profiles and service utilization for children accessing a mental health walk-in clinic versus usual...
TRANSCRIPT
Journal of Evidence-Based Social Work, 10:338–352, 2013
Copyright © Taylor & Francis Group, LLC
ISSN: 1543-3714 print/1543-3722 online
DOI: 10.1080/15433714.2012.663676
Profiles and Service Utilization for Children Accessing aMental Health Walk-In Clinic versus Usual Care
Melanie Barwick
Research Institute and Learning Institute, The Hospital for Sick Children; Department of
Psychiatry and Dalla Lana School of Public Health, University of Toronto, Toronto,
Ontario, Canada
Diana Urajnik
Department of Psychiatry & Behavioural Neurosciences, McMaster University, Hamilton,
Ontario, Canada
Linda Sumner and Sharna Cohen
Yorktown Child and Family Services, Toronto, Ontario, Canada
Graham Reid
Psychology and Family Medicine, University of Western Ontario, London, Ontario, Canada
Karen Engel
Yorktown Child and Family Services, Toronto, Ontario, Canada
Julie E. Moore
Knowledge Translation Program, Li Ka Shing Knowledge Institute, St. Michael’s Hospital,
Toronto, Ontario, Canada
Many children and adolescents with mental health problems do not receive the treatment they need.
Unmet need raises questions about specific barriers that may prevent service use, and/or the charac-
teristics of children and families who are less likely to receive care. Brief interventions or single–
session psychotherapy delivered in a highly accessible manner are methods of addressing the problems
associated with waitlists and limited access to care. In the current study the authors offer an exploratory
evaluation of the West End Walk-In Counseling Centre for children and youth with psychosocial
problems. Children 4 to 18 years of age who accessed the Walk-In Counseling Centre and a comparison
group of clients who accessed usual care were assessed at intake, post-treatment, and 3-month
follow-up on demographic characteristics, behavioral/emotional adjustment and functioning, client
satisfaction, and service use. Children in the walk-in group had more severe behavioral/emotional
adjustment and functioning than usual care clients at baseline. At post-treatment, walk-in clients
had lower scores on Total Mental Health Problems and Internalizing Behaviors, and exhibited fewer
Address correspondence to Melanie Barwick, Research Institute, The Hospital for Sick Children, 555 University
Avenue, Toronto, ON M5G 1X8, Canada. E-mail: [email protected]
338
WALK-IN CLINIC VERSUS USUAL CARE 339
problems across all scales at follow-up. Walk-in clients found the wait time for service more reasonable
and at follow-up, felt the service addressed concerns and had higher regard for counselor availability
and cultural sensitivity of the service than usual care clients. Service utilization, assessed at post–
treatment and 3-month follow-up, showed that both groups were more likely to access mental health
and education services rather than health or child welfare services, and were more likely to have used
services in the 12 months prior to service than the 3 months following service completion. Walk–
in clients had steeper rates of improvement compared to usual care clients despite equivalence in
psychosocial functioning at baseline. The walk-in model may be an effective alternative to usual care,
particularly for those clients only willing to wait up to 2 weeks for service.
Keywords: Service utilization, mental health, walk-in, child mental health
Many children and adolescents who suffer from mental health problems do not receive thetreatment they need (e.g., Burns et al., 1995; Farmer, Stangl, Burns, Costello, & Angold, 1999;Offord et al., 1987; Verhulst, & Van Der Ende, 1997). Multiple aspects of treating children withmental health problems require improvement, including overcoming barriers to care and increasingservice use (Blais, Breton, Fournier, St.-Georges, & Berthiaume, 2003; McKay, McCadam, &Gonzales, 1996). Recent estimates, based on a combination of epidemiological studies indicatethat of the 14% of children with mental health disorders, only 18% of children receive specializedservices for their difficulties (Waddell, Offord, Shepherd, Hua, & McEwan, 2002). Certain groupsof children, such as those with special needs, immigrant children, those living in certain geographicareas or in disadvantaged economic conditions, and those with different cultural backgrounds maybe further at risk of reduced service accessibility (Boydell & Pong, 2003). The implications ofuntreated mental health problems have become increasingly serious for children, their families, andsociety. Children who do not receive treatment are at risk for a host of negative outcomes, suchas school failure, inadequate family and social functioning, and poor physical health (Costello& Angold, 2000; Waddell et al., 2002). Approximately 50% of untreated childhood disorderspersist into adulthood (Hofstra, Van der, & Verhulst, 2000; Tremblay, 1992). This underscores theimportance of prevention and early intervention for children who are, or may be, at risk of mentalhealth problems.
The issues associated with the unmet need for children’s mental health services raises questionsabout specific barriers that may prevent service use, and/or the characteristics of children andfamilies who are less likely to receive care. Barriers that inhibit access to services includedistance to care, competing time or scheduling demands, and waiting for treatment (e.g., McKayet al., 1996). However, it is important to highlight that accessing children’s services is largelydependent upon parental recognition of, and help-seeking for their child’s problem. Factors thatimpact parental help-seeking have been identified in the literature, and include lack of parentalknowledge of available resources (Zwaanswijk, Van der Ende, Verhaak, Bensing, & Verhulst,2005), demographic factors (e.g., parent age, education, income; Pavuluri, Luk, & McGee, 1996),and parent psychosocial functioning (e.g., depression; Briggs-Gowan, Horwitz, Schwab-Stone,Leventhal, & Leaf, 2000). Furthermore, families who experience social adversity (e.g., familystress, lack of social support) may have difficulty in accessing care. Research shows that childrenin single-parent or impoverished homes, who experience trauma (e.g., child abuse), and whosefamilies are mobile, are significantly less likely to seek help for their mental health difficulties(Flisher et al., 1997; Kazdin et al., 1997). Perceptions of services—such as unrealistic treatmentexpectations and dissatisfaction with prior services—can also prevent parents from choosing touse services (McKay et al., 1996; Polgar et al., 2001).
Waiting for treatment is a particular focus of concern in the current behavioral health careenvironment. The use of waiting lists is conventionally viewed as necessary when service capacityis outstripped by demands for treatment (Brown, Parker, Godding, 2002). Health services managers
340 M. BARWICK ET AL.
are expected to set priorities based on patient need and evidence-based criteria (Ministry ofCommunity and Social Services, South West Region [MCSS-SW], 2001; Noseworthy et al., 2003;Smith, & Hadorn, 2002; Walker, 1998). However, lengthy waiting times for service remain asignificant barrier to receiving mental health treatment when and where children and familiesneed it most. Children endure a variety of costs when access to treatment is delayed or preventedthrough placement on a waiting list. At a minimum, waiting for treatment introduces an additionalobstacle to receiving care; it is likely that the use of waitlists compounds existing access difficulties.Waiting may exacerbate mental health conditions, prolong distress, and occasionally lead to deathin times of crisis. Many waitlists lack both organization and fairness, having been implementedquickly due to pressing situations and time constraints (Smith & Hadorn, 2002).
Given the issues associated with waitlists and the small percentage of children with mentalhealth disorders receiving appropriate care, it is clear that children’s mental health is an aspectof health care that could be improved. Difficulties with service accessibility and the utilizationof care for children with mental health difficulties has been emphasized in policy documentsaimed at addressing these issues (e.g., BC-Ministry of Children and Family Development [BC-MCFD], 2004; Children’s Mental Health Ontario [CMHO], 2004; United States Public HealthService [USPHS], 2000). Decision makers have indicated the need for evidence-based researchto advocate for improved services or different forms of services and support (e.g., CanadianHealth Services Research Foundation [CHSRF], 1999). Efforts to improve access to mental healthservices have been undertaken (see Pumariega & Winters, 2003), such as systems-of-care, wrap-around intervention (Kamradt, Gilbertson, & Lynn, 2005), and large-scale projects (e.g., FortBragg demonstration; Bickman, 2001). However, the dilemma faced by research and practicecommunities is how best to respond in a cost efficient and timely manner to rising demand andlack of access without compromising the quality of services (Brown et al., 2002; Kroll, 2003).This issue requires a change in thinking about current services in terms of intervention type andmode of delivery. There is a critical need for alternative and effective intervention models that arehighly accessible—particularly to capture those children who do not access mental health care.
Walk-In Treatment Model
Brief interventions or single session psychotherapy delivered in a highly accessible manner areone method of addressing the problems associated with waitlists and limited access to care (e.g.,Heather, 1995; Hoyt, 1995; Stallard, 1998); however few empirical studies have been conducted onthe effectiveness of single-session psychotherapy interventions and those that have been conductedare inconclusive (Bloom, 2001; Cameron, 2007). One such intervention is walk-in treatment, whichis an innovative, new model of mental health service delivery that addresses the growing problem ofbarriers to service delivery (Clouthier, Fennema, Johnston, Veenendaal, & Viksne, 1997; Miller, &Slive, 2004). Created in Calgary, Alberta under the umbrella of Woods Homes (Slive, MacLaurin,Oakarden, & Amundson, 1995), this unique form of intervention has evolved as service providershave responded to rapid societal change. Over time clients have had increased expectations ofconvenience and immediacy, which has been accompanied by an expanding need for service (Sliveet al., 1995; Talmon, 1990). It is within this framework that an easily accessible form of therapyhas been developed. Although no one therapeutic framework is employed, the walk-in modelof service delivery is based on a systemic and brief therapy orientation that emphasizes alreadyexisting client resources (e.g., social support, client strengths). Interventions are pragmatic, andaim to provide a clear outcome for clients when they leave their single session. The nature of theservice eliminates many of the barriers (e.g., waiting) that traditionally prevent access to mentalhealth care.
Evidence from clinical practice and prior evaluation work has suggested that mental healthwalk-in service delivery is successful in achieving better client outcomes (e.g., Cohen & Engel,
WALK-IN CLINIC VERSUS USUAL CARE 341
2000; Harper-Jaques, McElheran, Slive, & Leahey, 2008; Slive et al., 1995; Young, 2008; Young,Dick, Herring, & Lee, 2008) and has the potential to be an effective strategy at targeting minoritypopulations (Bobele, Lopez, Scamardo, & Solorzano, 2008). However, despite the relativelylengthy history of brief therapies and single-session counseling (e.g., Boyhan, 1996; Budman& Gurman, 1988; Clouthier, Fennema, Johnston, Veenendaal, & Viksne, 1996; Hoyt, Rosenbaum,& Talmon, 1992; Miller, 1998; Miller & Slive, 2004; Slive, McElheran, & Lawson, 2008), fewoutcome studies using standardized measures have focused on the effectiveness of walk-in servicefor children and youth presenting with psychosocial problems (Cameron, 2007; Perkins, 2006).
Yorktown Child and Family Centre: West End Walk-In Counseling Centre
The West End Walk-In Counseling Centre located at Yorktown Child and Family Centre (YCFC)was established in 1999 in response to the growing need for immediate and accessible treatment—particularly in the former City of York, which has traditionally been a high-risk and under-servicedarea. The walk-in service is operated as a partnership of children’s mental health agencies (YCFC,Oolagen Community Services, COSTI immigrant social service agency) and is partially fundedby the United Way. Adapted from the Slive et al. (1995) walk-in model (Calgary, Alberta, WoodsHomes), the goal of the service is to provide high-quality, accessible treatment. Service deliveryentails immediate access to culturally relevant counseling, provided at no cost to clients. The walk-in consultation format allows clients to receive help at their chosen time of need. An appointmentor referral is not necessary, there is no lengthy intake process, and the service operates duringevening hours. The model also emphasizes community capacity through a Community VolunteerTherapist Program. This program trains clinicians in the use of the walk-in model in exchangefor service. The nature of the service eliminates barriers (such as waiting for treatment) thattraditionally prevent access to mental health care.
Prior evaluations based on client satisfaction, self-report of symptoms, usefulness of services,and anecdotal evidence have suggested that this type of service delivery is successful (e.g., Cohen& Engel, 2000; Harper-Jaques et al., 2008; Miller, 2008; Slive et al., 1995; Young, 2008; Younget al., 2008). Preliminary evaluations found that the center provided an accessible, immediatetherapeutic response to a high level of need. A diverse range of ethno-specific and special needsclientele received help for a variety of mental health problems—at their chosen time of need.The center was an important first point of access for those children and families who had nothad previous counseling. Clients expressed a high level of satisfaction with treatment and animprovement in the problem that had brought them to the service (e.g., child behavior issues;YCFC, 2003; Miller, 2008; Miller & Slive, 2004). Clients were also largely satisfied with thestructure (e.g., no-cost, no appointment or waiting list) and culturally relevant/respectful nature ofthe service provided, and its usefulness in addressing their needs.
However, there is no clear and composite profile of the mental health characteristics of children/youth who access this model of care. Standardized assessment of the psychosocial adjustment/outcomes of children receiving walk-in service has not been undertaken (Miller & Slive, 2004).Few outcome studies have used standardized measures to assess walk-in service for children withpsychosocial difficulties (e.g., Perkins, 2006), despite the documented success of brief and single-session therapies (e.g., Boyhan, 1996; Budman, & Gurman, 1988; Clouthier et al., 1996; Hoytet al., 1992; Miller, 1998; Miller & Slive, 2004; Slive et al., 2008).
Current Study
The current study is an exploratory evaluation of the West End Walk-In Counseling Centre forchildren and youth with psychosocial problems. Through this study the authors contributes to the

342 M. BARWICK ET AL.
evidence base on alternative sources of mental health service delivery and help-seeking amongchildren and families. Delineating the service pathways of walk-in clients—in addition to thosewho have accessed usual care—can provide important information with which to inform effortsaimed at service accessibility and coordination. Moreover, the model may prove to be an effectivestrategy to reduce waitlist bottlenecks throughout the provincial system. The authors objectivesincluded: (1) describe the mental health characteristics of walk-in and the usual care child andyouth clients; (2) compare the psychosocial adjustment over a 3-month period of time of walk-inclients with those accessing standard care at Yorktown Child and Family Centre; and (3) describethe service utilization of walk-in clients prior to and following walk-in service delivery.
METHOD
Sample
Participants in the walk-in group were children and youth (4 to 18 years) who accessed the West-End Walk-In Counseling Centre, from October 11, 2006 to December 31, 2008. Of the 151 eligiblewalk-in clients, 112 agreed to participate, representing a 74.2% recruitment rate at baseline (parentand youth informants combined). Of the112 who participated at baseline, 68 completed the postservice measures at follow-up (60.7%). Forty-six of these clients continued with the 3-monthinterview (n D 40 parent informants, n D 6 youth informants with full assessment data). Fourteenof the 44 clients that did not complete the post interview completed the 3-month interview, for atotal of 60 interviews at the 3-month follow-up. Therefore, 53.6% of recruited clients completedthe study.
The comparison group or the YCFC usual care group was comprised of clients (4 to 18 years)who accessed service via the standard intake process at YCFC for the CORE Counseling Program.Among usual care clients, 60 of 157 of eligible clients agreed to participate (38.2%). Of theseclients, 32 completed the post interview, and 26 were interviewed at the 3-month assessment point(22 parents and 4 youth). Twelve additional clients who had not completed the post-test interviewcompleted the 3-month assessment for a total of 38 completed 3-month interviews (63.3% ofparticipants).
Procedure
Participants in the walk-in group were recruited on an iterative basis as they entered the West-End Walk-In Counseling Centre during two weekday evenings (Monday, Wednesday). Studyrecruitment for the usual care group occurred at intake; at Yorktown this is the client’s InitialClient Consultation (ICC) meeting with a therapist which typically occurs within two weeks ofthe initial call for service.
Measures
Demographic information. The Client Intake Information (CII) form is a standard intakesheet that gathers demographic data for walk-in center clients. Demographics characteristicsconsisted of child age, gender, parent/guardian age, gender, education, income, marital status,and cultural background. The form also captures information about the number of adults andchildren present, and whether the current visit is the first time the family has visited the walk-in clinic. Walk-in clients completed this form at intake. For the usual care group, demographicinformation was also collected at intake as part of the standard intake process (computerizedintake).
WALK-IN CLINIC VERSUS USUAL CARE 343
Brief Child and Family Phone Interview (BCFPI). The BCFPI version 3 (Cunningham,Pettingill, & Boyle, 2003) is a standardized measure of behavioral/emotional adjustment, andfunctioning for children 3 to 18 years of age. The measure has a total of 51 items which arecollapsed into four scales: Externalizing Behaviour (18 items), Internalizing Behavior (18 items),Impact on Child Functioning (8 items), and Impact on Family Functioning (7 items). The Ex-ternlizing and Internalizing Behavior scales combine to create a Total Mental Health Problemsscale (36 items). The Externalizing Behaviour scale is a composite measure that is made up ofthree subscales: Regulating Attention, Impulsiveness and Activity Level; Cooperativeness; andConduct. The Internalizing Behaviour composite scale includes three subscales: Separation fromAdults, Managing Anxiety, and Managing Moods. Impact on Child Functioning assesses theextent to which problems have adversely affected the child’s social participation, quality of socialrelationships, and school achievement. The Impact on Family Functioning Scale includes itemsdescribing family activities and family comfort and assesses how the child’s behavior affectsfamily interactions.
An interviewer administers the measure to a parent or adolescent by telephone or in-person,which takes approximately 30 minutes. The BCFPI was completed by parents or youth at baseline,via phone at post-test (two weeks after the baseline assessment) and at the 3-month follow-upassessment. The BCFPI’s items were derived from the survey measurement tools of the OntarioChild Health Survey (OCHS; Boyle et al., 1993; Boyle, Offord, Racine, Szatmari, & Fleming,1993). The psychometric properties of the measure have been well-established with samples ofcommunity and clinic referred children derived from the OCHS, with Cronbach’s alphas rangingfrom .75 to .86 (Cunningham & Boyle, 2006; Cunningham et al., 2002). Reliability for the currentstudy was in a similar range: Externalizing Behaviour (alpha D 0.82); Internalizing Behaviour(alpha D 0.86); Child Functioning (alpha D 0.74); and Family Functioning (alpha D 0.77). Theinstrument is a mandated tool in Ontario for approximately 110 funded providers of children’smental health services (Barwick, Boydell, Cunningham, & Ferguson, 2004), and thus providescomparison against provincial, regional, and Yorktown norms. The responses were normed to havea standardized distribution with a mean of 50, and a SD of 10; scores of 70—higher than 98%of the norming population—are considered to be significantly elevated, or within the “clinical”range.
Client satisfaction. A Client Satisfaction Questionnaire (CSQ) was used to assess participantsatisfaction with the services received from the walk-in center. Clients were asked to indicate: theextent of service usefulness, overall satisfaction, whether they would recommend the counselingcenter, whether the service was respectful of cultural values, the importance of being able to seea counselor without an appointment, and what they consider is a reasonable amount of time towait to get help. All responses were on a four-point scale, with high scores indicating greatersatisfaction, with the exception of an item that assessed perceptions of wait time for service(seven-point scale). Higher scores for this item represented a longer length of time. The CSQmeasured standard client care satisfaction. Participants completed the CSQ after the first sessionwith the clinician and at the 3-month follow-up.
Service use. Service use was captured through the use of a semi-structured interview (Reidet al., 2005). This interview assessed help-seeking behavior/trajectory of service use in thecommunity. Assessments of formal service utilization included: type of agency/provider (e.g.,Children’s Mental Health Centre, private practitioner), sector (e.g., education, health, mentalhealth), services received, and number of contacts with a service provider within the last 12months. Respondents also reported informal sources of help (e.g., help received from family).The interview items were guided by the Ontario Child Health Study-Revised (OCHS-R; Boyleet al., 1987), the Child and Adolescent Services Assessment (CASA; Ascher, Farmer, Burns, &
344 M. BARWICK ET AL.
TABLE 1
Demographic Characteristics by Group
Walk-In Group
N D 94
YCFC Group
N D 56
Group Differences
t-test
Youth age 10.5 (SD D 3.87) 10.4 (SD D 3.64) 0.20
Youth gender: Male 52.1% 64.3% 1.34
Youth immigrant 84.1% 85.5% 0.22
Parent age 39.0 (SD D 8.4) 38.9 (SD D 9.1) 0.05
Parent gender: Male 12.8% 5.4% 1.61
Parent immigrant 56.2% 48.2% 0.93
Family type: Single parent 58.5% 64.8% 0.75
Family income below $40,000 57% 70% 1.24
Note. No significant differences by group.
Angold, 1996), Services Assessment for Children and Adolescents (SACA; Stiffman et al., 2000).These widely used measures of service utilization (or service use items in the case of the OCHS-R), have well-established psychometric properties (e.g., Burns et al., 1995; Farmer et al., 1999;Waddell et al., 2002). Participants in the walk-in and usual care groups completed the measure ofservice use at post-test and the 3-month follow-up.
RESULTS
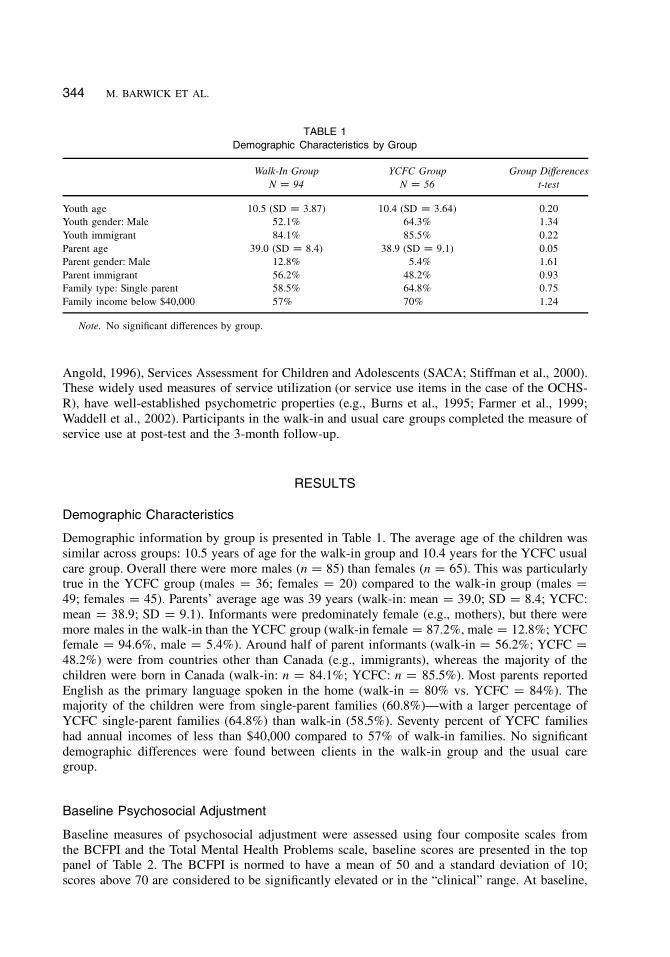
Demographic Characteristics
Demographic information by group is presented in Table 1. The average age of the children wassimilar across groups: 10.5 years of age for the walk-in group and 10.4 years for the YCFC usualcare group. Overall there were more males (n D 85) than females (n D 65). This was particularlytrue in the YCFC group (males D 36; females D 20) compared to the walk-in group (males D
49; females D 45). Parents’ average age was 39 years (walk-in: mean D 39.0; SD D 8.4; YCFC:mean D 38.9; SD D 9.1). Informants were predominately female (e.g., mothers), but there weremore males in the walk-in than the YCFC group (walk-in female D 87.2%, male D 12.8%; YCFCfemale D 94.6%, male D 5.4%). Around half of parent informants (walk-in D 56.2%; YCFC D
48.2%) were from countries other than Canada (e.g., immigrants), whereas the majority of thechildren were born in Canada (walk-in: n D 84.1%; YCFC: n D 85.5%). Most parents reportedEnglish as the primary language spoken in the home (walk-in D 80% vs. YCFC D 84%). Themajority of the children were from single-parent families (60.8%)—with a larger percentage ofYCFC single-parent families (64.8%) than walk-in (58.5%). Seventy percent of YCFC familieshad annual incomes of less than $40,000 compared to 57% of walk-in families. No significantdemographic differences were found between clients in the walk-in group and the usual caregroup.
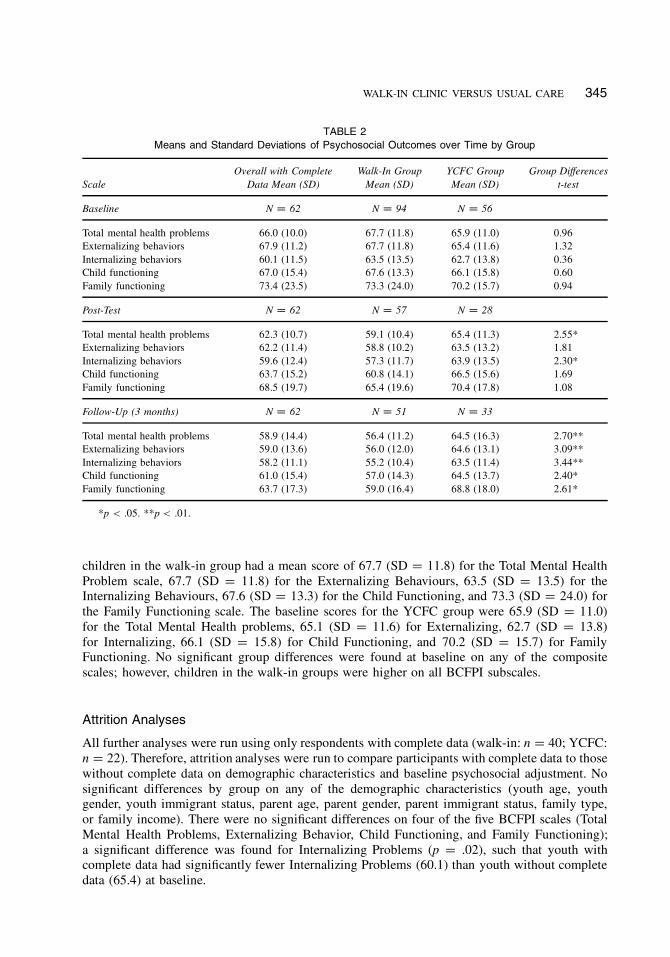
Baseline Psychosocial Adjustment
Baseline measures of psychosocial adjustment were assessed using four composite scales fromthe BCFPI and the Total Mental Health Problems scale, baseline scores are presented in the toppanel of Table 2. The BCFPI is normed to have a mean of 50 and a standard deviation of 10;scores above 70 are considered to be significantly elevated or in the “clinical” range. At baseline,
WALK-IN CLINIC VERSUS USUAL CARE 345
TABLE 2
Means and Standard Deviations of Psychosocial Outcomes over Time by Group
Scale
Overall with Complete
Data Mean (SD)
Walk-In Group
Mean (SD)
YCFC Group
Mean (SD)
Group Differences
t-test
Baseline N D 62 N D 94 N D 56
Total mental health problems 66.0 (10.0) 67.7 (11.8) 65.9 (11.0) 0.96
Externalizing behaviors 67.9 (11.2) 67.7 (11.8) 65.4 (11.6) 1.32
Internalizing behaviors 60.1 (11.5) 63.5 (13.5) 62.7 (13.8) 0.36
Child functioning 67.0 (15.4) 67.6 (13.3) 66.1 (15.8) 0.60
Family functioning 73.4 (23.5) 73.3 (24.0) 70.2 (15.7) 0.94
Post-Test N D 62 N D 57 N D 28
Total mental health problems 62.3 (10.7) 59.1 (10.4) 65.4 (11.3) 2.55*
Externalizing behaviors 62.2 (11.4) 58.8 (10.2) 63.5 (13.2) 1.81
Internalizing behaviors 59.6 (12.4) 57.3 (11.7) 63.9 (13.5) 2.30*
Child functioning 63.7 (15.2) 60.8 (14.1) 66.5 (15.6) 1.69
Family functioning 68.5 (19.7) 65.4 (19.6) 70.4 (17.8) 1.08
Follow-Up (3 months) N D 62 N D 51 N D 33
Total mental health problems 58.9 (14.4) 56.4 (11.2) 64.5 (16.3) 2.70**
Externalizing behaviors 59.0 (13.6) 56.0 (12.0) 64.6 (13.1) 3.09**
Internalizing behaviors 58.2 (11.1) 55.2 (10.4) 63.5 (11.4) 3.44**
Child functioning 61.0 (15.4) 57.0 (14.3) 64.5 (13.7) 2.40*
Family functioning 63.7 (17.3) 59.0 (16.4) 68.8 (18.0) 2.61*
*p < .05. **p < .01.
children in the walk-in group had a mean score of 67.7 (SD D 11.8) for the Total Mental HealthProblem scale, 67.7 (SD D 11.8) for the Externalizing Behaviours, 63.5 (SD D 13.5) for theInternalizing Behaviours, 67.6 (SD D 13.3) for the Child Functioning, and 73.3 (SD D 24.0) forthe Family Functioning scale. The baseline scores for the YCFC group were 65.9 (SD D 11.0)for the Total Mental Health problems, 65.1 (SD D 11.6) for Externalizing, 62.7 (SD D 13.8)for Internalizing, 66.1 (SD D 15.8) for Child Functioning, and 70.2 (SD D 15.7) for FamilyFunctioning. No significant group differences were found at baseline on any of the compositescales; however, children in the walk-in groups were higher on all BCFPI subscales.
Attrition Analyses
All further analyses were run using only respondents with complete data (walk-in: n D 40; YCFC:n D 22). Therefore, attrition analyses were run to compare participants with complete data to thosewithout complete data on demographic characteristics and baseline psychosocial adjustment. Nosignificant differences by group on any of the demographic characteristics (youth age, youthgender, youth immigrant status, parent age, parent gender, parent immigrant status, family type,or family income). There were no significant differences on four of the five BCFPI scales (TotalMental Health Problems, Externalizing Behavior, Child Functioning, and Family Functioning);a significant difference was found for Internalizing Problems (p D .02), such that youth withcomplete data had significantly fewer Internalizing Problems (60.1) than youth without completedata (65.4) at baseline.

346 M. BARWICK ET AL.
TABLE 3
Repeated-Measures ANOVA: Main Effects by Group and Time and Interaction of Time by Group
Scale Main Effect of Group Main Effect of Time Time by Group Interaction
Total mental health problems F D 5.17* F D 8.40*** F D 5.05**
Externalizing behaviors F D 4.47* F D 20.72*** F D 7.20**
Internalizing behaviors F D 4.33* F D 1.04 F D 8.63***
Child functioning F D 2.36 F D 3.47* F D 7.58**
Family functioning F D 0.77 F D 6.22** F D 7.69**
*p < .05. **p < .01. ***p < .001.
Psychosocial Adjustment over Time
Means and standard deviations for the BCFPI scales at post-test and follow-up are presented inthe bottom two panels of Table 2. Group comparisons were conducted with the walk-in group andthe YCFC group for each of the measures. At post-test, group differences were found for TotalMental Health Problems (p D .013) and Internalizing Behaviors (p D .024), such that children andyouth in the Walk-In group had lower scores on both scales. At follow-up there were significantgroup differences on all five scales (p < .05) with the walk-in group exhibiting fewer problemsthan the YCFC group for all scales.
A repeated measures ANOVA was used to assess changes in mental health outcomes over timeusing baseline, post-test, and 3-month follow-up assessments for the composite BCFPI scalesfor clients with complete data. The model included group as a between-subject factor, time asa within-subject factor, and the interaction between group and time. Table 3 presents the resultsof the repeated measures ANOVA. The interaction between time and group was significant forall domains: Total Mental Health (F2;120 D 5.05, p D .008, partial eta2
D .08); ExternalizingBehaviours (F2;120 D 7.20, p D .001, partial eta2
D .11); Internalizing Behaviours (F2;120 D
8.63, p D .000, partial eta2D .13); Child Functioning (F2;120 D 7.58, p D .001, partial eta2
D
.11); and Family Functioning (F2;120 D 7.69, p D .001, partial eta2D .12). When an interaction
is significant in a repeated-measures ANOVA, the main effects for the variables included in theinteraction should not be examined. As the interactions between time and group were significantfor all outcomes, the main effects for group and time will not be interpreted.
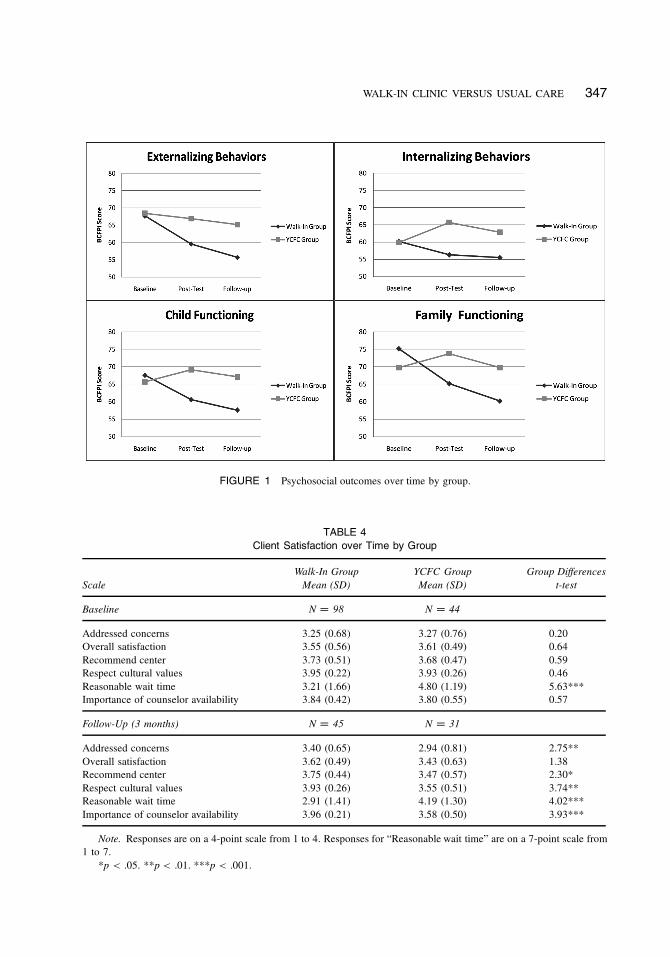
To interpret the results of the interactions, the means over time by group are presented inFigure 1 for each of the four composite scales. In all cases, the walk-in group had steeper rates ofdecline on the BCFPI than the YCFC group. This reflects the greater extent of improvement forthe walk-in children over time as compared to the YCFC clients. Furthermore, there was slippage(an increase in problems) for the Internalizing, Child Functioning, and Family Functioning scalesfor YCFC clients at the time of the second assessment.
Client Satisfaction
Participants completed the Client Satisfaction Questionnaire at baseline and at the three-monthfollow-up (Table 4). At baseline, only one of the items was significant, the length of time theclient feels is a reasonable amount of time to wait for help (p < .001). At follow-up five ofthe six questions were significantly different by group: compared to the YCFC group, walk-inclients were more likely to report that the center addressed their concerns (p D .007), that theywould recommend the center to a friend (p D .026), that the center was culturally respectful (p D
.001), and that they thought being able to walk in and see a counselor was important (p < .001).When asked how long they thought was reasonable to wait to get help, those in the walk-in group
WALK-IN CLINIC VERSUS USUAL CARE 347
FIGURE 1 Psychosocial outcomes over time by group.
TABLE 4
Client Satisfaction over Time by Group
Scale
Walk-In Group
Mean (SD)
YCFC Group
Mean (SD)
Group Differences
t-test
Baseline N D 98 N D 44
Addressed concerns 3.25 (0.68) 3.27 (0.76) 0.20
Overall satisfaction 3.55 (0.56) 3.61 (0.49) 0.64
Recommend center 3.73 (0.51) 3.68 (0.47) 0.59
Respect cultural values 3.95 (0.22) 3.93 (0.26) 0.46
Reasonable wait time 3.21 (1.66) 4.80 (1.19) 5.63***
Importance of counselor availability 3.84 (0.42) 3.80 (0.55) 0.57
Follow-Up (3 months) N D 45 N D 31
Addressed concerns 3.40 (0.65) 2.94 (0.81) 2.75**
Overall satisfaction 3.62 (0.49) 3.43 (0.63) 1.38
Recommend center 3.75 (0.44) 3.47 (0.57) 2.30*
Respect cultural values 3.93 (0.26) 3.55 (0.51) 3.74**
Reasonable wait time 2.91 (1.41) 4.19 (1.30) 4.02***
Importance of counselor availability 3.96 (0.21) 3.58 (0.50) 3.93***
Note. Responses are on a 4-point scale from 1 to 4. Responses for “Reasonable wait time” are on a 7-point scale from
1 to 7.
*p < .05. **p < .01. ***p < .001.
348 M. BARWICK ET AL.
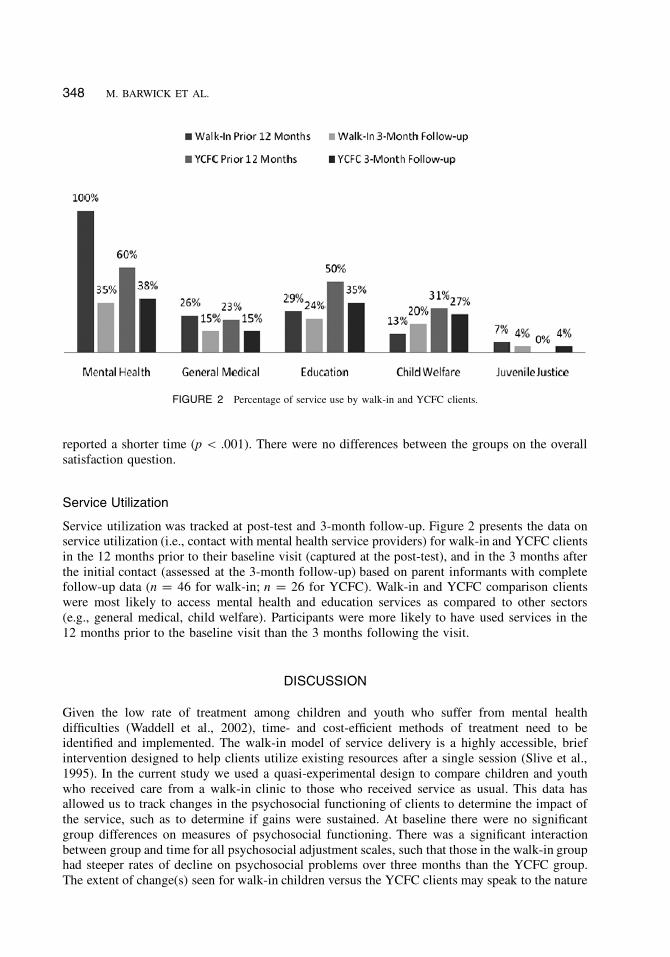
FIGURE 2 Percentage of service use by walk-in and YCFC clients.
reported a shorter time (p < .001). There were no differences between the groups on the overallsatisfaction question.
Service Utilization
Service utilization was tracked at post-test and 3-month follow-up. Figure 2 presents the data onservice utilization (i.e., contact with mental health service providers) for walk-in and YCFC clientsin the 12 months prior to their baseline visit (captured at the post-test), and in the 3 months afterthe initial contact (assessed at the 3-month follow-up) based on parent informants with completefollow-up data (n D 46 for walk-in; n D 26 for YCFC). Walk-in and YCFC comparison clientswere most likely to access mental health and education services as compared to other sectors(e.g., general medical, child welfare). Participants were more likely to have used services in the12 months prior to the baseline visit than the 3 months following the visit.
DISCUSSION
Given the low rate of treatment among children and youth who suffer from mental healthdifficulties (Waddell et al., 2002), time- and cost-efficient methods of treatment need to beidentified and implemented. The walk-in model of service delivery is a highly accessible, briefintervention designed to help clients utilize existing resources after a single session (Slive et al.,1995). In the current study we used a quasi-experimental design to compare children and youthwho received care from a walk-in clinic to those who received service as usual. This data hasallowed us to track changes in the psychosocial functioning of clients to determine the impact ofthe service, such as to determine if gains were sustained. At baseline there were no significantgroup differences on measures of psychosocial functioning. There was a significant interactionbetween group and time for all psychosocial adjustment scales, such that those in the walk-in grouphad steeper rates of decline on psychosocial problems over three months than the YCFC group.The extent of change(s) seen for walk-in children versus the YCFC clients may speak to the nature
WALK-IN CLINIC VERSUS USUAL CARE 349
of the walk-in model. For example, walk-in clients are choosing to attend the walk-in, to receivehelp immediately, and this may be indicative of higher readiness for change—a characteristicknown to be important relative to behavior change (Prochaska et al., 1994). Moreover, close to70% (23 of 34 responses) of walk-in clients were only willing to wait upwards of 2 weeks forservice, which could be indicative of their perceived sense of urgency. By comparison, usual careclients did not receive treatment immediately, and their baseline measures were taken at intake.Usual care clients have, therefore, not received treatment at the time of baseline, and some clientsmay still be waiting for treatment at the time of follow-up assessments. Within this context, morethan half (60%) of the usual care clients were willing to wait a month or more for treatment (9 of15 responses). In short, our data provide some empirical support for the immediate behavioralproblems and family crises commonly observed for families and children seen at the walk-in uponentry to service, and suggest that the walk-in model may be accessed more frequently by familieswith problems in these areas, although differences were not significant.
Service utilization data for both groups measured at post- and 3-month follow-up showed,not surprisingly, that both walk-in and YCFC usual care group clients reported seeking moretreatment from mental health and education services, than from the general medical sector andchild welfare prior to seeking service at YCFC. At follow-up, approximately one-third of bothgroups sought mental health support, suggesting that even walk-in clients still feel the need for,or require mental health services even after a single consultation. Caution must be exercised wheninterpreting the service use data, as the type or nature of “treatment” was not captured (e.g., couldbe brief treatment contacts, individual, family counseling).
Client satisfaction data suggests that the length of time clients are willing to wait for serviceis a defining feature, as stated above. Additionally, however, we find that walk-in clients perceivethe service addressed their concerns, respected cultural values, and was strengthened by counseloravailability compared to usual care clients who waited for service. Walk-in parents appear similarto those identified as Action oriented in a study of the information preferences of parents seekingchild mental health services that used a quantitative consumer preference modeling method.Cunningham and colleagues (2008) demonstrated that two out of three types of parents preferredto wait for child mental health information until their child was assessed or treated. A third groupof parents—the Action group—were more likely than the Overwhelmed or Information parentsegments to prefer information while waiting for treatment.
Among the limitations of this study, the biggest challenge was the rate of recruitment of YCFCusual care clients. The number of YCFC clients recruited for baseline assessment was below theplanned recruitment rate. There were several reasons for this occurrence, including a clinicianshortage that reduced case assignment expectations (e.g., staff turnover), a higher than expectedcancellation/no show rate for clients with existing appointments, clients who were not eligible toparticipate (e.g., due to study inclusion criteria), and clients that clinicians were unable to recruitdue to high-risk situations. To help solve this problem, the recruitment strategy was adapted forthis group to include clients recruited at the time of agency intake (clients’ first phone call forservice).
Additionally, there were issues with client retention to the study and collecting post-test andfollow-up data. The YCFC group was comprised of clients who attended intake/an initial clientmeeting, and does not necessarily reflect all clients initially coming to YCFC, or going into service.In other words, the composition of this group of clients who are subsequently placed on a waitlistfor service, may represent those who “self-select” (e.g., affected by motivational factors) to cometo an initial intake or consultation (“business”) meeting. It may also be that more impaired YCFCclients either go straight to service, or have difficulty in attending intake procedures (meetingincluded), and that these clients are not fully represented in our sample. A third issue relative torecruitment is that while parents, youth, and families have been increasingly using the Walk-InCounseling Centre, many of the clients accessing the center were adults and couples. Over 60%

350 M. BARWICK ET AL.
of clients accessing the walk-in during the study period presented with adult issues, and were noteligible for study participation. Lastly, the outcome results presented are based on study clientswith complete follow-up data. It is entirely possible that the pattern of results may be differentfor the whole sample, including those clients with missing follow-up data. All of these real-worldcontext sampling issues must be considered in the interpretation of our findings.
This study provides an encouraging view of walk-in service as an alternative to usual care forchild and youth mental health. In particular, it appears to provide a service option that may bemore desirable to a segment of the client population. Outcomes including psychosocial, serviceutilization, and client satisfaction are promising.
REFERENCES
Ascher, B. H., Farmer, E. M. Z, Burns, B. J., & Angold, A. (1996). The Child and Adolescent Service Assessment
(CASA): Description and psychometrics. Journal of Emotional and Behavioral Disorders, 4, 12–20.
Barwick, M., Boydell, K., Cunningham, C. E., & Ferguson, B. (2004). Overview of Ontario’s screening and outcome
measurement initiative in children’s mental health. The Canadian Child and Adolescent Psychiatry Review, 13, 105–109.
Bickman, L. (2001). A continuum of care—More is not always better. American Psychologist, 51, 689–701.
Blais, R., Breton, J. J., Fournier, M., St.-Georges, M., & Berthiaume, C. (2003). Are mental health services for children
distributed according to need? Canadian Journal of Psychiatry, 48, 176–186.
Bloom, B. L. (2001). Focused single-session psychotherapy: A review of the clinical and research literature. Brief Treatment
and Crisis Intervention, 1, 75–86.
Bobele, M., Lopez, S. S., Scamardo, M., & Solorzano, B. (2008). Single-session/Walk-In therapy with Mexican-American
clients. Journal of Systematic Therapies, 27, 75–89.
Boydell, K. M., & Pong, R. W. (2003). The rural perspective on continuity of care: Pathways to care for children with
emotional and behavioural disorders. Ottawa, ON: Canadian Health Services Foundation.
Boyhan, P. A. (1996). Clients’ perceptions of single session consultations as an option to waiting for family therapy.
Australian and New Zealand Journal of Family Therapy, 17, 85–96.
Boyle, M. H., Offord, D. R., Racine, Y., Fleming, J. E., Szatmari, P., & Sanford, M. (1987). The Ontario Child Health
Study, I: Methodology. Archives of General Psychiatry, 44, 826–831.
Boyle, M. H., Offord, D. R., Racine, Y., Fleming, J. E., Szatmari, P., & Sanford, M. (1993). Evaluation of the revised
Ontario Child Health Study Scales. Journal of Child Psychology and Psychiatry, 34, 189–213.
Boyle, M. H., Offord, D. R., Racine, Y., Szatmari, P., & Fleming, J. E. (1993). Evaluation of the original Child Health
Study Scales. Canadian Journal of Psychiatry, 38, 397–405.
Briggs-Gowan, M., Horwitz, S., Schwab-Stone, M. E., Leventhal, J., & Leaf, P. (2000). Mental health in pediatric settings:
Distribution of disorders and factors related to service use. Journal of the American Academy of Child and Adolescent
Psychiatry, 39, 841–849.
British Columbia Ministry of Children and Family Development. (July, 2004). Child and youth mental health plan for
British Columbia. BC: Mental Health and Youth Services, Author.
Brown, S. A., Parker, J. D., & Godding, P. R. (2002). Administrative, clinical, and ethical issues surrounding the use
of waiting lists in the delivery of mental health services. Journal of Behavioral Health Services and Research, 29,
217–228.
Budman, S. H., & Gurman. A. S. (1988). The practice of brief therapy: An introduction. In S. H. Budman & A. A.
Gurman (Eds.), Theory and practice of brief therapy (pp. 1–25). New York, NY: Guilford Press.
Burns, B. J., Costello, E. J., Angold, A., Tweed, D., Stangl, D. K., Farmer, E. M., & Erkanli, A. (1995). Children’s mental
health service use across sectors. Health Affairs, 14, 147–160.
Cameron, C. L. (2007). Single session and walk-in psychotherapy: A descriptive account of the literature. Counselling
and Psychotherapy Research, 7, 245–249.
Canadian Health Services Research Foundation. (1999). Issues in linkage and exchange between researchers and decision-
makers. National Workshop. Retrieved from http://www.chsrf.ca/other_documents/events/1999_e.php
Children’s Mental Health Ontario. (February, 2004). Towards a mental health policy for Ontario’s children and youth.
Toronto, ON: Author.
Clouthier, K., Fennema, D., Johnston, J., Veenendaal, K., & Viksne, U. (1996). Expanding the influence of a single-session
consultation program. Journal of Systemic Therapies, 15(4), 1–11.
Cohen, S., & Engel, K. (2000). Yorktown Child and Family Centre: “West End Walk-In Counselling Centre.” Toronto,
ON: Yorktown Child and Family Centre.
WALK-IN CLINIC VERSUS USUAL CARE 351
Costello, E. J., & Angold, A. (2000). Developmental psychopathology and public health: Past, present and future.
Developmental Psychopathology, 12, 599–618.
Cunningham, C. E., Pettingill, P., & Boyle, M. (2006). The Brief Child and Family Phone Interview (BCFPI-3): A
computerized intake and outcome assessment tool, interviewer’s manual. Hamilton, ON: Canadian Centre for the Study
of Children at Risk, Hamilton Health Sciences Corporation, McMaster University.
Farmer, E. M., Stangl, D. K., Burns, B. J., Costello, E. J., & Angold, A. (1999). Use, persistence, and intensity: Patterns
of care for children’s mental health across one year. Community Mental Health Journal, 35, 31–46.
Flisher, A. J., Kramer, R. A., Grosser, R. C., Alegria, M., Bird, H. R., Bourdon, K. H., : : : Hoven, C. W. (1997). Correlates
of unmet need for mental health services by children and adolescents. Psychological Medicine, 27, 1145–1154.
Harper-Jaques, S., McElheran, N., Slive, A., & Leahey, M. (2008). A comparison of two approaches to the delivery of
walk-in single session mental health therapy. Journal of Systemic Therapies, 27, 40–53.
Heather, N. (1995). Brief intervention strategies. In R. K. Hester & W. R. Miller (Eds.), Handbook of alcoholism treatment
approaches: Effective alternatives (2nd ed., pp. 105–122), Needham Heights, MA: Allyn & Bacon.
Hofstra, M. B., Van der, E. J., & Verhulst, F. C. (2000). Continuity and change of psychopathology from childhood
into adulthood: A 14-year follow-up study. Journal of the American Academy of Child and Adolescent Psychiatry, 39,
850–858.
Hoyt, M. (1995). Brief therapy and managed care: Readings for contemporary practice. San Francisco, CA: Jossey-Bass.
Hoyt, M., Rosenbaum, R., & Talmon, M. (1992). Planned single-session psychotherapy. In S. H. Budman, M. F. Hoyt, &
S. Friedman (Eds.), The first session in brief therapy (pp. 59–86). New York, NY: Guilford Press.
Kamradt, B., Gilbertson, S. A., & Lynn, N. (2005). Wraparound Milwaukee. In M. H. Epstein, K. Kutash, & A. J.
Duchnowski (Eds.), Outcomes for children and youth with emotional and behavioral disorders and their families
(2nd ed., pp. 307–328), Austin, TX: ProEd.
Kazdin, A. E., Holland, L., & Crowley, M. (1997). Family experience of barriers to treatment and premature termination
from child therapy. Journal of Consulting and Clinical Psychology, 65, 453–463.
Kroll, L. (2003). A brief consultation and advisory approach for use in child and adolescent mental health services: A
pilot study. Clinical Child Psychology and Psychiatry, 8, 503–512.
McKay, M., McCadam, K., & Gonzales, J. (1996). Addressing the barriers to mental health services for inner city children
and their caretakers. Community Mental Health Journal, 32, 353–361.
Miller, J. K. (2008). Walk-in single session team therapy: A study of client satisfaction. Journal of Systematic Therapies,
27, 78–94.
Miller, J. K., & Slive, A. (2004). Breaking down the barriers to clinical service delivery: Walk-in family therapy. Journal
of Marital and Family Therapy, 30, 95–103.
Ministry of Community and Social Services, South West Region. (2001). An ideal model for children’s mental health
services in South West Region. London, ON: Author.
Noseworthy, T. W., McGurran, J. J., Hadorn, D. C., & Steering Committee of the Western Canada Waiting List Project.
(2003). Waiting for scheduled services in Canada: Development of priority-setting scoring systems. Journal of Evaluation
in Clinical Practice, 9, 23–31.
Offord, D. R., Boyle, M. H., Szatmari, P., Rae-Grant, N., Links, P. S., Cadman, D. T., : : : Woodward, C. A. (1987). Ontario
child health study. Six-month prevalence of disorder and rates of service utilization. Archives of General Psychiatry,
44, 832–836.
Pavuluri, M. N., Luk, S. L., & McGee, R. (1996). Help-seeking for behavior problems by parents of preschool children:
A community study. Journal of the American Academy of Child and Adolescent Psychiatry, 35, 215–222.
Perkins, R. (2006). The effectiveness of one session of therapy using a single-session therapy approach for children and
adolescents with mental health problems. Psychology and Psychotherapy: Theory, Research and Practice, 79, 215–227.
Polgar, M., Stiffman, A., Horvath, V., Hadley-Ives, E., O’Neal, J., & Pescarino, R. (2001). What impedes youth mental
health service use? Presented at the 13th Annual Conference Proceedings—Research and Training Center for Children’s
Mental Health, Tampa, Florida.
Prochaska, J. O., Velicer, W. F., Rossi, J. S., Goldstein, M. G., Marcus, B. H., Rakowski, W., : : : Rossi, S. R. (1994).
Stages of change and decisional balance for 12 problem behaviors. Health Psychology, 13, 39–46. doi: 10.1037/0278-
6133.13.1.39
Pumariega, A. J., & Winters, N. C. (2003). The handbook of child and adolescent systems of care: The new community
psychiatry. San Francisco, CA: Jossey-Bass.
Reid, G. J., Evans, B., Belle Brown, J., Cunningham, C. E., Lent, B., Neufeld, R., : : : Shanley, B. (2005). Help—I
need somebody: The experiences of families seeking treatment for children with psychosocial problems and the impact
of delayed or deferred treatment. London, ON: Author. Retrieved from http://www.chsrf.ca/funding_opportunities/ogc/
2003/reid?e.php
Slive, A., MacLaurin, B., Oakander, M., & Amundson, J. (1995). Walk-in single sessions: A new paradigm in clinical
service delivery. Journal of Systemic Therapies, 14, 3–12.

352 M. BARWICK ET AL.
Slive, A., McElheran, N., & Lawson, A. (2008). How brief does it get? Walk-in single session therapy. Journal of Systemic
Therapies, 27, 5–22.
Smith, D. H., & Hadorn, D. C. (2002). Lining up for children’s mental health services: A tool for prioritizing waiting
lists. Journal of the American Academy of Child and Adolescent Psychiatry, 41, 367–377.
Stallard, P. (1998). An opt-in appointment system and brief therapy: Perspectives on a waiting list initiative. Clinical Child
Psychology and Psychiatry, 3, 199–212.
Stiffman, A. R., Horwitz, S. M., Hoagwood, K., Compton, W., Cottler, L., Bean, D. L., : : : Weisz, J. R. (2000). The
Services Assessment for Children and Adolescents (SACA): Adult and child reports. Journal of the American Academy
for Child and Adolescent Psychiatry, 39, 1032–1039.
Talmon, M. (1990). Single-session therapy: Maximizing the effect of the first (and often only) therapeutic encounter. San
Francisco, CA: Jossey-Bass.
Tremblay, R. E., Masse, B., Perron, D., Leblanc, M., Schwartzman, A. E., & Ledingham, L. E. (1992). Early disruptive
behavior, poor school achievement, delinquent behavior, and delinquent personality: Longitudinal analyses. Journal of
Consulting and Clinical Psychology, 60, 64–72.
United States Public Health Service (USPHS: 2000). Report of the Surgeon General’s conference on children’s mental
health: A national action agenda. Washington, DC: Department of Health and Human Services.
Verhulst, F. C., & Van Der Ende, M. S. (1997). Factors associated with child mental health service use in the community.
Journal of the American Academy of Child and Adolescent Psychiatry, 36, 901–909.
Waddell, C., Offord, D., Shepherd, C., Hua, J., & McEwan, K. (2002). Child psychiatric epidemiology and Canadian
public policy making: The state of the science and the art of the possible. Canadian Journal of Psychiatry, 47, 825–831.
Walker, S. (1998). Mental health. Wait not, want not? Health Service Journal, 108, 32–33.
Yorktown Child and Family Centre. (April, 2003). West End Walk-In Counselling Centre: Project evaluation. Toronto,
ON: Author.
Young, K. (2008). Narrative practice at a walk-in therapy clinic: Developing children’s worry wisdom. Journal of Systemic
Therapies, 27, 54–74.
Young, K., Dick, M., Herring, K., & Lee, J. (2008). From waiting lists to walk-in: Stories from a walk-in therapy clinic.
Journal of Systemic Therapies, 27, 23–39.
Zwaanswijk, M., Van der Ende, J., Verhaak, P., Bensing, J., & Verhulst, F. (2005). Help-seeking for child psychopathology:
Pathways to informal and professional services in the Netherlands. Journal of the American Academy of Child and
Adolescent Psychiatry, 44, 1292–1300.