pre(peri)-natal ω-3 pufa deficiency-induced hypertension and its broader implications
TRANSCRIPT

216 Current Nutrition & Food Science, 2008, 4, 216-225
1573-4013/08 $55.00+.00 © 2008 Bentham Science Publishers Ltd.
Albumin Infusion Therapy in Stroke, Sepsis and the Critically Ill
Undurti N. Das*
UND Life Sciences, 13800 Fairhill Road, #321, Shaker Heights, OH 44120, USA
Abstract: Albumin is a complex molecule that is a principal transporter of plasma fatty acids and binds to majority of the
drugs ingested. Albumin traps oxygen radicals and has anti-oxidant actions that exceed that of vitamin E. Vascular
endothelial cells express specific binding sites for albumin that may aid in its ability to prevent endothelial cell apoptosis.
Albumin regulates the enzyme pyruvate dehydrogenase in astrocytes and thus helps in the flux of glucose and lactate.
Thus, albumin could limit ischemia-induced neuronal damage. Recent studies showed that intravenous albumin
administration improved neurological function by reducing infarction volume and cerebral edema. In addition, albumin
seems to be useful in the treatment of in those who are critically ill due to due to medical and surgical conditions, and
sepsis. The cytoprotective action of albumin is due to an increase in the formation of protectins from docosahexaenoic
acid (DHA) and possibly, other polyunsaturated fatty acids.
Keywords: Sepsis, critical illness, albumin, docosahexaenoic acid, polyunsaturated fatty acids, lipoxins, resolvins, neuroprotectin D1, stroke, neuroprotection, cerebrovascular disease, free radicals, cytokines, tumor necrosis factor, interleukins, nitric oxide, reactive oxygen species, superoxide radical.
INTRODUCTION
Ischemic cerebrovascular disease is one of the major causes of morbidity and mortality. Although, preventive measures targeted at major risk factors did decrease the incidence of stroke and mortality rates [1] no specific therapies have been developed that are of significant benefit in reducing the effects and complications of stroke. The only exception being the administration of recombinant human tissue-type plasminogen activator (rh-tPA), a thrombolytic agent, that is of significant benefit when given within 3 hours of the onset of stroke [2]. Community practice surveys revealed that in actual practice only a very small proportion of patients with acute ischemic stroke actually receive rh-tPA therapy within 3 hours of the onset of stroke, and deviations from the recommended guidelines are frequent that resulted in high rates of intracerebral hemorrhage and in-hospital death [3]. These results suggest that more practical, simple, and yet effective measures need to be developed for the treatment of stroke.
Sepsis is a major cause of death in intensive care units. More than 750,000 cases of sepsis will be diagnosed per year, with crude mortality rates of 28% to 50% accounting for about 200,000 deaths per year in U.S.A. alone [4]. Sepsis is due to systemic inflammatory response to infection. When sepsis causes hypotension and multiorgan dysfunction, it results in septic shock. Noninfectious disorders such as trauma, pancreatitis, and following major abdominal and cardiovascular surgery also result in critical illness that resembles sepsis, due to inappropriate stimulation of the innate immune system. Mortality in sepsis is due to multiple organ dysfunctions (MODS = multiorgan dysfunction syndrome) that cause death among patients in non-coronary critical care units. Thus, prognosis of patients with sepsis is related to the severity of organ dysfunction [5]. Several
*Address correspondence to this author at the UND Life Sciences, 13800
Fairhill Road, #321, Shaker Heights, OH 44120, USA; Tel: 216-231-5548; Fax: 928-833-0316; E-mail: [email protected]
mechanisms contribute to the pathogenesis of MODS. Some of these include: bacterial toxins, inflammatory mediators secreted by neutrophils, macrophages, and T cells; endo-thelial injury, disturbed homeostasis, and microcirculatory failure. Sepsis impairs immune function by inducing defects in innate immunity and excessive lymphocyte apoptosis. Several clinical trials that studied the effect of agents that block the inflammatory cascade-corticosteroids, anti-endo-toxin antibodies, tumor necrosis factor antagonists, and interleukin-1-receptor antagonists, all of which failed to reduce deaths due to sepsis. Recent studies suggest that albumin could be of benefit in sepsis. This beneficial action could be due to the ability of albumin to trap oxygen radicals and its antioxidant actions.
TRADITIONAL USES OF ALBUMIN
Albumin accounts for approximately 50% of the serum proteins and is the major protein produced by hepatocytes in the liver [6]. Albumin is not stored in the liver and is immediately excreted into the hepatic lymph system or the sinusoids [7]. Albumin circulates from the intravascular space across the capillary wall into the interstitium and returns to the intravascular space via the lymphatic system. This circulation half-life is approximately 16 hours [8]. The degradation half-life of albumin is 17 to 20 days [9]. Traditionally albumin infusions are given for the mana-gement of hypoalbuminemia that is known to occur in cirrhosis of the liver, patients with severe malnutrition such as marasmus and kwashiorkor, and those who have lost protein due to severe burns, injuries, and following gastrointestinal surgeries. One of the functions of albumin is to maintain oncostatic pressure. Hence, loss of substantial amounts of albumin would result in dependent edema, hypotension, and, at times, circulatory collapse. In general, albumin produced in the liver is sufficient to meet normal body needs. But, in situations such as severe injuries as seen in war, burns involving large body surface area, and subs-tantial loss of blood during major gastrointestinal surgeries, loss of blood volume and the resultant hypoalbuminemia is

Albumin Infusion Therapy in Stroke, Sepsis and the Critically Ill Current Nutrition & Food Science, 2008, Vol. 4, No. 3 217
significant to produce hypotension and circulatory collapse. In these situations, to maintain blood pressure and tissue perfusion, one needs to resort to blood, plasma, and/or albumin transfusions. Hypoalbuminemia that occurs as result of hepatic damage as seen in cirrhosis of the liver is best corrected by giving albumin infusions till liver regains its capacity to synthesize albumin to meet body demands. On the other hand, hypoalbuminemia seen in conditions such as marasmus and Kwashiorkor are best treated by giving protein-rich diet rather than by albumin infusions, unless and otherwise, there is danger of hypotension and circulatory collapse due to low albumin levels, in which case albumin infusion could be resorted to. One of the advantages of albumin therapy is the fact that albumin has a prolonged half-life (~ 20 days) and it does not easily leave the intravascular space. Albumin is capable of increasing plasma oncotic pressure over prolonged periods of time [10] and is responsible for 80% of the plasma colloid oncotic pressure [11].
In the United States, the indications for which albumin
therapy are considered include hypovolemia or shock, burns,
hypoalbuminemia, surgery or trauma, cardiopulmonary
bypass, acute respiratory distress syndrome, hemodialysis, and sequestration
of protein-rich fluids [12]. The use of this
relatively expensive therapy accounts for up to 30% of the
total pharmacy budget in certain hospitals. Despite the use of
albumin therapy in different clinical situations
and its influence in morbidity and mortality, the use of albumin still remains controversial
in several clinical situations. Although
albumin infusions have been used extensively in patients with cirrhosis to improve renal function
and facilitate
elimination of ascites, the beneficial effects of albumin are
very modest and limited only to patients with slightly
impaired renal function who respond to conventional therapy. In contrast, albumin infusions
are effective in
preventing the deterioration in renal function associated with
large volume paracentesis or spontaneous bacterial perito-
nitis, conditions that cause impairment of
circulatory function in patients with cirrhosis and ascites. Moreover,
albumin infusions improve survival in patients with spontaneous
bacterial peritonitis. These data suggest that
albumin prevents renal impairment by maintaining effective
arterial blood volume in situations characterized by acute deterioration
in circulatory function [13]. On the other hand,
when circulatory dysfunction is already established, albumin
alone is not effective in improving renal function. The recent
demonstration that concomitant administration of albumin
and vasoconstrictor drugs acting preferentially in the splan-
chnic circulation normalizes almost completely circulatory
function and improves renal function in patients with cirrhosis
and hepatorenal syndrome opens a new indication
for albumin infusions in patients with liver
disease [14].
Albumin is the primary oxygen radical trapping agent and functions as major free radical quenching plasma molecule both against endogenously generated free radicals and against exogenous oxidizing substances. Albumin inhibits copper ion-dependent lipid peroxidation and retards the formation of hydroxyl radicals. In view of these beneficial properties, possible beneficial effects of albumin in stroke and sepsis are being studied. Although there are many other antioxidants in the body but are not
neuroprotective, the neuroprotective and cytopro-tective action of albumin could be attributed to its ability to mobilize docosahexaenoic acid (DHA) and, possibly, other polyunsaturated fatty acids (PUFAs) from liver and other tissues that, in turn, are converted to form protectins, lipo-xins and resolvins that are potent endogenous cytoprotective molecules.
ALBUMIN IN THE CRITICALLY ILL
Hypoalbuminemia is a common finding in critically ill patients. It has been well documented that hypoalbuminemic patients have a higher morbidity and mortality rate when compared with patients with a normal serum albumin. Consequently, hypoalbuminemic patients are commonly treated with exogenous albumin in the hope of improving their outcome. In this context, it is interesting to note that in a prospective, randomized trial of 25% albumin adminis-tration to hypoalbuminemic (serum albumin, less than 25 g/L [2.5 g/dL]), critically ill patients revealed no clinical benefit despite the fact that in the treatment group 25% albumin supplementation achieved and maintained serum albumin levels of 25 g/L (2.5 g/dL) or greater [15]. No significant differences in length of hospital stay, intensive care unit stay, ventilator dependence, or tolerance of enteral feeding, despite significant elevations of albumin in the treatment group was noted.
In contrast, in a prospective, controlled, randomized study of a mixed population of critically ill patients administration of albumin to correct hypoalbuminemia whose serum albumin concentration < or =30 g/L, albumin administration showed improved organ function. Patients who received albumin showed organ function improved due to a difference in respiratory, cardiovascular, and central nervous system components of the Sequential Organ Failure Assessment score. It was reported that albumin adminis-tration not only improved organ function in hypoalbu-minemic critically ill patients but also resulted in a less positive fluid balance and a better tolerance to enteral feeding [16].
On the other hand, when the efficacy of supplemental 25% albumin in reducing morbidity and mortality rates in surgical intensive care patients with circulating albumin concentration of <3.0 g/dL was evaluated in a prospective, randomized, unblended clinical study, no significant differences between the control and albumin treated groups was noted [17]. In another study, intravenous infusion of either human albumin or hydroxyethyl-starch (HES) in hypoalbuminemic critically ill were compared administration of human albumin was not associated with improvement of the clinical outcome [18].
These results coupled with the observation that fluid resuscitation with 4% albumin or saline in patients with a baseline serum albumin concentration of 25 g/l or less or more than 25 g/l in the critically ill did not show any significant benefit [19] suggests that one has to be careful in recommending the use of albumin infusion in the critical care units. In contrast, when low level albumin excretion (microalbuminuria), a marker of systemic capillary permeability, with mortality, Acute Physiologic And Chronic Health Evaluation (APACHE II) score, the Simplified Acute

218 Current Nutrition & Food Science, 2008, Vol. 4, No. 3 Undurti N. Das
Physiologic (SAP II) score, and their derived mortality probabilities in patients admitted to a general intensive care unit was studied in 140 consecutive patients (59 surgical, 48 medical, 22 trauma, and 11 burns), microalbuminuria within 15 mins of intensive care unit admission predicted death as well as APACHE II and SAP II scores calculated after 24 hrs only for surgical, trauma, and burn patients, but not medical patients [20]. These results suggest that microalbuminuria shows promise as a predictor of outcome.
These data suggest that treatment of critically ill with albumin is not without controversy. These controversial results could be attributed to several factors. Some of these include: heterogeneity of patients studied, presence of other illnesses in them such as infections, presence or absence of associated renal, liver or lung diseases, abnormalities in their immune responses to the underlying diseases or infections, variations in the cytokine profiles, endogenous concen-trations of polyunsaturated fatty acids and their products, their nutritional status, associated reactive hyperglycemia and insulin secretion and resistance, and possibly, differences in the dose of albumin employed [21-29]. Hence, one has to take into consideration several factors before abandoning the use of albumin in the critical care units. In this context, recent findings that albumin shows cytopro-tective actions by enhancing the formation of anti-inflam-matory molecules lipoxins, resolvins and neuroprotectin D1 (NPD1) is worth noting. Albumin complexed with polyunsa-turated fatty acids (PUFAs) such as docosahexaenoic acid (DHA) is particularly effective in enhancing the formation of anti-inflammatory lipoxins, resolvins and NPD1 suggesting that plain and simple fatty acid-free albumin may not be the right choice for the critically ill.
ALBUMIN HAS NEUROPROTECTIVE ACTIONS
Animal Studies
Animal studies revealed that high-dose human albumin therapy (2.0 to 2.5 g/kg), when administered within 2 hours after the onset of stroke, is effective in improving neurological status, as evident from the observation that there was both a reduction in infarction volume and cerebral edema [30-32]. Subsequent studies showed that human albumin is highly effective even when administered 4 hours after the stroke and in moderate doses. Sprague-Dawley rats given different doses of human albumin (0.63 or 1.25 g/kg) at different time intervals (2, 3, 4, or 5 hours after onset of middle cerebral artery occlusion), revealed that 1.25 g/kg albumin dose significantly improved the neurological score compared with control at 24, 48, and 72 hours whereas the 0.63 g/kg dose was effective at 72 hours. The moderate-dose albumin 1.25 g/kg was effective even when initiated as late as 4 hours after the onset of middle cerebral artery occlusion and markedly reduced infarct volumes in cortex (by 68%), subcortical regions (by 52%) and total infarct (by 61%), and virtually eliminated cerebral edema [33]. Although, several different doses of albumin is effective in improving neurological function, reducing the volume of cerebral infarction, and cerebral edema the optimum dose appears to be 1.25 g/kg. It was noted that albumin therapy not only diminished brain infarction and edema but also improved local perfusion to zones of critical blood flow reduction [32]. Focal ischemia-induced blood-brain barrier dysfunction
could permit albumin to penetrate into the brain parenchyma, where it was taken up by cortical neurons and thus, are protected by albumin from ischemic injury [34]. Albumin prevented necrosis of neurons in tissue zones of residual ischemic injury by preserving glial and endothelial elements. Albumin normalized diffusion coefficient of water even in zones of residual histological injury as measured by diffusion-weighted magnetic resonance technique [30]. Albumin regulates the enzyme pyruvate dehydrogenase in astrocytes and thus helps in the flux of glucose and lactate that aids in the limitation of neuronal damage due to cerebral ischemia. These evidences suggest that albumin has a direct protective effect on both parenchymal and vascular tissues of the brain. In animal models of transient global ischemia and fluid-percussion traumatic brain injury models, albumin was found to protect vulnerable neurons of the hippocampus from injury and diminished contusion volume [35, 36]. These neuroprotective actions of albumin encouraged its clinical evaluation for patients with stroke.
Albumin in Animal Models of Sepsis and other Critical Illness
In an infant rat model designed to study the ability of various rabbit antisera to protect against challenge by Haemophilus influenzae type b, it was observed that use of phosphate buffered saline (PBS) resulted in higher levels of bacteremia than PBS containing 0.5% bovine serum albumin (PBS-BSA). This suggested that BSA protected the rats from H. influenzae infection [37]. Although these results are interesting, the exact mechanism by which albumin protected against H. influenza infection is not clear.
Albumin has the ability to trap oxygen radicals including endogenously generated free radicals and exogenous oxidizing substances. Albumin inhibits copper ion-dependent lipid peroxidation and retards the formation of hydroxyl radicals. Nitric oxide (NO) is an endogenous vasodilator and modulator of inflammation. During endotoxemia, the beneficial effects of NO are overwhelmed by the inflam-matory cascade, resulting in a functional depletion of NO. S-nitroso-albumin (S-NO-alb) exists as a novel and highly stable NO thiol complex that slowly releases NO into the vascular micro-environment. In a porcine model of LPS-induced cardiopulmonary dysfunction, it was reported that pretreatment with intravenous S-NO-alb improved cardio-pulmonary dysfunction without adversely affecting systemic hemodynamics. S-NO-alb blunted LPS-induced hypoxemic response and reduced neutrophil activation. S-NO-alb did not, however, attenuate LPS-induced increases in lung MPO. This suggests that S-NO-alb selectively modulates endo-toxin-induced pulmonary dysfunction, attenuate neutrophil priming and block the early mortality [38].
Acute lung injury is a frequent complication of severe sepsis or blood loss and is often associated with an excessive inflammatory response requiring mechanical ventilation. Experimental studies revealed that human albumin solutions can prevent and benefit acute lung injury following shock/ resuscitation. In a rodent model of acute lung injury induced by intratracheal LPS, both cytokine-induced neutrophil chemoattractant messenger RNA concentrations and nuclear factor-kappaB (NF- B) translocation were diminished following 25% albumin resuscitation. Furthermore, 25%

Albumin Infusion Therapy in Stroke, Sepsis and the Critically Ill Current Nutrition & Food Science, 2008, Vol. 4, No. 3 219
albumin significantly decreased plasma lipid peroxidation, and exhibited protection from lung injury [39]. These studies suggest that 25% albumin acts as an anti-inflammatory agent in neutrophil-mediated diseases, such as acute respiratory distress syndrome ARDS). Rats subjected to either hemorrhage or endotoxemia for 1 hr required significantly smaller volume of fluids in the albumin-treated groups than in the Ringer's lactate groups. Furthermore, in this hemorr-hagic shock model, plasma concentrations of tumor necrosis factor- , interleukin-6, and macrophage inflammatory protein-2 were significantly lower and interleukin-10 was significantly higher in the albumin-treated groups compared with the Ringer's lactate-treated group. The decreased cytokine production was associated with a reduction of hydrogen peroxide formation with albumin resuscitation. Resuscitation with albumin reduced ventilator-induced lung injury after hemorrhagic shock, but not after endotoxic shock, suggesting that the mechanisms leading to ventilator-induced lung injury after hemorrhage differ from those after endotoxemia [40], which needs to be kept in mind while evaluating the role and utility of albumin in shock/sepsis. In this context, it is interesting that PEG-Alb (albumin covalently linked to polyethylene glycol) could be used as a potential resuscitative agent. PEG when covalently linked to human albumin at multiple sites on the protein, the effective volume of PEG-Alb is increased 13- to 16-fold compared with unmodified albumin. In an LPS (lipopolysaccharide) model of shock, rats treated with PEG-Alb showed better blood pressure, lower haematocrit consistent with haemodilution and less lung injury than rats treated with unmodified albumin or saline. In a CLP (caecal ligation and puncture) model of sepsis, PEG-Alb was more effective than albumin or saline in maintaining blood pressure and in decreasing haematocrit. Rats with LPS- or CLP-induced shock, PEG-Alb were retained within blood vessels, whereas albumin extravasates into the interstitial space [41]. Thus, PEG-Alb may be more effective in the clinical treatment of shock associated with capillary leak.
The beneficial action of albumin in critical illness is further supported by the observation that albumin resusci-tation improved decreased ventricular contractility and myocardial oxygenation by improving ventricular dysfunc-tion by reducing myocardial hypoxia in endotoxemic rats [42]. This beneficial action of albumin resuscitation on cardiomyocyte contractility could be attributed to an albumin-induced reduction in nitric oxide synthase II protein and messenger RNA expression following endotoxin injection [43]. These results coupled with the observation that resuscitation with PEG-Alb (2.5% weight/volume) infused at 16 mL/kg/hr (PEG-BSA-16) or at 24 mL/kg/hr (PEG-BSA-24) for 1 hr improves microcirculatory condi-tions in endotoxemia compared with dextran 70 (6% weight/volume) infused at 24 mL/kg/hr implies that albumin given at the right time and right dose is of benefit in sepsis. PEG-BSA provided significantly improved microvascular conditions as shown by restoration of functional capillary density that could be related to improved microvascular flow and perivascular and tissue P(O2), normalization of shear rate, and decreased perivascular nitric oxide concentration. These beneficial effects were related to improved fluid retention using PEG-BSA-24 as evidenced by the
significantly lower hematocrit at 24 hrs after resuscitation. Nitric oxide at 6 hrs after induction of sepsis achieved perivascular millimolar concentrations, which were reduced to normal values by PEG-BSA-24 treatment [44]. Thus, PEG-BSA produced improved microcirculatory conditions in the treatment of endotoxemia.
Human Studies
Despite the fact that resuscitations measures in animal models of sepsis have been fairly encouraging, similar studies performed in patients with sepsis have given contro-versial results. Rackow et al. [45] studied twenty consecutive patients with severe sepsis who were randomized to fluid challenge with 5% albumin or 10% low MW hydroxyethyl starch (pentastarch) solutions. Fluid challenge was administered intravenously as 250 ml of test colloid every 15 min until the pulmonary artery wedge pressure (WP) was greater than or equal to 15 mm Hg or a maximum dose of 2000 ml was infused. Both colloid infusions resulted in similar increases in cardiac output, stroke output, and stroke work, although pentastarch was associated with a 45% decrease in factor VIII:c. This led to the conclusion that pentastarch is equivalent to albumin for fluid resuscitation of patients with severe sepsis. Although all of the patients with a clinical diagnosis of septic ARDS had similar impairments in oxygenation and chest roentgenograms, those patients with a significantly increased pulmonary albumin flux (greater than 2 SD above control mean) had a markedly increased morbidity [46], suggesting that efforts made to decrease albumin flux could benefit these patients.
In a case-controlled study of inpatients who sustained burns of > or =20% total body surface area (TBSA), patients who received albumin during resuscitation because of increased fluid requirements showed decreased likelihood of mortality compared to those who did not receive albumin despite more severe systemic dysfunction [47]. In contrast, in a multicenter, randomized, double-blind trial in a hetero-geneous population of patients in the ICU, no significant differences between the groups in the mean numbers of days spent in the ICU, days spent in the hospital, days of mechanical ventilation, or days of renal-replacement therapy was noted [48]. These results suggest that in patients in the ICU, use of either 4 percent albumin or normal saline for fluid resuscitation results in similar outcomes at 28 days. Since resuscitation with albumin or saline in the intensive care unit does not depend on patients' baseline serum albumin concentration [19], whatever results that have been obtained with albumin resuscitation can be attributed to the infused dose of albumin. Despite these controversial results, potential use of albumin in critical illness cannot be set aside. This is so since, albumin has the ability to trap oxygen radicals and exogenous oxidizing substances, suppress the production of pro-inflammatory cytokines, and enhances endothelial NO generation [38-41, 43] that are desirable actions in the setting of sepsis and in the critically ill. To exploit these beneficial actions of albumin in the critically ill and sepsis, obviously more studies are needed to determine the exact dose, timing, and frequency of its administration. It is also important to know whether albumin by itself is sufficient or it need to be conjugated to other biologically active molecules such as PEG or NO to bring about its
220 Current Nutrition & Food Science, 2008, Vol. 4, No. 3 Undurti N. Das
beneficial actions. In this context, the recent observation that albumin when conjugated with docosahexaenoic acid (DHA) shows some novel beneficial actions especially in the treatment of stroke is particularly interesting.
Albumin Administration for Stroke
Ischemic cerebrovascular disease ranks among the leading causes of death and long-term disability. Several investigations of cerebral ischemia led to the identification of key biochemical and molecular mechanisms that contribute to the death of brain tissue some of which include: excito-toxicity [49], tissue calcium overload [50], oxygen radicals [51], and inflammatory mediators [52]. As already discussed above, high-dose human albumin therapy (2.0 to 2.5 g/kg), if administered within2 hours after stroke onset, is highly effective in improving neurological status and in reducing infarction volume and extent of brain swelling [30-36]. These studies were performed in a widely used, minimally invasive model of middle cerebral artery occlusion in the albino rat. Subsequent dose response studies revealed that even moderate dose of albumin (1.25 g/kg) given intravenously as late as 4 hours after onset of middle cerebral artery occlusion, improved the neurological score, reduced infarct volume in cortex (by 65%), subcortical regions (by 52%), and total infarct (by 61%) [33]. Although albumin is
useful in the prevention of brain damage, the exact mechanism by which this beneficial action is brought about is not clear. In this context, it is interesting to note that albumin administration induces a selective mobilization of n-3 polyunsaturated fatty acids (PUFAs) especially that of DHA (22:6) and docosapentaenoic acid (DPA, 22:5 n-3). Both DHA and DPA concentrations were selectively increased within 30 minutes of albumin administration in systemic venous plasma by their mobilization from the liver [53] so that PUFAs lost from neural membranes during ischemia are replenished [54].
Metabolism of Essential Fatty Acids and Formation of Lipoxins, Resolvins, and Neuroprotectin D1 that are
Cytoprotective and Neuroprotective in Nature
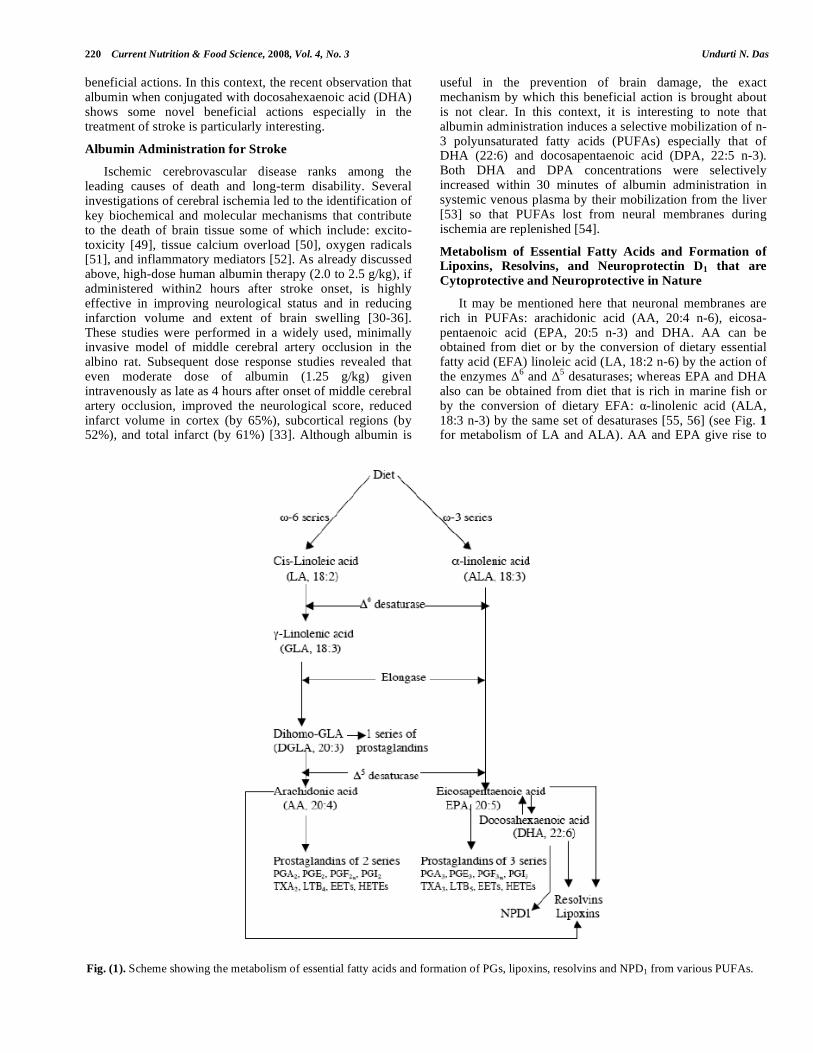
It may be mentioned here that neuronal membranes are rich in PUFAs: arachidonic acid (AA, 20:4 n-6), eicosa-pentaenoic acid (EPA, 20:5 n-3) and DHA. AA can be obtained from diet or by the conversion of dietary essential fatty acid (EFA) linoleic acid (LA, 18:2 n-6) by the action of the enzymes
6 and
5 desaturases; whereas EPA and DHA
also can be obtained from diet that is rich in marine fish or by the conversion of dietary EFA: -linolenic acid (ALA, 18:3 n-3) by the same set of desaturases [55, 56] (see Fig. 1 for metabolism of LA and ALA). AA and EPA give rise to
Fig. (1). Scheme showing the metabolism of essential fatty acids and formation of PGs, lipoxins, resolvins and NPD1 from various PUFAs.
Albumin Infusion Therapy in Stroke, Sepsis and the Critically Ill Current Nutrition & Food Science, 2008, Vol. 4, No. 3 221
the formation of various prostaglandins (PGs), thromboxanes (TXs) and leukotrienes (LTs) that are mainly pro-inflam-matory in nature (but it should be noted that PGE1 and PGI2 show anti-inflammatory actions under certain circums-tances). AA, EPA, and DHA also form precursors to anti-inflammatory molecules lipoxins (LXs), resolvins, and protectins that suppress inflammation. Thus, balance bet-ween these mutually antagonistic compounds formed from PUFAs could determine the final outcome of the disease process. Yet another series of biologically active compounds formed due to the nitration of unsaturated fatty acids called as nitrolipids have also been identified [55, 56]. Nitration of PUFAs by nitric oxide-derived reactive species forms novel derivatives called as nitrolipids that stimulates smooth muscle relaxation, blocks platelet activation, inhibits human neutrophil functions and suppresses inflammation.
Aspirin converts AA, EPA and DHA to form aspirin-triggered 15 epimer LXs (ATLs) that are potent inhibitors of acute inflammation [55-58]. Acetylation of COX-2 by aspirin prevents the formation of prostanoids, but the acetylated enzyme remains active in situ to generate 15R-hydroxy-eicosatetraenoic acid (15R-HETE) from AA that is released and converted by activated PMNs to the 15-epimeric LXs [57, 58]. This interaction between endothelial cells and PMNs leading to the formation of 15R-HETE and its subsequent conversion to 15-epimeric LXs by aspirin-acetylated COX-2 is a protective mechanism to prevent local inflammation on the vessel wall by regulating the motility of PMNs, eosinophils, and monocytes [55-58]. Endothelial cells oxidize AA (and possibly EPA and DHA) via P450 enzyme system to form 11, 12-epoxy-eicosatetraenoic acid (s) that blocks endothelial cell activation, suggesting that
COX-2 enzyme is essential for the formation of LXs. Deficiency or absence of LXs leads to interaction between PMN and endothelial cells as a result of which endothelial damage occurs that results in the initiation and progression of inflammation.
Compounds similar to 15R-HETE and 15-epimeric LXs are also formed from EPA and DHA. Neuronal cells transform enzymatically DHA to 17R series of hydroxy DHAs (HDHAs) that, in turn, is converted enzymatically by PMNs to di- and tri-hydroxy containing docosanoids [59] that have potent anti-inflammatory actions and induce resolution of the inflammatory process and hence are called “resolvins” (see Fig. 2). Resolvins inhibited cytokine gene-ration, leukocyte recruitment, leukocyte diapedesis, and exudate formation. AA, EPA, and DHA-derived resolvins from acetylated COX-2 are formed due to communication between endothelial cells and PMNs. Resolvins inhibit brain ischemia-reperfusion injury [60]. Thus, lipoxins and resol-vins formed from AA, EPA, and DHA have cardio-protec-tive, neuroprotective, and other cytoprotective actions.
Of the several 17-hydroxy-containing bioactive mediators derived from DHA that were termed docosatrienes and 17S series resolvins, 10,17S-dihydroxydocosatriene is termed as neuroprotectin D1 (NPD1) that reduced infiltration of PMNs, showed anti-inflammatory and neuroprotective properties [60, 61]. NPD1 inhibited oxidative stress-induced apoptosis of human retinal pigment epithelial cells [62]. Both LXs and NPD1 enhanced wound healing [63], and promoted brain cell survival via the induction of anti-apoptotic and neuroprotective gene-expression programs [64, 65] (Figs. 2-3).
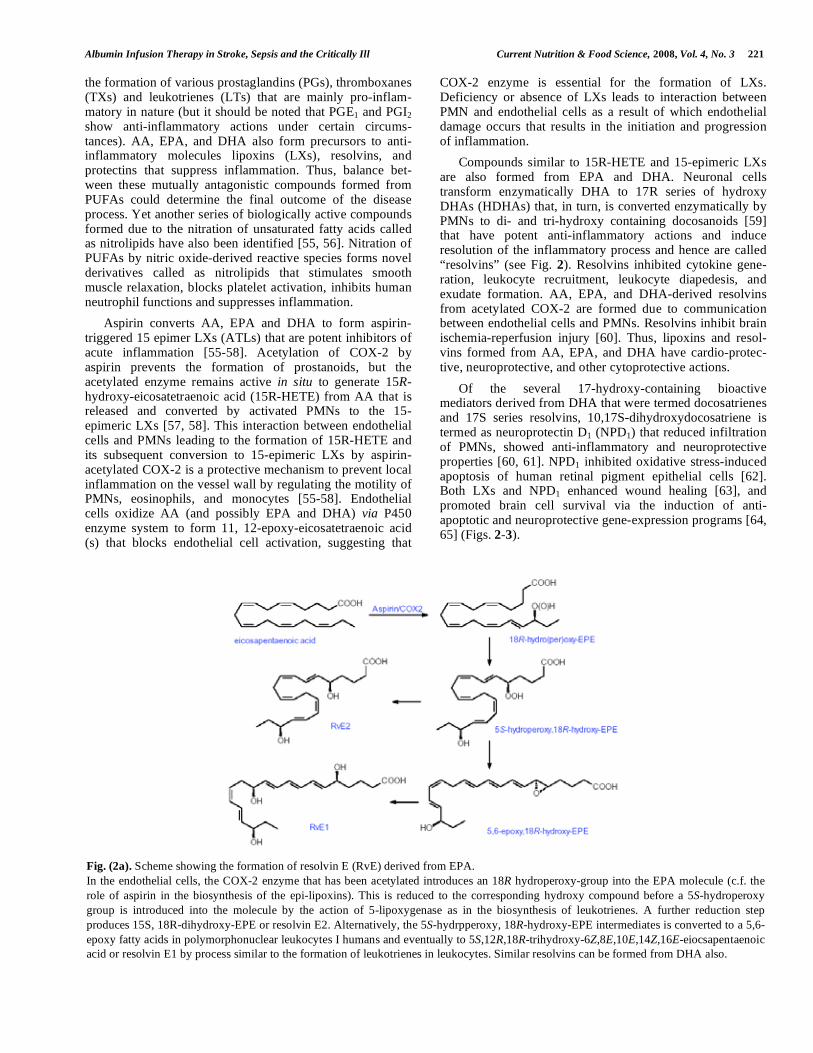
Fig. (2a). Scheme showing the formation of resolvin E (RvE) derived from EPA.
In the endothelial cells, the COX-2 enzyme that has been acetylated introduces an 18R hydroperoxy-group into the EPA molecule (c.f. the
role of aspirin in the biosynthesis of the epi-lipoxins). This is reduced to the corresponding hydroxy compound before a 5S-hydroperoxy
group is introduced into the molecule by the action of 5-lipoxygenase as in the biosynthesis of leukotrienes. A further reduction step
produces 15S, 18R-dihydroxy-EPE or resolvin E2. Alternatively, the 5S-hydrpperoxy, 18R-hydroxy-EPE intermediates is converted to a 5,6-
epoxy fatty acids in polymorphonuclear leukocytes I humans and eventually to 5S,12R,18R-trihydroxy-6Z,8E,10E,14Z,16E-eiocsapentaenoic
acid or resolvin E1 by process similar to the formation of leukotrienes in leukocytes. Similar resolvins can be formed from DHA also.
222 Current Nutrition & Food Science, 2008, Vol. 4, No. 3 Undurti N. Das
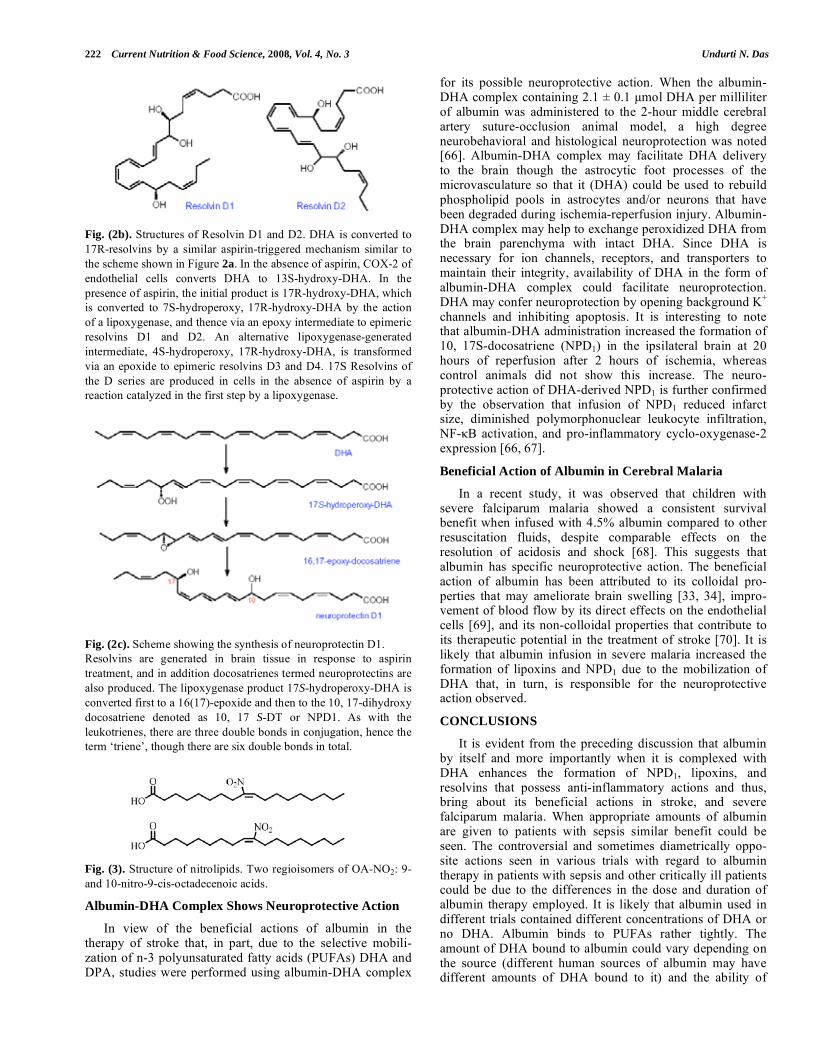
Fig. (2b). Structures of Resolvin D1 and D2. DHA is converted to
17R-resolvins by a similar aspirin-triggered mechanism similar to
the scheme shown in Figure 2a. In the absence of aspirin, COX-2 of
endothelial cells converts DHA to 13S-hydroxy-DHA. In the
presence of aspirin, the initial product is 17R-hydroxy-DHA, which
is converted to 7S-hydroperoxy, 17R-hydroxy-DHA by the action
of a lipoxygenase, and thence via an epoxy intermediate to epimeric
resolvins D1 and D2. An alternative lipoxygenase-generated
intermediate, 4S-hydroperoxy, 17R-hydroxy-DHA, is transformed
via an epoxide to epimeric resolvins D3 and D4. 17S Resolvins of
the D series are produced in cells in the absence of aspirin by a
reaction catalyzed in the first step by a lipoxygenase.
Fig. (2c). Scheme showing the synthesis of neuroprotectin D1.
Resolvins are generated in brain tissue in response to aspirin
treatment, and in addition docosatrienes termed neuroprotectins are
also produced. The lipoxygenase product 17S-hydroperoxy-DHA is
converted first to a 16(17)-epoxide and then to the 10, 17-dihydroxy
docosatriene denoted as 10, 17 S-DT or NPD1. As with the
leukotrienes, there are three double bonds in conjugation, hence the
term ‘triene’, though there are six double bonds in total.
Fig. (3). Structure of nitrolipids. Two regioisomers of OA-NO2: 9-
and 10-nitro-9-cis-octadecenoic acids.
Albumin-DHA Complex Shows Neuroprotective Action
In view of the beneficial actions of albumin in the therapy of stroke that, in part, due to the selective mobili-zation of n-3 polyunsaturated fatty acids (PUFAs) DHA and DPA, studies were performed using albumin-DHA complex
for its possible neuroprotective action. When the albumin-DHA complex containing 2.1 ± 0.1 μmol DHA per milliliter of albumin was administered to the 2-hour middle cerebral artery suture-occlusion animal model, a high degree neurobehavioral and histological neuroprotection was noted [66]. Albumin-DHA complex may facilitate DHA delivery to the brain though the astrocytic foot processes of the microvasculature so that it (DHA) could be used to rebuild phospholipid pools in astrocytes and/or neurons that have been degraded during ischemia-reperfusion injury. Albumin-DHA complex may help to exchange peroxidized DHA from the brain parenchyma with intact DHA. Since DHA is necessary for ion channels, receptors, and transporters to maintain their integrity, availability of DHA in the form of albumin-DHA complex could facilitate neuroprotection. DHA may confer neuroprotection by opening background K
+
channels and inhibiting apoptosis. It is interesting to note that albumin-DHA administration increased the formation of 10, 17S-docosatriene (NPD1) in the ipsilateral brain at 20 hours of reperfusion after 2 hours of ischemia, whereas control animals did not show this increase. The neuro-protective action of DHA-derived NPD1 is further confirmed by the observation that infusion of NPD1 reduced infarct size, diminished polymorphonuclear leukocyte infiltration, NF- B activation, and pro-inflammatory cyclo-oxygenase-2 expression [66, 67].
Beneficial Action of Albumin in Cerebral Malaria
In a recent study, it was observed that children with severe falciparum malaria showed a consistent survival benefit when infused with 4.5% albumin compared to other resuscitation fluids, despite comparable effects on the resolution of acidosis and shock [68]. This suggests that albumin has specific neuroprotective action. The beneficial action of albumin has been attributed to its colloidal pro-perties that may ameliorate brain swelling [33, 34], impro-vement of blood flow by its direct effects on the endothelial cells [69], and its non-colloidal properties that contribute to its therapeutic potential in the treatment of stroke [70]. It is likely that albumin infusion in severe malaria increased the formation of lipoxins and NPD1 due to the mobilization of DHA that, in turn, is responsible for the neuroprotective action observed.
CONCLUSIONS
It is evident from the preceding discussion that albumin by itself and more importantly when it is complexed with DHA enhances the formation of NPD1, lipoxins, and resolvins that possess anti-inflammatory actions and thus, bring about its beneficial actions in stroke, and severe falciparum malaria. When appropriate amounts of albumin are given to patients with sepsis similar benefit could be seen. The controversial and sometimes diametrically oppo-site actions seen in various trials with regard to albumin therapy in patients with sepsis and other critically ill patients could be due to the differences in the dose and duration of albumin therapy employed. It is likely that albumin used in different trials contained different concentrations of DHA or no DHA. Albumin binds to PUFAs rather tightly. The amount of DHA bound to albumin could vary depending on the source (different human sources of albumin may have different amounts of DHA bound to it) and the ability of
Albumin Infusion Therapy in Stroke, Sepsis and the Critically Ill Current Nutrition & Food Science, 2008, Vol. 4, No. 3 223
albumin to mobilize DHA. Since, in majority of instances, albumin mobilizes DHA from the liver, the amount of DHA stored in the liver could be another factor that influences the amounts of NPD1 formed. Furthermore, the activity of enzymes concerned with the formation of NPD1 may vary depending on the underlying clinical condition. These factors may lead to variations in the amount of DHA mobilized and the concentrations of NPD1 formed at the site of injury, and hence, variations in the response to albumin therapy observed.
In this context, it is interesting to note that albumin fully restored granulocyte-macrophage (CFU-GM) and erythro-cyte colony forming units to control values in experimental animals following trauma/hemorrhagic shock. This has been attributed to the binding of circulating toxic factors to albumin [71]. But, it is equally possible that albumin may enhance the formation of NPD1, lipoxins and resolvins that have cytoprotective actions and thus, could have prevented bone marrow suppression following trauma/hemorrhagic shock.
Another important aspect that needs serious conside-ration is the fact that albumin kinetics are altered in those with sepsis and critically ill. It was reported that the half-life time in septic group was shorter compared to control group
(8.2 ± 1.4 vs. 12.5 ± 1.7, P < 0.01), the transportation rate in the septic group was higher than that in the control group. These results suggest that in patients with severe sepsis, the distribution rate of albumin from vessel to tissue is increased and the decomposition rate of albumin was markedly improved [72].
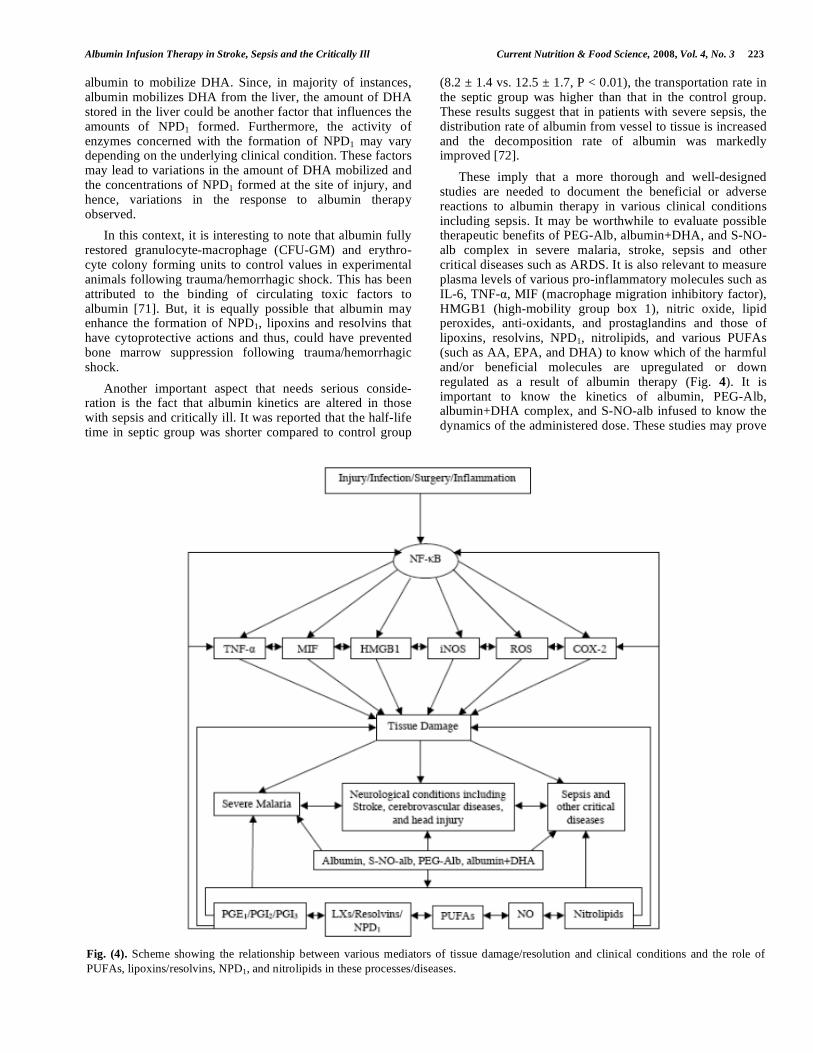
These imply that a more thorough and well-designed studies are needed to document the beneficial or adverse reactions to albumin therapy in various clinical conditions including sepsis. It may be worthwhile to evaluate possible therapeutic benefits of PEG-Alb, albumin+DHA, and S-NO-alb complex in severe malaria, stroke, sepsis and other critical diseases such as ARDS. It is also relevant to measure plasma levels of various pro-inflammatory molecules such as IL-6, TNF- , MIF (macrophage migration inhibitory factor), HMGB1 (high-mobility group box 1), nitric oxide, lipid peroxides, anti-oxidants, and prostaglandins and those of lipoxins, resolvins, NPD1, nitrolipids, and various PUFAs (such as AA, EPA, and DHA) to know which of the harmful and/or beneficial molecules are upregulated or down regulated as a result of albumin therapy (Fig. 4). It is important to know the kinetics of albumin, PEG-Alb, albumin+DHA complex, and S-NO-alb infused to know the dynamics of the administered dose. These studies may prove
Fig. (4). Scheme showing the relationship between various mediators of tissue damage/resolution and clinical conditions and the role of
PUFAs, lipoxins/resolvins, NPD1, and nitrolipids in these processes/diseases.
224 Current Nutrition & Food Science, 2008, Vol. 4, No. 3 Undurti N. Das
to be interesting since albumin when given in a dose range from 0.34 to 2.05 g/kg to patients with acute ischemic stroke is safe and well tolerated [73, 74].
ACKNOWLEDGEMENT
Dr. U N Das was in receipt of Ramalingaswami Fellowship of Department of Biotechnology, India during the tenure of this study.
REFERENCES
[1] Wolf PA, Kannel WB, D’Agostino RB. Epidemiology of stroke. In: Ginsberg MD, Bogousslavsky J, Eds. Cerebrovascular Disease:
Pathophysiology, Diagnosis, and Management. Malden, Mass; Blackwell Science 1998: 834-849.
[2] NINDS rt-PA Stroke Study Group. Tissue plasminogen activator for acute ischemic stroke. N Engl J Med 1995; 333: 1581-1587.
[3] Katzan IL, Furlan AJ, Lloyd LE, et al. Use of tissue-type plasminogen activator for acute ischemic stroke: the Cleveland area
experience. JAMA 2000; 283: 1151-1158. [4] Angus DC, Linde-Zwirble WT, Lidicker J, Clermont G, Carcillo J,
Pinsky MR. Epidemiology of severe sepsis in the United States: analysis of incidence, outcome, and associated costs of care. Crit
Care Med 2001; 29: 1303-1310. [5] Das UN. Critical advances in septicemia and septic shock. Crit Care
2000; 4: 290-294. [6] Vanek V. The use of serum albumin as a prognostic or nutritional
marker and the pros and cons of IV albumin therapy. Nutr Clin Pract 1998; 13: 110-22.
[7] Uhing MR. The albumin controversy. Clinics Perinatol 2004; 31: 475-488.
[8] Margarson MP, Soni N. Serum albumin: touchstone or totem? Anaesthesia 1998; 53: 789-803.
[9] Doweiko JP, Nompleggi DJ. Role of albumin in human physiology and pathophysiology. J Parenteral Enteral Nutr 1991; 15: 207-211.
[10] Halliwell B, Gutteridge JM. The antioxidants of human extracellular fluids. Arch Biochem Biophys 1990; 280: 1-8.
[11] Albright AL, Latchaw RE, Robinson AG. Intracranial and systemic effects of osmotic and oncotic therapy in experimental cerebral
edema. J Neurosurg 1984; 60: 481-489. [12] Foley EF, Borlase C, Dzik WH, Bistrian BR, Benotti PN. Albumin
supplementation in the critically ill. A prospective, randomized trial. Arch Surg 1990; 125: 739-742.
[13] Dubois MJ, Orellana-Jimenez C, Melot C, et al. Albumin administration improves organ function in critically ill
hypoalbuminemic patients: A prospective, randomized, controlled, pilot study. Crit Care Med 2006; 34: 2536-2540.
[14] Mendez CM, McClain CJ, Marsano LS. Albumin Therapy in Clinical Practice. Nutrition Clin Practice 2005; 20: 314-320.
[15] Gines P, Arroyo PV. Is there still a need for albumin infusions to treat patients with liver disease? Gut 2000; 46: 588-590.
[16] Uriz J, Gines P, Cardenas A, et al. Terlipressin plus albumin infusion: an effective and safe therapy of hepatorenal syndrome. J
Hepatol 2000; 33: 43-48. [17] Golub R, Sorrento JJ Jr, Cantu R Jr, Nierman DM, Moideen A,
Stein HD. Efficacy of albumin supplementation in the surgical intensive care unit: a prospective, randomized study. Crit Care Med
1994; 22: 613-619. [18] Veneman TF, Oude Nijhuis J, Woittiez AJ. Human albumin and
starch administration in critically ill patients: a prospective randomized clinical trial. Wien Klin Wochenschr 2004; 116: 305-
309. [19] SAFE Study Investigators, Finfer S, Bellomo R, McEvoy S, et al.
Effect of baseline serum albumin concentration on outcome of resuscitation with albumin or saline in patients in intensive care
units: analysis of data from the saline versus albumin fluid evaluation (SAFE) study. BMJ 2006; 333: 1044.
[20] Gosling P, Brudney S, McGrath L, Riseboro S, Manji M. Mortality prediction at admission to intensive care: a comparison of
microalbuminuria with acute physiology scores after 24 hours. Crit Care Med 2003; 31: 98-103.
[21] Roe PG. Liver function tests in the critically ill patient.lin Intens Care 1993; 4: 174-182.
[22] Gough DB, White M, Morrin M, et al. The relationship between a
nutritional index and acute physiology score in critical illness. Irish J Med Sci 1992; 161: 565-568.
[23] Dofferhoff AS, Bom VJ, de Vries-Hospers HG, et al. Patterns of cytokines, plasma endotoxin, plasminogen activator inhibitor, and
acute-phase proteins during the treatment of severe sepsis in humans. Crit Care Med 1992; 20: 185-192.
[24] Das UN. Lysophosphatidylcholine and -3 fatty acids in sepsis. Adv Sepsis 2004; 3: 121-128.
[25] Das UN. Can critical illness and sepsis be predicted or prognosticated? Adv Sepsis 2006; 5: 52-59.
[26] Das UN. Ethyl pyruvate in sepsis. Adv Sepsis 2007; 6: 10-15. [27] Das UN. Cytokines, NF-kB, activated protein C, oxidized
phospholipids, inducible cyclo-oxygenase eicosanoids, adenosine and insulin in sepsis and septic shock. Crit Care Shock 2003; 6: 40-
49. [28] Das UN. Current advances in sepsis and septic shock with
particular emphasis on the role of insulin. Med Sci Monit 2003; 9: RA181-RA192.
[29] Das UN. Insulin in sepsis and septic shock. J Assoc Physicians India 2003; 51: 695-700.
[30] Belayev L, Busto R, Zhao W, Clemens JA, Ginsberg MD. Effect of delayed albumin hemodilution on infarction volume and brain
edema after transient middle cerebral artery occlusion in rats. J Neurosurg 1997; 87: 595-601.
[31] Belayev L, Zhao W, Pattany PM, et al. Diffusion-weighted magnetic resonance imaging confirms marked neuroprotective
efficacy of albumin therapy in focal cerebral ischemia. Stroke 1998; 29: 2587-2599.
[32] Huh PW, Belayev L, Zhao W, Busto R, Saul I, Ginsberg MD. The effect of high-dose albumin therapy on local cerebral perfusion
after transient focal cerebral ischemia in rats. Brain Res 1998; 804: 105-113.
[33] Belayev L, Liu Y, Zhao W, Busto R, Ginsberg MD. Human albumin therapy of acute ischemic stroke: marked neuroprotective
efficacy at moderate doses and with a broad therapeutic window. Stroke 2001; 32: 553-560.
[34] Remmers M, Schmidt-Kastner R, Belayev L, Lin B, Busto R, Ginsberg MD. Protein extravasation and cellular uptake after high-
dose human-albumin treatment of transient focal cerebral ischemia in rats. Brain Res 1999; 827: 237-242.
[35] Belayev L, Saul I, Huh PW, et al. Neuroprotective effect of high-dose albumin therapy against global ischemic brain injury in rats.
Brain Res 1999; 845: 107-111. [36] Belayev L, Alonso OF, Huh PW, Zhao W, Busto R, Ginsberg MD.
Post-treatment with high-dose albumin reduces histopathological damage and improves neurological deficit following fluid
percussion brain injury in rats. J Neurotrauma 1999; 16: 445-453. [37] Loeb MR. Unexpected effects of absorbed normal rabbit serum and
bovine serum albumin on survival of Haemophilus influenzae type b in the infant rat. Microb Pathog 1988; 4: 9-13.
[38] Gluckman TL, Grossman JE, Folts JD, Kruse-Elliott KT. Modulation of endotoxin-induced cardiopulmonary dysfunction by
S-nitroso-albumin. J Endotoxin Res 2002; 8: 17-26. [39] Powers KA, Kapus A, Khadaroo RG, Marshall JC, Lindsay TF,
Rotstein OD. Twenty-five percent albumin prevents lung injury following shock/resuscitation. Crit Care Med 2003; 31: 2355-2363.
[40] Zhang H, Voglis S, Kim CH, Slutsky AS. Effects of albumin and Ringer's lactate on production of lung cytokines and hydrogen
peroxide after resuscitated hemorrhage and endotoxemia in rats. Crit Care Med 2003; 31: 1515-1522.
[41] Assaly RA, Azizi M, Kennedy DJ, et al. Plasma expansion by polyethylene-glycol-modified albumin. Clin Sci (Lond) 2004; 107:
263-272. [42] Tokunaga C, Bateman RM, Boyd J, Wang Y, Russell JA, Walley
KR. Albumin resuscitation improves ventricular contractility and myocardial tissue oxygenation in rat endotoxemia. Crit Care Med
2007; 35: 1341-1347. [43] Walley KR, McDonald TE, Wang Y, Dai S, Russell JA. Albumin
resuscitation increases cardiomyocyte contractility and decreases nitric oxide synthase II expression in rat endotoxemia. Crit Care
Med 2003; 31: 187-194. [44] Hangai-Hoger N, Nacharaju P, Manjula BN, et al. Microvascular
effects following treatment with polyethylene glycol-albumin in lipopolysaccharide-induced endotoxemia. Crit Care Med 2006; 34:
108-117.
Albumin Infusion Therapy in Stroke, Sepsis and the Critically Ill Current Nutrition & Food Science, 2008, Vol. 4, No. 3 225
[45] Rackow EC, Mecher C, Astiz ME, Griffel M, Falk JL, Weil MH.
Effects of pentastarch and albumin infusion on cardiorespiratory function and coagulation in patients with severe sepsis and systemic
hypoperfusion. Crit Care Me 1989; 17: 394-398. [46] Byrne K, Tatum JL, Henry DA, et al. Increased morbidity with
increased pulmonary albumin flux in sepsis-related adult respiratory distress syndrome. Crit Care Med 1992; 20: 28-34.
[47] Cochran A, Morris SE, Edelman LS, Saffle JR. Burn patient characteristics and outcomes following resuscitation with albumin.
Burns 2007; 33: 25-30. [48] Finfer S, Bellomo R, Boyce N, French J, Myburgh J, Norton R.
SAFE Study Investigators. A comparison of albumin and saline for fluid resuscitation in the intensive care unit. N Engl J Med 2004;
350: 2247-2256. [49] Choi DW. Excitotoxic cell death. J Neurobiol 1992; 23: 1261-1276.
[50] Tymianski M. The central role of calcium ions and calcium-permeable channels in ischemic brain injury. In: Ginsberg MD,
Bogousslavsky J, Eds. Cerebrovascular Disease: Pathophysiology, Diagnosis, and Management. Malden, Mass; Blackwell Science
1998: 371-390. [51] Chan H. Role of oxidants in ischemic brain damage. Stroke 1996;
27: 1124-1129. [52] Feuerstein GZ, Wang X, Barone FC. The role of cytokines in the
neuropathology of stroke and Neurotrauma. Neuroimmuno-modulation 1998; 5: 143-159.
[53] Rodriguez de Turco EB, Belayev L, Liu Y, et al. Systemic fatty acid responses to transient focal cerebral ischemia: influence of
neuroprotective therapy with human albumin. J Neurochem 2002; 83: 515-524.
[54] Bazan NG. Supply of n-3 polyunsaturated fatty acids and their significance in the central nervous system. In: Wurtman RJ,
Wurtman JJ, eds. Nutrition and the Brain. New York; Raven Press; 1990.
[55] Das UN. Essential fatty acids: Biochemistry, physiology, and pathology. Biotechnol J 2006; 1: 420-439.
[56] Das UN. Essential fatty acids- a review. Curr Pharm Biotechnol 2006; 7: 467-482.
[57] Claria J, Serhan CN. Aspirin triggers previously undescribed bioactive eicosanoids by human endothelial cell-leukocyte
interactions. Proc Natl Acad Sci USA 1995; 92: 9475-9479. [58] Chiang N, Gronert K, Clish CB, O’Brien JA, Freeman MW, Serhan
CN. Leukotriene B4 receptor transgenic mice reveal novel protective roles for lipoxins and aspirin-triggered lipoxins in
reperfusion. J Clin Invest 1999; 104: 309-316. [59] Serhan CN, Hong S, Gronert K, et al. Resolvins: A family of
bioactive products of omega-3 fatty acid transformation circuits initiated by aspirin treatment that counter proinflammation signals.
J Exp Med 2002; 196: 1025-1037. [60] Marcheselli VL, Hong S, Lukiw WJ, et al. Novel docosanoids
inhibit brain ischemia-reperfusion-mediated leukocyte infiltration
and pro-inflammatory gene expression. J Biol Chem 2003; 278:
43807-43817. [61] Hong S, Gronert K, Devchand PR, Moussignac RL, Serhan CN.
Novel docosatrienes and 17S-resolvins generated from docosa-hexaenoic acid in murine brain, human blood, and glial cells.
Autacoids in anti-inflammation. J Biol Chem 2003; 278: 14677-14687.
[62] Mukherjee PK, Marcheselli VL, Serhan CN, Bazan NG. Neuroprotectin D1: a docosahexaenoic acid-derived docosatriene
protects human retinal pigment epithelial cells from oxidative stress. Proc Natl Acad Sci USA 2004; 101: 8491-8496.
[63] Gronert K, Maheshwari N, Khan N, Hasan IR, Dunn M, Laniado Schwartzman M. A role for the mouse 12/15-lipoxygenase pathway
in promoting epithelial wound healing and host defense. J Biol Chem 2005; 280: 15267-15278.
[64] Calon F, Lim GP, Yang F, et al. Docosahexaenoic acid protects from dendritic pathology in an Alzheimer’s disease mouse model.
Neuron 2004; 43: 633-645. [65] Lukiw WJ, Cui J-G, Marcheselli VL, et al. A role for
docosahexaenoic acid-derived neuroprotectin D1 in neural cell survival and Alzheimer disease. J Clin Invest 2005; 115: 2774-
2783. [66] Belayev L, Marcheselli VL, Khoutorova L, et al. Docosahexaenoic
acid complexed to albumin elicits high-grade ischemic neuroprotection. Stroke 2005; 36: 118-123.
[67] Das UN. Biological significance of essential fatty acids. J Assoc Physicians India 2006; 54: 309-319.
[68] Akech S, Gwer S, Idro R, et al. Volume expansion with albumin compared to gelofusine in children with severe malaria: result of a
controlled trial. PLoS Clin Trials 2006; 1: e21. [69] He P, Curry FE. Albumin modulation of capillary permeability: role
of endothelial cell [Ca2+]i. Am J Physiol 1993; 265: H74-H82. [70] Koch S, Concha M, Wazzan T, Romano JG, Forteza A. High dose
human serum albumin for the treatment of acute ischemic stroke: A safety study. Neurocrit Care 2004; 1: 335-341.
[71] Osband AJ, Sifri ZC, Wang L, et al. Small volume albumin administration protects against hemorrhagic shock-induced bone
marrow dysfunction. J Trauma 2004; 56: 279-283. [72] Li WQ, Wang XY, Zhu H, et al. Albumin kinetics in patients with
severe sepsis. Zhonghua Wai Ke Za Zhi 2003; 41: 423-426. [73] Ginsberg MD, Hill MD, Palesch YY, Ryckborst KJ, Tamariz D.
The ALIAS Pilot Trial. A dose-escalation study of albumin therapy for acute ischemic stroke-I: physiological response and safety
results. Stroke 2006; 37: 2100-2106. [74] Palesch YY, Hill MD, Ryckborst KJ, Tamariz D, Ginsberg MD.
The ALIAS Pilot Trial. A dose-escalation and safety study of albumin therapy for acute ischemic stroke-II: neurologic outcome
and efficacy analysis. Stroke 2006; 37: 2107-2114.
Received: ???? 11, 2007 Revised: ???? 21, 2007 Accepted: ?????? 15, 2008