mechanical properties of aaa tissue
TRANSCRIPT

Journal of Biomechanics ] (]]]]) ]]]–]]]
Contents lists available at ScienceDirect
journal homepage: www.elsevier.com/locate/jbiomech
Journal of Biomechanics
0021-92
doi:10.1
n Corr
Comput
IA 5224
E-m
Pleasunru
www.JBiomech.com
Biomechanical failure properties and microstructural content of rupturedand unruptured abdominal aortic aneurysms
Madhavan L. Raghavan a,n, Mauro M. Hanaoka b, Jarin A. Kratzberg a,Maria de Lourdes Higuchi b, Erasmo Simao da Silva b
a Department of Biomedical Engineering, University of Iowa, Iowa City, IA, USAb University of S~ao Paulo Medical School, S~ao Paulo, SP, Brazil
a r t i c l e i n f o
Article history:
Accepted 3 June 2011Purpose: To test the hypothesis that ruptured abdominal aortic aneurysms (AAA) are globally weaker
than unruptured ones.
Keywords:
Abdominal aortic aneurysm
Failure properties
Mechanical testing
Rupture
90/$ - see front matter & 2011 Elsevier Ltd. A
016/j.jbiomech.2011.06.004
esponding author. Department of Biomedica
er-Aided Design, 1136 Seamans Center (SC), U
2-1527, USA. Tel.: þ1 319 335 5704; fax: þ1
ail address: [email protected] (M.L. Ra
e cite this article as: Raghavan, Mptured abdominal aortic aneurysms
a b s t r a c t
Methods: Four ruptured and seven unruptured AAA specimens were harvested whole from fresh
cadavers during autopsies performed over an 18-month period. Multiple regionally distributed
longitudinally oriented rectangular strips were cut from each AAA specimen for a total of 77 specimen
strips. Strips were subjected to uniaxial extension until failure. Sections from approximately the
strongest and weakest specimen strips were studied histologically and histochemically. From the load-
extension data, failure tension, failure stress and failure strain were calculated. Rupture site
characteristics such as location, arc length of rupture and orientation of rupture were also documented.
Results: The failure tension, a measure of the tissue mechanical caliber was remarkably similar
between ruptured and unruptured AAA (group mean7standard deviation of within-subject means:
11.272.3 versus 11.673.6 N/cm; p¼0.866 by mixed model ANOVA). In post-hoc analysis, there was
little difference between the groups in other measures of tissue mechanical caliber as well such as
failure stress (95728 versus 98723 N/cm2; p¼0.870), failure strain (0.3970.09 versus 0.3670.09;
p¼0.705), wall thickness (1.770.4 versus 1.570.4 mm; p¼0.470) , and % coverage of collagen within
tissue cross section (49.6712.9% versus 60.879.6%; p¼0.133). In the four ruptured AAA, primary
rupture sites were on the lateral quadrants (two on left; one on left-posterior; one on right).
Remarkably, all rupture lines had a longitudinal orientation and ranged from 1 to 6 cm in length.
Conclusion: The findings are not consistent with the hypothesis that ruptured aortic aneurysms are
globally weaker than unruptured ones.
& 2011 Elsevier Ltd. All rights reserved.
1. Introduction
Rupture of abdominal aortic aneurysm (AAA) is a poorlyunderstood phenomenon. Some aneurysms rupture as they growlarger, while many large ones do not. There has been considerableinterest in studying the mechanical characteristics of theselesions under the premise that rupture occurs when the tangen-tial tension and/or stretch on the AAA wall from blood pressureexceeds maximum allowable thresholds. Understanding the tol-erable threshold of force and stretch – the mechanical failureproperties – and the structural content that manifest in theseproperties can therefore be valuable in gaining insights into thephenomenon of rupture. Numerous studies have reported on the
ll rights reserved.
l Engineering and Center for
niversity of Iowa, Iowa City,
319 335 5631.
ghavan).
.L., et al., Biomechanical fa. Journal of Biomechanics (2
mechanical and structural properties of unruptured AAA tissue(Di Martino et al., 1998, 2006; He and Roach 1994; Raghavanet al., 1996; Vallabhaneni et al., 2004; Vorp et al., 1996, 2001;Thubrikar et al., 2001; Vande Geest et al., 2006a, 2006b). How-ever, there have been only two studies that reported on mechan-ical properties of ruptured AAA presumably because they rarelybecome available for studies (Di Martino et al., 2006; Raghavanet al., 2006). This limits our ability to reliably assess differencesbetween these lesions. A key question in this context is whetherthe aortic tissue in aneurysms that rupture is weaker and hencemore susceptible to failure under the same pressure-induced walltension than that in unruptured ones? This is the questionmotivating this study. A few additional, but related questionsare as follows: is the location and orientation of the tear in aruptured AAA consistent across patients or is it random? Howdoes tissue microstructure such as collagen, elastin or smoothmuscle cell content vary between ruptured and unruptured AAA?Further, what of regional variation in properties of AAA? Some
ilure properties and microstructural content of ruptured and011), doi:10.1016/j.jbiomech.2011.06.004

M.L. Raghavan et al. / Journal of Biomechanics ] (]]]]) ]]]–]]]2
studies have reported that the posterior wall is a preferredrupture site (da Silva et al., 2000; Darling et al., 1977). Is theAAA wall weaker on its posterior than its anterior in ruptured orunruptured AAA? This study aims to test the hypothesis thatruptured AAAs are on average weaker than unruptured AAAswhile also addressing some of the related questions posed here.
In this collaborative study between clinical investigators at theUniversity of S~ao Paulo, Brazil, and engineering investigators atthe University of Iowa, USA, unruptured and ruptured AAAs werewholly harvested during necropsy and the regional variations inwall thickness, mechanical properties and cellular content wereassessed. Investigators in Brazil performed specimen procure-ment and experiments. Investigators from the United Statesfabricated and installed the experimental apparatus in Brazil,and performed data analysis.
2. Methods
2.1. Specimen procurement and preparation
The study was approved by the institutional review board (Ethical Committee
of Clinics Hospital, S~ao Paulo University Medical School—#849/99). Whole AAA
specimens were excised from cadavers submitted to necropsy for the elucidation
of the cause of death at the Service for Confirmation of Deaths at S~ao Paulo
University School of Medicine. Specimens extended from a few centimeters
proximal to the renal arteries to a few centimeters distal to the iliac bifurcation.
Testing of specimen samples was completed within 24 h of harvest and within
48 h of death. The specimens were stored in saline at 4 1C where necessary during
this period. The harvested AAA was photographed using a custom-built 3601 view
camera system in order to document its surface shape. For this, the AAA was
hooked by three sutures inserted at a suprarenal site and hung in a static position
at the approximate center of rotation of the camera lever arm. A custom-built
large balloon device was inserted inside the AAA to have it under physiological
pressure during imaging (da Silva et al., 2000). The AAA was sectioned axially at
the anterior surface and intrasac thrombus was removed. Wall thickness was
measured along the exposed edge using digital calipers by a single investigator to
maintain consistency in the measurement. The measurement sites were labeled
on a suitable image from the 3601 image sequence. Multiple longitudinally
oriented rectangular strips of specimens were cut all around the circumference
of the AAA using a 4 mm wide cutting die. The location of the rectangular strips on
the AAA wall surface was also marked on the images. The study focused on
properties in the longitudinal orientation to maximize within-subject samples for
regional coverage while maintaining consistency in comparisons.
2.2. Mechanical testing
Mechanical extension tests were performed using an Instron Spec2200 table
top tester (Instron Corporation, Norwood, MA) with custom fabricated specimen
bath and custom soft tissue grips. Each specimen strip was clamped in the tissue
grips and attached to the crossheads of the test device. The specimen bath was
filled with saline at room temperature. The length (l0), the width (w0) and the
thickness (t0) of the specimen strip between the clamps were recorded. The zero
length was attained by placing a negligible preload on the specimen. Width and
thickness were measured at three sites and averaged. Preconditioning was
performed by loading and unloading the specimen to 5% extension at 20% of
specimen length/min. The strip was uniaxially extended also at 20%/min until
failure while recording the force and extension at an acquisition rate of 1 Hz. The
location of specimen failure with respect to the clamps was recorded in order to
identify and discard specimens that failed too close to the clamp (within 3 mm) as
these may have been due to tissue damage during clamping. The minor effect on
force from the gradually decreasing pressure head as the specimen rises through
the saline in the bath was documented and corrected by performing the test
without a specimen between the grips. All tests were performed by filling the
saline to the same level in order to have a consistent effect. The force-extension
data recorded without the specimen was subtracted from the data for tests with
each specimen in order to eliminate this linearly varying water bath pressure head
artifact during the test.
2.3. Histology and histochemical assessment
Tiny sections from specimen strips excised prior to mechanical tests were sent
to the Histology Laboratory, Division of Cardiology, University of S~ao Paulo, for
histology and histochemical analysis. Histology analysis included fixing in 10%
formalin and selective staining of tissue specimens (Verhoeff’s for elastin,
Please cite this article as: Raghavan, M.L., et al., Biomechanical faunruptured abdominal aortic aneurysms. Journal of Biomechanics (2
trichrome for collagen and T-Masson stain for smooth muscle cells) from which
the cross sectional area covered by each of collagen, elastin, smooth muscle cells
(SMC) and fat was recorded. Segments were visualized using a 20� magnification
and analyzed in an Image Analysis System, Quantimet 500 (Leica Inc., Germany).
Additionally, immunohistochemical reactions were performed in serial sections
from two fragments of each AAA—the weakest and/or strongest specimen strips
(based on Ff). The monoclonal antibodies against metalloproteinase MMP9,
C-reactive protein and inflammatory cells were used. For these, a semiquantifica-
tion evaluation was performed: 0 (absent), 1 (scarce and focal positivity), 2
(multifocal positivity) and 3 (diffuse positivity).
2.4. Data analysis
The AAA images and specimen locations were digitized. The locations of wall
thickness measurement sites and specimens were mapped to polar coordinates.
Custom algorithms were developed to geographically categorize the specimen
locations to facilitate regional classifications. The force-extension data from
mechanical testing was used to determine the peak load (Ff) and extension at
peak load (df). The failure properties calculated were failure tension (Tf), failure
stress (Sf) and failure strain (ef) as reported previously (Raghavan et al., 2006).
Failure strain (extension at peak load as a fraction of original length), ef ¼ df =l0Failure tension (peak load per unit width of specimen strip), Tf ¼
ðFf =w0Þffiffiffiffiffiffiffiffiffiffiffiffi1þef
pÞ
�
Failure stress (peak load per unit cross sectional area of specimen strip),
Sf ¼ ðFf =w0t0Þð1þef Þ
where, l0, w0 and t0 are the length, the width and the thickness of the specimen
strip between the clamps at zero load. The ef terms in above equations account for
the reduction in cross sectional area in case of stress calculations and reduction in
width for tension calculations (Raghavan et al., 1996). Rupture site characteristics
such as location, arc length of rupture and orientation of rupture were also
documented where present. Rupture site locations were regionally classified as
anterior (landmarked based on the celiac artery), left, posterior and right in the
circumferential direction. In the axial direction, they were classified as proximal,
mid-section and distal.
2.5. Statistical treatment
Since multiple but unequal number of specimens were harvested from each
subject, the between-group comparisons were done using mixed model ANOVA
with the grouping variable (e.g., rupture status) as a fixed effect and within-
subject specimens as random effects (Del Prete et al., 2004). Means reported are
the group means of the within-subject means while standard deviations are the
group standard deviations of the within-subject means. In the case of histochem-
ical measures – inflammation, C-reactive protein and MMP9 – given that only 1–2
within-subject measurements were collected, the within-subject means were
used to compare the groups by a Mann–Whitney test. The a priori hypothesis to
be tested was that ruptured AAAs are weaker (i.e., have a lower failure tension)
than unruptured ones with statistical significance at po0.05. All other group
comparisons (e.g., anterior versus posterior) were considered post-hoc and
exploratory.
3. Results
Over a period of 18 months, four ruptured and nine unrup-tured AAAs were harvested and studied. Table 1 lists demo-graphic, morphological and other relevant characteristics forthis study population. Photographs of all the AAAs in the studypopulation are shown in Fig. 1. A total of 145 specimen stripswere cut and tested in this study. Specimen strip orientationswere longitudinal for 4 of 4 ruptured and 7 of 9 unrupturedaneurysms. To enable post-hoc comparison of orientations, onlycircumferential strips were cut from 2 of 9 unruptured AAAs. Testdata from 32 specimen strips that failed at the clamp (i.e., thefailure location during extension test of the strip was less than3 mm from either clamp) were discarded. The location of stripsused for testing was approximately spread out all around the AAA(77) and where available, from the undilated neck (9), suprarenalaorta (14), iliacs (2) and the thoracic aorta (10). See Table 1 for thenumber of valid (i.e., no clamp tear) AAA strips tested for eachsubject. Within longitudinal specimens taken from ruptured andunruptured AAAs, the distribution of failure properties – failure
ilure properties and microstructural content of ruptured and011), doi:10.1016/j.jbiomech.2011.06.004
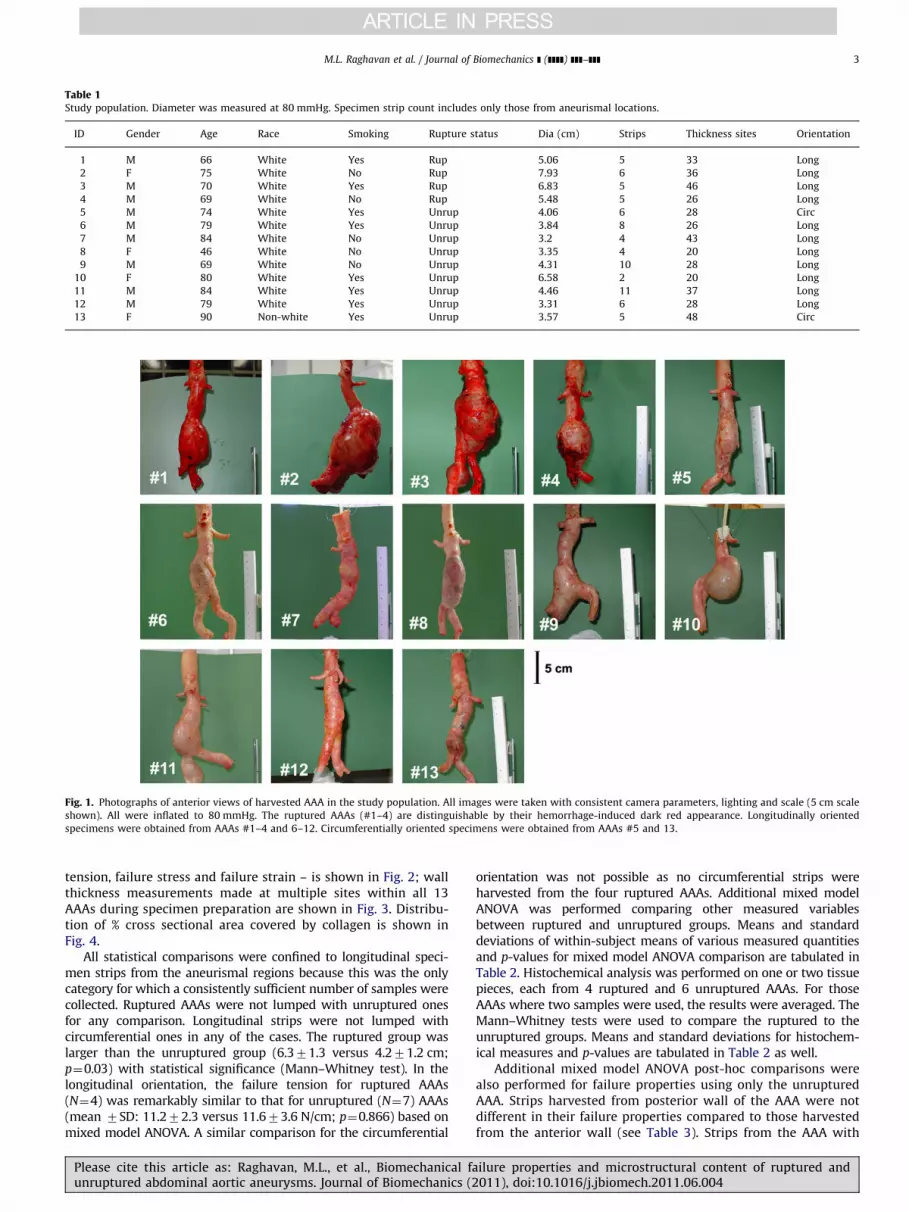
Fig. 1. Photographs of anterior views of harvested AAA in the study population. All images were taken with consistent camera parameters, lighting and scale (5 cm scale
shown). All were inflated to 80 mmHg. The ruptured AAAs (#1–4) are distinguishable by their hemorrhage-induced dark red appearance. Longitudinally oriented
specimens were obtained from AAAs #1–4 and 6–12. Circumferentially oriented specimens were obtained from AAAs #5 and 13.
Table 1Study population. Diameter was measured at 80 mmHg. Specimen strip count includes only those from aneurismal locations.
ID Gender Age Race Smoking Rupture status Dia (cm) Strips Thickness sites Orientation
1 M 66 White Yes Rup 5.06 5 33 Long
2 F 75 White No Rup 7.93 6 36 Long
3 M 70 White Yes Rup 6.83 5 46 Long
4 M 69 White No Rup 5.48 5 26 Long
5 M 74 White Yes Unrup 4.06 6 28 Circ
6 M 79 White Yes Unrup 3.84 8 26 Long
7 M 84 White No Unrup 3.2 4 43 Long
8 F 46 White No Unrup 3.35 4 20 Long
9 M 69 White No Unrup 4.31 10 28 Long
10 F 80 White Yes Unrup 6.58 2 20 Long
11 M 84 White Yes Unrup 4.46 11 37 Long
12 M 79 White Yes Unrup 3.31 6 28 Long
13 F 90 Non-white Yes Unrup 3.57 5 48 Circ
M.L. Raghavan et al. / Journal of Biomechanics ] (]]]]) ]]]–]]] 3
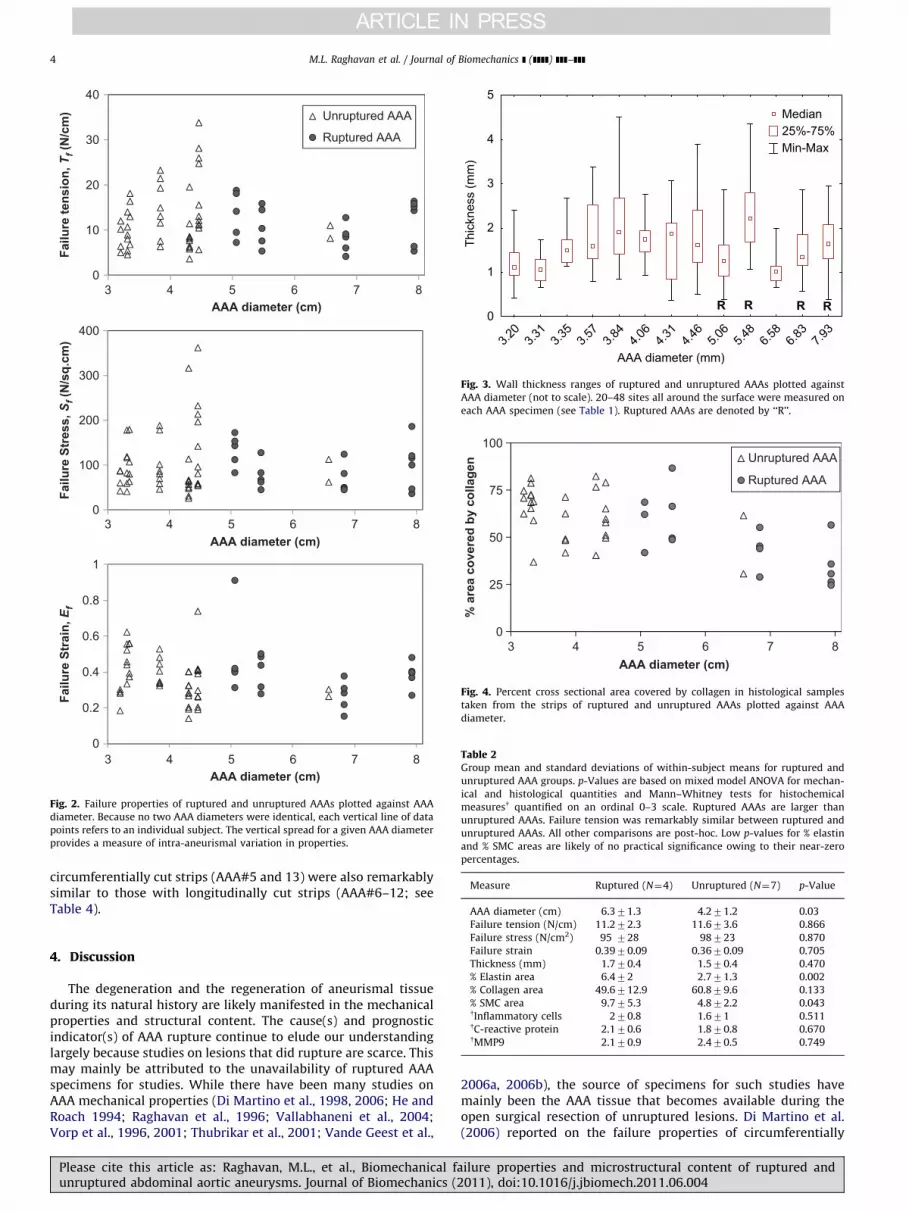
tension, failure stress and failure strain – is shown in Fig. 2; wallthickness measurements made at multiple sites within all 13AAAs during specimen preparation are shown in Fig. 3. Distribu-tion of % cross sectional area covered by collagen is shown inFig. 4.
All statistical comparisons were confined to longitudinal speci-men strips from the aneurismal regions because this was the onlycategory for which a consistently sufficient number of samples werecollected. Ruptured AAAs were not lumped with unruptured onesfor any comparison. Longitudinal strips were not lumped withcircumferential ones in any of the cases. The ruptured group waslarger than the unruptured group (6.371.3 versus 4.271.2 cm;p¼0.03) with statistical significance (Mann–Whitney test). In thelongitudinal orientation, the failure tension for ruptured AAAs(N¼4) was remarkably similar to that for unruptured (N¼7) AAAs(mean 7SD: 11.272.3 versus 11.673.6 N/cm; p¼0.866) based onmixed model ANOVA. A similar comparison for the circumferential
Please cite this article as: Raghavan, M.L., et al., Biomechanical faunruptured abdominal aortic aneurysms. Journal of Biomechanics (2
orientation was not possible as no circumferential strips wereharvested from the four ruptured AAAs. Additional mixed modelANOVA was performed comparing other measured variablesbetween ruptured and unruptured groups. Means and standarddeviations of within-subject means of various measured quantitiesand p-values for mixed model ANOVA comparison are tabulated inTable 2. Histochemical analysis was performed on one or two tissuepieces, each from 4 ruptured and 6 unruptured AAAs. For thoseAAAs where two samples were used, the results were averaged. TheMann–Whitney tests were used to compare the ruptured to theunruptured groups. Means and standard deviations for histochem-ical measures and p-values are tabulated in Table 2 as well.
Additional mixed model ANOVA post-hoc comparisons werealso performed for failure properties using only the unrupturedAAA. Strips harvested from posterior wall of the AAA were notdifferent in their failure properties compared to those harvestedfrom the anterior wall (see Table 3). Strips from the AAA with
ilure properties and microstructural content of ruptured and011), doi:10.1016/j.jbiomech.2011.06.004
0
10
20
30
40
3 4 5 6 7 8
3 4 5 6 7 8
3 4 5 6 7 8
Failu
re te
nsio
n, T
f (N
/cm
)
AAA diameter (cm)
Unruptured AAA
Ruptured AAA
0
100
200
300
400
Failu
re S
tres
s, S
f (N
/sq.
cm)
AAA diameter (cm)
0
0.2
0.4
0.6
0.8
1
Failu
re S
trai
n, E
f
AAA diameter (cm)
Fig. 2. Failure properties of ruptured and unruptured AAAs plotted against AAA
diameter. Because no two AAA diameters were identical, each vertical line of data
points refers to an individual subject. The vertical spread for a given AAA diameter
provides a measure of intra-aneurismal variation in properties.
Median 25%-75% Min-Max
3.20
3.31
3.57
3.84
AAA diameter (mm)
0
1
2
3
4
5
Thic
knes
s (m
m)
R R R R
4.06
4.31
4.46
5.06
5.48
6.58
6.83
7.93
3.35
Fig. 3. Wall thickness ranges of ruptured and unruptured AAAs plotted against
AAA diameter (not to scale). 20–48 sites all around the surface were measured on
each AAA specimen (see Table 1). Ruptured AAAs are denoted by ‘‘R’’.
0
25
50
75
100
3
% a
rea
cove
red
by c
olla
gen
AAA diameter (cm)
Unruptured AAA
Ruptured AAA
4 5 6 7 8
Fig. 4. Percent cross sectional area covered by collagen in histological samples
taken from the strips of ruptured and unruptured AAAs plotted against AAA
diameter.
Table 2Group mean and standard deviations of within-subject means for ruptured and
unruptured AAA groups. p-Values are based on mixed model ANOVA for mechan-
ical and histological quantities and Mann–Whitney tests for histochemical
measuresy quantified on an ordinal 0–3 scale. Ruptured AAAs are larger than
unruptured AAAs. Failure tension was remarkably similar between ruptured and
unruptured AAAs. All other comparisons are post-hoc. Low p-values for % elastin
and % SMC areas are likely of no practical significance owing to their near-zero
percentages.
Measure Ruptured (N¼4) Unruptured (N¼7) p-Value
AAA diameter (cm) 6.371.3 4.271.2 0.03
M.L. Raghavan et al. / Journal of Biomechanics ] (]]]]) ]]]–]]]4
circumferentially cut strips (AAA#5 and 13) were also remarkablysimilar to those with longitudinally cut strips (AAA#6–12; seeTable 4).
Failure tension (N/cm) 11.272.3 11.673.6 0.866
Failure stress (N/cm2) 95 728 98723 0.870
Failure strain 0.3970.09 0.3670.09 0.705
Thickness (mm) 1.770.4 1.570.4 0.470
% Elastin area 6.472 2.771.3 0.002
% Collagen area 49.6712.9 60.879.6 0.133
% SMC area 9.775.3 4.872.2 0.043yInflammatory cells 270.8 1.671 0.511yC-reactive protein 2.170.6 1.870.8 0.670yMMP9 2.170.9 2.470.5 0.749
4. Discussion
The degeneration and the regeneration of aneurismal tissueduring its natural history are likely manifested in the mechanicalproperties and structural content. The cause(s) and prognosticindicator(s) of AAA rupture continue to elude our understandinglargely because studies on lesions that did rupture are scarce. Thismay mainly be attributed to the unavailability of ruptured AAAspecimens for studies. While there have been many studies onAAA mechanical properties (Di Martino et al., 1998, 2006; He andRoach 1994; Raghavan et al., 1996; Vallabhaneni et al., 2004;Vorp et al., 1996, 2001; Thubrikar et al., 2001; Vande Geest et al.,
Please cite this article as: Raghavan, M.L., et al., Biomechanical faunruptured abdominal aortic aneurysms. Journal of Biomechanics (2
2006a, 2006b), the source of specimens for such studies havemainly been the AAA tissue that becomes available during theopen surgical resection of unruptured lesions. Di Martino et al.(2006) reported on the failure properties of circumferentially
ilure properties and microstructural content of ruptured and011), doi:10.1016/j.jbiomech.2011.06.004

M.L. Raghavan et al. / Journal of Biomechanics ] (]]]]) ]]]–]]] 5
oriented AAA tissue specimens harvested from anterior mid-section during surgical resection of 16 unruptured and 9 rupturedAAAs. They found that the failure stress, Sf, was lower in rupturedAAA, but without statistical significance (54 V s, 82 N/cm2;p¼0.04—not significant because Bonferroni correction for multi-ple hypotheses required po0.006 for significance). The currentstudy uses fewer subjects than the earlier report by Di Martinoet al. (2006) on ruptured versus unruptured AAAs, but accountsfor the key regional variations in properties with rigor. Further,while that study focused on circumferential properties, this studyfocused on longitudinal properties. Considering the considerableregional variations in failure properties possible in the AAA(Thubrikar et al., 2001; Raghavan et al., 2006), the comparisonbetween ruptured and unruptured AAAs is better done on awhole-AAA basis. Thus, to reliably assess ruptured AAA, cadaverstudies are likely the only alternative. Earlier, our group reportedon a preliminary exploratory study of three unruptured and oneruptured AAA harvested wholly from cadavers (Raghavan et al.,2006). One key limitation of that study – in addition to low studypopulation – was that the specimens were frozen for days toweeks prior to testing and this may have affected estimates. Thepresent study compared structural and mechanical propertiesbetween ruptured and unruptured aneurysms and reportedrigorous observations on the rupture site providing insights intokey questions regarding AAA rupture.
Table 3Comparison of failure properties between longitudinally oriented strips harvested
from the anterior and posterior surfaces of unruptured AAAs. Group mean and
standard deviations of within-subject means are shown. p-Values are based on
mixed model ANOVA.
Measure Anterior (N¼7) Posterior (N¼6a) p-Value
Thickness (mm) 1.570.3 1.670.3 0.410
Failure tension (N/cm) 11.674.7 12.275.0 0.933
Failure stress (N/cm2) 102728 100746 0.881
Failure strain 0.3570.09 0.470.10 0.587
a No posterior strips were obtained from one aneurysm.
Table 4Comparison of failure properties between unruptured AAAs from which only
longitudinally oriented strips were harvested and those from which only circum-
ferentially oriented strips were harvested. Group mean and standard deviations of
within-subject means are shown. p-Values are based on mixed model ANOVA.
Differences in failure stress can be attributed to incidental difference in strip
thickness between the groups. Note the similarity in failure tension and conse-
quently wall mechanical caliber.
Long (N¼7) Circ (N¼2) p-Value
Strip thickness (mm) 1.570.3 270.1 0.041
Failure tension (N/cm) 12.173.7 10.572.0 0.645
Failure stress (N/cm2) 103721 6579 0.099
Failure strain 0.3870.09 0.3870.07 0.978
Table 5Rupture site characteristics.
ID Rupture location Rupture length
(cm)
Ru
1 Left mid-section 2.5 Lo
2 Left; mid- to iliac-bifurcation 5.5 Lo
3 Site1: Left-posterior junction;
mid-iliac bifurcation; Site 2: right; mid-section
Site 1: 6.1;
Site 2: 2.25
Si
Si
4 Right; mid-section 2 Lo
Please cite this article as: Raghavan, M.L., et al., Biomechanical faunruptured abdominal aortic aneurysms. Journal of Biomechanics (2
4.1. Ruptured versus unruptured AAAs
The question motivating this study is whether the AAAs thatruptured are weaker (i.e., have a greater susceptibility to fail) thanthose that did not at the time of death. Perhaps the best measureof wall caliber is the failure tension, which lumps the contribu-tions from wall thickness and failure stress (Raghavan et al.,2006). It is conventional to focus on failure stress, but this wouldneedlessly normalize out a key determinant of vulnerability torupture, namely wall thickness, which we avoid here. Never-theless, it is noteworthy that the interpretations drawn are nodifferent if one were to focus on failure stress instead of failuretension (see Fig. 2). In the current study population of aneurysmsfrom which all strips were longitudinal, mean (of within-subjectmean) failure tension was remarkably similar between theruptured and unruptured groups (see Table 2). The results arenot consistent with the hypothesis that ruptured AAAs are weakerthan unruptured ones.
Additional post-hoc comparisons were also performed, mainlyto explore the data for any new hypothesis that may be tested infuture populations. There is little evidence of significant differ-ences between ruptured and unruptured AAAs for other proper-ties as well—failure strain, failure stress, wall thickness and %cross sectional area covered by collagen. Histological quantities, %area covered by elastin and SMC, did show low p-values, but theyare of little consequence because they are both quite depleted andof low percentage where small measurement errors inducesignificant noise. Note that the ruptured and unruptured groupsare not size-matched (ruptured dia versus unruptured dia:6.371.3 versus 4.271.2 cm; p¼0.03) as we cannot control thespecimens that became available in the study period. Just byvirtue of their larger size, the ruptured group should be predis-posed to be weaker, not stronger. Thus, while a size-matchedcomparison would have been preferable, the fact that rupturedAAAs were not any weaker despite being larger than the unrup-tured aneurysms only further underscores the lack of support forthe hypothesis that the former ones are globally weaker. A secondlimitation to consider is that a ruptured versus unrupturedcomparison was not performed for the failure properties in thecircumferential orientation. The choice of having all strips withlongitudinal orientation was to maximize the number of speci-men strips tested with a consistent orientation and becauseprevious studies found the longitudinal orientation to be of lowerfailure stress (Raghavan et al., 1996). Nevertheless, comparisonsbetween ruptured and unruptured AAAs in the circumferentialdirection would be valuable especially given that all ruptureswithin the AAAs had a longitudinal orientation (see Table 5 andFig. 5) suggesting that the circumferential tension may havebreached the circumferential failure tension. In this context, it isworthwhile to note that within the unruptured group, the stripstested in two AAAs (#5 and #13) had circumferential orientations(these were not included in any prior comparisons to rupturedAAAs). As apparent from Table 4, the failure tension in thecircumferential orientation did not significantly differ from that
pture orientation Comments
ngitudinal Rupture site sutured
ngitudinal
te 1: Longitudinal;
te 2: longitudinal
Site 1 is the primary rupture site; Site 2 is a dissection
followed by rupture
ngitudinal Site apparent only under inspection
ilure properties and microstructural content of ruptured and011), doi:10.1016/j.jbiomech.2011.06.004

543210
cm
Left-posteriorAAA #1
Anterior-leftAAA #2 AAA #3
Posterior Left-posteriorAAA #4
Right
Fig. 5. Photographs of ruptured AAAs under physiological balloon pressure (80–100 mmHg). All images are to the same scale (ruler on left) with consistent camera
parameters. White arrowheads point to the rupture sites. The circumferential view depicted in the photograph was chosen for best visualization of rupture site. Rupture
site in AAA #1 is sutured. For AAA #3, both primary and secondary rupture sites are shown.
M.L. Raghavan et al. / Journal of Biomechanics ] (]]]]) ]]]–]]]6
in the longitudinal orientation. This however needs to be con-firmed in an independent study.
AAA-wide averages aside, could it be that the weakest strip in theruptured AAA is much weaker than that in the unruptured AAA?After all, an aneurysm needs to have just one weak spot for ruptureto occur. In our study population, weakest strips in the rupturedAAA were not significantly weaker than the weakest strips in theunruptured AAA (group mean of within-subject minimumTf¼5.6 V s. 5.8 N/cm; p¼0.925 by Mann–Whitney test). It is how-ever worthnoting that while the strips tested do come from allaround the AAA, they do not cover every single spot in the aneurysmand particularly do not come from the rupture site itself—a practicalimpossibility. The weakest strip among those tested need notnecessarily be the weakest possible strip within a given AAA andtherefore caution is warranted in interpreting this latter result.
Overall, our findings have some interesting similarities anddifferences with the report by Di Martino et al. (2006), study designdifferences notwithstanding. Failure stresses are roughly in thesame range in both studies (20–200 N/cm2), but for outliers. Inboth studies, unruptured AAAs have a much wider range of failurestress values than ruptured AAAs. They found a much greaterdifference in average failure stress between ruptured and unrup-tured groups than in this study. The failure property ranges –failure tension, failure stress and failure strain – reported here arealso remarkably consistent with our earlier report (Raghavan et al.,2006) on a study population of four AAAs, but for a few outliers.These consistencies in values between independent studies addcredence to the experimental methodology adopted.
4.2. Characteristics of rupture site
All four ruptured AAAs were larger than 5 cm (see Table 1).One aneurysm (AAA #3) had two independent rupture sites,while the others had one each (see Table 5 and Fig. 5). Primaryrupture sites were on the lateral quadrants (left or right) with onerupture extending into the posterior. Previous reports on rupturelocation have classified them as just anterior or posterior (da Silvaet al., 2000; Darling et al., 1977). If a similar classification is used(based on whether rupture site is visible from the anterior orposterior views), then the primary rupture location is posterior inthree and either in one AAA (#2). Rupture lengths ranged from1 to 6 cm. Remarkably, all ruptures had a longitudinal orientationand appeared to follow a meridional geodesic line (shortest lineon a surface). In an earlier study where we reported on oneruptured AAA, we observed a progressive reduction in thicknessclose to the rupture site (a small 1 cm long rupture). In thecurrent population, progressive reduction in wall thickness mea-surements was not observed around the rupture sites.
Please cite this article as: Raghavan, M.L., et al., Biomechanical faunruptured abdominal aortic aneurysms. Journal of Biomechanics (2
4.3. Regional variation in properties
There was significant within-subject variation in all the AAAsstudied (see Fig. 2). Indeed, within-subject variation in the failureproperties was comparable to between-subject variation. Forfailure tension (Tf) in the longitudinal orientation, the averagewithin-subject variation (average of max–min within each sub-ject) was 12.1 N/cm while the between-subject variation ofaverages (max–min of within-subject averages for each AAA)was 9.3 N/cm. The posterior wall surface was not any weakerthan the anterior surface although AAAs in the patient populationexhibit preferential anterior bulge and rupture posteriorly (daSilva et al., 2000; Darling et al., 1977). Consistent with previousreports (Thubrikar et al., 2001; Raghavan et al., 2006), there wasno consistent perceptible pattern in mechanical properties or wallthickness around the circumference of the AAA on visualobservation.
5. Conclusion
In this study population, ruptured AAAs were not found to beweaker on average than unruptured ones. The small studypopulation and the limited number of sites where aortic walltissue caliber was assessed within each AAA warrant somecaution in drawing definitive conclusions.
Conflict of interest statement
The authors do not have any conflict of interest to declare inthis study.
Acknowledgments
This study was supported by a grant from the American HeartAssociation Heartland Affiliate Beginning grant-in-aid #0365408Z.Failure strength distribution of abdominal aortic aneurysm(to MLR).
References
Darling, R.C., et al., 1977. Autopsy study of unoperated abdominal aortic aneur-ysms. The case for early resection. Circulation 56 (Suppl. 3), II161–II164.
Del Prete, Z., et al., 2004. Viscoelastic properties of skin in Mov-13 and Tsk mice.J. Biomech. 37 (10), 1491–1497.
Di Martino, E., et al., 1998. Biomechanics of abdominal aortic aneurysm in thepresence of endoluminal thrombus: experimental characterisation and
ilure properties and microstructural content of ruptured and011), doi:10.1016/j.jbiomech.2011.06.004

M.L. Raghavan et al. / Journal of Biomechanics ] (]]]]) ]]]–]]] 7
structural static computational analysis. Eur. J. Vasc. Endovasc. Surg. 15 (4),290–299.
Di Martino, E.S., et al., 2006. Biomechanical properties of ruptured versuselectively repaired abdominal aortic aneurysm wall tissue. J. Vasc. Surg.43 (3), 570–576 (discussion).
da Silva, E.S., et al., 2000. Morphology and diameter of infrarenal aortic aneur-ysms: a prospective autopsy study. Cardiovasc. Surg. 8 (7), 526–532.
He, C.M., Roach, M.R., 1994. The composition and mechanical properties ofabdominal aortic aneurysms. J. Vasc. Surg. 20 (1), 6–13.
Raghavan, M.L., Webster, M.W., Vorp, D.A., 1996. Ex vivo biomechanical behaviorof abdominal aortic aneurysm: assessment using a new mathematical model.Ann. Biomed. Eng. 24 (5), 573–582.
Raghavan, M.L., et al., 2006. Regional distribution of wall thickness and failureproperties of human abdominal aortic aneurysm. J. Biomech. 39 (16),3010–3016.
Please cite this article as: Raghavan, M.L., et al., Biomechanical faunruptured abdominal aortic aneurysms. Journal of Biomechanics (2
Thubrikar, M.J., et al., 2001. Mechanical properties of abdominal aortic aneurysmwall. J. Med. Eng. Technol. 25 (4), 133–142.
Vallabhaneni, S.R., et al., 2004. Heterogeneity of tensile strength and matrixmetalloproteinase activity in the wall of abdominal aortic aneurysms.J. Endovasc. Ther. 11 (4), 494–502.
Vande Geest, J.P., et al., 2006a. A biomechanics-based rupture potential index forabdominal aortic aneurysm risk assessment: demonstrative application.Ann. NY Acad. Sci. 1085, 11–21.
Vande Geest, J.P., et al., 2006b. Gender-related differences in the tensile strength ofabdominal aortic aneurysm. Ann. NY Acad. Sci. 1085, 400–402.
Vorp, D.A., et al., 1996. Wall strength and stiffness of aneurysmal and nonaneur-ysmal abdominal aorta. Ann. NY Acad. Sci. 800, 274–276.
Vorp, D.A., et al., 2001. Association of intraluminal thrombus in abdominal aorticaneurysm with local hypoxia and wall weakening. J. Vasc. Surg. 34 (2),291–299.
ilure properties and microstructural content of ruptured and011), doi:10.1016/j.jbiomech.2011.06.004