psychiatric diagnoses, comorbidity, and functioning in national guard troops deployed to iraq
TRANSCRIPT

lable at ScienceDirect
Journal of Psychiatric Research 45 (2011) 126e132
Contents lists avai
Journal of Psychiatric Research
journal homepage: www.elsevier .com/locate/psychires
Psychiatric diagnoses, comorbidity, and functioning in National Guard troopsdeployed to Iraqq
Shannon M. Kehle a,b,c, Madhavi K. Reddy b,d, Amanda G. Ferrier-Auerbach b,c, Christopher R. Erbes b,c,Paul A. Arbisi b,c, Melissa A. Polusny a,b,c,*
aCenter for Chronic Disease Outcomes Research, Minneapolis, MN, USAbMinneapolis VA Medical Center, Minneapolis, MN, USAcUniversity of Minnesota Medical School, Minneapolis, MN, USAdAlpert Medical School of Brown University, Providence, RI, USA
a r t i c l e i n f o
Article history:Received 18 January 2010Received in revised form3 May 2010Accepted 7 May 2010
Keywords:Posttraumatic stress disorder (PTSD)TraumaMilitaryPsychiatric diagnosisQuality of life
q This research has not been previously published* Corresponding author. Minneapolis VA Medical C
Drive, Minneapolis, MN 55417, USA. Tel.: þ1 (612) 72727 5633.
E-mail address: [email protected] (M.A. Pol
0022-3956/$ e see front matter Published by Elseviedoi:10.1016/j.jpsychires.2010.05.013
a b s t r a c t
Objective: Over 1.8 million troops have been deployed to Iraq (OIF) and Afghanistan. Estimates of mentalhealth problems postdeployment have been based on screening instruments; no studies have examinedthe postdeployment mental health of troops returning from OIF using structured diagnostic interviews.The goal of the current study is to (a) report on rates of mental health diagnoses and comorbidity insoldiers after deployment to OIF using clinical interviews, and (b) examine the relationship betweenmental health diagnoses and overall functioning and quality of life.Method: Participants were 348 National Guard soldiers drawn from the Readiness and Resilience inNational Guard Soldiers (RINGS) study, a longitudinal study of mental health after deployment to OIFfrom March 2006 to July 2007. Participants completed clinical interviews, including the ClinicianAdministered PTSD Scale and the Structured Clinical Interview for the DSM-IV, and self-report measuresof social adjustment and quality of life 6e12 months following deployment.Results: Most participants did not meet criteria for a mental health diagnosis. Non-PTSD anxiety disor-ders and depressive disorders were the most common. Mental health diagnoses were associated withpoorer functioning and quality of life. PTSD had the strongest relationship with social functioning andquality of life. For those with PTSD, comorbid diagnoses were not associated with an incrementaldecrease in functioning or quality of life.Conclusions: The findings highlight the significant rate and burden of mental health disorders among thispopulation and suggest that while PTSD is relatively uncommon, it is a particularly deleterious disorder.
Published by Elsevier Ltd.
In recent years there have been increasing concerns regarding 12% for alcohol-related disorders (Jacobson et al., 2008; Milliken
the mental health of American soldiers returning from the currentwars in Afghanistan (OEF) and Iraq (OIF). Early data suggest highrates of posttraumatic stress disorder (PTSD), depression, andalcohol problems among OEF/OIF soldiers (Hoge et al., 2004, 2006;Jacobson et al., 2008; Seal et al., 2007). To date, most reports of OEF/OIF postdeployment mental health diagnoses involve rates ofprobable diagnoses based on the use of self-report measures(Grieger et al., 2006; Hoge et al., 2004, 2006). Using such meth-odology, estimated rates in returned OEF/OIF military personnelhave been reported at up to 25% for PTSD, 13% for depression, andor presented in any form.enter (116A9), One Veterans5 2000x3965; fax: þ1 (612)
usny).
r Ltd.
et al., 2007). The RAND Corporation recently conducted a largeepidemiological study of nearly 2000 OEF/OIF soldiers and esti-mated rates of both PTSD andmajor depression to be 14% (Tanielianand Jaycox, 2008).
While useful because of their ease of administration, self-reportassessment tools often result in inaccurate diagnoses and over-estimates of illness (Lowe et al., 2004; Terhakopian et al., 2008).Structured clinical interviews, while time intensive, are widelyconsidered to be the most accurate way of diagnosing mentalhealth conditions. We have previously explored rates of post-deployment PTSD in our sample and found that 7% of the troopsmet criteria using the Clinician Administered PTSD Scale (CAPS;Blake et al., 1995; Erbes et al., under review). To our knowledge, nostudy has examined the rate of other mental health diagnoses orcomorbidity, as assessed by structured clinical interviews, in mili-tary personnel who have recently returned from OEF/OIF. Thus, thegoal of this paper is to provide the first known report of rates of

S.M. Kehle et al. / Journal of Psychiatric Research 45 (2011) 126e132 127
mental health disorders and comorbidities, as diagnosed bystructured clinical interviews, in a sample of U.S. National Guardtroops who have recently returned from OIF.
Additionally, this paper will report on how mental healthdiagnoses impact the social functioning of these troops. Researchconducted with veterans of previous wars has shown that post-deployment mental health disorders are associated with impair-ments in functioning, decreased quality of life, increased healthcare costs, and significant financial burdens (The Iowa Persian GulfStudy Group, 1997; Jordan et al., 1991; Kang et al., 2003; Prigersonet al., 2002). PTSD alone is associated with an estimated $3 billiondollars of lost productivity per year, an average 3.6 days of work lostper month, a lowered likelihood of veterans working for pay, anda negative impact on veterans’ wages (Kessler, 2000; Savoca andRosenheck, 2000). In regards to OEF/OIF, the two-year cost ofpostdeployment PTSD and major depression is estimated to bebetween $4.0 and $6.2 billion dollars (Tanielian and Jaycox, 2008).Further, rates of comorbidity among individuals with PTSD havebeen estimated to be as high as 99% (Kulka et al., 1990) and previousstudies have shown the negative impact of PTSD is even greaterwhen another mental health diagnosis is present (Kessler andFrank, 1997). In line with previous research, we expected thatsoldiers who report a mental health diagnosis will report greaternegative impact on their functioning, and that comorbid mentalhealth diagnoses will have a cumulative negative impact on thesoldiers’ functioning.
1. Materials and methods
The National Guard command and the institutional reviewboards of the University of Minnesota Medical School, MinneapolisVeteran’s Affairs Medical Center, and Department of Defenseapproved the study protocol. The investigation was conducted inaccordance with the latest version of the Declaration of Helsinkiand written informed consent was obtained from participants priorto study enrollment and interview administration.
1.1. Participants and procedures
The study sample was drawn from the Readiness and Resiliencein National Guard Soldiers (RINGS) Study, a longitudinal investi-gation of risk and resilience factors predictive of postdeploymentmental health in troops deployed to OIF. Soldiers from a NationalGuard Brigade Combat Team (BCT) were surveyed one month priorto a 16-month deployment to Iraq and again 3 months followingreturn from deployment. As part of the postdeployment survey,a variety of psychological and deployment-related factors,including quality of life and social adjustment, were assessed usingstandard mailed survey methodology. All participants were alsoinvited to complete a postdeployment diagnostic interview. Inter-views were conducted between 6 and 12 months following troops’return from Iraq. Participants were compensated $130 forcompleting the interview.
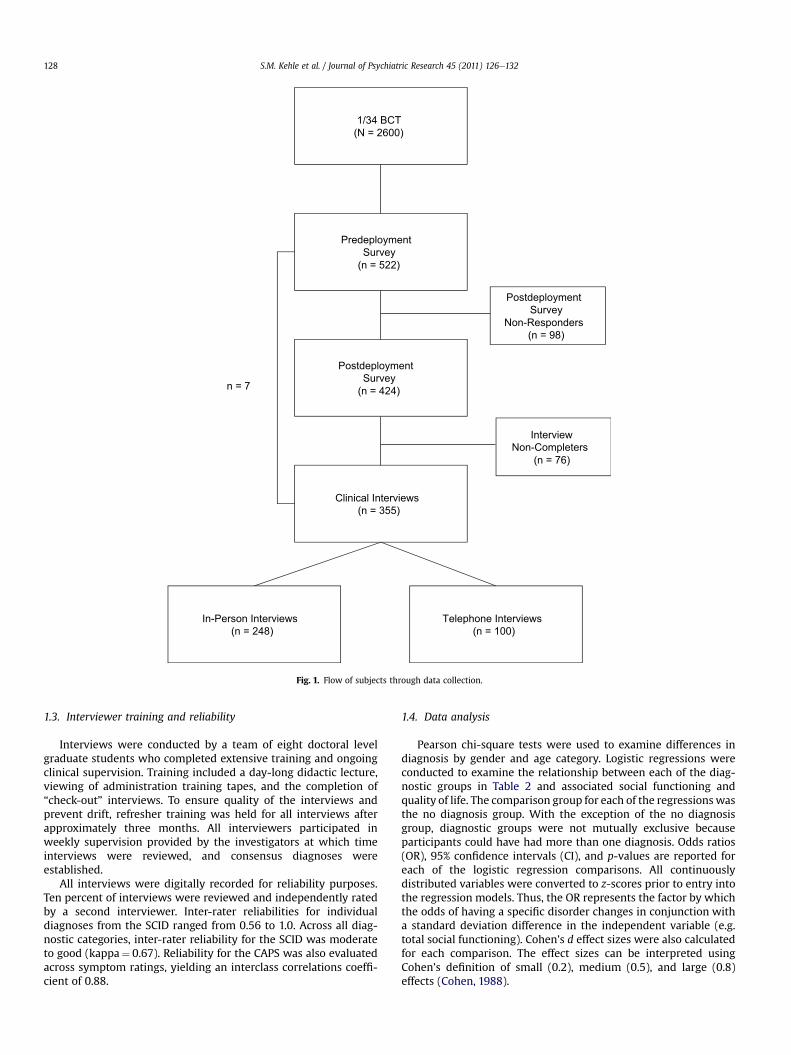
Fig. 1 details participation rates. Participants were originallycontacted approximately one month prior to deployment to OIFwhile completing a six-month mobilization training. Over thecourse of approximately 2½ weeks, soldiers were invited throughunit announcements and flyers to attend a group briefing sessionheld by investigators. Ultimately, 522 of the approximately 2600individuals in the total brigade completed the predeploymentsurvey. Those who participated predeployment were demograph-ically similar to the larger brigade (Table 1). Of the 522 soldiers whoparticipated predeployment, 424 participants (81%) completed thefollow-up survey. Postdeployment responders and non-respondersdid not differ on gender, ethnicity, or self-reported predeployment
distress. The responders were more likely to be officers(responders¼ 11%; non-responders¼ 4%), c2 (1, N¼ 522)¼ 4.43,p< 0.05, married (responders¼ 49%; non-responders¼ 31%), c2 (1,N¼ 522)¼ 10.65, p< 0.001, and older (responder M¼ 29.9,SD¼ 8.8; non-responder M¼ 25.6, SD¼ 6.9), t(520)¼�4.46,p< 0.001, than the non-responders.
Eighty-two percent (n¼ 348) of postdeployment surveyresponders completed a diagnostic interview. Seven participantscompleted an interview but not a follow-up survey and wereexcluded from current analyses. Therewere no differences betweensoldiers who completed or did not complete the interview on age,ethnicity, marital status, enlisted status, self-reported distress,social adjustment, or quality of life. Soldiers completing interviewswere more likely to report some college education (c2¼12.96,p< 0.001). Of those completing interviews, 248 soldiers (71%) wereinterviewed in-person and 100 soldiers (29%) were interviewed viatelephone. There were no differences between those interviewedin-person or by phone on demographics (age, ethnicity, maritalstatus, level of education), postdeployment PTSD or depressivesymptomology, number of diagnoses, quality of life, or socialadjustment. Female soldiers were more likely to participate in-person than by telephone (c2¼ 9.49, p¼ 0.002).
1.2. Measures
The Clinician Administered PTSD Scale (CAPS; Blake et al., 1995),considered to be the “gold standard” of PTSD diagnosis, consists of30-items, and corresponds to the Diagnostic and Statistical Manualof Mental Disorders 4th Edition (DSM-IV-TR; American PsychiatricAssociation, 2000) criteria for PTSD. Using original CAPS scoringcriteria (Blake et al., 1990), PTSD was diagnosed for participantswho experienced a traumatic event (criteria A1), reported at leastone reexperiencing symptom, three avoidance symptoms, and twohyperarousal symptoms each at a frequency rating of at least 1 andan intensity rating of at least 2, and reported and significantimpairment or distress. Subthreshold PTSD was diagnosed forparticipants who experienced a traumatic event (criteria A1),reported at least one avoidance, one reexperiencing, and onehyperarousal symptoms at a frequency rating of at least 1 and anintensity rating of at least 2, and reported significant impairment ordistress (Stein et al., 1997). Additional Axis I disorders were diag-nosed with the SCID-I/NP (Non Patient-Edition) Research Versioninterview (First et al., 2002). The following modules were admin-istered: Overview, Mood Episodes, Psychotic Disorders, MoodDisorders, Substance Use Disorders, Anxiety Disorders (withexception of PTSD questions), and Somatoform Disorders. Self-report survey data analyzed for the present report were collectedby two instruments: the Social Adjustment Scale-Self-Report (SAS-SR; Weissman, 1999) and Navy Quality of Life Survey (NQOLS;Wilcove et al., 2003). The SAS-SR contains 54-items which assessindividual’s functioning in 6 areas: work, social and leisure activi-ties, relationships with extended family, role as a marital partner,parental role, and role within the family unit including economicfunctioning perceptions. Each item is rated on a five point Likertscale, with higher scores indicating greater impairment. A domain-based approach for assessing soldiers’ quality of life was adaptedfrom the NQOLS. Domains assessed include leisure and recreation,friends and friendship, relationship with relatives, marriage/inti-mate relationships, relationships with children (if applicable),standard of living, and overall satisfaction with life experiences.Each item is rated on a seven point Likert scale, with higher scoresindicating greater satisfaction. We also used the “combat experi-ences” subscale of the Deployment Risk and Resilience Inventory toassess the presence or absence of a range of combat experiences(King et al., 2006).
1/34 BCT(N = 2600)
PredeploymentSurvey
(n = 522)
PostdeploymentSurvey
(n = 424)
In-Person Interviews(n = 248)
Telephone Interviews(n = 100)
PostdeploymentSurvey
Non-Responders(n = 98)
InterviewNon-Completers
(n = 76)
Clinical Interviews(n = 355)
n = 7
Fig. 1. Flow of subjects through data collection.
S.M. Kehle et al. / Journal of Psychiatric Research 45 (2011) 126e132128
1.3. Interviewer training and reliability
Interviews were conducted by a team of eight doctoral levelgraduate students who completed extensive training and ongoingclinical supervision. Training included a day-long didactic lecture,viewing of administration training tapes, and the completion of“check-out” interviews. To ensure quality of the interviews andprevent drift, refresher training was held for all interviews afterapproximately three months. All interviewers participated inweekly supervision provided by the investigators at which timeinterviews were reviewed, and consensus diagnoses wereestablished.
All interviews were digitally recorded for reliability purposes.Ten percent of interviews were reviewed and independently ratedby a second interviewer. Inter-rater reliabilities for individualdiagnoses from the SCID ranged from 0.56 to 1.0. Across all diag-nostic categories, inter-rater reliability for the SCID was moderateto good (kappa¼ 0.67). Reliability for the CAPS was also evaluatedacross symptom ratings, yielding an interclass correlations coeffi-cient of 0.88.
1.4. Data analysis
Pearson chi-square tests were used to examine differences indiagnosis by gender and age category. Logistic regressions wereconducted to examine the relationship between each of the diag-nostic groups in Table 2 and associated social functioning andquality of life. The comparison group for each of the regressionswasthe no diagnosis group. With the exception of the no diagnosisgroup, diagnostic groups were not mutually exclusive becauseparticipants could have had more than one diagnosis. Odds ratios(OR), 95% confidence intervals (CI), and p-values are reported foreach of the logistic regression comparisons. All continuouslydistributed variables were converted to z-scores prior to entry intothe regression models. Thus, the OR represents the factor by whichthe odds of having a specific disorder changes in conjunction witha standard deviation difference in the independent variable (e.g.total social functioning). Cohen’s d effect sizes were also calculatedfor each comparison. The effect sizes can be interpreted usingCohen’s definition of small (0.2), medium (0.5), and large (0.8)effects (Cohen, 1988).

Table 1Demographic characteristics of interview participants, overall readiness and Resil-ience in National Guard Soldiers (RINGS) cohort at baseline, and the Brigade CombatTeam population.
Demographiccharacteristic
Overall cohortat baseline(n¼ 522)
Panel participantsat follow-up(n¼ 348)
Brigade CombatTeam population(n¼ 2573)
SexMale, No. (%)a 462 (88) 304 (87) 2339 (91)Female, No. (%) 60 (12) 44 (13) 234 (9)
Age, mean (SD), y 29.1 (8.6) 31.3 (9.5) b
18e29 years, No. (%) 313 (60) 170 (49) 1672 (65)30þ years, No. (%) 209 (40) 172 (51) 901 (35)
Race/ethnicityWhite, non-Hispanic,No. (%)
484 (93) 325 (93) 2407 (95)
Non-white, No. (%) 37 (7) 23 (7) 134 (5)
RankEnlisted, No. (%) 471 (90) 303 (87) 2301 (90)Officer, No. (%) 51 (10) 44 (13) 270 (10)
Marital statusMarried, No. (%) 237 (45) 173 (48) 1006 (40)Not married, No. (%) 285 (55) 163 (52) 1515 (60)
a Percentages reported are the proportion of individuals within each demo-graphic subgroup who reported the outcome.
b Mean age for the brigade was not available.
S.M. Kehle et al. / Journal of Psychiatric Research 45 (2011) 126e132 129
Rates of psychiatric comorbidity were calculated for the entirepanel, for participants with a diagnosis of PTSD, and for participantswith a diagnosis of either PTSD or subthreshold PTSD. For the entirepanel, we conducted one-way analysis of covariance (ANCOVA) toexamine the association between total number of diagnoses andoverall social functioning and quality of life. We then conducteda second ANCOVA to examine the relationship between having nodiagnosis, onediagnosis, or twoormore diagnoses andoverall socialfunctioning and quality of life. Next, using only those with eitherPTSD or subthreshold PTSD, we again conducted an ANCOVA toexamine the association between number of diagnoses and overallsocial functioning and quality of life. Finally, using only those withPTSD or subthreshold PTSD, we conducted an ANCOVA to examinethe association between having a comorbidity (yes/no) and totalsocial adjustment and overall quality of life. Due to a response biaswithin our sample, we controlled for marital status, education level,age, and enlisted status in the regressions and ANCOVAs.
2. Results
2.1. Sample characteristics and deployment experiences
Interview completers were 87% male, 93% Caucasian, 50%married, 87% enlisted rank,with amean ageof 31.30 (SD¼ 9.5) years(Table 1). Four percent of the sample had a previous deployment to
Table 2Rates of psychiatric diagnoses among National Guard soldiers approximately six months
PTSD Subthreshold PTSD Depressive disorders Ot
Total n (%)a 23/348 (7) 30/348 (9) 51/348 (15) 46
GenderMale 17/304 (6) 25/304 (8) 39/304 (13) 35Female 6/44 (14) 5/44 (11) 12/44 (27) 1
Age18e29 14/170 (8) 20/170 (12) 25/170 (15) 1830e39 6/110 (6) 6/110 (6) 16/110 (15) 1740e49 3/48 (6) 3/48 (6) 7/48 (15)50e59 0/14 (0) 0/14 (0) 3/14 (21)
Abbreviations: PTSD, posttraumatic stress disorder.a Rows do not sum because participants can have more than one diagnosis.
OEF/OIF. Troops reported substantial exposure to combat and otherpotentially traumaticwar-relatedevents. A largemajority of soldiers(91%) reported participating in combat missions or patrols, 94%reported that theyoramemberof their unit received incoming smallarms fire, 55% were attacked by terrorists or civilians, and 22%thought they killed someone in combat. Ten percent of the samplereported being wounded or injured during deployment.
2.2. Rates of postdeployment psychiatric diagnoses
Table 2 displays rates of postdeployment psychiatric disorders.A majority (62%) of the sample did not meet criteria for a currentpsychiatric disorder at the time of assessment. Depressive disorderswere the most common diagnoses; major depressive disorder wasthe most frequent diagnosis in that category (n¼ 41). Non-PTSDanxiety disorders (other anxiety) and alcohol use disorders werealso relatively common. The most frequent disorders in the otheranxiety category were anxiety disorder not otherwise specified(NOS; n¼ 20), social anxiety disorder (n¼ 11), and generalizedanxiety disorder (n¼ 9). Of those who met criteria for an alcoholuse disorder, 73% were diagnosed with dependence. As we havepreviously reported, 7% of the sample met criteria for PTSD (Erbeset al., under review). When those with subthreshold PTSD wereincluded, the sample prevalence increased to 15%. Pain disorder,somatization disorder NOS, and psychotic disorder NOS were eachdiagnosed in one participant; these disorders were not included inthe analyses due to their low prevalence in the sample.
Women were more likely than men (52% vs 36%) to havea psychiatric diagnosis, c2¼ 4.40, p¼ 0.04. Specifically, femalesoldiers were more frequently diagnosed with PTSD (14% vs 6%;c2¼ 4.03, p¼ 0.04), depressive disorders (27% vs 13%; c2¼ 6.41,p¼ 0.01), and non-PTSD anxiety disorders (25% vs 12%; c2¼ 6.10,p¼ 0.01). Age was not significantly associated with the presence ofany diagnosis.
2.3. Functioning and quality of life associated with psychiatricdiagnoses
Table 3 displays the association between psychiatric diagnosesand overall functioning and quality of life among the panel of OIFdeployed troops. Drug use disorder was eliminated from theseanalyses due the small number of cases. Only participants in anintimate relationship (n¼ 157) were included in the marriage/intimate relationship analyses, while only those with children(n¼ 123) were included in the analyses related to parenting.Having a diagnosis of PTSD (M¼ 2.19, SD¼ 0.39), subthresholdPTSD (M¼ 2.17, SD¼ 0.56), depressive disorder (M¼ 2.14,SD¼ 0.48), non-PTSD anxiety disorder (M¼ 2.00, SD¼ 0.41), oralcohol use disorder (M¼ 1.98, SD¼ 1.20) was associated withlowered social functioning when compared with those without
following OIF deployment.
her anxiety Alcohol use disorders Drug use disorders No diagnosis
/348 (13) 45/348 (13) 4/348 (1) 216/348(62)
/304 (12) 38/304 (13) 3/304 (1) 195/304 (64)1/44 (25) 7/44 (16) 1/44 (2) 21/44 (48)
/170 (11) 23/170 (14) 1/170 (1) 105/170 (62)/110 (16) 15/110 (14) 3/110 (3) 67/110 (61)7/48 (15) 6/48 (13) 0/48 (0) 32/48 (67)3/14 (21) 0/14 (0) 0/14 (0) 9/14 (64)

Table 3Self-reported functioning and quality of life associated with psychiatric diagnoses among National Guard soldiers
PTSDa Subthreshold PTSD Depressive disorders Other anxiety Alcohol use disorders Any diagnosis
Adjusted odds ratiosb (95% confidence intervals)Total SAS-SR 3.03** (1.83e5.00) 2.58** (1.71e3.88) 2.76** (1.92e3.99) 2.19** (1.53e3.15) 2.12** (1.45e3.10) 2.16** (1.67e2.80)Total NQOLS 0.43** (0.28e0.66) 0.44** (0.31e0.64) 0.47** (0.34e0.65) 0.50** (0.35e0.70) 0.59 (0.43e0.81)** 0.53** (0.41e0.67)
Abbreviations: PTSD, posttraumatic stress disorder; SAS-SR, social adjustment scale e self-report; NQOLS, Navy quality of life scale.*p< 0.05. **p< 0.01.
a Reference group for all comparisons was no diagnosis.b Adjusted for age, marital status, education level, and enlisted status.
S.M. Kehle et al. / Journal of Psychiatric Research 45 (2011) 126e132130
a diagnosis (M¼ 1.72, SD¼ 0.35). In regards to PTSD, after adjustingfor age, marital status, enlisted status, and educational level, theodds of having PTSD increased three-fold for each standard devi-ation increase in impairment on the total social functioning score(Table 3). Impairments in social and leisure activities, extendedfamily relationships, and family role functioning were significantlyassociated with all diagnostic categories Impairment in self-reported functioning as a marital/intimate partner was associatedwith all diagnoses except PTSD and subthreshold PTSD. Parentalrole functioning was not associated with any diagnoses.
Overall quality of life was negatively associated with havinga diagnosis of PTSD (M¼ 4.35, SD¼ 1.04), subthreshold PTSD(M¼ 4.44, SD¼ 1.26), depressive disorder (M¼ 4.63, SD¼ 1.09),non-PTSD anxiety disorder (M¼ 4.81, SD¼ 0.99), or alcohol usedisorder (M¼ 4.90, SD¼ 1.20) when compared with those withouta diagnosis (M¼ 5.48, SD¼ 0.94). In regards to PTSD, for eachstandard deviation change in satisfaction with quality of life (rep-resenting increased satisfaction), the odds of having PTSDdecreased by a little over one-half (Table 3). Decreased quality oflife in leisure and recreational activities, relationships with rela-tives, and standard of living were significantly related to all diag-nostic categories. Decreased quality of life related to friends andfriendship was associated with all diagnoses except alcohol usedisorder. The subdomain of marriage/intimate relationships wassignificantly, negatively related to all diagnostic categories butPTSD and non-PTSD anxiety disorders. Finally, decreased satisfac-tion with relationships with children was only associated withPTSD and the depressive disorders.
An examination of effect sizes revealed that PTSD had thelargest association with disruptions in social functioning andquality of life. PTSD (d¼ 1.27 and d¼ 1.14 respectively),subthreshold PTSD (d¼ 0.96 and d¼ 0.94), and depressive disor-ders (d¼ 0.99 and d¼ 0.84) all had large associations with overallsocial functioning and quality of life. The effect sizes for non-PTSDanxiety (d¼ 0.73 and d¼ 0.69) and alcohol use disorders (d¼ 0.29and d¼ 0.54) were in the small to medium range.
2.4. Rates of psychiatric comorbidity
Twenty-three percent of the sample had only one diagnosis, 10%had two diagnoses, 3% had three diagnoses, and 2% had four ormore diagnoses. Among participants with PTSD, the averagenumber of diagnoses was 1.74 (SD¼ 1.36) with a range of zero tofive. Eighty-seven percent of those with PTSD had at least oneadditional diagnosis; 44% had one, 17% had two, 13% had three, and13% had four or more comorbid diagnoses. Table 4 shows rates ofspecific comorbid diagnoses among participants with a diagnosis ofPTSD and a diagnosis of either PTSD or subthreshold PTSD.
2.5. Impact of psychiatric comorbidity on functioning and quality oflife
For the entire panel, a one-way ANCOVA showed that number ofdiagnoses was associated with impairments in overall social
functioning, F(6, 337)¼ 9.97, p< 0.001, and quality of life, F(6,337)¼ 8.79, p< 0.001. Whenwe categorized participants into threegroups (no diagnosis, one diagnosis, two or more diagnoses), weagain found that number of diagnoses was associated with impair-ments in both overall social functioning F(2, 341)¼ 28.95, p< 0.001and quality of life F(2, 341)¼ 25.49, p< 0.001. Posthoc tests (LeastSignificantDifference) showed that each groupdiffered significantlyfrom each other (p� 0.002). For those with a diagnosis of PTSD orsubthreshold PTSD, a one-way ANCOVA showed that additionaldiagnoses were not related to further impairments in total func-tioning, F(5, 37)¼ 1.66, p¼ 0.22, or overall quality of life, F(5, 37)¼0.24, p¼ 0.64. Similarly, among individuals with PTSD orsubthreshold PTSD, there were no significant differences in socialfunctioning, F(1, 41)¼ 0.002, p¼ 0.96, or quality of life, F(1, 41)¼0.44, p¼ 0.44, between thosewith andwithout comorbid disorders.
3. Discussion
We found that a majority of National Guard soldiers recentlyreturned from a combat deployment to Iraq did not meet criteriafor a mental health disorder. However, overall rates were higher inthis panel than in epidemiological studies of community dwellingresidents, in which overall past-year prevalence among adults hasranged from 20 to 30% (Kessler et al., 1994; Narrow et al., 2002;Reiger et al., 1984). Rates of disorders were also substantiallyhigher in this postdeployment sample than in an epidemiologicalstudy of a general, non-OIF deployed, military cohort (Riddle et al.,2007). The soldiers had slightly higher rates than community andnon-deployed military samples across all diagnoses, with theexception of drug use disorders. Not surprisingly, the greatestelevation was in PTSD, which was double the population estimateof 3.6% (Kessler et al., 1994; Narrow et al., 2002). However, the rateof PTSD in our panel was similar towhat has been observed in othertrauma exposed populations (Breslau et al., 1998), and to recentestimates of PTSD among Vietnam veterans. While the NationalVietnam Veterans’ Readjustment Study (NVVRS) originally esti-mated that 15.2% of Vietnam veterans met criteria for PTSDapproximately 10 years after the end of the war (Kulka et al., 1990),reanalyses of those data resulted in an estimated prevalence of 9.7%(Dohrenwend et al., 2006). While rates of PTSD in our sample werelower than in other studies of OIF soldiers that relied on self-reportmeasures, self-report measures of depression and alcohol usedisorders yielded rates similar to those in our panel (Hoge et al.,2004; Jacobson et al., 2008; Milliken et al., 2007). Finally, comor-bidity was common. More than 85% of soldiers with a diagnosis ofPTSD had at least one additional mental health diagnosis, withdepressive disorders being the most common. These findings aresimilar to PTSD comorbidity rates in both the community andamong Vietnam veterans, which have estimated lifetime comor-bidity between 60 and 99% (Breslau et al., 1991; Davidson et al.,1991; Kessler et al., 1995; Kulka et al., 1990).
Over one-half of female soldiers had a mental health diagnosisand female soldiers were significantly more likely to have a mentalhealth diagnosis than male soldiers. Specifically, in our panel,

Table 4Rates of comorbidity among National Guard soldiers with a diagnosis of PTSD.
Depressive disorders Other anxiety Alcohol use disorders Drug use disorders No comorbid diagnosis
PTSD diagnosis n (%)a 16/23 (70) 8/23 (35) 5/23 (22) 0/23 (0) 3/23 (13)PTSD or subthreshold
PTSD diagnosis n (%)a27/53 (51) 15/53 (28) 10/53 (19) 1/53 (2) 10/53 (19)
Abbreviations. PTSD, posttraumatic stress disorder.a Rows do not sum because participants can have more than one comorbid diagnosis.
S.M. Kehle et al. / Journal of Psychiatric Research 45 (2011) 126e132 131
women were diagnosed with PTSD, depressive disorders, andnon-PTSD anxiety disorders at twice the rate of men. Thesediscrepancies are in line with epidemiological studies (both generalpopulation andmilitary); however, the overall rate of mental healthdisorders among female soldiers is substantially higher than infemales in the general population (Kessler et al., 1994). Further,these data reflect a shift in the roles and outcomes of deployedfemale soldiers, as data from NVVRS revealed that female Vietnamveterans had PTSD at one-half the rate of their male counterparts(Turner et al., 2007). Given this finding, the impact of combatdeployments on female soldiers’ mental health will be an impor-tant area of future study.
Soldiers with a mental health diagnosis reported significantimpairments in both social functioning and quality of life. All of thediagnostic categories were related to substantial impairments anddecreased quality of life. However, PTSD was associated with thegreatest impairments. Among Vietnam veterans, PTSD has beenassociated with impaired social and familial role functioning, poorhealth status, diminished well-being, and disruptions in workfunctioning (Carroll et al., 1985; Jordan et al., 1992; Zatzick et al.,1997). Our data suggest that the presence of PTSD is associatedwith similar problems among OIF soldiers as early as six monthspostdeployment. Contrary to our hypotheses, psychiatric comor-bidity among soldiers with PTSD was not related to further impair-ments in social functioning or quality of life. However, having morethan one diagnosis was related to higher levels of impairment in thefull panel. Previous epidemiological and clinic-based studies havefound that havingmore than one psychiatric diagnosis is associatedwith a greater disturbance in functioning and quality of life (Kesslerand Frank, 1997; Olfson et al., 1997; Ormel et al., 1994). While it isimportant to view the results regarding PTSD as preliminary due tothe small number of participants with PTSD, it may be that amongthis population, PTSD is particularly debilitating and those withPTSD are already experiencing such large disruptions that a “flooreffect” may be occurring, in which comorbid diagnoses do notfurther reduce quality of life and social functioning.
This study has a number of strengths, including the use of gold-standard clinical interviews and a large non-treatment seekingpopulation. However, participants were self-selected. Thus, whilethe panel demographics are similar to that of the overall brigade,this was not an epidemiological study and results may not gener-alize either to other National Guard units or the larger militarypopulation. Further, although our analyses suggest few differencesbetween responders and non-responders and we attempted tocontrol for response bias in the analyses, the findings may havebeen influenced by either postdeployment survey or interviewresponse biases. Our panel also had a very small number of soldierswith previous OEF/OIF deployments. The relationship betweenmultiple deployments, psychiatric diagnoses, and functioning is animportant area of future study. Also, a number of our diagnosticconditions had few participants, thus, we may have been under-powered to find differences between groups, particularly for anal-yses examining intimate relationships and parenting. Conclusionsregarding functioning and quality of life are based on self-reportand must be considered preliminary. It is possible that the self-report items measured a general sense of well-being, rather than
specific domains of functioning. As such, the findings requirefurther objective validation (e.g. collateral reports; objective workperformance data) in a larger sample. Finally, it is important to notethat we do not have predeployment diagnostic data, thus, wecannot conclude that the disorders are the result of deployment toa combat zone. Rather, the study highlights the overall post-deployment mental health burden of soldiers deployed to OIF.
This study is the first to provide diagnostic data for a communitysample of OIF soldiers. The data highlight the significant rate andburden of mental health disorders among this population. Further,while PTSD appears to be particularly deleterious, it is also relativelyuncommon. Thus, the findings highlight the importance of success-fully identifying and treating a range of mental health problems, notonly PTSD, in returning soldiers. If untreated, these disorders mayhave devastating effects, both for the soldier and for society.
Contributors
Shannon Kehle participated in study conceptualization anddesign, analysis and interpretation of data, drafting and revision ofthe manuscript, and statistical analysis. Madhavi Reddy partici-pated in acquisition of data, drafting and revision of themanuscript,and administrative support. Amanda Ferrier-Auerbach participatedin study conception and design, drafting and revision of themanuscript, and administrative support. Christopher Erbes partic-ipated in study conceptualization and design, acquisition of data,supervision, revision of the manuscript, and obtaining funding.Paul Arbisi participated in study conceptualization and design,acquisition of data, supervision, revision of the manuscript,administrative support, and obtaining funding. Melissa Polusnyparticipated in study conceptualization and design, acquisition ofdata, supervision, analysis and interpretation of data, revision ofthe manuscript, and obtaining funding.
Role of funding source
This research was supported by the Minneapolis VA MedicalCenter Research Service and grants toMelissa A. Polusny, PhD, fromMinnesota Medical Foundation (Grant #3662-9227-06) andDepartment of Defense Congressionally Directed Medical ResearchProgram (CDMRP) (W81XWH-07-2-003) and a grant to Christo-pher R. Erbes, PhD, from the Department of Veterans Affairs HealthService Research and Development program (RRP 08-385). None ofthe sponsors had any role in the following: design and conductof the study; collection, management, analysis, and interpretationof the data; and preparation, review, or approval of the manuscript.
Conflict of interestAll authors declare that they have no conflicts of interest.
Acknowledgements
The views expressed in this article are those of the authors anddo not reflect the official policy or position of the Department ofVeterans Affairs, Department of the Army, or the Departmentof Defense. This material is supported in part by the Department of
S.M. Kehle et al. / Journal of Psychiatric Research 45 (2011) 126e132132
Veterans Affairs, Veterans Health Administration, Office of Researchof Development, Health Services Research & Development.
References
AmericanPsychiatricAssociation.Diagnostic and statisticalmanual ofmental disorders(DSM-IV-TR). Washington, D.C.: American Psychiatric Association; 2000.
Blake DD, Weathers FW, Nagy LM, Kaloupek DG, Gustman FD, Charney DS, et al. Thedevelopment of a clinician-administered PTSD scale. Journal of Traumatic Stress1995;8:75e90.
Blake DD, Weathers FW, Nagy LM, Kaloupek DG, Klauminzer G, Charney DS, et al. Aclinician rating scale for assessing current and lifetime PTSD: the CAPS-1.Behavior Therapist 1990;13:187e8.
Breslau N, Davis GC, Andreski P, Peterson E. Traumatic events and posttraumaticstress disorders in an urban population of young adults. Archives of GeneralPsychiatry 1991;48:216e22.
Breslau N, Kessler R, Chilcoat HD, Schultz LR, Davis GC, Andreski P. Trauma andposttraumatic stress disorder in the community. Archives of General Psychiatry1998;55:626e32.
Carroll EM, Rueger DB, Foy DW, Donahoe CP. Vietnam combat veterans withposttraumatic stress disorder: analysis of marital and cohabitation adjustment.Journal of Abnormal Psychology 1985;94:329e37.
Cohen J. Statistical power analysis for the behavioral sciences. 2nd ed. Hillsdale, NJ:Lawrence Earlbaum Associates; 1988.
Davidson JRT, Hughes D, Blazer D, George LK. Posttraumatic stress disorder in thecommunity: an epidemiological study. Psychological Medicine 1991;21:1e19.
Dohrenwend BP, Turner JB, Turse NA, Adams BG, Koenen KC, Marshall R. Thepsychological risks of Vietnam for U.S. veterans: a revisit with new data andmethods. Science 2006;313:979e82.
Erbes CR, Polusny MA, Arbisi PA. Post-traumatic stress disorder and symptoms inNational Guard soldiers following combat deployment, under review.
First MB, Spitzer RL, Gibbon M, Williams JBW. Structured clinical interview forDSM-IV-TR axis I disorders, research version, non-patient edition. New York:Biometrics Research, New York State Psychiatric Institute; 2002.
Grieger TA, Cozza SJ, Ursano RJ, Engel CC, Hoge C, Martinez E, et al. Posttraumaticstress disorder and depression in battle-injured soldiers. America Journal ofPsychiatry 2006;163:1777e83.
Hoge CW, Auchterlonie JL, Milliken CS. Mental health problems, use of mentalhealth services, and attrition from military service after returning fromdeployment to Iraq or Afghanistan. Journal of the American Medical Association2006;295(9):1023e32.
Hoge CW, Castro CA, Messer SC, McGurk D, Cotting DI, Koffman RL. Combat duty inIraq and Afghanistan, mental health problems, and barriers to care. NewEngland Journal of Medicine 2004;351(1):13e22.
Jacobson IG, Ryan MAK, Hooper TI, Smith TC, Amoroso PJ, Boyko EJ, et al. Alcoholuse and alcohol-related problems before and after military combat deployment.Journal of the American Medical Association 2008;300(6):663e75.
Jordan BK, Marmar CR, Fairbank JA, Schlenger WE, Kulka RA, Hough RL, et al.Problems in families of male Vietnam veterans with posttraumatic stressdisorder. Journal of Consulting and Clinical Psychology 1992;60:916e26.
Jordan BK, Schlenger WE, Hough R, Kulka RA, Weiss D, Fairbank JA, et al. Lifetimeand current prevalence of specific psychiatric disorders among Vietnamveterans and controls. Archives of General Psychiatry 1991;48:207e15.
Kang HK, Natelson BH, Mahan CM, Lee KY, Murphy FM. Post-traumatic stressdisorder and chronic fatigue syndrome-like illness among Gulf War veterans:a population-based survey of 30,000 veterans. American Journal of Epidemi-ology 2003;157:141e8.
Kessler RC. Posttraumatic stress disorder: the burden to the individual and thesociety. Journal of Clinical Psychiatry 2000;61:4e21.
Kessler RC, Frank RG. The impact of psychiatric disorders on work loss days.Psychological Medicine 1997;27:861e73.
Kessler RC, McGonagle KA, Zhao S, Nelson CB, Hughes M, Eshleman S, et al. Lifetimeand 12-month prevalence of DSM-III-R psychiatric disorders in the UnitedStates. Archives of General Psychiatry 1994;51:8e19.
Kessler RC, Sonnega A, Bromet E, Hughes M, Nelson CB. Posttraumatic stressdisorder in the National Comorbidity Survey. Archives of General Psychiatry1995;52:1048e60.
King LA, King DW, Vogt DS, Knight JA, Samper RE. Deployment Risk and ResilienceInventory: a collection of measures for studying deployment-related experi-ences of military personnel and veterans. Military Psychology 2006;18:89e120.
Kulka RA, Schlenger WE, Fairbank JA, Hough RL, Jordan BK, Marmar CR, et al.Trauma and the Vietnam War generation: report of findings from the NationalVietnam Veterans Readjustment Study. New York: Brunner/Mazel; 1990.
Lowe B, Spitzer RL, Grafe K, Kroenke K, Quenter A, Zipfel S, et al. Comparativevalidity of three screening questionnaires for DSM-IV depressive disorders andphysicians’ diagnosis. Journal of Affective Disorders 2004;78(2):131e40.
Milliken CS, Auchterlonie JL, Hoge CW. Longitudinal assessment of mental healthproblems among active and reserve component soldiers returning from the Iraqwar. Journal of the American Medical Association 2007;298:2141e8.
Narrow WE, Rae DS, Robins LN, Regier DA. Revised prevalence estimates of mentaldisorders in the United States. Archives of General Psychiatry 2002;59:115e23.
Olfson M, Fireman B, Weissman MM, Leon AC, Sheehan DV, Kathol RG, et al. Mentaldisorders and disability among patients in a primary care group practice.American Journal of Psychiatry 1997;154:1734e40.
Ormel J, Von Korff M, Ustun B, Pini S, Korten A, Oldehinkel T. Common mentaldisorders and disability across cultures: results from the WHO collaborativestudy on psychological problems in general health care. Journal of the AmericanMedical Association 1994;272:1741e8.
Prigerson HG, Maciejewski PK, Rosenheck RA. Population attributable fractions ofpsychiatric disorders and behavioral outcomes associated with combat expo-sures among US men. American Journal of Public Health 2002;92:59e63.
Regier DA, Myers JK, Kramer M, Robins LN, Blazer DG, Hough RL, et al. The NIMHEpidemiologic Catchment Area program: historical context, major objectives,and study population characteristics. Archives of General Psychiatry1984;51:8e19.
Riddle JR, Smith TC, Smith B, Corbeil TE, Engel CC, Wells TS, et al. Millenniumcohort: the 2001e2003 baseline prevalence of mental disorders in the U.S.military. Journal of Clinical Epidemiology 2007;60:192e201.
Savoca E, Rosenheck R. The civilian labor market experiences of Vietnam-eraveterans: the influence of psychiatric disorders. Journal of Mental Health Policyand Economics 2000;3:199e207.
Seal KH, Bertenthal D, Miner CR, Sen S, Marmar C. Bringing the war back home:mental health disorders among 103,788 US veterans returning from Iraq andAfghanistan seen at Department of Veterans Affairs facilities. Archives ofInternal Medicine 2007;167(5):476e82.
Stein MB, Walker JR, Hazen AL, Forde DR. Full and partial posttraumatic stressdisorder: findings from a community survey. American Journal of Psychiatry1997;154(8):1114e9.
Tanielian T, Jaycox LH, editors. Invisible wounds of war: psychological and cognitiveinjuries, their consequences, and services to assist recovery. Santa Monica, CA:Rand Corporation, http://www.rand.org/pubs/monographs/MG720/; 2008[accessed 10.03.10].
Terhakopian A, Sinaii N, Engel CC, Schnurr PP, Hoge CW. Estimating populationprevalence of posttraumatic stress disorder: an example using the PTSDChecklist. Journal of Traumatic Stress 2008;21(3):290e300.
The Iowa Persian Gulf Study Group. Self-reported illness and health status amongGulf War veterans: a population-based study. Journal of the American MedicalAssociation 1997;277:238e45.
Turner JB, Turse NA, Dohrenwend BP. Circumstances of service and gender differ-ences in war-related PTSD: findings from the National Vietnam VeteransReadjustment Study. Journal of Traumatic Stress 2007;20:643e9.
Weissman MM. SAS-SR: social adjustment scale e self-report. Toronto, Ontario:MHS, Inc.; 1999.
Wilcove GL, Schewerin MJ, Wolosin DG. An exploratory model of quality of life inthe U.S. Navy. Military Psychology 2003;15:133e52.
Zatzick DF, Marmar CR, Weiss DS, Browner W, Metzler TJ, Golding JM, et al. Post-traumatic stress disorders and functioning and quality of life outcomes ina nationally representative sample of male Vietnam veterans. American Journalof Psychiatry 1997;154:1690e5.