p38 mapk inhibition reduces aortic ultrasmall superparamagnetic iron oxide uptake in a mouse model...
TRANSCRIPT
p38 MAPK Inhibition Reduces Aortic UltrasmallSuperparamagnetic Iron Oxide Uptake in a Mouse Model
of AtherosclerosisMRI Assessment
Joanne B. Morris, Alan R. Olzinski, Roberta E. Bernard, Karpagam Aravindhan, Rosanna C. Mirabile,Rogely Boyce, Robert N. Willette, Beat M. Jucker
Objective—Ultrasmall superparamagnetic iron oxide (USPIO) contrast agents have been used for noninvasive MRIassessment of atherosclerotic plaque inflammation. The purpose of this study was to noninvasively evaluate USPIOuptake in aorta of apoE�/� mice and to determine the effects of Angiotensin II (Ang II) infusion and chronicantiinflammatory treatment with a p38 MAPK inhibitor on this uptake.
Methods and Results—ApoE�/� mice were administered saline or Ang II (1.44 mg/kg/d) for 21 days. In vivo MRIassessment of USPIO uptake in the aortic arch was observed in all animals. However, although the Ang II group hadsignificantly higher absolute iron content (1103%, P�0.001) in the aortic arch compared with the saline group, the p38MAPK inhibitor (SB-239063, 150 mg/kg/d) treatment group did not (16%, NS). The in vivo MRI signal intensity wassignificantly correlated to the absolute iron content in the aortic arch. Histological evaluation of the aortic root lesionarea showed colocalization of USPIO with macrophages and a reduction in USPIO but not macrophage content withSB-239063 treatment.
Conclusion—The present study demonstrates that noninvasive assessment of USPIO uptake, as a marker for inflammationin murine atherosclerotic plaque, is feasible and that p38 MAPK inhibition attenuates the uptake of USPIO in aorta ofAng II–infused apoE�/� mice. (Arterioscler Thromb Vasc Biol 2008;28:000-000.)
Key Words: atherosclerosis � inflammation � magnetic resonance imaging � USPIO � apoE�/�� p38 MAPK
Although experimental evidence linking inflammatoryprocesses to the fate of the atherosclerotic plaque
development exists, it is difficult to examine these processesnoninvasively and to provide convincing links between pre-clinical and clinical studies. In this regard, ultrasmall super-paramagnetic iron oxide (USPIO) contrast agents, optimizedfor uptake by the mononuclear phagocytic system,1–3 are ofparticular interest for translational cardiovascular research.These agents have been used for noninvasive MRI assess-ment of atherosclerotic plaque inflammation in humans4–6 aswell as hypercholesterolemic balloon-injured NZW7 andWHHL8–11 rabbits. However, descriptions of USPIO use inextensively-studied murine genetic models of atherosclerosishave been limited. Investigators have used other targeted12,13
and nontargeted14 approaches to noninvasively assess plaqueburden or inflammation in atherosclerotic mouse models.Additionally, superparamagnetic iron oxide (SPIO) has beenused to quantify monocyte recruitment histologically inatherosclerotic lesions of the apolipoprotein E–deficient(apoE�/�) mouse.15 In that study, acute administration of
tumor necrosis factor (TNF), interleukin (IL)-1�, and inter-feron (INF)-� was shown to stimulate SPIO uptake by 4-foldin plaque. Although this study supports the hypothesis thatplaque targeting of the USPIO contrast agent in mouse isfacilitated by monocyte recruitment or activation of macro-phage phagocytosis, noninvasive assessment of USPIO up-take in mouse atherosclerotic lesions has not been reported.
Recent evidence suggests that a particularly aggressivemodel of atherosclerotic plaque development can be createdby elevating circulating Angiotensin II (Ang II) levels inapoE�/� mice.16 The addition of Ang II to apoE�/� micepromotes a marked increase in the number of macrophagespresent in the adventitia associated with vascular lesions. Inthe vessel wall, Ang II–induced vascular inflammation ismediated by AT type-1 receptors which in turn activateinflammatory signaling pathways, generate reactive oxygenspecies, and decrease NO bioavailability.17 Evidence suggeststhat reciprocal activation of p38 MAPK and NADPH oxidaserepresents an important amplification loop in vascular inflam-mation induced by Ang II.18,19 Therefore, the purpose of this
Original received July 3, 2007; final version accepted December 1, 2007.From Laboratory Animal Science (J.B.M.), Cardiovascular and Urogenital Center of Excellence in Drug Discovery (A.R.O., R.E.B., K.A., R.N.W.,
B.M.J.), and Safety Assessment (R.C.M., R.B.), GlaxoSmithKline, King of Prussia, Pa.Correspondence to Beat M. Jucker, PhD, GlaxoSmithKline, Mail Code: UW2510, 709 Swedeland Rd, King of Prussia, PA 19406. E-mail
[email protected]© 2007 American Heart Association, Inc.
Arterioscler Thromb Vasc Biol is available at http://atvb.ahajournals.org DOI: 10.1161/ATVBAHA.107.151175
1
by guest on September 5, 2016
http://atvb.ahajournals.org/D
ownloaded from
by guest on Septem
ber 5, 2016http://atvb.ahajournals.org/
Dow
nloaded from
by guest on September 5, 2016
http://atvb.ahajournals.org/D
ownloaded from
by guest on Septem
ber 5, 2016http://atvb.ahajournals.org/
Dow
nloaded from
study was to noninvasively evaluate USPIO uptake in aorta ofapoE�/� mice and to determine the effects of Ang II infusionand chronic antiinflammatory treatment with a p38 MAPKinhibitor.
Materials and MethodsAnimalsAll procedures were approved by the Animal Care and Use Com-mittee of GlaxoSmithKline and were specifically designed to mini-mize animal discomfort. Twenty-eight–week-old male apolipopro-tein E–deficient (apoE�/�) and background strain C57BL/6 mice(Taconic Farms, NY) were used in the study. ApoE�/� mice (n�28)were subjected to a subcutaneous infusion of either Angiotensin II(Ang II) or saline for a period of 21 days (Figure 1) via Alzet osmoticminipumps (model 2004; DURECT Corp). Minipumps were im-planted subcutaneously in the mid scapular region of mice anesthe-tized with 2% isoflurane (Abbott) delivered in 100% oxygen. Allanimals also received a single preoperative analgesic dose ofbanamine of 1.1 mg/kg, s.c.
Study Groups and Experimental ProtocolAnimals were assigned to 1 of 3 groups. Group 1 received a salineinfusion (Saline, n�9), group 2 received an Ang II infusion deliveredat 1.44 mg/kg/d (Ang II, n�10), and group 3 received Ang IIdelivered at 1.44 mg/kg/d�p38 MAPK inhibitor, SB-239063 at 150mg/kg/d, dietary dosing (Ang II�SB-239063, n�9). Dosing of thep38 MAPK inhibitor was initiated 1 week before Ang II adminis-tration (Figure 1). ApoE�/� mice were housed individually and wereallowed free access to chow. Osmotic minipumps were implanted onDay 0, and body weights and food consumption were recordedthroughout the study. Indirect blood pressure was collected onDay 18 before USPIO administration. On Days 19 and 20 allanimals received an i.v. administration of USPIO. The followingday (Day 21), in vivo MRI was performed. After in vivo imaging,whole blood was collected (EDTA) for determination of plasmalipid, cytokine, and drug concentrations. The heart and aortictrunk were removed after in situ formalin (10% neutral buffered)fixation. The aorta was submitted for absolute iron analysis andex vivo MRI was performed on the hearts on Day 22 followed byhistological evaluation (Figure 1).
Additional apoE�/� mice (n�10) and C57BL/6 mice (n�6) wereused as control groups in the study.
USPIO Contrast AgentUSPIO MRI contrast agent, Ferumoxtran-10 (Combidex), waskindly provided by Advanced Magnetics Inc (Cambridge, Mass) andwas administered at a dose of 1000 �mol/kg via tail vein injectionadministered on 2 consecutive days, 24 hours apart, and initiated 2days before imaging (Figure 1).
In Vivo MRIAfter 21 days of infusion and 24 hours after the second USPIOinjection (Figure 1), the animals were anesthetized with a mixture ofoxygen and isoflurane (1% to 2%) anesthesia. Imaging was per-
formed using a 9.4 Tesla imaging system (vertical, 89 mm borediameter, Bruker Medical). Both respiratory and ECG signal weremonitored, and the ECG signal was used to trigger the MRI pulsesequence. The animal’s core body temperature was maintained byadjusting the water cooled gradient set to 37°C. During each imagingsession a series of transverse, sagittal, and coronal scout imagesthrough the heart (FLASH sequence, TR/TE�50/2.7 ms, FOV�3�3cm, matrix�128�128, slice thickness�0.5 mm, number of averag-es�4) were acquired. An oblique 2D Time Of Flight (TOF) imageslice was positioned such that the image slice would capture theentire aortic arch from the root to the left subclavian arterial branch.A final high-resolution image was acquired in CINE (FLASHsequence, TR/TE�12/2.8 ms, FOV�2.5�2.5 cm, matrix�256�256, slice thickness�1.0 mm, number of averages�8).
Ex Vivo MRITo provide optimal spatial resolution, ex vivo imaging of the plaqueassociated with the aortic root was performed on the same 9.4 Teslasystem used for the in vivo studies. The perfused fixed heart wasflushed with 0.2% Gd-DTPA (Magnevist, Berlex Labs) and high-resolution images were acquired through the entire root using atransverse multi-slice spin echo (TR/TE�2000/10 ms,FOV�10�10 mm, matrix�256�256, slice thickness�0.3 mm,number of averages�2) sequence.
Image AnalysisAll images were analyzed using Analyze AVW software (Ana-lyzeDirect). Images were reconstructed to 512 pixels�512 pixelsbefore semiautomated trace analysis. The in vivo image analysis wasperformed on the single oblique slice containing the aortic arch. Thedata are presented as the signal loss area (%) with respect to theentire aortic arch area defined from the root to the left subclavianartery. The in vivo MRI signal loss thresholding criteria wasdetermined for each aorta by selecting a ROI in a region of aortadevoid of signal loss. From the measured signal intensity in this ROI,a 95% confidence interval was determined (ie, �2�SD). Thisconfidence level was now used as the thresholding level by whichsignal loss area (�2�SD signal loss) was determined. The ROItracing of the aorta remained similar for each aorta. All ex vivo aorticroot plaque volume measurements were performed by analyzing theregion of plaque deposition at the level of the aortic valve and theslice immediately cranial and caudal to it. Manually segmentedtracing of the aortic root plaque in all 3 slices was performed.
Blood Pressure, Histology, andAnalytical ProceduresPlease find these additional methods and materials in the online datasupplement section (http://atvb.ahajournals.org).
Statistical AnalysisAll data are expressed as mean�SEM. Survival curves were ana-lyzed using the Kaplan–Meier method. All other multiple compari-sons were made by ANOVA followed by a Tukey post hoc test. Allstatistical tests were performed using Prism software (GraphpadSoftware) and a value of P�0.05 was considered to be significant.
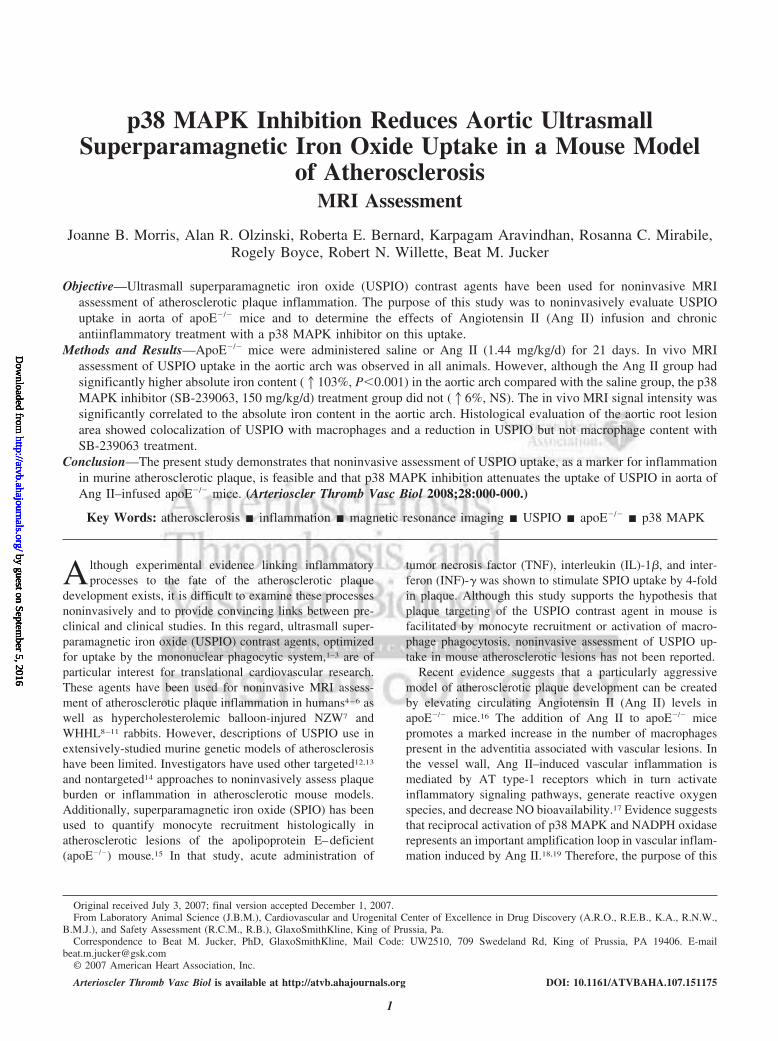
Day -7 Day 0 Day 18 Day 19 Day 20 Day 21 Day 22
•BeginSB-239063treatment
•ImplantInfusionPumps (Ang II orSaline)
•Indirect BloodPressure
•USPIO Injection
•USPIO Injection
•In Vivo MRI•Blood andTissue Collection
- Aorta removedfor absolute iron content analysis
- Heart removed for ex vivo MRI and histology
•Ex Vivo MRIof heart
Figure 1. Experimental study design. Dietary dos-ing of SB-239063 (150 mg/kg/d) was initiated 7days before either Saline or Ang II administrationvia osmotic minipump. Indirect blood pressurewas assessed on Day 18. Combidex (1000 �mol/kg/min) was administered on Day 19 and 20 ofAng II infusion, and animals were imaged on Day21. Tissue and blood were harvested on comple-tion of imaging on Day 21. The aorta wasremoved and analyzed for absolute iron content,and the heart was removed and examined by exvivo MRI on Day 22. Ater ex vivo MRI, heartswere sectioned for histological evaluation.
2 Arterioscler Thromb Vasc Biol February 2008
by guest on September 5, 2016
http://atvb.ahajournals.org/D
ownloaded from
ResultsPhysiology and PharmacokineticsThere were no differences in food consumption between thegroups throughout the duration of the study, and all groupsshowed a slight loss in body weight by the end of study(�1.4�0.4, �2.9�0.8, �2.7�1.5 g in Saline, Ang II, andAng II � SB-239063 groups, respectively). There was a 30%to 44% incidence of morbidity/mortality in the Ang IIadministered animals over the 21-day period, and there wasno effect of treatment on survival. The majority of deaths (5of 7) were attributable to rupture of the thoracic aorta(observed at necropsy). Blood pressure, measured on day 18,did not differ among groups. Additionally, there were nodifferences in plasma lipids (total cholesterol, HDL, LDL,and triglycerides) at the end of study (Table). The plasmaconcentration of SB-239063 at the end of study (479�62ng/mL; �1 �mol/L) was similar to efficacious concentrationsin a previous rodent cardiovascular study.20
Plasma CytokinesA variety of inflammatory cytokines (IL-1�, IL-1�, TNF-�,IL-6, G colony stimulating factor [CSF], MCP-1, MIP-1�,etc) were examined in plasma samples obtained from allgroups at the end of study. Only MCP-1 and MIP-1� wereincreased by Ang II infusion (Table). The significant eleva-tion of MCP-1 in the Ang II group (43.2�8.6 pg/mL) versusthe Saline group (24.7�1.7 pg/mL, P�0.05) was blunted inthe Ang II�SB-239063 treatment group (34.5�6.0 pg/mL).Additionally, SB-239063 treatment prevented the increase inMIP-1� observed in the Ang II group (20.3�2.7, 62.1�15.1,and 27.4�2.7 pg/mL in Ang II�SB-239063, Ang II, andSaline groups, respectively; P�0.01).
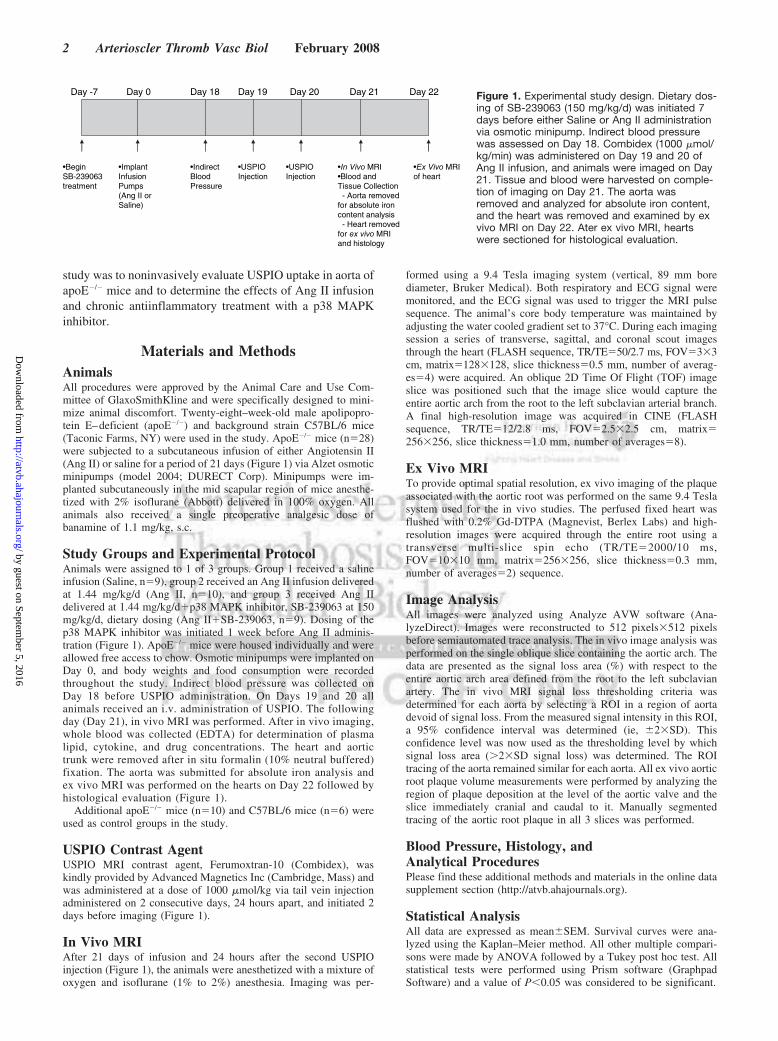
In Vivo MRI and Fe Analysis2D white blood, TOF, images that captured the aortic archincluding the aortic root, ascending, and the proximal de-scending aorta are shown in Figure 2A and 2B. In an apoE�/�
mouse that had not received any USPIO, the signal intensityof the arch is homogeneous and bright (Figure 2A). Figure 2Billustrates the nature of the focal signal loss regions associ-ated with USPIO deposition in atherosclerotic plaque regionsof the aorta in an apoE�/� mouse that had received USPIO.Figure 2C and 2D illustrates a transverse slice orientationthrough the aortic root at the level of the valves in represen-tative mice that did not receive or did receive USPIO,respectively. The signal loss region in the root was homoge-neous and represented a significant area of the root that wasassociated with atherosclerotic plaque burden. Because of thepromiscuous nature of macrophage deposition into regionsoutside of the vasculature including in the mediastinal lymphnode and attributable to the “blooming” nature of signal loss
Table. Plasma Lipid and Cytokine Profile at End of Study
Saline Ang II Ang II�SB-239063
Cholesterol, mg/dL 554�31 619�42 607�21
HDL, mg/dL 7�1 8�1 9�1
LDL, mg/dL 57�6 63�7 57�4
Triglycerides, mg/dL 63�5 73�12 86�16
MCP-1, pg/ml 24.7�1.7 43.2�8.6* 34.5�6.0
MIP-1�, pg/ml 27.4�2.7 62.1�15.1† 20.3�2.7
Plasma lipids and cytokines were measured in apoE�/� mice after 21 daysof Saline or Ang II administration. Data are presented as mean�SEM. *P�0.05vs Saline, †P�0.01 vs Saline and Ang II�SB-239063 groups.
Figure 2. In vivo imaging of the aorta in anAng II–infused apoE�/� mouse. Bright bloodTOF imaging was performed such that a 2Doblique slice was obtained through the aor-tic arch (A, B) and aortic root (C, D). Repre-sentative images from both control(�USPIO) (A, C) as well as (�USPIO) (B, D)administered mice are shown. In some invivo images of the aorta, signal loss wasdetected in the pulmonary artery (B) whichwas likely attributable to the susceptibilityartifact because of the significant ironuptake in the plaque from the lesser curva-ture of the aorta.
Morris et al p38 MAPK Inhibition Reduces Aortic USPIO Uptake 3
by guest on September 5, 2016
http://atvb.ahajournals.org/D
ownloaded from
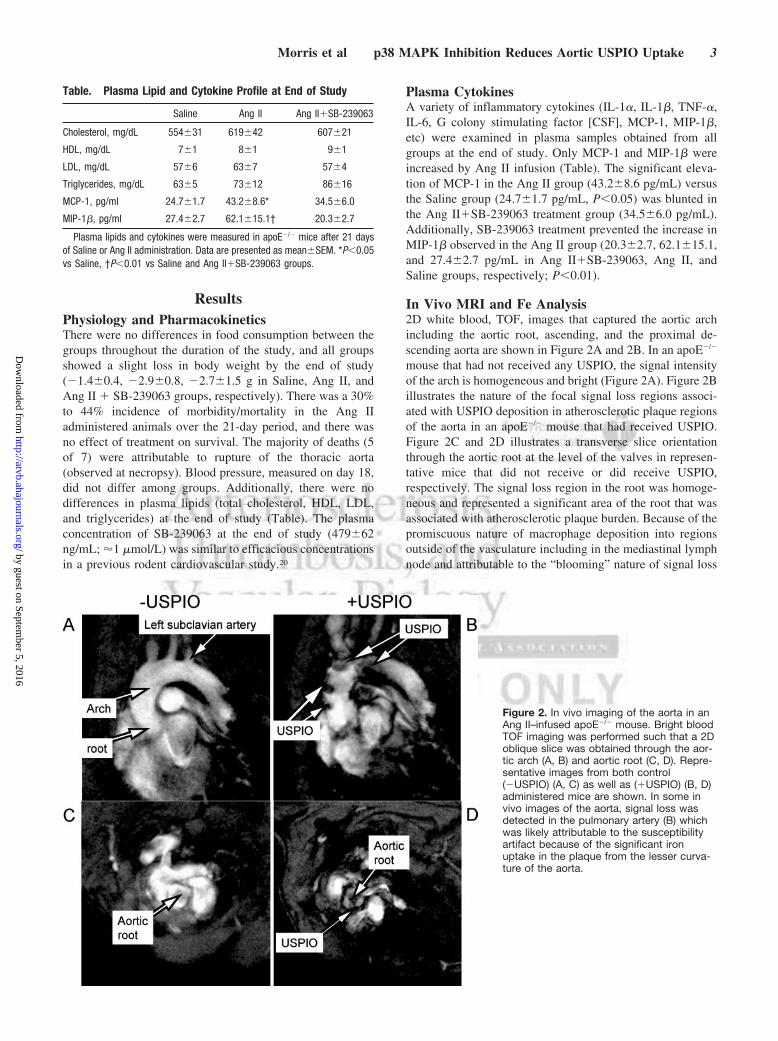
arising from USPIO particles, a group of C57BL/6 mice wereadministered USPIO and imaged to determine the degree ofsignal loss obtained in nonatherosclerotic aortas. Imageanalysis was performed by tracing the aortic arch from thelevel of the aortic root to the left subclavian artery. Thepercent signal loss area, using a signal loss threshold of �2� SDof blood pool signal intensity, in this region is shown inFigure 3A. Using this thresholding criteria, 2 groups ofcontrol mice (apoE�/��USPIO and C57BL/6�USPIO)showed minimal signal loss (3�1 and 5�3%, respectively).Although Ang II administration resulted in a 36�7% signalloss compared with saline administration (19�4% signalloss), Ang II�SB-239063 administration resulted in a nor-malization of the in vivo MRI signal loss (21�3% signal loss,P�0.05). The absolute iron in the aortic arch was measuredas a surrogate measure of USPIO deposition (Figure 3B). Theabsolute iron content in the aortas from the control mice(apoE�/��USPIO and C57BL/6�USPIO) was relatively low(178�25 and 165�65 ppm, respectively). The Ang II group(729�107 ppm) had a significantly higher iron level in theaortic arch compared with the Saline group (358�33 ppm,P�0.001). However, the Ang II�SB-239063 group had asignificantly lower Fe content (380�74 ppm, P�0.001)which was comparable to the Saline group. Additionally,there was a significant correlation between the absolute iron
content of the aortic arch and the proportion of in vivo MRIsignal intensity loss present in the aortic arch (r�0.80,P�0.001; Figure 3C) indicating that the in vivo imageanalysis was sensitive to differences in aortic uptake. Therewas significant adventitial hypertrophy that was present in theaortic arch on gross inspection in the Ang II–administeredmice. However, SB-239063 treatment resulted in a normal-ization of the aortic arch wet weight (3.0�0.1, 4.8�0.6, and3.2�0.5 mg in the Saline, Ang II, and Ang II � SB-239063groups respectively, P�0.05).
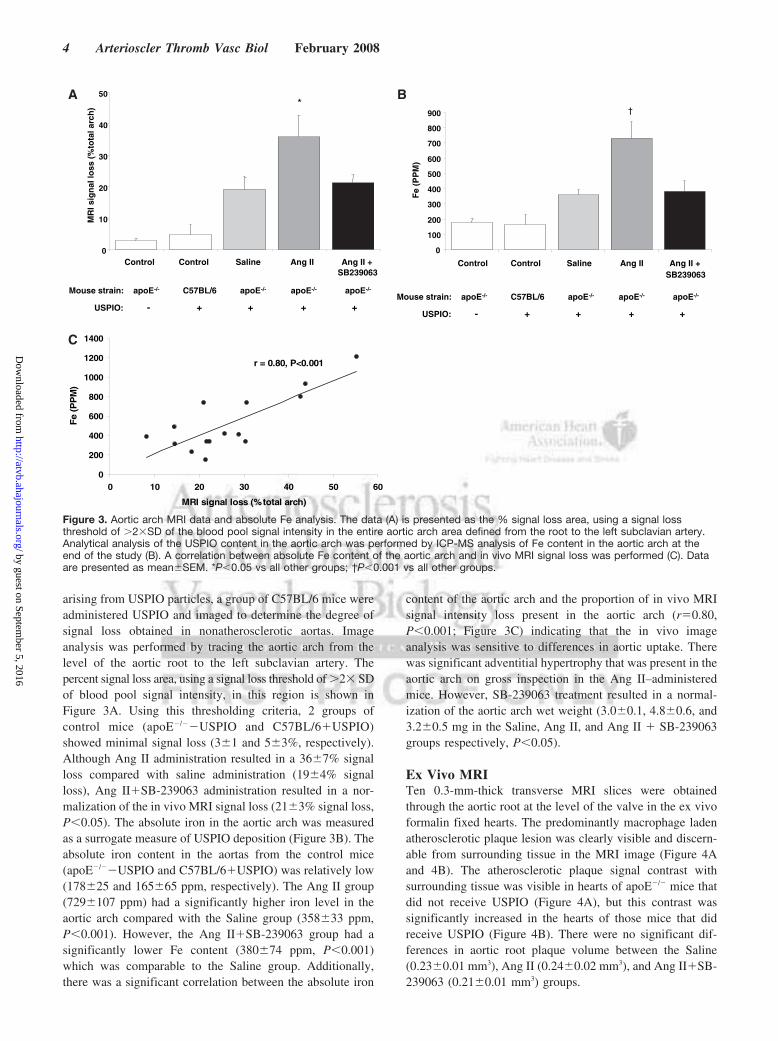
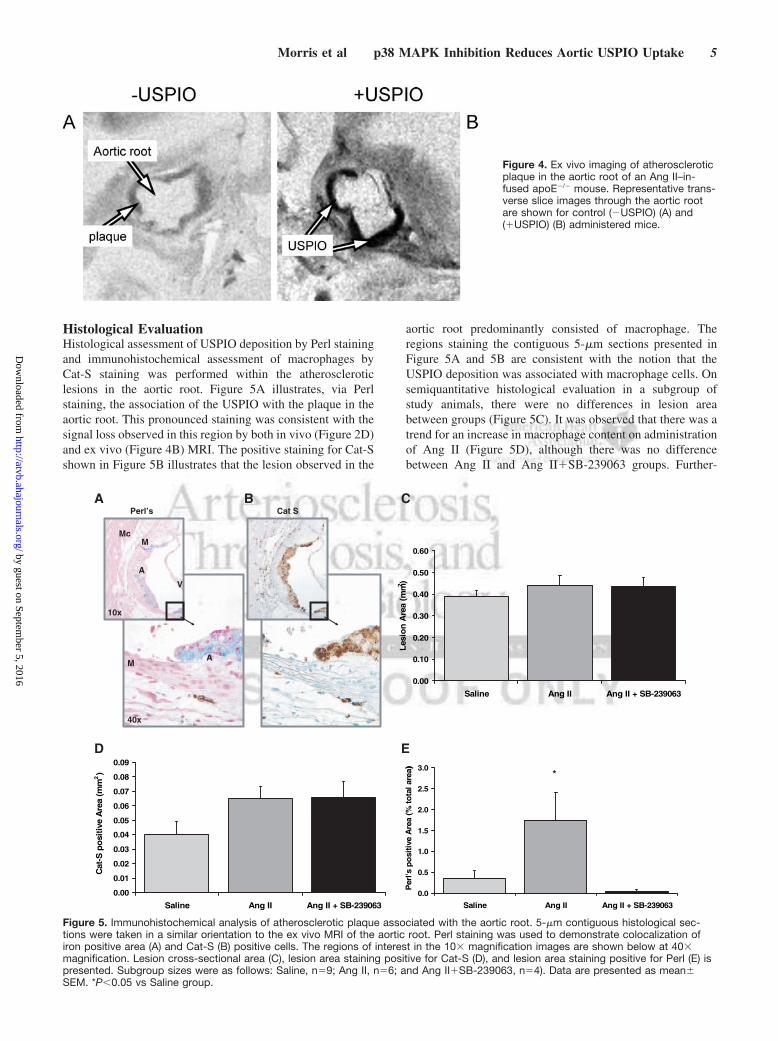
Ex Vivo MRITen 0.3-mm-thick transverse MRI slices were obtainedthrough the aortic root at the level of the valve in the ex vivoformalin fixed hearts. The predominantly macrophage ladenatherosclerotic plaque lesion was clearly visible and discern-able from surrounding tissue in the MRI image (Figure 4Aand 4B). The atherosclerotic plaque signal contrast withsurrounding tissue was visible in hearts of apoE�/� mice thatdid not receive USPIO (Figure 4A), but this contrast wassignificantly increased in the hearts of those mice that didreceive USPIO (Figure 4B). There were no significant dif-ferences in aortic root plaque volume between the Saline(0.23�0.01 mm3), Ang II (0.24�0.02 mm3), and Ang II�SB-239063 (0.21�0.01 mm3) groups.
USPIO: - + + + +
Mouse strain: apoE-/- C57BL/6 apoE-/- apoE-/- apoE-/-
0
10
20
30
40
50
Control Control Saline Ang II Ang II +SB239063
MR
I sig
nal
loss
(%
tota
l arc
h) *
USPIO: - + + + +
Mouse strain: apoE-/- C57BL/6 apoE-/- apoE-/- apoE-/-
†
0
100
200
300
400
500
600
700
800
900
Control Control Saline Ang II Ang II +SB239063
Fe
(PP
M)
r = 0.80, P<0.001
0
200
400
600
800
1000
1200
1400
0 10 20 30 40 50 60
MRI signal loss (%total arch)
Fe
(PP
M)
A
C
B
Figure 3. Aortic arch MRI data and absolute Fe analysis. The data (A) is presented as the % signal loss area, using a signal lossthreshold of �2�SD of the blood pool signal intensity in the entire aortic arch area defined from the root to the left subclavian artery.Analytical analysis of the USPIO content in the aortic arch was performed by ICP-MS analysis of Fe content in the aortic arch at theend of the study (B). A correlation between absolute Fe content of the aortic arch and in vivo MRI signal loss was performed (C). Dataare presented as mean�SEM. *P�0.05 vs all other groups; †P�0.001 vs all other groups.
4 Arterioscler Thromb Vasc Biol February 2008
by guest on September 5, 2016
http://atvb.ahajournals.org/D
ownloaded from
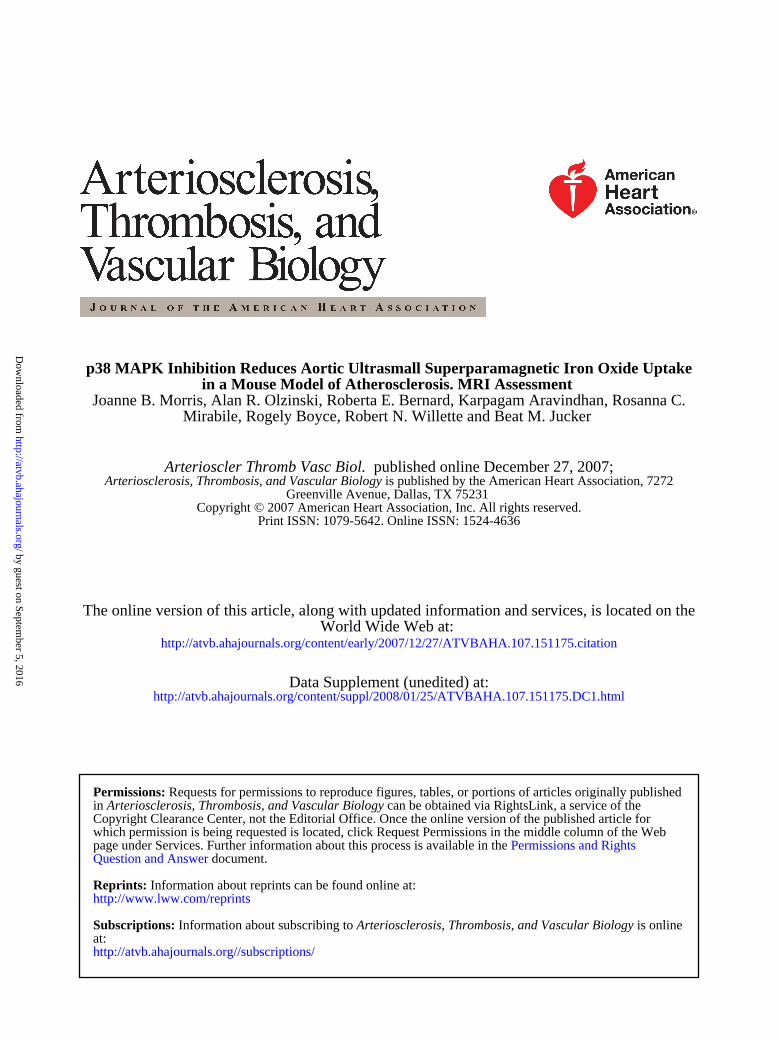
Histological EvaluationHistological assessment of USPIO deposition by Perl stainingand immunohistochemical assessment of macrophages byCat-S staining was performed within the atheroscleroticlesions in the aortic root. Figure 5A illustrates, via Perlstaining, the association of the USPIO with the plaque in theaortic root. This pronounced staining was consistent with thesignal loss observed in this region by both in vivo (Figure 2D)and ex vivo (Figure 4B) MRI. The positive staining for Cat-Sshown in Figure 5B illustrates that the lesion observed in the
aortic root predominantly consisted of macrophage. Theregions staining the contiguous 5-�m sections presented inFigure 5A and 5B are consistent with the notion that theUSPIO deposition was associated with macrophage cells. Onsemiquantitative histological evaluation in a subgroup ofstudy animals, there were no differences in lesion areabetween groups (Figure 5C). It was observed that there was atrend for an increase in macrophage content on administrationof Ang II (Figure 5D), although there was no differencebetween Ang II and Ang II�SB-239063 groups. Further-
Figure 4. Ex vivo imaging of atheroscleroticplaque in the aortic root of an Ang II–in-fused apoE�/� mouse. Representative trans-verse slice images through the aortic rootare shown for control (�USPIO) (A) and(�USPIO) (B) administered mice.
Perl’s Cat S
10x
40x
V
M
A
Mc
MA
0.00
0.10
0.20
0.30
0.40
0.50
0.60
Saline Ang II Ang II + SB-239063
mm(
aerA
noise
L2 )
0.00
0.01
0.02
0.03
0.04
0.05
0.06
0.07
0.08
0.09
Saline Ang II Ang II + SB-239063
mm(
aerA
evitiso
pS-ta
C2)
0.0
0.5
1.0
1.5
2.0
2.5
3.0
Saline Ang II Ang II + SB-239063
)a)eralatot
%(aer
Aevitis
op
s'lreP
*
A
D E
B C
Figure 5. Immunohistochemical analysis of atherosclerotic plaque associated with the aortic root. 5-�m contiguous histological sec-tions were taken in a similar orientation to the ex vivo MRI of the aortic root. Perl staining was used to demonstrate colocalization ofiron positive area (A) and Cat-S (B) positive cells. The regions of interest in the 10� magnification images are shown below at 40�magnification. Lesion cross-sectional area (C), lesion area staining positive for Cat-S (D), and lesion area staining positive for Perl (E) ispresented. Subgroup sizes were as follows: Saline, n�9; Ang II, n�6; and Ang II�SB-239063, n�4). Data are presented as mean�SEM. *P�0.05 vs Saline group.
Morris et al p38 MAPK Inhibition Reduces Aortic USPIO Uptake 5
by guest on September 5, 2016
http://atvb.ahajournals.org/D
ownloaded from

more, whereas the area staining positive for iron increased inthe Ang II group (P�0.05), this area was attenuated withSB-239063 treatment (Figure 5E).
DiscussionThe present study demonstrates that noninvasive assessmentof USPIO contrast agent uptake, used as an imaging markerof atherosclerotic plaque inflammation, is feasible in apoE�/�
mice administered Ang II. Additionally, although numerousinvestigators have evaluated USPIO uptake in both animal7–10
and human4–6 atherosclerotic plaque noninvasively usingMRI, the present study is the first to demonstrate a reductionof USPIO uptake in aorta after chronic treatment with a novelantiinflammatory therapy.
In the present study chronic Ang II administration wasused to accelerate vascular inflammation in apoE�/� mice. Ashas previously been shown,21 Ang II had neither an effect onblood pressure nor on the plasma lipid profile in the presentstudy. However, there were profound effects of Ang IIadministration on the morbidity and mortality observed in thestudy. Additionally, all of the animals that died or weremoribund had evidence of aortic rupture or aneurysm forma-tion, respectively. These findings are not surprising asDaugherty et al21 have shown that a relatively short Ang II(1000 ng/kg/min) exposure duration (28 days) promotedrapid atherosclerotic lesion development in the aorta, with adiscernable morphology in the abdominal aorta consistentwith characteristics of an aneurysm (ie, medial rupture, grossmacrophage, and collagen deposition). Although we observeda 30% to 44% incidence of morbidity/mortality in the presentstudy, there was no benefit of the p38 MAPK inhibitor on thisparameter. In rodent models of end organ dysfunction, p38MAPK inhibitors have been shown to be extremely effectivein eliciting a survival benefit in part via promoting endothe-lial protection.20,22,23 However in the present study, the deathsin the Ang II infused apoE�/� mice were most likely attrib-utable to aneurysm rupture initiated by matrix metallopro-teinase (MMP)/chymase activation.21,24,25
Ang II has been shown to activate the p38 MAPK signalingpathway in a number of vascular cell types18,19,26 includingmacrophages,27 and is an important signaling pathway for therecruitment of leukocytes.28 Additionally, the p38 MAPKsystem plays an important role in vascular inflammation andremodeling particularly in the medial and adventitial laminaof blood vessels.27,29 The mechanism by which Ang IIregulates p38 MAPK signaling and promotes vascular in-flammation is, in part, related to activation of vascularNADPH oxidase (NOX). In a variety of cellular systems, AngII–mediated AT-type 1 receptor modulation activates NOXand generates superoxide anion required for redox-sensitiveactivation of p38 MAPK.19,26 Recent in vivo evidence sug-gests that activation of vascular NOX and p38 MAPK islikely to be a reciprocal event, ie, the generation of reactiveoxygen species (ROS) activates p38 MAPK which in turnsleads to further ROS production.30 In that study, the increasedvascular production of ROS and enhanced expression ofNOX induced by hypertensive doses of Ang II were abol-ished after chronic treatment with a p38 MAPK inhibitor.Once activated, proinflammatory p38 MAPK–dependent pro-
cesses, ie, production of adhesion molecules (ie, vascular celladhesion molecule [VCAM]-1, intercellular adhesion mole-cule [ICAM]-1), chemokines (ie, MCP-1, MIP-1�) and cy-tokines (ie, IL-1, TNF-�), can contribute to monocyte recruit-ment, macrophage activation, and vascular remodeling.17,27,28
In addition, elevated ROS generation may also contribute tofurther oxidation of lipoproteins and reduced bioavailabilityof nitric oxide, both of which contribute to the developmentof atherosclerosis.31 Taken together, these observations sug-gest that p38 MAPK inhibitors reduce USPIO uptake inatherosclerotic plaque by reducing vascular inflammation.
Although the percent MRI signal loss area detected in theaortic arch of the Ang II�SB-239063 group was reducedversus the Ang II group and normalized to the Saline groupconsistent with the notion that there was decreased aorticlesion associated with the p38 MAPK inhibitor treatment, onecannot rule out the distinct possibility that a difference inmacrophage phagocytic activity rather than a difference in thenumber of macrophage present was responsible for thisobservation. There was no reduction in the Cat-S staining formacrophage while the Perl iron staining for USPIO wasreduced on p38 MAPK inhibition in the aortic root lesion inthe present study. Therefore the results suggest that the p38MAPK inhibitor treatment reduced phagocytic activity of theresident macrophages. USPIO phagocytosis by macrophagehas been shown in part to be facilitated via ScavengerReceptor-A (SR-A),3 and p38 MAPK inhibition reducesSR-A expression on Toll-like receptor stimulation in macro-phages.32,33 However, it has been shown that Ang II admin-istration to apoE�/� mice results in preferential promotion oflesion development in the aorta rather than in the aortic root.34
Indeed, there was no promotion of aortic root lesion devel-opment in the presence of Ang II assessed in the presentstudy. Although we did not have a quantitative readout ofatherosclerotic lesion development in the aorta because of thelogistics of the study (ie, ICPMS analysis of aorta), on grossinspection the wet weight of the aorta was significantlyelevated after Ang II administration and normalized with p38MAPK inhibitor treatment. However, it is not clear whetherthe increased adventitial hypertrophy or increased atheromadevelopment in the aorta was responsible for these dynamicchanges after Ang II administration. Additionally, Ang IIinfusion in the absence of USPIO administration did notincrease iron deposition in the aorta (data not shown).Therefore medial rupture of the vessel and thrombus devel-opment in the area of interest as a consequence of Ang IIadministration21 was not likely to have occurred as this wouldhave increased the absolute iron content measured.
In summary, the present study illustrates for the first timethat noninvasive MR imaging using USPIO as a contrastagent to target macrophage cells can be applied to a mouseatherosclerosis model. In addition, an antiinflammatory, ex-perimental therapeutic agent was beneficial in reducing thevascular uptake of the USPIO agent. These findings areunique and may reflect an exciting new opportunity fornoninvasive evaluation of therapeutic agents targeting mac-rophage presence or activity in the clinic.
6 Arterioscler Thromb Vasc Biol February 2008
by guest on September 5, 2016
http://atvb.ahajournals.org/D
ownloaded from

AcknowledgmentsWe thank Amy Grill for her expert technical assistance in handlingthe animals.
DisclosuresNone.
References1. Zimmer C, Weissleder R, Poss K, Bogdanova A, Wright SC, Enochs WS.
MR imaging of phagocytosis in expiremental gliomas. Radiology. 1995;197:533–538.
2. Dardzinski BJ, Schmithorst VJ, Holland SK, Biovin GP, Imagawa T,Watanabe S, Lewis JM, Hirsch R. MR imaging of murine arthritis usingultrasmall superparamagnetic iron oxide particles. Magnetic ResonanceImaging. 2001;19:1209–1216.
3. Raynal I, Prigent P, Peyramaure S, Najid A, Rebuzzi C, Corot C. Mac-rophage endocytosis of superparamagnetic iron oxide nanoparticles:mechanisms and comparison of ferumoxides and ferumoxtran-10. InvestRadiol. 2004;39:56–63.
4. Schmitz SA, Taupitz M, Wagner S, Wolf KJ, Beyersdorff D, Hamm B.Magnetic resonance imaging of atherosclerotic plaques using superpara-magnetic iron oxide particles. J Magn Reson Imaging. 2001;14:355–361.
5. Kooi ME, Cappendijk VC, Cleutjens KB, Kessels AG, Kitslaar PJ,Borgers M, Frederik PM, Daemen MJ, van Engelshoven JM. Accumu-lation of ultrasmall superparamagnetic particles of iron oxide in humanatherosclerotic plaques can be detected by in vivo magnetic resonanceimaging. Circulation. 2003;107:2453–2458.
6. Trivedi RA, Mallawarachi C, U-King-Im JM, Graves MJ, Horsley J,Goddard MJ, Brown A, Wang L, Kirkpatrick PJ, Brown J, Gillard JH.Identifying inflamed carotid plaques using in vivo USPIO-enhanced MRimaging to label plaque macrophages. Arterioscler Thromb Vasc Biol.2006;26:1601–1606.
7. Yancy AD, Olzinski AR, Hu TC, Lenhard SC, Aravindhan K, GruverSM, Jacobs PM, Willette RN, Jucker BM. Differential uptake offerumoxtran-10 and ferumoxytol, ultrasmall superparamagnetic ironoxide contrast agents in rabbit: critical determinants of atheroscleroticplaque labeling. J Magn Reson Imaging. 2005;21:432–442.
8. Hyafil F, Laissy JP, Mazighi M, Tchetche D, Louedec L, Adle-BiassetteH, Chillon S, Henin D, Jacob MP, Letourneur D, Feldman LJ.Ferumoxtran-10-enhanced MRI of the hypercholesterolemic rabbit aorta:relationship between signal loss and macrophage infiltration. ArteriosclerThromb Vasc Biol. 2006;1:176–181.
9. Schmitz SA, Coupland SE, Gust R, Winterhalter S, Wagner S, Kresse M,Semmler W, Wolf KJ. Superparamagnetic iron oxide-enhanced MRI ofatherosclerotic plaques in Watanabe hereditable hyperlipidemic rabbits.Invest Radiol. 2000;35:460–471.
10. Ruehm SG, Corot C, Vogt P, Kolb S, Debatin JF. Magnetic resonanceimaging of atherosclerotic plaque with ultrasmall superparamagnetic par-ticles of iron oxide in hyperlipidemic rabbits. Circulation. 2001;103:415–422.
11. Herborn CU, Vogt FM, Lauenstein TC, Dirsch O, Corot C, Robert P,Ruehm SG. Magnetic resonance imaging of experimental atheroscleroticplaque: comparison of two ultrasmall superparamagnetic particles of ironoxide. J Magn Reson Imaging. 2006;24:388–393.
12. Nahrendorf M, Jaffer FA, Kelly KA, Sosnovik DE, Aikawa E, Libby P,Weissleder R. Noninvasive vascular cell adhesion molecule-1 imagingidentifies inflammatory activation of cells in atherosclerosis. Circulation.2006;114:1504–1511.
13. Amirbekian V, Lipinski MJ, Briley-Saebo KC, Amirbekian S, AguinaldoJG, Weinreb DB, Vucic E, Frias JC, Hyafil F, Mani V, Fisher EA, FayadZA. Detecting and assessing macrophages in vivo to evaluate atheroscle-rosis noninvasively using molecular MRI. Proc Natl Acad Sci U S A.2007;104:961–966.
14. Jaffer FA, Nahrendorf M, Sosnovik D, Kelly KA, Aikawa E, WeisslederR. Cellular imaging of inflammation in atherosclerosis using magnet-ofluorescent nanomaterials. Mol Imaging. 2006;5:85–92.
15. Litovsky S, Madjid M, Zarrabi A, Casscells W, Willerson JT, Naghavi M.Superparamagnetic iron oxide-based method for quantifying recruitmentof monocytes to mouse atherosclerotic lesions in vivo. Circulation. 2003;107:1545–1549.
16. Nobuhiko A, Suganuma E, Babaev VR, Fogo A, Swift LL, Linton MF,Fazio S, Ichikawa I, Kon V. Angiotensin II amplifies macrophage-drivenatherosclerosis. Aterioscler Thromb Vasc Biol. 2004;24:2143–2148.
17. Allan R. Brasier, Adrian Recinos, III; Mohsen S Eledrisi. Vascularinflammation and the renin-angiotensin system. Arterioscler ThrombVasc Biol. 2002;22:1257–1266.
18. Ushio-Fukai M, Alexander RW, Akers M, Griendling KK. p38 mitogen-activated protein kinase is a critical component of the redox-sensitivesignaling pathways activated by angiotensin II. J Biol Chem. 1998;273:15022–15029.
19. Viedt C, Soto U, Krieger-Brauer HI, Fei J, Elsing C, Kubler W, KreuzerJ. Differential activation of mitogen-activated protein kinases in smoothmuscle cells by angiotensin II: involvement of p22phox and reactiveoxygen species. Arterioscler Thromb Vasc Biol. 2000;20:940–948.
20. Behr TM, Nerurkar SS, Nelson AH, Coatney RW, Woods TN, SulpizioA, Chandra S, Brooks DP, Kumar S, Lee JC, Ohlstein EH, AngermannCE, Adams JL, Sisko J, Sackner-Bernstien JD, Willette RN. Hypertensiveend-organ damage and premature mortality are p38 mitogen-activatedprotein kinase-dependant in a rat model of cardiac hypertrophy anddysfunction. Circulation. 2001;104:1292–1298.
21. Daugherty A, Manning MW, Cassis LA. Angiotensin II promotes ath-erosclerotic lesions and aneurysms in apolipoprotein E-deficient mice.J Clin Invest. 2000;105:1605–1612.
22. Ju H, Behm DJ, Nerurkar S, Eybye ME, Haimbach RE, Olzinski AR,Douglas SA, Willette RN. p38 MAPK inhibitors ameliorate target organdamage in hypertension: Part 1. p38 MAPK-dependent endothelial dys-function and hypertension. J Pharmacol Exp Ther. 2003;307:932–938.
23. Olzinski AR, McCafferty TA, Zhao SQ, Behm DJ, Eybye ME,Maniscalco K, Bentley R, Frazier KS, Milliner CM, Mirabile RC,Coatney RW, Willette RN. Hypertensive target organ damage isattenuated by a p38 MAPK inhibitor: role of systemic blood pressure andendothelial protection. Cardiovasc Res. 2005;66:170–178.
24. Daugherty A, and Cassis L. Angiotensin II-mediated development ofvascular disease. Trends Cardiovasc Med. 2004;14:117–120.
25. Manning MW, Cassis LA, Daugherty A. Differential effects of doxy-cycline, a broad-spectrum matrix metalloproteinase inhibitor, on angio-tensin II-induced atherosclerosis and abdominal aortic aneurysms.Arterioscler Thromb Vasc Biol. 2003;23:483–488.
26. El Bekay R, Alvarez M, Monteseirin J, Alba G, Chacon P, Vega A,Martin-Nieto J, Jimenez J, Pintado E, Bedoya FJ, Sobrino F. Oxidativestress is a critical mediator of the angiotensin II signal in human neu-trophils: involvement of mitogen-activated protein kinase, calcineurin,and the transcription factor NF-kappaB. Blood. 2003;102:662–671.
27. Ju H, Nerurkar S, Sauermelch CF, Olzinski AR, Mirabile R, ZimmermanD, Lee JC, Adams J, Sisko J, Berova M, Willette RN. Sustained acti-vation of p38 mitogen-activated protein kinase contributes to the vascularinjury response. The Journal of Pharmacology and ExperimentalTherapeutics. 2002;301:15–20.
28. Herlaar E, Brown Z. p38 MAPK signalling cascades in inflammatorydisease. Mol Med Today. 1999;10:439–447.
29. Zhan Y, Kim S, Izumi Y, Izumiya Y, Nakao T, Miyazaki H, Iwao H. Roleof JNK, p38, and ERK in platelet-derived growth factor-induced vascularproliferation, migration, and gene expression. Arterioscler Thromb VascBiol. 2003;23:795–801.
30. Bao W, Behm DJ, Nerurkar SS, Ao Z, Bentley R, Mirabile RC, JohnsDG, Woods TN, Doe CPA, Coatney RW, Ohlstein JF, Douglas SA,Willette RN, Yue T-L. Effects of p38 MAPK inhibitor on angiotensin II –dependent hypertension, organ damage and superoxide anion production.J Cardiovasc Pharmacol. In press.
31. Galle J, Hansen-Hagge T, Wanner C, Seibold S. Impact of oxidized lowdensity lipoprotein on vascular cells. Atherosclerosis. 2006;185:219–226.
32. Xu WY, Wang L, Wang HM, Wang YQ, Liang YF, Zhao TT, Wu YZ.TLR2 and TLR4 agonists synergistically up-regulate SR-A in RAW264.7through p38. Mol Immunol. 2007;44:2315–2323.
33. Doyle SE, O’Connell RM, Miranda GA, Vaidya SA, Chow EK, Liu PT,Suzuki S, Suzuki N, Modlin RL, Yeh WC, Lane TF, Cheng G. Toll-likereceptors induce a phagocytic gene program through p38. J Exp Med.2004;199:81–90.
34. Zhou Y, Chen R, Catanzaro SE, Hu L, Dansky HM, Catanzaro DF.Differential effects of angiotensin II on atherogenesis at the aortic sinusand descending aorta of apolipoprotein-E-deficient mice. Am JHypertens. 2005;18:486–492.
Morris et al p38 MAPK Inhibition Reduces Aortic USPIO Uptake 7
by guest on September 5, 2016
http://atvb.ahajournals.org/D
ownloaded from
Mirabile, Rogely Boyce, Robert N. Willette and Beat M. JuckerJoanne B. Morris, Alan R. Olzinski, Roberta E. Bernard, Karpagam Aravindhan, Rosanna C.
in a Mouse Model of Atherosclerosis. MRI Assessmentp38 MAPK Inhibition Reduces Aortic Ultrasmall Superparamagnetic Iron Oxide Uptake
Print ISSN: 1079-5642. Online ISSN: 1524-4636 Copyright © 2007 American Heart Association, Inc. All rights reserved.
Greenville Avenue, Dallas, TX 75231is published by the American Heart Association, 7272Arteriosclerosis, Thrombosis, and Vascular Biology
published online December 27, 2007;Arterioscler Thromb Vasc Biol.
http://atvb.ahajournals.org/content/early/2007/12/27/ATVBAHA.107.151175.citationWorld Wide Web at:
The online version of this article, along with updated information and services, is located on the
http://atvb.ahajournals.org/content/suppl/2008/01/25/ATVBAHA.107.151175.DC1.htmlData Supplement (unedited) at:
http://atvb.ahajournals.org//subscriptions/
at: is onlineArteriosclerosis, Thrombosis, and Vascular Biology Information about subscribing to Subscriptions:
http://www.lww.com/reprints
Information about reprints can be found online at: Reprints:
document. Question and AnswerPermissions and Rightspage under Services. Further information about this process is available in the
which permission is being requested is located, click Request Permissions in the middle column of the WebCopyright Clearance Center, not the Editorial Office. Once the online version of the published article for
can be obtained via RightsLink, a service of theArteriosclerosis, Thrombosis, and Vascular Biologyin Requests for permissions to reproduce figures, tables, or portions of articles originally publishedPermissions:
by guest on September 5, 2016
http://atvb.ahajournals.org/D
ownloaded from
Materials and Methods Supplement
Blood Pressure Measurements
Indirect blood pressure was determined in isoflurane anesthetized mice via tail
cuff measurement using a non-invasive blood pressure system (Harvard Apparatus,
Holliston, MA) after 18 days of Ang II or saline infusion (Figure 1). Animals were
acclimated to the device for two days prior to collection and measurements were recorded
on the third day (Day 18). A total of five readings per animal were recorded and the
mean value for each individual was analyzed.
Histological Procedures
Histology was performed on 5 µm sections cut through the aortic root in the heart.
After sections were deparaffinized, rehydrated and placed in 0.05M Tris buffer (pH=7.6),
they were stained on a DAKO Autostainer (DAKO Corporation, Carpenteria, CA) using
reagents from the Catalyzed Signal Amplification system provided by DAKO. Sections
were incubated with a cathepsin-S (Cat-S) goat polyclonal antibody, a marker of
macrophage cells (Santa Cruz Biotechnology Inc, Santa Cruz, CA). Additional 5 µm
sections were placed in hydrochloric acid-potassium ferrocyanide working solution for 30
minutes and counterstained with nuclear fast red for the Perl’s iron staining.
Quantification of lesion size and staining was performed using the Image-Pro Plus
version 4.1 software (Media Cybernetics, Inc., MD). Data are reported as a mean
analysis of three sections per heart including the aortic valve. Co-registration of Cat-S
and Perl’s positive staining areas was assessed in serial sections of atherosclerotic lesion.
Analytical Procedures
Absolute iron content was measured in the same section of aortic arch that was
assessed by in vivo MRI via inductively coupled plasma-mass spectrometry (ICP-MS)
analysis (Elemental Research Inc., North Vancouver, Canada) on nitric acid digested
tissue extracts. The absolute iron content was normalized to the dry tissue weight and
reported in parts per million (ppm). Plasma lipids were measured using an Olympus
AU640 chemical analyzer (Olympus Optical Company, Melville, NY). Pharmacokinetic
analysis of SB-239063 was performed on whole blood and a 50:50 mixture of blood: H2O
was used for LC/MS/MS analysis. Plasma cytokine concentrations were measured using
a Bio-Plex Mouse 23-Plex Panel Cytokine Assay (Bio-Rad Laboratories, Inc., Hercules,
CA).