neuropsychological outcome of gpi pallidotomy and gpi or stn deep brain stimulation in...
TRANSCRIPT

Brain and Cognition 42, 324–347 (2000)
doi:10.1006/brcg.1999.1108, available online at http://www.idealibrary.com on
Neuropsychological Outcome of GPi Pallidotomy and GPior STN Deep Brain Stimulation in Parkinson’s Disease
Lisa L. Trepanier,§,†,‡ Rajeev Kumar,§ Andres M. Lozano,†,i
Anthony E. Lang,§ and Jean A. Saint-Cyr*,†,‡, i**,§
†Toronto Western Hospital—Research Institute, and iDepartment of Surgery, Division ofNeurosurgery, University of Toronto and The Toronto Hospital; §Department of Medicine,Division of Neurology, University of Toronto and Morton and Gloria Shulman MovementDisorder Centre at The Toronto Hospital; ‡Department of Psychology, York University,North York, Ontario, Canada; and **Department of Psychology, University of Toronto,
Toronto, Ontario, Canada
This paper highlights the neuropsychological sequelae of posteroventral palli-dotomy (PVP) and deep brain stimulation (DBS) of the subthalamic nucleus (STN)and the internal segment of the globus pallidus (GPi) at 3/6 months postoperatively.Results are based on our extensive experience with PVP and our preliminary obser-vations with DBS. Patients with borderline cognitive or psychiatric functioning riskpostoperative decompensation. Nonlateralizing attentional and hemisphere-specificimpairments of frontostriatal cognitive functions followed unilateral PVP. ‘‘Fron-tal’’ behavioral dyscontrol was observed in approximately 25% of patients. Threecases of staged bilateral PVP suggest that premorbid factors may predict outcome,although lesion size and location are also critical. Older patients are at risk forsignificant cognitive and behavioral decline after bilateral STN DBS, while GPiDBS may be safer. 2000 Academic Press
Key Words: neuropsychology; Parkinson’s disease; pallidotomy; deep brain stim-ulation; basal ganglia; subthalamic nucleus; globus pallidus.
INTRODUCTION
The treatment of medically refractory symptoms in advanced Parkinson’sdisease (PD) patients by stereotactic neurosurgical interventions has enjoyeda renaissance (Gildenberg, 1995; Goetz & Diederich, 1996; Olanow, 1994).Success with these treatment approaches is attributable to the increasing un-derstanding of the pathophysiology of the basal ganglia, advances in micro-
Address correspondence and reprint requests to: Lisa L. Trepanier, Toronto Hospital—Western Division, 399 Bathurst Street, Centre for Movement Disorders, Edith Cavell Wing,2-026 Toronto, Ontario M5T 2S8, Canada. Fax: (416) 603-5321. E-mail: [email protected].
3240278-2626/00 $35.00Copyright 2000 by Academic PressAll rights of reproduction in any form reserved.
NEUROPSYCHOLOGICAL OUTCOME OF PVP AND DBS 325
electrode recording, neuroimaging and neurosurgical techniques, and thedemonstration of surgical alleviation of experimental parkinsonism, alongwith the growing awareness of the limitations of pharmacotherapyfor PD (Obeso et al., 1997; Wichman et al., 1995). This paper will discussthe neuropsychological impact of two major stereotactic neurosurgical ap-proaches to PD which are coming into widespread use (Baron et al., 1996;Benabid et al., 1996; Dogali et al., 1995; Krack et al., 1997; Laitinen 1995;Lang et al., 1997a, 1997b; Lozano et al., 1995; Kumar et al., 1998a, 1998b;Scott et al., 1998; Siegried & Lippitz, 1994): (1) ablative surgery (i.e., pal-lidotomy or PVP) and (2) deep brain stimulation (DBS) of the internal globuspallidus (GPi) and subthalamic nucleus (STN). This paper will not deal withneural transplantation or the specific treatment of tremor by thalamic DBSor lesions. In PD, the excessive inhibitory output from the GPi and substantianigra reticulata (SNr), caused largely by the excessive excitatory drive fromthe STN, reduces thalamic activation of the primary motor cortex, premotorcortex, and supplementary motor area (Alexander et al., 1990; Grafton &DeLong, 1997; Parent & Hazrati, 1995). Therefore, the functional goals oflesioning or blocking the neural activity of the GPi or the STN with DBSare to improve patients’ parkinsonian symptoms by reducing the inhibitoryaction of basal ganglia projections to the thalamus (Grafton & DeLong,1997).
Recent clinical outcome studies of unilateral pallidotomy and DBS havedemonstrated improvements in contralateral parkinsonian symptoms and lev-odopa-induced dyskinesias, with ipsilateral and axial benefits being less sig-nificant (Baron et al., 1996; Benabid et al., 1996; Dogali et al., 1995; Golbe,1998; Krack et al., 1997; Kumar et al., 1998a, 1998b, 1998c; Laitinen, 1995;Lang et al., 1997a, 1997b; Lozano et al., 1995; Olanow, 1996; Siegfried &Lippitz, 1994). DBS provides an alternative to pallidotomy and has the po-tential advantages of reversibility of adverse effects induced by stimulationand adaptability to individual patient needs because of flexibility in stimula-tion parameters and site (with a quadripolar electrode).
Although mostly in the form of conference abstracts, recent preliminaryreports of neuropsychological outcome of pallidotomy suggest either a lackof detrimental cognitive changes (Baron et al., 1996; Cahn et al., 1998; Cul-lum et al., 1997; Soukup et al., 1997) or a negative impact on specific fronto-striatal cognitive and functional processes. Specifically, deficits have beenfairly consistently observed in verbal phonemic or semantic fluencies, espe-cially after left-hemisphere lesions (Lucas et al., 1997; Manning et al., 1997;Masterman et al., 1997; Rilling et al., 1996; Riordan et al., 1997; Scott etal., 1998; Trepanier et al., 1998a,b; Uitti et al., 1997). Scott et al. (1998)reported verbal memory declines in their first 3 of 12 (25%) U-PVP patients(side not specified), whose lesions were large and extended vertically,whereas Trepanier et al. (1998a,b) found 9/15 (60%) of left PVP patients(and 1 right PVP) declined on verbal memory and none recovered by their
326 TREPANIER ET AL.
first year follow-up. Lang et al. (1997c), Masterman et al. (1997), and Scottet al. (1998) each noted further cognitive decline in 1 patient who was consid-ered preoperatively cognitively borderline. Riordan et al. (1997), Stebbins etal. (1997), and Trepanier et al. (1998a) reported further decline in executivefunctions, such as cognitive flexibility, working memory, abstract reasoning,or speed of processing. Baron et al. (1996) only noted these types of execu-tive changes in 2 of 12 patients who had iatrogenic small frontal subduralhematomas. Frontal behavioral dyscontrol has also been observed in somepatients (Dogali et al., 1995; Fazzini et al., 1997; Lang et al., 1997c; Shannonet al., 1998; Trepanier et al., 1998a,b).
With regard to the neuropsychological outcome of DBS, findings haveonly been reported following unilateral GPi stimulation in nine patients (sixleft and three right) (Troster et al., 1997). Declines were reported in semanticfluency and visuoconstructional abilities and were also seen in individualsfor phonemic fluency and the short- and long-term delayed free recall trialsof the CVLT (verbal learning).
Except for our long-term follow-up study of 42 PD patients postpalli-dotomy (Trepanier et al., 1998a), these outcome studies are unfortunatelylimited by small sample sizes, short-term follow-up, combining data fromright and left hemisphere pallidotomy surgeries, or potential practice effects.
This paper highlights our experience assessing the neuropsychologicaland behavioral outcomes of unilateral posteroventral pallidotomy (U-PVP),staged bilateral pallidotomy (B-PVP), and most recently of bilateral deepbrain stimulation of the globus pallidus (GPi-DBS) and subthalamic nucleus(STN-DBS) in advanced PD patients after their first follow-up evaluation (3or 6 months). A few comments regarding our long-term follow-up data willbe included. The preliminary nature of our DBS data must be emphasized.We are interested in examining which processes are differentially sensitiveto these procedures. Therefore, where sample size permits, highlights of sta-tistically significant cognitive effects within patient groups and average testscores pre- and 3/6 months postoperatively for the different groups willbe reported. In order to provide a clinical overview of individual trends inthe data, incidence of declining cognitive performance (.1 SD, except thePASAT, see Subjects and Methods) and frontal lobe behavioral changes fol-lowing these procedures will also be presented.
SUBJECTS AND METHODS
Selection Criteria
Patients with idiopathic Parkinson’s disease were considered for GPi pallidotomy or bilateralGPi or STN DBS implantation if they met the following inclusion criteria: substantial disabilitydue to motor fluctuations and levodopa-induced dyskinesias, despite optimization of antipar-kinson medications, and compliance with pre- and postoperative assessments. Exclusion crite-ria included: dementia, other neurological or unstable medical disorders, prior neurosurgical

NEUROPSYCHOLOGICAL OUTCOME OF PVP AND DBS 327
procedure, MRI evidence of other CNS disease, or current psychiatric complications compro-mising cooperation, failure to obtain informed consent, or incapacity to deal with managementand adjustment of the DBS device postoperatively.
Patients
Three groups of patients (demographics in Tables 1 and 2) who underwent either PVP orDBS, as well as a smaller number (n 5 3) who underwent staged bilateral PVP, are reportedhere. In the latter group, it should be noted that two patients had a history of diabetes andone of these had a history of clinical depression, treated with anti-depressant medication andelectroconvulsive shock therapy (ECT). These three patients were 47, 50, and 59 years of age;the first two had completed grade 12 and the latter had 24 years education. Premorbid/currentWAIS-R VIQs were 117/110 (modified slightly due to differences in cultural background),108/88 (difference due to depression, not dementia), and 125/128 preoperatively.
Surgical Procedures
The technique for microelectrode-guided PVP has been described in detail elsewhere (Lo-zano et al., 1996). Usually one or, rarely, two or three overlapping radiofrequency lesions,approximately 6 mm in diameter, were made with a thermistor-coupled probe, using tempera-tures up to 90°C for 60 s.
For STN or GPi DBS, the initial methods used for target selection were the same as thosefor pallidotomy (Lozano et al.,1996). Once the target was selected, a permanent four-channelDBS macroelectrode was implanted and then intraoperative test stimulation was carried outto optimize clinical effects and reduce adverse effects. After 1 week, the electrode cableswere internalized and connected to an internal pulse generator. Details of the procedures andequipment employed are described elsewhere (Kumar et al., 1998a, 1998b).
Clinical Motor Evaluation
A full description of the neurological evaluation protocol and related results from the pa-tients of the current pallidotomy and DBS studies (in part or in full) have been publishedelsewhere (Lang et al., 1997a, 1997b; Lozano et. al., 1995; Kumar et al., 1998a, 1998b).
Neuropsychological Evaluations: Baseline or Preoperative Evaluation
In order to assess suitability for trial inclusion, as well as to establish a baseline cognitiveprofile, a thorough neuropsychological evaluation was completed preoperatively on all pa-tients. Patients were then reassessed at 3, 6, and/or 121 months postoperatively (long-termfollow-up data are yet to be fully collected for the STN DBS trial). Not all patients were seenon all occasions, nor was it always possible to assess patients on all measures, but patientsreported in this review had at least one short-term follow-up assessment at 3 or 6 months.Patients were always evaluated in their optimal behavioral state on medication (i.e., in the‘‘on’’ state). Patients with DBS devices had their stimulators turned on during all assessments.There were no significant changes in the dosage of total dopaminergic medication postpalli-dotomy (Lang et al., 1997a, 1997b) or with bilateral GPi DBS (Kumar et al., 1998b), althoughtotal drug dosage was decreased for the bilateral STN DBS group (Kumar et al., 1998a).
Components of the full neuropsychological test battery were selected with three consider-ations in mind: the battery had to be relatively brief (3–4 h), evaluate the range of cognitivedomains often affected by PD, and include tests assessing aspects of cognitive, behavioraland emotional processes that were shown in the older literature to be affected by thalamotomyand/or pallidotomy (Kocher, Siegfried, & Perret, 1982; Ricklan et al., 1960; Vilkki & Laitinen,

328 TREPANIER ET AL.
TA
BL
E1
Patie
ntC
hara
cter
istic
sby
Gro
up
Est
imat
edD
isea
sePr
eope
rativ
ePr
eope
rativ
ePr
eope
rativ
edo
paE
duca
tion
prem
orbi
dC
urre
ntdu
ratio
nH
oehn
and
Hoe
hnan
deq
uiva
lent
sG
roup
nA
ge(y
ears
)IQ
WA
IS-R
VIQ
(yea
rs)
Yah
r(o
ff)
Yah
r(o
n)(m
g/da
y)a
Uni
late
ral
palli
dot-
4258
(8.2
)12
.6(5
)11
1(1
3.3)
108
(14.
2)12
.8(5
)3.
6(0
.9)
2.6
(0.7
)11
40.9
0(5
06)
omy
(42–
73)
(5–2
7)(7
8–13
2)(8
2–13
8)(4
–25)
(2.5
–5)
(1.5
–5)
(200
–225
0)B
ilate
ral
STN
967
.4(7
.5)
14(4
.9)
116.
4(1
2.3)
112.
2(1
2.9)
14.3
(3.5
)4
(1.2
)2.
6(0
.3)
1497
(659
)D
BS
(55–
75)
(3–2
0)(8
7-12
8)(9
4–13
0)(1
1–22
)(2
.5–5
)(2
–3)
(650
–237
5)B
ilate
ral
GPi
DB
S4
56(1
0.9)
11(1
.2)
109.
8(7
.2)
103.
5(9
)15
(5.3
)3.
9(1
)2.
6(1
)14
57(2
61)
(43–
69)
(10–
12)
(101
–117
)(9
5–11
5)(1
0–22
)(2
.5–5
)(2
–4)
(122
0–18
06)
Not
e.D
emog
raph
icch
arac
teri
stic
sar
epr
esen
ted
asth
em
ean
(sta
ndar
dde
viat
ion)
with
the
(ran
ge)
belo
w.
aT
otal
dopa
equi
vale
nts
5do
seof
regu
lar
levo
dopa
/car
bido
pa(o
rbe
nser
azid
e)1
0.75
3do
seof
cont
rolle
d-re
leas
ele
vodo
pa/c
arbi
dopa
110
3do
seof
brom
ocri
ptin
e1
1003
dose
ofpe
rgol
ide.
NEUROPSYCHOLOGICAL OUTCOME OF PVP AND DBS 329
TA
BL
E2
Neu
rops
ycho
logi
cal
Out
com
e3/
6M
onth
sFo
llow
ing
Uni
late
ral
PVP
and
Bila
tera
lD
BS
ofST
Nor
GPi
Uni
late
ral
Uni
late
ral
left
Uni
late
ral
righ
tB
ilate
ral
STN
Psyc
hom
etri
cte
sts/
palli
doto
my
palli
doto
my
(n5
18)
palli
doto
my
(n5
24)
Bila
tera
lST
ND
BS
(age
Bila
tera
lG
Pido
mai
n(R
&L
)(n
542
)(p
osth
ocan
alys
es)
(pos
thoc
anal
yses
)D
BS
(n5
9).
69)
(n5
5)D
BS
(n5
4)
Atte
ntio
n1.
PASA
T–3
″(%
53.8
86
38.8
63.4
635
.947
.16
40.6
566
35.0
40.4
635
.257
.96
17.1
corr
ect)
61.0
06
37.4
*68
.16
37.7
55.9
637
.848
.86
22.2
426
24.8
66.7
620
.4(n
524
)(n
510
)(n
514
)(n
58)
(n5
5)(n
53)
2.D
igit
Span
-6.
76
2.5
7.2
62.
46.
46
2.6
5.7(
2.3)
6(2.
8)6.
8(2.
2)B
ackw
ard
(raw
6.1
62.
2*6.
36
1.6*
6.0
62.
64.
7(2.
1)a
5.5(
3.5)
5.5(
1.3)
a
scor
e)(n
535
)(n
515
)(n
520
)(n
56)
(n5
2)(n
54)
Exe
cutiv
efu
nctio
ns3.
Tra
ilmak
ing
151.
26
95.6
120.
76
62.9
175.
36
110.
910
1.9(
30.5
)88
.5(2
7.1)
87(3
2)te
st—
B(s
econ
ds)
158.
06
109
135.
76
103.
317
5.6
611
2.9
135.
7(38
)*13
4.5(
36.8
)*88
(26)
(n5
34)
(n5
15)
(n5
19)
(n5
7)(n
55)
(n5
4)V
erba
lle
arni
ng(C
VL
T)
4.T
otal
scor
e(t
rial
s48
.36
12.7
54.3
68.
943
.16
13.4
416
12.3
40.2
613
.147
.56
0.7
1–5)
45.4
610
.0*
46.4
67.
2*44
.56
12.1
35.7
617
.533
.46
18.5
49.5
65
(n5
30)
(n5
14)
(n5
16)
(n5
7)(n
55)
(n5
2)5.
Shor
tde
lay
free
9.7
63.
811
.76
2.2
7.9
64
7.9
63.
77.
46
4.4
126
1.4
reca
ll(S
DFR
)8.
86
3.3a
9.7
62.
3*8.
16
3.8
5.7
65.
35
65.
4a10
61.
46.
Lon
gde
lay
free
10.2
64
12.1
62
8.5
64.
68.
76
47.
46
3.8
11.5
62.
1re
call
(LD
FR)
10.3
63.
311
.36
2.2
9.4
63.
95.
36
5.3*
4.8
65.
6a10
.56
0.7
7.L
ong
dela
ycu
ed10
.96
3.3
12.4
62.
29.
56
3.5
9.6
63.
39
63.
211
64.
2re
call
(LD
CR
)10
.66
2.9
11.6
62.
29.
86
3.2
6.9
64.
7*6
64.
6a11
.56
2.1

330 TREPANIER ET AL.L
angu
age:
Flue
ncy
8.Ph
onem
icflu
ency
33.4
616
.239
.96
15.3
28.5
615
.433
.56
11.7
37.6
612
.332
(FA
S/C
FL)
27.3
613
.6**
27.1
612
.1**
27.5
614
.921
.86
12.2
*23
.86
14.2
*20
(n5
35)
(n5
15)
(n5
20)
(n5
8)(n
55)
(n5
1)V
isuo
spat
ial
enco
ding
/le
arni
ng9.
Bat
tery
for
mem
-46
.76
10.4
47.1
68.
546
.36
14.1
47.2
612
.546
.66
16.2
48.7
62.
1or
yef
ficie
ncy
476
10.6
49.7
615
.344
.36
4.9
41.6
613
.1*
39.7
616
.1a
48.8
63.
9(B
EM
)(t
otal
(n5
6)(n
53)
(n5
3)(n
58)
(n5
5)(n
52)
scor
e)10
.B
EM
-RIE
(im
me-
6.3
62.
36.
86
2.6
5.8
62.
18.
96
2.4
9.1
62.
79.
26
0.8
diat
ere
call
ofco
m-
7.7
62.
2a8.
36
1.9
7.1
62.
77.
56
2.4*
7.1
63.
1*8
61.
4pl
exfig
ure)
(n5
8)(n
54)
(n5
4)(n
58)
(n5
5)(n
52)
11.
BE
M-A
L(s
eria
l6.
66
1.9
6.8
61.
96.
36
2.4
7.3
61.
87.
26
2.4
7.7
60.
3le
arni
ng—
127.
86
1.3
7.8
61.
87.
86
1.0
5.3
62.
5*4.
96
3*7.
86
0.4
desi
gns
inth
ree
(n5
6)(n
53)
(n5
3)(n
58)
(n5
5)(n
52)
tria
ls)
Not
e.In
each
data
cell,
the
top
line
isth
epr
e-m
ean
6SD
and
the
seco
ndlin
eis
the
post
-m
ean
6SD
.a
Indi
cate
str
ends
tow
ard
sign
ifica
ntch
ange
s,.0
5.
p#
.10.
*In
dica
tes
that
the
diff
eren
ces
are
stat
istic
ally
sign
ifica
ntat
p,
.05.
**In
dica
tes
that
the
diff
eren
ces
are
stat
istic
ally
sign
ifica
ntat
p,
.005
.

NEUROPSYCHOLOGICAL OUTCOME OF PVP AND DBS 331
1976) and which are commonly used in the neuropsychological evaluation of PD (Brown &Marsden, 1990; Dubois et al., 1991;Taylor & Saint-Cyr, 1995; Taylor, Saint-Cyr, & Lang,1986). Based on our experience with our evaluation of the U-PVP patients (Trepanier et al.,1998a), a selection of tests thought to be sensitive to the integrity of striatal circuits functionallylinked to the frontal lobes were chosen from the overall battery for the present comparisonof outcome of PVP and DBS.
Neuropsychological Tests and Questionnaires:
A full outline of the test battery can be found in Trepanier et al. (1998a). However, testsreported on here are as follows.
Intelligence. These measures were used only to establish premorbid and current verbal intel-lectual level (IQ) and to estimate cognitive weaknesses at baseline relative to the expectedPD cognitive profile (see Table 1): (i) American New Adult Reading Test (AMNART) and(ii) Wechsler Adult Intelligence Test—Revised: Verbal (WAIS-R VIQ).
Frontal executive tasks including attention, concentration, and problem solving. These in-cluded (i) the Paced Auditory Serial Addition Test (PASAT), 3″; (ii) the Digit Span—Back-ward (verbal subtest from the WAIS-R); (iii) the Trailmaking Test—part B; and (iv) the SpatialConditional Associative Learning Test (four-disk version).
Language. For language we used (i) the Semantic Category Fluency (‘‘Animals’’ trial) and(ii) the Controlled Oral Word Association Test (FAS & CFL versions).
Verbal memory and learning. We used the California Verbal Learning Test (CVLT: Forms1 and 2).
Visual memory and learning. This domain of function proved to be difficult to assess dueto the dyskinesias exhibited in many patients’ drawing hand as well as test sensitivity. In anattempt to circumvent these limitations, alternate methods for assessment of these functionswere explored over these series. (i) the Rey-Osterrieth (R/O) Complex Figure (copy) (usedonly for U-PVP-R group). (ii) the Battery for Memory Efficiency- 7 visual spatial subtests(BEM) make up the total score, and results from the immediate recall of a complex figure(RIE) and serial learning of 12 designs in three trials (AL) (both examining aspects of initialencoding).
Questionnaires. We used (i) the Frontal Lobe Personality Scale (FLOPS) and (ii) A clinicalfollow-up questionnaire regarding subjective experience of surgery by patient and caregiver.Descriptions of these tests can be found in Spreen and Strauss (1998), Signoret (1991), or inthe publications of Taylor, Saint-Cyr, and Lang, (1986, 1990). Care was taken not to confoundpractice effects with improvement in cognitive processing by using alternate forms (orderrandomized across patients), where available, to examine verbal memory (CVLT—forms 1and 2), and verbal phonemic fluency (FAS and CFL).
Statistical Analyses
Details regarding the analyses for the unilateral pallidotomy data are found in Trepanier etal. (1998a). In brief, pre- and postanalyses (i.e., 2 3 2 3 2 ANOVAS; side of lesion X pre-vs posttest score 3 time of post score; i.e., 3 or 6 months or paired t tests) were carried out.For the two DBS groups, the nonparametric Wilcoxon signed ranks test was used. In orderto maximize postoperative data for each measure and group, patients’ first follow-up scoresfrom either 3 or 6 months were employed.
Individual Patterns of Change
To evaluate test score changes among individual patients at their first follow-up evaluation,each reported test score was transformed to a standard (z) score, using published normative

332 TREPANIER ET AL.
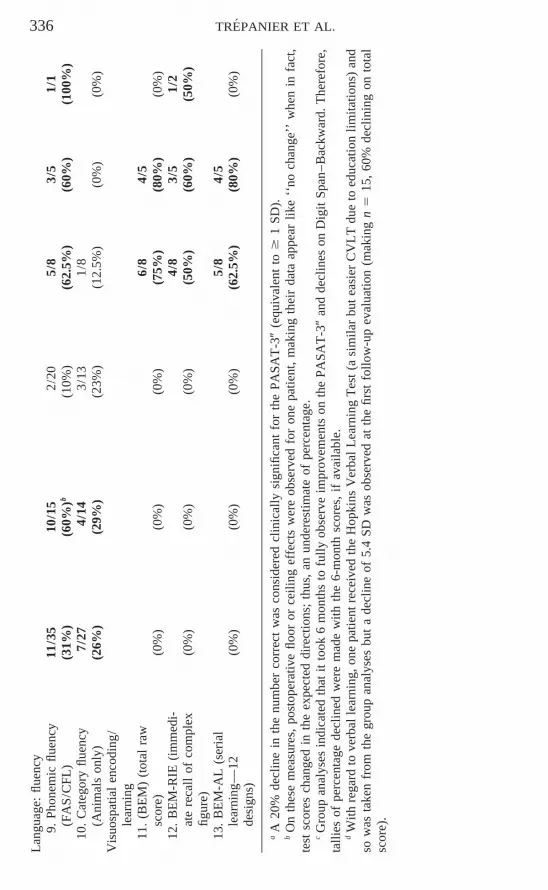
data for all measures except the PASAT 3″, where a conservative 20% decline in numbercorrect was considered clinically significant (≅ 0.5–1 SD, depending on the group; see Table2). This criterion was used for the PASAT due to high variability at baseline, because it isgreater than the mean change in our larger PVP group, and the fact that it is an experimentalbut clinically valid measure for this population. The clinical criterion of . 6 1 SD was em-ployed to tally improvements and declines, respectively, over the 3- to 6-month follow-up.Both levels of analyses were completed for the whole bilateral STN DBS group and for theolder ($ 69) subgroup.
RESULTS
Baseline Neuropsychological Profile
As seen in Table 1, there were no statistically significant differences be-tween premorbid and current IQs within the U-PVP and DBS study groups.Examination of other selected baseline psychometric tests indicated that thestudy groups had evidence of mild-moderate executive dysfunction), whichaffects processing across many cognitive domains, a neuropsychological pro-file comparable to that seen in other groups of PD patients with on/off fluc-tuations (eg. within 1 SD on CALT, TMT-B, FAS, and CVLT of means andSDs presented in Taylor, Saint-Cyr, & Lang, 1986; 1987).
Postoperative Course
As reported elsewhere (Lang et al., 1997a, 1997b; Lozano et. al., 1995;Kumar et al, 1998a, 1998b), clinically significant improvements in motorfunction were observed in patients undergoing each of the different surgicalprocedures, as of the first postoperative assessment. In summary, U-PVPresults in approximately 30% improvement in off-period ADL and motorUPDRS scores (with most of the improvement contralateral to the lesion).Although dyskinesias are reduced by 80% contralateral and 40% ipsilateralto the lesion, on-period motor functioning is otherwise not improved com-pared to the preoperative state. The results of bilateral PVP have not beenreported in large carefully studied groups of patients. Most centers havefound approximately 10% additional improvement in off-period functioningwith a second lesion and striking elimination of virtually all remaining levo-dopa-induced dyskinesias, but again no significant improvement in on-periodmotor functioning. The effects of unilateral and bilateral GPi DBS are similarto those of pallidotomy. In contrast, bilateral STN DBS has a greater effecton motor function and benefit may approximate that of levodopa, with 60%improvement in off-period motor scores and 30–40% improvement in off-period ADL scores. Unlike pallidal surgeries, bilateral STN DBS improveson-period motor scores by about 40%.
The acute cognitive morbidity of surgery may differ when operating onthe pallidum and the STN. Postoperative confusion was very uncommoneven in elderly patients undergoing pallidal surgery. However, there was a

NEUROPSYCHOLOGICAL OUTCOME OF PVP AND DBS 333
tendency toward intraoperative and postoperative confusion in the elderly($ 70 years) STN DBS patients (Kumar et al., 1998a, 1998b). Confusionalstates lasting 1 to 2 weeks postoperatively developed in 4 of our first 16 STNDBS patients (all $ 70 years), and 2 of these patients were still experiencingconfusional episodes at their 3-month follow-up assessment.
Neuropsychological Effects
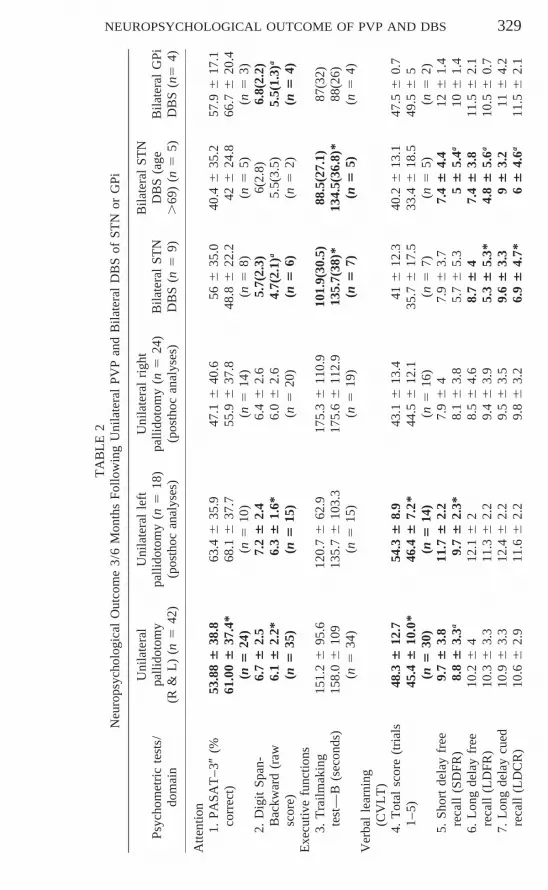
Posthoc analyses indicated significant age effects in the STN DBS group.Therefore, separate analyses are presented for the elderly subgroup. High-lights of our statistical results are reported by group in Tables 2 and 3. Table4 provides a summary of only the significant findings. Results will be pre-sented by functional domain. In Table 2, pre- and postoperative means, stan-dard deviations, sample sizes, and symbols denoting whether the group com-parisons demonstrated trends toward significance (used when sample sizewas small) or where statistically significant results are reported (i.e., @ 50.06 $ p # .10; * 5 p # .05; ** 5 p # .005). Table 3 indicates the incidenceof declining cognitive performance following the different procedures. Thefollowing applies to all groups except B-PVP.
Attention and Working Memory
As measured by the 3″ PASAT, attention significantly improved with U-PVP and a similar trend was seen in GPi DBS. No significant group changeswere noted with STN DBS but it should be mentioned that 37.5% of thesepatients and 20% of older STN DBS patients .69 declined in perfor-mance . 1 SD, although the elderly group started off at a lower level ofperformance. It is also worth mentioning that postoperative performance ofthe younger patients from this group was similar to that of the other groups.Working memory, as measured by Digit Span Backward, declined in allgroups but the change was significant only for U-PVP and for the left PVPsubgroup.
Executive Functioning
Set switching, as indicated by performance time on Trails B, declined forthe whole STN DBS group as well as for the older STN DBS subgroup.
There were no significant group changes in executive functioning, as mea-sured by the number of errors made on the Conditional Associative LearningTest (CALT 2 number of errors). However, Table 3 indicates that many ofthe STN and GPi DBS patients had more difficulty with the task postopera-tively.
Verbal Learning
Verbal learning effects were seen with the CVLT. The patients with leftpallidotomies had increased difficulty with initial encoding. In addition, they

334 TREPANIER ET AL.
were poorer in free recall at a short delay. By comparison, the STN DBSgroup (no age effect) were poorer in both free and cued recall at long inter-vals (consolidation phase) and generally had more difficulties with retrieval(Trials 1–5, LDFR) (see Tables 2–4). In contrast, although sample size waslimited, the GPi DBS patients did not experience encoding difficulties post-operatively but were similar to the STN DBS patients in that they were poorerin retrieval and the consolidation phase of learning (long delay free and cuedrecall).
Language (Phonemic and Semantic Category Fluency)
Controlled phonemic verbal fluency was significantly reduced for all pa-tient groups except the right PVP subgroup (Tables 2 and 4). This reducedperformance appears to be long-term in some patients, as indicated in 5/6U-PVP, 3/3 B-PVP, 2/5 STN DBS (both elderly), and 2/3 GPi DBS patientswho have had 121 month follow-up evaluations and at least one previouspostoperative assessment. Table 3 indicates that left PVP, STN DBS, andSTN DBS .69 patients are most susceptible to these difficulties. This mayalso be true of the GPi DBS but the numbers are too few to draw any conclu-sions.
In contrast, no groups had significant difficulties with semantic fluency,when only the ‘‘Animals’’ trial was given. Table 3 indicates that about 1/4of the U-PVP patients (regardless of lesion side) had difficulties. Althoughnot reported here, significant reductions were found in the STN DBS groupand the elderly subgroup when all three trials (Animals, Fruits, and Vegeta-bles) were employed.
Visual Learning & Memory
Visual–spatial functions were assessed with both the Rey-Osterrieth(R/O) Complex Figure (right PVP subgroup) and with the BEM (DBSgroups and some PVP patients who were later in our series). After a rightpallidotomy, patients had more difficulty accurately drawing the complexfigure (n 5 8; t 5 2.771, p 5 .028) but this improved to baseline levels after6 months. None of the small number of U-PVP patients tested with the BEMsubtests had postoperative difficulties. After STN DBS, the total score fromsix subtests, the immediate recall of a complex figure (simpler than theR/O), as well as the learning of a list of nonsense shapes were significantlyreduced. One of two GPi DBS had more difficulty recalling the BEM com-plex figure; otherwise, their performance was preserved.
Cognitive Effects of Staged B-PVP
Within the three cases of B-PVP at baseline, one patient demonstrated a11 SD (.15 points) difference between these IQ estimates. Two of our

NEUROPSYCHOLOGICAL OUTCOME OF PVP AND DBS 335
TA
BL
E3
Inci
denc
eof
Dec
linin
gC
ogni
tive
Perf
orm
ance
Follo
win
gU
nila
tera
lPV
Pan
dB
ilate
ral
DB
Sof
STN
orG
Pi
Uni
late
ral
Bila
tera
lST
Npa
llido
tom
yU
nila
tera
lle
ftU
nila
tera
lri
ght
Bila
tera
lST
ND
BS
(age
Bila
tera
lG
PiPs
ycho
met
ric
test
s/do
mai
n(R
&L
)(n
542
)pa
llido
tom
y(n
518
)pa
llido
tom
y(n
524
)D
BS
(n5
9).
69)
(n5
5)D
BS
(n5
4)
Dec
lined
Dec
lined
Dec
lined
Dec
lined
Dec
lined
Dec
lined
(.1
SD)
(.1
SD)
(.1
SD)
(.1
SD)
(.1
SD)
(.1
SD)
Atte
ntio
n1.
PASA
T-3
″(%
cor-
1/24
1/14
3/8
2/5
rect
)a(4
%)
(0%
)(7
%)
(37.
5%)b
(40%
)b(0
%)
2.D
igit
Span
-Bac
k-6/
352/
154/
201/
4w
ard
(raw
scor
e)(1
7%)c
(13%
)c(2
0%)c
(0%
)(0
%)
(25%
)E
xecu
tive
func
tioni
ng3.
Tra
ilmak
ing
test
—2/
342/
155/
75/
5B
(sec
onds
)(6
%)
(13%
)(0
%)b
(71%
)b(1
00%
)b(0
%)
4.C
ondi
tiona
las
soci
a-2/
302/
175/
84/
52/
3tiv
ele
arni
ngte
st(7
%)
(0%
)(1
2%)
(62.
5%)
(80%
)(6
6.7%
)(N
o.er
rors
)V
erba
lL
earn
ing
(CV
LT
)5.
Tot
alSc
ore
(tri
als
10/3
08/
141/
163/
73/
51–
5)(3
3.3%
)d(5
7%)d
(6%
)(4
3%)
(60%
)(0
%)
6.Sh
ort
dela
yfr
ee9/
307/
141/
163/
72/
52/
2re
call
(SD
FR)
(27%
)(5
0%)
(6%
)(4
3%)
(40%
)(1
00%
)7.
Lon
gde
lay
free
9/30
7/14
1/16
3/7
1/5
1/2
reca
ll(L
DFR
)(2
7%)
(50%
)(6
%)
(43%
)(2
0%)
(50%
)8.
Lon
gde
lay
cued
5/30
5/14
6/7
4/5
1/2
reca
ll(L
DC
R)
(17%
)(3
6%)
(0%
)(8
6%)
(80%
)(5
0%)
336 TREPANIER ET AL.L
angu
age:
fluen
cy9.
Phon
emic
fluen
cy11
/35
10/1
52/
205/
83/
51/
1(F
AS
/CFL
)(3
1%)
(60%
)b(1
0%)
(62.
5%)
(60%
)(1
00%
)10
.C
ateg
ory
fluen
cy7/
274/
143/
131/
8(A
nim
als
only
)(2
6%)
(29%
)(2
3%)
(12.
5%)
(0%
)(0
%)
Vis
uosp
atia
len
codi
ng/
lear
ning
11.
(BE
M)
(tot
alra
w6/
84/
5sc
ore)
(0%
)(0
%)
(0%
)(7
5%)
(80%
)(0
%)
12.
BE
M-R
IE(i
mm
edi-
4/8
3/5
1/2
ate
reca
llof
com
plex
(0%
)(0
%)
(0%
)(5
0%)
(60%
)(5
0%)
figur
e)13
.B
EM
-AL
(ser
ial
5/8
4/5
lear
ning
—12
(0%
)(0
%)
(0%
)(6
2.5%
)(8
0%)
(0%
)de
sign
s)
aA
20%
decl
ine
inth
enu
mbe
rco
rrec
tw
asco
nsid
ered
clin
ical
lysi
gnifi
cant
for
the
PASA
T-3
″(e
quiv
alen
tto
$1
SD).
bO
nth
ese
mea
sure
s,po
stop
erat
ive
floor
orce
iling
effe
cts
wer
eob
serv
edfo
ron
epa
tient
,m
akin
gth
eir
data
appe
arlik
e‘‘
noch
ange
’’w
hen
infa
ct,
test
scor
esch
ange
din
the
expe
cted
dire
ctio
ns;
thus
,an
unde
rest
imat
eof
perc
enta
ge.
cG
roup
anal
yses
indi
cate
dth
atit
took
6m
onth
sto
fully
obse
rve
impr
ovem
ents
onth
ePA
SAT
-3″
and
decl
ines
onD
igit
Span
–Bac
kwar
d.T
here
fore
,ta
llies
ofpe
rcen
tage
decl
ined
wer
em
ade
with
the
6-m
onth
scor
es,
ifav
aila
ble.
dW
ithre
gard
tove
rbal
lear
ning
,one
patie
ntre
ceiv
edth
eH
opki
nsV
erba
lL
earn
ing
Tes
t(a
sim
ilar
but
easi
erC
VL
Tdu
eto
educ
atio
nlim
itatio
ns)
and
sow
asta
ken
from
the
grou
pan
alys
esbu
ta
decl
ine
of5.
4SD
was
obse
rved
atth
efir
stfo
llow
-up
eval
uatio
n(m
akin
gn
515
,60
%de
clin
ing
onto
tal
scor
e).

NEUROPSYCHOLOGICAL OUTCOME OF PVP AND DBS 337T
AB
LE
4Su
mm
ary
ofSi
gnifi
cant
Cha
nges
inC
ogni
tion
Follo
win
gU
nila
tera
lPV
Pan
dB
ilate
ral
DB
Sof
STN
orG
Pi
Uni
late
ral
Bila
tera
lST
Npa
llido
tom
yU
nila
tera
lle
ftU
nila
tera
lri
ght
Bila
tera
lST
ND
BS
(age
Bila
tera
lG
PiPs
ycho
met
ric
test
s/do
mai
n(R
&L
)(n
542
)pa
llido
tom
y(n
518
)pa
llido
tom
y(n
524
)D
BS
(n5
9).
69)
(n5
5)D
BS
(n5
4)
Atte
ntio
n1.
PASA
T-3
″(%
cor-
↑re
ct)
2.D
igit
Span
-↓
↓↓*
↓*B
ackw
ard
(raw
scor
e)E
xecu
tive
func
tioni
ng3.
Tra
ilmak
ing
Tes
t-B
↓↓
(sec
onds
)V
erba
lle
arni
ng(C
VL
T)
4.T
otal
scor
e(T
rial
s↓
↓1–
5)5.
Lon
gde
lay
free
↓↓*
reca
ll(L
DFR
)6.
Lon
gde
lay
cued
↓↓*
reca
ll(L
DC
R)
Lan
guag
e:flu
ency
7.Ph
onem
icFl
uenc
y↓
↓↓
↓↓
(FA
S/C
FL)
Vis
uosp
atia
len
codi
ng/
lear
ning
8.(B
EM
)(t
otal
raw
↓↓*
scor
e)9.
BE
M-R
IE(i
mm
edi-
↑*↓
↓at
ere
call
ofco
mpl
exfig
ure)
10.
BE
M-A
L(s
eria
l↓
↓le
arni
ng—
12de
sign
s)
Not
e.(↓
)In
dica
tes
ade
clin
ein
perf
orm
ance
.(↑
)In
dica
tes
anin
crea
sein
perf
orm
ance
.*
Ref
ers
toa
tren
din
the
data
(i.e
.,0.
1#
p$
.051
)an
dpr
esen
ted
due
toth
epr
elim
inar
yna
ture
ofth
eD
BS
data
and
the
smal
lce
llsi
zes
for
som
em
easu
res/
grou
ps.

338 TREPANIER ET AL.
TABLE 5aPrevalence of Behavioral Complaints Post–Unilateral PVP
Prevalence of Complaint (x/N; %)
Behavioral description By patient By caregiver(s)
I. Environmental Dependency(i) Perseveration on actions or ideas 6/32 (19%) 11/27 (41%)
II. Psychosocial/emotional control(i) Unawareness of deficits 2/32 (6%) 11/27 (41%)(ii) Social judgment 1/32 (3%) 8/27 (30%)(iii) Lability (unipolar or bipolar) 6/32 (19%) 9/27 (33%)(iv) Depression (not reactive to PVP) 7/42 (17%) 7/27 (26%)(v) Impulsivity 2/32 (6%) 8/28 (29%)b
(vi) Sexually inappropriate behaviors 1/42 (2%) 3/27 (11%)(vii) personality change 1/42 (2%) 1/27 (4%)
III. Executive/cognitive(i) Word finding (fluency/quantity)a 17/42 (40%) 9/29 (31%)b
12/18 (67%) (L) 4/10 (40%) (L)6/24 (25%) (R) 5/19 (26%) (R)
(ii) Overall memory 12/42 (29%) 9/29 (31%)b
(iii) Concentration/distractibility 8/42 (19%) 5/29 (17%)b
(iv) Organizational abilities 5/32 (16%) 5/27 (19%)(v) increased confusion 2/42 (5%) (R only)b 2/29 (7%)b
(vi) dementia (general cognitive decline) 1/29 (3%)b
Note. L, left PVP; R, right PVP; otherwise, R 1 L. It was not until spontaneous reportingof complaints occurred that more systematic inquiry via the FLOPS and more detailed clinicalinterviewing was carried out, allowing for the possibility of an underestimate of the true inci-dence.
a These complaints were spontaneously reported during the clinical interview to haveworsened postoperatively.
b Data jointly collected from clinical interview and FLOPS. N’s increase if clinical interviewavailable, but not FLOPS.
three B-PVP patients experienced significant global cognitive decline subse-quent to their second pallidal lesion. Preoperatively, both of these patientshad atypical cognitive profiles for PD (i.e., impaired confrontational namingand extremely poor visual spatial integration or serial list learning and onehad functionally impaired intellectual capacities). Postoperatively, in all cog-nitive domains but especially executive functioning, performance for bothpatients was 1–3 SD below that seen prior to their second lesion. Both ofthese patients had problematic premorbid medical histories involving diabe-tes. One of the patients also had a history of psychiatric disturbance, alongwith a current verbal IQ .1 SD below premorbid estimates. This patientwas one of the earliest patients in our pallidotomy series. In contrast, thelast case in our series, who had a small second lesion, experienced onlytransient declines in certain aspects of executive functioning (working mem-ory, increased perseveration, and encoding of new material) post- second

NEUROPSYCHOLOGICAL OUTCOME OF PVP AND DBS 339
TABLE 5bPrevalence of Behavioral Complaints Post–Bilateral DBS of STN and GPi
Prevalence of complaint (individual tallies)
STN GPi
Patient Caregiver(s) Patient Caregiver(s)Behavioral description (n 5 9) (n 5 9) (n 5 4) (n 5 3)
I. Environmental dependency(i) perseveration (actions/ideas) 2 1 1 1
II. Psychosocial/emotional control(i) Unawareness of deficits 0 1 0 0(ii) Social judgment 1 1 0 0(iii) Lability (unipolar or bipolar) 1 1 3 1(iv) Depression (not reactive to DBS) 1 1 0 0(v) Impulsivity 2 1 1 1(vi) Sexually inappropriate behaviors 0 0 0 0(vii) Personality change 1 1 0 0
III. Executive/cognitive(i) Word-finding (fluency/quantity) 2 1 0 1(ii) Overall memory 8 4 1 1(iii) Concentration/distractibility 5 2 1 1(iv) organizational abilities 0 1 1 0(v) Increased confusion 2 2 0 0(vi) ‘‘General cognitive decline’’ 1 1 0 0(vii) Increased mental slowing 3 2 0 0
Note. Data were jointly collected from clinical interview and FLOPS.
lesion. Phonemic fluency had declined after the first lesion, never recoveredprior to the second lesion, but did not deteriorate further after the secondlesion.
‘‘Frontal Lobe’’ Behavioral Changes
Behavioral changes, in the three domains of Environmental Dependency,Psychosocial/Emotional Control, and Executive/Cognitive, are presented bygroup in Tables 5a–5c. Complaints were organized in this fashion basedon correlations with frontal lobe/executive functioning and the consistencyof observations reported by caregivers and some patients in the clinical inter-view and the FLOPS. Although most marked and persistent in two of thethree B-PVP, four U-PVP, and one STN DBS patient(s), behavioral changes,sufficiently noticeable to cause disturbance of family or social interactions,have been observed in all groups. Notably, lack of patient insight can beproblematic. Problems can vary from impulsivity and poor judgment to apa-thy and loss of initiative. Patients who became more physically independentpostoperatively, and who consequently attempted to resume their previousactivities, appeared to be the ones who experienced limitations and frustra-tions in this regard.
340 TREPANIER ET AL.
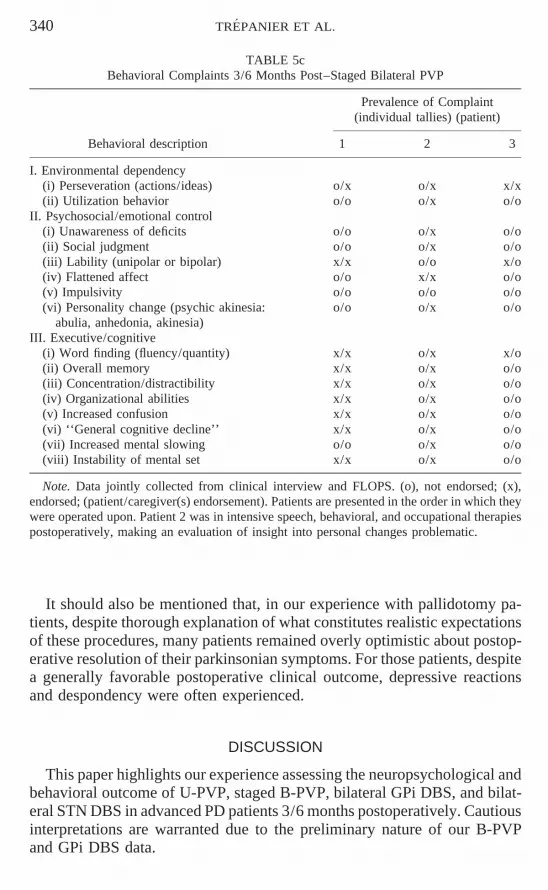
TABLE 5cBehavioral Complaints 3/6 Months Post–Staged Bilateral PVP
Prevalence of Complaint(individual tallies) (patient)
Behavioral description 1 2 3
I. Environmental dependency(i) Perseveration (actions/ideas) o/x o/x x/x(ii) Utilization behavior o/o o/x o/o
II. Psychosocial/emotional control(i) Unawareness of deficits o/o o/x o/o(ii) Social judgment o/o o/x o/o(iii) Lability (unipolar or bipolar) x/x o/o x/o(iv) Flattened affect o/o x/x o/o(v) Impulsivity o/o o/o o/o(vi) Personality change (psychic akinesia: o/o o/x o/o
abulia, anhedonia, akinesia)III. Executive/cognitive
(i) Word finding (fluency/quantity) x/x o/x x/o(ii) Overall memory x/x o/x o/o(iii) Concentration/distractibility x/x o/x o/o(iv) Organizational abilities x/x o/x o/o(v) Increased confusion x/x o/x o/o(vi) ‘‘General cognitive decline’’ x/x o/x o/o(vii) Increased mental slowing o/o o/x o/o(viii) Instability of mental set x/x o/x o/o
Note. Data jointly collected from clinical interview and FLOPS. (o), not endorsed; (x),endorsed; (patient/caregiver(s) endorsement). Patients are presented in the order in which theywere operated upon. Patient 2 was in intensive speech, behavioral, and occupational therapiespostoperatively, making an evaluation of insight into personal changes problematic.
It should also be mentioned that, in our experience with pallidotomy pa-tients, despite thorough explanation of what constitutes realistic expectationsof these procedures, many patients remained overly optimistic about postop-erative resolution of their parkinsonian symptoms. For those patients, despitea generally favorable postoperative clinical outcome, depressive reactionsand despondency were often experienced.
DISCUSSION
This paper highlights our experience assessing the neuropsychological andbehavioral outcome of U-PVP, staged B-PVP, bilateral GPi DBS, and bilat-eral STN DBS in advanced PD patients 3/6 months postoperatively. Cautiousinterpretations are warranted due to the preliminary nature of our B-PVPand GPi DBS data.

NEUROPSYCHOLOGICAL OUTCOME OF PVP AND DBS 341
Summary of Neuropsychological Effects
Patients with U-PVP lesions can experience improvements in allocationof attentional resources but can also suffer declines in working memory,certain aspects of executive functioning, and lateralized declines in verballearning and fluency post- left and visuoconstructional abilities post- rightlesions.
In our limited experience, staged B-PVP appears to potentially be the mostpsychologically toxic procedure. Two of three patients suffered major cogni-tive decompensation across all domains, but especially in the area of execu-tive functioning. However, optimal lesion placement and reduced lesion sizemay make this a viable option for selected patients (Scott et al., 1998).
Many aspects of cognitive functioning decline after STN DBS. Workingmemory, speed of mental processing, set switching, error rate on a condi-tional associative learning task (trend only), long delay free and cued recallof verbal material, phonemic fluency, and encoding of visuospatial materialcan decline in a clinically significant proportion of patients. Patients .69years of age are much more at risk for these cognitive changes (4/5 in ourseries so far), which appear to be progressive supranuclear palsy (PSP)-likein nature, especially with regard to the slowness of mental processing (seenext section for further discussion).
Our four GPi DBS patients (all , 70 years old) showed fewer of thedeleterious effects (working memory, executive functioning, long delay freeand cued recall on CVLT, FAS, RIE-BEM) seen in the other groups butthese observations are too preliminary to draw any conclusions.
Plausible Neuroanatomical Explanations for Neuropsychological Sequelae
These findings are consistent with the explanation that lesions or chronicstimulation within the frontal-striatal circuits (i.e., GPi and STN) are capableof causing further deterioration of processes normally thought to be depen-dent on the functional integrity of these circuits. Specifically, these cognitiveand behavioral/emotional changes may be due to alterations of ‘‘nonmotor’’pathways involving ‘‘dorsolateral’’ (affecting problem-solving, flexibility),‘‘orbitofrontal’’ (affecting inhibitory processes), or ‘‘anterior cingulate’’ (af-fecting initiation, motivation, and drive) striato-thalamo-cortical circuits (seeAlexander et al., 1990). Correlations between PVP lesion location and thesecognitive changes in a subset of our U-PVP patients have now been demon-strated (Lombardi, Gross, Trepanier, Lang, Lozano, & Saint-Cyr, in press).For a further discussion of this topic, please refer to Trepanier et al. (1998a).It should be mentioned that these neuropsychological changes were foundin our initial and consecutive series of pallidotomy patients. Subsequent pa-tients have had smaller and more carefully placed lesions, which may likelyresult in different motor and psychological consequences.
The PSP-like cognitive changes (especially mental slowness) observed

342 TREPANIER ET AL.
following STN DBS may be specifically due to chronic stimulation of theSTN, recalling that it is involved in the neuropathology of PSP (Parent &Hazrati, 1995; Weiner & Lang, 1989). Current spread to adjacent structuresas well as remote antidromic and orthodromic actions must also be consid-ered. Finally, nonspecific effects of surgery may also explain some of thecognitive changes. Specifically, bilateral frontal lobe trajectories or bilateraltrajectories through the thalamus, rather than specific stimulation of the STN,may be contributing factors. In order to determine if a microlesion/trajectoryeffect exists, patients would need to be tested off stimulation. However, inour practical experience, this would be very difficult as most patients havenot wanted their stimulators turned off due to the resumption of their motorsymptoms.
Comparisons with Other Studies
Unilateral pallidotomy. Our findings have been previously reported (Langet al., 1997c; Saint-Cyr et al., 1996; Trepanier et al., 1997, 1998a, 1998b)for this group and are indicative of some further postoperative decline inalready weakened frontal-striatal cognitive and functional processes. Thereare other centers also reporting some negative impact on specific aspectsof frontal-striatal processes, such as cognitive flexibility, working memory,abstract reasoning, or speed of processing (Riordan et al., 1997; Stebbins etal., 1997) (see Introduction for further details). Also similar to our findings,some centers have reported rare cases of frontal behavioral dyscontrol (i.e.,sexual disinhibition; see Tables 5a–5c for further examples) (Dogali et al.,1995; Fazzini et al., 1997; Shannon et al., 1998). Scott et al. (1998) is theonly other group who reported any patients who had difficulties with freerecall of verbal material. Last, similar to our observations, Masterman et al.(1997) and Scott et al. (1998) each noted further cognitive decline in a patientwho was preoperatively considered borderline cognitively, indicating a needfor caution when considering these surgical procedures for such patients.
Deep brain stimulation. With regard to the neuropsychological outcomeof DBS, findings have only been reported following unilateral GPi stimula-tion in nine patients (six left and three right) (Troster et al., 1997). Declineswere reported in semantic fluency and visuoconstructional abilities and werealso seen in individuals for phonemic fluency and the short- and long-termdelayed free recall trials of the CVLT (verbal learning). These findings areconcordant with our observations following bilateral GPi or STN DBS, ex-cept in the latter group, wherein we found patients’ difficulties to be moreextensive, especially if they were .69 years old (i.e., speed of processing,working memory, and executive functioning).
Staged-bilateral pallidotomy. The effects of staged bilateral pallidotomyhave not been well studied from either a neurological or a neuropsychologi-cal perspective, but our experience with three cases (Kumar, Trepanier, et

NEUROPSYCHOLOGICAL OUTCOME OF PVP AND DBS 343
al., in preparation; Galvez-Jiminez et al., 1996), along with the report of sixcases by Roberts and Heilbrun, (1997), suggests that although some aspectsof motor improvement can be seen, this procedure can carry a high risk ofunacceptible adverse effects in other aspects of motor, cognitive, and behav-ioral functioning. This is in direct contrast to the very recent and more opti-mistic study of Scott et al. (1998), reporting on the outcome of eight simul-taneous bilateral pallidotomy cases who, as a group, only experiencedreductions in phonemic and semantic verbal fluencies as well as decreasedspeech articulation rates. Their group also demonstrated significant improve-ments in functional outcome (similar to two of our three cases), although theydid report that one of eight patients (12.5%) suffered generalized cognitiveimpairment postoperatively.
Possible Explanations for Differential Findings
Differences between the neuropsychological outcome of PD patients oper-ated on in different centers may lie largely in the location and extent oflesions, on the one hand, or there may be other factors, such as age andpreoperative cognitive status, which influence outcome, on the other. Comor-bidity with other conditions (e.g., psychiatric history and diabetes, in ourgroup) probably plays an important role as well. Also of importance will beconsideration of test sensitivity and the use of alternate test forms, whenavailable. For example, we used the PASAT 5″ and 3″, the CVLT (two alter-nate forms), BEM subtests, phonemic fluency (FAS and CFL forms), andthe FLOPS, which have revealed impairments (or improvements) across allprocedures.
In our own studies, lack of group effects (despite significant individualchanges) could also be attributed to large variances (and SDs) and floor ef-fects on measures such as the Conditional Associative Learning Test, DigitSpan-Backward, and Trailmaking Test—B. When assessing semantic flu-ency, it appears more sensitive to use all three categories (i.e., Animals,Fruits, & Vegetables), rather than just ‘‘Animals’’ alone. When monitoringthe behavioral impact of these surgeries, a structured questionnaire, such asthe FLOPS, is needed, along with consultation with caregivers and patients.Sometimes, patients lack insight or the caregivers have some difficulty artic-ulating the nature of the behavioral problems, other than to report that theyare having more problems coping at home with their spouses, despite theirbeing more mobile, etc.
Conclusions
(1) Patients who have preexisting atypical cognitive profiles for PD orwho are borderline demented appear to be at high risk for postoperative be-havioral or cognitive decompensation.
(2) Unilateral GPi PVP is still clinically useful but caveats with regard to
344 TREPANIER ET AL.
preoperative status and the likelihood of neuropsychological sequelae mustbe taken into account. Our findings suggest that PVP can induce a furtherdecompensation in cognitive and behavioral areas which show preexistingimpairment in PD and can be hemisphere-specific. In our series, patientswith right lesions experienced fewer and only transient difficulties comparedto those with left lesions.
(3) In our experience, staged B-PVP can be the most problematic surgicalprocedure but careful patient selection with regard to premorbid cognitive,medical, and psychiatric profiles and care with lesion placement and/or sizemay make this a viable option.
(4) STB DBS is gaining the reputation of being the most clinically effec-tive method but older patients appear to be at risk for significant cognitiveand behavioral decline. We are still collecting long-term follow-up data todetermine whether these changes are permanent, but so far, speed of pro-cessing and verbal fluency appear to remain impaired. Larger patient samplesare also required to confirm these preliminary findings.
(5) The least neuropsychologically detrimental procedure may possiblybe bilateral GPi DBS but the numbers are too few to draw any conclusions.This treatment should probably be investigated further using random, blindedsurgical trials and evaluations.
(6) When deciding on any of these neurosurgical treatments, one needsto weigh the potential benefits and risks and hopefully to be prepared to offersustained and intensive postoperative follow-up, support, and managementfor any difficulties that arise. Education of patients and caregivers regardingstrategies to minimize cognitive losses has been very helpful. Also, whenpatients have experienced frontal lobe behavioral changes postoperatively,it has also been helpful to teach caregivers and family environmental man-agement skills to help organize and guide them so as to better manage poten-tially problematic situations.
REFERENCES
Alexander, G. E., Crutcher, M. D., & DeLong, M. R. 1990. Basal ganglia thalamocorticalcircuits parallel substrates for motor, oculomotor, ‘‘prefrontal’’ and ‘‘limbic’’ functions.[Review]. Progress in Brain Research, 85, 119–146.
Baron, M. S., Vitek, J. L., Bakay, R., Green, J., Kaneoke, Y., Hashimoto, T., Turner, R.,Woodard, J., Cole, S., McDonald, W., & DeLong, M. 1996. Treatment of advanced Par-kinson’s disease by posterior GPi pallidotomy: 1-year results of a pilot study. Annals ofNeurology, 40, 355–366.
Benabid, A. L., Pollack, P., Gao, D. M., Hoffmann, D., Limousin, P., Gay, E., Payen, I., &Benazzouz, A. 1996. Chronic electrical stimulation of the ventralis intermedius nucleusof the thalamus as a treatment of movement disorders. Journal of Neurosurgery, 84, 203–214.
Brown, R. G., & Marsden, C. D. 1990. Cognitive function in Parkinson’s disease: from descrip-tion to theory. Trends in Neurosciences, 13, 21–29.
Cahn, D., Sullivan, E., Shear, P., Heit, G., Lim, K., Marsh, L., Lane, B., Wasserstein, P., &
NEUROPSYCHOLOGICAL OUTCOME OF PVP AND DBS 345
Silverberg, G. 1998. Neuropsychological and motor functioning after unilateral anatomi-cally guided posterior ventral pallidotomy. Preoperative, performance and three-monthfollow-up. Neuropsychiatry, Neuropsychology and Behavioural Neurology, 11, 136–145.
Cullum, C. M., Lacritz, L. H., Frol, A. B., Brewer, K., Ciller, C., & Dewey, R. 1997. Effectsof pallidotomy on cognitive function in Parkinson’s disease. Journal of the InternationalNeuropsychological Society, 3, 61 [abstract].
Dogali, M., Fazzini, E., Kolodny, E., Eidelberg, D., Sterio, D., Devinsky, O., & Beric, A.1995. Stereotactic ventral pallidotomy for Parkinson’s disease. Neurology, 45, 753–761.
Dubois, B., Boller, F., Pillon, B., & Agid, Y. 1991. Cognitive deficits in Parkinson’s disease.In F. Boller & J. Grafman (Eds.), Handbook of Neuropsychology. Amsterdam: Elsevier.Pp. 195–240.
Fazzini, E., Dogali, M., Sterio, D., Eidelberg, D., & Beric, A. 1997. Stereotactic pallidotomyfor Parkinson’s disease: a long-term follow-up of unilateral pallidotomy. Neurology, 48,1273–1277.
Galvez-Jiminez, N., Lozano, A., Duff, J., Trepanier, L., Saint-Cyr, J., & Lang, A. 1996. Bilat-eral pallidotomy pronounced amelioration of incapacitating levodopa-induced dyskine-sias but accompanying cognitive decline. Movement Disorders, 11, 242.
Gildenberg, P. L. 1995. Management of movement disorders: an overview. Neurosurgery Clin-ics of North America, 6, 43–53.
Goetz, C. G., & Diederich, N. J. 1996. There is a renaissance of interest in pallidotomy forParkinson’s disease. Nature Medicine, 2, 510–514.
Golbe, L. I. 1998. Pallidotomy for Parkinson’s disease: hitting the target? Lancet, 351, 998–999.
Grafton, S. T., & DeLong, M. 1997. Tracing the brain’s circuitry with functional imaging.Nature Medicine, 3, 602–603.
Kocher, U., Siegfried J., & Perret, E. 1982. Verbal and nonverbal learning ability of Parkinsonpatients before and after unilateral ventrolateral thalamotomy. Applied Neurophysiology,45, 311–316.
Krack, P., Limousin, P., Benabid. A. L., & Pollack, P. 1997. Chronic stimulation of sub-thalamic nucleus improves levodopa-induced dyskinesias in Parkinson’s disease. Lancet,350, 1676. [letter]
Kumar, R., Lozano, A. M., Kim, Y. J., Hutchison, W., Sime, E., Halket, E., & Lang, A.April, 1998a. Double-blind evaluation of the effects of subthalamic nucleus deep brainstimulation in advanced Parkinson’s disease. Neurology, 51, 850–855.
Kumar, R., Lozano, A. M., Montgomery, E., & Lang, A. E. 1998b. Pallidotomy and deep brainstimulation of the pallidum and subthalamic nucleus in advanced Parkinson’s disease.Movement Disorders, 13 (Suppl. 1), 73–82.
Laitinen, L. V. 1995. Pallidotomy for Parkinson’s disease. Neurosurgery Clinics of NorthAmerica, 6, 105–112.
Lang, A. E., Lozano, A., Duff. J., Tasker, R., Miyasaki, J., Galvez-Jiminez, N., Hutchison,W., & Dostrovsky, J. 1997a. Medial pallidotomy in late-stage Parkinson’s disease andstriatonigral degeneration. In C. D. Marsden, J. A. Obeso, M. DeLong, C. Ohye (Eds.),Advances in understanding the basal ganglia and new surgical approaches for Parkin-son’s disease. New York: Lippincott–Raven. Pp. 199–211.
Lang, A. E., Lozano, A. M., Montgomery, E., Duff, J., Tasker, R., & Hutchison, W. 1997b.Posteroventral medial pallidotomy in advanced Parkinson’s disease. New England Jour-nal of Medicine, 337, 1036–1042.
Lang, A. E., Lozano, A., Tasker, A., Duff, J., Saint-Cyr, J., & Trepanier, L. 1997c. Neuropsy-

346 TREPANIER ET AL.
chological and behavioral changes and weight gain after medial pallidotomy. Archivesof Neurology, 41, 834–835. [letter]
Lombardi, W., Gross, R., Trepanier, L., Lang, A., Lozano, A., & Saint-Cyr, J. 2000. Relation-ship of lesion location to cognitive outcome following microelectrode-guided pallidotomyfor Parkinson’s Disease. Support for the existence of cognitive circuits in the humanpallidum. Brain, in press.
Lozano, A., Hutchison, W. D., Kiss, Z. H. T., Tasker, R. R., Davis, K. D., & Dostrovsky,J. O. 1996. Methods for microelectrode-guided posteroventral pallidotomy. Journal ofNeurosurgery, 84, 194–202.
Lozano, A. M., Lang, A. E., Galvez-Jimenez. N., Miyasaki, J., Duff, J., Hutchison, W. D., &Dostrovsky, J. O. 1995. Effect of GPi pallidotomy on motor function in Parkinson’sdisease. Lancet, 346, 1383–1387.
Lucas, J., Finton, M., Uitti, R., & Wharen, R. 1997. The effect of left unilateral pallidotomyon neuropsychological functioning in patients with Parkinson’s disease. Journal of theInternational Neuropsychological Society, 3, 207. [abstract]
Manning, C., Bennett, J., Wilkniss, S., Jones, M., & Laws, E. 1997. Comprehensive neuropsy-chological assessment of cognitive functioning pre- and post-unilateral posteroventralpallidotomy. Neurology, 48, A252. [abstract]
Masterman, D., Bronstein, J., DeSalles, A., Foti, D., & Cummings, J. 1997. Cognitive andbehavioral performance following unilateral ventroposterior pallidotomy. Neurology, 48,A252. [abstract]
Obeso, J. A., Rodriguez, M. C., Gorospe, A., Guridi, J., Alvarez, L., & Macias, R. 1997.Surgical treatment of Parkinson’s disease. Baillieres Clinical Neurology, 6, 125–145.
Olanow, C. W. 1996. GPi pallidotomy—Have we made a dent in Parkinson’s disease? Annalsof Neurology, 40, 341–343. [editorial]
Olanow, C. 1994. The role of surgery in the treatment of Parkinson’s Disease. In M. Stern(Ed.), Beyond the decade of the brain. Wells Medical. Pp. 157–175.
Parent, A., & Hazrati, L. 1995. Functional anatomy of the basal ganglia. I. The cortico-basalganglia-thalamo-cortical loop. Brain Research Review, 20, 91–127.
Ricklan, M., Diller, L., Weiner, H., & Cooper, I. S. 1960. Psychological studies on the effectsof chemosurgery of the basal ganglia in Parkinsonism. II. Aspects of personality. Archivesof General Psychiatry, 3, 267–275.
Rilling, L. M., Filoteo, J. V., Roberts, J. W., & Heilbrun, M. P. 1996. Neuropsychologicalfunctioning in patients with Parkinson’s disease pre- and post-pallidotomy. Archives ofClinical. Neuropsychology, 11, 442. [abstract]
Riordan, H. J., Flashman, L., Carroll, K., & Roberts, D. 1997. Neuropsychological functioningbefore and after stereotactic ventroposterolateral pallidotomy in Parkinson’s patients: Pre-liminary findings. Journal of the International Neuropsychological Society, 3, 60. [ab-stract]
Roberts, J. W., & Heilbrun, M. P. 1997. Staged bilateral ventroposterolateral pallidotomy forParkinson’s disease. Neurology, 48, A358.
Saint-Cyr, J., Trepanier, L., Lang, A., & Lozano, A. 1996. Neuropsychological outcome ofposteroventral pallidotomy in Parkinsonian patients. Movement Disorders, 11(Suppl.1),161. [abstract]
Scott, R., Gregory, R., Hines, N., Carroll, C., Hyman, N., Papanasstasiou, V., Leather, C.,Rowe, J., Silburn, P., & Aziz, T. 1998. Neuropsychological, neurological and functionaloutcome following pallidotomy for Parkinson’s disease: A consecutive series of eightsimultaneous bilateral and twelve unilateral procedures. Brain, 121, 659–675.
Shannon, K., Penn, R., Kroin, J., Adler, C., Janko, K., York, M., & Cox, S. 1998. Sterotactic
NEUROPSYCHOLOGICAL OUTCOME OF PVP AND DBS 347
pallidotomy for the treatment of Parkinson’s disease: Efficacy and adverse effects at 6months in 26 patients. Neurology, 50, 434–438.
Siegfried, J., & Lippitz, B. 1994. Bilateral chronic electrostimulation of ventropostero-lateralpallidum: A new therapeutic approach for alleviating all parkinsonian symptoms. Neuro-surgery, 35, 1126–1130.
Signoret, J-L. 1991. Batterie d’efficience mnesique. BEM 144. Paris: Elsevier.
Soukup, V. M., Ingram, F., Schiess, M. C., Bonnen, J. G., Nauta, H. J., & Calverley, J. R.1997. Cognitive sequelae of unilateral posteroventral pallidotomy. Archives of Neurology,54, 947–950.
Spreen, O., & Strauss, E. 1998. A compendium of neuropsychological tests: administration,norms, and commentary. 2nd ed. New York: Oxford Univ. Press.
Stebbins, G., Gabrieli, J., Goetz, C., Shannon, K., Penn, R., & Masciari, F. 1997. Impairedfronto-striatal memory functioning following pallidotomy in advanced Parkinson’s dis-ease. Neurology, 48, A252. [abstract]
Taylor, A. E., & Saint-Cyr, J. A. 1995. The neuropsychology of Parkinson’s disease. Brainand Cognition, 28, 281–296.
Taylor, A. E., Saint-Cyr, J. A., & Lang, A. E. 1986. Frontal lobe dysfunction in Parkinson’sdisease: The cortical focus of neostriatal outflow. Brain, 109, 845–883.
Taylor, A. E., Saint-Cyr, J. A., & Lang, A. E. 1987. Parkinson’s disease: Cognitive changesin relation to treatment response. Brain, 110, 35–51.
Taylor, A. E., Saint-Cyr, J. A., & Lang, A. E. 1990. Memory and learning in early Parkinson’sdisease: Evidence for a ‘‘Frontal Lobe Syndrome.’’ Brain and Cognition, 13, 211–232.
Trepanier, L., Saint-Cyr, J., Lang, A., & Lozano, A. 1997. Effect of GPi pallidotomy onneuropsychological function in Parkinson’s disease. Archives of Clinical Neuropsychol-ogy, 12, 419. [abstract]
Trepanier, L., Saint-Cyr, J., Lozano, A., & Lang, A. 1998a. Neuropsychological consequencesof posteroventral pallidotomy for the treatment of Parkinson’s disease. Neurology, 51,207–215.
Trepanier, L., Saint-Cyr, J., Lozano, A., & Lang, A. 1998b. Hemisphere-specific cognitiveand motor changes after unilateral posteroventral pallidotomy. Archives of Neurology,55, 881–883. [letter]
Troster, A. L., Fields, J. A., Wilkinson, S. B., Pahwa, R., Miyawaki, E., Lyons, K., & Koller,W. 1997. Unilateral pallidal stimulation for Parkinson’s disease: Neurobehavioral func-tioning before and 3 months after electrode implantation. Neurology, 49, 1078–1083.
Uitti R. J., Wharen, R. E., Turk, M. F., Lucas, J., Finton, M., Graff-Radford, N., Boylan, K.,Goerss, S., Kall, B., Adler, C., Caviness, J., & Atkinson, E. 1997. Unilateral pallidotomyfor Parkinson’s disease: Comparison of outcome in younger versus elderly patients. Neu-rology, 49, 1072–1077.
Vilkki, J., & Laitinen, L. V. 1976. Effects of pulvinotomy and ventrolateral thalamotomy onsome cognitive functions. Neuropsychologia, 14, 67–78.
Weiner, W. J., & Lang, A. E. (1989). Other akinetic-rigid and related syndromes. In Movementdisorders: A comprehensive survey. New York: Futura. Pp. 117–219.
Wichman, T., Vitek, J. L., & DeLong, M. R. 1995. Parkinson’s disease and the basal ganglia:Lessons from the laboratory and from neurosurgery. The Neuroscientist, 1, 236–244.