poststroke fatigue—a review
TRANSCRIPT

928 Journal of Pain and Symptom Management Vol. 38 No. 6 December 2009
Review Article
Poststroke FatiguedA ReviewAnners Lerdal, RN, PhD, Linda N. Bakken, RN, MSc,Siren E. Kouwenhoven, RN, MPhil, Gunn Pedersen, RN, Marit Kirkevold, RN,PhD, Arnstein Finset, Cand Psychol, PhD (C), and Hesook S. Kim, RN, PhDDepartment of Health Sciences (A.L., L.N.B., S.E.K., G.P., H.S.K.), Buskerud University College,
Drammen; Research Center (A.L.), Oslo University HospitaldAker, Oslo; Institute of Nursing Science
and Health Sciences (M.K.) and Department of Behavioral Medicine (A.F.), University of Oslo, Oslo,
Norway; and Institute of Public Health (M.K.), Aarhus University, Arhus, Denmark
Abstract
Although fatigue is a common complaint after stroke, relatively little is known about howpoststroke fatigue is experienced and what its related factors are. An in-depth understandingis necessary to develop effective and patient-centered poststroke rehabilitation programs. Thisreview was undertaken to provide a comprehensive synthesis of knowledge from the literatureconcerning the description, definition, and measurement of fatigue and its relationship tosociodemographic and clinical factors. A search in PubMed, CINAHL, EMBASE, andPsychInfo was performed using ‘‘stroke’’ or ‘‘cerebrovascular accident’’ as medical subjectheadings in combination with ‘‘fatigue’’ as a key word. Descriptions of fatigue revealedmultiple dimensions of the phenomenon. Although no specific theoretical definition of fatigueas a poststroke condition was found, a case definition has recently been published to be usedas a tool to determine the presence of fatigue in poststroke patients. Poststroke fatigue is mostfrequently measured by using the general fatigue scales such as the Fatigue Severity Scale anda Fatigue Visual Analogue Scale, as there is no scale developed to measure poststroke fatiguespecifically. Age, sex, living conditions, and personality were associated with poststrokefatigue, albeit with some conflicting findings. Conflicting results also were found in therelationships between fatigue and stroke-related characteristics such as stroke location/type,the number of strokes, and neurological deficits. There is an indication that prestroke andpoststroke fatigue are related. Possible antecedent components identified are personal factors,biomarkers, stroke characteristics, prestroke fatigue, and comorbidity. As knowledge regardingpoststroke fatigue remains limited, there is a need to continue empirical research with varioustheoretical orientations. J Pain Symptom Manage 2009;38:928e949. � 2009 U.S.Cancer Pain Relief Committee. Published by Elsevier Inc. All rights reserved.Key Words
Fatigue, stroke, review, etiology, rehabilitationThis project is funded by the Research Council ofNorway (RCN) for 2006e2010. Dr. A. Lerdal has re-ceived funding from the RCN (Grant 19256), theNorwegian Nurses Organization, and the U.S.-Nor-way Fulbright Foundation. This paper is a productstemming from the research project Post-Stroke Fa-tigue for which Dr. H. S. Kim is the project director
and Drs. Grethe Eilertsen, A. Lerdal, and HeidiOrmstad are the principal researchers.
Address correspondence to: Anners Lerdal, RN, PhD,Department of Health Sciences, BuskerudUniversity College, P.O.B. 7053, 3007 Drammen,Norway, E-mail: [email protected]
Accepted for publication: April 9, 2009.
� 2009 U.S. Cancer Pain Relief CommitteePublished by Elsevier Inc. All rights reserved.
0885-3924/09/$esee front matterdoi:10.1016/j.jpainsymman.2009.04.028

Vol. 38 No. 6 December 2009 929Poststroke Fatigue
IntroductionStroke is the third most common cause of
death in the world and the most frequentcause of disability in elderly people. Early mo-bilization and rehabilitation after the strokeare important strategies when trying to preventpermanent disability and help patients attainthe best possible level of functioning and qual-ity of life. Despite fatigue being one of themost common complaints after stroke, rela-tively little is known about how fatigue is expe-rienced after stroke; its related factors; and itsconsequences for the rehabilitation process,performance of activities of daily living(ADLs), and quality of life.1 Fatigue has beendescribed as a feeling of a lack of physicaland mental energy.2e4 However, as fatigue isgenerally a subjective feeling, it may coexistwith mental or physical symptoms and variousimpairments after stroke.1 The etiology of fa-tigue is often believed to be multifactorial,5
and the multidimensional nature of fatiguecreates difficulties for both clinicians andresearchers in describing and assessing thepatient’s condition and implementing thebest treatment.
Two methods have been used to measurefatigue in stroke patients: self-reported mea-sures and performance-based measures.Because of the subjective nature of the conceptof fatigue, different inventories of self-reportedmeasures are mostly used to estimate the magni-tude of the phenomenon, for example, theFatigue Severity Scale (FSS),6 the Fatigue ImpactScale,7 and the vitality subscale of the ShortForm-36 (SF-36).8 Some performance-basedmeasures are focused on either physical or cog-nitive outcome. In the research on fatigue in pa-tients with neurological diseases, manyinstruments have been used in adults with multi-ple sclerosis (MS). The instruments intended tomeasure physical fatigue indirectly rely ona physiological definition of the phenomenon,for example, motor fatigue as measured by theability to perform muscle contractions overtime.9 Cognitive fatigue may be measured usingtests of cognitive performance with sustainedattention.10 Performance-based measures focuson behavioral outcomes and rely on objectiveindicators.
Although there are several published reviewarticles regarding fatigue in stroke,1,11e13 these
articles are not based on a systematic review ofthe literature. To offer a comprehensive evalu-ation of the state of the knowledge on thistopic, this review was undertaken to addressthe following questions:
1) How is fatigue after stroke described,defined, and measured?
2) How is fatigue after stroke related to per-sonal factors, stroke characteristics, andpreexisting conditions?
3) What are the relationships of poststrokefatigue with coexisting clinical factorssuch as pain, depression, sleep distur-bance, cognitive status, motor function-ing, dependency, and anxiety?
4) How does fatigue affect the strokepatient’s life?
5) Is there research evidence for fatigue-relieving strategies?
Procedures for the Search and ReviewA computer-aided search in PubMed,
CINAHL, EMBASE, and PsychInfo was per-formed in August 2007, which was updated onJanuary 20, 2009. ‘‘Stroke’’ (in PubMed and EM-BASE), ‘‘cerebrovascular accidents’’ (in PsychIn-fo), and ‘‘cerebral vascular accident’’ (inCINAHL) were used as medical subject head-ings in combination with ‘‘fatigue’’ as a word inthe abstracts or the title in all four databases.The search retrieved 236 publications, with 191duplicates in one or two databases. Publicationsthat did not report findings based on empiricaldata were excluded.
All abstracts were reviewed by two re-searchers (AL and HSK). In addition, abstractsin the journals Stroke, Neurology, PsychosomaticResearch, and Journal of Neurology, Neurosurgery,and Psychiatry published between January1997 and January 2009 were manually reviewedin an effort to identify articles on fatigue instroke patients. The total set of identified pub-lished reports was then screened for inclusionin this review by the following criteria: 1) thereport must be concerned with poststrokefatigue, 2) it should report findings fromempirical research, 3) it was published beforeJanuary 20, 2009, and 4) it was published inEnglish or Norwegian. This report is basedon a review of 33 published articles(see Table 1) obtained through these proce-dures that met the inclusion criteria.
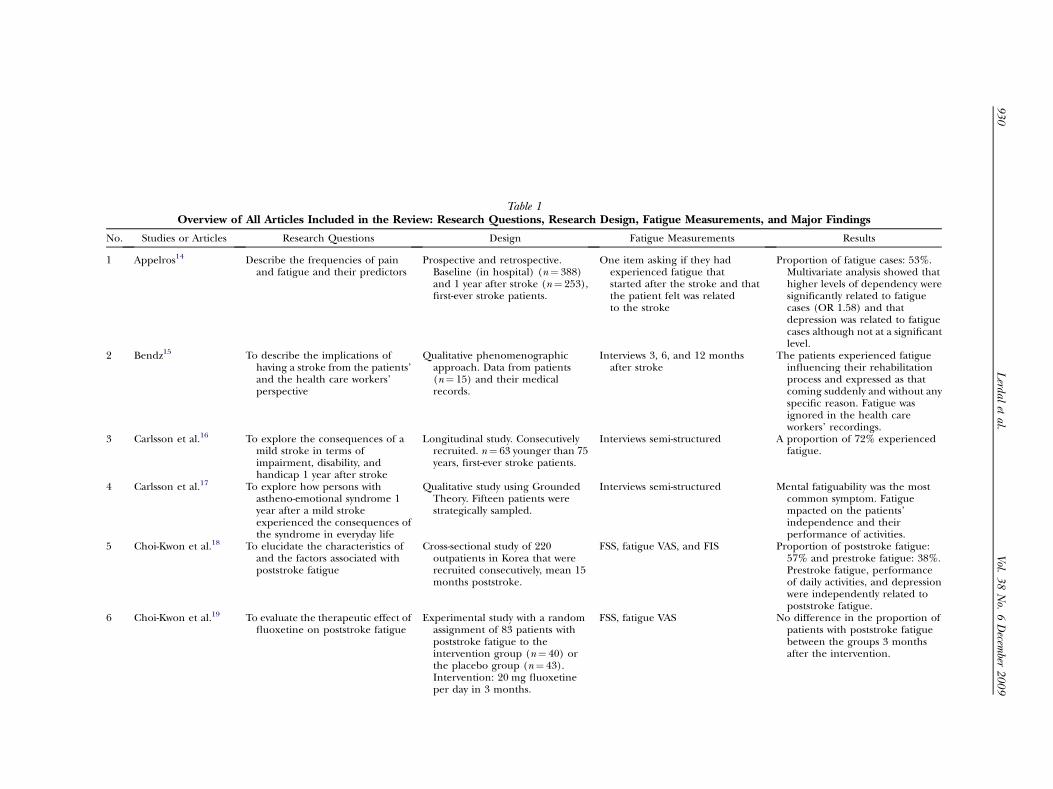
Table 1Overview of All Articles Included in the Review: Research Questions, Research Design, Fatigue Measurements, and Major Findings
Studies or Articles Research Questions Design Fatigue Measurements Results
Appelros14 Describe the frequencies of painand fatigue and their predictors
Prospective and retrospective.Baseline (in hospital) (n¼ 388)and 1 year after stroke (n¼ 253),first-ever stroke patients.
One item asking if they hadexperienced fatigue thatstarted after the stroke and thatthe patient felt was relatedto the stroke
Proportion of fatigue cases: 53%.Multivariate analysis showed thathigher levels of dependency weresignificantly related to fatiguecases (OR 1.58) and thatdepression was related to fatiguecases although not at a significantlevel.
Bendz15 To describe the implications ofhaving a stroke from the patients’and the health care workers’perspective
Qualitative phenomenographicapproach. Data from patients(n¼ 15) and their medicalrecords.
Interviews 3, 6, and 12 monthsafter stroke
The patients experienced fatigueinfluencing their rehabilitationprocess and expressed as thatcoming suddenly and without anyspecific reason. Fatigue wasignored in the health careworkers’ recordings.
Carlsson et al.16 To explore the consequences of amild stroke in terms ofimpairment, disability, andhandicap 1 year after stroke
Longitudinal study. Consecutivelyrecruited. n¼ 63 younger than 75years, first-ever stroke patients.
Interviews semi-structured A proportion of 72% experiencedfatigue.
Carlsson et al.17 To explore how persons withastheno-emotional syndrome 1year after a mild strokeexperienced the consequences ofthe syndrome in everyday life
Qualitative study using GroundedTheory. Fifteen patients werestrategically sampled.
Interviews semi-structured Mental fatiguability was the mostcommon symptom. Fatiguempacted on the patients’independence and theirperformance of activities.
Choi-Kwon et al.18 To elucidate the characteristics ofand the factors associated withpoststroke fatigue
Cross-sectional study of 220outpatients in Korea that wererecruited consecutively, mean 15months poststroke.
FSS, fatigue VAS, and FIS Proportion of poststroke fatigue:57% and prestroke fatigue: 38%.Prestroke fatigue, performanceof daily activities, and depressionwere independently related topoststroke fatigue.
Choi-Kwon et al.19 To evaluate the therapeutic effect offluoxetine on poststroke fatigue
Experimental study with a randomassignment of 83 patients withpoststroke fatigue to theintervention group (n¼ 40) orthe placebo group (n¼ 43).
FSS, fatigue VAS No difference in the proportion ofpatients with poststroke fatiguebetween the groups 3 monthsafter the intervention.
Intervention: 20 mg fluoxetineper day in 3 months.
93
0V
ol.3
8N
o.6
Decem
ber2
00
9L
erdalet
al.
No.
1
2
3
4
5
6

7 Christensen et al.20 To examine the associationsbetween patients’ characteristicsand poststroke fatigue and itscourse during 2 years
Longitudinal cohort study of 165first-ever stroke patients assessed10 days, 3 months, and 1 and 2years after stroke.
Multidimensional fatigue inventory The proportions of general severefatigue were 59%, 44%, 38%, and40% at different time points.Poor functional outcome wasassociated with higher levels offatigue. Poststroke fatigue wasmainly related to increased levelsof physical fatigue. No differencein the level of reduced motivationand mental fatigue between thestroke patients and the healthygeneral population.
8 Dam21 To examine the frequency ofdepression for affectivesymptoms and possible predictorsof depression 7 years after stroke
Cohort study. Reexamination of thestroke cohort (n¼ 166) andcontrols (n¼ 41).
One item concerning their changesin fatigue during the 7-yearperiod with four responsealternatives
Compared with controls, thepatients did not reportstatistically significant increase inthe level of fatigue during the last7 years, while they did reportmore subjective mood instabilityand irritability than the controls.
9 Dawes et al.22 To examine the perceived exertionin patients with brain injury(including stroke) and toexamine intensity andperformance and other possiblevariables influencing the exerciseintensity achieved
Case-control study. Patients withbrain injury (n¼ 30) recruitedconsecutively and a purposively,and a sample of healthy controls(n¼ 19) matched for age, sex,and habitual activity.
The Profile of Mood Statesdfatiguedomain
Level of fatigue predictedmaximum heart rate but not thepeak bicycle power output.
10 de Coster et al.23 Assess the sensitivity of individualdepressive symptoms and theircontribution to the diagnosis ofpoststroke depression
Longitudinal study. Patients withfirst-ever stroke (n¼ 206) wereinterviewed within the firstmonth after stroke and after 3, 6,9, and 12 months.
Fatigue assessed by item no. 13 inthe Hamilton Rating Scale fordepression
The proportion of fatigue was 70%at 3 months after stroke. Thefatigue item showed highdiscriminative properties inrelation to depression.
11 Gandiga et al.24 To evaluate the effect oftranscranial direct currentstimulation on health controlsand stroke patients
RCT. Patients with chronic stroke(n¼ 14) and healthy controls(n¼ 8) participated.
Fatigue VAS Elderly health controls reportedlower level of fatigue than thechronic stroke patients.
12 Glader et al.25 To determine the prevalence ofpoststroke fatigue and toexamine the impact of suchfatigue on daily life and onsurvival
Longitudinal prospective cohortstudy. Data from a nationalregistry of stroke patientsassessed at 3 months afterstroke and a 2-year follow-upquestionnaire (n¼ 3667).
Fatigue was measured by the oneitem: ‘‘Do you feel tired?’’ withfour response alternatives
High degree of dependency, beingsingle and being women wererelated to fatigue. Fatigue 2years after stroke was relatedto self-reported generalhealth, anxiety, pain, anddepressive symptoms.
More patients who were always tiredat 3 months had died at2-year follow-up.
(Continued)
Vol.
38
No.
6D
ecember
20
09
93
1P
oststrokeFatigu
e
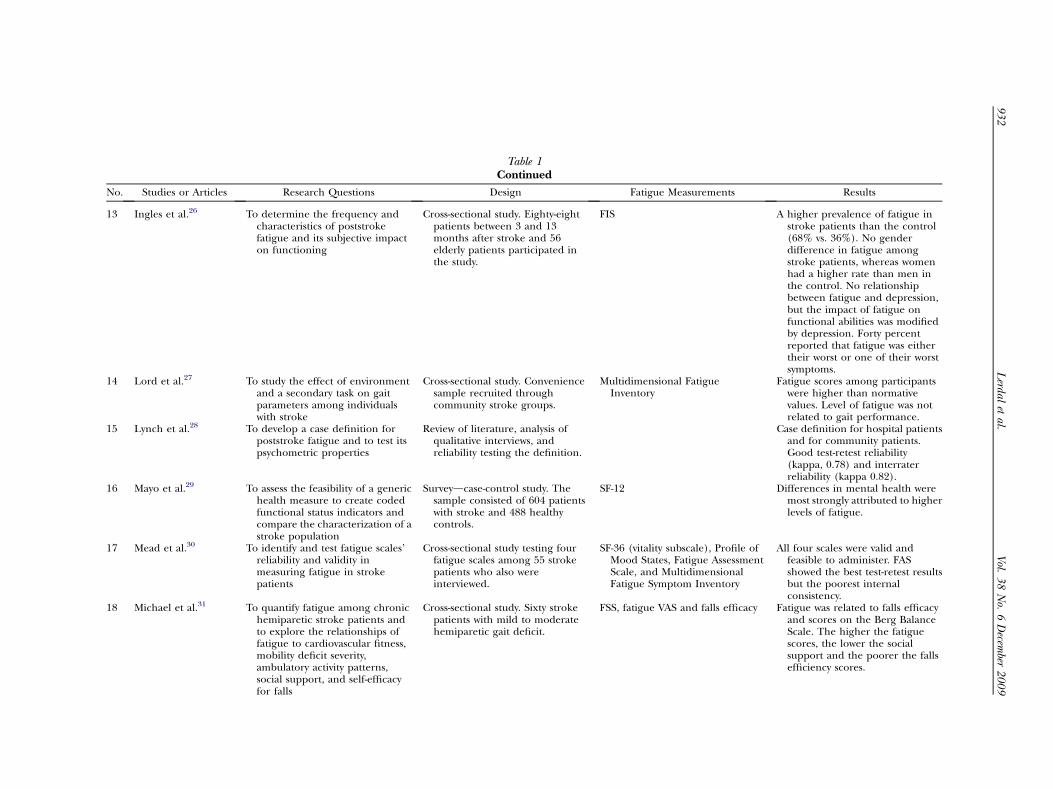
Table 1Continued
Studies or Articles Research Questions Design Fatigue Measurements Results
Ingles et al.26 To determine the frequency andcharacteristics of poststrokefatigue and its subjective impacton functioning
Cross-sectional study. Eighty-eightpatients between 3 and 13months after stroke and 56elderly patients participated inthe study.
FIS A higher prevalence of fatigue instroke patients than the control(68% vs. 36%). No genderdifference in fatigue amongstroke patients, whereas womenhad a higher rate than men inthe control. No relationshipbetween fatigue and depression,but the impact of fatigue onfunctional abilities was modifiedby depression. Forty percentreported that fatigue was eithertheir worst or one of their worstsymptoms.
Lord et al.27 To study the effect of environmentand a secondary task on gaitparameters among individualswith stroke
Cross-sectional study. Conveniencesample recruited throughcommunity stroke groups.
Multidimensional FatigueInventory
Fatigue scores among participantswere higher than normativevalues. Level of fatigue was notrelated to gait performance.
Lynch et al.28 To develop a case definition forpoststroke fatigue and to test itspsychometric properties
Review of literature, analysis ofqualitative interviews, andreliability testing the definition.
Case definition for hospital patientsand for community patients.Good test-retest reliability(kappa, 0.78) and interraterreliability (kappa 0.82).
Mayo et al.29 To assess the feasibility of a generichealth measure to create codedfunctional status indicators andcompare the characterization of astroke population
Surveydcase-control study. Thesample consisted of 604 patientswith stroke and 488 healthycontrols.
SF-12 Differences in mental health weremost strongly attributed to higherlevels of fatigue.
Mead et al.30 To identify and test fatigue scales’reliability and validity inmeasuring fatigue in strokepatients
Cross-sectional study testing fourfatigue scales among 55 strokepatients who also wereinterviewed.
SF-36 (vitality subscale), Profile ofMood States, Fatigue AssessmentScale, and MultidimensionalFatigue Symptom Inventory
All four scales were valid andfeasible to administer. FASshowed the best test-retest resultsbut the poorest internalconsistency.
Michael et al.31 To quantify fatigue among chronichemiparetic stroke patients andto explore the relationships offatigue to cardiovascular fitness,mobility deficit severity,ambulatory activity patterns,social support, and self-efficacyfor falls
Cross-sectional study. Sixty strokepatients with mild to moderatehemiparetic gait deficit.
FSS, fatigue VAS and falls efficacy Fatigue was related to falls efficacyand scores on the Berg BalanceScale. The higher the fatiguescores, the lower the socialsupport and the poorer the fallsefficiency scores.
93
2V
ol.3
8N
o.6
Decem
ber2
00
9L
erdalet
al.
No.
13
14
15
16
17
18

19 Michael and Macko32 To describe household andcommunity ambulatory activityprofiles, in terms of step countsand step intensity level, anddetermine whether these profilesare related to fitness or self-reported fatigue
A randomized exercise interventionstudy. Seventy-nine strokepatients with mild to moderatehemiparetic gait deficit.
FSS Forty-two percent of the samplerated their fatigue as severe(FSS $ 4). No statisticallysignificant association betweenfitness, step activity, and fatigue.
20 Naess et al.33 To analyze fatigue in young adultswith cerebral infarction andassociations with functional state,cognitive dysfunctions, andsocial factors
Case-control study. One hundredninety-two patients (15e49years), after primary or secondarystroke, 1.4e12.3 years after thestroke (mean 6.0), and 212healthy controls.
FSS Fatigue was higher in the strokepatients compared with thehealthy controls (51% versus32%).Fatigue was independentlyassociated with depression,reduced function, and basilarartery infarction.
21 Naess et al.34 To evaluate HRQoL among youngadults with ischemic stroke onlong-term follow-up
Case-control study. One hundredninety stroke patients (mean age47.8 years, 1.4e12.3 years afterthe stroke) and 215 healthycontrols (mean age 51.1 years).
FSS and SF-36 Fatigue was reported by 52% of thepatients. Those with fatigue hadlower SF-36 scores for allsubscales.
22 Purebl et al.35 To investigate the relationshipsbetween depressive symptomsand vital exhaustion amongpatients with cardiovasculardisorders
Cross-sectional survey. A subgroupof 1,749 with self-reportedcardiovascular disorders.
Hungarian adaptation of the 21-item Maastricht Vital ExhaustionQuestionnaire
The proportion of severe fatigueamong the respondents withstroke was 74.6%. Depression andexhaustion showed moderatecorrelation. Depressive symptomswere related to vital exhaustion.
23 Røding et al.36 To describe how younger strokepatients experiencedrehabilitation and the time afterstroke and to develop hypothesesabout their life situation
Qualitative, GT, descriptive studywith five young stroke patients(aged 37e54).
Interview Fatigue was an essential part in theirlivesdviewed to be overwhelmingand uncontrollable and createdfrustration. Impact on theirfamily, social life, sexuality, andability to work full time.
24 Schepers et al.37 To describe the course of fatigueduring the first year after strokeand determine the relationbetween fatigue at 1 year afterstroke and personalcharacteristics and poststrokeimpairments
Prospective longitudinal study.Patients (n¼ 228) recruitedconsecutively at a rehabilitationcenter. Data from 167 patientswere available for the analysis.
FSS (severe fatigue¼meanFSS scores> 4)
The proportions of severe fatiguewere 52% (baseline), 64% (6months), and 70% (12 months),with 17% with no fatigue at allmeasurement points. Twenty-nine percent of those with severefatigue at 1 year were depressed.In multivariate analysis, only age,depression, and level of locus ofcontroldpowerful others subscale(believe in physicians)dweresignificant predictors of higherlevels of fatigue.
25 Schuitemaker et al.38 To investigate whether vitalexhaustion is a precursor of firststroke while controlling for othercardiovascular risk factors
A prospective cohort study. Adultpopulation. One hundred sixty-seven participated in the RCTand 458 in the monitoring study.
Maastricht Interview VitalExhaustion scale
Feelings of vital exhaustionincreased the risk of stroke.Might be a side effect of otherrisk factors.
(Continued)
Vol.
38
No.
6D
ecember
20
09
93
3P
oststrokeFatigu
e

Table 1Continued
o. Studies or Articles Research Questions Design Fatigue Measurements Results
6 Shaughnessy et al.39 To test a hypothesized model thatconsidered the relationshipbetween self-efficacy andoutcome expectations forexercise, demographic variables,exercise history before stroke,and physician influences onphysical activity in patients afterstroke
A cross-sectional survey study.n¼ 312.
SSEE, SOEE Fatigue influences ADL and self-efficacy for exercise. Fatigue,race, and self-efficacy significantlyinfluenced outcome expectationsaccounting for 34% of thevariance.
7 Sorensen et al.40 To examine the quality of life andsocial prognosis after RIA
A long-term prospective study. Afterbaseline data were obtained, thepatients were approached at 6-month intervals. Median follow-up time was 58 months.
Interviews and questionnaires Fatigue was present in more than59% of the patients who only hadRIA. RIA was related topsychological dysfunction andquality of life.
8 Spalletta et al.41 To detect the frequency of clinicallyrated DSM-IV depressivesymptoms and the diagnosticvalidity of depressive disorders instroke patients suffering fromMDD, MIND, and NODEP
Cross-sectional. Two hundredfirst-ever stroke patients.Between 3 weeks and 3 monthsafter stroke.
DSM-IV (SCID-P) A gradient of severity of somaticsymptoms of depression, with thehighest severity found in MDDpatients and lowest severity inNODEP patients. Fatigue or lossof energy and insomnia werehigher in MIND patients than inNODEP patients.
9 Schwartz et al.42 To examine the synergism betweenvital exhaustion and cigarettesmoking in producing ischemicstroke
National prospective cohort studyin the United States of 13,066participants in the years 1987e1989 and 1990e1992.
MQdvital exhaustion Participants who scored in theupper quartile of vital exhaustionhad a risk for stroke compared tothose with a low score on vitalexhaustion.
0 Underwood et al.43 To study the changes in pain andfatigue status among peoplereceiving constraint-inducedmovement (CIM) therapy
Randomized 2-group design. Strokepatients with minimal elbow,hand, and wrist range of motionin extension. One group receivedCIM therapy for 2 weeksat 3e9 months after stroke(n¼ 18), the comparison groupat 1 year after stroke (n¼ 14).
Single-item VAS with rating 1e10,1¼ no fatigue and 10¼ absoluteexhaustion
The participants in the CIM therapydid not report any statisticallysignificant change in level offatigue during treatment, and nodifferences in level of fatiguebetween the two groups werefound.
1 van de Port et al.44 To identify clinical determinantsthat deteriorate mobilityafter stroke
Longitudinal prospective cohortstudy with 205 patients, 1 and 3years after first-time stroke.
Rivermead Mobility Index and FSS An association between mobilitydecline and fatigue was found.Fatigue predicted decline inmobility between 1 and 3 years.
93
4V
ol.3
8N
o.6
Decem
ber2
00
9L
erdalet
al.
N
2
2
2
2
3
3

32 van de Port et al.45 To determine the longitudinalassociation of poststroke fatiguewith ADL, instrumental ADL, andHRQoL
Prospective longitudinal cohortstudy. Stroke patientsconsecutively admitted forinpatient rehabilitation(n¼ 223). Data collected at 6, 12,and 36 months after first-everstroke.
FSS (severe fatigue defined asFSS> 4)
Fatigue was not related to ADL at 6and 36 months. Significantassociation with performance ofactivities. The proportion ofsevere fatigue was 68% (6months), 74% (12 months), and58% (36 months). Fatigue islongitudinally spuriouslyassociated with IADL andindependently with HRQoL.
33 van der Werf et al.46 To assess whether severe fatigue wasstill a frequent complaint in agroup of non-institutionalizedoutpatients who had suffered astroke at least 1 year before thestudydcompared with age-matched control group
Cross-sectional mailedquestionnaire survey. Patientswere asked to find an age-matching HC. One hundredthirty-eight patients received thequestionnaire. Sixty-five percentresponded and 37% of HC.
CIS 8-item range: 1e7 (CIS) cutoff40. BDI-PC (excluded somaticand performance items). Sevensubscales of the Sickness ImpactScale (SIP). These seven subscalescores were added together for atotal score (SIP-7-total). The SIPalertness behavior score was usedto measure experiencedneuropsychological problems
Fatigue was the main complaint in50% of the patients and among16% of the HC and elevatedfatigue in 51% of the strokepatients in contrast to 12% of theHC. The time since stroke wasnot related to fatigue. Nosignificant relationship betweenfatigue and depression. Only38% of the patients with extremefatigue had elevated depressionscores. In multivariate analysis,Sickness Impact Profile scaleexplained 34% of the variance inCIS fatigue, BDI-PC addedanother 11% and SIP alertnessadded 3%. BDI-PC explained themost variance in CIS fatigue(56%).
ADL¼ activities of daily living; BDI-PC¼ Beck Depression Inventory for Primary Care; CIS¼ checklist individual strength; DSM-IV¼Diagnostic and Statistical Manual for Mental Disorders, fourth edition;FIS¼ Fatigue Impact Scale; FSS¼ Fatigue Severity Scale; GT¼ grounded theory; HC¼ health control; HRQoL¼ health-related quality of life; IADL=instrumental ADL; MDD¼major depressive disorder;MIND¼minor depressive disorder; MQ¼Maastricht Questionnaire; NODEP¼ no depressive disorders; OR¼ odds ratio; RCT¼randomized controlled trial; RIA¼ reversible ischemic attacks; SF-12¼ ShortForm-12; SF-36¼ Short Form-36; SCI-P¼ Structured Clinical Interview for DSM-IV; SSEE¼ Short Self-Efficacy for Exercise scale; SOEE¼ short outcome expectations for exercise; VAS¼ visual analogue scale.
Vol.
38
No.
6D
ecember
20
09
93
5P
oststrokeFatigu
e

936 Vol. 38 No. 6 December 2009Lerdal et al.
The findings from the review are presentedaccording to the research questions in five sec-tions, with discussions regarding the findingsintegrated into each section.
The Characteristics of FatigueAfter Stroke
Although the general characterization offatigue seems to apply in describing poststrokefatigue, there were some differences in the waypoststroke fatigue was described in a few qual-itative studies carried out with poststroke pa-tients. Descriptions of fatigue revealeddifferent dimensions of the phenomenon,with problems related to self-control and emo-tional instability, reduced mental capacity, andperceived reduction in energy needed to reada book and participate in physical activities.17
Poststroke fatigue was characterized as startingor occurring without any specific exertion. Fa-tigue after stroke was characterized as a hiddendysfunction, invisible to other people, and asunpredictable, as the patient’s capacities werenot known or were variable or fluctuating,17
and has been reported as the most frequentsymptom three months after stroke.47
In a qualitative study of six women and ninemen interviewed at 3, 6, and 12 months aftera stroke event, a new form of fatigue was re-ported. This was related to the feeling of be-coming exhausted without any specificreason.15 Because of their fatigue after stroke,some stated that they had difficulty makingplans for the day. In addition, the patientsviewed fatigue as problematic during the reha-bilitation process, whereas the health careworkers did not address fatigue as a problem.15
Similarly, fatigue was viewed to play a centralrole and created frustration that was experi-enced as overwhelming and unable to be con-trolled in a descriptive study of five youngpatients aged between 37 and 54 years.36 Thesepatients became very emotional and sensitiveto what people said and it affected their totallife situation; when receiving a lot of informa-tion, they tired faster than before. Althoughthese findings suggest poststroke fatigue tohave somewhat distinct characteristics fromgeneral fatigue, there is a need for furtherclarification regarding the exact features that
may or may not differentiate poststroke fatiguefrom general fatigue.
The Definition and Measurement of Fatiguein Stroke
A theoretical definition of fatigue specificallyrelated to stroke was not found. In the area ofMS, however, a consensus conference of re-searchers and clinicians defined fatigue as ‘‘asubjective lack of physical and/or mental energythat is perceived by the individual or caregiver tointerfere with usual and desired activities.’’48
Even though this definition was developed to de-scribe fatigue in MS, it is generic in the way it de-scribes fatigue as a subjective experience and isconsistent with Staub and Bogousslavsky’s1 defi-nition of fatigue as ‘‘a feeling of early exhaustiondeveloping during mental activity, with weari-ness, lack of energy, and aversion to effort.’’ Fur-thermore, the subjective description impliesthat the patient’s self-reporting is the basis formeasuring the phenomenon. A case definitionhas recently been published to be used asa tool to determine the presence of fatigue inpoststroke patients in hospital and for patientsliving in the community.28
The different measures used in estimatingthe intensity of fatigue after stroke are shownin Table 2. The most frequently used instru-ments include the FSS and single items in theform of a 10 mm visual analogue scale (VAS).As the table shows, the different scales were de-veloped to measure different dimensions of fa-tigue such as concentration and motivation49
and the affective and somatic aspects50 of fa-tigue. None of the scales used in the strokepopulation have been developed specificallyfor measuring fatigue after stroke. A recentstudy30 in which 55 patients with stroke were in-terviewed evaluated the SF-36v2 (vitality subdi-mension), the Profile of Mood States, theFatigue Assessment Scale (FAS), and the Multi-dimensional Fatigue Symptom Inventory. Allfour scales were found to be valid and feasiblefor application to stroke patients. However,the FAS showed the highest test-retest reliabil-ity but the poorest internal consistency as as-sessed by Cronbach’s alpha values (0.58 at T1
and 0.62 at T2). These scales, in addition tothe Brief Fatigue Inventory, were chosen bythe research team based on their having thebest face validity of 52 fatigue scales. Surpris-ingly, the FSS, which is the most frequently

Table 2Self-Reported Fatigue Measurements Used in Stroke Populations
Measurement Developer Initial Population Dimensions and/or SubscalesNo. ofItems Stroke Studies
Checklist of IndividualStrenth (CIS)
Vercoulen et al.49 MS, CFS, HC 1) Subjective fatigue,2) concentration,3) motivation,4) physical activity level
24 van der Werf et al.46
Fatique AssessmentScale (FAS)
Michielsen et al.51 Workers Severity 10 Lynch et al.28 Mead et al.30
Fatique Severity Scale(FSS)
Krupp et al.6 MS and SLE Fatigue severity 9 Choi-Kwon et al.18 Choi-Kwon et al.19
Michael et al.30 Michael andMacko32 Naess et al.33 Naesset al.34 Schepers et al.37 van dePort et al.44 van de Port et al.45
Fatique ImpactScale (FIS)
Fisk et al.7 MS, CFS patients withhypertension
Perceived impact on1) cognitive,2) physical,3) psychological functioning
40 Choi-Kwon et al.18 Ingles et al.26
MasstrichtQuestionnaire (MQ)
Appels et al.52 Myocardial infarction Vital exhaustion: fatigue, irritability,stress (inability to cope), andfeeling of demoralization
Purebl et al.35 Schuitemaker et al.38
Schwartz et al.42
MultidimensionalFatigue Inventory(MFI-20)
Smets et al.50 Cancer patients, CFS and HC 1) General health,2) physical fatigue,3) mental fatigue,4) reduced motivation,5) reduced activity
20 Christensen et al.20
MultidimensionalFatigue SymptomInventory(MFISdgeneral)
Smets et al.50 Cancer patients 1) Global,2) somatic,3) affective,4) cognitive,5) behavioral symptomsof fatigue (not used in strokepatients)
6 Lord et al.27 Lynch et al.28
One-item questions For example, ‘‘.have youexperienced fatigue?’’
1 Appelros14 Dam21 de Coster et al.23
Glader et al.25 Shaughnessy etal.39 Sorensen et al.40
POMS McNair et al.53 1) Fatiguedinertia,2) vigordactivity,3) depressionddejection,4) tensiondanxiety,5) angerdhostility,6) confusiondbewilderment
65 Dawes et al.22 Lynch et al.28 Meadet al.30
SF-36/12 Vitalitysubscale
Ware et al.8 Patients with different chronicillnesses
Energy level and fatigue 4 Lynch et al.28 Mayo et al.29 Meadet al.30
VAS Used in many different types ofpopulations
1 Choi-Kwon et al.18 Choi-Kwon etal.19 Michael et al.31 Underwoodet al.42
CFS¼ chronic fatigue syndrome; CIS¼ checklist individual strength; HC¼ healthy controls; MS¼multiple sclerosis; MQ¼Maastricht Questionnaire; POMS¼ Profile of Mood States; SLE¼ systemic lupuserythematosus; SF-36/12¼ Short Form 36/12.
Vol.
38
No.
6D
ecember
20
09
93
7P
oststrokeFatigu
e

Table 3Overview of Studies Reporting Prevalence Rates of Severe Fatigue After Stroke
Study Sample and Sample Size Fatigue Instrument Used Prevalence of Fatigue Reported
Appelros14 Swedishdpopulation of first-everstroke in a municipality (253)
One item asking if they hadexperienced fatigue thatstarted after the stroke
53% at 1 year
Carlsson et al.16 First-ever stroke patients <75years consecutive admissionto a Swedish hospital (75)
AED 72% at 1 year
Carlsson et al.54 First-ever stroke patients andtheir spouses’ consecutiveadmission to a Swedishhospital (56)
AED 77% at 1 year
Choi-Kwon et al.18 Consecutive subjects froma Korean outpatient clinic (220)
VAS (severe¼ 7e10) FSS,FIS (cutoff value not given)
38% prestroke57% (between 3 and
27 months)Christensen et al.20 First-ever stroke patients’
consecutive admission to aDanish hospital (165)
MFI-20 (severe¼ generalfatigue sum score $ 12)
59% at 10 days44% at 3 months38% at 1 year40% at 2 years
Dam21 Follow-up study in Denmark (99) One item asking if theywere experiencing fatigue
de Coster et al.23 The Maastricht UniversityHospital Stroke Registry(206)
One item from the HAM-D 70% within 1 month
Ingles et al.26 Consecutively recruitedfrom a hospital (88)
FIS 68%, 3e13 months after stroke
Lynch et al.28 Patients in acute phase orrehabilitationdboth inpatients and from thecommunity (55)
Case definition 36%, 10e217 days after stroke
Michael et al.31 A community sample ofpatients with mild to moderatehemiparetic gait deficits inBaltimore (53)
FSS (mean> 4) VAS 46%, 6e166 monthsafter stroke (mean¼ 10.3months)
Michael and Macko32 Community sample of patientswith chronic hemipareticstroke in Baltimore (79)
FSS (mean> 4) 42%, 6e120 months after stroke(mean¼ 10 months)
Naess et al.33 Community sample in Norway,aged 15e49 years (192)
FSS (mean> 4) 51% (1.4e12.3 years after stroke)
Schepers et al.37 Dutchdconsecutive admissionsto rehabilitation center (228)
FSS (mean> 4) 51.5% at admission; 64.1% at 6months; 69.5% at 1 year
Purebl et al.35 Stroke patients identified in anational representative samplein Hungary (501)
MVEQ (mean 2.58) 74.6%
van de Port et al.45 Consecutive patients from aninpatient rehabilitation clinicin The Netherlands (223)
FSS (mean> 4) 68% at 6 months; 74%at 12 months; 58%at 36 months
van de Port et al.45 Consecutive patients from aninpatient rehabilitation clinicin The Netherlands (168)
FSS (mean> 4) 53% at 36 months
van der Werf et al.46 Stroke patients admitted to ahospital in The Netherlands(90)
CIS (sum score> 40) 50% (mean time since stroke¼ 2years)
AED¼ astheno-emotional disorder; CIS¼ checklist individual strength; FIS¼ Fatigue Impact Scale; FSS¼ Fatigue Severity Scale; HAM-D¼Hamilton Depression Rating Scale; MFI-20¼multidimensional fatigue inventory; MVEQ¼Maastricht Vital Exhaustion Questionnaire;VAS¼ Visual Analogue Scale.
938 Vol. 38 No. 6 December 2009Lerdal et al.
used instrument in stroke studies and whichhas shown high internal consistency (Cronba-ch’s alpha¼ 0.89),37 was not among the scalesevaluated in this report. Whether or not thegeneral fatigue scales are appropriate to cap-ture poststroke fatigue in reliable and validmanners is the question that needs to be ad-dressed in relation to the definition of
poststroke fatigue vis-a-vis the general defini-tion of fatigue. In addition, although various fa-tigue scales used in the poststroke fatiguestudies measure the degree or intensity, thequestion remains regarding the cutoff pointsfor determination of the presence of fatigueas many studies were concerned with preva-lence rather than the variation in intensity.

Vol. 38 No. 6 December 2009 939Poststroke Fatigue
Prevalence of FatigueFatigue is among the most prevalent symp-
toms after stroke,26,54 with prevalence ratesshown in Table 3.
In a study from The Netherlands focusing ondepression,23 70% of patients reported fatiguewithin the first month after a stroke. Scheperset al.37 demonstrated that 51% of patients re-ported fatigue when admitted to the hospital,whereas a longitudinal study from Denmarkshowed that 59% of the patients reported fa-tigue 10 days after stroke onset.20 These arethe only studies found that reported the preva-lence of fatigue in the acute phase.
In a Swedish sample at one year after stroke,53% of patients reported experiencing fatiguethat specifically started after the stroke.14 In twoother Swedish studies one year after stroke, theprevalence rate of having astheno-emotionalsyndrome diagnosed by a neurologist was72%e77%.16,54 In another Swedish follow-upstudy of 3,805 patients in the Swedish Riks-Stroke register examined two years aftera stroke, 39% reported that they ‘‘often’’ or‘‘always’’ felt tired,25 whereas 40% reportedfatigue at two-year follow-up in the Danishstudy.20 In a prospective study after patientswere diagnosed with reversible ischemic attacksover a median period of 58 months to identifythose who developed a stroke, 51% of those di-agnosed with stroke during the study period ex-perienced severe fatigue compared with 16% ofthose not diagnosed with stroke.40 The longitu-dinal cohort study from Denmark showed thatthe proportion of patients with severe fatiguevaried between 59% and 38% during the twoyears of follow-up.20 Various studies usingfatigue inventories have reported prevalencerates ranging from a low of 42% to a high of75%, and a study using a VAS format reported57% of patients classified as having fatigue(see Table 3).
Only two studies were found that trackedstroke patients’ fatigue experience over time.Although one of the studies showed that overthe course of their admission to the hospital,and six months and one year after stroke, theprevalence of fatigue increased over time,37
the proportion of fatigue cases was relativelystable over time except for a higher propor-tion in the acute phase in the second study.20
Only 17% of the patients did not have fatigue
at any time point, whereas 45% had sporadicfatigue (defined as having fatigue at one ortwo time points).37 The findings from alongitudinal case-control study indicated thatseven years after a stroke, patients retrospec-tively reported more change in fatigue thancontrols; however, this change was not statisti-cally significant.21 Conversely, in a cross-sec-tional study of Swedish stroke patients, theproportion of individuals with fatigue was rela-tively similar across poststroke time points at3e6, 7e9, and 10e13 months.26
As shown in Table 3, the prevalence offatigue ranges between 38% and 77%. An im-portant question is whether this variation isdue to the different measures and cutoffpoints used to distinguish between fatigueand no fatigue cases. FSS was the most fre-quently used fatigue measure in the strokestudies. All studies that reported the preva-lence of fatigue used mean FSS scores greaterthan 4.0 to indicate fatigue, although none ofthese studies explained the rationale for thiscutoff point. Interestingly, most recently pub-lished MS studies have used an FSS mean scoreof 5.0 as the cutoff value. In addition, fatiguein the general population in Norway hasbeen estimated using different cutoff values(4.0 and 5.0), suggesting possible overestima-tion of fatigue cases in the general popula-tion.56 As there is controversy regarding thecutoff value for the presence of fatigue whenusing FSS and other fatigue measurementtools, it is critical to standardize the cutoffvalue for use in descriptive comparison studies.
The literature indicates that fatigue is amajor issue confronting stroke patients, as sug-gested by the finding that more than one-thirdof stroke patients are likely to experience fa-tigue at some time after stroke. One area ofknowledge regarding prevalence that is lackingis the nature of modulation of the fatigue expe-rience in poststroke patients over time. In addi-tion, there is a lack of knowledge regarding thenature of the fatigue experience in strokepatients and how it might be similar to or differ-ent from general fatigue or fatigue in long-termconditions such as chronic fatigue syndrome. Itis critical to know about the specific characteris-tics of fatigue in stroke to begin to understandthe mechanisms and potential interventionsthat could be tested.

Table 4Studies Reporting on the Relationship Between Sociodemographic Variables, Stroke Characteristics,
Comorbidity, and Poststroke Fatigue
Antecedent Variables or Conditions Studies and Findings
Personal factors Age Appelros,14 NS; Carlsson et al.16 NS; Choi-Kwon et al.18 NS;Glader et al.25 P< 0.001; Ingles et al.26 NS; Lynch et al.28 NS;Naess et al.33 NS; Schepers et al.37 P¼ 0.02
Sex Appelros,14 NS; Carlsson et al.16 NS; Choi-Kwon et al.18 NS;Glader et al.25 women>men P¼ 0.01; Ingles et al.26 NS;Lynch et al.28 P¼ 0.02; Mayo et al.29 women>men;OR¼ 1.6; 95% CI: 1.1e2.2; Naess et al.33 NS;Purebl et al.35 NS; Schepers et al.37 NS
Marital status Glader et al.25 single>married/cohabitant P< 0.001;Schepers et al.37 NS
Employment status Carlsson et al.16 P¼ 0.05; Choi-Kwon et al.18 P< 0.05;Naess et al.33 P¼ 0.002
Cohabitant status Appelros,14 NS; Glader et al.25 living at home with socialsupport/in institution before the stroke> living alone,P< 0.01
Level of education Choi-Kwon et al.18 NS; Naess et al.33 NSStroke characteristics Location Appelros,14 NS; Carlsson et al.16 NS; Choi-Kwon et al.18 NS;
Ingles et al.26 NS; Lynch et al.28 NS; Naess et al.33 NS;Schepers et al.37 NS
Type Appelros,14 NS; Carlsson et al.16 NS; Schepers et al.37 NS;Glader et al.25 NS; Lynch et al.28 NS
Number of strokes Glader et al.25 recurrent> first ever, P¼ 0.003Time after stroke Ingles et al.26 NSNIHSS Appelros,14 facial palsy OR¼ 1.8; P¼ 0.04; arm paresis OR¼ 1.5;
P¼ 0.02SSS Carlsson et al.16 NSNeurological deficit Choi-Kwon et al.18 dysarthria, P< 0.01; inappropriate and
excessive laughing, P< 0.01; Ingles et al.26 NS; Naess et al.33 NSPrestroke fatigue Choi-Kwon et al.18 R¼ 33.46; P< 0.01; Choi-Kwon et al.19 r¼ 0.40;
P< 0.01; Schwartz et al.42 risk factor for stroke, P< 0.001;Schuitemaker et al.38 risk factor for stroke, P¼ 0.002
Lifestyle Cigarette smoking Choi-Kwon et al.18 P< 0.05; Naess et al.33 NSHigh use of alcohol Choi-Kwon et al.18 NSBMI Naess et al.33 NS
Primary ADLs before stroke Glader et al.25 dependency before the stroke, P< 0.001Comorbidity Cardiovascular diseases Appelros,14 NS; Choi-Kwon et al.18 NS; Naess et al.33 NS
Diabetes Appelros,14 NS; Choi-Kwon et al.18 NS; Naess et al.33 P¼ 0.008Migraine Naess et al.33 P¼ 0.003Primary ADLs before
strokeGlader et al.25 dependency before the stroke, P< 0.001
ADS¼ activities of daily living; BMI¼ body mass index; CI¼ confidence interval; NIHSS¼National Institutes of Health Stroke Scale; NS¼ notstatistically significant; OR¼ odds ratio; SSS¼ Scandinavian Stroke Scale.
940 Vol. 38 No. 6 December 2009Lerdal et al.
Fatigue in Relation to Personal Factors,Stroke Characteristics, and PreexistingConditions
Studiescorrelating factors that may beanteced-ents to poststroke fatigue are shown in Table 4.
Personal FactorsAlthough some studies have reported a
relationship between increasing age and therisk of fatigue 25,37, others have reported norelationship.14,16,18,26,29,33 Several studies offatigue in the general population show a higherproportion of fatigue among women;56,57 how-ever, there is conflicting evidence about the re-lationship between gender and poststroke
fatigue, as some researchers report no differ-ences between men and women,14,16,18,26,33
whereas others report a higher proportion offatigue among women.25,37 A higher propor-tion of fatigue cases among patients who are sin-gle compared with those who are married orcohabitate has been reported,25 whereasanother study reported no relationship.37
Findings from several studies indicated thatthose patients who experience fatigue afterstroke are more likely to be unemployed16,33
or have lost or changed jobs compared withthose with no fatigue after the stroke.18 Threestudies reported no significant relationshipbetween level of education and poststrokefatigue.18,33,35

Vol. 38 No. 6 December 2009 941Poststroke Fatigue
In a prospective study of stroke patientsfrom The Netherlands, researchers investi-gated the locus of control (i.e., the degree towhich the patients perceive the developmentof their health as an output of their own behav-ior) and its relationship to fatigue.37 The find-ings suggest that those who believed that theirhealth was determined largely by the actions ofphysicians reported higher levels of fatiguethan those who believed that their own actionswere more important.
Stroke CharacteristicsThe major stroke-related characteristics stud-
ied in relation to poststroke fatigue were strokelocation/type, number of strokes, and neuro-logical deficits. A study of young adults with ce-rebral infarction reported higher fatigue scoresamong patients with basilar artery infarction.33
No other studies showed any relationship be-tween fatigue and stroke location14,16,18,26,33,37
or fatigue and stroke type.14,16,25,37 One studyreported a relationship between the numberof strokes and fatigue,25 reporting a lower pro-portion of fatigue among patients who hada first stroke compared with those who had a re-current stroke.
Some studies have reported a significant re-lationship between neurological impairmentand fatigue,16,18 whereas others have notfound a significant relationship.14,26 Neurolog-ical deficits related to visual fields and facialpalsy were significant predictors of fatigue inone study.14 When stroke patients with fatiguein a Korean sample were compared with pa-tients with no fatigue, there was a higher pro-portion of dysarthria, decreased appetite, andinappropriate and excessive laughing in thefatigue group.18 Glader et al.25 found thatfatigue two years after stroke was less prevalentamong patients with no speech impairmentcompared with those with speech impairmentat admission, but there was no relationship tothe level of consciousness at admission.
Prestroke FatigueAs fatigue is a common experience in the gen-
eral population, there has been some interest inexamining the relationship between pre- andpoststroke fatigue to determine whether post-stroke fatigue is actually stroke related. In a ran-domized controlled study testing the effects offluoxetine on fatigue, the presence of prestroke
fatigue was related to fatigue after stroke(r¼ 0.40, P< 0.01).19 A surveyof220 consecutiveoutpatients conducted by the same Korean re-searchers showed that among the 57% who hadfatigue approximately 15 months after stroke,36% also had fatigue before the stroke.18 Amongpatients with prestroke fatigue, 58% experiencedan increase and 28% a decrease in fatigue sever-ity. In a longitudinal study of cardiovascular dis-ease in the United States, individuals whoreported higher levels of exhaustion had morethan twice the risk (hazard ratio [HR]¼ 2.42,P< 0.001) for stroke 5e7 years later than thosewho reported low exhaustion.42 That study alsoshowed that individuals with moderate exhaus-tion scores had a higher risk for stroke than thosewith lower exhaustion scores (HR¼ 1.66,P< 0.001). Furthermore, current smoking wasa significant risk among those with middle orhigh levels of exhaustion. Findings from a pro-spective survey in The Netherlands (mean fol-low-up time 50.9 months; range 9.5e62.7months) showed that feelings of exhaustion in-creased the risk of stroke (relative risk¼ 1.3).38
The association remained unchanged after con-trolling for confounding variables such as sex, to-tal cholesterol level, blood pressure, smokinghabits, and body mass index.
Preexisting MorbiditiesFew studies examined the relationship be-
tween preexisting morbidities such as cardiovas-cular disease, diabetes, other neurologicalconditions, and stroke or stroke-related experi-ences including fatigue. No significant relation-ships were found for cardiovascular disease, andconflicting findings were reported for diabe-tes.14,18,33 Naess et al.33 reported a significant re-lationship between migraine and poststrokefatigue.
In summary, the literature indicates inconclu-sive associations between poststroke fatigue andpersonal variables, stroke-related characteris-tics, and preexisting conditions. There are con-flicting findings regarding associations betweenpoststroke fatigue and personal and demo-graphic factors such as age, sex, level of educa-tion, living situation, and employment status.Furthermore, stroke-related factors such asstroke type, location, and number were shownto have inconclusive associations with post-stroke fatigue. There may be an association be-tween prestroke fatigue and poststroke
942 Vol. 38 No. 6 December 2009Lerdal et al.
fatigue. This association, however, is difficult tovalidate because of a high degree of unreliabil-ity in retrospectively obtained prestroke fatiguedata. It appears essential to evaluate possible re-lationships between pre- and poststroke fatigueto understand the component of fatigue that isspecifically stroke related. Therefore, it can beconcluded that the antecedents to poststroke fa-tigue are not well known, there appear to be noknown characteristics that differentiate pre-and poststroke fatigue, and the course of fatigueover time is not well understood.
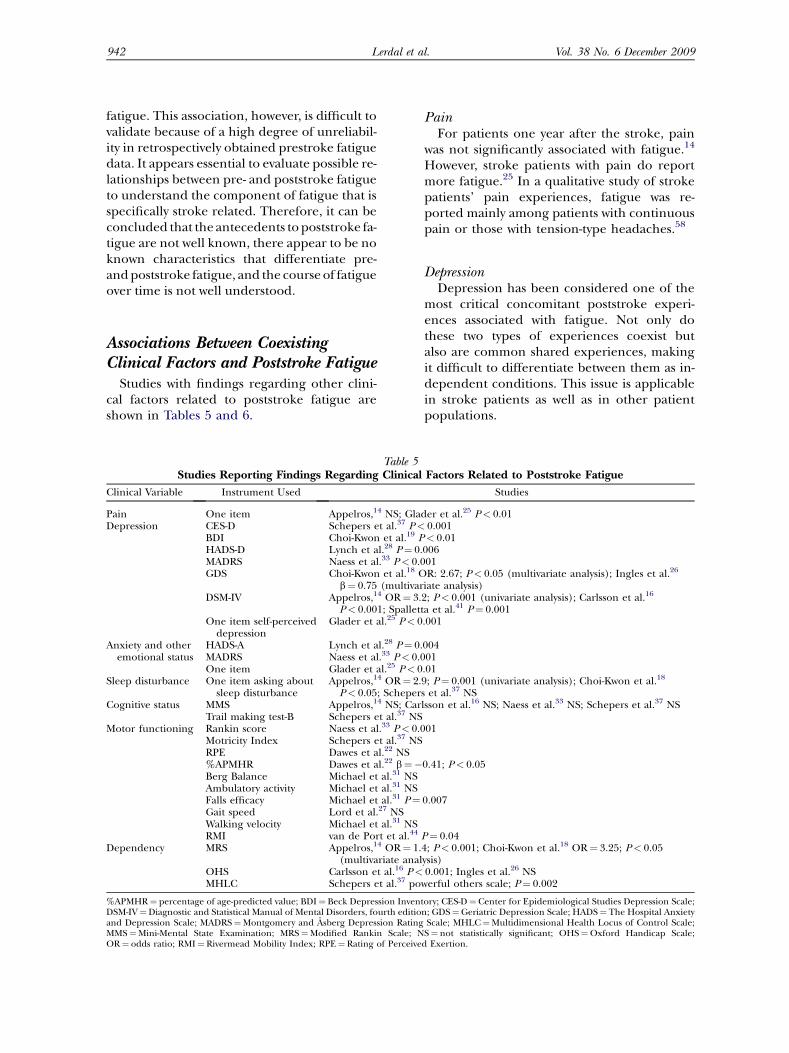
Associations Between CoexistingClinical Factors and Poststroke Fatigue
Studies with findings regarding other clini-cal factors related to poststroke fatigue areshown in Tables 5 and 6.
Table 5Studies Reporting Findings Regarding Clinical
Clinical Variable Instrument Used
Pain One item Appelros,14 NS; GlaDepression CES-D Schepers et al.37 P<
BDI Choi-Kwon et al.19 PHADS-D Lynch et al.28 P¼ 0.MADRS Naess et al.33 P< 0.0GDS Choi-Kwon et al.18 O
b¼ 0.75 (multivarDSM-IV Appelros,14 OR¼ 3.
P< 0.001; SpalletOne item self-perceived
depressionGlader et al.25 P< 0
Anxiety and otheremotional status
HADS-A Lynch et al.28 P¼ 0.MADRS Naess et al.33 P< 0.0One item Glader et al.25 P< 0
Sleep disturbance One item asking aboutsleep disturbance
Appelros,14 OR¼ 2.P< 0.05; Scheper
Cognitive status MMS Appelros,14 NS; CarTrail making test-B Schepers et al.37 NS
Motor functioning Rankin score Naess et al.33 P< 0.0Motricity Index Schepers et al.37 NSRPE Dawes et al.22 NS%APMHR Dawes et al.22 b¼�Berg Balance Michael et al.31 NSAmbulatory activity Michael et al.31 NSFalls efficacy Michael et al.31 P¼Gait speed Lord et al.27 NSWalking velocity Michael et al.31 NSRMI van de Port et al.44
Dependency MRS Appelros,14 OR¼ 1.(multivariate anal
OHS Carlsson et al.16 P<MHLC Schepers et al.37 po
%APMHR¼ percentage of age-predicted value; BDI¼ Beck Depression InvenDSM-IV¼Diagnostic and Statistical Manual of Mental Disorders, fourth editioand Depression Scale; MADRS¼Montgomery and Asberg Depression RatingMMS¼Mini-Mental State Examination; MRS¼Modified Rankin Scale; NOR¼ odds ratio; RMI¼ Rivermead Mobility Index; RPE¼ Rating of Perceive
PainFor patients one year after the stroke, pain
was not significantly associated with fatigue.14
However, stroke patients with pain do reportmore fatigue.25 In a qualitative study of strokepatients’ pain experiences, fatigue was re-ported mainly among patients with continuouspain or those with tension-type headaches.58
DepressionDepression has been considered one of the
most critical concomitant poststroke experi-ences associated with fatigue. Not only dothese two types of experiences coexist butalso are common shared experiences, makingit difficult to differentiate between them as in-dependent conditions. This issue is applicablein stroke patients as well as in other patientpopulations.
Factors Related to Poststroke Fatigue
Studies
der et al.25 P< 0.010.001< 0.01
00601R: 2.67; P< 0.05 (multivariate analysis); Ingles et al.26
iate analysis)2; P< 0.001 (univariate analysis); Carlsson et al.16
ta et al.41 P¼ 0.001.001
00401
.019; P¼ 0.001 (univariate analysis); Choi-Kwon et al.18
s et al.37 NSlsson et al.16 NS; Naess et al.33 NS; Schepers et al.37 NS
01
0.41; P< 0.05
0.007
P¼ 0.044; P< 0.001; Choi-Kwon et al.18 OR¼ 3.25; P< 0.05ysis)0.001; Ingles et al.26 NS
werful others scale; P¼ 0.002
tory; CES-D¼Center for Epidemiological Studies Depression Scale;n; GDS¼Geriatric Depression Scale; HADS¼ The Hospital Anxiety
Scale; MHLC¼Multidimensional Health Locus of Control Scale;S¼ not statistically significant; OHS¼Oxford Handicap Scale;
d Exertion.

Table 6Studies Reporting on the Impact of Poststroke Fatigue on Function and Quality of Life
Variables Instrument Used Studies
Quality of life HQoL Naess et al.34 physical functioning, P< 0.001; roledphysical, P< 0.001;bodily pain, P< 0.001; general health, P< 0.001; vitality, P< 0.001;social functioning, P< 0.001; mental health, P< 0.05
General health status Glader et al.25 P< 0.01Functioning ADLs Carlsson et al.16 NS; Glader et al.25 P< 0.001; Ingles et al.26 NS;
van de Port et al.45
IADLs Glader et al.25 P< 0.001; Mayo et al.29 P< 0.05; van de Port et al.45 NS(multivariable analyses)
FAI van de Port et al.45 P¼ 0.032Speech impairment Glader et al.25 P< 0.001General health Glader et al.25 P< 0.001Self-efficacy expectations Shaughnessy et al.39
SIP van der Werf et al.46 P< 0.001; van de Port et al.45 P< 0.001Fatality Glader et al.25 always> never/sometimes, OR: 1.85, P< 0.001
FAI¼ Frenchay Activity Index; HQoL¼ health-related quality of life; IADLs¼ instrumental activities of daily living; NS¼ not statistically signifi-cant; OR¼ odds ratio; SIP¼ Sickness Impact Profile Scale.
Vol. 38 No. 6 December 2009 943Poststroke Fatigue
In a study of 200 Italian patients with first-everstroke who were surveyed for depression threemonths after their stroke using the StructuredClinical Interview of the Diagnostic and Statisti-cal Manual for Mental Disorders, fourth edi-tion-P,41 the scores for fatigue or loss of energytended to be significantly higher amongpatients who had a minor depressive disorderthan among those who had no depressive disor-der. Similar findings were found in a Belgianstudy in which neurocognitive and somaticsymptoms were assessed in relation to their dis-criminant contribution to the diagnosis of post-stroke depression.23 The study showed thatreduced appetite, psychomotor retardation,and fatigue contributed significantly to identify-ing patients who had poststroke depression. Arelationship between depression and highlevels of fatigue has been shown in several otherstudies.19,25,33,37,45 The odds ratio for having fa-tigue one year after stroke when having depres-sion was 3.2 (95% confidence interval:1.7e6.0).14 In a Swedish study, 49% of patientswith fatigue one year after stroke werediagnosed with depression compared with39% in the total sample.16 This was similar ina Korean study, with 34% of patients depressedamong those with fatigue approximately 15months after stroke.18 When a stepwise linearregression analysis was performed separatelyfor the group of stroke patients and the groupof controls, and after controlling for sicknessimpact score on ambulation, depression scoresaccounted for 11% of the variance in fatiguescores for stroke patients compared with 56%of the variance for the control group.46 A
similar finding was reported in a multivariateregression analysis where the patients’ handi-cap score at discharge predicted their depres-sion score but not their fatigue score.25
AnxietyOnly a couple of studies examined the rela-
tionship between fatigue and anxiety. Gladeret al.25 reported that patients with anxiety alsohad a tendency to report more fatigue, whereasNaess et al.33 compared those with and withoutanxiety in their study of young adults with ische-mic stroke, noting that 71% had fatigue amongthose with anxiety and only 37% had fatigueamong those without anxiety. A Norwegianstudy of quality of life among young adultswith ischemic stroke showed that fatigue wasweakly related to mental health and morestrongly related to physical health.34
SleepFatigue is more likely in patients who report
sleep disturbance.14 Among patients with fa-tigue after stroke, 22% reported insomnia com-pared with 11% in the no fatigue group(P< 0.005).18 However, another study of pa-tients one year after stroke found no associationbetween fatigue and sleep problems.37 Self-report of sleep problems may be less valid andreliable than assessment of sleep problems byobjective measures, and the type of insomniamay vary with the patient’s fatigue experience.
One of the major points of discussion in thegeneral literature on fatigue is the possiblelink between fatigue and depression. As indi-cated by findings on poststroke fatigue, there

944 Vol. 38 No. 6 December 2009Lerdal et al.
is a trend for the co-occurrence of fatigue withdepression and fatigue with anxiety. However,the findings are not conclusive, and there isa need to differentiate the nature of subjectiveexperience and specific psychological andphysiological processes associated with fatigue,depression, and anxiety. This is critical becauseassociations found in the literature could beattributed to confounding effects from the in-struments used to measure these phenomena.Two other concomitant conditions that seemto be associated with fatigue in stroke, namely,sleep disturbances and daytime physical func-tioning, are important areas for further study,as an understanding of poststroke fatigueand patient experience is critical in developinginterventions.
Impact of Poststroke FatigueThe literature suggests that the major impact
of poststroke fatigue seems to be on patients’functioning and dependency. Although strokepatients are often affected by the presence of pa-ralysis in carrying out the ADLs, fatigue seems tofurther impact on their functioning in a varietyof ways.
A survey of exercise beliefs in the UnitedStates showed that patients with fatigue hadboth lower self-efficacy expectations and out-come expectations for exercise.39 Further-more, 68% of studied patients agreed orstrongly agreed that fatigue influenced theirdaily activities. Other studies also have shownthat those with a balance impairment andless confidence in performing ADLs withoutfalling (low falls efficacy) have higher fatiguescores31 and more perceived unmet de-mands.55 A study showed that those who havefatigue one year after a stroke have a higherdegree of dependency compared with thosewith no fatigue.14 Similar findings have beenreported two years after stroke.25 Furthermore,a study in The Netherlands of stroke patientstwo years after stroke showed that the patientswith higher perceived disability were morelikely to have higher fatigue scores.46 A pro-spective study of first-ever stroke patientsshowed that fatigue at one year after stroke in-dependently predicted a decline in mobilityfunction two years later.44 In a qualitative studyof the consequences of living with stroke, pa-tients described feelings about the need for
help and the lack of ability to master their dailylife due to fatigue.17 Family members tookmore responsibility for planning, organizing,and performing family-related activities be-cause of reduced physical capacity. A qualita-tive prospective study of 11 right hemispherestroke patients interviewed at one week, onemonth, three months, and six months afterstroke found that all patients described physi-cal and mental fatigue.59 Furthermore, fatiguewas the main reason for not engaging in activ-ities. Those who were inactive stated that theirlack of interest and tendency to tire easily werethe main reasons for inactivity. In contrast,others have shown that fatigue after strokewas not related to performance of daily activi-ties, as measured by the Barthel Index.16,45
However, contradictory findings withinthese studies were evident. Although a higherfatigue level was associated with a greater de-gree of handicap, there was also no relation-ship between fatigue and instrumentalADLs.16,45 The lack of association between fa-tigue and function as measured by the BarthelIndex, despite relationships between fatigueand more complex ADLs,16,45 indicates thatpoststroke fatigue might have more impacton performing activities that are more energyconsuming, such as shopping and going toparties, than less energy-demanding activities,such as getting dressed and going to the toilet.
The fatigue also affected their sexual activityand capacity to work full time.16 Other studieshave also found a decrease in sexual perfor-mance related to fatigue after stroke.18 Thesurvey showed that their satisfaction with lifeas a whole, their leisure situations, and theircontact with friends and acquaintances wereinfluenced by their fatigue one year after thestroke. Patients with high levels of fatigue afterstroke rated their general health lower thanthose with less or no fatigue.25
In an intervention study of patients withbrain injury (mainly stroke patients), generalfatigue level predicted the patient’s percent-age age-predicted maximal heart rate, indicat-ing that fatigue influenced the patient’s abilityto work hard.22 However, in a randomized fac-torial design study, patient fatigue did not haveany effect on gait performance in the hospitalcorridor, the suburban street, or in a mall.27
Similar findings were reported in a studyaimed at describing the relationship between

Vol. 38 No. 6 December 2009 945Poststroke Fatigue
household and community activity profiles, fa-tigue, and cardiovascular fitness.32 No statisti-cally significant relationship between fatigueand these variables was found, indicating thatfatigue is not directly related to the oxygenconsumption rate (VO2), at least in inactivestroke patients. Another study found that ahigher proportion of those stroke patientswho reported that they always felt tired haddied between one and three years after thestroke (17% vs. 7%).25
The findings in these reports suggest thatpoststroke fatigue seems to have impact onfunctioning in terms of the types of function-ing and activities. Poststroke fatigue also seemsto affect patients’ lives in relation to sexual, lei-sure, and social activities. However, the find-ings are inconsistent and lack theoreticalunderpinnings to explain the processes bywhich fatigue affects patients’ daily living.
Fatigue-Relieving InterventionsOnly one intervention study was found that
specifically targeted fatigue using a drug, inwhich the use of fluoxetine for fatigue wastested in a double-blind, placebo-controlledstudy.19 However, fluoxetine showed no effecton reducing poststroke fatigue, suggestingthat serotonergic system dysfunction is not a po-tential mechanism for poststroke fatigue.19 An-other study43 examined differences in pain andfatigue from constraint-induced movement
PersonalFactors
StrokeCharacteristics
BiophysiologicalMarkers
Fatigue
ChronicDiseases
Fatigue
Intensity
Quality
Timing
Trajectory
DepressionAnxiety
ANTECEDENTS FATIGUE EXPER
Fluctuation
Prestroke
Fig. 1. Biopsychosocial model
therapy designed to improve mobility betweena group receiving treatment in the subacutephase of stroke compared with a group receiv-ing this therapy in the chronic phase. Therewas no significant difference between thesetwo groups with regard to pain or fatigue, indi-cating that the timing for implementing con-straint-induced movement therapy was notcritical. This study, however, did not target fa-tigue for specific interventions. In chronic fa-tigue syndrome, where the evidence base islarger, cognitive behavioral therapy and, tosome degree, performing regular physical exer-cises have been shown to be effective in treatingfatigue.5 This paucity of studies examining in-tervention strategies for poststroke fatigue indi-cates the low level of attention to fatigue asa clinical problem that needs to be therapeuti-cally attended. It seems critical that there isa need to develop strategies to address post-stroke fatigue and test such strategies for theireffectiveness, given the high prevalence of post-stroke fatigue and its apparent effects on pa-tients’ lives.
SummaryThe literature on poststroke fatigue indi-
cates that knowledge regarding this phenome-non is still at a foundation stage. To developcomprehensive understanding to move towardeffective interventions, empirical research withvarious theoretical orientations must continue.
SleepDisturbances
Functioningin Daily Life
Quality ofLife
IENCES EFFECTS
of poststroke fatigue.

946 Vol. 38 No. 6 December 2009Lerdal et al.
The theory of unpleasant symptoms developedby Lenz et al60 is used to present a poststrokefatigue model. This model consists of threecomponents: antecedents, fatigue experiences,and effects, as shown in Fig. 1.
The antecedent component is represented byfive categories of factors: personal factors, bio-markers, stroke characteristics, prestroke fa-tigue, and chronic diseases. The key personalfactors are age, sex, living conditions, and per-sonality, as these are shown in the literature tohave some association with poststroke fatigue,albeit with some conflicting findings. Althoughassociations between fatigue and biophysiologi-cal markers have not been studied specifically inpoststroke fatigue, there is some evidence thatlevels of cytokines, selected proteins, and otherserum factors are involved in stress responsesand sickness behaviors such as apathy andsleepiness.61e64 Thus, it is necessary to includethis category as an antecedent. Various strokecharacteristics such as location, type, and num-ber of occurrences may be associated with post-stroke fatigue experience, as shown in somestudies. Two studies of patients with chronicfatigue syndrome have shown a reduction insubcortical gray matter when compared withhealthy controls.65,66 Similar studies on patientswith poststroke fatigue may discover possibleprecipitating factors. Prestroke fatigue as an an-tecedent factor is an important consideration inunderstanding poststroke fatigue, as there isevidence that they are related. However, the ex-act nature of the relationship is not clear. Thecomorbidities of stroke, especially chronic dis-eases such as cardiovascular disease, diabetes,chronic anemia, and chronic respiratory dis-ease, may have an impact on fatigue by eitheraggravating or masking it. These five categoriesof antecedent factors have been identified aspossible areas for further study.
The component of fatigue experience ad-dresses the conceptualization of fatigue in rela-tion to intensity, quality, timing, fluctuation,and long-term trajectory. Lenz et al60 identi-fied intensity, timing, distress, and quality asthe key dimensions of unpleasant symptoms.These five dimensions for poststroke fatigueencompass the experience associated withhow it is experienced at one time and how itis experienced over time. The fluctuation di-mension refers to how it changes throughoutthe day and night or during a certain specified
time, whereas the trajectory dimension refersto how the experience changes over a longpoststroke period. A longitudinal understand-ing is important because stroke is an illnesscondition with a specific trajectory.67 This com-ponent also includes possible concomitantsof stroke, including anxiety, depression, andsleep disturbance. Co-occurrence of these ex-periences, as well as differentiation of fatiguefrom these experiences, will further clarifythe nature of the poststroke fatigueexperience.
The third component of this model is out-comes or effects, consisting of two categories:functioning in daily life and one’s participa-tion in various ADLs, including physical, in-strumental, psychocognitive, and leisureactivities. As many stroke patients experiencedeficits in functioning because of the neuro-muscular insults of stroke, it is important tounderstand how fatigue further influencestheir functioning. In addition, it is importantto assess the impact of fatigue on quality oflife, as it may be associated with function aswell as with how one experiences fatigue inde-pendent of other factors.
This model is useful in reflecting on thestate of the science regarding poststroke fa-tigue and in specifying areas in need of furtherinvestigation. However, the model only servesas a framework for how fatigue is experiencedrather than as a theory of the mechanism ofhow poststroke fatigue develops.
AcknowledgmentsWe acknowledge the support and assistance
provided by various staff members of BuskerudHospital in Drammen and Oslo UniversityHospitaldAker in Oslo, Norway, in carryingout this research project.
References1. Staub F, Bogousslavsky J. Fatigue after stroke:
a major but neglected issue. Cerebrovasc Dis 2001;12:75e81.
2. Lerdal A. Energy, fatigue and perceived illness inindividuals with multiple sclerosis: A multi-method approach. Doctoral Dissertation, Depart-ment of Behavioural Science in Medicine, Universityof Oslo, Unipub AS, 2005.

Vol. 38 No. 6 December 2009 947Poststroke Fatigue
3. Krupp LB, Alvarez LA, LaRocca NG,Scheinberg LC. Fatigue in multiple sclerosis. ArchNeurol 1988;45:435e437.
4. Lee KA, Lentz MJ, Taylor DL, Mitchell ES,Woods NF. Fatigue as a response to environmentaldemands in women’s lives. Image J Nurs Sch 1994;26:149e154.
5. Prins JB, van der Meer JW, Bleijenberg G. Chronicfatigue syndrome. Lancet 2006;367:346e355.
6. Krupp LB, LaRocca NG, Muir-Nash J,Steinberg AD. The Fatigue Severity Scale. Applica-tion to patients with multiple sclerosis and systemiclupus erythematosus. Arch Neurol 1989;46:1121e1123.
7. Fisk JD, Ritvo PG, Ross L, Haase DA, Marrie TJ,Schlech WF. Measuring the functional impact of fa-tigue: initial validation of the fatigue impact scale.Clin Infect Dis 1994;18(Suppl 1):S79eS83.
8. Ware J, Snow KK, Kosinski M. SF-36 Health sur-vey: Manual and interpretation guide. Lincoln, RI:Quality Metric Incorporated, 2002.
9. Ponten EM, Stal PS. Decreased capillarizationand a shift to fast myosin heavy chain IIx in the bi-ceps brachii muscle from young adults with spasticparesis. J Neurol Sci 2007;253:25e33.
10. Schwid SR, Tyler CM, Scheid EA, et al. Cogni-tive fatigue during a test requiring sustained atten-tion: a pilot study. Mult Scler 2003;9:503e508.
11. Colle F, Bonan I, Gellez Leman MC, Bradai N,Yelnik A. Fatigue after stroke. Ann Readapt MedPhys 2006;49:361e364.
12. De Groot MH, Phillips SJ, Eskes GA. Fatigueassociated with stroke and other neurologic condi-tions: implications for stroke rehabilitation. ArchPhys Med Rehabil 2003;84:1714e1720.
13. Barker-Collo S, Feigin VL, Dudley M. Poststroke fatiguedwhere is the evidence to guide prac-tice? N Z Med J 2007;120:U2780.
14. Appelros P. Prevalence and predictors of painand fatigue after stroke: a population-based study.Int J Rehabil Res 2006;29:329e333.
15. Bendz M. The first year of rehabilitation aftera strokedfrom two perspectives. Scand J CaringSci 2003;17:215e222.
16. Carlsson GE, Moller A, Blomstrand C. Conse-quences of mild stroke in persons <75 yearsda1-year follow-up. Cerebrovasc Dis 2003;16:383e388.
17. Carlsson GE, Moller A, Blomstrand C. A qualita-tive study of the consequences of ‘hidden dysfunc-tions’ one year after a mild stroke in persons <75years. Disabil Rehabil 2004;26:1373e1380.
18. Choi-Kwon S, Han SW, Kwon SU, Kim JS. Post-stroke fatigue: characteristics and related factors.Cerebrovasc Dis 2005;19:84e90.
19. Choi-Kwon S, Choi J, Kwon SU, Kang DW,Kim JS. Fluoxetine is not effective in the treatment
of post-stroke fatigue: a double-blind, placebo-con-trolled study. Cerebrovasc Dis 2007;23:103e108.
20. Christensen D, Johnsen SP, Watt T, et al. Dimen-sions of post-stroke fatigue: a two-year follow-upstudy. Cerebrovasc Dis 2008;26:134e141.
21. Dam H. Depression in stroke patients 7 yearsfollowing stroke. Acta Psychiatr Scand 2001;103:287e293.
22. Dawes H, Scott OM, Roach NK, Wade DT.Exertional symptoms and exercise capacity in indi-viduals with brain injury. Disabil Rehabil 2006;28:1243e1250.
23. de Coster L, Leentjens AF, Lodder J, Verhey FR.The sensitivity of somatic symptoms in post-strokedepression: a discriminant analytic approach. Int JGeriatr Psychiatry 2005;20:358e362.
24. Gandiga PC, Hummel FC, Cohen LG. Transcra-nial DC stimulation (tDCS): a tool for double-blindsham-controlled clinical studies in brain stimula-tion. Clin Neurophysiol 2006;117:845e850.
25. Glader EL, Stegmayr B, Asplund K. Poststrokefatigue: a 2-year follow-up study of stroke patientsin Sweden. Stroke 2002;33:1327e1333.
26. Ingles JL, Eskes GA, Phillips SJ. Fatigue afterstroke. Arch Phys Med Rehabil 1999;80:173e178.
27. Lord SE, Rochester L, Weatherall M,McPherson KM, McNaughton HK. The effect of en-vironment and task on gait parameters after stroke:a randomized comparison of measurement condi-tions. Arch Phys Med Rehabil 2006;87:967e973.
28. Lynch J, Mead G, Grieg C, et al. Fatigue afterstroke: the development and evaluation of a casedefinition. J Psychosom Res 2007;63:539e544.
29. Mayo NE, Poissant L, Ahmed S, et al. Incorpo-rating the International Classification of Function-ing, Disability, and Health (ICF) into an electronichealth record to create indicators of function: proofof concept using the SF-12. J Am Med Inform Assoc2004;11:514e522.
30. Mead G, Lynch J, Greig C, et al. Evaluation offatigue scales in stroke patients. Stroke 2007;38:2090e2095.
31. Michael KM, Allen JK, Macko RF. Fatigue afterstroke: relationship to mobility, fitness, ambulatoryactivity, social support, and falls efficacy. RehabilNurs 2006;31:210e217.
32. Michael K, Macko RF. Ambulatory activity inten-sity profiles, fitness, and fatigue in chronic stroke.Top Stroke Rehabil 2007;14:5e12.
33. Naess H, Nyland HI, Thomassen L, Aarseth J,Myhr KM. Fatigue at long-term follow-up in youngadults with cerebral infarction. Cerebrovasc Dis2005;20:245e250.
34. Naess H, Waje-Andreassen U, Thomassen L,Nyland H, Myhr KM. Health-related quality of lifeamong young adults with ischemic stroke on long--term follow-up. Stroke 2006;37:1232e1236.

948 Vol. 38 No. 6 December 2009Lerdal et al.
35. Purebl G, Birkas E, Csoboth C, Szumska I,Kopp MS. The relationship of biological and psy-chological risk factors of cardiovascular disordersin a large-scale national representative communitysurvey. Behav Med 2006;31:133e139.
36. Røding J, Lindstrom B, Malm J, Ohman A. Frus-trated and invisibledyounger stroke patients’ expe-riences of the rehabilitation process. Disabil Rehabil2003;25:867e874.
37. Schepers VP, Visser-Meily AM, Ketelaar M,Lindeman E. Poststroke fatigue: course and its rela-tion to personal and stroke-related factors. ArchPhys Med Rehabil 2006;87:184e188.
38. Schuitemaker GE, Dinant GJ, Van Der Pol GA,Verhelst AF, Appels A. Vital exhaustion as a riskindicator for first stroke. Psychosomatics 2004;45:114e118.
39. Shaughnessy M, Resnick BM, Macko RF. Testinga model of post-stroke exercise behavior. RehabilNurs 2006;31:15e21.
40. Sorensen PS, Marquardsen J, Pedersen H,Heltberg A, Munck O. Long-term prognosis andquality of life after reversible cerebral ischemicattacks. Acta Neurol Scand 1989;79:204e213.
41. Spalletta G, Ripa A, Caltagirone C. Symptomprofile of DSM-IV major and minor depressive disor-ders in first-ever stroke patients. Am J Geriatr Psychi-atry 2005;13:108e115.
42. Schwartz SW, Carlucci C, Chambless LE,Rosamond WD. Synergism between smoking andvital exhaustion in the risk of ischemic stroke: evi-dence from the ARIC study. Ann Epidemiol 2004;14:416e424.
43. Underwood J, Clark PC, Blanton S, Aycock DM,Wolf SL. Pain, fatigue, and intensity of practice inpeople with stroke who are receiving constraint-induced movement therapy. Phys Ther 2006;86:1241e1250.
44. van de Port I, Kwakkel G, van WI, Lindeman E.Susceptibility to deterioration of mobility long-termafter stroke: a prospective cohort study. Stroke 2006;37:167e171.
45. van der Port I, Kwakkel G, Schepers VP,Heinemans CT, Lindeman E. Is fatigue an indepen-dent factor associated with activities of daily living,instrumental activities of daily living and health-related quality of life in chronic stroke? CerebrovascDis 2007;23:40e45.
46. van der Werf SP, van den Broek HL, Anten HW,Bleijenberg G. Experience of severe fatigue long afterstroke and its relation to depressive symptoms anddisease characteristics. Eur Neurol 2001;45:28e33.
47. Skaner Y, Nilsson GH, Sundquist K, Hassler E,Krakau I. Self-rated health, symptoms of depressionand general symptoms at 3 and 12 months aftera first-ever stroke: a municipality-based study in Swe-den. BMC Fam Pract 2007;8:61.
48. Multiple Sclerosis Council for Clinical PracticeGuidelines. Fatigue and multiple sclerosis: Eviden-ce-based management strategies for fatigue in mul-tiple sclerosis. Washington, DC: Paralyzed Veteransof America, 1998.
49. Vercoulen JH, Swanink CM, Fennis JF, et al.Dimensional assessment of chronic fatigue syn-drome. J Psychosom Res 1994;38:383e392.
50. Smets EM, Garssen B, Bonke B, de Haes JC. TheMultidimensional Fatigue Inventory (MFI) psycho-metric qualities of an instrument to assess fatigue.J Psychosom Res 1995;39:315e325.
51. Michielsen HJ, De VJ, Van Heck GL. Psychomet-ric qualities of a brief self-rated fatigue measure: theFatigue Assessment Scale. J Psychosom Res 2003;54:345e352.
52. Appels A, Hoppener P, Mulder P. A question-naire to assess premonitory symptoms of myocardialinfarction. Int J Cardiol 1987;17:15e24.
53. McNair DM, Lorr M, Dropplemann LF. Profileof Mood States (POMS). San Diego, CA: Educa-tional and Industrial Testing Service, 1992.
54. Carlsson GE, Forsberg-Warleby G, Moller A,Blomstrand C. Comparison of life satisfaction withincouples one year after a partner’s stroke. J RehabilMed 2007;39:219e224.
55. van de Port I, van den Bos GA, Voorendt M,Kwakkel G, Lindeman E. Identification of risk factorsrelated to perceived unmet demands in patients withchronic stroke. Disabil Rehabil 2007;29:1841e1846.
56. Lerdal A, Wahl A, Rustoen T, Hanestad BR,Moum T. Fatigue in the general population: a trans-lation and test of the psychometric properties of theNorwegian version of the Fatigue Severity Scale.Scand J Public Health 2005;33:123e130.
57. Loge JH, Ekeberg O, Kaasa S. Fatigue in thegeneral Norwegian population: normative dataand associations. J Psychosom Res 1998;45:53e65.
58. Widar M, Ek AC, Ahlstrom G. Coping withlong-term pain after a stroke. J Pain Symptom Man-age 2004;27:215e225.
59. Sisson RA. Life after a stroke: coping withchange. Rehabil Nurs 1998;23:198e203.
60. Lenz ER, Pugh LC, Milligan RA, Gift A, Suppe F.The middle-range theory of unpleasant symptoms:an update. ANS Adv Nurs Sci 1997;19:14e27.
61. Kelley ML, Sellick S, Linkewich B. Rural non-physician providers’ perspectives on palliative careservices in northwestern Ontario, Canada. J RuralHealth 2003;19:55e62.
62. Konsman JP, Parnet P, Dantzer R.Cytokine-induced sickness behavior: mechanismsand implications. Trends Neurosci 2002;25:154e159.
63. Capuron L, Gumnick JF, Musselman DL, et al.Neurobehavioral effects of interferon-alpha incancer patients: phenomenology and paroxetine

Vol. 38 No. 6 December 2009 949Poststroke Fatigue
responsiveness of symptom dimensions. Neuropsy-chopharmacology 2002;26:643e652.
64. Vollmer-Conna U. Acute sickness behaviour: animmune system-to-brain communication? PsycholMed 2001;31:761e767.
65. Okada T, Tanaka M, Kuratsune H, Watanabe Y,Sadato N. Mechanisms underlying fatigue:
a voxel-based morphometric study of chronic fa-tigue syndrome. BMC Neurol 2004;4:14.
66. de Lange FP, Kalkman JS, Bleijenberg G, et al.Neural correlates of the chronic fatigue syndrome:an fMRI study. Brain 2004;127:1948e1957.
67. Kirkevold M. The unfolding illness trajectory ofstroke. Disabil Rehabil 2002;24:887e898.