prevalence and risk factors of trachoma among children
TRANSCRIPT
Prevalence and Risk Factors of Trachoma EyobL 27
ORIGINAL ARTICLE
Prevalence and Risk Factors of Trachoma among Childrenof W oreillu W oreda, South W 0110 Administrative ZoneEyob Lemma, MD*
ABSTRACT
Background: Trachoma is still prevalent in large regions of Africa including Ethiopia,Crowded living condition, scarcity of water, poor hygiene and ownership of cattle wereincriminated as risk factors by studies in some countries. But the degree to which thesefactors contribute to the development of trachoma has not been well documented inEthiopia, especially in rural communities where the problem prevails.Methods: A cross-sectional study was conducted in Woreillu Woreda, South Wolloadministrative zone to determine the prevalence and factors associated with trachomaamong children of age 5 to 15years. A sample of 560 children in the age group of 5 to 7years of age were examined for the presence of trachoma. The World HealthOrganisation's (WHO) simplified classification scheme for assessing trachoma incommunity based surveys was used for the purpose. Prior to the examination aninterview was conducted with the mother or caretaker of each child using a structuredquestionnaire.Results: The prevalence of trachoma was found to be -10.9%. A totaL of 161(28.8%)children were found to have active trachoma (TF and/or TI). On multiple logisticregression older age group, not going to school, face washing habit less than once a dayand failure to seek eye care service were found to be associated with the presence oftrachoma in this study population. Other factors, which were independently andpositively associated with the presence of trachoma, include poor household andenvironmental conditions (animals living in the same room with people, cooking in theliving room, absence of proper waste disposal).Conclusion: An attempt at decreasing trachoma in the face of scarcity of resources,focusing on improving hygienic conditions both in the household and its surroundingsand changing people's behavior towards washing their face more frequently isrecommended.
Key words: Trachoma Risk Factors. Prevention. Face Washing.
INTROD UCTION
Trachoma is a term derived from a Greekroot meaning rough. referring to theappearance of the upper tarsal conjunctiva.It is a specific form of keratoconjunctivitis
that is communicable and usually ofchronic evolution. It's causative agentChlamydia trachomatis. is spread by directcontact. dirt and flies. The distraction overthe eyes ranges from conjunctivitis often
'Department of Community Health. Faculty ofMedicine ..Addis Ababa university. P.O. Box 101597 . Addis Ababa

28 Ethiop J Health Sci
follicular to most disabling forms ofentropion and trichiasis formation, cornealinfiltration, corneal scarring, completecorneal opacity and blindness.Identification of cases is relatively easy.Furthermore. the World HealthOrganization (WHO) has published asimple classification scheme for assessingtrachoma in community-based surveyswhich is reliable. easy and has been used ina number of studies (1,2).
The proportion of the population withfollicular trachoma (TF) and/orinflammatory trachoma (TI) represent thepresence of active disease. The stabilityand endemicity of the disease in thecommunity largely determines the agedistribution of the individual signs oftrachoma. In hyperendemic areas, activedisease is more common in pre-schoolchildren (3.4). The prevalence of activetrachoma decreases with increasing age.
Although trachoma has largelydisappeared from most of the westernworld. it continues to be a major cause ofblindness in developing countries (2)Trachoma IS more common inunderdeveloped areas. where good watersupplies and basic sanitation services arelacking. Even within hyperendemic areas.trachoma clusters both at the neighborhoodand at the household level (3,5.6).
Several risk factors were identified forthe disease transmission. Crowded livingconditions in the family unit specificallyincreasing number of persons per sleepingarea appears to increase the likelihood ofcontact with infected individuals (5.7-11).The association between the presence andseverity of trachoma and risk factors likepoor hygienic conditions due to lack ofavailable water. fly density III thehousehold or presence of flies on children'sfaces. and cattle have been documented(12-16). Trachoma is also common in theareas of the world characterized by lack ofhealth care/eye care services and isolation.
Vol. 11. No. 1 January 2001
lack of water and sanitation. excess of fliesand poverty.
As trachoma is a major public healthproblem there is an urgent need for itsprevention and control through systematicapproach. The establishment of prioritiesand. therefore the availability of adequateinformation are prerequisite for formulationand implementation of trachoma controlprogram strategies. The purpose of thissmall-scale community based survey wasto document the prevalence of trachoma inthe rural population of Woreillu Woredaand to identify important determinants ofthe occurrence of trachoma. which areamenable to change within the availableresources.
MA TERIALS AND METHODS
Study area and population: WoreilluWoreda is found in South WolloAdministrative Zone. The town Woreillu isfound 91 Kms Southwest of Dessie. thecapital of South Wollo Zone. The projectedtotal population for mid 1996 was 125,958of which 50.19% were females. Almost allpeople are Amharas and Christians byreligion. The staple diet is TefJ In the studyKebele springs and river water are the mainsource of water for the residents. Theaverage distance in time from a watersource to the center of the villages wasestimated to be 20 minutes both ways.There was only one functional communityhealth agent (CHA) in one of the Kebeles.The nearest health facility is Woreilluhealth center where there is no special eyecare clinic. Two elementary schools andthree adult literacy classes were also foundin these Kebeles. In addition two outreachEPI centers give services on a monthlybasis.
Lowland areas of the Woreda (District)were covered by these three Kebeles. with atotal population of 7.320. Children betweenthe ages of 5 to 15 years account for 29%
Prevalence and Risk Factors of Trachoma Evob L 29
of the total population. Using prevalence oftrachoma 58.7% obtained from a previouscommunity based survey (17) with 95%confidence interval. a power of 80% and amargin of error of 5% the sample size wascalculated to be 560. First a sketch map ofthe villages (locally known as "GoteY wasconducted to facilitate sampling ofhouseholds. The number of participants foreach Gote was determined proportional toits population size. Households with aneligible child (age 5 to 15 years) wereselected using WHO's EPI coverage clustersampling method (18). Field data collectionwas conducted from Januarv 22 to March07. 1997. -
Measurements: Each child had examinationof both eyes. A trained health assistantprior to the eye examination conducted astructured interview with themother/caretaker of the child using a pre-tested questionnaire. Data were collectedfor each index child including age. sex.household characteristics. face cleaninghabit. eye care service seeking habit. andtrachoma status. The steps of eveexamination and trachoma grading strictlvfollowed the WHO's simplified gradingscheme (L2) by a single examiner. Botheyes were examined in the same sequenceusing a magnification convergent 2.5xbinocular loupe adjustable to pupillarvdistance of the observer. Hygienicmeasures were also taken and results of theexamination were registered.
The research proposal was approved bvthe joint Save the Children Fund. (UK).and the Zonal Health Department researchsteering committee. An official letter waswritten to each of the study Kebeles fromthe Woreda Council prior to the datacollection. Finally. children who werefound to have trachoma were provided withthe standard treatment free of charge (19).Data analvsis: Data were edited andanalyzed using SPSS II statistical package.
Multiple logistic regression models wereused to estimate the independentcontributions of the risk factors to theoutcome.
RESULTS
Description of the Study Population:Results of the study showed that out of thetotal 560 children 267(47.7%) werefemales and the rest 293 (52.3%) weremales. The age distribution showed that29.80/0(167) of the children were betweenthe ages of 5 to 7 years. of which 53.9%were females (Table 1). The mean andmedian ages for females and males werefound to be 9.78 and 10 years respectively.Almost all were Christians by religion andtheir parents were farmers. Distribution ofthe study sample by literacy status showedthat 341(60.9%) were illit~rate. of which63.70/0(190) were above the age of 7 yearsand 30.2%(103) between the ages of 1iand15 years. From the total study participantsonly 18.8%(105) were enrolled at schoolfor the academic year (Table 1).
Distribution of risk factors: Nearly two-third of the children (60.7% to 61~8% offemales and 59.7% of males) of didn't havethe habit of face washing or wash their faceless than once a day. The rate of facewashing less than once per day amongthose who were not going to school was62.2%.
Nearly 33% of the total of thechildren live in households with properwaste disposal and only 10% of studvparticipants live in h~useholds wher~animals live inside the house with people.Concerning the cooking place, a total of505 (90 9%) children were living in houseswhere the family cook in the living room.Furthermore, only 30.7% of children andtheir family responded as having habit ofgoing to a health institution when havingeye problem (seek eve care services whenill). Yet. in 66.3%' of the total children
30 Ethiop J Health Sci Vol. 11. NO.1 January 2001
there was at least one other member of the mazz as the local people call it) [Table 1].family with symptoms of trachoma CAyne-
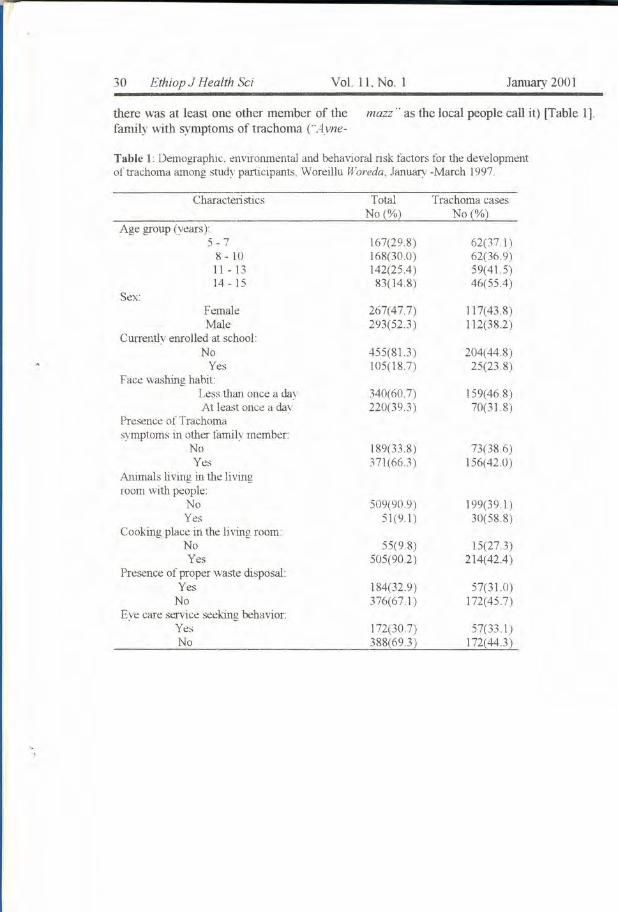
Table 1 Demographic, environmental and behavioral risk factors for the developmentof trachoma among study participants. Woreillu Woreda, January -March 1997.
Characteristics Total Trachoma casesNo(%) No(%)
Age group (years)5-7 167(29.8) 62(371 )
8 - 10 168(30.0) 62(36.9)11-13 142(25.4 ) 59(4l.5)14 - 15 83(14.8) 46(55.4)
Sex:Female 267(47.7) 117(43.8)Male 293(52.3) 112(382)
Currently enrolled at school:No 455(813) 204(448)
Yes 105(18.7) 25(23.8)Face washing habit:
Less than once a day 340(60.7) 159(468)At least once a day 220(39.3) 70(318)
Presence of Trachomasvmptoms in oilier family member:
No 189(33.8) 73(38.6)Yes 371(66.3) 156(42.0)
Animal s living in the Iivingroom with people:
No 509(90.9) 199(39.1 )Yes 51(9.1) 30(58.8)
Cooking place in the living roomNo 55(9.8) 15(27.3)Yes 505(902 ) 214(42.4)
Presence of proper waste disposal:Yes 184(32.9) 57(31.0)
No 376(67.1 ) 172(45.7)Eye care service seeking behavior:
Yes 172(30.7) 57(33.1 )No 388(69.3) 172(44.3)
.,.,
Prevalence and Risk Factors of Trachoma Evob L 31
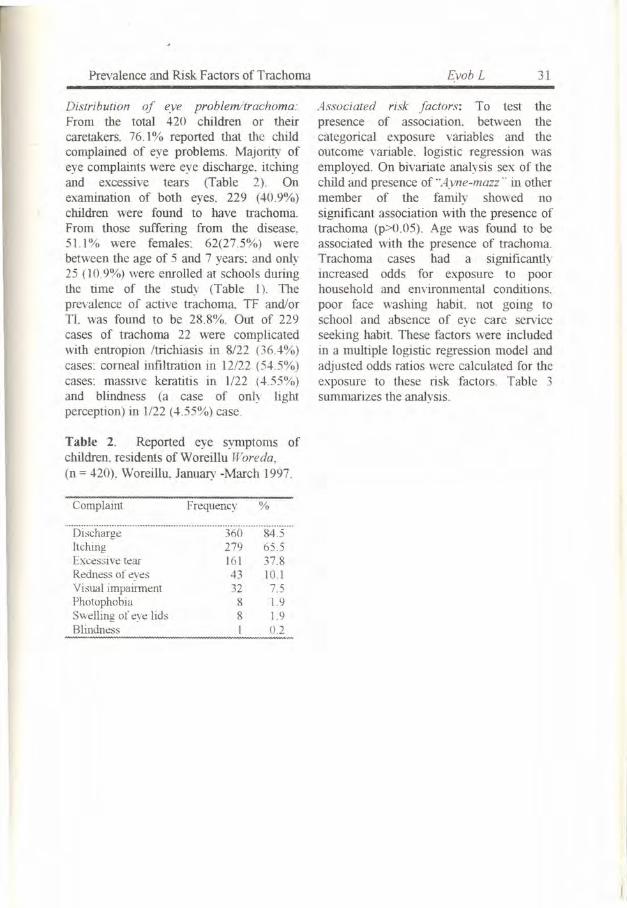
Distribution of eye problem/trachoma:From the total 420 children or theircaretakers. 76.1% reported that the childcomplained of eye problems. Majority ofeye complaints were eye discharge. itchingand excessive tears (Table 2). Onexamination of both eyes, 229 (40.9%)children were found to have trachoma.From those suffering from the disease,51.1 % were females: 62(27.5%) werebetween the age of 5 and 7 years: and only25009%) were enrolled at schools duringthe time of the study (Table I) Theprevalence of active trachoma TF and/orTI. was found to be 28.8%. Out of 229cases of trachoma 22 were complicatedwith entropion Itrichiasis in 8/22 (364%)cases~ corneal infiltration in 12122 (545%)cases: massive keratitis in 1/22 (455%)and blindness (a case of only lightperception) in 1/22 (455%) case.
Table 2. Reported eye symptoms ofchildren. residents ofWoreillu Woreda,(n = 420). Woreillu, January -March 1997.
Complaint Frequency %
DischargeItchingExcessive tearRedness of eyesVisual impairmentPhotophobiaSwelling of eye lidsBlindness
360 84.5279 65.5161 37.843 10.132 7.58 1.98 1.9I 0.2
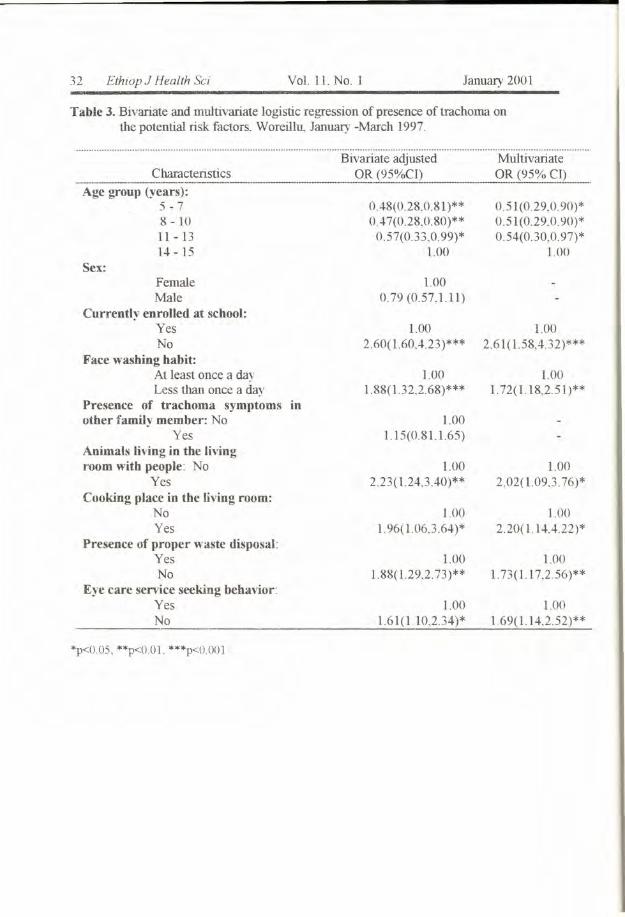
Associated risk factors: To test thepresence of association. between thecategorical exposure variables and theoutcome variable. logistic regression wasemployed. On bivariate analysis sex of thechild and presence of '"Ayne-mazz .. in othermember of the family showed nosignificant association with the presence oftrachoma (p>O.05). Age was found to beassociated with the presence of trachoma.Trachoma cases had a significantlyincreased odds for exposure to poorhousehold and environmental conditions.poor face washing habit not going toschool and absence of eye care serviceseeking habit. These factors were includedin a multiple logistic regression model andadjusted odds ratios were calculated for theexposure to these risk factors. Table 3summarizes the analysis.
32 Ethiop J Health Sci Vol. IL NO.1 January 2001
Table 3. Bivariate and multivariate logistic regression of presence of trachoma onthe potential risk factors. Woreillu.. January -March 1997.
Characteristics----_._--Age group (years):
5 - 78 - 1011-1314 - 15
Bivariate adjustedOR (95%CI)
0.48(0.28.0.81)**047(0.28.0.80)**
0.57(0.33.0.99)*1.00
Sex:FemaleMale
Currently enrolled at school:YesNo
Face washing habit:At least once a dayLess than once a day
Presence of trachoma symptoms inother family member: No
YesAnimals living in the livingroom with people No
YesCooking place in the living room:
NoYes
Presence of proper waste disposal:YesNo
Eye care service seeking behavior:YesNo
1000.79 (0.57.1.11)
LOO2.60(L60.4.23)***
1.001.88(1.32.2.68)***
1.001.15(0.81.1.65)
1.002.23(1.24,3.40)**
1.001.96( 1.06.3.64)*
1.001.88(1.29,2.73)**
LOO1.61(1.10,2.34)*
1.001.69(1.14.2.52)**
*p<O.05, **p<O.OL ***p<O.OOl
MultivariateOR (95% CI)
0.51(0.29,0.90)*0.51(0.29.0.90)*0.54(0.30,0.97)*
1.00
1.002.61(1.58.4.32)***
1.001.72(1.18,2.51)**
1.002.02(1.09.3.76 )*
1.002.20( L 14.·U2)*
1.001.73(117,2.56)**
Prevalence and Risk Factors of Trachoma Evob L 33
Keeping the other variables constant therisks of children being in the younger agegroup among the trachomatous group is50% less compared to the non-trachomatous group. Similarly. comparedto children without trachoma, the risks ofgetting children who didn't go to school orwho wash his/her face less frequently (lessthan once per day) is significantly higheramong the trachomatous children (2.61 and1.72 times higher respectively). Theseassociations were independently significantat 95% level.
Trachoma cases had independent andsignificantly increased odds of exposure topoor household and environmentalcondition. The difference in the exposure isnearly two times higher for children withtrachoma compared to those withouttrachoma. The strongest association wasfound between presence of trachoma andcooking place in the living room.Furthermore. the odds for absence ofproper waste disposal is 1.73 times higher(95% CI=1.17.2.56: P<O.OOI).
Another independent and positiveassociation was found between thepresence of trachoma and habits of seekingeye care service by the mother or caretakeror by the child in the case of older children.A 69% higher risk of not seeking theservice was detected in cases of trachomacompared to those without the disease. Thisassociation is also found to be statisticallysignificant (P<O.05).
DISCUSSION
This study indicates that trachoma has ahigh prevalence (40.9%). similar to studyfindings from other parts of the country(7.17. 20). But this figure may be higherthan the national figure (19). This can beattributed to the fact that the study includesonly the rural population where the healthservice facilities are poor and lowerenvironmental and personal hygiene
prevail. Scarcity of water is also the othercontributing factor.
The main sources for the spread of thedisease are children in the ages 1-10 years.who have highest prevalence of TF and TIand who are responsible for most shadingof chlamydial organism. Transmissionoccurs primarily within the family, betweenchildren and the older daughters lookingafter the small children. In the currentstudy, 55.6% of Trachoma cases werefound in children in the age group 5-10years. and 89% were not enrolled in anyschool at the time of the study.
A study in the rural highlandcommunity in Gondar region showedhyperendemicity. with prevalence rate of.+3%and the highest was identified in theage group of 5-9 years. accounting for59.8%. The lowest rate was found in thosewho wash their face regularly (27.4%) andamong educated (20.7%) compared to theilliterate which was 57.4% (20). Thisshowed that the above figures werecomparable with the current study findings.
Trachoma was complicated in 9.6%of the cases. The commonest sequel oftrachoma was found to be entropionItrichiasis 36.4%, comeal infiltration54.5%. keratitis and blindness each 4.5% ashas been found in other studies (20).
Risk factors for the development oftrachoma were also compatible with otherstudies in other parts of the country. Astudy in Gondar region in a new villagereported 80% prevalence showing astatistically significant inverse relationshipbetween face washing and literacy. Anotherstudy conducted in the rural areas ofSidamo showed increased risks of exposureamong trachoma cases for garbage disposalnear residential areas (7).
In the current study. unlike findingsfrom Sidamo (7). the presence of animalsin the living room is significantly andindependently associated with tlle presenceof trachoma. The presence of cattle and
34 Ethiop J Health Sci
cattle ownership has been associated withtrachoma in some African countries(12.16). In arid environments, cattledroppings create an optimal environmentfor breeding flies, and this has been theexplanation for the association of cattlewith trachoma, even if few studiesindicated these factors to be independentpredictors (12). On top of this, cattle alsomark families with traditional lifestyle whotend to have the poorest living conditions.
One potential source of infection isobviously the ocular and nasal secretions ofpreschool children. However. determiningthe frequency of face washing amongchildren is difficult and prone to bias. Asseen in some studies (2). self-reportedfrequency of washing children's face wasbelieved to be high. The lack of associationbetween this behavior and presence oftrachoma was also attributed to the lack ofvariance in this variable (7). As concerns tothe current study. face-washing habit atleast once per day is independently andsignificantly associated with the presenceof trachoma. A similar association was alsodocumented in other cross-sectional as wellas longitudinal intervention studies(12.21.22).
Eye care service seeking habit by thefamily of the children showed a protectiveeffect over the development of trachoma.Inquired reasons for failure of seeking eyecare service are of interesting combination.Health institution is too far. inconvenienttime. mother is too busy etc. shows thatthese families did not for some reason wantto reveal their reasons for failure of seekinghealth care sen;ices. Economical status(cost of treatment) and fate on thetreatment may play some role.
Changing the living standard of thesecommunities may be difficult consideringits direct relation with the economicalstatus. But in those who had both poor facewashing habit less than once per day andpoor household/environmental conditions
Vol. 11. No.1 January 2001
the occurrence of trachoma could beprevented through public health measures.These measures include health educationand changing the attitude and practice ofpeople regarding personal andenvironmental hygiene. Especially theeffect of regular face washing is welldocumented in intervention studies (21,22).
All in all trachoma is a communicabledisease. the transmission of which isheavily dependent on poor socio-economicand environmental conditions. In areaswhere it remains a blinding disease. acombination of encouraging regularprograms must be functional. In the studyarea it is recommended that. in addition toregular detection and treatment of peoplewith active trachoma. families andindividuals should be told to do somethingto protect themselves from the infection.That is teaching them to increase thenumber of times that their children washtheir face so as to remove discharge and toreduce flies that are attracted by dirt in theface. Assessing reasons behind poor facewashing will also be beneficial in thisregard.
The difficulty of carrying out behavioralinterventions is evident. but such anapproach is likely to be more sustainablethan the constant provision of antibiotictreatment. Based on the study findings itwas also indicated that, the other priorityareas for the zonal health departmentdonor agencies and the community tointervene will be improving water supply.sanitation and housing conditions toprevent trachoma altogether. Furthermore.evaluating the impact of socio-economicfactors and services at health institutions onhelp seeking behavior has to be conducted.Additional emphasis should focus on othercommon and preventable blinding diseases.Effort must be directed to improve theliteracy rate and at insertion of eye healthpromotion and education into schools'curricula.
Prevalence and Risk Factors of Trachoma EvobL 35
ACKNOWLEDGEMENTS
This study was financially supported bySave The Children Fund (UK) and theSouth Wollo Zonal Health Department. Iwould like to thank all the families of thestudy children in the study area and thecommunity health agent WIro AskaleTeshome who made the study possible.
REFERENCES
1. Thylefors B, Dawson CR, Jones BR, etal. A simple system for the assessmentoftrachoma and its complications. BullWId Health Org 1987: 65:477-83.
2. Munoz B, West S. Trachoma: theforgotten cause of blindness.Epidemiologic Review 1997: 19(2):205-217.
3. West Sk. Munoz B, Turner VM. et al.The epidemiology of trachoma incentral Tanzania. Int J Epidemiol1991: 20:1088-92.
4. Courtright P. Sheppard J, Schachter J.er al. Trachoma and blindness in theNile delta: current patterns andprojections for the future in the ruralEgyptian population. Br J Ophthalmol1989: 73:82-7.
5. Bailey R. Osmond C. Mabey DC. et al.Analysis of the household distributionof trachoma in a Gambian villageusing a Monte Carlo simulationprocedure. Int J Epidemiol 1989:18:944-51.
6. Katz 1. Zeger SL. Tielsch 1M. Villageand household clustering ofxerophthalmia and trachoma. In! JEpidemiol1988: 17:865-9.
7. Sahlu T. Larson C. The prevalence ofenvironmental risk factors formoderate and severe trachoma insouthern Ethiopia. J Trop Med Hyg1992: 95:36-41.
8. Assaad FA Maxwell-Lyons F.Sundaresan T. Use of local variation in
trachoma endemicity in depictinginterplay between socio-economicconditions and disease. Bull WIdHealth Org 1969: 41:181-94.
9. Taylor HR, Velasco FM. Sommer A.The ecology of trachoma: anepidemiological study in southernMexico. Bull WId Health Org 1985:63:559-67.
10. Congdon N. West S. Vitale S. et al.Exposure to children and risk of activetrachoma in Tanzanian women. Am JEpidemioI1993: 137:366-72.
11. Taylor CE, Gulati PV. Harinarian 1.Eye infections in a Punjab village. AmJ Epidemio/1990: 132:946-52.
12. Taylor HR. West SK. Mmbaga BBO.et al. Hygiene factors and increase inrisk of trachoma in central Tanzania.Arch Ophrha/moI1989: 107:1821-5.
13. West SK. Congdon N. Katala S, et at.Facial cleanliness and risk of trachomain families. Arch Optha/mol 1991:109:855-7.
14. Brechner RJ. West S. Lynch M.Trachoma and flies: individual Vsenvironmental risk factors. ArchOpthalmo/1992: 110:687-9.
15. West SK. Rapoza P. Munoz B, et al.Epidemiology of ocular chlamydialinfection in a trachoma-hyperendemicarea. J Infect Dis 199U63:752-6
16. De Sole G. Impact of cattle on theprevalence and severity of trachoma.BrJ Ophthalmo/1987: 71:873-6.
17. Cerulli L. Cedron C. Asefa C.Assessment of visual status in 7regions of Ethiopia. Report to theEthio-Italian Project. Office of theNational Programme for Prevention ofBlindness (NPPB). Addis Ababa.1981.
18. World Health Organisation. The EPIcoverage survey. WHOIEPIIMLMI91.10.1991.
36 Ethiop J Health Sci
19. Ministry of Health (MOH).Epidemiology and AIDS Department:Guideline for prevention of blindnessprogrammes in Ethiopia. Addis Ababa,1996.
20. Hans-Werner Kothe, Wolf-DeiterSittner: Trachoma: Frequency andtreatment in the Gondar region. EthiopMedJ 1987: 25: 55
Vol. 11.NO.1 January 2001
21. West SK Munoz B, Lynch M, et al.Impact of face-washing on trachoma inKongwa, Tanzania. Lancet 1995: 342(8943): 155-8.
22. Lynch M, West S, Munoz B,Kayongoya A, Taylor H, Mmbaga B.Face washing for trachoma prevention:a participatory strategy to changehygiene behavior. Trans Royal SocTrap Med Hyg 1994: 88: 513-17.