectTruth value
Applicability
Consistency
Neutrality
QualitativecriteriaCredibility
Transferability
Dependability
Confirmability
QuantitativecriteriaInternal validity
External validity
Reliability
Objectivity
QuestionaskedHave we reallymeasured whatwe set out tomeasure?
How applicableare our results toother subjects andother contexts?
Would our find-ings be repeatedif our researchwere replicated inthe same contextwith the samesubjects?
To what extentare our findingsaffected bypersonal interestsand biases?
TABLE 13.2 CRITERIA ASSESSING THE TRUSTWORTHINESS OF RESEARCHFINDINGS ACCORDING TO QUANTITATIVE AND QUALITATIVE
RESEARCH TRADITIONS
(From Dalgren, et al, 2003.7)

A Practical Guide for Researchers and Activists 215
no less able to generalize beyond their sam-ple than are epidemiologists. 7
In quantitative research, consistency orreliability of results is a key aspect of trust-worthiness. If another researcher con-ducted the same study using the same orsimilar methods on the same or similarpopulation, would the same results beobtained? Reliability is enhanced in quanti-tative research by such measures as accu-rate instruments and equipment,well-trained fieldworkers, and uniform datacollection procedures. In contrast, qualita-tive research is based on the premise thatresearchers and study participants are inti-mately related, and their interactioninevitably shapes the research process.Therefore, there is no pretense that thesame results could be achieved with differ-ent researchers and participants.
Accordingly, qualitative research isassessed by its dependability, or the degreeto which the researcher can describe andaccount for the way data were collected,interpreted, and how changing conditionswere addressed throughout the process.The research process may be documentedby means of an audit trail, including fieldnotes, raw data (such as transcripts anddiagrams) and process notes (procedures,designs, and strategies.) An audit trailshould allow another to follow the “deci-sion trail” used by the researcher.6
Finally, quantitative and qualitative tra-ditions diverge on the issue of neutrality.Quantitative researchers aspire to main-tain an objective attitude during theresearch process, and to avoid lettingtheir feelings or subjective views influ-ence the data collection or statisticalanalysis. Qualitative researchers arguethat subjectivity is unavoidable, and thatthe interaction between participants andresearchers actually enriches qualitativeresearch. The neutrality of the data ratherthan that of the researcher is sought,using the criteria of confirmability. Audit
trails also help establish confirmability. Ifthe research can be confirmed the auditorshould be able to find conclusionsgrounded in the data.6
1. Miles M, Huberman AM. Qualitative DataAnalysis: An Expanded Sourcebook. 2nd ed.Thousand Oaks, California: Sage Publications;1994.
2. Ulin P, Robinson E, Tolley E, McNeill E.Qualitative Methods: A Field Guide for AppliedResearch in Sexual and Reproductive Health.Research Triangle Park: Family HealthInternational; 2002.
3. Creswell JW. Research Design: Qualitative andQuantitative Approaches. Thousand Oaks,California: Sage Publications; 1994.
4. Shrader E, Sagot M. Domestic Violence: Women'sWay Out. Washington, DC: Pan American HealthOrganization; 2000.
5. Strauss A, Corbin J. Basics of QualitativeResearch: Grounded Theory Procedures andTechniques. Newbury Park, California: SagePublications; 1990.
6. Lincoln Y, Guba E. Naturalistic Inquiry. London,UK: Sage; 1985.
7. Dahlgren L, Emmelin M, Winqvist A. QualitativeApproaches for International Public Health.Umeå, Sweden: Umeå University; 2003.
8. Sandelowski M. The problem of rigor in qualita-tive research. Advances in Nursing Science.1986;8(3):27-37.
A N A LY Z I N G Q U A L I TAT I V E D ATA z

o
14PH
OTO
BY
HAF
M JA
NSE
N

A Practical Guide for Researchers and Activists 217
o
university-based researcherswho presented their resultsonly at international confer-ences or in academic journals.
Fortunately this approach isbeing supplanted by a newethic of research in whichresearchers and advocates joinforces to ensure that researchfindings are used for socialchange. This section includesseveral examples of how dif-ferent research teams haveused their findings strategi-cally to change laws, influ-ence policy, design serviceprograms, and place the issueof violence against women onthe public agenda.
The first step is to make a list of differ-ent constituent groups and individuals thatshould be made aware of the researchfindings. The study’s advisory group willbe particularly helpful in this regard. Next strategize about the different meansand venues available for reaching these
Research is a means to an end. Aresearcher’s task is only complete once thefindings from a research project are putinto the hands of the individuals andorganizations positioned to use them. Forviolence research, this generally includespolicy makers, legislators, advocacygroups, the academic community, serviceproviders, and the respondents themselves.
This chapter briefly highlights some cre-ative ways that different research teamshave approached these challenges.
OUTREACH TO KEYCONSTITUENCIES
Research can either be a positive force forchange or it can sit on a shelf, advancingonly the career paths of individual investi-gators. The field of international violenceresearch is filled with examples of both.
In the past, it was not uncommon forwomen’s groups and others working onviolence to be totally unaware that researchon violence had been conducted in theircountry, often by foreign investigators or
C H A P T E R F O U R T E E N
From Research to Action
Topics covered in this chapter:
Outreach to key constituenciesMatching your message to your audienceSharing findings with the communityReaching beyond your borders
Example of a Stakeholder List
• Ministry of Health• Office of Women’s Affairs• Members of Parliament,
especially Women’sCommissions
• Local women’s groups/net-works
• Local rape crisis center• Local journalists• School of Public Health• Department of Justice• Local radio—call-in show• School of Social Work• Catholic diocese• Municipal authorities

218 Researching Violence Against Women
C H A P T E R F O U R T E E Noaudiences. Also recognize that the type ofmessage and style of presentation that willbe persuasive to different audiences willlikely vary. (See Matching Your Message toYour Audience, below.)
Let’s Create Love and Peace inIntimate Relationships: Nationaldissemination of research findingsin ThailandIt may be possible to reach a number of tar-get groups at once by holding a stakeholdermeeting or a symposium at which the resultsare presented and discussed. Members ofthe Thai research team of the WHO multi-country study, for example, worked with theTask Force to End Violence Against Womenand the Coalition for Women’s Advancementto organize a month-long program of activi-ties on violence against women in Thailand.The month was kicked off with a press con-ference to present the Thai findings from theWHO multi-country study and to highlightcurrent activities of organizations working toeliminate violence and gender discriminationin Thailand.
To unify the campaign and project a posi-tive image, the researchers developed aneye-catching logo and printed 20,000 stickerswith the slogan “Let’s create love and peacein intimate relationships.” In addition, theteam distributed over 2,000 fact sheets andposters about violence against women (seeFigure 14.1). The key activity of the monthwas a two-day national seminar, held at theNational Women’s Council in Bangkok, andattended by more than 400 people. On thefirst day, the research team made an officialpresentation of the research and its findings.On the second day, six women with directexperiences of violence shared their ownstories of pain and survival followed by pre-sentations by other researchers and well-known experts in the field. Outside theseminar room, various concerned organiza-tions set up exhibit booths to advertise theirorganizations and services.
The research team evaluated the impact ofthe activities throughout the ensuing months,including tracking coverage of the findings inthe media. Overall, the research findings werepresented at events in more than 20 provinces.Significantly, findings on the prevalence offorced sex in marriage also proved critical toa legislative campaign to amend Article 276of Thailand’s criminal code that gave immu-nity to men who rape their wives.
Silence for the Sake of Harmony:Engaging local leaders in the dis-semination of results in IndonesiaThe SEHATI Research Project, a partner-ship between Gadjah Mada University andRifka Annisa Women’s Crisis Center (bothin Indonesia), Umeå University in Sweden,and PATH, carried out a prevalence studyin Central Java that showed that one in tenwomen had been physically abused by anintimate partner. To reach a wider audi-ence, researchers asked the Queen of theProvince of Yogyakarta in Central Java tohost the launch of their report. The launchwas attended by local authorities, media,
FIGURE 14.1 LET’S CREATE LOVE AND PEACEIN INTIMATE RELATIONSHIPS WAS THE
MESSAGE TIED TO THE DISSEMINATION OFSTUDY RESULTS IN THAILAND

A Practical Guide for Researchers and Activists 219
and religious and community leaders. TheQueen also wrote a preface to the vio-lence report, lending legitimacy to thisonce taboo area of research. A similar ses-sion was held in Jakarta, the capital ofIndonesia, hosted by the Minister ofHealth and the Minister of Women’sEmpowerment, both of whom also wroteprefaces for the report (Figure 14.2).
MATCHING YOURMESSAGE TO YOURAUDIENCE
A key to achieving impact is to tailor yourmessage to the various audiences that youseek to influence. The language, style, andmessage that may be persuasive to onegroup may be wholly unconvincing—orunintelligible—to another. The way thedata are presented also should vary. For
technical, academic, or policy audiences, itis important to follow scientific conventionand to include all required backgroundinformation so that others can evaluate thefindings, such as sample size, measures ofsignificance, and margins of error. Forother audiences, this information is merelyconfusing and detracts from the message.
Candies in Hell: Using research forsocial change in Nicaragua A good example of how the same informa-tion can be adapted to different audiencescomes from the Nicaraguan Network ofWomen Against Violence. The Networkcollaborated with researchers from theUniversity of Nicaragua in León andSweden’s Umeå University to conduct in-depth interviews of battered women and ahousehold survey on the rate of domesticviolence among women in León. The basic
F R O M R E S E A R C H T O A C T I O N o
FIGURE 14.2 STUDY REPORT FROM CENTRAL JAVA, WHICH INCLUDED PREFACES FROM THEQUEEN OF THE PROVINCE OF YOGYAKARTA, THE INDONESIAN MINISTER OF HEALTH,
AND THE MINISTER OF WOMEN’S EMPOWERMENT
(From Hakimi et al, 2002.1)

220 Researching Violence Against Women
finding of the study—that 52 percent ofever-married women ages 15-49 have beenhit, slapped, or beaten by a partner—waspresented in a variety of ways to make dif-ferent points to different audiences.
The results were presented in a publica-tion using graphs and charts to appeal tothe professional and scientific communities.
To influence health policy and the behaviorof health workers, researchers and theNetwork cosponsored a symposium at themedical school in León, where the resultswere presented to local providers, health-related NGOs, and ministry staff. The samepresentations were later repeated for anational audience at the public health
C H A P T E R F O U R T E E No
FIGURE 14.3 PRESENTING RESEARCH RESULTS IN DIFFERENT WAYS FORDIVERSE AUDIENCES IN NICARAGUA
(From Ellsberg et al, 19972 and Ellsberg et al, 1999.3)

A Practical Guide for Researchers and Activists 221
Several activities were also undertakento reach legislators and to use the resultsof the study to push for new domestic vio-lence legislation. The results were includedin the Preamble of the Draft Penal CodeReforms for the Prevention and Sanction ofFamily Violence, which was drafted andpresented to the National Assembly by theNational Network of Women AgainstViolence. But more significantly, the find-ings were translated into simple languageand incorporated into a national petitioncampaign asking legislators to approve thedomestic violence bill pending before theNational Assembly. Network members held“petition-signing parties” and reproducedthe petition as a full-page, tear-out ad inthe national newspaper. In a few months,more than 16,000 signatures were obtainedand presented in great packages to parlia-mentarians. They were so overwhelmed bythe public pressure, especially since it wasan election year, that they voted unani-mously to pass the law (Figure 14.4).
SHARING F INDINGS WITHTHE COMMUNITY
One step often overlooked in research isthe process of communicating findingsback to the community. Traditionallyresearch has been an “extrac-tive” process whereby resultsand insights derived from theresearch seldom make theirway back to the originalrespondents. In recent years,there has been a move toward“giving something back” to thecommunity in addition to shar-ing the results of research withpolicy makers, opinion leaders,and front-line providers. As the quote fromthe respondent in Papua New Guineamakes clear, community members appreci-ate the opportunity to see what comes ofthe time they invest with researchers.
F R O M R E S E A R C H T O A C T I O N
school in Managua. Here, the emphasis wason the health consequences of abuse andthe potential role of health workers inresponding to the problem.
These meetings helped launch severalinitiatives, including the production of aspecialized manual for health workers onresponding to abuse and the developmentof educational material on violence forincorporation into medical school andnursing curricula.
To reach community members, espe-cially women, the Network published thefindings in the form of a popular bookletentitled Ya No Quiero Confites en elInfierno (I No Longer Want Candies inHell). The booklet told the story of AnaCristina, one of the informants in the study,and the booklet’s margins included easy-to-understand statistics drawn from the survey. The booklet included basic infor-mation about where women could get help as well as questions to guide groupdiscussions (see Figure 14.3).
The prevalence data were also men-tioned in a pocket-sized card urging bat-tered women to get help, under the title“You are not alone: recent studies haveshown that one out of every two womenhas been beaten by her husband, and oneout of every four is beaten each year.”
o
“I would like to ask if youfind something to help us orto help us know more, canyou please come again? Donot take our stories withoutcoming back and telling uswhat you have learned.”Woman from Papua NewGuinea

222 Researching Violence Against Women
Sometimes this process of sharing cantake the form of directly communicatingthe findings back to the community viaworkshops or focus groups. Sharing pre-liminary results with community memberscan be an excellent way to test the validityof findings—do they ring true to thosewho participated in the research?Respondents may also be able to offerinsights that are helpful in interpreting sur-prising or unexpected findings.
Community Theater: Disseminating research findings in Liberia, Uganda, and KenyaInvestigators have also used a variety ofinnovative techniques to communicate theessence of research findings back to low-lit-eracy populations. In Liberia, for example,
researchers studying sexual coercion duringwar translated their findings into dramavignettes to communicate their results backto rural women. Based on survey findings,the researchers derived a profile that repre-sented the average experiences of thewomen surveyed. Local health promotersthen worked with researchers to develop astoryline that reflected the experiences ofthe majority of women in the survey. Thehealth promoters acted out the experiencesthat women discussed in the survey andthen the community discussed the “results.”4
Similar techniques were used in Uganda bythe organizations CEDOVIP and RaisingVoices (See Figure 14.5).
In Kenya, theater was used to communi-cate findings of a study carried out by theKenya Adolescent Reproductive Health
C H A P T E R F O U R T E E No
FIGURE 14.4 PETITION TO THE MEMBERS OF THE NATIONAL ASSEMBLY, CITING THELEÓN RESEARCH AND ASKING FOR A NEW DOMESTIC VIOLENCE LAW TO BE PASSED
These letters were distributed in community meetings, parties, and through the newspapers. The NationalNetwork of Women Against Violence collected more than 16,000 signatures in the space of a few weeks.
(From Ellsberg et al, 1997.2)
PHO
TO B
Y H
AFM
JAN
SEN

A Practical Guide for Researchers and Activists 223
Project (KARHP). The project was launchedto bring reproductive health education andsupport to communities in Vihiga andBusia districts. Dozens of parents, teachers,religious and political leaders, health clinicstaff, and hundreds of young people, cho-sen for their capacity to speak candidly totheir peers, were recruited by KARHP toreach out with information on sexual vio-lence, sexually transmitted diseases, andother reproductive health issues.
Like most development programs,KARHP used baseline and diagnostic stud-ies to evaluate its effect on the communi-ties it serves. But the question was how tocommunicate those findings to the relativestakeholders—people and organizations ina position to interpret, even improve onhow such information relates to our work.Using a new dissemination methodology,KARHP found two innovative ways:
1. The project implementation team drafteda summary report containing key findings
and presented them to stakeholders—many of whom did not speak English—in simple format and language.
2. The team then selected two local youththeatre groups—Visions 3000 based inKakamega and Mwangaza in Mambale
F R O M R E S E A R C H T O A C T I O N o
FIGURE 14.5 UGANDAN COMMUNITY THEATER GROUP PERFORMS A PLAY ON THE LINKBETWEEN HIV AND DOMESTIC VIOLENCE IN A KAMPALA MARKET
Dancers and drummersopening a street theaterperformance inKampala, Uganda.
PHO
TO B
Y M
. ELLS
BERG
PHO
TO B
Y M
. ELLS
BERG

224 Researching Violence Against Women
District—and trained them to presentkey learnings in an entertaining andvisually exciting manner. To prepare, theactors were provided with a presentationof the major findings, general informa-tion on adolescent reproductive health,and tips on communication skills. A the-ater consultant worked with both groupsto develop “storylines” for skits thatrequired audience participation.
Both the skits and the summary reportwere then presented in three locations inwestern Kenya to an audience thatincluded government staff, religious lead-ers, village elders, local groups, and com-munity members. Not only was theinformation shared with the community,but the researchers had an opportunity tovet their findings and ask the community ifthe skits represented their communities.These research dissemination sessionshelped the community to articulate theirsituation and own the problems. Then,
with everyone sharing a joint understand-ing of the situation, the community wasactively engaged in designing interventionsto respond to the challenges that youngpeople face today.5
Reaching communities through traditional art: The Jijenge! mural campaign against violence in Tanzania6, 7
In a similar effort, staff members at Jijenge!,a women’s health center in Mwanza,Tanzania, took great pains to convey backto the community the results of its needsassessment on domestic violence. (See Box5.2 for a description of the participatorystudy.) This was done through a workshopwith the community volunteers and aseries of community street meetings. Aspart of its multifaceted media campaignagainst violence, Jijenge! also appropriatedthe folk-art tradition of mural painting as ameans to communicate important messagesabout family violence and gender issues. Aseries of bright and colorful murals wasdesigned and painted on small walls out-side kiosks, shops, and buildings all overMwanza municipality. The images and sim-ple yet controversial messages wereintended to stimulate dialogue. Two pri-mary characters—a woman and man intheir early to mid-30s—were created andused in most of the murals. These charac-ters are shown in conversation with eachother and the audience (Figure 14.6). Onemural, for example, shows the womanwith her arm around her husband and thehusband confidently stating, “I don’t beatmy wife, we talk about our problemsinstead.” A rights statement such as“Women have a right not to be beaten!”appears in each mural to relate practicallife choices to the broader framework ofwomen’s rights. The murals address manyissues concerning violence against women,including emotional well-being, solidarityamong women, and causal factors of
C H A P T E R F O U R T E E No
CEDOVIP activists carry out informal
discussions with menunder a mural painting
on domestic violence inKampala, Uganda. PH
OTO
BY
M. E
LLSBE
RG

A Practical Guide for Researchers and Activists 225
violence such as inequality and economicdependence. Similar techniques are nowused successfully by the Ugandan organi-zations CEDOVIP and Raising Voices,which grew out of the Jijenge! experiencein Tanzania.
A disaster that men can prevent:A multimedia campaign targetingNicaraguan menIn other cases, research is used explicitlyas part of a communication for socialchange strategy. For example, findingsfrom the study on men’s violence inNicaragua (see Box 5.6) were incorporatedinto a mass media campaign using televi-sion and radio commercials, bumper stick-ers, T-shirts, community workshops, andbillboards. The messages targeted men,and referring to Hurricane Mitch that hadrecently devastated the region, suggestedthat “Violence against women is one disas-ter that we men can prevent” (Figure 14.7).
Matlakala’s Story: Communicationfor social change in South AfricaAnother example of how effective research
can be in social change efforts is providedby Soul City in South Africa. The Soul CityInstitute for Health and DevelopmentCommunication produces a prime time tel-evision drama, a radio drama in nine lan-guages, and full-color information bookletsto promote social change around a varietyof health and social issues. Soul City’sfourth series focused on gender-based vio-lence, including domestic violence andsexual harassment. In order to develop thestoryline about a woman named Matlakala,formative research was carried out withaudience members and experts in the fieldof gender-based violence. The story alsoincorporated findings from a survey onviolence recently carried out in threeprovinces by the South African MedicalResearch Council.8 Partnerships were estab-lished between Soul City and organizationsactive in the field, such as the NationalNetwork on Violence Against Women, acoalition of 1,500 activists and communica-tion organizations from rural and urbanareas. These partnerships aimed to ensurethat the messages developed conveyedappropriate and accurate information on
F R O M R E S E A R C H T O A C T I O N o
FIGURE 14.6. MURALS PAINTED ON COMMUNITY WALLS IN TANZANIA AND UGANDATO ENCOURAGE COMMUNITY DISCUSSION OF DOMESTIC VIOLENCE

226 Researching Violence Against Women
women’s rights, raising awareness of thetopic and promoting changes in attitudes,social norms, and practices around gender-based violence to help connect audiencesto needed services, including through atoll-free helpline; to promote individualand community action; to create an envi-ronment conducive to legislative change;and to develop training materials on gen-der-based violence for various audiences.
The Soul City series on violence thenenlisted independent researchers to evalu-ate the program through three studies:
■ A national survey carried out before theshow started, and nine months later,that included face-to-face interviewswith 2,000 respondents.
■ A sentinel site study conducted severaltimes in a rural and an urban site, with
a cohort sample of 500 respondents atbaseline, twice during the time that SoulCity’s fourth series was on the air, andpost intervention.
■ A national qualitative impact assessmentcomposed of 31 focus group interviewsand 30 semistructured interviews withcommunity leaders.
The evaluation found an associationbetween exposure to Soul City media andincreases in knowledge and awareness ofthe population regarding domestic vio-lence and domestic violence legislation.The results of the evaluation were pre-sented in numerous documents and peer-reviewed journals, as well as on aneasy-to-read fact sheet (Figure 14.8).9-11
Even more importantly, the show and theresearch findings helped create a positive
C H A P T E R F O U R T E E No
FIGURE 14.7 MEDIA CAMPAIGN FOR MEN CARRIED OUT BYPUNTOS DE ENCUENTRO FOUNDATION IN NICARAGUA BASED ON FINDINGS
OF QUALITATIVE RESEARCH ON MALE VIOLENCE AGAINST WOMEN

A Practical Guide for Researchers and Activists 227
social environment for reforming domesticviolence legislation.
Elsewhere, researchers have turned to the Internet to publicize findings ofdomestic violence research and seek inputand feedback from a broader constituency.The Thai team of the WHO multi-country
study posted the results of their survey on a local Thai-language web page thatincluded a “bulletin board” where viewerscould post their own comments and ques-tions. The web page received thousands ofhits and comments during its first monthof operation.
F R O M R E S E A R C H T O A C T I O N o
FIGURE 14.8 COMMUNICATION MATERIALS IN ENGLISH AND ZULU AND AN EVALUATION FACT SHEETPRODUCED BY SOUL CITY IN SOUTH AFRICA

228 Researching Violence Against Women
REACHING BEYOND YOUR BORDERS
In addition to local outreach, it is alsoimportant to consider reaching audiencesbeyond local borders. Given the generallack of data available on violence againstwomen, every research study is a poten-tially important addition to the globalknowledge base.
Consider publishing your results in theacademic literature, especially in a peer-reviewed journal indexed in one of thecomputerized services such as IndexMedicus, Psych-Lit, or POPLINE. Then,individuals who search for articles on vio-lence will be able to access your findings.
Additionally, the Center for CommunicationPrograms at Johns Hopkins University inBaltimore, Maryland, and the United NationsDevelopment Fund for Women (UNIFEM)have joined forces to produce a centraldepository for information on violenceagainst women, including documents, jour-nal articles, training materials, posters, and
TV and radio programs. Materials forwardedto the Center will be entered into theCenter’s online service, known as POPLINE,and will be featured on the Center’s EndViolence Against Women web site(http://www.endvaw.org). Individuals cansearch for materials using key words, andcopies will be sent to developing countrypractitioners free of charge.
C H A P T E R F O U R T E E No
The findings of theWHO study in Namibia
were published in thepopular women’s maga-
zine Sister Namibia.

A Practical Guide for Researchers and Activists 229
1. Hakimi M, Nur Hayati E, Ellsberg M, Winkvist A.Silence for the Sake of Harmony: DomesticViolence and Health in Central Java,Indonesia.Yogyakarta, Indonesia: Gadjah MadaUniversity, Rifka Annisa, PATH, Umeå University;2002.
2. Ellsberg M, Liljestrand J, Winkvist A. TheNicaraguan Network of Women Against Violence:Using research and action for change.Reproductive Health Matters. 1997;10:82-92.
3. Ellsberg MC, Peña R, Herrera A, Liljestrand J,Winkvist A. Wife abuse among women of child-bearing age in Nicaragua. American Journal ofPublic Health. 1999;89(2):241-244.
4. Swiss S, Jennings PJ, Aryee GV, et al. Violenceagainst women during the Liberian civil conflict.Journal of the American Medical Association.1998;279:625-629.
5. Folsom M. Using Theater to Disseminate ResearchFindings in Kenya. Personal Communication.Nairobi, Kenya; 2004.
6. Michau L. Mobilizing Communities to EndViolence Against Women in Tanzania. In:Haberland N, Measham D, editors. Responding toCairo: Case Studies of Changing Practice inReproductive Health and Family Planning. NewYork, New York: Population Council; 2002.
7. Michau L, Naker D. Mobilising Communities toPrevent Domestic Violence. Kampala, Uganda:Raising Voices; 2003.
8. Jewkes R, Penn-Kekana L, Levin J, Ratsaka M,Schrieber M. He Must Give Me Money, He Mustn'tBeat Me: Violence Against Women in Three SouthAfrican Provinces. Pretoria, South Africa: MedicalResearch Council; 1999.
9. Soul City Institute for Health and DevelopmentCommunication. Soul City 4 Impact Evaluation:Violence against Women, Vol. 1. Johannesburg:Soul City Institute for Health and DevelopmentCommunication; 2001.
10.Soul City Institute for Health and DevelopmentCommunication. Multi-Media Audience Reception.Johannesburg, South Africa: Soul City Institute forHealth and Development Communication; 2000.
11.Usdin S, Christofides N, Malepe L, Aadielah M.The value of advocacy in promoting socialchange: Implementing the new DomesticViolence Act in South Africa. Reproductive HealthMatters. 2000;8(16):55-65.
F R O M R E S E A R C H T O A C T I O N o

1
APH
OTO
BY
HAF
M JA
NSE
N

A Practical Guide for Researchers and Activists 231
1
and 802). Finally there are two questionsthat explore whether the woman herselfused violence against the most recent part-ner who used violence against her, andwhether this aggression was offensive or inself-defence (904 and 905). The instrumentdoes not aim to document every abusiveaction that a woman may experience, butrather aims to assess whether the respon-dent is likely to be experiencing ‘severe’and/or ‘moderate’ levels of abuse in herrelationship. The questions on injury con-tribute to providing a crude measure of theseverity of the violence. They should not beinterpreted as a measure of the healtheffects of violence as, in practice, the healtheffects of violence are far more wide-rang-ing than immediate injury. The questionsabout whether the respondent was everphysically violent herself toward her partnerand whether this violence was offensive orin self-defence, provide information criticalto interpreting the context of the violence.
Because of the complexity of definingand measuring emotional abuse in a waythat is relevant and meaningful across cul-tures, the questions regarding emotional vio-lence should be considered as a startingpoint, rather than a comprehensive measureof all forms of emotional abuse. Researchersare encouraged to add questions referring to
WHO VIOLENCE AGAINSTWOMEN INSTRUMENT
This instrument consists of two sets of ques-tions designed to capture information criticalto assessing the prevalence, frequency andseverity of different forms of violence againstwomen, perpetrated both by intimate part-ners and others. The first set of questionsfocuses on violence by intimate partners onlyand should be used in its entirety to measureviolence by intimate partners. The second setaddressing violence by others, can be addedonto the first set if violence against women isexplored in a broader context.
Violence against women by intimate partnersThe first set of questions focuses on vio-lence perpetrated against women by theirintimate partners (questions 703 to 706, 709,801, 802, 904 and 905 in the core question-naire). These questions on partner violenceexplore aspects of controlling behaviours,emotional abuse, physical violence, and sex-ual violence (703-706) as well as physicalviolence during pregnancy (709) by currentor former intimate partners. This sectionalso has questions for women who havesuffered physical violence by an intimatepartner, that assess the degree of injury (801
A P P E N D I X O N E
The WHO Multi-countryStudy on Women’s Healthand Domestic ViolenceAgainst Women

232 Researching Violence Against Women
A P P E N D I X O N E1
locally relevant forms of abuse. Because solittle is presently known about measuringemotional violence across cultures, theWHO Multi-country study does not includeemotional violence when reporting theprevalence of violence by intimate partners.Instead, the study reports lifetime and 12month prevalence of physical, sexual, andphysical or sexual violence by intimatepartners.
In the WHO study, this section of theinstrument is applied primarily to womenwho have had an intimate partner withwhom they have co-habitated. In countrieswhere it is common that women have inti-mate partnerships without co-habitating,the instrument can be used to capture “dat-ing” violence with only minor accommoda-tions in language.
Violence against women by others than intimate partnersThe second part of the instrument includes aset of questions (questions 1001-1003 and1201 in the core questionnaire) designed toaddress other types of violence that womenhave experienced outside of the context ofan intimate partner relationship. Questions1001-1003 enable the collection of minimaldata on the prevalence of sexual abuse inchildhood and on the prevalence of physicaland sexual violence in adulthood by peopleother than intimate partners. These questionsdo not capture physical, emotional or othertypes of neglect or maltreatment in child-hood. Question 1201 offers the respondentthe opportunity to report childhood sexualabuse in a linked concealed way. This sec-tion of the instrument may be asked of allwomen, regardless of relationship status.
USE OF WHO STUDY PROTOCOL AND QUEST IONNAIRE
The WHO Study questionnaire, togetherwith the protocol and other supporting
materials such as the training manuals anddata entry system, have been developed topermit the collection of standardised data,and thus facilitate cross-cultural compar-isons. To this end, wide dissemination andutilisation of the questionnaire is encour-aged. While recognising that some adapta-tion to local conditions may be necessary,these should be minimal, in order toensure that as far as possible, comparabil-ity can be maintained. This is particularlythe case for the questions that make upthe Violence Against Women Instrument.
Those using the WHO Study protocoland/or questionnaire are requested toacknowledge the WHO source documentsin all publications and/or documents thatarise from study (as detailed below). In addi-tion, WHO will make available to interestedparties all manuals, accompanying documen-tation and data entry programs developedfor use in the WHO Multi-country Study inexchange for a copy of the final, cleaneddata set, for cross-national comparison.
Some researchers may wish to generateprevalence estimates comparable to theWHO Multi-country Study, but may notwant to fully replicate the study. In order toensure that the prevalence data obtained iscomparable to the WHO study, investigatorsshould, at a minimum, incorporate theWHO Violence Against WomenInstrument (either the first section on part-ner violence alone, or also the questions onexperiences of violence by others). Again,for comparison purposes, the sample shouldenable the disaggregation of data to obtainprevalence estimates for a representativesample of ever-partnered women 15-49.
In addition to the WHO ViolenceAgainst Women Instrument, researchersmay choose to incorporate other questionsand/or entire sections from the WHO corequestionnaire. In such cases theresearchers should acknowledge the WHOquestionnaire in the following manner:
“This study adheres to the WHO

A Practical Guide for Researchers and Activists 233
ethical guidelines for the conduct ofviolence against women research anduses the WHO Violence Against WomenInstrument as developed for use in theWHO Multi-country Study on Women’sHealth and Domestic Violence AgainstWomen. Additionally it incorporatesquestions/sections from the WHO study
questionnaire (describe which ques-tions/section were used).”
For copies of the various documents mentionedabove, as well as further information on the studyand on arrangements to replicate the study can beobtained from Dr Claudia Garcia-Moreno, StudyCoordinator ([email protected]) or from DrHenriette Jansen, Epidemiologist to the Study([email protected]).
A P P E N D I X O N E 1
WHO VIOLENCE AGAINST WOMEN INSTRUMENT Incorporated in the Core Questionnaire Version 10
WHO Multi-country Study on Women’s Health and Domestic Violence Against Women20 September 2003
Hello, my name is *. I work for *. We are conducting a survey in STUDY LOCATION to learn about women’shealth and life experiences. You have been chosen by chance (as in a lottery / raffle) to participate in the study.
I want to assure you that all of your answers will be kept strictly secret. I will not keep a record of your name oraddress. You have the right to stop the interview at any time, or to skip any questions that you don’t want toanswer. There are no right or wrong answers. Some of the topics may be difficult to discuss, but many womenhave found it useful to have the opportunity to talk.
Your participation is completely voluntary but your experiences could be very helpful to other women in COUNTRY.
Do you have any questions?
(The interview takes approximately * minutes to complete). Do you agree to be interviewed?
NOTE WHETHER RESPONDENT AGREES TO INTERVIEW OR NOT
[ ] DOES NOT AGREE TO BE INTERVIEWED THANK PARTICIPANT FOR HER TIME AND END
[ ] AGREES TO BE INTERVIEWED
Is now a good time to talk?
It’s very important that we talk in private. Is this a good place to hold the interview, or is there somewhere else thatyou would like to go?
_______________________________________________________________________________________________
TO BE COMPLETED BY INTERVIEWER
I certify that I have read the above consent procedure to the participant.
Signed: ________________________________________________________________________________________
INDIVIDUAL CONSENT FORM

234 Researching Violence Against Women
A P P E N D I X O N E1
SECTION 7 RESPONDENT AND HER PARTNER
EVER MARRIED / EVER LIVING WITH A MAN / EVER SEXUAL PARTNER
[ ]
NEVER MARRIED / NEVER LIVED WITH A MAN / NEVER SEXUAL PARTNER
[ ] S.10
When two people marry or live together, they usually share both good and bad moments. I would now like to ask you somequestions about your current and past relationships and how your husband / partner treats (treated) you. If anyone interruptsus I will change the topic of conversation. I would again like to assure you that your answers will be kept secret, and thatyou do not have to answer any questions that you do not want to. May I continue?
703 I am now going to ask you about some situations that aretrue for many women. Thinking about your (current or most recent) husband / partner, would you say it isgenerally true that he: a) Tries to keep you from seeing your friends?b) Tries to restrict contact with your family of birth?c) Insists on knowing where you are at all times?d) Ignores you and treats you indifferently?e) Gets angry if you speak with another man?f) Is often suspicious that you are unfaithful?g) Expects you to ask his permission before seeking
health care for yourself?
a) SEEING FRIENDS b) CONTACT FAMILYc) WANTS TO KNOW d) IGNORES YOU e) GETS ANGRYf) SUSPICIOUS g) HEALTH CENTRE
YES
1 1 1 1 1 1 1
NO
2 2 2 2 2 2 2
DK
8 8 8 8 8 8 8
The next questions are about things thathappen to many women, and that your current partner, or any other partner may have done to you.
Has your current husband / partner, or any other partner ever….
A) (If YEScontinuewith B. If NO skipto next item)
YES NO
B)Has thishappened in thepast 12 months? (If YES ask Conly. If NO askD only)
YES NO
C)In the past 12 monthswould you say thatthis has happenedonce, a few times ormany times? (afteranswering C, go to next item) One Few Many
D) Before the past 12 months would you say that this hashappened once, afew times or many times?
One Few Many
704
a) Insulted you or made you feel badabout yourself?
b) Belittled or humiliated you in front of other people?
c) Done things to scare or intimidate you on purpose (e.g. by the way he lookedat you, by yelling and smashing things)?
d) Threatened to hurt you or someoneyou care about?
1 2
1 2
1 2
1 2
1 2
1 2
1 2
1 2
1 2 3
1 2 3
1 2 3
1 2 3
1 2 3
1 2 3
1 2 3
1 2 3

A Practical Guide for Researchers and Activists 235
A P P E N D I X O N E 1
Has he or any other partner ever….
A) (If YEScontinuewith B. If NO skipto next item)
YES NO
B)Has thishappened in thepast 12 months?(If YES ask Conly. If NO askD only)
YES NO
C)In the past 12 monthswould you say thatthis has happened once, a few times ormany times? (afteranswering C, go tonext item) One Few Many
D)Before the past 12months would yousay that this hashappened once, a fewtimes or manytimes?
One Few Many
705
a) Slapped you or thrown something atyou that could hurt you?
b) Pushed you or shoved you or pulledyour hair?
c) Hit you with his fist or with somethingelse that could hurt you?
d) Kicked you, dragged you or beat youup?
e) Choked or burnt you on purpose?f) Threatened to use or actually used a
gun, knife or other weapon against you?
1 2
1 2
1 2
1 2
1 2
1 2
1 2
1 2
1 2
1 2
1 2
1 2
1 2 3
1 2 3
1 2 3
1 2 3
1 2 3
1 2 3
1 2 3
1 2 3
1 2 3
1 2 3
1 2 3
1 2 3
A) (If YEScontinuewith B. If NO skipto next item)
YES NO
B)Has thishappened in thepast 12 months? (If YES ask Conly. If NO askD only)
YES NO
C)In the past 12 monthswould you say thatthis has happened once, a few times ormany times? (afteranswering C, go tonext item) One Few Many
D)Before the past 12months would yousay that this hashappened once, a fewtimes or manytimes?
One Few Many
706
a) Did your current husband/partner or any other partner ever physically force youto have sexual intercourse when you didnot want to?
b) Did you ever have sexual intercourseyou did not want to because you wereafraid of what your partner or any other partner might do?
c) Did your partner or any other partner ever forced you to do something sexualthat you found degrading or humiliating?
1 2
1 2
1 2
1 2
1 2
1 2
1 2 3
1 2 3
1 2 3
1 2 3
1 2 3
1 2 3
707 VERIFY WHETHER ANSWERED YES TO ANY QUESTION ON PHYSICAL VIOLENCE,SEE QUESTION 705
YES, PHYSICAL VIOLENCE .............................. 1NO PHYSICAL VIOLENCE ................................. 2
708 VERIFY WHETHER ANSWERED YES TO ANY QUESTION ON SEXUAL VIOLENCE,SEE QUESTION 706
YES, SEXUAL VIOLENCE .................................. 1NO SEXUAL VIOLENCE ..................................... 2
EVER BEEN PREGNANT[ ]
NUMBER OF PREGNANCIES [ ][ ]
NEVER PREGNANT [ ] S. 8
709 You said that you have been pregnant TOTAL times. Wasthere ever a time when you were slapped, hit or beaten by(any of) your partner(s) whilst you were pregnant?
YES ................................................................... 1NO ..................................................................... 2DON’T KNOW/DON’T REMEMBER ........... 8REFUSED/NO ANSWER............................... 9

236 Researching Violence Against Women
A P P E N D I X O N E1
SECTION 9 IMPACT AND COPING
I would now like to ask you some questions about what effects your husband /partner’s acts has had on you . With acts I mean…(REFER TO SPECIFIC ACTS THE RESPONDENT HAS MENTIONED IN SECTION 7).
IF REPORTED MORE THAN ONE PARTNER VIOLENCE, ADD: I would like you to answer these questions in relation to themost recent / last partner who was physically or sexually violent toward you..
WOMAN EXPERIENCED PHYSICALVIOLENCE [ ]
WOMAN HAS EXPERIENCED SEXUALVIOLENCE ONLY
[ ] sS.10
904 During the times that you were hit, did you ever fightback physically or to defend yourself?IF YES: How often? Would you say once or twice,several times or most of the time?
NEVER........................................................................1ONCE OR TWICE......................................................2SEVERAL TIMES......................................................3MANY TIMES/MOST OF THE TIME.....................4DON’T KNOW / DON’T REMEMBER....................8REFUSED / NO ANSWER........................................9
905
905 Have you ever hit or physically mistreated yourhusband/partner when he was not hitting or physicallymistreating you?IF YES: How often? Would you say once or twice,several times or many times?
NEVER........................................................................1ONCE OR TWICE......................................................2SEVERAL TIMES......................................................3MANY TIMES............................................................4DON’T KNOW / DON’T REMEMBER....................8REFUSED / NO ANSWER........................................9
SECTION 8 INJURIES
WOMAN EXPERIENCED PHYSICAL ORSEXUAL VIOLENCE
[ ]
WOMAN HAS NOT EXPERIENCED PHYSICAL OR SEXUAL VIOLENCE
[ ] S.10
I would now like to learn more about the injuries that you experienced from (any of) your partner’s acts that we havetalked about (MAY NEED TO REFER TO SPECIFIC ACTS RESPONDENT MENTIONED IN SECTION 7).By injury, I mean any form of physical harm, including cuts, sprains, burns, broken bones or broken teeth, or other things like this.
801 Have you ever been injured as a result of these acts by(any of) your husband / partner(s). Please think of theacts that we talked about before.
YES ..................................................................... 1NO ....................................................................... 2DON’T KNOW / DON’T REMEMBER.......... 8REFUSED / NO ANSWER............................... 9
S.9
802 a) In your life, how many times were you injured by (any of) your husband/partner(s)?Would you say once or twice, several times or many times?
ONCE/TWICE.................................................... 1SEVERAL (3-5) TIMES.................................... 2MANY (MORE THAN 5) TIMES ................... 3DON’T KNOW / DON’T REMEMBER.......... 8REFUSED / NO ANSWER............................... 9
802 b) Has this happened in the past 12 months? YES ..................................................................... 1NO ....................................................................... 2DON’T KNOW / DON’T REMEMBER.......... 8REFUSED / NO ANSWER............................... 9

A Practical Guide for Researchers and Activists 237
A P P E N D I X O N E 1
SECTION 10 OTHER EXPERIENCES
In their lives, many women experience different forms of violence from relatives, other people that they know,and/or from strangers. If you don’t mind, I would like to briefly ask you about some of these situations.Everything that you say will be kept private. May I continue?
1002
b) ASK ONLY FOR THOSE MARKED.How many times did this happen?Once or twice, a few times, or many times
1001a)
Since the age of 15, hasanyone (FOR WOMEN WITH CURRENT ORPAST PARTNER: other than your partner/husband) ever beaten or physicallymistreated you in any way?
IF YES:Who did this to you?
PROBE:How about a relative?How about someone atschool or work?How about a friend or neighbour?A stranger or anyone else?
NO ONE.......................................................A
FATHER ...................................................... B STEP FATHER............................................ C OTHER MALE FAMILY MEMBER .......DFEMALE FAMILY MEMBER: ________ E
TEACHER ....................................................FPOLICE/ SOLDIER ....................................GMALE FRIEND OF FAMILY ..................HFEMALE FRIEND OF FAMILY ...............I
BOYFRIEND................................................ JSTRANGER.................................................KSOMEONE AT WORK ...............................L PRIEST/RELIGIOUS LEADER ............... M
OTHER (specify): _______________ ......X
Once ortwice
1 1 1 1
1 1 1 1
1 1 1 1
1
A few times
2 2 2 2
2 2 2 2
2 2 2 2
2
Many times
3 3 3 3
3 3 3 3
3 3 3 3
3
1003b) ASK ONLY FOR THOSE MARKED.How many times did this happen?Once or twice, a few times, or many times
1002a)
Since the age of 15, hasanyone (FOR WOMEN WITH CURRENT ORPAST PARTNER: other than your partner/husband) ever forced you to havesex or to perform a sexualact when you did not wantto?
IF YES:Who did this to you?
PROBE:How about a relative?How about someone atschool or work?How about a friend or neighbour?A stranger or anyone else?
NO ONE.......................................................A
FATHER ...................................................... B STEP FATHER............................................ C OTHER MALE FAMILY MEMBER .......DFEMALE FAMILY MEMBER: ________ E
TEACHER ....................................................FPOLICE/ SOLDIER ....................................GMALE FRIEND OF FAMILY ..................HFEMALE FRIEND OF FAMILY ...............I
BOYFRIEND................................................ JSTRANGER.................................................KSOMEONE AT WORK ...............................L PRIEST/RELIGIOUS LEADER ............... M
OTHER (specify): __________________ .X
Once ortwice
1 1 1 1
1 1 1 1
1 1 1 1
1
A few times
2 2 2 2
2 2 2 2
2 2 2 2
2
Many times
3 3 3 3
3 3 3 3
3 3 3 3
3

238 Researching Violence Against Women
A P P E N D I X O N E1 1004
ASK ONLY FOR THOSE MARKED IN 1003ad) How many times did this happen?
b) How old were you when ithappened with thisperson for the firsttime? (more or less)
c) How old wasthisperson?
PROBE:roughly (more or less).
Once/twice
Few times
Many times
1003a) Before the age of
15, do you remember if anyone in your familyever touched you sexually, or madeyou do something sexual that you didn’t want to?
IF YES:Who did this toyou?
IF YES OR NO CONTINUE:How aboutsomeone at school?How about a friend or neighbour?Has anyone elsedone this to you?
IF YES:Who did this toyou?
NO ONE....................................................... A
FATHER .......................................................B STEP FATHER ............................................C OTHER MALE FAMILY MEMBER /(BROTHER, ETC) ________________.... DFEMALE FAMILY MEMBER: ________E
TEACHER ....................................................FPOLICE/ SOLDIER.................................... GMALE FRIEND OF FAMILY .................. HFEMALE FRIEND OF FAMILY ...............I
BOYFRIEND.................................................JSTRANGER ................................................ KSOMEONE AT WORK...............................L PRIEST/RELIGIOUS LEADER................M
OTHER (specify): _________________... X
[ ][ ] [ ][ ]
[ ][ ] [ ][ ]
[ ][ ] [ ][ ] [ ][ ] [ ][ ]
[ ][ ] [ ][ ] [ ][ ] [ ][ ]
[ ][ ]
[ ][ ] [ ][ ]
[ ][ ] [ ][ ]
[ ][ ] [ ][ ] [ ][ ] [ ][ ]
[ ][ ] [ ][ ] [ ][ ] [ ][ ]
[ ][ ] DK = 98
1 1
1 1
1 1 1 1
1 1 1 1
1
2 2
2 2
2 2 2 2
2 2 2 2
2
3 3
3 3
3 3 3 3
3 3 3 3
3
SECTION 12 COMPLETION OF INTERVIEW
1201 I would now like to give you a card. On this card are two pictures. No otherinformation is written on the card. The first picture is of a sad face, the second is of ahappy face.
No matter what you have already told me, I would like you to put a mark below the sad picture if, someone has ever touched you sexually, or made you do something sexualthat you didn’t want to, before you were 15 years old. Please put a mark below the happy face if this has never happened to you.Once you have marked the card, please fold it over and put it in this envelope. This willensure that I do not know your answer.
GIVE RESPONDENT CARD AND PEN. MAKE SURE THAT THERESPONDENT FOLDS THE CARD; PUTS IT IN THE ENVELOPE; AND SEALS THE ENVELOPE BEFORE GIVING IT BACK TO YOU. ON LEAVING THEINTERVIEW SECURELY ATTACH THE ENVELOPE TO THEQUESTIONNAIRE (OR WRITE THE QUESTIONNAIRE CODE ON THEENVELOPE).
CARD GIVEN FORCOMPLETION...... 1
CARD NOT GIVEN FORCOMPLETION...... 2

A Practical Guide for Researchers and Activists 239
A P P E N D I X O N E 1
SAMPLE OF CARD

240 Researching Violence Against Women
ACTIVITY 1: WHAT ISGENDER-BASED VIOLENCE?(30 MINUTES)
Step 1 Ask the participants to mention allthe different kinds of violence that arecommon in their community and writeup the answers on the flipchart orblackboard. An alternative is to handout cards for participants to write downtheir answers and then stick them upon the wall.
Step 2 Ask the group “Are all these acts ofviolence the same?” “What kinds of dif-ferences are there between them?”“What kinds of violence are more likelyto happen to women and girls than tomen and boys?” What do you think arethe effects on the health of women andgirls of this kind of violence?” If cardsare used, they can be grouped together,according to the types of violence (emo-tional, verbal, economic, sexual, orphysical), or according to which types ofviolence are suffered primarily bywomen and girls, which are mostly
experienced by men and boys, andwhich are suffered equally by men andwomen.
Step 3 Present overheads and distributehandouts on the definitions and charac-teristics of gender-based violence, wifeabuse and sexual coercion.
ACTIVITY 2: MYTHS ANDTRUTHS ABOUT VIOLENCE(30 MINUTES)
Step 1 Place three signs up around theroom with the words “I AGREE,” “I DIS-AGREE,” and “I DON’T KNOW.”
Step 2 Read out loud the following state-ments and ask participants to move tothe sign that represents their opinionabout the statement. Ask a few partici-pants on each side to explain their opin-ion. The facilitator may ask questions tostimulate discussion, but it is not neces-sary to provide “correct” answers, asthese will be discussed in greater depthlater on. On a flipchart the facilitator canwrite down the number of people agree-ing and disagreeing with each statement.
1 A P P E N D I X T W O
Exercises for Sensitizing Interviewers on Violence
Goal: To encourage participants tothink about different kinds of actsthat can constitute violence, and torecognize that violence can be physi-cal, verbal, emotional, sexual, andeconomic.
Goal: To challenge existing beliefsabout violence and to identify areasof consensus and disagreementwithin the group.

A Practical Guide for Researchers and Activists 241
■ Men are violent by nature.■ Violence is usually due to alcohol.■ Sometimes violence is a way of show-
ing affection.■ Boys who witness their father's violence
towards their mothers are more likely tobe violent when they grow up.
■ A woman should put up with violencein order to keep her family together.
■ Some women like to be beaten.■ Violence against women exists in every
society in the world.■ Violence is never justified.■ Girls who are sexually abused in child-
hood are more likely to drink and usedrugs when they are older.
■ Nobody deserves to be beaten. Violenceis always the responsibility of the per-son who uses it.
ACTIVITY 3: WHAT CAUSESVIOLENCE AGAINSTWOMEN? (1 HOUR)
Step 1 Place a circle or square at the centerof a blackboard or large sheet of paper,with the words “violence against women”in the middle. Ask participants to brain-storm possible causes of violence. Thesecan be immediate causes (for example“alcohol” or “economic problems” or largerproblems such as “cultural attitudes,”“machismo,” “unemployment,” “educationalsystem,” etc. Either write the answers onthe board or ask each participant to writethe causes on cards and place them on theboard with tape. All the problems consid-ered as “causes of violence” should beplaced on one side of the center circle,either above or to the side.
Step 2 For each problem identified, askthe group if it is related (either as acause or a result) to any other problemalready listed. If so, draw an arrowbetween the two boxes, indicating thedirection(s) of the relationship.
Step 3 After completing this side of theweb, ask the group to name importanteffects or consequences of violence.These can be any kind of problem,health, economic, or social — resultingfrom violence. It is a good idea to tryto discuss effects on individual womenfirst, and then on families, communi-ties, and society as a whole next.Again, for each problem, ask thegroups to examine possible relation-ships between different problems andto draw arrows between these issues,indicating the direction(s) of the relationship.
ACTIVITY 4: WHY DOESN’TSHE JUST LEAVE? (45 MINUTES)
Step 1 Show the group a small bird cageand ask them to imagine that inside is awomen living with violence. The barson the cage represent the different bar-riers that women confront when tryingto overcome abuse. Ask, “What aresome of the different reasons that keepwomen in abusive relationships?” Writethe different answers on the flipchart.
Step 2 Have participants read the storyCandies in Hell in small groups ofthree to four and discuss the followingquestions:
A P P E N D I X T W O 1
Goal: To identify the issues at the levelof both an individual and society thatperpetuate violence against women,and to examine the consequences ofviolence, not only for victims, but alsofor families and communities.
Goal: To understand some of the rea-sons that women stay in abusive rela-tionships and the barriers that theyface in seeking help.

242 Researching Violence Against Women
■ Is Ana Cristina’s story familiar to you?Has something like this ever happenedto any one you know?
■ Why do you think that Ana Cristinastayed in the marriage after her husbandbegan to beat her?
■ What do you think about the reactionsof Ana Cristina’s family and the police?
■ What do you think that the expression“Candies in Hell” means?”
■ What advice would you give AnaCristina if she were your friend?
Step 3 Have participants discuss in thelarger group what they have learned andsummarize their discussion. Presentoverheads on women’s experiences ofviolence and the stages of violent rela-tionships.
CANDIES IN HELL : THESTORY OF ANA CRIST INA
Ana Cristina was married at the age of 15to a man in his late 30’s. Her husband wasa soldier and that quickly earned him therespect and approval of Ana Cristina’smother. Shortly after the marriage, hebegan to beat Ana Cristina savagely andcontinued to do so regularly throughout thesubsequent five years. She learned to listenfor him at night and be ready to escapewith the children if necessary.
... I had to sleep in other people’s houses toavoid getting beaten when he came home. Iwould have to climb over the back wall withmy daughters when he arrived, and he wouldshoot at me. I escaped many times from hisbullets. I don’t know why I’m still alive…
…When I didn’t want to have sex withmy husband he simply took me by force...When he came home drunk he would beatme, and do what he wanted with me. ThenI fought with him, but what could I doagainst a man who was stronger than me?I couldn’t do anything, so I had to put upwith it and suffer…
...He used to tell me, “You’re an animal,an idiot, you are worthless.” That made mefeel even more stupid. I couldn’t raise myhead. I think I still have scars from this,and I have always been insecure ...I wouldthink, could it be that I really am stupid? Iaccepted it, because after a point ... he haddestroyed me by blows and psychologi-cally... …When he beat me, my daughterswould get involved in the fight. Then hewould throw them around in his fury andthis hurt me, it hurt me more than when hebeat me…
…Once, when I was recovering, becausehe had beaten me and he had left my eyesswollen and black, my daughter came up tome and said, “Mommy, you look like amonster” and she began to cry… It hurt meso much. It wasn’t so much the blows I had,but what really hurt me were her sobbingand the bitterness that she was feeling.
…He was so jealous, my grandmotherused to say, “If you stay with him he’s goingto put blinders on you like the horses thatpull carriages.” I couldn’t look at anyoneon the street, nor have either men orwomen friends, nor greet anyone. And if aman looked at me, he would smack meright there on the street.
…My mother would say to me, “Do youthink you’re the only one to live throughthis?” She told me not to leave, and mymother-in-law also told me that I shouldput up with it, ...” You have to maintainyour marriage, remember that you are hiswife and he is the father of your children.”
…Once I went to the police for help, butsince he was in the military they let him goright away and gave him a ride back to myhouse. That time he kicked down mydoor…
… After that, I didn’t know what to do. Ifelt trapped, a prisoner and I couldn’tescape…
…After the blows he always came back tocourt me, bought me clothes and afterwardshe always said, “forgive me, I won’t do it
A P P E N D I X T W O1

A Practical Guide for Researchers and Activists 243
again,” but then he always did the sameafterwards. And then my grandmotherwould say to me “Child, what are yougoing to do with candies in hell?”
Alternative exercise:After reading the story and discussing it ingroups, ask participants to write a letter ora poem to Ana Cristina. This is a verygood exercise for identifying stereotypicalreactions on the part of participants and forencouraging empathy for survivors of vio-lence. Following is a letter written to AnaCristina by a field worker in Peru duringher training:
Ana Cristina – you have the right tolive with dignity and to be happy
Dear Ana Cristina,My name is Rosalia Amada. I am a
social worker. I am grateful for the
chance to get to know you and accom-pany you on your journey to rebuildyourself. You are a very brave woman. Iknow it must have been difficult to shareyour story and remind yourself of oldwounds that must still hurt so much.
You have taken the first step, by recog-nizing the violence against you. You arelike so many women in Peru whodecided to live. Ana Cristina, you arebeautiful because you are freeing your-self daily from resignation, fear, andmanipulation. No one has the right todestroy our dreams, don’t ever forget that.
You are the star of your own journeyto freedom.
Good luck!Rosalia Amada
A P P E N D I X T W O 1
Monday Tuesday Wednesday Thursday Friday
1st week Gender and violence exercises Overview of study Question by question review of the instrument objectives and interviewing techniques/safety measures
2nd week Debriefing from Review of practice Practice household Field practice Debriefinginterviews Practice with survivors selection, first contactPractice in groups of three with case studies
3rd week Pilot testing Pilot testing Debriefing Pilot again if Debrief againnecessary
Start data entry with pilot data and debug data entry systemFinal questionnaire printed
4th week Field work begins For data typists: Start data entry with survey data and debug and finalize data entry system; familiarize them with all data management procedures
TRAINING PLAN FOR F IELD WORKERS FOR A POPULATION-BASED SURVEY

244 Researching Violence Against Women
The following resource materials have beencompiled to facilitate access to informationand organizations working on gender-based violence.
OVERVIEWS
Costs of Intimate Partner Violence atthe Household and Community Levels:An Operational Framework forDeveloping Countries. Duvvury N,Grown C, Redner J. Washington, DC,ICRW, 2004.
This publication summarizes studies thathave estimated economic costs of inti-mate partner violence against womenand lays out a framework to measure thecosts of intimate partner violence indeveloping countries, factoring in pre-vention, response, and opportunity costs. http://www.icrw.org/docs/2004_paper_costingviolence.pdf
Advancing the Federal ResearchAgenda on Violence Against Women.National Research Council SteeringCommittee for the Workshop in Issuesin Research on Violence AgainstWomen. Committee on Law andJustice, Division of Behavioral andSocial Sciences and Education.Washington, DC, The NationalAcademies Press, 2004.
This publication describes the efforts ofthe National Research Council since1998 and provides detailed information
about the interventions researchlaunched in the past few years (virtuallyall in the United States). It also includesdiscussion of methodological issues,challenges, gaps, and findings.
The Economic Dimensions ofInterpersonal Violence. World HealthOrganization, 2004.
This publication demonstrates that theconsequences of interpersonal violenceare extremely costly, prevention studiesshow evidence of cost effectiveness, andfor most of the developing world andmany developed countries, there is noteven descriptive information about thedirect costs of treating the consequencesof interpersonal violence.http://www.who.int/violence_injury_prevention/publications/violence/economic_dimensions/en/
How to make the Law Work?Budgetary Implications of DomesticViolence Policies in Latin America.ICRW, 2003.
The document analyzes national domes-tic violence laws and policies in sevenLatin American countries. One key find-ing of the report was that none of thecountries in the study had passed lawswith actual budgetary appropriations,which greatly limited the implementationof the programs and services.http://www.icrw.org
1 A P P E N D I X T H R E E
GBV Resources Section

A Practical Guide for Researchers and Activists 245
Intimate partner violence: causes andprevention. Jewkes R (2002). TheLancet 359:1423-1429.
This article presents a concise review ofavailable research on risk factors for inti-mate partner violence and the implica-tions of those findings for prevention.
Domestic Violence against Women andGirls. Innocenti Digest 6 United NationsChildren’s Fund (UNICEF), 2000.
This study on domestic violencedescribes the powerlessness of womenin situations of violence and notes thatup to half of the world’s female popula-tion may be victimized by those closestto them at some time in their lives.http://www.unicef-icdc.org/publications/pdf/digest6e.pdf
Ending violence against women. HeiseL, Ellsberg M, Gottemoeller M (1999).Population Reports 27(4).
This article describes an in-depth studyby the Johns Hopkins School of PublicHealth and the Center for Health andGender Equity. Based on over 50 popu-lation-based surveys and more than 500studies of domestic violence, the reportfinds that by far the greatest risk of vio-lence comes not from strangers, butfrom male family members, includinghusbands.In English:http://www.infoforhealth.org/pr/l11edsum.shtmlDownload pdf: http://www.infoforhealth.org/pr/online.shtml#lIn Spanish:http://www.infoforhealth.org/pr/prs/sl11edsum.shtml
Bringing Rights to Bear: An Analysis ofthe Work of the UN Treaty MonitoringBodies on Reproductive and SexualRight. Center for Reproductive Law andPolicy, 2002.
This report charts the collective work ofsix United Nations committees as theywork to translate international humanrights standards into state responsibilityon a broad spectrum of reproductiverights issues, including violence againstwomen.http://www.reproductiverights.org/pub_bo_tmb.html.
Gender-Based Violence: A HumanRights Issue. [Mujer y Desarrollo Series#16.] Economic Comisión for LatinAmerica and the Caribbean, 1996.
The study explores the various forms ofgender-based violence (GBV) and howgrowing awareness of the phenomenonin recent years has led to the establish-ment of new institutions and the adop-tion of legislative amendments, which inturn have served as a focal point for col-lective action by women.http://www.eclac.cl/publicaciones/UnidadMujer/7/lcl957/lcl957i.pdf
FEMALE GENITALMUTILAT ION (FGM)
Abandoning Female GenitalMutilation/Cutting: Information FromAround the World. PopulationReference Bureau, 2005.
This CD-ROM contains an extensivecompilation in English and French ofarticles and documents on FGM. http://www.prb.org
Female Genital Mutilation: ThePrevention and the Management of theHealth Complications. PolicyGuidelines for Nurses and Midwives.World Health Organization, 2001.
The purpose of these policy guidelinesis to promote and strengthen the caseagainst the medicalization of FGM tosupport and protect nurses, midwives,and other health personnel in adhering
A P P E N D I X T H R E E 1

246 Researching Violence Against Women
to WHO guidelines regarding the man-agement of FGM related complications.http://www.who.int/entity/gender/other_health/en/guidelinesnursesmid.pdf
Female Genital Mutilation - A jointWHO/UNICEF/UNFPA statement. WorldHealth Organization, 1997.
This joint statement by the World HealthOrganization, the United NationsChildren's Fund, and the United NationsPopulation Fund confirms the universallyunacceptable harm caused by femalegenital mutilation, or female circumcision,and issues an unqualified call for theelimination of this practice in all its forms.http://www.who.int/reproductive-health/publications/fgm/fgm_statement.html
GBV AND HEALTH
WHO Multi-country Study on Women’sHealth and Domestic Violence AgainstWomen: Initial Results on Prevalence,Health Outcomes and Women’sResponses. WHO. Geneva,Switzerland, 2005.
This report presents the results of amulti-country study of 10 countries and16 sites—findings on prevalence, healthoutcomes, and women’s responses to avariety of types of sexual and physicalviolence perpetrated by intimate partnersas well as non-partners.http://www.who.int/gender/violence/en/
Reproductive Health and Rights:Reaching the Hardly Reached. PATH,2002.
This publication is a compendium ofarticles that highlight the negative impactthat marginal status has on the healthand well-being of vulnerable groups.Various aspects of gender-based violenceare presented in several articles. http://www.path.org/publications/pub.php?id=503
Violence against women: effects onreproductive health. Shane B, EllsbergM (2002). Outlook 20(1): 1-8.
This issue presents an overview of vio-lence from a public health perspective.It provides examples from research andsuccessful programs and explores howthe health sector can take an active rolein the prevention and treatment of vio-lence against women. http://www.path.org/files/EOL20_1.pdf
World Report on Violence and Health.World Health Organization, 2002.
This publication provides a comprehen-sive and global review of evidencerelated to violence. Most relevant are thechapter devoted to violence by intimatepartners (Chapter 4) and the chapterdevoted to sexual violence (Chapter 6).Both chapters include a review of evi-dence on interventions to prevent vio-lence and care for survivors worldwide.http://www5.who.int/violence_injury_prevention/main.cfm?p=0000000682www.who.int/violence_injury_prevention/violence/world_report/wrvh1/en/In French and Spanish: www.who.int/violence_injury_prevention/violence/world_report/en/Summary_Spanish.pdf
Symposium 2001 Final Report: Gender-Based Violence, Health, and Rights inthe Americas. Pan American HealthOrganization, 2001.
This symposium brought together repre-sentatives from the ministries of health,women’s nongovernmental organizations(NGOs), civil society, and U.N. agenciesfrom 30 countries of the Latin Americanand Caribbean region as well as interna-tional donor agencies to identify priori-ties and formulate strategies forstrengthening the response of the healthsector to GBV. This report summarizesmany of the key recommendations andlessons learned from those reports, and
A P P E N D I X T H R E E1

A Practical Guide for Researchers and Activists 247
provides an overview of organizationsworking to improve policies in theregion.http://www.paho.org/English/HDP/HDW/Symposium2001FinalReport.htm
Annotated Bibliography on Violenceagainst Women: A Health and HumanRights Concern. World HealthOrganization, 1999.
This bibliography was commissioned bythe Global Commission on Women’sHealth and prepared by Rights andHumanity in collaboration with theWHO Women’s Health andDevelopment Unit and the GlobalCommission on Women’s Health.http://www.who.int/gender/documents/Annotated%20Bibliography%20green%20A4.pdf
Gender and Public Health Series This series published by PAHO containsthe following GBV-related topics:Nº1 Battered Women: A Working Guidefor Crisis Intervention, 1999Nº7 Helping Ourselves to Help Others:Self-Care Guide for Those Who Work inthe Field of Family Violence, 1999.http://www.paho.org/English/HDP/HDW/gphseries.htm
The Intimate Enemy: Gender Violenceand Reproductive Health. The PanosInstitute, 1998.
The report shows how local communi-ties around the world are providingmedical, legal, and counseling servicesfor victims of gender violence and lob-bying for changes in laws and customsto address the problem head-on.http://www.panos.org.uk/PDF/reports/IntimateEnemy.pdf
GBV AND HIV
Dying of Sadness: Sexual Violence andthe HIV Epidemic. United NationsDevelopment Program (UNDP), 2000.
This preliminary overview of availableliterature suggests that, within the con-text of gender and the HIV epidemic,sexual violence is a complex phenome-non with multiple determinants, conse-quences, and manifestations.http://www.undp.org/hiv/publications/gender/violencee.htm
The intersections of HIV and violence:Directions for future research andinterventions. Maman S, Campbell J,Sweat MD, Gielen AC, (2000). SocialScience and Medicine 50(4):459-478.
This article provides a comprehensiveoverview of current research on gender-based violence and HIV/AIDS.
REFUGEES/CONFL ICT
Interagency Manual on ReproductiveHealth in Refugee Situations: Sexualand Gender-Based Violence. UNFPA,2001.
Chapter 4 of this publication focuses onsexual violence against women. Mostreported cases of sexual violence amongrefugees involve female victims andmale perpetrators. It is acknowledgedthat men and young boys may also bevulnerable to sexual violence. http://www.unfpa.org/emergencies/manual/
Gender-based violence in refugee set-tings. Ward J, Vann B (2002). TheLancet Supplement, Vol. 360:(Supplement 1) s13-s14.
http://www.rhrc.org/pdf/lancet1.pdf
A P P E N D I X T H R E E 1

248 Researching Violence Against Women
Gender-Based Violence: EmergingIssues in Programs Serving DisplacedPopulations. Vann B. Arlington, VA,Reproductive Health Response inConflict Consortium, 2002.
http://www.rhrc.org/pdf/gbv_vann.pdf
If Not Now, When? Addressing Gender-Based Violence in Refugee, InternallyDisplaced and Post-Conflict Settings: AGlobal Overview. Ward J. New York,Reproductive Health Response inConflict Consortium, 2002.
http://www.rhrc.org/resources/gbv/ifnotnow.html
Gender-based Violence Tools Manualfor Assessment & Program Design,Monitoring and Evaluation in Conflict-affected Settings. Reproductive HealthResponse in Conflict Consortium, 2004.
http://www.rhrc.org/resources/gbv/gbv_tools/manual_toc.html
TRAFF ICKING
WHO Ethical and SafetyRecommendations for InterviewingTrafficked Women. World HealthOrganization, 2003.
http://www.who.int/gender/documents/en/final%20recommendations%2023%20oct.pdf
The health risks and consequences oftrafficking in women and adolescents:Findings from a European study.Zimmerman C, et al. London, LondonSchool of Hygiene & Tropical Medicine(LSHTM), 2003.
http://www.lshtm.ac.uk/hpu/docs/traffickingfinal.pdf
RESEARCHMETHODOLOGIES
The following texts provide excellentoverviews on methods for both quantita-tive and qualitative research.
Quantitative
Basic Epidemiology. Beaglhole R, et al.Geneva, WHO, 1993.
Research Design: Qualitative andQuantitative Approaches. Creswell J W.Thousand Oaks, CA, Sage Publications,1994.
Epidemiology for Public Health.Persson L-A, Wall, S. Umeå, Sweden,Umeå International School of PublicHealth, 2003.
Qualitative
Developing Focus Group Research:Politics, Theory and Practice. BarbourR, Kitzinger J, eds. London, SagePublications, 1995.
Doing Qualitative Research. CrabtreeB, Miller W. Newbury Park, CA, SagePublications, 1992.
Qualitative Inquiry and ResearchDesign: Choosing Among FiveTraditions. Creswell J W. ThousandOaks, CA, Sage Publications, 1998.
Qualitative Methodology forInternational Public Health. DahlgrenL, et al. Umeå, Sweden, UmeåUniversity, 2003.
Qualitative Data Analysis: AnExpanded Sourcebook. Second Edition.Miles M, Huberman A M. ThousandOaks, CA, Sage Publications, 1994.
A P P E N D I X T H R E E1

A Practical Guide for Researchers and Activists 249
Qualitative Evaluation and ResearchMethods 2nd ed. Patton M. NewburyPark, CA, Sage Publications, 1990.
Qualitative Methods: A Field Guide forApplied Research in Sexual andReproductive Health. Ulin P, et al.Research Triangle Park, NC, FamilyHealth International, 2002.
Embracing Participation inDevelopment: Wisdom From the Field.Shah M K, Kambou S D, Monahan B,eds. Atlanta, CARE, 1999.
http://www.careinternational.org.uk/resource_centre/civilsociety/embracing_participation_in_development.pdf
ETHICS
Putting Women First: Ethical and SafetyRecommendations for Research onDomestic Violence against Women.World Health Organization, 1999.
Research on violence against womenraises important ethical and methodolog-ical challenges. Researching abuse is notlike other areas of investigation—thenature of the topic means that issues ofsafety, confidentiality, and interviewerskills and training are even more impor-tant than in other forms of research.http://www.who.int/gender/violence/womenfirtseng.pdf
Bearing witness: ethics in domestic vio-lence research. Ellsberg M, Heise L(2002). The Lancet 359:1599-1604.
http://www.thelancet.com/journals/lancet/article/PIIS0140673602085215/fulltext
CONVENTIONS/LAWS
1950 Convention for the Suppression of the Traffic in Persons and of the Exploitation of the Prostitution of Othershttp://www.unhchr.ch/html/menu3/b/33.htm
1974 Declaration on the Protection ofWomen and Children in Emergencyand Armed Conflicthttp://heiwww.unige.ch/humanrts/instree/e3dpwcea.htm
1979 Convention on the Elimination of All Forms of Discrimination againstWomen http://www.un.org/womenwatch/daw/cedaw/
1989 Convention on the Rights of the Childhttp://www.unicef.org/crc/crc.htm
1993 World Conference on Human Rightshttp://www.unhchr.ch/html/menu5/wchr.htm
1993 Declaration on the Elimination ofViolence against Womenhttp://www.unhchr.ch/huridocda/huridoca.nsf/(Symbol)/A.RES.48.104.En?Opendocument
1994 Inter-American Convention on thePrevention, Punishment, andEradication of Violence against Women(Convention of Belém do Pará)http://www.undp.org/rblac/gender/osavio.htm
1994 International Conference onPopulation and Developmenthttp://www.un.org/popin/icpd2.htm
1995 Fourth World Conference on Women(Beijing) http://www.un.org/womenwatch/daw/beijing/platform/
A P P E N D I X T H R E E 1

250 Researching Violence Against Women
2000 Protocol to Prevent, Suppress, andPunish Trafficking in Persons,Especially Women and Children,Supplementing the United NationsConvention against TransnationalOrganized Crimehttp://www.uncjin.org/Documents/Conventions/dcatoc/final_documents_2/convention_%20traff_eng.pdf
2000 United Nations’ Security CouncilResolution 1325 on Women, Peace,and Securityhttp://www.un.org/events/res_1325e.pdf
INTERVENTIONS
Community-based
Addressing Gender-Based Violence in theLatin American and Caribbean Region:A Critical Review of Interventions.Morrison A, Ellsberg M, Bott S.Washington, DC, World Bank. PolicyResearch Working Paper 3438, 2004.
This paper examines good practiceapproaches to addressing gender-basedviolence in the Latin American andCaribbean regions justice, health, andeducation sectors, as well as multisec-toral approaches.http://web.worldbank.org/WBSITE/EXTERNAL/TOPICS/EXTGENDER/0,,contentMDK:20262193~pagePK:148956~piPK:216618~theSitePK:336868,00.html
Preventing and Responding to Gender-Based Violence in Middle and Low-income Countries: A Global Review andAnalysis. Bott S, Morrison A, EllsbergM. Washington, DC, World Bank. PolicyResearch Working Paper 3618, 2004.
This paper provides a global review ofpromising approaches to addressinggender-based violence in the justice,health, and education sectors, as well as
multisectoral approaches. The paperreviews existing evidence on successfulinterventions and offers a framework forassessing good practices.http://web.worldbank.org/WBSITE/EXTERNAL/TOPICS/EXTGENDER/0,,contentMDK:20262193~pagePK:148956~piPK:216618~theSitePK:336868,00.html
Not a Minute More: Ending ViolenceAgainst Women. UNIFEM, 2003.
In 1996, the UNIFEM Trust Fund beganfunding projects to address gender-based violence through advocacy,awareness raising, public education,legal advocacy, and youth projects. Thispublication describes these projects anddocuments their achievements, limita-tions, lessons leaned, and future chal-lenges. They provide examples of goodpractices as well as of strategies that didnot meet expectations. http://www.unifem.org/resources/item_detail.php?ProductID=7
With an End in Sight: Strategies fromthe UNIFEM Trust Fund to EliminateViolence Against Women. Spindel C,Levy E, Connor M. New York, UNIFEM,2000.
This publication documents sevenimportant programs dedicated to endingviolence against women in Bosnia andHerzegovina, Cambodia, Honduras,India, Kenya, Nigeria, and the WestBank and Gaza.http://www.unifem.org/index.php?f_page_pid=71
Mobilizing Communities to PreventDomestic Violence: A Resource Guidefor Organizations in East andSouthern Africa. Michau L, Naker D.Nairobi, Raising Voices, 2003.
This document is a resource guide out-lining a five-phase approach to produc-ing social change within a community.
A P P E N D I X T H R E E1

A Practical Guide for Researchers and Activists 251
This project uses a variety of strategies,including gathering baseline informationabout local attitudes and beliefs, raisingawareness about domestic violenceamong the whole community andamong key selected groups, buildingnetworks, and transforming institutions.http://www.raisingvoices.org/resourceguide.shtml
Beyond Victims and Villains:Addressing Sexual Violence in theEducation Sector. Panos Institute, 2003.
This is an excellent and extensivereview of the literature on sexual vio-lence in educational settings, includinginterventions and strategies that havebeen used in developing countries toaddress all forms of sexual violence inschools and universities.http://www.panos.org.uk/PDF/reports/Beyond%20Victims.pdf
Justice, Change, and Human Rights:International Research andResponses to Domestic Violence.Center for Development andPopulation Activities, 2000.
This paper employs both a human rightsand a development framework to iden-tify the limitations and strengths of eachapproach for understanding andresponding to domestic violence, as wellas to clarify the links that need to bemade between the frameworks.http://www.cedpa.org/publications/pdf/violenceprowid.pdf
La ruta crítica que siguen las mujeresafectadas por la violencia intrafamil-iar. Pan American HealthOrganization, 2000.
Translated into English as: DomesticViolence: Women’s Way Out.This research protocol addresses vio-lence against women and aims toimprove the services available forwomen affected by it.
Spanish:http://www.paho.org/Spanish/HDP/HDW/rutacritica.htmEnglish:http://www.paho.org/English/HDP/HDW/womenswayout.htm
Communications
Picturing a Life Free of Violence: Mediaand Communication Strategies to EndViolence against Women. UnitedNations Development Fund for Women(UNIFEM), 2001.
This report showcases a variety ofmedia and communications strategies tobe used to end violence against women.The report is a collaboration betweenUNIFEM and the Media MaterialsClearinghouse of the Johns HopkinsUniversity Center for CommunicationsPrograms.http://www.unifem.org/resources/item_detail.php?ProductID=8
Making a Difference: StrategicCommunications to End ViolenceAgainst Women. United NationsDevelopment Fund for Women(UNIFEM), 2003.
"Making a Difference" is an indispensa-ble tool for planning strategic communi-cations to raise awareness about andcombat gender-based violence.http://www.unifem.org/resources/item_detail.php?ProductID=6
Communication/Behaviour ChangeTools: Entertainment-Education. UNFPA.Programme Briefs No. 1, 2002.
This issue of Programme Briefs reviewsthe lessons learns from “entertainment-education” programs throughout theworld, many of which address the issueof violence against women. The issueprofiles programs such as Sexto Sentidoin Nicaragua and Soul City in South
A P P E N D I X T H R E E 1

252 Researching Violence Against Women
Africa, and provides a summary of thestate of knowledge about these efforts.www.unfpa.org/upload/lib_pub_file/160_filename_bccprogbrief1.pdf
Health Sector Response
Addressing Gender Based Violencefrom the Reproductive Health/HIVSector: A Literature Review andAnalysis. Guedes A. Washington, DC,Poptech, 2004.
This is an extensive review of existinginterventions to address gender-basedviolence in developing countries. Thereview is divided into six broad cate-gories: 1) behavior change communica-tion programs (2) communitymobilization programs (3) service deliv-ery programs (4) policy programs (5)youth programs and (6) programs work-ing with refugees and displaced popula-tions. The review includes a discussionof broad lessons learned as well as pro-files of “promising” interventions in eacharea. The profiles include details aboutevaluation as well as program design.http://www.poptechproject.com/pdf/04_164_020.pdf
Improving the Health Sector Responseto Gender-Based Violence: a ResourceManual for Health Care Managers inDeveloping Countries. Bott S, Guedes A,Claramunt C, Guezmes A. New York,IPPF/WHR, 2004.
IPPF/WHR coordinated a multi-site ini-tiative to improve the health sectorresponse to gender-based violencewithin four associations, Profamilia(Dominican Republic), INPPARES (Peru),and Plafam (Venezuela), with some par-ticipation from BEMFAM (Brazil). Thispublication is a compilation of all thelessons leaned, tools, and recommenda-tions that emerged from that collectiveeffort. It was published in English and
Spanish, and although the lessonslearned reflect the situation in selectedsites in Latin America and the Caribbean,the publication is designed to addressthe specific needs of health care man-agers in any resource-poor setting, par-ticularly those working innongovernmental organizations.http://www.ippfwhr.org/publications/publication_detail_e.asp?PubID=63
A Practical Approach to Gender-BasedViolence: A Program Guide for HealthCare Providers and Managers. UnitedNations Population Fund, 2001.
This publication contains practical stepsneeded to integrate gender-based vio-lence programming into reproductivehealth facilities. It is also meant to helpa wider range of readers understand theinterrelationships between reproductiveand sexual health and violence. http://www.unfpa.org/publications/detail.cfm?ID=69&filterListType=3
Diagnostic and Treatment Guidelineson Family Violence. American MedicalAssociation, 1999.
This publication presents separate mod-ules establishing guidelines on the fol-lowing seven aspects of violence: childphysical abuse and neglect and childsexual abuse, domestic violence, elderabuse and neglect strategies for the treat-ment and prevention of sexual assault,mental health effects of family violence,physician guide to media violence, and aphysician firearms safety guide.http://www.ama-assn.org/ama/pub/category/3548.html
National Consensus Guidelines: OnIdentifying and Responding toDomestic Violence Victimization.Family Violence Prevention Fund, 1999.
This is a multi-specialty, comprehensiveroutine screening document on domestic
A P P E N D I X T H R E E1

A Practical Guide for Researchers and Activists 253
violence. In addition to specific guide-lines for primary care, obstetrics andgynecologic, family planning, urgentcare, mental health, and in-patient set-tings, it includes an extensive bibliogra-phy, documentation forms, and otheruseful materials.http://endabuse.org/programs/healthcare/files/Consensus.pdf
Promoting Early and EffectiveIntervention to Save Women’s Lives.Family Violence Prevention Fund, 1999.
This kit contains a series of informationpackets for health care providers inter-ested in developing a comprehensivehealth care response to domestic vio-lence. Packets include: GeneralInformation on the Health CareResponse to Domestic Violence, TheEmergency Department Response toDomestic Violence, Screening Patientsfor Domestic Violence, MandatoryReporting of Domestic Violence byHealth Care Providers, and Violenceagainst People with Disabilities.http://endabuse.org/programs/display.php3?DocID=55
Building Data Systems for Monitoringand Responding to Violence againstWomen. CDC, 1998.
This report provides recommendationsregarding public health surveillance andresearch on violence against womendeveloped during a workshop held byCDC on 29–30 October 1998. http://www.cdc.gov/mmwr/preview/mmwrhtml/rr4911a1.htm
Improving the Health Care Responseto Domestic Violence: A ResourceManual for Health Care Providers.Family Violence Prevention Fund, 1996,revised 1998.
This manual includes information toeducate practitioners on screening,
identification, assessment, and interven-tions with victims of domestic violenceand their batterers. It offers practicaltools including a model hospital inter-vention packet outlining effective proto-cols and sample forms for screening,domestic violence/abuse assessment,documentation, safety planning, and dis-charge. Finally, it provides ideas to helpdevelop and implement response strate-gies and programs within a variety ofhealth care practices and settings.http://endabuse.org/programs/display.php3?DocID=238
Intimate Partner Violence and SexualAssault: A Guide to Training Materialsand Programs for Health CareProviders. CDC, 1998.
This guide was developed to help indi-viduals and organizations find appropri-ate materials for group or self-training.http://www.cdc.gov/ncipc/pub-res/ipvasa.htm
Intimate Partner Violence duringPregnancy: A Guide for Clinicians.American College of Obstetricians andGynecologists, 1998.
This guide was designed as a trainingtool for clinicians to increase under-standing of the role they can play inidentifying, preventing, and reducingintimate partner violence. It includes asituation report and potential areas ofaction for clinical staff.http://www.cdc.gov/reproductivehealth/violence/IntimatePartnerViolence/
Violence Against Women: The HealthSector Responds. Velzeboer M, EllsbergM, Clavel Arcas C, Garcia Moreno C,Washington, DC, Pan American HealthOrganization, PATH, 2003.
This book describes PAHO’s efforts toaddress gender-based violence (GBV) inseven countries of Central America. It
A P P E N D I X T H R E E 1

254 Researching Violence Against Women
includes the results of a participatoryreview that identifies the lessons learnedfrom activities conducted at the cliniclevel, the community, and the broaderlocal and national policy arena.http://www.paho.org/English/DPM/GPP/GH/VAWhealthsector.htm
Compendium of Indicators forEvaluating Reproductive HealthPrograms. Bertrand JT, Escudero G.MEASURE Evaluation Manual Series, No. 6. Washington DC, MeasureEvaluation, 2002.
This manual contains a concise subsec-tion on methodological issues related toevaluating interventions that address vio-lence against women, including thoseinterventions carried out in developingcountries. It is written from the perspec-tive of the health sector and primarilyfrom the perspective of local rather thannational initiatives.http://www.eldis.org/static/DOC13086.htm
Dilemmas and opportunities for anappropriate health-service response toviolence against women. Garcia MorenoC, (2002). The Lancet 359:1509-1514.
This article reviews what is knownabout the evidence from developingcountries on the effectiveness and limita-tions of programs that train providers toidentify and care for women who haveexperienced intimate partner violence.The article raises significant concernsabout introducing routine screening pro-grams in organizations that have notsucceeding in transforming the attitudesand beliefs of providers. http://www.thelancet.com/journals/lancet/article/PIIS0140673602084179/fulltext
International conference on the role ofhealth professionals in addressing vio-lence against women, 15th October2000, Naples, Italy, International
Journal of Gynecology & ObstetricsSupplement. [Garcia-Moreno C,Benegiano G, Guerra R (2002).]
This journal issue contains a collectionof papers from an international confer-ence devoted to the role of health pro-fessionals in addressing violence againstwomen. The collection includesdescriptions of programs and evaluationdata (when available) from developingcountries such as Bangladesh, Brazil,China, Russia, South Africa andThailand. In addition, it includes articlesthat present the ongoing efforts of inter-national organizations.
OTHER RESOURCES
Material Collections
End Violence against Women, JohnsHopkins University, Center forCommunications Programs
This site features an online collection ofmaterials and resources on preventingviolence against women. It is part of anongoing effort to share information withhealth professionals who seek informa-tion and resources on this subject.http://www.endvaw.org/
A Life Free of Violence: It’s Our Right(United Nations Inter-Agency Campaignon Women’s Human Rights in LatinAmerica and the Caribbean)
This site is part of the UNDP’s contribu-tion to the U.N. Inter-Agency Campaignon Women's Human Rights and providesa compilation of materials provided byall partner agencies.http://www.undp.org/rblac/gender/
Minnesota Center against Violence andAbuse (MINCAVA)
The MINCAVA Electronic Clearinghousestrives to provide a quick and easy accesspoint to the ever-growing number of
A P P E N D I X T H R E E1

A Practical Guide for Researchers and Activists 255
resources available online on the topic ofviolence and abuse. One focus of theClearinghouse is to assist faculty and staff in developing higher education cur-ricula on violence and abuse. TheClearinghouse shares in electronic formcurricula and syllabi used in violenceeducation programs at institutions ofhigher education across the United States.http://www.mincava.umn.edu
National Sexual Violence Resource Center
This clearinghouse provides information,resources, and research related to allaspects of sexual violence. Activitiesinclude collecting, reviewing, catalogu-ing, and disseminating informationrelated to sexual violence; coordinatingefforts with other organizations and proj-ects; providing technical assistance andcustomized information packets on spe-cific topics; and maintaining a websitewith up-to-date information.http://www.nsvrc.org
Reproductive Health Outlook (RHO)PATH’s RHO website provides links tonumerous sites of organizations address-ing violence against women andincludes sections on gender and menand reproductive health.http://www.rho.org/
Networks/Coalitions/Consortiums
GBV Prevention Network This network is a virtual community forthe 100+ member organizations in theHorn, East, and Southern Africa workingto prevent gender-based violence. Aresource for activists and practitioners inAfrica and beyond, it provides a richdatabase of regional programapproaches, communication materials,publications, reports, tools, and resources.There are also international documents,
resources, and links relevant to GBV pre-vention and opportunities to dialogue,contribute, and share experiences.www.preventgbvafrica.org
Coalition against Trafficking in Women The Coalition is composed of regionalnetworks and affiliated individuals andgroups and serves as an umbrella thatcoordinates and takes direction from itsregional organizations and networks inits work against sexual exploitation andin support of women’s human rights.http://www.catwinternational.org/
IntercambiosIntercambios is an alliance of interna-tional and national organizations basedin Latin America that aims to strengthenthe capacity of the public and privatehealth sectors to address gender-basedviolence through a public health andhuman rights approach. Intercambioscarries out activities on GBV in the fieldsof research, advocacy, training and com-munication.http://[email protected]
National Violence against WomenPrevention Research Center (NVAWPRC)
The Center serves as a clearinghouse forprevention strategies by keepingresearchers and practitioners aware oftraining opportunities, policy decisions,and recent research findings.http://www.vawprevention.org
Nursing Network on Violence againstWomen (NNVAW)
The NNVAW was formed to encouragethe development of a nursing practicethat focuses on health issues related tothe effects of violence on women’s lives.http://www.nnvawi.org/
A P P E N D I X T H R E E 1

256 Researching Violence Against Women
Reproductive Health for RefugeesConsortium (RHRC)
This Consortium is a partnership ofseven organizations dedicated to increas-ing access to a range of high-quality,voluntary reproductive health servicesfor refugees and displaced personsaround the world. Gender-based vio-lence is one of the four essential andcomplementary technical areas of repro-ductive health on which RHRC focusesits work. The website also features sev-eral links to reports and guides onaddressing gender-based violence inrefugee settings.http://www.rhrc.org/resources/gbv/index.html
Violence Against Women ElectronicNetwork (VAWnet)
This network provides support for thedevelopment, implementation, andmaintenance of effective violence againstwomen intervention and preventionefforts at the national, state, and locallevels through electronic communicationand information dissemination. VAWnetparticipants, including state domesticviolence and sexual assault coalitions,allied organizations, and individuals,have access to online databaseresources. http://www.vawnet.org
Organizations
Center for Women’s Global LeadershipThe 16 Days Campaign of ActivismAgainst Gender Violence is an interna-tional campaign originating in 1991.This 16-day period starts on November25, the International Day AgainstViolence Against Women, and ends onDecember 10, International HumanRights Day. The 16 Days Campaign hasbeen used as an organizing strategy byindividuals and groups around theworld to call for the elimination of all
forms of violence against women byraising awareness about gender-basedviolence as a human rights issue at thelocal, national, regional, and interna-tional levels. Since 1991, the 16 DaysCampaign has included the participationof over 1,700 organizations in approxi-mately 130 countries.http://www.cwgl.rutgers.edu/
Centre for Research on ViolenceAgainst Women and Children
The Centre is one of an alliance of fiveresearch centers in Canada whose pur-pose is to promote the development ofcommunity-centered action research onviolence against women and childrenand to facilitate individuals, groups, andinstitutions representing the diversity ofthe community to pursue research issuesand training opportunities related to theunderstanding and prevention of abuse.http://www.uwo.ca/violence/index.html
Family Violence Prevention Fund The Family Violence Prevention Fund,through the National Health Initiative onDomestic Violence (NHIDV), addressesthe health care response to domesticviolence through public policy reformand health education and preventionefforts. The NHIDV develops educa-tional resources, training materials, andmodel protocols on domestic violenceand screening to help health careproviders better serve abused women.http://endabuse.org/
International Planned ParenthoodFederation (IPPF), Western HemisphereRegion (WHR)
The IPPF/WHR website contains infor-mation on its GBV projects in LatinAmerica and the Caribbean. IPPF/WHRpublishes a quarterly newsletter called¡BASTA!, which can be accessed anddownloaded from its website. ¡BASTA!
A P P E N D I X T H R E E1

A Practical Guide for Researchers and Activists 257
reports on the efforts of IPPF affiliates inLatin America and the Caribbean toaddress GBV within the framework ofsexual and reproductive health andoffers practical information and tools toservice providers who wish to work inthis area.http://www.ippfwhr.org/
Isis InternacionalTogether with the Isis affiliate offices inManila and Kampala, Isis in Chile over-sees the Program on Violence againstWomen, an information and communica-tions initiative that provides informa-tional materials and resources toorganizations worldwide. (Information inSpanish only)http://www.isis.cl/
World Health Organization/PanAmerican Health Organization(WHO/PAHO)
The World Health Organization has sev-eral initiatives that deal with gender-based violence. The Department ofGender, Women and Health coordinatedthe WHO Multi-country Study onWomen’s Health and Domestic Violenceagainst Women, and it has several publi-cations on the effects of GBV onwomen’s health.http://www.who.int/gender/en/
WHO is also the coordinator of theSexual Violence Research Initiative (SVRI),a project that aims to strengthen thehealth-sector response to sexual violence. http://www.who.int/svri/en/
The Gender, Ethnicity and Health Unit ofthe Pan American Health Organization(PAHO) has numerous publications andfact sheets about GBV and health.http://www.paho.org/english/ad/ge/home.htm
PATHPATH is an international, nonprofitorganization that creates sustainable,culturally relevant solutions, enablingcommunities worldwide to break long-standing cycles of poor health. PATHpromotes gender equity in health andthe prevention of GBV using a systemsapproach to link communities, institu-tions, and policies. PATH works withlocal and international partners to carryout evidence-based advocacy and tostrengthen health systems and commu-nities to address GBV from a humanrights and public health perspective.http://www.path.org
United Nations Development Fund forWomen (UNIFEM)
UNIFEM provides financial and technicalassistance to innovative programs andstrategies that promote women’s humanrights, political participation, and eco-nomic security. The website featuresinformation about international resolu-tions concerning violence againstwomen, UNIFEM’s work, availableresources, and the application process.The UN Internet Gateway on theAdvancement and Empowerment ofWomen (WomenWatch) facilitates inter-net searching through UN organizationsfor materials on GBV. http://www.unifem.org/http://www.un.org/womenwatch/asp/user/list.asp?ParentID=3004
A P P E N D I X T H R E E 1

WHOAvenue Appia 20CH-1211 Geneva 27Switzerlandwww.who.int/gender/en
ISBN 92 4154647 6
PATH1800 K Street NWSuite 800Washington, DC 20006USAwww.path.org