maternal social capital and child health in vietnam
TRANSCRIPT
W O R K I N G P A P E R N O . 3 0
Maternal Social Capital and Child Health in VietnamTran TuanTrudy HarphamMary J De SilvaNguyen Thu HuongBill TodPham Thi LanTran Duc ThachSavitri Abeyasekera
In Vietnam there is growing concern about the potential social impact of rapid economic changes. The extent and type of social connectedness, or social capital, may be changing. Studies from other developing countries have demonstrated that social capital is often independently associated with various indicators of well-being, including some aspects of human capital (health and education status). In Vietnam there has only been one previous quantitative study of social capital and this did not consider associations with well-being. The Young Lives project in Vietnam allows the examination of the relationship between maternal social capital and child well-being. With a sample of 1,953 mothers of one-year-olds and 954 mothers of eight-year-olds across five provinces, this study examines whether maternal social capital is associated with child health.
This study found low levels of structural social capital (associational life) and citizenship and high levels of cognitive social capital (trust, etc) and support. While poorer women have even lower levels of structural social capital than their better-off peers, patterns across rural and urban areas are similar.
Maternal social support and high cognitive social capital show the most consistent associations with child health, while associations between maternal social capital and child health are stronger among one-year-old children than among eight-year-olds, with the exception of child mental health and risk of life-threatening illness. The most consistent associations were seen with the mental health of eight-year-olds, with all four indicators of social capital being significantly associated with mental health after other variables have been controlled for. Lastly, there was some evidence to suggest that active membership of formal organisations in Vietnam may be damaging to the health of eight-year-olds but not one-year-olds, with active participation in formal groups being significantly associated with an increase in stunting among eight-year-olds.
The main components of social capital associated with child health are social support and cognitive social capital. High levels of maternal social support are positively correlated with having an educated partner, living in an urban area and better maternal mental health. High cognitive social capital is positively correlated with living in a rural area, having an occupation other than agriculture and better maternal mental health.
There is a need to focus on maintaining the high levels of cognitive social capital and raising the current low level of maternal structural social capital in Vietnam.
Key words: social capital, child health, Vietnam, quantitative
Published by
Young Lives Save the Children UK 1 St John's Lane London EC1M 4AR
Tel: 44 (0) 20 7012 6796 Fax: 44 (0) 20 7012 6963 Web: www.younglives.org.uk
ISBN 1-904427-31-6 First Published: 2006
All rights reserved. This publication is copyright, but may be reproduced by any method without fee or prior permission for teaching purposes, though not for resale, providing the usual acknowledgement of source is recognised in terms of citation. For copying in other circumstances, prior written permission must be obtained from the publisher and a fee may be payable.
Designed and typeset by Copyprint UK Limited
Young Lives is an international longitudinal study of childhood poverty, taking place in Ethiopia, India, Peru and Vietnam, and funded by DFID. The project aims to improve our understanding of the causes and consequences of childhood poverty in the developing world by following the lives of a group of 8,000 children and their families over a 15-year period. Through the involvement of academic, government and NGO partners in the aforementioned countries, South Africa and the UK, the Young Lives project will highlight ways in which policy can be improved to more effectively tackle child poverty.

The Young Lives Partners Centre for Economic and Social Studies (CESS), India
Department of Economics, University of Addis Ababa, Ethiopia
Ethiopian Development Research Institute, Addis Ababa, Ethiopia
General Statistical Office, Government of Vietnam
Grupo de Análisis para el Desarrollo (GRADE), Peru
Institute of Development Studies, University of Sussex, UK
Instituto de Investigación Nutricional (IIN), Peru
London School of Hygiene and Tropical Medicine, UK
London South Bank University, UK
Medical Research Council of South Africa
RAU University, Johannesburg, South Africa
Research and Training Centre for Community Development, Vietnam
Save the Children UK
Statistical Services Centre, University of Reading, UK
Maternal Social capital and child health in VietnaM
Maternal Social capital and child health in Vietnamtran tuantrudy harphamMary J de Silvanguyen thu huongBill todpham thi lantran duc thachSavitri abeyasekera
WorKinG paper no.30
Maternal Social capital and child health in VietnaM
ii
ii
prefaceThispaperisoneofaseriesofworkingpaperspublishedbytheYoungLivesproject,aninnovativelongitudinalstudyofchildhoodpovertyinEthiopia,India(AndhraPradeshstate),PeruandVietnam.Between2002and2015,some2,000childrenineachcountryarebeingtrackedandsurveyedat3-4yearintervalsfromwhentheyare1until14yearsofage.Also,1,000olderchildrenineachcountryarebeingfollowedfromwhentheyareaged8years.
YoungLivesisajointresearchandpolicyinitiativeco-ordinatedbyanacademicconsortium(composedoftheUniversityofReading,theLondonSchoolofHygieneandTropicalMedicine,LondonSouthBankUniversityandtheSouthAfricanMedicalResearchCouncil)andSavetheChildrenUK,incorporatingbothinterdisciplinaryandNorth-Southcollaboration.
YoungLivesseeksto:
Producelong-termdataonchildrenandpovertyinthefourresearchcountries
Drawonthisdatatodevelopanuancedandcomparativeunderstandingofchildhoodpovertydynamicstoinformnationalpolicyagendas
Traceassociationsbetweenkeymacropolicytrendsandchildoutcomesandusethesefindingsasabasistoadvocateforpolicychoicesatmacroandmesolevelsthatfacilitatethereductionofchildhoodpoverty
Activelyengagewithongoingworkonpovertyalleviationandreduction,involvingstakeholderswhomayuseorbeimpactedbytheresearchthroughouttheresearchdesign,datacollectionandanalyses,anddisseminationstages
Fosterpublicconcernabout,andencouragepoliticalmotivationtoacton,childhoodpovertyissuesthroughitsadvocacyandmediaworkatbothnationalandinternationallevels.
Initsfirstphase,YoungLiveshasinvestigatedthreekeystorylines–theeffectsonchildwell-beingof(i)accesstoanduseofservices,(ii)socialcapital,and(iii)householdlivelihoods.Thisworkingpaperisoneofaserieswhichconsideranaspectofeachofthesestorylinesineachcountry.Asaworkingpaper,itrepresentsworkinprogressandtheauthorswelcomecommentsfromreaderstocontributetofurtherdevelopmentoftheseideas:youcancontactYoungLivesviathewebsitewww.younglives.org.uk
TheprojectreceivedfinancialsupportfromtheUKDepartmentforInternationalDevelopmentandthisisgratefullyacknowledged.
Forfurtherinformationandtodownloadallourpublications,visitwww.younglives.org.uk
•
•
•
•
•
Maternal Social capital and child health in VietnaM
iiiiii
abstractInVietnamthereisgrowingconcernaboutthepotentialsocialimpactofrapideconomicchanges.Theextentandtypeofsocialconnectedness,orsocialcapital,maybechanging.Studiesfromotherdevelopingcountrieshavedemonstratedthatsocialcapitalisoftenindependentlyassociatedwithvariousindicatorsofwell-being,includingsomeaspectsofhumancapital(healthandeducationstatus).InVietnamtherehasonlybeenonepreviousquantitativestudyofsocialcapitalandthisdidnotconsiderassociationswithwell-being.TheYoungLivesprojectinVietnamallowstheexaminationoftherelationshipbetweenmaternalsocialcapitalandchildwell-being.Withasampleof1,953mothersofone-year-oldsand954mothersofeight-year-oldsacrossfiveprovinces,thisstudyexamineswhethermaternalsocialcapitalisassociatedwithchildhealth.
Thisstudyfoundlowlevelsofstructuralsocialcapital(associationallife)andcitizenshipandhighlevelsofcognitivesocialcapital(trust,etc)andsupport.Whilepoorerwomenhaveevenlowerlevelsofstructuralsocialcapitalthantheirbetter-offpeers,patternsacrossruralandurbanareasaresimilar.
Maternalsocialsupportandhighcognitivesocialcapitalshowthemostconsistentassociationswithchildhealth,whileassociationsbetweenmaternalsocialcapitalandchildhealtharestrongeramongone-year-oldchildrenthanamongeight-year-olds,withtheexceptionofchildmentalhealthandriskoflife-threateningillness.Themostconsistentassociationswereseenwiththementalhealthofeight-year-olds,withallfourindicatorsofsocialcapitalbeingsignificantlyassociatedwithmentalhealthafterothervariableshavebeencontrolledfor.Lastly,therewassomeevidencetosuggestthatactivemembershipofformalorganisationsinVietnammaybedamagingtothehealthofeight-year-oldsbutnotone-year-olds,withactiveparticipationinformalgroupsbeingsignificantlyassociatedwithanincreaseinstuntingamongeight-year-olds.
Themaincomponentsofsocialcapitalassociatedwithchildhealtharesocialsupportandcognitivesocialcapital.Highlevelsofmaternalsocialsupportarepositivelycorrelatedwithhavinganeducatedpartner,livinginanurbanareaandbettermaternalmentalhealth.Highcognitivesocialcapitalispositivelycorrelatedwithlivinginaruralarea,havinganoccupationotherthanagricultureandbettermaternalmentalhealth.
ThereisaneedtofocusonmaintainingthehighlevelsofcognitivesocialcapitalandraisingthecurrentlowlevelofmaternalstructuralsocialcapitalinVietnam.
Keywords:socialcapital,childhealth,Vietnam,quantitative
Maternal Social capital and child health in VietnaM
iv
contents
Preface ii
Abstract iii
1. Introduction 1
1.1 economic growth, inequality, urbanisation and social exclusion in Vietnam 1
1.2 this study’s approach to social capital 2
2. Methods 4
2.1 Sample 4
2.2 Measures 4
2.3 Fieldwork and ethics 5
2.4 data analysis 5
3. Results 7
3.1 descriptive results 7
3.2 Multivariate results: the relationship between social capital and child nutrition 14
3.3 Multivariate results: the relationship between social capital and child health 17
3.4 determinants of maternal social capital 17
4. Discussionandconclusions 25
References 28
Maternal Social capital and child health in VietnaM
1
1. introduction
1.1 Economic growth, inequality, urbanisation and social exclusion in VietnamTherearecurrentlyanumberofdifferenteconomicanddemographicfactorsthatmayaffectsocialrelationsinVietnam.Rapideconomicgrowth,growinginequalities,urbanisationandsocialexclusionarebrieflyconsideredbelow.
Rapidnationaleconomic growthisoftenaccompaniedbyaweakeningofsocialties,orconnectedness(GrootaertandvanBastelaer,2002).VietnamisundergoingaperiodofrapideconomicchangeanditsachievementsintermsofpovertyreductionhavebeenheraldedbydonorsandbytheVietnamGovernmentasoneofthegreatsuccessstoriesofeconomicdevelopment(JointDonorReport,2003;GoV,2003).AdecadeofGDPgrowthfiguresaveragingaround7percentperannumhaveunderpinnedahalvingofincome-expenditure-consumptionpovertyfrom58percentofthepopulationin1993to29percentin2002.
Socialtiesbetweenandwithincommunitiescanalsobeseveredinacontextofgrowinginequalities.ThegapbetweenthepoorestquintileofVietnamandtherichesthasbeenwideningbothintermsofincomeandexpendituresince1993.TheGinico-efficientincreasedfrom0.35in1992/93to0.37in1997/98andwasupto0.41in2002(WorldBank,2003).Thesituationoftheminorityethnicpopulationisespeciallyworrying:whilethepovertyrateforthemajoritypopulationdeclinedfrom54percentin1993to29percentin2002,thepovertyrateforminorityethniccommunitiesremainshighandonlydeclinedfrom86percentto70percentinthesameperiod.Infact,followingimprovementsintheperiod1993-1998,severepovertyamongthepoorestminorityethniccommunitiesactuallyincreasedinmanyregionsfrom1998to2002(UNCT,2003).
Changesinsocialconnectednesscanalsoresultfromdemographicphenomenasuchasurbanisation,migrationandtheageingofapopulation.UrbanisationisaparticularlyimportantphenomenoninVietnam.By2020itisestimatedthat55percentofthepopulationwillliveincitiescomparedtolessthan25percenttoday(UNCT,2003).RecentestimateshavesuggestedthatonemillionpeopleayeararemigratingtoVietnam’scities(JointDonorReport,2003).Newmigrantstothecitiescurrentlyfaceadoubledisadvantageinthelossoftheirtraditionalsocialnetworksandthediscriminatorypolicieswithregardtoaccesstobasicservices,housingandpovertyalleviationprogrammes(SavetheChildrenUK,2003andJointDonorReport,2003).
Social exclusion inVietnamistackledheadonbyformalstatesafetynetstargetedattheexcluded,poorandvulnerable(forexample,theHungerEradicationandPovertyReductionprogramme–HEPR;andProgramme135).However,questionshavebeenraisedbythedonorcommunityabouttheeffectivenessofthetargetingandthesubsequentimpactoftheseformalsafetynets.Coverageratesarelow:itisestimatedthatProgramme135reaches28percentofthepoor,whileHEPRactivitiesonlyreach6-13percentofthepoor.Furthermore,findingsontheimpactofHEPRaccessaremixed:whileimprovementshavebeenfoundinschoolenrolment,nopositivecorrelationhasbeenfoundwithhouseholdexpenditureorwithbetterhealthoutcomes(JointDonorReport,2003).Communityconsultationscarriedoutinsixprovincesin2001inordertoformulatethegovernment’spovertyreductionstrategybasedonitsinterimPovertyReductionStrategy(i-PRSP)alsofoundwidespread
Maternal Social capital and child health in VietnaM
2
dissatisfactionwithsocialsafetynetcoverageandimpact–particularlyintermsoffeeexemptionpoliciesinhealthandeducation(ShanksandTurk,2002).Andanotherstudyconcludedthatwithrespecttothefinancingofsocialprotectionmeasures,themajorcostofriskmanagementispaidforbyhouseholdsandcommunities,andthemainbeneficiariesofstate-providedmeasuresaretherelativelywell-offratherthantherelativelypoor(ConwayandTurk,2002).Inthiscontextofincompletecoveragebyformalsocialsafetynets,theroleofinformalsocialsafetynets–orsocialsupport–becomesparticularlyimportant.
Opportunitiesforinformal(beyondfamilial)socialsupportinVietnammaybeincreasing.Vietnam’semergingcivilsocietyshowssignsofincreasingnon-state,voluntary,not-for-profit,civicorganisationsbuiltaroundcommoninterestsandissues,seekingtoimprovethewell-beingoftheirmembersorthewell-beingofothers.Thismayhavemoretodowitheconomicreformpolicysincedoimoi1in1985thanspecificlegislationregardingcivilsocietyorganisationsduringthesameperiod(WischermannandVinh,2003;Dalton,2002andPedersen,2001).Othersarelessoptimistic.Participatorypovertyassessmentscarriedoutin2003in43communesacrossallregionsofthecountrybyavarietyofdifferentorganisations,followingacommonframework,foundthattheparticipationoflocalpeopleinplanning,decision-makingandimplementationoflocaldevelopmentplansislimited(JointDonorReport,2003).Nevertheless,agrowingcivilsocietyaddressingsocialandeconomicproblemsoffersnewanddiversifiedopportunitiesforindividualstoformnewsocialrelationships,increasesocialconnectednessanddevelopinformalsafetynets.
Thepotentialforatleastaslowingdownofprogressonpovertyreduction,togetherwithworryingsignsofincreasinginequality,newsocialtrendsandinadequateformalsafetynets,suggeststhatthisisagoodtimetodeepenthedebateonhowsocialcapitalcanplayaroleinVietnam’sdevelopment,howsocialconnectionsbetweenindividuals,householdsandcommunities,andthesupportwhichmayflowfromthoseconnections,contributestohumandevelopment,povertyreduction,andinthisparticularcase,childwell-being.
1.2 This study’s approach to social capital
SocialcapitalismostcommonlyassociatedwiththeresearchofBourdieu(1986),Coleman(1990)andPutnam(1993).‘Inattemptingtofindnon-economicfactorstoexplainthesuccessofcertaineconomicprocesses,theseauthorsdrawonconceptssuchastrust,participationincivilsocietyandsocialnetworks,allofwhichformthe“social capital”ofagivencommunity’(vanKemenade,2002p.7).SocialcapitalisoneoffiveassetsinthelivelihoodsconceptualframeworkdevelopedbyDFID(theothersbeingphysical,human,naturalandfinancialassets).However,thereisongoingdebateastowhetheritistrulyaformof‘capital’(eg,seeArrow,2000).Researchhasshownittohaveanindependenteffectonvariouseconomicandotherwelfareindicators,includingphysicalandmentalhealth(GrootaertandvanBastelaer,2002;DeSilvaet al,2005).Socialcapitalcanbethoughtofasthe‘value’ofsocialrelationships,reflectingthequalityandquantityofsocialrelationshipsinagivenpopulation,mostcommonlythosewithinacommunity.Indeed,Quibria(2003)suggeststhatsocialcapitalhasbecomeshorthandfor‘community’.
1 Doi moimarksarenovationperiodstartingfrom1989whenaseriesofadjustmentreformswereinitiatedinordertoboosteconomicgrowthandreducepovertyinVietnam.
Maternal Social capital and child health in VietnaM
3
Althoughsomewritersclaimthatthenegativesideofsocialcapitalisstillignored(eg,Quibria,2003),mostsocialcapitalresearchthesedaysacknowledgesthathighlevelsofsocialcapital,insomecontexts,canbeassociatedwithexclusionofoutsiders,restrictionsonindividualfreedomsandreinforcementofharmfulnorms.Another,morefundamental,criticismofafocusonsocialcapitalisthatitemphasisesthe‘social’ofdevelopmentattheexpenseofthe‘economic’.However,many,includingthecurrentauthors,welcometheadditionalattentiontonon-marketsocialinteractions.
TheapproachtosocialcapitalinYoungLivesavoidsfocussingoneithertrust, norms,etc, or interactionsbutconsidersboth,asrecommendedbymostrecenttextsonsocialcapital(eg,DasguptaandSerageldin,2000).However,thisstudyrecognisestheimportanceofseparating outstructuralsocialcapital(objectivemeasuresofwhatpeople‘do’,suchasmembershipofnetworks)fromcognitivesocialcapital(subjectivemeasuresofwhatpeople‘feel’,suchasnotionsoftrustandreciprocity)(Harpham,GrantandThomas,2002).Itisimportanttoseparatetheseindicatorsofsocialcapitalastheymaynotbecorrelated.Allmeasuresrefertothe‘community’thereforethisstudyonlyaddressesbonding(withincommunity)socialcapitalandnotbridging(linkingtoothercommunitiesorinstitutions)socialcapital.Thisstudyalsoavoidscoveringboththecausesandconsequences(oroutcomes)ofsocialcapitalinthemeasureofsocialcapitalitself.AsPortes(1998)andQuibria(2003)pointout,thisstillhappensinsomestudies.
Currentresearchviewssocialcapitalasboththepropertyofindividuals(thedirectimpactofanindividualparticipatinginanetwork),andasanecologicalcharacteristic(theindirectimpactofnetworksirrespectiveofparticipationinthosenetworks).Individualsocialcapitalismeasuredbyaskinganindividualabouttheirownparticipationinnetworks(structural),andaboutthequalityofthosenetworks,forexamplewhethertheyaretrusting(cognitive).Ecologicalsocialcapitalismeasuredbyaskingarepresentativesampleofthecommunitytheaboveissues,andaggregatingtheanswerstothecommunitylevel,providingthesamescoreofsocialcapitalforeverypersoninthecommunity.Forthepurposesofthispaper,socialcapitalisregardedasacharacteristicofindividualsandnotasanecologicalvariable.
ThisstudyisthefirstquantitativeexaminationofmaternalsocialcapitalinVietnamthatconsidersthecorrelatesofmaternalsocialcapitalanditseffectuponchildhealth.Highlevelsofmaternalsocialcapitalmaypositivelyaffectchildhealthbyenablingmotherstoaccessmoreservices(health,education,childcare),byenablingthemtoaccessmoreassets(jobs,money,durables,etc),andbybeingpositivelyrelatedtomaternalphysicaland/ormentalhealth.Whilepreviousresearchindevelopedanddevelopingcountrieshasdemonstratedpositiveassociationsbetweenadultsocialcapitalandvariousadult(orhousehold)indicatorsofwell-being,theassociationbetweenmaternalsocialcapitalandchildhealthhasnotpreviouslybeenexamined(ProductivityCommission,2003).
Maternal Social capital and child health in VietnaM
4
2. Methods
2.1 Sample
ThisstudyusesdatafromtheYoungLivesproject,aninternationalstudyofchildhoodpovertyinEthiopia,India,PeruandVietnam.FulldetailsofthesampleselectionfortheVietnamesepartofthisstudycanbefoundatwww.younglives.org.uk.Briefly,arandomsampleof100one-year-oldsand50eight-year-oldswastakenfromeachof20sentinelsites,over-sampledtoincludepoorareas,makingatotalof2,000one-year-oldsand1,000eight-year-olds.These20sentinelsitescomprised31communes,orcommunities.Thechild’sprimarycaregiverwasinterviewed,andforthepurposesofthisstudythesamplewasrestrictedtobiologicalmothers,resultingin1,953mothersofone-year-olds,and954mothersofeight-year-olds.
2.2 Measures
SocialcapitalwasmeasuredusingashortenedversionoftheA-SCATtooldevelopedbyHarpham,GrantandThomas(2002)–aseriesoftenyes/noquestions.ThequestionnairehasbeenqualitativelyvalidatedinVietnam. Structural social capital wasmeasuredby(1)askingrespondentsaboutactivemembershipofformal(women’sunion,co-op,tradeunion,political/social)andinformal(religious,credit,lifeinsurance,sports)groupsintheircommunityduringthelastyear;(2)byrecordingsupportreceivedfrominformal(family,relatives,neighbours,friends,religiousleaders)andformal(communeleaders,governmentofficials,politicians,NGOs)networksduringthelastyear;and(3)byaskingaboutjoiningtogetherwithothercommunitymemberstoaddressanissue/problemandcommunicationwithcommunityleaders(seeTable3).Cognitive social capital wasmeasuredbyaskingrespondentsquestionsabouttrust,senseofbelonging,communityharmonyandperceivedfairness.
The health outcomes for one-year oldsincludenutritionalstatus,physicalhealthstatusperceivedbythemotherincomparisontootherchildren,perceivedlong-termhealthproblem,whetherthechildhasbeensosickthemotherthoughttheymightdie,injuryoraccidentssincebirth,andillnessinthelast24hours(measuredusingquestionsdevelopedbyWHOforscreeningdiarrhoeaandacuterespiratoryinfection(ARI).Threeindicatorswereusedtomeasurenutritionalstatus:weight-for-agez-scores(WAZ),height-for-agez-scores(HAZ),andweight-for-heightz-scores(WHZ).AllwerecomputedusingtheNutStatmoduleofEpiInfo2002withtheWHOInternationalGrowthReferenceasastandard,2andacut-offpointof–2SDusedtoclassifycasesofmalnutrition.
The health outcomes for eight-year-oldsincludeallthoselistedabove,andmentalhealth.ChildmentalhealthwasmeasuredusingtheStrengthsandDifficultiesQuestionnaire(SDQ)withaTotalDifficultiesScorerangingfrom0to40generatedbysummingthescoresfromfourscales(emotionalsymptomsscore,conductproblemscore,hyperactivityscoreandpeerproblemscore).Ascoreof<=13wasclassifiedas‘normal’,14-16‘borderline’and>=17‘abnormal’.
Otherfactorswhichmayconfoundtheassociationbetweenmaternalsocialcapitalandchildhealth,orbedeterminantsofmaternalsocialcapital,wereexplored.Thesecomprise:maternalfactors(age,religion,ethnicity,educationlevel,occupation,numberofyearslivedincommune,andmentalhealthstatusmeasuredusingtheSRQ20withacut-offof7/8todetermineaprobablecaseofcommon
2 NutStatisanutritionanthropometryprogrammethatcalculatespercentilesandz-scoresusingeitherthe2000CDCortheWHOgrowthreference(www.cdc.gov/EpiInfo/).InanalysisofYLVietnamchildnutritionalstatus,weusedtheWHOgrowthreferenceoption,asthe1983WHOReferenceGrowthChartscontinuetobepreferredforinternationalcomparison.

Maternal Social capital and child health in VietnaM
5
mentaldisorder);partnerfactors(partnerathome,age,education,occupation);householdfactors(householdwealth,numberofeconomicshocksinlastthreeyears,numberofchildrenunderfiveinhousehold);childfactors(age,sex)andcommunityfactors(rural/urban).
Householdwealthismeasuredusingahouseholdwealthindex(WI)–ascorebetweenzeroandoneconstructedasanaverageofthreecomponents:(1)housingquality,whichisthesimpleaverageofroomsperperson,floor,roofandwall;(2)consumerdurables,beingthescaledsumofnineconsumerdurables(radio,bicycle,TV,electricfan,motorbike,refrigerator,landline,mobilephoneandcar/truck);and(3)servicesofdrinkingwater,electricity,toiletandfuel.Thewealthindexisdividedintofourgroups:<0.25‘poorest’,0.25-<0.5‘verypoor’,0.5-<0.75‘lesspoor’,>=0.75‘betteroff ’.
2.3 Fieldwork and ethicsEthicalapprovalwasgrantedbytheVietnameseUnionofScientificandTechnologicalAssociations,LondonSouthBankUniversity,LondonSchoolofHygieneandTropicalMedicineandReadingUniversity,UK.Datawerecollectedinlate2002,withhouseholdinterviewsperformedbytheGeneralStatisticalOffice(GSO)staffandanthropometricmeasurementstakenbytheHanoiResearchandTrainingCenterforCommunityDevelopment(RTCCD)researchteam.
2.4 Data analysisDatawereanalysedusingthe‘surveycommands’inStata8.0(StataCorp,2003).Samplingweightfactor(pweight)wasthereverseoftheprobabilityofeligiblechildrenbeingsampledineachsentinelsite.Stratawasdefinedassentinelsite,andprimarysamplingunitasthehousehold.
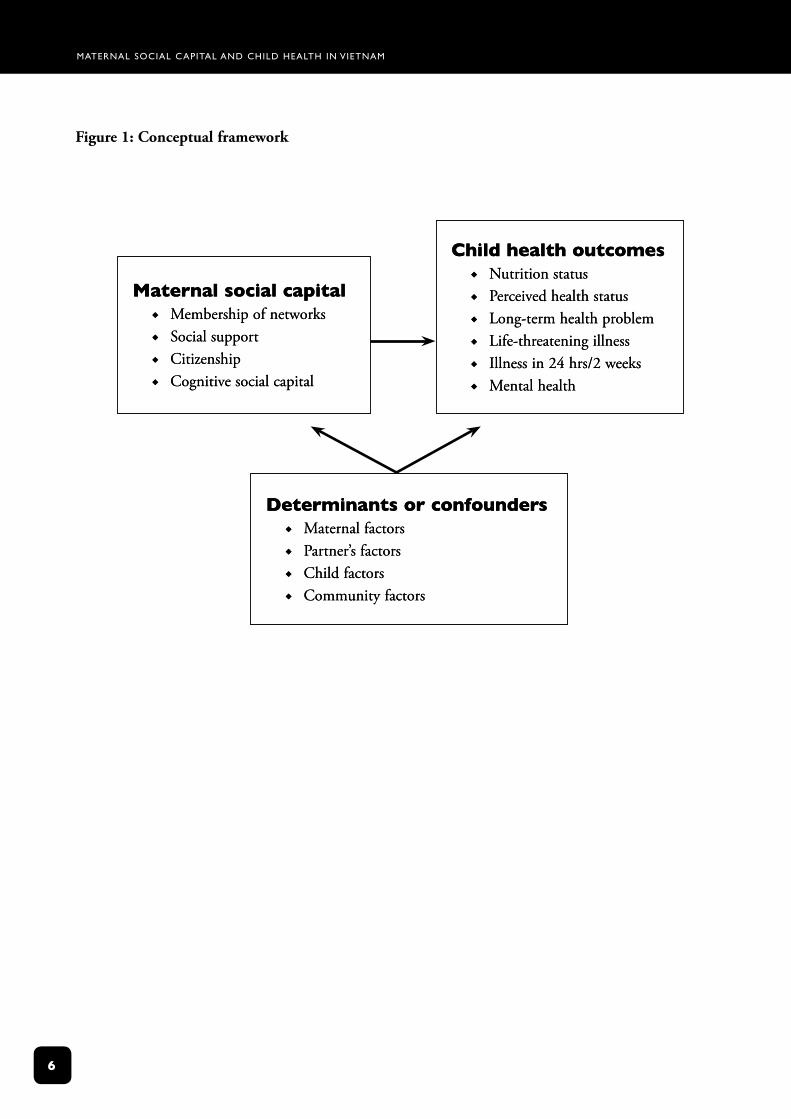
TheanalysisfollowedtheconceptualframeworkoutlinedinFigure1.Firstly,thedistributionofchildhealthoutcomesandmaternalsocialcapitalbyageofchild,location(rural/urban)andhouseholdwealthindexwasexploredusingPearsonchi-squaretestsforcategoricalvariablesandt-testsforcontinuousvariables,correctedforthesurveydesign.GiventhesituationinVietnam,wheretheroleofgovernmentincivilsocietylifehasbeenchangingsincethecountrymovedawayfromacentrallyplannedtowardsamarked-basedapproachtosocialdevelopment,theconceptsof‘formal’–belongingtothegovernment–and‘informal’–establishedandsustainedindependentlyfromthegovernment,groupornetwork,areusedinanalysingstructuralsocialcapital.Secondly,appropriatemultivariablemodels(eitherlinearorlogistic)foreachchildhealthoutcomewerefittedtoexploretheassociationbetweeneachspecificdimensionofmaternalsocialcapitalandchildhealthoutcomes,controllingforpotentialconfoundingfactors.Toclarifytheconceptofformal/informalgroupmembershipandsocialsupportreceived,modelswerebuiltwiththefollowingvariables:anyversusnone,anyformalversusnone,andanyinformalversusnone.
Thepredictorsofthosematernalsocialcapitalcomponentsfoundtobesignificantlyassociatedwithchildhealthoutcomesweresubsequentlyexploredinadditionalmultivariablemodels.
Maternal Social capital and child health in VietnaM
�
Figure 1: Conceptual framework
MaternalsocialcapitalMembershipofnetworksSocialsupportCitizenshipCognitivesocialcapital
Æ
Æ
Æ
Æ
MaternalsocialcapitalMembershipofnetworksSocialsupportCitizenshipCognitivesocialcapital
Æ
Æ
Æ
Æ
DeterminantsorconfoundersMaternalfactorsPartner’sfactorsChildfactorsCommunityfactors
Æ
Æ
Æ
Æ
DeterminantsorconfoundersMaternalfactorsPartner’sfactorsChildfactorsCommunityfactors
Æ
Æ
Æ
Æ
ChildhealthoutcomesNutritionstatusPerceivedhealthstatusLong-termhealthproblemLife-threateningillnessIllnessin24hrs/2weeksMentalhealth
Æ
Æ
Æ
Æ
Æ
Æ
ChildhealthoutcomesNutritionstatusPerceivedhealthstatusLong-termhealthproblemLife-threateningillnessIllnessin24hrs/2weeksMentalhealth
Æ
Æ
Æ
Æ
Æ
Æ
Maternal Social capital and child health in VietnaM
7
3. results
3.1 Descriptive results
Child health outcomesChildhealthoutcomeindicatorsarenecessarilydifferentforone-year-oldscomparedtoeight-year-olds.Theanalysesbelowwillthereforelinkchildoutcomestoeitherthesocialcapitalofthemothersofone-year-oldsorthemothersofeight-year-olds.
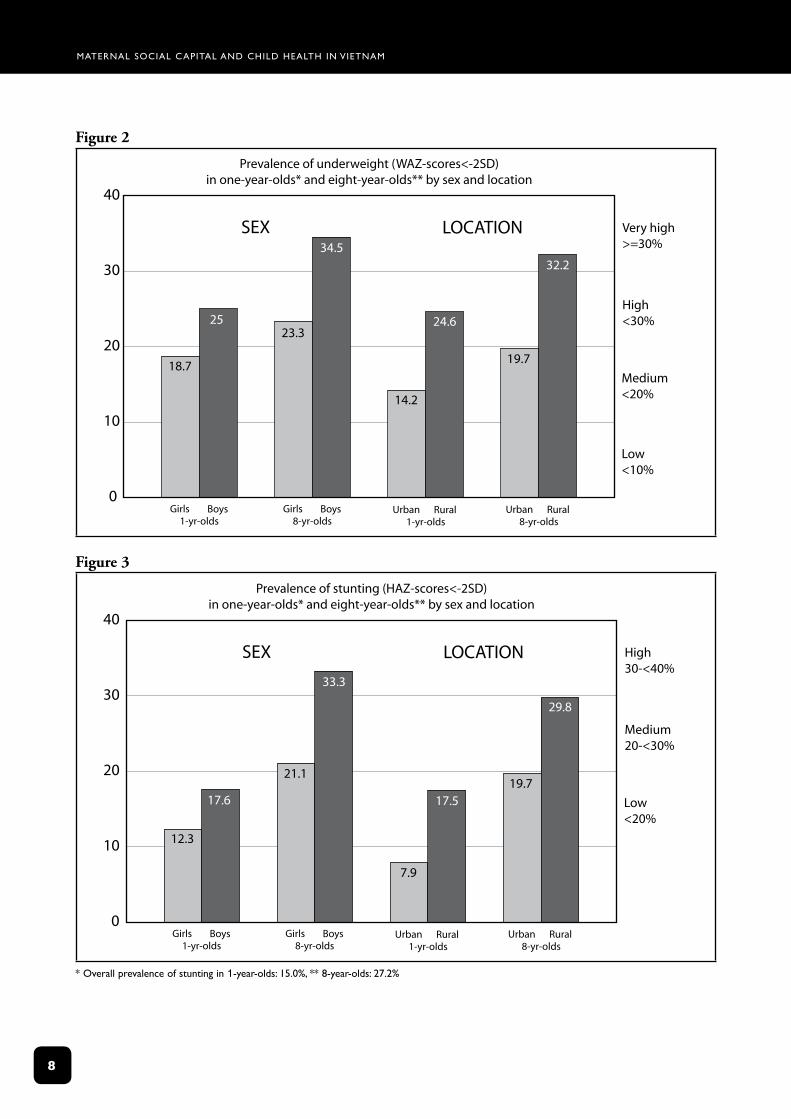
Figures2and3describenutritionaloutcomesbysexandlocationforeachchildagegroup.Accordingtointernationalstandards,theprevalenceofunderweightchildrenishighinbothone-andeight-year-oldgroups(from20to<30%WAZ<-2SD).Incontrast,stuntingratesarelow(<20%HAZ<-2SD)inone-year-oldsandmedium(from20to<30%)ineight-year-olds.Inbothagegroupsboysandchildrenlivinginruralareashaveworsenutritionalindicatorsthangirlsandchildrenlivinginurbanareas.
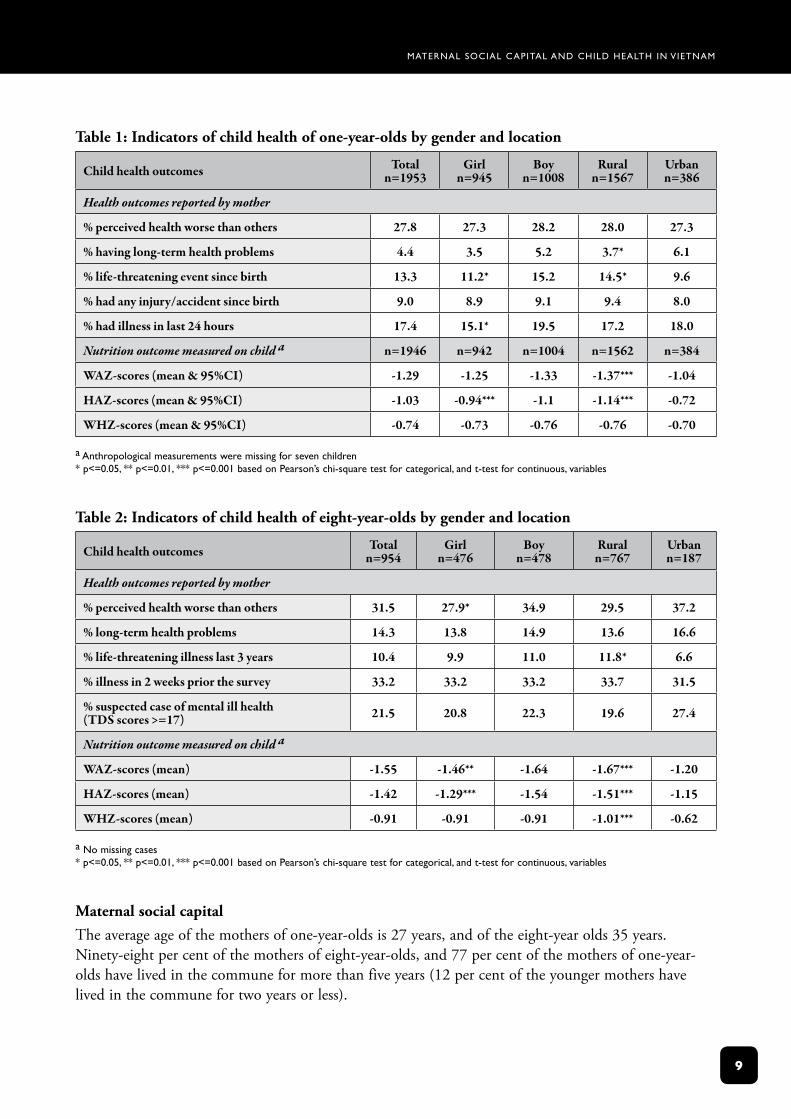
Tables1and2presentindicatorsofchildhealthbysexandlocationforone-year-oldsandeight-year-oldsrespectively.Eight-year-oldsaremorethanthreetimesmorelikelytosufferfromlong-termhealthproblemsthanone-year-olds,while21percentofeight-year-oldsareprobablecasesofmentalillness.Incontrasttothenutritionalindicators,fewsignificantdifferencesbetweenruralandurbanareas,orbetweengirlsandboysforeitheragegrouparefoundwiththephysicalhealthindicators.However,childrenofbothageslivinginruralareas,andone-year-oldboysratherthangirls,weremorelikelytohavesufferedfromalife-threateningillness.
Maternal Social capital and child health in VietnaM
8
Figure 2
40
30
20
10
0
18.7
2523.3
34.5
14.2
24.6
19.7
32.2
Prevalence of underweight (WAZ-scores<-2SD)in one-year-olds* and eight-year-olds** by sex and location
Very high>=30%
High<30%
Medium<20%
Low <10%
Girls Boys1-yr-olds
Girls Boys8-yr-olds
Urban Rural1-yr-olds
Urban Rural8-yr-olds
SEX LOCATION
Figure 3
40
30
20
10
0
12.3
17.6
21.1
33.3
7.9
17.519.7
29.8
Prevalence of stunting (HAZ-scores<-2SD)in one-year-olds* and eight-year-olds** by sex and location
High30-<40%
Medium20-<30%
Low<20%
Girls Boys1-yr-olds
Girls Boys8-yr-olds
Urban Rural1-yr-olds
Urban Rural8-yr-olds
SEX LOCATION
* overall prevalence of stunting in 1-year-olds: 15.0%, ** 8-year-olds: 27.2%
Maternal Social capital and child health in VietnaM
�
Table 1: Indicators of child health of one-year-olds by gender and location
Child health outcomes Total n=1953
Girl n=945
Boy n=1008
Rural n=1567
Urban n=386
Health outcomes reported by mother
% perceived health worse than others 27.8 27.3 28.2 28.0 27.3
% having long-term health problems 4.4 3.5 5.2 3.7* 6.1
% life-threatening event since birth 13.3 11.2* 15.2 14.5* 9.6
% had any injury/accident since birth 9.0 8.9 9.1 9.4 8.0
% had illness in last 24 hours 17.4 15.1* 19.5 17.2 18.0
Nutrition outcome measured on child a n=1946 n=942 n=1004 n=1562 n=384
WAZ-scores (mean & 95%CI) -1.29 -1.25 -1.33 -1.37*** -1.04
HAZ-scores (mean & 95%CI) -1.03 -0.94*** -1.1 -1.14*** -0.72
WHZ-scores (mean & 95%CI) -0.74 -0.73 -0.76 -0.76 -0.70
a anthropological measurements were missing for seven children * p<=0.05, ** p<=0.01, *** p<=0.001 based on pearson’s chi-square test for categorical, and t-test for continuous, variables
Table 2: Indicators of child health of eight-year-olds by gender and location
Child health outcomes Total n=954
Girl n=476
Boy n=478
Rural n=767
Urban n=187
Health outcomes reported by mother
% perceived health worse than others 31.5 27.9* 34.9 29.5 37.2
% long-term health problems 14.3 13.8 14.9 13.6 16.6
% life-threatening illness last 3 years 10.4 9.9 11.0 11.8* 6.6
% illness in 2 weeks prior the survey 33.2 33.2 33.2 33.7 31.5
% suspected case of mental ill health(TDS scores >=17) 21.5 20.8 22.3 19.6 27.4
Nutrition outcome measured on child a
WAZ-scores (mean) -1.55 -1.46** -1.64 -1.67*** -1.20
HAZ-scores (mean) -1.42 -1.29*** -1.54 -1.51*** -1.15
WHZ-scores (mean) -0.91 -0.91 -0.91 -1.01*** -0.62
a no missing cases * p<=0.05, ** p<=0.01, *** p<=0.001 based on pearson’s chi-square test for categorical, and t-test for continuous, variables
Maternal social capitalTheaverageageofthemothersofone-year-oldsis27years,andoftheeight-yearolds35years.Ninety-eightpercentofthemothersofeight-year-olds,and77percentofthemothersofone-year-oldshavelivedinthecommuneformorethanfiveyears(12percentoftheyoungermothershavelivedinthecommunefortwoyearsorless).
Maternal Social capital and child health in VietnaM
10
Table 3: Individual components of maternal social capital by child age group
Mothers of 1-year-olds
Mothers of 8-year-olds Combined
n=1953 %
n=954 %
n=2907 %
STRUCTURAl SoCIAl CApITAl
Group membership
In last year, been an active member of formal group
prof/trade union 7* 10 8
Co-op 5 6 5
Women's union 17*** 31 22
political/social group 1 2 1
In last year, been an active member of informal group
Religious group 1 2 1
Credit/life insurance group 6 7 6
Sports group 0.3 0 0.2
Social support received in the last year from
Formal networks
Commune leaders 15 17 16
politicians 0.1 0 0.1
Government officials 5 6 5
Non-government/charity officials 6* 9 7
other source 7*** 12 8
Informal networks
Family/relatives 94** 91 93
Neighbours 77* 81 78
Friends (not neighbours) 71 74 72
Religious leaders 1 2 1
Citizenship activities
Joined with other households to address a problem 30*** 50 36
Talked with commune leaders about a problem in the community 4*** 8 5
CoGNITIve SoCIAl CApITAl
In general, majority of people in commune can be trusted 83** 87 84
Majority of people in commune get along well 91* 94 92
Feel part of the commune 98** 99 98
Feel people would take advantage if they got the chance 9 7 9
* p<=0.05, ** p<=0.01, *** p<=0.001. pearson’s chi-square test is used to test for each category (dichotomous variable)
Maternal Social capital and child health in VietnaM
11
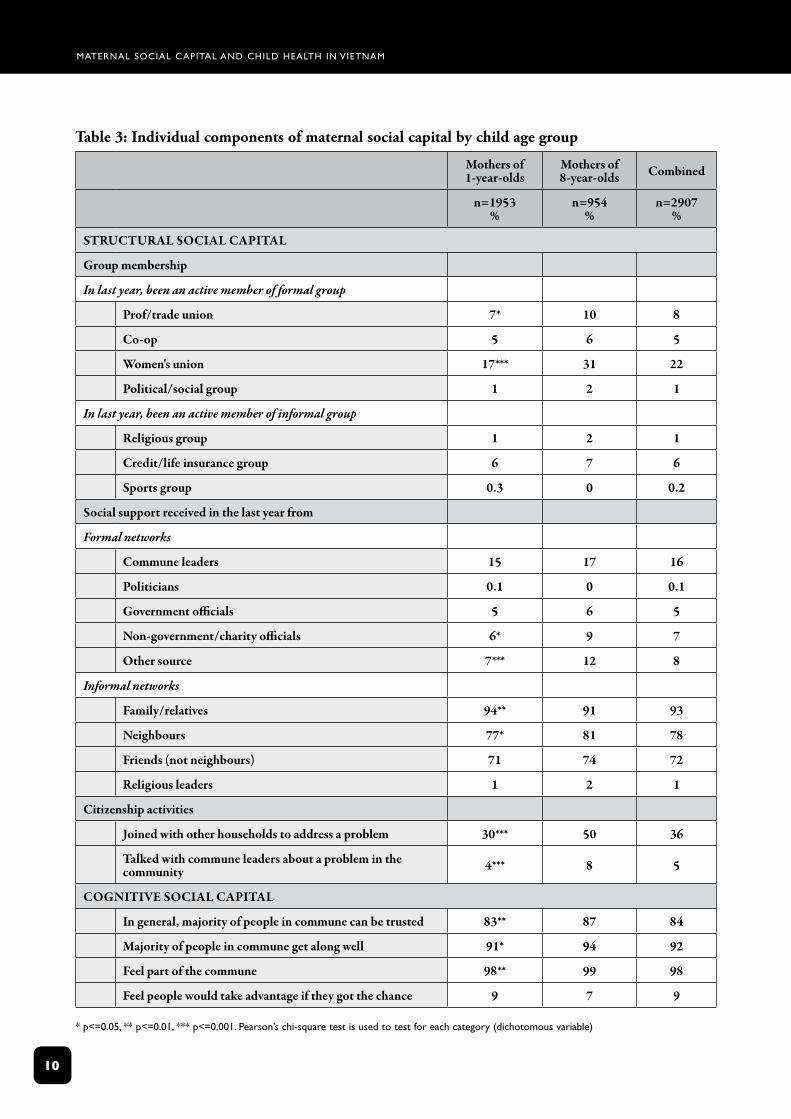
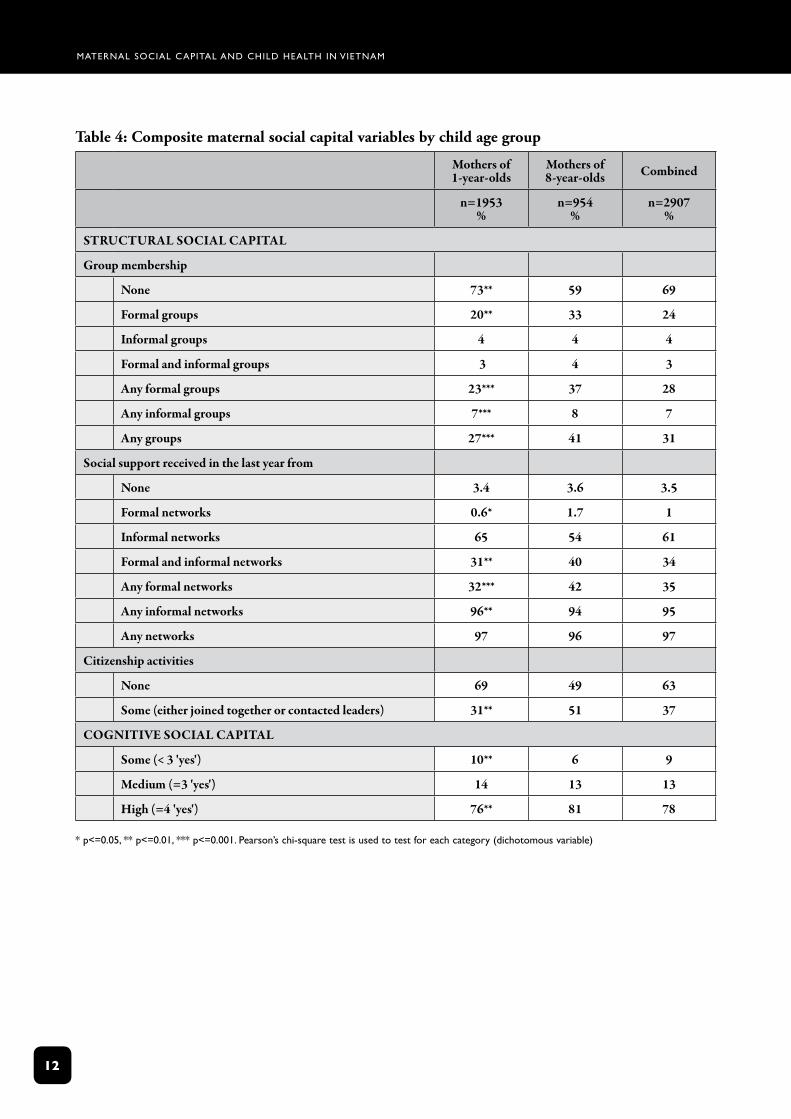
Table3describesthedistributionofeachaspectofmaternalsocialcapital,whileTable4presentscompositematernalsocialcapitalvariablesbychildagegroup.
Levelsofstructuralsocialcapitalarelow,particularlyamongmothersofone-year-olds.While73percentofmothersofone-year-oldsdonotparticipateinanygroup,thisfallsto59percentamongmothersofeight-year-olds(p<0.01).Inaddition,only31percentofmothersofone-year-oldsreceivesupportfrombothformalandinformalnetworks,comparedto40percentofmothersofeight-year-olds(p<0.01),andmothersofolderchildrenhavenearlytwicethelevelofcitizenship(p<0.01).Giventhecommunistpoliticalstructures,theoveralllevelofcitizenship(collectiveactionwithcommunityleaders)(37percent)issurprisinglylow.
Participationinwomen’sunionsaccountsforthemajorityofnetworkingactivitiescarriedoutbyallwomen,thoughagainparticipationisloweramongthemothersofone-year-olds(17percentcomparedto31percent,p<0.001).Whilesocialsupportfromformalnetworksislow(35percent),supportfrominformalnetworkssuchasfamily,friendsandneighboursisveryhigh(96percent,94percentand95percentrespectively).
Thefacevalidityofmeasuresofstructuralsocialcapitalappearsgoodasstatisticallysignificantdifferencesbetweenthegroupsonlyappearinquestionswhereonewouldexpectadifference.Forexample,olderwomen(mothersofeight-year-olds)aremorelikelytobeamemberofawomen’sunion(partoftheofficialCommunistParty’smassorganisations)andtohavecommunicatedwithcommuneleadersorjoinedwithothercommunememberstoaddressanissueorproblem(citizenship).Thisconcurswithexistingevidencethatshowsthatyoungergenerationsarelesslikelytoparticipateinmassorganisationsandothergroups(WischermannandVinh,2003).Itmayalsoreflectthedifferentneedsofolderandyoungerchildren–themothersofone-year-oldsprobablyhavelesstimetodevotetonetworkingactivities.
Incontrasttostructuralsocialcapital,levelsofcognitivesocialcapitalareveryhighamongbothgroups(76percentand81percent).Nevertheless,mothersofone-year-oldchildrendohavesignificantlylowerlevelsofgeneralisedtrust,senseofsocialharmonyandsenseofbelongingthanmothersofeight-year-oldchildren(p<0.01).Thiscouldbeduetotheirlowerparticipationratesoralowerdurationofresidenceinacommunity.
Thefacevalidityofthecognitivesocialcapitalquestionsisgoodasthe‘negatively’phrasedquestion‘Doyouthinkthatmostpeopleinthiscommunewouldtakeadvantageofyouifgiventheopportunity’getsalowpositiveresponseof9percent.
Maternal Social capital and child health in VietnaM
12
Table 4: Composite maternal social capital variables by child age group
Mothers of 1-year-olds
Mothers of 8-year-olds Combined
n=1953 %
n=954 %
n=2907 %
STRUCTURAl SoCIAl CApITAl
Group membership
None 73** 59 69
Formal groups 20** 33 24
Informal groups 4 4 4
Formal and informal groups 3 4 3
Any formal groups 23*** 37 28
Any informal groups 7*** 8 7
Any groups 27*** 41 31
Social support received in the last year from
None 3.4 3.6 3.5
Formal networks 0.6* 1.7 1
Informal networks 65 54 61
Formal and informal networks 31** 40 34
Any formal networks 32*** 42 35
Any informal networks 96** 94 95
Any networks 97 96 97
Citizenship activities
None 69 49 63
Some (either joined together or contacted leaders) 31** 51 37
CoGNITIve SoCIAl CApITAl
Some (< 3 'yes') 10** 6 9
Medium (=3 'yes') 14 13 13
High (=4 'yes') 76** 81 78
* p<=0.05, ** p<=0.01, *** p<=0.001. pearson’s chi-square test is used to test for each category (dichotomous variable)
Maternal Social capital and child health in VietnaM
13
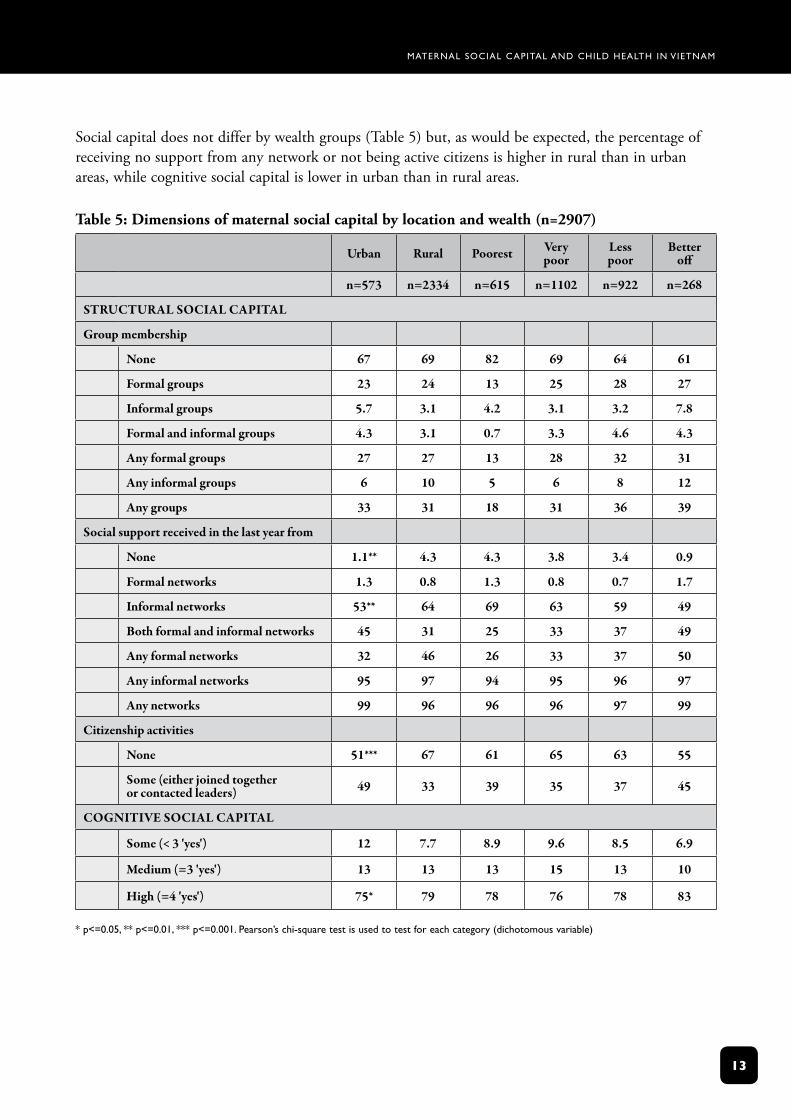
Socialcapitaldoesnotdifferbywealthgroups(Table5)but,aswouldbeexpected,thepercentageofreceivingnosupportfromanynetworkornotbeingactivecitizensishigherinruralthaninurbanareas,whilecognitivesocialcapitalislowerinurbanthaninruralareas.
Table 5: Dimensions of maternal social capital by location and wealth (n=2907)
Urban Rural poorest very poor
less poor
Better off
n=573 n=2334 n=615 n=1102 n=922 n=268
STRUCTURAl SoCIAl CApITAl
Group membership
None 67 69 82 69 64 61
Formal groups 23 24 13 25 28 27
Informal groups 5.7 3.1 4.2 3.1 3.2 7.8
Formal and informal groups 4.3 3.1 0.7 3.3 4.6 4.3
Any formal groups 27 27 13 28 32 31
Any informal groups 6 10 5 6 8 12
Any groups 33 31 18 31 36 39
Social support received in the last year from
None 1.1** 4.3 4.3 3.8 3.4 0.9
Formal networks 1.3 0.8 1.3 0.8 0.7 1.7
Informal networks 53** 64 69 63 59 49
Both formal and informal networks 45 31 25 33 37 49
Any formal networks 32 46 26 33 37 50
Any informal networks 95 97 94 95 96 97
Any networks 99 96 96 96 97 99
Citizenship activities
None 51*** 67 61 65 63 55
Some (either joined together or contacted leaders) 49 33 39 35 37 45
CoGNITIve SoCIAl CApITAl
Some (< 3 'yes') 12 7.7 8.9 9.6 8.5 6.9
Medium (=3 'yes') 13 13 13 15 13 10
High (=4 'yes') 75* 79 78 76 78 83
* p<=0.05, ** p<=0.01, *** p<=0.001. pearson’s chi-square test is used to test for each category (dichotomous variable)
Maternal Social capital and child health in VietnaM
14
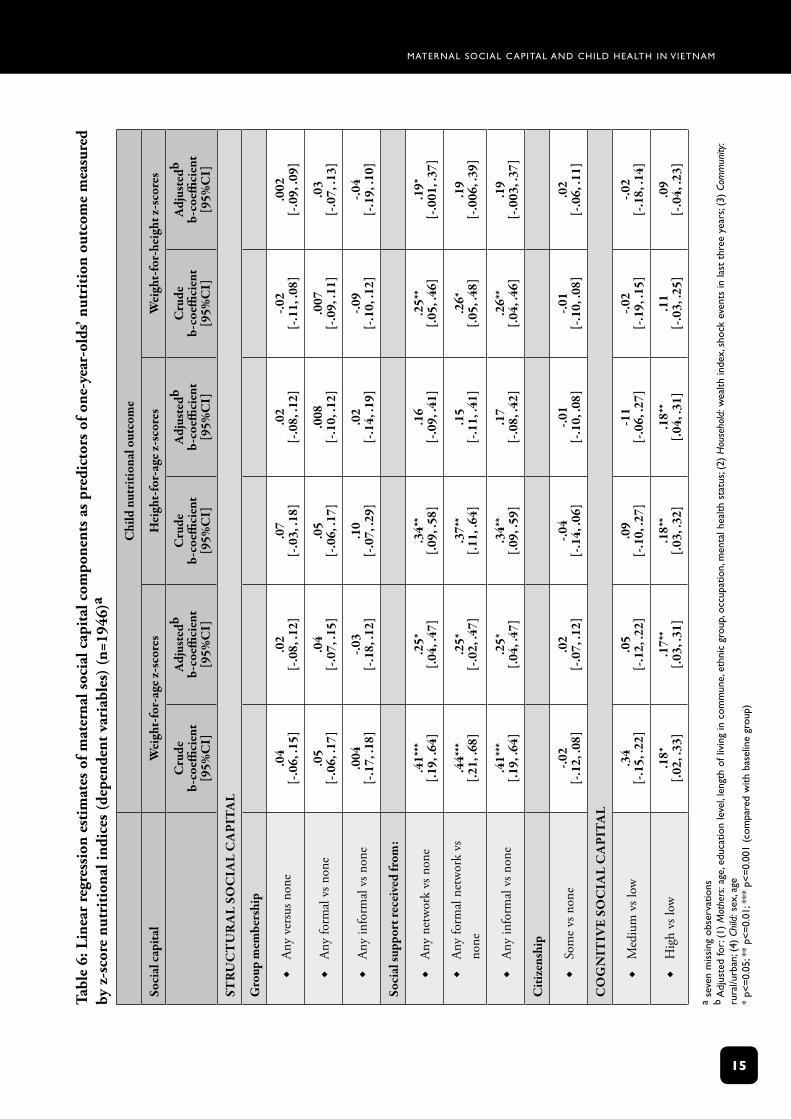
3.2 Multivariate results: the relationship between social capital and child nutritionAssociationsbetweenmaternalsocialcapitalandchildhealthoutcomesvarybyspecificoutcomesandbyspecificcomponentsofmaternalsocialcapital.Amongthefourcomponentsofmaternalsocialcapital,socialsupportandcognitivesocialcapitaldisplaythemoststatisticallysignificantassociationswithchildhealth.
Associationsbetweenmaternalsocialcapital(ie,socialsupportandcognitivesocialcapital)andchildnutritionwereapparentamongone-year-olds(Table6).Mothersofone-year-oldswhoreceivesupportfromeitherformalorinformalnetworkshavesignificantlybetterchildnutritionaloutcomesintermsofweight-for-age(β=0.25,P<0.05)andweight-for-height(β=0.19,P=0.05)aftercontrollingforanumberofotherfactors.Childrenofmotherswithhighcognitivesocialcapitalhavesignificantlyhigherweight-for-age(β=0.17,P<0.01)andheight-for-ageindices(β=0.18,P<0.01)thanthosewithlowcognitivesocialcapital.
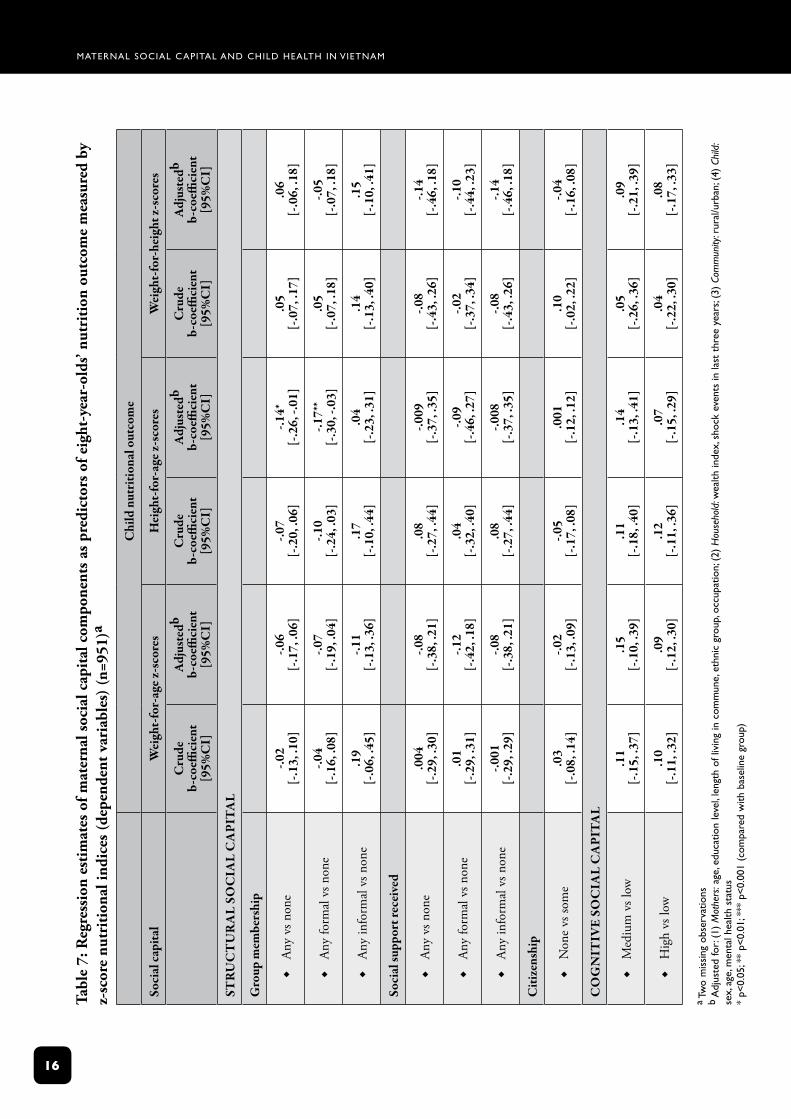
Amongeight-year-oldsveryfewconsistentassociationswerefoundbetweenmaternalsocialcapitalandchildnutrition.Onlymembershipofformalorganisationswassignificantlyassociatedwithchildnutrition,withmembershipofformalgroupsassociatedwith worse height-for-agez-scores(β=-0.17;95%CI-0.3,-0.03).
Maternal Social capital and child health in VietnaM
15
Tabl
e 6:
Lin
ear
regr
essi
on e
stim
ates
of m
ater
nal s
ocia
l cap
ital
com
pone
nts
as p
redi
ctor
s of
one
-yea
r-ol
ds’ n
utri
tion
out
com
e m
easu
red
by z
-sco
re n
utri
tion
al in
dice
s (d
epen
dent
var
iabl
es)
(n=1
946)
a
Chi
ld n
utri
tiona
l out
com
e
Soci
al ca
pita
lW
eigh
t-fo
r-ag
e z-s
core
sH
eigh
t-fo
r-ag
e z-s
core
sW
eigh
t-fo
r-he
ight
z-sc
ores
Cru
de
b-co
effici
ent
[95%
CI]
Adj
uste
db b-
coeffi
cien
t [9
5%C
I]
Cru
de
b-co
effici
ent
[95%
CI]
Adj
uste
db b-
coeffi
cien
t [9
5%C
I]
Cru
de
b-co
effici
ent
[95%
CI]
Adj
uste
db b-
coeffi
cien
t [9
5%C
I]
STR
UC
TU
RA
l So
CIA
l C
ApI
TA
l
Gro
up m
embe
rshi
p
Any
vers
usn
one
Æ.0
4 [-
.06,
.15]
.02
[-.0
8, .1
2].0
7 [-
.03,
.18]
.02
[-.0
8, .1
2]-.0
2[-
.11,
.08]
.002
[-.0
9, .0
9]
Any
form
alv
snon
eÆ
.05
[-.0
6, .1
7].0
4[-
.07,
.15]
.05
[-.0
6, .1
7].0
08[-
.10,
.12]
.007
[-.0
9, .1
1].0
3[-
.07,
.13]
Any
info
rmal
vsn
one
Æ.0
04[-
.17,
.18]
-.03
[-.1
8, .1
2].1
0[-
.07,
.29]
.02
[-.1
4, .1
9]-.0
9[-
.10,
.12]
-.04
[-.1
9, .1
0]
Soci
al su
ppor
t rec
eive
d fr
om:
Any
netw
ork
vsn
one
Æ.4
1***
[.19,
.64]
.25*
[.04,
.47]
.34*
*[.0
9, .5
8].1
6[-
.09,
.41]
.25*
*[.0
5, .4
6].1
9*[-
.001
, .37
]
Any
form
aln
etw
ork
vs
none
Æ.4
4***
[.21,
.68]
.25*
[-.0
2, .4
7].3
7**
[.11,
.64]
.15
[-.1
1, .4
1].2
6*[.0
5, .4
8].1
9[-
.006
, .39
]
Any
info
rmal
vsn
one
Æ.4
1***
[.19,
.64]
.25*
[.04,
.47]
.34*
*[.0
9, .5
9].1
7[-
.08,
.42]
.26*
*[.0
4, .4
6].1
9[-
.003
, .37
]
Citi
zens
hip
Som
evs
non
eÆ
-.02
[-.1
2, .0
8].0
2[-
.07,
.12]
-.04
[-.1
4, .0
6]-.0
1[-
.10,
.08]
-.01
[-.1
0, .0
8].0
2[-
.06,
.11]
Co
GN
ITIv
e So
CIA
l C
ApI
TA
l
Med
ium
vsl
owÆ
.34
[-.1
5, .2
2].0
5[-
.12,
.22]
.09
[-.1
0, .2
7]-1
1[-
.06,
.27]
-.02
[-.1
9, .1
5]-.0
2[-
.18,
.14]
Hig
hvs
low
Æ.1
8*[.0
2, .3
3].1
7**
[.03,
.31]
.18*
*[.0
3, .3
2].1
8**
[.04,
.31]
.11
[-.0
3, .2
5].0
9[-
.04,
.23]
a se
ven
mis
sing
obs
erva
tions
b
adj
uste
d fo
r: (1
) M
othe
rs: a
ge, e
duca
tion
leve
l, le
ngth
of l
ivin
g in
com
mun
e, e
thni
c gr
oup,
occ
upat
ion,
men
tal h
ealth
sta
tus;
(2)
Hou
seho
ld: w
ealth
inde
x, s
hock
eve
nts
in la
st t
hree
yea
rs; (
3) C
omm
unity
: ru
ral/u
rban
; (4)
Chi
ld: s
ex, a
ge
* p<
=0.
05; *
* p<
=0.
01; *
** p
<=
0.00
1 (c
ompa
red
with
bas
elin
e gr
oup)
Maternal Social capital and child health in VietnaM
1�
Tabl
e 7:
Reg
ress
ion
esti
mat
es o
f mat
erna
l soc
ial c
apit
al c
ompo
nent
s as
pre
dict
ors
of e
ight
-yea
r-ol
ds’ n
utri
tion
out
com
e m
easu
red
by
z-sc
ore
nutr
itio
nal i
ndic
es (
depe
nden
t var
iabl
es)
(n=9
51)a
Chi
ld n
utri
tiona
l out
com
e
Soci
al ca
pita
lW
eigh
t-fo
r-ag
e z-s
core
sH
eigh
t-fo
r-ag
e z-s
core
sW
eigh
t-fo
r-he
ight
z-sc
ores
Cru
deb-
coeffi
cien
t[9
5%C
I]
Adj
uste
dbb-
coeffi
cien
t[9
5%C
I]
Cru
deb-
coeffi
cien
t[9
5%C
I]
Adj
uste
dbb-
coeffi
cien
t[9
5%C
I]
Cru
deb-
coeffi
cien
t[9
5%C
I]
Adj
uste
dbb-
coeffi
cien
t[9
5%C
I]
STR
UC
TU
RA
l So
CIA
l C
ApI
TA
l
Gro
up m
embe
rshi
p
Any
vsn
one
Æ-.0
2 [-
.13,
.10]
-.06
[-.1
7, .0
6]-.0
7 [-
.20,
.06]
-.14*
[-
.26,
-.01
].0
5 [-
.07,
.17]
.06
[-.0
6, .1
8]
Any
form
alv
snon
eÆ
-.04
[-.1
6, .0
8]-.0
7 [-
.19,
.04]
-.10
[-.2
4, .0
3]-.1
7**
[-.3
0, -.
03]
.05
[-.0
7, .1
8]-.0
5 [-
.07,
.18]
Any
info
rmal
vsn
one
Æ.1
9 [-
.06,
.45]
-.11
[-.1
3, .3
6].1
7 [-
.10,
.44]
.04
[-
.23,
.31]
.14
[-.1
3, .4
0].1
5 [-
.10,
.41]
Soci
al su
ppor
t rec
eive
d
Any
vsn
one
Æ.0
04
[-.2
9, .3
0]-.0
8 [-
.38,
.21]
.08
[-.2
7, .4
4]-.0
09
[-.3
7, .3
5]-.0
8 [-
.43,
.26]
-.14
[-.4
6, .1
8]
Any
form
alv
snon
eÆ
.01
[-.2
9, .3
1]-.1
2[-
.42,
.18]
.04
[-.3
2, .4
0]-.0
9[-
.46,
.27]
-.02
[-.3
7, .3
4]-.1
0[-
.44,
.23]
Any
info
rmal
vsn
one
Æ-.0
01[-
.29,
.29]
-.08
[-.3
8, .2
1].0
8[-
.27,
.44]
-.008
[-.3
7, .3
5]-.0
8[-
.43,
.26]
-.14
[-.4
6, .1
8]
Citi
zens
hip
Non
evs
som
eÆ
.03
[-.0
8, .1
4]-.0
2[-
.13,
.09]
-.05
[-.1
7, .0
8].0
01[-
.12,
.12]
.10
[-.0
2, .2
2]-.0
4[-
.16,
.08]
Co
GN
ITIv
e So
CIA
l C
ApI
TA
l
Med
ium
vsl
owÆ
.11
[-.1
5, .3
7].1
5[-
.10,
.39]
.11
[-.1
8, .4
0].1
4[-
.13,
.41]
.05
[-.2
6, .3
6].0
9[-
.21,
.39]
Hig
hvs
low
Æ.1
0[-
.11,
.32]
.09
[-.1
2, .3
0].1
2[-
.11,
.36]
.07
[-.1
5, .2
9].0
4[-
.22,
.30]
.08
[-.1
7, .3
3]
a tw
o m
issi
ng o
bser
vatio
ns
b a
djus
ted
for:
(1)
Mot
hers
: age
, edu
catio
n le
vel,
leng
th o
f liv
ing
in c
omm
une,
eth
nic
grou
p, o
ccup
atio
n; (
2) H
ouse
hold
: wea
lth in
dex,
sho
ck e
vent
s in
last
thr
ee y
ears
; (3)
Com
mun
ity: r
ural
/urb
an; (
4) C
hild
: se
x, a
ge, m
enta
l hea
lth s
tatu
s *
p<0.
05; *
* p<
0.01
; ***
p<
0.00
1 (c
ompa
red
with
bas
elin
e gr
oup)
Maternal Social capital and child health in VietnaM
17
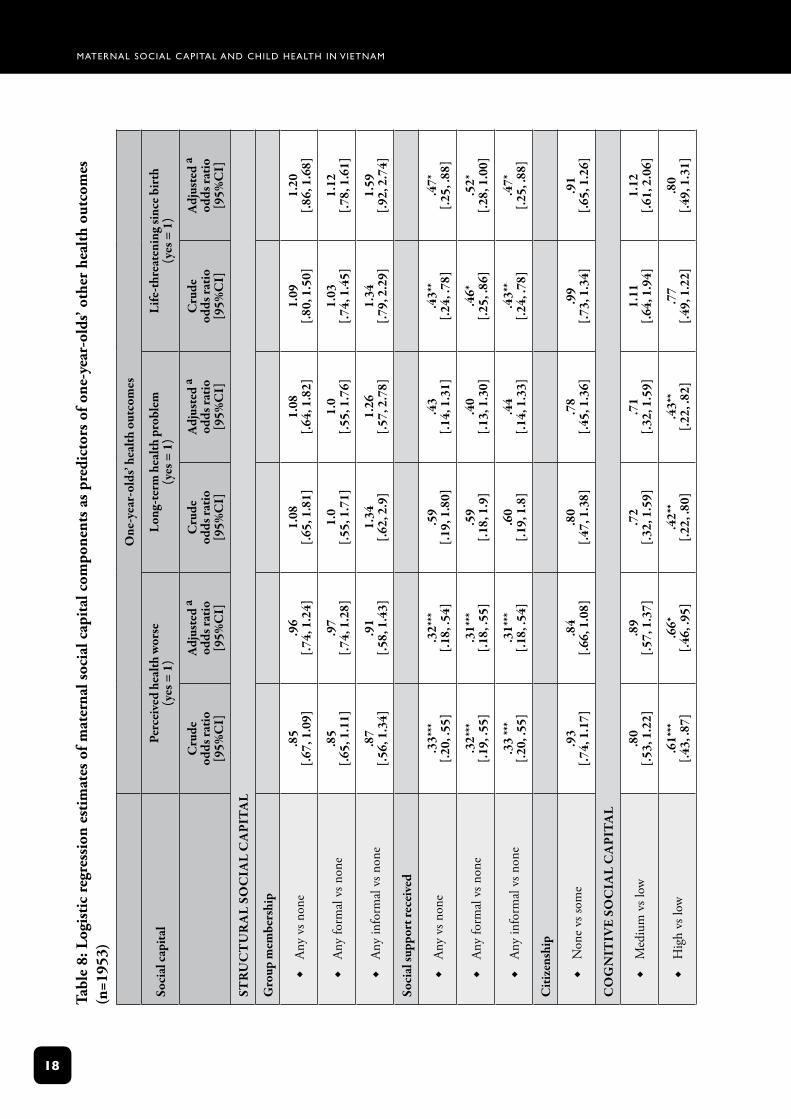
3.3 Multivariate results: the relationship between social capital and child healthAswithnutritionaloutcomes,socialsupportandcognitivesocialcapitalshowedthemostconsistentassociationswithchildphysicalhealthoutcomesamongone-year-olds.Childrenofmotherswhoreceivedsocialsupportfromeitherformalorinformalnetworkswerestrongerthanchildrenofmotherswhohadnosocialsupport(OR=0.31,P<0.001),andmotherswhoreceivedsocialsupportfromeitherformalorinformalnetworksreportedlesslife-threateningchildillnesscomparedtothosewithlittlesupport(OR=0.52and0.47respectively;P<0.05).Childrenofmotherswithhighcognitivesocialcapitalareatalowerriskofbothacuteillnessandlong-termhealthproblemsthanthosefrommotherswithlowcognitivesocialcapital(OR=0.66,P<0.05;OR=0.52,P<0.001;andOR=0.43,P<0.01,respectively)(Table8).
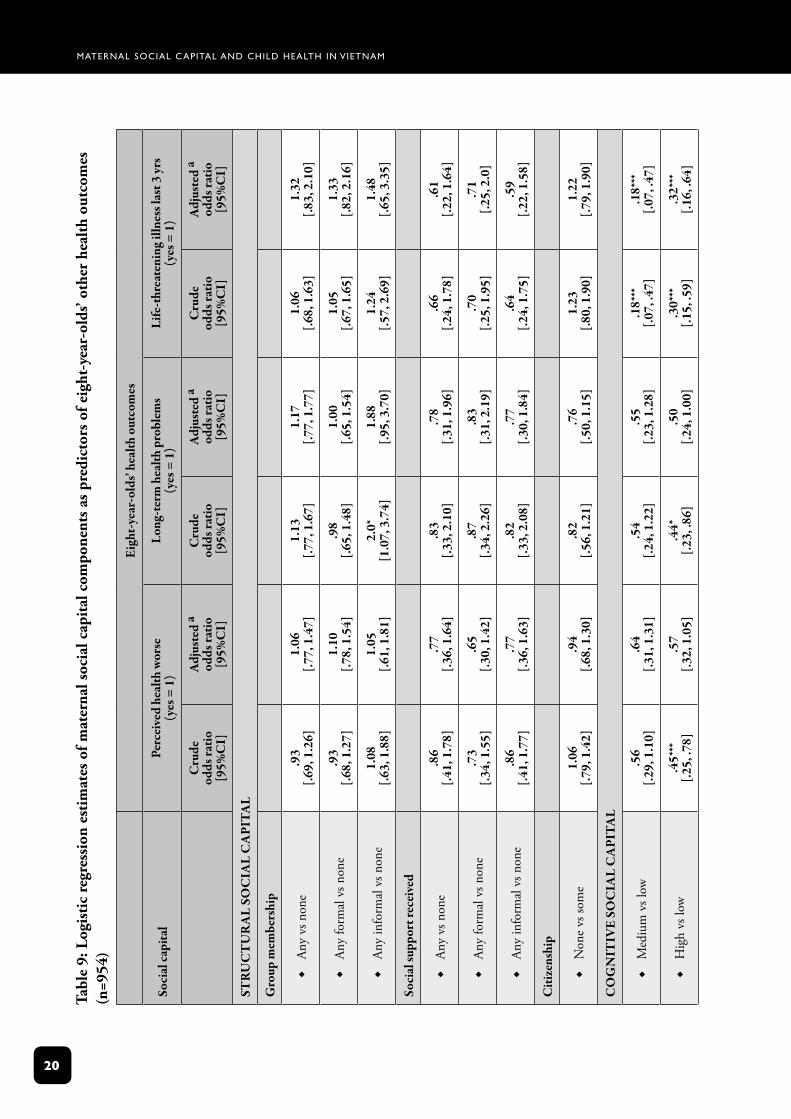
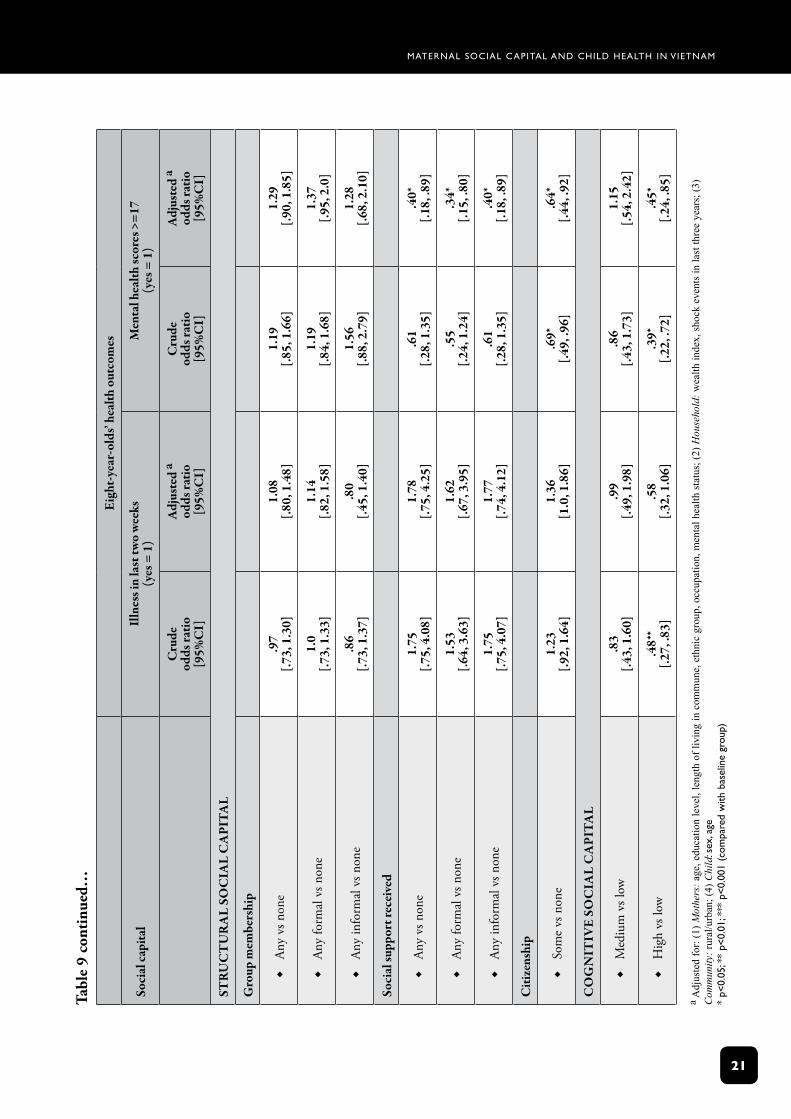
Amongeight-year-olds,themostconsistentassociationsarebetweengoodchildmentalhealthandhighlevelsofmaternalsocialcapital,wherebyexceptgroupmembership,allotherindicatorsofsocialcapitalaresignificantlyassociatedwithchildmentalhealth.Childrenofmotherswithhighlevelofcognitivesocialcapitalalsohaveloweroddsofhavingsufferedalife-threateningillness(Table9).Thecausalityofthisassociationmightruneitherway:hightrustandsenseofbelongingmayenableamothertoseekcaremoreeffectively,oraseriouslyillchildmayleadamothertobemorehouseboundandtonotbeabletoestablishtrustingrelationships.
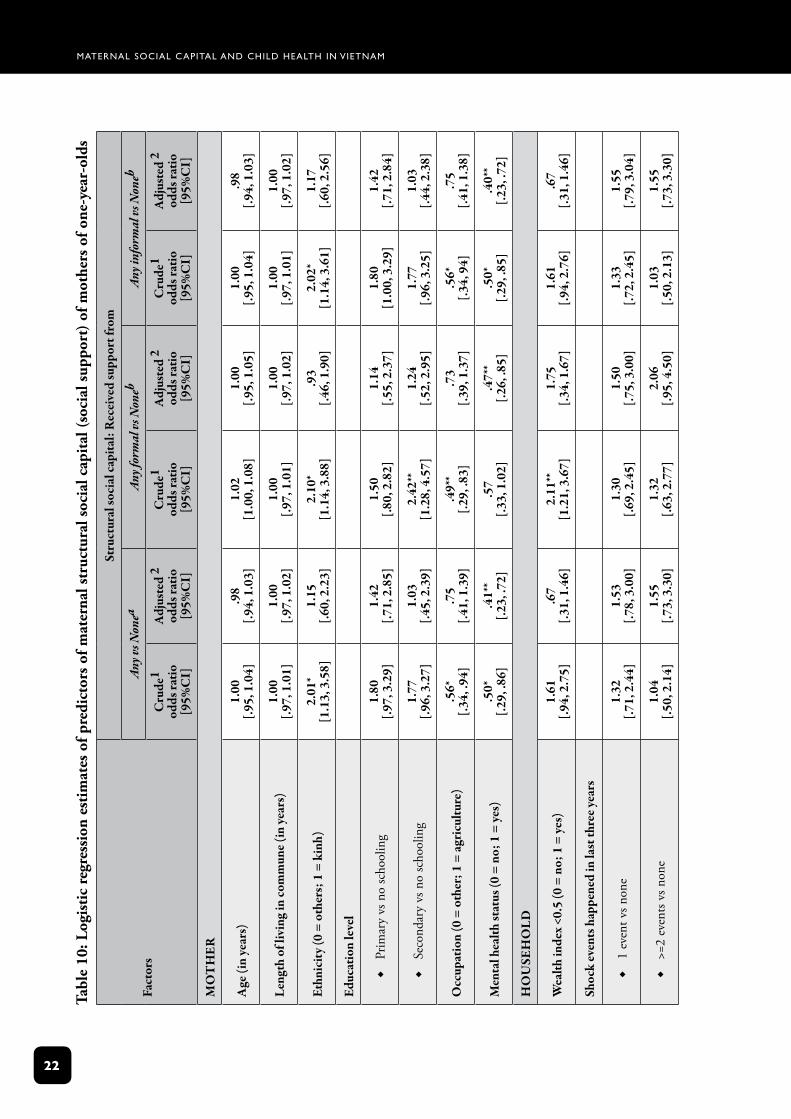
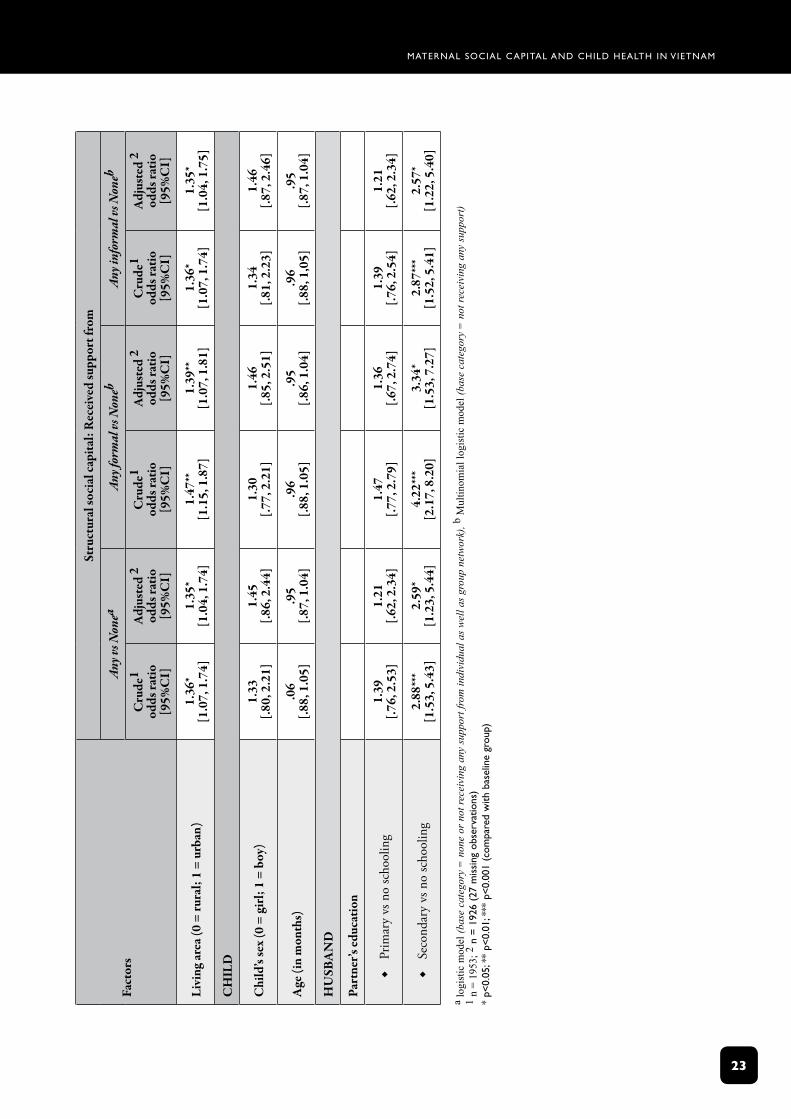
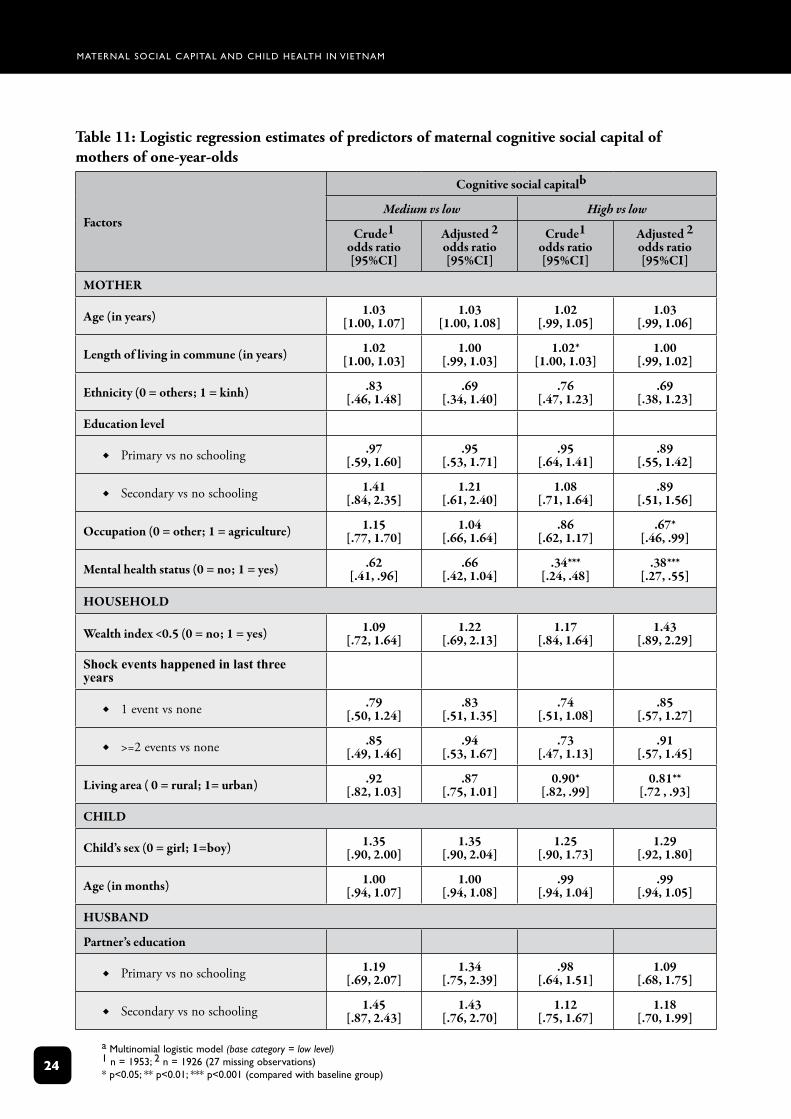
3.4 Determinants of maternal social capitalAsmaternalsocialcapitalinfluenceschildhealth,itisimportanttoknowwhatinfluencesmaternalsocialcapital.Thedeterminantsofsocialsupportandcognitivesocialcapitalamongthemothersofone-year-oldsweresubsequentlyexplored,asthesevariablesshowedthemostconsistentassociationswithchildhealth.Understandingsomethingofthedeterminantsofthesevariablesmayhelpindesigninginterventionprogrammestoimprovethem.
Predictorsofhavingsocialsupportarelivinginanurbanarea(OR=1.39and1.35respectivelyforanyformalandanyinformalsourcesofsupport;P<0.01andP<0.05),havingapartnerwhocompletedsecondaryschool(OR=3.34and2.57respectivelyforanyformalandanyinformal;P<0.05),andgoodmaternalmentalhealth(Table10).Notethatethnicity,lengthofresidenceincommune,maternaleducationstatus,maternaloccupation,householdwealthstatus,economicshocksandchild’ssexarenotassociatedwithhavingsocialsupport.
Predictorsofhighcognitivesocialcapitalaregoodmaternalmentalhealth,notworkinginagriculture,andlivinginaruralarea.Notethatmaternalage,ethnicity,lengthofresidence,maternaleducation,householdwealth,householdeconomicshocksandpartner’seducationarenotassociatedwithcognitivesocialcapital.
Maternal Social capital and child health in VietnaM
18
Tabl
e 8:
Log
isti
c re
gres
sion
est
imat
es o
f mat
erna
l soc
ial c
apit
al c
ompo
nent
s as
pre
dict
ors
of o
ne-y
ear-
olds
’ oth
er h
ealt
h ou
tcom
es
(n=1
953)
one
-yea
r-ol
ds’ h
ealth
out
com
es
Soci
al ca
pita
lpe
rcei
ved
heal
th w
orse
(y
es =
1)
long
-ter
m h
ealth
pro
blem
(y
es =
1)
life
-thr
eate
ning
sinc
e bir
th
(yes
= 1
)
Cru
de
odds
ratio
[9
5%C
I]
Adj
uste
d a
odds
ratio
[9
5%C
I]
Cru
de
odds
ratio
[9
5%C
I]
Adj
uste
d a
odds
ratio
[9
5%C
I]
Cru
de
odds
ratio
[9
5%C
I]
Adj
uste
d a
odds
ratio
[9
5%C
I]
STR
UC
TU
RA
l So
CIA
l C
ApI
TA
l
Gro
up m
embe
rshi
p
Any
vsn
one
Æ.8
5 [.6
7, 1
.09]
.96
[.74,
1.2
4]1.
08
[.65,
1.8
1]1.
08
[.64,
1.8
2]1.
09
[.80,
1.5
0]1.
20
[.86,
1.6
8]
Any
form
alv
snon
eÆ
.85
[.65,
1.1
1].9
7 [.7
4, 1
.28]
1.0
[.55,
1.7
1]1.
0 [.5
5, 1
.76]
1.03
[.7
4, 1
.45]
1.12
[.7
8, 1
.61]
Any
info
rmal
vsn
one
Æ.8
7[.5
6, 1
.34]
.91
[.58,
1.4
3]1.
34[.6
2, 2
.9]
1.26
[.57,
2.7
8]1.
34[.7
9, 2
.29]
1.59
[.92,
2.7
4]
Soci
al su
ppor
t rec
eive
d
Any
vsn
one
Æ.3
3***
[.20,
.55]
.32*
**[.1
8, .5
4].5
9[.1
9, 1
.80]
.43
[.14,
1.3
1].4
3**
[.24,
.78]
.47*
[.25,
.88]
Any
form
alv
snon
eÆ
.32*
**[.1
9, .5
5].3
1***
[.18,
.55]
.59
[.18,
1.9
].4
0[.1
3, 1
.30]
.46*
[.25,
.86]
.52*
[.28,
1.0
0]
Any
info
rmal
vsn
one
Æ.3
3 **
*[.2
0, .5
5].3
1***
[.18,
.54]
.60
[.19,
1.8
].4
4[.1
4, 1
.33]
.43*
*[.2
4, .7
8].4
7*[.2
5, .8
8]
Citi
zens
hip
Non
evs
som
eÆ
.93
[.74,
1.1
7].8
4[.6
6, 1
.08]
.80
[.47,
1.3
8].7
8[.4
5, 1
.36]
.99
[.73,
1.3
4].9
1[.6
5, 1
.26]
Co
GN
ITIv
e So
CIA
l C
ApI
TA
l
Med
ium
vsl
owÆ
.80
[.53,
1.2
2].8
9[.5
7, 1
.37]
.72
[.32,
1.5
9].7
1[.3
2, 1
.59]
1.11
[.64,
1.9
4]1.
12[.6
1, 2
.06]
Hig
hvs
low
Æ.6
1***
[.43,
.87]
.66*
[.46,
.95]
.42*
*[.2
2, .8
0].4
3**
[.22,
.82]
.77
[.49,
1.2
2].8
0[.4
9, 1
.31]

Maternal Social capital and child health in VietnaM
1�
Tabl
e 8
cont
inue
d…
one
-yea
r-ol
ds’ h
ealth
out
com
es
Soci
al ca
pita
lIn
jury
/acc
iden
t sin
ce b
irth
(yes
= 1
)Il
lnes
s in
last
24
hour
s(y
es =
1)
Cru
deod
ds ra
tio[9
5%C
I]
Adj
uste
d aod
ds ra
tio[9
5%C
I]
Cru
deod
ds ra
tio[9
5%C
I]
Adj
uste
d aod
ds ra
tio[9
5%C
I]
STR
UC
TU
RA
l So
CIA
l C
ApI
TA
l
Gro
up m
embe
rshi
p
Any
vsn
one
Æ1.
11[.7
6, 1
.61]
1.17
[.80,
1.7
1]1.
04[.7
9, 1
.38]
1.11
[.83,
1.4
8]
Any
form
alv
snon
eÆ
1.14
[.77,
1.6
8]1.
23[.8
2, 1
.85]
1.07
[.80,
1.4
4]1.
14[.8
4 , 1
.56]
Any
info
rmal
vsn
one
Æ1.
04[.5
4, 1
.98]
1.04
[.54,
1.9
9].9
6[.5
8, 1
.59]
1.04
[.62,
1.7
4]
Soci
al su
ppor
t rec
eive
d
Any
vsn
one
Æ.9
3[.4
0, 2
.13]
.92
[.38,
2.1
9].6
5[.3
6, 1
.17]
.61
[.33,
1.1
1]
Any
form
alv
snon
eÆ
.83
[.35,
2.0
].8
4[.3
4, 2
.11]
.62
[.33,
1.1
7].5
9[.3
1, 1
.12]
Any
info
rmal
vsn
one
Æ.9
3[.4
0, 2
.14]
.93
[.39,
2.2
1].6
5[.3
6, 1
.17]
.61
[.33,
1.1
1]
Citi
zens
hip
Non
evs
som
eÆ
.77
[.53,
1.1
2].7
4[.5
0, 1
.10]
.90
[.68,
1.1
9].8
8[.6
7, 1
.17]
Co
GN
ITIv
e So
CIA
l C
ApI
TA
l
Med
ium
vsl
owÆ
.71
[.38,
1.3
2].7
5[.4
0, 1
.41]
.95
[.60,
1.5
0]1.
00[.6
3, 1
.59]
Hig
hvs
low
Æ.5
8*[.3
5, .9
6].6
2[.3
7, 1
.05]
.49*
**[.3
3, .7
1].5
2***
[.35,
.77]
a a
djus
ted
for:
(1)
Mot
hers
: age
, edu
catio
n le
vel,
leng
th o
f liv
ing
in c
omm
une,
eth
nic
grou
p, o
ccup
atio
n, m
enta
l hea
lth s
tatu
s; (2
) H
ouse
hold
: wea
lth in
dex,
sho
ck e
vent
s in
last
thr
ee y
ears
; (3)
Com
mun
ity:
rura
l/urb
an; (
4) C
hild
: sex
, age
*
p<0.
05; *
* p<
0.01
; ***
p<
0.00
1 (c
ompa
red
with
bas
elin
e gr
oup)
Maternal Social capital and child health in VietnaM
20
Tabl
e 9:
Log
isti
c re
gres
sion
est
imat
es o
f mat
erna
l soc
ial c
apit
al c
ompo
nent
s as
pre
dict
ors
of e
ight
-yea
r-ol
ds’ o
ther
hea
lth
outc
omes
(n
=954
)
eigh
t-ye
ar-o
lds’
heal
th o
utco
mes
Soci
al ca
pita
lpe
rcei
ved
heal
th w
orse
(yes
= 1
)lo
ng-t
erm
hea
lth p
robl
ems
(yes
= 1
)li
fe-t
hrea
teni
ng il
lnes
s las
t 3 yr
s(y
es =
1)
Cru
deod
ds ra
tio[9
5%C
I]
Adj
uste
d a
odds
ratio
[95%
CI]
Cru
deod
ds ra
tio[9
5%C
I]
Adj
uste
d a
odds
ratio
[95%
CI]
Cru
deod
ds ra
tio[9
5%C
I]
Adj
uste
d a
odds
ratio
[95%
CI]
STR
UC
TU
RA
l So
CIA
l C
ApI
TAl
Gro
up m
embe
rshi
p
Any
vsn
one
Æ.9
3[.6
9, 1
.26]
1.06
[.77,
1.4
7]1.
13[.7
7, 1
.67]
1.17
[.77,
1.7
7]1.
06[.6
8, 1
.63]
1.32
[.83,
2.1
0]
Any
form
alv
snon
eÆ
.93
[.68,
1.2
7]1.
10[.7
8, 1
.54]
.98
[.65,
1.4
8]1.
00[.6
5, 1
.54]
1.05
[.67,
1.6
5]1.
33[.8
2, 2
.16]
Any
info
rmal
vsn
one
Æ1.
08[.6
3, 1
.88]
1.05
[.61,
1.8
1]2.
0*[1
.07,
3.7
4]1.
88[.9
5, 3
.70]
1.24
[.57,
2.6
9]1.
48[.6
5, 3
.35]
Soci
al su
ppor
t rec
eive
d
Any
vsn
one
Æ.8
6[.4
1, 1
.78]
.77
[.36,
1.6
4].8
3[.3
3, 2
.10]
.78
[.31,
1.9
6].6
6[.2
4, 1
.78]
.61
[.22,
1.6
4]
Any
form
alv
snon
eÆ
.73
[.34,
1.5
5].6
5[.3
0, 1
.42]
.87
[.34,
2.2
6].8
3[.3
1, 2
.19]
.70
[.25,
1.9
5].7
1[.2
5, 2
.0]
Any
info
rmal
vsn
one
Æ.8
6[.4
1, 1
.77]
.77
[.36,
1.6
3].8
2[.3
3, 2
.08]
.77
[.30,
1.8
4].6
4[.2
4, 1
.75]
.59
[.22,
1.5
8]
Citi
zens
hip
Non
evs
som
eÆ
1.06
[.79,
1.4
2].9
4[.6
8, 1
.30]
.82
[.56,
1.2
1].7
6[.5
0, 1
.15]
1.23
[.80,
1.9
0]1.
22[.7
9, 1
.90]
Co
GN
ITIv
e So
CIA
l C
ApI
TAl
Med
ium
vsl
owÆ
.56
[.29,
1.1
0].6
4[.3
1, 1
.31]
.54
[.24,
1.2
2].5
5[.2
3, 1
.28]
.18*
**[.0
7, .4
7].1
8***
[.07,
.47]
Hig
hvs
low
Æ.4
5***
[.25,
.78]
.57
[.32,
1.0
5].4
4*[.2
3, .8
6].5
0[.2
4, 1
.00]
.30*
**[.1
5, .5
9].3
2***
[.16,
.64]
Maternal Social capital and child health in VietnaM
21
Tabl
e 9
cont
inue
d…
eigh
t-ye
ar-o
lds’
heal
th o
utco
mes
Soci
al ca
pita
lIl
lnes
s in
last
two
wee
ks(y
es =
1)
Men
tal h
ealth
scor
es >
=17
(yes
= 1
)
Cru
deod
ds ra
tio[9
5%C
I]
Adj
uste
d a
odds
ratio
[95%
CI]
Cru
deod
ds ra
tio[9
5%C
I]
Adj
uste
d a
odds
ratio
[95%
CI]
STR
UC
TU
RA
l So
CIA
l C
ApI
TAl
Gro
up m
embe
rshi
p
Any
vsn
one
Æ.9
7[.7
3, 1
.30]
1.08
[.80,
1.4
8]1.
19[.8
5, 1
.66]
1.29
[.90,
1.8
5]
Any
form
alv
snon
eÆ
1.0
[.73,
1.3
3]1.
14[.8
2, 1
.58]
1.19
[.84,
1.6
8]1.
37[.9
5, 2
.0]
Any
info
rmal
vsn
one
Æ.8
6[.7
3, 1
.37]
.80
[.45,
1.4
0]1.
56[.8
8, 2
.79]
1.28
[.68,
2.1
0]
Soci
al su
ppor
t rec
eive
d
Any
vsn
one
Æ1.
75[.7
5, 4
.08]
1.78
[.75,
4.2
5].6
1[.2
8, 1
.35]
.40*
[.18,
.89]
Any
form
alv
snon
eÆ
1.53
[.64,
3.6
3]1.
62[.6
7, 3
.95]
.55
[.24,
1.2
4].3
4*[.1
5, .8
0]
Any
info
rmal
vsn
one
Æ1.
75[.7
5, 4
.07]
1.77
[.74,
4.1
2].6
1[.2
8, 1
.35]
.40*
[.18,
.89]
Citi
zens
hip
Som
evs
non
eÆ
1.23
[.92,
1.6
4]1.
36[1
.0, 1
.86]
.69*
[.49,
.96]
.64*
[.44,
.92]
Co
GN
ITIv
e So
CIA
l C
ApI
TA
l
Med
ium
vsl
owÆ
.83
[.43,
1.6
0].9
9[.4
9, 1
.98]
.86
[.43,
1.7
3]1.
15[.5
4, 2
.42]
Hig
hvs
low
Æ.4
8**
[.27,
.83]
.58
[.32,
1.0
6].3
9*[.2
2, .7
2].4
5*[.2
4, .8
5]
a A
djus
ted
for:
(1)
Mot
hers
: ag
e, e
duca
tion
leve
l, le
ngth
of
livin
g in
com
mun
e, e
thni
c gr
oup,
occ
upat
ion,
men
tal h
ealth
sta
tus;
(2)
Hou
seho
ld:
wea
lth in
dex,
sho
ck e
vent
s in
last
thre
e ye
ars;
(3)
C
omm
unity
: ru
ral/u
rban
; (4)
Chi
ld: s
ex, a
ge
* p<
0.05
; **
p<0.
01; *
** p
<0.
001
(com
pare
d w
ith b
asel
ine
grou
p)
Maternal Social capital and child health in VietnaM
22
Tabl
e 10
: Log
isti
c re
gres
sion
est
imat
es o
f pre
dict
ors
of m
ater
nal s
truc
tura
l soc
ial c
apit
al (
soci
al s
uppo
rt)
of m
othe
rs o
f one
-yea
r-ol
ds
Fact
ors
Stru
ctur
al so
cial
capi
tal:
Rec
eive
d su
ppor
t fro
m
Any v
s Non
eaAn
y for
mal
vs N
oneb
Any i
nfor
mal
vs N
oneb
Cru
de1
odds
ratio
[95%
CI]
Adj
uste
d 2od
ds ra
tio[9
5%C
I]
Cru
de1
odds
ratio
[95%
CI]
Adj
uste
d 2od
ds ra
tio[9
5%C
I]
Cru
de1
odds
ratio
[95%
CI]
Adj
uste
d 2od
ds ra
tio[9
5%C
I]
Mo
TH
eR
Age
(in
year
s)1.
00[.9
5, 1
.04]
.98
[.94,
1.0
3]1.
02[1
.00,
1.0
8]1.
00[.9
5, 1
.05]
1.00
[.95,
1.0
4].9
8[.9
4, 1
.03]
leng
th o
f liv
ing
in co
mm
une (
in ye
ars)
1.00
[.97,
1.0
1]1.
00[.9
7, 1
.02]
1.00
[.97,
1.0
1]1.
00[.9
7, 1
.02]
1.00
[.97,
1.0
1]1.
00[.9
7, 1
.02]
ethn
icit
y (0
= ot
hers
; 1 =
kin
h)2.
01*
[1.1
3, 3
.58]
1.15
[.60,
2.2
3]2.
10*
[1.1
4, 3
.88]
.93
[.46,
1.9
0]2.
02*
[1.1
4, 3
.61]
1.17
[.60,
2.5
6]
educ
atio
n le
vel
Prim
ary
vsn
osc
hool
ing
Æ1.
80[.9
7, 3
.29]
1.42
[.71,
2.8
5]1.
50[.8
0, 2
.82]
1.14
[.55,
2.3
7]1.
80[1
.00,
3.2
9]1.
42[.7
1, 2
.84]
Seco
ndar
yvs
no
scho
olin
gÆ
1.77
[.96,
3.2
7]1.
03[.4
5, 2
.39]
2.42
**[1
.28,
4.5
7]1.
24[.5
2, 2
.95]
1.77
[.96,
3.2
5]1.
03[.4
4, 2
.38]
occ
upat
ion
(0 =
oth
er; 1
= ag
ricu
lture
).5
6*[.3
4, .9
4].7
5[.4
1, 1
.39]
.49*
*[.2
9, .8
3].7
3[.3
9, 1
.37]
.56*
[.34,
94]
.75
[.41,
1.3
8]
Men
tal h
ealth
stat
us (0
= n
o; 1
= ye
s).5
0*[.2
9, .8
6].4
1**
[.23,
.72]
.57
[.33,
1.0
2].4
7**
[.26,
.85]
.50*
[.29,
.85]
.40*
*[.2
3, .7
2]
Ho
USe
Ho
lD
Wea
lth in
dex
<0.5
(0 =
no;
1 =
yes)
1.61
[.94,
2.7
5].6
7[.3
1, 1
.46]
2.11
**[1
.21,
3.6
7]1.
75[.3
4, 1
.67]
1.61
[.94,
2.7
6].6
7[.3
1, 1
.46]
Shoc
k ev
ents
hap
pene
d in
last
thre
e yea
rs
1ev
entv
snon
eÆ
1.32
[.71,
2.4
4]1.
53[.7
8, 3
.00]
1.30
[.69,
2.4
5]1.
50[.7
5, 3
.00]
1.33
[.72,
2.4
5]1.
55[.7
9, 3
.04]
>=2
even
tsvs
non
eÆ
1.04
[.50,
2.1
4]1.
55[.7
3, 3
.30]
1.32
[.63,
2.7
7]2.
06[.9
5, 4
.50]
1.
03[.5
0, 2
.13]
1.55
[.73,
3.3
0]
Maternal Social capital and child health in VietnaM
23
Fact
ors
Stru
ctur
al so
cial
capi
tal:
Rec
eive
d su
ppor
t fro
m
Any v
s Non
eaAn
y for
mal
vs N
oneb
Any i
nfor
mal
vs N
oneb
Cru
de1
odds
ratio
[95%
CI]
Adj
uste
d 2od
ds ra
tio[9
5%C
I]
Cru
de1
odds
ratio
[95%
CI]
Adj
uste
d 2od
ds ra
tio[9
5%C
I]
Cru
de1
odds
ratio
[95%
CI]
Adj
uste
d 2od
ds ra
tio[9
5%C
I]
livi
ng ar
ea (0
= ru
ral;
1 =
urba
n)1.
36*
[1.0
7, 1
.74]
1.35
*[1
.04,
1.7
4]1.
47**
[1.1
5, 1
.87]
1.39
**[1
.07,
1.8
1]1.
36*
[1.0
7, 1
.74]
1.35
*[1
.04,
1.7
5]
CH
IlD
Chi
ld’s
sex
(0 =
gir
l; 1
= bo
y)1.
33[.8
0, 2
.21]
1.45
[.86,
2.4
4]1.
30[.7
7, 2
.21]
1.46
[.85,
2.5
1]1.
34[.8
1, 2
.23]
1.46
[.87,
2.4
6]
Age
(in
mon
ths)
.06
[.88,
1.0
5].9
5[.8
7, 1
.04]
.96
[.88,
1.0
5].9
5[.8
6, 1
.04]
.96
[.88,
1,0
5].9
5[.8
7, 1
.04]
HU
SBA
ND
part
ner’s
educ
atio
n
Prim
ary
vsn
osc
hool
ing
Æ1.
39[.7
6, 2
.53]
1.21
[.62,
2.3
4]1.
47[.7
7, 2
.79]
1.36
[.67,
2.7
4]1.
39[.7
6, 2
.54]
1.21
[.62,
2.3
4]
Seco
ndar
yvs
no
scho
olin
gÆ
2.88
***
[1.5
3, 5
.43]
2.59
*[1
.23,
5.4
4]4.
22**
*[2
.17,
8.2
0]3.
34*
[1.5
3, 7
.27]
2.87
***
[1.5
2, 5
.41]
2.57
*[1
.22,
5.4
0]
a lo
gist
ic m
odel
(ba
se c
ateg
ory
= n
one
or n
ot r
ecei
ving
any
sup
port
from
indi
vidu
al a
s w
ell a
s gr
oup
netw
ork)
, b M
ultin
omia
l log
istic
mod
el (
base
cat
egor
y =
not
rec
eivi
ng a
ny s
uppo
rt)
1 n
= 19
53; 2
n =
192
6 (2
7 m
issi
ng o
bser
vatio
ns)
* p<
0.05
; **
p<0.
01; *
** p
<0.
001
(com
pare
d w
ith b
asel
ine
grou
p)
Maternal Social capital and child health in VietnaM
24
Table 11: Logistic regression estimates of predictors of maternal cognitive social capital of mothers of one-year-olds
Factors
Cognitive social capitalb
Medium vs low High vs low
Crude1odds ratio[95%CI]
Adjusted 2odds ratio[95%CI]
Crude1odds ratio[95%CI]
Adjusted 2odds ratio[95%CI]
MoTHeR
Age (in years) 1.03[1.00, 1.07]
1.03[1.00, 1.08]
1.02[.99, 1.05]
1.03[.99, 1.06]
length of living in commune (in years) 1.02[1.00, 1.03]
1.00[.99, 1.03]
1.02*[1.00, 1.03]
1.00[.99, 1.02]
ethnicity (0 = others; 1 = kinh) .83[.46, 1.48]
.69[.34, 1.40]
.76[.47, 1.23]
.69[.38, 1.23]
education level
PrimaryvsnoschoolingÆ.97
[.59, 1.60].95
[.53, 1.71].95
[.64, 1.41].89
[.55, 1.42]
SecondaryvsnoschoolingÆ1.41
[.84, 2.35]1.21
[.61, 2.40]1.08
[.71, 1.64].89
[.51, 1.56]
occupation (0 = other; 1 = agriculture) 1.15[.77, 1.70]
1.04[.66, 1.64]
.86[.62, 1.17]
.67*[.46, .99]
Mental health status (0 = no; 1 = yes) .62[.41, .96]
.66[.42, 1.04]
.34***[.24, .48]
.38***[.27, .55]
HoUSeHolD
Wealth index <0.5 (0 = no; 1 = yes) 1.09[.72, 1.64]
1.22[.69, 2.13]
1.17[.84, 1.64]
1.43[.89, 2.29]
Shock events happened in last three years
1eventvsnoneÆ.79
[.50, 1.24].83
[.51, 1.35].74
[.51, 1.08].85
[.57, 1.27]
>=2eventsvsnoneÆ.85
[.49, 1.46].94
[.53, 1.67].73
[.47, 1.13].91
[.57, 1.45]
living area ( 0 = rural; 1= urban) .92[.82, 1.03]
.87[.75, 1.01]
0.90*[.82, .99]
0.81**[.72 , .93]
CHIlD
Child’s sex (0 = girl; 1=boy) 1.35[.90, 2.00]
1.35[.90, 2.04]
1.25[.90, 1.73]
1.29[.92, 1.80]
Age (in months) 1.00[.94, 1.07]
1.00[.94, 1.08]
.99[.94, 1.04]
.99[.94, 1.05]
HUSBAND
partner’s education
PrimaryvsnoschoolingÆ1.19
[.69, 2.07]1.34
[.75, 2.39].98
[.64, 1.51]1.09
[.68, 1.75]
SecondaryvsnoschoolingÆ1.45
[.87, 2.43]1.43
[.76, 2.70]1.12
[.75, 1.67]1.18
[.70, 1.99]
a Multinomial logistic model (base category = low level) 1 n = 1953; 2 n = 1926 (27 missing observations) * p<0.05; ** p<0.01; *** p<0.001 (compared with baseline group)
Maternal Social capital and child health in VietnaM
25
4. discussion and conclusionsAswithallcross-sectionalstudies,causalitycannotbeattributedtotheassociationsfoundinthispaper.Inaddition,theover-samplingofpoorrespondentsfortheYoungLivesstudy,andthemeasurementofonlymaternalsocialcapital,meansthattheseresultscannotbegeneralisedtothepopulationofVietnamasawhole.
Thisstudyonlymeasuresthesocialcapitalofachild’smother.However,childrenarelikelytobeinfluencedbythesocialcapitalofothermembersofthehousehold,andindeedacompositemeasureof‘householdsocialcapital’mayshowstrongerassociationswithchildhealth.Theplaceofwomeninsocietymayaffectaccesstosocialcapital,forexamplebybeingamemberoffewerformalorganisationsorsocialgroupsthanmen.Inaddition,somemeasurementofthechild’ssocialcapital,particularlyoftheeight-year-olds,mayhelptoexplainsomeaspectsofchildhealth.
Fourmainconclusionscanbedrawnfromthisstudy.Firstly,maternalsocialsupportandhighcognitivesocialcapitalshowthemostconsistentassociationswithchildhealth.Thefactthatthesevariablesrelatetoamorenurturingenvironmentinwhichthechilddevelopsmayexplaintheimportanceofthesevariablesforchildhealth.
Secondly,associationsbetweenmaternalsocialcapitalandchildhealtharemuchstrongeramongone-year-oldchildrenthanamongeight-year-olds,withtheexceptionofchildmentalhealthandlife-threateningillness.Wehypothesisethatthisisbecauseinfantshavemuchgreatercontactwiththeirmother,andarethereforeinfluencedbythesocialworldinwhichshemovestoagreaterextent.Perhapsbytheageofeight,childrenhavebeguntodeveloptheirownsocialcapital,thoughtheiremotionaldevelopmentmaystillbeinfluencedbythesocialcapitaloftheirmother.
Thirdly,themostconsistentassociationsareseenwiththementalhealthofeight-year-olds,withthreeofthefourindicatorsofsocialcapitalbeingsignificantlyassociatedwithmentalhealthafterothervariableshavebeencontrolledfor.Otherstudieshaveshownsocialcapitaltobemoreconsistentlyassociatedwithmentalratherthanphysicalhealth(DeSilvaetal,2005);thequalityofthesocialenvironmentisperhapsexpressedmorereadilythroughemotionalthanthroughphysicalhealth.
Lastly,thereissomeevidencetosuggestthatactivemembershipofformalorganisationsinVietnammaybedamagingtothehealthofeight-year-oldsbutnotone-year-olds.Activeparticipationinformalgroupswassignificantlyassociatedwithanincreaseinstuntingamongeight-year-olds.Withthiscross-sectionaldataitisnotpossibletodeterminewhetherthecostsimposedonmothersparticipatinginformalgroupsleadtochildstunting,orwhethermotherswithastuntedchildaremorewillingtoparticipateinformalgroupsinordertoreceivesocialsupportfromthosegroups,thoughthiscanbeexploredinfutureroundsoftheYoungLivesproject.However,onepreviousstudydidfindanegativeimpactofmembershipofgroupsonmentalhealth,indicatingthepotentiallydamagingsidetogroupmembership(MitchellandLaGory,2002).Groupmembershipcandamagementalhealthbybeinganextraburdenontopoftheproductiveandreproductiverolesofwomenand/oritcanproducestigmaandpeerpressure,whichincreasestressorsuponawoman.Thishypothesiscouldbeusefullyexploredbyqualitativeresearchwhichtakescasesofmotherswithhighlevelsofparticipationwhohave
Maternal Social capital and child health in VietnaM
2�
malnourishedchildren.Themothers’perceptionsofparticipationasaburden/choreversusapositiveopportunitycouldbeexamined.
Structuralsocialcapitalisremarkablylowinacontextwheremassorganisationsstillexist.TheonlyotherquantitativestudyofsocialcapitalinVietnamfoundhigherlevelsofstructuralsocialcapitalbutitincludedmeninitssample.However,whenanalysingactivemembershipofgroups(aswasdoneinthisstudy)ageneral‘socialdisconnectedness’wasfound(DaltonandOng,2001).Thoughwomen’sunionsremainanimportantformalnetworkinVietnamwithapproximately20percentofmothersactivemembers,othertypesofinformalandformalgroupshaveamuchsmallerinfluence,inparticularinformalorganisationssuchasreligiousandsportsgroups.Theonlyassociationfoundinthisstudybetweenactivemembershipofgroupsandchildhealthwaswithnutritionalstatusofeight-year-oldsmeasuredbyheight-for-agez-scores,butthisstatisticalcorrelationhaslesspracticalimplications.
Apositiveassociationbetweensocialsupportfrominformalnetworksandthenutritionstatusofone-year-oldchildren(weight-for-age)wasfound.Thesenetworkscomprisefamily,friendsandneighboursandareastrongfeatureofVietnamesesociety,with96percentofmothersreceivingsupportfromthissource.For65percentofmothers,thisconstitutestheironlysourceofsupport.ConfuciantraditionsoftenpromotetrustinarelativelynarrowrealmoffamilyandtheVietnamesefamilyhasbeencharacterisedas‘residentiallynuclearbutfunctionallyextended’(Jones,1995p.189),withextensivesupportofferedbythefamily(Pham,1999).Daltonetal(2002)hypothesisethatdevelopmentinVietnamwillnotdiminishtraditionalfamilynetworksbutaddworkandfriendshipnetworkstothem:‘furtherdevelopmentinVietnamisnotsolikelytoexchangeonesetofsocialnetworksforanother,buttoexpandthenumberandactivitylevelsofthenetworksthatconnectindividualstosociety,andwhichhelpformtheirsocialandpoliticalidentities’(p.4).OnlylongitudinalresearchwillbeabletoaddressthishypothesisandYoungLivesiswellplacedtodoso.
Somepreviousstudieshaveshownlevelsofadults’generalisedtrusttobegenerallylowindevelopingcountries(ProductivityCommission,2003).Indeed,preliminaryresultsfromPeru,oneoftheothercountriestakingpartintheYoungLivesstudy,showlevelsofmaternalgeneralisedtrustinthecommunitytobeonly30percent(www.younglives.org.uk).Incontrast,Vietnamhasextremelyhighlevelsoftrust,with84percentofmothersbelievingthatpeopleingeneralcanbetrusted.Thisisechoedinthehighlevelsoftheotherindicatorsofcognitivesocialcapital:senseofcommunityharmony,senseofbelonging,andperceivedfairness.DaltonandOng(inpress),usingsimilarquestions,alsofoundhighlevelsoftrustinVietnam–higherthaninChinaandtheworldaverage.Highmaternalcognitivesocialcapitalisassociatedwithbetterchildhealthintermsofnutritionstatusandphysicalhealthamongone-year-olds,andinphysicalandmentalhealthamongeight-year-olds.
AsthisisonlythesecondstudytoconsidersocialcapitalinVietnam,andthefirsttostudymaternalsocialcapitalandchildwell-being,anyattempttoidentifypolicyimplicationsmustbeconsideredexploratory.Inaddition,thisstudywasnotabletoassesstherelativeimportanceofmaternalsocialcapitalasariskfactorforchildhealthasitdoesnotincludeallpotentialriskfactorsforchildhealth.Forexample,therelativeimportanceofmaternalsocialcapitalasariskfactorforchildmalnutritioncannotbeanalysedbecausewewereunabletoincludeallpossibleriskfactorsformalnutritioninthemodels(forexample,YoungLivesdoesnotmeasurefoodavailability).Asthisstudyhasestablishedthataspectsofmaternalsocialcapitalareassociatedwithsomechildhealthoutcomes,additionalstudies
Maternal Social capital and child health in VietnaM
27
areneededtoassessitsimportancerelativetootherknownriskfactorsforchildhealth(forexamplepoverty)andthereforeitspolicyimportance.However,raisingstructuralsocialcapital(butensuringthisdoesnotcreatedamagingburdenstowomen)andmaintainingthehighlevelsofcognitivesocialcapitalisobviouslyageneralpolicypriority.StrengtheningsocialcapitalinVietnamcanbeenvisagedintwo(mutuallysupporting)scenarios.Firstly,inaformalisingscenarioitisrecognisedthattraditionalsocialdynamicsarechanging(throughurbanisation,reductionofextendedfamilyandageingpopulation)andthatformalstructures,eg,massandnon-governmentalorganisationsandcommunity-basedorganisations(CBOs),willneedtostepintofacilitatesocialnetworksandsupport.Thoughtheirroleshavebeenincreasinglyrecognisedbythegovernmentandinthepublicdiscourse,thedevelopmentoftheseorganisationsis,however,constrainedbyanunsupportivelegalenvironment.Agovernmentdecreein2003(88/2003NC-CP)withregardstotheorganisationandmanagementofpeople’sassociationsinVietnamgivesapositivesignal.However,itfailstogiveclearoperationalguidelines,whichshouldbeapriorityforpolicydebateandformulation.Inaddition,givenaclearroleofengaginginsocialmobilisationworkandsecuringbenefitsfortheirownmembers,massorganisationscouldperformtheirrolebetterbytransformingthemselvesinordertoadapttosocialchanges.Thiscanbedone,andisbeingdoneinsomemassorganisations,bygoingbeyondmobilisingsupportforthecentralCommunistPartytomeetingtheneedsof,andadvocatingonbehalfof,theirmembership.Forexample,theyneedtodiversifytheiractivitiesinsuchawaythatcouldinterest,andmeetthevariousneedsof,theirmembers.Anexampleofthewomen’sunion’sdiversificationofactivitiesisthatthemeetingofwomen’suniongroupsshouldnotfocusonlyondiscussingtheirownproceduralactivitiesbutalsointegrateotheractivities(suchaslifeskillstraining,familyplanning,HIV/AIDS,businessplanning,etc)andcapacity-buildingfortheirlocalstaffinordertohandletheirnewrole.
Secondly,aninformalisingscenarioenvisagesnewindividualconnectionsandsupportarisingfromthenewsocialstructures.Strategiestorespondtothisscenariorequireactionsaimedatsupportinginformalstructuresratherthanformalinstitutions.InVietnam,thereisasupportivepolicyenvironmentforindividualstostrengthentheirinformalsocialcapitalandgeneralcitizenship.Theintroductionof‘Decree29’3anditsrecentrevisionthatwasbuiltonaprincipleof‘peopleknow,peoplediscuss,peoplemanage,andpeoplesupervise’indicatesgovernmentsupportinindividualcapacity-buildingandfacilitatinglocalpeople’sparticipationindecision-making.Accordingtothedecree,peopleareencouragedtodiscussandmakedecisionsonissuesthatconcernoraffectthem.Inaddition,theyareencouragedtoprovidefeedbackondecisionsmadebyrelatedstakeholdersandhigherauthorities.TheroleofCBOs/people’sorganisationswouldfitwellinthiscontextastheycouldfacilitatelocalpeopletospeakforthemselves,orlinkpeoplewithhigher-levelauthorities.Oneofthebiggestchallengesinimplementingthedecreeisthelackofpracticalguidanceandthedisincentiveoflossofpowerforlocalcivilservants(WorldBankandADB,2002).
ThisfirstquantitativestudyofmaternalsocialcapitalinVietnamhasshownittobeassociatedwithsomeaspectsofchildhealth.PolicydebateonstrengtheningsocialrelationsinadynamiccontextneedstobeinformedbythisdataandbyfutureroundsoftheYoungLivesstudythatwillproducedatacapableofexploringcausalrelationshipsaswellasthechangingsocialsituation.
3 Thisdecreeaimstostrengthentheparticipationofgrassrootspeopleinlocalplanninganddecision-making.
Maternal Social capital and child health in VietnaM
28
referencesArrow,K(2000)‘Observationsonsocialcapital’,inPDasguptaandISerageldin(eds)Social Capital: A multifaceted perspective,Washington,DC,WorldBank
Bourdieu,P(1986)‘Theformsofsocialcapital’,inJRichardson(ed)The Handbook of Theory and Researchfor the Sociology of Education, NewYork,GreenwoodPress
Coleman,JS(1990)Foundations of Social Theory,Cambridge,Mass.,BelknapPressofHarvardUniversityPress
Conway,TandCTurk(2002)Reducing Vulnerability and Providing Social Protection,Hanoi,PovertyTaskForce
Dalton,RandTOng(2001)The Vietnamese Public in Transition: The World Values Survey 2001,IrvineUSA,CenterfortheStudyofDemocracy
Dalton,R,PMinhHac,PThanhNghiandTOng(2002)‘SocialrelationsandsocialcapitalinVietnam:The2001WorldValuesSurvey’,Comparative Sociology,1,369-386
Dalton,RandTOng(inpress)‘CivilsocietyandsocialcapitalinVietnam’, inModernization and Social Change in Vietnam,Munich,MunichInstituteforSocialScience.www.democ.uci.edu/democ/papers/vietnam04.pdf
Dasgupta,PandISerageldin(eds)(2000)Social Capital: A multifaceted perspective,Washington,DC,WorldBank
DeSilva,M,KMcKenzie,SHuttlyandTHarpham(2005)‘Mentalillnessandsocialcapital:Asystematicreview’,Journal of Epidemiology and Community Health, 59,619-627
GoV(2003)Vietnam Growth and Reduction of Poverty: Annual progress report 2002-03,Hanoi,SteeringCommitteeoftheComprehensivePovertyReductionandGrowthStrategy(CPRGS),Inter-MinisterialWorkingGroup
Grootaert,CandTvanBastelaer(2002)Understanding and Measuring Social Capital: Amultidisciplinary tool for practitioners,Washington,DC,WorldBank
Harpham,T,EGrantandEThomas(2002)‘Measuringsocialcapitalwithinhealthsurveys:Somekeyissues’,Health Policy and Planning,17(1),106-111
JointDonorReport(2003)Vietnam Development Report 2004,Hanoi,JointDonorReporttotheVietnamConsultativeGroupMeeting
Jones,GW(1995)‘PopulationandfamilyinSoutheastAsia’,Journal of Southeast AsianStudies, 26(1),184-195
Mitchell,CandMLaGory(2002)‘Socialcapitalandmentaldistressinanimpoverishedcommunity’,City and Community,1(2),199-222
Pedersen,K(2001)Civil Society in the Context of Development Aid: The case of Vietnam,Copenhagen,CopenhagenBusinessSchoolWorkingPaper
Maternal Social capital and child health in VietnaM
2�
Pham,VB(1999)The Vietnamese Family in Change: The case of the Red River Delta,Surrey,UK,CurzonPress
Portes,A(1998)‘Socialcapital:Itsoriginsandapplicationsinmodernsociology’,Annual Review of Sociology,24,1-24
ProductivityCommission(2003)Social Capital: Reviewing the concept and its policy implications, Canberra,CommonwealthofAustralia
Putnam,R(1993)‘Theprosperouscommunity:Socialcapitalandpubliclife’,The American Prospect,4(13),27-40.www.prospect.org/print/V4/13/putnam-r.html
Quibria,M(2003)The Puzzle of Social Capital: A critical review,ERD(EconomicsandResearchDepartment)WorkingPaperNumber40,Manila,AsianDevelopmentBank
SavetheChildrenUK(2003)HCMC Participatory Poverty Assessment,London,SavetheChildrenUK/PovertyTaskForce
Shanks,EandCTurk(2002)Policy Recommendations from the Poor,Hanoi,PovertyTaskForce
StataCorporation(2003)Stata Statistical Software: Release 8.0,CollegeStation,TX,Stata
Tuan,T,THarpham,NTHuong,MDeSilva,VTTHuong,TTLong,NTVHaandDDewitt(2005)Measuring Social Capital and Mental Health in Vietnam: A validity study,YoungLivesWorkingPaper12
UNCT (2003) MDGs Closing the Millennium Gaps: Progress Report 2003,Hanoi,UNCT(UnitedNationsCountryTeam)
VanKemenade,S(2002)Social Capital as a Health Determinant: How is it defined?GovernmentServicesCanada,HealthPolicyResearchWorkingPaperSeries
Wischermann,JandNQVinh(2003)'TherelationshipbetweencivicorganizationsandgovernmentalorganizationsinVietnam',inGetting Organized in Vietnam,Singapore,InstituteofSouthEastAsianStudies
WorldBank(2003)Vietnam Development Report: Poverty,Hanoi,WorldBank
WorldBankandADB(2002)Vietnam, Delivering on its Promise,Hanoi,WorldBankandAsianDevelopmentBank

Maternal Social capital and child health in VietnaM
30
The Young Lives Partners Centre for Economic and Social Studies (CESS), India
Department of Economics, University of Addis Ababa, Ethiopia
Ethiopian Development Research Institute, Addis Ababa, Ethiopia
General Statistical Office, Government of Vietnam
Grupo de Análisis Para El Desarrollo (GRADE), Peru
Institute of Development Studies, University of Sussex, UK
Instituto de Investigación Nutricional (IIN), Peru
London School of Hygiene and Tropical Medicine, UK
Medical Research Council of South Africa
Queen Elizabeth House, University of Oxford
RAU University, Johannesburg, South Africa
Research and Training Centre for Community Development, Vietnam
Save the Children UK
South Bank University, UK
Statistical Services Centre, University of Reading, UK
W O R K I N G P A P E R N O . 3 0
Maternal Social Capital and Child Health in VietnamTran TuanTrudy HarphamMary J De SilvaNguyen Thu HuongBill TodPham Thi LanTran Duc ThachSavitri Abeyasekera
In Vietnam there is growing concern about the potential social impact of rapid economic changes. The extent and type of social connectedness, or social capital, may be changing. Studies from other developing countries have demonstrated that social capital is often independently associated with various indicators of well-being, including some aspects of human capital (health and education status). In Vietnam there has only been one previous quantitative study of social capital and this did not consider associations with well-being. The Young Lives project in Vietnam allows the examination of the relationship between maternal social capital and child well-being. With a sample of 1,953 mothers of one-year-olds and 954 mothers of eight-year-olds across five provinces, this study examines whether maternal social capital is associated with child health.
This study found low levels of structural social capital (associational life) and citizenship and high levels of cognitive social capital (trust, etc) and support. While poorer women have even lower levels of structural social capital than their better-off peers, patterns across rural and urban areas are similar.
Maternal social support and high cognitive social capital show the most consistent associations with child health, while associations between maternal social capital and child health are stronger among one-year-old children than among eight-year-olds, with the exception of child mental health and risk of life-threatening illness. The most consistent associations were seen with the mental health of eight-year-olds, with all four indicators of social capital being significantly associated with mental health after other variables have been controlled for. Lastly, there was some evidence to suggest that active membership of formal organisations in Vietnam may be damaging to the health of eight-year-olds but not one-year-olds, with active participation in formal groups being significantly associated with an increase in stunting among eight-year-olds.
The main components of social capital associated with child health are social support and cognitive social capital. High levels of maternal social support are positively correlated with having an educated partner, living in an urban area and better maternal mental health. High cognitive social capital is positively correlated with living in a rural area, having an occupation other than agriculture and better maternal mental health.
There is a need to focus on maintaining the high levels of cognitive social capital and raising the current low level of maternal structural social capital in Vietnam.
Key words: social capital, child health, Vietnam, quantitative
Published by
Young Lives Save the Children UK 1 St John's Lane London EC1M 4AR
Tel: 44 (0) 20 7012 6796 Fax: 44 (0) 20 7012 6963 Web: www.younglives.org.uk
ISBN 1-904427-31-6 First Published: 2005
All rights reserved. This publication is copyright, but may be reproduced by any method without fee or prior permission for teaching purposes, though not for resale, providing the usual acknowledgement of source is recognised in terms of citation. For copying in other circumstances, prior written permission must be obtained from the publisher and a fee may be payable.
Designed and typeset by Copyprint UK Limited
Young Lives is an international longitudinal study of childhood poverty, taking place in Ethiopia, India, Peru and Vietnam, and funded by DFID. The project aims to improve our understanding of the causes and consequences of childhood poverty in the developing world by following the lives of a group of 8,000 children and their families over a 15-year period. Through the involvement of academic, government and NGO partners in the aforementioned countries, South Africa and the UK, the Young Lives project will highlight ways in which policy can be improved to more effectively tackle child poverty.