rationale for anti-angiogenic therapy in pheochromocytoma and paraganglioma
TRANSCRIPT

1 23
Endocrine Pathology ISSN 1046-3976Volume 23Number 1 Endocr Pathol (2012) 23:34-42DOI 10.1007/s12022-011-9189-0
Rationale for Anti-angiogenic Therapy inPheochromocytoma and Paraganglioma
Judith Favier, Peter Igaz, NellyBurnichon, Laurence Amar, RossellaLibé, Cécile Badoual, Frédérique Tissier,Jérôme Bertherat, Pierre-FrançoisPlouin, et al.

1 23
Your article is protected by copyright and
all rights are held exclusively by Springer
Science+Business Media, LLC. This e-offprint
is for personal use only and shall not be self-
archived in electronic repositories. If you
wish to self-archive your work, please use the
accepted author’s version for posting to your
own website or your institution’s repository.
You may further deposit the accepted author’s
version on a funder’s repository at a funder’s
request, provided it is not made publicly
available until 12 months after publication.

Rationale for Anti-angiogenic Therapy in Pheochromocytomaand Paraganglioma
Judith Favier & Peter Igaz & Nelly Burnichon &
Laurence Amar & Rossella Libé & Cécile Badoual &Frédérique Tissier & Jérôme Bertherat &Pierre-François Plouin & Xavier Jeunemaitre &
Anne-Paule Gimenez-Roqueplo
Published online: 20 December 2011# Springer Science+Business Media, LLC 2011
Abstract Pheochromocytomas and paragangliomas are high-ly vascularized tumors which are candidates for anti-angiogenictherapies. Several studies have reported the association ofvascular endothelial growth factor (VEGF) overexpressionwith malignancy, but none took into account the genetic statusof the patients or tumors, which may have a major influenceon such observations. Transcriptome studies indeed revealed
that pheochromocytomas and paragangliomas can be classi-fied into two major clusters depending on their gene expres-sion profile: Cluster 1 comprises samples associated with ahypoxic signature such as SDHx- and VHL-related tumors andcluster 2 includes RET, NF1, and TMEM127-mutated tumors,as well as most of sporadic tumors. The aim of this study wasto provide a comprehensive rationale for the targeting of
For submission for the Proceedings of the 3rd InternationalSymposium on Pheochromocytoma and Paraganglioma
J. Favier (*) :N. Burnichon : L. Amar : C. Badoual :P.-F. Plouin :X. Jeunemaitre :A.-P. Gimenez-RoqueploINSERM, UMR970, Paris Cardiovascular Research Center,Paris, Francee-mail: [email protected]
J. Favier :N. Burnichon :C. Badoual : F. Tissier :X. Jeunemaitre :A.-P. Gimenez-RoqueploUniversité Paris Descartes, Faculté de Médecine,Paris, France
P. Igaz2nd Department of Medicine, Faculty of Medicine,Semmelweis University,Szentkirályi str. 46,1088 Budapest, Hungary
N. Burnichon :X. Jeunemaitre :A.-P. Gimenez-RoqueploAssistance Publique-Hôpitaux de Paris,Hôpital Européen Georges Pompidou,Service de Génétique,Paris, France
L. Amar : P.-F. PlouinAssistance Publique-Hôpitaux de Paris,Hôpital Européen Georges Pompidou,Service d’Hypertension Artérielle,Paris, France
R. Libé : F. Tissier : J. BertheratINSERM, U567, Département d’Endocrinologie,Métabolisme & Cancer, Institut Cochin,Paris, France
R. Libé : J. BertheratAssistance Publique-Hôpitaux de Paris, Hôpital Cochin,Centre de Référence Maladies Rares de la Surrénale,Service des Maladies Endocriniennes et Métaboliques,Paris, France
R. Libé : J. Bertherat : P.-F. Plouin :A.-P. Gimenez-RoqueploRare Adrenal Cancer Network-Cortico MédullosurrénaleTumeur Endocrine, Institut National du Cancer,Paris, France
C. BadoualAssistance Publique-Hôpitaux de Paris,Hôpital Européen Georges Pompidou,Service d’Anatomo-pathologie,Paris, France
F. TissierAssistance Publique-Hôpitaux de Paris, Hôpital Cochin,Service d’Anatomie Pathologique,Paris, France
Endocr Pathol (2012) 23:34–42DOI 10.1007/s12022-011-9189-0
Author's personal copy

angiogenesis in patients with malignant forms of the disease.We used in situ hybridization, immunohistochemistry, andmicroarray gene expression profiling to evaluate angiogenesisand the expression of several angiogenic factors in a largecohort of pheochromocytomas and paragangliomas. We alsostudied the activation of mTOR by assessing the phosphory-lation of its targets, P70 S6 kinase and 4E-BP1. These resultswere correlated with both malignancy and transcription sig-nature. Our results reveal that cluster 1 tumors display amarked increase in both vascularization and in the expressionofmajor angiogenicmolecules, includingVEGF, its receptors,HIF2α, Angiopoietin-2, and the endothelin receptors ETAand ETB. These overexpressions were observed in both be-nign and malignant samples of cluster 1 and thus appeared tobe mainly dependent on the pseudo-hypoxic status of thesetumors. The mTOR pathway was potentially activated in halfof the tumors studied, with a slight increase in cluster 2pheochromocytomas. Our results suggest that there is astrong rationale for anti-VEGF-based therapeutic strate-gies in malignant pheochromocytomas and paraganglio-mas, in particular in those associated with mutations inthe SDHB gene.
Keywords Pheochromocytoma . Paraganglioma .
Angiogenesis . VEGF. Hypoxia
Introduction
Pheochromocytomas (PCC) and paragangliomas (PGL) areneural crest-derived tumors that develop in the sympatheticand parasympathetic nervous systems. These rare tumors aregenetically determined in at least a third of cases [1] and arethen caused by a germline mutation in one of the tensusceptibility genes currently described: the RET proto-oncogene [2] and the NF1 [3], VHL [4], SDHA [5], SDHB[6], SDHC [7], SDHD [8], SDHAF2 [9], TMEM127 [10],and MAX [11] tumor suppressor genes. Around 10% ofpheochromocytomas and up to 40% of paragangliomas aremalignant, and to date, malignancy is still defined by theappearance of distant metastases (generally in lymph nodes,bone, liver, and lungs) [12]. Patients affected with malignantforms of the disease have a variable but mostly poor clinicalcourse resulting in a 5-year survival of <50%. The onlyvalidated risk factor for malignancy and poor prognosis isthe identification of a germline mutation in the SDHB gene[13, 14]. Hence, a meta-analysis of the literature has con-cluded that 36% of malignant PCC harbor a germline SDHBmutation and that around 50% of patients with an SDHBmutation are expected to develop a malignant form of thedisease [15]. After the diagnosis of the first metastasis,SDHB-mutated patients have a sixfold reduced survival than
that of patients without an SDHB mutation (median survivalof 42 months versus 244 months, respectively) [13].
Currently, the treatment of choice for themajority of patientsis the surgical removal of the tumor. Radiotherapies and che-motherapies can also be used, but with various and limitedefficiencies. Radiometabolic therapy using 131I-MIBG can beproposed for metastases that are positive at scintingraphy, withan objective response in up to 30% of cases [16]. The mosteffective chemotherapy seems to be the CVD combination(cyclophosphamide, vincristin, dacarbazine). However, thereis no significant demonstration that such treatment extends thesurvival of patients with metastatic disease. Nevertheless, CVDmay lead to partial remissions and does promote symptomrelief in up to 50% of patients.
Molecular targeted therapies are nowadays considered asthe most promising strategies for the management ofpatients with progressive malignant PCC or PGL. Amongthese approaches, and because PCC and PGL are classicallydescribed as highly vascularized tumors, anti-angiogenictherapies have recently been the subject of most attention.These therapies include targeting of the vascular endothelialgrowth factor (VEGF) pathway using either humanizedmonoclonal anti-VEGF antibodies (Bevacizumab) or smalltyrosine kinase inhibitors such as Sunitinib or Sorafenib, aswell as mTOR inhibitors such as Everolimus (RAD001).These molecules are already approved by the Food andDrug Administration for patients with advanced renal cellcarcinomas and gastrointestinal stromal tumors. The ratio-nale for the use of anti-angiogenic therapies in malignantPCC/PGL is based on a relatively abundant literature thatreported the evaluation of angiogenesis in PCC or PGLtissues. Although sometimes contradicted [17, 18], most ofthese reports suggested an overall increase in microvasculardensity (MVD) in malignant versus benign tumors [19–22],but MVD quantification did not appear as a robust predic-tive factor of malignancy. Accordingly, an overexpression ofVEGF was systematically described in malignant PCCwhen compared with non-metastatic tumors [18, 21–25].All these studies, however, presented a major weakness asnone included a comprehensive assessment of the geneticstatus of the patients studied. It is now well accepted thatSDHx and VHL-related PCC/PGL display a peculiar activa-tion of the pseudo-hypoxic pathway (for a review, see [26]),which, among other consequences, leads to an increasedvascularization potentially mediated by VEGF overexpres-sion. Following microarray gene expression studies, thesetumors are now commonly referred to as “cluster 1” tumors,while RET, NF1, TMEM127, or MAX-related tumors areenclosed in the so-called “cluster 2” group [27–29].SDHB-mutated tumors represent a large proportion of allmalignant PCC/PGL, and it is therefore unclear whether theobserved activation of the VEGF pathway was actuallyattributable to malignancy or to an unexplored SDHB-
Endocr Pathol (2012) 23:34–42 35
Author's personal copy

mutated status. In that context, the purpose of this study wasto reevaluate angiogenesis as well as the expression ofVEGF and its receptors in a cohort of patients for whom acomplete genetic testing had been performed. Moreover, asactivation of the mTOR signaling pathway had never beendescribed in PCC/PGL tissues, we analyzed the phosphory-lation of two mTOR targets, p70S6 kinase and 4E-BP1, inorder to obtain a comprehensive rationale for the targetingof angiogenesis in patients with malignant PCC/PGL.
Material and Methods
Patients
We analyzed 60 paraffin-embedded tumors collected from 55patients by the COMETE network in two referral centers inParis (Georges Pompidou European Hospital and Cochin Hos-pital). Forty of them were inherited and then caused by muta-tions in RET (n 0 6), SDHA (n 0 2), SDHB (n 0 15), SDHC (n 02), SDHD (n 0 1), and VHL (n 0 8) genes. Six patients werediagnosed with type 1 neurofibromatosis (NF1). Two tumorshad a somatic VHL mutation (VHLs) and one a RET somatic(RETs) mutation [29]. This series comprised 38 benign tumorsand 22 malignant ones (11 SDHB, 1 SDHC, and 1 VHLs).
Gene expression data were obtained from a previouslydescribed series of 188 tumor samples [29]. It comprised163 benign (including 9 NF1, 9 RET, 1 TMEM127, 1 SDHA,7 SDHB, 1 SDHC, 3 SDHD, 25 VHL, 8 VHLs, and 6 RETs)and 25 malignant (including 10 SDHB, 1 SDHC, 3 VHL and2 VHLs) cases. Six samples were ganglionic metastases. Theprocedures used for pheochromocytoma/paragangliomadiagnosis and genetic testing were in accordance withinstitutional guidelines [30].
In Situ Hybridization
Paraffin-embedded tissue samples were cut into 6-μm sectionsand mounted on Super Frost Plus slides. Slides were deparaffi-nized with xylene, rehydrated in decreasing concentrations ofethanol, and treated with proteinase K (8 pg/ml in PBS) for10 min. Pre-hybridization was performed by incubating thesections in hybridization buffer (1 × salt, 50% formamide,10% dextran sulfate, 10 mg of yeast RNA/ml, Denhardt solu-tion) for 4 h at 65°C in a humid chamber (50% formamide, 2XSSC). The hybridization solution containing the hybridizationbuffer and digoxigenin-labeled probe was then applied to thesections, covered with parafilm, and placed in a humid cham-ber overnight at 65°C. Slides were rinsed in 5X SSC at 65°Cand washed in a solution containing 2X SSC and 50% form-amide for 30 min at 65°C, and in TNE (10 mM Tris–HCl,pH 7.6, 500 mM NaCl, 1 mM EDTA) for 10 min at 37°C.Slides were treated with RNase A (20μg/ml, Roche) diluted in
TNE for 30 min at 37°C and washed once in TNE for 10 minat 37°C, once in 2X SSC for 20 min at 65°C, twice in 0.2XSSC at 65°C for 20 min, and twice in MABT [MAB (100 mMmaleic acid, 150 mMNaCl, 192 mMNaOH), 1.1%Tween 20]for 10 min at room temperature (RT). The sections werecovered with a blocking solution (MABT, 20% normal goatserum) at RT for 1.5 h and then incubated with anti-DIG(Roche) diluted 1:2,000 overnight at 4°C. After washing thesections twice for 5 min in MABT and once in NTMT(100 mM NaCl, 100 mM Tris–HCl, pH 9.5, 50 mM MgCl2,1% Tween 20) for 10 min, they were revealed using BMPPurple (Roche), 0.1% Tween 20, for 3–5 days to 2 weeks.Probes were as previously described [23] and were synthe-sized using the DIG RNA labeling kit (Roche) according tothe manufacturer’s protocol. All microscopic examinationswere performed on a Leica microscope. Vascular density wasmeasured on least five fields of 1,029 × 772 μm2 using theIPLab program (Scanalytics, Fairfax, VA).
Immunohistochemistry
Sections (6 μm thick) were cut from paraffin-embedded sam-ples and mounted on Superfrost plus slides. Immunohisto-chemistry was performed as previously described using ananti-CD34 (Clone QBEND 10, Immunotech, 1/100) antibody,an anti-eIF4BP1 (ab47467, Abcam, 1/500), an anti-eIF4BP1-phospho S64 (ab53686, Abcam, 1/500), an anti-p70 S6 kinase(sc-8418, Santa Cruz Biotechnologies, 1/100), and an anti-phospho p70 S6 kinase (Thr421/Ser424, sc-7984-R, SantaCruz Biotechnologies, 1/500) [31]. The protocol included aheat-mediated antigen retrieval step (10 mM citrate buffer,pH 6, 15 min), biotinylated secondary antibody (Vector Lab-oratories), an avidin–biotin–peroxidase complex (VectastainABC Elite, Vector Laboratories), and Histogreen (Abcys) as achromogen. eIF4BP1-phospho S64 and phospho p70 S6 ki-nase staining were graded blindly. A score was given as afunction of the percentage of positive cells and the stainingintensity. It was as the following: 0 0 no signal; 1 0 weak and/or <20% of positive cells; 2 0 moderate and/or 20–50% ofpositive cells; 3 0 high and/or more than 50% of positive cells;and 4 0 intense signal and or more than 80% of positive cells.
Microarray Analysis of Gene Expression
Tumor tissues (20–30 mg) were disrupted in liquid nitrogen.RNA was extracted using RNeasy Mini Kit (Qiagen). RNAquality was assessed by electrophoresis on a Bioanalyzer 2100(Agilent Technologies) and the quantity evaluated using aNanoDrop ND-1000 spectrophotometer (Labtech). Strict crite-ria for the quality of RNA were applied to exclude degradedsamples, and a 28:18 s ratio greater than 1.5 was required.Microarray analysis was performed with 3 μg of total RNAfrom each sample as the starting material and 10 μg cRNA for
36 Endocr Pathol (2012) 23:34–42
Author's personal copy

hybridization (GeneChip Fluidics Station 400, Affymetrix,Santa Clara, CA). Total RNA was amplified and labeledaccording to the manufacturer’s instructions with a one-cycletarget labeling protocol (http://www.affymetrix.com). The la-beled cDNAs were hybridized to HG-U133 Plus 2.0 Affyme-trix GeneChip arrays (Affymetrix ®) and the chips scannedwith GCOS 1.4.
Statistical Analysis
Statistical analyses were performed using the Stat View soft-ware (SAS Institute Inc.). Differences were evaluated byMann–Whitney test for vascular density and by ANOVA Bon-ferroni test for gene expression. Spearman correlation test wasperformed to compare individual expression data with tumorweight on the 147 samples for which both data were available.A p value <0.05 was considered statistically significant.
Results
Angiogenesis
We used CD34 immunohistochemistry to evaluate angio-genesis in PCC/PGL tissues. As previously reported by ourteam, we found that benign tumors presented a regulardistribution of capillaries in the tumor tissues (Fig. 1a, b),while malignant tumors displayed a very peculiar vasculararchitecture characterized by a highly heterogeneous densityof blood vessels and by the presence of vascular structuresforming arcs, parallels, and network (Fig. 1c). Such a vascularpattern, which may highlight components of the PASS score
such as large tumor Zellballen or diffuse tumor cell growth,did not allow performing a relevant quantification of micro-vascular density. We thus restricted the quantification of bloodvessels to benign tumors and compared cluster 1 (i.e., associ-ated with SDHx or VHL genes mutations) to cluster 2 (i.e.,associated with mutations in RET, NF1, or TMEM127 genes)tumors. Such analysis revealed a 2.5-fold increase in angio-genesis in cluster 1 tumors (p < 0.001, Fig. 1d)
VEGF System
The expression of VEGF and its receptors VEGFR-1 andVEGFR-2was first evaluated by in situ hybridization in a seriesof 60 pheochromocytomas or paragangliomas (Fig. 2a). Aspreviously reported, we observed that VEGF was expressedby tumor cells, while both its receptors were restricted tovascular endothelial cells. Although there were some importantvariations in their relative expression level between tumors, allthree genes were expressed in all the samples studied. With theaim of validating or infirming the dogma of an overexpressionof the VEGF system in malignant pheochromocytoma, wefurther evaluated the microarray RNA expression profile ofVEGF, VEGFR-1, and VEGFR-2 in our large series of 188PCC/PGL (Fig. 2b). In order to detect a potential pseudo-hypoxic effect, tumors were classified according to the malig-nant or benign diagnostic as well as to their presence in eithercluster 1 (C1) or cluster 2 (C2) in the unsupervised hierarchicalcluster analysis [29] (Table 1). As previously reported, we didobserve an overall overexpression of VEGF in malignant ver-sus benign tumors (50% increase, p < 0.01). However, thiseffect seemed to be solely caused by the overrepresentation ofSDHB-mutated tumors in the malignant group. It indeed
Fig. 1 Vascularization ofpheochromocytomas andparagangliomas.Immunostaining of bloodvessels with anti-CD34 anti-body reveals a regular vascularorganization in benign tumors(a, b), while malignant tumorsdisplay a heterogeneous vascu-lar architecture (c). Quantifica-tion of angiogenesis wasperformed on 17 cluster 1 (a)and 18 cluster 2 (b) benigntumors and revealed a 2.5-foldincrease in vascular density intumors associated with pseudo-hypoxia. Bar, 100 μm
Endocr Pathol (2012) 23:34–42 37
Author's personal copy

appeared that VEGF mRNA levels were markedly increased inboth benign and malignant samples of cluster 1 as comparedwith cluster 2 tumors (p < 0.0001). Inside C1 or C2, there wasno difference between benign and malignant tissues. VEGFreceptors were also significantly overexpressed in both benignand malignant tumors of cluster 1 as compared with benigntumors of cluster 2. However, their expression appeared to beslightly increased in malignant tumors of cluster 2 when com-pared with the benign tumors of this cluster. The expressionlevels did not correlate with tumor weight (data not shown).Interestingly, within the malignant group, mean expression ofVEGF, VEGFR-1, and VEGFR-2 was reduced in metastasis ascompared with primary tumors (relative mean values of 69%,36%, and 35%, respectively). These data were, however, notstatistically significant, probably because of the reduced tumorsample number (n 0 19 and n 0 6, respectively).
Other Angiogenesis-Related Pathways
In order to depict a comprehensive view of blood vesselformation in malignant pheochromocytomas and paragan-gliomas, we further studied the expression of several genes
involved in the regulation of angiogenesis (Fig. 3). Aspreviously reported, HIF1 was not differentially regulatedbetween groups [32], while EPAS1/HIF2 was significantlyoverexpressed in cluster 1 tumors versus benign tumors ofcluster 2 (p < 0.0001). Although it was not statisticallysignificant, it was also slightly increased in malignanttumors of cluster 2.
It is well established that the inactivation of a Tie-2-mediated stabilization of the vascular tree is a necessarystep prior to VEGF-mediated endothelial proliferation andmigration. Angiopoietin (ANGPT)-1, the Tie-2 agonistwhich promotes blood vessel maturation and stabilization,was significantly downregulated in all malignant tumors ascompared with benign ones regardless of their cluster position.In contrast, ANGPT-2, the Tie-2 antagonist, was markedlyoverexpressed in benign and malignant samples of cluster 1,but not in cluster 2 tumors.
We previously reported that endothelin receptors ETAand ETB were overexpressed in malignant pheochromo-cytomas [23]. Again, although there was a slight butnon-significant induction in malignant tumors of cluster2, this effect seemed to be principally mediated by the
Fig. 2 VEGF system in pheochromocytomas and paragangliomas. aIn situ hybridization reveals that VEGF is expressed in tumor cells andits receptors in endothelial cells. b Mean values of their mRNA
expression levels in all cluster 1 (C1) or cluster 2 (C2) benign andmalignant PCC/PGL. Data are means ± SEM. Bar, 50 μm
Table 1 Genotype of tumorsincluded in each group studiedin the microarray analysis
Group Mutation
Benign cluster 1 (n 0 50) 1 SDHA, 7 SDHB, 1 SDHC, 3 SDHD, 24 VHL, 8 VHLs, 6 non-mutated
Malignant cluster 1 (n 0 17) 10 SDHB, 1 SDHC, 3 VHL, 2 VHLs, 1 non-mutated
Benign cluster 2 (n 0 113) 9 NF1, 9 RET, 1 TMEM127, 1 VHL, 6 RETs, 87 non-mutated
Malignant cluster 2 (n 0 8) 8 Non-mutated
38 Endocr Pathol (2012) 23:34–42
Author's personal copy
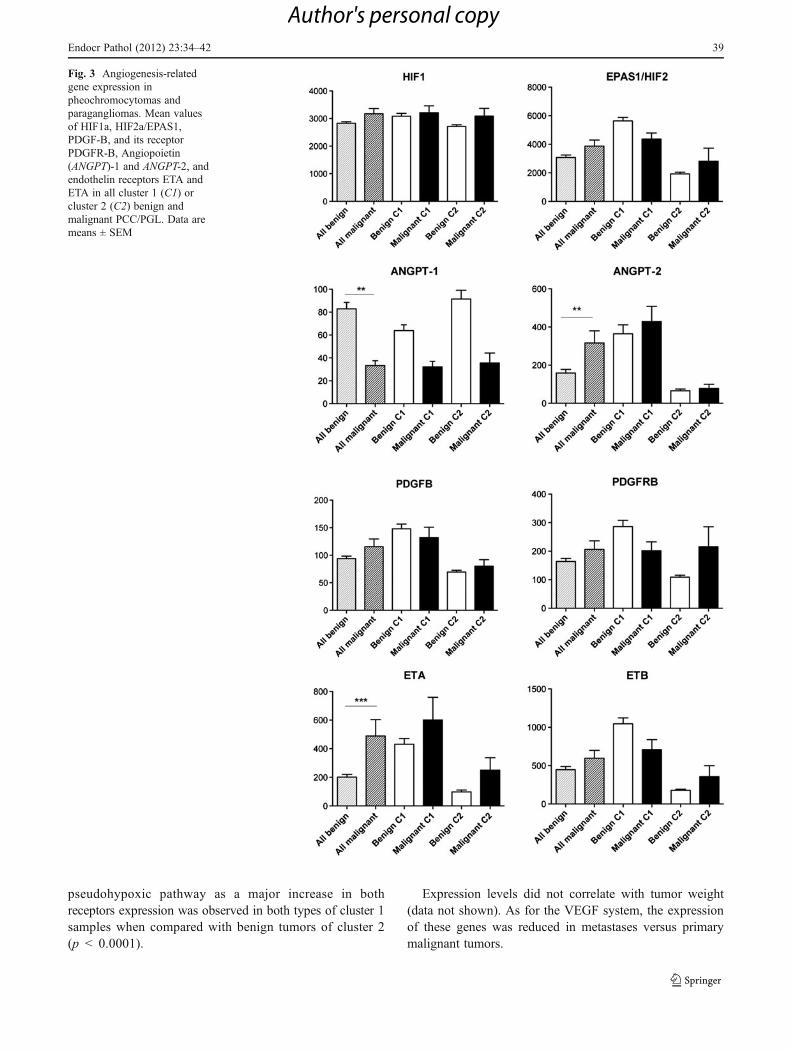
pseudohypoxic pathway as a major increase in bothreceptors expression was observed in both types of cluster 1samples when compared with benign tumors of cluster 2(p < 0.0001).
Expression levels did not correlate with tumor weight(data not shown). As for the VEGF system, the expressionof these genes was reduced in metastases versus primarymalignant tumors.
Fig. 3 Angiogenesis-relatedgene expression inpheochromocytomas andparagangliomas. Mean valuesof HIF1a, HIF2a/EPAS1,PDGF-B, and its receptorPDGFR-B, Angiopoietin(ANGPT)-1 and ANGPT-2, andendothelin receptors ETA andETA in all cluster 1 (C1) orcluster 2 (C2) benign andmalignant PCC/PGL. Data aremeans ± SEM
Endocr Pathol (2012) 23:34–42 39
Author's personal copy

mTOR Pathway
Activation of the mTOR pathway is a commonly observedtrait of human tumors and is expected to be particularlyincreased in cluster 2-related pheochromocytomas. We thusused immunohistochemistry to analyze the expression andthe phosphorylation of two major mTOR targets, namely,P70 S6 kinase and 4E-BP1, in 60 pheochromocytomas andparagangliomas. P70 S6 kinase was expressed at vari-able levels in 55 samples. Among these 55 tumors, 36were also positive for the phosphorylated form of theprotein (Fig. 4). Within cluster 1, a positive immunos-taining for phospho-P70 S6 kinase was detected in 7 of14 (50%) benign tumors and in 8 of 14 (57%) malig-nant ones. The level of labeling was higher in malignantthan in benign tumors (p < 0.05). Within cluster 2, apositive staining was observed in 16 of 19 (84%) benigntumors and in 5 of 7 (71%) malignant ones, at com-parable intensities. 4E-BP1 was only detected in 17tumors, nine of which also expressed the phosphorylated formof the protein. Such a reduced number did not allow anystatistical analysis.
Discussion
Targeted molecular therapies are expected to represent thefuture in the management of patients affected with malig-nant pheochromocytomas and paragangliomas. Among
these strategies, anti-angiogenic approaches are thought tobe highly promising. The rationale for targeting tumor vas-culature is first based on the well-established observationthat pheochromocytomas and parangangliomas are veryhighly vascularized tumors and, therefore, potentiallystrongly dependent on angiogenesis-mediated growth andsurvival. Targeting the VEGF pathway is the most common-ly used anti-angiogenic strategy in cancer and appeared asthe best candidate for inhibiting angiogenesis in PCC/PGL.Numerous studies have indeed reported the overexpressionof VEGF in malignant PCC/PGL, but none of them tookinto account the genetic status of the patients. In the presentstudy, we thus analyzed the expression of angiogenicfactors in correlation with patient/tumor genetic evaluation.Our observations reveal that VEGF and its receptors areindeed expressed in all PCC/PGL and therefore appear aspotentially implicated in the vascularization of these tumors.However, we show that in malignant tumors, the previouslyreported increase in VEGF levels actually reflected theoverrepresentation of SDHB-related tumors. Hence, anoverexpression of VEGF and its receptors was observedin both benign and malignant tumors of cluster 1. Incontrast, malignant tumors of cluster 2 did not present asignificant overexpression of these genes as comparedwith benign tumors of the same cluster. VEGF expressionin PCC/PGL thus appears to be mainly regulated by thepseudo-hypoxic status previously described in cluster 1tumors and is indeed associated with increased tumor vascu-larization. Comparable observations were made for other
Fig. 4 Activation of the mTOR pathway in pheochromocytomas andparagangliomas. Expression of p70 S6 kinase, 4E-BP1, and theirphosphorylated forms are revealed by immunohistochemistry. Graphs
illustrate individual values of the quantified signal for phospho-p70 S6kinase and phospho-4E-BP1 in patients presenting a positive stainingfor the corresponding total protein. Bar, 50 μm
40 Endocr Pathol (2012) 23:34–42
Author's personal copy

angiogenic factors such as HIF2a, Angiopoietin 2,PDFG-B, or endothelin receptors, which were all overex-pressed in cluster 1 tumors. It is, however, worth noting thatmalignant tumors included in cluster 2 did display an in-creased expression of VEGFR-2, ETA, ETB, or PDGFR-Bwhen compared with benign cluster 2 tumors. These obser-vations did not reach statistical significance, putativelybecause of the reduced size of this group of samples (n08),but do suggest that malignant tumors may overall present anincreased dependence to angiogenesis. Interestingly, we ob-served an overall decrease in the expression of angiogenicgenes in the group of metastases as compared with malignantprimary tumors, although these results did not reach statisticalsignificance. Such observations may reflect a decreased de-pendence of metastases on neovascularization, or, more likely,the fact that metastases are probably resected earlier thanprimary tumors in their natural history, thus restricting theestablishment of a hypoxic/angiogenic phenotype. mTOR isthe second target of choice for anti-angiogenic therapies. Inour study, we found that approximately half of PCC/PGLmaydisplay an activation of this signaling pathway, with a slighttendency toward an increase in cluster 2 tumors.
Altogether, our observations suggest that there is a strongrationale for anti-VEGF-based therapeutic strategies in ma-lignant PCC/PGL and in particular in those associated withmutations in the SDHB gene. In contrast, mTOR targetingdoes not appear as a first choice strategy and should only beused in a second intention, following analysis of the path-way in a sample of tumor tissue. These indications are inaccordance with the first reports using these kinds ofapproaches in the management of malignant PCC/PGL.Sunitinib-mediated inhibition of tyrosine kinase receptorsincluding VEGF receptors has indeed shown somepromising results (although, mainly partial responses)in six out of seven cases (including five SDHB andone VHL) reported during the past 2 years [33–37]. Incontrast, Everolimus (RAD001)-mediated inhibition ofthe mTOR protein was shown to be ineffective in four patientswith malignant PCC [38].
Although it is now clear that anti-angiogenic therapieswill not, in most cases, lead to complete responses in treatedpatients [39], they anyhow represent a true hope for patientsaffected with progressive, malignant PCC/PGL, which donot respond to chemotherapies. The probable developmentof resistance to these treatments will require case-by-caseadaptations, with modifications of the molecule/target basedon the analysis of relevant biomarkers [40] and implemen-tation of combinatorial “a la carte” treatments.
Acknowledgments This work was supported by the ProgrammeHospitalier de Recherche Clinique grant COMETE 3 (AOM 06 179)and by the Agence Nationale de la Recherche (ANR 08 GENOPATH029 MitOxy). This work is part of the national program ‘Cartesd’Identité des Tumeurs’ funded and developed by the ‘Ligue Nationale
contre le Cancer’ (http://cit.ligue-cancer.net). The authors thank DrJean-Marie Gasc and Pr Pierre Corvol for launching this study, morethan 10 years ago.
References
1. Gimenez-Roqueplo AP, Burnichon N, Amar L, Favier J, JeunemaitreX, Plouin PF Recent advances in the genetics of phaeochromocy-toma and functional paraganglioma. Clinical and experimental phar-macology & physiology 35: 376–379, 2008.
2. Mulligan LM, Kwok JB, Healey CS et al. Germ-line mutations ofthe RET proto-oncogene in multiple endocrine neoplasia type 2A.Nature 363: 458–460, 1993.
3. Wallace MR, Marchuk DA, Andersen LB et al. Type 1 neurofi-bromatosis gene: identification of a large transcript disrupted inthree NF1 patients. Science 249: 181–186, 1990.
4. Latif F, Tory K, Gnarra J et al. Identification of the von Hippel-Lindau disease tumor suppressor gene. Science 260: 1317–1320.,1993.
5. Burnichon N, Briere JJ, Libe R et al. SDHA is a tumor suppressorgene causing paraganglioma. Hum Mol Genet 19: 3011–3020,2010.
6. Astuti D, Latif F, Dallol A et al. Gene mutations in the succinatedehydrogenase subunit SDHB cause susceptibility to familialpheochromocytoma and to familial paraganglioma. Am J HumGenet 69: 49–54., 2001.
7. Niemann S,Muller UMutations in SDHC cause autosomal dominantparaganglioma, type 3. Nat Genet 26: 268–270, 2000.
8. Baysal BE, Ferrell RE, Willett-Brozick JE et al. Mutations inSDHD, a mitochondrial complex II gene, in hereditary paragan-glioma. Science 287: 848–851., 2000.
9. Bayley JP, Kunst HP, Cascon A et al. SDHAF2 mutations infamilial and sporadic paraganglioma and phaeochromocytoma.Lancet Oncol 11: 366–372, 2010.
10. QinY, Yao L, King EE et al. Germlinemutations in TMEM127 confersusceptibility to pheochromocytoma. Nat Genet 42: 229–233, 2010.
11. Comino-Mendez I, Gracia-Aznarez FJ, Schiavi F et al. Exomesequencing identifies MAX mutations as a cause of hereditarypheochromocytoma. Nat Genet 43: 663–667, 2011.
12. Lloyd R, Tischler A, Kimura N, McNicol A, Young JW. Adrenaltumours: Introduction. In: DeLellis RA LR, Heitz PU, Eng C, eds.WHO classification of tumours—Pathology and Genetics—Tumours of endocrine organs. IARC Press, Lyon, 2004.
13. Amar L, Baudin E, Burnichon N et al. Succinate dehydrogenase Bgene mutations predict survival in patients with malignant pheo-chromocytomas or paragangliomas. J Clin Endocrinol Metab 92:3822–3828, 2007.
14. Gimenez-Roqueplo AP, Favier J, Rustin P et al. Mutations in theSDHB gene are associated with extra-adrenal and/or malignantphaeochromocytomas. Cancer Res 63: 5615–5621, 2003.
15. Pasini B, Stratakis CA SDHmutations in tumorigenesis and inheritedendocrine tumours: lesson from the phaeochromocytoma-paraganglioma syndromes. Journal of internal medicine 266:19–42, 2009.
16. Chrisoulidou A, Kaltsas G, Ilias I, Grossman AB The diagnosisand management of malignant phaeochromocytoma and paragan-glioma. Endocr Relat Cancer 14: 569–585, 2007.
17. Ohji H, Sasagawa I, Iciyanagi O, Suzuki Y, Nakada T Tumourangiogenesis and Ki-67 expression in phaeochromocytoma. BJUInt 87: 381–385., 2001.
18. Salmenkivi K, Heikkila P, Liu J, Haglund C, Arola J VEGF in 105pheochromocytomas: enhanced expression correlates with malignantoutcome. Apmis 111: 458–464, 2003.
Endocr Pathol (2012) 23:34–42 41
Author's personal copy

19. Liu Q, Djuricin G, Staren ED et al. Tumor angiogenesis inpheochromocytomas and paragangliomas. Surgery 120: 938–942; discussion 942–933., 1996.
20. Rooijens PP, de Krijger RR, Bonjer HJ et al. The significance ofangiogenesis in malignant pheochromocytomas. Endocr Pathol 15:39–45, 2004.
21. Zielke A, Middeke M, Hoffmann S et al. VEGF-mediated angio-genesis of human pheochromocytomas is associated to malignancyand inhibited by anti-VEGF antibodies in experimental tumors.Surgery 132: 1056–1063; discussion 1063, 2002.
22. Feng F, Zhu Y, Wang X et al. Predictive factors for malignantpheochromocytoma: analysis of 136 patients. The Journal of urology185: 1583–1590, 2011.
23. Favier J, Plouin PF, Corvol P, Gasc JM Angiogenesis and vasculararchitecture in pheochromocytomas: distinctive traits in malignanttumors. Am J Pathol 161: 1235–1246, 2002.
24. Kolomecki K, Stepien H, Bartos M, Kuzdak K Usefulness of VEGF,MMP-2, MMP-3 and TIMP-2 serum level evaluation in patients withadrenal tumours. Endocrine regulations 35: 9–16, 2001.
25. Takekoshi K, Isobe K, Yashiro T et al. Expression of vascularendothelial growth factor (VEGF) and its cognate receptors inhuman pheochromocytomas. Life Sci 74: 863–871, 2004.
26. Favier J, Gimenez-Roqueplo AP Pheochromocytomas: The(Pseudo)-hypoxic hypothesis. Best Pract Res Clin EndocrinolMetab 24: 957–968, 2010.
27. Dahia PL, Ross KN, Wright ME et al. A HIF1alpha regulatoryloop links hypoxia and mitochondrial signals in pheochromocytomas.PLoS Genet 1: 72–80, 2005.
28. Lopez-Jimenez E, Gomez-LopezG, Leandro-Garcia LJ et al. Researchresource: Transcriptional profiling reveals different pseudohypoxicsignatures in SDHB and VHL-related pheochromocytomas. MolEndocrinol 24: 2382–2391, 2010.
29. Burnichon N, Vescovo L, Amar L et al. Integrative genomicanalysis reveals somatic mutations in pheochromocytoma andparaganglioma. Hum Mol Genet 20: 3974–3985, 2011.
30. Plouin PF, Gimenez-Roqueplo AP Initial work-up and long-term follow-up in patients with phaeochromocytomas and
paragangliomas. Best Pract Res Clin Endocrinol Metab 20:421–434, 2006.
31. Favier J, Kempf H, Corvol P, Gasc J Cloning and expressionpattern of EPAS1 in the chicken embryo. Colocalization withtyrosine hydroxylase. FEBS Lett 462: 19–24, 1999.
32. Favier J, Briere JJ, Burnichon N et al. The Warburg effect isgenetically determined in inherited pheochromocytomas. PloSone 4: e7094, 2009.
33. Jimenez C, Cabanillas ME, Santarpia L et al. Use of the tyrosinekinase inhibitor sunitinib in a patient with von Hippel-Lindaudisease: targeting angiogenic factors in pheochromocytoma andother von Hippel-Lindau disease-related tumors. J Clin EndocrinolMetab 94: 386–391, 2009.
34. Joshua AM, Ezzat S, Asa SL et al. Rationale and evidence forsunitinib in the treatment of malignant paraganglioma/pheochro-mocytoma. J Clin Endocrinol Metab 94: 5–9, 2009.
35. Park KS, Lee JL, Ahn H et al. Sunitinib, a novel therapy foranthracycline- and cisplatin-refractory malignant pheochromocy-toma. Jpn J Clin Oncol 39: 327–331, 2009.
36. Tuthill M, Barod R, Pyle L et al. A report of succinate dehydro-genase B deficiency associated with metastatic papillary renal cellcarcinoma: successful treatment with the multi-targeted tyrosinekinase inhibitor sunitinib. BMJ Case Rep 2009, 2009.
37. Hahn NM, Reckova M, Cheng L, Baldridge LA, Cummings OW,Sweeney CJ Patient with malignant paraganglioma responding tothe multikinase inhibitor sunitinib malate. J Clin Oncol 27: 460–463, 2009.
38. Druce MR, Kaltsas GA, Fraenkel M, Gross DJ, Grossman ABNovel and evolving therapies in the treatment of malignant phaeo-chromocytoma: experience with the mTOR inhibitor everolimus(RAD001). Horm Metab Res 41: 697–702, 2009.
39. Ebos JM, Kerbel RS Antiangiogenic therapy: impact on invasion,disease progression, and metastasis. Nat Rev Clin Oncol 8: 210–221, 2011.
40. Jain RK, Duda DG, Willett CG et al. Biomarkers of response andresistance to antiangiogenic therapy. Nat Rev Clin Oncol 6: 327–338, 2009.
42 Endocr Pathol (2012) 23:34–42
Author's personal copy