local immunosuppression prolongs survival of rpe xenografts labeled by retroviral gene transfer
TRANSCRIPT

Local Immunosuppression Prolongs Survival of RPEXenografts Labeled by Retroviral Gene Transfer
Chi–Chun Lai,1,5 Peter Gouras,1 Kentaro Doi,1 Stephen H. Tsang,2,3
Stephen P. Goff,2 and Paul Ashton4
PURPOSE. To determine whether local immunosuppression with Cyclosporin A can influence thesurvival of human fetal retinal pigment epithelium (RPE) xenografts in the rabbit’s subretinal space.
METHODS. Cultured human fetal RPE cells were transduced with the gene for green fluorescentprotein (GFP) using a lentiviral vector. The RPE was transplanted into the subretinal space of rabbitsthat received intravitreal cyclosporine either by weekly injections (0.25–0.5 mg) or by slow release(approximately 2 mg/d) from a capsule sutured into the vitreal cavity after prior cryopexy. Thetransplanted RPE was followed by GFP fluorescence scanning laser ophthalmoscopy and byhistology of the transplant site.
RESULTS. RPE xenografts in eyes receiving intravitreal cyclosporine survived longer (several months)than they did in control eyes without cyclosporine. Survival was as long with slow release capsulesas it was with weekly intravitreal injections at much higher concentrations of cyclosporine.
CONCLUSIONS. Local immunosuppression of the eye with cyclosporine prolongs the survival of RPExenografts in the subretinal space of rabbits, implying that rejection involves activated T lympho-cytes. Local immunosuppression with slow release capsules is as effective as weekly injections atmuch higher concentrations. (Invest Ophthalmol Vis Sci. 2000;41:3134–3141)
One problem with retinal pigment epithelium (RPE)transplantation is that the graft seems to be rejected inthe subretinal space, even though this is considered
an immunologically privileged site. Systemic immunosuppres-sion can counteract such rejection, but this has complicatingside effects, especially in older subjects in whom transplanta-tion might have its most therapeutic applicability. One way tocircumvent systemic complications is to immunologically sup-press only the eye in which the transplant has been placed.Intravitreally placed slow release capsules have been shown todeliver therapeutic levels of the immunosuppressive drug cy-closporine over relatively long periods of time.1 This mayprovide a way to prevent rejection in the subretinal spacewithout generalized immunosuppression.
We have tested local immunosuppression of the eye, usingRPE xenografts in the subretinal space of rabbits by trackingthe transplants with a reporter gene encoding green fluores-cent protein (GFP) introduced into these cells by retroviralgene transfer. Such labeled transplants can be followed nonin-
vasively with the scanning laser ophthalmoscope (SLO), whichgreatly facilitates carrying out such experiments because itprovides a means of continuously reexamining the transplantsin vivo. An abstract2 and a brief report3 of this research havebeen published.
METHODS
Human fetal RPE was cultured and transduced with the genefor GFP using a lentiviral vector.3 The virus was generated bycotransfection of human kidney–derived 293T cells by threeplasmids.3,4 The packaging construct contained the cytomeg-alovirus (CMV) promoter and the insulin polyadenylation sig-nal to express all the viral proteins in trans, except the enve-lope and Vpu. The second plasmid provided a vector with allthe cis-acting elements that allow transfer and integration intothe target cells. In this transducing vector, an expression cas-sette with the Rev responsive element and the CMV promoteris used to direct the expression of GFP. The third plasmidprovides the envelope protein from the vesicular stomatitisvirus glycoprotein to enhance the virus stability and the rangeof possible targets. The lentiviral titers were determined byinfection of 293T cells seeded in six-well plates at 1 3 105
cells/well the day before infection with serial dilution of theviral stock in the presence of 8 mg/ml polybrene. After over-night incubation, the culture medium was changed and thecells incubated for 2 more days. Fluorescent microscopyand/or a fluorescence-activated cell sorter (FACStar plus; Bec-ton–Dickinson, Mountain View, CA) identified GFP fluorescentcells. Titers ranged from 107 to 109. The cultures were exposedto the virus only once.
GFP fluorescent fetal human RPE was transplanted as asuspension, approximately 50,000 cells in 50 microliters,
From the Departments of 1Ophthalmology and 2Biochemistry andMolecular Biophysics, Columbia University, Howard Hughes MedicalInstitute, New York, New York; 3The Jules Stein Eye Institute, Univer-sity of California Los Angeles; and 4Tufts New England Medical Center,Boston, Massachusetts; 5Chang Gung Memorial Hospital, Taipei, Tai-wan.
Supported by Grant EY 03854, National Institutes of Health (Be-thesda, Maryland); and by Research to Prevent Blindness (New York,New York).
Submitted for publication October 28, 1999; revised March 6,2000; accepted April 13, 2000.
Commercial relationships policy: N.Corresponding author: Peter Gouras, Department of Ophthalmol-
ogy, Columbia University, 630 W. 168 Street, New York, NY [email protected]
Investigative Ophthalmology & Visual Science, September 2000, Vol. 41, No. 103134 Copyright © Association for Research in Vision and Ophthalmology

into the subretinal space of rabbits, anesthetized with ket-amine (20 mg/kg intramuscularly [IM]) and rompun (10mg/kg, IM). The cells selected for transplantation were fol-lowed in culture after transduction with lentivirus to assesstheir GFP fluorescence. The percentage of cells expressingGFP ranged from 40% to 80%. The transplanted cells werenot sorted for fluorescence before transplantation but wereused directly after they were removed from the culture plateby trypsinization, washed with balanced salt solution, andconcentrated by gentle centrifugation. A glass pipette with atip diameter of 100 to 150 mm was used to inject the cellsolution subretinally under microscopic control. Twenty-two rabbits received a transplant, occupying a space lessthan a millimeter in diameter, in each eye adjacent to themyelinated region of the optic nerve, which provides alandmark to find the transplant site by SLO.
Fourteen rabbits received an intravitreal injection of Cy-closporine A (CSA) weekly. Five rabbits received 0.25 mg/wkand nine rabbits 0.5 mg/wk. The solutions were obtained byvolumetrically diluting a stock solution of CSA, 50 mg/ml. Thisis a standard solution for the intravenous administration ofcyclosporine, which contains 0.65 g/ml castor oil as a solventand 33% ethyl alcohol as a preservative. The opposite eyereceived an intravitreal injection of an equal volume of abalanced salt solution in the controls.
Eight rabbits were used to study the effect of slow releasecapsules containing only cyclosporine. The slow release cap-sule was sutured through the sclera at the pars plana 2 weeksafter local cryopexy. Slow release capsules have been found todeliver approximately 2 mg of cyclosporine daily into thevitreal chamber.1 The other eye received a device consisting ofpolymers only without cyclosporine.
The rabbits were followed weekly by biomicroscopy,indirect ophthalmoscopy, and scanning laser ophthalmos-copy (SLO) using infrared, red and argon blue light, andfluorescence filtering for fluorescein emission. Survival ofthe transplant was judged by the presence of GFP fluores-cence in the transplant area. When no fluorescence wasdetected, the transplant was considered to have been re-jected.3 At this point the rabbit was killed and the eyesremoved for histology. Three rabbits were killed at 2 to 3weeks after all fluorescence had disappeared. One rabbitwas euthanatized while there was still strong GFP fluores-cence, and this rabbit was not considered in the survivaldata. The eyes were fixed in either 3% buffered glutaralde-hyde or 4% paraformaldehyde in phosphate-buffered salineat pH 7.2. The former eyes were processed for Epon em-bedding and thin sectioning and the latter for cryosectioningand fluorescence microscopy. For cryomicroscopy, the para-formaldehyde-fixed sections were immersed in ornithinecarbamoyltransferase compound and frozen by dry ice. Sec-tioning was performed on a Leica 1850 cryotome (LeicaInstruments, Nusslach, Germany). Sections were mountedon gelatinized glass slides with fluoromount-G and examinedby fluorescence microscopy.
The animals were treated in conformity with the Declara-tion of Helsinki, the Guiding Principles in the Care and Use ofAnimals (DHEW Publication, NIH 80-23), and the ARVO State-ment for the Use of Animals in Ophthalmic and Vision Re-search.
RESULTS
Figure 1A shows a patch of human fetal RPE in culture viewedby white light transillumination. The patch (asterisk) is heavilypigmented with nondividing RPE. Along the edge of the patchmigrating, dividing cells can be seen with much less pigmen-tation (arrowheads). Figure 1B shows the patch of RPE in thepresence of an additional strong blue light that induces GFPfluorescence. Despite their dense pigmentation, the fluores-cence is intense enough to make GFP-expressing cells quitevisible. Some cells (small arrows) are fluorescing more stronglythan others. Many cells are fluorescing too dimly to be seen inthe presence of the transilluminating white light but can beidentified and counted by fluorescence illumination alone. Thefraction of GFP-fluorescing cells in this patch was estimated tobe approximately 70%. The fraction of GFP fluorescence ob-tained by lentiviral transduction varied from 40% to 80%. Thisfluorescence remained stable in vitro.3
Figure 2 shows the appearance of a transplant site in aneye with a slow release capsule of cyclosporine at 2, 3, 4, and12 weeks after surgery. The upper set of photographs showsthe appearance of the transplant in blue light. The transplantsite is a darker structure just to the left of the highly reflectingmyelinated nerve fibers at the optic nerve head of the rabbit.There are several small, highly reflecting structures close to theperimeter of the transplant that are not always visible becausethey depend in large part on the angle of illumination (e.g.,they are not very visible in the photograph at 4 weeks aftertransplantation surgery). The lower set of photographs in Fig-ure 2 shows the fluorescent appearance of the retina. Hererelatively small, bright structures about the size of single epi-thelial cells (i.e., approximately 10–30 mm) can be seen withinand along the perimeter of the transplant. They do not corre-spond to the reflecting structures seen along the perimeter ofthe transplant in blue light, described previously. These GFPfluorescent structures remained similar in size, position, andbrightness for the entire 12-week period after transplantation.
Figure 3 shows a transplant in the opposite eye, in whichthere was only a polymer device without cyclosporine. Thetransplant site is a darker elliptical structure, which has a darkvitreal band extending to the retinotomy. The transplant isadjacent to the myelinated optic nerve, seen on the right in thephotograph (arrow) taken at 12 weeks after transplantationsurgery. The lower set of photographs in Figure 3 shows thefluorescent appearance of the retina. At 2 weeks after trans-plantation, numerous small fluorescent cell-like spots can beseen throughout the transplant site. At 3 weeks after transplan-tation, many of these fluorescent spots have disappeared. At 4weeks after transplantation, all the fluorescent spots have dis-appeared, which was our criterion for rejection.3 This is alsothe appearance at 12 weeks, although at that point somefluorescence is seen adjacent the transplant site. These fluores-cent spots are slightly larger, less bright, and more amorphousthan the GFP fluorescence. These structures show a yellowfluorescence in histologic sections and appear as lipofuscin-like particles in the host RPE layer by electron microscopy.
Figure 4 shows a transplant that has survived for 14 weeksafter transplantation. In the upper set of photographs, thereflected blue light image shows the transplant site adjacent tothe myelinated optic nerve. The dark spot on the right edge ofthe transplant is the retinotomy. In the lower set of photo-graphs, the fluorescence of the retina shows many brightly
IOVS, September 2000, Vol. 41, No. 10 Survival of RPE Xenografts 3135

FIGURE 1. Color photographs show-ing a patch of human fetal RPE in vitro(A). The darkly pigmented cells withinthe patch (asterisk) have not divided;lightly pigmented, migrating cells arevisible along the edge of the patch (ar-rowheads). (B) The same patchviewed with both fluorescence andtransillumination. Green fluorescenceof GFP is evident in a large proportionof the stationary cells in the patch.Some cells (arrows) fluoresce morestrongly than others. (C) A frozen sec-tion of rabbit retina shows GFP fluores-cent xenografts on the host RPE layer.There is a weak yellowish fluorescenceconsidered to be lipofuscin surround-ing black cytoplasmic melanin in thehost RPE (arrow). (D) A frozen sectionof rabbit retina, viewed with both flu-orescence and transillumination, showsGFP-fluorescent xenografts on top ofthe nonfluorescent host RPE layer (ar-row at the basal margin of this layer).(E) An Epon section of a transplantsite, which shows rejection. There is adense concentration of monocyteswithin the subretinal space (asterisk)and the adjacent choroid (C) directlyunder a disrupted host RPE layer (anarrow shows the basal edge of thislayer). The neural retina (NR) has fewmonocytes. The inflammatory responseis extremely local to this area of retina.(F) An Epon section of a transplantsite, which shows another example ofrejection. There are two foci of mono-cytes in the subretinal space (aster-isks) and the adjacent choroid (C). Anarrow shows the basal edge of thehost RPE layer. The neural retina (NR)has virtually no monocytes.
3136 Lai et al. IOVS, September 2000, Vol. 41, No. 10
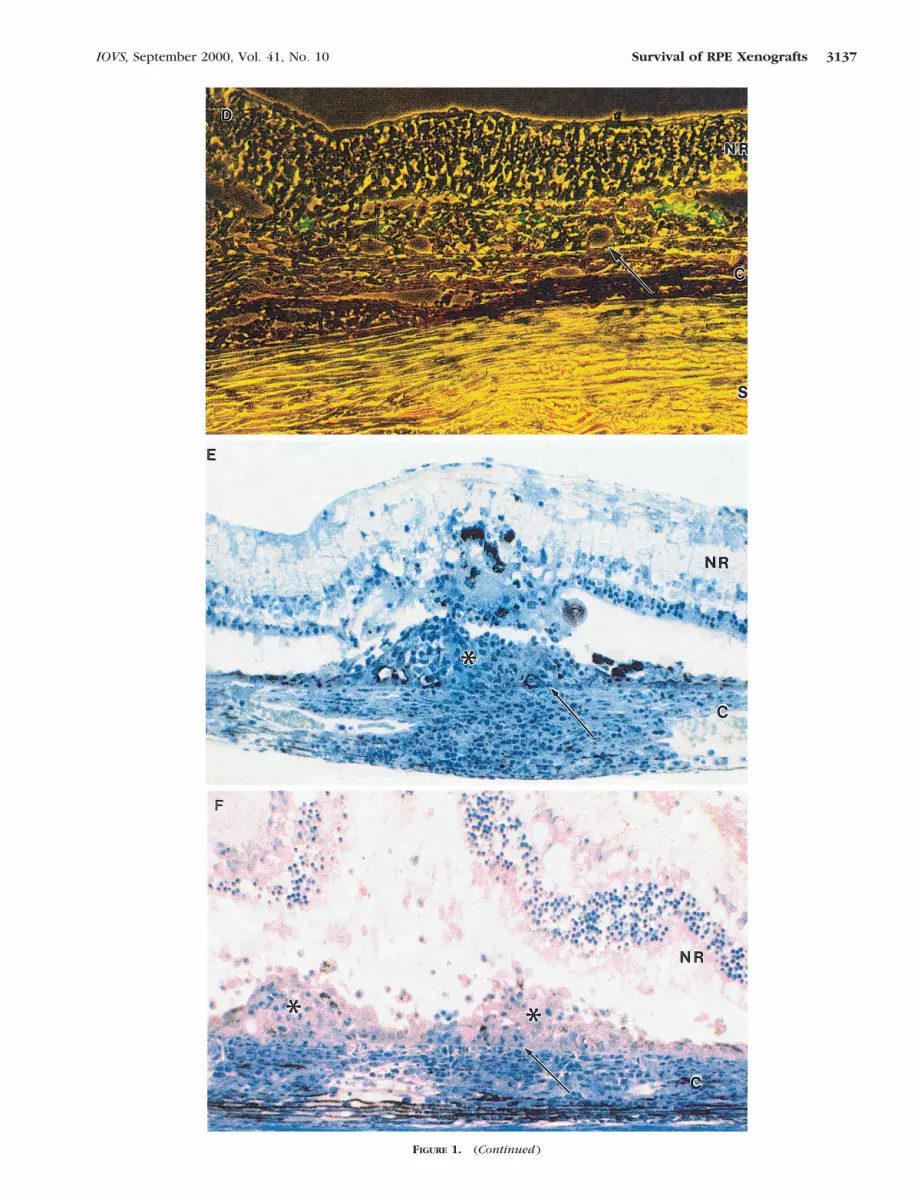
FIGURE 1. (Continued )
IOVS, September 2000, Vol. 41, No. 10 Survival of RPE Xenografts 3137

fluorescent spots, about the size of single retinal epithelialcells, within the transplant site. These fluorescent spots remainsimilar in size, shape, position, and brightness over time. Thiseye received 0.25 mg/wk of cyclosporine intravitreally.
Figure 5 illustrates a transplant that also survived for morethan 7 weeks after transplantation in an eye that contained a
slow release capsule of cyclosporine. In this case the retina isshown in blue, fluorescence, and infrared images. The bluelight image (upper set) shows the transplant site below themyelinated optic nerve fibers. There is a vitreal band extendingto the retinotomy. The transplant site is visible as a horizontalstructure with a light demarcation line around it. The fluores-
FIGURE 2. SLO views of a transplant site at 2, 3, 4, and 12 weeks after transplantation seen by reflected blue light (upper set) and fluorescence(lower set). The transplant, located adjacent to the myelinated optic nerve fibers, is seen as darker area surrounded by a light demarcation line inblue light and in fluorescence as a structure containing bright pointlike structures, which are considered to be GFP-expressing transplanted RPE.This eye had a slow release capsule of cyclosporine.
FIGURE 3. SLO views of the trans-plant site in the opposite eye of thatshown in Figure 2. This eye had acapsule without cyclosporine, and thetransplant shows evidence of rejectionat 3 weeks. The upper row shows thetransplant in reflected blue light; thetransplant is a darker structure sur-rounded by a lighter demarcation line.It is adjacent to the myelinated opticnerve fiber layer seen only in the right-most photograph (arrowhead). Thelower row shows the fluorescentview. At 2 weeks, GFP-fluorescingcells are visible within the transplant.At 3 weeks, the number of fluorescingcells is reduced. At 4 weeks all fluores-cence has disappeared. At 12 weeksthere is also no fluorescence withinthe transplant; some lipofuscin-like flu-orescence has developed outside thetransplant site (at the upper left).
3138 Lai et al. IOVS, September 2000, Vol. 41, No. 10

cent view (middle set) shows the GFP fluorescent transplantcells within the transplant site. These cells retain their shape,position, and brightness for the entire 7-week period. The
infrared view (lower set) reveals a dark band extendingthrough the entire transplant site. This darkness is consideredto represent the added density of the transplanted RPE cells
FIGURE 4. SLO views of a transplant site in an eye receiving weekly injections of cyclosporine (0.25 mg). The upper row shows the retina inreflected blue light. The transplant is visible by a faint demarcation line and mottling of the RPE layer; the retinotomy site is seen as a dark spotadjacent to the myelinated optic nerves on the right side of each photograph. The lower row shows the fluorescent view. GFP fluorescent cellscan be seen for 14 weeks after transplantation.
FIGURE 5. SLO views of a transplant site in an eye with a slow release capsule containing cyclosporine at 2, 3, and 7 weeks after transplantation.The upper row shows the retina in reflected blue light, the middle row in fluorescence, and the lower row in infrared light. GFP-fluorescing cellscan be seen for the entire time. The infrared view shows a darker reflected image within the transplant site produced by the increase due to thexenograft.
IOVS, September 2000, Vol. 41, No. 10 Survival of RPE Xenografts 3139

within the subretinal space, only a fraction of which exhibitGFP fluorescence.
This hypothesis was supported by the histology wheretransplanted cells identified by their GFP fluorescence could beseen on top of the host RPE layer (Figs. 1C, 1D). When rejec-tion occurred, GFP fluorescent cells were no longer found inthe retina, and when the transplant site was examined withinseveral weeks after the fluorescence had disappeared, therewas always clear evidence of rejection within the transplantsite. The rejection was characterized by intense collections ofmonocytes in the choroid and focal areas of host RPE andphotoreceptor damage (Figs. 1E, 1F). Many more monocyteswere always found in the choroid adjacent to the transplantsite than in the neural retina. The longer the time between thedisappearance of the GFP fluorescence in the retina and theeuthanatization of the rabbit, the less was the amount ofmonocytes detectable around the transplant site. In somecases, the major evidence for rejection was disruption of thehost RPE layer and loss of photoreceptors at the transplant site.
Figure 6 compares the survival of the xenografts in thepresence and absence of local cyclosporine immunosuppres-sion. Based on the criterion of complete loss of GFP fluores-cence as an indicator of rejection, locally immunosuppressedtransplants survived longer than those without immunosup-pression. Fifty percent of the RPE xenografts survived for atleast 5 weeks when associated with local immunosuppression.Without immunosuppression, 50% of the xenografts disap-peared in less than 1 month. The mean graft survival time forthe controls, slow release CSA, and 0.25 and 0.5 mg CSAweekly groups was 4, 11, 10, and 9 weeks, respectively. Theslow release of cyclosporine was as effective as repeated intra-vitreal injections of much greater concentrations. Survival of atransplant in one eye did not appear to be related to its survivalin the other eye. One RPE xenograft survived for at least 10weeks without immunosuppression, whereas all the othersdisappeared within 5 weeks. The loss of GFP fluorescence
occurred relatively quickly, disappearing within the course of1 week. In some cases, there was a more gradual loss offluorescence, and this seemed more common in the transplantsthat survived the longest. All the transplants surviving for 15weeks or longer had lost much of the fluorescence they orig-inally had.
DISCUSSION
These results indicate that local administration of cyclosporineprolongs the survival of human fetal RPE xenografts in thesubretinal space of rabbits. This supports the hypothesis thatclassic rejection plays a role in the survival of foreign trans-plants in the subretinal space. It implies that a T cell–mediatedresponse must be involved, because cyclosporine immunosup-presses mainly, if not exclusively, by inhibiting the calmodulin-dependent phosphatase, calcineurin in T cells.5 That a cellularform of rejection is involved in subretinal xenograft rejection issupported by the histology, which usually showed an intensemonocytic infiltration within and around the transplantsite.3,6,7 This cellular reaction appears to diminish with timeafter rejection. There is a report of only mild rejection ofhuman RPE xenografts in the rabbit8 and also evidence oftolerance of a fraction of human RPE grafts to the monkey foras long as 6 months.7 We have also observed survival of onetransplant for more than 2 months without immunosuppres-sion, whereas all the other control transplants rejected withinweeks after transplantation. These differences imply that sev-eral factors are involved in the viability of these grafts.
What is interesting is that immunosuppression can beeffective at a local level and with relatively low total concen-trations of cyclosporine. Local immunosuppression does notentirely eliminate rejection of these xenografts, however, be-cause virtually all disappear with time despite immunosuppres-sion. This may be because of either the inability of localimmunosuppression to completely stem the rejection processor of other factors that appear to influence the survival of thesexenografts.
RPE allografts in the subretinal space seem less prone torejection than xenografts. In mice, RPE allografts in the sub-retinal space survive longer than those placed in the conjunc-tiva and in addition induce a cell-mediated suppression ofdelayed hypersensitivity to graft antigen.9 There are reportsthat RPE allografts survive and continue to rescue photorecep-tors from degeneration in the Royal College of Surgeons rat forrelatively long times.10–12 On the other hand, there is evidencethat such allografts in rats are slowly rejected but in an atypical,noninflammatory manner.13 In rabbits, RPE allografts havebeen reported to survive with14 or to degenerate slowly with-out15 cyclosporine immunosuppression. Small human RPE al-lografts have been reported to survive when placed perifo-veally, but larger ones, especially those placed over areaswhere the blood–brain barrier has been disturbed, are rejectedwithout immunosuppression.16 That local cyclosporine immu-nosuppression could prolong the survival of RPE allograftswould seem to be a reasonable expectation, but evidence thata slow allograft rejection in the rabbit subretinal space appearsunaltered by systemic immunosuppression17 is evidence to thecontrary. Further research will be needed to determinewhether there are cyclosporine-resistant mechanisms mediat-ing allograft and xenograft rejection in the subretinal space.
FIGURE 6. The survival time of each transplant as judged by thecomplete absence of GFP fluorescence at the transplant site. Theordinate represents the percentage of transplants that survived, andthe abscissa represents the time after transplantation surgery in weeks.The controls received no CSA immunosuppression. The other threegroups received either 0.25 or 0.5 mg CSA by weekly intravitrealinjection or by a slow release vitreal capsule.
3140 Lai et al. IOVS, September 2000, Vol. 41, No. 10

Such research is greatly expedited by having an in vivomonitor, which provides a means to track the behavior andsurvival of these retinal transplants, noninvasively. It would bemuch more difficult and time-consuming to follow the fate ofthese transplants relying on postmortem histology alone. Theuse of the fluorescent marker GFP allows the same transplantto be followed over time, providing clues to the onset andextent of the rejection process. We expect that even greaterimprovements in the resolution of SLO imaging will provideeven more powerful means of following rejection and survivalin the living retina in the future.
References1. Pearson PA, Jaffe GJ, Martin DF, et al. Evaluation of a delivery
system providing long-term release of cyclosporine. Arch Ophthal-mol. 1996;114:311–317.
2. Lai C, Doi K, Gouras P, Ashton P, Tsang S, Goff S. Intravitreal slowrelease of cyclosporine prolongs survival of RPE xenografts mon-itored in vivo by gene transferred GFP fluorescence [ARVO Ab-stract]. Invest Ophthalmol Vis Sci. 1999;40(4):S858. Abstract nr4521.
3. Lai C, Gouras P, Doi K, et al. Tracking RPE transplants labeled byretroviral gene transfer with green fluorescent protein. InvestOphthalmol Vis Sci. 1999;40:2141–2145.
4. Naldini K, Blomer U, Gallay P, et al. In vivo gene delivery and stabletransduction of nondividing cells by a Lentiviral vector. Science.1996;272:263–267.
5. Rao A, Luo C, Hogan PG. Transcription factors of the NFAT family:regulation and function. Annu Rev Immunol. 1997;15:707–747.
6. Sheng Y, Gouras P, Cao H, et al. Patch transplants of human fetalretinal pigment epithelium in rabbit and monkey retina. InvestOphthalmol Vis Sci. 1995;36:381–390.
7. Berglin L, Gouras P, Sheng Y, et al. Tolerance of human fetalpigment epithelium xenografts in monkey retina. Graefes ArchClin Exp Ophthalmol. 1997;235:103–110.
8. He S, Wang HM, Ogden TE, Ryan SJ. Transplantation of culturedhuman pigment epithelium into rabbit subretina. Graefes ArchClin Exp Ophthalmol. 1993;231:737–742.
9. Jiang LQ, Jorquera M, Streilein JW. Immunologic consequences ofintraocular implantation of retinal pigment epithelial allografts.Exp Eye Res. 1994;58:719–728.
10. LaVail MM, Li L, Turner JE, Yasumura D. Retinal pigment epithelialcell transplantation in RCS rats: normal metabolism in rescuedphotoreceptors. Exp Eye Res. 1992;55:555–562.
11. Yamamoto S, Du J, Gouras P, Kjeldbye H. Retinal pigment epithe-lial cell transplants and retinal function in RCS rats. Invest Oph-thalmol Vis Sci. 1993;34:3068–3075.
12. Whitley SJO, Litchfield TM, Coffey PJ, Lund RD. Improvement ofthe pupillary light reflex of Royal College of Surgeons rats follow-ing RPE cell graft. Exp Neurol. 1996;140:100–104.
13. Zhang X, Bok D. Transplantation of retinal pigment epitheliumcells and immune response in the subretinal space. Invest Oph-thalmol Vis Sci. 1998;39:1021–1027.
14. Gouras P, Lopez R, Brittis M, Kjeldbye H. The ultrastructure oftransplanted rabbit retinal epithelium. Graefes Arch Clin Exp Oph-thalmol. 1992;230:468–475.
15. El Dirini AA, Wang H, Ogden TE, Ryan SJ. Retinal pigment implan-tation in the rabbit: technique and morphology. Graefes Arch ClinExp Ophthalmol. 1992;230:292–300.
16. Algvere PV, Gouras P, Dafgard–Kopp E. Long-term outcome of RPEallografts in non-immunosuppressed patients with AMD. Eur JOphthalmol. 1999;9:217–230.
17. Crafoord S, Seregard S, Dafgard–Kopp E, Algvere PV. CyclosporinA does not prevent RPE allograft failure in the rabbit subretinalspace [ARVO Abstract]. Invest Ophthalmol Vis Sci. 1999;40(4):S597. Abstract nr 3136.
IOVS, September 2000, Vol. 41, No. 10 Survival of RPE Xenografts 3141