reconstructive surgery for deep vein reflux in the lower limbs: techniques, results and indications
TRANSCRIPT

Author's personal copy
Reconstructive Surgery for Deep Vein Reflux in theLower Limbs: Techniques, Results and Indications
O. Maleti a, M. Perrin b,*
aHesperia Hospital, Via Arqua 80/A, 41124 Modena, ItalybClinique du Grand Large, Vascular Department, 26 Chemin de Decines, F-69680 Chassieu, France
Submitted 5 October 2010; accepted 13 February 2011Available online 30 March 2011
KEYWORDSDeep venous surgery;Venous valveincompetence;Chronic venousinsufficiency;Venous reflux;Post-thromboticsyndrome
Abstract Deep venous reflux (DVR) is defined as a reflux affecting the deep venous system.DVR essentially arises from two aetiologies, primary deep valve incompetence (PDVI) and post-thrombotic syndrome (PTS), and it is correlated with severe chronic venous insufficiency. DVRcorrection aims at reducing the increased ambulatory venous pressure, which results from re-flux in deep veins in orthodynamic conditions.
The results of DVR surgery are not easy to assess, as it is mostly associated with surgery forinsufficiency in the superficial venous system and/or perforators. In cases of primary insuffi-ciency, valvuloplasty, the operation of choice, is credited at 5 years follow-up with a 70%success rate in terms of clinical outcome and improved haemodynamic performance. In PTS,a meta-analysis of transpositions and transplants at more than 5 years estimates successfulclinical outcome and improved haemodynamic performance at 50%. The Maleti neovalveconstruction technique has achieved better results.
Indications for DVR surgery are based on clinical, haemodynamic and imaging data. Aeti-ology is a decisive factor in the choice of the technique.ª 2011 European Society for Vascular Surgery. Published by Elsevier Ltd. All rights reserved.
Deep venous reflux (DVR) in the lower limbs is defined asa reflux affecting the deep venous system. The reflux canbe segmental or axial. A deep segmental reflux is charac-terised by a limited reflux to a segment of the femoral,popliteal, crural or calf muscle vein, without continuityfrom groin to calf. Axial reflux means uninterrupted reflux
from the groin to calf. This axial reflux may affect only thedeep venous system or may also be a reflux involving boththe deep and superficial venous systems, which communi-cate via the perforators. In this situation, the reflux istermed ‘combined’.1 When the superficial system isaffected by an axial reflux in addition to axial DVR, themost appropriate term is ‘associated axial reflux’. There isa general consensus that the more extensive the venousreflux, the more severe is the chronic venous disease.2 Thisarticle will describe, from a technical viewpoint, thevarious techniques aimed at correcting DVR, as well as theiroutcome and indications.
To access continuing medical education questions on thispaper, please go to www.vasculareducation.com and click on ‘CME’
* Corresponding author. Tel.: þ33 (4) 72 05 72 66; fax: þ33 (4) 7205 72 74.
E-mail address: [email protected] (M. Perrin).
Eur J Vasc Endovasc Surg (2011) 41, 837e848
1078-5884/$36 ª 2011 European Society for Vascular Surgery. Published by Elsevier Ltd. All rights reserved.doi:10.1016/j.ejvs.2011.02.013

Author's personal copy
Aethiopathogenesis
DVR essentially arises from three aetiologies. According tothe CEAP (clinical, etiologic, anatomic and pathophysio-logic data) classification, they are: secondary Es (post-thrombotic syndrome, PTS), primary Ep (primary deepvalve incompetence) and congenital Ec (valve congenitalmalformation).
Es is the most common aetiology (60e85% of cases) incertain series,3 and Ep in others.2 In post-thrombotic aeti-ology, valve lesion is a consequence of thrombosis andinflammation of the vein wall. The former is followed bya recanalisation but as the valve has been completely orpartially damaged, it is usually retracted, fibrotic andadherent to the vein wall (Fig. 1). In PTS, the valves cannotusually benefit from direct repair.4
Primary deep valve incompetence (PDVI) is the secondcause of DVR. The cusps are present, but malfunctioning.The most frequent anomalies are abnormal, long, free edgeof each valve, which result in a prolapsed valve, dilatationof the valve ring with a widening of the commissures,asymmetrical insertion of the cusps or asymmetrical leaf-lets (Fig. 2). These valves anomalies can usually be repairedby direct surgery (valvuloplasty).5,6
The valve congenital malformation involves agenesis andhypoplasia associated or not with other vascular congenitalmalformations. Direct valve repair is possible in certaincases of congenital vascular malformations, but not in valveagenesis or hypoplasia where the valves are completelyabsent or rudimentary.7,8
Diagnosis
Ultrasound
Venous duplex scanning (VDS) provides data concerninganatomy and haemodynamics. The presence and theduration of a deep reflux can be detected at femoral,popliteal and crural levels. Perforator and gastrocnemialveins must also be investigated. The venous valve cusps,as well as their functioning, can be identified with B-Flowtechnology.9 VDS does not provide accurate informationon the deep femoral vein (DFV) that limits its reliability
for possible femoral transposition. Intravenous ultrasoundscanning (IVUS) is particularly useful to identify venousobstruction at cava and iliac level10 and is also ableto detect the best site for reconstructing a neovalve inthe femoro-popliteal vein axis as far as the vein iscatheterisable.
Plethysmography
Air plethysmography is useful in venous valve reconstruc-tion because comparison of preoperative and postoperativeparameters give information on the global effectivenessof surgical treatment. The residual volume fraction is incorrelation with ambulatory venous pressure,11 which isconsidered the gold standard for an overall haemodynamicevaluation.12
Venography
Venography is crucial before performing DVR surgery, as itprovides the most precise morphological data.
Ascending venography supplies data on anatomy andaetiology but little information on haemodynamics. Thedescending phlebography is performed placing the catheterin the controlateral femoral vein to avoid venous spasm andinterference due to the catheter itself. In cases of occlu-sion of the iliac axis, the ipsilateral femoral vein is used.The diagrams are detected in multiplanar view and in thesupine position with Valsalva manoeuvre.
Descending venography allows to quantify the extentof the reflux13 and provides precise information on themorphology of the valve, the competence of DFV and thepresence of possible double post-thrombotic channel (Figs.3 and 4). These data are crucial in determining whichtechnique can be used even if these data are inaccurate innearly 25% of cases. The phlebo computed tomography (CT)is an additional investigation particularly useful to evaluatelesions of the deep femoral and femoral veins as well as theiliocaval veins.Figure 1 Post-thrombotic lesions: the fibrotic process.
Figure 2 PDVI. Asymmetrical insertion of the cusps causingmalfunction of the valve itself.
838 O. Maleti, M. Perrin
Author's personal copy
Techniques (Video)
When a direct valve repair is possible, valvuloplasty is thebest option but when direct valve repair is not feasible,other techniques can be used:
- transposition of the femoral vein (FV) into the greatsaphenous vein (GSV) or into the DFV as far as theirterminal valve is competent;
- vein transplant (usually axillary vein transfer);- neovalve;- non-autologous artificial venous valve.
Supplementary video related to this article can be foundat doi:10.1016/j.ejvs.2011.02.013.
Valvuloplasty
The valvuloplasty aim is to restore the competence of thevalve by correcting the anatomical defect. This is the firstchoice operation in primary venous insufficiency.
Internal valvuloplastyFirst proposed by Kistner,5 this technique involves venot-omy and correction of the valve leaflet defects under directvisualisation.
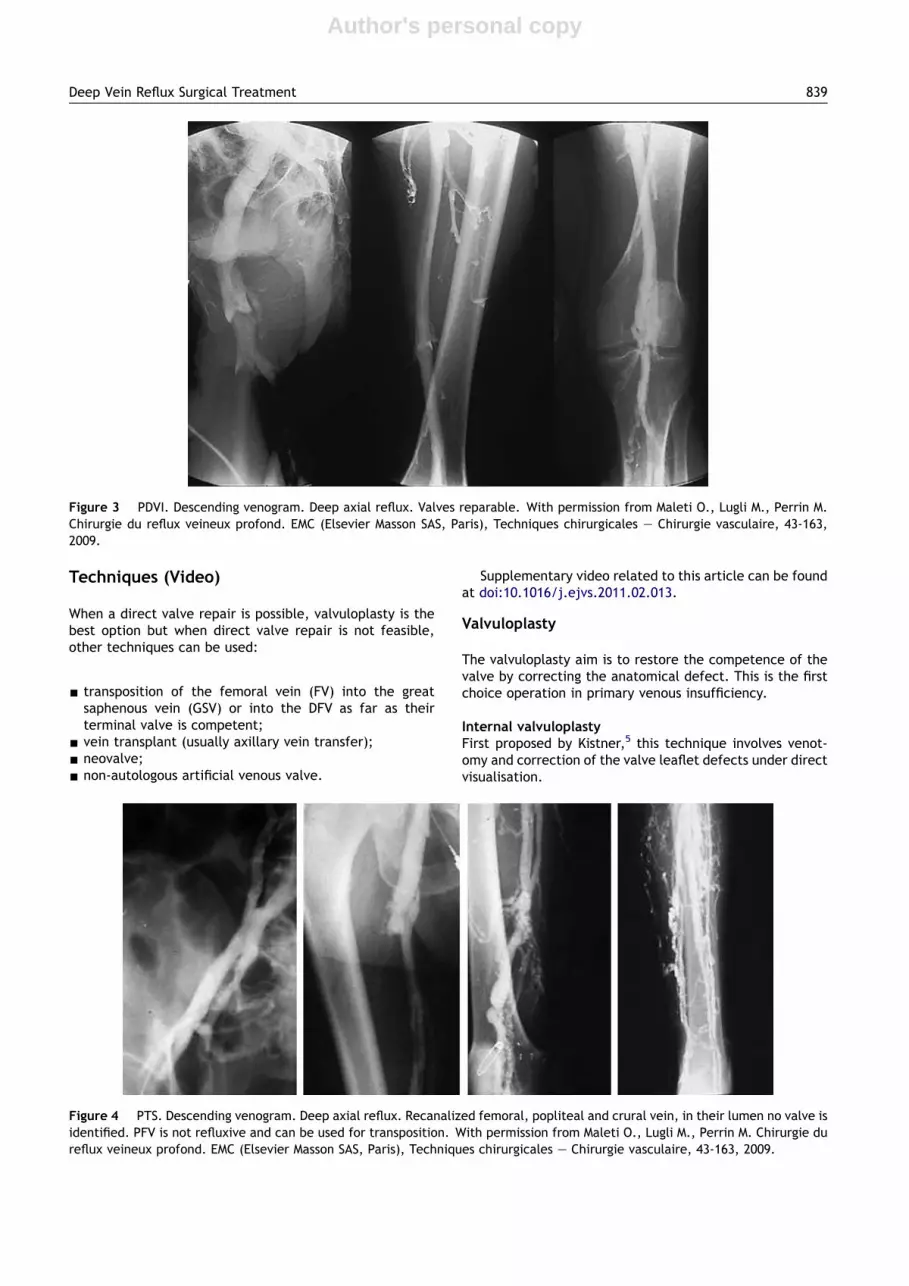
Figure 3 PDVI. Descending venogram. Deep axial reflux. Valves reparable. With permission from Maleti O., Lugli M., Perrin M.Chirurgie du reflux veineux profond. EMC (Elsevier Masson SAS, Paris), Techniques chirurgicales e Chirurgie vasculaire, 43-163,2009.
Figure 4 PTS. Descending venogram. Deep axial reflux. Recanalized femoral, popliteal and crural vein, in their lumen no valve isidentified. PFV is not refluxive and can be used for transposition. With permission from Maleti O., Lugli M., Perrin M. Chirurgie dureflux veineux profond. EMC (Elsevier Masson SAS, Paris), Techniques chirurgicales e Chirurgie vasculaire, 43-163, 2009.
Deep Vein Reflux Surgical Treatment 839

Author's personal copy
Advantages:
- perfect exposure of the overall valve apparatus;- valvuloplasty is easy to perform including a la carte
correction in presence of asymmetrical valve cusps.
Disadvantages:
- possible damage to the valve’s apparatus during thephlebotomy;
- difficulty to assess if the two free valve edges areperfectly in contact until the valvuloplasty is completed(Fig. 5).
Subsequent variations in the technique have beenproposed by Raju,14 Sottiurai15 (Fig. 6) and Thripathi16 toimprove the valve exposure and its surgical correction,mainly for reducing the risk of tearing the free edges duringthe phlebotomy.
External valvuloplastyValvuloplasty is also performable without phlebotomy bynarrowing the lumen with some stitches at the cusp inser-tion angle: transmural valvuloplasty (Fig. 7). Trans-commisural valvuloplasty has the same purpose but unlikethe former requires stitching of the cusp insertion. Externalvalvuloplasty can be made with17 or without endoscopicsupervision.
Advantage:- absence of venotomy.
Disadvantages:- less precision in the valve restoring;- modification of valvular apparatus shape that reduces
more or less its anti-reflux effect.9
External valve bandingRestoring valve competence without opening the vein isalso the purpose of external banding (or prosthetic sleeveor external cuffing).
This procedure can be used in association followingtransplant or other reconstructive techniques8 or in isolation.
The principle is to reduce the calibre of the vein so as torestore valve competence.18
This action is evident during vein dissection: when thevein spasm occurs the valve incompetence is corrected. Ifthe valve is absent (agenesis or PTS), the Venturi’s effectalone may play a transitional role. The Venturi’s effect isbased on the physical low whereby narrowing a vessel ina short portion one obtains an increased velocity in thenarrowed segment.
Different materials have been used for banding the vein:Dacron cuff, Venocuff I�, Venocuff II�, polytetrafluoro-ethylene (PTFE) and bovine pericardium.19e23
Advantage:- easy to perform.
Figure 5 Primary deep venous insufficiency after Kistner’svalvuloplasty. The valve competence is checked after throughthe distal part of the phlebotomy after proximal clamprelease.
Figure 6 Valvuloplasty according to Sottiurai, modified by Perrin. With permission from Maleti O., Lugli M., Perrin M. Chirurgie dureflux veineux profond. EMC (Elsevier Masson SAS, Paris), Techniques chirurgicales e Chirurgie vasculaire, 43-163, 2009.
840 O. Maleti, M. Perrin

Author's personal copy
Disadvantage:- potential risk of narrowing the vein lumen.
Femoral transposition
This technique was first described by Kistner.24 If ipsilateralDFV or GSV have a proximal competent valve and adequatecalibre, the transfer of femoral vein distal to the compe-tent valve can be performed (Fig. 8).
Although termino-lateral anastomosis is more common,end-to-end anastomosis of the FV into DFV or GSV can beused (Fig. 9).
When the FV is the seat of obstructive lesions and theDFV has become the axial vein, DFV can be transposed intocompetent proximal GSV.25
Advantages:- easy to perform;- no direct action on the valve apparatus.
Disadvantages:- adverse anatomy (calibre);- incompetent DFV or GSV terminal valve is frequently
associated with FV incompetence;- subsequent dilatation and reflux due to the different
structure of the DFV valve.25
Vein transplant
Vein transplant principle consists in inserting a segment ofa competent valvulated vein in the incompetent deepvenous network.
The donor segment can be the axillary vein or brachialvein (Fig. 10). The axillary vein transplant was firstdescribed by Raju26 and the brachial vein transplant byTaheri.27
The best-matched size for transplant at the femorallevel is the axillary vein, while the brachial vein can beused in a small-calibre popliteal vein.
Figure 7 Transmural external valvuloplasty according to Kistner. With permission from Maleti O., Lugli M., Perrin M. Chirurgie dureflux veineux profond. EMC (Elsevier Masson SAS, Paris), Techniques chirurgicales e Chirurgie vasculaire, 43-163, 2009.
Figure 8 Femoral vein transposition into the great saphenous vein. With permission from Maleti O., Lugli M., Perrin M. Chirurgiedu reflux veineux profond. EMC (Elsevier Masson SAS, Paris), Techniques chirurgicales e Chirurgie vasculaire, 43-163, 2009.
Deep Vein Reflux Surgical Treatment 841
Author's personal copy
The valve transplantation technique must be meticu-lous, avoiding any torsion, any tension and any stenosis ofthe sutures.
This technique can be associated with excision oftrabeculae inside the lumen of the host vein to obtaina sufficiently wide lumen in PTS.
Despite appropriate techniques, the valve transplantcan fail in the follow-up for non-identified reason.
Advantage:- to insert a segment with a competent valve at popliteal
level, below the FV and the possible re-entry of associ-ated refluxes (DFV).
Disadvantages:- 40% of axillary vein valves are incompetent and require
bench repair;- an external sleeve should be applied to prevent later
dilatation of the segment.
Neovalve
The principle is to construct an autologous valve by usingthe patient’s venous tissue. In Plagnol’s technique,28 theneovalve is created with the GSV termination, opportunelysectioned, shaped and invaginated into the femoral vein tofunction as a valve.
In Maleti’s technique,21,29 the neovalve is obtained bydissecting the vein wall to obtain a flap, which will work asa valve after adequate fixation (Figs. 11 and 13). The walldissection is performable thanks to the thickened post-thrombotic veinwall. Thepost-thrombotic lesions frequentlycreate an intraluminal fibrotic septum that facilitates neo-valve elaboration (Fig. 1). The technique for constructinga neovalve is not always the same; it depends on theanatomical condition of the wall and, therefore, the mostsuitable option is decided only after phlebotomy.
When the vein wall is thickened, the neovalve is createdaccording to the usual manner, by dissecting the veinwall.4,8 However, in presence of a double channel, the bestoption is to create a neovalve by using the intraluminalseptum (Fig. 12). If we find none of these conditions and inpresence of valve agenesis the vein wall is invaginated tocreate a flap featuring a valve and the vein itself isreconstructed with a bovine pericardium30 (Fig. 14) or with
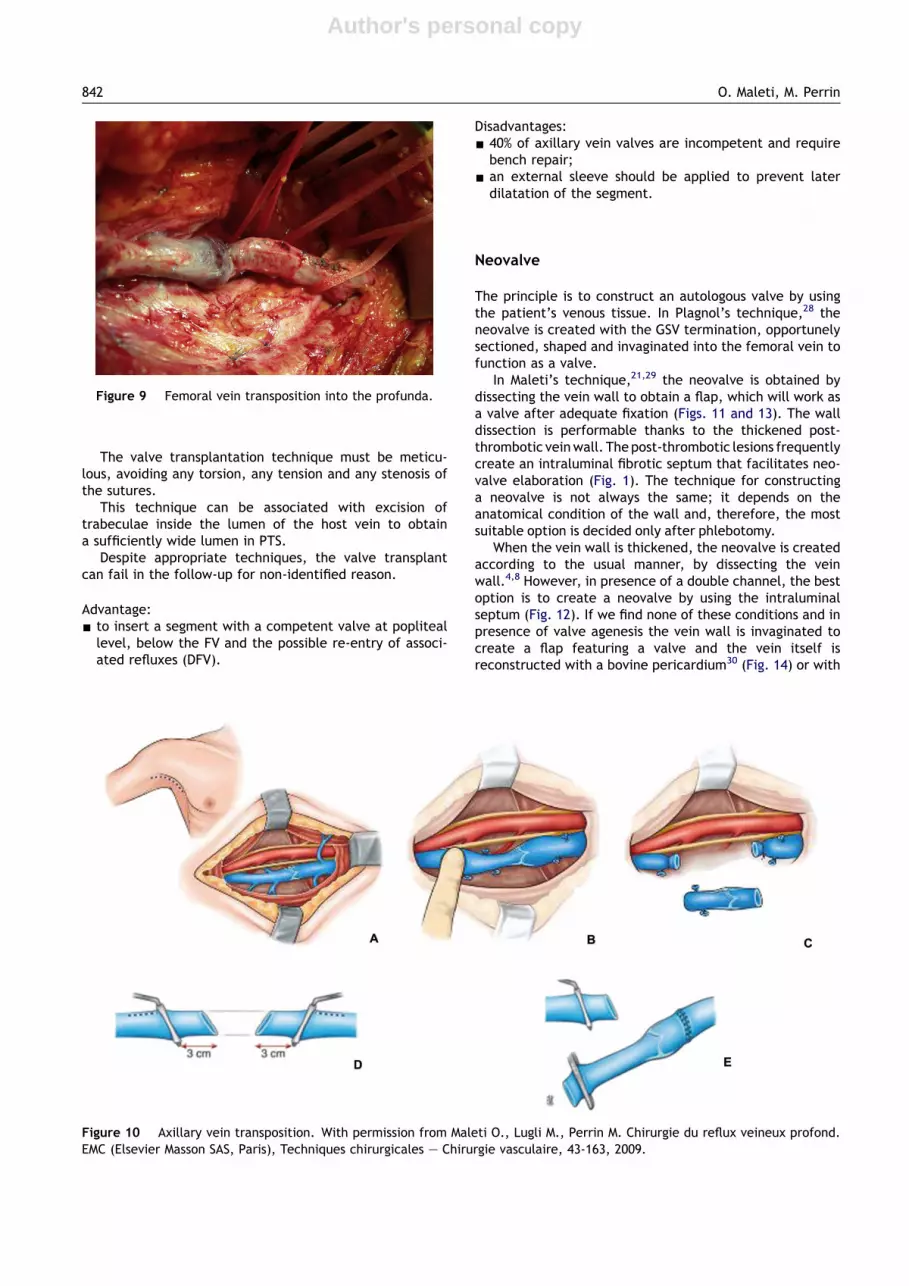
Figure 9 Femoral vein transposition into the profunda.
Figure 10 Axillary vein transposition. With permission from Maleti O., Lugli M., Perrin M. Chirurgie du reflux veineux profond.EMC (Elsevier Masson SAS, Paris), Techniques chirurgicales e Chirurgie vasculaire, 43-163, 2009.
842 O. Maleti, M. Perrin

Author's personal copy
PTFE.31 The flap has to be fixed at both corners to workcorrectly during the motion alternatively in semi-open andclosed position (Video).
Advantages:- to create an anti-reflux apparatus with the patient’s
venous tissue;- to offer a further possibility when vein transposition or
vein transplant is not performable.
Disadvantages:- technique not standardisable;- the best site to create the valve is not always preoper-
atively predictable;- it requires frequently an associated endophlebectomy.
Non-autologous artificial venous valve
Several attempts to create a non-autologous valve havebeen performed,32e35 but research is still underway andapplication in humans is not yet recommended.36
Outcome of Reconstructive SurgicalProcedures
Outcome is different in primary deep venous insufficiencywhen the valve is restorable compared with the outcome inPTS, where the valves are usually destroyed. It is some-times difficult to evaluate the results of deep venousreconstructive surgery for reflux and, generally, theoutcomes are based on: pain decrease, absence of ulcerrecurrence and restored valve competence.
In PDVI
The results of internal and external valvuloplasty in PDVIare shown in Table 1.37e45
Figure 11 Scheme of neovalve by dissection.
Figure 12 Neovalve can be performed utilising a doublechannel.
Figure 13 Neovalve by dissecting the thickened post-thrombotic wall. The valve competence is checked through thedistal part of the phlebotomy.
Figure 14 Neovalve in valve agenesis. Invagination of thevein wall and reconstruction with bovine pericardium.
Deep Vein Reflux Surgical Treatment 843

Author's personal copy
The valvuloplasty is credited of a success rate over 70%at 5 years follow-up. External valvuloplasty on the wholeachieved less satisfactory results, if we consider theabsence of ulcer recurrence and the competence ofrepaired valves. In all the published series, an excellentcorrelation can be noted between clinical outcome andvalve competence.
The outcome of other techniques, either angioscopy-assisted valvuloplasty17,46e48 or cuffing,19,20,23,40 (Table 2),is more difficult to assess, knowing that the follow-up is notlong enough, with the exception of the series reported byLane.20
In PTS
Transposition resultsThese are set out in Table 3.37e39,43,49,50 Successful clinicaloutcomes can be put at between 50% and 75% with valvecompetence between 40% and 77%.
Transplant resultsThese are given in Table 4.37,39,40,43,44,51-53,58,61,62
Successful outcome can be put at between 33% and 82%(follow-up period over 1 year) with valve competencebetween 16% and 87%, and haemodynamic performance
Table 1 Deep vein reconstruction results.
Author, Year SurgicalTechnique
Valvuloplasty results AetiologyPDVI/Total
Follow-upmonth (m)
Ulcer recurrenceor non healedulcer (%)
Haemodynamic results
Number of limbs(number ofvalves repaired)
CompetentValves (%)
AVP e VRT
Lehtola 2008 VIVE TransmurVI þ VE Transmur
1271
5/123/70/1
24e78 (54) / (55) /
Masuda, 1994 VI 32 27/32 48e252 (127) (28) 24/31 (77*) AVP [ 81% (m)VRT [ 50% (m)
Perrin, 2000 VI 85 (94) 65/85 12e96 (58) 10/35 (29) 72/94 (77) AVP normalized63% (m)
Raju, 1996 VI 68 (71) / 12e144 16/68 (26) 30/71 (42) /Raju, 1996 VE Transmur 47 (111) / 12e70 14/47 (30) 72/111 /Raju, 2000 VE Transco 141(179) 98/141 1e42 (37) (59) AVP [ 15% (m)
VRT normalized100%
Rosales, 2006 VE Transmur 17 (40) 17/17 3e122 (60) 3/7 (43) (52) AVP [ 50% (m)Sottiurai, 1996 VI 143 / 9e168 (81) 9/42 (21) 107/143
(75)/
Tripathi, 2004 VIVE Transmur
90 (144)12 (19)
118 (24) (32) (50) (79,8)(31,5)
//
Wang 2006 VE Transmur (40) 40/40 (36) / (91) VRT [ 50% (m)
VI: internal valvuloplasty; VE Transmur: external transmurale valvuloplasty; VE Transco: external transcommissurale valvuloplasty;*: reflux absence or moderate (<1 s); PDVI: primary deep venous insufficiency; AVP: ambulatory venous pressure; VRT: venous returntime; [: increased; m: mean.
Table 2 Banding, cuffing, external stent, wrapping results.
Author, year,material
Number of limbs(number ofvalves repaired)
Site AetiologyPDVI/Total
Follow-upmonth (m)
Ulcer recurrenceor non healedulcer (%)
Haemodynamic results
CompetentValves (%)
AVP e VRT
Akesson, 1999,Venocuff I�
20 (27) F,P 7/20 5e32 (19) 2/10 (20) PTS PVI 7/7 (100)PTS 7/10 (70)
PVI: AVP [ 10% (m)VRT [ 10% (m)PTS: AVP [ 10% (m)VRT [ 100% (m)
Camilli, 1994,Dacron�
54 F 54/54 4e63 / 41/54 (76) /
Lane, 2003,Venocuff II�
42 (125) F,P 36/42 64e141 (93) (20) (90) AVP [?VRT [ 100% (m)
Raju, 1996,Dacron�
(96) F,P,T / 12e134 6/22 (27) 60/72 (83) /
PDVI: primary deep venous insufficiency; PTS: post-thrombotic syndrome; F: femoral; P: popliteal; T: posterior tibial; AVP: ambulatoryvenous pressure; VRT: venous return time; [: increased; m: mean.
844 O. Maleti, M. Perrin

Author's personal copy
little changed. It would appear that transplant to thepopliteal vein yields better results.43,53 Transplant gener-ally achieves less satisfactory results than transposition.
Neovalve resultsNeovalve results are displayed in Table 5.8,28,31
One can be surprised by Opie’s results knowing that theflap is not fixed laterally on both sides; consequently, leakis inevitable.
Cryopreserved valves and bioprosthetic valvesThe results obtained with cryopreserved valves are notso satisfactory.32,33 Indeed, at 9 months, patency andcompetence are respectively 78% and 67%. The clinicaloutcomes are also difficult to assess knowing that post-operative thrombosis provisionally improves the patient’scondition by suppressing the reflux.
Concerning bioprostethic valves, a comprehensive studywas recently carried out.54 The Bioprosthetic Venous ValveIII (BVV III), developed by the Portland team, was the
subject of phase 3 clinical experimentation on 15 patients.At 1 year, none of the valves implanted was competent, butthe patients improved in clinical terms in 60% of cases.
Indications (Fig. 15)
Crucial points to obtain good results are:
- accurate diagnosis;- good clinical assessment;- planning strategic surgery.
As the purpose is to achieve an improved clinical stategiven the already compromised conditions of the lowerlimb, the first priority is to neutralise the axial DVR.55 Inassociated refluxes, superficial and deep, the former shouldbe corrected first, even if the persistence of deep reflux isa cause of varicose vein recurrence.56
Table 3 Transposition results.
Author, year Number oflimbs
AetiologyPTS/Total
Follow-upmonth
Ulcer recurrenceor non healedulcer (%)
Haemodynamic results
Competent Valves (%) AVP e VRT
Cardon, 1999 16 16/16 24e120 4/9 (44) 12/16 (75) /Johnson, 1981 12 12/12 12 4/12 (33) / AVP unchanged
VRT unchangedLehtola, 2008 14 12/14 24e78 / (43) /Masuda, 1994 14 / 48e252 7/14 (50) 10/13 (77) AVP [ 70% (m)
VRT [ 70% (m)Perrin, 2000 17 16/17 12e168 2/8 (25) 9/17 (53) /Sottiurai, 1996 20 / 9e149 9/16 (56) 8/20 (40) /
PTS: post-thrombotic syndrome; AVP: ambulatory venous pressure; VRT: venous return time; [: increased; m: mean.
Table 4 Transplantation results.
Author, Year Number of limbs(number of valvesrepaired)
Site AetiologyPTS/Total
Follow-upmonth (m)
Ulcer recurrenceor non healedulcer (%)
Haemodynamic results
Competent Valves (%) AVP e VRT
Bry, 1995 15 P / 15e132 3/14 (21) 7/8 (87) AVP unchangedVRT unchanged
Eriksson, 1988 35 F,P 35/35 6e60 / 11/35 (31) VRT unchangedLehtola, 2008 29 F,P 25/29 24e78 (54) / (16) /Mackiewicz, 1995 18 F / 43e69 5/14 (36) / VRT [?Nash, 1988 25 P 25/25 / 3/17 (18) 18/23 (77) AVP [ 18% (m)Perrin,2000 32 F 31/32 12e124 (66) 9/22 (41) 8/32 (25) VRT [ 19% (m)Raju, 1999 83 F,P,T 83/83 12e180 (40) 6 years (38) 4 years AVP unchangedRaju, 1996 54 F / 12e180 / 16/44 (36) /Rosales, 2008 22 including
3 double Tr2 Tr þ otherprocedure
F,P 22/22 6e108 / Tr GSV 14/26Tr AV 3/6
/
Sottiurai, 1996 18 F,P / 7e144 6/9 (67) 6/18 (33) /Taheri, 1986 71 F,P / / 1/18 (6) 28/31 (90) AVP [ 15% (m)Tripathi, 2004 35 F,P 35/35 24 (45) (41) /
Tr: transplantation; PTS: post-thrombotic syndrome; F: femoral; P: popliteal; T: posterior tibial; GSV: great saphenous vein; AV: axillaryvein; AVP: ambulatory venous pressure; VRT: venous return time; [: increased; m: mean.
Deep Vein Reflux Surgical Treatment 845

Author's personal copy
Clinical failure after suppression of superficial reflux or/and perforator insufficiency is an indication to correct thedeep reflux.57
The neutralisation of DVR requires an accurate evaluationof femoro-politeal axis andDFV. The isolated correction of FVreflux, does not improve haemodynamics if DFV is refluxive.58
In this event, the best site for surgery is at popliteallevel.
Indication for reconstructive surgery for DVR in thelower limbs is
- severe chronic venous insufficiency C4beC6 notcontrolled by conservative treatment (compression) inpatients with deep axial reflux or combined or associatedreflux involving superficial and perforator veins previ-ously treated (Fig. 15), especially in young patients withan efficient calf pump without:
- severe limited mobility of the ankle;- thrombophilia not corrigible.
Effectiveness of isolated incompetent perforator abla-tion is still debated when combined with superficial anddeep reflux.
Given that results are generally better in PDVI than inPTS, surgery to repair valve function is proposed to patientswhose condition is clinically less severe.
In cases of PDVI, the recommended technique is internalvalvuloplasty for the majority of authors.38,39,43,44
In PTS, a valvuloplasty is rarely feasible except inpatients whose proximal femoral vein valve has not beendamaged due to an early spontaneous lysis of thrombi.59
If valvuloplasty is not feasible, we favour in order:
- vein transposition that needs a DFV or GSV competentterminal valve;
- neovalve construction;- vein transplant.
The instrumental diagnosis has to identify the frequentlyassociated iliac obstruction that may be non-thrombotic(MayeThurner syndrome) or post-thrombotic. A persistentnon-identified obstruction at this level can nullify theaction of deep venous reconstructive surgery for reflux;therefore, in all cases when deep reflux is combined, veinobstruction should be treated first.60
A persistent DVR is themain cause of significant symptomsand trophic lesions; hence, when medical treatments andcompression therapy are not able to control symptoms, theserepresent an indication for deep vein reconstruction.38,39
When deep and superficial refluxes co-exist (associatedreflux), axial reflux in the superficial veins should be treatedfirst, and only clinical failure following treatment of super-ficial reflux is an indication for deep vein reconstruction.
Results of deep venous reconstructive surgery (DVRS) forreflux are satisfactory despite the fact that patients areusually treated by surgery usually in the advanced phases ofchronic venous insufficiency.
DVRS is able to improve the patient’s quality of life (QoL),reducing the venous clinical severity score with its relatedsocial costs. However, DVRS remains the domain of speci-alised centres. This point is worth explaining. The impor-tance of DVR in chronic venous disease is poorly understoodby angiologists and vascular surgeons, either in cases of PDVIor PTS.When it is identified, conservative treatment is nearlyalways recommended, despite its constraints and
Table 5 Neovalve results.
Author, year Technique Numberof limbs
AetiologyPTS/Total
Follow-upmonth (m)
Ulcer recurrenceor non healedulcer (%)
Haemodynamic results
CompetentValves (%)
AVP e VRT
Plagnol, 1999 Bicuspid neovalve 44 44/44 6e47 (17) 3/32 (17) 38/44 (86)Maleti-Lugli,2009
Monocuspidor bicuspid neovalve
19 þ 21 Z 40 36/40 2e78 (28.5) 7/40 (17) 13/19 (68)21/21 (100)
75 VRT improved
Opie, 2008 Monocuspid neovalve 14 / (48) 0/6 13/14 (92)
PTS: post-thrombotic syndrome; AVP: ambulatory venous pressure; VRT: venous return time; m: mean.
Figure 15 Indication for treating deep venous reflux. Diagram.
846 O. Maleti, M. Perrin

Author's personal copy
shortcomings. DVRS is not routinely taught in vascularsurgery academic hospitals for two reasons. First, they areoverloadedwith arterial surgery, and second because DVRS israrely indicated; it requires great precision and can betechnically difficult in some cases. It, therefore, demands anapprenticeship that is not easily acquired. In practice, it isperformed only in high-skilled and specialised centres.
Supplementary data
Supplementary video related to this article can be found atdoi:10.1016/j.ejvs.2011.02.013.
Conflict of Interest
None.
Funding
None.
References
1 Eklof B, Perrin M, Delis KT, Rutherford RB, Gloviczki P, VEINTERMTransatlantic Interdisciplinary Faculty. Updated terminology ofchronic venous disorders: the vein-term transatlantic interdis-ciplinary consensus document. J Vasc Surg 2009;49:498e501.
2 Danielsson G, Eklof B, Grandinetti A, Kistner RL, Masuda EM,Sato DT. Reflux from thigh to calf, the major pathology inchronic venous ulcer disease: surgery indicated in the majorityof patients. Vasc Endovasc Surg 2004;38:209e19.
3 Perrin M, Gillet JL, Guex JJ. Syndrome post-thrombotique.Angeiologie 2003;19(2040):12. EMC (Elsevier Masson SAS, Paris).
4 Maleti O. Venous valvular reconstruction in post-thromboticsyndrome. A new technique. J Mal Vasc 2002;27:218e21.
5 Kistner RL. Surgical repair of a venous valve. Straub Clin Proc1968;24:41e3.
6 Kistner RL. Surgical repair of the incompetent femoral veinvalve. Arch Surg 1975;110:1336e42.
7 Raju S. Operative management of chronic venous insufficiency.In: Rutherford RB, editor. Vascular surgery. Philadelphia: WBSaunders; 1995. p. 1851e62.
8 Lugli M, Guerzoni S, Garofalo M, Smedile G, Maleti O. Neovalveconstruction in deep venous incompetence. J Vasc Surg 2009;49:156e62.
9 Lurie F, Kistner RL, Eklof B, Kessler D. Mechanism of venousvalve closure and role of the valve in circulation. A newconcept. J Vasc Surg 2003;38:955e61.
10 Neglen P, Raju S. Intravascular ultrasound scan evaluation ofthe obstructed vein. J Vasc Surg 2002;35:694e700.
11 Criado E, Farber MA, Marston WA, Daniel PF, Burnham CB,Keagy BA. The role of air plethysmography in the diagnosis ofchronic venous insufficiency. J Vasc Surg 1998;27:660e70.
12 Nicolaides AN, Zukowsky AJ. The value of dynamic pressuremeasurement. World J Surg 1986;17:919e24.
13 Kistner RL, Ferris EB, Randhawa G, Kamida C. A method ofperforming descending venography. J Vasc Surg 1986;4:464e8.
14 Raju S. Venous insufficiency of the lower limb and stasisulceration: changing concepts and management. Ann Surg 1983;197:688e97.
15 Sottiurai VS. Technique in direct venous valvuloplasty. J VascSurg 1988;8:646e8.
16 Tripathi R, Ktenidis KD. Trapdoor internal valvuloplasty: a newtechnique for primary deep vein valvular incompetence. Eur JVasc Endovasc Surg 2001;22:86e9.
17 Gloviczki P, Merrell SW, Bower TC. Femoral vein valve repairunder direct vision without venotomy: a modified techniquewith use of angioscopy. J Vasc Surg 1991;14:645e8.
18 Hallberg D. A method for repairing incompetent valves in deepveins. Acta Chir Scand 1972;138:143e5.
19 Akesson H, Risberg B, Bjorgell O. External support valvuloplastyin the treatment of chronic deep vein incompetence of the legs.Int Angiol 1999;18:233e8.
20 Lane RJ, Cuzilla ML, McMahon CG. Intermediate to long-termresults of repairing incompetent multiple deep venous valvesusing external stenting. ANZ J Surg 2003;73:267e74.
21 Maleti O, Lugli M. Neovalve construction in postthromboticsyndrome. J Vasc Surg 2006;43:794e9.
22 Belcaro G, Nicolaides AN, Errichi BM, Incandela L, DeSanctis MT, Laurora G, et al. Expanded polytetrafluoroethylenein external valvuloplasty for superficial or deep vein incompe-tence. Angiology 2000;51:S27e32.
23 Camilli S, Guarnera G. External banding valvuloplasty of thesuperficial femoral vein in the treatment of primary deepvalvular incompetence. Int Angiol 1994;13:218e22.
24 Kistner RL, Sparkuhl MD. Surgery in acute and chronic venousdisease. Surgery 1979;85:31e43.
25 Raju S, Fountain T, Neglen P, Devidas M. Axial transformation ofthe profunda femoris. J Vasc Surg 1998;27:651e9.
26 Raju S. Discussion after late objective assessment of venousvalue surgery. Arch Surg 1981;116:1466.
27 Taheri SA, Lazar L, Elias S, Marchand P, Heffner R. Surgicaltreatment of postphlebitic syndrome with vein valve trans-plant. Am J Surg 1982;144:221e4.
28 Plagnol P, Ciostek P, Grimaud JP, Prokopowicz SC. Technique dereconstruction valvulaire autogene dans le syndrome de refluxpostphlebitique. Ann Chir Vasc 1999;13:339e42.
29 Maleti O, Lugli M, Maresi R, Meli M. Neovalvules dans le traite-ment des reflux veineux propfonds sous-inguinaux. In: Kieffer E,Chiche L, editors. Techniques modernes en chirurgie vascu-laire. Paris: AERCV; 2007.
30 Maleti O, Lugli M, Perrin M. Chirurgie du reflux veineux profond.In:Techniques chirurgicaleseChirurgie vasculaire, vol. 43e163.Paris: EMC, Elsevier Masson SAS, www.emc-consulte.com; 2009.
31 Opie JC. Monocusp-novel common femoral vein monocuspsurgery uncorrectable chronic venous insufficiency with aplas-tic/dysplastic valves. Phlebology 2008;23:158e71.
32 Dalsing MC, Raju S, Wakefield TW, Taheri S. A multicenter,phase I evaluation of cryopreserved venous valve allografts forthe treatment of chronic deep venous insufficiency. J Vasc Surg1999;30:854e66.
33 Neglen P, Raju S. Venous reflux repair with cryopreserved veinvalves. J Vasc Surg 2003;37:552e7.
34 Pavcnik D, Kaufman J, Uchida B, Correa L, Hiraki T, Kyu SC,et al. Second-generation percutaneous bioprosthetic valve:a short-term study in sheep. J Vasc Surg 2004;40:1223e7.
35 Pavcnik D. Update on venous valve replacement: long-termclinical results. Vascular 2006;14(Suppl. 1):S106.
36 Dalsing MC. Artificial venous valves. In: Gloviczki P, editor.Handbook of venous disorders. 3rd ed., cap. 43. Hodder Arnold;2009. p. 483e90.
37 Lethola A, Oinonen A, Sugano N, Alback A, Lepantalo M. Deepvenous reconstructions:long-term outcome in patients withprimary or post-thrombotic deep venous incompetence. Eur JVasc Endovasc Surg 2008;35:487e93.
38 Masuda EM, Kistner RL. Long-term results of venous valvereconstruction: a four to twenty-one year follow-up. J Vasc Surg1994;19:391e403.
39 Perrin M. Reconstructive surgery for deep venous reflux. Areport on 144 cases. Cardiovasc Surg 2000;8:246e55.
40 Raju S, Fredericks R, Neglen P, Bass JD. Durability of venousvalve reconstruction for primary and post-thrombotic reflux.J Vasc Surg 1996;23:357e67.
Deep Vein Reflux Surgical Treatment 847

Author's personal copy
41 Raju S, Berry MA, Neglen P. Transcommissural valvuloplasty:technique and results. J Vasc Surg 2000;32:969e76.
42 Rosales A, Slagsvold CE, Kroese AJ, Stranden E, Risum O,Jorgensen JJ. External venous valveplasty (EVVp) in patientswith primary chronic venous insufficiency (PVCI). Eur J VascEndovasc Surg 2006;32:570e6.
43 Sottiurai VS. Current surgical approaches to venous hyperten-sion and valvular reflux. Int J Angiol 1996;5:49e54.
44 Tripathi R, Sieunarine K, Abbas M, Durrani N. Deep venous valvereconstruction for non healing ulcers: techniques and results.ANZ J Surg 2004;74:34e9.
45 Wang SM, Hu ZJ, Li SQ, Huang XL, Ye CS. Effect of externalvalvuloplasty of the deep vein in the treatment of chronicvenous insufficiency of the lower extremity. J Vasc Surg 2006;44:1296e300.
46 Welch HJ, McLaughlin RL, O’Donnel Jr TF. Femoral vein valvu-loplasty: intra operative angioscopic evaluation and hemody-namic improvement. J Vasc Surg 1992;16:694e700.
47 Nishibe T, Kudo F, Flores J, Miyazaki K, Yasuda K. Femoral veinvalve repair with angioscopy-assisted anterior valve sinus plica-tion. Early results. J Cardiovasc Surg (Torino) 2001;42:529e35.
48 Sakuda H, Nakaema M, Kamada Y, Kuniyoshi Y, Koja K. Airplethysmography assessment of external valvuloplasty inpatients with valvular incompetence of the saphenous and thedeep veins. J Vasc Surg 2002;36:922e7.
49 Cardon JM, Cardon A, Joyeux A, Mangialardi N, Noblet D,Nguyen T, et al. La veine saphene interne comme transplantvalvule dans l’insuffisance veineuse post-thrombotique: resul-tats a long terme. Ann Chir Vasc 1999;13:284e9.
50 Johnson ND, Queral LA, Flinn WR, Yao JS, Bergan JJ. Lateobjective assessment of venous valve surgery. Arch Surg 1981;116:1461e6.
51 Bry JD, Muto PA, O’Donnell TF, Isaaacson LA. The clinical andhemodynamic results after axillary-to-popliteal valve trans-plantation. J Vasc Surg 1995;21:110e9.
52 Taheri SA, Heffner R, Bodd T, Pollack LH. Five years experiencewith vein valve transplant. World J Surg 1986;10:935e7.
53 Rosales A, Jorgensen JJ, Slagsvold CE, Stranden E, Risum O,Kroese AJ. Venous valve reconstruction in patients withsecondary chronic venous insufficiency. Eur J Vasc EndovascSurg 2008;36:466e72.
54 Pavcnik D, Uchida B, Kaufman J, Hinds M, Keller FS, Rosch J.Percutaneous management of chronic deep venous reflux:review of experimental work and early clinical experience withbioprosthetic valve. Vasc Med 2008;13:75e84.
55 Lurie F, Kistner R, Perrin M, Raju S, Neglen P, Maleti O. Invasivetreatment of deep venous disease. A UIP consensus. Int Angiol2010;29:199e204.
56 Perrin MR, Labropoulos N, Leon Jr LR. Presentation of thepatient with recurrent varices after surgery (REVAS). J Vasc Surg2006;43:327e34.
57 Perrin MR. Results of deep vein reconstruction. Vasc Surg 1997;31:273e5.
58 Eriksson I, Almgren B. Influence of the profunda femoris veinon venous hemodynamics of the limb: experience from thirty-one deep vein valve reconstructions. J Vasc Surg 1986;4:390e5.
59 Meisner MH, Manzo RA, Bergelin RO, Markel A, Strandness Jr DE.Deep venous insufficiency: the relationship between lysis andsubsequent reflux. J Vasc Surg 1993;18:596e608.
60 Raju S, Darcey R, Neglen P. Unexpected major role for venousstenting in deep reflux disease. J Vasc Surg 2010;51:401e8.
61 Mackiewicz Z, Molski S, Jundzill W, Stankiewicz W. Treatmentof postphlebitic syndrome with valve transplantation: 5 yearexperience. Eurosurgery ’95. Bologna Monduzzi; 1995:305e10.
62 Nash T. Long-term results of vein valve transplants placed inthe popliteal vein for intractable post-phlebitic venous ulcersand pre-ulcer skin changes. J Cardiovasc Surg 1988;29:712e6.
848 O. Maleti, M. Perrin