laparos: advanced computer assisted laparoscopic surgery training
TRANSCRIPT

II INTERNATIONAL CONFERENCE ON COMPUTATIONAL BIOENGINEERING H. Rodrigues et al. (Eds.)
Lisbon, Portugal, September 14-16, 2005
LAPAROS: ADVANCED COMPUTER ASSISTED LAPAROSCOPIC SURGERY TRAINING
Bricelis J. Urbina* Ernesto J. Coto* Omaira C. Rodríguez* Rodolfo E. Miquilarena** Miguel E. Cerrolaza***
* Computer Graphics Lab, Central University of Venezuela, Venezuela e-mail: { bricelis | ecoto | omaira }@opalo.ciens.ucv.ve
** Experimental Surgery Institute, Central University of Venezuela, Venezuela e-mail: [email protected]
*** Bioengineering Center, Central University of Venezuela, Venezuela e-mail: [email protected]
Keywords: Laparoscopy, Simulation, Virtual Reality, Surgery Training.
Abstract. Laparoscopic surgery training deals with the improvement of a new surgical technique where the working space is magnified. As well, surgeon movements are amplified and therefore they must be accurate and smooth. Moreover, the surgeon has to deal with the fulcrum effect, and learn how to manipulate instruments in a 3D space based only in 2D images. Therefore, training in laparoscopic surgery requires the stimulation of the visuospatial and motor skills of the surgeon. It should stress the manipulation of laparoscopic surgery instruments and the interpretation of 2D images of human internal organs and tissues. In this paper we present LAPAROS, a new laparoscopic surgery training system that allows the user to learn navigation inside the human body and interactively manipulate laparoscopic surgery instruments. The system is based on virtual reality technology and 3D computer graphics. We have also incorporated our own state-of-the-art mechanical simulator. LAPAROS provides the user with several training exercises displaying different skill levels. The system provides an evaluation tool and also keeps track of all training sessions for every user, so they can have a feedback on their overall improvement at any moment.

Bricelis J. Urbina, Ernesto J. Coto, Omaira C. Rodríguez, Rodolfo E. Miquilarena and Miguel E.Cerrolaza
1 INTRODUCTION
Open surgery requires an incision large enough for the surgeon to see directly and place his hands, fingers and instruments directly into the body. Frequently, reaching the target operating site leads to damage of skin, muscles, connective tissue and bones, resulting in longer recovery time, complications related to the surgical trauma as well as increased soreness for the patient. Minimally Invasive Surgery (MIS) limits the surgical trauma by reducing the size of the incisions or using catheters or endoscopes threaded through vessels, the gastrointestinal tract, or other tubular structures. MIS reduces the risk of complications and patient recovery is faster than with traditional surgery.
Laparoscopic surgery, or MIS of the abdomen, has shown a particularly rapid growth in the last years. In this procedure, a laparoscope is inserted through a 10 mm incision in the abdominal wall. A camera mounted on the laparoscope transmits the image to a monitor viewed by the surgical team. The surgeons handle the camera and the instruments inside the abdominal cavity, based on the visual feedback of the image displayed on the monitor, as shown in figure 1. Several laparoscopic instruments including graspers, scissors, staplers, and electrosurgical devices, are inserted through separate incisions [1].
Figure 1: Image of laparoscopic surgery in process at Experimental Surgery Institute, Central University of Venezuela (UCV), showing surgeons handling the instruments and a monitor displaying images from
the patient’s body.
Laparoscopic surgery has all the benefits of a MIS, but unfortunately, it also has pitfalls. The instruments reduce dexterity, eliminate tactile sensation, and reduce kinesthetic force feedback, reducing the perception of the surgeon during surgery [2, 3]. Several other factors increase the difficulty of the procedure, such as the lack of a stereoscopic image, geometric viewing distortions, and the limitations on resolution, contrast, and color inherent in video imaging [3].
Training in this technique requires the surgeons developing unusual skills, such as handling the camera and the instruments inside the abdominal cavity, based on the visual feedback of the image displayed on the monitor. This involves the capacity of interpreting two-dimensional images out of a three-dimensional real environment, corresponding to the abdominal cavity of the patient.
Bricelis J. Urbina, Ernesto J. Coto, Omaira C. Rodríguez, Rodolfo E. Miquilarena and Miguel E.Cerrolaza
MIS training is usually performed in animals, cadavers or real patients. However, animals do not have the same anatomy as a human being, cadavers have incorrect physiology and training on real patients involves risk to patient safety. For many years, Virtual Reality has been successfully used as a mean to simulate real environments for medical training [4], including laparoscopy surgery [4, 5, 6, 7]. Simulation of a laparoscopy surgery using virtual reality allows the surgeon to develop and acquire the skills demanded for this surgery through practice, therefore increasing surgeon’s experience and patient safety [8, 9].
Currently, there are several commercial simulation systems for laparoscopy surgery. These systems can be classified according to their technology as mechanical simulators [9, 10] or virtual reality simulators [5, 6, 7]. However, an effective training system should have not only technical components but also educational components, designed to provide the trainee with a feedback on the development of his surgical skills [11, 12, 13, 14].
In this paper we present LAPAROS, a virtual reality laparoscopic surgery simulator that includes a brand new educational component, to assist the surgeons in improving their skills on laparoscopy surgery. LAPAROS is setup with both hardware and software components. For the hardware component, we present our own state-of-the-art mechanical simulator [10]. For the software component, we exploit current technology in 3D computer graphics and virtual reality. In addition, we have included a brand new educational component that provides the user with a record of his training sessions and an evaluation of his skills. The medical trainer also benefits from the educational component, since he can keep track of the performance of his students. All of these components interacting together, makes of LAPAROS an advanced computer assisted laparoscopic surgery training system. LAPAROS is already being tested at the medical school of our university.
2 RELATED WORK
Current commercial applications on simulation of laparoscopy surgery can be classified as mechanical simulators [9, 10] or virtual reality simulators [11, 12, 13, 14].
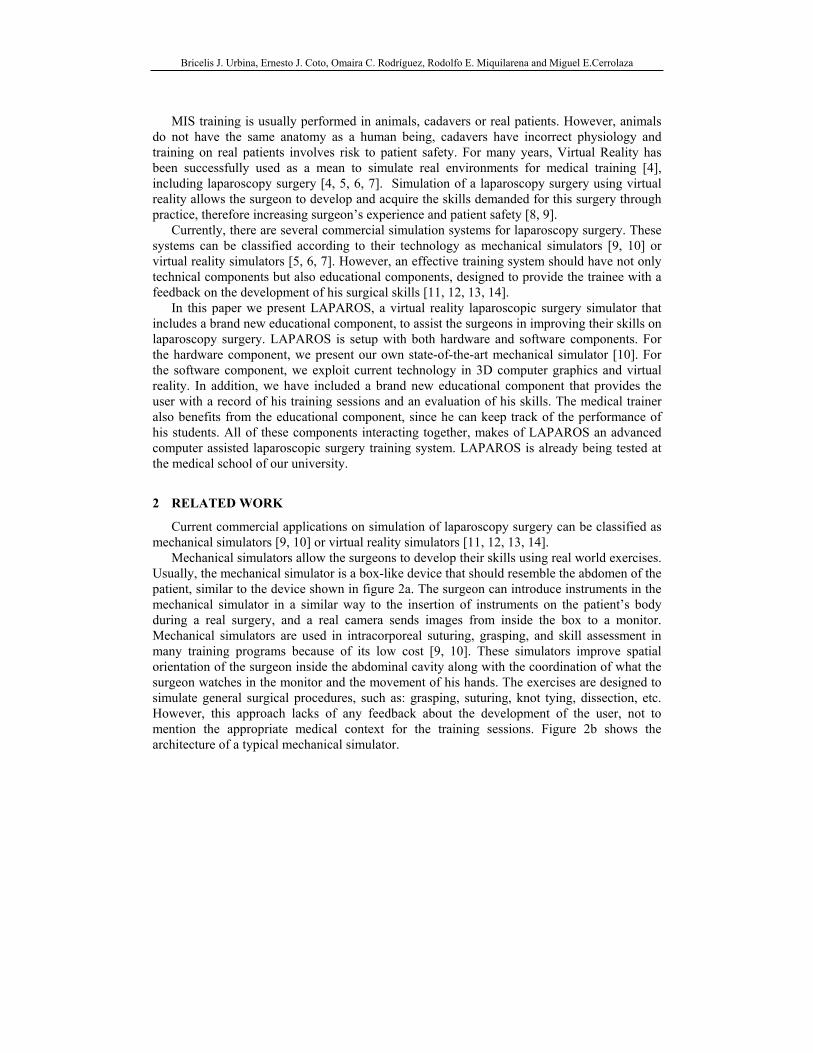
Mechanical simulators allow the surgeons to develop their skills using real world exercises. Usually, the mechanical simulator is a box-like device that should resemble the abdomen of the patient, similar to the device shown in figure 2a. The surgeon can introduce instruments in the mechanical simulator in a similar way to the insertion of instruments on the patient’s body during a real surgery, and a real camera sends images from inside the box to a monitor. Mechanical simulators are used in intracorporeal suturing, grasping, and skill assessment in many training programs because of its low cost [9, 10]. These simulators improve spatial orientation of the surgeon inside the abdominal cavity along with the coordination of what the surgeon watches in the monitor and the movement of his hands. The exercises are designed to simulate general surgical procedures, such as: grasping, suturing, knot tying, dissection, etc. However, this approach lacks of any feedback about the development of the user, not to mention the appropriate medical context for the training sessions. Figure 2b shows the architecture of a typical mechanical simulator.
Bricelis J. Urbina, Ernesto J. Coto, Omaira C. Rodríguez, Rodolfo E. Miquilarena and Miguel E.Cerrolaza
(a) (b)
Figure 2: (a) Ethicon Endo-Surgery© Endotrainer (b) Architecture of a mechanical simulator.
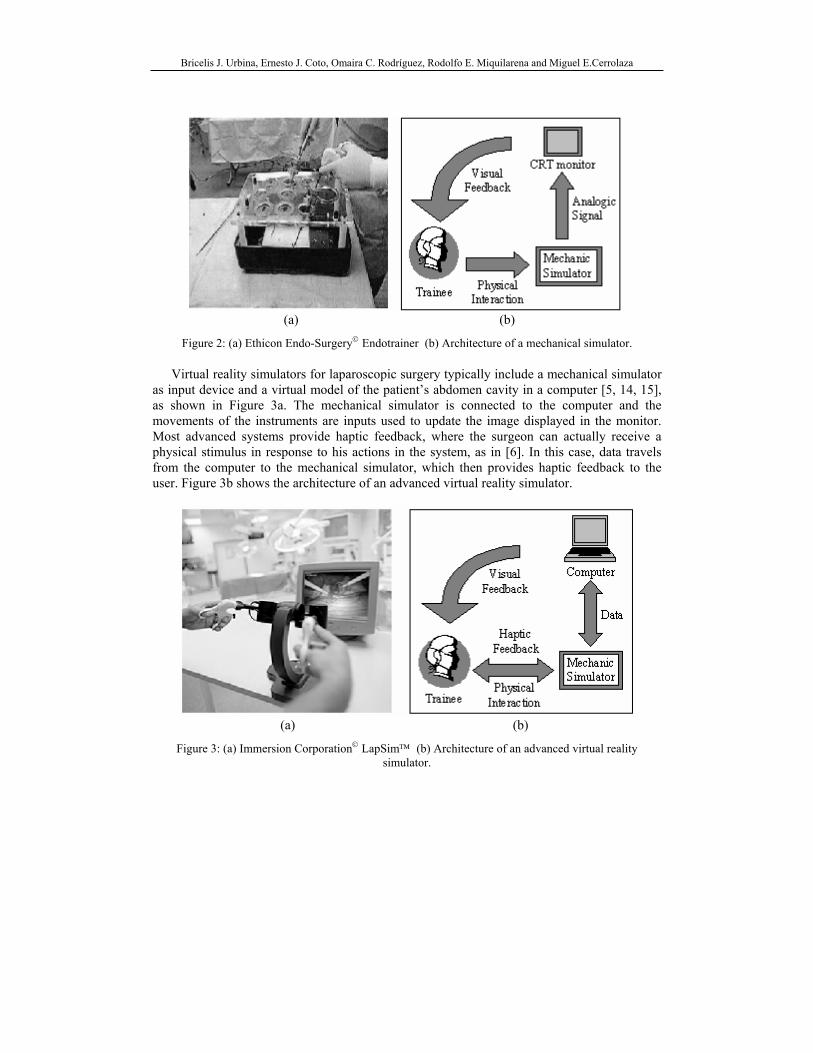
Virtual reality simulators for laparoscopic surgery typically include a mechanical simulator as input device and a virtual model of the patient’s abdomen cavity in a computer [5, 14, 15], as shown in Figure 3a. The mechanical simulator is connected to the computer and the movements of the instruments are inputs used to update the image displayed in the monitor. Most advanced systems provide haptic feedback, where the surgeon can actually receive a physical stimulus in response to his actions in the system, as in [6]. In this case, data travels from the computer to the mechanical simulator, which then provides haptic feedback to the user. Figure 3b shows the architecture of an advanced virtual reality simulator.
(a) (b)
Figure 3: (a) Immersion Corporation© LapSim™ (b) Architecture of an advanced virtual reality simulator.
Bricelis J. Urbina, Ernesto J. Coto, Omaira C. Rodríguez, Rodolfo E. Miquilarena and Miguel E.Cerrolaza
The visual feedback provided by the computer monitor is very similar to the feedback provided by the usual monitor used in real surgery, so the simulation is useful to improve the visual perception and the spatial orientation of the user.
Virtual reality laparoscopic surgery simulators are useful to simulate specific and general surgical procedures. For inexperienced users the system can even display a simple virtual world where the user just has to move or touch objects in order to improve their spatial location and manipulation of the instruments. For experienced users more advanced tasks can be carried out, like suturing or knot tying. Nevertheless, most virtual reality systems also lacks of any feedback about the development or improvement of the user.
3 THE LAPAROS SYSTEM
LAPAROS is an advanced virtual reality system for laparoscopic surgery simulation. As most virtual reality systems, it has a software component and a hardware component. The hardware component is mainly conformed of a mechanical simulator and a tracking subsystem. The software component is conformed of an information subsystem and a 3D graphics subsystem. Hardware components were developed at the Bioengineering Center and software components were developed at the Computer Graphics Lab. The system is already being tested at the Experimental Surgery Institute of our university.
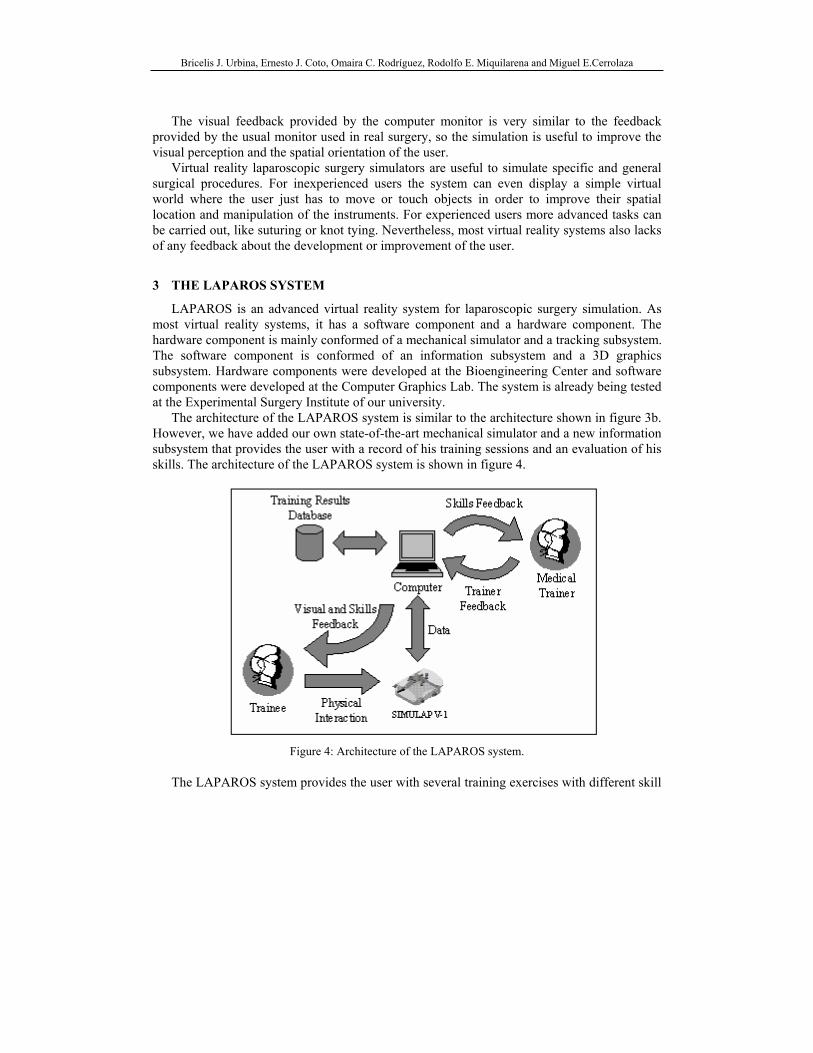
The architecture of the LAPAROS system is similar to the architecture shown in figure 3b. However, we have added our own state-of-the-art mechanical simulator and a new information subsystem that provides the user with a record of his training sessions and an evaluation of his skills. The architecture of the LAPAROS system is shown in figure 4.
Figure 4: Architecture of the LAPAROS system.
The LAPAROS system provides the user with several training exercises with different skill
Bricelis J. Urbina, Ernesto J. Coto, Omaira C. Rodríguez, Rodolfo E. Miquilarena and Miguel E.Cerrolaza
levels. The user can use the information subsystem to select an exercise and then start the 3D graphics subsystem. The trainee manipulates the instruments in the mechanical simulator, and his actions are transformed into data which is sent to the computer. The position and orientation of the instruments are transformed into data by the tracking subsystem. The 3D graphics subsystem receives the information and updates the image displayed on the screen. While the trainee is interacting with the 3D graphics subsystem, the information subsystem is keeping track of his performance. A screen showing the performance of the trainee is displayed once he finishes the exercise. This information is recorded in a database so the user can keep track of his improvement. The performance of the user can be supervised by an instructor, looking at the records of the exercises the trainee have done and suggesting to repeat an exercise (if necessary), increasing its complexity or trying a new exercise.
In the following sections we briefly describe the design of the hardware component and the training exercises we incorporated in LAPAROS, and how the performance of the trainee during the training sessions is measured.
4 THE MECHANICAL SIMULATOR
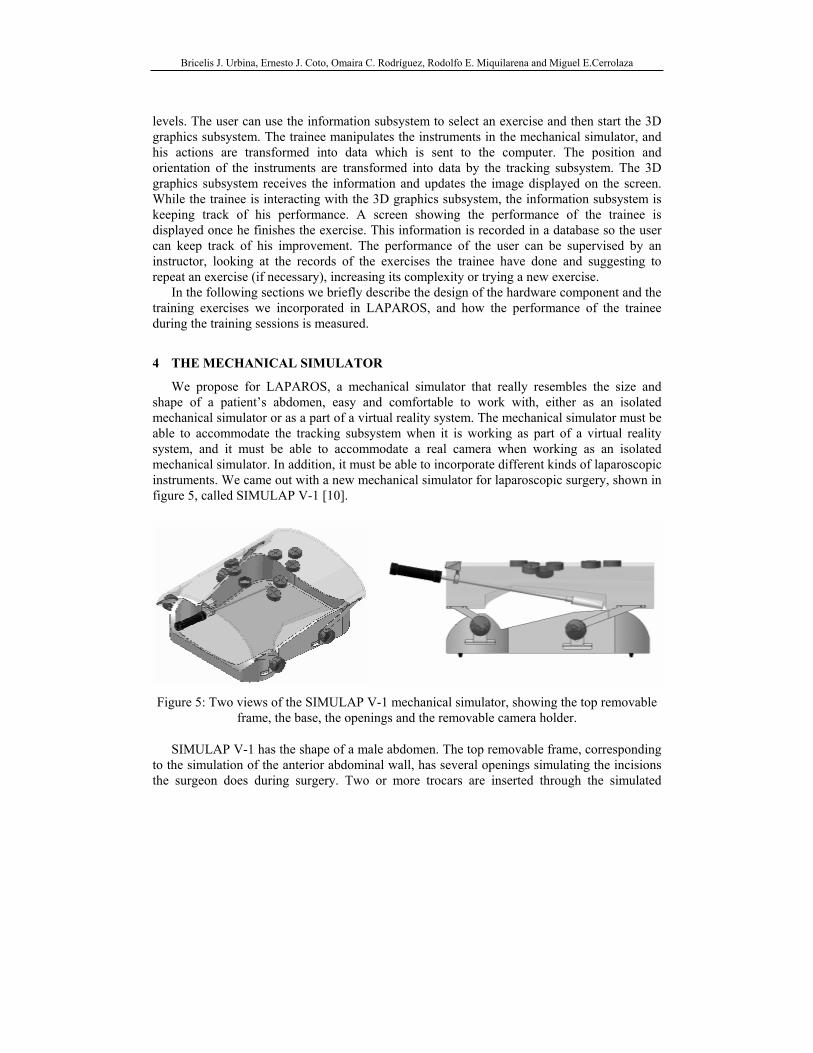
We propose for LAPAROS, a mechanical simulator that really resembles the size and shape of a patient’s abdomen, easy and comfortable to work with, either as an isolated mechanical simulator or as a part of a virtual reality system. The mechanical simulator must be able to accommodate the tracking subsystem when it is working as part of a virtual reality system, and it must be able to accommodate a real camera when working as an isolated mechanical simulator. In addition, it must be able to incorporate different kinds of laparoscopic instruments. We came out with a new mechanical simulator for laparoscopic surgery, shown in figure 5, called SIMULAP V-1 [10].
Figure 5: Two views of the SIMULAP V-1 mechanical simulator, showing the top removable frame, the base, the openings and the removable camera holder.
SIMULAP V-1 has the shape of a male abdomen. The top removable frame, corresponding to the simulation of the anterior abdominal wall, has several openings simulating the incisions the surgeon does during surgery. Two or more trocars are inserted through the simulated
Bricelis J. Urbina, Ernesto J. Coto, Omaira C. Rodríguez, Rodolfo E. Miquilarena and Miguel E.Cerrolaza
abdominal wall and instruments are introduced through them to conduct operative manipulations. The openings have special rubber gums that simulate the resistance of the tissue to the insertion of the instruments. The frame and the rubber gums provide enough resistance to make the trocars function similar as in a real body. The inclination of the frame can be easily changed through small knobs at the support of the frame, in order to simulate that the patient is lying on an inclined surgery table.
When used as an isolated mechanical simulator, a camera or a standard laparoscope can be easily accommodated. The scope is connected to a light source and camera monitor system as it would be in the operating room. Alternatively, the video monitor may be attached to a camcorder or a VCR to record exercise manipulations for review and analysis. When used as part of a virtual reality system, the simulated abdominal cavity is big enough to accommodate the tracking subsystem.
The top frame is made of acrylic, the base is made of glass fiber and the supports are made of aluminum. All materials have a low cost, are easily cleaned and maintained and have a low weight. All these features make of SIMULAP V-1 an excellent mechanical simulator that can also be used as part of a virtual reality system like LAPAROS.
5 TRAINING SESSIONS
Training sessions for medical students in laparoscopy surgery conducted at the Experimental Surgery Institute (UCV), were systematically observed and analyzed by our developing team. This experience allowed us to identified three training levels: basic, intermediate and advanced. All of them are designed to teach special abilities such as handling the camera, manipulation of instruments in a 3D space guided by a 2D image, coordination of both hands, basic navigation in a 3D space and special surgical skills. Each level associated with a set of exercises is designed to develop these specific abilities. Table 1 summarizes the abilities associated with each level.
Basic Intermediate Advanced
o Spatial orientation and perception. o Hand-eye coordination including
dominant and non-dominant hand. o Hand-inverse eye coordination.
o Camera navigation o Instruments handling o Grasping o Cutting
o Dissecting o Suturing
Table 1. Summary of abilities associated with each exercise level
Some exercises are developed using deformable models [16, 17] to simulate the deformation produced on a tissue by a specific action. Collision detection is used to provide a realistic visual feedback when, for instance, a virtual instrument touches an object simulating an organ. Surface models of the liver and gallbladder are generated by a fast segmentation procedure [18] from the visible male dataset [19]. In this work only the basic and intermediate levels were considered; the advanced level will be reported in a future work.
The system is designed in such a way that the instructor can make a combination of
Bricelis J. Urbina, Ernesto J. Coto, Omaira C. Rodríguez, Rodolfo E. Miquilarena and Miguel E.Cerrolaza
exercises from any of the three levels according to the expertise of the student. However, this training tool is a system that can be used either in the presence of the instructor or without it, since an advanced student will focus on improving the performance reported by the system.
An important aspect to consider in any training tool is the capability of evaluation. The main metrics used in our surgery training system are time performance and precision. The exercises proposed in our virtual environment have their own metric and their complexity can be increased. Other works have also proposed metrics to measure user’s skills [11, 12, 13].
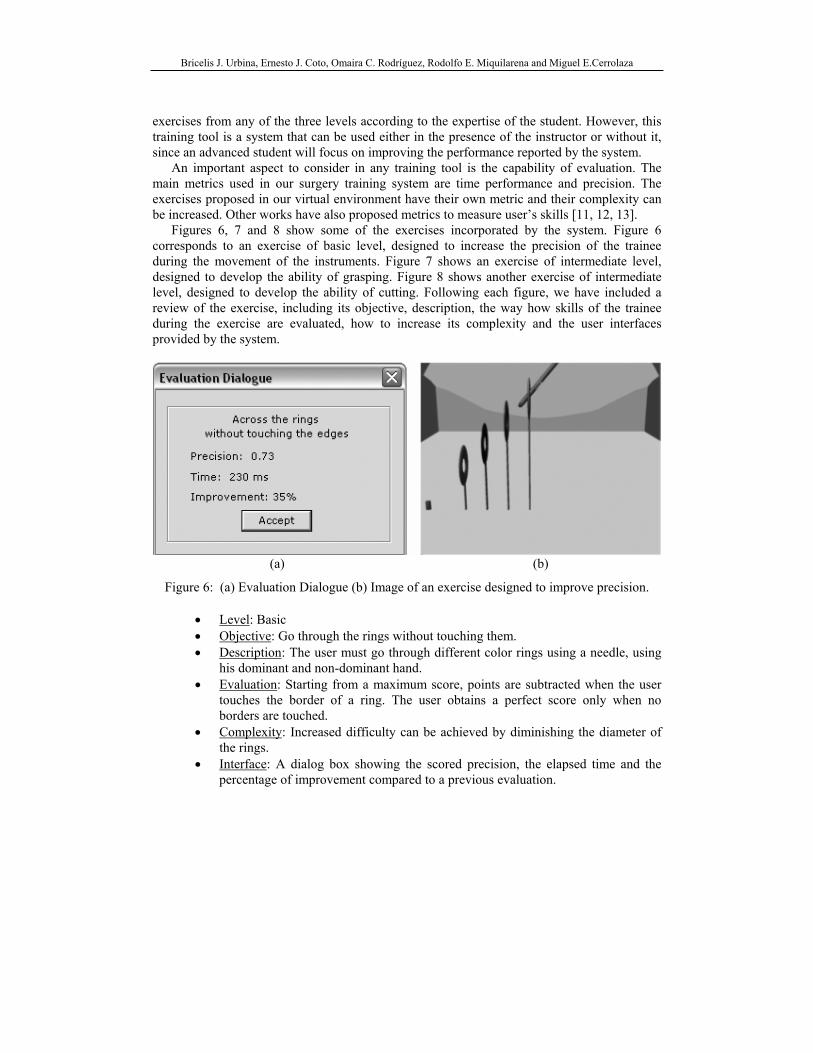
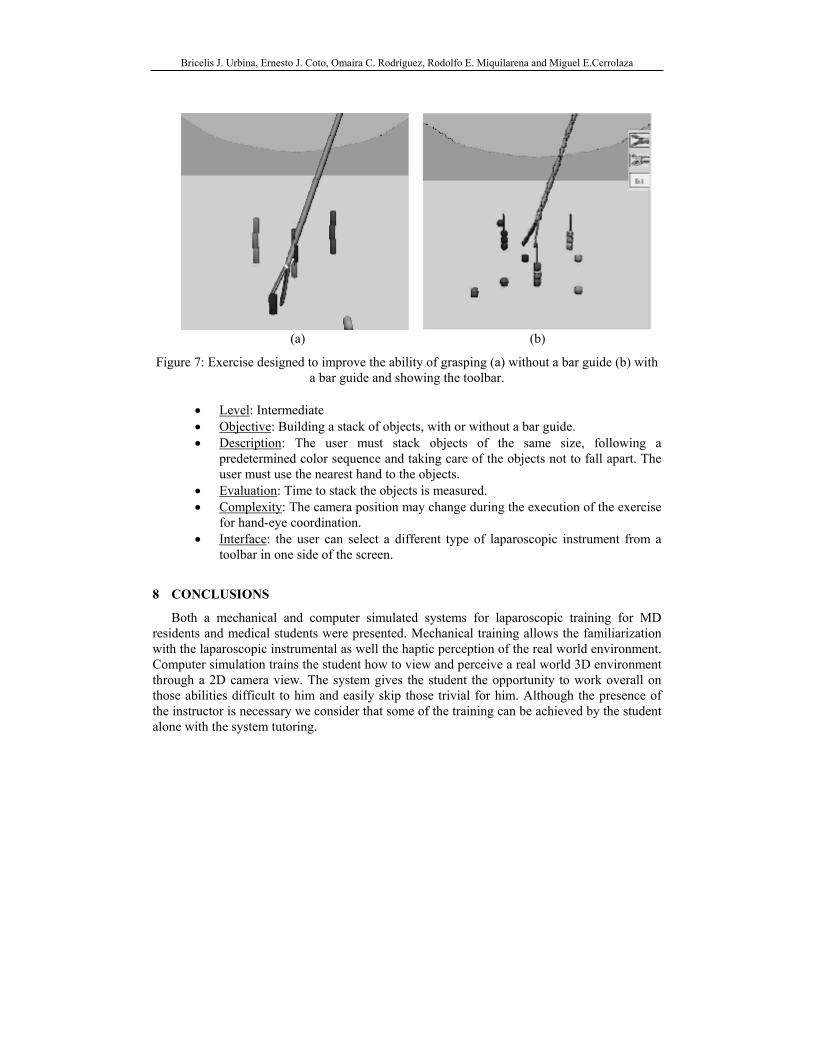
Figures 6, 7 and 8 show some of the exercises incorporated by the system. Figure 6 corresponds to an exercise of basic level, designed to increase the precision of the trainee during the movement of the instruments. Figure 7 shows an exercise of intermediate level, designed to develop the ability of grasping. Figure 8 shows another exercise of intermediate level, designed to develop the ability of cutting. Following each figure, we have included a review of the exercise, including its objective, description, the way how skills of the trainee during the exercise are evaluated, how to increase its complexity and the user interfaces provided by the system.
(a) (b)
Figure 6: (a) Evaluation Dialogue (b) Image of an exercise designed to improve precision.
• Level: Basic • Objective: Go through the rings without touching them. • Description: The user must go through different color rings using a needle, using
his dominant and non-dominant hand. • Evaluation: Starting from a maximum score, points are subtracted when the user
touches the border of a ring. The user obtains a perfect score only when no borders are touched.
• Complexity: Increased difficulty can be achieved by diminishing the diameter of the rings.
• Interface: A dialog box showing the scored precision, the elapsed time and the percentage of improvement compared to a previous evaluation.
Bricelis J. Urbina, Ernesto J. Coto, Omaira C. Rodríguez, Rodolfo E. Miquilarena and Miguel E.Cerrolaza
(a) (b)
Figure 7: Exercise designed to improve the ability of grasping (a) without a bar guide (b) with a bar guide and showing the toolbar.
• Level: Intermediate • Objective: Building a stack of objects, with or without a bar guide. • Description: The user must stack objects of the same size, following a
predetermined color sequence and taking care of the objects not to fall apart. The user must use the nearest hand to the objects.
• Evaluation: Time to stack the objects is measured. • Complexity: The camera position may change during the execution of the exercise
for hand-eye coordination. • Interface: the user can select a different type of laparoscopic instrument from a
toolbar in one side of the screen.
8 CONCLUSIONS
Both a mechanical and computer simulated systems for laparoscopic training for MD residents and medical students were presented. Mechanical training allows the familiarization with the laparoscopic instrumental as well the haptic perception of the real world environment. Computer simulation trains the student how to view and perceive a real world 3D environment through a 2D camera view. The system gives the student the opportunity to work overall on those abilities difficult to him and easily skip those trivial for him. Although the presence of the instructor is necessary we consider that some of the training can be achieved by the student alone with the system tutoring.
Bricelis J. Urbina, Ernesto J. Coto, Omaira C. Rodríguez, Rodolfo E. Miquilarena and Miguel E.Cerrolaza
9 ACKNOLEDGEMENTS
The work presented in this publication has been funded by the LAPAROS project, supported by the CDCH (Consejo de Desarrollo Científico y Humanístico) under the number PTP-08.12.5294.2004. We would like to thank our students Marvi Martinez and José Manuel Motezuma, for their invaluable contribution in the development of the 3D graphics subsystem.
REFERENCES
[1] L.W. Way, S. Bhoyrul, and T. Mori, Fundamentals of Laparoscopic Surgery, Churchill Livingstone, 1995.
[2] F. Tendick, R. Jennings, G. Tharp, and L. Stark, Sensing and manipulation problems in endoscopic surgery: Experiment, analysis and observation, Presence, 2(1), pp. 66-81, 1993.
[3] F. Tendick, S. Bhoyrul, and L. Way, Comparison of laparoscopic imaging systems and conditions using a knot tying task, Computer Aided Surgery, 2(1), 1997.
[4] A. Liu, F. Tendick, K. Cleary and C. Kaufmann, A Survey of Surgical Simulation: Applications, Technology, and Education, J. Presence, 12(6), pp. 599-614, 2003.
[5] R.S. Haluck, R.W. Webster, A.J. Snyder, M.G. Melkonian, B.J. Mohler, M.L. Dise and A. Lefever, A Virtual Reality Surgical Trainer for Navigation in Laparoscopic Surgery, Proc. of Medicine Meets Virtual Reality IX (MMVR’01), pp. 171-177, Newport Beach, CA, 2001.
[6] F. Tendick, M. Downes, T. Goktekin, M.C. Cavusoglu, D. Feygin, X. Wu, R. Eyal, M. Hegarty and L.W. Way, A Virtual Environment Testbed for Training Laparoscopic Surgical Skills, J. Presence, 9(3), pp. 236-255, 2000.
[7] M. Downes, M.C. Cavusoglu, W. Gantert, L.W. Way and F. Tendick, Virtual Environments for Training Critical Skills in Laparoscopic Surgery, Proc. of Medicine Meets Virtual Reality VI (MMVR'98), pp. 316-322, San Diego, CA, 1998.
[8] J.A. Jordan, A.G. Gallagher, J. McGuigan and N. McClure, Virtual reality training leads to faster adaptation to the novel psychomotor restrictions encountered by laparoscopic surgeons, Surgical Endoscopy 2001, 15(10), pp. 1080-1084, 2001.
[9] G.L. Adrales, U.B. Chu, D.B. Witzke, M.B. Donnelly, D. Hoskins, M.J. Mastrangelo, Jr., A. Gandsas and A.E. Park, Evaluating minimally invasive surgery training using low-cost mechanical simulations, Surgical Endoscopy 2003, 17(4), pp. 580-585, 2003.
[10] A. Zambrano and A. Piñango, Design and Manufacturing of a Laparoscopic Surgery Mechanical Simulator (in Spanish), Central University of Venezuela, Caracas, 2003.
Bricelis J. Urbina, Ernesto J. Coto, Omaira C. Rodríguez, Rodolfo E. Miquilarena and Miguel E.Cerrolaza
[11] F. Tendick and M.C. Cavusoglu, Human-Machine Interfaces for Minimally Invasive Surgery, Proc. of the 19th Annual International Conference of the IEEE Engineering in Medicine and Biology Society, pp. 2771-2776, Chicago, IL, 1997.
[12] S. Payandeh, A.J. Lomax, J. Dill, C.L. Mackenzie and C.G.L. Cao, On Defining Metrics for Assessing Laparoscopic Surgical Skills in a Virtual Training Environment, Proc. of Medicine Meets Virtual Reality X (MMVR’02), Newport Beach, CA, pp. 334-340, 2002.
[13] F. Tendick, M. Downes, M.C. Cavusoglu, W. Gantert, and L.W. Way, Development of Virtual Environments for Training Skills and Reducing Errors in Laparoscopic Surgery, Proc. of the SPIE International Symposium on Biological Optics (BIOS'98), San Jose, CA, pp. 36-44, 1998.
[14] R. Eyal and F. Tendick, Spatial Ability and Learning the Use of an Angled Laparoscope in a Virtual Environment, Proc. of Medicine Meets Virtual Reality IX (MMVR’01), Newport Beach, CA, pp. 146-152, 2001.
[15] U. Kühnapfel, H.K. Cakmak, H. Maaβ, Endoscopic surgery training using virtual reality and deformable tissue simulation, J. Computer & Graphics, 24(5), pp. 671-682, 2000.
[16] J.P. Gourret, N.M. Thalmann and D. Thalman, Simulation of objects and human skin deformation in a grasping task, Proc. of ACM SIGGRAPH’89, 23(3), pp. 21-31, Boston, Mass., 1989.
[17] M. Teschner, B. Heidelberger, M. Mueller, M. Gross, A versatile and robust model for geometrically complex deformable solids, Proc. of Computer Graphics International CGI’04, pp. 312-319, Crete, Greece, 2004.
[18] E. Coto and O. Rodríguez, T-Snakes and the Delaunay Triangulation for generation of anatomical structure meshes suitable for the Finite Element Method (In Spanish), Proc. of CIMENICS’04, pp. TC 11-18, 2004.
[19] M.J. Ackerman, The Visible Human Project, Proc. of the IEEE, 86(3), pp. 504-511, 1998.