modesty and the skin: why they shouldn't mix
TRANSCRIPT

January/February 2012 • Volume 10 • Issue 1
EDITORIALModesty and the Skin: Why They Shouldn’t Mix
Campbell and Parish
COMMENTARYOrigin and Evolution of Syphilis: Drifting Myth
Sehgal, Verma, Chatterjee, Chaudhuri, Chatterjee, and Rasool
ORIGINAL CONTRIBUTIONSA New Paradigm in the Treatment of Kerions:
Treat the InflammationDolder, O’Neill, O’Brien, Ross, Allen, and Allen
Pityriasis Rubra Pilaris: Evolution of Challenges in Promising Treatment Options
Sehgal, Srivastava, and Verma
REVIEWThe Role of Surgical Debridement in Healing of
Diabetic Foot UlcersGordon, Lebrun, Tomic-Canic, and Kirsner
CORE CURRICULUMCutaneous Tuberculosis: A Diagnostic DilemmaSehgal, Verma, Bhattacharya, Sharma, Singh, and Verma
DEPARTMENTSCOSMETIC SCIENCE
Repelling Insects With Safe and Effective Alternatives to DEET
Epstein
PERILS OF DERMATOPATHOLOGYIt’s Not Just Who You Are, It’s Also Where You Are:
The Cutaneous Leiomyosarcoma DilemmaTumer, Castilla, and Lambert
INFECTIOUS DISEASE CAPSULEIt May Be Vulgar, but It Isn’t a Bad Word
Saunders, Herchline, and Bernstein
CASE STUDIESUnusually Severe Case of Dermatosis Neglecta
Turrentine, Blalock, and Davis
Fixed-Drug Eruption Caused by Ashwagandha (Withania somnifera): A Widely Used Ayurvedic Drug
Sehgal, Verma, and Bhattacharya
Chronic Lymphocytic Leukemia Revealed by a Granulomatous Zosteriform Eruption
Trojjet, Hammami, Zaraa, Bouzguarrou, Joens, Haouet, Osman, and Mokni
CORRESPONDENCEMycobacterium marinum Cutaneous Infection With Sporotrichoid Distribution Treated With
Azithromycin MonotherapyRallis, Falidas, and Stavropoulos

RESULTS PATIENTS WANT IN A FORMULATION THAT DOES THE WORK—
PRESCRIBE DIFFERIN® LOTION, 0.1% TODAY!
DIFFERIN® (adapalene) LOTION, 0.1%—THE ONLY RETINOID IN A LOTION FORMULATION
Please see Brief Summary of Prescribing Information on adjacent page.
Important Safety InformationDifferin® Lotion, 0.1% is indicated for the topical treatment of acne vulgaris in patients 12 years and older. A thin fi lm of Differin® Lotion, 0.1% should be applied once per day to the face and other areas of the skin affected by acne. In clinical trials, the most common adverse event (>1%) reported with use of Differin® Lotion, 0.1% was mild to moderate skin dryness. Erythema, scaling, stinging and burning may also occur. Excessive exposure to sunlight and sunlamps should be avoided during treatment, and use of sunscreen products and protective clothing is recommended. Concomitant use of drying or irritating topical products (like products containing resorcinol, salicylic acid or sulfur) should be used with caution. Instruct patients to avoid the eyes, lips and mucous membranes when applying Differin® Lotion, 0.1%, and not to apply to areas that have been depilated with wax products. Differin® Lotion, 0.1% has not been tested in pregnant or nursing women, or with the elderly. Pregnancy Category C.
www.differin.com/HCP
* A 12-week, multicenter, randomized, double-blind, parallel-group study of patients 12 to 18 years of age with acne vulgaris (N=1075).†The most frequent adverse event reported was dryness. Erythema, stinging/burning, and scaling may also occur.1
ON THE JOBWITH GENTLE EFFICACY1
58.2% MEDIAN TOTAL LESION COUNT REDUCTION BY WEEK 121*
TOLERABILITY PROFILE SIMILAR TO DIFFERIN® (adapalene) CREAM, 0.1%1†
AVAILABLE IN AN EASY-TO-USE PUMP DISPENSER

DIFFERIN® Rx only(adapalene) Lotion 0.1%For Topical Use OnlyNot For Oral, Ophthalmic, or Intravaginal Use.BRIEF SUMMARYINDICATIONS AND USAGEDIFFERIN Lotion is a retinoid product indicated for the topical treatment ofacne vulgaris in patients 12 years and older.CONTRAINDICATIONSNone.WARNINGS AND PRECAUTIONSUltraviolet Light and Environmental Exposure: Avoid exposure to sunlightand sunlamps. Wear sunscreen when sun exposure cannot be avoided.Erythema, scaling, dryness, and stinging/burning may occur with use ofDIFFERIN Lotion.ADVERSE REACTIONSDry skin of mild to moderate severity was the most frequently reported(≥ 1%) treatment related adverse event. Erythema, scaling, dryness,burning/stinging were also seen during treatment.DRUG INTERACTIONSConcomitant use of topical products with a strong drying effect can increaseskin irritation. Use with caution, especially in using preparations containingsulfur, resorcinol, or salicylic acid in combination with DIFFERIN Lotion. Waxdepilation should not be performed on treated skin.PregnancyPregnancy Category C. There are no well-controlled trials in pregnant womentreated with DIFFERIN Lotion. Therefore, DIFFERIN Lotion should beused during pregnancy only if the potential benefit justifies the potential riskto the fetus. Animal reproduction studies have not been conducted withDIFFERIN Lotion. Furthermore, such studies are not always predictive ofhuman response.Human DataIn clinical trials involving DIFFERIN Lotion, 0.1% in the treatment of acnevulgaris, women of childbearing potential initiated treatment only after anegative pregnancy test. Two women became pregnant while using DIFFERINLotion, 0.1%. One patient delivered a healthy full term baby and the otherpatient electively terminated her pregnancy.Animal DataNo teratogenic effects were observed in rats treated with oral doses of 0.15to 5.0 mg adapalene/kg/day, up to 25 times (mg/m2/day) the maximumrecommended human dose (MRHD) of 2 grams of DIFFERIN Lotion.However, teratogenic changes were observed in rats and rabbits when treatedwith oral doses of ≥ 25 mg adapalene/kg/day representing 123 and 246 timesMRHD, respectively. Findings included cleft palate, microphthalmia,encephalocele and skeletal abnormalities in rats; and umbilical hernia,exophthalmos and kidney and skeletal abnormalities in rabbits.Dermal teratology studies conducted in rats and rabbits at doses of 0.6-6.0 mg adapalene/kg/day [25-59 times (mg/m2) the MRHD] exhibited nofetotoxicity and only minimal increases in supernumerary ribs in both speciesand delayed ossification in rabbits.Systemic exposure (AUC 0-24h) to adapalene at topical doses(6.0 mg/kg/day) in rats represented 101 times the exposure to adapalene inpatients with acne treated with DIFFERIN Lotion applied to the face, chestand back (2 grams applied to 1000 cm² of acne-involved skin).Nursing MothersIt is not known whether adapalene is excreted in human milk followinguse of DIFFERIN Lotion. Because many drugs are excreted in human milk,caution should be exercised when DIFFERIN Lotion is administered to anursing woman.Pediatric UseSafety and effectiveness of DIFFERIN Lotion in pediatric patients under theage of 12 have not been established.Geriatric UseClinical studies of DIFFERIN Lotion did not include sufficient numbers ofsubjects aged 65 and over to determine whether they respond differentlyfrom younger subjects.Carcinogenesis, Mutagenesis, Impairment of FertilityNo carcinogenicity, mutagenicity and impairment of fertility studies wereconducted with DIFFERIN Lotion.Carcinogenicity studies with adapalene have been conducted in mice attopical doses of 0.4, 1.3, and 4.0 mg/kg/day (1.2, 3.9, and 12 mg/m²/day),
and in rats at oral doses of 0.15, 0.5, and 1.5 mg/kg/day (0.9, 3.0, and9.0 mg/m2/day). In terms of body surface area, the highest dose levels are9.8 (mice) and 7.4 times (rats) the MRHD of 2 grams of DIFFERIN Lotion.In the rat study, an increased incidence of benign and malignantpheochromocytomas in the adrenal medulla of male rats was observed.No photocarcinogenicity studies were conducted with adapalene. However,animal studies have shown an increased tumorigenic risk with the useof pharmacologically similar drugs (e.g. retinoids) when exposed to UVirradiation in the laboratory or sunlight. Although the significance of thesefindings to humans is not clear, patients should be advised to avoid orminimize exposure to either sunlight or artificial irradiation sources.Adapalene did not exhibit mutagenic or genotoxic effects in vitro (Ames test,Chinese hamster ovary cell assay, mouse lymphoma TK assay) or in vivo(mouse micronucleus test).In rat oral studies, 20 mg adapalene/kg/day (120 mg/m2/day; 98 times theMRHD based on mg/m2/day comparison) did not affect the reproductiveperformance and fertility of F0 males and females, or growth, developmentand reproductive function of F1 offspring.PATIENT COUNSELING INFORMATION• Apply a thin film of DIFFERIN Lotion to the affected areas of the skin oncedaily, after washing gently with a mild soapless cleanser. Dispense a nickelsize amount of DIFFERIN Lotion (3-4 actuations of the pump) to cover theentire face. Avoid application to the areas of skin around eyes, lips andmucous membranes. DIFFERIN Lotion may cause irritation such aserythema, scaling, dryness, stinging or burning.
• Advise patients to cleanse the area to be treated with a mild or soaplesscleanser; pat dry. Apply DIFFERIN Lotion to the entire face or otheracne affected areas as a thin layer, avoiding the eyes, lips and mucousmembranes.
• Exposure of the eye to this medication may result in reactions such asswelling, conjunctivitis and eye irritation.
• Patients should be advised not to use more than the recommended amountand not to apply more than once daily as this will not produce fasterresults, but may increase irritation.
• Advise patients to minimize exposure to sunlight including sunlamps.Recommend the use of sunscreen products and protective apparel(e.g., hat) when exposure cannot be avoided.
• Moisturizers may be used if necessary; however, products containing alphahydroxy or glycolic acids should be avoided.
• This medication should not be applied to cuts, abrasions, eczematous, orsunburned skin.
• Wax depilation should not be performed on treated skin due to thepotential for skin erosions.
• This product is for external use only.
Marketed by:GALDERMA LABORATORIES, L.P., Fort Worth, Texas 76177 USAManufactured by:Galderma Production Canada Inc., Baie d’Urfé, QC, H9X 3S4 CanadaMade in Canada.GALDERMA is a registered trademark.P51503-0Revised: March 2010
Galderma is a registered trademark.©2010 Galderma Laboratories, L.P.Galderma Laboratories, L.P.14501 N. FreewayFort Worth, TX 76177DIFF-113 Printed in USA 09/10
Reference: 1. Data on file. Galderma Laboratories, L.P.
www.differin.com/HCP

2
TABLE OF CONTENTS
January/February 2012 • Volume 10 • Issue 1
EDITORIAL
Modesty and the Skin: Why They Shouldn’t Mix ................................................................................................ 6 Caren Campbell, BA; Lawrence Charles Parish, MD, MD (Hon)
COMMENTARY
Origin and Evolution of Syphilis: Drifting Myth .................................................................................................. 8 Virendra N. Sehgal, MD; Prashant Verma, MD; Kingshuk Chatterjee, MBBS; Anita Chaudhuri, MD; Gautam Chatterjee, MS; Farhan Rasool, MBBS
ORIGINAL CONTRIBUTIONS
A New Paradigm in the Treatment of Kerions: Treat the Inflammation ............................................................. 14 Sarah E. Dolder, MD; Brendan J. O’Neill, MD; Meghan M. O’Brien, MD; Amy S. Ross, MD; Robert A. Allen, MD; Herbert B. Allen, MD
Pityriasis Rubra Pilaris: Evolution of Challenges in Promising Treatment Options ............................................. 18 Virendra N. Sehgal, MD; Govind Srivastava, MD; Prashant Verma, MD
REVIEW
The Role of Surgical Debridement in Healing of Diabetic Foot Ulcers .............................................................. 24 Katherine A. Gordon, BS; Elizabeth A. Lebrun, MD; Marjana Tomic-Canic, PhD; Robert S. Kirsner, MD, PhD
CORE CURRICULUM
Cutaneous Tuberculosis: A Diagnostic Dilemma ............................................................................................. 28 Virendra N. Sehgal, MD; Prashant Verma, MD; Sambit N. Bhattacharya, MD; Sonal Sharma, MD; Navjeevan Singh, MD; Nishant Verma, MD
Self-Test Review Questions (p. 34)
DEPARTMENTS
COSMETIC SCIENCE
Howard A. Epstein, PhD, Section Editor
Repelling Insects With Safe and Effective Alternatives to DEET ....................................................................... 36 Howard A. Epstein, PhD
PERILS OF DERMATOPATHOLOGY
W. Clark Lambert, MD, PhD, Section Editor
It’s Not Just Who You Are, It’s Also Where You Are: The Cutaneous Leiomyosarcoma Dilemma ......................... 40 Gizem Tumer, MD; Carmen F. Castilla, BS; W. Clark Lambert, MD, PhD
INFECTIOUS DISEASE CAPSULE
Jack M. Bernstein, MD, Section Editor
It May Be Vulgar, but It Isn’t a Bad Word......................................................................................................... 42 David Saunders, MD;Thomas Herchline, MD; Jack M. Bernstein, MD
CASE STUDIESVesna Petronic-Rosic, MD, MSc, Section Editor
Unusually Severe Case of Dermatosis Neglecta .............................................................................................. 46 Jake E. Turrentine, BS; Travis W. Blalock, MD; Loretta S. Davis, MD
Fixed-Drug Eruption Caused by Ashwagandha (Withania somnifera): A Widely Used Ayurvedic Drug ................ 48 Virendra N. Sehgal, MD; Prashant Verma, MD; Sambit N. Bhattacharya, MD

3
TABLE OF CONTENTS
January/February 2012 • Volume 10 • Issue 1
EDITORIAL DIRECTOR Sarah D. Staats
COPYEDITOR Elizabeth Holcomb
MEDIA WEB DIRECTOR Joan Osgoodby
PUBLISHER Art Kalaka
ASSOCIATE PUBLISHER James R. Adams
PRESIDENTArthur Kalaka
CHIEF EXECUTIVE OFFICER Jo-Ann Kalaka-Adams
ABOUT OUR JOURNAL
SKINmed: Dermatology for the Clinician®, print ISSN 1540-9740, online
ISSN 1751-7125, is published bimonthly by Pulse Marketing & Com-
munications, LLC, located at 4 Peninsula Avenue, Sea Bright, NJ 07760.
Printed in the USA.
Disclaimer: The Publisher, Editors, and Editorial Board cannot be held
responsible for errors or any consequences arising from the use of infor-
mation contained in this journal; the views and opinions expressed herein
do not necessarily reflect those of the Publisher, Editors, and Editorial
Board, neither does the publication of advertisements constitute any en-
dorsement by the Publisher, Editors, and Editorial Board of the products
or services advertised. The Publisher, Editors, Editorial Board, Reviewers,
Authors, and Affiliated Agents shall not be held responsible or in any way
liable for the continued accuracy of the information or for any errors,
inaccuracies, or omissions of any kind in this publication, whether arising
from negligence or otherwise, or for any consequences arising thereafter.
Copyright: ©2012 Pulse Marketing & Communications, LLC. All rights
reserved. No part of this publication may be reproduced, stored, or trans-
mitted in any form or by any means without the prior permission in writ-
ing from the Publisher. Requests should be addressed to the Permissions
Editor at: Pulse Marketing & Communications, LLC, 4 Peninsula Av-
enue, Sea Bright, NJ 07760.
Abstracting & Indexing: The journal is indexed in Index Medicus/
MEDLINE and Embase.
To submit a manuscript for peer review, send as an e-mail attach-
ment to the Editor in Chief at [email protected]. Please
visit www.skinmedjournal.com for Information for Authors.
Pulse Marketing & Communications, LLC
4 Peninsula Avenue • Suite 401 • Sea Bright, NJ 07760
Tel (732) 747-6525 • Fax (732) 747-7010
Corporate
Publishing
Editorial
GENERAL COUNSEL Marianne Mckenzie
Chronic Lymphocytic Leukemia Revealed by a Granulomatous Zosteriform Eruption ....................................... 50 Sondes Trojjet, MD; Houda Hammami, MD; Inès Zaraa, MD; Alia Bouzguarrou, MD; Meriem Joens, MD; Slim Haouet, MD;
Amel Ben Osman, MD; Mourad Mokni, MD
CORRESPONDENCE
Mycobacterium marinum Cutaneous Infection With Sporotrichoid Distribution Treated With Azithromycin Monotherapy ............................................................................................................................ 54
Efstathios Rallis, MD, PhD; Evangelos Falidas, MD; Panagiotis Stavropoulos, MD, PhD

January/February 2012 EDITORIAL BOARD
4
Mohamed Amer, MD
Cairo, Egypt
Robert L. Baran, MD
Cannes, France
Anthony V. Benedetto, DO
Philadelphia, PA
Brian Berman, MD, PhD
Miami, FL
Jack M. Bernstein, MD
Dayton, OH
Sarah Brenner, MD
Tel Aviv, Israel
Joaquin Calap Calatayud, MD
Cadiz, Spain
Henry H.L. Chan, MB, MD, PhD, FRCP
Hong Kong, China
Noah Craft, MD, PhD, DTMH
Torrance, CA
Ncoza C. Dlova, MBChB, FCDerm
Durban, South Africa
Richard L. Dobson, MD
Mt Pleasant, SC
William H. Eaglstein, MD
Palo Alto, CA
Boni E. Elewski, MD
Birmingham, AL
Charles N. Ellis, MD
Ann Arbor, MI
Howard A. Epstein, PhD
Gibbstown, NJ
Ibrahim Hassan Galadari, MD, PhD, FRCP
Dubai, United Arab Emirates
Anthony A. Gaspari, MD
Baltimore, MD
Michael Geiges, MD
Zurich, Switzerland
Michael H. Gold, MD
Nashville, TN
Lowell A. Goldsmith, MD, MPH
Chapel Hill, NC
Aditya K. Gupta, MD, PhD, FRCP(C)
London, Ontario
Seung-Kyung Hann, MD, PhD
Seoul, Korea
Roderick J. Hay, BCh, DM, FRCP, FRCPath
London, UK
Tanya R. Humphreys, MD
Philadelphia, PA
Camila K. Janniger, MD
Englewood, NJ
Abdul-Ghani Kibbi, MD
Beirut, Lebanon
Andrew P. Lazar, MD
Highland Park, IL
Jasna Lipozencic, MD, PhD
Zagreb, Croatia
Eve J. Lowenstein, MD, PhD
New York, NY
George M. Martin, MD
Kihei, HI
Marc S. Micozzi, MD, PhD
Bethesda, MD
George F. Murphy, MD
Boston, MA
Oumeish Youssef Oumeish, MD, FRCP
Amman, Jordan
Joseph L. Pace, MD, FRCP
Naxxar, Malta
Art Papier, MD
Rochester, NY
Johannes Ring, MD, DPhil
Munich, Germany
Roy S. Rogers III, MD
Rochester, MN
Donald Rudikoff, MD
New York, NY
Robert I. Rudolph, MD
Wyomissing, PA
Vincenzo Ruocco, MD
Naples, Italy
Noah S. Scheinfeld, MD, JD
New York, NY
Virendra N. Sehgal, MD
Delhi, India
Charles Steffen, MD
Oceanside, CA
Alexander J. Stratigos, MD
Athens, Greece
James S. Studdiford III, MD
Philadelphia, PA
Robert J. Thomsen, MD
Los Alamos, NM
Julian Trevino, MD
Dayton, OH
Snejina Vassileva, MD, PhD
Sofia, Bulgaria
Daniel Wallach, MD
Paris, France
Michael A. Waugh, MB, FRCP
Leeds, UK
Wm. Philip Werschler, MD
Spokane, WA
Joseph A. Witkowski, MD
Philadelphia, PA
Ronni Wolf, MD
Rechovot, Israel
EDITOR IN CHIEF
EDITORIAL BOARD
DEPUTY EDITORS
William Abramovits, MD
Dallas, TX
W. Clark Lambert, MD, PhD
Newark, NJ
Larry E. Millikan, MD
Meridian, MS
Jennifer L. Parish, MD
Philadelphia, PA
Lawrence Charles Parish, MD, MD (Hon)Philadelphia, PA
Vesna Petronic-Rosic, MD, MSc
Chicago, IL
Marcia Ramos-e-Silva, MD, PhD
Rio de Janeiro, Brazil

©2010 Triax Pharmaceuticals, LLC. All Rights Reserved. Printed in USA TX-0610-02
A New Tretinoin TherapyFrom Triax Pharmaceuticals
%

January/February 2012 Volume 10 • Issue 1
6SKINmed. 2012;10:6–7 © 2012 Pulse Marketing & Communications, LLC
From the Jefferson Medical College of Thomas Jefferson University, Philadelphia, PA;1 and the Department of Dermatology and Cutaneous Biology, Jefferson Medical College of Thomas Jefferson University, Philadelphia, PA2
Address for Correspondence: Lawrence Charles Parish, MD, MD (Hon), 1760 Market Street, Suite 301, Philadelphia, PA 19103 • E-mail: [email protected]
Some years ago, the American Cancer Society first
mounted a campaign against modesty to publicize the
need for breast examinations. All too often, women
were not only too embarrassed to let their physicians fully
examine their chests, but they were also reluctant to perform
self-examination.
This was not the case of the young woman who presented with
a black lesion on her right breast. She was concerned about the
peculiarity of the lesion since its appearance 2 months prior
(Figure). Fortunately, modesty did not play a role in her situ-
ation. The lesion was quickly excised and proved to be a level
3 melanoma. How many other patients are not so fortunate to
have appropriate removal and treatment before it is too late?
CANCER SCREENING
Americans should be well informed on the importance of early
detection in skin cancer. Much emphasis has been placed on this
concept; however, while patients may be attuned to the idea of
cancer screening for other body systems, they do not grasp the
concept of the full body scan. This diagnostic procedure, need-
less to say, cannot be accomplished in a proper fashion without
disrobing, but many patients are reluctant to do so.
As any seasoned clinician can attest, melanomas and nonmela-
noma skin cancers can be found in any area of the body from the
breasts to the soles. They do not avoid the genitalia, let alone the
intertriginous areas. Curiously, primary cutaneous melanomas in
hidden anatomic sites are thicker than those in visible sites, likely
because of a delay in diagnosis.1,2 Additionally, the problem may
be compounded by UV radiation from indoor tanning. Many a
tanner disrobes completely to obtain his or her money’s worth at
the tanning parlor but is reluctant to have the dermatologist see
most of the body.
MODESTY AT WORK
Let’s reflect upon the skin examination. Isn’t its purpose to
find anything that might create a problem? The reason for the
procedure is to examine visually every skin surface. The act of
wearing any clothing only serves to hinder and prolong the
examination.
Modesty is a behavior, manner, or appearance intended to avoid
impropriety or indecency. During a physical examination, mod-
esty is not serving to avoid impropriety or indecency. It is a false
modesty. Much like the modesty panel underneath a desk or
nude-colored hosiery worn by women, it is a social construct.
The impropriety and judgment felt by the patient and others is
also created by society.
The subject of modesty has been examined in detail in other
disciplines. For example, one such study on modesty sought to
explore the role that culture played, finding that some perspec-
tives on modesty are accounted for by culture, while others are
not.3 Modesty was found to be driven by maturity/age, religion/
culture, or esteem/upbringing. For the maturity-driven group,
modesty did not play a role in the health care setting, while the
religiously/culturally driven group felt modesty should be con-
sidered in a health care setting. (Disrobing in this setting was not
an issue.) Most interestingly, the esteem-driven group posed the
greatest challenge to health care providers, as this group felt it
stressful and uncomfortable to undress in the health care setting
and would likely avoid screening for reasons of modesty.
Although not formally studied, one realizes that body image plays
a large role in patient modesty. Patients worry that as the physician
examines their skin they are secretly being judged on their lingerie
or less-than-ideal body weight. Here, the truth hurts—the clini-
cians are doing their job—to screen the patient for skin cancer.
There are many papers detailing ways to protect patient modesty,4–8
but just as important as the patient’s comfort is the necessity to per-
form a thorough examination. The most obvious way to accom-
plish an appropriate examination to detect malignancy, including
the scalp, oral cavity, genitals, and nails, would be disrobing.9
The patient may wear a gown to cover surfaces not being examined.
An alternative involves the patient disrobing one quadrant at a
time. It is both curious and unfortunate when a patient requests a
full body scan but only permits limited views of the skin.
EDITORIAL
Modesty and the Skin: Why They Shouldn’t MixCaren Campbell, BA;1 Lawrence Charles Parish, MD, MD (Hon)2

Modesty and the Skin: Why They Shouldn’t Mix
EDITORIALJanuary/February 2012
7SKINmed. 2012;10:6–7
REFLECTIONS
When reflecting upon the situation, the role of modesty in
prophylactic screening is raised. What stands out is a lack of com-
pliance in both breast and colon cancer screening due to mod-
esty.10,11 If patients are unwilling to undergo cancer screening
developed for the sole purpose of early detection and prevention,
we can only conclude that modesty should be considered
dangerous to their health.
Skin self-examination is one method that might prove an
alternative for those too modest to allow yearly examina-
tion of the entire skin’s surface. Self-examination taught to
both patient and partner improves self-efficacy for patients.12
Partnering with those trusted by the patient might improve
detection and outcomes for patients too modest for frequent
skin examination.
Isn’t there an old adage: Modesty killed the cat?
REFERENCES
1 Nagore E, Oliver V, Moreno-Picot S, Fortea JM. Primary cutaneous mela-noma in hidden sites is associated with thicker tumours—a study of 829 patients. Eur J Cancer. 2001;37:79–82.
2 Hemo Y, Gutman M, Klausner JM. Anatomic site of primary melanoma is associated with depth of invasion. Arch Surg. 1999;134:148–150.
3 Andrews CS. Defining and exploring modesty in Jewish American women. J Relig Health. 2010. http://www.springerlink.com.proxy1.lib.tju.edu:2048/content/r666v2x100160487/. Accessed April 23, 2011.
4 Baillie J. Making a difference to the patient experience. Health Estate. 2010;64:48–50, 52–55.
5 Wehbe-Alamah H. Bridging generic and professional care practices for Muslim patients through use of Leininger’s culture care modes. Contemp Nurse. 2008;28:83–97.
6 Yosef ARO. Health beliefs, practice, and priorities for health care of Arab Muslims in the United States. J Transcult Nurs. 2008;19:284–291.
7 Roberts KS. Providing culturally sensitive care to the child bearing Islamic family. Adv Neonatal Care. 2002;2:222–228.
8 Lawrence P, Rozmus C. Culturally sensitive care of the Muslim patient. J Transcult Nurs. 2001;12:228–233.
9 Craft N, Fox LP, Goldsmith LA. VisualDx: Essential Adult Dermatology. Philadelphia, PA: Lippincott Williams & Wilkins; 2010.
10 Denberg TD, Melhado TV, Coombes JM, et al. Predictors of nonadher-ence to screening colonoscopy. J Gen Intern Med. 2005;20:989–995.
11 Parsa P, Kandiah M, Abdul Rahman H, Zulkefli NM. Barriers for breast cancer screening among Asian women: a mini literature review. Asian Pac J Cancer Prev. 2006;7:509–514.
12 Robinson JK, Stapleton J, Turrisi R. Relationship and partner moderator variables increase self-efficacy of performing skin self-examination. J Am Acad Dermatol. 2008;58:755–762.
Figure. A level 3 melanoma found on the right breast.
HISTORICAL DIAGNOSIS & TREATMENTDiagnosis and treatments have advanced over the past century. This feature depicts conditions from a collection of steroptic cards published in 1910 by The Stereoscopic Skin Clinic, by Dr. S. I. Rainforth.
(continued on page 12)

January/February 2012 Volume 10 • Issue 1
8SKINmed. 2012;10:8–12 © 2012 Pulse Marketing & Communications, LLC
From the Dermato-Venereology (Skin/VD) Center, Sehgal Nursing Home, Panchwati, Delhi; Department of Dermatology and STD, University College of Medical Sciences, and Associated Guru Teg Bahadur Hospital, Shahdara, Delhi; Department of Dermatology, Burdwan Medical College and Associated Hospital, Burdwan; Apollo Nursing Home, Burdwan; Skin Institute and School of Dermatology, Greater Kailash New Delhi, India
Address for Correspondence: Virendra N. Sehgal MD, Dermato-Venerology (Skin/VD) Center, Sehgal Nursing Home, A/6 Panchwati, Delhi 110 033 India • E-mail: [email protected]
Syphilis, a treponemal disease, has undergone discernible
metamorphosis in its natural history. The diverse clinical
manifestations of syphilis are known to masquerade as
a spectrum of clinical entities, earning itself the reputation of
being the great imitator.1 Syphilis was even mentioned in Act 3
of Timon of Athens2 by William Shakespeare:
Live loathed and long,
Most smiling, smooth, detested parasites,
Courteous destroyers, affable wolves, meek bears,
You fools of fortune, trencher-friends, time’s flies,
Cap and knee slaves, vapours, and minute-jacks!
Of man and beast the infinite malady
Crust you quite o’er! What, dost thou go?
Soft! take thy physic first—thou too—and thou;—
Stay, I will lend thee money, borrow none.
The name for syphilis is derived from Fracastorius’ 1530 epic
poem in three parts, Syphilis sive morbus gallicus (“Syphilis or
The French Disease”), about a shepherd boy named Syphilus
who insulted the sun god of Haiti and was punished by that
god with a horrible disease. The poem suggests using mercury
and “guaiaco” as a cure.3,4 Oil of guaiac is a fragrance used in
soap, originating from the Palo Santo, sacred tree in Ecuador,
which provides an essential oil that heals both body and spirit.5
Syphilis, with its antiquity, has carried social stigma. In order
to avoid the cultural embarrassment, countries attempted “to
pass the buck to others.”6 Accordingly, variations in its nomen-
clature were likely; the English and the Germans called it the
“French disease”; the French called it the “Neapolitan sickness”;
the Russians, the “Polish sicknes”; the Poles, the “German
sickness”; Flemish, Dutch, Portuguese, and North Americans
called it the “Spanish sickness” or “Castilian sickness”; and
the Japanese, the “Canton rash” or “Chinese ulcer.” The term
Great pox was used for 2 centuries to differentiate syphilis from
Smallpox.7
Christopher Columbus, the great Italian voyager, whose pre-
cise date of birth is only speculated,8 left on his first voyage
at the age of 41 years (1492–1493). His journey initiated the
process of Spanish colonization, which foreshadowed the gen-
eral European colonization of the “New World.”9 The idea that
“Civilization is Syphilization” has historically stamped Colum-
bus as the importer of syphilis to Europe.10 The current contri-
bution attempts to review the more recent archeological reports,
dendrochronologic findings, and radiocarbon dating studies in
order to clarify the development of the disease. The origin and
evolution of syphilis is currently unknown11 and may continue
to puzzle researchers until a plausible consensus is developed.
COMMENTARY
Origin and Evolution of Syphilis: Drifting Myth Virendra N. Sehgal, MD; Prashant Verma, MD; Kingshuk Chatterjee, MBBS; Anita Chaudhuri, MD;
Gautam Chatterjee, MS; Farhan Rasool, MBBS
The venereal form of treponematosis, caused by the spirochete Treponema pallidum, plagued every major city in the preantibiotic era.
“Civilization means syphilization,” was an idea touted by Richard von Krafft-Ebing in the late 19th, and early 20th centuries that the
effects of modern life make men more susceptible to syphilis and other diseases. Christopher Columbus was thought of as an importer of
syphilis to Europe. Because his serendipitous voyages to the New World initiated the process of Spanish colonization, which foreshadowed
general European colonization of the New World, it is difficult to rule out the cultural and political animosity created by Columbus and
his men. These recent revelations are intriguing and may create dialogue that may subsequently challenge the age-old theory of “East to
West” spread of venereal syphilis. This contribution warrants the continuation of study in this direction, taking into account skeletal studies
that utilized radiocarbon dating technique and the phylogenetic analysis of the bacterial strains, offering a possible consensus on the origin
and evolution of syphilis.

Origin and Evolution of Syphilis
COMMENTARYJanuary/February 2012
9SKINmed. 2012;10:8–12
HYPOTHESIS OF THE ORIGIN OF SYPHILIS
THE UNITARIAN THEORY
Hudson12 has been credited with the unitarian theory, which
claims that treponemal diseases originating from one form,
free-living treponemes in the mud, ultimately evolve into
human saprophytes. “Yaws” appears to have first evolved in
Central Africa, from where it spread to engulf the east and
north, probably attributable to the importation of slaves to
Egypt in 30th century BCE.13,14 Yaws eventually spread to the
Arabian Peninsula and the valleys of the Tigris and Euphrates
rivers, where it was called Bejel.15 Dissemination of yaws into
Europe followed, peaking in the 8th century CE, when the
Crusades made the slave trade from Africa more popular by
transporting slaves for work to other countries.16,17 The Cru-
sades moved from Europe to the Holy Land between the 11th
and 14th centuries.
It was between the 17th and 19th centuries that a series of
yaws-like diseases, the endemic syphilis, and pinta were identi-
fied in individuals who had a poor rural background and over-
crowded living conditions. Endemic syphilis prevailed as the
Spirocolon of Greece, the hills of Bosnia, the Pian of Nerac
in South-West France, the Button scurvy of Ireland, the Sib-
bens of Scotland, the Radseyege of Scandinavia, Siti of Gam-
bia, Therlijevo of Croatia, Njovera of Zimbawe, Frenjak of
the Balkans, and nonvenereal endemic syphilis, Bejel disease.
The Dithmarsh evil of Jutland and Schlesweig-Holstein is yet
another entity. All of these diseases, including yaws, were con-
sidered to be a consequence of either direct or indirect social
contact, affecting all age groups. Children and family members
were the most susceptible.
The histories of Button scurvy and Sibbens have also been docu-
mented.18,19 These entities have been defined and classified into
endemic syphilis or treponarids, and are considered to be a form
of yaws modified by climatic conditions, clothing customs, and
even the sharing of drinking utensils. This seems plausible due to
the fact that yaws was later shipped via slaves from West Africa
to the West Indies. In addition, some treponemes adapted to
the conditions by thriving in the moist and warm areas of the
body and by mutating into more lethal organisms. The latter
was acquired by sexual contact and expressed as syphilis in the
contemporary context.
In the absence of any viable means to control the transmission
of treponemes, the advent of soap in the Arab peninsula and
Europe in the 7th and the 14th century, respectively, and its
widespread use was acknowledged as a possible mode for the
reduced survival of treponemes in treponarids.
NONUNITARIAN THEORY
An African origin hypothesis developed, with endemic trepo-
nemes originally acquired from apes, brought back to Europe by
the Portuguese during the Age of Exploration.6
Another theory for the post-1492 syphilis outbreak mentions
the role of a human immunodeficiency virus–like immunosup-
pressive agent causing an uncharacteristically severe variant of
syphilis, lues maligna.
PRE-COLUMBIAN PERCEPTION
The perception that treponemal infection existed in the pre-
Columbian civilization, which is now the southwestern part of
the United States, was documented by the lesions indicative of
treponematosis in a burial site found in the central Great House
of Chaco Canyon, Pueblo Bonito, New Mexico, an epicenter of
a broad culture system that spanned the Four Corners regions, in
contrast to numerous reports available from New World skeletal
burial remains. This is an interesting revelation, which may open
a venue for future workup.20–24
COLUMBIAN THEORY
It is speculated that treponematoses was absent in Europe
in the pre-Columbian era25 until the 13th century CE, when
yaws appeared as a possible result of slave trading.26 Berbers and
Moors, from North and North-West Africa, established them-
selves in Southern Europe, mostly in Spain, in the 15th century.
Half a century prior to Columbus’ first voyage (1492–1493),
Spanish and Portuguese sailors already competed with more
extensive journeys down the West coast of Africa and encouraged
the migration of the Africans.
Despite the efforts for quarantines, yaws spread to the European
continent. According to the Columbian theory, venereal syphilis
appears to have been brought from the New World and joined
so-called endemic syphilis. An outbreak of the epidemic resur-
faced upon the return of Columbus and his men from the New
World. A similar presentation of the disease was identified in the
indigenous people of the New World as well as in the members
of Columbus’ crew. The epidemic in the earliest years, popularly
called the Morbus gallicus, may have been the combination of
2 diseases; the newly arrived sexually acquired venereal syphilis
and the old socially acquired endemic syphilis forms of yaws.19
The changes in clinical presentation, particularly in the first half
of the 16th century, might be the result of expanding influ-
ences of the Renaissance, including improved personal hygiene.
Others explain the devastating Morbus gallicus as the relatively
benign venereal syphilis of the New World, afflicting people with
no previous contact with the condition and producing more

Origin and Evolution of Syphilis
COMMENTARYJanuary/February 2012
10SKINmed. 2012;10:8–12
obvious signs and symptoms, both the views commensurate
with the Columbian theory. Accordingly, the arguments for and
against the Columbian theory are listed below.
• Syphilis, as one form of pathologic treponematosis, has a
skeletal signature. Rothschild demonstrated that the osseo-
type characteristics of syphilis were absent in specimens
from pre-Columbian Europe, Africa, and Asia.27
• The sailors with Columbus in 1493 were said to have
brought the disease back to Spain. The Spanish fleet, when
they fought for King Alfonso II against the French forces of
Charles VIII of France in 1494–1495, heavily infected the
people of Naples. The illness spread rapidly around Europe
and mercenaries, who in 1496 joined Perkin Warbeck in
Scotland and with the support of James IV of Scotland,
invaded England, bore both arms and the grandgore (Old
French; grand gorre: grand = great + gore = syphilis), as it
was then called. In 1497, the Minutes of the Town Council
of Edinborough (Phil. Trans. XLII. 421) recognized: “This
contagious sickness call it the Grandgore.”28
• The osseous evidence documents the presence of syphilis
in Hispanola, where Columbus landed. Columbus’ crew
had the opportunity and means to contract and spread this
venereal disease.27
• In the work “Tractado contra el mal serpentino,” written
in 1510 and published in 1539, Ruy Diaz de Isla had
been thought to have cured, during the travel of return in
Europe, many members of the crew of Columbus, affec-
tions from certain luetic manifestations, and thought that
the new disease was imported from Hispanola. This view
was supported by Bartolomè de Las Casas.29
• The absence of evidence for congenital transmission of
the disease in pre-1492 North America suggests that this
treponemal disease was not the same venereal form we
know today.30
CONTEMPORARY SCENARIO
Several archeologic studies have taken cognizance of phylogenet-
ically diverse material at different geographic locations and have
gathered together enough evidence to suggest that the disease
existed in Europe, long before the birth of Columbus (Octo-
ber 31, 1451–May 20, 1506).31 The osseotype characteristics of
syphilis are absent in specimens from pre-Columbian Europe,
Africa, and Asia.32
A study was conducted on approximately 240 skeletons exhumed
at the site of a medieval friary in Hull. The skeletons were mostly
of Augustinian friars, Mendicants serving the local poor, and sea-
men and prostitutes. Of the 245 well-preserved skeletons found,
207 were relatively complete. Many were buried in wooden
coffins, prepared from the wood brought from the Baltic
countries. Dendrochronologic examination indicated that the
trees had fallen between 1340 and 1369. The interpretation of the
findings was, therefore, found to be confusing. Three skeletons
showed more variable and more widespread bony lesions. One
of these three, number 1216, was that of a man aged between
25 and 35 years. He showed signs of syphilitic stigmata; thick-
ening with areas of localized disease of thigh bones, sabre-like
thickening of shin bones, perforation of the palate, and ero-
sion of the skull’s frontal bone, a condition called caries sicca.
Caries sicca, a bony finding from gummatous syphilis has been
described as “The only reliable and pathognomonic lesion of
syphilis….”33 Other findings are of variable reliability.34
Carbon-dating of the skeleton showed it to have lived some-
time between 1300 and 1420, corresponding to about a century
before Columbus’ first voyage in 1492 to 1493. Three paleo-
pathologists opined on the skeleton number 1216. Charlotte
Roberts recognized it as treponemal disease but could not dis-
tinguish among them,35 while Rothschild suggested that the
population frequency of skeletal involvement was too high for
treponemal disease. Secondly, the pattern of disease in the Hull
site is classic for yaws. It matches in all details the reports of skel-
etal findings in yaws and is quite different than those for syphilis.
Much of what was diagnosed as disease appeared taphonomic.36
George Armalegos, with extensive experience in viewing New
World, pre-Columbian bones allegedly showing changes due to
syphilis, was impressed but wanted the confirmation in terms of
quantity rather than quality.
Support for the existence of venereal syphilis in pre-Colum-
bian Europe comes from Dr Mattie Hennenberg37 and his wife
based on the examination of 300 Greek skeletons buried in a
southern Italian port in 600 BCE, with the claim that many
of them showed changes similar to those of the Hull friary
skeletons, indicative of syphilis; however, taphonomy could be
a confounder. The term taphonomy (from the Greek taphos
[ταφος] meaning burial and nomos [vóμoς] meaning law) was
introduced to paleontology in 1940 by Russian scientist Ivan
Efremov to describe the study of the transition of remains, parts,
or products of organisms from the biosphere to the lithosphere,
that is a creation of fossil assemblages.38
Hennenberg, a dental specialist, claimed that the upper cen-
tral incisor teeth from two skeletons showed “grooves,” proof of
congenital syphilis. A second “dig” of old bones from a port near
Pompeii offers similar bony findings. Recent research based on
exhumed human skeletons from a cemetery at an East London
church, St Mary Spital, identified rough patches on skulls and

Origin and Evolution of Syphilis
COMMENTARYJanuary/February 2012
11SKINmed. 2012;10:8–12
limbs of some of the skeletons, pointing toward a syphilitic origin
for such findings. This study scores over its predecessors in terms of
executing radiocarbon dating of the exhumed samples, estimated
to be 95% accurate. Brian Connell, an expert from the Museum
of London who studied the bones, opined that the skeletons were
buried before the Columbus voyage. He said “We’re confident that
Christopher Columbus is simply not a feature of the emergence,
and timing of the disease in Europe.”39 Two of the syphilitic skel-
etons unearthed from the site were from 1200–1250, while the
other 5 were from 1250–1400, preceding Columbus’ birth. They
were buried with coins and other objects that helped the experts
corroborate the radiocarbon dating results.11,39
The Unitarian hypothesis, based on skeletal morphology data,40
has recently been challenged by analysis of the molecular evolu-
tion of the tpr C, D, I, K, G, and J genes in the pathogenic genus
Treponema.41 The elusive outcome of past research warrants future
exploration. The advent of phylogenetic systematic analysis may
prove beneficial in exploring the veracity of the findings. It is that
field of biology that deals with identifying and understanding the
evolutionary relationships among the many different kinds of life
on earth, both living (extant) and dead (extinct).
Evolutionary theory states that similarity among individuals or spe-
cies is attributable to common descent or inheritance from a com-
mon ancestor. Thus, the relationships established by phylogenetic
systematics often describe a species’ evolutionary history and, hence,
its phylogeny, the historical relationships among lineages or organ-
isms or their parts, such as their genes.42 This modality was made
use of to analyze the data from 21 genetic regions examined in 26
geographically disparate strains of pathogenic Treponema.43 Of all
the strains examined, the venereal syphilis–causing strains origi-
nated most recently and were more closely related to yaws-causing
strains from South America than to other nonvenereal strains.
Old World yaws–causing strains occupied a basal position on the
tree, indicating that they first arose in human history, and a sim-
ian strain of Treponema pallidum was found to be indistinguish-
able from them. These results lend support to the Columbian
theory of syphilis’ origin, while suggesting that the nonsexually
transmitted subspecies arose earlier in the Old World. In yet
another study,44 using an integrative phylogenetic and paleo-
pathologic approach, syphilis seems to have emerged in the time
span between 5000 years before present (yBP) and 16,500 yBP,
in the Americas, because the resulting evolutionary rate is com-
patible with those observed in other bacteria; however, these
studies relied on 2 bacterial isolates from individuals with alleged
yaws from a site where antibiotic treatment of yaws had altered
the picture. It is unclear what disease was present in the two
isolates on which they based their studies. The suggested time
span for origin of syphilis of 5000 to 16,500 yBP is still debat-
able, especially in view of skeletal evidence supporting origin
2000 to 1800 yBP. In contrast, if the claims of pre-Columbian
venereal syphilis outside the Americas are taken into account,
the place of origin remains unresolved.
REFERENCES
1 King A, Nicol C, Rodin P, eds. Yaws: endemic syphilis: Bejel: Pinta. In: Venereal Diseases. 4th ed. London, England: Balliere Tindall; 1980:333–345.
2 Soellner R. Timon of Athens: Shakespeare’s Pessimistic Tragedy. Colum-bus: Ohio State University Press; 1979.
3 Baumgartner L, Fulton JF. A Bibliography of the Poem Syphilis Sive Mor-bus Gallicus, by Girolamo Fracastoro of Verona. New Haven, CT: Yale University Press; 1935:157–159.
4 Opdyke DL. Bulnesia sarmientoi. Food Cosmet Toxicol. 1974;12:905
5 Essential Oils Desk Reference. 4th ed. Orem, UT: Essential Science Pub-lishing; 2007.
6 Rothschild BM. History of syphilis. Clin Infect Dis. 2005;40:1454–1463.
7 Heymann WR. The history of syphilis. J Am Acad Dermatol. 2006;54:322–323.
8 Dunn O, Kelly J. The Diario of Christopher Columbus’s First Voyage to America 1492–1493. Norman, OK: University of Oklahoma Press; 1991:333–343.
9 Stokes JH, Beerman H, Ingraham MR. Modern Clinical Syphilology. Philadelphia, PA: WB Saunders; 1945:1120–1121.
10 Miller H. Secrets of the Dead. London, England: Channel 4 Books: Mac-Millan; 2000:149–184.
11 Morton R, Rashid S. “The syphilis enigma”: the riddle resolved? Sex Transm Inf. 2001;77:322–324.
12 Hudson EH. Non-Venereal Syphilis: A Sociological and Medical Study of Bejel. Edinburgh and London: E & S Livingstone; 1958.
13 Hackett CJ. On the origin of the human treponematosis. Bull World Health Organ. 1963;29:7–41.
14 Scott HH. The influence of the slave trade in the spread of tropical dis-eases. Transcr R Soc Trop Med Hygiene. 1943;38:169.
15 Wedad M. Is Bejel, Yaws? (In Arabic). Bagdad, Iraq: Government Press; 1936.
16 Hudson EH. Treponematosis and African slavery. Br J Vener Dis. 1964;40:43–52.
17 Major RH. “Prince Henry the Navigator”: A Life. New Haven, CT: Yale University Press; 2000.
18 Morton RS. The buttons scurvy of Ireland. Br J Vener Dis. 1964;40:271–274.
19 Morton RS. A clinical look at the morbus gallicus. Eur J Sex Transm Dis. 1985;2:133–140.
20 Marden K, Ortner DJ. A case of treponematosis from pre-Columbian Chaco Canyon, New Mexico. Int J Osteoarchaeol. 2011;21:19–31.
21 Lahr MM, Bowman JE. Paleopathology of the Kechipawan site: health and disease in a southwestern Pueblo. J Archaeol Sci. 1992;19:639–654.
22 Ortner DJ, Tuross N, Stix AI. New approaches to the study of disease in ar-chaeological New World populations. Human Biology. 1992;64:337–360.
23 Verano JW. Advances in the paleopathology of Andean South America. J World Prehistory. 1997;11:237–268.
24 Baker BJ, Armelagos GJ. The origin and antiquity of syphilis: paleopatho-logical diagnosis and interpretation. Curr Anthropol. 1988;29:703–738.
25 Rothschild BM, Coppa A, Petrone PP. “Like a virgin”: absence of rheuma-toid arthritis and treponematosis, good sanitation and only rare gout in Italy prior to the 15th century. Reumatismo. 2004;56:61–66.

Origin and Evolution of Syphilis
COMMENTARYJanuary/February 2012
12SKINmed. 2012;10:8–12
26 Rothschild C, Rothschild BM. Patterns of periosteal reaction in England from Roman through Elizabethan epochs. J Paleopath 1995;7:130.
27 Rothschild BM. History of syphilis. Clin Infect Dis. 2005;40:1454–1463.
28 Pearce JMS. A note on the origins of syphilis. J Neurol Neurosurg Psy-chiatry. 1998;64:542.
29 Di Cicco CO. History of syphilis. J Eur Acad Dermatol Venereol. 2005;19:1–11.
30 Dutour O, Palfi G, Berato J, Brun JP. The Origin of Syphilis in Europe: Before or After 1493? Toulon: Centre Archéologique du Var; 1995.
31 Stirland, A. Evidence for pre-Columbian treponematosis in Medieval Eu-rope. In: L’Origine de la Syphilis en Europe Avant ou après 1493? Dutour O, Palfi G, Berato J, Brun JP, eds. Toulon, France: Centre Archéologique du Var; 1995:109–115.
32 Anderson T, Arcini C, Anda S, Tangerud A, Robertsen G. Suspected endemic syphilis (treponarid) in sixteenth-century Norway. Med Hist. 1986;30:341–350.
33 Virchow RLK. Beitrag zur geschichte der lues. Arch Dermatol. 1896;2:1–9.
34 Lahr MM, Bowman JE. Palaeopathoogy of Kechipawan Site: health and disease in a south western pueblo. J Archeolog Sci. 1992;19:639–654.
35 Roberts C, Millard A, Pearson G, Macpherson C, Nowell G. The origin and mobility of people with venereal syphilis buried in Hull, England in
the late medieval period. Poster presented at: the 18th Paleopathology Association European Meeting, Vienna, Austria; 2010.
36 Rothschild BM. History of syphilis. Clin Infect Dis. 2005;40:1454–1463.
37 Henneberg RJ, Henneberg M. Possible occurrence of treponematosis in the ancient Greek colony of Metaponto. Am J Phys Anthropol. 1995(suppl 163):107–108.
38 Efremov IA. Taphonomy: a new branch of paleontology. Pan-Am Geol. 1940;74:81–93.
39 Columbus Didn’t Sail Syphilis Back to Europe. Medieval Archives Illumi-nating the Dark Ages for the Digital World. Sci Technol. Oct 27, 2010.
40 Hudson EH. Treponematosis and man’s social evolution. Am Anthropol. 1965;67:885–901.
41 Gray RR, Mulligan CJ, Molini BJ, et al. Molecular evolution of the tprC, D, I, K, G, and J genes in the pathogenic genus Treponema. Mol Biol Evol. 2006;23:2220–2233.
42 Hillis DM, Moritz C, Mable BK, eds. Molecular Systematics. 2nd ed. Sunderland, MA; Sinauer Associates: 1996
43 Harper KN, Ocampo PS, Steiner BM, et al. On the origin of the trepone-matoses: a phylogenetic approach. PLoS Negl Trop Dis. 2008;2:e148.
44 de Melo FL, de Mello JC, Fraga AM, et al. Syphilis at the crossroad of phylogenetics and paleopathology. PLoS Negl Trop Dis. 2010;4:e575.
HISTORICAL DIAGNOSIS & TREATMENT: SYCOSIS (continued from page 7)
SYNONYMS: ACNE SYCOSIS; SYCOSIS BARBAE, SEU MENTI; SYCOSIS NON PARASITICA; MENTAGRA; FOLLICULITIS BARBAE, SEU PILORUM.Sycosis is a chronic inflammatory disease of hairy parts of the skin characterized by tubercles, papules and pustules, each of which is pierced invariably by the shaft of a hair. In the great majority of cases the disease is limited to the region of the beard in men, though it may occur on the eyebrows, scalp, axillae and pubes. On the face it starts usually as one or more ill defined patches and may remain confined in certain areas or spread so as to include in time the whole bearded region. The disease does not extend to non-hairy parts. The lesions may be discrete and relatively few in number, or, in very severe cases, so numerous and closely set as to form almost continu-ous patches of infiltration. The inflammation starts in the walls of the hair follicles and the first surface manifestations are pap-ules or tubercles situated at the orifices, with a hair passing through each little elevation. The papules and tubercles soon change into pustules. Occasionally in old patches, pustules develop about the hairs without preceding papulation. The pus-tules exhibit slight tendency to rupture, but the inflammatory exudate often escapes alongside the hairs from the mouths of the follicles and dries to form small crusts. When the lesions are closely set one crust may cover the openings of several follicles. The removal of such a crust does not expose a raw, oozing surface, but tears the top off a number of pustules. The amount of crusting is never very great. Burning and tension are usually the only subjective symptoms complained of. At the on-set of an attack traction on the hairs which issue from inflamed follicles causes considerable pain, but later the root sheaths become swollen with pus and the hairs loosen and may be easily extracted. At times they fall out spontaneously. The hair loss is seldom permanent, though in some cases the thinning
of the beard is quite noticeable. Untreated the disease persists indefinitely. Periods of quiescence alternate with exacerbations and the outbreak of acute symptoms is as a rule without any apparent cause. Sycosis on the upper lip, which is a favorite location, is often associated with chronic rhinitis. The nasal secretion may be the cause of the sycosis or the sycosis by extension may affect the vibrissae and cause the Schneiderian membrane to become swollen and exquisitely sensitive. Syco-sis sometimes develops from eczema of the bearded region. The disease is feebly contagious and in not infrequently trans-mitted by the barber shop razor. The pyogenic staphylococci are invariably present in the pus.
DIAGNOSIS: Numerous pustules pierced by hairs are almost pathognomonic of the disease. Trichophytosis barbae begins as a scaling spot and later produces a lumpy condition of the skin; from every node many hairs project and these may be twisted, split or broken. The spores are easily found with the microscope. In pustular eczema the pustules are not so accurately located about the hairs, the crusting is greater and the crusts cover raw, oozing surfaces. The disease spreads readily to non-hairy parts. Itching is severe.
TREATMENT: Epilation is the most essential part of the treat-ment. Each day all the hairs in a given area of the affected region should be extracted. Pasta zinci Lassar, N. F., is to be applied plentifully and kept as constantly as possible in close contact with the skin. In very obstinate cases with thickening of the skin the amount of salicylic acid may be increased to 10-15 per cent. Exposures to the X-rays carried to the point of producing a slight erythema and falling of the hair, have a brilliant curative effect, but every precaution must be observed not to cause dermatitis actinica.


January/February 2012 Volume 10 • Issue 1
14SKINmed. 2012;10:14–16 © 2012 Pulse Marketing & Communications, LLC
From the Department of Dermatology, Drexel University College of Medicine, Philadelphia, PA
Address for Correspondence: Herbert B. Allen, MD, Department of Dermatology, Drexel University College of Medicine, 219 North Broad Street, Philadelphia, PA 19107 • E-mail: [email protected]
We present two patients with kerions who are rep-
resentative of more than 3 dozen similar patients
seen in more than 2 decades of observation in our
clinic. Recognizing that kerions are delayed-type hypersensitivity
(DTH) reactions,1 we treated all our patients with short courses of
anti-inflammatory agents, and all had resolution of their lesions.
CASE 1
Patient 1 was a 7-year-old African American boy who was taking
oral cephalexin for a cultured methicillin-sensitive Staphylococcus
aureus markedly crusted, boggy, alopectic tumefaction on the left
lateral scalp that was associated with markedly enlarged postauricu-
lar and posterior cervical nodes. He had taken the antibiotic for
2 weeks without any resolution. A fungal culture obtained from a
scaling scalp site distant from the kerion was positive for Trichophy-
ton tonsurans, and the diagnosis was kerion. He was treated with
two drops (94 mg) of saturated solution of potassium iodide (SSKI)
three times daily2,3 and 2.5% selenium shampoo twice weekly.4 Two
weeks later, the crusting, swelling, and adenopathy had resolved,
and 2 months later the hair had regrown without scarring.
CASE 2
Patient 2 was a 9-year-old African American boy who had been
treated with adequate doses of griseofulvin for 4 weeks for a
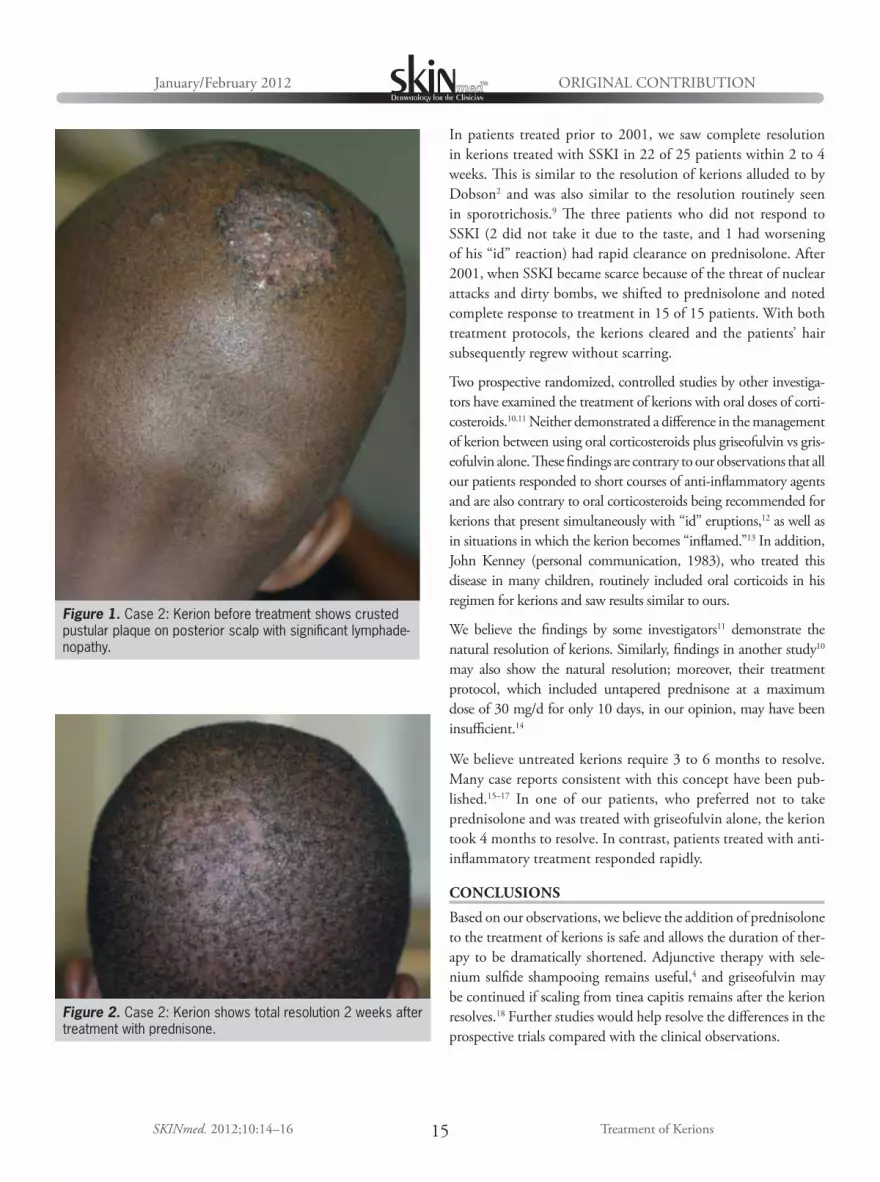
crusted, nodular, alopectic plaque on the posterior scalp (Figure 1)
along with a markedly enlarged posterior cervical node. Bacte-
rial and fungal cultures were negative. The clinical diagnosis was
kerion, and treatment with prednisolone 1 mg/kg/d and selenium
sulfide shampoo was instituted. Three weeks later, the plaque
had cleared and new hair started to regrow (Figure 2). Within
2 months, the hair had completely regrown without scarring.
DISCUSSION
Kerion formation is the inflammatory extreme of tinea capitis,
producing a large, painful, crusted plaque on the scalp, often with
purulent discharge and cervical lymphadenopathy. Kerions are
the result of a massive DTH reaction to a dermatophyte.1 Positive
DTH skin tests, lesional histopathology, and immunofluorescence
studies are all consistent with this concept,1,5,6 proposed originally
by Birt and Wilt7 in 1954 and later supported by Rasmussen and
Ahmed.8 Inasmuch as the kerion is an immunologic event, this
helps explain why antibiotics, whether antibacterial or antifun-
gal, are ineffective (in spite of positive cultures) and why all our
patients responded to anti-inflammatory treatment with complete
resolution of the kerions and subsequent regrowth of hair.
Treatment of kerions has been directed primarily toward the
underlying dermatophyte, often with protracted courses of gris-
eofulvin; however, we believe the inflammation, rather than the
infection, should be the initial focus of kerion treatment. The
clinical findings and treatment outcomes for our two patients
with kerion treated with short courses of anti-inflammatory
agents are representative and exactly similar to the other patients
with kerion seen in our clinic.
Kerions result from a massive delayed-type hypersensitivity reaction to a dermatophyte. Treatment traditionally has been directed primarily
toward the dermatophyte. The authors propose, however, that inflammation should be the initial target of treatment. Clinical findings and
treatment outcomes for two patients with kerions, treated with short courses of anti-inflammatory agents, are presented. Earlier studies
showing minimal effects with corticosteroid treatment of kerions may have had design flaws. The anti-inflammatory treatment of kerions
is both safe and effective and permits the duration of therapy to be shortened dramatically. (SKINmed. 2012;10:14–16)
ORIGINAL CONTRIBUTION
A New Paradigm in the Treatment of Kerions: Treat the Inflammation
Sarah E. Dolder, MD; Brendan J. O’Neill, MD; Meghan M. O’Brien, MD; Amy S. Ross, MD; Robert A. Allen, MD; Herbert B. Allen, MD
ABSTRACT
ORIGINAL CONTRIBUTIONJanuary/February 2012
15SKINmed. 2012;10:14–16 Treatment of Kerions
In patients treated prior to 2001, we saw complete resolution
in kerions treated with SSKI in 22 of 25 patients within 2 to 4
weeks. This is similar to the resolution of kerions alluded to by
Dobson2 and was also similar to the resolution routinely seen
in sporotrichosis.9 The three patients who did not respond to
SSKI (2 did not take it due to the taste, and 1 had worsening
of his “id” reaction) had rapid clearance on prednisolone. After
2001, when SSKI became scarce because of the threat of nuclear
attacks and dirty bombs, we shifted to prednisolone and noted
complete response to treatment in 15 of 15 patients. With both
treatment protocols, the kerions cleared and the patients’ hair
subsequently regrew without scarring.
Two prospective randomized, controlled studies by other investiga-
tors have examined the treatment of kerions with oral doses of corti-
costeroids.10,11 Neither demonstrated a difference in the management
of kerion between using oral corticosteroids plus griseofulvin vs gris-
eofulvin alone. These findings are contrary to our observations that all
our patients responded to short courses of anti-inflammatory agents
and are also contrary to oral corticosteroids being recommended for
kerions that present simultaneously with “id” eruptions,12 as well as
in situations in which the kerion becomes “inflamed.”13 In addition,
John Kenney (personal communication, 1983), who treated this
disease in many children, routinely included oral corticoids in his
regimen for kerions and saw results similar to ours.
We believe the findings by some investigators11 demonstrate the
natural resolution of kerions. Similarly, findings in another study10
may also show the natural resolution; moreover, their treatment
protocol, which included untapered prednisone at a maximum
dose of 30 mg/d for only 10 days, in our opinion, may have been
insufficient.14
We believe untreated kerions require 3 to 6 months to resolve.
Many case reports consistent with this concept have been pub-
lished.15–17 In one of our patients, who preferred not to take
prednisolone and was treated with griseofulvin alone, the kerion
took 4 months to resolve. In contrast, patients treated with anti-
inflammatory treatment responded rapidly.
CONCLUSIONS
Based on our observations, we believe the addition of prednisolone
to the treatment of kerions is safe and allows the duration of ther-
apy to be dramatically shortened. Adjunctive therapy with sele-
nium sulfide shampooing remains useful,4 and griseofulvin may
be continued if scaling from tinea capitis remains after the kerion
resolves.18 Further studies would help resolve the differences in the
prospective trials compared with the clinical observations.
Figure 2. Case 2: Kerion shows total resolution 2 weeks after treatment with prednisone.
Figure 1. Case 2: Kerion before treatment shows crusted pustular plaque on posterior scalp with significant lymphade-nopathy.

ORIGINAL CONTRIBUTIONJanuary/February 2012
16SKINmed. 2012;10:14–16 Treatment of Kerions
REFERENCES
1 Arenas R, Toussaint S, Isa-Isa R. Kerion and dermatophytic granu-loma. Mycological and histopathological findings in 19 children with inflammatory tinea capitis of the scalp. Int J Dermatol. 2006;45:215–219.
2 Dobson RL. In: Dobson RL, ed. Yearbook of Dermatology. Chicago, IL: Yearbook Publishers; 1979:124.
3 Sterling JB, Heymann WR. Potassium iodide in dermatology: a 19th cen-tury drug for the 21st century—uses, pharmacology, adverse effects, and contraindications. J Am Acad Dermatol. 2000;43:691–697.
4 Allen HB, Honig PJ, Leyden JJ, McGinley KJ. Selenium sulfide: adjunctive therapy for tinea capitis. Pediatrics. 1982; 69:81–83.
5 Woodfolk JA, Platts-Mills TA. The immune response to dermatophytes. Res Immunol. 1998;149:436–445; discussion 522–523.
6 Woodfolk JA. Allergy and dermatophytes. Clin Microbiol Rev. 2005;18:30–43.
7 Birt AR, Wilt JC. Mycology, bacteriology, and histopathology of suppura-tive ringworm. AMA Arch Derm Syphilol. 1954;69:441–448.
8 Rasmussen JE, Ahmed AR. Trichophytin reactions in children with tinea capitis. Arch Dermatol. 1978;114:371–372.
9 Sandhu K, Gupta S. Potassium iodide remains the most effective therapy for cutaneous sporotrichosis. J Dermatol Treat. 2003;14:200–202.
10 Honig PJ, Caputo GL, Leyden JJ, et al. Treatment of kerions. Pediatr Dermatol. 1994;11:69–71.
11 Hussain I, Muzaffar F, Rashid T, et al. A randomized, comparative trial of treatment of kerion celsi with griseofulvin plus oral prednisolone vs. gris-eofulvin alone. Med Mycol. 1999;37:97–99.
12 Alvarez MS, Silverberg NB. Tinea capitis. In: Kelly AP, Taylor SC, eds. Dermatology for Skin of Color. New York, NY: McGraw Hill; 2009:253.
13 Tinea capitis. In: James WD, Berger TG, Elston DM, eds. Andrews’ Diseases of the Skin: Clinical Dermatology. 10th ed. Philadelphia, PA: Elsevier; 2006:298.
14 Pomeranz AJ, Sabnis SS. Tinea capitis: epidemiology, diagnosis and management strategies. Paediatr Drugs. 2002;4:779–783.
15 Van Rooij P, Detandt M, Nolard N. Trichophyton mentagrophytes of rab-bit origin causing family incidence of kerion: an environmental study. Mycoses. 2006;49:426–430.
16 Schauder S. Itraconazole in the treatment of tinea capitis in children. Case reports with long-term follow-up evaluation. Review of the literature. Mycoses. 2002;45:1–9.
17 Gibbon KL, Goldsmith P, Salisbury JA, Bewley AP. Unnecessary surgical treatment of fungal kerions in children. BMJ. 2000;320:696–697.
18 Allen HB, Honig PJ. Scaling scalp diseases in children. Clin Pediatr (Phila). 1983;22:374–377.

Soothing and alcohol-free — part of a complete approach to acne treatment
TM C A L M I N G
WIPES(30 WIPES)
Complementary T3 Calming Wipes
A dual approach to acne care
ONE PRESCRIPTION.TWO POWERFUL EFFECTS.
The power to eradicate P acnesSignificant reduction in P acnes—even up to 3 weeks after discontinuation2
A decrease in P acnes can lead to a drop in pro-inflammatory cytokines and reduced inflammation1
Minimal resistance in an in vitro study
—The majority of tetracycline-resistant P acneswere cross-resistant to doxycycline—but sensitive to minocycline*3
The power to calm inflammatory acneInflammation is an important aspect in the pathophysiology of acne1
Both laboratory and clinical studies document the anti-inflammatory effects of minocycline1
+
The most common adverse events associated with MINOCIN are nausea, vomiting, and diarrhea. CNS adverse effects may includedizziness, vertigo, and headache.
References: 1. SapadinAN,Fleischmajer R.Tetracyclines:nonantibiotic properties and their clinical implications.JAmAcad Dermatol. 2006;54(2):258-265. 2. Leyden JJ,McGinley KJ,KligmanAM.Tetracycline and minocyclinetreatment.Arch Dermatol. 1982;118(1):19-22. 3. Hubbell CG,Hobbs ER,RistT,White JW Jr.Efficacy of minocycline compared with tetracycline in treatment of acne vulgaris.Arch Dermatol.1982;118(12):989-992.
*In vitro activity does not necessarily correlate to in vivo activity.
©2010 Triax Pharmaceuticals, LLC All rights reserved. Printed in USA. MN-0810-280
Important InformationThe most common adverse events associated with MINOCIN are nausea, vomiting, and diarrhea. Central nervous system adverse events includinglight-headedness, dizziness, or vertigo have been reported with minocycline therapy, but are generally transient in nature. Other adverse eventsinclude tinnitus, headache, sedation, and skin pigmentation, particularly on the face and mucous membranes. MINOCIN is contraindicated in personswho have shown hypersensitivity to any of the tetracyclines or to any of the components of the product formulation. WARNING: MINOCIN Pellet-Filled Capsules, like other tetracycline-class antibiotics, can cause fetal harm when administered to a pregnant woman. The use of drugs of thetetracycline class during tooth development (last half of pregnancy, infancy, and childhood to the age of 8 years) may cause permanent discoloration of teeth (yellow-gray-brown). Concurrent use of tetracyclines may render oral contraceptives less effective.
For more information, go to www.minocin-kit.com
The only pelletized form of Minocycline available...

January/February 2012 Volume 10 • Issue 1
18SKINmed. 2012;10:18–23 © 2012 Pulse Marketing & Communications, LLC
From the Dermato Venereology (Skin/VD) Center, Sehgal Nursing Home, Panchwati, Azadpur, Delhi, India;1 the Skin Institute and School of Dermatology, Greater Kailash, New Delhi, India;2 Department of Dermatology, and STD University College of Medical Sciences and Associ-ated Guru Teg Bahadur Hospital, Shahdara, Delhi, India3
Address for Correspondence: Virendra N. Sehgal MD, Dermato Venerology (Skin/VD) Center, Sehgal Nursing Home, A/6 Panchwati, Delhi, 110 033, India • E-mail: [email protected]
Pityriasis rubra pilaris (PRP) comprises a group of chronic
disorders that demonstrate circumscribed follicular
keratosis with palmoplantar keratoderma. Both famil-
ial and acquired forms have been recognized. The former is
infrequent and usually occurs in childhood. The bimodal or
trimodal distribution usually involves a peak case incidence
in the first and second decades of life,1,2 and it affects both
men and women. Its etiology and management has remained a
challenge. Occasionally, PRP is associated with other diseases,
and it was speculated that the disorder might be the result
of an abnormal immune response to some antigenic stimuli.
Familial occurrence of the disease might point to genes that
predispose the individual to develop the disorder after certain
precipitating events. The occurrence of PRP in patients with
the human immunodeficiency virus (HIV)/AIDS is a topic of
recent debate.3
METHODS
Medline/PubMed (1936–2010) was searched using the terms
“PRP” and “treatment.” Accordingly, this contribution out-
lines the published reports on the topic, with the objective to
focus on the evolution and challenges of promising treatment
options.
CLINICAL CRITERIA/CLASSIFICATION
Management of PRP varies according to the type, extent, and age
at onset of the disease. Thus, an understanding of the classification
of the disease offers insight into individualizing treatment.
Griffiths1 classified PRP into 6 types according to the age at on-
set, behavior, clinical appearance, and prognosis (Table I). Clas-
sic adult-onset PRP (type I) shows the characteristic generalized
rash with palmo-plantar keratoderma, whereas atypical adult-
onset PRP (type II) is chronic, with ichthyosiform and lamellar
scales on the palms and soles and alopecia of varying degrees. The
association of PRP and HIV infection has recently been identi-
fied as type VI PRP, and most of the cases have been reported in
young heterosexual/homosexual men. It is characterized by nod-
ulocystic and lichen spinulosus–like lesions, with poor prognosis
and resistance to treatment.2 Another classification5 divides the
disease into 4 types based only on physical findings (Table II);
however, Griffiths1 classification continues to be the mainstay in
practice for delineating the disease.
CHALLENGES AND PROMISING TREATMENTS
HISTORICALLY (ARCHIVE) IMPORTANT MODALITIES
The diagnosis and treatment of PRP have always been a source
of great interest. At present, there is no acclaimed treatment
ORIGINAL CONTRIBUTION
Pityriasis Rubra Pilaris: Evolution of Challenges in
Promising Treatment OptionsVirendra N. Sehgal, MD;1 Govind Srivastava, MD;2 Prashant Verma, MD3
ABSTRACT
Pityriasis rubra pilaris is an uncommon inflammatory dermatosis that is well recognized across the globe. Erythroderma is a common
presentation. A precise diagnosis of pityriasis rubra pilaris is based on morphologic features and is classified into 6 types: classic adult
onset (type I), atypical adult (type II), classic juvenile (type III), circumscribed juvenile (type IV), atypical juvenile (type V), and human
immunodeficiency virus–associated (type VI). Several conventional systemic and/or topical treatments are currently in use. Largely, their
results are unsatisfactory and limited by long-term toxicity. The authors investigate the efficacy of a wide spectrum of drugs by examining
historical (archive) and promising (modern) treatment modalities for the treatment of pityriasis rubra pilaris. (SKINmed. 2012;10:18–23)

January/February 2012
SKINmed. 2012;10:18–23
-
-
-
PROMISING (MODERN) MODALITIES
-
15–18 8
-
22
25
-
-
-
21 28 -
RETINOIDS/VITAMIN A DERIVATIVES21
-
-
Table I. Pityriasis Rubra Pilaris: Griffiths Clinical Classification
CLINICAL TYPE LESIONS’ DISTRIBUTION NATURAL COURSE PERCENTAGE OF CASES
55
5
10
25
5
Table II. Pityriasis Rubra Pilaris: Piamphongsant and Akaraphant Classification5
TYPES
168 PATIENTS
CLINICAL FEATURES ADULTS CHILDREN
11 21
20
10

January/February 2012
20SKINmed. 2012;10:18–23
IMMUNOSUPPRESSIVE THERAPY
-
31
32 -33
PHOTOTHERAPY
21
28
35
TOPICAL THERAPY
-
8
-
38
-8 10
11 12 and 13
BIOLOGICS
Table III. Pityriasis Rubra Pilaris: Challenges and Promising Treatment—Historical (Archive) Importance
AUTHOR(S) YEAR(S) RECOMMENDED DRUG(S) DOSAGE RESPONSE/RESULT PATIENTS
´ Good
8
10 Good –
11 – –
12
-
13 –

January/February 2012
21SKINmed. 2012;10:18–23
Table IV. Pityriasis Rubra Pilaris (PRP): Challenges and Promising Treatment—Modern Modalities
AUTHOR(S) YEAR RECOMMENDED DRUG(S) DOSAGE RESPONSE/RESULT PATIENTS
- – – –
30 –
31 Good
2000
25
-
28 2000
21 2000 –
2005 – –
- 2/mo on –
50 – –
- – –
2008
2008
2008
2008
2008
20
Continued »

January/February 2012
22SKINmed. 2012;10:18–23
-
-
-
-
FIVEYEAR VIEW
-
-
-
-
-
REFERENCES1 Griffiths WA. Pityriasis rubra pilaris–an historical approach. 2. Clinical
features. Clin Exp Dermatol. 1976;1:37–50.
2 Sehgal VN, Srivastava G, Dogra S. Adult onset pityriasis rubra pilaris. Indian J Dermatol Venereol Leprol. 2008;74:311–321.
3 -laris and human immunodeficiency virus infection. Br J Dermatol. 1995;133:990–993.
4and HIV infection: a part of the spectrum of HIV-associated follicular syndrome. Br J Dermatol. 1995;135:818–819.
5 Piamphongsant T, Akarphant R. Pityriasis rubra pilaris: a new proposed classification. Clin Exp Dermatol. 1994;19:134–138.
6 Petter MF. Pityriasis rubra pilaris, with particular reference to vitamin medication and dietary control. Penn Med J. 1936;39:864–866.
35
2010 a
a
b

January/February 2012
23SKINmed. 2012;10:18–23
7 Gunther S, Alston W. Follicular keratoses. Pilot studies of serum level of vitamin A and liver function tests during administration of retinoic acid in hyperkeratosis follicularis et parafollicularis (Kyrle’s disease), pityriasis rubra pilaris, and keratosis follicularis (Darier’s disease). Dermatologica. 1973;147:274–283.
8 Ayres S Jr, Mihan R, Scribner MD. Synergism of vitamin A and Cutis. 1979;23:600–603, 689–690.
9diseases. J Am Acad Dermatol. 1981;5:222.
10 Arch Dermatol Syphilol. 1941;43:42–61.
11 -ence in therapy with carotene and vitamin A. Arch Dermatol Syphilol. 1943;48:288–296.
12 Webster JR, Falk AB. Pityriasis rubra pilaris; clinical and laboratory observation on combined treatment with corticotropin and vitamin A. AMA Arch Dermatol Syphilol. 1952;65:685–700.
13 Irgang S. Pityriasis rubra pilaris responsive to ascorbic acid. Australas J Dermatol. 1968;9:211–217.
14drugs as possible therapeutic agents. Arch Dermatol. 1965;92:428–430.
15rubra pilaris. Arch Dermatol. 1981;117:749–750.
16the retinol binding protein. Br J Dermatol. 1981;104:253–256.
1713-cis-retinoic acid (isotretinoin). J Am Acad Dermatol. 1982;6:710–715.
18 -riasis rubra pilaris: unapproved use. Int J Dermatol. 2006;45:1238–1240.
19pilaris with calcipotriol. Br J Dermatol. 1994;130:675–678.
20 Vergilis-Kalner IJ, Mann DJ, Wasserman J, Petronic-Rosic V, Tsoukas MM. Pityriasis rubra pilaris sensitive to narrow band-ultraviolet B light therapy. J Drugs Dermatol. 2009;8:270–273.
21 Kirby B, Watson R. Pityriasis rubra pilaris treated with acitretin and Br J Dermatol. 2000;142:376–377.
22 Hanke CW, Steck WD. Childhood-onset pityriasis rubra pilaris treated with Cleve Clin Q. 1983;50:201–203.
23 Wetzig T, Sticherleng M. Juvenile pityriasis rubra pilaris: successful treatment with cyclosporine. Br J Dermatol. 2003;149:202–203.
24 Usuki K, Sekiyama M, Shimada T, et al. Three cases of pityriasis ru-bra pilaris successfully treated with cyclosporine A. Dermatology. 2000;200:324–327.
25pilaris. Arch Dermatol. 1985;121:105–106.
26rubra pilaris responsive to triple anti-retroviral therapy. Br J Dermatol. 1999;140:931–934.
27 Bonomo RA, Kormam N, Nagashima-Wholen I, et al. Pityriasis rubra pilaris–an unusual cutaneous complication of AIDS. Am J Med Sci. 1997;314:118–121.
28 radiation and acitretin therapy as a treatment option for pityriasis rubra pilaris. Br J Dermatol. 2000;142:574–575.
29for the treatment of erythrodermic pityriasis rubra pilaris. Arch Dermatol. 1999;135:475–476.
30 Aust J Dermatol. 1966;8:183–185.
31 Hunter GA, Forbes IJ. Treatment of pityriasis rubra pilaris with azathio-prine. Br J Dermatol. 1972;87:42–45.
32 Wetzig T, Sticherling M. Juvenile pityriasis rubra pilaris: successful treatment with ciclosporin. Br J Dermatol. 2003;149:202–203.
33pilaris with calcipotriol. Br J Dermatol. 1994;130:675–678.
34 -Clin
Exp Dermatol. 2004;29:244–246.
35therapeutic agents in pityriasis rubra pilaris. J Dtsch Dermatol Ges. 2010;8:354–356.
36 -ment of pityriasis rubra pilaris with pimecrolimus cream 1%. J Drugs Dermatol. 2007;6:340–342.
37 -scribed pityriasis rubra pilaris to topical tazarotene treatment. Pediatr Dermatol. 2008;25:125–126.
38 Raza N, Bari AU, Dar NR. Juvenile onset classical pityriasis rubra pilaris: every patient may not require systemic therapy. J Coll Physicians Surg Pak. 2007;17:564–565.
39Acta Derm Venereol.
2007;87:552–553.
40pilaris with etanercept. J Am Acad Dermatol. 2008;59:113–114.
41rubra pilaris. Br J Dermatol. 2008;158:642–644.
42 Barth D, Harth W, Treudler R, et al. Successful treatment of pityriasis
J Dtsch Dermatol Ges. 2009;7:1071–1073.
43treatment for adult-onset pityriasis rubra pilaris: case report and review of the literature on biologic therapy. J Am Acad Dermatol. 2008;59:65–70.
44J Eur Acad Dermatol Vene-
reol. 2008;22:117–118.
45 Garcovich S, Di Giampetruzzi AR, Antonelli G, Garcovich A, Didona B. Treatment of refractory adult-onset pityriasis rubra pilaris with TNF-alpha antagonists: a case series. J Eur Acad Dermatol. 2010;24:881–884.
46of pityriasis rubra pilaris with adalimumab treatment. Clin Exp Dermatol. 2009;35:e155–e156.
47 -mumab. Arch Dermatol. 2009;145:99–101.
48 Kerr AC, Ferguson J. Type II adult-onset pityriasis rubra pilaris suc-cessfully treated with intravenous immunoglobulin. Br J Dermatol. 2007;156:1055–1056.
49 Clin Exp Dermatol. 1991;16:181–184.
50pilaris with combination eternacept and acitretin therapy. Arch Dermatol. 2007;143:1597–1599.

January/February 2012 Volume 10 • Issue 1
24SKINmed. 2012;10:24–26 © 2012 Pulse Marketing & Communications, LLC
From the Department of Dermatology & Cutaneous Surgery, University of Miami Miller School of Medicine, Miami, FL
Address for Correspondence: Robert S. Kirsner, MD, PhD, Department of Dermatology & Cutaneous Surgery, University of Miami Miller School of Medicine, 1600 NW 10th Avenue, RMSB, Room 2023-A, Miami, FL 33136 • E-mail: [email protected]
A question commonly encountered when treating chronic
wounds is whether and when debridement is needed.
The 3 most common chronic wounds are the diabetic
foot ulcer (DFU), the venous leg ulcer, and the pressure or decu-
bitus ulcer. The former 2 chronic wounds have been more exten-
sively studied. Using DFU as an example, certainly the question
is of importance, considering that an estimated 15% of the 170
million people currently with diabetes mellitus will develop a
foot ulcer during their lifetime.1,2
The multifactor etiology of DFUs includes peripheral vascular dis-
ease along with sensory, motor, and autonomic neuropathy.3 DFUs
are a major cause of morbidity and mortality due to increased
amputations, infections, and hospitalizations in diabetic patients.4
At first glance it would seem to be a rather simple question.
Surgical debridement is a longstanding standard of care for
DFUs, aimed at removing necrotic, devitalized wound bed and
wound edge tissue that inhibits healing. Such tissue includes
hyperkeratotic epidermis (callus) and necrotic dermal tissue,
foreign debris, and harmful bacterial elements.5 Various debride-
ment methods exist, including surgery, wet-to-dry dressings,
biosurgery (ie, maggots), enzyme preparations, polysaccharide
beads or paste dextranomer polysaccharide, and hydrogels.3 This
contribution focuses on surgical debridement.
Debridement encourages healing by converting a chronic
nonhealing wound environment into a more responsive acute
healing environment.6 Debridement is included in multiple
guidelines for the care of DFUs, including the American Dia-
betes Association, the American College of Foot and Ankle
Surgeons, and the Wound Healing Society; however, herein lies
the issue: while the rationale for debridement seems logical, the
evidence to support its use in enhancing healing is scarce.
REVIEW OF CURRENT LITERATURE
Many studies on which clinicians have based their rationale for
debridement possess methodologic flaws, small sample sizes,
and bias.3 A recent paper7 systematically reviewed 5 published
clinical trials that investigated surgical debridement of DFUs
to enhance healing.5,8,9 These clinical trials were found to be
defective in their methodology, statistically insignificant, or
lacking in definitive scientific evidence for surgical debridement
in the treatment of DFUs.7 In addition, most existing studies
are not randomized clinical trials optimized to test the rela-
tionship between debridement of DFUs and wound healing.
A focused, well-designed study is needed, therefore, to eluci-
date the effect of surgical debridement on the healing status of
chronic wounds.
REVIEW
The Role of Surgical Debridement in Healing of Diabetic Foot Ulcers
Katherine A. Gordon, BS; Elizabeth A. Lebrun, MD; Marjana Tomic-Canic, PhD; Robert S. Kirsner MD, PhD
ABSTRACT
A critical question in the treatment of chronic wounds is whether and when debridement is needed. The three most common chronic
wounds are the diabetic foot ulcer (DFU), the venous leg ulcer, and the pressure or decubitus ulcer. Surgical debridement, aimed at re-
moving necrotic, devitalized wound bed and wound edge tissue that inhibits healing, is a longstanding standard of care for the treatment
of chronic, nonhealing wounds. Debridement encourages healing by converting a chronic nonhealing wound environment into a more
responsive acute healing environment. While the rationale for debridement seems logical, the evidence to support its use in enhancing
healing is scarce. Currently, there is more evidence in the literature for debridement for DFUs than for venous ulcers and pressure ulcers;
however, the studies on which clinicians have based their rationale for debridement in DFUs possess methodologic flaws, small sample
sizes, and bias. Thus, further studies are needed to develop clinical evidence for its inclusion in treatment protocols for chronic wounds.
Here, the authors review the scientific evidence for debridement of DFUs, the rationale for debridement of DFUs, and the insufficient data
supporting debridement for venous ulcers and pressure ulcers. (SKINmed. 2012;10:24–26)

Surgical Debridement in DFUs
REVIEWJanuary/February 2012
25SKINmed. 2012;10:24–26
SCIENTIFIC EVIDENCE FOR DFU DEBRIDEMENT
The biological and molecular basis for debridement has been
investigated in several studies.10,11 Molecular and histologic anal-
yses of biopsies from the nonhealing edge of a chronic wound
have been suggested to validate the use of debridement.10
Keratinocytes become activated following wounding and are key
players in restoring the epidermal barrier during wound healing.12
Keratinocytes and fibroblasts at the nonhealing edges of chronic
wounds were shown to exhibit not only a pathogenic phenotype
detrimental to healing but also a slowed migratory capacity.10–13 In
chronic wounds, the keratinocytes multiply at a higher rate than
usual (hyperproliferation), yet they are unable to migrate into the
wound as would be normally expected.10–13 Basically, keratino-
cytes on a chronic wound edge are capable of proliferating but are
unable to migrate properly.12 These nonhealing keratinocytes of the
chronic wound edge are marked by induction of c-Myc and nucle-
arization of β-catenin, which may contribute to the inhibition of
migration.10–12 Many clinicians visually identify this nonhealing
phenotype as a “callus,” indicating the need for removal to facilitate
wound healing.14 Debridement seems to be a reasonable solution
to the problem of nonmigratory tissue in the margins of chronic
wounds. Researchers suggest that debridement will be effective if
unresponsive cells are surgically removed, and cells responsive to
wound healing signals and topical agents are optimized.11
RATIONALE FOR DEBRIDEMENT OF DFUS
The benefits of debridement include removal of bacteria,
senescent cells, and hyperproliferative nonmigratory tissue and
stimulation of growth factor activity.15
Bacterial burden in a wound likely impedes healing,16 as greater
bacterial load and certain types of bacteria have been shown
to reduce healing responses.17,18 Bacteria in chronic wounds
stimulate a prolonged inflammatory response with a concomi-
tant release of free oxygen radicals and various lytic enzymes,
ultimately causing tissue damage.19 In addition, biofilms, which
are communities of bacteria and other organisms embedded
in an extrapolysaccharide matrix within the wound bed, show
increased resistance to antimicrobial agents and to the host
immune system.20,21 Debridement is an effective way to remove
bacterial burden and biofilms from nonhealing wounds.
Additionally, growth factors are reduced in chronic wounds,
including platelet-derived growth factor, fibroblast growth fac-
tor, epidermal growth factor, and transforming growth factor
β.22 Dead tissue within chronic wounds, which is removed by
surgical debridement, is unreceptive to growth factors.23 In addi-
tion, the bleeding and platelet activation caused by debridement
stimulates the production of blood-borne growth factors, further
promoting wound healing.24
Senescent cells have markedly decreased proliferation and protein
production.17 Chronic wound fibroblasts are less receptive to
growth factor stimuli,25 making these wounds less likely to heal
or respond to treatments.26 Overall, debridement removes both
the hyperproliferative edge and the senescent cells of the chronic
wound, thus allowing the remaining cells to undergo normal
proliferation, migration, response to treatment, and healing.
DEBRIDEMENT AND VENOUS ULCERS
Another example of a chronic wound is venous ulcer. Venous insuf-
ficiency is the most common cause of lower-extremity ulcers and
accounts for the development of approximately 1 million venous
ulcers in patients in the United States with venous insufficiency.27
There are many theories for the mechanism of venous ulcer develop-
ment, including pericapillary fibrin cuff deposition, abnormalities
of the fibrinolytic system, trapping of growth factors by macromole-
cules in the dermis, and leukocyte plugging in the vessels of the lower
extremities.28–30 The treatment modalities for venous ulcers include
bed rest with leg elevation31; compression therapy32; aspirin33; pent-
oxifylline34; skin grafting,35 including cultured epidermal autografts
and allografts36,37; superficial venous surgery38; and debridement.17,39
The data supporting debridement for venous ulcers are even
more sparse than for DFUs. The role of debridement in the
treatment of venous ulcers has not been proven, although it is
used as a standard of care.39 One controlled, prospective cohort
study involving 53 patients for 12 months evaluated sharp
debridement in combination with standard treatment regimens
for nonhealing venous leg ulcers.40 The study group contained
ulcers that had slough, nonviable tissue and no granulation tis-
sue, while the control group had ulcers with 15% to 20% granu-
lation tissue without slough or nonviable tissue. Although they
failed to reach statistical significance, the authors concluded that
sharp debridement was effective at initiating the healing process.
They found a 6-cm2 reduction in the mean surface area of the
study group ulcers, compared with a 1-cm2 reduction in the
control group in the first 4 weeks (P = .02).40
Clinical experience also dictates that venous ulcers are com-
monly more difficult to debride than most DFUs, and it is more
time-consuming for the clinician to achieve viable tissue margins
in these cases; therefore, chronic venous ulcers, much like DFUs,
are in need of evidence-based standardized treatment plans.
DEBRIDEMENT AND PRESSURE ULCERS
The most common cause of chronic wounds is the pressure
ulcer. While the rationale for debridement is excellent as part
of standard care when treating pressure ulcers, given the mul-
tiple comorbidities coexistent in patients with pressure ulcers,
the data supporting debridement for pressure ulcers are the least
substantial of the 3 common chronic wounds.
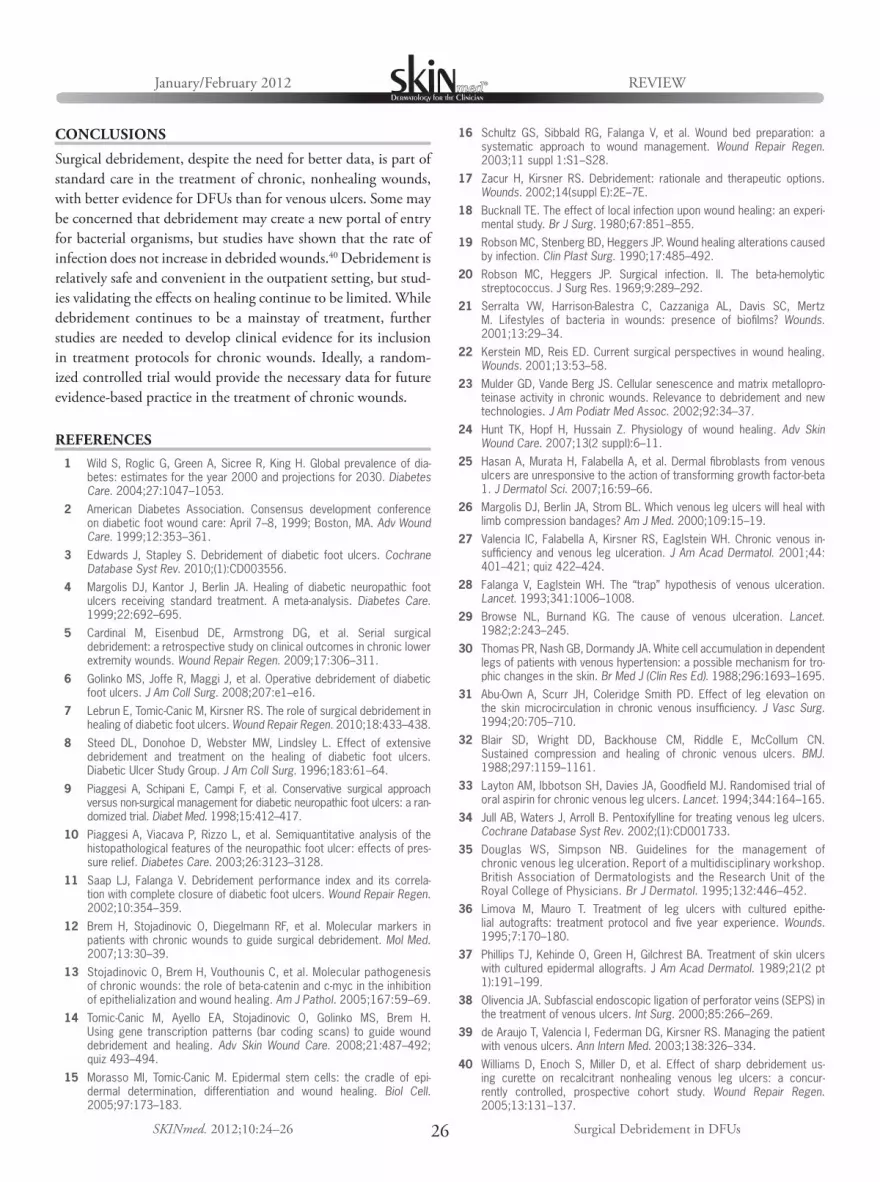
Surgical Debridement in DFUs
REVIEWJanuary/February 2012
26SKINmed. 2012;10:24–26
CONCLUSIONS
Surgical debridement, despite the need for better data, is part of
standard care in the treatment of chronic, nonhealing wounds,
with better evidence for DFUs than for venous ulcers. Some may
be concerned that debridement may create a new portal of entry
for bacterial organisms, but studies have shown that the rate of
infection does not increase in debrided wounds.40 Debridement is
relatively safe and convenient in the outpatient setting, but stud-
ies validating the effects on healing continue to be limited. While
debridement continues to be a mainstay of treatment, further
studies are needed to develop clinical evidence for its inclusion
in treatment protocols for chronic wounds. Ideally, a random-
ized controlled trial would provide the necessary data for future
evidence-based practice in the treatment of chronic wounds.
REFERENCES
1 Wild S, Roglic G, Green A, Sicree R, King H. Global prevalence of dia-betes: estimates for the year 2000 and projections for 2030. Diabetes Care. 2004;27:1047–1053.
2 American Diabetes Association. Consensus development conference on diabetic foot wound care: April 7–8, 1999; Boston, MA. Adv Wound Care. 1999;12:353–361.
3 Edwards J, Stapley S. Debridement of diabetic foot ulcers. Cochrane Database Syst Rev. 2010;(1):CD003556.
4 Margolis DJ, Kantor J, Berlin JA. Healing of diabetic neuropathic foot ulcers receiving standard treatment. A meta-analysis. Diabetes Care. 1999;22:692–695.
5 Cardinal M, Eisenbud DE, Armstrong DG, et al. Serial surgical debridement: a retrospective study on clinical outcomes in chronic lower extremity wounds. Wound Repair Regen. 2009;17:306–311.
6 Golinko MS, Joffe R, Maggi J, et al. Operative debridement of diabetic foot ulcers. J Am Coll Surg. 2008;207:e1–e16.
7 Lebrun E, Tomic-Canic M, Kirsner RS. The role of surgical debridement in healing of diabetic foot ulcers. Wound Repair Regen. 2010;18:433–438.
8 Steed DL, Donohoe D, Webster MW, Lindsley L. Effect of extensive debridement and treatment on the healing of diabetic foot ulcers. Diabetic Ulcer Study Group. J Am Coll Surg. 1996;183:61–64.
9 Piaggesi A, Schipani E, Campi F, et al. Conservative surgical approach versus non-surgical management for diabetic neuropathic foot ulcers: a ran-domized trial. Diabet Med. 1998;15:412–417.
10 Piaggesi A, Viacava P, Rizzo L, et al. Semiquantitative analysis of the histopathological features of the neuropathic foot ulcer: effects of pres-sure relief. Diabetes Care. 2003;26:3123–3128.
11 Saap LJ, Falanga V. Debridement performance index and its correla-tion with complete closure of diabetic foot ulcers. Wound Repair Regen. 2002;10:354–359.
12 Brem H, Stojadinovic O, Diegelmann RF, et al. Molecular markers in patients with chronic wounds to guide surgical debridement. Mol Med. 2007;13:30–39.
13 Stojadinovic O, Brem H, Vouthounis C, et al. Molecular pathogenesis of chronic wounds: the role of beta-catenin and c-myc in the inhibition of epithelialization and wound healing. Am J Pathol. 2005;167:59–69.
14 Tomic-Canic M, Ayello EA, Stojadinovic O, Golinko MS, Brem H. Using gene transcription patterns (bar coding scans) to guide wound debridement and healing. Adv Skin Wound Care. 2008;21:487–492; quiz 493–494.
15 Morasso MI, Tomic-Canic M. Epidermal stem cells: the cradle of epi-dermal determination, differentiation and wound healing. Biol Cell. 2005;97:173–183.
16 Schultz GS, Sibbald RG, Falanga V, et al. Wound bed preparation: a systematic approach to wound management. Wound Repair Regen. 2003;11 suppl 1:S1–S28.
17 Zacur H, Kirsner RS. Debridement: rationale and therapeutic options. Wounds. 2002;14(suppl E):2E–7E.
18 Bucknall TE. The effect of local infection upon wound healing: an experi-mental study. Br J Surg. 1980;67:851–855.
19 Robson MC, Stenberg BD, Heggers JP. Wound healing alterations caused by infection. Clin Plast Surg. 1990;17:485–492.
20 Robson MC, Heggers JP. Surgical infection. II. The beta-hemolytic streptococcus. J Surg Res. 1969;9:289–292.
21 Serralta VW, Harrison-Balestra C, Cazzaniga AL, Davis SC, Mertz M. Lifestyles of bacteria in wounds: presence of biofilms? Wounds. 2001;13:29–34.
22 Kerstein MD, Reis ED. Current surgical perspectives in wound healing. Wounds. 2001;13:53–58.
23 Mulder GD, Vande Berg JS. Cellular senescence and matrix metallopro-teinase activity in chronic wounds. Relevance to debridement and new technologies. J Am Podiatr Med Assoc. 2002;92:34–37.
24 Hunt TK, Hopf H, Hussain Z. Physiology of wound healing. Adv Skin Wound Care. 2007;13(2 suppl):6–11.
25 Hasan A, Murata H, Falabella A, et al. Dermal fibroblasts from venous ulcers are unresponsive to the action of transforming growth factor-beta 1. J Dermatol Sci. 2007;16:59–66.
26 Margolis DJ, Berlin JA, Strom BL. Which venous leg ulcers will heal with limb compression bandages? Am J Med. 2000;109:15–19.
27 Valencia IC, Falabella A, Kirsner RS, Eaglstein WH. Chronic venous in-sufficiency and venous leg ulceration. J Am Acad Dermatol. 2001;44:401–421; quiz 422–424.
28 Falanga V, Eaglstein WH. The “trap” hypothesis of venous ulceration. Lancet. 1993;341:1006–1008.
29 Browse NL, Burnand KG. The cause of venous ulceration. Lancet. 1982;2:243–245.
30 Thomas PR, Nash GB, Dormandy JA. White cell accumulation in dependent legs of patients with venous hypertension: a possible mechanism for tro-phic changes in the skin. Br Med J (Clin Res Ed). 1988;296:1693–1695.
31 Abu-Own A, Scurr JH, Coleridge Smith PD. Effect of leg elevation on the skin microcirculation in chronic venous insufficiency. J Vasc Surg. 1994;20:705–710.
32 Blair SD, Wright DD, Backhouse CM, Riddle E, McCollum CN. Sustained compression and healing of chronic venous ulcers. BMJ. 1988;297:1159–1161.
33 Layton AM, Ibbotson SH, Davies JA, Goodfield MJ. Randomised trial of oral aspirin for chronic venous leg ulcers. Lancet. 1994;344:164–165.
34 Jull AB, Waters J, Arroll B. Pentoxifylline for treating venous leg ulcers. Cochrane Database Syst Rev. 2002;(1):CD001733.
35 Douglas WS, Simpson NB. Guidelines for the management of chronic venous leg ulceration. Report of a multidisciplinary workshop. British Association of Dermatologists and the Research Unit of the Royal College of Physicians. Br J Dermatol. 1995;132:446–452.
36 Limova M, Mauro T. Treatment of leg ulcers with cultured epithe-lial autografts: treatment protocol and five year experience. Wounds. 1995;7:170–180.
37 Phillips TJ, Kehinde O, Green H, Gilchrest BA. Treatment of skin ulcers with cultured epidermal allografts. J Am Acad Dermatol. 1989;21(2 pt 1):191–199.
38 Olivencia JA. Subfascial endoscopic ligation of perforator veins (SEPS) in the treatment of venous ulcers. Int Surg. 2000;85:266–269.
39 de Araujo T, Valencia I, Federman DG, Kirsner RS. Managing the patient with venous ulcers. Ann Intern Med. 2003;138:326–334.
40 Williams D, Enoch S, Miller D, et al. Effect of sharp debridement us-ing curette on recalcitrant nonhealing venous leg ulcers: a concur-rently controlled, prospective cohort study. Wound Repair Regen. 2005;13:131–137.


January/February 2012 Volume 10 • Issue 1
28SKINmed. 2012;10:28–33 © 2012 Pulse Marketing & Communications, LLC
From the Dermato-Venereology (Skin/VD) Center, Sehgal Nursing Home, Panchwati, Delhi;1 the Departments of Dermatology and STD2 and Pathology,3 University College of Medical Sciences and Associated Guru Teg Bahadur Hospital, Delhi; and the Department of Microbiology, Maulana Azad Medical College and Associated Chacha Nehru Bal Chikitsalaya, Delhi,4 India
Address for Correspondence: Virendra N. Sehgal, MD, Dermato-Venerology (Skin/VD) Center, Sehgal Nursing Home, A/6 Panchwati, Delhi 110 033 India • E-mail: [email protected]
Tuberculosis (TB) is a common disease worldwide,1
and its clinical incidence has been impacted by the
emergence of the human immunodeficiency virus
(HIV), increased transmigration from endemic countries,
and its transmission in health care facilities, prisons, homeless
shelters, and other crowded settings.2–5 TB is largely an air-
borne infection; however, skin manifestations may be caused
by hematogenous spread or the contiguity from latent and/or
active foci of infection. Primary inoculation, although uncom-
mon, is another known mode of transmission. HIV infection,
intravenous drug abuse, diabetes mellitus, immunosuppressive
therapy, malignancies, end-stage renal disease, and infancy may
predispose to TB. Although cutaneous TB (CTB) is a well-
recognized clinical entity, it often poses a diagnostic dilemma
for physicians6; therefore, it is important to perform a careful
review of clinical presentations in each patient, which may prove
predictive of its diagnosis.7,8
CLASSIFICATION
The most widely accepted CTB classification is based on the
route of infection.6,9 Exogenous inoculation occurs after the
direct inoculation of Mycobacterium tuberculosis into the skin of a
person who is susceptible to infection (vide infra). This may cause
TB verrucosa cutis (TBVC), TB chancre, and some cases of lupus
vulgaris (LV), whereas endogenous infection is caused by either
lymphatic or hematogenous spread or a contiguous extension.
Occasionally, lymphatic spread is seen in LV. Hematogenous
spread, on the other hand, is responsible for acute miliary TB,
metastatic tubercular abscess, gummatous TB, papulonecrotic
tuberculid (PNT), and lupus vugaris. Contiguous extension
from the underlying lesion is a characteristic feature of both
scrofuloderma and TB cutis orificialis (TBCO).
In attempt to embellish the preceding classification, it has been
divided into multibacillary and paucibacillary variants based on
the bacterial load. The former is recognized by the characteris-
tic morphology of the organism in the tissue sections stained
with Ziehl-Neelsen method, complemented by in vitro recov-
ery of M tuberculosis, while sparse bacilli on histological exami-
nation and rare in vitro culture isolation2 identify the latter.
Unfortunately, it is difficult to distinguish the organisms in
paucibacillary TB.
CLINICAL FEATURES
Although the prevalence of CTB accounts for 1.5% of all cases
of TB, it is, nevertheless, important to consider the entity when
patients present with a suggestive clinical morphology. CTB has
many forms, including multibacillary and paucibacillary CTB,
which are defined in detail below.
MULTIBACILLARY CTB
TB CHANCRE/INOCULATION TBTuberculous chancre (primary inoculation TB) is a variant of
multibacillary CTB that results from direct introduction of
mycobacteria into the skin or mucosa of an individual who nei-
ther had tubercular infection in the past nor was immunized
with Bacille Calmette-Guérin (BCG). Trauma also facilitates the
entry of the organism into the skin.10,11
Face and other exposed areas are vulnerable sites of introduction.
The organism multiplies in tissue macrophages and migrates to
CORE CURRICULUM
Virendra N. Sehgal, MD, Section Editor
Cutaneous Tuberculosis: A Diagnostic Dilemma Virendra N. Sehgal, MD;1 Prashant Verma, MD;2 Sambit N. Bhattacharya, MD;2 Sonal Sharma, MD;3
Navjeevan Singh, MD;3 Nishant Verma, MD4
Cutaneous tuberculosis continues to be one of the most difficult conditions to diagnose. It is a challenge particularly in developing
countries due to the lack of resources. The authors define the classification and clinical manifestations considered predictive of its diagnosis.

CORE CURRICULUMJanuary/February 2012
29SKINmed. 2012;10:28–33 Cutaneous Tuberculosis
regional lymph nodes. An inflammatory papule develops in 2
to 4 weeks after inoculation that breaks down into a firm, non-
healing, shallow, nontender, undermined ulcer with a granulo-
matous base. Painless regional lymphadenopathy is a cardinal
sign, appearing after about 3 to 8 weeks. Numerous bacilli are
demonstrable at the inoculation site and regional lymph node.
The ultimate ulceroglandular lesion is a “mirror image” of the
Ghon’s complex. Its clinical course varies according to the host-
immune response.12
The primary lesion heals with scarring after 1 to 3 months;
however, with a less effective host-immune response, the bac-
terial load remains high, and healing may be delayed up to
12 months. Regional nodes may suppurate, erode, and perforate
the surface of overlying skin, resulting in scrofuloderma. Latent
foci of infection may persist at the site and progress to either
LV or TBVC despite evident tuberculin sensitivity. Hematog-
enous dissemination of mycobacteria from skin can result in TB
at other sites, particularly bones or joints, or progress to acute
miliary disease with poor outcome.
SCROFULODERMA (TB COLLIQUATIVE CUTIS)
Scrofuloderma (TB colliquative cutis) is the most common
form of CTB in children. It results from the direct extension
from an underlying TB focus, such as a regional lymph node
or infected bone or joint, to the overlying skin. Lesions present
as firm, painless, subcutaneous, red-brown nodules overlying an
infected focus, which gradually enlarge and suppurate, forming
ulcers and sinus tracts that drain watery, purulent, and/or case-
ous material. The ulcers heal with typical puckered scarring.13
TB CUTIS ORIFICIALIS
The lesions associated with TBCO are frequently characterized
by erythematous, edematous nodules, and/or plaques. Pain-
ful central ulceration covered by necrotic pseudomembranous
material with an irregular border is apparent. Constitutional
symptoms of TBCO include fever, malaise, weight loss, and
night sweats. The oral mucosa and tongue are the most com-
monly afflicted sites.2 The exact mechanism resulting in TBCO
is unknown; however, ingestion of bacilli in sputum from active
pulmonary TB, hematogenous and lymphatic spread, and direct
spread from adjacent organs has been alleged,14 with ingestion
of bacilli in sputum being the most accepted mode.15 There has
been a reported case of isolated perianal TB without pulmonary
or gastrointestinal involvement.16
DISSEMINATED MILIARY TB
Disseminated miliary TB is characterized by a wide dissemi-
nation of M tuberculosis in the body and shows a distinctive
pattern of millet-sized, multiple, tiny lesions on chest x-ray,
distributed throughout the lung fields. It may hematogenously
infect any number of organs including the lungs, liver, and
spleen in patients with advanced TB. There is a systemic fail-
ure of the cell-mediated immune system that allows and facili-
tates the spread of infection, resulting in rapid deterioration
and death.4,17,18 Certain events, infections, and medications
that suppress the body’s cell-mediated immune system may
precipitate this infection. Although miliary TB is rare and
well known for its occurrence in children, it is an increasingly
serious infection in immunosuppressed patients, such as those
infected with HIV and those on long-term oral corticoste-
roid therapy or other immunosuppressive therapies for organ
transplant or inflammatory and autoimmune conditions.
Cutaneous skin lesions associated with miliary TB consist of
small, erythematous to violaceous papules or pustules with
hemorrhagic necrosis and umbilication affecting a substantial
portion of the body. Healing is indicated by the presence of
atrophic, depressed scars surrounded by a brownish, hyperpig-
mented halo.
METASTATIC TUBERCULOUS ABSCESSES (GUMMA)
Metastatic tuberculous abscesses (gumma) may either arise
from the breakdown of an old healed tubercle that still has
live organisms or in immunocompromised individuals.2,4
Accordingly, it is usually seen in malnourished children and
immunosuppressed adults.6 Single or multiple, nontender, fluc-
tuant nodules develop, forming draining sinuses and abscesses
(Figure 1). Nodules may occur at any location without specific
predominance.
Figure 1. Metastatic tuberculous abscesses (gumma): a single, nontender, fluctuant nodule, draining sinus is apparent.
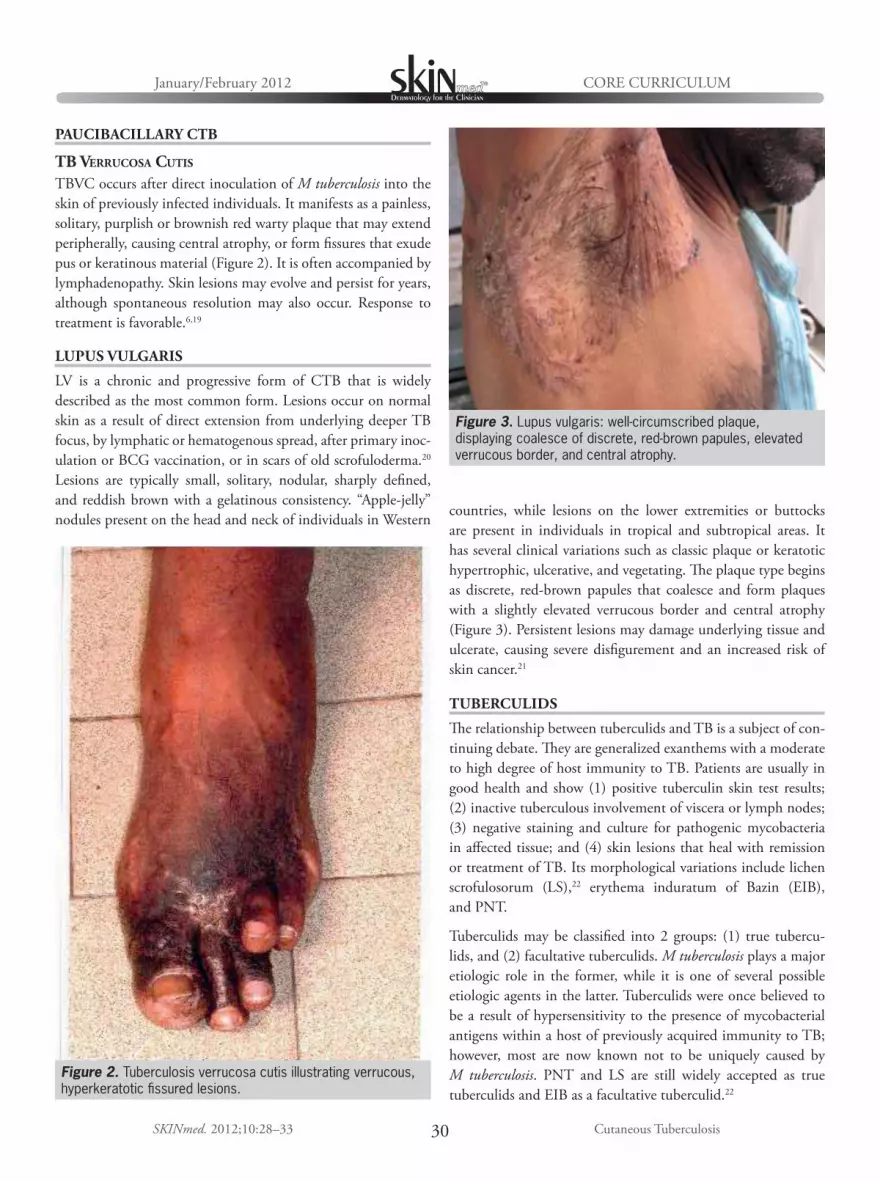
CORE CURRICULUMJanuary/February 2012
30SKINmed. 2012;10:28–33 Cutaneous Tuberculosis
PAUCIBACILLARY CTB
TB VERRUCOSA CUTIS
TBVC occurs after direct inoculation of M tuberculosis into the
skin of previously infected individuals. It manifests as a painless,
solitary, purplish or brownish red warty plaque that may extend
peripherally, causing central atrophy, or form fissures that exude
pus or keratinous material (Figure 2). It is often accompanied by
lymphadenopathy. Skin lesions may evolve and persist for years,
although spontaneous resolution may also occur. Response to
treatment is favorable.6,19
LUPUS VULGARIS
LV is a chronic and progressive form of CTB that is widely
described as the most common form. Lesions occur on normal
skin as a result of direct extension from underlying deeper TB
focus, by lymphatic or hematogenous spread, after primary inoc-
ulation or BCG vaccination, or in scars of old scrofuloderma.20
Lesions are typically small, solitary, nodular, sharply defined,
and reddish brown with a gelatinous consistency. “Apple-jelly”
nodules present on the head and neck of individuals in Western countries, while lesions on the lower extremities or buttocks
are present in individuals in tropical and subtropical areas. It
has several clinical variations such as classic plaque or keratotic
hypertrophic, ulcerative, and vegetating. The plaque type begins
as discrete, red-brown papules that coalesce and form plaques
with a slightly elevated verrucous border and central atrophy
(Figure 3). Persistent lesions may damage underlying tissue and
ulcerate, causing severe disfigurement and an increased risk of
skin cancer.21
TUBERCULIDS
The relationship between tuberculids and TB is a subject of con-
tinuing debate. They are generalized exanthems with a moderate
to high degree of host immunity to TB. Patients are usually in
good health and show (1) positive tuberculin skin test results;
(2) inactive tuberculous involvement of viscera or lymph nodes;
(3) negative staining and culture for pathogenic mycobacteria
in affected tissue; and (4) skin lesions that heal with remission
or treatment of TB. Its morphological variations include lichen
scrofulosorum (LS),22 erythema induratum of Bazin (EIB),
and PNT.
Tuberculids may be classified into 2 groups: (1) true tubercu-
lids, and (2) facultative tuberculids. M tuberculosis plays a major
etiologic role in the former, while it is one of several possible
etiologic agents in the latter. Tuberculids were once believed to
be a result of hypersensitivity to the presence of mycobacterial
antigens within a host of previously acquired immunity to TB;
however, most are now known not to be uniquely caused by
M tuberculosis. PNT and LS are still widely accepted as true
tuberculids and EIB as a facultative tuberculid.22
Figure 2. Tuberculosis verrucosa cutis illustrating verrucous, hyperkeratotic fissured lesions.
Figure 3. Lupus vulgaris: well-circumscribed plaque, displaying coalesce of discrete, red-brown papules, elevated verrucous border, and central atrophy.

Cutaneous Tuberculosis
CORE CURRICULUMJanuary/February 2012
31SKINmed. 2012;10:28–33
LICHEN SCROFULOSORUM
LS is an eruption of multiple, small, grouped, asymptomatic,
firm, perifollicular, lichenoid papules and/or plaques (Figure
4), most often affecting children or young adults, that pro-
gresses and subsides within weeks to months without scar-
ring.4,23 An association between LV, caries of the spine, LS,24
and its unusual occurrence in pulmonary TB25 has been
described in the past.
ERYTHEMA INDURATUM OF BAZIN
EIB is a TB-associated panniculitis that presents with multi-
ple, painful, recurring, ulcerated nodules that affect the legs of
women.4,6 Pre-existing vascular disease may predispose patients
to lesions during exposure to cold weather. Lesions are chronic,
slow to resolve (if at all), and result in atrophic hyperpigmented
scarring after several months (Figure 5). Although patients show
TB skin hypersensitivity, acid-fast bacilli (AFB) are rarely identi-
fied. A study from Spain demonstrated that about 10% of cases
were positive for M tuberculosis using polymerase chain reaction
(PCR).26 A case series and literature review revealed that organ-
isms, such as Mycobacterium bovis and Mycobacterium mari-
num, may also be involved in the etiology of EIB, although no
evidence of such was found during the investigation. It was
suggested that EIB has diverse etiologies with varying patho-
genesis, leading to similar histological changes, and the cases
analyzed may not have had an infectious etiology (suggesting a
facultative tuberculid picture).27
PAPULONECROTIC TUBERCULID
Papulonecrotic tuberculid occurs as a chronic and recurrent sym-
metric eruption of necrotizing skin papules appearing in clusters
and healing with varioliform scars (Figure 6). Tubercle bacilli are
difficult to demonstrate, but patients typically have an internal
focus of TB and are tuberculin sensitive, and skin lesions resolve
after anti-TB therapy. TB DNA has been detected in these
lesions using PCR amplification reactions.28 Lesions appear on
the exterior aspects of extremities, knees, elbows, buttocks, and
lower trunk in a symmetric distribution, often in clusters. Indi-
vidual lesions are asymptomatic, small, dusky red papules with
a central punctum or crust. Involution is common after 6 to 8
weeks.29
DIAGNOSIS
Diagnosis of CTB is based on relative and absolute criteria, in
addition to supportive immunologic evidence.30
Figure 5. Erythema induratum occupying the lower leg. Figure 6. Papulonecrotic tuberculid.
Figure 4. Lichen scrofulosorum: multiple, small, grouped, firm, perifollicular, lichenoid papules and/or plaques.

CORE CURRICULUMJanuary/February 2012
32SKINmed. 2012;10:28–33 Cutaneous Tuberculosis
RELATIVE DIAGNOSIS
CARDINAL MORPHOLOGIC FEATURES (VIDE SUPRA)A characteristic history of evolution of the disease is distinct
in re-infection and re-activation. In re-infection, a history
of primary infection or BCG vaccination must be obtained.
The latter forms an important component of the immuniza-
tion program in some countries, including India, and may be
identified by a BCG vaccination scar at the insertion point on
the left deltoid. In re-activation, on the other hand, a history
of TB, established by clinical and/or investigative procedures,
followed by cure and an asymptomatic period on completion
of specific anti-tubercular therapy. Often, the only evidence
of past infection may be pulmonary scarring and calcification
visible on radiography. Subsequently, any event that lowers
the cell-mediated immunity may re-activate the condition,
resulting in its relapse.
MANTOUX TEST
A positive Mantoux test indicates the cell-mediated skin hyper-
sensitivity to tuberculin. The response in re-infection may be
higher as compared with that in re-activation TB. This in vivo
test correlates well with the migratory index of lymphocytes to
tuberculin antigen, assayed through leukocyte migration inhi-
bition test. A strongly positive reaction, however, indicates
active TB. It has only a limited diagnostic application in coun-
tries where the infection is highly prevalent and BCG forms an
integral part of the immunization program and the majority of
adults are tuberculin positive; nevertheless, it may be a useful
adjunct in developed countries.
Microscopic examination of the tissue section may depict a
tuberculoid and tuberculous granuloma. The former, charac-
terized by a focal accumulation of epithelioid cells, a few giant
cells, and surrounding mantle of mononuclear cells, is a relative
parameter encountered in LV and TBVC. It also demonstrates
caseation necrosis in the center. It may be possible to demon-
strate AFB on Fite’s stain. This granuloma fulfills an absolute
criterion for diagnosis of TB and typifies scrofuloderma.
ABSOLUTE DIAGNOSIS
An absolute diagnosis consists in the demonstration of AFB on
Ziehl-Neelsen’s staining of the smear, prepared from material
from lesions. The colonies should be further subjected to bio-
chemical and pigment production tests to confirm M tuberculosis.
Recovery of M tuberculosis on inoculation of material from
lesions into guinea pigs.
In an effort to achieve universal access to high-quality diagnosis
and ultimate patient-centered treatment as envisaged by World
Health Organization (WHO), it is important to be aware of the
diagnostic modalities thus far available in the global arena.31
NONTUBERCULOUS MYCOBACTERIA
Physicians should be aware of nontuberculous mycobacteria
(NTMB) in the current context, because they are environmental
organisms capable of causing chronic disease in humans world-
wide. The prevalence of NTMB disease is steadily increasing and
has emerged in previously unrecognized populations. They, too,
are a diagnostic challenge.32 TB verrucosa cutis–like lesions may
be caused by M bovis.33
ATYPICAL MYCOBACTERIOSIS
Mycobacterium avium-intracellulare (MAI) is now a well-
established cause of cervical lymphadenitis, simulating scrofu-
loderma, especially in the pediatric age group in the developed
world.34 In addition, LV-like morphology may also be encoun-
tered following primary MAI infection.35
HIV INFECTION AND CTB
HIV-infected patients are vulnerable to contract TB.36 TB may pres-
ent as a rapidly progressive disease in immunosuppressed patients.
Miliary TB is common and may be associated with cutaneous
manifestations.37 Disseminated CTB may show a high yield of
mycobacterium from an unusual dermatitis in this group. Despite
the dissemination of the organism, the diagnosis of TB may be dif-
ficult.38,39 In addition, atypical presentations of oesophago-pleuro-
cutaneous and pleuro-cutaneous fistula may be seen.40,41
In addition to the decrease in tuberculin reactivity, atypical
chest radiographic patterns are common. Biopsy and aspirates
of peripheral and regional lymph nodes, liver, and bone mar-
row provide the highest yield and are used for early diagnosis.42
Co-lesional acquired immunodeficiency syndrome– associated
cutaneous Kaposi’s sarcoma and M tuberculosis–associated
granulomatous inflammation have recently been documented.43
Tuberculous gumma, new-onset cervical lymphadenopathy, and
worsening of the pre-existing lymphadenitis, yet another high-
risk immune reconstitution inflammatory syndrome, has previ-
ously been described.44
CONCLUSIONS
Reviewing the prevalence and variations in the clinical expres-
sion of CTB across the globe may assist in evolving a uniform
pattern of the disease vital for a core curriculum. The compre-
hension of the text is, therefore, crucial in developing treat-
ment strategy through the recommendations of WHO. WHO
believes that the same treatment regimen for pulmonary and/or
extrapulmonary TB should be used.45

Cutaneous Tuberculosis
CORE CURRICULUMJanuary/February 2012
33SKINmed. 2012;10:28–33
REFERENCES
1 Sehgal VN, Wagh SA. The history of cutaneous tuberculosis. Int J Dermatol. 1990;29:666–668.
2 Bravo FG, Gotuzzo E. Cutaneous tuberculosis. Clin Dermatol. 2007;25:173–180.
3 Fariña MC, Gegundez MI, Piqué E, et al. Cutaneous tuberculosis: a clinical, histopathologic, and bacteriologic study. J Am Acad Dermatol. 1995;33:433–440.
4 MacGregor RR. Cutaneous tuberculosis. Clin Dermatol. 1995;13:245–255.
5 Bhutto AM, Solangi A, Khaskhely NM, et al. Clinical and epidemiological observations of cutaneous tuberculosis in Larkana, Pakistan. Int J Der-matol. 2002;41:159–165.
6 Barbagallo J, Tager P, Ingleton R, et al. Cutaneous tuberculosis: diagno-sis and treatment. Am J Clin Dermatol. 2002;3:319–328.
7 Regnier S, Ouagari Z, Perez ZL, et al. Cutaneous miliary resistant tuber-culosis in a patient infected with human immunodeficiency virus: case report and literature review. Clin Exp Dermatol. 2009;34:e690–e692.
8 Rai VM, Shenoi SD, Gowrinath. Tuberculous gluteal abscess coexisting with scrofuloderma and tubercular lymphadenitis. Dermatol Online J. 2005;11:14.
9 Lai-Chong JE, Perez A, Tang V, et al. Cutaneous manifestations of tuber-culosis. Clin Exp Dermatol. 2007;32:461–466.
10 Glickman FS, Price E. Primary inoculation complex (tuberculous chan-cre). Arch Dermatol. 1969;100:646–647.
11 Ara M, Seral C, Baselga C, et al. Primary tuberculous chancre caused by Mycobacterium bovis after goring with a bull’s horn. J Am Acad Derma-tol. 2000;43:535–537.
12 Mataix J, Botella R, Herrero A, et al. Tuberculous primary complex of the skin. Int J Dermatol. 2008;47:479–481.
13 Kiliç A, Gül U, Soylu S, et al. Scrofuloderma: a forgotten disease? Skinmed. 2007;6:303–304.
14 Sharma MP, Bhatia V. Abdominal tuberculosis. Indian J Med Res. 2004;120:305–315.
15 Ichihashi K, Katoh N, Takenaka H, et al. Orificial tuberculosis: presenting as a refractory perianal ulcer. Acta Derm Venereol. 2004;84:331–332.
16 Akgun E, Tekin F, Ersin S, et al. Isolated perianal tuberculosis. Neth J Med. 2005;63:115–117.
17 Sehgal VN, Sharma S, Verma P, et al. Disseminated cutaneous tubercu-losis an atypical presentation of re-infection (secondary) tuberculosis in an immuno-competent individual. Am J Dermatopathol. 2011. Sep 13. [Epub ahead of print]
18 Regnier S, Ouagari Z, Perez ZL, et al. Cutaneous miliary resistant tuber-culosis in a patient infected with human immunodeficiency virus: case report and literature review. Clin Exp Dermatol. 2009;34:e690–e692.
19 Afshar K, Mundi M. Tuberculosis verrucosa cutis. Mayo Clin Proc. 2004;79:1562.
20 Marcoval J, Servitje O, Moreno A, et al. Lupus vulgaris. Clinical, histo-pathologic, and bacteriologic study of 10 cases. J Am Acad Dermatol. 1992;26:404–407.
21 Akoglu G, Karaduman A, Boztepe G, et al. A case of lupus vulgaris suc-cessfully treated with antituberculous therapy despite negative PCR and culture. Dermatology. 2005;211:290–292.
22 Frankel A, Penrose C, Emer J. Cutaneous tuberculosis: a practical case report and review for the dermatologist. J Clin Aesthet Dermatol. 2009;2:19–27.
23 Singal A, Bhattacharya SN. Lichen scrofulosorum: a prospective study of 39 patients. Int J Dermatol. 2005;44:489–493.
24 Sehgal VN, Srivastava G, Sharma VK. Lupus vulgaris, caries of the spine and lichen scrofulosorum—an intriguing association. Clin Exp Dermatol. 1987;12:280–282.
25 Seghal VN, Chander R, Logani K. Lichen scrofulosorum: an unusual expression of pulmonary tuberculosis in a child. J Eur Acad Dermatol Venereol. 1995;4:71–74.
26 Vieites B, Suárez-Peñaranda JM, Pérez Del Molino ML, et al. Recovery of Mycobacterium tuberculosis DNA in biopsies of erythema induratum—results in a series of patients using an improved polymerase chain reac-tion technique. Br J Dermatol. 2005;152:1394–1396.
27 Bayer-Garner IB, Cox MD, Scott MA, et al. Mycobacteria other than Mycobacterium tuberculosis are not present in erythema induratum/nodular vasculitis: a case series and literature review of the clinical and histologic findings. J Cutan Pathol. 2005;32:220–226.
28 Quirós E, Bettinardi A, Quirós A, et al. Detection of mycobacterial DNA in papulonecrotic tuberculid lesions by polymerase chain reaction. J Clin Lab Anal. 2000;14:133–135.
29 Freiman A, Ting P, Miller M, et al. Papulonecrotic tuberculid: a rare form of cutaneous tuberculosis. Cutis. 2005;75:341–346.
30 Sehgal VN. Cutaneous tuberculosis. Dermatol Clin. 1994;12:645–653.
31 The Regional Strategic Plan for TB Control 2006–2015. World Health Organization, Regional Office for South-East Asia, World Health House, Indraprastha Estate, Mahatma Gandhi Road, New Delhi 110002, India.
32 Griffith DE, Aksamit T, Brown-Elliott BA, et al. An official ATS/IDSA state-ment: diagnosis, treatment, and prevention of non tuberculous mycobac-terial diseases. Am J Respir Crit Care Med. 2007;175:367–416.
33 Wolff K, Tappeiner G. Mycobacterial diseases: tuberculosis and atypical mycobacterial infection. In: Fitzpatrick TB, Eisen AZ, Wolff K, eds. Dermatology in General Medicine. 3rd ed. New York, NY: McGraw Hill; 1987:2152–2170.
34 Starke JR. Management of nontuberculous mycobacterial cervical adeni-tis. Pediatr Infect Dis J. 2000;19:674–675.
35 Kullavanijaya P, Sirimachan S, Surarak S. Primary cutaneous infec-tion with Mycobacterium avium intracellulare complex resembling lupus vulgaris. Br J Dermatol. 1997;136:264–266.
36 Starke JR. Tuberculosis. In: Jenson HB, Baltimore RS, eds. Pediatric Infectious Diseases: Principles and Practices. Philadelphia, PA: WB Saunders; 2002:396–419.
37 Sharma SK, Mohan A, Sharma A, et al. Miliary tuberculosis: new insights into an old disease. Lancet Infect Dis. 2005;5:415–430.
38 Regnier S, Ouagari Z, Perez ZL, et al. Cutaneous miliary resistant tuber-culosis in a patient infected with human immunodeficiency virus: case report and literature review. Clin Exp Dermatol. 2009;34:e690-e692.
39 Corbett EL, Crossley I, De Cock KM, et al. Disseminated cutaneous Mycobacterium tuberculosis infection in a patient with AIDS. Genitourin Med. 1995;71:308–310.
40 Arif M. Oesophago-pleuro-cutaneous fistula in an HIV-positive patient. Braz J Infect Dis. 2010;14:183–185.
41 Gulinelli A, Toledo DO, Coelho-Neto AP, et al. Parasternum pleural- cutaneous fistula in a severely immunosuppressed HIV-positive patient. Braz J Infect Dis. 2010;14:183–185.
42 Shafer RW, Kim DS, Weiss JP, Quale JM. Extrapulmonary tuberculosis in patients with human immunodeficiency virus infection. Medicine (Baltimore). 1991;70:384–397.
43 Ramdial PK, Sing Y, Subrayan S, et al. Granulomas in acquired immunodeficiency syndrome-associated cutaneous Kaposi sarcoma: evidence for a role for Mycobacterium tuberculosis. J Cutan Pathol. 2010;37:827–834.
44 Sharma SK, Dhooria S, Barwad P, et al. A study of TB-associated immune reconstitution inflammatory syndrome using the consensus case-definition. Indian J Med Res. 2010;131:804–808.
45 World Health Organization. Treatment of tuberculosis guidelines. Treatment of extrapulmonary TB and of TB in special situations. 4th ed. Geneva 27, Switzerland; 2009: 95–99.
January/February 2012
34 © 2012 Pulse Marketing & Communications, LLC
Volume 10 • Issue 1
SELF-TEST REVIEW QUESTIONSW. Clark Lambert, MD, PhD, Section EditorInstructions: For each of the following numbered questions, choose the most appropriate lettered response(s) Unless directed to choose only one lettered response, all, some, or none of the responses may be correct.
1) Exogenous inoculation, due to the direct inoculation of Myco-
bacterium tuberculosis into the skin of a person who is sus-
ceptible to infection, may be responsible for: (Answer as
many as apply.)
a. acute military tuberculosis.
b. gummatous tuberculosis.
c. lupus vulgaris.
d. papulo-necrotic tuberculid.
e. tuberculous chancre.
f. tuberculosis verrucosa cutis.
2) Exogenous inoculation, due to the direct inoculation of Myco-
bacterium tuberculosis into the skin of a person who has
been previously infected but is susceptible to infection, is
most likely to be responsible for: (Choose the single best
response.)
a. acute military tuberculosis.
b. gummatous tuberculosis.
c. lupus vulgaris.
d. papulo-necrotic tuberculid.
e. tuberculous chancre.
f. tuberculosis verrucosa cutis.
3) Which of the following is widely described as the most com-
mon form of cutaneous tuberculosis? (Choose the single best
response.)
a. Acute military tuberculosis
b. Gummatous tuberculosis
c. Lupus vulgaris
d. Papulo-necrotic tuberculid
e. Tuberculous chancre
f. Tuberculosis verrucosa cutis
4) The most accepted mode of development of tuberculosis
cutis oroficialis is: (Choose the single best response.)
a. direct spread from adjacent organs.
b. hematogenous spread.
c. ingestion of bacilli in sputum.
d. lymphatic spread.
e. exogenous inoculation due to the direct inoculation of
Mycobacterium tuberculosis into the skin/mucosa of a
person who is susceptible to infection.
5) “Apple-jelly” nodules present on the head and neck of individu-
als in Western countries are most characteristic of: (Choose
the single best response.)
a. erythema induratum of Bazin.
b. lichen scrofulosorum.
c. lupus vulgaris.
d. papulonecrotic tuberculid.
e. tuberculosis verrucosa cutis.
ANSWERS TO SELF-TEST REVIEW QUESTIONS:
1) c, e, f; 2) f; 3) c; 4) c; 5) c
From the Departments of Pathology and Dermatology, UMDNJ-New Jersey Medical School, Newark, NJ
Address for Correspondence: W. Clark Lambert, MD, PhD, Room C520 MSB, UMDNJ-NJMS, 185 South Orange Avenue, Newark, NJ 07101 • E-mail: [email protected]
RESTLESS LEG SYNDROME
Drugs that may cause restless leg syndrome (RLS)
Alcohol Haldol Prozac Topamax
Caffeine Iron Remeron Ultram
Celexa Klonopin Risperdal Zoloft
Dilantin Neurotin Seroquel Zyprexa
Elavil Paxil
Adapted from Litt, JZ. Curious, Odd, Rare, and Abnormal Reactions to Medications. Fort Lee, NJ: Barricade Books; 2009:107.

Arnika Forte®
SPEED THE HEALING
Arnika Forte®
The New Gold Standardfor treating bruising,swelling, pain
1st and only combination of Arnica Montana 30x and Bromelain
One convenient capsuletwice a day
All natural, safe,physician - formulated
Speed the healing timefrom bruising, swelling andpain after surgery or dermalfiller injections
To Order Call 484-568-0306
�
�
�

January/February 2012 Volume 10 • Issue 1
36SKINmed. 2012;10:36–39 © 2012 Pulse Marketing & Communications, LLC
COSMETIC SCIENCEHoward A. Epstein, PhD, Section Editor
Repelling Insects With Safe and Effective Alternatives to DEET
Howard A. Epstein, PhD
In addition to the annoying itch that results from biting
insects, insect-borne diseases, including Lyme disease,
encephalitis, Rocky Mountain spotted fever, and West Nile
virus, are all causes of concern for many individuals who wish to
enjoy the outdoor environment during the warmer months of the
year. The military of various nations experienced the same prob-
lems and have conducted much research in developing repellents
to protect their soldiers. The Indian Army used oils of citronella,
camphor, and paraffin as repellents. These agents were effective
for limited periods and therefore the search for more effective
repellents continued. In 1953, N, N-diethyl-m-toluamide
(DEET) was discovered (Figure 1). As of 2007, it was estimated
that 15 million people in the United Kingdom, 78 million peo-
ple in the United States, and 200 million people globally use
DEET each year.1 Over the years, as cases of insect-borne dis-
eases continued to be reported in the news, so has the use of
DEET. Reports of adverse reactions associated with DEET have
increased with its use.
HEALTH-RELATED ISSUES AND CONSUMER CONCERNS
In 2004, the Oregon State University (OSU) Agricultural Experi-
ment Station issued a press release entitled “OSU Scientist Gives
Safety Tips for Use of DEET Against Mosquitoes & West Nile
Virus.” In the release, Dr Damiel Sudakin, an assistant professor
at OSU’s Department of Environmental and Molecular Toxicology
and toxicologist at the Agricultural Experiment Station was quoted
as expressing concern that hundreds of adverse reactions, most com-
monly affecting the skin, are reported each year. The majority of
these adverse reactions occur when DEET is overused or misused.2
In 2009, Science Daily published a paper entitled “Popular Insect
Repellent DEET Is Neurotoxic.”3 The contribution referenced a
study that concluded that DEET is not simply a behavior-modifying
chemical, but also inhibits the activity of a key central nervous sys-
tem enzyme, acetylcholinesterase, in both insects and mammals.4
In 2004, the Agency for Toxic Substances & Disease Registry issued
a report on the health effects of DEET in humans. The report men-
tioned 6 cases of DEET ingestion, 3 led to death after ingestion
of 15 mL to 50 mL of 47.5% to 95% DEET filled in bottles. In
2 of these cases, the individuals drank an unspecified amount of
alcohol. In the third case, the individual ingested an unspecified
number of pills with 50 mL of DEET. In yet another case, a woman
ingested 15 mL to 25 mL of 95% DEET and was admitted to a
hospital with right and left atrial enlargement that returned to nor-
mal within 24 hours. This woman survived with no further cardiac
abnormalities.5 From 1961 to 2002, the Agency reported 8 deaths
related to DEET exposure, 3 resulting from deliberate ingestion,
and 2 following dermal exposure to DEET. The remaining 3 cases
were girls aged 17 months, 5 years, and 6 years. All 3 children were
described as having “heavy, frequent, or nightly applications of
DEET.” The 6-year-old had congenital ornithine carbamoyl trans-
ferase deficiency, which may have contributed to her death.5 Two
other reported cases involved 2 men, aged 27 and 30 years, who
developed severe psychological effects from exposure to DEET. In
both cases, the men recovered after hospitalization.5
MILITARY AND GOVERNMENT PERSONNEL: DERMAL EFFECTS OF DEET EXPOSURE
Unique cutaneous side effects were reported in 15 soldiers who
applied military-issued DEET repellents. One soldier applied a
33% DEET repellent to his skin without washing it off at bedtime.
He developed a vesiculobullous eruption, which cleared after
14 days. Another soldier who went to bed without removing
DEET applied to his skin woke up 8 hours later complaining of
a burning sensation and skin eruptions. A 10-day treatment with
corticosteroids cleared the condition. Other soldiers reported
burning skin and erythema after application of 50% DEET
solution applied just before bedtime. Three soldiers were referred
to treatment by a dermatologist: 2 of the soldiers developed a
permanent scar and 1 required corrective surgery.5
From EMD Chemicals Inc, Gibbstown, NJ
Address for Correspondence: Howard A. Epstein, PhD, EMD Chemicals Inc, One International Plaza, Suite 300, Philadelphia, PA 19113 • E-mail: [email protected]

Alternatives to DEET
COSMETIC SCIENCEJanuary/February 2012
37SKINmed. 2012;10:36–39
Other controlled studies in which DEET was applied to 63 vol-
unteers with a gauze pad soaked in DEET determined that DEET
should be washed from skin prior to sleeping directly related to the
irritant effects of DEET.5 Additional studies involving 143 National
Park Service employees at Everglades National Park resulted in 36
of the workers having adverse health effects to the applied DEET.
The effects included skin or mucous membrane irritation, transient
numb or burning lips, dizziness, disorientation, and difficulty in
concentration. Headache and nausea were also reported.5
MULTIPLE CASE STUDIES OF DEET EXPOSURE
An analysis of phone calls to poison control centers in the United
States from 1985 to 1989 represented more than 6 million human
exposures to a variety of chemicals. Of these, 9086 were related to
DEET. Of the DEET-related calls, 54% of patients had no symp-
toms at the time of the call and 40% had symptoms thought
to be related to DEET exposure. The most commonly reported
exposure was inhalation of DEET or spray into the eyes. These
exposures were more likely to cause adverse reactions compared
with cases in which small quantities of DEET were ingested. Of
the individuals with symptoms, 88% did not require medical
attention, 35% had minor skin irritation, and 1% experienced
disorientation or brief seizures. There was a reported death from
deliberate consumption of an 8-oz bottle of DEET. Children
were not more likely to develop side effects than adults.5
CASE REPORTS OF CHILD EXPOSURES
During 1961 to 2002, 14 of the 17 reported cases of significant
DEET toxicity were in children younger than 8 years. The most
frequently reported symptoms of DEET toxicity in children
were lethargy, headaches, tremors, involuntary movements, sei-
zures, and convulsions.5 The common route of exposure in chil-
dren is frequently dermal or accidental ingestion. Adverse effects
have been reported in an 18.5-month child who was sprayed
with 20% DEET daily for 3 months and a 6-year-old who was
sprayed with 15% DEET on 10 occasions. Generally, children
recover from exposure. In 1989, there were 4 cases of children
ages 3 to 7 years and a 29-year-old man having generalized
seizures associated with the dermal application of DEET, with
fewer than 3 applications.5
ALTERNATIVES TO DEET
Picaridin, 1-piperidine carboxylic acid-2(2-hydroxxyethyl)-1-
methpropylester (Figure 2) was developed by Bayer in the 1980s.
It is a synthetic molecule chemically based on the active agent
in pepper (Piper sp). Picaridin was first registered with the US
Environmental Protection Agency (EPA) in 2001 and entered
the market in 2005. Picaridin has a favorable safety profile, most
likely because the compound has not been as commercially
available for as long as DEET, and therefore there is far less infor-
mation regarding adverse reactions.
The first report of a contact allergy during commercial use was
reported in 2005, in which a 39-year-old man experienced an
itchy erythematous reaction to a spray a few hours after applica-
tion to the skin.1 Australian soldiers evaluated 19.2% Picaridin
compared with 35% DEET in a gel formulation, with signifi-
cantly more soldiers reporting mild discomfort and irritation
with the use of the DEET gel. Published studies indicate that
Picaridin may be as effective as DEET. There are variations in
repellent efficacy depending on species of insect and levels of
use. The literature reports that Picaridin is aesthetically more
“elegant” than DEET in various formulations.1 It is registered
for use on the human body and clothing to repel biting flies,
ticks, chiggers, fleas, and mosquitoes.6
NATURAL AND EFFECTIVE ALTERNATIVES
IR3535, [3-(N-acetyl-N-butyl)aminopropionic acid ethyl ester]
(Figure 3) has been marketed by Merck KGaA, Darmstadt,
Germany, for the past 30 years. It was registered by the US EPA
in 1999. IR3535 is unique in that it is classified as a biopesti-
cide repellent. DEET and Picaridin are classified as conventional
insect repellent pesticides. The EPA defines a biopesticide as a
pesticide derived from natural materials including animal, plant,
bacteria, and minerals. Canola oil and baking soda have pesti-
cidal applications and are considered biopesticides.7 Biochemical
pesticides are naturally occurring substances that control pests
Figure 3. Ethyl butylacetylami-nopropionate (IR3535), Chemi-cal Abstracts Service registry number 52304–36–6.
N O
O O
Figure 2. Picaridin, Chemical Abstracts Service registry number 119515–38–7.
NC O
MeO
Et
OHCH2CH2
CH
Figure 1. DEET CAS 134–62–3.
N
O
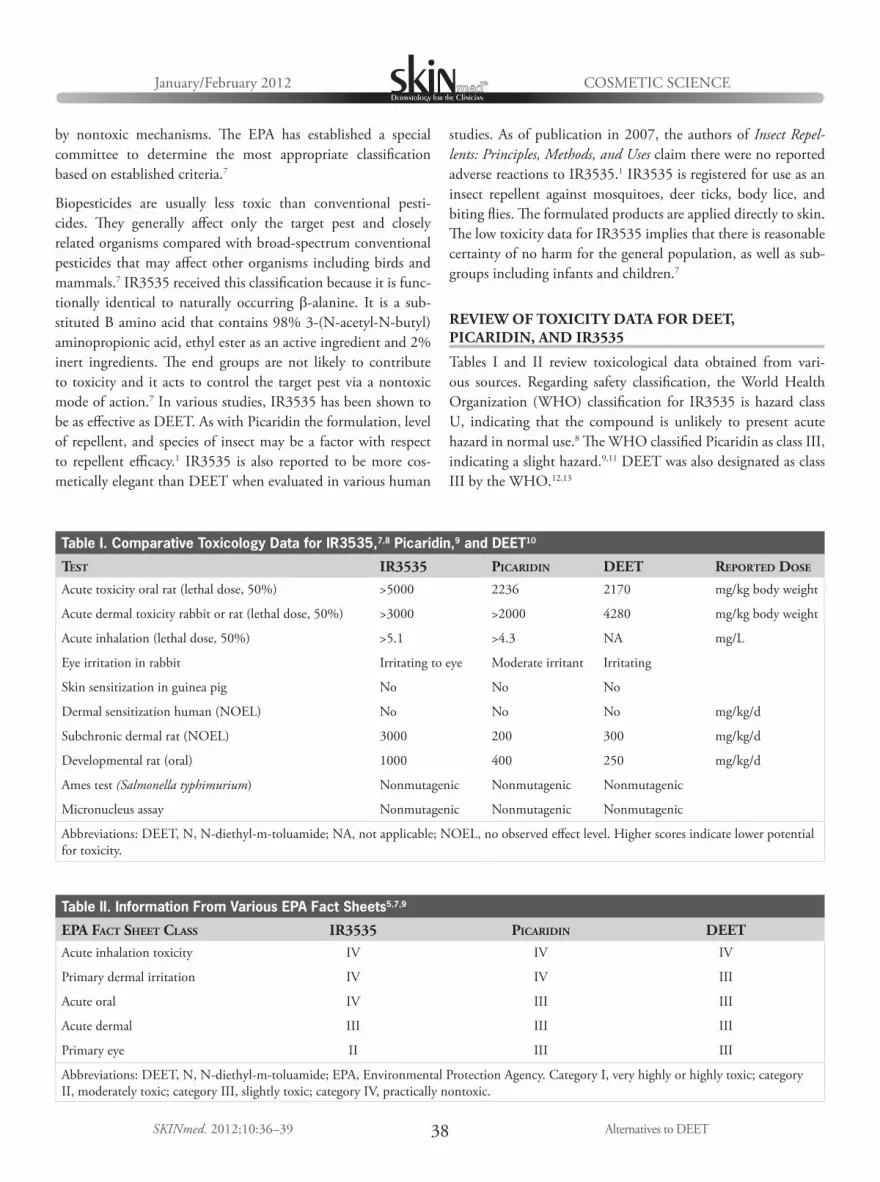
Alternatives to DEET
COSMETIC SCIENCEJanuary/February 2012
38SKINmed. 2012;10:36–39
by nontoxic mechanisms. The EPA has established a special
committee to determine the most appropriate classification
based on established criteria.7
Biopesticides are usually less toxic than conventional pesti-
cides. They generally affect only the target pest and closely
related organisms compared with broad-spectrum conventional
pesticides that may affect other organisms including birds and
mammals.7 IR3535 received this classification because it is func-
tionally identical to naturally occurring b-alanine. It is a sub-
stituted B amino acid that contains 98% 3-(N-acetyl-N-butyl)
aminopropionic acid, ethyl ester as an active ingredient and 2%
inert ingredients. The end groups are not likely to contribute
to toxicity and it acts to control the target pest via a nontoxic
mode of action.7 In various studies, IR3535 has been shown to
be as effective as DEET. As with Picaridin the formulation, level
of repellent, and species of insect may be a factor with respect
to repellent efficacy.1 IR3535 is also reported to be more cos-
metically elegant than DEET when evaluated in various human
studies. As of publication in 2007, the authors of Insect Repel-
lents: Principles, Methods, and Uses claim there were no reported
adverse reactions to IR3535.1 IR3535 is registered for use as an
insect repellent against mosquitoes, deer ticks, body lice, and
biting flies. The formulated products are applied directly to skin.
The low toxicity data for IR3535 implies that there is reasonable
certainty of no harm for the general population, as well as sub-
groups including infants and children.7
REVIEW OF TOXICITY DATA FOR DEET, PICARIDIN, AND IR3535
Tables I and II review toxicological data obtained from vari-
ous sources. Regarding safety classification, the World Health
Organization (WHO) classification for IR3535 is hazard class
U, indicating that the compound is unlikely to present acute
hazard in normal use.8 The WHO classified Picaridin as class III,
indicating a slight hazard.9,11 DEET was also designated as class
III by the WHO.12,13
Table II. Information From Various EPA Fact Sheets5,7,9
EPA FACT SHEET CLASS IR3535 PICARIDIN DEETAcute inhalation toxicity IV IV IV
Primary dermal irritation IV IV III
Acute oral IV III III
Acute dermal III III III
Primary eye II III III
Abbreviations: DEET, N, N-diethyl-m-toluamide; EPA, Environmental Protection Agency. Category I, very highly or highly toxic; category
II, moderately toxic; category III, slightly toxic; category IV, practically nontoxic.
Table I. Comparative Toxicology Data for IR3535,7,8 Picaridin,9 and DEET10
TEST IR3535 PICARIDIN DEET REPORTED DOSE
Acute toxicity oral rat (lethal dose, 50%) >5000 2236 2170 mg/kg body weight
Acute dermal toxicity rabbit or rat (lethal dose, 50%) >3000 >2000 4280 mg/kg body weight
Acute inhalation (lethal dose, 50%) >5.1 >4.3 NA mg/L
Eye irritation in rabbit Irritating to eye Moderate irritant Irritating
Skin sensitization in guinea pig No No No
Dermal sensitization human (NOEL) No No No mg/kg/d
Subchronic dermal rat (NOEL) 3000 200 300 mg/kg/d
Developmental rat (oral) 1000 400 250 mg/kg/d
Ames test (Salmonella typhimurium) Nonmutagenic Nonmutagenic Nonmutagenic
Micronucleus assay Nonmutagenic Nonmutagenic Nonmutagenic
Abbreviations: DEET, N, N-diethyl-m-toluamide; NA, not applicable; NOEL, no observed effect level. Higher scores indicate lower potential
for toxicity.

Alternatives to DEET
COSMETIC SCIENCEJanuary/February 2012
39SKINmed. 2012;10:36–39
CONCLUSIONS
Insect repellents are more effective at higher concentrations. In
addition to the level of actives in the formulation, the degree
of efficacy may be related to the species of insect to be repelled.
Another factor is proper use of the repellent. When there is
concern that label directions for use may not be properly fol-
lowed, the best option is to suggest the compound with the
least hazard risk. The WHO notes that classification criteria are
guide-points intended to supplement but never substitute for
special knowledge, sound clinical judgment, or experience with
a compound.13
REFERENCES
1 Debboun M, Frances SP, Strickman D, eds. Insect Repellents: Principles, Methods, and Uses. Boca Raton, FL: CRC Press; 2006.
2 Gewin V. OSU scientist gives safety tips for use of DEET against mosquitoes & West Nile virus. http://extension.oregonstate.edu/news/release/2004/08/osu-scientist. Accessed June 24, 2011.
3 Science Daily. Popular insect repellant DEET is neurotoxic. http://www.sciencedaily.com/releases/2009/08/090804193230.htm. Accessed June 24, 2011.
4 Corbel V, Stankiewicz M, Pennetier C, et al. Evidence for inhibition of cholinesterases in insect and mammalian nervous systems by the insect repellant deet. BMC Biology. 2009;7:47.
5 Agency for Toxic Substances & Disease Registry Division of Toxicology and Environmental Medicine. Health Effects in Humans: DEET (N,N-Diethyl-meta-toluamide). Atlanta, GA: Agency for Toxic Substances and Disease Registry; December 6, 2004. http://www.atsdr.cdc.gov/con-sultations/deet/health-effects.html. Accessed July 12, 2011.
6 National Pesticide Information Center. Picaridin Technical Fact Sheet. Corvalis, OR: Oregon State University; March 2009. http://npic.orst.edu. Accessed July 14, 2011.
7 United States Environmental Protection Agency. Pesticides: Regulating Pesticides. 3-[N-Butyl-N-acetyl]-aminopropionic acid, ethyl ester (113509) Technical Document. Washington, DC: United States Environmental Protec-tion Agency; February 1999. http://.epa.gov/opp00001/biopesticides/ingredients. Accessed July 13, 2011.
8 World Health Organization. Specifications and Evaluations for Public Health Pesticides. Ethyl Butylacetylaminopropionate also known as IR3535 3-(N-acetyl-N-butyl) aminopropionic acid ethyl ester. Geneva, Switzerland: World Health Organization; February 2006. htt://www.who.int/quality/en/. Accessed July 12, 2011.
9 United States Environmental Protection Agency. EPA New Pesticide Fact Sheet Picaridin. Washington, DC: United States Environmental Protec-tion Agency; May 2005. http://www.epa.gov/opprd001/factsheets/. Accessed July 12, 2011.
10 United States Environmental Protection Agency. Reregistration Eligibility Decision (RED) DEET. Washington, DC: United States Environmen-tal Protection Agency; September 1998. EPA738-R-010.
11 World Health Organization. Specifications and Evaluations for Public Health Pesticides. Icaridin, 1-piperidinecarboxylic acid 2-(2-hydroxxxyethyl)-1-methylpropylester also known as isobutyl piperidine carboxylate. Geneva, Switzerland: World Health Organization; October 2004. http://www.who.int/quality/en/. Accessed July 12, 2011.
12 World Health Organization. International Program on Chemical Safety PCS INCHEM. Data Sheet on Pesticide No. 80 DEET. Geneva, Switzerland: World Health Organization. WHO/VBC/DS/87.80. http://www.inchem.org/documents/pds/pds/pest80. Accessed June 24, 2011.
13 World Health Organization. IPCS, IOMC. The WHO Recommended Classification of Pesticides by Hazard and Guidelines to Classifica-tion 2009. Geneva, Switzerland: World Health Organization; 2010. http://www.who.int/ipcs/publications/pesticides_hazard. Accessed July 12, 2011.
VINTAGE LABEL
Courtesy of BuyEnlarge, Philadelphia, PA

January/February 2012 Volume 10 • Issue 1
40SKINmed. 2012;10:40–41 © 2012 Pulse Marketing & Communications, LLC
From the Departments of Dermatology and Pathology, UMDNJ-New Jersey Medical School, Newark, NJ
Address for Correspondence: W. Clark Lambert, MD, PhD, Room C520 MSB, UMDNJ-NJMS, 185 South Orange Avenue, Newark, NJ 07103 • E-mail: [email protected]
Leiomyosarcoma of the skin is a rare soft tissue neoplasm
of smooth muscle origin. Treatment and prognosis of
this lesion are dependent on its depth, with deep soft tis-
sue tumors carrying a significantly worse prognosis and requir-
ing more extensive surgery than cutaneous ones. It is essential
that all physicians involved know this. It is also critical that the
dermatopathologist report the depth of a leiomyosarcoma in
order for the clinician to render appropriate therapy. Failure to
report the location of this neoplasm and/or failure to compre-
hend the prognostic significance of this information, can lead to
inappropriate therapy and increased morbidity in patients.
CLASSIFICATION
Three classifications of smooth muscle tumors of the skin have
been described1:
• Atypical smooth muscle tumor of the dermis (purely dermal
lesion);
• Cutaneous leiomyosarcoma (dermal lesion with minimal
extension into the subcutis);
• Subcutaneous leiomyosarcoma.2
Microscopically, the cutaneous leiomyosarcoma lesion involves
the dermis and focally, the subcutis. It is composed of blunt-
ended, cigar-shaped fusiform neoplastic spindle cells with eosin-
ophillic cytoplasm forming fascicles and bundles.2–5 This neoplasm
may appear in two different architectural patterns: a fasciculated
growth pattern and a pilar-type architectural pattern (Figure 1 and
Figure 2). The latter generally represents a low-grade neoplasm
showing histologic features suggestive of pilar leiomyoma with the
addition of a variable degree of cytological atypia and mitoses.2
CLINICAL FINDINGS
Cutaneous leiomyosarcomas typically follow an indolent clinical
course. Local recurrence does occur; however, distant metastasis
is uncommon and mortality related to tumor progression
is unusual.2,6–10 In contrast to cutaneous leiomyosarcoma,
subcutaneous leiomyosarcoma presents as a larger mass of a
higher grade. Although still superficially located above the fascia,
the local recurrence rate and metastatic rate of subcutaneous
leiomyosarcoma is closer to the more ominous deep soft tissue
leiomyosarcoma.5,6,11
Based on the differences in their prognoses, investigators pro-
posed the term atypical intradermal smooth muscle neoplasm
instead of cutaneous leiomyosarcoma to highlight the benign
nature of cutaneous leiomyosarcoma vs the more aggressive
soft tissue leiomyosarcoma and subcutaneous leiomyosarcoma.
The same group also argued that grading primary dermal atypi-
cal smooth muscle neoplasms is inappropriate given the fact
that the only prognostic predictor is margin status at the time of
excision and no other reliable prognostic factor has been identi-
fied.5 While we respect these investigators’ opinion, we believe
that thus terming such lesions is a bit like a tail wagging the
dog. We believe it is more sensible to name a tumor in the most
logical way based on its histological features, and subsequently
to note if some subset of these lesions has a different prognosis.
TREATMENT
Treatments for cutaneous and deep soft tissue leiomyosarcoma
differ significantly. Unlike deep soft tissue leiomyosarcoma,
which requires extensive surgery, the standard treatment for
cutaneous leiomyosarcoma and subcutaneous leiomyosarcoma is
wide local excision, with margins ranging from 2 cm to 5 cm.12,13
Mohs’ micrographic surgery (MMS) has also been used for cuta-
neous leiomyosarcomas. This technique can be beneficial as it
provides the ability to examine all margins as the lesion is excised
while sparing normal tissue.9 At this time, only a few small stud-
ies investigating MMS have been reported and further studies
are required to investigate this technique.13–16
PERILS OF DERMATOPATHOLOGYW. Clark Lambert, MD, PhD, Section Editor
It’s Not Just Who You Are, It’s Also Where You Are: The Cutaneous Leiomyosarcoma Dilemma
Gizem Tumer, MD; Carmen F. Castilla, BS; W. Clark Lambert, MD, PhD
“To understand a name you must be acquainted with the particular of which it is a name.”—Bertrard Russell

January/February 2012
41SKINmed. 2012;10:40–41
PERILS OF DERMATOPATHOLOGY
It’s Not Just Who You Are
OBSERVATIONS
Due to the increased risk of metastasis and the worse prognosis of
subcutaneous leiomyosarcoma, an analysis of the subcutaneous
tissue is crucial when the diagnosis of cutaneous leiomyosarcoma
is made. Undergrading of the tumor may occur if a shave biopsy
is utilized to diagnose the lesion.
In contrast to deep soft tissue leiomyosarcomas, which may
require extensive surgery, overly aggressive treatment or mutilat-
ing surgeries are not warranted in cutaneous leiomyosarcoma.
The standard of care for cutaneous leiomyosarcoma remains
wide excisional biopsy; however, recent studies have shown ben-
efits to using MMS.
The dermatopathologist must report the depth of the tumor
and the closest distance from the margin in order to provide the
best therapeutic approach. The clinician must then understand
the significance of this interpretation. Failure to distinguish and
report the exact depth of this neoplasm or a failure of the clini-
cian to understand the significance of this information may lead
to inappropriate and aggressive treatment with excess morbidity.
REFERENCES
1 Hornick JL, Fletcher CD. Criteria for malignancy in nonvisceral smooth muscle tumors. Ann Diagn Pathol. 2003;7;60–66.
2 Massi D, Franchi A, Alos L, et al. Primary cutaneous leiomyosarcoma: clinicopathological analysis of 36 cases. Histopathology. 2010;56:251–262.
3 Mentzel T. Sarcomas in the skin of the elderly. Clin Dermatol. 2011;29:80–90.
4 De Giorgi V, Sestini S, Massi D, et al. Superficial cutaneous leiomyosar-coma: a rare, misleading tumor. Am J Clin Dermatol. 2008;9:185–187.
5 Kraft S, Fletcher CD. Atypical intradermal smooth muscle neoplasms: clinicopathologic analysis of 84 cases and a reappraisal of cutaneous “leiomyosarcoma.” Am J Surg Pathol. 2011;35:599–607.
6 Svarvar C, Böhling T, Berlin O, et al. Clinical course of nonvisceral soft tissue leiomyosarcoma in 225 patients from the Scandinavian Sarcoma Group. Cancer. 2007;109:282–291.
7 Brown MD. Recognition and management of unusual cutaneous tumors. Dermatol Clin. 2000;18:543–552.
8 Ikari Y, Tokuhashi I, Haramoto I, et al. Cutaneous leiomyosarcoma. J Dermatol. 1992;19:99–104.
9 Swanson PE, Stanley MW, Scheithauer BW, Wick MR. Primary cutane-ous leiomyosarcoma: a histological and immunohistochemical study of 9 cases, with ultrastructural correlation. J Cutan Pathol. 1988;15:129–141.
10 Fields JP, Helwig EB. Leiomyosarcoma of the skin and subcutaneous tissue. Cancer. 1981;47:156–169.
11 Massi D, Franchi A, Alos L, Cook M. Primary cutaneous leiomyosarcoma: clinicopathological analysis of 36 cases. Histopathology. 2010;56:251–262.
12 Tsut Sumido A, Yoshida T, Yamamoto Y, Itoh T. Management of superfi-cial leiomyosarcoma: a retrospective study of 10 cases. Plast Reconst Surg. 2005;116:8–12.
13 Humphreys TR, Finkelstein DH, Lee JB. Superficial leiomyosarcoma treat-ed with Mohs micographic surgery. Dermatol Surg. 2004;30:108–112.
14 Starling J 3rd, Coldiron BM. Mohs micrographic surgery for the treat-ment of cutaneous leiomyosarcoma. J Am Acad Dermatol. 2011;64:1119–1122.
15 Huether MJ, Zitelli JA, Brodland DG. Mohs micographic surgery for the treatment of spindle tumors of the skin. J Am Acad Dermatol. 2001;44:656–659.
16 Annest NM, Grekin SJ, Stone MS, Messingham MJ. Cutaneous leiomyosar-coma: a tumor of the head and neck. Dermatol Surg. 2007;33:628–633.
Figure 2. Spindle cell lesion with areas of mitosis (arrowheads).Figure 1. Subcutaneous skin biopsy of tumor cells composed of cigar-shaped spindle cells with mitotic figures (black arrows) (hematoxylin-eosin stain, original magnification ×20).

January/February 2012
42SKINmed. 2012;10:42–43
From the Department of Veterans Affairs Medical Center, Dayton, OH,1 and the Department of Medicine, Wright State University School of Medicine, Dayton, OH2
Address for Correspondence: Jack M. Bernstein, MD, Research (151), VA Medical Center, 4100 West Third Street, Dayton, OH 45428
INFECTIOUS DISEASE CAPSULEJack M. Bernstein, MD, Section Editor
It May Be Vulgar, but It Isn’t a Bad Word1,2 2 Jack M. Bernstein, MD1,2
A
-
-
-
and
-1
2
3
1
CLINICAL MANIFESTATIONS
4
-3
-
4
1
DIAGNOSIS
-
-
-
4
4
TREATMENT
8
Mycobacterium tuberculosis
3
CONCLUSIONS
-

January/February 2012
43SKINmed. 2012;10:42–43
REFERENCES1
J Am Acad Dermatol.
2 Dermatology in General
Medicine.
3 Int J Tuberc Lung Dis.
4
Int J Dermatol.
5 Int J Dermatol.
6
MMWR Recomm Rep.
7 JAMA.
8 N Engl J Med.
Figure 3. Figure 1.
Figure 2.



January/February 2012 Volume 10 • Issue 1
46SKINmed. 2012;10:46–47 © 2012 Pulse Marketing & Communications, LLC
From the Division of Dermatology, Medical College of Georgia, Augusta, GA
Address for Correspondence: Travis W. Blalock, MD, Medical College of Georgia, Division of Dermatology, 1004 Chafee Avenue, Augusta, GA 30904 • E-mail: [email protected]
The term dermatosis neglecta was originally coined in
1995 when three cases of an “unwashed dermato-
sis” were presented by L. Poskitt and colleagues.1
In all cases, the patients committed what Poskitt described
as “acts of omission” by failing to wash their skin in the
affected areas. The resulting hyperpigmented, hyperkeratotic
dermatosis resolved by vigorously washing with soap and
water or, in severe areas, by applying 5% salicylic acid in
aqueous cream twice daily. Our patient had a severe case that
responded well to salicylic acid followed by routine washing.
Because the patient was subsequently lost to follow-up, we were
unable to evaluate hair regrowth.
Periodic shedding of the outermost cellular layers is an essen-
tial component of normal keratinocyte development. In the
stratum corneum, protein-rich, lipid-depleted keratinocytes
are the “bricks” that are held together by hydrophobic intercel-
lular membranes and desmosomes, making up the “mortar.”2,3
Genetic defects in this system—either in the keratinocytes them-
selves or their intercellular molding—can lead to abnormal re-
tention of stratum corneum, causing disorders such as ichthyosis
vulgaris and recessive X-linked ichthyosis. Ichthyosis vulgaris
is caused by defective profilaggrin, a keratinocyte protein, and
recessive X-linked ichthyosis is caused by a deficiency in steroid
sulfatase, an enzyme in the intercellular domain.4 These genetic
abnormalities of adherent stratum corneum illustrate the impor-
tance of regular shedding of superficial keratinocyte layers.
Dermatosis neglecta represents a failure to cleanse adequately a
particular area of skin, leading to the buildup of adherent hyper-
pigmented scales. Thus, dermatosis neglecta can be understood
as a self-induced “defect” in normal keratinocyte shedding that
causes abnormal accumulation of cellular layers and debris. Der-
matosis neglecta typically occurs in an area of hyperesthesia or
prior trauma where the patient refuses to scrub the skin.5 Also,
as in our patient, dermatosis neglecta can develop in situations
where a patient is unable to properly care for an area of skin
because of physical or mental disability.
A similar condition described in the literature is terra firma forme
dermatosis (TFFD), which is a disorder of unknown etiology char-
acterized primarily by disordered keratinization.6–8 In TFFD, the
classic clinical finding is a dark, dirty-looking, slightly raised hy-
perkeratotic skin lesion that is completely asymptomatic. Cases of
TFFD respond to 70% isopropyl alcohol rubs but not to cleansing
with normal soap and water; therefore, TFFD can be distinguished
CASE STUDYVesna Petronic-Rosic, MD, MSc, Section Editor
Unusually Severe Case of Dermatosis NeglectaJake E. Turrentine, BS; Travis W. Blalock, MD; Loretta S. Davis, MD
An 18-year-old black woman with cerebral palsy was admitted for evaluation of an intrathecal baclofen pump site infection. The dermatology
service was consulted for treatment suggestions of a presumed diagnosis of chronic tinea capitis. Three courses of oral griseofulvin during
the past 2 years failed to resolve the patient’s chronic scalp dermatosis. Scalp lesions first began about 2 years earlier after hospitalization for
placement of an intrathecal baclofen pump. The patient was unable to care for her scalp due to her cerebral palsy, and her mother inter-
preted the scalp condition as infectious. No routine shampoo care, scalp care, or topical treatment was performed for more than 1½ years.
The mother felt that touching the patient’s scalp might cause pain and noted that the majority of her time was spent concentrating on more
critical medical issues. Physical examination revealed coalescing hyperkeratotic plaques extending dorsally from the anterior hairline to the
occipital scalp with small flecks of keratinous debris throughout the remaining hair (Figure 1). The plate-like plaques were devoid of hair,
except at a few fissures where a few tufts of hair emerged. No cervical lymph nodes were appreciated on palpation. Treatment was initiated
with compresses consisting of large warm water–soaked towels 4 times daily. Three times a day, a nursing staff applied 5% salicylic acid in
olive oil to the scalp under a shower cap for approximately 1 hour. Over the following 2 days, a significant reduction in keratinous debris
was appreciated. Within 2 weeks, the bulk of the plaques had been removed (Figure 2). At 6-week follow-up, the underlying scalp showed
areas of fibrosis and possible scarring with a few emerging tufts of hair. On the basis of history and response to treatment with salicylic acid
and routine scalp care, the patient was diagnosed with an unusually severe case of dermatosis neglecta.

Dermatosis Neglecta
CASE STUDYJanuary/February 2012
47SKINmed. 2012;10:46–47
clinically from dermatosis neglecta by the lack of response to normal
washing and, of course, the absence of historical clues of neglect.
Given its rapid response to inexpensive and simple treatment,
dermatosis neglecta should be considered in the evaluation of
a pigmented, hyperkeratotic skin lesion. If identified, a skin
biopsy can often be avoided. Physicians should always inquire
about skin care habits when gathering history about an unex-
plained skin lesion and should review and recommend normal
skin hygiene, when a patient fails to respond to a full course of
standard therapy for an alternate diagnosis.
REFERENCES
1 Poskitt L, Wayte J, Wojnarowska F, Wilkinson JD. “Dermatosis neglecta”: unwashed dermatosis. Br J Dermatol. 1995;112:827–829.
2 Elias PM. Epidermal lipids, barrier function, and desquamation. J Invest Dermatol. 1983;80:44s–49s.
3 Williams ML. Ichthyosis: mechanisms of disease. Pediatr Dermatol. 1992;9:365–368.
4 Elias PM, Crumrine D, Rassner U, et al. Basis for abnormal desquama-tion and permeability barrier dysfunction in RXLI. J Invest Dermatol. 2004;122:314–319.
5 Lucas JL, Brodell RT, Feldman SR. Dermatosis neglecta: a series of case reports and review of other dirty-appearing dermatoses. Dermatol Online J. 2006;12:5.
6 Akkash L, Badran D, Al-Omari AQ. Terra firma forme dermatosis: case series and review of the literature. J Dtsch Dermatol Ges. 2009;7:102–107.
7 Guarneri C, Guarneri F, Cannavo SP. Terra firma-forme dermatosis. Int J Dermatol. 2008;47:482–484.
8 Raveh T, Gilead LT, Wexler MR. Terra firma forme dermatosis. Ann Plast Surg. 1997;39:542–545.
Figure 2. Almost complete resolution of scalp plaque follow-ing 2 weeks of therapy.
Figure 1. Crusted, plate-like plaques on the scalp at initial presentation.
Courtesy of BuyEnlarge, Philadelphia, PA
VINTAGE LABEL

January/February 2012 Volume 10 • Issue 1
48SKINmed. 2012;10:48–49 © 2012 Pulse Marketing & Communications, LLC
Fixed-drug eruption, one of the most well-recognized
adverse drug reactions, is characterized by a peculiar,
sudden onset of round and/or oval, edematous, dusky
red macules/plaques on the skin and/or mucous membranes
accompanied by burning and/or itching.1 Several drugs
have been incriminated in its causation, the details of which
have been specifically recounted in a recent comprehensive
review.2 Ashwagandha belongs to an alternative system of
medicine and has a long medicinal history. It is an innocuous
agent that has not been associated with any cutaneous drug
reactions to date. Fixed-drug eruption following the use of
ashwagandha is an uncommon occurence; hence, the current
report.
Ashwagandha literally means “horse smell” (ashwa = horse,
gandha = smell), for its wet roots smell similar to horse’s urine.
Withania somnifera, also known as ashwagangha, Indian gin-
seng, winter cherry, ajagandha, kanaje hindi, and samm al
ferakh, the offending indigenous drug, is derived from a plant
in the Solanaceae or nightshade family.3 It is a beautiful, deli-
cate plant native to India, Pakistan, and Sri Lanka. It is con-
sidered the king of herbs among ayurvedic medicines. It has
a medicinal history of 4000 years and is a well-accepted, vital
drug in Ayurveda and Indian traditional medicine.4 It has
been conventionally used for calming the mind and relieving
weakness, nervous exhaustion, and arthritis. In addition, it
is used for building sexual energy. Ashwagandha root is said
to be beneficial in people who do physical labor or exercise
a lot, helping the body adapt to physical stress. In addition,
its paste is recommended for external use in the treatment
of carbuncles, ulcers, and nondescript swellings. Bedsores and
wounds are also amenable to topical application of ashwa-
gandha leaves.
CONCLUSIONS
Ashwagandha is said to possess anti-inflammatory, anti-tumor,
antistress, antioxidant, immunomodulatory, hemopoeitic, and
rejuvenating effects.5 In addition, it is thought to exert a posi-
tive influence on the endocrine, cardiopulmonary, and central
nervous systems.6 Ashwagandha’s mechanism of action is still
speculative, and toxicity studies have revealed it to be a safe com-
pound.7–9
REFERENCES
1 Sehgal VN, Bhattacharya SN, Verma P. Physiopathology of adverse cu-taneous drug reactions—applied perceptions: Part I. Skinmed. In press.
2 Sehgal VN, Srivastava G. Fixed drug eruption (FDE): changing scenario of incriminating drugs. Int J Dermatol. 2006;45:897–908
3 Winters M. Ancient medicine, modern use: Withania somnifera and its po-tential role in integrative oncology. Altern Med Rev. 2006;11:269–277.
CASE STUDY
Fixed-Drug Eruption Caused by Ashwagandha (Withania somnifera): A Widely Used Ayurvedic Drug
Virendra N. Sehgal, MD; Prashant Verma, MD; Sambit N. Bhattacharya, MD
From the Dermato-Venereology (Skin/VD) Center, Sehgal Nursing Home, Panchwati-Delhi, India; the Department of Dermatology and STD, University College of Medical Sciences and Guru Teg Bahadur Hospital, Shahdara, Delhi, India
Address for Correspondence: Virendra N. Sehgal, MD, Dermato-Venereology (Skin/VD) Center, Sehgal Nursing Home, A/6 Panchwati, Delhi 110 033, India • E-mail: [email protected]
A 28-year-old man with decreased libido received ashwagandha in the usual daily dosage of 5 g for 10 days. During this period, he
experienced a burning and/or itching sensation as well as discoloration of the skin/mucous membrane confined to the penis. He had a
similar type of eruption at the same site 6 months prior while taking ashwagandha. Examination of the skin surface was conspicuous and
marked by the presence of a dusky, erythematous, oval, eroded plaque of 3 cm, affecting the glans penis and prepuce (Figure). The drug
was withdrawn and topical 0.05% clobetasol propionate cream was administered along with cetrizine dihydrochloride, an H1-receptor
blocker, 10 mg daily for 1 month. There was a perceptible amelioration of the lesion, resulting in residual greyish white pigmentation. He
was prescribed oral drug provocation with 1 g of ashwagandha powder. Within 12 hours, a flare-up developed at the earlier site, confirm-
ing the causality.

CASE STUDYJanuary/February 2012
49SKINmed. 2012;10:48–49 Fixed-Drug Eruption Caused by Ashwagandha
4 Rasool M, Varalakshmi P. Protective effect of Withania somnifera root powder in relation to lipid peroxidation, antioxidant status, glycoproteins and bone collagen on adjuvant-induced arthritis in rats. Fundam Clin Pharmacol. 2007;21:157–164.
5 Mishra LC, Singh BB, Dagenais S. Scientific basis for the therapeutic use of Withania somnifera (ashwagandha): a review. Altern Med Rev. 2000;5:334–346.
6 Sehgal VN, Srivastava G. Traditional/ayurvedic pharmacotherapy of skin diseases. Skinmed. 2010;8:282–284.
7 Behl PN, Arora RB, Srivastava G. Traditional Indian Dermatology Concept of Past and Present. 1st ed. New Delhi, India: SISD Publication; 1992.
8 Behl PN, Srivastava G. Herbs Useful in Dermatological Therapy. 2nd ed. New Delhi, India: CBS Publishers; 2004.
9 Sehgal VN, Grangwani OP. Fixed drug eruptions: a study of epidemiological, clinical and diagnostic aspects of 89 cases from India. J Dermatol. 1988;15:50–54.
Figure. Fixed-drug eruption affecting the glans and prepuce of the penis.
VINTAGE LABEL
Courtesy of BuyEnlarge, Philadelphia, PA

January/February 2012 Volume 10 • Issue 1
50SKINmed. 2012;10:50–52 © 2012 Pulse Marketing & Communications, LLC
From the Department of Dermatology, La Rabat Hospital, Tunis Tunisia;1 the Faculté de Médecine de Tunis, Tunis El Manar University, Tunis, Tunisia;2 and the Department of Pathology, La Rabta Hospital, Tunis, Tunisia3
Address for Correspondence: Ines Zaraa, MD, Dermatology Department, La Rabta Hospital, Jabbari, Bab Saadoun, Tunis, 1007 Tunisia • E-mail: [email protected]
Various cutaneous lesions may appear at sites of prior
herpes zoster infection, such as annular granuloma, sar-
coidal granuloma, granulomatous vasculitis, Kaposi’s
sarcoma, and pseudolymphoma.1 These cutaneous lesions may
appear immediately after resolving vesicular lesions or at vary-
ing times after the acute eruption. We describe in this report an
unusual case of a granulomatous zosteriform eruption revealing
a B-cell chronic lymphocytic lymphoma.
Our patient is of special interest because she presented with a
granulomatous eruption arising after a probable latent zoster re-
vealing B-CLL. Unfortunately, varicella-zoster virus DNA detec-
tion was not performed in our case.
Granulomatous reactions and specific infiltrations at sites
of resolved cutaneous herpes zoster lesions in patients with
B-CLL have been described as a rare clinical event.2,3 The
cause of granulomatous reactions caused by varicella-
zoster virus remains to be elucidated.4 Type III and type
IV hyper sensitivity reaction,5 isotopic response,6,7 and viral
etiologies2are thought to be possible provoking factors.
A study of granulomatous reactions associated with herpes
zoster lesions for the presence of varicella-zoster virus
genome using the polymerase chain reaction suggested
that varicella-zoster virus DNA is detected in cases where
eruption occurred immediately in the wake of resolving
vesicular herpes zoster lesions.2 In this case, differential
diagnosis includes specific cutaneous infiltrates with
neoplastic B cells. The clinical resolution of the lesions after
treatment with acyclovir and topical steroids confirms the
benign nature of the granulomatous infiltration.
CASE STUDY
Chronic Lymphocytic Leukemia Revealed by a Granulomatous Zosteriform Eruption
Sondes Trojjet, MD;1 Houda Hammami, MD;1 Inès Zaraa, MD;1,2 Alia Bouzguarrou, MD;1 Meriem Joens, MD;1 Slim Haouet, MD;2,3 Amel Ben Osman, MD;1,2 Mourad Mokni, MD1,2
A 70-year-old woman presented with an atypical erythematopapular zosteriform eruption of 3 weeks’ duration. The patient had no his-
tory of previous vesicular eruption. She developed a painful burning sensation on the neck. Clinical examination revealed a cluster of small
erythematous firm papules and plaques in a zosteriform distribution on the left ear, face, neck, and shoulder (Figure 1A). The lesions were
unilateral and did not cross the midline. Multiple cervical and axillary lymph nodes were palpable. Laboratory tests revealed an increase
in white blood cells of 25,000/mm3, with 17,910/mm3 lymphocytes and a normal range of hemoglobin, platelets, creatinine, and liver
enzymes. Erythrocyte sedimentation rate was 87 mm. Blood smear results showed small, morphologically mature lymphocyte cells. In
immune phenotyping, lymphocyte cells co-express CD5 and B-cell–surface antigens CD19 and CD23, as well as a restriction of kappa
immunoglobulin light chains. The cells were CD22-, CD79b-, CD38-, CD10-, CD25- and FMC7-. Computed thoracoabominal tomog-
raphy revealed cervical, mediastinal, abdominal, and pelvic adenopathy confirming the diagnosis of B-cell chronic lymphocytic leukemia
(B-CLL) stage B. Histology of a skin biopsy from a papule showed a dense nodular granulomatous infiltrate in the dermis (Figure 2A).
The infiltrate contained epithelioid and giant cells surrounded by lymphocytes and plasma cells. Small monomorphic lymphocytes without
mitotic figures predominated (Figure 2B). The epidermis was irregularly thickened. Immunohistology revealed a polymorphous infiltrate
with a phenotype of reactive T lymphocytes (CD3, CD5 positive) (Figure 2C), B lymphocytes (CD20 positive) (Figure 2D). Epithelioid
and giant cells were positive for CD68 (Figure 2E). A latent herpes zoster infection with granulomatous reaction at the site of zoster lesions
was highly suspected as the patient reported a unilateral burning sensation without a history of vesicular zosteriform eruption. She received
treatment with intravenous acyclovir 10 mg/kg every 8 hours. The papular lesions resolved markedly (60%) on macular plaques at the end
of the treatment. Following topical treatment with corticosteroids, the lesions healed completely within 4 weeks (Figure 1B). Concerning
leukemia, our patient was monitored without therapy by the hematologist.

January/February 2012 CASE STUDY
51SKINmed. 2012;10:50–52 Chronic Lymphocytic Leukemia
CONCLUSIONS
An atypical zosteriform eruption should alert dermatopatholo-
gists to the possibility of an associated hematological dyscrasia,
mainly B-CLL.
REFERENCES
1 Requena L, Kutzner H, Escalonilla P, et al. Cutaneous reactions at sites of herpes zoster scars: an expanded spectrum. Br J Dermatol. 1998;138:161–168.
Figure 2A. Histology of skin papule showing a dense nodular granulomatous infiltrate in the dermis (hematoxylin and eosin stain, original magnification ×40).
Figure 2B. Granulomatous infiltrate containing small mature lymphocytes with no significant atypia, epithelioid, or giant cells (hematoxylin and eosin stain, original magnification ×100).
Figure 1A. Clustered erythematous papules and plaques on right neck and shoulder.
Figure 1B. Healing of clustered erythematous papules and plaques within 4 weeks.
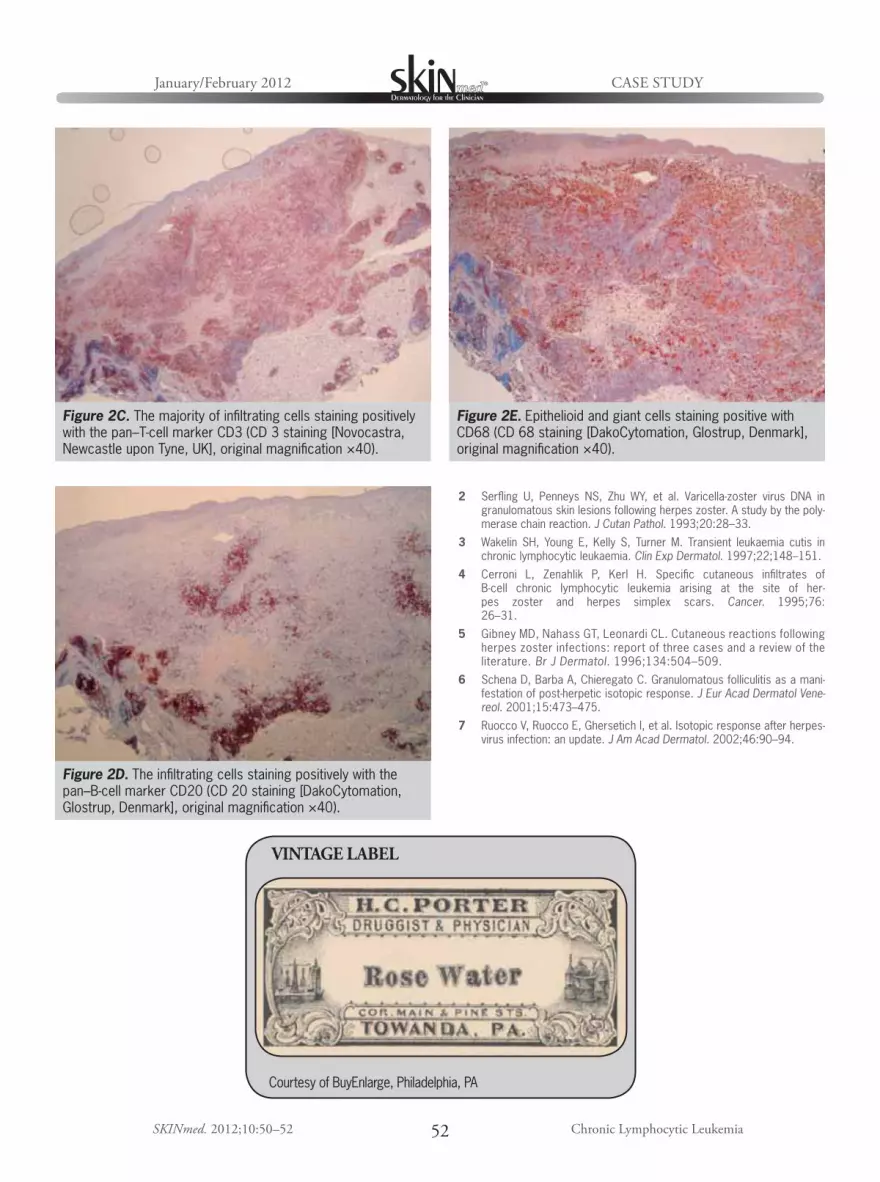
January/February 2012 CASE STUDY
52SKINmed. 2012;10:50–52 Chronic Lymphocytic Leukemia
2 Serfling U, Penneys NS, Zhu WY, et al. Varicella-zoster virus DNA in granulomatous skin lesions following herpes zoster. A study by the poly-merase chain reaction. J Cutan Pathol. 1993;20:28–33.
3 Wakelin SH, Young E, Kelly S, Turner M. Transient leukaemia cutis in chronic lymphocytic leukaemia. Clin Exp Dermatol. 1997;22;148–151.
4 Cerroni L, Zenahlik P, Kerl H. Specific cutaneous infiltrates of B-cell chronic lymphocytic leukemia arising at the site of her-pes zoster and herpes simplex scars. Cancer. 1995;76:26–31.
5 Gibney MD, Nahass GT, Leonardi CL. Cutaneous reactions following herpes zoster infections: report of three cases and a review of the literature. Br J Dermatol. 1996;134:504–509.
6 Schena D, Barba A, Chieregato C. Granulomatous folliculitis as a mani-festation of post-herpetic isotopic response. J Eur Acad Dermatol Vene-reol. 2001;15:473–475.
7 Ruocco V, Ruocco E, Ghersetich I, et al. Isotopic response after herpes-virus infection: an update. J Am Acad Dermatol. 2002;46:90–94.
Figure 2C. The majority of infiltrating cells staining positively with the pan–T-cell marker CD3 (CD 3 staining [Novocastra, Newcastle upon Tyne, UK], original magnification ×40).
Figure 2D. The infiltrating cells staining positively with the pan–B-cell marker CD20 (CD 20 staining [DakoCytomation, Glostrup, Denmark], original magnification ×40).
Figure 2E. Epithelioid and giant cells staining positive with CD68 (CD 68 staining [DakoCytomation, Glostrup, Denmark], original magnification ×40).
VINTAGE LABEL
Courtesy of BuyEnlarge, Philadelphia, PA

Grand Wailea, Maui • February 4–8, 2012
20
12
Featured Lectures Hot Topics • Cases for the Panel • Seminars • Workshops • Basic Science
Medical Dermatology: Basic Science, Hot Topics, Cases for the Panel, Point:Counterpoint, Seminars, “How I Do It” Cutaneous Oncology • Acne/Rosacea • Pediatric Dermatology • Infectious Diseases Psoriasis • Skin of Color • Life Threatening Dermatoses • Master’s CPC • Offi ce Surgery • Practice Management
Cosmetic Dermatology: From Basic Science to Case Based Discussion and “How I Do It” Botulinum Toxin A and Fillers • Lasers • Sclerotherapy
“Lunch with the Faculty” – Controversial Topics, Case-based Discussions Interactive WorkshopsSmall Group, Live Patient, Hands-On Demonstrations: Botulinum Toxins/Fillers, Sclerotherapy
February 4–8, 2012 Grand Wailea : Maui, Hawaii
Plan to attend the 8th Annual Maui Derm Conference! “Cutting edge, a great blend of science and clinical medicine and a world class faculty” describe Maui Derm 2012. Our faculty will share with you the most important developments in medical and cosmetic dermatology vital to your practice. Our live patient demonstration workshops in lasers, Botulinum Toxin A and fi llers have set the standard for “hands on” workshops. Our format has been specifi cally designed to allow optimal time for discussion with our faculty.We are certain that you will fi nd this to be an outstanding and memorable educational event that you will not want to miss. Put Maui Derm on your calendar for 2012!
Register Now for the 8th Annual Conference!2012 Faculty * Chairman:
Dr. George Martin
Matthew Avram, MDNeal Bhatia, MDAndrew Blauvelt, MDValerie Callender, MDJoel Cohen, MDLawrence Eichenfi eld, MDRebecca Fitzgerald, MDKeith T. Flaherty, MDSheila Friedlander Fallon, MDIlona Frieden, MDMichael Gold, MDMitchel Goldman, MDPearl Grimes. MDDerek Jones, MDArthur Kavanaugh, MDSuzanne Kilmer, MDDavid Laub, MDPhilip LeBoit, MDCraig Leonardi, MDStuart Maddin, MDAshfaq Marghoob, MD
Sam Moschella, MDStuart Nelson, MDKevin Pinski, MDPhoebe Rich, MDTed Rosen, MDE. Vic Ross, MDAlan Shalita, MDAva Shamban, MDDaniel Siegel, MDEggert Stockfl eth, MDBruce Strober, MD, PhDNeil Swanson, MDJames Treat, MDHensin Tsao, MDSandy Tsao, MDGuy Webster, MD, PhDWm. Philip Werschler, MDJohn Zone, MD
* Subject to Change
MAUI DERM 2012 HAS SPECIAL/REDUCED RATES AT THEGrand Wailea and the Wailea Marriott
For more details, visit our website at
www.acmd-derm-hawaii.com

January/February 2012 Volume 10 • Issue 1
54SKINmed. 2012;10:54–55 © 2012 Pulse Marketing & Communications, LLC
MYCOBACTERIUM MARINUM CUTANEOUS INFECTION WITH SPOROTRICHOID DISTRIBUTION TREATED WITH AZITHROMYCIN MONOTHERAPY
To the Editor:
Mycobacterium marinum is an aerobic, waterborne mycobacte-
rium commonly found in nonchlorinated water in a worldwide
distribution. It is also the most common atypical Mycobacte-
rium to cause infection in humans. Infection is not transmittable
from person to person, and skin infections due to M marinum
are rare.1
There is no established treatment of choice for M marinum
infection, probably because it is a multidrug-resistant species.
Its treatment has been based primarily on personal experience
without the benefit of large studies.2 To our knowledge, this is
the first case of cutaneous M marinum infection treated with
azithromycin monotherapy.
A 52-year-old-woman, a cleaning worker in our hospital, was
referred to our department because of the appearance of red
nodules on the left palm and left forearm in a sporotrichoid
distribution (Figure 1). She mentioned that the first lesion
appeared on her hand 6 months previously and new lesions
gradually appeared and increased in number and size during this
period. She also reported a private fish aquarium usually cleaned
by her without using hand protection. The remainder of her
medical history was unremarkable.
Routine laboratory tests including human immunodeficiency
virus test were within normal limits. The patient underwent
surgical skin biopsy of the nodule of the forearm, and histologic
examination revealed the presence of tuberculoid structures with
neutrophils and macrophages (Figure 2). Results from periodic
acid-Schiff and Ziehl-Neelsen stains were negative. Cultures taken
from the lesions were negative for bacilli or atypical mycobacteria.
Chest and right hand radiological evaluations were normal. The
patient reported an episode of headache after doxycycline intake,
a ciprofloxacin-associated morbilliform eruption, and frequent
gastrointestinal symptoms after drug administration. She told
us she could receive azithromycin without a problem; there-
fore, we decided to try azithromycin 500 mg (tabs Zinfect
500 mg, Verisfield, Athens, Greece) 3 times a week for 2 months
and re-evaluation. To our surprise, complete clinical cure was
obtained after 8 weeks of treatment (Figure 3). No relapse has been
observed after 10 months of follow-up.
M marinum infection, also called “fish tank granuloma,”
“aquarium granuloma,” or “swimming pool granuloma” seems to
represent an opportunistic disease and occurs after approximately
2 weeks of direct (traumatic) inoculation of the organism either
from fish fins and bites or from the handling of aquariums.1
Solitary red-to-violaceous plaques or nodules with an overlying
crust or verrucous and/or ulcerate surface is a common clinical
presentation in immunocompetent patients. Inflammatory
CORRESPONDENCE
Figure 2. Histologic examination revealed the presence of tuberculoid structures (hematoxylin and eosin stain, original magnification ×100).
Figure 1. Mycobacterium marinum skin infection of the left palm with sporotrichoid distribution on the left forearm.

CORRESPONDENCEJanuary/February 2012
55
nodules, abscesses with a sporotrichotic type of distribution,
followed by nodular lymphangitis can develop in severely immu-
nosuppressed patients.3 Over a period of months, involvement
of deeper soft tissues (tenosynovitis, arthritis, bursitis, and/or
osteomyelitis of the underlying bone) may be life- threatening.4
Lesions may be either painful or painless. Lung involvement,
disseminated infection, and bacteremia have been rarely
reported.1
The organism can be isolated from the lesion as well as from
infected fish or aquariums; however, in clinical practice,
diagnosis remains largely presumptive based on clinicohistologic
features. Histopathologic examination usually reveals a nonspe-
cific inflammatory infiltrate.1
Treatment of M marinum infections is challenging. In superficial
cutaneous infections, minocycline, clarithromycin, doxycycline,
trimethoprim sulfamethoxazole, and ciprofloxacine as mono-
therapy are usually effective treatment options. In severe infec-
tions, a combination of rifampicin and ethambutol seems to be
the recommended regimen. Surgical treatment is usually unnec-
essary, and where it should be performed must be cautiously
determined.1,2
Azithromycin shows good response in vitro against other than
Mycobacterium tuberculosis mycobacteria. There is only one
case of M marinum infection in a patient who underwent lung
transplantation successfully treated with surgical removal of the
lesions and a 12-month administration of a combination of
azithromycin and ethambutol.5
Azithromycin seems to be a promising option to treat M marinum
skin infections, although, further studies—or at least cases—are
needed to establish the effectiveness of the drug.
REFERENCES
1 Rallis E, Koumantaki-Mathioudaki E. Treatment of Mycobacterium marinum cutaneous infections. Expert Opin Pharmacother. 2007;8:2965–2978.
2 Edelstein H. Mycobacterium marinum skin infections. Report of 31 cases and review of the literature. Arch Intern Med. 1994;154:1359–1364.
3 Bartralot R, Garcia-Patos V, Sitjas, et al. Clinical patterns of cuta-neous nontuberculous mycobacterial infections. Br J Dermatol. 2005;152:727–734.
4 Wu TS,Chiu CH,Su LH et al. Mycobacterium marinum infection in Taiwan. J Microbiol Immunol Infect. 2002;35:42–46.
5 Torres F, Hodges T, Zamora MR. Mycobacterium marinum infection in a lung transplant recipient. J Heart Lung Transplant. 2001;20:486–489.
—Efstathios Rallis, MD, PhD, Department of Dermatology, Veterans Administration Hospital (NIMTS), Athens, • E-mail: [email protected]; Evangelos Falidas, MD, 1st Department of General Surgery, Veterans Administration Hospital (NIMTS), Athens; Panagiotis Stavropoulos, MD, PhD, Department of Dermatology, University of Athens, “A.Syggros”
Hospital, Athens, Greece
Figure 3. Complete clearance of the lesions was achieved after 8 weeks of azithromycin treatment.
FORMULARY OF DR GEORGE C. ANDREWS
Nail Bleach
Oxalic acid Gm xxx
Distilled water 2000 cc
Perfume Qs ad
The above may be irritating—ingredients should be on poison label with a word of caution.
Submitted by Douglas D. Altchek, MD, New York, NY

THE Aesthetic Show of the Year
World-Class FacultyPre-Show Educational SessionsAdvanced Hands-On Training
Patient Tx Workshops
To register visit www.aestheticshow.com or call + 1 (949) 830-5409
Register with Promo Code TAS3AD:
Aesthetic TV
THE Aesthetic Awards TM

Abstract submission deadline:O c to b e r 30 th , 2011
CANCUN 2012CANCUN 2012CANCUN 2012
+ (52 55) 5531- 0865+ (52 55) 5203- 6454
January 31st to February 4thCancun Quintana Roo, Mexico




Locoid Lipocream® Cream, 0.1% Rx Only(hydrocortisone butyrate 0.1% cream)For Topical Use Only
BRIEF SUMMARY
INDICATIONS AND USAGELocoid Lipocream is a topical corticosteroid indicated for: relief of the inflammatoryand pruritic manifestations of corticosteroid-responsive dermatoses in adults andthe treatment of mild to moderate atopic dermatitis in patients 3 months to 18 yearsof age.
WARNINGS AND PRECAUTIONSReversible hypothalamic-pituitary-adrenal (HPA) axis suppression may occur, withthe potential for glucocorticosteroid insufficiency. Consider periodic evaluations forHPA axis suppression if Locoid Lipocream is applied to large surface areas or usedunder occlusion. If HPA axis suppression is noted, reduce the application frequency,discontinue use, or switch to a lower potency corticosteroid. Systemic effects of topical corticosteroids may also include manifestations ofCushing’s syndrome, hyperglycemia, and glucosuria. Pediatric patients may be more susceptible to systemic toxicity due to their largerskin surface-to-body-mass ratios. Initiate appropriate therapy if concomitant skin infections develop. Discontinue use if irritation develops.
ADVERSE REACTIONSThe most common adverse reactions (>1%) are HPA axis suppression andapplication site reactions.The following additional local adverse reactions have been reported infrequentlywith topical corticosteroids, and they may occur more frequently with the use ofocclusive dressings and higher potency corticosteroids. These reactions included:irritation, folliculitis, acneiform eruptions, hypopigmentation, perioral dermatitis,allergic contact dermatitis, secondary infection, skin atrophy, striae, miliaria andtelangiectasia.
USE IN SPECIFIC POPULATIONSPregnancyPregnancy Category C. Corticosteroids have been shown to be teratogenic inlaboratory animals when administered systemically at relatively low dosage levels.Some corticosteroids have been shown to be teratogenic after dermal applicationin laboratory animals.There are no adequate and well-controlled studies inpregnant women. Therefore, Locoid Lipocream should be used during pregnancyonly if the potential benefit justifies the potential risk to the fetus.Please refer to full prescribing information for detailed information regardingsystemic embryofetal development studies.Nursing MothersSystemically administered corticosteroids appear in human milk and couldsuppress growth, interfere with endogenous corticosteroid production, or causeother untoward effects. It is not known whether topical administration ofcorticosteroids could result in sufficient systemic absorption to produce detectablequantities in human milk. Because many drugs are excreted in human milk, cautionshould be exercised when Locoid Lipocream is administered to a nursing woman.Pediatric UseSafety and efficacy in pediatric patients below 3 months of age have not beenestablished. Because of higher skin surface-to-body-mass ratios, pediatric patients are at agreater risk than adults of HPA axis suppression when they are treated with topicalcorticosteroids. They are therefore also at a greater risk of glucocorticosteroidinsufficiency after withdrawal of treatment and of Cushing’s syndrome while ontreatment. Eighty-six (86) pediatric subjects (5 months to less than 18 years of age) withmoderate to severe atopic dermatitis affecting at least 25% of body surface area(BSA) treated with Locoid Lipocream three times daily for up to 4 weeks wereassessed for HPA axis suppression. The disease severity (moderate to severeatopic dermatitis) and the dosing regimen (three times daily) in this HPA axis studywere different from the subject population (mild to moderate atopic dermatitis) andthe dosing regimen (two times daily) for which Locoid Lipocream is indicated. Five of the 82 evaluable subjects (6.1%) demonstrated laboratory evidence ofsuppression, where the sole criterion for defining HPA axis suppression was aserum cortisol level of less than or equal to 18 micrograms per deciliter aftercosyntropin stimulation. Suppressed subjects ranged in age from 5 months to 16 years and, at the time of enrollment, had 25% to 95% BSA involvement. Thesesubjects did not develop any other signs or symptoms of HPA axis suppression. At the first follow up visit, approximately one month after the conclusion oftreatment, cosyntropin stimulation results of all subjects had returned to normal,with the exception of one subject. This last subject recovered adrenal function bythe second post treatment visit, 65 days post-treatment. Cushing’s syndrome, linear growth retardation, delayed weight gain, andintracranial hypertension have also been reported in pediatric patients receivingtopical corticosteroids. Manifestations of adrenal suppression in pediatric patientsinclude low plasma cortisol levels to an absence of response to ACTH stimulation.Manifestations of intracranial hypertension include bulging fontanelles, headaches,and bilateral papilledema.
Geriatric UseClinical studies of Locoid Lipocream did not include sufficient numbers of subjectsaged 65 and over to determine whether they respond differently from youngersubjects.Carcinogenesis, Mutagenesis, Impairment of FertilityNo studies were conducted to determine the photococarcinogenic or dermalcarcinogenic potential of Locoid Lipocream.Hydrocortisone butyrate revealed no evidence of mutagenic or clastogenicpotential based on the results of two in vitro genotoxicity tests (Ames test andL5178Y/TK+ mouse lymphoma assay) and one in vivo genotoxicity test (mousemicronucleus assay).No evidence of impairment of fertility or effect on mating performance wasobserved in a fertility and general reproductive performance study conducted inmale and female rats at subcutaneous doses up to and including 1.8 mg/kg/day(0.7X maximum topical human dose [MTHD]). Mild effects on maternal animals,such as reduced food consumption and a subsequent reduction in body weight gain,were seen at doses ≥0.6 mg/kg/day (0.2X MTHD).
PATIENT COUNSELING INFORMATIONPatients using Locoid Lipocream should receive the following information and instructions:Apply a thin layer to the affected skin two or three times daily for corticosteroid-responsive dermatoses in adults. Consult with your physician to determine iftreatment is needed beyond 2 weeks. Apply a thin film to the affected skin areastwo times daily for atopic dermatitis in patients 3 months of age and older. Safety of Locoid Lipocream in pediatric patients has not been established beyond 4weeks of use.Rub in gently.Avoid contact with the eyes. Do not bandage, otherwise cover, or wrap the affected skin area so as to beocclusive unless directed by your physician.Do not use Locoid Lipocream in the diaper area, as diapers or plastic pants mayconstitute occlusive dressings.Do not use Locoid Lipocream on the face, underarms, or groin areas unlessdirected by your physician.If no improvement is seen within 2 weeks, contact your physician.Do not use other corticosteroid-containing products while using Locoid Lipocreamwithout first consulting your physician.
Store at 25°C (77°F); excursions permitted to 15-30°C (59-86°F) [see USP ControlledRoom Temperature]. Protect from freezing. Keep out of the reach of children.
Marketed and Distributed By:Triax Pharmaceuticals, LLCCranford NJ 07016www.Locoid.com
Manufactured for: Triax Pharmaceuticals, LLCCranford NJ 07016By: Ferndale Laboratories, Inc.Ferndale MI 48220
131B301Rev 11/09
Locoid Lipocream is a registered trademark of Astellas Pharma Europe BV licensed to Triax Pharmaceuticals, LLC.

Now younger eczema patients have something
to smile about
Now approved for use in children down to 3 months of age
(hydrocortisone butyrate 0.1%) Cream
Locoid Lipocream is indicated for the relief of the inflammatory and pruritic manifestations of corticosteroid-responsive dermatoses, including the treatment of mild to moderate atopic dermatitis in patients 3 months of age and older.Safety and effectiveness in pediatric patients below 3 months of age have not been established.Reversible HPA axis suppression may occur, with the potential for corticosteroid insufficiency. Consider periodic evaluations for HPA axis suppression if applied to large surface areas or used under occlusion . Systemic effects of topical corticosteroids may also includemanifestations of Cushing’s syndrome, hyperglycemia, and glucosuria. Pediatric patients may be more susceptible to systemic toxicity due to their large skin surface-to-body-mass ratios. Initiate appropriate therapy if concomitant skin infection develops. Discontinue use if irritation develops. Please see full Prescribing Information on adjacent page. Visit us at www.locoid.com
©2010 Triax Pharmaceuticals, LLC. All rights reserved. Locoid is a registered trademark of Astellas Pharma Europe B.V. licensed to Triax Pharmaceuticals, LLC. LOC-0410-01
The power of an ointment with the elegance of a cream