multiple sclerosis: disability profile and quality of life in an australian community cohort
TRANSCRIPT

Original article 87
Multiple sclerosis: disability profile and quality of life inan Australian community cohortFary Khana, Tracey McPhailb, Caroline Brandc, Lynne Turner-Stokesd andTrevor Kilpatricke
The objective of this study was to determine the
experience of disability and reported symptoms in multiple
sclerosis in an Australian community sample, comparing
the perceptions of patients, carers and treating doctors,
and to examine effects on quality of life, carer stress and
utilization of health services. The study design used a
prospective cross sectional community survey. The
participants were persons with a confirmed diagnosis of
multiple sclerosis, with quantified neurological, mobility
and cognitive deficits, from a tertiary hospital database
(n = 101), who lived at home, and their carers and doctors.
The study method used demographic, diagnostic and
disease severity data extracted from the database.
Structured interviews conducted at home included: (1)
open questionnaires for participant, carer and general
practitioner, prioritizing symptoms/problems affecting
daily living; and (2) standardized assessments for patient
quality of life, caregiver strain and perceived burden of
care. The mean age was 49 years (range 28–64). Those
more severely affected had a significantly reduced quality
of life and increased carer burden than those with milder
disability, but discordance between patients, carers and
doctors was noted in their perception of problems and
symptom experience. Rates of depression (67%) and
work-related problems were high, but vocational support
was rarely provided. Forty persons used interferon, of
whom 20 had secondary progressive multiple sclerosis;
39% reported difficulty in accessing rehabilitation services
and only 10% were referred to medical rehabilitation units.
In conclusion, the rates of disability and symptom
experience were similar to other series; however, access
and utilization of appropriate rehabilitation and support
services appears to be lacking. There were higher reported
rates of depression and poor quality of life. Opportunities
may possibly exist to re-deploy resources to develop
vocational support, counselling and rehabilitation.
Anhand der vorliegenden Studie sollte die Erfahrung mit
Behinderung und den gemeldeten Symptomen bei
multipler Sklerose am Beispiel einer australischen
Gemeinde und im Vergleich der Auffassungen von
Patienten, Betreuern und behandelnden Arzten ermittelt
und die Auswirkungen auf Lebensqualitat, Stress der
Betreuer und Benutzung der Gesundheitsdienste
untersucht werden. Dem Studienaufbau wurde eine
prospektiv randomisierte Querschnittsumfrage in der
Gemeinde zugrunde gelegt. Die Teilnehmer waren
Personen aus einer tertiaren Krankenhaus-Datenbank
(n = 101) mit diagnostizierter multipler Sklerose und
quantifizierbaren neurologischen, Mobilitats- und
kognitiven Ausfallen, die zu Hause lebten, sowie
ihre Betreuer und Arzte. Die Studie bediente sich
demographischer und diagnostischer Daten sowie Daten
zum Schweregrad der Erkrankung, die der Datenbank
entnommen wurden. Zu den strukturierten Interviews,
die zu Hause durchgefuhrt wurden, zahlten: (1) offene
Fragebogen fur Teilnehmer, Betreuer und praktischen Arzt,
die sich mit den Symptomen/Problemen befassen, die das
tagliche Leben erschweren; (2) Standardbeurteilungen der
Lebensqualitat des Patienten, der Stresssituation und der
wahrgenommenen Belastung des Betreuers. Das
Durchschnittsalter der Patienten lag bei 49 Jahren
(Altersspanne: 28–64 Jahre). Bei den starker behinderten
Patienten war eine stark verminderte Lebensqualitat und
eine hohere Belastung der Betreuer zu beobachten als bei
den leichter Behinderten, wobei jedoch Uneinigkeiten
zwischen Patienten, Betreuern und Arzten in ihrer
Sichtweise der Probleme und Symptome deutlich wurden.
Depressionen (67%) und Probleme im beruflichen Alltag
traten haufig auf, im Berufsfeld dagegen erfuhren die
Betroffenen jedoch selten Unterstutzung. Von den 40
Personen, die Interferon einnahmen, hatten 20 eine
sekundar progrediente multiple Sklerose; 39% gaben
Probleme bei der Benutzung von Reha-Einrichtungen an,
und nur 10% wurden an medizinische Reha-Zentren
verwiesen. Daraus folgt, dass der Schweregrad der
Behinderung und die Symptomerfahrung sich mit
anderen Versuchsreihen decken, der Zugriff auf die
entsprechenden Reha- und Supportdienste und deren
Benutzung jedoch mangelhaft zu sein scheint. Ein hoherer
Depressionsgrad und eine schlechtere Lebensqualitat
wurden beobachtet. Moglicherweise konnen die Ressourcen
fur die Entwicklung von Unterstutzungsmaßnahmen am
Arbeitsplatz, fur Beratungs- und Seelsorgedienste und fur
Reha-Maßnahmen neu verteilt werden.
El objetivo de este estudio fue determinar las experiencias
de individuos con esclerosis multiple en relacion con
la discapacidad y los sıntomas que presentan como
resultado de esta enfermedad, en una comunidad
australiana tomada como muestra, para lo que se comparo
las percepciones de los pacientes, y sus cuidadores y
medicos, y se examinaron los efectos que esta afeccion
tiene en la calidad de vida de los pacientes, en el grado de
estres de los cuidadores y en el uso de los servicios
de salud. La investigacion se realizo en forma de un
0342-5282 �c 2006 Lippincott Williams & Wilkins
Copyright © Lippincott Williams & Wilkins. Unauthorized reproduction of this article is prohibited.

estudio transversal prospectivo. Los participantes fueron
individuos residentes en sus hogares, con diagnostico
confirmado de esclerosis multiple, y con trastornos
neurologicos, de movilidad y cognitivos cuantificados,
tomados de la base de datos de un hospital de atencion
terciaria (n = 101); ası como los cuidadores y medicos de
estos. Se emplearon datos demograficos, diagnosticos y
sobre la gravedad de la enfermedad, extraıdos de la base
de datos. Entre las entrevistas estructuradas llevadas a
cabo en el hogar figuraron: (1) cuestionarios abiertos para
los participantes, sus cuidadores y medicos de cabecera,
en los que se evaluan principalmente los sıntomas y
trastornos que afectan la vida cotidiana; (2) evaluaciones
estandarizadas de la calidad de vida del pacientes, las
tensiones a las que de los cuidadores estan sometidos y la
carga percibida que representa el cuidado de estos
individuos. La edad promedio fue de 49 anos (intervalo de
28 a 64). Los individuos mas afectados por la enfermedad
experimentaron una calidad de vida significativamente
peor que aquellos con discapacidades moderadas, pero la
discordancia entre pacientes, cuidadores y medicos se
manifesto en la percepcion que cada uno de ellos tuvo de
los problemas y sıntomas relacionados con la enfermedad.
La incidencia de depresion (67%) y de problemas
relacionados con el trabajo fue alta, pero en muy pocos
casos se brindo apoyo vocacional. Cuarenta de estos
individuos utilizaron interferon, de ellos 20 padecıan
esclerosis multiple progresiva secundaria. El 39% de los
participantes manifestaron dificultades para tener acceso
a los servicios de rehabilitacion y solo al 10% de ellos se
remitio a los servicios de rehabilitacion profesional. En
conclusion, la incidencia de discapacidades y sıntomas fue
similar a la encontrada en otros estudios; sin embargo,
el acceso a los servicios de rehabilitacion y apoyo y la
utilizacion adecuada de estos servicios parecen estar
ausentes. La incidencia de depresion y mala calidad
de vida reportadas fue mas alta en este estudio.
Probablemente existan oportunidades de redistribuir el
uso de los recursos para desarrollar servicios de apoyo
vocacional, psicoterapia y rehabilitacion.
Cette etude avait pour objectif de determiner l’experience
du handicap et les symptomes signales dans les cas de
sclerose en plaques parmi un echantillon de la collectivite
australienne, en comparant les perceptions des patients,
des aides-soignants et des medecins traitants, et en
examinant les effets de la maladie sur la qualite de la vie, le
stress pour les personnes assurant les soins et l’utilisation
des services de sante. L’etude a ete concue en utilisant une
enquete prospective couvrant toutes les sections de la
collectivite. Les participants etaient des individus dont le
diagnostic de sclerose en plaques etait confirme et
presentant des deficits neurologiques, de mobilite
et cognitifs quantifies, confirmes par les informations d’une
banque de donnees hospitaliere tertiaire (n = 101), qui
vivaient a domicile, et leurs personnes soignantes et
docteurs. La methode d’etude utilisait des donnees
demographiques, de diagnostic et de severite de la
maladie extraites de la banque de donnees. Les entretiens
structures effectues a domicile incluaient: (1) des
questionnaires ouverts pour les participants, les personnes
soignantes et les medecins generalistes, definissant la
priorite des symptomes/problemes affectant la vie
quotidienne; (2) des evaluations standardisees de qualite
de la vie du patient, de stress de la personne soignante et
de la lourdeur percue des soins. L’age moyen etait de 49
ans (fourchette 28-64). Les personnes les plus severement
affectees presentaient une reduction plus significative de
leur qualite de vie et accroissaient plus notablement la
lourdeur des soins que les patients souffrant d’un handicap
moindre, mais des desaccords entre les patients, les
personnes soignantes et les docteurs ont ete notes dans
leur perception des problemes et leur experience
des symptomes. Les taux de depression (67%) et de
problemes lies au travail etaient eleves, mais une
assistance professionnelle etait rarement fournie.
Quarante personnes utilisaient l’interferon, dont 20
patients souffrant de sclerose en plaques progressive
secondaire, 39% signalaient des difficultes d’acces aux
services de rehabilitation et seulement 10% avaient ete
envoyes vers des unites de reeducation medicale.
En conclusion, le taux de handicap et l’experience
des symptomes etait similaire aux autres series,
toutefois l’acces aux services de reeducation et de
soutien appropries et leur utilisation semble etre
deficiente. On note des taux de depression plus importants
et une mauvaise qualite de la vie. Il pourra exister
des possibilites de redeployer les ressources en vue
de developper un soutien professionnel et des services
de conseil et de reeducation. International Journal of
Rehabilitation Research 29:87–96 �c 2006 Lippincott
Williams & Wilkins.
International Journal of Rehabilitation Research 2006, 29:87–96
Keywords: carer burden, disability, Expanded Disability Status Scale,health service utilization, multiple sclerosis, quality of life, rehabilitation
aDepartment of Rehabilitation Medicine, University of Melbourne, RoyalMelbourne Hospital, Melbourne, Australia, bPeter Macallum Cancer Centre,Melbourne, Australia, cDepartment of Clinical Epidemiology, Health ServiceEvaluation Unit, Royal Melbourne Hospital, Melbourne, Australia, dKings CollegeLondon, Regional Hospital Unit, Northwick Park Hospital, London, UK andeCentre for Neuroscience, University of Melbourne, Melbourne, Australia.
Correspondence and requests for reprints to F. Khan, c/o Building 21, RoyalMelbourne Hospital, Royal Park Campus, Poplar Road, Parkville, Victoria 3052,Australia.Tel: + 61 3 8387 2178; fax: + 61 3 8387 2506;e-mail: [email protected]
Sponsorship: This study was made possible by the 2005 Research Fellowshipgrant, made available by the Royal Australasian College of Physicians and theDepartment of Medicine, University of Melbourne, Australia. The supportingsources had no involvement, control nor influenced the decision to submit thefinal manuscript.
Received 26 August 2005 Accepted 21 October 2005
88 International Journal of Rehabilitation Research 2006, Vol 29 No 2
Copyright © Lippincott Williams & Wilkins. Unauthorized reproduction of this article is prohibited.

IntroductionMultiple sclerosis (MS) is a chronic disease of the central
nervous system associated with progressive disability and
cognitive dysfunction. It affects over 1 million young
adults worldwide, and is the third leading cause of
disability in adults between 20 and 50 years of age
(Dombovy, 1998). The prognosis is variable; 50% will
require a gait aid within 15 years of onset (Weinshenker
et al., 1989). Therefore, issues of progressive physical
disability, psychosocial adjustment, social reintegration,
financial strain, and impact on driving, work and family
occur over time (Frankel, 2001).
It has been recognized that doctors do not always
accurately estimate factors affecting health-related issues
in their patients (Slevin et al., 1988; Rothwell et al., 1997).
Patients themselves may underestimate their own care
needs (Donohoe et al., 1996) and access to community
services can bear little relationship to need (Freeman and
Thompson, 2000). The planning of appropriate services
for people with MS relies not only on epidemiological
figures for the condition itself, but also requires a good
understanding of the needs and priorities of the local MS
population.
There are at least 15 000 persons with MS in Australia
(MS Society Australia, 2005). MS is not a notifiable
disease so the actual figure is likely to be higher. The
prevalence of MS (per 100 000 people) has been
estimated at 40–80 in Victoria and Hobart, and 30–35 in
Perth and Newcastle (Hammond et al., 1988). Improved
physician awareness and imaging facilities (Stenager et al.,1991; Sadovnik and Ebers, 1993), and increase in MS
prevalence with age, will impact on health services due to
increased functional disability, as well as aging. However,
an extensive literature search revealed no published
Australian data on the prevalence of symptom and
disability profile in persons with MS, their access to
health care, carer burden or quality of life. Results from
other studies (Aronson et al., 1996; Stolp-Smith et al.,1998; Gottberg et al., 2002) cannot be extrapolated to
Australian conditions due to differences in healthcare and
rehabilitation services.
The aim of this study was therefore to document
disability, symptom experience and quality of life in an
Australian community-based sample of MS patients, and
to relate these to the severity and stage of disease. We
were also interested in comparing the perceptions of the
individuals, their carers and treating doctors, regarding
the priority of different symptoms and problems, and the
extent to which these impact on their daily living. Finally
we wished to ascertain their access to, and use of,
different services and to make recommendations for
future development of services to meet identified
priorities.
MethodsParticipants and setting
A community-based MS group was selected for this study,
who could ‘reliably’ report the main problems of living
with MS. The selection criteria included the recruitment
of younger persons with a confirmed diagnosis of MS,
made by a research neurologist based on Poser’s criteria
(Poser et al., 1983), and cerebral MRI findings consistent
with MS according to Paty’s criteria (Paty et al., 1988).
These persons were residing in their homes, were still
active in the community, and had known limitations in
neurological status, mobility and cognition, based on
Kurtzke’s Functional Systems (KFS) and Expanded
Disability Status Scale (EDSS) (Kurtzke, 1983). Partici-
pants needed to live within a feasible distance for home
interviews. Those who were bed bound and/or institu-
tionalized were excluded. Participant selection criteria
are listed in Table 1.
Participants were ascertained from the MS database held
at the Royal Melbourne Hospital (RMH), a large tertiary
referral centre in Victoria, Australia. Participants were
recruited through the MS Society as well as public and
private neurology clinics. Patient demographic data,
details of diagnosis (using Poser and Paty criteria) and
category per EDSS levels were entered in the database
after assessment by one of five neurologists with a
subspeciality interest in MS.
The severity of MS was determined by assigning a score
for each of the seven KFS (pyramidal, cerebellar,
brainstem, sensory, bowel and bladder, visual, cerebral)
and a single unifying score of the EDSS (Kurtzke, 1983),
quantifying disability from the seven functional system
scores. EDSS is a 20-step scale (using half steps) ranging
from 0 = normal to 10 = death due to MS.
Participant recruitment is outlined in Fig. 1. At the time of
recruitment for this study there were 1023 patients listed
on the RMH MS Database. Of these, 204 patients (20% of
the total sample) were identified as being eligible for this
study, based on a definite diagnosis of MS made by a
neurologist (subspecialty MS) using Poser and Paty criteria,
residing in their homes in the community within a 60-km
radius of metropolitan Melbourne. All were contacted by
mail and invited to participate in the project. The 104 who
replied affirmatively, and returned consent forms, were
telephoned by the primary researcher (F.K.) to explain the
study further and organize the interview appointment.
Their nominated preferred primary treating doctors were
then contacted by mail.
Recruitment and all interviews were undertaken between
December 2004 and February 2005. Twelve interviews
were conducted by the primary author (F.K.) and 92
(88.5%) were assessed by an independent trained
Multiple sclerosis: disability profile in an Australian community cohort Khan et al. 89
Copyright © Lippincott Williams & Wilkins. Unauthorized reproduction of this article is prohibited.

research assistant. Each participant was interviewed at
their home using a structured format. They completed an
open ended questionnaire (see below) and the Assess-
ment of Quality of Life (AQoL) questionnaire
(Hawthorne and Osborne, 2005). Interviews took ap-
proximately 1.5 h and appropriate rest breaks were
provided. The research assistant (and F.K.) provided
assistance for participants who had difficulty with
completing the questionnaires.
Twenty-four participants lived alone and had no carers.
Sixty-nine agreed to have their carers interviewed during
the same visit (Fig. 1) and completed their open-ended
questionnaire, the Care giver strain index (CSI) (Robinson,
1983) and Carer perceived burden, using the Visual
Analogue Scale (VAS) scored in mm along a 10-cm line
(score range 0–100). If concurrent carer interviews were not
possible, the two questionnaires were left for completion
and returned by post. The researchers also contacted (mail
and telephone) the patient’s treating medical practitioner or
neurologist to complete and return their open questionnaire
form.
Measurements
The following diagnostic information was obtained from
the RMH database:
(1) MS diagnosis.
(2) Stage of disease – classified as relapsing remitting
(RR), secondary progressive (SP) or primary
progressive (PP).
(3) EDSS scores.
Disease course, diagnosis and severity of MS symptoms
(EDSS scores) were confirmed by the treating neuro-
logists. Participants were divided into three groups:
mild (EDSS 0–3), moderate (EDSS 3.5–6) and severe
(EDSS 6.5–8.0).
Other information collected during the structured inter-
view included:
(1) Demographic data, including living arrangements,
work, driving and pension status.
(2) Medical history, medication use and relapses within
last 2 years. Relapse was defined as progressive and
persistent worsening of MS symptoms beyond 48 h
requiring hospitalization.
(3) Access to health and social care: the number and
frequency of visits annually to general practitioners or
specialists, allied health staff and others.
Questionnaires
Open self-report questionnaires were used for MS partici-
pants, their carers and treating medical practitioners, to gain
first-hand information about problems due to MS, without
prompting, using checklists or suggesting expected specific
problems. They were asked to list and prioritize up to a
maximum of 10 problems. Questionnaires were standar-
dized and designed to be similar in format to give parallel
perspectives from all three groups (questionnaires available
upon request from authors). If participants were not sure,
the interviewers asked them to outline the most pressing
problems they faced in everyday life. Carers and medical
practitioners were prompted to prioritize the problems they
identified in the participants.
The various symptoms, impairments and problems
identified by all three groups were categorized themati-
cally under major disability headings, then clarified and
confirmed with carers and medical practitioners. They
were listed in terms of importance under the following
headings: fatigue, mobility (weakness, spasticity), con-
tinence (bladder/bowel), depression, cognition, psycho-
social, pain, sexuality, work, transport and other (vision).
This study was approved by the University of Melbourne
and the RMH, Human Research and Ethics Committees.
Statistical analysis
All data were from a single centre and entered by a single
researcher (T.M). Statistics were calculated using SPSS
11.0 for Windows (SPSS, Chicago, Illinois, USA).
Results are described by mean and SD for continuous
non-skewed data, as median and interquartile range
(IQR) for continuous skewed data (as defined by
kurtosis > 2), and as frequency (%) for categorical data.
One-way ANOVA were used to evaluate statistically
significance differences between the three groups of
condition severity (defined by EDSS). Statistical sig-
nificance was determined by an a level of 0.05. AQoL
utility scores were calculated using SPSS according to
guidelines (Hawthorne and Osborne, 2005).
Table 1 Patient selection criteria
Inclusion criteriaAged 18–64 years (male and female patients)Diagnosis of clinically or laboratory-supported definite multiple sclerosis,confirmed by a neurologist according to Poser’s criteriaa and cerebral magneticresonance imaging findings as per Paty’s criteriab
Multiple sclerosis diagnosed a minimum of 2.5 years agoParticipants residing in their homesParticipants with documented neurological deficits based on Kurtzke’sFunctional Systems and Expanded Disability Status Scalec between 2 and 7.5for mobility, and between 0 and 2 for cognitive impairmentAble and willing to give informed consentLiving in metropolitan and greater Melbourne (within 60 km radius)
Exclusion criteriaSevere cognitive issues (Kurtzke’s Functional Systems cognitiongreater than 2)Exacerbation of multile sclerosis in the 3 months prior to recruitmentfor the studyInstitutionalized and bed-bound patients
aPoser et al. (1983).bPaty et al. (1988).cKurtzke (1983).
90 International Journal of Rehabilitation Research 2006, Vol 29 No 2
Copyright © Lippincott Williams & Wilkins. Unauthorized reproduction of this article is prohibited.

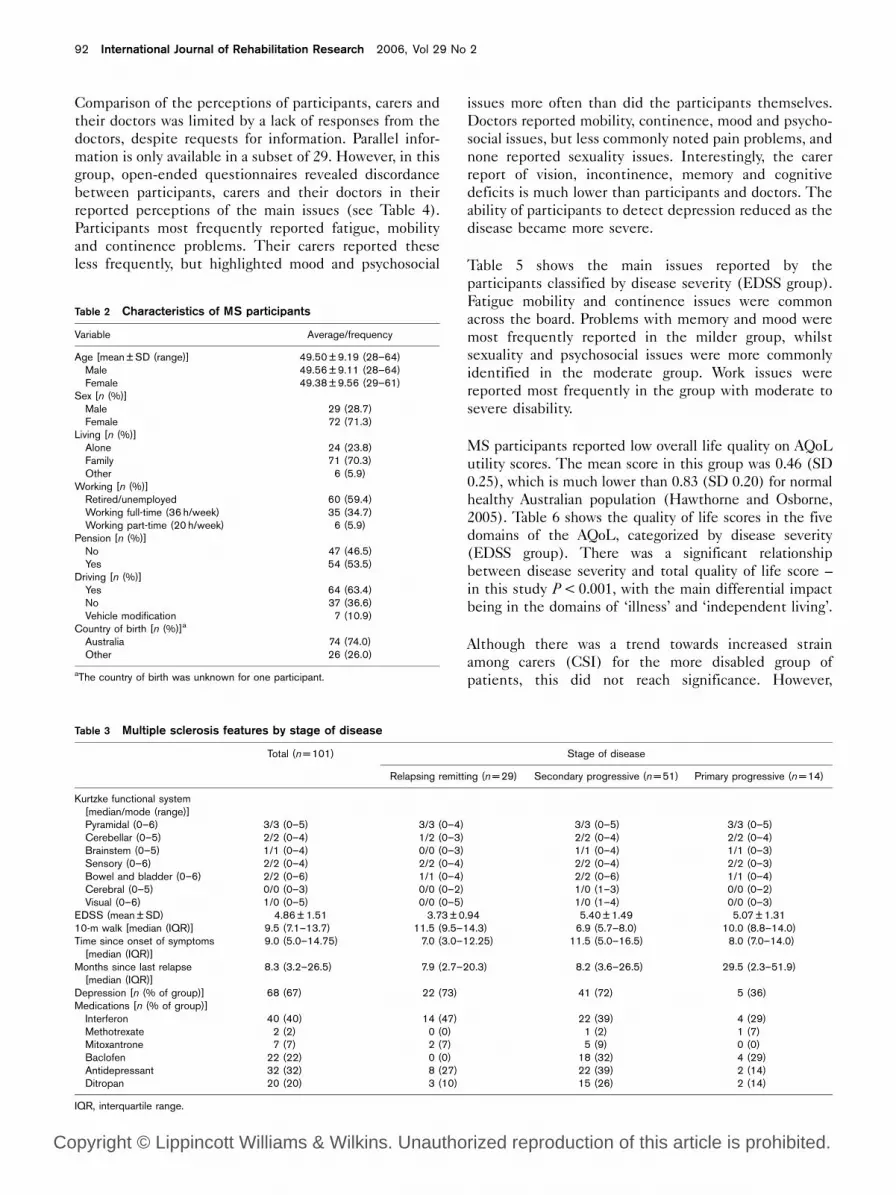
ResultsThe demographic characteristics of the sample are shown
in Table 2. The mean age was 49.5 years (SD 9.2),
female:male ratio approximately 3:1 and there was a mean
of 9 years since diagnosis. Only one-third (35%) were
still working full-time and almost half of those partici-
pants who were employed at the time of diagnosis had
modified their working hours, altered duties to lighter
work or stopped work. The main reasons for giving up
work were fatigue, mobility issues (difficulty in accessing
workplace and transport) and continence. Two-thirds
(63%) were still driving and only 11% had car modifica-
tions (e.g. spinner knob, adjusted brakes).
Table 3 lists the disease characteristics, functional
ability and treatment, categorized by stage of disease.
Two-thirds of the sample reported depression
(67%) and a third (32%) were taking antidepressant
medication.
Forty (40%) used interferon. An unexpected finding
was that 20 (39%) of these had secondary progressive MS,
with an average use of interferon of 8 years. This is
contrary to current authority Pharmaceutical Benefit
Scheme (PBS) guidelines (PBS, 2005), although some
participants reported that they believed the treatment to
be of benefit to them.
Fig. 1
MS database at RMH (n=1023)
Patients met study criteria and invited to participate (n=204)
Participants consented to participate and interviewed (n=101)
Of those not participating:
• 89 failed to respond • 2 declined to participate • 2 responded after analysis
was complete • 5 were unavailable (away) • 3 were excluded due to acute
exacerbation • 2 relocated to another state
Carers interviewed (n=69)
• 321 patients had incomplete information at the time of study
• 204 fulfilled all study criteria • 203 did not have a confirmed
diagnosis of MS as per Paty criteria.
• 161 were unlikely to have definite MS
• 105 were non-ambulant• 25 were excluded (residence too
distant)• 4 were deceased
Of participants with carers: • 6 participants did not want
their carer to be interviewed • 2 carers were not available • 24 lived alone (no carers)
General practitioners responded by mail/fax (n=39)
Of 101 general practitioners contacted:
• 10 had not seen patient in more than 12 months
• 7 were not contactable • 45 failed to respond
Flow chart of recruitment process. MS, multiple sclerosis; RMH, Royal Melbourne Hospital.
Multiple sclerosis: disability profile in an Australian community cohort Khan et al. 91
Copyright © Lippincott Williams & Wilkins. Unauthorized reproduction of this article is prohibited.
Comparison of the perceptions of participants, carers and
their doctors was limited by a lack of responses from the
doctors, despite requests for information. Parallel infor-
mation is only available in a subset of 29. However, in this
group, open-ended questionnaires revealed discordance
between participants, carers and their doctors in their
reported perceptions of the main issues (see Table 4).
Participants most frequently reported fatigue, mobility
and continence problems. Their carers reported these
less frequently, but highlighted mood and psychosocial
issues more often than did the participants themselves.
Doctors reported mobility, continence, mood and psycho-
social issues, but less commonly noted pain problems, and
none reported sexuality issues. Interestingly, the carer
report of vision, incontinence, memory and cognitive
deficits is much lower than participants and doctors. The
ability of participants to detect depression reduced as the
disease became more severe.
Table 5 shows the main issues reported by the
participants classified by disease severity (EDSS group).
Fatigue mobility and continence issues were common
across the board. Problems with memory and mood were
most frequently reported in the milder group, whilst
sexuality and psychosocial issues were more commonly
identified in the moderate group. Work issues were
reported most frequently in the group with moderate to
severe disability.
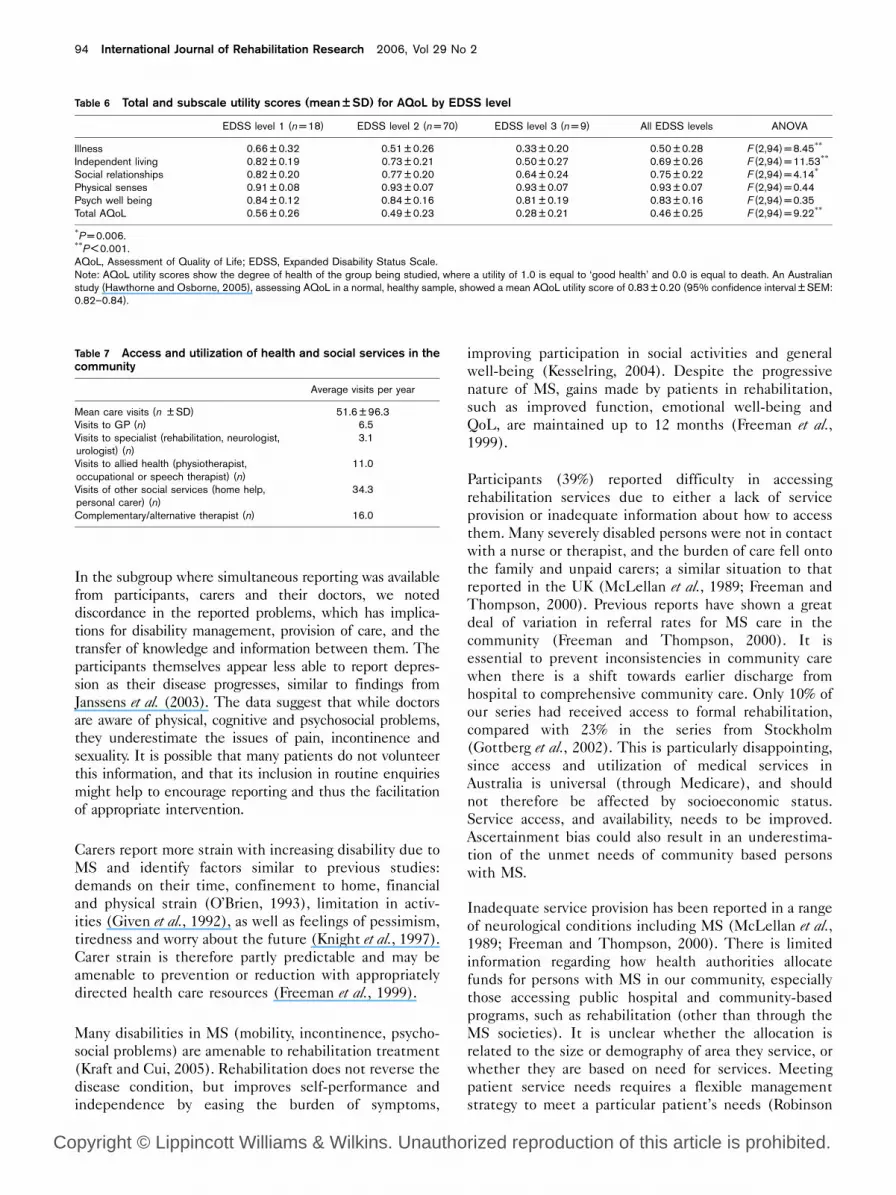
MS participants reported low overall life quality on AQoL
utility scores. The mean score in this group was 0.46 (SD
0.25), which is much lower than 0.83 (SD 0.20) for normal
healthy Australian population (Hawthorne and Osborne,
2005). Table 6 shows the quality of life scores in the five
domains of the AQoL, categorized by disease severity
(EDSS group). There was a significant relationship
between disease severity and total quality of life score –
in this study P < 0.001, with the main differential impact
being in the domains of ‘illness’ and ‘independent living’.
Although there was a trend towards increased strain
among carers (CSI) for the more disabled group of
patients, this did not reach significance. However,
Table 2 Characteristics of MS participants
Variable Average/frequency
Age [mean ± SD (range)] 49.50 ± 9.19 (28–64)Male 49.56 ± 9.11 (28–64)Female 49.38 ± 9.56 (29–61)
Sex [n (%)]Male 29 (28.7)Female 72 (71.3)
Living [n (%)]Alone 24 (23.8)Family 71 (70.3)Other 6 (5.9)
Working [n (%)]Retired/unemployed 60 (59.4)Working full-time (36 h/week) 35 (34.7)Working part-time (20 h/week) 6 (5.9)
Pension [n (%)]No 47 (46.5)Yes 54 (53.5)
Driving [n (%)]Yes 64 (63.4)No 37 (36.6)Vehicle modification 7 (10.9)
Country of birth [n (%)]a
Australia 74 (74.0)Other 26 (26.0)
aThe country of birth was unknown for one participant.
Table 3 Multiple sclerosis features by stage of disease
Total (n = 101) Stage of disease
Relapsing remitting (n = 29) Secondary progressive (n = 51) Primary progressive (n = 14)
Kurtzke functional system[median/mode (range)]Pyramidal (0–6) 3/3 (0–5) 3/3 (0–4) 3/3 (0–5) 3/3 (0–5)Cerebellar (0–5) 2/2 (0–4) 1/2 (0–3) 2/2 (0–4) 2/2 (0–4)Brainstem (0–5) 1/1 (0–4) 0/0 (0–3) 1/1 (0–4) 1/1 (0–3)Sensory (0–6) 2/2 (0–4) 2/2 (0–4) 2/2 (0–4) 2/2 (0–3)Bowel and bladder (0–6) 2/2 (0–6) 1/1 (0–4) 2/2 (0–6) 1/1 (0–4)Cerebral (0–5) 0/0 (0–3) 0/0 (0–2) 1/0 (1–3) 0/0 (0–2)Visual (0–6) 1/0 (0–5) 0/0 (0–5) 1/0 (1–4) 0/0 (0–3)
EDSS (mean ± SD) 4.86 ± 1.51 3.73 ± 0.94 5.40 ± 1.49 5.07 ± 1.3110-m walk [median (IQR)] 9.5 (7.1–13.7) 11.5 (9.5–14.3) 6.9 (5.7–8.0) 10.0 (8.8–14.0)Time since onset of symptoms
[median (IQR)]9.0 (5.0–14.75) 7.0 (3.0–12.25) 11.5 (5.0–16.5) 8.0 (7.0–14.0)
Months since last relapse[median (IQR)]
8.3 (3.2–26.5) 7.9 (2.7–20.3) 8.2 (3.6–26.5) 29.5 (2.3–51.9)
Depression [n (% of group)] 68 (67) 22 (73) 41 (72) 5 (36)Medications [n (% of group)]
Interferon 40 (40) 14 (47) 22 (39) 4 (29)Methotrexate 2 (2) 0 (0) 1 (2) 1 (7)Mitoxantrone 7 (7) 2 (7) 5 (9) 0 (0)Baclofen 22 (22) 0 (0) 18 (32) 4 (29)Antidepressant 32 (32) 8 (27) 22 (39) 2 (14)Ditropan 20 (20) 3 (10) 15 (26) 2 (14)
IQR, interquartile range.
92 International Journal of Rehabilitation Research 2006, Vol 29 No 2
Copyright © Lippincott Williams & Wilkins. Unauthorized reproduction of this article is prohibited.

perceived carer burden was markedly increased in the
severely disabled group, as compared with the mild and
moderate groups (P < 0.01).
Table 7 shows access and utilization of available health
and social services in the community. The average annual
number of health and social service visits was 51.6 (SD
96). Less than 10% of participants had been formally
referred to medical rehabilitation units and 39% reported
difficulty accessing rehabilitation intervention for MS
due to lack of services or information about how to access
them. Eight (8.1%) participants were visiting practi-
tioners of complementary medicine and using various
‘tonics’. The average number of annual visits to
allied health staff (physiotherapy, occupational therapy
or speech services) was 11 (often coordinated by
the MS society, Victoria) and, of these, about 2% of
participants self-funded private physiotherapy (gym
program, fitness instructor). The average number
of visits by services (personal care, home help)
organized through the local council and MS society was
35 per year.
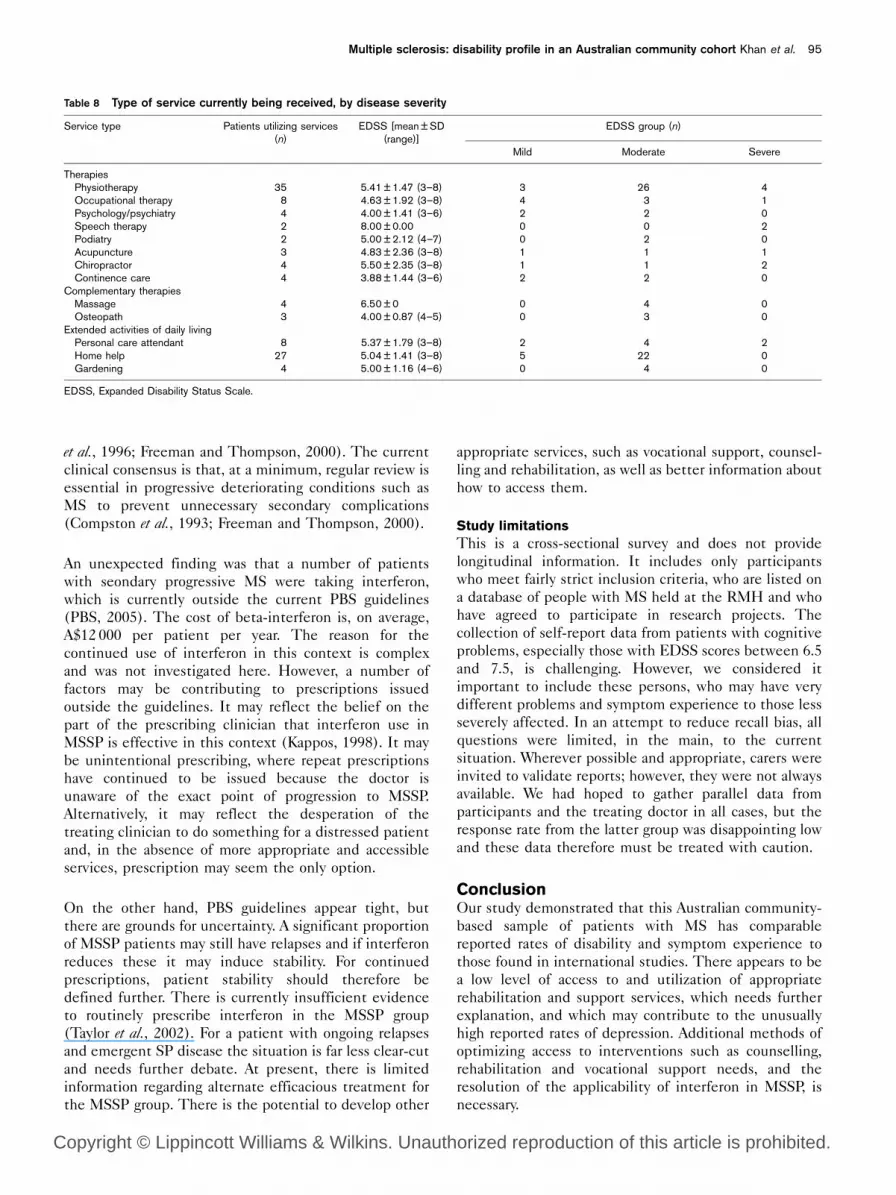
Table 8 outlines the type of service utilized by the MS
participants, categorized by severity. Overall, 35 regularly
received physiotherapy, and 27 had home help through
the local council and MS society, mainly amongst the
moderately affected individuals. Paradoxically the most
severe category of MS participants received the least
services; they were cared for by their carers and family,
and none attended a day centre. From the low utilization
rates there appears to be inadequate usage of existing
services across the board, particularly in the most severely
affected group.
DiscussionThe mean participant age, gender, time since diagnosis,
distribution of type, severity of disease (based on EDSS)
and disability in this group were similar to those reported
by others (Mathews et al., 1985; Kraft et al., 1986; Monks
and Robinson, 1989; Cockerill and Warren, 1990;
Sadovnick and Ebers, 1993; Aronson et al., 1996; Gottberg
et al., 2002). The participants represented a broad range
of disability and disease severity, with demographic and
diagnostic characteristics typical of MS (Weinshenker
et al., 1989). The problems reported have a clear impact
on quality of life, which was much lower in these MS
participants than in the normal Australian population.
In this study, two-thirds of the participants reported
depression, which is much higher than the 36% reported
by Janssens et al. (2003). Work-related problems were
common and in keeping with other studies (Kraft et al.,1986; Warren et al., 1986; Aronson et al., 1996). Gronning
et al. (1990) reported 16 years ago that approximately
50–80% of MS patients are unemployed within 10 years
of disease onset. Services do not seem to have improved
much since then; almost none of this series reported
having received specific interventions to support vocation
or to lessen the impact of unemployment.
Table 4 Main issues for multiple sclerosis patients, as reported by patient, carer and general practitioner
Total group For subgroup of 29
Patient (n = 101) Carer (n = 69) General practi-tioner (n = 39)
Patient Carer General practitioner
n % n % n % n % n % n %
Fatigue 82 81.2 32 46.4 19 48.7 24 82.8 11 37.9 15 51.7Mobility 80 79.2 32 46.4 31 79.5 21 72.4 23 79.3 23 79.3Bladder/bowel problems 61 60.4 17 24.6 14 35.9 20 69.0 6 20.7 10 34.5Memory/cognition 24 23.8 9 13.0 15 38.5 6 20.7 4 13.8 10 34.5Sexuality 16 15.8 12 17.4 0 0.0 8 27.6 8 27.6 0 0.0Work 16 15.8 6 8.7 2 5.1 6 20.7 3 10.3 1 3.4Vision 15 14.9 6 8.7 6 15.4 3 10.3 1 3.4 5 17.2Depression/anxiety/
emotional lability15 14.9 32 46.4 16 41.0 4 13.8 13 44.8 11 37.9
Psychosociala 13 12.9 24 34.8 11 28.2 3 10.3 13 44.8 8 27.6Pain 12 11.9 9 13.0 2 5.1 2 6.9 5 17.2 2 6.9Transportb 5 5.0 4 5.8 0 0.0 2 6.9 1 3.4 0 0.0
aPsychosocial problems: marital problems, lack of social activities.bTransport problems include inability to drive, lack of access to transport.
Table 5 Main issues reported by participants classified by diseaseseverity
Expanded disability status scale
Level 1 (0–3)n = 19 [n (%)]
Level 2 (3.5–6)n = 60 [n (%)]
Level 3 (6.5–8)n = 22 [n (%)]
Fatigue 17 (89.5) 48 (80.0) 17 (77.3)Mobility 13 (68.4) 46 (76.7) 21 (95.5)Pain 2 (10.5) 8 (13.3) 2 (9.1)Bladder/bowel 9 (47.4) 37 (61.7) 15 (68.2)Depression 8 (42.1) 7 (11.7) 0 (0.0)Sexuality 3 (15.8) 12 (20.0) 1 (4.5)Psychosocial 1 (5.3) 10 (16.7) 2 (9.1)Work 1 (5.3) 11 (18.3) 4 (18.2)Transport 1 (5.3) 3 (5.0) 1 (4.5)Memory 6 (31.6) 15 (25.0) 3 (13.6)Vision 3 (15.8) 11 (18.3) 1 (4.5)
Multiple sclerosis: disability profile in an Australian community cohort Khan et al. 93
Copyright © Lippincott Williams & Wilkins. Unauthorized reproduction of this article is prohibited.
In the subgroup where simultaneous reporting was available
from participants, carers and their doctors, we noted
discordance in the reported problems, which has implica-
tions for disability management, provision of care, and the
transfer of knowledge and information between them. The
participants themselves appear less able to report depres-
sion as their disease progresses, similar to findings from
Janssens et al. (2003). The data suggest that while doctors
are aware of physical, cognitive and psychosocial problems,
they underestimate the issues of pain, incontinence and
sexuality. It is possible that many patients do not volunteer
this information, and that its inclusion in routine enquiries
might help to encourage reporting and thus the facilitation
of appropriate intervention.
Carers report more strain with increasing disability due to
MS and identify factors similar to previous studies:
demands on their time, confinement to home, financial
and physical strain (O’Brien, 1993), limitation in activ-
ities (Given et al., 1992), as well as feelings of pessimism,
tiredness and worry about the future (Knight et al., 1997).
Carer strain is therefore partly predictable and may be
amenable to prevention or reduction with appropriately
directed health care resources (Freeman et al., 1999).
Many disabilities in MS (mobility, incontinence, psycho-
social problems) are amenable to rehabilitation treatment
(Kraft and Cui, 2005). Rehabilitation does not reverse the
disease condition, but improves self-performance and
independence by easing the burden of symptoms,
improving participation in social activities and general
well-being (Kesselring, 2004). Despite the progressive
nature of MS, gains made by patients in rehabilitation,
such as improved function, emotional well-being and
QoL, are maintained up to 12 months (Freeman et al.,1999).
Participants (39%) reported difficulty in accessing
rehabilitation services due to either a lack of service
provision or inadequate information about how to access
them. Many severely disabled persons were not in contact
with a nurse or therapist, and the burden of care fell onto
the family and unpaid carers; a similar situation to that
reported in the UK (McLellan et al., 1989; Freeman and
Thompson, 2000). Previous reports have shown a great
deal of variation in referral rates for MS care in the
community (Freeman and Thompson, 2000). It is
essential to prevent inconsistencies in community care
when there is a shift towards earlier discharge from
hospital to comprehensive community care. Only 10% of
our series had received access to formal rehabilitation,
compared with 23% in the series from Stockholm
(Gottberg et al., 2002). This is particularly disappointing,
since access and utilization of medical services in
Australia is universal (through Medicare), and should
not therefore be affected by socioeconomic status.
Service access, and availability, needs to be improved.
Ascertainment bias could also result in an underestima-
tion of the unmet needs of community based persons
with MS.
Inadequate service provision has been reported in a range
of neurological conditions including MS (McLellan et al.,1989; Freeman and Thompson, 2000). There is limited
information regarding how health authorities allocate
funds for persons with MS in our community, especially
those accessing public hospital and community-based
programs, such as rehabilitation (other than through the
MS societies). It is unclear whether the allocation is
related to the size or demography of area they service, or
whether they are based on need for services. Meeting
patient service needs requires a flexible management
strategy to meet a particular patient’s needs (Robinson
Table 6 Total and subscale utility scores (mean ± SD) for AQoL by EDSS level
EDSS level 1 (n = 18) EDSS level 2 (n = 70) EDSS level 3 (n = 9) All EDSS levels ANOVA
Illness 0.66 ± 0.32 0.51 ± 0.26 0.33 ± 0.20 0.50 ± 0.28 F (2,94) = 8.45**
Independent living 0.82 ± 0.19 0.73 ± 0.21 0.50 ± 0.27 0.69 ± 0.26 F (2,94) = 11.53**
Social relationships 0.82 ± 0.20 0.77 ± 0.20 0.64 ± 0.24 0.75 ± 0.22 F (2,94) = 4.14*
Physical senses 0.91 ± 0.08 0.93 ± 0.07 0.93 ± 0.07 0.93 ± 0.07 F (2,94) = 0.44Psych well being 0.84 ± 0.12 0.84 ± 0.16 0.81 ± 0.19 0.83 ± 0.16 F (2,94) = 0.35Total AQoL 0.56 ± 0.26 0.49 ± 0.23 0.28 ± 0.21 0.46 ± 0.25 F (2,94) = 9.22**
*P = 0.006.**P < 0.001.AQoL, Assessment of Quality of Life; EDSS, Expanded Disability Status Scale.Note: AQoL utility scores show the degree of health of the group being studied, where a utility of 1.0 is equal to ‘good health’ and 0.0 is equal to death. An Australianstudy (Hawthorne and Osborne, 2005), assessing AQoL in a normal, healthy sample, showed a mean AQoL utility score of 0.83 ± 0.20 (95% confidence interval ± SEM:0.82–0.84).
Table 7 Access and utilization of health and social services in thecommunity
Average visits per year
Mean care visits (n ± SD) 51.6 ± 96.3Visits to GP (n) 6.5Visits to specialist (rehabilitation, neurologist,urologist) (n)
3.1
Visits to allied health (physiotherapist,occupational or speech therapist) (n)
11.0
Visits of other social services (home help,personal carer) (n)
34.3
Complementary/alternative therapist (n) 16.0
94 International Journal of Rehabilitation Research 2006, Vol 29 No 2
Copyright © Lippincott Williams & Wilkins. Unauthorized reproduction of this article is prohibited.
et al., 1996; Freeman and Thompson, 2000). The current
clinical consensus is that, at a minimum, regular review is
essential in progressive deteriorating conditions such as
MS to prevent unnecessary secondary complications
(Compston et al., 1993; Freeman and Thompson, 2000).
An unexpected finding was that a number of patients
with seondary progressive MS were taking interferon,
which is currently outside the current PBS guidelines
(PBS, 2005). The cost of beta-interferon is, on average,
A$12 000 per patient per year. The reason for the
continued use of interferon in this context is complex
and was not investigated here. However, a number of
factors may be contributing to prescriptions issued
outside the guidelines. It may reflect the belief on the
part of the prescribing clinician that interferon use in
MSSP is effective in this context (Kappos, 1998). It may
be unintentional prescribing, where repeat prescriptions
have continued to be issued because the doctor is
unaware of the exact point of progression to MSSP.
Alternatively, it may reflect the desperation of the
treating clinician to do something for a distressed patient
and, in the absence of more appropriate and accessible
services, prescription may seem the only option.
On the other hand, PBS guidelines appear tight, but
there are grounds for uncertainty. A significant proportion
of MSSP patients may still have relapses and if interferon
reduces these it may induce stability. For continued
prescriptions, patient stability should therefore be
defined further. There is currently insufficient evidence
to routinely prescribe interferon in the MSSP group
(Taylor et al., 2002). For a patient with ongoing relapses
and emergent SP disease the situation is far less clear-cut
and needs further debate. At present, there is limited
information regarding alternate efficacious treatment for
the MSSP group. There is the potential to develop other
appropriate services, such as vocational support, counsel-
ling and rehabilitation, as well as better information about
how to access them.
Study limitations
This is a cross-sectional survey and does not provide
longitudinal information. It includes only participants
who meet fairly strict inclusion criteria, who are listed on
a database of people with MS held at the RMH and who
have agreed to participate in research projects. The
collection of self-report data from patients with cognitive
problems, especially those with EDSS scores between 6.5
and 7.5, is challenging. However, we considered it
important to include these persons, who may have very
different problems and symptom experience to those less
severely affected. In an attempt to reduce recall bias, all
questions were limited, in the main, to the current
situation. Wherever possible and appropriate, carers were
invited to validate reports; however, they were not always
available. We had hoped to gather parallel data from
participants and the treating doctor in all cases, but the
response rate from the latter group was disappointing low
and these data therefore must be treated with caution.
ConclusionOur study demonstrated that this Australian community-
based sample of patients with MS has comparable
reported rates of disability and symptom experience to
those found in international studies. There appears to be
a low level of access to and utilization of appropriate
rehabilitation and support services, which needs further
explanation, and which may contribute to the unusually
high reported rates of depression. Additional methods of
optimizing access to interventions such as counselling,
rehabilitation and vocational support needs, and the
resolution of the applicability of interferon in MSSP, is
necessary.
Table 8 Type of service currently being received, by disease severity
Service type Patients utilizing services(n)
EDSS [mean ± SD(range)]
EDSS group (n)
Mild Moderate Severe
TherapiesPhysiotherapy 35 5.41 ± 1.47 (3–8) 3 26 4Occupational therapy 8 4.63 ± 1.92 (3–8) 4 3 1Psychology/psychiatry 4 4.00 ± 1.41 (3–6) 2 2 0Speech therapy 2 8.00 ± 0.00 0 0 2Podiatry 2 5.00 ± 2.12 (4–7) 0 2 0Acupuncture 3 4.83 ± 2.36 (3–8) 1 1 1Chiropractor 4 5.50 ± 2.35 (3–8) 1 1 2Continence care 4 3.88 ± 1.44 (3–6) 2 2 0
Complementary therapiesMassage 4 6.50 ± 0 0 4 0Osteopath 3 4.00 ± 0.87 (4–5) 0 3 0
Extended activities of daily livingPersonal care attendant 8 5.37 ± 1.79 (3–8) 2 4 2Home help 27 5.04 ± 1.41 (3–8) 5 22 0Gardening 4 5.00 ± 1.16 (4–6) 0 4 0
EDSS, Expanded Disability Status Scale.
Multiple sclerosis: disability profile in an Australian community cohort Khan et al. 95
Copyright © Lippincott Williams & Wilkins. Unauthorized reproduction of this article is prohibited.

AcknowledgementsWe would like to thank all our participants with MS, their
carers and treating medical practitioners for their
assistance and cooperation. Ms L. Spooner and C. Paros
for data collection and interviews, M. Tanner and
J. Eckholdt for their assistance with the RMH database,
and Drs L. McDonald and P. Disler for their advice in
planning this study.
ReferencesAronson KJ, Goldenberg E, Cleghorn G (1996). Sociodemographics characteris-
tics and health status of persons with multiple sclerosis and their care givers.MS Management 3:5–15.
Cockerill R, Warren S (1990). Care for caregivers: the needs of family membersof MS patients. J Rehabil 56:41–44.
Compston DAS, Evans CD, Fenely RCL, McLellan DL, Pentland B,Roberts MHW, et al. (1993). Working party report of the British Society ofRehabilitation Medicine. London: The Stationery Office.
Dombovy ML (1998). Multiple sclerosis and Parkinson’s Disease rehabilitation.In: Lazar R (editor): Principles of neurological rehabilitation. New York:McGraw-Hill. pp. 173–197.
Donohoe KM, Wineman NM, O’Brian RA (1996). Are alternate long-termcare programs needed for adults with chronic disability? J Neurosci Nurs28:373–380.
Frankel D (2001). Multiple sclerosis. In: Umphred DA, (editor): Neurologicalrehabilitation. 4th ed. St Louis: Mosby. pp. 595–615.
Freeman JA, Thompson AJ (2000). Community services in MS: still a matter ofchance. J Neurol Neurosurg Psychiatry 69:728–732.
Freeman JA, Langdon DW, Hobart JC, Thompson AJ (1999). Inpatientrehabilitation in multiple sclerosis. Do the benefits carry over into thecommunity? Neurology 52:50–56.
Given CW, Given B, Stommel M, Collins C, King S, Franklin S (1992). Thecaregivers reaction assessment (CRA) for caregivers to persons withphysical and mental impairments. Res Nurs Health 15:271–283.
Gottberg K, Einarsson U, Fredrikson S, von Koch L, Holmqvist LW (2002).Multiple sclerosis in Stockholm county. A pilot study of utilization of healthcare resources, patient satisfaction with care and impact on family caregivers.Acta Neurol Scand 106:241–247.
Gronning M, Hannisdal E, Mellgren SI (1990). Multivariate analysis of factorsassociated with unemployment in people with multiple sclerosis. J NeurolNeurosurg Psychiatry 53:388–390.
Hammond SR, McLeod JG, Millingen KS, Stewart-Wynne EG, English D,Holland JT, et al. (1988). The epidemiology of multiple sclerosis in threeAustralian cities: Perth, Newcastle and Hobart. Brain 111:1–25.
Hawthorne G, Osborne R (2005). Population norms and meaningful differencesfor the Assessment of Quality of Life (AqoL) measure. Aust NZ J PublicHealth 29:136–142.
Janssens ACJW, van Doorn PA, van der Meche FGA, Passchier J, Hintzen RQ(2003). Impact of recently diagnosed multiple sclerosis on quality of life,anxiety, depression and distress of patients and partners. Acta Neurol Scand108:389–395.
Kappos L (1998). Placebo controlled multicentre randomized trial of InterferonBeta-1b in the treatment of secondary progressive multiple sclerosis. Lancet352:1491–1497.
Kesselring J (2004). Neurorehabilitation in MS – What is the evidence base?J Neurol 251:25–29.
Knight RG, Devereux RC, Godfrey HPD (1997). Psychosocial consequencesof caring for a spouse with multiple sclerosis. J Clin Exp Neuropsychol19:7–19.
Kraft GH, Cui JY (2005). In: Delisa JA (editor): Multiple sclerosis in physicalmedicine and rehabilitation: principles and practice. 4th ed. Philadelphia:Lippincott. pp. 1753–1769.
Kraft GH, Freal JE, Coryell JK (1986). Disability, disease duration andrehabilitation service needs in multiple sclerosis: patient perspectives. ArchPhys Med Rehabil 67:164–168.
Kurtzke JF (1983). Rating neurological impairment in multiple sclerosis: anexpanded disability status scale (EDSS). Neurology 33:1444–1452.
Mathews WB, Acheson ED, Batchelor JR, Wellor RO (1985). McAlpine’smultiple sclerosis. London: Churchill Livingstone.
McLellan DL, Martin JR, Roberts MHW, Spackman A, McIntosh-Michaelis S, Nichols S(1989). Multiple Sclerosis in the Southampton District. Southampton: Universityof Southampton Research Unit and Department of Sociology.
Monks J, Robinson I (1989). The characteristics of a national register of peoplewith multiple sclerosis: a comparison between the ARMS (Action forresearch into multiple sclerosis) register and 10 British MS populations.J Epidemiol Community Health 43:179–186.
MS Society Australia [online]. http://www.msaustralia.org.au. [Accessed 29 July2005]
O’Brien MT (1993). Multiple sclerosis: stressors and coping strategies in spousalcaregivers. J Community Health Nurs 10:123–135.
Paty DW, Oger JJ, Kastrukoff LF, Hashimoto SA, Hooge JP, Eisen AA, et al.(1988). MRI in the diagnosis of MS: a prospective study with comparison ofclinical evaluation, evoked potentials, oligoclonal banding and CT neurology.Neurology 38:180–185.
PBS (2005). Schedule of Pharmaceutical Benefit Scheme. Canberra:Australian Government Department of Health and Aging [online].http://www1.health.gov.au/pbs/scripts/search.cfm. [Accessed 30 July 2005].
Poser CM, Paty DW, Scheinberg L, McDonald WI, Davis FA, Ebers GC, et al.(1983). New diagnostic criteria for Multiple Sclerosis: guidelines for researchprotocols. Ann Neurol 13:227–231.
Robinson BC (1983). Validation of a Caregiver Strain Index. J Gerontology38:344–348.
Robinson I, Hunter M, Neilson S (1996). A dispatch from the front line: the viewsof people with multiple sclerosis about their needs. A qualitative approach.London: Brunnel Research Unit.
Rothwell PM, McDowell Z, Wong CK, Dorman PJ (1997). Doctors and patientsdon’t agree: cross sectional study of patients and doctors perceptions andassessments of disability in multiple sclerosis. BMJ 314:1580.
Sadovnik AD, Ebers GC (1993). Epidemiology of multiple sclerosis: a criticalreview. Can J Neurol Sci 20:17–29.
Slevin ML, Plant H, Lynch D, Drinkwater J, Gregory WM (1988). Who shouldmeasure the quality of life, the doctor or the patient? Br J Cancer 57:109–112.
Stenager E, Knudson L, Jensen K (1991). Multiple sclerosis: the impact ofphysical impairment and cognitive dysfunction on social and spare timeactivities. Psychother Psychosom 56:123–128.
Stolp-Smith KA, Atkinson EJ, Campion ME, O’Brien PC, Rodriguez M (1998).Health care utilization in multiple sclerosis: a population based study inOlmsted County, MN. Neurology 50:1594–1600.
Taylor I, Macdonell R, Coleman J (2002). Treatment of multiple sclerosis withnewer immune-modulating drugs. Australian Prescriber 25:32–35.
Warren S, Cockerill R, Paterson M, Patterson I (1986). Planning support servicesfor chronically sick in rural areas. Can J Public Health 77:19–23.
Weinshenker BG, Bass B, Rice GP, Noseworthy J, Carriere W, Baskerville J, et al.(1989). The natural history of multiple sclerosis: a geographically basedstudy. 2. Predictive value of early clinical course. Brain 112:1419–1428.
96 International Journal of Rehabilitation Research 2006, Vol 29 No 2
Copyright © Lippincott Williams & Wilkins. Unauthorized reproduction of this article is prohibited.