new members - de gruyter
TRANSCRIPT
New members
Abner, Susan, NYCOM '84; 93 Westgate Dr., Edison, NJ 08820
Asbury, Willard E., COPS '59; Bldg. E, Suite 590, 1049 S.W. Baseline, Hillsboro, OR 97123
Bass, Steven, UHSCOM '80; 5125 Beacon Hill Rd., Columbus, OH 43228
Beaumont, Roger W., KCOM '69; 15350 W. National Ave., New Berlin, WI 53151
Behnke, Allen W. , KCOM '55; 152 Castelwood Dr., Brooklyn, MI 49230
Bender, Charles R., PCOM '58; Suite 112, 5975 W. Sunrise Blvd., Sun-rise, FL 33313
Bentz, Robert L., PCOM '78; Suite 103, 2151 45th St. , West Palm Beach, FL 33407
Beson, James L., Capt., OCOMS '82; 5th General Hospital, APO, New York, NY 09154
Biggers, Jerel R., KCOM '78; Suite 101, 5409 N. Jim Miller, Dallas, TX 75227
Binder, Jeffrey E., OUCOM '81; No. 306, 24700 Lorain Rd., North Olmsted, OH 44070
Bishop, Donald W., UHSCOM '74; Suite 102, 710 E. Park Blvd., Plano, TX 75074-5432
Blanzy, John E., CCOM '60; 14319 Dix-Thledo Rd., Southgate, MI 48195
Blueskye, William C., KCOM '54; 7496 Mentor Ave., Mentor, OH 44060
Bowen, Ronald W., TCOM '85; 4058 Weber, Corpus Christi , TX 78415
Brickner, Kurt A. , CCOM '83; No. 101; 2385 E. Prater Way, Sparks, NV 89431
Brown, Wayne L, TCOM '82; 304 For-est Hill , Palestine, TX 75801
Burnett, R. James, III, UHSCOM '79; Box 361, Somerville, TN 38068
Buszek, Robert F., UHSCOM '69;
552
212 W. Michigan Ave., Ypsi-lanti, MI 48197
Carlstrom, Graydon J., UHSCOM '64; Box 271089, Dallas, TX 75227
Castiglia, Clare A. , COMP '84; 480 Sunset, Plymouth, MI 48170
Ching, Daniel T.Y. , KCOM '84; Box 70110, William Beaumont Army Medical Center, El Paso, TX 79920
Cicero, Steven, UHSCOM '83; 303 N. W. 59th Pl., Gladstone, MO 64118
Conley, Joseph P ., Jr., UNECOM '84; 250 Eddie Dowling Hwy., North Smithfield, RI 02895
Conway, Megan L., NYCOM '85; 36 Forsythia Dr. , E., Levittown, PA 19056
Corcoran, Marie E. , CCOM '78; 2134 Kentucky Ct., Wheaton, IL 60187
Costantino, Thomas G. , UOMHS '71; 14319 Dix Rd., Southgate, MI 48192
Curtwright, Lewis K. , UHSCOM '65; Box 555669, Orlando, FL 32855-5669
Dickerson, Margaret M. , PCOM '79; No. 7B., 3800 N. Lake Shore, Chi-cago, IL 60613-3313
Durose, Galen C. , UHSCOM '68; 817 E. Main, Lancaster, OH 43130
Eaton, James C., OCOMS '81 ; 322 E. 11th St., Baxter Springs, KS 66713
Esack, Richard B., PCOM '80; No. G-42, 10811 Indian Hills Ct., Largo, FL 34667
Everett, Roslein M. , UHSCOM '85; No. 4, 13025 102nd Ln., N.E. , Kirkland, WA 98034
Farinosi, James P., CCOM '85; 5200 S. Ellis Ave., Chicago, IL 60615
Fong, Jon W. , COMP '84; 12741 E. Alconbury, Cerritos, CA 90701
Frazier, Harold A., UHSCOM '55; 792 Graham Rd., Cuyahoga Falls, OH 44221
Fried, Harley Ann, Capt, NYCOM '84; 213 Cherry St., Panama City, FL 32404
Gabbert, Timothy B. , UHSCOM '82; Wetzel Clinic, Hwy. 13, North, Clinton, MO 64735
Galvin, William D. , UHSCOM '65; Box 447, Noel, MO 64854
Gilman, Michael H ., UOMHS '79; 4957 W. Fond DuLac Ave. , Mil-waukee, WI 53216
Gleba, Mark T. , TCOM '83; 1621 Em-erald St. , San Diego, CA 92109
Griffin, Rodney L., UHSCOM '66; 4231 Bay Th Bay Blvd., Tampa, FL 33609
Hayrynen, Thrry S., MSUCOM '84; Box 428, Roscommon, MI 48653-0428
Hazelip, Sandra J ., TCOM '84; Box 351, Eastland, TX 76448
Hill, Jimmie Sue M., OCOMS '85; 1524 W. Okmulgee, Muskogee, OK 74401
Howell , Michael George, UHSCOM OCOMS '85; Box 172, Ashland, MS 38603
Jackson, James, UOMHS '60; 2416 Peck St., Muskegon Heights, MI 49444-1431
Jelonek, EdwardJ.,Jr., Lt., UOMHS '84; 531 La Barca St. , Spring Val-ley, CA 92077
Juele, Nicholas J ., PCOM '79; 205 Thckerton Rd., Medford, NJ 08055
Koerner, Theodore G., PCOM '75; Box 1107, 1251 Blackhorse Pike, Thrnersville, NJ 08012
Lafferty, Linda D., MSUCOM '80; Suite 101, 2385 E. Prater Way, Sparks, NV 89431
Leitkam, Bruce C., UHSCOM '73; 5142 Miller Rd., Flint, MI 48507
Lubow, Allan, KCOM '82; 1040 S. Gaylord St. , Denver, CO 80209
Malina, Barry Drew, TCOM '84; 11627 S. Warcloud Ct. , Phoenix, AZ 85044
McElroy, David S.A., COMP '83; Box
April 1988/Journal of AOA/vol. 88/no .4

Hear news briefs about cholesterol studies and
treatment guidelines The rotating faculty of lipid experts includes:
Dr. DeWitt Goodman, Chairman of the National Cholesterol Education Program Panel on Detection, Evaluation, and Treatment of High Blood Cholesterol in Adults, summarizes the NIH guidelines for treating elevated blood cholesterol.
Dr. David Blankenhorn, Director of the Atherosclerosis Research Institute at the University of Southern California School of Medicine, describes his study indicating that lowering blood cholesterol leads to regression of atherosclerotic lesions.
Dr. William Castelli, Medical Director of the Framingham Heart Study, summarizes conclusive data from two landmark stud ies.
Dr. John LaRosa, Director of the Lipid Research Clinic at the George Washington University School of Medic ine, questions the common medical wisdom about treating elevated serum cholesterol levels.
Dr. Joseph Stokes, Coprincipal Investigator of the Framingham Heart Study, offers practical ways to motivate patients to lower their cholesterol.
Dr. Michael DeBakey, Chancellor and Chairman of the Department of Surgery at Baylor College of Med icine , defines the role of cholesterol lowering in an overall strategy to reduce the risk of heart disease.
Ca/11-800-MD-GOALS Your Cholesterol Connection
Call toll free 24 hours a day, 7 days a week. Programs change periodically.
An educational service for physicians sponsored by Merck Sharp & Dohme
MEVACOR is indicated as an adjunct to diet for the reduction of elevated total and LDL cholesterol levels in patients with primary hypercholesterolem ia (Types IIa and lib) when response to nonpharmacologic measures has been inadequate.
MEVACOR is con traindicated in patients hypersensitive to any component of the medication; in patients with active liver disease or unexplained persistent transaminase elevations; in pregnant or lactating patients; and in women of childbearing age, except when such patients are highly unlikely to conceive.
In many patients
EVACOR' (LOVASTATIN MSD)
Liver Dysfunction: Marked persistent increases (to more than three times the upper limit of normal) in serum transaminases occurred in 1.9% of adult patients who received lovastatin for at least one year. It is recommended that liver function tests be performed every 4
to 6 weeks during the first 15 months of therapy with lovastatin and periodically thereafter in all patients. In patients who develop elevated transaminase level s, measurements should be repeated promptly and performed more frequently. If the transaminase levels show evidence of progression, particularly
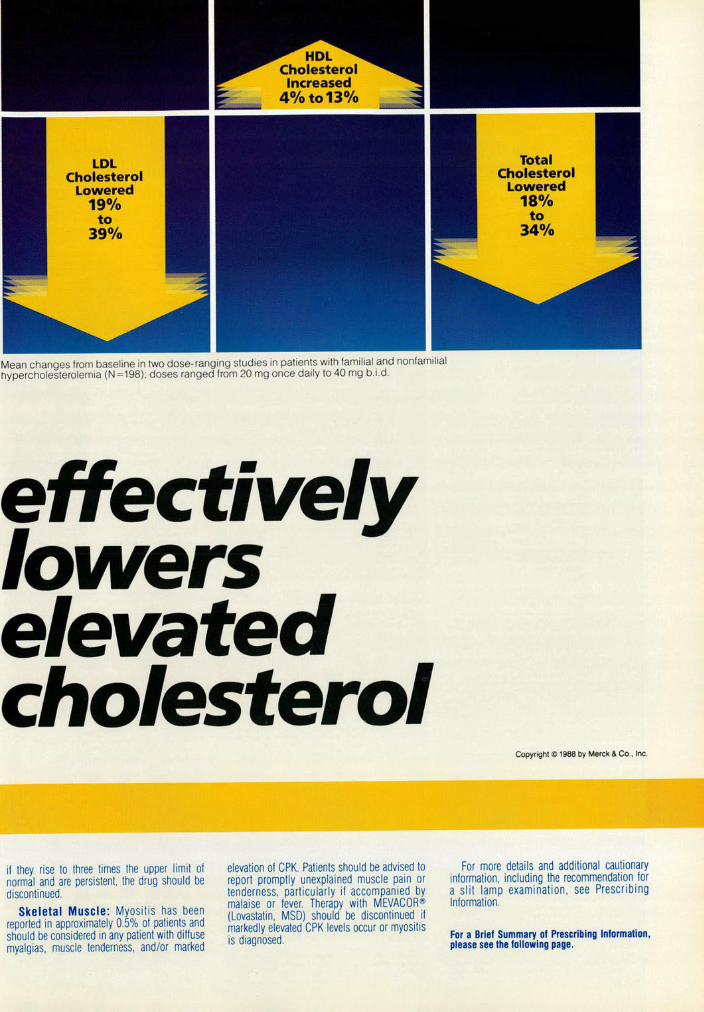
LDL Cholesterol
Lowered 19%
to 39%
Total Cholesterol
Lowered 18°/o
to 34%
Mean changes from baseline in two dose- ranging studies in patients with familial and nonfamilial
hypercholesterolemia (N =198); doses ranged from 20 mg once daily to 40 mg b.i.d.
effectively lowers elevated cholesterol
if they rise to three times the upper limit of normal and are persistent, the drug should be discontinued.
Skeletal Muscle : Myositis has been reported in approximately 0.5% of patients and should be considered in any patient with diffuse myalgias, muscle tenderness. and/or marked
elevation of CPK. Patients should be advised to report promptly unexplained muscle pain or tenderness, particularly if accompanied by malaise or fever. Therapy with MEVACQR® (Lovastatin, MSD) should be discontinued if markedly elevated CPK levels occur or myositis is diagnosed.
Copyright <C> 1988 by Merck & Co., Inc.
For more detai Is and additional cautionary information, including the recommendation for a slit lamp examination , see Prescribing Information.
For a Briel Summary of Prescribing Information, please see the following page .

MEVACOR (LOVASTATIN I MSD)
MEVACOR"' (Lovastatin I MSD) CONTRAINOICATIONS
Hypersensitivity to any component of this medication. Active liver disease or unexplained persistent elevations of serum
transaminases. Pregnancy and lactation . Atherosclerosis is a chronic process and the discontinuation of lipid-
lowering drugs during pregnancy should have little impact on the outcome of long-term therapy of primary hypercholesterolemia. Moreover, choles-terol and other products of the cholesterol biosynthesis pathway are essen-tial components for fetal development, including synthesis of steroids and cell membranes . Because of the ability of inhibitors of HMG-CoA reduc-tase such as MEVACOR to decrease the synthesis of cholesterol and possibly other products of the cholesterol biosynthesis pathway, MEVACOR may cause fetal harm when administered to a pregnant woman . Therefore, lovastatin is contraindicated during pregnancy. Lovastatin should be administered to women of childbearing age only when such patients are highly unlikely to conceive. If the patient becomes pregnant while taking this drug , lovastatin should be discontinued and the patient should be apprised of the potential hazard to the fetus .
WARNINGS Liver Dysfunction
Marked persistent Increases (to more than 3 times the upper limit ol normal) in serum transaminases occurred ln1.9%of adult patients who received fovastatin tor at least one year (see ADVERSE REACTIONS). When the drug was interrupted or discontinued in these patients, the transaminase levels usually fell slowly to pretreatment levels. The increases usually appeared 3 to 12 months after the start ol therapy with lovastatin and were not associated with jaundice or other clinical signs or symptoms . There was no evidence of hypersensitivity. A liver biopsy was done in one of these patients and showed areas of focal hepatitis. In this patient, transaminase levels returned to normal following discontinuation ol therapy. Some of these patients had abnormal liver function tests prior to lovastatin therapy and/or consumed substantial quantities of alcohoL
It Is recommended that liver function tests be performed every 4 to 6 weeks during the first 15 months ot therapy with lovastatin and periodically 1herealter in all patients. Special attention should be paid to patients who develop elevated serum transaminase levels , and in these patients , measurements should be repeated promptly and then performed more frequently. If the transaminase levels show evidence of progression , particularly if they rise to 3 times the upper limit of normal and are persistent. the drug should be discontinued . Liver biopsy should be con-sidered if elevations are persistent beyond the discontinuation of the drug.
The drug should be used with caution in patients who consume sub-stantial quantities of alcohol and/or have a past history of liver disease. Active liver disease or unexplained transaminase elevations are con-traindications to the use of lovastatin .
As with other lipid-lowering agents . moderate (less than 3 times the upper limit of normal) elevations of serum transaminases have been reported loll owing therapy with MEVACOR (see ADVERSE REACTIONS). These changes appeared soon after initiation ol therapy with MEVACOR, were often transient , were not accompanied by any symptoms , and interruption of treatment was not required . Skeletal Muscle
Myalgia has been associated with lovastatin therapy. Transient , mildly elevated creatine phosphokinase levels are commonly seen in lovastatin-treated patients. However, in clinical trials, approximately 0.5% of patients developed myositis , i. e., myalgia associated with markedly elevated CPK levels. In cardiac transplant patients who were receiving immunosup-pressive drugs including cyclosporine , there have been reports of severe rhabdomyolysis that precipitated acute renal failure. Myositis should be considered in any patient with diffuse myalgias , muscle tenderness, and/or marked elevation ol CPK. Patients should be advised to report promptly unexplained muscle pain or tenderness, particularly if accom-panied by malaise or fever. Lovastatin therapy should be discontinued il markedly elevated CPK levels occur or myositis is diagnosed .
Most of the patients who have developed myositis were receiving con-comitant therapy with immunosuppressive drugs or gemfibrozil. In clinical trials , about 30 percent of patients on immunosuppressive therapy including cyclosporine developed myositis within a year after starting lovastatin; the corresponding value for gemfibrozil was approximately 5 percent. It is not known whether the same phenomenon occurs with other fibrates. Therefore, the benefits and risks of using lovastatin con-comitantly with immunosuppressive or librate drugs shou ld be carefully considered .
Consideration should be given to temporarily withholding or discon-tinuing drug therapy in any patient with a risk factor predisposing to the development ol renal failure secondary to rhabdomyotysis , including: severe acute Infection, hypotension, major surgery, trauma , severe met-abolic, endocrine, or electrolyte disorders, and uncontrolled seizures.
PRECAUTIONS General
Before instituting therapy with MEVACOR, an attempt should be made to control hypercholesterolemia with appropriate diet , exercise, weight reduction in obese patients, and to treat other underlying medical prob-lems (see INDICATIONS AND USAGE).
Eye There was a high prevalence of baseline lenticular opacities in the
patient population included in the clinical trials with lovastatin . During these trial s the appearance of new opacities was noted . The causal relationship ollovastatin to these findings has not been established.
Of 431 patients examined with slit lamp at baseline and during therapy with lovastatin, 34 had opacities reported at the final examination (5 to 15 months alter starting lovastatin) that were not noted at baseline. On the other hand , in 45 patients, opacities observed at baseline were not noted at the final examination , so that the prevalence did not increase. There was no clinically significant change in visual acuity in the patients who had new opacities reported , nor was any patient, including those with opacities noted at baseline. discontinued from therapy because of a decrease in visual acuity. Nevertheless, until further experience is obtained , it is recom-mended that patients placed on lovastatin therapy be examined with a slit lamp before or shortly after in itiation ol treatment and annually thereafter.
MEVACOR"' (Lovastatin I MSD)
Homozygous Familial Hypercholesterolemia MEVACOR is less effective in patients with the rare homozygous familial
hypercholesterolemia, possibly because these patients have no functional LDL receptors. MEVACOR appears to be more likely to raise serum trans-aminases (see ADVERSE REACTION S) in these homozygous patients. Drug Interactions
Immunosuppressive Drugs, Gemfibrozil: See WARNINGS, Skeletal Muscle.
Antipyrine: Antipyrine is a model lor drugs metabolized by the micro-somal hepatic enzyme system (cytochrome P450 system). Because lovastatin had no effect on the pharmacokinetics of antipyrin e, interac-tions with other drugs metabolized via this mechanism are not expected .
Propranolol: In normal volunteers , there was no clinically significant pharmacokinetic or pharmacodynamic interaction with concomitant ad-ministration of single doses of lovastatin and propranolol .
Digoxin: In patients with hypercholesterolemia, concomitant admin-istration of lovastatin and digoxin resulted in no effect on digoxin plasma concentrations .
Warfarin: The concomitant administration of lovastatin and warfarin to a lew patients with hypercholesterolemia did not suggest an alteration of the anticoagulant action of warfarin .
Other Concomitant Therapy: Although specific interaction stud ies were not performed , in clinical studies, lovastatin was used concomitantly with beta blockers, calcium channel blockers, diuretics , and nonsteroidal anti-inflammatory drugs (NSAIDs) without evidence ol clinically significant adverse interactions.
Orug/Laborafory TeSIInteractions Lovastatin may elevate creatine phosphokinase and transaminase lev-
els (see ADVERSE REACTIONS). This should be considered in the differ-ential diagnosis of chest pain in a patient on therapy with lovastatin. Carcinogenesis, Mutagenesis. Impairment of Fertility
In a 21-month carcinogenic study in mice, a statistically significant (p< O.OS) increase in the incidence of hepatocellular carcinomas and adenomas was observed at doses of 500 mg/kg/day (312 times the maximum recommended human dose) of lovastatin. Th ese changes were not seen in mice given doses of 20 and 100 mg/kg/day (12.5 and 62.5 times the maximum recommended human dose).
A statistically significant increase (P"'0.05) in the incidence ol pulmo-nary adenomas was seen in female mice receiving 500 mg/kg/day (312 times the maximum recommended human dose) ; no similar changes were seen in males at any dose or in females receiving 20 or 100 mg/kgi day (12 .5 or 62.5 times the maximum recommended human dose). Because the incidence of pulmonary tumors was within the range of untreated animals in studies of similar duration , the relationship of this latter change to treatment is not known.
In addition , an increase in the incidence of papilloma in the non-IUCCIS~''' !~1e st~m_achwa!;observed in mice receiving 100 and day (62 .5 and 312 times the maximum recommended human crease was seen at a dosage ol20 mg/kg/day (12.5 times the
maximum recommended human dose). The glandular mucosa was not affected . The human stomach contains only glandular mucosa. Impor-tantly, there is a strong association between this change and hyperplasia of the squamous epithelium (acanthosis) in this region: acanthosis is a characteristic change observed in the non-glandular mucosa of rodents treated with HMG-CoA reductase inhibitors and is most probably a result of inhibition of the reductase in this tissue .
Similar squamous epithelium is found in the esophagus and anorectal junction of the mouse and rat; however, no evidence of a similar drug-induced hyperplastic response was observed in these tissues in stud ies of up to 21 months in the mouse given up to 500 mg/kgi day (312 times the maximum recommended human dose), or in a study of 24 months in the rat given 180 mg/kglday (112 times the maximum recommended human dose).
In a 24-month carcinogenicity study in rats , there was a positive dose response relationship for hepatocellular carcinogenicity in males (unad-justed p = 0.025). However, because the incidence ol hepatocellular carci-nogenicity observed in male rats in this study is similar to that observed spontaneously in this strain of rat, the implications of this finding are unclear.
No evidence of mutagenicity was observed in a microbial mutagen test using mutant strains of Salmonella typhimurium with or without rat or mouse liver metabolic activation . In addition , no evidence of damage to genetic material was noted in an in vitro alkaline elution assay using rat or mouse hepatocytes , a V-79 mammalian cell forward mutation study, an in vitro chromosome aberration study in CHO cells , or an in vivo ch ro-mosomal aberration assay in mouse bone marrow.
No drug-related effects on fertil ity were found in studies with rats. Pregnancy Pregnancy Category X
See CONTRAINDICATIONS. Lovastatin has been shown to produce skeletal malformations in the rat
let us at doses of 800 mg/kg/day (500 times the maximum recommended human dose). At similar doses in mice, an increase in skeletal malforma-tions was observed . These individual changes are within the range of those observed spontaneously in this strain of mouse. No drug-induced changes were seen in either species at doses ol up to 80 mg/kg/day (50 times the maximum recommended human dose). No evidence of malfor-mations was noted in rabbits at up to 15 mg/kg/day (highest tolerated dose- about 9 times the maximum recommended human dose). There are no data in pregnant women .
Nursing Mothers Studies in rats have shown that lovastatin is excreted in the milk. It is
not known whether th is drug is excreted in human milk. Because many drugs are excreted in human milk and because of the potential for serious adverse reactions in nursing infants from MEVACOR, women taking lovastatin should not nurse their infants (see CONTRAINDICATIONS). Pediatric Use
Safety and effectiveness in children have not been established. Because children are not likely to benefit from cholesterorlowering lor at least a decade and because experience with this drug is limited (no studies in
MEVACQR® (Lovastatin I MSD)
subjects below the age of 20 years), treatment of children with Iovas!< not recommended at this time.
ADVERSE REACTIONS MEVACOR is generally well tolerated; adverse reactions usually
been mild and transient. Less than 1% of patients were discontinued controlled clinical studies due to adverse experiences attributab MEVACOR. About 2% ol patients were discontinued from all st1 (controlled and uncontro lled) due to adverse experiences attributat MEVACOR; about one-third ol these patients were discontinued d1 increases in serum transaminases . Clinical Adverse Experiences
Adverse experiences reported in patients treated with MEVACO controlled clinical stud ies are shown in the table below:
MEVACOR Placebo Cholestyramlne Prol (N =o/.613) (N = 82) (N o/,88) (N :
Gastrointestinal Constipation 4.9 34.1 l Diarrhea 5.5 4.9 8.0 t\ Dyspepsia 3.9 13.6 Flatus 6.4 2.4 21 .6 Abdominal pain/ cramps 5.7 2.4 5.7 Heartburn 1.6 8.0 Nausea 4.7 3.7 9.1
Musculoskeletal Muscle cramps 1.1 1.1 Myalgia 2.4 1.2
Nervous System/Psychiatric Diuiness 2.0 1.2 Headache 9.3 4.9 4.5
Skin Rash/pruritus 5.2 4.5
Special Senses Blurred vision 1.5 1.1 Dysgeusia 0.8 1.1
Laboratory Tests Marked persistent increases of serum transaminases have been m
(see WARNINGS). About 11% ol patients had elevations ol creatine phosphokinase (C
levels of at least twice the normal value on one or more occasions. corresponding values for the control agents were cholestyramim percent and probucol, 2 percent. This was attributable to the noncan fraction ol CPK. Large increases in CPK have rarely been reported ( WARNINGS, Skeletal Muscle). Concomitant Therapy
In controlled clinical stud ies in which lovastatin was administt: concomitantly with chotestyram ine, no adverse reactions peculiar to · concomitant treatment were observed . The adverse reactions I occurred were limited to those reported previously with lovastatin or c lestyramine. Other lipid-lowering agents were not administered conco tantly with lovastatin during controlled clinical studies. In uncontro clinical studies, most ol the patients who have developed myositis • receiving concomitant therapy with immunosuppressive drugs or g£ librozil (see WARNINGS, Skeletal Muscle). Uncontrolled Clinical Studies
The adverse experiences observed in uncontrolled studies were sim to those seen in controlled clinical studies. Abnormal liver function te were observed at a higher incidence than in the controlled studies (' WARNINGS, Uver Dysfunction). Myositis (myalgia with marked C elevations) was reported in approximately 0.5% of patients (see WAF INGS, Skeletal Muscle). Causal Relationship Unclear
Nervous System: A single case ol peripheral neuropathy has bt reported: the relationship to lovastatin is uncertain. Visual evoked sponse , nerve conduction measurements, and electromyography in or 30 patients showed no evidence of neurotoxic effects of lovastatin .
Special Senses: Of 431 patients examined with slit lamp at baseline a during therapy with lovastatin, 34 had opacities reported at the li1 examination (5 to 15 months after starting lovastatin) that were not nol at baseline . On the other hand, in 45 patients, opacities observed baseline were not noted at the final examination, so that the prevalence t not increase (see PRECAUTIONS).
OVERDOSAGE There have been no cases ol overdosage with MEVACOR in humar
The oral L050 of MEVACOR in mice is 20 g/kg . DOSAGE AND ADMINISTRATION
The patient should be placed on a standard cholesterol-lowering d before receiving MEVACOR and should continue on this diet duri treatment with MEVACOR. MEVACOR should be given with meals .
The recommended starting dose is 20 mg once a day given with t evening meal. The recommended dosing range is 20 to 80 mg/day single or divided doses; the maximum recommended dose is 80 mg/di Adjustments ol dosage should be made at intervals of 4 weeks or mol Doses should be individualized according to the patient's response (s Tables I to IV under CLINICAL PHARMACOLOGY, Clinical Studies for do response results).
For those patients with severely elevated serum cholesterol levels (i.E >300 mg/dL (7.8 mmoi/L] on diet), MEVACOR may be initiated at 1
mg/day. Cholesterol levels should be monitored periodically and consideratit
should be given to reducing the dosage ol MEVACOR if cholesterol lev• fall below the targeted range.
HOW SOPPLIEO Tablets MEVACOR 20 mg are light blue , octagonal tablets, coded MS
731 on one side and MEVACOR on the other. They are MSI supplied in unit-of-use bottles of 60 and in unit-dose ~ packages of 100. 88:'r.l For more detai led information, consul1 your MSD Representative or Sl Prescribing Information, Merck Sharp & Dohme, Division ol Merck Co., INC., West Poin1, PA 19486.
JBMC201(50

386, Broken Arrow, OK 74728 McNamara, Thomas William,
CCOM '84; 219 Green Ct., Cas-tle Shannon, PA 15234
Meadow, Felice, TCOM '82; 20 Sunnyside Rd., Durham, NH 03824
Megna, Robert J., KCOM '85; Rt. 2, Box 195M, Waxahachie, TX 75165-9802
Melvin, Susan, Capt., COMP '84; 5865 Naples Plaza, l.Dng Beach, CA 90803
Mileke, Kevin, Capt., COMP '84; 21173 Martynia Ct., Riverside, CA 92507
Miranda, Armand G., KCOM '74; 135 S. Mine La Motte, Box 271 , Fredericktown, MO 63645
Monte, Michael B. , TCOM '77; Suite 140, 3434 Hwy. 67 E., Mesquite , TX 75150-2635
Morrill, Thomas R. , TCOM '86; No. 302, 5115 N. Galloway, Mes-quite, TX 75150
Murray, Shawne Elaine, WVSOM '86; Suite 1, 3875 Holcomb Bridge Rd., Norcross, GA 30092
Myers, Doris A., KCOM '81; Suite 206, 27155 Chardon Rd., Richmond Heights, OH 44143
Nathan, Michael D., KCOM '71 ; 380 Hillside Ave ., Allendale, NJ 07401
Ott, Paul D. , UHSCOM '78; Rt. 6, Box 585, 'fulsa, OK 74127
Payne, John B., Lt. Col., UOMHS '78; 6710 Cresta Bonita St., El Paso, TX 79912
Perez, Miguel A., MSUCOM '84; 106 Bel Air, No. 2A, Laredo, TX 78041-2301
Pierce, Allyn M., UOMHS '73 ; Box 1027, Corona, CA 91718
Pino, John A. , UOMHS '73; 12 Joyce St., Thms River, NJ 08753,
Ranta, James P., MSUCOM '84; 1256 Granada, N.W., Walker, MI 49504-2215
Schaffer, Robin M., UNECOM '83;
No. 8A, 4015 Bayshore Blvd., Tampa, FL 33611-1702
Silk, Marshall B., UOMHS '81 ; Star Route 610, Placitas, NM 87043
Subudhi, Manoj K., NYCOM '82; 247 Reed Ave. , Syracuse, NY 13207
Thdesco, J. Michael, PCOM '77; 534 Wyoming Ave, Kingston, PA. 18704
Thomas, Michael E., MSUCOM '83; 1953 Evergreen, S.E., Grand Rap-ids, MI 49506
Tischler, Jeffrey H., CCOM '77; Suite 4, 260 Godwin Ave., Wyckoff, NJ 07481
Vallad-Hix, Colleen M., KCOM '85; 4250 Davlind St. , Holt, MI 48842-6006
Weinstein, Mitchell 1. , UHSCOM '84; Apt. 14F, 200 Carman Ave., East Meadow, NY 11554
THE CHICAGO COLLEGE OF OSTEOPATHIC MEDICINE DEAN, VICE PRESIDENT FOR ACADEMIC AFFAIRS
The Chicago College of Osteopathic Medicine invites nominations and applications for the position of Dean, Vice President for Academic Affairs.
The DeanNice President is the Chief Academic and Administrative Officer of the Chicago College of Osteopathic Medicine and reports directly to the President of the College. The DeanNice President will provide leadership for planning, coordinating, and implementing the development of a new campus . This individual assumes extended administrative responsibilities as delegated by the President and plays a major role in representing the College to constituencies in the professional and scientific arenas , as well as to the community.
The DeanNice President must be a leader in the osteopathic profession, a scholar and teacher of acknowledged achievement with a vision for the future of osteopathic medicine. This individual must have experience appropriate for the Chief Academic and Administrative Officer.
The Chicago College of Osteopathic Medicine is located in the Hyde Park area of Chicago, IL. , along with the Chicago Osteopathic Medical Center. Additionally, there is a satellite teaching hospital in Olympia Fields, as well as a network of ambulatory clinical facilities throughout metropolitan Chicago. In September, 1988 the Chicago College of Osteopathic Medicine will move its pre-clinical facilities to a 105 acre campus in Downers Grove, a western suburb of Chicago. The College enjoys a reputation for excellence among osteopathic colleges and has the largest osteopathic postgraduate training program in the country.
The Search Committee will begin reviewing applications on March 1, 1988 and will continue until the position is filled .
The deadline date is April 20, 1988. Send curriculum vitae to: Dr. Jack B. Kinsinger President/CEO Chicago College of Osteopathic Medicine Office of the President 5200 South Ellis Chicago, Illinois 60615
The Chicago College of Osteopathic Medicine is an equal opportunity, affirmative action employer.

~PATIENT HEALTH GUIDE
~----------------~ Taking charge of your migraine
MARGARET REICH Senior Staff Editor
Stay home from work due to a co ld or stomach ache
and chances are you w i II receive plenty of sympathy.
But ca ll in with a migraine headache and you' re
likely to be scoffed at fo r such an "excuse ." After
all , everyone gets headaches, but most of us take two aspirins and forget about it.
Yet, for some 12 to 16 million persons, a migraine
is unfo rgettable. In its most severe form , bolts of lightning-like pain seem to flash through the eyes.
It's as if a vise has been placed on the head and the
screws are slowly tightened increasing the internal
throbbing pressure. To complicate matters, nausea
and vomi ting often accompany these symptoms. The
pain can be so debilitating that a migraine sufferer may be in bed fo r hours if not days.
Who gets a migraine?
While many famous, well-educated persons
throughout hi story reportedly suffered from thi s disorder (Aristotle, Madame Pompadour, and Ulysses
S. Grant), a high IQ or income is not a prerequisite
for migrai nes. Even long-held views that onl y
neurotic, perfectionists are suscepti ble to migraines
have been di sputed . It's poss ible that having to dea l w ith chronic pain is what causes some migraineurs
to develop these traits. What is certain is that
migraines are hereditary. About 70% to 75 % of
migraineurs have a family member w ho shares the
same disorder. Symptoms usuall y first appear between ages 5 to
35 . However, infants and toddlers are not immune
from the pain of a full -blown attack. In severe cases,
babies may bang thei r heads on the side of the crib or the floor during an epi sode. Often, parents
incorrectl y interpret thi s as a tantrum. Likewise, children with milder attacks are more
prone to motion sickness and stomache aches
accompanied by vomiting. Children often turn red
or blue during an attack. Swelling of hands and feet,
increased urination, and sweating are common
manifestati ons of migraine in adults and children.
Patient health guide
During childhood, both boys are girl s are equall y
susceptible. However, w ith the onset of ado lescence,
women have the dubious distinction of outnumbering
men 4 to 1. Estrogen appears to be a factor, although to what extent remains unknown . Thi s may explain
why some women taking birth contro l pill s experience migraines.
Classifying migraines
For diagnostic purposes, migraines tend to be pi geonholed according to symptoms. Keep in mind
that these categories are not set in stone. Symptoms frequently overl ap.
Classic
Like the finer things in life, a class ic migraine has
very di st inct qualiti es. In thi s case, neuro logic
symptoms ca ll ed an aura announce the fo rthcoming
throbbing pain about 30 minutes before it actually arri ves . Fl ashing lights and co lor, double v ision,
strange smell s, or halluc inations are an aura's
hallmark . Zig-zag lines appea r in the fi eld of v ision.
Areas of blind spots make words disappear from the printed page. Sometimes an increased sensitiv ity to
li ght occurs. Size perception may become distorted .
Migraineurs may also experi ence numbness,
wea kness, or cl umsi ness during th is phase. Intense moods are not uncommon either. Some may feel
euphoric a day or two before an attack, while others w ill be depressed.
O nly 20% to 30% actuall y experience an aura
beforehand . Conversely an aura ca n occur without
the actual headache. When a headache does ensue, the symptoms
assoc iated w ith the aura sometimes linger. Pai n, which starts out as a dull throb and increases to a
constant stream, is usuall y one-s ided. It may be felt
around the eyes, forehead, or travel to the cheeks,
jaws, or back and side of the head. There's loss of
appetite, nausea, and vomi ting. Constipati on,
diarrhea, and water retention are famili ar signs
exhibited during the early headache phase. Light and
no ise often aggravate the pain . Sometimes temporary hea ring loss or ringing noises in the ear may develop.
·It hurts just to touch the head, face, and neck.
W hen the attack w inds down, the need to urinate
increases as the body rids itse lf of the excess water
retained during the earlier stages. When it's all over-
561

PATIENT HEALTH GUIDE
anywhere from six to eight hours or, in some cases, one to two days later- the migraineur may feel spent or, depending on the individual , elated.
Frequency of attacks varies. Some persons may experience more than one a week, while others may go months, even years before onset of another migraine. By age 50, most sufferers are spared further incidents.
Common
As the name implies, this is the most frequently experienced migraine. Some sufferers report doing their best work just days before an attack.
Generally, the symptoms resemble the classic migraine without the aura . However, common migraineurs don't get off the hook that easily. Pain tends to be more intense than that experienced in the classic variety. Although often one-sided, it can occur in the front or on both sides of the head. This headache usually lasts about one to three days. Between attacks, the migraineur is generally a healthy person .
While these two types are the most prevalent, the varieties outlined below prove just as troublesome for their sufferers.
Basilar
This migraine primarily affects women under age 21. The basilar artery supplies blood to the brain stem and brain . Along with all the previous symptoms described, basilar migraineurs often appear confused, disoriented, or in a stupor. They have ringing in the ears and difficulty speaking. This confused state lasts about 45 minutes. Often it 's mistaken for signs of alcohol or drug intoxication . On rare occasions, a sufferer may become unconscious.
Ophthalmoplegic
Impaired eye movement and temporary partial or total blindness during the later stages of the headache signal this specific migraine. Young men are more likley to experience these symptoms. While these ophthalmologic characteristics usually disappear with age, the headache pa in remains.
Hemiplegic
Paralysis on one side of the body accompanies this migraine. Not surprisingly, sometimes this headache is confused with stroke symptoms. Muscle weakness persists for about an hour on the second or third day, but can last for one to two days. Depending on which side of the body is affected , speech may be impaired during this time.
562
Mixed headache
A tension headache due to strident neck and shoulder muscles can lead to migraine. The result delivers a combination one-two punch of pain. The typical person with mixed headache experiences a tension headache every day and a migraine one to two times a week.
Abdominal
Children and young adults who experience recurrent bouts of abdominal pain with stomach upset, nausea, and vomiting occurring regularly may not be suffering from a migraine headache. If your doctor finds no stomach or intestinal problems, the pain could be due to a stomach migraine.
What causes a migraine?
Trying to determine what causes migraine is about as easy as answering the question, "Which came first, the chicken or the egg?" About the only thing medical scientists agree on is that migraines are related to the stretching or dilation of blood vessels. What causes the stretching and the pain are the real sticklers .
The serotonin connection
The answer may lie with one of the body's chemicals-serotonin. This amine regulates the constriction and expansion of blood vessels (vasoconstriction and vasodilation), and acts as a neurotransmitter to the brain.
As a regulator of blood circulation, serotonin is stored in microscopic disc-like platelets. When you cut yourself, these blood platelets congregate, stopping the flow so you won't bleed to death . The serotonins in the platelets assist in the clotting by constricting the blood vessels . Increased serotonin levels are present during the preheadache stage of migraine.
Neurotransmitters to the brain tell the nerve cells when to fire and when to stop. Specifically, serotonin switches off nerve impulses. Serotonin levels fall during the headache stage making migraine sufferers particularly sensitive to outside stimuli.
Because of this , one theory suggests that the nervous system responds to a trigger causing a spasm in the small arteries in the brain . As a result, the blood vessels in the scalp and neck constrict, reducing blood flow. At the same time, the platelets begin releasing serotonin which further constricts blood vessels. Since its bloodline is being cut off, the brain becomes starved for oxygen. This may account for the dizziness and distorted speech often associated
April 1988/Journal of AOA/vol. 88/no.4

with the aura. To make up for the decreased blood flow, major
arteries and vessels in and around the brain tissue dilate, becoming engorged with blood . Most
probably pain occurs because of this vascular dilation
that is due to serotonin imbalance in the brain.
Non-food trigger mechanisms
Whether the misery is considered vascular or
neurologic seems irrelevant when you're in the midst of an attack. The trick is to identify those factors,
environmental and otherwise, which seem to trigger
an episode. Like most aspects of migraine, triggers
are very subjective. Why and how most work remain unknown. What's music to one person's ears sends
another under cover for peace and quiet. Determining your own triggers is a trial and error
process . Take heart, though. The following factors
have been found to cause a migraine in many
persons. This list, by no means complete, should help
single out your own triggers.
Post-adrenaline blues Contrary to popular belief, stress is not always a
precipitator. Sometimes, the let-down following that
week-long struggle to meet a deadline frequently brings on an attack over a seemingly stress-free
weekend.
The "write" light Flashing televison lights and sunlight, either glaring from the driver's rear window in front of you or
reflecting off snow, often spell trouble. Even
fluorescent office lighting can spark the beginnings
of a migraine. Looking at the world through rose-colored glasses
normally presents an unreal picture of your surroundings, but for migraineurs this eyewear could
thwart an attack caused by inside lighting. Wearing
sunglasses outdoors serves a similar purpose. Some sufferers report that writing with and on pastel-
colored paper instead of standard white stock
decreases glare and with it the frequency of attacks.
Silence is golden Noise doesn't have to be loud to send the headache
prone into a quiet, dark room seeking respite from
the surroundings. A vacuum in use, or vibrations from
your teenager's upstairs stereo are sufficient to
facilitate a headache.
Stay out of the kitchen
The old adage, "If you can't stand the heat, get out
Patient health guide
PATIENT HEALTH GUIDE
of the kitchen" offers sound advice for migraineurs.
Cooking odors, steam, smoke, and an unventilated room are the perfect ingredients for a migraine.
"Not tonight, dear ... "
The onset of a migraine in both men and women during or shortly after sex is common . Drastic
changes in blood flow along with muscle contraction
are responsible for the headache. If no organic causes are found, such as an aneurysm, medication can be
prescribed. Taken 15 to 20 minutes before intercourse, the drug should prevent an attack.
Rocky mountain high
Although considered seasonless, migraines occur
most frequently during the fall and spring, times when the barometric pressure fluctuates greatly. Weather
in general-winds, hot, humid conditions-can
forecast the oncoming storm of migraine pain.
Inhale, exhale Exercise tones up muscles and improves the
cardiovascular system. However, a workout can
work up to a migraine. But, don't use it as an excuse
to become a couch potato! Take a deep breath and choose an appropriate exercise. Stay away from
sports like football where head bashing is unavoidable . Likewise, while you may love tennis or badminton , watching the ball (or birdie) creates
eyestrain.
Early to bed, early to rise
Regular sleep patterns help prevent a migraine.
Burning the midnight oil only serves to usher in
fatigue, with headache not far. behind. On the other
hand, sleeping late on Sunday morning plays havoc with your blood sugar levels . Low sugar levels are
synonymous with migraine. On weekends, set the
alarm for your regular workday wakeup. Eat
something small and then go back to sleep. With
sugar levels back to normal you can rest your mind
and body without risking a headache. Balancing enough sleep with the proper diet are
the keys to avoiding most migraines. Determining
which foods are bad for you is similar to playing
Russian roulette: You don ' t always know if the food
you're eating contains chemicals that will trigger an
episode.
Eating right as a matter of course
Three square meals a day eaten at regular intervals
is sensible advice for everyone, not just migraineurs.
Especially for the headache prone, skipping a meal
563
PATIENT HEALTH GUIDE
or eating too late can produce a migraine. Preparing these daily dishes means keeping an eye
out for certain chemicals known to cause migraines, especially amines found in wine (most notably red) , aged cheeses (cheddar, Brie, Stilton), and chocolate. Tyramine, present in many of these foods, may trigger a migraine.
Another culprit is monosodium glutamate (MSG) a flavor enhancer frequently used in Chinese dishes, canned soups, meat tenderizers, and seasoned salts. This doesn 't mean staying away from your favorite Chinese restaurant. Eating a roll or salad before enjoying a Chinese dish may lessen the chance of migraine. Also many Oriental restaurants will serve MSG-free dishes upon request. As far as processed foods are concerned, remember to read the labels in search of MSG.
Shake that salt habit. The obvious culprits-chips, pretzels-are easy to avoid. Others may be inconspicuous-cheese, ham, bacon.
In additon to sa lt, nitrites found in cured meats (lunch meats, hot dogs, bacon) give meat an appetizing red color, but they can also give you a headache.
Skip the "Skippy" peanut butter and any kind of nuts, eaten alone, as part of dessert topping, or mixed in the batter. The same goes for coconut. Scratch bourbon and gin off your li st, too.
Sometimes milk and other dairy products-yogurt, ice cream-spell trouble. But warm milk may prove less harmful. Likewise small amounts of yogurt (1/2 a cup) should pose no problem. Ice cream lovers need not be discouraged. Small amounts of the frozen delight melting slowly on your tongue tickles the tastebuds without tormenting the cranial nerves that stimulate a headache.
Caffeine, a vasoconstrictor, is one of those can't-live-with-but- can't-live-without things. If you're used to drinking lots of coffee and then quit co ld turkey, you're likely to get a headache. But too much is not healthy either . A good rule of thumb is to limit caffeine to 200 milligrams (mg) a day. That averages out to about 2 cups of regular, freshly made coffee. Instant coffee has even less caffeine (about 60 mg/ cup) , but with only 3 mg a cup, decaffeinated java is best. Stay away from caffeine colas, too.
Not all of these foods affect everyone in the same way. Since it takes about 24 hours before you know whether or not a particular food caused your latest attack, it's best to keep a daily chart or menu of what and when you eat. Once you know what to avoid , you can control your migraines. In fact, 20% to 30% percent of migraineurs find rei ief through diet. If that doesn't work, biofeedback or drug therapy may prove
564
suitable alternatives.
Biofeedback
Frequently used as a first line of treatment for migraines, biofeedback therapy usually includes both temperature and muscular control techniques. That's because many migraines are often combined with muscle tension headache.
Thermal biofeedback
This methods involves controlling skin temperature using suggestive phrases like, " I am quite relaxed . Warmth is flowing into my hands." Such exercises are done with a thermistor attached to your index finger. This device lets you know when you have succeeded in raising your skin temperature.
Since skin temperature is related to the amount of blood flow, the warmer the hand gets, the more blood is ci rcu lating to the hand away from the head. Main head arteries and vessels return to normal size.
Thi s " hothand" approach relieves preheadache symptoms before they become full-fledged headaches. It can also alleviate acute ep isodes already in progress.
Thermal biofeedback training requires a bit of an imagination . Not surprisingly, children make th~ most suitable candidates for this method .
Muscle contro l
Biofeedback for muscle control operates much the same way as " hot hand" therapy . If combination biofeedback treatments are prescribed, muscle training follows thermal control. Electrodes are placed on each temple while you sit in a recl ining position . With tense facial , shoulder, and neck muscles a high pitch is hea rd . As you relax (aga in using phrases like those in thermal therapy), the pitch decreases in tone. Sensitivity of tone can be regulated making it harder for you to relax each time .
The goal of all biofeedback therapy is for you to recognize and control these automatic functions without using any mechanical devices. It can be done if you have a real desire to learn and practice the techniques faithfully .
Once you 've mastered biofeedback therapy, after eight to ten sessions, you may be able to decrease any migraine med ication you may be taking. This holds true especially for women who seem to learn the procedure faster than men .
Osteopathic manipulative treatment Another drugless treatment, espec ially usefu I for a mi xed headache, is osteopathic manipulative treatment (OMT). Manipulating the head and neck
April 1988/Journal of AOA/vol. 88/no.4
muscles by an osteopathic physician can bring relief
from an attack already in progress. In cases where the headache is related to r1 midback problem, OMT
can be used to treat the back malady and in the
process al leviate the headache. If you have a chron ic
back condition, OMT may serve to prevent the
headache in the first place.
Drug therapy For those who suffer an occasiona l mild attack,
aspirin or other analgesics do the trick. Most contain modest amounts of caffe ine. However, taking too many may irritate your stomach. Similarly, the
ongoing chemica l processes occurring during a
migraine may prevent aspi rin from being absorbed. When that happens, the drug becomes less effective
in providing pain relief. But, if you exper ience frequent more severe
attacks, your doctor may need to prescribe medicine that will prevent the migraine in the first place
(prophylactic) or stop the pain in progress (abortive).
As with all prescriptive drugs, close monitoring by your doctor is essential to avoid possibly harmfu l
side effects . Ergotamine tartrate constricts the blood vessels.
It's most effective when taken as soon as the headache symptoms, including aura, appear. This
drug should not be taken daily because it can cause rebound headaches. As your body bui lds a tolerance
to ergotam ine, you w ill f ind yourself taking more of
the drug. just like too much caffeine from coffee,
the ergotamine may end up causing headaches instead of preventing or stopping them. For this
reason, at least a four-day respite in between
treatment is advised. Side effects assoc iated with taking more than the
recommended dosage include nausea, vomiting,
cramps, and weakness in the legs-a ll the migraine
symptoms you were trying to allievate in the first
place. Similar to ergotamine, methysergide provides relief
from inflammation. Because it can permanently
constrict blood vesse ls, leading to kidney, heart, and lung problems, patients are usually taken off the drug
for six to eight weeks at a time. Certain drugs like cyproheptadine decrease the
serotonin and histamine leve ls in the blood. Because
of this, the body responds less to stimu li that would
otherwise trigger an attack. lnderal , a type of medication that slows heart rate
and decreases blood pressure (beta blocker), can help
old and young migraineurs with minimal side effects.
Unlike the other drugs, this beta blocker works to
Patient health guide
PATIENT HEAlTH GUIDE
stabi lize blood vessels and prevent migraines. Even
after you stop taking this drug, it may conti nue to prevent such headaches from coming back.
Situation serious but not hopeless ...
Obvious ly, migraines pose serious problems.
However, you should not let them take contro l of your life. Learn to recognize your personal triggers
and change your eating and sleeping habits accord ingly. Together with professional therapy,
relaxation techniques, and drugs, these modifications will help put you in contro l of you r migraines and your life .
(A ll material in the Patient Health Guide is reviewed by JAOA physician referees.)
References: The anti-headache diet. By Denise Foley. Prevention , vol. 36, pp. 60-66, June 1984
Biofeedback and operant conditioning. In The practic ing ph ys ician's approach to headache, ed. 4. By Seymour Diamond and Donald) . Dalessio. Will iams & Wilkins, Baltimore, MD, 1986
Biofeedback for headaches. By Peter M . Marzuk . Annals of Internal Medic ine, vol. 102, pp. 128-131, )an 1985
Control of migraine. By John B. Brainard . W.W. Norton & Company, Inc., New York , 1977
Coping w ith your headaches. By Seymour Diamond and Mary Franklin Epstein . Delai r Publi shing Company, Inc ., New York, 1982
Discussion, ideas abound in migra ine research; consensus remains elusive. By Tim Kirn . Journal of American Medica l Association , vo l. 257, pp. 9- 12, )an. 2, 1987
Doctors close in on the mechanisms behind headache. By Edw in Kiester, )r. Smithsonia n Magazine, vo l. 18, pp. 175-190, Dec. 1987
Headache. By eil H Raskin, and Otto Appenzeller. W.B. Saunders Company, Philadelphia, 1980
Headaches common, but not ordinary: Part 2 Migraine. Emergency Medicine, vo l . 16, Aug. 15, 1984, pp. 69-82
Headache: Hope through research. National Institutes of Health , Bethesda, MD, Sept. 1984
Headaches: New drugs and advancing research offer hope for 4S million chronic victims. By Matt Clark, et al. Newsweek, Dec. 7, 1987, pp. 76-82
How to find relief from migraine. By Rosemary Dudley and Wade Rowland. Beaufort Books, Inc., New York , 1982
Instructions for migraine patients (patient handout). By Jose Medina . The Neuro Center, Ch icago
Migraine headache: A ca ll for humane treatment (letter). By Anthony S. DiFatta . Journal of the America n Osteopathic Association, vol . 87, pp. 14-21, Sept. 1987
Migraine headache: Diagnos is and treatment. By R. Michael Gallagher and Frederick G. Freitag. Journal of Osteopa thic Medicine, vol. 1, pp. 36-43
Stopping the pain of migraine. By Lewis Vaughn . Prevention vol. 37, pp. 73-78, July 1985
565
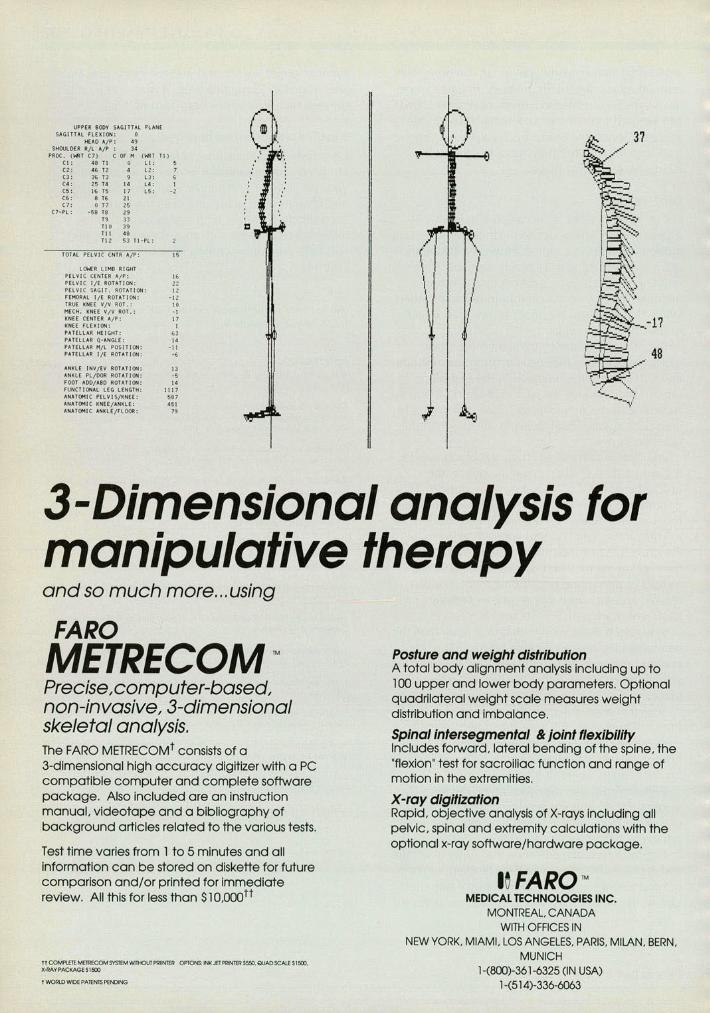
UPPER BODY SAGITTAL PLANE SAGITTAL FLEI<ION: 0
HEAD A/P: 49 SHOULDER R/l A/P : 34
PROC. ( ~T C7) C OF M (1-!RT Tl ) Cl: 48 Tl 0 L1: C2: 4& T:Z l2: C3: 36 T3 L3: C4: 25 T4 \4 L4: I C5: 16 T5 17 LS: - 2 C6: 8 T6 21 C7: 0 T7 25
C7-Pl: -58 TS 29 T9 33 Tl 0 39 Til 48 T\2 53 Tl - PL:
TOHL PELVIC CNTR AfP: 15
LO'WER LIMB RIGHT PELVI C CENtER " f P: 16 PELVIC 1/E ROTAT I ON: Z2 PELVI C SAG I T, ROTATION: 11 FEMORAL 1/E ROT ATION: - 11 TRUE KNEE VfV ROT.: 10 ME CH. KNE E VJV ROT .: - I KNEE CE NTER A/P: 17 KNEE FL EXION: I
~~ I
\ I PATELLAR HEIGHT: ., PATELLAR Q-ANGLE: I< PATELLAR M/l POS ITION: - II PATELLAR lj£ ROTATION: -· ANKlE INVfEV ROTATION: 13 ANKLE PLJDOR ROTA Tl ON: - 5 FOOT ADD/ABO ROTATION: I< FUNCTIONAL LEG LENGTH: 1117 ANATOMIC PELV I S/KNEE: 587 ANATOMIC KNEE/ANKLE: 451 ANATOMIC ANKLE/fLOOR: " J .l€1
3-Dimensional analysis for manipulative therapy and so much more ... using
FARO METRECOM ~ Precise ,computer-based, non-invasive, 3-dimensional skeletal analysis. The FARO METRECOMt consists of a 3-dimensional high accuracy digitizer with a PC compatible computer and complete software package. Also included are an instruction manual, videotape and a bibliography of background articles related to the various tests.
Test time varies from 1 to 5 minutes and all information can be stored on diskette for future comparison and/or printed for immediate review. All this for less than $10,000tt
tt COMPLETE METR€COM SYSTEM WllHOIJTPRIINTER OPTONS: INKJET PRINTER SS50. QUAD SCALE 51500, X-RAY PACKAGES1500
t WORLD WIDE PATENTS PENDING
Posture and weight distribution A total body alignment analysis including up to 1 00 upper and lower body parameters. Optional quadrilateral weight scale measures weight distribution and imbalance.
Spinal intersegmental & joint flexibility Includes forward, lateral bending of the spine, the "flexion" test for sacroiliac function and range of motion in the extremities.
X-ray digitization Rapid, objective analysis of X-rays including all pelvic, spinal and extremity calculations with the optional x-ray software/hardware package.
le FARo ~ MEDICAL TECHNOLOGIES INC.
MONTREAL, CANADA WITH OFFICES IN
NEW YORK. MIAMI. LOS ANGELES. PARIS, MILAN. BERN, MUNICH
1-(800)-361 -6325 (IN USA) 1-(514)-336-6063

Quick! Who has the hearing problem?
Jimmy? Joe? Mrs. Wilson?
It could be any one of them, and with a single AudioScope 3~M
you can screen them all. AudioScope 3. Now one instrument
can do the work of three. These days the demands on your
time and professional skills are greater than ever. That's why AudioScope 3 is quickly becoming the preferred method for screen ing for hearing loss. With AudioScope 3 you can screen your pa-tients quickly and accurately- and with more flexibi li ty. It's a simple procedure that takes on ly seconds. Not only is AudioScope 3 screen ing fast and easy, in many instances it is third party reimbursab le.
Because AudioScope 3 has 20. 25 and 40 dB HL levels in one unit. you can screen al l of your patients with a single instrument. And the tones are presented at random interva ls so your patients ca n't second guess their hea r-ing screen . This varied timing mea ns improved resu lts.
Welch Allyn has also built in a 1000Hz pretone. presented at 20 dB HL above the screening level. so your patients have the opportunity to "practice" listening before they're actua lly screened.
After the pretone your pat ient is given the easiest tones first. beginning at 1000Hz, enhancing the reliab ility of the patients' responses .
At Welch Allyn, we hear you! You told us you wanted a hearing
screen with . • three screening levels • varied timing • pretone And we've done something about
it. AudioScope 3 represents the latest in audiometric screening technology, combined wi th the reliability for which Welch Allyn has become known.
,,~~\
Welch Allyn
Welch Allyn , Inc. 434 1 State St reet Road PO. Box 220 Skaneateles Fa ll s. NY 13153-0220 (315 ) 685-835 1
r----------------------Welch Allyn, I hear you! I would like a demonstration of AudioScope 3 in my office. Name _________ ______ ________ __________ __ _
Address ____________ ___ __ __
City/State/Zip _ ______ _ ____ __ _
Phone( __________________ _
Best time to ca ll _______ ____ (AM) (PM.)
lA<
,,~~
Welch All} Welch Allyn .
4341 Sta te Street R P.O. Box
Skaneateles Falls. NY 13153-C (3151685-1
