prevalence of psychiatric morbidity in general hospital inpatients
TRANSCRIPT
THE PREVALENCE OF PSYCHIATRIC MORBIDITY IN GENERAL HOSPITAL INPATIENTS
David M. Clarke, I. Harry Minas and Geoffrey W. Stuart
The aim of this study was to examine the prevalence of psychiatric morbidity in a sample of medical and surgical inpatients in an Australian general hospital. Using the 60-item General Health Questionnaire, the estimated prevalence was 30% (previous studies have yielded estimates generally between 20 and 50%). The prevalence of morbidity was significantly higher in medical (45%) than in surgical (23%) inpatients. Twelve percent of patients (20% of medical patients and 8% of surgical patients) satisfied DSM-Ill criteria for a current Major Depressive Episode. Anxiety scores on the State-Trait Anxiety Inventory were higher than those reported in general population samples. There were no significant differences between males and females on any scores. The problems associated with the definition and identification of depressive and anxiety syndromes in medical and surgical inpatients are discussed, whilst the importance of this task is emphasized.
Australian and New Zealand Journal of Psychiatry 1991 ; 25:322-329
The Afli.c,tion.s, Mrhich he the sudden motions, and pertuhutions of the mynde, oirght not to he neglected of the phisition: hecause they he of greut might, and niuke great ulterution in ull the body. (Christopher Langton 1547 [ I ] )
Monash University, Department of Psychological Medicine, Monash Medical Centre, Prince Henry's Hospital, Melbourne, Vic
David M. Clarke MBBS. FRACGP, MPM, FRANZCP, Lecturer, Formerly Senior Psychiatry Registrar, St. Vincent's Hospital, Mel- bourne. Victorian Transcultural Psychiatry Unit.
1. Harry Minac MBBS, B Med Sci, DPM, FRANZCP, Director, Honorary Senior Lecturer, Monash University, Department of Paychological Medicine. Monash University, Department of Psychological Medicine
Geoffrey W. Stuart PhD, Professional Officer Correspond with Dr Clarke
That there is a relationship between psychological problems and physical illness has been believed for a long time [ 2 ] , and, although the nature of that relation- ship has not been well understood, it has been shown that attention to psychological and social factors is important for a good outcome in the care of the physi- cally il l [3-51. In addition, attention to psychosocial factors is cost effective in that it leads to reduced morbidity and mortality, reduced utilization of medi- cal services, and a lower rate of hospitalization [6]. In order to be able to pay appropriate attention to such factors it is important to identify the prevalence and nature of psychiatric disturbances in medical and sur- gical inpatients. It has been suggested that there is much psychiatric morbidity that is not being recog- nized 171.
In 1967 Lipowski 181 estimated that between 30% and 60% of medical inpatients had a psychiatric illness severe enough to warrant attention. Since then the development of structured clinical interviews has
Aus
t NZ
J Psy
chia
try D
ownl
oade
d fro
m in
form
ahea
lthca
re.c
om b
y Ro
yal A
ustra
lian
and
New
Zea
land
Col
lege
of P
sych
iatri
sts (R
AN
ZP)
For p
erso
nal u
se o
nly.
DAVID M. CLARKE, 1. HARRY MINAS. GEOFFREY W. STUART 323
Table I . Studies of psychiatric moi%idity in general hospital patients ~
Hospital Patients Number Screening Second of instruments stage
patients
Maguire eta/ Oxford General 1974 [ lo ] Medical
Moffic and Newhaven General Paykel Medical 1975[11]
Knights and Baltimore General Folstein Medical 1977 [12]
DePaulo eta/ Baltimore Neurology 1978 [13]
Fava eta/ Venice General 1982 [14] Medical
Cavanaugh Chicago General 1983 [15] Medical
Bridges and Manchester Neurology Gold berg 1984 [16]
Feldman eta/ Oxford General 1987 [I71 Medical
Deshpande New Delhi General ef a/ Medical 1989 [18]
a General Health Questionnaire [9]
230 GHQ60 a CIS e
b
150 BDI
57 GHQ30
126 GHQ30
325 CES-D
335 GHQ30 BDI
100 GHQ28 CIS
382 GHQ30 PSE
158 SRQ PSE
Threshold morbidity
45.3%
24% (Depression)
46%
5 0 ‘/o
58% (Depression)
61% 32% (Depression)
43%
30%
Beck Depression Inventory [19] CES-D, A Self Report Depression Scale 1201 Clinical Interview Schedule [22]
Self-Reporting Questionnaire 1211 Present State Examination [23]
Estimated prevalence
2 3 ‘/o
39%
15% (Affective disorders only)
3 4%
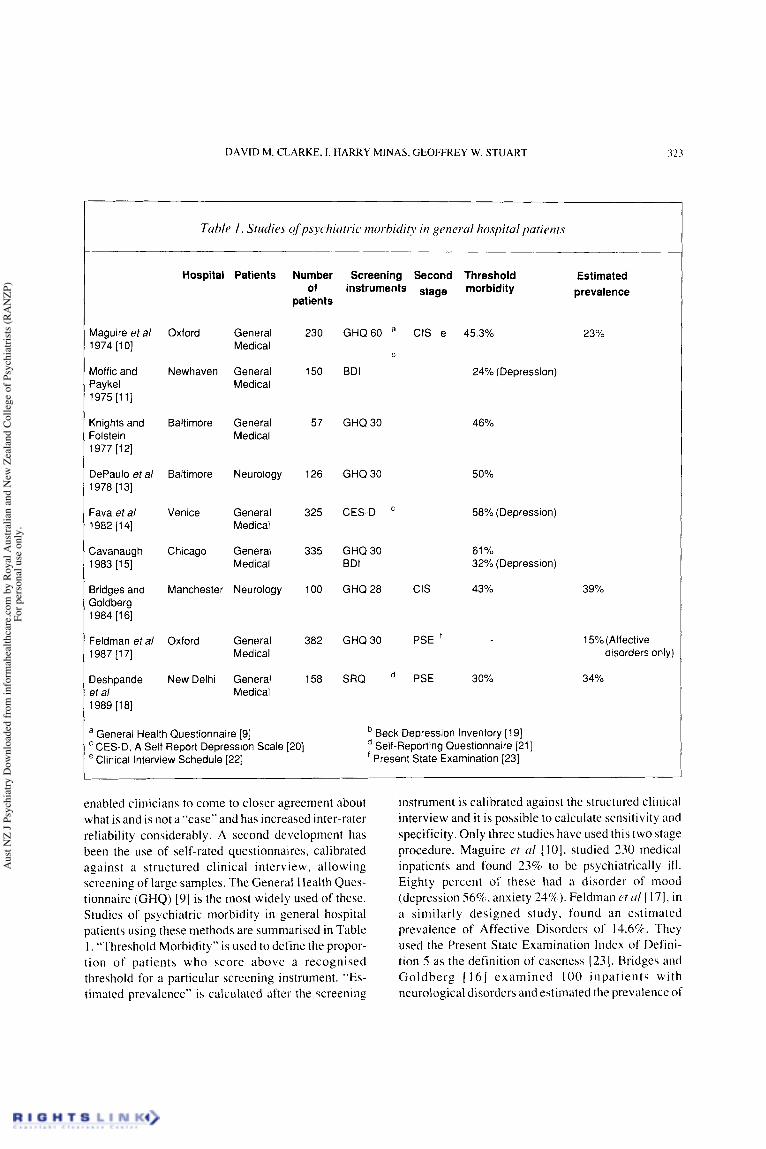
enabled clinicians to come to closer agreement about what is and is not a “case” and has increased inter-rater reliability considerably. A second development has been the use of self-rated questionnaires, calibrated against a structured clinical interview, allowing screening of large samples. The General Health Ques- tionnaire (GHQ) (91 is the most widely used of these. Studies of psychiatric morbidity in general hospital patients using these methods are summarised in Table I . “Threshold Morbidity” is used to define the propor- tion of patients who score above a recognised threshold for a particular screening instrument. “Es- timated prevalence” is calculated after the screening
instrument is calibrated against the structured clinical interview and it is possible to calculate sensitivity and specificity. Only three studies have used this two stage procedure. Maguire ct ul [ 101, studied 230 medical inpatients and found 23% to be psychiatrically i l l . Eighty percent of these had a disorder of mood (depression 56%, anxiety 24%)). Feldman ot 01 1171, in a similarly designed study. found an estimated prevalence of Affective Disorders of 14.6%. They used the Present State Examination Index of Defini- tion 5 as the definition of caseness (231. Bridges and Goldberg [ 161 examined 100 inpatients with neurological disorders and estimated the prevalence of
Aus
t NZ
J Psy
chia
try D
ownl
oade
d fro
m in
form
ahea
lthca
re.c
om b
y Ro
yal A
ustra
lian
and
New
Zea
land
Col
lege
of P
sych
iatri
sts (R
AN
ZP)
For p
erso
nal u
se o
nly.
324 PREVALENCE OF MORBIDITY IN GENERAL HOSPITAL INPATIENTS
Table 2. Studies of cognitive disorders in generul hospital patients -- - -
Patients Number of Case patients definition
Cases
Maguire et a/ 1974 [lo] General 230 GHQ and clinical assessment 3%
Knights and Folstein 1977 [12] General 57 MMS a 33% Medical
Medical DePaulo eta/ 1978 [131 Neurology 126 MMS 30%
Cavanaugh 1983 1151 General 335 MMS 28% Medical
Bridges and Goldberg 1984 [16] Neurology 121 GHQ and clinical assessment 2%
Feldman eta/ 1987 [17] General 453 CAS and review of notes 12% Medical
a MMS - Mini Mental State Examination: a brief rating scale (241, with a sensitivity of 87% and a specificity of 82% [25] CAS - Cognitive Assessment Scale: from the Clifton Assessment Procedure for the Elderly [26]
psychiatric morbidity to be 39%. Studies which have used the GHQ have usually found the threshold mor- bidity to be between 40% and 60%. The GHQ was designed to detect psychiatric disorders amongst com- munity, primary care and outpatient samples, where it has been found to have a high sensitivity and specificity. However, in the only reported study of hospital inpatients using the 60 item GHQ, it was found to have a high mis-classification rate, yielding a large number of false positives [ 101.
A number of researchers have studied depression in medical inpatients using interviewer-rated or self- rated scales. The prevalence of depression in such reports ranges from 30 to 60% (see table 1)[ 11,14,15]. The Beck Depression Inventory [19], in its original format, has 21 items. A cut-off of 13/14 is commonly used as the threshold. The CES-D [20] is a self-rated instrument which similarly measures depressive symptoms. These instruments essentially measure the seventy of symptoms, and do not take into account operational criteria currently used for the diagnosis of depressive syndromes.
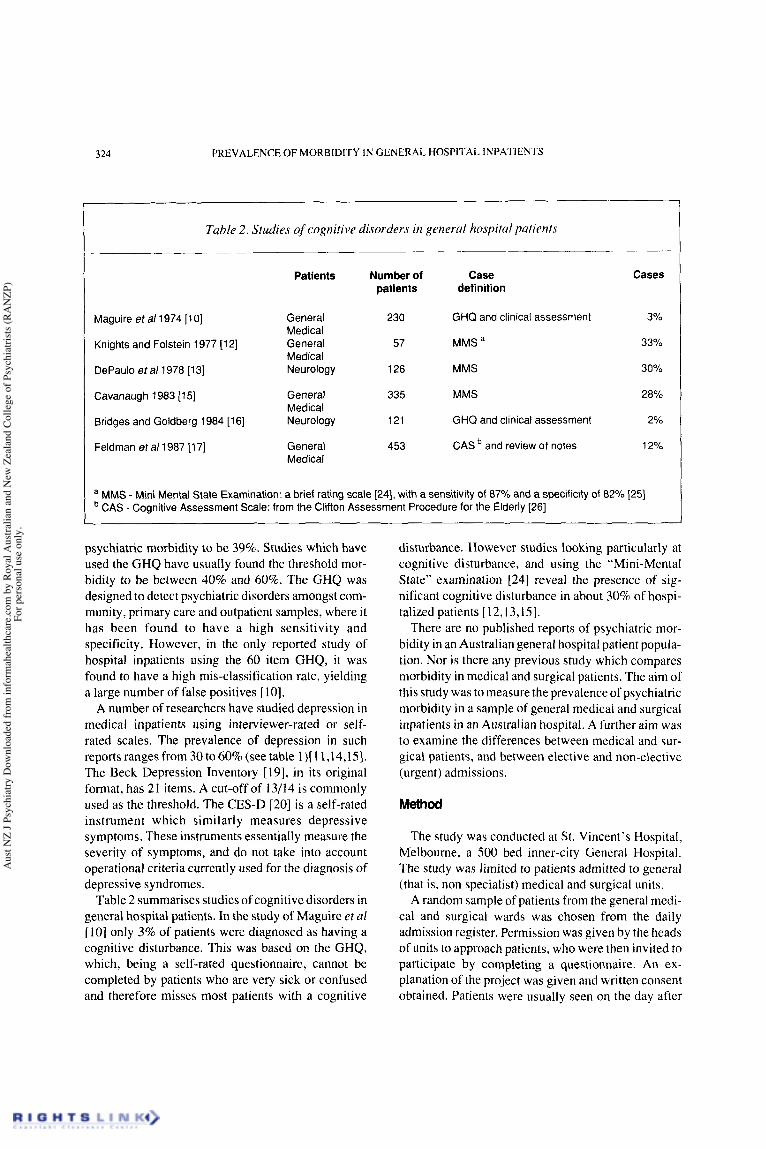
Table 2 summarises studies of cognitive disorders in general hospital patients. In the study of Maguire et a1 [ 101 only 3% of patients were diagnosed as having a cognitive disturbance. This was based on the GHQ, which, being a self-rated questionnaire, cannot be completed by patients who are very sick or confused and therefore misses most patients with a cognitive
disturbance. However studies looking particularly at cognitive disturbance, and using the “Mini-Mental State” examination [24] reveal the presence of sig- nificant cognitive disturbance in about 30% of hospi- talized patients [12,13,15].
There are no published reports of psychiatric mor- bidity in an Australian general hospital patient popula- tion. Nor is there any previous study which compares morbidity in medical and surgical patients. The aim of this study was to measure the prevalence of psychiatric morbidity in a sample of general medical and surgical inpatients in an Australian hospital. A further aim was to examine the differences between medical and sur- gical patients, and between elective and non-elective (urgent) admissions.
Method
The study was conducted at St. Vincent’s Hospital, Melbourne, a 500 bed inner-city General Hospital. The study was limited to patients admitted to general (that is, non specialist) medical and surgical units.
A random sample of patients from the general medi- cal and surgical wards was chosen from the daily admission register. Permission was given by the heads of units to approach patients, who were then invited to participate by completing a questionnaire. An ex- planation of the project was given and written consent obtained. Patients were usually seen on the day after
Aus
t NZ
J Psy
chia
try D
ownl
oade
d fro
m in
form
ahea
lthca
re.c
om b
y Ro
yal A
ustra
lian
and
New
Zea
land
Col
lege
of P
sych
iatri
sts (R
AN
ZP)
For p
erso
nal u
se o
nly.
DAVID M. CLARKE. 1. HARRY MINAS, GEOFFREY W. STUART 325
I I
Tuhlc 3 . Validity studies qf GHQ-60 (Threshold Score 11112). Comparison made with Clinical Interview Schedule
Setting Number Sensitivity Specificity of patients % YO
Goldberg and Blackwell [27] Primary care attenders, London 200 91 .o 94.1
Goldberg 1972 [28] Medical outpaitients, London 91 80.6 93.3
Maguire et a/ 1974 [I O] Medical inpatients, Oxford 230 88.2 73.0
Tennant 1977 [29] Primary care attenders, Sydney 120 90.0 90.0
admission. If a selected patient was unavailable they would be re-approached later. A number of patients were unable to participate because of inadequate English, or severe ill health, and, for them, demographic data only were recorded.
Instruments The questionnaire consisted of four parts: 1. Demographic data. The following data were
recorded: age, gender, marital status, country of birth, year of arrival in Australia if born overseas, education, occupation.
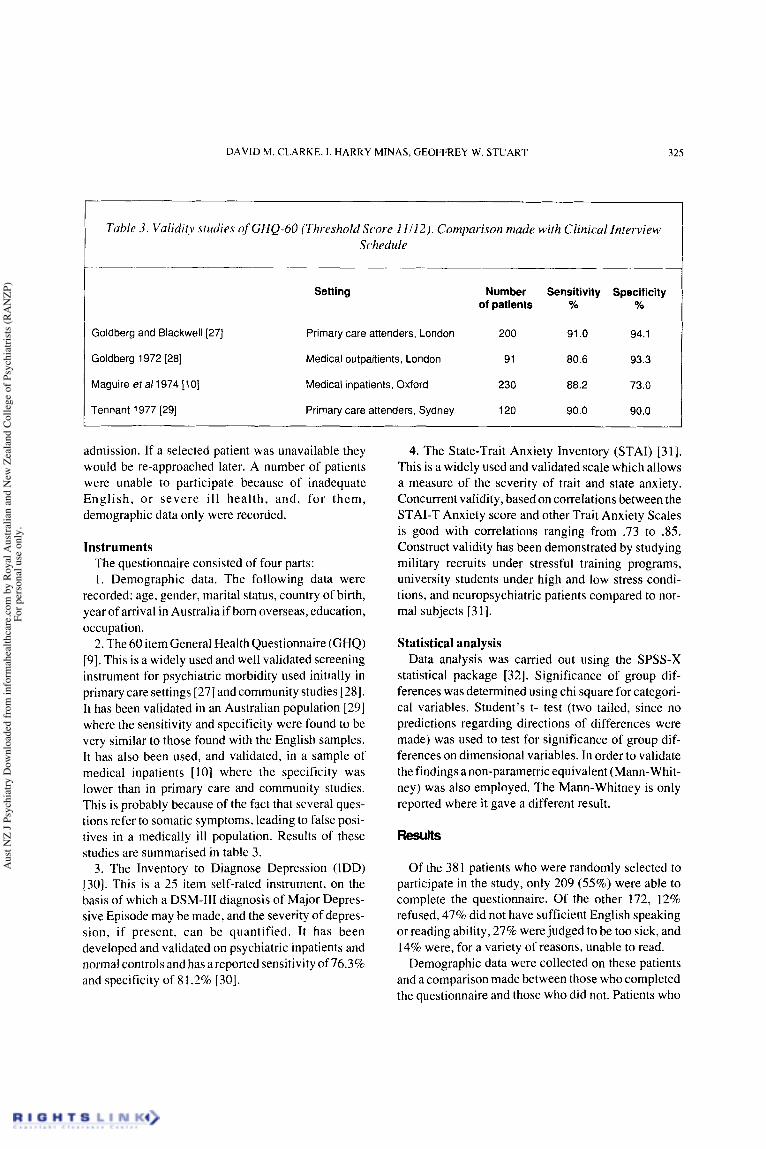
2. The 60 item General Health Questionnaire (GHQ) [9]. This is a widely used and well validated screening instrument for psychiatric morbidity used initially in primary care settings [27] and community studies [28]. It has been validated in an Australian population [29] where the sensitivity and specificity were found to be very similar to those found with the English samples. It has also been used, and validated, in a sample of medical inpatients [ 101 where the specificity was lower than in primary care and community studies. This is probably because of the fact that several ques- tions refer to somatic symptoms, leading to false posi- tives in a medically ill population. Results of these studies are summarised in table 3.
3. The Inventory to Diagnose Depression (IDD) [30]. This is a 25 item self-rated instrument, on the basis of which a DSM-111 diagnosis of Major Depres- sive Episode may be made, and the severity of depres- sion, if present, can be quantified. It has been developed and validated on psychiatric inpatients and normal controls and has a reported sensitivity of 76.3% and specificity of 8 1.2% [30].
4. The State-Trait Anxiety Inventory (STAI) [31]. This is a widely used and validated scale which allows a measure of the severity of trait and state anxiety. Concurrent validity, based on correlations between the STAI-T Anxiety score and other Trait Anxiety Scales is good with correlations ranging from .73 to 3 5 . Construct validity has been demonstrated by studying military recruits under stressful training programs, university students under high and low stress condi- tions, and neuropsychiatric patients compared to nor- mal subjects [31].
Statistical analysis Data analysis was carried out using the SPSS-X
statistical package [32]. Significance of group dif- ferences was determined using chi square for categori- cal variables. Student’s t- test (two tailed, since no predictions regarding directions of differences were made) was used to test for significance of group dif- ferences on dimensional variables. In order to validate the findings a non-parametric equivalent (Mann-Whit- ney) was also employed. The Mann-Whitney is only reported where it gave a different result.
Of the 38 1 patients who were randomly selected to participate in the study, only 209 (55%) were able to complete the questionnaire. Of the other 172, 12% refused, 47% did not have sufficient English speaking or reading ability, 27% were judged to be too sick, and 14% were, for a variety of reasons, unable to read.
Demographic data were collected on these patients and a comparison made between those who completed the questionnaire and those who did not. Patients who
Aus
t NZ
J Psy
chia
try D
ownl
oade
d fro
m in
form
ahea
lthca
re.c
om b
y Ro
yal A
ustra
lian
and
New
Zea
land
Col
lege
of P
sych
iatri
sts (R
AN
ZP)
For p
erso
nal u
se o
nly.
326 PREVALENCE OF MORBIDITY IN GENERAL HOSPITAL INPATIENTS
GHQ score % “threshold morbidity” Yo “estimated prevalence”
% “major depression” IDD depression score
State anxiety Trait anxiety
a t=2.00, df=205, pcO.05
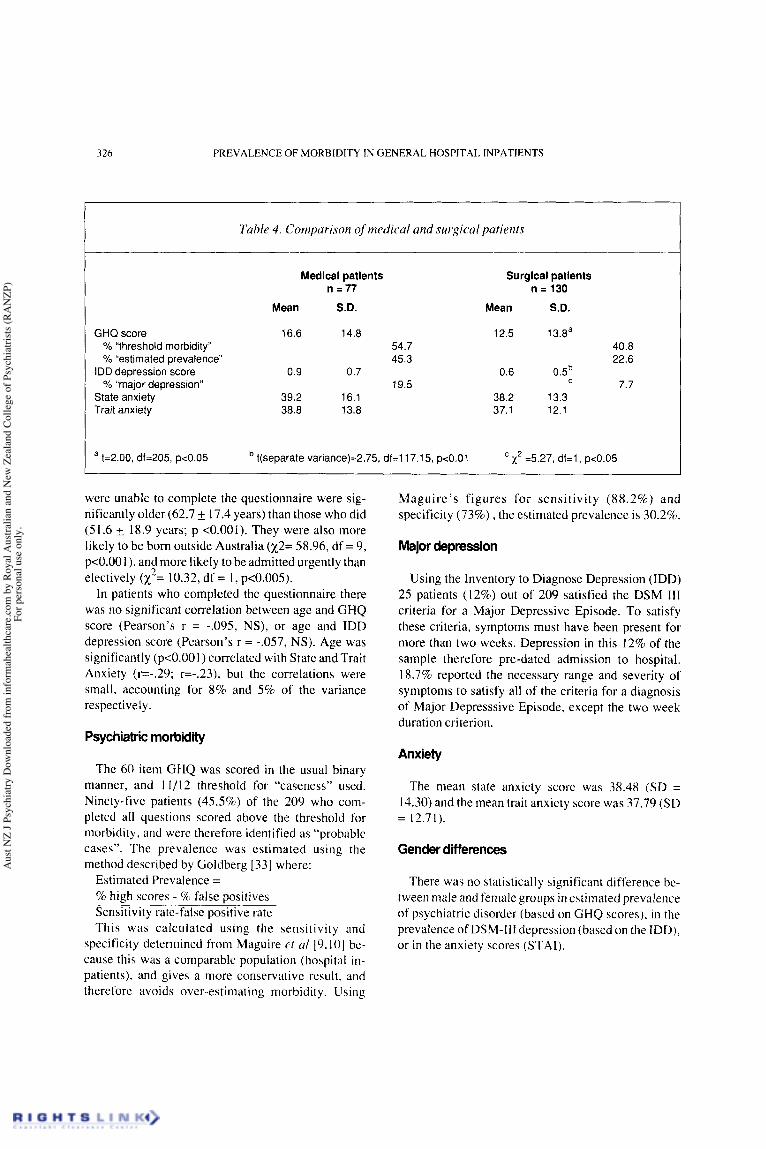
Table 4 . Comparison of medical and surgical patients -
Medical patients n = 77
Mean S.D.
16.6 14.8 54.7 45.3
19.5 0.9 0.7
39.2 16.1 38.8 13.8
t(separate variance)=2.75, df=ll7.15, p<O.Ol
Surgical patients n = 130
Mean S.D.
12.5 1 3Ba 40.8 22.6
7.7 0.5b 0.6
38.2 13.3 37.1 12.1
x2 =5.27, df=l, pc0.05
were unable to complete the questionnaire were sig- nificantly older (62.7 17.4 years) than those who did (51.6 18.9 years; p <0.001). They were also more likely to be born outside Australia (x2= 58.96, df = 9, p<O.OO I ) , and more likely to be admitted urgently than electively (x = 10.32, df = 1, p<O.OOS).
In patients who completed the questionnaire there was no significant correlation between age and GHQ score (Pearson’s r = -.095, NS), or age and IDD depression score (Pearson’s r = -.057, NS). Age was significantly (p<O.OO 1) correlated with State and Trait Anxiety (r=-.29; r=-.23), but the correlations were small, accounting for 8% and 5% of the variance respectively.
2
Maguire’s figures for sensitivity (88.2%) and specificity (73%) , the estimated prevalence is 30.2%.
Major depression
Using the Inventory to Diagnose Depression (IDD) 25 patients ( I 2%) out of 209 satisfied the DSM I11 criteria for a Major Depressive Episode. To satisfy these criteria, symptoms must have been present for more than two weeks. Depression in this 12% of the sample therefore pre-dated admission to hospital. 18.7% reported the necessary range and severity of symptoms to satisfy all of the criteria for a diagnosis of Major Depressive Episode, except the two week duration criterion.
Psychiatric morbidity Anxiety
The 60 item GHQ was scored in the usual binary manner, and 11/12 threshold for “caseness” used. Ninety-five patients (45.5%) of the 209 who com- pleted all questions scored above the threshold for morbidity, and were therefore identified as “probable cases”. The prevalence was estimated using the method described by Goldberg [33] where:
Estimated Prevalence = % high scores - %I false positives Sensitivity rate-false positive rate This was calculated using the sensitivity and
specificity determined from Maguire et a1 19,101 be- cause this was a comparable population (hospital in- patients), and gives a more conservative result, and therefore avoids over-estimating morbidity. Using
~ _______.
The mean state anxiety score was 38.48 (SD = 14.30) and the mean trait anxiety score was 37.79 (SD = 12.71).
Gender differences
There was no statistically significant difference be- tween male and female groups in estimated prevalence of psychiatric disorder (based on GHQ scores), in the prevalence of DSM-I11 depression (based on the IDD), or in the anxiety scores (STAI).
Aus
t NZ
J Psy
chia
try D
ownl
oade
d fro
m in
form
ahea
lthca
re.c
om b
y Ro
yal A
ustra
lian
and
New
Zea
land
Col
lege
of P
sych
iatri
sts (R
AN
ZP)
For p
erso
nal u
se o
nly.
DAVID M. CLARKE, I. HARRY MINAS, GEOFFREY W. STUART 327
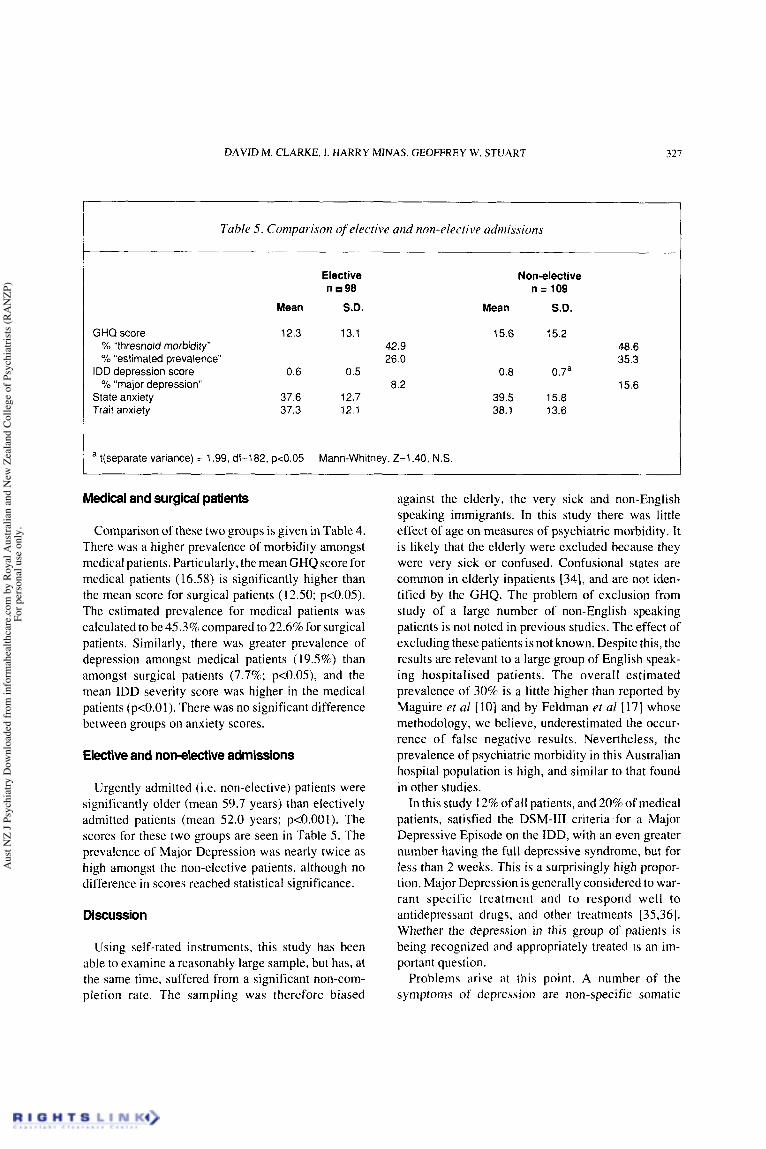
Tuhle 5. Comparison of elective and non-elective admissions
GHQ score % "threshold morbidity" % "estimated prevalence"
"major depression" IDD depression score
State anxiety Trait anxiety
Elective n 98
Mean S.D.
12.3 13.1 42.9 26.0
8.2 0.6 0.5
37.6 12.7 37.3 12.1
I a t(separate variance) = 1.99, df=182, pcO.05 Mann-Whitney, Z=1.40, N.S.
Non-elective n = 109
Mean S.D.
15.6 15.2 48.6 35.3
15.6 0.8 0.7a
39.5 15.8 38.1 13.6
Medical and surgical patients
Comparison of these two groups is given in Table 4. There was a higher prevalence of morbidity amongst medical patients. Particularly, the mean GHQ score for medical patients (16.58) is significantly higher than the mean score for surgical patients (12.50; p<O.OS). The estimated prevalence for medical patients was calculated to be 45.3% compared to 22.6% for surgical patients. Similarly, there was greater prevalence of depression amongst medical patients ( 19.5%) than amongst surgical patients (7.7%; p<O.OS), and the mean IDD severity score was higher in the medical patients (p<O.OI). There was no significant difference between groups on anxiety scores.
Elective and nonelective admissions
Urgently admitted (i.e. non-elective) patients were significantly older (mean 59.7 years) than electively admitted patients (mean 52.0 years; p<O.OOl). The scores for these two groups are seen in Table 5. The prevalence of Major Depression was nearly twice as high amongst the non-elective patients, although no difference in scores reached statistical significance.
Discussion
Using self-rated instruments, this study has been able to examine a reasonably large sample, but has, at the same time, suffered from a significant non-com- pletion rate. The sampling was therefore biased
against the elderly, the very sick and nowEnglish speaking immigrants. In this study there was little effect of age on measures of psychiatric morbidity. It is likely that the elderly were excluded because they were very sick or confused. Confusional states are common in elderly inpatients [34], and are not iden- tified by the GHQ. The problem of exclusion from study of a large number of non-English speaking patients is not noted in previous studies. The effect of excluding these patients is not known. Despite this, the results are relevant to a large group of English speak- ing hospitalised patients. The overall estimated prevalence of 30% is a little higher than reported by Maguire er a1 [ 101 and by Feldman et a1 [ 171 whose methodology, we believe, underestimated the occur- rence of false negative results. Nevertheless, the prevalence of psychiatric morbidity in this Australian hospital population is high, and similar to that found in other studies.
In this study 12% of all patients, and 20% of medical patients, satisfied the DSM-111 criteria for a Major Depressive Episode on the IDD, with an even greater number having the full depressive syndrome, but for less than 2 weeks. This is a surprisingly high propor- tion. Major Depression is generally considered to war- rant specific treatment and to respond well to antidepressant drugs, and other treatments [35,36]. Whether the depression in this group of patients is being recognized and appropriately treated is an im- portant question.
Problems arise at this point. A number of the symptoms of depression are non-specific somatic
Aus
t NZ
J Psy
chia
try D
ownl
oade
d fro
m in
form
ahea
lthca
re.c
om b
y Ro
yal A
ustra
lian
and
New
Zea
land
Col
lege
of P
sych
iatri
sts (R
AN
ZP)
For p
erso
nal u
se o
nly.

328 PREVALENCE OF MORBIDITY IN GENERAL HOSPITAL INPATIENTS
symptoms, which of course also occur in a variety of physical illnesses in the absence of depression. These include appetite and weight loss, disturbed sleep-wake cycle, and tiredness. In the absence of physical illness such symptoms, in association with a number of char- acteristic psychological symptoms, constitute the depressive syndrome. The significance of such symptoms (in relation to depression) is unclear in the presence of physical illness. Further, the presence of severe physical illness is frequently associated with psychological symptoms such as lowered mood, thoughts of death, preoccupations and sometimes im- paired concentration. The question then is whether the constellation of symptoms and signs, which in the absence of physical illness is recognised as an episode of depressive illness, has the same significance in terms of cause, course and response to treatment (eg. antidepressants) when it occurs in the presence of severe physical illness. In this situation errors of clini- cal judgement can be made in two directions. Depres- sive syndromes may be missed because of a predominant focus on somatic symptoms and, alterna- tively, lowered mood states may be inappropriately considered Major Depression. Depressive symptoms are common . Clarification of the depressive syndromes in the medically ill is required, and indica- tions for treatment made clear.
In this study STAI anxiety scores were considerably higher than scores reported for normal population samples [31]. This was so for medical and surgical, and elective and non-elective patients. Anxiety is a significant problem in hospitalized patients and im- portantly has been linked with post-operative mor- bidity and poor recovery [37]. More attention needs to be given to this area with examination of strategies for reducing this morbidity. What is the cause of the anxiety? What fears do patients have? Are they being addressed? Could improvements be made in ward procedures to reduce patient anxieties? Are resident medical staff adequately explaining procedures and operations? Are patients being properly informed? Is pain relief and night sedation adequate? Some means of assessing the presence and severity of anxiety is required and examination of the cause undertaken. Does the training or the workload of the residents allow this? Do the consultants model a concern in this area?
This study demonstrates that depression and anxiely are common in hospitalized patients. I t has previously been reported that these problems frequently are not
I
recognised 171. The extent to which psychiatric mor- bidity is recognized and patients referred for psychiatric assessment and treatment, and some of the factors influencing referral are the subject of a separate report [ 381.
Acknowledgements
The authors wish to thank Professor J.R.B. Ball and Professor G.C. Smith for helpful support, and the Board of Research of the Royal Australian and New Zealand College of Psychiatrists which provided fund- ing.
References
Langton C. A very brefe treatise, ordrely declaring the principle partes of phisick, that is to saye: thynges natural. Thynges not naturall. Thynges agaynst nature. London: Whitchurch, 1547. Reprinted in Hunter R, McAlpine 1. Three hundred years of Psvchiatrv 1535-1860. New York: Carlisle Publishine, 1982: 10. -
2. Wittkower ED. Historical perspective of contemporary Psychosomatic Medicine. International Journal of Psychiatry in Medicine 1974; 5: 309-319.
3. Farmer CJ, Bewick M, Parsons V, Snowden SA. Survival on home haemodialysis: its relationship with physical symptomatol- ogy, psychosocial background and psychiatric morbidity. Psychological Medicine 1979; 9: 5 15-523.
4. Simonton OC, Matthews-Simonton S. Cancer and Stress: Coun- selling the Cancer Patient. Medical Journal of Australia 1981; I :679-683.
psychosocial treatment on survival of patients with metastatic breast cancer. Lancet 1989; 2:888-891.
6. Mendelson G. Psychosocial factors and the management ofphyai- cal illness: A contribution to the cost-containment of medical care. Australian and New Zealand Journal of Psychiatry 1984; 18:21 1-216.
psychiatrists. Australian and New Zealand Journal of Psychiatry 1984; 18:128-133.
psychosomatic medicine. I1 clinical aspects. Psychosomatic Medicine 1967; 29:201-224.
9. Goldberg D. Manual of the General Health Questionnaire. NFER- Nelson, 1978.
10. Maguire GP, Juiier DL, Hawton KE, Bancroft JHJ. Psychiatric morbidity and referral on two general medical wards. British Medical Journal 1974; 1:268-270.
British Journal of Psychiatry 1975; 126:346-353.
disturbance in medical patients. Annals of Internal Medicine 1977; 87:723-724.
13. DePaulo JR, Folstein MF. Psychiatric disturhances in neurologi- cal patients: Detection, recognition, and hobpila1 course. Annals of Neurology 197X; 4:225-228.
5. Spiegel D, Bloom JR. Kraemer HG, Gottheil E. Effect of
7. Goldberg D. The recognition of psychiatric illness by non-
8. Lipowski ZJ. Review of consultation psychiatry and
1 I . Moffic HS. Paykel ES. Depression in medical in-patients.
12. Knights EB, Folstein MF. Unsuspected Emotional and Cognitive
Aus
t NZ
J Psy
chia
try D
ownl
oade
d fro
m in
form
ahea
lthca
re.c
om b
y Ro
yal A
ustra
lian
and
New
Zea
land
Col
lege
of P
sych
iatri
sts (R
AN
ZP)
For p
erso
nal u
se o
nly.

DAVID M. CLARKE, I. HARRY MINAS. GEOFFREY W. STUART 329
14. Fava GA. Pilow\ky I. Pierfederici A, Bernardi M. Pathak D. Dcpre\sive \ymptoms and abnormal illness behaviour in general hospital patients. General Hospital Psychiatry 1982; 4:171-178.
IS. Cavanaugh S VonA. The prevalence of emotional and cognitive dysfunction in a General Medical Population: Using the MMSE, GHQ, and BDI. Generd! Hospital Psychiatry 1983; 5: 15-24,
16. Bridges KW. Goldberg DP. Psychiatric illness in inpatients with neurological disorders: patients’ views on discussion of emotional problems with neurologists. British Medical Journal 1984;
17. Feldman E. Mayou R, Hawton K, Ardern M, Smith EBO. 289:656-658.
Psychiatric disorder in medical in-patients. Quarterly Journal of Medicine 1987; New Series 63, (241):405-412.
18. Deshpande SN, Sundaram KR, Wig NN. Psychiatric disorders among medical in-patients in an Indian hospital. British Journal of Psychiatry 1989; 154:504-409.
19. Beck AT, Ward CH, Mendelson M, Mock J, Erbaugh J. An in- ventory for measuring depression. Archives of General Psychiatry 196 I ; 4:56 1-57 I .
20. Radloff LS. The CES-D Scale. A self report depression scale for research in the general population. Applied Psychological Meas- urement 1977; 1:385-401.
21, Harding TW, DeArango HV, Baltazar J, e t a / . Mental disorders in primary health care - a study of their frequency and diagnosis in four developing countries. Psychological Medicine 1980; 10:231-242.
22. Goldberg DP, Cooper B, Eastwood MR, Kedward HB, Shepherd M. A standardized psychiatric interview for use in community sur- veys. British Journal of Preventive and Social Medicine 1970; 24: 18-23.
23. Wing JK, Cooper JE, Sartorius N. The Measurement and Clas- sification of Psychiatric Symptoms. London: Cambridge Univer- sity Press, 1974.
24. Folstein MF, Folstein SE, McHugh PR. Mini-mental State. A practical method for grading the cognitive state of patients for the clinician. Journal of Psychiatric Research 1975; 12: 189.198.
25. Anthony JC, LeResche L, Niaz U, Von Korff MR, Folstein MF. Limits of the “Mini-Mental State” as a screening test for demen- tia and delirium among hospital patients. Psychological Medicine 1982; 12:397-408.
26. Pattie AH, Gilleard CJ. Manual of the Clifton Assessment Proce- dures for the Elderly (CAPE). Sevenoaks: Hodder and Stoughton Educational, 1979.
27. Goldberg DP, Blackwell B. Psychiatric Illness in general prac- tice. A detailed study using a new method of case identification. British Medical Journal 1970 2:439-443.
28. Goldberg DP. The detection of Psychiatric Illness by Question- naire. Maudsley Mongraph, No21, Oxford University Press, 1972.
29.Tennant C. The General Health Questionnaire: A valid index of psychological impairment in Australian populations. Medical Journal of Australia 1977; 2:392-394.
scale to diagnose Major Depressive Disorder. Archives of General Psychiatry 1986; 43:1076-1081.
3 1. Speilberger CD. Manual for the State-Trait Anxiety Inventory (Form Y). Palo Alto: Consulting Psychologists Press, 1983.
32. SPSS lnc. SPSS-X User’s guide (2nd ed). Chicago; SPSS lnc, 1986.
33. Goldberg D. Estimating the prevalence of psychiatric disorder from the results of a screening test, in Wing er a/.(eds). What is a Case? London: Grant McIntyre, 1981. Ch. 13.
fusional states) in the elderly. American Journal of Psychiatry
35. Morris JB, Beck AT. The Efficacy of Antidepressant Drugs: A
30. Zimmerman M, Coryell W. Corenthal C, Wilson S. A self-report
34. Lipowski ZJ. Transient Cognitive disorders (delirium, acute con-
1983: 140: 1426-1436.
Review of Research (1958 to 1972) Archives of General Psychiatry 1974,30667474
36. Elkin 1, Shea T, Watkins JT. Imber SD, Sotsky SM, Collins JF, Glass DR, Pilkonis PA, Lober WR, Docherty JP, Fiester SJ, Par- loff MB. National Institute of Mental Health treatment of depres- sion collaborative research program: general effectiveness of treatments. Archives of General Psychiatry 1989;46:97 1-982
37. Kimball CP. Psychological responses to the experience of Open Heart Surgery: I. American Journal of Psychiatry 1969; 126:348- 359.
38. Clarke DM, Minas IH, McKenzie DP. Illness behaviour as a determinant of referral to a psychiatric consultationfliaison ser- vice. Australian and New Zealand Journal of Psychiatry 1991; 25:330-337
Aus
t NZ
J Psy
chia
try D
ownl
oade
d fro
m in
form
ahea
lthca
re.c
om b
y Ro
yal A
ustra
lian
and
New
Zea
land
Col
lege
of P
sych
iatri
sts (R
AN
ZP)
For p
erso
nal u
se o
nly.