radiologic evaluation of mesenchymal tumors of the female genital tract
TRANSCRIPT
RADIOLOGIC EVALUATIONOF MESENCHYMALTUMORS OF THE FEMALEGENITAL TRACT
Richard L. Zampolin, MDa, Ann Shi, MDa,b,*KEYWORDS� Mesenchymal tumors � Ultrasound � Computed tomography� Magnetic resonance imaging � Positron emission tomography � Female genital tract
ABSTRACT
M esenchymal neoplasms of the femalegenital tract are a diverse group of tumors,of which the most common are smooth
muscle tumors. There is a significant overlap inthe imaging characteristics of benign and malig-nant tumors and final diagnosis often requirespathologic correlation. However, familiarity withtypical radiologic features, common imagingpitfalls, and the utility of different imaging modali-ties can be valuable in the evaluation of mesen-chymal tumors. This article highlights the imagingfeatures of the most commonly encounteredmesenchymal tumors in the female genital tract.
OVERVIEW
THE FUNDAMENTALS OF IMAGING THE FEMALEGENITALTRACT
Ultrasound (US) is generally the first-line modalityfor imaging the uterus and adnexa. It is low cost,widely available, lacks ionizing radiation, andprovides excellent anatomic evaluation of theuterus and the ovaries. US allows for differentiationof solid from cystic structures and highlights differ-ences in tissue interfaces; however, there are alsoseveral important limitations to consider. It is tech-nologist dependent, linking the diagnostic qualityand sensitivity of the examination to the level ofexperience and diligence of the sonographer.
a Department of Radiology, Montefiore Medical Center,b Albert Einstein College of Medicine, Bronx, NY, USA* Corresponding author. Department of Radiology, MoNY 10467.E-mail address: [email protected] (A. Shi).
Surgical Pathology 2 (2009) 581–602doi:10.1016/j.path.2009.08.0131875-9181/09/$ – see front matter ª 2009 Elsevier Inc. All
Tissues with different histologic characteristicsmay have similar echotexture, making their differen-tiation difficult. Furthermore, when examining largemesenchymal tumors, restricted tissue penetrationoften limits accurate delineation of tumor size andextent of invasion. US does not provide adequateevaluation of metastatic disease and typically isonly an organ-specific examination.
The principal role of computed tomography (CT)in the initial evaluation of mesenchymal neoplasmsof the female genital tract is to delineate the extentof local disease and involvement of adjacent struc-tures. Furthermore, CT allows for evaluation ofmetastatic disease and secondary complicationssuch as ureteral obstruction or venous throm-bosis. It is a readily available, low-cost modalityof imaging that is also suited to evaluateposttreatment changes and monitoring diseaserecurrence. The disadvantages of CT includeexposure to ionizing radiation, potential of contrastreaction, and limited use of contrast in patientswith renal disease secondary to the risk ofcontrast-induced nephropathy. In addition, thesensitivity of CT for detecting early, localizeddisease is limited because of its poor soft tissuecontrast resolution.
For exquisite soft tissue contrast resolution andanatomic detail, pelvic magnetic resonanceimaging (MRI) is the key imaging modality. Itemploys a wide array of imaging parameters andallows for differentiation of many tissue types. Itis sensitive in detecting early local disease and
111 E210th Street, Bronx, NY 10467, USA
ntefiore Medical Center, 111 E210th Street, Bronx,
rights reserved. surg
path
.thec
lini
cs.c
om

Zampolin & Shi582
provides accurate local tumor staging. Theanatomic detail and multiplanar capability of MRImake it the modality of choice for presurgicaland pretreatment planning and for posttreatmentfollow-up. The downsides of MRI include its lackof widespread and timely availability, high cost,and limited use in patients with claustrophobiaor with certain metallic hardware or foreignbodies. Increased awareness of the rare, butdeadly, and currently untreatable complication ofnephrogenic systemic fibrosis has limited theuse of gadolinium-enhanced MRI in patients withrenal failure.
In general, one of the problems with standardradiologic techniques when imaging tumors of thefemale genital tract is lack of specificity. Positronemission tomography (PET) and PET/CT addressthese issues by incorporating evaluation of physio-logic activity. Malignant tumors generally demon-strate increased metabolic activity and, thus,more uptake of fluorine-18 fluorodeoxyglucose(FDG) than benign tumors on PET. The use of PETand CT together combines functional imaging andprecise anatomic localization to advance the initialdiagnosis and staging of malignancies, and post-treatment surveillance. Despite limited experiencewith PET in mesenchymal tumors of the femalegenital tract, several studies have shown that PETcan increase specificity in distinguishing betweenbenign and malignant uterine smooth muscletumors,1 and is highly sensitive in detecting recur-rent sarcomas.2 Interpretation of PET and PET/CTof the female genital tract requires familiarity withcommon pitfalls. For example, increased uptakeon FDG-PET has been reported in many benignpelvic processes, including uterine fibroids andendometriosis, and even in endometrium duringthe normal menstrual cycle.3,4 Inflammatorychanges from recent surgery and radiation, andfocal physiologic radiotracer activity in bowel loopsand the urinary system, can all lead to false-positiveinterpretations. False-negative interpretationresults when the tumor is not FDG avid. Cost, avail-ability, and limited sensitivity for small lesions areother factors to be considered before obtaininga PET or PET/CT examination.
GENERAL PRINCIPLES OF TISSUE
CHARACTERIZATION BY IMAGING
Smooth muscle is typically hypoechoic on US,demonstrates soft-tissue density on CT, and itssignal characteristics on MRI often parallel thoseof striated muscle. Cystic or myxoid change is hy-poechoic on US, shows low density on CT, and is
hypointense (dark relative to muscle) on T1-weighted MRI and hyperintense (bright relative tomuscle) on T2-weighted images. Blood productshave a variable appearance on imaging dependingon their age, but typically have slightly higherdensity than muscle on CT, and subacute hemor-rhage (methemoglobin) is most easily recognizableas hyperintense signals on T1-weighted MRI.Lipid-containing tissues are echogenic on US,show low attenuation on CT, and are hyperintenseon T1- and fast-spin echo (FSE) T2-weightedimages. Fat signal is suppressed with short tauinversion recovery (STIR) and fat saturationsequences. Fibrous tissues are usually hypoe-choic on US, demonstrate soft tissue attenuationon CT, and are hypointense on T2-weighted MRIimaging. The degree of enhancement on CT andMRI following contrast administration reflects thevascularity of the tumor.
UTERUS
LEIOMYOMA
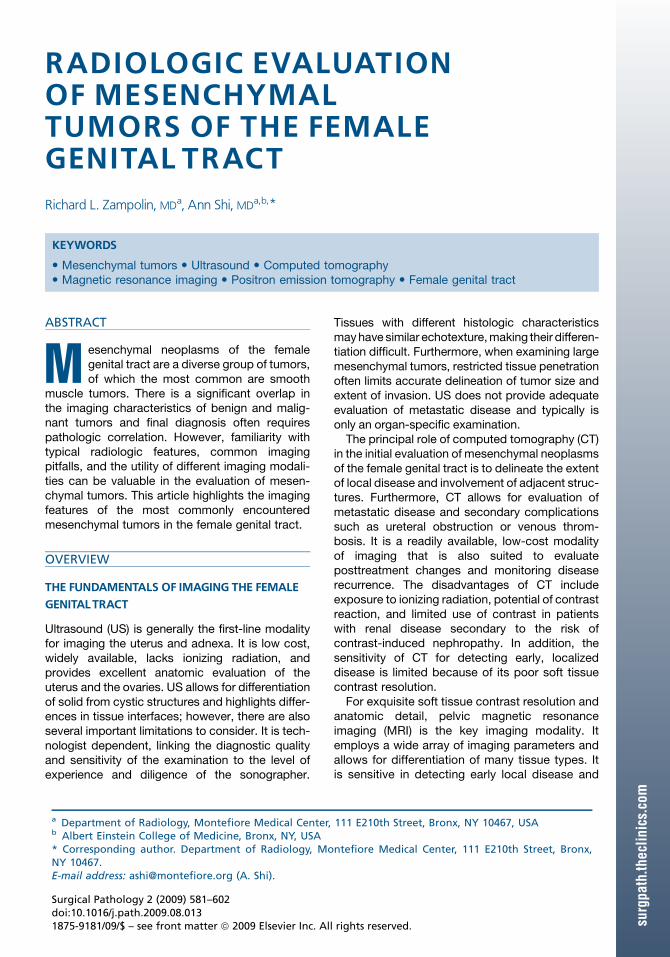
The most common benign neoplasm of the uterusis leiomyoma, which occurs most commonly inmiddle-aged women, with a prevalence of 20%to 30% in patients older than 30 years.5 Leiomyo-mas are classified as intramural, submucosal, sub-serosal, or cervical depending on their location.Imaging evaluation of leiomyomas often beginswith US. The typical leiomyoma is seen as a well-circumscribed, hypoechoic, solid mass (Fig. 1).However, the sonographic appearance can bevariable, ranging from echogenic, caused by calci-fications, to mixed solid and cystic, caused bydegeneration when the leiomyoma outgrows itsblood supply.6,7 Sonographic evaluation of theheavily myomatous uterus can be limited byincreased US attenuation, making full character-ization and accurate sizing of these lesionsdifficult. Multiple small uterine leiomyomas cancause the uterine parenchyma to have a heteroge-nous, echogenic appearance, which can beindistinguishable from adenomyosis.7 On a non–contrast-enhanced CT, uterine leiomyomasusually demonstrate attenuation similar to themyometrium.8 The appearance of the uterus canrange from normal in size and contour to markedlyenlarged and irregular, with multiple nodular struc-tures.8 Calcification is not uncommon, and whencoarse and clustered it is characteristic of leio-myomas (Fig. 2). Contrast-enhanced CT generallydemonstrates avid enhancement. Degenerationadds complexity to the evaluation of leiomyomas
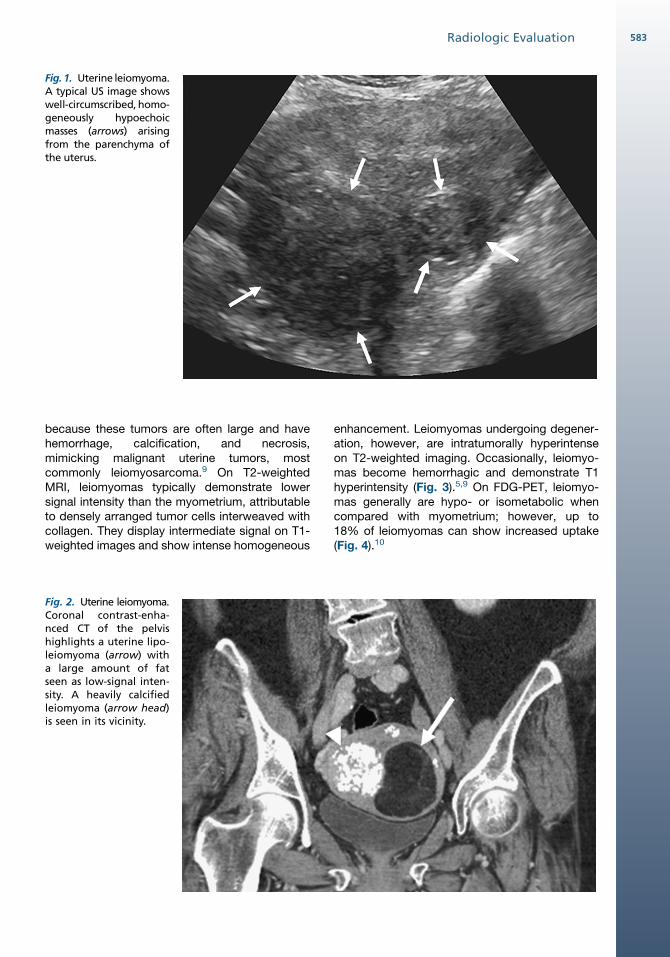
Fig. 1. Uterine leiomyoma.A typical US image showswell-circumscribed, homo-geneously hypoechoicmasses (arrows) arisingfrom the parenchyma ofthe uterus.
583Radiologic Evaluation
because these tumors are often large and havehemorrhage, calcification, and necrosis,mimicking malignant uterine tumors, mostcommonly leiomyosarcoma.9 On T2-weightedMRI, leiomyomas typically demonstrate lowersignal intensity than the myometrium, attributableto densely arranged tumor cells interweaved withcollagen. They display intermediate signal on T1-weighted images and show intense homogeneous
Fig. 2. Uterine leiomyoma.Coronal contrast-enha-nced CT of the pelvishighlights a uterine lipo-leiomyoma (arrow) witha large amount of fatseen as low-signal inten-sity. A heavily calcifiedleiomyoma (arrow head)is seen in its vicinity.
enhancement. Leiomyomas undergoing degener-ation, however, are intratumorally hyperintenseon T2-weighted imaging. Occasionally, leiomyo-mas become hemorrhagic and demonstrate T1hyperintensity (Fig. 3).5,9 On FDG-PET, leiomyo-mas generally are hypo- or isometabolic whencompared with myometrium; however, up to18% of leiomyomas can show increased uptake(Fig. 4).10
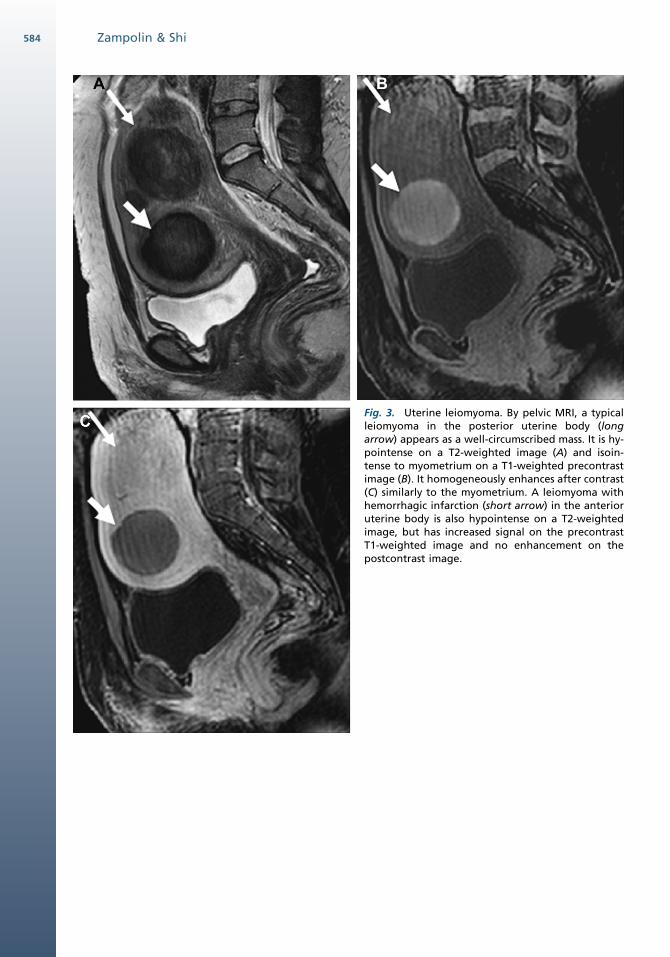
Fig. 3. Uterine leiomyoma. By pelvic MRI, a typicalleiomyoma in the posterior uterine body (longarrow) appears as a well-circumscribed mass. It is hy-pointense on a T2-weighted image (A) and isoin-tense to myometrium on a T1-weighted precontrastimage (B). It homogeneously enhances after contrast(C) similarly to the myometrium. A leiomyoma withhemorrhagic infarction (short arrow) in the anterioruterine body is also hypointense on a T2-weightedimage, but has increased signal on the precontrastT1-weighted image and no enhancement on thepostcontrast image.
Zampolin & Shi584
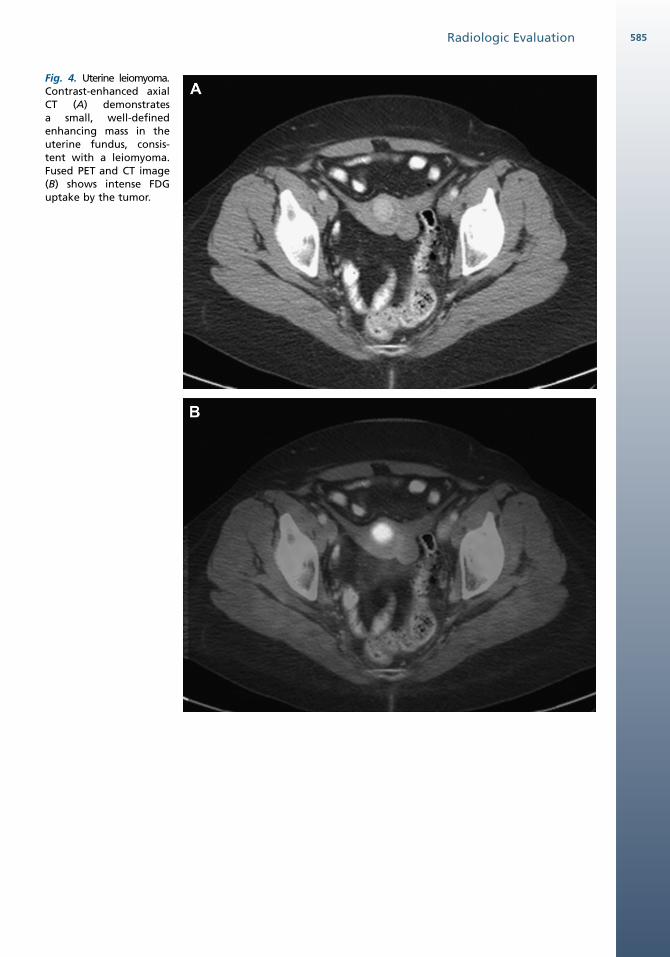
Fig. 4. Uterine leiomyoma.Contrast-enhanced axialCT (A) demonstratesa small, well-definedenhancing mass in theuterine fundus, consis-tent with a leiomyoma.Fused PET and CT image(B) shows intense FDGuptake by the tumor.
Radiologic Evaluation 585
Zampolin & Shi586
Lipoleiomyoma, a variant of leiomyoma, can bedefinitively characterized by imaging. These arerare, benign tumors composed histologically of vari-able amounts of smooth muscle, fat cells, andfibrous tissue, thought to arise from fatty metamor-phosisof smoothmuscle cells in leiomyomas. Theseare well-circumscribed tumors that are hyperechoicon US. On CT and MRI, lipoleiomyomas containeasily identifiable areas of fat (see Fig. 2).11,12
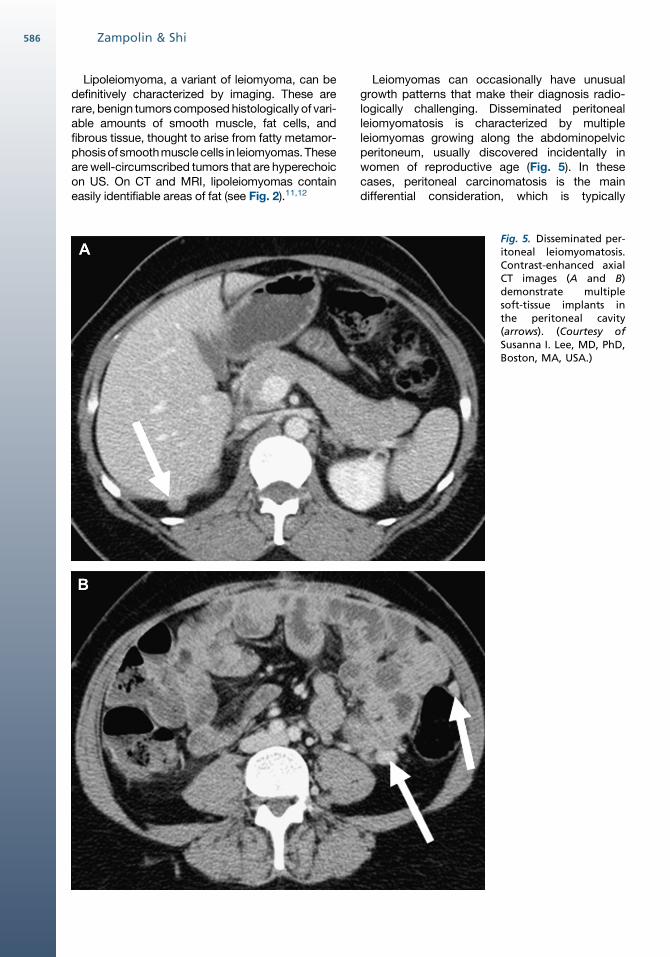
Leiomyomas can occasionally have unusualgrowth patterns that make their diagnosis radio-logically challenging. Disseminated peritonealleiomyomatosis is characterized by multipleleiomyomas growing along the abdominopelvicperitoneum, usually discovered incidentally inwomen of reproductive age (Fig. 5). In thesecases, peritoneal carcinomatosis is the maindifferential consideration, which is typically
Fig. 5. Disseminated per-itoneal leiomyomatosis.Contrast-enhanced axialCT images (A and B)demonstrate multiplesoft-tissue implants inthe peritoneal cavity(arrows). (Courtesy ofSusanna I. Lee, MD, PhD,Boston, MA, USA.)
Radiologic Evaluation 587
associated with weight loss, ascites, and diseaseprogression.13,14 Other entities that should beconsidered in the differential diagnoses are meso-thelioma, lymphoma, tuberculous peritonitis, anddesmoid tumor, which can be radiologically indis-tinguishable from disseminated peritoneal leio-myomatosis. Benign metastasizing leiomyoma ischaracterized by the presence of single ormultiple nodules, usually pulmonary, composedof benign-appearing smooth muscle in womenwho have had typical uterine leiomyomas, orrarely leiomyomas with vascular invasion or intra-venous leiomyomatosis.15 Other sites affectedinclude retroperitoneal and mediastinal lymph no-des, soft tissue, bone, and skin. These distantlesions are easily confused with metastaticdisease by imaging studies because of their loca-tion. Rarely, benign smooth muscle proliferationscan grow in uterine or systemic veins (intravenousleiomyomatosis) and may extend into the inferiorvena cava (IVC) and even into the heart.16 Onimaging, when intravenous leiomyomatosisextends beyond uterine vessels, it may mimica uterine sarcoma with extrauterine extension orvascular spread. If IVC involvement is seen, a leio-myosarcoma arising from the wall of the IVCshould be included in the differential diagnosis.Nontumor or tumor-related thrombi (ie, renal cellcarcinoma) can usually be excluded based onlack of enhancement or lack of a primary lesion.Parasitic leiomyoma is another rare entity thatcan mimic an ovarian mass or lymphadenopathy.It occurs when a subserosal leiomyomaundergoes torsion and twists off from its uterinepedicle; the now ‘‘free’’ leiomyoma develops neo-vascularization to surrounding structures such asthe broad ligament or omentum and thusbecomes ‘‘parasitic.’’ In all these unusualgrowths, a high degree of suspicion is needed,in the presence of coexistent uterine fibroids ora history of surgery for uterine fibroids, to makethe correct diagnosis and avoid unnecessarysurgery. Typical features of leiomyoma onimaging and lack of FDG avidity on PET imagingcan suggest the diagnosis.17 Nevertheless,a definitive diagnosis usually requires histologicexamination.
UTERINE SARCOMAS
Uterine sarcomas are a rare group of tumors, consti-tuting up to 6% of all uterine malignancies.18 Thethree most common histologic types are leiomyo-sarcoma, malignant mixed mullerian tumor, andendometrial stromal sarcoma. In general, uterinesarcomas are characterized by their aggressivenature, propensity for early metastasis, and poor
clinical outcomes.18 Differentiation among thevarious types of sarcomas and differentiation ofuterine sarcomas from other uterine neoplasmscannot reliablybeaccomplishedonclinicalgrounds,as they all commonly present with nonspecificabdominal pain and postmenopausal or dysfunc-tional uterine bleeding.19 Imaging is useful to narrowthe differential diagnosis and aids in pretreatmentstaging and monitoring posttreatment response.
Leiomyosarcoma comprises approximately40% to 50% of all uterine sarcomas, with a peakincidence in women between 40 and 60 years ofage.20 Leiomyosarcoma typically arises de novo21
and only rarely from a preexisting leiomyoma.22
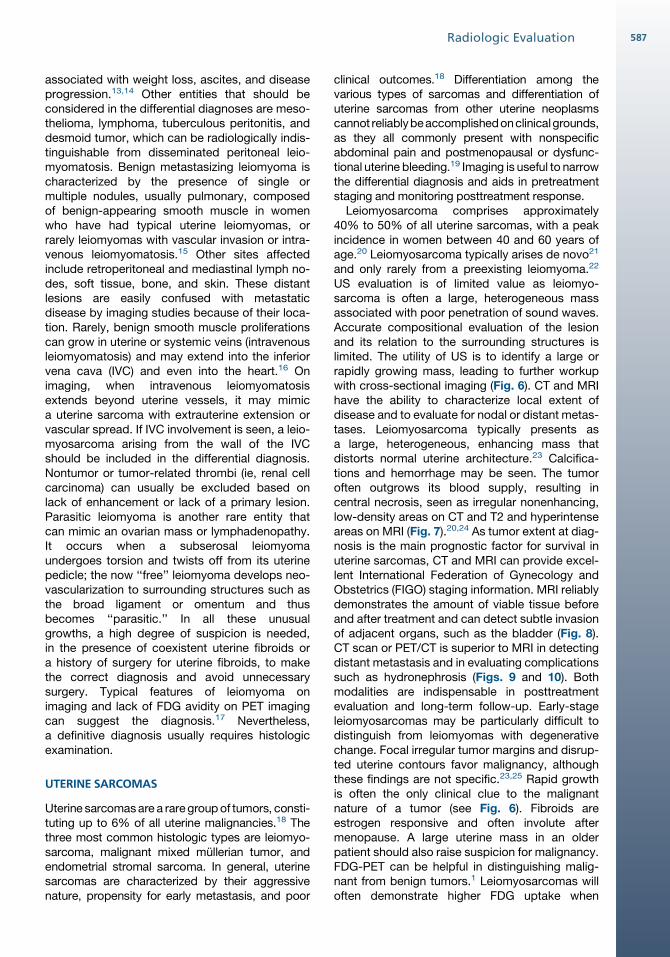
US evaluation is of limited value as leiomyo-sarcoma is often a large, heterogeneous massassociated with poor penetration of sound waves.Accurate compositional evaluation of the lesionand its relation to the surrounding structures islimited. The utility of US is to identify a large orrapidly growing mass, leading to further workupwith cross-sectional imaging (Fig. 6). CT and MRIhave the ability to characterize local extent ofdisease and to evaluate for nodal or distant metas-tases. Leiomyosarcoma typically presents asa large, heterogeneous, enhancing mass thatdistorts normal uterine architecture.23 Calcifica-tions and hemorrhage may be seen. The tumoroften outgrows its blood supply, resulting incentral necrosis, seen as irregular nonenhancing,low-density areas on CT and T2 and hyperintenseareas on MRI (Fig. 7).20,24 As tumor extent at diag-nosis is the main prognostic factor for survival inuterine sarcomas, CT and MRI can provide excel-lent International Federation of Gynecology andObstetrics (FIGO) staging information. MRI reliablydemonstrates the amount of viable tissue beforeand after treatment and can detect subtle invasionof adjacent organs, such as the bladder (Fig. 8).CT scan or PET/CT is superior to MRI in detectingdistant metastasis and in evaluating complicationssuch as hydronephrosis (Figs. 9 and 10). Bothmodalities are indispensable in posttreatmentevaluation and long-term follow-up. Early-stageleiomyosarcomas may be particularly difficult todistinguish from leiomyomas with degenerativechange. Focal irregular tumor margins and disrup-ted uterine contours favor malignancy, althoughthese findings are not specific.23,25 Rapid growthis often the only clinical clue to the malignantnature of a tumor (see Fig. 6). Fibroids areestrogen responsive and often involute aftermenopause. A large uterine mass in an olderpatient should also raise suspicion for malignancy.FDG-PET can be helpful in distinguishing malig-nant from benign tumors.1 Leiomyosarcomas willoften demonstrate higher FDG uptake when
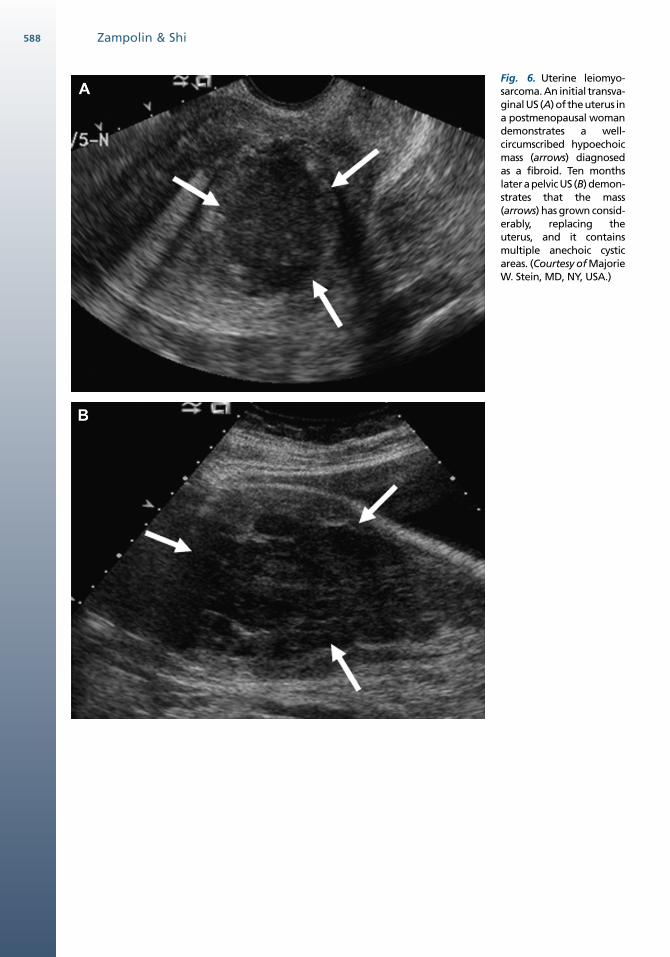
Fig. 6. Uterine leiomyo-sarcoma. An initial transva-ginalUS (A)of theuterus ina postmenopausal womandemonstrates a well-circumscribed hypoechoicmass (arrows) diagnosedas a fibroid. Ten monthslaterapelvicUS (B)demon-strates that the mass(arrows) has grown consid-erably, replacing theuterus, and it containsmultiple anechoic cysticareas. (Courtesy of MajorieW. Stein, MD, NY, USA.)
Zampolin & Shi588
Fig. 7. Uterine leiomyosarcoma. On axial contrast-enhanced CT (A), a large, heterogeneously enhancing masswith nonenhancing, necrotic central areas is seen. Sagittal T2-weighted MRI (B) and sagittal T1-weighted post-contrast MRI (C) demonstrate a large heterogeneous, enhancing mass replacing the uterus. After embolization(D) there is decreased enhancement of the tumor. (Courtesy of Susanna I. Lee, MD, PhD, Boston, MA, USA.)
589Radiologic Evaluation
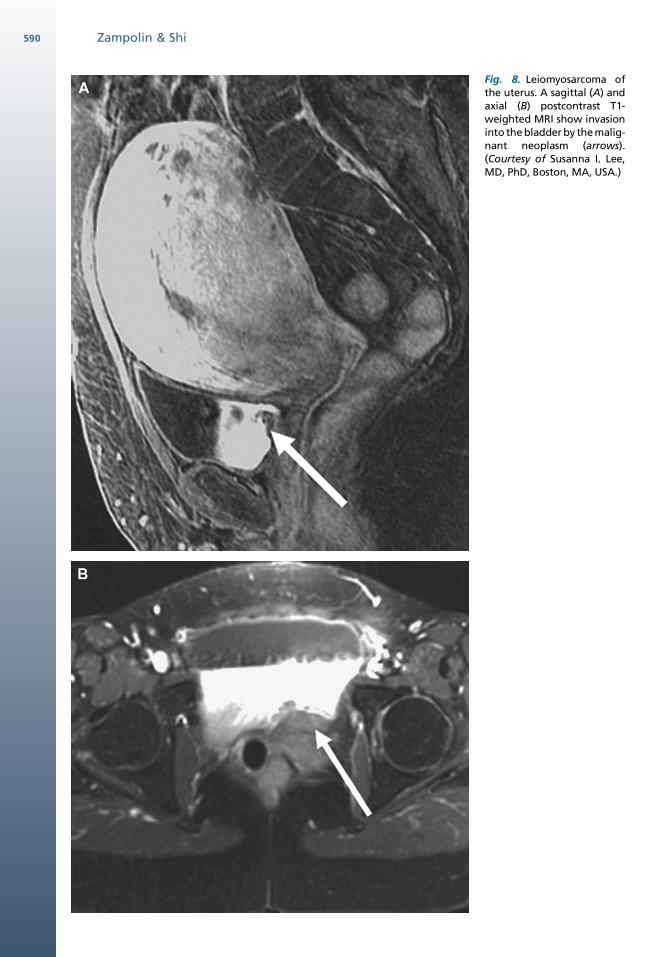
Fig. 8. Leiomyosarcoma ofthe uterus. A sagittal (A) andaxial (B) postcontrast T1-weighted MRI show invasioninto the bladder by the malig-nant neoplasm (arrows).(Courtesy of Susanna I. Lee,MD, PhD, Boston, MA, USA.)
Zampolin & Shi590
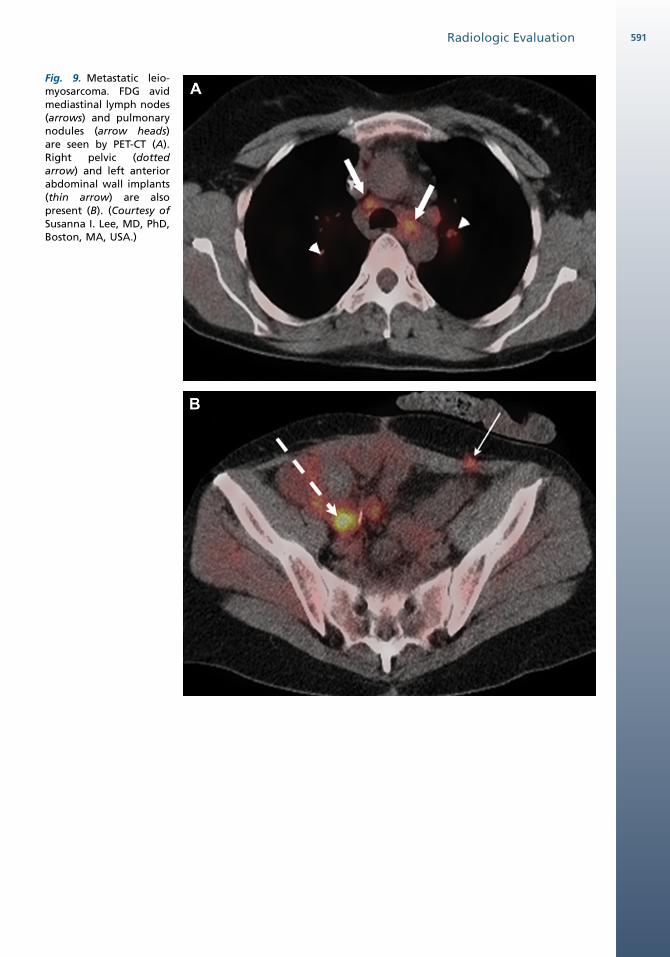
Fig. 9. Metastatic leio-myosarcoma. FDG avidmediastinal lymph nodes(arrows) and pulmonarynodules (arrow heads)are seen by PET-CT (A).Right pelvic (dottedarrow) and left anteriorabdominal wall implants(thin arrow) are alsopresent (B). (Courtesy ofSusanna I. Lee, MD, PhD,Boston, MA, USA.)
Radiologic Evaluation 591
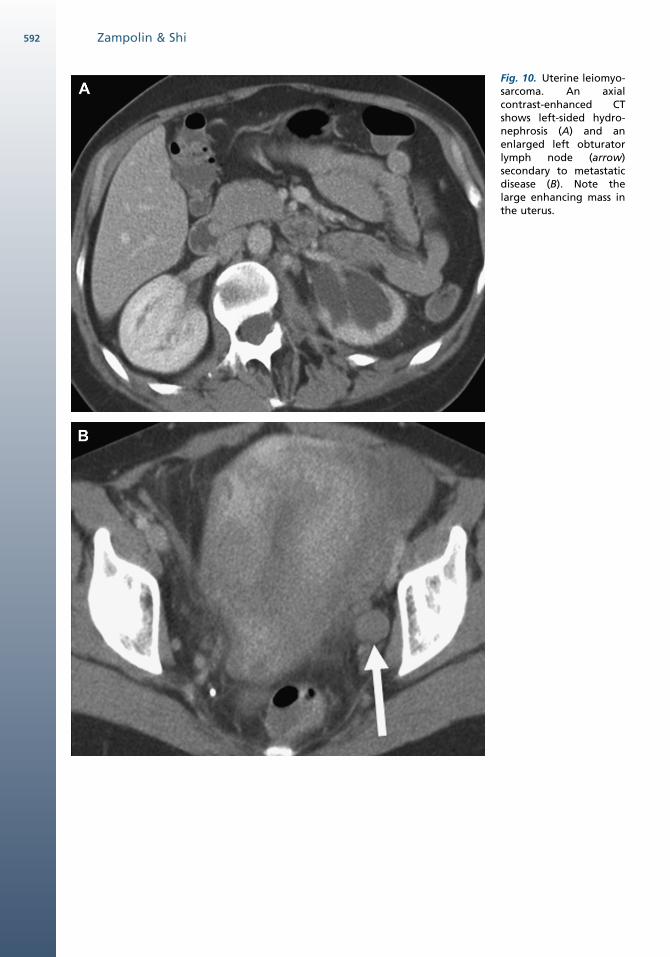
Fig. 10. Uterine leiomyo-sarcoma. An axialcontrast-enhanced CTshows left-sided hydro-nephrosis (A) and anenlarged left obturatorlymph node (arrow)secondary to metastaticdisease (B). Note thelarge enhancing mass inthe uterus.
Zampolin & Shi592
Radiologic Evaluation 593
compared to leiomyomas. Ring accumulation oftracer activity suggests intratumoral necrosis,whereas heterogeneous accumulation suggeststhe presence of areas with of different morphol-ogies.26,27 New agents may increase the useful-ness of PET in evaluating uterine sarcomas. Forexample, combining the use of FDG and 16a-[18F]fluoro-17b-estradiol (FES) to study the rela-tionship between estrogen receptor expressionand glucose metabolic activity in benign andmalignant uterine tumors, leiomyomas demon-strate significantly higher uptake of FES thanFDG, whereas sarcomas demonstrate the oppo-site tendencies in tracer uptake.28
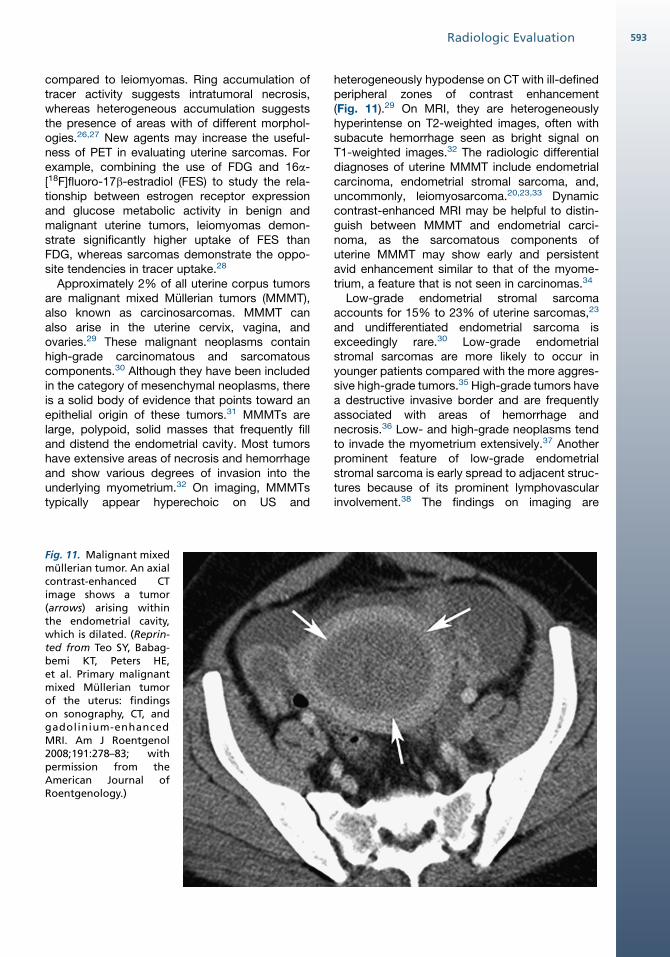
Approximately 2% of all uterine corpus tumorsare malignant mixed Mullerian tumors (MMMT),also known as carcinosarcomas. MMMT canalso arise in the uterine cervix, vagina, andovaries.29 These malignant neoplasms containhigh-grade carcinomatous and sarcomatouscomponents.30 Although they have been includedin the category of mesenchymal neoplasms, thereis a solid body of evidence that points toward anepithelial origin of these tumors.31 MMMTs arelarge, polypoid, solid masses that frequently filland distend the endometrial cavity. Most tumorshave extensive areas of necrosis and hemorrhageand show various degrees of invasion into theunderlying myometrium.32 On imaging, MMMTstypically appear hyperechoic on US and
Fig. 11. Malignant mixedmullerian tumor. An axialcontrast-enhanced CTimage shows a tumor(arrows) arising withinthe endometrial cavity,which is dilated. (Reprin-ted from Teo SY, Babag-bemi KT, Peters HE,et al. Primary malignantmixed Mullerian tumorof the uterus: findingson sonography, CT, andgadolinium-enhancedMRI. Am J Roentgenol2008;191:278–83; withpermission from theAmerican Journal ofRoentgenology.)
heterogeneously hypodense on CT with ill-definedperipheral zones of contrast enhancement(Fig. 11).29 On MRI, they are heterogeneouslyhyperintense on T2-weighted images, often withsubacute hemorrhage seen as bright signal onT1-weighted images.32 The radiologic differentialdiagnoses of uterine MMMT include endometrialcarcinoma, endometrial stromal sarcoma, and,uncommonly, leiomyosarcoma.20,23,33 Dynamiccontrast-enhanced MRI may be helpful to distin-guish between MMMT and endometrial carci-noma, as the sarcomatous components ofuterine MMMT may show early and persistentavid enhancement similar to that of the myome-trium, a feature that is not seen in carcinomas.34
Low-grade endometrial stromal sarcomaaccounts for 15% to 23% of uterine sarcomas,23
and undifferentiated endometrial sarcoma isexceedingly rare.30 Low-grade endometrialstromal sarcomas are more likely to occur inyounger patients compared with the more aggres-sive high-grade tumors.35 High-grade tumors havea destructive invasive border and are frequentlyassociated with areas of hemorrhage andnecrosis.36 Low- and high-grade neoplasms tendto invade the myometrium extensively.37 Anotherprominent feature of low-grade endometrialstromal sarcoma is early spread to adjacent struc-tures because of its prominent lymphovascularinvolvement.38 The findings on imaging are
Key FeaturesUTERINE TUMORS
Differential diagnosis
Leiomyoma, leiomyosarcoma, MMMT, endome-trial stromal sarcoma, lymphoma, endometrialcarcinoma, metastasis, adenomyosis
Imaging pearls
Leiomyomas are typically well circumscribed,hypoechoic on US, and hypointense on T2-weighted images
Lipoleiomyoma can be definitively diagnosedbased on imaging
Features that favor malignancy include largesize, irregular margin, rapid growth, and olderage
PET and PET/CT are useful in distinguishingbenign versus malignant mesenchymal tumors
Uterine sarcomas appear as large masses withextensive hemorrhage and necrosis by imagingand demonstrate rapid growth on serialimaging
MMMT and endometrial stromal sarcomas aremore likely to be centered within and expand-ing the endometrium, whereas leiomyosarco-mas typically arise from the myometrium
Imaging pitfalls
Degenerative leiomyoma can have overlappingimaging features with malignant tumors
Leiomyomas with unusual growth patterns:
Disseminated peritoneal leiomyomatosis mimicsperitoneal carcinomatosis, mesothelioma,lymphoma, tuberculous peritonitis, and des-moid tumor
Benignmetastasizing leiomyomamimicsameta-static malignant tumor
Intravenous leiomyomatosis can simulatea uterine malignancy or IVC sarcoma
Parasitic leiomyoma can be confused with anovarian mass or lymphadenopathy
Key FeaturesVAGINAL AND VULVARMESENCHYMAL
TUMORS
Differential diagnosis
Leiomyoma, leiomyosarcoma, aggressive an-giomyxoma, angiomyofibroblastoma, cellularangiofibroma, peripheral nerve sheath tumor,malignant fibrous histiocytoma, liposarcoma
Imaging pearls
Leiomyoma and angiofibroblastoma are wellcircumscribed
A large tumor with infiltrative margins tendsto be malignant
A whorled pattern of signal intensity on T2-weighted images is reported to be typical ofaggressive angiomyxoma
Imaging pitfalls
Tumor infiltration may be difficult to discernwith smaller tumors
Zampolin & Shi594
nonspecific and variable, ranging from a discretemass to multiple masses associated with diffuseinfiltration of the myometrium. Bands of low-signalintensity can be observed within the areas of myo-metrial involvement, corresponding to preservedbundles of myometrium on pathologic examina-tion.36 Some investigators have demonstratedthat especially high-grade sarcomas are likely topresent as large endometrial masses with irregular
margins, peripheral nodularity, and myometrialnodules on MR imaging. In addition, increasedenhancement, in at least a part of the tumor, ismore commonly observed in endometrialstromal sarcoma compared with endometrialcarcinoma.35
VAGINA AND VULVA
LEIOMYOMA
The most common benign mesenchymal tumor ofthe vagina and vulva is the leiomyoma. Its radio-logic features are similar to those described inuterine leiomyomas. Vaginal leiomyomas usuallypresent as a single solid nodule most frequentlyarising from the midline anterior wall and rarelyfrom the posterior wall, whereas vulvar tumorsare typically subcutaneous.39 Myxoid degenera-tion can occur, especially in pregnancy, and inthese cases the imaging features may overlapwith those seen in other tumors.
SARCOMAS
Sarcomas account for less than 3% of primaryvaginal malignancies and they are even rarer inthe vulva. Primary vaginal leiomyosarcoma is themost common vaginal soft-tissue sarcoma inadults.40 It accounts for less than 2% of all primaryvaginal cancers, with a wide age range (25–86years).41 Leiomyosarcomas may develop after

Radiologic Evaluation 595
radiation therapy. They are thought to originatefrom the rectovaginal septum and mainly involvethe upper vagina, grossly appearing as bulkysubmucosal tumors.41 US and CT have limitedutility in assessment of the primary tumor becauseof poor soft-tissue contrast. MRI provides superiorsoft-tissue resolution and displays the perinealstructures with exquisite detail being the modalityof choice in evaluating size, location, and extent oftumor. Vaginal and vulvar leiomyosarcomas aresimilar to uterine leiomyosarcomas on MRI.42,43
Differentiating leiomyosarcoma from its benigncounterpart can be difficult on imaging. A largetumor with infiltrative margins is more likely to bemalignant, whereas leiomyomas are typicallywell-defined, homogeneous, and enhance vividlyafter contrast administration.44
In children, sarcoma botryoides (embryonalrhabdomyosarcoma) is a rare aggressive tumoroccurring typically in girls. It grows as a grapelikemass with mixed high and low intensity on T2-weighted MR, and significant enhancement.45
The imaging features of adult rhabdomyosar-comas have not been well studied. They havebeen reported to show a large uterine tumor withintermediate marbled background of T2-signalintensity with pockets of high T2-signal intensity.
Fig. 12. Aggressive angio-myxoma. A T2-weightedMR image shows a tumorextending from perineumto the upper pelvis. Notethe characteristic whorledpattern of alternating brightand dark signal intensity(black arrows). (Reprintedfrom Outwater EK, Marche-tto BE, Wagner BJ, et al.Aggressive angiomyxoma:findings on CT and MRimaging. AJR Am J Roent-genol 1999;172:435–8; withpermission from theAmerican Journal ofRoentgenology.)
T1-weighted images reveal a homogenous low-signal intensity mass.20
OTHERMESENCHYMALTUMORS
Aggressive angiomyxoma (AA) is a distinctiveneoplasm that occurs in young women, character-ized by a large size, an infiltrative growth pattern,and a myxoid matrix. It usually grows along tissueplanes, displacing rather than invading the pelvicorgans.46 On CT, it appears as a well-defined,moderately enhancing mass within the pelvis orperineum that is iso- or hypoattenuating relativeto muscle. On MRI, it is iso- or hypointense onT1-weighted images and hyperintense on T2-weighted images.47,48 The high-signal intensityseen on T2-weighted images reflects the highmyxomatous content of these tumors. A whorledpattern of signal intensity on T2-weighted imageshas been reported as a typical feature of this tumor(Fig. 12).49–51 Strong contrast enhancementreflects the inherent vascularity of this lesion.
Angiomyofibroblastoma (AMFB), first describedby Fletcher and colleagues as a distinct entity fromAA,52 occurs predominantly in the vulva of middle-aged women. In the scant literature on its radio-logic findings, it has been reported that the tumor

Key FeaturesOVARIANMESENCHYMALTUMORS
Differential diagnosis
Epithelial tumors, granulosa cell tumors,fibroma/fibrothecoma, Sertoli-Leydig celltumors, metastasis, leiomyoma, sarcomas
Imaging pearls
Fibroma/fibrothecoma are characteristically darkon T2-weighted MRI
A ‘‘spongelike’’ appearance is characteristic ofgranulosa cell tumor
Ovarian leiomyoma enhances avidly, whereasfibroma/fibrothecoma demonstrate weak enhance-ment
Imaging pitfalls
Brenner cell tumor may mimic the radiologicappearance of a fibrothecoma
Zampolin & Shi596
has intermediate to hypertense signal on T2-weighted MRI and enhances homogeneously, inaccordance with its prominent vascularity. In onecase, nodular and curvilinear dark T2-signal inten-sities have been observed, which corresponded toareas of hypocellularity and abundant collagenousstroma as seen on the pathologic specimen.53–55
As AMFBs may have microscopic fat, chemicalshift (in-phase, opposed-phase) MRI studies maybe helpful in its diagnosis.56 AMFBs may be diffi-cult to differentiate from AA because they occurin similar locations and the imaging features mayoverlap. Recognition of the well-circumscribedappearance of AMFB is an important radiologicdifferential diagnostic criterion. AA tends to belarger and shows more infiltrative margins54;however, infiltration may be difficult to evaluate insmaller tumors. Cellular angiofibroma, anothermesenchymal tumor of the vulva and perineum,should also be included in the differential diag-nosis; however, no radiologic findings have yetbeen reported for these tumors. Smooth-muscleneoplasms can also mimic AA or AMFB. The differ-ential diagnoses of soft-tissue tumors occurring inthe vagina, vulva, and perineum in an adult womanalso include other rare neoplasms such as periph-eral nerve sheath tumor, malignant fibrous histio-cytoma, and liposarcoma. These tumors mayhave myxoid contents and thus, they may be indis-tinguishable from the entities discussed earlierbased on imaging.
OVARY
LEIOMYOMA
Leiomyoma of the ovary is one of the rarest solidtumors of the ovary, constituting only 0.5% to1% of benign ovarian neoplasms.57,58 Theycommonly occur in middle-aged women, areusually unilateral, and frequently (80%) coexistwith uterine leiomyomas.57 Imaging features aresimilar to leiomyomas elsewhere. Ovarian tumorssuch as fibroma or fibrothecoma are the mostimportant entities to consider in the differentialdiagnoses.59 The early contrast enhancement ofleiomyomas may help differentiate them fromthese other ovarian tumors, which tend to enhanceweakly.59
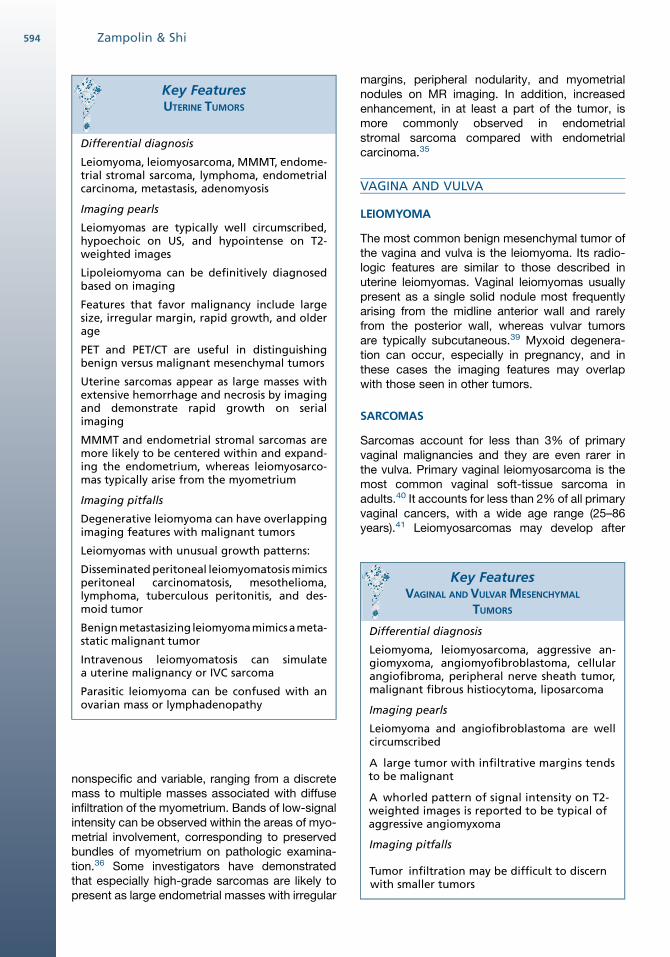
FIBROTHECOMATOUS TUMORS
Fibroma, fibrothecoma, and thecoma are a spec-trum of benign tumors that as a group comprise4% to 6% of all ovarian neoplasms and areconsidered the most common solid primaryneoplasm of the ovary and the most common
stromal tumors. Pure thecomas, composed ofa single population of lipid-rich thecal cells, areuncommon.60 They have imaging features thatare non-specific on US and CT, similar to othersolid ovarian neoplasms.61,62 On MR, pure theco-mas demonstrate relatively high signal on T1- andT2-weighted imaging and can display chemicalshift artifacts on opposed-phase imaging.61,63
The majority of tumors are composed of a mixedpopulation of fibroblasts (which predominate)with scant interspersed collagenous connectivetissue and thecal cells.64 This admixture providesa characteristic appearance on MRI. Homoge-neous, markedly hypointense signal on T2-weighted images is highly suggestive of this entity.Fibrothecomas may be slightly hypointense onT1-weighted images and demonstrate variable,but generally weak enhancement depending onthe amount of fibrous tissue (Fig. 13). On US,they appear as well-circumscribed, homoge-neously hypoechoic solid masses often with signif-icant sound attenuation.65,66 However,fibrothecomas can have variable US appearances,ranging from hyperechoic to hypoechoic withincreased through transmission.67 On CT, theyare well-circumscribed soft tissue density massesand commonly have calcifications (Fig. 14). Largetumors may have areas of edema and degenera-tion.61 Fibrothecomas can be difficult to differen-tiate from leiomyomas and other sex cordstromal tumors. Among the latter, granulosa celltumors (adult and juvenile) most commonly appearas large, unilateral, multiseptated cystic masseswith multiple thickened, irregular septations
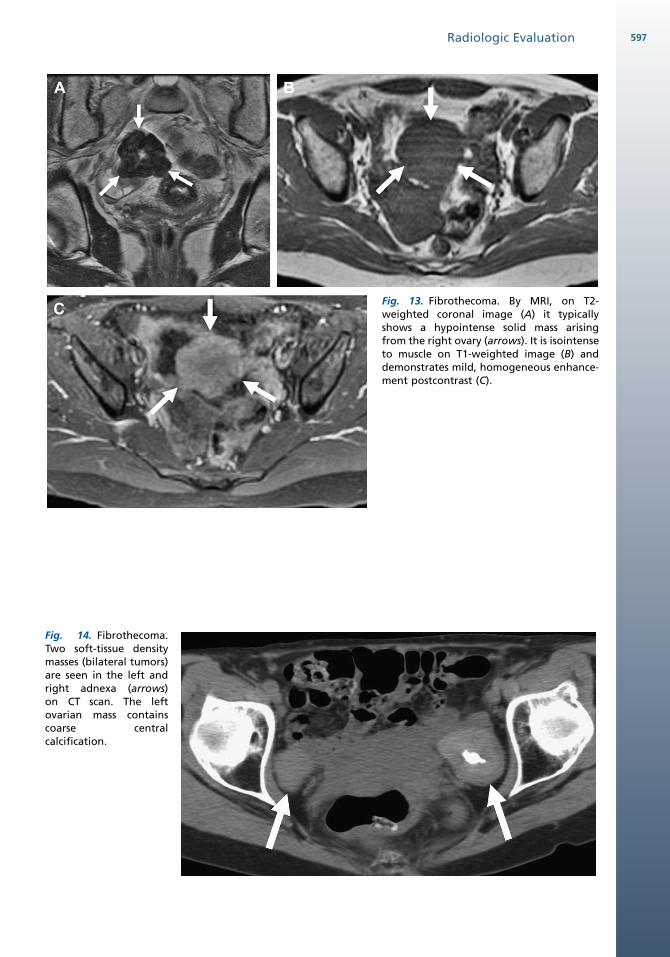
Fig. 13. Fibrothecoma. By MRI, on T2-weighted coronal image (A) it typicallyshows a hypointense solid mass arisingfrom the right ovary (arrows). It is isointenseto muscle on T1-weighted image (B) anddemonstrates mild, homogeneous enhance-ment postcontrast (C).
Fig. 14. Fibrothecoma.Two soft-tissue densitymasses (bilateral tumors)are seen in the left andright adnexa (arrows)on CT scan. The leftovarian mass containscoarse centralcalcification.
Radiologic Evaluation 597
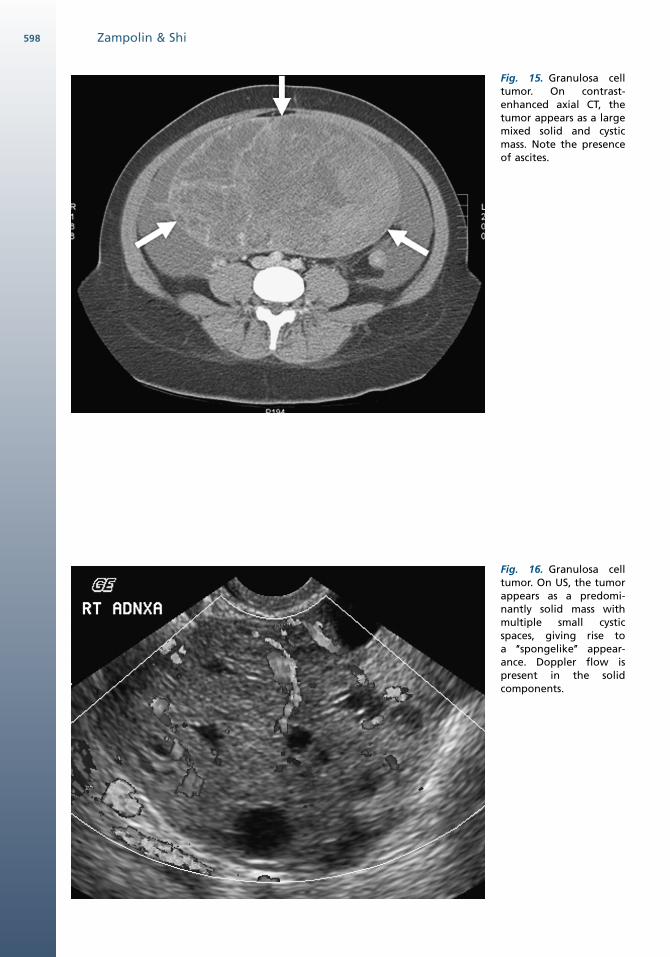
Fig. 15. Granulosa celltumor. On contrast-enhanced axial CT, thetumor appears as a largemixed solid and cysticmass. Note the presenceof ascites.
Fig. 16. Granulosa celltumor. On US, the tumorappears as a predomi-nantly solid mass withmultiple small cysticspaces, giving rise toa ‘‘spongelike’’ appear-ance. Doppler flow ispresent in the solidcomponents.
Zampolin & Shi598
Radiologic Evaluation 599
interspersed with solid components (Fig. 15).68 A‘‘spongelike’’ appearance with solid componentsinterdigitated with innumerable cystic spaces ischaracteristic of granulosa cell tumors, thoughtto reflect its macrofollicular pattern of growth(Fig. 16).61,68 Frequent hemorrhage into thesecystic spaces is common. The solid componentsof granulosa cell tumors tend to be hypointenseon T1- and T2-weighted images, reflecting theirrich fibrous stroma. Brenner tumor, classified asan epithelial neoplasm, may also appear as a solidT2 hypointense lesion on MRI because of its
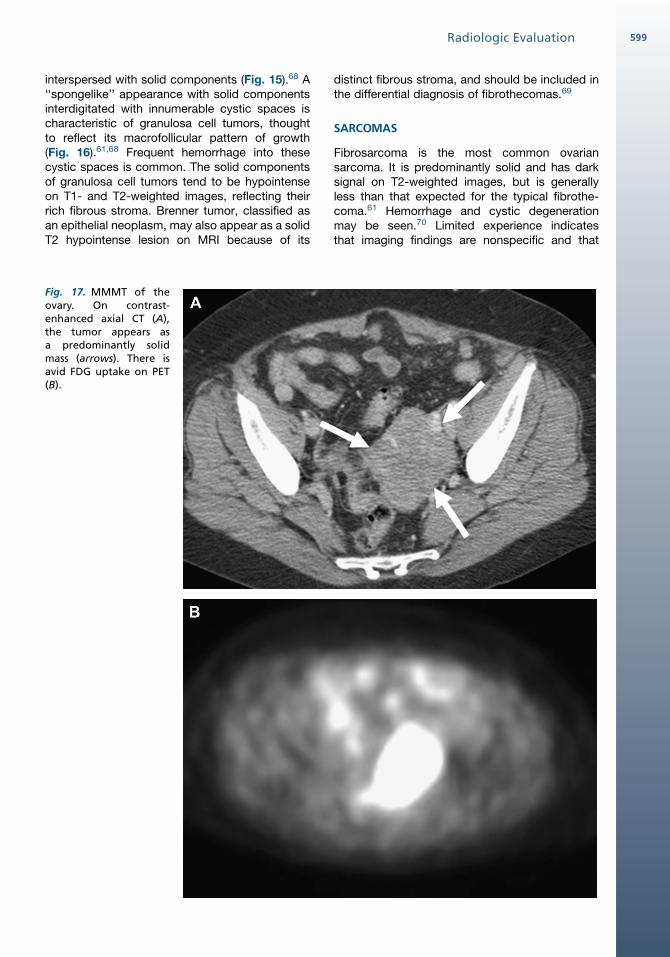
Fig. 17. MMMT of theovary. On contrast-enhanced axial CT (A),the tumor appears asa predominantly solidmass (arrows). There isavid FDG uptake on PET(B).
distinct fibrous stroma, and should be included inthe differential diagnosis of fibrothecomas.69
SARCOMAS
Fibrosarcoma is the most common ovariansarcoma. It is predominantly solid and has darksignal on T2-weighted images, but is generallyless than that expected for the typical fibrothe-coma.61 Hemorrhage and cystic degenerationmay be seen.70 Limited experience indicatesthat imaging findings are nonspecific and that

Zampolin & Shi600
histology is required for accurate diagnosis.Malignant mixed Mullerian tumor of the ovary israre. It usually presents as aggressive, bilateral,large, solid, and cystic tumors associated withascites, frequent peritoneal seeding, and adjacentorgan invasion (Fig. 17).71 FDG-PET is helpful inconfirming its hypermetabolic, and therefore likelymalignant nature. Leiomyosarcoma, another rareovarian sarcoma, has no specific imagingfeatures.
REFERENCES
1. Yoshida Y, Kurokawa T, Sawamura Y, et al. Compar-
ison of 18F-FDG PETand MRI in assessment of uterine
smooth muscle tumors. J Nucl Med 2008;49:708–12.
2. Park JY, Kim EN, Kim DY, et al. Role of PET or PET/
CT in the post-therapy surveillance of uterine
sarcoma. Gynecol Oncol 2008;109:255–62.
3. Strauss LG. Fluorine-18 deoxyglucose and false
positive results: a major problem in the diagnostics
of oncologic patients. Eur J Nucl Med 1996;23:
1409–15.
4. Garcia Velloso MJ, Boan Garcia JF, Villar Luque
Lerman H, et al. Normal and abnormal 18F-FDG
endometrial and ovarian uptake in pre- and post-
menopausal patients: assessment by PET/CT.
J Nucl Med 2004;45:266–71.
5. Szklaruk F, Tamm EP, Choi H, et al. MR Imaging of
common and uncommon large pelvic masses.
Radiographics 2003;23:403–24.
6. Karasick S, Lev-Toaff A, Toaff ME. Imaging of uterine
leiomyomas. Am J Roentgenol 1992;158:799–805.
7. Hulka CA, Hall DA, McCarthy k, et al. Sonographic
findings in patients with adenomyosis: can sonog-
raphy assist in predicting extant of disease? Am J
Roentgenol 2002;179:379–83.
8. Casillas J, Joseph RC, Guerra JJ. CT appearance of
uterine leiomyomas. Radiographics 1990;10:
999–1007.
9. Hricak H. MRI of the female pelvis: a review. Am J
Roentgenol 1986;146:1115–22.
10. Saksena MA, Blake MA, Brachtel E, et al. Uterine
fibroid 18F-fluorodeoxyglucose (FDG) uptake on
combined PET-CT: genitourinary—imaging the
male and female pelvis with CT, MRI, and ultra-
sound. Am J Roentgenol 2006;186(Suppl 4):A20–4.
11. Tsushima Y, Kita T, Yamamoto K. Uterine lipoleio-
myoma: MRI, CT and ultrasonographic findings. Br
J Radiol 1997;70:1068–70.
12. Ishigami K, Yoshimitsu K, Honda H, et al. Uterine lip-
oleiomyoma: MRI appearances. Abdom Imaging
1998;23:214–6.
13. Fasih N, Prasad Shanbhogue AK, Macdonald DB,
et al. Leiomyomas beyond the uterus: unusual loca-
tions, rare manifestations. Radiographics 2008;28:
1931–48.
14. Papadatos D, Taourel P, Bret PM. CT of leiomyoma-
tosis peritonealis disseminata mimicking peritoneal
carcinomatosis. Am J Roentgenol 1996;167:475–6.
15. Lee HJ, Choi J, Kim KR. Pulmonary benign metasta-
sizing leiomyoma associated with intravenous leio-
myomatosis of the uterus: clinical behavior and
genomic changes supporting a transportation
theory. Int J Gynecol Pathol 2008;27:340–5.
16. Kocica MJ, Vranes MR, Kostic D, et al. Intravenous
leiomyomatosis with extension to the heart: rare or
underestimated? J Thorac Cardiovasc Surg 2005;
130:1724–6.
17. Cohen DT, Oliva E, Hahn PF, et al. Uterine smooth-
muscle tumors with unusual growth patterns: imaging
with pathologic correlation. Am J Roentgenol 2007;
188:246–55.
18. Lurain JR. Uterine cancer. In: Berek JS, Adashi EY,
Hillard PA, editors. Novak’s gynecology. Philadel-
phia: Williams & Wilkins; 1991. p. 1057–110.
19. Lin JF, Slomovitz BM. Uterine sarcoma 2008. Curr
Oncol Rep 2008;10(6):512–8.
20. Sahdev A, Sohaib SA, Jacobs I, et al. MR imaging of
uterine sarcomas. Am J Roentgenol 2001;177:
1307–11.
21. Crum CP. The female genital tract. In: Contan RS,
Kumar V, Collins T, editors. Robbins: pathologic
basis of disease. 6th edition. Philadelphia: WB
Saunders; 1991. p. 1064–5.
22. Janus CJ, White M, Dottino P, et al. Uterine leiomyo-
sarcoma: magnetic resonance imaging. Gynecol
Oncol 1989;32:79–81.
23. Rha SE, Byun JY, Jung SE, et al. CT and MRI of
uterine sarcomas and their mimickers. Am J Roent-
genol 2003;181:1369–74.
24. Kaphanpaa KV, Wahlstrom T, Grohn P, et al.
Sarcomas of the uterus: a clinicopathologic study
of 119 patient. Obstet Gynecol 1986;67:417–24.
25. Pattani SJ, Kier R, Deal R, et al. MRI of uterine
leiomyosarcoma. Magn Reson Imaging 1995;13:
331–3.
26. Karube M, Minagawa Y, Shizukuishi K, et al. FDG-
PET findings of uterine leiomyosarcoma: correlative
analysis with MR images and pathology. J Nucl
Med 2007;48:387P Meeting Abstract.
27. Umesaki N, Tanaka T, Miyama M, et al. Positron
emission tomography with (18)F-fluorodeoxyglucose
of uterine sarcoma: a comparison with magnetic
resonance imaging and power Doppler imaging.
Gynecol Oncol 2001;80:372–7.
28. Tetsuya T, Yoshio Y, Tetsuya M, et al. Uterine tumors:
pathophysiologic imaging with 16a-[18F]fluoro-17b-
estradiol and 18F fluorodeoxyglucose PET—initial
experience. Radiology 2008;248:599–605.
29. Smith T, Moy L, Runowicz C. Mullerian mixed
tumors: CT characteristics with clinical and patho-
logic observations. Am J Roentgenol 1997;169:
531–5.
Radiologic Evaluation 601
30. Tavassoli FA, Devilee P, editors. World Health Organi-
zation classification of tumours. Pathology and
genetics of tumours of the breast and female genital
organs. Lyon (France): IARC Press; 2003. p. 233–84.
31. McCluggage WG. Malignant biphasic uterine
tumours: carcinosarcomas or metaplastic carci-
nomas? J Clin Pathol 2002;55:321–5.
32. Teo SY, Babagbemi KT, Peters HE, et al. Primary
malignant mixed Mullerian tumor of the uterus: find-
ings on sonography, CT, and gadolinium-enhanced
MRI. Am J Roentgenol 2008;191:278–83.
33. Shapeero LG, Hricak H. Mixed mullerian sarcoma of
the uterus: MR imaging findings. Am J Roentgenol
1989;153:317–9.
34. Ohguri T, Aoki T, Watanabe H, et al. MRI findings
including gadolinium-enhanced dynamic studies of
malignant, mixed mesodermal tumors of the uterus:
differentiation from endometrial carcinomas. Eur
Radiol 2002;12:2737–42.
35. Oliva E, Clement PB, Young RH. Endometrial stromal
tumors: an update on a group of tumors with a protean
phenotype. Adv Anat Pathol 2000;7:257–81.
36. Ueda M, Otsuka M, Hatakenaka M, et al. MR
imaging findings of uterine endometrial stromal
sarcoma: differentiation from endometrial carci-
noma. Eur Radiol 2001;11:28–33.
37. Koyama T, Togashi K, Konishi I, et al. MR imaging of
endometrial stromal sarcoma: correlation with patho-
logic findings. Am J Roentgenol 1999;173:767–72.
38. Chang KL, Crabtree GS, Lim-Tan SK, et al. Primary
uterine endometrial stromal neoplasms: a clinico-
pathologic study of 117 cases. Am J Surg Pathol
1999;14:415–38.
39. Nielsen GP, Rosenberg AE, Koerner FC, et al.
Smooth-muscle tumors of the vulva. A clinicopatho-
logical study of 25 cases and review of the literature.
Am J Surg Pathol 1996;20:779–93.
40. Morrow CP, Curtin JP. Tumors of the vagina. In:
Morrow CP, Townsend DE, editors. Synopsis of
gynecological oncology. 5th edition. Philadelphia:
Churchill Livingstone; 1998. p. 89–105.
41. Tavassoli FA, Norris HJ. Smooth muscle tumors of
the vagina. Obstet Gynecol 1979;53:689–93.
42. Cantisani V, Mortele KJ, Kalantari BN, et al. Vaginal
metastasis from uterine leiomyosarcoma. Magnetic
resonance imaging features with pathological
correlation. J Comput Assist Tomogr 2003;27(5):
805–9.
43. Parikh JH, Barton DPJ, Ind TEJ, et al. MR imaging
features of vaginal malignancies. Radiographics
2008;28:49–63.
44. Betts MT, Huo EJ, Miller FH. Gastrointestinal and
genitourinary smooth-muscle tumors. Am J Roent-
genol 2003;181:1349–54.
45. Kobi M, Khatri G, Edelman M, et al. Sarcoma bo-
tryoides: MRI findings in two patients. J Magn Reson
Imaging 2009;29:708–12.
46. Nielsen GP, Young RH. Mesenchymal tumors and
tumor like lesions of the female genital tract. Int J
Gynecol Pathol 2001;2:105–27.
47. Davani M, Chablani VN, Saba PR. Aggressive
angiomyxoma of pelvic soft tissues: MR imaging
appearance. Am J Roentgenol 1998;170:1113–4.
48. Outwater EK, Marchetto BE, Wagner BJ, et al.
Aggressive angiomyxoma: findings on CT and MR
imaging. AJR Am J Roentgenol 1999;172:435–8.
49. Jeyadevan NN, Sohaib SA, Thomas JM, et al.
Imaging features of aggressive angiomyxoma. Clin
Radiol 2003;58:157–62.
50. Chien AJ, Freeby JA, Win TT, et al. Aggressive angio-
myxoma of the female pelvis: sonographic, CT and
MR findings. AJR Am J Roentgenol 1998;171:530–1.
51. Sinha R, Verma R. Case 106: aggressive angiomyx-
oma. Radiology 2007;242:625–7.
52. Fletcher CD, Tsang WY, Fisher C, et al. Angiomyofi-
broblastoma of the vulva. A benign neoplasm
distinct from aggressive angiomyxoma. Am J Surg
Pathol 1992;16:373–82.
53. Kitamura H, Miyao N, Sato Y, et al. Angiomyofibro-
blastoma of the female urethra. Int J Urol 1999;6:
268–70.
54. Mortele KJ, Lauwers GJ, Mergo PJ, et al. Perineal
angiomyofibroblastoma: CT and MR findings with
pathologic correlation. J Comput Assist Tomogr
1999;23:687–9.
55. Lim KJ, Moon JH, Yoon DY, et al. Angiomyofibro-
blastoma arising from the posterior perivesical
space: a case report with MR findings. Korean J
Radiol 2008;9:382–5.
56. Demir MK, Genchellac H, Ozdemir H, et al. Perineal
angiomyxomas: can a differential diagnosis be
made with imaging studies? Radiology 2007;245:
612–3.
57. Lerwill MF, Sung R, Oliva E, et al. Smooth muscle
tumors of the ovary: a clinicopathologic study of 54
cases emphasizing prognostic criteria, histologic
variants, and differential diagnosis. Am J Surg
Pathol 2004;28:1436–51.
58. Doss BJ, Wanek SM, Jacques SM, et al. Ovarian
leiomyomas: clinicopathologic features in fifteen
cases. Int J Gynecol Pathol 1999;18:63–8.
59. Tamada T, Sone T, Tanimoto D, et al. MRI appear-
ance of primary giant ovarian leiomyoma in a hyster-
ectomized woman. Br J Radiol 2006;79(946):
e126–8.
60. Scully RE, Young RH, Clement PB. Sertoli-stromal
cell, mixed and unclassified sex-cord stromal
tumors. In: Scully RE, editor. Tumors of the ovary,
maldeveloped gonads, fallopian tube and broad
ligament. 3rd edition. Washington, DC: Armed
Forces Institute of Pathology; 1998. p. 169–226.
61. Outwater EK, Wagner BJ, Mannion C, et al. Sex
cord-stromal and steroid cell tumors of the ovary.
Radiographics 1998;18:1523–46.

Zampolin & Shi602
62. Sutton CL, McKinney CD, Jones JE, et al. Ovarian
masses revisited: radiologic and pathologic correla-
tion. Radiographics 1992;12:853–77.
63. Tanaka YO, Saida TS, Minami R, et al. MR findings of
ovarian tumors with hormonal activity, with emphasis
on tumors other then sex cord-stromal tumors. Eur J
Radiol 2007;62(3):317–27.
64. Crum CP. The female genital tract. In: Cotran RS,
Kumar V, Collins T, editors. Robbins: pathologic
basis of disease. 6th edition. Philadelphia: WB
Saunders; 1991. p. 1076–7.
65. Stephenson WM, Laing FC. Sonography of ovarian
fibromas. Am J Roentgenol 1985;144:1239–40.
66. Bazot M, Ghossain MA, Buy J-N, et al. Fibrotheco-
mas of the ovary: CT and US findings. J Comput
Assist Tomogr 1993;17:754–9.
67. Athey PA, Malone RS. Sonography of ovarian
fibromas/thecomas. J Ultrasound Med 1987;6:431–6.
68. Kim SH, Kim SH. Granulosa cell tumor of the ovary:
common findings and unusual appearances on CT
and MR. J Comput Assist Tomogr 2002;26(5):756–61.
69. Outwater EK, Siegelman ES, Talerman A, et al.
Ovarian fibromas and cystadenofibromas: MRI
features of the fibrous component. J Magn Reson
Imaging 1997;7:465–71.
70. Testa H, Gaurilcikas A, Licameli A, et al. Sono-
graphic features of primary ovarian fibrosarcoma:
a report of two cases. Ultrasound Obstet Gynecol
2009;33:112–5.
71. Cho I, Park CM, Park SW, et al. Malignant mixed
mullerian tumor of the ovary: imaging findings. Eur
Radiol 2001;11:1147–50.