rbgo - gynecology & obstetrics - febrasgo
TRANSCRIPT

RBGO Gynecology & Obstetrics
ISSN 0100-7203eISSN 1806-9339
Revista Brasileira de Ginecologia e Obstetrícia Number 2 • Volume 42 • Pages 65–119 • February 2020

RBGO Gynecology and ObstetricsRevista Brasileira de Ginecologia e Obstetrícia
ISSN 0100-7203
Editor in Chief
Marcos Felipe Silva de Sá Universidade de São Paulo, Ribeirão Preto, SP, Brazil
Former Editors
Jean Claude NahoumRio de Janeiro, RJ (1979–1989)
Clarice do Amaral FerreiraRio de Janeiro, RJ (1989–1994)
Sérgio Pereira da CunhaRibeirão Preto, SP (1994–1997)
Jurandyr Moreira de AndradeRibeirão Preto, SP, Brazil (1997–2015)
Associated Editors
Agnaldo Lopes da Silva FilhoUniversidade Federal de Minas Gerais,Belo Horizonte, MG, Brazil
Alessandra Cristina MarcolinUniversidade de São Paulo,Ribeirão Preto, SP, Brazil
Ana Katherine da Silveira GonçalvesUniversidade Federal do Rio Grande doNorte, Natal, RN, Brazil
Andréa da Rocha TristãoUniversidade Estadual Paulista“Júlio de Mesquite Filho”, Botucatu, SP, Brazil
Antonio Rodrigues Braga NetoUniversidade Federal do Rio de Janeiro, Rio de Janeiro, RJ, Brazil
Corintio Mariani NetoUniversidade Cidade de São Paulo, São Paulo, SP, Brazil
Daniel Guimarães TiezziUniversidade de São Paulo,Ribeirão Preto, SP, Brazil
Diama Bhadra Andrade Peixoto do ValeUniversidade Estadual de Campinas, Campinas, SP, Brazil
Eddie Fernando Candido MurtaUniversidade Federal do Triângulo Mineiro, Uberaba, MG, Brazil
Edward Araujo JúniorUniversidade Federal de São Paulo,São Paulo, SP, Brazil
Eliana Aguiar Petri NahasUniversidade Estadual Paulista“Júlio de Mesquita Filho”, Botucatu, SP, Brazil
Fabrício da Silva CostaMonash University, Melbourne, Victoria, Australia
Fernanda Garanhani de Castro SuritaUniversidade Estadual de Campinas, Campinas, SP, Brazil
Fernando Marcos dos ReisUniversidade Federal de Minas Gerais,Belo Horizonte, MG, Brazil
Gerson Botacini das DoresGustavo Salata Romão
Universidade de Ribeirão Preto, Ribeirão Preto, SP, Brazil
Helena von Eye CorletaUniversidade Federal do Rio Grande do Sul, Porto Alegre, RS, Brazil
Ilza Maria Urbano MonteiroUniversidade Estadual de Campinas, Campinas, SP, Brazil
José Geraldo Lopes RamosUniversidade Federal do Rio Grande do Sul, Porto Alegre, RS, Brazil
José Guilherme CecattiUniversidade de São Paulo, Campinas, SP, Brazil
José Maria Soares JúniorUniversidade de São Paulo, São Paulo, SP, Brazil
Julio Cesar Rosa e SilvaUniversidade de São Paulo, Ribeirão Preto, SP, Brazil
Lucia Alves da Silva LaraUniversidade de São Paulo, Ribeirão Preto, SP, Brazil
Lucia Helena Simões da Costa PaivaUniversidade Estadual de Campinas, Campinas, SP, Brazil
Luiz Carlos ZeferinoUniversidade Estadual de Campinas,Campinas, SP, Brazil
Luiz Gustavo Oliveira BritoUniversidade de São Paulo,Campinas, SP, Brazil
Maria Celeste Osório WenderUniversidade Federal do Rio Grande do Sul, Porto Alegre, RS, Brazil
Maria Laura Costa do NascimentoUniversidade Estadual de Campinas, Campinas, SP, Brazil
Mila de Moura Behar Pontremoli Salcedo Universidade Federal de Ciências da Saúde de Porto Alegre, Porto Alegre, RS, Brazil
Omero Benedicto Poli NetoUniversidade de São Paulo, Ribeirão Preto, SP, Brazil
Patrícia El BeituneUniversidade Federal de Ciências da Saúde de Porto Alegre, RS, Brazil
Paula Andrea de Albuquerque Salles NavarroUniversidade de São Paulo,Ribeirão Preto, SP, Brazil
Ricardo Carvalho CavalliUniversidade de São Paulo,Ribeirão Preto, SP, Brazil
Rosana Maria dos ReisUniversidade de São Paulo, Ribeirão Preto, SP, Brazil
Rosiane MattarUniversidade Federal de São Paulo, São Paulo, SP, Brazil
Rodrigo de Aquino CastroUniversidade Federal de São Paulo,São Paulo, SP, Brazil
Silvana Maria QuintanaUniversidade de São Paulo, Ribeirão Preto, SP, Brazil
Sophie Françoise Mauricette DerchainUniversidade Estadual de Campinas,Campinas, SP, Brazil
Editorial Board
Alex Sandro Rolland de SouzaInstituto de Medicina Integral Prof. Fernando Figueira, Recife, PE, Brazil
Ana Carolina Japur de Sá Rosa e SilvaUniversidade de São Paulo, Ribeirão Preto, SP, Brazil
Aurélio Antônio Ribeiro da CostaUniversidade de Pernambuco, Recife, PE, Brazil
Belmiro Gonçalves PereiraUniversidade Estadual de Campinas, Campinas, SP, Brazil
Carlos Augusto Alencar JuniorUniversidade Federal do Ceará, Fortaleza, CE, Brazil
Carlos GrandiUniversidad de Buenos Aires, Buenos Aires, Argentina

Cesar Cabello dos SantosUniversidade Estadual de Campinas, Campinas, SP, Brazil
Délio Marques CondeHospital Materno Infantil de Goiânia, Goiânia, GO, Brazil
Dick OepkesUniversity of Leiden, Leiden, The Netherlands
Dino Roberto Soares de LorenziUniversidade de Caxias do Sul, Caxias do Sul, RS, Brazil
Diogo de Matos Graça Ayres de CamposUniversidade do Porto, Porto, Portugal
Eduardo Pandolfi PassosUniversidade Federal do Rio Grande do Sul, Porto Alegre, RS, Brazil
Edmund Chada BaracatUniversidade de São Paulo, São Paulo, SP, Brazil
Eliana Martorano AmaralUniversidade Estadual de Campinas, Campinas, SP, Brazil
Francisco Edson Lucena FeitosaUniversidade Federal do Ceará, Fortaleza, CE, Brazil
George CondousNepean Hospital in West Sydney, Sidney, Australia
Giuseppe RizzoUniversità degli Studi di Roma“Tor Vergata”, Roma, Italy
Gutemberg Leão de Almeida FilhoUniversidade Federal do Rio de Janeiro,Rio de Janeiro, RJ, Brazil
Iracema de Mattos Paranhos CalderonUniversidade Estadual Paulista“Júlio de Mesquita Filho”, Botucatu, SP, Brazil
João Luiz Pinto e SilvaUniversidade Estadual de Campinas, Campinas, SP, Brazil
João Paulo Dias de SouzaUniversidade de São Paulo, Ribeirão Preto, SP, Brazil
João Sabino Lahorgue da Cunha FilhoUniversidade Federal do Rio Grande do Sul, Porto Alegre, RS, Brazil
José Carlos PeraçoliUniversidade Estadual Paulista “Júlio de Mesquita Filho”, Botucatu, SP, Brazil
José Juvenal LinharesUniversidade Federal do Ceará, Campus de Sobral, Fortaleza, CE, Brazil
Joshua VogelDepartment of Reproductive Health and Research, World Health Organization, Geneva, Switzerland
Juvenal Soares Dias-da-CostaUniversidade Federal de Pelotas, Pelotas, RS, Brazil
Laudelino Marques LopesUniversity of Western Ontario, London, Ontario, Canada
Luciano Marcondes Machado NardozzaUniversidade Federal de São Paulo, São Paulo, SP, Brazil
Luis Otávio Zanatta SarianUniversidade Estadual de Campinas, Campinas, SP, Brazil
Luiz Claudio Santos ThulerInstituto Nacional do Câncer, Rio de Janeiro, RJ, Brazil
Luiz Henrique GebrimUniversidade Federal de São Paulo, São Paulo, SP, Brazil
Manoel J. B. Castello Girão, Universidade Federal de São Paulo, São Paulo, SP, Brazil
Marcelo ZugaibUniversidade de São Paulo, São Paulo, SP, Brazil
Marcos Desidério RicciUniversidade de São Paulo, São Paulo, SP, Brazil
Maria de Lourdes BrizotUniversidade de São Paulo, São Paulo, SP, Brazil
Marilza Vieira Cunha RudgeUniversidade Estadual Paulista “Júlio de Mesquita Filho”, Botucatu, SP, Brazil
Newton Sergio de CarvalhoUniversidade Federal do Paraná, Curitiba, PR, Brazil
Nuno Henrique Malhoa Migueis ClodeFaculdade de Medicina de Lisboa, Lisboa, Portugal
Olímpio Barbosa Moraes FilhoUniversidade de Pernambuco, Recife, PE, Brazil
Paulo Roberto Nassar de CarvalhoInstituto Fernandes Figueira-Fiocruz, Rio de Janeiro, RJ, Brazil
Renato Augusto Moreira de SáUniversidade Federal Fluminense, Niterói, RJ, Brazil
Rintaro MoriNational Center for Child Health and Development, Tokyo, Japan
Roberto Eduardo BittarUniversidade de São Paulo, São Paulo, SP, Brazil
Rosane Ribeiro Figueiredo AlvesUniversidade Federal de Goiás, Goiânia, GO, Brazil
Roseli Mieko Yamamoto NomuraUniversidade Federal de São Paulo, São Paulo, SP, Brazil
Rossana Pulcinelli Vieira FranciscoUniversidade de São Paulo, São Paulo, SP, Brazil
Ruff o de Freitas JuniorUniversidade Federal de Goiás, Goiânia, GO, Brazil
Sabas Carlos VieiraUniversidade Federal do Piauí, Teresina, PI, Brazil
Sebastião Freitas de MedeirosUniversidade Federal do Mato Grosso, Cuiabá, MT, Brazil
Selmo GeberUniversidade Federal de Minas Gerais, Belo Horizonte, MG, Brazil
Silvia DaherUniversidade Federal de São Paulo, São Paulo, SP, Brazil
Shaun Patrick BrenneckeUniversity of Melbourne Parkville, Victoria, Australia
Técia Maria de Oliveira MaranhãoUniversidade Federal do Rio Grande do Norte, Natal, RN, Brazil
Toshiyuki HataUniversity Graduate School of Medicine, Kagawa, Japan
Wellington de Paula MartinsUniversidade de São Paulo, Ribeirão Preto, SP, Brazil
Editorial Offi ce
Bruno Henrique Sena Ferreira
Editorial Production
Thieme Medical Publishers
Federação Brasileira das Associações de Ginecologia e ObstetríciaBrazilian Federation of Gynecology and Obstetrics Associations
ISSN 0100-7203
Society Board (2020–2024)
PresidentAgnaldo Lopes da Silva Filho (MG)
Administrative Director Sérgio Podgaec (SP)
Scientifi c Director César Eduardo Fernandes (SP)
Financial DirectorOlímpio B. de Moraes Filho (PE)
Professional Status DefenceMaria Celeste Osório Wender (RS)
Vice-president of North RegionRicardo de Almeida Quintairos (PA)
Vice-president of Northeast Region Carlos Augusto Pires C. Lino (BA)
Vice-president of Middle West Region Marta Franco Finotti (GO)
Vice-president of Southeast Region Marcelo Zugaib (SP)
Vice-president of South Region Almir Antônio Urbanetz (PR)
Presidency and Executive Staff
Av. Brigadeiro Luís Antônio, 3421 - Sala 903 - Jardim Paulista, São Paulo, SP, BrazilCEP: 01401-001Phone.: (+55 11) [email protected]
RBGO Editorial Offi ce
editorial.offi [email protected]

RBGO Gynecology and ObstetricsRevista Brasileira de Ginecologia e Obstetrícia
Volume 42, Number 2/2020
online www.thieme-connect.com/products
Editorial
65 Impact of Vaginal Delivery on Pelvic FloorCássia Raquel Teatin Juliato
Original Articles
Obstetrics
67 Factors Associated with Inadequate Birth Intervals in the BRISA Birth Cohort, BrazilRaphael Barbosa, Maria Teresa Seabra Soares Britto Alves, Ian Nathasje, Deysianne Chagas, Vanda Ferreira Simões, and Leonardo Silva
High Risk Pregnancy
74 Gestational Outcomes in Patients with Severe Maternal Morbidity Caused by Hypertensive SyndromesDaisy de Lucena Feitosa Lins Pinheiro, Francisco Edson de Lucena Feitosa, Edward Araujo Júnior, and Francisco Herlânio Costa Carvalho
Gynecological Endocrinology
81 Increased Sympathetic Cardiac Autonomic Modulation after Two Consecutive Tilt Tests in Women with Polycystic Ovary SyndromeVictor Barbosa Ribeiro, Gislaine Satyko Kogure, Rafael Costa Silva, Hugo Celso Dutra Souza, Rui Alberto Ferriani, and Rosana Maria Reis
Quality of Life/Endometriosis
90 Quality of Life in Women with Deep Endometriosis: A Cross-Sectional StudyDaniela Angerame Yela, Iuri de Paula Quagliato, and Cristina Laguna Benetti-Pinto
Lower Genital Tract Diseases
96 Infl uence of Gender and Undergraduate Course on the Knowledge about HPV and HPV Vaccine, and Vaccination Rate among Students of a Public UniversityMarília Biselli-Monteiro, Amanda Canato Ferracini, Luis Otávio Sarian, and Sophie Françoise Mauricette Derchain
Integrative Review
106 Genital Injuries: Are They Telling us Something about Sexual Violence?Carolina Orellana-Campos
Case Report
114 Metachronic Breast and Cerebellar Neoplasm in a Young PatientJéssika de Oliveira Nascimento, Lara Caroline Anastacio Haro, Rafael da Silva Sá, and Rebeca Espelho Storch
Thieme Revinter Publicações Ltda

Some of the product names, patents, and registered designs referred to in this publication are in fact registered trade marks or proprietary names even though specifi c reference to this fact is not always made in the text. Therefore, the appearance of a name without designation as proprietary is not to be construed as a representation by the Publisher that it is in the public domain.
All rights, including the rights of publication, distribution, and sales, as well as the right to translation, are reserved. No part of this work covered by the copyrights hereon may be reproduced or copied in any form or by any means—graphic, electronic, or mechanical, including photocopying, recording, taping, or information and retrieval systems—without written permission of the Publisher.
Important Note: Medical knowledge is ever-changing. As new research and clinical experience broaden our knowledge, changes in treatment and drug therapy may be required. The authors and editors of the material here-in have consulted sources believed to be reliable in their efforts to provide information that is complete and in accord with the standards accepted at the time of publication. However, in view of the possibility of human er-ror by the authors, editors, or publisher of the work herein, or changes in
medical knowledge, neither the authors, editors, or publisher, nor any other party who has been involved in the preparation of this work, warrants that the information contained here in is in every respect accurate or complete, and they are not responsible for any errors or omissions or for the results obtained from use of such information. Because of rapid advances in the medical sciences, independent verification of diagnoses and drug dosages should be made. Readers are encouraged to confirm the information con-tained herein with other sources. For example, readers are advised to check the product information sheet included in the package of each drug they plan to administer to be certain that the information contained in this publi-cation is accurate and that changes have not been made in the recommended dose or in the contraindications for administration. This recommendation is of particular importance in connection with new or infrequently used drugs.
Although all advertising material is expected to conform to ethical (medical) standards, inclusion in this journal does not constitute a guar-antee or endorsement of the quality or value of such product or of claims made by its manufacturer.
Copyright © 2020 by Thieme Revinter Publicações Ltda Inc. RBGO Gynecology and Obstetrics/Revista Brasileiro de Ginecologia e Obstetrícia is published monthly by Thieme-Revinter Publicações Ltda., Rua do Matoso, 170, Rio de Janeiro 20270-135, Brazil.
Editorial comments should be sent to [email protected]. Articles may be submitted to this journal on an open-access basis. For further informa-tion, please send an e-mail to [email protected]. The content of this journal is available online at www.thieme-connect.com/products. Visit our Web site at www.thieme.com and the direct link to this journal at www.rbgo.com.br.
Revista Brasileiro de Ginecologia e Obstetrícia is an official publication of the Federação Brasileira das Associações de Ginecologia e Obstetrícia (Brazilian Federation of Association of Gynecology and Obstetrics, Febrasgo), It is listed in Isi - Web of Science, Web of Knowledge (Emerging), MEDLINE /PubMed, Index Medicus, Scopus (Sci Verse), SCImago, SciELO (Scientific Electronic Library Online), LILACS (Literatura Latino-Americana e do Caribe em Ciências da Saúde, Index Medicus Latino Americano), and Portal de Periódicos Capes (Coordenação de Aperfeiçoamento de Pessoal de Nível Superior). Thieme Medical Publishers is a member of the CrossRef initiative.
ISSN 0100-7203
Complementary material is available online at www.rbgo.org.br.

Editorial
Impact of Vaginal Delivery on Pelvic FloorCássia Raquel Teatin Juliato1
1Universidade Estadual de Campinas, Campinas, SP, Brazil
Rev Bras Ginecol Obstet 2020;42(2):65–66.
Pelvic floor disorders (PFDs) include urinary incontinence(UI), overactive bladder (OAB), fecal incontinence (FI) andpelvic organ prolapse (POP).1 Although the pathophysiologyof PFDs is multifactorial, two of the main associated factorsare the gestational period and the delivery route.2,3
The pregnancy period demands several modifications inthe woman’s body in order to allow fetal development andchildbirth. These physiological, anatomical, biomechanicaland hormonal changes alter the functioning of the pelvicfloor, mainly by increasing the elasticity of structures.4 Theincrease in body weight and uterine size leads to a higherabdominal pressure that overloads pelvic floor structures5
and provides the occurrence of injuries.Despite the impact of pregnancy on the pelvic floor, the
main factor associated with pelvic floor injuries and PFDs ischildbirth, even though no consensus on the impact of thedelivery route and PFDs is available in the literature.
Inour service,weevaluatedacohortofprimiparouswomen12-24months after delivery and found no difference betweenthe prevalence of UI and the delivery route.6 Another studyfollowed women for five years and also found no associationbetween UI and the delivery route, although this study hadonly 18% of cesarean sections, which limited the results.7
Some studies followed postpartum women for longerperiods, one of which showed that the peak risk for stressurinary incontinence (SUI) was five years after delivery,while the peak for POP was 20 years after childbirth.8 Thisfinding is especially important, because it justifies the dis-crepancy in the literature, since studies with less than fiveyears (SUI) and 20 years (POP) might not reveal the magni-tude of changes caused by childbirth.
Handa et al.9 evaluated a longitudinal cohort with 1011women five to ten years after childbirth and observed a 2.9times greater risk of presenting SUI (OR 2.9; 95% CI 1.5-5.5)and 5.6 times greater risk of presenting prolapse (OR 5.6; 95%CI 2.2-14.7) after vaginal delivery compared to cesareandelivery without labor. Instrumental deliveries (such asforceps) were associated with an increase in all PFDs, espe-cially POP, with a 7.5-fold increase (OR 7.5; 95% CI 2.7-20.9).The study also demonstrated that for every 6.8 instrumentaldeliveries or 8.9 spontaneous vaginal deliveries, there is anincrease of one case of prolapse.9
This same cohort of women was monitored for up to nineyears, resulting in a publication in 20188 that showed anaccumulated 15-year incidence of 34.3% of SUI (95% CI; 29.9%-38.6%); 21.8% of OAB (95% CI; 17.8% -25.7%); 30.6% of FI (95%CI; 26.4% -34.9%) and 30.0% of POP (95% CI; 25.1% -34.9%)after the first delivery. The association between the deliveryroute and the PFD was significant, but especially the associ-ation between vaginal delivery and POP. In addition, thisstudy showed that cesarean delivery was significantly asso-ciated with lower risk scores for PFD.8
Regarding the effect of cesarean section on PFDs, 12-yearfollow-up studies from the United Kingdom and New Zea-land have shown an association between cesarean sectionand lower risk for urinary incontinence, and that POP is lessfrequent in women who have had cesarean section.10,11 Asystematic review study showed that cesarean sectionsreduce the risk for SUI from 16 to 9.8% or from 22 to 10%.The number of cesarean sections required to prevent a case ofSUI was estimated at 10 to 15. However, the risk for severeSUI and urge incontinence was not different when compar-ing the delivery routes.12
Thepathophysiology that explains the effect of childbirthonPFDs involves several aspects such as decreased support ofpelvic organs, damage to the levator ani muscle and pudendalnerve. In relation toperinealmusculature,women’spelvicfloorwas evaluatedwith a perineometer in a study. It was found thatwomenwith reducedmuscle strength and at least one vaginaldelivery were associatedwith a shorter interval for presentingPFD, compared to women who had cesarean sections. Inaddition, the decrease in muscle strength was associatedwith a higher risk for SUI, 16%; OAB, 27%: and POP, 43%.13 Ina systematic review, a decrease in muscle strength was alsoconfirmed in women with vaginal delivery compared to thosewithcesareansections.14Womenwithcomplaintsofdecreasedstrength of pelvic floor muscles had avulsion of the levator animuscle, found after evaluation by means of translabial ultra-sound, and the study conducted by our research group showedan association between avulsion and vaginal delivery.7 Inaddition, 1/3ofwomenwitha levatorani injuryhavedecreasedmuscle strength.15 The relationship with loss of strength isextremely important after vaginal delivery because it allowsthe adoption of a preventive strategy in women after delivery.
Address for correspondenceCássia Raquel Teatin Juliato,Universidade Estadual deCampinas, Campinas, SP, Brazil(e-mail: [email protected]).
DOI https://doi.org/10.1055/s-0040-1709184.ISSN 0100-7203.
Copyright © 2020 by Thieme RevinterPublicações Ltda, Rio de Janeiro, Brazil
THIEME
Editorial 65

DeLancey16 compared the stage of POP and hiatal area bypredicting that the larger the hiatal area, the greater the levelof POP.15 This shows the importance of hiatal area and therisk for PFDs. Our research team conducted a review study inwhich all articles included demonstrated an increase inhiatal area evaluated by 3D ultrasound after delivery, espe-cially after vaginal delivery.15 The increase in hiatal area is animportant risk factor for all PFDs, and an enlarged hiatal areacan be considered a risk marker for POP over time.
Injuries to the levator ani are also associated with theappearance of POP, but some injuries are not so evidentimmediately after delivery. Studieswith 3D ultrasound showthere may be injury to the levator muscle in 13% of womenafter a vaginal delivery,17 although these injuries can takeyears to develop into POP.
Bladder neck hypermobility is also associated with PFDs,specifically SUI. However, our review article showed no differ-encebetweenbladderneckhypermobilityanddelivery route.15
PFDs seem to be closely related to vaginal delivery, espe-cially cases of instrumental delivery. Cesarean section isassociated with a reduction in the risk for PFDs, althoughthe routine performance of this procedure does not eliminatethe risk for dysfunctions because the pathophysiology ismultifactorial. The pelvic floor undergoes several changesduring pregnancy and, especially, postpartum. Some injuries,such as injuries to the levator ani, are not routinely diagnosed.Knowledge of the pathophysiology and diagnosis of pelvicfloor injuries are crucial for actions that can recover thismusculature and reduce the impact of childbirth and PFDs.
Conflict of InterestsThe authors have no conflict of interests to declare.
References1 Haylen BT, Ridder D, Freeman RM, Swift SE, Berghmans B, Lee J,
et al; International Urogynecological Association; InternationalContinence Society. An International Urogynecological Associa-tion (IUGA)/International Continence Society (ICS) joint report onthe terminology for female pelvic floor dysfunction. NeurourolUrodyn. 2010;29(01):4–20. Doi: 10.1002/nau.20798
2 Ulmsten U, Ekman G, Giertz G, Malmström A. Different biochem-ical composition of connective tissue in continent and stressincontinent women. Acta Obstet Gynecol Scand. 1987;66(05):455–457. Doi: 10.3109/00016348709022054
3 Falconer C, Ekman G, Malmström A, Ulmsten U. Decreased colla-gen synthesis in stress-incontinent women. Obstet Gynecol.1994;84(04):583–586
4 Lavin JM, Smith ARB, Anderson J, Grant M, Buckley H, Critchley H,et al. The effect of the first pregnancy on the connective tissue ofthe rectus sheath. Neurourol Urodyn. 1997;16(05):381–382
5 Herbert J. Pregnancy and childbirth: the effects on pelvic floormuscles. Nurs Times. 2009;105(07):38–41
6 Araujo CC, Coelho SSA, Martinho N, Tanaka M, Jales RM, JuliatoCRT. Clinical and ultrasonographic evaluation of the pelvicfloor inprimiparous women: a cross-sectional study. Int Urogynecol JPelvic Floor Dysfunct. 2018;29(10):1543–1549. Doi: 10.1007/s00192-018-3581-y
7 Viktrup L. The risk of lower urinary tract symptoms five yearsafter thefirst delivery. Neurourol Urodyn. 2002;21(01):2–29. Doi:10.1002/nau.2198
8 Blomquist JL, Muñoz A, Carroll M, Handa VL. Association ofdelivery mode with pelvic floor disorders after childbirth.JAMA. 2018;320(23):2438–2447. Doi: 10.1001/jama.2018.18315
9 Handa VL, Blomquist JL, Knoepp LR, Hoskey KA, McDermott KC,Muñoz A. Pelvic floor disorders 5-10 years after vaginal orcesarean childbirth. Obstet Gynecol. 2011;118(04):777–784.Doi: 10.1097/AOG.0b013e3182267f2f
10 MacArthur C, Glazener C, Lancashire R, Herbison P, Wilson D;ProLong study group. Exclusive caesarean section delivery andsubsequent urinary and faecal incontinence: a 12-year longitudi-nal study. BJOG. 2011;118(08):1001–1007
11 Glazener C, Elders A, MacArthur C, Lancashire RJ, Herbison P,Hagen S, et al; ProLong Study Group. Childbirth and prolapse:long-term associations with the symptoms and objective mea-surement of pelvic organ prolapse. BJOG. 2013;120(02):161–168.Doi: 10.1111/1471-0528.12075
12 Press JZ, Klein MC, Kaczorowski J, Liston RM, von Dadelszen P.Does cesarean section reduce postpartum urinary incontinence?A systematic review. Birth. 2007;34(03):228–237. Doi: 10.1111/j.1523-536X.2007.00175.x
13 Blomquist JL, Carroll M, Muñoz A, Handa VL. Pelvic floor musclestrength and the incidence of pelvic floor disorders after vaginaland cesarean delivery. Am J Obstet Gynecol. 2020;222(01):62.e1–62.e8. Doi: 10.1016/j.ajog.2019.08.003
14 Yang XJ, Sun Y. Comparison of caesarean section and vaginaldelivery for pelvic floor function of parturients: a meta-analysis.Eur J Obstet Gynecol Reprod Biol. 2019;235:42–48. Doi: 10.1016/j.ejogrb.2019.02.003
15 de Araujo CC, Coelho SA, Stahlschmidt P, Juliato CRT. Does vaginaldelivery cause more damage to the pelvic floor than cesareansection as determined by 3D ultrasound evaluation? A systematicreview. Int Urogynecol J Pelvic Floor Dysfunct. 2018;29(05):639–645. Doi: 10.1007/s00192-018-3609-3
16 DeLancey JO. The hidden epidemic of pelvic floor dysfunction:achievable goals for improved prevention and treatment. Am JObstet Gynecol. 2005;192(05):1488–1495. Doi: 10.1016/j.ajog.2005.02.028
17 Shek KL, Dietz HP. Intrapartum risk factors for levator trauma.BJOG. 2010;117(12):1485–1492. Doi: 10.1111/j.1471-0528.2010.02704.x
Rev Bras Ginecol Obstet Vol. 42 No. 2/2020
Editorial66

Factors Associated with Inadequate BirthIntervals in the BRISA Birth Cohort, Brazil
Fatores associados a intervalos inadequados denascimentos na coorte de nascimentos BRISA, BrasilRaphael Barbosa1 Maria Teresa Seabra Soares Britto Alves1 Ian Nathasje1 Deysianne Chagas1
Vanda Ferreira Simões1 Leonardo Silva1
1Department of Public Health, Universidade Federal do Maranhão,São Luís, MA, Brazil
Rev Bras Ginecol Obstet 2020;42(2):67–73.
Address for correspondence Maria Teresa Seabra Soares Britto Alves,MD, Universidade Federal do Maranhão, São Luís, MA 65080-805,Brazil (e-mail: [email protected]).
Keywords
► birth interval► birth► women’s health► family planning► reproductive health
Abstract Objective To determine the prevalence of inadequate birth interval and its associatedfactors in the BRISA study.Methods Cross-sectional study using data from the BRISA cohort. Birth interval wascategorized into “adequate” (� 2 years or< 5 years between births), “short interval” (<2 years) and “long interval” (� 5 years). The analysis of the factors associated with shortand long birth intervals used multinomial logistic regression.Results The prevalence of adequate birth intervals was 48.3%, of long intervals,34.6%, and of short intervals, 17.1%. Skin color, age, education level, economic status,type of delivery, number of prenatal visits, parity, blood pressure, diabetes, and anemia(p-value was< 0.2 in the univariate analysis) proceeded to the final model. The variable� 3 births (odds ratio [OR]¼1.29; confidence interval [CI]: 1.01–1.65) was associatedwith short intervals. Age<20 years old (OR¼0.48; CI: 0.02–0.12) or � 35 years old(OR¼ 2.43; CI: 1.82–3.25), � 6 prenatal visits (OR¼ 0.58; CI: 0.47–0.72), � 3 births(OR¼ 0.59; CI: 0.49–0.73), and gestational diabetes (OR¼0.38; CI: 0.20–0.75) wereassociated with long intervals.Conclusion Older mothers were more likely to have long birth intervals, and higherparity increases the chances of short birth intervals. Furthermore, gestational diabetesand adequate prenatal care presented higher chances of having adequate birthintervals, indicating that health assistance during pregnancy is important to encouragean adequate interval between gestations.
Resumo Objetivo Determinar a prevalência de intervalo inadequado de nascimento e seusfatores associados no estudo BRISA.Métodos Estudo transversal com dados da coorte BRISA. O intervalo de nascimentofoi categorizado em “adequado” (� 2 anos ou<5 anos entre os nascimentos),“intervalo curto” (< 2 anos) e “intervalo longo” (� 5 anos). A análise dos fatoresassociados aos intervalos de nascimento curtos e longos utilizou regressão logísticamultinomial.
receivedMay 30, 2019acceptedDecember 12, 2019
DOI https://doi.org/10.1055/s-0040-1701463.ISSN 0100-7203.
Copyright © 2020 by Thieme RevinterPublicações Ltda, Rio de Janeiro, Brazil
THIEME
Original Article 67

Introduction
The World Health Organization (WHO) recommends waitingbetween 18 to 24months, but<5 years, after a livebirth beforeattempting another pregnancy.1,2 Birth intervals<24 monthsare considered short and intervals>5 years are consideredlong.1–5 Both short and long intervals are considered inade-quate. This recommendation aims to reduce the risk of adversematernal, perinatal, and infant health outcomes and is consis-tent with the WHO/UNICEF recommendation that breastfeed-ing should be maintained for at least 2years.2,6
Research has shown that long and short interpregnancyintervals are independently associated with an elevated riskof adverse maternal, perinatal, and infant health outcomes.3
Adverse maternal health outcomes include anemia, gesta-tional hypertension, and maternal death.4–7
Literature on this topic has tended to focus on the con-sequences of short and long birth intervals for perinataloutcomes. The effects of birth spacing on maternal mortalityand morbidity have received less attention. Therefore, rela-tively little is known about its consequences and associatedfactors.2,6,8–11
Short interpregnancy intervals areassociatedwith increasedadverse maternal health outcomes, such as risk of prematurerupturing of membranes, preterm birth, uterine and placentalbleeding, and gestational diabetes,3,6,8–10,12 while longintervals can increase the risk of gestational hypertension orpreeclampsia.7,9–13
The length of birth interval is influenced by socioeconomic,demographic, and reproductive health factors. In this respect,studies have shown that factors related to short intervalsinclude low socioeconomic status, postpartumstress, unstablelifestyles, and access to health services, while advancedmater-nal age, maternal illness, infertility, unplanned pregnancy, andfamily and social break-ups are potential factors associatedwith long intervals. These factors can influence maternalhealth independently of their effect on birth interval.6,8–10
Studies have also investigated the influence of prenatal careon maternal and reproductive health and, by association,the relationship between this factor and birth interval.13–15
The aimof prenatal care, besides providing adequate assistanceduring pregnancy, is to promote maternal, family, and infanthealth.13–17 Prenatal care can also facilitate fertility planningbecause it represents an opportunity for pregnant women tokeep in contact with health and social services. However, theinfluenceof this factoron future reproductivebehavior remainsunclear.13,14
AmongwomeninAfrica, inadequatebirthspacingwasratedasmore risky forwomen’shealth thanotherpregnancy-relatedevents, like contraceptive methods.18
In view of the above, it is essential to gain a deeperunderstanding of the factors influencing birth intervals andthe association between these intervals andmaternalmorbid-ity. The aim of the present study was, therefore, to determinebirth intervals and to investigate the socioeconomic andreproductive health factors and maternal morbidities associ-ated with inadequate birth intervals in São Luís, state ofMaranhão, in the northeastern region of Brazil.
Methods
A cross-sectional population-based study was conductedusing data on hospital births in São Luís from the BRISAbirth cohort. The present study was conducted in 10 publicand private hospitals and maternity facilities in the munici-pality of São Luís using a representative sample (one-third) ofbirths in these facilities in 2010. The total sample comprised5,067 births after the exclusion of stillbirths and twins.19
A stratified sampling designwas used, inwhich the size ofeach stratum was proportional to the number of births ineach maternity facility. The births from each maternityfacility were selected systematically from a list of all birthsthat occurred in the facility sorted in chronological order,using a sampling interval of three and a random starting
Resultados A prevalência de intervalos adequados de nascimento foi de 48,3%, longade 34,6% e curta de 17,1%. A cor da pele, idade, escolaridade, status econômico, tipo departo, número de consultas pré-natais, paridade, pressão arterial, diabetes e anemia(valor-p<0,2 na análise univariada) prosseguiram para o modelo final. A variável � 3nascimentos (odds ratio [OR]¼1,29; intervalo de confiança [IC]: 1,01–1,65) esteveassociada a intervalos curtos. Idade<20 anos (OR¼0.48; CI: 0.02–0.12) ou � 35 anos(OR¼ 2.43; CI: 1.82–3.25), � 6 consultas pré-natais (OR¼ 0.58; CI: 0.47–0.72), � 3nascimentos (OR¼ 0.59; CI: 0.49–0.73), e diabetes gestacional (OR¼0.38; CI:0.20–0.75) foram associados a longos intervalos.Conclusão As mães mais velhas apresentaram maior probabilidade de ter longosintervalos de nascimento, e uma paridade maior aumenta as chances de intervaloscurtos de nascimento. Além disso, o diabetes gestacional e o pré-natal adequadoapresentaram maiores chances de ter um intervalo adequado ao nascimento, indi-cando que a assistência à saúde durante a gravidez é importante para incentivar umintervalo adequado entre as gestações.
Palavras-chave
► intervalo denascimento
► nascimento► saúde da mulher► planejamento
familiar► saúde reprodutiva
Rev Bras Ginecol Obstet Vol. 42 No. 2/2020
Factors Associated with Inadequate Birth Intervals in the Brisa Birth Cohort, Brazil Barbosa et al.68

point between one and three. Starting with the randomstarting point, we counted down the list selecting each thirdbirth until the desired number of births was selected.19
Data was collected using a standardized questionnaire an-swered by mothers, preferably in the first 24hours after birth.Information on prenatal care was obtained from verbal reportsof the mothers or from maternity records, when available.
The questionnaire was divided into 11 blocks. Blocks Cand G contained questions about socioeconomic status anddemographic characteristics, and maternal morbidities dur-ing pregnancy, respectively, while block H included ques-tions about the current pregnancy and prenatal care.
The following variableswere analyzed: birth interval, skincolor, age, economic status, education level, type of delivery,number of deliveries, number of prenatal visits, high bloodpressure, diabetes, bleeding in the 3rd trimester, and anemia.
Birth interval was calculated by using the differencebetween the current age of the mother and her age in thelast pregnancy. The data were self-reported and were catego-rized into “adequate” (� 2years or<5 years between births),“short interval” (< 2 years), and “long interval” (� 5 years)based on recommendations proposed by the Report of a WHOTechnical Consultation on Birth Spacing.1 Skin color was self-reported and categorized into white (participants whoresponded “white”) and nonwhite (those who responded“black,” “brown/mulatto/cabocla/morena,” “yellow/oriental,”or “indigenous”). Age was divided into three categories:<20years old, 20 to 34years old, and � 35years old. Economicstatus was classified according to the Brazilian Criteria ofEconomic Classification into groups A, B, C, D, and E17,20 andregrouped into three categories: A-B, C, and D-E. Educationlevelwas assessed based onyears of studyanddivided into twocategories:<9 years and>9 years.
With regard to reproductive health variables, deliverytype was classified as natural birth and cesarean section,while number of deliveries was grouped into 2 deliveries and� 3 deliveries. The number of prenatal visits was definedaccording to the minimum number recommended by theBrazilian Ministry of Health20 and was categorized into<6and>6 visits. Maternal morbidities, such as high bloodpressure, diabetes, anemia, and bleeding in the 3rd trimester,were assessed in relation to the current pregnancy.
For the present article, the minimum sample size wasdetermined based on an expected prevalence of 50%, preci-sion of 2%, and 95% confidence interval (CI), resulting in 2,396women. From the total sample of the BRISA study, all womenwho reported more than one delivery, live birth, and single-ton pregnancies were included in this analysis.
Data analysis was conducted using the statistical softwarepackage Stata 14.0 (Statacorp, College Station, TX, USA). Adescriptive analysis of the data was conducted to determinethe frequencies andpercentages of the variables. The analysisof the factors associated with short and long birth intervalsused multinomial logistic regression, using the adequateinterval as the reference category.
Univariate analysis was conducted first to determineunadjusted odds ratios (ORs) adopting a 95% CI. The inde-pendent variables that obtained a p-value<0.20 were in-
cluded in the multivariate analysis. A significance level of 5%was adopted.
In accordance with the provisions of Resolution 196/96 oftheNationalHealthCouncil, thepresentstudywasapprovedbythe Ethics Committee of the Hospital Universitário PresidenteDutra (application number 4771/2008–30 and 223/2009).
Results
The final sample was comprised of 2,751 mothers who gavebirth in maternity facilities in São Luís, state of Maranhão,Brazil (►Fig. 1). The prevalence of adequate birth intervals(48.3%) was higher than that of long (34.6%) and short(17.1%) intervals (►Table 1).
Themajority of thewomenwere nonwhite, from economicgroup C, aged between 20 and 24years old, had at least 9 yearsof education, had 2 lifetime births, had vaginal births, and hadat least 6 prenatal care visits; 15.6% of the respondents hadhigh blood pressure during pregnancy, 2.2% had diabetes,49.5% had anemia, and 9.4% had had at least one bleedingepisode in the 3rd trimester of pregnancy (►Table 2).
In the univariate analysis for short birth intervals, a signifi-cant associationwas foundwith� 3 deliveries (OR¼1.38; 95%CI 1.11–1.70). For long intervals, a significant association wasobservedwithage<26yearsold (OR¼0.05; 95%CI: 0.02–0.12)or � 35years old (OR¼2.66; 95%CI: 2.04–3.46);>9 years ofeducation (OR¼1.43; 95%CI: 1.19–1.71); economic status C(OR¼0.76; 95%CI: 0.60–0.98) or D/E (OR¼0.41; 95%CI:0.32–0.53); cesarean section (OR¼1.50; 95%CI: 1.26–1.77);� 6 prenatal visits (OR 0.45; 95%CI: 0.37–0.53);� 3 births (OR0.68; CI95%: 0.57–0.81); and gestational diabetes (OR¼0.25;
Fig. 1 Flowchart of the selection of eligible participants and finalsample of the BRISA study.
Table 1 Women’s birth interval in the BRISA study
Birth interval n (%)
Adequate interval 1,328 (48.3)
Short interval 471 (17.1)
Long Interval 952 (34.6)
Rev Bras Ginecol Obstet Vol. 42 No. 2/2020
Factors Associated with Inadequate Birth Intervals in the Brisa Birth Cohort, Brazil Barbosa et al. 69

95%CI: 0.13–0.46). No significant association was foundbetween the other variables studied (►Table 3).
The variables skin color, age, education level, economicstatus, type of delivery, number of prenatal visits, number ofbirths, high blood pressure, diabetes, and anemia, whose p-valuewas<0.2 intheunivariateanalysis,proceededto thefinalmodel. In the adjusted analysis, only the variable � 3 births(OR¼ 1.29; CI: 1.01–1.65) was associated with short intervals.Age<20yearsold (OR¼0.48;CI:0.02–0.12),�6prenatalvisits(OR¼0.58;CI:0.47–0.72),�3births (OR¼0.59;CI:0.49–0.73),and gestational diabetes (OR¼0.38; CI: 0.20–0.75) wereinverselyassociatedwith long interval independently.Age�35
years old (OR¼2.43; CI: 1.82–3.25) was a factor associatedwith long birth intervals (►Table 4).
Discussion
Birth intervals were predominantly adequate. However,approximately one third of the participating women hadlongbirth intervals. Only thevariable�3birthswasassociatedwith short intervals. Age <20 years old, � 6 prenatal visits,� 3 births, andgestational diabetes decreased the likelihoodoflong intervals. Age up to 35years oldwas associatedwith longintervals.
Table 2 Socioeconomic and reproductive health characteristics and maternal morbidity during the last pregnancy
Variables Adequate interval Short interval Long interval Total
n (%) n (%) n (%) n (%)
Skin color
White 223 (16.8) 62 (13.2) 181 (19.0) 466 (17.0)
Nonwhite 1,103 (83.2) 409 (86.8) 770 (81.0) 2,282 (83.0)
Age (years old)
< 20 154 (11.6) 42 (8.9) 6 (0.6) 202 (7,3)
20–34 1,078 (81.2) 391 (83.0) 765 (80.4) 2,234 (81.2)
� 35 96 (7.2) 38 (8.1) 181 (19.0) 315 (11.5)
Education level (years)
< 9 476 (36.1) 192 (41.3) 268 (28.3) 936 (34.3)
� 9 842 (63.9) 273 (58.7) 678 (71.7) 1,793 (65.7)
Economic status
A – B 180 (14.3) 57 (13.6) 193 (21.4) 430 (16.6)
C 617 (49.0) 209 (49.8) 506 (56.0) 1,332 (51.6)
D – E 462 (36.7) 154 (36.7) 204 (22.6) 820 (31.8)
Type of delivery
Normal 816 (61.4) 284 (60.3) 491 (51.6) 1,591 (57.8)
Cesarean section 512 (38.6) 187 (39.7) 461 (48.4) 1,160 (42.2)
Number of prenatal visits
< 6 395 (30.2) 116 (25.4) 458 (49.2) 969 (36.0)
� 6 913 (69.8) 341 (74.6) 472 (50.8) 1,726 (64.0)
Number of births
2 751 (56.6) 229 (48.6) 625 (65.7) 1,605 (58.3)
� 3 577 (43.4) 242 (51.4) 327 (34.3) 1,146 (41.7)
High blood pressure
Yes 195 (14.7) 69 (14.7) 166 (17.4) 430 (15.6)
No 1,132 (85.3) 402 (85.3) 786 (82.6) 2,320 (84.4)
Diabetes
Yes 13 (1.0) 11 (2.3) 37 (3.9) 61 (2.2)
No 1,312 (99.0) 460 (97.7) 915 (96.1) 2,687 (97.8)
Bleeding in 3rd trimester
Yes 118 (8.9) 46 (9.8) 94 (9.9) 258 (9.4)
No 1,209 (91.1) 425 (90.2) 857 (90.1) 2,491 (90.6)
Anemia
Yes 671 (50.8) 41 (51.3) 446 (46.9) 1,358 (49.5)
No 650 (49.2) 229 (48.7) 505 (53.1) 1,384 (50.5)
Rev Bras Ginecol Obstet Vol. 42 No. 2/2020
Factors Associated with Inadequate Birth Intervals in the Brisa Birth Cohort, Brazil Barbosa et al.70

Maternal morbidities were determined based on the self-reports of the mothers and on maternity records, whenavailable, without considering their medical records, healthprofessionals’ reports, or laboratory tests. This may be consid-ered a limitation of the present study and is likely to have
influenced the true prevalence of morbidities across thesample. Furthermore, mothers were considered to have highblood pressure if they reported being diagnosed with thecondition during pregnancy, without making any distinctionfor different types of hypertension (chronic high blood pres-sure, preeclampsia, and gestational hypertension, etc.).21 Wepoint out that the BRISA Study is a population-based researchwith a large sample size. In addition, as previouslymentioned,this survey was conducted in maternity facilities in São Luísand may have peculiar results due to the profile of thepopulation.
The predominance of long intervals was found by otherstudies, which showed that the prevalence was higher for
Table 3 Univariate analysis of short and long birth intervals,socioeconomic and reproductive health variables, andmaternalmorbidity
Variables Short interval� Long interval� p-value
OR (95%CI) OR (95%CI)
Skin color 0.02
White Ref. Ref.
Nonwhite 1.33 (0.98–1.80) 0.86 (0,69–1,06)
Age (years old) < 0.01
< 20 0.75 (0.52–1.08) 0.05 (0.02–0.12)
20–34 Ref. Ref.
� 35 1.09 (0.74–1.62) 2.66 (2.04–3.46)
Educationlevel (years)
< 9 Ref. Ref. < 0.01
� 9 0.80 (0.65–1.00) 1.43 (1.19–1.71)
Economic status < 0.01
A–B Ref. Ref.
C 1.07 (0.76–1.50) 0.76 (0.60–0.98)
D–E 1.05 (0.74–1.49) 0.41 (0.32–0.53)
Type of delivery < 0.01
Normal Ref. Ref.
Cesareansection
1.05 (0.85–1.30) 1.50 (1.26–1.77)
Number ofprenatal visits
< 0.01
< 6 Ref. Ref.
� 6 1.27 (1.00–1.62) 0.45 (0.37–0.53)
Number ofbirths
< 0.01
2 Ref. Ref.
� 3 1.38 (1.11–1.70) 0.68 (0.57–0.81)
High bloodpressure
0.17
No Ref. Ref.
Yes 1.00 (0.75–1.35) 0.82 (0.65–1.02)
Diabetes < 0.01
No Ref. Ref.
Yes 0.41 (0.18–0.93) 0.25 (0.13–0.46)
Bleeding in3rd trimester
0.69
No Ref. Ref.
Yes 0.90 (0.63–1.29) 0.89 (0.67–1.18)
Anemia 0.13
No Ref. Ref.
Yes 0.98 (0.79–1.21) 1.17 (0.99–1.38)
Abbreviations: CI, confidence interval; OR, odds ratio.�Reference category: adequate birth interval.
Table 4 Multivariate analysis of short and long birth intervals,socioeconomic and reproductive health variables, andmaternalmorbidity
Variables Short interval� Long interval�
OR (95%CI) OR (95%CI)
Skin color
White Ref. Ref.
Nonwhite 1.39 (1.00–1.95) 1.02 (0.80–1.30)
Age (years old)
< 20 0.84 (0.56–1.28) 0.48 (0.02–0.12)
20–34 Ref. Ref.
� 35 1.00 (0.65–1.55) 2.43 (1.82–3.25)
Education level (years)
< 9 Ref. Ref.
� 9 0.83 (0.64–1.07) 0.84 (0.67–1.05)
Economic status
A–B Ref. Ref.
C 0.91 (0.62–1.33) 1.25 (0.95–1.65)
D–E 0.83 (0.54–1.26) 0.82 (0.59–1.14)
Type of delivery
Normal Ref. Ref.
Cesarean section 1.20 (0.93–1.54) 0.95 (0.77–1.17)
Number of prenatal visits
< 6 Ref. Ref.
� 6 1.21 (0.92–1.60) 0.58 (0.47–0.72)
Number of births
2 Ref. Ref.
� 3 1.29 (1.01–1.65) 0.59 (0.49–0.73)
High blood pressure
No Ref. Ref.
Yes 0.93 (0.68–1.28) 0.89 (0.69–1.14)
Diabetes
No Ref. Ref.
Yes 0.44 (0.19–1.03) 0.38 (0.20–0.75)
Anemia
No Ref. Ref.
Yes 0.99 (0.79–1.25) 0.99 (0.83–1.20)
Abbreviations: CI, confidence interval; OR, odds ratio.�Reference category: adequate birth interval.
Rev Bras Ginecol Obstet Vol. 42 No. 2/2020
Factors Associated with Inadequate Birth Intervals in the Brisa Birth Cohort, Brazil Barbosa et al. 71

birth or pregnancy-spacing intervals of>5 years.9,12,21–23
The increased intervals between pregnancies may have beencaused by the implementation of public policies on familyplanning in the last decades and an increase in the autonomyof the women over their own reproductive health.24
The univariate and multivariate analyses revealed a sta-tistically significant association between the number ofprenatal visits and birth intervals, whereby mothers whohad at least 6 visits had 58% less chance of having long birthintervals. A study conducted with Arab women in 2012showed that the number of prenatal visits during the 1st
trimester of pregnancywas lower amongmothers with shortbirth intervals.25 Similarly, women who had inadequateprenatal care were more likely to have a short subsequentbirth interval than those who had adequate care.13 Thehigher contact with health professionals enables healtheducational actions, which promote healthier attitudes andimprovements in family planning. It is worth highlightingthat adequate prenatal care is associatedwithmore favorableoutcomes in maternal and infant health, especially when theprenatal care group included a multidisciplinary team.26,27
The multivariate analysis also showed statistically signif-icant association between age and long birth intervals. Age<20 years old decreases the chances of long birth intervals,whereas age� 35 years old increases this chance by 43%. Therelationship between age and parity is well described in theliterature. Often, women with more children are older.Women who have had � 3 births had 29% more chance ofhaving short birth intervals. The negative impact of shortbirth intervalsmayonly occur in high parity births, usually inolder women. This finding is consistent with the concept ofmaternal depletion as the underlying cause of increasedadverse child outcomes.28
The univariate analysis showed a statistically significantassociation between diabetes and birth interval. Having ges-tational diabetes proved to be a factor associatedwith long andshort birth intervals. After adjustment for socioeconomicvariables, age, and parity, the association with long intervalswas maintained. A systematic review of the effects of birthinterval onwomen’s healthhighlighteda cross-sectional studyundertaken in Latin America that did not find a significantassociation between diabetes and birth interval.2,11 Afteradjustment for age, number of prenatal visits, and economicstatus, the association between diabetes and short birthintervalwas notmaintained. In an updated systematic review,there was evidence that short birth intervals were associatedwith increased risks of subsequent gestational diabetes, butnot long intervals.29 In the BRISA study, having gestationaldiabetes was inversely associated with long intervals whencompared with adequate birth intervals. A possible explana-tion for this finding is the potential of prenatal care inmonitoring gestational morbidities.26
No association was found between prevalence of anemiaduring pregnancy and birth interval. Despite the fact thatanemia is common during pregnancy, the findings in theliterature are inconclusive.2,11,25,30 Studies conducted inLatin America reported a 30% increase in the risk of anemiaamong women with birth intervals of<6 months, while a
study undertaken in Nigeria found an increased risk ofanemia in birth intervals of<2 years. However, studiesconducted in Bangladesh and Singapore did not find astatistically significant association.2,11,25,30 Supporting ourfindings, the same aforementioned updated review pointedthat no study reported outcomes related tomaternal anemiaand short birth intervals.29
There is emerging evidence that women with long birthintervals are at increased risk for labor dystocia, and thatshort intervals are associated with increased risks of uterinerupture in women attempting vaginal birth after previouscesarean delivery and uteroplacental bleeding disorders(placental abruption and placenta previa).2 A recent system-atic review including 15 studies shows that birth intervalslonger than 18 months were related to decreased risk ofmaternalmorbidity and failed vaginal delivery after previouscesarean section.31
The high number of women included in the present studyand the recruitment strategy increased the possibility ofgeneralization of thefindings forwomenwho reside in capitalsin thenortheastern regionofBrazilwithsimilar characteristics.
Recent studies indicate the importance of identifyingfactors associated with birth intervals due to different pat-terns of association shown for preterm birth compared withmaternal outcomes. This suggests that increasing maternalage may have discordant effects on associations betweenshort birth intervals and adverse perinatal and maternaloutcomes.32
Conclusion
Most of the women in the sample were nonwhite, fromeconomic group C, aged between 20 and 24years old, hadat least 9 years of education, had 2 lifetimebirths, had naturalbirths, and had at least 6 prenatal care visits. With respect tomaternal morbidity, 15.6% of the mothers had high bloodpressure, 2.2% had diabetes, 49.5% had anemia, and 9.4% hadexperienced at least one bleeding episode in the 3rd trimesterof pregnancy. The prevalence of adequate birth intervals washigher than that of long and short intervals. However,approximately one third of the participating women hadlong intervals. A statistically significant association wasmaintained between the variable � 3 births and short birthinterval with multivariate analysis. In this respect, womenwho were � 35 years old were more likely to have long birthintervals. Age<20 years old, � 6 prenatal visits, � 3 births,and gestational diabetes decreased the chances of long birthintervals. Moreover, women with gestational diabetes andadequate prenatal care had higher chances of adequate birthinterval, indicating that health assistance during pregnancyis extremely important to encourage adequate intervalsbetween gestations.
ContributorsAll of the authors contributed with the project and datainterpretation, the writing of the article, the criticalreview of the intellectual content, and with the finalapproval of the version to be published.
Rev Bras Ginecol Obstet Vol. 42 No. 2/2020
Factors Associated with Inadequate Birth Intervals in the Brisa Birth Cohort, Brazil Barbosa et al.72

Conflict of InterestsThe authors have no conflict of interests to declare.
AcknowledgmentsWe thank the interviewers and the mothers who kindlyagreed to participate in the study. The funding agencies:CNPq (Brazilian National Research Council: Grants PROC-ESSON°47923/2011–7), Fapema(MaranhãoStateResearchFoundation: Grants FAPEMA PRONEX N° 00035/2008) andFAPESP (São Paulo State Research Foundation: GrantsFAPESP PROCESSO N° 2008/53593–0).
References1 World Health Organization. Report of a WHO technical consulta-
tion on birth spacing: Geneva, Switzerland 13–15 June 2005.Geneva: World Health Organization; 2007
2 Conde-Agudelo A, Rosas-Bermúdez A, Kafury-Goeta AC. Effects ofbirth spacing onmaternal health: a systematic review. Am J ObstetGynecol 2007;196(04):297–308. Doi: 10.1016/j.ajog.2006.05.055
3 Conde-AgudeloA,Rosas-BermudezA,CastañoF,NortonMH.Effectsof birth spacing on maternal, perinatal, infant, and child health: asystematic review of causal mechanisms. Stud Fam Plann 2012;43(02):93–114. Doi: 10.1111/j.1728-4465.2012.00308.x
4 King JC. The risk of maternal nutritional depletion and poor out-comes increases in early or closely spaced pregnancies. J Nutr 2003;133(05, Suppl 2):1732S–1736S. Doi: 10.1093/jn/133.5.1732S
5 Razzaque A, Da Vanzo J, Rahman M, Gausia K, Hale L, Khan MA,et al. Pregnancy spacing and maternal morbidity in Matlab,Bangladesh. Int J Gynaecol Obstet. 2005;89(Suppl 1):S41–S49.Doi: 10.1016/j.ijgo.2005.01.003
6 Erickson JD, Bjerkedal T. Interval between pregnancies. Lancet1979;1(8106):52. Doi: 10.1016/s0140-6736(79)90502-6
7 Rousso D, Panidis D, Gkoutzioulis F, Kourtis A, Mavromatidis G,Kalahanis I. Effect of the interval between pregnancies on thehealth ofmother and child. Eur J ObstetGynecol Reprod Biol 2002;105(01):4–6. Doi: 10.1016/s0301-2115(02)00077-5
8 Klebanoff MA. The interval between pregnancies and the out-come of subsequent births. N Engl J Med 1999;340(08):643–644.Doi: 10.1056/NEJM199902253400809
9 Conde-Agudelo A, Belizán JM, Norton MH, Rosas-Bermúdez A.Effect of the interpregnancy interval onperinatal outcomes in LatinAmerica. Obstet Gynecol 2005;106(02):359–366. Doi: 10.1097/01.AOG.0000171118.79529.a3
10 Wendt A, Gibbs CM, Peters S, Hogue CJ. Impact of increasing inter-pregnancy interval on maternal and infant health. Paediatr PerinatEpidemiol 2012;26(Suppl 1):239–258. Doi: 10.1111/j.1365-3016.2012.01285.x
11 Winikoff B. The effects of birth spacing on child and maternalhealth. Stud Fam Plann 1983;14(10):231–245
12 Li DK, Wi S. Changing paternity and the risk of preeclampsia/eclampsia in the subsequent pregnancy. Am J Epidemiol 2000;151(01):57–62. Doi: 10.1093/oxfordjournals.aje.a010122
13 Teitler JO, Das D, Kruse L, Reichman NE. Prenatal care andsubsequent birth intervals. Perspect Sex Reprod Health 2012;44(01):13–21. Doi: 10.1363/4401312
14 LiuCM,ChangSD,ChengPJ. Relationshipbetweenprenatal care andmaternal complications inwomenwith preeclampsia: implicationsfor continuity and discontinuity of prenatal care. Taiwan J ObstetGynecol 2012;51(04):576–582. Doi: 10.1016/j.tjog. 2012.09.013
15 de Oliveira RL, da Fonseca CR, Carvalhaes MABL, Parada CMGL.Evaluation of pre-natal care from the perspective of differentmodels in primary care. Rev Lat Am Enfermagem 2013;21(02):546–553. Doi: 10.1590/S0104-11692013000200011
16 Lutenbacher M, Gabbe PT, Karp SM, Dietrich MS, Narrigan D,Carpenter L, et al. Does additional prenatal care in the homeimprove birth outcomes for women with a prior preterm deliv-ery? A randomized clinical trial. Matern Child Health J. 2014;18(5):1142–1154. Doi: 10.1007/s10995-013-1344-4
17 Associação Brasileira de Empresas de Pesquisa [Internet]. CritérioBrasil 2008. 2010 [cited 2018 Dec 10]. Available from: http://www.abep.org/criterio-brasil
18 Schwandt HM, Skinner J, Hebert LE, Cobb L, Saad A, Odeku M.Inadequate birth spacing is perceived as riskier than all familyplanning methods, except sterilization and abortion, in a qualita-tive study among urban Nigerians. BMC Womens Health 2017;17(01):80. Doi: 10.1186/s12905-017-0439-2
19 Silva AAM, Batista RFL, SimõesVMF, Thomaz EB, Ribeiro CC, Lamy-Filho F, et al. Changes in perinatal health in two birth cohorts(1997/1998 and 2010) in São Luís, Maranhão State, Brazil. CadSaude Publica. 2015;31(7):1437–1450. Doi: 10.1590/0102-311X00100314
20 Ministério da Saúde. Secretaria de Atenção à Saúde. Departamentode Ações Programáticas Estratégicas. Área Técnica Saúde da Pessoacom Deficiência. A pessoa com deficiência e o Sistema Único deSaúde. Brasília (DF): Editora do Ministério da Saúde; 2006
21 Almeida MMG. Intervalo entre partos: condiconantes e conse-quência. Salvador-Bahia. Rev Baiana Enferm. 1995;8(1/2):37–55
22 Zhu BP, Grigorescu V, Le T, Lin M, Copeland G, Barone M, et al.Labor dystocia and its association with interpregnancy interval.Am J Obstet Gynecol. 2006;195(1):121–128. Doi: 10.1016/j.ajog.2005.12.016
23 Bener A, Saleh NM, Salameh KMK, Basha B, Joseph S, Samson N,et al. The impact of the interpregnancy interval on birth weightand other pregnancy outcomes. Rev Bras Saúde Mater Infant.2012;12(3):233–241. Doi: 10.1590/S1519-38292012000300003
24 Osamor PE, Grady C. Women’s autonomy in health care decision-making in developing countries: a synthesis of the literature. Int JWomens Health 2016;8:191–202. Doi: 10.2147/IJWH.S105483
25 Singh K, Fong YF, Arulkumaran S. Anaemia in pregnancy–a cross-sectional study in Singapore. Eur J Clin Nutr 1998;52(01):65–70.Doi: 10.1038/sj.ejcn.1600517
26 Allen AJ, Snowden JM, Lau B, Cheng Y, Caughey AB. Type-2 diabetesmellitus:doesprenatal care affectoutcomes? JMatern FetalNeonatalMed 2018;31(01):93–97. Doi: 10.1080/14767058.2016.1276558
27 Ickovics JR, Lewis JB, Cunningham SD, Thomas J, Magriples U.Transforming prenatal care: Multidisciplinary team scienceimproves a broad range of maternal-child outcomes. Am Psychol2019;74(03):343–355. Doi: 10.1037/amp0000435
28 Kozuki N, Walker N. Exploring the association between short/longpreceding birth intervals and childmortality: using reference birthinterval children of the same mother as comparison. BMC PublicHealth 2013;13(Suppl 3):S6. Doi: 10.1186/1471-2458-13-S3-S6
29 Hutcheon JA, Nelson HD, Stidd R, Moskosky S, Ahrens KA. Shortinterpregnancy intervals and adversematernal outcomes in high-resource settings: An updated systematic review. Paediatr PerinatEpidemiol 2019;33(01):O48–O59. Doi: 10.1111/ppe.12518
30 De Oliveira AC, De Barros AM, Ferreira RC. [Risk factors associatedamong anemia in pregnancywomen of network public health of acapital of Brazil Northeastern]. Rev Bras Ginecol Obstet 2015;37(11):505–511. Doi: 10.1590/SO100-720320150005400
31 Ye L, CaoW, Yao J, PengG, ZhouR. Systematic reviewof the effects ofbirth spacing after cesarean delivery on maternal and perinataloutcomes. Int J Gynaecol Obstet 2019;147(01):19–28. Doi: 10.1002/ijgo.12895
32 Haight SC, Hogue CJ, Raskind-Hood CL, Ahrens KA. Short inter-pregnancy intervals and adverse pregnancy outcomes by mater-nal age in the United States. Ann Epidemiol 2019;31:38–44. Doi:10.1016/j.annepidem.2018.12.002
Rev Bras Ginecol Obstet Vol. 42 No. 2/2020
Factors Associated with Inadequate Birth Intervals in the Brisa Birth Cohort, Brazil Barbosa et al. 73

Gestational Outcomes in Patients with Severe MaternalMorbidity Caused by Hypertensive Syndromes
Resultados gestacionais em pacientes com morbidadematerna grave causada por síndromes hipertensivasDaisy de Lucena Feitosa Lins Pinheiro1 Francisco Edson de Lucena Feitosa1
Edward Araujo Júnior2,3 Francisco Herlânio Costa Carvalho1
1Department of Obstetrics and Gynecology, Faculdade de Medicina,Universidade Federal do Ceará, Fortaleza, CE, Brazil
2Department of Obstetrics, Escola Paulista de Medicina, UniversidadeFederal de São Paulo, São Paulo, SP, Brazil
3Medical Course, Universidade Municipal de São Caetano do Sul, SãoPaulo, SP, Brazil
Rev Bras Ginecol Obstet 2020;@42(2):74–80.
Address for correspondence Edward Araujo Júnior, PhD,Departmento de Obstetrícia, Escola Paulista de Medicina,Universidade Federal de São Paulo, Rua Napoleão de Barros, 875, VilaClementino, São Paulo, SP, 04024-002, Brazil(e-mail: [email protected]).
Keywords
► pregnancycomplications
► maternal morbidity► high-risk pregnancy► hypertensive
disorders
Abstract Purpose To evaluate the impact of the presence of criteria for severe maternalmorbidity and maternal near miss associated with hypertensive disorders on maternaland perinatal outcomes in a maternity school.Methods The present is a sub-analysis of a larger study involving 27 centers in Brazilthat estimated the prevalence of serious maternal morbidity and near miss. It is ananalytical and cross-sectional study with a quantitative approach, involving 928womenwho were cared for at Maternidade Escola Assis Chateaubriand (MEAC, in Portuguese),Universidade Federal do Ceará (UFC, in Portuguese), from July 2009 to June 2010. Thewomen were diagnosed with near miss according to the World Health Organization(WHO) criteria. The sample was divided into 2 groups: patients with (n¼ 827) andwithout hypertension (n¼ 101). The results were considered statistically significantwhen p< 0.05. The Pearson chi-squared and Fisher Exact tests were used for thecategorical variables, and the Mann–Whitney U test was used for the continuousvariables.Results In total, 51 participants with maternal near miss criteria were identified, and36 of them had hypertensive disorders. Of these, 5 died and were obviously excludedfrom the near miss final group. In contrast, we observed 867 cases with non-near missmaternal morbidity criteria. During this period, there were 4,617 live births (LBs) in theinstitution that was studied.Conclusion In the severe morbidity/maternal near miss population, the presence ofhypertensive complications was prevalent, constituting a risk factor for both themother and the fetus.
receivedMay 24, 2019acceptedNovember 22, 2019
DOI https://doi.org/10.1055/s-0040-1701464.ISSN 0100-7203.
Copyright © 2020 by Thieme RevinterPublicações Ltda, Rio de Janeiro, Brazil
Original ArticleTHIEME
74

Introduction
Arterialhypertension isaseverepublichealthproblem,and it isa frequent cause of gestational complications worldwide.1–3
Hypertensive disorders have the potential to increase otherclinical complications3- to25-fold,whichmay lead todeath.4,5
Hypertensive disorders are responsible for � 50 thousandcases of globalmaternal deathsper year, and theyare themaincause of maternal death in Latin America and the Caribbean.Estimates indicate that this problem represents a quarter ofthe total number of these deaths.6,7 In Brazil, it is the primarycause of direct maternal death, with a prevalence of 37% ofthese cases; additionally, the ratio is higher in the Northernand Northeastern regions of Brazil compared with the South-eastern, Southern and Midwestern regions.7–9
Studyingmaternal death is a step to improve the obstetricalcare process, as it can signal potential problems in the healthsystem and enable the development of strategies to improvethe quality of maternal assistance.10 However, an importantpiece of data to increase the information related to maternalhealth is the identification and analysis of cases involvingwomenwho survived severe complications during pregnancy,parturition and the puerperium – which are called maternalnear miss –, because they allow us to understand the aspectsthat the survivors have in commonwith those who died fromthese complications, facilitating the gathering of information.Thepatients themselvesaresourcesof informationaboutwhattruly happened during their medical care, reporting potentialdifficulties with referrals and delayed care.11,12
Near misses occur more often than maternal death. Theidentification and knowledge of these cases enables thedevelopment of strategies to reduce the number of maternaldeaths for reasons that could be avoided.13
The present study aimed to evaluate the impact of thepresence of criteria for severe maternal morbidity andmaternal near miss associated with hypertensive disorderson maternal and perinatal outcomes in a maternity schoolthat is a reference in tertiary care.
Methods
The present is an analytical and cross-sectional study with aquantitative approach, involving 928 women who were caredfor at Maternidade Escola Assis Chateaubriand (MEAC, in Por-tuguese), Universidade Federal do Ceará (UFC, in Portuguese),from July 2009 to June 2010; the patients were diagnosedwithnearmiss according to theWorldHealthOrganization (WHO)14
criteria and/or thenon-nearmissmaternalmorbiditycriteria ofthe Brazilian Ministry of Health. Severe morbidity cases due toabortionwere excluded, cases in which the parturition did notoccur in the institution, as well as cases in which the medicalrecordswere unavailable for consulting. This is a sub-analysis ofa larger study involving 27 centers that estimated the preva-lence of severe maternal morbidity and near miss in Brazil.15
The variables that were studied include: age, schooling,race/ethnicity, marital status, number of pregnancies, parity,previous abortion, previous cesarean section, process of par-turition, preexistent clinical conditions, perinatal outcome
Resumo Objetivo Avaliar o impacto da presença de critérios de morbidade materna grave epotencial evento adverso materno associados a distúrbios hipertensivos nos desfechosmaternos e perinatais em uma maternidade escola.Métodos Trata-se de uma subanálise de um estudo maior, envolvendo 27 centros,que estimou a prevalência de morbidade materna grave e potencial evento adverso noBrasil. Realizou-se um estudo analítico e transversal, com abordagem quantitativa,envolvendo 928 mulheres atendidas na Maternidade Escola Assis Chateaubriand(MEAC), na Universidade Federal do Ceará (UFC), no período de julho de 2009 a junhode 2010, diagnosticadas com potencial evento adverso de acordo com os critérios daOrganizaçãoMundial da Saúde (OMS). A amostra foi dividida em dois grupos: pacientescom (n¼827) e sem hipertensão (n¼101). Os resultados foram consideradosestatisticamente significativos quando p<0,05. O teste do Qui-quadrado de Pearsone o teste exato de Fisher foram usados para as variáveis categóricas, e o teste U deMann-Whitney, para as variáveis contínuas.Resultados Foram identificados 51 participantes com critérios de potencial eventoadverso materno, sendo 36 mulheres com distúrbios hipertensivos. Destas, 5 morre-ram e foram obviamente excluídas do grupo final do potencial evento adverso. Foramobservados 867 casos com critérios de morbidade materna que não caracterizavampotencial evento adverso. Nesse período, houve 4.617 nascidos vivos (NVs) nainstituição estudada.Conclusão Na população commorbidade grave/potencial evento adversomaterno, apresença de complicações hipertensivas é prevalente, constituindo fator de risco para obinômio materno-fetal.
Palavras-chave
► complicações nagestação
► morbidade materna► gestação de alto
risco► distúrbios
hipertensivos
Rev Bras Ginecol Obstet Vol. 42 No. 2/2020
Gestational Outcomes in Patients with Severe Maternal Morbidity Pinheiro et al. 75

(birth weight, Apgar score and death) and maternal outcome(severematernalmorbidity, including nearmiss andmaternaldeath).
The sample was divided in two groups: patients with(n¼827) and without hypertension (n¼101). Out of the 827participants who had a diagnosis of hypertensive syndrome,49 had chronic hypertension, 20 had preeclampsia withoutsignsofseverity,616hadpreeclampsiawithsignsof severity, 60had eclampsia, and 82 had hemolysis, elevated liver enzymes,and a low platelet count (HELLP) syndrome. Chronic hyperten-sion was considered when the hypertension diagnosis (�140�90mmHg) occurred before the 20th gestational week in theabsence of proteinuria. Preeclampsia was considered whenhypertension was identified after the 20th gestational weekin the presence of proteinuria (� 300mg of protein in 24-hoururine or in labstix isolated samples with two crosses in a singleepisode or two identifications of a cross). Preeclampsia wasclassified as severe when the hypertension was�160�100mm Hg, creatinine�1.2mg/dl, oliguria (< 400ml within24hours), or signs of impending eclampsia were observed(nausea, vomiting, turbidity or visual scotomas, occipital head-ache and epigastralgia). The diagnostic criteria used at the timewere ratified by the International Society for The Study ofHypertension in Pregnancy (ISSHP) in 2014.16
For the statistical analysis, the International BusinessMachines Statistical Package for the Social Sciences (IBMSPSS Statistics for Windows, IBM Corp., Armonk, NY, US)software, version 22.0, was used. The results were consideredstatistically significant when p<0.05. The Pearson chi-squaredand theFisherexact testswereused for thecategoricalvariables, and the Mann–Whitney U test was used for thecontinuous variables.
The project was approved by the Ethics in ResearchCommittee of UFC under number 1.783.162. The free andinformed consent forms of the women were not obtainedindividually. The information of interest was gathered frommedical records without identifying the patient’s name;instead, the record number was used.
Results
The sociodemographic data of the cases classified as severematernalmorbiditywith or without hypertension are shownin►Table 1. No difference between the groupswas observed,except regarding race/ethnicity, with three patients self-declaring as white, and 925 self-declaring as non-white.Most women did not have partners. Additionally, thewomenwerebetween 20 and 34 years old, and hadmore than 8 yearsof schooling.
In relation to the obstetrical characteristics, there was ahigher number of primiparous women (p¼0.005) and sub-jects without previous abortions (p¼0.024) in the group ofpatients with hypertension (►Table 1). Most parturitionswith hypertensive complications occurred through cesareansection: 635. Among the severe maternal morbidity indica-tors, there were 110 intensive care unit (ICU) admissions, 80blood transfusions (29 requiring at least 5 units of packed redblood cells), 42 hospitalizations for more than 7 days post-
partum, 33 hysterectomies, and 17 intubations (unrelated toanesthesia), with no significant difference between thegroups with and without hypertension. Among the caseswith potentially life-threatening conditions (n¼142, some
Table 1 Epidemiological and clinical characteristics of thepatients identified as cases of severe maternal morbidity withand without hypertension
Hypertension
Variables Yesn (%)
Non (%)
p-value
Age (years) 0.061�
10–19 178 (21.5) 13 (12.9)
20–34 511 (61.8) 74 (73.3)
35 or older 138 (16.7) 14 (13.9)
Schooling 0.081�
> 8 years 450 (63) 31 (51.7)
� 8 years 264 (37) 29 (48.3)
Marital status 0.603�
With a partner 194 (27.4) 18 (30.5)
Without a partner 515 (72.6) 41 (69.5)
Pregnancies 0.005�
1 403 (48.7) 32 (31.7)
2–3 294 (35.6) 47 (46.5)
> 3 130 (15.7) 22 (21.8)
Births 0.336�
1 195 (53.1) 32 (53.3)
2–3 138 (37.6) 19 (31.7)
> 3 34 (9.3) 9 (15)
Previous cesareansections
0.832�
1 133 (70.4) 15 (68.2)
� 2 56 (29.6) 7 (31.8)
Abortions 0.024�
None 639 (77.5) 68 (67.3)
> 1 186 (22.5) 33 (32.7)
Number of live births 0.023�
1 197 (55.3) 29 (50)
2–3 119 (33.4) 15 (25.9)
> 3 40 (11.2) 14 (24.1)
Years since thelast birth
0.436�
1 4 (6.7) 18 (5)
2–3 7 (11.7) 65 (18.1)
> 3 49 (81.7) 276 (76.9)
Prenatal care visits 0.092�
< 6 236 (44.4) 32 (56.1)
� 6 295 (55.6) 25 (43.9)
Note: �Pearson chi-squared test.
Rev Bras Ginecol Obstet Vol. 42 No. 2/2020
Gestational Outcomes in Patients with Severe Maternal Morbidity Pinheiro et al.76

patients had more than 1 condition), the following werehighlighted: premature detachment of the placenta (n¼44);placenta accreta/percreta (10); shock (24); respiratory fail-ure (23); sepsis (23); postpartum hemorrhage (23); endo-metritis (6); acute pulmonary edema (2); ectopic pregnancy(9); and uterine rupture (1), with no significant differencebetween the groups with andwithout hypertension. Magne-sium sulfate was used in 682 cases, all of which were in thehypertensive group. In total, 51 participants with maternalnear miss criteria were identified, 36 of whomwere womenwith hypertensive disorders. From this group, 5 died; there-fore, they were obviously excluded from the final near missgroup. We observed 867 cases of non-near miss maternalmorbidity criteria. During this period, there were 4,617 livebirths (LBs) in the institution that was studied, with amaternal near miss ratio of 55.55/1,000 LBs, a non-nearmiss maternal morbidity ratio of 190.6/1,000 LBs, and amaternal morbidity ratio of 238.2/1,000 LBs. We observed
that the number of women at risk for death was 51, and theratio was 11.2/1,000 LBs. ►Table 2 shows the maternal out-comes of the women classified with severe maternal mor-bidity with and without hypertension.
Among the 10 cases of maternal death, all involvedhospitalization in the ICU, and 7 patients received bloodproducts. Among the cases with hypertensive syndromes,there were two cases of severe preeclampsia, and three ofeclampsia. None of the patients with HELLP syndrome died.Sepsis was diagnosed in two of these cases. In the groupwithout hypertension, four women died of hemorrhagicsyndromes (two with premature placental detachment andtwowith a previous placenta accreta) and one case of severesepsis was observed. Perinatal death was more prevalent inthe groupwithout hypertension (19.8% versus 5%, p<0.001)(►Table 3).
No significant differences in the near miss criteria betweenthe participants with and without hypertensive disorderswere observed, except for cyanosis (72% versus 28%,p¼0.038) and cardiopulmonary resuscitation (76% versus24%, p¼0.011), which were more prevalent in the groupwith hypertension (►Table 4).
Discussion
The present study evaluated severe maternal morbidity/maternal near miss in women with or without hypertensionduring pregnancy. It was performed in a reference center forobstetric and neonatal care over one year. We observed thepresence of hypertension in most the participants (89.1%)who met the severe criteria.
Hypertensive syndromes are widely understood as themain cause of complications in prenatal care, occurring in2% to 26% of gestations.16,17 Hypertensive disorders areresponsible for nearly 45,000 cases of maternal death everyyear worldwide, and are the main cause of maternal healthin Latina America and the Caribbean. Estimates indicatethat this problem represents a quarter of the total numberof these deaths.7,8 These observations make the study of theincidence of hypertension and its related causes relevant tounderstanding its relationship with maternal near miss.
Vidal et al18 performed a study whose goal was to identifythe factors associated with maternal near miss in the city ofBarbacena, state of Minas Gerais, Brazil. This study identifiedthat in a sample of 276 women, which included 92 cases and184 controls, the parturient womenwith a previous history ofhypertension had a greater risk of developing severe maternalmorbidity, such as preeclampsia and HELLP syndrome. In thisgroup, 10.1% had severe hypertension, followed by 9.4% withsevere preeclampsia, 0.4% with severe preeclampsia and se-vere hypertension, and 0.4% with eclampsia.
Studies point to hypertensive syndromes as frequentcauses related to maternal near miss. In a study by Souzaet al,19 57% of the women had hypertensive disorders. In astudy by Morse et al,20, nearly 70% of the women hadpreeclampsia, HELPP syndrome and eclampsia. This evidenceemphasizes the need for and importance of prevention, earlydetection and treatment of these complications to control
Table 2 Maternal near miss and death among the patientsidentified with severe maternal morbidity associated or notwith hypertensive syndromes
Hypertension
Variables Yesn (%)
Non (%)
p-value
Near miss criteria < 0,0007�
Yes 36 (71) 15 (29)
No 86 (91) 81 (9)
Maternal death < 0.001�
Yes 5 (0.6) 5 (4.9)
No 822 (99.4) 96 (95.1)
Note: �Pearson chi-squared test.
Table 3 Perinatal outcomes of women identified with severematernal morbidity criteria with and without hypertensivesyndromes
Hypertension
Variables Yesn (%)
Non (%)
p-value
Perinatal death < 0.001�
Yes 41 (5) 20 (19.8)
No 786 (95) 81 (80.2)
Average birthweight (g)(mean� SD)
2,723.6� 837.7 2,848.1� 742.3 0.569��
Low birthweight
0.817�
Yes 278 (36.8) 26 (38.2)
No 477 (63.2) 42 (61.8)
Prematurity 0.759�
< 37 weeks 281 (37.2) 27 (39.7)
� 37 weeks 474 (62.8 41 (60.3)
Notes: �Pearson chi-squared test; ��Mann–Whitney test.
Rev Bras Ginecol Obstet Vol. 42 No. 2/2020
Gestational Outcomes in Patients with Severe Maternal Morbidity Pinheiro et al. 77

and reduce the risk of maternal near miss related to hyper-tensive causes.
We found that a lower frequency of the subjects in thispopulation group evolved to more severe cases, as a lowerfrequency of subjects whomet thematernal near miss criteriaand a lower frequency of maternal and perinatal deaths wereobserved when compared with cases who met the morbiditycriteria that were not associated with hypertensive disorders.
A possible explanation for these findings is that, as the twogroups (with and without hypertension) were epidemiologi-cally similar, there may be differences in the expertise of theinstitution’s clinical body in managing cases with gestationalhypertensive syndromes. The assistance protocols, which areoften updated and based on the available scientific evidence,are widely disseminated in written form in virtual environ-ments and on banners in every maternity sector wherepatients with hypertensive complications are cared for.
There was a prioritization in recent years of the dissemina-tion of knowledge on gestational hypertensive pathologieswith the development of multiprofessional protocols adaptedto local realities,becausethis is themostprevalentpathology in
cases of perinatal andmaternal deaths. Themagnesium sulfateprotocols were associated with improvements in maternalindicators, as they are widely known and often implementedwhen they are recommended, and they lead to lower lethalityin thesecases. It is important tonote thatMEAC-UFC is themainreference point for gestational complications in the state ofCeará, Brazil –with a profile of following risky pregnancies.
The results of the present study showed that the maternalnear miss ratio was of 55.55/1,000 LBs. These data arecompatible with those found in the literature, which rangefrom 0.7 to 101.7 cases per 1,000 births.4,5,15 Souza et al19
performed a study with 2,929 women, and identified asevere maternal morbidity ratio from 15 to 42 cases/1,000births. In the same study, the estimated near miss morbiditywas of 44.3/1,000 LBs. It is important to point out that moststudies work with the number of births in the denominatorof the maternal morbidity ratio, whereas the WHO recom-mends using LBs, as wehave done in our study. Themortalityratio in the maternal near miss cases was of 18%, which iscompatible with what is found in the literature11,19–22 forcountries with low and medium socioeconomic levels.
Table 4 Maternal near miss criteria among the participants with and without hypertensive disorders
Hypertension
Clinical criteria Yesn (%)
Non (%)
p-value
Acute cyanosis 20 (72) 8 (28) 0.038�
Respiratory rate> 40 or< 60 bpm 16 (70) 7 (30) 0.542�
Oliguria unresponsive to fluids and diuretics 19 (66) 8 (34) 0.197�
Shock 18 (75) 6 (25) 0.053�
Coagulation disorders 20 (71) 8 (29) 0.038�
Loss of consciousness for 12 hours or more 13 (62) 8 (38) 0.398�
Absence of consciousness and absence of pulsations or cardiac beats 15 (62) 9 (38) 0.333�
Cerebrovascular accident 17 (65) 9 (35) 0.704�
Uncontrolled convulsion 16 (62) 10 (38) 0.129�
Jaundice in the presence of preeclampsia 18 (64) 10 (36) 0.301�
Laboratorial criteria
Saturation and oxygen< 90% for 60minutes or more 18 (67) 9 (33) 0.516�
PaO2/FiO2< 200mm Hg 18 (67) 9 (33) 0.516�
Creatine�3.5mm Hg/dL or� 300 µMol/1 18 (67) 9 (33) 0.516�
Bilirubin� 6.0mg/dL or> 100 µMol/1 15 (60) 10 (40) 0.283�
pH<7,1 20 (65) 11 (35) 0.112�
Acute thrombopenia (< 50,000/mm3) 11 (61) 7 (38) 0.641�
Handling criteria
Continuous use of vasoactive drug 12 (75) 4 (25) 0.515�
Puerperal hysterectomy by infection and hemorrhage 23 (70) 10 (30) 0.882�
Transfusion� 5 units of red-blood cell concentrate 22 (76) 7 (24) 0.127�
Intubation and ventilation for�60minutes not related to anesthesia 13 (76) 4 (24) 0.389�
Dialysis for acute renal insufficiency 26 (76) 8 (24) 0.011�
Cardiopulmonary resuscitation (CPR) 21 (70) 9 (30) 0.849�
Note: �Pearson chi-squared test.
Rev Bras Ginecol Obstet Vol. 42 No. 2/2020
Gestational Outcomes in Patients with Severe Maternal Morbidity Pinheiro et al.78

It is necessary todevelop apublic policy to protectmaternaland child health throughout all of the care levels to preventcomplications or evolution into severe cases.23 A severe prob-lemassociatedwith the developmentof complications and theevolution of severity in the puerperal pregnancy cycle aredelays in obstetrical assistance, whether they are related topatients, families, access difficulties, inefficient reference-counter reference systems, or care units and their staff (latediagnosis, delay in theappropriate and timelyestablishmentofa therapy). An explanatory model was described by Thaddeusand Maine in 1994.24
Unfortunately, these delays were not evaluated in thepresent study, and they may explain the worse evolutionand higher lethality found in the cases associated withhypertension when compared with the cases that did notshow this association. Another cause of maternal morbidity/mortality are hemorrhagic syndromes, in which little time isavailable to avoid more severe complications and maternaland perinatal deaths.
A high frequency of cesarean sections (nearly 81%) wasobserved among our study participants. This result is similarto what was observed in other studies.20 It is assumed thatthis occurs due to the risk of complication in the clinical stateof the patients.
In relation to prenatal care, most patients in the presentstudy had fewer than six prenatal care visits. In a study byMantel et al,25 the authors identified that between 21% and30% of the women had not even been examined once duringtheir prenatal care. When considering the results, it isimportant to note the number of visits that these pregnantwomen had. According to theWHO, the appropriate numberof prenatal visits should be equal to or greater than six;however, this number may be lower in low-risk patients.Nevertheless, adequate prenatal assistance enables the earlydetection of and intervention for gestational complications,and it is a fundamental tool in reducing the risk of stillbirthsand problems during pregnancy. The lack or the inadequacyof prenatal care is contemplated in level 1 and level 2 delaysby Thaddeus and Maine.24
Some limitations in the present studymust be recognized.The study was performed in a single unit; however, thematernity school is a reference for third-level care, and thesampling involved a significant number of patients. Anotherlimitation was that the data were collected from recordswithout applying a direct contact tool with the women,which could have broadened the range of information,such as information related to prenatal care and delaysin the path through the health system when a patient needshospital and medical care. We suggest that this tool be usedin further studies.
The main limitation of the study is that the data collectionperiod tookplace�9years ago;however, dataonnearmiss andmaternal morbidity in the institution are now presentedannually as amanagement report, and are very similar to thosedatathatwerecollected.Additionally, thesedatawerecollectedwith a rigorousmethodology, andwere approved by the ethicscommittee for collection and therefore publication. Thesewerefactors for us in reporting this longstanding data.
The data found here have the potential to aid in thesurveillance of maternal near miss cases and risk factors.They point out the importance of adequate prenatal care andassistance, as they present a determining factor in thereduction of the risk of hypertensive complications andsubsequent cases of maternal near miss, which could beavoided.
Conclusion
In summary, in the severe morbidity/maternal near misspopulation, the presence of hypertensive complications wasvery prevalent, constituting a risk factor for pregnantwomen and their fetuses. Among the women with hyper-tensive syndromes, we observed a lower presence ofmaternal near miss criteria and lower maternal and peri-natal mortality rates when compared with women withouthypertensive problems.
ContributorsAll of the authors contributed with the project and datainterpretation, the writing of the article, the criticalreview of the intellectual content, and with the finalapproval of the version to be published.
Conflict of InterestsThe authors have no conflict of interests to declare.
References1 Antza C, Cifkova R, Kotsis V. Hypertensive complications of
pregnancy: A clinical overview. Metabolism 2018;86:102–111.Doi: 10.1016/j.metabol.2017.11.011
2 Mbachu II, Udigwe GO, Okafor CI, Umeonunihu OS, Ezeama C,Eleje GU. The pattern and obstetric outcome of hypertensivedisorders of pregnancy in Nnewi, Nigeria. Niger J Med 2013;22(02):117–122
3 Ye C, Ruan Y, Zou L, Li G, Li C, Chen Y, et al. The 2011 surveyon hypertensive disorders of pregnancy (HDP) in China: pre-valence, risk factors, complications, pregnancy and perinataloutcomes. PLoS One 2014;9(06):e100180. Doi: 10.1371/journal.pone.0100180
4 Shah S, Gupta A. Hypertensive disorders of pregnancy. CardiolClin 2019;37(03):345–354. Doi: 10.1016/j.ccl.2019.04.008
5 Sutton ALM, Harper LM, Tita ATN. Hypertensive disorders inpregnancy. Obstet Gynecol Clin North Am 2018;45(02):333–347. Doi: 10.1016/j.ogc.2018.01.012
6 BrownMA,Magee LA, Kenny LC,Karumanchi SA,McCarthy FP, SaitoS, et al. International Society for the Study of Hypertension inPregnancy (ISSHP). Thehypertensive disorders of pregnancy: ISSHPclassification, diagnosis & management recommendations for in-ternational practice. Pregnancy Hypertens 2018;13:291–310. Doi:10.1016/j.preghy.2018.05.004
7 Say L, Chou D, Gemmill A, Tunçalp Ö, Moller AB, Daniels J, et al.Global causes of maternal death: a WHO systematic analysis.Lancet Glob Health 2014;2(06):e323–e333. Doi: 10.1016/S2214-109X(14)70227-X
8 Alkema L, Chou D, Hogan D, Zhang S, Moller AB, Gemmill A, et al.United Nations Maternal Mortality Estimation Inter-AgencyGroup collaborators and technical advisory group. Global, region-al, and national levels and trends in maternal mortality between1990 and 2015, with scenario-based projections to 2030: asystematic analysis by the UN Maternal Mortality Estimation
Rev Bras Ginecol Obstet Vol. 42 No. 2/2020
Gestational Outcomes in Patients with Severe Maternal Morbidity Pinheiro et al. 79

Inter-Agency Group. Lancet 2016;387(10017):462–474. Doi:10.1016/S0140-6736(15)00838-7
9 Zanette E, Parpinelli MA, Surita FG, Costa ML, Haddad SM, SousaMH, et al. Brazilian Network for Surveillance of Severe MaternalMorbidity Group. Maternal near miss and death among womenwith severe hypertensive disorders: a Brazilian multicenter sur-veillance study. Reprod Health 2014;11(01):4. Doi: 10.1186/1742-4755-11-4
10 Bandali S, Thomas C, Hukin E, Matthews Z, Mathai M, Ram-achandran Dilip T, et al. Maternal Death Surveillance andResponse Systems in driving accountability and influencingchange. Int J Gynaecol Obstet 2016;135(03):365–371. Doi:10.1016/j.ijgo.2016.10.002
11 Smith H, Ameh C, Roos N, Mathai M, Broek NVD. Implementingmaternal death surveillance and response: a review of lessonsfrom country case studies. BMC Pregnancy Childbirth 2017;17(01):233. Doi: 10.1186/s12884-017-1405-6
12 Souza JP, Gülmezoglu AM, Carroli G, Lumbiganon P, Qureshi Z;WHOMCS Research Group. The world health organization multi-country survey on maternal and newborn health: study protocol.BMC Health Serv Res 2011;11:286. Doi: 10.1186/1472-6963-11-286
13 Souza JP, Cecatti JG, Haddad SM, Parpinelli MA, Costa ML, Katz L,et al. Brazilian Network for Surveillance of Severe MaternalMorbidity Group; Brazilian Network for Surveillance of SevereMaternal Morbidity. The WHO maternal near-miss approach andthe maternal severity index model (MSI): tools for assessing themanagement of severematernalmorbidity. PLoSOne 2012;7(08):e44129. Doi: 10.1371/journal.pone.0044129
14 Say L, Souza JP, Pattinson RC; WHO working group on MaternalMortality and Morbidity classifications. Maternal near miss–towards a standard tool for monitoring quality of maternal healthcare. Best Pract Res Clin Obstet Gynaecol 2009;23(03):287–296.Doi: 10.1016/j.bpobgyn.2009.01.007
15 Cecatti JG, Souza JP, Parpinelli MA, Haddad SM, Camargo RS,Pacagnella RC, et al. Brazilian Network for Surveillance of SevereMaternal Morbidity. Brazilian network for the surveillance ofmaternal potentially life threatening morbidity and maternalnear-miss and a multidimensional evaluation of their long termconsequences. Reprod Health 2009;6:15. Doi: 10.1186/1742-4755-6-15
16 Tranquilli AL, Dekker G, Magee L, Roberts J, Sibai BM, Steyn W,et al. The classification, diagnosis and management of the hyper-tensive disorders of pregnancy: A revised statement from theISSHP. Pregnancy Hypertens 2014;4(02):97–104. Doi: 10.1016/j.preghy.2014.02.001
17 ACOG Practice Bulletin No. 202: Gestational Hypertension andPreeclampsia. Obstet Gynecol 2019;133(01):e1–e25. Doi:10.1097/AOG.0000000000003018
18 Vidal CE, Carvalho MAB, Grimaldi IR, Reis MC, Baêta MCN, GarciaRB, et al. [Severe maternal morbidity in the microregion ofBarbacena, Minas Gerais state, Brazil]. Cad Saude Colet 2016;24(02):131–138. Doi: 10.1590/1414-462X201600020181
19 Souza JP, Cecatti JG, Parpinelli MA, Serruya SJ, Amaral E. Appro-priate criteria for identification of near-miss maternal morbidityin tertiary care facilities: a cross sectional study. BMC PregnancyChildbirth 2007;7:20. Doi: 10.1186/1471-2393-7-20
20 Morse ML, Fonseca SC, Gottgtroy CL, Waldmann CS, Gueller E.Severe maternal morbidity and near misses in a regional refer-ence hospital. Rev Bras Epidemiol 2011;14(02):310–322. Doi:10.1590/s1415-790X2011000200012
21 Lima HM, Carvalho FH, Feitosa FE, Nunes GC. Factors associatedwith maternal mortality among patients meeting criteria ofsevere maternal morbidity and near miss. Int J Gynaecol Obstet2017;136(03):337–343. Doi: 10.1002/ijgo.12077
22 Vogel JP, Souza JP, Mori R, Morisaki N, Lumbiganon P, LaopaiboonM, et al. WHO Multicountry Survey on Maternal and NewbornHealth Research Network. Maternal complications and perinatalmortality: findings of the World Health Organization Multicoun-try Survey on Maternal and Newborn Health. BJOG 2014;121(Suppl 1):76–88. Doi: 10.1111/1471-0528.12633
23 Luz BG, Soares LT, Grillo VT, Viola BM, Laporte IC, BinoDB, et al. [Theprofile of high risk pregnantwomena clinic ofDivinópolis, inMinasGerais,Brazil, in thebiennium2013/14. JHealthBiol Sci2015;3(03):137–143. Doi: 10.12662/2317-3076jhbs.v3i3.177.p137-143.2015
24 Thaddeus S, Maine D. Too far to walk: maternal mortality incontext. Soc Sci Med 1994;38(08):1091–1110. Doi: 10.1016/0277-9536(94)90226-7
25 Mantel GD, Buchmann E, Rees H, Pattinson RC. Severe acutematernal morbidity: a pilot study of a definition for a near-miss.Br J Obstet Gynaecol 1998;105(09):985–990. Doi: 10.1111/j.1471-0528.1998.tb10262.x
Rev Bras Ginecol Obstet Vol. 42 No. 2/2020
Gestational Outcomes in Patients with Severe Maternal Morbidity Pinheiro et al.80

Increased Sympathetic Cardiac AutonomicModulation after Two Consecutive Tilt Tests inWomen with Polycystic Ovary Syndrome
Aumento da modulação autonômica cardíaca simpáticaapós dois testes de inclinação consecutivos em mulherescom síndrome dos ovários policísticosVictor Barbosa Ribeiro1,2 Gislaine Satyko Kogure1 Rafael Costa Silva1
Hugo Celso Dutra Souza3 Rui Alberto Ferriani1 Rosana Maria Reis1
1Department of Gynecology and Obstetrics, Medical School ofRibeirão Preto, Universidade de São Paulo, Ribeirão Preto, SP, Brazil
2 Insituto Federal de São Paulo, Jacareí, SP, Brazil3Department of Biomechanics, Medicine and Locomotive ApparatusRehabilitation, Faculdade de Medicina de Ribeirão Preto,Universidade de São Paulo, Ribeirão Preto, SP, Brazil
Rev Bras Ginecol Obstet 2020;42(2):81–89.
Address for correspondence Victor Barbosa Ribeiro, PhD,Department of Gynecology and Obstetrics, Medical School of RibeirãoPreto, Universidade de São Paulo, Ribeirão Preto, SP 14049-900, Brazil(e-mail: [email protected]).
Keywords
► polycystic ovarysyndrome
► cardiac autonomicmodulation
► hyperandrogenism► spectral analysis► symbolic analysis
Abstract Objective The present study aimed to analyze cardiac autonomic modulation viaspectral and symbolic analysis of heart rate variability (HRV) in women with polycysticovary syndrome (PCOS) who were subjected to two consecutive tilt tests.Methods A total of 64 women were selected and divided into 2 groups: control(without PCOS), and PCOS. Concentrations of follicle-stimulating hormone, luteinizinghormone, prolactin, estradiol, homocysteine, sex hormone-binding globulin, thyroidstimulating hormone, fasting insulin, testosterone, androstenedione, and 17-hydrox-yprogesterone levels, triglycerides, free androgen index (FAI), and homeostasisassessment model (HOMA-IR) were assessed. Cardiac autonomic modulation wasevaluated by spectral and symbolic analyses during two consecutive tilt tests (twomoments) and supine moments before, between and after (three moments) the tilttests.Results Women with PCOS had higher fasting insulin, HOMA-IR indexes, testosteroneand FAI. Additionally, we observed that the PCOS group had greater sympatheticautonomic cardiacmodulation in supine 2, tilt 1, and supine 3moments comparedwithcontrols.Conclusion Women with PCOS had higher autonomic sympathetic cardiac modula-tion even after a second tilt test. No adaptation to this provocative test was observed.Spectral analysis was more sensitive for identifying differences between groups thanthe symbolic analysis.
receivedAugust 6, 2019acceptedNovember 22, 2019
DOI https://doi.org/10.1055/s-0040-1701467.ISSN 0100-7203.
Copyright © 2020 by Thieme RevinterPublicações Ltda, Rio de Janeiro, Brazil
THIEME
Original Article 81

Introduction
Polycystic ovary syndrome (PCOS) is a disease of endocrineorigin that affects� 5 to 16% ofwomen of childbearing age.1 In2003, the Rotterdam consensus proposed that PCOS could bediagnosed after excluding other causes ofmenstrual irregular-ity, the presence of ovary cysts, and hyperandrogenism,2 andtheir healthcare providers must be aware of the possible risksand complications of PCOS including those related to thecardiovascular system, and endocrine, metabolic, and bodycomposition parameters.2–6
The cause and effect relationship between increasedinsulin resistance (IR) and excess testosterone is evident inPCOS. This has been associated with increased visceral fatandmetabolic syndrome,4–7which predisposes to the devel-opment of metabolic chronic diseases2,6,7 and of cardiovas-cular disorders that directly impair the physiology of normalheart function and are often accompanied by impairments incardiac autonomic control.8–10 It has been demonstratedthat there is a cardiovascular autonomic imbalance in wom-enwith PCOS,with increased autonomic sympathetic cardiacmodulation and reduced parasympathetic modulation,which increases the risk of cardiovascular disease.3,10,11
Noninvasive, reproducible, and low-cost tests have beenused to evaluate autonomic function, specifically, heart ratevariability (HRV),12–15 which can be analyzed in both a linearand in a nonlinear manner. On the other hand, the tilt test,which involves autonomic provocations by means of posturalchanges from supine to orthostatic positions (standing, 90°;passively or actively), allows a better evaluation of the auto-nomic modulation.16,17
To our knowledge, there are no data available onHRVaftera second of two consecutive tilt tests, nor on whethersymbolic analyses would express results similar to those ofspectral analyses. An adaptation of HRV to the second con-secutive test in the PCOS group could represent an auxiliaryform of training that controls the modulation of the cardiacautonomic cardiovascular system. Thus, the present studyaimed to analyze the behavior of cardiac autonomic modu-lation via spectral and symbolic analyses of HRV in womenwith PCOS subjected to two consecutive tilt tests.
Methods
Participants and MethodsIn the present case-control study, women with PCOS andcontrols with regular menstrual cycles were included. Thestudy sample comprised 64 women, 32 with PCOS and 32controls (without PCOS), aged between 18 and 37years old,with body mass indexes (BMIs) between18 and 39.9kg/m2
who did not engage in regular supervised physical activity.Womenwith PCOSwere selected fromoutpatient clinics of theHumanReproduction Sector of theDepartment of Gynecologyand Obstetrics, Ribeirão Preto Medical School, University ofSão Paulo, Ribeirão Preto, state of São Paulo, Brazil, and thehealthy control group (CG) participants were recruited fromthe women who had routine gynecological examinations atBasicHealthClinics. Polycystic ovary syndromewasdiagnosedusing the criteria established by the Rotterdam consensus andwas based on the presence of at least two of the followingconditions: oligomenorrhea or amenorrhea; clinical and/orbiochemical signs of hyperandrogenism; polycystic ovaries
Resumo Objetivo O presente estudo teve como objetivo analisar a modulação autonômicacardíaca por análise espectral e simbólica da variabilidade da frequência cardíaca (VFC)emmulheres com síndrome dos ovários policísticos (SOP) que foram submetidas a doistestes consecutivos de inclinação.Métodos Um total de 64 mulheres foram selecionadas e divididas em 2 grupos:controle (sem SOP) e SOP. Concentrações de hormônio folículo-estimulante, hormônioluteinizante, prolactina, estradiol, homocisteína, globulina de ligação a hormôniossexuais, hormônio estimulante da tireóide, insulina em jejum, testosterona e andros-tenediona e níveis de 17-hidroxiprogesterona, triglicerídeos, índice de andrógeno livre(FAI) e homeostase modelo de avaliação (HOMA-IR) foram avaliados. A modulaçãoautonômica cardíaca foi avaliada por análises espectrais e simbólicas durante doistestes de inclinação consecutivos (dois momentos) e momentos supinos antes, entre eapós (três momentos) os testes de inclinação.Resultados Mulheres com SOP apresentaram insulina em jejuM, índices HOMA-IR,testosterona e FAI mais altos. Além disso, observamos que o grupo PCOS apresentoumaior modulação cardíaca autonômica simpática nos momentos supino 2, inclinado 1e supino 3 em comparação aos controles.Conclusão Mulheres com SOP apresentaram modulação cardíaca simpática autonô-mica mais alta mesmo após um segundo teste de inclinação. Nenhuma adaptação aesse teste provocativo foi observada. A análise espectral foi mais sensível paraidentificar diferenças entre os grupos do que a análise simbólica.
Descritores
► síndrome dos ováriospolicísticos
► modulaçãoautonômica cardíaca
► hiperandrogenismo► análise espectral► análise simbólica
Rev Bras Ginecol Obstet Vol. 42 No. 2/2020
Increased Sympathetic Cardiac Autonomic Modulation Ribeiro et al.82

detected by pelvic ultrasound.2 The inclusion criteria for CGwere:without PCOS,menstrual cycles occurring at intervals ofbetween 22 and 35 days; duration of menses from 3 to7 days.18 The exclusion criteria for both groups were: othersystemic diseases, smoking, pregnancy, use of medicationsthat might interfere with the hypothalamus–pituitary–ovari-an axis, and drugs that definitively interfered with the hypo-thalamic-pituitary-axis or cardiac autonomic modulation.
The present study was conducted in accordance with theethical standards set forth in theHelsinki Declaration of 1975andwas approved by the Human Research Ethics Committeeof the Clinical Hospital of the School of Medicine of RibeirãoPreto, University of São Paulo, Ribeirão Preto, state of SãoPaulo, Brazil (case HCRP N. 13475/2009).
Pelvic UltrasonographyAll of the women underwent transvaginal pelvic ultrasonog-raphy examinations using a Voluson 730 Expert machine (GEMedical Systems, Zipf, Austria) to evaluate for polycysticovaries.19
Biochemical MeasurementsThe concentrationsof follicle-stimulatinghormone (FSH), lutei-nizing hormone (LH), prolactin, estradiol, homocysteine, sexhormone-binding globulin (SHBG), thyroid stimulating hor-mone (TSH), and fasting insulin were determined using achemiluminescence assay (IMMULITE 2000 Immunoassay Sys-tem; Siemens, Munich, Germany). Testosterone, androstenedi-one, and 17-hydroxyprogesterone (17- OHP) levels weremeasuredusing radioimmunoassay (IMMULITE1000;Siemens,Munich, Germany), and glucose levels were assessed using theglucose oxidase method. Total cholesterol (TC), high-densitylipoprotein cholesterol (HDL), and triglycerides (TG) wereassessed using an enzymaticmethod, and low-density lipopro-tein cholesterol (LDL) was calculated using the Friedewaldformula: [LDL¼TC - (HDLþTG/5)].20 The free androgen index(FAI) was determined using total testosterone [(nmol/L�1)/SHBG (nmol/L�1)�100],21 and IR (insulin resistance) wasquantified using the homeostatic model assessment of IR(HOMA-IR) ([fasting glycemia level (mg/dL�1) _ 0.05551] x[fasting insulin level (μIU/Ml�1)]/22.5).22
Anthropometry and Body FatAnthropometric measurements were obtained according tothe recommendations of the International Society for theAdvancement of Kinanthropometry.23–28Height was recordedto the nearest 0.1 cm using a standard anthropometer, andweight to the nearest 0.5 kg using a weight scale (Filizola, SãoPaulo, SP, Brazil). Anonelasticflexiblemeasuring tapewasusedto measure waist, hip, and abdominal circumferences, with allmeasurements taken by a single evaluator and recorded to thenearest 0.1 cm.Waist circumference (WC)wasmeasured at themid-point between the lower ribs and the iliac crest. Hipcircumference was measured around the greatest circumfer-ence of the gluteal region,while abdominal circumferencewasmeasured just under the umbilicus (umbilicalwaist circumfer-ence). The following anthropometric indices were calculated:BMI (kg/m2), calculated by dividing body weight by the square
of the height, and the waist-to-hip ratio (WHR), calculatedby dividing WC (cm) by hip circumference (cm). The body fatpercentage (%)was assessed using a QDR Discovery Series dualenergy- X-ray absorptiometry (DXA) device (Hologic, Marl-borough; MA, USA) and the 5 Discovery Wi model software(S/N 84826) version 13.0 provided by the manufacturer(Waltham, MA).
Heart Rate Variability AnalysisSpectral and symbolic analyses of HRV were conducted toevaluate cardiac autonomic modulation, using a custom-made computer software (CardioSeries version 2.4; http://sites.google.com/site/cardioseries). The volunteers were askednot to consume alcohol and caffeine or participate in exerciseand to maintain a regular diet over the 48hours before theexamination. Recordings for the spectral and symbolic analysisof HRV were performed using ECG signals (AD Instruments,Sydney, Australia) between 8:00 and 11:00hours over a60-minute period according to the following protocol:20minutes in the supine position on a special motorized tilttable (orthostatic table), and 10minutes of recording withinitial adaptation of the phase followed by 10minutes ofrecording in the supine position. Subsequently, the table motorwas switchedonand thevolunteersweremovedpassively fromthe supine position to the orthostatic position (90°) for10minutes, returning to the supine position for another10minutes. Finally, the volunteers were moved passivelya second time, from the supine position to the orthostaticposition (90°) for 10minutes, and returning once more to thesupine position, where they remained for another 10minutes.
For the spectral analysis, the R-R interval (RRi) valuesobtained were resampled (3Hz) using cubic spline interpola-tion to adjust the time interval between heartbeats. Thesewere divided into segments of 512 values each with 50%overlap (Welch protocol). Each RRi stationary segment wassubjected to fast Fourier transform, after applying a Hanningwindow function. The oscillatory components were classifiedas either low frequency (LF: 0.04–0.15Hz) or high frequency(HF: 0.15–0.5Hz). The mean values of the power spectraldensities of RRi in both bands (LF and HF) are expressed inabsolute units (ms2). The relative power (%), also known asnormalized units (n.u.) in each frequency band, as well as theLF/HF ratio powers, were calculated by subtracting the verylow frequency (VLF<0.04Hz) values. The normalizationtended to minimize the effect of changes in total poweron the LF and HF component values.12,24 For this reason, inaddition, an individualized analysis of the LF/HFratiowasusedto verify the predominance of sympathetic and parasympa-thetic autonomic modulation in women with metabolicsyndrome of both groups, in all the five moments, in orderto minimize the effects of confouders.
For the symbolic analysis, the methodology used wasdescribed previously,13 where the lowest iRR of the highestRRiwas subtracted and the resulting deltawas divided by six,generating six levels with identical intervals (0 to 5). Subse-quently, the distribution of the iRR series was performedaccording to its duration of time. Each symbolic sequenceconsisted of the sequential values of three iRRs (a symbolic
Rev Bras Ginecol Obstet Vol. 42 No. 2/2020
Increased Sympathetic Cardiac Autonomic Modulation Ribeiro et al. 83

crack) that were transformed into symbols (0, 1, 2, 3, 4, and5), according to the level that fit each value of iRR. For thefinal analysis, the following cracking patterns were used: 1)0V: unchanged patterns, with three equal symbols, forexample (2,2,2) or (5,5,5); 2) 1V: patterns with one variation,that is, patterns with two equal consecutive symbols and theremaining ones were different symbols, for example (3,2,2)and (3,3,2); 3) 2LV: patterns with two variations, with thethree symbols forming an ascending or descending ramp, forexample, (5,4,2) or (1,2,4); and 4) 2ULV: patterns with twovariations in reverse, where the three symbols formed a peakor a trough, such as (3,5,3) or (4,1,2). At the end, the 2LV and2ULV values were summed and presented as 2V. Previousstudies have shown that 0% represents sympathetic cardiacautonomic modulation, 2V% represents parasympatheticmodulation, and 1V represents simultaneity of the twomodulations.13,15
Statistical AnalysisThe Shapiro-Wilk test was used to analyze the distribution ofquantitative data, with 95% significance in each of theanalyzed variables. For comparison of the anthropometric,biochemical, and HRV variables between groups (inter-group), the t-test was used to analyze the parametric data,and the Mann-Whitney U test was used for nonparametricdata. For comparisons between the bench press, tilt 1, benchpress 2, tilt 2, and bench press 3 (intragroup), a one-wayanalysis of variance (ANOVA)was used. Data are presented asmeans� standard errors of the means (SEMs). The differ-ences were considered significant when p<0.05. SigmaStat11.0 software (Systat Software Inc., San Jose, CA, USA) wasused for the statistical analysis.
Results
The comparison between PCOS and CG groups with respectto anthropometric data, body fat percentiles, and biochemi-cal parameters are shown in ►Table 1. The PCOS group hadhigher values of fasting insulin (p¼0.014), testosterone(p¼0.036), and HOMA-IR (p¼0.012) and FAI (p¼0.010)scores comparable to the CG. No differences were observedin the other parameters.
►Table 2 shows the comparison between the PCOS and CGgroupswith respect to the HRV data evaluated at the supine 1,supine 2, and supine 3 moments. No differences were identi-fied at supine moment 1. At supine 2, the PCOS group hadhigher values for LF (n.u.) (p¼0.030) and the LF/HF ratio(p¼0.030), and a lower value for HF (n.u.) (p¼0.30). Thissuperiority in thePCOSgrouppersisted at supine3 for all threevariables: LF (n.u.) (p¼0.020) andLF/HFratio, (p¼0.020) andalower value for HF (n.u.) (p¼0.20). In addition, there wassuperiority of the PCOS group in the LF value (ms) (p¼0.002).
►Table 3 shows the comparisons between thePCOS andCGgroupswith respect to theHRVdataevaluated at tilt 1 and tilt 2moments. At tilt 1, thePCOS grouphadhigher values of LF (ms)(p¼0.025), LF (n.u.) (p¼0.009), and LF/HF ratio (p¼0.009),and variance (ms) (p¼0.026) and lower HF (n.u.) (p¼0.009).No differences were observed between groups at tilt 2.
►Table 4 shows the HRV comparisons (intergroup)between supine 1, tilt 1, supine 2, tilt 2, and supine 3moments in the CG group. The tilt 1 and tilt 2 momentpresented higher values of LF (n.u.), LF/HF, 0V (%), and 0V/2V,and lower values in the square root of the squaremean of thedifferences between adjacent normal RR intervals (RMSSD)and iRR HF (ms), HF (n.u.), variance, 2 LV, 2UV, 2 total Vwhen
Table 1 Comparisonof anthropometry, body fat andbiochemicalparameters among women in the control group (CG) withoutPolycystic Ovary Syndrome and women with Polycystic OvarySyndrome (PCOS)
Comparison CG (n¼32) PCOS (n¼ 32)
Anthropometry parameters
Age, years 29.4 (0.90) 27.0 (0.93)
Weight, Kg 69 (2.57) 75 (3.04)
Height, m 1.61 (0.01) 1.62 (0.01)
BMI 26.8 (1.02) 28.8 (1.15)
WC, cm 78 (2.00) 89 (2.45)
HC, cm 105 (1.91) 108 (1.94)
WHR 0.74 (0.01) 0.76 (0.01)
Body Fat, % 38.8 (1.23) 40.5 (0.92)
Biochemical parameters
Total Cholesterol, mg/dL 195 (8.99) 198 (6.36)
Triglycerides, mg/dL 95 (6.86) 128 (12.87)
LDL, mg/dL 123 (7.36) 119 (5.29)
HDL, mg/dL 52 (2.10) 54 (2.04)
Fasting Insulin, mg/dL 5.88 (0.95) 9.34 (1.16)�
Fasting Glycemia, mg/dL 97 (3.22) 100 (3.45)
Homa-IR 1.42 (0.26) 2.36 (0.33)�
Homocysteine, µmol/L 7.37 (0.25) 7.86 (0.40)
TSH, uIU/mL 2.01 (0.98) 2.48 (1.27)
PRL, ng/ml 13.9 (6.58) 16.1 (16.1)
17-OHP, ng/dL 105 (63) 113 (62)
FSH, uIU/mL 4.26 (0.43) 4.72 (0.50)
LH, uUI/mL 5.58 (1.19) 6.96 (1.21)
Testosterone, ng/dL 66 (4.67) 86 (6.68)�
Androstenedione, ng/dL 102 (5.98) 112 (8.72)
SHBG, nmol/L 65 (6.52) 56 (7.64)
FAI 4.65 (0.54) 7.90 (0.91)�
Abbreviations: %, percentage; µmol/L / L - micromole / liter; 17-OHP - 17-hydroxyprogesterone; BMI, body mass index; CG, control group; cm, centi-meters; FAI, free androgen index; FSH, follicle stimulating hormone; HC, hipcircumference; HDL, High Density Lipoproteins; HOMA-IR, homeostaticmodel assessment; LDL, Low Density Lipoproteins; LH, luteinizing hormone;mg/dL, milligrams / decilitre; ng / dL, nanogram / deciliter; ng / ml, nano-grams per milliliters; nmol / L, nanomol / Liter; PCOS, polycystic ovarysyndrome; PRL, prolactin; SHBG, sex hormone binding globulin; TSH, thyroidstimulating hormone; uIU / mL, international microunits / milliter; WC, waistcircumference; WHR, hip waist ratio.The data are presented in mean and standard deviation.�p< 0.05.
Rev Bras Ginecol Obstet Vol. 42 No. 2/2020
Increased Sympathetic Cardiac Autonomic Modulation Ribeiro et al.84

compared with supine 1, supine 2, and supine 3 moments.When comparing the supine moments 1, 2, and 3 with eachother, bench press 3 presented higher values those of thansupine 1 in RMSSD, iRR, HF (ms) and variance, and lowervalues than those of 1Vand 2 UV, in addition to a lower valuefor 2UV in comparison to supine moment 2. Supine moment2 was superior compared with supine 1 in RMSSD, iRR, HF(ms), variance, and values<1V. Regarding the comparisonbetween tilt 1 and tilt 2, tilt 2 showed higher values for LF (n.u.), the LF/HF ratio, 0V, 2UV, and the 0V/2V ratio, and lowervalues for HF (n.u.).
►Table 5 shows the HRV comparisons between supine 1,tilt 1, supine 2, tilt 2 and supine 3 moments in the PCOSgroup. The tilt 1 and tilt 2 moments presented higher valuesfor LF (n.u.), LF/HF, 0V, and 0V/2V, and lower values forRMSSD, iRR, HF (ms), HF (n.u.), variance, 2 LV, 2UV, 2 total Vwhen compared with the supine 1, supine 2, and supine 3moments. Only LF (ms) and 1V tilt 2 presented inferior andsuperior values, respectively, in relation to supinemoment 2.When comparing supine moments 1, 2, and 3 with eachother, supine 3 values were higher than those of supine 1 forRMSSD, iRR, LF (ms), variance (ms), 0V, 2UV, and 2V total andlower values than 1V, in addition to higher values for LF (ms)and variance (ms) in relation to supine moment 2. Supinemoment 2 presented superiority in relation to supine 1 in theRMSSD, iRR, LF (ms), HF (ms), variance (ms), 2UVand 2V totaland values lower than those of 0V and 1V. Regarding thecomparison between tilt 1 and tilt 2, tilt 2 showed higher
values for variance, 0V, and the 0V/2V ratio, and lower valuesthan those of 2LV, 2UV, and 2UV total.
►Table 6 shows the LF/HF ratio of the spectral analysiscomparisons during supine 1, tilt 1, supine 2, tilt 2 and supine3 moments in the GC and PCOS group in women in bothgroups with and without metabolic syndrome. There was nodifference between the groups.
Discussion
The present study suggests that there is a significant increasein sympathetic autonomic cardiac modulation at differenttimes and in different positions among women with PCOSwho underwent two consecutive tilt tests. Our spectral andsymbolic analyses of HRVwere performed simultaneously inwomenwith PCOS andwere compared with those of womenwith regular menstrual cycles. Similar to other studies, bothgroups showed increases in sympathetic cardiac modulationafter changes from the supine positions.16,17 However, wenoted that the responses to the position changes weredifferent between groups and moments.
At the time of bench press 1, therewas no difference in theHRV indices between the groups; however, in supine 2 andsupine 3, the women with PCOS had greater sympatheticautonomic cardiac modulations compared with those of theCG group.We observed that the PCOS group had higher LF (%)and LF/HF ratio, and lower HF (%). At tilt times, it wasobserved that this difference only occurred in tilt 1, and
Table 2 Comparison of cardiac autonomic modulation through spectral and symbolic analysis in the supine 1, supine 2 and supine3 periods among control women (CG) without Polycystic Ovary Syndrome and women with Polycystic Ovary Syndrome (PCOS)
Supine 1 Supine 2 Supine 3
CG PCOS CG PCOS CG PCOS
Spectral Analysis
RMSSD, ms 55 (6.3) 54 (5.2) 72 (7.1) 69 (6.7) 70 (6.2) 75(7.5)
iRR, ms 896 (20) 901 (15) 967 (21) 972 (16) 978 (23) 978(17)
LF, ms2 728 (145) 883 (113) 910 (152) 1220 (162) 1053 (189) 1582 (193)B
HF, ms2 1520 (433) 1378 (250) 2385 (570) 2073 (404) 2046 (384) 2367 (478)
LF, n.u. 38 (2.5) 44 (2.7) 35 (2.8) 43 (3.0)A 37 (2.4) 47 (3.2)B
HF, n.u. 62 (2,5) 56 (2.7) 65 (2.8) 57 (3.0)A 63 (2.4) 53 (3.2)B
LF/HF ratio 0.70 (0.08) 0.95 (0.12) 0.69 (0.13) 1.02 (0.19)A 0.69 (0.09) 1.34 (0.31)B
Variance, ms2 2942 (633) 3279 (405) 4181 (750) 4428 (626) 4139 (629) 5643 (753)
Symbolic Analysis
0 V, % 9.7 (1.3) 11 (1.39) 7.8 (1.0) 10 (2.41) 8.7 (1.2) 12 (1.69)
1 V, % 40 (1.2) 44 (0.9) 37 (1.1) 39 (1.1) 38 (1.1) 39 (1.0)
2 LV, % 20 (1.1) 17 (1.0) 20 (1.4) 17 (1.1) 18 (1.2) 17 (1.0)
2 UV, % 36 (2.3) 27 (1.6) 36 (2.2) 33 (1.9) 30 (2.3) 32 (2.0)
2 V Total, % 50 (2.2) 45 (2.0) 54 (2.0) 51 (2.2) 54 (2.0) 49 (2.4)
0V/2V ratio 0.26 (0.06) 0.35 (0.08) 0.18 (0.05) 0.28 (0.07) 0.21 (0.05) 0.34 (0.06)
Abbreviations: %, percentage; CG, control group; HF, High Frequency; LF, Low Frequency; ms, milliseconds; n.u., normalized units; PCOS, polycysticovary syndrome.The data are presented in mean and standard error.Supine 2 - CG vs PCOS (A p< 0.05); Supine 3 - CG vs PCOS (B p< 0.05).
Rev Bras Ginecol Obstet Vol. 42 No. 2/2020
Increased Sympathetic Cardiac Autonomic Modulation Ribeiro et al. 85

Table 3 Comparison of cardiac autonomic modulation through spectral and symbolic analysis in the supine 1, supine 2 and supine3 periods among control women (CG) without Polycystic Ovary Syndrome and women with Polycystic Ovary Syndrome (PCOS)
Tilt 1 Tilt 2
CG PCOS CG PCOS
Spectral Analysis
RMSSD, ms 24 (3.0) 21 (1.6) 25 (3.6) 21 (1.7)
iRR, ms 720 (17) 711 (12) 712 (17) 708 (13)
LF, ms2 595 (115) 759 (82)A 860 (130) 863 (140)
HF, ms2 367 (107) 251 (42) 422 (150) 237 (43)
LF, n.u. 66 (2.7) 76 (2.2)A 73 (2.5) 78 (2.3)
HF, n.u. 34 (2.7) 24 (2.2)A 27 (2.5) 22 (2.3)
LF/HF ratio 2.54 (0.30) 4.88 (0.73)A 3.98 (0.49) 5.44 (0.69)
Variance, ms2 1579 (246) 1896 (172)A 2217 (367) 2206 (231)
Symbolic Analysis
0 V, % 29 (2.4) 34 (2.10) 33 (2.3) 38 (2.05)
1 V, % 45 (0.9) 46 (0.8) 45 (0.8) 44 (0.6)
2 LV, % 13 (1.0) 10 (0.9) 11 (0.9) 9.2 (0.9)
2 UV, % 9.9 (1.3) 9.6 (0.9) 12 (1.4) 8.6 (0.9)
2 V Total, % 25 (2.2) 20 (1.6) 21 (2.0) 18 (1.6)
0V/2V ratio 2.39 (0.68) 2.74 (0.52) 2.70 (0.50) 3.13 (0.46)
Abbreviations: %, percentage; CG, control group; HF, High Frequency; LF, Low Frequency; ms, milliseconds; n.u. normalized units; PCOS, polycysticovary syndrome.Tilt 1 - CG vs PCOS (A p< 0.05).The data are presented in mean and standard error.
Table 4 Cardiac autonomic modulation through spectral and symbolic analysis in the supine 1, tilt 1, supine 2, tilt 2 and supine 3periods among control women (CG) without Polycystic Ovary Syndrome
CG (n¼32)
Supine 1 Tilt 1 Supine 2 Tilt 2 Supine 3
Spectral Analysis
RMSSD, ms 55 (6.3) 24 (3.0)J 72 (7.1)HI 25 (3.6)EG 70 (6.2)ACD
iRR, ms 896 (20) 720 (17)J 967 (21)HI 712 (17)EG 978 (23)ACD
LF, ms2 728 (145) 595 (115) 910 (152) 860 (130) 1053 (189)
HF, ms2 1520 (433) 367 (107)J 2385 (570)HI 422 (150)EG 2046 (384)ACD
LF, n.u. 38 (2.5) 66 (2.7)J 35 (2.8)H 73 (2.5)EFG 37 (2.4)AC
HF, n.u. 62 (2.5) 34 (2.7)J 65 (2.8)H 27 (2.5)EFG 63 (2.4)AC
LF/HF ratio 0.70 (0.08) 2.54 (0.30)J 0.69 (0.13)H 3.98 (0.49)EFG 0.69 (0.09)AC
Variance, ms2 2942 (633) 1579 (246)J 4181 (750)HI 2217 (367)EF 4139 (629)ACD
Symbolic Analysis
0 V, % 9.7 (1.3) 29 (2.4)J 7.8 (1.0)H 33 (2.3)EFG 8.7 (1.2)AC
1 V, % 40 (1.2) 45 (0.9)J 37 (1.1)HI 45 (0.8)EG 38 (1.1)ACD
2 LV, % 20 (1.1) 13 (1.0)J 20 (1.4)H 11 (0.9)EG 18 (1.2)AC
2 UV, % 36 (2.3) 9.9 (1.3)J 36 (2.2)H 12 (1.4)EFG 30 (2.3)ABCD
2 V Total, % 50 (2.2) 25 (2.2)J 54 (2.0)H 21 (2.0)EFG 54 (2.0)AC
0V/2V ratio 0.26 (0.06) 2.39 (0.68)J 0.18 (0.05)H 2.70 (0.50)EFG 0.21 (0.05)AC
Abbreviations: %, percentage; CG, control group; HF, High Frequency; LF, Low Frequency; ms, milliseconds; n.u., normalized units.The data are presented in mean and standard error.Supine 3 vs Tilt 2 (A p< 0.05); Supine 3 vs Supine 2 (B p< 0.05); Supine 3 vs Tilt 1 (C p< 0.05); Supine 3 vs Supine 1 (D p< 0.05); Tilt 2 vs Supine 2 (E p< 0.05);Tilt 2 vs Tilt 1 (F p< 0.05); Tilt 2 vs Supine 1 (G p< 0.05); Supine 2 vs Tilt 1 (H p< 0.05); Supine 2 vs Supine 1 (I p< 0.05); Tilt 1 x Supine 1 (J p< 0.05).
Rev Bras Ginecol Obstet Vol. 42 No. 2/2020
Increased Sympathetic Cardiac Autonomic Modulation Ribeiro et al.86

again, the PCOS group demonstrated elevated sympatheticcardiac autonomic modulation comparedwith the CG group,also due to the higher LF (%) and LF/HF ratio and lower HF (%).In fact, this phenomenon is noteworthy, since the PCOSgroup, in addition to maintaining a predominance of sym-pathetic cardiac autonomic modulation in relation to the CGduring tilt 1, maintained this predominance in the tworeturns to the supine position (supine 2 and supine 3).
This alteration of sympathetic autonomic cardiac modula-tion inwomenwithPCOSmaybeassociatedwithhigher serum
concentrations of testosterone and fasting insulin, as well ashigh FAI and HOMA-IR values. Although we did not perform acorrelation analysis, previous studies have reported that theincrease in sympathetic cardiac autonomic modulation inwomen with PCOS occurs due to endocrine-metabolicchanges, especially hyperandrogenism and insulin resistance,whicharebothprevalent inPCOS.3,25Throughdifferent testsofshort-term HRV, the heart rate and standing blood pressureresponse after deep breathing and isometric grip, Kuppusamyet al26 found in women with PCOS an inverse relationship
Table 5 Cardiac autonomicmodulation through the spectral and symbolic analysis in the supine 1, tilt 1, supine 2, tilt 2 and supineperiods among women with Polycystic Ovary Syndrome (PCOS)
PCOS (n¼ 32)
Supine 1 Tilt 1 Supine 2 Tilt 2 Supine 3
Spectral Analysis
RMSSD, ms 54 (5.2) 21 (1.6)J 69 (6.7)HI 21 (1.7)EG 75 (7.5)ACD
iRR, ms 901 (15) 711 (12)J 972 (16)HI 708 (13)EG 978 (17)ACD
LF, ms2 883 (113) 759 (82) 1220 (162)HI 863 (140)E 1582 (193)ABCD
HF, ms2 1378 (250) 251 (42)J 2073 (404)HI 237 (43)EG 2367 (478)ACD
LF, n.u. 44 (2.7) 76 (2.2)J 43 (3.0)H 78 (2.3)EG 47 (3.2)AC
HF, n.u. 56 (2.7) 24 (2.2)J 57 (3.0)H 22 (2.3)EG 53 (3.2)AC
LF/HF ratio 0.95 (0.12) 4.88 (0.73)J 1.02 (0.19)H 5.44 (0.69)EG 1.34 (0.31)AC
Variance, ms2 3279 (405) 1896 (172)J 4428 (626)HI 2206 (231)EFG 5643 (753)ABCD
Symbolic Analysis
0 V, % 11 (1.39) 34 (2.10)J 10 (2.41)HI 38 (2.05)EFG 12 (1.69)ACD
1 V, % 44 (0.9) 46 (0.8) 39 (1.1)HI 44 (0.6)E 39 (1.0)ACD
2 LV, % 17 (1.0) 10 (0.9)J 17 (1.1)H 9.2 (0.9)EFG 17 (1.0)AC
2 UV, % 27 (1.6) 9.6 (0.9)J 33 (1.9)HI 8.6 (0.9)EFG 32 (2.0)ACD
2 V Total, % 45 (2.0) 20 (1.6)J 51 (2.2)HI 18 (1.6)EFG 49 (2.4)ACD
0V/2V ratio 0.35 (0.08) 2.74 (0.52)J 0.28 (0.07)H 3.13 (0.46)EFG 0.34(0.06)AC
Abbreviations: %, percentage; HF, High Frequency; LF, Low Frequency; ms, milliseconds; n.u., normalized units; PCOS, polycystic ovary syndrome.The data are presented in mean and standard error.Supine 3 vs Tilt 2 (A p< 0,05); Supine 3 vs Supine 2 (B p< 0.05); Supine 3 vs Tilt 1 (C p< 0.05); Supine 3 vs Supine 1 (D p< 0.05); Tilt 2 vs Supine 2 (E
p< 0.05); Tilt 2 vs Tilt 1 (F p< 0.05); Tilt 2 vs Supine 1 (G p< 0.05); Supine 2 vs Tilt 1 (H p< 0.05); Supine 2 vs Supine 1 (I p< 0.05); Tilt 1 x Supine 1 (J
p< 0.05).
Tabela 6 Comparison of cardiac autonomic modulation by LF/HF ratio of spectral analysis in the supine 1, tilt 1, supine 2, tilt 2, andsupine 3 periods between control women (CG) without Polycystic Ovary Syndrome (with and without Metabolic Syndrome) andwomen with Polycystic Ovary Syndrome (PCOS) (with and without Metabolic Syndrome)
Position CG PCOS Metabolic Syndrome (MS)
Without MSn¼ (26)n (%)
MSn¼ (6)n (%)
Without MSn¼ (24)n (%)
MSn¼ (8)n (%)
CGn¼ (6)n (%)
PCOSn¼ (8)n (%)
Supine 1 0.64 (0.07) 0.97 (0.33) 0.86 (0.10) 1.25 (0.38) 0.97 (0.33) 1.25 (0.38)
Tilt 1 2.64 (0.32) 2.10 (0.80) 5.51 (1.89) 3.00 (0.94) 2.10 (0.80) 3.00 (0.94)
Supine 2 0.56 (0.07) 1.27 (0.61) 0.75 (0.09) 1.81 (0.68) 1.27 (0.61) 1.81 (0.68)
Tilt 2 3.80 (0.50) 4.74 (1.53) 5.99 (0.81) 3.75 (1.20) 4.74 (1.53) 3.75 (1.20)
Supine 3 0.59 (0.06) 1.12 (0.61) 0.96 (0.13) 2.49 (1.14) 1.12 (0.61) 2.49 (1.14)
Abbreviations: CG, control group; MS, metabolic syndrome; PCOS, polycystic ovary syndrome.The data are presented in mean and standard error.
Rev Bras Ginecol Obstet Vol. 42 No. 2/2020
Increased Sympathetic Cardiac Autonomic Modulation Ribeiro et al. 87

between insulin resistance and the LF/HF ratio, and increasedsympathetic autonomiccardiacmodulation, reducedHRV,andincreased biochemical factors, including insulin and testoster-one. Other researchers have also found, similar to our results,an increase in sympathetic modulation in womenwith PCOS;however, they measured HRV after a different test that wasrelated to mental stress.27 More recently, in animal experi-mentation, the simple neonatal exposure to excess androgenspredisposed the animals studied to autonomic imbalance, dueto an increase in sympathetic tone. Excess androgen was alsoassociated with cardiometabolic disorders.28
It is known that hyperandrogenism and insulin resistanceare associated with increased obesity and metabolic disor-ders,2,6,7,28,29 and these changes, over time, can predisposepatients to the development of cardiovascular diseases.16,26
Therefore, metabolic alterations such as obesity, diabetes, andvisceral fat increase are directly linked to autonomic imbal-ances, especially increases in sympathetic cardiac autonomicmodulation.16,26,30,31 However, in our study, we did notobserve differences in body fat distribution or percentilebetween the PCOS group and the CG. In addition, althoughmetabolic syndrome (MS) is a confounding factor, as it mayreduce HRV,32 in our study we did not observe differenceswhen assessing the LF/HF ratio in women with and withoutMS. However, in the present study, the number of womenanalyzedwithMS is low comparedwith the others. Therefore,we suggest that further studies be conducted to assess HRV inwomen with PCOS and MS.
The increase in cardiac sympathetic autonomicmodulationin women with PCOS was found in several studies,3,16,26,31
which encouragedus to evaluate the response of thesewomentoasecondconsecutive tilt test, and toconduct twomethodsofanalysis, one linear and one nonlinear. After our analysis andcomparison between the groups, only the spectral analysisshoweddifferencesbetween them,with agreater sensitivityofthe spectral analysis compared with the symbolic analysis.However, when the intragroup evaluation was performed atdifferent moments and with changes in posture, it wasobserved that for both the CG and PCOS groups, 0V and the0V/2V ratio increasedwhen the volunteers leaned tomaintainstanding position, similar to LF (n.u.) and the LF/HF ratio,conferring to these variables the postulation of sympatheticcardiac autonomic modulation measurements. On the otherhand, it occurred in an opposite way with the HF (n.u.), 2UV,2LV, and 2V total, that is, they decreased as the volunteerstilted and maintained the standing posture. This finding isconsistent with the literature, since at rest there is a predomi-nance of parasympathetic autonomic cardiac modulation,with a reverse of this predominance with changes to standingpostures.16,17
In the intra-group analyses, we observed that cardiacsympathetic autonomic modulation was higher in tilt 2 com-paredwith tilt 1 in both groups, after detection of LF (%), LF/HFratio andHFreduction (%) in the CG group and0V increase and0V/2V ratio and reduction of 2UVand 2V total in the PCOS andCG groups. However, as reported, on returning to supineposition 3, thePCOS groupmaintained a sympathetic predom-inance compared with the CG. As previously mentioned,
hyperandrogenism and insulin resistancemay have contribut-ed to this response in the PCOS group.16,25,26,31 Dutra et al33
showed that there are important differences between theautonomic cardiac modulation between men and women,with lower sympathetic modulation (lower LF) and higherparasympatheticmodulation (higherHF) inwomen comparedwith men. In view of this, we suggest that women with PCOSexhibit a cardiac autonomic modulation response to the tilttest that is more similar to that of men, with greater sympa-thetic heart modulation and lower parasympathetic modula-tion compared with the CGwomen. This “masculinization” ofthe cardiovascular system in womenwith PCOS has also beensuggested by other authors.33,34
In our study, one of the objectives was to identify whetherthe response to a second consecutive tilt test would promotemodifications or adaptations in the cardiovascular autonomicresponses that might allow the PCOS group to show valuessimilar to those found in the CG. The literature shows thatamong people with autonomic alterations, especially thosewith symptoms of vasovagal syncope, one of the forms oftreatment has been repeated tilt training,which could, in part,facilitate improved control of autonomic cardiac modulation.In our study, despite repeating the test, we observed that theincrease in sympathetic modulation in the PCOS group per-sisted compared with the control group on the bench press 3.Thus, the present study showed that repeating the tilt test isnot sufficient to alter the autonomic control among womenwith PCOS similar to that observed in women without PCOS.
The present study was innovative in evaluating the effectof two tilt tests inwomenwith PCOS. However, it was limitedbecause it was not randomized. Thus, we suggest that futurestudies carry out the randomization process as well asinvestigate and compare the effect of two tilt tests on otherpopulations.
Conclusion
We conclude that women with PCOS had higher autonomicsympathetic cardiac modulation even after a second tilt test,and no adaptation to this provocative test was observed. Inaddition,we observed that the linear spectral analysismethodwas more sensitive for identifying differences between thegroups than the non-linear method of symbolic analysis.
ContributionsAll authors were involved in the design and interpretationof the analyses, contributed to the writing of the manu-script, read and approved the final manuscript.
Conflict of InterestsThe authors have no conflicts of interest to declare.
References1 Ding T, Hardiman PJ, Petersen I, Wang FF, Qu F, Baio G. The
prevalence of polycystic ovary syndrome in reproductive-agedwomen of different ethnicity: a systematic review and meta-analysis. Oncotarget 2017;8(56):96351–96358. Doi: 10.18632/oncotarget.19180
Rev Bras Ginecol Obstet Vol. 42 No. 2/2020
Increased Sympathetic Cardiac Autonomic Modulation Ribeiro et al.88

2 Rotterdam ESHRE/ASRM-Sponsored PCOS Consensus WorkshopGroup. Revised 2003 consensus on diagnostic criteria and long-term health risks related to polycystic ovary syndrome. FertilSteril 2004;81(01):19–25. Doi: 10.1016/j.fertnstert.2003.10.004
3 Ribeiro VB, Kogure GS, Reis RM, Gastaldi AC, De Araújo JE, MazonJH, et al. Polycystic ovary syndrome presents higher sympatheticcardiac autonomic modulation that is not altered by strengthtraining. Int J Exerc Sci 2016;9(05):554–566
4 Chan JL, Kar S, Vanky E, Morin-Papunen L, Piltonen T, Puurunen J,et al. Racial and ethnic differences in the prevalence of metabolicsyndrome and its components of metabolic syndrome in womenwith polycystic ovary syndrome: a regional cross-sectional study.Am J Obstet Gynecol 2017;217(02):189.e1–189.e8
5 Jena D, Choudhury AK, Mangaraj S, Singh M, Mohanty BK,Baliarsinha AK. Study of visceral and subcutaneous abdominalfat thickness and its correlation with cardiometabolic risk factorsand hormonal parameters in polycystic ovary syndrome. Indian JEndocrinol Metab 2018;22(03):321–327. Doi: 10.4103/ijem.IJEM_646_17
6 Pasquali R. Metabolic syndrome in polycystic ovary syndrome.Front Horm Res 2018;49:114–130. Doi: 10.1159/000485995
7 Dargham SR, Shewehy AE, Dakroury Y, Kilpatrick ES, Atkin SL.Prediabetes and diabetes in a cohort of Qatariwomen screened forpolycystic ovary syndrome. Sci Rep 2018;8(01):3619. Doi:10.1038/s41598-018-21987-6
8 Kleiger RE, Miller JP, Bigger JT Jr, Moss AJ. Decreased heart ratevariability and its associationwith increasedmortality after acutemyocardial infarction. Am J Cardiol 1987;59(04):256–262. Doi:10.1016/0002-9149(87)90795-8
9 Glintborg D, Rubin KH, Nybo M, Abrahamsen B, Andersen M.Cardiovascular disease in a nationwide population of Danishwomen with polycystic ovary syndrome. Cardiovasc Diabetol2018;17(01):37. Doi: 10.1186/s12933-018-0680-5
10 Gui J, Wang RH. Cardiovascular autonomic dysfunction in womenwith polycystic ovary syndrome: a systematic review and meta-analysis. Reprod Biomed Online 2017;35(01):113–120. Doi:10.1016/j.rbmo.2017.03.018
11 Saranya K, Pal GK, Habeebullah S, Pal P. Assessment of cardio-vascular autonomic function in patients with polycystic ovary syn-drome. J Obstet Gynaecol Res 2014;40(01):192–199. Doi: 10.1111/jog.12154
12 Task Force of the European Society of Cardiology and the NorthAmerican Society of Pacing and Electrophysiology. Heart ratevariability: standards of measurement, physiological interpreta-tion and clinical use. Circulation 1996;93(05):1043–1065. Doi:10.1161/01.CIR.93.5.1043
13 Porta A, Guzzetti S, Montano N, Furlan R, Pagani M, Malliani A,et al. Entropy, entropy rate, and pattern classification as tools totypify complexity in short heart period variability series. IEEETrans Biomed Eng 2001;48(11):1282–1291
14 Abad CC, Nascimento AM, Gil S, Kobal R, Loturco I, Nakamura FY,et al. Cardiac autonomic control in high level Brazilian power andendurance track-and-field athletes. Int J Sports Med 2014;35(09):772–778. Doi: 10.1055/s-0033-1363268
15 Porta A, Tobaldini E, Guzzetti S, Furlan R, Montano N, Gnecchi-Ruscone T. Assessment of cardiac autonomic modulation duringgraded head-up tilt by symbolic analysis of heart rate variability.Am J Physiol Heart Circ Physiol 2007;293(01):H702–H708. Doi:10.1152/ajpheart.00006.2007
16 Freeman R, Chapleau MW. Testing the autonomic nervous sys-tem. Handb Clin Neurol 2013;115:115–136. Doi: 10.1016/B978-0-444-52902-2.00007-2
17 Laranjo S, Geraldes V, Oliveira M, Rocha I. Insights into thebackground of autonomic medicine. Rev Port Cardiol 2017;36(10):757–771. Doi: 10.1016/j.repc.2017.01.007
18 Fraser IS, Critchley HO, Munro MG, Broder M; Writing Group forthis Menstrual Agreement Process. A process designed to lead tointernational agreement on terminologies and definitions used to
describe abnormalities of menstrual bleeding. Fertil Steril 2007;87(03):466–476. Doi: 10.1016/j.fertnstert.2007.01.023
19 Griffin IJ, Cole TJ, Duncan KA, Hollman AS, Donaldson MD. Pelvicultrasound measurements in normal girls. Acta Paediatr 1995;84(05):536–543. Doi: 10.1111/j.1651-2227.1995.tb13689.x
20 Friedewald WT, Levy RI, Fredrickson DS. Estimation of the con-centration of low-density lipoprotein cholesterol in plasma,without use of the preparative ultracentrifuge. Clin Chem 1972;18(06):499–502
21 Cascella T, PalombaS,TauchmanovàL,MangusoF,DiBiaseS, LabellaD, et al. Serumaldosterone concentration and cardiovascular risk inwomenwith polycystic ovarian syndrome. J Clin Endocrinol Metab2006;91(11):4395–4400. Doi: 10.1210/jc.2006-0399
22 Matthews DR, Hosker JP, Rudenski AS, Naylor BA, Treacher DF,Turner RC. Homeostasis model assessment: insulin resistance andbeta-cell function from fasting plasma glucose and insulin con-centrations in man. Diabetologia 1985;28(07):412–419. Doi:10.1007/bf00280883
23 International Society for the Advancement of Kinanthropometry.International standards for anthropometric assessment. Potch-efstroom: The International Society for Advancement of Kinan-thropometry; 2001
24 Malliani A, Pagani M, Lombardi F, Cerutti S. Cardiovascular neuralregulation explored in the frequency domain. Circulation 1991;84(02):482–492. Doi: 10.1161/01.cir.84.2.482
25 Shorakae S, Ranasinha S, Abell S, Lambert G, Lambert E, deCourten B, et al. Inter-related effects of insulin resistance, hyper-androgenism, sympathetic dysfunction and chronic inflamma-tion in PCOS. Clin Endocrinol (Oxf) 2018;89(05):628–633. Doi:10.1111/cen.13808
26 Kuppusamy S, Pal GK, Habeebullah S, Ananthanarayanan PH, Pal P.Association of sympathovagal imbalance with cardiovascularrisks in patients with polycystic ovary syndrome. Endocr Res2015;40(01):37–43. Doi: 10.3109/07435800.2014.920350
27 Di Domenico K, Wiltgen D, Nickel FJ, Magalhães JA, Moraes RS,Spritzer PM. Cardiac autonomic modulation in polycystic ovarysyndrome: does the phenotype matter? Fertil Steril 2013;99(01):286–292. Doi: 10.1016/j.fertnstert.2012.08.049
28 Nohara K, Waraich RS, Liu S, Ferron M, Waget A, Meyers MS, et al.Developmental androgen excess programs sympathetic tone andadipose tissue dysfunction and predisposes to a cardiometabolicsyndrome in female mice. Am J Physiol Endocrinol Metab 2013;304(12):E1321–E1330. Doi: 10.1152/ajpendo.00620.2012
29 Barber TM, Vojtechova P, Franks S. The impact of hyperandrogen-ism in female obesity and cardiometabolic diseases associatedwith polycystic ovary syndrome. Horm Mol Biol Clin Investig2013;15(03):91–103. Doi: 10.1515/hmbci-2013-0014
30 De Angelis C, Perelli P, Trezza R, CasagrandeM, Biselli R, PannitteriG, et al. Modified autonomic balance in offsprings of diabeticsdetected by spectral analysis of heart rate variability. Metabolism2001;50(11):1270–1274. Doi: 10.1053/meta.2001.27225
31 de Sá JC, Costa EC, da Silva E, Zuttin RS, da Silva EP, Lemos TM, et al.Analysis of heart rate variability in polycystic ovary syndrome.Gynecol Endocrinol 2011;27(06):443–447. Doi: 10.3109/09513590.2010.501881
32 Kangas P, Tikkakoski A, UittoM, Viik J, Bouquin H, Niemelä O, et al.Metabolic syndrome is associated with decreased heart ratevariability in a sex-dependent manner: a comparison between252 men and 249 women. Clin Physiol Funct Imaging 2019;39(02):160–167. Doi: 10.1111/cpf.12551
33 Dutra SGV, Pereira APM, Tezini GCSV, Mazon JH, Martins-PingeMC, Souza HC. Cardiac autonomic modulation is determined bygender and is independent of aerobic physical capacity in healthysubjects. PLoS One 2013;8(10):e77092. Doi: 10.1371/journal.pone.0077092
34 Sandhu KS, Khan P, Panting J, Nadar S. Tilt-table test: its role inmodern practice. Clin Med (Lond) 2013;13(03):227–232. Doi:10.7861/clinmedicine.13-3-227
Rev Bras Ginecol Obstet Vol. 42 No. 2/2020
Increased Sympathetic Cardiac Autonomic Modulation Ribeiro et al. 89

Quality of Life in Women with DeepEndometriosis: A Cross-Sectional Study
Qualidade de vida de mulheres com endometrioseprofunda: Estudo de corte transversalDaniela Angerame Yela1 Iuri de Paula Quagliato1 Cristina Laguna Benetti-Pinto1
1Department of Gynecology and Obstetrics, School of MedicalSciences, Universidade de Campinas, Campinas, SP, Brazil
Rev Bras Ginecol Obstet 2020;42(2):90–95.
Address for correspondence Daniela Angerame Yela, MD, PhD,Universidade de Campinas, Campinas, SP, 04111-070, Brazil(e-mail: [email protected]).
Keywords
► endometriosis► quality of life► pelvic pain► dysmenorrhea
Abstract Objective To describe clinical and sociodemographic characteristics of women withdeep infiltrating endometriosis (DIE) and assess their quality of life (QOL) during6 months of medical treatment.Methods A descriptive cross-sectional study of 60 women diagnosed with DIE eitherby surgery or image methods (ultrasound or magnetic resonance), who receivedclinical treatment for at least 6 months in the Universidade de Campinas, Campinas,state of São Paulo, Brazil. Both the SF-36 and the EHP-30 questionnaires were used toassess the quality of life.Results The mean age of the patients was 37.7�6.0 years old, with 50% presentingdysmenorrhea; 57% dyspareunia; and 50% chronic pelvic pain. The SF-36 and the EHP-30 revealed impaired quality of life. In the SF-36, the worst domains were limitation dueto emotional aspects (40.2� 43.1) and self-esteem and disposition (46.1�24.8),whereas in the EHP-30 they were social well-being (50.3�30.6); infertility(48.0�36.3); and sexual intercourse (54.0� 32.1).Conclusion Although clinically treated, women with deep endometriosis presentimpairment in different domains of quality of life regardless of the questionnaire usedfor evaluation.
Resumo Objetivo Descrever características clínicas e sociodemográficas de mulheres comendometriose profunda infiltrativa e avaliar sua qualidade de vida dentro de 6meses detratamento clínico.Métodos Estudo de corte transversal descritivo com 60 mulheres em seguimentoambulatorial na Universidade de Campinas, Campinas, SP, Brasil, com endometrioseprofunda infiltrativa diagnosticada por cirurgia ou métodos de imagem (ultrassono-grafia ou ressonância magnética), em tratamento clínico há pelo menos 6 meses. Paraavaliar a qualidade de vida, foram utilizados os questionários SF-36 e EHP-30.Resultados A média etária das mulheres foi de 37,7�6,0 anos; 50% delas apresen-taram dismenorreia, 57% dispareunia e 50% dor pélvica crônica. O SF-36 e o EHP-30mostraram comprometimento da qualidade de vida destas mulheres. No SF-36, os
receivedAugust 21, 2019acceptedJanuary 13, 2020
DOI https://doi.org/10.1055/s-0040-1708091.ISSN 0100-7203.
Copyright © 2020 by Thieme RevinterPublicações Ltda, Rio de Janeiro, Brazil
Original ArticleTHIEME
90

Introduction
Endometriosis is characterized by the presence of endo-metriotic tissue beyond the uterine cavity, mainly in theovaries and other pelvic organs.1Womenwith endometriosismay be asymptomatic or may report symptoms of dysme-norrhea; deep dyspareunia; chronic pelvic pain; urinary painor intestinal pain; and infertility.2
Although all types may cause pain, deep lesions are usuallyrelated to amore severe clinical status, impairing quality of life(QOL);dailyworkactivities;social relationships;and frequentlythe fertility of thesewomen.3–5 Studies report a reduction in�38%of theworkproductivityof thesewomen,mainlyattributedto pelvic pain.4 Furthermore, � 88% of these women hadanxiety disorders or depression.6 The disease was also highlyrelevant in the area of human reproduction, since 50% ofpatients diagnosed with endometriosis had some fertilitydisorder, due to chronic inflammation and the formation ofpelvic adhesions.7
Studies have shown that endometriosis has a negativeimpact on QOL.4,8,9 However, with surgical and/or medicaltreatment, QOL is improved.10–14 The majority of studies inthe literature did not evaluate women according to thedisease stage, although few studies show a poorer QOL inlater stages.15 In addition, women with chronic pain have alower QOL due to both physical and psychological fac-tors.16,17 The literature also shows that pain reduction isgenerally not related to the improvement of psychologicaldisturbances.18 A recent study with women with deependometriosis has shown that it affects these women glob-ally and that more studies are needed to better understandthe whole context.19 Therefore, because endometriosis cannegatively affect QOL, particularly in more advanced stages,the main goal of the present study is to assess QOL inwomenwith deep infiltrating endometriosis (DIE).
Methods
A descriptive cross-sectional study was performed with 60women undergoingmedical treatment for at least 6months atthe Universidade de Campinas (UNICAMP, in the Portugueseacronym), Campinas, State of São Paulo, Brazil, for DIE, diag-nosed surgically or by imaging (nuclear magnetic resonanceimaging [NMRI] or transvaginal ultrasoundwith bowel prepa-ration). Deep infiltrating endometriosis was characterizedwhen imaging exams showed lesions in the retrocervicalregion (uterosacral ligaments and uterine torus), the vagina,
the intestine (rectum, sigmoid, ileum and appendix), thebladder and theureter.Womenwhowere surgically diagnosedhad performed the procedure for>2 years and had recurredfrom the injuries after surgery. Those included in the studywere exclusively on drug treatment. Women with cognitiveimpairment, incapable of understanding the instruments, andwomenwith other chronic diseases such as neoplasias; lowerback pain; psychiatric disorders; rheumatologic diseases;among others that could impact the QOL, were excluded.
ThediagnosisofDIEwasconsideredsurgicalwhenasurgicaldescription of deep endometriosis was presented along with aconfirmatory anatomopathological report (20 women hadsurgical diagnosis). All of the women with surgical diagnosiswere on hormonal treatment to prevent recurrence and tocontrol pain. Clinical diagnosis was performed by transvaginalultrasound with bowel preparation or NMRI (40 women hadimagingdiagnosis). Thediagnosis ofdeependometriosis estab-lished by imaging was performed through transvaginal sonog-raphy with bowel preparation or NMRI, always performed bythe same expert during the diagnosis. All of the women hadpainsymptomsand20womenhad infertility, andat the timeofthe interview 9 were asymptomatic.
The variables analyzed were: QOL; age; color (white, non-white); school education (illiterate, elementary school level,high school level, university level); family income;professionalactivity (unemployed, employed); marital status (with a part-ner, without a partner); religion (atheist, catholic, protestantand other); number of pregnancies; parity; body mass index(BMI) (calculated by weight in kilograms divided by height insquare meters, classified as underweight<20kg/m2, normal20 to 25kg/m2, overweight 25 to 30kg/m2, and obese� 30kg/m2); treatment used, symptoms of endometriosis(dysmenorrhea, dyspareunia, chronic pelvic pain, pain tourinate and pain to defecate), smoker (yes or no), surgicalhistory (any previous surgeries such as abdominal surgeriesor cesareans). Treatments used for pain control werehormonal (progestin alone – 53 women, or combined oralcontraceptives – 5 women) or non-hormonal (nonsteroidalanti-inflammatory agents – 2 women).
Pain symptomswere evaluated according to the pain visualanalog scale (VAS) on a scale of 0 to 10, where 0 representedabsence of pain and 10 indicated maximum pain. Pain wasclassified as mild when the score was 1 to 3, moderate whenthe score was 4 to 6 and severe when it was>7.20
To assess QOL, two questionnaires were used: the Endome-triosis Health Profile Questionnaire (EHP-30) and the ShortForm – 36 (SF-36). The EHP-30 questionnaire was developed
piores domínios foram os aspectos emocionais (40,2�43,1) e a autoestima edisposição (46,1� 24,8), enquanto que no EHP-30 foram o bem-estar social(50,3�30,6), a infertilidade (48,0�36,3) e as relações sexuais (54,0�32,1).Conclusão Embora tratadas clinicamente, as mulheres com endometriose profundaapresentaram comprometimento em diferentes domínios da qualidade de vidaindependente do questionário utilizado para avaliação.
Palavras-chave
► endometriose► qualidade de vida► dor pélvica► dismenorreia
Rev Bras Ginecol Obstet Vol. 42 No. 2/2020
Quality of Life in Women with Deep Endometriosis Yela et al. 91

by Jones et al, in 200121 and was validated to BrazilianPortuguese in 2008 byMengarda et al.22 It consists of 30 itemscovering five dimensions: pain; control and capacity to copewith the disease (hopelessness); emotional well-being; socialsupport and self-image; and a modular questionnaire with 23items distributed in six scales: sexual intercourse; work;doctor x patient relationship (medical profession); infertility;relationship with children and treatment. Each item isassessed on a 4-point scale (never¼0, rarely¼1, sometimes¼2,many times¼3, always¼4). Scoring is transformed into a0 to 100 scale, where the lowest score means a better QOL.
The SF-36 questionnaire was developed by Ware et al in199223 and was validated to Brazilian Portuguese in 1999 byCiconelli et al.24 It assesses 8 dimensions: functional aspects;physical aspects; pain; general health status; vitality; socialaspects; emotional aspects; and mental health. It presents afinal score of 0 to 100, in which zero corresponds to a worsegeneral health status and 100 to a better general healthstatus. Among the eight scales, three (functional capacity,physical aspects and pain) correspond to the Physical Com-ponent Summary (PCS), and the Mental Component Sum-mary (MCS )includes mental health scales, emotional andsocial aspects. Two of the scales (vitality and general health)do not correlate with either component.23
All of the participants in the study signed an informedconsent agreement. The present study was approved by theResearch Ethics Committee of the Institution (number:43715915.4.0000.5404).
Statistical AnalysisTo calculate the sample size, the method used to compare theaverage QOL score between 2 evaluations in a longitudinalstudy (before and after intervention) with a quantitativevariable, was according to Browner et al,25 setting the signifi-cance level of α or type I error at 5% (α¼0.05) (or 95%confidence interval [CI]), and sample power at 80% (or 20%type II error [β¼0.20]), and obtaining themean and standarddeviation (SD) values of delta (difference of scores betweenbefore and after intervention) from a literature study.26 It wasestimated that a sample of 63womenwould be representativeto comparethephysicalQOLscoreafter6monthsof treatment,with a 5% significance level and 80% sample power.
Descriptive analysis expressed in relative frequencies wasused for statistical analysis, for the categorical variables andfor the continuous variables the analysis was expressed inmean and SD.
Results
We evaluated 60women treated clinically, out of which 2wereexcluded due to the use of anti-inflammatory treatment, leav-ing 58 women who underwent hormonal clinical treatment.
The mean age of the patients was 37.2�6.0 years old(minimum: 26years old and maximum: 49years old); 55%were nulliparous and 75% of the cases had already undergoneprevious surgery. Regarding clinical factors, 91% were under-going progestin treatment; 51% had chronic pelvic pain; 58%had dyspareunia; 53% had dysmenorrhea, 13% had pain on
urination and 43% had pain when defecating (►Table 1).Regarding pain intensity, we observed that women reportedscores of 7.5�4.9 for dysmenorrhea, 7.4�4.9 for dyspareunia,7.2�4.4 for chronic pelvic pain, 6.6�4.9 for pain whendefecating and 5.7�0.7 for pain when urinating.
Table 1 Percentage distribution of women with deepinfiltrating endometriosis according to sociodemographic andclinical characteristics (n¼ 58)
Characteristic n (%)
Color
White 44 (75.86)
Non-white 14 (24.14)
Marital status
With a partner 37 (63.79)
Without a partner 21 (34.21)
Profession
Employed 15 (25.86)
Unemployed 43 (74.14)
Education
Illiterate 1 (1.73)
Elementary school level 14 (24.14)
High school level 28 (48.27)
University level 15 (25.86)
Gestation
Nulliparous 32 (55.17)
Multiparous 26 (44.83)
BMI (kg/m2)
� 20 4 (6.89)
20 -25 24 (41.39)
25–30 16 (27.58)
� 30 14 (24.14)
Smoking
Yes 5 (8.63)
No 53 (91.37)
Previous surgery
Yes 44 (75.86)
No 14 (24.14)
Treatment
Progestin 53 (91.37)
Estrogen with progestin 5 (8.63)
Pain symptoms
Dysmenorrhea 31 (53.44)
Chronic pelvic pain 30 (51.72)
Dyspareunia 34 (58.62)
Intestinal pain 25 (43.10)
Urinary pain 8 (13.79)
Abbreviation: BMI, body mass index.
Rev Bras Ginecol Obstet Vol. 42 No. 2/2020
Quality of Life in Women with Deep Endometriosis Yela et al.92

The SF-36 exhibited median scores for all domains. Thewomen had scores � 50 on average in the physical domainsof the SF-36, such as functional capacity; limitation due tophysical aspects; pain; and general health status. Psycholog-ical domains (self-esteem 46.1�24.8; disposition and emo-tional aspects 40.2�43.1) affected the QOL in these womenmore intensely; although other psychological domains, suchas social aspects and mental health, scored>50 (►Table 2).
In the EHP-30, some questions from the domains work;children; sexual intercourse; doctor patient relationship;treatment and infertility were not answered by all of thewomen, because they did not feel empowered to respond(they had not experienced the questions asked or felt con-strained in responding).
The EHP-30 showed a greater impairment in QOL in socialdomains (social well-being 50.3�30.6; social support48.0�36.2), capacity to cope with the disease (44.7�33.7)and fertility (48.0�36.3). These women had a good doctor-patient relationship (18.1�23.8). Only 21 out of 58 womenresponded to the children domain, since these patients wereeither nulliparous or felt uncomfortable talking about thesubject (►Table 3).
Discussion
Assessment of QOL, by applying questionnaires, allows themeasuring of the general impact of chronic diseases, such asendometriosis, on the lives of women. Two questionnaireswere used in the current study, generic and specific, the SF-36and the EHP-30, respectively, to observe whether the resultswere similar. The decision to apply both questionnaires isbased on the fact that both address physical (pain) andpsychological aspects that can influence the QOL in womenwith a chronic disease. However, the EHP-30 addresses somespecific aspects of endometriosis that affect the QOL of thesewomen, such as their sexual function; the question of moth-erhood; the relationship between doctor and patient; and thetreatment of the disease. A recent review shows that endome-triosis affects negatively the QOL of women with endometri-osis but there is still no consensus on what would be the bestinstrument to evaluate it.27
In a review published in 2017 that evaluated 26 studies onendometriosis and QOL, only one used the EHP-30 and SF-36questionnaires.28 And recently, a Brazilian study addressedQOL in women with deep endometriosis using the twoquestionnaires.18
Approximately half of the women in the study had goodpain control, but those with this symptom had moderate tosevere pain. Furthermore, on evaluation of their QOL, thesewomen had better results in the physical domains than in thepsychological domain. It is also important to highlight thatthese women had deep endometriosis. In the literature,studies usually do not assess QOL according to disease stage.
Studies in the literature have shown that women with amore severe pain level have a worse QOL, although physicalQOL is only related to physical pain. According to models ofmediation, increasing physical pain and difficulties in emo-tion regulation result in increased psychological stress,which is associated with deterioration in QOL. The maingoal of the treatment is to reduce pain symptoms andimprove QOL, decreasing the societal burden and healthcare costs related to endometriosis.27,29
A review of 18 articles published in the past 5 yearsshowed that understanding by the part of family membersand partners may help women cope with this disease. Inaddition, pharmacological and surgical treatment may con-tribute toward pain control. However, other alternativeshave been associated with the therapeutic management ofendometriosis, such as lifestyle changes; physical exercise;diet; and sleep.30
A Brazilian study was performed in 2008 to investigate therelationshipbetweenclinical aspectsandQOL inagroupof130women with endometriosis. Data was collected using the SF-36 questionnaire, showing that patients with endometriosishad lower QOL scores than the general population.27
The term QOL should encompass three main dimensions:mental health; physical; and social functioning. Both ques-tionnaires addressed these issues and apparently presentedsimilar results. It has been observed that medical treatmenthelps a woman to improve in some items, since it waseffective in pain control. Although management is not
Table 2 Descriptive analysis of questionnaire domains SF-36
Domains n mean SD
Functional capacity 58 56.2 23.7
Limitation due tophysical aspects
58 50.0 42.9
Pain 58 55.1 59.4
General health status 58 60.8 22.4
Self-esteem and disposition 58 46.1 24.8
Social aspects 58 57.8 29.5
Limitation due toemotional aspects
58 40.2 43.1
Mental health 58 51.1 24.0
Abbreviation: SD, standard deviation.
Table 3 Descriptive analysis of questionnaire domains EHP-30
Domains n Mean SD
Pain 58 40.4 31.1
Control and capacity to copewith the disease
58 44.7 33.7
Social well-being 58 50.3 30.6
Social support 58 48.0 36.2
Self-image 58 41.2 34.2
Work 47 27.5 31.4
Children 21 33.9 37.3
Sexual intercourse 52 54.0 32.1
Doctor x patient relationship 56 18.1 23.8
Treatment 51 35.3 31.1
Infertility 39 48.0 36.3
Abbreviation: SD, standard deviation.
Rev Bras Ginecol Obstet Vol. 42 No. 2/2020
Quality of Life in Women with Deep Endometriosis Yela et al. 93

effective at obtaining an excellent QOL, it still exerts asignificantly negative impact on QOL.
Studies have emphasized the central role of pain associatedwith endometriosis, which is negatively correlated with QOL;sexual functioning; quality of relationship with partner;mood; work; and social role functioning. Chronic pain mayresult in social isolation and can also negatively affect emo-tionalwell-being. Endometriosis is associatedwith psycholog-ical problems; anxiety; depression, and a weak capacity tocope with difficulty. It is noteworthy that there is a positiverelationship between the level of anxiety symptoms and painintensity. A decrease in the level of depressive symptoms isobserved after pain treatment.28 Furthermore; it is worthmentioning that women with asymptomatic endometriosismay not report impairment of QOL and mental health.31
Another study showed greater improvement in physical do-main scores than in those ofmental domains for patientswithdeep endometriosis.11
In the SF-36 questionnaire, the domain due to emotionalaspects and self-esteem/disposition had amean score of 40.2and 46.1, respectively, once again pointing to the mentalhealth issue, which is not frequently addressed duringmedical consultations. Another Brazilian study of 128 wom-en performed in 2007 suggested that psychological supportwith group intervention was a good adjunct to conventionaltreatment, since scores of pain and emotional aspects de-creased.32 A recent study shows that women with deependometriosis have worse physical and mental QOL thanwomen with rheumatoid arthritis.33
The limitation of the present study is not having includeda control group in the analysis. The literature shows thatmedical or surgical treatment may improve pain over time.The QOL in a woman with deep endometriosis is stillunsatisfactory and inferior in comparison to the QOL of thegeneral population, since other aspects (psychological, socialand sexual) are not addressed.
Somestudies in the literatureshowanoverall improvementin the QOL of clinically treated women with endometri-osis.26,34 All of these studies were prospective and womenwere followed for at least 1year. This makes us infer whethermedical care could help improve the psychological aspects ofQOL. The fact that our study evaluates women at just onemoment of their lives may not reflect all aspects of QOL and,therefore, these women present a deterioration of their QOLmainly in relation to psychological aspects.
Conclusion
Both questionnaires used in the current study addressedthese issues and apparently produced similar results. It hasbeen observed that medical treatment can help womenimprove in some aspects. Management is not effective atobtaining an excellent QOL, as endometriosis still exerts asignificantly negative impact on a patient’s QOL.
ContributorsAll of the authors contributed with the project and datainterpretation, the writing of the article, the critical
review of the intellectual content, and with the finalapproval of the version to be published.
Conflict of InterestsThe authors have no conflict of interests to declare.
AcknowledgmentsThe present study was financed in part by the São PauloResearch Foundation (FAPESP, in the Portuguese acronym).
References1 Bulun SE. Endometriosis. N Engl J Med. 2009;360(03):268–279.
Doi: 10.1056/NEJMra08046902 Crispi CP, Oliveira FMM, Damian JC Junior, Oliveira MAP. Endome-
triose. In: Crispi CP, Oliveira FMM, Damian JC Junior, Oliveira MAP.Tratado de videoendoscopia e cirurgia minimamente invasiva emginecologia. 2a ed. Rio de Janeiro: Revinter; 2007:295–327
3 Fourquet J, Gao X, Zavala D, Orengo JC, Abac S, Ruiz A, et al. Patients’report on how endometriosis affects health, work, and daily life.Fertil Steril. 2010;93(07):2424–2428. Doi: 10.1016/j.fertnstert.2009.09.017
4 NnoahamKE,Hummelshoj L,WebsterP, d’HoogeT, deCiccoNardoneF, de Cicco Nardone C, et al; World Endometriosis Research Founda-tionGlobal StudyofWomen’sHealth consortium. Reprint of: Impactof endometriosis on quality of life and work productivity: a multi-center study across ten countries. Fertil Steril. 2019;112(4S1, Suppl1)e137–e152. Doi: 10.1016/j.fertnstert.2019.08.082
5 The Whoqol Group. The development of the World Health Orga-nization quality of life assessment instrument (theWHOQOL). In:Orley J, Kuyken W, editors. Quality of life assessment: interna-tional perspectives: proceedings of the joint-meeting organizedby the World Health Organization and the Fondation IPSEN inParis, July 2–3, 1993. BerlinSpringer1994:41–57
6 Sepulcri RdeP, do Amaral VF. Depressive symptoms, anxiety, andquality of life in women with pelvic endometriosis. Eur J ObstetGynecol Reprod Biol. 2009;142(01):53–56. Doi: 10.1016/j.ejogrb.2008.09.003
7 Holoch KJ, Lessey BA. Endometriosis and infertility. Clin ObstetGynecol. 2010;53(02):429–438. Doi: 10.1097/GRF.0b013e3181db7d71
8 SouzaCA,OliveiraLM,ScheffelC,GenroVK,RosaV,ChavesMF,CunhaFilho JS. Quality of life associated to chronic pelvic pain is indepen-dent of endometriosis diagnosis–a cross-sectional survey. HealthQual Life Outcomes. 2011;9:41. Doi: 10.1186/1477-7525-9-41
9 DunselmanGAJ,VermeulenN,BeckerC,Calhaz-JorgeC,D’HoogeT,DeBie B, et al; European Society of Human Reproduction and Embryol-ogy. ESHRE guideline: management of women with endometriosis.Hum Reprod. 2014;29(03):400–412. Doi: 10.1093/humrep/det457
10 Ferrero S, Abbamonte LH, Giordano M, Ragni N, Remorgida V.Deep dyspareunia and sex life after laparoscopic excision ofendometriosis. Hum Reprod. 2007;22(04):1142–1148. Doi:10.1093/humrep/del465
11 Ribeiro PAAG, Sekula VG, Abdalla-Ribeiro HSA, Rodrigues FC, AokiT, Aldrighi JM. Impact of laparoscopic colorectal segment resec-tion on quality of life in women with deep endometriosis: oneyear follow-up. Qual Life Res. 2014;23(02):639–643. Doi:10.1007/s11136-013-0481-y
12 Silveira da Cunha Araújo R, Abdalla Ayroza Ribeiro HS, Sekula VG,da Costa Porto BT, Ayroza Galvão Ribeiro PA. Long-term outcomeson quality of life in women submitted to laparoscopic treatmentfor bowel endometriosis. J Minim Invasive Gynecol. 2014;21(04):682–688. Doi: 10.1016/j.jmig.2014.02.005
13 Florentino AVA, Pereira AMG, Martins JA, Lopes RGC, Arruda RM.Qualityof life assessment by the endometriosishealthprofile (EHP-30) questionnaire prior to treatment for ovarian endometriosis in
Rev Bras Ginecol Obstet Vol. 42 No. 2/2020
Quality of Life in Women with Deep Endometriosis Yela et al.94

Brazilian women. Rev Bras Ginecol Obstet. 2019;41(09):548–554.Doi: 10.1055/s-0039-1693057
14 Vannuccini S, Reis FM, Coutinho LM, Lazzeri L, Centini G, Petraglia F.Surgical treatment of endometriosis: prognostic factors for betterquality of life. Gynecol Endocrinol. 2019;35(11):1010–1014. Doi:10.1080/09513590.2019.1616688
15 Comptour A, Pereira B, Lambert C, Chauvet P, Grémeau AS, PoulyJL, et al. Identification of predictive factors in endometriosis forimprovement in patient quality of life. J Minim Invasive Gynecol.2019:S1553-4650(19)30227-4
16 Rush G, Misajon R, Hunter JA, Gardner J, O’Brien KS. The relation-ship between endometriosis-related pelvic pain and symptomfrequency, and subjective wellbeing. Health Qual Life Outcomes.2019;17(01):123. Doi: 10.1186/s12955-019-1185-y
17 Marqui ABT. [Use of questionnaires for evaluation of the quality oflife in endometriosis]. Rev Bras Qual Vida.. 2014;6(02):104–114.Doi: 10.3895/S2175-08582014000200005
18 Cagnacci A, Della Vecchia E, Xholli A. Chronic pelvic pain improve-ment: impact on quality of life and mood. Gynecol Endocrinol.2019;35(06):502–505. Doi: 10.1080/09513590.2018.1540571
19 de Freitas Fonseca M, Aragao LC, Sessa FV, Dutra de Resende JA Jr,Crispi CP. Interrelationships among endometriosis-related painsymptoms and their effects on health-related quality of life: asectional observational study. Obstet Gynecol Sci. 2018;61(05):605–614. Doi: 10.5468/ogs.2018.61.5.605
20 Martinez JE,GrassiDC,Marques LG. Análisedaaplicabilidadede trêsinstrumentos de avaliação de dor em distintas unidades de atendi-mento: ambulatório, enfermaria e urgência. Rev Bras Reumatol.2011;51(04):304–308. Doi: 10.1590/S0482-50042011000400002
21 Jones G, Kennedy S, Barnard A, Wong J, Jenkinson C. Developmentof an endometriosis quality-of-life instrument: The Endometri-osis Health Profile-30. Obstet Gynecol. 2001;98(02):258–264.Doi: 10.1016/s0029-7844(01)01433-8
22 Mengarda CV, Passos EP, Picon P, Costa AF, Picon PD. [Validation ofBrazilian Portuguese version of quality of life questionnaire forwomen with endometriosis (Endometriosis Health Profile Ques-tionnaire–EHP-30)]. Rev Bras Ginecol Obstet. 2008;30(08):384–392. Doi: 10.1590/S0100-72032008000800003
23 Ware JE Jr, SherbourneCD.TheMOS36-itemshort-formhealthsurvey(SF-36). I. Conceptual framework and item selection.Med Care. 1992;30(06):473–483. Doi: 10.1097/00005650-199206000-00002
24 Ciconelli RM, Ferraz MB, Santos W, Meinão I, Quaresma MR.Tradução para a língua portuguesa e validação do questionário
genérico de avaliação de qualidade de vida SF-36 (Brasil SF-36).Rev Bras Reumatol. 1999;39(03):143–150
25 Browner WS, Newman TB, Hulley SB. Estimating sample size andpower: applications and examples. In: Hulley SB, Cummings SR,Browner WS, Grady DG, Newman TB. Designing clinical research.3rd ed. Philadelphia: Lippincott, Williams &Wilkins; 2007:65–96
26 Leonardo-Pinto JP, Benetti-Pinto CL, Cursino K, Yela DA. Dienogestand deep infiltrating endometriosis: The remission of symptoms isnot related to endometriosis nodule remission. Eur JObstetGynecolReprodBiol. 2017;211:108–111.Doi: 10.1016/j.ejogrb.2017.02.015
27 MarinhoMCP,Magalhaes TF, Fernandes LFC, Augusto KL, BrilhanteAVM, Bezerra LRPS. Quality of life in women with endometriosis:an integrative review. J Womens Health (Larchmt). 2018;27(03):399–408. Doi: 10.1089/jwh.2017.6397
28 Márki G, Bokor A, Rigó J, Rigó A. Physical pain and emotionregulation as themain predictive factors of health-related qualityof life inwomen living with endometriosis. HumReprod. 2017;32(07):1432–1438. Doi: 10.1093/humrep/dex091
29 Vercellini P, Barbara G, Abbiati A, Somigliana E, Viganò P, Fedele L.Repetitive surgery for recurrent symptomatic endometriosis:what to do? Eur J Obstet Gynecol Reprod Biol. 2009;146(01):15–21. Doi: 10.1016/j.ejogrb.2009.05.007
30 Moradi M, Parker M, Sneddon A, Lopez V, Ellwood D. Impact ofendometriosis on women’s lives: a qualitative study. BMC Wom-ens Health. 2014;14:123. Doi: 10.1186/1472-6874-14-123
31 Facchin F, Barbara G, Saita E, et al. Impact of endometriosis onquality of life andmental health: pelvic painmakes the difference.J Psychosom Obstet Gynaecol. 2015;36(04):135–141. Doi:10.3109/0167482X.2015.1074173
32 Lorençatto C, Vieira MJN, Marques A, Benetti-Pinto CL, Petta CA.[Evaluation of pain and depression inwomenwith endometriosisafter a multi- professional group intervention]. Rev Assoc MedBras (1992). 2007;53(05):433–438. Doi: 10.1590/S0104-42302007000500020
33 Verket NJ, Uhlig T, Sandvik L, Andersen MH, Tanbo TG, Qvigstad E.Health-related quality of life in women with endometriosis, com-pared with the general population and women with rheumatoidarthritis. Acta Obstet Gynecol Scand. 2018;97(11):1339–1348. Doi:10.1111/aogs.13427
34 Caruso S, IraciM, Cianci S, Vitale SG, Fava V, Cianci A. Effects of long-term treatment with Dienogest on the quality of life and sexualfunction of women affected by endometriosis-associated pelvicpain. J Pain Res. 2019;12:2371–2378. Doi: 10.2147/JPR.S207599
Rev Bras Ginecol Obstet Vol. 42 No. 2/2020
Quality of Life in Women with Deep Endometriosis Yela et al. 95

Influence of Gender and Undergraduate Course on theKnowledge about HPV and HPV Vaccine, and VaccinationRate among Students of a Public University
A influência do gênero e do curso de graduação noconhecimento sobre o HPV e sua vacina, e taxa devacinação em estudantes de uma universidade públicaMarília Biselli-Monteiro1 Amanda Canato Ferracini1 Luis Otávio Sarian1
Sophie Françoise Mauricette Derchain1
1Department of Obstetrics and Gynecology, Medical School,Universidade Estadual de Campinas, Campinas, SP, Brazil
Rev Bras Ginecol Obstet 2020;42(2):96–105.
Address for correspondence Marília Biselli-Monteiro, MD,Universidade Estadual de Campinas, Cidade Universitária ZeferinoVaz - Barão Geraldo, Campinas, SP, 13083-970, Brazil(e-mail: [email protected]).
Keywords
► humanpapillomavirus
► vaccine► students► knowledge► vaccination rate
Abstract Objective To evaluate the knowledge related to human papillomavirus (HPV) infec-tion and the rate of HPV vaccination among undergraduate freshmen and seniorstudents of medicine, pharmacy, speech therapy, nursing and physical education in aBrazilian university.Methods A questionnaire concerning sociodemographic aspects, sexual background,and knowledge about HPV and its vaccine was filled out by 492 students. Threemonthslater, a second questionnaire, concerning the new rate of vaccination, was applied to233 students.Results Among the 290 women who answered the first questionnaire, 47% of thefreshmen and 13% of the seniors stated they were not sexually active, as well as 11% ofthe 202 freshman and senior male students. Although the knowledge about HPV washigher among women, they reported a lower use of condoms. More than 83% of thewomen and 66% of themen knew that HPV can cause cervical cancer, but less than 30%of the students knew that HPV can cause vulvar, anal, penile and oropharyngeal cancer.Less than half of the students knew that HPV causes genital, anal and oropharyngealwarts. Comparing the students, the seniors hadmore knowledge of the fact that HPV issexually transmitted, and that HPV infection can be asymptomatic. The rate ofvaccination was of 26% for women, and of 8% for men, and it increased to 52% and27% respectively among the 233 students evaluated in the second questionnaire.Conclusion As almost half of freshman women declared being sexually inactive, theinvestment in public health information programs and easier access to the HPV vaccineseem to be a useful strategy for undergraduate students.
receivedJuly 5, 2019acceptedNovember 22, 2019
DOI https://doi.org/10.1055/s-0040-1701466.ISSN 0100-7203.
Copyright © 2020 by Thieme RevinterPublicações Ltda, Rio de Janeiro, Brazil
Original articleTHIEME
96

Introduction
Current academic knowledge pertaining to human papilloma-virus (HPV) infection and its relationship with human pathol-ogy is vast and well established. Decades of cumulativeinvestigation led to a firm amalgam of information concerningthe biological basis for the different effects of HPV infection onthe cervix, vulva, penis, anus and oropharynx.1 In essence, HPVis themajorcausal factor forgenitalwarts andmultiple cancerssuchascervical, vulvar, vaginal, oropharyngeal, penileandanalcancer.2 Cervical cancer is the third most prevalent neoplasmand the fourth leading cause of death by cancer amongwomen.3ThepreventionofHPV infection canbeaccomplishedthrough prophylactic vaccines, which, administered prior tothe contact with the virus, provide almost 100%of efficacy. Thevaccines are prophylactic, and have their greatest benefitin boys and girls who have not yet started their sexualactivity. Sexually active adolescents and young adults arealso vaccinated to catch up.2 The first vaccine against HPVhas been approved by the US Food and Drug Administration(FDA) in 2006; however, the global vaccination rate for girlsaged 10 to 20years by 2015 was of 6.1%.4
In spite of the unequivocal progress obtained in thediagnosis, treatment and prevention of HPV infection, sever-
al studies suggest that the awareness and knowledge aboutthe infection, its causes and risk factors among the popula-tion is surprisingly limited. Alarmingly, it is known thathigher knowledge about HPV and its consequences is relatedto a higher propensity to take the vaccine,5 and ignorance onthe part of the general population about the implications ofHPV infection to general health is highly associated with thefailure of prevention initiatives. McCusker et al6 applied aquestionnaire concerning knowledge about HPV to freshmanmedicine students at a university in Scotland. The studentsparticipated later in a public health information (PHI) cam-paign that described the role of HPV in the development ofcervical cancer. After the PHI, they observed a significantincrease in the rate of HPV vaccination among girls: in 2008,before the campaign, no girl had taken all three doses of thevaccine; however, one year after the intervention, more than58% were vaccinated. They also reported that after thiscampaign, 94% of the vaccinated girls understood that theyshould remain in the screening program.6
It is therefore clear that awareness about HPV infection andits consequences among the general population is surprisinglylow considering the consolidated academic knowledge aboutit, its clinical implications, and the ample amountofdiagnosticand therapeutic tools currently available. Evenmore alarming,
Resumo Objetivo Avaliar o conhecimento sobre a infecção pelo vírus do papiloma humano(human papillomavirus, HPV, em inglês) e a taxa de vacinação entre estudantes calourose veteranos do quarto ano dos cursos de medicina, farmácia, fonoaudiologia,enfermagem e educação física de uma universidade brasileira.Métodos Um primeiro questionário sobre aspectos sociodemográficos, anteceden-tes sexuais e conhecimento sobre o HPVe sua vacina foi aplicado a 492 estudantes. Trêsmeses depois, foi aplicado um novo questionário, a 233 estudantes, que avaliava a novataxa de vacinação entre eles.Resultados Entre as 290 mulheres que responderam ao questionário, 47% dascalouras e 13% das veteranas negaram início de atividade sexual. Entre os 202 calourose veteranos do sexo masculino avaliados, essa taxa foi de 11%. Apesar de o conheci-mento sobre o HPV ter sido maior entre as mulheres, elas declararam menor uso depreservativo. Mais de 83% das mulheres e 66% dos homens sabiam que o HPV causacâncer de colo de útero, mas menos de 30% de todos os alunos sabiam que o HPV podecausar câncer de vulva, ânus, pênis e orofaringe, e menos de 50% sabiam que o HPVpode causar verrugas genitais, anais e orofaríngeas. Comparando calouros e veteranos,houve um aumento no conhecimento de que o HPV é sexualmente transmitido, e deque sua infecção pode ser assintomática, entre os veteranos em comparação com oscalouros. Pela taxa de vacinação analisada no segundo questionário, identificou-se que,antes do início da pesquisa, 26% das mulheres e 8% dos homens haviam sido vacinados,e, no momento da aplicação do segundo questionário, essas taxas subiram para 52% e27%, respectivamente, entre os 233 alunos avaliados.Conclusão Quase metade das calouras relataram não ser sexualmente ativas, e amaioria delas ainda não era vacinada contra o HPV. O ingresso no Ensino Superiorparece um momento oportuno para a realização de campanhas governamentais deconscientização e vacinação contra o HPV.
Palavras-chave
► vírus do papilomahumano
► vacina► estudantes► conhecimento► taxa de vacinação
Rev Bras Ginecol Obstet Vol. 42 No. 2/2020
Influence of Gender and Undergraduate Course on the Knowledge about HPV and HPV Vaccine Biselli-Monteiro et al. 97

a few pioneering studies suggest that in the developed anddevelopingworld, young adults studying in healthcare-relatedundergraduate programsmay display unacceptable low levelsof knowledge about HPV infections as well. Our hypothesis isthat freshman students go to college between the ages of 18and25years, and, therefore, are at a high risk forHPV infection,but only a small proportion of those students are vaccinatedagainst HPV. Our objective was to perform a comprehensivelongitudinal evaluation of the knowledge related to HPV andHPV vaccination, among freshman and senior undergraduatestudents of medicine, pharmacy, speech therapy, nursing andphysical education in an extremely competitive Brazilianuniversity. We also evaluated the proportion of studentsalready vaccinated before the questionnaire, and the propor-tion of thosewho took the vaccinewithin threemonths of theapplication of the questionnaire.
Methods
The present was an observational cohort study. After approvalby the Ethics in Research Committee of Universidade Estadualde Campinas (Unicamp, in Portuguese) (under CAAE64275917.4.0000.5404), a questionnairewasapplied inAugust2017 to freshman and senior undergraduate students aged� 18years of the courses ofmedicine, nursing, speech therapy,pharmacy and physical education of Unicamp. All subjectssigned the free and informed consent form. The questionnairewas composed of 79 multiple-choice, true or false, and shortanswers; it included sociodemographic aspects, sexual back-ground, knowledge on HPV and the vaccine, and the rates ofvaccination and of intention to indicate the vaccine to girls andboys in their professional future. After the students filled outthequestionnaire, a sheetwith the correct answerswasofferedto them. A second questionnaire with 5 questions was appliedin November 2017 to 233 students, with the objective ofanalyzing the vaccination rate of the medicine and pharmacyundergraduates, and to evaluate if those who had participatedin thefirst partof the surveyweremore likely to get vaccinated.The transcription of the questionnaire data was performedusing the REDCap (Vanderbilt University, Nashville, TN, US)web application. The data was then exported and analyzedusing the R Environment for Statistical Computing (R Founda-tion for Statistical Computing, Vienna, Austria).7 The Chi-squared test for trends and the t-test were used to evaluatedifferences in knowledge across the groups of students, aswellas the changes in the vaccination rate before and after theapplication of the questionnaires. Due to the small number ofstudents and the similarity in the sociodemographic character-istics, the data obtained from the speech therapy and nursingstudents were grouped.
Results
Sociodemografic FactorsAmong the 492 students included in the present study, therewere 290 women and 202 men. In total, there were 196medicine students, 63 pharmacy students, 39 speech therapystudents, 44 nursing students, and 147 physical education
students. There were 279 (56.7%) freshmen and 213 (43.3%)seniors. The proportion of female students was significantlyhigher in the nursing (97.7%) and speech therapy (94.9%)courses compared with pharmacy (79.7%), medicine (57.4%)and physical education (31.3%) (p<0.001). A significantlylarger proportion of medical students reported living alone,in boarding homes or with friends, compared with those ofother courses, who most often reported living with theirparents. The rate of students who declared themselves asfollowers of a religion was higher among the nursing andspeech therapy students when compared with those of othercourses (p<0.05). Most students reported having graduatedfrom high school in a public or technical school, excluding thepharmacy students. The proportion of students who had atleast one parent that was a college graduate was significantlyhigher among the pharmacy (74.2%) and medicine (77.6%)students compared with the physical education (61%) andnursing/speech therapy (50%) students (p<0.01) (►Table 1).
Sexual Background►Table 2 shows that although most women self-declared asheterosexuals, there was a significantly higher proportion ofbisexuals among freshman students (13.2%) when comparedto the seniors (4%) (p<0.05). There was no difference in theproportion of heterosexuals, homosexuals and bisexualsamong female and male students (p>0.05). Only 63% offreshmen women reported having started sexual activity,and, among the seniors, 13.4% of women reported they werenot yet sexually active. Among the freshman and senior malestudents, more than 89% reported they were sexually active.The proportion of sexually active men (89%) among thefreshman males was significantly higher when comparedwith that of women (p<0.001). The reported age of initiationof sexual activity was significantly lower among men whencomparedwith women (p<0.001). Women reported a higherrate of stable relationships than men (p<0.05). We observedthatwomen reportedmorevisits to thegynecologist thanmento the urologist (p<0.001), andhaving or not health insurancewasnot associatedwithahigher rateofconsultations. Condomusewas reportedbymore than90%of the freshmanand seniormale students and by only 61.8% of freshman female studentsand 57.3% of senior female students.
Knowledge about HPV and the Vaccine►Table 3 shows theproportion of correct responses to specificquestions evaluating HPV-related knowledge. Of the 14 pro-posed questions, the proportion of senior female studentsanswering correctly was significantly higher for 9 questionscomparedwith their freshman counterparts, regardless of theundergraduate course. For men, in 12 out of the 14 questions,the proportion of senior students answering correctly washigher than that of their freshman counterparts. Comparingmale and female students, regardless of class and course, in6/14questions theproportionofwomenanswering correctlyaquestion was higher than that of men. In general, ►Table 3
shows a clear progression of HPV-related knowledge through-out the years and a higher level of HPV-related educationamong women compared with men. For instance, the rate of
Rev Bras Ginecol Obstet Vol. 42 No. 2/2020
Influence of Gender and Undergraduate Course on the Knowledge about HPV and HPV Vaccine Biselli-Monteiro et al.98

knowledge that HPV is a sexually transmitted infection (STI)was high among freshman and senior female students (91.4%and 95.3% respectively) and among freshman and senior malestudents (82.3% and 94.2% respectively), being significantlylower among freshman male students (p<0.05). The rate ofknowledgethatHPVcancausecervical cancerwasof82.2%and85.8% among female freshmen and seniors respectively, and of63.5% and 69.8% male freshmen and seniors respectively(p<0.001). However, concerning the knowledge of othercancers related to HPV infection, such as vulvar, vaginal,anal, penile and oropharyngeal cancers, the accuracy ratewas lower than 40% for both genders, with a significantincrease in correct answers among senior students(p<0.001). The percentage of students who knew that HPVcan cause different types of wartswas lower than the percent-age of students who knew HPV could cause cervical cancer.However, this knowledge was higher among the senior com-pared with the freshman female students (62.7% and 37.4%respectively), and among the senior compared with the fresh-man male students (58.1% and 22.6% respectively).
We observed a trend in general HPV-related knowledgeamong female andmale students.►Fig. 1A shows the compar-
ison between thewomen of the different courses:we observedthat physical education students know less aboutHPV infectionand its consequences than those of speech therapy andnursing,whoknowless thanpharmacystudents,who, in turn, knowlessthan medical students (p-trend<0.001). The accuracy rate inthe questions that stated that HPV is an STI that can affect bothgenders and can cause cervical cancer was higher than60%amongall of thewomen,andobeyedtheproposedstandard(p-trend<0.001). On theother hand, knowledge thatHPV has ahigher prevalence among young adults aged 15 to 25years didnot show any difference between the courses (p-trend>0.05).Knowledge thatHPV infection ismost often asymptomatic, thatthe infection may become latent and cause genital, anal andoropharyngeal warts showed a large difference among courses(p-trend<0.001). Only 32.6% of physical education studentsknew that HPV can be asymptomatic, compared with 52.5% ofspeech therapy/nursing students, 74.5% of pharmacy students,and 77% of medicine students. As for the knowledge thatwarts can be caused by HPV, 30.4% of physical educationstudents, 40.5% of speech therapy/nursing students, 47.1% ofpharmacystudents,and61.9%ofmedicinestudentsknewaboutthis correlation. Regarding the other cancers related to HPV
Table 1 Sociodemographic characteristics of the study sample
Sociodemographiccharacteristics
Physicaleducationn(%)
Speechtherapyn(%)
Nursingn(%)
Nursing andspeech therapyn(%)
Pharmacyn(%)
Medicinen(%)
p-value
Gender
Male 101(68.7) 2(5.1) 1(2.3) 3(3.6) 12(19) 83(42.3) p<0.001
Female 46(31.3) 37(94.9) 43(97.7) 80(96.4) 51(81) 113(57.7)
Class
Freshman 90(61.2) 23(59) 29(65.9) 52(62.7) 32(50.8) 104(53.1) p>0.05
Senior 57(38.8) 16(41) 15(34.1) 31(37.3) 31(49.2) 92(46.9)
Residence situation
Living with parentsor guardians
90(62.9) 20(52.6) 21(48.8) 41(50.1) 29(49.2) 43(22.3) p<0.001
Living alone or in afraternity/sorority
53(37.1) 18(47.4) 22(51.2) 40(49.9) 30(50.8) 150(77.7)
Follower of a religion
Yes 90(61.6) 32(82.1) 34(79.1) 66(80.5) 36(58.1) 122(62.2) p<0.05
No 56(3.4) 7(17.9) 9(20.9) 16(19.5) 26(41.9) 74(37.8)
High school institution
Public school 44(29.9) 13(34.2) 15(34.1) 28(34.2) 11(17.5) 64(32.7) p >0.05
Technical school 38(25.9) 10(26.3) 10(22.7) 20(24.4) 15(23.8) 44(22.4) p>0.05
Private school 65(44.2) 15(39.5) 19(43.2) 34(41.4) 37(58.7) 88(44.9) p<0.05
Schooling of the parents
Higher education 89(61) 18(46.2) 23(53.5) 41(50) 46(74.2) 152(77.6) p<0.001
High school 45(30.8) 17(43.6) 13(30.2) 30(36.6) 10(16.1) 38(30.8) p<0.05
Did not graduatefrom high school
12(8.2) 4(10.3) 7(16.3) 11(13.4) 6(9.7) 6(3.1) p<0.001�
Notes: p: comparison of all courses. � The analyses were compromised due to less than 5 answers. Because of the similarity between the data fromnursing and pharmacy students, and the small number of students in those groups, the courses were grouped for the sake of analysis. ��Thepercentages were calculated based on the number of students that answered the question.
Rev Bras Ginecol Obstet Vol. 42 No. 2/2020
Influence of Gender and Undergraduate Course on the Knowledge about HPV and HPV Vaccine Biselli-Monteiro et al. 99
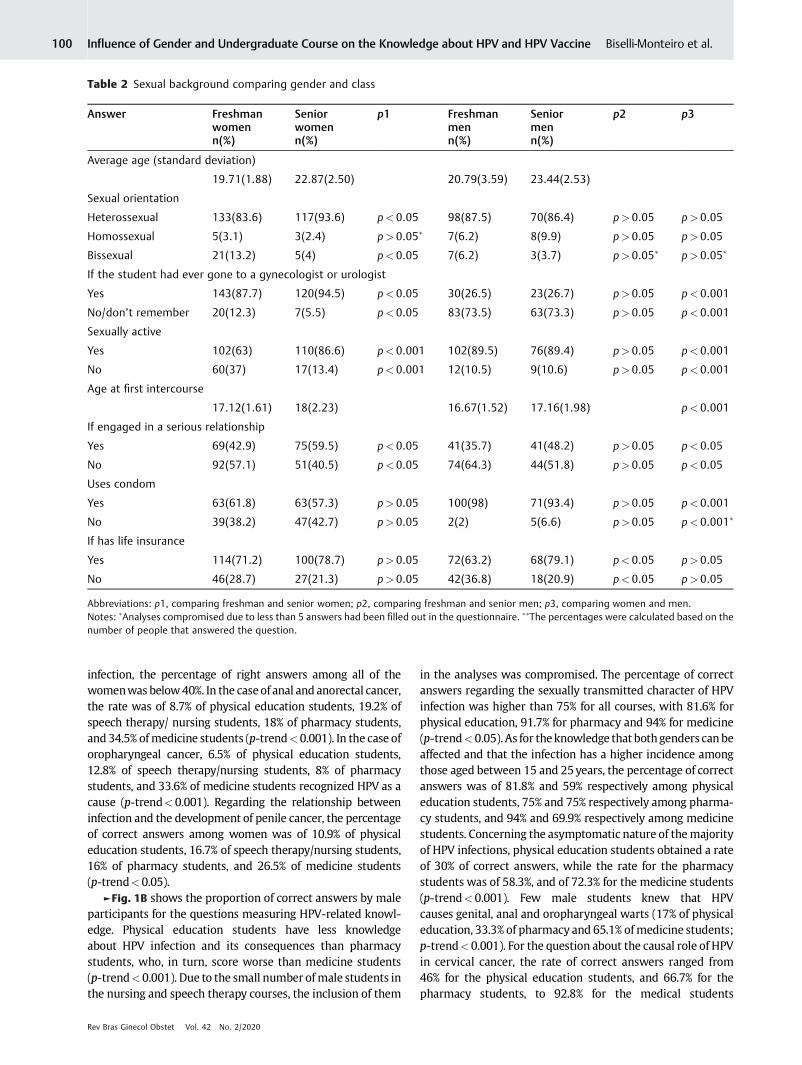
infection, the percentage of right answers among all of thewomenwas below40%. In the caseof anal and anorectal cancer,the rate was of 8.7% of physical education students, 19.2% ofspeech therapy/ nursing students, 18% of pharmacy students,and 34.5% ofmedicine students (p-trend<0.001). In the case oforopharyngeal cancer, 6.5% of physical education students,12.8% of speech therapy/nursing students, 8% of pharmacystudents, and 33.6% of medicine students recognized HPV as acause (p-trend<0.001). Regarding the relationship betweeninfection and the development of penile cancer, the percentageof correct answers among women was of 10.9% of physicaleducation students, 16.7% of speech therapy/nursing students,16% of pharmacy students, and 26.5% of medicine students(p-trend<0.05).
►Fig. 1B shows the proportion of correct answers by maleparticipants for the questions measuring HPV-related knowl-edge. Physical education students have less knowledgeabout HPV infection and its consequences than pharmacystudents, who, in turn, score worse than medicine students(p-trend<0.001). Due to the small number ofmale students inthe nursing and speech therapy courses, the inclusion of them
in the analyses was compromised. The percentage of correctanswers regarding the sexually transmitted character of HPVinfection was higher than 75% for all courses, with 81.6% forphysical education, 91.7% for pharmacy and 94% for medicine(p-trend<0.05). As for theknowledge that bothgenders canbeaffected and that the infection has a higher incidence amongthose aged between 15 and 25years, the percentage of correctanswers was of 81.8% and 59% respectively among physicaleducation students, 75% and 75% respectively among pharma-cy students, and 94% and 69.9% respectively among medicinestudents. Concerning the asymptomatic nature of themajorityof HPV infections, physical education students obtained a rateof 30% of correct answers, while the rate for the pharmacystudents was of 58.3%, and of 72.3% for the medicine students(p-trend<0.001). Few male students knew that HPVcauses genital, anal and oropharyngeal warts (17% of physicaleducation, 33.3% of pharmacy and 65.1% ofmedicine students;p-trend<0.001). For the question about the causal role of HPVin cervical cancer, the rate of correct answers ranged from46% for the physical education students, and 66.7% for thepharmacy students, to 92.8% for the medical students
Table 2 Sexual background comparing gender and class
Answer Freshmanwomenn(%)
Seniorwomenn(%)
p1 Freshmanmenn(%)
Seniormenn(%)
p2 p3
Average age (standard deviation)
19.71(1.88) 22.87(2.50) 20.79(3.59) 23.44(2.53)
Sexual orientation
Heterossexual 133(83.6) 117(93.6) p< 0.05 98(87.5) 70(86.4) p>0.05 p>0.05
Homossexual 5(3.1) 3(2.4) p> 0.05� 7(6.2) 8(9.9) p>0.05 p>0.05
Bissexual 21(13.2) 5(4) p< 0.05 7(6.2) 3(3.7) p>0.05� p>0.05�
If the student had ever gone to a gynecologist or urologist
Yes 143(87.7) 120(94.5) p< 0.05 30(26.5) 23(26.7) p>0.05 p<0.001
No/don’t remember 20(12.3) 7(5.5) p< 0.05 83(73.5) 63(73.3) p>0.05 p<0.001
Sexually active
Yes 102(63) 110(86.6) p< 0.001 102(89.5) 76(89.4) p>0.05 p<0.001
No 60(37) 17(13.4) p< 0.001 12(10.5) 9(10.6) p>0.05 p<0.001
Age at first intercourse
17.12(1.61) 18(2.23) 16.67(1.52) 17.16(1.98) p<0.001
If engaged in a serious relationship
Yes 69(42.9) 75(59.5) p< 0.05 41(35.7) 41(48.2) p>0.05 p<0.05
No 92(57.1) 51(40.5) p< 0.05 74(64.3) 44(51.8) p>0.05 p<0.05
Uses condom
Yes 63(61.8) 63(57.3) p> 0.05 100(98) 71(93.4) p>0.05 p<0.001
No 39(38.2) 47(42.7) p> 0.05 2(2) 5(6.6) p>0.05 p<0.001�
If has life insurance
Yes 114(71.2) 100(78.7) p> 0.05 72(63.2) 68(79.1) p<0.05 p>0.05
No 46(28.7) 27(21.3) p> 0.05 42(36.8) 18(20.9) p<0.05 p>0.05
Abbreviations: p1, comparing freshman and senior women; p2, comparing freshman and senior men; p3, comparing women and men.Notes: �Analyses compromised due to less than 5 answers had been filled out in the questionnaire. ��The percentages were calculated based on thenumber of people that answered the question.
Rev Bras Ginecol Obstet Vol. 42 No. 2/2020
Influence of Gender and Undergraduate Course on the Knowledge about HPV and HPV Vaccine Biselli-Monteiro et al.100

(p-trend<0.001). As ofother cancers related toHPV, the rate ofcorrectanswerswas low,withpenilecancerbeing reportedasapossible consequence of HPV infection by 10.1% of physicaleducation students, 41.7% of pharmacy students, and 37.3% ofthose studying medicine.
Attitude toward the Vaccine among Non-immunizedStudents and Intention to Indicate the Vaccine►Table 4 shows that the rate of women (26%) who had takenthe HPV vaccine prior to the application of the first ques-tionnaire was significantly higher than that of men (8%)(p<0.001), regardless of the class and course. As for age atvaccination, therewas a higher rate of freshmanwomenwhotook the vaccine until age 17, and only 10 women took thevaccine until age 14 (data not shown). There was no differ-ence in the proportion of girls vaccinated against HPVamongthe courses (data not shown). Non-vaccinated freshmanwomen reported a greater interest in taking the vaccine(74.3%) than the seniors (61.4%) (p<0.05). The intention totake the vaccine did not differ between women accordingto the course (data not shown). The intention to take thevaccinewas significantly higher amongunvaccinatedwomenthan among unvaccinated men (p<0.05). Among men whodid not take the vaccine, there was a higher proportion ofpharmacy students that intended to take the vaccine com-pared with those of other courses (data not shown). Mostmen and women who answered the questionnaire wouldrecommend the vaccine for both genders, and this propor-tion was higher among senior women (75.6%) than amongfreshman women (60.7%) (p<0,05).
Vaccination against HPV before and after Filling outthe First QuestionnaireAmong the 233 students who answered the second question-naire, which was applied 3 months after the first one, 39women (28medicine and 11 pharmacy students) and 15men(14 medicine and 1 pharmacy student) had already takenthe vaccine before the beginning of the research. Among thestudents who had filled out the first questionnaire and werenot previously vaccinated, 34 women (30 medicine and 4pharmacy students) and 10 male medicine students wereeventually vaccinated against HPV. Concerning these twocourses evaluated, there was an increase in the rate of vacci-nation. Between the 140 women that answered the secondquestionnaire, the rateof vaccinationdeclared prior to thefirstquestionnaire was of 28%, and it increased to 52% when weincluded women vaccinated in the three-month gap betweenquestionnaires (p<0.05). For men, the rate was of 16%, and itincreased to 27% (p>0.05).
Discussion
Afterhavingapplying thequestionnaire to almost500Brazilianmale and female university students, we observed that therewas a greater knowledge related to HPV infection and itsconsequences amongwomen, especially those in themedicinecourse. This knowledge was higher among senior students.In all courses and regarding both genders, the majority ofthe students were able to identify the sexually transmittednature of the HPV infection, and they were aware that theprevalence of HPV infection peaks between the ages of 15 and
Table 3 Knowledge about HPV comparing gender and class
Questions Freshmanwomenn(%)
Seniorwomenn(%)
p1 Freshmanmenn(%)
Seniormenn(%)
p2 p3
HPV is a sexually transmitted infection 149(91.4) 121(95.3) p>0.05 93(82.3) 81(94.2) p<0.05 p<0.05
HPV is common 134(82.7) 109(85.8) p>0.05 68(59.6) 71(82.6) p<0.001 p<0.001
Both genders can be affected by HPV 144(88.3) 115(90.6) p>0.05 95(83.3) 77(89.5) p>0.05 p>0.05
The incidence of HPV is higherbetween 15 and 25 years old
115(70.6) 105(82.7) p<0.05 69(60) 63(73.3) p<0.05 p<0.05
Most infections are asymptomatic 82(50.3) 100(78.7) p<0.001 40(34.8) 58(67.4) p<0.001 p<0.05
The infection can become latent 101(62) 94(74) p<0.05 63(54.3) 63(73.3) p<0.05 p>0.05
The infection can persist 121(74.2) 90(70.9) p>0.05 73(62.9) 66(76.7) p<0.05 p>0.05
HPV can cause genital,anal and oropharyngeal warts
61(37.4) 79(62.7) p<0.001 26(22.6) 50(58.1) p<0.001 p<0.05
HPV can cause cervical cancer 134(82.2) 109(85.8%) p>0.05 73(63.5) 60(69.8) p>0.05 p<0.001
HPV can cause vaginal cancer 27(16.8) 46(36.5) p<0.001 11(9.6) 28(32.6) p<0.001 p>0.05
HPV can cause analand anorectal cancer
22(13.7) 45(35.7) p< 0.001 9(7.9) 34(39.5) p<0.001 p>0.05
HPV can cause penile cancer 17(10.6) 39(31) p<0.001 14(12.3) 32(37.2) p<0.001 p>0.05
HPV can cause oropharyngeal cancer 15(9.3) 40(31.7) p<0.001 8(7) 25(29.1) p<0.001 p>0.05
The types of HPV that cause warts aredifferent from those that cause cancer
18(11) 54(42.5) p<0.001 9(7.8) 32(37.2) p<0.001 p>0.05
Abbreviations: p1, comparing freshman and senior women; p2, comparing freshman and senior men; p3, comparing women and men.Note: The percentages were calculated based on the number of people that answered the question.
Rev Bras Ginecol Obstet Vol. 42 No. 2/2020
Influence of Gender and Undergraduate Course on the Knowledge about HPV and HPV Vaccine Biselli-Monteiro et al. 101

25years. Although most students knew about the relationshipbetween HPV infection and cervical cancer, most were unableto identify the associationbetweenHPVandothercancers suchas vulvar, vaginal, anal, anorectal, penile, and oropharyngealcancer. Likewise, few students knew about the relationshipbetween genital, anal and oropharyngeal warts and HPVinfection. Most students interviewed had not previouslybeen vaccinated against HPV, and, even after being exposedto the correct answers to the questions, the vaccination rateincreased only to 52% for women and 27% for men within thesubsequent threemonths. It is interesting to report that duringthis period the vaccine was available at no cost to adults up to26years of age by the Brazilian UnifiedHealth System (SistemaÚnico de Saúde, SUS, in Portuguese).
The importance of HPV education and its vaccine is toenable the public to make a conscious choice about vacci-nation, knowing the risks of HPV infection and vaccineprotection.8 Similar to what was shown in our study, Ballaet al9 observed that among high-school seniors in Hungary,few had sufficient knowledge regarding HPV infection:although most acknowledged its association with cervicalcancer, their knowledge of other diseases was limited.
Those authors also reported better knowledge on the partof female students. For Monteiro et al,10 the gender com-parison showed a higher vaccination rate among women,which was similar to the findings made by Cooper et al11
that the knowledge and vaccination rate of men in highereducation was low: only three quarters had prior knowl-edge of HPV, and just over half had knowledge about thevaccine. Because cervical cancer is a preventable diseaseand affects only women, national campaigns have beenconducted for years in Brazil and worldwide, focusing ontracking cervical lesions and essentially educating women.Likewise, HPV vaccination was initially targeted at womenin Brazil and worldwide, which also favored female educa-tion. We also found that 90% of the women interviewed hadalready gone to the gynecologist, which can be anothercause of the higher knowledge.
In our study, the knowledge regarding almost all aspectsrelated toHPV infectionwas higher amongmedical students,regardless of gender, when compared with nursing, speechtherapy and pharmacy students, which is in line with thestudy by Chawla et al,12who found greater knowledge aboutlow-riskHPVand its relation to condylomaswhen comparing
Fig. 1 Knowledge about HPV comparing the percentage of right answers for the female (A) and male (B) students of the courses analyzed.
Rev Bras Ginecol Obstet Vol. 42 No. 2/2020
Influence of Gender and Undergraduate Course on the Knowledge about HPV and HPV Vaccine Biselli-Monteiro et al.102

Indian gynecologists with paramedics. Yam et al13 also foundgreater knowledge among Hong Kong medical students inrelation to other courses. In Brazil, Monteiro et al10 detectedthe same gap between literature and medicine students. Thelack of knowledge related to HPV is even greater whenconsidering courses not related to health care. In all of thequestions in our questionnaire, physical education studentsperformed poorly regardless of gender.
In our study, for both genders, senior students presentedbetter knowledge when compared with freshman students.Similar data have been found in other studies12,14with univer-sity students, mainly in health care courses. This may beattributed not only to formal exposure to HPV-related infor-mation as part of the curriculum of the courses, but also tocumulative acquisition of HPV-related information from othersourcesof information, suchas laymedia. Themajority (90%)ofthe studentswere awareof the sexually transmissible natureofHPV. This finding is in linewith those frommost of the studiesperformed with young university students globally.6,9,14,15
Cervical cancer is unequivocally caused by high-oncogenic-risk HPV infection, and this type of cancer is the third mostprevalent neoplasm and the fourth leading cause of cancerdeath among women.3 In our study, 76% of the participantswere aware of the causal nature of HPV in cervical carcinogen-esis. This question has been examined by severalauthors5,9,14–16 among students from a variety of courses,with the rate of correct answers ranging from 48 to 98%.Regarding the knowledge that HPV is related to other cancers,the proportion of correct answers did not exceed 40% for anytype of cancer. This knowledge gap was found in otherstudies9,17 for women and men. When we analyzed therelationship between HPV infection and the development ofwarts in our study and in the literature, knowledgewas higheramong higher-education students and among women.15,17
According to our expectation, only a small proportion ofstudents hadbeenvaccinatedagainstHPV: the rate of studentsevaluated in thefirst part of the survey was of 26% for womenand of 8% for men, being higher among medicine students.
Even within three months of the application of the question-naire, the vaccination rate increased only to 52% for womenand 27% for men. In Brazil, the quadrivalent vaccine wasapproved by the federal regulatory agency (Agência NacionaldeVigilância Sanitária, Anvisa, in Portuguese) in 2006, and it isrecommended for adolescents and young adults. In the firstyears after the approval, theavailabilityof theHPVvaccinewasrestricted to private clinics, and began to be offered by the SUSin 2014 for girls aged between 11 and 13years. Since January2017, its usehas been extended togirls aged9 to 14years, boysaged 11 to 14years, andmen andwomen aged between 9 and26years who are HIV positive, transplanted or oncologicalpatients on chemotherapy. Data from 2017 showed thatvaccination coverage rate among girls aged 9 to 14years inBrazilwasof82.6%for thefirstdose, andof52.8% for theseconddose. Amongboys aged12 to 13years, thevaccination ratewasof 43.8% for the first dose.17 In addition to not being easilyaccessible, concerns about the associationwith sexually trans-mitted infections (STIs), promiscuity, adverse effects, lowrecommendation of the vaccine by professionals, costs andlackofknowledgehave ledtothe lowrateofHPVvaccination inthe target population.13,16 Increased awareness had a positiveeffect on the intention to take the vaccine, and women weremore likely to have a positive attitude toward vaccination.9,15
Likewise, forMonteiro et al,10morewomenwere interested intaking the vaccine and, in general, higher-education studentswere more interested in the vaccination. In addition, only athird of the students had interest in taking the vaccine, andthose were essentially the ones with the higher knowledgeabout HPV.
However, in the present study, data from the question-naire applied three months after the first one showed aninsufficient improvement in the proportion of vaccinatedstudents. A study conducted in Scotland by McCusker et al6
evaluated the vaccination rate among medical students in2008 and 2009. In 2008, no female students had taken allthree doses of the HPV vaccine, and, in 2009, after an intensepublic campaign forHPV vaccination, 58% of the students had
Table 4 Attitude toward taking the vaccine and to whom the students would recommend the vaccine comparing gender and class
Answers Freshman womenn(%)
Senior womenn(%)
p1 Freshman menn(%)
Senior menn(%)
p2 p3
Vaccinated 44(27) 31(24.4) p>0.05 10(8.6) 7(8.1) p<0.05� p<0.001
Not vaccinated 104(63.8) 89(70.1) 80(69) 73(84.9)
Did not know 15(9.2) 6(4.7) 23(19.8) 2(2.3)
If not vaccinated (or doesn’t know), would get vaccinated after answering this questionnaire
Yes 78(74.3) 54(61.4) p<0.05 42(53.9) 46(61.3) p>0.05 p<0.05
No 27(25.7) 34(38.6) 36(46.2) 29(38.7)
Would recommend the vaccine
To both genders 99(60.7) 96(75.6) p<0.05 76(65.5) 60(69.8) p>0.05 p>0.05
Only to women 58(35.6) 27(21.3) p<0.05 30(25.9) 19(22.1) p>0.05 p>0.05
Only to men – – 2(1.7) 2(2.3) p>0.05� p<0.05�
Abbreviations: p1, comparing freshman and senior women; p2, comparing freshman and senior men; p3, comparing women and men.Notes: �Analyses compromised due to less than 5 answers had been filled out in the questionnaire. The percentages were calculated based on thenumber of people that answered the question.
Rev Bras Ginecol Obstet Vol. 42 No. 2/2020
Influence of Gender and Undergraduate Course on the Knowledge about HPV and HPV Vaccine Biselli-Monteiro et al. 103

taken all three doses. For Attia et al,17 the vaccination ratewill onlygrowsignificantlywhen the vaccine is administeredin programs designed and organized to do so, such as schoolprograms.
Thehelp of governmental andnon-governmental organiza-tions working in the health sector is necessary to increase theknowledge on the part of the various health professionals andthe general population regarding the various cancers andwarts induced by HPV.12 Campaigns on the efficacy and safetyof the vaccine are also required. The HPV vaccine is alreadyproven to be responsible for the decrease in cases of cervical,oropharyngeal, penile, anal, vulvar and vaginal cancer. Like-wise, a significant reduction in genital warts in vaccinatedpopulations is observed. It is extremely important to increasethe rate of vaccination among young people, especially beforethe beginning of sexual activity.18
The present study has some limitations. First, due to thefact that some of the courses had already finished thesemester, the second questionnaire was only applied tostudents from two of the five courses that had filled out tothefirst questionnaire. Second, a homogenization of answerscould have occurred by students comparing answers in class.The researchers reinforced the importance of individualanswers to minimize this problem. Another limitation isthat as the research included only students from healthcourses, we cannot conclude that the findings of our studyrepresent all university students.
Conclusion
So far, we conclude that knowledge and vaccination ratesagainst HPV are still low among the university studentsevaluated in the present study. After we conducted the study,it became clear that higher knowledge is associated with ahigher desire to get vaccinated. We hope that the resultspresentedmay lead to an investment in PHI programs, first toimprove the vaccination rate, and, second, to guide the newuniversity students about the risks of the infection and themethods to prevent it. The moment of starting universityseems to be an openwindowof opportunity for campaigns ofawareness once there is a gap in knowledge. It is also anopportunity to improve the rate of vaccination, as almost halfof the freshmanwomen declared being sexually inactive andwould highly benefit from the vaccination, along with sexu-ally active students who could be vaccinated in an attempt tocatch up.
ContributorsBiselli-Monteiro M developed the study design, plannedthe analyses, collected the data, performed the literaturesearch, the statistical analyses, prepared the tables andfigures, contributed to the interpretation of data, andwrote the manuscript. Ferracini AC collected the data,contributed to the interpretation of data, and writing andrevision of the article. Sarian LO performed the statisticalanalyses, prepared the tables, contributed to the interpre-tation of data, and to the revision of the article. DerchainSFM contributed to study design, planned the analyses,
performed the literature search, contributed to the inter-pretation of data, and wrote the manuscript. All authorsapproved the final submitted version.
Conflict of InterestsThe authors have no conflict of interests to declare.
AcknowledgmentsThe present research was supported by Fundação deAmparo à Pesquisa do Estado de São Paulo (Fapesp, inPortuguese) (under number 2017/03323–6) and by Con-selhoNacional deDesenvolvimentoCientífico e Tecnológico(CNPq, in Portuguese) (under number303742/2018–6). Theresearch was only possible due to the help of the directorsand professors of the courses of pharmacy, speech therapy,nursing, physical education and medicine of Unicamp.
References1 de Sanjosé S, Brotons M, Pavón MA. The natural history of human
papillomavirus infection. Best Pract Res Clin Obstet Gynaecol.2018;47:2–13. Doi: 10.1016/j.bpobgyn.2017.08.015
2 Castle PE, Maza M. Prophylactic HPV vaccination: past, present,and future. Epidemiol Infect. 2016;144(3):449–468. Doi:10.1017/S0950268815002198
3 Forman D, de Martel C, Lacey CJ, Soerjomataram I, Lortet-TieulentJ, Bruni L, et al. Global burden of human papillomavirus andrelated diseases. Vaccine. 2012;30(Suppl 5):F12–F23. Doi:10.1016/j.vaccine.2012.07.055
4 Bruni L, Diaz M, Barrionuevo-Rosas L, Herrero R, Bray F, Bosch FX,et al. Global estimates of human papillomavirus vaccinationcoverage by region and income level: a pooled analysis. LancetGlob Health. 2016;4(7):e453–e463. Doi: 10.1016/S2214-109X(16)30099-7
5 Nagpal J, Linares LO, Weiss J, Schlecht NF, Shankar V, Braun-Courville D, et al. Knowledge about human papillomavirus andtime to complete vaccination among vulnerable female youth.J Pediatr. 2016;171:122–127. Doi: 10.1016/j.jpeds.2015.12.070
6 McCusker SM, Macqueen I, Lough G, Macdonald AI, Campbell C,Graham SV. Gaps in detailed knowledge of human papillomavirus(HPV) and the HPV vaccine among medical students in Scotland.BMC Public Health. 2013;13:264. Doi: 10.1186/1471-2458-13-264
7 R Core Team. R: a language and environment for statisticalcomputing [Internet]. Vienna: R Foundation for Statistical Com-puting; 2018 [cited 2018 Aug 10]. Available from: https://www.R-project.org/
8 Ragin CC, Edwards RP, Jones J, Thurman NE, Hagan KL, Jones EA,et al. Knowledge about human papillomavirus and the HPVvaccine–a survey of the general population. Infect Agent Cancer.2009;4(Suppl 1):S10. Doi: 10.1186/1750-9378-4-S1-S10
9 Balla BC, Terebessy A, Tóth E, Balázs P. Young Hungarian students’knowledge about HPVand their attitude toward HPV vaccination.Vaccines (Basel). 2016;5(1):1–9. Doi: 10.3390/vaccines5010001
10 Monteiro DLM, Brollo LCS, Souza TP, Santos JRPD, Santos GR,Correa T, et al. Knowledge on the HPV vaccine among universitystudents. Rev Inst Med Trop São Paulo. 2018;60:e46. Doi:10.1590/s1678-9946201860046
11 Cooper DL, Zellner-Lawrence T, Mubasher M, Banerjee A, Her-nandez ND. Examining HPV awareness, sexual behavior, andintent to receive the HPV vaccine among racial/ethnic malecollege students 18–27 years. Am J Men Health. 2018;12(6):1966–1975. Doi: 10.1177/1557988318803163
12 Chawla PC, Chawla AK, Shrivastava R, Shrivastava A, Chaudhary S.Situation analysis of existing facilities for screening, treatmentand prevention of cervical cancer in hospitals/primary health
Rev Bras Ginecol Obstet Vol. 42 No. 2/2020
Influence of Gender and Undergraduate Course on the Knowledge about HPV and HPV Vaccine Biselli-Monteiro et al.104

centers of Delhi-NCR region, India. Asian Pac J Cancer Prev. 2014;15(13):5475–5482. Doi: 10.7314/apjcp.2014.15.13.5475
13 Yam PWA, Lam PL, Chan TK, Chau KW, Hsu ML, Lim YM, et al. Across sectional study on knowledge, attitude and practice relatedto human papillomavirus vaccination for cervical cancer preven-tion between medical and non-medical students in Hong Kong.Asian Pac J Cancer Prev. 2017;18(6):1689–1695. Doi: 10.22034/APJCP.2017.18.6.1689
14 Jelastopulu E, Fafliora E, Plota A, Babalis V, Bartsokas C, Poulas K,et al. Knowledge, behaviours and attitudes regarding HPV infec-tion and its prevention in female students inWest Greece. Eur RevMed Pharmacol Sci. 2016;20(12):2622–2629
15 Chiang VC, Wong HT, Yeung PC, Choi YK, Fok MS, Mak OI, et al.Attitude, acceptability and knowledge of hpv vaccination amonglocal university students in Hong Kong. Int J Environ Res PublicHealth. 2016;13(5):486. Doi: 10.3390/ijerph13050486
16 Sherman SM, Bartholomew K, Denison HJ, Patel H, Moss EL,Douwes J, et al. Knowledge, attitudes and awareness of the humanpapillomavirus among health professionals in New Zealand. PLoSOne. 2018;13(12):e0197648. Doi: 10.1371/journal.pone.0197648
17 Attia AC, Wolf J, Núñez AE. On surmounting the barriers to HPVvaccination: we can do better. Ann Med. 2018;50(3):209–225.Doi: 10.1080/07853890.2018.1426875
18 Ministério da Saúde. Secretaria de Vigilância em Saúde. Departa-mento de Vigilância das Doenças Transmissíveis. Coordenação-Geral do Programa Nacional de Imunizações [Internet]. Informetécnico da ampliação da oferta das vacinas papiloma vírushumano 6, 11, 16 e 18 (recombinante) –vacina HPV quadrivalentee meningocócica C (conjugada). Brasília, DF: Ministério da Saúde;2018 [cited 2018 Dec 02]. Available from: http://portalarquivos2.saude.gov.br/images/pdf/2018/marco/14/Informe-T–cnico-HPV-MENINGITE.pdf
Rev Bras Ginecol Obstet Vol. 42 No. 2/2020
Influence of Gender and Undergraduate Course on the Knowledge about HPV and HPV Vaccine Biselli-Monteiro et al. 105

Genital Injuries: Are They Telling us Somethingabout Sexual Violence?Carolina Orellana-Campos1,2
1Pediatric and Adolescent Gynecology Unit, Roberto del RíoChildren’s Hospital, Santiago, Chile
2Pediatric and Adolescent Gynecology Unit, Santa María Clinic,Santiago, Chile
Rev Bras Ginecol Obstet 2020;42(2):106–113.
Address for correspondence Carolina Orellana-Campos, MD,Roberto del Río Hospital, Santiago, Chile(e-mail: [email protected]).
Introduction
In the usual context of medical practice, the clinicians assess,diagnose, document and treat body injuries according to themedical needs of the patients. When a victim of sexualviolence is evaluated in the forensic context,much of the effortis puton the genital examination, giving toomuch emphasis tothe presence of the genital lesions as evidence to take a legalaction. For this reason, the forensic importance of genitallesions after a sexual assault has been subject to discussionand research among professionals working in this field.
Albeit understanding the psychosocial context and conse-quencesof sexualviolence is crucial forabettermanagementofthe victims, the aims of the present manuscript is, on the onehand, to refer only to genital injuries in adult females as anevidence of sexual assault. On the other hand, the presentreview intends to clarify the research in this area, which is fullof uncontrollable variables, and therefore, it is not possible tomake reliable conclusions considering genital lesionas theonlyevidence, even when they may be present after a consentedintercourse. Before analyzing this current research and delin-eating the importance of genital lesions, it seems pertinent toclarify some terms and characteristics of this forensic field.
Forensic Sexual Examination
The victim of sexual abuse requires to be examined by acompetent clinician with a comprehensive knowledge of
his/her forensic and therapeutic role. Essential componentsof a sexual forensic examination (►Table 1)must be describedin a standardized medico-legal report, with objective terms,providing expert opinion in legal proceedings, but in alanguage readable by police and lay people.1
It is important consider the clinical context in which theclinical environment in which physical and genital examina-tions were performed, and the expertise of the clinician. It isclear that clinicians or nurseswith different training levelswillbring different competencies to the clinical forensic examina-tion, and this will influence their findings. The venue can be areferral unit, center or any variant of this model care (e.g.,emergency unit). Both examiner and place heterogeneitiesmay explain the different outcomes that a sexual forensicexamination can have.2
The forensic examination can be done with several techni-ques towatch thegenitalzone, someof themallowcovering theskinandmucosawithdifferent solutions. Somepeopleonlyusenaked-eye inspection; others use the magnification given by acolposcopy, adding or not toluidine dye.3 As result, the tech-nique has a key influence on the frequency of found injuries,and therefore, it is necessary to be cautious on its interpreta-tion. Colposcopy has been shown to be statistically superior togross visualization alone,4 which may be increased with tolui-dine blue staining.5 However, the latter might be overestimat-ingmicroscopic injuries causedbyordinarywiping, insertionoftampons, sport activity or otherday-to-day personal routines.6
Indeed, one study7 confirmed the suspicion that minor vaginal
Keywords
► sexual assault► rape► genital injury
Abstract Genital injury has a forensic relevance after a sexual assault and it has been discussed andinvestigated among professionals whowork in this field. To analyze the studies published inthe last decades, the present review examines different factors that may influence thisfinding,first clarifying termsof the forensicfield, such as the peculiarity of the legalmedicalexamination, and the distinction of the terms “legal” and “anatomical” vagina. Finally, itanalyses if it is possible that the existence of these injuries in victims explain the lack ofconsent in sexual contact, and to clarify the meaning of the absence of injuries.
receivedJune 5, 2019acceptedNovember 22, 2019
DOI https://doi.org/10.1055/s-0040-1701465.ISSN 0100-7203.
Copyright © 2020 by Thieme RevinterPublicações Ltda, Rio de Janeiro, Brazil
Integrative ReviewTHIEME
106

conditions,whichdonotdeserve tobeclassifiedas ‘lesions’, arefairly common in women under normal circumstances.
Pubertal Changes of the Genitalia
The vaginal epithelium is characteristically thin in childhood,but after puberty, it begins to thicken in response to estrogenstimulation with progressive cellular proliferation andgrowth that results in the formation of intermediate andsuperficial layers of cells,8which couldmake the vaginamoreresistant to friction. Although it could be deduced thatchildrenmay get genital injuries easily, most sexually abusedchildren will not have signs of genital or anal injury, espe-cially when examined non-acutely.9 Moreover, the primarypredictor of diagnostic findingswas not the age, timing of theexamination, or the history told by the adult, but the historyreported by the child.10
The legal frame
Prior to continuing, it is important to define a legal frame ofsexual violence. Jewkes et al11 define sexual violence as “Anysexual act, attempt to obtain a sexual act, unwanted sexualcomments or advances, or acts to traffic, or otherwise directed,against a person’s sexuality using coercion, by any personregardless of their relationship to the victim, in any setting,including but not limited to home and work” (p. 140). Govern-ments in the Latin America and the Caribbean (LAC) regionbegan to revise national legislations to address violence againstwomen in the 1990s. Many countries incorporated specializedlegislation based on a gender perspective, and reformed theircivilandcriminal codesaccordingly.Manyadvanceswere linkedto implementing international agreements at the nationallevel.12 Besides the adoption of legislation, most countries oftheregionhaveformulatedplansandprogramsorientedtowardthe prevention and eradication of violence against women,
boys, girls and adolescents. Moreover, in some countries, legis-lative reforms have also addressed sexual harassment, sexualexploitation or violence in conflict settings.13
In many cases, legal reforms have reframed sexualviolence as a criminal rather than a moral offense - as itwas historically conceptualized in many LAC legal systems.In some settings, discriminatory clauses against the victimshave been eliminated, such as allowing victims to be ques-tioned about their previous sexual history, their conductduring the attack or their “honour.” Also, legal reforms haveintroduced marital rape as a criminal offense, which did notexist before in some countries, such as Mexico. For instance,in Brazil in 1983, Maria da Penha Maia, who was a womanwho survived to two murder attempts by her husband. Shebecame a paraplegic as a result of the abuse. She battled fortwenty years to bring her case to justice, appealing tointernational organizations such as the Inter American Com-mission on Human Rights. The story gained internationalattention and finally the national domestic violence law inBrazil was signed in 2006 and named “Maria da Penha” in herrecognition. The law specifically defines sexual violence as acrime, and includes preventive, punitive and protective legalmechanisms. It is considered one of the most advanced lawsin the world addressing violence against women.12
Despite significant improvements to the laws addressingsexual violence in LAC, sexual violence still remains as amajor concern. While in some countries marital rape is notaddressed by the legal code and others still consider rape andsexual assault as an offense against “morals” or honor ratherthan a criminal act against the individual woman,13 in mostdeveloped countries the argument is the lack of consent.
Otherwise, it is quite interesting the difference betweenmedical and legal definitions of vagina in some countries, asthe UK, which may guide to confusion and error amongstprofessionals involved in rape allegation. The medical defi-nition considers the vagina as a muscular tube that has thecervix as its proximal end and the hymen (or hymenalremnants) as the distal end. The British legal definitionaccording to the Sexual Offenses Act 2003 (point 9, section79, part 1) considers the distal end of the vagina as thebeginning part of the vulva, therefore, “vagina” includes thevulva (between the labia). For legal purposes, penetration ofthe vagina does not have to involve penetration of thehymen.By contrast, in other nations there is no difference betweenboth meanings in their domestic law.14
Evidence about Genital Injuries in SexualViolence
Thewide variations found in the literature are attributable todiverse examination variables such as inconsistent defini-tions of “findings,” variable time span from sexual inter-course to examination, inclusion criteria of complainants,and divergent statistical methods. These variations demon-strate the difficulty of interpreting the findings in a group ofvictims, and it is even harder to try to compare them.15
Therefore, I will focus the analysis on genital and/or analinjuries only.
Table 1 Components of the forensic examination
1. Informed consent
2. Medical and gynecological background
3. History of the aggression
4. General physical examination• Search and collection of biological material
5. Genito-anal examination• Inspection:• Naked eye• Colposcopy• With blue toluidine dye• Search and collection of biological material
6. Documentation of injuries and other findings• Interpret and report the findings
7. Chain of custody
8. Management:• Prophylactic treatment of sexually transmitted
infections• Emergency contraception• Derive
Rev Bras Ginecol Obstet Vol. 42 No. 2/2020
Genital Injuries: Are They Telling us Something about Sexual Violence? Orellana 107

The prevalence of genital injuries reported after sexualassault ranges between 5 and 87%, according to a meta-analysis conducted by Kennedy.2 The same study found amean prevalence of 34.8%. However, the authors claimedthat they were unable to draw firm conclusions about theprecise prevalence of genital injuries due to the heterogeneityof researchmethodologies. Inamore recentandbiggerwork,16
genital injuries were detected in 22.0% of women examined ata sexual assault referral center (SARC). Nevertheless, whilegenital injuries were found in 24.5% of women who allegedcomplete vaginal penetration, only 13.2% of women withsuspected sexual assault but no clear type of penetrationhad similar findings.
To improve the accuracy of interpretation of physicalfindings, some years ago a pattern of genital injuries infemale victims was defined, whose acronym is TEARS17:Tears (lacerations), Ecchymosis (bruises), Abrasions, Rednessand Swelling. Another classification considers abrasions,bruises and wounds, which can be lacerations or incisions.18
Many studies, however, have excluded erythema, rednessand swelling when calculated injury rates as they are moresubjective. These studies tend to have lower injury rates thanthose using the TEARS system,making comparison difficult.3
The frequency and type of injury also vary according to theregion of penetration.16 In vaginal penetration, laceration,abrasion and bruise were observed in 13.1%, 11% and 5.7% ofwomen, respectively. In anal penetration, abrasion and bruisewere similarly found (8.6%, 2.9%, respectively), but lacerationwasmore frequent (21.3%). The commonest sites, with at leastone injury in vaginal penetration, were the posterior four-chette (7.4%), the fossa navicularis (6.8%), the labia minora(6.1%) and the hymen/hymenal remnant (6.0%). When pene-trationwas anal, the frequent siteswere theperianal (19%), theanus (9.8%) and the rectum (2.9%).
Another issue to consider is the timing of sexual assault andhealing. The knowledge of injury healing may assist to decidethe urgencywithwhich an examination is performed. In somecases, the age of an injurymight assist in determiningwhohadaccess to the victim during the specified timeframe. Police orthe court may ask the clinician to consider how old a genitalinjury is, and this may help to determine whether it was aresult of previous consensual intercourse or a later allegedassault. On the other hand, many studies did not stipulateinjury rates as genitalia tend to heal quickly.3
In terms of healing times, the evidence has shown thatnon-hymenal genital injuries heal at diverse rates dependingon the type, location and severity. Nonetheless, there is nostatistical difference in the rate of healing between pre- andpostpubertal girls. In case of laceration, its depth determinedthe time required to heal. While superficial vestibular lacer-ations seemed to heal in 2 days, deep perineal lacerationsrequired up to 20 days.19
The timing of examination determines the diagnostic ratesof genital injuries,20 andwomen examined�72hours after anassault have significantly more injuries than those examined>72hours. Andersonet al21 studied thechanges in thepatternofgenital injuries according totype, site, areaandnumberat48and 72hours of consensual vaginal intercourse using several
techniques. In thosewomen examined at 24hours, they founda significantly higher number of injuries, and bigger surfaceareas of injury, both total and in the posterior fourchette, andbigger surfaceareasofabrasionsandredness. Similarly, Zilkenset al16 found that the odds of observing a genital injurydecreased with a delayed examination. Considering the tech-niques, the median survival time for lesions was 24, 40 and80hours using the naked eye, colposcope and toluidine bluedye, respectively.22
From a therapeutic and forensic perspective, a differentialdiagnosis is crucial. In both settings, the professional could beasked whether the genital findings resulted from an allegedassault or have another explanation. Therefore, awareness ofmedical conditions that affect the genitals can significantlyreduce stress inpatients and their surroundings, and lead to anaccurate diagnosis. There are several conditions that might beconfused with injuries such as allergy, eczema, psoriasis,infections (e.g., candida), and normal anatomical variations,amongst others. Consequently, obtaining a full history, whenindicated, is a critical element to establish the context inwhichthese findings should be interpreted.3,23
How to Interpret Genital Injuries when theConsent of the Victim is Questioned?
Knocking Down MythsDecades ago, there was a wrong view about the “normal”response of women in consensual intercourse. This includedvaginal lengthening, increased lubrication and changes inmuscular tension, which protected her from genital injury.24
By contrast, the use of force and the absence of this “normalphysiological process” during sexual assault would make inju-ries inevitable. As result, a female genital injury would betreatednotonlyas evidenceof sexual contact, but alsoas lackofconsent.25,26 Indeed, this hypothesis is still in the popularimagination in some countries and their justice systems.
Another myth that must be tackled is that rapes or sexualassaults are necessarily violent. Modern legal definitionshave now replaced the ‘use of force’ with ‘lack of consent’as the defining feature of rape. In the Sexual Offenses Act2003, a person consents if he/she agrees by choice, and hasthe freedom and capacity to make that choice,27 whichrequires active participation. This has changed how thecrime of rape is conceptualized and prosecuted legally, andsocieties are also assimilating the basic awareness that theuse of force is not a prerequisite for unconsented intercourse,and that physical resistance is not a universal response ofthe victims.6
Specifically about resistance, many women feel paralyzedwhen are attacked, especially when they fear for their life.28
In addition, it is frequent that women who did not respondaggressively blame themselves, and therefore, are lesswillingto talk about their experiences with others. Although aDanish study29 found that some women who resistedverbally during their assault were more likely to suffer aphysical injury, no correlation was found between physicalresistance and the risk of sustaining an anogenital injury.However, the lack of information about the time from assault
Rev Bras Ginecol Obstet Vol. 42 No. 2/2020
Genital Injuries: Are They Telling us Something about Sexual Violence? Orellana108

to examination, and the differentiation between genitaland anal injuries makes difficult to draw a firm conclusionfrom it.
The likelihood of injury in the first intercourse of a womandeserves a special mention. During many years, the bleedingfrom the first hymenal laceration has had sociological/reli-gious significances in many cultures across the world. Never-theless, hymenal injury is not always present, as 40 to 80% ofwomen do not bleed in the initial coitus,6 and the hymenwasobserved intact in 52% of adolescents who admitted pastintercourse.30 Indeed,whenpregnant adolescentswere exam-ined for sexual abuse, 82% of the examinations were normaland only 7% were definitive for penetrating trauma.31 Hence,the likelihood of sustaining a genital injury is not related to theconsent, resistance or prior sexual experience.
Was the Sexual Contact Consented?This is the most crucial question, which is not alwaysanswered ‘beyond reasonable doubt’. This situation usuallyfrustrates prosecutors of sexual crime as it might explain lowconviction rates for rape.6 The prevalence and location ofgenital injuries provide only a partial description of thenature of genital trauma, and the use of refined strategiesof injury measurements has not assured this nature.32 Forthis reason, it is necessary to analyze studies where com-plainants of rape were compared with a control group, thatis, consensual intercourse.
Systematic Reviewof Case-control Studies ofGenital Lesions
All case-control studiespublisheduntil31stDecember2018 inPubMed, CINAHL and EMBASE databases were retrieved usingthe terms case-control OR case AND “control” OR “consensual”AND “nonconsensual” AND genital OR anal OR genitoanal ORvagina OR vulva OR vulvar AND lesion OR injury AND sexualabuseOR sexual violenceOR rapeOR sexual assault. The searchretrieved 49 different articles, 41 of themwere excluded aftertitle and abstract reading, and full-text readingwasperformedfor the remaining 8 articles, independently of the language.Finally, 6 articles were included considering the followinginclusioncriteria1: case-control studies,2 theprimaryoutcomewas the analysis of female genital lesions,3 cases werewomenwho underwent sexual violence and controls were womenwho consented to sexual intercourse.
►Table 2 analyses three of the most recent studies inwhich victims of a sexual assault were compared with acontrol group.McLean et al33 have found that the presence ofinjurieswas significantly greater in the victims. However, theaverage time for the exam was significantly longer for thecontrol group, and the only factor that showed an increasedrisk of injury was the relationship with the attacker, specifi-cally with a close one. Astrup et al34 also found that thefrequency of injuries was significantly higher in the victims,who have injuries in different places, are larger and morecomplex ones in comparison to the control group. However,the groups are small to generalize. Finally, Lincoln et al35 alsofound that the frequency of injuries was significantly higher
in the victims, and the abrasions and bruises were observedexclusively in the cases. However, the average time fromsexual penetration to examinationwas longer in the consen-sual group, even higher than showed by MacLean et al.33
Since genital lesions heal quickly, these conclusions may bequestionable. In a retrospective research, Jones et al36
defined clearly that the presence of anogenital traumasuggests that penetration has occurred and that nothing tellsabout consent. In addition, anogenital injury is not aninevitable consequence of sexual assault – the lack of genitalinjury does not imply consent by the victim or lack ofpenetration by the assailant. But their results are biased as15% of the nonconsensual group had had consensual inter-course within 72hours of the reported assault. It is possiblethat anogenital injuries attributed to the sexual assault wereactually secondary to prior consensual intercourse.
Despite the works of Anderson et al37 and Kongtanajar-uanun et al38 having been case-control studies, the way inwhich the results were delivered is too heterogeneous, andtherefore, they cannot be added to►Table 2. The former gaveresults on the pattern of injuries according to the number ofsites and areas affected instead of the number of patients.Although the latter research provided information on thelocation and pattern of lesions, the latency of the examina-tion was too broad to compare its results with those previ-ously analyzed. In addition, it did not make clear reference tothe total number of patients affected in each group.
Factors Associated to Genital Injuries
Researchers have been motivated to determine whetherfactors associated with genital injury can assist in obtainingevidence, to corroborate something that typically occursbetween two people without direct witnesses.
Pattern or Severity of Genital InjuryBased upon the theory that genital injuries might be morelikely to occur or be more severe in those cases withoutconsent, the presence, pattern and/or severity of genital injurymight be helpful in answering the question about consent.However, this hypothesis is outdated. Although the aforemen-tioned studies done by Astrup et al34 and by Lincoln et al35
reported that cases had significantly more abrasions andbruises, and a higher frequency of multiple lesions, the smallsamplesizeof theformer and thedelayedcasesexaminationofthe latter affect this presumption. Anderson et al37 shows thatthere were differences in the types of injuries and the totalnumbers of injuries between the nonconsensual and theconsensual groups. Except for redness, there were more sitesof injury in the nonconsensual group than in the consensualgroup, where lacerations, ecchymosis, and abrasions weregreater in the nonconsensual than in the consensual group.One remaining chance to keepthis hypothesis aspartially validis the use of standardized scales such as the Genital InjurySeverity Scale developedbyKelly et al15 to define andmeasureexternal genital injury after sexual intercourse. However, theyneed to be validated prospectively in an unbiased/unselectedpopulation.
Rev Bras Ginecol Obstet Vol. 42 No. 2/2020
Genital Injuries: Are They Telling us Something about Sexual Violence? Orellana 109
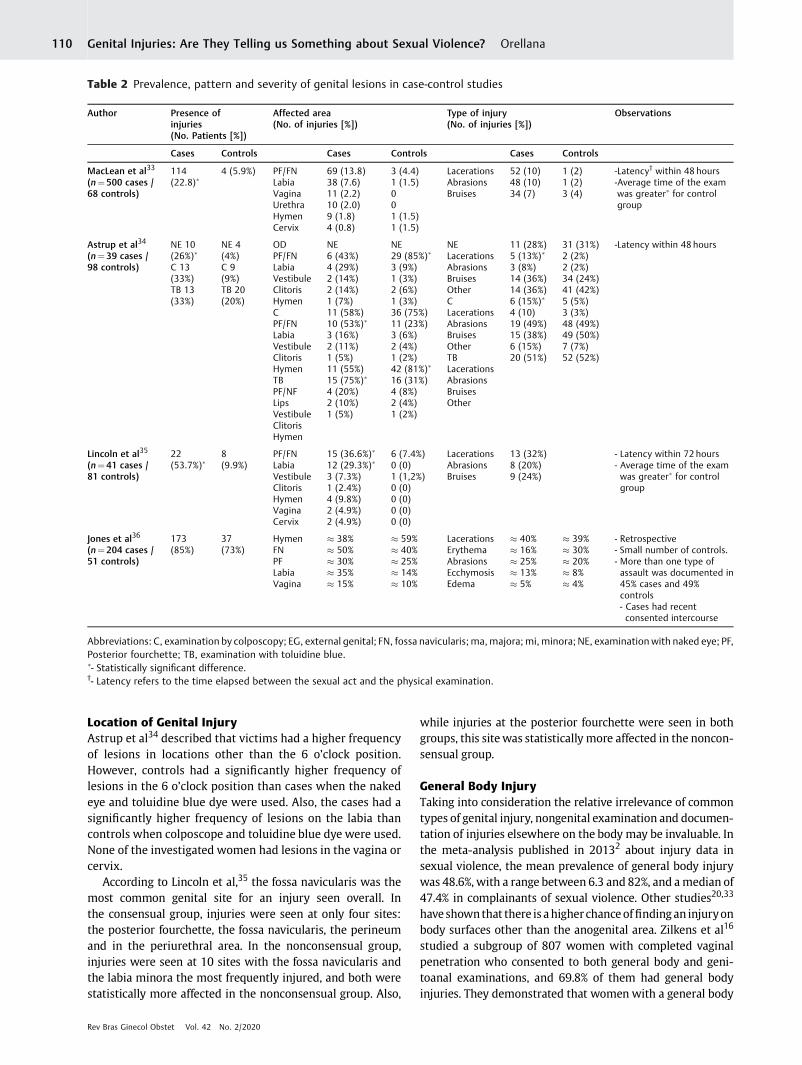
Location of Genital InjuryAstrup et al34 described that victims had a higher frequencyof lesions in locations other than the 6 o’clock position.However, controls had a significantly higher frequency oflesions in the 6 o’clock position than cases when the nakedeye and toluidine blue dye were used. Also, the cases had asignificantly higher frequency of lesions on the labia thancontrols when colposcope and toluidine blue dye were used.None of the investigated women had lesions in the vagina orcervix.
According to Lincoln et al,35 the fossa navicularis was themost common genital site for an injury seen overall. Inthe consensual group, injuries were seen at only four sites:the posterior fourchette, the fossa navicularis, the perineumand in the periurethral area. In the nonconsensual group,injuries were seen at 10 sites with the fossa navicularis andthe labia minora the most frequently injured, and both werestatistically more affected in the nonconsensual group. Also,
while injuries at the posterior fourchette were seen in bothgroups, this sitewas statistically more affected in the noncon-sensual group.
General Body InjuryTaking into consideration the relative irrelevance of commontypes of genital injury, nongenital examination and documen-tation of injuries elsewhere on the body may be invaluable. Inthe meta-analysis published in 20132 about injury data insexual violence, the mean prevalence of general body injurywas 48.6%, with a range between 6.3 and 82%, and amedian of47.4% in complainants of sexual violence. Other studies20,33
haveshownthat there is ahigherchanceoffindingan injuryonbody surfaces other than the anogenital area. Zilkens et al16
studied a subgroup of 807 women with completed vaginalpenetration who consented to both general body and geni-toanal examinations, and 69.8% of them had general bodyinjuries. They demonstrated that women with a general body
Table 2 Prevalence, pattern and severity of genital lesions in case-control studies
Author Presence ofinjuries(No. Patients [%])
Affected area(No. of injuries [%])
Type of injury(No. of injuries [%])
Observations
Cases Controls Cases Controls Cases Controls
MacLean et al33
(n¼ 500 cases /68 controls)
114(22.8)�
4 (5.9%) PF/FNLabiaVaginaUrethraHymenCervix
69 (13.8)38 (7.6)11 (2.2)10 (2.0)9 (1.8)4 (0.8)
3 (4.4)1 (1.5)001 (1.5)1 (1.5)
LacerationsAbrasionsBruises
52 (10)48 (10)34 (7)
1 (2)1 (2)3 (4)
-Latency† within 48 hours-Average time of the examwas greater� for controlgroup
Astrup et al34
(n¼ 39 cases /98 controls)
NE 10(26%)�
C 13(33%)TB 13(33%)
NE 4(4%)C 9(9%)TB 20(20%)
ODPF/FNLabiaVestibuleClitorisHymenCPF/FNLabiaVestibuleClitorisHymenTBPF/NFLipsVestibuleClitorisHymen
NE6 (43%)4 (29%)2 (14%)2 (14%)1 (7%)11 (58%)10 (53%)�
3 (16%)2 (11%)1 (5%)11 (55%)15 (75%)�
4 (20%)2 (10%)1 (5%)
NE29 (85%)�
3 (9%)1 (3%)2 (6%)1 (3%)36 (75%)11 (23%)3 (6%)2 (4%)1 (2%)42 (81%)�
16 (31%)4 (8%)2 (4%)1 (2%)
NELacerationsAbrasionsBruisesOtherCLacerationsAbrasionsBruisesOtherTBLacerationsAbrasionsBruisesOther
11 (28%)5 (13%)�
3 (8%)14 (36%)14 (36%)6 (15%)�
4 (10)19 (49%)15 (38%)6 (15%)20 (51%)
31 (31%)2 (2%)2 (2%)34 (24%)41 (42%)5 (5%)3 (3%)48 (49%)49 (50%)7 (7%)52 (52%)
-Latency within 48 hours
Lincoln et al35
(n¼ 41 cases /81 controls)
22(53.7%)�
8(9.9%)
PF/FNLabiaVestibuleClitorisHymenVaginaCervix
15 (36.6%)�
12 (29.3%)�
3 (7.3%)1 (2.4%)4 (9.8%)2 (4.9%)2 (4.9%)
6 (7.4%)0 (0)1 (1,2%)0 (0)0 (0)0 (0)0 (0)
LacerationsAbrasionsBruises
13 (32%)8 (20%)9 (24%)
- Latency within 72 hours- Average time of the examwas greater� for controlgroup
Jones et al36
(n¼ 204 cases /51 controls)
173(85%)
37(73%)
HymenFNPFLabiaVagina
� 38%� 50%� 30%� 35%� 15%
� 59%� 40%� 25%� 14%� 10%
LacerationsErythemaAbrasionsEcchymosisEdema
� 40%� 16%� 25%� 13%� 5%
� 39%� 30%� 20%� 8%� 4%
- Retrospective- Small number of controls.- More than one type ofassault was documented in45% cases and 49%controls- Cases had recentconsented intercourse
Abbreviations: C, examination by colposcopy; EG, external genital; FN, fossa navicularis; ma,majora; mi, minora; NE, examination with naked eye; PF,Posterior fourchette; TB, examination with toluidine blue.�- Statistically significant difference.†- Latency refers to the time elapsed between the sexual act and the physical examination.
Rev Bras Ginecol Obstet Vol. 42 No. 2/2020
Genital Injuries: Are They Telling us Something about Sexual Violence? Orellana110

injuryweremore likely topresentagenital injury, althoughtherisk was only 1.6-fold.
Vaginal Penetration by Body Parts other than thePenisPenetration with finger(s) and possible pre-existing genital‘infection’ were found to be significantly associated with thepresence of genital injury in the univariate analysis per-formed by Lincoln et al.35 Logistic regression demonstratedthat a penetration that included finger(s) was 4.2-fold morelikely to result in� 1 genital injury than penetrationwithoutfingers.While the presence of lacerationswas less likely thanother injuries if penetration involved finger(s) or if a womanwas penetrated exclusively with finger(s), abrasions weremore likely to occur than other injury types in the samescenario. Similarly, Zilkens et al16 reported that genital injurywas more likely with multiple types of penetrants (5.0-fold)other than the penis such as finger(s) or hand.
Vaginal Penetration by an ObjectAlthough in the Lincoln et al35 study there were no womenexclusively penetrated with an object, five women gave apenetration history that included an object. Four of these 5women were penetrated consensually and none of themsustained any injury; the nature of the object was notrecorded in the consensual group. One woman was pene-trated nonconsensually with an object, who described it as a‘toilet-roll holder’ andwas found to have three bruises on thelabia minora and hymen. Zilkens et al16 also reported thatgenital injury was more likely with multiple types of pene-trants, among them an object.
Age of VictimHilden et al39 reported that age was significantly related tothe occurrence of anogenital injury. Women � 19 years-oldand >50 years-old had the highest risk. Nevertheless, otherstudies33–35 showed that age is not an important factor forhaving genital injuries in sexual intercourse, either consen-sual or not.
Previous Sexual ActivityWhenWhite et al40 compared thefindings in virgin and non-virgin adolescents (12–17 years old) seen at a SARC after anallegation of nonconsensual intercourse, they did not findsignificant differences for the presence of genital or nongen-ital injuries overall. When different genital sites were takeninto account, 50.6% of the participants from the virgin grouphad a hymen injury, but only 12.4% of adolescents from thenonvirgin group had it. Other sites were similarly affected.Nonetheless, the virgin adolescents consulted later than thenonvirgin group (90 versus 44hours), which may affect theinjury rate.
Recently, Zilkens et al16 found that 52.1% of virgin womenwho reported completed vaginal penetration had genitalinjury. This represented a 4.7-fold risk of genital injury ifthere was no history of prior vaginal intercourse, which wasthe highest factor. However, this research did not havecontrol cases.
Nearness of the Aggressor to the VictimWhile Hilden et al39 found that assaults by strangers wereless likely to cause anogenital injury, although this was notstatistically significant, McLean et al33 demonstrated that if awoman knew her assailant, then there was a statisticallysignificant higher change of sustaining an injury whencompared with women who did not know their assailant.In the same way, Maguire et al20 found that to be a victimof sexual violence by an acquaintance increased the risk ofgenital injury 2.3-fold. Hence, it seems that the nearness ofthe victim to her attacker may be a factor to consider.
Other FactorsBoth thestudiesbyAstrupet al34andbyLincoln et al35analyzedother factors such as time since intercourse, use of condoms/lubricants, insertion of a tampon in 72hours preceding theexamination, usual pattern of sexual activity, roughness ofintercourse, and previous vaginal deliveries. None had anysignificant influence on the presence or type of lesions irre-spective of the examination technique. Concerning alcoholconsumption and sedatives by the victim previous to theassault, Hilden et al39 found that>50%of the sexually assaultedwomen in their study were influenced by alcohol. When theamount of alcohol drunk was enough to induce amnesia, thenthe anogenital injury rate was lower. A lesser resistanceimposed by the victim could explain this. Nonetheless, Maguireet al20 concluded that alcohol usehadnoeffecton the frequencyof genital injury. Also, Zilkens et al16 reported that the presenceof a genital injury was less likely with sedative use. Genitalinjury was not found to be significantly associated with aprevious history of vaginal delivery, obstetric genital injury,surgery, or if women had a pigmented skin.33,35 Regarding theeffects of hormonal contraception on the presence of genitalinjuries, the evidence is contradictory. While Lincoln et al35 didnot detect a significant relationship between hormonal contra-ception and the presence of injury, another study20 that includ-ed the use of colposcopy found a significantly higher rate ofgenital injury in those women who were not taking hormonalcontraception. Finally, it has been reported that females indorsal decubitus with thighs flexed, and male/female genitaldisproportion,wouldbepredisposing factors tovaginal injury inboth nonconsensual and hurried consensual intercourse.41
Lack of Injuries
The percentage of participantswithout bodyor genital injuryin diverse studieswas extremelywide, between 18 and 68%.2
This may be explained by several factors, some of themdetailed above, which must be kept in mind. Therefore, theforensic clinician must collect all data, consider differentialdiagnoses, and then assess if the available evidence is com-patible or not with the history provided by a complainant.3
It is known that police approach to the rape crime issignificantly influenced by the presence of injuries. However,the examiner clinicianmust emphasize in his/her report that“the absence of genital trauma does not preclude the possi-bility of nonconsensual sexual intercourse.” As health careproviders, we have an important obligation in ensuring that
Rev Bras Ginecol Obstet Vol. 42 No. 2/2020
Genital Injuries: Are They Telling us Something about Sexual Violence? Orellana 111

police officers fully understand the meaning and the signifi-cance of this assertion. Therefore, the same analysis that isdiscussed about genital injuries should be provided to thepolice, lawyers, the judiciary and the general public.42
Discussion
Many factors influence the presence or absence of genitalinjuries during a sexual assault, and therefore, they are notstrong evidence for this type of crime per se, but the exis-tence of a mutual consent among two – or more – peopleinvolved in an intercourse. Although two serious studiesdemonstrated a significant difference between consentedand nonconsented intercourse groups in prevalence of geni-tal injury, they have serious methodological issues that maybe affecting these results. Therefore, the presence or absenceof genital injury should not be used to render an opinionregarding consent to sexual intercourse.
There are many reports in the literature concerning theprevalence of genital injury following alleged sexual assault.Unfortunately, the variety of examination/visualization tech-niques, participant inclusion criteria, injury definitions, andtime to examination seen in these studies make them diffi-cult to assess and get to a convincing conclusion.16 Thus, it iscrucial to standardize the means used for detecting genitalinjuries, and to agree on injury definitions and examinationprotocols. The macroscopic genital examination may be theonly reliable way to detect differences in injury typology andpattern if they exist.35 Also, it must be emphasized theimportance of the time from sexual assault to examinationas it is used in trials as well.21
Regarding the severity or pattern of genital injuries andtheir association with the consent, some skepticism must beapplied to all research that tries to prove this association.25
Nevertheless, as a couple of studies reported that certaintype of injuries and their location were seen exclusively inthe nonconsensual group, further research is necessary toconfirm this. On the other hand, the presence of lesions inother parts of the body may be of greater importance thanminor genital injuries. Hence, this reinforces the idea that acomplete physical examination is neededwhenwe care for avictim of sexual violence.
Finally, the lack of injuries highlights the importance ofensuring that all those who are involved in these cases, suchas medical and legal professionals, police officers, and thepublic in general, are aware that injury is absolutely not anecessary outcome of sexual violence.2
Conclusion
In conclusion, it is important to emphasize that the absenceof genital lesions does not translate the absence of sexualviolence. This is something that we, as healthcare profes-sionals, must be sensitive to and aware of, especially know-ing the reality of the legal framework in our LAC region.Therefore, the forensic examination, although relevant, mustbe accompanied by other social, psychological, medical, etc.evaluations and care by the corresponding professionals to
give evidence of the occurrence of a sexual assault as well asto give a comprehensive, holistic management to the victim.
Conflict of InterestsThe author has no conflict of interests to declare.
References1 Ingemann-Hansen O, Charles AV. Forensic medical examination
of adolescent and adult victims of sexual violence. Best Pract ResClin Obstet Gynaecol 2013;27(01):91–102. Doi: 10.1016/j.bpob-gyn. 2012.08.014
2 KennedyKM.Heterogeneity of existing research relating to sexualviolence, sexual assault and rape precludes meta-analysis ofinjury data. J Forensic Leg Med 2013;20(05):447–459. Doi:10.1016/j.jflm.2013.02.002
3 WhiteC.Genital injuries inadults.BestPractResClinObstetGynaecol2013;27(01):113–130. Doi: 10.1016/j.bpobgyn.2012.08.011
4 Lenahan LC, Ernst A, Johnson B. Colposcopy in evaluation of theadult sexual assault victim. Am J EmergMed 1998;16(02):183–184
5 Kelly DL, Larkin HJ, Paolinetti LA. Intra- and inter-rater agreementof the Genital Injury Severity Scale. J Forensic Leg Med 2017;52:172–180. Doi: 10.1016/j.jflm.2017.09.011
6 Walker G. The (in)significance of genital injury in rape and sexualassault. J Forensic Leg Med 2015;34:173–178. Doi: 10.1016/j.jflm.2015.06.007
7 Fraser IS, Lähteenmäki P, ElomaaK, LacarraM,MishellDR Jr, AlvarezF, et al. Variations in vaginal epithelial surface appearance deter-minedbycolposcopic inspection inhealthy, sexually activewomen.Hum Reprod 1999;14(08):1974–1978. Doi: 10.1093/humrep/14.8.1974
8 Colvin CW, Abdullatif H. Anatomy of female puberty: The clinicalrelevance of developmental changes in the reproductive system.Clin Anat 2013;26(01):115–129. Doi: 10.1002/ca.22164
9 Adams JA, Farst KJ, KelloggND. Interpretation ofmedicalfindings insuspected child sexual abuse: an update for 2018. J Pediatr AdolescGynecol 2018;31(03):225–231. Doi: 10.1016/j.jpag.2017.12.011
10 Gallion HR, Milam LJ, Littrell LL. Genital findings in cases of childsexual abuse: genital vs vaginal penetration. J Pediatr AdolescGynecol 2016;29(06):604–611. Doi: 10.1016/j.jpag.2016.05.001
11 Jewkes R, Sen P, Garcia-Moreno C. Sexual violence. In: Krug EG,Dahlberg LL, Mercy JA, Zwi AB, Lozano R, editors. World report onviolence and health. Geneva: World Health Organization; 2002:147–181
12 Contreras JM, Bott S, Guedes A, Dartnall E. Sexual violence in LatinAmerica and the Caribbean: a desk review [Internet]. Pretoria:Sexual Violence Research Initiative; 2010 [cited 2019 Aug 25].Available from: http://www1.paho.org/hq/dmdocuments/2010/sexual_violence_LA_Caribbean_e.pdf
13 Montaño S, Alméras D, Aranda V. No more! The right of women tolive a life free of violence in Latin America and the Caribbean[Internet]. 2007 [cited 2019 Aug 25]. Available from: https://repo-sitorio.cepal.org/bitstream/handle/11362/2863/S2007616_en.pdf?sequence=1
14 Ministerio de Justicia. Ley N° 19.617 de 02 de julio de 1999.Modifica el Codigo Penal, el Codigo de Procedimiento Penal y otroscuerpos legales en materias relativas al delito de violación.Santiago: Ministerio de Justicia; 1999
15 Kelly DL, Larkin HJ, Cosby CD, Paolinetti LA. Derivation of theGenital Injury Severity Scale (GISS): a concise instrument fordescription and measurement of external female genital injuryafter sexual intercourse. J Forensic Leg Med 2013;20(06):724–731. Doi: 10.1016/j.jflm.2013.04.012
16 Zilkens RR, Smith DA, PhillipsMA,Mukhtar SA, Semmens JB, KellyMC. Genital and anal injuries: A cross-sectional Australian studyof 1266 women alleging recent sexual assault. Forensic Sci Int2017;275:195–202. Doi: 10.1016/j.forsciint.2017.03.013
Rev Bras Ginecol Obstet Vol. 42 No. 2/2020
Genital Injuries: Are They Telling us Something about Sexual Violence? Orellana112

17 Slaughter L, Brown CRV, Crowley S, Peck R. Patterns of genitalinjury in female sexual assault victims. Am J Obstet Gynecol 1997;176(03):609–616. Doi: 10.1016/s0002-9378(97)70556-8
18 Dalton M, Ed. Forensic gynaecology: advanced skills series. Cam-bridge: Cambridge University Press; 2015
19 McCann J, Miyamoto S, Boyle C, Rogers K. Healing of nonhymenalgenital injuries in prepubertal and adolescent girls: a descriptivestudy. Pediatrics 2007;120(05):1000–1011. Doi: 10.1542/peds.2006-0230
20 MaguireW,Goodall E,MooreT. Injury in adult female sexual assaultcomplainants and related factors. Eur J Obstet Gynecol Reprod Biol2009;142(02):149–153. Doi: 10.1016/j.ejogrb.2008.10.005
21 Anderson SL, Parker BJ, BourguignonCM. Changes in genital injurypatterns over time in women after consensual intercourse.J Forensic Leg Med 2008;15(05):306–311. Doi: 10.1016/j.jflm.2007.12.007
22 Astrup BS, Ravn P, Lauritsen J, Thomsen JL. Nature, frequency andduration of genital lesions after consensual sexual intercourse–implications for legal proceedings. Forensic Sci Int 2012;219(1-3):50–56. Doi: 10.1016/j.forsciint.2011.11.028
23 American Academy of Pediatrics. Supplemental Information Ap-pendix. Conditions that may be mistaken for child sexual abuse.Pediatrics 2013;132(02):s1–s8
24 Masters WH, Johnson VE. The human female: anatomy of sexualresponse. Minn Med 1960;43:31–36
25 Anderson JC, Sheridan DJ. Female genital injury following con-sensual and nonconsensual sex: state of the science. J Emerg Nurs2012;38(06):518–522. Doi: 10.1016/j.jen.2010.10.014
26 Anderson S, McClain N, Riviello RJ. Genital findings of womenafter consensual and nonconsensual intercourse. J Forensic Nurs2006;2(02):59–65. Doi: 10.1111/j.1939-3938.2006.tb00060.x
27 Rook P,Ward R. Rook andWard on sexual offences: law& practice.5th ed. London: Sweet & Maxwell; 2016
28 Gidycz CA, Van Wynsberghe A, Edwards KM. Prediction of wom-en’s utilization of resistance strategies in a sexual assault situa-tion: a prospective study. J Interpers Violence 2008;23(05):571–588. Doi: 10.1177/0886260507313531
29 Larsen ML, Hilden M, Lidegaard Ø. Sexual assault: a descriptivestudy of 2500 female victims over a 10-year period. BJOG 2015;122(04):577–584. Doi: 10.1111/1471-0528.13093
30 Adams JA, Botash AS, Kellogg N. Differences in hymenal morphol-ogy between adolescent girls with and without a history of
consensual sexual intercourse. Arch Pediatr Adolesc Med 2004;158(03):280–285. Doi: 10.1001/archpedi.158.3.280
31 Kellogg ND, Menard SW, Santos A. Genital anatomy in pregnantadolescents: “normal” does not mean “nothing happened”. Pedi-atrics 2004;113(1 Pt 1):e67–e69. Doi: 10.1542/peds.113.1.e67
32 Sommers MS. Defining patterns of genital injury from sexualassault: a review. Trauma Violence Abuse 2007;8(03):270–280.Doi: 10.1177/1524838007303194
33 McLean I, Roberts SA, White C, Paul S. Female genital injuriesresulting from consensual and non-consensual vaginal inter-course. Forensic Sci Int 2011;204(1-3):27–33. Doi: 10.1016/j.forsciint.2010.04.049
34 Astrup BS, Ravn P, Thomsen JL, Lauritsen J. Patterned genitalinjury in cases of rape–a case-control study. J Forensic Leg Med2013;20(05):525–529. Doi: 10.1016/j.jflm.2013.03.003
35 Lincoln C, Perera R, Jacobs I, Ward A. Macroscopically detectedfemale genital injury after consensual and non-consensual vagi-nal penetration: a prospective comparison study. J Forensic LegMed 2013;20(07):884–901. Doi: 10.1016/j.jflm.2013.06.025
36 Jones JS, Rossman L, Hartman M, Alexander CC. Anogenitalinjuries in adolescents after consensual sexual intercourse.Acad Emerg Med 2003;10(12):1378–1383. Doi: 10.1197/S1069-6563(03)00555-4
37 Anderson SL, Parker BJ, Bourguignon CM. Predictors of genitalinjury after nonconsensual intercourse. Adv Emerg Nurs J 2009;31(03):236–247. Doi: 10.1097/TME.0b013e3181afd306
38 Kongtanajaruanun N, Teerapong S, Janpanichjaroen A. Femalegenital injury resulting from consensual and non-consensualvaginal intercourse at Police General Hospital. J Med Assoc Thai2018;101(01):7–12
39 Hilden M, Schei B, Sidenius K. Genitoanal injury in adult femalevictims of sexual assault. Forensic Sci Int 2005;154(2-3):200–205.Doi: 10.1016/j.forsciint.2004.10.010
40 White C, McLean I. Adolescent complainants of sexual assault;injury patterns in virgin and non-virgin groups. J Clin ForensicMed 2006;13(04):172–180. Doi: 10.1016/j.jcfm.2006.02.006
41 Hoffman RJ, Ganti S. Vaginal laceration and perforation resultingfrom first coitus. Pediatr Emerg Care 2001;17(02):113–114. Doi:10.1097/00006565-200104000-00009
42 Kennedy KM. The relationship of victim injury to the progressionof sexual crimes through the criminal justice system. J ForensicLeg Med 2012;19(06):309–311. Doi: 10.1016/j.jflm.2012.04.033
Rev Bras Ginecol Obstet Vol. 42 No. 2/2020
Genital Injuries: Are They Telling us Something about Sexual Violence? Orellana 113

Metachronic Breast and Cerebellar Neoplasm ina Young Patient
Neoplasias mamária e cerebelar metacrônicas em umapaciente jovemJéssika de Oliveira Nascimento1 Lara Caroline Anastacio Haro1 Rafael da Silva Sá1
Rebeca Espelho Storch1
1Universidade do Oeste Paulista, Presidente Prudente, SP, Brazil
Rev Bras Ginecol Obstet 2020;42(2):114–119.
Address for correspondence Jéssika de Oliveira Nascimento, Studentof Medicine, Rua Albert Scheitzer, 965, Vila Formosa, Universidade doOeste Paulista, Presidente Prudente, SP 19050-030, Brazil(e-mail: [email protected]).
Keywords
► medulloblastomadesmoplastic
► breast cancer► carcinoma mucinous
mammary► Li-Fraumeni
syndrome
Abstract Several factors trigger the development of genetic mutations that are responsible forcausing a neoplasm. Medulloblastoma is a malignant and invasive cerebellar neoplasm,that affects children and young adults. Mucinous carcinoma is a special type of breastcancer. Being a special atypical subtype of invasive carcinoma, it most frequentlyaffects women of advanced age and represents 1 to 7% of all breast cancers. Thereported case aims to show the rarity of the occurrence of desmoplastic medulloblas-toma and mammary mucinous carcinoma in a young patient in a short period of time,in different sites, without direct anatomical attachment and without occurrence ofmetastasis. Initially, this patient had a desmoplastic medulloblastoma and was treatedwith lumpectomy and radiotherapy. After 13months, the patient was diagnosed with amucinous breast carcinoma, underwent mastectomy, adjuvant chemotherapy and iscurrently undergoing endocrinotherapy. We conclude, based on the metachronouscharacteristic of the neoplasia and clinical characteristics, that the patient is likely tohave Li-Fraumeni syndrome, an autosomal dominant disease withmutation of the TP53gene, which is the the main involved. Because the patient does not present all thecharacteristics of the phenotype of the syndrome, she can thus be classified as havingLi-Fraumeni variant or Li-Fraumeni-like syndrome.
Resumo Diversos fatores desencadeiam o desenvolvimento de mutações genéticas que sãoresponsáveis por originar uma neoplasia. Omeduloblastoma é uma neoplasia cerebelarmaligna e invasiva que acomete crianças e adultos jovens. O carcinomamucinoso é umtipo de câncer de mama especial por ser um subtipo atípico de carcinoma invasivo, queacomete com maior frequência mulheres de idade avançada e representa entre 1 a 7%do total de neoplasias mamárias. O caso relatado tem como objetivomostrar a raridadeda ocorrência do meduloblastoma desmoplásico e carcinoma mucinoso mamário emuma paciente jovem em um curto período de tempo, em diferentes sítios sem ligaçãoanatômica direta e sem ocorrência de metástase. Inicialmente, esta paciente possuíaum meduloblastoma desmoplásico e foi tratada com tumorectomia e radioterapia.
receivedAugust 6, 2019acceptedNovember 25, 2019
DOI https://doi.org/10.1055/s-0040-1701456.ISSN 0100-7203.
Copyright © 2020 by Thieme RevinterPublicações Ltda, Rio de Janeiro, Brazil
Case ReportTHIEME
114

Introduction
Neoplasias originate from the union of several factors:genetic, psychological, environmental, habits, and addic-tions. The association of these factors leads the individualto develop mutations in the genes, generating a rapid cellproliferation and, consequently, forming a tumor mass.1
Neoplastic cells have mutations in the mechanisms of cellcycle control, especially the structures involved in DNArepair, and in the mechanism of apoptosis, thus occurringto the proliferation of a damaged cell. The stimulus for thisproliferation inmost neoplasias is still unknown.2 Cancer canbe considered an isolated genetic disease, being character-ized by hereditary cancer syndromes, which created thedominant autosomal disorders (50% of the chance of trans-mission of genes related to one of the offspring syndromes ineach pregnancy), that make malignant neoplasms prevalentin individuals from the same family. Some characteristics areassociated with hereditary cancer, such as early age atdiagnosis, more than one neoplasm in the same individual,several members of the same family presenting the same orrelated neoplasms, and multiple generations affected.3,4
Patients with more than one type of neoplasia can beclassified intotwotypes: synchronous tumorormetachronoustumor. Metachronic tumors are found in the follow-up ofpatients already submitted to surgical resection, evidentlyexcluding the possibility of undiagnosed lesion at the timeofdiagnosis or recurrenceof theoperated tumor.5Theprimarysynchronic tumor is defined when it occurs simultaneouslywith the index tumor (thefirst tumor identified in the patient)or when it is identifiedwithin 6 months after discovery of theindex tumor. When this period exceeds 6 months, the case isconsidered as a primary metachronous tumor.6 Multipleprimary tumors present an incidence of 2 to 17%, and someof the risk factors are: changes in germ line, exposure totherapies, occupational risks, and lifestyle influences.7
Medulloblastoma is a malignant and invasive cerebellarneoplasm that manifests in children and young adults withdissemination through the cerebrospinal fluid.8,9 Amongadults, 80% occur between 21 and 40 years of age. Accordingto the World Health Organization (Louis et al, 2007),10
medulloblastomas are classified histologically into 5 types:desmoplastic/nodular (pale islands, highly proliferative cells,nodules with reduced cellularity), extensive nodular, classic,large cell, and anaplastic.11,12
The nodular/desmoplastic medulloblastoma has charac-teristics that distinguish it from typical tumors, since it isusually well circumscribed, contains a large amount ofreticulin fibers and, when completely removed, has a betterprognosis.13 It is mainly located in the cerebellar hemispherebut may also be located in the cerebellar vertebra.14 Someauthors consider less aggressive histological alterations dueto the lower occurrence of necrosis, lower mitotic index, andnuclear alterations are classified as mild when comparedwith the group of classical medulloblastomas.13
The clinical picture is insidious and progressive, makingthe patient complain of lumbar or radicular pain, seizures,cranial hypertension, and focal medullary or encephalicsymptoms due to neoplastic implants. Headache appearsas a predominant symptom in adults with this type of tumor.Imbalance, gait disturbance, dizziness, and/or nausea andvomiting are common. Other symptoms rarely referred to inadults are diplopia, loss of limb strength, tinnitus, deafness,photophobia, secondaryamenorrhea,mental confusion, syn-cope, visual blurring or blindness, drowsiness, nuchal anddorsal pain, dysarthria, dysphagia, maxillary, urinary incon-tinence, weight loss, and partial or generalized epilepticseizures.15 Surgery is the most important aspect of medul-loblastoma treatment, and tumor resection is ideal.12
Breast cancer is the secondmost common type of cancer inthe general population, just behind basal -cell skin cancer. TheNational Cancer Institute estimates that 59,700 new cases ofbreastcancerwill beexpected in2018, corresponding to29%offemale cancers, in Brazil.16 Mucinous cancer, also known ascolloid carcinoma of the breast, is considered an atypicalsubtype of invasive carcinoma; it affects more frequentlywomen of advanced age and represents 1 to 7% of the totalof mammary neoplasias9. Mucins are complex carbohydratesreleased by connective tissue cells and mainly by specializedepithelial cells. They represent themain constituent of mucusand play a protective role in tissues composed of epithelialcells. In addition to the protection factor, they are involved inprocesses of epithelial differentiation, cellular signaling andcellular adhesionmodulation.17Within themucinous tumors,there is differentiation between carcinoma of pure form andcarcinoma of mixed form. The carcinoma of pure form showsthe mucinous arrangement in practically the entire tumoralextent, while the carcinoma of mixed form has a greaterextension of neoplastic cells not surrounded by mucin. Thehigher the amount of mucin the better the prognosis.9
Após 13 meses, a paciente foi diagnosticada com carcinoma mucinoso de mama,sendo submetida a mastectomia, quimioterapia adjuvante e atualmente está sendotratada com endocrinoterapia. Concluímos, com base na característica metacrônica daneoplasia e características clínicas, que a paciente apresenta a síndrome de Li-Fraumeni, doença autossômica dominante com mutação do gene TP53, que é oprincipal gene envolvido nesta síndrome. Por não apresentar as característicascompletas do fenótipo da síndrome, a paciente pode assim ser classificada comoportadora de uma variante da síndorme de Li-Fraumeni ou síndrome do tipo Li-Fraumeni.
Palavras-chave
► meduloblastomadesmoplásico
► câncer de mama► carcinoma
mucinoso mamário► síndrome de Li-
Fraumeni
Rev Bras Ginecol Obstet Vol. 42 No. 2/2020
Metachronic Breast and Cerebellar Neoplasm in a Young Patient Nascimento et al. 115

The objective of the present work is to identify andanalyze the relationship between a nodular/desmoplasticmedulloblastoma (grade IV) and the subsequent develop-ment of intermediate grade mammary mucinous carcinomain a young patient, considering that there was no metastasisinvolved between the distinct anatomical periods and loca-tions and that there was no direct correlation.
The case report was approved by the local Research EthicsCommittee under CAAE 04155318.6.0000.5515 and CEPOpinion Number 3,193,241.
Case Description
The patient is female, 29 years old, Caucasian, single, hair-dresser, natural and from Sandovalina, SP. Patient deniesfamily history of neoplasms. She consulted with a neurolo-gist due to a complaint of headache, vertigo, blurred vision,ataxia, without episodes of syncope or lipothymia. Magneticresonance imaging (MRI) of the skull revealed an expansivelesion in the posterior fossa with epicenter in thecerebellar/IV ventricle, which was a cystic and solid, causingerasure of the IV ventricle and a mild/moderate supraven-tricular hydrocephalus. After anatomopathological exami-nation (macroscopy reveals an irregular portion of tissue,measuring 2.5�2 cm, with a smooth grayish surface. At cuts,the surface is whitish and firm-elastic in consistency, alsoaccompanied by several irregular tissue fragments, measur-ing 2�1 cm together and of light brown color and firmconsistency (►Fig. 1). On microscopy, we observed thepresence of malignant neoplasia consisting of oval cellswith hyperchromatic nuclei, well-marked nuclear mem-
branes, and scarce cytoplasmwith pseudo-rosettes; the cellsexhibited several atypical figures of mitoses, the vascularnetwork consisted of thin capillary vessels, and there waspresence of irregular areas of necrosis (►Fig. 2). In theimmunohistochemistry (GCDFP-15 antigen negative, Ki-67antigen indicating high cell proliferation index and synapto-physin antigen diffusely positive) examination, there wascompatibility with nodular/desmoplastic medulloblastoma.The patient was submitted to lumpectomy with adjuvantradiotherapy, which was started 4 months after the surgicalprocedure (29 sessions).
Thirteen months after the neurological lesion, the patientwas referred to the division of mastology due to palpablelump in the left breast. The bilateral mammography report,performed 3 months previously, presented microcalcifica-tions with discrete grouping in the upper left quadrant andan imagewith nodular effect in the upper left quadrant to theleft of themean density and partially defined contours, beingclassified as category 3 of the breast, imaging, reporting anddata system (BI-RADS). Physical examination showed ahardened nodule in the periareolar left lateral quadrantmeasuring 3 cm, free axillae and absence of papillary effu-sion (clinical staging: T2N0M0 - IIA). The histopathologicalpattern (multifocal lesion, being larger than 2.5 cm andsmaller than 0.9 cm in diameter, all whitish colors, finelygrainy surface, firm consistency and unctuous appearance)associated with the immunohistochemical profile (CerbB-2oncoprotein antigen negative [score 1], Ki-67 antigen mod-erate cell proliferation index, estrogen receptor antigenpositive in 90% of neoplastic cells, progesterone receptorantigen positive in 50% of neoplastic cells) was compatiblewith mammary mucinous carcinoma, intermediate grade,infiltrative, with approximate molecular classification ofluminal A. Due to its location, tumor size and tumor-breastratio, the patient underwent a mastectomy associated withthe left sentinel lymph node biopsy (benign to biopsy) andadjuvant chemotherapy (4 cycles of doxorubicin 108mg andcyclophosphamide 1,080mg combined with 4 cycles of
Fig. 2 Cerebellar tumor slide (600x magnification) showing oval cellswith hyperchromatic nuclei, well-marked nuclear membranes, andscarce cytoplasm with pseudo-rosettes.
Fig. 1 Magnetic resonance imaging of the skull shows expansivelesion in the posterior fossa with epicenter in the cerebellar vermis/IVventricle, solid and cystic.
Rev Bras Ginecol Obstet Vol. 42 No. 2/2020
Metachronic Breast and Cerebellar Neoplasm in a Young Patient Nascimento et al.116

docetaxel 100mg / m2). Currently, tamoxifen is being usedcontinuously (20mg/day).
Discussion
Medulloblastoma has a strong tendency of disseminationalong the cerebrospinal pathways. The extraneural or sys-temic spread is rare; when it occurs, the most common sitesare bone marrow, bones, peritoneum, lungs, and liver, re-spectively.18 Therefore, medulloblastoma metastasis tobreasts tissue is considered uncommon. However, in 2010,Ternier et al19 described the case of a 29-year-old womanwho developed a medulloblastoma and later breast carcino-ma. The results of the immunohistochemistry establishedthat metastasis had occurred, confirming the primary site.
In the clinical description of the case discussed in thepresent study, one patient presented breast mucinous lumpcancer posterior to the medulloblastoma, and, according tothe literature, extraneural dissemination of this tumor israre. The possibility that this patient was a case of meta-stasizationwas ruled out choice of use distinct bonds, havinga different immunohistochemistry and showing no relationbetween the tumors. Consideration should be given to thepossibility of the patient having a genetic mutation ofimportant cell division regulating genes, namely: growthpromoters, cell growth inhibitors, andgenes that regulate the
cell cutting program.20 Among them, we highlight the cellgrowth inhibitory genes, also called tumor suppressors, inwhich themain alteration is in the TP53 gene (encoder of p53protein—this protein has several antitumor effects, remainsgenetic, and inhibits angiography through cellular apopto-sis). Therefore, with a mutation of this gene, there is noefficient DNA repair, thus contributing to the formation ofabnormal cells.20,21
Due to the fact that the patient presented tumors indifferent primary sites, a hypothesis was formed that thepatient was a carrier of the Li-Fraumeni syndrome (LFS), anautosomal dominant disease in which the TP53 mutation isthe main gene involved.22 Li-Fraumeni syndrome relates tothe diagnosis of various types of tumors in young patients,multiple primary tumors, and a characteristic pattern offamily grouping of a variety of cancers (central tumorsincluding: bone and soft tissue sarcomas, central nervoussystem tumors, leukemia, adrenocortical carcinoma, andbreast cancer). This syndrome differs from other hereditarycancer syndromes because it is not related to a specific typeof cancer, but to a broad spectrum of tumors.23 Syndromevariants include LFS1, LFS2 and LFS-like (LFSL).21
In the South and Southeast regions of Brazil, there is ahigh frequency of Li-Fraumeni and Li-Fraumeni-like syn-dromes, because most of the population in these areas is ofEuropean origin. The hypothesis of a possible founding
Table 1 Clinical criteria for Li-Fraumeni and Li-Fraumeni-like syndromes
Clinical criteria Description
Classical Li-Fraumeni I-sarcoma diagnosed in childhood/young adulthood (� 45 years) andII-first-degree relative with any cancer in young adulthood (� 45 years) andIII-first- or second-degree relative with any cancer diagnosed in young adulthood (� 45 years) orsarcoma diagnosed at any age.
Li-Fraumeni-like – criteriaof Birch
I-childhood cancer (at any age) or sarcoma, CNS (tumor, or ACC in young adulthood (� 45 years) andII-first- or second-degree relative with LFS-spectrum cancer (sarcoma, breast cancer, CNS tumor,ACC, leukemia) at any age andIII-first- or second-degree relative with any cancer diagnosed at age< 60 years
Li-Fraumeni-like – criteriaof Eeles 1, Eeles 2
I-at least 2 first- or second-degree relatives with LFS-spectrum cancer (sarcoma, breast cancer, CNStumor, ACC, leukemia, melanoma, prostate cancer, pancreatic cancer) diagnosed at any ageII-sarcoma diagnosed at any age andIII-at least 2 other tumors diagnosed in one or more first- or second-degree relatives: BC at age< 50years; CNS tumor, leukemia, ACC, melanoma, prostate cancer, pancreatic cancer at age< 60 years;or sarcoma at any age.
Li- Fraumeni-like – criteriaof Chompret
I-diagnosis of sarcoma, CNS tumor, breast cancer, ACC at age< 36 years andII-first- or second-degree relative with any of the above cancers (except BC if proband had BC) orrelative with multiple primary tumors at any age orIII-multiple primary tumors, including two of the following: sarcoma, CNS tumor, BC, or ACC, withthe first tumor diagnosed at age<36 years regardless of family history; orIV-ACC at any age, regardless of family history.
Li-Fraumeni-like – criteriaof Modified Chompret
I-index case with LFS-spectrum cancer (sarcoma, breast cancer, CNS tumor, ACC, leukemia,bronchioloalveolar carcinoma) occurring at age<46 years andII-a first- or second-degree relative with LFS-spectrum cancer occurring at age< 56 years (except BCif the index case has BC as well), or multiple tumors; orIII-index patient with multiple tumors, at least two of which are in the LFS spectrum, the firstoccurring at age<46 years; orIV-ACC or choroid plexus carcinoma occurring at any age or BC occurring at age<36 years withoutBRCA1 or BRCA2 mutations.
Abbreviations: ACC, adrenocortical carcinoma; BC, breast cancer; CNS, central nervous system; LFS, Li-Fraumeni syndrome.Source: Giacomazzi et al.23
Rev Bras Ginecol Obstet Vol. 42 No. 2/2020
Metachronic Breast and Cerebellar Neoplasm in a Young Patient Nascimento et al. 117

mutation, also called the founding effect, was raised, that is,there was a first carrier of the mutation that spread to thepopulations of the South and Southeast of Brazil. This factcan be explained by the Brazilian colonization. At the end ofthe 17th century, the southern region received Portugueseimmigrants, known as “drovers;” they created routes to-ward the southeastern region to trade cattle and consumergoods. Thus, although the insertion of a mutant Portugueseallele in the colonization period took place when thepopulation was small, it led to a currently significantprevalence in the population.22,24
The patient in this report does not have complete char-acteristics of the phenotype of the syndrome, and can thus beclassified as having Li-Fraumeni variant or Li-Fraumeni-like(individuals with no detectable mutations in the P53 proteinof the gene TP53), subclassified by the Chompret criteria,which is characterized by multiple primary tumors, with atleast 2 tumors being in the group: sarcoma, a tumor of thecentral nervous system, breast cancer, or adrenocorticalcarcinoma, regardless of family history; these should bediagnosed before 36 years of age.21,22 Other clinical criteriafor diagnosis of the syndrome are briefly described in►Table 1.
The most frequent tumors in the TP53 gene mutation are,respectively, breast, soft-tissue sarcomas, adrenocortical,and central nervous system, among others. Up to 30% ofwomen with the syndrome are affected, characterizing agreat importance in the diagnosis of breast cancer in womenwith the syndrome and mutation of the TP53 gene.22 It isrecommended that these patients are referred to a geneticist,seek a detailed family register, perform a screening for newcancers and clarify the risks. Psychologicalmonitoring is veryimportant as it can cause anxiety or depression.21
Conclusion
Due to the metachronous characteristic of the neoplasia andthe clinical presentation displayed by the patient, we con-cluded that she probably carries Li-Fraumeni syndrome, anautosomal dominant disease. However, the patient of thisreport does not have complete characteristics of the pheno-type of the syndrome, and can thus be classified as having Li-Fraumeni variant or Li-Fraumeni-like syndrome; however, asa consequence of the lack of local resources of the UnifiedHealth System (it does not offer the service of medicalgenetics), it was not possible to confirm the mutation ofthe TP53 gene. The positivity of the test would be very usefulto the family of this patient, to hereditary investigation andprimary and secondary prevention of some neoplasias in-cluded in the Li-Fraumeni syndrome group. Unfortunately,the reality is discordant: few medical centers outside thestate capitals have the ability to perform genetic mutationtests. In fact, this case report has relevance for the medicalcommunity to elucidate a pathology little known among thepopulation.
Conflict of InterestsThe authors have no conflicts of interest to declare.
References1 Borges ADVS, Silva EF, Mazer SM, Toniollo PB, Valle ERM, Santos
MA. Percepção da morte pelo paciente oncológico ao longo dodesenvolvimento. Psicol Estud 2006;11(02):361–369. Doi:10.1590/S1413-73722006000200015
2 Rubin E, Gorstein F, Rubin R, Schwarting R, Strayer D. Rubin,patologia: bases clinicopatológicas da medicina. 4a ed. Rio deJaneiro: Guanabara Koogan; 2006
3 Dantas ELR, Sá FHL, Carvalho SMF, Arruda AP, Ribeiro EM, RibeiroEM. Genética do câncer hereditário. Rev Bras Cancerol 2009;55(03):263–269
4 Lassance FAC, Lassance PMS, Garicochea B, Cotti GCC, Cutait R.Câncer colorretal e síndromes hereditárias. Rev Medicina SaúdeBrasília 2012;1(01):34–50
5 Andrade SMS, Pereira FL. Câncer colorretal sincrônico: relato decaso e revisão de literatura. Rev Bras Coloproctol 2007;27(01):69–79. Doi: 10.1590/S0101-98802007000100010
6 Dedivitis RA, Castro MAF, Denardin OVP. Tumores primáriosmúltiplos em pacientes com câncer de cabeça e pescoço. RevBras Cir Cabeça Pescoço. 2009;38(04):211–214
7 MartinM, Sabari JK, Turashvili G, Halpenny DF, Rizvi H, Shapnik N,et al. Next-generation sequencing based detection of germlineand somatic alterations in a patient with four metachronousprimary tumors. Gynecol Oncol Rep 2018;24:94–98. Doi:10.1016/j.gore.2018.04.004
8 Martin M, Sabari JK, Turashvili G, Halpenny DF, Rizvi H, Shapnik N,et al. Assistência multiprofissional ao paciente adulto portadorde meduloblastoma em terapia intensiva: um relato de caso. RevHCPA [Internet]. 2008 [cited 2018 Apr 23];28 Supl:76. Availablefrom: http://www.lume.ufrgs.br/bitstream/handle/10183/14592/000660369.pdf?sequence=1
9 Coeli GNM, Reis HF, Bertinetti DR, Faria FM, Tiezzi DG, OliveiraTMG. Mucinous carcinoma of the breast: iconographic essay withhistopathological correlation. Radiol Bras 2013;46(04):242–246.Doi: 10.1590/S0100-39842013000400011
10 Louis DN, Ohgaki H, Wiestler OD, Cavenee WK, Burger PC, AnneJouvet A, et al. The 2007 WHO classification of tumours of thecentral nervous system. Acta Neuropathol 2007;114(02):97–109.Doi: 10.1007/s00401-007-0243-4
11 Almeida GC. Análise das frequências dos subgrupos molecularesdos meduloblastomas e associações com possíveis fatores prog-nósticos [tese]. São Paulo: Universidade de São Paulo; 2014
12 Alves HB, Alves HB, Soares ARAP, Soares GC, Nascimento WG.Caracterização tumoral do meduloblastoma acometido na faseinfanto-juvenil [Internet]. Anais do 2° Congresso Brasileiro deCiências da Saúde; 2017 Jun 14–16 [cited 2018 Apr 23]; CampinaGrande, Brasil. Available from:https://editorarealize.com.br/revis-tas/conbracis/trabalhos/TRABALHO_EV071_MD1_SA11_ID1168_15052017204719.pdf
13 Stávale JN, Cruz JRS. Meduloblastoma desmoplásico: fatoreshistológicos de prognóstico. Arq Neuropsiquiatr 1993;51(04):487–490. Doi: 10.1590/S0004-282X1993000400010
14 FonteMVM, Amaral RPG, CostaMOR, Garcia OtaduyMC, Lucato LT,Reed UC, et al. Medulloblastoma: correlation among findings ofconventional magnetic resonance imaging, diffusion-weighted im-aging and proton magnetic resonance spectroscopy. Radiol Bras2008;41(06):373–378. Doi: 10.1590/S0100-39842008000600006
15 Franco CMR, Malheiros SMF, Gabbai AA. Meduloblastoma emadultos. Rev Neurociênc 1999;7(03):129–135
16 Ministério da Saúde. Instituto Nacional de Câncer José AlencarGomes da Silva. Estimativa 2018: incidência de câncer no Brasil.Rio de Janeiro: INCA; 2017
17 Zanetti JS, Ribeiro-Silva A. Carcinoma mucinoso invasor da mamae seus diagnósticos diferenciais em biópsia por agulha grossa:revisão da literatura. J Bras Patol Med Lab 2010;46(02):99–104.Doi: 10.1590/S1676-24442010000200005
18 Muoio VMF, Shinjo SO, Matushita H, Rosemberg S, Teixeira MJ,Marie SKN. Extraneural metastases in medulloblastoma. Arq
Rev Bras Ginecol Obstet Vol. 42 No. 2/2020
Metachronic Breast and Cerebellar Neoplasm in a Young Patient Nascimento et al.118

Neuropsiquiatr 2011;69(2B, 2b)328–331. Doi: 10.1590/S0004-282X2011000300012
19 Ternier F, Hadjaj D, Jacquemier J. Sonographic appearance of ametastasis to the breast from a cerebellar medulloblastoma. J ClinUltrasound 2010;38(06):335–337. Doi: 10.1002/jcu.20698
20 Pinto FN, Prudente FVB, Gonçalves MS, Silva PDV, Giglio A.Mutação do gene p53 induzindo predisposição hereditária aocâncer: relato de um caso da síndrome de Li-Fraumeni. Rev Med(São Paulo) 2002;81(1/4):42–46
21 Aedma SK, Kasi A. Li Fraumeni syndrome [Internet]. TreasureIsland (FL)StatPearls2019 [cited 2019 Sep 09]. Available from:https://www.ncbi.nlm.nih.gov/books/NBK532286/
22 Achatz MIASW. Modificadores de penetrância de mutações ger-minativas no gene TP53 em famílias brasileiras com diagnósticoclínico da síndrome de Li-Fraumeni e Li-Fraumeni like: impactodos polimorfismos intragênicos do TP53 e de genes [tese]. SãoPaulo: Universidade de São Paulo; 2008
23 Giacomazzi CR, Giacomazzi J, Netto CBO, Santos-Silva P, Selistre SG,Maia AL, et al. Pediatric cancer and Li-Fraumeni/Li-Fraumeni-likesyndromes: a review for the pediatrician. Rev Assoc Med Bras(1992) 2015;61(03):282–289. Doi: 10.1590/1806-9282.61.03.282
24 Achatz MI, Zambetti GP. The inherited p53 mutation in theBrazilian population. Cold Spring Harb Perspect Med 2016;6(12):a026195. Doi: 10.1101/cshperspect.a026195
Rev Bras Ginecol Obstet Vol. 42 No. 2/2020
Metachronic Breast and Cerebellar Neoplasm in a Young Patient Nascimento et al. 119

Instructions to AuthorsScope and policyAll content of the journal, except where otherwise noted, is licensed under a Creative Commons License.
The material submitted for analysis cannot be simultaneously submitted for publication in other journals or previously published. In the selection of man-uscripts for publication, are evaluated the originality, relevance of the theme, quality of the methodology used, and adequacy to the editorial standards adopted by the journal. The published material becomes intellectual prop-erty of the Brazilian Journal of Gynecology and Obstetrics and Febrasgo.
Manuscripts evaluation
The manuscripts submitted to the journal are received by the Editorial Offi ce that checks the mandatory documentation and examines if the edi-torial norms contained in the Instructions to Authors have been fulfi lled. If the process is in compliance, the manuscript is sent to the Editor-in-Chief, who will make a merit evaluation of the material. If the Editor-in-Chief concludes the work is in favorable scientifi c and technical conditions, the manuscript is forwarded to the Associate Editors, who will designate re-viewers (double mind process) to evaluate it. Then, the reviewers’ opin-ions and editor’s instructions are sent to authors to inform them about changes to be made. Then, the authors resubmit the text with the sug-gested changes within the requested deadline. When resubmitting the manuscript, the requested corrections should be highlighted in yellow. In cases of disagreement with the suggestions, observations should be included in the comments balloons. Be assertive and punctual with the inquiry, and support the hypothesis with references.
IMPORTANT! Authors must comply with the deadlines, since non-attend-ance will result in delay of manuscript publication or even archiving of the process. At any point in the process of analysis and editing of the text, the authors may request the process suspension and withdrawal of the manuscript, except when it is accepted for publication. The concepts and statements contained in the articles are of the authors’ responsibility.
Preparing a manuscript for submission
Mandatory submission documents
When submitting a manuscript to RBGO, attach the documents listed below on the ScholarOne submission platform. Note that not attach-ing the documents will result in cancellation of the submitted process. Mandatory documentation for online submission:
• Authorization of copyright transfer signed by all authors (scanned and attached as supplementary document) Model;
• In accordance with chapter XII.2 of Res. CNS 466/2012, in Brazil, research involving human subjects needs to inform the registration number referring to the Certifi cate of Ethical Assessment (CAAE) or the approval number of the research (CEP/CONEP) in the Ethics Committee. International manuscripts must present local ethical documentation to proceed with the submission process;
• Cover Letter: written to justify the publication. The authors should be identifi ed, together with the title of the team that intends to pub-lish, origin institution of the authors and intention of publication;
• Title page;
• Manuscript.
Title Page
• Title of the manuscript in English with a maximum of 18 words;
• Authors’ full name without abbreviations (maximum six);
• Corresponding author (full name, professional mailing address and contact email);
• Institutional affi liation of each author. Example: Faculty of Medicine, University of São Paulo, Ribeirão Preto, SP, Brazil;
• Confl icts of interest: authors should report any potential confl icts of interest whether political, economic, of resources for research execution or intellectual property;
• Acknowledgements: restricted to people and institutions that contrib-uted to research development in a relevant way. Any fi nancial support provided by development agencies or private companies should be men-tioned in the section Acknowledgments. For Brazilian authors, RBGO re-quests the citation of CNPq, Capes, FAPESP and other fi nancing agencies, together with the number of research process or granted scholarships.
• Contributions: according to the criteria for scientifi c authorship of the International Committee of Medical Journal Editors (ICMJE), authorship credit must be based on three conditions met in full: 1. Substantial contributions to conception and design, data collection or analysis, and interpretation of data; 2. Writing of the article or critical review of the in-tellectual content; and 3. Final approval of the version to be published.
ManuscriptInstructions to Authors
The Brazilian Journal of Gynecology and Obstetrics publishes the follow-ing categories of manuscripts:
Original Articles, complete prospective, experimental or retrospec-tive studies. Manuscripts containing original clinical or experimental research results have priority for publication.
Case Reports, of great interest and well documented from the clinical and laboratorial point of view. In the letter of referral, authors should in-dicate new or unexpected aspects in relation to already published cases. The text of Introduction and Discussion sections should be based on an updated bibliographic review.
Review Articles, including comprehensive reviews, meta-analysis or systematic reviews. Spontaneous contributions are accepted. The meth-ods and procedures adopted for obtaining the text should be described, and based on recent references, including the current year. As this sub-ject is still subject to controversy, the review should discuss the trends and lines of research under way. In addition to the text of the review, there should be an abstract and conclusions. See the ‘Instructions to Authors’ section for information on the text body and title page;
Letters to the Editor, dealing with editorial matters or not, but presenting relevant information to readers. Letters can be summarized by the editor, but maintaining the main points. In case of criticism to published works, the letter is sent to the authors so their reply can be published simultaneously;
Editorial, only at the publisher’s invitation.
Title
When writing a scientifi c article, the researcher should focus on the manuscript title, which is the business card of any publication. It should be elaborated very carefully, and preferably written only after the article fi nalization. A good title adequately describes the manuscript content. Generally it is not a phrase, because it does not contain the subject, only verbs and arranged objects. Titles rarely contain abbreviations, chemical formulas, adjectives, names of cities, among others. The title of manu-scripts submitted to RBGO must contain a maximum of 18 words.
Abstract
The abstract should provide the context or basis for the study, establish the objectives, basic procedures, main outcomes and key fi ndings. It should emphasize new and important aspects of the study or observa-tions. Since the abstract is the only substantive part of the article in-dexed in many electronic databases, authors should ensure it refl ects the article content in an accurate and highlighted manner. Do not use abbreviations, symbols and references in the abstract. In case of original articles from clinical trials, authors must inform the registration number at the end of the text.

Informational abstract of structured type of original articles
Abstracts of original articles submitted to RBGO must be structured in four sections and contain a maximum of 250 words:
Objective: What was done; the question posed by the investigator.
Methods: How it was done; the method, including the material used to achieve the objective.
Results: What was found, the main fi ndings and, if necessary, the sec-ondary fi ndings.
Conclusion: The conclusions; the answer to the question asked.
Informational abstract of structured type of systematic review articles
Among the included items are the review objective to the question asked, data source, procedures for selecting the studies and data collec-tion, the results and conclusions. The abstracts of systematic review ar-ticles submitted to RBGO must be structured in six sections and contain a maximum of 250 words:
Objective: Declare the main purpose of the article.
Data sources: Describe the data sources examined, including the date, indexing terms, and limitations.
Selection of studies: Specify the number of studies reviewed and the criteria used in their selection.
Data collection: Summarize the conduct used for data extraction and how it was used.
Data synthesis: State the main results of the review and the methods used to obtain them.
Conclusions: Indicate the main conclusions and their clinical usefulness.
Informational abstract of unstructured type of review articles, except systematic reviews and case studies
It shall contain the substance of the article, covering the purpose, method, results and conclusions or recommendations. It exposes enough details so readers can decide on the convenience of reading the full text (Limit of words: 150).
Keywords
The keywords of a scientifi c paper indicate the thematic content of the text they represent. The main objectives of the aforementioned terms are the thematic content identifi cation, indexing of the work in databases, and rapid location and retrieval of contents. The keyword systems used by RBGO are DeCS (Health Sciences Descriptors - Lilacs Indexer) and MeSH (Medical Subject Headings - MEDLINE-PubMed Indexer). Please choose fi ve descriptors that represent your work on these platforms.
Manuscript body (Manuscripts submitted to RBGO must have a maximum of 4000 words. Note that tables, charts and fi gures in the Results section and References are not counted).
Introduction
The Introduction section of a scientific article has the purpose of in-forming what was researched and the reason for the investigation. This part of the article prepares the reader to understand the investigation and justification of its realization. The content informed in this sec-tion should provide context or basis for the study (i.e. the nature of the problem and its importance); state the specific purpose, research objective, or hypothesis tested in the study or observation. The study objective usually has a more precise focus when formulated as a ques-tion. Both the primary and secondary objectives should be clear, and any analyzes in a pre-specified subgroup should be described; provide strictly relevant references only and do not include data or conclusions of the work being reported.
MethodsAccording to the Houaiss dictionary, Methods “is an organized, logical and systematic process of research”. The method comprises the ma-terial and procedures adopted in the research in order to respond to the central research question. Structure the Methods section of RBGO starting with the study design; research scenario (place and period in
which it was performed); sample of participants; data collection; in-tervention to be evaluated (if any) and the alternative intervention; statistical methods used and the ethical aspects of the study. When thinking about the writing of the study design, refl ect if it is appropri-ate to achieve the research objective, if the data analysis refl ects the design, and if what was expected with use of the design was achieved to research the theme. Following, the guidelines used in clinical or epi-demiological research that should be included in the section Methods of manuscripts sent to RBGO:
Types of study (adapted from Pereira, 2014*):
Case Report (Case study): In-depth investigation of a situation in which one or a few people are included (usually up to ten);
Case series: A set of patients (for example, more than ten people) with the same diagnosis or undergoing the same intervention. In general, these are consecutive series of patients seen in a hospital or other health institu-tion for a certain period. There is no internal control group formed simul-taneously. The comparison is made with external controls. The name of external or historical control is given to the group used to compare the results, but that was not constituted at the same time within the study: for example, the case series is compared with patients from previous years.
Transversal (or Cross-sectional) study: Investigation to determine prevalence; examine the relationship between events (exposure, dis-ease, and other variables of interest) at any given time. Cause and eff ect data are collected simultaneously: for example, the case series is com-pared with patients from previous years.
Case-control study: Particular form of etiological investigation of ret-rospective approach in which the search of causes starts from the ef-fects. Groups of individuals, respectively with and without a particular health problem are compared in relation to past exposures in order to test the hypothesis that exposure to certain risk factors is the contrib-uting cause of the disease. For example, individuals affl icted with low back pain are compared with an equal number of individuals (control group) of the same sex and age, but without low back pain.
Cohort study: Particular form of investigation of etiological factors in which the search of eff ects starts from the cause; therefore, the oppo-site of case-control studies. A group of people is identifi ed, and perti-nent information on the exposure of interest is collected, so the group can be monitored over time, checking those who do not develop the disease in focus, and if the prior exposure is related to occurrence of disease. For example, smokers are compared to nonsmoker controls; the incidence of bladder cancer is determined for each group.
Randomized study: This has the connotation of an experimental study to evaluate an intervention hence the synonym of intervention study. Can be performed in a clinical setting; sometimes referred to simply as clini-cal trial or clinical study. It is also conducted at the community level. In clinical trials, participants are randomly assigned to form groups called study (experimental) and control (or testimony), whether submitted or not to an intervention (for example, a drug or vaccine). Participants are monitored to verify the occurrence of outcome of interest. This way, the relationship between intervention and eff ect is examined under controlled observation conditions, usually with double-blind evaluation. In the case of a randomized study, inform the number of the Brazilian Registry of Clinical Trials (REBEC) and/or the number of the International Clinical Trials Registration Platform (ICTRP/OMS) on the title page.
Ecological study: Research performed with statistics: the unit of observa-tion and analysis is not constituted of individuals, but of groups of individuals hence the synonyms: study of groups, aggregates, clusters, statistics or com-munity. For example, research on the variation of mortality coeffi cients for diseases of the vascular system and per capita consumption of wine among European countries.
Systematic Review and Meta-analysis: Type of review in which there is a clearly formulated question, explicit methods are used to critically iden-tify, select and evaluate relevant research, and also to collect and analyze data from the studies included in the review. There is use of strategies to

limit bias in the localization, selection, critical evaluation and synthesis of relevant studies on a given topic. Meta-analysis may or may not be part of the systematic review. Meta-analysis is the review of two or more stud-ies to obtain a global, quantitative estimate of the question or hypothesis investigated; and employs statistical methods to combine the results of the studies used in the review.
Source: *Pereira MG. Artigos Científi cos – Como redigir, publicar e avaliar. Rio de Janeiro: Guanabara-Koogan; 2014.
Script for statistical review of original scientifi c papers
Study objective: Is the study objective suffi ciently described, including pre-established hypotheses?
Design: Is the design appropriate to achieve the proposed objective?
Characteristics of the sample: Is there a satisfactory report on the selection of people for inclusion in the study? Has a satisfactory rate of responses (valid cases) been achieved? If participants were followed up, was it long and complete enough? If there was a pairing (eg. of cas-es and controls), is it appropriate? How did you deal with missing data?
Data Collection (measurement of results): Were the measurement methods detailed for each variable of interest? Is there a description of comparability of the measurement methods used in the groups? Was there consideration of the validity and reproducibility of the methods used?
Sample size: Has adequate information on sample size calculation been provided? Is the logic used to determine the study size described, includ-ing practical and statistical considerations?
Statistical Methods: Was the statistical test used for each comparison informed? Indicate if the assumptions for use of the test were followed. Was there information about the methods used for any other analysis? For example, subgroup analysis and sensitivity analysis. Are the main results accompanied by accuracy of the estimate? Inform the p value and confi dence interval. Was the alpha level informed? Indicate the al-pha level below which the results are statistically signifi cant. Was the beta error informed? Or indicate the statistical power of the sample. Has the adjustment been made to the main confounding factors? Were the reasons that explained the inclusion of some and the exclusion of oth-ers described? Is the diff erence found statistically signifi cant? Make sure there are suffi cient analyzes to show the statistically signifi cant diff er-ence is not due to any bias (eg. lack of comparability between groups or distortion in data collection). If the diff erence found is signifi cant, is it also relevant? Specify the clinically important minimal diff erence. Make clear the distinction between statistically relevant diff erence and relevant clinical diff erence. Is it a one- or two-tailed test? Provide this information if appropriate. What statistical program is used? Inform the reference where to fi nd it, and the version used.
Abstract: Does the abstract contain the proper article synthesis?
Recommendation on the article: Is the article in acceptable statistical stand-ard for publication? If not, can the article be accepted after proper review?
Source: *Pereira MG. Artigos Científi cos – Como redigir, publicar e avaliar. Rio de Janeiro: Guanabara-Koogan; 2014.
IMPORTANT!
RBGO joined the initiative of the International Committee of Medical Journal Editors (ICMJE) and the EQUATOR Network, which are aimed to improve the presentation of research results. Check the following international guides:
Randomized clinical trial: http://www.consort-statement.org/downloads/consort-statement
Systematic reviews and meta-analysis: http://www.scielo.br/pdf/ress/v24n2/2237-9622-ress-24-02-00335.pdf
Observational studies in epidemiology: strobe-statement.org/fi lead-min/Strobe/uploads/checklists/STROBE_checklist_v4_combined.pdf
Qualitative studies: http://intqhc.oxfordjournals.org/content/19/6/349.long
Results
The purpose of the Results section is to show the study fi ndings. It is the original data obtained and synthesized by the author with the aim to answer the question that motivated the investigation. For the writing of the section,
present the results in logical sequence in the text, tables and illustrations, fi rst mentioning the most important findings. Do not repeat all information of the tables or illustrations in the text. Emphasize or summarize only important ob-servations. Additional or supplementary materials and technical details may be placed in an appendix where they will be accessible without interrupting the flow of the text. Alternatively, this information may be published only in the electronic version of the Journal. When data are summarized in the results section, provide numerical results not only in derived values (eg. percentages), but also in absolute values from which the derivatives were calculated, and specify the statistical methods used for their analysis. Use only the tables and figures necessary to explain the argument of the work and evaluate its foundation. When scientifically appropriate, include data analysis with variables such as age and sex. Do not exceed the maximum limit of fi ve tables, fi ve charts or fi ve figures. Tables, charts and/or figures should be included in the body of the manuscript and do not count the requested limit of 4000 words.
ATTENTION!In Case Studies, the Methods and Results sections should be replaced by the term Case Description.
DiscussionIn the Discussion section, emphasize the new and important aspects of the study and the conclusions derived therefrom. Do not repeat details of data or other information presented in the introduction or results sections. For experimental studies, it is useful to begin the discussion by briefly summarizing the main findings, comparing and contrasting the results with other relevant studies, stating the limita-tions of the study, and exploring the implications of the findings for future research and clinical practice. Avoid claiming precedence and referring to incomplete studies. Do not discuss data not directly related to the results of the presented study. Propose new hypotheses when justifiable, but qualify them clearly as such. In the last paragraph of the Discussion section, cite which information of your work contributes relatively to advancement of knowledge.
ConclusionThe Conclusion section has the function of relating the conclusions to the objectives of the study, but authors should avoid unfounded statements and conclusions not adequately supported by data. In particular, authors should avoid making statements about economic benefits and costs unless their original includes economic analysis and appropriate data.
ReferencesA study is based on the results of other research that preceded it. Once published, it becomes support for future work on the subject. In the report of their research, authors state the references of prior works consulted that they deem pertinent to inform readers, hence the im-portance of choosing good References. Properly chosen references lend credibility to the report. They are a source for convincing readers of the validity of facts and arguments presented.Attention! For manuscripts submitted to RBGO, authors should num-ber the references in order of entry into the manuscript and use those numbers for text citations. Avoid excessive references by selecting the most relevant for each statement and giving preference to the most recent work. Do not use hard-to-reach quotations, such as abstracts of papers presented at congresses, theses or restricted publications (non-indexed). Seek to cite the primary and conventional references (ar-ticles in scientifi c journals and textbooks). Do not use references such as ‘unpublished observations’ and ‘personal communication’. Authors’ publications (self-citation) should be used only if there is a clear need and relationship with the topic. In this case, include in bibliographical references only original works published in regular journals (do not cite chapters or revisions). The number of references should be 35, in ex-ception review articles. Authors are responsible for the accuracy of data contained in the references.Please check the Vancouver Citation Style to format your references.

*The Instructions to Authors of this journal were elaborated based in the literary work Artigos Científi cos: Como redigir, publicar e avaliar de Maurício Gomes Pereira, Editora Guanabara Koogan, 2014.
Submission of papers
The articles must, necessarily, be submitted electronically, accord-ing to the instructions posted on the site: http://mc04.manuscript-central.com/rbgo-scieloThere is no fee for submission and review articles.
Revista Brasileira de Ginecologia e ObstetríciaAddress: Brigadeiro Luiz Antonio Avenue, 3421, 01401-001, 903 room, Jardim Paulista, São Paulo, SP, Brazil. Phone: + 55 11 5573.4919 E-mail: editorial.offi [email protected] Home Page: https://www.thieme.com/rbgo