relapsing nephrotic syndrome in childhood - core
TRANSCRIPT
Kidney International, Vol. 16 (1979), pp. 75-85
NEPHROLOGY FORUM
Relapsing nephrotic syndrome in childhoodPrincipal Discussant: WARREN E. GRUPE
Harvard Medical School and Children's Hospital Medical Center, Boston, Massachusetts
Case presentation
A 13.5-year-old boy with relapsing nephrotic syndromewas first treated for nephrosis at the age of 21 months. Atthat time, clinical signs included facial edema, edema ofthe extremities, and a distended abdomen. Blood pres-sure and renal function were normal, but he had severehypoalbuminemia (1 g/100 ml), hypercholesterolemia,and heavy proteinuria; 12-hour urine protein excretionwas 8.6 g. He was treated with a single 25 U dose of ad-renocorticotropic hormone (ACTH), and prednisone wasadministered in a divided dosage of 50 mg/day, for 2weeks, and 60 mg, every other day, thereafter. Within Iweek, urine protein excretion decreased to zero and ede-ma remitted. The patient was discharged on a regimen ofpenicillin prophylaxis and prednisone.
Over the next 8 months, the dosage of prednisone wasslowly tapered from 60 mg, every other day, to 10 mg,every other day. Three to four days following onset of aviral upper respiratory infection, however, proteinuria,hypoalbuminemia, and edema recurred. The dosage ofprednisone was again increased to 60 mg, every otherday, and a clinical remission again resulted with qualita-tive protein excretion decreasing to negative." Similarrelapses occurred at ages 3 and 4.5 years. During the lat-ter episode, the proteinuria did not disappear for the 2months during which prednisone was administered in a
75
dosage of 60 mg, every other day, but did subsequentlydisappear following a 2-week regimen of 100 mg of pred-nisone, every other day.
Six months later at age 5 years, proteinuria again re-curred (24-hour urine protein excretion, 1.2 to 1.5 g) whilethe patient was still receiving prednisone in a dosage of 50mg, every other day. Azathioprine was administered for 2weeks in a dosage of 50 mg/day but was stopped becauseof an intercurrent episode of pneumonia. Over the next 6months, proteinuria reappeared whenever the dosage ofprednisone was tapered to less than 30 mg, every otherday. Azathioprine was given for 3 months in a dosage of50 mg/day, and prednisone was slowly tapered; onemonth following institution of azathioprine therapy, the24-hour urine protein excretion was 10 mg. Azathioprinetherapy was discontinued because mild leukopenia devel-oped; prednisone was stopped as well, and the patient re-ceived no medication for the next 3 months.
At age 6 years immediately following the onset of sys-temic complaints related to a viral syndrome, the ne-phrotic syndrome recurred (24-hour urine protein excre-tion, 10.5 g). With no treatment, however, quantitativeprotein excretion decreased within 2 weeks to 3.2 g and inthe following 3 weeks to undetectable levels. At age 7 years,a partial relapse (24-hour urine protein excretion, 0.5 g)prompted a brief course of prednisone therapy; the pa-tient then remained in remission (24-hour urine proteinexcretion, undetectable) for the next 1.5 years.
At age 8.5 years, heavy proteinuria reappeared. Ad-ministration of prednisone in a dosage of 60 mg, everyother day, decreased 24-hour urine protein excretion to33 mg within 2 weeks. The prednisone dose was taperedand therapy was stopped after approximately 18 months.One month later at age 10 years, 24-hour urine protein
Presentation of the Forum is made possible by grants fromHoechst-Roussel Pharmaceuticals Inc., Smith Kline & FrenchLaboratories, G. D. Searle & Co., Warner-Lambert Pharma-ceuticals Division, Burroughs Wellcome Company, GeigyPharmaceuticals Inc., and Boehnnger Ingelheim Ltd.
0085-2538/79/0016—0075 $02.20© 1979 by the International Society of Nephrology
The Nephrologv Forum is designed to relatethe principles of basic science to clinical prob-lems in nephrology.
EditorsJORft\N J. Coiii NJOHN 1. HARRv'c IONJEROME P. KX5SIRER
it England .% kdh a I Center HospitalBoston I lOS s(i(/lt(S(tt1i
76 Nephrology Forum
excretion increased again to 10 g. A 1-month course ofprednisone in a dosage of 60 mg, every other day, had noeffect nor did a second month of prednisone therapy at anincreased dosage of 120 mg, every other day; prednisonetherapy was therefore stopped. Eight months later at age10.7 years, cyclophosphamide (75 mg/day) and predni-sone (20 mg/day) were administered for 4 months. Theprednisone dosage was increased to 120 mg, every otherday, for the final 2 weeks of the therapeutic period andthen rapidly tapered. Twenty-four-hour urine protein ex-cretion was 9.6 g before and 3.8 g following this regimen.
Over the 2 to 2.5 years since that last relapse and itstreatment with cyclophosphamide and prednisone, 24-hour urine protein excretion has slowly decreased to itsmost recent level of 130 mg. The patient's blood pressureis normal, serum creatinine concentration is 0.7 mg, andserum albumin concentration is 4.8 g/l00 ml. Growth anddevelopment appear to be normal; the patient's heightand weight are just below the mean for his age.
Discussion
DR. WARREN E. GRUPE (Associate Professor ofPediatrics, Harvard Medical School, Director ofPediatric Nephrology, Children's Hospital): Thisyoung man has experienced 12 years of steroid re-sponsive, but relapsing, nephrotic syndrome,treated at one time or another with ACTH, predni-sone, azathioprine, and cyclophosphamide. Insome periods relapses were frequent and in othersinfrequent; at times he was steroid dependent and atother times he demonstrated spontaneous remis-sions. The one surprise is that his long associationwith an active university nephrology group did notresult in his having a renal biopsy.
The first question to answer is what particular va-riety of nephrotic syndrome he has and whether arenal biopsy is indeed necessary for that definition.In this regard, we pediatricians have a distinct ad-vantage over our internist colleagues. In the pediat-
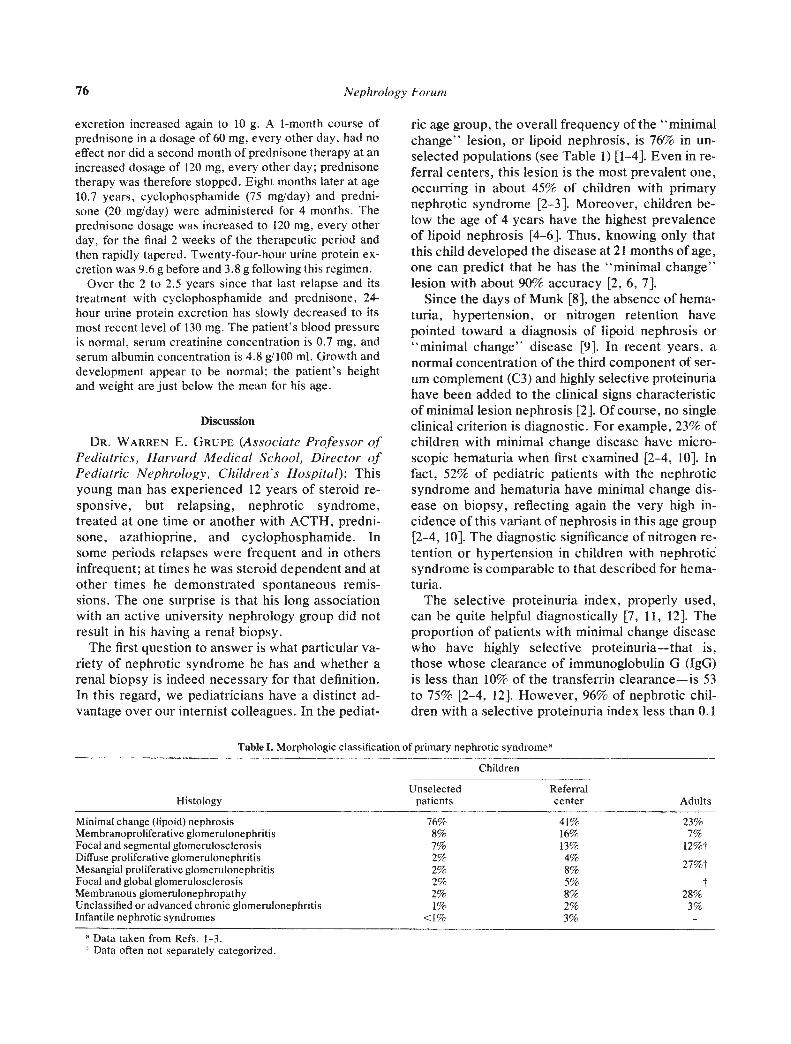
nc age group, the overall frequency of the "minimalchange" lesion, or lipoid nephrosis, is 76% in un-selected populations (see Table 1) [1—4]. Even in re-ferral centers, this lesion is the most prevalent one,occurring in about 45% of children with primarynephrotic syndrome [2-3]. Moreover, children be-low the age of 4 years have the highest prevalenceof lipoid nephrosis [4-6]. Thus, knowing only thatthis child developed the disease at 21 months of age,one can predict that he has the "minimal change"lesion with about 90% accuracy [2, 6, 7].
Since the days of Munk [8], the absence of hema-tuna, hypertension, or nitrogen retention havepointed toward a diagnosis of lipoid nephrosis or"minimal change" disease [9]. In recent years, anormal concentration of the third component of ser-um complement (C3) and highly selective proteinuriahave been added to the clinical signs characteristicof minimal lesion nephrosis [2]. Of course, no singleclinical criterion is diagnostic. For example, 23% ofchildren with minimal change disease have micro-scopic hematuria when first examined [2-4, 10]. Infact, 52% of pediatric patients with the nephroticsyndrome and hematuria have minimal change dis-ease on biopsy, reflecting again the very high in-cidence of this variant of nephrosis in this age group[2-4, 10]. The diagnostic significance of nitrogen re-tention or hypertension in children with nephroticsyndrome is comparable to that described for hema-tuna.
The selective proteinuria index, properly used,can be quite helpful diagnostically [7, 11, 12]. Theproportion of patients with minimal change diseasewho have highly selective proteinuria—that is,those whose clearance of immunoglobulin G (IgG)is less than 10% of the transferrin clearance—is 53to 75% [2—4, 12]. However, 96% of nephrotic chil-dren with a selective proteinuria index less than 0.1
Table I. Morphologic classification of primary nephrotic syndromea
Histology
Children
AdultsUnselected
patientsReferralcenter
Minimal change (lipoid) nephrosis 76% 41% 23%Membranoproliferative glomerulonephritis 8% 16% 7%Focal and segmental glomerulosclerosis 7% 13% 12%tDiffuse proliferative glomerulonephritisMesangial proliferative glomerulonephritis
2%2% 8% 279°
Focal and global glomerulosclerosis 2% 5% tMembranous glomerulonephropathy 2% 8% 28%Unclassified or advanced chronic glornerulonephritis 1% 2% 3%Infantile nephrotic syndromes <1% 3% -
a Data taken from Refs. 1-3.Data often not separately categorized.

Relapsing nephrotic syndrome in childhood 77
have minimal change disease on biopsy [4, 12].Thus, the finding of highly selective proteinuria is arather good predictor of morphology in childreneven though the p:resence of "poorly" selectiveproteinuria by no means excludes this diagnosis(see Table 2). Parenthetically, neither does poorlyselective proteinuria preclude a response to steroidtherapy.
Certain clinical criteria when taken collectivelydefine with surprising accuracy a subgroup of chil-dren who have a favorable outlook. The criteria forinclusion in this favorable subgroup are (1) ages ito10, (2) absence of nitrogen retention, (3) absence ofhematuria, (4) absence of hypertension, (5) normalserum concentration of C3, and (6) highly selectiveproteinuria; approximately 95% of such childrenhave minimal change disease on renal biopsy, re-spond to steroid therapy, and have a good prognosis[2, 7, i2]. Given the age of onset, the presentingsigns, the response to steroids, and the persistenceof normal renal function after 12 years of disease inthe patient described here, we can presume a diag-nosis of minimal lesion nephrosis with an accuracythat approaches that of renal biopsy. Thus, a biopsyin the early stages of his disease could be consid-ered unnecessary. In part, this analysis explainswhy fewer pediatric patients are subject to renalbiopsy than are adults.
Assuming that this patient has a minimal changelesion, let's turn to a review of our current under-standing of the mechanisms of glomerular injury inthis particular histopathologic type of nephrosis. Itis fair to say that the pathogenesis remains totallyunknown [13]. Despite many attempts to implicatehumoral processes in the etiology, neither con-vincing nor reproducible evidence exists. At onetime or another, various immunoglobulins wereconsidered important in the pathogenesis of this dis-
Table 2. Idiopathic nephrotic syndrome of childhood:Relationship of selected clinical characteristics to complete
response to steroidsa
Clinical parameter Prevalence
Complete responseto steroids
if parameter
Present Absent
Hematuria (microscopic) 23% 33% 87%Nitrogen retention 7.4% 33% 78%Hypertension 8.1% 36% 78%SPI <0.l 56% 38% 97%Serum C3 reduced 9.3% 0% 75%
a Data taken from Ref. 7.SPI = selective proteinuria index.
order. The evidence, however, is not convincing.Earlier reports of glomerular deposition of IgE havenot been confirmed consistently [14]. Nor is thereconvincing indication that the reported alterationsin serum immunoglobulin concentrations—particu-lary elevation of 1gM—follow a consistent pattern,bear any specific relation to disease activity, or areunique to minimal change disease [15, 16]. Besides,it is difficult to interpret serum immunoglobulin con-centrations in the presence of heavy proteinuriawithout studies of synthesis and turnover. It seemslikely that alterations of immunoglobulin patternsare only secondary manifestations of the disease.
Convincing evidence that the complement systemis involved is likewise lacking [13]. Early reportssuggested reduced concentrations of total hemo-lytic complement (CH5O) in patients with lipoidnephrosis" [17]. More recent reports in patientswith biopsy-proven minimal change disease, how-ever, have failed to show abnormal concentrationsof CH5O [13]. Serum concentrations of C3 arerarely, if ever, decreased [4, 7, 13] and C4 levels arelikewise normal [13]. Reports of reduced Ciq con-centrations have not been confirmed [13]. Faint orfocal deposits of glomerular C3 have been reportedbut are of doubtful significance. In fact, most neph-ropathologists now include the absence of glomeru-tar deposits by immunofluorescence in the morpho-logic definition of minimal change disease.
It has been reported that immunoconglutinin be-comes elevated in minimal change disease within 48hours of a relapse and this finding has been thoughtto have pathogenetic significance [18]. This eleva-tion may be related to some other factors, however,such as intercurrent infection. For example, one re-port indentified 15 occasions in 30 patients in whichimmunoconglutinin concentrations were raised; ononly two occasions was a high titer associated withrelapse [13].
The paucity of evidence supporting classical im-munological mechanisms, coupled with the lack ofovert structural damage to the glomeruli, suggeststhat some factor related to capillary permeabilitycould be responsible. This hypothesis would also beconsistent with the rapid appearance and reversal ofsigns and symptoms of the disease, as well as thevariety of stimuli ranging from allergy to infectionthat are associated with relapses. Evidence is begin-ning to appear from several laboratories that suchcirculating factors may indeed play a key role.
In one recent study, a factor was found in theserum of 39 patients with steroid-responsive neph-rotic syndrome that inhibited the agglutination of la-

78 Nephrology Forum
tex particles coated with human IgG [19]. Presentin relapse, this factor gradually disappeared withsuccessful steroid therapy. By Sepharose chroma-tography, this factor contains "heavy" IgG; it hasbeen proposed that it represents a circulating im-mune complex without complement activating ac-tivity. Another study demonstrated that preformedimmune complexes, solubilized by exposure to ex-cessive amounts of antigen and infused into saline-loaded rats, produced oliguria and transient protein-uria [20]. No complex deposition was demonstratedin the glomeruli of these animals by immuno-fluorescence. The authors suggested that such tran-sient changes could be mediated by kinin activa-tion, though no evidence for activation of this sys-tem was presented. A factor has also been found inthe supernatants of cultured, stimulated lympho-cytes from nephrotic patients in relapse that in-creased vascular permeability in the guinea pig andhad kinin-like properties [21].
Recently, a lymphocytotoxic response towardepithelial cells derived from trypsinized renal epi-thelial cell cultures was demonstrated in 9 of 12 pa-tients with minimal change disease [22]. The effectin these patients was notably greater than that seenin 12 patients with proliferative glomerulonephritis.This difference was not thought to be attributable tothe phagocytic cells in the cellular preparations.The relevance of these observations, however, isnot certain. For one thing, renal biopsies from pa-tients with minimal change disease show little or noevidence of epithelial cell damage from lympho-cytes.
Using the leukocyte migration inhibition test ineight patients with minimal change disease, Mallicket al demonstrated what was considered to be T-cellsensitization to an antigen obtained from a homoge-nate of neonatal human kidney cortex [23]. A simi-lar observation was made in other glomerular dis-eases as well. In another group of patients with min-imal change disease, 21 of 29 patients showedevidence of lymphocyte sensitization to neonatalkidney before receiving therapy for relapse as wellas during remission. Similar sensitization to adulthuman kidney was not demonstrated, which raisesthe question of whether these lymphocytes might beresponding to a persistent fetal antigen.
Some evidence suggests that T-cell function maybe suppressed in minimal change disease. Ooi wasable to demonstrate "cold" lymphocytotoxins inthe sera of five of eight patients with lipoid nephro-sis and in six of ten patients with diffuse prolifera-tive glomerulonephritis [24]. These lymphocytotox-
ins, thought to represent autoantibodies, have alsobeen described in systemic lupus erythematosus,rheumatoid arthritis, pernicious anemia, allograftedanimals, pregnant women, and aging populations;however, they are not found in patients with otherrenal lesions, such as acute tubular necrosis, renalcalculi, or polycystic disease. Therefore, a specificrelationship to minimal change disease, or for thatmatter any proteinuric state, is in doubt. Anotherstudy found that plasma from patients with minimallesion nephrosis in relapse inhibited autologouslymphocyte responses to phytohemagglutin and al-logenic lymphocytes [25]. This plasma factor wasnot demonstrable in remission.
These several phenomena may reflect alterationsin T-cell function [26], but no evidence has clearlyestablished T-cell activity or suppression as a directmediator of altered glomerular permeability. Thesestudies do not yet follow a predictable pattern noryield a completely understandable role for the T-cell in nephrotic syndrome [13]. Many of the phe-nomena are not unique to minimal change diseasesince some activity, suppression, or altered func-tion is also detected in other forms of glomerulardisease or in diseases having no clear glomerular in-volvement. The present evidence for T-cell in-volvement in lipoid nephrosis is therefore sugges-tive, exciting, and clearly worthy of further pursuiteven though currently somewhat incoherent.
The characteristic propensity for minimal changedisease to respond repeatedly to steroid therapy of-fers no further insight into the nature of the gb-merular injury. Despite the absence of prospective,controlled studies, corticosteroids have becomefully accepted therapy for children with minimalchange disease [2—4, 10, 12]. Steroids have not,however, been totally accepted for adults [27]. It isnot at all clear, however, how corticosteroids alterthe manifestations of the disease. These drugs arecalled anti-inflammatory, yet there is no evidence ofglomerular inflammation in minimal change disease.These drugs are likewise immunosuppressive, yet,as discussed before, there is little evidence that im-munoglobulins are in any way responsible for thedisease. There is no evidence for a direct steroideffect on the glomerular basement membrane. It isclear that corticosteroids affect lymphocytes; how-ever, there is no indication that this is the mecha-nism by which steroids reverse proteinuria.
Let us now turn to the therapeutic issues. Retro-spective clinical studies suggest a beneficial long-term effect of steroid therapy in children, and somepediatric nephrologists believe that the improved

Relapsing nephrotic syndrome in childhood 79
survival rate in childhood is related to the bettercontrol of the disease with steroid therapy [4, 12,28]. Because of this widespread belief, it is difficultto acquire data concerning the frequency of sponta-neous remissions in children; from previous workwe suspect the rate is as high as 25% [28—30]. Thepatient presented today did have a spontaneous re-mission on at least one occasion.
Using prednisone dosages of 60 mg/M2/day in di-vided doses, 85% of children with minimal changedisease become protein-free within 3 to 4 weeks(see Table 3) [4, 7]. Eight percent require more than4 weeks and 4V2% take as long as 12 weeks [4, 7]. Inthis latter group, it is not clear that steroids actuallycontribute to the response. Following an initialclearing of proteinuria, several clinical courses arepossible. Fifteen to twenty percent of these childrenrequire no further treatment and never have a re-lapse of the disease; this is true despite the reintro-duction in some cases of what might have been theprecipitating stimulus for that individual—for ex-ample, infection or an allergic reaction [7, 30—33].Eighty to eighty-five percent of children have sub-sequent relapses, 55% having five or more relapsesof heavy proteinuria [7]. The frequency of relapsetends to decrease as the child gets older [32]. Twen-
Initial Maintenance
ty-five to forty percent manifest steroid dependen-cy—that is, proteinuria recurs whenever steroidsare discontinued [3, 4, 34, 35]; 3 to 10% eventuallybecome steroid resistant [7, 32].
This young man's course demonstrates the diffi-culty of predicting the outcome for a given individ-ual from group data. His initial response to steroidswas prompt and complete. He averaged one relapseper year for the first 4 years of his disease, respond-ing to medication given only every other day. Dur-ing his third relapse he took a longer time to re-spond; whether the remission would have been in-duced more rapidly if he had been taking 60 mg/M2/day in divided doses is uncertain. It has been theexperience of many pediatric nephrologists that ahigher proportion of patients respond to divideddaily doses than to the same amount of medicationgiven every other day.
At age 5, he developed what appears to have beena steroid-dependent state, which was partially al-tered coincident with short-term azathioprine thera-py. The evidence that azathioprine is effective inthis disease is mixed. Several uncontrolled studiesusing relatively large doses of the drug seemed toindicate that it was efficacious [36—38]. In 1970—infact, shortly after this child was treated withazathioprine—one controlled trial was reported inwhich steroid-resistant patients were randomly allo-cated to receive either intermittent prednisone ther-apy plus azathioprine in a dosage of 60 mg/M2/day orintermittent prednisone plus placebo for 90 days[39]. Another group of frequently relapsing patientswas similarly allocated for 180 days of therapy [39],This study failed to demonstrate an advantage ofadding azathioprine either in eliminating proteinuriain nonresponsive patients or in altering the courseof patients with frequent relapses. As a result,azathioprine is rarely used today in the managementof pediatric patients with relapsing nephrotic syn-drome.
By contrast, in controlled studies the alkylatingagents cyclophosphamide and chlorambucil havebeen clearly demonstrated to be effective in steroid-dependent nephrotic syndrome [35, 40, 42]. In onestudy, prednisone was given to all patients in a dos-age of 60 mg/M2/day until proteinuria ceased, fol-lowed by a similar dose given every other day for 4months [40]. Cyclophosphamide in a dosage of 2.5mg/kg/day was added to one group of such patientsbut not to another group. During a follow-up periodof 14 to 39 months, over 90% of the patients treatedwith prednisone alone experienced relapses, ascompared with only 17% of the patients treated with
Table 3. Therapy of minimal change nephrotic syndrome'
PrednisoneFirst attack I to 2 mg/kg/day or None
60 mg/M2/day(maximum—80 mg/day) in divided dosesuntil urine negativefor protein for 2weeks
Relapse Ito 2 mg/kg/day or 3 mg/kg60 mg/M2/day (maximum—80 mg)(maximum—80 mg/ as single morningday in divided doses dose every otheruntil urine negative day for 4 to 6 weeksfor protein for 2 more of a proteinweeks, negative urine, then
gradually reducedose over another 4to 6 weeks untildiscontinued 3months after initialtherapy
Cyclophosphamide2 to 3 mg/kg/day orally, together with steroids, for 8 to 10 weeksmaximum
Chlorambucil0.2 to 0.3 mg/kg/day orally, together with steroids, for 10 to 12weeks maximum
a Data taken from Ref. 10.
80 Nephrology Forum
both drugs. Another study compared the same totaldose of cyclophosphamide given over two periodsof time [35]. One group received cyclophosphamidein a dosage of 2.5 mg/kg/day for 90 days, while asecond group received 5 mg/kg/day for 45 days.Prednisone was given throughout the period of cy-clophosphamide therapy. The duration of remissioninduced was similar in both groups. The frequencyof acute toxic side effects, however, was signifi-cantly higher in the group receiving the larger dailydose of cyclophosphamide. It also should be notedthat cyclophosphamide, given together with ster-oids, will occasionally convert an initially steroid-unresponsive patient to steroid responsive.
It is clear that the development of leukopenia orother toxicity is not required to achieve a therapeu-tic response from cyclophosphamide; moreover,the duration of the subsequent remission does notdepend on producing marrow suppression. There issome evidence, however, that the duration of re-mission following a course of therapy may be re-lated to the duration of therapy [41]. In patientstreated for less than 6 weeks, as few as 27%remainin remission beyond the first year. Currently theusual course of therapy consists of cyclophospha-mide and prednisone given for 2 months. With thisregimen, one can expect a remission rate of 58% at2 years and 44% at 4 years [41]. If treatment is ex-tended to 3 months, about two-thirds of patientswill be in remission 5 years or more after therapy[41]. As noted in the case report, the patient wastreated in this manner for 4 months and in fact is inremission 2.5 years later.
There is only one report of a prospective, con-trolled study using chlorambucil [42]. In this study,21 children with either steroid-dependent or fre-quently relapsing nephrotic syndrome were exam-ined. All control patients treated with prednisonealone continued the same pattern and rate of re-lapse; in all such patients, proteinuria returned by 7months. The group which received prednisonealong with chiorambucil for 6 to 12 weeks remainedin complete remission without further medicationduring the 12 to 34 months of observation. A com-parison with published reports of cyclophospha-mide suggested that the remission induced by chlo-rambucil was more "stable." A subsequent studyshowed that 84% of children so treated were in re-mission 3 years later and 78% at 5 years [43]. Fur-ther evaluation shows that a total chlorambucil dosein excess of 14 mg/kg or daily doses in excess of 0.3mg/kg for treatment periods in excess of 12 weeksconfer no additional benefit and thus are no longer
warranted [43, 44]. As in the case of cyclophospha-mide, there is no evidence that leukopenia is neces-sary to attain a therapeutic effect. One of the appar-ent advantages of chlorambucil has been its minimalimmediate toxicity when compared with cyclophos-phamide. It may be, however, that this low immedi-ate toxicity is a major disadvantage because it per-mits the use of doses far in excess of those neededto alter the course of the disease. Current recom-mendations are to limit the daily dose of chlorambu-cil to 0.2 mg/kg and to continue therapy for no morethan 10 to 12 weeks. Even this dosage may be morethan necessary.
Acute and chronic toxicity remain a major con-cern with cytotoxic agents [10, 42, 45]. Toxicity in-cludes marrow depression, infection, alopecia, nau-sea and vomiting, tumor induction, chemical cys-titis, hepatitis, phlebitis, oral ulceration, andsterility. Alopecia and chemical cystitis are muchmore common with cyclophosphamide than withchlorambucil. Both appear to be dose related, butwith currently recommended dosage schedulesthese complications should not be a major problem.Bladder fibrosis may develop in patients treatedwith cyclophosphamide, but has usually been aproblem with high doses used over time periodslonger than that necessary to achieve an effect inminimal change disease. Gastrointestinal irritationis generally minor and has not seriously limited theuse of either of these drugs. We have seen no ex-amples of hepatitis, phlebitis, or oral ulceration atthe doses we have outlined.
Sterility has been reported in both sexes with cy-clophosphamide [41, 46]. The male appears to bemore at risk than the female, and the effect seems tobe related to both dose and the duration of treat-ment. Doses below 5 mg/kg/day for less than 60days do not seem to produce azoospermia, whilesimilar doses for longer than 89 days are routinelyfollowed by this complication [46]. The thresholdfor cyclophosphamide-induced azoospermia seemsto be a cumulative dose above 250 mg/kg or ex-posure for greater than 60 days [46]. With chlo-rambucil, azoospermia occurs in both prepubertaland pubertal males with cumulative doses in excessof 7 mg/kg when given without steroids or at greaterthan 17 mg/kg when given with steroids [47, 48]. Ata cumulative dose in excess of 25 mg/kg, azoo-spermia is virtually certain to occur [48]. Recoveryof spermatogenesis has been reported after discon-tinuing the drugs in both cases [49, 50].
Malignant tumors rarely develop after therapywith both drugs. Solid tumors complicate therapy

Relapsing nephrotic syndrome in childhood 81
with cyclophosphamide, and leukemia complicatestherapy with chlorambucil; these malignancies usu-ally appear within 3 years of drug therapy [51]. Fourcases of leukemia have been reported in childrenfollowing treatment with chlorambucil [52]. Threeof the four patients also received other cytotoxicdrugs, and all were treated with either higher dosesor for longer durations than that which we currentlyrecommend. We have followed 35 children for long-er than 3 years and fortunately none has developeda malignancy [43].
Focal seizures occur in about 6% of childrentreated with chlorambucil [53]. These seizures aretransient and unrelated to age, underlying disease,duration of illness, dose, or duration of therapy.
The multiple serious complications of therapywith alkylating agents make it critically important toestablish the lowest minimum effective dose forboth medications and mandate careful selection ofpatients to receive this therapy. We restrict the useof these drugs to children with established steroiddependence or resistance, who are experiencing thesevere side effects of corticosteroid therapy; oftensuch patients fail to grow and are debilitated by thecombined effects of steroid treatment and the per-sistent protein-losing state [42]. We do not use thesemedications in children for whom steroids have be-come only a nuisance. With current selection cri-teria, I doubt that we would have selected this pa-tient for treatment with alkylating agents.
In contrast to steroids, it is clear that these drugsalter the course of minimal change nephrosis inchildhood [10], but as just noted, the complicationsof therapy with cytoxic agents are worrisome. Forthis reason some investigators have sought to altersteroid regimens to achieve a better therapeutic ef-fect with less toxicity. In one ongoing study in chil-dren with frequent relapses, the Mid-European Ste-roid Trial, intermittent steroid therapy was com-pared with alternate day steroid therapy [54].Progress reports from this study indicate that alter-nate day prednisone in a dosage of 35 mg/M2!48hours is more effective than intermittent prednisonein a dosage of 40 mg/M2, for 3 out of every 7 days, inreducing the relapse rates [54]. The children returnto their familiar pattern of frequent relapses, how-ever, when treatment is stopped. Thus, one may beable to suppress relapses with long term alternateday therapy, but this effect does not appear to alterthe course of the disease.
Another approach to this problem has come fromHelsinki. Using the 2-hour ACTH-stimulated corti-sol level as a probe, this group has shown that chil-
dren with long remissions had significantly higherplasma cortisol responses both before and afterprednisone therapy than children with frequent re-lapses [55, 56]. A normal response to ACTH pre-dicted a remission of 6 months or longer, whereas asubnormal response predicted a relapse within a 6-month period. These results imply that patientswith frequent relapses have a suppression of the hy-pothalamic-pituitary-adrenal (HPA) axis and sug-gest that this suppression, possibly induced by ste-roid therapy, may promote a relapse. There is noindication yet, however, that allowing the HPA axisto return to normal has any effect on the course ofthe disease or the frequency of relapses.
What does the future hold for this young man?His protein excretion is only slightly increased forhis age and size, he has normal renal function, andhe is growing and developing normally. He may re-main symptom-free for many years, develop occa-sional relapses, or indeed develop frequent relapsesonce more. Should this be the case, a second courseof cyclophosphamide or chlorambucil could be con-sidered. Over the long term, however, we mustkeep things in perspective; although the mortalityfor all nephrotic children is 7 to 12% [10], while themortality for children with minimal lesion, steroid-responsive disease, as this boy has, should not ex-ceed 1 to 2% [7, 10].
In closing, we might keep our therapeutic reli-gions also in perspective by reviewing one morestudy. This report describes a follow-up study of 26children who had the nephrotic syndrome for 2 to 5years or more [28]. Although 27% died, only 15%had persistent proteinuria and 50% recovered com-pletely with no evidence of the disease. The date ofthe report—1929; the form of treatment—kidneydecapsulation.
Questions and Answers
DR. J. T. HARRINGTON: Dr. Grupe, I should liketo make two comments and then ask a question.First, for the reasons you mentioned at the outset ofthe discussion, I chose not to perform a renalbiopsy in this patient but simply assumed that hehad minimal change disease. Second, with the ex-ception of the first 2 weeks, I chose not to use dailysteroid therapy in this child because of my concernabout the side effects of prednisone. My question is,have any studies demonstrated measurable differ-ences in the incidence of side effects in pediatric pa-tients treated either with daily or every other daytherapy?
82 Nephrology Forum
DR. W. E. GRUPE: I am unaware of a publishedstudy that prospectively compares the various ste-roid programs in that manner. No one of the manytreatment programs in the literature that vary indosage, duration of initial therapy, and use of main-tenance therapy has emerged as clearly superior ineither short or long-term results [10]. The publishedstudies using alternate day steroids as initial treat-ment claimed it was as effective in producing a com-plete remission as daily therapy but with less tox-icity [57, 58]. These were studies in a heterogeneousgroup of unbiopsied patients, however, and long-term outcome was not included. Other pediatricnephrologists found alternate day steroids to be su-perior maintenance therapy but not as effective asinitial treatment. The practice failed to gain wide ac-ceptance in pediatrics.
The patients with frequent relapses or steroid de-pendency are a major concern since they are atgreater risk for more steroid toxicity, and in childrenfor more growth problems. Early studies in Belgiumsuggested these patients might have emerged be-cause of steroid therapy [59]. Steroid scheduleswith less suppressive effect may need to be devisedfor even the initial episode. This is what is impliedin the Finnish studies that relate frequent relapsesto suppression of the HPA axis [55, 56].
DR. BORIS SENIOR (Chief, Pediatric Endocrinolo-gy, New England Medical Center Hospital): Haveyou had any experience with the use of methyl-prednisolone intravenously?
DR. W. E. GRUPE: No we have not. There is avery preliminary indication, however, that methyl-prednisolone administered intravenously is as ef-fective as prednisone taken orally for the inductionof a remission [60]. Whether the subsequent courseof the disorder will prove to be any different re-mains to be seen.
DR. B. SENIOR: Do you think parenteral methyl-prednisolone provides any advantages in the patientwho has not responded to daily prednisone in anadequate dose?
DR. W. E. GRUPE: I don't believe there are suf-ficient data to indicate that methylprednisolone ad-ministered intravenously is any more effective thansteroids taken orally in the nonresponsive patientwith minimal change disease.
DR. DAVID BUSHINSKY tRenal Fellow, New Eng-land Medical Center Hospital): Given the poten-tially serious complications of treatment, the pauci-ty of evidence that therapy alters the natural historyof the disease, and our capacity to treat the diseasesymptomatically with diuretics, are we in fact justi-
fled in treating these young patients with steroids,let alone the cytotoxic agents you described?
DR. W. E. GRUPE: That is a very good point, andit is really at the crux of the conceptual differencebetween adult and pediatric patients. In children,we are concerned with growth and developmentand think of survival in terms of many decades.Even though the adult with minimal change diseasemay respond as readily as a child to steroid therapy[27], there are many whose edema can be controlledwith diuretics alone; it is my impression that controlof edema with diuretics alone is more difficult toachieve in the child. In addition, diuretic therapydoes not control the proteinuria, hypoproteinemia,and hyperlipidemia. The child with massive protein-uria and hypoproteinemia does not grow. Finally,the long-term effects of prolonged diuretic therapyare not really known in such children, particularlyin terms of growth and development.
If we return to the presteroid, preantibiotic peri-od, only one-third of these patients survived thefirst 5 years [28, 30]. After the introduction of anti-biotics, survival doubled [28, 30]. With the currentcontrol of the disease with steroids, plus better anti-biotics and more potent diuretics, death at 5 years isnow only 1.5 to 6% [10]. Whether that could beachieved in children with diuretics and antibioticsalone is not known, and I know of no one who reallywants to withhold steroids to find out.
I would insert another caution about diuretictherapy. High doses of potent diuretics in a severelyhypovolemic child may produce more contractionof the plasma volume without necessarily producinga significant change in plasma oncotic pressure or ashift of extracellular fluid to the plasma space. Ourconcern is that either venous or arterial thrombosiscould be enhanced by volume contraction in thesepatients.
Even if we accept steroid therapy as reasonable,there seems to be no long-term advantage to usinghigh doses for prolonged periods. I would hope wewould all examine steroid therapy more carefully.
DR. J. P. KASSIRER: I have the same concernsabout therapy with cytotoxic drugs per se, and Iwas about to ask a similar question. I have resistedgiving children with steroid-dependent nephroticsyndrome anything but steroids, particularly out ofconcern for their becoming sterile. I haven't feltthat this cost was worth the marginal benefit. Howdo you select patients for therapy with theseagents?
DR. W. E. GRUPE: I agree that cytotoxic drugsshould be used with caution. We restrict their use to

Relapsing nephrotic syndrome in childhood 83
patients for whom continued use of steroids is es-sential, but they are becoming a real danger [42, 53].Many patients with steroid dependency or frequentrelapses can be maintained on low dose alternateday steroid therapy in complete remission with nor-mal growth and development. A smaller subgroup,however, requires higher doses or more frequentdaily therapy resulting in serious steroid toxicityand growth arrest. It is this high-risk problem groupthat we have included in our chlorambucil program[42].
DR. J. T. HARRINGTON: I should like to commentbriefly on some of the reasons we treated this pa-tient on so many occasions. I believe there are oftena number of psychosocial reasons beyond protein-uria that may make it reasonable to use cytotoxicdrugs in appropriate doses. For instance, when thispatient relapsed and became severely edematous,he was reluctant to go to school because the otherchildren made fun of him. In addition, he was a verygood hockey player and when he relapsed duringthe hockey season he became so edematous that hecould not play, which was very detrimental to hismorale and general well-being.
DR. LAWRENCE FEINGOLD (St. Luke's Hospital,New Bedford, Massachusetts): How long do youwait after a child relapses for spontaneous remis-sion to occur? Do you treat soon after a relapse?
DR. W. E. GRUPE: We generally allow 10 days to2 weeks of proteinuria before restarting steroids,particularly when the relapse was initiated by an in-tercurrent infection. I am not sure that we wait longenough; maybe spontaneous remissions would bemore frequent if we allowed a longer interval. Ouraim, however, is to avoid edema and hospital-ization.
DR. J. J. COHEN: I wonder if you would elaboratefurther about the pathogenesis of this fascinatingcondition. Histologically, there appears to be noevidence for an immunologic basis, yet the onlycommon denominator linking the two classes of ef-fective therapeutic agents, namely steroids andcytotoxic drugs, is that they are immunosup-pressive.
DR. W. E. GRUPE: They are indeed immuno-suppressive, but they can affect other cells as well.It is conceivable that they impede the function of agroup of cells producing a factor that alters gb-merular permeability in a nonimmunologic way.
DR. J. J. COHEN: Would that relate in any way tothe observation that infections often seem to precip-itate a relapse of proteinuria in this condition?
DR. W. E. GRUPE: There is not an all inclusive orcohesive hypothesis as yet. Infections, like allergy,
bee stings, or poison ivy, may be a nonspecific stim-ulus to whatever it is that alters glomerular per-meability.
DR. J. J. COHEN: One of the most exciting newconcepts about gbomerular function, as everyone isaware, is the influence of electrical charge on thepermeability of macromolecules. This raises the ob-vious possibility that this disease is the result ofsome alteration in the fixed negative charges. Isthere any evidence that this might be the case?
DR. W. E. GRUPE: The negatively charged gly-cocalyx covering the epithelial cell is one of fourpotential barriers to protein molecules in the gb-merular capillary wall. The other three are theendothelial cell, the basement membrane, and theepithelial slit diaphragm. In the experimental ani-mal, neutralization of the negative charge with pro-tamine produces a reversible spreading and fusionof the foot processes and an increase in proteinuria[61, 62]. Obviously, this is very similar to that seenin a variety of proteinuric states and suggests thatsuch an electrical barrier is important to the perm-selectivity of the glornerular capillary wall.
It is not clear whether changes in the glycocalyxare primary or secondary, however. Like the slit di-aphragm, the glycocalyx is on the wrong side of thebarrier to be the effective primary filter [63]. Like-wise, preliminary studies in early autobogous im-mune complex nephritis in rats have shown a loss ofcolloidal iron staining subjacent to very small sub-epithelial deposits before an increase in protein ex-cretion could be demonstrated [64]. Other studiesalso suggest that changes elsewhere in the capillarywall are primary while the loss of intrinsic negativecharge is contributory [65]. Of further interest, itappears that the two lamina rarae are also rich inpolyanionic radicals [66].
As might be expected, a decrease in glomerularglycocalyx staining has been seen in human lipoidnephrosis concomitant with proteinuria [67]. It isstill possible, however, that a primary change in thebasement membrane has allowed increased per-meability, which has then led to alterations on theepithelial side, including loss of the glycocalyx,curling and wrinkling of the slit diaphragm, andpodocyte fusion.
DR. J. J. COHEN: Are there any therapeutic ma-neuvers available to alter glomerular charge?
DR. W. E. GRUPE: Not to my knowledge, unlessthat is what prednisone does.
DR. KENNETH SHAPIRO (Renal Fellow, NewEngland Medical Center Hospital): Dr. Grupe, younoted that in the group of patients who didn't re-spond to prednisone there was a high mortality.
84 Nephrology Forum
Have those patients been biopsied, and if so, whatis the most common lesion found in that group ofyoungsters?
DR. W. E. GRUPE: The two most common steroidresistant lesions in children are focal segmentalsclerosis and membranoproliferative glomerulone-phritis (see Table 1). In children, these are also themost frequent reasons for progression to renal in-sufficiency. In the adult, the most common lesion, Ibelieve, is extramembranous glomerulonephropa-thy.
DR. J. T. HARRINGTON: It was my understandingthat even children whose nephrotic syndrome ulti-mately becomes steroid-resistant still have a greaterchance of having minimal change disease than anyother pathologic entity given the very high a prioriprobability of minimal change disease in children.
DR. W. E. GRUPE: I would agree with that, but Iwould caution that any biopsy diagnosis of minimalchange disease is not an absolute. It is not that un-usual for a focal lesion to be missed [68]; even serialsections of the tissue may fail to disclose a lesion,particularly if the biopsy is superficial. I am skepti-cal of morphologic diagnoses based solely on lightmicroscopy. I think a good number of patients with"biopsy proven" minimal change disease with ei-ther steroid resistance or progression to renal fail-ure represent other morphologic variants hidden inan inadequate biopsy [10].
Reprint requests to Dr. Warren E. Grupe, Division of Nephrol-ogy, Children's Hospital Medical Center, 300 Longwood Ave-nue, Boston, Massachusetts 02115.
References
1. CHURG J, HABIB R, WHITE RHR: Pathology of the nephroticsyndrome in children. A report for the International Study ofKidney Disease in Children. Luncet 1:1299, 1970
2. WHITE RHR, GLASGOW EF, MILLS Ri: Clinicopathologicalstudy of nephrotic syndrome in childhood. Lancet 1:1353,1970
3. HABIB R, KLEINKNECHT C: The primary nephrotic syn-drome of childhood: Classification and clinicopathologicstudy of 406 cases, in Pathology Annual, edited by S0M-MERS SC, New York, Appleton-Century-Crofts, 1971, p.417
4. International Study of Kidney Disease in Children. Nephrot-ic syndrome in children: Prediction of histopathology fromclinical and laboratory characteristics at time of diagnosis.Kidney fat 13:159, 1978
5. SHARPSTONE P, OGG CS, CAMERON iS: Nephrotic syn-drome due to primary renal disease in adults. I. Survey ofincidence in Southwest England. Br Med J 2:533, 1969
6. SCHLESINGER ER, SULTZ HA, MOSHER WE, FELDMAN JG:The nephrotic syndrome. Its incidence and implications forthe community. Am J Dis Child 116:623, 1968
7. MAKKER SP, HEYMANN W: The idiopathic nephrotic syn-drome of childhood: a clinical re-evaluation of 145 cases. AmJ Dis Child 127:830, 1974
8. MUNK F: Die Nephrosen. Med KIm 12:1019, 1916
9. BARNETT HL, FORMAN CW, LAUSON HD: The nephroticsyndrome in children, in Advances in Pediatrics edited byLEVINE SA, Chicago, Yearbook Medical Publishers, mc,1952, Vol. 5, p. 53
10. GRuim WE: Primary nephrotic syndrome in childhood, inAdvances in Pediatrics edited by BARNESS LA, Chicago,Year Book Medical Publishers, mc, 1980 (in press)
11. CAMERON iS: Histology, protein clearances and response totreatment in nephrotic syndrome. Br Med J 4:352, 1968
12. WHITE RHR: The nephrotic syndrome, in Recent Advancesin Pediatrics, Edition 4, edited by GAIRDNER D and HULLD, London, J. & A. Churchill, 1971, p. 281
13. MALLICK NP: The pathogenesis of minimal change nephrop-athy. Clin Nephrol 7:87, 1977
14. GERBER MA, PARONETTO F: IgE in glomeruli of patientswith nephrotic syndrome. Lancet 1:1097, 1971
15. GIANGIACOMO J, CLEARY TG, COLE BR: Serum immuno-globulins in the nephrotic syndrome: A possible cause ofminimal change nephrotic syndrome. N Engi J Med 293:8,1975
16. INGELFINGER JR, LINK DA, DAVIS AE, GRUPE WE: Serum
immunoglobulins in idiopathic minimal-change nephroticsyndrome. N Engl J Med 294:50, 1976
17. LANGE K, CRAIG F, OBERMAN J, SLOBODY L, OGURG, Lo-cASTO F: Changes in serum complement during the courseand treatment of glomerulonephritis. Arch Intern Med88:433, 1951
18. NOV JL, BARRATT TM, SOOTHILL JF: Immunoconglutininand complement changes in steroid sensitive relapsing ne-phrotic syndrome of children. Clin Exp Immunol 6:109, 1970
19. LEVINSKY RJ, MALLESON PH, BARRATT TM, SOOTHILL iF:Circulating immune complexes in steroid responsive ne-phrotic syndrome. N Engl J Med 298:126, 1978
20. O'REGAN S. SMITH M, DRUMMOND KN: Immune complexinfusion in the rat. Renal functional and morphologicchanges. Clin Exp Immunol 24:110, 1976
21. LAGRUE G, BRANELLEC A, BLANC C: A vascular per-meability factor in lymphocyte culture supernatants from pa-tients with nephrotic syndrome; II, pharmacological andphysiochemical properties. Biomedicine 23:73, 1975
22. EYRES KE, MALLICK NP, TAYLOR G: Evidence for cell me-diated immunity to renal antigens in minimal change ne-phrotic syndrome. Lancet 1:1158, 1976
23. MALLICK NP, WILLIAMS Ri, MCFARLANE H, TAYLOR G,WILLIAMS G: Cell mediated immunity in nephrotic syn-drome. Lancet 1:507, 1972
24. 001 BS, ORLINA AR, MASAITIS L: Lymphocytotoxins in pri-mary renal disease. Lancet 2:1348, 1974
25. MOORTHY AV, ZIMMERMANN SW, BURKHOLDER PM: Inhi-
bition of lymphocyte blastogenesis by plasma of patientswith minimal change nephrotic syndrome. Lancet 1:1160,1976
26. SHALHOUB Ri: Pathogenesis of lipoid nephrosis: A disorderof T-cell function. Lancet 2:556, 1974
27. CAMERON iS, TURNER DR, OGG CS: The nephrotic syn-drome in adults with minimal change glomerular lesions. 0 JMed 171:461, 1974
28. ARNEIL GC: The nephrotic syndrome. Pediatr Clin N Amer18:547, 1971
29. ARNEIL GC: One hundred and sixty-four children with ne-phrosis. Lancet 2:1103, 1961
30. CORNFELD D, SCHWARTZ MW: Nephrosis: A long termstudy of children treated with corticosteroids. J Pediatr68:507, 1966
31. ARNEIL GC. LAM CN: Long term assessment of steroidtherapy in childhood nephrosis. Lancet 2:819, 1966
Relapsing nephrotic syndrome in childhood 85
32. SIEGEL NJ, GOLDBERG B, KRASSNER LS, HAYSLETT JP:Long-term follow-up of children with steroid-responsivenephrotic syndrome. J Pediatr 81:251, 1972
33. SCHWARTZ MW, SCHWARTZ GJ, CORNFELD D: A 16 yearfollow-up study of 163 children with nephrotic syndrome.Pediatrics 54:547, 1974
34. WHITE RHR: Cytotoxic drug therapy in steroid-resistantglomerulonephritis,. Proc Roy Soc Med 60:1164, 1967
35. MCCRORY WW, Ssnuy.& M, Lu WH, LEWY JE: Therapeu-tic and toxic effects observed with different dosage programsof cyclophosphamide in treatment of steroid-responsive butfrequently relapsing nephrotic syndrome. J Pediatr 82:614,1973
36. GRUPE WE, HEYMANN W: Cytotoxic drugs in steroid-resist-ant renal disease. Am J Dis Child 112:448, 1966
37. WHITE RHR, CAMERON JS, TROUNCE JR: Immuno-suppressive therapy in steroid-resistant proliferative glomer-ulonephritis accompanied by the nephrotic syndrome. BrMed J 2:853, 1966
38. MICHAEL AF, VERNIER RL, DRUMMOND KN: Immuno-suppressive therapy of chronic renal disease. N Engi J Med273:943, 1967
39. ABRAMOWICZ M, BARNETT HL, EDELMANN CM: Con-trolled trial of azathioprine in children with nephrotic syn-drome. Lance! 1:959, 1970
40. International Study of Kidney Disease in Children: Prospec-tive, controlled trial of cyclophosphamide therapy in chil-dren with the nephrotic syndrome. Lance! 2:423, 1974
41. RANCE CP, Ausus GS, BALFE JW: Management of thenephrotic syndrome in children. Pediatr Clin N Amer23:735, 1976
42. GRUPE WE, MAKKER SP, INGELFINGER JR: Chlorambuciltreatment of frequently relapsing nephrotic syndrome. NEngl J Med 295:746, 1976
43. WILLIAMS SA, MAKKER SP, INGELFINGER JR, GRUPE WE:Long-term evaluation of chlorambucil, including effects ofdose, in idiopathic nephrotic syndrome of childhood PediatrRes 11:560, 1977
44. BALUARTE Hi, HINER L, GRUSKIN AB: Chiorambucil dos-age in frequently relapsing nephrotic syndrome. A con-trolled clinical trial. J Pediatr 92:295, 1978
45. MILLER JJ, WILLIAMS GF, LEISSRING JC: Multiple late com-plications of therapy with cyclophosphamide, includingovarian dysfunction. Am J Med 50:530, 1971
46. ETTELDORFJN, WEST CD, PITCOCKJA, WILLIAMS DL: Go-nadal function, testicular histology, and meiosis followingcyclophosphamide therapy in patients with nephrotic syn-drome. J Pediatr 88:206, 1976
47. RICHTER P, CALAMERA JC, MORGENFELD MC, KIERSZEN-BAUM AL, LAVIERI JC, MANCINI RF: Effect of chiorambucilon spermatogenesis in the human with malignant lymphoma.Cancer 25:1026, 1970
48. GUESRY P, LENOIR G, BROYER M: Gonadal effects of chlor-ambucil given to prepubertal and pubertal boys for nephroticsyndrome. J Pediatr 92:299, 1978
49. BUCHANAN JD, FAIRLEY KF, BARRIE JV: Return of sperma-togenesis after stopping cyclophosphamide therapy. Lancet2:156, 1975
50. CHEVIAKOFF 5, CALAMERA JC, MORGENFELD M, MANCINIRE: Recovery of spermatogenesis in patients with lym-phoma alter treatment with chiorambucil. J Reprod Fert33:155, 1973
51. CAMERON S: Chlorambucil and leukemia. N Engi J Med296:1065, 1977
52. WESTBERG NG, SWOLIN B: Acute myeloid leukemia appear-ing in two patients after prolonged continuous chlorambuciltreatment for Wegener's granulomatosis. Acta Med Scand199:373, 1976
53. WILLIAMS SA, MAKKER SP, GRUPE WE: Seizures: Clinicalsignificant side effect of chlorambucil therapy in children. JPediatr 93:516, 1978
54. BRODEHL J, KROHN HP: Steroid trial in frequently relapsingnephrotic syndrome in children, in Glomerulonephritis. In-ternational Conference on Pathogenesis, Pathology andTreatment edited by KLUTHE R, VOGT A, BATSFORD SR,Stuttgart, George Thieme Publishers, 1976, p. 210
55. LEISTI S, VILSKA J, HALLMAN N: Adrenocortical in-sufficiency and relapsing in idiopathic nephrotic syndrome inchildhood. Pediatrics 60:334, 1977
56. LEISTI S, K0sKIMIEs 0, RAPOLA J: Association of post-med-ication hypocortisolism with early relapse of idiopathicnephrotic syndrome. Lance! 2:795, 1977
57. SOYKA LF, SAXENA KM: Alternate-day steroid therapy fornephrotic children. J.4MA 192:225, 1965
58. SOYKA LF: Treatment of the nephrotic syndrome in child-hood. Use of an alternate-day prednisone regimen. Am J DisChild 113:693, 1967
59. vANACKER KJ, H00FT C: The influence of hormone treat-ment on the natural evolution of the idiopathic nephroticsyndrome in childhood. Acta Paediatr Scand 57:479, 1968
60. MCLEAN RH: Personal communication, 197861. SElLER MW, RENNKE HG, VENKATACHALAM MA: Patho-
genesis of polycation induced alterations ( fusion") of gb-merular epithelium. Lab Invest 36:48, 1977
62. RooT ER, CONLEY SB, ROBSON AM: Effect of glomerularpolyanion removal on proteinuria. PediatrRes 11:555, 1977
63. SCHNEEBERGER EE, GRUPE WE: The ultrastructure of theglomerular slit diaphragm in autologous immune complexnephritis. Lab Invest 34:298, 1976
64. SCHNEEBERGER EE, O'BRIEN MA, GRUPE WE: Altered gb-merular permeability in Munich-Wistar rats with autologousimmune complex nephritis. Lab Invest 40:227, 1979
65. RENNKE HG, COUSER WG, PATEL Y, VENKATACHALAMMA: Membranous nephropathy. Fractional clearances ofanionic, neutral and cationic horseradish peroxidase in Lew-is rats with autologous immune complex nephntis. Abstr IntCongr Nephrol, Montreal, 1978, p. X2
66. KANWAR YS, FARQUHAR MG: Characterization of anionicsites in the glomerular basement membrane (GBM). KidneyInt 14:713, 1978
67. BLAU EB, HAAS DE: Gbomerular sialic acid and proteinuriain human renal disease. Lab Invest 28:477, 1973
68. JA0 W, POLLACK YE, NORRIS YE: Lipoid nephrosis: an ap-proach to the clinicopathologic analysis and dismembermentof idiopathic nephrotic syndrome with minimal glomerularchanges. Medicine 52:445, 1973
The editors should like to expand the scope of these exercises by encouraging active partici-pation of the journal's readership in Nephrology Forum. Questions or comments pertaining tothis month's discussion may be submitted to Nephrology Forum, Box 212, New England Medi-cal Center Hospital, 171 Harrison Avenue, Boston, Massachusetts 02111. To be eligible forpublication correspondence must be received by August 31, 1979.