quantitative insulin analysis using liquid chromatography-tandem mass spectrometry in a...
TRANSCRIPT

Quantitative Insulin Analysis Using LiquidChromatography–Tandem Mass Spectrometry in a
High-Throughput Clinical LaboratoryZhaohui Chen,1 Michael P. Caulfield,1 Michael J. McPhaul,1 Richard E. Reitz,1 Steven W. Taylor,1
and Nigel J. Clarke1*
BACKGROUND: Circulating insulin concentrations re-flect the amount of endogenous insulin produced bythe pancreas and can be monitored to check for insulinresistance. Insulin is commonly measured using im-munochemiluminometric assays (ICMA). Unfortu-nately, differing crossreactivities of the various ICMAantibodies have led to variability in assay results. Incontrast, liquid chromatography–tandem mass spec-trometry (LC-MS/MS)-based approaches can providea highly specific alternative to immunoassays.
METHODS: Insulin was extracted from patient serum andreduced to liberate the insulin B chain. Subsequent reso-lution of the peptide was achieved by LC coupled to triple-quadrupole MS. Selected-reaction monitoring of B-chaintransitions was used for quantification. Recombinant hu-man insulin was used as a calibrator and was comparedagainst the National Institute for Biological Standards andControl (NIBSC) reference standard. Bovine insulin anda stable isotopic-labeled (13C/15N) human insulin B chainwere used and compared as internal standards.
RESULTS: The LC-MS/MS assay described herein hasbeen validated according to CLIA guidelines with alimit of detection of 1.8 �IU/mL (10.8 pmol/L) and alimit of quantitation of 3 �IU/mL (18.0 pmol/L).A correlation between the LC-MS/MS assay and a USFood and Drug Administration-approved ICMA wascompleted for patient samples and the resulting Dem-ing regression revealed good agreement. A referenceinterval for the assay was established.
CONCLUSIONS: A simple, high-throughput, quantitativeLC-MS/MS insulin assay traceable to the NIBSC stan-dard has been successfully developed and validated.© 2013 American Association for Clinical Chemistry
The detection of individuals with prediabetes and dia-betes may be achieved by measurement of fasting glu-cose, glycohemoglobin, and fasting insulin concentra-tions and glucose concentrations following an oralglucose load. Each of these methods is effective, buteach has drawbacks. Fasting glucose concentrationsthat are not within reference intervals reflect a physio-logical state in which early diabetes has already devel-oped. Increases in hemoglobin A1C can reflect eitherthe latter stages of prediabetes or overt diabetes. Oralglucose tolerance testing may identify insulin resis-tance earlier, but it involves a more involved dynamictesting and may not always be amenable to the clinicaltesting environment.
The measurement of fasting serum insulin hasbeen suggested as potentially providing a rapid andreadily accessible test to complement other existingmethodologies. Indeed, numerous studies have dem-onstrated increased concentrations of fasting insulin inpatients with prediabetes, even in the absence of in-creases of fasting glucose and hemoglobin A1C (1–5 ).In a limited number of circumstances, the utility offasting insulin measurements to detect early insulin re-sistance has been suggested (2, 6 ).
Immunological techniques have been widely usedfor insulin quantification, initially through radioim-munoassay, and more recently by commercially avail-able immunochemiluminometric assays (ICMAs)2 onautomated platforms (7 ). However, no internationalreference method for insulin has yet been established.The major hurdle in establishing such a method stemsfrom the variability in insulin values measured acrossdifferent immunoassays and platforms. Measured val-ues can differ by a factor of 2 for the same WHO humaninsulin standard (7 ). The differences in results fromvarious ICMA platforms are likely caused by differingcross-reactivities of the assay antibodies used. Further-
1 Quest Diagnostics Nichols Institute, San Juan Capistrano, CA.* Address correspondence to this author at: Quest Diagnostics Nichols Institute,
33068 Ortega Hwy, San Juan Capistrano, CA, 92675. Fax 949-728-4872; [email protected].
Received November 20, 2012; accepted April 26, 2013.Previously published online at DOI: 10.1373/clinchem.2012.199794
2 Nonstandard abbreviations: ICMA, immunochemiluminometric assays; MS,mass spectrometry; SRM, selected reaction monitoring; LC-MS/MS, liquidchromatography-tandem MS; TCEP, tris-(2-carboxyethyl) phosphine; NIBSC, Na-tional Institute for Biological Standards and Control; IS, internal standard; FDA,US Food and Drug Administration; SPE, solid-phase extraction; LOD, limit ofdetection; LOQ, limit of quantitation.
Clinical Chemistry 59:91349–1356 (2013)
Endocrinology and Metabolism
1349

more, auto- or heterophilic antibodies present withinthe patient’s sample may cause biases in reported insu-lin concentrations.
Mass spectrometry (MS)-based protein/peptideassays have recently been developed as important alter-native strategies for clinical analysis of biomolecules(8 ), including insulin. Because the insulin is present inhuman blood in very low concentrations, most previ-ously developed MS methods for the polypeptide’s de-tection and quantification have been dependent on im-munological capture methodologies (9 –15 ). However,recent improvements in the sensitivity of MS negatethe requirement of antibody-based enrichment with-out compromising high specificity. Accordingly, theapproach we have developed requires no capture anti-body while still providing a highly specific and sensitiveassay for human insulin through selected-reactionmonitoring (SRM) analysis on a triple-quadrupolemass spectrometer.
Mature human insulin (molecular weight, 5808Da) consists of 2 peptide chains (A and B) linked by 2disulfide bonds. The insulin A (molecular weight, 2377Da) and B chains (molecular weight, 3431 Da) can beseparated using suitable reducing agents. The insulin Bchain has been studied extensively; however, a quanti-tative assay for the peptide has not been developed(12, 16, 17 ). Our aim was to develop an assay for quan-tification of total insulin concentrations in human se-rum via quantifying the B chain after reduction andliberation from the intact molecule. Herein, we reportthe validation of this assay and reference interval stud-ies to support the high-throughput clinical measure-ment of insulin by liquid chromatography–tandem MS(LC-MS/MS).
Materials and Methods
STANDARDS AND REAGENTS
HPLC-grade acetonitrile, isopropanol, ethanol, ace-tone, and water were from Burdick and Jackson; meth-anol and bond-breaker tris-(2-carboxyethyl) phos-phine (TCEP) solution were from Thermo FisherScientific. High-purity formic acid was from Fluka.WHO human insulin standard (code: 66/304) wasfrom the National Institute for Biological Standards(NIBSC). Recombinant human insulin was from Mil-lipore. Bovine insulin (�95% purity) and 1.5 mol/LTris (Trizma) base solution were from Sigma. Fullysynthetic, isotopically labeled insulin B chain was fromAnaspec (see Fig. 1 in the Data Supplement that ac-companies the online version of this report at http://www.clinchem.org/content/vol59/issue9). Hypo-Opticlearstripped human serum free of insulin was from Bio-cell laboratories. All protein components were fullycharacterized by gel electrophoresis, HPLC, and MS
by the manufacturers. Amino acid analysis was per-formed by AAA Service Laboratory Inc. to confirmprotein content before use.
PREPARATION OF CALIBRATORS, CONTROLS, AND INTERNAL
STANDARDS
A stock solution of human insulin standard (recombi-nant human insulin unless otherwise stated) at 1IU/mL (6 �mol/L) was prepared in 0.2% formic acidsolvent and stored at �80 °C until use. Immediatelybefore assay, the stock solution was thawed and an ali-quot diluted into insulin-free human stripped serum ata final concentration of 4000 �IU/mL (24 nmol/L).Dilutions were subsequently performed to generate acalibration series at concentrations of 5.0, 10, 15, 25,50, 100, 200, and 300 �IU/mL (30.0 –1800 pmol/L).
In-house QC stocks were prepared using recombi-nant human insulin from Millipore, dissolved in 0.2%formic acid and stored at �80 °C. The concentration ofinsulin in these stocks was verified by amino acid anal-ysis before dilution. Five determinations were per-formed over a period of 6 months with a CV of 3%. QCcontrols (8, 16, 40, and 80 �IU/mL, or 48 – 480pmol/L) were made by spiking Human Hypo-Opticlear stripped serum to the target concentrationsand then storing them in aliquots at �80 °C. The newlymade insulin QC controls and calibrators were assessedby comparison to NIBSC reference material. EachQC aliquot was used only once after thawing to avoidfreeze–thaw cycles.
The internal standards (ISs) were prepared in 0.2%formic acid at a concentration of 10 �mol/L. Bovine in-sulin (350 pmol) was added to serum during the extrac-tion (before reduction) and isotopically labeled human Bchain (115 pmol) added to reduced extract before LC.
HUMAN STUDY PARTICIPANTS APPROVAL
Serum samples were obtained from healthy study par-ticipants following informed consent and stored at�80 °C until use (Western Institutional Review Boardapproval #1085473). The use of anonymized discardedsamples in these studies was reviewed by the WesternInstitutional Review Board and deemed exempt.
CLINICAL SAMPLE COLLECTION
Unless otherwise stated, blood was collected intobarrier-free serum preparation tubes (red top) and al-lowed to clot. The resulting serum was immediatelyprocessed then stored at �80 °C until analysis.
SAMPLE PREPARATION
Patient serum was thawed and vortex mixed, and 150�L was vigorously mixed with 350 �L of basic ethanol(85% ethanol, 15% Tris base) and allowed to incubatefor 60 min at �20 °C. The resulting precipitate was
1350 Clinical Chemistry 59:9 (2013)

pelleted by centrifugation for 10 min at 5200g. Clarifiedsupernatant (250 �L) was then mixed with 20 �L ofbond-breaker TCEP solution (Thermo Fisher Scien-tific) which was used per the manufacturer’s directionsto liberate the insulin A and B chains through reduc-tion of their disulfide bonds.
AUTOMATED PREPARATIVE AND ANALYTICAL
CHROMATOGRAPHY
Analytical separation of insulin B chain from matrixcomponents before MS was achieved with a Turbo-Flow Aria TLX-4 (Thermo Fisher), a fully automatedonline LC system. The 4 columns in this LC system areoperated in parallel, facilitating high throughput. Thesample cleanup and enrichment was performed by on-line solid-phase extraction (SPE) using an Oasis HLBcartridge column (2.1 � 20 mm, 25 �m) (Waters) (seeonline Supplemental Fig. 2). Chromatographic resolu-tion was accomplished using a Magic C4 column(2.1 � 50 mm, 5 �m, 300 Å) (Bruker- Michrom). Forboth SPE and analytical columns, we used the samesolvent A (water, 0.2% formic acid) and B (acetonitrile,0.2% formic acid). After injection of the extract (225�L) at 4 mL/min, the cartridge was washed with 12% Bsolvent for a further 60 s. The analytes were then back-flushed off the extraction cartridge with a step gradientof 35% solvent B at 0.8 mL/min and refocused onto theanalytical column, by means of a T valve with a 3:1 ratioof flow rates between eluting (0.6 mL/min) and loading(0.2 mL/min) pumps, respectively. Finally, the analyteswere resolved using a fast, linear gradient from 12% to42% solvent B at 0.5 mL/min over 3 min.
DATA ACQUISITION AND PROCESSING
A TSQ Vantage (ThermoFisher) triple quadrupolemass spectrometer interfaced to the TLX-4 system withan ESI probe served as the MS/MS detector. The datawere acquired using SRM in positive ion mode underthe following conditions: ionization voltage, 4800 V;sheath gas pressure, 50 (arbitrary units); auxiliary gaspressure, 25 (arbitrary units); capillary temperature,250 °C. Instrument settings in Xcalibur included posi-tive scan mode with the Chrom filter enabled and set at10; scan width, 0.5 m/z; scan time, 0.1 s; collision gas,1.5 mTorr; and both Q1 and Q3 peak widths set to 0.7.
The unique nature of the amino acid sequence forthe insulin B chain was confirmed by running a BLAST(Basic Local Alignment Search Tool) search (18 )(http://blast.ncbi.nlm.nih.gov/Blast.cgi). In this assay,we consider the retention time and the ratio of the masstransitions (1:1, with tolerance of �20%) to supportB-chain identification. For quantitative analysis, themost intense isotopic peak of the MH5
�5 ion of insulinchain B [m/z 686.9 (0.2)] was used as the precursor ion(see online Supplemental Fig. 3). Transitions to b14
�2
[768.5 (0.2)] and y13�2 [753.2 (0.2)] from insulin B
chain, with optimal collision energies of 21 and 19 V,respectively, were monitored by SRM to enhance selec-tivity. The corresponding transitions for the ISs were680.8 (0.2) to 768.5 (0.2), 738.3 (0.2) for bovine insu-lin, and 688.1 (0.2) to 768.5 (0.2), 756.0 (0.2) for isoto-pically labeled human insulin B chain. To enhance sen-sitivity, the peak areas for each transition were summedfor each peptide. The ratio of the peak area of the ana-lyte to the IS (unless otherwise stated, isotopically la-beled human insulin B chain was employed as the IS)was used to calculate the concentrations from the stan-dard curve. A weighted linear model (1/x) was used forgeneration of the standard curve by linear regression. Re-sults were reported as the concentration of insulin(�IU/mL or pmol/L; 1 �IU/mL � 6 pmol/L). Softwaretools used were TSQ Vantage 2.0.0, Tune Master V 2.0.0,Xcalibur V 2.0.7. SP1, LC Quan V 2.5.6. SP1, and XReport2.0.7. SP1 and ARIA OS V 1.6.1 (ThermoFisher) wereused for all the data acquisition and processing.
METHOD COMPARISON
The LC-MS/MS method was compared to a US Foodand Drug Administration (FDA)-approved commer-cial (Beckman Access� ICMA) platform [limit of de-tection (LOD) 0.13 �IU/mL; limit of quantitation(LOQ) 0.3 �IU/mL] for measurement of insulin in pa-tients (n � 89). These patient samples were deidenti-fied discards submitted previously for routine clinicaltesting. Concentrations measured covered the ex-pected human insulin reference intervals and beyondfrom low to very high insulin concentrations. Correla-tion of the 2 methods was evaluated through the use ofa Deming regression.
REFERENCE INTERVAL DETERMINATION
A reference interval for the LC-MS/MS assay was de-termined using sera collected in red top tubes from 97carefully selected healthy volunteers (51 females, 46males ages 18 – 65 years, employees and nonemployeesof Quest Diagnostics).The following inclusion criteriawere used: apparently healthy, ambulatory, commu-nity dwelling, nonmedicated adults. The exclusion cri-teria were as follows: any endocrine disorders, fastingglucose �100 mg/dL (�5.55 mmol/L), and abnor-mally high free insulin (�20 �IU/mL, or 120 pmol/L)detected by the current ICMA platform.
SAMPLE TYPE AND STABILITY
Six types of collection tubes (plain red top serum, se-rum separator tubes, EDTA plasma, sodium heparinplasma, lithium heparin plasma, and sodium citrateplasma) were assessed using samples drawn from 10 in-dividuals and analyzed in the LC-MS/MS assay. Samplestability was evaluated in serum over time at the following
Quantitative Analysis of Insulin
Clinical Chemistry 59:9 (2013) 1351

temperature ranges: ultralow frozen (�60.0 to�90.0 °C), frozen (�10.0 to �30.0 °C), refrigerated(2.0–8.0 °C), and room temperature (18.0–26.0 °C).Freeze–thaw stability was evaluated using 10 individualpatient serum samples. An initial sample with no freezing(cycle 0) was collected and 5 additional aliquots were sub-jected to repeated freeze–thaw cycles (1–5). Sample sta-bility was completed by assessing the mean difference be-tween the baseline value and the time/temperaturesample value within an acceptable range of 80%–120%.
Results
EFFECTIVENESS OF IS
The labeled B chain of insulin was initially favored forthe assay because it is chemically a match for the en-
dogenous B chain. The labeled peptide was spiked intoall extracted samples, QCs, and calibrators as describedin the Materials and Methods before analysis onthe LC-MS/MS system and was used to normalize thequantitative MS results. However, to correct for thepossibility of incomplete reduction of insulin, we alsoused intact bovine insulin as a surrogate IS added at thebeginning of sample preparation to account for anyprocedural losses during the extraction and reductionprocesses. Fig. 1 shows the SRM chromatograms cor-responding to coeluting bovine, endogenous human,and isotopically labeled human insulin B chain, respec-tively. Both ISs exhibited consistency in signal responseover time, and Deming regression of 51 patients sug-gested equal suitability (see online Supplemental Fig.4). We ultimately chose bovine insulin as the default IS
Fig. 1. Example of chromatograms in a patient’s serum (40.6 �IU/mL or 243.6 pmol/L).
Actual retention time is 4.8 min. RT, retention time; AA, area; SN, signal-to-noise ratio; BP, base peak; NL, normalized largest;TIC, total ion current.
1352 Clinical Chemistry 59:9 (2013)

because it has superior peak intensity and cost in addi-tion to correcting for the possibility of incomplete re-duction. The benefit of using an IS is demonstrated inonline Supplemental Fig. 5. The correlation of LC-MS/MS results with the ICMA assay results by Demingregression was observed to dramatically improve withslope, decreasing from 1.36 (no IS) to 1.07 (bovine IS).
ASSAY PERFORMANCE
Analytical performance specifications are summarizedin Table 1. The assay demonstrates a linear relationshipwithin the reportable range of 5 to 300 �IU/mL (30 –1800 pmol/L), with R2 of 0.9989. We determined theinsulin LOQ by assaying 6 different samples at concen-trations close to the expected LOQ [1.25, 2.5, 5, 10, 15,and 25 �IU/mL (1 �IU/mL � 6 pmol/L)] and thenevaluating the intraassay reproducibility in 7 runs. Thelowest concentration that yielded acceptable perfor-mance was 3 �IU/mL (18 pmol/L), for which the 95%CI for the CV remained below 20%. A blank was mea-sured 14 times and the resulting area ratios were back-calculated to establish an LOD (4 SDs from the zeroconcentration) of 1.8 �IU/mL (10.8 pmol/L) for insu-lin and a limit of blank (2 SDs from the zero concen-tration) of 1.4 �IU/mL (8.4 pmol/L) for insulin instripped serum. Confirmation of insulin B-chain iden-tity was established as described in the Methods. Masstransition ratios outside the stated tolerance limitswere found in �3% of patient samples. No detectablecarryover was found for concentrations below 500�IU/mL (3000 pmol/L). Intraassay precision and accu-racy for QC were generated by assaying 8 replicates. TheCVs ranged from 3.0% to 7.9%, with the intraassay accu-racy ranging from 80%–92%. The interassay variation
over 5 days ranged from 7.1% to 14.0% and the interassayaccuracy range from 87% to 96%. Assay performance wasalso assessed by spike and recovery experiments in patientserum and was found to have an overall recovery of 94%–113% across the measured range (Table 1).
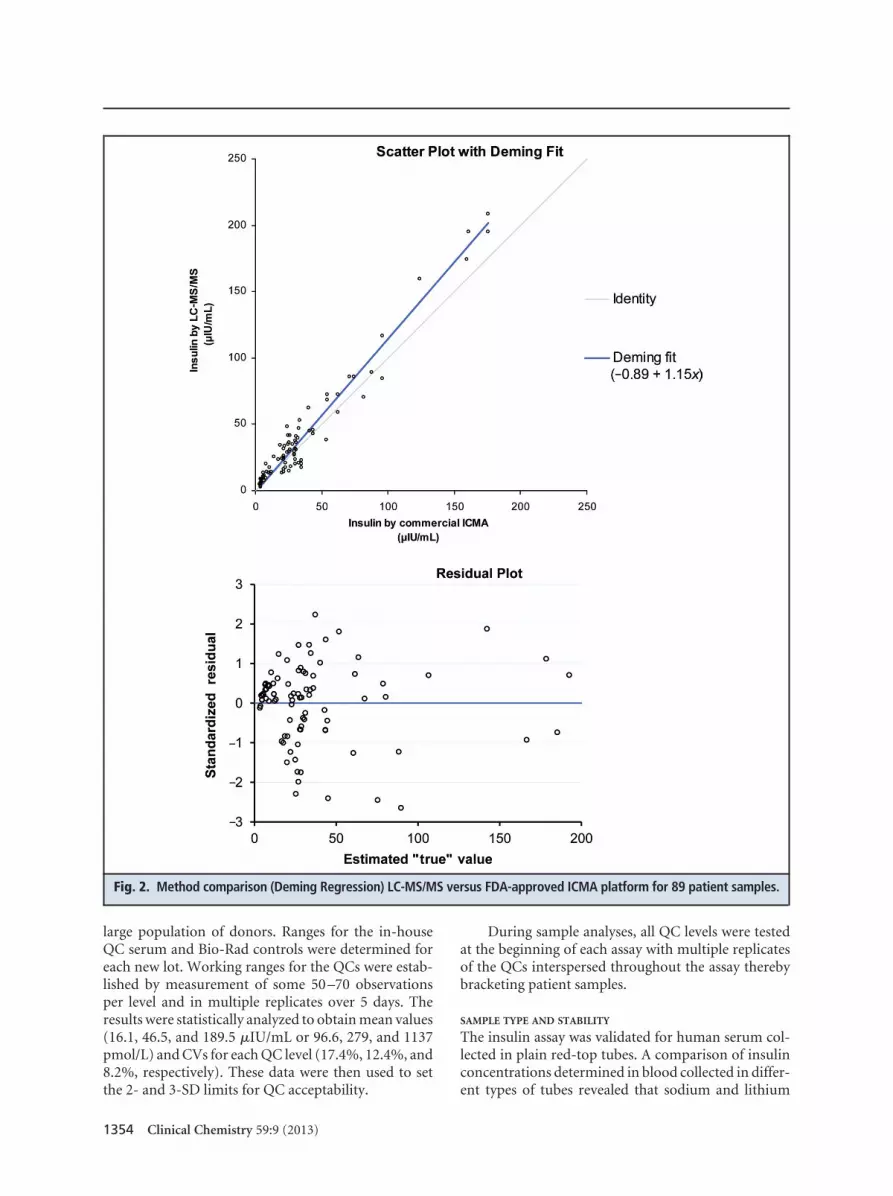
METHOD COMPARISON
To benchmark the assay, we completed an analysis ofcorrelations between the LC-MS/MS assay and anFDA-approved ICMA assay using 89 deidentified pa-tient discards across the insulin concentration range of3–180 �IU/mL (18 –1080 pmol/L). Deming regressionfrom this study revealed good agreement between thenew LC-MS/MS method with the ICMA assay (y �1.15x � 0.89) (Fig. 2).
REFERENCE INTERVAL DETERMINATION
In this investigation, we used samples from 97 carefullyselected healthy donors to complete a reference inter-val study (Fig. 3). The data were found to be nongauss-ian. The 95th percentile data were used to establish areference interval of �13.7 �IU/mL (82.2 pmol/L).
ASSAY QC
We used QC procedures according to Westgard ruleswithin the assay to allow determination of passing vsfailing runs as well as to identify biases within the dataattributable to analytical issues. QC controls were eval-uated from 2 different sources. The first were Bio-RadImmunoassay/TDM controls, QC serum samples withknown concentrations of insulin. The second type ofQC sample was a low insulin concentration in-houseserum pool that we prepared by determining the insu-lin concentration after combining the serum from a
Table 1. Performance of the LC-MS/MS assay for insulin.
Sensitivity LOBa LOD LOQ
1.4 �IU/mL (8.4 pmol/L) 1.8 �IU/mL (10.8 pmol/L) 3.0 �IU/mL (18.0 pmol/L)
Precision Insulin in stripped serum,�IU/mL (pmol/L)
Interassay %CV,accuracy (n � 8)
Intraassay %CV,accuracy (n � 8)
8 (48) 14.0, 91.3 7.0, 80.0
12 (72) 10.2, 91.2 7.9, 92.2
20 (120) 10.0, 87.0 6.0, 86.5
40 (240) 7.5, 87.7 4.0, 87.6
80 (480) 7.1, 96.3 3.0, 92.1
Recovery Insulin in serum, �IU/mL (pmol/L) Mean (SD) % recovery (n � 3)
8 (48) 93.8
20 (120) 113.3
48 (288) 99.4
a LOB, limit of blank.
Quantitative Analysis of Insulin
Clinical Chemistry 59:9 (2013) 1353
large population of donors. Ranges for the in-houseQC serum and Bio-Rad controls were determined foreach new lot. Working ranges for the QCs were estab-lished by measurement of some 50 –70 observationsper level and in multiple replicates over 5 days. Theresults were statistically analyzed to obtain mean values(16.1, 46.5, and 189.5 �IU/mL or 96.6, 279, and 1137pmol/L) and CVs for each QC level (17.4%, 12.4%, and8.2%, respectively). These data were then used to setthe 2- and 3-SD limits for QC acceptability.
During sample analyses, all QC levels were testedat the beginning of each assay with multiple replicatesof the QCs interspersed throughout the assay therebybracketing patient samples.
SAMPLE TYPE AND STABILITY
The insulin assay was validated for human serum col-lected in plain red-top tubes. A comparison of insulinconcentrations determined in blood collected in differ-ent types of tubes revealed that sodium and lithium
Fig. 2. Method comparison (Deming Regression) LC-MS/MS versus FDA-approved ICMA platform for 89 patient samples.
1354 Clinical Chemistry 59:9 (2013)

heparin gave equivalent results and therefore are ac-ceptable sample types (data not shown). Sample stor-age conditions were evaluated in terms of reproducibil-ity in quantification over time with acceptablemeasurements falling within �20% of day 0 (see onlineSupplemental Fig. 6). Insulin in patient serum was sta-ble for at least 86 days at �80 °C. However, at �20 °C itwas observed that measured insulin concentrations in aportion of serum samples dropped after samples werestored for 35 days. Insulin was stable in serum for only 1day at room temperature. Furthermore, insulin concen-trations in some samples appeared to decline on the sec-ond day of storage at refrigerated temperatures, as indi-cated by the increased SD, whereas samples from otherpatients showed exemplary stability. After analyzing allthe stability results it was determined that samples for theLC-MS/MS insulin assay should be stored and shippedfrozen at �20 °C or lower for the short term (less than 1month). Longer-term storage should be at �80 °C orlower. Finally, the data indicate that insulin concentra-tions were unchanged by 5 freeze–thaw cycles (see onlineSupplemental Fig. 6).
INTERFERENCE STUDIES
We performed interference studies by examiningstripped sera from different sources as well as testingover 100 patient samples to look for nonspecific inter-ferences. The effects of varying degrees of hemolysis,lipemia, and bilirubin (mild, moderate, or gross) onthe accuracy of insulin measurements were also inves-tigated. The effects of hemolysis/lipemia/bilirubin oninsulin determinations were evaluated by spiking dif-
ferent concentrations of insulin in patient samples withlow, medium, and high hemolysis/lipemia/bilirubin.An acceptance level of 80%–120% recovery was used toassess whether the assay was adversely impacted byinterference. No dependence between insulin concen-trations and the level of lipemia or concentration ofbilirubin was observed. In contrast, there were unac-ceptable recoveries of insulin from grossly hemolyzedsera. Thus, hemolysis constituted a criterion for samplerejection (data not shown).
Discussion
The application of HPLC interfaced with MS for pro-tein and peptide analysis in the clinical laboratory en-vironment has always been very challenging comparedto the current antibody-based automated immunoas-says. Insulin proved to be no exception to this observa-tion. First, any new assay is required to provide excel-lent selectivity and specificity regardless of thecomplexity of the human serum. Second, the usualconcentration range for insulin in human blood isquite low; some immunoassays have lower LOQs aslow as 2 �IU/mL, equivalent to 1.8 fmol of insulin inthe 150 �L of serum we use for our assay. Third, any assaythat is going to be routinely used in a clinical laboratorymust be simple and highly reproducible as well as beingrobust and able to accommodate high sample through-put. Each LC run takes �8 min, and by multiplexing theassay, data can be obtained for each sample in 2 min. Onaverage, a 96-well plate takes �4 h to run. Sample prepa-ration throughput is determined by extraction and reduc-tion incubation steps (about 2 h). Thus, we have devel-oped an LC-MS/MS method which meets all the criteriafor routine use in a clinical laboratory.
A unique feature of the LC-MS/MS insulin assayreported here is the consistency and harmonization ofthe NIBSC insulin standard and the synthesized re-combinant human insulin. Reference to the gold stan-dard WHO reference reagent purchased directly fromNIBSC with a designated biological activity of 3 IU pervial should help to avoid the standardization issues thathave plagued the currently available antibody-basedimmunoassays, which each use their own workingstandards developed by the manufacturers. The assayhas been validated, meeting internal policy in compli-ance with CLIA 88 493.1253 guidance, with an LOD of1.8 �IU/mL (10.8 pmol/L) and lower LOQ of 3�IU/mL (18.0 pmol/L). To confirm the applicability ofthis assay, a correlation between the LC-MS/MS assayand an FDA-approved ICMA was completed, and theresulting Deming regression revealed good agreementbetween both methods in the lower concentrationrange. A new reference interval has also been estab-lished for the LC-MS/MS assay.
Fig. 3. A reference interval for insulin determined byLC-MS/MS for 97 healthy donors.
Quantitative Analysis of Insulin
Clinical Chemistry 59:9 (2013) 1355

The methodology for this assay involves reduction ofintact insulin and measurement of the free B chain. Thisapproach provides valuable information for distinguish-ing the endogenous insulin from therapeutic insulin ana-logs. All the commercial synthetic forms of insulin havealterations affecting the C-terminal amino acids on the Bchain. The SRM mass filters used provide molecularstructural details confirming the authenticity of the insu-lin B chain signal being measured, while ignoring the syn-thetic analogs which are routinely detected as insulin withthe use of immunological methods (unpublished). In ad-dition, the requirement that proinsulin not be recognizedby the immunoassays is also fulfilled by the selectivity ofthe SRM-based quantification method (19).
Conclusion
A simple, high-throughput, quantitative LC-MS/MSinsulin assay traceable to the NIBSC standard has beensuccessfully developed and validated to CLIA guide-lines. The method combines molecular specificity withquantitative performance and standardized analysisand provides reference intervals, making this approacha candidate to be considered as a reference method forinsulin testing (19, 20 ).
Author Contributions: All authors confirmed they have contributed tothe intellectual content of this paper and have met the following 3 re-quirements: (a) significant contributions to the conception and design,acquisition of data, or analysis and interpretation of data; (b) draftingor revising the article for intellectual content; and (c) final approval ofthe published article.
Authors’ Disclosures or Potential Conflicts of Interest: Upon man-uscript submission, all authors completed the author disclosure form.Disclosures and/or potential conflicts of interest:
Employment or Leadership: Z. Chen, Quest Diagnostics; M.P. Caul-field, Quest Diagnostics; M.J. McPhaul, Quest Diagnostics NicholsInstitute; R.E. Reitz, Quest Diagnostics Nichols Institute; S.W. Tay-lor, Quest Diagnostics; N.J. Clarke, Quest Diagnostics.Consultant or Advisory Role: None declared.Stock Ownership: Z. Chen, Quest Diagnostics; M.P. Caulfield,Quest Diagnostics; R.E. Reitz, Quest Diagnostics; N.J. Clarke, QuestDiagnostics.Honoraria: None declared.Research Funding: None declared.Expert Testimony: None declared.Patents: Z. Chen, Quest Diagnostics, 20120164741 (application);N.J. Clarke, Quest Diagnostics, 20120164741 (application).
Role of Sponsor: No sponsor was declared.
References
1. Dankner R, Chetrit A, Shanik MH, Raz I, Roth J.Basal-state hyperinsulinemia in healthy nor-moglycemic adults is predictive of type 2 diabetesover a 24-year follow-up: a preliminary report.Diabetes Care 2009;32:1464–6.
2. Johnson JL, Duick DS, Chui MA, Aldasouqi SA.Identifying prediabetes using fasting insulin lev-els. Endocr Pract 2010;16:47–52.
3. Wang H, Shara NM, Calhoun D, Umans JG, LeeET, Howard BV. Incidence rates and predictors ofdiabetes in those with prediabetes: the StrongHeart Study. Diabetes Metab Res Rev 2010;26:378–85.
4. Drzewoski J, Czupryniak L. Concordance betweenfasting and 2-h post-glucose challenge criteria forthe diagnosis of diabetes mellitus and glucoseintolerance in high risk individuals. Diabet Med2001;18:29–31.
5. Kim SH, Abbasi F, Reaven GM. Impact of degreeof obesity on surrogate estimates of insulin resis-tance. Diabetes Care 2004;27:1998–2002.
6. Dankner R, Chetrit A, Shanik MH, Raz I, Roth J.Basal state hyperinsulinemia in healthy nor-moglycemic adults heralds dysglycemia aftermore than two decades of follow up. DiabetesMetab Res Rev 2012;28:618–24.
7. Manley SE, Stratton IM, Clark PM, Luzio SD.Comparison of 11 human insulin assays: implica-tions for clinical investigation and research. ClinChem 2007;53:922–32.
8. Hoofnagle AN, Wener MH. The fundamentalflaws of immunoassays and potential solutions
using tandem mass spectrometry. J ImmunolMethods 2009;347:3–11.
9. Kippen AD, Cerini F, Vadas L, Stocklin R, Vu L,Offord RE, Rose K. Development of an isotopedilution assay for precise determination of insulin,C-peptide, and proinsulin levels in non-diabeticand type II diabetic individuals with comparisonto immunoassay. J Biol Chem 1997;272:12513–22.
10. Stocklin R, Vu L, Vadas L, Cerini F, Kippen AD,Offord RE, Rose K. A stable isotope dilution assayfor the in vivo determination of insulin levels inhumans by mass spectrometry. Diabetes 1997;46:44–50.
11. Darby SM, Miller ML, Allen RO, LeBeau M. Amass spectrometric method for quantitation ofintact insulin in blood samples. J Anal Toxicol2001;25:8–14.
12. Thevis M, Thomas A, Delahaut P, Bosseloir A,Schanzer W. Qualitative determination of syn-thetic analogues of insulin in human plasmaby immunoaffinity purification and liquidchromatography-tandem mass spectrometry fordoping control purposes. Anal Chem 2005;77:3579–85.
13. Rodriguez-Cabaleiro D, Van Uytfanghe K, StoveV, Fiers T, Thienpont LM. Pilot study for thestandardization of insulin immunoassays withisotope dilution liquid chromatography/tandemmass spectrometry. Clin Chem 2007;53:1462–9.
14. Van Uytfanghe K, Rodriguez-Cabaleiro D, StocklD, Thienpont LM. New liquid chromatography/
electrospray ionisation tandem mass spectrome-try measurement procedure for quantitative anal-ysis of human insulin in serum. Rapid CommunMass Spectrom 2007;21:819–21.
15. Hess C, Thomas A, Thevis M, Stratmann B,Quester W, Tschoepe D, et al. Simultaneous de-termination and validated quantification of hu-man insulin and its synthetic analogues in humanblood serum by immunoaffinity purification andliquid chromatography-mass spectrometry. AnalBioanal Chem 2012;404:1813–22.
16. Thevis M, Thomas A, Schanzer W. Mass spectro-metric determination of insulins and their degra-dation products in sports drug testing. MassSpectrom Rev 2008;27:35–50.
17. Thevis M, Thomas A, Schanzer W. Insulin. In:Thieme D, Hemmersbach P, ed. Handbook ofexperimental pharmacology. Berlin: Springer-Verlag; 2010. p 209–26. Vol. 195.
18. Altschul SF, Gish W, Miller W, Myers EW, LipmanDJ. Basic local alignment search tool. J Mol Biol1990;215:403–10.
19. Miller WG, Thienpont LM, Van Uytfanghe K, ClarkPM, Lindstedt P, Nilsson G, et al. Toward stan-dardization of insulin immunoassays. Clin Chem2009;55:1011–8.
20. Marcovina S, Bowsher RR, Miller WG, Staten M,Myers G, Caudill SP, et al. Standardization ofinsulin immunoassays: report of the AmericanDiabetes Association Workgroup. Clin Chem2007;53:711–6.
1356 Clinical Chemistry 59:9 (2013)