loss of cd11b exacerbates murine complement-mediated tubulointerstitial nephritis
TRANSCRIPT

The significance of C4d staining
with minimalhistologic abnormalitiesMark Haas
Department of Pathology & Laboratory Medicine,Cedars-Sinai Medical Center, Los Angeles, California,USA
Correspondence to Mark Haas, MD, PhD, Departmentof Pathology & Laboratory Medicine, Cedars-SinaiMedical Center, 8700 Beverly Blvd., Los Angeles, CA90048, USATel: +1 310 248 6695; fax: +1 310 423 5881;e-mail: [email protected]
Current Opinion in Organ Transplantation 2010,15:21–27
Purpose of review
C4d deposition within peritubular capillaries (PTCs) in renal allograft biopsies is a
specific marker for interaction of antibody with the graft, and is an extremely useful tool
for the diagnosis of antibody-mediated rejection (AMR). Whereas PTC C4d itself is not
diagnostic of AMR, it is usually accompanied by histologic features of acute and/or
chronic AMR. However, some biopsies, mainly from ABO-incompatible renal allografts,
show C4d staining without histologic findings of AMR or cell-mediated rejection. The
significance of such C4d staining remains a topic of debate, and this finding may have
different implications in ABO-incompatible versus conventional renal allografts.
Recent findings
In biopsies of ABO-incompatible renal allografts (particularly protocol biopsies), C4d
deposition in the absence of histologic evidence of rejection is a common finding, is not
associated with an increased risk of graft scarring, and may even indicate a decreased
risk of scarring, at least in the short term. By contrast, in positive cross-match and
conventional renal allografts such C4d deposition is uncommon, and may indicate
potentially reversible graft injury. However, a state of C4d staining without associated
graft injury may be inducible in positive cross-match grafts by complement inhibition.
Summary
C4d staining without associated histologic findings of rejection may represent a marker
for stable graft accommodation, at least in ABO-incompatible renal allografts. However,
further studies are clearly needed to determine what the long-term implications of such
C4d deposition are.
Keywords
ABO-incompatible, accommodation, antibody-mediated rejection, complement, renal
transplantation
Curr Opin Organ Transplant 15:21–27� 2010 Wolters Kluwer Health | Lippincott Williams & Wilkins1087-2418
IntroductionDuring the past two decades, the role of alloantibodies
in both acute and chronic rejection of renal allografts
has become increasingly documented [1–4,5�,6�]. Still,
whereas certain histologic features of acute rejection in
the presence of donor-specific antibody (DSA), such as
margination of neutrophils in peritubular capillaries, have
long been recognized [1,2], such findings are not specific
for antibody-mediated rejection (AMR), nor are these
seen in all cases of AMR [7��,8].
For these reasons, immunostaining of renal allograft
biopsies for C4d has represented such an important
development in the field of renal allograft pathology.
C4d is a degradation product of complement factor C4,
a component of the classical complement pathway that is
typically initiated by antibody bound to antigen. After
cleavage of remaining C4 domains, C4d remains cova-
1087-2418 � 2010 Wolters Kluwer Health | Lippincott Williams & Wilkins
lently bound at sites of C4 activation, and is thus a
relatively long-lived marker of a humoral response
[9,10]. Furthermore, C4d is easily detected in biopsy
specimens by indirect immunofluorescence on frozen
sections using a monoclonal antibody [8,10] or by immu-
nohistochemistry (IHC) on paraffin sections of formalin-
fixed tissue using a polyclonal antiserum [11], both of
which are now commercially available.
Feucht et al. [10], in a study of 93 renal allografts biopsied
for early dysfunction (mean 11 days post-transplantation),
first demonstrated an association between C4d staining
in peritubular capillaries (PTCs) by indirect immuno-
fluorescence and reduced graft survival. Feucht et al. [10]
also found an association between PTC C4d staining and
both re-transplants and elevated panel-reactive anti-
bodies (PRAs), suggesting an association between such
staining and humoral immunity, and indeed several
groups [8,11–13] later documented a strong correlation
DOI:10.1097/MOT.0b013e3283342ebd
22 Mechanisms of rejection
between C4d staining of renal allograft biopsies and the
presence of DSA in serum, as well as histologic findings
previously shown to be present in acute rejection epi-
sodes associated with the presence of DSA [2]. Additional
studies [13–15] established an association between C4d
staining and morphologic findings of chronic rejection,
including transplant glomerulopathy and PTC basement
membrane multilayering, leading to further work clearly
documenting the association between these findings and
DSA [13,14,16,17,18��].
The strong association between histologic changes
including margination of leukocytes (neutrophils and/or
monocytes/macrophages) in PTC and/or glomerular
capillaries and (less commonly) arterial fibrinoid necrosis,
PTC C4d staining, and the presence of anti-HLA DSA
has led to the Banff consensus process formulating
criteria for the diagnosis of active AMR based on the
presence of this triad of histologic, immunohistologic, and
serologic findings [19]. In ABO-incompatible renal allo-
grafts, however, PTC C4d staining and antibodies to
donor blood group antigens are commonly seen in the
absence of histologic findings of acute or chronic rejection
[20,21��,22��], and cases of C4d staining without histo-
logic evidence of rejection have also been reported in
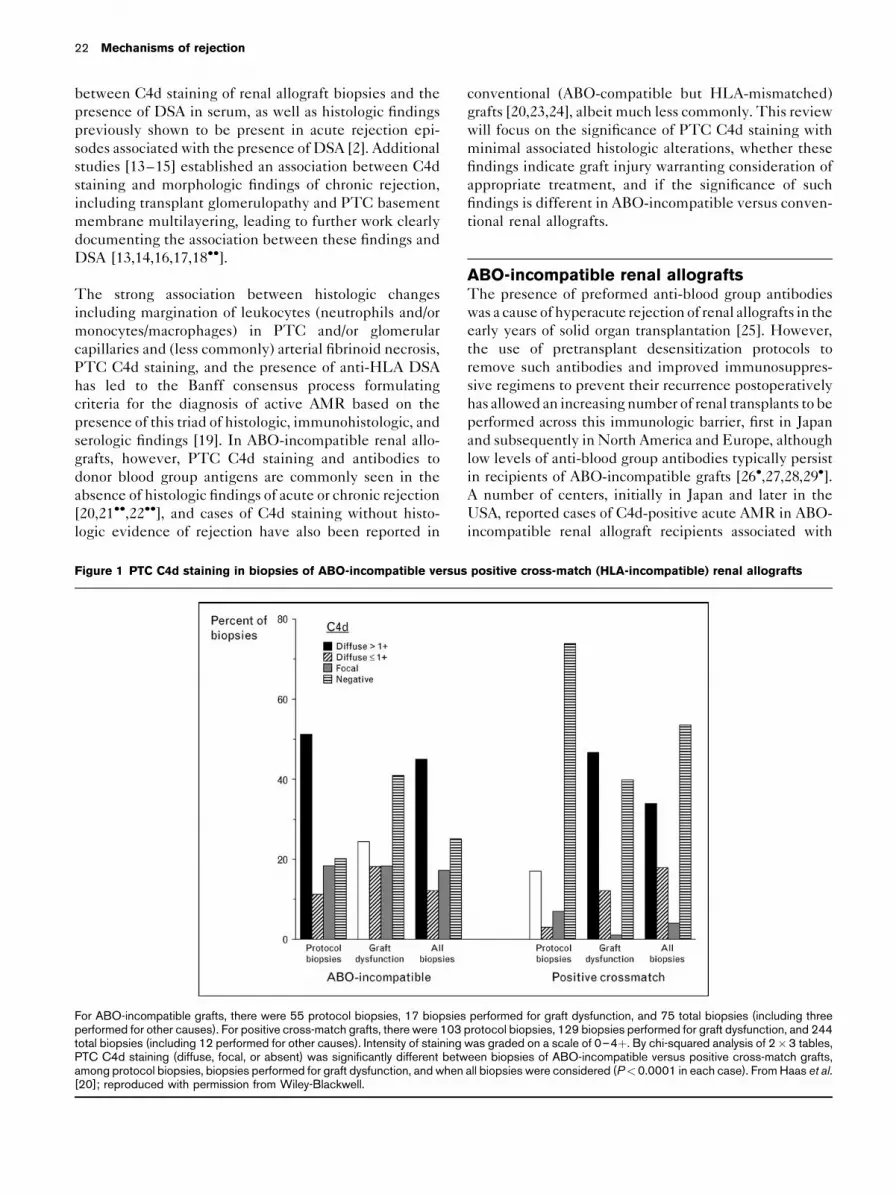
Figure 1 PTC C4d staining in biopsies of ABO-incompatible versus
For ABO-incompatible grafts, there were 55 protocol biopsies, 17 biopsiesperformed for other causes). For positive cross-match grafts, there were 103total biopsies (including 12 performed for other causes). Intensity of stainingPTC C4d staining (diffuse, focal, or absent) was significantly different betwamong protocol biopsies, biopsies performed for graft dysfunction, and when[20]; reproduced with permission from Wiley-Blackwell.
conventional (ABO-compatible but HLA-mismatched)
grafts [20,23,24], albeit much less commonly. This review
will focus on the significance of PTC C4d staining with
minimal associated histologic alterations, whether these
findings indicate graft injury warranting consideration of
appropriate treatment, and if the significance of such
findings is different in ABO-incompatible versus conven-
tional renal allografts.
ABO-incompatible renal allograftsThe presence of preformed anti-blood group antibodies
was a cause of hyperacute rejection of renal allografts in the
early years of solid organ transplantation [25]. However,
the use of pretransplant desensitization protocols to
remove such antibodies and improved immunosuppres-
sive regimens to prevent their recurrence postoperatively
has allowed an increasing number of renal transplants to be
performed across this immunologic barrier, first in Japan
and subsequently in North America and Europe, although
low levels of anti-blood group antibodies typically persist
in recipients of ABO-incompatible grafts [26�,27,28,29�].
A number of centers, initially in Japan and later in the
USA, reported cases of C4d-positive acute AMR in ABO-
incompatible renal allograft recipients associated with
positive cross-match (HLA-incompatible) renal allografts
performed for graft dysfunction, and 75 total biopsies (including threeprotocol biopsies, 129 biopsies performed for graft dysfunction, and 244was graded on a scale of 0–4þ. By chi-squared analysis of 2�3 tables,een biopsies of ABO-incompatible versus positive cross-match grafts,all biopsies were considered (P<0.0001 in each case). FromHaas et al.

Significance of C4d staining with minimal histologic abnormalities Haas 23
elevated levels of anti-blood group antibodies [30–33].
However, with the growing utilization of routine C4d
staining in the diagnostic work-up of renal allograft bio-
psies, particularly those from recipients felt to be at
increased risk of developing AMR, it became apparent
that PTC C4d staining in biopsies of ABO-incompatible
grafts was far more commonly seen than in biopsies
of ABO-compatible grafts, including those in recipients
who were desensitized prior to transplantation to remove
preformed anti-HLA antibodies (positive cross-match
transplants). In a study of 32 recipients of ABO-incompa-
tible renal allografts from the Mayo Clinic, Fidler et al. [33]
found that 13 (41%) developed AMR, nine with associated
graft dysfunction and four subclinical, diagnosed on a
protocol biopsy. Notably, eight of the nine patients diag-
nosed with clinical AMR had a protocol biopsy done 1–
7 days prior to the biopsy showing AMR, and five of these
protocol biopsies were C4d-negative, indicating that
the C4d associated with AMR was recently deposited.
In addition to the patients with clinical or subclinical
AMR, Fiedler et al. [33] also noted four patients who
had diffuse PTC C4d staining on a protocol biopsy done
approximately 1 year post-transplantation but no histologic
evidence of acute AMR or transplant glomerulopathy.
Figure 2 Correlation between PTC C4d staining and histologic findi
positive cross-match renal allografts
Among biopsies of ABO-incompatible grafts, 34 showed diffuse, >1þ PTCnegative). Among biopsies of positive cross-match grafts, 83 showed diffuse,(C4d-negative). All 20 positive cross-match biopsies and one of two ABO-incshowed PTC neutrophil margination. The kappa statistic was used to assesbetween categories of PTC C4d staining (diffuse >1þ, diffuse <1þ or focalnone). For biopsies of ABO-incompatible grafts, kappa was –0.01 with PP<0.0001. From Haas et al. [20]; reproduced with permission from Wiley
Figure 1 shows C4d staining results in 55 protocol biopsies
done during the first year post-transplantation in 24 reci-
pients of ABO-incompatible renal allografts at Johns Hop-
kins Hospital. We found PTC C4d staining in 80% of these
biopsies, with strong (>1þ on a 0–4þ scale) and diffuse
staining in 51% [20]. By contrast, 76/103 protocol biopsies
from recipients of ABO-compatible, positive cross-match
grafts were C4d-negative (Fig. 1). Furthermore, unlike the
case in positive cross-match grafts in which the vast
majority of C4d-positive biopsies are associated with
histologic features of AMR, including neutrophil and/or
mononuclear leukocyte margination in peritubular and/or
glomerular capillaries or less commonly changes of throm-
botic microangiopathy, most C4d-positive biopsies of
ABO-incompatible grafts show no histologic evidence of
AMR (Fig. 2) or cell-mediated rejection [20]. Subsequent
studies of protocol biopsies of ABO-incompatible renal
allografts from Japan [21��] and Switzerland [34�] have
confirmed that most such biopsies show PTC C4d staining,
diffuse in the majority of cases, without histologic features
of AMR.
We investigated whether diffuse PTC C4d deposi-
tion in the absence of histologic features of AMR or
ngs suggestive of AMR in biopsies of ABO-incompatible versus
C4d, 22 diffuse, �1þ or focal PTC C4d, and 19 no PTC C4d (C4d->1þPTCC4d, 29 diffuse,�1þ or focal PTCC4d, and 132 no PTCC4dompatible biopsies that showed thrombotic microangiopathy (TMA) alsos the degree and significance of correlation (probability of agreement), negative) and those of neutrophil margination (>1þ and/or TMA, trace,¼0.55; for biopsies of positive cross-match grafts kappa was 0.65,-Blackwell.
24 Mechanisms of rejection
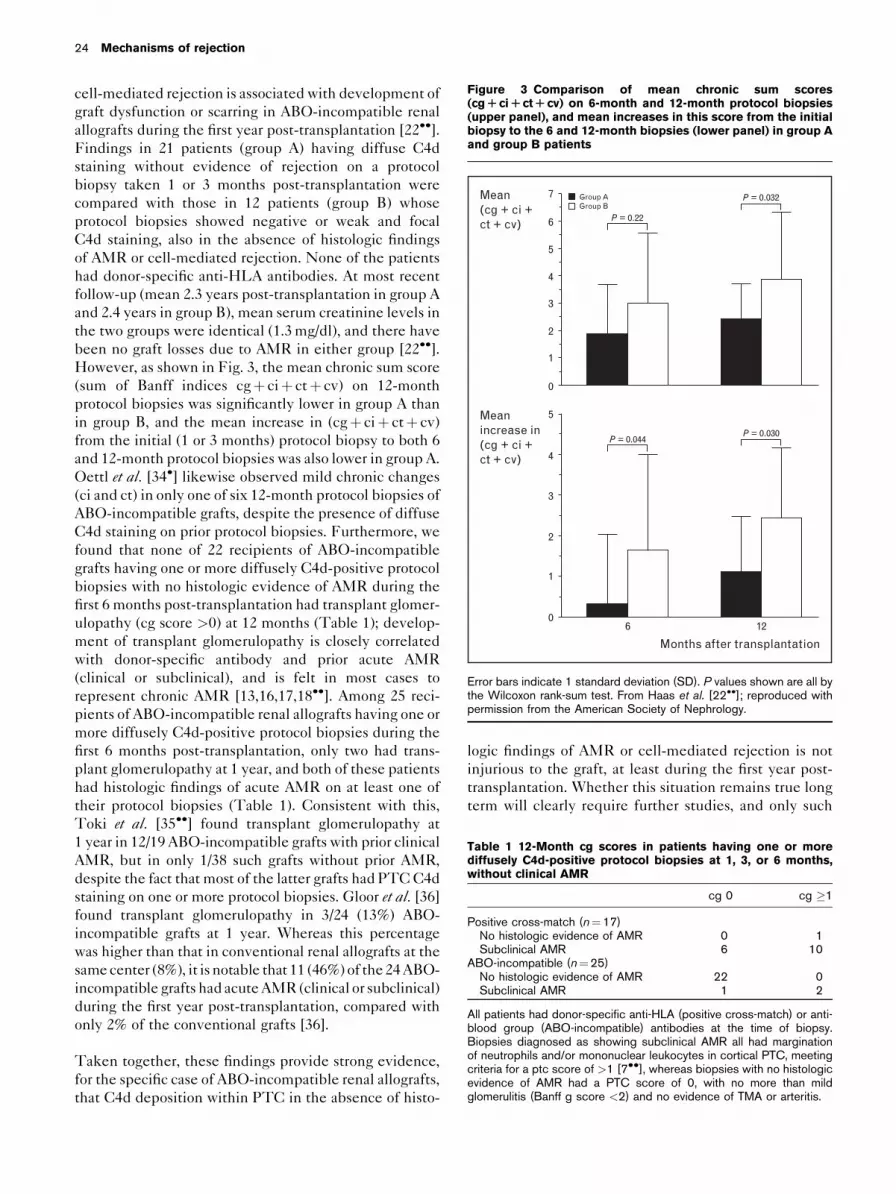
Figure 3 Comparison of mean chronic sum scores
(cgR ciR ctR cv) on 6-month and 12-month protocol biopsies
(upper panel), and mean increases in this score from the initial
biopsy to the 6 and 12-month biopsies (lower panel) in group A
and group B patients
7
6
5
4
3
2
1
0
5
4
3
2
1
06 12
Group AGroup B
P = 0.22
P = 0.032
P = 0.030P = 0.044
Months after transplantation
Meanincrease in(cg + ci +ct + cv)
Mean(cg + ci +ct + cv)
Error bars indicate 1 standard deviation (SD). P values shown are all bythe Wilcoxon rank-sum test. From Haas et al. [22��]; reproduced withpermission from the American Society of Nephrology.
Table 1 12-Month cg scores in patients having one or more
diffusely C4d-positive protocol biopsies at 1, 3, or 6 months,
without clinical AMR
cg 0 cg �1
Positive cross-match (n¼17)No histologic evidence of AMR 0 1Subclinical AMR 6 10
ABO-incompatible (n¼25)No histologic evidence of AMR 22 0Subclinical AMR 1 2
All patients had donor-specific anti-HLA (positive cross-match) or anti-blood group (ABO-incompatible) antibodies at the time of biopsy.Biopsies diagnosed as showing subclinical AMR all had marginationof neutrophils and/or mononuclear leukocytes in cortical PTC, meetingcriteria for a ptc score of >1 [7��], whereas biopsies with no histologicevidence of AMR had a PTC score of 0, with no more than mildglomerulitis (Banff g score <2) and no evidence of TMA or arteritis.
cell-mediated rejection is associated with development of
graft dysfunction or scarring in ABO-incompatible renal
allografts during the first year post-transplantation [22��].
Findings in 21 patients (group A) having diffuse C4d
staining without evidence of rejection on a protocol
biopsy taken 1 or 3 months post-transplantation were
compared with those in 12 patients (group B) whose
protocol biopsies showed negative or weak and focal
C4d staining, also in the absence of histologic findings
of AMR or cell-mediated rejection. None of the patients
had donor-specific anti-HLA antibodies. At most recent
follow-up (mean 2.3 years post-transplantation in group A
and 2.4 years in group B), mean serum creatinine levels in
the two groups were identical (1.3 mg/dl), and there have
been no graft losses due to AMR in either group [22��].
However, as shown in Fig. 3, the mean chronic sum score
(sum of Banff indices cgþ ciþ ctþ cv) on 12-month
protocol biopsies was significantly lower in group A than
in group B, and the mean increase in (cgþ ciþ ctþ cv)
from the initial (1 or 3 months) protocol biopsy to both 6
and 12-month protocol biopsies was also lower in group A.
Oettl et al. [34�] likewise observed mild chronic changes
(ci and ct) in only one of six 12-month protocol biopsies of
ABO-incompatible grafts, despite the presence of diffuse
C4d staining on prior protocol biopsies. Furthermore, we
found that none of 22 recipients of ABO-incompatible
grafts having one or more diffusely C4d-positive protocol
biopsies with no histologic evidence of AMR during the
first 6 months post-transplantation had transplant glomer-
ulopathy (cg score >0) at 12 months (Table 1); develop-
ment of transplant glomerulopathy is closely correlated
with donor-specific antibody and prior acute AMR
(clinical or subclinical), and is felt in most cases to
represent chronic AMR [13,16,17,18��]. Among 25 reci-
pients of ABO-incompatible renal allografts having one or
more diffusely C4d-positive protocol biopsies during the
first 6 months post-transplantation, only two had trans-
plant glomerulopathy at 1 year, and both of these patients
had histologic findings of acute AMR on at least one of
their protocol biopsies (Table 1). Consistent with this,
Toki et al. [35��] found transplant glomerulopathy at
1 year in 12/19 ABO-incompatible grafts with prior clinical
AMR, but in only 1/38 such grafts without prior AMR,
despite the fact that most of the latter grafts had PTC C4d
staining on one or more protocol biopsies. Gloor et al. [36]
found transplant glomerulopathy in 3/24 (13%) ABO-
incompatible grafts at 1 year. Whereas this percentage
was higher than that in conventional renal allografts at the
same center (8%), it is notable that 11 (46%) of the 24 ABO-
incompatible grafts had acute AMR (clinical or subclinical)
during the first year post-transplantation, compared with
only 2% of the conventional grafts [36].
Taken together, these findings provide strong evidence,
for the specific case of ABO-incompatible renal allografts,
that C4d deposition within PTC in the absence of histo-
logic findings of AMR or cell-mediated rejection is not
injurious to the graft, at least during the first year post-
transplantation. Whether this situation remains true long
term will clearly require further studies, and only such

Significance of C4d staining with minimal histologic abnormalities Haas 25
longer-term studies will enable us to assess whether
ABO-incompatible grafts showing C4d in PTC without
margination of leukocytes within these capillaries or
other histologic evidence of rejection represents a state
of stable graft accommodation. It is notable, however,
that the great majority of our ABO-incompatible grafts
with these findings showed persistent, diffuse PTC C4d
on each protocol biopsy taken during the first year post-
transplantation together with persistent low levels of
circulating anti-blood group antibodies [22��]. This find-
ing clearly contrasts with findings of Fidler et al. [33] in
ABO-incompatible grafts developing acute AMR; as noted
above the majority of these grafts were C4d-negative
during the week prior to the diagnosis of AMR. Likewise,
in conventional grafts, C4d associated with late AMR and
development of transplant glomerulopathy appears to
cycle on and off the graft, with persistent C4d positivity
on serial biopsies of the same graft being the exception
rather than rule [15].
Conventional and positive cross-match renalallograftsIn our experience, the overwhelming majority of C4d-
positive biopsies of ABO-compatible, HLA-mismatched
renal allografts, irrespective of whether there was a pre-
transplant positive cross-match requiring desensitization,
exhibit margination of leukocytes in PTC and/or other
histologic findings of AMR [20]. This situation is true for
both for-cause and protocol biopsies, although our experi-
ence with the latter has been limited to positive cross-
match and ABO-incompatible grafts (Figs. 1 and 2). We
feel that the combination of PTC C4d staining, leukocyte
margination in PTC and/or glomerular capillaries on a
protocol biopsy of a normally functioning graft, and the
presence of DSA represents subclinical AMR [37], and
indeed have found that for positive cross-match grafts this
triad is frequently associated with subsequent develop-
ment of chronic changes within the graft, including
transplant glomerulopathy (Table 1), just as has been
found for clinical AMR [14–17,18��].
In a study of 551 protocol biopsies of conventional renal
allografts from three European centers, Mengel et al. [23]
found PTC C4d staining (by immunohistochemistry on
paraffin sections, which is somewhat less sensitive than
immunofluorescence on frozen sections [38]) in 4.4%,
with diffuse staining in 2.0%. Notably, 86% of biopsies
showing diffuse C4d staining had PTC leukocyte mar-
gination, although the latter was seen in only 38% of
biopsies showing focal C4d staining. Thus, it appears
that, as with positive cross-match grafts, diffuse C4d
staining in protocol biopsies of conventional grafts
appears to reflect subclinical AMR in the great majority
of cases. However, in a small fraction of conventional
grafts there is C4d staining, usually focal, in the absence
of histologic features of AMR. Dickenmann et al. [24]
studied clinical outcomes in 22 patients with convention-
al renal allografts who had C4d-positive (by immuno-
fluoresence) biopsies lacking histologic features of AMR
or cell-mediated rejection; all biopsies were done for graft
dysfunction and in 21/22 the C4d staining was focal. Five
of the 22 patients received additional immunosuppres-
sive therapy following the biopsy, whereas the remaining
17 continued to receive just maintenance immunosup-
pression. Whereas mean serum creatinine (SCr) levels at
the time of biopsy were virtually identical in these two
patient groups, at 4 weeks post-biopsy the mean SCr was
significantly lower in the patients receiving additional
immunosuppression. Furthermore, graft survival at 3 years
post-biopsy was 100% in the patients receiving additional
immunosuppression compared with 69% in the remaining
patients, although this difference did not reach statistical
significance [24]. Nonetheless, these findings suggest that,
unlike the case in ABO-incompatible grafts, C4d staining
without histologic findings of rejection in conventional
renal allografts is associated with the potential for short-
term and longer-term graft injury, and should be treated
as such.
Therapeutic effects and implicationsPrevention of complement-mediated injury to the graft
can potentially be accomplished by two means: pharma-
cologic inhibition of the complement cascade or up-
regulation of endogenous complement regulatory
proteins, such as CD59 (protectin), which inhibits the
formation of the membrane attack complex (MAC), and
CD55 (decay-accelerating factor), which accelerates the
decay of C3 and C5 convertases. There is presently
evidence from both human renal allografts and rodent
xenografts that complement inhibition via these different
pathways has the potential to induce a state of C4d
positivity without clinical or histologic evidence of rejec-
tion, and possibly stable accommodation of these grafts.
In a preliminary study of 50 patients with positive cross-
match renal allografts from the Mayo Clinic, treatment
with the anti-C5 antibody eculizumab did not reduce the
fraction of C4d-positive biopsies (10/17 in eculizumab-
treated patients versus 18/45 in controls); however, none
of the 10 C4d-positive biopsies in the eculizumab group
showed histologic features of AMR, compared with 11
(61%) of the C4d-positive biopsies in controls [39�].
Furthermore, 22/45 biopsies in the control group (includ-
ing 15 of the 18 C4d-positive biopsies) but none of the
biopsies in the eculizumab group showed reactive
changes of the glomerular endothelium by electron
microscopy during the first year post-transplantation
[39�]; such ultrastructural changes may first become
apparent during the initial 1–3 months post-transplan-
tation and are associated with subsequent development
of transplant glomerulopathy [13]. In a rat-to-mouse

26 Mechanisms of rejection
model of heart xenograft accommodation [40�], the
latter process was found to be associated with strong
up-regulation of CD55 and CD59 on the graft endo-
thelium with prevention of endothelial C5 deposition
and histologic changes of rejection despite the binding of
antidonor IgG [40�].
ConclusionDiffuse PTC C4d deposition with circulating anti-blood
group antibodies in the absence of clinical or histologic
evidence of rejection is a common finding in ABO-
incompatible renal allografts. Furthermore, in these
grafts such C4d staining is not associated with an
increased risk of graft scarring, and may even indicate
a somewhat decreased risk of scarring, at least in the short
term. However, it will be important to determine if this
persists over the long term; if true such findings would
strongly suggest a state of stable graft accommodation.
Unlike the case in ABO-incompatible grafts, in positive
cross-match and conventional renal allografts C4d depo-
sition in the absence of histologic evidence of AMR
appears to be uncommon, and may indicate potentially
reversible graft injury. However, a state of C4d staining
without associated graft injury may be inducible in such
grafts by inhibition of the complement cascade at one or
more points subsequent to C4 cleavage but prior to C5
cleavage and formation of the MAC. Further develop-
ment of such approaches should increase our understand-
ing of humoral immunity in solid organ transplantation,
and may well improve long-term outcomes for transplant
recipients, especially those who are highly sensitized and
most at risk for AMR.
AcknowledgementsOriginal work of the author presented in this article was supported inpart by a grant from the Kidney & Urology Foundation of America, Inc.The author has no commercial associations or financial relationshipsthat might pose a conflict of interest in connection with any of thematerial presented in this article.
References and recommended readingPapers of particular interest, published within the annual period of review, havebeen highlighted as:� of special interest�� of outstanding interest
Additional references related to this topic can also be found in the CurrentWorld Literature section in this issue (p. 133).
1 Halloran PF, Wadgymar A, Ritchie S, et al. The significance of the anti-class Iantibody response. I. Clinical and pathologic features of anti-class I-mediatedrejection. Transplantation 1990; 49:85–91.
2 Trpkov K, Campbell P, Pazderka K, et al. Pathologic features of acute renalallograft rejection associated with donor-specific antibody. Transplantation1996; 61:1586–1592.
3 Lederer SR, Kluth-Pepper B, Schneeberger H, et al. Impact of humoralalloreactivity early after transplantation on the long-term survival of renalallografts. Kidney Int 2001; 59:334–341.
4 Colvin RB. Antibody-mediated renal allograft rejection: diagnosis and patho-genesis. J Am Soc Nephrol 2007; 18:1046–1056.
5
�Gloor J, Cosio F, Lager DJ, et al. The spectrum of antibody-mediated renalallograft rejection: implications for treatment. Am J Transplant 2008; 8:1367–1373.
This paper is a brief but informative review focusing on the treatment of acute AMRand long-term implications of exposure of renal allografts to DSA.
6
�Terasaki PI, Cai J. Human leukocyte antigen autobodies and chronic rejection:from association to causation. Transplantation 2008; 86:377–383.
This paper is a review of recent studies supporting the authors’ hypotheses of acausal connection between anti-HLA DSA and chronic rejection, and that humoralrather than cellular immunity is the major cause of allograft failure. Graft failure wasnot only strongly correlated with the presence of DSA, but also with serum titers ofthese antibodies.
7
��Gibson IW, Gwinner W, Brocker V, et al. Peritubular capillaritis in renalallografts: prevalence, scoring system, reproducibility and clinicopathologiccorrelates. Am J Transplant 2008; 8:819–825.
This paper describes an in-depth study of peritubular capillary leukocyte margina-tion in 688 renal allograft biopsies, and its correlation with C4d staining, glomer-ulitis, and cell-mediated rejection.
8 Mauiyyedi S, Crespo M, Collins AB, et al. Acute humoral rejection in kidneytransplantation: II. Morphology, immunopathology, and pathologic classifica-tion. J Am Soc Nephrol 2002; 13:779–787.
9 Baldwin WM III, Kasper EK, Zachary AA, et al. Beyond C4d: other comple-ment-related diagnostic approaches to antibody-mediated rejection. Am JTransplant 2004; 4:311–318.
10 Feucht HE, Schneeberger H, Hillebrand G, et al. Capillary deposition of C4dcomplement fragment and early renal graft loss. Kidney Int 1993; 43:1333–1338.
11 Bohmig GA, Exner M, Habicht A, et al. Capillary C4d deposition in kidneyallografts: a specific marker of alloantibody-dependent graft injury. J Am SocNephrol 2002; 13:1091–1099.
12 Herzenberg AM, Gill JS, Djurdjev O, et al. C4d deposition in acute rejection:an independent long-term prognostic factor. J Am Soc Nephrol 2002;13:234–241.
13 Wavamunno MD, O’Connell PJ, Vitalone M, et al. Transplant glomerulopathy:ultrastructural abnormalities occur early in longitudinal analysis of protocolbiopsies. Am J Transplant 2007; 7:1–12.
14 Mauiyyedi S, Della Pelle P, Saidman S, et al. Chronic humoral rejection:identification of antibody-mediated chronic allograft rejection by C4d depos-its in peritubular capillaries. J Am Soc Nephrol 2001; 12:574–582.
15 Regele H, Bohmig GA, Habicht A, et al. Capillary deposition of complementsplit product C4d in renal allografts is associated with basement membraneinjury in peritubular and glomerular capillaries: a contribution of humoralimmunity to chronic allograft rejection. J Am Soc Nephrol 2002; 13:2371–2380.
16 Sis B, Campbell PM, Mueller T, et al. Transplant glomerulopathy, late anti-body-mediated rejection and the ABCD tetrad in kidney allograft biopsies forcause. Am J Transplant 2007; 7:1743–1752.
17 Gloor JM, Sethi S, Stegall MD, et al. Transplant glomerulopathy: subclinicalincidence and association with alloantibody. Am J Transplant 2007; 7:2124–2132.
18
��Cosio FG, Gloor JM, Sethi S, et al. Transplant glomerulopathy. Am J Trans-plant 2008; 8:492–496.
This paper is a concise review documenting the association between transplantglomerulopathy and anti-HLA antibodies, particularly antibodies to HLA class IIantigens, and the impact of transplant glomerulopathy on graft survival.
19 Racusen LC, Colvin RB, Solez K, et al. Antibody-mediated rejection criteria:an addition to the Banff ’97 classification of renal allograft rejection. Am JTransplant 2003; 3:1–7.
20 Haas M, Rahman MH, Racusen LC, et al.C4d and C3d staining of biopsies ofABO- and HLA-incompatible renal allografts: correlation with histologicfindings. Am J Transplant 2006; 6:1829–1840; 2006.
21
��Setoguchi K, Ishida H, Shimmura H, et al. Analysis of renal transplant protocolbiopsies in ABO-incompatible kidney transplantation. Am J Transplant 2008;8:86–94.
This paper describes a retrospective analysis comparing histologic findings andC4d staining in 89 protocol biopsies from 48 ABO-incompatible renal allograftswith those from 250 protocol biopsies of 133 ABO-compatible grafts in patientsgiven equivalent maintenance immunosuppression.
22
��Haas M, Segev D, Racusen LC, et al. C4d deposition without rejectioncorrelates with reduced early scarring in ABO-incompatible renal allografts.J Am Soc Nephrol 2009; 20:197–204.
The findings in this retrospective study indicate that in ABO-incompatiblerenal allografts, diffuse PTC C4d staining without associated histologic findingsof AMR or cell-mediated rejection is not associated with development ofgraft scarring or transplant glomerulopathy within the first 12 months post-transplantation.

Significance of C4d staining with minimal histologic abnormalities Haas 27
23 Mengel M, Bogers J, Bosmans J-L, et al. Incidence of C4d stain in protocolbiopsies from renal allografts: results from a multicenter trial. Am J Transplant2005; 5:1050–1056.
24 Dickenmann M, Steiger J, Descoeudres B, et al. The fate of C4d positivekidney allografts lacking histological signs of acute rejection. Clin Nephrol2006; 65:173–179.
25 Williams GM, Hume DM, Hudson RP Jr, et al. ‘Hyperacute’ renal-homograftrejection in man. N Engl J Med 1968; 279:611–618.
26
�IchimaruN, TakaharaS. Japan’s experiencewith living-donor kidney transplanta-tion across ABO barriers. Nature Clin Pract Nephrol 2008; 4:682–691.
This paper reviews the extensive Japanese experience with ABO-incompatiblerenal transplantation, comprising over 1000 transplants at 92 institutions.
27 Gloor JM, Lager DJ, Moore SB, et al. ABO-incompatible kidney transplantationusing both A2 and non-A2 living donors. Transplantation 2003; 75:971–977.
28 Tyden G, Donauer J, Wadstrom J, et al. Implementation of a protocol for ABO-incompatible kidney transplantation: a three center experience with 60 con-secutive transplantations. Transplantation 2007; 83:1153–1155.
29
�Montgomery RA, Locke JE, King KE, et al. ABO incompatible renal trans-plantation: a paradigm ready for broad implementation. Transplantation 2009;87:1246–1255.
This article summarizes the Johns Hopkins Hospital experience with ABO-incom-patible renal transplantation over a 9-year interval comprising two separate eraswith respect to desensitization and immunosuppression. The article presents keypathologic as well as clinical data.
30 Onitsuka S, Yamaguchi Y, Tanabe K, et al. Peritubular capillary deposition ofC4d complement fragment in ABO-incompatible renal transplantation withhumoral rejection. Clin Transplant 1999; 13 (Suppl 1):33–37.
31 Kato M, Morozumi K, Takeuchi O, et al.Complement fragment C4d depositionin peritubular capillaries in acute humoral rejection after ABO blood group-incompatible human kidney transplantation. Transplantation 2003; 75:663–665.
32 Kanetsuna Y, Yamaguchi Y, Horita S, et al. C4d and/or immunoglobulinsdeposition in peritubular capillaries in perioperative graft biopsies in ABO-incompatible renal transplantation. Clin Transplant 2004; 18 (Suppl 11):13–17.
33 Fidler ME, Gloor JM, Lager DJ, et al. Histologic findings of antibody-mediatedrejection in ABO blood-group-incompatible living-donor kidney transplanta-tion. Am J Transplant 2004; 4:101–107.
34
�Oettl T, Halter J, Bachmann A, et al. ABO blood group-incompatibleliving donor kidney transplantation: a prospective, single-centre analysisincluding serial protocol biopsies. Nephrol Dial Transplant 2009; 24:298–303.
This paper describes a prospective clinical and pathologic study of 10 recipients ofABO-incompatible renal allografts in Basel, Switzerland from 2005 to 2007.Patients underwent protocol biopsies at the time of transplantation and at 7 days,and 3, 6, 12, and 18 months post-transplantation.
35
��Toki D, Ishida H, Setoguchi K, et al. Acute antibody-mediated rejection in livingABO-incompatible kidney transplantation: long-term impact and risk factors.Am J Transplant 2009; 9:567–577.
This study analyzes clinical and serologic risk factors for development of acuteAMR in 57 recipients of ABO-incompatible renal allografts, and examines theimpact of AMR on long-term survival of these grafts.
36 Gloor JM, Cosio FG, Rea DJ, et al. Histologic findings one year after positivecrossmatch or ABO blood group incompatible living donor kidney transplan-tation. Am J Transplant 2006; 6:1841–1847.
37 Haas M, Montgomery RA, Segev DL, et al. Subclinical acute antibody-mediated rejection in positive crossmatch renal allografts. Am J Transplant2007; 7:576–585.
38 Seemayer CA, Gaspert A, Nickeleit V, et al. C4d staining of renal allograftbiopsies: a comparative analysis of different staining techniques. Nephrol DialTransplant 2007; 22:568–576.
39
�Cornell LD, Burns JM, Stegall MD. Prevention of endothelial activation with C5inhibition in positive-crossmatch kidney transplants. Am J Transplant 2009; 9(Suppl 2):304.
This is an abstract of a study from the Mayo Clinic presented at the 2009 AmericanTransplant Congress meeting. Biopsies from 4 recipients of positive cross-matchrenal allografts receiving the C5 inhibitor eculizumab were compared with biopsiesfrom 46 recipients of positive cross-match grafts not receiving this drug; electronmicroscopy was performed on all biopsies to assess endothelial injury and earlychanges of transplant glomerulopathy.
40
�Ding JW, Zhou T, Ma L, et al. Expression of complement regulatory proteins inaccommodated xenografts induced by anti-a-Gal IgG1 in a rat-to-mousemodel. Am J Transplant 2008; 8:32–40.
This study examines the expression of the complement regulatory proteins CD55,CD59, and Crry in the endothelium of accommodated versus rejecting heart graftsin a xenograft model in which baby Lewis rat hearts are transplanted into Rag/GT-deficient mice, and accommodation is induced by repeated injections of low-doseanti-a-Gal IgG1.