ozone therapy for the treatment of dental caries
TRANSCRIPT

Ozone therapy for the treatment of dental caries (Review)
Rickard GD, Richardson RJ, Johnson TM, McColl DC, Hooper L
This is a reprint of a Cochrane review, prepared and maintained by The Cochrane Collaboration and published in The Cochrane Library2004, Issue 3
http://www.thecochranelibrary.com
Ozone therapy for the treatment of dental caries (Review)
Copyright © 2008 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

T A B L E O F C O N T E N T S
1HEADER . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
1ABSTRACT . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
2PLAIN LANGUAGE SUMMARY . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
2BACKGROUND . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
3OBJECTIVES . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
3METHODS . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
4RESULTS . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
6DISCUSSION . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
8AUTHORS’ CONCLUSIONS . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
8ACKNOWLEDGEMENTS . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
9REFERENCES . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
13CHARACTERISTICS OF STUDIES . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
21DATA AND ANALYSES . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
21ADDITIONAL TABLES . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
22APPENDICES . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
23WHAT’S NEW . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
23HISTORY . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
23CONTRIBUTIONS OF AUTHORS . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
23DECLARATIONS OF INTEREST . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
24SOURCES OF SUPPORT . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
24INDEX TERMS . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
iOzone therapy for the treatment of dental caries (Review)
Copyright © 2008 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

[Intervention Review]
Ozone therapy for the treatment of dental caries
George David Rickard1 , Robin J Richardson2 , Trevor M Johnson3, David C McColl4, Lee Hooper5
1Dorking, UK. 2Sutton Coldfield, UK. 3Yorkshire Area, Faculty of General Dental Practice, York, UK. 4Dental Surgery, Govan Hill
Health Centre, Glasgow, UK. 5School of Medicine, Health Policy & Practice, University of East Anglia, Norwich, UK
Contact address: George David Rickard, Old Sandstone Dental Practice, The Chine, Dorking, Surrey, RH4 1QT, UK.
Editorial group: Cochrane Oral Health Group.
Publication status and date: Edited (no change to conclusions), published in Issue 4, 2008.
Review content assessed as up-to-date: 13 May 2004.
Citation: Rickard GD, Richardson RJ, Johnson TM, McColl DC, Hooper L. Ozone therapy for the treatment of dental caries.
Cochrane Database of Systematic Reviews 2004, Issue 3. Art. No.: CD004153. DOI: 10.1002/14651858.CD004153.pub2.
Copyright © 2008 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.
A B S T R A C T
Background
Dental caries is a bacterially mediated disease characterised by demineralisation of the tooth surface, which may lead to cavitation,
discomfort, pain and eventual tooth loss. Ozone is toxic to certain bacteria in vitro and it has been suggested that delivering ozone
into a carious lesion might reduce the number of cariogenic bacteria. This possibly could arrest the progress of the lesion and may,
in the presence of fluoride, perhaps allow remineralisation to occur. This may in turn delay or prevent the need for traditional dental
conservation by ’drilling and filling’.
Objectives
To assess whether ozone is effective in arresting or reversing the progression of dental caries.
Search methods
We searched the Cochrane Oral Health Group’s Trials Register (to 7 November 2003); Cochrane Central Register of Controlled
Trials (CENTRAL) (The Cochrane Library 2003, Issue 3); MEDLINE and PREMEDLINE (OVID) (1966 to November 2003);
EMBASE (OVID) (1980 to November 2003); CINAHL (OVID) (1982 to November 2003); AMED (OVID) (1985 to November
2003). Quintessence was handsearched through 2002 and KaVo were contacted as manufacturers of the HealOzone apparatus for any
additional published or unpublished trials.
Selection criteria
Inclusion was assessed independently by at least two reviewers. Trials were only included if they met the following criteria: randomisation
in a controlled trial; single surface in vivo carious lesion accessible to ozone application; clear allocation concealment; ozone application
to the lesions in the intervention group; no such application of ozone in the control group; outcomes measured after at least 6 months.
Data collection and analysis
Reviewers independently extracted information in duplicate. A paucity of comparable data did not allow meta-analytic pooling of the
included studies.
1Ozone therapy for the treatment of dental caries (Review)
Copyright © 2008 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Main results
Three trials were included, with a combined total of 432 randomised lesions (137 participants). Forty-two conference papers, abstracts
and posters were excluded (from an unknown number of studies). The risk of bias in all studies appeared high. The analyses of all
three studies were conducted at the level of the lesion, which is not independent of the person, for this reason pooling of data was
not appropriate or attempted. Individual studies showed inconsistent effects of ozone on caries, across different measures of caries
progression or regression. Few secondary outcomes were reported, but one trial reported an absence of adverse events.
Authors’ conclusions
Given the high risk of bias in the available studies and lack of consistency between different outcome measures, there is no reliable
evidence that application of ozone gas to the surface of decayed teeth stops or reverses the decay process. There is a fundamental need
for more evidence of appropriate rigour and quality before the use of ozone can be accepted into mainstream primary dental care or
can be considered a viable alternative to current methods for the management and treatment of dental caries.
P L A I N L A N G U A G E S U M M A R Y
Ozone therapy for the treatment of dental caries
There is no evidence that ozone therapy can reverse or stop tooth decay.
Tooth decay can be painful, is expensive to treat and can lead to the loss of teeth. It has been suggested that treatment of a decayed
tooth with ozone will stop or reverse the decay process. This review of trials found no sound evidence that ozone is capable of reversing
or stopping the progression of tooth decay. High quality research is needed to show whether or not it works. Ozone should not be
considered an alternative to current treatment methods in dental practices.
B A C K G R O U N D
Dental caries is a multifactorial, bacteriologically mediated,
chronic disease that can damage the dentition of both children
and adults. Caries is widespread across all cultural groups and is
one of the most common diseases to affect the world’s population
(WHO 1990). Tooth decay accounts for almost half of all dental
extractions in the UK (NHS CRD 1999). However, patterns of
dental disease in the UK are changing (Kelly 2000), with less decay
being experienced by younger age groups. In the next two decades
there is likely to be a corresponding change in patterns of den-
tal treatment. The demand for traditional restorative treatment
(drilling and filling) may fall if preventive care is embraced or may
increase with the average age of the population as people retain
more disease susceptible teeth into older age. There has already
been a change in treatment philosophy. The emphasis in treatment
planning has shifted from the restoration of carious teeth to the
prevention of decay with minimal intervention. The early cari-
ous lesion is reversible (Silverstone 1983), a dynamic equilibrium
between demineralisation and remineralisation especially in the
presence of fluoride (Marinho 2002A; Marinho 2002B; Marinho
2003). Dental caries should be managed by preventive treatment
to encourage the remineralisation of non-cavitated lesions and the
need for restorative treatment can then be delayed or minimised
(Burke 2003).
Much of the research into dental caries diagnosis and manage-
ment has been inadequate. Current clinical diagnosis of caries in
practice is commonly subjective and new diagnostic tools have
not been widely embraced due to a variety of reasons, cost, lack
of familiarity and training, resistance to change, lack of validity,
specificity and reliability (NIHC statement 2001; Bader 2001).
Recent government policy outlined in ’Modernising NHS Den-
tistry - Options for Change’ (Options for Change) introduced a
mandate to promote novel or innovative methods to treat tooth
decay in the UK population. Drilling has always been associated
with some patient trepidation or fearfulness, but failure to inter-
vene may allow further progression towards the pulp and consid-
erable pain. Secondary dental caries can occur when a restoration
(filling) fails and the decay process reoccurs at the margin of a
restoration. Once restorations are in place they eventually fail and
require repetitive replacement, with further drilling away of tooth
material each time, which may eventually lead to total tooth loss.
2Ozone therapy for the treatment of dental caries (Review)
Copyright © 2008 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Ozone is a naturally occurring compound consisting of three oxy-
gen atoms produced by the ultraviolet conversion of oxygen into
the activated, but unstable and short lived form of oxygen. It is a
very powerful oxidising agent and in high concentrations is toxic
to living systems, causing damage to cell membranes (Timbrell
1987). This toxicity has led ozone to be suggested as an agent for
the disinfecting of dental unit water lines (Pankhurst 1998), but
may also be implicated in causing respiratory symptoms in chil-
dren with asthma (Gent 2003).
It has been suggested (PRWeb 2004; Midentistry 2004) that the
application of ozone to carious dental lesions will arrest or reverse
these lesions and that the use of ozone will provide an alternative
to conventional drilling and filling. Theoretically using ozone to
reduce the bacterial count in active carious lesions may temporarily
arrest progression of caries. This may prevent or delay the need
to restore the tooth surface, which would be of benefit to the
public, healthcare providers and to dentists. This review assesses
the effectiveness of ozone application(s) in the management of
caries in vivo.
O B J E C T I V E S
To assess the effectiveness of ozone in arresting or reversing the
progression of dental caries.
The review tested the null hypothesis that there is no difference in
caries progression following the application of ozone or no such
application/placebo.
M E T H O D S
Criteria for considering studies for this review
Types of studies
Randomised controlled trials, with a follow up of at least 6 months
were considered for inclusion. Split-mouth studies were appropri-
ate for inclusion. We originally intended to only include studies
with masked outcome assessment, however it was difficult to as-
certain whether masking occurred or whether it was adequate, so
a post-hoc decision was made not to exclude on this basis.
Types of participants
People, of any age, with caries (including demineralisation in non-
cavitated carious lesions). The caries may have affected any single
tooth surface accessible to the intervention.
Types of interventions
Intervention group: ozone either alone or in combination with
health promotion/oral hygiene plus conventional therapy (when
appropriate).
Control group: no ozone/placebo in combination with health pro-
motion/oral hygiene plus conventional therapy (as in the inter-
vention group).
Types of outcome measures
All outcomes, except for adverse events, were to be assessed at least
6 months from initial treatment.
Primary outcomes
Progression/regression of caries in unrestored cases (assessed clini-
cally or by any other recognised method (Bader 2001) or progres-
sion or regression of secondary caries in restored cases (assessed ra-
diographically against baseline radiograph, pain, failure of restora-
tion assessed clinically or any other method (Bader 2001)).
Secondary outcomes
• Further conventional dental treatment (filling and drilling)
(binary yes/no).
• Time to intervention.
• Pain (assessed by the patient).
• Cost.
• Adverse events.
• Patient satisfaction.
Search methods for identification of studies
The search strategy was developed for MEDLINE on OVID, and
adapted for the other databases. The MEDLINE strategy can be
found in Appendix 1.
The search was run on:
• The Cochrane Oral Health Group’s Trials Register
(November 2003)
• The Cochrane Central Register of Controlled Trials
(CENTRAL) (The Cochrane Library 2003, Issue 3)
• MEDLINE and PREMEDLINE (OVID) (1966 to
November 2003)
• EMBASE (OVID) (1980 to November 2003)
• CINAHL (OVID) (1982 to November 2003)
• AMED (OVID) (1985 to November 2003)
• The internet search engine Google (December 2002).
3Ozone therapy for the treatment of dental caries (Review)
Copyright © 2008 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Handsearching
Quintessence International: preliminary searches suggested that
this journal was a useful source of articles on ozone therapy in
dentistry. Handsearching has been completed by Albert Yeung for
1996 to 2001, the reviewers handsearched 2002.
English and non-English language articles were included and at-
tempts were made to obtain translations of non-English language
articles. Both published and unpublished materials were sought,
unpublished studies and abstracts were only included where they
provided enough methodological detail for them to be appropri-
ately assessed for inclusion.
Experts in the field and manufacturers were contacted in an at-
tempt to find further studies.
Data collection and analysis
Results of all searches were screened by at least two reviewers, inde-
pendently. Full copies of all studies meeting, or potentially meet-
ing, the inclusion criteria were obtained for detailed assessment by
at least two reviewers independently. Where inclusion was unclear
(generally due to randomisation being uncertain) attempts were
made to contact study authors. Where such information was not
obtained, and the original report was in the form of a conference
abstract only, the trial was excluded due to inadequate informa-
tion. Such trials may be included in updates of this review if fur-
ther information becomes available.
Data extraction and validity assessment were conducted inde-
pendently by at least two reviewers. Disagreements were resolved
through discussion by the review team. The authors of included
randomised controlled trials (RCTs) were contacted to ask for
missing information or clarification of data where necessary.
Assessment of validity included the following criteria:
• Randomisation: generation of sequence (yes/no/unclear).
• Allocation concealment (yes/no/unclear).
• Masking of participants/use of placebo (yes/no/unclear).
• Masking of outcome assessors (yes/no/unclear).
• Drop outs accounted for (yes/no/unclear).
• Good measure of interrater reliability reported (yes/no/
unclear).
• Baseline comparability (yes/no/unclear).
• Intention-to-treat analysis used (yes/no/unclear).
It is intended in future updates of this review that the presence
(or otherwise) of commercial sponsorship will be assessed, but this
has not been carried out for this version of the review.
Overall assessment of methodological quality was made on the
following basis: if allocation concealment, masking of outcome
assessors and participants and caries assessment were all adequate,
then the study was considered to be at low risk of bias. If masking
of participants or outcome assessors, or allocation concealment,
was not considered adequate, or was unclear then the study was at
high risk of bias.
Data on all discussed studies were tabulated.
Assessment of heterogeneity
It was planned that a check would be made for clinical heterogene-
ity by examining characteristics in the table of included studies. If
pooling was felt to be reasonable then the random-effects method
would be used, and statistical heterogeneity would be assessed us-
ing Chi2 test (P < 0.1). If heterogeneity existed, this was to be
investigated through subgrouping.
Choice of summary statistic
Binary data were to be presented as risk ratio (RR) with 95%
confidence intervals. Continuous data were presented as weighted
mean differences (WMD).
Combining the trials
Studies with an additional oral hygiene regimen, health promotion
and/or dental health education were to be combined separately
from those using ozone alone.
It was planned that subgroup analyses would be based on the fol-
lowing variables: method of caries assessment; lesion type; baseline
level of caries, plaque or caries risk.
Sensitivity analyses
Sensitivity analyses were to be carried out to assess the sensitivity
of the results to the influence of studies with a high risk of bias.
R E S U L T S
Description of studies
See: Characteristics of included studies; Characteristics of excluded
studies.
Two formally published studies, a large number of conference ab-
stracts, two PhD theses and a submitted manuscript were either
located during the electronic search of databases or the internet,
or provided by Professor E Lynch, a Professor of Restorative Den-
tistry and Gerodontology of the Queen’s University, Belfast, and
were assessed for inclusion. It was unclear from the abstracts how
many potentially relevant randomised trials were in progress, and
clarification of the number of trials was not provided. It may be
that some of these trials will be suitable for inclusion, but this
cannot be assessed until fuller published data become available.
Main reasons for exclusion of the abstracts were: intervention in
extracted teeth rather than people with teeth in situ; randomisa-
tion not stated; less than 6 months data available or supplied; no
4Ozone therapy for the treatment of dental caries (Review)
Copyright © 2008 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

relevant outcomes; no further data supplied by the authors within
the time frame of this review.
Three studies were included (Abu-Naba’a 2003; Abu-Naba’a
2003pilot; Baysan 2003) and are described in the table of
Characteristics of included studies.
Abu-Naba’a 2003
Ninety participants with 258 primary occlusal pit and fissure car-
ious lesions were included in this split-mouth study (129 received
ozone, 129 did not but the numbers of ozone and no ozone le-
sions were not necessarily equal in each mouth). Participants were
aged over 12, 88% were under 32 years of age, 39% were male.
They were all attending the Restorative Department of the School
of Dentistry, Queen’s University, Belfast with at least two carious
lesions (accessible to intervention) in their permanent dentition.
Included lesions were assessed and then individually randomised
to either ozone therapy or no ozone groups. Lesions randomised
to receive ozone had 10 seconds of ozone (2100 ppm ozone at
the start of the study, falling to 630 ppm, only 30% of the full
dose, by the end; this reduction in dose was not intended and it
is not clear why it occurred) at baseline, 1, 3, 6 and 9 months.
Lesions randomised to ozone, and to no ozone were sprayed with
a reductant containing fluoride and xylitol at each appointment.
All participants also received a toothbrush, preventive advice and
fluoride containing toothpaste.
Caries progression and regression were measured by change in
clinical severity scores, mean log(e) DIAGNOdent readings and
mean log(e) ECM (electric caries meter) scores at baseline, 1, 3,
6, 9 and 12 months. Patient satisfaction was also assessed.
Abu-Naba’a 2003pilot
Eight participants with 38 primary occlusal pit and fissure carious
lesions were included in the study (19 lesions received ozone, 19
did not). Inclusion criteria were identical to those in Abu-Naba’a
2003.
Included lesions were assessed and then individually randomised
to either ozone therapy or no ozone. Lesions randomised to receive
ozone had 40 seconds of ozone (dose unclear) at baseline, 1, 3 and
6 months. Reductant was sprayed onto ozone and no ozone lesions
(as in the main study). All participants also received a toothbrush,
preventive advice and fluoride toothpaste.
Caries progression and regression were measured by change in
clinical severity scores, mean log(e) DIAGNOdent readings, mean
log(e) ECM scores and other clinical indices (surface destruction,
hardness, visual index, colour of lesion, perceived treatment need,
frostiness of enamel, and enamel undermining) at baseline, 1, 3
and 6 months.
Baysan 2003
Seventy-nine participants with either two or four primary root car-
ious lesions (PRCLs) were randomised to either root sealant or no
root sealant in this split-mouth study. Only the participants ran-
domised to ’no root sealant’ (39 participants) are included in this
review. Lesions of individuals in the ’no root sealant’ group were
randomised to ozone or no ozone, so one lesion received ozone
and one did not, or two received ozone and two did not, within
each individual. Overall, 68 PRCLs received ozone treatment, and
68 PRCLs did not.
The mean age of all 79 participants was 65 years (range 30 to 72),
62% were male (details were not provided separately for partici-
pants not receiving sealant) and all were attending Queen’s Univer-
sity Belfast School of Dentistry. People with advanced periodontal
disease, with active root caries, who were pregnant, had partic-
ipated in another trial within the last 3 months, or had a cross
infection risk were excluded. All included PRCLs were leathery
(severity index two) and accessible to treatment.
Lesions randomised to receive ozone were cleaned with a sterile
toothbrush and water, dried with sterile cotton wool and given
ozone for 10 seconds. After removal of the ozone the cup was filled
with reductant (containing xylitol and fluoride) for 5 seconds.
Treatment was repeated at 3 and 6 months (and a further follow-
up appointment with reductant but no ozone was included at 1
month) and the trial was planned to continue to 1 year. At these
appointments the control lesions also received reductant, and did
not receive ozone (it is unclear whether they were cleaned or dried).
All participants were provided with toothpaste (1100 ppm sodium
fluoride), soft toothbrushes, extensive oral hygiene and preventive
dietary advice.
Caries progression or regression was measured by visual inspection
(per cent of lesions becoming hard) and electrically by an electric
caries monitor (ECM) or DIAGNOdent. Number of fillings were
recorded, and pain, adverse events and satisfaction were assessed
by patient questionnaire.
Risk of bias in included studies
The methodological quality of the three studies is detailed in the
table of Characteristics of included studies.
Given that effective masking of outcome assessors was unclear
(as the outcome assessor was also the operator at the same visit),
masking of participants was absent (as no placebo was provided),
and allocation concealment was unclear, all three trials were judged
to be at high risk of bias.
Effects of interventions
The analyses of all three studies were conducted at the level of the
lesion, which is not independent of the person and is therefore an
inappropriate analysis. A correct analysis would take the clustering
of the lesions within an individual into account (Macfarlane 1999).
For this reason pooling was not appropriate or attempted, and
caution should be exercised interpreting what the studies report as
”significant differences” between teeth treated or not treated with
ozone.
Data were not provided by any study on the number of lesions
requiring restorations performed to 6 months or later.
5Ozone therapy for the treatment of dental caries (Review)
Copyright © 2008 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Data for each outcome measure and each study are presented in
Table 1. No consistent trend indicating a healthcare benefit or
harm following the application of ozone to carious teeth was seen
across the outcome measures from any of the three studies.
Secondary outcomes
No data were provided in any of the included trials on the nature or
occurrence of any further conventional treatment or other dental
interventions, time to intervention, pain or costs.
Adverse events
Baysan 2003 stated that no adverse events were reported to 6
months, no information is provided by Abu-Naba’a 2003 or Abu-
Naba’a 2003pilot.
Patient satisfaction
Abu-Naba’a 2003 reports on participants’ state of anxiety, asking
participants to compare ozone treatment to traditional dental in-
terventions including dental injection, drilling, filling and scaling
and polishing. Participants had lesions randomised to both ozone
and no ozone treatments in their mouths but no injections or
drilling and filling occurred (as far as we are aware). No-one was
randomised between ozone or drilling and filling so that the results
of this questionnaire do not provide valid comparative informa-
tion.
D I S C U S S I O N
Three trials were included with a combined total of 137 partic-
ipants, with 432 lesions. The risk of bias in all studies appeared
high. Changes from baseline of clinical severity index, log(e) Elec-
tric Caries Monitor and log(e) DIAGNOdent scores were pro-
vided at 6 and 12 months (or end measurements at 6 months); no
consistent advantage or disadvantage of ozone on caries was seen
across outcome measures in any study. Few secondary outcomes
were reported, but one trial reported an absence of adverse events.
There is no reliable evidence that the application of ozone gas to
the surface of decayed teeth is effective in arresting or reversing the
progress of dental caries. It is as yet unclear whether there is merit
in this avenue of research and the reviewers would like to encour-
age sound research. Any future trials must be of high quality and
capable of withstanding rigorous independent review.
The difficulties of designing studies to investigate experimental
interventions for the management of dental caries are well docu-
mented (Bader 2001), as are the principles underlying a well de-
signed clinical trial (Petrie 2002A; Petrie 2002B). It is important
that the efficacy of experimental interventions be evaluated under
conditions that are replicable by other researchers, easily general-
isable to primary dental care and where threats to internal validity
are known, they are reported in detail and controlled. The diffi-
culties of caries diagnosis and monitoring (Kidd 1984; Elderton
1985), masking (of participants, operators and assessors), pairing
of lesions, appropriate placebo treatment, allocation concealment,
examiner reliability, interrater reliability, attrition (loss of partic-
ipants from follow up), adequate follow up and sufficient power
to detect clinically important differences in outcomes all need to
be addressed in future studies.
Many of these criteria appear essential for strong and reliable data.
Our included studies did not mask participants, did state that out-
come assessors were masked (but this would appear unlikely as
the same individual operator provided treatment and completed
outcome assessments at the same visit), did use several outcome
measures but only used a single outcome assessor and did not in-
clude power calculations. For these reasons the discussed trials’ re-
sults can be considered highly susceptible to bias. Therefore overall
there was no reliable evidence that ozone treatment was superior
to no treatment for management of pit and fissure or root caries.
The early carious lesion is reversible in vivo and the progress of
active lesions is slow. It may take 6 years for the early enamel le-
sion to progress through enamel to dentine, and up to 53% of pit
and fissure lesions remain unchanged or may reverse in a 21 to
41 month period (Elderton 1985). Any new treatment modalities
designed to arrest or reverse the carious process must be shown to
be effective over the lifetime of the lesion. To be considered signif-
icant any change in caries progression should be demonstrated to
be effective over a 2 to 6 year period. The discussed studies were
therefore much too short to appropriately investigate if the appli-
cation of ozone does or does not arrest the progression of dental
caries.
It is known to be difficult to diagnose the presence of caries, and
to assess the progress of the carious lesion objectively (Elderton
1985; Kidd 1984). The carious lesion occurs in a small highly
mineralised structure and can occur in a variety of different sites
each of which has a unique configuration and rate of spread. These
difficulties make it unlikely that any one diagnostic modality will
have adequate sensitivity and specificity for all sites (Bader 2001).
Where studies are being designed to assess the effectiveness of new
treatment modalities for the management of caries any measures
or techniques used to assess the progress of the lesion must be
demonstrated to be reliable, reproducible, sensitive and specific
due to the dynamic nature of the demineralising and remineralis-
ing process within the carious lesion. In the absence of such mea-
sures any change in caries progression must be validated by several
techniques and several examiners in the context of a controlled
trial not in the wider population. Many of the caries diagnostic
methods mentioned here are not used widely in general dental
practice.
6Ozone therapy for the treatment of dental caries (Review)
Copyright © 2008 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

The reviewers have some concerns with regard to the data analyses
of all three studies being conducted at the level of the lesion.
This level is not independent of variables relating to the person
and is therefore an inappropriate analysis which may introduce
inaccuracy and bias. A more appropriate level of analysis would
take the clustering of the lesions within an individual into account
(for more detailed discussion see Macfarlane 1999). For this reason
pooling was not appropriate or attempted, and caution should
be exercised interpreting what the studies report as ’significant
differences’ between teeth treated or not treated with ozone which
may be in fact in a small number of individuals.
It has been suggested that the application of ozone to carious den-
tal lesions will reverse these lesions and provide an alternative to
conventional drilling and filling. Ozone may disrupt the dental
bacterial plaque and arrest progression of the lesion however ozone
per se will not reverse the lesion, rather it may produce an envi-
ronment in which arrest of the carious lesion could occur.
In the presence of early carious lesions with no cavitation it has long
been understood that current preventative dental treatments can
be used to reverse or halt the demineralisation process, shifting the
ionic exchange at the tooth surface in favour of remineralisation.
Simple measures involving disruption of the dental plaque, which
have been shown to be effective, include: professional prophylaxis;
restriction of the bacterial substrate by modification of the diet
(DHHS 1999); the use of sugar free chewing gum (Machiulskiene
1999); and use of fluoride toothpaste (Marinho 2003). The use
of self applied fluoride supplements has been shown to be effec-
tive at reducing caries in high risk children who are compliant
(Riordan 1999), as have self applied fluoride rinses in high risk
children, adolescents, adults and the elderly (Davies 2003). The
application of professionally applied fluoride varnishes and gels
has been shown beneficial in high risk children, adolescents and
adults (Davies 2003; Marinho 2002A; Marinho 2002B). There-
fore, on the basis of the research currently available, the applica-
tion of ozone conveys no additional benefit to the preventative
treatments outlined above. Additionally where cavitation has al-
ready occurred conventional treatment will be still be required to
facilitate effect plaque removal .
The reviewers found significant failings in reporting in this review’s
three studies. Firstly no quantification of ozone output from the
HealOzone unit was reported (and appears in one of the included
studies to have failed). Secondly only passing mention was made
of the content of the ’reductant’, a solution applied after ozone
treatment to the carious tooth surface by the single operator in
both the treatment and control groups (in many of the studies).
On clarification from the manufacturers, KaVo, reductant was
identified as a 2% solution of sodium fluoride and 5% xylitol.
Given the evidence above the reporting of the use of the reductant
lacked detail particularly in the control groups. The reviewers felt
it would be far more enlightening to compare the use of ozone/
placebo in masked groups with/without fluoride reductant in a
well designed and conducted trial minimising bias to elucidate the
efficacy of ozone gas application as a treatment for dental caries.
Additionally the interaction between ozone and topical fluoride is
unknown and needs to be investigated. It was felt a very detailed
level of reporting would be helpful to determine the role of the
reductant solution, pre or post treatment oral hygiene instruction
and the use and application of fluoride containing dentifrice at
home on the outcomes measured.
The application of topical fluoride is cheap, simple and effective.
The clinical effectiveness, cost effectiveness and ease of application
of ozone need to be elucidated and may by comparison be much
more expensive. Abu Naba’a (Abu-Naba’a 2003) suggests that the
application of ozone is most effective following three applications
in 3 months, that with less frequent application it becomes less
effective and that poor compliance in terms of attendance reduces
effectiveness. If this is shown to be the case, the acceptability to
patients of such frequent attendance, and the cost implications,
need to be investigated. A recent paper (Holmes 2003E) suggested
that a single tooth ozone treatment should be costed at £68 in
the UK (equivalent to 122 US dollars or 101 Euros), and a full
mouth ozone treatment at UK £245 (equivalent to US$438 or
365 Euros). This will put this treatment modality out of reach of
a substantial percentage of the population at risk including those
in high risk groups, such as the socially deprived.
The clinical effectiveness and cost effectiveness of ozone applica-
tion is unknown. It is not known what the optimal concentration
of ozone might be, how long it should be applied for, how long
any effects might last, how deep into the lesion it might penetrate,
or whether ozone has any other effects. Further research is needed
to answer these questions, but it must be of adequate quality to
provide good evidence. Presently there is no good evidence that
the application of ozone gas to the surface of decayed teeth is effec-
tive in arresting or reversing the progression of dental caries, and
ozone should not be considered an alternative to current methods
for the management and treatment of dental caries.
The reviewers felt it would have been more appropriate to compare
anxiety levels with preventive dental procedures such as topical flu-
oride application, fissure sealing or placement of preventive resin
restorations within a study. The comparison with more invasive
restorative procedures such as injection and drilling is irrelevant.
In summary
Overall this systematic review of all relevant randomised controlled
trials found no good evidence that ozone treatment was superior
to no treatment for management of pit and fissure or root caries.
Across the results of the three trials included in this review there
is no consistent pattern of efficacy of ozone. There is no good ev-
idence that the application of ozone gas to the surface of decayed
teeth is effective in arresting or reversing the progression of dental
7Ozone therapy for the treatment of dental caries (Review)
Copyright © 2008 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

caries. The available studies investigating the effectiveness of ozone
in management of dental decay appear to be at high risk of bias.
There is no evidence to disprove the null hypothesis that there
is no difference in caries progression following the application of
ozone. There is a fundamental need for more evidence of appro-
priate rigour and quality before the use of ozone can be accepted
into mainstream primary dental care or can be considered a viable
alternative to current methods for the management and treatment
of dental caries.
A U T H O R S ’ C O N C L U S I O N S
Implications for practice• There is no good evidence that ozone application is
effective in arresting or reversing the progression of dental caries.
• There is no good evidence to support the use of ozone in a
primary care setting.
• Evidence of appropriate rigour and quality must become
available before ozone can be widely accepted. Ozone therapy
should not gain acceptance nor be used in general practice unless
valid evidence of its clinical effectiveness and (ideally) cost
effectiveness becomes available.
• Dental care providers or users of dental services should not
advocate the use of ozone gas on the sole basis of high patient
acceptability or desirability as compared to less attractive
conventional dental injection local anaesthesia, filling and
drilling.
• This group of reviewers wish to encourage an evidence-
based approach to the management of dental caries particularly
in the primary care setting of general dental practice despite the
barriers to its use such as lack of available clinical time and
financial constraints (Iqbal 2002).
Implications for research
There are currently no peer reviewed trials or papers published in
journals of repute on the efficacy of the use of ozone in dentistry.
There appear to be several longitudinal RCTs in progress but their
quality is unknown at the time of this review. A substantive update
of this review will be carried out when a body of published peer
reviewed data becomes available.
There is a need for well-conducted, valid studies to assess the
effectiveness of ozone in the management of dental caries. The
following issues will need to be addressed in future trials of ozone
for caries management:
• New treatments designed to arrest or reverse the carious
process must ideally be shown to be effective over the lifetime of
the lesion. To be considered significant any change in caries
progression should be demonstrated to be effective over at least a
2 to 6 year period.
• The development and use of a standard set of valid criteria
for the diagnosis and the assessment of progression of early
carious lesions would be desirable. Where studies are being
designed to assess the effectiveness of new treatments for the
management of caries any measures or techniques used to assess
the progress of the lesion must be demonstrated to be reliable,
reproducible, sensitive and specific. In the absence of such
measures any change in caries progression must be validated by
several techniques and several examiners (Bader 2001; Cohen
1968; Streiner 1990).
• Use of sample size calculations, to ensure that studies are
adequately powered to show clinically relevant effects if they
exist, should be encouraged.
• Allocation concealment should be adequate (Schulz 1995).
• Lesions should be randomised so that equal numbers of
intervention and placebo lesions exist in each mouth, and
analyses should provide outcome data per person rather than per
tooth (Macfarlane 1999).
• Robust masking of participants (using an appropriate
placebo treatment), operators and outcome assessors is essential
(Everitt 1995; Fyffe 2000).
• Assessment of examiner reliability and interrater reliability,
with the use of several masked assessors, is necessary in high
quality trials (Tranaeus 2002).
• Better reporting of adverse events, for example asthma
incidents, is required.
• The availability of new funding in the primary care setting
may in future need to be linked to quality assurance in research
design.
A C K N O W L E D G E M E N T S
This review came about as a direct result of a small number of
general dental practitioners and members of the Dental Defence
Agency enrolling on the inaugural Evidence Base for Effective
Clinical Practice Module of the recently developed pathway to the
Fellowship of the Faculty of General Dental Practitioners (UK)
by assessment. Thank you to the Faculty, in particular Malcolm
Pendlebury and 3M/ESPE for their support, vision and develop-
ment of this initiative in continuing professional development and
lifelong learning for general dental practitioners. Our thanks go to
the conveners of the course, Dr Jan Clarkson for her skills of per-
suasion and leadership, Professor Helen Worthington for her en-
lightenment on statistics, and Anne-Marie Glenny for her course
8Ozone therapy for the treatment of dental caries (Review)
Copyright © 2008 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

contribution and literature searching skills. We would also like to
thank course-member Anita Davies who first posed the question
about the effectiveness of ozone and the following researchers who
replied to our requests for additional information about their tri-
als: Professor E Lynch, Dr Layla Abu-Naba’a, Dr Aylin Baysan and
Mr P Stinson. Thanks also for the handsearching skills of Albert
Yeung.
R E F E R E N C E S
References to studies included in this review
Abu-Naba’a 2003 {published and unpublished data}
Abu-Naba’a L. Management of Primary Occlusal Pit and
Fissure Caries Using Ozone. Report by RKS Consultancy,
PO Box 81, 1250 AB Laren NH, The Netherlands 32.
Abu-Naba’a L, Al Shorman H, Lynch E. Ozone management
of occlusal pit and fissure caries (PFC): 12-month review
[abstract]. Provided by Prof E Lynch, source unclear
undated. [: Abst]
Abu-Naba’a L, Al Shorman H, Lynch E. Ozone Treatment
of Primary Occlusal Pit and Fissure Caries: 12-month ECM
Results and Clinical Implications [abstract]. Presented at
the 50th Annual Congress of European Organization for
Caries Research. Konstanz, Germany, 2–6 July 2003. [:
AbstORCAkonstanz2]
Abu-Naba’a L, Al Shorman H, Stevenson M, Lynch E.
Ozone Treatment of Pit and Fissure Caries: 6-month
Results [abstract]. Presented at the AADR meeting. San
Antonio, USA, March 2003.∗ Abu-Naba’a LA. Management of primary occlusal pit and
fissure caries using ozone [PhD Thesis]. Belfast, UK: Faculty
of Medicine and Health Sciences, Queen’s University, 2003.
Abu-Naba’a 2003pilot {published data only}
Abu-Naba’a LA. Management of primary occlusal pit and
fissure caries using ozone [PhD Thesis]. Belfast, UK: Faculty
of Medicine and Health Sciences, Queen’s University, 2003.
Baysan 2003 {published and unpublished data}
Baysan A. Management of primary root caries using ozone
therapies [PhD Thesis]. London: Department of Adult Oral
Health, Bart’s and The London Queen Mary’s School of
Medicine and Dentistry, 2003.
Baysan A, Lynch E. Clinical reversal of root caries using
ozone [abstract]. AADR Conference Abstracts 2002:
http://iadr.confex.com/iadr/2002SanDiego/techprogram/
(accessed Feb 2002).∗ Baysan A, Lynch E. Management of root caries using
ozone. American Journal of Dentistry [submitted]. [:
electronic ABO3CariesRes]
References to studies excluded from this review
Abu-Naba’a 2001 {published data only}
Abu-Naba’a L, Lynch E, Jonavonski V, Zou L, Cunnigham
L. Fissure Sealant Quantification by 3-D C0-Ordinate
Analysis [abstract]. Presentation at the 48th Annual
Scientific Meeting of the Irish and British divisions of
IADR. 9–12 April 2001.
Abu-Naba’a 2002A {published data only}
Abu-Naba’a L, Al Shorman H, Lynch E. In-vivo treatment
of occlusal caries with ozone: immediate effect and
correlation of diagnostic methods [abstract]. Presented at
the 49th Annual Congress of the European Organization
for Caries Research. Naantali, Finland, 3–6 July 2002.
Abu-Naba’a 2002B {published data only}
Abu-Naba’a L, Al Shorman H, Lynch E. Efficacy of ozone in
the treatment of pit and fissure caries [abstract]. Presented at
the 19th Annual Scientific Meeting. IADR, Irish Division.
Cork, Ireland, 25–26 January 2002.
Abu-Naba’a 2002C {published data only}
Abu-Naba’a L, Al Shorman H, Lynch E. Ozone efficacy in
the treatment of pit and fissure caries [abstract]. The First
Pan European Festival of Oral Sciences. Cardiff, UK, 2002.
Abu-Naba’a 2002D {published data only}
Abu-Naba’a L, Al Shorman H, Lynch E. The effect of
ozone application on fissure caries QLF readings [abstract].
AADR Conference Abstracts. San Diego: AADR, 2002:
http://iadr.confex.com/iadr/2002SanDiego/techprogram/
abstract_20059 (accessed March 2003).
Abu-Naba’a 2003A {published data only}
Abu-Naba’a L, Al Shorman H, Lynch E. Clinical indices
changes in ozone treatment of pit and fissure caries
[abstract]. AADR Conference Abstracts. 2003:http:
//iadr.confex.com/iadr/2003SanAnton/techprogram/
abstract_27273.htm (accessed February 2003). [: 1173]
Abu-Naba’a 2003B {published data only}
Abu-Naba’a L, Al Shorman H, Lynch E. 6-month Clinical
Indices Changes after Ozone Treatment of Pit and Fissure
Caries (PFC) [abstract]. Presented at the Annual Scientific
Meeting of IADR. Goteborg, Sweden, June 2003.
Abu-Salem undated {published data only}
Abu-Salem OT, Marashdeh MM, Lynch E. Ozone Efficacy
in Treatment of Occlusal Caries in Primary Teeth [abstract].
Oral Health Care research Center, Queen Elisabeth
University, Belfast, Northern Ireland. undated, source
unclear, provided by Prof. E Lynch.
Al Shorman 2002 {published data only}
Al Shorman H, Abu-Naba’a L, Lynch E. Patients’ Attitude to
Treatment of Pit and Fissure Caries with Ozone [abstract].
9Ozone therapy for the treatment of dental caries (Review)
Copyright © 2008 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Presented at the 49th Annual Congress of European
Organization for Caries Research. Naantali, Finland, 3–6
July 2002.
Al Shorman undated {published data only}
Al Shorman H, Abu-Naba’a L, Coulter WA, Lynch E.
Primary Colonization of DUWL by P. aeruginosa and
its Eradication by Ozone [abstract]. Provided by Prof E
Lynch, Queen’s University Belfast, United Kindom, source
unknown Undated.
Baysan 2000 {published data only}
Baysan A, Whiley RA, Lynch E. Antimicrobial effect
of a novel ozone-generating device on micro-organisms
associated with primary root carious lesions in vitro. Caries
Research 2000;34(6):498–501.
Baysan 2001 {published data only}
Baysan A, Lynch E. Management of primary root carious
lesions using ozone in vivo. Journal of Dental Research.
2001; Vol. 80, issue AADR Abstract:37.
Baysan 2003A {published data only}
Baysan A, Lynch E. Effect of ozone on the oral microbiota
and clinical severity of primary root caries. American
Journal of Dentistry 2003 [in press].
Cardon 2002 {published data only}
Cardon BE, Eleazer PD, Miller RD, Staat RH. Low
concentration ozone treatment insufficient to control
DUWL biofilm [abstract]. AADR Conference Abstracts.
2002:http://iadr.confex.com/iadr/2002SanDiego/
techprogram/ (accessed Feb 2003).
Chang undated {published data only}
Chang HH, Fulton C, Lynch E. Antimcirobial efficacy of
ozone on enterococcus faecalis [abstract]. Provided by Prof
E Lynch, source unknown Undated. [: 36760]
Claxson 2002 {published data only}
Claxson A, Smith C, Turner M, Silwood C, Lynch
E, Grootveld M. Oxidative Modification of Salivary
Biomolecules with Therapeutic Levels of Ozone [abstract].
AADR Conference Abstracts. 2002:http://iadr.confex.com/
iadr/2002SanDiego/techprogram/ (accessed Feb 2003).
Clifford undated {published data only}
Clifford C. Successful use of Airbrasion in Conjunction
with Ozone Treatment [abstract]. Provided by Prof E
Lynch, source unknown Undated.
Daly 2003 {published data only}
Daly T, Lynch E. Reversal of Occlusal Pit and Fissure Caries
by Ozone [abstract]. AADR Conference Abstracts. 2003:
http://iadr.confex.com/iadr/2003SanAnton/techprogram/
abstract_27531.htm (accessed Feb 2003).
Daly undated {published data only}
Daley T, Lynch E. Reversal of Occlusal Pit and Fissure
Caries by Ozone. Private Practice, Harwich. United
Kindom. Undated, source unknown, provided by Prof E
Lynch.
Domingo 2002 {published data only}
Domingo H, Abu-Naba’a L, Al Shoreham H, Holmes J,
Marashdeh MM, Abu-Salem OT, et al.Reducing barriers
to care in patients managed with ozone [abstract]. IADR
Electronic Abstract Submission Form. Cardiff: IADR,
2002.
Domingo 2003 {published data only}
Domingo H, Abu-Naba’a L, Al Shorman H, Holmes
J, Marashdeh M, Abu-Salem O. Reducing Barriers to
Care in Patients Managed with Ozone [abstract]. AADR
Conference Abstracts. 2003:http://iadr.confex.com/iadr/
2003SanAnton/techprogram/abstract_27392.htm (accessed
Feb 2003).
Holmes 2003A {published data only}
Holmes J, Lynch E. Arresting Occlusal Fissure Caries using
Ozone [abstract]. AADR Conference Abstracts. 2003:
http://iadr.confex.com/iadr/2003SanAnton/techprogram/
abstract_27455.htm (accessed Feb 2003). [: 0678]
Holmes 2003B {published data only}
Holmes J, Grootveld M, Smith C, Claxson A, Lynch
E. Bleaching of Components Responsible for Extrinsic
Tooth Discoloration by Ozone [abstract]. AADR
Conference Abstracts. 2003:http://iadr.confex.com/iadr/
2003SanAnton/techprogram/abstract_27410 (accessed
February 2003).
Holmes undated {published data only}
Holmes J. Clinical Reversal of Primary Occlusal Fissure
Carious Lesions (POFCLs) Using Ozone in General Dental
Practice. Web site: http://www.the-o-zone.cc/research/
fsd02.doc (undated) (accessed October 2003).
Jackson 2003 {published data only}
Jackson P, Lynch E. Healing of Pit and Fissure Caries after
Using Ozone [abstract]. AADR Conference Abstracts.
2003:http://iadr.confex.com/iadr/2003SanAnton/
techprogram/abstract_28324.htm (accessed Feb 2003). [:
1174]
Johnson 2003A {published data only}
Johnson N, Johnson J, Johnson K, Abu-Naba’a L, Al
Shorman H, Freeman R, et al.Patients’ Attitudes to Dental
Treatment using Ozone vs. Conventional Treatment
[abstract]. AADR Conference Abstracts. 2003:http:
//iadr.confex.com/iadr/2003SanAnton/techprogram/
abstract_27466.htm (accessed Feb 2003).
Johnson 2003B {published data only}
Johnson N, Johnson J, Lynch E. Cost Benefit Assessment
of a Novel Ozone Delivery System vs. Conventional
Treatment [abstract]. AADR Conference Abstracts. 2003:
http://iadr.confex.com/iadr/2003SanAnton/techprogram/
abstract_27588.htm (accessed Feb 2003).
Johnson 2003C {published data only}
Johnson N, Johnson J, Johnson K, Lynch E. Effective
Treatment of Occlusal Fissure Caries Using Ozone
[abstract]. AADR Conference Abstracts. 2003:http:
//iadr.confex.com/iadr/2003SanAnton/techprogram/
abstract_27377.htm (accessed Feb 2003). [: 0676]
Johnson 2003D {published data only}
Johnson N, Johnson J, Domingo H, Lynch E. Comparison
of Conventional Treatment vs Ozone for Occusal Caries
with Ozone Therapy [abstract]. Proceedings of the Annual
10Ozone therapy for the treatment of dental caries (Review)
Copyright © 2008 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Scientific Meeting of IADR. Goteborg, Sweden: http://
iadr.confex.com/iadr/2003Goteborg/techprogram/abstract_
36903.htm, 25–28 June 2003.
Lynch 2003 {published data only}
Lynch E, Johnson N, Johnson J, Johnson K. Effective
Treatment of Occlusal Fissure Caries Using Ozone
[abstract]. Proceedings of the Annual Scientific Meeting of
IADR. Goteborg, Sweden, 25–28 June 2003. [: 36975]
Lynch undated {published data only}
Lynch E, Baysan A, Silwood CJ, Mills B, Grootveld M.
Oxidation of root caries biomolecules by an anti-bacterial
ozone-generating device [abstract]. Source unclear, provided
by Prof E Lynch, December 2002.
Marashdeh 2003 {published data only}
Marashdeh M, Abu-Salem O, Lynch E. Ozone Treatment
of Occlusal Caries in Primary Teeth: Immediate Effects
and Correlation of Diagnostic Methods [abstract]. AADR
Conference Abstracts. 2003:http://iadr.confex.com/iadr/
2003SanAnton/techprogram/abstract_27576.htm (accessed
Feb 2003). [: 0683]
Megighian 2003A {published data only}
Megighian GD, Bertolini L. Invivo Treatment of Occlusal
Caries with Ozone: One and Two Months’ Effect with
Light-induced Fluorescence (QLF) as Diagnostic Methods
[abstract]. Proceedings of the Annual Scientific Meeting of
IADR. Goteborg, Sweden, 25–28 June 2003. [: Abstract
ID 36918]
Megighian 2003B {published data only}
Megighian GD, Dal Vera MV. Patients’ Attitudes toward
and Satisfaction with Managing Caries with Ozone as a
Routine Treatment in Dental Private Practice [abstract].
Proceedings of the Annual Scientific Meeting of IADR.
Goteborg, Sweden, 25–28 June 2003. [: 36937]
Morrison 2003A {published data only}
Morrison R, Lynch E. Remineralization of Occlusal Pit
and Fissure Caries After Using Ozone [abstract]. AADR
Conference Abstracts. 2003:http://iadr.confex.com/iadr/
2003SanAnton/techprogram/abstract_27482.htm (accessed
February 2003). [: 0680]
Morrison 2003B {published data only}
Morrison R. Clinical reversal of occlusal pit and fissure
caries after using ozone [abstract]. Proceedings of the
Annual Scientific Meeting of IADR. Goteborg, Sweden,
25–28 June 2003.
Reaney 2003 {published data only}
Reaney D, Lynch E. Clinical Reversal of Pit and Fissure
Caries After Using Ozone [abstract]. AADR Conference
Abstracts 2003:http://iadr.confex.com/iadr/2003SanAnton/
techprogram/abstract_27352.htm (accessed Feb 2003).
Reaney undated {published data only}
Reaney D, Lynch E. Clinical Reversal of Pit and Fissure
Caries After Using Ozone. PowerPoint slide GKT, King’s
College Dental Institute, London, England undated.
Sandhaus 1965 {published data only}
Sandhaus S. Ozone therapy in odontstomatology, especially
in treatments of infected root canals [L’Ozonetherapie en
odontostomatologie particulierement dans les traitments
des canaux radiculaires infectes]. Revue Belge de Medecine
Dentaire 1965;20(6):633–46.
Stinson 2003A {published data only}
Stinson P, Al Shorman H, Abu-Naba’a L, Lynch E. Clinical
Reversal of Occlusal Pit and Fissure Caries After Using
Ozone [abstract]. AADR Conference Abstracts. 2003:
http://iadr.confex.com/iadr/2003SanAnton/techprogram/
abstract_27499.htm (accessed Feb 2003).
Stinson 2003B {published data only}
Stinson P. Clinical Reversal of Occlusal Pit and Fissure
Caries After Using Ozone [abstract]. Proceedings of the
Annual Scientific meeting of IADR. Goteborg, Sweden,
25– 28 June 2003.
Stinson undated {published data only}
Stinson P, Al Shorman H, Abu-Naba’a L, Lynch E. Clinical
Reversal of Occlusal Pit and Fissure Caries after Using
Ozone. PowerPoint slide, submitted by Prof E Lynch.
Queen’s University, Belfast, UK undated.
References to studies awaiting assessment
Abu-Salem 2003 {published data only}
Abu-Salem O, Lynch E. Ozone Efficacy in Treatment of
Occlusal Caries in Primary Teeth [abstract]. 81st General
Session of the International Association for Dental Research.
Goteborg, Sweden, 2003.
Abu-Salem O, Marashdeh M, Lynch E. Ozone efficacy in
treatment of occlusal caries in primary teeth [abstract].
AADR Conference Abstracts. 2003:http://iadr.confex.com/
iadr/2003SanAnton/techprogram/abstract_27686.htm
(accessed Feb 2003).
Al Shorman 2003 {published data only}
Al Shorman H, Abu-Naba’a L, Coulter WA, Lynch E.
Primary colonization of DUWL by P.aeruginosa and its
eradication by ozone [abstract]. 81st General Session of the
International Association of Dental Research. Goteborg,
Sweden, 2003.
Chang 2003 {published data only}
Chang HH, Fulton C, Lynch E. Antimicrobial efficacy of
ozone on enterococcus faecalis [abstract]. 81st General
Session of the International Association of Dental Research.
Goteborg, Sweden, 2003.
Clifford 2003 {published data only}
Clifford C. Successful use of airbrasion in conjunction with
ozone treatment [abstract]. 81st General Session of the
International Association of Dental Research. Goteborg,
Sweden, 2003.
Cronshaw 2003 {published data only}
Cronshaw MA. Treatment of primary occlusal pit and
fissure caries with ozone: six month results [abstract]. 81st
General Session of the International Association of Dental
Research. Goteborg, Sweden, 2003.
11Ozone therapy for the treatment of dental caries (Review)
Copyright © 2008 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Hamid 2004 {published data only}
Hamid A. Clinical reversal of occlusal pit and fissure caries
using ozone. 82nd General Session of IADR/AADR/
CADR. Hawaii, 2004.
Holmes 2003C {published data only}
Holmes J. Clinical reversal of occlusal pit and fissure
caries using ozone [abstract]. 81st General Session of the
International Association of Dental Research. Goteborg,
Sweden, 2003. [: 36308]
Holmes 2003E {published data only}
Holmes J. Clinical reversal of root caries using ozone,
double-blind, randomised, controlled 18-month trial.
Gerodontology 2003;20(2):106–14.
Lynch 2003b {published data only}
Lynch E, Silwood C, Smith C, Grootveld M. Oxidising
actions of an anti-bacterial ozone-generating device towards
root caries biomolecules [abstract]. 81st General Session of
the International Association of Dental Research. Goteborg,
Sweden, 2003.
Morrison 2003C {published data only}
Morrisson R, Lynch E. Efficacy of ozone to reverse occlusal
caries [abstract]. 81st General Session of the International
Association of Dental Research. Goteborg, Sweden, 2003.
Additional references
Bader 2001
Bader JD, Shugars DA, Rozier G, Lohr KN, Bonito AJ,
Nelson JP, et al.Diagnosis and management of dental caries:
evidence report. Research Triangle Institute, University
of North Carolina at Chapel Hill, USA, Evidence-
Based Practice Center. Agency for Healthcare Research
and Quality , Rockville, MD, 2000; Vol. Technology
Assessment no 36, issue Publication no 01–E056. [:
contract no: 290–97–0011]
Burke 2003
Burke FJ. From extension for prevention to prevention of
extension: (minimal intervention dentistry). Dental Update
2003;30(9):492-8, 500, 502.
Cohen 1968
Cohen J. Weighted kappa: nominal scale agreement
with provision for scaled disagreement or partial credit.
Psychological Bulletin 1968;70:213–20.
Davies 2003
Davies RM. The prevention of dental caries and periodontal
disease from the cradle to the grave: what is the best
available evidence?. Dental Update 2003;30(4):170-6, 178-
9.
DHHS 1999
Committee on Medical Aspects of Food Policy. Dietary
Sugars and Human Disease. DoH. HMSO London, UK,
1999.
Elderton 1985
Elderton RJ. Assessment and clinical management of
early caries in young adults: invasive versus non-invasive
methods. British Dental Journal 1985;158(12):440–4.
Everitt 1995
Everitt BS. The analysis of repeated measures: a practical
review with examples. The Statistician 1995;44:113–35.
Fyffe 2000
Fyffe HE, Deery C, Nugent ZJ, Nuttall NM, Pitts
NB. Effect of diagnostic threshold on the validity and
reliability epidemiological caries diagnosis using the Dundee
Selectable Threshold Method for caries diagnosis (DSTM).
Community Dentistry & Oral Epidemiology 2000;28:42–51.
Gent 2003
Gent JF, Triche EW, Holford TR, Belanger K, Bracken
MB, Beckett WS, et al.Association of low-level ozone and
fine particles with respiratory symptoms in children with
asthma. JAMA 2003;290(14):1859–67.
Holmes 2003D
Holmes J. New Technologies for Dental Care. Independent
Dentistry 2003;April:76–82.
Iqbal 2002
Iqbal A, Glenny AM. General dental practitioners’
knowledge of and attitudes towards evidence based practice.
British Dental Journal 2002;193(10):587–91.
Kelly 2000
Kelly M, Steele J, Nuttall N, Bradnock G, Morris J, Nunn J,
et al.Adult Dental Health Survery: Oral Health in the United
Kingdom 1998. London, UK: The Stationery Office, 2000.
Kidd 1984
Kidd EA. The diagnosis and management of the ’early’
carious lesion in permanent teeth. Dental Update 1984;11
(2):69-70, 72-4, 76-8.
Macfarlane 1999
Macfarlane TV, Worthington HV. Some aspects of data
analysis in dentistry. Community Dental Health 1999;16(4):
216–9.
Machiulskiene 1999
Machiulskiene V, Nyvad B, Baelum V. A comparison of
clinical and radiographic caries diagnoses in posterior teeth
of 12-year-old Lithuanian children. Caries Research 1999;
33(5):340–8.
Marinho 2002A
Marinho VCC, Higgins JPT, Logan S, Sheiham A. Fluoride
varnishes for preventing dental caries in children and
adolescents. Cochrane Database of Systematic Reviews
2002, Issue 1. [Art. No.: CD002279. DOI: 10.1002/
14651858.CD002279]
Marinho 2002B
Marinho VCC, Higgins JPT, Logan S, Sheiham A. Fluoride
gels for preventing dental caries in children and adolescents.
Cochrane Database of Systematic Reviews 2002, Issue 1. [Art.
No.: CD002280. DOI: 10.1002/14651858.CD002280]
Marinho 2003
Marinho VCC, Higgins JPT, Logan S, Sheiham A. Fluoride
toothpastes for preventing dental caries in children and
adolescents. Cochrane Database of Systematic Reviews
2003, Issue 1. [Art. No.: CD002278. DOI: 10.1002/
14651858.CD002278]
12Ozone therapy for the treatment of dental caries (Review)
Copyright © 2008 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Midentistry 2004
Ozone: minimal intervention dentistry. http://
www.midentistry.com/aus_OZ_CLINIC.html (accessed
May 2004) undated.
NHS CRD 1999
NHS CRD. Dental restoration: what type of filling?.
Effective Healthcare 1999;5(2):1–12.
NIHC statement 2001
NIHC. National Institutes of Health Centre Consensus
Statement: Diagnosis and Management of Dental Caries
Throught Life. http://consensus.nih.gov/cons/115/115_
statement.htm. 2001; Vol. 18, issue 1:1–24.
Options for Change
Department of Health. Options for Change. http:
//www.doh.gov.uk/cdo/optionsforchange/ 2002
(accessed November 2003). [: www.doh.gov.uk/cdo/
optionsforchange]
Pankhurst 1998
Pankhurst CL, Johnson NW, Woods RG. Microbial
contamination of dental unit waterlines: the scientific
argument. International Dental Journal 1998;48(4):359–68.
Petrie 2000
Petrie A, Sabin C. Medical statistics at a glance. Oxford, UK:
Blackwell Science., 2000.
Petrie 2002A
Petrie A, Bulman JS, Osborn JF. Further statistics in
dentistry. Part 4: Clinical trials 2. British Dental Journal
2002;193(10):557–61.
Petrie 2002B
Petrie A, Bulman JS, Osborn JF. Further statistics in
dentistry, Part 3: Clinical trials 1. British Dental Journal
2002;193:495–8.
PRWeb 2004
Ozone treatment in Minimal Intervention Dentistry.
PRWeb at http://www.prweb.com/releases/2004/2/
prwebxml108000.php May 2004.
Riordan 1999
Riordan PJ. Fluoride supplements for young children: an
analysis of the literature focussing on benefits and risks.
Community Dentistry & Oral Epidemiology 1999;27(1):
72–83.
Schulz 1995
Schulz KF, Chalmers I, Hayes RJ, Altman DG. Empirical
evidence of bias. Dimensions of methodological quality
associated with estimates of treatment effects in controlled
trials. JAMA 1995;273(5):408–12.
Silverstone 1983
Silverstone LM. Remineralisation and enamel caries: new
concepts. Dental Update 1983;10(4):261–73.
Streiner 1990
Streiner GL, Norman DR. Health Measurement Scales: A
Practical Guide to their Development and Use. Oxford, UK:
Oxford University Press, 1990.
Timbrell 1987
Timbrell JA. Principles of biochemical toxicology. London,
UK: Taylor & Francis Ltd, 1987.
Tranaeus 2002
Tranaeus S, Shi XQ, Lindgren LE, Trollsas K, Angmar-
Mannsson B. In vivo repeatability and reproducibility of
the quantitative light-induced fluorescence method. Caries
Research 2002;36(1):3–9.
WHO 1990
WHO. Diet, Nutrition and Prevention of Chronic Diseases.
World Health Organisation: Geneva 1990.∗ Indicates the major publication for the study
13Ozone therapy for the treatment of dental caries (Review)
Copyright © 2008 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

C H A R A C T E R I S T I C S O F S T U D I E S
Characteristics of included studies [ordered by study ID]
Abu-Naba’a 2003
Methods Study type: RCT, lesions individually randomised to either ozone therapy or no ozone groups according to
computer generated random sampling digit tables (exact method unclear). Teeth were allocated to ’ozone’
and to ’no ozone’ in every mouth, though not always in equal numbers. In some participants teeth were
also allocated to ’ozone plus sealant’ or ’no ozone plus sealant’ (results in these teeth are not reported in
this systematic review).
Allocation concealment: stated as concealed but appears to use an open random number table.
Masking of patient and/or parent: not done, no placebo ozone treatment was given.
Masking of outcome assessors: unclear. While the authors state that outcome assessment was masked it is
unclear how effective this was, given that the assessor was also the operator at the same visit.
Interrater reliability: not done, single operator/ assessor.
Groups comparable at baseline: no, differences exist in clinical severity scores at baseline (50% scored 1
in the ozone group, 62% in the no ozone group).
Drop outs: 58 of 90 participants attended all visits, one subject missed all visits after the initial visit (and
was excluded from the study). 25 participants missed one visit, four missed two and two missed three
visits.
ITT: no (those without readings at a visit were excluded from analysis).
Other treatments equivalent: yes.
Participants Inclusion criteria: attending School of Dentistry, Queen’s University, Belfast. Male or female aged over
12 years, with at least two primary pit or fissure lesions (without cavitation) in permanent posterior teeth
accessible to diagnostic procedures (ECM and DIAGNOdent). Clinical severity scores were 1 to 3 and
DIAGNOdent readings = 10. Participants were considered reliable attenders and available for the duration
of the study.
Exclusion criteria: where participants had an odd number of lesions suitable for inclusion the lesion with
the lowest DIAGNOdent reading was excluded from randomisation. Participants were excluded for the
presence of advanced periodontal disease, participation in another study in past month or any condition
that in the opinion of the investigator would preclude participation by the subject (e.g. cross infection
risk).
Randomised: 90 participants, 258 lesions (129 in the ozone group, 129 in the no ozone group), 61%
female.
Mean age: not stated. Most were teenagers and young adults. Five subjects were aged 12 to 15, 74 were
aged 15 to 31, 11 were older than 31 years.
Baseline level of caries: clinical severity averaged 1.6 in the ozone treated lesions, 1.4 in the no ozone
lesions. ECM scores averaged 11.6 in the ozone treated lesions, 15.2 in the no ozone lesions. Participants
had 2 to 14 included lesions, often with numerous filled teeth and some decayed beyond the inclusion
criteria.
Caries risk assessment: not stated.
Interventions Intervention lesions: at 0, 1, 3, 6 and 9 months the lesions were disclosed, cleaned with an air abrasion
system (PROPHYflex), outcomes assessed, ozone applied for 10 seconds, then reductant sprayed on. At
the 12 month final visit no ozone was applied.
Control lesions: at 0, 1, 3, 6, 9 and 12 months the lesions were disclosed, cleaned with an air abrasion
system (PROPHYflex), outcomes assessed, then reductant sprayed on.
All participants: extensive oral hygiene and dietary advice was provided, a toothbrush and toothpaste (1,
14Ozone therapy for the treatment of dental caries (Review)
Copyright © 2008 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Abu-Naba’a 2003 (Continued)
100 ppm fluoride) were provided at each appointment.
Operator: single operator/assessor (Layla Abu-Naba’a).
Outcomes Caries progression or regression measured by clinical severity index, ECM, and DIAGNOdent. Anxiety
assessed
Notes Reductant (containing xylitol at = 5% by weight and fluoride at 1100 ppm, as well as other compounds)
was used for each lesion at each visit (0, 1, 3, 6 and 9 months).
This study also randomised lesions in some participants to receive the interventions above plus a sealant,
these lesions have been excluded from the current analysis.
The authors stated in correspondence that blinded outcome assessment occurred, however a single operator
was responsible for both outcome assessment and ozone delivery to appropriate lesions at 0, 1, 3, 6 and
9 months.
The actual level of ozone delivered was correct at the start of this study, but very much lower than expected
at the end. It is unclear how many full strength doses were actually delivered
Risk of bias
Item Authors’ judgement Description
Allocation concealment? Unclear B - Unclear
Abu-Naba’a 2003pilot
Methods Study type: RCT, lesions individually randomised to either ozone therapy or no ozone groups according to
computer generated random sampling digit tables (exact method unclear). Teeth were allocated to ’ozone’
and to ’no ozone’ in every mouth, though not always in equal numbers.
Allocation concealment: unclear.
Masking of patient and/or parent: not done, no placebo ozone treatment was given.
Masking of outcome assessors: unclear. While the authors state that outcome assessment was masked it is
unclear how effective this was, given that the assessor was also the operator at the same visit.
Interrater reliability: not done, single operator/assessor.
Groups comparable at baseline: no, differences exist in clinical severity scores at baseline (21% scored 1,
42% scored 2 in the ozone group, 21% scored 1 and 58% scored 2 in the no ozone group).
Drop outs: 13 of 19 lesions randomised to ’ozone’ and 12 of the 19 lesions randomised to ’no ozone’
attended the 6 month follow up.
ITT: no (those without readings at a visit were excluded from analysis).
Other treatments equivalent: yes.
Participants Inclusion criteria: attending School of Dentistry, Queen’s University, Belfast. Male or female aged over 12
years, with at least two primary pit or fissure caries (including cavitated lesions) in permanent posterior
teeth accessible to diagnostic procedures (ECM and DIAGNOdent). Clinical severity scores were 1 to
3 and DIAGNOdent readings = 10. Participants were considered reliable attenders and available for the
duration of the study.
Exclusion criteria: where participants had an odd number of lesions suitable for inclusion the lesion with
the lowest DIAGNOdent reading was excluded from randomisation. Participants were excluded for the
presence of advanced periodontal disease, participation in another study in past month or any condition
that in the opinion of the investigator would preclude participation by the subject (e.g. cross infection
15Ozone therapy for the treatment of dental caries (Review)
Copyright © 2008 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Abu-Naba’a 2003pilot (Continued)
risk).
Randomised: 8 participants, 38 lesions (19 in the ozone group, 19 in the no ozone group).
Mean age: not stated.
Baseline level of caries: (See under comparability at baseline).
Caries risk assessment: not stated.
Interventions Intervention lesions: at 0, 1, 3 and 6 months the lesions were cleaned, outcomes assessed, ozone applied
for 40 seconds, then reductant sprayed on.
Control lesions: at 0, 1, 3, and 6 months the lesions were cleaned, outcomes assessed, then reductant
sprayed on.
All participants: preventive advice was provided, as were a toothbrush and toothpaste (1100 ppm fluoride)
.
Operator: single operator/assessor (Layla Abu-Naba’a).
Outcomes Caries progression or regression measured by clinical severity index, ECM, DIAGNOdent and other
clinical indices (surface destruction, hardness, visual index, colour of lesion, perceived treatment need,
frostiness of enamel, enamel undermining). Anxiety assessed, but not as part of the randomised trial
Notes Reductant (containing xylitol at = 5% by weight and fluoride at 1100 ppm, as well as other compounds)
was used for each lesion at each visit.
The authors stated in correspondence that blinded outcome assessment occurred, however a single operator
was responsible for both outcome assessment and ozone delivery to appropriate lesions at 0, 1, 3 and 6
months.
The actual level of ozone delivered was unclear (see notes under main study)
Risk of bias
Item Authors’ judgement Description
Allocation concealment? Unclear B - Unclear
16Ozone therapy for the treatment of dental caries (Review)
Copyright © 2008 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Baysan 2003
Methods Study type: RCT, sequence generated by statistitian at Queen’s University, 2 or 4 primary root carious
lesions randomised, with equal numbers to intervention and control, in each mouth.
Allocation concealment: stated as concealed by author (however sequence presented in thesis as an open
list).
Masking of patient and/or parent: not done.
Masking of outcome assessors: unclear. While the authors state that outcome assessment was masked it is
unclear how effective this was, given that the assessor was also the operator at the same visit.
Interrater reliability: not done (single operator).
Groups comparable at baseline: unclear.
Drop outs: 4 people dropped out by 3 months, unclear how many lesions this represents, or number of
drop outs at 6 months.
ITT analysis: unclear.
Other treatment equivalent: unclear. The submitted paper suggests that the teeth receiving ozone were
cleaned before ozone and the reductant were applied, but the teeth not receiving ozone were not cleaned
before the reductant was applied. However, the PhD implies that in control group the teeth were cleaned
before caries measurements were taken, and so were cleaned before the reductant was applied
Participants Inclusion criteria: male and female at least 18 years old, with leathery root carious lesions (severity index 2)
on at least two surfaces and accessible for diagnostic procedure (electronic caries meter and Diagnodent).
Exclusion criteria: participants with advanced periodontal disease, who had participated in another dental
study in past 3 months, were pregnant or had any condition precluding participation (e.g. cross infection
risk).
Randomised: 39 participants, 68 teeth in intervention, 68 in control group, each participant had equal
numbers of intervention and control lesions (2 or 4 in total).
Mean age: unclear.
Baseline level of caries: not stated.
Caries risk assessment: not stated.
Interventions Intervention lesions: at initial visit tooth surface cleaned with sterile toothbrush and water, dried, ozone
applied for 10 seconds into cup, suction applied for 10 seconds, reductant applied for 5 seconds. Repeated
at 1 month (with no ozone), 3 months and 6 months (both with ozone for 10 seconds).
Control lesions: at initial visit no ozone (or placebo) applied, and no cleaning occurred, but reductant
applied for 5 seconds. Repeated at 1, 3 and 6 months.
All participants: standard dentifrice (1100 ppm sodium fluoride) and soft toothbrushes were provided to
all participants during the study.
Duration of follow up: 12 months stated intent, but results found for 6 months maximum.
Operator: Aylin Baysan, single operator.
Outcomes Caries progression or regression (’% lesions becoming hard’, Electric Caries Meter and DIAGNOdent
readings). It was stated that further dental interventions, pain, patient satisfaction and adverse events were
recorded, but these have not been reported at 6 months or later
Notes Reductant (containing xylitol at = 5% by weight and fluoride at 1100 ppm, as well as other compounds)
was used at each visit (0, 1, 3 and 6 months).
Protocol states that if participants present with discomfort the primary root carious lesions would be
immediately treated by drilling and filling.
The same study also randomised participants to receive the interventions above plus a sealant, these
participants have been excluded from the current analysis.
Study included as authors stated in correspondence that blinded outcome assessment occurred, however
17Ozone therapy for the treatment of dental caries (Review)
Copyright © 2008 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Baysan 2003 (Continued)
a single operator was responsible for outcome assessment and ozone delivery to appropriate lesions at 0,
3 and 6 months
Risk of bias
Item Authors’ judgement Description
Allocation concealment? Unclear B - Unclear
Characteristics of excluded studies [ordered by study ID]
Study Reason for exclusion
Abu-Naba’a 2001 In vitro study.
Abu-Naba’a 2002A Less than 6 months follow up.
Abu-Naba’a 2002B Less than 6 months follow up.
Abu-Naba’a 2002C Less than 6 months follow up.
Abu-Naba’a 2002D In vitro study.
Abu-Naba’a 2003A Not a randomised controlled trial.
Abu-Naba’a 2003B Not a randomised controlled trial.
Abu-Salem undated Less than 6 months follow up.
Al Shorman 2002 Primary outcome not assessed.
Al Shorman undated No relevant outcome measured (study in water lines, not teeth)
Baysan 2000 In vitro study.
Baysan 2001 No control group (all lesions given ozone).
Baysan 2003A No control group (all lesions given ozone), less than 6 months follow up
Cardon 2002 Not assessing effect of ozone on caries (in dental unit water lines)
Chang undated No teeth or caries involved, in vitro.
Claxson 2002 In vitro study.
18Ozone therapy for the treatment of dental caries (Review)
Copyright © 2008 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

(Continued)
Clifford undated No assessment of the effect of ozone on caries, no control group
Daly 2003 Less than 6 months follow up.
Daly undated Less than 6 months follow up.
Domingo 2002 Not 6 months follow up (immediate effects only).
Domingo 2003 Not a randomised controlled trial.
Holmes 2003A Follow up less than 6 months.
Holmes 2003B Did not assess the effect of ozone on caries (nor on teeth).
Holmes undated No control group, follow up less than 6 months.
Jackson 2003 Less than 6 months follow up.
Johnson 2003A Not a randomised controlled trial.
Johnson 2003B Cost benefit study, less than 6 months follow up.
Johnson 2003C Less than 6 months follow up.
Johnson 2003D Time expenditure study, not a controlled trial.
Lynch 2003 Less than 6 months follow up.
Lynch undated No assessment of effect of ozone on caries.
Marashdeh 2003 Less than 6 months follow up.
Megighian 2003A Less than 6 months follow up.
Megighian 2003B Attitude and satisfaction survey, no randomisation.
Morrison 2003A Less than 6 months follow up.
Morrison 2003B Less than 6 months follow up.
Reaney 2003 Less than 6 months follow up.
Reaney undated Less than 6 months follow up.
Sandhaus 1965 Not a randomised trial.
Stinson 2003A Less than 6 months follow up.
19Ozone therapy for the treatment of dental caries (Review)
Copyright © 2008 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

(Continued)
Stinson 2003B Less than 6 months follow up.
Stinson undated Less than 6 months follow up.
20Ozone therapy for the treatment of dental caries (Review)
Copyright © 2008 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

D A T A A N D A N A L Y S E S
This review has no analyses.
A D D I T I O N A L T A B L E S
Table 1. Results of the included studies, caries regression and progression
Study Measure Ozone N, mean (SD) Control N, mean (SD)
Abu-Naba’a 2003 main Clinical severity index*, change
from baseline, 6 months follow up
102, 0.22 (0.65) 102, 0.29 (0.68)
Abu-Naba’a 2003 main Log(e) ECM score*, change from
baseline, 6 month follow up
104, 0.29 (1.55) 104, -0.23 (1.45)
Abu-Naba’a 2003 main Log
(e) DIAGNOdent score*, change
from baseline, 6 month follow up
100, 0.05 (0.44) 103, 0.09 (0.50)
Abu-Naba’a 2003 main Clinical severity index*, change
from baseline, 12 months follow
up
106, 0.28 (0.64) 106, 0.44 (0.74)
Abu-Naba’a 2003 main Log(e) ECM score*, change from
baseline, 12 month follow up
109, 0.02 (1.40) 109, 0.07 (1.61)
Abu-Naba’a 2003 main Log(e) DIAGNOdent score*,
change from baseline, 12 month
follow up
105, 0.10 (0.58) 107, 0.08 (0.54)
Abu-Naba’a 2003 pilot Clinical severity score* Baseline: 19, 2.2 (0.76) 6 months:
13, 2 neg ranks, 0 pos ranks, 11
ties
Baseline: 19, 2.0 (0.67) 6 months:
12, 5 neg ranks, 0 pos ranks, 7 ties
Abu-Naba’a 2003 pilot Log
(e) DIAGNOdent score*, change
from baseline, 6 month follow up
Baseline: 19, 3.2 (0.92) Change to
6 months: 12, 0.1, 0.28
Baseline: 19, 2.2 (0.76) Change to
6 months: 11, -0.05, 0.27
Abu-Naba’a 2003 pilot Log(e) ECM score*, change from
baseline, 6 month follow up
Baseline: 19, 1.1 (0.91) Change to
6 months: 12, 0.3, 1.39
Baseline: 19, 0.8 (0.83) Change to
6 months: 11, 0.4, 0.63
Abu-Naba’a 2003 pilot Visual index, (1 = sound, 2 = car-
ious, 3 = arrested)
6 months: 13, 0 neg ranks, 8 pos
ranks, 5 ties
6 months: 12, 0 neg ranks, 1 pos
ranks, 11 ties
Abu-Naba’a 2003 pilot Colour of lesion (1 = yellow, 2 =
light brown, 3 = grey, 4 = dark
brown, 5 = black)
6 months: 13, 2 neg ranks, 3 pos
ranks, 8 ties
6 months: 12, 6 neg ranks, 2 pos
ranks, 4 ties
21Ozone therapy for the treatment of dental caries (Review)
Copyright © 2008 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.
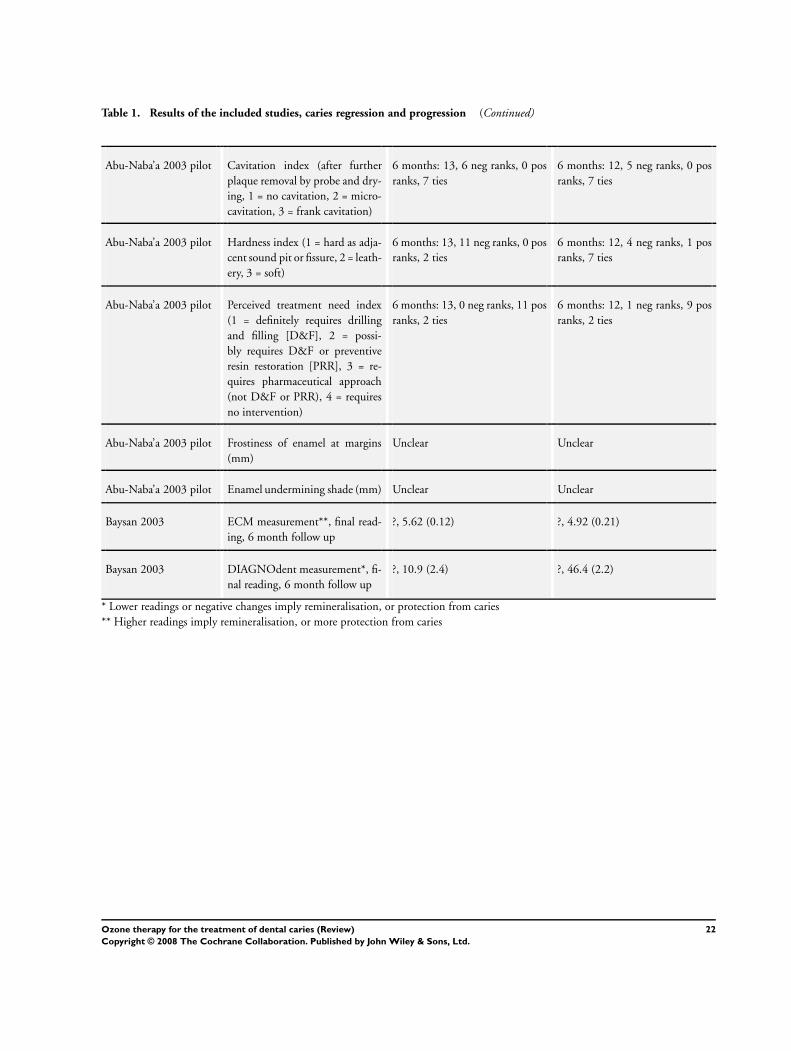
Table 1. Results of the included studies, caries regression and progression (Continued)
Abu-Naba’a 2003 pilot Cavitation index (after further
plaque removal by probe and dry-
ing, 1 = no cavitation, 2 = micro-
cavitation, 3 = frank cavitation)
6 months: 13, 6 neg ranks, 0 pos
ranks, 7 ties
6 months: 12, 5 neg ranks, 0 pos
ranks, 7 ties
Abu-Naba’a 2003 pilot Hardness index (1 = hard as adja-
cent sound pit or fissure, 2 = leath-
ery, 3 = soft)
6 months: 13, 11 neg ranks, 0 pos
ranks, 2 ties
6 months: 12, 4 neg ranks, 1 pos
ranks, 7 ties
Abu-Naba’a 2003 pilot Perceived treatment need index
(1 = definitely requires drilling
and filling [D&F], 2 = possi-
bly requires D&F or preventive
resin restoration [PRR], 3 = re-
quires pharmaceutical approach
(not D&F or PRR), 4 = requires
no intervention)
6 months: 13, 0 neg ranks, 11 pos
ranks, 2 ties
6 months: 12, 1 neg ranks, 9 pos
ranks, 2 ties
Abu-Naba’a 2003 pilot Frostiness of enamel at margins
(mm)
Unclear Unclear
Abu-Naba’a 2003 pilot Enamel undermining shade (mm) Unclear Unclear
Baysan 2003 ECM measurement**, final read-
ing, 6 month follow up
?, 5.62 (0.12) ?, 4.92 (0.21)
Baysan 2003 DIAGNOdent measurement*, fi-
nal reading, 6 month follow up
?, 10.9 (2.4) ?, 46.4 (2.2)
* Lower readings or negative changes imply remineralisation, or protection from caries
** Higher readings imply remineralisation, or more protection from caries
22Ozone therapy for the treatment of dental caries (Review)
Copyright © 2008 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

A P P E N D I C E S
Appendix 1. MEDLINE (OVID) search strategy
1 ozone$.mp.
2 exp OZONE/
3 O3.mp.
4 (curozone$ or healozone$).mp.
5 1 or 2 or 3 or 4
6 exp Tooth Demineralization/
7 (caries or carious or deminerali$ or de-minerali$).mp
8 exp Dentistry, Operative/
9 ((teeth or tooth or dental or enamel or dentin$) and (caries or carious or decay$ or lesion$ or deminerali$ or reminerali$ or white
spot lesion$)).mp
10 ((caries or “dental caries” or decay or enamel) and (prevent$ or control$ or reminerali$ or arrest$)).mp
11 exp Dental Caries Activity Tests/
12 exp Dental Caries Susceptibility/
13 exp Dental Enamel Solubility/
14 6 or 7 or 8 or 9 or 10 or 11 or 12 or 13
15 5 and 14
W H A T ’ S N E W
Last assessed as up-to-date: 13 May 2004.
Date Event Description
12 August 2008 Amended Converted to new review format.
H I S T O R Y
Protocol first published: Issue 2, 2003
Review first published: Issue 3, 2004
C O N T R I B U T I O N S O F A U T H O R S
George David Rickard (GDR), Robin Richardson (RR), Trevor Johnson(TJ), David McColl (DM) and Lee Hooper (LH) designed
the review and wrote the protocol with Anne-Marie Glenny (AMG) and Jan Clarkson. GDR co-ordinated the review. LH and AMG
developed the search strategy and undertook searches. GDR, RR, TJ, DM and LH screened the search results. LH organised retrieval
of papers. GDR, RR, TJ, DM and LH screened retrieved papers against inclusion criteria. GDR, RR, TJ, and LH appraised study
quality and extracted data from included papers. GDR, RR, and LH wrote to authors for additional information. GDR managed the
review data. GDR, RR and LH wrote the body of the review, and interpreted the data. GDR, RR, TJ and DM wrote the discussion.
23Ozone therapy for the treatment of dental caries (Review)
Copyright © 2008 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

D E C L A R A T I O N S O F I N T E R E S T
None known. None of the authors has ever acted as a consultant for, or been funded in any way by Kavo Dental GmbH & Co. KG the
company that manufactures the ozone delivery equipment. The faculty course was sponsored by 3M/ESPE (who have had no input
into or influence on, this review).
S O U R C E S O F S U P P O R T
Internal sources
• Cochrane Oral Health Group, UK.
• University of Manchester, UK.
• Central Manchester and Manchester Children’s University Hospitals NHS Trust, UK.
External sources
• 3M sponsored several places on the course that lead to this systematic review being developed, UK.
I N D E X T E R M S
Medical Subject Headings (MeSH)
Cariostatic Agents [∗therapeutic use]; Dental Caries [∗drug therapy]; Dental Fissures [drug therapy]; Ozone [∗therapeutic use]; Ran-
domized Controlled Trials as Topic
MeSH check words
Humans
24Ozone therapy for the treatment of dental caries (Review)
Copyright © 2008 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.