neural correlates of recognition and naming of musical instruments
TRANSCRIPT
NeuropsychologyNeural Correlates of Recognition and Naming of MusicalInstrumentsAmy M. Belfi, Joel Bruss, Brett Karlan, Taylor J. Abel, and Daniel Tranel
Online First Publication, February 22, 2016. http://dx.doi.org/10.1037/neu0000273
CITATION
Belfi, A. M., Bruss, J., Karlan, B., Abel, T. J., & Tranel, D. (2016, February 22). Neural Correlates ofRecognition and Naming of Musical Instruments. Neuropsychology. Advance online publication.http://dx.doi.org/10.1037/neu0000273

Neural Correlates of Recognition and Naming of Musical Instruments
Amy M. BelfiUniversity of Iowa College of Medicine
Joel Bruss, Brett Karlan, and Taylor J. AbelUniversity of Iowa College of Medicine
Daniel TranelUniversity of Iowa and University of Iowa College of Medicine
Objective: Retrieval of lexical (names) and conceptual (semantic) information is frequently impaired inindividuals with neurological damage. One category of items that is often affected is musical instruments.However, distinct neuroanatomical correlates underlying lexical and conceptual knowledge for musicalinstruments have not been identified. Method: We used a neuropsychological approach to explore theneural correlates of knowledge retrieval for musical instruments. A large sample of individuals with focalbrain damage (N � 298), viewed pictures of 16 musical instruments and were asked to name and identifyeach instrument. Neuroanatomical data were analyzed with a proportional MAP-3 method to createvoxelwise lesion proportion difference maps. Results: Impaired naming (lexical retrieval) of musicalinstruments was associated with damage to the left temporal pole and inferior pre- and postcentral gyri.Impaired recognition (conceptual knowledge retrieval) of musical instruments was associated with amore broadly and bilaterally distributed network of regions, including ventromedial prefrontal cortices,occipital cortices, and superior temporal gyrus. Conclusions: The findings extend our understanding ofhow musical instruments are processed at neural system level, and elucidate factors that may explain whybrain damage may or may not produce anomia or agnosia for musical instruments. Our findings also helpinform broader understanding of category-related knowledge mapping in the brain, as musical instru-ments possess several characteristics that are similar to various other categories of items: They areinanimate and highly manipulable (similar to tools), produce characteristic sounds (similar to animals),and require fine-grained visual differentiation between each other (similar to people).
Keywords: musical instruments, naming, recognition, brain lesions
Retrieval of lexical (names) and conceptual (semantic) informa-tion about items, both unique (e.g., famous faces, landmarks,melodies) and nonunique (e.g., tools, animals, musical instru-ments) is often impaired in individuals with neurological damage.Certain categories of items have been associated with specificneuroanatomical correlates; for example, impaired naming ofunique entities has often been associated with the left temporalpole (LTP; Belfi & Tranel, 2014; H. Damasio, Grabowski, Tranel,
Hichwa, & Damasio, 1996; Drane et al., 2008; Gorno-Tempini &Price, 2001; Tranel, 2006). A long track of research, in fact, hasshown that individuals with focal brain damage can develop re-markably specific category-related defects in retrieving lexical andconceptual information for various items (Crutch & Warrington,2003; Hart, Berndt, & Caramazza, 1985; Hillis & Caramazza,1991; Warrington & Shallice, 1984).
One category that has been frequently included in studies ofobject naming is musical instruments. However, research on mu-sical instruments has been inconclusive, perhaps owing to theunusual aggregation of attributes in the musical instrument cate-gory. One striking example is that musical instrument naming doesnot always follow the well-established living/nonliving distinction.In classic work of this type, it was frequently found that individ-uals who are impaired at naming living entities (e.g., animals,fruits/vegetables) are often unimpaired at naming nonliving enti-ties (e.g., tools, vehicles). However, the category of musical in-struments often does not track in orderly fashion with the living/nonliving dichotomy. For example, individuals who showimpairments in naming living entities often show impairments inmusical instruments, while they are unimpaired in other nonlivingitems (Basso, Capitani, & Laiacona, 1988; A. Damasio, 1990;Dixon, Piskopos, & Schweizer, 2000; Gainotti, 1996; Gale, Done,& Frank, 2001; Masullo et al., 2012; Stewart, Parkin, & Hunkin,1992; Warrington & Shallice, 1984). At the same time, somestudies have identified patients with abnormal naming of living
Amy M. Belfi, Interdisciplinary Graduate Program in Neuroscience, andDepartment of Neurology, University of Iowa College of Medicine; JoelBruss and Brett Karlan, Department of Neurology, University of IowaCollege of Medicine; Taylor J. Abel, Department of Neurosurgery, Uni-versity of Iowa College of Medicine; Daniel Tranel, InterdisciplinaryGraduate Program in Neuroscience and Department of Psychology, Uni-versity of Iowa, and Department of Neurology, University of Iowa Collegeof Medicine.
Amy M. Belfi is now at the Department of Psychology, New YorkUniversity.
We would like to acknowledge Ken Manzel for his help in collectingpatient data. This work was supported by McDonnell Foundation Collab-orative Action Award #220020387.
Correspondence concerning this article should be addressed to Amy M.Belfi, Department of Psychology, New York University, 6 WashingtonPlace Room 275, New York, NY 10003. E-mail: [email protected]
Thi
sdo
cum
ent
isco
pyri
ghte
dby
the
Am
eric
anPs
ycho
logi
cal
Ass
ocia
tion
oron
eof
itsal
lied
publ
ishe
rs.
Thi
sar
ticle
isin
tend
edso
lely
for
the
pers
onal
use
ofth
ein
divi
dual
user
and
isno
tto
bedi
ssem
inat
edbr
oadl
y.
Neuropsychology © 2016 American Psychological Association2016, Vol. 30, No. 3, 000 0894-4105/16/$12.00 http://dx.doi.org/10.1037/neu0000273
1

items but intact musical instrument naming (De Renzi & Lucchelli,1994; Hanley, Young, & Pearson, 1989; Kolinsky et al., 2002; forreview, see Capitani, Laiacona, Mahon, & Caramazza, 2003).Perhaps because of this inconsistent evidence, the category ofmusical instruments has often been omitted from studies of objectnaming (Capitani, Laiacona, Barbarotto, & Trivelli, 1994; Cop-pens & Frisinger, 2005; Garrard et al., 2001; Garrard, Patterson,Watson, & Hodges, 1998; Laws, 1999). Due to the potentiallyunique nature of musical instruments, however, a thorough inves-tigation of the neural correlates of musical instrument recognitionand naming is warranted.
A previous large-scale study reported on the neural correlates ofrecognition and naming for five categories of items: people, ani-mals, tools/utensils, fruits/vegetables, and musical instruments (H.Damasio, Tranel, Grabowski, Adolphs, & Damasio, 2004). Indi-viduals with focal brain damage were shown pictures of items ineach of the five categories and were asked to identify the items. Ifa participant was unable to name an item, the participant was askedto provide information about that item, that is, defining featuresand characteristics. For example, if a participant was shown apicture of Abraham Lincoln and could not come up with the name,the participant might demonstrate accurate recognition by statingthat “He was the President of the United States during the CivilWar.” The categories of people, animals, tools/utensils, and fruits/vegetables were examined in considerable depth in the H. Damasioet al. study, and have also received detailed attention in otherstudies (e.g., H. Damasio et al., 1996; Gainotti, 2005; Grabowski,Damasio, & Damasio, 1998; Tranel, Grabowski, Lyon, & Dama-sio, 2005; Tranel, 2009). By contrast, the category of musicalinstruments received less attention, and the findings that werereported were not entirely definitive. Impaired naming of musicalinstruments was associated with the LTP, insula, and inferior pre-and postcentral gyri. Impaired recognition of musical instrumentswas associated with damage in the left insula and frontal opercu-lum, and the right angular gyrus and temporo-occipital junction(H. Damasio et al., 2004). While these results are suggestive andinteresting, they were explicitly not the focus of the analyses anddiscussion in previous publications, including the extensive H.Damasio et al. study. As such, a more systematic examination ofmusical instruments is warranted. Here, we replicated and ex-tended the findings of the H. Damasio et al. study in a sample ofnew individuals with focal brain damage, focusing specifically ondeficits in musical instrument naming and recognition.
Method
Participants
Participants were chosen from the Patient Registry of the Divi-sion of Behavioral Neurology and Cognitive Neuroscience in theDepartment of Neurology. Participants were divided into twogroups: those who were reported in the previous study (H. Dama-sio et al., 2004; n � 128; “old”) and those who are new to thecurrent study (n � 170; “new”). Combining the old and newgroups, a total of 298 individuals (159 male, 139 female) withfocal brain damage were included. Lesions were located in the lefthemisphere (n � 172), right hemisphere (n � 93) or bilaterally(n � 33) and were caused by cerebrovascular disease (n � 212),herpes simplex encephalitis (n � 10), head trauma with focal
contusion (n � 5), benign tumor resection (n � 19), or resectionfor medically intractable epilepsy (n � 51). Participants wereeither right-handed (n � 252), left-handed (n � 15), or of mixedhandedness (n � 31).
Patients in the old and new groups were derived from thesame basic population (mainly persons from Iowa referred tothe tertiary health care system at the University of Iowa Hos-pitals for definitive management of neurological injury), and assuch, the two groups are demographically very similar. The newgroup consisted of a total of 170 individuals (102 male, 68female) with focal lesions in the left hemisphere (n � 89), righthemisphere (n � 48), or bilaterally (n � 33), caused by cere-brovascular disease (n � 110), head trauma with focal contu-sion (n � 3), benign tumor resection (n � 19), or resection formedically intractable epilepsy (n � 32). Participants were eitherright-handed (n � 135), left-handed (n � 12), or of mixedhandedness (n � 23). Participants had on average 13.54 yearsof education (SD � 2.83). The old group consisted of a total of128 individuals (56 male, 72 female) with focal lesions locatedin the left hemisphere (n � 83) or right hemisphere (n � 45),caused by cerebrovascular disease (n � 102), herpes simplexencephalitis (n � 4), head trauma with focal contusion (n � 2),benign tumor resection (n � 1), or resection for medicallyintractable epilepsy (n � 19). Participants were either right-handed (n � 117), left-handed (n � 3), or of mixed handedness(n � 8). Participants had on average 13.26 years of education(SD � 2.98). Lesion overlap maps depicting lesion locations forthe old, new, and combined groups can be seen in Figure 1.
All participants were screened to ensure that none had generalintellectual impairment (participants with IQ scores below 80 wereexcluded; IQ was determined by Wechsler Adult IntelligenceScale–Third Edition and/or Fourth Edition testing; Wechsler,2008). All data were obtained in the chronic phase of recovery,when participants were at least 3 months post lesion onset. In thesame manner as previous studies, all participants were screened toensure valid cooperation with the experimental protocol. Somerecovered aphasics were included in the sample, although noparticipants had residual aphasia severe enough to interfere withtheir ability to produce scorable responses on the experimental task(see below). To define normal performance, we used data from 55normal comparison participants (as reported in detail in previousstudies; see H. Damasio et al., 2004). The current study wasapproved by the Institutional Review Board and all participantsgave informed consent in accordance with the requirements of theHuman Subjects Committee.
Stimuli and Procedure
The musical instrument stimuli (n � 16), which have been usedin previous studies of musical instrument naming and recognition,consist of 10 black-and-white line drawings and six black-and-white photographs (H. Damasio et al., 2004; Snodgrass & Vander-wart, 1980). For examples of stimuli, see Figure 2; a list of allstimuli is included in Table 1. Procedures used here have beenreported elsewhere (H. Damasio et al., 2004). Musical instrumentstimuli were included in a larger set of stimuli including famousfaces, animals, tools/utensils, and fruits/vegetables. The adminis-tration order was the same for all participants, but the ordering hada mixture of items from various categories (so that the 16 musical
Thi
sdo
cum
ent
isco
pyri
ghte
dby
the
Am
eric
anPs
ycho
logi
cal
Ass
ocia
tion
oron
eof
itsal
lied
publ
ishe
rs.
Thi
sar
ticle
isin
tend
edso
lely
for
the
pers
onal
use
ofth
ein
divi
dual
user
and
isno
tto
bedi
ssem
inat
edbr
oadl
y.
2 BELFI, BRUSS, KARLAN, ABEL, AND TRANEL
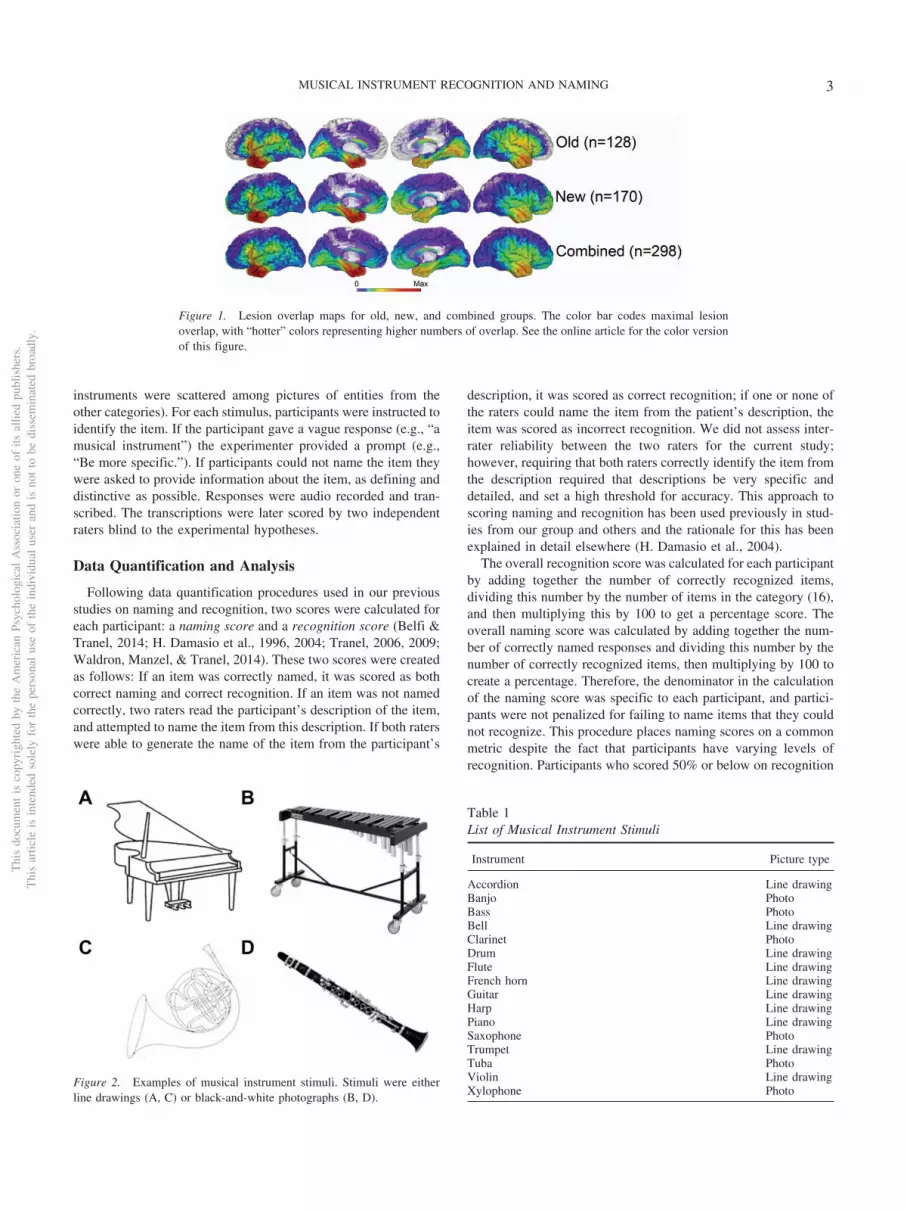
instruments were scattered among pictures of entities from theother categories). For each stimulus, participants were instructed toidentify the item. If the participant gave a vague response (e.g., “amusical instrument”) the experimenter provided a prompt (e.g.,“Be more specific.”). If participants could not name the item theywere asked to provide information about the item, as defining anddistinctive as possible. Responses were audio recorded and tran-scribed. The transcriptions were later scored by two independentraters blind to the experimental hypotheses.
Data Quantification and Analysis
Following data quantification procedures used in our previousstudies on naming and recognition, two scores were calculated foreach participant: a naming score and a recognition score (Belfi &Tranel, 2014; H. Damasio et al., 1996, 2004; Tranel, 2006, 2009;Waldron, Manzel, & Tranel, 2014). These two scores were createdas follows: If an item was correctly named, it was scored as bothcorrect naming and correct recognition. If an item was not namedcorrectly, two raters read the participant’s description of the item,and attempted to name the item from this description. If both raterswere able to generate the name of the item from the participant’s
description, it was scored as correct recognition; if one or none ofthe raters could name the item from the patient’s description, theitem was scored as incorrect recognition. We did not assess inter-rater reliability between the two raters for the current study;however, requiring that both raters correctly identify the item fromthe description required that descriptions be very specific anddetailed, and set a high threshold for accuracy. This approach toscoring naming and recognition has been used previously in stud-ies from our group and others and the rationale for this has beenexplained in detail elsewhere (H. Damasio et al., 2004).
The overall recognition score was calculated for each participantby adding together the number of correctly recognized items,dividing this number by the number of items in the category (16),and then multiplying this by 100 to get a percentage score. Theoverall naming score was calculated by adding together the num-ber of correctly named responses and dividing this number by thenumber of correctly recognized items, then multiplying by 100 tocreate a percentage. Therefore, the denominator in the calculationof the naming score was specific to each participant, and partici-pants were not penalized for failing to name items that they couldnot recognize. This procedure places naming scores on a commonmetric despite the fact that participants have varying levels ofrecognition. Participants who scored 50% or below on recognition
Table 1List of Musical Instrument Stimuli
Instrument Picture type
Accordion Line drawingBanjo PhotoBass PhotoBell Line drawingClarinet PhotoDrum Line drawingFlute Line drawingFrench horn Line drawingGuitar Line drawingHarp Line drawingPiano Line drawingSaxophone PhotoTrumpet Line drawingTuba PhotoViolin Line drawingXylophone Photo
Figure 1. Lesion overlap maps for old, new, and combined groups. The color bar codes maximal lesionoverlap, with “hotter” colors representing higher numbers of overlap. See the online article for the color versionof this figure.
Figure 2. Examples of musical instrument stimuli. Stimuli were eitherline drawings (A, C) or black-and-white photographs (B, D).
Thi
sdo
cum
ent
isco
pyri
ghte
dby
the
Am
eric
anPs
ycho
logi
cal
Ass
ocia
tion
oron
eof
itsal
lied
publ
ishe
rs.
Thi
sar
ticle
isin
tend
edso
lely
for
the
pers
onal
use
ofth
ein
divi
dual
user
and
isno
tto
bedi
ssem
inat
edbr
oadl
y.
3MUSICAL INSTRUMENT RECOGNITION AND NAMING

(n � 6) were excluded from the naming analyses, in order toeliminate participants in whom a recognition deficit was so ex-treme that there would be only a few items on which to judgenaming abilities, making the naming score susceptible to beingunreliable.
Following previous work, we classified each participant into an“impaired” or “unimpaired” group (H. Damasio et al., 2004).Specifically, we calculated for each participant how far their scoredeviated from the mean of the 55 normal comparison participants,in standard deviation (SD) units. Scores that were two or more SDsbelow the mean were classified as impaired. As mentioned in ourprevious work (H. Damasio et al., 2004), the classification intoimpaired and unimpaired groups based on scores greater than twoSD beyond the mean is somewhat arbitrary. In the present exper-iment, we tried various ways of dividing the groups, includingvisual inspection of the distribution of scores to find a naturaldivision point. Regardless of how the groups were subdivided, thefindings converged on the same structures. Therefore, we reporthere the groups divided using the 2-SD method.
Neuroanatomical Data Quantification and Analysis
Neuroanatomical analysis was based on data obtained during thechronic epoch of recovery. MRIs were acquired in a 1.5-T GESigna scanner (General Electric, Milwaukee, WI) with a two-dimensional spoiled gradient recalled echo sequence (1.5 mmcontiguous T1 weighted coronal cuts). If participants were unableto undergo MRI scanning (n � 30 participants in the presentstudy), computerized axial tomography data were collected. Le-sion maps were created using the MAP-3 method, in which lesionlocations are visually identified on MRI/computerized tomographyscans and manually transferred onto a normal reference brain (P.C.local standard space; resolution, 0.94 � 0.94 � 1.6 mm) based onthe identification of anatomical landmarks (Fiez, Damasio, &Grabowski, 2000; Frank, Damasio, & Grabowski, 1997). Lesiondelineation and transfer were done using Brainvox (Frank et al.,1997). This procedure circumvents the problems of interindividualregistration encountered with lesion data and the difficulties ofcombining participants scanned with different imaging modalities.An additional advantage of this approach is that it preservesanatomical boundaries in mapping lesions onto the reference brain,enabling group-level analysis. After manual transfer to normal
template space, the template brain was warped to the MontrealNeurological Institute (MNI152) standard 1-mm T1-weighted atlas(Collins, Neelin, Peters, & Evans, 1994; Evans, Dai, Collins,Neelin, & Marrett, 1991; Mazziotta et al., 2001) using BRAINS-DemonWarp (Johnson & Zhao, 2009). This transform, from thelesion template to the MNI152 template, was applied to each of thelesion maps.
To create voxelwise lesion proportion difference maps, we usedwhat we have called the “proportional MAP-3” (PM3) method(Rudrauf et al., 2008). PM3 expresses, for every voxel, the pro-portion of individuals whose lesion includes the voxel and whohave a deficit (NLD) relative to the total number of individuals witha deficit (ND), minus the proportion of individuals with a lesion atthe voxel and no deficit (NLnD) relative to the total number ofindividuals with no deficit (NnD). The formula can be expressedwith the equation Prob (L | D) – Prob (L | nD), the conditionalprobability of a lesion (L) given a deficit (D) minus the conditionalprobability of a lesion given no deficit (nD). It should be noted thatthe PM3 maps that we present are maps of descriptive, not infer-ential, statistics.
Results
All participants (N � 298) were included in the recognitionanalysis. After removing participants from the naming analysiswho scored below 50% correct recognition (n � 6), there were 292participants in the naming analysis. There were 78 participantswho were impaired in naming and 135 who were impaired inrecognition. See Figure 3 for overlap maps depicting impaired andunimpaired groups for naming and recognition.
Naming
PM3 maps for musical instrument naming for the old, new, andcombined groups are depicted in Figure 4. Overall, findings be-tween the old and new samples were very consistent. In our newsample, we replicated the previous finding that impaired naming ofmusical instruments is associated with damage to the LTP. We alsoreplicated the finding that impaired naming of musical instrumentsis associated with damage in the left inferior pre- and postcentralgyri. However, in our new sample, this finding was stronger thanin the previous sample. There was greater overlap in the inferior
Figure 3. Impaired and unimpaired naming and recognition for the combined group. See the online article forthe color version of this figure.
Thi
sdo
cum
ent
isco
pyri
ghte
dby
the
Am
eric
anPs
ycho
logi
cal
Ass
ocia
tion
oron
eof
itsal
lied
publ
ishe
rs.
Thi
sar
ticle
isin
tend
edso
lely
for
the
pers
onal
use
ofth
ein
divi
dual
user
and
isno
tto
bedi
ssem
inat
edbr
oadl
y.
4 BELFI, BRUSS, KARLAN, ABEL, AND TRANEL
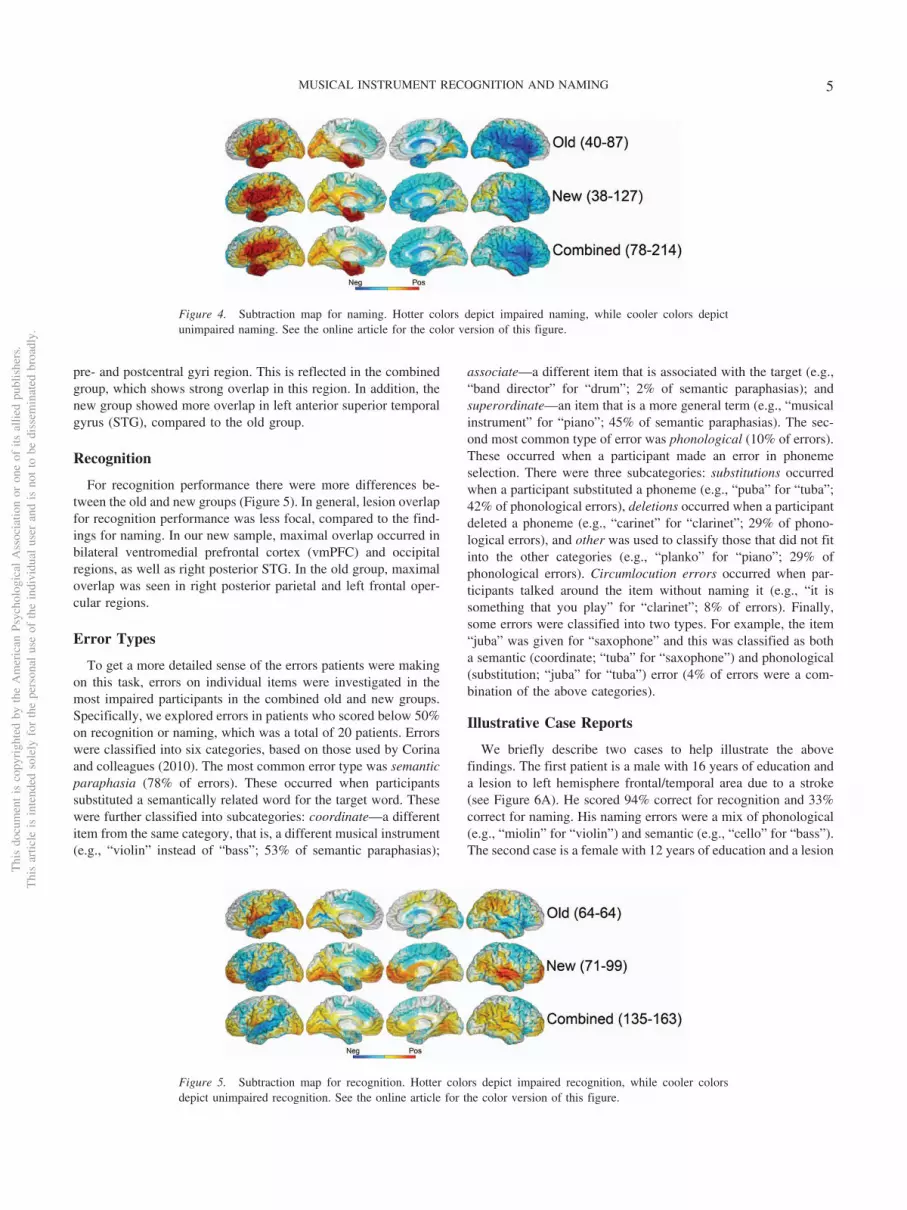
pre- and postcentral gyri region. This is reflected in the combinedgroup, which shows strong overlap in this region. In addition, thenew group showed more overlap in left anterior superior temporalgyrus (STG), compared to the old group.
Recognition
For recognition performance there were more differences be-tween the old and new groups (Figure 5). In general, lesion overlapfor recognition performance was less focal, compared to the find-ings for naming. In our new sample, maximal overlap occurred inbilateral ventromedial prefrontal cortex (vmPFC) and occipitalregions, as well as right posterior STG. In the old group, maximaloverlap was seen in right posterior parietal and left frontal oper-cular regions.
Error Types
To get a more detailed sense of the errors patients were makingon this task, errors on individual items were investigated in themost impaired participants in the combined old and new groups.Specifically, we explored errors in patients who scored below 50%on recognition or naming, which was a total of 20 patients. Errorswere classified into six categories, based on those used by Corinaand colleagues (2010). The most common error type was semanticparaphasia (78% of errors). These occurred when participantssubstituted a semantically related word for the target word. Thesewere further classified into subcategories: coordinate—a differentitem from the same category, that is, a different musical instrument(e.g., “violin” instead of “bass”; 53% of semantic paraphasias);
associate—a different item that is associated with the target (e.g.,“band director” for “drum”; 2% of semantic paraphasias); andsuperordinate—an item that is a more general term (e.g., “musicalinstrument” for “piano”; 45% of semantic paraphasias). The sec-ond most common type of error was phonological (10% of errors).These occurred when a participant made an error in phonemeselection. There were three subcategories: substitutions occurredwhen a participant substituted a phoneme (e.g., “puba” for “tuba”;42% of phonological errors), deletions occurred when a participantdeleted a phoneme (e.g., “carinet” for “clarinet”; 29% of phono-logical errors), and other was used to classify those that did not fitinto the other categories (e.g., “planko” for “piano”; 29% ofphonological errors). Circumlocution errors occurred when par-ticipants talked around the item without naming it (e.g., “it issomething that you play” for “clarinet”; 8% of errors). Finally,some errors were classified into two types. For example, the item“juba” was given for “saxophone” and this was classified as botha semantic (coordinate; “tuba” for “saxophone”) and phonological(substitution; “juba” for “tuba”) error (4% of errors were a com-bination of the above categories).
Illustrative Case Reports
We briefly describe two cases to help illustrate the abovefindings. The first patient is a male with 16 years of education anda lesion to left hemisphere frontal/temporal area due to a stroke(see Figure 6A). He scored 94% correct for recognition and 33%correct for naming. His naming errors were a mix of phonological(e.g., “miolin” for “violin”) and semantic (e.g., “cello” for “bass”).The second case is a female with 12 years of education and a lesion
Figure 4. Subtraction map for naming. Hotter colors depict impaired naming, while cooler colors depictunimpaired naming. See the online article for the color version of this figure.
Figure 5. Subtraction map for recognition. Hotter colors depict impaired recognition, while cooler colorsdepict unimpaired recognition. See the online article for the color version of this figure.
Thi
sdo
cum
ent
isco
pyri
ghte
dby
the
Am
eric
anPs
ycho
logi
cal
Ass
ocia
tion
oron
eof
itsal
lied
publ
ishe
rs.
Thi
sar
ticle
isin
tend
edso
lely
for
the
pers
onal
use
ofth
ein
divi
dual
user
and
isno
tto
bedi
ssem
inat
edbr
oadl
y.
5MUSICAL INSTRUMENT RECOGNITION AND NAMING
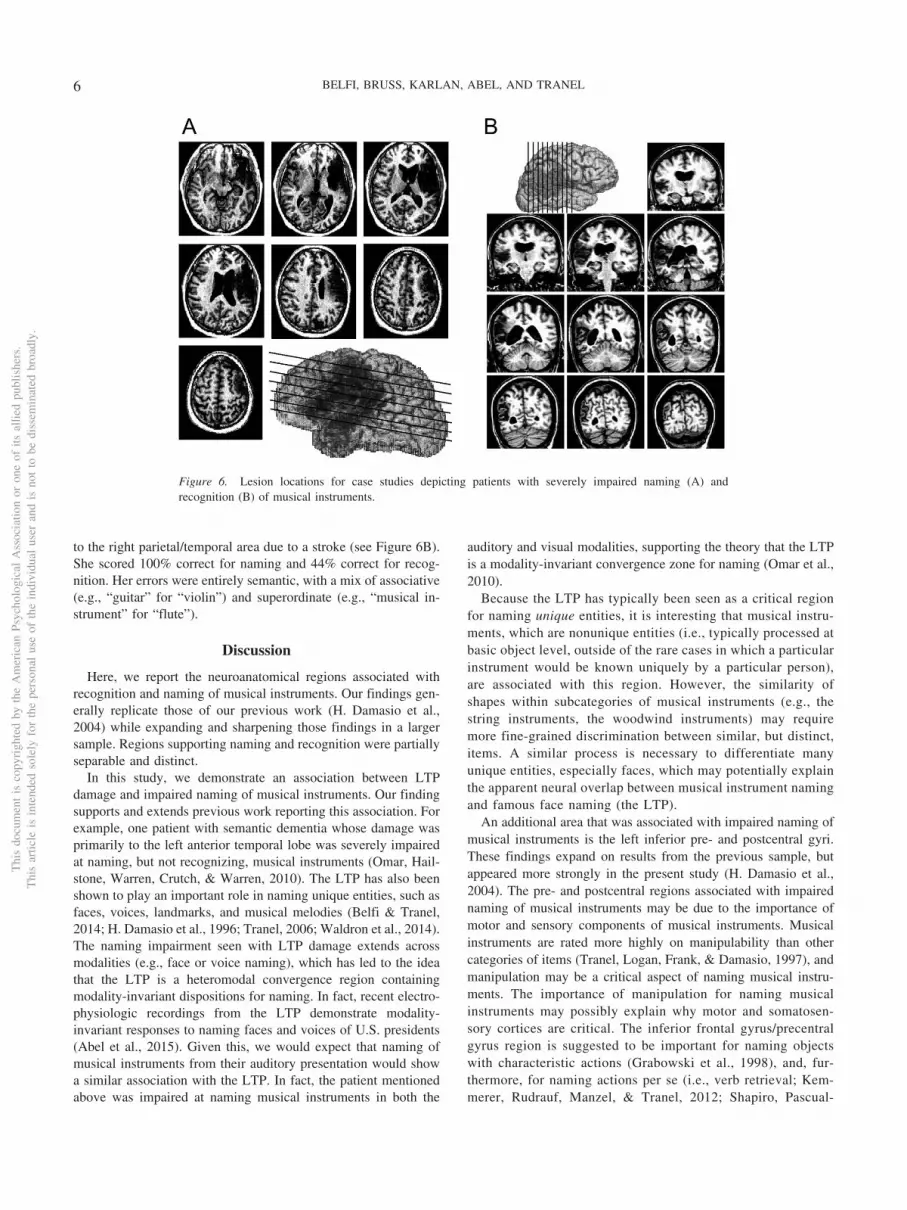
to the right parietal/temporal area due to a stroke (see Figure 6B).She scored 100% correct for naming and 44% correct for recog-nition. Her errors were entirely semantic, with a mix of associative(e.g., “guitar” for “violin”) and superordinate (e.g., “musical in-strument” for “flute”).
Discussion
Here, we report the neuroanatomical regions associated withrecognition and naming of musical instruments. Our findings gen-erally replicate those of our previous work (H. Damasio et al.,2004) while expanding and sharpening those findings in a largersample. Regions supporting naming and recognition were partiallyseparable and distinct.
In this study, we demonstrate an association between LTPdamage and impaired naming of musical instruments. Our findingsupports and extends previous work reporting this association. Forexample, one patient with semantic dementia whose damage wasprimarily to the left anterior temporal lobe was severely impairedat naming, but not recognizing, musical instruments (Omar, Hail-stone, Warren, Crutch, & Warren, 2010). The LTP has also beenshown to play an important role in naming unique entities, such asfaces, voices, landmarks, and musical melodies (Belfi & Tranel,2014; H. Damasio et al., 1996; Tranel, 2006; Waldron et al., 2014).The naming impairment seen with LTP damage extends acrossmodalities (e.g., face or voice naming), which has led to the ideathat the LTP is a heteromodal convergence region containingmodality-invariant dispositions for naming. In fact, recent electro-physiologic recordings from the LTP demonstrate modality-invariant responses to naming faces and voices of U.S. presidents(Abel et al., 2015). Given this, we would expect that naming ofmusical instruments from their auditory presentation would showa similar association with the LTP. In fact, the patient mentionedabove was impaired at naming musical instruments in both the
auditory and visual modalities, supporting the theory that the LTPis a modality-invariant convergence zone for naming (Omar et al.,2010).
Because the LTP has typically been seen as a critical regionfor naming unique entities, it is interesting that musical instru-ments, which are nonunique entities (i.e., typically processed atbasic object level, outside of the rare cases in which a particularinstrument would be known uniquely by a particular person),are associated with this region. However, the similarity ofshapes within subcategories of musical instruments (e.g., thestring instruments, the woodwind instruments) may requiremore fine-grained discrimination between similar, but distinct,items. A similar process is necessary to differentiate manyunique entities, especially faces, which may potentially explainthe apparent neural overlap between musical instrument namingand famous face naming (the LTP).
An additional area that was associated with impaired naming ofmusical instruments is the left inferior pre- and postcentral gyri.These findings expand on results from the previous sample, butappeared more strongly in the present study (H. Damasio et al.,2004). The pre- and postcentral regions associated with impairednaming of musical instruments may be due to the importance ofmotor and sensory components of musical instruments. Musicalinstruments are rated more highly on manipulability than othercategories of items (Tranel, Logan, Frank, & Damasio, 1997), andmanipulation may be a critical aspect of naming musical instru-ments. The importance of manipulation for naming musicalinstruments may possibly explain why motor and somatosen-sory cortices are critical. The inferior frontal gyrus/precentralgyrus region is suggested to be important for naming objectswith characteristic actions (Grabowski et al., 1998), and, fur-thermore, for naming actions per se (i.e., verb retrieval; Kem-merer, Rudrauf, Manzel, & Tranel, 2012; Shapiro, Pascual-
Figure 6. Lesion locations for case studies depicting patients with severely impaired naming (A) andrecognition (B) of musical instruments.
Thi
sdo
cum
ent
isco
pyri
ghte
dby
the
Am
eric
anPs
ycho
logi
cal
Ass
ocia
tion
oron
eof
itsal
lied
publ
ishe
rs.
Thi
sar
ticle
isin
tend
edso
lely
for
the
pers
onal
use
ofth
ein
divi
dual
user
and
isno
tto
bedi
ssem
inat
edbr
oadl
y.
6 BELFI, BRUSS, KARLAN, ABEL, AND TRANEL

Leone, Mottaghy, Gangitano, & Caramazza, 2001; Tranel,Kemmerer, Adolphs, Damasio, & Damasio, 2003). Correctnaming of musical instruments may therefore require neuralstructures underlying movement. Damage to motor and somato-sensory cortices involved in playing musical instruments maytherefore lead to impairments in naming these instruments.
Our findings for impaired recognition of musical instrumentswere less consistent between the old and new samples. In the newgroup, impaired recognition was associated with damage to bilat-eral vmPFC and occipital regions. The reason we identified theseregions in our new sample may be due to differing exclusioncriteria between the old and new samples. The new sample in-cluded individuals with bilateral lesions while the previous studydid not. Notably, damage to the vmPFC and occipital lobe oftenoccurs bilaterally. Therefore, the inclusion of these individualslikely influenced our results.
In the new sample we also identified a region of maximaloverlap in posterior STG that was associated with impaired rec-ognition of musical instruments. Previous research has shown thatdamage to STG impairs musical instrument recognition fromsound (Peretz et al., 1994). This may have more to do withperceptual deficits than deficits in semantic representations ofmusical instruments. However, it is consistent with our findingsthat impaired recognition of musical instruments, even in thevisual modality, is associated with damage to the right STG. Arecent study used functional MRI to investigate the neural struc-tures involved in retrieval of conceptual knowledge of musicalinstruments in a population of musicians and nonmusicians (Hoe-nig et al., 2011). The authors identified a region in right STG thatwas more active in musicians when retrieving conceptual knowl-edge about musical instruments. The authors attribute this findingto increased familiarity of musical instruments in musicians, whichleads to richer conceptual knowledge representations in sensorycortices. While the musical experience of our current participantswas not evaluated, the stimuli used in the present experiment havebeen rated as highly familiar (mean rating of 3.74 out of 5); theselevels of familiarity are similar to those shown for other standardcategories (e.g., animals; Tranel et al., 1997). In addition, previousresearch has shown that viewing pictures of musical instrumentsactivates auditory association areas even in nonmusicians (Down-ing, Chan, Peelen, Dodds, & Kanwisher, 2006). Our findingssuggest that STG may be critical for recognition of musical in-struments, regardless of prior musical experience.
Our study has limitations. For one, we did not address howparticipants performed in other categories of items. While this iscertainly an interesting issue, to do this scientific justice is farbeyond the scope of the current paper. The current data are notmeant to illustrate regions that are associated only with deficits inmusical instruments, and not other categories, but provide evi-dence for neural regions that are critical for naming and recogniz-ing musical instruments in general. A second limitation of thepresent study is that the PM3 method provides descriptive, thoughnot inferential statistical maps. An additional limitation is thatmusical experience of the participants, which could influenceperformance on the task, was not systematically measured. Giventhat expertise can affect neural representation of items, we expectthat musical experience may influence the neural structures under-lying naming and recognizing musical instruments. A final con-cern is that of ceiling effects, which is acknowledged in our
previous work (H. Damasio et al., 2004). In the previous study,ceiling effects were particularly present in the category of musicalinstruments. However, the study presented here greatly expands onthe sample size and includes a larger number of patients perform-ing below ceiling. This allows for more meaningful division intoimpaired and unimpaired groups and provides a necessary im-provement on our previous work.
Overall, the findings from our current sample replicated andextended previous findings. Naming and recognition of musicalinstruments are served by partially separable neural structures,although the structures underlying naming appear to be moredistinctive than those for recognition. Structures underlying nam-ing were localized to the left hemisphere, while those underlyingrecognition were more bilaterally distributed. Musical instrumentnaming appears to share neural structures underlying namingunique entities, as well as structures important for motion andsomatosensation. Musical instrument recognition is associatedwith structures important for audition, such as the right STG.These findings illustrate that neural regions likely associated withplaying and listening to music are critical for naming and recog-nizing musical instruments. Overall, our results provide a morethorough account of the neural structures underlying musical in-strument knowledge than has been available in the literature todate.
References
Abel, T. J., Rhone, A. E., Nourski, K. V., Kawasaki, H., Oya, H., Griffiths,T. D., . . . Tranel, D. (2015). Direct physiologic evidence of a hetero-modal convergence region for proper naming in human left anteriortemporal lobe. The Journal of Neuroscience, 35, 1513–1520. http://dx.doi.org/10.1523/JNEUROSCI.3387-14.2015
Basso, A., Capitani, E., & Laiacona, M. (1988). Progressive languageimpairment without dementia: A case with isolated category specificsemantic defect. Journal of Neurology, Neurosurgery, and Psychiatry,51, 1201–1207. http://dx.doi.org/10.1136/jnnp.51.9.1201
Belfi, A. M., & Tranel, D. (2014). Impaired naming of famous musicalmelodies is associated with left temporal polar damage. Neuropsychol-ogy, 28, 429–435. http://dx.doi.org/10.1037/neu0000051
Capitani, E., Laiacona, M., Barbarotto, R., & Trivelli, C. (1994). Livingand non-living categories. Is there a “normal” asymmetry? Neuropsy-chologia, 32, 1453–1463. http://dx.doi.org/10.1016/0028-3932(94)90117-1
Capitani, E., Laiacona, M., Mahon, B., & Caramazza, A. (2003). What arethe facts of semantic category-specific deficits? A critical review of theclinical evidence. Cognitive Neuropsychology, 20, 213–261. http://dx.doi.org/10.1080/02643290244000266
Collins, D. L., Neelin, P., Peters, T. M., & Evans, A. C. (1994). Automatic3D intersubject registration of MR volumetric data in standardizedTalairach space. Journal of Computer Assisted Tomography, 18, 192–205. http://dx.doi.org/10.1097/00004728-199403000-00005
Coppens, P., & Frisinger, D. (2005). Category-specific naming effect innon-brain-damaged individuals. Brain and Language, 94, 61–71. http://dx.doi.org/10.1016/j.bandl.2004.11.008
Corina, D. P., Loudermilk, B. C., Detwiler, L., Martin, R. F., Brinkley,J. F., & Ojemann, G. (2010). Analysis of naming errors during corticalstimulation mapping: Implications for models of language representa-tion. Brain and Language, 115, 101–112. http://dx.doi.org/10.1016/j.bandl.2010.04.001
Crutch, S. J., & Warrington, E. K. (2003). The selective impairment of fruitand vegetable knowledge: A multiple processing channels account of
Thi
sdo
cum
ent
isco
pyri
ghte
dby
the
Am
eric
anPs
ycho
logi
cal
Ass
ocia
tion
oron
eof
itsal
lied
publ
ishe
rs.
Thi
sar
ticle
isin
tend
edso
lely
for
the
pers
onal
use
ofth
ein
divi
dual
user
and
isno
tto
bedi
ssem
inat
edbr
oadl
y.
7MUSICAL INSTRUMENT RECOGNITION AND NAMING
fine-grain category specificity. Cognitive Neuropsychology, 20, 355–372. http://dx.doi.org/10.1080/02643290244000220
Damasio, A. R. (1990). Category-related recognition defects as a clue tothe neural substrates of knowledge. Trends in Neurosciences, 13, 95–98.http://dx.doi.org/10.1016/0166-2236(90)90184-C
Damasio, H., Grabowski, T. J., Tranel, D., Hichwa, R. D., & Damasio,A. R. (1996). A neural basis for lexical retrieval. Nature, 380, 499–505.http://dx.doi.org/10.1038/380499a0
Damasio, H., Tranel, D., Grabowski, T., Adolphs, R., & Damasio, A.(2004). Neural systems behind word and concept retrieval. Cognition,92, 179–229. http://dx.doi.org/10.1016/j.cognition.2002.07.001
De Renzi, E., & Lucchelli, F. (1994). Are semantic systems separatelyrepresented in the brain? The case of living category impairment. Cor-tex, 30, 3–25. http://dx.doi.org/10.1016/S0010-9452(13)80322-X
Dixon, M. J., Piskopos, M., & Schweizer, T. A. (2000). Musical instrumentnaming impairments: The crucial exception to the living/nonliving di-chotomy in category-specific agnosia. Brain and Cognition, 43, 158–164.
Downing, P. E., Chan, A. W.-Y., Peelen, M. V., Dodds, C. M., & Kan-wisher, N. (2006). Domain specificity in visual cortex. Cerebral Cortex,16, 1453–1461. http://dx.doi.org/10.1093/cercor/bhj086
Drane, D. L., Ojemann, G. A., Aylward, E., Ojemann, J. G., Johnson, L. C.,Silbergeld, D. L., . . . Tranel, D. (2008). Category-specific naming andrecognition deficits in temporal lobe epilepsy surgical patients. Neuro-psychologia, 46, 1242–1255. http://dx.doi.org/10.1016/j.neuropsycholo-gia.2007.11.034
Evans, A., Dai, W., Collins, L., Neelin, P., & Marrett, S. (1991). Warpingof a computerized 3-D atlas to match brain image volumes for quanti-tative neuroanatomical and functional analysis. Proceedings of the In-ternational Society of Optical Engineering (SPIE): Medical Imaging,1445, 236–246.
Fiez, J. A., Damasio, H., & Grabowski, T. J. (2000). Lesion segmentationand manual warping to a reference brain: Intra- and interobserver reli-ability. Human Brain Mapping, 9, 192–211. http://dx.doi.org/10.1002/(SICI)1097-0193(200004)9:4�192::AID-HBM2�3.0.CO;2-Y
Frank, R. J., Damasio, H., & Grabowski, T. J. (1997). Brainvox: Aninteractive, multimodal visualization and analysis system for neuroana-tomical imaging. NeuroImage, 5, 13–30.
Gainotti, G. (1996). Cognitive and anatomical locus of lesion in a patientwith a category-specific semantic impairment for living beings. Cogni-tive Neuropsychology, 13, 357–390. http://dx.doi.org/10.1080/026432996381944
Gainotti, G. (2005). The influence of gender and lesion location on namingdisorders for animals, plants and artefacts. Neuropsychologia, 43, 1633–1644. http://dx.doi.org/10.1016/j.neuropsychologia.2005.01.016
Gale, T. M., Done, D. J., & Frank, R. J. (2001). Visual crowding andcategory specific deficits for pictorial stimuli: A neural network model.Cognitive Neuropsychology, 18, 509–550. http://dx.doi.org/10.1080/02643290125912
Garrard, P., Lambon Ralph, M. A., Watson, P. C., Powis, J., Patterson, K.,& Hodges, J. R. (2001). Longitudinal profiles of semantic impairmentfor living and nonliving concepts in dementia of Alzheimer’s type.Journal of Cognitive Neuroscience, 13, 892–909. http://dx.doi.org/10.1162/089892901753165818
Garrard, P., Patterson, K., Watson, P. C., & Hodges, J. R. (1998). Categoryspecific semantic loss in dementia of Alzheimer’s type. Functional-anatomical correlations from cross-sectional analyses. Brain: A Journalof Neurology, 121, 633–646. http://dx.doi.org/10.1093/brain/121.4.633
Gorno-Tempini, M. L., & Price, C. J. (2001). Identification of famous facesand buildings: A functional neuroimaging study of semantically uniqueitems. Brain: A Journal of Neurology, 124, 2087–2097. http://dx.doi.org/10.1093/brain/124.10.2087
Grabowski, T. J., Damasio, H., & Damasio, A. R. (1998). Premotor andprefrontal correlates of category-related lexical retrieval. NeuroImage, 7,232–243. http://dx.doi.org/10.1006/nimg.1998.0324
Hanley, J. R., Young, A. W., & Pearson, N. A. (1989). Defective recog-nition of familiar people. Cognitive Neuropsychology, 6, 179–210.http://dx.doi.org/10.1080/02643298908253418
Hart, J., Jr., Berndt, R. S., & Caramazza, A. (1985). Category-specificnaming deficit following cerebral infarction. Nature, 316, 439–440.http://dx.doi.org/10.1038/316439a0
Hillis, A. E., & Caramazza, A. (1991). Category-specific naming andcomprehension impairment: A double dissociation. Brain: A Journal ofNeurology, 114, 2081–2094. http://dx.doi.org/10.1093/brain/114.5.2081
Hoenig, K., Müller, C., Herrnberger, B., Sim, E.-J., Spitzer, M., Ehret, G.,& Kiefer, M. (2011). Neuroplasticity of semantic representations formusical instruments in professional musicians. NeuroImage, 56, 1714–1725. http://dx.doi.org/10.1016/j.neuroimage.2011.02.065
Johnson, H., & Zhao, Y. (2009). BRAINSDemonWarp: An application toperform demons registration. The Insight Journal. Jan–June, 1–16. Re-trieved from http://www.insight-journal.org/browse/publication/312
Kemmerer, D., Rudrauf, D., Manzel, K., & Tranel, D. (2012). Behavioralpatterns and lesion sites associated with impaired processing of lexicaland conceptual knowledge of actions. Cortex, 48, 826–848. http://dx.doi.org/10.1016/j.cortex.2010.11.001
Kolinsky, R., Fery, P., Messina, D., Peretz, I., Evinck, S., Ventura, P., &Morais, J. (2002). The fur of the crocodile and the mooing sheep: Astudy of a patient with a category-specific impairment for biologicalthings. Cognitive Neuropsychology, 19, 301–342. http://dx.doi.org/10.1080/02643290143000196
Laws, K. R. (1999). Gender affects naming latencies for living and non-living things: Implications for familiarity. Cortex, 35, 729–733. http://dx.doi.org/10.1016/S0010-9452(08)70831-1
Masullo, C., Piccininni, C., Quaranta, D., Vita, M. G., Gaudino, S., &Gainotti, G. (2012). Selective impairment of living things and musicalinstruments on a verbal “Semantic Knowledge Questionnaire” in a caseof apperceptive visual agnosia. Brain and Cognition, 80, 155–159.http://dx.doi.org/10.1016/j.bandc.2012.06.002
Mazziotta, J., Toga, A., Evans, A., Fox, P., Lancaster, J., Zilles, K., . . .Mazoyer, B. (2001). A probabilistic atlas and reference system for thehuman brain: International Consortium for Brain Mapping (ICBM).Philosophical Transactions of the Royal Society of London Series B,Biological Sciences, 356, 1293–1322. http://dx.doi.org/10.1098/rstb.2001.0915
Omar, R., Hailstone, J. C., Warren, J. E., Crutch, S. J., & Warren, J. D.(2010). The cognitive organization of music knowledge: A clinicalanalysis. Brain: A Journal of Neurology, 133, 1200–1213. http://dx.doi.org/10.1093/brain/awp345
Peretz, I., Kolinsky, R., Tramo, M., Labrecque, R., Hublet, C., Demeurisse,G., & Belleville, S. (1994). Functional dissociations following bilaterallesions of auditory cortex. Brain: A Journal of Neurology, 117, 1283–1301. http://dx.doi.org/10.1093/brain/117.6.1283
Rudrauf, D., Mehta, S., Bruss, J., Tranel, D., Damasio, H., & Grabowski,T. J. (2008). Thresholding lesion overlap difference maps: Applicationto category-related naming and recognition deficits. NeuroImage, 41,970–984. http://dx.doi.org/10.1016/j.neuroimage.2007.12.033
Shapiro, K. A., Pascual-Leone, A., Mottaghy, F. M., Gangitano, M., &Caramazza, A. (2001). Grammatical distinctions in the left frontal cor-tex. Journal of Cognitive Neuroscience, 13, 713–720. http://dx.doi.org/10.1162/08989290152541386
Snodgrass, J. G., & Vanderwart, M. (1980). A standardized set of 260pictures: Norms for name agreement, image agreement, familiarity, andvisual complexity. Journal of Experimental Psychology: Human Learn-ing and Memory, 6, 174–215. http://dx.doi.org/10.1037/0278-7393.6.2.174
Thi
sdo
cum
ent
isco
pyri
ghte
dby
the
Am
eric
anPs
ycho
logi
cal
Ass
ocia
tion
oron
eof
itsal
lied
publ
ishe
rs.
Thi
sar
ticle
isin
tend
edso
lely
for
the
pers
onal
use
ofth
ein
divi
dual
user
and
isno
tto
bedi
ssem
inat
edbr
oadl
y.
8 BELFI, BRUSS, KARLAN, ABEL, AND TRANEL

Stewart, F., Parkin, A. J., & Hunkin, N. M. (1992). Naming impairmentsfollowing recovery from herpes simplex encephalitis: Category-specific? The Quarterly Journal of Experimental Psychology, 44, 261–284. http://dx.doi.org/10.1080/02724989243000037
Tranel, D. (2006). Impaired naming of unique landmarks is associated withleft temporal polar damage. Neuropsychology, 20, 1–10. http://dx.doi.org/10.1037/0894-4105.20.1.1
Tranel, D. (2009). The left temporal pole is important for retrieving wordsfor unique concrete entities. Aphasiology, 23, 867–884. http://dx.doi.org/10.1080/02687030802586498
Tranel, D., Grabowski, T. J., Lyon, J., & Damasio, H. (2005). Naming thesame entities from visual or from auditory stimulation engages similarregions of left inferotemporal cortices. Journal of Cognitive Neurosci-ence, 17, 1293–1305. http://dx.doi.org/10.1162/0898929055002508
Tranel, D., Kemmerer, D., Adolphs, R., Damasio, H., & Damasio, A. R.(2003). Neural correlates of conceptual knowledge for actions. CognitiveNeuropsychology, 20, 409 – 432. http://dx.doi.org/10.1080/02643290244000248
Tranel, D., Logan, C. G., Frank, R. J., & Damasio, A. R. (1997). Explain-ing category-related effects in the retrieval of conceptual and lexicalknowledge for concrete entities: Operationalization and analysis offactors. Neuropsychologia, 35, 1329–1339. http://dx.doi.org/10.1016/S0028-3932(97)00086-9
Waldron, E. J., Manzel, K., & Tranel, D. (2014). The left temporal pole isa heteromodal hub for retrieving proper names. Frontiers in Bioscience,6, 50–57. http://dx.doi.org/10.2741/S413
Warrington, E. K., & Shallice, T. (1984). Category specific semanticimpairments. Brain: A Journal of Neurology, 107, 829–854. http://dx.doi.org/10.1093/brain/107.3.829
Wechsler, D. (2008). Wechsler Adult Iltelligence Scale, fourth edition. SanAntonio, TX: Pearson.
Received November 19, 2015Revision received January 22, 2016
Accepted January 25, 2016 �
Thi
sdo
cum
ent
isco
pyri
ghte
dby
the
Am
eric
anPs
ycho
logi
cal
Ass
ocia
tion
oron
eof
itsal
lied
publ
ishe
rs.
Thi
sar
ticle
isin
tend
edso
lely
for
the
pers
onal
use
ofth
ein
divi
dual
user
and
isno
tto
bedi
ssem
inat
edbr
oadl
y.
9MUSICAL INSTRUMENT RECOGNITION AND NAMING