post-hearing briefing book congressional hearing 11 april 1994
TRANSCRIPT

L Post-Hearing Briefing Book
for Congressional Hearing 11 April 1994
RCC1.950005.000
UCCM / RCCl.95OOO5.001
April 12, 1994
MEMORANDUM FOR RECORD
SUBJECT: Trip Report -- Congressional Hearing on Saenger Research, Cincinnati, Ohio, April 11 , 1994
1. The Subcommittee on Administrative Law and Government Relations, ,chaired by Representative John Bryant of the House Judiciary Committee, convened "Hearings on Radiation Experiments Conducted By the University of Cincinnati Medical School with Department of Defense Funding" at 1O:OO a.m., Monday, April 11, 1994, in U.S. District Courtroom Number 822, U.S. Post Office/Federal Courthouse Building, Fifth and Walnut Streets, Cincinnati, Ohio. A copy of the hearing's agenda is at Tab A. Subcommittee members in attendance were Representative Bryant and Representative David Mann (of Cincinnati). Representative Robert Portman (also from the Cincinnati area), although not a Committee member, was invited to sit on the panel since his district includes the University of Cincinnati.
2. In his opening statement Representative Bryant explained the Subcommittee's interest. I was not able to obtain a copy of Representative Bryant's opening statement. The following summary is from my notes. He stated that the Committee has jurisdiction over compensation issues for the Government and that the Committee had already conducted hearings (February 2, 1994) that included testimony on the Cincinnati experiments. He viewed these experiments as serious and "most egregious'' with one of the fundamental issues being informed consent. Representative Bryant expected the committee to be involved with this subject for a while to come and that more hearings would be conducted before there was a markup for any legislation.
3. At Tab B are copies of Representatives Mann's and Portman's opening statements. Representative Mann's statement identified two primary issues of concern: "1) Did the patients knowledgeably consent to the experiments? And (2) Was this type of treatment appropriate for the types of illnesses suffered by the patients. By this I mean, absent the $8,000 - $10,000 per patient in Department of Defense funding would whole body radiation have been an appropriate therapy?"
Representative Portman also stated two issues of concern to the Federal government in his opening statement. "The first is the appropriateness of the Federal government compensating the victims and their families. If it is determined that the patients involved were not clearly informed in accordance with the standards for informed consent in force at the respective times of the experiments, or that these experiments became vehicles primarily for testing not treatment, then compensation, in my view, would be appropriate.

Representative Bryant said, if the information was important why didn't the Department of Defense (DoD) fund work on its own people, or would the DoD not have funded research such as this on its own people. Dr. Soper cited the 1953 directive on use of military personnel in research. He was then asked if DoD attempted to find out what was going on with patients when contracts were modified or renewed. The lack of records, which Dr. Soper pointed out was due in part to regulatory-based destruction criteria, did not indicate this was done. Representative Bryant then asked if project officers monitored effects on patients. Again, Dr. Soper's response was that the available records did not indicate such, although the DoD has been trying to locate project officer files. He did relate his own experiences as a contracting officer at DNA as an example of what was required in the 1970s/1980s. In response to the question of whether any of the contract officers were still alive, Dr. Soper said that one officer is dead, one officer is medically impaired, and that one he spoke with offered little information.
u
When his turn at questioning came, Representative Mann asked if anyone in the Pentagon cared where the patients came from, their race, IQ, and their socio-economic background. Dr. Soper responded that nothing in the files indicated such concern. Dr. Soper was then asked if total body radiation experiments were done at the University of Cincinnati prior to and after the cessation of Pentagon funding. Dr. Soper indicated that similar research was being conducted at Baylor University and Sloan-Kettering Hospital. Dr. Soper referred again to the Sloan-Kettering and Baylor studies later when asked if he was aware of any other studies funded by DoD. Representative Mann then asked how a proposal was submitted to the Pentagon in the 1950s. Dr. Soper replied that he was not completely familiar with the procedures in force then, but did describe current policy. He was then asked by Representative Mann if the 1953 document, which was once Top Secret, was now unclassified and, if so, wanted a copy for the record. Dr. Soper said a copy would be provided. Representative Mann also asked if the informed consent provision of this memo, which Dr. Soper pointed out contained detailed information, applied in the case of the Cincinnati experiments. Dr. Soper said no because it did not cover medical research conducted under contract. Representative Mann also wanted to know if the DoD knew why the National Institutes of Health (NIH) discontinued its support of the experiments in the 1960s because of "moral concerns". Dr. Soper replied that the DoD was trying to find information on this matter.
+ *
.-c-
Preceding his questions, Representative Portman expressed his concerns about the DoD's efforts in regard to contacting former DoD personnel involved with the Saenger research and the need to redouble efforts to identify DoD's role. Representative Portman then asked if there was any documentary evidence that the radiation was for the purpose of treating cancer. Dr. Soper replied that early documents do not reflect treatment of cancer, but that it is open for interpretation and that the Advisory Committee will make an evaluation. When asked if there should have been more oversight Dr. Soper said absolutely yes. Representative Portman then wondered why there was no DoD-produced summary report on the experiments once they were discontinued and asked if the lack of a report was unusual. Dr. Soper replied a report would have been helpful. Representative Portman then wanted to know if there are any documents out there that Dr. Soper was aware of that have not been released. Dr. Soper replied not to his knowledge and reiterated the Department's desire to bring things out in

I believe the second issue from the federal government's standpoint is one of disclosure -- disclosure by the Department of Defense and the Cincinnati General Hospital and all other's involved -- of all relevant information concerning the cases."
- Congressman Portman raised subsidiary issues of
"full disclosure and safeguards". He noted that the House Government Operations Committee, of which he is a member, ''has been exploring the possibility of holding hearings on disclosure of government information and safeguards."
4. Once the Committee's opening statements were completed the hearing began. The hearing was structured so that four panels (grouped by subject, for lack of a better term) appeared before the Committee. Panel I consisted of patient relatives. Panel I1 consisted of the research sponsodsupporters. Panel I11 members were those critical of the research. Panel IV was Dr. Saenger.
5. The general format allotted each panel member five minutes for an opening statement. Once witness opening statements were completed, each Committee member was allowed to question the witness. In some cases there were two rounds of questions. For the remainder of this report I will focus on the testimony of Dr. Soper, who appeared as part of Panel 11.
6 . Dr. Soper was accompanied by CAPT Robert L. Bumgarner, MC, USN, Director of the Armed Force Radiobiology Research Institute and Col. John F. Glenn, U.S. Army Medical Service Corps, who Dr. Soper identified as an expert on Federal, Department of Defense, and Army rules on the use of humans in research. I met Dr. Soper in the lawyer's lounge in the courthouse. I introduced myself, told him I was from JAYCOR and the RECC, and informed him I would be in the audience. I then introduced myself to CAPT Bumgarner and Col. Glenn.
-
7. Dr. Soper was the first witness from Panel I1 to speak before the Committee. A copy of Dr. Soper's statement with three attachments are at Tab C. Two of the attachments are the chronologies developed by RECC. It appeared that the five minute constraint on opening statements caused Dr. Soper to paraphrase his opening statement. Dr. Soper did emphasize that the Cincinnati research was to be reviewed by the President's blue ribbon advisory committee. He was followed by Dr. Cox, an expert witness who spoke favorably of the research. The final member of the panel to speak was Dr. Joseph Steger, President of the University of Cincinnati, who essentially pleaded the Fifth Amendment because of litigation over these matters.
8. After the witnesses completed their prepared statements, they were questioned by the committee. As a subjective observation, of all the witnesses who appeared, Dr. Soper received the most extensive questioning, except for, possibly, Dr. Egilman of Panel IV.
7. A summary of the question and answer session with Dr. Soper follows. The quality of the sound system in the hearing room was poor and I could not clearly hear some of what was said from where I was sitting.

open. No documents were to be retained and all that can be found will be released.
Representative Bryant ended Dr. Soper’s questioning by returning to the NIH issue.
8. Highlights of other testimony:
a. Dr. Egilman charged that there was a DoD conspiracy that provided funds to targeted hospitals that served poor whites or African Americans, thus exploiting them for nefarious purposes.
b. Dr. Saenger essentially reiterated the points made in his final report. He did provide a clear description on how DoD funds were used. He explained that in the cost of a hospital stay there are expenses for the bed the patient occupies in the hospital, medication received, etc. DoD funds did not pay for these costs, only for supplementary tests and lab work. When asked if he would have gone ahead with the experiments if he had not received DoD funding, Dr. Saenger said yes he would have. He reiterated his claim that it was an unsolicited proposal but did acknowledge that he may have received information that DoD was interested in the type of research he proposed from talking to some people. He said, however, these people did not encourage or tell him to submit a research application.
c. From comments by Representatives Bryant and Portman additional hearings on this particular issue and radiation experimentation in general appears to be a foregone conclusion.
W d. Issues that witnesses were questioned about involved informed consent, DoD funding, doses, patient reactions, the validity of the research methodology, patient selection, patient isolation techniques, Federal liability, the purpose of the research, the relationship between DoD and research institutions, oversight, and project officer responsibilities. I imagine that these issues will be relevant, in varying degrees, at other hearings and for other experiments.
e. At least one of the family witnesses alleged that her grandmother’s signature on the consent form was forged. Representative Portman asked Dr. Steger if steps were being taken to protect the records in the possession of the University of Cincinnati. As best as I could hear Dr. Steger replied steps have or will be taken to protect the sanctity of the records.
f. In my opinion Dr. Soper acquitted himself very well in an environment that was not friendly.
g. It appeared that both Representatives Mann and Portman relied heavily on the documents provided them by RECC through Dr. Soper. Representative Mann seemed to frequently use and reference the University of Cincinnati’s Ad Hoc Committee Report of 1972.
h. Representative Portman questioned Dr. Soper sharply about the existence of additional records relating to these experiments. This issue might be a potential time bomb for DoD. I do not know the extent of the file search at Suitland or the National Archives, but

Y
if somebody goes to either place and finds a sizable cache of DoD files that contain information about the research, which may not be marked project officer or contract files, the DoD’s entire effort might be open to question from less than friendly sources.
i. The hearing room was full and media coverage was intense. It was the lead story on the local five o’clock news that I saw in the airport, with more coverage promised later in the newscast.
j . I will do an in-depth review of the material at the tabs when the review of this report has been completed.
9. Dr. Saenger was the last witness. The hearing adjourned at approximately 3:OO p.m.
Research Branch RECC


UCCM / RCCl.950005.002
TABS
A - Hearing Agenda
B - Opening statements of Representatives Mann and Portman
C - Dr. Soper’s opening statement with attachments
D - Panel I statements (Mr. Joe Larkins, Gloria Nelson, and Ms. Catherine 0. Hager)
E - Remainder of Panel I1 statements (Dr. James D. Cox, M.D., Dr. Joseph Steger)
F - Panel 111 statements (Dr. David Egilman, M.D., Dr. Martha Stevens)
G - Dr. Saenger’s statement with attachments.


UCCM I RCCl.950005.003
HOUSE JUDICIARY CONNITTEE
SUBCOMMITTEE ON ADMINISTRATIVE L A W AND GOVERBMENTAL RELATION6
BEARINQ ON RADIATION BXPERIHENTB CONDUCTED BY THE UNIVERSITY OF CINCINNATI MEDICAL SCHOOL WITH DEPARTMENT OF DEFENSE PUNDIXO
-s . .I _. J .
APRXIL 11, 1994 10800 A.M. COURTROOM 2, Roon 822
L
WITNBS8BS . . .. 1 .
JOSEPH LARKINS survivor son
GLORIA NELSON Survivor granddaughter
CATHERINE HAQER Survivor daughter
4.-
DEPARTNEHT OF DEFENSE Dr. Gordon K. Soper, Principal Deputy to the Assistant to the Secretary for Atomic Energy
JAMBS COX, M.D. Professor of Radiotherapy, M.D. Anderson Cancer Center, Chairman, Radiation Therapy Oncology Group . .
President, University of Cincinnati ~, .
w.
JOSEPH BTEQIR ;. . % i t > .
C . . . I . A , . & . - , - I" ., . . -?-!*'
PANBL I11
DAVID EGILMN, MOD. Clinical Assistant Professor, Department of Community Medicine Brown University
WARTHA STEPHENS, PhoDo Professor of English, University of Cincinnati

-2-
(continued)
PANEX4 IV
EUOBNB SAENOER, M.D. Professor Emeritus of Radiology, University of Cincinnati Hospital
I .

I--
\
1

UCCM / RCCl.950005.0Ma
NEWS from Congressman David Mann
First District - Ohio The Statement of
The Honorable David Mann April 11, 1994
Mr. Chairman, I would like to thank you for agreeing to convene this hearing today. the facts with regard to the radiation tests performed at Cincinnati General Hospital in the 1960s and 1970s and I believe that this hearing will help to uncover evidence previously unknown and put some logical order to the information already available to us.
As you know, I have been working very hard to uncover
I would like to thank the witnesses who have agreed to testify before us today. My heart goes out to all of the family members of the patients we will discuss during this hearing. I know that reliving the illnesses of your loved-ones some twenty years ago has brought you real pain. Three of you will sit at the witness table today, but 1 know many more of you would have liked to share your stories. I would like to ask for unanimous consent that all of the written statements submitted to the Subcommittee and our offices be included in the record
L for today's proceedings.
I would also like to recognize and voice my appreciation for witnesses who will present their candid views of the radiation studiesi Dr. Egilman, Dr. Stephens, and Dr. Cox. I would like to thank Dr. Soper from the Department of Defense for presenting testimony on the DOD record retrieval process and President Steger for his testimony on the University's efforts to help investigate this matter. And I would like to thank Dr. Saenger for his willingness to present his views on the radiation experiments and to answer the many questions this Subcommittee will pose.
What we know to date, Mr. Chairman, is that some 87 patients received whole and partial body radiation in experiments funded in part by the Department of Defense. ,We know that the patients involved were diagnosed with various forms of cancer believed to be terminal. We also know that while they may have consented to the treatment, many or perhaps all of them were unaware of the Department of Defense interest in their conditions and many or perhaps all were unaware of the potential side effects of the radiation. We also know that written consent forms were not used until the mid 1 9 6 0 s .
( over)
- WASHINGTON OFFICE DISTRICT OFFICE
503 Cannon H.O.B. 2210 Kroger Building Washington, D.C. 20515 1014 Vine Street
(202) 225-2216 Cincinnati, OH 45202 (5 13) 684-2723 =esQ~~

But lets get to the heart of the matter. We also know that the orginial University of Cincinnati proposal to the Pentagon, the contract between U.C. and the Pentagon and the first five reports about the project from U.C. to the Pentagon all describe the purpose of the project in terms of the Pentagon's needs - - particularly its need for a biological test of radiation exposure - - and not in terms of therapy for patients. Each of the first five reports (covering the period from February 1960 to April 1967) labeled the project as IIMetabolic Changes in Humans Following Total Body Irradiationll . "Theraputic Efforts" do not even become a part of the title of the reports to the Pentagon until 1968 when the title becomes '!Radiation Effects in Man: Manifestations and Theraputic Efforts."
Note also that this project was conducted while the contract with the Pentagon and the Pentagon's money continued. Whole body radiation under this project neither preceeded nor outlived the Pentagon contract.
d
The two primary issues that I believe we need to resolve, Mr. Chairman, are (1) Did the patients knowledgeably consent to the experiments? And, ( 2 ) Was this type of treatment appropriate for the types of illnesses suffered by the patients. By this I mean, absent the $8,000 - $10,000 per patient in Department of Defense funding, would whole body radiation have been an appropriate medical therapy?
If we find that the answer to either of these questions is IInoIl then I believe we have no choice but to conclude that the radiation experiments were SIMPLY WRONG and that the government owes a huge apology to the victims, their families and the nation as a whole!
Again, Mr. Chairman, I appreciate the hard work you and your staff have put into preparing for this hearing. I believe that the testimony we hear today will enable us to craft a fair and just compensation bill in the weeks and months ahead. Thank you.

UCCM / RCCl.950005.0Ub
1
STATEMENT OF HONORABLE ROB PORTMAN
SUBCOMMITTEE ON ADMINISTRATIVE LAW AND GOVERNMENTAL RELATIONS
APRIL 11, 1994
Mr. Chairman, first, let me thank you for coming to
Cincinnati to hold this important hearing and for including me as
a panelist.
issues addressed here impact many people who live in the District
I represent. In particular, some of the patients involved lived
in what is now the Second District and many of the family members
- including some we will be hearing from today - are my constituents.
Although I am not a member of the Subcommittee, the
This matter has a long, but unfortunately incomplete,
history of public scrutiny.
that relate to not only the critical aspect of how people and
their families were treated, but also the role of the federal
government in supporting such experiments on human beings.
There remain unanswered questions
Although there are many issues that will be addressed by the
various parties involved, in my mind, there are two cardinal
issues that we as federal officials can and must address.

2
The first is the appropriateness of the federal government
compensating the victims and their families. If it is determined
that the patients involved were not clearly informed in
accordance with the standards for informed consent in force at
the respective times of the experiments, or that these
experiments became vehicles primarily for testing not treatment,
then compensation, in my view, would be appropriate. This is so
especially in light of the many potential legal barriers to
recovery, including the statute of limitations under the Federal
Tort Claims Act, sovereign immunity, and possible immunity of
government contractors. Chairman Bryant's subcommittee has
jurisdiction over the compensation issue, and I understand that
there is some precedent for compensation when the facts so merit
it. Because I am not on the subcommittee or committee, I will
not have the opportunity to vote upon this issue at the Committee
level. However, I would have the chance to consider any proposal
for compensation on the Floor of the House of Representatives.
I believe the second issue from the federal government's
standpoint is one of disclosure -- disclosure by the Department of Defense and the Cincinnati General Hospital and all others
involved -- of all relevant information concerning these cases. In addition to reviewing the merit of compensating potential
victims, I believe the government and the government contractors

3
have an obligation to be fully forthcoming, to admit mistakes if
mistakes have been made, and to ensure that safeguards are put in
place with respect to any experiments that may be conducted today
or in the future. The issues of full disclosure and safequards
may not be directly related to this forum. However, I have
particular interest in these issues, and the Government
Operations Committee upon which I serve has been exploring the
facts of the UC cases and the possibility of holding hearings on
disclosure of government information and safeguards.
Finally, I am here to listen - and to continue to learn as
much as I can about what happened 2 and 3 decades ago. This is
not a court of law; we are not here to press charges. We also
are not here to politicize a sensitive and emotional topic. I
view our role as fact finders who want to ensure that the federal
government acts responsibly and fairly with respect to the
patients and their families, to the investigators and to the DOD
officials involved in the study.
I commend all of the witnesses who have agreed to testify
before us today and very much look forward to their testimony.
Thank you Mr. Chairman.

UCCM / RCCl.950005.0Mc
OPENING REMARKS
REP. JOHN BRYANT, CHAIRMAN
SUBCOMMITTEE ON ADMINISTRATIVE L A W AND GOVERNMENTAL RELATIONS
HEARING ON RADIATION ,EXPERIMENTS CONDUCTED BY THE UNIVERSITY OF CINCINNATI MEDICAL SCHOOL WITH
DEPARTMENT OF DEFENSE FUNDING
GOOD MORNING LADIES AND GENTLEMEN AND
DISTINGUISHED GUESTS.
ORDER.
ON ADMINISTRATIVE L A W AND GOVERNMENTAL RELATIONS
MEETS TODAY I N CINCINNATI TO TAKE TESTIMONY
CONCERNING THE WHOLE AND PARTIAL BODY RADIATION
EXPERIMENTS CONDUCTED AT CINCINNATI GENERAL HOSPITAL
AND THE UNIVERSITY OF CINCINNATI MEDICAL CENTER
BETWEEN 1960 AND 1971 AND PARTIALLY FUNDED BY THE
THE SUBCOMMITTEE WILL COME TO
THE HOUSE JUDICIARY COMMITTEE'S SUBCOMMITTEE
-
DEPARTMENT OF DEFENSE.
THIS SUBCOMMITTEE HAS JURISDICTION OVER
COMPENSATION FOR CLAIMS AGAINST THE FEDERAL
GOVERNMENT BASED ON THE FEDERAL GOVERNMENT'S

L 2 WRONGDOING, AND CONSIDERED PREVIOUS COMPENSATION
LEGISLATION, SUCH AS THE CIVIL LIBERTIES ACT OF 1988, WHICH COMPENSATES JAPAN€$€-AMERICANS WHO WERE
IN INTERNMENT CAMPS DURING WORLD WAR 11, AND THE
RADIATION EXPOSURE COMPENSATION ACT OF 1990, WHICH
COMPENSATES THE RESIDENTS WHO LIVED DOWNWIND FROM
THE NEVADA NUCLEAR TEST S I T E AND THE WORKERS WHO
PARTICIPATED I N THOSE TESTS OR MINED URANIUM FOR THE
GOVERNMENT .
ON FEBRUARY 2, 1994, THE SUBCOMMITTEE HELD A
HEARING EXAMINING THE ISSUE OF GOVERNMENT-SPONSORED
EXPERIMENTS PERFORMED ON HUMANS WHO D I D NOT GIVE
INFORMED CONSENT TO THE EXPERIMENTS -- INCLUDING
SEPARATE TESTS INVOLVING RADIATION, MUSTARD GAS, LSD
AND OTHER CHEMICAL AGENTS.
THE ALLEGATIONS REGARDING THE CINCINNATI
RADIATION EXPERIMENTS ARE VERY SERIOUS. I F THEY ARE

L 3 TRUE, THESE HUMAN EXPERIMENTS COULD BE AMONG THE
MOST EGREGIOUS THAT HAVE BEEN BROUGHT TO LIGHT YET.
OUR TASK I S TO EXAMINE THESE TESTS, WHETHER THE
SUBJECTS GAVE INFORMED CONSENT TO PARTICIPATING I N
SUCH TESTS, WHAT HARM RESULTED FROM THE TESTS, AND
WHETHER COMPENSATION I S APPROPRIATE.
I WOULD LIKE TO THANK CONGRESSMAN DAVID MANN, A
MEMBER OF THIS SUBCOMMITTEE, FOR BRINGING THE
CINCINNATI RADIATION EXPERIMENTS TO THE
SUBCOMMITTEE‘S ATTENTION I COMMEND CONGRESSMAN
MANN’S COMMITMENT AND PERSISTENCE I N BRINGING THE
ISSUE OF THESE EXPERIMENTS TO THE FOREFRONT I N THE
CONGRESS AND THE ADMINISTRATION.
WORKING CLOSELY WITH THE HUMAN RADIATION INTERAGENCY
WORKING GROUP ESTABLISHED BY PRESIDENT CLINTON TO
ASSURE THAT THESE EXPERIMENTS GET SERIOUS
EXAMINATION AS PART OF THAT GROUP’S CONSIDERATION.
L-
I KNOW HE ALSO IS

4 THE SUBCOMMITTEE ALSO WOULD L I K E TO WELCOME
CONGRESSMAN ROB PORTMAN TO THIS SUBCOMMITTEE
HEARING. WHILE CONGRESSMAN PORTMAN IS NOT A MEMBER
OF THE JUDICIARY COMMITTEE OR T H I S SUBCOMMITTEE, AND
THE JUDICIARY COMMITTEE’S POLICY DOES NOT ALLOW NON-
MEMBERS TO QUESTION WITNESSES AT COMMITTEE HEARINGS,
I THINK I T IS APPROPRIATE I N THIS INSTANCE FOR
CONGRESSMAN PORTMAN TO S I T WITH THE SUBCOMMITTEE,
BASED ON H I S EXTENSIVE INVOLVEMENT WITH THIS ISSUE.
-- I THINK CONGRESSMAN PORTMAN’S INVOLVEMENT I N THIS
HEARING IS AN UNUSUAL CASE, AND I DO NOT INTEND FOR
H I S INVOLVEMENT TO BE A PRECEDENT FOR FUTURE
SUBCOMMITTEE OR COMMITTEE HEARINGS.
THE SUBCOMMIllEE EXPECTS TO BE INVOLVED I N THE
HUMAN TESTING ISSUE FOR SOME TIME TO COME. TODAY’S
HEARING I S JUST A STEP I N THE PROCESS, AND DOES NOT
FOCUS ON ANY PARTICULAR LEGISLATION.
HAVE MORE HEARINGS BEFORE WE CONSIDER WHETHER TO
WE EXPECT TO

5 - LEGISLATE I N THIS AREA, AND WILL BE WORKING CLOSELY
WITH THE CLINTON ADMINISTRATION I N FASHIONING AN
APPROPRIATE RESPONSE .
WE APPRECIATE THE PRESENCE TODAY OF ALL OUR
WITNESSES AND COMMEND THEM FOR THEIR PREPARATION.
WE REALIZE THAT WITH SO MANY WITNESSES THERE WILL
LIMITED TIME FOR MAKING YOUR STATEMENTS AND
ANSWERING QUESTIONS TODAY . HOWEVER, ADDITIONAL
MATERIALS AND ANSWERS MAY BE SUBMITTED AT A LATER
DATE . Y
I NOW RECOGNIZE CONGRESSMAN DAVID MANN TO MAKE
AN OPENING STATEMENT.
CONGRESSMAN PORTMAN, WOULD YOU L IKE TO MAKE AN
OPENING STATEMENT?


L
L
UCCM / RCCl.950005.005a
STATEMENT OF
GORDON K. SOPER, PRINCIPAL DEPUTY ASSISTANT TO THE SECRETARY OF DEFENSE
FOR ATOMIC ENERGY BEFORE THE
SUBCOMMITTEE ON ADMINISTRATIVE L A W AND GOVERNMENT RELATIONS
APRIL 11, 1994 CINCINNATI, OHIO
Mr. Chairman and Members of the Subcommittee, I am Gordon Soper the Principal Deputy in the Office of the Assistant to the Secretary of Defense for Atomic Energy. I am here to support your request of March 24th to conduct hearings on radiation experiments performed by the University of Cincinnati Medical School which were funded in part by the Department of Defense (DoD) .
If I may, Mr. Chairman, I'd like to provide a prelude to my testimony in order to put our efforts into context. Since early January, when the White House called for the formation of a senior level Interagency Working Group to coordinate the government-wide effort to uncover the nature and extent of any government sponsored experiments on individuals involving intentional exposure to ionizing radiation, the Department of Defense has been engaged in an extensive effort to discover the facts surrounding DoD sponsored human radiation experiments.
It goes without saying that the Department takes this action seriously, that it has the complete support of Secretary Perry and that we pledge to you our unqualified commitment to a thorough and complete search of all available records and the full public release of the pertinent information in those records. As Dr. Harold Smith, the Assistant to the Secretary of Defense for Atomic Energy, and the DoD focal point for this action, testified to you at your February 2 hearing on this subject, the retrieval of records is a discovery process requiring time intensive "detective work"--we are well into that process now and beginning to make excellent headway. I would be glad to take any questions that you might have regarding the Interagency Working Group process and the results we have obtained so far.
With that as background, I'd like to provide you with as complete a report as I can on the role that the Department of Defense played in the human radiation experiments conducted at the University of Cincinnati College of Medicine from 1960-1972 which were led by the principal investigator, Dr. Eugene L. Saenger, MD. My report to you is based on documents, reports and files that we have thus far been able to locate from wide and
1

varied sources--some of the official Department of Defense records were destroyed long ago as part of the normal regulatory
L instructions for disposal of contract files.
What I am going to report to you is really not newly uncovered information. The entirely unclassified University of Cincinnati studies have been previously reported in ten technical reports, 17 publications, and 26 presentations at scientific meetings; they were the subject of peer reviews at the University of Cincinnati; discussion of this work appears in the Congressional Record in 1971 and 1972; they were the subject of a report by the Comptroller General of the United States in 1972 for Senator Edward Kennedy, Chairman of the Senate Health Subcommittee; they were the subject of a separate investigation in a report by the American College of Radiology in 1972, at the request of U.S. Senator Mike Gravel; and they were--and continue to be--the subject of news articles in the press and other media reports.
In addition, Mr. Chairman, these studies will be further reviewed by the Advisory Committee on Human Radiation Experiments which just recently established by President Clinton. This Committee is composed of eminent scientists, physicians, legal experts and medical ethicists. Its purpose is to advise and guide the government on the larger questions of ethical and scientific standards of any government sponsored experiments which involved the intentional exposure to ionizing radiation. Specifically, as stated in the Executive Order issued by President Clinton in January: "The Advisory Committee shall consider whether (A) there was a clear medical or scientific purpose for the experiments; (B) appropriate medical follow-up was conducted; and (C) the experiments' design and administration adequately met the ethical and scientific standards, including standards of informed consent, that prevailed at the time of the experiments and that exist today." A major goal of DoD's "detective work" regarding the University of Cincinnati research is to provide a complete record for review by the Advisory Committee.
Next I want to run through a brief chronology of this research, based on the record compiled to date, focusing on the Department of Defense sponsorship.
In September, 1958 Dr. Eugene L. Saenger of the Department of Radiology, University of Cincinnati College of Medicine, as the principal investigator, submitted an unsolicited research proposal to the Research and Development Division of the Army Surgeon General's Office. the University of Cincinnati and not solicited by the Department of Defense. changes in humans following total body irradiation for the purpose of determining whether the presence of amino-aciduria in
The research proposal was initiated by
The application proposed to research metabolic
2

'cr
humans after radiation would provide a reliable biological marker of radiation exposure. Restated less technically, the original goal was to try to develop a simple urine test to detect the amount of radiation exposure. requested approximately $25,000 for the first year and $21,000 for two subsequent years. The proposal stated that Dr. Saenger was at that time also conducting pediatric cancer research funded by the National Institutes of Health, and preparing a Handbook on Medical Aspects of Radiation Accidents, under contract from the U.S. Atomic Energy Commission.
The University of Cincinnati
This unsolicited proposal was reviewed over the next year within the Department of Defense. reveals that at least five Army Medical Corps officers reviewed the proposal. application. Atomic Support Agency (DASA) recommended that DASA negotiate a contract with the University of Cincinnati for the study of the metabolic changes in humans following total body irradiation.
Available documentation
They recommended approval of the contract In October 1959 staff elements of the Defense
At that time a need existed within the Department of Defense to be able to determine the biological, statistical and clinical features of radiation injury. This was based on the requirements of our military commanders in the field to predict the outcome of human exposure to ionizing radiation, to predict the number of persons requiring hospitalization and to estimate the decrement in work capacity after radiation exposure on a nuclear battlefield. Remembering the context of the late 1950's, where fallout shelters were common in homes and schools and superpower tensions dominated public affairs, this was a real possibility of that time. Furthermore, such information would aid civil defense authorities in their efforts to combat the effects of nuclear explosions on the civilian population. I believe the fairly recent Chernobyl nuclear power reactor explosion underscores the importance of being able to ascertain radiation exposure effects and also understand its impact on a subject population.
So, in early 1960, a contract (DA-49-146-XZ-029, dated 1 January 1960)-was signed between DASA and the University of Cincinnati Board of Directors. The contract provided $25,085 for the study. This contract, with supplements and modifications, funded the study through February, 1964. Another contract (DA-49-146-XZ-315) carried the research until April, 1969. The final contract (DASA-01-69-C-0131), effective May, 1969, funded the research until March, 1972 when the University of Cincinnati refused DASA's offer for additional contract funding. Through 1971, the DoD spent $651,482.79 on this research.
While the search for a biological marker of radiation exposure was one steadfast aim of the University's research effort over the life of the contract, the goals of the Department of Defense were to also understand better the influence of
3

L.
radiation on the combat effectiveness of troops and to develop more suitable methods of diagnosis, prognosis, prophylaxis and treatment of radiation injuries. In order to obtain this information, the Department of Defense provided funds for laboratory, psychological and psychiatric tests to assess the effects of varying doses of whole and partial body irradiation for the treatment of cancer patients. No funds were paid to the University of Cincinnati for direct patient care nor did the Department of Defense play any part in patient selection or choice of treatment.
The University of Cincinnati College of Medicine submitted ten reports to the Department of Defense from 1961 through 1972 in accordance with the terms of the contract. I have provided the committee a copy of these ten reports as well as a number of other relevant documents that we have in our possession. Attachment 1 to my statement is a chronology summarizing major parts of the record compiled to date.
In reviewing these materials, we at DoD can understand the controversy that arose in the early 1 9 7 0 ' ~ ~ involving the University community, the press, and the Congress, and that which has reemerged this year, regarding this research. Some of the records, especially from the viewpoint of 30 years later, are troubling and raise very understandable concerns. Examples of these include statements in the University's early progress reports to the effect that only patients with non-radiosensitive tumors were selected for the research, which some see as evidence of a non-therapeutic purpose, and that symptoms and side effects were not described to the patients, which some see as evidence of the inadequacy of the informed consent procedures. On the other hand, for example, the 1972 peer review of the American College of Radiology, carried out at the request of Senator Mike Gravel, concluded that the research was validly conceived and executed, that the patient selection conformed with good medical practice, and that consent procedures complied with applicable standards. We at DoD do not at this point seek to resolve these apparent contradictions. Rather, our sole focus regarding this task is to compile a complete record and to make it available to the President's Advisory Committee and to the public.
Before concluding my statement, I want to address the constraints which the Department of Defense imposes on human subject experiments today and how we would respond to an unsolicited proposal, like the 1958 proposal from the University of Cincinnati College of Medicine, for experiments in which humans would participate.
Formal DoD policy for the protection of human subjects in research date back to at least 1953, when a then TOP SECRET Memorandum was sent to the Secretaries of the Services from Secretary of Defense C.E. Wilson, titled "Use of Human Volunteers
4

L.
L
in Experimental Research". This memorandum authorized the voluntary participation of military personnel and civilian employees in DoD conducted research for atomic, biological and chemical warfare defense and established specific standards for informed consent, minimization of risk of harm to subjects, and other matters.
Over the years, more detailed procedures were established, including incorporation in 1991 of the 1974 Department of Health and Human Services regulations for the Protection of Human Subjects, 45 C.F.R. Part 46.
Today, DoD-supported research is governed by the so-called "Common Rule''--the Federal Policy for the Protection of Human Subjects--which is part of DoD regulations at Title 32, Code of Federal Regulation, Part 219. A copy of this regulation is attached to my statement. DoD is a full partner in the government's commitment to this standard and has further defined its human use regulation in DoD Directive 3216.2, "Protection of Human Subjects in DoD Supported Research," January 7, 1983 and Department of Defense Guidance for Assurance of Compliance with the Federal Policy for the Protection of Human Subjects, June 10, 1993.
Under these regulations, a proposal like that from the University of Cincinnati would require much more supporting documentation and justification to be considered for funding. This includes the following:
1. The therapy itself, separate from the research, would require more information on the possible benefits and the known side effects.
2. Several local committees (specifically, scientific, radiation and Institutional Review Boards, or IRBs), would have to review the proposed research protocol package, with proposed consent forms, before DoD would review the proposal for acceptance.
3. It would be required that the sponsor's Institutional Review Board be made up of people from diverse backgrounds, including non-scientific perspectives, who could objectively and fully assess the proposal.
design is sound, that risks to subjects are minimized, that the selection of subjects is equitable, and that, if applicable, special protections have been adopted for any vulnerable groups mentioned.
4. The IRB record would have to document that the research
5. A written consent form signed by the patient/subject would be required for participation in the research. This
5

L
'v
consent form would require an explanation of the proposed therapy, all procedures and studies to be performed, and all expected outcomes and side effects in laymen's terms. The consent form must also state that the patient has been counseled about all of the above, and space provided for the patient to sign stating this has occurred and that the patient understands it.
6. The protocol would be required to justify withholding radiation in the control group of patients if such radiation therapy were the standard of care for the cancer each patient had.
7. The investigator would be required to give a more in
In other words, Mr. Chairman, we believe we have in place a
depth description of the known and suspected risks and the intended benefits of the research for the subject.
set of guidelines for human use experimentation that will preclude 30 years from now, hearings like we are conducting today.
So in summary, Mr. Chairman, the DoD received from the University of Cincinnati College of Medicine in 1958 an unsolicited proposal, which resulted in a contract from 1960 to 1971 supporting a human radiation experiment. DoD played no role in the selection of subjects, decisions regarding treatments, or the day-to-day conduct of the research. DoD received a series of reports describing the research results, none of which were ever classified. Data that we obtained from the University of Cincinnati studies were used to enhance our knowledge about the biological response to nuclear warfare--knowledge that we all hope will never have to be put to use. We well understand the controversy regarding this research, but make no effort at this time to resolve apparent contradictions in the voluminous record compiled to date. Our goal is to compile a complete record for the use of the President's Advisory Committee and ultimate release to the public.
That concludes my prepared remarks. I would be happy to take your questions.
6

UCCM / RCCl.950005.005b
CHRONOLOGICAL SUMMARY - - DASA/DNA REPORTS
‘cc 1. General Observations:
a. Dr. Saenger submitted ten reports to DASA/DNA from 1961 through 1972 in accordance with the terms of his contract.
research’s scope, increased sophistication of techniques, and ambitiousness of future plans. they stated the purpose of and criteria for the research, research structure and techniques, how the work was conducted, the results of the experiments, observations and analysis of the data, plans for future study, and individual case histories of patients observed during the reporting period.
2 . General information about DoD sponsorship of radiation experiments at the University of Cincinnati 1960-1971.
b. The reports provide a means to trace the expansion of the
The reports were similar in that
1958
1958-1959
1960
In September, 1958 Dr. Saenger submitted an unsolicited research application to the Research and Development Division of the Army Surgeon General’s Office. The application proposed to research metabolic changes in humans -following total body radiation for the purpose of ‘ determining whether the presence of amino-acidura in humans after radiation would provide a reliable biological marker of radiation exposure. Dr. Saenger requested approximately $25,000 for the first year and $21,000 for two subsequent years.
Over the next year the proposal was reviewed within the Defense Department and a contract negotiated. Available documentation reveals that at least four Army Medical Corps and one Medical Service Corps officer reviewed the proposal. recommended the contract application be approved. In October, 1959 the Defense Atomic Support Agency’s (DASA) Deputy Chief of Staff, Weapons Effects and Test requested, thru the Chief, DASA, the Contract Management Branch, Directorate of Logistics negotiate a contract with the University of Cincinnati for the study of the metabolic changes in humans following total body radiation.
In early 1960 a contract (DA-49-146-XZ-029, dated 1 January 1960) was signed between DASA and the University of Cincinnati Board of Directors. The contract provided $25,085 for the study. contract, with supplements and modifications,
They
This
1

1961
1961
1962
funded the study through February, 1964.
The first contract stated the technical scope of the research was "to study the phenomen of amino- acidura following irradiation, a condition which has been reported in humans and animals, to clarify some of the mechanisms responsible for amino-acidura and to determine whether it is a practical biological test of radiation exposure." The search for a biological marker of radiation exposure was one constant of Dr. Saenger's research effort over the next decade.
On 28 February 1 9 6 1 the Cincinnati project's contract was modified for the first time. The contract was modified to establish a new date for work completion to provide additional time for research on amino-aciduria following irradiation; amended the technical scope of the work to meet additional objectives of the government; provided additional funds to meet research requirements under the amended scope of work; altered portions of the contract to bring the contract in accordance with Armed Services Procurement Regulations that became effective subsequent to the signing of the original contract. contract amount increased almost $30,000 from $25 ,000 to $54 ,000 and the length of the project was extended from February, 1 9 6 1 to April, 1 9 6 2 . The scope of the work was expanded by three requirements: a breakdown of desoxyribonucleic acid and is derivatives in patients receiving total body radiation; DNA studies on patients who received partial irradiation and radiomimetic chemotherapeutic agents; and preliminary determination of appropriate psychometric tests.
The
In June, 1961 the contract was modified for the second time. An additional $650 was allocated to use the technical services of a French authority on radiobiology at a Whole Body Radiation Conference to be held by DASA at the University of Cincinnati in October, 1961.
In April, 1962 the project's contract was modified for the third time. The contract total was increased approximately $39 ,000 to $ 9 4 , 4 0 0 . project completion date was extended to April 30 , 1 9 6 3 . The scope of work was also further expanded. Additional studies were to be made of--increasing the upper range of radiation dose to 1 5 0 - 2 0 0 rad,
The
Three additional objectives were added.
I.
2

1963
1964
1965
and single doses of nitrogen mustard or other radiomimetic drug using .4mg/kilo. The following tests were to be conducted for 9 days post- treatment--urinary taurine for correlation with leukocyte count, BAIBA in urine, Kynurenic and xanthurenic acids, deoxycytidine, DNA fragments in urine, et al, xanthine and hypoxanthine in urine, urinary phosphate, and glutathione. The test were to be done over a 30 day period--routine electrophresis, immunoelectrophoresis, quantitative precipitin studies, serum urea nitrogen and/or serum creatine once weekly, urinalysis once weekly and as needed, routine hematology, and completion of the manuscript of the DASA Conference on Total Body Irradiation of October, 1961.
On April 1, 1963 the contract was modified for the fourth time. The contract was extended through April 30, 1964. Funding was increased $40,000 to $134,56. The scope of the work was further amended. Test to be conducted over a 30 day period between March 1, 1962 and February 28, 1963 were to be: (1) routine electrophesis, ( 2 ) immunoelectrophesis, (3) quantitative precipitin studies, (4) serum urea nitrogen and/or serum creatine once weekly, (5) urinalysis once weekly or as needed, and (6) routine hematology. During the same year the following tests were to be conducted over a 42 day period included 3,4,,5,6 and chromosome cultures of peripheral blood.
Contract DA-49-146-XZ-315 came into effect and funded the research from February, 1964 to April, 1969.
Ralph C. Rursiek and Dr. Eugene L. Saenger wrote a letter, dated May 17, 1965, to Director, Defense Atomic Support Agency, ATTN: STMD requesting that NWER No. 03.009 be funded at an estimated cost of $45,000 for FY65. The overall objective was to study various phenomena of desoxyribonucleic acid breakdown and other abnormalities following whole or partial body irradiation of human beings. were to be studied. The project intended to study patients for 5-14 days prior to irradiation and for as long as possible after to evaluate clinical hematological and psychological changes. Investigation of the metabolism and urinary excretion of deoxycytidine was to be continued. Bone marrow was also to be stored prior to
Fifteen patients
3

1967
1969
1971
1960-1971
irradiation. All serum was to be sent to Dr. Luzzio at Fort Knox.
In 1967 a member of the University of Cincinnati research team, Dr. James G. Kereiakes, attended an Atomic Energy Commission sponsored conference at Oak Ridge, Tennessee. A purpose of the conference was to refine the dosimetric aspects of whole and partial body irradiations being used by the medical community to treat leukemia and widely disseminated cancers. The aim of the conference was to standardize the dosimetry being used to report patient dose. Information developed at the conference revealed 1,835 patients at about 35 institutions had received whole or partial body irradiations for the palliation or treatment of cancers. The use of radiation was widely spread and acknowledged as an effective modality.
The final contract (DASA-01-69-C-0131), effective May, 1969 funded the research until March, 1972 when the University of Cincinnati refused DASA’s offer for additional contract funding.
Dr. Eugene L. Saenger wrote a letter, March 22, 1971, to Dr. Robert Loind, DASA, Attn: STMD. The cover letter with attachments forwarded the projects proposal for FY 73. The proposal requested $70,000 for a study entitled “An Appraisal of Human Studies In Radiobiological Aspects of Weapons Effectsll. description of the study’s philosophy, the role of future human research in relation to the remainder of the radiobiology program, specific areas of endeavor (eight--clinical evaluation, metabolic effects, behavioral effects, dose response studies, partial body studies, prognosis, therapeutic methods, use of healthy volunteers), and future plans regarding funding.
Through 1971 DoD ultimately spent over $650,000 on Dr. Saenger’s endeavors which treated 85 adults whole- or partial-body radiation. with localized Ewing‘s tumor were also treated with whole-body radiation. DoD funds were provided for laboratory, psychological and psychiatric tests to assess the effects of varying doses of whole and partial body irradiation. funds were paid to the University of Cincinnati for direct patient care.
A six page
Three children
No
3 . Report Summaries
4

1960-1961
1961-1963
The report for the first research period (February 19, 1960 to October 31, 1961) was DASA 1422 Supplement, which was entitled Metabolic Chanqes in Humans Followins Total Body Irradiation. This title was used for the reports through 1967. The report provides a detailed itemization of the investigations and study projects. The aim of the studies was "to obtain new information about the metabolic effects of total body and partial body irradiation so as to have a better understanding of the acute and subacute effects of irradiation in the human." During this period ten patients received total body irradiation in doses that ranged from 16 to 150 rads. Patients were selected for the study were those with llproven metastatic or far advanced cancer . . . in relatively good nutritional status, i.e., able to maintain their body weight . . . . [and] have normal hematological values." An explanation of one of the study's technique stated "the patient is told that he is to receive treatment to help his sickness. There is no discussion of subjective reactions resulting from the treatment. Other physicians, nurses and ward personnel are instructed not to discuss these aspects with the patient." The remainder of report discussed on-going studies, clinical observations, dosimetry, and other study techniques supplemented with tables and patient case histories.
The second report, DASA 1422 reported on the research from November, 1961 to April, 1963. Ten patients were treated with total body radiation in doses that ranged from 150-200 rad during the report period. The study's statement of aims was identical to that of the previous report except that it was expanded. The added aim stated "This information is necessary to provide knowledge of combat effectiveness of troops and to develop additional methods of diagnosis, prognosis, prophylaxis and treatment of these injuries." Patient selection criteria was more refined. In addition to those already stated new criteria was that "patients with lymphoma [were] excluded . . . Patients with solid neoplasms not radiosensitive are sought." The technique reported previously remained in use. Verbal consent of the patients was obtained prior to treatment.
involved complications in trying to determine the One of the issues the researchers encountered
5

.-
effects of radiation. the report stated "Physicians assess patient to be certain that the underlying disease can be evaluated. Thus, there was difficulty in selection of patients for assessment of radiation effects because of underlying disease. Patients previously treated by radiation or chemotherapy were excluded because previous treatment confounded the response to radiation in several early patients."
Throughout the narrative and near the conclusion with the researchers thoughts on "Human Effectiveness Following Whole-Body Irradiation". Several of their observations included:
"Marked hematological changes occur generally between the 25th and 35th day following exposure. Maximum recovery to be obtained generally requires about 100 days."
"Human beings recover slowly and are quite sensitive to radiation with multi-system involvement.
"Prodromal acute effects such a nausea, vomiting, anorexia, and lassitude are of the duration hours. Intermediate effects such as hematologic complications are to be conceived of in weeks.
"A previous dose of radiation does influence the incidence of acute effects. Therefore the incidence of 'combat effectiveness' will be significantly increased on re-exposure of an individual.
"...individuals with previous exposure to radiation will be less tolerant of subsequent exposures. hence troops previously exposed to 150-300r of whole body radiation will tend to show more combat ineffectiveness in the prodromal period than will those who are unexposed."
"This field of investigation has obvious important implications. Breakdown of DNA has long been implicated as the fundamental biochemical change of radiation and there is an impressive literature bearing on this point . . . The observation cited above of decrease of DOC after the administration of protective agents indicates the possibility of the use of specific prophylactic agents for the protection of humans in nuclear warfare. I I
6

A final observation was offered on future study:
"It is our opinion that human radiation studies need to be expanded.
We propose to establish facilities for withdrawal, storage, and reinfusion of autologous bone marrow. As indicated elsewhere in this report we have encountered significant hematological difficulties with a dose range of 200-325r. Therefore, to proceed with higher doses, we feel the need to protect our patients even if we might sacrifice their value for hematological evaluation after 2-3 weeks since the hematological effects are well documented. Once this technique has been developed as a support procedure we then anticipate increasing doses to higher levels.
Tables, figures and case histories rounded out the report.
1963-1964
1964-1966
DASA 1633 was the report submitted for the period May 1, 1963 to February 29, 1964 during which six patients were treated with total body radiation doses between 100 to 150 rad. The aims of the study remained as previously reported. "Normal renal function' was added to patient selection criteria. The technique to limit subjective reactions treatment was unchanged. Proposals for human study expanded on the previous report's discussion of autologous bone marrow reinfusion. The report stated:
"Storage and reinfusion of autologous bone marrow will be accomplished in the facility which has been established . . . The purpose of marrow storage and reinfusion is to protect subjects who receive doses in excess of 150 rad in the event of bone marrow failure. We hope to utilize doses between 200-300 rad."
Tables and case histories once again accompanied the report.
DASA 1844 covered not only the study years 1964 to 1966 but also provided a summary of the first six years of the experiment. Midway through the decade the aims of the project were stated as:
"This program is designed to obtain new
7

information regarding the metabolic, physiologic, immunologic, hematologic, and biochemical effects of TBR and PBR in human beings. It will then be possible to understand better the influence of radiation on combat effectiveness of troops and to develop more suitable methods of diagnosis, prognosis, prophylaxis and treatment of radiation injuries. It is our belief that information concerning radiation effects in the human being can be determined as well or better in these subjects as in the laboratory animal even though the characteristic of cancer must be kept in mind in the evaluation of the data."
On page 2 the aims were once again addressed in terms of the original scope of the study:
"A major objective of these studies has been a search for a suitable biological indicator of radiation dose in human beings . . . . At this time the urinary excretion of deoxycytidine seems to be promising as a biological indicator."
Another aim was stated on pages 2 and 3.
"Psychological and psychiatric testing has been started in 14 patients . . . . This approach will provide information on another important parameter of combat effectiveness of troops.ll
Later in the report an aspect of the psychiatric evaluation is further discussed.
'!One of the most difficult aspects of radiation injury requiring evaluation is that of performance decrement. This term is loosely used but in our laboratory it is defined as any decrease in ability to carry out assigned tasks."
Patient selection criteria was more specific:
"Patients with metastatic or incurable neoplasms are given whole partial body radiation for palliative treatment of their disease. Patients for the studies described in this report are selected from patients treated as described above providing that they satisfy the following criteria:
1. The patients have solid tumors.
2. Relatively good nutritional status Patients with lymphoma are excluded.
8

1966-1967
(ability to maintain weight). 3. Normal renal function 4. Stable hemogram in the control
period.
Twenty three additional patients were treated during the research period between 1964 and 1966. Of these patients 13 received total body radiation treatments with dosages between 25 and 150 rads. Partial body radiation doses between 100 and 300 rads were used in the treatment of 10 patients.
discussions of subjective reactions remained the same.
The technique to lfisolaterr patients from
Discussion of hematology stated:
"Since severe hematological depression was found in most patients who expired, autologous bone marrow storage has been performed for 13 patients. In only two patients has infusion been carried out. The method is being refined so as to include filtration prior to infusion. Although we have not encountered morbidity . . . filtration appears to decrease the probability of incidence of pulmonary emboli.
Accompanying the 35 page report were 122 pages of tables, and case histories of the all patients treated to date.
DASA 2179 described the treatment of four patients between May 1, 1966 and April 3 0 1967. Of the four patients treated one received total body radiation (150 rad) while the other three received partial body radiation doses in the range of 1 0 0 - 200 rad. Aims, patient selection criteria, and technique remained as previously reported. Three accomplishments were reported. The first involved "the completion of an infusion filtration system for reinfusion of autologous stored human bone marrow." As a result of the development the researchers stated "Since this instrumentation will make infusion of marrow a safer and more easily controlled procedure we feel that earlier infusion to prevent the hematological depression from radiation should be investigated." The text noted that the methods were described in a paper presented in Paris, France which cited DASA support.
The second accomplishment was the llperfection
9

1967-1968
1968-1969
by Dr. I-Wen Chen of a new, much improved method for the determination of deoxycytidine (CdR) in urine from humans and from rats."
of phage on synthetic culture medium." This development made it "possible to titrate antibody production in experimental animals and man before and after irradiation."
Future plans included the evaluation of llalterations in antibody production and /or destruction in human beings due to radiation." Observations of this nature on "the effects of radiation exposure will yield a better understanding for military planning and triage."
supplemented the text.
The third involved "the growth of two strains
Tables, figures, and case histories
The report for the period May 1, 1967 to April 30, 1968 was DASA 2168. The report's title changed to Radiation Effects in Man: Manifestations and Therapeutic Efforts. Reports carried this title for the remainder of research. This report recounted the treatment of seven patients. Four patients were treated with total body radiation doses between 100 and 200 rad. Three patients were treated with lower body partial body radiation doses of 200 to 300 rad. The report's forward noted "these studies were performed in conformation with the 'recommendations guiding doctors in clinical research' as stated in the Declaration of Helsinki of the World Medical Association (1964). Reported aims, criteria and techniques were as previously reported. Updated information from the psychiatric-psychological team noted "the number of patients who have been evaluated by the psychiatric-psychological team now totals 20." Hematology research continued. The researchers reported "seven patients received autologous bone marrow transfusions at completion of DADA 2168. Guidelines for quantity of marrow cells to be infused for successful transfusion and bone marrow protection were developed."
Case histories and tables provided additional information.
The research over the period between May 1, 1968 and April 30, 1969 was the subject of DADA 2428. Eight patients were treated during this period. Total body radiation doses of 100-200 rad were given to six patients. Two patients were treated with 200-300 rad doses of partial body radiation.
10

1969-1970
Once again the forward noted that the studies conformed to the recommendations of the Declaration of Helsinki. Aims and goals remained unchanged. In the field of hematology the report stated llsuccess has finally been obtained in autologous marrow infusion which will permit us to employ higher doses of radiation in the coming year. Several new biological dosimeters are under evaluation.Il Tables and case histories accompanied the report.
DASA 2599 reported on the research based on observations of twelve patients between May 1, 1969 and April 30, 1970. The recommendations of the Declaration of Helsinki were once again noted. A presentation by Dr. Edward B. Silberstein on the team's earlier work and the data contained in this report at the IAEA-WHO Conference in Paris on 24 June 1970 was reported.
with doses of 100-230 rad of total body radiation. The other six patients received partial body radiation doses between 150 to 300 rad. Regarding these patients the report stated "Most of the patients had inoperable metastatic carcinoma which was not amenable to conventional chemotherapy. Nevertheless, these patients were all clinically stable, many of them working daily. Several of the subjects, apparently tumor free and clinically normal after regression of regionally irradiated tumors (Ewing's tumor), received prophylactic whole body radiation."
biological dosimetry, was discussed. Several biological dosimetry issues were discussed.
During this period six patients were treated
Hematological work, specifically related to
"We are pursuing this goal at whole-body radiation doses up to 250 rad with even higher doses planned with the support of marrow autotransfusions and laminar-flow 'sterile' rooms. Large-volume partial-body irradiation is also being performed to learn more about the efficacy of chromosome aberrations as a radiation dosimeter in the more frequent situation of inhomogeneous exposure. With a linear accelerator, we hope to study the effects of various dose rate in vivo as well.
As for the continued research into the utility of deoxycytidine the report noted Ildeoxycytidinuria appears to be related to general
11

. L
1970-1971
tissue catabolism from several causes, including radiation. Other problems in using urinary CdR include variations in excretion due to race (57) and age (63) . [Note: Numbers in 0 are bibliographic reference numbers.]
Tables and case histories were included with the report. Table XI1 provided 'la summary of demographic and other pertinent data . . . for the entire group of 36 patients" observed since the start of testing.
DNA 2751T was the report for the period May 1, 1970 to April 30, 1971. Eight patients underwent treatment. Three received total body radiations dosages of 100-200 rad. Five underwent partial body radiation with doses of 300 rad. The research aims were restated.
"The University of Cincinnati studies in radiation effect in man continues as a carefully inteqrated effort to maximize clinical, psychiatric, therapeutic, biochemical, and theoretical approaches to whole and partial therapeutic irradiation as given for palliation of certain selected cancers."
To achieve these aims "the methods of applying radiation have remained essentially the same since the inception of these studies."
Acknowledgement was made of guidance provided.
"The nature of the specific projects undertaken in our laboratories reflects the consideration of many of our faculty and the thoughts and problems of the other DNA conferences organized over the past several years by Col E.J. Huycke. Valuable interchange of ideas have been stimulated by visitors from Department of Defense laboratories who give our staff a more practical insight into military problems than we might otherwise have.
Future plans were described.
"Many of the new directions in our investigation stem from concurrent advances in cytogenics, organ transplantation, bio-chemical aspects of molecular biology, and clinical aspects
12

1971-1972
of cancer therapy. 'I
"A renewed interest is manifested in chromosome aberrations as being eventually an index of 'effective radiation dose,' particularly since almost all exposures encountered in nontherapeutic circumstances will have varying degrees of nonuniformity of dose rate and dose distribution.
"As an outgrowth of our needs to afford maximum protection to patients receiving doses in the LD,, range, some new technical advances have been developed in bone marrow transfusion in patients.
Regarding biological dosimetry the report stated:
deoxycytidine ((deoxycytidine excreted in urine)) occurs late (in 2 to 4 weeks) and in the several patients studied the levels seemed directly related to the extent and depth of the burn. Radiation induced deoxycytidinuria when found occurs within 2 - 3 days and then disappears. Additional studies may suggest this test as a way of differentiating relative contribution of these two modalities of injury.
"Yet in severely burned individuals
The usual tables and case histories supplemented the narrative.
The final report in the series was DNA 3024F which was to be for the period April 1, 1971 to March 31, 1972. However, its was really a summary of the entire research effort and was a "scientific communication presented at the meeting of the American Roentgen Ray Society in Washington on 3 October 1972." It was further noted that Ilthis report has been accepted for publication in the American Journal of Roentgenology, Radium Therapy, and Nuclear Medicine."
As stated in this report the research were "to improve the treatment and general clinical management and if possible the length of survival of patients with advanced cancer. effects of radiation therapy have been given particular attention in our work."
Systemic
The issue of informed consent was addressed.
"All patients gave informed consent in
13

1971-1972
accordance with directives of the Faculty Research committee of the University of Cincinnati College of Medicine and those of the National Institutes of Health. forms in this study antedated the above requirements by two years. reviewed and approved regularly by the above committee.
The report noted that "patients become eligible for this form of treatment if they have advanced cancer for whom cure could not be anticipated....Chief among the reasons for elimination was an indication in the pretreatment phase that some risk from wide-filed radiation might ensue or that another method of treatment was considered preferable."
can identify eight cases in which there is a possibility of the therapy contributing to the mortality.
A comparison is later made between times of death of those that entered the study and received radiation treatments, and those that entered the study and did not receive radiation treatments. From this comparison the report noted:
The use of formal informed consent
The project is
From an analysis of radiation mortality "one
"Fisher's exact probability test yields a p value of 0.16, difference between the two groups. Therefore, one may conclude that in other patients described, the effect of whole- and partial-body radiation therapy was less important in contributing to death than was the extent of disease in these patients. physician selecting far advanced cancer patients for a given treatment would have about the same degree of difficulty in selecting any form of treatment for these very ill patients."
did a section entitled IIThermography as a Radiobiological Dosimeter".
indicating that there is no
Another interpretation would be that a
Tables and figures accompanied the report as
Issues arise that lead to the termination of the contractual relationship between DNA and the University of Cincinnati.
14

UCCM / RCCl.950005.005~ , '
Project Chronolow October 1971 - January 1973
L
October 8, 1971 - - An article appeared in T h e Washington Post, "Pentagon Has Contract to Test Radiation Effect on Humans", by Stuart Auerbach and Thomas O'Toole that prompted the subsequent governmental investigations of the Cincinnati project.
October 11, 1971 - - Dr. Eugene L. Saenger, Dr. Clifford G. Grulee, Dean of the University of Cincinnati College of Medicine, and Dr. Edward A. Gall, Vice President of the University of Cincinnati and Director of the University of Cincinnati Medical Center, were present at a press conference the subject of which was the impending Senate and Government Accounting Off ice (GAO) investigations of the conduct of the Cincinnati project.
October 11, 1971 - - A follow up article appeared in The Washington Post, IIPentagon's Radiation Experiments Defended". The article featured Dr. Saenger explaining the process of patients selection and Department of Defense (DOD) funding of the project.
Mid-October 1971 - - DOD developed a Fact Sheet on the Cincinnati project that discussed its contractual arrangements with the University of Cincinnati. A copy of the Fact Sheet was later entered into the Congressional Record on December 15, 1971 as an attachment to a letter from the Assistant Secretary of Defense (Legislative Affairs) to Senator Robert Taft, Jr.
November 10, 1971 - - Senator Mike Gravel wrote a letter to Dr. Robert W. McConnell, President of the American College of Radiology (ACR) requesting the ACR to conduct an evaluation of the Cincinnati Project.
November 12, 1971 - - Dean Clifford G. Grulee appointed an Ad Hoc committee to review the "whole-body radiation study" which Dr. Eugene L. Saenger had been conducting at the University of Cincinnati Medical Center. The Ad Hoc committee, chaired by Dr. Raymond Suskind, Director, Environmental Health, University of Cincinnati, was made up of eleven members and was charged with reviewing the scientific content, methodology, and data treatment of this study, as well as other aspects which the committee deemed appropriate. All eleven committee members were professors at the University of Cincinnati. Ten committee members were medical doctors and one was a Ph.D. in Physiology.
December 6, 1971 - - Mr. Ellis R. Mottur, Science Adviser to the Senate subcommittee on Health, Senate Committee on Labor and Public Welfare and Dr. Caper, both of Senator Kennedy's staff interviewed Dr. Edward B. Silberstein, University of Cincinnati Medical Center, Dr. Eugene L. Saenger, and others at Cincinnati General Hospital.
December 6, 1971 - - Dr. Robert S. Daniels, Professor and Director, Department of Psychiatry, University of Cincinnati, wrote a letter

L
L
to Dr. Raymond Suskind. The letter forwarded a list of question to Dr. Suskind for inclusion in a "our [Ad Hoc Review Committee] report on 'Total Body Radiation' project".
December 7, 1971 - - Mr. Ellis R. Mottur of Senator Kennedy's staff requested the opportunity to conduct interviews with surviving project subjects.
December 7, 1971 - - Dr. Eugene L. Saenger wrote a letter to Dr. Raymond Suskind, which discussed the impending arrival of the ACR Committee to review the project.
December 13, 1971 - - The subject of interviewing patients was broached in a letter from Senator Edward Kennedy, acting in his role as Chairman of the subcommittee on Health, Senate Committee o n Labor and Public Welfare, to Dr. Warren Bennis, president University of Cincinnati.
December 17, 1971 - - Dr. Eugene L. Saenger wrote a letter to Dr. Charles Barrett, Department of Surgery, University of Cincinnati Medical Center. The letter details Dr. Saenger's objections and concerns about providing patients to be interviewed.
December 20, 1971 - - Dr. Eugene L. Saenger authored "Comments on Differences Between Therapeutic andNon-Therapeutic Investigation". Dr. Saenger generally defended his research and methods by citing legal and medical opinions. He then went on to refute specific allegations that relate to DoD funding, informed consent techniques (Dr. Saenger made the point that since 1968 patients were told the information gained might be of use on the battlefield), follow-up, alleged contributory effects of radiation to patient deaths, racial composition of study group, and the below average intelligence level of the project subjects.
December 21, 1971 - - Dr. Eugene L. Saenger wrote a letter to Dr. Edward A. Gall. The letter was a response to Dr. Gall's request that Dr. Saenger identify patients that might be suitable for interviews by Mr. Mottur.
January 1972 - - The Ad Hoc Review Committee chaired by Dr. Raymond Suskind of the University of Cincinnati communicated its report to the Dean of the College of Medicine concerning Dr. Saenger's project. The Report contains seven sections,two of which are pertinent to DOD involvement; Section IV Financial Support of Proqram and Section V Informed Consent and Human Riqhts.
In Section IV it is reported that the request for financial support for the project was initiated by the University of Cincinnati. The systematic investigation of whole body radiation did not begin until the project was funded by the Defense Atomic Support Agency (DASA). Through March 1972 DASA had granted $651,483, 13% to 15% of the budget of the Radioisotope Division. Section IV also details the breakdown of expenditures. There is no evidence that the DASA funding was made contingent on work, ideas,

?
or suggestions proposed by DASA and that all the information reported to DASA was kept unclassified and publicly available. The
L work was also carried out by the University researchers with complete scientific freedom.
In Section V it was stated that the procedures for informed consent followed by Dr. Saenger's partial and whole body radiation project reflected the process characteristic of the University of Cincinnati and the nation. As the idea of informed consent developed nationally in the 1960's from informal, oral, and non- specific to formal, written, and more detailed, Dr. Saenger's project appropriately updated their procedure for informed consent to meet the more stringent levels required for good medical research.
January 3 , 1972 - - The ACR responded to Senator Mike Gravel's request to conduct an inquiry into the whole-body radiation therapy project supervised by Dr. Eugene L. Saenger. The ACR Report concluded that the Cincinnati project was validly conceived, stated, executed, controlled and followed up. The process of patient selection was based upon clinical considerations and conformed with good medical practice. The procedures for obtaining patient consent was valid and consistent with the recommendations of the National Institutes of Health and with the practice of most cancer centers. The ACR Report indicated procedures for obtaining informed consent were likely performed better than the average institution because of the volume of projects generated by the medical facility and the quality of the people involved. ACR urged Senator Gravel to support the projects continuation. The ACR Report also noted that DOD funds were used to support the laboratory and psychological studies, but not the treatment or the care of the patients. The ACR Report discusses at length the subject selection procedures and notes that in both race and IQ the group is representative of the patients served at Cincinnati General Hospital. The ACR Report also agreed with Dr. Saenger that
. . it seems reasonable to continue [whole-body radiation] therapy for the gravely ill individual since this method of treatment is less elaborate and with no greater risk than many present forms of chemotherapy."
January 11, 1972 - - Senator Edward Kennedy wrote a letter to Dr. Warren Bennis in reference to the University's refusal to identify patients to be interviewed by the committee. The Senator pointed out that some patients appeared in a documentary produced by National Education Television in September, 1971, and it was difficult to understand why the University allowed them to appear on TV and not before a Senate Subcommittee. Senator Kennedy stated that the University's decision was unfortunate because Ifthe most crucial element in the inquiry is the patient's perception and understanding of the experiments in which they were participating.. .
L
January 19, 1972 - - Dr. Edward A. Gall wrote a letter to Senator Kennedy responding to the Senator's January 11, 1972 letter. Dr.

1
L
Gall stated that names were provided to NET with the consent of the patients but points out that the situation had subsequently changed. In response to the Senator's request the University was sending letters to surviving patients to ask them if they would give their consent to being questioned by representatives of the subcommittee. He said that experts were consulted and they were of the opinion that any such questioning may have led to some unfavorable medical implications. Dr. Gall also asked the Senator if he would consent to a meeting with senior university officials.
January 21, 1972 - - Mr. Ellis R. Mottur wrote a letter to Dr. Edward A. Gall requesting copies of the letter (with names omitted) sent to patients or parents of surviving patients asking if they would consent to interviews.
January 25, 1972 - - Dr. Edward A. Gall wrote a letter to Mr. Ellis R. Mottur, Science Adviser, Senate Committee Labor Public Welfare, that forwarded the requested copies of letters sent to patients or parents to request interviews.
February 4, 1972 - - In a letter to Dr. Robert W. McConnell Senator Mike Gravel indicated his displeasure with the results of the ACR Report released on January 3 , 1 9 7 2 . Senator Gravel felt the report was deficient in relevant information and poorly organized. The Senator pointed out the ACR report "confirms that the patients were not thoroughly informed about the extra discomfort, the military aspects, or the possible lethal effects."
February 4, 1972 - - Mr. Myrton Tom Stewart and Mr. Robert Murphy of the General Accounting Officer (GAO) met with Dr. Eugene L. Saenger. Dr. Saenger was asked nine questions: when did the project start; did he approach DoD or vice versa [he approached]; how were parts of research funded; where were Federal funds used, etc. In response to question 4 which asked about the use of federal funds for patient care, Dr. Saenger replied that [nlo DOD funds under these contracts were at any time used for payment of patient days in any hospital. DOD funds were used for technical help, support of a biochemist, physicians, physicists and for psychological and psychiatric studies." In response to question 6 which asked if treatments were given for the benefit of the patients or DOD, Saenger responded, "that in all cases the treatment was given for the palliation of cancer of the patients and information for the Dod was a byproduct.Il
February 16, 1972 - - Dr. Warren Bennis wrote a letter to Senator Kennedy referring to meeting with the Senator and Ohio Governor Gilligan on February 24, 1 9 7 2 . Dr. Bennis included a copy of the Ad Hoc Review Committee's report, and advised the Senator that Dr. Gall would be responding within a few days to the Senator's request for an evaluation of the report by the Junior Faculty Association. The letter concluded with the promise that he was willing to cooperate with the Subcommittee in any way consistent with the health and legal rights of the patients.

L
February 17, 1972 - - Dr. Edward A. Gall wrote a letter to Senator Edward Kennedy which provided a copy of the Ad Hoc Committee Report and other documentation. Regarding the Junior Faculty Report, Dr. Gall wrote that since the Ad Hoc Committee report addressed the points raised by the Junior Faculty Association he considered the Ad Hoc report !'a complete and authoritative response.ll He also informed the Senator that they had received responses from all the surviving patients and the parents of the children treated regarding interviews. All responses had declined to be interviewed. Dr. Gall further expounded on the point made in his January 19, 1972 letter that two cancer experts (not local and not associated with the University) had given as their opinion that there would be unfavorable medical implications if patients were interviewed.
February 17, 1972 - - Dr. Edward A. Gall wrote a letter to Dr. Warren Bennis forwarding the consultant opinions from the two cancer experts. Dr. Gall noted they were in concurrence with their own physicians about the undesirability of subjecting the patients to interviews.
February 22, 1972 - - Mr. Cyril W. Kupferberg, Chair of Radiation Response Team, wrote a letter in response to an individual who requested to know if a family member was part of the experiment that was reported to DoD. The individual was not a subject of Dr. Saenger. The letter included attachments - University of Cincinnati Guideline for releasing medical information on deceased patients, an authorization for release of information form, and an example of a IIConsent for Special Study and Treatment" form.
March 31, 1972 - - The Cincinnati project contract number DASA-01- 69C-0131 expired. The University of Cincinnati had earlier indicated that it did not want to continue conducting research under this contract with the Defense Nuclear Agency.
July 5 , 1972 - - Dr. Eugene L. Saenger wrote a letter to Dr. Edward A. Gall. The three page letter appears to be Dr. Saenger's response to an article published in the Cincinnati Post on April 25, 1972. Dr. Saenger's response focuses on several points: University procedures for seeking Federal grants/contracts, issues associated with seeking DoD funds for research in FY 74 and the terminating of research utilizing FY 73 funds.
August 1, 1972 - - Several pieces of correspondence relating to the Cincinnati project were entered into the Congressional Record, including a letter from the Comptroller General of the United States to Senator Edward Kennedy summarizing the results of the GAO investigation of DOD policy regarding the protection of humans used in medical research projects and DOD responses to questions from Senate Staffers concerning DOD policy relative to human experimentation policies and procedures. The letter from the Comptroller General indicated that DOD policy was set forth by DOD
L Instruction 5030.29, dated May 12, 1964. Instruction 5030.29 states that '!The Department of Defense assumes full responsibility

L
for the protection of humans involved in research under its sponsorship whether this involves investigational drugs or other hazards." The letter also states, [cloncering the contract with the University of Cincinnati . . . [DNA] stated that the cost of radiation treatment and patient case had not been borne by their agency. They also stated that funds of the Defense Nuclear Agency had been used only to pay for supplementary laboratory analyses of patients who had received whole-body irradiation in order for the Defense Nuclear Agency to gain information in areas that were relative to national defense."
The questions from Senate staffers focused on (1) the level of human experimentation funded by DOD, ( 2 ) what authorization was needed to conduct human experiments, ( 3 ) the adequacy of information given to prospective subjects and ( 4 ) were there differing standards applied to military personnel than to civilians. DOD responded to question one that only a very small portion of its medical R&D budget was given to human experimentation. In response to question two DOD stated that although there was no standardized authorization process, all human experimentation was guided by DOD instructions and service regulations and instructions. In response to question three DOD stated that informed consents was a primary ethical and legal requirements for all DOD use of human volunteers. In response to question four DOD responded that in terms of supervision, volunteering, informed consent and freedom to terminate there was no difference.
January 11, 1973 - - Mr. Lawrence Elish released a 26 page paper titled, "Legal Rights of Human Subjects in the University of Cincinnati Whole-Body Radiation Study", that examined the legal and ethical implications of the Saenger experiments.
L-

UCCM / RCCl.950005.0054
\
3 219.101
PART 219-PROTECTION OF HUMAN SUBJECTS
DEPARTMENT OF DEFENSE
IMPLEMENTATION OF THE
"COMMON RULE" --
FEDERAL POLICY FOR THE
PROTECTION OF HUMAN
SUBJECTS
32 C.F.R. PART 219
Sec. 219.101 To what does this policy apply? 219.102 Definitions. 219.103 Assuring compliance with this
policy-research conducted or supported by a n y Federal Department or Agency.
219.104-219.106 [Reservedl 219.107 IRB Membership. 219.108 IRB functions and operations. 319.109 IRB review of research. 219.110 Expedited review procedures for
certain kinds of research involving no more than minimal risk, and for minor changes in approved research.
219.111 Criteria for IRB approval of re- search
219.112 Review by institution. 219.113 Suspension or termination of IRB
approval of research. 219.114 Cooperative research. 219.115 IRB records. 219.116 General requirements for informed
consent. 219.117 Documentation of informed con-
sent. 219.118 Applications and propossls lacking
definite plans for involvement of human subjects.
219.119 Research undertaken without the intention of involving human subjects.
219.120 hraluation and disposition of ap- plications and proposals for research LO be conducted or supported by a Federal Department or Agency.
219.121 [Reservedl 219.122 Use of Federal funds. 219.123 Early termination of research SUP-
port: Evaluation of applications and pro- posals.
219.124 Conditions. AVTHORITY: 5 U.S.C. 301: 42 U.S.C. 300v-
l (b) .
SOURCE 56 FR 28012.28021. June 18, 1991, unless otherwise noted.
Q219.101 To what does this policy apply? (a) Eicept as provided in paragraph
(b) of this section. this policy applies to all research involving human sub- jects conducted, supported or other- wise subject to regulation by any fed- eral department or agency which takes appropriate administrative action to make the policy applicable to such re- search. This includes research con- ducted by federal civilian employees or military personnel, except that each department or agency head may adopt such procedural modifications as may
289
8 219.101 32 CFR Ch. I (7-1-93 Edition)
(i) The human subjects are elected or appointed public officials or candi- dates for public office; or (W federal statutets) requirets) without exception that the confidentiality of the person- ally identifiable information will be maintained throughout the research and thereafter.
(4) Research, involving the collec- tion or study of existing data, docu- ments, records, pathological speci- mens, or diagnostic specimens, if these sources are publicly available or if the information is recorded by the investi- gator in such a manner that subjects cannot be identified, directly or through identifiers linked to the sub- jects.
(5) Research and demonstration projects which are conducted by or subject to the approval of department or agency heads, and which are de- signed to study, evaluate, or otherwise examine:
(i) Public benefit or service pro- grams; (ii) procedures for obtaining benefits or services under those pro- grams; (iii) possible changes in or al- ternatives to those programs or proce- dures; or (iv) possible changes in meth- ods or levels of payment for benefits or services under those programs.
(6) Taste and food quality evaluation and consumer acceptance studies, (i) if wholesome foods without additives are consumed or (ii) if a food is consumed that contains a food ingredient at or below the level and for a use found to be safe, or agricultural chemical or en- vironmental contaminant at or below the level found to be safe, by the Food and Drug Administration or approved by the Environmental Protection Agency or the Food Safety and Inspec- tion Service of the U.S. Department of Agriculture.
tc) Department or agency heads retain f i n a l judgment as to whether a particular activity is covered by this policy.
(d> Department or agency heads may require that specific research ac- tivities or classes of research activities conducted, supported, or otherwise subject to regulation by the depart- ment or agency but not otherwise COV- ered by this policy, comply with some or all of the requirements of this policy.
I
I I
I
w I
~
I
be appropriate from an administrative standpoint. It also includes research conducted, supported, or otherwise subject to regulation by the federal government outside the United States.
(1) Research that is conducted or supported by a federal department or agency, whether or not it is regulated as defined in 5 219.102te1, must comply with all sections of this policy.
(2) Research that is neither conduct- ed nor supported by a federal depart- ment or agency but is subject to regu- lation as defined in 8219.102te) must be reviewed and approved, in compli- ance with 8219.101. 0219.102, and 8 219.107 through 8 219.117 of this policy, by an institutional review board (IRB) that operates in accord- ance with the pertinent requirements of this policy.
(b) Unless otherwise required by de- partment or agency heads, research activities in which the only involve- ment of human subjects will be in one or more of the following categories are exempt from this policy:
(1) Research conducted in estab- lished or commonly accepted educa- tional settings, involving normal edu- cational practices, such as (i) research on regular and special education in- structional strategies, or (ii) research on the effectiveness of or the compari- son among instructional techniques, curricula, or classroom management methods.
(2) Research involving the use of educational tests (cognitive, diagnos- tic, aptitude, achievement), survey procedures, interview procedures or observation of public behavior, unless:
(i) Information obtained is recorded in such a manner that human subjects can be identified, directly or through identifiers linked to the subjects; and (ii) any disclosure of the human sub- jects’ responses outside the research could reasonably place the subjects a t risk of criminal or civil liability or be damaging to the subjects’ financial standing. employability, or reputation.
(3) Research involving the use of educational tests (cognitive, diagnos- tic, aptitude, achievement 1. survey procedures, interview procedures, or observation of public behavior that is not exempt under paragraph (b)(2) of this section. if:
290

Office of the Secretary of Defense 5 219.102
L
L.
(e) Compliance with this policy re- quires compliance with pertinent fed- eral laws or regulations which provide additional protections for human sub- jects.
( f ) This policy does not affect any state or local laws or regulations which may otherwise be applicable and which provide additional protec- tions for human subjects.
(g) This policy does not affect any foreign laws or regulations which may otherwise be applicable and which provide additional protections to human subjects of research.
(h) When research covered by this policy takes place in foreign countries, procedures normally followed in the foreign countries to protect human subjects may differ from those set forth in this policy. [An example is a foreign institution which complies with guidelines consistent with the World Medical Assembly Declaration (Declaration of Helsinki amended 1989) issued either by sovereign states or by an organization whose function for the protection of human research subjects is internationally recognized.3 In these circumstances, if a depart- ment or agency head determines that the procedures prescribed by the insti- tution afford protections that are at least equivalent to those provided in this policy, the department or agency head may approve the substitution of the foreign procedures in lieu of the procedural requirements provided in this policy. Except when otherwise re- quired by statute. Executive Order, or the department or agency head, no- tices of these actions as they occur will be published in the FEDERAL REGISTER or will be otherwise published as pro- vided in department or agency proce- dures.
(i) Unless otherwise required by law, department or agency heads may waive the applicability of some or all of the provisions of this policy to spe- cific research activities or classes of re- search activities otherwise covered by this policy. Except when otherwise re- quired by statute or Executive Order, the department or agency head shall forward advance notices of these ac- tions to the Office for Protection from Research Risks, Department of Health and Human Services (HHS), and shall
also publish them in the FEDERAL REG- ISTER or in such other manner as pro- vided in department or agency proce- dures. C56 FR 28012. 28021. June 18, 1991. as amended at 56 FR 29756, June 28,19911
9 219.102 Definitions. (a) Department or agency head
means the head of any federal depart- ment or agency and any other officer or employee of any department or agency to whom authority has been delegated.
(b) Institution means any public or private entity or agency (including federal, state, and other agencies).
tc) Legally authorized representative means an individual or judicial or other body authorized under applica- ble law to consent on behalf of a pro- spective subject to the subject’s par- ticipation in the procedurets) involved in the research.
(d) Research means a systematic in- vestigation, including research devel- opment, testing and evaluation, de- signed to develop or contribute to gen- eralizable knowledge. Activities which meet this definition constitute re- search for purposes of this policy, whether or not they are conducted or supported under a program which is considered research for other pur- poses. For example, some demonstra- tion and service programs may include research activities .
(e) Research subject to regulation, and similar terms are intended to en- compass those research activities for which a federal department or agency
1 Institutions with HHS-approved Bssur- ances on file will abide by provisions of title 45 CFR part 46 subparts A-D. Some of the other Departments and Agencies have in- corporated all provisions of title 45 CFR part 46 into their policies and procedures as well. However, the exemptions at 45 CF’R 46.10Ub) do not apply to research involving prisoners, fetuses, pregnant women, or human in vitro fertilization. subparts B and C. The exemption at 45 CF’R 46.101(b)(2), for research involving survey or interview procedures or observation of public behav- ior, does not apply to research with chil- dren, subpart D, except for research involv- ing observations of public behavior when the investigatorts) do not participate in the activities being observed.
291

L
8 219.103
has specific responsibility for regulat- ing as a research activity, (for exam- ple, Investigational New Drug require- ments administered by the Food and Drug Administration). It does not in- clude research activities which are in- cidentally regulated by a federal de- partment or agency solely as part of the department’s or agency’s broader responsibility to regulate certain types of activities whether research or non- research in nature (for example, Wage and Hour requirements administered by the Department of Labor).
( f 1 Human subject means a living in- dividual about whom an investigator (whether professional or student) con- ducting research obtains
(1) Data through intervention or interaction with the individual, or
(2) Identifiable private information. Intervention includes both physical procedures by which data are gathered (for example, venipuncture) and ma- nipulations of the subject or the sub- ject’s environment that are performed for research purposes. Interaction in- cludes communication or interpersonal contact between investigator and sub- ject. “Private information” includes information about behavior that occurs in a context in which an indi- vidual can reasonably expect that no observation or recording is taking place, and information which has been provided for specific purposes by an individual and which the individual can reasonably expect will not be made public (for example, a medical record). Private information must be individually identifiable (Le., the iden- t i ty of the subject is or may readily be ascertained by the investigator or as- sociated with the information) in order for obtaining the information to constitute research involving human subjects.
(g) IRB means an institutional review board established in accord with and for the purposes expressed in this policy.
(h) IRB approval means the deter- mination of the IRB that the research has been reviewed and may be con- ducted at an institution within the constraints set forth by the IRB and by other institutional and federal re- quirements.
32 CFR Ch. I (7-1-93 Edition)
(i) Minimal risk means that the probability and magnitude of harm or discomfort anticipated in the research are not greater in and of themselves than those ordinarily encountered in daily life or during the performance of routine physical or psychological ex- aminations or tests.
<j> CertVication means the official notification by the institution to the supporting department or agency, in accordance with the requirements of this policy, that a research project or activity involving human subjects has been reviewed and approved by an IRB in accordance with an approved assurance.
§ 219.103 Assuring compliance with this policy-research conducted or support- ed by any Federal Department or Agency.
(a) Each institution engaged in re- search which is covered by this policy and which is conducted or supported by a federal department or agency shall provide written assurance satis- factory to the department or agency head that it will comply with the re- quirements set forth in this policy. In lieu of requiring submission of an as- surance. individual department or agency heads shall accept the exist- ence of a current assurance, appropri- ate for the research in question, on file with the Office for Protection from Research Risks, HHS, and ap- proved for federalwide use by that office. When the existence of an HHS- approved assurance is accepted in lieu of requiring submission of an assur- ance, reports (except certification 1 re- quired by this policy to be made to de- partment and agency heads shall also be made to the Office for Protection from Research Risks, HHS.
(b) Departments and agencies will conduct or support research covered by this policy only if the institution has an assurance approved as provided in this section, and only if the institu- tion has certified to the department or agency head that the research has been reviewed and approved by an IRB provided for in the assurance, and will be subject to continuing review by the IRB. Assurances applicable to fed-
292

L
i
I
I L
Office of the Secretory of Defense 0 219.103
erally supported or conducted re- ous IRB review: and (iii) for ensuring search shall at a minimum include: prompt reporting to the IRB of pro-
(1) A statement of principles govern- posed changes in a research activity, ing the institution in the discharge of and for ensuring that such changes in its responsibilities for protecting the approved research, during the period rights and welfare of human subjects for which IRB approval has already Of research conducted at or sponsored been given, may not be initiated with- by the institution, regardless of out IRB review and approval except whether the research is subject to fed- when necessary to eliminate apparent era1 regulation. This may include an immediate hazards to the subject. appropriate existing code, declaration, (5 Written procedures for ensuring or statement of ethical principles, or a prompt reporting to the IRB, appro- Statement formulated by the institu- priate institutional officials, and the t i O n itself. This requhement does not department Or agency head of (i) any Preempt Provisions Of this Policy aP- unanticipated problems involving risks plicable to department- or agency-sup- to subjects Or others Or any serious or ported or regulated research and need continuing noncompliance with this not be applicable to any research ex- policy or the requiremenu or determi- empted or waived under 8 219.101 (b) nations of the IRB and (ii) any or (i). pension or termination of IRB approv-
(2) Designation of one or more IRBs ala established in accordance with the re- quiremenu of this Policy, and for tc) The assurance shall be executed
by an individual authorbed to act for which provisions are made for meeting the institution and to aSSume on space and sufficient staff to support behalf of the institution the obliga- the IRB’s review and recordkeeping tions imposed by this policy and shall
be filed in such form and manner as duties. (3) A list of IRB members identified the department Or agency head pre- by name; earned degrees; representa- scribes. tive capacity; indications of experience (d) The department or agency head such as board certifications, licenses, will evaluate all assurances submitted etc., sufficient to describe each mem-
ber’s chief anticipated contributions to in accordance with this policy through IRB deliberations; and any such Officers and emplOyeeS Of the de- ment or other relationship between partment or agency and such experts each member and the institution; for or consultants engaged for this Pur- example: full-time employee. part-time pose as the department or agency employee, member of governing panel head determines to be appropriate. or board, stockholder, paid or unpaid The Or agency head’s eval-
Changes in IRB member- uation W i l l take into consideration the ship shall be reported to the depart- adequacy of the proposed IRB in light merit or agency head, unless in accord Of the anticipated Scope Of the i n s t i t U - with 9 219.103(a) of this policy, the ex- tion’s research activities and the types istence of an HHS-approved w u a n c e Of subject POpUhtiOns likely to be in- is accepted. In this case, change in volved, the appropriateness of the pro- IRB membership shall be reported to posed initid and Continuing review the Office for Protection from Re- procedures in light of the probable search Risks, HHS. risks, and the size and complexity of
(4 ) Written procedures which the the institution. IRB will follow ( i ) for conducting its (e) On the basis of this evaluation, initial and continuing review of re- the department or agency head may search and for reporting its findings approve or disapprove the assurance, and actions to the investigator and the or enter h t o negotiations to develop institution; (ii) for determining which an approvable one. The department or projects require review more often agency head may limit the period than annually and which projects during which any particular approved need verification from sources other assurance or class of approved assur- than the investigators that no materi- ances shall remain effective or other- al changes have occurred since previ- wise condition or restrict approval.
293

Y
3 219.107
(f 1 Certification is required when the research is supported by a federal de- partment or agency and not otherwise exempted or waived under Q 219.101 (b) or (i). An institution with an ap- proved assurance shall certify that each application or proposal for re- search covered by the assurance and by Q 219.103 of this Policy has been re- viewed and approved by the IRB. Such certification must be submitted with the application or proposal or by such later date as may be prescribed by the department or agency to which the ap- plication or proposal is submitted. Under no condition shall research cov- ered by p 219.103 of the Policy be sup- ported prior to receipt of the certifica- tion that the research has been re- viewed and approved by the IRB. In- stitutions without an approved assur- ance covering the research shall certi- fy within 30 days after receipt of a re- quest for such a certification from the department or agency, that the appli- cation or proposal has been approved by the IRB. If the certification is not submitted within these time limits, the appiication or proposal may be re- turned to the institution. (Approved by the Office of Management and Budget under control number 9999- 0020)
C56 FR 28012, 28021, June 18. 1991, as amended at 56 FR 29756, June 28,19911
99 219.104-219.106 [Reserved]
0 219.107 IRB membership. (a) Each IRB shall have at least five
members, with varying backgrounds to promote complete and adequate review of research activities commonly conducted by the institution. The IRB shall be sufficiently qualified through the experience and expertise of its members, and the diversity of the members, including consideration of race, gender. and cultural backgrounds and sensitivity to such issues as com- munity attitudes, to promote respect for its advice and counsel in safeguard- ing the rights and welfare of human subjects. In addition to possessing the professional competence necessary to review specific research activities. the IRB shall be able to ascertain the ac- ceptability of proposed research in terms of institutional commitments
32 CFR Ch. (7-1-93 Edition)
and regulations. applicable law, and standards of professional conduct and practice. The IRB shall therefore in- clude persons knowledgeable in these areas. If an IRB regularly reviews re- search that involves a vulnerable cate- gory of subjects, such as children, pris- oners, pregnant women, or handi- capped or mentally disabled persons, consideration shall be given to the in- clusion of one or more individuals who are knowledgeable about and experi- enced in working with these subjects.
(b) Every nondiscriminatory effort will be made to ensure that no IRB consists entirely of men or entirely of women, including the institution’s con- sideration of qualified persons of both sexes, so long as no selec-ion is made to the IRB on the basis L.; gender. No IRB may consist entirely of members of one profession.
(c) Each IRB shall include at least one member whose primary concerns are in scientific areas and at least one member whose primary concerns are in nonscientific areas.
(d) Each IRB shall include at least one member who is not otherwise af- filiated with the institution and who is not part of the immediate family of a person who is affiliated with the insti- tution.
(e) No IRB may have a member par- ticipate in the IRB’s initial or continu- ing review of any project in which the member has a conflicting interest, except to provide information request- ed by the IRB.
( f ) An IRB may, in its discretion. invite individuals with competence in special areas to assist in the review of issues which require expertise beyond or in addition to that available on the IRB. These individuals may not vote with the IRB.
§ 219.108 IRB functions and operations. In order to fulfill the requirements
of this policy each IRB shall: (a) Follow written procedures in the
same detail as described in 8 219.103(b:(4) and, to the extent re- quired by. Q 219.103(b)(5).
(b) Except when an expedited review procedure is used (see $219.110), review proposed research at convened meetings at which a majority of the
294

Office of the Secretary of Defense 0 219.1 11
!
members of the IRB are present, in- cluding at least one member whose primary concerns are in nonscientific areas. In order for the research to be approved, it shall receive the approval of a majority of those members present at the meeting. Q 219.109 IRB Review of Research.
(a) An IRB shall review and have au- thority to approve, require modifica- tions in (to secure approval), or disap- prove all research activities covered by this policy.
(b) An IRB shall require that infor- mation given to subjects as part of in- formed consent is in accordance with 8219.116. The IRB may require that information, in addition to that specif- ically mentioned in 8 219.116, be given to the subjects when in the IRB’s judgment the information would meaningfully add to the protection of the rights and welfare of subjects.
tc) An IRB shall require documenta- tion of informed consent or may waive documentation in accordance with 8 219.117.
(d) An IRB shall notify investigators and the institution in writing of its de- cision to approve or disapprove the proposed research activity, or of modi- fications required to secure IRB ap- proval of the research activity. If the IRB decides to disapprove a research activity, it shall include in its written notification a statement of the reasons for its decision and give the investiga- tor an opportunity to respond in person or in writing.
(e) An IRB shall conduct continuing review- of research covered by this policy at intervals appropriate to the degree of risk, but not less than once per year, and shall have authority to observe or have a third party observe the consent process and the research. (Approved by the Office of Management and Budget under control number 9999- 0020)
Q 219.110 Expedited review procedures for certain kinds of research involving no more than minimal risk, and for minor changes in approved research.
(a) The Secretary, HHS, has estab- lished, and published as a Notice in the FEDERAL REGISTER, a list of catego- ries of research that may be reviewed
by the IRB through an expedited review procedure. The list will be amended, as appropriate after consul- tation with other departments and agencies, through periodic republica- tion by the Secretary, HHS, in the F ~ E R A L REGISTER. A copy of the list is available from the Office for Protec- tion from Research Risks, National In- stitutes of Health. HHS, Bethesda, Maryland 20892.
(b) An IRB may use the expedited review procedure to review either or both of the following:
(1) Some or all of the research ap- pearing on the list and found by the reviewerh) to involve no more than minimal risk,
(2) Minor changes in previously ap- proved research during the period (of one year or less) for which approval is authorized. Under an expedited review procedure, the review may be carried out by the IRB chairperson or by one or more ex- perienced reviewers designated by the chairperson from among members of the IRB. In reviewing the research, the reviewers may exercise aU of the authorities of the IRB except that the reviewers may not disapprove the re- search. A research activity may be dis- approved only after review in accord- ance with the non-expedited proce- dure set forth in 8 219.108(b).
(c) Each IRB which uses an expedit- ed review procedure shall adopt a method for keeping all members ad- vised of research proposals which have been approved under the procedure.
(d) The department or agency head may restrict, suspend, terminate, or choose not to authorize an institu- tion’s or IRB’s use of the expedited review procedure. 0219.111 Criteria for IRB approval of re-
(a) In order to approve research cov- ered by this policy the IRB shall de- termine that all of the following re- quirements are satisfied: (1) Risks to subjects are minimized:
(i) By using procedures which are con- sistent with sound research design and which do not unnecessarily expose subjects to risk, and (ii) whenever ap- propriate, by using procedures already
search.
295

6 219.1 12
being performed on the subjects for diagnostic or treatment purposes.
(2) Risks to subjects are reasonable in relation to anticipated benefits, if any, to subjects. and the importance of the knowledge that may reasonably be expected to result. In evaluating risks and benefits, the IRB should consider only those risks and benefits that may result from the research (as distinguished from risks and benefits of therapies subjects would receive even if not participating in the re- search). The IRB should not consider possible long-range effects of applying knowledge gained in the research (for example, the possible effects of the re- search on public policy) as among those research risks that fall within the purview of its responsibility.
(3) Selection of subjects is equitable. In making this assessment the IRB should take into account the purposes of the research and the setting in which the research will be conducted and should be particularly cogniwrnt of the special problems of research in- volving vulnerable populations, such as children, prisoners, pregnant women, mentally disabled persons, or economically or educationally disad- vantaged persons.
(4) Informed consent will be sought from each prospective subject or the subject’s legally authorized represent- ative, in accordance with, and to the extent required by 0 219.116.
(5) Informed consent will be appro- priately documented, in accordance with, and to the extent required by 9 219.117.
(6) When appropriate, the research plan makes adequate provision for monitoring the data collected to ensure the safety of subjects.
(7) When appropriate, there are ade- quate provisions to protect the privacy of subjects and to maintain the confi- dentiality of data.
(b) When some or all of the subjects are likely to be vulnerable to coercion or undue influence, such as children, prisoners, pregnant women, mentally disabled persons, or economically or educationally disadvantaged persons, additional safeguards have been in- cluded in the study to protect the rights and welfare of these subjects.
32 CFR Ch. I (7-1-93 Edition)
0 219.112 Review by institution. Research covered by this policy that
has been approved by an IRB may be subject to further appropriate review and approval or disapproval by offi- cials of the institution. However, those officials may not approve the research if it has not been approved by an IRB. S 219.113 Suspension or termination of
An IRB shall have authority to sus- pend or terminate approval of re- search that is not being conducted in accordance with the IRB’s require- ments or that has been associated with unexpected serious harm to subjects. Any suspension or termination of ap- proval shall include a statement of the reasons for the IRB’s action and shall be reported promptly to the investiga- tor, appropriate institutional officials, and the department or agency head. (Approved by the Office of Management and Budget under control number 9999- 0020)
§ 219.114 Cooperative research. Cooperative research projects are
those projects covered by this policy which involve more than one institu- tion. In the conduct of cooperative re- search projects, each institution is re- sponsible for safeguarding the rights and welfare of human subjects and for complying with this policy. With the approval of the department or agency head, an institution participating in a cooperative project may enter into a joint review arrangement, rely upon the review of another qualified IRB, or make similar arrangements for avoiding duplication of effort. § 219.115 IRB records.
(a) An institution, or when appropri- ate an IRB, shall prepare and main- tain adequate documentation of IRB activities. including the following:
(1) Copies of all research proposals reviewed, scientific evaluations, if any, that accompany the proposals, ap- proved sample consent documents, progress reports submitted by investi- gators, and reports of injuries to sub- jects.
(2) Minutes of IRB meetings which shall be in sufficient detail to show at-
IRB approval of research.
296

I Office of the Secretary of Defense 5 219.1 16
tendance at the meetings; actions taken by the IRB; the vote on these actions including the number of mem- bers voting for, against, and abstain- ing; the basis for requiring changes in or disapproving research: and a writ- ten summary of the discussion of con- troverted issues and their resolution.
(3) Records of continuing review ac- tivities.
(4) Copies of all correspondence be- tween the IRB and the investigators.
(5) A list of IRB members in the same detail as described is 8 219.103(b)(3).
(6) Written procedures for the IRB in the same detail as described in § 219.103(b)(4) and ff 219.103(b)(5).
(7 1 Statements of significant new findings provided to subjects, as re- quired by 8219.116(b)(5).
(b) The records required by this policy shall be retained for at least 3 years, and records relating to research which is conducted shall be retained for at least 3 years after completion of the research. All records shall be ac- cessible for inspection and copying by authorized representatives of the de- partment or agency at reasonable times and in a reasonable manner. (Approved by the Office of Management and Budget under control number 9999- 0020)
Q 219.116 General requirements for in-
Except as provided elsewhere in this policy, no investigator may involve a human being as a subject in research covered by this policy unless the inves- tigator has obtained the legally effec- tive informed consent of the subject or the subject’s legally authorized repre- sentative. An investigator shall seek such consent only under circum- stances that provide the prospective subject or the representative sufficient opportunity to consider whether or not to participate and that minimize the possibility of coercion or undue in- fluence. The information that is given to the subject or the representative shall be in language understandable to the subject or the representative. No informed consent, whether oral or written, may include any exculpatory language through which the subject or the representative is made to waive
formed consent.
or appear to waive any of the subject’s legal rights, or releases or appears to release the investigator, the sponsor, the institution or its agents from li- ability for negligence.
(a) Basic elements of informed con- sent. Except as provided in paragraph tc) or (d) of this section, in seeking in- formed consent the following informa- tion shall be provided to each subject:
(1) A statement that the study in- volves research, an explanation of the purposes of the research and the ex- pected duration of the subject’s par- ticipation, a description of the proce- dures to be followed, and identifica- tion of any procedures which are ex- perimental;
(2) A description of any reasonably foreseeable risks or discomforts to the subject:
(3) A description of any benefits to the subject or to others which may reasonably be expected from the re- search;
(4) A disclosure of appropriate alter- native procedures or courses of treat- ment, if any, that might be advanta- geous to the subject;
(5) A statement describing the extent, if any, to which confidentiality of records identifying the subject will be maintained;
(6) For research involving more than minimal risk, an explanation as to whether any compensation and an ex- planation as to whether any medical treatments are available if injury occurs and, if so, what they consist of, or where further information may be obtained:
(7) An explanation of whom to con- tact for answers to pertinent questions about the research and research sub- jects’ rights, and whom to contact in the event of a research-related injury to the subject: and
(8) A statement that participation is voluntary, refusal to participate will involve no penalty or loss of benefits to which the subject is otherwise enti- tled, and the subject may discontinue participation at any time without pen- alty or loss of benefits to which the subject is otherwise entitled. (b) Additional elements of informed
consent. When appropriate, one or more of the following elements of in-
297

9 219.1 17
formation shall also be provided to each subject: (1) A statement that the particular
treatment or procedure may involve risks tu the subject tor to the embryo or fetus, if the subject is or may become pregnant) which are currently unforeseeable;
(2) Anticipated circumstances under which the subject’s participation may be terminated by the investigator without regard to the subject’s con- sent;
(3) Any additional costs to the sub- ject that may result from participa- tion in the research;
(4) The consequences of a subject’s decision to withdraw from the re- search and procedures for orderly ter- mination of participation by the sub- ject;
(5) A statement that significant new findings developed during the course of the research which may relate to the subject’s willingness to continue participation will be provided to the subject; and
(6) The approximate number of sub- jects involved in the study.
tc) An IRB may approve a consent procedure which does not include, or which alters, some or all of the ele- ments of informed consent set forth above, or waive the requirement to obtain informed consent provided the IRB finds and documents that:
( 1) The research or demonstration project is to be conducted by or sub- ject to the approval of state or local government officials and is designed to study, evaluate, or otherwise examine: (i) Public benefit of service programs: (ii) procedures for obtaining benefits or services under those programs; (iii) possible changes in or alternatives to those programs or procedures; or (iv) possible changes in methods or levels of payment for benefits or services under those programs; and
(2) The research could not practica- bly be carried out without the waiver or alteration.
(d) An IRB may approve a consent procedure which does not include, or which alters, some or all of the ele- ments of informed consent set forth in this section, or waive the requirements to obtain informed consent provided the IRB finds and documents that:
32 CFR Ch. I (7-1-93 Edition)
(1) The research involves no more than minimal risk to the subjects:
(2) The waiver or alteration will not adversely affect the rights and welfare of the subjects;
(3) The research could not practica- bly be carried out without the waiver or alteration: and
(4) Whenever appropriate, the sub- jects will be provided with additional pertinent information after participa- tion.
(e) The informed consent require- ments in this policy are not intended to preempt any applicable federal, state, or local laws which require addi- tional information to be disclosed in order for informed consent to be legal- ly effective.
(f 1 Nothing in this policy is intended to limit the authority of a physician to provide emergency medical care, to the extent the physician is permitted to do so under applicable federal, state, or local law. (Approved by the Office of Management and Budget under control number 9999- 0020)
Q 219.117 Documentation of informed con- sent.
(a) Except as provided in paragraph (c) of this section, informed consent shall be documented by the use of a written consent form approved by the IRB and signed by the subject or the subject’s legally authorized represent- ative. A copy shall be given to the person signing the form.
(b) Except as provided in paragraph tc) of this section, the consent form may be either of the following:
(1) A written consent document that embodies the elements of informed consent required by 9 219.116. This form may be read to the subject or the subject’s legally authorized represent- ative, but in any event, the investiga- tor shall give either the subject or the representative adequate opportunity to read it before it is signed; or
(2) A short form written consent document stating that the elements of informed consent required by Q 219.116 have been presented orally to the sub- ject or the subject’s legally authorized representative. When this method is used, there shall be a witness to the
298

L
I
L
Office of the Secretary of Defense
oral presentation. Also, the IRB shall approve a written summary of what is to be said to the subject or the repre- sentative. Only the short form itself is to be signed by the subject or the rep- resentative. However, the witness shall sign both the short form and a copy of the summary, and the person actually obtaining consent shall sign a copy of the summary. A copy of the summary shall be given to the subject or the representative, in addition to a copy of the short form.
tc) An IRB may waive the require- ment for the investigator to obtain a signed consent form for some or all subjects if it f inds either: (1) That the only record linking the
subject and the research would be the consent document and the principal risk would be potential harm resulting from a breach of confidentiality. Each subject will be asked whether the sub- ject wants documentation linking the subject with the research, and the sub- ject’s wishes will govern: or
(2) That the research presents no more than minimal risk of harm to subjects and involves no procedures for which written consent is normally required outside of the research con- text.
In cases in which the documentation requirement is waived, the IRB may require the investigator to provide subjects nlth a written statement re- garding the research. (Approved by the Office of Management and Budget under control number 9999- 0020)
§ 219.118 Applications and proposals lack- ing definite plans for involvement of human subjects.
Certain types of applications for grants, cooperative agreements, or contracts are submitted to depart- ments or agencies with the knowledge that subjects may be involved within the period of support, but definite plans would not normally be set forth in the application or proposal. These include activities such as institutional type grants when selection of specific projects is the institution’s responsibil- ity: research training grants in which the activities involving subjects remain to be selected: and projects in which human subjects’ involvement will
8 219.120
depend upon completion of instru- ments, prior animal studies, or purifi- cation of compounds. These applica- tions need not be reviewed by an IRB before an award m a y be made. Howev- er, except for research exempted or waived under 8 219.101 (b) or (0, no human subjects may be involved in a n y project supported by these awards until the project has been reviewed and approved by the IRB, as provided in this policy, and certification submit- ted, by the institution, to the depart- ment or agency.
Q 219.119 Research undertaken without the intention of involving human sub- jects.
In the event research is undertaken without the intention of involving human subjects, but it is later pro- posed to involve human subjects in the research, the research shall first be re- viewed and approved by an IRB, as provided in this policy, a certification submitted, by the institution, to the department or agency, and final ap- proval given to the proposed change by the department or agency.
§ 219.120 Evaluation and disposition of applications and proposals for research to be conducted or supported by a Fed- eral Department or Agency.
(a) The department or agency head will evaluate all applications and pro- posals involving human subjects sub- mitted to the department or agency through such officers and employees of the department or agency and such experts and consultants as the depart- ment or agency head determines to be appropriate. This evaluation will take into consideration the risks to the sub- jects, the adequacy of protection against these risks, the potential bene- f i t s of the research to the subjects and others, and the importance of the knowledge gained or to be gained. (b) On the basis of this evaluation,
the department or agency head may approve or disapprove the application or proposal, or enter into negotiations to develop an approvable one.
299

0 219.122
0 219.121 [Reserved]
L-
§ 219.122 Use of Federal funds. Federal funds administered by a de-
partment or agency may not be ex- pended for research involving human subjects unless the requirements of this policy have been satisfied.
§ 219.123 Early termination of research support: Evaluation of applications and proposals.
(a) The department or agency head may require that department or agency support for any project be ter- minated or suspended in the manner prescribed in applicable program re- quirements, when the department or agency head finds an institution has materially failed to comply with the terms of this policy. (b) In making decisions about sup-
porting or approving applications or proposals covered by this policy the department or agency head may take into account, in addition to all other eligibility requirements and program criteria, factors such as whether the applicant has been subject to a termi- nation or suspension under paragarph (a) of this section and whether the ap- plicant or the person or persons who would direct or has have directed the scientific and technical aspects of an activity has have, in the judgment of the department or agency head, mate- rially failed to discharge responsibility for the protection of the rights and welfare of human subjects (whether or not the research was subject to federal regulation).
Q 219.124 Conditions. With respect to any research project
or any class of research projects the department or agency head may impose additional conditions prior to or at the time of approval when in the judgment of the department or agency head additional conditions are neces- sary for the protection of human sub- jects.
300


UCCM / RCCl.950005.006a
The Testimony of Joe Larkins
April 11, 1 9 9 4
My name is Joe P. Larkins. I am now 52 years old. My Father, Willard L. Larkins, passed away in 1971. I was 30 years o l d at the time. My family consisted of myself, an older sister and my parents. When my Father passed away, he and my Mother were in the process of raising a grandchild (my sister's son). Neither of my patents were well-educated, but my Father was hard-working and honest. We always had clean and decent clothes to go to school in and we always had ample Food on the table. It doesn't take a well-educated person to be hard-working or honest. If Cincinnati General Hospital and the Doctor's therein had been honest, there is of course, the possibility that my Father could have lived for several more years. Instead, he went from a fairly able-bodied middle-aged Father and Husband to a premature death caused by an "experiment". My Father did not know that he was being used as a guinea pig; my Mother did not know; as his children, we were not informed of the procedures to be used nor of the risks involved.
I feel as though Dr. Saenger and the other "Doctors"involved, if you will, knew that the high levels of radiation which they administered to these patients had the very real probability of being fatal, Oh, how right that is! My Father was very much a family man, yet these people killed him as surely as if they had put a gun to his head and pulled the proverbial trigger. These "Doctors" left my Mother, with no job skills, to raise a grandchild as best as she could. My Mother lived until 1983, but she was a broken woman after my Father's premature and unexpected death.
I know that my Father knew that something was very wrong with the treatments being given to him at Cincinnati General. He even asked me "Son, what are they doing to me? They're trying to kill me!" That's how bad the pain he endured after the treatment was. He suffered so needlessly. What really .gets me about this situation is the fact that the Pentagon contracted with these Doctors and this hospital to test the effects of radiation on the human body. Everyone realizes that Cincinnati General Hospital, now the University of Cincinnati Hospital, treated many low-education, low-income patients. I guess they felt that in some way, the fact that these patients were not rich, upper-class citizens, gave them the right to experiment with

their bodies without informed consent. NOT SO! I feel sure these physician/researchers were well-paid for their part and it would be very interesting to know the types and dollar amounts of the grants given to Cincinnati General by the Federal government. I feel sure that all parties, with the exception of the poor, unsuspecting patients and their families, were well-compensated. But since when, in our society, does one man or even a group of them, have the right to play God? A very good example of this is our 20th century "assisted suicide Doctor". This man is contacted by terminally-ill patients who wish to end their own lives with dignity and choose, by their own voilition, not to suffer needlessly for years. These people make the decision to die in peace, yet our great judicial system, along with the medical community, brought this compassionate physician up on charges. The differences in these deaths and the death of my Father are that my Father did not choose to die - someone else made that decision for him, without consulting or informing him and they were amply compensated for it. I feel that the price they should be required to pay to the families of the people they killed, should be exceedingly high. I also feel that the Federal government should be named as a co-conspirator in this case, because that's exactly what it was - a conspiracy. No person, and I emphsize 'NO', person would willingly consent to a treatment with any degree of fatality involved. People, both you and I, simply value life too much. I think that is the big thing here - the patients were not informed. I know that behavior of this sort would not be tolerated by the medical community today. But then again, this entire mess was surrounded by a thick veil of secrecy on both the doctors' part and on the part of Cincinnati General Hospital. It is still being closely guarded and kept under yet another veil of secrecy to this very day by the University of Cincinnati, in that they have yet to provide the medical records of the patients involved in this experiment/ I beseige you to order the University of Cincinnati to release the patient records, in their entirety, to the next of kin immediately. They are hedging to save their own skin. I was promised my Father's complete medical file over a month ago; as of this writing, I have nothing.
I only hope that you, the Congressional Committee, see fit, as members of the human race, to break this matter wide open here and now and award just compensation to the families of the victims. 'I feel that the Physicians involved and also the federal government (the Pentagon) should pay and a l s o I beg you to strip any and all of the Doctors involved of all their medical credentials that they hold. If justice prevails in this matter, and I have faith that it will, a strong message will be sent to our government officials and the private physicians (to whom people entrust their lives and the lives of their loved ones) that behavior of this

sort will simpley not be tolerated, that justice will in fact be both swift and severe. I pray that a situation s u c h as this will never again Le faced by a group of people. If this statement to y o u , the Congressional Committee, does anything to help in the name of justice, then my Father’s death and the sorrow and hardships that his familty faced, will not have been completely in vain.
Thank you.
c

1 UCCM I RCCI .950005.006b
The Testimony of G l o r i a N e l s o r l
~ I I I A SACXSON PATIZbPP btb - 67
On October 21, 1966, after being dj.s&arged for General Hospital, Ws Jackson was a very weak ill woman, care of herself properly, and depended on the family for all her basic needs. She experienced bleeciing from her rectum, loss of appetite, nausea, vomit.ing, weight loss, and was in constant pain. Her condition never improved.
She was unable to take
Within a few weeks she was readmitted to General Hospital. The family was informed she should be transferred to Drake Hospital. Ms Jackson indicated she was afraid and wanted to return home. She was transported hone, where she was loved and cared for by us until she died on Mardl 25, 1967.
The family of Amelia Jiickson would like far this committee to know, that for the entire 163 days after receiving the irradiation, her condition continued t o deteriorate. We feel that the 100 rads of psrtial-body irradiation administered to her was cruel and didn't help her condition i n any way. It's our belief that she may have lived longer if this experiment had not taken place.
A doctor is someone you trust. H i s job is to do everything in his power to alleviate your pain and suffering. However, this was not the case. She was altr'ays crying, moaning, groaning, and in excruciating pain. Me Jackson was used to fur ther DE, Saeger'a professional goals. Neither Ms Jackson nor the family were informed or consented to her being used in an frxperiment conducted by Dr. Saegrr, and funded by the Department of Defense. There has clearly been a cover up by means of the Government, General Hospital, D r . Saeger and City of Cincinnat:.. We cannot: believe that they consented to such atrocities to be financed by the government; utilizing Ms Jackson's and the fam:ily's tax paying dollars.
\
It was purely an ambitious and callous act.

'c
Ms. Catherine 0. Hager 590 Delta Avenue Cincinnati, OH 45226 5 1 3-87 1-8773
April 7, 1994
UCCM / RCCl.950005.006~
To: Total Body Radiation Subcommittee and Whom it may concern;
In January, 1994 I began noticing articles in The Cincinnati Enquirer regarding Total 80dy Radiation experimentation done on cancer patients in the 1960's at Cincinnati General Hospital. Since I knew my father, Joseph Mitchell, was treated at that hospital for cancer during that period of time, I contacted Linda'Reeves at The Cincinnati Enquirer. After a brief discussion with Linda, it was determined that my father had indeed been involved in the Total Body Radiation experimentation as patfent Rt051, the first patient to be identified. From this point, my husband and I, along with the assistance of the news media attempted to piece together any records available regarding my father's treatments at the hospital.
In October, 1963, my father was diagnosed with lung cancer in the right lung, and was admitted to Cincinnati General Hospital. Surgery was scheduled for November, 1963. Although there is no notation of this scheduled surgery in his medical records, we have a letter which was written by my father to my sister detailing the planned operation. For some unknown reason the surgery was canceled on the day it was scheduled to take place, with no explanation. The surgery was never rescheduled. Instead, my father was given a schedule of dates to return to the hospital for Cobalt Treatments. At this point, I asked the doctor why the surgery was canceled. He told me he was too weak for surgery and decided to opt for the Cobalt Treatments instead.
In reality, my father was not in a weakened state at that time but was in relatively good health, still working and living a normal life. It wasn't until the Cobalt Treatments started that my father began to go down hill. After 35 days of treatments my father was so weak that he had to retire from work and move closer to my family so we could help care for him.
In early 1965, my father was again admitted to Cincinnati General Hospital with severe chest pains. It was at this time he was subjected to the Total Body Radiation. H e immediately started on a drastic downhill spiral. After much suffering, my father died on July 14, 1965 - 74 days after the Total Body Radiation.

.
Total Body Radiation Subcommittee
Page 2 - April 7, 1994
Since Total Body Radiation had not been performed on cancer patients at Cincinnati General Hospital prior to the Government funding of 1960, I feel that my father, along with other cancer patients, were hand picked and used in Total Body Radiation; not as a treatment for cancer, as they had been told, but as a cover-up for a study performed for the Department of Defense to determine possible effects on soldiers in nuclear warfare.
It might be noted that at the time my father died, two of my brothers were in the US. Air Force. One in Vietnam in the war zone. The Red Cross had to locate him and bring him home for the funeral. Both brothers have since retired from the Air Force.
Isn't it ironic that two of my brothers were serving this country in the military, while at the same time The United States Government was sponsoring experiments which shortened or ended their father's life.
Respectfully,
- Catherine 0. Hager (Mitchell)
C0H;cmh
Enclosure
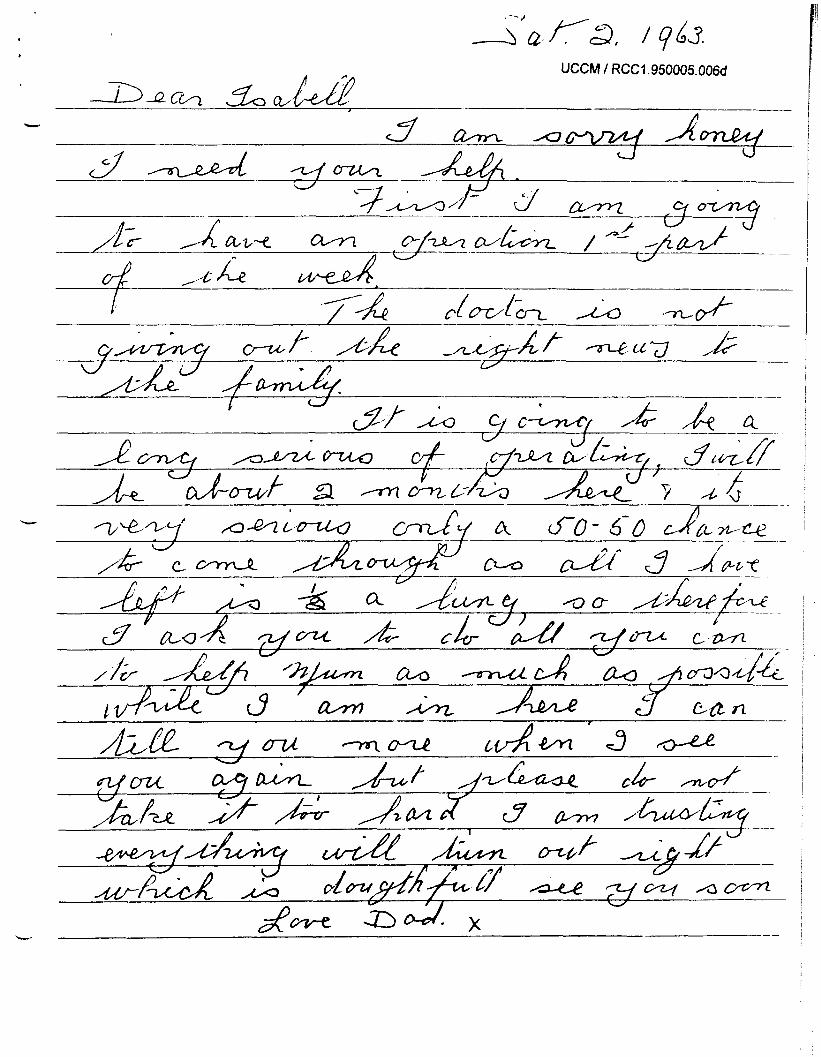
UCCM / RCCl.950005.006d
i 3 a Z 4 2 z Q b L -



UCCM / RCCI .950005.007a
SUBCOMMITTEE ON ADMINISTRATIVE LAW AND GOVERNMENTAL RELATIONS L
COMMITTEE ON THE JUDICIARY
HOUSE OF REPRESENTATIVES
SUMMARY STATEMENT OF JAMES D. COX, M.D.
Radiation therapy is an important part of the armamentarium of physicians in the care of
patients with cancer. Because of its effectiveness in the treatment of local-regional tumors, whole
body irradiation has been a subject of research for decades. At present, total body irradiation
followed by bone marrow transplantation is considered a standard part of treatment of many
patients with leukemia, lymphoma, and Hodglun’s disease, and is under investigation for
myeloma and cancer of the breast. In the era prior to the establishment of bone marrow
transplantation to support such treatment, lower (sublethal) doses of total body irradiation were
explored for patients with advanced cancer as a possible alternative to no treatment or treatment
with cytotoxic chemicals or hormones. The University of Cincinnati studies of total body
irradiation, conducted between 1960 and 1971 were based on a reasonable hypothesis, were
conducted and reported in the scientific literature in keeping with clinical investigations of that
period, and seem to have used the accepted standards of informed consent for that period. One
might judge them harshly from a perspective 20 years later, but they were reviewed and
repeatedly approved by peers of the investigators at the time the studies were conducted.
L

L
SUBCOMMITTEE ON ADMINISTRATIVE LAW AND GOVERNMENTAL RELATIONS COMMITTEE ON THE JUDICIARY
HOUSE OF REPRESENTATIVES BIOGRAPHY OF JAMES D. COX, M.D.
PRESENT TITLE & AFFILIATION:
BIRTH DATE & PLACE:
OFFICE ADDRESS:
EDUCATION: Undergraduate:
Graduate:
POSTGRADUATE TRAINING: 1963 - 1964:
1965 - 1966:
1966 - 1969:
1969 - 1970:
L
Professor of Radiotherapy Hubert L. and Olive Stringer Chair in Oncology in Honor of Sue Gribble Stringer Coordinator, Interdisciplinary Program Development The University of Texas M.D. Anderson
Houston, Texas 77030 Cancer Center
July 16, 1938; Steubenville, OH
The University of Texas M.D. Anderson
Interdisciplinary Program Development (Box 3 12) 15 15 Holcombe Boulevard Houston, Texas 77030
Cancer Center
(7 13) 792-2260
1960, Kenyon College, Gambier, OH
1965, University of Rochester School of Medicine and Dentistry, Rochester, NY
Fellow: Clinical Oncology and Therapeutic Radiology, Penrose Cancer Hospital, Colorado Springs, CO
Intern: (mixed with major in Medicine), University of Chicago, Chicago, IL
Resident: Therapeutic Radiology, Penrose Cancer Hospital, Colorado Springs, CO
Fellow: Therapeutic Radiology, Institute Gustave-Roussy, Villejuif, France
Page 1. Biographical Sketch of James D. Cox, M.D.

SPECIALTY BOARDS: 1966:
1971:
MILITARY SERVICE: 1970 - 1972:
ACADEMIC & PROFESSIONAL
APPOINTMENTS:
FACULTY: 1972 - 1974:
1974 - 1977:
1977 - 1982:
1982 - 1985:
1985 - 1988:
1988 - 1992:
1992 -
LOCAL:
1992 -Present: NATIONAL:
1972 - 1974: 1983 - 1987:
Diplomate, National Board of Medical
American Board of Radiology (Therapeutic Examiners
Radiology)
Major, US Army, Walter Reed General Hospital, Washington, DC Honorable Discharge
Assistant Professor of Radiology Georgetown University Hospital Washington, DC
Associate Professor of Radiology Medical College of Wisconsin
Professor of Radiology Medical College of Wisconsin
Professor and Chairman Department of Radiation Oncology Medical College of Wisconsin
Department of Radiation Oncology Columbia University College of Physicians and Surgeons
Care and Physician-in-Chief, The University of Texas M.D. Anderson Cancer Center
Professor of Radiotherapy; Coordinator, Interdisciplinary Program Development, The University of Texas M.D. Anderson Cancer Center
W
Professor and Chairman
Professor of Radiotherapy; Vice President for Patient
Texas Radiation Advisory Board Member
National Cancer Institute (NCI) Visiting Physician, Medicine Branch Cancer Research Manpower Review
Committee, Division of Extramural Activities
Biographical Sketch of James D. Cox, M.D. Page 2.

L 1987 - 1991:
1987 - Present:
1990 - 1993:
1985 - 1986: 1986 - 1987:
1981 - 1987:
1981 - 1987: 1987 - 1993: 1987 - 1993:
1981 - 1987: 1987 -Present:
1979 - 1989:
198 1 -Present:
1974 - 1979:
1978 - 1980:
EDITORIAL BOARDS: 198 1 -Present:
Board of Scientific Counselors Division of Cancer Treatment
Committee of Clinical Trials Cooperative Group Chairs
Chairman, Committee of Clinical Trials Cooperative Group Chairs
American Society for Therapeutic Radiology and Oncology (ASTRO) President Chairman, Board of Directors
American College of Radiology (ACR) Chairman, Committee of Radiotherapeutic
Steering Committee of the Council Chancellor Chairman, Commission on Radiation
Oncology
Research and Development
Radiation Therapy Oncology Group (RTOG) Vice Chairman for Research Strategies Chairman, RTOG
American Board of Radiology (ABR) Subcommittee for Written Examination
Examiner, Oral Examination in Radiation Oncology in Radiation Oncology
Veterans Administration Lung Group (VALG) Chairman, Radiotherapy Committee Executive Committee
Council of Radiation Oncology Committee Chairpersons (CROCC) Member
Editorial Consultant: AMERICAN JOURNAL OF CLINICAL ONCOLOGY CANCER CHEST INTERNATIONAL JOURNAL OF RADIATION
ONCOLOGY, BIOLOGY, PHYSICS JOURNAL OF CLINICAL ONCOLOGY NEW ENGLAND JOURNAL OF MEDICINE
giographical Sketch of James D. Cox, M.D. Page 3.

1985 -Present:
1990 -Present:
1990 - Present:
HONORS & AWARDS:
1960: 1965: 1983:
1984:
1985:
1986:
1987:
1988:
1989:
1992: 1992:
1992:
1993 :
1994:
Editor, INTERNATIONAL JOURNAL OF
Site Editor for Rapid Communica- RADIATION ONCOLOGY, BIOLOGY, PHYSICS
tions Section, INTERNATIONAL JOURNAL OF RADIATION ONCOLOGY, BIOLOGY, PHYSICS
Editorial Board, LUNG CANCER
AB: Magna Cum Laude, Phi Beta Kappa MD: With Honor Fellow of the American College of
Radiology (FACR) Robert Fowler Fellow of the Anti-Cancer
Council of Victoria, Australia President: American Society for
Therapeutic Radiology and Oncology (ASTRO)
University of Michigan
30th Anniversary, Department of Radiology, Hiroshima University Medical School
Radiation-Oncology
Physicians and Surgeons of Canada
William Caldwell Memorial Lecture, The University of Wisconsin
Hubert L. and Olive Stringer Chair in Oncology in Honor of Sue Gribble Stringer
Annual Oration in Radiation Oncology, Radiological Society of North America
Invited Lecturer, 7th International Symposium of the Foundation for Cancer Research.
Sixth Isadore Lampe Lecture
International Guest Lecturer,
Honorary Member, Belgian Association for
W. G. Cosbie Lecture, Royal College of
Gillies Memorial Lecture, The University of Iowa
In addition, Dr. Cox is the author of 212 peer-reviewed journal articles, book chapters, and books. Copies of the bibliography are available upon request.
Page 4. Biographical Sketch of James D. Cox, M.D.

c UCCM / RCCl.950005.007b
TESTIMONY
COMMITTEE ON JUDICIARY
SUBCOMMITTEE ON ADMINISTRATIVE
LAW AND GOVERNMENTAL RELATIONS
APRIL 11, 1994
MR. CHAIR, MEMBERS OF THE COMMITTEE, I AM JOSEPH L
A. STEGER, PRESIDENT, UNIVERSITY OF CINCINNATI.
I APPRECIATE THE OPPORTUNITY TO HAVE A CHANCE TO
PRESENT THE ACTIONS TAKEN BY THE UNIVERSITY OF
CINCINNATI RELATIVE TO THE WHOLE BODY RADIOTHERAPY
STUDIES CONDUCTED, AT THE THEN GENERAL HOSPITAL,
SOME TWENTY TO THIRTY YEARS AGO.
-
THERE HAVING BEEN SOME SEVEN INDEPENDENT
L INVESTIGATIONS OF THESE STUDIES MOSTLY 20 TO 30

YEARS AGO, WHEN THE CURRENT UNIVERSITY WAS ASKED BY
THE PRESS AND THE FAMILIES TO SUPPLY DOCUMENTS OR
RECORDS, WE BEGAN TO COMPILE IMMEDIATELY ALL THE
RECORDS WE HAD RELATIVE TO THE STUDY. MUCH TO OUR
SURPRISE, ALTHOUGH I T WAS A COMPLICATED TASK, WE
S T I L L HAD I N OUR ARCHIVES OR WE FOUND SOME 8,200
'v
PAGE OF DOCUMENTS--ALL OF WHICH WE HAVE MADE PUBLIC.
AND WITH THE HELP OF SENATOR GLENN AND CONGRESSMAN
MANN, WE SECURED THE ORIGINAL D.O.D. CONTRACT.
AT THE SAME TIME THAT WE WERE UNDERTAKING TO - LOCATE AND REPRODUCE DOCUMENTS, WE BEGAN A SEARCH
FOR THE PATIENTS' FAMILIES (SOME 88 FAMILIES). AS
OF T H I S DATE, WE HAVE LOCATED 38 SURVIVING RELATIVES
AND WE ARE S T I L L TRYING TO LOCATE 50 OTHER PATIENTS'
CLOSE RELATIVES .
WE ALSO ESTABLISHED A HOT L I N E SO THAT PEOPLE
COULD CHECK TO SEE I F THEY OR A RELATIVE HAD
PARTICIPATED I N THE STUDIES. WE HAVE HANDLED OVER

L
1,000 CALLS AND CROSS CHECKS TO ASCERTAIN BY PATIENT
RECORDS (OF THESE 1,000 SOME CALLS) I F ANY OF THE
INQUIRERS OR THEIR RELATIVES HAD BEEN I N THE STUDY--
OBVIOUSLY FEW HAD .
WE ALSO FEEL A SOCIETAL OBLIGATION TO THE
SURVIVING RELATIVES. ALTHOUGH WE ARE NO LONGER THE
SAME ENTITY UNDER WHICH THE STUDIES WERE CONDUCTED,
WE HAVE OFFERED SOCIAL WORK SUPPORT AND/OR PASTORAL
COUNSELING SHOULD THEY WISH.
WE AS A PUBLIC ENTITY SHALL CONTINUE TO COOPERATE
I N ANY WAY WE CAN TO PROVIDE INFORMATION SHOULD WE
UNCOVER ANY ADDITIONAL DOCUMENTS. AT T H I S TIME, WE
ARE 90% CERTAIN THAT WE DO NOT HAVE ANY OTHER
DOCUMENTS THAT HAVE NOT BEEN REPORTED.
THANK YOU FOR ALLOWING MY TESTIMONY. I SHALL BE
GLAD TO ANSWER ANY OF YOUR QUESTIONS.


UCCM / RCCl.950005.008a
Statement to Congress, Subcommittee on Administative law and Governmental Relations, April 11, 1994 by David S. Egilman MD, MPH, 759 Granite Street, Braintree, Massachusetts.
Chairman Bryant, Subcommittee Members, Good Afternoon
My name is David Egilman. I am a physician. I am primarily a practicing doctor in Braintree, Massachusetts. I am also a member of the faculty at Brown University. In that role I teach and conduct research on the history of the development of medical knowledge in the 20th century.
I want to thank the Subcommittee for inviting me here to speak. For almost ten years I have tried to raise my voice about some of the experiments conducted by our Government on its own citizens, and I am grateful for this opportunity today.
I would like to begin by reviewing some contemporaneous comments of the colleagues of the University of Cincinnati (UC) researchers. There is little that I can add to these, however some still defend these experiments so I will endeavor to explain the bases of the criticisms later in my comments.
'It is not certain from the [consent form] narrative whether the patient is advised that no specific benefit will derive to him and that there are, indeed risks involved in the procedure proposed." - Edward Gall MD, May, 1966
'I believe a twenty-five percent mortality is too high." All patients should be informed not only that a 'risk exists" but of, "a 1 in 4 chance of death within a few weeks" of treatment - George Shields MD, 1967
'The applicants have apparently already administered 150-200 rads to some 18 patients with a variety of malignancies and to their satisfaction have not found a beneficial effect. In fact, as I understand it, they found considerable morbidity associated with this high dose of radiation. Why is it now logical to expand this study?
-
Even if this study is expanded, its current design will not yield meaningful data. ... It will be difficult if not impossible to observe a beneficial effect in such a small sample containing a variety of diseases all of which share only CANCER in common.
This gross deficiency in design will almost certainly prevent making meaningful observations. When this deficiency in experimental method is placed next to their previously observed poor result and high morbidity with this type of treatment in a 'variety of neoplasms' I think it is clear that the study as proposed should not be done.
I have the uneasy suspicion, shoed up by the revised statement of objectives, that this revised protocol is a subterfuge to allow the investigators ... to test the ability of autologous marrow to 'take' in patients who have received high doses of total body radiation. This latter question may be an important one to answer but I can't justify 200 rad total body radiation simply for this purpose, 'even in terminal case material'. - Thomas Gaffney MD - 1967
... "the acceptability of our general consent form for human volunteers participating in research was questioned" - Evelyn Hess MD - 1969 commenting on the reason for rejection of two grant applications by the National Institutes of Health.
Box G , Brown University, Providenq Rhode Island 02912 Tel. (401) 863-3 172

In my statement I will cover four areas.
1. What were the experiments?
The whole body radiation (WBR) experiments conducted at the University of Cincinnati (UC) were designed to provide information to the military. They were not in any way cancer treatment or palliation. Some of those studies resulted in the deaths of their subjects.
2. Were the experiments conducted according to the ethical standards of their time?
The answer to this question is a firm no.
3. Why did it take until 1994 for these activities to reach the national consciousness?
Why did these experiments occur and continue over a considerable period of time?
There was a lack of oversight and we are all responsible.
4. We must do our best to right past wrongs and prevent this from happening again.
I would argue that this necessitates taking several long and short-term steps, including the following:
A. We must document and assess what happened. B. Those harmed should receive compensation. C. Appropriate actions should be taken against researchers who acted improperly. D. We must establish permanent mechanisms to assure that this type of experiments will not
occur again.
In my opinion, they could occur again, they may occur again, and we need to establish a system of checks and balances to assure that hearings such as these are not held again. Never again.
2

The University of Cincinnati Experiments 1961-1 972
A. Ethics and Informed Consent L
On November 28, 1950, Dr. Joseph Hamilton wrote a letter to Shields Warren MD, Director Division of Biology and Medicine, The Atomic Energy Commission (AEC) concerning the ability of irradiated soldiers to function. (AEC) researchers wanted to determine the dose that might limit a soldier's "capacity to execute intricate tasks for which physical well being is essential.' He discussed the difficulties of performing such a research study, and suggested that "For both politic and scientific reasons, ... it would be advantageous to secure what data can be obtained by using latge monkeys such as chimpanzees which are somewhat more responsive than lower mammals.' If the research was to be done on humans, Dr. Hamilton predicted that "those concerned in the (AEC) would be subject.to considerable criticism, as admittedly this would have a little of the Buchenwald touch ... The volunteers should be on a freer basis than inmates of a prison. At this point, I haven't any very constructive ideas as to where one would turn for such volunteers should this plan be put into execution.'
Despite Hamilton's "political" sensitivity to a possible adverse public reaction to this research, the DOD funded studies similar to those described in his letter. Eugene Saenger MD and his fellow researchers at the University of Cincinnati conducted these experiments between 1960 and 1971. In all researcher irradiated 88 cancer patients during those years. Dr. Saenger and coworkers published some of their findings in 1969 in the Archives of General Psychiatry. The article was titled, 'Total and Half Body Irradiation, Effect on Cognitive and Emotional Processes."
Cancer therapy was not the purpose of this research. Recently some defenders of this work have stated that the experiments met the ethical standard of their day. This is not true.
L As they say, the devil is in the details. In their 1969 paper the researchers stated, that preirradiation analysis of the experimental subjects revealed that the researchers would have had difficulty in obtaining true informed consent from the study participants. "Relevant intellectual characteristics of the patient sample were as follows: a low-educational level (ranging from 63 to 112 on the full-scale of the Wechsler-Bellevue which has a mean of 84.5), and a strong evidence of cerebral organic deficit in the baseline (preradiation) measure of most patients.' Thirteen of sixteen subjects were 'Negro,' three were White.
These researchers like others involved in similar experiments funded by the DOE and NASA, selected the most vulnerable of our citizens as subjects, the poor, the mentally and emotionally impaired, and African-Americans. UC researchers knew or should have known that their patient population was incapable of giving informed consent even if had they were informed of the experimental risks (which they were not). The UC researchers did not give the subjects all the facts on the side effects of the radiation. Therefore, if the patients consented to the experiments, the consent was not informed. According to the UC investigation of this research (Suskind report) a review of 27 of 33 patient charts between 1960-1964 did not contain any notation that the patients were informed about anything. Six of the patient charts contained information indicating that the patient 'was informed about the nature of the treatment and its possible benefits." The patient charts did not contain any notation on the risks of the experiments. It must be assumed from comments of relatives of survivors and the lack of notation that 27 of 33 patients received little or no information of the risks. The researchers own contradictory statements about informed consent provide the best evidence that they violated the ethical and moral standards of both the sixties and the nineties.
UC researchers in their 1969 research paper revealed these contradictory elements themselves. The report included both of the following statements: "In each case the patient was advised that the therapy might be beneficial to him but that it was experimental in nature. Informed consent was obtained in all cases." And, "There was no discussion with the patient of possible subjective reactions resulting from the treatment, Other physicians, nurses, technicians and
3 I
i

ward personnel were instructed not to discuss post irradiation symptoms or reactions with the patient. This precaution was carefully followed so as to standardize and minimize 'iatrogenic' factors in influencing whatever subjective reactions the patients might have to radiation." Iatrogenic means doctor induced. The researchers claim they did not tell the patients about the possible side effects because this information could have induced nausea and vomiting in the patients. This is further evidence that the study was a study of the side effects of radiation not of the treatment of cancer. It is obviously impossible to obtain informed consent without giving information on the side effects of the treatment.
In response to a junior faculty report critical of the research, the UC researchers claimed that they had informed the patients of the risks involved and the possibilities of complications. They even produced a consent form allegedly used and signed by every adult patient in the study from 1965 onward. However, in addition to the detailed information on the lack of informed consent presented in the 1969 paper a 1973 publication that outlined the study methods stated specifically that the researchers did not tell the patients of the severe nausea or vomiting that could result from therapy. The researchers clearly understood that informed consent represented the standard of the day. They felt obligated to include a statement on informed consent in the paper they published. Did they lie about receiving informed consent from the patients when the story broke or did they lie about not giving them information required to receive informed consent in their published papers? If their published papers correctly report their failure to advise patients about the possible experimental risks, their stated conclusion that they received informed consent is surely wrong. Having failed to provide informed consent, (how could their patient population possibly give informed consent?) they had to lie about it when the experiments became public. There is no better evidence that they violated their own and our own ethical and moral standards.
The researchers were so aware of the importance of informed consent that they stated they received it from the participants in the experiment even though it is clear they did not.
In 1966 Saenger and Lushbaugh (in charge of studies of WBR at Oak Ridge funded in part by NASA), combined the results of their WBR research and published a joint paper. The paper reported the amount of radiation it took to kill half of the recipients. That same year, a review panel of the AEC suggested that Oak Ridge conduct experiments similar to those conducted by UC researchers. In reviewing a suggestion that patients with carcinoma of the breast, gastrointestinal tract, and urogenital tract should be treated by total body irradiation, the panel made the following statement: "These groups of patients have been carefully considered for such therapy, and we are very hesitant to treat them because we believe there is so little chance of benefit to make it auestionable ethically to treat them. Lesions that require moderate or high doses of local therapy for benefit, or that are actually resistant (gastrointestinal tract) are not helped enough by total body irradiation to justify the bone marrow depression that is induced. Of course, in one way these patients would make good subjects for research because their hematologic responses are more nearly like those of normals than are the responses of patients with hematologic disorders." (Emphasis added) The argument that these experiments were appropriate from the ethical standards of the 1960's lacks both scientific and historic accuracy.
In their 1967 report to the DOD, UC researchers said that they followed ethical standards as set forth in Declaration of Helsinki. Again, this is not true. The Declaration clearly states:
inherent risks in comparison to foreseeable benefits to the subjects or to others.
subject by the doctor.
1. (4) Every clinical research project should be preceded by careful assessment of
Ill. (2) The nature, the purpose and the risk of clinical research must be explained to the
4

L
Ill. (3) ... the responsibility for clinical research always remains with the research worker; it never falls on the subject, even after consent is obtained.
There is no question that the research failed to meet the ethical standards of the late 1940's as expressed in the first part of the Nuremberg code, "The voluntary consent of a human subject is absolutely essential." The code states that the subjects must have sufficient understanding of their situation, and must be capable of making an informed decision as to their participation in the research. The research conducted by UC researchers did not meet this standard established for prisoners of War.
Informed consent was the ethical standard of Dr. Saenger's day, and was the medical standard since the 1890s. On April 8, 1899, an editorial in the Joumal of American Medical Association asserted that "the rule of conduct in this matter is for the physician to put himself in the patient's place with all his natural feelings and desires. Even consent on the part of the subject can not justify an experiment that needlessly puts his health or life in peril, or diminish the responsibility of the one who performs or permits it." (Emphasis added)
The legal importance of informed consent was established in 1914, when Justice Cardozo wrote that, 'Every human being ... has a right to determine what shall be done with his own body and a surgeon who performs an operation without his patient's consent commits an assault for which he is liable in damages." Schloendorf v. Societv of New York HosDital, 21 1 NY 125 (1914).
The courts aaain clearly stated the standard of informed consent in 1960. This decision stated that, "A man is master of his own body .... A doctor may well believe that ... treatment is desirable or necessary, but the law does not permit him to substitute his own judgment for that of the patient by any form of artifice or deception." Natanson v. Kline, 350 P 2d 1093 (Kansas 1960). Deception is precisely what occurred. "The patient is told that he is to receive treatment to help his disease," wrote the authors in another DOD report, despite the fact that they selected patients with non-treatable cancers for the experiments. The researchers denied some of the patients potentially effective treatments.
The human experimentswhich Dr. Hamilton discussed in his 1950 letter, and which Dr. Saenger designed in Cincinnati, were an atrocious example of medicine gone wrong.
B. Cancer therapy was not the purpose of this research.
Researchers tested the efficacy of whole body irradiation in the 1 930'~-50's at several centers, including Memorial-Sloan Kettering in New York City. WBR was not useful in the treatment of solid tumors. Researchers found that the so-called 'non-radiosensitive cancers" such as those that UC researcher irradiated, were unresponsive to whole-body radiotherapy. The medical utility of this study was suspect and disguised, and as a result the research resulted in the deaths of at least eight, and probably more than twenty of the participants.
In a separate article titled "Whole Body Radiotherapy of Advanced Cancer," Dr. Saenger et al., wrote, "If one assumes that all severe drops in blood cell count and all instances of hypocellular or acellular marrow at death were due only to radiation and not influenced by previous therapy, then one can identify 8 cases in which there is a possibility of the therapy contributing to mortality." Suskind states that up to 19 may have died as a result of the radiation.
In 1905, Dessauer first used irradiation of the entire body for purposes of the experimental therapy of disease. Physicians used whole-body irradiation for treatment of a wide variety of benign conditions including asthma, migraine, and arthritis (Scott 1940) reports of adverse effects from radiation (Brues 1955, Furth and Lorenz 1954) quickly narrowed the use of the treatment to metastatic tumors.
5
I

Physicians conducted a set of clinical trials of whole-body irradiation for cancer out at Memorial Sloan-Kettering in New York from 1931 through the 1940's. These trials involved high total dose irradiation given over a period of days. Physician designed the low-dose rate irradiation to minimize side-effects such as radiation sickness and bone marrow suppression. Low-dose rate irradiation exposed the cancer cells to radiation during the entire cycle of cell division in order to irradiate each cell at the most vulnerable stage in its division. Physicians published progress reports of the experiments performed at Memorial in 1932, 1934, and 1942. The reports were in agreement with other literature from that time. The technique of whole-body irradiation showed some promise with leukemias and lymphomas, but 'little or no benefit follows its use in the treatment of aeneralized carcinoma or sarcoma." (Emphasis added) (Medinger and Craver 1942). In the same study, Medinger and Craver explained why the therapy did not work on carcinomas (the type of cancer selected for the UC experiments): 'The results in these generalized carcinoma cases were discouraging. The reason for this is quickly apparent. Carcinomas are much more radioresistant than lymphomatoid tumors, and by total body irradiation the dose cannot be nearly large enough to alter these tumors appreciably." The reason the dose cannot be large enough is that a dose that will kill the tumor will also kill the patient.
Later studies found similar results. Jacobs and Marasso reported in 1965 on 52 patients treated with whole-body irradiation when 'other modalities had failed or could not be employed." They found that in patients with radioresistant tumors, "In no Datient was there evidence that total-body irradiation affected the disease." (Emphasis added) In contrast to the Memorial Hospital studies, these studies administered the radiation at higher doses, and much more rapidly.
4
Interestingly Dr. Aron, one of the UC researchers and a member of the UC committee that investigated the appropriateness of this work in the early 1970's, recently stated, 'In Cincinnati, the patients' disease had spread throughout their bodies, and most were given a life expectancy of six months. The effect of the study was a short prolongation of their lives. All who had the
exposure." If this was therapy and it worked, why did the researchers stop it when it became public? Did the researchers stop the experiments because they became public? If the radiation did not help, the subjects, who lived an average of 15 months after being irradiated, were not really suffering from terminal cancer. They were not. The researchers reported that until they were irradiated most of the patients were in, 'relatively good health." Suskind's report indicated that the researchers excluded terminal patients from the study, 'Some of the reasons for patient rejection included advanced stage of malignancies leading to disorientation, stupor, and/or coma, and terminal advanced malignant disease in which the life expectancy was only a few weeks." (pg. 27) At least nine and probably more than twenty subjects died as a result of the experiment.
treatment have died of their cancers. They lived an average of fifteen months after the radiation -
The studies at the University of Cincinnati began and continued after the medical literature clearly reflected that whole-body irradiation was inappropriate. UC researchers knew about the acute and chronic toxicity of whole-body irradiation; they knew that only leukemias and lymphomas responded to the treatment; they knew that radioresistant tumors would require a dose that would be lethal to the patient in order to affect the tumor. In the literature review of the paper by UC researchers in 1973, the authors cite the study by Medinger and Craver, and note that Yhirty-five patients with advanced carcinoma and sarcoma were included in this series". UC researchers preferentially selected patients with tumors that were not treatable by whole-body irradiation (cancer of the colon, breast, and lung) and then told the patients that they would receive therapy for their disease.
It is important to note that the ill-effects of successful irradiation conSist of symptoms from the radiation and from the widespread destruction of the tumor cells (which release cellular chemicals and cause symptoms from the body's effort to remove the dead tumor cells). Irradiating patients with radioresistant tumors allowed the investigators to state that the
destruction. This is the reason the patients with radioresistant tumors received high dose rate symptoms the patients experienced were caused by the radiation and not by the effects of tumor 4
6

L
irradiation. The experiment mimicked the effects of nuclear war on soldiers. The purpose of the experiments was as described in the researchers reports to the Department of Defense, These studies are designed to obtain new information about the metabolic effects of total body and partial body irradiation so as to have a better understanding of the acute and subacute effects of irradiation in the human .... The long-term program envisions carrying out the various obsetvations at dose levels of 100 to 150, and 300 rad. Eventually doses up to 600 rad are anticipated.' These doses were potentially and were in fact lethal. Other physicians established decades before the UC researchers conducted these experiments. A dose of 250 rads would kill up to 50% of those who received it. A 600 rad dose would kill almost everyone who received it.
The treatment methods
An examination of the treatment methods reveals much about the true purpose of the experiments. Patients received treatment in a sitting position with legs raised, and head tilted slightly forward. This position mimics that of a soldier in a protective fetal position. The powerful single doses resembled the dose rate of a nuclear blast. "Whenever possible unidirectional radiation will be attempted since this type of exposure is of military interest," the researchers wrote in 1969. This was not the way radiation physicians used in therapeutic applications. Physicians give real therapy slowly and from as many different directions as possible to minimize side effects and maximize efficacy.
In addition, the UC researchers denied the patients treatment for nausea and vomiting. This was apparently so anathema to the hospital staff used to caring for patients that the researchers had to create a special form to ensure that the doctors, nurses and other personnel would not perform their usual function of caring for sick patients. This form instructed hospital staff not to ask about the symptoms and signs of radiation poisoning. "DO NOT ASK THE PATIENT WHETHER HE HAS THESE SYMPTOMS," the form said. The form went on to instruct the staff to record the time, duration and severity of these symptoms. The researchers offered no treatment.
From another DOD report we find that the researchers sought to psychologically isolate the patients, "There is no discussion of possible subjective reaction resulting from the treatment with the patient. Other physicians, nurses, technicians and ward personnel are instructed not to discuss post-irradiation symptoms or reaction with the patient. This 'isolation' is carried out carefully so as not to influence any objective reactions of the patient which might be attributable to radiation.' Patients resided in the psychiatry unit instead of the tumor ward, "The environment is far more attractive and there are no other patients receiving radiation therapy with whom the patient can exchange experiences." What manner of cancer treatment seeks to psychologically isolate patients and deny them treatment for nausea and vomiting?
7

II. Assessing Responsibility
In my opinion the responsibility for these experiments rests on many shoulders. These include: the government agencies that funded them and failed to provide adequate ethical safeguards; the Congress which failed to provide adequate oversight; the researchers who violated their HippocraUc oaths and their sacred trust with their patients; the universlties which failed to provide adequate oversight of their researchers; the journals that published the work without comment, or review of the ethical issues that the research raised.
4
The research conducted by UC researchers was clearly unethical and resulted in the deaths of many of the irradiated patients. Dr. Stephens revealed this information to the public in 1971. Dr Thomas Gall brought this information to the attention of University personnel in 1966.
We must address several if we are to assure ourselves that similar experiments will not occur in the future.
1. If the research was wrong and people knew it was wrong when it was done, why wasn't it stopped sooner? In fact, the Suskind committee suggested that the research should continue in a modified form.
2. public?
Why was there no outcry, apology or thorough investigation after the research became
There are several answers to these questions.
1.
There are several reasons for this.
There was a lack of appropriate oversight by the University.
A.
B.
C.
D.
E.
F.
G.
No one likes to admit they made mistakes or apologize.
Dr. Saenger and his colleagues were well known and respected. It is hard to criticize the powerful and famous. Dr. Mossman, head of the Health Physics Society, told me at the last Congressional hearing that he would not criticize Dr. Saenger because he was a 'big man."
-
Physicians do not like to criticize their peers especially if they work at the same institution.
The University ignored the timely criticisms of is own faculty. (letters by Drs. Gaffney and Gall - 1967)
The University allowed the research to continue from 1966-1 971 without the approval of its own human subjects review board established in March 1966. The UC research review board granted a protocol limited to WBR and bone marrow transplantation provisional approval in May 1967. The approval granted in 1967 was provisional and requested that three modifications be made to the original protocol. A final revised protocol was not approved until August 1971. The experiments continued during this entire period.
At least two of the researchers were members of the University committee (Suskind report) that investigated the research. The UC burdened the researchers with the evaluation of their own work. This is a clear conflict of interest and a situation that is not likely to result in an objective evaluation of the research. (See below)
The University chose to attack the messenger by using McCarthyite tactics against the critiques of the research. This has continued to date. 4
8

7. There was lack of appropriate oversight by the Medical Community
a. The United States Senate requested that an "outside review" be carried out by the American College of Radiology (ACR). Dr. Robert McConnell a 'long time fishing partner" of Dr. Saenger conducted this 'review". In his report to the Senate Dr. McConnell noted that Dr. Saenger was a member of the American College of Radiology. He neglected to mention his personal friendship with the principle investigator or the fact that Dr. Saenger was at the time of the investigation a member of five different committees of the American College of Radiation, including the Commission on Radiological Units, Standards, and Protection, the Committee on Research and Development in Nuclear Medicine, the Commission on Public Health, the Subcommittee on Nuclear Medicine Technology, and the Committee on Efficacy. Prior to the investigation Saenger also served as a member of the Subcommittee on Radiological Aspects of Disaster Planning. These relationships constituted a conflict of interest and a situation that is not likely to result in an objective evaluation of the research.
b. Two UC researchers were members of the UC committee that reviewed the research for the University. This is an obvious conflict of interest.
c. The Ohio board of medical licensure has to date not investigated any of the physicians involved in this series of experiments.
d. The Cincinnati Medical Society has not investigated this series of experiments.
3. There was lack of appropriate oversight by the Congress.
Senator Taft vigorously obstructed a potential Senate investigation.
4. There was lack of appropriate oversight by the Department of Defense.
Who reviewed this work while it was conducted? Is there a current investigation of this research?
5. Were there violations of Medicare or Medicaid rules?
If it is true that the DOD only funded researcher salaries, overhead and travel money then public funds paid for these experiments.
6.
The press, the last link in the chain that must protect our citizens from its government failed to cover the story. The press permitted the uncontroverted comments of the researchers and universities to stand alone as reports on these experiments.
The press failed in its oversight role.
7. problems.
The previous investigations were inadequate and filled with conflict of interest
It is important to consider the University's evaluation of these experiments (Suskind report). When these experiments again reached the public consciousness this year, the University claimed the review agencies had found the experiments to be ethical and appropriate. It is my opinion that the reviews were inadequate and wrong. Nonetheless the University, the researchers, and the DOD have used the reviews to protect themselves from scrutiny. The reviews were part of an organized effort to mislead the public about the research. A careful
9

examination of the Suskind report reveals the inadequacies of the University's analysis of the radiation experiments and the unethical nature of the experiments themselves.
a. What were the objectives of the study?
The only protocol that preceded the experiments indicates that the purpose was to provide, 'information [that] is necessary to provide knowledge of combat effectiveness of troops and to develop additional methods of diagnosis, prognosis, prophylaxis and treatment of these injuries." (pg. 1 DOD report 1963)
After the research was publicly criticized, the researchers claimed the DOD protocol was an add- on to a cancer treatment program. A cancer treatment protocol was produced in 1966 and approved on August 9,1971. Perhaps because UC researchers never implemented any protocol while the study was conducted, friendly reviewers have had differing conclusions about the purpose of the experiments.
The ACR stated that the experiment was a Phase I study of the toxicity of whole body radiation in humans. American College of Radiology: 'The committee viewed the project as it was designed - as a clinical investigation of a modality for the care of cancer patients with extensive and incurable disease. Phase one investigations follow basic animal work and always precede randomized clinical trials which may or may not be justified on the basis of the first human applications." (pg. 3)
Suskind found the experiment to be a Phase II cancer study of the efficacy of treatment. Suskind's report states that the hazards of whole body radiation were well established before the UC studies were started, "the hazard [bone marrow suppression] is well documented in the available literature and the dose relationship to side effects well understood." (pg. 9) Suskind then states that the study was some type of Phase II study of the efficacy of bone marrow transplant and radiation. However, of the 87 patient's treated only 13 received a bone marrow transplant. In addition, Suskind notes, 'The committee, however, was unable to find any written protocol in which the purpose of the study was to determine palliative effects of whole body radiation until ... 1967."(pg. 14) He latter notes, "No plan for a systematic study of palliative effects was made." (pg. 64)
Only the researchers' own words fully explain the experiments. They explained ihat the purpose was military. Only this purpose explains the experimentardesign, that included psychological isolation, organized denial of treatment for nausea and vomiting, and no plan for analysis of cancer palliation or treatment efficacy. Since treatment was not the intent of the study there was no need to organize the study so that treatment outcomes could be evaluated.
b. Was there a need to test whole body radiation for cancer treatment?
Suskind reviewed the prior studies of WBR to try to see if physicians had conducted adequate Phase ll trials prior to the UC experiments. They report universal failure. "Medinger and Craver (1942) - Results were described as discouraging in this group of patients 'except for transient relief of pain in a few cases'." Jacobs and Marasco (1965) - 11 of 16 'died within one month of treatment; the remaining 5 having survivals of 1-1/2, 2, 3, 4, and 9 months. The statement suggesting the need for further evaluation of this form of treatment refers most probably to the radiosensitive, widespread neoplasms rather than the results in the 16 patients with radioresistant cancers.' (pg. 10-1 1) In addition, Suskind could not find anyone else performing
radiosensitive tumors, no information is available to the committee which indicates that this form of treatment is used elsewhere in radioresistant, disseminated or localized cancers as used at the University of Cincinnati.' (pg. 12)
- similar experiments, 'Although whole body radiation is widely used for many forms of
10

Suskind notes that in 1966, 'This proposal received a critical internal review and was submitted to the NIH in an application for a research grant. The application was not approved and the reasons for this decision were not disclosed.' (pg. 42) This was not true. In 1969, Evelyn Hess MD, the chairwoman of the faculty committee on research wrote that NIH had rejected two research grants because, ?he acceptability of our general consent form for human volunteers participating in research was questioned."
Suskind concluded that, 'The Phase II criteria for whole body radiation were not adequately satisfied at the time the original protocol was designed in 1960 and evidence for its effectiveness was incomplete. The results which were available for interpretation were not encouraging. Hence, the need for mounting a Phase II study at that time was indicated.' (pg. 11)
If, after reviewing the dismal results of previous studies examining WBR use for radioresistant tumors and faculty criticisms of the WBR experiments at UC, Suskind really thought another study was necessary, there is something fundamentally wrong with the way UC researchers evaluate medical treatment and research needs. This is perhaps a more important area of investigation than the original studies themselves.
It may indicate that there is still a problem in this area at UC today. If the University authorities cannot recognize that the WBR experiments were wrong and apologize to the community, how can the community trust them to evaluate current experimental programs?
c. Quality of care
Suskind: "The thoroughness of the psychological support is apparent from the report of the psychological staff." (pg. 28)
DOD report: 'There is no discussion of possible subjective reaction resulting from the treatment with the patient. Other physicians, nurses, technicians and ward personnel are instructed not to discuss post-irradiation symptoms or reaction with the patient. This 'isolation' is camed out carefully so as not to influence any objective reactions of the patient which might be attributable to radiation." (pg. 4)
If denial of treatment for nausea and vomiting and psychological isolation is good quality of care perhaps there is a current problem at UC in this area as well.
d. Ethics
Suskind: 'Patients and families were not informed about the possibility of transient nausea and vomiting since such symptoms may be induced by suggestion. Typically, such side effects can occur a few days after treatment." (pg. 50)
Suskind: 'Were there patients, whose IQ was subsequently determined to be 75 or below, who signed the consent form themselves?
Yes there were ten patients. There was no reason to believe that they did not understand the conditions of the project. The Committee also questions the significance of the scores of intelligence tests in this group of patients who were dying of far advanced cancer.' (pg. 51) It was precisely these IQ scores that formed part of the basis for the DOD cognitive effects research.
Suskind: 'Informed consent should be obtained as it is now. Revisions of the consent forms should be considered in relation to the use of the phrase 'sound mind and body'. The procedure for withdrawal from the project should be improved." (pg. 56)
11
If it is Suskind's (and the University's) opinion that sick patients with IQ's less than 75 who are not told about side effects like nausea, vomiting and a 25% death rate within weeks of treatment can provide informed consent there is a serious problem at the University.
e. Research quality
Suskind noted, 'It is uncertain whether this study and similar studies reported in the medical literature are truly comparable in all major factors that influence survival, such as selection of patients and ancillary medical management. Therefore, the significance of comparisons of survival rates is doubtful, unless marked differences are found."(pg. 59)
'Since the manner in which the data on palliative effects was developed was inadequate, no conclusions can be drawn from them." (pg. 66)
Despite these comments Suskind concluded, 'Since the Committee cannot at this time rule out a positive effect of whole body radiation, a well-designed study to compare whole body radiation with other forms of therapy is necessary if the investigator wished to continue." (pg. 66)
Is this the current type of analysis UC uses to evaluate research and researchers?
111. Why did this happen?
That's a list of who but the answer to why this occurred is a more subtle and important issue. Our population views the United States as a unique country, and it is. It is uniquely democratic; these hearings are an example of that. It is my belief that we in the United States have a certain belief in the infallibility of our own history and our own behavior. We tend to believe that our actions could only have good intentions. I am afraid this is not so. We have at times done the wrong thing for the wrong reasons just as many other countries have done. The history of medical science, replete with the use of certain marginalized groups in our society for harmful experimentation, offers some examples of repugnant actions performed in this country. Perhaps these experiments will serve as a turning point and provide us with a fresh look at ourselves. A look that recognizes that the United States is the greatest country on earth but also recognizes that it is not an infallible country. That not everything we have done has been with good intentions or with good results, and therefore we, like other countries, must remain vigilant of our government, and our citizens and our companies. We must continue to maintain and buttress our system of checks and balances to assure us that these types of experiments will never go on again.
12

4
L
IV. What should be done?
A. Short term
1. The University should apologize.
2. The victims or their families should be compensated.
3. State Medical boards should investigate.
4. Criminal investigations should occur.
5. A single Congressional investigation should occur.
6. The DOD should investigate their role and oversight procedures
7. Medicare and Medicaid agencies should investigate the possible use of patient care funds for research.
8. The Association of Occupational and Environmental Clinics should provide an independent non-govemmental evaluation of all of the DOD, NASA and DOE research.
B. Long term
1. Medical review boards must be composed of >SO% independent and unrelated researchers and lay people.
2. Medical journals should have ethical reviewers.
.-
3. NIH must inform appropriate authorities when they find that a research project violates ethical standards. Their silence must stop.
13

Some people have asked why I am here. To paraphrase Thoreau, the question should not be why am I here, but why aren't other responsible parties here? It is every physician's duty to speak out when medicine goes wrong.
To quote from Pastor Niemdler about the Holocaust:
'In Germany the Nazis came for the communists, and I did not speak up since I was not communist. Then they came for the Jews, and I did not speak up since I was not a Jew. Then they came for the trade unionists, and 1 did not speak up since I was not a trade unionist. Then they came for the Catholics, and I was a Protestant so I did not speak up. Then they came for me, and by that time no one was left to speak up.
Thanks
My wife Helene, my students, my staff, my friends at NIOSH, Mitch Singal, and Bill Halperin, and my friends, particularly Mike Donahue.
14

Contemporaneous comments of colleagues
"It is not certain from the (consent form) narrative whether the patient
is advised that no specific benefit will derive to him and that there are,
indeed risks involved in the procedure proposed." - Edward Gall MD,
1966
"I believe a twenty-five percent mortality is too high." All patients
should be informed not only that a "risk exists" but of, "a 1 in 4 chance
of death within a few weeks" of treatment - George Shields MD, 1967 -
Statement to Congress April 11, 1994 by David S. Egilman MD, MPH.

Contemporaneous comments of colleagues
"The applicants have apparently already administered 150-200 rads
to some 18 patients with a varietv of malignancies and to their
satisfaction have not found a beneficial effect. In fact, as I understand
it, they found considerable morbidity associated with this high dose of
radiation. Why is it now logical to expand this study?
Even if this study is expanded, its current design will not yield
meaningful data. ... It will be difficult if not impossible to observe a
beneficial effect in such a small sample containing a variety of
diseases all of which share only CANCER in common.
This gross deficiency in design will almost certainly prevent making
meaningful observations. When this deficiency in experimental
method is placed next to their previously observed poor result and
high morbidity with this type of treatment in a 'variety of neoplasms' I
think it clear that the study should not be done. - Thomas Gaffney - MD - 1967
Statement to Congress April 11, 1994 by David S. Egilman MD, MPH. 2

Contemporaneous comments of colleagues
....” the acceptability of our general consent form for human volunteers
participating in research was questioned” - Evelyn Hess MD - 1969
commenting on the reason for rejection of two grant applications by
the National Institutes of Health.
Statement to Congress April 11, 1994 by David S. Egilman MD, MPH. 3

Overview
1. First I will the describe the whole body radiation (WBR) experiments that were conducted at
the UC. These were designed to provide information to the military. They were not in any
way cancer treatment or palliation. Some of those studies resulted in the deaths of their
subjects.
2. Secondly, I will address the question of whether the experiments were conducted according
to the ethical standards of their time. The answer to this question is a firm no.
3. Third, I think we should consider why these experiments were allowed to occur and continue
over a considerable period of time. Why did it take until 1994 for these activities to reach
the national consciousness?
4. Fourth, we must do our best to right past wrongs. We must accurately assess responsibility
for these studies if we are to address my final concern: how can we prevent this from
happening again? I would argue that this necessitates taking several long and short-term
steps, including the following:
A. We must document and assess what happened.
B. Compensation should be provided to those who were harmed.
C. Appropriate actions should be taken against researchers who acted improperly.
D. We must establish permanent mechanisms to assure that this type of experiments will not
occur again.
Statement to Congress April 11, 1994 by David S. Egilman MD, MPH. 4

The University of Cincinnati Experiments 1960-1 972
a. Ethics and Informed Consent
On November 28 1950 Dr. Joseph Hamilton wrote a letter to Shields Warren
MD., Director Division of Biology and Medicine, The Atomic Energy Commission
(AEC).
(AEC) researchers wanted to determine the dose that might limit a soldier’s
“capacity to execute intricate tasks for which physical well being is essential.”
Hamilton discussed the difficulties of performing such a research study, and
suggested that “For both politic and scientific reasons, ... it would be
advantageous to secure what data can be obtained by using large monkeys
such as chimpanzees which are somewhat more responsive than lower
mammals.”
-
If the research was to be done on humans, Dr. Hamilton predicted that “those
concerned in the (AEC) would be subject to considerable criticism, as
admittedly this would have a little of the Buchenwald touch ... The volunteers
should be on a freer basis than inmates of a prison. At this point, I haven’t any
very constructive ideas as to where one would turn for such volunteers should
this plan be put into execution.”
Statement to Congress April 1 I, 1994 by David S. Egilman MD, MPH. 5

The University of Cincinnati Experiments 1960-1 972
a. Ethics and Informed Consent
2. Selection of subjects
a. b.
c. Brain dysfunction (did not
d radiation therapy. e.
f.
Uneducated - average 4th grade Low intelligence - average IQ 84 (many mentally retarded
know how to follow instructions) Patients with tumors that were resistant to
“They must be in relatively good nutritional status and with a stable hemogram. 54 of 88 patients African-American
These researchers, like others involved in similar experiments
funded by the DOE and NASA, selected the most vulnerable of
our citizens as subjects, the poor, the mentally and emotionally
impaired, and African-Americans.
Statement to Congress April 11, 1994 by David S. Egilman MD, MPH. 6

The University of Cincinnati Experiments 1960-1 972
a. Ethics and Informed Consent
I)
informed consent.
Patient population was incapable of giving
2)
experimental risks.
Patient population not informed of the
Statement to Congress April 11,1994 by David S. Egilman MD, MPH. 7

The University of Cincinnati Experiments 1960-1 972
a. Ethics and Informed Consent
3. Researchers were aware of Informed consent requirements-
a. Researchers claimed - patients informed of the
risks and complications.
b. Researchers reported -Only 6 of first 33
patients received any information on the nature of the experiment
C. Researchers claimed = they received informed
consent in the paper they published.
d. Researchers reported - they did not tell the
patients of the risks.
If their published papers correctly report their failure to advise patients
about the possible experimental risks, their stated conclusion that they
received informed consent is surely wrong.
There is no better evidence that they violated their own
and our own ethical and moral standards.
Statement to Congress April 11, 1994 by David S. Egilman MD, MPH. 8

The University of Cincinnati Experiments 1960-1 972
a. Ethics and Informed Consent
3. Researchers were aware of Informed consent requirements
a. Researchers were aware of the Helsinki code
The Declaration states:
(4) Every clinical research project should be preceded by
careful assessment of inherent risks in comparison to foreseeable
benefits to the subjects or to others.
I I (2) The nature, the purpose and the risk of clinical research
must be explained to the subject by the doctor.
II (3) ... the responsibility for clinical research always remains
with the research worker; it never falls on the subject, even after
consent is obtained.
Statement to Congress April 11, 1994 by David S. Egilman MD, MPH. 9

The University of Cincinnati Experiments 1960-1972
a. Ethics and Informed Consent
4. Researchers were aware research was “questionable ethically”
a. Similar experiments were rejected in 1966.
“The suggestion is made that we should treat carcinoma of the breast,
gastrointestinal tract, and urogenital tract by total body irradiation. These
groups of patients have been carefully considered for such therapy, and we are
very hesitant to treat them because we believe there is so little chance of
benefit to make it westionable ethicallv to treat them. Lesions that require
moderate or high doses of local therapy for benefit, or that are actually
resistant (gastrointestinal tract) are not helped enough by total body
irradiation to justify the bone marrow depression that is induced.”
(emphasis added)
The argument that these experiments were appropriate from the ethical
standards of the 1960’s lack both scientific and historic accuracy.
Statement to Congress April 11 1994 by David S. Egilman MD, MPH. 10

The University of Cincinnati Experiments 1960-1 972
Cancer therapv was not the purpose of this research. b.
1) Result of previous research - Dismal
a) “little or no benefit follows its use in the treatment of
generalized carcinoma or sarcoma.” (emphasis added) (Medinger and Craver
1942).
“The results in these generalized carcinoma cases were discouraging. The
reason for this is quickly apparent. Carcinomas are much more radioresistant
than lymphomatoid tumors, and by total body irradiation the dose cannot be
nearly large enough to alter these tumors appreciably.”
b) In no patient was there evidence that total-bodv irradiation
affected the disease.” [with radioresistant tumors] (emphasis added)
(Jacobs and Marasso 1965).
A dose which will kill the tumor will also kill the patient.
Statement to Congress April 11, 1994 by David S. Egilman MD, MPH. 11

The University of Cincinnati Experiments 1960-1 972
b. Cancer therapv was not the purpose of this research.
2.
experiments in their reports to the Department of defense.
The Researchers themselves described the purposes of the
The purpose was, ‘‘ to provide knowledge of combat
effectiveness of troops and to develop additional methods of
diagnosis, prognosis, prophylaxis and treatment of these
i n j u ri es . ”
Statement to Congress April 11, 1994 by David S. Egilman MD, MPH. 12

Issue
The University of Cincinnati Experiments 1960-1 972
b. Cancer therapv was not the purpose of this research.
TREATMENT FOR NAUSEA AND VOMITING
PSYCHOLOGICAL AND PEER COUNSELING
DOSE RATE
DOSE DIRECTION
Real Medicine
PROVIDED
PROVIDED
MULTI- DIRECTIONAL
What manner of cancer treatment psychologically
isolates patients and deny them treatment for nausea
and vomiting?
Statement to Congress April 11, 1994 by David S. Egilman MD, MPH. 13

The University of Cincinnati Experiments 1960-1 972
C. Assessing Responsibilitv
1. Government agencies that funded them and failed to provide
adequate ethical safeguards - DOD, ?Medicare and Medicaid.
2. Congress failed to provide adequate oversight.
3. Researchers violated their trust with their patients.
4. Universities failed to provide adequate oversight.
5. Journals that published the work without comment failed to
provide adequate oversight.
6. NIH refused to fund the work on ethical grounds kept silent.
Statement to Congress April 11,1994 by David S. Egilman MD, MPH. 14

The University of Cincinnati Experiments 1960-1 972
D. Explaininq the continuance of the experiments in the face
of ethical questions
1. There was a lack of appropriate oversight by the University.
2. There was lack of appropriate oversight by the Medical
Community
a) ACR The fishing buddy reviewer
b) The Ohio board of medical licensure
c) The Cincinnati Medical Society
Statement to Congress April 11, 1994 by David S. Egilman MD, MPH. 15

The University of Cincinnati Experiments 1960-1 972
D. Explainincr the continuance of the experiments in the face
of ethical questions
3. There was lack of appropriate oversight by the Congress
Senator Taft vigorously obstructed a potential senate investigation.
There was lack of appropriate oversight by the Department of Defense.
Who reviewed this work while it was being conducted? Is there a current investigation of
4.
this research?
5. Were there violations of medicare or medicaid rules?
If it is true that the DOD only funded researcher salaries, overhead and travel money
then public funds paid for these experiments.
6. The press failed in its oversight role.
Permitted the uncontroverted comments of the researchers and universities to stand
alone as reports on these experiments.
Statement to Congress April 11, 1994 by David S. Egilman MD, MPH. 16

The University of Cincinnati Experiments 1960-1 972
D. Explaining the continuance of the experiments in the face
of ethical questions
7. Previous investigations inadequate, filled with conflict of interest, incomplete
research and bizarre analysis.
The Reviewers’ views:
a) What were the objectives of the study?
i) The ACR - phase I study of the toxicity of whole body radiation in humans.
ii) Suskind -phase II cancer study of the efficacy of bone marrow transplant and
radiation.
iii) The UC researchers stated purpose was ignored.
b) Was there a need to test whole body radiation for cancer treatment?
I) Suskind reviewed the prior dismal studies of WBR
ii) Suskind found that no one else anywhere in the world is doing this.
iii) Suskind found that in 1966 NIH rejected the proposed research -
Suskind concluded, “the need for mounting a Phase II study at that time was indicated.”
If the University authorities cannot recognize that the WBR experiments were wrong and
apologize to the community, how can the community trust them to evaluate current
experimental programs?
Statement to Congress April 11, 1994 by David S. Egilman MD, MPH. 17

The University of Cincinnati Experiments 1960-1 972
D. Explaining the continuance of the experiments in the face
of ethical questions
7.
problems, incomplete research and bizarre analysis.
The previous investigations were inadequate and filled with conflict of interest
c) Quality of care
Suskind: "The thoroughness of the psychological support is apparent from the report of the
psychological staff." (pg. 28)
DOD report: The patients were psychologically isolated and denied treatment for nausea and
vomiting.
If denial of treatment for nausea and vomiting and psychological isolation is good quality
of care perhaps there is a current problem at UC.
Statement to Congress April 11, 1994 by David S. Egilman MD, MPH. 18

The University of Cincinnati Experiments 1960-1 972
D. Explaininq the continuance of the experiments in the face
of ethical questions
7.
problems, incomplete research and bizarre analysis.
The previous investigations were inadequate and filled with conflict of interest
d)Ethics
Suskind: "Patients and families were not informed about nausea and vomiting .... Typically, such side effects can occur a few days after treatment." (pg. 50)
Suskind: Patients, with IQ's 75 or below [mentally retarded] can "understand the conditions of
the project" and provide informed consent.
If it is Suskind's (and the University's) opinion that sick patients with IQ's less than 75
who are not told about side effects like nausea, vomiting and a 25% death rate within
weeks of treatment can provide informed consent there is a serious problem at the
University.
Statement to Congress April 11, 1994 by David S. Egilman MD, MPH. 19

The University of Cincinnati Experiments 1960-1 972
D. Explaininq the continuance of the experiments in the face
of ethical questions
7.
problems, incomplete research and bizarre analysis.
The previous investigations were inadequate and filled with conflict of interest
e) Research quality
Suskind noted, ...” the significance of comparisons of survival
rates is doubtful, unless marked differences are found.”(pg. 59)
“Since the manner in which the data on palliative effects was
developed was inadequate, no conclusions can be drawn from
them.” (pg. 66)
Despite these comments Suskind concluded a modified
study could continue. (pg. 66)
Is this the current type of analysis UC uses to evaluate research and researchers?
Statement to Congress April 11, 1994 by David S. Egilman MD, MPH. 20

V. What should be done? A. Short term
1. The University should apologize.
2. The victims or their families should be compensated.
3. State Medical boards should investigate.
4. Criminal investigations should occur.
5. A single Congressional investigation should occur.
6. The DOD should investigate their role and oversight procedures.
7. Medicare and Medicaid and the city should investigate the diversion of patient care monies to research.
8. There should be an investigation by the Association of Occupational and Environmental clinics.
B. Long term
1. Medical review boards must be composed of >50% independent and unrelated researchers and lay people.
2. Medical journals should have ethical reviewers.
3. Thanks
NIH should abandon its a code of silence.
My wife Helene, my students, my staff, my supervisors at NIOSH, Mitch Singal, and Bill Halperin, and my friends particularly Mike Donahue.
Statement to Congress April 11, 1994 by David S. Egilman MD, MPH. 21

ERRATA
The University of Cincinnati Experiments 1960-1972
On page 4, paragraph 3, line 6 the sentence should read: "In
reviewing a suggestion that patients with carcinoma of the breast,
gastrointestinal tract, and urogenital tract should be treated by
total body irradiation, the Oak Ridqe researchers made the
following statement ... II
Statement to Congress April 11,1994 by David S. Egilman IUD, MPH.

UCCM / RCC1.950005.008b
Statement for House Judiciary Committee -- Hartha Stephens
Q- How did you f i rs t f ind out about the radiat ion pro ject a t U. C.?
A- In the f a l l of 1971 I was s ta r t ing my f i f th year i n the University of Cincinnati English Department. I was thirty-four, an Assistant Professor.
When I f i rs t began t o look i n t o these experiments, I had no idea anyone had died o f the radiation. In the corr idor o f Mctlicken Hall one day, a fr iend in the department, Dave Logan (now the d i rector o f Prospect House, an alcohol treatment center i n Cincinnati), showed me a b r ie f report from the VWuge Voiceabout experiments being done a t U. C. f o r the Defense Department, using poor cancer patients. The reporter was questioning whether or not the patients knew they were i n an experiment; he said some were being i r radiated over their whole bodies and were suffering nausea and vomit ing f o r several days afterward.
This was a l l we knew when a group of us i n the Junior Faculty Association decided we should look i n to the matter, We were l i v i ng i n the tail-end of the sixties, a f te r all, not long af ter the bombing of Cambodia and so on, and we should remember that many Americans had developed a profound d is t rus t o f everything that issued f rom the Defense Department.
I had a research leave coming up in the winter, w i th t ime t o study th is issue, and I went over t o see Edward 6al1, who was then director of the tledical Center. I remember v is i t ing h im several t imes and trying out various arguments on h im t o try t o get information; he was courteous, but f o r quite a whi le nothing was forthcoming f rom him. I remember h i s saying that the f i l es on the pro ject were long and complicated and would not mean much t o people who were not doctors. He said, 'I'm sure you wouldn't want them all-. I said, 'We do though. We would l i ke t o see them al l . If everything i s a l l right, as you say, Dr. Gall, and we have no reason t o doubt your word, then perhaps i t would be useful t o have a campus organization c lear up the matter.' One day I went back over t o his of f ice and there was a large p i l e o f documents on h is desk. These papers were copies of the typescript reports the doctors were sending t o the DOD, and I would l a te r f ind that they to ld a t ragic and ter r ib le ta le- Even now, I do not know why 6a l l surrendered these papers t o me, and I l a te r real ized I was quite possibly the f i r s t person outside the tledical School and the Defense Department t o see them.

2 This set of documents tha t has now been copied and re-copied i n Cincinnati and elsewhere.
campus drive, up on our h i l l w i t h i t s beauti ful lawn stretching down t o C l i f ton Avenue, and pulled these papers out on my lap t o see what I had. I saw that individual pat ient h is tor ies were attached t o the backs of each of the nine reports, and I began reading these histories. I read f o r about an hour, and when I got out of the car, i t was as i f I could hardly recognize what was around me. Everything I saw looked d i f ferent t o me.
I was used t o reading i n plays and novels about t ragic deaths, full o f p i t y and sorrow, but I was not used t o lhfspity, th issorrow- I f e l t that these experiments had t o be stopped, and of cuurse in due t ime they were stopped.
Over that ChriStm8S holiday, I spread these papers oui i a te a t night over my dining room table, a f t e r our children were put t o bed, and I wrote a summary o f what had happened t o the eighty-seven individuals that had been irradiated, I wrote about how they died.
I presented my f indings t o a meeting of the Junior Faculty Association on January 14, and the group decided t o have a press conference, and this we d id on January 26 o f 1972. I feel now, as I look into the whole mat ter again, that our report was actual ly a conservative one. t ly fr iends i n the JFA had gone over w i th me every sentence of it. We knew i t had t o be clear and i t had t o be right. I introduced a number of qual i fying phrases, everywhere we had the least idea tha t an assertion could be challenged. Today I would not be as hesitant; but a t that t ime i t was as i f I could hardly believe myself what I was putting down on paper. S t i l l , this report t o ld a l l the basic truths of the case; i t to ld the truth, and i t examined every possible argument the doctors could use t o just i fy what they had done-
In some ways i t i s even more astonishing t o me today t o re f lec t on what transpired and t o image up the whole scene f rom the point o f view of the patients that were used. Even now, a f te r so much discussion of these fe l low ci t izens of ours, we don't know a l l t he i r names o r where they lived, what they d id fur CI l iving, what they personally went through, the weys in which their loved ones suffered -- CIS they themselves waited helplessly f o r word of this o r that f rom doctors and nurses that usually could not be found, o r stood a t bedsides i n crowded wards, of ten dirty wards, as various hospital users o f those years have test i f ied.
I - -
discussions about this project. I'm thinking, f o r instance, o f a man w i th
I drove back over t o tlctl icken Hall that day, and I sat out on the
- - - , - - These families I'm speaking of have been 3 ;_.-... - = the inv is ib le people inhabit ing a l l our debates and

3 w c e r who, a f te r h i s irradiat ion, never came back t o the hospital,
bore h is painful disease wi thout help, as fa r as we know, not w i l l i ng t o be treated again a f te r such an experience, I think of an eighty-year-old African American woman, -H. B.,’ who had lung cancer and suffered a stroke on the operating table in 1969, having her bone marrow aspirated i n preparation f o r her irradiat ion. She died s ix days afterwards -- ’an anesthesia-related death,’ as the doctors themselves describe i t- Did she volunteer t o be in an experiment that might end her l i f e ?
Q. How many patients died? We know that a t least 8 pat ients died o f bone marrow failure as a
direct resul t of radiation; f o r these patients the doctors provide the blood scores that a l low us t o document these cases o f classic radiat ion in jury- Then there were cases l i ke that o f fl. 8. mentioned above. Some of the histories, however, t e l l more than the others; i n the l a te r period, blood scores are no longer being studied and we are not generally to ld how much bone marrow depression existed a t t ime o f death. But there are altogether 26 individuals who died within 60 days of being i r radiated and whose deaths were almost certainly hastened by radiation. For some o f these short survivors we need t o see the i r fu l l hospital charts and follow-up i n the c l in ics and hospitals t o know exactly how they died.
Q. Were these cancer pat ients terminal? Were they people expected t o l i ve only a few months, as the medical school has said?
The patients who survived the radiat ion of ten l ived several years. One woman w i t h cancer o f the tongue was i r radiated i n 1961 and l ived a t least f i ve years a f te r the radiat ion- We i n fac t do not know when she died-
A l a te r group o f subjects were chosen speci f ical ly because they were i n re la t ive ly good shape, were not elderly, and could be interviewed in the i r homes o r workplaces about coming i n f o r this ‘treatment.’ They were working, eating normally, w i t h good blood counts. Def in i te ly not bed-ridden, extremely feeble, or about t o die-
0. Who were ihe doctors? It was not a question of one or two o r three individuals performing
a deadly r i t e that very few other doctors knew about, A projec c wac QOeS O n fo r eleven years and involvca the 3crctning and Cofi3idcmtion of a t least 1 1 1 patients had t o be known t o a great many people. There were ihirteen d m i w s o n th i s team over the years, co-authoring the reports and publications, and many more who assisted i n various ways
6 .La.

4 and were sometimes closely involved, i n the complex test ing of i r radiated subjects f o r mental functioning, f o r instance. Then we have the doctors who were staf f ing the Tumor Cl in ic a t the hospital and w i l l i ng t o hand over pat ients t o the chief investigator and his associates, as we l l as s ta f f a t several other hospitals; a t least three subjects were ‘recruited’ f rom Drake, t o use the doctors’ term, and three youngsters w i th Ewing’s sarcomi were brought over os ’volunteers’ f rom Children’s.
os i f he were an uninvolved o r neutral spokesman, he was himself a member of the team f o r the f i na l two years of the project. This doctor also served on the medical School‘s internal review which cleared the project o f any wrong-doing-
i n the defendant’s box also s i t t ing on the jury.
Cullege uf R d . o l m didnut find angthig offmim in these in-883 and in fbcl twmed them ‘jr)Gyrgjc. ’
What should we think about the long l i s t o f important medical journals which published the findings of these doctors over the years? How d id the i r editors and readers regard the deaths they learned about i n these reports? What were the at t i tudes o f the local hospital authorities, the s tate l icensing board?
Though Dr. Bernard Aron has been put forward by the tledical School
In general, I believe we do not expect t o have the individual who i s
Where i n fac t does the compl ic i ty begin and end? Thedmen-cun
Why did the review cammiiiees ut & C fui?? I n Cincinnati, i t can also be said, not one m. d. i n the tledical
School came forward t o o f fe r help t o the facul ty group studying the project in 1971, or simply t o examine their resul ts wi th an independent eye, though one research biologist d id consult w i t h our group -- anonymously.
No doctor in the greater medical community of the town openly expressed any doubts about what had been done.
This i s tha t wider complicity that SliOU’l+ 3’lZiTii iiS E G G ikii anything else, and here i n 1994 -- when things are supposed t o be ‘better’ -- the same situa%on exists. A4? dbCtum m i h g fwwuint I believe i t i s correct t o say that no reporter here i n town has been able t o f ind a single local doctor t o examine what our facul ty group found.
In 1995 on m. d. working here f o r NIOSH got i n touch w i t h me about this project and examined some o f the medical h istor ies i n my home one night, Since then this individual, David Egilman, has attempted t o draw at tent ion t o these trials; he bears out the findings o f the JFA and has publ ic ly explained the s tate of medical knowledge about whole body radiat ion f o r cancer as i t existed a t the t ime of the U- C. tests. He finds

no reason f o r the doctors t o have believed that radio-resistant tumors such as most of t he i r patients suffered f rom could have been helped by the 'treatments' administered; the doses given, as deadly as they proved t o be f o r many subjects, .) not high enough t o reduce tumors o r stop the spread of cancer-
Q. Why did the tledical School succeed i n drawing a curtain over th i s whole af fa i r in 19723 If the case against the doctors was as clear as i t sounds, why was there not a lawsu i t from subjects o r a cr iminal investigation?
One needs t o understand the ro le o f the media i n Cincinnati (and i n many other American towns). When the JFA press conference took place, the W8sh@7iunPusi sent a reporter and the flew Y@r& Times A crew came from CES. Our report was entered into the CungressiunuM%m?trdby Senator Kennedy- But there was no rea l coverage in Cincinnati -- no way f o r any of the subjects o r t he i r fami l ies t o know what had taken place. No one here broached the words 'radiation death-'
The tledical School was never compelled t o acknowledge any wrong-doing, and yet there was a tac i t acknowledgement that such work could no longer be tolerated, fo r a f te r a l l the pro ject was stopped. No pat ient was i r radiated a f te r the f a l l o f 1971, even though i n the report that would prove t o be the i r l as t t o the DOD, the doctors had announced the i r plans f o r more experiments i n the year t o come.
Q- Was there a cancer study being carr ied out using these patients? There was no publication o r report on cancer study during the
eleven years o f the project. No design f o r a cancer study was ever produced during the actual
course o f the experiments, although a study on cancer was issued a f te r the fac t and os a resul t o f publ ic revelations. There i s no reference t o an ongoing cancer project i n the DOD reports. There i s no evidence of close follow-up by the team o f the patients who survived more than 60 days. When the team had completed i t s radiat ion-injury tests, i t seemed t o have no more in terest i n the patients o r their cancers.
If there was a cancer project, who were the doctors, where i s the design, by whom was i t funded, what were i t s resul ts and how were they being reported?
9- Didn't some people a t the universi ty object t o what you and your group were doing, feel ing that the act iv i t ies of your medical colleagues were none of your business?

6 A. Of course. But surely events l i k e these are everyme's business.
working people; the great ma jo r i t y o f them we now know were paying taxes; they were helping t o Pay the salaries of those of us i n the JFA, and the salaries of the doctors. They were helping t o fund this public hospital, not t o mention the U. S- war machine of those days (as they do today). One can say that t he i r taxes helped t o pay the salary o f Ohio 6overnor John Gilligan, who came, not t o the i r defense, but t o the defense o f the tledical School and assisted i n the cover-up- Gil l igan convinced Senator Kennedy t o drop U. C. f rom the hearings on human experimentation which fol lowed the U. C. revelations and those about Tuskegee (where beginning i n the th i r t i es men i n Alabama w i t h syphi l is were denied treatment f o r their whole l i fet imes, and many died of syphil is-related disease or became insane).
I grew up among ordinary working people. My father worked f o r the railroads; my mother had only an eighth grade education. Hany of us in the JFA were individuals who tended t o side w i t h common people against leaders and experts who wanted t o control everything. I think people l i k e oursetves are s t i l l hoping that we i n the U. S. can grow in to a t rue democracy, that common c i t izens w i l l take the lead and assume control over their own society.
We are a class-ridden country, and actual ly i t should not surprise us when our class conf l i c t resul ts i n grievous actions l i k e those of the U. C. doctors, actions, that is, of one potent and protected class against another that i s powerless. It was a question here of a conf l i c t between wealthy doctors and administrators -- in a public i ns t i t u t i on insulated against public accountabil ity -- and common working people who could not a f fo rd doctors of t he i r own choosing.
The people who used General Hospital were most ly Cincinnati
Q. What changes should come out o f these revelations?
A. F i r s t of all, surely i t ought t o occur t o us that i f we had had national health insurance of a single-payer kind, that is, of the Medicare type that a l lows people t o choose the i r own doctors, these fe l l ow ci t izens of ours would not have been trapped in a publ ic hospital w i th nowhere else t o turn.
children o f the wealthy? of ten the children o f doctors, whose incomes, a f te r all, are within the top one o r t w o percent of U. S. incomes? There should be a public examination of a l l our admission practises around the c o u n t y and the way that medical schools are funded and how doctors are trained-
We need t o see who i s going t o medical school- Is i t only the

I
I
I
G

UCCM / RCCl.950005.009
Statement of Eugene L. Saenger, M. D. Before the House Judiciary Committee
Subcommittee on Administrative Law and Governmental Re la t ions
April 11, 1994 Cincinnati, Ohio
E.L Saenger, M.D.
April 11. 1994 Page 1

SUMMARY
Several important points are presented summarizing our work:
a One purpose of the study was the treatment of patients with far advanced cancer for whom the goal was the relief of pain, shrinkage of cancer and improvement in well being.
b. A second purpose was to study the systemic effects of radiation on the patient.
C. Treatment was given only if benefit to the patient was anticipated.
d Patients were chiefly from the Cincinnati General Hospital. Selection was made only based on the presence of advanced cancer and where no other therapy was considered to be as or more efficacious than that currently available chemotherapy. Race, IQ, or socioeconomic standing were not selection factors.
e. Treatment was paid for by Cincinnati General Hospital and the National Institutes of Health. No Department of Defense funds were used for treatment or patient care or decisions regarding therapy or patient reimbursement.
f. Patients were told that the treatment might help them and were cautioned that it migM not. Some patients chose not to be treated.
0 There was nothing secret about our work. There was nothing secret as to its bemg conducted. There was nothing secret about the findings obtained.
E L Saenger, M.D.
April 11, 1994 Page 2

1 am Eugene L. Saenger, M. D. of Cincinnati. It is a privilege for me to speak before this distinguished sub-committee of the Judiciary Committee of the U.S. House of Representatives to present a summary of our work on the treatment of far advanced cancer and the effects of wide field radiation therapy, work which I was privileged to direct and the results of which I am proud. The participation and support of the highly qualified physicians, allied scientists and associated health professionals is gratefully acknowledged. My Curriculum Vitae is attached. (See Appendix 1)
I am a graduate of Walnut Hills Hlgh School, Harvard College, 1938, cum laude and University of Cincinnati, College of Medicine 1942. My training in Radiology was at Cincinnati General Hospital completed in 1945. I am a Diplomate of the American Board of Radiology and the American Board of Nuclear Medicine.
My major appointments at University of Cincinnati College of Medicine include rising from Assistant Professor of Radiology to Professor of Radiology from 1949-1 987 and Professor Emeritus since then. I was the founder and director of (what continues today) the Eugene L. Saenger Radioisotope Laboratory from 1950 to 1987. I was Radiology Therapist at Children's Hospital from 1947 to 1987.
1 have given over 40 guest and invited lectures in the U.S. and elsewhere. I have received the De Hevesy Nuclear Pioneer Award of the Society of Nuclear Medicine and the Gold Medal of the Radiological Society of North America and the Daniel Drake Award of the University of Cincinnati College of Medicine, these being the highest honors of these organizations.
My consultant appointments to my government encompass both domestic and international service, and include among others requests from the Department of Justice; Department of Energy; Environmental Protection Agency; Department of Health and Human Services; National institutes of Health; Department of Defense; Food and Drug Administration: International Atomic Energy Agency; Oak Ridge Affiliated Universities; Surgeon General of the Air Force; the U. S. Public Health Service and numerous government administered hospitals. Additionally, I was proud to serve my country as an officer in the United States Army, attaining the rank of Major prior to my honorable discharge.
My principal appointments at the University of Cincinnati College of Medicine range from Assistant Professor of Radiology in 1949 rising to Professor, and from 1987, the rank of Professor Emeritus. I am a member of 29 medical and scientific societies and the Founding President of the Society for Medical Decision Making. In addition to being an honorary member of the National Council on Radiation Protection and Measurement (NCRP), I delivered the Sixth Lauriston Taylor Lecture--the highest honor of this organization. The NCRP is an organization chartered by Congress that develops recommendations for radiation safety used by Federal Agencies for protection of the public.
E L Saenger, M.D.
April 11, 1994 Page 3

Wfi my colleagues, I am the author of 187 publications in the scientific literature, the majority being in refereed journals.
t C C C C t . C t .
I, Introduct ion
Several important points are presented summarizing our work:
A One purpose of the study was the treatment of patients with far advanced cancer for whom the goal was the relief of pain, shrinkage of cancer and improvement in well being.
B. A second purpose was to study the systemic effects of radiation on the patient.
C Treatment was given only if benefit to the patient was anticipated.
D. Patients were chiefly from the Cincinnati General Hospital. Selection was based only on the presence of advanced cancer and where no other therapy was considered to be as or more efficacious than then available chemotherapy. Race, IQ, or socioeconomic standing were not selection factors.
E Treatment was paid for by Cincinnati General Hospital and the National Institutes of Health. No Department of Defense funds were used for treatment or patient care or decisions regarding therapy or patient reimbursement.
F. Patients were told that the treatment might help them and were cautioned that it might not Some patients chose not to be treated.
G There was nothing secret about our work. There was nothing secret as to its Wmg conducted. There was nothing secret about the findings obtained.
11, What Was The Purpose of The Total Body Irradiation (TBI)/Partial Body lrradia!ion (PBI) Study:
The primary goal of the study was to improve the treatment and general clinical management by increasing, if possible, survival of patients with advanced cancer and palliation of symptoms. (Palliation is treatment directed at relief but not cure.) In addition, observations and laboratory tests were carried out to seek effects of radiation on cancer patients and on the changes that could be ascribed to radiation.
The palliative effects of TBI were considered to be at least equal to and very likely to be superior to the chemotherapy available in the period from 1960 - 1970. Also the treatment methods
EL Saenger, M.D.
April 11, 1994 Page 4

were thought to be less stressful to the patients than chemotherapy then in use, especially in terms of initial symptomatology following administration of the dose, as for example, the painful mouth ulcers from methotrexate and 5-fluorouracil, drugs used at that time.
The background for this project originated in my observations over the prior 20 years that cancer patients treated with radiation might be benefitted by a more careful evaluation of the effects of this kind of treatment on the total patient.
It seemed to me at that time that the approach to the total management of the cancer patients receiving radiation therapy was not as well studied as was that of the same patient who would be treated surgically. In addition, the effect on the cancer patient of doses of radiation given through large fields in relation to systemic effects was not being adequately considered, even though much work was being done on the radiation effects on the tumor and its immediate substrate.
The scientific indications that these goals might be achievable were based on two levels of evidence one from animal studies and one from human studies.
a ) Animal studies indicated better tumor regression when total body irradiation was preceded by localized radiation than when localized radiation therapy was given alone both for lymphoma and carcinoma in mice.
b ) Studies in human beings: Human studies for treatment of far advanced solid tumors prior to 1960 suggested the value of TBI. It was employed in several American centers and internationally. Treatment was given with success in relieving pain, shrinking tumors and, in some cases, prolonging survival. (See Appendix 2)
A major reason that we could begin TBI and PBI resulted from several important developments. The cobalt 60 teletherapy unit was installed at General Hospital in 1958, the first in Ohio. Harold Perry, M. D. was the first full time radiation therapist at our hospital. He had come from Memorial Sloan Kettering Cancer Center in New York Hospital and was familiar with TBI and PBI techniques and indicators. James G. Kereiakes, Ph.D., a physicist, joined the Department of Radiology in 1959. He calculated the doses, dose rate and distribution of radiation.
I believed that there could be implications from this treatment for well individuals exposed to radiation under other circumstances. In 1958, I submitted an unsolicited application to DOD because there had been no studies on the metabolic effects of radiation and funds were available. This proposal was reviewed by J. A. Isherwood, M. D. for the Army Medical Research and Development Command. He made the following comments: “Any correlation of tumor response to total dose of irradiation by such means as proposed in this project would be of great value in the field of cancer. In addition if by some means such as those proposed accurate knowledge of the total dose of radiation received could be determined it would be of inestimable value in case of atomic disaster or nuclear warfare.” (See Appendix 3)
E L Saenger, M.D.
April 11, 1994 Page 5

111. The Study
A Typical of medical investigations, this study progressed through phases. These phases are defined as follows:
Phase I studies are to determine whether the treatment is toxic.
Phase II is to determine in patients without controls but with measurable disease, whether the treatment is effective. Our studies included Phase II.
Only then are Phase Ill studies with controls and ideally with randomization conducted to determine therapeutic values. Although a Phase 111 study was proposed, we did not reach this level.
B. Patient selection: Patients were not recruited. Patients were referred for consideration for this form of therapy mostly from the Tumor Clinic (outpatient) and the Tumor Service (in-patient). I was not involved in patient selection or in determination of extent of therapy or dosage. These decisions were made solely by the attending physicians, internists and surgeons, and by radiation therapists. There were 24 patients entered into the study who were not given TBI or PBI. Some were rejected because it was thought that the patient would not benefit. Several patients and their families declined treatment.
1. Eligibility for therapy was spelled out in our 1962 document to DOD:
a There is a reasonable chance of therapeutic benefit to the patient.
b. The likelihood of damage to the patient is not greater than that encountered from comparable therapy of another type.
c. The facilities for support of the patient and complications of treatment offer all possible medical services for successful maintenance of the patient's well being.
2. Race was not a factor in selection--only the type of cancer and its extent. A statistical analysis, done only after the program was terminated, confirmed that the patients in this s!udy did not differ from the patient population of Cincinnati General Hospital.
3. IQ was not a factor in patient selection.
JV, lnformed Consent
As m selection of patients, informed consent for therapy was obtained by the attending physicians.
E L Saenger. M.D.
April 11, 7994 Page 6

In the 1940's and 1950's informed consent was verbal except for the general brief informed consent required by the hospital from all patients to be hospitalized irrespective of the treatment to be administered.
In this project, the purpose and actual treatmeat and the possible outcomes were discussed with the patient and often included family members.
In April 1965, the use of written informed consent, both for radiation and bone marrow harvesting and reinfusion, were developed by this project. These forms clearly indicated that risks of treatment were discussed. At that time, DHEW and DOD did not require written informed consent. As a result of a number of helpful suggestions from the University of Cincinnati faculty Research Committee, several revisions to the form were made between 1967 and 1971 (See Appendix 4). Furthermore, this written informed consent that we developed preceded any written requirements of the University of Cincinnati Medical Center by two (2) years.
One criticism of our work stemmed from the instructions to the attending personnel not to inquire concerning nausea, vomiting and diarrhea in the first few days after treatment. We were particularly interested in the frequency of these manifestations. Since both nausea and vomiting could be induced by suggestive questions, we requested that no questions be asked as to how the patient felt. This restriction did not in any way restrict the administration of drugs such as Compazine to relieve symptoms. This care is amply documented in patients' charts. Of interest is that after treatment 39 patients (44%) had no nausea and vomiting, that 23 (27%) had symptoms for three (3) hours or less and that 12 patients (14%) had symptoms for six (6) hours or less. These responses are comparable to chemotherapy at the time, e.g., methotrexate, 5-fluorouacil and Chlorambucil.
V, Funding
As noted earlier, most costs of treatment were paid by Cincinnati General Hospital. An estimate of the expenditures for direct patient care for about 3,804 days at about $114 per day with some additional cost estimates gave a total calculated amount of $483,222. There were no professional costs or physician fees for patient care.
Some funding was obtained from the NIH. Some patients were maintained on the General Clinical Research Center of Cincinnati General Hospital; this unit was supported by NIH. The protocols and records of each patient so hospitalized were submitted to the NIH and approved. In addition, several of the Post Graduate Fellows supported by the Radiation Training Grant of the National Jnstitute of General Medical Sciences (NIH) participated in some phases of the DASA program.
DOD funding was utilized solely for observation of patient symptoms and signs and for the extensive laboratory tests (See Appendix 5). DOD funds had no relation to choice of dose, choice of patient or patient care, in any way. No patient was compensated or reimbursed or paid for
€L Saenger, M.D.
April 11, 1994 Page 7

treatment. A Congressional General Accounting Office audit documented all of this in 1972. The Wial DOD contract for FY 1960 through FY 1971 was $671,482.79.
W, Success of the TBI study
Mortality. In the group of patients who received radiation, there were three categories in which there were enough patients to compare with other patients of the Cincinnati General Hospital treated differently or with comparable groups reported in the refereed medical literature. The cancers were those of the breast, lung and colon. The death rates were comparable to those treated by other means.
An important question is whether radiation was the factor leading to the early death of a patient. These patients had far advanced cancers which were growing exponentially. In the course of the disease, patients received chemotherapy and/or localized radiation therapy both before and immediately afier TBI or PBI. For these reasons, it is not possible to identify a single form of treatment or the rapid growth of cancer as being the single contributing cause of death. It most likely would be the rate of growth of the cancer itself.
There were 20 cases in which patients survived longer than one year. Except for the one patient with Ewing's tumor who remains alive after 25 years, the longest survivor lived 9 years. Two other relatively long survivors lived five years.
Palliation was successful with relief of pain in 31% of patients. Some decrease in tumor size occurred in 31% and an increase in well being was found in 30%. No change was observed in 31%. (In some patients there was more than one indication of improvement; thus the percentages exceed 100%). (See Appendix 6).
Because of radiation induced hematological depression, autologous bone marrow storage and reinfusion began in 1964. With improvement in technique to include harvest of the marrow under general anesthesia and replacement immediately after TBI it became possible to avoid the characteristic depression of the white blood cells in five patients. This promising development was stopped at the time of termination of the contract.
VIL Review by Others
A Faculty Research Committee. Our protocol was submitted to this newly formed committee in March of 1966. Provisional approval was given in 1967 with recommendations for review of therapeutic efficacy, bone marrow infusion as a supportive measure and some revision in the study design. At no time was the project disapproved by the Faculty Research Committee as it received exhaustive and critical reviews.
B. The ad hoc Committee of the University of Cincinnati (the Suskind Report) undertook a complete review of the TBI project. Among the findings were that Phase Ill -dies should be initiated with better criteria for the determination of palliative effects and
E L Saenger, M.D.
April 11, 7994 Page 8

that bone marrow transplantation be pursued. The study was judged to be adequate for support of the critically ill patients because of the development of skilled team management especially with the help of the psychiatrist and psychologist coupled with home visits.
C. American College of Radiology. At the request of Senator Mike Gravel, the American College of Radiology formed an expert committee of Dr. Henry Kaplan, Chairman of Radiology at Stanford University, Dr. Frank Hendrickson, Chairman of Radiation Therapy at Rush-Presbyterian Hospital, Chicago and Dr. Samuel Taylor, Ill, a medical oncologist at Rush- Presbyterian Hospital, Chicago. This distinguished group made two visits to our hospital. Their major findings were as follows:
followed up.
conforms with good medical practice.
and commendable.
and consistent with the recommendations of the National Institutes of Health and with the practice of most cancer centers.
committees in some fashion, we would urge your support for its continuation. (See Appendix 7)
1.
2.
3.
4.
The project is validly conceived, stated, executed, controlled and
The process of patient selection based on clinical considerations
The records, publications and patient follow-up are voluminous
The procedure used for obtaining patient consent is valid, thorough
5. Should this project come before the Senate or one of its
D. At the request of Senator Edward Kennedy, the Government Accounting Office reviewed the accounts of the Cincinnati General Hospital to determine whether there had been any intermingling of DOD funds used for patient care, since we had pointed out from the star! of our work that no DOD funds would be used for this purpose.
An excerpt from the letter dated May 26, 1972 from the Comptroller General to Senator Kennedy follows: "Concerning the contract with the University of Cincinnati, officials of the Defense Nuclear Agency stated that the cost of radiation treatment and patient care had not been borne by their agency. They stated also that funds of the Defense Nuclear Agency had been used only to pay for supplementary laboratory analyses of patients who had received whole body irradiation in order for the Defense Nuclear Agency to gain information in areas that were relative to national defense." (See Appendix 8)
E National Institutes of Health (DHEW). D.T. Chalkley, Ph.D., Chief, Office for Protection from Risks, Office of the Director NIH, was very supportive of our work. In a letter copied to Senators Nunn and Talmadge, he comments that "It is to be regretted that this incident has halted what promised to be a very significant addition to our armamentarium against metastatic cancer." He also wrote directly to Senator Nunn pointing out that "...the patients were treated individually for the diseases they had." (See Appendix 9)
F. Secrecy. This study received widespread publicity in the early 70's. We responded to all questions about it at the time including at an open press conference. The study
EL Saenger, M.D.
April 11, 1994 Page 9

resulted in numerous unclassified presentations at open medical meetings and in published papers and reports (See Appendix 10).
V111. Total Body Irradiation & Partial Body Irradiation Since 1971
It is apparently a common misunderstanding that the use of TBVPBI as a therapeutic agent has been discontinued. In the period from 1970 to the present there have been major changes in the use of TBI and PBI (See Appendix 2). Doses have risen from the low levels of 100-300 rad TBI and up to 300 rad PBI used by us from 1960 to 1970. Doses now range from 600 to 1200 rad in single or divided doses of TBI and with sequential HBI in these same dose ranges. fractionation has replaced single large doses (1 200 rad) because of the complication of radiation pneumonitis. Among the solid tumors treated during these two decades have been cancer of breast, prostate, lung, colon and some sarcomas.
At the University of Cincinnati Department of Radiation Oncology beginning in 1979, TBI and PBI were administered to adults and children for leukemias, lymphomas, cancers of breast and prostate and neuroblastoma. Nonmalignant diseases treated included aplastic anemia and congenital anomalies.
E L Saenger, M.D.
April 11, 1994 Page 10

--I
1

UCCM / RCC1.950005.009a
CURRICULUM VITAE
EUGEME L. SAENGER, M.D. PROFESSOR EMERITUS OF RADIOLOGY
UNIVERSITY OF CINCINNATI COLLEGE OF MEDICINE
Personal
Date of Birth: March 5, 1917
Place of Birth: Cincinnati, Ohio (Hamilton County)
Home Address: 9160 Given Road Cincinnati, Ohio 45243 (513) 793-1373
Office Address: University of Cincinnati Hospital 234 Goodman Street - M.L. #569 Cincinnati, Ohio 45267-0569 Telephone: (513) 558-9042 Facsimile: (513) 558-4715
Married: Sue R. Saenger
Education:
A , B , - Cum Laude, Biochemical Sciences, Harvard University, 1938 M,D, - University of Cincinnati College of Medicine, 1942 Internship, Cincinnati General Hospital, 1942-43
Assistant Resident and Resident in Radiology, Cincinnati General Hospital, 19 4 3 -46
Diplomate, American Board of Radiology, 1946
Diplomate, American Board of Euclear Medicine, 1972
Appointments
Professor Emeritus of Radiology, University of Cincinnati College of Medicine, September 1987
Professor of Radiology, University of Cincinnati College of Medicine, 1962-1987
Director, Eugene L. Saenger Radioisotope Laboratory, University of Cincinnati College of Nedicine, 1950-1987
Vice-chairman, Department of Radiology, University of Cincinnati College of Medicine, i975-1987

2
Assistant and Associate Professor of Radiology, University of Cincinnati College of Medicine, 1949-1962
Radiation Therapist, Children's Hospital Medical Center, Cincinnati, Ohio, 1947-Present
Major, U.S. Army Medical Corps; Chief, Radioisotope Laboratory, Brooke Army Hospital, Ft. Sam Houston, Texas, 1953-1955
Consultant in Radiology, Brooke Army Hospital, Ft. Sam Houston, Texas, 1956-1977
Consultant, Oak Ridge Operations Office, Division of Biology, U.S. Atomic Energy Commission, Oak Ridge, Tennessee, 1958-Present
Consultant, Division of Compliance, U.S. Atomic Energy Commission (now U.S. Nuclear Regulatory Commission), Washington, D . C . , 1962-1987
Consultant in Radiology, Lackland AFB Hospital, Lackland AFB, Texas, 1959-1975
Consultant, Radiological Health Research Activities, USFHS, Taft Engineering Center, 1964-1969
Consultant, Medical Advisory Committee, Defense Atomic Support Agency, Washington, D.C., 1965-1971
Network, Environmental Protection Aqency, 1968-1984 Representative fer State of Ohio to the Medical Liaison Officer
Consultant on Radiology Training, DHEW/PHS, National Institute of General Medical Sciences, NIH, Eethesda, Maryland, 1967-1970
Consultant to the Office of the Director, DHHS/PHS/FDA, Center for Devices and Radiological Health, Rockville, blaryland, 1969-Present
Consultant, Radiation Bio-Effects and Epidemiology Advisory Committee, DHE\7/PHS, P7zshington, D.C., 1970-1971
Consultant, Radiation Science & Protection Fellowship Board, Oak Ridge Associated Universities, Oak Ridge, Tennessee, 1970-Present
Consultant to Surgeon General, U.S. Air Force, in Nuclear Medicine, 1970-1975
Consultant, Wright-Patterson Air Force Base, Ohio, 1977-Present
Board of Directors, Center of Science and Industry, Cincinnati, Ohio, 1964-1969

Chairnizn, Radiation Safety Ccxrm.ittee, Uriiversity of Cincinnati, 1964-1985; Nember, 1985-1389
Board of Trustees, Community Chest & Council, Cincinnati, Ohio, 1364-1970; Executive Committee, 1970
President, Public Health Federation, Cincinnati, Ohio, 1965-1969
Executive Committee, Health Planning Association of the Central Ohio River Valley (CORVA), 1970-1972
Environmental Health Planning Committee of the Central Ohio Fiver Valley (CORVA) 1970-1972
Advisory Committee to the Federal Radiation Council, National Academy of Sciences, Washington, D.C., 1964-1972
Associate Editor, Journal of Nuclear Medicine, 1960-1970
Prcgram Director in Radiological Sciences (National Cancer Institute and National Institute of General Medical Sciences, M I H ) Training Program, University of Cincinnati, 1359-1970
Program Director for stueies in metabolism of radiation following whole-body irradiation (Department of Defense) 1960-1971
Co-investiqator, Biomedical Computing Center, University of
Chairman, Cancer Control Council, Public Health Federation,
Cincinnati College of Medicine, 1962-1966
Cincinnati, Ohio, 1961-1968
Board cf Directors, Cancer Control Council, Cincinnati, Ohio, 1964-1970
Eoard of Governors, Ohio V a l l e y Chapter of the Arthritis and Rheumatism Foundation, 1961-1968
Eoard, Hamilton County Chapter of the American Cancer Society, 1963-1967
Governor's Advisory Eoard on Atomic Energy, State of Ohio,
Member, Medical Advisory Committee to Departnent of Health, State
Member, Honorary Editorial Advisory Boar2 of the Journal - of
Radiation Research Society, Member - Finance Committee, 1977-1981
1963-1972
of Ohio, 1962-1969
Applied Radiology, 1972

H e a l t h P h y s i c s S o c i e t y , Chai rman - L e g i s l a t i o n C c m i t t e b , 1968-1369
E e a l t h P h y s i c s S o c i e t y , r.lember - Board of D i rec to r s , 13G6-1969
l ? a t i o n a l C o r n i t t e e o n R a d i a t i o n P r o t e c t i o n , N a t i o n a l Bureau o f S t a n d a r d s , Member Subcommi t t ee o n Radium, Coba l t -60 and Cesium-137, 1952-1965
Nat iona l C o u n c i l on R a d i a t i o n P r o t e c t i o n a n d Measurements I N C R P ) , Board of D i rec to r s , 1967-1983; H o n o r a r y Member s t a t u s 1983
NCRP, Member - Subcommi t t ee f o r R e v i s i o n of Handbook 7 3 , 1966
NCRP, Chai rman - Budge t a n d F i n a n c e Committee, 1368-1973
MCRP, Chai rman - S c i e n t i f i c Committee 4!29 on B r a c h y t h e r a p y Devices, 1968-1972
ECP9, Chai rman - A d Hoc T h y r o i d B l o c k i n g C o m m i t t e e , 1972-1978
NCRP, M e m b e r - S c i e n t i f i c Committee # 4 4 on R a d i a t i o n A s s o c i a t e ? w i t h Medical E x a m i n a t i o n s , 1 .973-Present
NCRP, Cha i rman - Resources Deyrelopment P rogram,
Amer ican f ioen tgen Ray S o c i e t y , R e p r e s e n t a t i v e t o t h e H a t i o n a l
1986-1990
C o u n c i l on R a d i a t i o n P r o t e c t i o n a n d !4ezsurements , 1 9 6 0 - P r e s e n t
S o c i e t y of Nuc lea r N e d i c i n e , Member - Board of D i rec to r s , 1966-1969
S o c i e t y of PJuc lear M e d i c i n e , Nember - R a d i a t i o n P r o t e c t i o n Committee, 1966-1969
S o c i e t y of R u c l e a r M e d i c i n e , Chai rman - Subcommi t t ee on P o s t
S o c i e t y of Nuc lea r M e d i c i n e , Member - By-Laws Committee,
Soc ie ty of N u c l e a r F e d i c i n e , Menber - C o r n i t t e e on E d u c a t i o n and T r a i n i n g , 1969-1971
Socie ty of N u c l e a r Medic ine , Chai rman - C o r m i t t e e on P u b l i c H e a l t h a n d E f f i c a c y , 1972-1984; Member, 1984-1987
S o c i e t y of Nuc lea r M e d i c i n e , Member - S u b c o r m i t t e e on R i s k s o f
S o c i e t y of Nuc lea r Medic ine , P r i n c i p a l I n v e s t i g a t o r - U . S .
G r a d u a t e T r a i n i n g i n N u c l e a r Kedic ine , 1969-1971
1969- i972
Low Leve l I o n i z i n g R a d i a t i o n , 1 9 8 0 - P r e s e n t
D e p a r t m e n t of E n e r g y C o n t r a c t , "The E f f i c a c y o f C l i n i c a l D i a g n o s t i c P r o c e d u r e s U t i l i z e d i n N u c l e a r M e d i c i n e " , 1977-1983

5
American College of P.adiology, XenSer - Subcommittee on RaZiological Aspects of Disaster Planning, 1964-1969
American College of Radiology, Member - Commission on F.adiologic Units, Standards, and Protection, 1969-1988; Chairman, 1989-Present
American College of Radiology, Chairman - Committee or. Research and Development in Nuclear Medicine, 1969-1372
American College of Radioloqy, Member - Commission on Public Health, 1969-1971
American College of Radiology, Member - Subcommittee on “uclcar Medicine Technology, 1969-1975
American College of Radiology, Member - Committee on Quality Assurance and Efficacy, 1972-Present
American College of Radiology, Member - Comittee on Radiation Physics, 1977-1982
American College of Radiology, Member - Coxmission on i :uc lear Medicipe, 1977-1986
American College of Radiology, Member - Medical L e q n l C o r r m i t t e e , 1986-Present
National Consultant, Office of the Radiation Safeti7 O f f i c e r of the Veterans Administration, 1974
Member, A d Hoc Cqwittee to Evaluate the Health and S a f e t y L Aspects of Pu in the Environment Adjacent to the Yound
Laboratory, 1975
Argonne National Laboratory, Member - Review Committee for the Radiological and Environmental Research Division, 1976-1977
International Conmission an Radiological Protection, Member - Committee # 3 on Protection in Medicine, 1977-1984
Federated Council of Nuclear Medicine Organizations, Representative - Americm College of f:uclear Physicians, 1977-1980
FeJeratcd Council of Nuclear Medicine Organizations, Secretary-Treasurer, 1978-1980
33EIR Report (The Effects on Populations of Exposure to L o w Levt?!1c of Ionizing Radiation), National Academy of Sciences, l!ational Research Council, Member of Ccmmittee, 1 9 7 2

G
Reactcr S a f e t y S tudy (lJASE-?4OO) , Ar. Assessment of Acc iden t R i s l r s U n i t e d i n U.S. Corrrnercial K u c l e a r Power P l a r t s , Appendix IV,
S t a t e s Nuclear R e g u l a t o r y Commission, Oc tobe r 1975, Menber- Advisory Group on H e a l t h E f f e c t s
C o n s u l t a n t , Pan Americ3.r. H e a l t h O r q a n i z a t i c n , World H e a l t h C r g a n i z a t i o n , Mexico C i t y , Mexico, December 1380
Co-founder and P r e s i d e n t , Societ:r f o r l4ediczl D e c i s i o n b:aking, September 1973; H i s t o r i a n 1979-1385
Member, O v e r s i g h t C o r n i t t e e on t h e Radioepidemiologic T a b l e s (OCRET) , N a t i o n a l Research C o u n c i l , Commission on L i f e S c i e n c e s , Augcs t 1983-Gacuary 1985
Eember, U . S . D e p a r t c e n t o f Energy Ad Hoc Cornt i t tee on ILTeutrcn
Chairman, AZvisory C o r n i t t e e of t h e C h a r l e s 1.1. Barre t t Cancer
Q u a l i t y F 'zctor , January-December 1985
C e n t e r , U n i v e r s i t y of C i n c i n n a t i , 1384-1986
f f e a l t h E f f e c t s Model f o r K u c l e a r Power P l a n t Acc iden t CoRsecuence Analysj-s , (NUREC/CR-4214) P r e p a r e d by S a n d i a N a t i o n a l L a b o r a t o r i e s , Albuquerque, ??IC for t h e D i v i s i o n of Risk A n a l y s i s and O p e r a t i o n s , U . S . K u c l e a r R e g u l a t o r y Ccrmiss ion , j u l y 1 9 8 5 , Member, Advisory Committee
C o n s u l t a n t , 7 t h Medical Command, U.S. Army, H e i d e l b e r g , F 3 e r ; t Gemany, i,iay 1 9 8 6
Fember , AbV\ C o n n i t t e e on Gon-Mil i ta ry Kad ia t ion Emergencies , August 1986; c o n f e r e n c e November 1 5 - 2 1 , 1986
C i r e c t o r , F.egion I, Carcer Con tzo l Ccnsortiurri of Ohio ( C C C O ) , 1985-1989
Honorary menber, F'ledical Acac5ep.y of S R C r o a t i a , Feb rua ry 1 9 8 8
Ad H c c C o n s u l t a n t t o : U . S . U.S. U . S . U.S. U.S.
Department of &Tust ice Depar tnen t of Enerc;:i E n v i r o c r e n t a l P r o t e c t i o n AgeEcy Department of Defecse Department of E e a l t h and IIuman Ser-Jices, Food and Grug A d m i n i s t r a t i o n
I n t e r n a t i o n a l Atomic Er.ergy Agenc'i M e m b e r , E x p e r t C o m L t t e e o f IAEA t o t h e USSR t o e v a l u a t e t h e l a t e e i i e c t s o f Chernobyi , Guly 1330
Marquis ' Who ' s Who
American Men and Komen of S c i e n c e

7
Lectczeships :
Annual Oration, "Radiologists, Medical Radiation and the Public Eealth", presented at the Radiological Society of North Americs., Chicago, Illinois, December 4, 1968
Aubrey 0. Hampton Lecture, "Radiation 1971 - Just How Safe?", Harvard Eledical School, Massachusetts General Hospital, Boston, April 4 , 1971
Wright H. Langham Memorial Lecture, "Radiation Accidents - 3 Decades of Facts and Fancies", University of Kentucky tledicai Center, Lexington, Kentucky, November 15, 1977
Annual Failla Lecture, "Benefits vs Risks of Medical Radiation: N e w Concepts and Frcblems", presented to the Greater New Yor!; Chapter of the Health Physics Society, Columbia University, New York, December 7, 1 9 7 7
Brookhaven National Laboratory, "'Safe' Tracer Dose in Human Experimentation", Islip, New York, April 7, 1978
Tenth Annual CGnference cn Radiation Cor,trol, "Efficacy of Nuclezr Medicine Przc2duresf', fiarricburq, Pennsylvania, April 30-!lay 4 , 1978
Harvard University School of Public Health, Planning for Muclear Enerqencies, (seminar), "Nedical-Legal Aspects of Radiation Exposure", Boston, ?4assachusetts, May 8-12, 1 9 7 8 (through 1386)
Society of Nucl-ear Medicine Refresher Course, "Radiation Effects and Radiation Protection", Anaheim, California, Jure 1978
Radiological Society cf fiorth American Refresher Course, "Recent Advances in Radiation Epidemioloql-." , Chicago, Illinois, November 1976 (repeated 1979, 19SO!
Food and Drug Administration, Bureau of Radiological Health, "Efficacy Studies in Lung Scanning: Desicjn and Implementation", Rockville, Maryland, Xarch 20, 1373
Armed Forces Radicbiological Research Institute (AFRRI) , "The Experienced Effects of Ionizing Radiation on the Body", Bethesda, Maryland, May 2 3 , 1979
Guest Lecturer, "Efficacy and Efficiency of the Diagnostic Application of Radiation and Radionuclides", organized by the Government of the Federal Republic of Germany and the World Health Organization, Neuherberg, West Germany, December 5 - 7 , 197'3
Literary Club, "Perceptions of Risk", Cincinnati, Ohio, February 18, 1980

8
S c c i e t y of N u c l e a r Med ic ine C o n t i n u i n g Educatior, Course, "Muclear Power , N u c l e z r M e d i c i n e and t h e P u b l i c " , Det ro i t , Elichiqar!, J u n e 25, 1 9 8 0
G u e s t L e c t u r e r , "Low Level R a d i a t i o n R i s k s " , U n i v e r s i t y of Texzs H e a l t h S c i e n c e C e n t e r , Hous ton , T e x a s , J u l y 2 5 , 198G
G u e s t L e c t u r e r , l J u c l e a r R a d i ? t i o n R i s k s - A U t i l i t y - M e d i c a l D i a l o g u e , "Case Histories of L a w s u i t s f o r O v e r e x p o s u r e " , s p o n s o r e d by t h e I n t e r n a t i o n a l I n s t i t u t e o f S a f e t y and H e a l t h , Wash ing ton , D . C . , September 22-23, 1980
"Hospital P r e p a r a t i o n f o r t h e Management o f R a d i a t i o n A c c i c l e n t s " , c o u r s e p r e s e n t e d by t h e E.L. S a e n q e r R a d i o i s o t o p e L a b o r a t o r y , Sep tember 29-30, 1980 ( r e p e a t e d S e p t e m b e r , 1981)
G u e s t L e c t u r e r and Banquet A d d r e s s , Los A l a m o s S c i e n t i f i c L a b o r a t o r y , L i f e S c i e n c e s Symposium, "Med ica l A s p e c t s of R a d i a t i o n : R a d i a t i o n B u r n s " , L o s A l a m o s , N e w Mexico, Oc tobe r 8-10, 1980
"Aspects o f N u c l e a r M e d i c i n e " , Medical S o c i e t y of t h e D i s t r i c t of C o l u m b i a Annual S c i e n t i f i c Assembly, Whi t e S u l p h u r S p r i n g s , West V i r g i n i a , O c t o b e r 2 4 - 2 6 , 1 9 8 0
S o c i e t y o f N u c l e a r Med ic ine R e f r e s h e r C o u r s e , "What Y u c l e a r M e d i c i n e P r o f e s s i o n a l s S h o u l d Know About. N u c l e a r W a r f a r e " , L c s Vegas , Nevada, J u n e 1 7 , 1981
G u e s t L e c t u r e r and Member o f F a c u l t y , " R e g i o n a l Senir.ar c n G e n e r a l P r o c e d u r e s t o Manage P e r s c n s R e c e i v i n g Whole o r P a r t i a l Body I r r a d i a t i o n " , co - sponsored by t h e Pan imerican H e a l t h O r g a n i z a t i o n and t h e Government o f B r a z i l , I t a i p a v a , B r a z i l , December 1 1 - 2 2 , 1982
G u e s t L e c t u r e r , "The P.ole of t h e P h y s i c i a n i n X e d i c o - l e g a l C l a i m s A s s o c i a t e d w i t h R a d i a t i o n I n j u r y ' ' , s p o n s o r e d by t h e P a c i f i c - S i e r r a C o r p o r a t i o n , i n A-lbuquerque, N e w Mexico, March 4-6, 1 9 8 2
S i x t h Annual L a u r i s t o n S . T a y l o r L e c t u r e , " E t h i c s , T r a d e - o f f s a n d M e d i c a l R a d i a t i o n " , p r e s e n t e d t o t h e E a t i o n a l C o u n c i l o n R a d i a t i o n P r o t e c t i o n and Measurements , Wash ing ton , D . C . , A p r i l 6 , 1982
"Hiyh Level R a d i a t i o n " , i n v i t e a Grand R o u ~ d s p r e s e n t a t i o n , Hamot Medical C e n t e r , E r i e , P e n n s y l v a n i a , A p r i l 2 9 , 1982
G u e s t L e c t u r e r , "Medical Management of R a d i a t i o n I r . j u r i e s " , s p o n s o r e d by t h e Radia t ion Management C o r p o r a t i o n o f P h i l a d e l p h i a , i n A t l a n t i c C i t y , New J e r s e y , May 6 , 1982

9
G u e s t L e c t u r e r , "Medical Maxagernent of R a d i a t i o n Czsualties" , s p o n s o r e d by t h e R E M C o r p o r a t i o n o f A lbuquerque , i n S o u t h Haver,, M i c h i g a n , May 2 4 - 2 6 , 1 9 8 2
S o c i e t y of N u c l e a r N e d i c i n e C o n t i n u i n g E d u c a t i o n C o u r s e , "ALhFA - What is R e a s o n a b l e " , M i a m i Beach , F l o r i d a , J u n e 1 7 , 1 9 8 2
" D i a g n o s t i c E f f i c a c y - Lung Imaging as a Model. The S o c i e t y of N u c l e a r M e d i c i n e E f f i c a c y S t u d y " , 2 9 t h Annual Mee t ing of t h e S o c i e t y of N u c l e a r M e d i c i n e , F l i a m i Beach , F l o r i d a , J u n e 15-18, 1 9 8 2
G u e s t L e c t u r e r , A Symposium: H e a l t h A s p e c t s of N u c l e a r Power P l a n t I n c i d e n t s , " R e g i o n a l O r g a n i z a t i o n of Nedical Care" , s p o n s o r e d by t h e N e w York Academy of Med ic ine and t h e N e w York State Depar tmen t of H e a l t h , N e w York, New York, A p r i l 7 - 8 , 1 9 8 3
G u e s t L e c t u r e r , 23rd Annual Symposium on Trauma, " I r r a d i a t i o c Trauma", s p o n s o r e d by t h e Mich igan Committee on Trauma, T h e American College of S u r g e o n s , L a k e s h o r e C o n t i n u i n g Medical E G u c a t i o n , I n c . and Muskegon County Medical F o u n d a t i o n , Muskegon, M i c h i g a n , Sep tember 2 1 , 1983
Guest L e c t u r e r , I n t e r n a t i o n a l C o n f e r e n c e o n N u c l e a r E?edicir.e, " E f f i c a c y A n a l y s i s i n N u c l e a r M e d i c i n e - Lung S c a n n i n g a s a Model" a h d " P o t e n t i a l s f o r TC-99m M y o c a r d i a l ~ Imaging A g e n t s " , Rhodes, Greece, A p r i l 2 4 - 2 9 , 1 9 8 4
G u e s t Lec tu re r , Medical/Legal A s p e c t s of R a d i a t i o n Induced. C a n c e r , " I m p a c t of Compensa t ion L e g i s l a t i o n on f . l e d i c a i S c i e n c e s ' ' , s p o n s o r e d by t h e R a d i a t i o n Ilanagement C o r p o r a t i o n , Philadelphia, P e n n s y l v a n i a , September 5-7, 1 9 8 4
G u e s t L e c t u r e r , " F r o b a b i l i t y of C a u s a t i c n " , sponscrec! by E l e c t r i c B o a t Company, G r o t o n , C o n n e c t i c u t , l May 1 4 , 1 9 8 5
G u e s t L e c t u r e r , " D e t e r m i n a t i o n of C l i n i c a l E f f i c a c y : N u c l e a r M e d i c i n e as A p p l i e d t o Lung S c a n n i n g " , s p o n s o r e d b y U n i v e r s i t y of C o n n e c t i c u t , F a r m i n g t o n , C o n n e c t i c u t , May 15 , 1985
G u e s t L e c t u r e r , Nedical A s p e c t s of R a d i a t i o n E m e r q e n c i e s , " N e w T r e n d s i n T r i a g e and T r e a t m e n t of t h e A c c i d e n t V i c t i m " , s p o n s o r e d b y Yale U n i v e r s i t y S c h o o l of N e d i c i n e , Lawrence b Memorial H o s p i t a l s , N e w London, C o n n e c t i c u t , May 1 6 , 1985
G u e s t L e c t u r e r , Emergency Planninc j a n d Response , "Case S t u d i e s of: H a d i a t i o n A c c i d e n t s " a n d "Legal I m p l i c a t i o n s : Long Term R i s k and Compensa t ion" , H e a l t h P h y s i c s Summer S c h o o l , E v a n s t o n , I l l i n o i s , June 3 - 7 , 1 9 8 5

10
Guest Lecturer, 1985 International Congress of Radioloqy, - - "Efficacy and Cost Effectiveness of Diagnostic Tests: Lung Scans f o r Pulmonary Embolism", "Medical-Legal Problems for the Radiologist a s a Consultant"; also served as co-moderator of session entitled "Decision Making and Image Selection", Honolulu, Hawaii, July 8-12, 1985
Guest Lecturer, Advanced Management of Radiation Accidents, "Early Medical Decisions", and "Legal Aspects-A Physician's View" sponsored by the University of New Mexico School of Medicine, Albuquerque, New Mexico, October 3-5, 1985
Guest Lecturer, Toxicology: Basic Science and Clinical Research, "New Thoughts About Radiation Accidents", sponsored by the University Association for Emergency Medicine and the International Research Institute for Emergency Medicine, San Francisco, California, February 13-14, 1986
Guest Lecturer, "Should There Be a Limit of Patient Exposure Based on Risk?", sponsored by Brookhaven National Laboratory, Upton, L.I., New York, April 7, 1986
Guest Lecturer, "Nuclear Accident Management", Society of Nuclear hIediclne Annual Xeeting refresher course, presented. in June of 1986, 1987 and 1988
Guest Lecturer, "Acute Effects of Radiation", International Conference on Non-Military Radiation Emergencies, sponsored by the American Xedical Association, Washington, D.C., !:ovember 1 9 - 2 1 , 1986
Recipient of the 2 8 t h George Charles de Hevesy Nuclear Pioneer Award, presented at the 34th Annual Fleeting of the Society of 1:uclear Nedlcine, Toronto, Ontario, Canada, June 2, i987
Co-chair, Special Session: Chernobyl, "Diagnosis and Treatment of Acute Radiation Injury'', presented at the Health Physics Society Annual Meeting, Salt Lake City, UT, July 5-10, 1387
Keynote ad?ress, Physician's Role in Nuclear !lass Casualties: Applications of the Chernobyl EXDerienCe, "The Physician's Role in PJuclear Energy", sponsored by the Department of Radiation Therapy, Hospital of the University of Pennsylvania and Radiation Management Consultants, Cincinnati, OH, September 11-13, 1987
Guest Lecturer, "Benefit, Risk and Cost-Effectiveness in Medical Radiation", sponsored by the U.S. Food and Drug Administration, Center f o r Drug Evaluation and Research, Rockville, ED, October
Recipient of the Daniel Drake Award, the most prestigious award given by the University of Cincinnati College of Medicine for outstanding contributions to medicine and science, June 1988
28, 1 3 8 7

11
Amy Bowles Lawrence D i s t i n g u i s h e d S c i e n t i s t i n Research b l ed ic ine , a t t h e Donner L a b o r a t o r y and t h e Lawrence B e r k e l e y L a b o r a t o r y of t h e U n i v e r s i t y of C a l i f o r n i a , B e r k e l e y , CA, J u n e 13-15, 1988 ( D r . S a e n g e r w a s t h e i n a u g u r a l Lawrence L e c t u r e r )
C l a r e n c e C . Lushbaugh L e c t u r e on C o n t r o v e r s i a l R a d i a t i o n C o n c e p t s , "The N I M B Y Syndrome", a t t h e Oak Ridge A s s o c i a t e d U n i v e r s i t i e s , Oak Ridge , TN, Oc tobe r 21, 1 9 8 8 ( D r . Saenge r w a s t he i n a u g u r a l Lushbaugh L e c t u r e r )
G u e s t L e c t u r e r , T o p i c s i n R a d i o l o g i c a l H e a l t h f o r P h y s i c i a n s , " N e d i c a l Manaqement of I r r a d i a t e d P a t i e n t s " , sponsored by t h e M e d i c a l College of Ohio , T o l e d o , O H , J a n u a r y 1 9 - 2 0 , 1 9 9 0 -
G u e s t L e c t u r e r , "Is t h e Environment Around DOE P l a n t s as Hazardous as Represen ted? ' " , s p o n s o r e d by t h e E a s t e r n C h a p t e r , H e a l t h P h y s i c s S o c i e t y , Oak Ridge , TN, March 2 0 , 1 9 3 0
G u e s t L e c t u r e r , O c c u p a t i o n a l H e a l t h i n N u c l e a r F a c i l i t i e s , "Counse l ing t h e R a d i a t i o n Worker and Fami ly" , sponsored by REAC/TS, Oak Ridge A s s o c i a t e d U n i v e r s i t i e s , Oak R i d g e , T N , Augus t 17, 1990
G u e s t L e c t u r e r , C l i n i c a l ApDrOaCheS t o FIedicinc i n t h e ?!uclear I n d u s t r y , "Medica l Management o f t h e I r r a d i a t e d P a t i e n t " , s p o n s o r e d by R a d i a t i o n Management C o n s u l t a n t s , h e l d i n O r l a n d o , FL, O c t o b e r 11, 1 9 9 0
G u e s t L e c t u r e r , 2 6 t h Radio logy Congres s of t h e German Democra t ic R e p u b l i c , "Acute L o c a l R a d i a t i o n I n j u r y " , " D i a g n o s i s ami T r e a t m e n t of t h e Acu te R a d i a t i o n Syndrome" and "Late E f f e c t s from R a d i a t i o n " , H e r i n g s d o r f , E a s t Germany, Oc tobe r 2 3 - 2 4 , 1990
G u e s t L e c t u r e r , S o v i e t Refugee H e a l t h and X e n t a l I f e a l t h : T:dentyr Yea r s of S o v i e t R e s e t t l e m e n t , "Chernobyl : F a l l o u t R e v i s i t e d " , s p o n s o r e d by t h e O f f i c e of Refugee H e a l t h , O f f i c e of t h e A s s i s t a n t S e c r e t a r y of H e a l t h , D H H S , Chicago , I L , December 1 0 - 1 2 , 1 9 9 1
G u e s t L e c t u r e r , R a d i a t i o n P r o t e c t i o n i n Med ic ine , " I m p l i c a t i o n s of t h e N e w R i sk E s t i m a t e s " . Annual m e e t i n g 0 2 t h e N a t i o n a l C o u n c i l on R a d i a t i o n P r o t e c t i o n and Measurements , A r l i n g t o n , Vil , A p r i l 1 - 2 , 1 9 9 2
"Medico L e g a l 1ssue.s A s s o c i a t e d w i t h I o n i z i n g R a d i a t i o n " , p r e s e n t e d a t t h e a n n u a l m e e t i n g of t h e American Roentgen Ray S o c i e t y , San F r a n c i s c o , C a l i f o r n i a , A p r i l 2 5 - 3 0 , 1993
Recipient of the 1993 Gold Medal of the Radiological Society of North American (RSNA), the highest honor of the Society, p r e s e n t e d at the R S N A Annual Meeting, Chicago, Illinois, November 30, 1993

1 2
Profess iona l S o c i e t i e s :
Academy of Medicine of Hamilton County Alpha Omega Alpha American Association f o r the Advancement of Science American College of Nuclear Physicians American College of Radiology American Medical Association American Radium Society American Roentgen Ray Society Cinc inna t i Radiation Society Greater Cinc inna t i Radiological Society Health Physics Society O h i o S t a t e Medical Association Ohio S t a t e Radiological Society Ra6iation Research Society Radiological Society of North America Sigma X i Soc ie ty f o r Medical Decision Making Society of Nuclear Kedicine Socie ty of P e d i a t r i c Radiology

13
Publications
1947
Unilateral Paraspinal Abscess, Radiology 4 8 : 256-259, March
1949
-
Pyarthrosis in Infancy, Ohio State Medical Journal 45: 453-458, May with J.V. Greenebaum and J.A. Frieberg
1950
Spondylarthritis in Children, American Journal of Roentgen., Rad. Therapy and Nuclear Medicine, LXIV: 20-31, July
1952
Results of Therapy with Radioactive Iodine-131 in Hyperthyroidism, Ohio State Medical Journal 50: 26-27, January, with R.E. Goldsmith
Letterer-Siwe's Disease: Problems in Diagnosis and Treatments, American Journal Roentgen., Rad. Therapy and Nuclear Medicine, LXII, No. 3 , March, with R.J. Johansmann
Protection Against Radiations from Radium, Cobalt-60 and Cesium-137, National Bureau of Standards Handbook 54, Section 9: Accidents entailing radiation hazards, September
EmergeRcy Measures and Precautions in Radium Accidents, Journal of the American Medical Association 149: 813-815, with R.G. Gallaghar, D.S. Anthony and P.J. Valaer
1955
Roentgen Ray Epilation under Anesthesia, A.M.A. Archives of Dermatologv 71: 116, January
1956
Carcinoma of the Prostate: Therapy with Radioactive Colloidal Gold, U.S. Armed Forces Medical Journal, VII: 469, April, with P.D. Beach and D.V. Becker
A Method for Monitorinq Backqround by Means of Statistical Control Chart, American Journal of Roentgen., Rad. Therapy and Nuclear Medicine, LXXV: June, with C.M. Herbert
A Method for Labeling the Lone Star Tick with Radioactive Indicator (P-3?), Journal of Economic Entomology 4 9 : 393, June, with S.E. Knapp, C.J. Farinacci and C.M. Herbert

R a d i G t i o r : 1iazz.l-ds i n t h e P r h c t i c e o f S u r g e r l r , The Amer ican S u r g e o n 2 2 : 6 7 6 , w i t h C.M. B a r r c t t
1 9 5 7
R a d i u m Ca2su;es a n d t h e i r Associated Hazards, Amer ican Zournzl of R o e n t g e n . , Rad. T h e r a p y a n d EJuclear M e d i c i n e 7 7 : 511-523, March , with R . G . G a l l a g h a r
1959
P l a n n i n g f o r 2 E i a d i a t i o n A c c i d e n t , Amer ican I n d u s t r i a l I!>’qiene A s s o c i a t i o n J o u r n a l 2 0 : No.6, December
1960
I n c i d e n c e of N e o p l a s i a F o l l o w i n g T h e r a p e u t i c I r r a d i a t i o n for B e n i g n C o n d i t i o n s i n C h i l d r e n , R a d i o l o g y 7 4 : 8 8 9 - 9 0 2 , J u n e , b!o. 6
R a d i a t i o n A c c i d e n t s , Amer ican J o u r n a l R o e n t g e n o l o g y , R a d i a t i o n Therapy a n d I !uc lear M e d i c i n e 84: 7 1 5 - 7 2 8 , O c t o b e r
1 3 6 2
R a d i a t i o n E p i d e m i o l o g y , C a n c e r 15: 4C9-503, May-June, No. 3
1 9 6 3
b!edical Aspects of R a d i a t i o n A c c i d e n t s : h Handbook F G r P h y s i c i a n s , E e a l t h P h y s i c i s t s a n d I n d u s t r i a l Hygienists, published by t h e U.S. Government P r i n t i n g O f f i c e , February
Cosp i t a l P l a n n i n g t o Coribzt R a d i o a c t i v e C o n t a p . i n s t i o n , J c u r n a i ~l t h e Amer ican Fedica l A s s o c i a t i o n 185 : 5 7 8 - 5 8 1 , A u g u s t 17
Deoxyc-,7tidine i n U r i n e of Humar-s A f t e r Nhole-Sodv I r r a d i a t i o n , - - S c i e n c e 1 4 2 : 396-398, O c t o b e r 1 8 , N o . 3590 , with-1I.K. B e r r y , A . P e r r y , B . I . F r i e d m a n , J . G . Kereiakes a n d C . S c h e e l
Robot Data S c r e e n i n g : P r o c e e d i n g s of t h e C o R f e r e n c e on Data A c q u i s i t i o n a n d P r o c e s s i n g i n B i o l o g y a n d l d e d i c i n e , P e r g a n o n Press, w i t h T . D . S t e r l i n g a n d M . Gleser
Robot T r e a t m e n t P l a n n i n g : Proceedirqs of t h e C o n f e r e n c e o n D a t a A c q u i s i t i o n a n d P r o c e s s i n g i n B i o l o q y a n d M e d i c i n e , Pergamon Press, w i t h T.D. S t e r l i n g , H . P e r r y a n d J . Weinkam
Some P l a i n Fac ts Abou t C o m p u t e r - O r i e n t e d P r o g r a m s i n Medical C e n t e r s , P r o c e e d i n g s of t h e C o n f e r e n c e e n Data A c q u i s i t i o n a n d P r o c e s s i n g i n B i o l o g y a n d M e d i c i n e , Pergamon P r e s s
L i v e r S c a n n i n g i n t h e D i a g n o s i s of Hematobilia, R a d i o l o g y 81: 380-983

15
Carcinogenic Effects of Iodine-131 compared with X-Irradiation - A Review, Health Physics 9: 1371, with R. Seltzer, T.D. Sterling and J.G. Kereiakes
Liquid Scintillation Counting of 1-131 in a Clinical Laboratory, Journal of Nuclear Medicine 4: 426-438, with H. Horwitz, J.G. Xereiakes and T. Selkirk, Jr.
1964
Radiation Casualties: Newer Aspects of Mass Casualty Care, New York State Journal of Medicine 64: No. 2, with M.L. Boone
Radiation Therapy: Chapter 79, pp 684-796, Pediatric Therapy, editor: Harry C. Shirkey, published by C.V. Mosby, with J.P. Dorst
-
Radiation Exposure from Radioiodine Compounds in Pediatrics, Radiology 8 2 : 486-494, with R.A. Seltzer, J.G. Kereiakes, and D.H. Myers
Radiation Exposure from Radioisotopes in Pediatrics, New England Journal of Medicine 271: 84-90, with R.A. Seltzer and J.G. Xereiakes
Endoreduplication in Leucocyte Chromosomes - Preliminary Report of Its Relation to Cancer and Whole Body Irradiation, The Lancet, September 5, pp 494-495, with €3.1. Friedman and M.S. Kreindler
Epidemiology and the Practicing Physician, Cincinnati Journal of Medicine 45: 397-338
Experiences with 1-131 in the Management of Carcinoma of the Thyroid, Radiology 83: 892, with C.M. Barrett, J.W. Passino, R.A. Seltzer and W.D. Dooley
Implications to Man of Irradiation by Internally Deposited Strontium-89, Strontium-90 and Cesium-137. A Report of the Advisory Committee to the Federal Radiation Council, December 31, 1’364. Division of Medical Sciences, National Academy of Sciences - National Research Council, Washington, D.C. 1965
Continuing Use of the Whole Body Counter - The Nature of the Problems, reprinted from Radioactivity in Man, editor: G.R. Meneely, pp 450-461, published by Charles C. Thomas, with J.G. Kereiakes
Do Malignancies Result from Diagnostic and Therapeutic Radiation, from Genetics and the Epidemiology of Chronic Diseases, Part IV, pp 355-371, Public Health Service Publication No. 1163, U.S. Government Printing Office, Superintendent of Documents, Washington, D.C., with T. Sterling and R.A. Seltzer

Ra?,ionucli.de Doses t o I 2 f a r . t ~ and C h i l d r e n : A ? l e a For a Standzrc‘ C h i l d , H e a l t h P h y s i c s 11: 993-1004, w i t h R.A. S e l t z e r , J . G . K e r e i a k e s and B. B lackburn
T r e a t i n g t h e R a d i a t i o n C a s u a l t y , Summary of P r o c e e d i n g s 1 6 t h N a t i o n a l Confe rence on D i sas t e r Medica l Care , Oc tobe r 3G-31, 1 9 6 5
1966
S p e c i f i c P r o t e i n s i n Serum o f Total-Body I r r a d i a t e d Hmar.s, - The J o u r p a l of Immunology 96: 6 4 - 6 7 , w i t h B . I . F r i e d p a n , A.J. Luzzio and J . G . K e r e i a k e s
H e m a t o l o g i c a l and Dosimetric F i n d i n g s i n Human Be ings Rece iv ing V?hole and Hal f Body R a d i a t i o n , a b s t r a c t e d i n R a d i a t i o n Research 2 7 : 5 3 0 , w i t h J.G. K e r e i a k e s , B . I . Friedman asd Ii. P e r r y
1967
A S e n s i t i v e Technique for Measur ing T h y r o i z a l Uptake of 1-131 I c d i n e , J o u r n a l o f Nuclear Medic ine 9: 8 6 - 9 6 , w i t h H . N . Wellman, J.G. K e r e i a k e s , T .B. Yeager and C . G . Karches
Treatmer?t of Acute R a d i a t i o n I n j u r y u n d e r K e d i c a l l y F.usterc C o n d i t i o n s , p r e p a r e d by TRIFIAC C o r n t i t t e e ( E . L . Saenge r m m b e r o f Commit tee) a t t h e request of t h e O f f i c e o f C i v i l D e f e n s e , Depar tment of Defense and t h e N a t i o n a l R a d i o l o g i c a l Defense L a b o r a t o r y , San F r a n c i s c o , C a l i f o r n i a , OCD S u b t a s k 2 4 3 1 F , April
E f f e c t s of T o t a l and P a r t i a l Bod.;’ T h e r a p e u t i c I r r a d i a t i c n i n :.ian: P r o c e e d i n g s of t h e 1st I n t e r n a t i o n a l Symposium o n t h e E i o l o q i c a l I n t e r p r e t a t i o n of Dose from A c c e l e r a t o r - P r o d u c e d f i a d i a t i o n : U.S. A t c m i c Energy Commission, D i v i s i o n o f T e c h n i c a l I n f o r m a t i o n , CONF-670305
The R o l e of t h e C i t i z e n i n E jea l th P l a n n i n g , C i n c i n n a t i J o u r n a l of Med ic ine page 6 2 , ( f i r s t i n a t h r e e - p a r t p r e s e R t a t i o n g i v e n by E.L. S a e n g e r , M . D . , P r e s i d e n t of t h e P u b l i c E e a l t h F e d e r a t i o n , a s t h e k e y n o t e a d d r e s s a t t h e Golden C e n t e n n i a l C e l e b r a t i o n of t h e P u b l i c E e a l t h F e d e r a t i o n and C i n c i n n a t i H e a l t h Depar tment , Kovember 1 6 , 1 9 6 7 )
N e w Meeds and Trends i n N u c l e a r FIedicine (keyr .o te a d d r e s s ) , p r e s e n t e d a t t h e symposium, Reduc t ion of R a d i a t i o n Expcsure i n N u c l e a r Med ic ine , h e l d a t K i c h i g a n S t a t e U n i v e r s i t y , E a s t La:ising, Michigan , Augus t 7 -9 , p u b l i s h e d i n Snv i ronmen ta l H e a l t h S e r i e s , R a d i o l o g i c a l H e a l t h , U . S . Department of H e a l t h , E d u c a t i o n a n d Welfare, PHS, P u b l i c a t i o n #999-RH-30
1968
Colo r ime t r i c A n a l y s i s of D e o x y c y t i d i n e i n U r i n e a f t e r S e p a r a t i o n b y Ion-Exchange Column Chromatography, J o u r n a l of Ana ly t i ca l_ B i o c h e m i s t r y 2 3 : 2 3 0 , w i t h I . W . Chen, J . G . K e r e i a k e s and B . I . F r iedman

17
Radiopharmaceutical Dosimetry in Pediatrics, Radiology 3 0 : 925-930, with J.G. Kereiakes, H.N. Wellman and J. Tieman
Clinical Experience with Oblique Views in Pulmonary Perfusion Scintiphotoqraphy in Normal and Pathological Anatomy, Journal of Nuclear Medicine 9: 374, with H.N. Wellman, J.F. Mack and B.I. Friedman
Studies of Preliminary Experience with the Use of Iodine-123 for Thyroid Function and Scanning Compared to Iodine-131, Journal of Nuclear Medicine 9: 359
A New Concept in Dynamic-Function Studies - Quantitative Cinescintivideography, Journal of Nuclear Medicine 9: 420, with H.N. Wellman, J.G. Kereiakes and D. Hunkar
The Use of Computers in Nuclear Medicine: Proceedings of Conference on the Use of Computers in Radiology, held October 20-23, published April 1968, University of Missouri
Incidence of Leukemia Following Treatment of Hyperthyroidism, JAMA 205: 147-154, with G.E. Thoma and E.A. Tompkins (A cooperative study)
Radiation Exposure of Uranium Miners. A Report of the Advisory Committee to the Federal Radiation Council, National Academy of Sciences, Washington, D.C., August 27, 1968
Radiation-Induced Urinary Excretion of Deoxycytidine by Rats and Humans, Radiology 91: 345-348, with I.W. Chen, J.G. Kereiakes and B.I. Friedman
Status of Research in Diagnostic Radiology. A Report by the Radiology Training Committee of the National Institute of General Medical Sciences, National Institutes of Health, (E.L. Saenqer, Nember of Committee) , Bethesda, Maryland, 1968 llanagement of the Early Phase of Radioactive Contamination in Human Beings: reprinted from Diagnosis and Treatment of Deposited Radionuclides, Proceedings of a Symposium held at Richland, Washington, May 15-17, Excerpta Medica Foundation pp 600-607
1969
Radiologists, Medical Radiation and the Public Health, Annual Oration presented at the Radiological Society of North America, Chicago, Illinois, December 4, published in Radiology (special edition) 9 2 : 681-699, March
Medulloblastoma - A Review of Prognosis and Survival, British Journal of Radiology 42: 198-214, with D.R. McFarland, H. Horwitz and G.K Bahr

1 8
C l i n i c a l E x p e r i e n c e with Gblique V i e w s i n Camera- imaging i n Norral a n a P a t h o l o g i c a l 8 9 7 - 9 0 2 , w i t h J . F . l.lack, E .N. Ve l lman ar.d
P u h - , ~ r ; i r y F e r f u s i o n Anatomy, R a d i o l o q y 9 2 : R . I . Frieciman
T o t a l and Hal f -Body I r r a d i a t i o n : E f f e c t o n C o g n i t i v e a n d E m o t i o n a l P r o c e s s e s , A r c h i v e s of G e n e r a l P s y c h i a t r y 21: 574-580, w i t h L . A . G o t t s c h a l k , R. K u n k e l , T.H. Wohl a n d C . N . Winge t
P a t i e n t a n d P e r s o n n e l Dcse d u r i n g R a d i o i s o t o p e P r o c e d u r e s . P r o c e e d i n g s of a C o n f e r e n c e h e l d a t B a y l o r U n i v e r s i t y C o l l e g e o f Medic ine , H o u s t o n , T e x a s , November 21-22 p u b l i s h e d i n Medical R a d i a t i o n I n f o r m a t i o n f o r L i t i g a t i o n , DMRE 69-3 , p 1 5 3 , j u l y 1 9 6 9 , w i t h J . G . K e r e i a k e s , H . H o r w i t z , H . N . Wellman a n d V . J . Sodd
1 9 7 0
T h e F u t u r e of R a d i o i s o t o p e s i n M e d i c i n e : B e n e f i t s vs R i s k s , p u b l i s h e d i n Medical R a d i c n u c l i d e s : R a d i a t i o n Dose a n d E f f e c t s , e d i t o r s : R . J . C l o u t i e r , C . L . Edwards , W.S. S n y d e r . U.S. A t o m i c E n e r g y Commiss ion , D i v i s i o n of T e c h n i c a l I n f o r m a t i o n , p p 491-507, J u n e 1 9 7 0 , p r o c e e d i n g s of a S l ~ , p o s i u m h e l d a t t h e Oak R i d g e Associated U n i v e r s i t i e s , December 8-11, 1969
N a t i c n a l Uses and. E!eeds for Skzm2ard Ra2icact ive r h t e r i a l s . A R e p o r t by a n A d Hoc P a n e l of t h e Committee o n N u c l e a r S c i e n c e , N a t i o n a l R e s e a r c h C o u n c i l , N a t i o n a l Academy of S c i e n c e s , W a s h i n g t o n , D . C . , 1 3 7 0 , E . L . S a e n g e r , Member of P a n e l
1 9 7 1
R a d i a t i o n a n d L e u k e n i a Xates, l e t t e r t o S c i e n c e 1 7 1 : 1 0 9 6 - 1 C 9 8 , N o . 3976 , !,larch 1 9 , w i t h E . Tor ,pk ins a n d G . E . Thoma
C y t o l o q i c - B i o c h e m i c a l I i z 6 i a t i o n D o s i m e t e r s i n !:an, B i o c h e m i c a l I n d i c a t o r s of R a d i a t i o n I n j u r y i n . M a n , I n t e r n a t i o n a l A t o m i c E n e r g y F-gency, V i e n n a , ( P L - 4 @ 9 / 1 3 ) , p p 181-214, w i t h E . B . S i l b e r s t e i n , I . W . Chen ar,d J . G . K e r e i a k e s
E s t i m a t e of Manpower ?Ieeds o f Medical P h y s i c i s t s i n t h e U n i t e d S t a t e s , Amer ican A s s o c i a t i o n of P h y s i c i s t s i n M e d i c i n e 5 ( 2 ) : 129-131, w i t h L.H. Larzl a n d J . G . K e r e i a k e s
A Head-Hold ing D e v i c e f o r Improved B r a i n S c i n t i g r a p h y , J o u r n a l o f N u c l e a r M e d i c i n e 1 2 : 305-306, J u n e , w i t h R.A. B e r k e
Care of P a t i e n t s I n v o l v e d i n R a d i a t i o n A c c i d e n t s : R e c e n t Advances . D e r S t r a h l e n u n f a l l und s e i n e B e h a n d l u n g , vom. 1 9 - 2 0 , J u n i 1 9 7 0 i n Z u r i c h , p u b l i s h e d by George Thieme Verlag, S t u t t g a r t , p p 54-78

19
The Safe Tracer Dose in Nedical Investigation, reprinteci from Progress in Atomic Medicine: Recent Advances in Nuclear Medicine, Chapter 5 , Vol. 3, pp 139-165, editor, John H. Lawrence, by Grune . -
and Stratton, Inc., with J.G. Kereiakes
1972
Protection Against Radiation from Brachytherapy Sources, NCRP Report No. 40 (National Council on Radiation Protection an2 Measurements), March 1972. E.L. Saenger, M.D., Chairman of Committee preparing report
Active Bone-Marrow Dose Relaigd to Hematological Changes in Whole-Body and Partial-Body Co Gamma Radiation Exposures, Radiology 103: 651-656, with J.G. Kereiakes, W. Van de Tiet, C. Born, E.B. Silberstein, and C. Ewing
Human Skeletal Scanning with a Stable 99mTechnetium-Tin-Phosphate Agent, Southern Medical Journal 65: 1407, with E.B. Silberstein, H. Park and G.W. Alexander
A Study of the Parameters Influencing the Clinical Use of Iodine-123, Angiography/Scintigraphy - Symposium of the European Association of Radiology, Editor L. Diethelm, Sprinaer-Verlag, Berlin, pp 129-137, with H.N. Wellman, J.F. Mack, R.E. Goldsmith and V.J. Sodd
Radiopharmaceutical Dosimetry in Pediatrics, Seminars in Nuclear Medicine 2: (no.4 - October), 316-327, with J.G. Kereiakes, H.N. Wellman and G. Simmons
The Effects on Populations of Exposure to Low Levels of Ionizicg Radiation (BEIR Report), National Academy of Sciences, National Research Council, Washington, D.C., November, E.L. Saenger, Member of Committee
A Fixed Format Lexicon for Nuclear Medicine Reports, DHEW Pub. No. (FDA) 74-8009, with R.G. Hoops, V.J. Sodd, G.W. Alexander
1973
A Multiple-Dose 133Xe Solution "Generator" : The Disposable Glass Ampule Equilibration Chamber, Journal of Nuclear Medicine 14, with R.G. Carroll, R.A. Berke, R.T. Anger, G. Levine, and H.N. We 1 lman
Radiation Dose to Breast-Feeding Child after Mother has 99nTc-MAA Lung Scan, Journal of Nuclear Medicine 14: 51-52, with R.A. Berke, R.C. Hoops and J.G. Kereiakes

2 0
Pediatric Radiopharmaceutical Dosbetry, Prcceedings of the XI11 (13th) International Congress of Radiology, p. 238, Ns.drid, October 15-20, with J.G. Kereiakes and V.J. Sodd
Whole and Partial Body Radiotherapy of Advanced Cancer, American Journal Roentgenology, Radiation Therapy and Nuclear Xedicine 117: (3) 670-685, Presented at the 73rd Annual Meeting of the American Roentgen Ray Society, Washington, D.C., October 3-6, 1972, with E.B. Silberstein, B . Aron, H. Horwitz, Z.G. Kereiakes, G.K. Bahr, H. Perry and B.I. Friedman
Radiation-Induced Change in Serum and Urinary Amylase Levels in Man, Radiation Research 54: 141-151, April, with I.W. Chen, J.G. Xereiakes, B.S. Aron and E.B. Silberstein
Clinical Evaluation of Radioimmunoassay of Digoxin, Journal of Nuclear Nedicine 14: 17) 531-533, julv, with 1i.M. Park, 1.K.
4 . ~ . . Chen, A. Lower:J and G.T. Planitasas
Radiation Cose to Various Organ Sites in a Tissue-Equivalent HumTg7Phantom Resulting from Implantation of a Promethium 147 (Pm ) Intracardiac Nuclear Pzcemaker, American Journal of Roentqenoloqy, Radiation Therapy and Nuclear Medicine 118 : ( 4 ) 768-776, A-ugust, with IV. Arnold, 2 . G . Kereiakes, G.K. Bzhr and J.W. Spickler
Prospects for Dose Reduction and Assessment in Fluclear I,Iedicine, presented at Second International Symposium on P?uclear Medicir.e, Carlsbad, NM, with H.N. Wellman, V.J. Sodd, J. Rcbbins, B . X . Branson and J . G . Kereiakes
1974
Scintiscanning with Galliun? Citrate 67, Diagnosis of f!ead and Neck llalignant Neoplasms, Archives of Otolaryngology 100: 201-206, September, with A . D . Rornblut, E.B. Silberctein and D . A . Shumr ick
A ComDarison of 1231 and I3’I for Thyroid Imaging Using Various Collihators , International J o u r n a l of Nuclear-Medicine- and Biology 1: 2 0 1 - 2 0 4 , with H. Nishiyama, A . B . Ashare, P.. Shafie and V.J. Sodd
14C-Tripalmitin Breath Test as a Diagnostic Aid for Fat l~lalabsorption due to Pancreatic Insufficiency, Jounal of N u c l e a r Medicine 15 (12): 1125-1129, with 1.N. Chen, A. Kambiz ana A.i.1. Conne 11
Efficacy Studies in tluclear Medicine, reprinted from Proceedings of the XI11 International Congress of Radiology, Excerpta Medica 1: 45-48, Amsterdam
Evaluation of Clinical Value of 1231 and 13’1 in Thyroid Disease, Journal of Nuclear Medicine 15: 261, with H. Nishiyama, V.J. Sodd, and R.A. Berke

2 1
Quantification of Myocardial Infarction by Scintigraphy: i i ~ Autopsy Correlated Study, Journal of Nuclear Medicine 15: 475, (abstract) with A . B . Ashare, D.W. Romhilt, V.J. Sodcl, N.I. Levicson, R.J. Adolph, and L.S. August
Detection and Evaluation of Pulmonary Malignancies Using I
Recent Advances in Nuclear Medicine, Proceedings of the First World Congress of Nuclear Medicine, Ohkawa Printing Company, Yokohama, p. 255, Tokyo, September, with H. Nishiyama and V . J . Sodd
1 2 3 c s
An Investigation of the Disposal of Radiopharmaceuticals in the Cincinnati Sewage System, Recent Advances in Nuclear Medicine, Proceedings of the First World Congress of Nuclear Medicine, Ohkawa Printing Ccmpany, Yokohama, p. 298, Tokyo, September, with V . J . Sodd and R.J. Velten
1975 c__
Some Possible Consequences of Recertification, Radiology 114: 745-746, March
The Use of Nuclear Medicine in Evaluating Liver Disease, Seninars in Roentgenology 10: (3) 215-222, July, with L.E. Holder
1 2 5 ~ a n 2 Cqpcentrations of Medically Useful Radionuclides ( Tc, 99m I) at a Large Metropolitan Waste Water Treatment Plant, Health 131
Physics 28: 355-359, with V.J. Sodd and R. Velten
Evaluation of Radiochemical Protectors Using Urinary Deoxycytidine Levels, International Journal of Radicltion B . i o l ~ $ : ~ 28: (2) 117-124, with D.E. Wrede, 1.N. Chen and J . G . Kereiakes
The Gamut Approach to Scintigram Interpretation - Diagnostic and Teaching Method, Journal of Nuclear Medicine 16: ( 1 2 ) , December, with L.E. Holder, A.B. Ashare, T. Tomsick, D . P . Colley, 31. Fernandez-Ulloa, and Z. Catz
Reactor Safety Study ( W A S H - 1 4 0 0 ) , An Assessment of Acciderit Risks in U.S. Corpmercial Nuclear Power Plants, Appendix VI, United States Nuclear Regulatory Commission, October, E.L. Saenger, Member of Advisory Group on Health Effects
Interpretation of Radionuclide Liver Images: Do Training ar.d Experience Ikke a Difference?, Journal of Nuclear Nedicine 16, with H . Nishiyama, J.T. Lewis, and A . B . Asharc
Intercomparison of Myocardial Imaging A g e n t s , Journal of Nuclear Medicine 16: 553 , with H. Nishiyama, V.J. Sodd, J.T. Lewis ar,d R . J . Adolph
Inadequacies of Gamma Camera Performance and Quality Control, Journal of Nuclear Medicine 16: 564 (abstract), with V.J. Sodd, J.G. Kereiakes and R.J. Van Tuinen

2 2
C l i n i c a l Expe r i ence w i t h I2’Xe, C o n t i n u i n g E d u c a t i o n Lec tu res , P r o c e e d i n q s o f t h e 1 6 t h Annual Xeet ing o f t h e S o u t h e a s t e r n C h a p t e r o f t h e S o c i e t y of Nuclear M e d i c i n e , page 6 , ( a b s t r a c t ! , w i t h E. Nishiyama, V . J . Sodd, J . T . L e w i s and R.A. Neff
Imaging o f Pulmonary Tumors w i t h . R a d i o p h a r m a c e u t i c a l s , Subraman ian , e t a l . , e d i t o r s . S o c i e t y of N u c l e a r M e d i c i n e , N e w Y o r k , p . 1 2 5 , w i t h H . Nish iyama, V . J . Sodd, T . J . S c h r e i b e r and R.G. Loudon
1 2 g c s
1976
C y s t o u r e t h r o g r a p h y P r o c e d u r e s i n C h i l d r e n : E v a l u a t i o n o f B e r e f i t s v e r s u s Dose, Rad io louv 118: 123-128, w i t h J . G . X e r e i a k e s , D . J . Cavanaugh, J . L . H a l l and W. Eiseman
Breas t Cancer S c r e e n i n g - B e n e f i t and R i sk f o r t h e F i r s t Annual S c r e e n i n g , Rad io logy 120: 4 3 1 - 4 3 2 , w i t h M . Moskowitz, J . G . R e r e i a k e s , S . Pemmaraju, A. Kumar and G . T a f e l
The Use of R a d i o a c t i v e C e s i u m C h l o r i d e f o r Imaging o f M a l i g n m t and Benign Pulmonary L e s i o n s , S u r g e r y , Gynecoloqy and O b s t e t r i c s 1 4 3 : 575-580, w i t h FI. Nishiyama, J . T . L e w i s and R . C . Hoops
Imaging o f Pulmonary Tumors w i t h 1 2 g C s , R a d i o p h a r m a c e u t i c a l s , pp 482-490, w i t h H . Nishiyarna, V . J . Sodd, T . J . S c h r e i b e r a n a R . G . Loudon
I n t e g f c m p a r i s o n o f Myoca rd ia l Imaging Agen t s : 2 c 1 T l , 129cs, 4 3 K
and R b , J o u r n a l of N u c l e a r Eledicine 17: 880-889, w i t h I i . N i sh iyama , V.J. Sodd, R . J . Adolph, 2.T. L e w i s and 1.1. Gabel
Lack o f S p e c i f i c i t y f o r D e t e c t i o n of Breast L e s i o n s w i t h Rac2icac t ive Cesium C h l o r i d e , S u r g e r y , Gynecology and O b s t e t r i c s 1 4 3 , w i t h H . Nish iyama, M . Moskowitz, 2 . T . L e w i s , and R . G . Hoops
R a d i a t i o n C o n t a m i n a t i o n and A c u t e R a d i a t i o n I n j u r y , i n I n i t i a l Management o f t h e Trauma P a t i e n t , e d i t o r C h a r l e s F r c y , p u b l i s h e d by L e e and F e b i g e r , P h i l a d e l p h i a , pp 203-228
R a d i o b i o l o g y and D o s i m e t r y o f P e d i a t r i c Nuclear Med ic ine , i n The P e d i a t r i c N u c l e a r Med ic ine Club: A B i b l i o g r a p h y o f P e d i a t r i c Muclear Med ic ine L i t e r a t u r e , Sear le RadFcgraph ics , I n c . , pp 1 6 0 1 - 1 6 5 9 , w i t h N.J. G e l f a n d
-
- -
Ceuium-137 Body Burdens and H a l f - L i f e i n a Group of A d u l t Males i n C i n c i n n a t i , Oh io , H e a l t h P h y s i c s 30 , w i t h J . T . L e w i s , L.W. Grossman, and J . G . K e r e i a k e s
KUMEDACON: Nuclear Med ic ine Repor t and Data S t o r a g e Sys tem, P r o c e e d i n g s 6 t h Symposium on S h a r i n g o f Computer Programs and Technology i n N u c l e a r M e d i c i n e , p . 1 1 8 , w i t h R . G . Hoops, M.L. Yudofsky, A.B. Asha re and V . J . Sodd

23
Radiopharmaceutical Dosimetry in Pediatrics, Proceedings of the 62nd Scientific Assembly and Annual Meeting of the Radiological Society of North America (RSNA), with J.G. Kereiakes, S.R. Thomas, F.A. Ascoli, M.J. Gelfand, P.A. Feller, V.J. Sodd, P. Paras, 2 . W . Poston, G.G. Warner and R.L. Shoup
1977
Quantitative External Counting Techniques Enabling Improved Diaqnostic and Therapeutic Decisions in Patients with Weli-Differentiated Thyroid Cancer, Radioloqv 122: 731-737, with S.R. Thomas, H.R. Maxon and J.G. Kereiakes
"The Developing Role of Short-Lived Radionuclides in Nuclear Medicine", A Report of the Task Force on Short-Lived Radionuclides for Medical Applications to the Bureau of Radiological Health, Food and Drug Administration, U.S. Department of Health, Education and Welfare, August. E.L. Saenger, Chairman of Committee
NCRP Report No. 5 5 , "Protection of the Thyroid Gland in the Event of Releases of Radioiodine", Recommendations of the National Council on Radiation Protection and Measurements, E.L. Saenger, Chairman of Committee
A Comparison of Technetium Etidronate and Pyrophosphate for Acute Myocardial Infarct Imaging, Journal of Nuclear Medicine 18: 905-909, with C. Williams, H. Nishiyama, R. Adolph, M. Gabel, D. Romhilt and V.J. Sodd
Radiation-Associated Thyroid Carcinoma, editor Leslie J. DeGroot, M.D., E.L. Saenger contributing editor, Grune and Stratton, New York, 1977
Ionizing Irradiation and the Induotion of Clinically Significant Disease in the Human Thyroid Gland, The American Journal of Medicine 63: 967-978, with H . R . Maxon, S . R . Thomas, C.R. Buncher and J.G. Kereiakes
se to the Metaphyseal Growth Complexes in Children Undergoing ""Tc-EHDP Bone Scans, Radiology 126: 193-196, with S.R. Thomas, M.J. Gelfand, J.G. Kereiakes, F.A. Ascoli, H.R. Maxon, P.A. Feller, V.J. Sodd and P. Paras
1978
Radiation Induced Thyroid Cancer, Cincinnati Journal of Medicine 3: 59, March
--
Benefit/Risk Analysis of Aggressive Mammographic Screening, Radiology 128: 359-365, with S.H. Fox, M. Moskowitz, J.G. Kereiakes, J. Milbrath and M.W. Goodman

E v a l u a t i o n cf Diseases of t h e Thlrroid Gland w i t h t h e In-i.Tivo C;se of R a d i o n u c l i d e s , J o u r n a l o f N u c i e a r N e d i c i n e 13: 1 0 7 - 1 1 2 , ; : i t h Task F o r c e on Shor t -L ived R a d i o n u c l i d e s , Bureau o f R a d i o l o q i c a l I!ealth, Food and Drug A d n i n i s t r a t i o n , U . S . Department of f i e a l t h , E d u c a t i o n and W e l f a r e
Sarcoma B o t y r o i d e s of t h e Vagina i n Ch i ldhood , T r e a t e d b17 I r r a d i a t i o n and V a g i n a l R e c o n s t r u c t i o n , American Zoi i rnal af O b s t e t r i c s and Gynecology 132: 339-340, O c t o b e r , w i t h R.D. Pa t c h e 11
D i a g n o s t i c R a d i a t i o n f o r a Young Woman, JMLA 2 4 0 : 1 6 4 1 , O c t o b e r , w i t h J . G . Kereiakes
1 9 7 9
R a d i o t h e r a p e u t i c Agents : P r o p e r t i e s , Dos ime t ry , and R a d i o b i o l o g i c C o n s i d e r a t i o n s , Seminars i r , : Juclear N e d i c i n e 3 : ( 2 ) 7 2 - & 4 , l i i t ' n
J . G . K e r e i a k e s , V.J. Sodd and R . David
Med ica l R a d i a t i o n Exposure Dur ing P regnancy , JWA 2 4 2 : 1 6 6 3 , O c t o b e r , w i t h J . G . K e r e i a k e s
1929
R a d i a t i o n E f f e c t s and R a d i a t i o n P r o t e c t i o n , i n Nuclear ' !edicire Review S y l l a b u s , e d i t o r P e t e r T . K i r c h n e r , M . D . , Societ:,? of TJuclcar Med ic ine I n c . , 4 7 5 P a r k Avenue S o u t h , N e w York, YY l O O I F , w i t h R.T. Anger , A . R . a e n e d e t t o and R.L . W i t c o f s k i
C l i n i c a l E x p e r i e n c e s i n 1 4 C - t r i ~ a l m i t i n R r c a t h T e s t f c r Y n t 1"- N a l a b s c r p t i o n , American Gourna l of Gastroenterolcg-,-, pp -,/-231,
Narch , w i t h H.E. Meeker, I.W. Chen and A.M. C o n n e l l
C l i n i c a l l y I m p o r t a n t R a d i a t i o n - A s s o c i a t e d Thyro id D i s e a s e - A C o n t r o l l e d S t u d y , J A M A 2 4 4 : 1802-1505, Octobe r 1 7 , with €!.P,. Maxon, S.R. Thomas, C . R . Buncher, J . G . K e r e i a k e s , M.L. S h a f e r and C.A. KcLaughl in
R e f l e c t i o n s on Cancer Treatment and t h e F e d e r a l Agency.' R e g u l a t i o n s , Radio logy 1 3 7 : 8 6 5 - 8 6 6 , December, w i t h J . G . K e r e i a k e s
E f f i c a c y and E f f i c i e n c y of t h e D i a g n o s t i c A p p l i c a t i o n s of R a d i a t i o n and R a d i o n u c l i d e s , Repor t o f a m e e t i n g oxganizec! b : ~ t h e World H e a l t h O r g a n i z a t i o n and t h e Government of t h e F e d e r a l R e p u b l i c of Germany, Neuherbe rg , FRG, Dec. 5-7 , 1 9 7 9 ; p r o c e e d i n g s p u b l i s h e d A p r i l 1 9 8 0
C l i n i c a l Course and Dos imet ry of Acute Hand I n j u r i e s t o I n d u s t r i a l R a d i o q r a p h e r s from M u l t i c u r i e S e a l e d Gamma S o u r c e s , i n - - The Med ica l Bas is f o r R a d i a t i o n A c c i d e n t P r e p a r e d n e s s , K.F. Hubner and S.A. F r y , e d s . , E l s e v i e r Nor th Ho l l and , I n c . , 1 9 8 0 , w i t h J.G. K e r e i a k e s , N . Wald and G.E. Thoma

2 5
Biological Risks of Medical Irradiations, edited by G.D. Fullerton, D.T. Knopp, R.G. Waggener, E.W. Webster. E.L. Saenger contributing author: "Methods of Risk Reduction in Nuclear Medicine" with J.G. Kereiakes and S . R . Thomas: "Dose Evaluation in Nuclear Medicine" with J.G. Kereiakes, S.R. Thomas, M.J. Gelfand and H.R. Maxon. American Association of Physicists in Medicine, Medical Physics Monograph # 5
Survey of Technetium-99m Contamination of Laboratory Personnel: Its Degree and Routes, Radiology 135: 467-471, with H. Nishiyama
Radiation-Associated Carcinoma of the Salivary Glands: A Controlled Study, Annals of Otolaryngology 90: 107-108, with H.R. Maxon, S.R. Thomas, M.L. Shafer, C.R. Buncher, J.G. Kereiakes and C.A. McLaughlin
Once to Every Man...An Introduction, Medical Decision Making 1: (1) page 1
Evaluation of LAD Blockage: Hazard of Repeated Radiation Exposure, JAMA 246: 2754, December
1982
"Ethics, Trade-offs and Medical Radiation", Lauriston S. Taylor Lecture Series in Radiation Protection and Measurements, Lecture No. 6. NCRP Publications, 7910 Woodmont Avenue, Suite 1016, Bethesda, MD 20814
Protection of the Patient in Diagnostic Radiology, ICRP Publication 3 4 . E.L. Saenger, Chairman of Task Group preparing report. Annals of the ICRP, Volume 9, No.2/3. Pergamon Press, New York
Development and U s e of a New Tc-99m Nyocardial Perfusion Agent - DMPE. Proceedings of the Third World Congress of Nuclear Medicine and Biology, C. Raynaud, ed., Pergamon Press Vol. No. 2, Paris, France, pp 2255-2260, with V . J . Sodd, E.A. Deutsch, H. Nishiyama, R.J. Adolph, L.W. Grossman, K.L. Scholz, K. Libson, D.L. Fortman and J.L. Vanderheyden
Nuclear Orthopedics, "Dosimetry", edited by E.B. Silberstein, with J . G . Kereiakes, S.R. Thomas, M . J . Gclfand and C.C. Williams, New York, Futura Publishers
Basal Kinetic Studies of Tc-99m DNPE as a Myocardial Agent in the Dog, Journal of Nuclear Medicine 23: 1093-1102, with H. Nishiyama, E.A. Deutsch, R.J. Adolph, V.J. Sodd, K. Libson, M.C. Gerson, M. Gabel, S.J. Lukes, J.L. Vanderheyden, D.L. Fortman, K.L. Scholz, L.W. Grossman and C.C. Williams

Tc-99m DMPE a s a R e s t i n u Elyocardial Imaging A g e n t . J o u r n a l of Mucleer EIed ic ine 2 3 ( 5 ) : 1 2 ( a b s t r a c t ) , w i t h H . N i s h i y a m a , E.A. D e u t s c h , R . J . A d o l p h , V . J . S d d , IC. L i b s o n , S . J . L u k e s , 1.1. G a b e l , M.C. Gerson and J . L . Vanderheyden
1 9 8 3
M y o c a r d i a l P e r f u s i o n Imag ing w i t h 99%c-D14PE i n Man. E u r o p e a n J o u r n a l of Nuc lea r M e d i c i n e 8 : 371-374, w i t h b!.C. G e r s o n , E . A . D e u t s c h , H . N i s h i y a m a , K.F. L i b s o n , R . J . Ado lph , L.W. Grossman, V.J. Sodd , D.L. F o r t m a n , J . L . V a n d e r h e y d e n , and C . C . W i l l i e m s
R e l a t i o n Between E f f e c t i v e R a d i a t i o n Dose a n d Outcome of R a d i o i o d i n e T h e r a p y f o r T h y r o i d C a n c e r . N e w Eng land J o u r n a l o f Medic ine 309: 937-S41, w i t h H . R . MaXon, S . R . Thomas, V . S . H e r c z b e r g , J . G . K e r e i a k e s , I . W . Chen , and E i . 1 . S p e r l i n g
R e g i o n a l O r g a n i z a t i o n o f Medical Care. B u l l e t i n of t h e N e w York Academy of M e d i c i n e 59: 1095-1107
" D o s i m e t r y of Bone-Seeking R a d i o p h a r m a c e u t i c a l s " , i n Bone S c i n t i g r a p h y , w i t h J . G . K e r e i a k e s , S.R. Thomas, f 4 . J . G e l f a n d , C . C . V i i l l i a m s . E . B . S i l b e r s t n i n , e d i t o r , F u t u r a P u b l i s h i n g Companyr, P l t . Kisco, NY
NCRP Report N o . 7 3 , " P r c t e c t i o n i n N u c l e a r Medicine a n d U l t r a s o u n d D i a g n o s t i c P r o c e d u r e s i n C h i l d r e n " , E . L . S a t n g e r , committee member. MCRP P u b l i c a t i o n s , 7910 Woodmont Avenue , S u i t e 1 0 1 6 , B e t h e c d a , MD 20814
1 9 8 4
Low- leve l I n t e r n a l R a d i o n u c l i d e C o n t a m i n a t i o n : U s e of Gamma C a m e r a f o r D e t e c t i o n . R a d i o l o g y 1 5 0 : 2 3 5 - 2 4 0 , w i t h I!. P:ishiyama and S.J . Lukes
A Guide t o t h e H o s p i t a l l l anaqement of I n j u r i e s A r i s i n g f rom E x p o s u r e t o o r I n v o l v i n g I o n i z i n g R a d i a t i o n , E .L . S a e n g e r , M . C . , m e m b e r CSA A d v i s o r y P a n e l , Amer ican Medical A s s o c i a t i o n , C h i c a g o , I l l i n o i s , J a n u a r y
F a m i l y H i s t o r y of C a n c e r i n a R a d i a t i o n T e c h n o l o g i s t . JAMA 2 5 1 : 1 9 0 1 - 1 9 0 2 , A p r i l 1 3
"The N u c l e a r P h y s i c i a n ' s Role i n P l a n n i n g f o r a n d H a n d l i n g R a d i a t i o n A c c i d e n t s " i n , N u c l e a r M e d i c i n e Annual 1 3 8 4 , L.M. Freeman and H.S. Weissman, eds . , Raven P r e s s , New York , 1 9 8 4 , pp 1 - 2 2
Myocardial S c i n t i g r a p h y w i t h 99%c- t r i s -Dl~lPE i n J o u r n a l of Nuc lea r Medic ine 9 :403-407, w i t h M.C D e u t s c h , K.F. L i b s o n , R.J . A d o l p h , A .R . K e t r i n g V a n d e r h e y d e n , and C.C . Wi l l i ams
Man. E u r o p e a n G e r s o n , E . A . J . L .

27
Assigned Share for Radiation as a Cause of Cancer, Review of Radioepidemiological Tables Assigning Probabilities of Causation. Final Report: Oversight Committee on Radioepidemiologic Tables (OCRET), Board on Radiation Effects Research, Commission on Life Sciences, National Research Council. National Academy Press, Washington, D.C. E.L. Saenger, M.D., member of OCRET Committee
1985
Accidental Cs-137 Contamination, Radiology 154: 513-517, with H.Nishiyama, L.W. Grossman and S.J. Lukes
NCRP Report No. 80, "Induction of Thyroid Cancer by Ionizing Radiation", Recommendations of the National Council on Radiation Protection and Measurements. E.L. Saenger, M.D., Advisor to Task Group
Determination of Clinical Efficacy: Nuclear Medicine as Applied to Lung Scanning, Journal of Nuclear Medicine 26: 793-806, with C.R. Buncher, B.L. Specker and R.A. McDevitt
Application of an Information-Theoretic Method for Efficacy Assessment, Journal of Nuclear Medicir.e 26: 807-811, with D.A. Gift, 1d.R. Schonbein and E.J. Potchen
"Health Effects Model for Nuclear Power Plant Accident Consequence Analysis" (NUREG/CR-4214), J . S . Evans, D.W. Moeller, D.W. Cooper, eds., U.S. Government Printing Office, P.O. Box 37082, Washington, D.C. 20013, July. E.L. Saenger, M.D., Member of Advisory Group
1986
Cost-Effectiveness of Screening Mammography in Low-Risk Patients, - JAMA 256: 406-407, July 18, with M. Moskowitz
The Reactor Accident at Chernobyl: A Nuclear Medicine Practitioner's Perspective, Seminars in Nuclear Medicine 1 4 ( 3 ) : 224-230, July, with J.G. Kereiakes and S.R. Thomas
Radiation Accidents, Annals of Emergency Medicine 15: 1061-1066, September (Proceedings of the 1986 UAEM/IRIEM Research Symposium on Toxicology)
Comparison of 1231 and "?c Pertechnetate in Nodular Goiter Imnging, Radiologia Iugoslavica 20 (suppl.111): 47-49, with S. Spaventi, Z. Kusic and D.V. Becker
1987
Radiation Exposure, in Current Therapy in Emergency Medicine, M. Callaham, ed., B.C. Decker Inc., pp 922-927, with H. Mishiyama

C f f i c a c i r a n d Cost-Ef f e c t i v e n e s s of IauiIg S c a n s , i n P u h o n a r y -- X u c l e a r P!e? ic ine , !-1. Lolien, ed . , A p p l e t o n a n d T,ange, ;)p 1 3 3 - 1 4 1 , v i t h R . Specker
NCRP R e p o r t >Io. 9 1 , "Reco ,we? .da t ions on L i m i t s f o r E x p o s u r e +n I o n i z i n g R a d i a t i o n " , E . L . S a e n g e r , c o m m i t t e e member. f7CP.P P u b l i c a t i o n s , 7910 Woodxcnt Avenue , S u i t e 1 0 1 6 , Bethesr2a, !.:D 20E14
P u l m o n a r y E m b o l i s m a n d Lunq S c a n n i n g : C o s t - E f f e c t i v e n e s s ar:d B e n e f i t : R i s k , J o u r n a l -- of ?!\?clear N e d i c i n e 2 C : 1521-1530 , w i t h R . L . S p e c k e r , C . R . Runche r a n d l?.A. I - I c D e G i t t
P r o t e c t i o n of t h e F a t i e n r , i n W u c l e a r I l e d i c i n c , ICRP P u S l i c a t i o r 5 2 . E . L . S a e n q e r , Chai rman of Task Group p r e p a r i n q r eoor t . A n n a l s of the ICRP, Volume 1 7 , No. 4 . Pergamon P r e s s , :?mi Yor?
D o n ' t Disn iss L i a b i l i t v Poter.tLa?- of ?!edical R a d i a t i o n E : < n c s u r ~ , D i a q n o s t i c I m a q i n q 3 ( 1 2 ) : 1 2 0 - 1 2 5
NCRr R e p o r t 110. 3 2 , " T o n i - : ..-1?9 R a d i a t i o n E x p o s u r e of t h e P o p u l a t i o n of t h e U n i t e d S t a t e s " , E.1,. S a e n g e r , committee zer ibcr . VCFP P u b l i c a t i o n s , 7 3 1 0 Voodmont Avenue , S u i t e 1 0 1 6 , B c t h e s d a , :.ID 2 0 8 1 4
1 3 5 9
"RaSiation A c c i d e n t s " , p r e p a r e d by "_!le k n e r i c a n College of F a d i o l o g y A d Roc Committee c n P a d i a t i c r A c c i d e n t s , E.1, . S a e n q e r , committee member. Amer ican Col leac- of Rac?iolog;l, 1 8 9 1 P r e s t o n W h i t e D r i v e , R e s t o n , VA 22091
1990 -- E v a l u a t i o n of Extent cf T n j u r y , i n _ _ _ ~ . ?!e<ical Y a n a g e n e n t o f R a 6 i a t i o n Accir ' ,entr,, P . A . : . I e t t l e r , Z r . , C . A . KeLsey a n d R . C . R i c k s , ec ls . , CRC Press, pp 67-78
"Eealth E f f e c t s Models f o r N u c l e a r Power P l a n t . A c c i d e n t C o n s e q u e n c e A n a l y s i s , Low LET R a d i a t i o n . P a r t I: I n t r o d u c t i o n , I n t e g r s t i o n , and Summary" (NUREG/CR-4214; SAND85-7185, R e v . 1 , P a r t I ) . J . S . E v a n s , e d . , U . S . Government P r i n t i n q O f f i c e , P.O. Fox 37082 , P!ash ington , D . C . 2 0 0 1 3 , J a n u a r y . E .L. S a e n g e r , A d v i s o r y Committee member

29
Comparison of Technetium-99m and Iodine-123 Imaging of Thyroid Nodules: Correlation with Pathologic Findings, Journal of Nuclear Medicine 31: 393-399, with 2 . Kusic, D.V. BeckeE P. Paras, T. Wesseler and S. Spaventi
Radiation and the NIMBY Syndrome, in The Medical Basis for Radiation Accident Preparedness 11: Clinical Experience and Follow-up Since 1979, R.C. Ricks and S.A. Fry, eds., Elsevier Science Publishing Company, New York
1991
Radiation Exposure, in Current Practice of Emergency Medicine, M. Callaham, ed., 2nd edition, B.C. Decker, Philadelphia, with E.B. Silberstein
Perception of Radiation Injury vs. Radiogenic Effect, in The Medical Basis for Radiation-Accident Preparedness I11 : T h e Psychological Perspective, R.C. Ricks, M.E. Berger and F.I.1. O'Hara, eds., Elsevier, New York, with J. Hinnefeld
1992
Discitis, in The Spine, R.H. Rothman and F.A. Simeone, Founding Editors, 3rd edition, W.B. Saunders Company, with J.L. Stambough
Thyroid Nodules in the Population Living Around Chernobyl, JMIA 268 (5): 616-619, with F.A. Mettler Jr, M.R. Williamson, H.D. Royal, J.R. Hurley, F. Khafagi, M.C. Sheppard, V. Beral, G. Reeves, N. Yokoyama, V. Parshin, E.A. Griaznova, M. Taranenko, V. Chesin and A. Cheban
Administration of Stable Iodide to the Population Around the Chernobyl Nuclear Power Plant, Journal of Radiological Protection 12 (3): 159-165, with F.A. Flettler Jr, H.D. Royal, J.R. Hurley, F. Khafagi, M.C. Sheppard, V. Beral, G. Reeves, N. Yokoyama, V. Parshin, E.A. Griaznova, M. Taranenko, V. Chesin and A. Cheban
1993
Reflections on NCRP Statement No. 7, "The Probability that a Particular Malignancy May Have Been Caused by a Specified Irradiation", Health Physics 64 ( 5 ) : 549, invited editorial
Comments on the NCRP Statement No. 7, "The Probability that a Particular Malignancy May Have Been Caused by a Specified Irradiation", Radiation Research 134: 396-397, invited editorial

30
"Implications of the New Risk Estimates" in Froceedinqs of the 28th Annual Meeting of the >:z.tional Comcil on Radiation Protection and Neasurements entitled Radiation Frotection in Medicine, NCRP Publications, 7910 Woodmont Avenue, Bethesda I4D 20814
2

UCCM / RCC1.950005.009b
REFERENCES
I . Before 1970:
Heublein, Arthur C., M. D., 'A Preliminary Report on Continuous Irradiation of the Entire Body", m, Vol. XVII, No. 6, Pages 1051-1062, June, 1932.
Jacobs, Melville L., M. D. & Marasso, Fred J. M. D., 'A Four-Year Experience with To!al-Body Irradiation", , Vol. 84, No. 3, Pages 452-456, 463, March 1965.
Jenkin, R.D.T., M. B., Rider, W.D., M.B., F.F.R., et al, "Ewing's Sarcoma A Trial of Adjuvant Total-Body Irradiation", -, Vol. 96, Pages 151 -1 55, July 1970.
King, Captain E. Richard, M.C., U. S. Navy, 'Use of Total-Body Radiation in the . . Treatment of Far-Advanced Malignancies", Journal of the American Medical , VOl. 177, No. 9, Pages 610-613, September 2, 1961.
Loeffler, R. Kenneth, M. D. & Puterbaugh, Myron R., M. D. 'The Therapeutic Use of Fractionated Subtotal Body Irradiation", -an Journal of RoentaeOPlPglL Rad ium T h e r u and Nuclear Me-, Vol. 123, No. 1, Pages 170-178, January, 1975.
Medinger, Fred G., M. D. & Craver, Lloyd F. M. D., 'Total Body Irradiation", &ner ican al of R o m o l o a v . Rad ium Therap and Nuclear Me w, Vol. 48, No. 5, Pages 651-
671, November, 1942.
Millburn, Lowell F., M. D., O'Grady, Lois, M. D. et al, "Radical Radiation Therapy and Total Body Irradia!ion in the Treatment of Ewing's Sarcoma", Carica, Vol. 22, Pages 919-925, November, 1968.
Miller, Lowell S, Fletcher, Gilbert H., et al "Radiobiologic Observations on Cancer , Vol. 4, Pages 150-165, Patients Treated with Whole-Body X-Irradiation", Radlatlon Research
1968.
. .
Newcomer, Earl H., "A New Cytological and Histological Fixing Fluid", $&me, Vol. 118, Pages 161-163, August 7, 1953.
Rider, W. D., & Hasselback, R., "The Symptomatic and Haematological Disturbance
I Health. Public Health Service P u b w n No. 999-RH-39, Pages 139-144, Following Total Body Radiation of 300-Rad Gamma-Ray Irradiation", U S B u r U
1968.
. .
Page #1

Rubin, Philip, M. D., Salazar, Omar, M. D., et al, "Systemic Hemibody Irradiation for Overt and Occult Metastases", Cancer, Vol. 55, Pages 221 0-2221, Supplement, May 1, 1985.
11. 1970 to Present:
A Total Body Irradiation
Armitage, James O., M. D., "Bone Marrow Transplantation", The New F n w d Journal of Medicine, Vol. 330, No. 12, Pages 827 - 838, March 24, 1994.
Armitage, James O., M. D. & Gale, Robert Peter, M. D., "Bone Marrow Autotransplantation", Jhe -rial of Me W e , Vol. 86 Pages 203-205, February, 1989.
August, Charles S., Serota, Frederic T., et al, "Treatment of Advanced Neuroblastoma with Supralethal Chemotherapy, Radiation, and Allogeneic or Autologus Marrow
, Vol. 2., No. 6, Pages 609-616, June, 1984. Reconstitution", u n a 1 of Clinical Onc- . .
Byhardt, Roger W., M. D., Cox, James D., M. D., et al, "Total Body Irradiation vs. Chemotherapy as a Systemic Adjuvant for Small Cell Carcinoma of the Lung",-
nc&&v. WialpQv & Phv&, Vol. 5, No. 11 and No. 12, Pages 2043- 2048, 1979.
Douer, Dan, M. D., Champlin, Richard E., M. D. et al, "High-Dose Combined-Modality Therapy and Autologous Bone Marrow Transplantation in Resistant Cancer", The A m e r b -, Vol. 71, Pages 973-976, December 1981. . .
Franzone, P., Scarpati, D., et al, "Chemo-radiotherapy and Autologous Bone Marrow Transplantation in Poor Prognosis Neuroblastoma", m p v and Oncology , Supplement 1, Pages 102-1 04, 1990.
Huys, John V., M. D., Simons, Maria J., M. D. et al, "Total Body Irradiation with 8 MeV X-rays in Generalized Malignant Disease", Cancer, Vol. 39, Pages 1435-1 438, 1977.
Kramer, Simon, M. D., "Fraactionated Total-Body Irradiation", Cancer, Vol. 37, Pages 2120-21 22, April 1976.
Livingston, Robert B., M. D., Schulman, Susan, et al, "Combination Chemotherapy and ystemic Irradiation Consolidation for Poor Prognosis Breast Cancer", Cancer, Vol. 59, Pages 7249-1254, 1987.
Page #2

Loeffler, Kenneth R., M. D. Therapeutic Use of Fractionated Total Body and Subtotal Body Irradiation", Cancer, Vol 47, Pages 2253-2258, 1981.
Marcus, Robert B., Jr., M.D., Graham-Pole, John R., M. D., et al, "High-Risk Ewing's Sarcoma: End-Intensification Using Autologous Bone Marrow Transplantation", international
1 of -. RiolQgy & Phv .*, Vol. 15, Pageas 53-59, July 1988. . .
Rostom, A. Y., "A Review of the Place of Radiotherapy in Myeloma with Emphasis on Whole Body Irradiation", He-cal Oncology , Vol. 6, Pages 193-198, 1988.
Socie, G., M. D., Devergie, A., M. D., et ai, "Influence of the Fractination of Total Body Irradiation on Complications and Relapse Rate for Chronic Myelogenous Leukemia",
March 1991. I of Radlatlon 0 n c o l o a v . v & P h v u , Vol. 20, Pages 397-404, . .
Stjernsward, J., M. D., "Adjuvant Radiotherapy Trials in Breast Cancer", Cancer, Vol. 39, Pages 2846-2867, 1977.
Vriesendorp, H. M., "Prediction of Effects of Therapeutic Total Body Irradiation in Man", -and Oncology , Supplement 1, Pages 37-50, 1990.
Vriesendorp, H. M., Herman, M. G., et ai, "Future Analyses of Total Body Irradiation", lnte-nal J o w l of w o n 0-v. BiolQgy & P w Vol. 20, Pages 635-637, March, 1991.
. .
Zablow, Andrew, M. D., Stabile, R. J., et al, "Single High Dose-Large Field Irradiation", flew Jersev Me-, Vol. 85, No. 1, Pages 39-42, January 1988. . .
B. Partial Body Irradiation
Aziz, H., M. D., Choi, K., M. D., et al, "Comparison of 32P Therapy and Sequential Hemibodfy Irradiation (HBI) for Bony Metastases as Methods of Whole Body Irradiation",
of C u O n c o l o g y CCCI, Vol. 9, No. 3, Pages 264-268, 1986. . .
Eichhorn, H.-J., Prof. Dr. Med., Huttner, J., Dr. Med., et al, "Preliminary Report on 'One-Time' and High Dose Irradiation of the Upper and Lower Half-Body in Patients with Small
* , Vol 9, Pages Cell Lung Cancer", -rial of w o n Oncology&&gv & Phvsics 7459-1465. October 1983.
. .
Page #3

Epstein, Lonnie M., Stewart, Bruce H., et al, "Half and Total Body Radiation for Carcinoma of the Prostate", & m a l of Uroloay, Vol. 122, Pages 330-332, 1974.
Fitzpatrick, Peter J., M. B., F.R.C.R., FRCP, & Rider, Walter D., M. B., F.R.C.R., FRCP., . . "Half Body Radiotherapy",- Journal of R~&$QD 0 n c o l o a v . v ti Phv &, VOl, 1. No. 3-4, Pages 197-207, 1976.
Green, Alexander A., M. D., Hustu, H. Omar, M. D., et al, "Total-Body Sequential Segmental Irradiation and Combination Chemotherapy for Children with Disseminated Neuroblastoma", m c e r , Vol. 38, Pages 2250-2257, 1976.
Jenkin, R.D.T., M. B., & Berry, M. P., M. B., "Sequential Half-Body Irradiation in Childhood", Interwonal Journal of m n Onc&gy. Blolq~v & Phv &, Vol. 9, Pages . . 1969-1 971, 1983.
Montebello, Joseph F., M. D. & Hartson-Eaton, Mary, Ph. D., "The Palliation of Osseous Metastasis with 32P or 89Sr Compared wtih External Beam and Hemibody Irradiation: A Historical Perspective", W c e r lnve m, Vol. 7 No. 2 Pages 139-160, 1989.
Payne, David G., M. D., F.R.C.P., Yeoh, Lim, M. D., F.R.C.P., et al, "Upper Half Body Irradiation (UHBI) For Extensive Small Cell Carcinoma of the Lung", -rial U n a 1
n c w 81 Phv&, Vol. 9, Pages 1571-1574, 1983.
Poulter, C. A., M. D., Cosmatos, D., Dr. et al, "A Report of RTOG 8206: A Phase Ill Study of Whether the Addition of Single Dose Hemibody Irradiation to Standard Fractionated Local Field Irradiation is More Effective than Local Field Irradiation Alone in the Treatment of Symptomatic
ioloav & Phvs ir& Vol. 23, Osseous Metastases", a n Onc- B Pages 207-214, 1992.
. .
Powell, Bayard, M. D., Jackson, Don V., Jr., M. D., et al, "Sequential Hemibody and Local Irradiation with Combination Chemotherapy for Small Cell Lung Carcinoma: A Preliminary Analysis",lnternational Journal of Rad iation O n c o l o m & Ph. w, Vol. 11, Pages 457- 462, 1985.
Qasim, M. M., "Half Body Irradiation (HBI) in Metastatic Carcinomas", Clinical Radloloav. Vol. 32, Pages 215-219, 1981.
Rowland, C. G., Bullimore, Jill A., et al, "Half-body Irradiation in the Treatment of Metastatic Prostatic Carcinoma", Britis Joyrnal of UrolQgy , Vol. 53, Pages 628-629, 1981.
Rubin, Philip, M. D., Salazar, Omar, M. D., et al, "Systemic Hemibody Irradiation for
Page #4

Overt and Occult Metastases", Cancer, Vol. 55, Pages 221 0-2221, 1985.
Rubin, Philip, M. D., & Heilmann, Hans-Peter, M. D., "Large Field Trials", of -n OncQlQQy R i o u v & Phv&, Vol. 124, Pages 565-576, . .
1988.
Salazar, Omar M., M. D., Rubin, Philip, M. D., et al, "Single-Dose Half-Body Irradiation for Palliation of Multiple Bone Metastases from Solid Tumors", Cancer, Vol. 58, Pages 29-36, 1986.
Thatcher, Nick, Ph. D., FRCP, Anderson, Heather, M. D., MRCP, et ai, "Treatment of Metastatic Melanoma by 24-Hour DTlC Infusions and Hemibody Irradiation", Cancer, Vol. 57, Pages 2103-21 07, 1986.
Urtasun, R. C., M. D., Belch, A., M. D., et al, "Hemibody Radiation, an Active Therapeutic Modality for The Management of Patients with Small Cell Lung Cancer", m n a l
ncolQgv. Biobav & Phu-, Vol. 9, Pages 1575-1578, 1983.
Page #5


UCCM / RCCl.958206.005a
50 I Chief, Rodiologiwl Service Walter Reod Amy Mcdical Center
DATE: 20 October 1958
: A s a t Chief, 9iophysic3 and Astronautics Research Branch, U. S, -- M o d i d Research and Developmnt C m d .
SmJLC=: Application for Research Contract ,
q.
1. The hclosed 'copy of research proposal e n t i t l e d , nl.leMxlic Chanl;es in R n - s ? o l l o r r i n ~ T o t a l Body Endlation,'t has been suka i t t ed f o r our consideretion by
- Dz. EhEeno L, .%cnger of the University of Chc inna t l , College of Hedicine, . ' Cinc3nrxt t i , cplio. - .
2. Request review of the at tached proposal and please give yuur recarr;-,endaticn as to vhether or not this study should be supported by the grnY Medical Servica.
1 L C X
1=,7a m: A s s t Ch, Bio7hysics & Astronautics FROM: C h i & , Radiological DATZ: 22 Oct 195:
Research BrancS, US Kedical svc, URAH - C o l I ~ h e m o d / r u 6 ; Research & Developcent C o m d
O?SG Fo13 108
- 1. ~eco=ne/ni approval.
2, ?!uch work has been done on the e f f ec t s of total b d y i r r a d i a t i o n izi ar-3 There hts been no real e f f o r t t o da te for s i n i l n r s tud ie s on hmans. Of t h e a s s m ? t i o n t h a t a n i n a l r eac t ion is i d e n t i c a l wi th t h a t in,htnaru is weir assmpt ion . Thcre is def i&te need f o r basic vork i n this f i e ld . Any c o r r r l a t l c a Of t u o r response t o t o t a l dose of i r r a d i a t i o n by auch meam a1 p p s e d i n tkLs P r0.j e C t would be of g r e a t value =ears t ach a s those proposed accurate knowledge of t h e t o t a l dose of r a d i a t i o n receive2 could be deternined it w u l d be of inest imable value In case Of a-c disaster o r nuclear uarfare . Thc appl icant , D r . Ssenger, I s ueu q d c : e d *a conduct such rasearch, tbr a b i l i t y to stizrulatc his covorkers and a s s i s t a n t s . z i n d and i8 an excel lent organizer and adminis t ra tor .
he has available are well adapted t o t h e project. f h d s spent on such a pro jec t are u e l l w r t h u h i l e .
The validity
t h e f i e l d o f cancer. In addi t ion tC b7
He is not only an en thus i a s t i c 4 t i r e l e s3 worker b~: b s He ha8
It is bddovad
U U s u l a u l f i : : c I believe t he f a ~ 9 i ' - i e a
1 zncl p l o n e l , MC
W e f , Radiological S e d c e

4

RCCl.958026.001
COXSEXT FOR SPECIAL STL'D'f LYD ' i X E A I E i i
, do hereby g ive my consent . t o the members of t h e p r o f e s s i o n a l s t a f f of t he C inc inna t i General Hosp i t a l ,
Un ive r s i ty of Cinc inna t i College of Nedicine, t o admin i s t e r t o me whole or b a r t i a l
body i r r a d i a t i o n on o r about
0 . .
196 . -.
The n a t u r e and purpose of t h i s therapy, p o s s i b l e a l t e r n a t i v e methods of
t r ea tmen t , t h e risks involved, t h e p o s s i b i l i t y of complicat ions, and prognzsis have
been fully e x p l a h e d t o me.
ment has been d iscussed wi th me and is understood by me.
. . The s p e c i a l s tudy and research n a t u r e of t h i s treat-
Consent is given f o r photographs and p u b l i c a t i o n f o r t h e advancemmt of
n e d i c a l educa t ion .
S igna tu re . . Witnesses t o s i g n a t u r e :
Or ig ina l : t o p a t i e r i t ' s c h a r t Copies: t o Ca-60 f i l e
t o TBR f i l e
Re la t ionsh ip ( p a t i e n c o r g i ia r i ian)
AM Date P bl
(Mo. Day Yr.) . . .
- Place (Ward - C l i n i c - 'Jni:)
Chart So. . . ,
5/1/65

CONSENT FOR SPECIAL STUDY AYD T?UlXl3T
1, , do hereby g i v e ny consent
t o the members o f the p r o f e s s i o n a l s t a f f of the Cincinnati General H o s p i t a l ,
university of C i n c i n n a t i Col lege of Xedic ine , t o per form a bone narrow a s p i r a t i c n
and t o s t o r e mv bone marrow on o r about . . . . . .
, 196 - . ' . The n a t u r e and purpose of t h i s t he rapy , t h e risks involved , t h e p o s s i 5 i l i t y
of compl ica t ions , and prognos is have been f u l l y exp la ined t o ne. The s p e c i a l
study and r e s e a r c h n a t u r e o f t h i s t r ea tmen t has been d i scussed w i t h ne and is
Consent is a l s o g iven for r e i n f u s i o n (g iv ing t h e marrow back t o m e ) when t h e
members o f the p r o f e s s i c n a l s -caf f recomnend it .
Consent is given f o r photographs and p u b l i c a t i o n f o r :he advancement of
medica l educa t ion .
S i gnat u r e - .
Witnesses to s i g n a t u r e :
. -
Orig ina l : t o p a t i e n t ' s c h a r t Copies: t o CO-60 f i l e
- t o TBR f i l e
- R e l a t i o n s h i p . ( p a t i e n t o r g u z r d i t n )
AM Date PM
(No. Day Yr.)
P l a c e . (Ward - C l i n i c - U n i t )
Chart No.

,
Uh'IVERSITY OF CfNCIhYATI IEDICAL CEYTER FACULTY CO?MITTEE ON RESEARCH
VOLLTTARY COSSEXT STATE!.IEST
*I of ( P a t i e n t ) . (normal s u b j e c t ) - ( p l a c e - c i t y )
b e i n g of t h e age o f n a j o r i t y and o f sound mind and body, v o l u n t a r i l y and w i t h o u t f o r c e or d u r e s s , c o n s e n t t o p a r t i c i p a t e i n a s c i e n t i f i c i n v e s t i g a t i o n which is n o t d i r e c t e d specical l . ] t o my own b e n e f i t , b u t i n c o n s i d e r a t i o n f o r t h e expec ted advancement of medica l knowledge, which may r e s u l t f o r t h e b e n e f i t o f mankind.
I have b e e n i n f o m e d of and unders tand t h e n a t u r e , d u r a t i o n , and purpose D f t h e s t u d y , t h e method and means by which i t is t o b e conducted, t h e inconvenience and h a z a r d s t o be e x p e c t e d , and t h e e f f e c t s upon ny h e a l t h and p e r s o n which may p o s s i b l y come from p a r t i c i p a t i c n i n t h e exper iment , as f o l l o w s :
Purpose: on b l o o d and u r i n e :
To k i l l tumor ce l l s and a t t h e same time s t u d y t h e e f f e c t s of r a d i a t i o n
Procedure:
Risks: plant, drugs, o r t r a n s f u s i o n as needed.
R s d i a t i o n o f t h e whole body.
The chance of i n f e c t i o n o r mi ld b l e e d i n g t o b e t r e a t e d w i t h marrcw t r a n s -
I unders tand t h a t I may, a t any time d u r i n g t h e c o u r s e o f t h e e x p e r i n e n t , revoke ny c o n s e n t , i n w r i t i c g , and withdraw from t h e esper i insn t .
I acknoxledge t h a t no g u a r a n t e e o r a s s u r a n c e h a s been made t o m e a s t o t h e r e s d t s t h a t may. b e o b t a i n e d , and I hereby waive any and a l l claims f o r l i a b i l i t y , e x c e p t f o r n e g l i g e n c e , o n - t h e p a r t o f t h e medical p e r s o n n e l i n v o l v e d , t h e U n i v e r s i t y o f C i n c i n n a t i , i ts H o s p i t a l and its X e d i c a l School , v h i c h o t h e m i s e might h a e i n u r e d TO me or my h e i r s , 3s a r e s u l t o f t h i s F e d i c a l procedure .
I cer t i fy t 5 a t 'I have r e a d and am competent to f u l l y u n d e r s t a n d t h i s consent and t h a t t h e e x p l a m t i o n s l i s t e d above were, i n f a c t , nade.
Volunteer Date
I n v e s t i g a t o r Date
Date . . Witness (1)
+In case of s u b j e c t under age , t h e p a r e n t o r g u a r d i a n s h o u l d be t h e r e s p o n s i b l e p a r t y and s h o u l d s i g n on h i s b e h a l f .
h'm: Copy to P a t i e n t / n o r m a l s u b j e c t , Research F i l e and P a t i e n t ' s Chart .

- -- .
I certify that I have read and am conpetcnt to understand this cowenc and that the explanation listed above
Volunteer Date
wae, in fact, =de.
Investigator Date
Witness (1) Date
* 'Incase of subject under age, the parent or guardian should be the responsible party and should sign on h i s behalf.
NOTE: Copy to Patient/Nonnal subject, Research F i l e and Patient'e Chart. .
-.
- + . .
.
'.
n.-. e' . I .. .
' .
..

c
1 t
.. FACULTY COXIITTEX ON RESEIIRQI . '.- - I
' / VOLUIITARY C0:;S EliT STXTE!EZTT
*I of ( P a t i e n t ) (>lorma1 s u b j e c t )
being of t h c age of m a j o r i t y and of sound mind and body, v o l u n t a r i l y and w i t h o u t f o r c e o r d u r e s s , c o n ~ e n t t o p a r t i c i p a t e in a e c f e n t i f i c i n v e s t i - g a t i o n which I s n o t on ly d i r e c t e d s p e c i f i c a l l y t o my o m b e n e f i t , b u t also i n c o n s i d e r a t i c n for t h e expected advanccncnt of medica l knowledge, which may r e s u l t f o r t h e b e n e f i t of mankind.
I have been infonncd of and unders tand the n a t u r a , d u r a t i o n , and purFose of thc e tudy , t h c method and maans by which i t i a t o be conducted, t h e inconvenience and haza rds t o b c expcc tcd , and t h e e f f e c t a upon my h c o l t h and pe r son which nay p o s s i b l y come from p a r t i c i p a t i o n i n t h e exper iment , as follows:
e
. Purpose: t h e e f f e c t s of r a d i a t i o n on blood and u r i n e .
To k i l l tumor ce l l s and a t t h e same t i m e e tudy i
* Procedure: Rad ia t ion of t h e whole body.
Risks: Radia t ion t r c n t n e n t employed is used t o kill tumor c e l l s but a t t h e sane time other , n o m a l , ce l l s of your body w i l l l e a f f e c t e d . The only ce l l s a f f e c t s d which would cnusc any risk t o you are t h o s e c e l l s i n your bone marrow. Thc bone marrow is a "blood f a c t o r y " where whicc c e l l s t h a t f i g h t i n f c c t i o n , t hc p l a t e l e t s which h e l p blood c l o t , and t h c red c e l l s which c a r r y oxygen t o your t i s s u c s a r a a i d e . The bone marrou'o a b l l i t y t o make t h e s e c e l l s w i l l bc decrzascd for f o u r o r f l v c wesks a f t e r you r e c c i v c y o u r r a d i a t i o n . I f you r c c c i v c a dose of r a d i a t i o n 'of 200 rads o r more, trhich your doc to r will t e l l you, your blood c o u n t s will f a l l t o l e v e l s where i n f c c t i o n or b l e e d i n g could be a problem. and p l a t e l e t s and t h e i n f a c c l o n by a n t i b i o t i c s . I n a d d i t i o n , ue I
preven: such low blood cocncs u i t h t h e usc of a bone ciarrow t r a n s - p l a n t which w i l l b e d i s c u s s e d w i t h you i n a separate v o l u n t a r y consen t s ta te rcent . If your r a d l a t l o n dose is only g i v e n to p a r t of t h e body t h e r e is no r i s k of danger or unusua l ly low b lood counts .
The b l e e d i n s can be t r c a t c d by t r a n s f u s i o n of r e d c c l l s
I under s t and t h a t I n a y , a t any t i n e dur ing t h e course of the c x p c r i n c n t , revoke my c o n s e n t , in w r i t i n g , and withdraw from the experiment .
I acknowledge t h a t no gua ran tec or assu rance has been made t o m c as t o t h c r e s u l t s t h a t nay b e o b t a i n e d , and I hereby waive any and all claims f o r
- - l i a b i l i t y , excep t f o r n c g l i g s n c s , on t h e p a r t of t h z nadical pcrconnc l i n v o l v e d , t h e Un ive r s i ty of Cfnc inna t f i t s HDspital and its lhx!ical Schoo l , which o t h e r v i s e might have inu red t o me o r my h e i r s , as a r c s u l t of this medica l procedure.
-
- - a
. . .
. .
I
I 1
!
I
1
~
I
I !
i 1
i

i
. . I rcrtlfy that Xihave read and,= cnmpetcnt to understand this conrcwt rind (Itat the explanation ll&tcd ~ L O V C vag, ln i n c t , mde.
Yoluntrcr Date
fnvcst 1p;ucor Dote
* Icicasc o f subject under age, thc parcnt or guartilnr, should bc thc r c n p ~ ~ i s l b l c - p a t t y aad should t3fF;t l on his b c h l i .
NOTE: Copy t o Psticnt/Konnal subjec t , Itcscnrch File and Patient’o Chort.
.
.
‘.
/ i I
.

. L - \ '..
.- .- .
i UNIVERSITY OF CINCINNATI MEDICAL CENTER
FACULTY CO>lHIT'tlX ON RKSEARCIl
*I of i (Pa t i en t ) (Normal sub j c c t )
. being of t he age of ma jo r i ty and of sound mind and body, v o l u n t a r i l y and c without fo rce o r d u r e s s , consent t o p a r t i c i p a t e i n a s c i e n t i f i c i n v e s t i -
ga t ion which is no t only d i r c c t c d s p e c i f i c a l l y t o my orm b c n c f i t , b u t a l s o i n coiisidcrntion €or the cxpcctcd advnnccincnt of medical knovlcdgc, . which may result f o r t h e b c n c f i t of nian1:inll.
I have been informed of and understand the n a t u r e , d u r a t i o n , and purpose of tlic s tudy , t hc mctliod and nicms by which i t is t o bc conduclcd, t h c incoiivcnicnce: and liazarcls t o IC cxpcctcd, and thc e f f e c t s upon my i i ca l th as fo l lous :
; I ' -- Purpose: - .--- of' your body.
--_- Procedure: Bone marrow t r a n s p l a n t a t i o n .
To prevent low blood counts fo l lowing r a d i a t i o n
-.
--- R i s k s : - You w i l l b e pu t t o sleep i n t h c ope ra t ing room w h i l e npproximatcly onc p i n t of honc, nnrrw is rcmovcd by ncedlcs from your pe lv ic boncs a n d l , r c a s t b o n c . tlicrc is no c u t t i n g . The proccclurc would b c p a i n f u l i f you wcrc not p u t t o s l c c p a t this t i i i i c ! . Thcrc is alniost no r i s k i n gcncra l anastlicsicl. A f t c r you awd;cn, your lovcr back and clicst may b c somcwliat s o r e and w i l l bc t r c a t c d w i t h p a i n k i l l e r s i f you so d c s i r c . mcnt trliilc l y i n g on a s t r c t c h c r m J hc tnlccii back to your rooni. A t t h i s tirnc, your hone mnrrov vi11 bc givci i back t o you through a v e i n j u s t as ony.blood t r a n s f u s i o n 11ouli1. cc iv ing your own blood is zcro. I n ttic bone mnrrov t h c r c arc many g lobules of f a t and t i n y p i cccs o i hone a l l of which arc ' f i l t c r c d o u t of tlic bone marrow rncltcriol which you w i l l p x c i v c bcfo rc i t c n t c r s your ljody.
No opcra t ion is performed -
You w i l l tticil rcccivc your r a d i a t i o n trcat-
l'tic r i s k of rc-
I understand t h a t I may, at any time dur ing t h e course of t h e experiment, revokc my consent , i n m i t i n g , and u i t l d r m from t tic expcrimcnt .
. I acknowlcdge t h a t no gua ran tee or a s su rance has been made t o mc as t o t h e results t h a t may b e ob ta ined , and I licrcby traivc any and a l l clainis f o r l i a b i l i t y , except f o r ncg l igcncc , on tlic par t of t h c medical pcr- sonncl involvcd, t h c Un ive r s i ty of C l n c i c n a t i , i t s Hosp i t a l and its Medical Scliool, which otlicrtrisc xniglrt have i n u r e d t o uic o r my h c i r g ,
' h s w r c s u l t o f t h e medical proccdurc.

CONSENT FOR SPECIAL STUDY AND TREATMENT
- . * , do hereby give my consent
. . . . - - 2 . . . . 1,
t o t h e members of t h e profess iona l s t a f f of the Cincinnat i General Hospi ta l ,
Universi ty of Cinc inna t i College of Medicine, t o adminis ter t o m e whole o r
par t ia l body i r r a d i a t i o n
- - .- - _ - . - .
. .
and marrow auto t ransplan t on or about S
196-.
The n a t u r e and purpose of t h i s therapy, poss ib l e a l t e r n a t i v e methods of
t reatment , the r i s k s involved, the p o s s i b i l i t y of complications, and prognosis
have been f u l l y explained t o me. The s p e c i a l s tudy and research n a t u r e of t h i s
treatment has been discussed wi th me and is understood by me .
Consent is given f o r photographs and publ ica t ion f o r t h e advancement of
qed ica l education.
W i tnes se s t o s igna tu re : . .
Original : t o p a t i e n t ' s cha r t Copies: t o CO-60 f i l e
t o TBR f i l e
5/1/65
Sign a t u r e
Relat ionship - (pa t i en t or guardian)
AM PM Date
- (Mo. Day Yr.)
Place (Ward - C l i n i c - Unit)
Chart No.
'.
. .

5

UCCM / RCC1.950005.009e
1.
2.
3.
4.
5 .
6.
7.
8.
9 .
10.
1 1 .
12.
13.
14.
15.
BIOCHEMICAL AND BIOLOGICAL TESTS FOR PATIENTS UNDERGOING TOTAL BODY IRRADIATION AND PARTIAL BODY IRRADIATION
Pre and Post Radiation Observations'
Complete history and physical examination
Hematocrit, hemoglobin, leukocyte count and differential
Electrocardiogram, chest X-ray, urinalysis
Sequential multiple analyses (SMA-12) for blood chemistry determination, prothrombin time, creatinine phosphokinase levels, partial thromboplastin time
Blood and urine amylase
Ultraviolet absorbing compounds in urine
Bone marrow aspiration
Blood typing and cross matching if bone marrow transfusion is to be done
Tritiated thymidine uptake for lymphocyte viability
Histochemistry and electron microscopy of bone marrow pre and post etiocholanolone
Chromosome analysis
Nitroblue tetrazolium study of granulocyte function
Serum glycoprotein assay
Serum amino acid assay
Bacteriophage titers

1 6.
17. Psychological testing
1 8 .
19. BAIBA in urine
20. Kynurenic and xanthurenic acids
2 1 . Deoxycytidine
22.
23. Urinary phosphate
24. Glutathione
25. Routine electrophoresis and immunoelectrophoresis
26. Quantitative precipitin studies
Urinalysis for hydroxyproline levels
Urinary taurine for correlation with leukocyte count
Xanthine and hypoxanthine in urine.
These observations and tests have varied as some tests do not seem useful and new ones suggest that they may be valuable.
file: PositiorVAppendix 4

6

RCCl.95O321.010
Reprinted from Tk Amrricm / o u d of R o n t g r n o l o g y , Radium T h r w p y ond Nwlmr bftdinw
Vol. CXVII, KO. 3. March, 1973 r.'..(* r.-
WHOLE BODY AND PARTIAL BODY RADIOTHERAPY OF ADVANCED CANCER*
BT EUGENE L SAENGER, M.D., EDWARD B. SILBERSTEIY, hl.D., BERNARD ARON, M.D., HARRY HORtVITZ, M.D.,
J A M B G. KERELSKES, PH.D., GUSTAVE K. BAHR, PH.D., HAROLD PERRY, M.D.,t ond
BEN I. FRIEDMAN, M.D.$ CINCINWATI, OHIO; DTTIOIT, MICHIGAN; AND )rfEM+'HIJ, TLNYLSJEL
T H E P urpose of these investigations has been to improve the treatment and
general clinical management and i f possible the length of survival of patients with ad- vanced cancer. Systemic effects of radiation therapy have been given particular atten- tion in our work.
In the period-February 19,1960, through August 31, 1971, 85 adults were given whole or partial body radiation as therapy for far advanced cancer.
This paper will report on the survival of patients in 3 categories: colon; lung; and breast.
Prophylactic whole body radiation ther- apy was given to 3 children with localized Ewing's sarcoma and this experience will be discussed br idy.
Investigations of biochemical, cytologic and psychologic tests have been reported elsewhere.8.~1~10 Our experience with the adjuvant use of
autologous bone marrow will also be desai bed.
A N I M 4 L STUDIES
The animal investigations basic to our work stem from the studies of Hollcroft et ui.Ia-'* These authors demonstrated bet- ter tumor regression when whole body ir- radiation was preceded by localized radia- tion therapy than when localized radiation therapy was given alone both for Iym- phoma and carcinoma in mice. T h e studies of Jacobson et aL1'.l' showed the impor-
tance of shielding of the spleen and other organs and parts of the body in preventing high dose radiation lethality in the mouse.
B R I E F REVIEW OF TOTAL BODY IRRADIATION IN MAN
Total body irradiation was first em- ployed in 1923 by Chaoul and Lange.' Its use in 270 cases over the next zo years was reviewed by Medinger and Craver.n These authors found the greatest palliation in the lymphomas and myeloproliferative diseases, but also noted improvement in multiple myeloma. Thirty-five patients with ad- vanced carcinoma or sarroma were in- cluded in this series, most of them receiving their total body radiation between 1931 and 193:.
Loefler et ~ 1 . ' ~ compared total body irradiation in single doses up to 150 r with nitrogen mustard and triethylene melamine and found that neither chemotherapy nor radiotherapy differed in hematologic ef- fects, but that the patients receiving radia- tion did not experience the malaise of vaT- ing sctperity noted by all patients receiving the chemotherapeutic agents. Subjective improvement was noted only in the radio- therapy s o u p .
Collins and L d e r ' gave total body irradiation in single exposure up to 200 roentgens and found this form of systemic rherapy "a useful addition to the manage- ment of advanced cancer." The malipnan- cies treated included lymphoma, chronic

671 voL. 117, N ~ . 3 - Whole Body Radiotherapy of Advanced Cancer
myelogenous leukemia and multiple mye- loma.
Interest in total body irradiation in the treatment of Ewing’s sarcoma, a tumor of children which carries a high mortality, has been aroused by reports from Milburn ti af.,* Jenkins t r a].,= and Rider and Hasselback?g In a small series so treated, survival appeared to be moderately im- proved compared to larger series treated by conventional local radiotherapy and/or ablative surgery. These groups felt further evaluation of this form of therapy to be most important.
Additional data have been published by the Rledical Division of Oak Ridge Ass& ciated Universities,’ concerning total body radiation therapy of lymphoproliferativr and mveloproliferative disease.
Summaries of the frequent use of total body irradiation for the therapy of leu- kemia appear in an article by Bu-k L ner et af.‘ and in a comprehensive review of bone marrow transplantation by Bortin.a
Whole body radiation in routine clinical therapy has been and is currently used for leukemia,p.u Iymphoma,s?-26*Y Hodgkin’s disease,’ polycythemia vera,’ cancer of breast,” cancer of thyroid,’ cancer of pros. tate,’O*sl and multiple mye l~ma .~ .~ ’ Such therapy may be given by external radiation therapy (as in this particular study) or in the form of various radionuclides.
STUDY DESIGN
The studies reported h u e were initially considered as being in Phase I (to deter- mine whether the treatment was toxic or not) and subsequently as Phase I1 (whether treatment appears effective or not but without controls). In reviewing these data it has been possible to find some compara- ble material in the literature. In one catG gory, cancer of bronchus, comparable data were available in our institution.
INrOIYLD CONSENT AND INmTUTIONAL IEVILU’
All patients gave informed consent in accordance with directives of the Faculty Research Committee of the University of
Cincinnati College of Medicine and those of the National Institutes of Health. The use of formal informed consent forms in this study antedated the above require- ments by 2 years. The project is reviewed and approved regularly by the above Commi ttee.
ELlClBlLrrY OF PATIENTS
Patients become eligible for this form of treatment i f they have advanced cancer for which cure could not be anticipated. Three children with localized Ewing’s tumor at Children’s Hospital were given whole body radiation as part of the curative attempt after the primary tumor had been ablated with local radiotherapy.
Biopsy proof of the malignancy has been established in all instances. Clinical data in each case have been reviewed by several physicians to be certain that the tumor had indeed extended from its primary site and that curative therapy was not applicable. This preliminary evaluation is followed by an observation period of 7-14 days to o b serve the general condition of the patient and to carry out baseline laboratory tests to be as certain as possible that the condi- tion of the patient is relatively stable. Fre- quently this determination is difficult since the patients have serious illnesses of long standing and often have had considerable previous therapy.
Patients remain in the hospital as long as is necessary. Prior to the use of autologous bone marrow transfusion, hospi talization was occasionally as long as 8-10 weeks. Length ofstay was also dependent upon the severity of the clinical manifestations stun- ming from the cancer. With the use of par- tial body irradiation and bone marrow infu- sion, hospitalization has been greatly short- ened. The follow-up procedure is continu- ous during the lifetime of the patient.
A total of 112 subjects were initially entered in the study through August 31, 1971. During the screening p e n 4 of 7-14 days, 2,+ of them (ax per cent) were not continued in the study and did not receive whole or partial body irradiation. Chief

672 Saenger et a/. MALCU, r973
among the reasons for elimination was an indication in the pretreatment phase that some risk from widsfield radiation might ensue or that another method of treatment was considered preferable. In some, a very rapid progress of the disease made inclusion undesirable. The treatment was completed in 85 adults and 3 children between April 1960 and August 31, 1971. Three patients have received 2 separate courses of treat- ment in this program. Follow-up time for survivors is reported through August 31, 1972.
PATIEST DOSIMETRY
The radiation is delivered by a cobalt 60 teletherapy unit under the following expo- sure conditions: The beam is directed hori- zontally a t a wall 342 cm. away with the midline of the patient a t 286 cm. from the source. For whole body exposures, the radi- ation beam size for the 60 per cent isodose curve a t the patient midline distance is a square approximately I 2 0 cm. X I 20 cm. The patient is placeci in the sitting position with legs raised and head tilted slightly forward. Radiation is given by delivering half the specified exposure laterally through one side of the patient, the patient is then turned and the other half exposure deliv- ered laterally through the ocher side. The combined dose of the 2 radiation fields provides a good homogeneous dose distri- bution through the patient. The maximum variation in lateral dose distribution was - + 13 per cent for I patient who had a lateral trunk dimension of 36 cm.
The exposure to the patient is deter- mined using a percentage depth dose table corrected for the sourccto-skin distance used for the patient. Using the corrected depth dose a t patient midline ( 1 / 2 lateral dimension a t the trunk in the plane of the xiphoid) and a conversion factor of 0.957 rads/roentgen for cobalt 60 gamma radia- tion, the midline air exposure required to give a desired midline absorbed dose in rads is calculated. The validity of this pro- cedure was established with measurements in an' Alderson Rando Phantom using
thermoluminescence dosimeters. Over the course of the study, the air exposure rates a t the distance indicated above varied from 3 to 6 per minute.
For individuals receiving partial body radiation, the teletherapy collimator is used to restrict the beam. The xiphoid is used as the boundary of the field for upper and lower body exposures. The lateral dimen- sions of the patient in the plane of the xiphoid is again used for calculating the desired midline dose. As for the whole body exposure, the dose is delivered bilaterally. Additional information on the dosimetry aspects of this study has been published by Kereiakes ct al."
ANALYSIS OF SURVIVAL DATA
In considering the survival data there was a lack of consistent selection bias both in recommendation that a patient be eiigi- ble for treatment and in regard to the dose. The principal investigator had no part in determination of therapy in any given case except for outlining the general principles of the therapeutic regime. The choice in the case of each patient was made by several radiation therapists, 3 having been asso- ciated with the project during the IO year period. In addition, 2 internists have had active roles in the selection and medical care of each patient. The dose of radiation to be given was decided upon by the radia- tion therapist in consultation with the internist.
There are 3 categories of patients (those with carcinoma of the colon, lung and breast) which are large enough to permit some analyses of survival. Each group will be discussed separately.
Survival data are given in days from the diagnosis of far advanced disease, since this convention has been used frequently in the literature and permits comparison of our survival data with published reports.
CANCER or THE COLOE AND RECTUM
Twenty-nine patients with this tumor comprised the largest single category (Ta- ble x). In dl cases the patients were classed

Vor. 117. No. J Whole Body Radiotherapy of Advanced Cancer 673
TABLE I CANCLL or COLON-ALL c A s u av LEN- or SURVIVAL or ADVANCED DISEASE
(29 Patients)
i
I
as far advanced and in a few instances as terminal. Four patients were not included in the study for medical reasons, or because the patients themselves declined participa- tion in the study.
In order to make an appropriate com- parison, several published series were re- viewed. Series of cases of colon cancer metastatic to liver were utilized, since they were the best found by us with appropriate time periods of metastasis available for comparison. Steams and Binkley,(l in 32 patients with colon cancer with liver metas
tases, found a median survival time of X I months after palliative resection of the primary tumor; in 28 of their patients in whom only biopsy or diversion was per- formed, the median survival was 8 months. In 353 patients with untreated colon cancer metastatic to liver, Pestana et uLn reported a median survival of g months. Figure I presents an analysis of 177 patients with liver metastases and no subsequent therapy reported by Jaffe et d.*' There is also a group of 61 patients reported by Rappor t and Burleson*' treated with 5-fI uorouracil.

674 Saenger et ai.
90
SURVNAL coMpARlsoNs CANCER OF COLON METASTATIC TO LJER
The 22 patients in ouflseries with proven metastatic carcinoma of the colon to the liver treated by irradiation are also shown in Figure I.
The median survival time for untreated patients was 146 days; for patients treated only with 5-fluorouracil, 255 days; and, among our patients with liver metastases, 391 days (Table 11). A life table analysis was performed and indicates that the treat- ment given to our patients was approxi- mately equivalent to the group given 5- fluorouracil. There was no evidence that the median survival time was shortened by total or partial body irradiation (Fig. I). It should be appreciated that 5 of our pa- tients had received or are receiving 5-fluoro- uracil in addition to the radiation therapy (3 of these with liver metastases).
The median survival for the entire group of 29 patients (22 with liver metastases) was 327 days.
CANCER or rnL BRONCHUS
This group of I 5 patients (Table 111) had far advanced disease with distant metas- tases a t the time of treatment. The best comparison group was from our own insti- tution reported by Horwitz et ai." The median survival of the 1 5 patients receiving whole body irradiation was 193 days from the time of diagnosis. The median survival of 61 patients seen a t Cincinnati General Hospital from December, 1961, to June, 1964, was 135 days. In 15 of the 17 cases with distant metastases excluded by Hor- witz t t a/. from their study (see caption to Fig. 2), the median survival was 32 days.
This last group of patients with distant metastases constitutes the most appropri- a te comparison group. \\'hen the median survival* of 15 patients mentioned by Horwitz et ai.*' is compared with the 15
Two of the 17 patients excluded in the Horwitz rr d." study were m a t e d by rhok body radiation.

Yor. 117, No. 3 Whole Body Radiotherapy of Advanced Cancer 67 5
patients treated by whole body irradiation, the survival times are significantly different (Chi square I 1.63, p <o.005) (Fig. 3).
TABLE 111 LUNG CANCER-SURVIVAL I N DAYS A n E R D,
(15 Patients)
EWING'S TUMOR
This subgroup of 3 patients constituted the only one in which an attempt a t cura- tive therapy was made; all 3 patients are surviving. The times of survival are 854, 1,243 and 1,553 days from the time of diag- nosis to August 31, 1972. The patient with the longest survival has recently developed a solitary pulmonary metastasis. The use of whole body irradiation to eliminate small clumps of cells in the disease has been reported by others.21*"
A fourth patient with Ewing's tumor had pulmonary metastases when first seen. Therapy in that case was only palliative.
TABLE I1 CANCER O T COLON--CASES WITH
METASTASES TO LIVER
(22 Patients) ~~~ ~~
Study Survival After Survival After No.. D. (days) R. (days)
40 116
I 26 136 I43 192 161
29 5 3 27 347 434 45 I 583 631
98 2 983
I 1258 I 1161 1,437 1,691
I20
912
See foornotc to fable 1. Median ruwiral-~~ d ~ m
Survival Survival Dose %:dJ After D. After R, (rads)
(days) (days)
053 57 18 200 056 103 38 100 UB 086 116 20 I 0 0 078 I 16 61 1CO 08 8 '35 7 150 08 I I 4 4 14 I00 0 5 1 163 74 1 5 0 070 193 68 150 I02 166 21 100 Trunk 018 333 044 349 196 01 I 419 3 23 100 I I1 683 403 IO3 0 2 5 797 33 150 084/097 855 643 300 L'B+ioo
200 298 100
See footnote ro Table I. Median rurvival--r9j daw
CANCER or THE BXEAST
In 15 cases treated by us the median survival from diagnosis to death was 479 days and after treatment to death was 446 days (Table IV). Two comparable reports in the literature include the one by the Committee on Estrogens and AndrogensU and the other by Samp and Ansfield using j-fluor~uracil .~~ Again a life table analysis was done for our 1 5 patients and indicates that the survival of our patients appears somewhat better than that of the patients treated solely by estrogens and androgens, but not quite as good as the group treated with 5-fluorouracil (Fig. 4). The patients survive longer than those receiving the "standard therapy" as described by Samp and A n ~ f i e l d ; ~ ~ this includes appropriate administration of estrogen and androgen, oophorectomy, local irradiation, adrenalec- tomy and hypophysectomy.
OTHER CAWCEXS
A remaining group of 25 cases reflected several different kinds of cancer. It is not

Saenger et a/. MAKE, 1973 676
IO0
Bo-
bo.
?e
69 - 8 - j 50. Y)
# 40-
30-
20-
Jo-
97 x ------------------_ _ _ _ _ s 8 s t
12 ma. Survival ’t8 8 s- Pmbabillty 1 c
UIcrrtohty Ban Show21 Standard E m 10 x
1 I I I I I I I I I I I
0 I 2 3 4 5 6 7 8 9 10 I 1 12
possible to make an analysis of these at this point since the individual case groups are too small to warrant this
DISCUSSION
RELATION Or RADIATION THERAPY TO P A T I E S T DEATH
Some analyses can be made which give information on this point.
The doses of whole body radiation given could initiate only the hematologic form of the acute radiation syndrome. In the healthy individual, after prodromal s y m p
toms of malaise and vomiting lasting about 6-48 hours, there is a latent period lasting until 18-21 days after exposure. At this time there is a marked rapid fall in white blood cells and platelets and a less rapid fall of red blood cells reaching a nadir a t 3-40 days and then recovering. These changes are associated frequently with episodes of infection and bleeding. Epila- tion will occur at doses over 300 rads.
Manv of these patients had received much radiation and chemotherapy prior to total or partial body treatment and in

VOL. 117, No. J Whole Body Radiotherapy of Advanced Cancer 677
SURVIVAL COMPARISONS CANCER OF BRONCHUS WITH METASTASES
SURVIVL T Y E IN MONTHS
FIG. 3.
many cases this treatment was followed immediately by planned local therapy to various portions of the body.
If one assumes that all severe drops in blood cell count and all instances of hypo- cellular or acellular marrow a t death were due only to radiation and not influenced by the tvpe or extent of cancer and effects of previous therapy, then one can identify 8 cases in which there is a possibility of the therapy contributing to mortality. Of this subgroup, 2 patients received localized radiation between total body irradiation and death a t 31 and 32 days, respectively. Two had extensive previous chemotherapy and I also had local radiotherapy. In 2 other cases, autologous marrow transfusion was unsuccessful because the pruadiation marrow was hypocellular. Both of these latter patients had had intensive localized irradiation and I had received intensive chemotherapy.
TArrr IV
(15 Patients) CANCEL OF BLLAI1L5UIYIVAL POST D,
I .
I

67 8 Saenger CI of.
SURVIVAL COMPARISONS CAKSER GF BREAST WITH METASTASES
STD. ERROR 0 IS T . R . 0 RX. PTS. (U.CJ
I S IO 6 m V A L T I M IN MONTHS
FIG. 4.
Of the 19 patients who died within 2 d j o days, I I showed clear evidence of well func tioning marrow with steady or rising white blood cell counts and absence of bleeding and infection at the time of death.
The time from diagnosis to death of the z.+ patients entered in the study who were not treated has been analyzed. There were 4 who died in a 20-60 day interval:
Patients Total No. of rumiving m
in dying at 0 t h times
Patients not given radiation 4 20 14
Patients given radiation 19 63 82
Fisher’s exact probability test yields a p value of 0.16, indicating that there is no difference between the 2 groups. Therefore one may conclude that in other patients described, the effect of whole and partial body radiation therapy was less important in contributing to death than was the a-
tent of disease in these patients. Another interpretation would be that a physician selecting far advanced cancer patients for a given treatment would have about the same degree of difficulty in selecting any form of treatment for these very ill pa- tients. The same probabilities, p = o . ~ g , 0.2 and 0.21 are found for patients dying between o and 20 days post treatment, from djo days, and from 20-40 days, when compared to the untreated group. Current status of survival for these 88 treated pa- tients is as follows:
Prophylactic therapy @wing’s tumor) 3 Others surviving I s of August 31, 1972 7 Deaths possibly attributable to irradiation 8 Deaths attributable to tumor 70
88 -
REACTIONS nou TREATMENT AND ErrEcrs O t PALLIATION
The acute radiation syndrome develops in stages. In the prodromal stage, nausea and vomiting of a transient nature occur.

VOL. 117, No. 3 Whole Body Radiotherapy of Advanced Cancer 679
These complaints are often highly subjec tive; therefore, they are not discussed with the patient before treatment.
The analysis of our 88 treated patients shows that 44 per cent experienced no symptoms a t all, that 27 per cent had tran- sient nausea and vomiting within 3 hours, 14 per cent within 6 hours and 3 per cent within 1 2 hours. In only 4 patients (4 per cent) were the nausea and vomiting of a severe nature (Table v) .
These symptoms are no greater than found after surgery or after treatment with cancer chemotherapy drugs, the reactions of which are often far more severe than those from these kinds oi radiation therapy. Lahtri et observed that when 5-fluorcr ura . I is given orally a t a dose of 1 5 mg./kg. daily for 6 days, and then weekly a t the same dose, nausea, vomiting, diarrhea or stomatitis are found in 5s per cent of the patients treated, and marrow depression is observed in 50 per cent. A recent study by the \Yestern Cooperative Cancer Chemo- therapy Group, employing 5-fluorouracil without a loading dose a t 15 mg./kg./wk. for ii month, reported mild to major gastrcr intestinal or liematologic toxicity in 85.5 per cent of430 patients." Higyins rt aL1* in treating cancer of the colon using 12 mg./ kg. of fluorouracil intravenously for 5 successive days, observed that 27.9 per cent of 359 patients experienced a toxic reaction. T h e same group reported one or more sur- gical complications following resection of colon carcinoma in 29.6 per cent of 433 patients. Parson~etn l . '~ note that 61-72 per cent of patients suffering from so-called radiation sickness responded favorably to placebo medication, indicating that sug- gestibility may have a big part to play in the appearance and control of these symp- toms. Mukherji et nLs' in evaluating the effectiveness of a combination of 4 drugs in the treatment of 23 patients with lympho- sarcoma and reticulum cell sarcoma found severe myelosuppression in 4 patients (17 per cent) and possibly attributed this de- pression to their deaths from infection.
Dur;ng the latent period of 18-21 days
TABLE V INCIDENCE or N A U S E A AWD VOMITING I N 88 CANCER
PATIENTS RECEIVING W H O L E AND/OR PARTIAL BODY RADIATIOW T H E R A P Y
Patients Per Cent
39 44 No nausea or vomiting Nausea and/or vomiting up to
Nausea and/or vomiting up to
Nausea and/or vomiting up to
Nausea and/or vomiting up to
Nausea and/or vomiting up to
Nausea and/or vomiting 48
3 hours after R. 23 27
I2 1 4 6 hours after R.
3 3 I z hours after R,
24 hours after R, 7 8
- 48 hours after R. 0
hours + 4 4 - - 88 1 0 0
the patient is asymptomatic. The period oi manifest illness then begins with evidence of malaise, infection and bleeding. These findings occur only with whole body irradi- ation and not with partial body treatment. Also when marrow is successfully replaced these findings do not occur.
In regard to palliation, a review of pa- tient records shows that some palliation was achieved in 56 per cent and that 31 per cent were made neither better nor worse (Table VI). In another 3 cases we were unable to obtain follow-up history concerning pallia- tive effects. The 3 cases of Ewing's tumor are not included in this table as therapy was prophylactic.
POSSIBLE UXIQUE MECHASISLlS Or W H O L E A I D PARTIAL BODY IRRADIATION
\Vhole body irradiation in the doses reported herein could be effective against cancer in several ways: ( I ) alteration of the immune mechanism of the body altering the balance in favor of the host; (2) by a direct effect on the metabolism of the can- cer cells. In this case wide-field radio- therapy would have one advantage over drug therapy, since it would reach all can- cer cells without depending upon blood
.

680 * Saengv et a!. MARCB, r973
TABLE VI PALLIATIVE EFFECTS. O F TREATMENT
(85 Patientst)
Per Cent
Relief of pain 31 Decrease i n tumor sire 3’ Increase in activity 13 Increase in well being (weight gain, a p
petite improvemenr, subjective rtate- ment by patient) 30
One or more of the above 56
KO change 31 Lost to follow-up for evaluation of palli-
ation 4 Death between 20 and 60 days possibly
attributable to radiation 9
In oome of the patienu there was more than one indication of
t 3 children rich Ewing’s tumor reaired pmphykt ic treat- impraremeat; thus, the percencagcs exceed 100 per cent.
m a t and ut not included in this analysis.
supply, or chemical and pharmacologic distribution.
Partial body irradiation could be com- pared to regional isolation perfusion with antineoplastic drugs, again being certain to reach ail tumor cells within the irradiated volume and lacking the more hazardous systemic effects of total body irradiation.
The effectiveness of both methods may be explained by the fact that small tumor foci are more sensitive to treatment than large foci ar.d that single cancer cells are more susceptible than clumps of cells.
PSYCHOLOGIC AND PSYCHIA7WC EVALUATION OF PATIENTS
A unique and important aspect of the research work in this project has been the attempt to evaluate and distinguish bG tween the manifestations of cancer and the etTects of radiation therapy in regard to psychologic and psychiatric changes. For example, others have reported on personal- ity types in certain cancers,’ but no studies were presented investigating the effects of
In 1969, we reponed on the effect of trUtmCnt.
total and partial body irradiation on the cognitive and motional processes of 16 patients.” This number has been increased to 43. These studies consisted of adminis- tration of a battery of tests to each patient in the pretreatment phase, during sham and actual treatment and during a 6 week post-treatment period. Tests which have been utilized included the Halstead Bat- tery, Rechsler-Bellevue Adult Intelligence Scale, some tests of intellectual impairment modified from Reitan, and the 5 minute verbal content test of Gottschalk and Gleser. There has been some change in the several tests which we have been using during this phase of the total project; i.e., not all tests have been used continually.
In the baseline data of39 patients tested, the median intelligence quotient was 87 and the mean also 87. There were 41 per cent of subjects with I.Q. values of 95-1 16,47 per cent between 71-35, and IZ per cent be- tween 63-70. The distribution of intelli- gence factors as measured by several tests is representative of the population served by the General Hospital.
I t is clear that the intensive study and the above testing have had a helpful effect in increasing the level of motivation to cooperate, as exhibited by all patients so studied.
The need for careful handling of the cancer patient by all members of the medi- cal team is emphasized by the consistent evidence of depression over the 7 week study period. The depression is lessened with clinical improvement and attention to patient needs. I t is also less in patients with long survival (over IOC, days) as would be expected. Similarly, hope is directly re- lated to survival. Anxiety dips sharply during sham treatment; i t increases just prior to actual treatment, then decreases and levels off. Outward hostility tends to increase a t the time of post sham treat- ment, then dips and remains quite stable. Hope as measured by the content analysis of verbal behavior is related to satisfactory human relations in the patient’s life situa- tion.

VOL. 1x7, No. 3 Whole Body Radiotherapy of Advanced Cancer 68 I
U S E OF AUTOLOGOUS BONE MARROW
TRANS PLA NTATION
Because of radiation-induced hemato- logic depression, autologous bone marrow storage and reinfusion were instituted in 1964. Employing the method of Kurnick,” marrow was removed from the posterior iliac crest under local anesthesia, to an average value approximating 300 cc. I t was mixed with Ospod-glycerol medium and stored a t -83” C. following a programmed temperature reduction of I’ C. per minute. Prior to rtinfusion dextrose was added, and then the marrow was given intravenously, initially without filtration, a t a rate of 50 to 62 cc. per minute. The first 2 patients who received a marrow transfusion in our study, Patients 051 and 053, were infused with frozen marrow 24 and 19 days post irradiation, respectively, a t a time when the marrow sinusoids were relatively empty of precursor cells, with the expectation that there would be more room for the trans- plant to take. hiarrow viability in these 2 procedures was 5 5 and 57 per cent.45
Patient 05 I experienced moderate herno- globinuria not seen in Patient 053 after infusion. Rlarrow was given in both cases 2 to 3 weeks post irradiation; hence, it was impossible to distinguish spontaneous mar- row recovery from successful marrow auto- transfusion.
Because hemoglobinuria had been noted, a triple filter system was developed and marrow iutotransplantations on Patients O ~ O , O ~ ~ , W ~ , O ~ ~ , W + O ~ I ~ 9 5 , ~ 8 , 0 9 9 , 137 and 1 1 1 have all been performed em- ploying this filter system.‘*
In marrow transplants of Patients 070, 077, and 078, the delay between the re- moval of marrow and transfusion was i I , 2 and o days, respectively. The platelet count of Patient 078 never fell below 1 2 5 , m per rnm.s, brit the white blood cell count dropped as low as goo, suggesting possible effectiveness of the technique for the first time.
For the ncxt 8 patients the technique was therefore modified, so that a larger volume of marrow (coo cc.) was removed
from the parient under general anesthesia. The patient was then irradiated and the marrow replaced intravenously on the same day as it was removed. The results in Table VIX indicate the success attendant on the modification of this procedure. Five pa- tients receiving 200 rads of whole body radiation showed mean white blood counts to be 2,820 & 804 cells per mm.’at the nadir. In .7 patients given the same dose but no autograft, the level a t the nadir was 850 f380 cells per mm.’, the 2 means being significantly different (Table vm). The first patient transplanted with our new technique (Patient 087) was followed in the Clinical Research Center, Cincinnati Chil- dren’s Hospital, for over 6 weeks without any evidence of illness. Subsequently pa- tients receiving these whole body doses have only been hospitalized for a total of 5 days or less. The degree of marrow depres- sion in the successfully transplanted pa- tient is such that hemorrhage and infection are not observed.
The 3 failures in the revised transplanta- tion technique have been Patient qo, ogg and 107. Patient ogo suffered a cerebro- vascular accident unrelated to her tumor or her radiotherapy. The latter 2 patients (ogg, 107) had had widespread radicr therapy which had affected the reticulo- endothelial framework necessary for stem cell development, and preliminary cell aspirates in allegedly unirradiated areas did appear hypocellular. Patient 107 ap- peared to possess normal granulocyte re- serves, one of our marrow screening param- eters, only because we were given an in- correctly high body weight on which to base our etiocholanolone dosage, thus falsely elevating the marrow granulocyte reserves. From this unfortunate experience we now insist that a candidate for marrow autotransplantation have a normal iliac marrow aspirate histologically, a normal bone marrow scan employing technetium ggm sulfur colloid, and normal granulocyte reserves measured with etiocholanolone (after we weigh the patient) as indicators of normal marrow function, ,4t autopsy, Pa-
c
L

68 2 Sacnger et af. M A ~ C M , 1973
TABLE VI1 WHOLE BODY IRRADIATION WITH YARROW TRANSPLANTATION
051 Auro 150 4/6/65 5/1/65 5/15/65 1 . 6 X I d 55% Y a t)kmagkbinuri.far Did not uke d.T
053 Auto am I/ 4/65 I/ 8/65 5/17/65 1.4 X 1 d n% Y a Woac Did mot take
40 Auto 1 5 0 I/ 4/65 3/ 1/67 3/13/67 o . n X i d 68% Y a Noac Did mu take ~~~
Auto am 10/31/67 I I / 7/67 I I / 9/67 o . i r X r d 48% Y a Huoapbbiauriaforra Did not ukc haur
4 8 Auto am I I / 4/67 la/ 5/67 la/ 5/67 4 . 1 6 X i d 96% No Nmc
087 1- am 3/ 3/69 a/ri /69 3/ 3/69 4 . 3 8 X r d 99% No Noac Take
TABLE VI11 KESULTS 01 SUCCJSSTUL 110- AND AUTOTUNS?LANTS Or YARROW A n E .
200 LADS XIDLINE WHOLE BODY IKKADIATION
Nadir Nadir '--I1- ' Study No.
4 7 26 2,Ioo 091 25 4,100 095 33 9,700 098 28 2,- 1 x 1 31 3 ,-
M a n 28.6 2, 8mf 804 t M u n of Con&* 24 85of380t
1.6Xrd 1.3X1d 0.6Xro' I. 7 X 10' I .4X 1d I.~XId -

683 VOL. 117, NO. J Whole Body Radiotherapy of Advanced Cancer
tient ogg, who died on Day 31 post irradia- tion, had widespread carcinoma of the pancreas. Patient 107 survived her pancy- topenia without any evidence of sepsis. Patient I I I had no significant cytopenia and her hospitalization (including auto- transplant) lasted only 4 days.
This technique has been of advantage in simplifying the patient’s course and elimi- nating the long period of hospitalization needed prior to transfusion. The possibility of reinfusing tumor cells in the untreated marrow exists, but the elimination of this problem awaits the development of suc- cessful methods of marrow allotransplanta- tion.
S L‘MMA RY
I . Whole and/or partial body radiation therapy given in single doses has shown beneficial effects in the control of certain advanced cancers. T h e palliative cffects compare favorably with results using anti- cancer drugs as commonly reported in the medical literature.
Irradiation certainly seems to improve survival in the untreated patient with cancers of colon, lung and breast.
2. The use of autologous marrow reinfu- sion immediately after radiation therapy minimizes the characteristic marrow de- pression otherwise observed. The degree of illness following infusion is greatly lessened and hospitalization greatly shortened.
Eugene L. Saenger, M.D. Radioisotope Laboratory Cincinnati General Hospital Cincinnati, Ohio 45219
REFERENCES
I. ASDREWS, G.A., COMAS, F. V., EDWARDS, C. L., KNISELEY, R. M., LUSHSAVGH, C. C., and VOWPICK H. Hematologic and therapeutic effects of total-body irradiation (5oR-1ooR) in paticntl with malignant lymphoma, chronic lymphocytic and granulocytic leukemias, and polycythemia vem. USAEC. Division of Technical Information Extension, Oak Ridge, Tennessee, ORAU-I 12, Biology and Medicine, T l D - 4 5 ~ , December, 1970.
1 BAHNSOS, C. B. Second conference on psycho-
physiological aspects of cancer. Ann. New l’mk A d . Sc., 1g&,164,307-6;4.
3. BORTIN, M. Compendium of bone marrow trans. plantation. Tranrp&nfafion, 1970, 9, 571-587.
+ BUCKNER, C. D., EPSTEIN, R., RUDOLPH, R., CLITT, R., STORE, R., and THOMAS, E. Allo. genic marrow engraftment following whole body irradiation in patient with leukemia. Blood, 1970,35, 741-750.
5. BEIERWALTES, W. H., HAYKIT, T. P., and No- PAL, M. hi. Treatment of thyroid carcinoma with lUI: results at fourteen years. Y.A.M.A., 1963, f J3,30?34.
6. CAHPBLLL, A., GODLEE, J. N., EMERY, E. W., and PRASKERD, T. A. Diagnosis and treat- ment of primary polycythemia. Loncet, 1970, I, 1074-1077.
7. CHAOUL, H., and LANCE, K. Ueber Lympho. granulcrnatose und ihre Behandlung mit R6ncgcnstnhlen. Mtinchcn. mrd. Wchnschr.,
8. CHEN, LIVEN, KEREIAKES, J. G., FRIEDMAS, B. I., and SAESGER, E. L. Radiation-induced urinary excretion of deoxycytidine by nu and humans. Radiology, 1968,91,343-348.
9. COLLISS, V. P., and LOEPFLER, R. E(. Thcrapeu- tic use oi single doses of total body radiation. AM. J. RQENTGESOL., RAD. THERAPY 8: S u -
IO. CORWIX, S. H. Phosphorus 32 in advanced car- cinoma of prostate. 7. Urol., 1970, 104, 745- 748.
XI. GOITSCHALK. L. A., KUNKEL, R., WOHL, T. H., SAENGER, E. L., and WISGET, C. N. T o d and half body irradiation: effect on cognitive and emotional processes. Arch. Cm. Prychiat.,
12. HICGISS, G. A., DWIGHT, R. W., SMITH, J. V., and MEEHS, R. J. Fluorouracil as adjuvant to surgery in carcinoma of colon. A.M.A. Arch. sm., 1971,f02,339-343.
13. HOLLCROFT, J., LORENZ, E., and HUKsnCEx, H. Effect of ionizing radiations on transplanted lymphosarcoma. 7. hkI. Cancer Inst., 1950, 11, 1-16.
14. HOLLCROET, J., LORENZ, E., and MATHEW, M. Factors modifying effect of x-irradiation on re- gression of tnnsplantcd lymphosarcoma. 7. Nut. Cancer lnjt . , 195% 11,751-763.
15. HOLLCROFT, J., and MATHEWS, M. Effect of ionizing irradiation treatments on tumor re- gression. 3. Nut. Cancer Inst., 1953, f/, 5 2 7
535. 16. Horwln, H., WRIGHT, T. L, PERRY, H., 8nd
B A R R ~ , C. M. “Suppressive” chemothempy in bronchogenic carcinoma-mndomizcd pr~r- p c t i v e clinical trial. AM. J. ROE~TCENOL., RAD. Tnrurr 81 ~ U C L E A R him., 1965, 93, 61 5-638.
1923,70,725-717*
CLEAR hf ED., 1956,75, 542-547.
1963,2l, 5-74-90.
..

684 Sacnger et al. M A ~ C H , 1973
17. JACOBS, E. M.,REEvu,W. J., WOOD, D. A., PUCH, R., BMUNWALD, J., and BATWAN, J. R. Treatment of cancer Gth weekly intra- venous 5-fluorouracil. Cuncrr, 1971,27, 1302- 1305.
18. JACOBSOS,L.O., hfARKs, E. K., ROBSON, M.J., GASTOS, E., and ZXRKLE, R. E. Effect of spleen protection on mortality following x- irradiation. 7. Lob. &? Clin. Mcd., 1949, 34, 153&1543*
19. JACOBSOS, L . O . , S I U M O S S , E . L . , ~ ~ A R K S , E . K., and ELDREDGE, J. H. Recovery from radiation injury. Science, 1951, rr3, 51cr511.
and S P R A ~ , J. S. Factors influencing survival in patients with untreated hepatic metastases. surg., Gynec. e Ob~t . , 1968, 127, 1-1 I .
21. JESUSS, R. D. T., RIDER, W. D., and SOKLEY, Xi . R. Ewing's sarcoma-trial of adjuvant total-body irradiation. Radiology, 1970, 96, 151-1SS.
22. JOHESOS, R . E. Ray of hope in lymphosarcoma. Medical World Ncws, 1970, rr, 23.
2;. JOHSSOS, R. E. Total body irradiation of chronic lymphocytic leukemia: incidence -nd duration of remission. Cuncrr, 1970, 25, 5 2 s 5-30.
q- JOHSSON, R. E. Total-body irradiation with fractionated dosage schedules. FrontirrJ Rad. Therap. ~ O n c o l . , 1968,3,152-162. S. Karger,
20. JAFFE, B. hf., DOSEGAS, I\'. L., \\'ATSON, F.,
.
A.G.,'Basel. 15. JOHSSOS, R. E., FOLEY, H. T., SWAIS, R. W.,
and O'COKKOR, G. T. Treatment of lympho- sarcoma with fractionated total-body irradia- tion. Cancer, 1967,20,482-485.
26. JOHKSOS, R. E., O'Cosson, G. T., and LEVIS, D. Primary management of advanced lymphosarcc,na with radiotherapy. Cunccr, 1.9% 25, 78779r-
27. KEREIAKES, J. G., VAN DE RIET, R., BORN, C., Errsc, C., SILBERSTEIN, E. B., and SAENGER, E. L. Active bone-marrow dose related to hematological changes in whole-body and partial body %o gamma radiation exposures. Rodiolou, 1971, ro3,65 1-656.
28. KurNIcrg N. B. Autologous and isokgous bone marrow storrge and infusion in treatment of rnyelosuppmion. Transfusion, 1962, 2, 178- 187.
29. LAHIRI, S. R., BOILEAU, G., and HALL, T. C. Treatment of metastatic colorectal carcinoma with fluorouracil by mouth. Cancrr, 1971, &901--906-
3. L o E r n E R , R. K., Coiilxs, V. P., and HY- MAN, G. Comparative & ~ t s of total body ir- radiation, nitrogen mustard and methylene- melamine on hematopoietic system of terminal cancer patients. Science, 1953, rr8,161-163.
31. MAxnzLD, J. R., JR. UK of radioactive phoc phonu and cutoatcrone in tracment of
metastatic lesions in bone from breast and prostate. Int. 7. Appl. Rad. U IJOIO~CI, I 956, 1, 133-134.
31. MEDINCER, F. G.,and CRAVER,L. F. Total body irradiation with review of cases. AM J. ROEKTCESOL. & RAD. THERAPY, 1942 48, 651-671.
33. hfiLBuus, L. F., O'GRADY, L., and HESDYICK- SON, F. R. Radical radiation therapy and total body irradiation in treatment of Ewing's sar- coma. Cancer, 1968,22,91g-g15.
34. MUKHERJI, B., YACODA, .4., O E ~ G E S , H. F., and KRAKOFF, I. H. Cyclic chemotherapy in lymphoma. Canccr, 1g:1,28, 866-893.
35. PARSONS, J. A., \VCBSTER, J. H., and DOWD, J . E. Erahation of placeboeffect in treatment of radiation sickness. Artu radio/., 1961, 56. 12p-1+0.
36. PECG, D. E. Bone hlarrow Transplantatim. Year Book Publishers, Inc., Chicago, 19%. pp. 102-1 12.
37. PESTAFA, C., REITEMEIER, R., hloEuTu, C.. JL'DD, E., and DOCKERTEY, hi. Natural h:>- tory of carcinoma of colon and rectum. Am. 7. Surg., 1964, 108, 826-829.
38. RAPOPORT, A., and BURLESOS, R. Survival cf patients treated with systemic fluorourat i t
for hepatic metastases. Surg., Cynec. e Obn.. 1970, f30,773-777.
39. RIDER, W. D., and HASSELBACK, R. The symp- tomatic and hematological disturbance follou- ing total body radiation of 300 rad gamma-rap irradiation. In: International Conference on Guidelines to Radiological Health, published as #999-RH-33, U. S. Bureau of Radiological Health, USPHS, Rockville, hlaryland, 1968, PP. 139-144-
40. SAEWER, E. L. Metabolic changes in humans following total body irradiation: report for period February, 1960, through October, 1961. Defense Atomic Support Agency Report.
41. SAESCER, E. L. Metabolic changes in humans following total body irradiation: report for period November, 1961, through April, 196;. Defense Atomic Support Agency Report, DASA 1411.
42. SAENGER, E. L., FRIEDMAS, B. I., KEREIAKES, J. G., and PERRY, H. Metabolic changes in humans following total body irradiation: re- port for period May, 1963, through February, 1 964. Defense Atomic Support Agency Report, DASA 1633.
43. SAENCER, E. L., FRIEDMAN, B. I., KEREXAKES, J. C., and PERRY, H. Metabolic chanqer in humans following total body irradiation: re- port for period February, 1960, through May. 1966. Defense Atomic Support Agency Re- port, DASA 1 8 6
u. SAENCER, E. L., FRIEDMAN, B. I.,Horu*m, H., KERE~KU, J. G., and PERRT, H. Metabolic

c-
V o r . 2 1 7 , No. 3 Whole Body Radiotherapy of Advanced Cancer
changes in humans following total body ir- radiation: report for period May, 1966, through April, 1967. Defense Atomic Support Agency Report, DASA 2179.
45. SAENCER, E. L., FLIEDMAN, B. I., HORWITL, H., and KEREIAKES, J. G. Radiation effects in man: manifesudons and thenpeunc efforts: report for period May, 1967, through April, 1968. Defense Atomic Support Agency Re- port, D.4SA 2168.
46. SAENCER, E. L, SILBERSTEIN, E. B., HOR- wm, H., KERLIAKES, J. G., CHEN, I-WEN, WINCET, C., GLESER, G. C., and KUNKEL, R. L. Radiation effects in man: manifestations and therapeutic efforts: report for period May, 1968, through April, 1969. Defense Atomic Support Agency Report, DASA 1428.
47. SAEHCER, E. L., SILBERSTEIN, E. B., AROK, B. S., HORWIIZ, H., KEREIAKES, J. G., CHEK, I-WEK, WIKCET, C., and GLESER, G. C. Ra- diation effects in man: manifestations and therapeutic efforts: report for period May, 1969, through April, 1970. Defense Atomic Support Agency Report, DASA 1599.
48. SAESCER, E. L., SILBERSTEIX, E. B., AROX, B. S., H o n w ~ n , H., KEREIAKES, J. G., CHES, I -W'ES,WISCET,C. ,~~~ G L E S E R , ~ . C. Radiation effects in man: manifestations and therapeutic efforts: report for period May.
685
1970, through April, 1971. Defense Nuclear Agency (formerly Defense Atomic Support Agency) Report DNA 2751 T.
49. SAHP, R. J., and A N S ~ E L D , F. J. Breast cancer created with fluorouracil. Y.A.M.A., 1966, Jp8,724-730.
50. SILBERSTEIN, E. B., CHEN, I-WEN, SALNCER, E. L., and KEREIAKES, J. G. Cytologic-bio- chemical radiation dosimeters in man. In: Bio- chemical Indicators of Radiation Injury in Man. Intern. Atomic Energy Agency, Vienna, 1971, pp. 181-114.
51. STEARNS, M., and BINKLEY, G. Palliative sur- gery for cancer of rectum and colon. Conrcr,
52. Subcommittee on Breast and Genital Cancer. Androgens and estrogens in treatment of dis- seminated mammary carcinoma-retrospec- tive study of 949 patients. Council on Drugs. Y.A.M.A., 1960,~7.?, 1271-1283.
53. THOMAS, E. D., BUCKSER, C. D., RUDOLPH, R. H., FEFER, A., STORB, R., NEIMAN, P., BRYAXT, J., CHARD, R., C L I ~ ~ , R.,EPSTEIK, R., FIALKOW, P., FUNK, D., GIBLEIT, E., LER- K E R , K., REYNOLDS, F., and SLICHTER, S. AI- logeneic marrow grafting for hematologic ma- lignancy using HLA matched donor-recipient sibling pairs. Blood, 1971,38, 167-287.
195-47, 1016101g.


UCCM / RCC 1.958099.001
(COPY)
AMERICAN COLLEGE OF RADIOLOGY: 20 NORTH WACKER DRIVE CHICAGO, I U l N O l S 60606 (312) 2364963 WASHINGTON OFFICE: 6900 WISCONSIN AVENUE CHEW CHASE. MARYLAND 2001f (301) 651-6900
The Honorajle :.like Gravel 1251 X e d Senats Off ice Building Washington, 3. C.
Dear Senator Gravel:
This l e t t e r reprasents our response t o your r ecues t of u s t o inqxi re i n t o t h e whole-body zaEi+ticr. therapv s z o j e c t heir,? conducted by O r . Eugene L. Saenaer and h i s col leacues a t :he i lniversit ir cf Cinc inna t i . :.!e have male our ir.quiry and our broad conclusions a r e as follows:
1.
2 .
3 .
4.
5.
I n =?e ~cr r r r s l c m t e x t of a c l i n i c a l i nves t iqa t ion , t he p ro jec t i s v a l i e l y conceived, s t a t e d , executed, cont ro l led and followed u_o. me appropriate s c i e n t i f i c a d profess icna l conni t tees of t h e Univers i ty of Cincinnat i have pe r fomed t h e i r funcrions during the ccurse of the projec t .
The ?recess o f p a t i e n t s e l e c t i o n based uton c l in ica l considerat ions confoms w i t h good medical p rac t i ce .
The records, publ ica t ions and s a t i e n t f01lo-~-cp are voluminous and ccrzendable.
The Fzocedure used f o r ob ta in ing p a t i e n t csnsent is v a l i d , t!!oron:n a!?& cons i s t en t -..:it:? t he r e z c x e n c a t i o n s of the : :a t ionzl I n s t i r L t e s of Healt' 2nd w i t h t he p r a c t i c e of nos: cancer centers .
Should t!is p r o j e c t come before the Senate o r one of i ts co rn i t t ee s i n some fashion, we would urge your s u p o r t f o r i t s cont inuat ion.
Thouah rhys ic i r r . s Bo no t i nva r i ab lv share w i t 5 t!!e p u b l i c the ways i n which they rezci-i p rofess iona l conclusiozs , w e th ink it approgr ia te t o your inquiry t o d e t a i l belcv the wzy i n ;;;iich we reached t!!ese conclusions. of your reques t ras based 'iaon t'-e r e a l i z a t i o n cha t s ena to r s have need of exper t , in - r t ia l x e z i c a l a d scientific aBl-ice i n eva lxa t inq cm.plex biomedical sroblems. Should you d e s i r e f u r t h e r in forzzz ion , w e w i l l again endeavor t o be responsive.
Our accc3tznce
'Pie c o r i t t a e
As I noted i n 2; e a r l i e r l e t t e r t o you, the College i s seldorn c a l l e d uFon t o inves t iqa t e the s c i e n t i f i c e f f o r t s of arf of i ts members and thus has no s tanding c o m i t t e e wit5 suck a charge. and a t h i r d d is t inguished physician t o undertzke the inqui ry . They are:
Ins tead , I asked t w o leading r a d i a t i o n t h e r a p i s t s

P Page 2
D r . Henry Kaplan, chaiLza3 ar.d c r o f e s s o r of radiology a t S tanford 'Jni;-er,e:t.l Medical Scliool i n Pa lo X l t 3 , t a l i f 3 r n i a . Dr. Kanlan is i n t e r n a t i c n a l l y k?.c;:n f c r h i s p ioneer ing ;:ork i n s e v e r a l arsas of cancer thera7.l. va r ious cancer s tgdv and advirory grca?s i ac lud ing t h e Coz- l i t t s s of C o r , r u l t ~ ~ , r i l s t o Conquer Crncer :,*Zich r e c e n t l y advised the Ssna te .
o f p a t i e n t s . C r . Xaplan i s c u r r e n t l y chzi-man o f oc r Cax i i s s ion on c a n c e r .
E e h a s S s ~ n a s e r j z r c f
iiis exter?sive Sibl iccra>- , ; l inc ludes d e s c r i 3 t i c n s of h i s Kork on Eoeqkin's d i sease involv izq extezci;-e r ~ c ~ t ; : = : _ .
O r . F rank R. Hendrickson, c h a i m a n of the 2eFartment of r a d i a t i c n therapy a t C h i c a ~ o ' s ? r s s = y t 2 r i m - S t . LILke's i-iosnital. O r . Eenzrickson is 2150 a fac:::t-? mer-ker of t:;e u n i v e r s i t y of I l l i r . o i s CollcTe of ?!edicine and t h e ?ush :.:nfic11 College as we11 a s a c m s u l t m t t o tP.e V e t e r m s Adn in i s t r a t ion and a ? .=xer 0 5 var i cus x t i c n a l c a ~ c e r 503ies. ?is b i b l i o c r a $ i y incl-ic?es rec3rts of h i s trz:z.-.~zz of c h i l d r e n a f f i i c t e d *,rich Z:.rina's sarcoid with r a z i a t i o n . i-le i s t h e ? r e s e n t chaim.an of ou r C m z i s s i o n on 7.adiation Therapy.
O r . Sanuel Taylor, 111, a d i s t i n * p i s h e d i n t e r n i s t and o n c o l o g i s t a t PzesbyteriLn- S t . ~ u k e ' s Hos?rtnl i n ChicaTo. Ae i s thc founder of t h e a e r i c a n Col?eqe of Phys ic ians cancer 2rogra-T. !ie i s a ? ro fes so r of rtcdicine a t Xusn. S r . T a y l o r ' s wide experience as a s e n i o r inves t iqaLor i n t!ie f i e l d of cancer provided u s v i 5 a view f r o a ano tne r d i s c i 2 l i c s . ne i s a long t i n e e x p e r t i n checotkerasy of. disseainatec? cancer .
!4r. Otha Linton, d i r e c t o r of ou r Xashinqton Df f i ce , provided s t a f f suppor t t o t!.e grour, and coord ina ted t.?eir i n q u i r y with O r . Saenger and h i s c o l l r a q u e s .
D r s . %plan and Xendrickscz ar.d X r . Linton net w i t h Dr. Saenger and 3 r . Ckarlz; !,I. Barret t , d i r e c t o r of r s d i a t i c n tAera?y a t t h e Univers i ty of Cincir,.-.ati, ::ay;e:.z?~- 29 i n Chicaqo. The d i s c u s s i o n covered the back3round of t h e pro?e!ct and cbe purposes , o b j e c t i v e s and. achievenents of the e r ' for t t o d a t e . D r . Szer,ger tk.er. provicied the c c m i t t e e wi th pUjlis!ied Fapzrs and suzmar-r r a t e r i a l s about <-&e p r o j e c t .
Cn Decenker 16 , D r s . Kaplan, Hendrickson and Taylor met i n CiRcirinati *:it5 C r . Saenqer , o t h e r mexbers of h i s tea? , tVA.o neyhers of the Un ive r s i ty of C:?: : : .Y- . - - human i a v e s t i q a t i o n cc r rn i t t ee , an2 the c h i n a 3 of the s p e c i a l universr::! cz.---i t tes which vas c r e a t e d by t h e p r e s i d e n t t o review *.e p r o j e c t .
_ _ - 7
Those i n t e n i e w e d were, f r o 3 t h e UC Xunan Research Comrillttee, D r . Eveivn T!. Cess, p r o f e s s o r of ned ic ine and D r . Harvey C. Knowles, Jr., g r o f e s s o r of medicine, f r c n t h e s p e c i a l u n i v e r s i t y c o n n i t t c e t o zeview t h e Sacnger p r o j e c t , Dr. Raymond ?..
Suskind, F r c f e s s o r of envlror.:.i2ntal k .oa l th and nedic inc , from t h e de;a::r.ezZ ~f radiolo9. i ar.d t h e s tudy tezm, Drs. Char les M. B a r r e t t , Harry !!o-mitz, Ber-ard S . Aron and Zd..-aru B. S i l j e r s t e i n , p h y s i c i s t s , Drs. I-Wen Chen and Janss G . i :er i ixes , and t h e psychologis t , ;4rs. Carolyn N. Singet .

P Page 3
D r . Saenqer and everyclne a t the u n i v e r s i t y were Wil l ing t o recognize our competence and t o coo_zera% f'1ll:l w i t ; ? o u r i nqu i ry . were extended f u l l cooaera t ion a n d can concl*ida t h a t they a??r i sed <- .CSP:T;?~
of the s i t u a t i o n t o the saze e x t e n t t h a t they vculd have nee2ed t o 23 2s menbers of an NIX s t u d y s e c t i o n o r s i t e revie?.< tean. Each se*er of t h e co------.= . - . . .L----
has served i n s u c h a capac i ty .
The COFinltt2e c e - k e r s
The c o m i t t e e viewed tkie p r o j e c t as it was d s s i ~ n e d - - - a s a c i i n i c a l InvestiTz'iz-.
Phase one in- res t iqac ions f o l l o : ~ b a s i c a n i x a l work and al-..rays preced? r z r i i : . ~ . ~ ~ ~ ? c l i n i c a l t r i a l s wnich cay o r nay not be j u s t i f i e d on t h e basis of the firs'; ?.--.- a p p l i c a t i o n s .
of a modzlit:J f o r t he c z r e o f cancer 3 s t i e n t s wit:? ex ta3s ivc and i n c i r b j l z C L Z ~ : C S . . .
I n the o p i z i c n of t he co'l--.ittee, t h e t e a ? a t C inc inna t i had abundant 5ases :n :?.e l i t e r a t u r e f o r c-dsrtakir ,q i t s stad-!. m e p a r t i c i p a n t s a r e fu l l l r q i a l i f i 9 j . :Q
undertake t h e i n v e s t i c a t i o n , 3of-1 f r o 3 the v i e + o i n t of ?cod s a t i e n t c z r e &?:
im2or tan t ly the p o s s i k i l i t g t h a t new and va luab le c l i n i c a l i n f o m a t i o n coalci 22 obta ined .
Our c o m i t t e e d i d not concern i t s e l f wi th t h e imp l i ca t ions which have been r z i s z d concerning p a r t i a l funding of t h e e f f o r t 5:' t ho Decarment of Defense. :u'e 2 id note t h a t EO3 fuzds were used on ly to s u p z o r t t n e l a b o r a t o r y and psychologica l s t u d i e s b u t n o t t k t r e a a e n t o r t h e care of Lhe ? a t i e n t . The b a s i c c o s t s w e r ? borne by t h e u n i v e r s i t y and i t s teacning h o s p i t a l s .
Because of th2 p e v a l e n c e of cancer which has been noted sa r e c e n t l y by t5.2 Senate , t he Eouse of Zepr s sen ta t ives and the P r e s i d e n t , t??ose charaed . . ~ i t h :?.e care of canc.er p a t i s n t s have n2ed f o r every ? o s s i 5 l e b i t cf i n f o n a t i o n c~r.c:r-.zr.; t h e rr,ethods and moda l i t i e s w!?ich we u s e t o t r e a t these p z t i e n t s . I n o x o? ln l c r . , t h i s g r o j e c t has t h e F o s s i S i l i t y of c o n t r i b u t i n g usef-11 c l i n i c a l in for r .= t ion .
I t is worth no t ing t h a t i f o t h e r s have had access on ly t o t h e r e p o r t s nade t o X? on its p a r t of t!!e p r o j e c t or i f thoy sonefiaw f a i l e d t o understand t h a t the Eayc of ex tens ive followup i n no way depa r t ed o r de t r aczed frorn fundanental preceszs of good s a t i e n t care, then it fo l lows t h a t they might reach conclus ions c i i fL~; - .nc- from those of o u r committee.
h e na tu re cf cancer i n v e s t i q a t i o n s and t r o a t 2 e n t
I n c l i n i c a l i n v e s t i g a t i o n s of cancer , tie are concerned both with the b a s l c c i r .zer p rocess and wit!! i t s m a n i f s s t a t i o n s i n huiians and s p e c i f i c a l l y i n t ! e r z t r ~ . - : s who p r e s e n t t h e m e l v e s f o r ca re . The t r e a t T e n t of 3n i n d i v i d u a l repres2nt-s 3 series of choices f o r h i s -hys i c i ans which are based u3on d i a g n o s t i c f i n i r i n g 5 37.2
t h e i r b e s t jud;eaent. Since hunans respond t o t h e a s s a u l t of cancer and ;3 ;:fe-:f t o t r e a t it a s uniquely a s +hey do to n o s t o t h e r t h i n g s , g e n e r a l i z a t i o n s b.e:? h:2ve s t a t i s t i ca l va lue b u t limited a 2 p l i c a t i o n t o ind iv idua l s .

Phys ic ians have th roe f?x2aTienta l z o d a l i t i s s which may be used s i n q l v c r cr .kir .e5 to a t t e n ? t t o cure o r c o n t r o l cancers . r a d i a t i c n and chemicals. of c e r t a i n c a t e r s involv ing the e d o c r i n e sys t en .
These a r e axtir2a:ive sar:ery, h i s ; ? er.=:;lr 2ozzones also ars used t o atter?.?t t o a l t .er t h e C C ~ U ~ C S
The choice of t r e a t r e n t m u s t be decided f a r each p a t i e n t . The 2ecFsicn i s k a s ~ e uPon the tyge of cancer , i t s l o c a t i m , i t s s i z e , i L s degree of s=.reed ar.6 ss2n t h e age and c s n e r a l h e a l t h of =?e p a t i e n t . ICeally, t he t h e r a p + a t i c Eecislcn ii Eade i n 3 cancer confer tnce invol*rinq 2n:isicians f r o 3 tho, d i f f z r e n t e i sc i? l inPi a s g r o ? r i a t s to t h e ~ r o b l e n a t hand. 9y t!!e nacure or' tha disease, m y cancez therany r u s t be re7ardaa as h e m i c . T?I~ caccer p a t i e n t n u s t a c c e e i l e s s e r p r c b a b i l i t i e s 3: success and ?.>re s t r i n g e n t s i d e e f f e c t s of treat?lgnt t5sn usua l ly b e f a l l s u f f e r e r s f r o 3 o t h e r d i s e a s e s .
T h i n g i s a l l i n p o r t a n t i n t!e t r e a t z e n t of most czncers . A small? e a r l v czncsr may be removed s u q i r a l l y o r destrovea wi th r a d i a t i o n . But i f t he cancer has begun t o s s r s a d beyond i t s o r i g i n a l s i t e and beyond t!!s s u r g i c a l o r r a d i a t i g n f i e l d , t \e d e s t r u c t i o n of t he prima,? l e s i o n w i l l no t s u f f i c e t o save the payient .
Unfor tuna te ly , nany p a t i e n t s s t i l l a r e diagnosed is having fa . r advanced c?ncer wnich r u s t b e judgsd u n l i k e l y to respond t3 any s t anda rd c u r a t i v e . eEf3rt. :?.25e
p a t i e n t s riay have uzderqone va r ious t r e a t z e n t s wi thout success . C r they nsy h?.:c- had a " s i l e n t " prirnary cancer wnich w a s d iagnased only az te r it Lcgan t o s;rca, through t h e body.
The phys ic i an having t h e care of a p a t i e n t with advanced cancer has t k e e _nrac:,:&i1 choices . One is to do noty ing , a l l o x i n g %!e d i s e a s e t o t a k e i t s c o u ~ c e . >..n,-z:-.zr is to a t t e n p t g a l l i a t i o n , an e f f o r t t o r e t a r d t h e tuztor growth and/or t o ease rc.5 p a i n of Lye p a t i e n t . The t h i r d is t o &:tc.?,t d r a s t i c or radical t t e a t r i n r s r.2:
cormonly accea ted as r e l i a b l e o r e f f i c a c i o u s f o r a a t i e n t s havisq a g r e a t e r E?.:-. 1 2
of success . The t h i r d apgroach c d f r i e s t h e lonc-shot F o s s i b i l i t y of d i r e c t ;J:-~-:=
g a i n . be learnecf f t o n t h e e f for t .
The 2oc to r and p a t i e n t :,nust agree t h a t something of b e n e f i t to o t k e r s 71:'
Thus, t h e e f f o r t t o improve cancer t r e a t x e n t s has been based upon t!!e f i r s t a g g l i c a t i o n of new o r qges t ionzb le tecnniques t o those Fat ieats having nothi:.: t o lose by t h e i r f a i l u r e because t h e r e is no known t r e a t m n t a v a i l a b l e . Ofzc? . , the e f f e c t i v e n s s s of t h e technique gcst bo neasured i n t i m e of s w v i v a l , r e l i c : L L pa in , o r froa c e r t a i n body seasurements , ra ther than i n terms of o v e r t t ux r d e s t r u c t i o n . E f f o r t s n u s t be made t=, i s o l a t e and ceasure t h e s p e c i f i c t i r r i nc , dosages, procedures and r e s t r a i n t s which czn be observed t o a l t e r the course '-: the d i s e a s e . >ken a form of t r e a t y e n t h a s besn shown t o have some neasuraol? b e n e f i c i a l e f f e c t on f a r advanced p a t i e n t s it can be corlsidared f o r gerieral : s e .

P Page 5
The na ture of cancer i n v e s t i c a t i o n r ecu i r e s t h a t nore t5an one t \ e r a p i s t - G : Z
undertake a neu noda l i ty a t each s t a5e cf i t s 6evelcpz.ent becore it c;n be 3ccz;zi. f o r genera l usage. such a s the advent of sugervol taqe r a d i a t i o n Sources then previous s t u d i s s r.&y be repeated w i t h T r o f i t .
I f an in;rOvemCn' i n scze tool ot resource becores a':aiLi3Lc,
Both the hiqh er.erqy r a d i a t i o n and the seve ra l chemicals now used i n cancer t?,erz;- have h a - n f u l e f f t c t s upon F a t i m t s . So does r a e i c l l surqery. The choice x s t 5s made t o r e f r e i n f rz r t curazivo e f f s z t s when the Ckstructior. of 5 s tiL:Cir :.:.=1il?
involv? u n a c c e ? z r j l e side e f f e c t s of a loca l i zed or sys tcTic naturc?. Tl-.us, e f c z z t r t o control o r r e l i e v e s i d e e f f e c t s are equal ly s i z n i f i z a n t with those t 2 destroy the tumor.
When r ad ia t ion i s used as t h e t m o r i c i d a l agent , t ! e e f f o r t is nade m iinit- its e f f e c t s by ta i lor in . ; t he dose t o the s u s F e c t z r ?a and k:r usinq a s e r i e s of t 3 1 e r q z - exposurss t o des t roy the ccncer c e l l s without dzraging v i t a l 0rqzr.s and a5)zcer.: noma1 t i s s u e s . I: a cancer i s widespread, then a t unor i c ida l dose of rs2iiz:cn presents pro3ler.s xhich, f o r t?.e r o s t p a r t , remain unsolved. Lesser arounts of r a d i z t i o n hive been used i n various ways as p a r t of e f f o r t s t o r e t a r d tumr q x - i t b . , t o r e l i e v e s a i n o r t o a l t e r t h e p a t t e r n of cancer development.
The l i t e r a t u r e of r a d i a t i o n therapy o f f e r s s u b s t a n t i a l n t z e r s of c i t a t i o n s of e f f o r t s t o use :;:?ole or F a r t i a l body r a d i a t i o n for the p a l l i a t i o n of advanced cancers. The conc l*s ion , broadly, must be t h a t t9e c m c e p t has not b?en s u f f i c r e ? z product ive to reczxaend gene ra l ly nor so l ack ing i n effect to be abandoned 2s an approach.
The Cincinnat i ?reject
The a c t u a l t r e a t y e n t of p a t i e n t s was begun i n 1960 by D r . Saenger and ?.is C O l i S d 7 ' . l F t
as a c l i c i c a l assessnent of the us2 of sublet!!al :;hole body r ad ia t ion f o r 2 . 2 p a l l i a t i o n of F a t i e n t s witS a v a r i e t y of disseminated cancers. The ? rer . i s s ;.as t h a t the l e v e l of r ad ia t ion s e i e c t e d would nave a retardar.t e f f e c t upon t h e crzitr. of t he t m o r c e l l s tkroughout the body and t h a t =?.e p a t i e n t , f o r t he m s t ?arc,, could t o l e r a t e t k e s i d e e f f e c t s of systemic r ad ia t ion .
The second p a r t of &the pre-ise was t h a t g a t i e n t s who were c l o s e l y fo l lo*<ed after t h e i r cancer t roatments could izci icate both the 2hys ica l and psychologi c a l r??c::c:.? to t h e the rageu t i c e f f o r t over a Fer iod of s e v e r a l weeks. provided a new dinension t o previous s t u d i e s of the use of whole body rad ia t rcn .
Beginning i n 1964 , t he group began t o use t he techniqu? of autologcus bote *=fr=v t r a n s p l a n t s as a Ceans of overconing the marrow ee9ress ion otharwise inescaTl-:e a f t e r :.:hole 5cC.y r a d i e t i o n . e x t r a c t i o n of 300 t o 600 cubic c e n t i z e t e t s (about a p i n t o r so) Of ; I a r f C w f x : l
the posterior i l i a c c r e s t j u s t before +he r a d i a t i o n -?sure. marrow i s f i l t e r e d and r e i n j e c t e d i n t o t he p a t i e n t . has succeeded i n ave r t ing most of the exter.ded r a d i a t i o n syndrome e f f e c t s observed i n p a t i e n t s i n t h i s series and i n o'-,her whole body s t u d i e s .
This c l i n i c a l assesx-?n:
??io t e c k i q u e a f t e r sore zodif i c a t i o n ir.volves c:.e
The sane da:!, ' I?c As a c l i n i c a l p r?ccd=r l , =?.:S
?re . r i ? ' L = :

Effcr t s t o minimize l a t e e f f e c t s , such as t h e drop i n w1:ite c e l l s and p l ~ t d ~ : ~ and the decrease i n red blood C e l l s which arb cl-assic t o xadiayion syz?r;3-y:~, =s;ar: i n 1965. t he raay , became p r a c t i c a l e a r l y i n 1969
T h i s method us ing autologous bone marrow i m e d i a t e l y a f t e r radiar-ion
The concept of whole body r a d i a t i o n as a ne thod of tr23ti;?? cmcsr i s n o t XIJ
with the C i n c i n n a t i ?reject.'
t o hunan t ux r s . e f f o r t s i n 1923. X review of r e z o r t s t o 1942 shsrizd a3re than 270 _ = . a t l e n t 5 t-;:; t r e a t e d r;ith f a i r l y l i t t l e e n t o u r a g e x n t . S ince these z s t i o n t s ir. a l l ctszs :-.i2 disseminated t~?.crs and t h e r a d i a t i c n sources a v a i l a j l e .#:?re i n t h e orti;ovoltz:? range, t h e r e s u l t s Tiere n o t s u r 2 r i s i n g .
The advent of s u ~ e r v o l t a q 2 g e n e r a t o r s end p a r t i c a l a r l y c3balt 63 E O ' J r t e i crs-.=ztc! a d d i t i o n a l s t u 2 i e s t o a s s e s s t h e e f f e c t o f h ighe r energy r a d i a t i o n ar , l l e 3 t:, 2
new rcund of s t u d i e s . I n 1953, '1. E). C o l l i n s and R. i;. L o e f f l e r cc l l -?d <..e vsc of 200 rocntqens xhole body "a u s e f c l a d d i t i o n t o t h e 2anagement of advznced cancer."
There i s voluninous l i t e r a c u r e r e ; o r t i ~ l ~ ;C:ZTS i1.l-d animal e x s e r i x n t s ?...5ic:? =re hi;hly u s e f u l bu t no t ineiczciyra or - . n;rx.p. :esl=nscs
The l i t e r a t u r e r e c o r t i n q on hmsr . e.u;csures dates Cazic t c
A c u r r e n t b ib l iography con ta ins scme 86 s c i e n t i f i c a r t i c l e s on the s . h j c c t , excluding D r . Saenqer ' s c o n t r i b u t i o n s . Vhole bo6y p r o j e z t s have beer. unaertzker. i n more than 4 2 U. S. s e d i c a l c e n t e r s . A t p r s s e n t , e f f o r t s a r e urc?eroray usi;.?.' whole o r ? a r t i a l bsey r a d i a t i o n for <?e c o n t r o l of l e d i e n i a , i iodqsin's d i s e a s e . po lycythea ia ve ra , m u l t i p l e z p l o m a , and disserninated cancers of <-.e b r e i s t , t hy ro id and p r o s t a t e . In very s m l l crou=)s, whole body r a d i a t i o n b s been used s u c c e s s f u l l y i n curac ive e f f o r t s a g a i n s t E:v.ing's sarcoma, a bone tunor ? ~ i . ? ? a r i l y o f ch i ld ren .
The Cinc inna tL s tudy through t h e end of 1970 involvod a t o t a l of 196 c , a= ien ta r e f e r r e d f r c 3 t h e Tun.or C l i n i c of t3.e C i c c i n n a t i G i n e r a l 2ospitaal. These i ' = ! r ~ p a t i e n t s found by Sio3sy and c l i n i c a l exmi? . a t ion to have 51 ss2ni?.ated ~ ~ - 0 r . i . They "were chosen because they s u f f e r e d from advanced and widespread neopLastic disease such t h a t cure could not be a n t i c i p a t e d , " i n D r . Saenger ' s WOK*.
All o f t h e p a t i e n t s unciement a 7 t o 1 4 day a s ses snen t c e r i o d t o r e a f t i n :he d iagnos i s and t o determine whether t h e i r disease and tiieir g e n e r a l healt .? w.ou;a r a k e t h e r z 3 i a t i o n a t teza t f e a - e i t l e . Sone 24 p a t i e n t s were r e l e c t e d and r ~ c e : . ~ ? d no r a d i a t i o n on t!e b a s i s of t h e i r c l i n i c a l assessnenc. Some o f ti-ie e2 FacienEs l a t e r t r e a t e d r ece ived sham r a d i a t i o n s e s s i o n s dur ing t h e assessxerr t per iod k-.;: none ac tua- l ly were exposed u n t i l a f t e r a d e c i s i o n by t h e team which dsterniced the t r e a t m e n t muld ba b e n e f i c i a l .
The p a t i e n t s had a v a r i e t y of t w o r s . The Larges t group was 25 with cancers o r i g i n a t i n g i n t h e colon and rectum. X second group of 14 had tmcrs of the bronchus. F i f t e e n women nad d i s s e n i n a t e d b r e a s t cater. There were 23 pa t i en t ; w i th misce l laneous tLxors. Three c h i l 2 r e n had Ewi.?g's sarcoina and were t r e s z e l f o r c u r a t i v e e f f e c t . One of t!!e 25 p a t i e n t s w i th n i sce l i aneous tumors had E w i r . 3 ' ~ sarcoma wi th metastases t o o widespread f o r a c u r a t i v e e f f o r t .

Page 7
Discussions wit!! t he p a t i e n t s and members of t h e i r f a m i l i e s are s t anda rd i n a:iy cancer therapy s i t u a t i o n a d were a p a r t of t h i s p r o j e c c from i t s beginninq. S p e c i f i c p a t i e n t ccnsent f o m s have Seen 'used s i n c e 1965, when t h i s s t e ? was reconmmded by t h e Nation'al I n s t i t u t e s of Health.
Since 1363, p a t i e n t s s e l e c t e d for t h e s tudy v e r e intenriewed on succeedicg t!a:~s by t he i n t e r n i s t i n t he p r 3 j e c t before bcing asked t o s i g n a c m s c n t fo -7 f o r :?.e thera?y. ?,%en - w s s i b l e and i n a l l cases of ch i ld ren , t h e in t e rv i ew inclu222 cr.e or nore n e r k e r s c f t h e f c i l : r who a l s o conser,ted t o t h e t r e a t m i n t . t he t h r e e c h i l d r e n wi th C*.;.i.?g's s a rcoza , a l l *>rere t o l d t h a t t!!eir caccerr :?a? been dsfinecl a s i n c u r s j l e an3 t h a t t h e t r e a t T 2 n t would be aCte?.?ted i n an e f f s r : to prolor,.; t h e i r l i v e s and ?3ss iS ly to r e t a r d or sh r ink t h e 2 c o r s . t o l d t h a t t h e infom.a t ion Tained from t h e s tudy w a s hoped to be h e l 2 f u l t o oc?.or S a t i e n t s . m i l i t a r y as w e l l as c l i n i c a l s i g n i f i c a n c e .
Exce?: f o r
They were
In t h e l a s t few yea r s they were t o l d t h a t t h e information n i g h t have
The p a t i e n t s were t o l d t h a t t!!ere could be s o l e s i d e e f f e c t s fron t h e r a d i a t i o n exposure and t h a t t he tea- :could wish t o kee? i n c l o s e touch wi th then f o r a p e r i o d of veeks t o s tudy t h e i r r e a c t i o n s both t o the advances i n t h e i r d i sease and t o the ir,?act of t h e r a d i a t i o n . The p o s s i b l e s i d e e f f e c t s were n o t descr ibed i.1 d e t a i l no r emphasized t o avoid s u b j e c t i v e inducement of the s p p t o m s .
So f a r a s the s i d e e f f e c t s were conccraed, t h e team r e p o r t e d t ba t 4 5 percen t had no von i t inq o r nacsea a f t o r v o n i t i z q and r euscz w i t h i n t!ree ?.cars and a n c t h e r 17 3 e r c e n t had tke SL-2 S ~ : . > ~ S - . E
w i t h i n 1 2 hours of e x p s u r e . Anotker 9 g e r c e n t cont inued -orniting up t o 2 3 ?,:surs. Only f i v e p e r c e n t had _trolonged and severe vomiting and nausea.
r a l i a t i c n . SCZE 24 g e r c e n t ex2erFence d trw.srz7.z
I t is worth no t inq t h a t t h e s e syrngtons are c e r t a i n l y no g r e a t e r than thcse experienced by p a t i e n t s t r e a t e d e i t h e r by su rqe ry o r by any of t h e s y s t e q i c i r i lgs now be ing used c l i n i c a l l y on d isseminated cancers .
The p a t i e n t s were selected by c l i n i c i a n s a t t h e C i n c i n n a t i General I iospi ta l fro3 the p o p l a t i o n served by t h a t i n s t i t u t i o n s o l e l y on t h e b a s i s o f their t ' s o z diagriosis . S ince CGH is a i n s t i t u t i o n , none of t h e p a t i e n t , were p r i v 3 t e c a t i e n t s . The t h r e e c h i l d r z n with Ewinq's sa rcona were r e f e r r e d by phys ic ians at t h e a f f i l F a L Cina inn3 t i Cinildren's Hosp i t a l .
Extens ive psychologica l s t u d i e s were Zone on 39 p a t i e n t s . It vas Foss iS le t o e s t a b l i s h t h e i r IQs. The median on t h e s t t ld ied grcup w a s 87. The r a c e ..ias frcn 116 t o a l o w of 63. Some 31 of the t r e a t e d p a t i e n t s were Caucasian ar.d 5 1 :;ere negro. I n both race and IQ t h e group w a s r e p r e s e n t a t i v e of the p a t i e n t s served by CGH.
The three c h i l d r e n who were t reated d e f i n i t i v e l y f o r Ewing's sarcoma rer?ainc:! a l i v e f r o n one t o fou r y e a r s a f t e r t reakTent . From t h e o t h e r 79 , for whom cnly , a l l i a t i c w a s expected, f i v e others su rv ived as of October of 1971, t h e longes t by nore than s i x y- ears.

F
Page 8
In t e r n s of s u r v i v a l , t h e C i n c i n n a t i qrcu, r e3or t ed r 2 s x l t s showing an extep._cion of days over u n t r e a t e d ? ,a t ien ts i n each of t h e V r . o r c e t s q o r i e s . Ko'xever, x e s c l t s were n3t csz:;aaly s u ? e r i o r t o t h e s u r v i v a l r e s u l t s r egor t ed by oth.or i n v e s t i q a x r s u s inq various chemicals o r o t h e r co rb ina t ions .
The s u r v i v a l f i g u r e s are clo-icied by t h e f a c t t !a t nany of t h e p a t i e n t s inclu2s.l i n t h e smr le had a l r eady uneergcno on? o r more tyges of t r e a t n e n t unsuccess<u:l;J, o f t e n only a s>.ort t i n e 5efore t h e i r i z c l u s i o n i n tile s tudy . Sore o f t h e _catif::_= : t h e stu+ alsc reze ived e x t s p s i v e followup t r e a t z a n t , s s a e t l n e s invol-?in.; f c r t ' - . c r r a d i a t i o n of t ! e p r i n a r y t u . o r area.
Thus, t?e patients recsis.cd a t h e r a p e u t i c reginon *&ich w a s c l i n i c a l l y jcdzecl 7 . Z i l t
e f f i c a c i c u s f o r t h s i r sur'Jiva1 and p a l l i a t i o n , hc:.:ever mucn t!!e added e f fo rzs b l u r r a d the c k s e r v a t i o n of t h e e f f e c t s of t n e s i n g l e whoie body ex_cosure,
I n s p e c i f i c terr.s of s u r v i v a l , D r . Saenger was able t o dras rough cor .?ar iz?rr which i n d i c a t e d the b e n s f i t of some t r e a t n e n t o v s r none. He found t h a t !!is r e s u l t s cornzared t o those ga ined by o t h e r i n v e s t i g a t o r s us inq s u r s i c z l resscz- =?.SI
drugs such a s 5 - f l u o r o u r a c i l and, f o r Lye b r e a s t cancer p a t i e n t s , e s t r cgens 27.5 androgens.
I n Dr. Seer..;er's words, "The r e l a t i v e l y small nur3ers of p a t i e e t s i n t!!esi! c:c-rs (his and the ories com?ared from the l i t e r a t u r e ) preclude any claim t o th2z2y?i:i= s u p e r i o r i t y . 3n t h e o t h e r hand, i t s c m s reasonable to ccn t inue t h e r a y fcr S T . F . S ~
g r a v e l y ill i n d i v i d u a l s s i n c e t? , is r.et?.od of t r c a t n e n t is less elabora=e and ..\L::I
no g r e a t e r r i s k than many p r e s e n t foms of chmotherapy."
I n this conclus ion , t h e ACR co.?rmittee would concur. The! c o r m i t t e e would a l s c observe L9at the p r o t o c o l s , reviews by a o p r o 9 r i a t e i n s t i t u t i o n a l a u t ' l o r i t i e s , a t t e n t i o n t o F a t i e n t in terests and r c s s o n s i b i l i t i e s and r e p o r t i n g are all ccnsls:er.t with accepted sood clinical and s c i e n t i f i c p r a c t i c e .

Page 9
Responses t o Senator Gravel ' s ques t ions
Some of the p o i n t s r a i s e d i n the qt1estior.s i n your l e t t e r of.!iover>er 10 2 ~ 2 covered a t l s a s t i n genera l aSove. SoCz a r e not. Hence, t he ques t ions ene s p e c i f i c responses a r e d e t a i l e d below.
ANSKZR: t r i a l s of whole bod:/ r a d i a t i o n for a v a r i e t y of ?ur?oses. appended. Alnost alwavs, c l i n i c a l r e s e c c h e r s have had t h e b e n e f i t of a n r e l .:;rk t o tes t t i e t o x i c i t y or' t h e i r n a t e r i a l s and t o develop gene ra l p a t t e r n s o f b i o l c g i c a l ressonse. iio::'ever, s ince in t e r - s?ec ie s d i f f e r e n c e s never ailow ?.e t o t a l t r z n s f e r of anizal d s t a t o hcnan usace, it i s necessary t o u n d e r t a e c l i n i c a l t r i a l s undar ?ro?er cond i t i cns :a t e s t any new thera?:? o r aqent . It is n o t necessary for a c l in i ca l researcher himsel f to undertake aninal work i f he has access to and 2 good uniers tanding of t3e l i t e r a t u r e on t h e sub jec t . Tzrs was t h e cas? of O r . Saonger and h i s col leagues.
The l i t o , r a t u r e on r a d i a t i c n Sioloq:? is s u b s t a n t i a l v i t h reqard t o 2 : L - i l
One bibl iograzhy 1s
As an exzzple of t ! ! e aop l i ca t ion of a n i s a l s t u d i s s to h . a n uses , t h e use of autoloc.3.;; Sqne m3zrow t r a n s g i m t s czd t h e b a s i c understandina of tke infl:::::: cf marrov s t o n c e l l s 3n n x n a l i a n s* i rv iva i a f t e r :?hole Sody r a f i a t i c n exz7cs':r5 were worked o u t i n an ina l oxnerinents . T n e narrow tri;n.sslants a r e a m s t im-portant ?art of t k e C inc inna t i i nves t iga t ion . me Zetailed Sioc3.oTistr:/ :.E c only pe-zsits a ?ore c c o l e t e a n a l y s i s of t h z res?onse of these ca t i en ta Su= -1:: could po in t the -;ray t o o t h e r researzhczs :<?.o a r e a t ten? t ing r y s t e n i c theray.: with r a d i a t i o n and with. i n v e s t i c a t i v e cheTicals.
I t was a necessary p a r t of L l e c l i n i c a l i nvss t iqa t ion for Dr. Saenger t o 22:er:?.o the o p t i n a l =.out of marrow t o e x t r a c t , t!!e xost e f z e c t i v e :Jay to har.dle it ?r.: the best t h i n g for its r e i n j s c t i c n i n t o the pa t i en t . A t the keginnin? of '.:I-:
work, D r . Sacncjer aad 5is q m c ? e:r.trscts? tF.2 zarrow and f roze it to re?.ai:. -: i z r t!!e 18 to 21 days dxrinq x h i c h blooci :ii?ite and red c e l l l e v e l s a r e ex?ecte= ' - 7
decl ine . With- subsequent Gat i en t s , they a e t e m i n e d that: the grompt rein;ec:: :n of t h e marrowthe sa?e day tha r ad ia t ion was adminis tered ave r t ed much 02 t i e blood dzpletinq effect of t h e r ad ia t ion .
Since Dr. daenqer i n t k i s i n s t ance sup l i ed t o t h e Department of Defense, r?.-- r than ano the r fur.ding agency, f o r tk .e s2T;or': for t h e ex tens ive biochenical . :- -:; which would provide the "new" e l enen t cf i n fo rna t i cn f r o m the survey, h i s p r e 2 a r a t i s n s preceded <!e 1960 d a t a a t v;aicn t h e actual p r o j e c t was fun6ed DY COD and 2 3 t i z n t tzest!!.ent begzn. ks r .~%d, t ! !e sup-mrt for the p a t i e n t t reatment and manageqent was provided by t h e Universit.=* of Cincinnat i and 1:;
hosgitals. t h e psychological t a s t i n g xhich allo:.:cd a mre coy?lete assessment of t h e e : : : r:.
The DOD funds were appl ied oniy t o t he b i o c h e n i s t r l and subse=.ci.-.::.: - -

@
Page 10
2 . MLW,iuP sTJDIES: Eow dces Dr. Saenger f o l l c r up h i s O',X p a t i e n t s t3 f i n d o u t i f h i s " t r e a t 7 e n t " has been n e l p f u l o r ha-nfnl to the.?? h e measure the tunor s he hoped t o reduce, for in s t anze?
C J ~ S
?U?S:TER: than is p o s s i b l e f o r most t m o r c l i n i c s . obse rva t ions zn2 d i a g r o s t i c s t u Z i e s and f r equen t doc to r -pa t i en t c sn taccs jet:.:een both the i n t e r n i s t s and the r a d i a t i o n t h e r a p i s t s on t!!e team wit!! t h e 2 a t i e x t s who had been t r e a t e d . I n a d d i t i o n , t h e team psychologis t zaint-inscl c o n t i c t , r?ct only for h e r t x t s b u t also as a f u r t h e r suppor t ive nezsure.
AS noted, t h e followup on these p a t i e n t s is cznsider=.bl:J more cxp le t - . The follo:mu=, c o n s i s t s d of c l i n i c a l
h e data on S iochen ica l responses and upon psycholoqicz l r e a c t i o n s is v a l s a l l e b u t s i n l y t t o ex=:..nsive i n te-ns 05 manpower an:! labcl-ator! f z c i l i t i e s t o Le p o s s i b l e f o r c-ret.1 cancer c s t i e n t , e v m i n t h e b e s t of cancsr c e n t e r s .
The assessment of r e s u l t s was ma6e by c l i n i c a l obse rvz t ions of 'the p a t i e n t :ihich i n d i c a t e t h e e l e r ~ e n c s of veil-being and systemic func t ion p l u s l abora to ry ar.aivses o f blood con5Ltion and void ing func t ions F lus x-ray d i a j n o s i s t o check the s i z e and p e n e t r a t i o n o f s o l i d tumors. had been exc i sed s u r g i c a l l y o r treated previous ly wit!! a p r o c h y l a c t i c dose o f r a d i a t i o n , l ezv ing cm-.age:?.cnt of t h e Zetastases 25 the rayor c l i n i c a l mnce rn . I t is warL& n0tir.g t h a = o n l y 4 p e r c e n t of t h e 82 p a t i e n t s i n t k e l O - y e a r series xeze l o s t to c c n ~ k t o , follawup. X detailed re-wrt on these results is c i t z d i n Lhe preceding sec?i.cn.
In many of the F a t i e n t s , ths primary Y a o r
3 . CONTFgL G?.CU?S: Gaat c o n t r o l grougs .does D r . Saenger have, or has k.e a r ranged f o r a t our g r e a t czncer r e sea rch i m i t i t u t e s , so t h a t h e EL:: d e t e r n i n e how h i s s 2 e c i a l " t rea tment" is working?
AZISXR: usua l ly ar ise u n t i l a f t e r the com?letion and e v a l u a t i o n cf t h e type af s tudy c u r r e n t l y m<a%a:? by Dr. Saenger. H e adv i ses t h a t p l a n i n g foz a nore e:a-,cratc phase t h r e e s t c d y beqan l a s t June on t h e bas i s of a s s e s f a e n t of t he 10-yezr r e s u i t c of t h e ? r e s e n t ef 'lort.
The ques t ion of s p e c i f i c c o n t r o l grougs and .rmSoinized sm?les does mt
The l i t e r a t u r e c o n t a i n s s u f f i c i e n t s t u d i e s of s h i l a r p t i e n t s and corn?araSle s i z e d s m p l e s treated by o t h e r nethods to a l low basic c;a?ar isons of t u o r r eg res s ion , pos t - t r ea tmrn t s>m?toas and s u r v i v a l times a f t e r p z l l i a t i o n .
Again, it is worth no t ing t h a t t h e e x t e n t of p r e p a r a t i c n s and f o l l o m p cn each p a t i e n t znd t\o, nZr!Acr of cancer D a t i e n t s at CG9 v3.0 axe s u i t a b l e fo r an ac;;ro,ssiv.e p a l l i a t i o n study kava cor5 ined t o l i n i t t h e s ize of the group under investiG2:;un. A phase three stud.:* ayoears- f e a s i b l e a t C i n c i n n a t i b u t sill req.Jire a s S s t a r . t : a l coxni t r ient of s t a f f i n 3 and f inanc ing from some source other t han ?a t ien t , tare f-?ks.
4. PRIVATE PkTfENTS: Does D r . Saenger treat an? p r i v a t e cancer patients, cr o f f e r c o n s u l t a t i o n on pr ivr l te cases? or whDle-SoZy r a Z i a t i o n "thcra?y" on paying p t i c n t s ? doctor who does?
Does he r?corfiend o r use ?-.is r 3 f t i a ' Daes he Lnov AI*.?

Page 11
ANSWER: Unive r s i ty of C inc inna t i Col leqe of !:edicine snd hav.*e r.3 2 r i v a t e p r a c t i c e in 57.5
ord ina ry sense. a t the c i ty -c?e ra t ed C i n c i m a t i Gecetal Xospi ta l and i z s a f f i l i a t e d i n s t i t c c i o z s . A very fev F a t i e n t s :isre x s f e r r e d t o %!e Qz3u3 fzcn d o c t x s a t the !?Dl-.es Hc;?lt?l, a privat;. prsccice i n s t i t i J t i o n a f f i l i a t e d wit3 the u n i r s r s i t y . Eo:7esretl %\os? p a t i e n t s :.:era c o t chzrqed f o r tde t rea tment and n e d i c a i care involved i;l t!\eir p a r t i c i p z t i o n i n the s tudy .
D r . Saenger and h i s co l l eagues are f u l l - t i c e f c c u l t y merhers of tb.e
The i r p a t i e n t ca re r e s y n a i b i l i t i e s +=% r e s t r i c t e d tc p a t i t r . = s
h t this poi.??, 3r. Saer.Ter Zoes n o t use h i s t r ea t -on t cn "paying ? a t i e n t s " Secause 5s :?as ecns. Ze CCPS noc recornend h i s technizvie t o o t h e r chysiciar.a because the i n v e s t i c c t i o n is n o t y e t c a x s l e t a &?a t;ie r e s u l t s are Rot i r . f ic=tLve of i x - . e x L x m c l i c n t i x i :a c l i n i c a l siL--.~itic~.s asar t $=on a r e sza rch eEfo r t . O r . Sesye r m u l a e:c3*Lz=qo, oc:io,r q u a l i f i e d resezrc5crs t o 8 u 9 l i c a t e h i s p r o j i c c or to c c d i f y h i s teci?niqc:..s on t he basis t h a t r e s u l t s to date are s u f f i c i e n t l y promising t o warran t f u r t h e r i n v e s t i g a t i o n both by h i s gro.;o and by o t h e r s .
_ .
As noted akove, so%? type of c a r t i a l o r whole boey r a d i a t i o n is used i n mors than 42 d i f z e r e n t U. S. n e d i c a l c e n t e r s . X t o t a l l i s t of t h e s e is n c t a v a i l a b l e , b u t they 23 i i ic lzde both p u b l i c i n s t i t u t i o n s l i k e f:e L 'nivezsi tp of C i n c i n n a t i and o r i v a t e cnes *.-:here n c s t patie?.ts are charTed for t?.eir care and t r ca t t l en t . Thus, it i s l i k e l y t k a t instances could be foux i i n which F a t i e n t s diO gay fsr t!!is t r e r t z e n t al;nrozch. :io:fever, t5.e s c i e n t i f i c l i t e r a t u r e does n o t x e i n a r i l y c i t e the c_*.xstix~ cf _sstimt ca;c.snz i n r e s o r t i n g 3n c l i n i c a l research . The X P . committee :-:as n o t i n a p o s i t i o n t o make any extprided i zqu i ry on this Faint.
5. TRICYSRY: Is there any t r ickery of the p a t i c z t s involved?
D o t h e p a t i e n t s r e a l l y nnderstand the exczrircant i s l a r 7 e l y to help t h e Defense 3 e p a r t n e n t _ore?are for r.?lclp,zr warfare?
Do you c o n s i e e r t h e release t h e p a t i e n t s s i g n to be s u f f i c i e n t evidence that they umiers tand?
Do t h e p a t i e n t s understand t h a t t h e experiment may cause them severe d i s c o x f o r t , sucn as nours of v m i r i n g ?
Do t h e p a t i e n t s unders tand t h a t ga r t i a l o r whole-body i r r a d i a t i o n may shor t en t!!eir l i v e s , and i f so, by how much?
D o the p a t i e n t s mdesszand whether o r not t h e r e e x i s t s any b a s i s for suqges t ing C i a t the " t r e a t c e n t " may rcduce t h e size of their tunors o r re2uce t h e i r g a i n (as Dr. Saenqar sugges t s i n the Washinaton Pos t , O c t . 8 , 19711?
The q u e s t i o n of i a f o m e d consent was i n v e s t i g a t e d extensively by the ACR c c r c i t t e s . l 3 e Uriiv?rs i ty of Cir,cir .nati Co;?nitteo for Hu~an I n v e s i i p a t i o n vas forced i n 1965, as it was i n most o t h e r i a s t i t u t i o n s , arrd has hzd a parallel d e v e l o 3 e n c under C-2 quie .c l inss of t5= ? k t i o n a l i n s t i t u t e s of IIealth. have bsen q r a d u a l l y rnodir'ie8 ove r t!!e yea r s ar,d Lhe s o p h i s t i c a t i o n of t h e i r review has i nc reased i n a p a r a l l a l r'&s!iim.
Their cansen t foms

P
?age 12
I t is t h e oc in ion of t h e AC3 c c m i t t e e t h a t a t t!!e p r e s e n t tizie and thtouch the yea r s t h e UC c o p z i t t e e has f u n c t i m e d e f f e c t i v e l y and c=r.;ar3bly t o siT,ii=r co rmi t t ees a t ar.y of the o t h e r l ead ing i n s t i t u t i c r s vkich co$act cancez r e s e i r c h . I t is l i k e l y tha t the U\= c i m i t t e e h a p e r f o r z s a i t s r'unction b e t t e r than the average groL;p because of t h e V O ~ L ? . ~ of p r o j e c t s cane ra t ad by t h e medical f a c u l t y and t h e professional c n T e t e n c e of the people involved.
The c u r r e n t consent seeking 2rocedure was reviewed by t h e P.CX corn-it t ie. The teaT i n t e r z i s t (3r. Sil5s:stoin) in te rv iows p a t i e n t s t v o t i n e s a t l e a s t 2 4 h o u r 3 a-zart and d i s c x s e s in sxz2slsLve & ? t a i l t5e Sracedzres t i a t w i l l Se cndorcakea. Th i s is Zsn-:! r a t only f a r the z e t i z n t b u t also f D r cerbers or' his f a z i l y , ..<:?2n
e v a i l a b l e . 7.1e s a e c i f i c a>= f s t a i l a d consent E t n s are n c t ? resentee tc 2.2 rat12r.z tL?til ?ha ccns l e t - im 3: = A c sccond in tc rv iew. Tke fo-ri i n use is modi f i e i f z r s p e c i f i c i L y f z m t h e basic ozes _cre?ared by t h e : :ationdl I n s t i t c t e s of Sealt-h.
- .
Except i n t h e case of t h e t h e e c h i l d r e n w i t h Ewing's sarcma who were t r e a t e d carnt ive ly , Cis p a t i e n t s knew b e f o r e being r e f e r z e d to *.e study tam that t k e y had mclirnant disease for which no c u r a t i v e t r ea tmen t is poss ib le , They kr.e-4 t h a t t h e effor ts of t!!e s tudy team were n o t o f f e r e d as c u r a c i v e l
:-:any p a t i e n t s ex2ressed a dl-sire to p a r t i c i p a t e i n +he s tudy and 2oss iS ly t o he12 t h a plichr, or' 0 t h ~ ~ : sazctr g a t i e s t s i n t h e f u t u r e . The do,x?ented gsycholcgicz s t u d i e s which xere incc-r=orsted i n t h e croject bea inning i n 1965 g ive t h e s t u i y grou, c o r e than the usua l a s su rance that t h e i r exp lana t ions and t he r equ i r ed ~O-T.S
were understood by the F a t i e n t s and by the i r fa;.ulics. ,
The AC3. comi .2 t ee felt t h a t t h e 2 a t i e n t s were adequazel-/ infom.ed about t h e na::ire of t h e Fro?csed t5orapy and about the consecuencos. were n3t i>fo-T.sd i n & t a i l a j o ~ t t h e si& e f f a c t s of r a d i a t i o n beceus i of 5ie psycho loq ica l inz luence of expecza t icn involved. i n both nallsea and vczit1r.g. nent ioned i n the p r o j e c t f i a x a t i v e , &out h a l f of t h e p a t i e n t s d i d n o t Ex-,eris.izt: unc leasan t s i d t effects and n o s t of t h e o t h e r s had only t r a n s i e n t s:=ctor.s.
t r e a t z e n t s , o f t e n invo lv ing r a d i a t i o n o r sys te - ic L!enicals, they were avare frc- p rev ious cxce r i ence of t h e t.ypes of s e q u e l l a e which might be encouncered.
As s?oted above, %!e ?ati??.ts
.'-..s
IC sho\;ld also tc noted t h a t s i n c e c o s t of t h e p a t i e n t s had underaone p r - a V l ' r - . , . . .,La ZZ.C:CST
The p a t i e n t s wsre adviscd t h a t t h o p r o j e c t w a s &signed i n t h e hope t h a t t h e r a d i a t i o n would r e l i e v e t k e Fa in of t ! e i r cencer , t h a t it n i q h t shrizk t h e s i z e of t h e g r i x r y tuTor o r recard t he develcpzznt of netastases. of a?y o f those r e s u l t s a s r ~ o i f c r e ? .
!:o guzrar.cees
In the ACR committee's view, the a s s e r t i o n i n qJestion 5 a, that the experiner , t "is largely'tg hel_o' the Defense CeFartztent Dre3are for nuclear xarfare" i s acc carrect. T h i s is n o t thc crir?.ary Fur rose of tkc effort and to have advised t h e pa t ien ts t o t ! a t e f f e c t srould have been misleading,

rage 1 3 P
The p a t i e n t s were n o t s s e c i f i c a l l y i n f o m e d t h a t t h e p a r t i a l s u p r o r t cane frcn DOD any more t!!an o t 3 e r p a t i e n t s i n O C m t s t u d i e s at C i n c i n n a t i cr else;.-hero are advised of t h e s a e c i f i c agency sucpott of ?rejects i n which they a r e invol-,*z?. The C inc inna t i G a t i e n t s were t o l d that supgor t cme i n p a 2 fron a n a t i o n a l ac;sr.=y.
?it the t i m e the p a t i s n t s were counseled p r i o r t o the r e q u e s t * f o r execut icn c f tL.e i n f o r r i d consent fom, they were advised tha% t h e p s s i b l e f i n d i r q s zay have :=YO
than c!.inical i ? .? l i=a t ions and could be k e l p f u l t o persons tecoFvin-J whole 503.' r a d i a t i o n i n i n 3 u s t r i a l acc idan t s , m i l i t a r y a e t i v i t i a s o r as f a l l c u t f r o n a nuc lea r de tona t ion .
The ques t ion of t h s source of suppor t for a oroject is n o t cons t rued by t h e x?. co ,mi t t ee o r Sy mst zeCical i n v e s t i g a t o r s as be ing t o l e v a n t t o t h e issse ~f i n f o c e d cmsest. I n t h i s case , the E D exezc ised no c o n t r o l over s a t i s n t se1ecti.t: o r c l i n i c a l t r?a txsz t L?Q indeed d i d n o t r e q u i r e d e s c r i p t i o n s of t h a t 22z t of t k e project been d i r e c t e e o r i n d r i l y to..lrard t h e a s sossnen t of whole Sod:? e f f e c t s of r a d i a t i o n r a t h e r than t h s nanagezent of d i s s e n i n a t e d cancer by r a d i a t i o n , t h e study group could n o t have inco-orated t!!e autologous marrow t r a n s p l a n t s which so d r a s t i c a l l y al tered t h e classic r a d i a t i o n response.
.
Though t h i s l e t t e r has extended t o s u 5 s t a n t i a l leRgth, it obviously r e p r e s e n t s a s u m a r y of t h e facts of the C i n c i n n a t i s tudy and a precis of t h e op in ions j€ tho Colleg.r ' s c o x d t t e o , ne7hers on t h a t s tudy and on the basic i s s u e s of cancer i n v e s t i s a t i o n i n h ~ t a n s . As WB i n d i c a t a d a t t ! e keginning or' the l e t t e r , w e would. 50 hz2;y t3 actL?,?t f u r t h e r d i s c u s s i c n of any p o i n t on which you ray s t i l l have concern.
S ince re ly ,
Robert K. ::cConnell, N. D. P r e s i d e n t M e t i c a n Col lege cf 9acXology

8

\
I3- l G 4 03 L ( 2 )
Dczr Hr. Chairman:
P u r s u a n t t o your request o f December 23, 1371, and d i s - c:rssiojis with y o u r o f f i c e , we o b t a i n e d docur;lents r e l a t i n g t o (1) t ! : c wholc-body i r r a d i a t i o n p r o g r m a t the Univcrsity of C i n c i n n a t i bIcdic31 C c n t e r and ( 2 ) the policy of the DeFzrt- ncn t of Defense on t h e subject o f the p r o t c c t i o n of hutnans used in z e d i c a l research p r o j e c t s under con t r sc t . The mi- c l o s u r c t o t h i s l e t t e r identifies tlie docuocnts obta ined by
. us and made a v a i l a b l c t o your o f f i c e d u r i n g o u r work.
C m c e r n i n g t h c p o l i c y on t h s subjsct of t h e p r o t e c t i o n of h m a n s used in m d i c a l rescarch p r o j e c t s , an official of *,lie I IcpLrznent adv i sed us t h a t ’ t!re p o l i c y of tkc 2 c p a r t m n t rrns s e t f o r t h in Department of Defense Instruction S 0 3 0 . 2 9 , d z t c d ).ifiy 12, 1964. The i n s t r u c t i b n , which is applicable to 311 coiJpancnts of the Departrent and to its ccnt rac tors or g r a n t e e s , s t a t e s t h a t : e.
“Thc Dcoartxcnt of Dcfcnsa assuflcs f u l l rcsponsi- b i l i t y f o r the p r c t c c t i o n of hmsns involvcd i n rescsrch under its sponsorsliip vhethzr this involves. invcstigational drcgs o r other hazards.
“Each Il!ilitrrry D c p a r t m n t will cs tzb l i s f i v i t h i n t!;c o f f i c z of its Surgeon Gcrxral a f o r z a l I:c>3ricv Board 0 5 p r o f c s s i o r a l pcrscr.ne1 t o c o n s i d e r c a c ! ~ research ~ i ~ o p o s r t l f r o 2 i : i t i i in t h r t Xili t3i-y flq?artr,r?nt or frorn its coatractors or e r s n t c e s a..-iii.ch zay i nvo lve the UTIC o f human subjects i n t!ic clinical invcstigs- tion o f ’ R C W d x q s . BcEni-c a cI.inScs1 t e s t with in i n v c z t i z a t t o x l drug nay bc p c r f o r m d md::r tlic sponsorship o f a f 4 i I i t n r y D c p a r t m n t - -
“I. t h e p l a o f the &st nnd other pertinent d c t a i l s rwst be S t i b n i t Z c G to the a p p r o p r i - ate Rcvi e\,* Cczrd,
“2. thc Board nust i n d i c s t c i t s z p p r a w l , ar,d.
I
I I L i r
I f

B-164031(2)
14ith the csccption of c e r t a i n reports t h z t \:'ere rcqQired t o bc f i l e d w i t h t h e Food and Drug A c h i n i s t r a t i o n of thc Da- p n r t n m t of Health, Educat ion, and XelEarc i n the case of in- vestigational ne\< drugs, no proccciurcs liere s p e c i f i e d in the i n s t r u c t i o n with regard' t o the use of hunati subjects f o r o t h e r research purposes. The reports to be f i l e d w i t h t h e Foot1 and Drug Administration were s e t forth in a Iknorendum of U n d c r - stancllny, bctween thc Departrent of Health, Education, and If'elfare and the Dopar tcent of Cefcnse, dated February 196.4, which contained tlic proccdurcs to be fo11ov;cil t o ensure t h a t tlzc rcquircneti ts of the Federa l Faod, Drug, znd Cosnet ic A c t , as mended (21 U . S . C . 355), 2nd the regulations i ssued wzdcr thc a c t are EuIly net . .
Although the instructicn sppeareO to be directed p r i - marily toward the i n v s s t i g a t i o n a l use of cirussI an official of t h e Dcpa r tmnt of Dcfcnse zdvised LIS t h a t t h e i n s t ruc t ion appl i ed t o a l l ncCicaL research p r o j e c t s . lie s t a t e d a l s o Zhat c a d i service d i r e c t e d its o m research p r o j e c t s \ i i t h o u t con- trol from tlic Departcent .
4. t'fc contacted o f f i c i a l s of the Cepz r tncn t s of the Am'y, t : a v y , end Air Force and of the Dcfcnse ihx-lear ,igcncy, for- ncrLy I;ilown as t h c , Dcfensc Atoxic Support A g e m y ( t h e o r g m i -
' r a s i o n n l e n t i t y w i t h i n t h e ~ i ? p a r t m n t of rkfcnr;C t h t had coiltracts wirh t h e Uiliversity of C i ~ i c i r ~ i a e i rs!.sting to the uhoie-body irradiztian proxran) , to d e t c m i n c \:i;ether t h e y bad any i n s t r u c t i o i z s or r e g u l c t i o n s t h z t m r e applicsb-le to t h o us8 oE hunans in nctiical research \:ark t m d e r cox t rLc t . *-:. i I I c
. o f f i c i c l s were n o t 3.warc of m y i n s t r u c t i o n s or rcgu?.atiorts, o t h e r t h a n the i.llstrl1cticris m a regulations i ~ q l . e z m t i I i g 1i:- s t n i c t i on 5030.29 , i n v o l v i n - ~ t ! : e use of h*z.z&i subjects t hs t w u l d app ly t o c o n t r a c t o r s c o n d u c t i n g medical research f o r - t h e i r o r g a n i z a t i o n s ,
US thr,t. t.hc Air For-cc d i d n o ~ c c n t u c t ncri ical research c i d e r c o n t r a c t . Of f i c i a l s of tile De?art;>c;l ts of the X r n y and Kavy S t z ~ t c d t h a t , alt!l01:gh iyiost: rxciical rcscarch h a d been colid\)C'cr?d in -house , s o ~ e i!zd been pcrfformd under con t r i l c t . l h c y s t z t e d a l s o t h a t , ~ J i c n work i s t o bc per io rncd u~lc'lsr C O n t r t t C t , they ~ t u s t b 2 s a t i s f i e d t:liat p z t i c n t consen t f ' o r ~ s \.;iI.l bc US?^ ?ad t h a t hunzn. subj C C ~ S \:ill bc ndequztcly protected before a coil- t r a c t is rxecutcr?.
/in o f i i c i s l o f the Dzps;-er;cnt c ~ f * the Air Force advised
.

* . b
/
An o f f i c i a l of thc Dcfense Nuclcar AEcrtcy adviscd us t h a t , alt i ioagh t h e Defense Nuclear Agency d i d R o t have m y contracts f o r the use of Irunan subjects for medical research, the folloying langxage hsd bcen included in all ncdical coj1- trncts a f t e r August 1971.
"The COR [Contracting Officer's I k : ~ r c s c n t a ' t i ~ c ] shall be infom.ed in w r i t i n g of m y prtj;c.st p h n s on the part O P the Contractor t o cnploy new, expc r i zen - tal, and i n v e s t i g a t i o n a l drucs or o the r hazards in research involving h w s n s u b j e c t s , and such c q e r i - menta t ion s h a l l be spec i f i ca l ly auzhoritcd by tho Contracting OCficer in w r i t i n g pricrr to t h e prosecu- ticn of st?cli research. Without t h e concurrence mid authorization by the C o n t r a c t i n g Officer f o r t h e spec i f ied drug or ot?ier hazard involved, such re- search shall n o t be pcrforncd. c l ause is t o i n s u r e conpiiance w i t h tho Depcrtncnt of Dcfense Instructicn, 5 0 2 0 . 2 3 , 19G4 !-by 12, en- t i t l e d s Ti lves t iga t iona l Use of Drugs o r O t h e r l i a z s x l s by the Dcpartccnt of Dcfcnse' , a copy of ::hich is furn ished to t h c Contractor v i t h this Contract)."
(The purpose of this
.. i ..

contcnts of t t i z r c p o r t . li'e t rus t these coments will servc t h e purpose of your i n q u i r y .
Sincerely yours,
Conptrol Ic r Gencrnl of the Urritcd S t a t e s
Exlosure
The lionorable Edward bf. Kcnnedy Cl~airt :an, S u S c m x i t t c e on IlszPth Connittec on Lzbor and P u b l i c Vcl.fare United S t n t e s S e m t e

9

.
! . .
MRS. LL
OTCATUR. GEORGIA aooso 165 WOODLAWN AVENUE
Novembe r 7, 1974
Department o f Heal th, Education and Welfare Washington, D.C. 20214
Gen t lernen :
I f i n d the attached almost beyond b e l i e f . STOP THIS!
Where i s the hea l th , education, o r we l fa re i n a program that t rea ts a human as i t would a protozoan? federal money be used i n such programs a t a l l ? We should n o t a l low such progrgms, much less f inance them.
Why s h o u l d
Thousands o f cancer victimswho read t h i s w i l l s u f f e r the uncer ta in ty o f the nature o f the treatments they receive, many apparent ly w i t h reason. Research on human fetuses, aborted o r otherwise, should never be allowed. You csn- no t poss ib ly dare to continue o r a l l ow to cont inue such i m r a l and depraved crimes against c i t i z e n s whether aborted, menta l ly ill v ic t ims o f our soc ie ty , o r o t h e r innocents; c e r t a i n l y no t i n the name of the peop!e o f the Uni ted States.
Stop it. I n the name o f God.
S i n ce r e 1 y ,
a
cc: Senators Nunn and Talmadge Representative Blackburn Secretary o f the Army Callaway

1 RCC 1.958204.006~ /

RCCI .950005.009i
Dawcbcr 9 , 1974
Batortole SPQ Fmn United Stater Scnatc: ;lo&hinpton, 0.C. 26510
Ubolc-body t a d l a t l m ut levels of fed hundred reds f 6 1c t3 t l only uhcn it destroys the S ~ C O J tsildfn; cctlr of the borre s&rrOil. cf t h e t e pstfcatr * ihO had vldcoprerd mctratotic cariccr, 8 lcr&c par t of the marrw g a c ~ f irat mawwed, t)ic patiant v10 then crested End tho csrrw ratutocd.
In t 5 c Crcatneat
Notla of the jx~tfcntr Lr.volvcd Jfed fsoa radfatfim sfcknaro.
.

t2mw.h t;o of tkeo d i d d i e v i t h unusually X w w % i blo d cell counts. In a l l instsneer, donth i l ia clezrly atttibutobro t o tfia adrzrncc of cnncer, or t o fntcrcurtent Gisctte tasociated w l t i i sZvsnced crncer.
Dbctor Xx=gcr f n l l c t o note tkc ffcdirp. by tCla A%?rfcsn Collcqa of k d l o l m y that c!lfs treatrest s e s A t l emt 2s effective os drug t!:crsr.y for ccrta1.t types o € cezcex- find, In the cc4se of K*:fzg'a czzcma, ti child'mod b u m csxecr, appeared t o be z'sr superior t o rny other crentdimnt ther ovri lsble .
D. 2. C:nltrley, ?h.D. Clifcf, Gfffce for tkatcctfon Era-? 1Icgcarcb X 1 ; b OffLcc of t h e Director

RCC 1.958204.006a *e.%,
. - - DEPARTMENT OF HEALTH. EDUCATION, AND WELFARE
h - - - > PUBLIC HEALTH SERVICE
NATIONAL INSTITUTES OF HEALTH 1 . ol; - 3c\ - - - - -
? I
EETHESDA M A R Y L A N D 20014 - . _ _ .. C ? ' n - - r
.. +- 2 - December 13, 1974 . 6.
-e.. h - - ,.,- . - - _ - &a. Lloyd B. Wilford 0 ' -
Decatur, Georgia 30030 -~ __ . 7 ~ .
Dear k s . Wilford: .,. --- : - . - - . 7 - - ' .. ,: - i ^ ' -
In typ ica l bureaucrat ic fashion i t i s h ighly probable t h a t U L O A ~ of the copies of your November 7, 1974, l e t t e r to t h e Department of Health, Education, and Welfare w i l l end up on my desk. probably rece ive r eve ra l e s s e n t i a l l y i d e n t i c a l responses.
165 Woodlava Avenue 7 - * -
- .. .--- . . ~ -,,,.-,., - - -. - , - . . 3 - . C - - - - 7 - - 7 . -
You v i l l , a8 a consequence,
We are enclosing a copy of our r ep ly t o Senator Nunn and copies of the enclosures . does no t propose, permit, o r countenance research t h a t coufuses patients v i t h paramecium. these i ssues . I w i l l be g lad t o send you copier of our pol icy issuances da t ing back a s f a r as 1953, f f you a r e in t e re s t ed . t he i n t e r e s t s of irPmora1 and depraved pers0118.
As an old protozoologis t , I can assure you t h a t the Department
I t r u s t t h a t the l e t t e r i nd ica t e s ou r long concern w i t h
They do not r e f l e c t
Doctor Metzgcr appears to have r e l i e d on newspaper "morgue" mater ia l t h a t vas years o ld and g ross ly inaccura te . i n such a sloppy fashion we would s t i l l be glving mothers thalidomide. The accusat ions a r e a l i b e l on both the Department of Defense and the Universi ty of Cincinnat i .
I f medical rc rearch was c a r r i e d s u t
Senator Kennedy's concerns were u ide ly c i r c u l a t e d i n the Cincinnat i papers , y e t none of the p a t i e n t s of their survivors made any i s sue of the matter. The Universi ty refused to r e l e a s e the p a t i e n t s ' names not only because af l ega l r e s t r i c t i o n s , but because of severe surv ivors ' reac t ions t o a previous attempt by a T.V. network t o document the study with the Un ive r s i ty ' s coopera t ion .
Several of the Psing 'a sarcoma cases t r e a t e d a t the h o s p i t a l are s t i l l e l b e and w e l l s eve ra l years a f t e r t reatment , though the average rurvfve l of such pa t i en t s i r less then 6 Plonths. has ha l t ed what promised to be a very s i g n i f i c a n t addi t ion to our anmamen- tariurn aga ins t me tas t a t i c cancer. and i n fu tu re years t h i s country may w e l l move even fu r the r ahead of ud i n t he f i e l d of radiotherapy.
It I s t o be r eg re t t ed t h a t t h i s inc ident
Similar work is going ahead i n Canada,
Sincere ly yours,
D. T. Chalkley, Ph.D. Chief, Off ice for R o t e c t i o n from Research Risks Off ice of the Director
Enclosure

, - - . - * , . -
I * . - .
. . cc : Dr. Eugene Saenger Depertment of Radiology '
College of Medicine University of Cincinnati i . . . ... Eden end Bethesda Avenues Cincinnati, Ohio 45219 . . . . . . . . . . . . . .
Col. Lsweyne Stromberg .. - r:,;::-b. . . . . Armed Forces Radiobiology Rtstarch I n s t i t u t e Grounds of the National Naval Medical Center :: T; :,. . . . . Building No, 42 Betherds; Maryland 20014 . . . .,! : . . . . .
, ' - -. -
. I . .
. . . * . . - e'.. .: . -. ..
..& . .
- . f ' " L ) . . . . - . . . _ . . ... . ... . -* ,. ,; '. -.., - c . . 5 ? . - - . . - . . . - . . - . . . _ _ ..- - - - * . . . . .. .i: V; L .. - . - - '. r , . ..
5 - ... ..L 6 , , , . - . t - C - ~ - I . . . . . ~ .; _- . . - . . = T - ...'..- - . .. '..:;-#,. ..... -
... " .
. .
10

UCCM / RCCl.950005.009j
Published in Scientific Literature
PUBLISHED PAPERS - Under DASA Contract - Radiation Effects in Cancer Patients
Comparison of Serum Phenylalanine Levels with Growth in Guthries's Inhibition Assay in Newborn Infants. Carolyn Scheel and Helen K. Berry. The Jour. of Pediatrics, Vol. 61, No. 4, pp. 610-616, October 1962.
Deoxycytidine in Urine of Humans after Whole-Body Irradiation. Helen K. Berry, Eugene L. Saenger, Harold Perry, Ben I. Friedman, James G. Kereiakes and Carolyn Scheel. Science, October 18, 1963, V O ~ . 142, NO. 3590, pp. 396-398.
Deoxycytidine Levels in the Urine of X-irradiated Rats. James G. Kereiakes, Eugene L. Saenger, and Helen Berry. Abstracted in Radiation Research, Vol. 22, No. 1, May 1964.
Urinary Excretion of Amino Acids and Nucleosides by Cancer Patients Following Whole-Body Irradiation. E.L. Saenger, J.G. Kereiakes and Helen Berry. Abstracted in Radiation Research, Vol. 22, No. 1, May 1964.
Endoreduplication in Leucocyte Chromosomes: Preliminary Report of its Relation to Cancer and Whole-Body Irradiation. Ben I. Friedman, Eugene L. Saenger and Michael-S. Kreindler. The Lancet, September 5, 1964, pp. 494-495.
Specific Proteins in Serum of Total-Body Irradiated Humans. A.J. Luzzio, B.I. Friedman, J.G. Kereiakes and E.L. Saenger. The Jour. of Immunology, Vol. 96, No. 1, pp. 64-67, 1966.
Hematologic Effects of Total-Body Radiation in the Human Being. Gould A. Andrew, C.C. Lushbaugh, Ralph J. Kniseley, David A. White and Ben I. Friedman. This paper was presented at the InLernational Atomic Energy Agency Panel on the Effects of Various Types of Ionizing Radiation from Different Sources on the Haematopoietic Tissues, meeting in Vienna, Austria, May 17-20, 1966. Published in Proceedings by IAEA, Vienna, 1967, STI/PUB/134, pages 75-83.

Effects of Whole and Half Body Irradiation in Human Beings w i t h Cancer. E.L. Saenger, B.I. Friedman, J.G. Kereiakes and H. Perry. Congress of Radiation, Cortina d'Ampezzo, Italy, June 26-July 2, 1966, p. 191, abstract #759.
Published in the Proceeding of the Third International
Effects of Total Partial Body Therapeutic Irradiation in Man. Eugene L. Saenger. Published in Proceedings of the 1st International Symposium on the Biological Interpretation of Dose from Accelerator-Produced Radiation - Held at the Lawrence Radiation Laboratory, Berkeley, California, March 13-16, 1967. Published U.S. Atomic Energy Commission/Division of Technical Information, CONF-670305, p. 114-227.
Colorimetric Analysis of Deoxycytidine in Urine After Separation by Ion-Exchange Column Chromatography. I-Wen Chen, James G. Kereiakes, Ben I. Friedman and Eugene L. Saenger. Analytical Biochemistry, Vol. 23, No. 2, May 1968, pp. 230-240.
Radiation-Induced Urinary Excretion of Deoxycytidine by Rats and Humans. I-Wen Chen, James G. Kereiakes, Ben I. Friedman and Eugene L. Saenger. Radiology, Vol. 9 No. 2, pp. 343-348, August 1968.
Total and Half Body Irradiation: Effect on Cognitive and Emotional Processes. Louis A . Gottschalk, Robert Kunkel, Theodore H. Wohl, Eugene L. Saenger and Carolyn N. Winget. Arch. Gen. Psychiat. Vol. 21, pp. 574-580, Nov. 1969.
Cytologic-Biochemical Radiation Dosimeters in Man. E.G. Silberstein, I-Wen Chen, E.L. Saenger and J.G. Kereiakes. Published in Proceedings "Biochemical Indicators of Radiation Injury in Man "International Atomic Energy Agency, PL-409/13, pp. 181-214, Vienna, 1971.

PRESENTATIONS
Bone Marrow Dosimetry in a Cobalt 60 Irradiated Tissue Equivalent Human Phantom. presented by James G. Kereiakes at the Second International Conference on Medical Physics, Boston, Massachusetts August 1 1 - 1 5 , 1969.
Effect of Total and Partial Body Radiation on Cognitive- Intellectual Functioning and Emotional Reactions, C.C. Gleser, C.N. Winget, R.L. Kunkel and E.L. Saenger. Presented at the DASA Medical Coordination Conference "Radiation-Induced Incapacitation/Performance Decrement", Armed Forces Radiobiology Research Institute, Bethesda, Md. 18-19 November 1969.
Cytologic-Biochemical Indicators of Radiation Injury in Man. Presented by E.B. Silberstein at the WHO/IAEA Conference, Paris, June 22-26, 1970.
The Changing Picture of Bone Marrow Granulocyte Reserves in Irradiated Patients. Presented at the Experimental HernLtology Society by E.B. Silberstein, November 12-13, 1970, Pittsburgh.
Presentations listed below were made by staff of the Radioisotope Lab. at the Joint Oak Ridge Associated Universities-Defense Atomic Support Agency Information Exchange Program "Radiation Effects on Biological Systems," Oak Ridge, Tenn. March 29-30, 1971.
A Closed System for Marrow Transplantation - E.B. Silberstein
Chromosome Aberrations as a Dosimeter of Whole Body Irradiation - E.B. Silberstein
Active Bone Marrow Doses in Whole-Body and Partial Body Exposures - J.G. Kereiakes
Serum and Urinary Amylase Activities in Irradiated Cancer Patients - E.L. Saenger
The Relationship of Nausea and Vomiting to Radiation Dose - E.L. Saenger
In vitro studies of Chromosome aberrations caused by Irradiation - E.B. Silberstein

Ultraviolet-Absorbing Compounds in Urine of Two Irradiated Cancer Patients as Determined by High- Resolution Column Chromatography - E.L. Saenger
Active Bone Marrow Dose Related to Hematological Changes in Whole Body and Partial Body Exposures - J.G. Kereiakes, E.B. Silberstein, E.L. Saenger, W.G. Van De Riet and C. Born - submitted for presentation at the Annual Meeting of the Radiological Society of North American in December 1971.
Bone Marrow Dose in Whole and Partial Body Cobalt 60 tissue- equivalent human phantom. C. Born, J.G. Kereiakes, G.K. Gahr and G.H. Simmons, presented at the annual meeting of the AAPM, Houston, Texas, July 1971.
PRESENTATION - Made under DASA contract - Radiation effects on cancer patients
Radiation Casualties-Newer Aspects of Mass Casualty Care. Presented by Eugene L. Saenger and Max L.M. Boone, at the Thirteenth County Medical Societies Conference on Disaster Medical Care, American Medical Association, Chicago, Illinois, November 4, 1962.
Deoxycytidine Levels in the Urine of X-irradiated Rats. Presented by James G. Kereiakes at the Annual Meeting of the Radiation Research Society, May 1964, Miami Beach, Florida.
Urinary Excretion of Amino Acids and Nucleosides by Cancer Patients Following Whole-Body Irradiation, presented by E.L. Saenger at the Annual Meeting of the Radiation Research Society, May 1964 at Miami Beach, Florida.
Autologous Bone Marrow Storage and Infusion in Patients Receiving Whole Body Radiation. Presented by Ben I. Friedman at the American College of Physicians Regional Meeting in Pittsburgh on November 20, 1965.
Effect of Whole and Half-Body Irradiation in Human Beings with Cancer. Presented by Eugene L. Saenger at the Third International Congress of Radiation Research, Cortina d"Ampezzo, Italy, June 26, July 2, 1966.
Hope and Denial in Metastatic Carcinoma - A Preliminary Report. Presented by Dr. Robert L. Kunkel at a Psychosomatic Meeting in New Orleans, 1966.
Effects of Total and Partial Body Therapeutic Irradiation in Man. Presented by Eugene L. Saenger at the Proceedings of the 1st International Symposium on the Biological Interpretation of Dose from Accelerator-Produced Radiation. Held at the Lawrence Radiation Laboratory, Berkeley, California, March 13-16, 1967.

Quantitive Analysis of Deoxycytidine in the Urine of Irradiated Cancer Patients and Rats. Presented by James G. Kereiakes at the DASA Symposium, U.S. Naval Radiological Defense Laboratory, San Francisco, California, April 9-11, 1968.
The Management of the Acute Radiation Syndrome in Man. Presented by Eugene L. Saenger at the DASA Symposium, U.S. Naval Radiological Defense Laboratory, San Francisco, California, April 9-11, 1968.
Bone Marrow Dosimetry in a Cobalt 60 Irradiated Tissue-Equivalent Human Phantom. Presented by James G. Kereiakes at the DASA Medical Coordination Conference, Air Force Weapons Laboratory, Kirkland Air Force Base, New Mexico, May 27-29, 1969.
Radiation-Induced Urinary Excretion of Deoxycytidine by Rats and Humans. Presented by I-Wen Chen at the Annual Meeting of the Radiological Society of North America, Chicago, Illinois, December, 1967.

TECHNICAL REP 0 RTS
Report Period
Feb. 1960 thru Oct. 1961
Nov. 1961 thru Apr. 1963
May 1963 thru Feb. 1964
Feb. 1960 thru Apr. 1966
May 1966 thru Apr. 1967
May 1967 thru Apr. 1968
day 1968 thru Apr. 1969
May 1969 thru Apr. 1970
May 1970 thru Apr. 1971
Submitted by University of Cincinnati to Defense Nuclear Agency (DNA) formerly DASA
Title
Metabolic Changes in Humans Following Total Body Radiation
Metabolic Changes in Humans Following Total Body Radiation
Metabolic Changes in Humans Following Total Body Radiation
Metabolic Changes in Humans Following Total Body Radiation
Metabolic Changes in Humans Following Total Body Radiation
Radiation Effects in Man; Manifestations and Therapeutic Efforts
Radiation Effects in Man; Manifestations and Therapeutic Efforts
Radiation Effects in Man; Manifestations and Therapeutic Efforts
Radiation Effects in Man; Manifestations and Therapeutic Efforts
Contract No.
DA-49-146-XZ-029
DA-49-146-XZ-029
DA-49-146-XZ-029
DA-49-146-XZ-315
DA-49-146-XZ-315
DA-49-146-XZ-315
DA-49-146-XZ-315
DASAO1-69-C-0131
DASAO1-69-C-0131
DASA Report No.
None Assigned
DASA 1422
DASA 1633
DASA 1844
DASA 2179
DASA 2163
DASA 2428
DASA 2599
DNA 2751T

- ,
RCC 1.950922.00 1
RADIATION EXPERIMENB CONJM’IED BY THE UNlvERsFTy OF CINCINNATI MEDICAL SCHOOL WITH DEPARTMENT OF DEFENSE FUNDING
4
I L! HEARING
BEFORE THE
SUBCOMMITTEE ON ADMINISTRATIVE LAW AND GOVERNMENTAL RELATIONS
OF THE
COMMITTEE ON THE JUDICIARY HOUSE OF REPEESENTATIVES
ONE HUNDRED THIRD CONGRESS SECOND SESSION
APRIL 11, 1994
Serial No. 67
Printed for the use of the Committee on the Judiciary
U.S. OOVEFWMENT PRINTING OFFICE
84-514 WASHINGTON : 1994
For sale by the U S Government Pnnting Office Supenntendent of Documents. Congressional Sales Office. Washington, DC 20402
ISBN 0-16-046348-3

ua 1
the
COMMIrnE ON THE JUDICLARY

C O N T E N T S
HEARING DATE
.
J
3
April 11, 1994 ........................................................................................................... OPENING STATEMENT
Bryant, Hon. John, a Representative in Congress from the State of Texas, and chairman, Subcommittee on Administrative Law, and Governmental Relations ...............................................................................................................
WITNESSES
Cox, James D., M.D., professor of radiothera y, M.D. Anderson Cancer Cen- ter, and chairman, Radiotherapy Oncology &roup ............................................
E ‘lman, David, M.D., clinical assistant professor, Department of Community
Ha er, Catherine, survivor daughter ..................................................................... Sedicine, Brown University ................................................................................ L a t i n s , Joseph, survivor son .................................................................................
Atomic Energy, Department of 8efense .......................................................
Stephens, d r t h a , Ph.D., professor of English, University of Cincinnati ..........
Nelson, Gloria, survivor granddaughter ................................................................ Saenger, Eugene, M.D., professor emeritus of radiology, University of Cin-
cinnati ................................................................................................................... So r, Dr. Gordon K., Principal De uty to the Assistant for the Secretary
Ste er, Joseph, president, University of Cincinnati, accompanied by Stanley hf Chesle ............................................................................................................
LETTERS, STATEMENTS, ETC., SUBMITTED FOR THE HEARING
Bryant, Hon. John, a Representative in Congress from the State of Texas, and chairman, Subcommittee on Administrative Law, and Governmental Relations: Opening statement .............................................................................
Cox, James D., M.D., professor of radiothera y, M.D. Anderson Cancer Cen- ter, and chairman, Radiotherapy Oncology &roup: Prepared statement ........
E ‘lman, David, M.D., clinical assistant professor, Department of Community Sedicine, Brown University: Prepared statement ............................................
Ha r, Catherine, survivor dau hter: Prepared statement ................................. Mann, Hon. bavid, a Representative in Congress from the State of Ohio:
Openin statement ............................................................................................... Nelson, Gloria, survivor anddaughter: Pre ared statement ............................. Portman, Hon. Rob, a gpresentative in Ebngress from the State of Ohio:
Saenger, Eugene, M.D., professor emeritus of radiology, University of Cin-
So r, Dr. Gordon K., Principal De uty to the Assistant for the Secretary E Atomic Energy, Department of Lfense: Prepared statement .................... Steger Jose h resident, University of Cincinnati: Prepared statement .......... Stephcks, d art ’ l! a, Ph.D., professor of English, University of Cincinnati: Pre-
Lagins, Jose h, survivor son: &pared statement .............................................
Prepared statement .............................................................................................. cinnati: Prepared statement ................................................................................
pared statement ...................................................................................................
Material submitted for the hearing ........................................................................ APPENDIX
5
68
107 19 17 19
171
27
81 147
5
70
111 297 294
10 293
14
177
30 83
150
293

RADIATION EXPERINIENTS CONDUCTED BY THE UNIVERSITY OF CINCINNATI MEDICAL SCHOOL WITH DEPARTMENT OF DEFENSE FUNDING
MONDAY, APRIL 11,1994
HOUSE OF REPRESENTATIVES, SUBCOMMITTEE ON ADMINISTRATIVE LAW
AND GOVERNMENTAL RELATIONS, COMMITTEE ON THE JUDICIARY,
Cincinnati, OH. The subcommittee met, pursuant to notice, at 10 a.m., in court-
mom 2, mom 822, U.S. Post Ofice and Courthouse, Fifth and Wal- nut Streets, Cincinnati, OH, Hon. John Bryant (chairman of the subcommittee) presiding.
Present: Representatives John Bryant and David Mann. Also present Representative Rob Portman. Staff present: David Naimon, assistant counsel; Nichole Jenkins,
assistant counsel; and Ray Smietanka, minority counsel.
OPENING STATEMENT OF CHAIRMAN BRYANT Mr. BRYANT. Good morning, ladies and gentlemen and distin-
guished guests. The subcommittee will come to order. The House Judiciary's Subcommittee on Administrative Law and
Governmental Relations meets today in Cincinnati to take testi- mony concerning the whole and partial body of radiation experi- ments conducted in Cincinnati General Hospital and the University of Cincinnati Medical Center between 1960 and 1991, and partially funded by the Department of Defense. This subcommittee has jurisdiction over com ensation for claims
ment's wrongdoing and considered previous com ensation legisla-
Japanese-Americans who were in internment camps during World War 11, and the Radiation Exposure Compensation Act of 1990, which compensates the residents who lived downwind from a Ne- vada nuclear test site and participated in those tests by the Gov- ernment.
On February 2, 1994, the subcommittee held a hearin examin-
humans who did not give informed consent to the experiments, in- cluding separate tests involving radiation, mustard gas, LSD, and other chemical agents.
(1)
against the Federal Government based on t K e Federal Govern-
tion such as the Civil Liberties Act of 1988, w R ich compensates
ing the issue of Government-sponsored experiments pe B ormed on
' I I

2
The allegations the Cincinnati radiation experiments are very serious. these human ex riments could be the most
Our task is to examine these tests, determine whether the sub- ects gave informed consent to partici ating in such tests, and what
priate. I would like to thank Congressman David Mann, a member of
this subcommittee, for bringmg the Cincinnati radiation experi- ments to the subcommittee’s attention. 1 commend Congressman Mann’s commitment and persistence for brin ‘ng these e eri-
Clinton administration. I know he also has worked closely with the working group estab-
lished by President Clinton to ensure these experiments get serious examination as part of that group’s consideration.
The subcommittee would also like to welcome Rob Portman to this subcommittee. While he is not a member of this specific sub- committee and the Judiciary committee does not allow nonmembers to question witnesses at committee hearings, as chair- man I think it is ap ropriate in this instance for Congressman
volvement with this issue. I think Congressman Portman’s involve- ment in this hearing is an unusual case and it does not set a prece- dent for future subcommittee or committee olicies elsewhere.
issue for some time to come. Today’s hearing is just a ste in that process. It does not focus on any particular legislation, w%ch has not yet been written by this subcommittee. We expect to have more hearin s before we consider whether to legislate in this area, and we wi If be working closely with the Clinton administration in fash- ioning an appropriate response.
We ap reciate the presence today of all of our witnesses and
witnesses there will be limited time for makin statements and an-
swers may be submitted at a later date. I am informed that I said 1960 through 1991 while referring to
those experiments. As everyone knows, it was 1960 through 1971. I would like, before concluding my statement, to say a very pro-
found thank ou to Jud e Webber for the use of his courtroom. I
logistical develo ment in making this possible.
Mr. MANN. Thank you, Mr. Chairman. Welcome to Cincinnati. We are proud that you are here and I am proud to serve on your subcommittee. I enjoy very much working with you and I admire your leadership.
I think this is an important hearing. As you know, I have been working on this subject for some months now, as this entire com- munit has been focused increasingly on the experiments that oc-
light and help focus the issue as this subcommittee takes up the question of compensation.
been brought to lig g. t yet.
B arm resulted from the tests, and w t ether compensation is appro-
ments to the forefront of the Congress and to t a e attention o 7 the
Portman to sit with t R e subcommittee based on his extensive in-
The subcommittee expects to be involv e l in the human testing
commen 0 them for their preparation. We realize that with so many
swering questions today. However, addition 3 materials and an-
would also li l e to give t anks to Betsy Brockmeyer for all of her
At this time, P recognize Congressman Mann.
cu J between 1961 to 1971. I hope this hearing will cast new
I

3
I too would like to thank the witnesses who have agreed to tes- tify today. My heart goes out to all of the family members of the patients we will be discussing during this hearing. I know that re- living the illnesses of your loved ones some 20 years ago has brought you real pain. Three of you will sit at the witness table today. But I know many more of you would have liked to share your stories.
I would like to ask unanimous consent, Mr. Chairman, that all the written statements submitted to the subcommittee, whether by witnesses or otherwise, be included in the record for today’s pro- ceedings.
Mr. BRYANT. Without objection, so ordered. Mr. MANN. I would like to voice my appreciation for all witnesses
other than family members who will be participating today, includ- ing Dr. Saenger.
What we know to date, Mr. Chairman, is that some 87 patients received whole or partial body radiation. We know the patients in- volved were diagnosed with various forms of cancer believed to be terminal.
We also know while they may have consented to the treatment, many or perhaps all of them were unaware of the Department of Defense interest in their conditions and many or perhaps all were unaware of the potential side effects of the radiation.
We also know that written consent forms were not used until the mid-1960’s.
But let’s get to the heart of the matter. We also know that the original University of Cincinnati proposal to the Pentagon, the con- tract between the University of Cincinnati and the Pentagon, and the first five reports about the project from the University of Cin- cinnati to the Pentagon all describe the purpose of the project in terms only of the Pentagon’s needs, particularly its need for biologi- cal tests of radiation exposure, and not in terms of therapy for pa- tients.
Each of the first five reports covering the period from February 1960 to April 1967 label the project as “metabolic changes in hu- mans following total body irradiation.”
The term “therapeutic efforts” does not even become a part of the title of the reports to the Pentagon until 1968 when the title be- comes “Radiation Effects in Man: Manifestations and Therapeutic
It is also important to understand and keep focused on the fact that this project was conducted while the contract with the Penta- gon and while the Pentagon’s money continued. Whole body radi- ation under this project neither preceded nor outlived the Penta- gon’s contract.
The two primary issues that I believe we need to resolve, Mr. Chairman, are, first, did the patients knowledgeably consent to the experiments? And by “knowledgeably,” I mean were they fully in- formed of all the facts and circumstances and possible con- sequences to them and funding.
And second, was this type of treatment a propriate for the types of illnesses suffered by the patients? By t&s I mean, absent the $8,000 or $10,000 per patient provided by the Department of De-
= -
Efforts.”
4
fense, would whole body radiation have been an appropriate medi- cal thera y for these patients?
believe we have no choice but to conclude t at the radiation ex ri- ments were simply wrong and that the Government owes a E g e apology to the victims, their families, and the Nation.
ain, Mr. Chairman, I appreciate the hard work ou and the
to the testimony here today. h a n k you very much.
R If we P ind the answer to any of these uestions is "no," then I
s 3 have put into preparin for this hearing and I P ook forward
[The opening statements of Messrs. Bryant and Mann follow:]

5
OPENING REMARKS REP. JOHN BRYANT, CHAIRMAN
SUBCOMMITTEE ON ADMINISTRATIVE LAW AND GOVERNMENTAL RELATIONS
HEARING ON RADIATION EXPERIMENTS CONDUCTED BY THE UNIVERSITY OF CINCINNATI MEDICAL SCHOOL WITH
DEPARTMENT OF DEFENSE FUNDING
GOOD MORNING LADIES AND GENTLEMEN AND DISTINGUISHED GUESTS. ORDER. ON ADMINISTRATIVE LAW AND GOVERNMENTAL RELATIONS MEETS TODAY IN CINCINNATI TO TAKE TESTIMONY CONCERNING THE WHOLE AND PARTIAL BODY RADIATION EXPERIMENTS CONDUCTED AT CINCINNATI GENERAL HOSPITAL AND THE UNIVERSITY OF CINCINNATI MEDICAL CENTER BETWEEN 1960 AND 1971 AND PARTIALLY FUNDED BY THE DEPARTMENT OF DEFENSE.
THE SUBCOMMITTEE WILL COME TO THE HOUSE JUDICIARY COMMITTEE’S SUBCOMMITTEE
THIS SUBCOMMITTEE HAS JURISDICTION OVER COMPENSATION FOR CLAIMS AGAINST THE FEDERAL GOVERNMENT BASED ON THE FEDERAL GOVERNMENT’S

6
2 WRONGDOING , AND CONSIDERED PREVIOUS COMPENSATION
LEGISLATION, SUCH AS THE C I V I L LIBERTIES ACT OF
1988, WHICH COMPENSATES JAPANESE-AMERICANS WHO WERE
I N INTERNMENT CAMPS DURING WORLD WAR 11, AND THE
RADIATION EXPOSURE COMPENSATION ACT OF 1990 , WHICH
COMPENSATES THE RESIDENTS WHO LIVED DOWNWIND FROM
THE NEVADA NUCLEAR TEST S I T E AND THE WORKERS WHO
PARTICIPATED I N THOSE TESTS OR MINED URANIUM FOR THE
GOVERNMENT.
ON FEBRUARY 2, 1994, THE SUBCOMMITTEE HELD A
HEARING EXAMINING THE ISSUE OF GOVERNMENT-SPONSORED
EXPERIMENTS PERFORMED ON HUMANS WHO D I D NOT GIVE
INFORMED CONSENT TO THE EXPERIMENTS -- INCLUDING
SEPARATE TESTS INVOLVING RADIATION, MUSTARD GAS, LSD
AND OTHER CHEMICAL AGENTS.
THE ALLEGATIONS REGARDING THE CINCINNATI
RADIATION EXPERIMENTS ARE VERY SERIOUS. IF THEY ARE
Y

7
3 TRUE, THESE HUMAN EXPERIMENTS COULD BE AMONG THE
MOST EGREGIOUS THAT HAVE BEEN BROUGHT TO LIGHT YET.
OUR TASK I S TO EXAMINE THESE TESTS, WHETHER THE
SUBJECTS GAVE INFORMED CONSENT TO PARTICIPATING I N
SUCH TESTS, WHAT HARM RESULTED FROM THE TESTS, AND
WHETHER COMPENSATION I S APPROPRIATE.
I WOULD LIKE TO THANK CONGRESSMAN DAVID MANN, A
MEMBER OF THIS SUBCOMMITTEE, FOR BRINGING THE
CINCINNATI RADIATION EXPERIMENTS TO THE
SUBCOMMITTEE’S ATTENTION. I COMMEND CONGRESSMAN
MANN’S COMMITMENT AND PERSISTENCE I N BRINGING THE
ISSUE OF THESE EXPERIMENTS TO THE FOREFRONT I N THE
CONGRESS AND THE ADMINISTRATION. I KNOW HE ALSO I S
WORKING CLOSELY WITH THE HUMAN RADIATION INTERAGENCY
WORKING GROUP ESTABLISHED BY PRESIDENT CLINTON TO
ASSURE THAT THESE EXPERIMENTS GET SERIOUS
EXAMINATION AS PART OF THAT GROUP’S CONSIDERATION.

B
8
4 THE SUBCOMMITTEE ALSO WID LIKE TO WELCOME
CONGRESSMAN ROB PORTMAN TO THIS SUBCOMMITTEE
HEARING.
OF THE JUDICIARY COMMITTEE OR THIS SUBCOWITTEE, AND
THE JUDICIARY COMMITTEE’S POLICY DOES NOT ALLOW NON-
MEMBERS TO QUESTION WITNESSES AT COMMITTEE HEARINGS,
I THINK I T I S APPROPRIATE I N THIS INSTANCE FOR
CONGRESSMAN PORTMAN TO S IT WITH THE SUBCOMMITTEE,
BASED ON HIS EXTENSIVE INVOLVEMENT WITH THIS ISSUE.
I THINK CONGRESSMAN PORTMAN’S INVOLVEMENT IN THIS
HEARING I S AN UNUSUAL CASE, AND I W NOT INTEND FOR
HIS INVOLVEMENT TO BE A PRECEDENT FOR FUTURE
SUBCOWITTEE OR COMMITTEE HEARINGS.
WHILE CONGRESSMAN PORTMAN I S NOT A MEMBER **
4
THE SUBCOWITTEE EXPECTS TO BE INVOLVED I N THE
HUMAN TESTING ISSUE FOR SOME TIME TO COME. TODAY‘S
HEARING I S JUST A STEP I N THE PROCESS, AND DOES NOT
FOCUS ON ANY PARTICULAR LEGISLATION.
HAVE MORE HEARINGS BEFORE WE CONSIDER WHETHER TO
WE EXPECT TO

c
9
5
LEGISLATE IN THIS AREA, AND WILL BE WORKING CLOSELY WITH THE CLINTON ADMINISTRATION IN FASHIONING AN APPROPRIATE RESPONSE.
WE APPRECIATE THE PRESENCE TODAY OF ALL OUR WITNESSES AND COMMEND THEM FOR THEIR PREPARATION. WE REALIZE THAT WITH SO MANY WITNESSES THERE WILL BE
LIMITED TIME FOR MAKING YOUR STATEMENTS AND ANSWERING QUESTIONS TODAY. HOWEVER, ADDITIONAL MATERIALS AND ANSWERS MAY BE SUBMITTED AT A LATER DATE.
I NOW RECOGNIZE CONGRESSMAN DAVID MANN TO MAKE AN OPENING STATEMENT.
CONGRESSMAN PORTMAN, WOULD YOU LIKE TO MAKE AN OPENING STATEMENT?

10
NEWS from Congressman David Mann
First District - Ohio The Statement of
Th. Ilonorabl~ David Yurn April 11, 1994
Mr. Chairman, I would like to thank you for agreeiag to convene this hearing today. As you bow, I have been working very hard to uncover the facts with regard to the radiation tests performed at Cincinnati General Hospital in the 1960s and 1970s and I believe that this hearing will help to uncover evidence previously unknown and put some logical order to the information already available to us.
before ua today. My heart goes out to all of the family members of the patients we will discuss during this the illnesses of your loved-ones sane twenty years ago has brought you real pain. Three of you will sit at the witness table today, but I know many more of you would have liked to share your stories. I would like to ask for unanimous conaent that all of the written statemcnta submitted to the Subcdttee and our offices be included in the record for today's proceedings.
I would also like to recognize and voice my appreciation €or witnesses who will present their candid views of the radiation studies, Dr. Bgilman, Dr. Stephens, and Dr. Cox. I would like to thank Dr. Soper from the Department of Defense for presenting testimony on the DOD record retrieval process and President Steger for his testimony on the University's efforts to help investigate this matter. And I would like to thank Dr. Saenger for his willingness to present his view on the radiation experiments and to anewer the many question. this Subcommittee w i l l pose.
What we know to date, Mr. Chairman, is that some a7 patients received whole and partial body radiation in experiments funded Fn,part by the Department of Defense. We know that the patients involvedhre diagnosed with various forms of cancer believed to be termiwl. 'ke also know that while they may have consented to the treatment, many or perhaps all of them were unaware of the Department of Defense interest in their conditions and many or perhaps all were unaware of the potentiaL side effects of the radiation. consent forma were not used until the mid 1960s.
I would like to thank the witnesses who have agreed to testify
hearing. I know that reliving
We also know that written
(over)
WASHINGTON OFFICE DlsFlllcTomcE 2210 Ymser BuMln8
1014 Vns Slncl C i w m . OH 45m2
(S13) 684-2723
m3 Cannon H 0 B Wuhmpon. D C M51S
(202) 225-2216 .Ir.*
1 I .
I
I

11
But lets get to the heart of the matter. We also know that the orginial University of Cincinnati proposal to the Pentagon, the contract between U.C. and the Pentagon and the first five reports about the project from U.C. to the Pentagon all describe the purpose of the project in tern of the Pentagon's needs - - particularly its need for a biological test of radiation exposure - - and in tern of therapy for patients. Each of the first five reports (covering the period from February 1960 to April 1967) labeled the project as "Metabolic Changes in Humans Following Total Body Irradiation". "Theraputic Efforts" do not even become a part of the title of the reports to the Pentagon until 1968 when the title becomes "Radiation Bffects in Man: Manifestations and Theraputic Efforts."
Note also that this project was conducted while the contract with the Pentagon and the Pentagon's money continued. whole body radiation under this project neither preceeded nor outlived the Pentagon contract.
The two primary issues that I believe we need to resolve. M r . Chainnan, are (1) Did the patients knowledgeably consent to the experiments? And, ( 2 ) Was this type of treatment appropriate for the types of illnesses suffered by the patients. By this I mean, absent the $8,000 - $10,000 per patient in Department of Defense funding, would whole body radiation have been an appropriate medxal therapy?
I believe we have no choice but to conclude that the radiation experiments were SIMPLY WRONO and that the government owes a huge apology to the victims, their families and the nation as a whole!
Again, M r . Chairman, I appreciate the hard work you and your staff have put into preparing for this hearing. I believe that the testimony we hear tpday will enable us to craft a fair and just compensation bill in the weeks and months ahead.
If we find that the answer to either of these questions is "no" then
Thank you.

12
Mr. BRYANT. Mr. Portman. Mr. PORTMAN. Mr. Chairman, thank you for coming to Cincinnati
to hold this important hearing and also for including me as a an- elist. As you noted, I am not a member of the subcommittee; Row- ever, I do have a long commitment to this issue. I have been heav- ily involved in the issue for the past several months, and also the issues impact the people who live in my district. In particular, some of the patients involved lived in what is now the Second Dis- trict of Ohio. Many of the family members, including at least one who will be testifLing here today, currently live in the district I re resent. bs matter has a long but unfortunately incomplete history of public scrutiny. There remain unanswered questions that relate not only to the critical aspect of how le and their families were treated, but also the role of the Fe Trap e Government in conducting such experiments on human beings.
Although there are many issues that will be addressed by the various parties involved, in my mind, there are two cardinal issues that we, as Federal officials, can and must address. The first is the appropriateness of the Federal Government compensating the vic- tims and their families. If it is determined that the patients in- volved were not clearly informed in accordance with the standards for informed consent in force at the respective times of the experi- ments, or that these ex riments became vehicles primaril for testing, not treatment, tg. en compensation, in my view, wou r d be ap ropriate. k s is so especially in light of the many potential legal barriers to recovery, including the statute of limitations under the Federal Tort Claims Act, sovereign immunity, and possible immunity of Government contractors.
Chairman Bryant’s subcommittee has jurisdiction over the com- pensation issue, and I understand that there is some precedent for compensation when the facts so merit it. Because I am not on the subcommittee or committee, I will not have the opportunity to vote upon this issue at the committee level.
I believe that the second issue from the Federal Government’s standpoint is one of disclosuredisclosure by the De artment of Defense and the Cincinnati General Hospital and al P others in- volved-of all relevant information concerning these cases. In addition to reviewing the merit of compensating potential vic-
tims, I believe the Government and the Government contractors have an obligation to be hlly forthcoming, to admit mistakes if mistakes have been made, and to ensure that safeguards are put in place with respect to any experiments that may be conducted today or in the future.
The issues of full disclosure and safeguards may not be directly related to this forum. However, I have particular interest in these issues, and the Government Operations Committee upon which I serve has been exploring the possibility of having additional hear- in s on those two issues.
knally, I am here to listen and to continue to learn as much as I can about what happened two and three decades ago. This is not a court of law; we are not here to press charges. We are also not here to politicize what is a sensitive and emotional topic.

13
I view our role as factfmders who want to ensure that the Fed- eral Government ads responsibly and fairly with respect to the pa- tients and their families, to the investigators and to the DOD offi- cials involved in the study.
I commend all of the witnesses for bein here today. I commend
timony. Thank you, Mr. Chairman. [The prepared statement of Mr. Portman follows:]
you for agreeing to testify and very much f ook forward to your tes-

14
1
STATEMENT OF HONORABLE ROB PORTMAN
SUBCOMMITTEE ON ADMINISTRATIVE LAW AND GOVERNMENTAL RELATIONS
APRIL 11, 1994
Mr. Chairman, first, let me thank you for coming to
Cincinnati to hold this important hearing and for including me as
a panelist. Although I am not a member of the Subcommittee, the
issues addressed here impact many people who live in the District
I represent. In particular, some of the patients involved lived
in what is now the Second District and many of the family members
- including some we will be hearing from today - are my constituents.
This matter has a long, but unfortunately incomplete,
history of public scrutiny.
that relate to not only the critical aspect of how people and
their families were treated, but also the role of the federal
government in supporting such experiments on human beings.
There remain unanswered questions
Although there are many issues that will be addressed by the
various parties involved, in my mind, there are two cardinal
issues that we as federal officials can and must address.
h

15
2
The first is the appropriateness of the federal government
compensating the victims and their families. If it is determined
that the patients involved were not clearly informed in
accordance with the standards for informed consent in force at
the respective times of the experiments, or that these
experiments became vehicles primarily for testing not treatment,
then compensation, in my view, would be appropriate. This is so
especially in light of the many potential legal barriers to
recovery, including the statute of limitations under the Federal
Tort Claims Act, sovereign immunity, and possible immunity of
government contractors. Chairman Bryant's subcommittee has
jurisdiction over the compensation issue, and I understand that
there is some precedent for compensation when the facts so merit
it. Because I am not on the subcommittee or committee, I will
not have the opportunity to vote upon this issue at the Committee
level. However, I would have the chance to consider any proposal
for compensation on the Floor of the House of Representatives.
I believe the second issue from the federal government's
standpoint is one of disclosure -- disclosure by the Department of Defense and the Cincinnati General Hospital and all others
involved -- of all relevant information concerning these cases. In addition to reviewing the merit of compensatinq potential
victims, I believe the government and the government contractors

16
3
have an obligation to be fully forthcoming, to admit mistakes if
mistakes have been made, and to ensure that safeguards are put in
place with respect to any experiments that may be conducted today
or in the future. The issues of full disclosure and safequards
may not be directly related to this forum. However, I have
particular interest in these issues, and the Government
Operations Committee upon which I serve has been exploring the
facts of the UC cases and the possibility of holding hearings on
disclosure of government information and safeguards.
Finally, I am here to listen - and to continue to learn as much as I can about what happened 2 and 3 decades ago. This is
not a court of law; we are not here to press charges. We also
are not here to politicize a sensitive and emotional topic. I
view our role as fact finders who want to ensure that the federal
government acts responsibly and fairly with respect to the
patients and their families, to the investigators and to the DOD
officials involved in the study.
I commend all of the witnesses who have agreed to testify
before us today and very much look forward to their testimony.
Thank you Mr. Chairman.

.
17
Mr. BRYANT. At this time we would invite to come to the witness table the first three witnesses on our panel.
First, Joseph Larkins, survivor son; Gloria Nelson, survivor granddaughter; and Katherine Hager, survivor daughter.
We would ask that each of you, as well as all of the witnesses who come behind you, limit your statement to 5 minutes in order that we might ask you questions and have time for all the wit- nesses to speak.
I will begin on my left with Mr. Larkins. Mr. Larkins, thank you very much for coming here today. Please proceed.
STATEMENT OF JOSEPH LARKINS, SURVIVOR SON Mr. LARKws. All right. Well, m name is Joe Larkins. I am 62
At that time, I was 30. My family consisted of myself, an older sis- ter, and my parents. When my father passed away he and my mother were in the process of raising a grandchild, my sister‘s son. Neither of my parents were well educated, but my father was hard working and honest. If Cincinnati General Hospital and the doctors therein had been honest, there is, of course, the possibility that my father could have lived for several more years. Instead, he went from a fairly able-bodied, middle-a@ father, and husband to a premature death caused by an expenment. My father did not know that he was being used .as q guinea ig; my mother did not know;
or of the risks involved. and the other doctors involved, if
of radiation which they admin- very real probabilit of being
fatal. Oh, how right that is! My father was very muc a family man, yet these eople killed him as surely as if they had put a
my mother, with no job skills, to raise a andchild as best as she
after my father‘s premature and unexpected death. I know that my father knew that something was very wrong with
the treatments being given to him at Cincinnati General. He even asked me, “Son, what are they doing to me? They’re trying to kill me.” That is how bad the pain he endured after the treatment was. He suffered so needlessly.
What really gets me about this situation is the fact that the Pen- tagon contracted with these doctors and this hospital to test the ef- fects of radiation on the human body. Everyone realizes that Cin- cinnati General Hospital, now the University of Cincinnati Hos- pital, treated many low-education, low-income patients. I guess they felt that in some way the fact that these patients were not rich, upper class citizens gave them the right to experiment with their bodies without informed consent. Not so. I feel sure these physician-researchers were well paid for their art, and it would be
amounts of the ts given to Cincinnati General by the Federal Government. I E sure that all parties, with the exception of the poor,
unsuspecting patients and their families, were well compensated.
years old now. My father, Will aKT Larkins, passed away in 1971.
as his children, we were not inforpl e l of the procedures to be used
Y to his head an B pulled the trigger themselves. These doctors eft
could. My mother lived until 1983, but s a e was a broken woman
E
very interesting to know the types and dolar P

18
But since when, in our society, does one man or even a group of them, have the right to play God?
A very good example of this is our 20th century “assisted-suicide doctor.” This man is contacted by terminally ill patients who wish to end their own lives with dignity and choose, by their own voli- tion, not to suffer needlessly for years. These people make the deci- sion to die in peace, yet our great judicial system, along with the medical community, brought this compassionate physician up on charges.
The differences in these deaths and the death of my father are that my father did not choose to diesomeone else made that deci- sion for him without consulting or informing him, and they were amply compensated for it.
I feel that the price they should be required to pay to the fami- lies of the people they killed should be exceedingly high. I also feel that the Federal Government should be named as a coconspirator in this case, because that is exactly what it was, a conspiracy.
No person-and I emphasize “no” person-would willingly con- sent to a treatment with any degree of fatality involved. People, both you and I, simply value life too much. I think that is the big thing here, the patients were not informed. I know that behavior of this sort would not be tolerated by the medical community today.
But then again, this entire mess was surrounded by a thick veil of secrecy on both the doctors’ part and on the part of Cincinnati General Hospital. It is still being closely guarded and kept under yet another veil of secrecy to this very day by the University of Cincinnati, in that they have yet to provide the medical records of the patients involved in this experiment-but they have, as of now. At the time of this statement they were n o t i n the entirety, to the next of kin immediately.
They are hedging to save their own skin. I was promised my fa- ther‘s complete medical file over a month ago; as of this writing, I have nothing. But like I said, we do have them now.
I only hope that you, the congressional committee, see fit, as members of the human race, to break this matter wide open here and now and award just compensation to the families of the vic- tims. I feel that the physicians involved and also the Federal Gov- ernment, the Pentagon, should pay; and also I beg you to strip any and all of the doctors involved of all their medical credentials that they hold. If justice prevails in this matter-and I have faith that it will-a strong message will be sent to our government officials and the private physicians, to whom people entrust their lives and the lives of their loved ones, that behavior of this sort will simply not be tolerated, that justice will, in fact, be both swift and severe.
I pray that a situation such as this will never again be faced by a group of people. If this statement to you, the congressional com- mittee, does anything to help in the name of justice, then my fa- ther‘s death and the sorrow and hardships that his family faced, will not have been completely in vain.
Thank you. Mr. BRYANT. Thank you, Mr. Larkins. Ms. Nelson.
19
STATEMENT OF GLORIA NELSON, SURVIVOR GRANDDAUGmR
MS. NELSON. Amelia Jackson, patient number 67. On October 21, 1966, after bein discharged from General Hos-
take care of herself properly and depended on the family for all of her basic needs. She experienced bleeding from her rectum, loss of a petite, nausea, vomiting, weight loss, and was in constant pain. &r condition never improved.
Within a few weeks, she was readmitted to General Hospital. The family was informed she should be transferred to Drake Hos-
ital. MS. Jackson indicated she was afraid and want to return fl ome. She was transported home, where she was loved and cared for by us until she died on March 25, 1967.
The famil of Amelia Jackson would like for this committee to know that Zr the entire 163 days after receivin the irradiation,
of partial-body irradiation administered to her was cruel, and didn't he1 her condition in any wa It is our belief that she may
A doctor is someone you trust. His 'ob is to do everything in his
the case. She was always crying, moaning, groaning, and in excru- ciating pain. MS. Jackson was used to further Dr. Saengeis rofes- sional oals. It was urely an ambitious and callous act. Pfeither
used in an experiment conducted b Dr. Saenger, and funded by the Department of Defense. There gas clear1 been a coveru by
city of Cincinnati. We cannot believe that they consented to such atrocities to be financed by the Government utilizing the Jacksons' and the family's taxpaying dollars.
pital, MS. Jackson was a very we 2 , ill woman. She was unable to
her condition continued to detenorate. We feel t f at the 100 rads
have live c! longer if this experiment t a d not taken place.
power to alleviate your pain and su fi ering. However, this was not
MS. Jac 5 son nor the F amily was informed or consented to her being
means of the Government, General Hospital, 6r. Saenger, an a the
Mr. BRYm.,Thank you, MS. Nelson. MS. Hager. STATEMENT OF CATHERINE HAGER, SURVIVOR DAUGHTER MS. HAGER. To.the+total body radiation subcommittee and whom
it may concern: In January 1994, I be an noticing articles in The Cincinnati
cancer patients in the 1960's at Cincinnati neral Hos ital. Since I knew my father, Joseph Mitchell, was treated at that ospital for cancer during that period of time, I contacted Linda Reeves at the Cincinnati Enquirer. After a brief discussion with Linda, it was de- termined that my father had indeed been involved in the total radi- ation ex erimentation as patient No. 51, the first patient to be identifiex. From this point, my husband and I, along with the as- sistance of the news media, attempted to piece to ether any records available regarding my father's treatment at the os ital.
the right lung, and was admitted to Cincinnati General Hospital. Surgery was scheduled for November 1963. Although there is no notation of this scheduled surgery in his medical records, we have a letter which was written by my father to my sister detailing the
R (!c Enquirer regarding total % ody radiation ex rimentation done on
In October 1963, my father was diagnosed with f p ung cancer in

20
planned operation. For some unknown reason, the surgery was can- celed on the day it was scheduled to take place, with no expla- nation. The surgery was never rescheduled. Instead, my father was given a schedule of dates to return to the hospital for cobalt treat- ments. At this point, I asked the doctor why the surgery was can- celed. He told me he was too weak for surgery and decided to opt for the cobalt treatments instead.
In reality, my father was not in a weakened state at that time, but was in relatively good health, still working, and living a normal life. It wasn’t until the cobalt treatments started that my father began to go downhill. After 35 days of treatments, my father was so weak that he had to retire from work and move closer to my family so we could heip care for him.
In early 1965, my father was again admitted to Cincinnati Gen- eral Hospital with severe chest pains. It was at this time he was subjected to the total body radiation, 150 rads. He immediately started on a drastic downhill spiral. After much suffering, my fa- ther died on July 14, 1965, 74 days after the total body radiation.
Since total body radiation had not been performed on cancer pa- tients at Cincinnati General Hospital prim to the Government funding of 1960, I feel that my father, along with other cancer pa- tients, were handpicked and used in total bod radiation, not as a
a study performed for the Department of Defense to determine pos- sible effects on soldiers in nuclear warfare.
It might be noted that at the time my father died, two of my brothers were in the U.S. Air Force, one in Vietnam in the war zone. The Red Cross had to locate him and bring him home for the funeral. Both brothers have since retired from the Air Force. Isn’t it ironic that two of my brothers were serving this country in the military, while at the same time the Government was sponsoring experiments which shortened or ended their father’s life?
I would like to read the little note that my father sent to my sis- ter, which was written November 2, 1963.
DEAR ISABELL: I am very sorry, hone ; I need your help. First, I am going to have an o eration, first part of the week. ‘de doctor is not giving out the right news to the f m l y . It is going to be a long, serious operation. I will be about two months here, and it is very serious. Only a 50/50 chance to come throu h, as al l I have left is half a lung. So therefore I ask you to do all you can to hefp mom as much as possible, while I am in here.
I can tell you more when I see you again, but please do not take it to heart. I am trusting everything wil l turn out okay, which is doubtful. See you soon.
treatment for cancer, as they had been told, by u t as a coverup for
Love, DAD.
Thank you very much. Mr. BRYANT. Thank you, Ms. Hager. Mr. Larkins, let me start with you by asking, when did you or
your representative request your relative’s records from the Uni- versity of Cincinnati?
Mr. LARKINS. A little over a month ago. Mr. BRYANT. Have you received them yet? Mr. LARKINS. Yes, I finally got them today. Mr. BRYANT. Did you make the same request, Ms. Nelson? Ms. NELSON. Yes. Mr. BRYANT. And have you received them also?

21
MS. NELSON. Yes, I received them Friday. Mr. BRYANT. How long ago did you make the request? Ms. NELSON. Over a month ago. Mr. BRYANT. A month ago. Ms. Hager, did you request the records? Ms. HAGER. Yes, I did. But I don't think we have all of them. We
Ms. NELSON. Same here. MS. HAGER. You feel so, too? Ms. NELSON. Yes. The are not all there.
Me. HAGER. When did we receive ours, Bob? Mr. BOB HAGER. Approximately 3 weeks ago. Mr. BRYANT. Sir, would ou ident' yourself?
Mr. LARKINS. Can I sa sometLg else? Mr. BRYANT. Yes, Mr. Lkins. Mr. LARKINS. When we were going throu h my dad's files, we
found charts from 1971, December. He d i 3 in June of 1971. I would like to know how that can be.
Mr. BRYANT. Did you find anythin else unusual?
A couple of them are, but not all of them. Ma. NELSON. "he signatures on my grandmother's papers, they
are not hers either. Mr. BRYANT. You say they are not? Ms. NELSON. No. Mr. BRYANT. Does it purport to be her signature, but it is not her
writing? Ms. NELSON. Ri ht. And also I found documents in my grand-
That person's name is scratched out. Her name put in and a dif- ferent number put in.
Mr. BRYANT. Can you tell us, Mr. Hager, what type of harm your relatives suffered from the radiation treatment that was not a nor- mal result of cancer treatment?
Mr. Larkina-1 am so ; I spoke the wrong n a m r w h a t type of
a normal result of cancer treatment? Mr. LARKINS. Well, I guess the f a c t j u s t the way he went down-
hill. He was hoping to et well, but he was telling me, deep down, I ess that he knew, fike I said, that something was wrong. He dig% know what. He wasn't getting no better. He was getting worse.
Mr. BRYANT. I should say obviously we don't expect you to know what is the normal result of cancer, since you are not a doctor. But in terms of a layman's observation. Mrs. Nelson.
Ms. NELSON. My grandmother lost over 30 pounds after she had her radiation treatments, within a 3-month period.
Mr. BRYANT. MS. H er.
total body radiation. He had it on May 1. think he came home- he had it on May 1. He came home on May 8, 1965, he came home, and we had to take care of him. He was bedridden. We had to give
got some, but I still think there are more there.
Mr. BRYANT. When di B you get yours, Ms. Hager?
Mr. BOB HAGER. I am d r. Ha er, 2 atherine's husband.
Mr. LARKINS. The Signatures on f alf of the papers are not his.
mother's records t % at were originally made out for someone else.
harm did your father su 7 er from radiation treatment that was not
P Ms. HAGER. My fat x er was burnt prett bad after he had his

22
him baths. The Red Cross had to come and take him back and forth to the hospital every day. A nurse came every day and took a blood test from his finger.
I mean, he was just-he couldn’t eat. He couldn’t sit up. He had to-whatever came out of him, whatever kind of spittle came out of him, we used to have to save that and take it back to the hos- pital.
Mr. BRYANT. OK. Let me ask you a question. You spoke in your testimony about the fact that your father’s
surgery was called off, and instead he was given cobalt treatments. After 35 days---
Ms. HAGER. He had 35 days of cobalt treatment plus the whole body radiation also.
Mr. BRYANT. But the whole body radiation took place about 2 years later; is that correct?
Ms. HAGER. That is correct. Mr. BRYANT. And the letter from your father was dated 1963, im-
plying that you- Ms. HAGER. That was the first surgery he was su posed to have,
day, an J the nurse come in the same day and said-they started taking the things off of him.
I said, what are you doing? And she said, they canceled the sur- gery. He is not going to have surgery today.
And I said, well, who do we talk to to find out what is going on? And she said, you will have to get a hold of his doctor.
We sat there all day and no doctor came into the room to talk to us to explain anything.
Mr. BRYANT. Mr. Mann. Mr. MANN. I want to thank each of you for taking the time to
be with us. I know that it is not easy going over a sad chapter in your life. And it is of immense value to us.
Mr. Larkins, were you or any member of your family ever present when the radiation treatment, the radiation experiments were discussed with your father by any of the doctors at the hos- pital?
Mr. LARKINS. No, sir; I wasn’t. Mr. MANN. Did he ever talk with ou about the radiation that
he was going to have administered to Hm? Mr. LAR.KINS. He didn’t talk to me about it, but he talked to me
after. I was out there a couple of times after his treatments. That is the one time he asked me what they were trying to do with him. He received 300 rads of the radiation. I understand he got the most of anybody.
Mr. MANN. Do you know why he asked the question that way, what are they trying to do to me?
Mr. LARKINS. I think he was scared that he was dyin from it.
that led him to make that comment? Mr. LARKINS. To me, he was suffering all over. I mean, he was
just hurting all over. He didn’t know what to think about what was going on. He wanted to get well, but I guess that is what he had in the back of his mind, was that eventually he would get well, but he didn’t. He was only 55 years old, 3 years older than I am now.
that the did not give him. They had him prepared P or surgery that
Mr. MANN. Was he suffering in a particular way at t fl at point

23
Mr. m. Ms. Nelson, your grandmother, how old were you
Ms. NELSON. I was 20. Mr. IMANN. Were you or an other family members present when
Id. ELSON. No. We didn't even know that she had the treat- ment until I had read that in the En uirer, and we pieced to-
and all that. That is when we found out that this was my grand- mother. All the had was H.A
Mr. IMANN. E& there was no discussion that they had with any member of the family, that you are aware?
Me. NELSON. No. Mr. IMANN. Did she ever say anything about the radiation? Me. NELSON. She never said anything about the radiation nor did
g about the three cobalt treatments she received,
Mr. hrlANN. Basically, she was doing what the doctors rec- ommended to her?
Ms. NELSON. Right. She didn't know an better. Mr. IMANN. Me. H er, our father, in&s treatment, did ou or
any member of the Y d y - w e r e you present when the dbctors were lainin what the wereproposin
Ms.YLGER.50. me Joctors never tof: us anything. me only thing the doctor told me was when I went out there, when they canceled the surgery, I made an appointment to go out there and talk to the doctor, and all he told me was that they wanted to build him up and make him a little stronger. He was only 5-foot-2 and weighed 116 pounds. He was doing this normal work every day, and I mean, you know, you listen to what the doctor says and you don't question it. So I figured, well, maybe the want to fatten him u a little bit
he said, we are going to go with the cobalt treatment, and we are going to let it go at that for now.
And that is the only-that is the only time I met with the doctor on any of this. And I used to go with him when he would get his treatments; I was there every time with him. They woul take him away from me; I would sit in the hall, and then they would come out and say, well, your dad is a little sick for a while; we are oing to hold him for a little bit, then we can release him and come
tome Him and I rode the bus together. But they never let ou go back
and see what they did; they made you sit in the hall an i wlut. Mr. IMANN. Did he ever ex res8 concern to you about what was
hap ening to him or wonde J whethe- Id. J~AGER. No. He trusted the doctor. He trusted the doctor. Whatever the doctor said, that is what he did, because he thought the doctor was
Mr. IMANN. &ch doctors do you have contact with? Do you re- member the names?
Ms. HAGER. Sir, I wish I could remember. I asked for the doctors in charge. Whoever they gave me, I have no idea.
Mr. m. Did you ever meet Dr. Saenger?
when she died?
the ro sed treatment was d: ' s c u d w i t h h e r ?
gethe-d the date of her death, and t 1 e condition of her cancer
that she say I foun =P in her records.
more than 116 pounds to do t i: e surgery they wante 1 to do; and
ing to make him better.

24
Ms. HAGER. Sir, I couldn't tell you. I don't know if I did or not. Mr. MANN. Dr. Silberstein. Ms. HAGER. Like I said, I couldn't tell you. Mr. MANN. Dr. Aron. Ms. HAGER. I have no idea. Mr. MANN. Dr. Horowitz. Ms. HAGER. I have no idea. I met one doctor at one time. I don't
know who it was. Mr. MANN. Mr. Larkins, do you remember meeting any of those
doctors, the names I just gave? Mr. LARKINS. No. 1 think I remember seeing Dr. Saenger, but I
never met him. The only people I talked to was like nurses and or- derlies, sometimes.
Mr, MANN. Where did you see Dr. Saenger? Mr. LARKINS. In the tunnels and General Hospital. Mr. MANN. Did you talk to him? Mr. LARKINS. No. He was pointed out to me by someone else. Mr. MANN. Pointed out to you as what? Mr. LARKINS. As the doctor in charge. Mr. MANN. Ms. Nelson, do you recall meeting any of the doctors? Ms. NELSON. Never saw any of the doctors, never talked to them.
Whenever I went with my grandmother to the hospital, there were just the nurses around.
Mr. MANN. Thank you, Mr. Chairman. Mr. BRYANT. Mr. Portman. Mr. PORTMAN. Thank you, Mr. Chairman. Thank you all for being here today. It takes a lot of courage to
do what you are doing. It is difficult, I know, to talk about it. I just have a few questions.
Mr. Larkins, first, my question to you is really whether you know whether your father knew anything about the military study that was going on. Did he ever talk about that?
Mr. LARKINS. He never knew anything about that. Me and my dad were pretty close, and I think he would have talked to me about it. He probably would have said, hey, man, they have got the Government on us, and they are really going to do some good ac- tion. They really did.
Mr. PORTMAN. How did you and your mother first learn about the military aspect of the study?
Mr. LARKINS. In the paper, when it first started to come out this year.
Mr. PORTMAN. This year? Mr. LARKINS. Yes. Mr. PORTMAN. On the consent side, did your father ever talk
about the various options he had before him? Do you know if he was apprised of the risks and benefit+
Mr. LARKINS. The only thing he ever told me was, "they have got their treatment schedule for me; they have got another treatment schedule for me." That is all he would say.
Mr. PORTMAN. So in terms of whether he consented to the treat- ment in an informed way, do you know whether he was told what the risks and benefits of the treatment were?
Mr. LARKINS. I don't think he was. He waa kind of like me, or I guess I am like him. I want to know what is facing me. He would

2s
have told me, Joe, I have got chances of dying. We would have talked about it. He didn't say nothing like that.
He said, they have got another treatment scheduled for me. They are going to use me again. That is one time he said that, "They are going to use me again." What he meant at that time, I didn't know. Mr. PORTMAN. At the end of your testimony you talked about the
compensation issue. I just wondered if you could 've us a sense
I have no idea, but I think it should be something just. I have no idea what to say. Mr. POkTMAN. Thank you again for being here and for your
statement. Ms. Nelson, your grandmother, Mrs. Jackson, went through a
tough time. You gave us a lot of
was discharged in 1966. When did she first become involved in the radiation experiments; do you know?
MS. NELSON. In October 1966. do ou believe that she Mr. PORTMAN. October 1966? OK
understood the risks involved and t e beneits involved in the treatment that she received? Ms. NELSON. No. If she was told anything about it, she didn't un-
derstand it. Mr. PORTMAN. Did she? Ms. NELSON. She was illiterate. She couldn't read or write. Mr. PORTMAN. Did she ever talk to you or other family members
about it? Ms. NELSON. She never mentioned it. We never knew anything
about it until we read it in The Enquirer. That is when we were first informed of it. Mr. PORTMAN. And in terms of the Government's role, the De-
artment of Defense's role, did she ever bring that up, or did you ave any inklin of that?
anything about any of that until we read about it in The Enquirer. Mr. PORTMAN. So it was not until this year that you had any in-
kling of that? Ms. NELSON. That is right. Mr. PORTMAN. Thank you. Ms. Hager, do you know whether your dad was ever told about
the existence of a military study? Ms. HAGER. No. He had two sons in the military, and I am sure
if he had been told, he would have told us. He told me just about everything he signed. He told me just about everything that they did to him. Him and I were very close right at the end, and he told me pretty much of what was going on. He knew nothing of this at all. Mr. PORTMAN. He knew nothing of the DOD involvement? Ms. J~AGER. Of the Government beiig involved. He knew nothin
told him that, you know, Mr. Mitchell, you are not go' wpelive: maybe a couple of more months or so, and they would
of what you might think just com nsation would T e in this case. Mr. LARKINS. Bring him back, g. ut I know that is not possible.
Just in terms of getting the P ates straight, you mentioned she information.
%- P
Ms. NELSON. B he never talked about any of that. We never heard E
of that. I am sure if they would have come and talked to him an f

c
26
plained this to him, he might have said, well, you know, go ahead and do it. But with him not knowin , no.
he would have wanted to spend as much time as he had le with his-with my mother. Because he h a t e d 4 d he not want to leave her behind. That was his one main thing of getting better; is he did not want to leave her behind.
Mr. PORTMAN. Just one specific question. It relates to the letter he wrote to your sister, Isabell. He says in the letter that the doc- tor is not giving out the ri ht news to the family. Chairman Bryant
the initial operation that never took place. But how did you read that? Does that mean that he thought the doctors were trying to mislead the family, or that the doctors just didn't have good news for the family concerning his condition?
Ms. HAGER. What he didn't know was the doctors were not tell- ing the family anything. The doctors did not tell us about the oper- ation that he was going to have. The doctors never told us any- thing. This letter that my sister showed me, she showed me the week we had the meeting with David Mann. I knew no idea of this letter. I could have told him, dad, the doctors are not telling the family nothing. We know nothing. They are not keeping us in- formed at all.
I asked the nurse every night I left his room, I would make it a point to go to the nurse's station and sa if m father ets worse,
mother there, and J want to be there. W e lived 10 minutes from Cincinnati General Hospital. I never received one phone call, noth- ing.
When my dad passed away, my brother made a trip to the hos- ital. He found him in a private room. When we left him the night E efore, he was in a ward. We left him; they let me stay there that
night until 9:30, quarter to 10, to be with him. When my brother went back the next day, he was in a private room. He said, my fa- ther was in a private room-my dad was in a private room. I said, your dad has never been in a private room.
But they moved him when they know that he was dyin they never picked up the phone and they never called me to et me know that my dad was dying. And 1 begged them to let me know.
Two days before he died, he begged me to bring him out of that hos i d . He said, they are not doing what is right with me. Take
our dad, go along with what your dad said, because he can't go ome. And I had to leave him. They didn't do what was right by my dad and by any other pa-
tient that was in there connected with this treatment. They were . They know the were wrong. And it is about time they
Mr. PORTMAN. Thank you, Ms. Hager. Mr. BRYANT. On behalf of the subcommittee, I would like to
thank each of you for coming forward and giving us a personal angle on this whole matter and taking the time to take off in the middle of the week and come up here and let the subcommittee see exactly how this has impacted your individual families.
x He was a man that loved his wi f e and he loved his famil , and
talked about the timing o f this. I understand this is in relation to
please call me, no matter what time, c d m e , {,cause f want my
K' But
me K ome. And the nurse pulled me aside and said, just agree with
K Stan ""If up and they say t K ey were wrong.

/ 27
I thank each of you for being here. Mr. BRYANT. At this time we would like to ask the second panel
to come forward, which consists of Dr. Gordon K. Soper, Principal Deputy to the Assistant to the Secretary for Atomic Energy in the De artment of Defense; Dr. James Cox, professor of radiotherapy, M.6. And erson Cancer Center, and chairman, Radiation Therapy Oncology Group; and Dr. Joseph Steger, president of the University of Cincinnati.
Dr. Steger, you are also accompanied by Mr. Stan Chesley, cor- rect?
Mr. STEGER. Yes. Mr. CHESLEY. I am here as counsel, Mr. Congressman, Congress-
man Bryant, just here as an assistant, to assist Dr. Steger in any way I can.
Dr. Soper, please w e d . Mr. BRYANT. Dr. & per, can we begin with you?
STATEMENT OF DR GORDON Id SOPER, PRINCIPAL DEPUTY TO THE ASSISTANT TO THE SECRETARY FOR ATOMIC EN- ERGY, DEPARTMENT OF DEFENSE Mr. SOPER. Thank you very much, Mr. Chairman, members of
the subcommittee. I am Gordon Soper and I represent the Depart- ment of Defense at this hearing.
With me are two of my colleagues from the De artment of De- fense. Capt. Robert Bumgarner, Medical Corps, $$. Navy, is the Director of the Armed Services Radiobiology Research Institute and is an expert in milita medicine. It may also be useful to hear
partment of Defense, and Army’s rules on human use experimen- tation.
You have already commented on the extensive effort the adminis- tration is conducting to uncover the facts surrounding past radi- ation experiments. I can only tell you, the Department of Defense pledges to ou our unqualified commitment to a thorough and com-
se today is to rovide you with a summary of the role
1972. M report to ou is based upon re orts, files and documents
Most of the official Department of Defense records were retired and then destroyed long ago as part of the normal regulato in- structions for disposal of contract files. And as such, what? am going to tell you or summarize for you is not newly uncovered in-
from Col. John Fraser 8 lenn, who is an expert on the Federal, De-
plete seam c of all of the records.
that we L ve been a i le to locate from wi c f e and varied sources.
artment of IY efense played in the human radiation at the University of Cincinnati from 1960 to
formation. - The entirely unclassified University of Cincinnati studies have
been extensivGly reported in the open-literature. They have been a subject of peer review, review by the American College of Radiol- ogy, congressional hearings, and all of ou know, a series of
in one way or another addressed the Department of Defense’s in- volvement.
Now these studies will be further reviewed by a blue ribbon advi- sory committee on human radiation experiments, which was just
news articles starting as far back as 1971; d of these reviews have
I

28
recently established by President Clinton. This committee is com- posed of eminent scientists, physicians, legal ex erts, and medical
on the larger questions of ethical and scientific standards of any Government-sponsored experiments which involved the intentional exposure of humans to ionizing radiation.
A major goal of what we have been doing in DOD is to retrieve as many of the records as we possibly can of all DOD involvement in human experimentation, particularly that of the University of Cincinnati, and to provide a complete record of this to the advisory committee for their review.
of the Department of
terested, a more detailed chronology is attached to my submitted testimony. As you all know, in September 1958, Dr. Eugene Saenger of the
Department of Radiology, University of Cincinnati College of Medi- cine, as the princi al investigator, submitted what was called an
the Army Surgeon General‘s office; and as you have already stat- ed, the application roposed to research metabolic changes in hu-
sim le urine or blood test to detect how much radiation an individ-
This unsolicited proposal was reviewed over the next year within the Department of Defense, and the available remaining docu- mentation reveals that at least five Army Medical Corps officers re- viewed the proposal and recommended approval of the contract ap- plication.
In October 1959, st& elements of what we call the Defense Atomic Sup ort Agency recommended that they negotiate a con-
1960, I think it was the first of Janu 1960, a contract was en-
the Defense Nuclear Agency, and the University of Cincinnati board of directors.
The contract provided $25,058 for the initial study, and over the contract period-there were three separate contracts-between 1960 and 1971, a little more than $650,000 was spent on this ef- fort.
Let me say just a few words about the reason for the Department of Defense involvement. The search for a biological marker of radi- ation exposure was one steadfast aim of the University’s research for the Department of Defense over the life of these contracts. And I will also say that the results of the research contributed in a gen- eral way to a better understanding of the influence of radiation ex- posure on the combat effectiveness of military personnel, and it provided a more suitable method for diagnosis, prophylaxis and treatment of radiation effects on the nuclear battlefield, a very fearful possibility at that time.
Department of Defense funds were used for laboratory studies and psycholo ‘cal and psychiatric tests of cancer patients that re-
disease. No Department of Defense funds were used for direct pa-
ethicists; and their purpose is to advise and gui B e the Government
I would like to give you a brief summa Defense support to this research, and for t x ose of you who are in-
unsolicited propos 3 to the Research and Development Division of
mans following to taP body irradiation, so that we could develop a
ual Yl ad received.
tract with t R e University of Cincinnati for the study. So in early
tered into between the Defense Atomic ? upport Agency, now called
ceived this w f ole or partial body radiation for treatment of their
r

29
tient care, nor did the Department of Defense play any part in pa- tient selection or their choice of treatment.
The University of Cincinnati submitted 10 reports to the Depart- ment from 1961 to 1972; they are a part of the record. I have pro- vided a copy of these reports to your ofices along with other rel- evant documents in our possession.
Certainly, in reviewing these materials, Mr. Chairman, we at DOD can understand the controvers that arose in the early 1970’s
Mann said, especially from the viewpoint of 30 years later, are troubling and raise understandable concerns. Examples include statements in the University’s early progress re orts to the DOD
which some see as an indication of nontherapeutic purpose. Some see the inadequacy of the informed consent procedures. On
the other hand, for example, in 1972 the American College of Radi- ology concluded that the research was validly conceived and carried out, the patient selection conformed with good medical and that consent procedures complied with applicable stan ards.
We in the Department do not at this point seek to resolve these apparent contradictions. Our main focus, Mr. Chairman, is to com- pile as complete a record as we can, make it available to the Presi- dent’s Advisory Committee and to the public for their study.
Today, DOD-supported research is governed by the so-called com- mon r u l e t h e Federal Policy for Protection of Human Subjects- and a copy of this regulation is attached to my statement. DOD is a full partner in the Government’s commitment to this standard.
Under these regulations, today, a proposal like that from the University of Cincinnati in 1958 would require much more support- ing documentation and justification to be considered for funding support by the Department of Defense.
During the course of these hearings, perhaps I could have the op- portunity to expand upon this point more thoroughly.
So, Mr. Chairman, I have given you a very top-level summary of what we know so far. We are continuing to track down further in- formation.
We sincerely appreciate the openness of the University of Cin- cinnati in sharing with us their records. We appreciate the local
a contribution to the knowledge-gathering process. We agree, in the Department of Defense, with the need to air
once again the issues surrounding this early chapter of our Govern- ment’s human use research. Our sincere goal is to pull together as complete a record as we can of our involvement and provide it to the President’s Advisory Committee for their detailed study and ul- timate release to the public.
Thank you for your attention, sir. Mr. BRYANT. Thank you. [The prepared statement of Dr. Soper follows:]
and continues to this day. Some o P the records, as Congressman
that only nonradiosensitive tumors were selecte B for the research
Bradice9
- press sharing their records with us also. This hearing will also be
1
84-514 0 - 94 - 2
30
STATEMENT OF
GORDON K. SOPER, PRINCIPAL DEPUTY ASSISTANT TO THE SECRETARY OF DEFENSE
FOR ATOMIC ENERGY BEFORE THE
SUBCOMMITTEE ON ADMINISTRATIVE LAW AND GOVERNMENT RELATIONS
CINCINNATI, OHIO APRIL 11, 1994
Mr. Chairman and Members of the Subcommittee, I am Gordon Soper the Principal Deputy in the Office of the Assistant to the Secretary of Defense for Atomic Energy. I am here to support your request of March 24th to conduct hearings on radiation experiments performed by the University of Cincinnati Medical School which were funded in part by the Department of Defense (DoDl .
If I may, Mr. Chairman, I'd like to provide a prelude to my testimony in order to put our efforts into context. Since early January, when the White House called for the formation of a senior level Interagency Working Group to coordinate the government-wide effort to uncover the nature and extent of any government sponsored experiments on individuals involving intentional exposure to ionizing radiation, the Department of Defense has been engaged in an extensive effort to discover the facts surrounding DoD sponsored human radiation experiments.
seriously, that it has the complete support of Secretary Perry and that we pledge to you our unqualified commitment to a thorough and complete search of all available records and the full public release of the pertinent information in those records. As Dr. Harold Smith, the Assistant to the Secretary of Defense for Atomic Energy, and the DoD focal point for this action, testified to you at your February 2 hearing on this subject, the retrieval of records is a discovery process requiring time intensive "detective work"--we are well into that process now and beginning to make excellent headway. I would be glad to take any questions that you might have regarding the Interagency Working Group process and the results we have obtained so far.
With that as background, I'd like to provide you with as complete a report as I can on the role that the Department of Defense played in the human radiation experiments conducted at the University of Cincinnati College of Medicine from 1960-1972 which were led by the principal investigator, Dr. Eugene L. Saenger, MD. My report to you is based on documents, reports and files that we have thus far been able to locate from wide and
It goes without saying that the Department takes this action

31
varied sources--some of the official Department of Defense records were destroyed long ago as part of the normal regulatory instructions for disposal of contract files.
What I am going to report to you is really not newly uncovered information. The entirely unclassified University of Cincinnati studies have been previously reported in ten technical reports, 17 publications, and 26 presentations at scientific meetings; they were the subject of peer reviews at the University of Cincinnati; discussion of this work appears in the Congressional Record in 1971 and 1972; they were the subject of a report by the Comptroller General of the United States in 1972 for Senator Edward Kennedy, Chairman of the Senate Health Subcommittee; they were the subject of a separate investigation in a report by the American College of Radiology in 1972, at the request of U.S. Senator Mike Gravel; and they were--and continue to be--the subject of news articles in the press and other media reports.
reviewed by the Advisory Committee on Human Radiation Experiments which just recently established by President Clinton. This Committee is composed of eminent scientists, physicians, legal experts and medical ethicists. Its purpose is to advise and guide the government on the larger questions of ethical and scientific standards of any government sponsored experiments which involved the intentional exposure to ionizing radiation. Specifically, as stated in the Executive Order issued by President Clinton in January: "The Advisory Committee shall consider whether (A) there was a clear medical or scientific purpose for the experiments; (B) appropriate medical follow-up was conducted; and (C) the experiments' design and administration adequately met the ethical and scientific standards, including standards of informed consent, that prevailed at the time of the experiments and that exist today." A major goal of DoD's "detective work" regarding the University of Cincinnati research is to provide a complete record for review by the Advisory Committee.
Next I want to run through a brief chronology of this research, based on the record compiled to date, focusing on the Department of Defense sponsorship.
In September, 1958 Dr. Eugene L. Saenger of the Department of Radiology, University of Cincinnati College of Medicine, as the principal investigator, submitted an unsolicited research proposal to the Research and Development Division of the Army Surgeon General's Office. The research proposal was initiated by the University of Cincinnati and not solicited by the Department of Defense. The application proposed to research metabolic changes in humans following total body irradiation for the purpose of determining whether the presence of amino-aciduria in
2
In addition, Mr. Chairman, these studies will be further

32
humans after radiation would provide a reliable biological marker of radiation exposure. Restated less technically, the original goal was to try to develop a simple urine test to detect the amount of radiation exposure. The University of Cincinnati requested approximately $25,000 for the first year and $21,000 for two subsequent years. The proposal stated that Dr. Saenger was at that time also conducting pediatric cancer research funded by the National Institutes of Health, and preparing a Handbook on Medical Aspects of Radiation Accidents, under kontract from the U.S. Atomic Energy COUimiSSiOn.
within the Department of Defense. reveals that at least five Army Medical Corps officers reviewed the proposal. They recommended approval of the contract application. In October 1959 staff elements of the Defense Atomic Support Agency (DASA) recommended that DASA negotiate a contract with the University of Cincinnati for the study of the metabolic changes in humans following total body irradiation.
At that time a need existed within the Department of Defense to be able to determine the biological, statistical and clinical features of radiation injury. This was based on the requirements of our military commanders in the field to predict the outcome of human exposure to ionizing radiation, to predict the number of persons requiring hospitalization and to estimate the decrement in work capacity after radiation exposure on a nuclear battlefield. Remembering the context of the late 1 9 5 0 ' ~ ~ where fallout shelters were common in homes and schools and superpower tensions dominated public affairs, this was a real possibility of that time. Furthermore, such information would aid civil defense authorities in their efforts to combat the effects of nuclear explosions on the civilian population. I believe the fairly recent Chernobyl nuclear power reactor explosion underscores the importance of being able to ascertain radiation exposure effects and also understand its impact on a subject population.
So, in early 1960, a contract (DA-49-146-XZ-029, dated 1 January 1960) was signed between DASA and the University of Cincinnati Board of Directors. The contract provided $25,085 for the study. This contract, with supplements and modifications, funded the study through February, 1964. Another contract (DA-49-146-XZ-315) carried the research until April, 1969. The final contract (DASA-01-69-C-0131), effective May, 1969, funded the research until March, 1972 when the University of Cincinnati refused DASA's offer for additional contract funding. Through 1971, the DoD spent $651,482.79 on this research.
While the search for a biological marker of radiation exposure was one steadfast aim of the University's research effort over the life of the contract, the goals of the Department of Defense were to also understand better the influence of
This unsolicited proposal was reviewed over the next year Available documentation
3 .

33
radiation on the combat effectiveness of troops and to develop more suitable methods of diagnosis, prognosis, prophylaxis and treatment of radiation injuries. In order to obtain this information, the Department of Defense provided funds for laboratory, psychological and psychiatric tests to assess the effects of varying doses of whole and partial body irradiation for the treatment of cancer patients. No funds were paid to the University of Cincinnati for direct patient care nor did the Department of Defense play any part in patient selection or choice of treatment.
The University of Cincinnati College of Medicine submitted ten reports to the Department of Defense from 1961 through 1972 in accordance with the terms of the contract. I have provided the committee a copy of these ten reports as well as a number of other relevant documents that we have in our possession. Attachment 1 to my statement is a chronology summarizing major parts of the record compiled to date.
controversy that arose in the early 1970rs , involving the University community, the press, and the Congress, and that which has reemerged this year, regarding this research. Some of the records, especially from the viewpoint of 30 years later, are troubling and raise very understandable concerns. Examples of these include statements in the University's early progress reports to the effect that only patients with non-radiosensitive tumors were selected for the research, which some see as evidence of a non-therapeutic purpose, and that symptoms and side effects were not described to the patients, which some see as evidence of the inadequacy of the informed consent procedures. On the other hand, for example, the 1972 peer review of the American College of Radiology, carried out at the request of Senator Mike Gravel, concluded that the research was validly conceived and executed, that the patient selection conformed with good medical practice, and that consent procedures complied with applicable standards. We at DoD do not at this point seek to resolve these apparent contradictions. Rather, our sole focus regarding this task is to compile a complete record and to make it available to the President's Advisory Committee and to the public.
Before concluding my statement, I want to address the constraints which the Department of Defense imposes on human subject experiments today and how we would respond to an unsolicited proposal, like the 1958 proposal from the University of Cincinnati College of Medicine, for experiments in which humans would participate.
research date back to at least 1953, when a then TOP SECRET Memorandum was sent to the Secretaries of the Services from Secretary of Defense C.E. Wilson, titled "Use of Human Volunteers
In reviewing these materials, we at DoD can understand the
Formal DoD policy for the protection of human subjects in
, 4
I

,
34
in Experimental Research". This memorandum authorized the voluntary participation of military personnel and civilian employees in DoD conducted research for atomic, biological and chemical warfare defense and established specific standards for informed consent, minimization of risk of harm to subjects, and other matters.
Over the years, more detailed procedures were established, including incorporation in 1991 of the 1974 Department of Health and Human Services regulations for the Protection of Human Subjects, 45 C.F.R. Part 46.
Today, DoD-supported research is governed by the so-called "Common Rule"--the Federal Policy for the Protection of Human Subjects-which is part of DoD regulations at Title 32, Code of Federal Regulation, Part 219. A copy of this regulation is attached to my statement. DoD is a full partner in the government's commitment to this standard and has further defined its human use regulation in DoD Directive 3216.2, "Protection of Human Subjects in DoD Supported Research," January 7, 1983 and Department of Defense Guidance for Assurance of Compliance with the Federal Policy for the Protection of Human Subjects, June 10, 1993.
Under these regulations, a proposal like that from the University of Cincinnati would require much more supporting documentation and justification to be considered for funding. This includes the following:
1. The therapy itself, separate from the research, would require more information on the possible benefits and the known side effects.
radiation and Institutional Review Boards, or IRES), would have to review the proposed research protocol package, with proposed consent forms, before DoD would review the proposal for acceptance.
3. It would be required that the sponsor,s Institutional Review Board be made up of people from diverse backgrounds, including non-scientific perspectives, who could objectively and fully assess the proposal.
design is sound, that risks to subjects are minimized, that the selection of subjects is equitable, and that, if applicable, special protections have been adopted for any vulnerable groups mentioned.
would be required for participation in the research. This
2. Several local committees (specifically, scientific,
4. The IRB record would have to document that the research
5. A written consent form signed by the patient/subject
5

- I
E
consent form would require an explanation of the proposed therapy, all procedures and studies to be performed, and all expected outcomes and side effects in laymen's terms. The consent form must also state that the patient has been counseled about all of the above, and space provided for the patient to sign stating this has occurred and that the patient understands it.
6. The protocol would be required to justify withholding radiation in the control group of patients if such radiation therapy were the standard of care for the cancer each patient had.
7. The investigator would be required to give a more in
In other words, Mr. Chairman, we believe we have in place a
depth description of the known and suspected risks and the intended benefits of the research for the subject.
set of guidelines for human use experimentation that will preclude 30 years from now, hearings like we are conducting today.
So in summary, Mr. Chairman, the DoD received from the University of Cincinnati College of Medicine in 1958 an unsolicited proposal, which resulted in a contract from 1960 to 1971 supporting a human radiation experiment. DoD played no role in the selection of subjects, decisions regarding treatments, or the day-to-day conduct of the research. DoD received a series of reports describing the research results, none of which were ever classified. Data that we obtained from the University of Cincinnati studies were used to enhance our knowledge about the biological response to nuclear warfare--knowledge that we all hope will never have to be put to use. We well understand the controversy regarding this research, but make no effort at this time to resolve apparent contradictions in the voluminous record compiled to date. Our goal is to compile a complete record for the use of the President's Advisory Committee and ultimate release to the public.
take your questions. That concludes my prepared remarks. I would be happy to
6

. 7
36
1. General Observations:
a. Dr. Saenger submitted ten reports to DASA/DNA from 1961
b. The reports provide a means to trace the expansion of the
through 1972 in accordance with the terms of his contract.
research's scope, increased sophistication of techniques, and ambitiousness of future plans. The reports were similar in that they stated the purpose of and criteria for the research, research structure and techniques, how the work was conducted, the results of the experiments, observations and analysis of the data, plans for future study, and individual case histories of patients observed during the reporting period.
2. General information about DoD sponsorship of radiation experiments at the University of Cincinnati 1960-1971.
1958 In September, 1958 Dr. Saenger submitted an unsolicited research application to the Research and Development Division of the Army Surgeon General's Office. The application proposed to research metabolic changes in humans following total body radiation for the purpose of determining whether the presence of amino-acidura in humans after radiation would provide a reliable biological marker of radiation exposure. Dr. Saenger requested approximately $25,000 for the first year and $21,000 for two subsequent years.
1958-1959 Over the next year the proposal was reviewed within the Defense Department and a contract negotiated. Available documentation reveals that at least four Army Medical Corps and one Medical Service Corps officer reviewed the proposal. They recommended the contract application be approved. In October, 1959 the Defense Atomic Support Agency's (DASA) Deputy Chief of Staff, Weapons Effects and Test requested, thru the Chief, DASA, the Contract Management Branch, Directorate of Logistics negotiate a contract with the University of Cincinnati for the study of the metabolic changes in humans following total body radiation.
In early 1960 a contract (DA-49-146-XZ-029, dated 1 January 1960) was signed between DASA and the University of Cincinnati Board of Directors. The contract provided $25,085 for the study. This contract, with supplements and modifications,
1960
1

37
funded the study through February, 1964.
The first contract stated the technical scope of the research was "to study the phenomen of amino- acidura following irradiation, a condition which has been reported in humans and animals, to clarify some of the mechanisms responsible for amino-acidura and to determine whether it is a practical biological test of radiation exposure." The search for a biological marker of radiation exposure was one constant of Dr. Saenger's research effort over the next decade.
On 28 February 1961 the Cincinnati project's contract was modified for the first time. The contract was modified to establish a new date for work completion to provide additional time for research on amino-aciduria following irradiation; amended the technical scope of the work to meet additional objectives of the government; provided additional funds to meet research requirements under the amended scope of work; altered portions of the contract to bring the contract in accordance with Armed Services Procurement Regulations that became effective subsequent to the signing of the original contract. The contract amount increased almost $30,000 from $25,000 to $54,000 and the length of the project was extended from February, 1961 to April, 1962 The scope of the work was expanded by three requirements: a breakdown of desoxyribonucleic acid and is derivatives in patients receiving total body radiation; DNA studies on patients who received partial irradiation and radiomimetic chemotherapeutic agents; and preliminary determination of appropriate psychometric tests
In June, 1961 the contract was modified for the second time. An additional $650 was allocated to use the technical services of a French authority on radiobiology at a Whole Body Radiation Conference to be held by DASA at the University of Cincinnati in October, 1961.
In April, 1962 the project's contract was modified for the third time. The contract total was increased approximately $39,000 to $94,400. The project completion date was extended to April 30, 1963. The scope of work was also further expanded. Three additional objectives were added. Additional studies were to be made of--increasing the upper range of radiation dose to 150-200 rad,
1961
1961
1962
2

38
1963
1964
1965
and single doses of nitrogen mustard or other radiomimetic drug using .4mg/kilo. The following tests were to be conducted for 9 days post- treatment--urinary taurine for correlation with leukocyte count, BAIBA in urine, Kynurenic and xanthurenic acids, deoxycytidine, DNA fragments in urine, et al, xanthine and hypoxanthine in urine, urinary phosphate, and glutathione. The test were to be done over a 30 day period--routine electrophresis, immunoelectrophoresis, quantitative precipitin studies, serum urea nitrogen and/or serum creatine once weekly, urinalysis once weekly and as needed, routine hematology, and completion of the manuscript of the DASA Conference on Total Body Irradiation of October, 1961.
On April 1, 1963 the contract was modified for the fourth time. The contract was extended through April 30, 1964. Funding was increased $40,000 to $134,56. The scope of the work was further amended. Test to be conducted over a 30 day period between March 1, 1962 and February 28, 1963 were to be: (1) routine electrophesis, (2) immunoelectrophesis, ( 3 ) quantitative precipitin studies, (4) serum urea nitrogen and/or serum creatine once weekly, (5) urinalysis once weekly or as needed, and (6) routine hematology. During the same year the following tests were to be conducted over a 42 day period included 3,4,,5,6 and chromosome cultures of peripheral blood.
Contract DA-49-146-XZ-315 came into effect and funded the research from February, 1964 to April, 1969.
Ralph C. Rursiek and Dr. Eugene L. Saenger wrote a letter, dated May 17, 1965, to Director, Defense Atomic Support Agency, ATTN: STMD requesting that NWER No. 03.009 be funded at an estimated cost of $45,000 for FY65. The overall objective was to study various phenomena of desoxyribonucleic acid breakdown and other abnormalities following whole or partial body irradiation of human beings. Fifteen patients were to be studied. The project intended to study patients for 5-14 days prior to irradiation and for as long as possible after to evaluate clinical hematological and psychological changes. Investigation of the metabolism and urinary excretion of deoxycytidine was to be continued. Bone marrow was also to be stored prior to
3

39
1967
1969
1971
irradiation. All serum was to be sent to Dr. Luzzio at Fort Knox.
In 1967 a member of the University of Cincinnati research team, Dr. James G. Kereiakes, attended an Atomic Energy Commission sponsored conference at Oak Ridge, Tennessee. A purpose of the conference was to refine the dosimetric aspects of whole and partial body irradiations being used by the medical community to treat leukemia and widely disseminated cancers. The aim of the conference was to standardize the dosimetry being used to report patient dose. Information developed at the conference revealed 1,035 patients at about 35 institutions had received whole or partial body irradiations for the palliation or treatment of cancers. The use of radiation was widely spread and acknowledged as an effective modality
The final contract (DASA-O1-69-C-0131), effective May, 1969 funded the research until March, 1972 when the University of Cincinnati refused DASA's offer for additional contract funding.
Dr. Eugene L. Saenger wrote a letter, March 22, 1971, to Dr. Robert Loind, DASA, Attn. STMD. The cover letter with attachments forwarded the projects proposal for FY 73. The proposal requested $70,000 for a study entitled "An Appraisal of Human Studies In Radiobiological Aspects of Weapons Effects". A six page description of the study's philosophy, the role of future human research in relation to the remainder of the radiobiology program, specific areas of endeavor (eight--clinical evaluation, metabolic effects, behavioral effects, dose response studies, partial body studies, prognosis, therapeutic methods, use of healthy volunteers), and future plans regarding funding.
1960-1971 Through 1971 DoD ultimately spent over $650,000 on Dr. Saenger's endeavors which treated 05 adults whole- or partial-body radiation. Three children with localized Ewing's tumor were also treated with whole-body radiation. DoD funds were provided for laboratory, psychological and psychiatric tests to assess the effects of varying doses of whole and partial body irradiation. NO funds were paid to the University of Cincinnati for direct patient care.
3 . Report Summaries
4

I
40
1960-1961 The report for the first research period (February 19, 1960 to October 31, 1961) was DASA.1422
2. This Supplement, which was entitled &!&olic
title was used for the reports through 1967. The report provides a detailed itemization of the investigations and study projects. The aim of the studies was "to obtain new information about the metabolic effects of total body and partial body irradiation so as to have a better understanding of the acute and subacute effects of irradiation in the human." During this period ten patients received total body irradiation in doses that ranged from 16 to 150 rads. Patients were selected for the study were those with "proven metastatic or far advanced cancer ... in relatively good nutritional status, i.e., able to maintain their body weight.. . . [andl have normal hematological values.' An explanation of one of the study's technique stated "the patient is told that he is to receive treatment to help his sickness. There is no discussion of subjective reactions resulting from the treatment. Other physicians, nurses and ward personnel are instructed not to discuss these aspects with the patient." The remainder of report discussed on-going studies, clinical observations, dosimetry, and other study techniques supplemented with tables and patient case histories.
1961-1963 The second report, DASA 1422 reported on the research from November, 1961 to April, 1963. Ten patients were treated with total body radiation in doses that ranged from 150-200 rad during the report period. The study's statement of aims was identical to that of the previous report except that it was expanded. The added aim stated "This information is necessary to provide knowledge of combat effectiveness of troops and to develop additional methods of diagnosis, prognosis, prophylaxis and treatment of these injuries." Patient selection criteria was more refined. In addition to those already stated new criteria was . that "patients with lymphoma [were] excluded ... Patients with solid neoplasms not radiosensitive are sought." The technique reported previously remained in use. Verbal consent of the patients was obtained prior to treatment.
involved complications in trying to determine the One of the iseues the researchers encountered
5 c

I I
41
effects of radiation. the report stated "Physicians assess patient to be certain that the underlying disease can be evaluated. Thus, there was difficulty in selection of patients for assessment of radiation effects because of underlying disease. Patients previously treated by radiation or chemotherapy were excluded because previous treatment confounded the response to radiation in several early patients."
Throughout the narrative and near the conclusion with the researchers thoughts on "Human Effectiveness Following Whole-Body Irradiation". Several of their observations included:
"Marked hematological changes occur generally between the 25th and 35th day following exposure. Maximum recovery to be obtained generally requires about 100 days."
"Human beings recover slowly and are quite sensitive to radiation with multi-system involvement. 'I
'IProdromal acute effects such a nausea, vomiting, anorexia, and lassitude are of the duration hours. Intermediate effects such as hematologic complications are to be conceived of in weeks. 'I
"A previous dose of radiation does influence the incidence of acute effects. Therefore the incidence of 'combat effectiveness' will be significantly increased on re-exposure of an individual. 'I
"...individuals with previous exposure to radiation will be less tolerant of subsequent exposures. hence troops previously exposed to 150-300r of whole body radiation will tend to show more combat ineffectiveness in the prodromal period than will those who are unexposed."
"This field of investigation has obvious important implications. Breakdown of DNA has long been implicated as the fundamental biochemical change of radiation and there is an impressive literature bearing on this point ..The observation cited above of decrease of DOC after the administration of protective agents indicates the possibility of the use of specific prophylactic agents for the protection of'humans in nuclear warfare 'I
6

42
A final observation was offered on future study:
"It is our opinion that human radiation studies need to be expanded.
We propose to establish facilities for withdrawal, storage, and reinfusion of autologous bone marrow. As indicated elsewhere in this report we have encountered significant hematological difficulties with a dose range of 200-325r. Therefore, to proceed with higher doses, we feel the need to protect our patients even if we might sacrifice their value for hematological evaluation after 2-3 weeks since the hematological effects are well documented. Once this technique has been developed as a support procedure we then anticipate increasing doses to higher levels. ''
out the report. Tables, figures and case histories rounded
1963-1964 DASA 1633 was the report submitted for the period May 1, 1963 to February 29, 1964 during which six patients were treated with total body radiation doses between 100 to 150 rad. The aims of the study remained as previously reported. "Normal renal function' was added to patient selection criteria. The technique to limit subjective reactions treatment was unchanged. Proposals for human study expanded on the previous report's discussion of autologous bone marrow reinfusion. The report stated:
marrow will be accomplished in the facility which has been established. ..The purpose of marrow storage and reinfusion is to protect subjects who receive doses in excess of 150 rad in the event of bone marrow failure. We hope to utilize doses between 200-300 rad."
Tables and case histories once again
"Storage and reinfusion of autologous bone
accompanied the report.
1964-1966 DASA 1844 covered not only the study years 1964 to 1966 but also provided a summary of the first six years of the experiment. Midway through the decade the aims of the project were stated as:
"This program is designed to obtain new
7

43
information regarding the metabolic, physiologic, immunologic, hematologic, and biochemical effects of TBR and PBR in human beings. It will then be possible to understand better the influence of radiation on combat effectiveness of troops and to develop more suitable methods of diagnosis, prognosis, prophylaxis and treatment of radiation injuries. It is our belief that information concerning radiation effects in the human being can be determined as well or better in these subjects as in the laboratory animal even though the characteristic of cancer must be kept in mind in the evaluation of the data."
On page 2 the aims were once again addressed in terms of the original scope of the study:
"A major objective of these studies has been a search for a suitable biological indicator of radiation dose in human beings . . . . At this time the urinary excretion of deoxycytidine seems to be promising as a biological indicator."
Another aim was stated on pages 2 and 3 .
"Psychological and psychiatric testing has been started in 14 patients . . . . This approach will provide information on another important parameter of combat effectiveness of troops.''
Later in the report an aspect of the psychiatric evaluation is further discussed.
"One of the most difficult aspects of radiation injury requiring evaluation is that of gerformance decrement. This term is loosely used but in our laboratory it is defined as any decrease in ability to carry out assigned tasks."
Patient selection criteria was more specific:
"Patients with metastatic or incurable neoplasms are given whole partial body radiation for palliative treatment of their disease. Patients for the studies described in this report are selected from patients treated as described above providing that they satisfy the following criteria:
1. The patients have solid tumors.
2 . Relatively good nutritional status Patients with lymphoma are excluded.
8

(ability to maintain weight).
period.
Twenty three additional patients were treated during the research period between 1964 and 1966. Of these patients 13 received total body radiation treatments with dosages between 25 and 150 rads. Partial body radiation doses between 100 and 300 rads were used in the treatment of 10 patients.
discussions of subjective reactions remained the same.
3. Normal renal function 4. Stable hemogram in the control
The technique to “isolate” patients from
Discussion of hematology stated:
“Since severe hematological depression was found in most patients who expired, autologous bone marrow storage has been performed for 13 patients. In only two patients has infusion been carried out. The method is being refined so as to include filtration prior to infusion. Although we have not encountered morbidity . . . filtration appears to decrease the probability of incidence of pulmonary emboli.“
Accompanying the 35 page report were 122 pages of tables, and case histories of the all patients treated to date.
1966-1967 DASA 2179 described the treatment of four patients between May 1, 1966 and April 30 1967. Of the four patients treated one received total body radiation (150 rad) while the other three received partial body radiation doses in the range of 100- 200 rad. Aims, patient selection criteria, and technique remained as previously reported. Three accomplishments were reported. The first involved “the completion of an infusion filtration system for reinfusion of autologous stored human bone marrow.” As a result of the development the researchers stated “Since this instrumentation will make infusion of marrow a safer and more easily controlled procedure we feel that earlier infusion to prevent the hematological depression from radiation should be investigated.” The text noted that the methods were described in a paper presented in Paris. France which cited DASA support.
The second accomplishment was the “perfection
9

45
by Dr. I-Wen Chen of a new, much improved method for the determination of deoxycytidine (CdR) in urine from humans and from rats."
of phage on synthetic culture medium." development made it "possible to titrate antibody production in experimental animals and man before and after irradiation."
Future plans included the evaluation of "alterations in antibody production and /or destruction in human beings due to radiation." Observations of this nature on "the effects of radiation exposure will yield a better understanding for military planning and triage."
supplemented the text.
The third involved "the growth of two strains This
Tables, figures, and case histories
1967-1968 The report for the period May 1, 1967 to April 30, The report's title changed to 1968 was DASA 2168:
tip Effo-. Reports carried this title for the remainder of research. This report recounted the treatment of seven patients. Four patients were treated with total body radiation doses between 100 and 200 rad. Three patients were treated with lower body partial body radiation doses of 200 to 300 rad. The report's forward noted "these studies were performed in conformation with the 'recommendations guiding doctors in clinical research' as stated in the Declaration of Helsinki of the World Medical Association (1964). Reported aims, criteria and techniques were as previously reported. Updated information from the psychiatric-psychological team noted "the number of patients who have been evaluated by the psychiatric-psychological team now totals 20." Hematology research continued. The researchers reported "seven patients received autologous bone marrow transfusions at completion of DADA 2168. Guidelines for quantity of marrow cells to be infused for successful transfusion and bone marrow protection were developed."
Case histories and tables provided additional information.
BBdlatlon Effects in Man: MaaL&&auons and
1968-1969 The research over the period between May 1, 1968 and April 30, 1969 was the subject of DADA 2428. Eight patients were treated during this period. Total body radiation doses of 100-200 rad were given to six patients. Two patients were treated with 200-300 rad doses of partial body radiation.

46
Once again the forward noted that the studies conformed to the recommendations of the Declaration of Helsinki. Aims and goals remained unchanged. In the field of hematology the report stated "success has finally been obtained in autologous marrow infusion which will permit us to employ higher doses of radiation in the coming year. Several new biological dosimeters are under evaluation." Tables and case histories accompanied the report.
1969-1970 DASA 2599 reported on the research based on observations of twelve patients between May 1, 1969 and April 30, 1970. The recommendations of the Declaration of Helsinki were once again noted. A presentation by Dr. Edward B. Silberstein on the team's earlier work and the data contained in this report at the IAEA-WHO Conference in Paris on 24 June 1970 was reported.
with doses of 100-230 rad of total body radiation. The other six patients received partial body radiation doses between 150 to 300 rad. Regarding these patients the report stated "Most of the patients had inoperable metastatic carcinoma which was not amenable to conventional chemotherapy. Nevertheless, these patients were all clinically stable, many of them working daily. Several of the subjects, apparently tumor free and clinically normal after regression of regionally irradiated tumors (Ewing's tumor), received prophylactic whole body radiation."
Hematological work, specifically related to biological dosimetry, was discussed. Several biological dosimetry issues were discussed.
"We are pursuing this goal at whole-body radiation doses up to 2 5 0 rad with even higher doses planned with the support of marrow autotransfusions and laminar-flow 'sterile' rooms. Large-volume partial-body irradiation is also being performed to learn more about the efficacy of chromosome aberrations as a radiation dosimeter in the more frequent situation of inhomogeneous exposure. With a linear accelerator, we hope to study the effects of various dose rate in vivQ as well. 'I
As for the continued research into the
During this period s i x patients were treated
utility of deoxycytidine the report noted "deoxycytidinuria appears to be related to general
11

47
tissue catabolism from several causes, including radiation. Other problems in using urinary CdR include variations in excretion due to race (57) and age (63) ." [Note: Numbers in 0 are bibliographic reference numbers.]
the report. Table XI1 provided "a summary of demographic and other pertinent data . . . for the entire group of 36 patients" observed since the start of testing.
Tables and case histories were included with
1970-1971 DNA 2751T was the report for the period May 1, 1970 to April 30, 1971. Eight patients underwent treatment. Three received total body radiations dosages of 100-200 rad. Five underwent partial body radiation with doses of 300 rad. The research aims were restated.
"The University of Cincinnati studies in radiation effect in man continues as a carefully integrated effort to maximize clinical, psychiatric, therapeutic, biochemical, and theoretical approaches to whole and partial therapeutic irradiation as given for palliation of certain selected cancers. I'
To achieve these aims "the methods of applying radiation have remained essentially the same since the inception of these studies."
provided.
undertaken in our laboratories reflects the consideration of many of our faculty and the thoughts and problems of the other DNA conferences organized over the paet several years by Col E.J. Huycke. Valuable interchange of ideas have been stimulated by visitors from Department of Defense laboratories who give our staff a more practical insight into military problems than we might otherwise have.
Future plans were described.
investigation stem from concurrent advances in cytogenics, organ transplantation, bio-chemical aspects of molecular biology, and clinical aspects
Acknowledgement was made of guidance
"The nature of the specific projects
"Many of the new directions in our
12

48
of cancer therapy. 'I
'A renewed interest is manifested in chromosome aberrations as being eventually an index of 'effective radiation dose,' particularly since almost all exposures encountered in nontherapeutic circumstances will have varying degrees of nonuniformity of dose rate and dose distribution."
"As an outgrowth of our needs to afford maximum protection to patients receiving doses in the LD,, range, eome new technical advances have been developed in bone marrow transfusion in patients. 'I
Regarding biological dosimetry the report stated:
"Yet in severely burned individuals deoxycytidine ((deoxycytidine excreted in urine)) occurs late (in 2 to 4 weeks) and in the several patients studied the levels seemed directly related to the extent and depth of the burn. Radiation induced deoxycytidinuria when found occurs within 2-3 days and then disappears. Additional studies may suggest this test as a way of differentiating relative contribution of these two modalities of injury."
The usual tables and case histories supplemented the narrative.
1971-1972 The final report in the series was DNA 3024F which was to be for the period April 1, 1971 to March 31, 1972. However, its was really a summary of the entire research effort and was a "scientific communication presented at the meeting of the American Roentgen Ray Society in Washington on 3 October 1972.' It was further noted that "this report has been accepted for publication in the American Journal of Roentgenology, Radium Therapy, and Nuclear Medicine."
As stated in this report the research were "to improve the treatment and general clinical management and if possible the length of survival of patients with advanced cancer. effects of radiation therapy have been given particular attention in our work."
Systemic
The issue of informed consent was addressed.
"All patients gave informed consent in
13

49
accordance with directives of the Faculty Research committee of the University of Cincinnati College of Medicine and those of the National Institutes of Health. The use of formal informed consent forms in this study antedated the above requirements by two years. The project is reviewed and approved regularly by the above committee."
The report noted that "patients become eligible for this form of treatment if they have advanced cancer for whom cure could not be anticipated .... Chief among the reasons for elimination waa an indication in the pretreatment phase that some risk from wide-filed radiation might ensue or that another method of treatment was considered preferable."
can identify eight cases in which there 1s a possibility of the therapy contributing to the mort a1 i ty . 'I
A comparison is later made between times of death of those that entered the study and received radiation treatments, and those that entered the study and did not receive radiation treatments. From this comparison the report noted:
"Fisher's exact probability test yields a p value of 0.16, indicating that there is no difference between the two groups. Therefore, one may conclude that in other patients described, the effect of whole- and partial-body radiation therapy was less important in contributing to death than was the extent of disease in these patients. Another interpretation would be that a physician selecting far advanced cancer patients for a given treatment would have about the same degree of difficulty in selecting any form of treatment for these very ill patients."
From an analysis of radiation mortality "one
Tables and figures accompanied the report as did a section entitled "Thermography as a Radiobiological Dosimeter".
1971-1972 Issues arise that lead to the termination of the contractual relationship between DNA and the University of Cincinnati.
14

Proi ec t Chronolouy October 1971 - January 1973
October 0. 1971 - - An article appeared in The Washington Post, "Pentagon Has Contract to Test Radiation Effect on Humans", by Stuart Auerbach and Thomas O'Toole that prompted the subsequent governmental investigations of the Cincinnati prolect.
October 11, 1971 - - Dr. Eugene L. Saenger, Dr. Clifford G. Grulee, Dean of the University of Cincinnati College of.Medicine, and Dr Edward A. Gall, Vice President of the University of Cincinnati and Director of the University of Cincinnati Medical Center, were present at a press conference the subject of which was the impending Senate and Government Accounting Office (GAO) investigations of the conduct of the Cincinnati project.
October 11, 1971 - - A follow up article appeared in The Washington P o s t , "Pentagon's Radiation Experiments Defended". The article featured Dr. Saenger explaining the process of patients selection and Department of Defense (DOD) funding of the project.
Mid-October 1971 - - DOD developed a Fact Sheet on the Cincinnati project that discussed its contractual arrangements with the University of Cincinnati. A copy of the Fact Sheet was later entered into the Congressional Record on December 15, 1971 as an attachment to a letter from the Assistant Secretary of Defense (Legislative Affairs) to Senator Robert Taft, Jr.
November 10, 1971 - - Senator Mike Gravel wrote a letter to Dr. Robert W. McConnell, President of the American College of Radiology (ACR) requesting the ACR to conduct an evaluation of the Cincinnati Project.
November 12, 1971 - - Dean Clifford G Grulee appointed an Ad Hoc committee to review the "whole-body radiation study" which Dr Eugene L. Saenger had been conducting at the University of Cincinnati Medical Center. The Ad Hoc committee, chaired by Dr. Raymond Suskind, Director, Environmental Health, University of Cincinnati, was made up of eleven members and was charged with reviewing the scientific content, methodology, and data treatment of this study, as well as other aspects which the committee deemed appropriate. All eleven committee members were professors at the University of Cincinnati. Ten committee members were medical doctors and one was a Ph.D. in Physiology.
December 6, 1971 - - Mr. Ellis R. Mottur, Science Adviser to the Senate subcommittee on Health, Senate Committee on Labor and Public Welfare and Dr. Caper, both of Senator Kennedy's staff interviewed Dr. Edward E. Silberstein, University of Cincinnati Medical Center, Dr. Eugene L. Saenger, and others at Cincinnati General Hospital.
December 6, 1971 - - Dr. Robert S . Daniels, Professor and Director, Department of Psychiatry, University of Cincinnati, wrote a letter

51
to Dr. Raymond Suskind. The letter forwarded a list of question to Dr. Suskind for inclusion in a "our [Ad Hoc Review Committee] report on 'Total Body Radiation' project".
December 7. 1971 - - Mr. Ellis R. Mottur of Senator Kennedy's staff requested the opportunity to conduct interviews with surviving project subjects.
Decembar 7 , 1971 - - Dr. Eugene L. Saenger wrote a letter to Dr. Raymond Suskind, which discussed the impending arrival of the ACR Committee to review the project.
December 13, 1971 - - The subject of interviewing patients was broached in a letter from Senator Edward Kennedy, acting in his role as Chairman of the subcommittee on Health, Senate Committee on Labor and Public Welfare, to Dr. Warren Bennis, Presi3ent University of Cincinnati.
December 17, 1971 - - Dr. Eugene L. Saenger wrote a letter to Dr. Charles Barrett, Department of Surgery, University of Cincinnati Medical Center. The letter details Dr. Saenger's objections and concerns about providing patients to be interviewed.
December 20, 1971 - - Dr. Eugene L. Saenger authored "Comments on Differences Between Therapeutic and Non-Therapeutic Investigation". Dr. Saenger generally defended his research and methods by citing legal and medical opinions. He then went on to refute specific allegations that relate to DoD funding, informed consent techniques (Dr. Saenger made the point that since 1968 patients were told the information gained might be of use on the battlefield), follow-up, alleged contributory effects of radiation to patient deaths, racial composition of study group, and the below average intelligence level of the project subjects.
Dacamber 21, 1971 - - Dr. Eugene L. Saenger wrote a letter to Dr. Edward A. Gall. The letter was a response to Dr. Gall's request that Dr. Saenger identify patients that might be suitable for interviews by Mr. Mottur.
January 1972 - - The Ad Hoc Review Committee chaired by Dr. Raymond Suskind of the University of Cincinnati communicated its report to the Dean of the College of Medicine concerning Dr. Saenger's project. The Report contains seven sections,two of which are pertinent to DOD involvement; Section IV Financial Surmort sf Proarm and Section V Informed Consent and Human Riahtg.
In Section IV it is reported that the request for financial support for the project was initiated by the University of Cincinnati. The systematic investigation of whole body radiation did not begin until the project wa8 funded by the Defense Atomic Support Agency (DASA). Through March 1972 DASA had granted $651,483, 13% to 15% of the budget of the Radioisotope Division. Section IV also details the breakdown of expenditures. There is no evidence that the DASA funding was made contingent on work, ideas,

52
or suggestions proposed by DASA and that all the information reported to DASAwas kept unclassified and publicly available. The work was also carried out by the University researchers with complete scientific freedom.
In Section V it was stated that the procedures for informed consent followed by Dr. Saenger's partial and whole body radiation project reflected the process characteristic of the University of Cincinnati and the nation. AS the idea of informed consent developed nationally in the 1960's from informal, oral, and non- specific to formal, written, and more detailed, Dr. Saenger's project appropriately updated their procedure for informed consent to meet the more stringent levels required for good medical research.
January 3 , 1972 - - The ACR responded to Senator Mike Gravel's request to conduct an inquiry into the whole-body radiation therapy project supervised by Dr. Eugene L. Saenger The ACR Report concluded that the Cincinnati prolect was validly conceived, stated, executed, controlled and followed up. The process of patient selection was based upon clinical considerations and conformed with good medical practice. The procedures for obtaining patient consent was valid and consistent with the recommendations of the National Institutes of Health and with the practice of most cancer centers. The ACR Report indicated procedures for obtaining informed consent were likely performed better than the average institution because of the volume of prolects generated by the medical facility and the quality of the people involved. ACR urged Senator Gravel to support the projects continuation The ACR Report also noted that DOD funds were used to support the laboratory and psychological studies, but not the treatment or the care of the patients. The ACR Report discusses at length the subject selection procedures and notes that in both race and IQ the group is representative of the patients served at Cincinnati General Hospital. The ACR Report also agreed with Dr. Saenger that ' I . . . it seems reasonable to continue [whole-body radiation] therapy for the gravely ill individual since this method of treatment is less elaborate and with no greater risk than many present forms of chemotherapy.''
January 11, 1972 - - Senator Edward Kennedy wrote a letter to Dr. Warren Bennis in reference to the University's refusal to identify patients to be interviewed by the committee. The Senator pointed out that some patients appeared in a documentary produced by National Education Television in September, 1971, and it was difficult to understand why the University allowed them to appear on TV and not before a Senate Subcommittee. Senator Kennedy stated that the University's decision was unfortunate because "the most crucial element in the inquiry is the patient's perception and understanding of the experiments in which they were participating.. ." January 19, 1972 - - Dr. Edward A. Gall wrote a letter to Senator Kennedy responding to the Senator's January 11, 1972 letter. Dr

Gall stated that names were provided to NET with the consent of the patients but points out that the situation had subsequently changed. In response to the Senator's request the University was sending letters to surviving patients to ask them if they would give their consent to being questioned by representatives of the subcommittee. He said that experts were consulted and they were of the opinion that any such questioning may have led to some unfavorable medical implications. Dr. Gall also asked the Senator if he would consent to a meeting with senior university officials.
J.puary 21, 1972 - - Mr. Ellis R. Mottur wrote a letter to Dr. Edward A. Gall requesting copies of the letter (with names omitted) sent to patients or parents of surviving patients asking if they would consent to interviews.
January 25, 1972 - - Dr. Edward A. Gall wrote a letter to Mr. Ellis R. Mottur, Science Adviser, Senate Committee Labor Public Welfare, that forwarded the requested copies of letters sent to patients or parents to request interviews.
February 4, 1972 - - In a letter to Dr. Robert W. McConnell Senator Mike Gravel indicated his displeasure with the results of the ACR Report released on January 3, 1972. Senator Gravel felt the report was deficient in relevant information and poorly organized. The Senator pointed out the ACR report "confirms that the patients were not thoroughly informed about the extra discomfort, the military aspects, or the possible lethal effects."
F e b r u a r y 4, 1972 - - Mr. Myrton Tom Stewart and Mr. Robert Murphy of the General Accounting Officer (GAO) met with Dr. Eugene L. Saenger. Dr. Saenger was asked nine questions: when did the project start; did he approach DoD or vice versa [he approached]; how were parts of research funded; where were Federal funds used, etc. In response to question 4 which asked about the use of federal funds for patient care, Dr. Saenger replied that "[nlo DOD funds under these contracts were at any time used for payment of patient days in any hospital. DOD funds were used for technical help, support of a biochemist, physicians, physicists and for psychological and psychiatric studies.'' In response to question 6 which asked if treatments were given for the benefit of the patients or DOD, Saenger responded, "that in all cases the treatment was given for the palliation of cancer of the patients and information for the Dod was a byproduct."
Pebru8ry 16, 1972 - - Dr. Warren Bennis wrote a letter to Senator Kennedy referring to meeting with the Senator and Ohio Governor Gilligan on February 24, 1972. Dr. Bennis included a copy of the Ad Hoc Review Committee's report, and advised the Senator that Dr. Gall would be responding within a few days to the Senator's request for an evaluation of the report by the Junior Faculty Association. The letter concluded with the promise that he was willing to cooperate with the Subcommittee in any way consistent with the health and legal rights of the patients.

54
P.bnaary 17, 1972 - - Dr. Edward A. Gall wrote a letter to Senator Edward Kennedy which provided a copy of the Ad Hoc Committee Report and other documentation. Regqding the Junior Faculty Report, Dr. Gall wrote that since the Ad Hoc Committee report addressed the points raised by the Junior Faculty Association he considered the Ad Hoc report "a complete and authoritative response." He also informed the Senator that they had received responses from all the surviving patients and the parents of the children treated regarding interviews. All responses had declined to be interviewed. Dr. Gall further expounded on the point made in his January 19, 1972 letter that two cancer experts (not local and not associated with the University) had given as their opinion that there would be unfavorable medical implications if patients were interviewed.
February 17, 1972 - - Dr. Edward A. Gall wrote a letter to Dr. Warren Bennis forwarding the consultant opinions from the two cancer experts. Dr. Gall noted they were in concurrence with their own physicians about the undesirability of subjecting the patients to interviews.
Fobrurry 22, 1972 - - Mr. Cyril W. Kupferberg, Chair of Radiation Response Team, wrote a letter in response to an individual who requested to know if a family member was part of the experiment that was reported to DoD. The individual was not a subject of Dr. Saenger. The letter included attachments - University of Cincinnati Guideline for releasing medical information on deceased patients, an authorization for release of information form, and an example of a "Consent for Special Study and Treatment" form.
%arch 31, 1972 - - The Cincinnati project contract number DASA-01- 69C-0131 expired. The University of Cincinnati had earlier indicated that it did not want to continue conducting research under this contract with the Defense Nuclear Agency.
July 5, 1972 - - Dr. Eugene L. Saenger wrote a letter to Dr. Edward A. Gall. The three page letter appears to be Dr. Saenger's response to an article published in the Cincinnati P o s t on April 25, 1972. Dr. Saenger's response focuses on several points: University procedures for seeking Federal grants/contracts, issues associated with seeking DoD funds for research in FY 74 and the terminating of research utilizing FY 73 funds.
Auguat 1. 1972 - - Several pieces of correspondence relating to the Cincinnati project were entered into the Congressional Record, including a letter from the Comptroller General of the United States to Senator Edward Kennedy summarizing the results of the GAO investigation of DOD policy regarding the protection of humans used in medical research projects and DOD responses to questions from Senate staffers concerning W D policy relative to human experimentation policies and procedures. The letter from the Comptroller General indicated that DOD policy was set forth by DOD Instruction 5030.29, dated May 12, 1964. Instruction 5030.29 states that "The Department of Defense assumes full responsibility

for the protection of humans involved in research under its sponsorship whether this involves investigational drugs or other hazards." The letter also states, "[cloncering the contract with the University of Cincinnati . . . [DNA] stated that the cost of radiation treatment and patient case had not been borne by their agency. They also stated that funds of the Defense Nuclear Agency had been used only to pay for supplementary laboratory analyses of patients who had received whole-body irradiation in order for the Defense Nuclear Agency to gain information in areas that were relative to national defense."
The questions from Senate staffers focused on (1) the level of human experimentation funded by DOD, ( 2 ) what authorization was needed to conduct human experiments, ( 3 ) the adequacy of information given to prospective subjects and ( 4 ) were there differing standards applied to military personnel than to civilians. DOD responded to question one that only a very small portion of its medical R&D budget was given to human experimentation. In response to question two W D stated that although there was no standardized authorization process, all human experimentation was guided by W D instructions and service regulations and instructions. In response to question three DOD stated that informed consents was a primary ethical and legal requirements for all DOD use of human volunteers. In response to question four W D responded that in terms of supervision, volunteering, informed consent and freedom to terminate there was no difference.
January 11, 1973 - - Mr. Lawrence Elish released a 26 page paper titled, "Legal Rights of Human Subjects in the University of Cincinnati Whole-Body Radiation Study", that examined the legal and ethical implications of the Saenger experiments.

56
9 219.101
PAW 2 1 9 4 R O m O N OF HUMAN SUBJECTS
sec. 219.101 To what doea this policy apply? 219.102 Defirutions. 219.103 Assunhg compliance with this
policy-research conducted or supported by any Federal Department or Agency.
219.104-219.106 [ R ~ r v e d l 219.107 IRB Membership. 219.108 IRB functions and operations. 219.109 IRB review of research. 219.110 Expedited review procedures for
certain kin& of research involving no more than mintmnl r u t and for rmnor changes m approved research.
219.111 C n t e ~ for IRB approval of re- search
219.112 Review by mtitutioh 219.113 Suspension or terrnlnation of IRB
approval of mearch. 219.114 Cooperative research. 219.115 IRBneOrds. 219.118 General requirements for informed
consent. 219.117 Documentation of informed con-
sent. 219.118 Applhtiom and PrOpOdS lacking
definite p h for mvolvement of human subjects.
219.119 Research undertaken without the intention of Involving human subjects.
219.120 Evaluation and disposition of ap- plications and pro- for mearch to be conducted or supported by a Federal Department or Agency.
219.121 [Reservedl 219.122 Use of Federal funds. 219.123 Early ternunation of research sup.
port: Evaluation of applications and pro- P d .
219.124 Conditions.
l(b). A m o n m 5 U.S.C. 301: 42 U.S.C. 300v-
Somm 58 FR 28012.28021. June 18. 1991. unleas otheransc noted
1219.101 To what docr this policy apply? (a) F&ept as provided in paragraph
(b) of this section. this policy applies to all research involvtng human sub- jects conducted. supported or other- wise subject to regulation by any fed- eral department or agency which takes appropriate administrative action to make the policy applicable to such re- search. This includes research con- ducted by federal civilian employees or military personnel. except that each deDartmentoragencyheadmay adopt such procedural modVlcations ae may
289_
DEPARTMENT OF DEFENSE
IMPLEMENTATION OF THE
"COMMON RULE" --
FEDERAL POLICY FOR THE
PROTECTION OF HUMAN
SUBJECTS
3 2 C F R PART219

57
8 219.101
be appropriate from an sdmlnfstrrrtsve standpoint. It also includes research conducted. supported, or otherwise subject to regulation by the federal government outride the United States.
(1) Resevch that is conducted or supported by a federal department or agency. whether or not it is regulated 88 defined in t 219.102te). must comply
(2) Research that is neither conduct- ed nor supported by a federal depsrt- ment or agency but is subject to regu- lation LB defined in i 219.102te) must be reviewed and approved, in compli- ance Wfth 02lg.101, 1219.102, and 0219.10? through [email protected]? of this policy. by an Institutional review board (IRB) that operates in accord- ance With the pertinent requirements of this policy.
(b) Unless othenvbe re~ulred by de- partment or agency heads, research acttvities in which the only Involve- ment of human subjects wil l be In one or more of the followine categories are exempt from this polky:
(1) Fbearch conducted in estab- Wed or commonly accepted educa- tional settings, involving normal edu- cational practices, such as (1) research on regular and special education in- structional strategies. or (11) research on the effectiveness of or the compari- son among instructional techniques. curricula, or classroom management methods.
(2) Research involving the use of educational teats tcognItive, diagnos- tic. aptitude. achievement). survey procedures. Interview procedures or observation of public behavior. unless:
(1) Information obtained Is recorded In such a manner that human subjects can be identified, directly or through identifiers linked to the subjects and (ti) any diaclosure of the human sub- jects’ responses outride the research could reasonably place the subjects at rWr of cllminrrl or civil liability or be damagin# to the subjects’ financial standing. employability. or repuution.
(3) Research involving the use of educational tests (cognitive. diagnos- tic. aptitude, achievement). survey procedures, intervlew procedures. or obatnntion of public behavIor that 1. not exempt under psrrWlrph tbX2) of thk Isction. iI:
With all & O M Of this poliCg.
32 CFR ch. I (7-1-93 m) (i) The hurmrn subjects ~n e l m
or appointed public officials or can&. dates for public office; or (ti) fedem statutets) r e ~ u i r e t s ) without exception that the wnfidentictlity of the pemn- ally identifiable information will be mslntalned throughout the re8earch and thereafter.
(4) F&aearch, involving the all=. tion or study of existin# data, docu. mente. records. patholoqical speci- mens, or diagnostic specimen& if these sources are publicly available or if the information is recorded by the Inveeti- gator in such a manner that subjects cannot be Identifled, dlrectly or through identifiers linked to the sub- JW.
(5) Research and demonstration projects which are conducted by or subject to the approval of department or agency hee\is. and which are de- signed to study. evaluate, or otherwise examine:
(1) Public benefit or service pro- grams: (ii) procedures for obtaining beneftts or eervlces under those pro- grams; (111) possible changes In or al- ternatives to those proprams or proce- dures; or tlv) posrrible changes in meth- ods or levels of payment for beneflts or services under those programs.
(6 ) Taste and food Quality evaluatlon and consumer acceptance studies, (1) if wholesome foods without addltlves are consumed or (U) if a food is consumed that contains a food ingredient at or below the level and for a use found to be safe, or agricultural chemical or en- vironmental contaminant at or below the level found to be safe, by the Food
by the Environmental Protection Agency or the Food Safety and Inspec- tion Service of the U.S. Department of Agriculture.
tc) Department or agency h e w retain final judgment as to whether a particular activity ls covered by this poUCY.
(d) Department or agency he- may require that specific research ac- tivities or classes of research rctivltier conducted supported, or otherwise subject to regulation by the deport. ment or agency but not otherwine W V - ered by thk policy, comply with some or all of the requinmentr of thfr pouw.
and Drug Administration or approved
390
I

58
Offkm of the Secretory of Defenra 9 219.102
(e) Compliance with this policy re- quires compliance with mrtinent fed- eral laws or regulations which provide additional protections for human sub- jects.
( f ) This policy does not affect any state or local laws or rehulations which may otherwise be applicable and which provide additional protec- tions for human subjects.
(g) This policy does not affect any foreign laws or regulations which may otherwise be applicable and which provide additional protections to human subjects of research.
(h) When research covered by this policy takes place in foreign countries, procedures normally followed in the foreign countries to protect human subjects may differ from those set forth in this policy. [An example is a foreign Lnstitution which complies with guidelines consistent with the World Medical Assembly Declaration (Declaration of Helsinki amended 1989) issued either by sovereign states or by an organization whose function for the protection of human research subjects is internationally recognized.1 In these circumstances, if a depart- ment or agency head d e t e m e s that the procedures prescribed by the insti- tution afford protections that are at least equivalent to those provided in this policy, the department or agency head may approve the substitution of the foreign procedures m lieu of the procedural requirements provided in this policy. Except when otherwise re- quired by statute. Executive Order, or the department or agency head, no- tices of these actions as they occur will be published in the Fbm REGISTER or will be otherwise published as pro- vided in department or agency proce- dures.
(i) Unless o t h e m e required by law. department or agency heads may waive the applicability of some or all of the provisions of this policy to spe- cific research activities or classes of re- search activities otherwise covered by this policy. Except when otherwise re- quired by statute or Executive Order, the department or agency head shall forward advance notices of these ac- tions to the Office for Protection from Research Risks, Department of Health and Human Services (HHS), and shall
also publish them in the F ~ E R A L REO- IS- or in such other manner as pro- dded in department or agency proce- dures. 156 FR 28012. 28021. June 18. lOB1. as amended at 56 FR 20756, June 28,10011
0 219.102 Mnitiom. (a) Department or agency head
means the head of any federal depart- ment or agency and any other officer or employee of any department or agency to whom authority has been delegated.
(b) Znrtitution m e w any public or private entity or agency (including federal, state, and other agencies).
tc) LegaUy authonzed tepreaentatiue means an individual or judicial or other body authorized under applica- ble law to consent on behalf of a pro- spective subject to the subject's par- ticipation in the procedurets) involved in the research.
(d) Reseatch means a systematic in- vestigation, including research devel- opment, testing and evaluation, de- signed to develop or contribute to gen- eralizable knowledge. Activities which meet this definition constitute re- search for purposes of this policy. whether or not they are conducted or supported under a program which is considered research for other pur- poses. For example, some demonstra- tion and service programs may include research activities.
(e) Research subject to regulation, and similar terms are intended to en- compass those research activities for which a federal department or agency
1 Institutions with HHS-approved Bbsur- ances on file will abide by provisions of title 45 CFR part 46 subparts A-D. Some of the other Departmenta and Agencies have in- corporated all provisions of title 45 CFR part 46 Into their policies and procedures as well. However. the exemptions at 45 CFR 46.101Cb) do not apply to research involving prmners. fetuaes. pregnant women, or human in vitro fertilization. subparts B and C. The exemption at 45 CFR 46.101(b)(2), for reaearch involvin~ survey or interview procedure6 or observation of public behav- ior, does not apply to research with chil- dren, subpart D. except for research involv- ing obeervations of public behavior when the invdgntor(s) do not partlcivate In the activities bemg observed.
29 1

59
9 219.103
has specific mponslbillty for regula& In0 as a research activity. (for exam- ple, Investigational New Drug require- ments administered by the Food and DNg Administration). It does not in- clude research activities which are In- cidentally regulated by a federal de- partment or agency solely ns part of the department’s or agency’s broader responsibillty to regulate certaln types of activities whether research or non- research in nature (for example. Wage and Hour requirements administered by the Department of Labor).
( f ) Human subject means a living in- dividual about whom an investigator (whether professional or student) con- ducting research obtains
(1) Data through intervention or interaction with the individual. or
(2) Identlfiable private Information. Interventton includes both physical procedures by which data are gathered (for example. venipuncture) and ma- nipulations of the subject or the sub- ject’s environment that are performed for research purposes. Interaction in- cludes communfcation or interpersonal contact between investigator and sub- ject. “Private information” includes mformation about behavior that occm in a context in which an indi- vidual can reasonably expect that no observation or recording is taking place. and Information which has been provided for specific purposes by an individual and which the individual can reasonably expect will not be made public (for example, a medical record). Private Information must be individually identifiable (Le.. the iden- ti ty of the subject is or may readlly be ascertained by the investigator or as- sociated wtth the Information) in order for obtaining the information to constitute research Involving human subjects.
(8) IRE means an institutional review board established in accord with and for the purposes expressed in this policy.
(h) IRB approvcrl m e w the deter- mination of the IRB that the research has been reviewed and may be con- ducted at an institution within the constraints set forth by the IRB and by other institutional and federal re- quirements.
32 CFR Ch. I (7-1-93 Edition)
(1) Minima4 risk means that the probability and maonftude of harm or discomfort anticipated in the research are not greater in and of themselves than those ordinarily encountered in daily life or durfng the performance of routine physical or psychological ex- aminations or tests.
(1) CettfAcation means the official notification by the institution to the supporting department or agency. in accordance with the requirements of this policy, that a research project or activity involving human subjects has been yeviewed and approved by an IRB in accordance with an approved assurance. bI 219.103 hsurlng compliance with this
policy-research conducted or rupport- ed by any Federal Department or Agency.
(a) Each institution engaged in re- search which is covered by this policy and which is conducted or supported by a federal department or agency shall provide written assurance satis- factory to the department or agency head that it wil l comply with the re- quirements set forth in this policy. In lieu of requiring submission of an as- surance. individual department or agency heads shall accept the exist- ence of a current assurance. appropri- ate for the research In question. on file with the Office for Protection from Research Risks. HHS. and ap- proved for federalwide use by that office. When the existence of an HHS- approved assurance is accepted in lleu of requiring submission of an assur- ance. reports (except certification) re- quired by this policy to be made to de- partment and agency heads shall also be made to the Office for Protection from Research Risks. Ha8.
(b) Departmenta and agencies will conduct or support research covered by this policy only if the institution has an assurance approved as provided La this section, and only if the hstitu- tion has certifled to the department or agency head that the research has been reviewed and approved by M IRB provided for in the assurance. and will be subject to continuing review by the IRB. Assurances applicable to fed-
292

60
Offico of tho kcrotary of Dofonro
erally supported or conducted re- search shall at a minimum include:
( 1 ) A statement of principles govern- ing the institution in the discharge of its responsibilities for protecting the rights and welfare of human subjects of research conducted at or sponsored by the institution, regardless of whether the research is subject to fed- eral regulation. This may include an appropriate existing code, declaration, or statement of ethical principles, or a statement formulated by the institu- tion itself. This requirement does not preempt provisions of this policy ap- plicable to department- or agency-sup- ported or regulated research and need not be applicable to any research ex- empted or wmved under 5 219.101 (b) or (i).
(2) Designation of one or more IRBs established in accordance with the re- quirements of this policy, and for which provisions are made for meeting space and sufficient staff to support the IRB’s review and recordkeeping duties.
(3) A list of IRB members identified by name; earned degrees; representa- tive capacity; indications of experience such as board certifications, licenses, etc.. sufficient to describe each mem- ber’s chief anticipated contributions to IRB deliberations: and any employ- ment or other relationship between each member and the institution: for example: full-time employee, part-time employee, member of governing panel or board, stockholder, paid or unpaid consultant. Changes m IRB member- ship shall be reported to the depart- ment or agency head, unless m accord with 5 219.103ta) of this policy. the ex- istence of an HHS-approved assurance is accepted. In this case, change in IRB membership shall be reported to the Office for Protection from Re- search Risks. HHS.
(4) Written procedures which the IRB will follow ( I ) for conducting its initial and continuing review of re- search and for reporting its findings and actions to the investigator and the institution; (11) for determining which projects require review more often than annually and which projects need verification from sources other than the investigators that no materi- al changes have occurred since previ-
3 219.103
ous IRB review; and (110 for ensuring prompt reporting to the IRB of pro- posed changes in a research activity, and for ensuring that such changes in approved research, during the period for which IRB approval has already been given, may not be initiated with- out IRB review and approval except when necessary to eliminate apparent immediate hazards to the subject.
(5) Written procedures for ensuring prompt reporting to the IRB. appro- priate institutional officials, and the department or agency head of (i) any unanticipated problems involving risks to subjects or others or any serious or continuing noncompliance with this policy or the requirements or determi- nations of the IRB and (ii) any sus- pension or termhation of IRB approv- al.
tc) The uu rance shall be executed by an individual authorlzed to act for the institution and to assume on behalf of the institution the obliga- tions imposed by this policy and shall be filed in such form and manner as the department or agency head pre- scribes.
(d) The department or agency head will evaluate all assurances submitted in accordance with this policy through such officers and employees of the de- partment or agency and such experts or consultants engaged for this pur- pose as the department or agency head determines to be appropriate. The department or agency head’s eval- uation will take into consideration the adequacy of the proposed IRB in light of the anticipated scope of the institu- tion’s research activities and the types of subject populations likely to be m- volved. the appropnateness of the pro- posed initial and continuing review procedures in light of the probable risks, and the size and complexity of the institution.
(e) On the basls of this evaluation. the department or agency head may approve or disapprove the assurance, or enter into negotiations to develop an approvable one. The department or agency head may limit the period during which any particular approved asaur8nce or class of approved assur- ances shall remlun effective or other- wise condition or restrict approval.
293

61
9 219.107 (f) Certification is muired when the
research is supported by a federal de- partment or agency and not otherwise exempted or waived under 1219.101 (b) or (1). An institution with an ap- proved assurance shall certify that each application or proposal for re- search covered by the assurance and by 1 219.103 of this Policy has been re- viewed and approved by the IRB. Such certification must be submitted with the application or proposal or by such later date as may be prescribed by the department or agency to which the ap- plication or proposal is submitted. Under no condition shall research cov- ered by 1 219.103 of the Policy be sup- ported prior to receipt of the certdica- tion that the research has been re- viewed and approved by the IRB. In- stitutions without an approved assur- ance covering the research shall certi- fy within 30 days after receipt of a re- quest for such a certification from the department or agency, that the appli- cation or proposal has been approved by the IRB. If the certification is not submitted within these time lunits, the application or proposal may be re- turned to t9e institution. (Approved by the Office of Management and Budget under control number 9999- 0020) C56 F R 28012. 28021. June 18. 1991. 8s amended at 56 FR 29756. June 28.19911
88 219.104-219.106 [Reservedl
8219.107 IRB membership. (a) Each IRB shall have at least five
members, with varying backgrounds to promote complete and adequate review of research activities commonly conducted by the institution. The IRB shall be sufficiently qualified through the experience and expertise of its members, and the diversity of the members, including consideration of race, gender, and cultural backgrounds and sensitivity to such issues as com- munity attitudes, to promote respect for its advice and counsel in safeguard- mg the rights and welfare of human subjects. In addition to possessing the professional competence necessary to review specific research activities, the IRB shall be able to ascertain the ac- ceptability of proposed research in terms of institutional commitments
32 CFR Ch. I(7-1-93 Edition)
and regulations. applicable law, and standards of professional conduct and practice. The IRB shall therefore in- clude persons knowledgeable in these areas. If an IRB regularly reviews re- search that involves a vulnerable cate- gory of subjects. such as children, pns- oners. pregnant women, or handi- capped or mentally disabled persons, consideration shall be given to the in- clusion of one or more individuals who are knowledgeable about and experi- enced in working with these subjects.
(b) Every nondiscriminatory effort will be made to ensure that no IRB consists entirely of men or entirely of women, including the institution's con- sideration of qualified persons of both sexes, so long as no selec-ion is made to the IRB on the basis L - gender. No IRB may consist entirely of members of one profession.
tc) Each IRB shall include at least one member whose primary concerns are in scientific areas and at least one member whose pnmary concerns are in nonscientific areas.
(d) Each IRB shall include at least one member who 1s not otherwise af- filiated with the mstitution and who is not part of the immediate family of a person who is affiliated with the insti- tution.
(e) No IRB may have a member par- ticipate in the IRB's initial or continu- ing review of any ProJect m which the member has a conflicting interest, except to provide mformation request- ed by the IRB.
( f ) An IRB may, in its discretion. mvite mdividuals with competence in special areas to asslst in the review of issues which requre expertise beyond or in addition to that available on the IRB. These indinduals may not vote with the IRB.
8 219.108 IRB functions and operations. In order to fulfill the rtquirements
of this policy each IRB shall: (a) Follow written procedures in the
same detail as described in 5 219.103(b:(4) and, to the extent re- quired by. 1 219.103(b)(5).
(b) Except when an expedited review procedure is used (see 4219.110). review proposed research at convened meetings at which a majority of the
294
84-514 0 - 94 - 3

62
Offico of tho Swotary of Dohnro
members of the IRB are present, in- cluding at least one member whose primary concerns are in nonscientific areas. In order for the research to be approved. it shall receive the approval of a majority of those members present at the meeting. (I 219.109 IRB Review of Reaearei
(a) An IRB shall review and have au- thority to approve, require modifica- tions in (to secure approval). or disap- prove all research activities covered by this policy.
(b) An IRB shall require that infor- mation given to subjects as part of in- formed consent is in accordance with 0210.116. The IRB may require that information, in addltion to that specif- ically mentioned in 0 210.116. be given to the subjects when in the IRBs judgment the information would meaningfully add to the protection of the rights and welfare of subjects.
tc) An IRB shall require documenta- tion of informed consent or may waive documentation in accordance with 0 210.117.
(d) An IRB shall notify investigators and the institution In writing of its de- cision to approve or disapprove the proposed research activity, or of modi- fications required to secure IRB ap- proval of the research activity. If the IRB decides to disapprove a research activity. it shell include in its written notification a statement of the re880118 for its decision and give the investiga- tor an opportunity to respond in person or in writing.
(e) An IRB shall conduct continuing review- of research covered by this policy at intervals appropriate to the degree of risk, but not leas than once per year, and shall have authority to observe or have a third party observe the consent process and the research. (Amroved by the Offla of Management and Budget under control number goOP o o m (I 219.110 Expedited review pmeedum for
certain kin& of research involving no more than minimal rirk. and for minor c h ~ w in approved research.
(a) The Secretary, HR8. has estab- lbhed. and published a8 a Notice In the R ~ I S R R . a list of catego- rlea of research that may be reviewed
0 219.1 11
by the IRB through an expedited review procedure. The list will be amended, as appropriate after consul- tation with other departments and agencies. through periodic republica- tion by the Secretary. HEIS. in the FEDPUL REGISTER. A copy of the list is available from the Office for Protec- tion from Research Risks. National In- stitutes of Health, HIIS. Bethesda, Maryland 20802.
(b) An IRB may use the expedited review procedure to review either or both of the following:
(1) Some or ell of the research ap- pearing on the list and found by the reviewerts) to involve no more than minLmal risk.
(2) Minor changes in previously ap- proved research durlng the period (of one year or lese) for which approval is authorized. Under an expedited review procedure, the review may be carried out by the IRB chairperson or by one or more ex- perienced reviewers designated by the chairperson from among members of the IRB. In reviewing the research. the reviewers may exercise all of the authorities of the IRB except that the reviewers may not disapprove the re- search. A research activity may be &- approved only after review in accord- ance with the non-expedited proce- dure set forth in 0 219.108(b).
tc) Each IRB which uses an expedlt- ed review procedure shall adopt a method for keeping all members ad- vised of research proposals which have been approved under the procedure.
(d) The department or agency head nay restrict. suspend. terminate. or choose not to authorize an institu- tion's or IRB's use of the expedited review procedure. II 219.111 Criteria for IRB approval of re-
(a) In order to approve research cov- ered by thts policy the IRB shrll de- termine that ell of the following re- quirements are satisfied:
(1) Risks to subjects are minimized: ( i ) By using procedures whlch are con- sistent with sound research design and which do not urine expose subjectr to risk, and (Ill whenever aP- propriate. by using procedure8 already
search.
295

-
t
63
being performed on the subjects for diagnostic or treatment purposes.
(2) Risks to subjects are reasonable in relation to anticipated benefits. if any, to subjects, and the importance of the knowledge that may reasonably be expected to result. In evaluating risks and benefits. the IRB should consider only those risks and benefits that may result from the research (as distinguished from risks and benefits of therapies subjects would receive even if not participating in the re- search). The IRB should not consider possible long-range effects of applying knowledge gained in the research (for example, the possible effects of the re- search on public policy) as among those research risks that fall within the purview of its responsibility.
(3) Selection of subjects is equitable. In making this assessment the IRB should take into account the purposes of the research and the setting in which the research will be conducted and should be particularly cognizant of the special problems of research in- volving vulnerable populations, such as children, prisoners, pregnant women, mentally disabled persons. or economically or educationally disad- vantaged persons.
(4) Informed consent will be sought from each prospective subiect or the subject's legally authorized repreaent- ative. in accordance with, and to the extent required by 4 219.116.
(5) Informed consent an11 be appro- priately documented. in accordance wth. and to the extent requued by 5 219.117.
(6) When appropriate. the research plan makes adequate prowion for monitoring the data collected to ensure the safety of subjects.
(7) When appropriate, there are ade- quate provisions to protect the privacy of subjects and to maintain the confi- dentiality of data.
(b) When some or all of the subjects are likely to be vulnerable to coercion or undue influence, such as chlldren. prisoners, pregnant women. mentally disabled persons, or economically or educationally disadvantaged persons, additional safeguards have been in- cluded in the study to protect the rights and welfare of these subiects.
32 CFR Ch. I (7-1-93 Edition)
ff 219.112 Review by idht ion. Research covered by this policy that
has been approved by an IRB may be subject to further approprlate review and approval or disapproval by offi- cials of the institution. However, those officials may not approve the research if it has not been approved by an IRB. ff 210.113 Surpenaion or termination of
An IRB shall have authority to sus- pend or terminate approval of re- search that is not being conducted in accordance with the IRB's require- ments or that has been associated with unexpected serious harm to subjects. Any suspension or termination of ap- proval shall include a statement of the reasons for the IRBs action and shall be reported promptly to the investiga- tor, appropriate institutional officials. and the department or agency head. proved by the Offlce of Management and Budget under control number @e@@- 0020)
$210.114 Cooperative research. Cooperative research projects are
those projects covered by thts polfcy which involve more than one Institu- tion. In the conduct of cooperative re- search projects, each institution is re- sponsible for safeguarding the rights and welfare of human subjects and for complying with this policy. With the approval of the department or agency head, an institution participating in a cooperative project may enter lnto a Joint review arrangement, rely upon the review of another qualified IRB. or make similar arrangements for avoiding duplication of effort. ff 219.115 IRB recorda.
(a) An institution. or when appropri- ate an IRB. shall prepare and main- tain adequate documentation of IRB activities, including the followmg:
(1) Copies of all research proposals reviewed, scientific evaluations. if any. that accompany the proposals. BP- proved sample consent documents. progress reports submitted by investi- gators, and reports of injuries to sub- Jects.
(2) Minutes of IRB meetings which shall be in sufficient detail to show at-
IRB approval of research.
296

64
ottk. of tho kcntary of Dohnu
tendance at the meetings; actions taken by the IRB: the vote on these actions Including the number of mem- bers voting for. m t , and abstain- ing: the basis for requiring changes in or disapproving r e s e e and a writ- ten summary of the discusion of con- troverted issues and their resolution.
(3) Records of continuin@ review ac- tivities.
(4) Copies of all correspondence be- tween the IRB and the investigators.
(5) A list of IRB members in the same detail as described is 0 219.103(b)(3).
(6 ) Written procedures for the IRE in the same detail as described in @ 219.103(b)(4) and @ 219.103(b)(S).
(7) Statements of significaut new
quired by @ 219.116(bMS). (b) The records required by this
policy shall be retained for at least 3 years, and records relating to research which is conducted shall be retalned for at least 3 yeare after completion of the research. All records shall be ac- cessible for inspection and copying by authorized representatives of the de- partment or agency at reasonable times and In a reasonable manner. (Approved by the Office of Manasement and Budge$ under contml number gooS 0020)
$219.116 General requiremcntr for in-
Except as provided elsewhere in this policy. no investigator may involve a human being as a subject in research covered by this policy unless the inves- tigator has obtained the legally effec- tive informed consent of the subject or the subject's legally authorized repre- sentative. An investigator shall seek such consent only under clrcum- stances that provide the prospective subject or the representative sufficient opportunity to consider whether or not to participate and that mMmize the possibility of coercion or undue in- fluence. The information that is given to the subject or the representative shall be in language understandable to the subject or the representative. No informed consent, whether oral or written, may include any exculpatory language through which the subject or the representative is made to walve
fIn- Provided to Subjects. as re-
formed colucnt.
8 219.1 16
or appear to walve any of the subject's legal rights, or rele- or appears to release the investigator. the sponsor. the lnstitution or its agents from li- ability for negligence.
(a) Basic elements of informed con- sent. Except as provided In paragraph tc) or (d) of this section. in seeking In- formed consent the following informa- tion shall be provided to each subject:
(1) A statement Chat the study in- volves research, an explanation of the purposes of the research and the ex- pected duration of the subject's par- ticipation, a description of the proce- dures to be followed. and identifica- tion of any procedures which are ex- perimental;
(2) A description of any reasonably foreseeable risks or discomforts to the subject:
(3) A description of any benefits to the subject or to others which may reasonably be expected from the re- search;
(4) A disclosure of appropriate alter- native procedures or courses of treat- ment. if any. that might be advanta- geous to the subject:
(5) A statement describing the extent, if any, to which confidentiality of records identifying the subject will be maintained:
( 6 ) For research involving more than minimal risk. an explanation as to whether any compensation and an ex- planation as to whether any medical treatments are available if Injury OCC- and, if SO, what they C O M i s t Of, or where further information may be obtained:
(7) An explanation of whom to con- tact for answers to pertinent questions about the research and research sub- jects' rights. and whom to contact in the event of a research-related Injury to the subject: and
(8) A statement that participation is voluntary, refusal to participate will involve no penalty or loss of benefits to which the subject is otherwise enti- tled. and the subject may discontinue participatlon at any time wtthout pen- alty or loss of benefits to which the subject is otherwise entitled.
(b) Additional elements of informed consent. When appropriate, one or more of the following elements of In-
29'7

8 219.1 17
65
32 CFR Ch. I(7-1-93 Edition)
.
?
formation shall also be provided to each subject:
(1) A statement that the particular treatment or procedure may involve risks to the subject tor to the embryo or fetus, if the subject is or may become pregnant) which are currently unforeseeable:
(2) Anticipated circumstances under which the subject's participation may be termhated by the investigator without regard to the subject's con- sent:
(3) Any additional costs to the sub- ject that may result from participa- tion in the research:
(4) The consequences of a subject's decision to withdraw from the re- search and procedures for orderly ter- mlnation of participation by the sub- ject;
(5) A statement that significant new findings developed during the course of the research which may relate to the subject's willinmess to continue participation will be provided to the subject; and
(6) The approximate number of sub- jects involved in the study.
tc) An IRB may approve a consent procedure which does not include, or which alters, some or all of the ele- ments of informed consent set forth above, or waive the requirement to obtain informed consent provided the IRB finds and documents that:
(1) The research or demonstration project is to be conducted by or sub- ject to the approval of state or local government officials and is designed to study. evaluate. or o t h e m e examme: (i) Public benefit of service programs: (ii) procedures for ob tahng benefits or services under those programs; (iii) possible changes in or alternatives to those programs or procedures: or (iv) possible changes in methods or levels of payment for benefits or services under those programs; and
(2) The research could not practica- bly be carried out without the waiver or alteration.
(d) An IRB may approve a consent procedure which does not include, or which alters, some or all of the ele- ments of informed consent set forth in this section, or waive the requlrements to obtain informed consent provided the IRB finds and documents that:
(1) The research involves no more than minimal risk to the subjects:
(2) The waiver or alteration will not adversely affect the rights and welfare of the subjects: (3) The research could not practica-
bly be carried out without the waiver or alteration: and
(4) Whenever appropriate, the sub- jects wil l be provided with additional pertinent information after participa- tion.
(e) The informed consent require- ments in this policy are not intended to preempt any applicable federal, state, or local laws which require addi- tional information to be disclosed in order for informed consent to be legal- ly effective.
( f ) Nothmg in this policy is intended to limit the authority of a physician to provide emergency medical care. to the extent the physician is permitted to do so under applicable federal, state, or local law. (Approved by the Office of Management and Budget under control number 9999- 0020)
B 219.117 Documentation of informed con- sent.
(a) Except as provided in paragraph tc) of this section. informed consent shall be documented by the use of a written consent form approved by the IRB and signed by the subject or the subject's legally authorned represent- ative. A copy shall be given to the person signing the form.
(b) Except as provlded in paragraph (c) of this section. the consent form may be either of the following:
(1) A written consent document that embodies the elements of informed consent required by 4 219.116. This form may be read to the subject or the subject's legally authorized represent- ative, but in any event, the investiga- tor shall gwe either the subject or the representative adequate opportunity to read it before it is signed; or
(2) A short form written consent document stating that the elements of informed consent required by 4 219.116 have been presented orally to the sub- ject or the subject's legally authorized representative. When this method is used. there shall be a witness to the
298

66
oral presentation. Also. the IRE shall approve a written summary of what is to be sudd to the subject or the repre- sentative. Only the short form itself is to be signed by the subject or the rep- resentative. However. the witness shall e lm both the short form and a copy of the summary. and the person actually obtalnine consent shall sign a copy of the summary. A copy of the summary shall be given to the subject or the representative. in additlon to a copy of the short form.
tc) An IRB may waive the require- ment for the investigator to obtain a slmed consent form for some or all subjects K it finds either.
(1) That the only record linking the subject and the research would be the consent document ar.d the principal risk would be potential harm resulting from a breach of confidentiality. Each subject wil l be asked whether the sub- ject wanm documentation linking the subject with the research. and the sub- ject‘s wishes will govern, or
(2) That the research presents no more than minimal risk of harm to subjects and involves no procedures for whlch written consent is normally required outside of the research con- text.
In csses in whlch the documentation requirement is waived. the IRB may require the investigator to provide subjects with a written statement re- garding the research. (AppIUVed by the Office of Management and Budget under control number 9999- 0020)
S 219.118 Applications and p ~ - ~ p o ~ l s lack- ing definite plans for involvement of human subject&
Certain types of applications for grants. cooperative agreements, or contracts are submitted to depart- menta or agencies with the knowledge that subjects may be involved anthin the period of support, but definite plans would not normally be set forth in the application or proposal. These include activities such as institutional type granta when selection of specific projects is the Institution’s responsibll- ity: research training grants in which the activities involving subjects remain to be selected: and projecta in which human subjects’ involvement will
9 219.120
depend upon completion of instru- ments, prior animal studies. or purfii- cation of compounds. These applica- tions need not be revlewed by an IRE before an award may be made. Howev- er, except for reswch exempted or waived under #[email protected] (b) or (1). no human subjects may be involved in any project supported by these awards until the project has been reviewed and approved by the IRB, as provided in this policy, and certification submit- ted, by the institution, to the depart- ment or agency.
$219.119 Rcrcueh undertaken without the intention of involving human rub-
In the event research is undertaken wfthout the intention of involvlng human subjects. but it is later pro- posed to involve human subjecta in the research. the research shall first be re- viewed and approved by an IRB, as provided in this policy, a certification submitted. by the lnstltution. to the department or agency, and final ap- proval given to the proposed change by the department or agency.
S 219.120 Evaluation and disposition of applicationr and pmp04~ for research to be conducted or supported by a Fed- eral Department or Agency.
(a) The department or agency head Will evaluate all apDlications and pro- posals involving human subjects sub- mitted to the department or agency through such officers and employees of the department or agency and such experts and consultants as the depart- ment or agency head determines to be appropriate. This evaluation will take into consideration the risks to the sub- jects. the adequacy of protection against these rlsks. the potential bene- fi ts of the research to the subjects and others, and the importance of the knowledge gained or to be gamed.
(b) On the basis of this evaluation, the department or agency head may approve or dlsapprove the application or p r o m , or enter into negotiations to develop an approvable one.
)-
299
I

f
67
.
.
5 219.122
(r 219.121 [Renemed]
@ 219.122 Use of Federrrl funds. Federal funds administered by a de-
partment or agency may not be ex- pended for research involving human subjects unless the requirements of this policy have been satisfied.
ff 219.123 Early termination of research suppork Evaluation of applications and propoulr.
(a) The department or agency head may require that department or agency support for any project be ter- minated or suspended in the manner prescribed in applicable program re- quirements, when the department or agency head finds an institution has materially failed to comply with the terms of this policy.
(b) In making decisions about sup- portmg or approving applications or proposals covered by this policy the department or agency head may take into account. in addition to all other eligibility requlrements and program criteria factors such as whether the applicant has been subject to a termi- nation or suspension under paragarph (a) of this section and whether the ap- plicant or the person or persons who would direct or has have drected the scientific and technical aspects of an activity has have, in the Judgment of the department or agency head, mate- nally failed to discharge responsibility for the protection of the rights and welfare of human subjects (whether or not the research was subject to federal regulation).
ff 219.124 Conditions. With respect to any research project
or any class of research proJecta the department or agency head may impose additional conditions prior to or at the time of approval when in the judgment of the department or agency head additional conditions are nett% sary for the protection of human sub- l a .
300

68
Mr. BRYANT. Dr. Cox.
STATEMENT OF JAMES D. COX, MD, PROFESSOR OF RADIO- THERAPY, M.D. ANDERSON CANCER CENTER, AND CHAIR- MAN, RADIOTHERAPY ONCOLOGY GROUP Dr. COX. Mr. Chairman, I am James Cox, a physician involved
in the treatment of patients with cancer and clinical research deal- ing with radiation oncology and other cancer treatments.
My remarks will center on cancer treatments in the 19608, the use of total body irradiation in cancer treatment, including the Cin- cinnati project, the status of clinical trials for the treatment of can- cer dunng the period in question, and the evolution of informed consent.
The treatment of patients who were found to have cancer in the 1960s was centered on the use of surgical removal or radiation therapy, which were the only known means to cure cancer. "he drugs available to treat widespread cancer in patients at that time were minimally affected by current standards. Virtually all cancer treatments considered standard in the early 1960s had evolved without formal clinical trials.
Patients whose spread of cancer was be ond local re 'onal tu-
tients was to alleviate symptoms without any expectation of pro- longing the atient's life.
palliative treatments, or attempting experimental treatments, pa- tients frequently wished to do something unproven rather than doing nothing.
Radiation therapy was known to produce predictable responses in most forms of cancer, and it was often curative-is often cura- tive for Hodgkin's disease, cervical cancer, advanced cancer of the mouth, throat, et cetera. Its limitation was that it could be applied only to local or re 'onally advanced tumors. Total body irradiation
chronic leukemias and lymphomas. It was reasonable to hypothesize that total body irradiation
might have some benefit in widely disseminated cancer of other types. Enthusiasm for total body irradiation increased as the tech- nology evolved to reinfuse bone marrow to overcome potentially le- thal bone marrow depletion.
Published data from the University of Cincinnati indicate that the total body irradiation trials were undertaken to determine the tolerance and effectiveness of this treatment in several types of cancer. The total body irradiation doses differed range from 100 to 200 rads and were not considered in the range that would cause death. All but three patients had advanced cancer not considered curable by local reeonal treatments.
Total body irradiation was given as an adjunct to three children considered at extremely high risk to the threat of metastasis.
The study at the University of Cincinnati went under several lev- els of review by the National Institutes of Health, the editors of sci- entific journals. In addition, a special review, already alluded to, by Dr. Henry Kaplan of Stanford University, Frank Hendrickson in
mors were considered incurable. The aim o P treatment o P such pa-
Faced wit K the choices of doing nothing and administering local
had been used wit t some success in the treatment of patients with

69
Chicago, was requested by the American College of Radiology in re- sponse to an inquiry by Senator Mike Gravel in 1972.
Clinical trials which compared experimental treatments to stand- ard treatments for patients with cancer were begun in the United States only in the mid-to-late 1950s. As these studies evolved, the concept of informed consent evolved. Formalization of informed con- sent by the National Institutes of Health was begun in the 1960s, and has continued to evolve to this day.
In a 1973 publication of the Cincinnati studies by Dr. Saenger and colleagues, a statement is included which says,
All patients ave informed consent in accordance with the directives of the Fac- ulty Research Eommittee of the Universit of Cincinnati College of Medicine and those of the National Institutes of Head . The use of formal, informed consent forms in this study antedated the above requirements by two years.
In conclusion, radiation therapy is an important part of the ar- mamentarium of physicians in the care of patients with cancer. Be- cause of its effectiveness in the treatment of local regional tumors, whole body irradiation has been the subject of research for decades. At present, total body irradiation followed by bone marrow trans- plantation is considered a standard part of the treatment of many patients with leukemia, lymphoma and Hodgkin’s disease, and it is under investigation still for other diseases.
In the era prior to the establishment of bone marrow transplan- tation to support such treatment, lower, sublethal doses of total body irradiation were explored for patients with advanced cancers as a possible alternative to no treatment or to treatment with cytotoxic chemicals or hormones.
The University of Cincinnati’s studies of total body irradiation conducted between 1960 and 1971 were based on a reasonable hy- pothesis were conducted and reported in the scientific literature in a manner consistent with other clinical investigations, and seem to have used the accepted standards of informed consent for that pe- riod.
One might judge them harshly from a perspective 20 years later, but they were reviewed and re eatedly approved by peers of the in- vestigators at the time the stuiies were conducted.
Thank you. Mr. BRYANT. Thank you. [The prepared statement of Dr. Cox follows:]

70
SUBCOMMITTEE ON ADMINISTRATIVE LAW AND GOVERNMENTAL RELATIONS
COMMITTEE ON THE JUDICIARY
HOUSE OF REPRESENTATIVES
SUMMARY STATEMENT OF JAMES D. COX, M.D.
Radiation therapy is an important part of the armamentarium of physicians in the care of
pattents wth cancer. Because of its effechveness m the treatment of local-regional tumors, whole
body irrdahon has been a subject of research for decades. At present, total body trradiahon
followed by bone marrow transplantation is considered a standard part of treatment of many
patients with leukemia, lymphoma, and Hodgkin's disease, and IS under Investigahon for
myeloma and cancer of the breast. In the era prior to the establishment of bone marrow
transplantation to support such treatment, lower (sublethal) doses of total body imdiahon were
explored for patients w th advanced canm as a possible alternative to no treatment or treatment
with cytotoxic chemicals or hormones. The Umversrty of Cincinnati studies of total body
d i a h o n , conducted between 1960 and 1971 were based on a reasonable hypothesis, were
conducted and reported III the scientific literature in keepmg with clinical investlgations of that
period, and seem to have used the accepted standards of informed consent for that period. One
mght judge them harshly from a pempective 20 years later, but they were reviewed and
repeatedly approved by peers of the investigators at the hme the studies were conducted.

71
SUBCOMMITTEE ON ADMINISTRATIVE LAW AND GOVERNMENTAL RELATIONS COMMITTEE ON THE JUDICIARY HOUSE OF REPRESENTATIVES
BIOGRAPHY OF JAMES D. COX, M.D.
PRESENT TITLE & AFFILIATION: .
BIRTH DATE & PLACE:
OFFICE ADDRESS:
EDUCATION Undergraduate
Graduate
POSTGRADUATE TRAINING: 1963 - 1964.
1965 - 1966
1966 - 1969:
1969 - 1970.
Professor of Radiotherapy Hubert L. and Olive Stringer Char in Oncology in Honor of Sue Gribble Stringer Coordinator, Interdisciplinary Program Development The University of Texas M D Anderson
Houston, Texas 77030
July 16, 1938, Steubenville, OH
The Umversity of Texas M.D Anderson
Interdisciplinary Program Development (Box 3 12) 15 15 Holcombe Boulevard Houston, Texas 77030
Cancer Center
Cancer Center
(713) 792-2260
1960, Kenyon College, Gambier, OH
1965, University of Rochester School of Medicine and Dentistry, Rochester, NY
Fellow Clinical Oncology and Therapeutic Radiology, Penrose Cancer Hospital, Colorado Springs, CO
Intern (mixed w~th major in Medicine), University of Chicago, Chicago, IL
Resident Therapeutic Radiology, Penrose Cancer Hospital, Colorado Springs, CO
Fellow: Therapeutic Radiology, Institute Gustave-Roussy, Villejuif, France
Biographical Sketch at Jam- U Cox, M 0 Page I

72
SPECIALTY BOARDS: 1966:
1971.
MILITARY SERVICE 1970 - 1972'
ACADEMIC & PROFESSIONAL
APPOINTMENTS:
FACULTY: 1972 - 1974:
1974 - 1977
1977 - 1982
1982 - 1985:
1985 - 1988.
1988 - 1992:
1992 - .
LOCAL:
1992 -Present. NATIONAL:
1972 - 1974. 1983 - 1987.
Diplomate, National Board of Medical
American Board of Radiology (Therape.Uk Examiners
Radiology)
Major, US Army, Walter Reed General Hospital, Washington, DC Honorable Discharge
Assistant Professor of Radiology Georgetown University Hospital Washington, DC
Associate Professor of Radiology Medical College of Wisconsin
Professor of Radiology Medical College of Wisconsin
Professor and Chairman Department of Radiahon Oncology Medical College of Wisconsin
Department of Radiation Oncology Columbia University College of Physicians and Surgeons
Care and Physician-in-Chef, The University of Texas M D Anderson Cancer Center
Professor of Radiotherapy, Coordinator, Interdisciplinary Program Development, The University of Texas M.D Anderson Cancer Center
Texas Radiation Advisory Board Member
National Cancer Institute (NCT) Visihng Physician, Medicine Branch Cancer Research Manpower Review
Professor and Chairman
Professor of Radiotherapy; Vice President for Patient
Committee, Division of Extramural Activihes

1987 - 1991.
1987 - Present
1990 - 1993.
1985 - 1986 1986 - 1987
1981 - 1987
1981 - 1987. 1987 - 1993. 1987 - 1993
1981 - 1987' 1987 -Present.
1979 - 1989
1981 -Present.
1974 - 1979.
1978 - 1980
EDITORIAL BOARDS: 1981 -Present
Board of Scientific Counselors Division of Cancer Treatment
Committee of Clinical Trials Cooperative Group Chairs
Charman, Committee of Clinical Trials Cooperative Group Chairs
American Society for Therapeutic Radiology and Oncology (ASTRO) President Chairman. Board of Directors
American College of Radiology (ACR) Chauman, Committee of Radiotherapeutic
Steenng Committee of the Council Chancellor Charman, Commission on Radiation
Oncology
Research and Development
Radiation Therapy Oncology Group (RTOG) Vice Chairman for Research Strategies Chairman. RTOG
American Board of Radiology (ABR) Subcommittee for Wntten Examination
Examiner, Oral Examination in Radiation Oncology
Veterans Administration Lung Group (VALG) Chairman, Radiotherapy Committee Executive Committee
Council of Radiation Oncology Committee Chairpersons (CROCC) Member
in Radiation Oncology
Editorial Consultant. AMERICAN JOURNAL OF CLINICAL ONCOLOGY CANCER CHEST INTERNATIONAL JOURNAL OF RADIATION
ONCOLOGY, BIOLOGY, PHYSICS JOURNAL OF CLINICAL ONCOLOGY NEW ENGLAND JOURNAL OF MEDICINE

74
1985 -Present:
1990 -Present:
1990 - Present
HONORS & AWARDS:
1960. 1965 1983
1984
1985
1986
1987.
1988.
1989:
1992. 1992.
1992.
1993
1994
Editor, INTERNATIONAL JOURNAL OF
Site Editor for Rapid Communica- RADIATION ONCOLOGY, BIOLOGY, PHYSICS
tions Section, INTERNATIONAL JOURNAL OF RADIATION ONCOLOGY, BIOLOGY. PHYSICS
Editorial Board, LUNG CANCER
AB: Magna Cum Laude, Phi Beta Kappa MD: With Honor Fellow of the American College of
Radiology (FACR) Robert Fowler Fellow of the Anti-Cancer
Council of Victoria, Australia President: American Society for
Therapeutic Radiology and Oncology (ASTRO)
University of Michigan
30th Anniversary, Department of Radiology, Hiroshima Umversity Medical School
Radiation-Oncology
Physicians and Surgeons of Canada
William Caldwell Memonal Lecture, The Umversity of Wisconsin
Hubert L. and Olive Stringer C h r in Oncology in Honor of Sue Gribble Stringer
Annual Oration in Radiation Oncology, Radiological Society of Ncrth America
Invited Lecturer, 7th International Symposium of the Foundation for Cancer Research
Sixth Isadore Lampe Lecture
International Guest Lecturer,
Honorary Member, Belgian Association for
W. G. Cosbie Lecture, Royal College of
Gillies Memonal Lecture., The University of Iowa
In addition, Dr. Cox is the author of 212 peer-reviewed journal articles, book chapters, and books Copies of the bibliography are available upon request

75
SUBCOMMITTEE ON ADMINISTRATIVE LAW AND GOVERNMENTAL. RELATIONS
COMMITTEE ON THE JUDICIARY
HOUSE OF REPRESENTATIVES
PREPARED STATEMENT OF JAMES D: COX, M.D.
The following comments are submrttcd at the request of Congressman Jack Brooks, Chair,
House of Representatives Committee on the Judiciary. They pertain to hearings on radiation
expenments performed by the University of Cincinnati Medical School. My formal remarks wll
center on.
1) Cancer treatment in the 1960’s;
2) The use of total body irradimon in cancer treatment, including the Cicinnat~
PmJWC
3) The status of climcal trials for the treatment of cancer during the penod in
queshon and the evolution of mformed consent.
Status of Cancer Treatment Durine the 1960’s
The treatment of patients who were found to have cancer UI the 1960’s was largely
centered on the use of surgical removal or radiation therapy Such treatments were the only
known means to cure cancer. Hormonal therapy and systermc cytotoxlc chemotherapy were
undergoing inveshgation: wth rare exception, such systemic treatments were used wth palhatwe
RpMd SwCmnt O f J n a D Cor. M D p w I

76
intent or to retard progression of uniformly fatal diseases. The drugs available to treat
widespread cancer in patients m the 1960's were minimally effective by current standards.
Cancer of the bronchus or the colon infrequently responded to the available drugs, and breast
cancer was only slightly more responsive.
Virtually all standard cancer treatment in the 1960's evolved by clinical applications of
best known therapies without fonnal clinical trials. Standard surgical procedures for cancer such
as radical mastectomy, laryngectomy, resections of the large bowel, stomach and esophagus had
not been tested in formal clinical trials. Similarly, radiation therapy considered standard, such
as that for cervical cancer, had not been studied in c l i ca l trials, but had proven to be curative
over several decades.
Patients whose tumors had sprcad beyond local-regional me8115 of treatment (surgery and
radiation therapy) were considered incurable. The aim of treatment of such patients WIW to
alleviate symptoms such as pain, bleeding and obstnrction of natural passages. Such palliative
treatments were not undertaken with an expectation of prolonging the patient's life. Faced with
the choices of doing nothmg, administering local palliative treatment, or attempting highly
experimental unproven treatments, the patient would ftquently express a desire to do something
unproven rather than doing nothing.

d .
77
T otal Bodv Irradiation in Cancer T c e a t m ~
The responsiveness of tumors to ionizing radiations demonstrated soon after the discovery
of x-rays by Roentgen iF 1895 d t e d in a sttady increase in the usc of such hratmeata By
the early 195O’s, high-energy photona became available for cancer treatment with Cobalt 60
teletherapy units, betatrons, and linear accelerators, and the usc of d a t i o n therapy expanded
rapidly.
Radiation therapy was known to produce predictable responses in most fomu of cancer
and was o h curative for Hodgkin’s disease. cervical cancer, advanced cancer of the mouth,
phpryox (throat) and larynx (voice box), etc. IO limitation was that it could be applied only to
local or regionally advanced tumors. Total body irradiation had been used with some success in
the treatment of patients with strikingly doresponsive diseases such w chronic and acute
leukemias and lymphomas. It was reasonable to hypothesk that total body irradiation might
have some benefit in widely disseminated cancer.
Even greciter enthusiasm for total body irradiation as a component of cancer treatment
developed as the technology to remove. store and reinfuse bone marrow to overcome the
potentially lethal effects of high-dose systemic treatment was explored. E. D o d l Thomas,
M.D., of the University of Washington, was awarded the Nobel Prize in Physiology and Medicine
in 1990 for pioneering treatments which included total body irradiation with doses so high aa to

78
be lethal were it not for bone marrow transplantation.
Published data from the Umversity of Cincinnatl indicate that the total body irradiation
trials were undertaken as phase I (to d e t e m e maxunum tolerated dose) and phase I1 (to
determine anti-tumor effect with specific diseases). The total body irradiation doses delivered
ranged from 100 to 200 rads and were carefully calculated and measured. The trials involved
three major forms of cancer--carcinoma of the colon, bronchus and breast. All but three patients
had advanced cancer not curable by local-regional treatments. Total body irradiation was given
as an adjuvant to local uradiation for three chldren with Ewing’s sarcoma of the bone
(considered at extremely high risk for the presence of distant metastasis). The treatment team
consisted of radiation oncologists, two specialists in internal medicine and a medical physicist.
The Umversity of Cincinnati project underwent several levels of peer review. h addition
to concurrence with the protocol by the participating members of the team, the were
rewewed by the Faculty Research Committee of the University of Cincinnati College of
Medicine. They also underwent review by the National Institutes of Health, editors of scienbfic
journals, and a special review by Drs. Henry Kaplan of Stanford University, Frank Hendrickson
of Chicago’s Presbyterian St. Luke’s Hospital, and Samuel Taylor, 111, of the Presbyterian St.
Luke’s Hospital at the request of Robert W. McConnell, President, Amencan College of
Radiology, in response to a request by Senator Mike Gravel in 1972.
I

79
Cancer Clinical Trials and Informed Come nt
The history of medicine is filled with clinical experiments undertaken with the intent to
benefit individual patients or all mankind. Clinical trials which compared experimental m e n @
to standard treatments for patients with cancer were begun in England in the 1940's and in the
rmd to late 1950's in the United States. Seventeen clinical woperative groups were established
in 1956 with funding from the National Cancer Instilute. The conceptual framework leading
from phase I (toxicity) to phase I1 (efficacy) to phase 111 (comparisons with standard treatment)
was first formalized in the early 1960's at the National Cancer Institute.
As studies in these cancer clinical cooperative gmups evolved, the wnccpt of informed consent
evolved. Prior to 1965, patients enrolled in clinical trials were obviously asked to consent and
such consent was usually documented in the medical mod, formalition of this process began
in the 1960's and has wntinued to evolve to the pnsent time. Current standards include a
description to the patient of the experimental treatment off& specifics risks that such treatment
might entail, statements to the. effect that all r i h are not fully understood and unexpected effects
might occur, the possible benefits to the patients and society as a whole, and the express
willingness of the physicians to treat the patient outside the protocol with the best standard
treatments if the patient declines participation. It is now customary to provide the patient written
information (usually two or three pages long); to let the patient keep a copy of this information

80
so he or she may discuss it wth family or friends, and, after opportunibes for questions, to ask
the patient to sign a consent form. The patient always has the nght to withdraw from
investigational treatment at any time, and to receive the best standard care
In a 1973 publication of the Cincinnati studies by Eugene L. Sanger, et al (“Whole Body
and Partial Body Radiotherapy of Advanced Cancer”, &nerican Journal o f Roentaenoloev.
Radium Theram. and Nuclear Medicine. Vol 117; 670-68S), the following statement is included.
All patients gave informed consent in accordance with the directives of the Faculty Resemh
Committee of the University of Cincinnati College of Medicine and those of the National
Institutes of Health. The w e of formal, informed consent f o m in this stu@ antedated the
above requirements by two years.
Radiation therapy is an important part of the armamentarium of physicians m the care of
patients wth cancer. Because of its effectweness m the treatment of local-regional tumors, whole
body irradiation has been a subject of research for decades At present, total body irradiahon
followed by bone marrow transplantation is considered a standard part of treatment of many
patients wth leukemia, lymphoma, and Hodglun’s disease, and is under investigation for
myeloma and cancer of the breast. In the era prior to the establishment of bone marrow
transplantation to support such treatment, lower (sublethal) doses of total body irradiation were

81
Mr. BRYANT. Mr. Steger. STATEMENT OF JOSEPH STEGER, PRESIDENT, UNIVERSITY OF
CINCINNATI, ACCOMPANIED BY STANLEY M. CHESLEY Mr. STEGER. Thank you, Mr. Chairman and members of the com-
mittee. I am Joseph A. Steger, president, University of Cincinnati. Stan Chesley has joined the University as an adviser, not really as- sistant, and he is former chairman of our board, and more than willing to help in this instance.
I appreciate the o portunity to have a chance to present the ac-
body radiation studies conducted at the then General Hospital some 20 to 30 ears ago.
There have een some seven inde ndent investigations of these studies mostly 20 to 30 years ago, w en the current University was asked by the press and the families to supply documents or records, we be an voluntaril to compile immediately all of the
task. The records were not in one place. The records were in writ- ten forms, some were written, some were microfiche. And much of it, in order to copy it, we had to send to the State of Washington, to a special company that then took the microfiche and turned it into printed documents.
Although we did this, we still had in our archives or we found some 11,233 pages of documented1 of which we have made pub- lic. We have made them public in terms of the press, in terms of inquiries, in terms of Government officials; and we will continue to make anything we find public.
The atient records, however, we have not made ublic. They are
long time. Most of them are on microfiche, and it took us several months to get the microfiche into print.
With the help of Senator Glenn and Con essman Mann, we se- cured the original DOD contract, which we r id not have.
At the same time that we were undertakin to locate and repro-
patients’ families, some 88 families. As of this date, we have lo- cated 38 surviving relatives, and we are still tryin to locate 50
have exhausted different search techniques to find these families. We have also established a hot line so that people could check
to see if they or a relative had participated in the studies. We have handled over 2,857 calls and cross-checks with the records to ascer- tain if any of the inquirers or their relatives had been in the study. Obviously, few had.
We also feel a societal obligation to the surviving relatives. Al- though we are no longer the same entity under which the studies were conducted, we have offered social work support andor pas- toral counseling, should the families wish. As a public entity, we shall continue to cooperate in any wa we
ments. At this time, we are fairly certain, in the sense of 90 to 100 ercent, that we do not have any other documents that have not
Eeen reported, because we have contacted the departments in the
tions taken by the rJ niversity of Cincinnati relative to the whole
F i:
records we ha c f relative to t E e study. It was a very complicated
being, K owever, given to the families. I apologize i F it has taken a
duce documents, we began-again, voluntari Y y-to search for the
other patients’ close relatives. We will continue to d o so until we
can to provide information, should we uncover any additional B ocu-

82
studies, we have gone through all our archives, we have contacted every individual associated with the studies, and as far as we are concerned, we cannot find any other documents.
Thank you for allowing my testimony. I shall be glad to answer any of your questions. We will continue to cooperate in any way we
Mr. BRYANT. Thank you. [The prepared statement of Mr. Steger follows:]
C a n .

TESTIMONY COMMITTEE ON JUDICIARY
SUBCOMMITTEE ON ADMINISTRATIVE L A W AND GOVERNMENTAL RELATIONS
APRIL 11, 1994
MR. CHAIR, MEMBERS OF THE COMMITTEE, I AM JOSEPH A. STEGER, PRESIDENT, UNIVERSITY OF CINCINNATI.
I APPRECIATE THE OPPORTUNITY TO HAVE A CHANCE TO PRESENT THE ACTIONS TAKEN 8Y THE UNIVERSITY OF CINCINNATI RELATIVE TO THE WHOLE BODY RADIOTHERAPY STUDIES CONDUCTED, AT THE THEN GENERAL HOSPITAL, SOME TWENTY TO THIRTY YEARS AGO.
THERE HAVING BEEN SOME SEVEN INDEPENDENT INVESTIGATIONS OF THESE STUDIES MOSTLY 20 TO 30

84
YEARS AGO, WHEN THE CURRENT UNIVERSITY WAS ASKED BY
THE PRESS AND THE FAMILIES TO SUPPLY DOCUMENTS OR
RECORDS, WE BEGAN TO COMPILE IMMEDIATELY ALL THE
RECORDS WE HAD RELATIVE TO THE STUDY. MUCH TO OUR
SURPRISE, ALTHOUGH I T WAS A COMPLICATED TASK, WE
S T I L L HAD I N OUR ARCHIVES OR WE FOUND SOME 8,200
PAGE OF DOCUMENTS--ALL OF WHICH WE HAVE MADE PUBLIC.
AND WITH THE HELP OF SENATOR GLENN AND CONGRESSMAN
MANN, WE SECURED THE ORIGINAL D.O.D. CONTRACT.
AT THE SAME TIME THAT WE WERE UNDERTAKING TO
LOCATE AND REPRODUCE DOCUMENTS, WE BEGAN A SEARCH
FOR THE PATIENTS' FAMILIES (SOME 88 FAMILIES). AS
OF T H I S DATE, WE HAVE LOCATED 38 SURVIVING RELATIVES
AND WE ARE S T I L L TRYING TO LOCATE 50 OTHER PATIENTS,
CLOSE RELATIVES.
WE ALSO ESTABLISHED A HOT L I N E SO THAT PEOPLE
COULD CHECK TO SEE I F THEY OR A RELATIVE HAD
PARTICIPATED I N THE STUDIES. WE HAVE HANDLED OVER I

1,000 CALLS AND CROSS CHECKS TO ASCERTAIN BY PATIENT
RECORDS (OF THESE 1,000 SOME CALLS) I F ANY OF THE
INQUIRERS OR THEIR RELATIVES HAD BEEN I N THE STUDY--
OBVIOUSLY FEW HAD.
WE ALSO FEEL A SOCIETAL OBLIGATION TO THE
SURVIVING RELATIVES. ALTHOUGH WE ARE NO LONGER THE
SAME ENTITY UNDER WHICH THE STUDIES WERE CONDUCTED,
WE HAVE OFFERED SOCIAL WORK SUPPORT AND/OR PASTORAL
COUNSELING SHOULD THEY WISH.
WE AS A PUBLIC ENTITY SHALL CONTINUE TO COOPERATE
I N ANY WAY WE CAN TO PROVIDE INFORMATION SHOULD WE
UNCOVER ANY ADDITIONAL DOCUMENTS. AT THIS TIME, WE
ARE 90% CERTAIN THAT WE DO NOT HAVE ANY OTHER
DOCUMENTS THAT HAVE NOT BEEN REPORTED.
THANK YOU FOR ALLOWING MY TESTIMONY. I SHALL BE
GLAD TO ANSWER ANY OF YOUR QUESTIONS.

86
Mr. BRYANT. Dr. Soper, in your written statement, you said one of the reasons the Department was interested in the experiments was to understand the influence of radiation on combat effective- ness. Why couldn’t the Department fund an experiment using its own healthy servicemen as opposed to innocent civilian cancer pa- tients that were used in these studies?
Dr. SOPER. I can’t, Mr. Bryant, give you a direct answer to that. I know that in developing the types of criteria for battle, whether it is on a conventional, a chemical, or a nuclear battlefield, infor- mation is gathered from many sources-from animal studies, for example, and I think, also from studies with people in uniform and civilian members of the Department of Defense. This information that we obtained from the University of Cin-
cinnati, sir, was one part from many different sources. We put to- gether those manuals that perhaps are offensive to some, but those manuals are required by the commander on a nuclear battlefield to fight in a hostile environment. Like it or not, that is the business I am in; and I am doing that the best that I can. All the members of the Department of Defense are.
Mr. BRYANT. Did the Department of Defense carry out any such experiment on healthy servicemen?
Dr. SOPER. I will have to answer that, for the record, I don’t know of any.
[The information follows:l Our record search is stil l ongoing, but to date we have not discovered any such
experiments. Dr. SOPER. Let me say, I do know of other experiments besides
the Cincinnati experiments that were done, reported in the lit- erature, having to do with total body irradiation, as Dr. Cox point- ed out-that contributed to our overall data base. But, I do not know the answer to your specific question.
Mr. BRYANT. If the Department received a proposal for such an experiment on healthy servicemen, would it have been funded?
Dr. SOPER. There are a series of protocols through which funding for human-use experiments must pass. The rules for that in the Department of Defense started as early as 1953, with a then top secret memorandum from Secretary of Defense Charles Wilson to the Secretaries of the military services, which outlined in some spe- cific detail the rules for human-use experimentation of healthy sol- diers and civilian members.
Mr. BRYANT. The Department did not pay $651,000 up front for the experiments. Rather, it paid $25,000 for the initial contract, and then increased the amount for close to 10 years as the contract was renewed and modified?
Dr. SOPER. Yes, sir. Mr. BRYANT. Before approving the contract or its modifications,
did the Department of Defense officials inquire as to the potential harm being caused to patients being administered such high doses of radiation?
Dr. SOPER. I don’t know the answer to that. The available surviv- ing records do not show any such inquiry. I have a few of the docu- ments, I think you have them as well, that have survived, these many years; and the approval process in the Department of De-

87
fense is, as far as that documentation is concerned, rather super- ficial.
Let me be more specific. I have been able to find nothing in the records of specific questions sent back to the University of Cin- cinnati with regard to informed consent or patient selection cri- teria. It was our purpose to use the information from the psycho- logical and psychiatric tests and blood and urine tests.
Mr. BRYANT. Did the project officer monitor the effect on patients as part of his responsibilities?
Dr. SOPER. There is no indication that the project officer, what we call the contracting officer's representative, (COR) did so. As a matter of fact, some of the records suggest that the University a m - mented on the fact that they had total scientific freedom with re- spect to their work.
Now, I was a contracting officer's representative at the Defense Nuclear Agency for much of my career, sir, and I was responsible for and expected to do exactly that, be a contractin officer's rep-
ican taxpayer was getting what he paid for. That is not to say that it wasn't done, there is just nothing in
the record. If you are interested, we have made repeated attempts at locating a nondestroyed file. As I said, as part of the normal con- tract destruction process that occurs by law 6Y2 years after the con- tract is terminated, the file is destroyed. We have called people that we have known, we have tried to locate somewhere in some- one's desk drawer a contracting officer's representative (COR) file that would give us some indication of that.
Now, there is no indication either that there was or there wasn't influence by the contracting officer's representative.
Mr. BRYANT. Are any of the project officers alive? Isn't anybody around that was involved?
Dr. SOPER. The gentleman at the Defense Nuclear Agency, the senior official, is dead. At least two of the people whose names ap- pear on the forms about which I just s oke have died. I spoke with
for this hearing, and his recollection of involvement was of no help. The contractin officer at the Defense Nuclear Agency, while still
have tried. Mr. BRYANT. My time has expired. Mr. Mann. Mr. MANN. Thank you, Mr. Chairman. I want to pursue first the
line that is similar to what Mr. Bryant has been pursuing. I read with some care the original proposal by Dr. Saenger, the original contract, the periodic reports that were sent to the Department of Defense; and nowhere can I find any evidence that anybody at the Pentagon or with the Government had the least bit of concern about where the patients were coming from, what the consequences to them might be of the administration of whole body irradiation that was being reported from the Pentagon perspective at great length and great detail insofar as the various parameters that were being used in the study.
resentative, ask the technical questions and ensure t fl at the Amer-
another gentleman on the telephone t R e other day in preparation
living, is medi ca5 y impaired and is not able to contribute. So we

88
I mean, didn’t somebody at some point ask at least in their own mind, I wonder who these people are and what else is happening to them?
Dr. SOPER. Congressman Mann, I agree with what you are say- ing. There is nothing in the file that has remained that suggests that that was done. That is not to say it wasn’t. But I can find nothing, either.
Mr. MANN. You make the point in the attachment to your state- ment that the title of the report was changed in 1968, whereas pre- viously the report had talked totally about metabolic changes, now we are talking also about therapeutic efforts.
Do you have any knowledge of the reason for that title change? Dr. SOPER. No, I do not. I do note it, however. Mr. MANN. To your knowledge, were whole body radiation experi-
ments of the kind that the Pentagon paid for conducted at the Uni- versity of Cincinnati either before or after the period of the con- tract with the Pentagon?
Dr. SOPER. There is reference in the file to experiments at the Sloan-Kettering Cancer Research Institute at the University of Baylor School of Medicine, and at the M.D. Anderson Clinic, I be- lieve. There are those references in the file of related whole body irradiation experiments as contributory to Department of Defense needs.
And after that, I do not know of any. Perhaps we can call Cap- tain Bumgarner in a moment.
Mr. MANN. Did any of that work involve Dr. Saenger or any of his personnel?
Dr. SOPER. No, I don’t think the work at Sloan-Kettering or at M.D. Anderson did. Dr. Saenger‘s work is referenced, along with others, in military documents that relate to military radiobiology.
Mr. MANN. Can you tell us how often in the 1950s an unsolicited proposal such as Dr. Saenger‘s would have come to the Pentagon?
Dr. SOPER. I don’t know, but I will give you my experience begin- ning at the Defense Nuclear Agency in 1972, primarily a research and development organization funded by 6.2 money, if that means anything-it was primarily research and development funds. A sig- nificant portion-that is, better than 10 percent of the work that was done in the early 1970s when I was there-was done as a re- sult of unsolicited proposals.
The Department came under criticism by Members of Congress and others that there was an indication that these weren’t unsolic- ited, perhaps they were solicited unsolicited proposals. So it nor- mally happened that the contracting requirements were tightened UP.
There is no indication, sir, that this was a solicited unsolicited proposal.
Mr. MANN. Are you aware of any other studies similar in the overall purpose or scope to the one that we are looking at today, that was funded by the Department of Defense at any time?
Dr. SOPER. Yes, I believe mention is made of the work at Sloan- Kettering and M.D. Anderson. I have information on that. I will provide that for the record.
[The information follows:]

4
We have identified several studies supported by the Department of Defense in which radiation effects on humans were studied.
In our records there are three reports that cover research conducted at Sloan-Kettering Institute €or Cancer Research in New York during the 1950's and early 1960's. The work at Sloan-Kettering exposed patients with widespread cancer to low-level doses of total body irradiation to study post-irradiation syndrome in humans and to evaluate the effects on the modification of tumor response.
Hospital in Houston, Texas evaluated the systemic and clinical effects induced in 263 cancer patients by whole body x-irradiation with nominal air doses of 15r to 200r. Another study was conducted at the Baylor University College of Medicine. also in Houston, from 1954 to 1964. This research studied the effect of total body irradiation on the immunologic tolerance of bone marrow and homografts of other living tissue. A third study in Texas during the same general time period (1956 to 1962) was conducted by the University of Texas to study the effects of total body irradiation and local irradiation on the metabolism of the hematopoietic system in humans.
1960 until 1963 at the University of Southern California. The research was conducted to observe the effect in humans of 250-300r of total body irradiation. Also, from 1972 to 1916 at the Armed Forces Radiobiology Research Institute, leukemia patients were treated with total-body irradiation to ablate their bone marrow so that a bone marrow transplant could be done to cure their leukemia.
and that our record search continues.
In the early to mid-1950's research at M.D. Anderson
Another study we have identified was conducted from
I want to reiterate that this is current information

.
90
Mr. MANN. Those were DOD-funded? Dr. SOPER. Yes, they were. In fact, supported by the Defense
Atomic Support Agency. Mr. MANN. For the same question, developing a biological indica-
tor to indicate--- Dr. SOPER. Yes. Mr. MANN. Let me get the timing. That was before or after or
during the UC-1960 to 1971? Dr. SOPER. I have a report here on the work at Baylor University
College of Medicine. It is the final report for February 1, 1963, to January 31, 1964, entitled “The Effect of Total Body Irradiation on Immunologic Tolerance of Bone Marrow and Homographs of Other Living Tissue, Tables and Charts Therein.”
I also have a paper by M.D. Anderson Hospital Tumor Institute, entitled “Systemic and Clinical Effects Induced in 263 Cancer Pa- tients b Whole Body Irradiation with Nominal Air Doses of 15 to
Mr. MANN. What hospital did you say it was? What institution 200 RaL.”
did you say it was? Dr. SOPER. Radiology Department, University of Texas, M.D. An-
derson HosDitd Tumor Institute. TX. This was done for the De- partment of Radiology, School of Aviation Medicine, U.S. Air Force. As art of the record, I have, and I think I gave it to you or at
Col. Arthur Sullivan, Assistant Chief of Biophysics and Astronau- tics. The Saenger proposal has received favorable comment from Colonel Maupin, Colonel Isherwood, Colonel Hutgerhang, I think he died, and Colonel Cox. In the opinion of the undersigned, the work being done by Dr. Collins at Baylor and the Sloan-Kettering Institute, who are working with human-
Mr. MANN. I know Sullivan’s name. I don’t think I have that par- ticular document. I would like to have it. I guess, expanding on Mr. B ant’s question, would any of those five people be alive and be ab Y e to offer information to us?
Dr. SOPER. We are trying to track those people down. I think Dr. Sullivan, we found, died a month or so ago. But we are still trying to track those people down, sir.
Mr. MANN. Finally, Dr. Soper, ou mentioned there was a 1953
consent. Is that something you can now-I assume that is not still
least P hope I did, a memorandum of November 12, 1958, from Lt.
top secret document that set fort i specific standards for informed - _
classified. Dr. SOPER. It is not. I t was unclassified in 1975 or 1979. Mr. MANN. Have you had the occasion to ponder whether the in-
formed consent procedures that were used in this particular project meet the standards in that memorandum?
Dr. SOPER. Good question. I have it here, and I will search for it if you don’t have it, the memorandum from the Secretary of De- fense, Mr. Charles Wilson, in 1953, was specifically for human use of military people, in uniform, and Department of Defense civilian workers, and it did not speak to the issue of contracted studies like the work here a t the University of Cincinnati.
Mr. MANN. Could you give us a flavor of what information would be given to a member in uniform, the serviceman, before an experi- ment?

91
Dr. SOPER. Yes, if I can find it. Mr. Wuw. OK. Dr. SOPER. The copy I have here is dated February 26, 1953; it
was declassified, I can't read when i t k a s , 1975; and it speaks to a number of criteria. The voluntary consent of the human subject is absolutely essential, and it gives three very specific subpara- gra hs with respect to the criteria for voluntary consent.
&e experiment, that was number A, B, the experiment should be such as to yield fruitful results for the good of society, un rocurable by other methods or means of study, and not random
be kept to a minimum. an 8 unnecessary in nature. C, the number of volunteers used shall
I will go through the others if you wish. Mr. 1MANN. If you could, give us a copy of that for the record. Dr. SOPER. Of course. [The information follows:]

SECRLTAEY CY ~ t r r ~ s c Was hi ngl on ,.
26 Fob 1953
IIIEbIOPANDUIl FOR TiIE SBCRETAEY 01-’ THC ARilY SECRETACY 01‘ TIIE i:AVY SECHEl’ARY OF TlK AIR FORCE
SUBJECT. Usc of Hunan Voluritct?rs i n Experimental Rcswirch .) i
1. Dascd upon z rucommcnlation of t h e Armed r o r c c s Medical Po l i cy Counci l , t h a t hwwii subjcctr ; bc cmpleycd, undcr rc~orjiri::-d s a f c g u a r J s , as the on ly Crar:iLle nic.uis foi- rea l i s t ic cvrrli.stioi1 an4/or CicvLlopincnt o i e f f c r t : vc Fit’vcntJvr! measures or 4nfn;ic,e arjiinsi: a t u v i c , h io log ic r l l or clicmical aqcn ta , t h e po l i cy sct fort.1, ba1v.r w i l l . govc r i i t l iv u z r of Iiumnri vo lun tde r s by thc Dcportment of Defensc i n c::pei.imcntal resc:;\rch i n t h e f le l t i ; of atomic, b i o l o g i c a l and./or chemical warfare .
2. By reason of t h e hdsi.c medical. r e s p o n s i k i l i t y i n conncct jon w ~ t h t h o dcvelopment or rk fenso of a11 typcs a g a i n s t a tomic, b i o l o g i c a l and/or chemical m r i a r c nqonts , Arnet Scrvi cns r)?rso-n.cl and/or c iv i l . i dn r on du ty a t i r i s t a l l . i t i ons engagr d i n s m h r r s - a rch shc*!!.l ijc permi t t ed t o a c t i v e l y p a r t i c i p 3 t c i n a l l pn.iscs ut Lhe p.-uqrav, such p a r t i c i p a t i o n s h a l l bc s u b j c c t t o the io l lo~rj conciit i u s :
a. The vo lun ta ry consent of Chc human u b j e c t is a b s o l u t e l y c s s e n t i a l .
(1) Th i s means t h a t t h e person invo l cd sheul* have l c g a l c a p a c i t y t o g i v e consent : shoulr: be SO s i t i i a t c d as t o be a b l e t o c v e r c i s e f ee poi\e1- of cho ice , without thr i n t c r v c n t i o n of ny elc:wnt of
. forc:e, r r aud , *emit , clurcss, ovcr-r . ,achinq, or otler u l t e r i o r form of const:riimi. o r c o e x 1 o n ; arA shoi:ld have suf f i c i r i l r i~~irmlcdcjc and r:ompre.i.-nnicr 01 t’ic elements of the s t ib j ac t ma t t e r involved ab to cnab lc him t o ,.iakc an undcrstcinAmy and en11 qhtc*n?:l d e c i s i o n . Th;s l a t c c ~ ’ rlcmcnt rcqujres t h a t I J ~ P C I I - O t h e acccptancc? of an ciiEfxnativc d e c i s i o n by il‘c experimental s u b l e c t t h r i c shoald bo nado knowir t o him t h e n a t u r e , d u r a t i o n , and purpose of t h e experiment: Clrc metlidd and-means by
-_

93
. u which il; is t o I x , conrlucti-A; a1 1 iiiconvcnic9nrc:n
and IiitLards rcosonnl,ly Lo bc cupcc tcd ; and tlre c f f e c t r upon h a s h e a l t h or pcrsoti r ~ h j c h may p o s s i b l y comc from h i s p a r t i c i p a t i o n i n t h e experiment.
( 2 ) The conccpt of the human s u b l e c t s h a l l be i n w r i t i n g , h i s sirjn,iLrim s h a l l bc a f f i x e d t o i~ w r j t t r n ins tument sctting f o r t h s u b s t a n t i a l l y t h e a fo re - mentioned requi rcec .n ts and s h a l l b e s igned i n t h e p rc sencc of i t lcast onc w i t n c s s G who s h a l l a t t c s t to such s i g n a t u r c in m i t i n y . ts-an one S e r v i c e a r e involvcd t h e S e c r c t a r y of t h e S e r v i c e which i s c k e r c i s i n g prinrary r e s p o n s i b i l i t y Cor conduct inq t h e cxpar tment i s des igna ted t o pre- p a r e such an ins t r ime l i t and c o o r d i n a t e it f o r usc by all t h e S e r v i c e s having human v o l u n t e e r s involved i n the exper iment .
(3) The d u t y and r c s p o n s i b i l i t y for a s c e r t a i n i n g t h e q u a l i t y of t h c consen t rests upon each i n d i v i d u a l who i n i t i a t e s , d i r e c t s or ciigages i n t h e cxperimcnt. It i s a per sona l du ty and r c s p o n s i b i ; i t y which may n o t be d e l e g a t c d t o ano the r w i th impunity.
(a) In cxucr imcnts whcrc pc r sonne l from more
I
b. Thc exper iment should bc such ds to y i e l d f r i i iLru1 r e s u l t s f o r t h c good o f s o c i e t y , unprocuroble by o t h c r methods o r means oC s t u d y , and not random and unneccssary i n na tu rc .
c. The number of v o l u n t e c r s used s h i > l l be k e p t a t a minimum c o n s i s t e n t w i th i t e m b . , above.
d. The expcr imcnt should be so d c s i t n c d and based on t h e r e s u l t s o f an imal exper in icn ta t ion and a k n o w h i g e of t h e n a t u r a l h i s t o r y o f t h e d i s e a s e or o t h c r problem uadcr s t u d y t h a t t h e an t i c ipa t - cd r e s u l t s w i l l j u s t i f y t h e pe r fo r~nance of t h e cxpcrimcnt.
unnecossary p h y s i c a l and menta l suf Coring and x j u r y . E . Thc exger imcnt should be so conducted as t o avoid a l l
f . NO exper iment choitld l x conducted whcrc t h c r c jr. an a p r i o r i rtmson t o b o l j c v c t h a t clc.it11 or d i s a b l i n g i n j u r y w i l l o ccu r .
g . The dcgree o f r i s k t o ba tcr1:en shou ld never exceed t h a t de te rmined by t h e 1iumanitarian.importanc.e of tho problem to bo solvod by t h o oxporimont.
2
84-514 0 - 94 - 4
. .
Downgradcd t o UNCLASSIF1i:D 22 Aug 1 5

94
- J' . h. Propcr p rcpa ra t ion sliorild bc niadc and adcqri-tc
facilities provided to p r a t c c t tlio oxpc r inen ta l sub ject egainst evcn rcmotc p o s s i b i l i t i e s of i n j u r y , d i n n b l l i t y , or death.
c a l l y q u a l i f i c d pcrsons. should bc r c q u i r c d through a11 stagon of t h e experiment of t h o s e who conduct o r cngagc i n t l ic cxpcrimcnt.
sliould I]? at l i b e r t y to b r ing the cxpyximcnt to an end i f hc has reachcd tho phys ica l or mcfital s t a t e whcro c o n t i n u a t i o n of t h c experimcnt seems t o him t o be impossible .
cha rge m u s t be prepared to t e rmina te thc cxpcriment a t any s t a g e , i f he has probable causc to b o l i e v c , i n the e x e r c i s e of t h e good f a i t h , s u p r r i o r s k i l l and c a r e f u l judgment r e q u i r e d o f him tha t a c o n t i n u a t i o n of t h e experirmnt i o l i k e l y to r e s u l t i n i n j u r y , d l s - a b i l i t y , o r doatb t o t h e experimental s u b j e c t .
p r i s o n c r s of war i n human exporimentat ion, is cont inued and they
i. The experiment should be co.iducted o n l y by s c i c n t i f i - The h i q h c s t degrcc of s k i l l and c a m
j. During tlie cour se of tlrc experiment t h e huilian subject:
- k. During t h e cour se of t h e experiment t h e s c i o n t i s t i n .
1. The e s t a b l i s h e d p o l i c y , which p r o h i b i t s t h e use of
w i l l n o t be used under any circumstances. il
3. The S e c r e t a r i e s of the Army, Navy and hir Forcc are au tho r ixcd to conduct experlmenta j 11 connnction wi th t h e devclopnlirt of Bcfcnoes of all typcs cgo ino t a tomic, b i o l o g i c a l and/or chemical warfare iir;c:its involving the uco of hunian s u b j e c t s w i t tnn thc l i m i k s p r e sc r ihcd above.
I n cach i n s t a n c c i n which an experiment is proposed pur- suan t to t h i s memorandum, t h e n a t u r e and purpose of t h e propoucd
such cxpcriincnt shall bo s u b n i t t c d f o r approval to t h e Sec re t a ry of t h e m i l i t a r y Bepartmmont i n vh ich t h c l'roposcti experiment 1s tc be conducted. No such cxpcri i i~cnt s h a l l bc undertaken u n t i l such S e c r e t a r y has approved i n w r i t l n g t h e experiment proposcd, t h e person who w i l l be i n charge o f conduct ing it, as w e l l as informing t h e Scc,rctary of Defense.
5. wi th t h e p rov i s ions of t h i s mcmornndum wiLlrin t h e i r r e s p e c t i v e Servicco.
!
1 4 .
kexpcrimcnt and t h c name of t h e person who v j l l be i n chdrgc of
The addres ses w i l l be r c s p o n s i b l c f o r i n s u r i n g compliancc
/ s i g m a / C.E. WILSON
Copies fu rn i shed : J o i n t c h i c f s of S t a f f Research 2nd Development Board
Downgraded Lo UNCLTISSII'I I :D 22 hug ? 5
3

95
Mr. MANN. Finally, in this round, Dr. Soper, there came a oint in time when, as I understand it-maybe we will have more a etail later-the project at UC had multiple funding sources in terms of the dollars that were necessary to treat the patients. At some point in the 1960s, before the rojed ended, NIH, at least for a period,
body else’s characterization. Was the Pentagon aware of that refusal by NIH at the time? Dr. SOPER. At the time, the records don’t show that they were
or they weren’t. I am in contact with HHS. Part of the interagency working group has allowed senior members of each one of the De- partments to meet together on a very re lar basis and talk seri-
in
to the second round.
declined to offer funding B ased on some moral issues, that is some-
ously about these issues, and the senior o F icial at HHS is research-
t r . MANN. Mr. C R airman, I have other questions, but I will wait that for us. I ho e to have an answer to that question.
Mr. BRYANT. Mr. Portman. Mr. PORTMAN. Thanks, Mr. Chairman. Dr. Soper, thank you for the help you have provided me and my
staff over the last couple of months. I know our dialogue will con- tinue.
Dr. SOPER. I hope so. Mr. PORTMAN. I really want to echo some of the concerns the
chairman raised in terms of the efforts you are making to contact people who were directly involved at the time. It sounds as though you have made some efforts, and we have talked about that. I would just hope that we would redouble those efforts now, to try to find out as much as we can about what the DOD role was, how much oversight there might have been or not have been. The records, as you indicate, are very sparse in that regard.
That is an issue that I know this subcommittee, as well as the Congress as a whole, is intensely interested in.
With regard to documentation between the Cincinnati General Hos ital and DOD, let me ask you, was there any evidence, par-
ation proposed to be administered to patients was expressly de- signed to treat cancer?
Dr. SOPER. Quite to the contrary. I think the information that you see in the early documentation-the first reports, I have their
the reports. As I said early, those earlier reports, for those of us who are looking at them for the first time, are certainly troubling.
And, as I have talked about this issue with medical ethicists in the De artment of Defense and other places-my younger brother is a ra&ologist and I have talked with him about this-is open for interpretation.
It is one element that I hope the advisory committee, that is made up of ethicists and radiologists like those that are here at the table today, will look at and come to a view on. Perhaps it was just a badly written report. I can’t judge; I am not qualified to judge that.
Mr. PORTMAN. Getting back to the documents for a moment, how about the 1958 proposal from the University to the DOD with re- gard to this issue?
ticu P arly in the documents from the earlier years, that the radi-
numbers-clearly does not state treatment of cancer as a part of

d I
96
Dr. SOPER. There is certainly an early indication that we have an appraisal of human studies and the radiobiological aspects of weapon effects. The word weapon appears. The report was written by Dr. Saenger and Dr. Friedman. It was prepared for the Defense Atomic Support Agency.
The date I have here is November 14, 1962, and this is an ap- praisal, I presume at that time, of the work that is being performed by the Department of Defense. They talk about the adequacy or the inadequacy of animal data. And it says,
Nevertheless it is essential to consider M e r well-planned studies in patients as long as the following criteria are fulfill& There is a reasonable chance of thera- peutic benefit to the patient; the likelihood of damage to the patient is no greater than that encountered from comparable therapy of another type; and the facilities for support of the patient and complications of treatment offer all possible medical services for successtid maintenance of the patient's well-being. So this, Mr. Portman, is in 1962, written word from a Depart-
ment of Defense-supported document written with Department of Defense funds, that speaks to the therapeutic issue associated with these experiments. It is the earliest one that I can find on the record.
Mr. PORTMAN. This is not directly related to the then General Hospital situation? This was a general document with regard to DOD-funded projects?
Dr. SOPER. Oh, no. This was supported by DOD. This was work, an appraisal of the work, that they were performing, prepared for the Defense Atomic Support Agency under contract; and the num- ber of the contract was one of the three contracts that the Depart- ment of Defense had with the University of Cincinnati.
Mr. PORTMAN. You mentioned earlier that you were a contracting officer's representative yourself in a previous life?
Dr. SOPER. Yes, sir. I would like to go back. Mr. PORTMAN. It is too late. Dr. SOPER. Yes, you are right. Mr. PORTMAN. I would like to ask you a general question, and
that is, should there have been more oversight, from what you have been led to believe, from the discussions with people and from the documents?
Dr. SOPER. Absolutely. It is the responsibilit of the contracting
that, but one of the tenets of doing a good job at the Defense Nu- clear Agency, or the Defense Information Systems Agency, or the CIA, or any agency in representing taxpayers' money is to be an informed buyer. I took courses early on in my career that told me how to be a good COR, what to ask for, and what to expect in re- sponse.
Mr. PORTMAN. Let me ask you then a follow-up question. This is something that I found very unusual in looking through the docu- ments.
Should there not have been a DOD report at the conclusion of this study? Should there not have been a DOD report at the conclu- sion of the study in 1971?
Dr. SOPER. Let me ask for clarification. Do you mean when the contract was terminated, a report by the Department of Defense
*
officer's representative. You don't raise your i and and swear to

97
saying, we, the Department of Defense, spent $650,000 of your money, this is what we got for it A, B, C?
Mr. PORTMAN. Exactly. I am not aware of the existence of any such report.
Dr. SOPER. I am not either. The information we paid for appears throughout radiobiology and military medical radiobiology lit- erature. So it was used extensively in reparing documents like I
Mr. PORTMAN. Do you find it unusual that there was not a report at the end of the study?
Dr. SOPER. It is a good question. I am now trying to think in my career, whether or not each contract that ended, ended with a re- port, and the DOD provided a report on this as to what we got or didn’t get. I am not sure that wouldn’t have been the norm. I think that would not have been the norm.
have before me regarding military radio i! iology, et cetera.
.
S
Mr. PORTMAN. Not have been the norm? Dr. SOPER. No, sir. Mr. PORTMAN. One final question, Mr. Chairman, and that is
simply, are there any documents out there of which you are aware, classified or unclassified, that DOD has not yet disclosed?
Dr. SOPER. Oh, le- Mr. PORTMAN. Of which you are aware. Dr. SOPER. There are no documents of which I am aware, classi-
fied or unclassified, that aren’t going to be a part, that are not, or will be a part of the record retrieval process and the documents that we submit to the advisory committee for their review. The ad- visory committee, by the way, is meeting for the first time on April 21 and 22, I am expected to brief them on the results of the DOD record retrieval process, I believe this will be a major element.
Mr. PORTMAN. One follow-up, then, to that. Are you saying then that the working group or the advisory committee to the working group may receive documents that this subcommittee does not re- ceive, or the public does not receive?
Dr. SOPER. No. No. Mr. PORTMAN. When you say- Dr. SOPER. What I am saying is that the process throu h which
advertised as intensive and providing a view into the cold war ex- perimentation, good or bad, sir, we will provide to you, as well as
Mr. PORTMAN. Thank you. Mr. BRYANT. Dr. Soper, I think it is important to pursue this
question about the NIH. Apparently, the National Institutes of Health was asked to fund experiments, and they refused to do so because of the moral concerns; at least that is what the indications are.
Was it your testimony that the Department of Defense did not know about that refusal?
Dr. SOPER. I do not know the answer, specifically. I think we did not, but if I can leave it at that, I think we did not-and I am re- searching t h a t 4 will supply that answer for the record.
[The information follows:l
we are going, this interagency working group, is open. It fl as been
e to the advisory committee, the records that we find.
The University of Cincinnati Ad Hoc Committee Report of January 1972 noted that a proposal entitled Protection of Humans with Stored Autologous Marrow was

98
submitted to NIH in 1966 or 1967 by Dr. Ben Friedman, one of Dr. Saenger's re- search colleagues. The re rt further noted that the application was not a proved and that reason for this %&ion was not disclosed. Our efforts, and cons$tations with HHS and NIH, have not revealed additional information on this matter. How- ever, documents rovided by the University of Cincinnati do reveal that durin this same time p e d Dr. Saenger had three research contracts with HEW (two? and NIH (one).
Mr. BRYANT. Dr. Cox, ou talked about the peer reviews that
Radiology. Were they aware that the National ealth had refused to participate in experiments
all t h 's activity, including one sought by the
Institutes of based upon moral concerns?
Dr. COX. Not to the best of my knowledge. Mr. BRYANT. Were you aware of it before this morning? Dr. COX. I was not. Dr. SOPER. May I ask a question? Mr. BRYANT. Yes. Dr. SOPER. Is this NIH refusal, does that appear in the written
record for the first time in the Universit of Cincinnati ad hoc com-
Mr. BRYANT. Yes, that is correct. That is exactly where it ap- pears.
Dr. SOPER. Thank you. Mr. BRYANT. We are seeking more information from the National
Institutes of Health about it. They have not yet constructed their response.
Dr. Cox, your statement quotes a 1973 article by Dr. Saenger saying that all patients gave informed consent to the radiation ex- periments. Do you have any evidence as to whether the statement in the article is accurate?
Dr. COX. I have no corroborating evidence. Mr. BRYANT. Did the individuals in these experiments have can-
cers that would benefit from radiation treatment? Dr. COX. Many of them, as expressed by one of the earlier family
members, su gested that local irradiation was used for some of the
riod, 2-year interval to the time when the total body irradiation was given that it may have been of benefit. So the local radiation that was given to these patients would very likely have been of benefit.
The total body irradiation was experimental, and was presum- ably undertaken on the hypothesis that it might have been a bene- fit to patients for whom no other systemic treatment was available.
Mr. BRYANT. We understood that portion of your testimony. Some of this was-as you testified, was experimental, and ill patients with very little hope of survival were willing to undergo the tests.
Let me ask ou, what types of cancer were radio sensitive or were known to e radio sensitive at the time?
Dr. COX. A wide variety. The exception were those that were not considered radio sensitive. However, they required high doses to produce control of the disease, and such high doses could only be given locally. The could not be given to the entire body. So the
whole body, and that was the hypothesis.
mittee report? I mean, I have a copy o f t K at.
patients, an f even suggested from, I believe, maybe a 2-year pe-
question was, cou P d lower doses be of some benefit if given to the
Mr. BRYANT. What types of cancers are radio resistant?

J
99
Dr. COX. The ones that are relatively radio resistant are certain tumors of bone, cartilage, and soft tissues. Most of the rest are con- sidered sensitive or moderately radio sensitive. Some are exquis- itely radio sensitive-the leukemias, lymphomas, Hodgkin’s dis- ease; there is a long list. The others are of intermediate radio sen- sitivity and require higher doses.
Mr. BRYANT. I guess my question is whether the individuals that were the subject of these ex eriments had cancer which might logi-
based upon what you knew at the time. Dr. COX. The published information indicates that the studies
were being done, the whole body irradiation and half-body irradia- tion studies were being done-were being done for diseases where the tumors were considered intermediate radio sensitivity, not ex- tremely radio sensitive. See, there is a gradation from extremely radio sensitive to pretty radio resistant, and these were intermedi- ate. They are curable, when local treatments-where radiations can be given and the tumor is only localized, so in that sense they are sensitive.
You are asking a very difficult question from a radiation biology perspective.
Mr. BRYANT. Are colon, lung and breast cancer radio resistant or radio sensitive?
Dr. COX. When they are localized and treated with radiation therapy alone, they are curable. They can be eradicated penna- nently. When they have s read widely, the doses are usually con- sidered such that you coul8n’t give them for the whole body.
But they were investigating that. That was exactly the subject of the study in the 1960s.
Mr. BRYANT. I think the logical extension of that is, would it not, therefore, be unreasonable to assume that perhaps whole body ra- diation at an acceptable level might have an impact on them if they had spread?
report states that patients were not s cifically informed that tg partial financial support, this is for
patients were told that support came in part from a national agen- cy.
The uestion of the source for support of a project is not con- committee or most
medical investigators as being relevant to t e issue of informed consent. That is all in the uote.
agency is funding the experiments he or she may be taking part in?
Dr. COX. They may or ma not be told which agency is funding
most informed consent, because for clinical investigations-because the approval process is one that is independent of the funding source. The approval process within any institution, and in adher- ence with the NIH guidelines, is independent. It is in each institu- tion and is independent of the funding source. That is what drives the informed consent.
cally be assumed to have i een sensitive to radiation treatment,
Dr. Cox. Exactly. Mr. BRYANT. The radiolo
t K“ e experimentation, came from the Department of Defense. The
strued 1 y the American College of Radiolo gx With the standard of in 9 ormed consent, is the patient told what
the experiments. I don’t real Y y believe that it is a standard part of

100
Mr. BRYANT. Mr. Mann. Mr. 1MANN. Thank you, Mr. Chairman. Dr. Cox, my understanding of the way that the project was orga-
nized is that the Pentagon dollars were used for laboratory work that had to do with the things the Pentagon was interested in. And patient care and cost of administering radiation and so forth were paid from separate sources. So I guess the question is, if this was an appropriate experi-
mental therapy from a medical perspective, could it have been done without the Pentagon funding? In other words, if the lab work is purely to support what the Pentagon is interested in, why were they merged together; and would it have been appropriate to pro- ceed without any Pentagon involvement, and on the same budget?
You wouldn’t need the Pentagon dollars if my hypothesis is cor- rect.
Dr. COX. I can’t really speculate on the thinking at the time. I can say that the support for clinical research is very meager. Even from the National Cancer Institute at the present time, there is an average of $50 per new patient diagnosed each year to sup ort clin-
with institutional support, or they may seek any number of oppor- tunities to get funding if such funding might be available.
And it usually, if there is any outside support, it comes from multiple sources, but it only covers a very tiny amount of the cost. So my guess is, based both on what was going on then and what I know now, the experiments probably would have been done much as they were; maybe not all those measurements of interest to the Department of Defense might have been made, but I think the total body irradiation experiments would have been done anyhow.
Mr. MANN. That is not the way it was done. It was done coinci- dentally, timewise, with the contract with the Pentagon. Obviously, the question that we are all struggling with is, would it have hap- pened without the Pentagon dollars and what was driving the re- search?
Your statement closes with this sentence, “One might judge them harshly from a perspective of 20 years later, but they were re- viewed and approved by peers and directors at the time the studies were conducted.” Are you one of those that would judge them harshly from a 1994 perspective?
Dr. COX. With the evolution of informed consent between that time and now, I think we would bend over backwards to be much more clear in what is made available to the patients and their fam- ilies. I think we would provide written information to them before they were ever asked to give informed consent to describe the ex- periment, and let them take such information home and discuss it with anyone that they wish.
I think we would provide them with repeated opportunities to discuss this with anyone they wish, including the referring physi- cian, includin any other physicians. That is pretty much the
That was not the standard at that time. And so in that sense I think, sure, we would not do informed consent today anything like what they did then, like what we did then. The half-body irradia-
ical research. So investigators usually either do it on t hp eir own
standard of to % ay.

7
101
tion experiments are going on right now in exactly the same way, with NCI funding. So I think there is little question that those would not be consid-
ered out of the ordinary by current standards. The total body irradiation experiments would only be done now-
adays with the help of bone marrow support, either bone marrow transplants from other individuals or from other family members or from the atient's own blood, or more modern techniques to use
So we would not undertake those studies of whole body irradia- tion now without havin the supportive structure to assure us that
that was given to these patients, with bone marrow rescue; and it is not always successful.
And those are the nature of the clinical experiments that are going on.
Mr. MANN. Some of that work now is in the experimental cat- egory?
Dr. COX. Yes, sir. Mr. MANX. In the later years of this project it did, as I under-
stand, involve bone marrow transplants, typically by taking mar- row before the irradiation from the patient and reinserting it, whatever the proper term is.
You have reviewed the ACR, American College of Radiology, re- port from 1972. Do you agree with what that report, says?
Dr. COX. I have no reason to disagree. Nothing else has come to my attention that would cause me to chan e the opinion which was
Mr. MANN. Do ou have any professional relationship with Dr.
Dr. COX. No. Mr. MANN. Dr. Steger, we appreciate your presence, and I guess
I want to make sure I understand exactly what the stance is of the University of Cincinnati today.
Obviously, you made very clear that you are making every effort to be as completely forthcoming with the documents as possible. I think that is important. "here are those in the community who are saying that it is a propriate for someone to say we are sorry. And the uestion is, w E at responsibility is the university assuming for a ju a gment today on the appropriateness of using 1960s values and standards of what was done at the University of Cincinnati?
Mr. STEGER. Well, there are certainly two sides of the story, when you read the evidence and listen to witnesses. Unfortunately, we are under litigation, so I really can't respond to that other than to say I think that the university would like to see investigations done-that you are doing, that outsiders are doing-because we are suspect, frankly. And so we invite you to answer that question; we invite other groups to study and answer the question.
And that is the stance we are taking. I think it is the only one we can take.
Mr. MANN. Thank you. Mr. BRYANT. Mr. Portman. Mr. PORTMAN. Thank you, Mr. Chairman.
. peripheral b P ood stem cells.
the bone marrow woul C f be reconstituted. But high-dose, otherwise 9
lethal, therapy is given now, now with doses far above anything
rendered by Drs. Kaplan, Hendrickson, an 3 Taylor at that time.
Saenger, just for t E e record?

102
Dr. Cox, thank you for coming to Cincinnati. We appreciate your erspective as an expert on oncology and also radiation therapy rom a very distinguished medical institution.
I would really like to build on the earlier questions with regard to informed consent. I think you answered very well what today's standards are. I think you answered less well what the standards were in place at the time of the experiments.
You said in your testimony that they seemed to have used the appropriate standards of informed consent, in response to questions from my colleague. You mentioned that you thought that standards had evolved significantly, as they surely have. I just wonder if you could fill us in a little further as to what the standards actually were in 1960 or in 1966, or indeed in 1971.
Dr. Cox. Well, the standards underwent an evolution during that time, not only in terms of clinical experiments, such as this one, but in terms of what one told the patient that was being treated with standard therapy.
There was literature in the early 1960s from prestigious univer- sities that defended the idea of not telling the patient they had cancer at all because it would harm them. In so histicated institu-
So there was an evolution in what you told cancer patients about their disease and of course about their treatment. In the middle 19608, the National Institutes of Health quite a propriately, even at that time we thought appropriately, demandel, because most of us advocated complete honesty with patients all alon advocate that if they were to be involved in clinical research, tfat we tell them everything that we could about the experimental treatment about what they had, about what benefits they might receive, and about what benefits mankind might gather from such treatments.
More and more and more, those demands have become increas- ingly arduous, but the basics of them were there, and it was really more a matter of how you documented them. And so what we told patients then, in m experience, was not profoundly different.
and for such hearings as this has become far more rigorous. Mr. PORTMAN. With regard to whole body radiation, you s oke
earlier about the fact that it continues to be used today at 8 oses higher even than doses which were administered in this experi- ment. Going back to the 1960s a n, which is the relevant time
thought to actually be helpful either in curing cancer or to reduce the symptoms related to the cancer?
Dr. Cox. Yes. Mr. PORTEXAN. And that obviously would include the Ewing sar-
coma, as you talked about earlier, and would include the cancers in your discussion with Chairman B ant that are more subject to
Dr. COX. No. I don't think I could answer yes to the fact that they would-that that would be considered the standard at the time. That was what was being experimented. What was done, standard treatment, was most1 with leukemias, lym homas, espe-
f!
tions in other countries, that is still the standar B today.
The degree to w h 'ch i t was documented for the medical record
period for our inquiry, was whoe Y body radiation at that time
metastasism, s reading throughout x t e body, but would that also be true with al P the cancers in this study, to your knowledge?
cially chronic leukemias, acute T eukemias of childhoocf
L

L
.
103
The other types of cancers, such as total body irradiation would be considered investigational.
Mr. PORTMAN. With regard to the doses that were given in the 1960’s, do you believe that those were at the appropriate level? You had mentioned earlier some levels that you deemed to be nonlethal versus lethal.
In your study of this matter, do you believe the doses given were appropriate?
Dr. Cox. The doses given, I believe, were probably selected be- cause they were the highest doses that could be given without bone marrow support, as I described, that would not be lethal. So the doses that were administered that I have read would be considered sublethal.
But they were as high as one could hope to achieve for tumors that were not exquisitely radio sensitive. So it seems to me that they were reasonable doses for the experiments that were done.
Mr. PORTMAN. Thank you, Dr. Cox. Mr. Steger, again, thank you for being here today. Earlier, we
heard from Gloria Nelson that her grandmother‘s name may not have been correctly signed. In other words, it might not have been her grandmother’s signature on some of the forms.
I have not had an opportunity to look at all the patient records. 1 understand those records have now been released to family mem- bers that have been identified.
But do you have any procedure in place to be sure there is not any tampering with the existing records, such as they are?
Mr. STEGER. Yes. We have formed a particular group that are now the custodians of all the records surrounding the whole body radiation studies, and they are now kept in one place under lock and key and only one individual, myself, essentially can release those. So that I would hope that they are currently very well pro- tected.
Mr. PORTMAN. University Hospital is a teaching hospital, a re- search hospital, well-known throughout the country. I t seems to me one of your jobs is to provide information, research, data, and so on, to agencies like the Department of Defense from time to time.
You have another job, which is to treat patients. And I guess my general question for you is whether in looking at the facts in the record from 1960 to 1971, the then General Hospital, do you think that General Hospital became too concerned with the providing of information and not concerned enough with the treatment of the patients at the time?
Mr. STEGER. Well, again, since we are under litigation, I can’t answer that question.
Mr. CHESLEY. Let me just volunteer as a former chairman of the board of the university. There has been, just as Dr. Cox has talked about, an evolution. The evolutionary aspect of the university, since the days when it was Cincinnati General Hospital, under the city of Cincinnati as a municipal university, has been a miracle as far as evolution.
I am not taking anything away, but from my role as chairman of the board for 5 years and on the board of trustees for 9 :-ears, just what I saw as far as the movement forward toward the 21st

104
century relative to that institution and the medical complex has been phenomenal.
It is very, very difficult to compare back, Congressman Portman, and I think it is an excellent question, it is almost impossible to compare back to what it was like in the 1960s as far as a teaching university, which it was, as compared to today, where it is one of the real crown jewels in this community and a crown jewel region- ally as one of the finest medical complexes in the country, irrespec- tive of the fact that we are in litigation, the university is in litiga- tion.
I think it is very significant that here is a defendant, I am usu- ally on the other side, a defendant in litigation coming forward, which we have, the university in the last month or so, and put all of the documents forward on a volunteer basis when it was not in any way required, because I believe, Dr. Ste er believes that that is the role of this teaching university, whic % is that information which we have, at least from an archives standpoint, must go for- ward to the public and be put.
In response to the question on the signature, we will look into that because all of the patient records are on microfiche, so if there is a different signature on that medical record of those unfortunate individuals that would have been contemporaneous when that doc- ument was put on microfiche. And we want to take a look at it.
I am glad-I forgot which one of the women it was-brought it forward to our attention so we can take a look at it and find out what the facts are.
Mr. PORTMAN. Thank you for that commitment and thank you for that ex lanation.
Thank you, Mr. Chairman. Mr. BRYANT. Dr. Steger or Mr. Chesley, either of you who wish
to respond, one of our purposes, of course, our essential pu ose in this hearing, is to determine if we have inherited responsib3ity for actions that might have been illegal or wrong from the previous
faith, to compensate people for damage that might have been one to them.
It would be helpful if you could tell us the nature of the litigation you are involved with right now.
Mr. CHESLEY. Let me respond. I have purposely stayed out of any aspect of the litigation. I happen to be, by job description, an attor- ney, but in this role I am an adviser, I like to call myself his assist- ant.
We, the University of Cincinnati, has been sued in a number of cases, I believe there are presently pending three class actions, none of those classes have been certified, and a class action, as you know, Mr. Chairman, means that there are la ers who are sug- gesting that they represent all of the victims an 7 all of the claims, and that may very well end up being. So the way we are looked at it in the university is that the Uni-
versity of Cmcinnati at present is a defendant on behalf of every person, whether they have individual counsel or are a participant as part of a class. So theoretically, that is 88 claims against the University of Cincinnati. The same claimants have also brought
I re a f ly have no further questions.
Yd eneration of leadership, that require us, in order to show

105
lawsuits against Dr. Saenger, he and his counsel can speak about that, and the other 8 or 10 physicians and professionals who were part of that original team.
ending here in the United States That litigation is presently District Court. I believe it is t L ee separate lawsuits, if that is of help to you.
Mr. BRYANT. And what have the alleged? Mr. CHESLEY. They have allege tr violation of-and I think one of
, .
the-two of the plahtiffs’ l aGers are here. They can probably speak clearer about it. As I say, I am not counsel for the university. I t is my understanding that they have alleged violation of civil rights. They have alleged violation of medical malpractice claims and sundry other claims of conspiracy, fraud, and so forth that are all encompassed.
One of the significant claims bringing it into the Federal Court was the violation of the individual’s civil rights.
Do I not kmw-and maybe counsel can speak as to whether or not the Department of Defense is presently a defendant in those lawsuits. I would ask if you would speak to one of the attorneys that are here and the could-I know there is someone here, I
and he is seated right behind some of the people that testified, and maybe the could give you more specificity or in the alternative, I think the i est thing to do is to see to it that we get this panel a copy of the present lawsuits that are pending, we can get that for you today.
Mr. BRYANT. Obviously my wheels are turning about whether or not these individuals are going to receive the most thorough pos- sible hearing in a Federal courtroom, and therefore, having this en- tire matter adjudicated without this committee having to look at it.
Mr. STEGER. 1 believe what you and Congressman Mann and Congressman Portman are doing is very, very important. It may have other issues over and above when a lawsuit will or will not be heard what the facts are, and an opportunity to have all sides aired.
Unfortunately, litigation, while it is very, very complete, in the final potential resolution, it is slow in going forward, and these are issues that I think you are bringing together with President Clin- ton’s admission that are issues that I think are important for the university to be brought forward.
I think it is very important for us to be able to say, we are here to cooperate irrespective of the litigation, irrespective of the law- suit, and we will continue that cooperation with Congress, the interagency commissions, President Clinton’s commission.
Dr. Cox, the severest critics of this entire matter re-
for a very long time. I am looking at the peer reviews that took place here and wondering, how should we view these peer reviews of the actions of 20,30 years ago?
Are they dispositive of the issues of responsibility here? Should they be read as a clear approval of what went on in terms of hav- ing given the patients adequate information, and any other ele- ments of responsibility or not?
know Mr. Newman is E ere. He represents some of the plaintiffs,
Mr. BRYANT. Very well. Final1
main-t t e ones on the next panel are those who have been critics

106
Dr. COX. I can say that I believe the only way of being fair is to ’udge them by the standards of the time, not the standards of to d ay. To do otherwise would be to treat them unfairly. To ’udge cancer treatments of the time by the standards of today
woul be to ‘udge them unfairly. We have evolved. Medicine has evolved and t e mess of informed consent has evolved.
Mr. BRYANT. ou mentioned the studies reviewed by the Faculty Research Committee of the Cincinnati University College of Medi- cine.
I think it is fair to say we might set that aside, inasmuch as they are, I would think, an interested party.
Dr. COX. I would take exce tion to that, sir. I believe that that
Board, and that that is a standard part of the review process. As a matter of fact, key to the review process to this day. So I
was interpreting that as being a specific term for the general term of what we would call the IFU3 or Institutional Review Board, and that is absolutely critical to this, but the standards have changed relative to the IRB today relative to what they were then.
Mr. BRYANT. I agree we should stick to the standards at the time in judgin everybody’s intent at the time. You say they were also reviewed % y the National Institutes of Health. We have now found that ap arently the refused to participate in this. Is that relevant?
Dr. 8 OX. I took t t at from the footnote to Dr. Saenger‘s paper of 1973, where it said that this was supported in part by the Depart- ment of Health and Human Services. I don’t know any other a en-
that would have supported it in whole or in part except N d at gat time. Mr. BRYANT. What do you mean by support? Dr. COX. 1- Mr. BRYANT. You mean help pay for the research? Dr. COX. I assumed that is what it meant. Is it possible that the
NIH approved and supported this for a period of time and then withdrew its sup ort?
was included in the publication. You will have to ask others. Mr. BRYANT. We are asking others, but this reference that you
made on page 4 of your testimony, and is in the list of things which you characterize as peer review.
My uestion is, if this matter underwent peer review by the Na-
it could be that they did not participate. There is indication they didn’t partici ate, and at the same time came back and gave this
Dr. COX. I made that statement based on this uote from Dr.
NIH General Research Support Grant of the College of Medicine in Cincinnati.” Maybe the grant was through the University in a broad sense and not specifically to this project. But it would have undergone review by NIH as a part of the review of the University of Cincinnati’s grant from MH.
Mr. BRYANT, Have you seen a review of this that went back to judge whether or not it was handled in a proper way?
Dr. COX. No.
k g d
is the title for what we wou P d now call the Institutional Review
I don’t know t I& e answer to that, but I was just going by what
tional 1 nstitutes of Health, it is a fair question for us to ask how
a clean bill o P health in the peer review process.
Saenger‘s paper of 1973: “Supported in part by U ’5 PH RR-5408,

107
Mr. BRYANT. So I wonder if it is appropriate that you list it under peer review in your testimony here. Perhaps you are just as- suming they would have reviewed it if they had a role in it, and now we doubt that they even had a role in it.
Dr. COX. 1 am just taking it from the publication that is-that is where that came from. I took it from the quote in the publication by Dr. Saenger's report, Dr. Saenger and colleague's report from 1973.
Mr. BRYANT. Let's go to the one conducted by the American Col- lege of Radiology at the request of Senator Gravel in 1972.
Would that have taken place over the telephone? Would that have been everybody exchanged written data and read it over in their office, or would that mean a visit to Cincinnati? What would that mean?
Dr. Cox. From the reDort that I have. which I really only have two documents that s&ve as background for this, -one -is Dr. Saenger's paper, the one is the report from Drs. Kaplan, Hendrickson and Taylor, through the American College of Radiol- ogy, to Senator Lavelle.
In that report, they indicate that they first had a preliminary meeting in Chicago, and after that paid a site visit to the Univer- sity of Cincinnati and reviewed records, discussed with a wide vari- ety of people here, and did that which we would consider standard for a site visit today and they did it in the context, as they wrote, of what they would consider a study section or a peer review at NZH at that time. So they were approaching it as if they were peer reviewers, as
they would review any grant that had been submitted to them for review at NIH. They were all experienced reviewers. So they both reviewed the documents and they paid a site visit.
Mr. BRYANT. Any further questions? I would like to thank all the panelists, particularly Dr. Soper and
Dr. Cox who traveled a long way, and Dr. Steger and Mr. Chesley for taking your time in coming forward and helping us in this in- quiry.
Thank you very much. At this time, the committee would invite the third panel to come
forward, which consists of Dr. David Egilman, clinical assistant professor, Department of Community Medicine, Brown University; and Dr. Martha Stevens, professor of English at the University of Cincinnati.
We thank both of you for being here today. As with the other wit- nesses, we ask you to hold your opening statement to five minutes so that we might go right to the questions.
We will start on the left of the committee, Dr. David Egilman.
STATEMENT OF DAVID EGILMAN, M.D., CLINICAL ASSISTANT PROFESSOR., DEPARTMENT OF COMMUNITY MEDICINE, BROWN UNIVERSITY Dr. EGILMAN. Chairman Bryant, committee members, thank you
very much for inviting me here. I am a private physician, practic- ing in Braintree, MA. I am on the faculty at Brown University.

108
I teach a course on the development of medical and scientific knowledge and history of the 20th century that includes the issue of the development of ethical standards during that time.
For 10 years or so, I have been trying to get the research funded by our Government on its own citizens that was performed here and at other institutions for purposes of military research inves- tigated. I ap reciate this opportunity today.
of the previous panel. Dr. Cox was asked whether or not he could find confirmatory evidence of informed consent in the 1973 paper. Well, there is some evidence on page 678.
I want to E egin first by responding to a question that was asked
It says, The acute radiation syndrome develops in stages. In the prodromal stage, nausea
and vomiting of a transient nature occur. These complaints are not discussed with the patient before treatment.
The comments I make are not a retrospective look at the 1960’s by 1970’s standards or 1980’s standards or 1990’s standards. They are rather a look at the 1960’s and 1970’s by the standards of the 1890’~~ the 1940’~~ and the 1950’s. As I begin with comments of physicians who reviewed this research for the University of Cin- cinnati, on the faculty of the University of Cincinnati, at the time the work was going on, that will be clear.
Dr. Gall, first in 1966, in a letter, stated that the informed con- sent form was inadequate. Dr. Shields, also writing about the in- formed consent form, in 1967, wrote “I believe a 25 percent mortal- it is too high.” He also made a small comment about the adequacy
that a risk exists, but of a one in four chance of death within a few weeks of treatment.”
Eve1 Hess, writing in 1969, stated “The acceptability of our generrconsent form for human volunteers participating in re- search was questioned.”
Dr. Thomas GafTney, in 1967, wrote: The applicants have ap arently already administered 150 to 200 rads to some 18
patients with a variety o?malignancies and to the researcher‘s themselves’ satisfac- tion, have not found a beneficial effect. In fact, as I understand it, they found con- siderable morbidity associated with this high dose of radiation. Wh is it now logical to expand this study? Its current design wil l not yield meaningddata. The study should not be done.
Dr. Gaffney was on the faculty of the Universit of Cincinnati re-
and established long before, with reference to this type of an exper- iment. In 1950, Dr. Hamilton wrote describing similar work to Dr.
Shields Warren, and said that this type of experiment had a little bit of the Buchenwald touch.
My father was at Buchenwald. I can assure you by 1950 it was well known what it meant to say that an experiment had a little of the Buchenwald touch.
The subjects were uneducated, had poor education, low IQs, and many had brain dysfunction because of their disease. They were unable to give informed consent. Rose Strom was diagnosed as re- sectable sarcoma in April 1970. She received a course of chemo- therapy.
o P the therapy for cancer. “All patients should be informed not only
viewing these experiments. But the ethical stan g ards were known

109
Chemotherapy was given for colon cancer in this time period. It was and still is to date palliative therapy for colon cancer. She was readmitted to the CGH on December 14,1970.
According to Mrs. Strom’s records, at 2 p.m. on that date, she re- ceived 10 milligrams of morphine IM, intramuscularly. Also at 2 p.m. she signed a consent form for radiation. She was then irradi- ated. This was immediately followed by nausea and vomiting that
lasted for 3 hours. She vomited repeatedly for 3 days. Antinausea medicine was withheld until the staff noted she was depressed to the point of crying and that she said, “I am so sick.”
Withholding thera y for nausea and vomiting is not then nor is
The researchers knew that informed consent was the standard of the day. As you have heard in the paper we read, they claimed they received informed consent. Despite that fact, only six of the first three patients received any information on the nature of the experiment, and none were informed of possible risks. If their pub- lished papers correctly report their failure to advise their patients about the possible experimental risks, their stated conclusion that they received informed consent is surely wrong.
The researchers were aware of informed consent requirements. They said the met the informed consent requirements of the Hel-
one of the researcheis colleagues and when advised of the research in 1966 when it was suggested that the same thing be done at Oak Ridge University.
Oak Ridge researchers said, we are hesitant to treat these can- cers because we believe there is so little chance of benefit to make it questionable ethically to treat them. Lesions that require mod- erate or a high dose of local therapy for benefit or are actually radio-resistant such as gastrointestinal cancer, just to help Dr. Cox, are not helped enough by total body irradiation to justitjl the bone marrow depression that is induced.
The argument that these experiments were appropriate from the ethical standards of the 1960s lack both scientific and historic accu- racy.
In addition, cancer therapy was not the purpose of this research. Previous research had already been done. In 1942, it was pub- lished, “Little or no benefit follows its use,” that is radiation, whole body radiation, “in the treatment of generalized carcinoma or sar- coma.”
That is the kind of cancer in this study. “In no patient was there evidence that total body irradiation affected disease, 1965.“ In the kinds of cancers in this study.
Cancer therapy was not the purpose of the research. The re- searchers themselves described the purpose of the research: “To provide knowledge of combat effectiveness of troops.” In real medi- cal research, in real therapy, treatment for nausea and vomiting is provided. In military research in the U.S. experiments, it was de- nied until the patients had severe nausea and vomiting.
In real research, in real cancer therapy, psychologic and peer counseling is provided. In this work, in this military research, in
it now part of norma P cancer treatment.
sinki Code pu i lished in 1962. Similar experiments were rejected by

110
these U.C. experiments, patients were intentionally psychologically isolated.
In real medicine, in real radiation therapy, the radiation is given slowly and from many directions to improve effect and reduce side effects. In military research, in these experiments, the radiation was given fast and unidirectional, in the words of the researchers, because that was the radiation of military ixiterest.
On February 9, 1971, Mr. Willard Larkins was noted to either have a lymphoma or adnocarcinoma of the colon. According to the hospital notes written by Dr. Aron and Dr. Rau, if he had a lymphoma, radiation would be indicated, while if an adnocarcinoma chemotherapy would “probably be in order.”
On February 19, Mr. Larkins was found to have adnocarcinoma and Dr. Rau said, “Radiotherapy was definitely out of the picture and the patient may be a candidate for 5FU.” 5FU is chemo- therapy.
Five days later, he got the radiation. He never got the chemo- therapy. There were four or five informed consents signed in Mr. Larkin’s chart for surgical procedures. There was no informed con- sent signed for radiotherapy like this. This was 1971, well into the period where people claim all the
patients signed informed consents, well into the period when people claim the standard was a signed informed consent should be given.
Who was res nsible? I think we find here we still have a prob- lem. The fact t F at the representatives of the ACR, admittedly ap-
arently from an institution that did similar work, could still come tere and claim that this work was appropriate means that we have a problem in the medical community in this country. I t is a prob- lem that is a current problem. It is not an old problem.
The fact that there is an attempt to let you think that this was in some way not previously found to be inappropriate therapy means we have a roblem in this country.
It is in the mezical community. “he fact that the University of Cincinnati’s report reported almost everything I said and then said they had no problem means that there is a problem at the Univer- sity of Cincinnati and at other universities. The fact that NIH de- nied the funding and then didn’t tell anybody it was because of eth- ical reasons means we have a problem.
Thank you. Mr. BRYANT. Thank you. [The prepared statement of Dr. Egilman follows:]

111
B R 0 W N DEPARTMENT OF COMMUNITY HEALTH
U N I V E R S I T Y Division of Biology and Medicine
Statement to Congrsss, Subcommittee on Administative law and Governmental Relations, April 11,1094 by David S. Egilman MD, MPH, 759 Granite Street. Braintree, Massachubetts.
Chairman Bryant. Subcommittee Memben. Good Afternoon
My name is David Egilman. I am a physician. I am primarily a practicing dodor in Braintree, Massachusetts. I am also a member of the faculty at Blorm Univerrlty. In that role I teach and conduct m a r c h on the hdory of the development of medical knowledge In the 20th century.
I want to thank the Subcommittee for inviting me here to speak. For almost ten yean I have tried to raise my voice about some of the experiments conducted by our Government on its own cituens, and I am Qratefui for thls opportunity today
I would like to w i n by reviewing some contemporaneous comments of the colleagues of the University of Cincinnatl (UC) researchers. There is IitUe that I can add to these. however some still defend these experiments so I will endeavor to explain the bases of the critidsms later In my comments.
'It is not certain from the [consent form] narrative whether the patient is advised that no spedflc benefil will derive to him and that there are, indeed risks involved in the procedure proposed.' - Erhvard Gall MD, May. 1966
'I believe a twenty-five percent mortality Is too high.' All patients should be informed not only that a 'risk exists' but of, .a 1 in 4 chance of death within a few weeks' of treatment - George Shields MD. 1967
The applicants have apparently already administered 150-200 rads to some 18 patients wnth a y&& of malignancies and to their satisfaction have not found a beneficial effect. In fact, as I understand it. they found considerable morbidity associated with this high dose of radiation.
Even if this study is expanded, its current design will not yield meaningful data. ... It will be d i f f i l if not impossible to observe a beneficial effed in such a small sample containing a variety of diseases all of which share only CANCER in common
This gmss deficiency in design will almost certainly prevent making meaningful observations. When this deficiency in experimental method is piaced next to their previously observed poor result and high morMdity with thls type of treatment in a 'variety of neoplasms' I think it is dear that the study as proposed should not be done.
I have the uneasy Juspicion. shoed up by the revised statement of objectives, that this revised protocol is a suMerfuge to allow the investigaton .. to test the ability of autologous ma- to lake' in patients who have received high doses of total body radiation. This latter question may be an important one to answer but I can? justify 200 rad total body radiation simply for this purpose, 'even in terminal case material'. -Thomas Gaffney MD - 1967 . .We acceptability of our general consent form for human voluntgen participating in research was questioned' - Evelyn Hess MD - 1969 commenting on the reason for rejection of two grant applications by the National Institutes of Health.
Why is it now logical to expand this study?
1
Box G, Brown University, Providmcg Rhode Island 02912 Tel. (401) 863-3 172

112
In my statement I wilt cover four areas.
1 What were the experiments?
The whole body radiation (WBR) experiments conduded at the University of Cincinnati (UC) were designed to provide information to the military. They were not in any way cancer treatment or palliation. Some of those studies resulted in the deaths of their subjects
2. Were the experiments conducted according to the ethical standards of their time?
The answer to this question is a firm no.
3 Why did il take until 1994 for these activities to reach the national consciousness?
There was a lack of oversigM and we are all responsible.
4
I would argue that this necessitates taking several long and short-term steps, including the following:
A We must document and assess what happened. 6. Those harmed should receive compensation C Appropriate actlons should be taken against reseamhen who acted improperly. D. We must establish permanent mechanisms to assure that this type of experiments will not
o a r aQaln
In my opinion, they could occur again, they may occur again, and we need to establish a system of checks and balances to assure that hearings such as these are not held again. Never again.
why dd these experiments occur and continue over a conslderable period of time?
We must do our best to nght past m n g s and prevent this from happening again
2

113
The University of Cincinnati Experiments 1961-1972
A. Ethic8 and Informed Consent
On November 28,1950, Dr. Joseph Hamilton wrote a letter to Shields Warren MD. Diredor Division of Biology and Medicine. The Atomic Energy Commission (AEC) concerning the ability of irradiated soldiers to function. (AEC) researchen wanted to determine the dose that might limn a soldlets 'capacity to execute intricate tasks for which physical well being is essential.' He discusJed the difficulties of performing such a research study, and suggested that 'For both politic and scientific reasons, ... it would be advantageous to secure what data can be obtained by using large monkeys wch as chimpanzees which are somewhat more responsive than lower mammals.' If the research was to be done on humans, Dr. Hamilton predicted that 'those concerned in the (AEC) would be subject to considerable Criticism, as admittedly this would have a little of the Buchenwald tou ch... The volunteers should be on a freer basis than inmates of a prison. At this point, I haven't any very construdive Meas as to where one would tum for such volunteers should this plan be put into execution.'
Despite Hamilton's .polillcar sensitivity to a possible adverse public readion to this research, the DOD funded studies similar to those dexribed in his letter. Eugene Saenger MD and his fellow researchers at the University of Cincinnati conduded these expenments behwen 1980 and 1971. In all researcher ifradiated 88 cancer patients during those years. Dr. Saenger and cowodcers published some of their findings in I969 in the Archives of General Psychiatry. The article was titled, Total and Half Body Irradiation, Effed on Cognitive and Emotional Processes.'
Cancer therapy was not the purpose of this research. Recently some defenders of this worlc have stated that the experiments met the ethical standard of their day. This is not true.
As they say, the devil is in the details In their 1969 paper the researchers stated, that preiriadiation analysis of the experimental subjeds revealed that the researchers would have had diffculty in obtaining true informed consent from the study participants. "Relevant intelledual charaderistics of the patient sample were as follows. a loweducational level (ranging from 63 to 112 on the full-scale of the Wechsler-Bellevue which has a mean of 84.5). and a strung evidence of cerebral organic deficit in the baseline @reradiation) measure of most patients.' Thirteen of sixteen subjeds were 'Negro.' three were Whine.
these researchers like olhers involved in similar experiments funded by the DOE and NASA, seleded the most vulnerable of our citizens as subjeds, the poor, the mentally and emotionally impairad, and African-Americans. UC researchers knew or should have known that their patient population was incapable of glving informed consent even if had they were Informed of the experimental rkks (which they were not). The UC researchers did not give the subjects all the fects on the side effects of the radiation. Therefore, if the patients consented to the expdments. the consent was not informed. According to the UC invesligation of this research (Suskind report) a review of 27 of 33 patient charts between 1960-1984 did not contain any notaUon that the patients wen, informad about anything. slx of the patient charts contained infonation indicating that the patient 'was informed about the nature of the treatment and its possible benefits.' The w e n t charts did not contain any notation on the risks of the experiments. It must be assumed from comments of relatives of survivors and the lack of notation that 27 of 33 patients received little or no information of the risks. The researchers own contradictory statements about informed consent provide the best evidence that they violated the ethical and moral standards of both the sixties and the nineties.
UC researchers in their 1969 research paper revealed these contradictory elements themselves. The report induded both of the following statements: 'In each case the patient was advised that the therapy mbht be beneficial to him but that it was experimental in nature. Informed consent was obtained In all cases." And, There was no discussion with the patient of possible subjective readions resulting from the treatment. Other physicians. nurses, technicians and
3

114
ward personnel were instruded not to diswss post irradiation symptoms or reactions wtth the patient. This precaution was carefully followed so as to standardize and minimize 'iatrogenic' factors in influencing whatever subjedive readions the patients might have to radiation." Iatrogenic means dodor induced. The researchen claim they did not tell the patients about the possible side effeds because this information couid have induced nausea and vomiting in the patients. This Is further evidence that the study was a study of the side effects of radiation not of the treatment of cancer. It is obviously impossrble to obtain informed consent without giving information on the side effects of the treatment.
In response to a junior faculty report critical of the research, the UC researchers claimed that they had informed the patients of the risks involved and the possibiltties of complications. They even produced a consent form allegedly used and signed by every adult patient in the study from 1965 onward. However, in addttion to the detailed information on the lack of informed consent presented in the 1969 paper a 1973 publication that outlined the study methods stated specifically that the researchers did not tell the patients of the severe nausea or vomiting that could result from therapy. The researchers clearly understood that informed consent represented the standard of the day. They felt obligated to include a statement on informed consent in the paper they published Did they lie about receiving informed consent from the patients when the story broke or did they lie about not giving them information required to receive informed consent in their published papers? If their published papers comdly report their failure to advise patlents about the possible experimental nsks, their stated conclusion that they received informed consent Is surely wmng. Having failed to provide informed consent. (how could their patient population possibly give informed consent?) they had to lie about it when the experiments became public. There is no better evidence that they violated their own and our own ethical and moral standards.
The researchers were so aware of the importance of informed consent that they stated they received it from the partiupants in the expenment even though it is clear they did not
In 1968 Saenger and Lushbaugh (in charge of studies of WBR at Oak Ridge funded in part by NASA), combined the results of their WBR research and published a joint paper. The paper reported the amount of radiation it took to kill half of the recipients. That same year, a review panel of the AEC suggested that Oak Ridge conduct experiments similar to those conduded by UC researchers In reviewing a suggestion that patients with carcinoma of the breast, gastrointestinal tract, and urogenital tract should be treated by total body irradiation, the panel made the following statement: 'These groups of patients have been carefully considered for such therapy, and we am very hesitant to treat them because we believe them is SO Iittla chance of benefit to make it $a#est/on able ethlcallyto treat them. Lesions that require moderate or high doses of local therapy for beneffi, or that am actually resistant (gastrointestinal tract) am not helped enough by total body Irradiation to justify the bona marrow depression that is induced. Of coune. in one way these patients would make good subjeds for research because their hematologic responses are more nearly like those of normals than are the responses of patients with hematologic disorders.' (Emphasis added) The argument that these experiments were appropriate from the ethical standards of the 1960's l a d s both scientific and historic accuracy.
In their 1967 report to the DOD, UC researchers said that they followed ethical standards as set forth in Declaration of Helsinki. Again, this is not true. The Declaration clearly states:
inherent risks in comparison to foreseeable bene- to the subjects or to others.
subjed by the dodor.
1. (4) Every clinical research project should be preceded by careful assessment of
111. (2) The nature, the purpose and the risk of clinical research must be explained to the
4

115
111. (3) ... the responsibility for clinical research always remains wlih the research worker. 4 never falls on the subject. even after consent is obtained.
There is no question that the m a r c h failed to meet the ethical standards of the late 1940's as expresed in the first part of the Nuremberg code, The voluntary consent of a human subject is absolutely essential.' The code states that the subjacts must have sufficient understanding of their situation, and must k, capable of making an informed deusion as to their participation in the research. The research conducted by UC researchers did not meet this standard established for prisoners of War.
Informed consent was the ethical standard of Dr. Saengefs day, and was the medical standard since the 1890s. On April 8.1899. an editorial in the Journal of American Medical Assodation asserted that We rule of conduct in this matter is for the physician to put himself in the patient's place with all his natural feelings and desires. Even consent on the part of the subject can not justify an experiment that needlessly puts his health or IWe in peril, or diminish the mrponsibility of the one who pefioms or permit. it.' (Emphasis added)
The legal importance of Informed consent was estabiished in 1914. when Justice Cardozo mote that, 'Every human being ... has a right to determine what shall be done with his own body and a surgeon who performs an operation without his patient's consent commits an assault for which he is liable in damages." Schloendorf v. SOCI 'etv of New Yolk HOSD it& 211 NY 125 (1914).
The coults that, "A man is master of his own body .... A doctor may well believe that ... treatment is desirable or necessary, but the law does not permit him to substitute his own judgment for that of the patient by any form of artifice or deception.' 1960). Deception is pcisely what occulrad. The patient IS told that he is to receive treatment to help his disease.' wmte the authors in another DOD report, desplte the fact that they seleded patients with non-treatable cancers for the expenments. The researchers denied some of the patients potentially effedive treatments.
The human experiments which Dr Hamilton discussed in his 1950 letter, and which Dr. Saenger designed In Cincinnati. were an atrocious example of medicine gone mong.
B.
Researchers tested the efficacy of whole body irradiation in the 193O'sSO's at several centers, induding MemoriaCSloan Kettering in New Yolk City. WBR was not useful In the treatment of solid tumors. Researchers found that the so-called %on-radiosenskive cancers' such as those that UC researcher irradiated. were unresponsive to whole-body radiotherapy. The medical utility of this study was suspect and dsquised, and as a result the research resulted in the deaths of at least eigM. and probably more than twenty of the participants
In a separate artide titled 'Whole Body Radiotherapy of Advanced Cancer," Or. Saenger et al., mote. 'If one assumes that all severe dmps in Mood cell count and all instances of hypocellular or acellular mamm at death were due only to radiation and not infiuenwd by previous therapy, then one can Identify 8 cases in which there is a possibility of the therapy contributing to mortality.' Suskind states that up to 19 may have died as B result of the radiation.
In 1905, Dessauer first used inadiation of the entire body for purposes of the experimemlal therapy of diseasei. Physicians used whole-body irradiation for treatment of a wide varidy of benbn conditions induding asthma, migraine, and allhriti (Scott 1940) reports of adverse effects hom radiation @rues 1955, Furth and Lorenz 1954) quickly narmwBd the use of the treatment to metastatic tumors.
dearly stated the standard of informed consent In 1980. This decision stated
' ,350 P 2d 1093 (Kansas
Cancer therapy was not the purpose of this msearch.
5

116
Physicians conduCed a set of clinical trials of whole-body irradiation for cancer out at Memorial Sloan-Keitering in New Yo& from 1931 through the 1840's. These trlals involved high total dose irradiion given over a period of days. Physician designed the I d o s e rate irradiation to minimize side-effects such as radiation slckness and bone m a w suppression. L d o s e rate irradiation exposed the cancer cells to radiation during the entire cycle of cell division in order to irradiate each cell at the most vulnerable stage in its division Physicians published progress reports of the experiments performed at Memorial in 1932,1934. and 1942. The reports were in agreement with other liierature from that time. m e technique of Mole-body irradiation showed some promise with leukemias and lymphomas, but 'little or no benefit follows its use in the
1942). In the same study, Medinger and Craver explained why the therapy did not work on carcinomas (the type of cancer selected for the UC experiments): 'The results in these generalked carcinoma cases wem discouraging. The reason for this is quickly apparent. Carcinomas are much more rediomsklant than lymphomatoid tumors, and by total body irradiation the dose cannot be nearly large enough to aHer these tumors appreciably.' The reason the dose cannot be large enough is that a dose that will kiii the tumor wlll also kill the patient.
Later studies found similar results. Jacobs and Marasso reported in 1965 on 52 patients treated with whole-body irradiation when 'other modalities had failed or could not be employed.' They
m i a t i o n affected the d iseasq.' (Emphasis added) In contrast to the Memorial Hospital studies. these studies administered the radiation at higher doses, and much more rapidly.
Interestingly Dr Aron, one of the UC researchers and a member of the UC committee that Investigated the appropriateness of this work in the early 1970's, recently stated, 'In Cincinnati, the patients' disease had spfead throughout their bodies, and most were given a life expectancy of six months. The effect of the study was a short prolongation of their lives All who had the treatment have died of their cancers They lived an average of fifteen months afler the radiation exposure.' If this was therapy and it worked, why did the researchers stop lt when it became public? Did the researchers stop the experiments because they became public? If the radiation did not help, the subjects. who lived an average of 15 months after being irradiated, were not really suffering from terminal cancer. They were not. The researchers reported that until they were irradiated most of the patients were in. 'relatively good health " Suskind's report indicated that the researchers excluded terminal patients from the study, 'Some of the reasons for patient rejection included advanced stage of malignancies leading to disorientation, stupor, and/or coma, and terminal advanced malignant disease in whichfhe life expectancy was only a few weeks.' (pg. 27) At least nine and probably more than twenty subjects died as a resul of the experiment.
m e studies at the University of Cincinnati began end continued afler the medical liierature deariy refkcled that wholabody irradiation was inappropriate. UC researchers knew about the acute and chronic toxicity of whole-body irradiation; they knew that only leukemias and lymphomas responded to the treatment; they knew that radioresistant tumors would require a dose that would be lethal to the patient in order to affect the tumor. In the literature review of the paper by UC mearchers in 1973, the authors cite the study by Medinger and Craver, and note that Thirty-five patients with advanced carcinoma and sarcoma were included In this series'. UC researchers preferentially selected patients with tumors that were not treatable by whole-body irradiation (cancer of the colon, breast. and lung) and then told the patients that they would receive therapy for their disease.
It is important to note that the ill-effects of successful irradiation consist of symptoms from the radiation and from the widespraad destruction of the tumor cells (which release cellular chemicals and cause symploms from the body's effort to remove the dead tumor cells). Irradiating patients with radioresistant tumors allowed the investigators to state that the symptoms the patints experienced were caused by the radiation and not by the effects of tumor destrucbon. This is the reason the patients with radioresistant tumors received high dose rate
watment of Denera lized carcin oma or sarcom a: (Emphasis added) (Medinger and Craver
found that in patients with radioresistant tumors. . j j y I-
6

117
irradiation. The experiment mimicked the effects of nuclear war on soldiers. The purposs of the experiments was as described in the researchers reports to the Department of Defense, These studies are designed to oblain new information about the metabolic effeds of total body and partial body irradiation so as to have a better understanding of the acute and subacute effects of irradiation in the human. ... The long-term program envisions canying out the various observations rt dose levels of 100 to 150, and 300 red. Eventually d w s up to 600 rad are anticipated.' These doses were patentlally and wen in fact lethal. Other physicians established decades W o n the UC researchers conducted these experiments. A dose of 260 rads would kill up to LOW of those who received it. A 600 rad dose would kill almosl eveworm who received it.
The tmatment methods
An examination of the treatment methods reveals much about the true purpose of the experiments. Patients neceived treatment in a silting posltion with legsiaised, and head tilted slightly fornard. This position mimics that of a soldier in a protective fetal position. The powerful single doses resembled the dose rate of a nuclear blast. 'Whenever possible unidirectional radiation will be attempted since this type of exposure is of military interest,' the researchers wrote in 1989. This was not the way radiation physicians used In therapeutic applications. Physicians give real therapy slowly and from as many different directions as possible to minimize side effects and maximize emcacy.
In addition, the UC researchers denied the patients treatment for nausea and vomitino This was apparently so anathema to the hospital staff used to caring for patients that the researchers had to create a special form lo ensure that the doctors. nurses and other pemnnei would not perform their usual function of caring for sick patients This form instructed hospital staff not to ask about the symptoms and sons of radiation poisoning. p0 NOT ASK THF PAT IENT WHETHFR HF M S THESE SYMPTOMS,' the form said. The form went on to instruct the staff to record the time, duration and seventy of these symptoms. The researchers offered no treatment.
From another DOD report we find that the researchen sought to psychologicaiiy isolate the patients, 'There is no discussion of possible subjective readion resulting from the treatment with the patient. Other physicians, nums. techniuans and ward personnel are instructed not to d m s s post-irradiation symptoms or reaction with the patient. This 'isolation' is carried out carefully so as not to influence any objective reactions of the patient which might be attributable to rudiation.' Patients resided in the psychiatry unit instead of the tumor ward. The environment is far more attractive and there are no other patients receiving radiation therapy with whom the patient can exchange experiences. What manner of cancer treatment seeks to psychoiogically isolate patients and deny them treatment for nausea and vomiting?

118
II. Assessing Responsibility
In my opinion the rorponsibiitiy for these experiments rests on many shouidets. These include: the government agencies that funded them and filled to provide adequate ethlcol safeguards; the Congmss which filled to p d d e adequate ovoTsIoM; the mearchers who vldstrd their H i m c oaths and their sac& tnmt with their patients; the unlvvsMTsr which filled to pmvide adequate owsight of thdr msearchws; the joumek that publkhed the work without comment, or review ofthe ethical LrsuoJ that the mearch rahd.
The m a r c h conducted by UC researchers was cleariy unethical and resulted in the deaths of many of the irradiated patients. Or Stephens revealed this information to the public in 1971. Dr. Thomas Gall brought this information to the attention of Universlty personnel in 1968.
We must address several if we are to assure ourselves that similar expenments will not occur in the future.
I. If the research was wrong and people knew it was wrong when d was done, why wasnY it stopped soonen In fad. the Suskind committee suggested that the research should continue in a modified form.
2 why was there no outcry, apology or thorough investigation after the research became public?
There are several answers to these questions.
1.
There are several reasons for this.
Them was a lack of appropriate oversight by the University.
A.
B.
C.
0.
E.
F.
G.
No one likes to admn they made mistakes or apologize.
Or. Saenger and his colleagues were well known and respected. It is hard to criticize the powedul and famous. Or. Mossman, head of the Health Physics Society. told me at the last Congressional heanng that he would not criticize Dr Saenger because he was a 'big man.
Physicians do not like to cntidze their peers especially if they work at the same instnution
The University ignored the timely cnticisms of is own faculty. (letters by Drs Gaffney and Gall - 1967)
The Univefsly allowed the research to continue from 1986-1971 without the approval of its am human subjects review board established in March 1966. The UC research review board granted a protocol limited to WBR a bone marrow transplantation provisional approval in May 1867. The approval granted in 1967 was provisional and requested that three modifications be made to the original protocol A final revised protocol was not approved until August 1971. The expenments continued during this entire period.
At least two of the researchers were members of the University committee (Suskind report) that investigated the research. The UC burdened the researchers wth the evaluation of their own work. This is a clear conflict of interest and a situation that is not likely to result in an objective evaluation of the research. (See below)
The University chose to attack the messenger by using McCalthyite tactics against the critiques of the research. This has continued to date

7. Them was lack of approprhte wenight by the Medical Community
a. The United states Senate requested that an 'outside revievC be carried out by the American College of Radiology (ACR). Dr. Robert McConnell a 'long time fwling partner of Dr. Saenger conducted this 'reviewf. In his report to the Senate Dr. McConnell noted that Dr. Saenger was a member of the American College of Radiology. He neglected to mention his personal friendship with the principle investigator or the fact that Dr. Saenger was at the time of the Investigation a member of five different committees of the American College of Radiation, including the Commission on Radiological Units, Standards. and Protection. the Committee on Research and Development in Nudear Medicine. the. Commission on Public Health, the Subcommittee on Nuclear Medicine Technology. and the Committee on Efficacy. Prior to the investigation Saenger also served as a member of the Subcommittee on Radiological AspeUs of Disaster Planning. These relationships constituted a conflict of Interest and a situation that is not likely to resuit in an objective evaluation of the research.
b. Two UC researchers w r e members of the UC committee that reviewed the research for the University. This is an obvious conflict of interest.
c. The Ohio board of medical licensure has to date not Investigated any of the physicians Involved in this series of experiments.
d. The Cincinnati Medical Society has not investigated this series of experiments.
Them was lack of approprlate oversight by the Congmss. 3.
Senator Tafl vigorously obstructed a potential Senate investigation.
4.
who reviewed this work while it was conducted? Is there a current investigation of this research?
6.
If it is true that the DOD only funded researcher salaries, overhead and travel money then public funds paid for these experiments.
6.
The press, the last link in the chain that must protect our citizens from its government failed to cover the story. The press permitted the uncontroverted comments of the researchers and universities to stand alone as reports on these experiments.
7. problems.
n is knpoltent to consider the. University's evaluation of these experiments (Suskind report). When these experiments again reached the public consciousness thk year, the U n l v e w claimed the review agencies had found the experiments to be ethical and appropriate. It is my opinion that the reviews were inadequate and m n g . Nonetheless the Unlvetsity. the mearchen. and the DOD have used the reviews to pmted themselves from scrutiny. The reviews were part of an otganized effort to mislead the public about the research. A careful
Them was lack of approprlate oversight by the DeparmMnt of Defanse.
Wen them violations of Medicare or Medicaid rules?
The pmss failed in its oversight role.
The pmvious investigations were inadequate and fllled with conflict of lntemst
9

120
examination of the Suskind report reveals the inadequacies of the University's analysis of the radiation experiments and the unethical nature of the experiments themselves.
a.
The only protocol that preceded the experiments indicates that the purpose was to provide, 'information [that] is necessary to provide knowledge of combat effectiveness of troops and to develop addilional methods of diagnosis, prognosis, pmphylaxis and treatment of these injuries.' @a. 1 DOD report 1963)
After the m a r c h was publicly criticized. the researchen claimed the DOD protocol was an add- on to a cancer treatment program. A cancer treatment protocol was produced in 1966 and approved on August 9,1971. Perhaps because UC researchers never implemented any protocol while the study was conducted, friendly reviewers have had differing conclusions about the purpose of the experiments
The ACR stated that the experiment was a Phase I study of the toxidy of whole body radiation in humans. American College of Radiology: The committee viewed the project as il was designed - as a clinical investigation of a modality for the care of cancer patients with extensive and incurable disease. Phase one investigations follow basic animal worlc and always precede randomized dinical trials which may or may not be justified on the basis of the first human applications ' (pg 3)
Suskind found the expenment to be a Phase II cancer study of the efficacy of treatment Suskind's report states that the hazards of whole body radiation were well established before the UC studies were started. The hazard [bone marrow suppression] is well documented in the available literature and the dose relationship to side effects well understood.' (pg. 9) Suskind then states that the study was some type of Phase II study of the efficacy of bone m a m transplant and radiation. However. of the 87 patient's treated only 13 received a bone marrow transplant. In addtion. Suskind notes, The committee. however, was unable to find any wntten protocol in which the purpose of the study was to determine palliative effects of whole body radiation until. .1967.'@a. 14) He latter notes, 'No plan for a systematic study of palliative effects was made (pg 64)
Only the researchers' own words fully explain the experiments. They explained that the purpose was military. Only this purpose explains the experimental desgn, that included psychological isolation, organized denial of treatment for nausea and vomiting, and no plan for analysis of Cancer palliation or treatment efficacy. Since treatment was not the intent of the study there was no need to organize the study so that treatment outcomes could be evaluated
b.
Suskind reviewed the prior studies of WBR to try to see if physicians had conducted adequate Phase II trials prior to the UC expenments. They report universal failure. 'Medinger and Craver (1942) - Results were described as discouraging in this group of patients 'except for transient relief of pain in a few cases'.. Jacobs and Marasw (1965) - 11 of 16 'died within one month of treatment; the remaining 5 having survivals of 1-1/2. 2. 3.4. and 9 months The statement suggesting the need for further evaluation of this form of treatment refers most probably to the radiosensitive, widespread neoplasms rather than the results in the 16 patients with radioresistant cancers.' @a. Wll) In addition, Suskind could not find anyone else performing similar experiments, 'Ailhough whole body radiation is widely used for many forms of radiosensilive tumon. no information is available to the committee which indicates that this form of treatment is usedelsewhere in radioresistant, disseminated or localized cancers as used at the Univesity of Cincinnati.' @a. 12)
What were the objectives of the study?
Was there a need to test whole body radiation for cancer treatment?
10

121
Suskind notes that In 1908. This proposal recslved a critical Internal review and was submitted to the NIH in an application for a research grant. The application was not approved and the reasons for this deddon were not disclosed.' (pg. 42) This was not true. In 1980, Evelyn Hess MD, the chairnoman of the faculty committee on research mots that NIH had rejected two research grants because, ?he acceptability of our general consent form for human volunteera participating in research was questioned.'
Suskind conduded that, The Phase II uiteria for whole body radiation were not adequately satisfied at the time the oalnal protocol was designed In 1960 and evidence for its effediveness was incomplete. The results which were available for Interpretation were not encouraging. Hence, the need for mounting a Phase I1 study at that time was indicated.' @e. 11)
If, after reviewing the dismal resuits of previous studies examining WBR use for radloreslst.nt tumon and faculty utUcisms of the WBR experiments at UC, SUsMnd really thought another study was necessary, there is something fundamentally wrong with the way UC researchen evaluate medical treatment and research needs. This is perhaps a mom Important area of Investigation than the original studies themselves.
it may indicate that there is stili a problem In this area at UC today. If the University authorities cannot recognize that the WBR experiments were wrong and apologize to the community, how can the community trust them to evaluate currant experimental programs?
c. Quality of care
Suskind: The thoroughness of the psychological support is apparent from the report of the psychological staff.' @o. 28)
W D report: 'There Is no discussion of possible subjective reaction resulting from the treatment with the patient. Other physicians. nuws, technicians and wad personnel are Instructed not to discus post-lrrediatlon symptoms or reaction with the patient. This 'isolation' is canled out carefully so 8s not to Influence any objective reactions of the patient which might be aMbutaMe to radiation (pg. 4)
If denial of treatment for nausea and vomiting and psychological isolation is good quality of care pemaps there is a current problem at UC In this area as well.
d. Ethics
Suskid Patients and families were not informed about the possibility of transient nausea and vomiting since such symptoms may be induced by suggeslion. Typcally, such stde effects can ocwr a few days afler treatment.' (pg. 50)
Susklnd: 'Were there patients. whose 10 was subsequently determined to be 75 or below, who signed the consent form themselves?
Yes there were ten patients There was no reason to believe that they did not understand the conditions of the prolad. The Committee also questions the significance of the s ~ r e s of intelligence tests in this group of patients who were dying of far advanced cancer.' (pg. 51) ll was precisely these IQ scores that formed part of the basis for the DOD mgnitive effects research.
Suskind' 'Informed consent should be obtained as it is now. Revisions of the consent forms should be consklered in relation to the use of the phrase 'sound mind and body'. The procedure for withdrawal from the proled should be improved.' @o. 56)

122
If it is Suskind's (and the University's) opinion that sick patients with IQ's less than 75 who are not told about side effects like nausea, vomiting and a 25% death rate within weeks of treatment can provide informed consent there is a serious problem at the University.
e Research quality
Suskind noted, 'ff is uncertain whether this study and similar sludies reported in fhe medical literature are truly comparable in all major factors that influence survival, such as selection of patients and ancillary medical management. Therefore, the signiflcance of comparisons of survival rates is doubtful, unless marked differences are found.'(pg. 59)
'Since the manner k, WMCh the Ma on palliative efiea was developed was kurdequcr!e, no conclusions can be drawn from them.' @a. 66)
Despite these commenfs Suskind concluded. Since the Commitfee cannot at this time rule out a positive effect of whole body radiation, a welkdesigned study to compare whole body radiation W h other forms of therapy is necessary if the investigator wshed to continue.' @a. 66)
Is this the current type of analysis UC uses to evaluate research and researchers?
111. Why did this happan?
That's a llst of who but the answer to why this occurred is a more subtle and Important issue. Our population views the United States as a unbue country. and tl k. I! IS unrquely democratic; these heanngs are an example of that It is my belief that we in the United States have a certain belief in the infallibility of our own history and our own behavior We tend to believe that our adions could only have good intentions. I am afraid this is not so. We have at times done fhe m n g thing for the wrong reasons just as many other countries have done. The history of medical sclence, replete with the use of certain marginalized groups in our soaety for harmful experimentation, offers some examples of repugnant actions performed in this country. Perhaps these experiments will serve as a turning point and provide us with a fresh look at ounelves A
that II is not an infallible country. That not everything we have done has been with good intentions or with good results, and therefore we, like other countries, must remain vigilant of our government, and our citizens and our companies. We must continue fo maintain and buttress our system of checks and balances to assure us that these types of experiments will never go on again
look that recognizes th8t Ih8 United States iS the greatest W U n t r y On earth but dS0 r e c O g n Z 8 S
12
123
N. What should ba done?
A. Shortterm
1. The University should apologize
2. The victims or their families should be compensated.
3 State Medical boards should investigate.
4. Criminal investigations should occur.
5. A single Congressional investiiation should occur.
6. The DOD should investigate their role and overnight procedures
7 Medicare and Medicad agencies should investigate the possible use of patient care funds for research.
8. The Association of Occupational and Environmental Clinics should provide an independent nongovernmental evaluation of all of the DOD, NASA and DOE research
B. Long term
1. Medical review boards must be composed of ~ 5 0 % independent and unrelated researchen and lay people.
2. Medical journals should have ethical reviewers
3 NIH must inform appropriate authonties when they find that a research project violates ethical standards Their silence must stop
13

124
Some people have Wed why I am here To paraphrase Thoreau, the question should not be why am I here, but why aren’t other responsible parties here? If is every phpldanb duty to speak out when medicine ooes m n g .
To quote from Pastor Nlemdler about the Holocaust:
‘In Germany the Nazis came for the communists. and I did not speak up since I was not communist. Then they came for the Jews, and I did not speak up since I was not a Jew. Then they came for the trade unionlsts. and I did not speak up since I was not a trade unionist Then they came for the Catholics, and I was a Protestant so I did not speak up Then they came for me, and by that time no one was leR to speak up.
Thanks
My wife Helene, my students. my staff, my fnends at NiOSH, Mitch Singal, and Bill Halperin, and my friends, particularly Mlke Donahue.
14

125
Contemporaneous comments of colleagues
'It is not certain from the (consent form) narrative whether the patient
is advised that no specific benefit will derive to him and that there are,
indeed risks involved in the procedure proposed." - Edward Gall MD,
1966
'I believe a twenty-five percent mortality is too high." All patients
should be informed not only that a 'risk exists' but of, "a 1 in 4 chance
of death within a few weeks" of treatment - George Shields MD, 1967
e
Statomd to Congress Aprll 1 1 ,1994 by Davld S. Egilman MD, MPH. - 1 1 . .
84-514 0 - 94 - 5
1

126
Contemporaneous comments of colleagues
T h e applicants have apparently already administered 150-200 rads
to some 18 patients with a variety of malignancies and to their
satisfaction have not found a beneficial effect. In fact, as I understand
it, they found considerable morbidity associated with this high dose of
radiation. Why Is it now logical to expand thls study?
Even if this study is expanded, Its current deslgn wlll not yleld
meanlngful data. ... lt will be difficult if not impossible to observe a
beneficial effect in such a small sample containing a variety of
diseases all of which share only CANCER in common.
This gross deficiency in design will almost certainly prevent making
meaningful observations. When this deficiency in experimental
method is placed next to their previously observed poor resutt and
high morbidity with this type of treatment in a 'variety of neoplasms' I
think It dear that the study should not be done. - Thomas Gamey
MD - 1967
2

127
Contemporaneous comments of colleagues
....' the acceptability of our general consent form for human volunteers
participating in research was questioned" - Evelyn Hess MD - 1969
commenting on the reason for rejection of two grant applications by
the National Institutes of Health.
3

128
Overview
1. FLst I w(u the descrlk, the whole body nrdletion (WBR) experiments that were conducted at
the UC. These WIU deslgnd to provide informsuon to the mUltary. They were not In any
way cancertmatnmt OT pallkith. Some ofthose studies resulted In the deaths of thelr
-.
2. Seamdly, I will addmthe question of WhSuHHthe experlmentswem conducted occdkrg
tothe ethical standards ofthdrtime. The answer to thisquestlon is a firm no.
3. Thkd. I thlnk we should cons#er why these ~ r i m s n l s wem allawsd to occur and conUnw
owra c o d d m b k prbd oftime. Why did It take until 1oQ) forthese actMUesto mch
thenrtionr(-?
.

129
e
.
The University of Cincinnati Experiments 1960-1 972
a. Ethics and informed Consent
On November 28 1950 Dr. Joseph Hamilton wrote a letter to Shields Warren
MD., Director Division of Biology and Medicine, The Atomic Energy Commission
WC) .
(AEC) researchers wanted to determine the dose that might limit a soldier's
"capacity to execute intricate tasks for which physical well being is essential.'
Hamilton discussed the difficulties of performing such a research study, and
suggested that 'For both politic and scientific reasons, . it would be
advantageous to secure what data can be obtained by using large monkeys
such as chimpanzees which are somewhat more responsive than lower .-
mammals' -
If the research was to be done on humans, Dr. Hamilton predicted that 'those
concerned in the (AEC) would be subject to considerable criticism, as
admittedly this would have a /&/e of the Buchenwald touch ... The volunteers
should be on a freer basis than inmates of a prison. At this point, I haven't any
very constructive ideas as to where one would turn for such volunteers should
this plan be put into execution.'
slotemcmt to COngmSS April 11.1994 by David S. Egilman MD. MPH. I -
S

130
The University of Cincinnati Experiments 1960-1972
a. Ethics and Informed Consent
2. Selection of subjects
a. Uneducated - average 4th grade b. Low intelligence - average IQ 84 (many mentally
retarded c. Brain dysfunction (did not
know how to follow instructions) d Patients with tumors that were nrSlstan( to radiation therapy. e. 'They must be in relatively good nutritional
status and with a stable hemogram. f. 54 of 88 patients African-American
These researchers, like others involved in similar experiments
funded by the DOE and NASA, selected the most vulnerable of
our citizens as subJects, the poor, the mentally and emotionally
impaired, and African-Americans.

131
The University of Cincinnati Experiments 1960-1 972
a. Ethics and Informed Consent
e 1) Patient population was incapable of giving
m informed consent.
2)
experimental risks.
Patient population not informed of the

I
132
The University of Cincinnati Experiments 1960-1972
a Researchers claimed’- p.tl.nbim-~o(th.
rkkrmdcomplk8uonm.
b. Researchers reported - 6 ol- =
canrmt in th. p8perth.y publidled.
d Researchers reported - ti^ did not wi th.
and our own ethical and moral standards.
a
. a

133
The University of Cincinnati Experiments 1960-1 972
a. Ethics and informed Consent
3. Researchers were aware of Informed consent requirements
a. Researchers were aware of the Helsinki code
The Declaration states:
(4) Every clinical research project should be preceded by
careful assessment of inherent risks in comparison to foreseeable
benefits to the subjects or to others.
II (2) The nature, the purpose and the risk of clinical research
must be explained to the subject by the doctor.
I I (3) ... the responsibility for clinical research always remains
with the research worker; it never falls on the subject, even after
consent is obtained.
Statement to Congnus April 11,1994 by David S. Egilman MD, MPH. .-c
9

134
The University of Cincinnati Experiments 1960-1972
a. Ethics and Informed Consent
4. Researchers were aware research was 'questionable ethically"
a. Similar experiments were rejected in 1966.
'The suggestion is made that we should treat carcinoma of the breast,
gastrointestinal tract, and urogenital tract by total body irradiation. These
groups of patients have been carefully considered for such therapy, and we are
very hesitant to treat them because we believe there is SO little chance of
benefit to make it uuestionable ethical& to treat them. Lesions that require
moderate or high doses of local therapy for benefit, or that are actually
resistant (gastrointestinal tract) are not helped enough by total body
inadiation to justify the bone mamw depression that is induced.'
(emphasis added)
The argument that these experiments were appropriate from the ethical
standards of the 1960's lack both scientific and historic accuracy.
Shtemcd to ~ O ~ ~ K J S S Aprll 1 1,1994 by Drvid S. @ilman MD. MPH. /I \_-a. a . 10
i N

135
The University of Cincinnati Experiments 1960-1 972
Cancer theraw was not the Dumose of this research. b.
1) Result of previous research - Dismal
e or no b e neflt follow its us e In the treatme n t of a) m m o e ~ l l z ~ cam lnoma or sarcoma.’ (emphasis added) (Medinger and C r a w
1942).
7he results in these generalized carcinoma cases were discouraging. The
reason for this is quiddy apparent. Carcinomas are much more radioresistant
than lymphomatoid tumors, and by total body irradiation the dose cannot be
nearly large enough to alter these tumors appreciably.’
b) in no Datient was there evidence that total-body irradiation
the disease.‘ wth radioresistant tumors] (emphasis added)
(Jacobs and Marasso 1965).
A dose which will kill the tumor will also kill the patient Y
Statemd tk -rag Apil 11,1994 by Davld S. QWmn MD. MPH. 11

136
The University of Cincinnati Experiments 1960-1972
- . . I
B. Can- r theraw was not the n u m e o f this res earch.
2.
eucperiments in their reports to the Department of defense.
The Researchers themselves described the purposes of the .
The purpose was, to provide knowledge of combat
dfecthmneu of troops and to develop additional methods of
dlagnoek, prognosis, prophylaxis and treatment of these
InJurks."
l2

137
The Unlverrrity of Cincinnati Experiments 1960-1 972
9 j ! j f I
Issue Real Medicine
ANDVOMITING
PSYCHOLOGICAL AND PEER COUNSELING
DOSE DIRECTION DIRECTIONAL
What manner of cancer treatment psychologically
isolates patients and deny them treatment for nausea
and vomiting?
~
WItanenl to AprH 11.199) by D.vW S Eglltnan MD. MPH 13
.

138
The University of Cincinnati Experiments 1960-1972
C. Assessina ResDonsibilQ
1. Government agencies that funded them and failed to provide
adequate ethical safeguards - DOD, ?Medicare and Medicaid.
2. Congress failed to provide adequate oversight
3. Researchers violated their trust with their patients.
4. U~ivemltles failed to provide adequate oversight.
5. Journals that published the work without comment failed to
pmvide adequate oversight.
6. NIH refused to fund the work on ethical grounds kept silent.
14

139
The University of Cincinnati Experiments 1960-1 972
D. blainina the continuance of the exneriments in the face
of ethical auestions
1. There was a lack of appropriate oversight by the University.
2. There was lack of appropriate oversight by the Medical
Community
a) ACR The fishing buddy reviewer
b) The Ohio board of medical licensure
c) The Cincinnati Medical Society

_.
140
The Unhremity of Cincinnati Experiments 1960-1972 *
p. Exolainina the co ntinuance o f the exoen 'ments in the faca pf ethical auest iong

141
The University of Cincinnati Experiments 1960-1 972
D. ExDlainina the continuance of the emeriments in the face
of ethical auestiom
&aelmnl to coqpss &Ill 11,1994 by 0.Vid 8. E@nal MD, MPH. 17

142
The University of Cincinnati Experiments 1960-1 972
p. bla in ina the continuance of the exmriments in the face
i
18
I

143
The University of Cincinnati Experiments 1960-1 972
P. - lainina the continuance of the erne riments in the fa-
19

L
144
The University of Cincinnati Experiments 1960-1 972
g. ExDlainina the continuance of the emeriments in the face
7. Th. pmlow &)-OM WWW IrUd.gWt0 M d RIW wlth ContliCt Of Int.R.1
pmblmna, bKompktr nrurch and Mum uulysb.
Suskind noted, ..." the significance of comparisons of survival
rates Is doubtful, unless marked differences are found."(pg. 59)
'Since the manner in which the data on palliative effects was
developed was inadequate, no conclusions can be drawn from
them." (pg. 66)
Despite these comments Suskind concluded a modified
study could continue. (pg. 66)
Is this the current type of analysis UC uses to evaluate research and researchers?
to April 11, loo) by DMd 8. EgUm8n MD, MPH.

146
V. What should be done? A. Shorttwin
I. TheunhmlanyshouldIpdogize.
2. The vidhs w thdr families should be compensated.
3. State Medical boards should Investigate.
4. Cllmlnal Invmtbatbm should occur.
5. A tlngkt Can~rsrdoMl invoslbation should occur.
6. The 000 should investigate their role and ovemi~ht procedures.
7. Medicus and Medicaid and the City should invealigate the dhrenlon of patient care monk to rewrrreh.
8. Them should tie an InvostbaUon by the Aswdrlkn of Occuprtlonrl and Envimnmentr( dinks.
6.Longtwin
1. Medicrl IWIOW boards must be compolsed of >50% independent and unralated t8seaFchsn .ndkY*.
2. Medkal journals should haw SUIkal reviewers.
3. NIH 8hould &don r15 a cade of silence. Thsnk
My wife Helene. my 8tudmts. my ataff, my wpenrfsors at NIOSH. Milch Singal, and BiH Halpdn, urd my frbndzi pamlady Mike Donahue.
21

146
ERRATA
The University of Cincinnati Experiments 1960-1972
On page 4, paragraph 3, line 6 the sentence should read: "In
reviewing a suggestion that patients with carcinoma of the breast,
gastrointestinal tract, and urogenital tract should be treated by
total body irradiation, the Oak Ridae researchers made the
following statement ..."

147
Mr. BRYANT. Dr. Stephens. STATEMENT OF MARTHA STEPHENS, Ph.D., PROFESSOR OF
ENGLISH, uNI[vERSITY OF CINCINNATI Dr. STEPHENS. I have been somewhat disappointed that we
couldn’t hear from more family members. I would like to look at some of the medical charts.
The family of the peo le who spoke to us toda suffered. I think
sick for several days-intensely, usually. Many had to go into the hospital for this treatment. They were taken out of their homes, called up, told to come to the hospital fopthis treatment.
No matter how long they lived after the radiation, they suffered. The doctors tell us in fact that it can take up to 100 days to recover from whole body or partial body radiation. For those who didn’t die directly of the radiation, nevertheless they all suffered, were made ill, possibly were sicker than they would have been for up to 100 days, the ones that lived that long.
Now, we did not hear this morning from any of the so-called short survivors, and we must remember that there were at least eight people who died directly of radiation. We can document this from the doctors’ reports. They give us the blood scores for those patients. These patients died within 40 days. We know that they suffered from bone marrow failure. And when that happens, you are wide open to infection. Infection swoops down and takes you away because you have no white and red blood cells to fight it with.
Thus, I wish we could have heard from a lot more families. Let’s remember this: 26 people died within 60 days. Their lives were al- most certainly hastened by radiation. As the years went on, the doctors stopped telling us what the
blood scores were, because they were no lon er studying what was found out that
with 200 rads of radiation, you have a good chance of dying of it. They knew what would happen, and they kept on doing it.
So we don’t know, for all of those 26 peo le-that is, until we
which Dr. Egilman now is studying and others will be studying- we don’t know exactly how all of them died. I am sure we will find that many more than eight also suffered severe bone marrow de- pression.
The question has been raised, were these patients terminal? My view is, many were not what we would in common parlance today call terminal. Early on in the experiments, a woman was irradiated who had had cancer of the tongue. She was given a high dose of radiation that she might have died from. She was submitted to that lethal risk, but she recovered.
You usually either die or begin to get better within about 40 days of having total body radiation.
She survived. She got very sick, but she survived. She lived after that over 5 years. In fact, we don’t know the date of her death. I don’t think she could be considered terminal at the time she re- ceived this high, possibly lethal dose of radiation.
I have been particularly interested in one patient, No. 090, be- cause of those 26 patients who died between 6 and 59 days after
everybody that was in t K ese experiments suffereb: They were made
happening to the blood scores. They had aready 9
study the medical records which we have on P y recently gotten and

148
they were irradiated, she is the shortest survivor of all. She lived only 6 days after her radiation. She was an 80-year-old African- American woman who lived in Hillsboro, OH.
I did not know until last Friday when I went to a meeting of the families in attorney Bob Newman’s ofice that her family have been identified. I had wondered all of these years who they were. I didn’t know her name. Her name is Margaret Bacon. Here is what hap- pened to her. First I should say that we have heard a good bit about bone marrow transplantation and whether this could have helped protect the people who were receiving the higher doses in the later years of the project. I t wasn’t even tried until mid-way through the project, and at that time, even, it was experimental. The doctors were not sure they could make it work.
So Margaret Bacon had an operation to have her bone marrow removed so that it could then be replaced after her irradiation, to give her a chance of her bone marrow recovering. On the operating table-and this was a severe, serious operation, to have your bone marrow removed, it was another ordeal that people had to go through, it took up to 2 hours with general anesthesia-on the op- erating table or shortly thereafter she suffered a stroke.
She still was irradiated that very day, at 2. They probably did not know that she had suffered a cerebral accident. We read in her patient history, she was shammed, that is, given fake radiation to “see whether that would have any psychological effects, on June 2, 1969. On June 4, bone marrow was aspirated from the posterior and anterior sternum with ease.
At approximately 2 in the afternoon, the patient received 150 rads midline tissue dose total body irradiation.
She experienced only mild nausea and vomiting. Following irradiation, the bone marrow was infused. The patient tolerated the procedure well. No fever, chills, were noted.
On June 9, 1969, the patient was noted to have left sided facial weakness. This is just a few days later. Suggestive of a cerebral vascular accident.
On June 10, the next day, six days post TBR, she expired. In that same report that the doctors submitted, which contains
this history, we read as follows. The second death (patient 090) was anesthesia related. Four days, they say here,
after the procedure, that is, the bone marrow aspiration.
I could read-maybe I will have a chance later on, to look at these statements from her family, her nephew, her great niece and her great nephew, who appeared at our meeting on Friday, and they have submitted to you three statements.
They, like the others, do not know anything of an experiment being carried out on their aunt.
If I may return to the question of informed consent, there is no evidence of any kind of consent for the first 5 years, written, oral, otherwise. There is no evidence that has ever been put forward. When consent forms were introduced-and after all we do have these, I saw them years ago, we do have the consent forms-none of them ever stated the real risk to the patients, that is, none said to the patient, ‘You may die of this treatment, do you really wish to have it?” None ever said that.
I have two recommendations I would like to make, if there is time.

;r -.
149
Mr. BRYANT. You might summarize them so we can begin to ask
Dr. STEPHENS. Maybe I will 8ave those. Can I save those? Mr. BRYANT. Very well. Thank you very much. [The statement of Dr. Stephens fol1ows:l
questions.

Statement for House Judiciary Committee -- Martha Stephens
p. How did you first find out about the radiation project a t U. C.?
A. I n the f a l l of 1971 I was starting my f i f th gear in the University of Cincinnati English Department. I was thirty-four, an Assistant Professor.
When I f i r s t began to look in to these experiments, I had no idea anyone had died of the radiation. I n the corridor of ncnicken Hall one day. a friend i n the department, Dave Logan (now the director of Prospect House, an alcohol treatment center i n Cincinnati), showed me a br ief report from the #7bp YBicaabout experiments being done a t U. C. f o r the Defense Department, using poor cancer patients. The reporter was questioning whether or not the patients knew they were in an experiment; he said some were being irradiated over the i r whole bodies and were suffering nausea and vomiting fo r several days afterward.
This was a l l we knew when a group of us in the Junior Faculty Association decided we should look in to the matter. We were l iv ing in the tail-end of the sixties, a f ter all, not long af ter the bombing of Cambodia and so on. and we should remember that many Americans had developed a profound distrust of eveything that issued from the Defense Department.
I had a reseamh leave coming up i n the winter, w i th t ime to study th is issue, and I went over to see Edward 6011, who was then director of the Medical Center. I remember v is i t ing him several times and t y i n g out various arguments on him t o try t o get information; he was courteous, but fo r quite a while nothing was forthcoming from him. I remember his saying that the f i l es on the project were long and complicated and would not mean much t o people who were not doctors. He said, 'I'm sure you wouldn't want them all-' I said, 'We do though. We would l i ke t o see them all. If eveything i s a l l right, as you sag. Dr. 6011, and we have no reason t o doubt your word, then perhaps i t would be Useful t o have a campus organization clear up the matter.' One day I went back over t o his of f ice and there was a large p i le of documents on his desk. These papers were copies of the typescript reports the doctors were sending t o the DOD, and I would la ter find. that they to ld a tragic and terrible tale. Even now, I do not know why 6011 surrendered these Ospsrs t o me, and I later realized I was quite possibly the first person outside the nodical School and the Defense Department to see them.

161
2 This set of documents that has now been copied and re-copied in Cincinnati and elsewhere.
campus drive, up on our hill wi th i t s beautiful lawn stretching down to Clifton Avenue, and pulled these papers out on my lap to see what I had. I saw that individual patient histories were attached to the backs of each of the nine reports, and I began reading these histories. I read for about an hour, and when I got out of the car. i t was as i f I could hardly recognize what was around me. Everything I saw looked different t o me-
I was used to reading i n plays and novels about tragic deaths, fu l l of pity and sorrow, but I was not used to IMspity. IMssorrow. I f e l t that these experiments had to be stopped, and o f course i n due time they ware stopped.
Over that Christmas holiday, I spread these papers out late at night over my dining room table, after our children were put to bed, and I wrote a summary o f what had happened to the eighty-seven individuals that had been irradiated. I wrote about how they died.
I presented my findings to a meeting o f the Junior Faculty Association on January 14, and the group decided to have a press conference, and this we did MI January 26 of 1972. I feel now, as I look into the whole matter again, that our report was actuelly a conservative one. ny friends i n the JFA had gone over with me every sentence of it. We knew it had to be clear and It had to be right. I introduced a number of qualifying phrases. everywhere we had the least idea that an assertion could be challenged. Today I would not be as hesitant; but at that time it was as i f I could hardly believe myself what I was putting down on paper. Still, this report told a l l the basic truths of the case; it told the truth, and it examined every possible argument the doctors could use to just i fy what they had done.
In some ways it i s even more astonishing t o me today to reflect on what transpired and t o image up the whole scene from the point of view of the patiehts that were used. Even now, after sa much discussion of these fellow citizens of ours. we don't know a l l their names or where they lived. what theM did fw a living, what thew personally went through, the ways i n which their loved ones suffered -- as they themselvas waited helplessly for word of this or that from doctors and nurses that usually could not be found, or stood at bedsides i n crowded wards, often &dgwards, as various hospital usem of those years have testified.
I .- - -I the invlsibte peo~ le inhabiting a l l our debates and discussions about this project. I'm thinking, for instance, of a man with
I drove back over to ncnicken Hall that day, and I sat out on the
. , - - * These families I'm speaking of have been '-. -;1--.:: - . -

152
3. M c e r who, af ter h is irradiation, never came back to the hospital,
bore his painful disease without help, as fa r as we know, not wi l l ing to be treated again af ter such an experience. I think of an eighty-year-old African American woman, -H. 6.; who had lung cancer and suffered a stroke on the operating table in 1969. having her bone marrow aspirated in preparation for her irradiation. She died six days afterwards -- 'an anesthesia-related death,' as the doctors themselves describe it. Did she volunteer to be i n an experiment that might end her l i f e?
9. How many patients died? We know that a t least 8 patients died of bone marrow failure as a
direct result of radiation; f o r these patients the doctors provide the blood scores that allow us t o document these cases of classic radiation injury. Then there were cases l i ke that of ?I. 8. mentioned above. Some of the histories, however, t e l l more than the others; in the later period, blood scores are no longer being studied and we are not generally to ld how much bone marrow depression existed at t ime of death. But there are altogether 26 individuals who died within 60 days of being irradiated and whose deaths were almost certainly hastened by radiation. For some of these short survivors we need to see the i r full hospital charts and follow-up i n the clinics and hospitals to know exactly how they died.
0. Were these cancer patients terminal? Were they people expected to l i ve only a few months, as the medical school has said?
The patients who survived the radiation often l ived several years. One woman w i th cancer of the tongue was irradiated in 1961 and lived at least f ive years af ter the radiation. We in fact do not know when she died.
A la ter group of subjects were chosen specifically because they were in relatively good shape, were not elderly, and could be interviewed i n their homes or workplaces about coming i n fo r th is 'treatrhent.' They were working. eating normally, w i th good blood counts. Definitely not bed-ridden, extremely feeble, or about to die.
Q. Who were the doctors? It was not a question of one or two or three individuals performing
a deadly r i t e that very few other doctors knew about. A project ::6: goes On for eleven yeors ond inrol+as the screening and CohSidsrotion of a t least 11 1 patients had t o be known to a great many people. There were t&fHm BBclerson this team w e r the years, co-authoring the reports and publications, and many more who assisted i n Various ways

153
4 and were sometimes closely involved, i n the complex testing of irradiated subjects for mental functioning, for instance. Then we have the doctors who were staffing the Tumor Clinic at the hospital and wil l ing t o hand over Patients to the chief investigator and his associates, as well as staff et several other hospitals; at least three subjects were 'recruited' from Omke. t o use the doctors' term, and three youngsters with Erring's samoma were brought over as 'volunteers' from Children's.
as i f he were an uninvolved or neutral spokesman, he was himself a member of the team for the final two years o f the project. This doctor also served on the Iledical School's internal review which cleared the project of any wrong-doing.
i n the defendant's box also sit t ing on the jury.
Cull- of RMulqy tWmt fi& q t M @ uffeasftw ia tibass trtels ss8
What should we think about the long l ist of important medical journals which published the findings of these doctors over the years? How did their editors and readers mgerd the deaths they learned about in these reports? What were the attitudas of the local hospital authwi t i es, the state 1 icensi ng board?
Mtg did trbs m i u w cammittem et LL C ieil? In Cincinnati, i t can also be said, not one m. d. i n the Medical
School came forrrard to offer help to the faculty group studying the project i n 1971, or simply to examine their results with an independent eye, though one research biologist did consult with our group -- anonymousli.
No doctor in the greater medical community of the town openly expressed ang doubts about what had been done.
This i s that wider compltcity that should alam iit i ~ m tk8a anytbing else, and here in 1994 -- when things are supposed to be 'bettef -- the same situa3on exists. Ak rbclm -#u# /.rand I believe i t i s correct to say that no reporter here i n town has been able to find a single local doctor t o examlne what our faculty group found.
In 1985 an m. d. working here for WIOSH got in touch with me about this project and examined some of the medical hlstories i n my home one night. Since then this individual, David Egllman, has ettempted to draw attention to these trials; he bears out the findin#s of tbe JFA and has publicly explained the state of medical knowledge about whole body mdiation for cancer as i t existed a t the time of the U. C. tests. He finds
Though Or. Bernard Aron has been put forward by the Radical School
In general, I believe we do not expect to have the tndlvidual who i s
Where tn fact does the complicity begin and end? 7hAmuHce#
hl f H f t d -fC '
..

154
5 no reason fo r the doctors t o have believed that radio-resistant tumors such as most of their patients suffered from could have been helped by the 'treatments' administered; the doses given, as deadly as they proved to be for many subjects. m not high enough to reduce tumors or stop the spread of cancer.
9. Why did the tledical School succeed in drawing a curtain over this whole affair in 19727 If the case against the doctors was as clear as i t sounds, why was there not a lawsui t from subjects o r a criminal investigation?
One needs to understand the role of the media i n Cincinnati (and in many other American towns). When the JFA press conference took place, the W , j w t # PBSl sent a reporter and the M w Pant T i m A crew came from CBS. Our report was entered in to the C t q p - e s s j m l M b y Senator Kennedy. But there was no real coverage i n Cincinnati -- no way fo r any of the subjects or the i r families to know what had taken place. No one here broached the words 'radiation death.'
The tledical School was never compelled to acknowledge any wrong-doing, and yet there was a tac i t acknowledgement that such work could ne longer be tolerated, f o r a f ter a l l the project was stopped. No patient was irradiated af ter the f a l l of 1971, even though i n the report that would prove t o be their l as t t o the DOD, the doctors had announced their plans fo r more experiments i n the year t o come.
0. Was there a cancer study being carried out using these patients? There was no publication o r report on cancer study during the
eleven years of the project. No design fo r a cancer study was ever produced during the actual
course of the experiments, although a study on cancer was issued af ter the fact and as a result of public revelations. There i s no reference to an ongoing cancer project i n the DOD reports. There i s no evidence of close follow-up by the team o f the patients who survived more than 60 dags- When the team had completed i t s radiation-injury tests, i t seemed t o have no more interest in the patients or their cancers.
If there was a cancer project, who were the doctors, where i s the design, by whom was i t funded, what were I t s results and how were they being reported?
9. Didn't some people at the university object t o what you and your group were doing, feeling that the act iv i t ies of your medical colleagues were none of your business?

6 A. O f course. But surely events l i ke these are enYp~G's business.
working people; the great major i ty of them we now know were paying taxes; they were helping t o pay the salaries of those of us i n the JFA, and the salaries of the doctors. They were helping to fund this publfc hospital, not t o mentton the U. S. war machine of those days (as they do today). One can say that the i r taxes helped t o pay the salary of Ohio 6overnor John 6illigan. who came, not t o the j r defense, but t o the defense of the Hedical School and assisted i n the cover-up. 6i11igan convinced Senator Kennedy t o drop U. C. from the hearings on human experimentation which followed the U. C. revelations and those about Tuskegee (where beginning in the th i r t ies men in Alabama w i th syphilis were denied treatment fo r the i r whole lifetimes, and many died of syphilis-related disease or became insane).
I grew up among ordinary working people. tly father worked fo r the railroads; my mother had only an eighth grade education. tlany of us i n the JFA were individuals who tended to side w i th common people against leaders and experts who wanted to control everything. I think people l i k e ourselves are s t i l l hoping that we in the U. S. can grow in to a true democracy, that common citizens w i l l take the lead and assume control over their own society.
We are a class-ridden country, and actually it should not surprise us when our class conf l ic t results in grievous actions l i ke those of the U. C. doctors, actions, that is, of one potent and protected class against another that i s powerless. It was a question here of a conf l ic t between wealthy doctors and administrators -- i n a public inst i tut ion insulated against public accountability -- and common working people who could not af ford doctors of the i r own choosing.
0. What changes should come out of these revelations?
A. F i rs t of all, surely i t ought to occur to us that i f we had had national health insurance of a single-payer kind, that is, of the Hedicare type that allows people to choose the i r own doctors, these fel low citizens of ours would not have been trapped in a public hospital with nowhere else t o tun.
children of the wealthy? often the children of doctors, whose incomes, af ter all. are within the top one or two percent of U. S. incomes? There should be a public examination of a l l our admission practises around the country and the way that medical schools are funded and how doctors are trained. .
The people who used General Hospital were mostly Cincinnati
We need t o see who i s going t o medical school. Is i t only the

156
7 We ought to know, f inal ly now, that we mrtst have ordinary citizens
of a l l walks of l i f e wel l represented on medical boards, hospital boards, university boards and so on.
In the same year (1972) that the U. C. radiation project was f i r s t exposed, a group called the People's Health Movement was attempting to change the way the General Hospital Board was formed. It was asking fo r a c i t y amendment that would allow fo r common people to be elected t o the board; many hospital workers were involved i n th is struggle, and a massive pet i t ion drive was launched to place an amendment to th is effect on the ballot, but the c i t y fathers saw to i t that citi+s were never able to vote on th is measure.
We need common citizens on the hospital board today and on the Board of Trustees of the university. A t present the U. C. board i s made up largely of wealthy business-people and attorneys.
We need to struggle in every way we can to a l ter the general class-ism and e l i t ism of our medical system (and indeed of our whole society). I believe we could have good doctors, h t t w d o c t o r s i n fact, without the need to have doctors who are r ich and powerful. Possibly in t ime we w i l l even come to recognize that medicine f o r prof i t i s not such a good idea anyway and that i t doesn't have to be th is way. Perhaps our current health care cr is is and the recognized need fo r universal access to humane medicine w i l l lead to some of the changes we need.
9. Didn't we need, during the Cold War, t o protect ourselves from our enemies abroad, and wasn't that why the U. C. doctors decided t o do what they did?
[d from the fact that the Cold War was -- as I see i t anyway, and *A&&$ a d more Americans are coming to realize -- largely an inaention of those who wanted t o benefit from the arms race, we might ask this: if smriiices were becessssrgL wlQy cevldnnt the investijaton ~ ~ ~ t ~ ~ ~ t ~ ~ t ~ . . . ~ # t ~ ~ ~ ~
MARTHA STEPHENS i s a Professor of English at the University of Cincinnati, teaching modem literature, creative writing, and courses in literature and society. She i s the author of a study of the Georgia wr i t e r Flanney OConnor. two novels set amongst working people i n south Georgia, and many shorter wr i t ings in f ic t ion and on l iterature and the arts, as wel l as reports on social issues fo r newspapers and magazines. She has been involved in peace and justice movements i n this country and in Central America.
. .

157
Mr. BRYANT. The Chair recognizes itself for 5 minutes. Dr. Egilman, in our experience did any of these patients have
Dr. EGILMAN. In some cases, if treated locally, some of them had cancers that were radioresistant to whole body radiation but would have responded to some local radiation, so that not all of the radi- ation they got was inappropriate. Only the whole body radiation they received was inappropriate.
The three Ewing‘s cases got what was thought to be correct care at the time, and there were other studies on that.
The total body radiation applied to the rest of the patients was ina propriate and had been tested before in the 1940s and 1950s
The possibility of usin bone marrow replacement was an inter-
So it is hard to argue that the a proach to cancer therapy using
And in those 13 it was universally a failure. I don’t think you wait until 13, until you have stopped doing the
work. I think one or two or three should be more than enough if it is a cancer treatment examination.
Mr. BRYANT. I guess you are saying the sum total of your lengthy study of this matter and our concern for 20 years about this mat-
is that correct?
cancers that would % enefit from cancer radiation treatment?
v
an cp was known to be inappropriate and not to work.
esting possibility, but, o f the 88 patients, it was only tried on 13.
bone marrow replacements was t K e reason this study was done.
0
ter, the essence of it is t x at there was no informed consent, first;
Dr. EGILMAN. That is correct. Mr. BRYANT. Because of illiteracy? Dr. EGILMAN. No. In part because of their mental status. Not
only were they illiterate, but they also were ill. They could not fol- low simple instructions.
For the military part of the experiment that related to the psy- chological testing, normally the questionnaire was self-adminis- tered. These patients could not fill out the self-administered ques- tionnaire as part of the psychological testing. It had to be adminis- tered by the investigator. So they were not able to follow simple in- structions because of their-for a variet of reasons.
said, that they might d i e t h e r e was some chance they might die within a few weeks.
Dr. EGILMAN. It was recommended at the time that that is what the informed consent form said.
Mr. BRYANT. But it didn’t say that? Dr. EGILMAN. It didn’t say anything about any risk. Mr. BRYANT. You said it was recommended at the time. Who rec-
Mr. BRYANT. Second, they weren’t P ully informed, I think you
e
ommended that? Dr. EGILMAN. That recommendation was by Dr. Shields in 1967. Mr. BRYANT. And who is he? Dr. EGILMAN. He was a University of Cincinnati physician, a re-
Mr. BRYANT. Is there a record- Dr. EGILMAN. He wrote a letter. That is in his letter. Mr. BRYANT. Is there any indication of why they chose not to in-
clude his advice and follow his advice and include that information in the consent form?
viewer of the research.
84-514 0 - 94 - 6

158
Dr. EGILMAN. The research protocol was not finally approved at the University of Cincinnati until 1971, in August. There was a progressional approval given in 1967 but no final protocol was ap- proved until 1971. The research was allowed to continue without approval, as far as I could tell, reading Dr. Suskind’s evaluation.
Mr. BRYANT. This is a little harsh, but it seems to be your con- clusion that they also carried out radiation tests on these individ- uals in order to obtain information for the Defense Department that were not therapeutic, that did not hold a promise of curing these people. Is that accurate?
Dr. EGILMAN. Curing, for sure. They never even thought that a cure was a possibility. At best, it was thought-the best they can argue now was to reduce the size of the tumor and reduce pain. That is a hard argument because, as Dr. Suskind noted, there was never a protocol written to evaluate the effect of the therapy on palliation. There was never a study protocol to look at the effect of this therapy on what they now claim was the purpose.
Mr. BRYANT. When you say palliation, you mean reduction of pain?
Dr. EGILMAN. It means reduction of pain. Or reduction of size of the tumor, et cetera. Or life expectancy. All that was done in retro- spect. This 1973 paper was a retrospective after the study was criticized by Dr. Stevens.
Mr. BRYANT. In the medical community, does the lack of such protocol lead to the absolute conclusion that was not the intent of their work at the time?
Dr. EGILMAN. I don’t know. Only a mind reader could know what was absolutely in their mind. I think that it wouldn’t have been viewed as reasonable research. If there is no way to evaluate the question because there is no protocol for evaluating palliative ef- fects, how can you say it was research to look at the effects of palliation?
That was Dr. Suskind‘s comment. The University’s own analysis of the roject said that there was no protocol that would allow one
when it was criticized, is they went back and quickly tried to put the data together.
Mr. BRYANT. You are asserting-I am not going to ut words in
they did military research on people who didn’t know what was happening to them. That was not done for the benefit of the patient but for the benefit of the Defense Department, is that what you are saying?
Dr. EGILMAN. That is what they say. And I am agreeing with them. That is what they said in their reports to the Defense De- partment, and I agree with them.
Mr. BRYANT. Maybe you better elaborate on that. You say that is what they say.
Dr. EGILMAN. In the reports to the Defense De artment they say
ation on soldiers who might be in a nuclear war. That is what the researchers said. There is no cancer treatment mentioned in the first five or six years of this study at all, anywhere. Nowhere. It is their words, not mine.
<
I
to ev ap uate the effects on palliation. What they tried to do was,
your mouth; I am just trying to boil it down here--t R at basically J
i+
the purpose of the research was to determine t R e effects of radi-

159
Mr. BRYANT. Mr. Mann. Mr. MANN. Thank you, Mr. Chairman. Dr. Egilman, 'ust to clarify, could you lay out exactly where it
Dr. EGILMAN. Sure. I took a few notes. Thank you for that ques- tion.
He said the doses were not meant to be lethal. Well-or not known to be lethal. That is not true. Neither was true. The doses were given up to 300 rads. It was known after Hiroshima-from Hiroshima that the lethal dose that would kill 50 percent of the population was 300 rads.
Not only that, the researchers themselves used this information, combined with the research information at Oak Ridge where they were irradiating radiosensitive tumors, to ublish a little abstract
used their information to revise the estimate of how much it too to kill someone. So for sure they knew that the dose was sufficient to kill some of the people.
They themselves found that eight of the people died as a result of the radiation. I t is written as a cause of death at least in one of the medical charts that I have reviewed. I haven't reviewed them all.
So certainly the researchers at the time knew that the doses could be lethal to some of the individuals.
Mr. MANN. I am trying to focus-excuse m-n exactly where it is that you and Dr. Cox, who had no part in the project, disagree.
Dr. EGILMAN. He said that the doses were not known to be le- thal.
Mr. 1MANN. So, No. 1, he said the doses are not, and you say they are.
Dr. EGILMAN. I say they are, and they were known to the re- searchers to be so. And I explained why he said it was reasonable to test the hypothesis that with whole body radiation what would not work.
I disagree. I t had previously been shown in the 1940s and 1950s not to work. Shields Warren wrote an article in Scientific Amer- ican, in case you weren't reading the general medical literature in 1959, that specifically said whole body radiation should not be used for gastrointestinal tumors and other radioresistant tumors. He didnt even have to read the medical literature. You could get Sci- entific American at good magazine stores. Clearly, it was known to be ineffective by the time this research started and not to be indi- cated.
And there are reasons for that. This radioresistant tumor takes a high dose to kill it. And if it is spread throughout the body, the high dose that will kill the tumor will kill the patient for sure. The dose that is are given here, 300 rads is a low number. If you have a cervical cancer or a breast cancer, you are going to get 5,000 rads. That is what it takes to kill a radioresistant tumor.
You couldn't give 5,000 rads to a person. You couldn't even give 600 rads. Six hundred rads would kill everybody. So the thing is the radiosensitive tissue, the bone marrow, is af-
fected by a much lower dose. You kill the radiosensitive tumor; you kill the patient. You can't get to a dose high enough to kill the
is that you and 13 r. Cox disagree?
z to help people understand how much it too K to kill people. So the

160
radioresistant tumor that is spread throughout the body. That was known and commented on and said in 1942.
Mr. m. That is the second difference. What else? Dr. EGILMAN. Well, the informed consent, I think I explained
that one. And then the issue about the fact that it is used now. Now, that
is a use of 1990s standards looking at the 1960. It is used now be- cause we have perfected bone marrow transplants. It is a misrepre- sentation to say because whole body radiation is used now it was OK to use it then. We use it now because we know how to deal with the bone marrow suppression. We didn’t then.
Mr. MANN. How did we learn? Dr. EGILMAN. We didn’t learn from this study. We learned from
other studies. Mr. MANN. How do you go about moving from where you are to
where you are today? You said something had been perfected. What is that? Not the result of experiments?
Dr. EGILMAN. It was, but it was well-controlled studies that were looking at that for a particular reason. And when you do those studies you inform people, OK?
I am not critical of doing research. I am critical of doing research that doesn’t inform people of potential risks of the facts at the time that were known.
It is true. What you said is true. Science must do research. Some of the research may be lethal to some of the peo le. And that was
know. Mr. MANN. Anything else, in terms of differences between you
and Dr. Cox? Dr. EGILMAN. Well, I guess the only one would have been some-
thing he didn’t say but something that came out. I think it would have been important to announce that the institution from whence he came did similar work funded by the same agency. That I think to me is a relevant piece of information in evaluating the com-
*
true then and that is true now. But when you B o it you let them
, ments.
Mr. MANN. University of Texas? Dr. EGILMAN. M.D. h d e r s o n is one of the institutions that got I
funding from the same agency to do the same work. I think that is important. I
Mr. W. Anything else? Dr. EGILMAN. That is all I can think of right now. Mr. MANN. Let me ask you to help me. I am, obviously, not a
radiotherapist who, obviously, is trained in the field. As I under- stood your earlier testimony, you are an internist. You are a part- time faculty member at Brown, teaching medical ethics. Why should I believe you and not him or vice versa?
Dr. EGILMAN. I think you need to read the documents. I think they speak for themselves. I read you from some of the patient records. The physicians at the time thought that in the case of Mr. Larkins that he should receive chemotherapy. They wrote that down. Those are their words, not mine. According to them radio- therapy was definitely out of the picture.
I
physician. I practiced law for 25 years. We have got a 1

16 1
I don’t think you need to be a physician to evaluate that. I don’t think you need to be a physician to evaluate someone vomiting 3 days and not getting treatment. I think you can read the records in most of these cases.
Read the Suskind report. Ignore his conclusions. Read him for the facts. Suskind’s analysis of the facts are quite similar to mine.
Mr. MAIVN. His conclusion is quite different. Dr. EGILMAN. His conclusions are quite different, but the facts
are the same.
I trust the public to make up their own mind about the conclusions. Mr. MANN. I have and will, I am sure, continue to spend a lot
of time trying to understand the facts. Your testimony is helpful. But it certainly is-I am unable at this oint to reach a conclusion with quite the certainty that you can. ?!his is part of the purpose of today and whatever happens after today.
You talked about palliation, if that is the right pronunciation. The Suskind ad hoc committee report criticizes the protocol but doesn’t disagree with the conclusions.
Do you disagree with the conclusions of the final report that in some ercentage of the patients the result of whole body radiation
tients pain was lessened in some percentage t e patients? The length of life after their whole body radiation was longer than what would have been projected for the alternative chemotherapy that mi h t have been used? Or even what could have been projected h a i no whole body radiation or chemotherapy been applied?
Dr. EGILMAN. Well, here I am an expert, being an epidemiologist in addition to an internist.
In terms of the evaluation of the outcomes, Dr. Suskind says the data was insufficient to compare the outcomes of these patients to any other similar patients.
But, of course, the historian part would refer you to the com- ments of, I think, Dr. GafTney, who said that you couldn’t evaluate the data and you couldn’t ho e to evaluate the data because there
cancers. And there weren’t enough cancers to come up w i x any conclusions about what went on in terms of impacting on treat- ment.
In order to answer the beginning part about whether you could retros ectively analyze this data for palliation, I don’t know until I go t R rough all the records. As you know, I only got the records on Friday, and I haven’t had time to-I have gotten time to get a few things out of them, but I haven’t had time to do a statistical analysis of those uestions.
the question because you need to compare. How can you know if these people benefitted when there was no comparison group and there was no systematic way of recording the data? You just have to go throughout charts and see what you can get.
I would need maybe-if the university wants to provide me with redacted records on 300 similar patients and we can see what was reported on those patients, we could compare how much pain those patients who had normal treatment versus the ones who had mili-
w So if you believe that there is no disagreement about the facts,
e
R was t K e tumor size was reduced? That in some ercentage of pa-
were no controls given and t R e cancers were all different t es of
r
But I don’t thin R there is going to be any ability to really answer

162
tary research performed on them did in terms of palliation. I think that is the only way to look at that question.
Mr. MANN. As you know, the Suskind report says no plan for sys- tematic study of palliative effects was made in a retrospective re- view of the charts, following the data where elicited. So it looks like the Suskind group at least did that. Thirty percent had a decrease in tumor size of 50 percent or greater. That is objective, I guess.
Dr. EGILMAN. I haven’t seen-in the records I have seen, I don’t see that information. So I don’t know where it comes from.
Mr. W. You have been working on this, Dr. Egilman. How long have you had an interest in this project and how did you first learn about the issues that we are discussing today?
Dr. EGILMAN. I first learned about it when I was here in 1984 from Dr. Stevens.
Mr. m. I have other questions, but I will yield until the sec- ond round.
Mr. BRYANT. Mr. Portman. Mr. PORTMAN. Thank you, Mr. Chairman. Thank you for being here, Dr. Egilman. You state very clearly in your testimony that cancer therapy was
not the purpose of the research project. In fact, you went so far in your response to Mr. Bryant as to say there is no cancer research mentioned anywhere.
I am looking at the 1958 response back from the Department of Defense regarding the proposal, which was really the approval of the project, and I quote, “Any correlation of tumor response to total dose of irradiation by such means as proposed in this project would be of great value in the field of cancer.”
And it goes on to say, “In addition, if by such means the dose could be determined it would be of inestimable value in the case of atomic or nuclear warfare.”
Have you seen this? Dr. EGILMAN. I haven’t, but that doesn’t contradict what I have
said. That is a reviewer’s comment, isn’t it? Mr. PORTMAN. It is a comment from the DOD reviewing the re-
search contract. I
Dr. EGILMAN. Right. I t is not from the contract. It is not part of the proposal.
I could read the proposal and say, gee, if I didn’t know anything about the previous research that had been done that showed this wasn’t true, that it didn’t work, and I looked at this, just relying on what the researchers said, I might think that, too. There is no evidence that that reviewer knew about the other articles that I talked about from 20 years before.
Just because4 mean, could you look at the research now and say, gee, maybe it was helpful, maybe it could have been helpful, as Dr. Cox did? Of course. I have reviewed the previous research, and I know that if you had done that at the time you would have seen that this was not an effort in cancer treatment because it had already been tried and failed.
Mr. PORTMAN. This was in 1958. This wasn’t looking retrospec- tively. I think it is inaccurate to say there is no mention anywhere in the record. This is something I just found looking in the record here.
I
I
j 1
163
The issue of informed consent is, of course, one of the ones that we are very interested in, and it is something that you addressed very articulately in your testimony, your written testimony. You have not had the o portunity to address what you view as the ac- tual standards in p ace at eat length, but you mentioned various
stand, from 1967 from a physician at the General Hospital. What in your view were the standards that were in place, taking
into account the Hippocratic Oath, taking into account all the var- ious standards that were out there, for that critical time period, particularly in the early 1960s?
Dr. EGILMAN. The standards would have been to verbally inform them of the risks, at least, and to record for medicalllegal reasons, if no other, that the person had been informed of those risks. And certainly by 1965 there was a university committee established that required formal signed informed consent forms. So that by then we know that the atient would have signed a consent form,
said that the risks should be explicit. All I can-I mean, I am not trying to put a 1990’s face on this.
I am telling you that Dr. Gaffney and others at the time said that the informed consent was inadequate and made specific rec- ommendations about how it would be changed. I think the rec- ommendations that they made at the time were the standard of the time and were adequate for the time and, in fact, would be ade- quate for now.
Mr. PORTMAN. Written consent, as you note, I think, in your tes- timony, was used then. In fact, some have said that it antedated or predated that requirement or that recommendation to the uni- versity by 2 years. But in your res onse a ain, to Chairman Bry-
And we just talked about informed consent. We talked about how verbal consent in that period, particularly in the early 1960s, might have been appropriate. Dr. Cox, in fact, testified that there was, in his view, a requirement I think for verbal consent, not written, in 1960, at least.
I just wonder, do you know whether there was verbal consent or not during that eriod? You have said that people were not in-
interviewed people to know whether there was, in fact, verbal con- sent during that period?
Dr. EGILMAN. Well, the researchers in the Suskind reporGSus- kind comments on that. And let me just see what he says about that. “Patients and families were not informed about the possibility of transient nausea and vomiting since such symptoms may be in- duced by suggestion. Typically, such side effects can occur a few da s after treatment.”
h a t is a quote from the paper that I just said. So the research- ers themselves said the atients weren’t told of that. That was art
study. Mr. PORTMAN. Part of your concern is about the demographics of
the patient group, which is a concern of mine as well. We have heard from others that the study reflected the general patient pop-
indicia of what that p r might ave been, including a letter, as I under-
T
0
and I think that I wou f d agree with the people at the time who
ant you had said that none were in P ormed , P o possible risks.
formed of the ris K s. Have you interviewed the doctors? Have you r
.
of their study. It would R ave messed up the military aspects o P the

164
ulation at the General Hospital. Would that change your view as to the study grou
Dr. EGILMAN. I$? 0. This was a national problem. The DOD sought people here and at Charity and Tulane. NASA sought people at Oak Ridge. As far as I can tell, Afro-Americans were their first choice. When
they couldn’t find them, they accepted poor whites. I believe that that was a national policy, not a local policy, and that the site se- lections were not random by any means.
I think they picked people who they thought were powerless, and that is why they picked eo le who had low educational level and
African-Americans. They didn’t want to be questioned by the pa- tients.
If it was cancer therapy, if people really thought that this was a way to cure cancer, there are lots of hospitals in this town that take care of affluent white people. Those hospitals could have been selected.
Mr. PORTMAN. Just to be specific here, you said in a couple of in- stances that DOD selected the patients. That is not my under- standing and that certainly isn’t what we are hearing from DOD in 1994.
Dr. EGILMAN. They selected institutions. Institutions. I mean, look, you can say, oh, that is what happened to be at the institu- tion, which is apparently what you are saying. What I am telling you is it was no secret who was at the institution. It wasn’t some random selection of institutions around the country that happened to serve predominantly poor peo le and African-Americans. Those
Mr. PORTMAN. Having been associated with U.C. Hospital in 1984, as you said, are there other research institutions, to your knowledge, at that time, in 1960, that would have been appropriate for this kind of research?
Dr. EGILMAN. I don’t think the research was appropriate. You mean in 1984? What is the tim+
Mr. PORTMAN. I am saying you have some knowledge of the Uni- versity Hospital and General Hospital. You indicate that DOD se- lected the hospital. -
It is my understanding that it was an unsolicited proposal, one; and, two, that at that time, in 1960-and I would certainly think that continues today-that the then General Hospital, University Hospital, was the preeminent research facility in Cincinnati. Is that your understanding or not?
Dr. EGILMAN. That is my understanding. But in the paper yesterday I saw some advertisements for people.
If you had sinus infections, there is a research protocol. And you can go to two or three different places and get in a research proto- col for sinus infections.
So if you have a real research project and you want to do a lot of patients-after all, this was 88 patients over 12 years, not real fast. You need a lot more patients than that to do a research project. You could always advertise. And if you can’t advertise, if the DOD won’t fund your small ad in the Inquirer, you could al- ways call your colleagues up at the other institutions.
who had low IQs. And I t R E in that was also the reason for selecting
are the places they picked to do t R e work, for the most part.

165
Certainly Children’s was able to appropriately send patients from Children’s to the University of Cincinnati.
These patients, as I saw from the records, took a bus. Presum- ab1 the bus went from affluent areas of town to the university.
idn’t just go from the university to the oor areas of town. So if it was good cancer research, unfortunatey, the white, af’fluent people in town were deprived of the ability to participate in it.
Mr. PORTMAN. Thank you. I have no further questions. Mr. BRYANT. Dr. Egilman, I am curious to know your view of the
Federal Government’s role in this. As I understand it, the Univer- sity of Cincinnati solicited the support of the Defense Department in funding this study.
Dr. EGILMAN. Ri ht. Mr. BRYANT. Is t at correct? Dr. EGILMAN. That is what I understand. Mr. BRYANT. And the Defense Department contributed to it, as-
suming I am sure-and correct me if this assumption is wrong- that they would not be the only source of funding.
Dr. EGILMAN. That part I don’t know. I think they were not the only source. I think that the University used this other general re- search find-
By the way, that is another area of disagreement. I don’t think NIH ever approved this consent form. There was general research, as I understand, at the University, and some of those funded the treatment.
Now, some of those funds-and also it is here from some of the charts-medicare funding was used. Now, it is my understanding- 1 don’t know if this was true at the time. Medicare doesn’t fund clinical research, only treatment. So that one of the Federal questions I think that is involved here
is were medicare and medicare funds diverted to clinical research. That is a Federal question.
Mr. BRYANT. In view of all of that, doesn’t that auger a little bit against the assertion that this is ex licitly military research being
cinnati solicited help in funding this from the Department of De- fense but, as you just stated, had other sources involved in funding the research as well.
Dr. EGILMAN. The research would not have gone on like this had the military not wanted it to go on. The fact that civilian money were used doesn’t miti ate the fact that it appears completely to
purposes and not medical purposes. The fact that they diverted money from general research monies or from medicare or medicaid funding doesn’t seem to mitigate the purpose of the research or change the purpose of the research.
It might have been funded by some private foundation and still had a military purpose. The purpose doesn’t depend on the funding. I don”t criticize it because the Defense Department funded it.
Mr. BRYANT. Do you think that this totally lacked‘ therapeutic purpose?
Dr. EGILMAN. Oh, yes. Mr. BRYANT. You don’t think there was ever any intent to de-
vel0 a way to solve cancer problems through whole body irradia-
P It C F
I
e a
done on people? I mean, it was-a P ter all, the University of Cin-
. have been done for miitary f
tion. B

166
Dr. EGILMAN. Not at this time, not with this therapeutic modal- ity, not when there were only 13 of the 75 who received bone mar- row transplants.
What about the other 75? It was known not to work on them. Mr. BRYANT. That is a pretty strong position you take. You are
basically saying Dr. Saenger and those others that attempted in subsequent years to characterize this as a way to try to find a way to cure or make more comfortable cancer patients were not telling the truth and what they were really trying to do was get informa- tion for the armed services.
Dr. EGILMAN. Well, look, no cancer therapy study was published until it was criticized. No cancer therapy protocol was written until 1966, and that was limited to the bone marrow radiation combina- tion.
So, I mean, as they say, the facts speak for themselves. No re- search started until the Defense Department agreed to fund it, and it was stopped when the Defense Department withdrew funding.
I don't think those are all coincidences. Perhaps I am a cynic, but I think there is a relationship there.
Mr. BRYANT. Very well. Mr. Mann. Mr. MANN. Dr. Stevens, you indicated you had a couple of rec-
ommendations that you were interested in making. I would be pleased to hear that.
Dr. STEPHENS. All right. If I might just make a few other com- ments first.
Mr. MANN. Sure. Dr. STEPHENS. I would just like to clear this up.
r The doctors did not give 300 rads of total body radiation, as I am sure they will remind us. Three hundred referred to partial body radiation. And there was only one person who received 250 rads of total body radiation. The high dosages were 150 and 200 rads.
With regard to the cancer study, if I might just read part of the statement I gave you:
Was a cancer study being carried out? "here was no publication or report on cancer study during the 11 years of the
study. No design for cancer study was ever produced during the actual c o w of the experiments, although a study on cancer was issued after the fact and as a result of public revelations. There is no reference to an ongoing cancer project in the DOD reports. "here is no evidence of close follow-up by the team of the patients who sur- vived more than 60 days-and often less than that.
When the team had completed its radiation injury test it seemed to have no more interest in the patients or their cancers. If there was a cancer project, who were the doctors? Where is the design? By whom was it funded? What were its results and how were they being reported?
I know it has been said that we were in the cold war and maybe we needed to do this kind of research to protect ourselves against enemies abroad. But I say even if that was t r u e a n d sometimes I think the cold war was an invention of people who wanted to ben- efit from the arms race anyway-but if that was true, then maybe these doctors should have experimented on other doctors or on themselves, which is not unprecedented, actually, in the history of human experimentation.
But-I am sorry. You asked me--
1 -i; I

L
167
Mr. MAN-N. You indicated, Dr. Stevens, you had a couple of rec- ommendations for us.
Dr. STEPHENS. Yes, I did. I think if we regard these experiments just as an anomaly of the cold war we may be missing the point. I think there was abuse of patients in those days, and there is abuse today.
Let’s consider it this way. If people had had in those days na- tional health insurance, and especially of the medicare or single-
ayer kind where you can choose your doctors, they would not have Eeen trapped in a chant hospital, or even, let’s say, in a cheap
That is-I want to look at what we are oing today and see what this project of the sixties helps us to understand about today.
I would appeal to you, the three of you, to consider, this matter closely, to search our hearts and minds to see if you can support
doing. I am not quite sure whether any of you are alread sup ort- ing a single-payer system. It would have solved the proilem tack then. This would not have happened.
Mr. BRYANT. Will the gentleman yield? I guess I don’t understand-and I definitely do not want to get
into a discussion about national health insurance here. I have had two weeks of that at home, and I would like to talk today about this matter.
But I don’t understand what the point you are making is. We are talking here about experimentation which was defended by the University as having been for therapeutic purposes. Many of the facts seem to indicate otherwise, as has been laid out by Dr. Egilman.
Dr. STEPHENS. With health insurance, people would not have had to go to that public hospital. These people had no choice. They had no national health insurance such as nearly all developed countries did have at that time and do have today.
Mr. BRYANT. You are saying that-I guess you are ignoring or findin less than-I guess you are assuming that the statements
undergo very risky treatment was not credible. Dr. STEPHENS. No, I don’t see any contradiction there. I am just
saying that they would have been able to go to their own doctors. They wouldn’t have been the victims of this kind o medi- cal violence by researchers. That is a recommendation I have.
Mr. MANN. Did you have a second one, Dr. Stephens? Dr. STEPHENS. Yes, I do. I think neither one of these may be ter-
ribly popular, but I hope some people at least will think about them. I think that we need to have common citizens, users of insti- tutions, on all our bodies on hospital boards, on review boards, on university boards, where now we have almost entirely wealthy businessmen and attorneys.
After all, the university board could have played a part in stop- ping these tests much sooner than they did, and in recent months they could have res onded to the desperate pleas of families to
on them and when they had no choice. They allowed over 600 peo-
d HMO, which may also to 2 ay not be giving ood care.
a people’s nationa P health insurance as many of your colleagues are
that t E ese people had a hopeless circumstance and were willing to
private
know what hap ene B to them several months before they did re- spond. They o n y P responded because of enormous public pressure

168
ple to wonder for many weeks whether their families had been irra- diated or not.
So I think if we had had users, common citizens, nonspecialists, on these boards, on the board of the hospital, for instance, things might have been different. And I just appeal to you that whatever legislation regarding medical matters comes before you, surely this is something to consider. I think we must learn these kinds of things, from what happened in that public hospital.
Mr. MANN. Thank you. I have one more question of Dr. Egilman. You refer to this 1950
letter from Dr. Hamilton. Could you share a copy of that with us? And who was he?
Dr. EGILMAN. He was a physician in California. He wrote the let- ter to Shields Warren, who-was the head of the Atomic Energy Commission. And he was discussing the research needs similar to the ones that were conducted here.
Mr. MANN. Was he a researcher? Dr. EGILMAN. He was a hysician researcher. He is the gen-
Mr. MANN. Hamilton did? Dr. EGILMAN. Hamilton, before he wrote that letter. He wasn’t
concerned about the ethics. He was concerned that it might become public and that the public would be concerned about the ethics.
Mr. MANN. Thank you, Mr. Chairman. Mr. BRYANT. Mr. Portman. Mr. PORTMAN. Thank you, Mr. Chairman. Dr. Stephens, thank you for being here today. Just a couple of
quick questions. No. 1, you had said in response to Mr. Bryant, my view is that
many of the patients were not terminally ill. Dr. STEPHENS. Right. Mr. PORTMAN. If you could just tell us a little further what you
base that on, number one, and then tell us whether you have any medical training, whether you have had any experience in that field. I am not sure what your field is. I believe you are a professor at the University in English.
Dr. STEPHENS. Right. Mr. PORTMAN. If you could just expand on that in terms of the
question as to whether the patients were terminally ill or not. Dr. STEPHENS. Well, I didn”t bring the file of patient histories
that I have with me. I can’t skim through them and see just how many might be considered to be in that category. But I do remem- ber very clearly that two people stand out that would not have seemed, I think, to most people to be terminal.
The woman I mentioned, was irradiated in the first group of pa- tients and lived 5 years after receiving the high dose of radiation, at least 5 years. We don’t have her date of death. It is hard to con- sider that she was terminal.
And then I remember another woman shortly after that irradia- tion who lived over 3 years. And there were a ood many who lived
ple. You either begin to get better or die, generally, within about 40 days.
tleman who started injecting R ealthy patients with plutonium.
a couple of years. Again, these are eople w a o might have died. Some of those people received the hig K doses that were killing peo-

169
I am sorry I don’t have figures on how many people this might be. Of course, in some cases it is hard to tell.
We have discovered already, by the way, that there are problems and errors in the patient histories that I originally examined 22 years ago when I wrote the JFA report. When I examine the ori - medical records, there are discrepancies.
Mr. PORW. Getting back to my favorite issue of informed con- sent, just to further flesh out, again, your comments to Mr. Bryant in that re ard, you had said that there is absolutely no evidence
Dr. STEPHENS. Of the first 5 years. Mr. PORTMAN. Of the first 5 ears. Some patients, of course, in
Dr. STEPHENS. I am sorry. I am not aware of that. Mr. PORTMAN. The records that we have indicate that some a-
Dr. STEPHENS. Well, I am sorry. I didn’t remember that. Mr. PORTMAN. I ’ust wonder if there was no information given
Dr. STEPHENS. Where do you find that? Is that in one of the so- called DOD reports?
Mr. PORTMAN. It is in several documents that I have seen, Dr. Saenger‘s report.
Dr. STEPHENS. Oh, Dr. Saenger‘s. OK. Well- Mr. PORTMAN. We will find that out and let you know. I think
I saw it in the ad hoc re ort, but I am not sure.
Mr. PORTMAN. It is an interesting issue in terms of the consent. There was no written consent, as you say, during that time period.
Dr. STEPHENS. Yes, no evidence of any kind of consent. Let’s don’t forget that in their own reports the doctors say the patients were told “they were being treated for their disease.” That is a di- rect quote. I have included this in my original analysis. There are several such direct quotes, more than several, in those first five years of reports to the DOD. A number of times we read the pa- tient is being told he is being treated for his disease.
nal summaries and we compare them to what we now have in t f? e
of informe % consent. Some patient-
those 5 years said no. Why did x ey say no?
tients were asked to participate, and they said that they di c r n’t
as to the risks and is enefits, how that decision would have been-
want to.
Dr. STEPHENS. I woul C Y like to see it.
Mr. PORTMAN. Thank ou, Professor Stephens.
Mr. BRYANT. I have no further questions. Would you like to add anything? We would be happy to hear it. Dr. EGILMAN. Just with respect to the last question. Dr. Suskind noted that the researchers excluded terminal pa-
tients from the study. “Some of the reasons for patient rejection in- cluded advanced stage of malignancies leading to disorientation, stupor and/or coma and terminal advanced malignant disease in which the life expectancy was only a few weeks.”
Mr. BRYANT. Leading to a conclusion tha- Dr. EGILMAN. Well, we know the therapy didn’t help them, so
there is only two conclusions. Some of the people lived a consider- able amount of time. We know the therapy didn’t help them. There is only one conclusion left then, that they weren’t terminal when they were irradiated. That is the only conclusion.
No further questions, L r. Chairman.

170
Otherwise, there are two possibilities. One is they were terminal, and the therapy helped them. If that is true, then we have spent 20 years-we were wrong. They were right. But we have denied people this great therapy for 22 years. I don’t think that is what we have been doing.
Clearly, the patients were not terminal. The therapy didn’t help them. And that is from the life expectancy on the charts.
Mr. MANN. Dr. Egilman, you started that comment quoting some- thing from Dr. Suskind‘s report. Where is that?
Dr. EGILMAN. Page 27. Mr. MANN. Yes, sir. Dr. EG~LMAN. Wait a minute. Mr. MANN. You were making the point that patients who were
so advanced that their life expectancy was only a few weeks were excluded from the study.
Dr. EGILMAN. That is what Suskind said. Mr. MANN. But you are not disagreeing-at least the information
that we have--or are you disagreeing-all the information we have indicates you weren’t even qualified to be a part of the study unless your cancer was advanced and you were terminal and alternative therapies were not thought to be beneficial.
Dr. EGILMAN. Well, you have to be a little careful here. We are all terminal, Congressman Mann. We will all die.
Terminal from a medical sense means, as they defined it, within several weeks or certainly within six months. And many of the pa- tients, perhaps most of the patients, would not have been consid- ered to be terminal within weeks or months, and so, therefore, would not be defined as medically terminal. They were terminal the way we are all terminal. We all die. It is a question of how soon.
Mr. MANN. Are you suggesting that having cancer was not a pre- requisite for being in the study?
Dr. EGILMAN. No. They all had cancer. And they all had cancer that was likely to result in their death. It is a question of how long. People can live with cancer for months, years.
Mr. MANN. It was more subtle than that. It was cancer that had spread in the body, as I understand it. And it was cancer that, at least if you accept the premise of the research, was not going to urrlicxiivlriicrlapy waa i i v b g v i i i ~ LO uv aiiyuiiii6 C A W Z ~ L pciuapu ai - .I
rest the speed of the cancer, the speed of death. And they argue-and this is part of what we are trying to find
colon cancers. And they themselves wrote that that is the preferred treatment in 1971. That is their opinion. That has got to be the
I
. , * 3 1 , . 8 . current stanaara at tne time. The second question is how reasonable is it to think that whole
body radiation might have helped the others. For that I refer you

17 1
to what I already read about the previous studies that had looked at this and those patients that had shown it wasn’t effective.
In addition, you have heard that radiosensitive tissues, bone marrow, get destroyed with 100 to 300 rads, certainly 400 or 500 rads. You have also heard that radioresistant tumors like GI can- cer and breast, the ones that were treated here, take thousands of rads to kill the tissue, to kill the cancer.
So it was not medically reasonable, it was not scientifically rea- sonable to think that giving someone 300 rads half body or 150 rads whole body would in any way touch the radioresistant malig- nant spread of cancer without wiping out their bone marrow first.
The dose differences between radioresistant and radiosensitive are quite high, thousands versus hundreds. So there wasn’t a medi- cal rationale and scientific rationale, and that fact was noted in 1942.
I am not telling you something that I figured out last week. I am telling you something that was published. This scientific rationale, this medical thinking, was published by Craver in 1943.
Dr. STEPHENS. May I reply again to your question about my own specialty not being medicine?
Mr. PORTMAN. Sure. Dr. STEPHENS. May I do so? Mr. PORTMAN. Yes, ma’am. Dr. STEPHENS. It relates to my recommendation that we have
common citizens on all boards that decide how hospitals and uni- versities and medical services shall be organized. If we can’t do that, we are not a democracy, in my opinion.
I am an English professor, all right. Medicine is not a magic science. I t is not a body of knowledge different from all other bodies of knowledge that only certified people can understand.
Mr. PORTMAN. I appreciate that response. I asked that question, in the context of your statement as to the patients being terminally ill or not, which is in my mind a medical issue and a diagnostic issue.
We asked about-where it said the patients had not agreed, on page 26 of the ad hoc report, you see something about two patients did not agree to be treated. That is what I was referring to.
Dr. STEPHENS. May I say that I am extremely happy that I have been able to work lately with Dr. Egilman, because, of course, I am not a physician. There is a great deal I don’t know about cancer.
Mr. PORTMAN. Thank you very much. Mr. BRYANT. Thank you very much for your testimony. Thank you, Dr. Egilman, for traveling here today. At this time we will ask our fourth panelist to come forward,
which consists of Dr. Eugene Saenger, Professor Emeritus of Radi- ology, University of Cincinnati.
Dr. Saenger, thank you very much for being here today. At this time, we would ask you to proceed.
STATEMENT OF EUGENE SAENGER, M.D., PROFESSOR EMERITUS OF RADIOLOGY, UNIVERSITY OF CINCINNATI
Dr. SAENGER. Thank you, Mr. Chairman.

172
There is a great deal to respond to in this hearing, and I will begin by stressing the important points that we wish to bring out concerning our work.
One purpose of the study was the treatment of patients with far advanced cancer to whom the goal was the relief of pain, shrinkage of cancer and improvement in well-being.
A second purpose was to study the systematic effects of radiation on the patient, the systemic effects.
The third and most important, treatment was given only if bene- fit to the patient was anticipated.
Patients were chiefly from the General Hospital. Selection was based only on the presence of advanced cancer and where no other therapy was considered to be as or more effective than the avail- able chemotherapy.
Race, IQ or socioeconomic standing were not selection factors. Treatment was paid for by the Cincinnati General Hospital and the National Institutes of Health. No Department of Defense funds were used for treatment or patient care or decisions regarding ther- apy or patient reimbursement. Patients were told that the treat- ment might help them and were cautioned that it might not. Some patients chose not to be treated.
There was nothing secret about our work. There was nothing se- cret as to its being conducted. There was nothing secret about the findings obtained.
The primary goal of the study was to improve the treatment and general clinical management by increasing, if possible, survival of patients with advanced cancer and palliation of symptoms.
In addition, observations in laboratory tests were carried out to seek effects of radiation on cancer patients and on the changes that could be ascribed to radiation.
The background for this project originated in my observations over the previous 20 years that cancer patients treated with radi- ation might be benefited by more careful evaluation of the effects of this kind of treatment. The scientific indications that these goals might be achievable were based on two levels of evidence, one from animal studies and one from human studies.
Animal studies indicated better tumor regression by localized ra- diation followed by total body irradiation for lymphoma and car- cinoma in mice. Human studies for treatment of advanced cancer, for far advanced solid tumors prior to 1960 suggested the value of total body radiation.
I t was employed in several American medical centers and inter- nationally. Treatment was given with success in relieving pain, shrinking tumors and, in some cases, prolonging survival.
A major reason that we could begin this work resulted from sev- eral developments. First, the cobalt 60 teletherapy unit was in- stalled in General Hospital in 1958, the first in the State of Ohio.
Harold Perry, M.D., our first full-time radiation therapist, came from Memorial Sloan-Kettering Cancer Institute in New York and was familiar with total and partial body radiation techniques. James G. Kereiakes, Ph.D., a physicist, joined the department in 1959. He performed the calculations regarding the administration of the doses prescribed by the treating physician.

173
I believe that there could be implications of this treatment for in- dividuals exposed to radiation under other circumstances.
In 1958, I submitted an unsolicited application to DOD because there had been no studies on the metabolic effects of radiation, and funds were available. The Army recognized the importance of can- cer therapy in this regard.
This pro osal was reviewed by J. A. Isherwood, M.D., for the
quote, Army Me B ical Research and Development' Command. And, to
Any correlation of tumor response to total dose of irradiation by such means as proposed in this roject would be of great value in the field of cancer.
In addition, if%y some means such as those proposed accurate knowledge of the total dose of radiation received could be determined, it would be of inestimable value in case of atomic disaster or nuclear warfare.
Patients were not recruited. Patients were referred for this form of therapy mostly from the tumor clinic, outpatient or inpatient. I was not involved in patient selection or in determination of the ex- tent of dose or the regions involved. These decisions were made solely by the attending physicians, internists and surgeons and by radiotherapists.
There were 24 patients entered into the study who were not given total or partial body irradiation. Some were rejected because it was thought the patient would not benefit. Several patients and their families declined treatment. Some were treated by other means.
In 1962, we developed for the DOD a document concerning the eligibility of patients for therapy-in 1962. And it stated,
There is a reasonable chance of therapeutic benefit to the patient. The likelihood of damage to the patient is not greater than that encountered from comparable ther- apy of another type. The facilities for support of the patient and complication of treatment offer all possible medical services for successful maintenance of the pa- tient's well-being.
Race was not a factor in selection, on1 the type of cancer and
minated confirmed that the patients in this study did not differ from the patient population of the Cincinnati General Hospital.
Again, I& was not a factor in patient selection. The subject of informed consent-I believe we sort of fell in a pe-
riod when there was a change in the general understanding of in- formed consent. In our study, informed consent for therapy was ob- tained by the attendin physicians. In the 1940s and 19509, in-
formed consent required by the hos ital from all patients who were hospitalized for whatever services t ey re uired.
sible outcomes were discussed with the patient and often included family members.
In April, 1965, this project began the use of written informed consent 2 years before it was required in our medical center. I t clearly indicated that the risks of treatment were discussed.
One criticism of our work stems from the instructions of the at- tend personnel not to inquire concerning nausea, vomiting and di- arrhea in the first few days after treatment. Since both nausea and vomiting could be induced by suggestive questions, we requested
extent. A statistical analysis done only a x er the program was ter-
formed consent was ver % al, except for the general brief signed in-
In this project, the purpose and { B q actu treatment and the pos-

174
that no questions be asked as to how the patient felt within these first few days. This restriction did not in an way restrict the administration of
after treatment, 44 percent of the patients who were treated had no nausea and vomiting, 27 percent noted it for three hours or less, and 14 percent had symptoms for 6 hours or less. These responses are comparable to chemotherapy at the time.
Funding. As noted earlier, most costs of treatment were paid by the Cincinnati General Hospital. This amounts to about $483,000. There were no professional costs or physicians fees for patient care. Some funding was obtained from the NIH through the General Clinical Research Center of our hospital, which was a unit funded by the NIH.
The records of each patient in the hospital on that service were submitted to the NIH and approved. In addition, several of the postgraduate fellows in another NIH training grant of our depart- ment participated in this study. - had no relation to choice of dose, choice of patient or patient care in any way. No patient was compensated or reimbursed or paid for treatment.
The total DOD contract was about $671,000. Mortalities. In the group of patients who received radiation there
were three categories in which there were enough atients to com-
comparable groups described in the refereed medical literature. The cancers were those of the breast, lung, and colon. The death rates were comparable to those treated by other means. This can be seen clearly in our 1973 paper and the graphs that are there.
A n important question is whether radiation was the factor lead- ing to the early death of a patient. These patients had far advanced cancers which were owing exponentially. In the course of disease,
both before and immediately after total or artial body irradiation.
treatment or the ra id growth of cancer as being the sin le contrib-
cancer itself, There were 20 cases in which patients survived longer than 1
year. Except for the one patient with Ewing's sarcoma who remains alive after 25 years, the lon est survivor lived 9 years. Two other
Palliation was successful with relief of pain in 31 percent of pa- tients. There was decrease in tumor size in 31 percent and an in- crease in well-being found in 30 percent. No change was observed in 31 percent.
Because of the radiation induced hematological depression, bone marrow storage and reinfusion began in 1964. With the improve- ment in techniques to include harvest of the marrow under general anesthesia and replacement immediately after total body irradia- tion, it became possible to avoid the characteristic depression of the white cells in five patients.
drugs such as Compazine to re E 'eve symptoms. Of interest is that,
DOD finding was utilized solely for observation of patient s toms and for the extensive laboratory tests carried out. DOD F% un s
pare with other patients in our hospital treated di I! erently or with
the patients receive !r chemotherapy and/or local radiation therapy
For these reasons, it is not possible to i (P entify a single form of
uting cause of deat E . It most likely would be the rate o F growth of
relatively long survivors live % 5 years each.
I

175
This promising development was stopped at the time of the ter- mination of the contract. This pioneering use of bone marrow has been and is being used today.
Review by others. The UC Faculty Research Committee. Our pro- tocol was submitted to this newly formed committee in March 1966. Provisional approval was given in 1967, with recommenda- tions for review of therapeutic efficacy, bone marrow infusion as a supportive measure and some revisions in the study design. At no time was the project disapproved by the faculty research committee as it received exhaustive and critical reviews, and it was approved again in 1971.
The ad hoc committee of the University of Cincinnati began a complete review of this project in 1971. Among the findings were that phase I11 studies should be initiated with better criteria for the determination of palliative effects and that bone marrow trans- plantation should be pursued. The study was judged to be adequate for support of the critically ill patients because of the development of skilled team management, especially with the help of a psychia- trist and psychologist, coupled with home visits.
The American College of Radiology. You have already heard of the three gentlemen who visited us, This distinguished group made two visits to our hospital. Their major findings were as follows:
One, the project is validly conceived, stated, executed, controlled and followed up. Two, the patient’s selection based on clinical consideration conforms with good
medical practice. Three, the records, publications, the patient-follow-up are voluminous and com-
mendable. Four, the procedure used for obtaining patient consent is valid, thorough and con-
sistent with the recommendations of the National Institutes of Health and with the practice of most cancer centers.
And, five, should this project come before the Senate or one of its committees in some fashion, we would urge your support for its continuation.
At the request of Senator Edward Kennedy, the Government Ac- counting Ofice reviewed the accounts of the Cincinnati General Hospital to determine whether there had been any intermingling of DOD funds used for patient care since we have pointed out from the start of our work that no DOD funds would be used for this purpose.
An excerpt from the letter dated May 26, 1972, from the Comp- troller General to Senator Kennedy, follows:
Concerning the contract with the University of Cincinnati, officials of the Defense Nuclear Agency stated that the cost of radiation treatment and patient care have not been borne by their agency. They stated also that funds of the Defense Nuclear Agency have been used only to pay for supplementary laboratory analyses of pa- tients who had received whole body irradiation in order for the Defense Nuclear Agency to gain information in areas that were relevant to national defense.
From the National Institutes of Health, D.T. Chalkley, Ph.D., Chief, Office of Protection from Risks, was very supportive of our work. In a letter copied to Senators Nunn and Talmadge, he com- ments that,
It is to be regretted that this incident has halted what promised to be a very sig- nificant addition to our armamentarium against metastatic cancer.
He also wrote directly to Senator Nunn, pointing out that, “The patients were treated individually for the diseases that they had.”

176
Secrecy. This study received widespread publicity in the 1970's. We responded to all questions about it at the time, including an open press conference. The study resulted in 13 published papers, nine DASA reports and 24 scientific resentations.
What about the status of total boly irradiation and partial bod irradiation since 1971? It is ap arentl a common misunderstan2
been discontinued. This statement is incorrect. Doses. Our doses were at a low level of 100 to 200 rads total vol-
ume. I might state there-that in the documents that you have there is a typo. It says, 300. It should be 200. And up to 300 rads partial body radiation between 1960 and 1970.
In other centers, doses now range from 600 to 1,200 rads in sin- gle or divided doses of total body and with sequential hemibody ra- diation in these same dose ranges.
Fractionation, that is the splittin of these doses over a period
because of the complication of ratfiation pneumonitis. Among the solid tumors treated during these two decades have
been cancers of the breast, prostate, lung, colon, and some sarco- mas.
At the University of Cincinnati De artment of Radiation Oncol-
tered to adults and children for leukemias, lymphomas, cancers of the breast, prostate, and neuroblastoma.
Nationally, uses of total bod and partial body irradiation have
ever before. To conclude this presentation of several decades, I speak to you
as a survivor of cancer, having been treated with radiation and sur- gery.
Our work has contributed significantly to the better treatment of patients with far advanced cancer and to our better understanding of the effect of radiation on humans in a time when nuclear war- fare once again seems possible.
ing that the use of these met R P ods o treatment for therapy has
of several days, has replaced sin le f arge doses of, say, 1,200 rads,
ogy, from 1979 on, total and partial E ody radiation were adminis-
grown steadily since 1970 an J are used more widely today than
Thank you. Mr. BRYANT. Thank you, Dr. Saenger. [The prepared statement of Dr. Saenger follows:]

177
Statement of Eugene L. Saenger, M. D. Before the House Judiciary Committee
Subcommittee on Administrative Law and Governmental Relations
April 11, 1994 Cincinnati, Ohio
E.L Saenger. M.D.
April 11. 1994 Page 1

178
SUMMARY
Several Important points are presented summarizing wr wok
One purpose of the study was the treatment of patients with far advanced cancer for whom the goal was the relief of pain, ShrinkaQe ol cancer and improvement in well being.
A second purpose was to study the systemic effects of radiation on the paUent.
Treatment was given only if benefit to the patienl was antklpated.
Patients were chiefly from the Cincinnati General Hospital. Selection was made only based on the presence of advanced cancer and where no other therapy was considered to be as or more efficadous than that currently available chemotherapy. Race, IQ. or socioeconomic standing were not selection factors.
a
b.
c
d
a Treatment was paid for by Cindnnatf General Hospital and the National Institutes of Health. No Department of Defense funds were used for treatment or patient care or decisions regarding therapy or patient reimbursement.
Patients were told that the treatment might help them and were cautioned that it might not. Some patients chose not to be treated.
There was nothing w e t about our work. There was nothing secret as to its being conducted. There was nothing secret about the findings obtained.
1.
0
EL Saenger, M.D.
April 11, 1994

179
I am Eugene L. Saenger. M. 0. of Cincinnati. It is a privilege for me to speak before this distinguished sub-commitlee of the Judiciary Committee of the US. House of Representatives to present a summary of our work on the treatment of far advanced cancer and the effects of wide fmld radiation therapy, work which I was privilegd to direct and the results of which I am proud. The participation and support of the highly qualified physicians, allied dentists and associated health professionals is gratefully acknowledged. My Curriculum Vitae is attached. (See Appendix 1)
I am a graduate of Walnut Hills Hlgh School, Harvard College, 1938. cum laude and University of Cincinnati, College of Medicine 1942. My training in Radiology was at Clncinnati General Hospital completed in 1945. I am a Diplomate of the American Board of Radiology and the American Board of Nuclear Medicine.
My major appointments at University of Cincinnati College of Medicine include rising from Assistant Professor of Radiology to Professor of Radiology from 1949-1987 and Professor Emeritus since !hen. I was the founder and director of (what continues Way) the Eugene L Saenger Radioisotope Laboratory from 1950 to 1987. I was Radiology Therapist at Children's Hospital from 1947 to 1987.
I have given over 40 guest and invited lectures in the U.S. and elsewhere. I have received the De Hevesy Nudear Pioneer Award of the society of Nuclear Medicine and the Gold Medal of the Radiological Society of North America and the Daniel Drake Award of the University of Clncinnati College of Medicine. these being the highest honon of these organizations.
My consultant appointments to my government encompass both domestic and international service. and include among others requests from the Department of Justice; Department of Energy; Environmental Protection Agency; Department of Health and Human Services; National Institutes of Health; Department of Defense; Food and Drug Administration: international Atomic Energy Agency; Oak Ridge Affiliated Universities; Surgeon General of the Air Force; the U. S. Public Health Service and numerous government administered hospitals. Additionally, I was proud to serve my country as an o f f i r in the United States Army, attaining the rank of Major prior to my honorable discharge.
My principal appointments at the University of Cincinnati College of Medicine range from Assistant Professor of Radiology In 1949 rising to Professor, and from 1987, the rank of Professor Emeritus. I am a member of 29 medical and scientifc societies and the Founding President of the Society for Medical Decision Making. In addition to being an honorary member of the National Council on Radiation Protection and Measurement (NCRP). I delivered the Sixth Laudston Taylor Lecture-the highest honor of this organization. The NCRP is an organization chartered by Congress that develops recommendations for radiation safely used by Federal Agencies for protection of the public.
E.L Saenger, M.D.
April 11. 1994 Page 3

180
wldh my colleagues, I am the author of 187 publicetbns in the scientific literature, the majority being in refereed Journals.
1. lntroductlon
Several Important points am presented summarizing our work:
One purpose of the study was the treatment of patients wivl far advanced cancer lor whom the goal was the relief of pain, shrinkege of c a m r and Improvement in weii being.
A second purpose was to study the systemic effects of radiation on the patient.
Treatment was given only if benefit to the patient was anticlpated.
Patients were chietly from the Cincinnati General Hospital. Selection was based only on the presence of advanced cancer end where no other therapy was considered to be as or more efficedous than then available chemotherapy. Race, IQ. or socioeconomic standing were not selectbn factors.
Treatment was paid for by Cincinnati Qeneral Hospnai and the National Institutes of Health. No Department of Defense funds were used for treatment or patient care or decisions regarding therapy or patient reimbursement.
Patients were toid that the treatment migM help them and were cautioned that it might not. Some patients chose not to be treated.
Them was nothing secret about our work. There was nothing secret as to its being conducted. mere was nothing SBCret about the findings obtained.
..........
A
B.
C
0.
E
F.
(3
I I . Whal Was The Purpose of The Total Body Irradiation (TBI)/Partial Body Irradlallon (Pel) Study:
The prtmary goal of the study was b improve the treatment and general clinical management by inaeashg, if possible, survival of patients with advanced cancer and palliation of symptoms. (Pallietkn k treatment directed at relief but not cure.) In additbn. observations and leboratory tests were carried out to seek effects of radiation on cancer patients and on the changes that could be ascribed to radiah.
The paniadhre effects of TBi were considered to be at least equal to and very likely to be superior 10 the chemotherapy available in the period from 1960 - 1970. Also the treatment methods
EL Sasnger. M.D.
April 11. I994 page4

181
were thought to be less stressful to the patients than chemotherapy then in use, especially in terms of Initial symptomatology follwving administration of the dose, as for example, the painful mouth ulcers from methotrexate and 5-tluorouredl. ~ N Q S used at that time.
The background for this project orlginated in my observations over the prior 20 years that cancer patients treated with radiation might be benefitled by a more careful evaluation of the effects of this kind of treatment on the total patient.
It seemed b me at that time that the approach to the total management of the cancer patients receiving radiatbn therapy was not as well studied as was that of the same patient who would be treated surgically. In addition. the effect on the cancer patient of doses of radiation given through large fields In relation lo systemic effects was not being adequately considered. even though much work was being done on the radiation effects on the tumor and its immediate substrate.
The scientific indications that these goals might be achievable were based on two levels of evidence one from animal studies and one from human studies.
a) Animal studies indicated belter tumor regression when total body irradiation was preceded by localized radiation than when localized radiation therapy was given alone both for lymphoma and carcinoma in mice.
Studies in human beings: Human studies for treatment of far advanced solid tumors prior to 1960 suggested the value of TBI. It was employed in several American centers and internationally. Treatment was given with SUCC~SS in relieving pain, shrinking tumors and, in some cases, prolongi~ survival. (See Appendix 2)
A major reason that we could begin TBI and PEI resuited from several important developments. The cobalt 60 teletherapy unit was installed at General Hospital in 1958, the first in Ohio. Harold Perry, M. D. was the first full time radiatbn therapist at our hospital. He had come from Memorial Sloan Keltering Cancer Center in New Yo* Hospital and was familiar with TBI and PBI techniques and indicators. James 0. Kereiakes, Ph.D., a physicist. joined the Department of Radiology in 1959. He calculated the doses, dose rate and distribution of radiation.
I believed that there could be implications from this treatment for well individuals exposed to radiation under other circumstances. In 1958, I submitted an unsolicited application to DO0 because there had been no studies on the metabolic effects of radiatbn and funds were available. This proposal was reviewed by J. A. Isherwood. M. D. for the A m y Medical Research and Development Command. He made the following comments: ‘Any correlation of tumor response to total dose of irradiation by such means as proposed in this project would be of great value in the field of cancer. In addition if by some means such as those proposed accurate knowledge of Ihe total dose of radiation received could be determined it would be of inestimable value in case of atomic disaster or nuclear warfare.’ (See Appendix 3)
b )
E.L Saenger. M.D.
April 11. 1994 Page 5

182
111. The Study
phases are defined as follows: A Typlcal of medical investigations. this study ptqressed through phases. These
Phase I studies are to determine whether the treatment is toxk.
Phase I I Is to determine in patrents without controls but with measurable
Only then are Phase 111 studies wlth controls and ideally with randomization
disease, whether the treatment is effective. Our studies included Phase 11.
conducted to determine therapeutic values. Although a Phase 111 study was proposed. we did not reach this level.
8. Patient selection: Patients were not recruited. Patients were referred for consideration for this form of therapy mostly from the Tumor Clink (outpatient) and the Tumor Service (in-patient). I was not inwhred in patient selection or in determination of extent of therapy or dosage. These dedsions were made solely by the attending physicians. internists and surgeons. and by radiatbn therapists. There were 24 patients entered into the study who were not given TBI or PBI. Some were rejected because it was thought that the patient would not benefit. Several patients and their families declined treatment.
1. Eligibility for therapy was spelled out in our 1962 document lo DOD:
a
b.
There is a reasonable chance of therapeutic benetlt to the patient.
The liielihood of damage to the patient is not greater than that
The facilities for support of the patient and complications of
encountered from comparable therapy of another type.
treatment offer all possible medical services for successful maintenance of the patient's well being.
Race was not a factor in selection-only the type of cancer and its extent. A statistical analysis, done only after the program was terminated, confirmed that the patients in this study did not differ from the patient population of Cincinnati General Hospital.
IO was not a factor in patient selection.
c.
2.
3.
IV. Informed Consent
As in selectbn of patients, informed consent for therapy was obtained by the attending physicians.
E.L Saenger. M.D.
-6 April 11, 1994

183
In the 1040s and 1950s informed consent was vetbal except for the general brief informed consent required by the hospital from all patients to be hospitalized irrespective of the treatment to be administered.
In thls project, the purpose and actual treatmeqt and the possible outcomes were discussed with the patient and often included family members.
In A@ 1965. the use of written informed consent, both for radiation and bone marrow harvesting and reinfusion, were developed by this project. These forms clearly indicated that risks of treatment were discussed. At that time. DHM and DOD did not require written informed consent As a result of a number of heQtul suggestions from the University of Cincinnati Faculty Research Committee, several revisbns to the form were made between 1967 and 1971 (See Appendix 4). Furthermore, thls written Informed consent that we developed preceded any mitten requirements of the Unhrenity of Cindnnati Medical Center by two (2) Y e w
One aitidsm of our work stemmed from the Instructions lo the attending personnel not to inquire concerning nausea, vomiting and diarrhea in the first few days afler treatment. We were particularly Interested in the frequency of these manifestations. Since both nausea and vomiting could be induced by suggestive questions, we requested that no questions be asked as to how the patient felt. This restriction dd not in any way restrict the administration of drugs such as Compazine to relieve symptoms. This care is amply documented in patlents' charts. Of interest Is that after treatment 39 patients (44%) had no nausea and vomiting, that 23 (27%) had symptoms for three (3) hours or less and that 12 patients (14%) had symptoms for six (6) hours or less. These responses are comparable to chemotherapy at the time, e.9.. methotrexate, 5-fluorouacil and Chlorambucil.
V. Funding
As noted earlier. most costs of treatment were paid by Cincinnati General Hospital. An estimate of the expenditures for direct patient care for about 3.804 days at about $1 14 per day with some additional cost estimates gave a total calculated amount of $483,222. There were no professional costs or physician fees for patient care.
Some funding was obtained from the NIH. Some patients were maintained on the General Clinical Researdr Center of Cincinnati General Hospital; this unit was supported by NIH. The protocols and records of each patient so hospitalized were submitted to the NIH and approved. In addition, several of the Post Graduate Fellows supported by the Radiation Training Grant of the National Institute of General Medical Sciences (NiH) participated in some phases of the DASA program.
DOD funding was utilized solely for observation of patient symptoms and signs and for the extonshre laboratory tests (See Appendix 5). DOD funds had no relation to choice of dose, choice of pallent or patient care, in any way. No patient was compensated or reimbuned or paid for
&L Saenger. M.O.
April 11. 1994 -7

184
treatment. A Congressional General Accounting Office audit documented all of this in 1972. The mal DOD contract for FY 1960 through FY 1971 was $671,482.79.
VI. Success of the TBI study
Mortality. In the group of patients who received radiation, there Were three categorles in which there were enough patients to compare with other patients of the Cincinnati General Hospital treated differently or with comparable groups reported in the refereed medical literature. The cancers were those of the breast, lung and cobn. The death rates were comparable to those treated by other means.
An Important question Is whether radiation was the factor leading to the early death of a patient. These patients had far advanced ~ ~ l l ~ e r s which were growing exponentialiy. in the come of the disease, patients received chemotherapy andlor bcaiired radiation therapy both before and immediately after TBI or PBI. For these reasons, it is not possible to Identify a single form of treatment or the rapid growth of cancer as being the single contributing cause of death. It most likely would be the rate of growth of the cancer itself.
There were 20 cases in which patients survived longer than one year. Except for the one patient with Ewing's tumor who remains alive after 25 years, the longest survivor lived 9 years. Two other relatively long survivors lived five years.
Palliation was successful with relief of pain in 31% of patients. Some decrease in tumor size occurred In 31% and an increase in well being was found in 30%. No change was observed in 31%. (In some patients there was more than one indication of improvement; thus the percentages exceed 100%). (See Appendix 6).
Because of radiation Induced hematological depression. autologous bone marrow storage and reinfusion began in 1964. With improvement in technique to include harvest of the marrow under general anesthesia and replacement immediately after TBI it became possible to avoid the characteristic depression of the white Mood cells in five patients. This promising development was lopped at the time of termination of the contract.
VII. Review by Others
A Faculty Research Committee. Our protocol was submitted to this newly formed committee in March of 1966. Provisional approval was given In 1967 with recommendations for review of therapeutic efficacy. bone marrow infusion as a supportive measure and some revision in the study design. AI no time was the project disapproved by the Faculty Research Committee as it received exhaustive and critical reviews.
6. The ad hoc Committee of the University of Cincinnati (the Suskind , Report) underlook a complete review of the TBI project. Among the findings were that Phase 111 studies should be initiated with better criteria for the determination of palliative effects and
LL Saenger, M.D.
Aprll 11, 1994 P a w 8

185
that bone marrow transplantation be pursued. The study was jud~ed to be adequate for support of the critically ill patients because of the development of skilled team management especially with the help of the psychlatrist and psvchobglst coupled with home visits.
American College of Radiology. AI the request of Senator Mike Gravel, the American College of Radiology formed an expert committee of Dr. Henry Kaplan. Chairman of Radiology at Stanford University, Dr. Frank Hendrickson, Chairman of Radiation Therapy at Rush-PresbyterIan Hospital, Chlcago and Or. Samuel Taylor, 111, a medical oncologist at Rush- Presbyterian Hospital, Chlcago. This distinguished group made Iwo visits to our hospital. Their major findings were as follows:
The project is validly conceived, stated, executed. controHed and fdlowed up.
The process of patient selecriOn based on cNnical considerations conforms with good medical practice.
The records. publications and patient follow-up are voluminous and commendable.
The procedure used for obtaining patient consent is valid, thorough and consistent with the recommendations of the National Institutes of Health and wlth the practice of most cancer centers.
5. Should this projecl come before the Senate or one of its committees in some fashion, we would urge your support for its continuation. (See Appendix 7)
At the request of Senator Edward Kennedy, the Government Accounting ORiCe reviewed the accounts of the Clndnnati General HospHal to determine whether there had been any intermingling of DOD funds used for patient care. since we had pointed out from the start of our work that no DOD funds would be used for this purpose.
An excerpt from the letter dated May 26, 1972 from the Comptroller General to Senator Kennedy follows: Toncerning the contract with the University of Cincinnati, officials of the Defense Nudear Agency stated that the cost of radiation treatment and patient care had not been bome by their agency. They stated also that funds of the Defense Nuclear Agency had been used only to pay for supplementary laboratory analyses of patiits who had received whole body irradiation in order for the Defense Nudear Agency to gain information in areas that were relathre to national defense.' (See Appendtx 8)
C.
1.
2.
3.
4.
D.
E National Institutes of Health (DHEW). D.T. Chalkley. Ph.D.. Chief, Orlice for Protectlon from Rlsks. Ofbe of the Director NIH. was very supportive of our work. In a letter copied to Senators Nunn and Talmadge. he comments that *It is to be regretted that this lnddent has halted what promised to be a very signifmnt additbn to our armamentarium against metastatic cancer." He also wrote directly to Senator Nunn pointing out that '...the patients were treated individually for the diseases they had: (See Appendix 9)
responded to all questions about it at the sme including at an open press conference. The study F. Secrecy. This study received widespread publiily in the early 70s. We
E.L Saenger, M.D.
April 11, 1994 -9

186
resulted in numerous undessHled presentatbns at open medical meetings and in published papem and reports (See Appendix 10).
VIII . Total Body Irradiation 6 Partial Body irradiation Since 1971
It is apparently a common misunderstending that the use of TEVPEI as a therapeutic agent has been discontinued. In the petiod from 1970 to the present there have been major changes in the use of TEI and PBI (See Appendix 2). Doses have risen from the low levels of 100-300 rad TBI and up to 300 rad PBI used by us from 1960 to 1970. Doses now range from 600 to 1200 rad In single or divided doses of TBI and wlth sequemial HBI in these same dose ranges. Fractbnatbn has replaced dingle lafge doses (1200 rad) because of the compllcatbn of radiatbn pneumonitis. Among the solid tumors treated during these two decades have been cancer of breast, prastate. lung. colon and some satcornas.
At the Unhrersity of Cindnnati Department of Radiatbn Oncobgy beginning in 1979, TEI and PBI were administered to adults and children for ieukemias, lymphomas, cancers of breast and proslate and neuroblastoma. Non-mdlgnant diseases treated hcluded aplastic anemia and congenital anomalies.
E.L Saenger, M.D.
Page 10 April 11. 1994

187
CURRICULUM VITAE
EUGENE L. SAENGER, M.D. PROFESSOR EMERITUS OF RADIOLOGY
UNIVERSITY OF CINCINNATI COLLEGE OF MEDICINE
Personal
Date of Birth: March 5, 1917
Place of Birth: Cincinnati, Ohio (Hamilton County)
Home Address: 9160 Given Road Cincinnati, Ohio 45243 (513) 793-1373
Office Address: University of Cincinnati Hospital 234 Goodman Street - M.L. (1569 Cincinnati, Ohio 45267-0569 Telephone: (513) 558-9042 Facsimile: (513) 558-4715
Married: Sue R. Saenger
Education:
A.B. - Cum Laude, Biochemical Sciences, Harvard University, 1938 M.D. - University of Cincinnati College of Medicine, 1942 Internship, Cincinnati General Hospital, 1942-43
Assistant Resident and Resident in Radiology, Cincinnati General Hospital, 1943-46
Diplomate, American Board of Radiology, 1946
Diplomate, American Board of Nuclear Medicine, 1972
Appointments
Professor Emeritus of Radiology, University of Cincinnati College of Medicine, September 1987
Professor of Radiology, University of Cincinnati College of Medicine, 1962-1987
Director, Eugene L. Saenger Radioisotope Laboratory, University of Cincinnati College of Medicine, 1950-1987
Vice-chairman, Department of Radiology, University of Cincinnati College of Medicine, 1975-1987

188
2
Assistant and Associate Professor of Radioloqy, University of Cincinnati College of Medicine, 1949-1962
Radiation Therapist, Children's Hospital Medical Center, Cincinnati, Ohio, 1947-Present
Major, U.S. Army Medical Corps; Chief, Radioisotope Laboratory, Brooke Army Hospital, Ft. Sam Houston, Texas, 1953-1955
Consultant in Radiology, Brooke Army Hospital, Ft. Sam Houston, Texas, 1956-1977
Consultant, Oak Ridge Operations Office, Division of Biology, U.S. Atomic Energy Commission, Oak Ridge, Tennessee, 1958-Present
Consultant, Division of Compliance, U.S. Atomic Energy Commission (now U.S. Nuclear Regulatory Commission), Washington, D.C., 1962-1987
Consultant in Radiology, Lackland AFB Hospital, Lackland AFB,
Consultant, Radiological Health Research Activities. USPHS, Taft
Texas, 1959-1975
Engineering Center, 1964-1969
Agency, Washington, D.C., 1965-1971 Consultant, Medical Advisory Committee, Defense Atomic Support
Representative for State of Ohio to the Medical Liaison Officer
Consultant on Radiology Training, DHEWIPHS. National Institute of General Medical Sciences, NIH, Bethesda. Maryland, 1967-1970
Network, Environmental Protection Aqency, 1968-1904
Consultant to the Office of the Director, DHHS/PHS/FDA, Center for Devices and Radiological Health, Rockville, Maryland, 1969-Present
Consultant, Radiation Bio-Effects and Epidemiology Advisory Committee, DHEIJ/PHS, Washington, D.C., 1970-1971
Consultant, Radiation Science & Protection Fellowship Board, Oak Ridge Associated Universities, Oak Ridge, Tennessee, 1970-Present
Consultant to Surgeon General, U.P. Air Force, in Nuclear
Consultant, Wright-Patterson Air Force Base, Ohio, 1977-Present
Board of Directors, Center of Science and Industry, Cincinnati.
Medicine, 1970-1975
Ohio, 1964-1969

189
3
Chairnian, Radiation Safety Committee, University of Cincinnati,
Board of Trustees, Community Chest & Council, Cincinnati, Ohio,
President, Public Health Federation, Cincinnati, Ohio, 1965-1969
Executive Committee, Health Planning Association of the Central
1964-1985; Member, 1985-1989
1964-1970; Executive Committee, 1970
Ohio River Valley (CORVA) , 1970-1972
Valley (CORVA) 1970-1972
Academy of Sciences, Washington, D.C., 1964-1972
Environmental Health Planning committee of the Central Ohio River
Advisory Committee to the Federal Radiation Council, National
Associate Editor, Journal of Nuclear Medicine, 1960-1970
Program Director in Radiological Sciences (National Cancer Institute and National Institute of General Medical Sciences, NIH) Training Program, University of Cincinnati, 1359-1970
Program Director for studies in metabolism of radiation following whole-body irradiation (Department of Defense) 1960-1971
Co-investigator, Biomedical Computing Center, University of Cincinnati College of Medicine, 1962-1966
Chairman, Cancer Control Council, Public Health Federation, Cincinnati, Ohio, 1961-1968
Board of Directors, Cancer Control Council, Cincinnati, Ohio, 1964-1970
Board of Governors, Ohio Valley Chapter of the Arthritis and Rheumatisn Foundation, 1961-1968
Board, Hamilton County Chapter of the American Cancer Society, 1963-1967
Governor's Advisory Board on Atomic Energy, State of Ohio, 1963-1972
Member, Medical Advisory Committee to Department of Health, State of Ohio, 1962-1969
Applied Radiology, 1972 Member, Honorary Editorial Advisory Board of the Journal Of
Radiation Research Society, Member - Finance Committee, 1977-1981
84-514 0 - 94 - 7

4
Health Physics Society, Chairman - Legislation Committee,
Health Physics Society, Member - Board of Directors, 1966-1969 National Committee on Radiation Protection, National Bureau of
1968-1 969
Standards, Member Subcommittee an Radium, Cobalt-60 and Cesium-137, 1952-1965
Board of Directors, 1967-1983: Honorary Member status 1983 National Council on Radiation Protection and Measurements (NCRP),
NCRP, Member - Subcommittee for Revision of Handbook 73, 1966 NCRP, Chairman - Budget and Finance Committee, 1368-1973 NCRP, Chairman - Scientific Committee (29 on Brachytherapy
NCPS, Chairman - Ad Hoc Thyroid Blocking Committee, 1972-1978 NCRP, Member - Scientific Committee #44 on Radiation Associated
Devices, 1968-1972
with Medical Examinations, 1973-Present
NCRP, Chairman - Resources Development Program, 1986-1990 American Roentgen Ray Society, Representative to the Iiational
Council on Radiation Protection and Measurements, 1960-Present
Society of Nuclear Medicine, Member - Board of Directors, Society of Nuclear Medicine, Member - Radiation Protection
Society of Nuclear Medicine, Chairman - Subcommittee on Post
Society of Nuclear Medicine, Member - By-Laws Committee, Society of Nuclear Medicine, Member - Conmittee on Education and
1966-1969
Committee, 1966-1969
Graduate Training in Nuclear Medicine, 1969-1971
1969-1972
Training, 1969-1971
Society of Nuclear Medicine, Chairman - Committee on Public Health and Efficacy, 1972-1984: Member, 1984-1987
Low Level Ionizing Radiation, 1980-Present
Department of Energy Contract, .The Efficacy of Clinical Diagnostic Procedures Utilized in Nuclear Medicine',
Society of Nuclear Medicine, Member - Subcommittee on Risks of Society of Nuclear Medicine, Principal Investigator - U.S.
1977-1983

191
5
American College of Radiology, Menber - Subcommittee on Radiological Aspects of Disaster Planning, 1964-1969
American College of Radiology, Member - Commission on Radiologic Units, Standards, and Protection, 1969-1988; Chairman, 1909-Present
American College of Radiology, Chairman - Committee on Research
American College of Radiology, Member - Commission on Public and Development in Nuclear Medicine, 1969-1972
Health, 1969-1971
American College of Radiology, Member - Subcommittee on Nuclear Medicine Technology, 1969-1975
American College of Radiology, Member - Committee on Quality Assurance and Efficacy, 1972-Present
Physics, 1977-1982 American College of Radiology, Kember - Committee on Radiation
American College of Radiology, Member - Cormission on Iiuclear Medicine, 1977-1986
American College of Radiology, Member - lledical Legal Cormittee, 1986-Present
National Consultant, Office of the Radiat-on S a f e t y Officer of the Veterans Administration, 1974
Member, Ad Hoc Cqwittee to Evaluate the Health and Safety Aspects of Pu in the Environment Adjacent to the Wound Laboratory, 1975
Argonne National Laboratory, Member - Review Committee for the Radiological and Environmental Research Division, 1976-1977
International Commission on Radiological Protection, Member - Committee # 3 on Protection in Medicine, 1977-1984
Federated Council of Nuclear Medicine Organizations, Representative - American College of Nuclear Physicians, 1977-1980
Federated Council of Nuclear Medicine Organizations, Secretary-Treasurer, 1978-1980
of Ionizing Radiation), National Academy of Sciences, National Research Council, Member of Committee, 1972
BEIR Report (The Effects on Populations of Exposure to Low Levels

192
6
Reactor Safety Study (WASE-lGOO), An Aooeosment of Accident Rioks in U.S. Commercial Nuclear Power Plants, Appendix IV, United States Nuclear Regulatory Conrmiasion, October 1975, Member- Advisory Group on Health Effects
Consultant, Pan American Health Organization, World Health Organization, Mexico City, Mexico. December 1980
Co-founder and President, Society for Medical Decision Making, September 1979; Historian 1979-1985
Member, Oversight Committee on the Radioepidemiologic Tables (OCRET), National Research Council, Commission on Life Sciences, August 1983-January 1985
Eember, U.S. Department of Energy Ad Hoc Committee on Neutron Quality Fzctor, January-December 1985
Chairman, Advisory Committee of the Charles 14. Barrett Cancer Center, University of Cincinnati, 1984-1986
Kealth Effects Model for Nuclear Powet Plant Accident Consequence Analysis, (NUREC-/CR-4214) Prepared by Sandia National Laboratories, Albuquerque, NN for the Division of Risk Analysis and Operations, U.S. Kuclear Regulatory Ccmnission, July 1985, Member, Advisozy Committee
Germany, 1-iay 1986
August 1986; conference November 13-21, 1986
Consultant, 7th Medical Command, U.S. Army, Heidelberg, West
Kenber. AUA Cornittee on h'on-Military Radiation Emergencies,
Cirector, Region I, 1985-1989
Cancer Control Consortium of Ohio
Honorary member, Medical Academy of SR Croatia, February 1988
Ad Hoc Consultant to: U.S. Department of Justice U.S. Department of Energy U.S. Environmental Protection Agency U.S. Department of Defense U.S. Department of Eealth and Human Services, Food and Drug
International Atomic Energy Agency
Administration
Member, Expert Committee of IAEA to the USSR to evaluate the late effects of Chernobyl, Zuly 1990
Marquis' Who's Who
American Men and Women of Science

I
193
.
Lectcreships:
Annual Oration, "Radiologists, Medical Radiation and the Public Health", presented at the Radiological Society of North America, Chicago, Illinois, December 4 , 1968
Aubrey 0 . Hampton Lecture, "Radiation 1971 - Just How Safe?", Harvard Medical School, Massachusetts General Hospital, Boston, April 4 , 1971
Wright H. Langham Memorial Lecture, "Radiation Accidents - 3 Decades of Facts and Fancies", University of Kentucky Medical Center, Lexington, Kentucky, November 15, 1977
Annual Failla Lecture, "Benefits vs Risks of Medical Radiation: New Concepts and Problems", presented to the Greater New York Chapter of the Health Physics Society, Columbia University, New York, December 7, 1977
Brookhaven National Laboratory, "'Safe' Tracer Dose in Human Experimentation", Islip, New York, April 7, 1978
Tenth Annual Conference on Radiation Control, "Efficacy of Nuclear Medicine Procedures", Harrisburg, Pennsylvania, April 30-May 4 , 1978
Harvard University School of Public Health, Planning for Nuclear Emerqencies. (seminar), "Medical-Legal Aspects of Radiation Exposure", noston, Massachusetts, May 8-12, 1978 (through 1986)
Society of Nuclear Medicine Refresher Course, "Radiation Effects and Radiation Protection", Anaheim, California, June 1978
Radiological Society of Iiorth American Refresher Course, "Recent Advances in Radiation Epidemiology", Chicago, Illinois, November 1978 (repeated 1979, 19801
Food and Drug Administration, Bureau of Radiological Health, "Efficacy Studies in Lung Scanning: Design and Implementation", Rockville, Maryland, March 20, 1979
Armed Forces Radiobiological Research Institute (AFRRI), "The Experienced Effects of Ionizing Radiation on the Body", nethesda, Maryland, May 23, 1979
Guest Lecturer, "Efficacy and Efficiency of the Diagnostic Application of Radiation and Radionuclides', organized by the Government of the Federal Republic of Germany and the World Health Organization, Neuherberg, West Germany, December 5-7, 1979
Literary Club, "Perceptions of Risk", Cincinnati, Ohio, February 18, 1980

194
8
Scciety of Nuclear Medicine Continuing Education Course, "Nuclear Power, Nuclear Medicine and the Public", Detroit, Michigan, June 25, 1980
Guest Lecturer, "Low Level Radiation Risks', University of Texas Health Science Center, Houston, Texas, July 25, 1980
Guest Lecturer, Nuclear Radiation Risks - A Utility-Medical Dialogue, 'Case Histories of Lawsuits for Overexposure", svonsored bv the International Institute of Safetv and Health. Whshington,-D.C., September 22-23, 1980
"Hospital Preparation for the Management of Radiation Accidents", course presented by the E.L. Saenger Radioisotope Laboratory, September 29-30, 1980 (repeated September, 1981)
Guest Lecturer and Banquet Address, Los Alamos Scientific Laboratory, Life Sciences Symposium, "Medical Aspects of Radiation: Radiation Burns', Los Alamos. New Mexico, October 8-10, 1980
"Aspects of Nuclear Medicine", Medical Society of the District of Columbia Annual Scientific Assembly, White Sulphur Springs, West Virginia, October 24-26, 1980
Society of Nuclear Medicine Refresher Course, "What Nuclear Medicine Professionals Should Know About Nuclear tlarfare", Las Vegas, Nevada, June 17, 1981
Guest Lecturer and,Member of Faculty. "Regional Seminar on General Procedures to Manage Persons Receiving Whole or Partial Body Irradiation", co-sponsored by the Pan American Health Organization and the Government of Brazil, Itaipava, Brazil, December 11-22, 1982
Guest Lecturer, "The Pole of the Physician in Medico-legal Claims Associated with Radiation In ]u ry" , sponsored by the Pacific-Sierra Corporation, in Albuquerque, New Mexico, March
Sixth Annual Lauriston S. Taylor Lecture, "Ethics, Trade-offs and Medical Radiation", presented to the P!ational Council on Radiation Protection and Measurements, Washington, D.C., April 6, 1982
"High Level Radiation", invited Grand Rounds presentation, Hamot Uedical Center, Erie, Pennsylvania, April 29, 1982
Guest Lecturer, "Medical Management of Radiation Injuries", sponsored by the Radiation Management Corporation of Philadelphia, in Atlantic City, New Jersey, May 6, 1982
4-6, 1982

195
9
.
Guest Lecturer, "Medical Management of Radiation Casualties", sponsored by the =IS Corporation of Albuquerque, in South Haven, Michigan, May 24-26, 1982
Society of Nuclear Medicine Continuing Education Course, "ALARA - What is Reasonable", Miami Beach, Florida, June 17, 1982
"Diagnostic Efficacy - Lung Imaging as a Model. Nuclear Medicine Efficacy Study", 29th Annual Meeting of the Society of Nuclear Medicine, Miami Beach, Florida, June 15-18, 1982
Guest Lecturer, A Symposium: Health Aspects of Nuclear Power Plant Incidents, "Regional Organization of Medical Care", sponsored by the New York Academy of Medicine and the New York State Department of Health, New York, New York, April 7-8, 1983
Guest Lecturer, 23rd Annual Symposium on Trauma, "Irradiation Trauma", sponsored by the Michigan Committee on Trauma, The American College of Surgeons, Lakeshore Continuing Medical Education, Inc. and Muskegon County Medical Foundation, Muskegon, Michigan, September 21, 1983
The Society of
Guest Lecturer, International Conference on Nuclear Medicim, "Efficacy Analysis in Nuclear Medicme - Lung Scanning as a Model" and "Potentials for TC-99m Myocardial Imaging Agents", Rhodes, Greece, April 24-29, 1984
Guest Lecturer, Medical/Legal Aspects of Radiation Induced Cancer, "Impact of Compensation Legislation on Nedical Sciences", sponsored by the Radiation Wanaqement Corporation, Philadelphia, Pennsylvania, September 5-7, 1984
Guest Lecturer, "Probability of Causation", sponsored by Electric Boat Company, Groton, Connecticut,. May 14, 1985
Guest Lecturer, "Determlnatlon of Clinical Efficacy: Nuclear Medicine as Applied to Lung Scanning", sponsored by University of Connecticut, Farmington, Connecticut, May 15, 1985
Guest Lecturer, Medical Aspects of Radiation Emergencies, "New Trends in Triage and Treatment of the Accident Victim", sponsored by Yale University School of Cledicine, Lawrence & Memorial Hospitals, New London, Connecticut, May 16, 1985
Guest Lecturer, Emergency Planninq and Response, "Case Studies ot Radiation Accidents" and "Legal Implications: Long Term Risk and Compensation" Health Physics Summer School, Evanston, Illinois, June 3-7, 198;

10
Guest Lecturer, 1985 International Congress of Radiology, "Efficacy and Cost Effectiveness of Diagnostic Tests: Lung Scans for Pulmonary Embolism", "Medical-Legal Problems for the Radiologist as a Consultant") also served as co-moderator of session entitled "Decision Making and Image Selection", Uonolulu, Hawaii, July 8-12, 1985
Guest Lecturer, Advanced Managenent of Radiation Accidents, "Early Medical Decisions", and "Legal Aspects-A Physician's View" sponsored by the University of New Mexico School of Medicine, Albuquerque, New Mexico, October 3-5, 1985
Guest Lecturer, Toxicology: Basic Science and Clinical Research, "New Thoughts About Radiation Accidents", sponsored by the University Association for Emergency Medicine and the International Research Institute for Emergency Medicine, San Francisco, California, February 13-14, 1986
Guest Lecturer, "Should There Be a Limit of Patient Exposure Based on Risk?*, sponsored by Brookhaven National Laboratory, Upton, L.I., New York, April 7. 1986
Guest Lecturer, "Nuclear Accident Management", Society of Nuclear Kedicine Annual Meeting refresher course, presented in June of 1986, 1987 and 1988
Guest Lecturer, "Acute Effects of Radiation", International Conference on Non-Military Radiation Emergencies, sponsored by the American Medical Association, Washington, D.C., November
Recipient of the 28th George Charles de Hevesy Nuclear Pioneer Award, presented at the 34th Annual Meeting of the Society of Nuclear Medicine, Toronto, Ontario, Canada, June 2, 1987
Co-chair, Special Session: Chernobvl, "Diagnosis and Treatment of Acute Radiation Injury", presented at the Health Physics Society Annual Meeting, Salt Lake City, UT, July 5-10, 1987
Keynote address, Physician's Role in Nuclear Kass Casualties: Avplications of the Chernobyl Experience, "The Physician's Role rn Nuclear Energy", sponsored by the Department of Radiation Therapy, Hospital of the University of Pennsylvania and Radiation Management Consultants, Cincinnati, OH, September 11-13, 1987
Guest Lecturer, "Benefit, Risk and Cost-Effectiveness in Medical Radiation", sponsored by the U.S. Food and Drug Administration, Center for Drug Evaluation and Research, Rockville, HD, October 28, 1987
Recipient of the Daniel Drake Award, the most prestigious award given by the University of Cincinnati College of Medicine for outstanding contributions to medicine and science, June 1988
19-21, 1986

197
11
Amy Bowles Lawrence Dlstinguished Scientist in Research Medicine, at the Donner Laboratory and the Lawrence Berkeley Laboratory of the University of California, Berkeley, CAI June 13-15, 1988 (Dr. Saenger was the inaugural Lawrence Lecturer)
Clarence C. Lushbaugh Lecture on Controversial Radiation Concepts, "The NIMBY Syndrome", at the Oak Ridge Associated Universities, Oak Ridge, TN, October 21, 1988 (Dr. Saenger was the inaugural Lushbaugh Lecturer)
Guest Lecturer, Topics in Radiological Health for Phvsicians, "Medical Management of Irradiated Patients", sponsored by the Medical College of Ohio, Toledo, OH, January 19-20, 1990
Guest Lecturer, "Is the Environment Around DOE Plants as Hazardous as Represented?", sponsored by the Eastern Chapter, Health Physics Society, Oak Ridge, TN, March 20, 1990
Guest Lecturer, Occupational Health in Nuclear Facilities, "Counseling the Radiatlon Worker and Family", sponsored by REAC/TS, Oak Ridge Associated Universities, Oak Ridge, TN, August 17, 1990
Guest Lecturer, Clinical Approaches to Medicine in the Nuclear Industr , "Medical Management of the Irradiated Patient", sponsorzd by Radiation Management Consultants, held in Orlando, FL, October 11, 1990
Guest Lecturer, 26th Radiology Congress of the German Democratic Republic, "Acute Local Radiatlon In~ury", "Diagnosis and Treatment of the Acute Radiation Syndrome" and "Late Effects from Radiationn, Heringsdorf, East Germany, October 23-24, 1990
Guest Lecturer, Soviet Refugee Health and Mental Health: Twentr Years of Soviet Resettlement, "Chernobyl: Fallout Revisited", sponsored by the Office of Refugee Health, Office of the Assistant Secretary of Health, DHHS, Chicago, IL, December 10-12, 1991
Guest Lecturer, Radiation Protection in Medicine, "Implications of the New Risk Estimates". Annual meeting 0: the National Council on Radiation Protection and Measurements, Arlington, VA, April 1-2, 1992
"Medico Legal Issues Associated with Ionizing Radiation", presented at the annual meeting Of the American Roentgen Ray Society, San Francisco, California, April 25-30, 1993
Recipient of the 1993 Gold Medal of the Radiological Society of North American (RSNA), the highest honor of the Society, presented at the RSNA Annual Meeting, Chicago, Illinois, November 3 0 , 1993

198
12
Professional Societies:
Academy of Medicine of Hamilton County Alpha Omega Alpha American Association for the Advancement of Science American College of Nuclear Physicians American College of Radiology American Medical Association American Radium Society American Roentgen Ray Society Cincinnati Radiation Society Greater Cincinnati Radiological Society Health Physics Society Ohio State Medical Association Ohio State Radiological Society Radiation Research Society Radiological Society of North America Sigma Xi Society for Medical Decision Making Society of Nuclear Medicine Society of Pediatric Radiology
Y

1
199
13
a
.
Publications
1947
Unilateral Paraspinal Abscess, Radioloqy 48: 256-259, March
1949
Pyarthrosis in Infancy, Ohio State Medical Journal 45: 453-458, May with J.V. Greenebaum and J.A. Frieberg
1950
-
-
- Spondylarthritis in Children, American Journal of Roentgen., Rad. Therapy and Nuclear Medicine, LXIV: 20-31, July
1952
Results of Therapy with Radioactive Iodine-131 in Hyperthyroidism, Ohio State Medical Journal 50: 26-27, January, with R.E. Goldsmith
Letterer-Siwe's Disease: Problems in Diagnosis and Treatments, American Journal Roentgen., Rad. Therapv and Nuclear Medicine, LXII, No. 3, March, with R.J. Johansmann
Protection Against Radiations from Radium, Cobalt-60 and Cesium-137, National Bureau of Standards Handbook 54, Section 9: Accidents entailing radiation hazards, September
-
Emergency Measures and Precautions in Radium Accidents, Journal of the American Medical Association 149: 813-815, with R Y Gallaghar, D.S. Anthony and P.J. Valaer
1955 - Roentgen Ray Epilation under Anesthesia, A.M.A. Archives of Dermatology 71: 116, January
1956
Carcinoma of the Prostate: Therapy with Radioactive Colloidal Gold, U.S. Armed Forces Medical Journal, VII: 469, April, with P.D. Beach and D.V. Becker
-
A Method for Monitoring Background by Means of Statistical Control Chart, American Journal of Roentqen., Rad. Therapy and Nuclear Medicine, LXXV: June, with C.M. Herbert
A Method for Labeling the Lone Star Tick with Radioactive Indicator (P-32), Journal of Economic Entomolo 49: 393, June, with S.E. Xnapp, C.J. Farinacci and C.M. Herbe2

14
Radiation Hazercis in the Practice of Surgery, The American Surqeon 22: 6 7 6 . with C.M. Barrctt
1957
Radium Capsules and their Associated Hazards, American Journal of Roentqen., Rad. Therapv and Nuclear Medicine 77: 511-523, March, with R.G. Gallaghar
1959
Planning for a Radiation Accident, iherican Industrial ltyqiene Association Journal 20: No.6, December
1960
Incidence of Neoplasia Following Therapeutic Irradiation for Benign Conditions in Children, Radiolow 14: 889-902, June, No. 6
-
-
-
Radiation Accidents, American Journal Roentgenoloqv, Radiation Therapy and Nuclear Medicine 84: 715-728, October
1962 - Radiation Epidemiology, Cancer 15: 4119-503, May-June, No. 3
1963 - Uedical Aspects of Radiation Accidents: A Handbook :or Physicians, Eealth Physicists and Industrial Hygicni., published by the U . S . Government Printing Office, February
Bospital Planning to Combat Radioactive Contamination, Jcornal of the American Medical Association 185: 5711-581, August 17
Deoxycytidine in Urine of Humans After Whole-Body Irradiation, Science 142: 396-398, October 18, No. 3590, with H.K. Berry, H. Perry, B.I. Friedman, J.G. Rereiakes and C. Scbesl
Robot Data Screening: Proceedings of the Conference on Data Acquisition and Processing in Biology and Medicine, Pergamon Press, with T.D. Sterling and M. Gleser
Robot Treatment Planning: Proceedings of the Conference on Data ACqUiSitiOn and Processing in Biology and Medicine, Pergamon Press, with T.D. Sterling, H. Perry and J. Weinkam
Some Plain Facts About Computer-Oriented Programs in Medical Centers, Proceedings of the Conference on Data Acquisition and Processing in Biology and Medicine, Pergamon Press
Liver Scanning in the Diagnosis of Bematobilia, Radiology 81: 980-983
t

201
15
Carcinogenic Effects of Iodine-131 compared with X-Irradiation - A Review, Health Physics 9: 1371, with R. Seltzer, T.D. Sterling and J.G. Kereiakes
Liquid Scintillation Counting of 1-131 in a Clinical Laboratory, Journal of Nuclear Medicine 4: 426-438, with H. Horwitz, J.G. Xereiakes and T. Selkirk, Jr.
1964 - Radiation Casualties: Newer Aspects of Mass Casualty Care, New York State Journal of Medicine 64: No. 2, with M.L. Boone
Radiation Therapy: Chapter 79, pp 684-796, Pediatric Therapy, editor: Harry C. Shirkey, published by C.V. Mosby, with J.P. Dorst
Radiation Exposure from Radioiodine Compounds in Pediatrics, Radiology 82: 486-494, with R.A. Seltzer, J.G. Kereiakes, and D.H. Myers
Radiation Exposure from Radioisotopes in Pediatrics, New England Journal of Medicine 271: 84-90, with R.A. Seltzer and J.G. Kereiakes
Endoreduplication in Leucocyte Chromosomes - Preliminary Report of Its Relation to Cancer and Whole Body Irradiation, The Lancet, September 5, pp 494-495, with B.I. Friedman and M.S. Kreindler
Epidemiology and the Practicing Physician, Cincinnati Journal of Medicine 45: 397-338
Experiences with 1-131 in the Management of Carcinoma of the Thyroid, Radiology 83: 892, with C.M. Barrett, J.W. Passino, R.A. Seltzer and W.D. Dooley
Implications to Man of Irradiation by Internally Deposited Strontium-89, Strontium-90 and Cesium-137. A Report of the Advisory Committee to the Federal Radiation Council, December 31, 1964. Division of Medical Sciences, National Academy of Sciences - National Research Council, Washington, D.C. 1965 - Continuing Use of the Whole Body Counter - The Nature of the Problems, reprinted from Radioactivity in Man, editor: G.R. Meneely, pp 450-461, published by Charles C. Thomas, with J.G. Kereiakes
Do Malignancies Result from Diagnostic and Therapeutic Radiation, from Genetics and the EDidemioloav of Chronic Diseases. Part IV, - --- -- - - . .. _ _ _ ~ ~- pp 355-371, Public Health Servicg Publication No. 1163, U.S. Government Printing Office, Superintendent of Documents, Washington, D.C., with T. Sterling and R.A. Seltzer
-
16
RaCionuclide Doses to Infants and Children: A Plea For a Standard Child, Health Physics 11: 999-1004, with R.A. Seltzer, J . G . Kereiakes and B. Blackburn
Treating the Radiation Casualty, Summary of Proceedings 16th National Conference on Disaster Medical Care, October 3G-31, 1965
1966
Specific Proteins in Serum of Total-Body Irradiated Humans, The Journal of Immunology 96: 64-67, with B.I. Friedman, A.J. L u z o and J.G. Kereiakes
Hematological and Dosimetric Findings in Human Beings Receiving Whole and Half Body Radiation, abstracted in Radiation Research 27: 530. with J . G . Kereiakes, B.I. Friedman and H. Perry
1967
-
- A Sensitive Technique for Measuring ThyroiZal Uptake of 1-131 Iodine, Journal of Nuclear Medicine 8: 86-96, with H.N. Wellman, J.G. Kereiakes, T.B. Yeager and C.Z. Karches
Treatment of Acute Radiation Injury under Medically Austere Conditions, prepared by TRIMAC Committee fE.L. Saenger member of Committee) at the request of the Office of Civil Defense, Department of Defense and the National Radiological Defense Laboratory, San Francisco, California, OCD Subtask 243tF, April
Effects of Total and Partial Body Therapeutic Irradiaticn in Man: Proceedings of the 1st International Synposium on the Biological Interpretation of Dose from Accelerator-Produced Radiation: U.S. Atomic Energy Commission, Division of Technical Information, CONF-670305
The Role of the Citizen in Health Planning, Cincinnati Journal of Medicine page 62, (first in a three-part presentation g i v e n b y E.L. Saenger, M.D., President of the Public Iiealth Federation, as the keynote address at the Golden Centennial Celebration of the Public Eealth Federation and Cincinnati Health Department, November 16, 1967)
New Needs and Trends in Nuclear l-ledicine (keynote address), presented at the symposium, Reduction of Radiation Exposure in Nuclear Medicine, held at Michigan State University, East Lansing, Michigan, August 7-9, published in Environmental Health Series, Radiological Health, U.S. Department of Health, Education and Welfare, PHS, Publication 1999-RH-30
Colorimetric Analysis of Deoxycytidine in urine after Separation by Ion-Exchange Column Chromatography, Journal of Analytical_ Biochemistr 23: 230, with I.W. Chen, J.G. Kereiakes and B.I. d

203
17
Radiopharmaceutical Dosimetry in Pediatrics, Radiologv 90: 925-930, with J.G. Kereiakes, H.N. Wellman and J. TieGan
Clinical Experience with Oblique Views in Pulmonary Perfusion Scintiphotography in Normal and Pathological Anatomy, Journal of Nuclear Medicine 9: 374, with H.N. Wellman, J.F. Mack and B.I. Friedman
Studies of Preliminary Experience with the Use of Iodine-123 for Thyroid Function and scanning Compared to Iodine-131, Journal of Nuclear Medicine 9: 359
A New Concept in Dynamic-Function Studies - Quantitative Cinescintivideography, Journal of Nuclear Medicine 9: 420, with H.N. Wellman, J.G. Kereiakes and D. Hunkar
The Use of Computers in Nuclear Medicine: Proceedings of Conference on the Use of Computers in Radiology, held October 20-23, published April 1968, University of Missouri
Incidence of Leukemia Following Treatment of Hyperthyroidism, - JAMA 205: 147-154, with G.E. Thoma and E.A. Tompkins (A cooperative study )
Radiation Exposure of Uranium Miners. A Report of the Advisory Committee to the Federal Radiation Council, National Academy nf Sciences, Washington, D.C., August 27, 1968
Radiation-Induced Urinary Excretion of Deoxycytidine by Rats and Humans, Radiology 91: 345-348, with I.W. Chen, J.G. Kereiakes and B.I. Friedman
Status of Research in Diagnostic Radiology. A Report by the Radiology Training Committee of the National Institute of General Medical Sciences, National Institutes of Health, (E.L. Saenger, Member of Committee), Bethesda, Maryland, 1968
Management of the Early Phase of Radioactlve Contamination in Human Beings: reprintei from Diagnosis and Treatment of Deposited Radionuclides, Proceedings of a Symposium held at Richland, Washington, May 15-17, Excexpta Medica Foundation pp 600-607
1969 - Radiologists, Medical Radiation and the Public Health, Annual Oration presented at the Radiological Society of North America, Chicago, Illinois, December 4, published in Radiology (special edition) 92: 681-699, March
Medulloblastoma - A Review of Prognosis and Survival, British Journal of Radiology 42: 198-214, with D.R..McFarland, H. Horwitz and G.K Bahr

18
Clinical Experience with Oblique Views in Pulrmr.ary Perfusion Camera-Imaging in Normal and Pathological Anatomy, Radiology 92: 897-902, with J.F. Mack, H.N. Wellman acd R.I. Friedman
Total and Half-Body Irradiation: Effect on Cognitive and Emotional Processes, Archives of General Psychiatry 21: 574-580, with L.A. Gottschalk, R. Kunkel, T.H. Wohl and C.N. Winget
Patient and Personnel Dose during Radioisotope Procedures. Proceedings of a Conference held at Baylor University College of Medicine, Houston, Texas, November 21-22 published in Medical Radiation Information for Litigation, DMRE 69-3, p 1 5 3 m 1969, with J . G . Kereiakes, H. Homitz, H.N. Wellman and V.J. Sodd
1970 - The Future of Radioisotopes in Medicine: Benefits vs Risks, published in Medical Radionuclides: Radiation Dose and Effects, editors: R . J . Cloutier, C.L. Edwards, W.S. Snyder. U.S. Atomic Energy Commission, Division of Technical Information, pp 491-507, June 1970, proceedings of a Symposium held at the Oak Ridge Associated Universities, December 6-11, 1969
National Uses and Needs for Standard Radioactive E.!aterials. A Report by an Ad Hoc Panel of the Committee on Nuclear Science, National Research Council, National Academy of Sciences, Washington, D.C., 1970, E.L. Saenger, Member of Panel
1971 - Radiation and Leukenia Rates, letter to Science 171: 1096-1098, No. 3976, March 19, \?ith E. Tompkins and G . E . Thoma
Cytologic-Biochemical Radiation Dosimeters in Nan, Biochemical Indicators of Radiation Injurv in.Man, International Atomic Energy Agency, Vienna, (PL-409/13), pp 181-214, with E.B. Silberstein,-I.W. Chen and J.G. Kereiakes
Estimate of Manpower Needs of Medical Physicists in the United States, American Association of Physicists in Medicine 5 (2): 129-131, with L.H. L a m 1 and J.G. Kereiakes
A Head-Holding Device for Improved Brain Scintigraphy, Journal of Nuclear Medicine 12: 305-306, June, with R.A. Berke
Care of Patients Involved in Radiation Accidents: Recent Advances. Der Strahlenunfall und seine Behandlung, vom. 19-20, Juni 1970 in Zurich, published by George Thieme Verlag, Stuttgart, pp 54-78

19
The Safe Tracer Dose in Medical Investigation, reprinted from Progress in Atomic Medicine: Recent Advances in Nuclear Medicine. Chapter 5, Vol. 3, pp 139-165, editor, John H. Lawrence, by Grune and Stratton, Inc., with J.G. Kereiakes
1972 - Protection Against Radiation from Brachytherapy Sources, NCRP Report No. 40 (National Council on Radiation Protection and Measurements), March 1972. E.L. Saenger, M.D., Chairman of Committee preparing report
Active Bone-Marrow Dose Relaggd to Hematological Changes in Whole-Body and Partial-Body Co Gamma Radiation Exposures, Radiology 103: 651-656, with J.G. Kereiakes, W. Van de Tiet, C. Born, E.B. Silberstein, and C. Ewing
H u m a n Skeletal Scanning with a Stable 99%echnetium-Tin-Phosphate Agent, Southern Medical Journal 65: 1407, with E.B. Silberstein, A. Park and G.W. Alexander
A Study of the Parameters Influencing the Clinical Use of Iodine-123, AngiographylScintisraphy - Symposium of the European Association of Radiology, Editor L. Diethelm, Sprinqer-Verlag, Berlin, pp 129-137, with H.N. Wellman, J.F. Mack, R.E. Goldsmith and V.J. Sodd
Radiopharmaceutical Dosimetry in Pediatrics, Seminars in Nuclear Medicine 2: (no.4 - October), 316-327, with J.G. Kereiakes, H.N. Wellman and G. Simmons
The Effects on Populations of Exposure to Low Levels of Ionizing Radiation IBEIR Report), National Academy of Sciences, National Research Council, Washington, D.C., November, E.L. Saenger, Member of Committee
A Fixed Format Lexicon for Nuclear Medicine Reports, DHEW Pub. No. (FDA) 74-8009, with R.G. Hoops, V.J. Sodd, G.W. Alexander
1973
A Multiple-Dose 133Xe Solution "Generator" : The Disposable Glass Ampule Equilibration Chamber, Journal of Nuclear Medicine 14, with R.G. Carroll, R.A. Berke, R.T. Anger, G. Levine, and H.N. Wellman
Radiation Dose to Breast-Feeding Child after Mother has "%c-MAA Lung Scan, Journal of Nuclear Medicine 14: 51-52, with R.A. Berke, R.C. Hoops and J.G. Kereiakes
-

206
20
Pediatric Radiopharmaceutical Dosimetry, Proceedings of the XI11 (13th) International Congress of Radiology, p. 238, Madrid, October 15-20, with J.G. Kereiakes and V.J. Sodd
Whole and Partial Body Radiotherapy of Advanced Cancer, American Journal Roent enolo Radiation Thera y and Nuclear Medicine I d Annual Meeting of the American Roentgen Ray Society, Washington, D.C., October 3-6, 1972, with E.B. Silberstein, B. Aron, H. Horwitz, J.G. Kereiakes, G.K. Bahr, H. Perry and B . I . Friedman
Radiation-Induced Change in Serum and Urinary Amylase Levels in Man, Radiation Research 54: 141-151, April, with I.W. Chen, J.G. Kereiakes, B.S. Aron and E.B. Silberstein
Clinical Evaluation of Radioimmunoassay of Digoxin, Journal of Nuclear Medicine 14: (7) 531-533, Zuly, with H.M. Park, I.W. Chen, A. Lowery and G.T. Manitasas
Radiation Dose to Various Organ Sites in a Tissue-Equivalent Humpg,Phantom Resulting from Implantation of a Promethium 147 (Pm”’) Intracardiac Nuclear Pacemaker, American Journal of Roentqenoloqy, Radiation Therapy and Nuclear Medicine 118: (4) 768-776, August, with W. Arnold, J.G. Kereiakes, G.K. Bahr and J.W. Spickler
Prospects for Dose Reduction and Assessment in presented at Second International Symposium on Carlsbad, NM, with H.N. Wellman, V.J. Sodd, J. Branson and J.G. Kereiakes
1974 -
Nuclear Pledicine, Nuclear Medicine, Robbins, D . M .
Scintiscanning with Gallium Citrate 67, Diagnosis of Head and Neck Malignant Neoplasms, Archives of Otolaryngology 100: 201-206, September, with A.D. Kornblut, E.B. Sllberstein and D.A. Shumrick
A Comparison of 1231 and 13’1 for Thyroid Imaging Using Various Collimators, International Journal of Nuclear Medicine and Biology 1: 201-204, with H. Nishiyama, A.B. Ashare, A. Shafie and V.J. Sodd
14C-Tripalmitin Breath Test as a Diagnostic Aid for Fat Malabsorption due to Pancreatic Insufficiency, Journal of Nuclear Medicine 15 (12): 1125-1129, with I.W. Chen, A. Kambiz and A.M. Connell
Efficacy Studies in Nuclear Medicine, reprinted from Proceedings of the XI11 International Congress of Radiology, Excerpta Medica 1: 45-40, Amsterdam
Evaluation of Clinical Value of 12’1 and 13’1 in Thyroid Disease, Journal of Nuclear Medicine 15: 261, with H. Nishiyama, V.J. Sodd, and R.A. Berke
1
’ I

21
Quantification of Myocardial Infarction by Scintigraphy: An Autopsy Correlated Study, Journal of Nuclear Medicine 15: 475, (abstract) with A.B. Ashare, D.W. Romhilt, V.J. Sodd, N.I. Levinson, R.J. Adolph, and L.S. August
Detection and Evaluation of Pulmonary Malignancies Using "'Cs, Recent Advances in Nuclear Medicine, Proceedings of the First World Congress of Nuclear Medicine, Ohkawa Printing Company, Yokohama, p. 255, Tokyo, September, with H. Nishiyama and V.J. Sadd
An Investigation of the Disposal of Radiopharmaceuticals in the Cincinnati Sewage System, Recent Advances in Nuclear Medicine, Proceedings of the First World Congress of Nuclear Medicine, Ohkawa Printing Company, Yokohama, p. 298, Tokyo, September, with V.J. Sodd and R.J. Velten
1975 - Some Possible Consequences of Recertification, Radiology 114: 745-746, March
The Use of Nuclear Medicine in Evaluating Liver Disease, Seminars in Roentgenology 10: (3) 215-222, July, with L.E. Holder
fqfcentrations of Medically Useful Radionuclides fg9%c, 1251 and I) at a Large Metropolitan Waste Water Treatment Plant, Health
Physics 28: 355-359, with V.J. Sodd and R. Velten
Evaluation of Radiochemical Protectors Using Urinary Deoxycytidine Levels, International Journal of Radiation Biology 28: (2) 117-124, with D.E. Wrede, I.W. Chen anc! 2.G. Rerciakes
The Gamut Approach to Scintigram Interpretation - Diagnostic and Teaching Method, Journal of Nuclear Medicine 16: (121, December, with L.E. Holder, A.B. Ashare, T. Tomsick, D.P. Colley, M. , Fernandez-Ulloa, and Z. Cat=
Reactor Safety Study (WASH-1400), An Assessment of Accident Risks in U.S. Commercial Nuclear Power Plants, Appendix VI, United States Nuclear Regulatory Commission, October, E.L. Saenger, Member of Advisory Group on Health Effects
Interpretation of Radionuclide Liver Images: Do Training and Experience Wake a Difference?, Journal of Nuclear Hedicine 16, vith B. Nishiyama, J.T. Lewis, and A . B . Ashare
Intercomparison of Myocardial Imaging Agents, Journal of Nuclear Medicine 16: 553, with H. Nishiyama, V.J. Sodd, J.T. Lewis and R.J. Adolph
Inadequacies of Gamma Camera Performance and Quality Control, Journal of Nuclear Medicine 16: 564 (abstract), with V.J. Sodd, J.G. Kereiakes and R.J. Van Tuinen

208
22
Clinical Experience with 127Xe, Continuing Education Lectures, Proceedinqs of the 16th Annual Meeting of the southeastern Chapter of the Society of Nuclear Medicine, page 6, (abstract), with H. Nishiyama, V.J. Sodd, Z.T. Lewis and R.A. Neff
Imaging of Pulmonary Tumors with 12’Cs. Radiopharmaceuticals , Subramanian, et al., editors. Society of Nuclear Medicine, New York, p. 125, with H. Nishiyama, V.J. Sodd, T.J. Schreiber and R.G. Loudon
1976 - Cystourethrography Procedures in Children: Evaluation of Ber.efits versus Dose, Radiolog 118: 123-128, with J.G. Kereiakes, D.J. Cavanaugh, J.LT Hall and W. Eiseman
Breast Cancer Screening - Benefit and Risk for the First Annual Screening, Radiolog 120: 431-432, with M. Moskowitz, J.G. Kereiakes, S. Pemmazaju, A. Kumar and G. Tafel
The Use of Radioactive Cesium Chloride for Imaging of Malignant and Benign Pulmonary Lesions, Surgery, Gynecoloay and Obstetrics 143: 575-580, with H. Nishiyama, J.T. Lewis and R.C. Hoops
Imaging of Pulmonary Tumors with 12’Cs, Radiopharmaceuticals, pp 482-490, with H. Nishiyma, V.J. Sodd, T.J. Schreiber and R.G. Loudon
Integfomparison of Myocardial Imaging Agents: 2@1T1, 12’Cs, 43X and Rb, Journal of Nuclear Kedicine 17: 880-889. with H. Nishiyama, V.J. Sodd, R.J. Adolph, J.T. Lewis and 1.1. Gabel
Lack of Specificity for Detection of Breast Lesions with Radioactive Cesium Chloride, Surgery, Gynecology and Obstetrics 143, with H. Nishiyama, M. Moskowitz, Z.T. Lewis, and R.G. Hoops
Radiation Contamination and Acute Radiation Injury, in Initial Management of the Trauma Patient, editor Charles Frey, published by Lee and Febiger, Philadelphla, pp 203-228
Radiobiology and Dosimetry of Pediatric Nuclear Medicine, in The Pediatric Nuclear Medicine Club: A Biblioqraphy of Pediatric - Nuclear Medlcine Literature, Searle Radiographics, Inc., pp 1601-1659, with M.J. Gelfand
Cesium-137 Body Burdens and Half-Life in a Group of Adult Males in Cincinnati, Ohio, Health Physics 30, with J.T. Lewis, L.W. Grossman, and J.G. Kereiakes
NUMEDACON: Nuclear Medicine Report and Data Storage System, Proceedings 6th Symposium on Sharing of Computer Programs and Technology in Nuclear Medicine, p. 118, with R.G. HOOPS, M.L. Yudofsky, A.B. Ashare and V.J. Sodd

209
23
Radiopharmaceutical Dosimetry in Pediatrics, Proceedings of the 62nd Scientific Assembly and Annual Meeting of the Radiological Society of North America (RSNA), with J.G. Kereiakes, S.R. Thomas, F.A. Ascoli, M.J. Gelfand, P.A. Feller, V.J. Sodd, P. Paras, J.W. Poston, G.G. Warner and R.L. Shoup
1977
Quantitative External Counting Techniques Enabling Improved Diagnostic and Therapeutic Decisions in Patients with Well-Differentiated Thyroid Cancer, Radiology 122: 731-737. with S.R. Thomas, H.R. Maxon and J.G. Kereiakes
"The Developing Role of Short-Lived Radionuclides in Nuclear Medicine", A Report of the Task Force on Short-Lived Radionuclides for Medical Applications to the Bureau of Radiological Health, Food and Drug Administration, U.S. Department of Health, Education and Welfare, August. E.L. Saenger, Chairman of Committee
NCRP Report No. 55, "Protection of the Thyroid Gland in the Event of Releases of Radioiodine", Recommendations of the National Council on Radiation Protection and Measurements, E.L. Saenger, Chairman of Committee
A Comparison of Technetium Etidronate and Pyrophosphate for Acute Myocardial Infarct Imaging, Journal of Nuclear Medicine 18: 905-909, with C. Williams, A. Nishiyama, R. Adolph, M. Gabel, D. Romhilt and V.J. Sodd
Radiation-Associated Thyroid Carcinoma, editor Leslie J. DeGroot, M.D., E.L. Saenger contributing editor, Grune and Stratton, New York. 1977
-
Ionizing Irradiation and the Induotion of Clinically Significant Disease in the Human Thyroid Gland, The American Journal of Medicine 63: 967-978, with H.R. Maxon, S.R. Thomas, C.R. Buncher and J.G. Kereiakes
e to the Metaphyseal Growth Complexes in Children Undergoing 89% c-EHDP Bone Scans, Radiology 126: 193-196, with S.R. Thomas, M.J. Gelfand, J.G. Kereiakes, F.A. Ascoli, H.R. Maxon, P.A. Feller, V.J. Sodd and P. Paras
1978 - Radiation Induced Thyroid Cancer, Cincinnati Journal of Medicine 3: 59, March
Benefit/Risk Analysis of Aggressive Mammographic Screening,
Kere a es J . Hilbrath and M.W. Goodman Radiolo 128: 359-365, with S.H. FOX, M. Moskovitz, J.G.

210
24
Evaluation of Diseases of the Thyroid Gland with the In-Vivo Use of Radionuclides, Journal of Nuclear Medicine 13: 107-112, with Task Force on Short-Lived Radionuclides, Bureau of Radiological Health, Food and Drug Adninistration, U.S. Department of Health, Education and Welfare
Sarcoma Botyroides of the Vagina in Childhood, Treated by Irradiation and Vaginal Reconstruction, American Journal-of Obstetrics and Gynecology 132: 339-340, October, with R.D. Patchell
Diagnostic Radiation for a Young Woman, JAElA 240: 1641, October, with 3.G. Kereiakes
1979 - Radiotherapeutic Agents: Properties, Dosimetry, and Radiobiologic Considerations, Seminars in Nuclear Medicine 9: (2) 12-04, 111th 3.G. Kereiakes, V.J. Sodd and R. David
Medical Radiation Exposure During Pregnancy, JAMA 242: 1669, October, with J.G. Kereiakes
Radiation Effects and Radiation Protection, in Nuclear ?!edicine Review Syllabus, editor Peter T. Kirchner, M.D., Society of Nuclear Medicine Inc., 475 Park Avenue South, New York, SY 10016, with R.T. Anger, A.R. Benedetto and R.L. Witcofski
Clinical Experiences in 14C-tripalrnitin Rrcath T e s t fcr r e t Malabsorption, American Journal of Gastroenterolcqy, p p 327-231, March, with H.E. Meeker, 1.14. Chen and A.M. Connell
Clinically Important Radiation-Associated Thyroid Disease - A Controlled Study, JAMA 144: 1802-1805, October 17, with H.R. Maxon, S . R . Thomas, C.R. Bunchcr, J.G. Xereiakes, N.L. Shafer and C.A. McLaughlin
Reflections on Cancer Treatment and the Federal Agency Regulations, Radiologr 137: 865-866, December, with J.G. Kereiakes
Efficacy and Efficiency of the Diagnostic Applications of Radiation and Radionuclides, Report of a meeting organized by the World Health Organization and the Government of the Federal Republic of Germany, Neuherberg, FRG, Dec. 5-7, 1979; proceedings published April 1980
Clinical Course and Dosimetry of Acute Hand Injuries to Industrial Radioaranhers from Multicurie Sealed Gamma Sources. in ~~ _ _ The Medical Basi; fbr Radiation Accident Preparedness, K.F.
.
HUbnaK and S.A. F r y , eds., Elsevier North Holland, Inc., 1980, with J.G. Kereiakes, H. Wald and G.E. Thoma

25
Biological Risks of Medical Irradiations, edited by G.D. Fullerton, D.T. Knopp, R.G. Waggener, E.W. Webster. E.L. Saenger contributing author: "Methods of Risk Reduction in Nuclear Medicine" with J.G. Kereiakes and S.R. Thomas; "Dose Evaluation in Nuclear Medicine" with J.G. Kereiakes, S.R. Thomas, M.J. Gelfand and H.R. Maxon. American Association of Physicists in Medicine, Medical Physics Monograph 15
Survey of Technetium-99m Contamination of Laboratory Personnel: Its Degree and Routes, Radiology 135: 467-471, with H. Nishiyama
Radiation-Associated Carcinoma of the Salivary Glands: A Controlled Study, Annals of Otolaryngolog 90: 107-108, with H.R. Maxon, S.R. Thomas, M.L. Shafer, C.R. Bunzher, J.G. Kereiakes and C.A. McLaughlin
Once to Every Man...An Introduction, Medical Decision Makinp 1: (11 page 1
Evaluation of LAD Blockage: Hazard of Repeated Radiation Exposure, JAMA 246: 2754, December
1982 - "Ethics, Trade-offs and Medical Radiation", Lauriston S. Taylor Lecture Series in Radiation Protection and Measurements, Lecture No. 6. NCRP Publications, 7910 Woodmont Avenue, Suite 1016, Bethesda, MD 20814
Protection of the Patient in Diagnostic Radiolog , ICRP Publication 34. E.L. Saenger, Chairman of Task &oup preparing report. Annals of the ICRP, Volume 9, No.2/3. Pergamon Press, New York
Development and Use of a New Tc-99m Myocardial Perfusion Agent - DMPE. Proceedings of the Third World Congress of Nuclear Medicine and Biology, C. Raynaud, ed., Pergamon Press Vol. NO. 2, Paris. France, pp 2255-2260, with V.J. Sodd, E.A. Deutsch. A. Nishiyama, R.J. Adolph, L.W. Grossman, K.L. Scholz, K. Libson, D.L. Fortman and J.L. Vanderheyden
Nuclear Orthopedics, "Dosimetry", edited by E.B. Silberstein, with J.G. Kereiakes, S.R. Thomas, M.J. Gelfand and C.C. Williams, New York, Futura Publishers
Basal Kinetic Studies of Tc-99m DMPE as a Myocardial Agent in the Dog, Journal of Nuclear Medicine 23: 1093-1102, with 8. Nishiyama, E.A. Deutsch, R.J. Adolph, V.J. Sodd, K. Libson, H.C. arson, M. Gabel, 6.J. Lukes, J.L. Vanderheyden, D.L. Fortman, K.L. Scholz, L.W. Groesman and C.C. Williams

212
26
Tc-99m DMPE as a Resting Myocardial Imaging Agent. Journal of Nuclear Fredicine 23(5): 12 (abstract), with H. Nishiyama, E.A. Deutsch, R.J. Adolph, V.J. Soda, K. Libson, S.J. Lukea, 1.1. Gabel, M.C. Gerson and J.L. Vanderheyden
1983
Myocardial Perfusion Imaging with 99?!c-DWPE in Man. European Journal of Nuclear Medicine 8: 371-374, with H.C. Gerson. E.A. Deutsch, H. Nishiyama, K.F. Libson, R.J. Adolph, L.W. Grossman, V.J. Scdd, D.L. Fortman, J.L. Vanderheyden, and C.C. Williams
Relation Between Effective Radiation Dose and Outcome of Radioiodine Therapy for Thyroid Cancer. New England Journal of Medicine 309: 937-S41, with H.R. Maxon, S.R. Thomas, V.S. Hertzberg, J.G. Kereiakes, I.W. Chen, and Fr .1 . Sperling
Regional Organization of Medical Care. Bulletin of the New York Academy of Medicine 59: 1095-1107
"Dosimetry of Bone-Seeking Radiopharmaceuticals", in Done Scintigraphy, with J.G. Kereiakes, 8.R. Thomas, M.J. Gelfand, C.C. Williams. E.B. Silberstein, editor, Futura Publishing Company, Ilt. Kisco, NY
NCRP Report No. 73, "Protection in Nuclear Medicine and Ultrasound Diagnostic Procedures in Children", E.L. Saenger, committee member. NCRP Publications, 7910 Woodmont Avenue, Suite 1016, Bethesda, MD 20814
1984 - Low-level Internal Radionuclide Contamination: Use of Gamma Camera for Detection. Radiology 150: 235-240, with 8 . Nishiyama and S.J. Lukes
A Guide to the Hospital IIanaqement of In]uries Arising from Exposure to or Involving Ionizing Radiation, E.L. Saenger, M . C . , member CSA Advisory Panel, American Medical Association, Chicago, Illinois, January
Fanily History of Cancer in a Radiation Technologist. JAMA 251: 1901-1902, April 13
"The Nuclear Physician's Role in Planning for and Handling Radiation Accidents" in, Nuclear Medicine Annual 1984, L.M. Freeman and H.S. Weissman, eds., Raven Press, New York, 1984, pp 1-22
Myocardial Scintigraphy with 99%7c-tris-D14PE in Man. Journal of Nuclear Medicine 9:403-407, with fl.C. Gerson, E.A. Deutsch. K.F. Libson. R.J. Adolph, A.R. Ketring, J.L.
European
Vanderheyden, and C.C. Williams-
213
27
Assigned Share for Radiation as a Cause of Cancer, Review of Radioepidemiological Tables Assigning Probabilities of Causation. Final Report: Oversight Committee on Radioepidemiologic Tables (OCRET), Board on Radiation Effects Research, Commission on Life Sciences, National Research Council. National Academy Press, Washington, D.C. E.L. Saenger, M.D., member of OCRET Committee
1985
Accidental Cs-137 Contamination, Radiolo 154: 513-517, with E.Nishiyama, L.W. Grossman and 5.-
NCRP Report No. 80, "Induction of Thyroid Cancer by Ionizing Radiation", Recommendations of the National Council on Radiation Protection and Measurements. E.L. Saenger, M.D., Advisor to Task Group
-
Determination of Clinical Efficacy: Nuclear Medicine as Applied to Lung Scanning, Journal of Nuclear Medicine 26: 793-806, with C.R. Buncher, B.L. Specker and R.A. McDevitt
Application of an Information-Theoretic Method for Efficacy Assessment, Journal of Nuclear Medicine 26: 807-811, with D.A. Gift, W.R. Schonbein and E.J. Potchen
.Health Effects Model for Nuclear Power Plant Accident Consequence Analysis" (NUREG/CR-4214). J.S. Evans, D.W. Moeller, D.W. Cooper, eds., O.S. Government Printing Office, P.O. Box 37082, Washington, D.C. 20013, July. E.L. Saenger, M.D., Member of Advisory Group
1986
Cost-Effectiveness of Screening Mammography in Low-Risk Patients, - JAMA 256: 406-407, July 18, with M. Moskowitz
The Reactor Accident at Chernobvl: A Nuclear Medicine
-
Practitioner's Perspective, Seminars in Nuclear Medicine 14 (3) : 224-230, July, with J.G. Kereiakes and S.R. Thomas
Radiation Accidents, Annals of Emergency Medicine 15: 1061-1066, September (Proceedings of the 1986 UAEM/IRIEM Research Symposium on- Toxicology)
Comparison of lZ3I and 99%c Pertechnetate in Nodular Goiter Imaging, Radiologia Iugoslavica 20 (suppl.111): 47-49, with S. Spaventi, 2. Kusic and D.V. Becker
1987
Radiation Exposure, in Current Therapy in Emergency Medicine, M. Callaham, ed., B.C. Decker Inc., pp 922-927, with H. Nishiyama
-

Efficacy and Cost-Effectiveness of Lung Scans, in Pulmonarv Xuclear Medicine, bl. Loken, ed., Appleton and J.ange, pp 133-141, with R. Specker
NCRP Report NO. 91, "Recomer.dations on Limits for Exposure to Ionizing Radiation", E.L. Saenger, committee member. NCRP Publications, 7910 Woodr.ont Avenue, Suite 1016, Bethesda, MD
Pulmonary Embolism and Lunq Scanning: Cost-Effectiveness and Benefit:Risk, Journal of ?!nclear Medicine 28: 1521-1530, with B.L. Specker, C.R. Runcher and R.A. blcDevitt
Protection of the Patient in Nuclear I!edicinc, ICRP Publicatior 52. E.L. Saenger, Chairman of Task Group preparing report. Annals of the ICRP, Volume 17, KO. 4 . Peryamon Press, ?1ev York
Don't Disniss Liability Potential of >!edical Radiation Exposuri?, Diagnostic Xmaginq 9 (12): 120-115
NCRP Report No. 3:, "Ionizing Radiation Exposure of the Population of the United States", E.!,. Saenger, committee member. NCRP Publications, 7910 Woodmont Avenue, Suite 1016, Brthesda, I.ID 20814
20814
1989 - WCRP Report t!o. 100, "3:posure of the U.S. Population from Diagnostic !!edicnl Radiat:nn", 7.L. Saenser, com!i';tr-r ?PF~R?. NCRP Publications, 7910 Yioodmont Avenue, Suite 1016, nethcsrla, PiD 2 0 8 1 4
"Radiation Accidents", prepared by ?!le American College of Radiology Ad Hoc Committee on Radmticn Accidents, E . I . . Saenyer, committee member. American CollegP of Radiology, 1091 Preston White Drive, Reston, VA 2209:
1990
Evaluation of Extent of Injury, in >lzd-ical b!anagement of Radiation Accidents, F.A. blettler, Jr., C.A. Kelney and R.C. Ricks, eds., CRC Press, pp 67-78
"Health Effects Models for Nuclear Power Plant Accident Consequence Analysis, Low LET Radiation. Part I: Introduction, Integration, and Summary" (NUREG/CR-4?14: BAND85-7185, Rev.1, Part I). J.S. Evans, ed., U.S. Government Printin9 Office, P.O. Box 37082, Washington, D.C. 20013, January. E.L. Saenger, Advisory Committee member
-

0 4
216
29
Comparison of Technetium-99m and Iodine-123 Imaging of Thyroid Nodules: Correlation with Pathologic Findings, Journal of Nuclear Medicine 31: 393-399, with 2 . Kusic, D.V. Becker, P. Paras, T. Wesseler and S. Spaventi
Radiation and the NIMBY Syndrome, in The Medical Basis for Radiation Accident Preparedness 11: Clinical Experience and Follow-up Since 1979, R.C. Ricks and S.A. Fry, eds., Elsevier Science Publishing Company, New York
1991
Radiation Exposure, in Current Practice of Emergency Medicine, M. Callaham, ed., 2nd editlon, B.C. Decker, Philadelphia, with E.B. Silberstein
-
Perception of Radiation Injury vs. Radiogenic Effect, in The Medical Basis for Radiation-Accident Preparedness 111: T h e Psychological Perspective, R.C. Ricks, M.E. Berger and F.M. O'Hara, eds., Elsevier, New York, with J. Hinnefeld
1992 - Discitis, in The S ine R.H. Rothman and F.A. Simeone, Founding Editors, 3rd d 6 . B . Saunders Company, with J.L. Stambough
Thyroid Nodules in the Population Living Around Chernobyl, JAMA 268 (5): 616-619, with F.A. Mettler Jr, M.R. Williamson, H.D. Royal, J.R. Hurley, F . Khafagi, M.C. Sheppard, V. Beral, G. Reeves, N. Yokoyama, V. Parshin, E.A. Griaznova, M. Taranenko, V. Chesin and A. Cheban
Administration of Stable Iodide to the Population Around the Chernobyl Nuclear Power Plant, Journal of Radiological Protection 12 (3): 159-165, with F.A. Mettler Jr, H.D. Royal, J.R. Hurley, F. Khafagi, M.C. Sheppard, V. Beral, C. Reeves, N. Yokoyama, V. Parshin, E.A. Griaznova, M. Taranenko, V. Chesin and A. Cheban
1993 - Reflections on NCRP Statement No. 7, "The Probability that a Particular Malignancy May Have Been Caused by a Specified Irradiation-, Health Physics 64 ( 5 ) : 549, invited editorial
Comments on the NCRP Statement No. 7. "The Probability that a Particular Malignancy May Have Been Caused by a Specified frradiation", Radiation Research 134: 396-397, invited editorial

216
30
"Implications of the New Risk Estxmates" in Proceedings of the 28th Annual Meeting of the t!ational Council on Radiation Protection and Measurements entitled Radiation Protection in Medicine, NCRP Publications, 7910 Woodmont Avenue, Bethesda MD 20814

217
1. Be- 1970
Hsllblein, kthw C., M. D, 'A Prellminay Rspoct on Continuow lnadakn of (he
Jacob. MeMle L, M. D. 6 Marasso. Fred J. M. D.. 'A Four-Year Expmbnm with
Jenkh. R.D.T., M. B., Rlder. W.D.. M.B.. F.F.R.. el al. 'Ewkrg's Saranna A T M of
Mbs eody. Aadiabcrv. Vd. XVII. NO. 6, 1051-1062. h. 1932.
Totdgody Imdhtkn', Rlldialwv. Vol. 84, No. 3. Plper 452456.463. Man21 1985.
TotaCBody Imdiatkn'. Radiolaav. Vd. 96, Pager 151-155, July 1970.
Khg. ceptein E. Richard M.C., U. S. NW, ylse of Totel-Body Radietbn In the Tmlmnent Of F a r - A d v m MaligfUnck~~, VOl. in. NO. 9. P- eio813, sepember 2, imi.
Loeffler. R Kenneth, M. D. & PuWmgh. M~KWI R., M. D. The Therapeutic Use of
Vd. 123. NO. 1, paOer 170-178. January. 1975. Freetbnatecl SuMotal Body Inaaakn',
Mednger. Fred G.. M. D. & Crcnrer, uoyd F. M. D., Total Body Inadbtbn', Amerlcan 1 Vd. 46, No. 5. Pager 651- 671. November. 1942.
Mllbum.~F..M.D.,OYirady,~.M.D.etal.'RadlcelRadietbnTheraWand Tog( Novemb#. 1988.
hdktbt~ in UW T m W Of W S Senxmur, Vol. 22. P m 919-925,
Miller, Lowel S, Fleichw. Gilbe~I H.. et al 'Radobbbgic observatbns on Cancer PaUmts Treated with Whole-Body X-Irradiation', 1968.
Vd. 4, P- 150-185,
Nemxrmer. Earl H.. .A New Cyl~kglcal and His(dogicd Fixhg Flulb, sdence. vel. 118, P m 161-163, AuQUSt 7, 1953.
R W . W. D.. & Hasdback, R.. The and Haemaldogicd DisiudmfICe folorvho lotd Body Redietbn of =Rad Qamlnnw Inadhtion.. ll&mmlA
P m 139-144, 1968.

218
RubIn. Philip, M. D., Salazar, Omar, M. D., et d. 'Systemic Hemibody Irradiation for Overt and Occult Metastases., Cancer, Vol. 55. Pages 22162221, Supplement, May 1. 1985.
11. 1970 to Present:
A Total Body lmdlation
ArmRage. James 0.. M. D.. 'Bone Marrow Transplantation',
Armitage, James 0.. M. D. & Gale, Robert Peter, M. D., "Bone Mamw
bi&i&e. Vol. 330, No. 12. Pages 827 - 838, March 24, 1994.
Autotransplantation', -e, Vol. 86 Pages 203-205, February, 1989.
August Charles S., Semta, Frederic T., et al, 'Treatment of Advanced Neumblastoma WHh Supralethal Chemolherapy, Radiation. and Allogeneic or Autoiogw Marrow Reconstllutbn', Vol. 2.. No. 6, Pages 809-616, June, 1984.
Chemotherapy as a Systemic Adjuvant for Small Cell Cadnoma of the b n g m ~ 1, Vol. 5, No. 11 and No. 12, Pages 2043- 2048. 1979.
Therapy and A u t o ~ u s Bone Marrow Transplantation in Resistant Cancer, I h & m & ~
Byhardt. Roger W., M. D., Cox, James D., M. D., et al, 'Total Body Irradiation vs.
Douer, Dan, M. D., ChampUn, Richard E.. M. D. et al. 'High-Dose Combined-Modallty
Vol. 71, Pages 973-976, December 1981.
Franzone. P., Scarpati, D., et ai, Zhemo-radiotherapy and Autologous Bone Marrow Tmsplantation in Poor Prognosis Neuroblastoma', Pages 102-104, 1990.
Huys. John V.. M. D., Simons, Maria J.. M. D. et ai, Total Body Irradiation with 8 MeV X-rays in Generalized Malignant Disease". Qm& Vol. 39. Pages 1435-1438. 1977.
Kramer, Simon, M. D , 'Fraactionated Total-Body Irradiation', Vol. 37, Pages 2120-2122. April 1976.
Uvingston. Robert B.. M. D., Schulman. Susan, et al, 'Combination Chemotherapy and ystemic lrradiatkn Consolidation for Poor Prognosis Breast Cancer, w, Val. 59, Pages
Supplement 1,
1240-1254, 1987.

219
Loeffler. Kenneth R., M. D. 7herapeutic Use of Fradbnated Total Bo&y and Subtotal Body Lrradiatbn', Cancer. V d 47. Pages 2253-2258, 1961.
Uarcus. Robert B., Jr., M.D.. Graham-Pole, John R., M. D.. et al, 'Hlgh-Risk €wing's SaraMIII: End-lntenslkatbn Uslng Autobgous Bone Manow Transplantatbn*, international
Vol. 15. Pageas 53-59. July 1988.
Fhtorn. A. Y., 'A Review of the place of Radbtherapy in Myeloma with Emphasis on
Sode. 0.. M. D.. Devergle, A., M. D.. el al, Ynfluence of the Fractinatbn of Total Body
whde Body l r r a d i a t b n D ~ Vol. 8, Pages 193-198, 1988.
IrradIaUon on Compllcatkns and Relapse Rate for Chronic Myelogenous Leukemia',
LAerch 1991. Vd. 20. Pages 397-404,
!3jemsrmrd. J.. M. D.. 'Adjuvant Radbtherapy Trials in Breast Cancer, Ea0r;er. Vol.
Vrlesendorp. H. M.. 'Predklbn of Effects of Therapeutic Total Body lnadiatbn in
WMesendorp. H. M., Herman. M. G.. el al. 'Future Analyses of Total Bndy Irradatbn'.
39, Pages 2846-2867. 1977.
uan'. Supplement 1, Pages 3750.1990.
s my&& Vol. 20, Pages 635-637, LJarch. 1991.
h#orr. Andrew, M. D., Stabile. R. J., et al, %Ingle Hbh Dose-Large Field Inadiatlon'. Vd. 85, No. 1. Pages 3942, January 1988.
R PddBodylnadiatbn
Ark, H.,M. D.,Choi. K .M.D . .e ta l .~nrper lsond32P~andSequenth l Hembodly lnadiaakn (HBI) for Bony Metastases as Methods ot Whole Body Inadia(kn',
Vd. 9, No. 3. Pages 264-268.1986.
Flchhan. H.J., Prof. Dr. Med., Hultner, J.. Dr. Med., el al, T m Y m h ~ Report on DnalhW.nd Hbh DOW lnadlatbn dthe Llpperad Lower Hslf-Body In Petientswiul Small c d m - , v vol 9, PaQea 1459-1465. October 1983.

220
Epsteln. Lonnie M., Stewart. Bruce H., et al, 'Half and Total Body Radiatkn for
FkpatrW, Peter J., M. B., F.R.C.R., FRCP, & Rlder, Walter D., M. B., F.R.C.R., FRCP..
Carcinoma of the Prostate', Vol. 122. Pages 330-332, 1974.
Valf Body R a d i o t h e r a p y * ~ 9 Val, 1. No. 3-4, Pages 197-207, 1976.
Segmental Inadation and Comblnatbn Chemotherapy for Children with Disseminated Neuroblastoma'. m, Vol. 38. Pages 2250-2257. 1978.
Jenkin. R.D.T., M. €3.. & Berry, M. P.. M. E.. Sequential Half-Body Irradiation In Chiidhood'# , Vol. 9, Pages
Green, Alexander A., M. D., Hustu. H. Omar. M. D.. et al, Total-Body Sequential
1969-1971. 1983.
Montebello. Joseph F.. M. D. & Hartson-Eaton, Mary, Ph. D., The Palliatbn of Osseous Metastasis with 32P or WSr Compared wHh External Beam and Hemibody Irradietion: A Historical Perspective", CancerInvestiaation, Vol. 7 No. 2 Pages 139-160, 1989.
lrradlation (UHBI) For Extensive Small Cell Carcinoma of the Lung', Payne. David G., M. D., F.R.C.P., Yeoh, Um. M. D., F.R.C.P.. et al. 'Upper Half Body
& Ph-, Vol. 9, Pages 1571-1574, 1983.
Poulter. C. A., M. D., Cosmatos, D.. Dr. et ai, .A Reporr of RTOG 8206: A Phase 111 Study of Whether the Addition of Single Dose Hemibody irradiation to Standard FractiDnated Local Flew lnadlatbn is More Effectbe than Local Field Irradiation Alone in the Treatment of Symptomatic Osseow Metastases', Pages 207-214. 1992.
Powell. Bayard, M. D., Jackson. Don V., Jr., M. D., et al, 'Sequential Hemibody and Local lnadiation with Combination Chemotherapy for Small Cell Lung Carcinoma: A Preliminary
, Vol. 11, Pages 457- Analysis-- 462. 1985.
, Vol. 23. . .
. .
Qashn. M. M.. "Half Body Irradiation (HBI) in Metastatic Carcinomas'.-
Rwrland. C. G., Bullimore. Jill A.. et al, 'Half-body Irradiation in the Treatment of
- Voi. 32, Pages 215-219, 1981.
Metaslatic Prostatic Carcinoma'. , Voi. 53. Pages 628-629. 1981.
RuMn. Philip, M. D., Saiazar, Omar, M. D., et ai, Systemic Hemibody Irradiation for
Page U4

221
.
c
Overt and Occult Metastases'. Gancu, Vol. 55, Pages 2210-2221, 1985.
Rubin. Philip, M. D.. & Heilmann. Hans-Peter, M. D., 'Large Field Trials'. Vol. 124, Pages 565-576,
1988.
Salazar, Omar M., M. D.. Rubin, Philip, M. D., et ai, Single-Dose Half-Body Irradiation for Palliation of Multiple Bone Metastases from Solid Tumors", w, Vol. 58, Pages 29-36. 1986.
Metastatic Melanoma by 24-Hour DTlC Infusions and Hemibody Irradiation'. w, Voi. 57. Pages 2103-2107. 1986.
Modalii for The Management of Patients with Small Cell Lung Cancer",
Thatcher, Nick. Ph. D., FRCP, Anderson, Heather, M. D.. MRCP. et al, 'Treatment of
Urtasun, R. C., M. D., Belch, A.. M. D.. et al. 'Hemibody Radiation, an Active Therapeutic
Vol. 9, Pages 1575-1578, 1983.
Page W5
84-514 0 - 94 - 8

222
. 50 8 Chief, Radiolo&al Service ' DATE: zo &totar 1958 W o l t a r Reod k y Mcdlcal Center
Asat chief, Slophyalca and AstroMutiu Rereuch Brurch, 11. S. .cr;pr U o & d Research and Dsvelopaont C d
=OX I .
W W r Appllcatlon for Research Contract . 1. The inclosed' copy of research proposd entltled, "Mehbollc -ea in
b- Follouinc Total Body PadlatlM,n he18 been sutzaltted for our consldor6tion by . It.. m e n o L. .%eager of the UnSversitY of Cincinnati, Collage of 14adlcln0, I
.: ! cincinnatl, axlo.
2. Requast m i e v of the attadrsd proposal and planas elm your ree-htlcn aa to vhether or not t h l o atudy ahould be *upportad by tbo Amy Medical senrice.
~~~
ELM Z33r Aast Ch, Bio$yrlcs L. Astmnrrutfcs FRUK: chi&, Radlologid DATE: 22 Oct 195
Bssearch Branch, US h z y Kedlcal svo, VRRA . ColIohenmod/rWb. Research B D s n l o ~ n t oormrnd
1. Ree&+d approval.
2. Much vork hrs been done on the effects of btnl kody l r radlat ion '9 ar-s mere has been DO r e d effort t o d6te f o r s l n i l n r studles on luzmaa. Of the asrmfion that aninul reaction io identicel with that in,&nana I t Fur& 8snnption. There is d e f a t s need f o r b o l e vork in this field. Any cor=rlatlon Of t-r response to total dose of lrradlation by such mema an prepred in this P fD e C t Muld be of great v a l u in the f i e ld of cancer. =earn wch as those propsad accurate knowledge of the total dose of rrdiatZon reccitnd could be determined it would be of 1 n e s t h U e d u e in easa of a e c dlsaster or nuclear mrfare. I b c applicant, Dr. hanger, l a veL1 qualUled to W&+uct 3uch rosearch. the a b i l l t t to s t h u l a - his co-wrkera and arsistanta. tkrd .nd 18 sa excellent organizer and admLcLstrator. *& h S 8Vallahle are v e l l adapted to the project. -S wt 081 such project am ve l l wrthvhlle.
me vd ld i ty
In addltlon' i i b y14
Re is not only sa anthuriastic d t i re less wrker hrt h a Hs bas LD UnUsusl a d Y = i : t
It 1s bollevod tka t rq. 1 bellava the facFlit ies
,
1 krd 4 c
Chlaf, Radiologlcsl Service

r
223
COXSENT FOR SPECIAL STI'M AXD TXATXENT
, do hereby give my consene % . t o the pambers of the professional s t a f f of the Cincinnati General Hospital.
l lniversity of Cincinnati College of Xedicine. t o administer t o ma whole OK a a r t i a l
bo- i r r ad ia t ion on or about , 1 9 s .
The nature and purpose of t h i s therapy. possible alternaeive methods of
treatm+nt. the risks involved, the poss ib i l i ty of complications. and prognssis have
been fully explained t o me. The special study and research nature of th i s treat-
uent bas been discussed v i t h me and is understood by ma.
Consent is given f o r photographs and publication fo r the advancemert of
m d i c a l education.
Uitnesres t o signature:
Original: to pat ien t ' s chart Copies: t o Ca-60 file
t o TBR f i l e
5/1/65
Signature
Relationship (patient or grardian)
An Date PH
(Ho. Day Yr.1 . . Place
(Ward - Clinic - !mi:) Chart l o .

224
do br&Y l i v e my C O I U M t . . . . 1.
to th U0b.r~ of tta professional s taf f of the Cincinnati General Uoapttal,
Xhinrsity of CincSmuti College of ~ d i c i n e . to perform a bone carrow eeDiration
d to stem m bone mrrw 011 or &our . .
I 196-. . . 'zb. M~Q- and purpoae of Chi. therapy, the rirlu involved. the poaeibili*.
of uql%utinu. Md prognosis have been ful ly explained to 011. The apecial
ibrg sad rarearch natura of chi. treatsent k u b a n dbcuseed with 011 mud is
amdaatood by. m.
w n t i a also given for reinfusion (giving, the Iarrw back to ma) when the
d c r s o f the professional s t a f f recommend it.
W e n t 1. given for photographs and publication for tbe advancement of
rd.lu1 education.
Signature
liltncssca t o slpnarure:
. _
OrLgbal: to parienr's chart Copies: t o Co-60 f i l a . to TBR file
Relationship (patient or guardionl- AM
nata PH (Moo. Day Yr.)
- (Ward - Clinic - Unit)
Chart Iso.

I
225
,
+I of Oatimt) ( n o d subject) . (place - c i t y )
being of the age of majority and of sound mind and body, vo luntar i ly m d without force o r duress. c m e n t to p a r t i c i p a t e in a a c i e n t i f i c inves t iga t ion which Is not d i rec ted apec ica l l7 t o my ova benef i t , b u t in coaaider.*ion f o r the expected advancemenr of medical knowledge, which may r e s u l t f o r the benef i t of mankind.
I have been infomed of and understand the nature, duration, and purpose i f the study, the method .nd mew by which It is t o b e conducted, the inconvenience and hazards t o be expected, end the e f f e c t s upon ny heal th and person which my possibly come from p a r t i c i p a r i c n i n the experiment, as follows:
Purpose: on blood m d urine:
h e d u r e :
Rirlrs: plant, drugs, o r transfusion as needed.
I understand t h a t I may, a t any time during the course of the experinent, revoke ray consent, in w r i t i z ; , and withdraw from the experiment.
I acknurledge t h a t no guarantee o r assurance has been made to me as to the r e s b l t s that -3 be obtained. and I hereby waive any and a l l claims f o r l i a b i l i t y , except f o r negligence, on,thr par t of the nedical personnel involved, the University of Cindrmi t i . its Hospital and its Xedical School. rh ich othenrise might have inured LO M or my h e i r s , i s a r s s u l t of t h i s ced ica l procedure.
I c e r t i f y t h a t I have read and am competent t o fully understand t h i s consent and that the explaclltions l i s t e d above w e r e . in f a c t , reade.
Volunteer Date
Inves t iga tor Date
Wtness (1) Date
To k i l l tumor c e l l s and a t the same time study the e f f e c t s of rad ia t ion
Radiation of the whole body.
‘Ihe chance of in fec t ion or mild bleeding t o be t rea ted with marrow trans-
-
*In cese of subjec t under aee. the parent o r guardian should be the responsiblc party and should s i p on h i s behalf .
XLITE: C q q t o P a t i e n t h o m a 1 subjcct. Research F i l e and Pa t ien t ’s Chart.

1 e8rCify C h 8 t COM8Of 8d Ch8L C h a . rp luurion Il8c8d ~bw8
hrrn rud .ad .p cwatont to nnd8r8t.nd thi8 w u . in fect . u d e .
Voluncc~r Data
Inrr8tig)cor Data
uitOf.8 (1) b C 8
he888 of d j e c t under .&e. the parat or guardian 8hould be th8 mmpomible party 8ad 8hould 8ign on h i s behalf.
m: COW LO P8ti8nL/Normd 8ubjQct. a8a8rch File and PatianC'8 a r t .

227
I ,. FACULTY ~'CIIT'TEE ON RESEARCll * . d .
' I VOLUNTARY C0::SEKT STATUEKT
- *I of (Pa t ien t ) (lorm~l s u b j e c t )
being of t h c age of P a j o r i t y and of sound mind and body, v o l u n t a r i l y and wi thout f o r c e o r duress . consent t o p a r t i c i p a t e in a s c i e n t i f i c i n v e s t i - gation which is not only d i r e c t e d s p e c i f i c a l l y to ny own b e n e f i t , b u t also i n cons idera t ion f o r t h e expected advanccacnt of amdical knowledge. M c h may r e s u l t f o r t h c b e n e f i t of mankind.
1 have been informcd of and understand tho naturo. durat ion. and purpose of tha study. t h e method and maans by which i t i a to be conducted, t h e inconvenience and hazards t o be expcctcd. and t h e e f f e c t 0 upon my h e a l t h .ad person which nay poss ib ly COW from p a r t i c i p a t i o n i n t h e experiment, u follows:
. Purpose: the e f f e c t s of r a d i a t i o n on blood and ur ine.
To k i l l tunor c e l l s and a t t h e some t i m e e tudy i .
Procedure: Radiat ion of t h e whole body.
Risks: b u t a t t h c sane t i m e othcr . noreal . c e l l s of your body w i l l le a f f e c t e d . you a r e those c e l l s i n your bonc narrow. The bone marrow is a "blood factory" where v h l t c c a l l s chat f i g h t i n f e c t i o n . t h c platelets which he lp blood c l o t , and t h a red c e l l s which c a r r y oxygen t o your t i s s u a s a r c made. The bonc marrow'o ab i l iLy t o make t h e s e c e l l s w i l l bc dccraascd f o r four o r f i v c waeks a f t c r p u r e c e i v c your r a d i a t i o n . I f you r c c c i v c a dosc of r a d i a t i o n o f 200 rads or more, which your doctor w i l l t e l l you. your blood counts w!ll f a l l t o l c v c l s where i n f e c t i o n or blccdlng could be a problem. and p l a t e l e t s and the i n f e c t i o n by a n t l b l o t i c s . I n addi t ion . vc 0
prevcnc such lov blood cocnts with t h c use of a bonc clarrow t rans- plant which w i l l be discusscd with you i n a s e p a r a t e voluntary consent s t a t e n c n t . part of t h e body t h e r e is no r i s k of dangcr o r unusual ly low blood counts .
Radiat ion t r e a t u c n t employed is used t o k i l l t m o r c e l l s
The only cclls a f f e c t e d which would cousc any r i s k to
The b lccdins can bc t r e a t e d by t ransfus ion of red c e l l s
I f your r a d i a t i o n dose is only givcn to '
I understand t h a t I may, a t any t i u e d u r i n s t h e course of the expcrlmcnt, revoke my consent , i n w r i t i n g , and withdraw from the experiment.
1 a c k n w l e d g e t h a t no guarantee or assuTance has been made t o m e as t o the r e s u l t s t h a t nay be obta ined , and I harcby waive any and a l l claims f o r
involved, t h e Universi ty of Clnc inna t l its H l s p i t a l and its I lcdical School, which othcrwisc might have inured t o m e o r my h e i r s , as a r c s u l t of this medical procedure.
- - l i a b i l i t y , except f o r negl igencc. on the par r of the n e d i c a l pcroonnel , s

. I ecrtlfy that I'have read ond am CaIUpQtQnt t o undoretond thin COM&-IIC and I I ~ C tho explanation I luted irLnvo
%%l~ItWr DOC0
was. in ioct. made.
Inrest IRutor Date
U1tae.s (1). Data
tucasc of 8ubjecc under age. tho parent or guardian 0110uld bo tho r r s p ~ l b l c party urrd rboulll eiji~r on Mol boltalf.
nmE: &py t o P.ltlQnt/th8ial o u b j ~ c t , RC60Jreh Fila ond Patlent'o Chart.
r
i

BIOCHEMCALANDBKXOOlCALTESTS~PATIENTSWERGC#G TOTAL BODY IRRADIATION AND PARTIAL BODY 1RRADIATK)N
Pre and Post Radiation Observations'
1.
2.
3. Electrocardiogram, chest X-ray, urinalysis
4.
Complete history and physical examination
Hematocrit, hemoglobin, leukocyte count and differential
Sequential multiple analyses (SMA-12) for blood chemistry determination, prothrombin time, creatinine phosphokinase levels, partial thromboplastin
5.
6.
7.
8.
9.
10.
11.
12.
13.
14.
15.
time
Blood and urine amylase
Ultraviolet absorbing compounds in urine
Bone marrow aspiration
Blood typing and cross matching i f bone marrow transfusion is to be done
Tritiated thymidine uptake for lymphocyte viabllity
Histochemistry and electron microscopy of bone marrow pre and post etiocholanolone
Chromosome analysis
Nitroblue tetrazolium study of granulocyte function
Serum glycoprotein assay
Serum amino acid assay
Bacteriophage titers

18.
17.
18.
19.
20.
21.
22.
23.
24.
25.
26.
Urinalysis for hydroxyproline levels
Psychological testing
Urinary taurine for correlation with leukocyte count
BAIBA in urine
Kynurenic and xanthurenic acids
Deoxycytidine
Xanthine and hypoxanthine in urine.
Urinary phosphate
Glutathione
Routine electrophoresis and Immunoelectrophoresis
Quantitative precipitin studies
These observatbns and tests have varied as some tests do not seem useful and new ones suggest that they may be valuable.

231
Reprinted fmm The A- J o v r d of Rontgmology. Rndim Thrmpy a d Nvlcor Mrdrrkr
VoL CXVII. No. 3. March, 1973 ..Q....
"I.
WHOLE BODY AND PARTIAL BODY RADIOTHERAPY OF ADVANCED CANCER*
B? EUGENE L SAENGER, M.D., EDWARD B. SILBERSTEIN. M.D.. BERNARD ARON, M.D., HARRY HORWITZ, M.D..
JAMES G. KEREIAKES, F'n.D., GUSTAVE K. BAHR, PH.D., HAROLD PERRY, M.D..t and
BEN I. FRIEDMAN. M.D.8 C I N U N N A n , OH10; DETROIT, NICHIGAN; AND bIUI1'HlS, TCNI(CSSLE
T H E P urpose of these investigations has been to improve the treatment and
general clinical management and if possible the length of survival of patients with ad- vanced cancer. Systemic effects of radiation therapy have been given particular atten- tion in our work.
In the peridFebruary 19,1960, through August 31, 1971, 85 adults were given whole or partial body radiation as therapy for far advanced cancer.
This paper will report on the survival of patients in 3 categories: colon; lung; and breast
Prophylactic whole body radiation ther- apy was given to 3 children with localized Ewing's sarcoma and this experience will be discussed briefly.
Investigations of biochemical, cytologic and psychologic tests have been reported elsewhere.' fl*'O
Our experience with the adjuvant use of autologous bone marrow will also be described.
ANIMkL STUDIES
The animal investigations basic to our work stun from the studies of Hollcroft et aI.n-1' These authors demonstrated bet- ter tumor regression when whole body ir- radiation was preceded by localized rrdia- tion therapy than when localized radiation therapy was given alone both for Iym- phoma and carcinoma in mice. The studies of Jacobson et af."*1* showed the impor-
tance of shielding of the spleen and other organs and parts of the body in preventing high dose radiation lethality in the mouse.
BRIEF REVIEW OF TOTAL BODY IRRADIATION IN HAN
Total body irradiation was first em- ployed in 1923 by Chaoul and Lange.' Its use in 270 cases over the next 20 years was reviewed by Medinger and Graver.- These authors found the greatest palliation in the lymphomas and myeloproliferative diseases, but also noted improvement in multiple myeloma. Thirty-five patients with ad- vanced carcinoma or aarmma were in- cluded in this series, most of them receiving their total body radiation berwcen 1931 and 1933.
Loeffler et a P compared total body irradiation in single doses up to 150 r with nitrogen mustard and triethylene melamine and found that neither chemotherapy nor radiotherapy differed in hematologic ef- fects, but that the patients receiving radia- tion did not experience the malaise of vary- ing severity noted by all patients receiving the chemotherapeutic agents. Subjective improvement was noted only in the radio therapy group.
Collins and LodRer* gave total body irradiation in single exposure up to 200 roentgens and found this form of systemic therapy ''a useful addition to the manage ment of advanced cancer." The malignan- cies treated included lymphoma, chronic

232
vob. 117, N ~ . 3 - Whole Body Radiotherapy of Advanced Cancer 671
myelogenous leukemia and multiple m y 5 lomr.
Interest in total body irradiation in the treatment of Ewing's sarcoma, a tumor of children which carries a high mortality, has been aroused by reports from Milburn et 0 1 . ~ ~ Jenkins et and Rider and Hassclback.ag In a small series so treated, survival appeared to be moderately im- proved compared to larger series treated by conventional local radiotherapy and/or ablative surgery. T h e groups felt further evaluation of this form of therapy to bc most important.
Additional data have been published by the Medical Division of Oak Ridge A s s dated Universities,' concerning total body radiation therapy of lymphoprolifvativc and myeloproliferative disease.
Summaries of the frequent use of total body irradiation for the therapy of leu- kemia appear in an article by Buikner et 01.' and in a comprehensive review of bone marrow transplantation by Bortin.'
Whole body radiation in routine clinical therapy has been and is currently used for l ~ u k e m i a , ~ . ~ Ipphoma,~"*" Hodgkin's disease: polycythemia vera: cancer of breastP cancer of thyroid: cancer of pros tate,'o*J' and multiple Such therapy may be given by external radiation therapy (as in this particular study) or in the form ofvarious radionuclides.
STUDY DESXQN
The studia reported here were initially considered as being in Phase I (to deter- mine whether the treatment was toxic or not) and subsequently as Phase I1 (whether treatment appurs effective or not but without con&). In reviewing these data it has ken possible to find some compara- ble material in the literature. In one ute p r y , cancer of bronchus, comparable data rere avmihble in our institution.
IN.OuILD C O N S U T A I D I N ~ O l I A L . m C W
All natients nave infonned conseat in
Cincinnati College of Medicine and t h w of the National Institutes of Health. The use of formal informed consent forms in this study antedated the above require- ments by 2 years. The project is reviewed and approved regularly by the above Committee.
W G I I I ~ or PATIIWIY
Patients become eligible for this form of treatment if they have advanced cancer for which cure could not be anticipated. Three children with localized Ewing's tumor at Children's Hospital were given whole body radiation as part of the curative attempt after the primary tumor had been ablated with local radiotherapy.
Biopsy proof of the malignancy has been established in all instances. Clinical data in each case have been reviewed by several physicians to be certain that the tumor had indeed extended from its primary site and that curative therapy was not applicablc This preliminary evaluation is followed by an observation period of 7-14 days to ob serve the general condition of the patient and to urry out baseline laboratory tests to be as certain as possible that the condi- tion of the patient is datively stable. Fra quently this determination is difficult s ine the patients have urious illnesses of long standing and often have had considerable previous therapy.
Patients remain in the hospital u long as is necessary. Prior to the use of autolopus bone marrow transfusion, hospitalization was occasionally as long as 8-10 weeks. Lcngth of stay was also dependent upon the severity of the clinical manifestations stan- ming from the cancer. With the use of par- tial body irradiation and bone murow i n b Jon, hospitalization has been greatly hor~ e n d The fdlor-up procedure is continu. ous during the l i f e h e of the paen>.
A total of 1x2 Nbjeca rae h b d y entered in the study rhrough Aupust 31, 1971. During the screening period of 7-14 daw. ZA of than (21 w cent) were not

233
Saenger et al. MAU., I973
among the reasons for elimination was an indication in the pretreatment phase that some risk from widsfield radiation might ensue or that another method of treatment was considered preferable. In some, a very rapid progress of the disease made inclusion undesirable. The treatment was completed in 85 adults and 3 children between April 1960 and August 31, 1971. Three patients have received 2 separate courses of treat- ment in this program. Follow-up time for survivors is reported through August 31, 1972.
?AnEhT W S l W L T I Y
The radiation is delivered by a cobalt bo teletherapy unit under the following upo- sure conditions: The beam is directed hori- zontally a t a wall 342 cm. away with the midline of the patient a t 286 cm. from the source. For whole body exposures, the radi- ation beam size for the 60 per cent isodose curve a t the patient midline distance is a square approximately I 20 cm. X 120 cm. The patient is placed in the sitting position with legs raised and head tilted slightly forward. Radiation is given by delivering half the specified exposure laterally through one side of the patient, the patient is then turned and the other half exposure deliv- ered laterally through the other side. The combined dose of the 2 radiation fields provides a good homogeneous dose distri- bution through the patient. The maximum variation in lateral dose distribution was f 13 per cent for I patient who had a lateral aunk dimension of 36 cm.
The exposure to the patient is deter- mined using a percentage depth dose table corrected for the sourccto-skin distance used for the patient. Using the corrected depth dose at patient midline (1/2 lateral dimension at the trunk in the plane of the xiphoid) and a conversion factor of 0.957 rads/rocntgen for cobalt 60 gamma radia- tion, the midline air exposure rquircd to give a daired midline absorbad dose in rads is calculated. The validity of this pro. cedure was established with measurements in an' Aldenon Rando Phantom using
thermoluminescence dosimeters. Over the course of the study, the air exposure rates at the distance indicated above varied from 3 to 6 per minute.
For individuals receiving partial body radiation, the teletherapy collimator is used to restrict the beam. The xiphoid is used as the boundary of the field for upper and lower body exposures. The lateral dimen- sions of the patient in the plane of the xiphoid is again used for calculating the desired midline dose. As for the whole body exposure. the dose is delivered bilaterally. Additional information on the dosimetry aspects of this study has been published by Kereiakes et al.n
AKALYSIS Or IUIVII'AL DATA
In considering the survival data there was a lack of consistent selection bias both in recommendation that a patient be eligi- ble for treatment and in regard to the dose. The principal investigator had no part in determination of therapy in any given case except for outlining the general principles of the therapeutic regime. The choice in the case of each patient was made by several radiation therapists, 3 having been asso- ciated with the project during the JO year period. In addition, 2 internists have had active rola in the selection and medical care of each patient. The dose of radiation to be given was decided upon by the radia- tion therapist in consultation with the internist.
There are 3 categories of patients (those with carcinoma of the colon, lung and breast) which are large enough to permit some analysca of survival. Each group will be discussed separately.
Survival data are given in days from the diagnosis of far advanced disease, since this convention has been used frquently in the literature and permits comparison of our survival data with published reports.
CANCZU or m c COUJK AKD aLcTm(
Twenty-nine patients with this tumor comprised the largest single category (TP, ble I). In 1 case the patients were d a d

as far dvanccd and in a fen instances as tamiaal. Four patients were not included in the study fa medical v, or bccaur the patients themselves declrned pamapt don in the study. In der to make an appropriate corn-
prison, md published d a were re- viewed. series of cases of colon cancer metastatic to liver were utilited, since they were the best found by us with appropriate time paiodr of metastasis available for compuison. Sturnr and Binkky,a in 32 pstienarith dom eurcerwith lirmmeue
ura, found a median survival time of 11 months 8ftU palliative raecuon of the primary tumor; in 28 of their patients in whom only biopsy a diversion w u per- formed, thc median m d v d wu 8 months. In 353 patientswith untruted d o n anew metastatic to liver, Pestana et .Ip reponed a median survival of 9 months. F i I
~metastascsandaombscquatthmpy nponcdby J $ e r r d a T h a e i s . I r o r
of 61 paeena rrponcd by hpoport
ts UI analysis of r77 patients wirk
~ur laonut ru ted with ~-i?UomUruiL
*
k

235
a74 . Saenger et 01.
The 22 patients in our series with proven metastatic carcinoma of the colon to the liver treated by irradiation are also shown in Figure I.
The median survival time for untreated patients was 146 days; for patients treated only with fluorouracil, 255 days; and, among our patients with liver metastases, 391 days (Table 11). A life table analysis was performed and indicates that the treat- ment given to our patients was approxi- mately equivalent to the group given 5- fluorouracil. There was no evidence that the median survival time was shortened by total or partial body irradiation (Fig. I). It should be appreciated that 5 of our pa- tients had received or are receiving 5-fluoro- uracil in addition to the radiation therapy 0 of these with liver metastases).
The median survival for the entire group of zy patients (22 with liver metastases) was 327 days.
CANCER 01 THE 1RONCWVS
This group of I 5 patients (Table 111) had far advanced disease with distant metas tam a t the time of treatment. The best comparison group was from our own insti- tution reported by Horwju r! al.” The median survival of the 15 patients receiving whole body irradiation was 193 days from the time of diagnosis. The median survival of 61 patients seen a t Cincinnati General Hospital from December, 1961, to June, 1964, was 135 days. In 15 of the 17 CPKS with distant metastases excluded by Hor- wits et a/. from their study (see caption to Fig. 2), the median survival was 32 days.
This last groiip of patients with distant metastases constitutes the most appropri- ate comparison group. When rhe median survival* of 15 patients mentioned by Horwin rf ai.” is compared with the 15
‘T-ofrhr #7 yaneccbdd m rk Horn= ~ d ~ s t u d r nn m.mJ b, rhde body d a c h a .

236
Pbr. #it. Ne. I Whole Body Radiotherapy of Advanced Cancer
patients treated by whole body irradiation, the survival times are significantly different (Chi quare 11.63, p <oms) (Fig. 3).
EWNO'S TUYOi
This subgroup of 3 patients constituted the only one in which an attempt a t cura- tive therapy was made; dl 3 patients arc aurviving. The times of survival are 854, 1,33 and 1,153 days from the time of diag- nous to August 31,1972. The patient with the longest survival has recently developed a solitary pulmonary metastasis. The use of whole body irradiation to eliminate small dumps of cells in the disease has been reported by othcrs.n*'
A fourth patient with Ewing's tumor had pulmonary metastases when first seen. Therapy in that case was only palliative.
TABLE I1 CANCU or COWN-CASU amr
(a i Patima) YEIASTASU 50 L I V U
Study Survival After S u r n d After No.. U (dam) R. (dam)
n 103 116 I 16 '35 144 163 193 166 333 349 419 683 197 855
CANCU 01 IWL B R U I T
In 15 cases treated by w the median survival from diagnosis to d u t h was 479 days and after treatment to d u t h was 446 days (Table IV). Two comparable reports in the literature indude the one by the Committee on Estrogens and AndrogcnP and the o tha by S a p and Ansfield using ~-fluor~uraal.~* Again a life table analysis was done for our 15 patients and indicates that the survival of our patients appears somewhat better than that of the patients treated solely by estrogens and androgens, but not quite u good u the group treated with 5-fluorourral (Fig. 4). The patients survive longer than those meivin the "standard therapy" as described by Bamp and Ansfieldf' this induda appropriate administration of estrogen and androgen, oophorectany, Id irradiation, adrcnalec tomy and hypophyrcctomy.
OIWIZI CANCCU
A remaining group of 25 cues reflected ~ v e r d different kinds of cancer. It is not

237
t
L I I I I I I I @ 1 o I L a 4 s 6 7 (I e IO II 12
M d l U Fro. z The d v d by 8Cnnri.l a d p i s is r h o m for 8 cod of 61 pCienta rith a&ams of the bmnchue
.nd disanr metastases, who presented knwen December. 1961 8nd June, I& at Ci&nmti General Hapid . The only phta excluded fmn chis group are thor in whom diranr metastases wae p m n c at the omc of di .pMia (17 ptiena). If they were to be included, the I year nmid figure vould drop to about 7 p1 me. IC u emphaized dut thae figum take ~ C C O U D ~ of d c u a wen (including thae apparently "early" d ~ C I U M C to emrplcm ~ 1 g i 4 rrrenjon). Although other reported may be mewhat higher, diff- ue more realistidy amibuable to bidec faem nther dun to tbapy.=
possible to make an analysis of there at this point since the individual use groups are too small to warrant this
DISCUSSION
I U A I I O J OT IADIATION T H t l l A I Y 10 PATICYI DEATH
Some analyla can be made which give information on this point.
The d a e r of whole body radiation given could initiate only the hematologic form of the acute radirdon syndrome. In the bedthy individual, after prodromal rymp
toms of mdaire and vomiting lasting about 6-48 hours, then is a latent period lasting until 18-21 days after exporun. At this time thw is a marked rapid fall in white blood cells and platelets and a leu rapid fall of red blood cells ruching a nadir at p 4 0 days and then recovering. " h u e changea arc urociatcd frequently with episodes of i n f d o n and bleeding. Epila- tion will occur at daer ova Many of the patients had d v e d
much radiation and chemotherapy pnw to total or partial body autment and in
rads.

238
VOL. 117. NO. J Whole Body Radiotherapy of Advanced Cancer 677
SURVIWL COMPYUZISONS CANCER OF BRONCHUS WITH MET-S
URHWL TYE IN MONTHS
ha. 3.
many cases this treatment was followed immediately by planned local therapy to
If one assumes that dl severe drops in
TABU IV
(15 htirntl) C A X C L ~ 01 ILIA-VITIVAL n m
various portions of the body.
blood cell count and dl instances of hypo- surrirrl surrinl . cellular or acellular mamnv at death were ;$ After D. After (&)
due only to radiation and not influenced by ( d a d (d.d 16 2m TN& the type or extent of cancer and effects of
previous therapy, then one can identify 8 055 175 156 2 m U B y cases in which there is a possibility of the 019 28s 15% 150 therapy contributing to mortality. Of this 060 316 P 150 subgrou~, 2 patients received localized 2: :i: radiation between total body irradiation - 473 and death at 31 and 32 days, respectively. 031 419 446 100 Two had extensive previous chemotherapy 079 554 109 100 and I also had local radiotherapy. In I 0 x 0 783 4 otba cases, autologous marrow transfusion co8 1*056
marrow was hypocellular. Both of these 083 1,og8 loo
chcmochmpy. Y.Bu-m(.lr
d9 Iol
as I p 10 150 - PI
354 150 Tmak
100 zoo 91
859 150 I ,& was unsuccertf~l because the prcmiiation 2: 1 , 4 3 loo
latter patients had had intensive localized 09% 1,3d 1.143 * tjoTrUnL irradiation and I had rcccived intensive .Slboorlor.Ulr

FIO.
Of the 19 patients who died within 20-60 days, I I showed dear evidence of well b c tioning m m with steady or rising white blood Etll counts and absence of bleeding and infection at the time of duth. The time from diagnosis to d u t h of the
y patients entered in the study who were not treated has been analyzed. Thac were 4 who dicd in a & day interval:
No.$ '?? &&;m Mnmnfr Total &&,' d!i*rU
lima Rtialtl not
#i.o&doa 4 '10 a* Plrima #iwn &ti00 19 63 82
Fisher's exact probability test yields a p vdw of 0.16, indiunng that there is no diffbeace between the z groups. Therefm m e may condude that in other patients dacribed, the &cct of whole urd putid body &ation therapy was lcrr important in coatributiq to death than was &e QC
4.
tent of disease in thw patients. Another interpretation would be that a physician selecting far dvmccd cancer patients for a given wmtment wodd have about the rune degree of difljculty in selecting any form of treatment for these very ill pa- tients. T h e rune probabiitia, p=0.!9, 0.2 and O.ZI a n found for patienu dying between o and 10 days port trutment, from 0-60 days, urd from a0-e days, when compued to the untmtcd group. Cumnt status of survivd for thoe 88 trutcd pa- tients is as follows:
Prophfictic b p y @wing's tumor) 3 Othcn &via u d A m t 31. ~ q r 7 D a h paribly amihabk to imducion 8 Dah amibable to tumor P
88 -
~ U C n O N I ; ?ROY TBCATUllIT A I D E?- 0. cAusAnou
T h e a&te radiation syndmme develops in staga. In the prodromal stage, nausea urd vwnidng of a transient nature occur.

L
240
VOL. lay. No. J Whole Body Radiotherapy of Advanced Cancer 679
These complaints are often highly subjec tive; therefore, they are not discussed with the patient before treatment.
The analysis of our 88 treated patients shows that 44 per cent experienced no symptoms a t all, that 27 per cent had tran- sient nausea and vomiting within 3 hours, 14 per cent within 6 houn and 3 per cent within 12 hours. In only 4 patients (4 per cent) were the nausea and vomiting of a Severe nature CTable v).
These symptoms are no greater than found after surgery or after treatment with cancer chemotherapy drugs, the reactions of which are often far more severe than those from these kinds oiradiation therapy. Lahvi d d*’ observed that when S-fluorw lira is given orally a t a dose of 15 mg./kg. daily for 6 days, and then weekly a t the same dose, nausea, vomiting, diarrhea or stomatitis are found in 55 per cent of the patients treated, and marrow depression :E observed in 50 per cent. A recent study by the \Vestern Cooperative Cancer Chemo- therapy Group, employing 5-fluorouracrl without a loading dose at 15 mg.Ikg./wk. for a month, reported mild to major gastro- intestinal or hematologic toxicity in 85.5 per cent of430 patients.” Higgins rr al.” in treating cancer of the colon using IZ mg./ kg. of 5-fluorouracil intravenously for 5 succes4ve days, observed that 27.9 per cent of 359 patients experienced a toxic reactioa. The same group reported one or more sur- gical complications following resection of colon carcinoma in 29.6 per cent of 433 patients. PanonsefaLJ’note that 61-72 per cent of patients suffering from swcalled radiation sickness responded favorably to placebo medication, indicating that sug- gestibility may have a big part to play in the appearance and control of these s y m p toms. Mukherji et a/.” in evaluating the effectiveness of a combination of 4 drugs in the treatment of 23 patients with lymphs sarcoma and reticulum cell sarcoma found severe myelosuppmsion in 4 patients (17 per cent) and possibly attributed this de- pression to their deaths from infection.
Dut;ng the latent period of 18-21 days
TABLE V
PATIsWzs ~ECLIVING WHOLE AWD/OL PARTIAL 1NClDENCL Or NAUSEA A X 0 VOMITING I W 88 CINCLR
BODY IADIATION THERAPY - Patients Per Cent
No nausea or vomttmg 39 44
3 houn after R, 23 a7
IZ hours after R 3 3
houn after R. 7 8
48 houn after R. 0 -
houn -+ 4 4
Nausea and/or vomiting up to
Nausea and/or vomiting up to
Nausea and/or vomiting up to
Nausea and/or vomiang up to
Nausu and/or vomiting up to
Nausea and/or vominng 48
6 houn after R. t a 14
- - 88 1 0 9
the patient is asymptomatic. The period of manifest illness then begins wtth evidence of malaise, infection and bleeding. These findings occur only with whole body irradi- ation and not with partial body treatment. Also when marrow is successfully replaced thew findings do not occur.
In regard to palliation, a review of pa- tient records shows that some palliation was achieved in 56 per cent and that 31 per cent were made neither better nor worse (Table VI). In another 3 cases we were unable to obtain follow-up history concerning pallia- ’ tive effects. The 3 cases of Ewing’s tumor
are not included in this table as therapy was prophylactic.
wsaraLc uxrquc MECWAXISUS or WHOLE AL’D
\\‘hole body irradiation in the doses reported herein could be effective against cancer in several ways: (I) alteration of the immune mechanism of the body altering the balance in favor of the host; (2) by a direct effect on the metabolism of the can- cer cells. In this case widcficld radic- therapy would have one advantage over drug therapy, since it would reach all can- cer cells without depending upon blood
PARTIAL BODY IRlADlATlOX

241
680
supply, or chemical and pharmacologic distribution.
Partid body irradiation could be corn- pared to regional isolation perfusion with antineoplastic drugs, again being certain to reach all tumor cells within the irradiated volume and lacking the more hazardous systemic effects of total body irradiation.
The dFcctivenert of both methods may be explained by the fact that nnd tumor foci arc more sensitive to trutment than h g c fod wad that sin(& cancer celb arc more NIcepable t h ~ dumps of cells.
nycnouwc AID ?sycnurmc tvALuAnon or m - m m s
A unique and important aspect of the raarrh wort in this project has been the attempt to evaluate and distinguish bc tween the murifestations of cancer and the dats of radiation therapy in regard to psychologic .nd psychiatric ch.nga. For cnmpk, others have reportal on PaOnJ ity types in ccnrin uncast but no sndio rae pmented iavatig.dag the dats of bt.tmmt
h r & n r r p a c s d - t h e & c r o f
total and put id body irradiation on the cognitive and motional procewr of 16 patients=” This number has been i n d to 43. These studies consisted of rbninic tration of a battery of tests to each patient in the pretreatment phase, during sham and actual treatment and during a 6 week posttreatment period. Tests which have been utilized included the Hdstead B a t tery, Wcchsler-Bclkvuc Adult Intclligcncc Scale, some tests of intellectual impairment modified from Reitan, and the 5 minute verbal content tat of Gottschalk and Glou. There has been m e change in the several tests which we have been using during this phue of the total project; Le., not id tests have been used continually.
In the b.seline data of jg patients tested, the median intelligence quotient was 87 and the m u n also 87. There were 41 per cent of subjects with I.Q. values of 95-1 ~ 6 , 4 7 pcr cent between 71-91, and 11 per cent be- tween 6370. Th e distribution of intelli- gence factors as measured by several tests is representative of the population served by the General Hospital.
I t is clear that the intensive study .nd the above testing have had a helpful effect in increasing the level of motivation to coopcrate, as exhibited by all patients so studid
The need for careful handling of the cancer patient by all members of the medii c d turn is emphasized by the consistent evidence of depression over the 7 week study period. The depression is lessened with clinical improvement and attention to patient needs. I t is also less in patients with long ourvival (over 100 days) as would be apected. Similarly, hope is directly rr- Iated to survival. Anxiety dips sharply during sham treatment; i t incnucr just prior to actual treatment, then dmuKI and lev& off. outward hordlity tends to increase at the time of post sham treat meat, then dips and remaim quite s t ~ b k Hope as musured by the content analysir of vabd behavior is d a t e d to utirfactary hum- d a b in the padeat’s fife anu riaa.

242
V O L 117. NO. f Whole Body Radiotherapy of Advanced Cancer 68 I
USE OT AUTOLOGOUS BONE MARROW TMNSPWNTATION
Because of radiation-induced hemato- logic depnruon, autologous bone marrow storage and reinfusion wen instituted in 1964. Employing themethod of Kurnick?' marrow was removed from the posterior iliac crest under local anesthesia, to an average value approximating 3co cc. It was mixed with Ckgood-glycerol medium and stored a t -83' C. following a programmed temperature reduction of 1' C. per minute. Prior to rtinfusion dextrose was added, and then the marrow was given intravenously, inirially without filtration, a t a rate of 50 to 6c cc. per minute. The fint z patients who received a marrow transfusion in our study, Patients 051 and 053, were infused with frozen marrow @ and 19 days post irradiation, mpectivelp, a t a time when the marrow unusaids were relatively empty ofprecursor cells, with the expectation that there would be more room for the trans- plant to rake. Marrow viability in t h w z procedures was 55 and 57 per cent."
Patient 051 experienced moderate hem5 globinuriin not seen in Patient 053 after infusion. Marrow was given in both cases 2 to 3 weeks post irradiation; hence, it was impossible to distinguish spontaneous mar- row recovery from successful marrow auto- transfusion.
Because hemoglobinuria had been noted, a triple filter system was developed and marrow iutotransplantations on Patients 070,077,078,0871 390, 0 9 1 , 095. 098,0991 107 and I I I have all been performed em- ploying this filter system."
In marrow transplants of Patients 070, 077, and 078, the delay between the re- moval of marrow and transfusion was I I , z and o days, respectively. The platelet count of Patient 078 never fell below 125,cm per mm.'. but the white blood cell count dropped as low as goo, suggesting possible effectiveness of the technique for the fint rime.
For thr next 8 patients the technique was therefore modified, so that I larger volume of marrow (.coo cc.) was removed
from the patient under general anesthesia. The patient was then irradiated and the marrow replaced intravenously on the same day as it was removed. The results in Table VXI indicate the success attendant on the modification of this procedure. Five pa- tients receiving 2- rads of whole body radiation showed mean white blood counts to be 2,820 & 804 cells per mm.' at the nadir. In 7 patients given the same dose but no autograft, the level a t the nadir was 850 f380 cells per mm.', the 2 m a n s being significantly different (Table VIII). The first patient transplanted with our new technique (Patiento87) was followed in the Clinical Research Center, Cincinnati Chil- dren's Hospital, for over 6 weeks without any evidence of illness. Subsequently pa- tients receiving these whole body doses have only been hospitalized for a total of 5 days or less. The degree of marrow depres- sion in the successfully transplanted pa- tient is such that hemorrhage and infection are not observed.
The 3 failures in the revised transplanta- tion technique have been Patient op, 099 and 107- Patient o p suffered a cerebra vascular accident unrelated to her tumor or her radiotherapy. The latter 2 patients (ogg, 107) had had widespread radio- therapy which had affected the reticula endothelial framework necessary for stern cell development, and preliminary cell aspirates in allegedly unirradiated areas did appear hypocellular. Patient 107 a p peared to possess normal granulocyte re- serves, one of our marrow screening param- eters, only because we were given an in- correctly high body weight on which to base our etiocholanolone dosage, thus falsely elevating the marrow granulocyte reserves. From this unfortiinate experience we now insist that a candidate for marrow autotranzplantation have a normal iliac marrow aspirate histologically, a normal bone marrow scan employing technetium ggm sulfur colloid, and normal granulocyte reserves measured with etiocholanolone (after we weigh the patient) as indicators of normal marrow function. .4t autopsy, Pa-

682
1.6Xid r.jxid 0.6Xid 1.7Xid r.4Xid r.sXid -

244
Vu. 117. NO. 3 Whole Body Radiotherapy of Advanced Cancer
tient 099, who died on Day 31 post irradie tion, had widespread cardnoma of the pancreas. Patient 1q survived her pancy- topenia without any evidence of sepsis. Patient I I I had no significant cytopenia and her hospitalization (including auto- transplant) lasted only 4 days.
This technique has been of advantqe in simplifying the patient’s course and Jimi- nating the long period of hospitalization needed prior to transfusion. The possibility of reinfusing tumor cells in the untreated marrow exists, but the elimination of this problem awaits the development of suc casful methods of marrow allotransplanta- tion.
SUMMARY
I. Whole and/or partial body radiation therapy given in single doses has shown beneficial effects in the control of certain advanced cancers. The palliative effects compare favorably with results using anti- cancer drugs as commonly reported in the medical literature.
Irradiation certainly seems to improve survival in the untreated patient with cancers of colon, lung and breast.
P. The use of autologous marrow reinfu- sion immediately after radiation therapy minimizes the characteristic marrow d e prasion otherwise observed. The degree of illness following infusion is greatly lessened and hospitalization greatly shortened. Eugene L S.cnpr, M.D. Radiarorope Lbontory Cinonmti General Horpid Cincinnati. Ohio 49ag
REFERENCES I. Asoacu*s, G.A., C0u~s.F. V., EDWARDS. C. L.,
VODOPICK H. Hemacolcuic and thenautic KKlSELtT, R. M., LWSHBAUCH, C. C., and
cfieca of cot~-body imiiation (SOR-~OOR) in patients with malignant Iymphonu, chronic lymphocytic and gnnulocytic leukemias, and pdycythunia ven. USAEC. Division of Technical Information Extenion. Oak R i d h TCIIWSSCC,ORAU-II~,B~~~~UUIMC~~~~~C,
683
phy.idagial upcu c cancer. Ann. N#o York Aced. Sc.. 1969, ~64,307434.
J. Born*, M. Compendium of bone marrow tram plantation. TmnipLntatim, 1970,9,571-587.
+ BUCKJIE~, C. D.. EPSTUN, R.. Rucmrw, R., C L I ~ , R , Sroar, R., and THOUAS. E Allo- genic marrow engraftment following whole body irradiation in patient rslth leukemia. B I o 4 1970.55 741-7~0.
5. BUEaWALTCS. W. H., HAYKIE, T. P., and Xo- rAL, M. M. Treatment of thyroid urcinoma with “1: rcauih at fourteen yean. 7.A.M.A.. 1963, J83,303-M.
6. CAuraiLr, A.. GODLEE, J. N., Ewrru, E. W., and PLANKCID, T. A. Diagnosis and mat- mcnt of primary polycythemia. hnce t , 1970, I, w r l o ? 7 .
7. CHAOUL, H., and LANCE, K. Uebcr Lympho- pnulomatore und ihrc Behandlung mit RBnlgcnsmhlen. Mfinclun. nrd. Wchnrehr..
B. I., and SAcscEa, E. L. Wadiatiorunduced u r i ~ r y excretion of deoxyxytidine by mu and humans radiata^, 1968,9r, 343-348.
9. COLLISS, Y P., and LorrrLsr, R. K. Thenpcu- nc ux oi angle dac r of toul body radiation. Au. J. RormcrsoL., RAD. TH~XAPY & Nu- CLTAL hlco., 19~6,75,54%-$47.
IO. CO~WIK, S. H. Phmphomr 32 in advanced u r - cinoma of pmstarc. 7. Urd.., 1974 104,745-
I 1. G ~ ~ C H A L K . L A.. KWNKEL, R.. WOHL, T. H., SAENGER, E. L, and WINGET, C. N. Toul and half body irradiation: effect on cognitive and emotional procnm. Arch. Cm. PJJC~~U..
I% HICGISS. G A., DWIGHT, R. W.. S m , J. V., and KEEHX, R. J. Fluomuncil as adjuvant to surgery in carcinoma of colon. ANA. Arrh. sm, 1971, I O 4 33p.343.
13. H O L L C R O ~ , J., L~REKZ, E., and Hunnota, H. Effm of tonizing ndianom on mnsplanlcd lymphourcoma. 7. Nu. Cancrr Inst., 1950. II, 1-16.
14. H O L L C R O ~ ~ , J., Lortwz, E., and MATHEWS, M. Factors modifying eflect of x-imdiation on IC- W i o n of mnsplantcd lymphosarcoma. 3: Nu. Canerr Init., rgp, I*, 751-763.
15. HOLLC~OIT, J., and MAT HEW^. M. Effect of ionizing imdiat:on a a r m c n o on tumor R- gmrion. 7. Nat. Cancer Ins:., 19~3.14, sap 535.
16. Hoanrz, H., Waim, T. I.., Purr. H.. and BABRCTT. C. M. “SupprrPive”chemothcnpy in bmchcgcnic um~8-rlndmiZd proc oective dinid mal. AM. I. ROESTQCNOI...
I913r 70,?~5-717. 8. CHEN, I- \ iEN, KESEIAKES, J. G., FllEDUAK,
748.
194,zt , $74-580.

245
. 153bl543-
ip JACODSDS. L. 0.. Sryuoxr, E. L. MA~KS, E. K., and Emarwr . I. H. R a o m r fknn radiation .- injury. Science. 1951. rr3, 5ic-5sIs..
24 JArrc, B. M., b x r c * x , W. L.. !\ATSOW, F., and Slum, J. S. Fumn influenang auwivd in ptieno .nth unwaccd hepatic meuatUQ
ai. Jrxuxr. R. D. T.. RIDER, W. D.. and SOKLCY. M. R. En'ng'r urcoma-md of adjuvant total-body irradiation. RJiolou. 1974 pb, 1 ~ 1 - 1 ~ 5 .
ax Jonxrox, R. E. Ray of hope in lymphourcoma. Medical W a d hTtw~, 1970, JJ. 1%
13. JonxSOX, R. E. Total body irradiation of chronic lymphocytic leukemia: incidence and duration of mimion. Cancer, 1954 as, sap 5 s
2+ Jonxrow, R. E. Total-body i d i a d o n with fractionated daagc acheduln. F r o d m I&d. T k a p . U O n ~ ~ l . , 1968,j,15a-16% S. K a m , A.G., E d .
y. Jonxror, R. E., FOLEY, H. T., SWAIS, R. W., and O'Cou~oa, G. T. Tramat of I>mpho- YIEQII~ .til fnctiolutcd toul-body imdia- t h . t h c t r , 1967. rO.481-485.
26. JOHKJOX, R. E.. O'Coxuor, C. 7.. and Lcvrs, D. Primary management of advanced lymphwucc.na with radiotherapy. Cancer,
7. YE~CIAKU, J. G., VAN DI Rim, W., b a n , C., EWWG, C, SILDC~STCIW, E. B.. and SArwcra. E L Active b m e - m a m d a c related to henudogid changes in whde-body and pamid body "Co gunma radiation cxporurn. Uidov. 191% r03.651-656.
a6. Koamcx, N. B. A u d q o u r and irdagous bone numow and infuaion in treatment of rnydosuppradon. l h q f n n o n , 1965 2, 178- 187.
zp b m u , S. R., BDUUV, G., and HALL, T. C. Traanenc of mcuautic colorecul a re inma rith s.homuncil by mouth. Curer, 1971.
L o r m y R. K., Corutr, V. P., and HY- MAS, G. Canpntirr &eta of toal body ir- &tion. n i c q a m u r d and methylene- md.miae on henumpoietic amtan d t c n n i d -ptients. Srinur, 1953. J J ~ , 161-163.
p h a u .ad 01ta term~ in f r a ~ n t d
sy., CJneC. CdmJf., 1968, J V , 1-11.
r m % 78r?9!.
rd, 902-906
31- b n E L D , J. R., Ja. uw of ndibd*e ph-
mcraaatie krionr in bone fmn h t and prmuce. Inr. 3. Appl. RJ. W imp^, 1956,
imdiarion with review of UICL &I J. ROIXTGEXOL. & RAD. Tnunrr. ip*a 4, 65 1-67 I.
u. MILDVRX, L F.. O'Gimv. L. and HEKDIIICG row, F.R. R d i u l radiation thmpy and coal body i d i a t i o n in trurmcnt of Ewing'i YT- coma.C.lrcer,ig68,rr,9iwr~.
3~ Murwrrjr. E., PAGODA, A., Omccx, H. F., and Kurorr. I. H. Cyclic chcmochcrapi in lymphoma. Cancer, igji. 28,886893.
J. E. Erdrution ofplaccboeffect in t r a m e n t of radiation richas. ACU did., 1 ~ 6 1 . 9 . I1!P.r*a
36. PLGG, D. E. Bone Marrow Tranaplantao.m. Yur Book Publiahen. Inc., Chicago, 19/16. pp. I O l - l l l .
37. PESTAXA, C., REITCUCIC~. R., hfousrq C.. JVDD, E., and DOCICERTEY, M. Katunl h:.. tory of cardnomi of colon and rectum. An. 3. S y . , I&, 108, 8a6-8ag.
38. RAPOPOW, A.. and BuaLraox, R. Survival cf patieno treated with ayatcmic fluomntil for hepatic mcuatua. Snv.. Cjner. B ~ J I . 1974 JP, i73-m.
39. RIDER, W. D.. and HASSCLDACK, R. T h e rymp- comatic and hematdogiul disturbance Idlow- ing mu1 body radiation of 300 rad gunmamy imdiaaon. In: International Conference on Guiddinn to Radidcgial Health. pbliial aa kgP-RH-33. U. S. Bureau of Radidogical Health, USPHS. Rockvilk. hfar)lland, 1+3. PP. I39-144.
40. SAEXGE~, E. L. Metabolic changer in humina Idlowing coal body irradiation: ~ p o n f a period February, I*, throughOctober, 1961. Dcfense Atomic Support Agency Repon
41. SAESCER, E. L. Meubdic changer in humanr following ~ c . 1 body imdiacion: rrpon for period S-k, 1961, thmugh April, 1963. Dcknac DASA 1412 Atomic Support Agency Repon.
4% SACNGER, E. L. FUCDNAIC, E. I., KFAUAKCS. J. G., and P n w , H. Mctabdic c h a w in humanr fdlovlng mu1 body irradiation: IC- port for penod May, r963. through Febnury. 1 9 4 Dcfenr AmmicSupponAga~cy Repan, DASA 1633.
43. SAEWOL~. E. L, FUCDUAW, B. I., KUUAKU. J. G.. and Pcaar. H. Metabolic chuya in humans following mal body irndiatim: IC- port f a period February, 1964 thmugh May. 1966. Defense Atomic Support Re- port, DASA 18-
SACNGC.~. E. L, FNCDUAN, B. I., H o a n n . H.. K~UKCS. J. G.. and Pcrar. H. Mctabalic
I, l3W.W 3% M c D I w G K ~ , F . G . , ~ ~ ~ C ~ A V ~ L F . T O ~ ~ body
31. PARS0S.S. J. A., tVEDSTZl, J. H., and DowD.

246
Vor. 817, No. J Whole Body Radiotherapy of A d v a n d Cancer 685 dunge, in hununs following toul body it. dation: report for p o d May. 1966, thmugh April. 1967. Defenr Atomic Support ASUKY Re- D m 1179-
45. SACNCC~, E. L, FUUIWAN, B. I., HORT H., and KERUAKCS, J. G. h d i a a o n decb in man: nunifatations d thenputic &om: report for pried May, 1967, through April, 1968. De& Atomic Support Agency Re- port, DASA 1168.
.nsr, H., K E ~ U A K C J , J. G.. CHEN, I-WEN,
R. L Radiation deco in man: nunifesations and thcnpcutic dorm report for priod May, 1968. through April. 1969. Defense Atomic Support Agency Repon. DASA -18.
47. SACNGCR. E. L, SMCRSTCIN, E. B., AROK. B. S., Hoawnr, H., KCRCIAK~S. J. G., CHCI. I-WrK. WINGET, C.. a d GLUEI, G. c. R8- diation deco in man: manifestations and thenpuac doru: report for period May, 1969, through April. 1 9 7 ~ Defense Atomic Support Agency Report, DASA 0599.
B. S., Hoawnr, H., KC~CIAKES, J. G., CHES, I-Wrx,\V~scrr, C., and GLISSCR, G. C. Radiation decu in man: manifestations d rhmputic efforts: repon for period May.
46. SAENCER, E L. SILDEBSTUN, E. B., HOR-
WINGET, c.. GLCJEI. G. c.. and KUNKEL,
48. SAESGER, E. L., SILDLRSTUK, E. B., AMOK,
1970, through April, 1971. Dekm Nudur Agency (formerly Defense Atomic Support Agency) Report DNA 1751 T.
49. SAUP, R. J., and ANSnCLD, F. J. B m t cancer treated with Buorouncil. y.A.Md,, 1966, W&7t4-190.
5Q ~ I L B E R S T ~ N ~ E. B., CHLN, I-WEN, SACNCCR, E. L, and KERUACU. J. G. Cytologic-bre chemical mdiaaon dodmccm in man. In: Bio. chemical Indiacon of Radiation Injury in Man. Incun. Atomic Energy Agency, Vienna.
$1. STCA~NS, M.. and BINKLEY, G. Palliative sur- gery for cancer of reefurn and d o n . Canre, 1954,7,1or61019.
5% Subcommittee on Bruat and Gcniul Cancer. A n d q c n s and auogens in treatment of d l e seminated mammary amnoma-retmrpc- tive study of 949 p t i e n a Council on Drugs. Y.A.M.A., 1960,r74 iqr-ra8j.
53. THOMAS, E. D., Bucurcn, C. D., RUDOLPH, R. H., F r r n , A., SYURD, R., NUUAN, P., BRYAxr, ] . ,CHA1D,R. ,CLlrr ,R. .E~IW,R. , FIALKOW. P.. FUNK, D., GIDLrrr, E., Lca- I E a , li., REYNOLDS, F., and Sucnrra. S. AI- lqwxic manow grafting for hematologic ma- lignancy using HLA matched donor&picnt sibling pin. Blood, 1971.jB,n67-187.
1971, Pp. 181-114.

J w 3. 1972
mi8 1.tt.x ~ w a a 8 n t a oar reapona8 to your remust of tu to inquire into tha WhOlcLWdY Xac?iatiOn theraw groject b i n q conducted by Dr. Euq8ne L. Saenqer md N a collmawes a t -A8 'Jniv8raity of Cincinnati. Y. haw m a l our inquiry md our :rod conclusions arm aa f o l l m z
1. In t h ncrmal cantext of a c l in ica l inwsti~ation. the project i a valiely conwiwd, s ta ted , 8ueut8d. controlled and f o o l l a d up. me appropriau sc i8nt i I ic .nd prof8~s io1ul comittus of e!! Uaiwrsity of Cincinnati haw P.rt0-d their fWClons durinq th8 mYLI8 Of the p m j 8 a .
1. zh. p r o m s of patient selaction b a d upn clinical mnsid8ratioru conform dM qood mdical pract in .
Ih. record.. publ iu t iona urd patlult tollwwup arm voluminous and -nabla.
h a proc8durm used for obuin inq p . t ien t consent is valid, thorough and ~011sist8nt rir! tha rescsanC.tioru of rh8 : : a t i o ~ l Instieate. of male!! and d t h th. practica of uns: CMC.C c8nt.r..
Should :!La projact cou before the Senat. or OM of i t a c0zmitt.e. in a- fashion. wn would urqe your suFport for its m t i n w t i o n .
3.
4-
5.
m h #%ySiCi&M do M t invAnablv ShAr8 W i t h L!8 public th8 W a Y . i n NhiCh thq rwch prOf8aaional conclusions, H chink it appropriate to your inquily to d e t a i l belev L!8 way i n pnica v. reached of your r8qU8.t vu baaed u.xn Lh8 raalizatton -&at s8natOl. h.w ne8d Of Up8rt. hputial r C i u l LTd ScientiLic a f v i n i n 8val'xating caml8x blm8dic.l ?-*lanm. Should you d e s k 8 furtnar LntomAZion. y. rill again 8ndeaME to b8 reapruiV8.
meclusioru. Our acCOptLnn
-8
I noted i n ziy a u l i e r l e t t e r t o you, the Collepe i a selba ul l8d uwn to
IMt.ad, I asked tV0 l8.dinp radiation MeraPlStI in-atisat. +h. a c i m t i f i c of for ta of any of i t a aab.n and thus has no atandin9
md a th i rd distinguished physician to undertake e!!. inquiry. e t - 8 dh SUC! A chug..
Thy a n :

Page 2 .-
Dr. Hen- -plan, chair?a? and professor of rbdiolcqy a t Stanford g n i v s r r i t y Medical School in Palo .Uta, California. D r . :<dpldn is In te rndt rcna l ly t r c . i f c r h i s pioneering rork in severa l areas of cancer theraay. various cancer stJCy and advisory grcu?s including the Cox-dttee of CoTcultants t o Conquer Czncer Anich recent ly advrsed the Ssnate. includes descr i? t icns of h i s work on tlodqkrn's disease rnvo1v;ng exte-sivc radra:~:: of pat ien ts . Cr. Kapbn IS curren t ly chcirnan of ocr Ca.mission on cancer.
Dr. Prank R. Hendrickson. chaimdn of t l r CcFartment of radxation therapy a t . Chica'jo's Presiytcra3n-St. Luke's Hospledl. Dr. Icndrackson is also a facd1t.w
W a r of U e CnLversi?! of ILlir.ois Colle?e of Yedicine and the Push ' 'edicrl Colleqe as well a s a consultant t o the Veterans A b i n i s t r a t r o n and a i3STser of various nat iona l ca icer bo3:es. ?is bibliocra.pny incl3des r e p r t a of h i s t r s a e s r t of chxldren a i f l z c t e d d i t \ Zwina's sarco-a with radiation. ae is the present chairman of our Co?nission on Radiation Therapy.
Dr. Smuel Taylor, II:, a dittinlu:s%ed i n t e r n i s t and oncologist a t Presbyterian- .)
St. Luke's Hospital i n Chicaso. de is t x founder of the Amencan College of Physicians caffcer srogran. Sa is a professor of rcdicine at Rush. SI. Taylor 's wide experience a s a sen ior investrqaLor rn %le f i e l d of cancer provided us with a view frcn another d i sc ip l ine . ne is a long time expert i n hero therapy of dzsseainated cancer.
,Q. otha Linton. d i r e c t o r of our ::ashinqton Office. provided s t a f f s u p w r t to tL.e grou? and cwrdxnated r:eir rnciuiri with Dr. Saenqer and h i s collsaques.
He has been a nerbor of
P i s extensive bib1rocrr;:y
Rature of %Ye ircllim-
Drs. Yaplan and Bendricksor. ar.d nr. Linton net with Dr. Saenqer and 5z. Charla? M. Bdrrett , d i r e c t o r of rad ia t ion L.era?y a t the University of C:ncinnd:i, : srCnce: 29 i n C h i c a ~ o . The discussion covered the back?rou?d of tha pro jec t and m e purposes, 0b:ectives &?d acnibvenents of tne e z f o r t to date. Dr. Szenger taien provided the co.%nittee with ptwlrshed papars and s r n a r f l ra te r ra l s atou: c?e project.
On Decc-lber 16, Drs. Ka?lan. Hendrickson and Taylor met i n Cincinnatr "it5 D;. Saenger, otner mersers of h i s Lea?, t'm ne-.oers of tns univers i ty of C:-~i;?:?ti human i sves t lga t ion c o r n i t t e e , and :le A a i n a a of the spacra l univer8;ty c o . t i t t e € whic!! was crea ted by Llc pres ident to review the pmjec t .
mose interviewed were, frm the UC Swan Research Comm:ttee, Dr. Evelw '1. YeSS. professor of m d i c i n e and D r . Harvey C. raovles, Jr., proteasor of medicine. :Kc9 the s p e c i a l un ivers i ty couni t tee to review the Sao.wer pro jac t , DT. R a m n d 3. Srukmd. grofessor of anvrrorJJenta1 Pealth and ne&cino, fmm the d e p a r a e n t 3f
r a d i o l w f and t h e stu3y team, D r s . Charles H. Bamtt, Harry K o O l u i t Z . mr?ard 5 . A r o n urd 6duard 8. S i l h r s t e i n , physrc i r t s , Dra. 1-n.n Chen and J m s G. Ie r rMes , and tha p a y e o l o g i s t , xis. C a r o l y n X. Xrwet.

Dr. Saenger and everyone a t *.e un ivers i ty warm w i l l i n g to recognize our mmwtence and t o coogeeate fXl1.l with our inquiry. w o r m extended ful l coo?erat:on and CM concl.de tha t they appriaed e.ea,se:ver Of the s i tua t ion to the S a m ehtant tha t M a y would have neeCed t o b as numbers of an NIH study soction or s i t e raview tsma. hm served i n such a Capacity.
me comaittee viewed the pro jec t dS i t Was dasiqwd---as d c l i n i c a l invtstiTat:c-. of a modality for the cnre of cancer pat ients vith extnssLve and i n c j r e l a C L S J ~ S ~ . Phase one in*mstlgacions f O l l O r basic animal work and alvays precede rzaec - i r e C C l i n i C A l t r i l l s which ray O r Clay not b. j us t i f i ed on tbe basis of t e f i r s t h-u-ax applications.
In the opinion of the cox- i t tet , the team a t Cincinnat i had abundant bases i n t k e l i t e r a t u r e for undert ik in? i t s stuCy. undertake the invest icat ioa, EO:\ from the v i w p o i n t of q w d pat ient care ar.? im-prtant ly tbe poss ia i l i t p tha t new and valuable c l i n i c a l in fo rua t ion c o d d od obtained.
The corni t tee Fentees
Each ;ac*er of t h m =mitt>.
??Ie par t i c ipants are cull:^ qxa1i:icd to
cemi t tee d i d not concon a tse l f w i t h the implications w h i c h have been ralscd concerning p a r t i a l funding of the e f f o r t by the MFarment of Dafense. 'de d i d nota that Do3 funds were used only to support the laboratory and payr\oloqical studies b u t no t the t r e a c n n t or the care of %!e y t i a n t . T h m basic costs were bo- by the un ivers i ty and i t s tmacnrnq hospitals.
Becdusm of %!e prevalence o t CI.3cer whim ha9 been notsd so recent ly Sy the Sendte, the Rouse of i epr isan ta t i ver and tho Ptesidont, those chargee '81th c.Le care of cmcer pat ients haw need for every p s r r b l e b i t of infomaczon coice-ir? t h e mtkoods and modal i t ies t&i& we use t o t rmst these pat imes. this pro jec t has the poss ib i l i t y of contr ibut ing Uaef'Al c l m i c a l infoorrcatron.
It i s worth not inq t i rat i f others haw had acasa only t o tka reports Dade t o 3% on its part of &%e pro jec t or if thry .ocrhm :ail& to understand tha t the f r rc of extensive C o l l w p i n no way departed or datraczzd from Cundurntal prece;zs of good p . t i en t cam, then i t follows that a e y might reach concluarons &ffsieic fm theem of our solai t tee.
I n our ooinxr.,
me nature of cancer invest isat ions and t raahen t
In c l i n i c a l invest igat ions oL cancer, we are concerned both with t h e basic ct?z4+ process Md wit! i t s manifortations in hunms Md spec i f i ca l l y i n t!!e Fatit-'.r who present theeselves Cor care. ?5e treatsmnt of UL i nd iv idua l represents Series Of choices for h i s -physiCiAnt Vflich a m based Wmn d iagMl t rC f i V h 3 g S A?.& their h a t judgment. to t rea t i t as uniquely AS they do to nost other t h l n q s , generalizations k8:. h o v ~ s t a t i s t i c a l value bu t 1Imit.d ai?plr:at?on to ind iv iduak .
Since humans respond to th assault of UnNr auu! ;e .::9-?t

Page 4
There are many forma of cancer. ccn t ro l u-wn rnich normal cells depend t o regulate t h e i r qrow%h. The cancers d i f f e r i n c e l l u l a r types and i n tne s i t t of oriTln of a pnnarl, l es ioa wltazn the body as w a l l as the bodily ?athrays t?roug? vhicn they nay spread. example. t!!e ;robla, ol defining and t rea t iap a aolrd t m o r Q&Y d i f t e e radiZa1,y frcm *.e ag?roach t o a form of l e u k s d a .
Physician6 have tnree fwda?ental >odalit i$s vhich nay be used singlv c r c o r 3 i r ~ d to dt ten3t t o curt or con:rol caacers. rad ia t icn and chenicals. of cer ta in can:ers involving h e endocrine systen.
The choice of t r e a w e n t nus t be decided f o r ea:h patieqt. u p n the t y p of cancer, its louacion, i t s size, i c s dcqrre of s-read and asan the age u r O general h a l t 7 of t i e patient. nade i n a caTcer conference involving gh'picians :son the d i f fe ren t Crsca?lines appropriate t o the problm a t hand. theraw trust be reqardaa as heroic. proba3~li:fes af success and r a r e s t r ingent s ide e f f e c t s of treat-ent Lbnn usually b e f a l l suf fe rers from o t h e r diseases.
T h i n g is a l l inportant i n the treat-ant 0: r o s t Cancers. may be r a o v e d st.rgically or dertroved w i t ? radiation. But i f the cancer has begun t o spread beyond i ts or ig ina l s i t e and beyond L!$ surp ica l or rad ia t ion f i e l d , %+e destruction of t..e prmary l es ion w i l l not s u f f i c e t o save the pat ien t .
Unfortunately, many pa t ien ts still are diaqnoscd LT having f a r advanced cmcer which Jus t be pdged unlikely to respond t a any standard curative e f f o r t . patien- qay have undergone various treat-,enti without success. had a "s i len t" p r i i c r y cancer nnicll was diagnosed only a f t e r it bogan to sgrca; through the body.
"he physician having the care of a pat ien t with advanced cancer has three ?r.tcti:.il choices. One is to do n~t!!ing, allowing %e disease t o take i t s course. Anatc?: i a to a t t e n p t p a l l i a t i o n , an e f f o r t t o re ta rd c!e t m o r grout!! and/or to easa t--+ pain of t . e pa t ien t . comonly a c c e g e d as r e l i a b l e or efficacious f o r 9a t ien ts having a 9 r s a t e r c - z - : ? of succems. Tne t h i r d approach carr'les the long-snot poss ib i l i ty of d i r e c t ?.?z:.-c gain. be leamet fmn the e f f o r t .
%a, t h e e f f o r t t o improve cancer t rea txents has been based upon t h e f i r s t appl ica t ion of new or quesciondde tecnniquer t o those pa t ien ts taving nothi-5 to loa. by their f a i l u r e oecause the:. i s no known treatment availaale. Oft$-i , the effactivenesa of the technique nust b+ neatured i n t i n e Df survival. r e l i t : :I pain, or fne c e r t a i n body neasuranents, ra ther tnan i n terms of over t tunor destruction. S f f o r t s must ba mada t a i s o l a t e and Beasure t h e s p e c i f i c t r m 7 c , doaages. procedures urd r e s t r a i n t s which czn be ooserved to a l t e r the course the disease. :%en a form of t rea t7ent !as been show to have some m a ~ . u r a n l ~ tQMficia1 e f f e c t on f a r advanced pa t ien ts x t can be mnsidered f o r qnneral z e .
Each t 'ee has i n caiwon the l o s s of intzaze1p":a:
Thus. :*.r
There are cwtirpative sur5e~:. nigh e-s:g., <omones also are used t o atteT?t t o a l t e r the course
The decision is haszd
Ideally. the thera;aJtic decis;c? 1s
9y L!S naeura of tna disease, any cancee m e cu.cLz pa t ien t m u s t accepc l e s s e r
A small, e a r l v CMCDT
?%se O r they m y n3.e
%e t h r d is t o aZtC-pt d r a s t i c or rad ica l treat,-ents rcz
me Coctor and p a t i e n t -.use agree L5at someL!ing of benef r t t o others - 3

261
Page 5 ,. c
Ihe nature of cancer inveatigation r emi res tha t more than one therapist r ~ i t undertake a ner modality a t each Stage cf its develowcnt becore it can be acceptc for general usage. such as t!!e advent of aupezvolta5s radiation sources then previous studies nay be r e p a t a d with profit .
Both +he high e n e m radiation and the several chemicals now used in cancer therz:. have hamful e f fec ts upon patlants. made t o re f ra in 5 - 3 curativa e5f?rts when the Cescructisn of %he t-mor .so*~lc involve uxacceetble side e f fec ts of a localized or aystemic nature. t o control or relieve side e f fec t r are equally a ign i fkan t wit!! thoae t a dertmy the tunor.
When radiation is used as %!e tucoricidal agent. t !e e f fo r t is nsde to l i n I t its ef fec ts by t a i lo rmq the dose to the suspect ar3s and by using a ser ies of t o k r a s - exposures to destray the cancer cells without dwagang v i t a l oeqar.a and adja=e-.r noma1 t issues. I: a cancer is widespread, then h tmo:icidal 6oae of radia:tcn presents proble-s wnich. for r2e Fost part . ranrin unsolved. Lesser Mounts 0 5 radiation have cecn used in varioUs ways aa par t of e f io r t s t o re ta rd tumor pro.&*., t o re l ieve pain or to a l t e r the pattern Of Cancer development.
The literature of radiation therapy offers s u b a t a t i a l nube ra of c i t a t ions of efforts to use sf\ole o r p a r t i a l M y radiation for the pal l ia t ion of advancsd cancer.. productive to recollrrend generally nor so lacking i n e f fec t ta be abandoned as an approach.
If an insrovemen: in sme t-1 or resource becones a ia i las le ,
So Coes radical rurqery. The cholce -ust be
n u s , effozt-
h e concluaicn, Sraadly. must b. t ha t %!e concept ha, not been sufficiei- .
The Cincinnati a ro iec t
me actual t r e a e e n t of patient. waa bequn in 1960 by Dr. Saenper and his collernuet aa a c l in ica l assessnent of tha uae of sublet9al whole %dy radiation for LIE pal l ia t ion of Battents wit!! a variety of disseminated cancerr. ZIE pre-xss *as t ha t the level of radiation selected would have a retardant e f fec t upon the ar - i tc of the tunor cells t!!rouqnout t!\e body and that tke patient. Cor tt.e asst part . could to le ra te %?e si& effect. of systemic radiation.
I h e second pa r t of t h o premise was t ha t patient. who uem closaly followed a f t c r their cancer traatmenta could ir.dicate both the phyaical and psycholopica1 ~ * ~ c . I I o ~ * to thc therap.utic e f fo r t over a Feriod of several WOKS. pr0rid.a a m dhenaion to previous atudios of Uu u n of uhoh body radiation.
Beginning in 1964, the group began t o us. the to.clniqus of autolwcua bone -a.sr?+ truraplant. aa a Ceana of overconing the mmrrow &pmsLon 0-hanrfao inelcdpa2:e a f t e r who10 b o C g radiation. extraction of 300 t o 600 cubic centimeters (&ut a p in t or ao) of s a r m fro-i ttu posterior i l iac c rea t j u s t before +h radIatLon oxpzmulr. Th. s u w day. %?e mrrw is f i l t e s s d and reinjected in to tho patient. haa succeeded in averting most of t!m extended radiation iyndmrr e f i ec t r pre-ii-u:' observed in patianta i n thia aariea and In o*her w%olo body atudies.
?hi. cl inical uaerrsrens
The techcique a f t e r acas &ificetion involvea c'.c
As c l in i ca l pr?cedues. tX1

252
4 E f f c r t r t o mininrze l a t e e f fec ts . such as the drop i n w x t e c e l l s &?d p l a t e l e t s and the decrease i n red blood c e l l s khich aea c l a s s i c t o rad ia t ion s > n d r r s s , tsqm in 1965. therapy. b c . ~ p r a c t i c a l early i n 1969.
The concept of whole ixdy rad ia t ion as a nethod of t r s a t i n ? cancer is not m w with the Cincinnati p m i e c t . There is volminous 1itssacL-e reportin, ccr.:eclled anlnal ex?erirents mien are higlrlv usefu l but not ind:cctive of h z c r rs~~:- ,5es to human tW.Ors. The l i t e r a t u r e re;orring on hunan exacsures dates ha:\ t c e f f o r t s i n 1923. A review of regor t s t o 1942 shohcd mare L!an 270 pat-ents ?-,-3 t reb ted w l t n f a i r l y l i t t l e encourage~ent. Since t!!ese pa t izn ts i n a l l C.LPEJ - I d d i s s m i n a t c d tL-ozs an3 :Te rad ia t ion sources ava i lab le dIpre i n the orriovil1ta;e range, the r e s u l t s bere not s u e r i s i n g .
The advent OF supervoltaae generators and p a r t i c a l a r l y c s b a l t 60 so ,xcss p r ~ 5 : c d addi t iona l s tud ies t o assess t!\e e f f e c t of higher energy rad ia t ion ant led tJ 3 no1 round of s tudies . In 1953, '1. P. Collins and R. K. Laeff le r c z l l s d the m e of 200 roentgens h o l e boby "a usefu l addi t ion t o the maiagament of advaxed cancer."
A curren t bibliography contains scme 86 s c i e n t i f i c a r t i c l e s on the a b j e c t . excluding ne. Saenger's contributions. Whole body proje:ts havo bean undertaken in more than 42 U. 5 . r e d i c a l centers. A t present, e fFor t s are urdeeway usiqz whole or p a r t i a l b& rad iar ion for L\e cont ro l of leu!<enia, dodqtin's Iiseane. pIyCyt!!aib vera, n u l t i p l e ?yeloma, and d isse i ina ted ca icers of L\e breas t , thyroid and prostate. In very r i a l 1 groups, wnola body r a b a t i o n bas been used successfu l ly i n cura t ive e f f o r t s aga ins t Ewing's sarcoma, a tone t w r ?,r:mariiy of cnilbrcn.
The Cincinnati' study through the end of 1970 involved a t o t a l of 106 pazients re fer red froa the %-or C l i n i c of t!!e Cincinnair General Josp i ta l . 3 e s e .&re p a t i e n t s found by baossy and c l i n i c a l exminat ion -a have di sscnnatsd iu-ori . They 'vera chomn because they suf fered from advanced and wibesgread neopiastic diaear auch t h a t cure could not be anticipated." in Dr. Saenger's wor3s.
All of the p r t i e n t s undawent a 7 to 14 day assessment 0o:iod to reaffrrn t!!% diaqnosis M d to d e t e d n e whether therr disease and t ielr general hea1t.l wouia make the rad ia t ion a t t u ? t feas ib le . no rad ia t ion on t h e basia of t h e i r c l i n i c a l a s s e s s a n t . Some of the e2 ga t ien ts l a t a r t r e a t e d received sham rad ia t ion sessions during *.e arsassuent period k4: nom ut--l ly uera erpord u n t i l a f t e r a declaion by t h e tebm which datemined th. treatrunt OULd b s benef ic ia l .
The patient. hed a var ie ty of tumrs. o r i g i n a t i n g in the colon and rectum. bronchus. F i f teen women had d i s s m i n q t e d b r e a s t cancer. There were 25 p a t i e n t s with miscellaneous tli.aora. Three chil&en had Wing's sarcoma and were t re l te r l f o r cura t ive e f f e c t . One of the 25 p a t i e n t s with niscellbneous tmn had E w i r - l ' s abrcnma w i t h matastasea tco widespread f o r a curative e f for t .
Thia mothod using autolo9Olu tone mrrw i m e d i a t e l y a f t e r rad ia t ion
Sone 24 p a t i e n t s w+re r e l t c t e d and rtceived
The l c r g e s t group waa 25 with cancers A second group of 14 had tIEbc:s of me

253
paqe 7
Discursiona w i t 5 the pat ien ts and members of t h e i r families ara standard i n m y cancer thera-p s i t u a t i o n and were a part of this pmjecc from i ts beginning. Spcc i f ic p a t i e n t ccnsent f o m have been.used s ince 1965, when t h i s s t e p was r e m e n d e d by the National I n s t i t u t e s of Health.
Since 1363, patienta se lec ted f o r the study were interviewed on succeeding days by the i n t e r n i s t i n tne pro jec t before oein? asked t o sign a consent fom f o r t'Le therapy. ;Ben possible and i n a l l cases of c i i ld ren , the interview included one or m r e met-kers of t?e fb-ily who a lso consented t o the treatmsnt. Except for the three children with Edir.g's sarcccm, a l l were to ld t h a t t h e i r cancers i a d been defined a s incue?.de and t 5 a t the t r e a m e n t would be arteppted i n a? effor-t to prolong t h e i r l i v e s and ?ossibly t o re ta rd or shrink the t c o r s . They were t o l d that the infornation rained fmn t b e study was hoped t o be helpful t o o t h s r Tatienta. In the last fev :/ears Lhey bere t o l d t h a t t h e information nignt have mi l i ta ry as well as c l i n i c a l significance.
The pa t ien ts were t o l d tnat t i a r a could be some s ide e f f e c t s fron the radiation expasure and t h a t Lie t e a would wisn t o keep i n close touch with them for a period of weeks t o stul:f t h e i r reactions both t o the advances i n their disease and t o the i n j a c t of the radiation. in detail nor emphasized to avoid subjective inducement of the symptoms.
So far as t h e s i d e e f f e c t s were concerned, the team reported khat 45 percent had no voniting or nausea a f t e r t'ie radiation. vonitinp and nausea within t i r e e b u r s and ancther 17 percent had the sa-B r:-:to~r within 12 hours of exposure. only f i v e percent had Prolonged and ssvere vomiting and nausea.
It is worth noting t h a t these symptoms me c e r t a m l y no grea te r than those experienced by oat ien ts t r e a t e d e i t h e r by surgery or by m y of t h e systemic drugs DQV being used c l i n i c a l l y on disseminated cancers.
The pat ien ts were se lec ted by c l in ic ians a t the Cincinnati General tiospital fro= the population served by t h a t i n s t r t u t i o n so le ly on the bas is of t h e i r t L i O Z diagnosis. Since CGH is a i n s t i t u t i o n , none of the patient.. were pr iva te pa t ien ts . me three children with m i n e ' s sarcona were referred by physicians a= t i e af fz l iaL Cinaanniti Children's Hospital.
Extensive psychological studiDs were *one on 39 patients. e s t a b l i s h t h e i r Ips. The median on the studied group was 07. The ranqe has from 116 t o a low of 63. negro.
The possible r i d e e f f e c t s were not described
sone 24 percent experienced t r a n s i e ~ :
Another 9 percent continued vaxiting up t o 1 4 i surs .
.
It was possible t o
some 31 of the t rea ted pa t ien ts were caucaaian afid 51 r e r e I n both race and I Q the group w.g representative of the pa t ien ts served
by azJ.
?h. three children who were t r e a t e d duf in i t ive ly for Ewinq's sarcoma renamed a l i v e fmm one t o tour years a f t e r treaLTent. Prom t h e o ther 79, for whom Only p a l l l a t i c was expected, f i v e o thers survived a s of October of 1971, the longest by moie than six ytars .
84-514 0 - 94 - 9

-
254
sage 8
The c l l n i u l assessment of t h e e f r o r t indicated t h a t Isrrfl overlapping ?erce:iri?tii 29 percent f e l t r e l i e f of Fain. 10 percent showed a Te?SUrable d6crease i n ; r~ -er : tMwr size, 11 percent reported an increase i n dc:rvre:i on mcir o m par t f o l l w i n q treat-ent and -? Fercent re;orted dn tnsrearr i n "well-b9ir.g ." ; h L t 29 percent sno.ed no evidence of Lm?rovenent or c7an-e. FoLr percenz w*re ?US=
to follol-.p. after tne +bola t o d y exposure.
It is not possible t o determine p s i t i v e l y t h a t thout gatLents r*o *ied w i t 5 i ~ 60 days of the Crea=?ent would not have succmbed to - 2 . e ~ d i t e i s e r i t - i n tPa t period, even %-.04n e s c l i n i c a l assersnent had been t l iat t h e i r disease cas s t a b l e ens;qn t o justify their ixclusion i n c e ¶eddy. the follo.-q s tud iar t h e twdr bone Mrrw function was s u b n o m l ar.d .&.*AS r e l a t a b l e t o rad ia t ion rindroan.
I n terns of survival. the Cincinnati pmg? reported remlts skawinq M extension of days over untreated pa t ien ts i? each of the t.i-or c i tegor ies . Cowever. acsu l t s were n5t na:*<e61? suy;erxor t o the rurvrval r e s u l t s reported by other investigators using various chemicals or other cmblmtiaas.
The survival fiquros are cloJded by the f a c t m e t nany of t3e o e t i e n t s i n c l u i e l i n t h e s m ~ l e had already undsrqone on+ or more types of t r r a m e n t unsuccesn:u:?y, o f t a n only a s h o r t t i m e before t n e l e rnclusion i n the stud?. the stuclj a l s o re-eived extensxve followup t red taent , soaetines involvin? fcrt-,e: rad ia t ion of %?e prmdry tumr area.
Thua. t h e pa t ien ts received a tnerapeutic reqinen 'rhich was c l i n i c a l l y j u d j c i ? ? s t efflcdcious for :!-air rurvaval and palliation, hcdeevar nucn the added efZoorts blur red the oilaarvatzon of the ef fec ta of tnc single whoie body exposure,
In s p e c i f i c t e r s of survival, Or. Saengar vaa able +A d:a..) rough m m ~ a r i r ~ r r t h i c h ind ica ted the b e n t f i t of some t r c a m e n t over none. He found t h d t )?IS r e s u l t a con;ared to tt.ose gained by other investiqdtors using surgical resec-'2-sr drugs such as I-fluorouracil and, for me breas t cdncer pat ien ts , estrogens ::.a dndrgens . I n vr. Seenser's wards, "me r e l a t i v e l y small nu-hrs of pat ien ts i n c'ese o m - ~ s (his and tie ones -Fared from the Iiteraturel greclUda dny claim t o L?er2;S-:LC auperiority. gXaWly ill individuals s ince this r;..:-.od of t r c a m e n t is less e l a h r a t e and .~=.l
M graater risk than many present foms oC ch~aoeher6w.~
In this concluaion, t h e ACR cozmittee would concur. The committee would a l ~ o &sew* that t!!e protocols, revieus by s w r o n r i a t * i n s t i t u t i o n a l a u t l o r i t i e r . a t t8n t ion e0 g e t i e n t i n t e r e s t s and re -ons ib i l l t i es and npoetiw a m a11 cC?s:s%St w i t h acceptad 5& clinical and s c i e n t i f r c practice.
& qrcu? 02 10 sescent or e iqnt patLents Lied frm 20 to 60 days
no-revel. it -*as PO:+< ZEC-
Soea of the patie5tS .
3n the o t h e r \and. i t i o c 3 s reasonabln to continue t!erdgy for --+E¶

255
Rasponsea t o Senator Gravel's questions
Scurd of the poin ts ra i sed i n the qieotio?s i n your l e t t e r of Novuber 10 as2 covered a t l e a s t i n general above. Sor.2 are not. Hence, the questions m d .pacific responses are deta i led below.
1. AN1:U DATA: Don't experimental aninal t r i a l s as A r u l e Free@?< m-ez t r i a l s i n the t es t ing of nw.1 v d i c a l therapies and drugs? hat ari-:l t r i a l s using p a r t i a l or h!ole-to&: i r rad ia t ion t o t r e a t c m c t r . e r e comoleted tezore cr. l a e y e r began h i s h a a n ex;errr%ntat-on> C:d 3:. Saenges begin h i s scec ia l "thera?]" before or a f t e r Defense Csgar%--t>i rugpart?
mSER: t r i a l s of whole body rad ia t ion for a var ie ty of jur-ses. appended. A h s t alwavs, c l i n i c a l researchers have had the benef i t of ani?aL .jrt to tcst the tox;city of their n a t e r i a l s and t o develop general patterns of biological res-xnse. 1imever. since inter-SDecies l i f fe rcnces never ailow :%e t o t a l t ransfer of m i x 1 data t o hunan usace. i t is necessary t o undnrtake c l i n i c a l t r i a l s und+r pro?er conditicns .o t e s t any new thera?:i or agent. I t i a not necessaq for a c l i n i c a l researcner h inse l f to undertakn aninal work i f he has access to and a good un.'erstnndin? of tbe l i t e r a t u r e on the subject. T-:s w u th5 cam of Dr. Samqcr and h t s colleagues.
As an exa..jle of the application of aninal studie9 t o hman uses, the use of autoloqou9 bono narrow transFiants ~ r d the bas ic undsrnzandiny of L-.e int1-z. z : of marrow s ten c e i l s on naznal im sltrvivai a f t e r * h o l e 5ody r a s i a t i c n ex-csIzz wre w r r e d o u t In aninal e:.yerinents. w r t a n t .part of t!!e Cincinnati investigation. Thc d e t a i l e d biochcaistry -:= only pexaita a nom co=jlete ana1ys:s oi che rssjonse of these gacrents bu: i - 5 3 could poin t the vay tc o t h e r researchers 120 are attem?ting systemic therd:: with rad ia t ion and with inves t iga t ive c i e i i c a l s .
It vas a neceasuy p a r t of the c l i n i c a l investiqation ?or D r . Saenqer t o de:er:rn the optiaal &ununt of m u m v to ext rac t , L!e most e f f e c t i v e vay to hu.dle i: ?-:
the bast timing for i t a r e i n p x t i o n i n t o the patient. .z wrk, D r . Saenqer aad h i s qrx? entr3cto2 tha ;iarrow and froze it to retali . .: i3.r th. 18 to 21 day. d-urinq rnich blood w i C e and red c e l l levels are emectes ..: &cline. With-mubs.qrunt s a t i e n t s . they detennined t h a t the prompt rain]ec:.-i of the mrrrortha s e e &y t%e radiation was administered averted much of tne blood dnplerslr, e f f e c t of tha radiation.
S i n a Or. Saengcr i n &!is instance a p j l i e d t o *.e Department of Defense. r>: than another furding agency, for t h s3:;or: for the extensive b iochmlca l - _ -:? which wmld provide the "ne"" element of r?fomaticn frop *e survey. h i s preparations preceded t?e 1980 data a t rnich the ac tua l pm]eCt was funded by COD and Tat ian t t r e a 3 e x begm. hs r.oCed. t5e s u p w i t for the pat ien t t rea tnunt and manag-nt was provided by the Universief of Cincinnati And i t 3 hosjdtals. the p.ycholoqical taa t inq *ich a11cwce a aore m p l e t e assesscent of the e$:-:=.
me l i t e r a t u s e on radiation b:olopl is subs tan t ia l *fit! reDard t o a-:-sl One bibliograsny i s
Tne i3rm.f t r m s p l a n t s aze a l o s t
A t the teq'inning of
:
The 000 funds were apslied oniy t o the biocheaistr? and SUbSC=Lh.:: '

- 256
1. FOLLOIUP STJDIES: f ind out i f h i s "tZeat!mt. ha. been helpful or h a n f u l t o thu? he m u m the t w r a he hoped to reduce, foz inatanso?
liov doe. Dr. Saenqer f o l l c r up hi. ovn pat ian ta t o OJcs
WSCRx than i a poaaiole f o r moat t w r clinic.. observations m d dinqroa t ic atudiea and frequent &acto--patient cGntacea between both the i n t e r n i r t a and the radiation thmra9iat.a on t h t a m w i t h the pat ien ts who had been treated. In d d i t i o n . the team _oaycholog:ct min tz inod con-act, no'. only for her t x t a b u t a lao aa a fur ther supportive measure.
Ihe data on biochhiical reaponaea and upon payohologiul reaction. is valuaXe
paaaible for e'mry cancar patient. even in the bas t of cmur centers.
Ih* aaaeaamnt of m a u l t a WAS made by C l i n i C A l obaematione Of the pat ien t rclich indicate the e l m a n t a of well-baing and a y a t d o func+fon plus 1Aboratory Anaiysea of blood condition and voidinq function. p lus x-ray d i a p o a i a to chock the sire and penetration of aol id t w r a . In many of the patients, t!!~ pr- tumor h d barn excised aUrqiCAlly OK t rea ted previously Vi%\ A pKOphylACtfc doae O$ rad ia t ion , leaving aar.agezcnt of the =etaataaea AS the rajor c l i n i c a l concwn. It i a worth not i rq that only 4 parcmnt o i the 82 p ~ t i m t ~ i n the 10-ye.r aerie. vera l o a t to cm?le tc ~ o l l o v u p . pracadfnq iac:ion.
3. C O ~ L GPWPS: m a t cont ro l qmupa &ea ~ e . saenqer h a w , or hAS he
Aa noted. the followup on theae patient. is ccnaidernbly mora c a l e t a The f o l l w u p conaisted of c1:niul
bu t SfmplY to0 eX=e.UiVe i n t e N Of mMpW*K M$ labo+AtOr! f a c i l i t i e l to be
X deta i led repor t on them r e s u l t s i a i n tho
ur.anqcd tor A t OUK g r e a t C M C e r KeSeAKC!! i c S t i t U U S . d.te&na how hi. SwCi.1 . t K e A C P . n + ' ilwKkhcl?
M t h a t be can
AXSZRz usually arise u n t i l after the ccapletion and evaluation of the tup. af stuCy currently mCu&ay by or. Sunqor. phaae throe at=&/ beqan l a a t J w on the baaia of a a a u m e n t of the 10-year resu l tg of the 2raaent effort.
The quaation of specific cont ro l g m u g and rmSoIuired .Amplea &ea no=
Ha adviaea that pl iv l inq for A mro .:.;orate
l i t e r a t u r e contain. s u f f i c i a n t atudiaa of a L n i l u wttents uid c a ~ ~ ~ ~ b l e aized amplea t rea ted by other methods to a l b v baa ic m ; A r i M n l Of t w r ragraaaion, poat-tnatmant ap.?tcma m d survival times After pa l l ia t ion .
again, it is wrth notinq t h a t the extan t of prrp.rarion?r ud followU~ on e x 7 p a t i a t and the n-cr of cancer - p t i a n t a a t CG!l *!LO LI. aui tab le for an wsraasive p a l l i a t i o n ahlCy zave cocbmed to l i m i t tha air. of the gmup
comribwnt of a t a f i i n g d fimncinq frcm wma wuTa ether than p a t i r n t Care f.-aZI.
imreati:i-.lon. li MU. thm atudy appECrl t e u i b l e A t C i n C i M A u but V i 1 1 K*q.JiK* SubStAr.::rl
4. PRIVATE PATIENTS: 0.s Dr. Saenqer tmat q p d V a U CUlCer patients, OK offer consultation on private casea? or whole-body rad ia t ion "thorapy' on paying ~ i t i o n t a ? &xitor who &ea?
00.. he rg-nd or uae his !Xrtia: he L n w AI:;'
257
P.9.11
iUISWF.R: University of Cincinnati Colleqe of !:edicine and have ro przvate prac t ice in =+, ordinary aense. a t the city-operated CincinaatL General Rospital and 1-0 a f f i l i a t e d ins t i tuc ioas . A very few pa t ien ts *&ere r r t e r r e d t o the qssup Zrc~. doczars at the B?LTes n o s ~ i t ~ l , a pr iva t9 g a c t i c e i n s t i t u t i o n a f f i l i a t e d wit!! the university. Eouever, *os? pat ien ts **:e co t c5arqed f o r tne t r e a m e n t and maciicai care involved i a the i r par t ic ipa t ion i n the study.
h t tnis Wrqt, Jr. Saer3er does not use h i s t r e a e e n t cn "paying ?atients" because he ?as none. r'a eces ROC recomend h i s tec?niTie t o o ther nhysicianr because :?e inves t iga t ion is not y e t cborrlrfe and t!e r e s u l t s are not iY5icative of i y e i i c z a a p g l x a t i a n -2 c l i n i c a l sz:~ztiozs apar t fzon a research ef5ort . Dr. Saa.-ger xould ennuragt other c u a l i f i e d researcnars t o duplicate his pro$rcc or to rodify h i s technigu3s on the bas i s :'tat r e s u l t s to da te are suf f ic ien t ly pmmisinp to warrant f u r t h e r investiqation both by h i s qrosp and by others.
As noted abbove, son9 type of p a r t i a l or whole body radiation i a used i n nore than 42 d i f f e r e n t U. 5 . nedica l centers. d t o t a l l ist of these is not available, bu t they es include bot3 p u l i c ins t i tuk ions l i k e t ? e h i v a r s i t y of Cincinnati and p r i v a t e cnes vhcre ncse pa t ien ts a r e charqed for rhir care and t r e a m n t . Thus. it is l i k e l y t h a t ins:ances could be found i n m r c h Fa t ien ts d id pay far t h i s t r e a e e n t approach. dudever, t!%e s c z e n t i i i c l i t e r a t u r e does not arCinarily c i t e t!\e q i e s t i a n of p a t i e n t pa7;ent in regor t iaq on c i i n i c a l research. The ACP c m m t t e e waa not i n a pos i t ion to m k e any extended i rqui ry on this point.
5. TRICKERY: 1s there any t r ickery of t h e pa t icz ts involved?
De. Saenqer and h i s Colleagues a re f u l l - t i n e i r ~ l t y nerbers of the
Their p a t i e n t care respons ib i l i t i es L-4 r e s t r i c t e d to pa t icn ts
a.) Do tha p a t i e n t s r e a l l y understand t h e exczrirrsnt is l a rge ly t o he lp tne Defense 3epartnent prepare Cor ruc lear wartare?
Do you consiZer the re lease the pa t ien ts s ign to be s u f f i c i e n t evidence t h a t tSey understand?
0 t h e p a t i e n t s understand t h a t the experment may cause them severe discomfort, sucn as hours of vonirinq?
b.)
c.)
d.) Do me p a t i e n t s understand t h a t p a r t i a l or x*ole-body i r rad ia t ion pay ahorten t!eir l i v e s , and if so, by how much?
Do the pa t ien ts ,mders=and whet!!er or not there e x i s t s any basi'l for suqqestinq that the " t r a a w n t " may rtduce the si+e of t h e i r tumora o r reduce their pain (as Dr. Saenger suggests i n the Hasl-inuton Post, Oct. 8 , 1971)?
e.)
Tha quastion of iilforned consent was investigated extenei'mly by the &CR mcmit te t . Ihe Univ+rsity of Cincicnati Conmittee for H w a n Investiqation vaa foxred i n 1965. as it vas i n mst o t h s r i n s t i t u t i o n s , &?d has had a p a r a l l e l eevalopnent under t h e quiCe1ines of L.e Sat iona l I n s t i t u t e s of Health. have been qradually modified over tk.e years and the sopnistication of t h e i r review has increased i n a p a r a l l e l fishion.
Their consent f o n s

It 1. the opinion of the ACCX n n n i t t e e that a t th!e preseqt t ine and throuGh t!!~ )urn the UC C(CPittee h u functioced effectively and cmparxbly to a i x l s r canmitteea a t my of tAe o*.er leading ina t i t u t i c r s whic! mnCact cancer reneirch. It 1. l ikely %'a+ tha UC amzi t t ee haa mrfoensd i t a function bet ter than the
and th. professional ccapetence of the pwple involved.
The current conaent seeking procedure waa ravirred bv tho ACR coumittae. teaa inter?.ist IJr. Sil ters te inl intervitws patients t m t i m a a t l ea s t 24 hours apart an< diamssea in rxrinsive & t a l l tL.0 procedcrea ebnt w i l l be un0ertaten. T.nia i a dam ra t only tor tae patient but also for e e r s of h i s f w i l y , +.en available. un t i l the c=-;letioa ot --1o second intervrev. :fie fon. in use is mo6i:ied fcr a w c l t i c i t y fzax tne basic oms preaared by the ::ationdl Inst i tutes of Hedlt!!.
mpt ia th c u e of the three children with Eving'e aar- rho w n t n a t d curatively, Lie patiant. kn.y before baing referrd to the atudy team t na t t h y had maUqmnt diaeaae for which no curativm t reaO.nt i a p o a s i b l c Thw knm t h a t the efforu of t!!e atudy teaa w e n not offered as curat i tnr
m n y patient. ex3msaed a dr r i r e to pdrticipate i n the study dnd -msaibly to help the pliqnc of ot5er cancer patient. i n the f u t u n . a t u d l a unicn were incora0rat.d l n tho pOjee t b#?lnning i n I965 qitn the etudy grar? rare tun the u a u l assurance t ha t their oxpluutiona and tha requirod form wore dram by the patient. and by Cieir fwi l ioa .
m r q e gZOC? b.CAlU* Of thhe -1- Of pmjecta qOIimZAted b/ the -dial faculty
The
3 e specitic &!A i e t a i l ed conaent f c D a a m not greaantec! t c tho 8ntier.Z
The docuruntod pwcholoqicr
, T% x x coml t t ae f e l t t ha t t!!e gatienta were ac!.qua'rkj informed about the natxre of the propoad therapy dnd -ut L!e conrwuencra. X. noted above, %!e -Wticntl sure wt i n f o r e d i n de t a i l &out t!e aide oftoeta of radiation because of tile ,
paycholoqical inil lunca of expc ta t ion lnvolvcd i n bot? nausea and wait inq. mentioned i n t i e project narrative, &ut half of the patient. did not cx-,erie.icr unploaaant aide ef:ects and m a t of the others had only tranaient ay7stot-s. ahould alao bo noted that since coat o f the patient. had unde-one prtvious ztacer treat=.nta. o t t e i involvinq radiation or ayate-ic &rsicr la , tnay b%r¶ avare f r o m p r r V i a U w r i e n c e of the t y p s of seqUellA0 S h i h might be encountered.
Ru patient. w e n advised tha t t t e project vaa C8aigned i n &!e hop. t!at the radiation d d relieve t!!e Farn of t'eir cancer, that it afght ahrrak Vie ais. of tha p r i m tuaar or ratard the d e v e l c p n t of n r t u e u e a . 0; m y of those reaults wars offered.
In th. AQ M t t . . ' a viw, the usertion in question 5 a. that tbe cxp.rfrur.t -in l u g d y - t o help the Dafanae cep-nt p m p . ~ ~ f o r nuclear .warfare. La not comet. %ia i a not tho @ s a q pur?wse of tke effort and to ham advlaed the p.?imU to that effect u u l d haw been afalelaino-
.Is
rl:
::o guaraneaer

259
Page 13
Y
t
"ha pat ien t . vera not sgecirical'y informed t h a t the partial support came rrm DOD any more than ot'ter Pat ian ts i n ocher s tudies a t Cincinnati or e l s e i h e n are advised of the s p e c i f i c agency su%ort of p-wjects i n vhich they are involmd. The Cincinnati pa t ien ts were t o l d that s u p p x t came i n part froa a national agzscy.
a t t h m t i m e t h e pa t ien ts were counseled prior to the request f o r executicn cf e e inforred consent form, the)'uere advised t h a t t h e psaaible findinqs cay have r i r e than c1in:cal :-?l::ations and could t e helpful t o persona receiving wholu bas? rad ia t ion i n i n d u s t r i a l accidents. mi l i ta ry a:tivitlru or as f a l l o u t fron a nuclear detonation.
me question of thu source of su-rt for a projec t is not construed by the XCR carunittee or Ly most r a d i c a l investigators u being relevant t o :ie issue of infomed cansent. In t h i s case, the DOD exercised M control over J a t i e n t SelfCtiCr or c l i n i c a l tr%atz!ent md indeed d i d not require descr ip t ions of t h a t par t of t>.e projec t been di rec t& p r b r i l y b a r d the assus.P.nt of whole bad? e f f e c t s of rad ia t ion ra ther than the Mnrgenent of diSSmfMtEd cancer by r&diation, the study gmup oauld not have incorporatad t h e autologous rmtr01 transplant. which SO
d r a a t i c a l l y a l t e r e d the clusic radia t ion response.
Though this l e t t e = haa extendmd t o s u 5 s t m t i a l length, it obviously represents a s ~ r c m r y of the !&c:s of t n e Cincinnati study and a prec is of :!e opinions gf the Colleg+'s Cobslittau ne?bers on t h a t study and 0-1 :he basic issuer of canO.r inves t iqa t ion in hI2zMa. As YE indicated at the begiMiw of the letter, v. would b t hapy:. t i att%z?t further discussion of m y pornt on which you m y still have concern.
Sincerely,
Rohert IC. ::cCanne11, w. D. President m r i c a n College cf ?.adiology

I
Q. lay 2 0 1972
'p: * D o u r ~ a e m u i ~ r r r r r u w r m p e r a ~ p q j w ~ M o m 4 0 0 . 1 w *;+
B-I6d051(2]
Dear M r . Chairman:
Pursuant t o your rcqucst of December 25, 1971, and d i s - cussions wi th your o f f i c c , we obtaincd docuncnts r e l a t i n g t o (1) thc whole-body i r r a d i a t i o n program a t t h e Univcrsity of Cincinnati Medical Ccnter and (2) t h c po l i cy of t he Dopart- #sent of Defense on the subject of t h e pro tccr ion of humans utcd i n medical research p ro jcc t s under contract . The en- c losure t o this le t ter i d e n t i f i e s t h e documents obtained by
Concerning thc pol icy on t h e s u b j e c t of thc p ro tcc t ion OP hmans used i n medical rescarch p r o j c c t s , an o f f i c i a l of tlie Depcirtment advised us t ho t t he pol icy of tho DcpartGent stas set forth in Doportnent of Defense Instruct ion 5030.29, dated Way 1 2 , 19G4. The in s t ruc t ion , which is applicabla t o a l l coraponents of t he Departncnt and t o i ts ccntrnctors o r Prantccs, s t a t e s tha t :
"Tho Departincnt of Dcfensc assumes f u l l responsi- -
b i l i t y for t h e pro tec t ion of hunsns involvod i n rescsrch undcr its sponsorship whethcr t h i s involves. i nvcs t iga t ionn l drugs or o the r hazards.
"Each Mi l i t a ry Ucpartmnt w i l l os t=b l i sh v i t h i n t!ic o f f i c e of its Surgcon Gcnoral a fomal Gevicw Board of profcss ionnl porsonntl t o cons ider cec!~ research
from i t s cont rac tors o r grantees xhiclr ray involve the usc of hunan subjec ts i n t!ie c l i n i c a l inves t igs - t i on of ' new drucs. lrefnre a clinical test with an invcs t iga t ionz l drug nay bc pcr fomcd under tho sponsorship o f a Military l)epnrtncnt--
. us and made available t o your o f f i c e during our work.
. proposal fron wi th in thot Mil i t a ry Departcent o r
-
~~~, the plan of the tcst and o t h e r pe r t inen t d e t a i l s rmst bc submittc4 t o thc approprF- a t e Hcvicw Coord,
"2. ' t lm Board nust indiclntc i ts approval, and.
"3. t hc approval nust be c t n f i m c d by tlic re- spcc t ivc Surgeon Gc;iurnI.."

261
8-164031(2) .
With t h e c s c c p t i o n of c c r t n i n r e p o r t s t h a t were rcqr r i rcd t o bc f i l e d w i t h t h c Food and Drug A d i i i n i s t r a t i o n of t h e Do- p a r t n c n t of Heal th , Educat ion, and Welfare i n t h e case of i n - v c s t i g a t i b n a l new d r u g s , no proccdurcs were s p c c i f i c d i n the i n s t r u c t i o n w i t h regard ' t o t h e u s e of huaan s u b j e c t s f o r o t h e r r e s e a r c h purposes . The r e p o r t s t o be f i l e d w i t h t h e Food and Drug A d m i n i s t r a t i o n were s e t f o r t h i n a Menorandum of Under- s t a n d i n g bctween t h c Department o f H e a l t h , Educat ion, and h'elfaro and the Deportnent of Defense, d a t e d February 1964, nh ich c o n t a i n e d t h c procedures t o bc fo l lowed t o c n s u r e t h a t tho requi rements o f t h e Federal Food, Drug, and Cosractic A c t , as amended ( 2 1 U.S.C. 355). and t h e r e g u l a t i o n s i s s u e d undar t h c a c t are fully not . .
Although t h e i n s t r u c t i o n appeared to bo d i r e c t e d p r i - m a r i l y toward t h e i n v e s t i g a t i o n a l use of d r u g s , an o f f i c i a l of t h o Dcpar tnent of Defense a d v i s e d u s t h a t the i n s t r u c t i o n a p p l i e d t o a l l medical research p r o j e c t s . He s t a t e d a l s o t h a t each s e r v i c e d i r e c t e d i ts o m r e s e a r c h p r o j e c t s w i t h o u t con- t r o l from t l ic Dcpar taent .
a Wc c o n t a c t e d o f f ic ia l s o f the Depnr tncnts of t h e A n y , Kavy, and A i r Force and of t h e Defense Muclear Agency, for- n c r l y known as the. Dcfensc ACoaic Suppor t Ageccy ( t h e or j iani-
' z n t i o n n l c n t i e y w i t h i n t h e Ucpartncnt of Dafcnse t h a t had c o i i t r n c t s w i t h t h e U n i v e r s i t y of C i n c i r a n t i r e l a t i n g t o t b c whole-body i r r a d i a t i o n program) , t o d e t e r n i n c xi ie ther they had any i n s t r u c t i o n s or r e g u l a t i o n s t l i e t wcro q p l i c s b t o t o t h o use of humans i n n c d i c a l research ~ o r k under coat r t ic t . Tho
. o f f i c i a l s ir'erc n o t OWJTC of any i n s t r u c t i o n s or r e E i i 1 a t i o m , o t h e r than the, i n s t r u c t i o n s and repu1at ior . s i i q l e m e n t i n g Iil- s t r u c t i o n 5030.29, involv inp t h c use of h*aiUi s u b j c c t s t h n t would apply t o c o n t r a c t o r s conduct ing n o d i c a l r e s e a r c h f o r - t h e i r o r g a n i z a t i o n s . - .
An o f f i c i a l of t h e Dopaitmcnt o f . t h e A i r Forcc advisccl US t h a t t h c Air Forcc d i d ,?Ci conrluct n e d i c a l rcsdzrch widor c o n t r a c t . O f f i c i a l s of tilc Separtne; i ts of the Army and lhvy ' s t s t c d t h a t , a l though i m s t r -edical r c s e a r c h hod becn conductnd in-house , soze I m i m e n p c r f o r a c d c n b c r c o n t r a c t . lhcy srzted also t h a r . when work i s to \IC perforsmd u n d c r c o n t r a c t , t h e y ms t be s a t i s f i e d t h a t p a t i e n t conscrit for t i s v i 1 1 be uscd m d t h a t human s u b j e c t s w i l l bc ndequatc ly p r o t e c t c d b e f o r e a con- t r ac t is cxecutcd .

262
E- I540 31 (2)
An o f f i c i a l of t he Dcfcnse Nuclear Agcncy adviscd us t h a t , although t h e Defcnse Nuclcnr Agency d i d not have any cont rac ts f o r tho use o f hman sub jec t s €or medical research , tho following language had been included i n a l l medical colt- t r a c t s a f t e r August 1971.
"The COR [Contracting O f f i c e r ' s Rcprosenfativc] s h a l l bo i n fonwd in wri t ing of any p r o j e c t plens on the p a r t of t h e Contractor to enploy new, exporinon- t a l , and invo i t ige t iona l drugs o r other hazards i n research invorving hugan s u b j e c t s , and such cxpori- mentation s h o l l be s p e c i f i c a l l y au thor ized by t h e Contracting Of f i ce r i n wr i t i ng p r i o r t o the protccu- t i o n of such research. Without t h e concurronco and au thor i za t ion by the Contracting Of f i ce r fo r t h e spec i f i ed drug or other hazard involved, such re- search s h a l l not be performed. c lause is to insurc conplizncc with the Departaont of Dcfcnse Ins t ruc t ion , 5030.29, 1964 !?ay 12, 0n- t i t l e d g I~ ;vcs t iga t iona l Use pf Drugs o r Other Iiazs:ds by t h e Dcpartncnt of Uefcnse , a copy of which is furnished to Tho ConZractot wi th t h i s Contract) ." . Concerning the cont rac t wi th the Univorsi t y of Cinc inna t t ,
o f f i c i a l s of tho Dcfcnso Nuclear Agency state6 L5ut tho c a n t o f r ad ia t ion t .reatlont znd pa t i en t c a r e had noc been borr~c by t h e i r agency. Tlicy s t a t e d a l so t h a t funds of the Defenss Nuclcnr hecncy had been uscd only t o pay f o r supplcnentary laboratory anol rscs of p a t i e a t s who had rcce ived whole-Body i r r a d i a t i o n i n order f o r the DcCense Nuclear Xgoccy t o gain informafion i n a reas thot wcrc r e l a t i v e t o na t iona l JcTcnsa. -
We p lan t o make n3 fur ther d i s t r i b u t i o n of t h i s r c p o r t unlcss copies a r e s p e c i f i c z l l y rcqucsted, an3 then ne s h n l l mako d i s t r i b u t i o n only a f t e r your agrccrmtt tias been obts inod o r publ ic announccocnt has been nacie by you concerning tho
(Tho purpose o f t h i s
.I

263
B-164031(2)
contents of the report. Ve trust these cornelits w i l l scrvc the purposc of your inquiry.
Sincerely yours,
Comptroller General of the Urri tnd Sta tes
Enclosure
The Honorable Edvard M. Kennedy Cliairnsn, Subconnittee on Hsalth Connittee on Lcbor and Public Vclfore United S t a t e s Senste

I
264
Docmbcr 9, 1974
E o u x ~ b l a Sno k n
Ua&hingtm, D.C. 2GSlO
lrur Senator Nunu:
m r k 7ou for foar note8 of Fow*f 20. 1974, d d r e ~ e e d to rhe Departpmt of IkHIta . Educsrioa. and littf.ta 6nd LO ihe h p l r t i a n t vf ;)ofonre, encloriup: Cfrm. L:;.yd 8 . < i l f o r d ' r l c t t r r c oZ::w+tzh,ar I and. p t r t f c u l n r l y , for
United Stom. S C M C R
L .
Dr. 8. h L Q t 1 i l t t ; W ' G l l i @ l Y f B Z C C W l t a C O l U a l fCoJ C'W ctl*ntll J C U n l S I .
TBC regulatory icsuai?cc. dcccrlbrd by Doctor $kCrFcr as aowthinf i '. . . t!ic V.S. Rprracnt of il.oltn, iidr.cntio~. ai.& iclforc (XL:). 5-5s f lnrr l ly conc up with . . . . EI'C pro;roscd 1+7$ emndlbfnla to cnlrclcp. 1913 rc~ulations which fit t u r n codi f ied a 1971 deoart-rccrrnl policy wcich grad out of e hrS1lc l!calth Service pol5ey C3tLab back to 1956 ar;d t-zrllec p a r s . Iter+ prc-cxisrfna policic. re€ lcc tcd c5e sa= co.~errnc rslord in -tor )L'r:i:cr ' m article. ir'e are enclosing t*e r o l c w n t fsm~:nccr and tSe Zacr i tuLfmrl Culdc . . .'. to t!its Foltcp waLcS Loucb on Mny OE Laeet ioaitcs. Your attmtian i s a p c c l f i r a l l v callrii to t b e requirement rb f ic e l l of our crantccr: n d w t rlirfr OJO moral sad crirlcsl codon t o pcido chclr ccscarcIi, and to L:m l a g l i n t of .:I& codes OD tSc l rs t ra;;rr of the Cufdc. hir grrrnlb a d coaL7~ctm support w s e o t c h i n a vide s p e c t r u of rcli&irvs cod s e c u l a r l y c o n t r o l Icd sciwtlfic tasti tatlonm.
fba eolloorr by Doctor tht ry.er dwells a t CCCFP lcngtb odi an allaged sbucc of rr8asrcb praeedurcr a t t!ic Ciifverifty of Clncinn~i t l i.etzccn 1430 nnd 1971. kcountfcg Office faf lcd to dlcclore m y tulr8tcntive drrceistloa tctvcaa Dcpnrtncnt of li .olt2. b0ucnrfon. cod kklr=rc and Dcprrtmast of Pe€cme
fha C i n c f l m t t patfmts. T!ie Cdvermity =ever accoptad &Lens. fwda t o
DJctor tSetr;ct does cot c m t l o n L h t . dn i G V c s 1 ~ ~ 6 C i O ~ by tee Ccacral
ta8t.rCh oCuVi t iQ0 S t t h i s l * t l t u t i a *Id t L 8 CoCO-by-c8S8 t r c a t r s o t of
mp" FlithIC8. !I58 p8tfCnt. uere t r8e t8d lRdiVldua11~ €Or t h e d i O C U O 8 bad.
ybole-body red lo t ion st Ieocls of fov bundrcd rad. i s Ic rbol on ly vben S t destroy t h e blood bulldfn; calls of tlia bmt wrrou. aL these pstlaatr ubo h 6 widespread a t a r c o t i c cacrer. a lerse pnst et :ha mrrm va8 first rcooPed, t!!e pactooc vas then crested cnd tho oarroy rstutoed.
Ia t5c trcoLaaat
of tho patient. 1r.volwd dlrd from raJ1mUoa 81CknOa8.

265
P8go 2 - Uoaorrblo Sann Num
thouEh tdo of tkea did d ie ufth ururually I o v d i t e blood cell caunts. b a11 instmccr. dcnth una closrly srtributoblo t o tho rdvroce of ~sncet , m to intercurrent dleeose amxiatrd w i t h fhoacad cancer.
Tho l r c t por;r$rspb of Coetor )Wrgcr'c rrtielo contain8 the basic error-- ther eke gatientr ver8 O d n g gtrca ul:olc-baig radiuLioa for j-q-cc~!~~ cancer. 1;othir~ cmld be fart!tcr froa tho rrutb. A l l oE tbo prticntr bad had prior--and ur.ruecarsful--rargery for l@s:allred cancer, moot of them had bpd 8ddftioiinl surgery or loenlired raliarion, a11 by nbr bad Vid88pr8rd mtutsaea =king further curgcry or locclizrd radlatlon ineffective.
Ooctot &trgcr f a i l s t o n3tC tho fifidirp. by t?8 A a ? t i C 6 n Collcfp of bdiolopy that t h i r treatmest YBD a t l eaat 8s ef€cctivc oa Grul: t!rcruny for ccrtaia type. o t ccncer and, in the c8.e of P.vlna'a cli:co~a, E c : ~ f ~ C ~ o o d bono cancer, appeared t o kc far mperior KO m y other t f 8 a t n ~ t then ovcilsblo.
-
Sincerely JMKS.
D. T. 0 ~ 1 ~ 1 ~ ~ . &.D. Olcf, GCCfce for Protcction frm I'.ercarc5 Birlu Office of tho Dircctor

266
DEPARTMENT OF HEALTH. EDUCATION. AND WELFARE . r -
o . - - i ' - - ol; . to - - - -
1 9 - 3.- - - .,. ? I
o - l . _ . .
e,:
PUELlC HEALTH SERVICE NATIONAL INSTITUTES OF HEALTH .,
- - - W C I W L . O I . U M V U W WD14
- c De, . , - -,. ._.- . . - Docaber 13. 1914 . I. .
. . - Ws. Lloyd 1. Yilford - _ . -
mtur, ceagia 30030
Dear Ihr. Uilfardr - - -".. ~ * ._. '- - - - ,,_L ", - 8 - ' o -. , r.,- - ,' . _ I . _ - In typical buruucra t fc fashion it i 8 highly probable t h t ' o o a t o f the copies of yarr Mov&er 7 . 1974. letter to the Departmnt of b e l t h , Education, and Welfare wi l l m d up on my derk. prubbly receive several es8eot i s l ly ident ica l ruponses.
Ue u e enclosing a copy of our reply t o Senator Nuno end copies of the enclosure.. doer not propose. permit, or countenence research that coofwes patieots w i t h paramecim. these irrues. I w i l l be glad t o send you copiar; of our policy isrusncer dating back as f a r as 1953. i f you are interested. the in t e re s t s of itmoral sod depraved pcrrooa.
Doctor Metzger appears t o have r e l i ed on newspaper "morgue" mmterial tha t vas years old .ad grossly inaccurate. in such a sloppy f a sh im ve vould s t i l l be giving mothers thalidomide. The a c c w a t i m s are a libel on both the Department of Defense nod tha University of Cincinnati.
Senator Kennedy's concerns vere widely circulated in the Cincinnati papers, ye t none of the patients of t he i r rurvivors ude m y issue of the metter The Oniverrity refused t o release the patients ' namas not only bueuse of legal restrictiats, but becatma of eevere survfvors' reactions to 8 previous a t t a q t by a T.V. network t o document the . t u g with the b i v e r r i t y 8 coopara tion.
Several of the laing'e sarcoma carer treated st the holp i ta l are still alive aad w e l l several years a f t e r t r e a t m t , though the average s&vd of ouch pa t icn t r ir less than 6 .onths. bu helted what promired to be a very significant additioa to our arumen- terium against metastatic cancer. and io future years this carn t ry r y w e l l m e even further ahead of u. in the f i e l d o f radiotherapy.
165 Uoodlnm Avenue ~" _-. - ~ .. 7 -
. a . , - - ,. <-,,e . "', * . - ' .- , -
You vill . as a conrequence.
h en old protozoologist, I can assure you tha t the Departmnt
I t r u s t tha t the letter indicates our long concern wit6
They do not r e f l ec t
I f medical rerearch VU carried nat
It i s t o be regretted thet t h i s incident
Similar work ir going aherd in anad. .
Sincerely purr, a
D. t. Qalkley. B . D . Qlief, Office for Protection from Reaesrch Risk# Office of the D i r e c t o r

Mas. UOVD 6. WILroaD 165 WOODLAWN AVENUL
DLCATUR. QWRGI4 ¶OO¶O
November 7, 1974
Department o f H e a l t h , Educat ion and Welfare Washington, D.C. 20214
Gen t 1 emen :
I f i n d t h e a t t a c h e d almost beyond b e l i e f . STOP THIS!
Where i s t h e h e a l t h , e d u c a t i o n , or w e l f a r e i n a program t h a t t rea t s a human as i t would a pro tozoan? Why s h o u l d f e d e r a l money be used i n such programs a t a l l ? n o t a l l o w s u c h programs, much less f i n a n c e them.
We SI-auld
Thousands of c a n c e r victimswho r e a d t h i s w i l l s u f f e r t h e u n c e r t a i n t y o f t h e n a t u r e of t h e t r e a t m e n t s t h e y r e c e i v e , many a p p a r e n t l y w i t h reason. Research on human f e t u s e s , a b o r t e d or o t h e r w i s e , s h o u l d n e v e r be al lowed. You cm- n o t p o s s i b l y d a r e to c o n t i n u e or a l l o w to c o n t i n u e such immoral and depraved cr imes a g a i n s t c i t i z e n s whether a b o r t e d , m e n t a l l y i l l v i c t i m s of o u r s o c i e t y , or o t h e r i n n o c e n t s ; c e r t a i n l y n o t i n t h e n- of t h e peop!e of t h e United S t a t e s .
S t o p i t . In t h e name of God.
S i n cere1 y ,
cc: S e n a t o r s Nunn and Talmadge R e p r e s e n t a t i v e B1 ackburn S e c r e t a r y of t h e Anny Callaway
J


269
Published in Scientific Literature
PUBLISHED PAPERS - Under DASA Contract - Radiation Effects in Cancer Patients
Comparison of Serum Phenylalanine Levels with Growth in Guthries's Inhibition Assay in Newborn Infants. Carolyn Scheel and Helen K. Berry. The Jour. of Pediatrics, Vol. 61, No. 4, pp. 610-616, October 1962.
Deoxycytidine in Urine of Humans after Whole-Body Irradiation. Helen K. Berry, Eugene L. Saenger, Harold Perry, Ben I. Friedman, James 0. Kereiakes and Carolyn Scheel. Science, October 18, 1963, Vol. 142, NO. 3590, pp. 396-398.
Deoxycytidine Levels in the Urine of X-irradiated Rats. James G. Kereiakes, Eugene L. Saenger, and Helen Berry. Abstracted in Radiation Research, V o l . 22, No. 1, May 1964.
Urinary Excretion of Amino Acids and Nucleosides by Cancer Patients Following Whole-Body Irradiation. E.L. Saenger, J.G. Xereiakes and Helen Berry. Abstracted in Radiation Research, Vol. 22, No. 1, May 1964.
Endoreduplication in Leucocyte Chromosomes: Preliminary Report of its Relation to Cancer and Whole-Body Irradiation. Ben I. Friedman, Eugene L. Saenger and Michael S . Kreindler. The Lancet, September 5 , 1964, pp. 494-495.
Specific Proteins in Serum of Total-Body Irradiated Humans. A.J. Luzzio, B.I. Friedman, J.G. Kereiakes and E.L. Saenger. The Jour. of Immunology, Vol. 96, No. 1, pp. 64-67, 1966.
Hematologic Effects of Total-Body Radiation in the Human Being. Gould A. Andrew, C.C. Lushbaugh, Ralph J. Kniseley, David A. White and Ben I. Friedman. Incernational Atomic Energy Agency Panel on the Effects of Various Types of Ionizing Radiation from Different Sources on the Haematopoietic Tissues, meeting in Vienna, Austria, May 17-20, 1966. Published in Proceedings by IAEA, Vienna, 1967, STI/PUB/134, pages 75-83.
This paper was presented at the

Effects of Whole and Half Body Irradiation in Human Beings with Cancer. E.L. Saenger, B.I. Friedman, J . G . Kereiakes and H. Perry. Published in the Proceeding of the Third International Congress of Radiation, Cortina d'Ampezzo, Italy, June 26-July 2 , 1966, p. 191, abstract #759.
Effects of Total Partial Body Therapeutic Irradiation in Man. Eugene L. Saenger. Published in Proceedings of the 1st International Symposium on the Biological Interpretation of Dose from Accelerator-Produced Radiation - Held at the Lawrence Radiation Laboratory, Berkeley, California, March 13-16, 1967. Published U.S. Atomic Energy Commission/Division of Technical Information, CONF-670305, p. 114-227.
Colorimetric Analysis of Deoxycytidine in Urine After Separation by Ion-Exchange Column Chromatography. I-Wen Chen, James G. Kereiakes, Ben I. Friedman and Eugene L. Saenger. Analytical Biochemistry, Vol. 23, No. 2, May 1968, pp. 230-240.
Radiation-Induced Urinary Excretion of Deoxycytidine by Rats and Humans. I-Wen Chen, James G. Kereiakes, Ben I. Friedman and Eugene L. Saenger. Radiology, Vol. 9 No. 2, pp. 343-348, August 1968.
Total and Half Body Irradiation: Effect on Cognitive and Emotional Processes. Louis A. Gottschalk, Robert Kunkel, Theodore H. Wohl, Eugene L. Saenger and Carolyn N. Winget. Arch. Gen. Psychiat. Vol. 21, pp. 574-580, Nov. 1969.
Cytologic-Biochemical Radiation Dosimeters in Man. E.G. Silberstein, I-Wen Chen, E.L. Saenger and J.G. Kereiakes. Published in Proceedings "Biochemical Indicators of Radiation Injury in Man "International Atomic Energy Agency, PL-409/13, pp. 181-214, Vienna, 1971.

Bone Marrow Dosimetry in a Cobalt 60 Irradiated Tissue Equivalent Human Phantom. presented by James G. Kereiakes at the Second International Conference on Medical Physics, Boston, Massachusetts August 11-15, 1969.
Effect of Total and Partial Body Radiation on Cognitive- Intellectual Functioning and Emotional Reactions, C.C. Gleser, C.N. Winget, R.L. Kunkel and E.L. Saenger. Presented at the DASA Medical Coordination Conference "Radiation-Induced Incapacitation/Performance Decrement", Armed Forces Radiobiology Research Institute, Bethesda, Md. 18-19 November 1969.
Cytologic-Biochemical Indicators of Radiation Injury in Man. Presented by E.B. Silberstein at the WHO/IAEA Conference, Paris, June 22-26, 1970.
The Changing Picture of Bone Marrow Granulocyte Reserves in Irradiated Patients. Presented at the Experimental Hematology Society by E.B. Silberstein, November 12-13, 1970, Pittsburgh.
Presentations listed below were made by staff of the Radioisotope Lab. at the Joint Oak Ridge Associated Universities-Defense Atomic Support Agency Information Exchange Program "Radiation Effects on Biological Systems," Oak Ridge, Tenn. March 29-30, 1971.
A Closed System for Marrow Transplantation - E.B. Silberstein
Chromosome Aberrations as a Dosimeter of Whole Body Irradiation - E.B. Silberstein Active Bone Marrow Doses in Whole-Body and Partial Body Exposures - J.G. Kereiakes
Serum and Urinary Amylase Activities in Irradiated Cancer Patients - E.L. Saenger The Relationship of Nausea and Vomiting to Radiation Dose - E.L. Saenger In vitro studies of Chromosome aberrations caused by Irradiation - E.B. Silberstein

272
Ultraviolet-Absorbing Compounds in Urine of Two Irradiated Cancer Patients as Determined by High- Resolution Column Chromatography - E.L. Saenger
Active Bone Marrow Dose Related to Hematological Changes in Whole Body and Partial Body Exposures - J.G. Kereiakes, E.B. Silberstein, E.L. Saenger, W.G. Van De Riet and C. Born - submitted for presentation at the Annual Meeting of the Radiological Society of North American in December 1971.
Bone Marrow Dose in Whole and Partial Body Cobalt 60 tissue- equivalent human phantom. C. Born, J.G. Kereiakes, G.K. Gahr and G.H. Simmons, presented at the annual meeting of the AAPM, Houston, Texas, July 1971.
PRESENTATION - Made under DASA contract - Radiation effects on cancer patients
Radiation Casualties-Newer Aspects of Mass Casualty Care. Presented by Eugene L. Saenger and Max L.M. Boone, at the Thirteenth County Medical Societies Conference on Disaster Medical Care, American Medical Association, Chicago, Illinois, November 4, 1962.
Deoxycytidine Levels in the Urine of X-irradiated Rats. Presented by James G. Kereiakes at the Annual Meeting of the Radiation Research Society, May 1964, Miami Beach, Florida.
Urinary Excretion of Amino Acids and Nucleosides by Cancer Patients Following Whole-Body Irradiation, presented by E.L. Saenger at the Annual Meeting of the Radiation Research Society, May 1964 at Miami Beach, Florida.
Autologous Bone Marrow Storage and Infusion in Patients Receiving Whole Body Radiation. Presented by Ben I. Friedman at the American College of Physicians Regional Meeting in Pittsburgh on November 20, 1965.
Effect of Whole and Half-Body Irradiation in Human Beings with Cancer. Presented by Eugene L. Saenger at the Third International Congress of Radiation Research, Cortina d"Ampezzo, Italy, June 26, July 2, 1966.
Hope and Denial in Metastatic Carcinoma - A Preliminary Report. Presented by Dr. Robert L. Kunkel at a Psychosomatic Meeting in New Orleans, 1966.
Effects of Total and Partial Body Therapeutic Irradiation in Man. Presented by Eugene L. Saenger at the Proceedings of the 1st International Symposium on the Biological Interpretation of Dose from Accelerator-Produced Radiation. Held at the Lawrence Radiation Laboratory, Berkeley, California, March 13-16, 1967.

Quantitive Analysis of Deoxycytidine in Cancer Patients and Rats. Presented by DASA Symposium, U.S. Naval Radiological Francisco, California, April 9-11, 1968.
the Urine of Irradiated James 0 . Kereiakea at the Defense Laboratory, San
The Management of the Acute Radiation Syndrome in Man. Presented by Eugene L. Saenger at the DASA Symposium, U.S. Naval Radiological Defense Laboratory, San Francisco, California, April
Bone Marrow Dosimetry in a Cobalt 60 Irradiated Tissue-Equivalent Human Phantom. Presented by James 0 . Kereiakea at the DASA Medical Coordination Conference, Air Force Weapons Laboratory, Kirkland Air Force Base, New Mexico, May 27-29, 1969.
Radiation-Induced Urinary Excretion of Deoxycytidine by Rats and Humans. Presented by I-Wen Chen at the Annual Meeting of the Radiological Society of North America, Chicago, Illinois, December. 1967.
9-11, 1968.

274
TECHNICAL REPORTS
Submmed by Unwerslty of Cmannah to Defense Nudear Agency (DNA) formerly DASA
Repori Period
Feb 1960 thN OCt 1961
Nov 1961 Mru Apr 1963
May 1963 thw Feb. 1964
Feb. 1960 Mru Apr 1966
M y 1966 thN Apr 1987
May 1 9 6 7 M r u A p r 1968
my ism mru Apr 1969
May 1969 rnm Apr 1970
May 1970 thn, Apf 1971
m e Metabolic Changes In Humans Follomng Total Body Radiation Metabolic Changes in Humans Follomng Total Body Radiation Metabolic Changes in Humans Followng Total Body Radiation
Metabolic Changes in Humans Followng Total Body Radiation
Metabolic Changes in Humans Followng Total Body Radlatlon
Radtatton Effects In Man, Manllestations end Therapeutic Efforts
Radimon Effects in Man, Manllestations and Therapeutic Efforts Radiation Effects in Man, Manifestations and Therapeutic Efforts Radiation Effects m Man, Manifestations and Therapeutic Efforts
Contra* No DA-49-146-WMg
DA-49-146-W-029
DA-49-146-XZ-028
DA-49-146-XZ-315
DA-49-146-XZ-315
DA-49-146-XZ-315
DA-49-146-w-315
DASAOl.6oc-0131
DASAOl -69-C-0131
DASA Report No
None Assigned
DASA 1422
DASA 1633
DASA 1044
DASA 21 79
DASA 2163
DASA 2420
DASA 2599
DNA 2751T

- f- 275
Mr. BRYANT. You testified that funding was obtained from the National Institutes of Health and that most costs were paid by Cin- cinnati General Hospital.
We have found one indication, as I mentioned earlier today, that the National Institutes of Health refused to participate on the grounds of its concern about the moral implications of going for- ward.
Dr. SAENGER. Yes. I mentioned in my resentation the National
for the purpose of metabolic study which was available to any pro- gram within the medical center which would satisf their require-
ted one bed there for a perio%of time. And we had several patients on this service.
And in order for us to maintain that servicemaintain that availability, it was required that we submit the protocol and the course of these patients. And we used this in great part for our de- velopment of autologous marrow harvesting and reinfusion.
And this-this was-these were the reports that Dr. Chalkley of the Office of Risk Protection at the NIH responded to in his com- ments to a letter that he had received. Did I make that clear?
Mr. BRYANT. Not exactly. You might elaborate a little bit. Dr. SAENGER. The NIH maintained a service, a ward, in our hos-
pital, which they paid for totally. When a patient was put in that ward the funds were supplied totally by the NIH. This ward was there for conducting nutritional balance studies, looking at meta- bolic studies for a variety of purposes.
And we put several of our atients in this particular service so
plantation technique that we were working out. It took us some time to do that before we were successful in the five patients to
Institutes of Health maintained a Gener af Clinical Research Center
ments. One had to submit a rotocol and so on. An l we were allot-
that we could study particular P y the autologous bone marrow trans-
whom I referred. In order that the NIH could maintain this funding we had to give
them re orts of the protocol and the progress of the patients, and
Now the other research projects that we submitted to the NIH were turned down for pu oses which I don’t recall exactly at this moment. They accepted ‘ph t is work that we did with the General Clinical Research Center.
Mr. BRYANT. Are you sayin that this-I am looking for some clarification. We have had impfication from some of the documents we saw that the NIH refused to go along with the whole body radi- ation treatment experiments because of moral questions. Does your answer indicate they did go along with it?
Dr. SAENGER. They did o along in the studies of these several
For additional funding after our contract with the DO was termi- nated. And it was those-that was that proposal I think that they declined.
we did t K at. And these were approved.
5 atients that we reported. I n d we then made a subse uent request
Mr. BRYANT. On the grounds that they had some moral- Dr. SAENGER. I do not know the grounds. Mr. BRYANT. Well, our indications are that they were concerned
Dr. SAENGER. As to what? about the moral implications of it. Is that a surprise to you?

276
Mr. BRYANT. About the moral indications. Dr. SAENGER. I think there was some difference of opinion about
informed consent. I might say, in that regard, from the time we de- veloped the first informed consent in 1965 we submitted several additional informed consents which I believe you have in your doc- uments. These were done at the request of the Human Research Committee and were approved.
Our final informed consent technique that we used was a 2-day informed consent where the patient would be-where the study would be explained to the patient and/or his family or other-min- ister, lawyer, whoever-n one day. And on a second day we would again repeat this process. And if the patient agreed to it then it would be a signed, informed concept.
So we went through a rather elaborate series of improvements on informed consent.
Mr. BRYANT. The first question would be, did these people have the capacity to understand what was being told to them and to give consent? That was one of the criticisms raised, that they were not capable of understanding what you were asking them about and, therefore, not able to give informed consent. Could you respond to that?
Dr. SAENGER. My response to tha t -our physicians who carried out the informed consent procedure were very careful to explain this work to the patients in most if not in all cases prior to the written informed consent period. We had one of our nurses or other research associates accompany the physician with the patient so that this explanation would be carried out so that they would un- derstand it.
And we do have several recordings where we had taped the in- formed consent procedure with the patients.
Mr. BRYANT. Dr. Egilman further pointed out there was a 25 per- cent chance of very rapid death from the whole body radiation treatment. I ask the question, why weren’t these people told they might die rather than in several months or years but instead in a few weeks?
Dr. SAENGER. I have looked at a great many written informed consent procedures that have been developed over the years. I have yet to see one in which the risk of death is explicitly stated in the written informed consents that I have reviewed.
Mr. BRYANT. Well, I don’t wish to impose a standard, a 1994 standard on actions back in the 1960’s and early 1970’s, but it does seem to me to be a fairly simple concept that if a person is ill and is probably going to live many more months or probably even a cou- ple of years, if they run a significant risk of dying immediately or within a few weeks, that that is something that you would just nor- mally tell them.
Dr. SAENGER. I think we explained to the patients that they might benefit and they very well may not benefit from the treat- ment. I don’t think that we could be guarantors of results because, as you can see from our studies, we had some 20 patients who lived longer than a year.
And I think that it is really impossible to determine in any single case how long a patient will survive. We had some patients who we

277
thought would not survive, and they seemed to improve tremen- dously and live for several months.
Mr. BRYANT. I think you are confirming Dr. Egilman’s statement that these patients were not told that they would, 88 a result of the whole body radiation, die much more rapidly due to the treatment.
Dr. SAENGER. I don’t think that in anyone’s experience it is pos- sible to foretell the exact time of death after any treatment which is given. We gave this treatment with the understanding that it would improve the patient’s welfare either by prolonging survival- we did the best we could in that regard-and we gave them the very best we were capable of in terms of shrinking tumors, improv- ing well-being.
We got many statements from these patients which support what I am saying to you.
Mr. BRYANT. Mr. Mann. Mr. MANN. Mr. Chairman, thank you. Just to follow up on that point, Dr. Saenger, do you agree with
Dr. Shields’ statement that Dr. Egilman quoted that there was 25 percent mortality?
Dr. SAENGER. I do not agree with that at all. Mr. MANN. So how-what was the risk then of death within a
few weeks of treatment? Dr. Shields said one in four. How would you-
Dr. SAENGER. I think there was a risk of death within a short period of time after treatment. But the question is what was the risk due to. In our opinion, in reviewing these charts over and over again, it seemed to us that the primary reason for death within a few weeks after the treatment or in a few cases within a few days was the growth and the-the rapid growth of a tumor rather than the treatment.
If you look at the amount of radiation which we gave to these people in light of the further development of whole and partial body radiation, we find the patients today are living with doses of 600 to 1,200 rads, and our doses of up to 200 rads were really at a very low dose compared to what we see in survival today.
And it is not reasonable to assign radiation as the sole or major contributing cause of death in this series of patients.
Mr. MANN. Your paper that you published in 1973 does suggest that eight of the patients may have had their death accelerated as a result of the whole body radiation. Isn’t that true?
Dr. SAENGER. What we said in that paper was if one assumes that all severe drops in blood cell count and all instances of hypocellular or acellular death were due only to radiation and not influenced by the type or extent of cancer and the effects of pre- vious therapy, then one can identify eight cases in which there is a possibility of therapy contributing to mortality.
The fact that-that was the statement in the paper. The fact is that these patients did have far advanced cancer and
had other forms of therapy before and after. And, therefore, the as- sumption is just that. It is not what actually occurred. We have looked at these charts recently and find the course of these pa- tients-the downhill course of these patients to have been due to cancer.

278
Mr. IMANN. It is no longer possible that those eight died because of treatment?
Dr. SAENGER. I a m sorry? Mr. m. Are you saying that the statement in the paper of 20
years ago that it was possible that those eight had mortality ad- vanced because of treatment is no longer, in your opinion, the case?
Dr. SAENGER. That is my opinion. May I continue? Mr. m. Yes, I am sorry. Dr. SAENGER. Also, statistically, we would have found the mortal-
ity of these patients would have differed from the mortality of pa- tients treated by other means.
In our patients, it does not differ. That we can see in the survival curves in our 1973 paper.
Mr. IMANN. Now, I want to go to your own documents, which I think are the most difficult part of all this, at least for me,
I have looked at your 1958 proposal to DOD, the contract with DOD, as I indicated in my opening comments, the reports that were made periodically from the beginning of the study in Feb- ruary 1960 until April 1967. And in none of those documents can I find any indication that there is any purpose to the study what- ever other than to identify a biological marker or biological link that would allow the Department of Defense to administer simple tests and determine how much radiation a soldier in battle had re- ceived.
And the question I think we all have is, if this was about treat- ment and this was about therapy, why would there be no mention in all these documents for all those years?
Dr. SAENGER. I would like to refer you to our 1962 document pre- pared for the Defense Atomic Agency.
Mr. MANN. I have it. Yes, sir. Dr. SAENGER. The eligibility for patients entering this treatment
was spelled out. “There is a reasonable chance of therapeutic bene- fit to the patient. The likelihood of damage to the patient is no greater than that encountered in comparable therapy of another type.”
Furthermore, I would refer you to the statement of J.A. Isher-
Mr. -. That we discussed earlier? Dr. SAENGER. Yes, that was discussed earlier. That clearly identi-
fies the attempt to improve the condition of cancer patients with that therapy.
Mr. m. Focusing on that, your 1958 proposal says nothing about pa\ient therapy. And Dr. Isherwood sort of gratuitously starts talking about the project will be of great value in the field of cancer. How would he know that? What did he have beyond the proposal that would allow him to reach such a conclusion? Dr. SAENGER. Well, I really can’t answer that except to say to
you that we had discussed this proposal with the Department of Defense people involved, so that I think we had indicated that this was the primary intent of our work. The reason that we hrased
that was what they were interested in and that is what we tried to tell them about.
wood-
our reports to the Department of Defense in the way we di c r is that

279
But that did not have anything to d-that did not interfere in any wa with the therapeutic intent of the program.
Mr. &ANN. Doctor, you referred to a 1962 document that you submitted to DOD. For what reason-what were the circumstances that led to the drafting and submittal of that document?
Dr. SAENGER. My recollection was that the DOD had requested us to give them an overview of where we thought this whole pro- gram was goin , and at the time we made that report.
the re rts, we are saying, other t an the 1962 document, were ti- tling t k e project, metabolic changes in humans following total body irradiation and the aims and sco of the project had continued-
to April 1963. This information is necessary to provide knowled e
of diagnosis, pro osis, prophylaxis, and treatment of injuries that would be su f fe re r as I understand, from radiation.
That continues to be pretty much the way it is all characterized until suddenly the report that was released after April 1968, the title is changed. The title now is, “Radiation Effects in Man: Mani- festations and Therapeutic Efforts.” That was the title that was used for the reports that were submitted for the period of the project, May 1967 until March 1972.
What was the reason for the change in title? Dr. SAENGER. I think part of that developed from our work with
autologous bone marrow transplantation and our effort to be able to control the de ression of bone marrow.
We also foun c f at that time, in that work, that with the use of autologous bone marrow infusion, reinfusion, that the patients did not seem, at least clinical1 to me, to et as sick as they did before
course was ameliorated by the fact that their blood count came back to normal much more quickly than they did before we used that technique.
Mr. MANN. So the therapeutic efforts would be describing the use of bone marrow transplant?
Dr. SAENGER. If you look at our initial proposal in 1958 to the development of this entire project, I like to think we became more and more so histicated in what we were doing and became more
great deal more about the therapeutic benefits that we were achieving.
Mr. MANN. There is one last report that covers the time period April 1971 to March 1972. This continues to have this new title. But it also-and I think it is the first time that the purpose of the study is described in this way.
The purpose of these investigations has been to im rove the treatment and gen- eral clinical management and, if possible, the l e v or survival of patients with ad- vanced cancer since systemic effects of radiation erapy have been given particular attention in our work.
In fact, there is virtually no mention of Pentagon interest or Pen- tagon purpose. Now why was the purpose of the work characterized so dramatically differently in March 1972?
% Mr. MANN. B ust tracking throu h what we have here so that-
Let me just read from one o f t I? e reports. This is November 1961,
of combat effectiveness of troops and to develop additional metho 8 s
in the period immediatey 1y after ra % iation. And certainly their
knowledgeab P e about the effects of radiation, and we understood a
March 1972, the purpose is as follows:

280
Dr. SAENGER. May I get a copy of that? Mr. MANN. Yes, sir. Dr. SAENGER. That was the April 1971 to 197- Mr. MANN. April 1971, to March 1972, yes, sir. Dr. SAENGER. I think, Congressman, you will find that to be al-
most the exact duplicate of the published paper in 1971. Mr. MANN. I think that is true. But, as I understand, this is the
final report of which I am aware to the Department of Defense. And the question is why the purposes of the work are so dramati- cally transformed or at least stated in such a dramatically different fashion.
Dr. SAENGER. I thought it was a pretty good report. I summa- rized what we had learned over the 10-year period.
Mr. MANN. I am not questioning that. The question is-I read to you what the purpose was stated to
be of the work in your earlier reports. And it was all focused on the battlefield and so forth. And, suddenly, the battlefield and the Pentagon is not mentioned. I was curious.
The question is, what is the reason for the different characteriza- tion?
Dr. SAENGER. I think part of the reason for the characterization is that we-this whole research came under a great deal of criti- cism, and we were pointing out what the value and the benefits of our therapeutic part of the study was, in addition to the informa- tion which we gave to the Department of Defense.
Mr. MANN. Thank you. Now, I want to ask a few questions out of Dr. Suskind‘s study.
Dr. Suskind is present, I notice. We appreciate his presence. But on page 12 of the report-I am quoting-although whole
body radiation is widely used for many forms of radiosensitive tu- mors, no information is available to the committee which indicates that this form of treatment is used elsewhere in radioresistant or localized cancers as used at the University of Cincinnati. The first one is, do you agree with that statement?
Dr. SAENGER. Well, there are three references that are cited there. We have cited in the documents that we have prepared for this a great many papers on this subject. And this was written by the committee. It was not written by me.
Mr. MANN. Do you disagree with his statement, sir? Dr. SAENGER. All I can say is it is the committee’s opinion. I did
not write this report. Mr. MANN. Yes, sir. Do you agree or disagre+ Dr. SAENGER. I don’t have to agree or disagree with it. Their sur-
vey of the literature is their survey. Mr. MANN. I am asking you, sir, whether, in your professional
judgment or professional opinion, do you-you-I am asking you to develop an opinion. Do you agree or not agree?
Dr. SAENGER. This says that the committee didn’t find-it says, the committee-no information is available to the committee. I was not a member of the committee, and I did not review this report. If they didn’t find information in this regard, which we have sup- plied in our bibliography, submitted to this-to your committee, I don’t know what to say about it.

28 1
Mr. W. So you believe, in your opinion, the treatment was being used elsewhere in radioresistant or localized cancers?
Dr. SAENGER. In the diseases that we treated, I would say yes. Mr. m. Quoting again from the study, this is page 1 4
The committee, however, was unable to find any written protocol in which the purpose of the study, which is determined palliative effects of whole body irradia- tion until the rotocol entitled, The Therapeutic Effect of Total Body Irradiation Follbwed by I& ion of Stored Analogous Marrow in Humans was resubmitted to the Chairman of the research committee by Dr. Ben Friedman, then principal inves- tigator, on April 13,1967.
Dr. SAENGER. Again, I would have to refer you to our statement made to DASA in 1962. I cannot say whether Dr. Suskind’s com- mittee was familiar with that statement or not.
Mr. MANN. So your 1962 document to DOD is a written protocol? Dr. SAENGER. I think it is fairly explicit. Mr. MANN. All right, sir. I am going to yield for the moment. I Mr. BRYANT. Mr. Portman. Mr. PORTMAN. Thank you, Mr. Chairman. Dr. Saenger, thank you for agreeing to be before us today. Just to back up, again. My view is that the role of this sub-
committee is to help determine the appropriateness of compensa- tion for the families, and it is in that context that I ask these ques- tions.
And first, of course, informed consent. You have mentioned in your response to Mr. Bryant and I believe in your testimony that the attending physicians were responsible for providing information as to risks, benefits and so on. I just wondered-perhaps this is in the record. I haven’t seen it. And there are many documents I have reviewed. But who were these people that were informing the pa- tients-who were these the internists or radiologists? Who were the attending physicians?
Dr. SAENGER. The principal ones I have identified: Dr. Harold Perry, who was responsible for the radiotherapy in our institution from about 1957 until about 1965; Dr. Horowitz, a radiation thera- pist, who was from about 1965 to 1968; Dr. Ben Friedman, an in- ternist and hematologist who was with us from about 1963 to 1965 or 1966-1 can’t give you these exact dates; I don’t have them-Dr. Silberstein, who began in 1967, I believe; and Dr. Bernard Aron, who began in about 1966.
Now these are all board certified specialists in their fields either of radiation oncology or internal medicine, nuclear medicine. And I think they are very responsible ph sicians and have been very
br. PORTMAN. Further, on the issue of informed consent, having heard a lot about that today and having looked at it quite a bit over the last few months, there is a lot of conflict, I believe, out there between, as an example, the Hippocratic Oath on the one hand, and codes that were adopted later, the various radices of hospitals and so on. We have heard today that standar B s of disclo- sure were evolving durin this time period, the 1950s and 1960s.
at that time?
will pick up on the second round.
hi hly regarded in this community an if nationally.
My question to ou is, d o you believe that the experiments devi- ated in any way P rom the standards that govern informed consent

282
Dr. SAENGER. Absolutely not. I think we complied fully with in- formed consent. I think we were in the advance of techniques of in- formed consent throughout this study.
Mr. PORTMAN. There has been discussion today about radiation doses being lethal or close to lethal. You stated earlier in response to Mr. Bryant’s question that today there continue to be whole body radiation treatments. You indicated that the rads were higher, al- though I am a little confused as to the intervals. If you could per- haps flesh that out a little further and then just give us your o in- ion as a radiologist as to the question of lethal or nonlethal l ose in the period of 1971.
Dr. SAENGER. When we began our works we were feeling our way very gingerly, and we believed that somewhere around 150 to 200 rads of whole body radiation was about as high as we could go without getting into trouble.
After our project was terminated, at the point when we were able -to maintain better control of the patients with our autologous bone marrow infusion, we then find from looking at the literature that other centers continuing in this work, many treating the same and different cancers, were using doses of two, three and four times the size, the amount that we were using, with success.
If you go back and look at what we were doing, it would seem to indicate very strongly that the doses that we were considering as getting pretty close to a danger point were really not. And this is one of the reasons that we were able to conclude that the deaths in many of these patients, as they died, were due to the progress of their cancer, which was growing exponentially, rather than as a result of the comparatively small doses of radiation that we were giving both whole body and artial body.
to today’s practices in terms of levels of-I believe you talked about levels in the 600 to 1,200 range but indicated that treatment would perhaps be given at intervals. This is today’s practice.
Dr. SAENGER. Today’s practice in some institutions, they still will give 1,000 to 1,200 rads as a single dose. Now what is found in those patients is that they don’t die of the acute radiation syn- drome. They die of a subsequent radiation pneumonitis.
And in order to get around the problem of dying of radiation pneumonitis and still accomplish the intended therapy, which is to either treat the cancers or ablate the bone marrow, it has been found that one can fractionate the dose. And by that you would perhaps give four doses of 300 rads, say, a day or every other day, for a period of time. You would give 200 rads a day times five to g e e f o r five days to get to 1,000 rads.
Furthermore, in today’s treatment of cancer, these patients now are getting several series over a period of weeks of intensive chem- otherapy, then getting this total body therapy and then goin back
radiation which are damaging to the bone marrow are really in terms of what we were doing back in the 1960’s. It is sort of, I guess, fantastic. And patients are surviving this.
Mr. PORTMAN. The final question in the area of informed consent. This has to do with the selection of the patients. Many patients had a lower level of education. Many are indigent.
Mr. PORTMAN. Again, cou P d you just flesh out a little further as
to intensive chemotherapy. So that the amount of chemic af s and

I-- -
- 283
I know in response to an earlier question you indicated you weren’t involved in the selection. If you have anything further on that, I would be happy to hear about it.
But my concern is, really, do you think that that is relevant? Does that bear on the informed consent question specifically? Would that same patient group be selected today, even with the evolving higher standards of informed consent?
Dr. SAENGER. I would like to respond to that because I think it is a very important question. It has been of great interest to me to first listen to several of the taped consent interviews which we have with several of our patients. And irrespective of their IQs or level of illness and so on, I can tell you that from my experience of some 50 years in handling cancer patients, that these patients were thoroughly aware of their situation. They understood that we were going to try and do something for them which might be help- ful and might not.
In addition to that, we did something that is unique in the field of studying radiation effects in cancer patients. We had a very elaborate program of investigating the psychological and psy- chiatric reactions of these patients to their treatment. And part of this consisted of 5-minute interviews where the psychologist would simply take a tape-recorder and put this in front of the patient and say, talk for 5 minutes about anything you want to.
Now, what happens in these situations was that these patients are first interviewed in that fashion immediately when they began on our study program. That took us usually 2 or 3 weeks to get them all prepared, worked up, as we say, tested with our various laboratory tests and undergoing sham radiation, which wt? did carry out. And each time we had this interview.
Then the patients were interviewed just before they were treat- ed, just after they were treated, and for a 3-day interval, I believe, a 7-day interval, as long sometimes as 6 weeks.
I have only listened to a few of these tapes, and I can tell you that these patients are understanding, sensitive and alert to their conditions, to their treatment, to their progress, to the fact that their tumors are growing, that sometimes they feel better, some- times they feel worse, and they are as sensitive as any individual in this room today.
And I do not believe that all of this talk about the poor and uneducated and low IQs and so on had anything to do with their ability to perceive their situation in life and how it is progressing.
Mr. PORTMAN. The next major issue is the DOD role, the Govern- ment role in all of this.
I, too, have questions about your reports back to DOD. Congress- man Mann quoted from a couple of those reports.
I wish DOD were still at the panel because 1 would like to hear- and perhaps we can now, Dr. Soper, hear from you later about other examples where DOD responded with an institution’ in terms of the effects versus the treatment, because it seems to me that Dr. Saenger‘s statement that this is what DOD was interested in and concerned about and, therefore, that was what was in the report might be something that we should look into in terms of other re- porting that was done in other experiments around the country.
- - 3

284
But my general question, I suppose, is, would you have gone
Dr. SAENGER. Yes. We had Dr. Perry. We had Dr. Kereiakes. We ahead without DOD?
had the physical equipment and so on. And we would have pro- ceeded whether or not we had DOD’s support. DOD’s support was not used for the treatment of the patients. As we have emphasized, the GAO investigated this uestion, and
entirely separate from the therapy of the patients. Mr. PORTMAN. My final question really is how DOD used the in-
formation. There is very little in the file that I find, at least as to DOD reporting back on how it used the information that the ex- periments in Cincinnati provided to them. Are you aware of any DOD reports generated during the study period or after the study period as to how they used the information that was provided?
Dr. SAENGER. I cannot give you the exact times that I met with DOD people, the DNA personnel and other Army and other com- mands. But there were several meetings which I attended. There was data that I worked on with them to develop the manuals which they use in the field for the commanders and for the person- nel in the field in the event of nuclear warfare.
I don’t have the information that Dr. Soper had about the exact manuals today. But I have participated in these, and I know-at least I am led to believe that our information was useful to the DOD in this regard.
I know that some of the studies, the psychological studies were of some help in interpreting what they find is a very important consideration of performance.
Mr. PORTMAN. And you are led to believe that some of the infor- mation provided was useful in compilin manuals-
with DOD personnel. The only thing I can’t tell you today is the exact date, location of those meetings. I think I could find some of this information.
Mr. PORTMAN. I think some of that is relevant-at least in my mind it is relevant to the issue of the DOD role.
Thank you very much, Dr. Saenger. Mr. BRYANT. Dr. Saenger, you mentioned a moment ago-I am
sorry. Dr. Egilman referred earlier and you made some reference to this business of treatment for nausea. And his comment was to the effect that ill patients who were nauseated were not given nau- sea treatment for up to three days, which was not the normal prac- tice, as he stated it. Would you repeat what you said earlier about that?
Dr. SAENGER. What I said earlier about that was that we asked the ward personnel and the attending people not to ask specifically are you nauseated, do you feel like vomiting, because we found, as I think many of us observe in raising children and so on, if you ask leading questions you very often elicit responses, particularly for things which are somewhat suggestible such as nausea and vomit- ing.
On the other hand, we have taken a great deal of pride in the quality of our nursing care on the tumor wards of the General Hos- pital over a period of some 50 years that I have been associated
I think the conclusion is inescapable that the DOD 1 unction was
Dr. SAENGER. I attended some con B erences from time to time

285
with that institution. And I can tell you at that these patients were not left all alone and completely neglected and so on. That is sim- ply not so.
I think, on the other hand, you have to realize the situation of people who are desperately ill. They have very unpleasant things happen to them. They get sick. They throw up. They lose control of their bodily functions. They don’t immediately always have someone to come and clean them up. And when family members come in and see them in these rather sad states, everybody gets pretty upset. And I have had this personal experience with mem- bers of my family, and I am sure all of you have.
But these patients under no consideration were abandoned or left out in a field and so on. I t is just not so. That is not the quality of medical care that has been given in our institution during my entire career, earlier or later.
Mr. BRYANT. If a patient was nauseated, were they given anti- nausea medication?
Dr. SAENGER. If they complained. All they had to do was say, I don’t feel good, and the patients were given whatever therapy-I mean, whether it was Compazine or some other antiemetic or cracked ice.
Mr. BRYANT. So your only policy in this regard was don’t go and ask them?
Dr. SAENGER. Just don’t ask the leading question. That was the only thing that we requested. And we only requested that for a pe- riod of 3 or 4 days. This was not something that would go on for a period of weeks.
Mr. BRYANT. So for a period of 3 or 4 days, during their course of these whole body-
Dr. SAENGER. Immediately after the irradiation. Immediately after the total body irradiation.
Mr. BRYANT. You made reference also to psychological isolation of the patient. Do you recall any instructions that the patients be put in rooms all by themselves and left alone?
Dr. SAENGER. I do not recall that specific incident. The wards in which the patient were hospitalized were at that time generally open wards. There would be maybe anywhere from 2 to 5 to 10 beds on these wards, more or less.
became critically and terminally ill, having a lot of things going on, if there was a single room in the wards of the hospital the patient sometimes was moved in it for two reasons: one, that the family
from the nurses; and also so they would not disturb the other pa- tients who were less sick on the ward.
That was the general, I guess, nursing practice at the hospital. Mr. BRYANT. But that would be, I assume, the policy for all pa-
tients at all times, would it not? Dr. SAENGER. That is my impression. I don’t think there was
anything particular-I think the patients that we treated were treated as well, hopefully better, than any other patient in the hos- pital but certainly not less well. They were certainly not isolated or disregarded.
L
. It was the custom from the time I was an intern when a patient
s could be there, that they could get some care from the family and
84-514 0 - 94 - 10

286
Mr. BRYANT. Finally, the reference to what the Defense Depart- ment paid for. I don't understand how you segregate the different parts of this treatment. A patient is ill, has what you diagnose as terminal cancer, and they are given whole body radiation treat- ment, which they are informed in advance is experimental. What did the Defense Department pay for?
Dr. SAENGER. What was the DOD getting? Mr. BRYANT. Not what were they getting. What were they paying
for? Dr. SAENGER. What they were paying for was a detailed observa-
tion of the progression of the manifestations of radiation, the mani- festations that could be related to radiation such as nausea, vomit- ing, diarrhea, weakness and so on, and for a long string of labora- tory tests which are included in the material which you have in one of the appendices.
Mr. BRYANT. The cost of hospitalization and cost of treat- m e n 6
Dr. SAENGER [continuing]. Was not paid for by DOD. In other words, in those days, as I recall, at General Hospital, you would come in and you would be charged, say, $100 a day that would cover everything that happened to you. You did not have these rather elaborate accounting systems that we have in hospitals today.
That money was paid by the General Hospital. That was part of-the General Hospital was supported at that time by the general revenues of the city of Cincinnati. And they allotted so much money and then you could apportion that by what wa+
Mr. BRYANT. What portion of the treatment was funded by the Department of Defense?
Dr. SAENGER. No portion of the treatment was funded by the De- partment of Defense. If a patient got penicillin because of an infec- tion, if they got intravenous fluids, if the patient had to have an infected area operated upon, et cetera, if the patient was irradi- ated, that was not paid for by DOD.
Mr. BRYANT. You had a grant from D O G Dr. SAENGER. The grant paid for statisticians-I am sorry-for
clerical people, technologists, doing laboratory tests, some super- visory care by various Ph.D.8. I think occasionally M.D.s would get some small funds in that regard, but the treating physicians were not paid by DOD.
Mr. BRYANT. Therefore, the US. Government, through the De- partment of Defense, played a role in this only insofar as they funded research on the results of the treatment which otherwise were paid for by the hospital; is that correct?
Dr. SAENGER. I think you stated probably better than I did. Mr. BRYANT. Was my statement correct? Dr. SAENGER. I think it is correct. Yes, sir. Mr. BRYANT. Mr. Mann. Mr. MANN. Dr. Saenger, 'ust continuing in that same line, you
stated a few moments ago t at the Pentagon funding in no way in- fluenced the study. The study would have taken place either way. My understanding-
Dr. SAENGER. The therapy.

287
Mr. M,om. Yes, sir. My understanding is that the course of ther- apy, the application of radiation, whole body radiation of these tu- mors, did not, in fact, start before the Pentagon fundin fact, stopped when the Pentagon funding stopped; isn’t t at true?
Dr. SAENGER. The therapy did not start before the DOD funding. By the time we got all of our activities in place, the tests and
so on, we wanted to train our technologists, train our physicians and so on, in what we wanted to do, it took about a year to get ourselves together.
somehow in our records cannot find what was done in total body radiation and partial body radiation in our hospital until 1979. From 1979 on, this form of therapy was used in a variety of condi- tions, which I described in my presentation. So t h a t w e do have a gap in that period which is mostly one of recovery of records, so I can’t answer your question from 1970 to 1979.
From 1979 on, these patients weren’t treated. Mr. MANN. So the use of whole body radiation in treating pa-
tients at U.C. did not begin until the Pentagon funding began. And we have no evidence that between 1971, when the Pentagon began funding the program, and when your participation in that program ended in 1979, that whole body radiation was continued.
Dr. SAENGER. I can’t answer that. From 1979 on, this method of therapy was continued.
Mr. MANN. We have no evidence, so we don’t know. Dr. SAENGER. That is right. Mr. MANN. Now, earlier with Dr. Soper we were talking about
the difference between solicited and unsolicited proposals. Had there been discussions with DOD before you submitted a formal proposal?
Dr. SAENGER. I believe we had had discussions, but I don’t have any documents for that. Our proposal was considered in the cat- egory which was in common parlance then as an unsolicited pro- posal. In other words, they did not come to me and say, Dr. Saenger, will you consider to do the things that we did? I said to them, I think we can find information which will be of help to you in this particular thing, as we described in the proposals.
Mr. NIANN. I want to refer to the report that was done by the American College of Radiologists which talked about the fact that
are suitable for an aggressive palliation study have limited the size of the group under investigation. Do you agree with that state- ment?
Dr. SAENGER. Yes, I do. Mr. M,om. Now, given that the purpose of this research, as you
have indicated to us, in your opinion was to advance medical knowledge and so forth and it also held out some benefit, you told us, for atients that had the opportunity to participate, did you
of the work with other hospitals in Cincinnati? Dr. SAENGER. We did not-no, we did not go to other hospitals. Mr. Dr. SAENGER. In getting our patients, you may recall that we
said-the patients were referred to us. Now, by the time the pa-
fi and, in
P Now, since 1970, or 1971 when the project was terminated, we
a the number of cancer patients at Cincinnati General Hospital who
*
ever m aR e an attempt to find suitable patients who met the criteria
Is there a reason for that?

288
tient ot to us, the patient was considered for chemotherapy, per-
a limited group o atients finally into the study. And even after t t about, roughly, a quarter of the patients who
were admitted into the study, we never did treat for various rea- sons, as I mentioned. Either we didn’t think after we analyzed them and worked them up that they would benefit from the treat- ment or we should treat them otherwise or they declined. There was always the option that the patient could withdraw from the study.
Mr. MANN. I guess my point is if this was a therapy that held out hope or advance for a patient who partici ated and then, from
to have more patients. I am not sure I understand wh you weren’t
pitals in Cincinnati so that patients who meet the criteria could be asked to participate. This would deal with the concerns expressed about the demographice of this population.
Dr. SAENGER. In looking over our records it appears there were five rivate atients who were referred and then became part of the Ckneral fiosptal study. They did come from private physicians.
Mr. MANN. Ho mes Hospital or- Dr. SAENGER. I think one or two were from Holmes. Another two
or three were from outside and were admitted to the service of the General Hospital.
Mr. MANN. Five out of the 8- Dr. SAENGER. Then the three children, too. Mr. MANN. They are included in the five or in addition to the
Dr. SAENGER. In addition to the five. Mr. MANN. So five adults and three children. Dr. SAENGER. We did not have a vigorous solicitation campaign.
You know, if you take the 88 patients whom we treated over a e- riod of 10 years, at eight patients a year we are n o t 1 mean, t R is isn’t a tremendous4 mean, this is not what we would consider a very high volume of people being studied.
Mr. MANN. Let me go back to some of the things that others have said and just ask you to comment.
In the ad hoc committee re ort chaired by Dr. Suskind, the state- of the
study to measure the palliative effects of whole body rag t ion or partial body radiation was unstructured and not uniformly applied, particularly as regards uniform definition and methods of report-
%o you disagree with that statement? Dr. SAENGER. I would say there is nothing that we did in the
study that couldn’t have been im roved. We were trying to improve
search Committee had made some comments along that line. We tried to improve the recording of palliative effects.
e 61 and page 64.
that these design problems make it difficult now to-or at the time it made it dinticult to measure what you were accomplishing from
% haps B or surgery, rhaps for no therapy whatsoever. And so we got
the standpoint of your research goals, it wou P d have been helpful
making the program in which you were known to t i e other hos-
five?
ment is made on page 59 t R at, prior to 1966, the desi
it as we went along. Statements P ike that-I think our Human Re-
Of course, this speaks to the point that Dr. 8Y gi man was making, Mr. IMANN. Similar statements are made on

289
a palliative perspective. He would argue-I guess that supports his conclusion that that was never much of a purpose at all.
Do you care to comment on that point? Dr. SAENGER. Well, I have participated over my career in design-
ing quite a few studies, some of them interinstitutional, some of them involvin tens of thousands of patients, and the problem of
There a ave been a number of critics of our studies who point out the deficiencies in the design, and I myself always have had prob- lems in saying that the design is adequate or inadequate to some degree, and it is something to which all of us have to suffer. We have to improve our design and so on. And I can’t disagree with what Dr. Suskind‘s committee said.
All I can say is that our design was the best we could do at the time, and, you know, in retrospective it may or may not have been inadequate. I thought the information we got out of it in the final analysis was prett good. Whether it was as good as other people
Mr. m. Dr. G a n e f s letter was read at length by Dr. Egilman. Do you know who T. Gaffney is?
Dr. SAENGER. Yes, I do. Mr. m. I take it he was involved in the review that UC con-
ducted of the bone marrow transplant aspect of the project. Is that your understanding?
Dr. SAENGER. I am sorry? Mr. W. My understanding is-I was asking if it is true that
Dr. G d n e y was involved in the UC review of the bone marrow transplant part of the project. Is that true?
Dr. SAENGER. I don’t know what you are quoting from. If you say it is true, I don’t know-I wouldn’t dispute he was involved.
I would only say this. If you look at all the comments that were made by-the fact that the research committee at that time, they at no time disapproved our project. In 1971, at the time that the president of the university terminated the DOD contract, we re- ceived a letter of approval from the faculty research committee and from the dean of the medical school, so that we must have done something that was right.
None of these things-this problem of determining this autologous bone marrow reinfusion. We worked on that from 1964 until 1968 until we got some good results. This was at the very early stages of these techniques, at least at our institution.
designin stu Cf ies is always a very difficult one.
might have done, t K at is an individual matter.
Mr. m. Thank you, Dr. Saenger. Mr. BRYANT. Mr. Portman. Mr. PORTMAN. I just have a few additional questions really relat-
ed primarily to DODs role. We have heard different analyses of the DOD funding. It seems
to me that Chairman Bryant has gone into that in enou h detail.
you don’t know this off the top of your head-but what percent of the total funding for the project, the $651,400, came from the De- Dartment of Defense?
But my question is, what percent, if you could tell us-an % perhaps
a Dr. SAENGER. Are you talking about the combination of therapy and the DOD?
Mr. PORTMAN. Yes.

290
Dr. SAENGER. We estimated-this is a very crude e s t i m a b 1 think it would be some $416,000. I gave a figure-I don't want to contradict myself, bu+
Mr. PORTMAN. $43,422--- Dr. SAENGER. $483,000. I don't want to tell you this is the best
estimate I could possibly make. In terms of the General Hospital at that period of time, our ac-
counting system was, to say the least, rudimentary, and we made an estimate based on the average cost of a hospital day and then we added on some figures because of the additional cost for the ra- diation therapy and extra-some additional medication and so on, multiplied it by the number of patients, and that is how you got the number.
But I must tell you it was a very crude fi re. If you take that,
whatever fraction- Mr. PORTMAN. Almost 40 percent. Dr. SAENGER. Forty
cians costs or professional fee+ Dr. SAENGER. I want to clarify that all of us who worked at the
General Hospital were on salary. Whether I treated one of the pa- tients you heard about this morning or I treated you, I was neither richer nor poorer for this service. We were on straight salary. Whatever we did was part of the job.
Mr. PORTMAN. The second question on the DOD side is, to the extent patients were told about the milita uses of the data that
they told of the military use of the data. Dr. SAENGER. This was really sort of a mixed bag. We had asked,
along with not asking about nausea and vomiting, the patients were not told, to my knowledge, were not told that they were being-that this information was being used by the Department of Defense.
Unbeknownst to me, several of the physicians who were attend- ing the patients and obtaining the informed consent had mentioned to these that there may be some use of the information for prob- lems in a radiation accident. So that there was some knowledge.
Now, this is by word of mouth, as the informed consents were, and we cannot document this in writing. They were told of the risks. It was only, I think, in about 1967 or so that mention was made that this information would be used for people in the battle- field. So that this is somewhat-
Now, you must understand that in terms of what other patients were told in other studies, there were no people, no patients to my knowledge, certainly in that era and even today who are told the funding source or necessarily what the purpose of the study was. That varies with different investigators. Perhaps today that is more explicit than it was.
But, certainly, talking to many investigators in internal medi- cine, surgery and other fields, they never disclosed the funding source for some purpose of the study other than whatever it was they told the patient about the benefits and risks.
the $483,000 and the $650,000, it comes to a I? out a million one and
Mr. PORTMAN. But t R" e figure of $483,000 does not include physi- rcent one, 60 percent the other.
was being compiled, how much were y p 7 e told and when were
Mr. PORTMAN. Thank you, Dr. Saenger.
29 1
That is all I have, Mr. Chairman. Mr. BRYANT. I just have a couple of final questions. You indicated that the proposal to have the Department of De-
fense participate with you was unsolicited. How did you all know that the Department of Defense funds were available?
Dr. SAENGER. I am s u r e a g a i n , I can’t give you a firm answer, but I am sure that this developed from some conversations which I had with members of the Department of Defense saying this- these were my interests. And they said, well, you know, we are sort of interested in the same things you are interested in. And then I made my unsolicited proposal.
Mr. BRYANT. Were you searching for funding, calling a whole lot of agencies at once? How did you-
Dr. SAENGER. In those days I think we were all searching for funding. This was a general problem, and I think it is true today. People are looking for funding.
Mr. BRYANT. Also, if the Department of Defense was really only buying results from you-and correct me if I am wrong but that is kind of what I read what you are saying as being-they weren’t paying for any of this activity. They were paying for the lab work and for the studies and for the results of it. Is that correct?
Dr. SAENGER. Well, that is what-I don’t understand your ques- tion, Congressman.
Mr. BRYANT. The actual administering of the treatment to these patients that has been the subject of controversy here today was paid for by the hospital.
Dr. SAENGER. By the hospital, right. Mr. BRYANT. And as I understood what you said-I understood
what you said to be that the Department of Defense was paying for results, in effect.
Dr. SAENGER. Well, we weren’t guaranteeing them results. We were trying to elicit changes, either biochemical or chromosomes, blood counts, et cetera, et cetera, that we thought we could predict knowing what the effects of radiation might be. And, as you can see, we tried a number of different things.
We did not guarantee them-or , for instance, let’s say we had a contract to build an airplane. We would guarantee at some period the plane would be available. But this was a research in which the outcome was not a guaranteed-
Mr. BRYANT. I didn’t mean to imply results-pay you to accom- plish a stated goal. I mean to pay for the results of the information, the findings from this work. That is what they were paying for, is that correct?
a 10-year period-n an annual basis over a 10-year period. I just wondered if that is consistent with that explanation.
Dr. SAENGER. There were contracts. We submitted new proposals as our work developed. We submitted new proposals. We got-we stopped doing certain tests. We instituted new tests. We instituted this whole program of psychological and psychiatric testing and so on.
And the project gradually changed. We finally got into some as- pects of the bone marrow preservation and so on.
Dr. SAENGER. Yes, that is what we put in our reports. t Mr. BRYANT. I am curious why they made their payments over

292
I don’t know if I am answering our question.
today and testi@ing on this matter. We would like to evress our thanks once again to Judge Weber
and his staff for makmg the courtroom available to us and all of those who have been helpful in making this hearin a success.
I mean, this was a changing project. It wasn’t a static proposal.
Mr. BRYANT. Dr. Saenger, tz ank you very much for appearing
With that, the subcommittee hearing is adjourn 3 . Whereupon, at 255 p.m., the subcommittee adjourned.]

A P P E N D I X
MATERIAL SUBMITTED FOR THE HEARING
The Testimony of Gloria N e l s o r i
on Oc+ober 21, 1966, aftor boing disohargod for Genoral Hospital, Mm JaOluon was a vary weak ill woman. aaro of harsolf proper1 and deponded on the family for all her bamic n0.d.- appotito, nauaoa, vomiting, weight lose, and was in aomant pain. Rer aondition nmvor improved.
Within a f e w weok she was readmitted to General Rospital. family was informod sha should bo trawferred to Drako Xospital. Ma Jaokson indicated she was afraid and wanted to roturn home. She Wa8 trawprtod holm, wboro 8hs was lovod and aared for by us until a0 dfod on March PI, 1967.
Ihe family oi Amelia Jiickson would lib for this oommitteo to know, that for the ontlrs 163 days aftor rooeivlng tho irradiation, hor condition aontinued to detoriorato. We foe1 that tho t o 0 rad. of partial-body irradiation administorod to hor was crud and didn't hslp her condition in any way. It's our boliof that she may havo lived longor i f this oxporimont had not taken place.
A doctor is 8omeone you trumt. His job is to do everything in h i s powor to alleviato your pain an8 auiforing. Eow~vez., this was not the cas.. She was alrays orying, moaning, groaning, and in
she was unablo to tako
8hr exper%xed bleoding from her rectum, lose of
Tho
suah atrwitios to be financed by tho government; utilising Ms Jackmon's and tho FaPa:ily*e tax paying dollars.
(293)

The Testimony of Joe Larkins
April 11, 1994
My name is Joe P. Larkins. I am now 52 years old My Father, Willard L. Larkins, passed away in 1971 I was 30 years old at the time. My family consisted of myself, an older sister and my parents. When my Father passed away, he and my Mother were in the process of raising a grandchild (my sister's son). Neither of my patents were well-educated, but my Father was hard-working and honest. We always had clean and decent clothes to go to school in and we always had ample food on the table. It doesn't take a well-educated person to be hard-working or honest. If Cincinnati General Hospital and the Doctor's therein had been honest, there is of course, the possibility that m Father could have li-ved for
mor . -Tinst~df-Tii7Sit. '--from'-% TilIFm ' s i d i : u m i z g e d Father and Husband to a premature death caused by an "experiment". MY Father did not know thqt
- _ he --- .being usg&a_8. a. guinc~a.-a_pig;.Nokbez. BLd- not know, as his children, we were n_ot 4,nforw.d af.Lh-qrooeduirQe--to 'be usea m -dp-€hS risks involved.
I feel as though Dr. Saenger and the other "Doctors"involved, if you will, knew that the high levels of radiation which they administered to these patients had the very real probability of being fatal. Oh, how right that is! My Father was very much a family man, yet these people killed him as surely as if they had put a gun to his head and pulled the proverbial trigger. These Doctors" left my Mother, with no Job skills, to raise a grandchild as best as she could. My Mother lived until 1983, but she was a broken woman after my Father's premature and unexpected death.
-.I____ /- - -- c
I know that my Father knew that something was very wrong' with the treatments being given to him at Cincinnati General. He even asked me "Son. what are they doing to me? . They're trying to kill me!" That's how bad the pain, he endured after the treatment was. He suffered so needlessly. What really gets me about this situation is the fact that the Pentagon contracted with these Doctors and this hospital to test the effects of radiation on the human body. Everyone realizes that Cincinnati General . Hospital, now the University of Cincinnati Hospital, treated many low-education, low-income patients. I guess they felt that in some way, the fact that these patients were not rich, upper-class citizens, gave them the right to experiment with

their bodies without informed consent NOT SO! I feel sure these physlciari/resaarchers were well-paid for their part and it would be very interesting to know the types and dollar amounts of the grants given to Cincinnati General by the Federal government I feel sure that all parties, with the exception of the poor, unsuspecting patients and their families, were well-compensated But since when, in our society, does one man or even a group of them, have the right to play God? A very good example of this is our 20th century "assisted suicide Doctor" This man is contacted by terminally-ill patients who wish to end their own lives with digrrlty and choose, by their own voilition, not to suffer needlessly for years These people make the decision to die in peacse, yet our great judicial system, along with the medical community, brought this compassionate physician up on charges. The differences in these deaths and the death of my Father are that my Father did not choose to die - someone else made that decision for him, without consulting or informing him and they were amply compensated for it. I feel that the price they should be required to pay to the families of the people they killed, should be exceedingly high I also feel that the Federal government should be named as a co-conspirator in this case, because that's exactly what it was - a conspiracy. No person, and I emphsize 'NO', person would willingly consent to a treatment with any degree of fatality involved People, both YOU and I, simply value life too much I think that is the big thing here - the patients were not informed. I know that behavior of this sort would not be tolerated by the medical community today But then again, this entire mess was surrounded by a thick veil of secrecy on both the doctors' part and on the part of Cincinnati General Hospital. It is still being closely guarded and kept under yet another veil of secrecy to this very day by the University of Cincinnati, in that they have yet to provide the medical records of the patients involved in this experiment/ I beseige you to order the University of Cincinnati to release the patient records, in their entirety, to the next of kin immediately They are hedging to save their own skin I was promised my Father's complete medical file over a month ago; as of this writing, I have nothing
i
I only hope that you, the Congressional Committee, see fit, as members of the human race, to break this matter wide open here and now and award just compensation to the families of, the victims. I feel that the Physicians involved and also the federal government (the Pentagon) should pay and also I beg you to strip any and all of the Doctors involved of all their medical creaentials that they hold. If justice prevails in this matter, and I have faith that it will, a strong message will be sent to our government officials and the private physicians (to whom people entrust their lives and the lives of their loved ones) that behavior of this .

sort will simpley not be tolerated, that Justice will in fact be both swift and severe. I pray that a situation such 6 4 this will nrvr l a a a ~ r i Le f.accJ b y d group of people If this statement to ynii, the Congressional Committee, does anything to help in the name of justice, then my Father's death and the sorrow and hardships that his familty faced, will not have been completely in vain.
Thank you.

297
MS. Catherine 0. Hager 590 Delta Avenue Cincinnati, OH 46226 61 3-871-8773
April 7, 1994
To:
In January, 1994 I began noticing articles in The Cincinnati Enquirer regarding Total Body Radiatlon experimentation done on cancer patients in the 1960's at Cincinnati General Hospital. Since I knew my father, Joseph Mitchell, was treated at that hospital for cancer during that period of time, I contacted Linda Reeves at The Cincinnati Enquirer. After a brief discussion with Unda, It was determined that my father had Indeed been involved in the Total Body Radiation experimentatlon as patient 1051, the flrst patient to be identified. From this point, my husband and I, along with the assistance of the news media attempted to piece together any records available regarding my father's treatments at the hospital.
In October, 1963, my father was diagnosed with lung cancer in the right lung, and was admitted to Cincinnati General Hospital. Surgery was scheduled for November, 1963. Although there Is no notation of this scheduled surgery in his medical records, we have a letter which was written by my father to my sister detailing the planned operation. For some u n k n o w n _ ~ g _ a a r r a ~ ~ ~ ~ s ~ e ~ ~ w a s ~ c ~ ~ e J e d on the day it was -- tion. The surgery was never rescheduled. i tbr wazgiven e schedule of dates t o ~ ~ b ~ e ~ t ~ ~ o r ( M a l t
-At this point, I asked the d o c t o r ~ e e _ s ~ ~ ~ a a c a n c e l a d . . t l a t o l d - -. me he was t o d ~ a r ( - f o ~ ~ ~ ~ r i - ~ n d d ~ c i d e d to. opt. for ItmCahaU-Treatmep
instead. I In reality, my father was not in a weakened state at that time but was In relatively good health, still working and living a normal life. It wasn't until the Cobalt Treatments started that my father began to go down hill. After 35 days of treatments my father was so weak that he had to retire from work and move closer to my family so we could help care for him.
In early 1965, my father was again admitted to Cincinnati General Hospital with severe chest pains. It was at this time he was subjected to the Total Body Radiation. He Immediately started on a drastic downhill spiral. After much suffering, my father died on July 14, 1965 - 74 days after the Total Body Radiation. / / zjo r
Total Body Radiation Subcommkee and Whom it may concern;
L * 5 )

298
Total Body Radiatlon Subcommittee April 7, 1994 Page 2
Since Total Body Radlation had not been performed on cancer patients at Clncinlrati General Hospital prior to the Government funding of 1960, I feel that my father, along with other cancer patients, were hand picked and used in Total Body Radlatlon; not as a treatment for cancer, as they had been told, but as a cover-up for a study performed for the Department of Defense to determine possible effects on soldiers In nuclear warfare.
It might be noted that at the tlma my father died, two of my brothers were in the US. Air Form. One In Vietnam In the war zone. The Red Cross had to lacate him and bring him home for the funeral. Both brothers have since retired from the Air Force.
Isn't It ironic that two of my brothers were serving this country in the military, while at the same time The Unlted States Government was sponsoring experiments which shortened or ended their father's life.
Respectfully.
Catherine 0. Hager (Mitchell)
C0H;cmh
Enclosure
E

I

300

301
A REPORT TO THE CAMPUS C O I W U N I ~ bc&4t4. --_-- - - S i n c e l a s t October a committee of t h e J u n i o r Pacul& Aasoc- pmw i a t i o n of t h e Un ive r sa ty o f C inc inna t i has been i n v e s t i q a t i n t h e r a d i a t i o n expe r imen t s a t the Un ive r s i ty Medical Center . Ue have in t e rv i ewed d o c t o r s involved, and we have studied with c a r e t h e report8 of t h e research t ea l to the Defense Department, as -11 as the taaa's p u b l i c a t i o n s on r a d i a t i o n i n medical j o u r n a l s , and many o t h e r p e r t i n e n t documents. Our committee has had e x t e n s i v e he lp €ma MllbOrs o€ the ($kmab medical community.
For reasons t h a t we w i l l preuent below, w have mme to t h e conc lus ion t h a t many p a t i e n t s i n t h i a p r o j e c t pa id ueverely for t h e i r p a r t i c i p a t i o n and o f t e n without even knowinq t h a t t hey were part of a n experiment. W e f e e l that t h e evidence c l e a r l y c a l l a i n t o q u e s t i o n t h e manner i n which theue human experiments were des igned and c a r r i e d o u t . We t h e r e f o r e urge t h e p r e s i d e n t of t h e Universi ty t o t e r m i n a t e t h i s p r o j e c t and t o i n s t r u c t the Medical C e n t e r t o coope ra t e f u l l y w i t h t h e c o n q r e r s i o n a l hearings to be h e l d next month.
Ue are addres s inq o u r s e l v e s i n t h i s report to what we b e l i e v e t o be the three most c r u c i a l ques t ions t o be auked about t h i s project:
(1)
( 2 )
( 3 ) D i d t h e p a t i e n t s g ive their informed consent t o
Was c a n c e r s t u d y t h e main o b j e c t of t h e
What were t h e real risks t o t h e p a t i a n t s ?
beinq used as expe r i aen ta l a u b j e c t u ?
To beqin wi th , im have been unable to f i n d any evidence of a planned. s y s t e m a t i c c a n c e r study. I t seams u n l i k e l y t h a t the team would n o t have mentioned, somewbere i n t h e 900 pages o f the Department of Defense (DODI r ep r t s , the f a c t t h a t t hey were conduc t ing t h e DOD p r o j e c t i n conjunct ion r i c h a specific c a n c e r r e sea rch s tudy , had t h i B indeed been t-e case . Nor h a s the team made pub lzc , even during the r e c e n t months, a d e s i g n f o r cancer s t u d y i n any way comparable t o t h e d e t a i l e d p ropoaa l s f o r DOD r a d i a t i o n s t u d i e s p roposa l s r i c h have been r e p e a t e d l y and p a i n s t a k i n g l y modif i id and a r p l i f i e d ove r t h e e l even y e a r s o f t h e p ro )ec t .
Y e a l s o p o i n t o u t t h a t there is no ev idence i n t h e DOD r e p r t s t h a t any p a t i e n t s -re i r r a d i a t e d be fo re t h e beqinning of the WD p r o j e c t i n February 1960: the two p r o j e c t s , r e sea rch on c a n c e r and r e sea rch on r a d i a t i o n i n j u r y fit indeed t h e r e were " t w o " ) , aeea t o have been coterminous.

2
C o n s i s t e n t l y th roughou t t he r epor t s t o t h e DOD t h e d o c t o r s make s t a t e m e n t s t h a t i n d i c a t e t h a t t he s e l e c t i o n af p a t i e n t s and t h e r a d i a t i o n dose given them was a t l e a s t p a r t l y t a i l o r e d t o t h e needs o f t h e DOD p ro lec t . For i n s t ance , w f i n d t h a t i n t n e f i r s t desc r ip t ion of t h e i r p r o j e c t t he team s t a t e s t h a t t hey w i l l gene ra l ly no t i r r a d i a t e women with a c t i v e mens t rua l cyc le s . The menstrual c y c l e , they say , a f f e c t s t h e appearance of amino a c i d s i n the u r ine and a t t h i s t i m e t h e t e a m is studying amino a c i d s i n t h e u r i n e of i r r a d i a t e d S u b j e c t s i n hopes of f ind ing an ind ica to r f o r r a d i a t i o n i n j u r y . Such a statement a s t h e fol lowing, which appea r s i n the 1970 report., po in t s c l e a r l y t o the f a c t t h a t t h e main r eason f o r i nc reas ing the dose ove r t he years was t o improve t h e data--not on cancer treatment--but on r ad ia - t i o n i n j u r y :
C l e a r l y much more i n vivo data a r e r equ i r ed [ f o r i n d i c a t o r s t u d i e s 1 with good d o s i m e t q [where t h e r a d i a t i o n exposure can be c o n t r o l l e d l . We a r e pu r su ing t h i s goa l a t whole-body r a d i a t i o n doses up t o 250 r a d s with even higher doses planned with t h e s u p p o r t o f marrow au to - t r ans fus ion and laminar-flow "sterile" rooms. Large-volume pa r t i a l -body i r r a d i - a t i o n is a l s o being performed t o l e a r n more about t h e e f f i c a c y o f chromosome a b e r r a t i o n s a s a radi- a t i o n dos ime te r . . . . L1970, page 221
Also, c o n s i d e r t h e wording i n t h i s i n i t i a l sentence of a 1964 p u b l i c a t i o n on dosimeters by t h e Saenger team in Radiat ion Research: "In an e f f o r t t o e v a l u a t e t h e metabolic e f f e c t s o f s i n g l e doses of h o l e body r a d i a t i o n i n the human be ing , p a t i e n t s a b l e t o maintain t h e i r n u t r i t i o n with disseminated neoplasms were given t h e r a p e u t i c doses of whole body r a d i a t i o n with Cobalt-60 t e l e the rapy . " And i n t h e 1971 D3D report w e f i n d these p a r t i c u l a r l y c h i l l i n g l i n e s :
T h i s l r e p o r t l b r i n g s t o 43 t h e t o t a l number of p a t i e n t s wiio have undergone assessment f o r the e f f e c t s o f t o t a l o r p a r t i a l body i r r a d i a t i o n on t h e i r cogni- t i v e - i n t e l l e c t u a l funct ioning and emotional r eac t ions . In t e r m s of t h e c h a r a c t e r i s t i c s of t h e o v e r a l l sample t h e a d d i t i o n o f t h e new p a t i e n t s w i l l s e rve t o improv; t h e r a t i o of wh i t e s t o Negroes, t o increase s l i g h t l y t h e ave rage educa t iona l a t t a inmen t . and t o decrease t h e a v e r a s e aae. The t r end noted i n the 1969-70 r e p o r t t oGard - rec ru i t i nq p a t i e n t s comuaratively b e t t e r p h y s i c a l cond i t ion has cont inued.
c1971, page 721
F i q a l l y , w e r e p e a t t h e now r a t h e r well-known f a c t t h a t t h e r e has been no p u b l i c a t i o n by t h i s team s p e c i f i c a l l y on t o t a l

303
3
or p a r t i a l body r a d i a t i o n as cancer t reatment . One of t h e d o c t o r s , D r . Edward S i l b e r s t e i n , wrote to t h e chairman o f t h e JFA committee l a s t November 14 as fol lows:
I hope I made c l e a r t o you on Monday t h a t we have n o t y e t publ ished t h e r e s u l t s of therapy because of t h e v a r i a b l e d u r a t i o n o f p a t i e n t s ' c l i n i c a l c o u r s e wi th c a n c e r fol lowing t r ea tmen t and t h e need t o have a n adequa te sample of p a t i e n t s be fo re one maker any s t a t e m e n t s about t h e e f f i c a c y o f one ' s therapy. S i n c e I am l i m i t e d to t r e a t i n g 7 or 8 pat ient . a y e a r , I canno t , as a r e spons ib l e s c i e n t i s t , i s s u e claims about what we can do t h e r a p e u t i c a l l y f o r p a t i e n t s ove r a s h o r t pe r iod o f t i m e .
Is it conce ivab le t h a t i n an a u t h e n t i c cancer r e sea rch s t u d y , no r e s u l t s would be r epor t ed a f t e r e l even yea r s and t h e r a d i a t i o n o f 87 p a t i e n t s ? I f no p a t t e r n had emerged a f t e r t h e i r r a d i a t i o n of 87 pat ients-- indeed a f t e r 10 or 20-- would t h i s i n i t s e l f no t have been worth communicating t o o t h e r c a n c e r s p e c i a l i s t s ? W e a l s o ques t ion why, if t h i s were a s e r i o u s s tudy o f t h e e f f e c t s o f r a d i a t i o n on c a n c e r , so few a u t o p s i e s were performed.
W e c an o n l y conclude t h a t t h e purpose of i r r a d i a t i n g c a n c e r p a t i e n t s a t General Hosp i t a l w a s p r imar i ly t o s tudy r a d i a t i o n i n j u r y f o r t h e DOD and t h a t i ncu rab le cance r p a t i e n t s were used because ( a ) they were going t o die anyway and (b) they "might" b e n e f i t from t h e r a d i a t i o n i n terms of reducing p a i n or slowing t h e sp read of cancer .
W e move now t o t h e q u e s t i o n o f t h e real r i s k s t o t h e p a t i e n t s and t h e e f f e c t s on them o f t h e r a d i a t i o n . W e beqin with t h i s c r u c i a l statistic: o f t h e 87 i r r a d i a t e d s u b i e c t r h i s t o r i e s are given i n t h e DOD rewrts. 21 d ied wi th in 38 %--or zZC What is even more s e r i o u s is t h a t o f t h e f i r s t 40 p a t i e n t s g iven to t a l -body r a d i a t i o n be fo re t h e advent of bone marrow t r a n s p l a n t s , 7 of t h e 18 r e c e i v i n g t h e h ighe r doses (150 or 200 r a d s ) d i ed within 38 days--or 39%. That t h e h ighe r d o s e s were much more l e t h a l than t h e lower doses i s c l e a r l y bo rne o u t by t h e f a c t t h a t of t h e 2 2 p a t i e n t s r ece iv ing 100 r a d s or under , on ly 10% succumbed within t h e 38-day pe r iod . The f u l l s t a t i s t i c s on t h i s e a r l y per iod of t h e p r o j e c t , a s w e have a b s t r a c t e d them from the reports, a r e a s fo l lows :
I

4
--- F i r s t 40 t o t a l -body s u b i e c t s (1960-66):
Of t h o s e r ece iv ing 200 r ads , 2 of 6 d i e d wi th in 38 d t y s I, I, 150 r a d s , 5 of 1 2 " "
I, ,a 100 r a d s . 1 of 14 " '* " "
I , 8 , "unde r 100 r ads ; 1 o f 8 " " " "
150 r ads or over : 7 of 18 under 150 rads: 2 of 22
~~
Of t h e t o t a l 87 p a t i e n t s , it may be added t h a t 4 d i e d within 10 d a y s , 7 within 20 days.
These s t a t i s t i c s a r e a l l t h e more alarming d e n one juxta- poses them with t h e d o c t o r s ' d e s c r i p t i o n s of the p a t i e n t s a t t h e t ime o f r ad ia t ion . Throughout t h e W D documents t h e d o c t o r s r e p o r t t h a t though a l l t h e i r s u b j e c t s a r e p a t i e n t s w i th i n c u r a b l e cancer t hey a r e no t i n t h e f i n a l s t a g e s o f d i s e a s e or c l o s e t o death. P a t i e n t s a s a g rcup a r e descr ibed o v e r and ove r again a s having " r e l a t i v e l y good n u t r i t i o n a l s t a t u s . " "normal r ena l f u n c t i o n , " and " s t a b l e hemograns." W e o f f e r t h i s sentence from t h e W D report o f 1969: "The p a t i e n t s who a r e i r r a d i a t e d . a l l of whom have inoperable . m e t a s t a t i c carcinoma but a r e r e l a t i v e l y good h e a l t h , p r o v i d e u s with an oppor tun i ty t o s tudy mul t ip l e f a c e t s o f t h e e f f e c t s of r a d i a t i o n i n man r a t h e r t han i n experimental a n i m a l s , " (page 1). In t h e 1970 r epor t t h e doc to r s write:
Seve ra l of t h e s u b j e c t s were tumour-free and e s s e n t i a l l y normal ( fo l lowing radiat ion-induced tumour r eg res s ion ) r ece iv ing p rophy lac t i c whole- body r ad ia t ion . The rest had metastatic carcinomas which were inoperable and no t amenable t o conven- t i o n a l chemotherapy. Neve r the l e s s , t h e s e p a t i e n t s were a l l c l i n i c a l l y s t a b l e , of them workin dally. T1970. d
Even of t h e group desc r ibed above, 2 d i e d within a month-- one on day 31 and one on day 2 2 .
I n r ega rd t o poss ib l e b e n e f i t s , w e assume t h a t any b e n e f i t s t h a t would balance ou t t h e s e enormous r i s k s would have t o be ve ry p l a i n and dramatic. Yet t h i s is no t a t a l l the c a s e . The American College o f Radiology (ACR) team s t a t e d t h a t abou t a t h i r d of t h e p a t i e n t s r epor t ed a decrease of p a i n ( t h e medical h i s t o r i e s show, by t h e way, t h a t some p a t i e n t s had an inc rease of pain fol lowing r a d i a t i o n ) and a g r e a t e r "sense of well-being" and t h a t a t h i r d had decrease i n pr imary tumor s i ze . D r . Saenger has said t h a t he f e e l s t h e s t a t i s t i c s f o r long-term survivors--a small number of p a t i e n t s l i v e d seve ra l y e a r s a f t e r r ad ia t ion -wi l l show

5
t h a t t o t a l and p a r t i a l body r ad ia t ion is "promising" as cancer t reatment . But even t h a t much is clouded by ( a ) t h e f a c t t h a t many s u b j e c t s received o the r k inds of t he rapy be fo re O K a f t e r r a d i a t i o n and ( b ) the f a c t t h a t t h e Saenger team used no c o n t r o l group. The doctors s t a t e i n t h e l a t e r WD repor t s t h a t t hey a r e ca r ry ing o u t t h e i r experiments in conformity with t h e H e l s i n k i Code (which d a t e s from 1964) : y e t t he code c l e a r l y states t h a t t he h e a l t h of t h e p a t i e n t m u s t always be t h e first considerat ion i n t r y i n g o u t new k inds of therapy:
1.4. Every c l i n i c a l research p r o j e c t should ba preceded by c a r e f u l assessment o f i nhe ren t r i s k s i n comparison to fo reseeab le b e n e f i t s t o t h e s u b j e c t or t o o t h e r s .
But l e t us assume f o r t h e moment t h a t t h o s e w e add res s a r e not convinced, even by t h e number of s h o r t s u r v i v o r s p l u s t h e pa t i en t s ' c o n d i t i o n s a t time of r a d i a t i o n , t h a t many d i e d of r a d i a t i o n i n j u r y r a t h e r than s imply from t h e i r d i sease . There is y e t another kind of evidence t h a t r ad ia - t i o n in ju ry was a major cause of death. I t has been known f o r some t i m e t h a t a major i n j u r i o u s e f f e c t of r a d i a t i o n is bone marrow f a i l u r e . The bone marrow's a b i l i t y t o make wh i t e and red blood cells can begin t o f a i l a s e a r l y a s 6 days pos t r ad ia t ion : t h e c r i t i c a l per iod f o r marrow f a i l u r e then comes from 25 t o 40 days pos t r ad ia t ion . I n summarizing i n 1966 t h e marrow problems for t h e i r f i r s t f i f t y p a t i e n t s , t h e doctors themselves make t h e fol lowing s ta tement: "The t o t a l white count f a l l s t o a low po in t 25 t o 40 days a f t e r i r r a d i a t i o n . There w a s a p e r s i s t e n t lymphopenia A i c h p e r s i s t e d f o r 40 to 60 days" (page 31). Can it be merely a coincidence t h a t t h e s h o r t su rv ivo r s a r e bunched in e x a c t l y t h a t c r i t i c a l 25-40-day per iod?-- that , f o r i n s t ance . no l e s s than 9 s u b j e c t s d i e d from 31-38 days? In t h i s same 1966 r epor t , in f a c t , t h e doc to r s s t a t e o u t r i g h t t h a t "severe hematologic dep res s ion was found in most p a t i e n t s who expired," and they note t h a t because of t h i s . they a r e beginning work on bone marrow t r a n s p l a n t s - - f a r t oo l a t e , i n our opinion. In t h e 1963 r e p o r t , they w r i t e t h a t "Delin- e a t i o n of d i s e a s e s c o r e [a r a t i n g f o r blood problems1 r ad ia t ion s c o r e [ t h e r a t i n g ad jus t ed a f t e r r ad ia t ion1 'and t o t a l continued t o be o f value i n a s c r i b i n g the imwr tance --- of r ad ia t ion i n p r e c i D i t a t i n g demise" (page
A d i s t r e s s i n g a s p e c t o f t h e doc to r s ' p u b l i c d i s c l o s u r e s about t h i s p r o j e c t h a s been t h e i r misleading s t a t emen t s concerning t h e p r o t e c t i o n given t h e p a t i e n t s by bone marrow t r ansp lan t s . It h a s no t been made c l e a r t h a t of t he f i r s t 50 p a t i e n t s on ly 2 r ece ived t r a n s p l a n t s and t h a t n e i t h e r of t hese t r a n s p l a n t s was a c l e a r succes8 ( t h e f i r s t s u b j e c t d i ed . i n s p i t e of t h e in fus ion , 28 days pos t r a d i a t i o n ) .

306
6
The team from t h e American Co l l ege o f Radiology reported t h a t i t f e l t t h e r e s e a r c h team could n o t be censu red f o r not g i v i n g bone marrow t r a n s p l a n t s du r ing t h e e a r l y y e a r s f o r t h e s imple reason t h a t t h e technique had n o t t h e n been p e r f e c t e d . But s i n c e t h e d o c t o r s cou ld not p r o t e c t t h e p a t i e n t s from bone marrow f a i l u r e . were they j u s t i f i e d i n g iv ing t h e h ighe r doses of r a d i a t i o n ? Among those f i r s t 50 p a t i e n t s , w e po in t o u t a g a i n , 7 of t h e 18 high-dose s u b j e c t s d i d not l i v e beyond 38 days.
Why d i d t h e d o c t o r s n o t d i s c o n t i n u e h igh dose r a d i a t i o n as soon as t hey began t o lose p a t i e n t s from bone marrow f a i l u r e ? I t is p e r f e c t l y c l e a r t h a t i n t h e f irst s i x y e a r s o f t h e p r o j e c t , t h e l e s s r a d i a t i o n g lven the b e t t e r t h e p a t i e n t was l i k e l y t o do. It h a s , i n f a c t , on ly been wi th in t h e l a s t yea r o r so t h a t t h e d o c t o r s have had much success wi th t h e t r a n s p l a n t s : i t is s t i l l no t completely c l e a r t h a t bone marrow t r a n s p l a n t s o f f e r a c e r t a i n way of p r o t e c t i n g a l l p a t i e n ts . We move now t o t h e t h i r d ques t ion : D i d t h e p a t i e n t s g i v e t h e i r informed consent to being used a s experimental s u b j e c t s ? We n o t e t o begin wi th t h a t du r ing t h e f i r s t f i v e y e a r s o f t h e p r o j e c t no consen t form seems t o have been used a t a l l ; none is mentioned i n t h e W D r e p o r t s f o r t h e s e y e a r s , and t h e absence o f w r i t t e n consent I S corroborated by t h e ACR. In f a c t , i t is clear from t h e DOD reports t h a t du r ing t h e s e y e a r s t h e d o c t o r s were n o t a t t empt ing t o j u s t i f y t h e r a d i a t i o n as experimental cancer t r e a t m e n t b u t simply a s " therapy" o r " p a l l i a t i o n t r ea tmen t . " as it is i n t h e s e words t h a t t h e r a d i a t i o n is c o n s t a n t l y described. P a t i e n t s seem t o have been t o l d notning except t h a t t h e r a d i a t i o n was p a r t o f t h e i r t r ea tmen t . Over and o v e r aga in i n t h e reports we f i n d such l i n e s a s t hese :
The p a t i e n t is t o l d t h a t he is t o r e c e i v e t r ea tmen t t o h e l p h i s s i c k n e s s . C1961, page 31
The p a t i e n t is t o l d t h a t he is t o r ece ive t r e a t m e n t t o h e l p h i s d i s e a s e . C1961, page 41
In 1965 a s h o r t consen t form was i n i t i a t e d , bu t it made no mention of s p e c i f i c r i s k s from r a d i a t i o n i n j u r y , merely a sk ing t h e p a t i e n t t o s t a t e t h a t " t h e r i s k s involved" and " t h e p o s s i b i l i t y of compl i ca t ions" had been exp la ined and t h a t " t h e s p e c i a l s tudy and r e sea rch n a t u r e of t h i s t r e a t - ment h a s been d i scussed wi th m e and is understood by me." For what t h e p a t i e n t s were t o l d we have only t h e d o c t o r s ' w3rd. Another form, used as l a t e a s December 1970, s t a t e s t h e r i s k s a s fol lows: "The chance of i n f e c t i o n o r mild b l eed ing to be t r e a t e d with marrow t r a n s p l a n t , d r u g s , or t r a n s f u s i o n a s needed," and t h e f i r s t l i n e of t h a t form
T

307
r eads
7
a s fol lows:
I ( t h e s u b j e c t ) being of the age o f m a j o r i t y and of sound mind and body. vo lun ta r i ly and wi thou t fo rce o r du res s , c o n s e n t - t o p a r t i c i p a t e i n a SClen t l f lC i n v e s t i g a t i o n which is not d i r e c t e d s P e c i f i c a 1 1 ~ my o m b e n e f i t , b u t i n cons ide ra t ion f o r t h e expected advancement of medical knowledge, which m y r e s u l t f o r t he b e n e f i t of mankind.
Tne l a t e s t consent form, a r ev i s ion of t h e above made last s p r i n g and s igned by o n l y a handful of p a t i e n t s . i nc ludes under " R i s k s " a long paragraph regarding bone marrow problems and a l t e r s t he l e a d sen tence t o read "no t Only d i r e c t e d s p e c i f i c a l l y t o my own b e n e f i t , but a l s o i n c o n s i d e r a t i o n f o r t h e expected advancement o f medical knowledge. . . ." I t is a very unhappy f a c t t h a t i t was t h i s l a s t form, on ly in use f o r a f e w months, t h a t Dr. Edward G a l l , d i r e c t o r o f t h e Medical Center , chose t o r e l e a s e t o t h e newspapers. Th i s form was p r i n t e d e n t i r e in t he C i n c i n n a t i poSr, with a s t a t emen t saying it was s igned by "every a d u l t p a t i e n t " o f t h e p r o l e c t .
In our view none of t h e consent forms p r o p e r l y s t a t e s t h e real r i s k t o t h e p a t i e n t s - - t h a t i s , t h e r i s k of dea th from bone marrow f a i l u r e wi th in 40 days. W e f e e l , i n f a c t , t h a t no conceivable consen t form, p a r t i c u l a r l y in view o f t h e s u b j e c t s ' low leve l o f educa t ion , would have j u s t i f i e d t h e d o c t o r s i n s u b j e c t i n g t h e p a t i e n t s t o t h e h i g h e r doses of r a d i a t i o n .
In conc lus ion , we want t o comment on t h e recent r e p o r t by t h e American Co l l ege of Radiology, which f i n d s nothing whatever t o c r i t i c i ze i n t h e s e experiments and u rges t h a t t hey be continued. W e a r e conf iden t t h a t t h i s report w i l l not be taken s e r i o u s l y by anyone p rope r ly informed about t h i s p r o j e c t . The ACR omits from t h e i r report t h e more damaging s t a t i s t i c s on p a t i e n t su rv iva l . The on ly s t a t i s t i c t hey g i v e is a s fo l lows : "A group of 10 p e r c e n t o r e i g h t p a t i e n t s d i e d from 20 t o 60 days a f t e r t h e whole body expo- su re . " We f i n d 14 to t a l -body s u b j e c t s who d i e d within t h i s per iod ( n o t t o mention 5 par t i a l -body) - -o r 23%. and of cour se t h i s f i g u r e t akes no account of the 7 s u b l e c t s who died wi th in t h e f i r s t 20 days. The ACR d o c t o r s c o n t r i b u t e , i n o t h e r words, t o t h e d e c e p t i v e impression t h a t t h e main s i d e e f f e c t s from r a d i a t i o n were nausea and vomit ing within t h e f i rs t few days.
A s f o r t h e s p e c i a l committee appointed by t h e p r e s l d e n t , we r e g r e t very much t h a t t h e ex i s t ence of such a committee was kept s e c r e t f o r so long and t h a t even today t h e names of t h e committee members have not been revealed. I t h a s been

308
a
impossible f o r us. or any o t h e r p a r t y i n t e r e s t e d i n t h e p r o j e c t o r having s p e c i a l information about it. t o communi- c a t e with t h e committee. W e hope t h a t even i n t h i s unprom- i s i n g c o n t e x t , however, t h e committee w i l l s e r i o u s l y addres s i t s e l f t o t h e r e a l ques t ions surrounding t h l s p r o j e c t and w i l l make a recommendation t h a t we a l l can support .
The J u n i o r Facu l ty Assoc ia t ion committee h a s not been s e c r e t , and w e have asked i n t h e campus newspaper for t h e a s s i s t a n c e of a l l i n t e r e s t e d parties. W e a l s o succeeded f i n a l l y i n having a f u l l set of t h e EOD r e p o r t s made a v a i l a b l e i n t h e r e fe rence room of t h e UC l i b r a r y f o r a l l t o i n s p e c t , and a l l a r e i n v i t e d t o check our f a c t s and f i g u r e s i n t h e s e p u b l i c documents.
We a r e c o n f i d e n t t h a t those who examine t h e evidence f o r themselves w i l l j o i n with us i n urging t h e p r e s i d e n t t o t e rmina te t h i s p r o j e c t and t o a s s u r e t h e p u b l i c t h a t t h e Medical Cen te r w i l l make a f u l l d i s c l o s u r e of a l l t h e f a c t s a t t h e congres s iona l hea r lngs .
P r i n t e d a t JFA expense.

Date: April 4, 1994
To: Robert B. Newman, Attorney at Law
From: Members of the Maude Jacobs Family
Subject: Radiation Testing at UC (Cincinnati General Hospital)
This correspondence is regarding Maude Jacobs, a female Caucasian, who was an unsuspecting victim cf the radiation tests conducted by the University of Cincinnati. Maude was born in Whitesburg, Kentucky on June 7, 1916. The third grade was her final year of formal education. By the time she was thirteen years old, she was married and had given birth to her first child. She bore seven children in all, six girls and one son. She was a beautiful woman with a lovely radiant smile. She was impeccable about her children's appearance, as well as her own. Her devotion to her family was obvious to anyone who knew her. Maude lived her life below the poverty level, but was a proud and dignified woman. She was genuinely happy with the simple things in life. Her delight was cooking and caring for her children. When she died she was a widow and left three minor children at home.
According to information from CGH (Cincinnati General Hospital), Maude was diagnosed with breast cancer on July 17, 1964. A treatment of hexamethylmelamine began on July 27,1964 and was completed on August 18, 1964. With this medication her primary tumor receded markedly. On November 7 . 1964 total body irradiation was administered. The midline absorbed tissue dose was 150 rad (250 r midline air dose). At the termination of the treatment she had severe vomiting for twenty-four hours, in spite of intramuscular comparine. Before treatment she had a normal hemogram. Seven days after treatment the white blood count began to fall. The platelet count fell around fourteen days after treatment. The WBC was 1,000 and platelet count was 80,000 twenty-three days after treatment. On the twenty-fourth day, the WBC was 850 and platelet count was 38,000. Maude died December 2, 1964. Twenty-five days after total body irradiation. She was study number 045. (Documentation from CGH attached.)
Two letters written by Maude to her sister Arlie less than two months before her death describes how she felt, and also indicates she thought the doctors did not know what was wrong with her. She talks of living near her oldest daughter, Lillian, who is very helpful to Maude. She also is pleased to be home with her children, but feels sorry because she is too tired in the evenings after preparing dinner to watch television with them. She refers to the expense of her medication and said prayer helps her more than the doctors. These letters demonstrate her education level, but also reveal her devotion to her children. Maude had no knowledge of the seriousness of her cancer much less knowledge of the radiation

310
treatment. She did not expect to die. I f she had, she would have discussed the future care of her minor daughters with the rest of the family. Her death was so sudden and unexpected the family was totally Unprepared. The three young daughters eventually were put in St. Aloysius Orphanage. (The two letters from Maude to her sister are attached.)
The family was NEVER informed of the radiation test or it's purpose. Nor was anyone ever asked to sign a consent form or give verbal permission for testing. Some of the memories which were dismissed without attaching importance now make sense OK at least raise suspicion. Her daughter Irene was seven months pregnant at the time and was having a difficult pregnancy. She remembers Maude's bright smile and cheerfulness, then remembers a private room and no more smiles OK happy faces. Irene remembers being afraid of going into that room. Maude asked her to feel her head and when she did it felt full of soft tumors. Her body felt like sand. Even in the hallway she could hear Maude's delirious talk.
Maude's daughter Sherry was twelve years old and remembers the private room, but at the time didn't know it was uncommon for a person without insurance. Sherry remembers the orphanage and being split up from her two younger sisters. The youngest girl, Kim, eventually went to a foster family.
Robert Murphy, one of Maude's grandson's, remembers thinking how nice it was to have a private room without insurance. Bill Murphy, another grandson recalls visiting her in the private room, but,,not wondering why she was there. He remembers her conversation as out of her head".
Her oldest daughter, Lillian Murphy Pagano, lived downstairs from Maude and was her primary care provider. Lillian was never contacted or consulted about her mother's treatment. She remembers a drastic mood change associated with rapid physical deterioration. She too recalls the private room at the end. She remembers thinking her body felt like sand. She was concerned too for Irene, because of her pregnancy and the worsening of their mother's health so rapidly. Lillian's concern grew as Maude quickly became disoriented and no longer recognized anyone. She was violently ill and talking utter nonsense. Maude died before her time everyone felt. Her family lived for the next twenty-nine plus years with the sadness of her death, but also had warm memories to console them.
Since the details of the experiments became public, the entire family has been drastically affected. Now guilt has replaced the sadness and coments like "I should have known" OK ''I should have asked" are commonplace. Reliving Maude's last days over and over, remembering differently now why she was so violently ill, how she suffered, and now a reason for the private room. Her death is now a nightmare. She died without comfort and dignity. She was discriminated against and selected because of her background. No benefit was ever planned for Maude. She was a number, a statistic.

311
Her children want an apology. They want to know nothing they could have done would have altered the results. They want Maude to know they are sorry if they disappointed her because she suffered needlessly without intervention from them. They also need a quick resolution so this too can be a memory. Already too much damage has been realized.
Lillian Murphy Pagano (Maude's oldest daughter) feels personally responsible for her death. She became obsessed with Maude's death, often calling other family members several times a day to go over some part of her last days again and again. She was found several times at three or four o'clock in the morning with a fixed stare and silent sobs. Eventually she was rushed to the hospital with a suspected heart attack. After a short stay of a few days, some testing, several prescriptions, and instructions to avoid stressful situations, she was permitted to go home. Anxiety struck again within a few weeks. This time she was gone. Lillian's daughter found her, called 911, and received over the phone guidance for delivering CPR. When paramedics arrived, she was given multiple shock treatments to revive her. It is estimated she was dead for four minutes. She was on a respirator and in a coma; she also had several seizures. The doctor's gave her a 50% chance of pulling through, but warned all about the possibility of permanent brain damage. She has regained consciousness, but is still in critical condition at this writing. She recognizes family members, but is mentally unstable. The extent of damage is still unknown. Her family has been told she will need twenty- four care and cannot be exposed to Ally stressful situations. She doesn't talk about Maude now. She doesn't even remember who visited her an hour ago.
The ordeal with the UC experiments must come to a swift conclusion. This is the saga of only one family, there is supposed to be eighty-seven more victims with families. It's amazing how something that was a remote, barely thought of memory, now is resurrected and grown into an unwelcome demanding problem. A problem that can consume your days and affect people from twenty-nine years of family growth --- people Maude never could have known. This letter was compiled from the hearts and thoughts of Maude Jacob's children: Lillian Murphy Pagano (nee Phillips) Irene Froman (nee Phillips) Bob Phillips Betty Wolfe (nee Phillips) Sherry Brabant (nee Jacobs) Janet Baker (nee Jacobs) Kim Swedo ( nee Jacobs)
Attachments

312
My Aunt Louise Richmond passed away from Colon Cancer in March, 1968. She was only 49 years of age. My Mother Viola Macklin (one of Louise's older sister) brought her from Cleveland, Ohio to Cincinnati, Ohio for medical care of her cancer at the General Hospital.
Instead of medical treatment, my Aunt Louise, unknowingly was used as an experimental subject at General Hospital in their radiation experiment. Within weeks of her admission, her health rapidly and painfully deteriorated and ultimately leading to her death.
Regrettably, the news of the General Hospital Radiation experiment has recalled many agonizing memories for myself and my family. The death of a loved one, under normal circumstances is difficult, but now with the added knowledge of my Aunt sacrificial involvement in the radiation experiment, my family members must relive the misery, now with twice the anguish.
Various family members can vividly recall the evening visits to the hospital as we accompanied our mother to visit Aunt Louise. The torturing cries of pain that greeted us as we entered into the hospital ward had become all to familiar to us. She would be lying in her hospital bed trembling and shaking from her agonizing pain so forcefully that the bed itself would be visibly vibrating.
Throughout the visit, my Aunt Louise would cling on to my mother's arm crying and begging her to take her home. She would repeatedly say, "please Viola take me home with you, I['m in so much pain, they are hurting me, they are trying to kill me".
The visits would always end with my mother tearing herself away from my Aunt Louise only to hear her cry in pleading desperation as we walked away. For seemly, hours after we left the hospital and even after reaching home my mother would cry from the guilt she felt for my Aunt's severe pain and suffering. My mother would routinely rock herself to sleep while crying and humming spiritual songs to relieve the burdensome feeling of her most recent experiencdvisit to my Aunt Louise.
After my Aunt Louise' death in March, 1968, my mother would often ask us if they (the Doctors at General Hospital) were really giving her the correct treatments for cancer.
We had no idea Aunt Louise was a part of a Defense Department experiment We're sure if she had known she was a guinea pig, she would not have participated.
My mother would often recall the visit and continued to blame herself for the pain and anguish my Aunt Louise had experienced. My mother carried this unwarranted guilt to her death, and now we have been forced to carry this guilt as well in memory of my mother and aunt.

Study#WS N.C. crwt # CctH $09-278
My mothcps name was Nina L. Cline, a loving and Caring m o k , whoaeonly hope was to sict ha grandchild betixc she d i d . Shc did 10 months Wore her dceth. She was also very close to her sister, and her a;ittan children, who wcxc all very hdpfd with my mother ddnghercancer.
My mothtt was diagnod with c~flo# in 1962, she put a lot of hope and faith in her doctors and oencral Hoopftal who were t r d n g her. She d e n talked to me and other family members about her
trratment, but at no time did she mention being apart of any experiments for the govanmeat. She would have talked to me and other family manbcra b8fm ever conssndng to any arpcrimcnts.
I am appstlled to think that Dr. Eugene Saenger, his associates and ow Fedmd Government would join is such an inhumane act. I dm belleve Dr. Eugene Sacnger Violated his moral and ethical obligation toward his patimu.
We weta taught as c h 3 h and young adult, to bcliwe in our Federal Oovemment, that they would make all the right decisions amceming ow welfim as people. For the government to sponsor a xadiarian cxperimont of this nature, on my mother and other patients wu Qbsly immoral.
Hehect F. Vuln (Son)

814
* I Cb.irper80Zl O f the C a m g r a 8 8 i O M l C o u m i t t e O I m: The Partial and Whole Body Radiation
)now: I l r . W o o d y P l a i r and F d l y of M r m . Beatriae Plair
rxperimont C o z i d u c t d troa 1960-1971
This letter was very difficult to write for us, the family I
9f our departed wife, mother and grandmother.
many traumatic thoughts and feelings regarding our loss.
We conversed of
Herein is the summation of our collective thoughts and
feelings. Dr. Saenger states that the patients and familiea gave
!heir conrent to receive partial or whole body radiation.
dhe record, our mother loved life and she would have never given
her coneent to any treatment that would have shortened her life
or cause her the pain, we observed. She never knew she was part
For
of the Cold War Radiation Experiment. As a family, we were never
old o f her participation in partial or whole radiation. We J ould have not given our consent €or her participation in an experiment.
did anyone tell our father nor her children that she was part of
9 dangerous and life threatening experiment.
At no point in the eupposed treatments of our mother
t
What we can say to the Sub-committee is that we remember our
dother complaining of increared pain, especially following the
dadiation exposuree.
felt am though she was on "fire" or "burning all overn. We can
!ell this committee, we resent our mother being used a8 a human
Guinea Pig and the implication by Dr. Saenger that our mother
agreed to have her body exposed to radiation injury that would
lead to serious pain and shortening of her life.
We can told you how our mother told us she

316
The PLair family asked thie Sub-cornittee to help UE ta !
bring the people w h o we feel shortened our mothet’o l i f e to
juetice.
! rorth less and lees, we and other familiea are depending on this
In a society where life, especially human life appears to be
!hb-committse to send a clear meseage to Dr. Saangcr and
?eeociatea, the University of Cincinnati Medical Center and the
$efense Department that human life is still important.
I
We must let the world know that here in America, what makes
$6 different and greater than othar countries is that we truly
value each and every human being regerdleee of their I.Q.,
iducation, race, creed, color or poeition in our eociety.
$110~ this travesty of justice to go unchallenged others may be
w o w i n g l y experimented upon in the future.
Tf wc
Respectfully submitted,
Wr. Woody Plair and Family

316
qo )(lro Will tri.t-t I : I wae 30 yeare old when my mother was stricken with cancer.
iho had oix other children, three very young at home, the oldeet
dae 12. I dent to the Second Qrade of Urade School, waa married at 13 years
df age. Bsr husband had
dnly been dead a short time and ehe walr struggling to care €or
der three girle at home.
had left enjoying her three daughters.
out-patient at General Hospital.
She wae born ( m y mother) in Whitesburg, KY, 1916, only
When cancer struck she had no money.
She wanted to epend am much time ae ehe I
8he was being treated an
One day near tho end nurse
dalled told her to come to hospital clinic.
&cause no one was available to drive her. She came home weak
She took a taxi
vomiting. She was admitted to hospital and only laeted lees
than a month. When we (the family) found out recently about the
450 Rad she had received my older sister felt ehe was to blame
Acauae ehe did not go with her in taxi to clinic.
yepitalized herself and may need constant care.
dieter has M.S. and hae not been told for fear she won't be able
t~ cope with it. I'm muse all the other families that are still
I
I I
She had to bt I A younger
+live I are having arimilar problems. My prayers are with them too.
you can tell from my letter, I don't have a good education.
4ould I be afraid to be treated in a hospital? Afraid of being
deed for teeting eome other chemical to benefit our government.
Or carry a Donor'e Card EO if they wanted an organ they could I take I it at will? Something needr to be done it ie up to you.
I
! Thank you. !
y ' m helplens. I
Bob Phillips Son of Maud Jacobs #45

1055 Lillie Wright
4
.
Chart No. 4 4 1 7 4 t
1
My mother Lillie Wright was admitted to Cincinnati
qeneral Hospital Aug 23, 1965. She was sent there for a
qiospy. She warn confined to the hospital for one 1 week.
, The summary I recieved of her illness revealed that
4er biospy was performed. AUT 30, 1965 diagnosis was
qarcinoma of the breast. On September she was given partial
lpody irrodation 200 rad midline. On October 8, 1965 local
*-ray therapy began. In 5 3 days she( Lillie Wright) had
recieved 2000 r8dS to her l e f t and right chest.
On December 1, 1965 x-ray was begun on the I lmtermammsry chain and to the anterior and posterior above
the collarbone region (supraclavicular). She received 4000
+n 40 days. Her white blood cell count fell to a low of
2200 on December 3, 1965. These doses o f radiation in I ~y opinion was enough to destroy bone marrow and white
blood cells and even the patient.
1 We the family of Lillie Wright was not notified about
,there radiation treatments or any other proceduree, which
bay have taken place. We d i d not sign any pager6 to permit
this experiment to be done on her( Lillie Wright).
’
84-514 0 - 94 - 11

The doctor at the hospital gave her sample tubes o f I qniment to use on her breasts, her back and abdomen.
$tr skin Was burned on both breast. Her back and abdomen.
*here was raw flesh exposed where once there were skin.
I had to apply this onimant to those exposed areas.When
applied this oniment to those raw areas she was in such
$xcruciating pain Z cried. She was given enough oniment I for 1 week. She was given Morphine which last lor 2 weeks.
1 do not recall the name on the oniment tubes ( 3 1 but both
I
gf these product was given to her around December of 1965.
Neither of these medication helgod her. When a person
ill I waa under the impression someone have to
ign €or meUication such as morphine for a patient which
is terminally ill. She was kept in the dark about the
treatments she wa5 receiving. She never talked about it.
It’s not fair to treat another human being as a guinea
pig because they are poor and uneducated. Some of our
parent. didn‘t have the privilegea we are blessed with
I
” f” . I
f
today.

319
I took my mother back to the horpital Peb 1 2 , 1965
around 10x30 or 1 1 : O O . My nephew and I stayed a t the
horpital u n t i l 3:OO ant I asked the receptionist if they
were re-admitting her and she said y e s w e should go home
and get some rest. When I return home my husband callcd
me from his job and told me my mother had died. The people
at the hospital never did call me t o inform me.of her death.
I ' m her daughter, I should have been informed about
her death before I left the hospital. I was at the hospital
at 3:OO am the death certificate states she died at this
tine. Feb 1 3 , 1966 . I thought the nearest relative was
to be informed first. ! I

How I feel about my mother participating in the exwriaant. I
I ' m very'angry about this doctor taking it upon himself
to use poor live, uneducated human beings for his personal
famu and pain. These human being5 had the right to
iive the test of their lives until God wa6 ready €or them
90 die. Not to d i e because man want to find out what effect
i t would have on eoldiers in the war zone. I
My family have been deprived of what days my mother I could have lived. I know she wasn't educated but she knew
domething was wrong but she didn't know what it wats.
I don't L i k e it because she Lillie Wright was kept I in the dark about this experiment. It's a disgrace to
use high doses of radiatlon on anyone why didn't you
qxperiment on your love one? No bsCaUae they are spacial
$0 you. Remember aoatday you will reap your just reward.

321
to 1 \ 1 , C O L L
LOCAWON:
TELEPHONE NUMRER:
bAm
I h M B E R OF PACES (INCLUDING COVER SHEET):
.

322
? r w s Nembera of tho Maude Jacob8 Family
Bubjbct: Radiation Testing aC UC (Cincinnati General Hospital)
?hi#] corronpondenae is regarding Maude Jacobs, a female caucaaian, who was an unsuspecting victim of the radiation tests conducted by the University of Cincinnati. Maude was born in Whitesburg, Kentucky on June 7, 1916. The third grade was her final yoar of formkl education. By the time she wan thirteen yearr old, she was nurrled and had givon birth to her first child. She bore aevan children in all, nix girls and one son. 8hm war a beautiful woman with' a lovely radiant smile. She waa impoccable about hor ohildren's appearance, as well aa her own. Hmr devotion to her family w8a obvious to anyone who know her. Maude livod hor life bolo* the poverty level, but was a proud and dignified woman. She was genuinely happy with the simple things in life. Her delight was hooking and caring for her ohildren. When she diod shm was a ridolr 8nd left throo minor children at home.
Aocotding to information from COH (Cincinnati General tioapital), Waude was diagnosed with breast cancer on July 17, 1964. A treakmont of hsxamethylmelamine began on July 27,1961 and waa complmtod on August 18, 1964. With this medicatfon her primary tumor recedod markodly. On November 7 , 1964 total body irradiation was administered. Tho midline absorbed tiroue dose was 150 rad (250 r midline air doso). At the termination o f the trmatmont mh m had seve e vomiting for tuonty-four hours, in spite of intramuscular omp sine. Before treatment ahm had a normal hemogram. 8w.n days afte f treatmont the white blood count bogan to fall. The platelot count fell around fourtoon days after treatment. The WBC was 1,000 and platelet count was 80,000 tuanty-throe days after treatment. On the twenty-fourth day, tho WOBC was 850 and platelet count was 38,000. Maude died December 2, 1964..Twent - ' d after total bo irradiati on. She-- number 045,- from cati A b e d . )
Two letters writton by Maude to her sister Arlio loss than two months bofore her doath describes how she felt, and also indicate# she thought thm dootors did not know what uaa wrong with hor. Bho talks of living near her oldest daughter, Lillian, who is very helpful to Maude. aha also is pleased to be home with hor ahildron, but feelo sorry booauas ahe is too tired in the evenings after preplring dinner to watch tcleviaion with them. %he refera to the O X Q ~ ~ I S ~ of her medication and said prayor holpr hor mor. than the d o r t h r r . Thann l n t t p r a dpmnnatrrtc ~ h c r cAiirrt+nn l rvr l hiit r l s n

doctors. These letters dmonrtrate her educltton lovol, but-81so rovo~l her dovotion to her children. Maude had no knowlodge of the meriousnoss of her cancer much less knowlodge of the r8dirtion
I

824
trodtmont. She did not expect to dio. If she had, she would havo di8du88.d the future care of her minor daughters wlth the rest of the funfly. Ror death was (IO sudden and unaxpocted the family wa8 totdlly unprepared. The three young daughters evontumlly were put in 4t. Aloy8ius orphanage. (The two tettero from Maude to her s i n t p r mre attached.)
me 'family warn HEVER informed of the radiation test or it'8 purpbee. NOK waa angone tver asked to nign a coneent form or give verwl permiasion for testing. Some o f the memories which wera disTiesed without attaching importanca now make sense or at least r d e e suspicion. BOK daughter Irene was revon months pragnant at the 'time and was having a difficult pregnancy. She remembera Maudp's bright #milo and cheerfutness. then romambars a private room' and no more smiles o r happy faces. frons remambars being afrasd of going into that room. Maude asked her to foe1 her haad and hen she did it felt full of soft tumots. Her body folt liko s a n d Evrn in the hallway she could hear Maude's delirious talk.
M a d ' s daughtrr Sherry was twolvo yoars old and remembers the privht. room, but at the time didn't know it waa uncomon for a person without insurance. Sherry remembers the orphanage and baing mplib up from her two younger 8istora. The youngest g i r l , Kim, evo&tuaIly went to 1 fostor family.
nice it was to have a private room without insurance. Bill Murphy, another grandson recalls visiting her i n the private room, but not wondtering why 8ho w8s thoro. He rcmomborm her conversation as "out o t tibr head".
R e r ,oldest daughter, Lillian Murphy pagan^, lived doun8tairs from Waudk and was bar p'rimry care provider. Lillian waa novor coat' cted or conoultcd about her methar's treatment. 8ha remembers a dr s t i c mood change associatedwith rapid physical datarioration.
hrr body tolt like sand. She was concerned too for Irene, because of lpr pragnancy and the worsenhg of their mother's health 8 0 rapidly. Lillian's concern grew as Maude quickIy became disoriented and ho longer recognized anyone. She waa violently ill and talking uttek nonsenec. Maude died before her time ovoryono folt. Her family. lived for tha noxt tuonty-nina plus years with the sadness of hkr death, but also had warm memories to console them. Bin& the details of the experiments became public, the ontiro f a m i l y ha8 been dra8tically affected. Now guilt has replacod tho sadnosm and o m o n t s liko ''I should havo known" OK "I should havo ask+" are oommonplaee, Reliving Maude's last days ovar and ovor, rmwtnbcciag differently aou why she was so violently i l l , how she
now a reaaon for tho private room. Hor death i8 now She died without comfort and dignity. She was
Rob a t Murphy, one of Maudo's grandmon'a, remembcra thinking how
She f 00 recalls tho privata room at the end. She remembers thinking
_ _

325
Her ohildren want an apology. Thoy want to know nothing thoy could hrvo don. would have altered tho rosults. They want Maude to know they are sorry if they disappointed hct bocause she suffered m e lessly without intervention from them. They also need a quick
beer( realircd. res f lution so this too can be a momory. Already too much damage has Lill'ian Murphy Pagano (Maude's oldest daughter) feels personallp ro~ponsfb~e for her death. She became obsessed with Maude's death, oftda calling othor family members ssvcral times a day to go ovor somd part of her last days again and again. she was found several timds at three or four o'clock in the morning with a fixed stare rnd 'silent sobs. Eventually she was rushed to the hospital with a suspected heart attrck. After a short s t a y of a few days, dome tcst'inq, reveral grescriptions, and instructions to avoid stressful situations, she was permitted to go home. Anxiety atruck again within a few weeks. This timo she was gone. Lillian's daughtor found her, called 911, and received over the phone guidance f o r deli'vering CPR. When paramedics arrived, she was given multiple s h o d treatments t o revive her. It is estimated she was dead for four'minutes. She was on a respirator and in a coma; she also had several seizures. The doctor's gave her a 50% chance of pulling through, but warned all about tho pos8ibility of permanent brain dadgo. She has regained consciousness, but is still in critical conqition at th ia writing. 8ho rocogniror family members, but i s mentally unstable. The extent of damage is still unkncwn. Her fad'ly has been told she will need twenty- four car. and cannot be exposed to MR stressful situations. She dosrn't talk about Haudo now.< she doesn't even remember who visited bet an hour ago.
The brded with the UC experiments must come to a awift conclusion. This is the saga of only one family, there is supposed to be eigqtjy-seven more victim6 with familios. It'r amaeing how eommthing that unm a romote, baroly thought of memory, now is resurrected and group into an unuolcomo demanding problem. A problem that crn consume your days and affect people from twenty-nine YO8r8 of family growth --- people Maude never could have known. Thim, letter was compiled from the hearts and thoughts of Maude J~COII'B children: Lillian Murphy Pagano (nee Phillips) Ire L Froman (nee Phillips) Bob khillip8 Bott Wolfr (no. Phillips) she& Brabant (nee Jacobs) Jan#t Baker (nee Jacob6) Kim pwodo ( not Jacobm)
!
It t Jchmen tr

326
I
-.. . . . - . . , .. .,. _ _ - .. _. a -
,
.i


II- c
4
328

I
&CATION:
FAX NUMBER a 0-2- - 3 2 5 363-3
DATE:
I NUMBER OF PACES (INCLUDING COVER S H E m
CJOMMJEIYTS:
I I

WN.* OI .U.O..IU 1nVInm.lu.
I

381
s 4400.00 - - 4000.00 I 1000.00 Udv. ckrti.
1000.00 1523.03 8 ) ; 2000.00 ' I 1'
'I ' 1
I 500-00 I I I

332
r a A - iw a- N. ((na44 DECARTYENT OI THL 1 I Y V
o m c i or THE S U R G E O ~ GENCRAL I L S U I C W AN0 DWCLOCYENT DIVISION
WASHINGTON IS 0 C
.
\



_--
APPLICATION FOR RESEARCH CONTRACT - PART 111
O' -c51 . :b&buc ciuagca k ii:U;-Jno L.'ol&*: rotd Lorly In&oa
. ,. I .;
0 FORM ...-- .. - . .. - .. ... ..... . . ... '

F a r A . c m d Dmdnt - No 19 Rl.1 OEPAXTYENT OF THE ARM*
O m C E Of THE SURGEON G E Y E R l L R L I U R C H AND DNELOPMEMT DIVISION
WASHINGTON 2% D. C

I APPLICATION FOR RESEARCH CONTRACT. PART 111


r- APWM DWflRTHfNT OF THE ARUY
R m U R C H AN0 OEVELO?MENT DIdISlON WASHINOTON 2% D. C.
Bud.., Bvmm Ne 4s R ? U omcE OF THE SURGEON GENERAL

340
I

341
7435 Pair Oaks Drive Cincinnati, OH 45237 April 6, 1994
Dear Congressman M ~ M ,
considered by your ctmrmittee as an addition to the oral testimony that you will be hearing in conanittee.
I am a retired oncology nurse. University Hospital. in Radiation Oncology.
experiments that were under the supervision of Dr. Eugene Sanger.
was obvious to me that she knew that she was on an experimental treatment. her treatment. This indicated to me that she was a willing and knowledgeable participant. Her family was also present. The day that I took care of her she was also being interviewed by a psychologist associated with the project. This would also indicate that this was a treatment and an experiment that she had consented to.
While it is not always possible to draw general conclusions from a particular event, it seems unlikely that they would only get informed consent from this particular patient. It is more likely that this was the procedure for all patients on the study.
In addition there were three children treated, one of whom is still living. At the time that these children were treated, a diagnosis of Bwing sarcoma was usually a death sentence. Frequently these children suffered mutilating surgery to no avail. When Children8 Hospital sends a child for radiation it is only after much deliberation by the physician and appropriate discussions with parents. send a child without the parents consent.
high ethical, professional and caring manner. criticism that has been thrust upon them.
I am writing this letter as requested by your office, to be
I worked for twenty-five years at Ten years were as a staff nurse and fifteen years
M y employment covered the time frame of some of the Radiation
I did have personal contact with one of the study patients, and it
She spoke openly and appropriately about her illness and
They would never
I feel that the physicians involved conducted their work in a very They do not deserve the
Yours truly,
Sonya G. Margalia, R.N., O.C.N.

d 342


344
$ 4400.03 4000.00 1000.00
, 2000.00 1000. 00 1523.09
mn
mu mourn

345

346


348
I h a ..lor. I-
- - - - - -- -. ___________ .- -- .. .__ .
r- AP- I I m d n l B a o m No 4Y8244 1 DEPARTYEW OF THE ARMY OIFlCE 01 TH5 SURGECN GLhERAL
RUEARCH AN> DEVELOPVENT ClVlSlON WASHINGTON 25. D L

349
APPLICATION FOR RESEARCH CONTR4CT. PART 111
84-514 0 - 94 - 12

350


352
3 .,.......a .,...I..*,., I.IC,..'_l -~ IC FGlU i m s i l06C


354
TAFT. STETTINIUS 6 HOLLISTER , 1800 STAR mANK CENTER 426 WALNUT STREET
CINCINNhTI. OHIO 46202-SO67
Nichole Jenkins, Esq. Staff counsel to the House Judiciary Corrmittee
Subcommittoe on Administrative l a w and Governmental Relations
2138 Raybum House Office Bldg., Room B35U Washington, DC 20515
Re: House Judiciary Couittee Subcommittee on Administrativo Law and Governmental Relations Hearing on Radiation Experiments Conducted By the
01
b a r 11.. Jenkins:
It appeared to me from some coxmente I read in the pross that not all of the eubcornittee members vera avare that the Department of Dofense had been told very clearly in 1962 that pationt selection vas rada only if there was a "reasonablo chance of therapeutic benefit to the patient."
obeervation of radiation effects vera being chosen from a group roceiving therapy is roinforc.d by the reference on p. I that the use of patients recoiving thorapeutic radiation may bo introducing unrocognisod biasos into the investigation. Those statennts vera mad0 at a t i n vhon thoro vas no aontrovorsy surrounding this investigation or the source of funds for tho post-treatment observations. bofore the existence of a faculty research couitteo. The statements, therefore, are entitled to a great deal of voight, and there is no legitimate reason to challenge their crodibility.
The fact that pationts chosen for the post-treatment
Thin report vas authorod long

Nichole Jenkins April 22, 1994 Page 2
I would like this letter and the 1962 Report included as
Thank you for your help.
part of tho rucord.
wP:vra Encl.:
cc: Eugenm L. Saenger, W.D.
"An Appraisal of Human Studies In Radiobiological Aspects of Weapons Effects" November 14, 1962
Congrmsslan John Bryant (w/encl.) Congruoman David llann (v/encl.) Congressman Rob Portman (v/encl.)

. . .

357
A N APPRATSAL OF HVMAN STVDm IN
,RADIOB~OLffilCU ASPECTS OF WEAPONS EFFECTS
A. Introductlon
h th. inlskl considoratton of thore ho catogoriee om c u rearo-bly a d g n dfectr on tho oko-ryatome to groupe oth.r thp tho Defeme Atomic Support Agency. These etudter of effecte on dl typos of nor. rad fauna are of great knport.lue md little coneldoratba b e kea riven to tho bag tom effecti of high doeee of radhtba,
T& prlmaq problom of hpara effects of h i p &me# - bo& uute and chrodc - rsquiree corulderable further analyela h regard to propor Uobaent of reeearch h c and dart. Tho obviooe Cotrernh tho dlvlrion of #upport between rpiaul awl humaa invamtlgattoa.
B. PhlloeophT of Approach
la aay problem h rdiokdology o m le iaterarted k two arpeetr. Th. first ia th. diecovsry of general law. or prhclplee which are eesanri.lly the e u n e for a l l u r k n a l m . .I1 mammalc, all large aa inde , otc. Tho accord aepct is the documantatlon of epctllc Information eoocemlag mea. If a general prklpls can ba domoantrated h several type. Of d e , O m nUy then a0IPme Ut It 1I FrJkJbly true for humaw. For example, reputod e W e e Iuw ahown t h t U M .rJmP 1. placed under eevere atreem. e. g., eurciee to uhuetbn or thermal b r M . ite roleranee to a ylven dose of r4Jktlon la I0.s than M rphul lacklng the e u n e etroee. It is reaao9.ble to aeeuum that b a a b i n g e d e r etreee t0ler.t. radktlon lese wall thn a hoalthy hdlvIdryL MLt. t lwly eueh a concept 18 of great d u e l quadtatlvmly it 1. Of L O W U p S h e 0- 1. Mt able to ext.Apoht* the epclflc etres. etfacta to Werent epoclee d &ale or to people. Nor 1. o w able to predict the effect of a given etrea. h a buram be- after obemrvlsg It in UI anLnal. Anderson (1) e t ~ t a e t h t tha use of labratory W e In radfation rerearch programme. ie necerrary h order to obtain a batter uaderetandloz Of a nrnrhr of the breie changer reeulttog from radktton &I-. Extrapolation bom anunal to man Le Wereat lf not Lnporelble. ,
It is. however. qat. apparent thu may Ugh dore effectr rknply cannot b. studled h humsue kcrt lee of obvio9. hclpunit.rlm coreideratioru. Cns Cannot subject poopla to wbole body Qeee of 800 rad .Itheugh .ucL a etudy would be

358
rt - entirely fearlble In aa anhrd. Thus many ~.p.~-h.nt~ of rbdloblological iotereet w i l l contirmm. to k doam b d a d s .
Neverflulesr. i le e a r e a t i d to conalder furthor r o l l pluPrud studlea h patients so lory u the iollovisp criteria are WUedr
1. Tkn l a a reasomable chnge d thrrapwlic haofit to the patieat.
2. T L . UhlJhod of dmnage to tba p a a t ia no greater thn . that smcoantered from compar.ble tbrapy of typo. 3. Tbe kcil ikiea for mupport of tba p.tIaot and c - p l k a t b ~ of
tmatm.nt offer all poesible m e d W eervkem for ruccesrful rs rk t .uoce d tho patlent’s well be-.
.
c .
T h type of prH~a w.s~LIy selectrd for whole body radiation expomure Is an Individual with cancer rtich i s far enough abed either by direct rxteruton of m o r or by metastatic o p r r d so as to eUmlnrte conaideration oi attempts at curdve therapy. UssaUy tb.re prtieute receivo IpnspcIfic eu~portive treatment o t paLlf.t#w treatment by sur!pry, radlatbn or chernlerlr. The conrequence of thome forms of therapy a n usually helpful but rosnetimes tho requslre or complicatioru 01 the varbme treatanentr are in tharaselrer 1110 threat~rdug and ronatute a hazard tlwrapy Ls no more Llkely to produes untoward s e q u o l ~ e than ~ n ) . other currently accepted treatments d o t h r typo#. I . I
rrdirtios actually potsri5ate tbe otlect oi subsequent radlatlon Biven locally to tumor a ~ s a ~ . In acute rwhtiom In:-- of humma Interest&l( ~ ~ n t r i b u t i ~ ~ tar. been made by A .amber of wrkers. Hempelmurn et al (3) h v e described the features ot acute radiation injury and these obeemttoau bave been .mpriUcd by Andrerr et al / I) S5l;maa (5). Hodand et .I ( 6 ) and 0th.r.. A n excellant let ThoPu and W a d . [ I )
the patlaat. X.rue. ahoh body radi.Uan
Aninrbl studies (t) hare su:seatod Uut -al l doses of vlrJ1m. body
certain aew dirgnoetic criteria was prerentrd by
Obee?ntbnm d0l:Orfol therapmtio rholo body radltion hvw bosn nude by Collins (8) . Xing (91 uui Muller et al (IO).
Mtbouih OD0 few FUentr have b o a treatod by whoh body radiatton at tho Unlverrity of ChdanrCi College to bo *.lid statistically, we h w s mads rereral loterertiq obmmtionm. In generJ. there rtudler have demonatrated tho rolrtive lnnocwue nahrs of doeem at or below 100 rad and h v e continued to confirm the well burn hsmct8lo:ical chan~sa. At 150 ?.:A at LOO rad v o h v e h d responses to tadktion of t!m typo .*OD In group fl of the acute radL.tion syndrome. We lure had tvo c u e # , one at 150 .rd one st 2120 rad. orpire whOe

359
-3-

360
-4.
D. Specific Area# of Endeeror:
1. Clinical Edautlon - All patient. r h o receive wbole hody radktlon far any purpoeca mould b. evrluated,caretJly utUlaing all clinical .nd laboratory ObrcrvatioM whfch can b. reaeolubly 0bL.io.d. clinical pattarn# related to do#.. coexiatlag diaeare. nutrItlon and other parametera may thur k Identified.
It d d # e m import.nt to c u r y there obrerrr(iona further at nrtoue &#e h V d # ae moat pluminD lor capabllltlea of humma deer eaporure depend on a b l a d g e of mnir upacted parlornuace.
2. Mctabollc Effect. - Contlrariry metabolic r n d i e e are needed. Little le Lsown oi nutritional requirements and fluid and electrolytr c i u q c e in h u r n ~ ~ ~ . Liane invertizatora auto th.1 &ear arpectm are not importrnt in r.dktbn injury om th. -1s of mknal etudlee. Tbore b e mt k e n e m g h human reaurch in W a area to provide convincing data at any &#e level. Suea idormrtion la orrent id In pLnninr patient care. ,
Change# in DXA-RNA eyetune Ln a 0 complex a mammal a# man may be difficult to firrd. S u a e prellmkury obaenntloar in our laboratory tdicate that m e r ehrdl00 in t M a general -ea MY b. frdtful. H.ny other oyateue miaht b. Boggerted u ahown by the ObBerVntloM of h r k r et al (11) regarding crsatln- a r k bet. h b o b u t y r l c acid and hydro- proline. T h UBO of labeled precursor. k mggertod alaso at 10s. time it will k neceeeary to determlna rhetker ccrtJn c-ca follodng irradhcion uo due to apoclfic biochmfcal alteration# oz are Qu to mnap.cUic rtreaa.
Chngae Ln the immune eyBt.m b.re to date eluded mort obaervere who h v e aouyht them. W i t h the renewed hterrat in knmUrrol0,r centering boa about tho lpphocyte a d thymu#. new techniqwa of # M y B h o t J d be *ought.
3. , Ectrviord EIfecte - One of the quertlone moat frequently aaked by fndivldwlr reaponalble io? plrcp ly Lor nuclear warfare ConCerM the offect of a glven &eo of rubtion on aubrequent capabllity and parionnrrur of UI
lndividwl or group. It La apparently mt e u y to find a rdtable Wet or battay of teats which meamre the knportant human fuactiow ol periorarase or decision m&hg m u c h ribat o m or more teat. could br uaed beform and after expoawe to rdiatlon.
p.rf?rrmoce tertr ahodd b. developed or sdapted. There tort# Sb=eri to #ubJect# b.fOr. md after O x p o B W e 0 a # C O M C u e . b th. capability ol th. M1vidu.l.
4. Core R e a w n s o St-l.lios - Lioat atudha have been carried out d21 r a m w h t?;t t l e dose i8 CcUvered vsthto 30-300 &to#. 1l d o B 0 Of 200 rad 1. dellvercd in approximately 9'2 minuter and producer glvcn effect it b8coz.a.

361
C
84-514 0 - 94 - 13

. . .
362
-6-

363

1
April 2, 1994
To Whom It May Concern:
My name is Josef Jerome Kahr. I am one of five great nephews of the late Margaret Bacon. She vas partially responsible for my upbringing. She vas also an intricle part of my life for 13 wonderful years. She shared a residence vith myself and her sister, Lillian Joan Kahr, who was my grandmother and my legal guardian.
The death of my great aunt was a very hard matter for me to accept. The heartfelt joys that we shared turned into faded memories. All the happy times we spent together turned into heartaches and sorrow. Her death felt like a lethal weapon that wounded my soul and left an emptiness that will never go away.
The thought of my great aunt suffering through needless and un- authorized radiation treatments is totally repugnant. Nothing will ever bring QY great aunt back, but I feel something should be done to those parties that are responsible for doing radiation experiments on her without her consent.
It is unthinkable that a hospital misused and prematurely ended the life of my great aunt, Margaret Bacon.
The hospital had no right to play God!
Sincerely,

April 8,1994
TO Whom IT May Concern:
+
c
My Name is Margaret J. Willis. I am the great niece of the
late Margaret Bacon. She was a very inportant part of my life
and upbringing. She also had a hand in the upbringing of my
late mother Ella Margaret Willis. In her latter years she
she shared a residence with her sister, Lillian Joan Kahr,
my grandmother.
When my Aunt Margaret became ill my mother,grandmother,and
other members of the family had to talk her into going into
the hospital. That is when I found out she had cancer. MY
mother, grandmother and myself went to the hospital to visit
Aunt Bacon ,and I wondered why she was laying wlth blood over
her sheet.
I think this may of had something to do with why my mother
refused treatment of cancer-due to the death of her aunt.
Just the thought of my great aunt suffering through needless
and unauthorized radiation treatments is totally repugnant.
Nothing will ever bring back my Aunt Margaret, I do feel some-
thing should be done to those parties responsible for the
radiation experiments with out consent.
This in it self makes you very leary of going to a hospital
that would let this 99 on.
Si neem lv,, 4

366
April 4, 1994
On Oatober 21, 1966, after being disahargad for General Xospital, X. Jeakson VIU a v u y uerlc ill woman. a r e of hersolf prap.rl and aOp.ndod on the fmily tor all her basic mode. amtito, neuna, Maittng, rniqht loss, and was in aonstant pain. R e r oondition nawor brov6d.
Within a few sleek. 8he waa readnittad to General Hospital. The family was informed shr should b8 transferred to Drake Hospital.
Jackson indicated stre was afraid and wanted to return homo. She was transported ham, aero she was loved and oared for by US until she died on March 2S, 1967.
The family of Amelia Jackson would l ike for this committee to how, that for the ontlre t 6 3 day8 aftor reoaiving the irradiation, hor condition oontinued to deteriorate. We foe1 that tho 100 ra& of petal-body irradiation administera3 to her was cruel and didn't h8lp hor condition Ln any way. It's our baliof that she may havo lived longer if this uporimnt had not taken place.
A dootor 1s somaone you trust. His job is to do everything in his pover to alleviate your pain and suffering. E~wevor, this vas not the case. She -5 aluays orying. moaning, groaning, and in excruciating pain. Xa Jacluon wae used to further Dr. Saeger's professional goals. It vas purely an ambitious and callous eat. Neither XC Jaokson nor tho family were informad or oonsented to her being used in an tqmriment conducted by Dr. Baeqor, and funded by the Vapartmmt of Defmao. mer0 has clearly beon a cover up by mans of the oovunmtnt, General Hoepital, Dr. Saeger and City of Cineinnat:.. We aannot believo that they oonsantod to suah atrocities to be Slnanoed by the government; utiliting Ms JaCkSOn'E and tho f-:Lly'e tax paying dollars.
She was unable to taka
oh. -XI&- bleeding f r a her rectum, loss of

L
My Aunt Louise Richmond passed away from Colon Cancer in March, 1968. She was only 49 years of age. M y Mother Viola Macklin (one of Louise's older sister) brought her from Cleveland, Ohio to Cincinnati, Ohio for medical care of her cancer at the General Hospital.
Instead of medical treatment, my Aunt Louise, unknowingly was used as an experimental subject at General Hospital in their radiation experiment. Within weeks of her admission, her health rapidly and painfully deteriorated and ultimately leading to her death.
Regrettably, the news of the General Hospital Radiation experiment has recalled many agonizing memories for myself and my family. The death of a loved one, under normal circumstances is difficult, but now with the added knowledge of my Aunt sacrificial involvement in the radiation experiment, my family members must relive the misery, now with twice the anguish.
Various family members can vividly recall the evening visits to the hospital as we accompanied our mother to visit Aunt Louise. The torturing cries of pain that greeted us as we entered into the hospital ward had become all to familiar to us. She would be lying in her hospital bed trembling and shaking from her agonizing pain so forcefully that the bed itself would be visibly vibrating.
Throughout the visit, my Aunt Louise would cling on to my mother's arm crying and begging her to take her home. She would repeatedly say, "please Viola take me home with you, I r m in 50 much pain, they are hurting me, they are trying to kill me".
The visits would always end with my mother tearing herself away from my Aunt Louise only to hear her cry in pleading desperation as we walked away. for seemly, hours after we left the hospital and even after reaching home my mother would cry from the guilt she felt for my Aunt's severe pain and suffering. My mother would routinely rock herself to sleep while crying and humming spiritual songs to relieve the burdensome feeling of her most recent experiencdvisit to my Aunt Louise
After my Aunt Louise' death in March, 1968, my mother would often ask us if they (the Doctors at General Hospital) were really giving her the correct treatments for cancer.
We had no idea Aunt Louise was a part of a Defense Department experiment. We're sure if she had known she was a guinea pig she would not have participated.
My mother would often recall the visit and continued to blame herself for the pain and anguish my Aunt Louise had experienced. My mother carried this unwarranted guilt to her death, and now we have been forced to carry this guilt as well in memory of my mother and aunt.

368
Date:'hpril 4, 1994
To: Robert 8. Newman, Attorney at Law
Prom: Uembcrs of the Maude Jacobs Family
Subject: Radiation Testing at UC (Cincinnati General Hospital)
This correspondence is regarding Maude Jacobs, a female Caucasian, who was an unsuspecting victim of the radiation tests conducted by the University of Cincinnati. Maude was born in Whitesburg, Kentucky on June 7, 1916. The third grade was her final year of formal education. By the time she was thirteen years old, she was married and had given birth to her first child. She bore seven children in all, six girls and one son. She was a beautiful woman with a lovely radiant smile. She was impeccable about her children's appearance, as well as her own. Her devotion to her family was obvious to anyone who knew her. Maude lived her life below the poverty level, but was a proud and dignified woman. She was genuinely happy with the simple things in life. Her delight was cooking and caring for her children. When she died she was a widow and left three minor children at home.
According to information from CGH (Cincinnati General Hospital), Maude was diagnosed with breast cancer on July 17, 1964. A treatment of hexamethylmelamine began on July 27,1964 and was completed on August 18, 1964. With this medication her primary tumor receded markedly. On November 7, 1964 total body irradiation was administered. The midline absorbed tissue dose was 150 rad (250 r midline air dose). At the termination of the treatment she had severe vomiting for twenty-four hours, in spite of intramuscular compazine. Before treatment she had a normal hemogram. Seven days after treatment the white blood count began to fall. The platelet count fell around fourteen days after treatment. The WBC was 1,000 and platelet count was 80,000 twenty-three days after treatment. On the twenty-fourth day, the WBC was 850 and platelet count was 38,000. Maude died December 2, 1964. Twenty-five days after total body irradiation. She was study number 045. (Documentation from CGH attached.)
Two letters written by Maude to her sister Arlie less than two months before her death describes how she felt, and also indicates she thought the doctors did not know what was wrong with her. She talks of living near her oldest daughter, Lillian, who is very helpful to Maude. She also is pleased to be home with her children, but feels sorry because she is too tired in the evenings after preparing dinner to watch television with them. she refers to the expense of her medication and said prayer helps her more than the doctors. These letters demonstrate her education level, but also reveal her devotion to her Children. Maude had no knowledge of the seriousness of her cancer much less knowledge of the-radiation

treatment. She did not expect to die. If she had, she would have discussed the future care of her minor daughters with the rest of
. the family. Her death was so sudden and unexpected the family was totally unprepared. The three young daughters eventually were put in St. Aloysius Orphanage. (The two letters from Maude to her sister are attached.)
The family was NEVER informed of the radiation test or it's purpose. Nor was anyone ever asked to sign a consent form or give verbal permission for testing. Some of the memories which were dismissed without attaching importance now make sense or at least raise suspicion. Her daughter Irene was seven months pregnant at the time and was having a difficult pregnancy. She remembers Maude's bright smile and cheerfulness, then remembers a private room and no more smiles or happy faces. Irene remembers being afraid of going into that room. Maude asked her to feel her head and when she did it felt full of soft tumors. Her body felt like sand. Even in the hallway she could hear Maude's delirious talk.
Maude's daughter Sherry was twelve years old and remembers the private room, but at the time didn't know it was uncommon for a person without insurance. Sherry remembers the orphanage and being split up from her two younger sisters. The youngest girl, Kim, eventually went to a foster family.
Robert Murphy, one of Maude's grandson's, remembers thinking how nice it was to have a private room without insurance. Bill Murphy, another grandson recalls visiting her in the private room, but,,not wondering why she was there. He remembers her conversation as out of her head".
Her oldest daughter, Lillian Murphy Pagano, lived downstairs from Maude and was her primary care provider. Lillian was never contacted or consulted about her mother's treatment. She remembers a drastic mood change associated with rapid physical deterioration. She too recalls the private room at the end. She remembers thinking her body felt like sand. She was concerned too for Irene, because of her pregnancy and the worsening of their mother's health so rapidly. Lillian's concern grew as Maude quickly became disoriented and no longer recognized anyone. She was violently ill and talking utter nonsense. Maude died before her time everyone felt. Her family lived for the next twenty-nine p l u s years with the sadness of her death, but also had warm memories to console them.
Since the details of the experiments became public, the entire family has been drastically affected. Now guilt has replaced the sadness and comnents like "I should have known" or "I should have asked" are commonplace. Reliving Maude's last days over and over, remembering differently now why she was so violently ill, how she suffered, and now a reason for the private room. Her death is now a nightmare. She died without comfort and dignity. She was discriminated against and selected because of her background. No benefit was ever planned for Maude. She was a numberFa statistic.

370
Her children want an apology. They want to know nothing they could have done would have altered the results. They want Maude to know they are sorry if they disappointed her because she suffered needlessly without intervention from them. They also need a quick resolution so this too can be a memory. Already too much damage has been realized.
Lillian Murphy Pagano (Maude's oldest daughter) feels personally responsible for her death. She became obsessed with Maude's death, often calling other family members several times a day to go over some part of her last days again and again. She was found several times at three or four o'clock in the morning with a fixed stare and silent sobs. Eventually she was rushed to the hospital with a suspected heart attack. After a short stay of a few days, some testing, several prescriptions, and instructions to avoid stressful situations, she was permitted to go home. Anxiety struck again within a few weeks. This time she was gone. Lillian's daughter found her, called 911, and received over the phone guidance for delivering CPR. When paramedics arrived, she was given multiple shock treatments to revive her. It is estimated she was dead for four minutes. She was on a respirator and in a coma; she also had several seizures. The doctor's gave her a 50% chance of pulling through, but warned all about the possibility of permanent brain damage. She has regained consciousness, but is still in critical condition at this writing. She recognizes family members, but is mentally unstable. The extent of damage is still unknown. Her family has been told she will need twenty- four care and cannot be exposed to ANY stressful situations. She doesn't talk about Maude now. She doesn't even remember who visited her an hour ago.
The ordeal with the UC experiments must come to a swift conclusion. This is the saga of only one family, there is supposed to be eighty-sevenmore victims with families. It's amazing how something that was a remote, barely thought 0.f memory, now is resurrected and grown into an unwelcome demanding problem. A problem that can consume your days and affect people from twenty-nine years of family growth --- people Maude never could have known. This letter was compiled from the hearts and thoughts of Maude Jacob's children: Lillian Murphy Pagano (nee Phillips) Irene Froman (nee Phillips) Bob Phillips Betty Wolfe (nee Phillips) Sherry Brabant (nee Jacobs) Janet Baker (nee Jacobs) Kim Swedo ( nee Jacobs)
Attachments

--.
March 31, 1994
i
To Whom It May Concern:
-.r38Yi3 8'3 2 5 9 - 5/33
My name is Joe P. Larkins. I am now 52 years old My Father, Willard L . Larkins, passed away in 1971. I was 30 years old at the time. My family consisted of myself, an older sister and my parents. When my Father passed away, he and my Mother were in the process of raising a grandchild (my sister's son). Neither of my patents were well-educated, but my Father was hard-working and honest. We always had clean and decent clothes to go to school in and we always had ample food on the table. It doesn't take a well-educated person to be hard-working or honest If Cincinnati General Hospital and the Doctor's therein had been honest, there is of course, the possibility that my Father could have lived for several more years. Instead, he went from a fairly able-bodied middle-aged Father and Husband to a premature death caused by an 'experiment" My Father did not know that he was being used as a guinea plg; my Mother did not know; as his children, we were not informed of the procedures to be used nor of the risks involved.
I feel as though Dr. Saenger and the other "Doctors"involved, if you will, knew that the high levels of radiation which they administered to these patients had the very real probability of being fatal Oh, how right that is! My Father was very much a family man, yet these people killed him as surely as if they had put a gun to his head and pulled the proverbial trigger. These "Doctors" left my Mother, with no job skills, to raise a grandchild as best as she could. My Mother lived until 1983, but she was a broken woman after my Father's premature and unexpected death
I know that my Father knew that something was very wrong with the treatments being given to him at Cincinnati General. He even asked me "Son, what are they doing to me? They're trying to kill me!' That's how bad the pain he endured after the treatment was. He suffered 80 needlessly. What really gets me about this situation is the fact that the Pentagon contracted with these Doctors and this hospital to test the effects of radiation on the human body. Everyone realiaes that Cincinnati General Hospital, now the University of Cincinnati Hospital, treated many lou-education. low-income patients. I guess they felt that in some way, the fact that these patients were not rich, upper-class citizens, gave them the right to experiment with

872
their bodies without informed consent. NOT SO! I feel sure these physician/researchers were well-paid for their part and it would be very interesting to know the types and dollar amounts of the grants given to Cincinnati General by the Federal government. I feel sure that all parties, with the exception of the poor, unsuspecting patients and their families, were well-compensated. But since when, in our society, does one man or even a group of them, have the right to play God? A very good example of this is our 20th century “assisted suicide Doctor’ This man is contacted by terminally-ill patients who wish to end their own lives with dignity and choose, by their own voilition, not to suffer needlessly for years. These people make the decision to die in peace, yet our great judicial system, along with the medical community, brought this compassionate physician up on charges. The differences in these deaths and the death of my Father are that my Father did not choose to die - someone else made that decision for him, without consulting or informing him and they were amply compensated for it. I feel that the price they should be required to pay to the fahilies of the people they killed, should be exceedingly high I also feel that the Federal government should be named as a co-conspirator in this case, because that’s exactly what it was - a conspiracy. No person, and I emphsize ’NO’, person would willingly consent to a treatment with any degree of fatality involved. People, both you and I, simply value life too much. I think that is the big thing here - the patients were not informed. I know that behavior of this sort would not be tolerated by the medical community today. But then again, this entire mess was surrounded by a thick veil of secrecy on both the doctors’ part and on the part of Cincinnati General Hospital. It is still being closely guarded and kept under yet another veil of secrecy to this very day by the University of Cincinnati, in that they have yet to provide the medical records of the patients involved in this experiment/ I beseige you to order the University of Cincinnati to release the patient records, in their entirety, to the next of kin immediately. They are hedging to save their own skin. I was promised my Father’s complete medical file over a month ago; as of this writing, I have nothing.
I only hope that you, the Congressional Committee, see fit, as members of the human race, to break this matter wide open here and now and award just compensation to the families of the victims. I feel that the Physicians involved and also the federal government (the Pentagon) should pay and also I beg you to strip any and all of the Doctors involved of all their medical credentials that they hold. If justice prevails in this matter, and I have faith that it will, a strong message will be sent to our government officials and the private physicians (to whom people entrust their lives and the lives of their loved ones) that behavior of this

sort will simpley not be tolerated, that justice will in fact be both swift and severe. I pray that a situation such as this will never again be faced by a group of people. If this statement to you, the Congressional Committee, does anything to help in the name of justice, then my Father’s death and the sorrow and hardships that his familty faced, will not have been completely in vain.
Thank you
.
.

374
To: Chairpermon of the CongremmioPrl C d t t e e
R E X Th. P a r t i a l md Whole Body Radiation mrrirmt C o n d u c t e d f rom 1960-1971
Mr. Woody P l a i r and P d l y of Mrtl. B e a t r i c e P l a i r
This letter was very difficult to write for us, the family
of our departed wife, mother and grandmother. We conversed of
many traumatic thoughts and feelings regarding dur loss.
Herein is the summation of our collective thoughts and
feelings. Dr. Saenger states that the patients and families gave
their consent to receive partial or whole body radiation. For
the record, our mother loved life and she would have never given
her consent to any treatment that would have shortened her life
or cause her the pain, we observed. She never knew she was part
of the Cold War Radiation Experiment. As a family, we were never
told of her participation in partial or whole radiation. We
would have not given our consent for her participation in an
experiment. At no point i n the supposed treatments of our mother
did anyone tell our father nor her children that she was part of
a dangerous and life threatening experiment.
What we can say to the Sub-committee is that we remember our
mother complaining of increased pain, especially following the
radiation exposures. We can told you how our mother told us she
felt as though she was on "fire" or "burning all over". We can
tell this committee, we resent our mother being used as a human
Guinea Pig and the implication by Dr. Saenger that our mother
agreed to have her body exposed to radiation injury that would
lead to serious pain and shortening of her life.

The Plair family asked this Sub-committee to help us to
bring the people who we feel shortened our mother's life to
just ice.
In a society where life, especially human life appears to be
worth less and less, we and other families are depending on this
Sub-committee to send a clear message to Dr. Saenger and
associates, the University of Cincinnati Medical Center and the
Defense Department that human life is still important.
We must let the world know that here in America, what makes
us different and greater than other countries is that we truly
value each and every human being regardless of their I.Q.,
education, race, creed, color or position in our society. If we
allow this travesty of justice to go unchallenged others may be
unknowingly experimented upon in the future.
Respectfully submitted,
Mr. Woody Plair and Family

To (louool Who Will Lfmt.nc
I was 30 years old when my mother was stricken with cancer.
She had six other children, three very young at home, the oldest
was 12. She was born (my mother) in Whitesburg, KY, 1916, only
went to the Second Grade of Grade School, was married at 13 years
of age. When cancer struck she had no money. Her husband had
only been dead a short time and she was struggling to care for
her three girls at home. She wanted to spend as much time as she
had left enjoying her three daughters.
an out-patient at General Hospital. One day near the end nurse
called told her to come to hospital clinic. She took a taxi
because no one was available to drive her. She came home weak
and vomiting. She was admitted to hospital and only lasted less
than a month. When we (the family) found out recently about the
150 Rad she had received my older sister felt she was to blame
because she did not go with her in taxi to clinic. She had to be
hospitalized herself and may need constant care. A younger
sister has M.S. and has not been told for fear she won't be able
to cope with it. I'm sure all the other families that are still
alive are having similar problems. My prayers are with them too.
As you can tell from my letter, I don't have a good education.
Should I be afraid to be treated in a hospital? Afraid of being
used for testing some other chemical to benefit our government.
Or carry a Donor's Card so if they wanted an organ they could
take it at will? Something needs to be done it is up to you.
I'm helpless.
She was being treated as
Thank you
Bob Phillips Son of Maud Jacobs #45
J

To : Congressional committe!e FROM Herbat F. Varin DATE: lrpril4,1994
StudyXO75 N.C. ChacttCGH 409-278
My mothem name was Nina L. Cline, a loving and caring mother, whose only hope was to see her grandchild befan she died. Shedid 10 months before her death. She was also vay b to her sister, and her sisters children, who wem all very helpful with my mother during her cancer.
My mother was diagnosed with cancer in 1962, she put a lot of hope and faith in her doctors and General Hospital who were treating her. She often talked to me and other family members about her
treatment, but at no time did she mention being apart of any experiments for the government. She would have talked to me and other family members before ever consenting to any experiments.
I am appalled to thiik that Dr. Eugene Saenger, his associates and our Federal Government would join is such an inhumane act. I also believe Dr. Eugene Saenger violated his moral and ethical obligation toward his patients.
We were taught as children and young adult, to believe in our Federal Government, that they would make all the right decisions concerning our welfare as people. For the government to sponsor a radiation experiment of this nature, on my mother and other patients was totally immoral.
Herbert F. Varin (Son)

378
R A O I A T I O N EXPERIMENTS
TO WHOM I T MAY CONCERN!
BACON WAS MY MOTHERS SISTER.WHICH I S MY AUNT. I A L S 0 , L I K E MANY OF OUR R E L A T I V E S WAS Pf iRTLY R A I S E D B Y MY AUNT MARGARET BACON OF WHOM I HFIVE VERY FONO MEMORIES OF.
MY NAME I S J O E KAHR SR..MRS MARGARET
I W A S ENCOURAGED B Y HER H O S P I T A L DOCTOR TO CONVINCE HER ( S I N C E SHE D I D NOT WANT TO ENTER A H O S P I T A L ANYWAY)THAT GENERAL H O S P I T A L ( T H E H O S P I T A L SHE WAS I N A T THAT TIME),HAD THE BEST R A D I A T I O N F A C I L I T I E S I N THE C I T Y WHICH COULD HELP HER S I T U A T I O N IMMENSELY. AFTER A WHILE,SHE AS WELL AS I BOTH B E L I E V E D THE DOCTOR - I F YOU KNEW T H I S FAMILY,THEN YOU WOULD KNOW THAT WE ARE THE L A S T OF ANY I N D I V I D U A L S TO COMPLAIN. HOWEVER WHEN I T REACHES T H I S POINT,THEN WE CAN NO LONGER R E M A I N THE S I L E N T I N D I V I D U A L S THAT WE ARE. SHE NEVER ASKEO FOR MUCH.NOR D I D I T TAKE MUCH TO S A T I S F Y HER. tiOWEVER.BE1NG A HUMAN R A D I A T I O N GUINEA P I G I N T H I S TYPE OF DEATHLY S I T U A T I O N I S DESPICABLE,WHEN ONE SUCH AS HER LOVED L IFE AS SHE 010.
I H E F I R S T T H I N G MY AUNT AND I NOTICED AS WE ENTEREO THE C I N C I N N A T I GENERAL HOSPITAL,WAS THE AMAZING U N I V E R S A L I S M WHICH WAS EXPRESSED I N SUCH PROFOUND ELOQUENT AND EQUIVALENT LANGUAGE.THE D I G N I T Y AND WORTH OF A L L PATIENTS,WHICH THEN WAS MENTIONED THAT A L L P A T I E N T S WERE TREATED EQUALLY. ON ONE H A N 0 , I T WAS PROFESSED TO US,THE NOBLE P R I N C I P A L S AND EXPECTATIONS OF THE HOSPITAL. BUT I T SEEMS THAT ON THE OTHER HAND THAT SOMEONE WAS SADLY P R A C T I C I N G THE VERY OPPOSITE OF THOES EXPECTATIONS THAT WE WERE ORIENTATED WITH.
I A M SURE THAT SHE A S WELL A S OTHERS WANTED TO BE CONTENT BUI I T SEEMS THAT SHE WAS USED AS AN EXPERIMENTAL OBJECT AND BECAME THE VETERAN OF CREATED SUFFERING. I NEVER DREAMED THAT T H I S F A M I L Y WOULD EVER BE EXPOSED OR WRONGED B Y SUCH AN IMMORAL AND UNJUST S I T U A T I O N . I F E E L THAT I MUST SPEAK NOW BEFORE I T I S TAKEN FOR GRANTED THAT WE ARE S T I L L ONE B I G HAPPY FAMILY,NOW OPPOSED TO WHAT W E USE TO BE.
I T SEEMS THAT T H I S NOW IS THE K I N D OF ENVIROMENT I N WHICH WE L I V E . HOW CAN WE A V O I D B E I N G DEPRESSEO WHEN WE DISCOVER THAT A L L P R I O R GENUINE CODE OF E T H I C S ARE SLOWLY CHANGING +FOR THE WORST. WE A L L AS LOVED ONES ARE INVOLVED I N A NETWORK OF M U T U A L I T Y . T I E 0 I N A S I N G L E PROMINENCE OF OESTINEY. WHAT EVER EFFECTS ONE F A M I L Y DIRECTLY, EFFECTS A L L F A M I L I E S I N D I R E C T L Y . WE CAN ONLY AND WILL ONLY S U R V I V E T H I S EMOTIONAL

CATASTROPHE.BECAUSE IT 'SEEMS THAT WE HAVE NO ALTERNAT-IVE IF, W E WISH TO KEEP OUR SANITY,
, . I !
I T I S A TORTUROUS LOGIC TO USE THE TRAGIC RESULTS OF THE:' HOSPITAL OR GOVERNMENTS REASONING AS AN ARGUMENT FOR THE::
' - , _
. , I
CONTINUATION,OF RADIATION EXPERIMENTS DURING.THAT TIME<*cY.. . , I
WE SHOULD HOPE.THAT NEVER AGAIN SHOULD WE OR ANYONE ELSE :; HAVE TO RESIGN OURSELVES TO SUCH AN OUTRAGE. ' ' ,
THE TORMENTED AND UNHAPPY FAMILY OF MRS MARGARET BACON.

April 8, 1994
To Whom It May Concern:
It is our feeling that our mother was not informed of the true nature of the radiation she received at Cincinnati General Hospital. It was her belief and ours that the radiation “therapy” was being performed to (1) reduce the pain due to her cancer and (2) to kill tumor cells in order to possibly extend her life expectancy. This is what we were led to believe by the physicians and other health professionals in charge of our mother’s care. We all were led to believe that the radiation therapy would also benefit mankind in determining the ef f icacy of these treatments, to help cancer patients in the future.
As a family, one small consolation in watching our mother die a slow and painful death from cancer was the fact that her participation in the treatments would represent a positive outcome from her death in the form of her helping others who shared her fate.
Having found out the truth about what really happened to our mother has not only brought back painful memories of seeing her suffering, we must now live with the knowledge that this Suffering (excruciating physical pain, intense fear, despair, and many other terrible effects of the treatments) was intensified and not alleviated by these radiation experiments. This has caused even greater pain and suffering knowing that our mother was treated no better than a laboratory animal thereby robbing her of her human dignity and the right to live out her final days as comfortably as possible. We believe her life was shortened immeasurably by these physicians making god-like choices which they had no right to make.
Sincerely, :+- a.3 w d 3 , l?yg T Daltg
Elyse A. Feltrup Daughter of Rose E. Strohm
Stephen G. Strohm Son of Rose E. Stroh Date

381
.-- 1
382
March 29, 1994
TO THE CONGRESSIONAL COMMITTEE OF MR. DAVID MANN:
I, Doris Baker, only have a few things to say. One is why were we kept in the dark about my great grandmother and the other i s why didn’t they tell her about it? Her life, was her‘s and God‘s, not their’s.
I had to take care of her as a young pregnant 17 year old mother day and night. They said she didn’t return, she couldn’t even walk by herself. I had to lift her to the bathroom. I watched her slowly die. She tried to fight it; even when they told her she was dying. At times, she was in so much pain. I would ask her what was wrong and she would say nothing, but I saw the tears in her eyes and the pain.
You know, I almost lost my baby, because I was tired and run down from taking care of my grandmother. My child was born on 10J20164 and only weighed 2 pounds. Please someone tell me why?
That lady was my life, for personal reasons. After 30 years i s st i l l hurts, because she was my protector. So you see she never would have agreed to be a guinea pig for no one, because she loved life. When you shortened her life, you caused my brother and I alot of pain until this day. So please someone be honest with my family and I. Because no one was honest with Mrs. Gertrude Newell. She was just a case number and a piece of meat to them to experiment on for their use.
Sincerely,
Doris J. Baker

383
# 0 5 5 Lillie Wright
Chart No. 4 4 1 7 4
My mother Lillie Wright was admitted to Cincinnati
General Hospital Aug 23, 1 9 6 5 . She was sent there for a
biospy. She was confined to the hospital for one 1 week.
The summary I recieved of her illness revealed that
her biospy was performed. Aug 30, 1 9 6 5 diagnosis was
Carcinoma of the breast. On September she was given partial
body irrodation 200 rad midline. On October 8, 1 9 6 5 local
x-ray therapy began. In 53 days she( Lillie Wright) had
reciaved 2000 rads to her left and right chest.
On December 1 , 1 9 6 5 x-ray was begun on the
imtermammary chain and to the anterior and posterior above
the collarbone region (supraclavicular). She received 4000
in 4 0 days. Her white blood cell count fell to a low of
2200 on December 3, 1965 . These doses of radiation in
my opinion was enough to destroy bone marrow and white
blood cells and even the patient.
We the family of Lillie Wright was not notified about
these radiation treatments or any other procedures which
may have taken place. We did not sign any papers to permit
this experiment to be done on her( Lillie Wright).

384
The doctor at the hospital gave her sample tubes of
oniment to use on her breasts, her back and abdomen.
Her skin was burned on both breast. Her back and abdomen.
There was raw flesh exposed where once there were skin.
I had to apply this oniment to those exposed areas.When
I applied this oniment to those raw areas she was in such
excruciating pain I cried. She was given enough oniment
for 1 week. She was given Morphine which last lor 2 weeks.
I do not recall the name on the oniment tubes ( 3 ) but both
of these product was given to her around December of 1965 .
Neither of these medication helped her. When a person
IS r3al 111 I was under the impression someone have to
sign for medication such as morphine for a patient which
is terminally ill. She was kept in the dark about the
treatments she was receiving. She never talked about it.
It's not fair to treat another human being as a guinea
pig because they are poor and uneducated. Some of our
parents didn't have the privileges we are blessed with
today.

. c
I took my mother back to the hospital Feb 12, 1965
around 10:30 or 11:OO. My nephew and I stayed at the
hospital until 3:OO am I asked the receptionist if they
were re-admitting her and she said yes we should go home
and get some rest. When I return home my husband called
me from his job and told me my mother had died. The people
at the hospital never did call me to inform me of her death.
I'm her daughter, I should have been informed about
her death before I left the hospital. I was at the hospital
at 3:OO am the death certificate states she died at this
time. Feb 13, 1966. I thought the nearest relative was
to be informed first.

--
How I feel about my mother participating in the experiment.
I'm very angry about this doctor taking it upon himself
to use poor live, uneducated human beings for his personal
fame and gain. These human beings had the right to
live the rest of their lives until God was ready for them
to die. Not to die because man want to find out what effect
it would have on soldiers in the war zone.
My family have been deprived of what days my mother
could have lived. I know she wasn't educated but she knew
something was wrong but she didn't know what it was.
I don't like it because she Lillie Wright was kept
in the dark about this experiment. It's a disgrace to
use high doses of radiation on anyone why didn't you
experiment on your love one? No because they are special
to you. Remember someday you will reap your just reward.

387

388

npril 1. 1994
STATEWENT FOR CoNoRE'iSIoNAL HEARING REGARDING EXCES'i l l A D I A T I f f l USAOE AT C I N C I M T I GENERAL bOSPITM
~~ ~~ ~- - ~
BY: Pewy Carboina (Brooksbank) Granddaughter of John Edgar W a t e r 1049 Belvoir Lam Cincinnsti. Ohio 45238 ( 513) 451-8427
Rcgardinq nr. John Edpar Uebster ~ ~~ ~ - -
John Edqar Webster. father of Luc i l le H. Webster Ermksbank was admitted t o Gcncral I losptial around January or February of 1967. tie was t o l d he had cancer at that timc. A l s o durinq t h i s timu m y wandtather was l i v i n s wfth us. meanina my mother. father and brother6 and sisters. I recal l my mother t e l l i n g us that the hospital had a now t r e a t r r i l for cancer pntionts l i k e my grandfather. Thnt t h i s treatment w i l l cure hi!; cancer. My mother was extrcsmly excited af ter hearing the nswa o f t h i s M W ~ Y discovered treatment. She. as uull a8 a l l of us was led t o b e l i w e that th is treatment was the miracle ut the century. Never uas any family member adviscd that t h i s treatmcnt was an experimental venturc with thc United States Government. I r cca l i my qrandfathcr arilttns t o mc that a t tcr h is caiicer wan curd wiLh t h i s now proc:edi,re he w a n noim t o take il t r i p t o Cali lornio t o viuiL hln eldest son whom he had riot wen i n four yeart?. Before Lliat treatments bcgan. my grandfattior was comvlctcly mobile, and tunctioned riormolly. Thcn the treat men t besn n . n f ta r my grandfather.. cancer treatment. he uaa vcry mak. confined t o h i s hospital bed and could not keep any food down inrludinq water. He wan i n constant nevcre pain. Ue visted my grandfather on a da i ly basis. Prior t o h is treatment we would give him back rubs. huw. whatever. After the treatment we were advised by hosptial o f f i c i a l s not t o touch h is body. k begari tu lose weight rapidly. We watched him physically deteriorate to ta l l y . However. hio mind otaycd a l c r l . lic would cry duc L n ouch pain. We hoard him pray that tiod would take him so thc pain would elup.
On the day m y grandfather died. we were getting rcacly t o on Lhe the hosptial whcn thc hospital called and adviscd my mottier that wandpa w a s dying and that wc shniild hurry. As wc arrived t o the floor wc uere met by nurses i n front of h is room t e l l i n g us that my grandfather wan dead. MY mother wanted to ass my srandfather's body. The nurse refused. MY mother advised the nurse that she wasn't a f ra id of him while he was alive. why would she be afra id o f him doad. The nurse n t i l l refused. MY mother pushed tha nurue aside and uc entered h is r o o m . As w e looked at him we noticed he had a yellowish-green color. Mot a grey dead look. MY mother asked the nurse why he was so dis- colored. She stated suae pewle I w k that way at thc time o f the i r death. My mother advised that there was t o be no autopsy. It w a s n ' t unt i l t h i s invest- igation bepan d i d I diecover that an autopsy was Porformed against the wishes o t my mther. Neucr were wc adviscd that thir; radiaLion trootllent was an experiment i n any fashion. Nor were any papers granting such an arperi- an t signed. I strongly believe that the victims o f these treatments were used as laboratory animale t o see Just how much radiation the humn body could take.
0

c
ISBN 0-1 6-046348-3