methadone maintenance and drug-related crime
TRANSCRIPT

METHADONE MAINTENANCE AND DRUG-RELATED CRIME
JAMES BELL* The Prince of Wales Hospital
RICHARD MATTICK University of New South Wales
ANNA HAY The Prince of Wales Hospital
JENNIFER CHAN WAYNE HALL
University of New South Wales
ABSTRACT: Using duta from nn evaluation of methadone maintenance treatment,
this study investigated factors associated with continued involvement in crime during
treatment, and in particular whether there appeared to be diflerences in effectiveness of treatment between diflerent methadone clinics. The methodology was an observa-
tional study, in which 304 patients attending three low-intervention, private methadone
clinics in Sydney were interviewed on three occasions over a twelve month period. Out-
come mea,sures usere self-reported criminal activity and police department records of
convictions. By self-report, crime dropped promptly and substantially on entry to treat-
ment, to a level of acquisitive crime about one-eighth that reported during the last addiction period. Analysis of oflicial records indicated that rates of acquisitive convic-
tions were significantly lower in the in-treatment period compared to prior to entry to
treatment, corroborating the changes suggested by self-report. Persisting involvement
in crime in treatment wa.s predicted by two,factors: the cost of persisting use of illicit
*Direct n/l correspondence to: James Be//, Drug and Alcohol Unit. The Prince of Wales Hospital. High Street,
Randwick, NSW 2031, Australia; E-mail: jumes.bell~uns~.edu.au
JOURNAL OF SUBSTANCE ABUSE, Volume 9, pages 15-25. Copyright 0 1997 by Ablex Publishing Corporation All rights of reproduction in any form reserved. ISSN: 0899-3289

16 JOURNAL OF SUBSTANCE ABUSE Vol. 9/l 997
drugs, particularly cunnahis, und ASPD symptom count. Treutment fuctors ulso we’re
independently predictive of continued involvement in crime. By both self-report und
ofJicia1 records, and adjusting for subject factors, treatment at one clinic M’US associ-
ated with greater in\&tement in crime. This clinic operuted in a chaotic und poor!\
orgunized way. It is concluded that crime during methadone treatment is suhstantiall~
lower thun during street addiction, although the extent of reduction depends on the
quality of treutment king delivered.
INTRODUCTION
In the USA in the last four decades, heroin use largely has been restricted to an addict subculture of marginalized young people (Inciardi, 1979; Nurco, Ball, Shaffer, & Hanlon, 1985). A similar situation pertains in Australia (Hall, Bell, & Carless, 1993), and appears
to have developed in the United Kingdom (Hammersley, Forsyth, & Lavelle, 1990: MacGregor, 1990). Antisocial behavior and acquisitive crime are common in this group, frequently preceding heroin use (Hall et al., 1993). Once individuals become dependent on heroin, the cost of maintaining a heroin habit contributes to an escalating involvement in income-generating crime, reinforcing the relationship between heroin use and criminal
activity (Dobinson & Ward, 1987; Hammersley, Forsyth, Morrison, & Davies, 1989). One possible antecedent factor linking drug use and crime is the constellation of person-
ality traits and behaviors which constitute the diagnostic entity antisocial personality disorder (ASPD). A pattern of behavior characterized by behavioral traits such as deceit- fulness, impulsivity, irresponsibility, and lack of remorse, ASPD is strongly associated with drug use and crime (Darke, Hall, & Swift, 1994). It seems probable that drug use helps relieve the dysphoric moods-particularly pervasive frustration and boredom-experi- enced by many individuals who fulfill the diagnostic criteria for ASPD.
There have been several research reports documenting the association between metha- done treatment and lower involvement in crime by heroin addicts (Ball & Ross, 1991:
Hubbard et al., 1989). The current study extends this research by seeking to identify factors associated with continuing involvement in crime, particularly treatment factors. The reason for this is to identify the mechanisms by which methadone treatment produces any benefi- cial changes. This is particularly pertinent to methadone treatment, as changes in treatment delivery have frequently run ahead of research evidence of efficacy. In Australia in the last decade, there has been a very large expansion of methadone treatment, and a change in the approach to delivering treatment. Driven by funding from Australia’s system of universal health insurance, two models of methadone treatment have evolved, each based on care being delivered by medical practitioners. In the first model. methadone is prescribed by primary care physicians in office practice, with the patient receiving the daily dose of methadone from a retail pharmacy. In the second model, patients are dispensed methadone
from private clinics, and have regular scheduled appointments with the methadone prescriber at the clinic. Patients pay fees; clinics operate for profit. Both systems represent minimal approaches to treatment in that access to psychosocial and welfare services are not part of the structure of treatment. One concern underlying this study is whether the low- threshold, low-intervention clinics are effective in reducing involvement in crime by those
in treatment.

Methadone Maintenance and Drug-Related Crime 17
METHODS
Patients attending three private methadone clinics were recruited. The clinics were selected on the basis that they had been in continuous operation at the same site for at least three years. Clinic managers were approached, and their consent to participate was sought. Within each clinic, it was planned to interview 100 of the 120 patients being treated by one prescribing doctor. Most patients were interviewed on three occasions over a 12 month period. All subjects participated in the study voluntarily. Clinic staff were not involved in the recruitment of subjects, other than to provide research interviewers with a list of the names of current patients. Recruitment and interviewing was conducted by contract researchers who spent many months working in each clinic. The study was approved by the ethics committee of the Eastern Sydney Area Health Service.
At the first interview, a structured psychosocial history was taken. Subjects were also asked the number of days in the previous month on which they had been involved in illicit drug selling and other income generating crime, and about their involvement in these activ- ities during their last addiction period prior to entering treatment. At the first and third interview, patients were administered the crime scale of the Opiate Treatment Index (OTI; Darke, Hall, Heather, Wodak, & Ward, 1992). This scale comprises detailed questions covering a range of criminal activities over the preceding 30 days. This scale does not quantitate the number of offenses, but attempts to rate the extent of involvement in crime on a set of Likert scales.
At the second interview, conducted about one month after the initial interview, subjects were administered the Diagnostic Interview Schedule (DIS; Robins, Helzer, Croughan, & Ratcliff, 1981). This provided the number of current ASPD symptoms (lifetime and 12 month). Interviewers were trained in the administration of the DIS. To check on quality of interviews and interpretation of responses, all interviews were audiotaped and 20% were randomly selected and rerated for psychiatric morbidity by an assessor qualified in admin- istering the DIS. Agreement on diagnoses was in excess of 97%.
A third interview was conducted 12 months after the initial interview to provide an indi- cation of changes in drug use and social functioning over time in treatment.
To estimate changes in criminal activity on entry to treatment, descriptive statistics were tabulated on involvement in crime in the month prior to interview, and in the last month of each subject’s last addiction period. Subjects with one month or less in treatment were treated as a separate group, as their self-reported crime in the month prior to interview covered crime committed prior to entering treatment.
Statistical analysis of conviction rates prior to methadone treatment, and during metha- done treatment, was used to complement the self-report measures of change on entry to treatment. At the first interview, as part of the process of consenting to participate in the research, subjects were specifically asked to consent to their criminal records being exam- ined. Police records provided an external reference point against which to validate self- report data. Offenses from police records were divided into property offenses (covering all acquisitive crime except drug dealing), drug offenses (possession, self-administration, and trafficking), and other offenses (such as offensive behavior and traffic offenses).
The differences between treatment delivered in the three clinics was assessed by two approaches. Staff completed questionnaires regarding treatment philosophy and goals, staff training and attitudes, stated policies and procedures, and differences in workloads. A

18 JOURNAL OF SUBSTANCE ABUSE Vol. 9/l 997
random sample of clinical files was reviewed in each clinic. In addition, a senior research
assistant spent considerable time in each clinic observing operations, providing a qualita-
tive account of interactions in the clinic. In order to deal with differences in treatment, it
was decided to use two variables to describe treatment-methadone dose and “clinic’‘-as
predictor variables in regression analyses. In analyses in which “clinic” was included as a
predictor variable, subjects with one month or less of treatment were excluded, as their
self-reported crime in the month prior to interview includes a period of time when they
were not in treatment. Analysis of factors associated with continued involvement in crime was performed using
linear regression. Variables which were significant or approached significance in univari-
ate models were included in multivariate models.
RESULTS
Management of the first three private clinics invited to participate all consented. One clinic
was in an outer suburb, and two were in inner-suburban areas. For initial interview, 304
patients were recruited. Characteristics of the subjects are shown in Table 1. In terms of age, education, employment and pre-treatment involvement in crime,
samples from the three clinics did not differ. However, there were differences in the sex
distribution in the three clinics, with Clinics 1 and 2 having approximately equal numbers
of male and female subjects, while the sample from Clinic 3 was 70% male. Subjects’ self reported involvement in drug dealing and in other acquisitive crime is
tabulated in Table 2, along with their reported involvement in their last period of street
addiction. Patients with a history of being in treatment less than one month are tabulated
separately, as their self-reported crime covers a variable non-treatment period. Fewer people in treatment for at least one month report involvement in crime, and their
level of criminal activity was much lower than their reported crime during their last addic-
TABLE 1 Subject Characteristics and Self-Reported Drug Use
Females Males Total n 131 173 304
Mean Age (years) 18 31 30
Employed (c/c) 49 46 1x
Months in Study Clinic I? 16 I5
Ever Imprisoned (96) 36 56 47
<IO Years Education (p/c) 56 62 59
Diagnosis of ASPD (%I 42 44 43
Heroin Use (o/r)* 50 44 47
Cannabis Use (c/j Sh 6s s9
Benzodiazepine Use (%) 3.5 33 34
Amphetamine Use (‘i;) 17 20 I8
* Figures for drug use refer 10 the proportion of ubjects who rcportrd having used the drug or drug type in the month prior to interwew. Because heroin use fell nhruptly on entry to trealment. wherea\ uw of other
drug types did not change. ligures for heroin use are hased on the proportion of whJects with more than I month of treatment who reported heroin we.
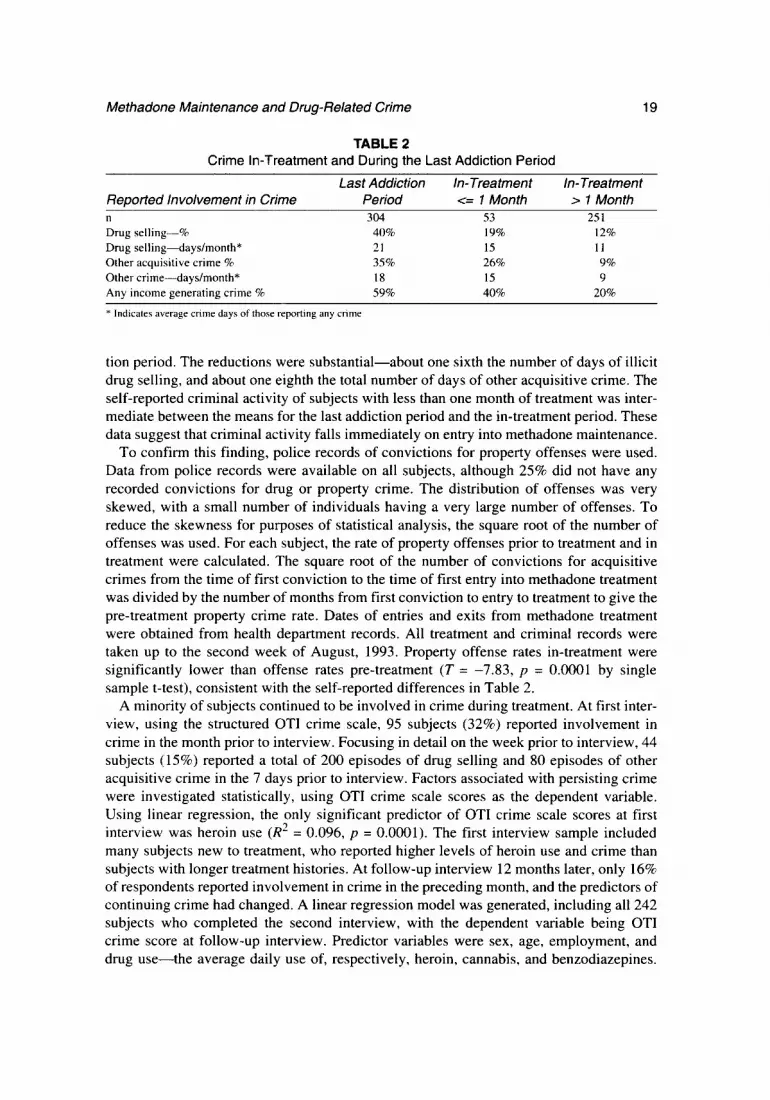
Methadone Maintenance and Drug-Related Crime 19
TABLE 2 Crime In-Treatment and During the Last Addiction Period
Last Addiction In-Treatment In-Treatment Reported involvement in Crime Period c= 1 Month > 1 Month n 304 53 251 Drug selling-% 40% 19% 12%
Drug selling-days/month* 21 15 11
Other acquisitive crime % 35% 26% 9%
Other crimedays/month* 18 1.5 9
Any income generating crime % 59% 40% 20%
* Indicates average cnme days of those reportmg any crime
tion period. The reductions were substantial-about one sixth the number of days of illicit drug selling, and about one eighth the total number of days of other acquisitive crime. The self-reported criminal activity of subjects with less than one month of treatment was inter- mediate between the means for the last addiction period and the in-treatment period. These data suggest that criminal activity falls immediately on entry into methadone maintenance.
To confirm this finding, police records of convictions for property offenses were used. Data from police records were available on all subjects, although 25% did not have any recorded convictions for drug or property crime. The distribution of offenses was very skewed, with a small number of individuals having a very large number of offenses. To reduce the skewness for purposes of statistical analysis, the square root of the number of offenses was used. For each subject, the rate of property offenses prior to treatment and in treatment were calculated. The square root of the number of convictions for acquisitive crimes from the time of first conviction to the time of first entry into methadone treatment was divided by the number of months from first conviction to entry to treatment to give the pre-treatment property crime rate. Dates of entries and exits from methadone treatment were obtained from health department records. All treatment and criminal records were taken up to the second week of August, 1993. Property offense rates in-treatment were significantly lower than offense rates pre-treatment (T = -7.83, p = 0.0001 by single sample t-test), consistent with the self-reported differences in Table 2.
A minority of subjects continued to be involved in crime during treatment. At first inter- view, using the structured OTI crime scale, 95 subjects (32%) reported involvement in crime in the month prior to interview. Focusing in detail on the week prior to interview, 44 subjects (15%) reported a total of 200 episodes of drug selling and 80 episodes of other acquisitive crime in the 7 days prior to interview. Factors associated with persisting crime were investigated statistically, using OTI crime scale scores as the dependent variable. Using linear regression, the only significant predictor of OTI crime scale scores at first interview was heroin use (R2 = 0.096, p = 0.0001). The first interview sample included many subjects new to treatment, who reported higher levels of heroin use and crime than subjects with longer treatment histories. At follow-up interview 12 months later, only 16% of respondents reported involvement in crime in the preceding month, and the predictors of continuing crime had changed. A linear regression model was generated, including all 242 subjects who completed the second interview, with the dependent variable being OTI crime score at follow-up interview. Predictor variables were sex, age, employment, and drug use-the average daily use of, respectively, heroin, cannabis, and benzodiazepines.

20 JOURNAL OF SUBSTANCE ABUSE Vol. 9/l 997
TABLE 3 Predictors of Crime Scale Scores Including Role of ASPD Symptom Count
Variable Estimate SEM p-L&lie Sex -0. I87 0.4 I x 0.7 Age 0.00 I 0.032 0.0
Employment -0.49 0.40 0.22 Average BDZ Use 0.060 0.0x2 0.5 Cost of Drugs 0.002x 0.0007 0.000 I Lifetime ASPD Symptom Count 0.08’~ 0.03 I 0.00s
Overall, the regression was significant (R’ = 0.138). The only significant predictors of crime in this model were heroin use @ = 0.01) and cannabis use (p = 0.0001). In estimating the relative contribution of heroin and cannabis, two models were developed. When the variable cannabis use was removed as a predictor, the resulting regression was not signifi-
cant (R’ = 0.03). However, when heroin use was removed as a predictor, the regression remained highly significant (R’ = 0.115). It is clear that at the follow-up interview.
cannabis use had become the major predictor of continued involvement in crime. Valid interview data on psychiatric comorbidity was available on only 229 subjects, and
therefore a separate set of analyses was performed to investigate the role of antisocial personality disorder as a predictor of continued involvement in crime. Subjects with a posi- tive diagnosis of ASPD had higher rates of conviction prior to entering treatment. and had been arrested at an earlier age. Univariate analysis indicated that the diagnosis of ASPD was not associated with more self-reported crime while in treatment. However. the contin- uous variable “lifetime ASPD symptom count” was significantly associated with continued in-treatment involvement in crime.
The findings in relation to heroin and cannabis use suggested that it is the cost of main- taining a habit on illicit drugs which drives continued involvement in crime. In investigating the role of ASPD symptom count, the variable “cost of drugs” was included in the regression. This variable represents the estimated average daily cost of street drugs for each subject. It was generated by multiplying the average daily use of heroin, amphet- amines, and cannabis by their respective unit prices. Given that prices are variable, this represents at best a rough estimate. Adding ASPD lifetime symptom count to the linear regression model incorporating age, sex. employment, benzodiazepine use and cost of drugs, ASPD symptom count was independently predictive of crime scores. Overall. the regression was significant (R’ = 0.125). The model, based this time on the 229 subjects for whom all variables were available, is shown in Table 3.
This indicates that ASPD symptom count and cost of illicit drug use are independently predictive of continued crime during methadone treatment. while other predictor variables did not approach significance.
Role of Treatment Factors Influencing Involvement in Crime
The role of treatment factors in influencing level of involvement in crime was investi- gated by including “clinic” as a predictor variable, while controlling for subject
characteristics. In univariate analyses, the variable “methadone dose” did not approach significance, and was omitted from final models. For these analyses, subjects with less than

Methadone Maintenance and Drug-Related Crime 21
TABLE 4 Predictors of In-Treatment Crime Rates
Variable Estimate Standard Error p-Value
Pre-Treatment Property Offense Rates 0.193 0.044 0.0001
Months in Treatment -0.001 0.0005 0.049
Clinic I 0.070 0.026 0.009
Clinic 3 0.042 0.026 0.10
one month of treatment were excluded, since their level of crime in the month prior to inter-
view did not reflect their treatment experience. This left a sample of 251. At the three
clinics, 35%, 20%, and 25% of respondents, respectively, reported any crime in the month
prior to interview. Using linear regression, the influence of clinic was examined in the 25 1 subjects in treatment for at least one month. Potential predictor variables in the regression
were age, sex, employment, duration of previous imprisonment, average daily use of
heroin, benzodiazepines, and cannabis, and clinic. Overall, the regression was significant
(R2 = 0,085). The significant predictors of involvement in crime were average daily heroin
use 01 = O.Ol), and treatment at Clinic 1 (at which self-reported criminal activity was
significantly higher, p = 0.02). Lifetime ASPD symptom count offers another way to control for possible differences
between the clinics in the population being treated. When ASPD symptom count was
included in a linear regression model, along with clinic, sex, age, employment, and average
use of heroin, amphetamines, benzodiazepines, and cannabis, the overall regression was
significant (R2 = 0.15). The significant predictors of crime were ASPD symptom count (p
= O.OOS), heroin use (p = 0.0002), and treatment at Clinic 1 (p = 0.03). Thus, there is consistent evidence that after adjusting for subject variables, subjects from
Clinic 1 reported more crime than those from the other two clinics. On self-report data,
crime was least at Clinic 2, but this did not differ significantly from Clinic 3. Results from police criminal records were used to confirm the differences between the
clinics apparent in self-reported crime data. For this analysis, subjects who in total received
less than three months total treatment are excluded, leaving a sample of 288 subjects. The
pre-treatment rates of offending were very similar for the three clinics. In-treatment
offense rates were lowest in Clinic 2, and highest in Clinic 1. Using pre-treatment property
offense rates, duration of treatment , and “clinic” as predictor variables, and in-treatment
offense rates as the dependent variable, the role of treatment was analyzed by linear regres-
sion. The overall regression was significant (R2 = 0.10). In this model, Clinic 2 served as
the reference clinic. Pre-treatment property offense rates were significantly predictive of in-treatment offense
rates. Longer duration of treatment was associated with lower crime rates. Adjusting for
these factors, Clinic 1 differed significantly from Clinic 2 0, = 0.009) in having higher rates
of offending. Clinic 3 was also higher than Clinic 2, but again the differences between
Clinic 3 and the other clinics did not reach significance. These figures provide an external reference point against which to compare the self-
report data. By both self-report and official records, the lowest rate of offending was at
Clinic 2, and the highest at Clinic 1, which on both measures differed significantly from

22 JOURNAL OF SUBSTANCE ABUSE Vol. 9/l 997
Clinic 2. The data suggest that both the duration of treatment, and the way it is delivered, predicted continued involvement in crime.
Differences in Treatment Delivered in the Three Clinics
In terms of formal delivery of treatment, the three clinics were very similar. In all three clinics, patients saw their doctor for regular, brief interviews. There was no other counsel- ing or other service provided in each clinic. Dispensing staff were all nurses, with similar training and experience working in methadone clinics. The mean daily methadone doses in the three clinics were 58,53, and 76 mg respectively. The goals of treatment enunciated by the three medical practitioners were very similar, and in none of the clinics were patients involuntarily discharged for continued drug use during treatment. Indeed, during the period of the study, only one patient was discharged involuntarily from one clinic (for non- payment of fees).
However, while superficially similar in the way treatment was delivered, and in the number and training of staff, the clinics differed markedly in “ambiance”. Clinic 3 was businesslike, a dispensing operation in which the manager conducted regular time and motion studies to ensure that a daily dose of methadone was dispensed efficiently. The clinic was well run, but there was little sense that it was a treatment service. An air of toler- ance, almost cynicism, was apparent in the staff-client interaction. Marijuana use was tolerated, and patients openly discussed their involvement in “rorts”-illegal activities-in earshot of staff. In contrast, Clinic 2 had a “treatment” ethos. It had the best maintained and most comprehensive files, and a more individualized approach to treatment. Although there were no punitive sanctions against drug use, the prescribing doctor urged patients to avoid use of cannabis and benzodiazepines, and placed emphasis on the need for patients to seek employment.
Clinic 1 stood out in having a prevailing atmosphere of chaos. The daily dispensing of methadone took place in an atmosphere of intense pressure, accompanied by loud and public interactions between staff and patients over issues such as payment of fees, take- away doses, and topics unrelated to treatment. Although officially there was a queuing system, whereby patients took a ticket on arrival in order to be dosed in order, in practice the system was ignored and patients thronged around the entrance to the dispensing area. The clinic had a computerized dosing system, but none of the staff had been trained in the use of the system, and whenever a problem arose (which was on most days) there was no- one who could remedy the problem. In the longer term, no efforts were made to avoid these problems by training staff or discussing what was occurring.
DISCUSSION
Interpretation of these results needs to take into account the pattern of illicit drug use in treatment in these three clinics. On entry to treatment, there was a prompt and substantial drop in heroin use reported in all clinics. Although there were marked differences between the clinics, at first interview about 50% of subjects reported having used heroin in the month prior to interview, and about 60% reported having used cannabis. By the third inter- view, just under 30% of respondents reported having used heroin, but there were still 60% reporting cannabis use. Furthermore, average daily cannabis use actually increased over

Methadone Maintenance and Drug-Related Crime 23
the 12 months between interviews. Thus, both heroin use and acquisitive crime dropped on entry to treatment, and continued to fall with increasing duration of treatment. However, as heroin use fell, cannabis use emerged as the predictor of continued acquisitive crime.
These changes were not uniform across the three clinics. At first interview, heroin use was highest at Clinic 1, and did not fall with increasing duration of treatment. At third interview, the proportion of respondents at Clinic1 still reporting heroin use had actually increased. In both other clinics, heroin use was significantly lower at third interview than at initial interview. Furthermore, subjects from Clinic 2 reported significantly lower cannabis use (5 1% of respondents) than subjects from Clinic 1 (65%) and Clinic 3 (67%). These differences go some way to explaining why subjects from Clinic 2 had greater reductions in criminal activity than subjects at the other two clinics.
This appears to have been a treatment effect rather than a result of selection bias. All employed the same criteria for eligibility for treatment-opioid dependence-and there was nothing in the client characteristics to suggest selection bias contributed to differences in outcomes between the clinics. Although the three clinics were located in different socio- economic areas, the clientele in the clinics were very similar in terms of age, education, employment, and pre-treatment criminality. All analyses adjusted for subject variables. Most importantly, interpretation of the findings in relation to crime needs to take into account other differences in treatment outcomes between the clinics. There was consistent evidence that Clinic 1 had many problems. Subjects treated at that clinic reported the high- est rate of heroin, cannabis, and benzodiazepine use, were more likely to drop out of treatment, and rated their treatment less highly than subjects from the other two clinics (Bell et al., 1995). Thus, the findings in relation to greater involvement in crime did not come in isolation, but were part of a consistent picture of less effective treatment delivered at this clinic. Thus the important finding-that after controlling for drug use and for sever- ity of ASPD, subjects from Clinic1 reported significantly higher involvement in crime- not only is supported by analysis of official records, but occurs in a context of consistently worse outcomes. It represents strong evidence that the differences in crime at the three clin- ics were the result of differences in the way treatment was delivered.
The cost of illicit drugs was the major factor identified in this study as driving involve- ment in acquisitive crime, and the effectiveness of treatment in reducing crime appears to be largely a function of the extent to which illicit drug use is reduced. In addition, particular individuals appear to be consistently more involved in property crime, as demonstrated by the finding that pre-treatment property conviction rates were highly predictive of in-treat- ment rates. This observation is consistent with previous reports from the USA (Ball, Shaffer, & Nurco, 1983; Nurco, Hanlon, Kinlock, & Duszynski, 1989). Lifetime ASPD symptom count also was predictive of persisting involvement in crime. Although recent involvement in crime may contribute to ASPD symptom count, the majority of behaviors explored in the DIS cover such criteria as impulsivity, irritability, reckless disregard for safety, and consistent irresponsibility, are not directly met by engaging in acquisitive crime. Thus it seems reasonable to conclude that temperament and personality traits are factors predisposing to continued involvement in crime.
The high prevalence of ASPD in this sample is a reminder of the severity and complexity of the problems being addressed in methadone treatment. For people with a long history of poor impulse control, limited social skills, and pervasive moods of frustration, it is unreal- istic to expect an immediate transformation on entry into treatment. Continuing

24 JOURNAL OF SUBSTANCE ABUSE Vol. 9/l 997
involvement in illegal and antisocial acts should be seen not as a failure of treatment, but
as an expression of the severity of the problems of those in treatment. Viewed in this
context, the dramatic reduction in crime, and progressive reduction with increasing dura- tion of treatment, represent a powerful argument for the effectiveness of methadone clinics
in reducing crime. There are two broad limitations to the data. The first is that measures of crime-both
self-report and official records-are biased. Self-report is subject to expectancy bias. over generalization, and the vagaries of memory. Official records are an insensitive measure of
an individual’s involvement in crime. Nonetheless, there was good agreement between the two measures, with both approaches confirming both the effectiveness of treatment over-
all, and the differences in effectiveness between the clinics. The second weakness is that conclusions about the effectiveness of treatment are more
robust if drawn from controlled trials rather than from an observational study. However,
observational studies have one advantage-they permit us to see treatment as it is actually delivered, and to identify problems with it. It is difficult to imagine setting up a trial in
which some patients are randomized to receive treatment in a chaotic and poorly managed clinic. The observation that organization and management style appeared to be the chief
factors differentiating the clinics came as a surprise during this research, and one which points the way to relatively simple approaches to improving treatment efficacy.
REFERENCES
Ball. J.C.. Shaffer, J.W.. & Nurco. D.N. ( 1983). The day-to-day criminality of heroin addicts in Bal- timore: A study in the continuity of offense rates. Dqq cmtl Alcohol Dqxvu~enc~r. 12. I 19-142.
Ball, J.C., & Ross, A. (199 1). Thr r~~~cti~~n~.s.s c~fmethudonr~ maintrnuncc trcutmcnt: Putirnt.s, pry
grurns, .srrvicrs, and outcome. New York: Springer-Verlag. Bell. J.R., Ward, J., Mattick, R.P.. Hay. A.. Chan, J., & Hall, W. (1995). An evaluation of private
methadone clinics. National Drug Str&cgy Monograph No. 4. Canberra. Australia: Australian Governrnent Publishing Service.
Darke. S., Hall, W. Heather. N.. Wodak, A., & Ward. J. (1992). Development and validation of a multi-dimensional instrument for assessing outcome of treatment among opioid users: The Opiate Treatment Index. British Journal of Addictiorl, 87, 593-602.
Darke. S.. Hall, W.. & Swift, W. (I 994) Prevalence. symptoms, and correlates of antisocial person- ality disorder among methadone maintenance clients. Drug and Alcohol Drprndencc~, 34. ?53-
257. Dobinson. I., & Ward, P. (1987). Drugs und Crime--Phus~, II. Sydney, Australia: New South Wales
Bureau of Crime Statistics and Research. Hall, W., Bell, J.. & Carless, J. (1993). Crime and drug use among applicants for methadone mainte-
nance. Drug and Alcohol Dqx~d~u~. 31. 123- 129. Hammersley. R., Forsyth. A, & Lavelle. T. (1990). The criminality of new drug users in Glasgow.
British Journul qf Addiction, HS. 1583-I 594. Hammersley. R.. Forsyth, A., Morrison. V.. & Davies. J.B. (1989). The relationship between crime
and opioid use. British Journal ofAddiction, 84, 1029-1043. Hubbard, R.L., Marsden, M.E., Rachal. J.V.. Harwood. H.J.. Cavanagh, E.R., & Ginsberg. H.M.
(1989). Drug ahu.se trCutment: A national SW!\. of .$~ctivene.ss. USA: University of North Carolina Press.
Inciardi. JA. (1979). Heroin use and street crime. Crime crnd Drlinyucvxy. 25, 335346.

Methadone Maintenance and Drug-Related Crime 25
MacGregor, S. (1990). Could Britain inherit the American nightmare? British Journal ofAddiction,
85,863~872. Nurco, D.N., Ball, J.C., Shaffer, J.W., & Hanlon, T.E. (1985). The criminality of narcotic addicts.
Journal ofNervou.s and Mental Diseases, 173, 94-102.
Nurco, D.N., Hanlon, T.E., Kinlock, T.W., & Duszynski, K.R. (1989). The consistency of types of criminal behavior over preaddiction, addiction, and nonaddiction status periods. Comprehen- sire Psychiatry, 30, 39 1402.
Robins, L.N., Helzer, J.E., Croughan, J., & Ratcliff, K. (1981). National Institute of Mental Health Diagnostic Interview Schedule. Its history, characteristic, and validity. Archives of General Psychiatry, 38. 381-389.