potentially avoidable hospital readmissions report and
TRANSCRIPT
Working together to improve health care quality, outcomes, and affordability in Washington State.
Potentially Avoidable Hospital Readmissions
Report and Recommendations
July 2014
Adopted by the Bree Collaborative, July 17th, 2014. Page 1 of 20
Table of Contents
Executive Summary and Recommendations ................................................................................................ 2
Background Information ............................................................................................................................... 3
Dr. Robert Bree Collaborative Background ............................................................................................... 3
Problem Statement ................................................................................................................................... 4
National Hospital Readmissions Data ....................................................................................................... 4
Washington State Hospital Readmissions Data ........................................................................................ 6
Interventions ................................................................................................................................................. 9
State-Wide Readmission Efforts in Washington ..................................................................................... 10
Potentially Avoidable Readmissions Workgroup ........................................................................................ 12
Dissolution .............................................................................................................................................. 12
Reconvening ............................................................................................................................................ 13
Recommendations ...................................................................................................................................... 14
Collaborative Model................................................................................................................................ 14
Tools and Techniques Used in Washington State ................................................................................... 15
Recommended Measurement ................................................................................................................ 16
References .................................................................................................................................................. 19
Appendices:
Appendix A: List of Bree Collaborative Members Appendix B: Potentially Avoidable Readmissions Charter and Roster
Appendix C: Accountable Payment Models Workgroup Background Appendix D: Reconceived Workgroup Roster Appendix E: Washington State Hospital Association’s Reducing Readmissions: Care Transitions Toolkit, Second Edition Appendix F: Qualis Health Community Organization Profile Appendix G: Draft Community Collaborative Charter
Adopted by the Bree Collaborative, July 17th, 2014. Page 2 of 20
Executive Summary and Recommendations
The Robert Bree Collaborative was established in 2011 to provide a forum in which public and private health
care stakeholders can work together to improve quality, health outcomes, and cost-effectiveness of care in
Washington State. Reducing hospital readmissions was identified as a priority for Washington State and the
Bree Collaborative elected to form a workgroup to address the issue. The workgroup met from May 2012 to
September 2012 and reconvened with different membership in April 2014 to develop recommendations.
This report discusses national and Washington State-specific data, the evidence base around interventions
to reduce readmissions, organizations and initiatives in Washington State working to reduce avoidable
hospital readmissions, and recommends three items:
I. Support for the collaborative model as used in Washington State. The Bree Collaborative
recommends that at a minimum, Hospital Readmissions Collaboratives be recognized by the
following three items:
a. Formally writing a charter that includes a list of participating organizations, shared
expectations for best practices, and measures of success.
b. Demonstrating evidence of participation in recurring meetings.
c. Recognition by the Washington State Hospital Association (WSHA) or Qualis Health as an
active member. WSHA or Qualis Health will recognize collaboratives for a period of one year
after which time the organizations will reevaluate their roles.
II. Support for the tools and techniques to reduce readmissions in Washington State, especially the Washington State Hospital Association’s Care Transitions Toolkit, the work done by Qualis Health, and the work done by the Washington Health Alliance. The Bree Collaborative recognizes the consensus work based on best available evidence that went into the Care Transitions Toolkit and recommends that hospitals adopt the Toolkit in its entirety. It is understood that some variation may be appropriate based on clinically compelling reasons.
III. Two hospital-specific measures are recommended: Percent of inpatients with diagnosis of acute myocardial infarction (AMI), heart failure (HF), community acquired pneumonia, chronic obstructive pulmonary disease (COPD), and stroke for which there is: a. Patient discharge information provided to the primary care provider (PCP) or aftercare
provider within three business days of discharge, and b. A documented follow-up phone call after discharge within three business days.
Reducing potentially avoidable hospital readmissions will require multiple strategies on the part of all
community stakeholders. This report represents a first step toward reducing readmissions.
Adopted by the Bree Collaborative, July 17th, 2014. Page 3 of 20
Background Information
Dr. Robert Bree Collaborative Background
The Robert Bree Collaborative was established in 2011 by Washington State House Bill 1311 “…to provide a
mechanism through which public and private health care stakeholders can work together to improve quality,
health outcomes, and cost effectiveness of care in Washington State.” The Bree Collaborative was modeled
after the Washington State Advanced Imaging Management (AIM) project and named in memory of Dr.
Robert Bree, a pioneer in the imaging field and a key member of the AIM project.
Members are appointed by the Washington State Governor and include public health care purchasers for
Washington State, private health care purchasers (employers and union trusts), health plans, physicians and
other health care providers, hospitals, and quality improvement organizations. The Bree Collaborative is
charged with identifying up to three health care services annually that have substantial variation in practice
patterns, high utilization trends in Washington State, or patient safety issues. For each health care service,
the Bree Collaborative identifies and recommends best-practice evidence-based approaches that build upon
existing efforts and quality improvement activities aimed at decreasing variation.a See Appendix A for a list
of current Bree Collaborative members.
Recommendations are then sent to the Washington State Health Care Authority for review and approval.
The Health Care Authority oversees Washington State’s largest health care purchasers, Medicaid and the
Public Employees Benefits Board Program, as well as other programs. The HCA uses the recommendations
to guide state purchasing for these programs. The Bree Collaborative also strives to develop
recommendations to improve patient health, health care service quality, and the affordability of health care
for the private sector but does not have the authority to mandate implementation of recommendations.
For more information about the Bree Collaborative, please visit: www.breecollaborative.org.
a In the bill, the legislature does not authorize agreements among competing health care providers or health carriers as to the price or specific level of reimbursement for health care services. Furthermore, it is not the intent of the legislature to mandate payment or coverage decisions by private health care purchasers or carriers.

Adopted by the Bree Collaborative, July 17th, 2014. Page 4 of 20
Problem Statement Avoidable hospital readmissions are common and costly events, negatively impacting patients’ health and wellbeing. The estimated national cost for unplanned Medicare hospital readmissions was $17.4 billion in 2004.1 Unplanned and potentially avoidable hospital readmissions are a complex problem with multiple influences. Readmissions are reflective of a local health care system’s ability to coordinate care for patients across settings and are often a sign of inadequate discharge planning, lack of coordination with community-based care, and lack of follow-up with patients.2 Additional drivers of poor transitions from the hospital to the community are lack of information transfer, especially across-settings to the primary care provider (e.g., delays, inaccuracies, missing information), lack of standard and known processes at the hospital (e.g., patient discharge, hand-over, internal work flow), poor communication between provider and patient (e.g., understanding medications), and lack of patient and family activation (e.g., health literacy, self-management skills and tools, motivation, locus of control).3,4,5 Individual and neighborhood socioeconomic status, income inequality, as well as low education, being older, and being unmarried have been found to be associated with higher readmission rates.6,7,8,9 Studies have also shown that some patients may preferentially seek care in the hospital rather than the primary care setting and therefore are more likely to be readmitted.10 Poor transitions between health care settings (e.g., hospital, skilled nursing facility, home) can lead to adverse events post discharge, which can be common.11,12 One study found that 49% of discharged patients experienced at least one medical error and were then 6.2 times more likely to be rehospitalized within three months of discharge.13 While not all hospital readmissions are preventable, reducing readmission rates through greater community collaboration among diverse stakeholders, implementation of standard processes within the hospital, and better communication between the hospital and community health care providers and the hospital, patients, and family represents a great opportunity to improve health care quality, patient health outcomes, and the affordability of health care in Washington State.
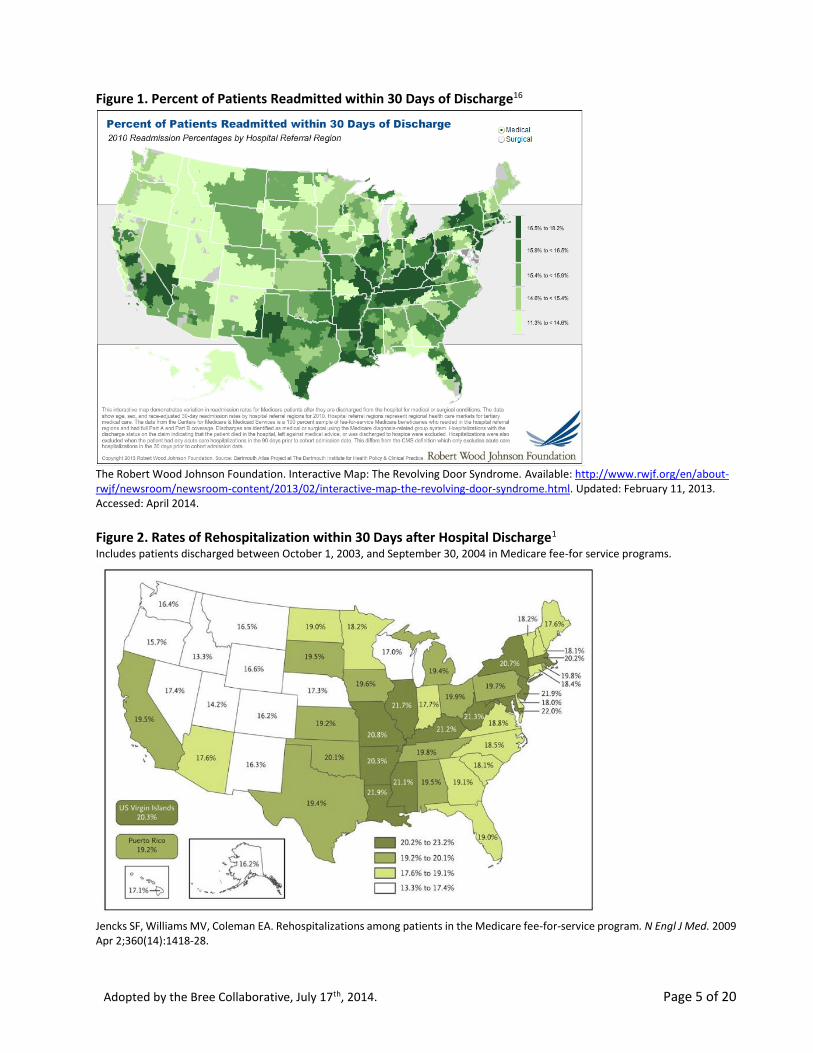
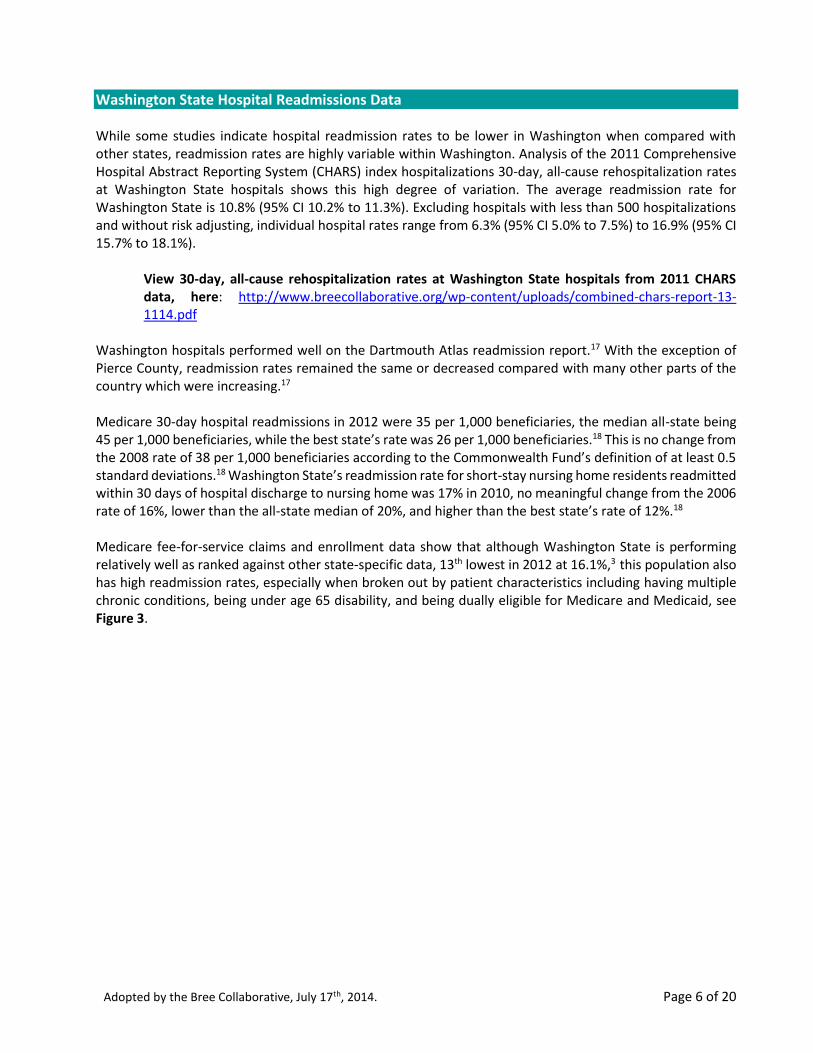
National Hospital Readmissions Data Hospital readmissions vary widely between and within states, see Figure 1, and Figure 2 for Medicare-specific rates. This variation is at least partially attributable to characteristics of the community in which the hospital is located rather than individual hospital characteristics, indicating the importance of community engagement in any intervention meant to reduce hospital readmissions.14 Analysis of 30-day all-payer hospital readmissions shows high rates for more complicated but less frequent procedures (e.g., kidney transplants and ileostomy or other enterostomy, both at 29.1%).15 Hospital readmissions rates for more common procedures such as amputation of lower extremity are 22.8%, debridement of a wound, infection or burn at 19.1%, and heart valve procedures at 18.5%.15 The 2011 Dartmouth Atlas Report found that little progress has been made in reducing 30-day readmission rates from 2004-2009 despite significant effort and identified a link between high hospital utilization and readmission rates, Figure 1.16 For many parts of the country, rates are increasing, indicating an opportunity to improve patient care, outcomes, and lower costs.
Adopted by the Bree Collaborative, July 17th, 2014. Page 5 of 20
Figure 1. Percent of Patients Readmitted within 30 Days of Discharge16
The Robert Wood Johnson Foundation. Interactive Map: The Revolving Door Syndrome. Available: http://www.rwjf.org/en/about-rwjf/newsroom/newsroom-content/2013/02/interactive-map-the-revolving-door-syndrome.html. Updated: February 11, 2013. Accessed: April 2014.
Figure 2. Rates of Rehospitalization within 30 Days after Hospital Discharge1 Includes patients discharged between October 1, 2003, and September 30, 2004 in Medicare fee-for service programs.
Jencks SF, Williams MV, Coleman EA. Rehospitalizations among patients in the Medicare fee-for-service program. N Engl J Med. 2009 Apr 2;360(14):1418-28.
Adopted by the Bree Collaborative, July 17th, 2014. Page 6 of 20
Washington State Hospital Readmissions Data While some studies indicate hospital readmission rates to be lower in Washington when compared with other states, readmission rates are highly variable within Washington. Analysis of the 2011 Comprehensive Hospital Abstract Reporting System (CHARS) index hospitalizations 30-day, all-cause rehospitalization rates at Washington State hospitals shows this high degree of variation. The average readmission rate for Washington State is 10.8% (95% CI 10.2% to 11.3%). Excluding hospitals with less than 500 hospitalizations and without risk adjusting, individual hospital rates range from 6.3% (95% CI 5.0% to 7.5%) to 16.9% (95% CI 15.7% to 18.1%).
View 30-day, all-cause rehospitalization rates at Washington State hospitals from 2011 CHARS data, here: http://www.breecollaborative.org/wp-content/uploads/combined-chars-report-13-1114.pdf
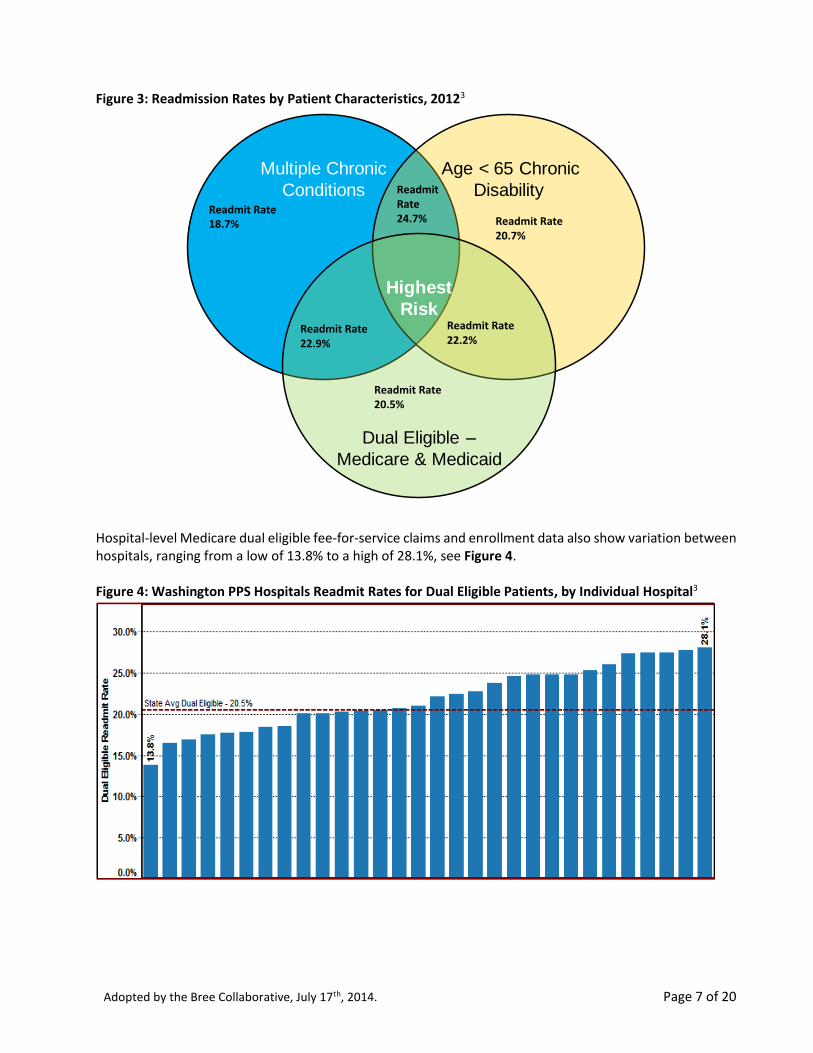
Washington hospitals performed well on the Dartmouth Atlas readmission report.17 With the exception of Pierce County, readmission rates remained the same or decreased compared with many other parts of the country which were increasing.17 Medicare 30-day hospital readmissions in 2012 were 35 per 1,000 beneficiaries, the median all-state being 45 per 1,000 beneficiaries, while the best state’s rate was 26 per 1,000 beneficiaries.18 This is no change from the 2008 rate of 38 per 1,000 beneficiaries according to the Commonwealth Fund’s definition of at least 0.5 standard deviations.18 Washington State’s readmission rate for short-stay nursing home residents readmitted within 30 days of hospital discharge to nursing home was 17% in 2010, no meaningful change from the 2006 rate of 16%, lower than the all-state median of 20%, and higher than the best state’s rate of 12%.18 Medicare fee-for-service claims and enrollment data show that although Washington State is performing relatively well as ranked against other state-specific data, 13th lowest in 2012 at 16.1%,3 this population also has high readmission rates, especially when broken out by patient characteristics including having multiple chronic conditions, being under age 65 disability, and being dually eligible for Medicare and Medicaid, see Figure 3.
Adopted by the Bree Collaborative, July 17th, 2014. Page 7 of 20
Figure 3: Readmission Rates by Patient Characteristics, 20123
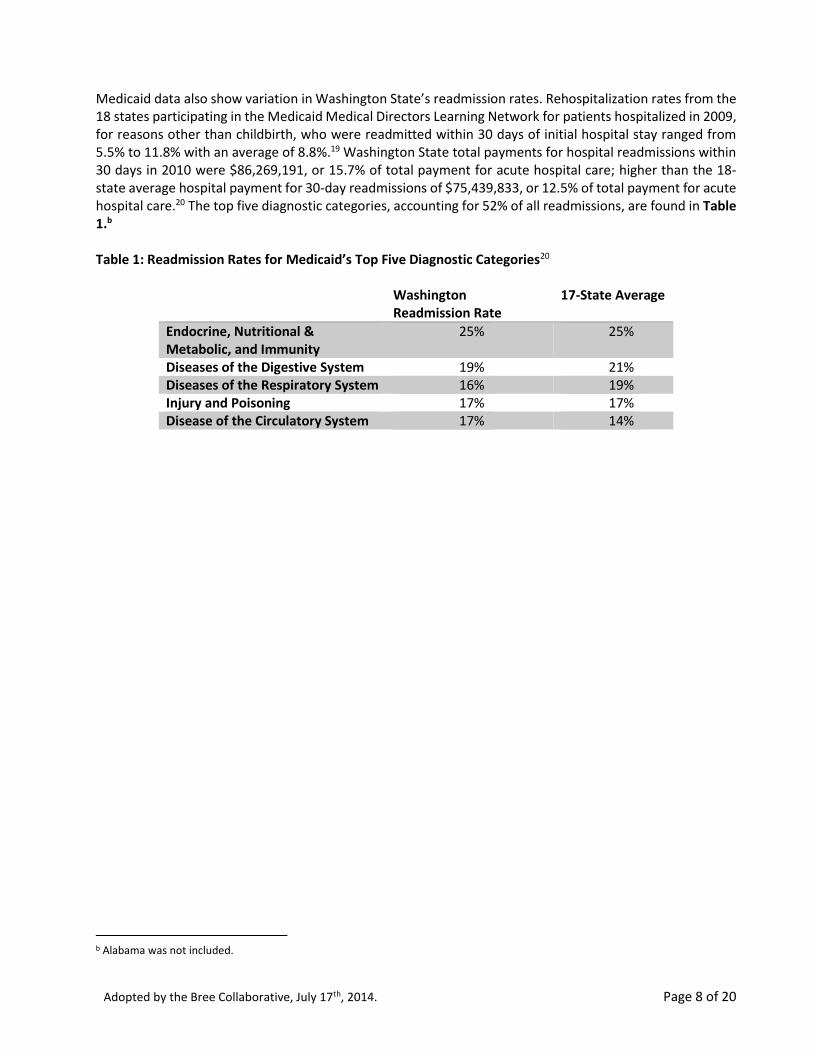
Hospital-level Medicare dual eligible fee-for-service claims and enrollment data also show variation between hospitals, ranging from a low of 13.8% to a high of 28.1%, see Figure 4. Figure 4: Washington PPS Hospitals Readmit Rates for Dual Eligible Patients, by Individual Hospital3
Multiple Chronic
Conditions
Age < 65 Chronic
Disability
Highest
Risk
Dual Eligible –
Medicare & Medicaid
Readmit Rate 20.7%
Readmit Rate 22.2%
Readmit Rate 20.5%
Readmit Rate 24.7%
Readmit Rate 22.9%
Readmit Rate 18.7%
Adopted by the Bree Collaborative, July 17th, 2014. Page 8 of 20
Medicaid data also show variation in Washington State’s readmission rates. Rehospitalization rates from the 18 states participating in the Medicaid Medical Directors Learning Network for patients hospitalized in 2009, for reasons other than childbirth, who were readmitted within 30 days of initial hospital stay ranged from 5.5% to 11.8% with an average of 8.8%.19 Washington State total payments for hospital readmissions within 30 days in 2010 were $86,269,191, or 15.7% of total payment for acute hospital care; higher than the 18-state average hospital payment for 30-day readmissions of $75,439,833, or 12.5% of total payment for acute hospital care.20 The top five diagnostic categories, accounting for 52% of all readmissions, are found in Table 1.b Table 1: Readmission Rates for Medicaid’s Top Five Diagnostic Categories20
Washington Readmission Rate
17-State Average
Endocrine, Nutritional & Metabolic, and Immunity
25%
25%
Diseases of the Digestive System 19%
21%
Diseases of the Respiratory System 16%
19%
Injury and Poisoning 17%
17%
Disease of the Circulatory System 17%
14%
b Alabama was not included.
Adopted by the Bree Collaborative, July 17th, 2014. Page 9 of 20
Interventions Interventions across the United States to reduce hospital readmission rates have found success through multi-faceted approaches, the majority of which focus on facilitated care during the transition from the hospital to community or other care setting, patient education and self-management, patient management by a multidisciplinary team, and end of life planning.21 Many include a combination of coordinating discharge plans with community providers, educating patients, reconciling medication, following-up with individual patients, and comparing data across project sites.22 Project Re-Engineered Hospital Discharge (RED), which utilizes nurse discharge advocates to administer the in-hospital component of the program and a clinical pharmacist to call participants two to four days post discharge, saw hospital utilization within 30 days decrease by about 30% in the intervention group.23 The Better Outcomes for Older Adults through Safe Transitions (BOOST) includes mentoring between sites, team development, patient teach-back, and written discharge instructions.22,24 Implementation of the BOOST program in 11 hospitals resulted in a relative rehospitalization reduction of 13.6%.25 The Care Transitions intervention includes medication self-management, patient understanding of the medical record, recommending a primary care visit post discharge, and educating the patient about red flags (e.g., condition is worsening).26 The program resulted in lower rehospitalization rates in control patients (8.3% vs 11.9%) 30 days post-discharge.26 The Interventions to Reduce Acute Care Transfers (INTERACT) quality improvement program which focuses on reducing nursing home resident hospitalization through managing patient conditions proactively within the nursing home has also been successful in reducing hospitalizations, indicating the potential for impact from within community care facilities.27,28 In Washington State, the Reducing Readmissions Care Transitions Toolkit (the Toolkit), second edition, was developed by the Washington State Hospital Association (WSHA) with the support of a multitude of other community organizations. The Toolkit includes learnings from community projects to reduce hospital readmissions and is intended as a resource for hospitals and primary care providers. WSHA conducted a pilot program to test components of the Toolkit in Pierce County from August 2012 to September 2013 in seven hospitals.29 Data from WSHA’s validation of the Toolkit are shown in Table 2. Selected practices tested components of the toolkit, including:
Admit notification to the patient’s primary care provider. All of the notifications occurred via Epic inbasket to the primary care providers affiliated with the system. If the notification is incorrect, the clinic responds to the hospital and the hospital corrects the information in the system.
Discharge summary: Outpatient clinics can access case management discharge summaries and risk assessment score.
Follow-up appointments: Follow-up appointments with the primary care provider are made for all of the intensive and high-risk patients prior to the patient leaving the hospital.
Follow-up phone calls: Follow-up phone calls with the patient that are prioritized based on risk.
Risk for readmission assessment.
Adopted by the Bree Collaborative, July 17th, 2014. Page 10 of 20
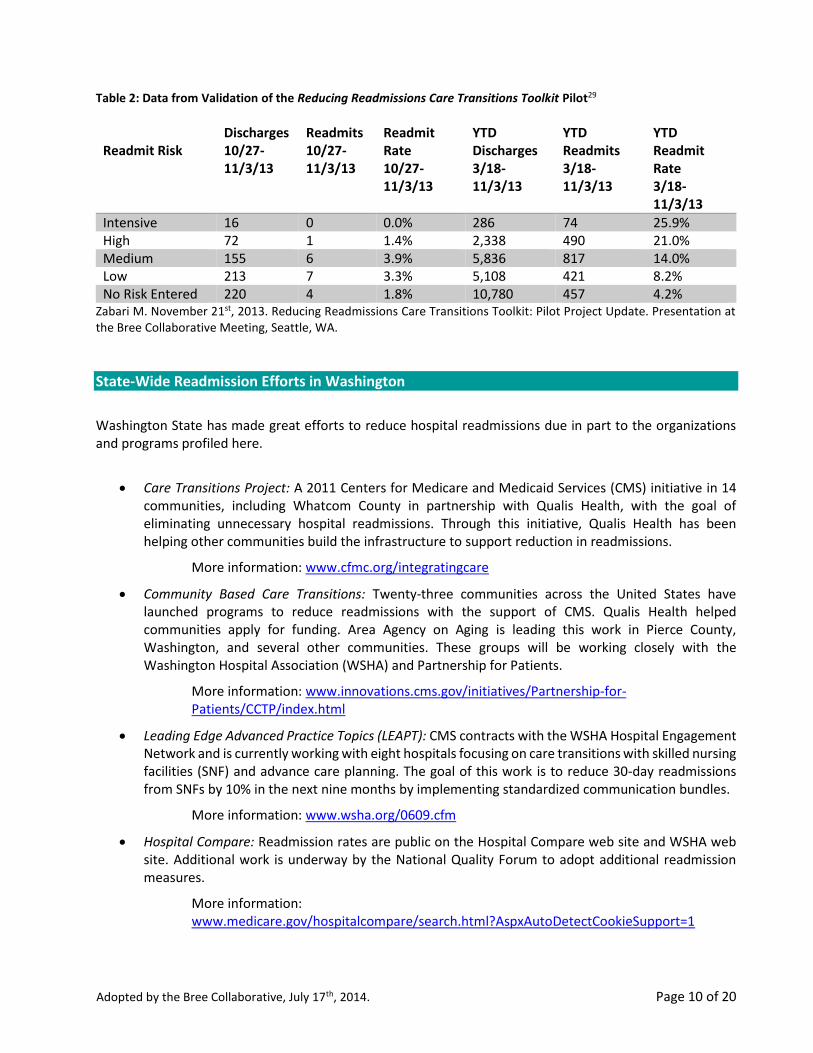
Table 2: Data from Validation of the Reducing Readmissions Care Transitions Toolkit Pilot29
Readmit Risk
Discharges 10/27-11/3/13
Readmits 10/27-11/3/13
Readmit Rate 10/27-11/3/13
YTD Discharges 3/18-11/3/13
YTD Readmits 3/18-11/3/13
YTD Readmit Rate 3/18-11/3/13
Intensive 16 0 0.0% 286 74 25.9% High 72 1 1.4% 2,338 490 21.0% Medium 155 6 3.9% 5,836 817 14.0% Low 213 7 3.3% 5,108 421 8.2% No Risk Entered 220 4 1.8% 10,780 457 4.2%
Zabari M. November 21st, 2013. Reducing Readmissions Care Transitions Toolkit: Pilot Project Update. Presentation at the Bree Collaborative Meeting, Seattle, WA.
State-Wide Readmission Efforts in Washington
Washington State has made great efforts to reduce hospital readmissions due in part to the organizations and programs profiled here.
Care Transitions Project: A 2011 Centers for Medicare and Medicaid Services (CMS) initiative in 14 communities, including Whatcom County in partnership with Qualis Health, with the goal of eliminating unnecessary hospital readmissions. Through this initiative, Qualis Health has been helping other communities build the infrastructure to support reduction in readmissions.
More information: www.cfmc.org/integratingcare
Community Based Care Transitions: Twenty-three communities across the United States have launched programs to reduce readmissions with the support of CMS. Qualis Health helped communities apply for funding. Area Agency on Aging is leading this work in Pierce County, Washington, and several other communities. These groups will be working closely with the Washington Hospital Association (WSHA) and Partnership for Patients.
More information: www.innovations.cms.gov/initiatives/Partnership-for-Patients/CCTP/index.html
Leading Edge Advanced Practice Topics (LEAPT): CMS contracts with the WSHA Hospital Engagement Network and is currently working with eight hospitals focusing on care transitions with skilled nursing facilities (SNF) and advance care planning. The goal of this work is to reduce 30-day readmissions from SNFs by 10% in the next nine months by implementing standardized communication bundles.
More information: www.wsha.org/0609.cfm
Hospital Compare: Readmission rates are public on the Hospital Compare web site and WSHA web site. Additional work is underway by the National Quality Forum to adopt additional readmission measures.
More information: www.medicare.gov/hospitalcompare/search.html?AspxAutoDetectCookieSupport=1
Adopted by the Bree Collaborative, July 17th, 2014. Page 11 of 20
Medicaid Medical Directors Learning Network. A program led by the Agency for Healthcare Research and Quality is focused on sharing best practices nationally since 2005. Learning communities allow State Medicaid medical directors to learn from one another, share data, and implement quality improvement projects.
More information: www.ahrq.gov/policymakers/measurement/quality-by-state/mmdln.html
Partnership for Patients: A Centers for Medicare and Medicaid Services initiative targeting preventable injuries and hospital-acquired conditions in ten areas including readmission. In 2011, WSHA, the Washington State Medical Association (WSMA), and the Washington Health Alliance have convened three community groups in Pierce, Spokane, and Yakima as pilot sites designed to test care transition practices. The learnings from these groups has been used to develop the WSHA Care Transitions Toolkit. New community groups recently started in Seattle, WA and Vancouver, WA. This collaboration has been a contributor in a 23% reduction in readmissions per 1000 Medicare beneficiary.
More information: www.wsha.org/partnershipforpatients.cfm
State Action on Avoidable Rehospitalization (STAAR) Project: The Institute for Healthcare Improvement's STAAR project goal is to reduce rehospitalization rates by 30% and improve patient satisfaction with care coordination. Four states, Washington, Michigan, Ohio, and Massachusetts, were selected. WSHA is the lead in Washington State, focusing on coordinating discharge process and creating landmark reports in collaboration with Qualis Health to inform improvement work. These efforts have involved providers from across setting and purchases through the state-wide steering committee. Early results from the program are promising.30
More Information: www.ihi.org/Engage/Initiatives/Completed/STAAR/Pages/Materials.aspx
State Demonstrations to Integrate Care for Dual Eligible Individuals: Washington State Department of Health is working to design new approaches to better integrate care for dual eligible patients as part of a CMS funded 15 state pilot program.
More information: www.cms.gov/medicare-medicaid-coordination/04_StateDemonstrationstoIntegrateCareforDualEligibleIndividuals.asp
Washington State Rehospitalization Steering Committee: A statewide committee, assembled by WSHA, consisting of payers, providers from settings along the continuum, state agencies, and other stakeholders, is meeting to improve and coordinate work between organizations working in this area. The core focus is alignment of payment incentives, data and analysis, and improvement including smooth transitions.
Adopted by the Bree Collaborative, July 17th, 2014. Page 12 of 20
Potentially Avoidable Readmissions Workgroup The Bree Collaborative approved the Potentially Avoidable Readmissions (PAR) workgroup charter in May 2012. See Appendix B for the original PAR workgroup charter and roster. The workgroup met from May to September 2012 and identified three strategies:
1. Alignment with Local Readmissions Activities: Identify alignment opportunities where the Collaborative can promote and augment current evidence-based, quality improvement initiatives aimed at reducing PARs including effective communication, coordination of care, and ‘patient hand-offs’ during transitions in care settings.
2. Measurement, Transparency, and Reporting: Support use of current process and outcome measures for reducing PARs and transparency of methodologies and readmissions rates, by hospital and physician group, in a semi-public manner.
3. Accountable Payment Model: Research and recommend components and structures essential to creating a successful PAR accountable payment model that aligns incentives, including warranty pricing, bundled payments, and other innovative payment methodologies. See Appendix C for a summary of the Accountable Payment Models Workgroup.
Dissolution By September 2013, four of the nine original members, including the Chair, left the Bree Collaborative or no longer served on the workgroup. Replacement members were not identified and no Bree Collaborative members volunteered to serve as the new workgroup chair. This substantially decreased the effectiveness of the workgroup causing the PAR to meet only twice in 2013. In this time, the workgroup made two recommendations approved by Collaborative members:
1. Endorsing WSHA and its community partners’ work to develop a standardized toolkit and process that both hospitals and community providers can use to reduce the rate of readmissions.
2. Requesting that 30-day, all-cause readmission results, by hospital, be publicly available.
The Washington Health Alliance hosted a meeting in July 2013 to review hospital-specific, unblinded 30-day, all-cause readmissions CHARS data, purchased by the Foundation for Health Care Quality from the Washington State Department of Health. Bree Collaborative staff hired a statistician to conduct analysis. The Bree Collaborative elected to add sample sizes and confidence intervals to the charts before further distribution and approved posting a final version of the unblinded, hospital-specific data on the Bree Collaborative website on September 25th, 2013.
View 30-day, all-cause rehospitalization rates at Washington State hospitals from 2011 CHARS data, here: www.breecollaborative.org/wp-content/uploads/combined-chars-report-13-1114.pdf.
Additionally, the Accountable Payment Models workgroup posted blinded CHARS readmissions data following total knee and total hip replacement surgery. Hospitals can request unblinded information for their institution by contacting Bree Collaborative staff at [email protected].
Adopted by the Bree Collaborative, July 17th, 2014. Page 13 of 20
View blinded readmission rates for total knee and total hip replacement procedures in Washington State, from 2011 CHARS data, here: www.breecollaborative.org/wp-content/uploads/bree_summary_CHARS_Analysis.pdf.
In May 2013, the PAR workgroup reported a hiatus and a plan to wait for the WSHA toolkit to be finalized and pilot results to be known before supporting operationalization and development of incentives to encourage standardized implementation of the toolkit across Washington State. The PAR workgroup was dissolved at the November 21st, 2013 meeting with unanimous support of Bree Collaborative members. Rick Goss, MD, medical director at Harborview Medical Center and Bree Collaborative member, volunteered as PAR champion to work with Bree Collaborative staff to identify potential opportunities for the Bree Collaborative to support WSHA’s toolkit and pilots and the work done by Qualis Health.
Reconvening The PAR workgroup was reconvened after the March 19th, 2014 Bree Collaborative meeting and met in April and June 2014, chaired by Dr. Goss. See Appendix D for a list of reconvened members. The workgroup voted to recommend three primary items:
I. Support for the collaborative model as used in Washington State.
II. Support for the tools and techniques to reduce readmissions in Washington State, especially the Washington State Hospital Association’s Care Transitions Toolkit, second edition (Appendix E), the work done by Qualis Health (Appendix F), and the work done by the Washington Health Alliance.
III. Two hospital-specific measures are recommended: Percent of inpatients with diagnosis of acute myocardial infarction (AMI), heart failure (HF), community acquired pneumonia, chronic obstructive pulmonary disease (COPD), and stroke for which there is: a. Patient discharge information provided to the primary care provider (PCP) or aftercare
provider within three business days of discharge, and b. A documented follow-up phone call after discharge within three business days.
Adopted by the Bree Collaborative, July 17th, 2014. Page 14 of 20
Recommendations
These recommendations represent a first step for our community working together to reduce potentially
avoidable hospital readmissions. The workgroup recognizes that additional tools and techniques (e.g.,
behavioral health interventions, home health, structured medication reconciliation, quality improvement
and follow-up around hospital acquired infections) could also greatly impact readmissions but are currently
out of the scope of this report.
Collaborative Model Groups collaborate to reach common goals, in the case of reducing potentially avoidable hospital readmissions, the goal is to improve safety during transitions through learning from different facilities and optimally using collective knowledge. Individual members of any one collaborative may be different from site to site and may include many different community stakeholders such as hospitals, skilled nursing facilities, organizations representing patients or individual patient representatives, home health, primary care, and others.
In the case that Hospital Readmissions Collaboratives wish to build upon their work in a more formalized and systematic way, the Bree Collaborative suggests that groups work to follow the Institute for Healthcare Improvement’s (IHI) collaborative model as defined in the Breakthrough Series: IHI’s Collaborative Model for Achieving Breakthrough Improvement. Collaboratives are defined as including the following elements:31
Choosing an area of interest through use of data, examination of an evidence base, and stakeholder analysis.
Recruiting technical experts to identify and review suggested changes and metrics.
Recruiting organizations and/or teams with pre-work calls that include buy-in from organizational leadership. The pre-work calls should clarify expectations, the collaborative’s process, create aim statements, and determine goals.
Learning sessions, traditionally face-to-face, during which the teams submit data, learn from one another, and learn how to test and implement a change package with specific, actionable, testable changes associated with each topic, (e.g., increasing patient activation/engagement as a change concept, using teach back as a suggested change). Suggestions for optimal learning sessions are as follows:
o Three learning sessions with an optional fourth “outcomes congress.”
The Bree Collaborative recommends that at a minimum, Hospital Readmissions Collaboratives be recognized by the following three items:
1. Formally writing a charter, see appendix G for a draft charter, that includes a list of participating organizations, shared expectations for best practices, and measures of success.
2. Demonstrating evidence of participation in recurring meetings. 3. Recognition by WSHA or Qualis Health as an active member. WSHA or Qualis Health will
recognize collaboratives for a period of one year after which time the organizations will reevaluate their roles.
Adopted by the Bree Collaborative, July 17th, 2014. Page 15 of 20
o The first and second learning sessions are about eight weeks apart, second – third three months apart; an outcomes congress often three – six months after learning session three and includes a standard agenda.
o Learning sessions are often a whole day in length. o The standard learning session agenda includes review of progress on measures, change
concept overview by the collaborative chair (a technical expert); all-teach, all-learn presentations by teams, storyboard review, “team time” in which teams sit together to plan next plan-do-study-act (PDSA) cycles, and quality improvement concept review (e.g., MFI, PDSA, metrics, spread/sustainability).
o Specific roles for faculty members at each learning session (e.g., system leader, collaborative chair, day-to-day leader, metrics support, administrative support).
Action periods between learning sessions in which the teams test, implement, and collect data. Optimally, reports of the data are generated monthly that also includes summary of the PDSA cycles and case studies of what has worked exceptionally well at particular sites. There may also be phone calls, webinars, or peer site visits between learning sessions.
The IHI recommends the Model for Improvement, an approach for organizing improvement work that includes four components:31
o Specific, measurable aims, o Tracking measures for improvement over time, o Changes to the system or process to result in improvement, and o Multiple testing cycles.
Tools and Techniques Used in Washington State The Bree Collaborative acknowledges the work of the Washington State Hospital Association to develop, disseminate, and support the Care Transitions Toolkit (the Toolkit); Qualis Health’s data reports and technical assistance; and the Washington Health Alliance’s work to increase data transparency to reduce potentially avoidable hospital readmissions and supports the continuation of this work.
Washington State Hospital Association The Washington State Hospital Association (WSHA) is a membership organization representing hospitals and other health-related organizations.32 WSHA has many programs, including the Patient Safety program that works with hospitals to adopt evidence-based protocols to improve safety and increase quality. The Care Transitions Toolkit, second edition, can be found here: www.wsha.org/files/177/CareTransitions_Toolkit_Version2_Feb%2024%202014_Final.pdf
More information: www.wsha.org
The Bree Collaborative recognizes the consensus work based on best available evidence that went into the Care Transitions Toolkit and recommends that hospitals adopt the Toolkit in its entirety. It is understood that some variation may be appropriate based on clinically compelling reasons.
Adopted by the Bree Collaborative, July 17th, 2014. Page 16 of 20
Qualis Health Qualis Health has been working to reduce avoidable hospital readmissions through care transitions quality improvement since 2008 with community engagement as an area of focus. Qualis Health provides quarterly data reports at the community, hospital, skilled nursing facility, and home health agency level. Data is used as a prompt to do further local analysis, identify risk, and other quality improvement activities. Qualis Health then facilitates community building and engages in direct one-to-one technical assistance (e.g., teach-back, INTERACT). More information: www.qualishealth.org Washington Health Alliance The Washington Health Alliance (the Alliance) works to share data on health care quality and value in Washington State to help providers, patients, employers and union trusts make informed decisions about health care.33 The Alliance is part of the Robert Wood Johnson Foundation’s Aligning Forces for Quality initiative, disseminates the annual Community Checkup report that “highlights health care quality and value at medical groups and hospitals in Washington State,” and is part of the Choosing Wisely campaign.
More information: www.wahealthalliance.org More information: www.wacommunitycheckup.org More information: http://oyh.wacommunitycheckup.org/choosingwisely/
Recommended Measurement The Bree Collaborative recognizes that many factors contribute to potentially avoidable hospital readmissions, including community factors and individual patient socioeconomic factors, and recommends two hospital specific measures as a first step toward a state-wide impact in reducing hospital readmissions.
Applies to adult and pediatric hospitals. Medical patients were selected for this measure as they are the patients where there are the highest readmission rates. The five conditions were selected to align with the Medicaid Quality Incentive Program to reduce the reporting burden for individual hospitals. Three business days was selected. As an example, a patient discharged on Thursday should have the discharge information and follow-up phone call completed by the next Tuesday. See the ICD-9 population eligibility grid, here: www.wsha.org/files/318/MQI_Readmissions_Eligible_Population_UpdatedJuly2014.pdf
Two hospital-specific measures are recommended: Percent of inpatients with diagnosis of acute myocardial infarction (AMI), heart failure (HF), community acquired pneumonia, chronic obstructive pulmonary disease (COPD), and stroke for which there is:
Patient discharge information provided to the primary care provider (PCP) or aftercare provider within three business days of discharge, and
A documented follow-up phone call after discharge within three business days.
Adopted by the Bree Collaborative, July 17th, 2014. Page 17 of 20
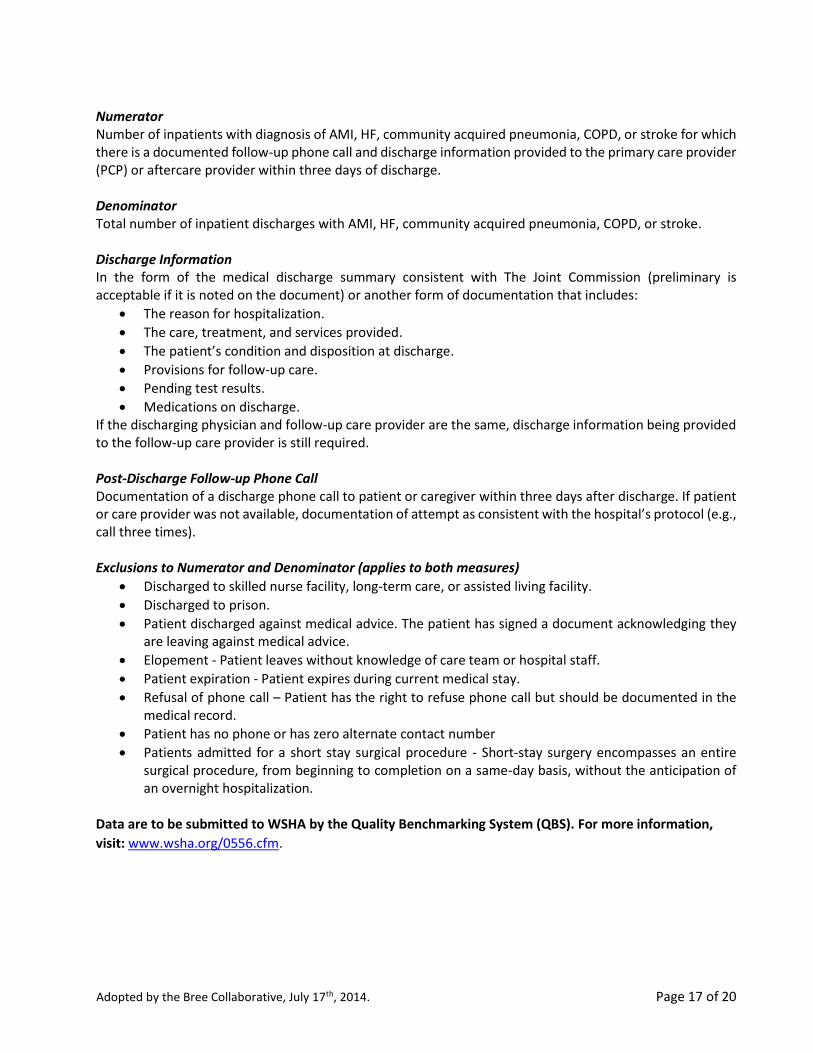
Numerator Number of inpatients with diagnosis of AMI, HF, community acquired pneumonia, COPD, or stroke for which there is a documented follow-up phone call and discharge information provided to the primary care provider (PCP) or aftercare provider within three days of discharge. Denominator Total number of inpatient discharges with AMI, HF, community acquired pneumonia, COPD, or stroke. Discharge Information In the form of the medical discharge summary consistent with The Joint Commission (preliminary is acceptable if it is noted on the document) or another form of documentation that includes:
The reason for hospitalization.
The care, treatment, and services provided.
The patient’s condition and disposition at discharge.
Provisions for follow-up care.
Pending test results.
Medications on discharge. If the discharging physician and follow-up care provider are the same, discharge information being provided to the follow-up care provider is still required.
Post-Discharge Follow-up Phone Call Documentation of a discharge phone call to patient or caregiver within three days after discharge. If patient or care provider was not available, documentation of attempt as consistent with the hospital’s protocol (e.g., call three times). Exclusions to Numerator and Denominator (applies to both measures)
Discharged to skilled nurse facility, long-term care, or assisted living facility.
Discharged to prison.
Patient discharged against medical advice. The patient has signed a document acknowledging they are leaving against medical advice.
Elopement - Patient leaves without knowledge of care team or hospital staff.
Patient expiration - Patient expires during current medical stay.
Refusal of phone call – Patient has the right to refuse phone call but should be documented in the medical record.
Patient has no phone or has zero alternate contact number
Patients admitted for a short stay surgical procedure - Short-stay surgery encompasses an entire surgical procedure, from beginning to completion on a same-day basis, without the anticipation of an overnight hospitalization.
Data are to be submitted to WSHA by the Quality Benchmarking System (QBS). For more information,
visit: www.wsha.org/0556.cfm.

Adopted by the Bree Collaborative, July 17th, 2014. Page 18 of 20
The timeline of implementation will be as follows:
Ramp up period – July 1st – July 31st, 2014. Step 1 – Hospital will begin submission of monthly data to WSHA on August 1st, 2014. Submission of monthly data is in alignment with data collection already underway.
Step 2 – Hospitals will have the opportunity to test the measures and employ methods for improvement between August 1st and December 31st, 2014.
Step 3 – In 2015, the readmission measurement process will be evaluated for ongoing value and impact on care improvement. Determination will be made what data or measures will be reported and shared on the WSHA public website. The process, measures, and data will be reviewed again after a year to evaluate the value to continue the project.
Adopted by the Bree Collaborative, July 17th, 2014. Page 19 of 20
References
1 Jencks SF, Williams MV, Coleman EA. Rehospitalizations among patients in the Medicare fee-for-service program. N Engl J Med. 2009 Apr 2;360(14):1418-28.
2 Goodman DC, Fisher ES, Chang CH, The Dartmouth Institute for Health Policy and Clinical Practice. After Hospitalization: A Dartmouth Atlas Report on Post-Acute Care for Medicare Beneficiaries. Available: www.dartmouthatlas.org/downloads/reports/Post_discharge_events_092811.pdf. Accessed: April 2014.
3 Eloranta S. Care Transitions Update. April 23, 2014. Presentation at the Potentially Avoidable Hospital Readmissions Workgroup, Seattle, WA.
4 Kripalani S, Jackson AT, Schnipper JL, Coleman EA. Promoting effective transitions of care at hospital discharge: a review of key issues for hospitalists. J Hosp Med. 2007 Sep;2(5):314-23.
5 Kripalani S, LeFevre F, Phillips CO, Williams MV, Basaviah P, Baker DW. Deficits in communication and information transfer between hospital-based and primary care physicians: implications for patient safety and continuity of care. JAMA. 2007 Feb 28;297(8):831-41.
6 Hu J, Gonsahn MD, Nerenz DR. Socioeconomic status and readmissions: evidence from an urban teaching hospital.
Health Aff (Millwood). 2014 May;33(5):778-85. 7 Lindenauer PK1, Lagu T, Rothberg MB, Avrunin J, Pekow PS, Wang Y, Krumholz HM. Income inequality and 30 day
outcomes after acute myocardial infarction, heart failure, and pneumonia:retrospective cohort study. BMJ. 2013
Feb 14;346:f521.
8 Arbaje AI1, Wolff JL, Yu Q, Powe NR, Anderson GF, Boult C. Postdischarge environmental and socioeconomic factors
and the likelihood of early hospital readmission among community-dwelling Medicare beneficiaries.
Gerontologist. 2008 Aug;48(4):495-504.
9 Foraker RE1, Rose KM, Suchindran CM, Chang PP, McNeill AM, Rosamond WD. Socioeconomic status, Medicaid
coverage, clinical comorbidity, and rehospitalization or death after an incident heart failure hospitalization:
Atherosclerosis Risk in Communities cohort (1987 to 2004). Circ Heart Fail. 2011 May;4(3):308-16.
10 Kangovi S1, Barg FK, Carter T, Long JA, Shannon R, Grande D. Understanding why patients of low socioeconomic
status prefer hospitals over ambulatory care. Health Aff (Millwood). 2013 Jul;32(7):1196-203. 11 Forster AJ, Clark HD, Menard A, Dupuis N, Chernish R, Chandok N, Khan A, van Walraven C. Adverse events among
medical patients after discharge from hospital. CMAJ. 2004 Feb 3;170(3):345-9.
12 Forster AJ, Murff HJ, Peterson JF, Gandhi TK, Bates DW. The incidence and severity of adverse events affecting patients after discharge from the hospital. Ann Intern Med. 2003 Feb 4;138(3):161-7.
13 Moore C, Wisnivesky J, Williams S, McGinn T. Medical errors related to discontinuity of care from an inpatient to an outpatient setting. J Gen Intern Med. 2003 Aug;18(8):646-51.
14 Herrin J, St Andre J, Kenward K, Joshi MS, Audet AM, Hines SC. Community Factors and Hospital Readmission Rates. Health Serv Res. 2014 Apr 9.
15 Agency for Healthcare Research and Quality. Readmissions to US Hospitals by Procedure, 2010. Statistical Brief #154. Health Care Cost and Utilization Project. Available: http://www.hcup-us.ahrq.gov/reports/statbriefs/sb154.pdf. Accessed: June 2014.
16 The Robert Wood Johnson Foundation. Interactive Map: The Revolving Door Syndrome. Available: http://www.rwjf.org/en/about-rwjf/newsroom/newsroom-content/2013/02/interactive-map-the-revolving-door-syndrome.html. Updated: February 11, 2013. Accessed: April 2014.
Adopted by the Bree Collaborative, July 17th, 2014. Page 20 of 20
17 Washington State Hospital Association. Flashpoint Details: Consumer Reports, Dartmouth Atlas Release
Readmission Data. Available: www.wsha.org/flashpointDetails.cfm?EID=2011-09-28%2000%3A00%3A00%2E0. Updated: September 28, 2011. Accessed: April 2013.
18 Radley DC, McCarthy D, Lippa JA, Hayes SL, Schoen C. Aiming Higher: Results from a Scorecard on State Health System Performance, 2014. The Commonwealth Fund. May 2014. Available: www.commonwealthfund.org/Publications/Fund-Reports/2014/Apr/2014-State-Scorecard.aspx.
19 Medicaid Medical Directors Learning Network. Hospital Readmissions 18-State Summary. Available: www.hca.wa.gov/medicaid/ebm/Documents/eru_ahrq_mmdln_states.pdf. Accessed: May 2014.
20 Medicaid Medical Directors Learning Network. Hospital Readmission Washington. Available: www.hca.wa.gov/medicaid/ebm/Documents/eru_ahrq_mmdln_wa.pdf. Accessed: May 2014.
21 Boutwell A, Hwu S. Effective Interventions to Reduce Rehospitalizations: A Survey of the Published Evidence. Cambridge, Massachusetts: Institute for Healthcare Improvement; 2009.
22 Enderlin CA, McLeskey N, Rooker JL, Steinhauser C, D'Avolio D, Gusewelle R, Ennen KA. Review of current conceptual models and frameworks to guide transitions of care in older adults. Geriatr Nurs. 2013 Jan-Feb;34(1):47-52.
23 Jack BW, Chetty VK, Anthony D, Greenwald JL, Sanchez GM, Johnson AE, Forsythe SR, O'Donnell JK, Paasche-Orlow MK, Manasseh C, Martin S, Culpepper L. A reengineered hospital discharge program to decrease rehospitalization: a randomized trial. Ann Intern Med. 2009 Feb 3;150(3):178-87.
24 Society of Hospital Medicine. BOOST Fact Sheet: Improving the Care of Patients as They Transition from Hospital to Home. Available: www.hospitalmedicine.org/ResourceRoomRedesign/RR_CareTransitions/PDFs/Project_BOOST_Fact_SheetFinal.pdf. Accessed: May 2014.
25 Hansen LO, Greenwald JL, Budnitz T, Howell E, Halasyamani L, Maynard G, Vidyarthi A, Coleman EA, Williams MV. Project BOOST: effectiveness of a multihospital effort to reduce rehospitalization. J Hosp Med. 2013 Aug;8(8):421-7.
26 Coleman EA, Parry C, Chalmers S, Min SJ. The care transitions intervention: results of a randomized controlled trial. Arch Intern Med. 2006 Sep 25;166(17):1822-8.
27 Ouslander JG1, Lamb G, Tappen R, Herndon L, Diaz S, Roos BA, Grabowski DC, Bonner A. Interventions to reduce hospitalizations from nursing homes: evaluation of the INTERACT II collaborative quality improvement project. J Am Geriatr Soc. 2011 Apr;59(4):745-53.
28 Ouslander JG1, Lamb G, Perloe M, Givens JH, Kluge L, Rutland T, Atherly A, Saliba D. Potentially avoidable hospitalizations of nursing home residents: frequency, causes, and costs. J Am Geriatr Soc. 2010 Apr;58(4):627-35.
29 Zabari M. November 21st, 2013. Reducing Readmissions Care Transitions Toolkit: Pilot Project Update. Presentation at the Bree Collaborative Meeting, Seattle, WA.
30 Boutwell AE, Johnson MB, Rutherford P, Watson SR, Vecchioni N, Auerbach BS, Griswold P, Noga P, Wagner C. An early look at a four-state initiative to reduce avoidable hospital readmissions. Health Aff (Millwood). 2011 Jul;30(7):1272-80.
31 The Breakthrough Series: IHI’s Collaborative Model for Achieving Breakthrough Improvement. IHI Innovation Series white paper. Boston: Institute for Healthcare Improvement; 2003.
32 Washington State Hospital Association. About WSHA. Available: www.wsha.org/aboutWSHA.cfm. Accessed: May 2014.
33 Washington Health Alliance. About Us. Available: wahealthalliance.org/about-us/. Accessed: May 2014.
Appendix A: Bree Collaborative Members
Member Title Organization
Roki Chauhan MD Senior Vice President & Chief Medical Officer
Premera Blue Cross
Susie Dade MS Deputy Director Washington Health Alliance Gary Franklin MD, MPH Medical Director Washington State Department of
Labor and Industries Stuart Freed MD Medical Director Wenatchee Valley Medical Center Tom Fritz Chief Executive Officer Inland Northwest Health Services,
Spokane Joe Gifford MD Chief Executive, ACO of
Washington
Providence Health and Services
Richard Goss MD Medical Director Harborview Medical Center – University of Washington
Steve Hill (Chair) Retired Previously Director, Department of Retirement Systems, and Chair, Puget Sound Health Alliance
Christopher Kodama MD Medical Vice President, Clinical Operations
MultiCare Health System
MaryAnne Lindeblad RN, MPH
Director, Medicaid Program Health Care Authority
Greg Marchand Director, Benefits & Policy and Strategy
The Boeing Company
Robert Mecklenburg MD Medical Director, Center for Health Care Solutions
Virginia Mason Medical Center
Carl Olden MD Family Physician Pacific Crest Family Medicine, Yakima Mary Kay O’Neill MD, MBA
Executive Medical Director Regence Blue Shield
John Robinson MD, SM Chief Medical Officer First Choice Health Terry Rogers MD (Vice Chair)
Chief Executive Officer Foundation for Health Care Quality
Jeanne Rupert DO, PhD Director of Medical Education Skagit Valley Hospital Kerry Schaefer Strategic Planner for Employee
Health King County
Bruce Smith MD Associate Medical Director, Strategy Deployment
Group Health Physicians
Lani Spencer RN, MHA Vice President, Health Care Management Services
Amerigroup
Jay Tihinen Assistant Vice President Benefits Costco Wholesale Carol Wagner RN, MBA Senior Vice President for Patient
Safety The Washington State Hospital Association
Shawn West MD Family Physician Edmonds Family Medicine
Appendix Page 1 of 13
Appendix B: Potentially Avoidable Readmissions Charter and Roster
(Updated 10/26/12)
Problem Statement
Potentially avoidable readmissions (PARs) are common and costly events. It is estimated that nationally, the cost for unplanned or PARs in 2004 was $17.4 billion. The PAR rate is increasingly seen as a reflection of a local health care system’s ability or inability to coordinate care for patients across the health care continuum, and a high PAR rate is often a sign of inadequate discharge planning during transitions of care. Reducing PAR is an opportunity to improve quality and reduce health care costs in Washington State.
Aim
To reduce the number of potentially avoidable readmissions in Washington State.
Purpose
The purpose of the PAR workgroup is to propose recommendations to the full Bree Collaborative on how to reduce PARs within the following three general strategies identified by the Bree Collaborative:
1. Alignment with local readmissions activities. Identify alignment opportunities where the BreeCollaborative can promote and augment current evidence-based, quality improvement initiativesaimed at reducing PARs, including effective communication, coordination of care and ‘patient hand-offs’ during transitions in care settings.
2. Measurement, Transparency, and Reporting. Support use of current process and outcome measuresfor reducing PARs and transparency of methodologies and readmissions rates, by hospital andphysician group, in a semi-public manner.*
3. Accountable Payment Model. Research and recommend components and structures essential tocreating a successful PAR accountable payment model that aligns incentives, including warrantypricing, bundled payments, and other innovative payment methodologies.
Duties & Functions
The PAR workgroup shall:
Report directly to the Bree Collaborative; present recommendations in a report.
Provide updates at Bree Collaborative meetings.
Research national and regional readmissions quality improvement initiatives and strategies thatbetter align incentives, reduce costs, and improve quality of care.
Consult members of WSHA, WSMA, other stakeholder organizations and subject matter experts forfeedback.
Create and oversee subsequent subgroups to help carry out the work.
Appendix Page 2 of 13

Post recommendations on the Bree Collaborative website for public comment prior to sending tothe Bree Collaborative for approval and adoption.
* Semi-public refers to the direct sharing of results with provider organizations, purchasers of healthcare (employers, union trusts), health plans and other health-related organizations directly working on these initiatives. It does not include posting results to a public website or other distribution vehicles that result in the information being broadly shared with the general public.
Structure
The PAR workgroup will consist of individuals appointed by the chair of the Bree Collaborative, and confirmed by the Bree Collaborative steering committee. Individuals must have in-depth knowledge and expertise in at least one of the following: readmissions, payment reform, the health care delivery system, benefit design, and quality improvement. There must be at least one representative from each stakeholder group: employer, health plan, hospital, provider (including a specialist), and quality improvement organization.
The chair of the PAR workgroup will be appointed by the chair of the Bree Collaborative.
The Bree Collaborative project manager will staff and provide management and support services for the PAR workgroup.
Less than the full PAR workgroup may convene to: gather and discuss information; conduct research; analyze relevant issues and facts or draft recommendations for the deliberation of the full workgroup. A quorum shall be a simple majority and shall be required to accept and approve recommendations to the Bree Collaborative.
Meetings
The PAR workgroup will hold meetings as necessary.
The PAR workgroup chair will conduct meetings and arrange for the recording of each meeting, and will distribute meeting agendas and other materials prior to each meeting.
Appendix Page 3 of 13
PAR Workgroup Roster
Name Title Organization
Susie Dade Deputy Director Puget Sound Health Alliance Sharon Eldoranta, MD Medical Director, Quality and
Safety Initiatives Qualis Health
Joe Gifford, MD Chief Strategy and Innovation Officer for Western Washington
Providence Health and Services
Mary Gregg, MD Director, Quality and Patient Safety Swedish Health Services Tony Haftel, MD VP Quality & Associate Chief
Medical Officer Franciscan Health Systems
Bob Mecklenburg, MD Medical Director, Center for Health Care Solutions
Virginia Mason Medical Center
Kerry Schaefer Strategic Planner for Employee Health
King County
Peter Valenzuela, MD Medical Director PeaceHealth Medical Group Committee Staff Steve Hill Chair Bree Collaborative Rachel Quinn Project Manager Bree Collaborative
Appendix Page 4 of 13
Appendix C: Accountable Payment Models Workgroup Background
In November 2012, the Collaborative formed an Accountable Payment Model (APM) subgroup to make recommendations to the PAR workgroup in the third focus area, research and recommend components and structures essential to creating a successful PAR accountable payment model that aligns incentives, including warranty pricing, bundled payments, and other innovative payment methodologies. The APM workgroup started by creating an accountable payment model for total knee and hip replacements (TKR/THR) surgery. The model is an attempt to align purchasing and payment with best practices that lead to safe care, better outcomes, and lower costs. The final products will serve as a guide for quality- and value-based purchasing for both public and private sectors. The surgical bundle defines the expected components of pre-operative, intra-operative, and post-operative care needed for successful TKR/THR surgery. It includes both clinical components (disability due to osteoarthritis despite conservative therapy, fitness for surgery, repair of the osteoarthritic joint, and post-operative care and return to function) and quality standards. The Bree Collaborative formally adopted the TKR/THR surgical bundle at the November 21st, 2013 meeting.
Read the TKR/THR Surgical Bundle: www.breecollaborative.org/wp-content/uploads/tkrthr_bundle.pdf
The TKR/THR warranty defines complications and time-frames after surgery during which complications should be attributed to the original surgery. The purpose of the warranty is to track clinical and financial accountability for the extra care needed to diagnose, manage, and resolve those complications. The intent is to distribute financial risk across professional and facility components in proportion to the revenue generated by the procedure. The warranty was formally adopted by the Bree Collaborative at the July 18th, 2013 meeting.
Read the TKR/THR Warranty Model: www.breecollaborative.org/wp-content/uploads/bree_warranty_tkr_thr.pdf
Both the TKR/THR surgical bundle and warranty were approved by the Health Care Authority Director in April 2014.
Read the letter: www.breecollaborative.org/wp-content/uploads/hca_letter_accepting_spine_tkrthr.pdf
At the November 21st, 2013 Bree Collaborative meeting, the APM subgroup was promoted to a workgroup and encouraged to continue work beyond the total knee and total hip replacement topic.
Appendix Page 5 of 13
Appendix D: Reconvened Roster
Name Title Organization
Rick Goss, MD, MPH (Chair)
Medical Director Harborview Medical Center
Sharon Eloranta, MD Medical Director, Quality and Safety Initiatives
Qualis Health
Stuart Freed, MD Medical Director Wenatchee Valley Medical Center Leah Hole-Marshall, JD Medical Administrator Washington State Department of Labor
and Industries Dan Lessler, MD, MHA Medical Director Washington State Health Care
Authority Bob Mecklenburg, MD Medical Director, Center for Health
Care Solutions Virginia Mason Medical Center
Amber Theel, RN, MBA, CPHQ
Director, Patient Safety Practices Washington State Hospital Association
Committee Staff Ginny Weir Program Director Bree Collaborative, Foundation for
Health Care Quality
Appendix Page 6 of 13
Appendix E: Washington State Hospital Association’s Reducing Readmissions: Care Transitions Toolkit,
Second Edition
Due to size issues this document has been posted separately. The document is available:
Here: www.breecollaborative.org/wp-content/uploads/Appendix-C-WSHA-Toolkit.pdf
OR
Here: www.wsha.org/files/177/CareTransitions_Toolkit_Version2_Feb%2024%202014_Final.pdf
Appendix Page 7 of 13
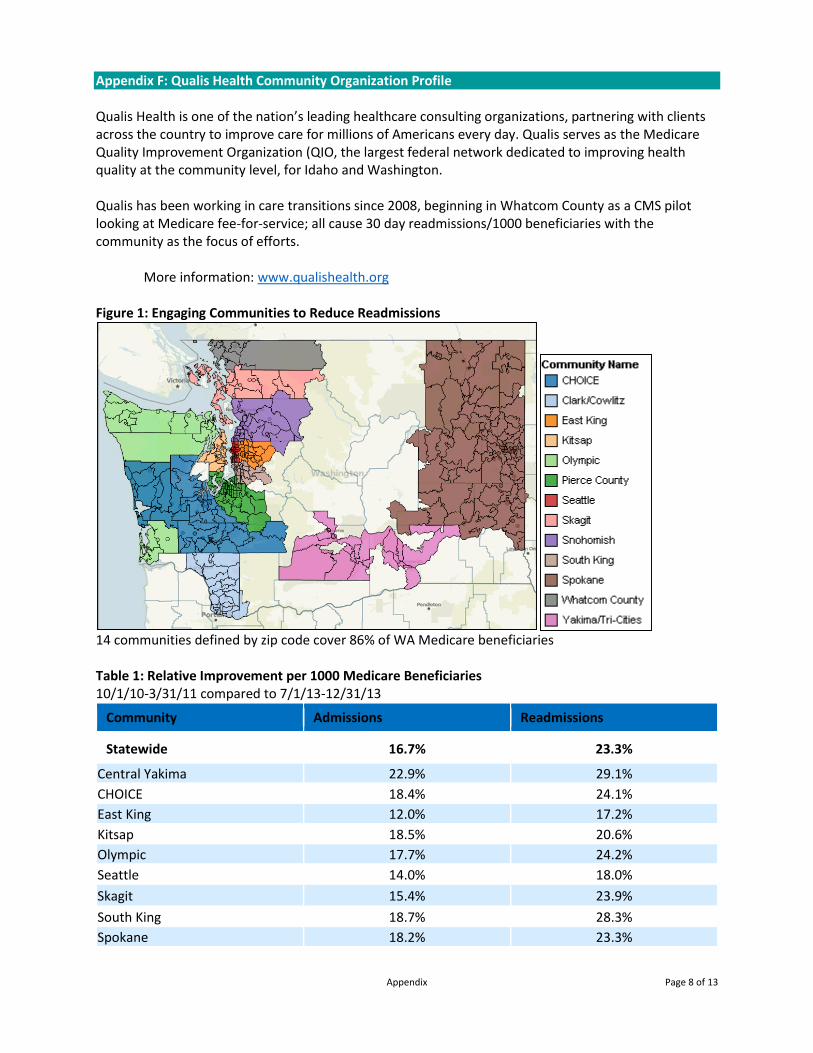
Appendix F: Qualis Health Community Organization Profile Qualis Health is one of the nation’s leading healthcare consulting organizations, partnering with clients across the country to improve care for millions of Americans every day. Qualis serves as the Medicare Quality Improvement Organization (QIO, the largest federal network dedicated to improving health quality at the community level, for Idaho and Washington. Qualis has been working in care transitions since 2008, beginning in Whatcom County as a CMS pilot looking at Medicare fee-for-service; all cause 30 day readmissions/1000 beneficiaries with the community as the focus of efforts. More information: www.qualishealth.org Figure 1: Engaging Communities to Reduce Readmissions
14 communities defined by zip code cover 86% of WA Medicare beneficiaries Table 1: Relative Improvement per 1000 Medicare Beneficiaries 10/1/10-3/31/11 compared to 7/1/13-12/31/13
Community Admissions Readmissions
Statewide 16.7% 23.3%
Central Yakima 22.9% 29.1% CHOICE 18.4% 24.1% East King 12.0% 17.2% Kitsap 18.5% 20.6% Olympic 17.7% 24.2% Seattle 14.0% 18.0% Skagit 15.4% 23.9% South King 18.7% 28.3% Spokane 18.2% 23.3%
Appendix Page 8 of 13
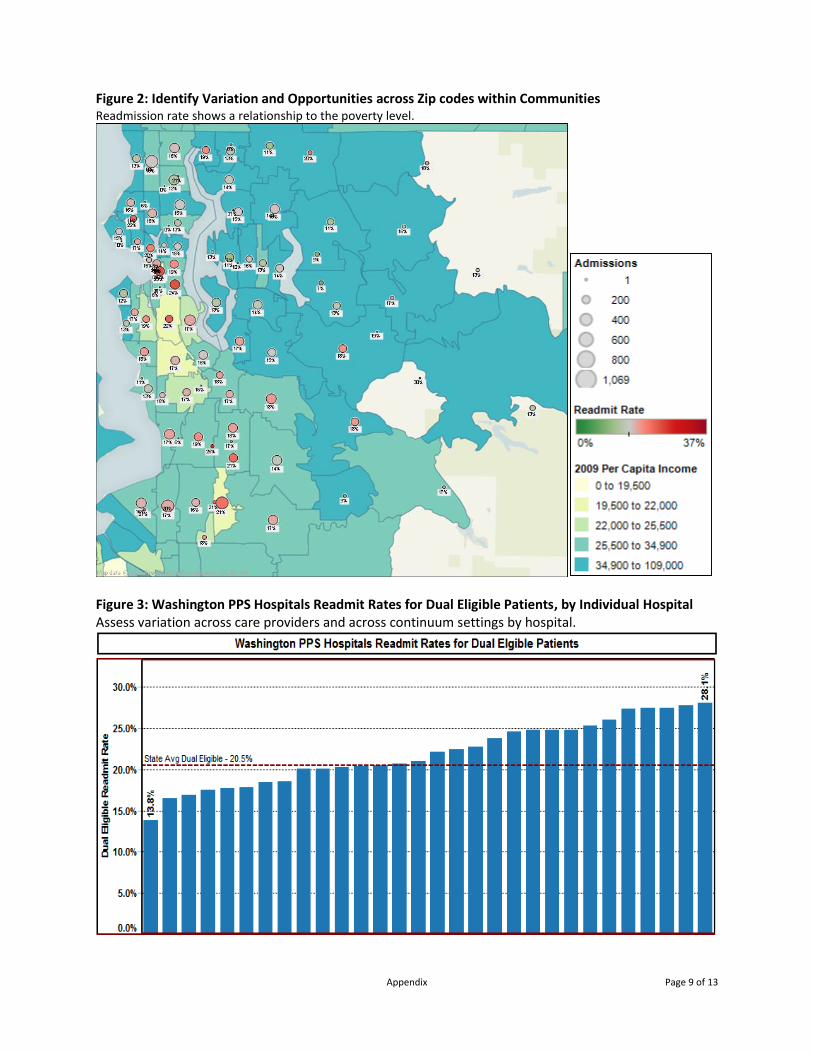
Figure 2: Identify Variation and Opportunities across Zip codes within Communities Readmission rate shows a relationship to the poverty level.
Figure 3: Washington PPS Hospitals Readmit Rates for Dual Eligible Patients, by Individual Hospital Assess variation across care providers and across continuum settings by hospital.
Appendix Page 9 of 13
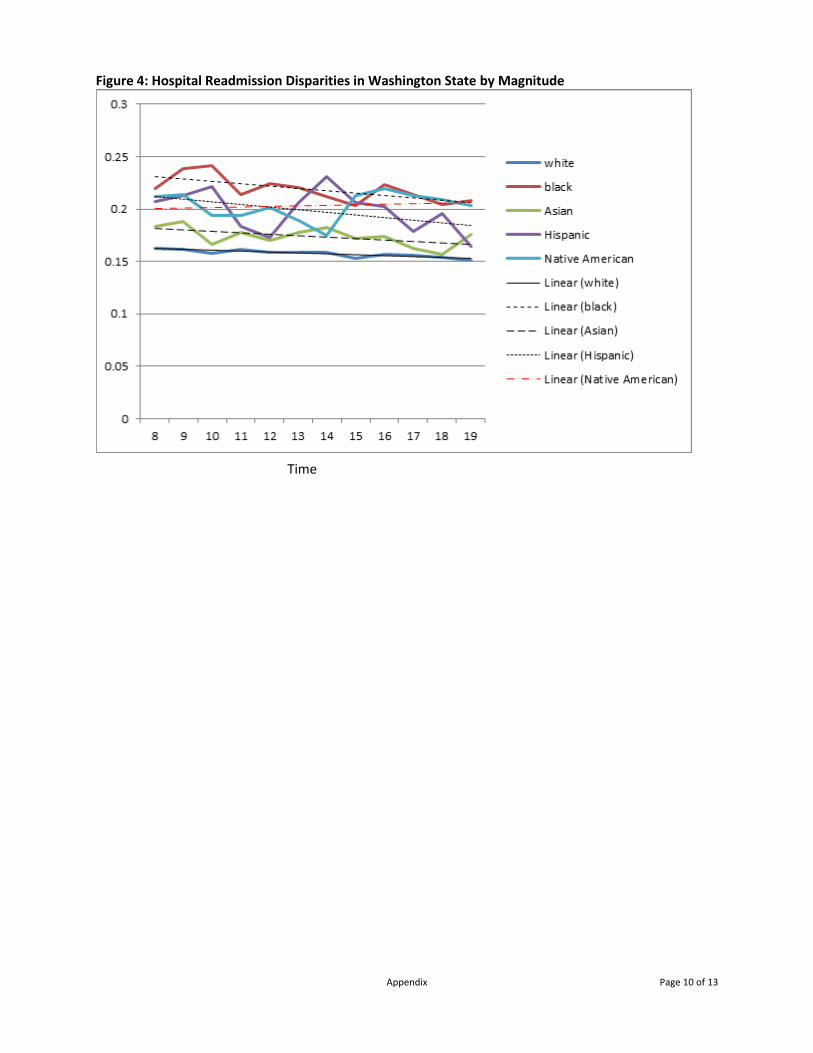
Figure 4: Hospital Readmission Disparities in Washington State by Magnitude
Time
Appendix Page 10 of 13
Community Coalition Charter(Template – please adjust as needed for your community)
(10th SOW Section C.8.1.C.2.b) Article I – Name
The name of this Coalition shall be [name].
Article II – Mission & Vision
The mission of the [Coalition Name] is…
The coalition will… [Include commitment to reduce 30 day readmission rates by 20% over three years & consider adding a statement about whether the community intends to apply for a formal care transitions program]
Article III – Purpose
Examples: 1. To build and sustain a community coalition with a focus on improving transitions of care for
Medicare beneficiaries 2. To be a vehicle for the patient and family voice3. To encourage person-centered and person-directed models of care4. To collaborate and encourage efforts of organizations with shared visions5. To advance public policies that further the vision
Article IV – Participation
Section I – Collaboration Participation in the [Coalition Name] is open to organizations and individuals interested in fostering the vision by actively engaging in the planning and work of the Coalition.
Charter members should join in a commitment to: • Share best practices and knowledge• Mentor partners and providers• Share data and support analyses• Promote implementation of evidence-based interventions
Participant categories may include: • Healthcare Providers (hospitals, skilled nursing facilities, physician practices, home health
agencies, dialysis facilities, hospice organizations, palliative care organizations, etc.) • Provider Associations• Consumer Advocacy Organizations• Government Organizations (Health department, Area Agency on Aging, etc.)• Quality Improvement Organizations• Educational Organizations• Professionals• Consumers• Funding Organizations• Academics
Appendix G: Draft Community Collaborative Charter
Appendix Page 11 of 13
Section II – Coalition Participant Responsibilities
Meeting Attendance. Coalition Members agree to attend in person or by teleconference a minimum of fifty (50) percent of scheduled meetings each year with not more than two (2) consecutive unexcused absences.
Committees. Coalition Members agree to actively participate in committee work, and are expected to volunteer their services for Coalition projects.
Article V – Committees
Section 1. The activities of the Coalition will take place within its committees and all Active Participants are expected to select the committee or committees on which they wish to serve during any given year.
Section 2. The standing committees of the Coalition are [list committees]. Other Task Forces may be formed on an ad hoc basis as needed.
Section 3. Committees are chaired by Active Participants, chosen by the Coalition.
Section 4. The term of service for the committee chairs shall be one year. In the event a chair cannot complete a term, the Coalition shall appoint a replacement to complete the term of office.
Section 5. No member shall hold more than one committee chairmanship at a time.
Article VI – Meetings
Section 1. Annual Meeting There shall be an Annual Meeting of the Coalition, at which time the Coalition will review membership, committee reports, develop annual goals, and other business.
Section 2. Regular Meetings Meetings of the Coalition shall be held at least quarterly. Meetings may take place in person or remotely.
Article VII –Procedural Policies
Section 1. Conflicts No one may profit financially from membership in the Coalition by sales or solicitation at meetings or workshops. Participants will disclose any actual or potential conflicts of interest to QIO or other designee.
Section 2. Decision Making In the spirit of the [Coalition Name] vision, all Coalition business shall be conducted based on the philosophy of mutual respect. Simple majority rules will apply. Coalition Participants are entitled to one vote per member.
Section 3. Voting Voting on the business of the Coalition may be conducted by those in attendance at the meeting either in person or by teleconference. Proxy voting via email is permissible.
Appendix Page 12 of 13
Signatures [please revise as needed for your community]:
________________________________ ________________________________
________________________________ ________________________________
________________________________ ________________________________
________________________________ ________________________________
________________________________ ________________________________
________________________________ ________________________________
________________________________ ________________________________
________________________________ ________________________________
________________________________ ________________________________
________________________________ ________________________________
________________________________ ________________________________
________________________________ ________________________________
________________________________ ________________________________
________________________________ ________________________________
________________________________ ________________________________
________________________________ ________________________________
Appendix Page 13 of 13