kink health project: stigma, coming out and healthcare access
TRANSCRIPT

Two community-based research organizations in the leather/BDSM/kink communities:
CARAS TASHRA

www.tashra.org

https://carasresearch.org

Our outline Kink Health Project outline Preliminary Results on Access Preliminary Results on Stigma Preliminary Results on Coming Out to
Healthcare Providers
What are Alternative Sexualities?
Alternative sexualities A diverse group of sexual practices,
expressions, and identities that fall outside of the sexual mainstream
Generally includes various types of “kinky” sex, BDSM, and sexual fetishism
Covers consensual non-monogamy, sexual orientation and gender identity as they intersect with alternative sexuality practices.
What is BDSM? BDSM is a compound acronym,
standing for: Bondage and Discipline (B/D) Dominance and Submission (D/s) Sadism and Masochism (S/M)
“It serves as an umbrella label for forms of sexuality which incorporate restraint, pressure, intense sensation, and elements of power exchange between the engaged parties.” (Ortmann & Sprott, 2012)
Common Types of BDSM Play Impact/Sensation/Pain Play – e.g. Spanking, flogging, whipping, caning, touch, tickling, hot/cold.
Bondage/Restraint – Restraining, restricting, or tying a person up.
Psychological/Role-play – Intense mental/emotional stimulation, eroticized roles, rituals, rule compliance.
Edge Play – Denotes greater risk, higher intensity, or considered more transgressive than common play.

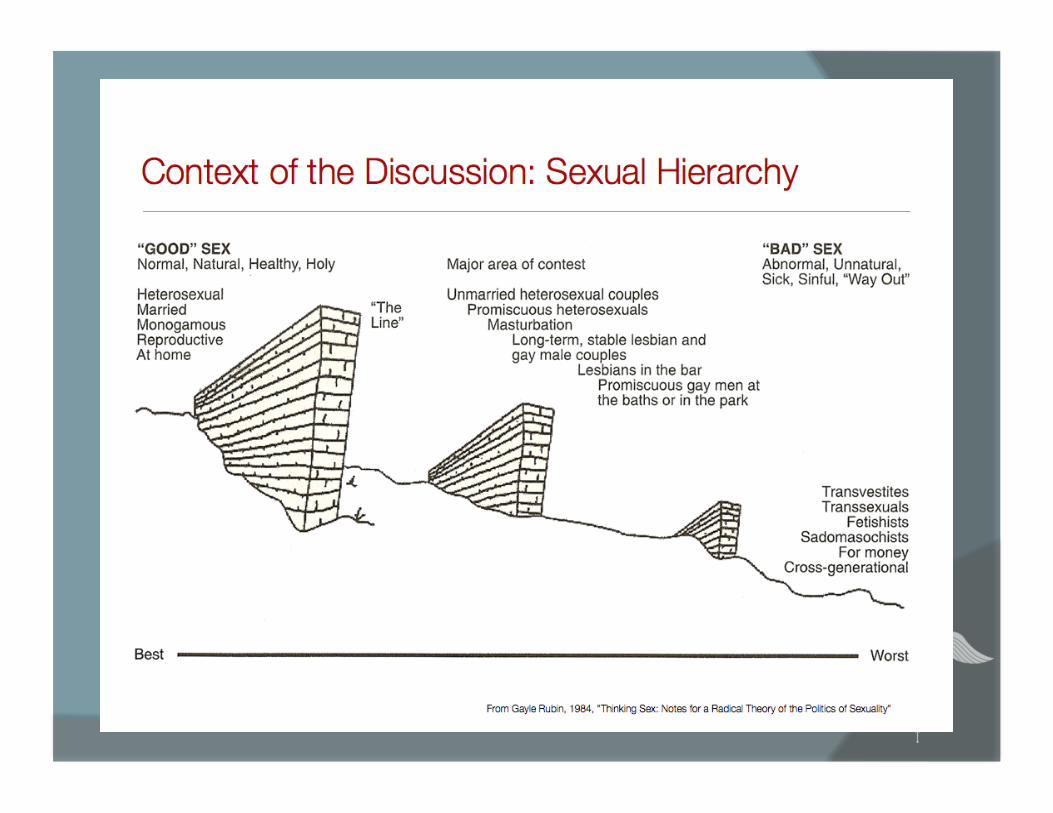
The context for the discussion
Stigma and Stereotype Alternative sexualities are anti-social
BDSM is violence BDSM is abuse Poly / swinging is hedonistic Poly / swinging is narcissistic
Alternative sexualities are mental disorders These people are alone, isolated These people cannot function at higher levels of
psychological maturity Alternative sexualities are easy to spot
So, how many people are kinky?
Kink is not that uncommon: 10-15% of the U.S. population engages
in non-traditional sexual practices. 1-2% self-disclose and self-identify as
“kinky”
BDSM Prevalence • 14% of men & 11% of women in US have had experience with SM (national sample, n = 2,742) (Janus & Janus, 1993).
• From Durex’s 2005 online survey of 317,000 people: • 10% of Americans have experienced sadomasochism. • 5% worldwide have experienced SM.
• Australia: 2% of sexually active men, 1.4% of women engaged in BDSM in the past year (Richters et al., 2008).
Demographic Trends • May be more prevalent in LGBT populations. • Participants often report higher education & income. • More likely to have broader sexual experience/repertoire.
Are they mentally ill?
Selected Research • From Australian nationally representative sample:
• BDSM engagement not significantly related to any sexual difficulties or higher psychological distress. Men had sig. lower psych. distress.
(Richters et al., 2008)
• Recent comparison of Dutch BDSM participants (n=902) to controls (n=434). BDSM participants:
• Big 5: Less neurotic, more extraverted, more open to new experiences, more conscientious, less agreeable.
• Had either similar or better attachment scores than controls. • Less sensitive to rejection. Higher subjective well-being.
(Wismeijer & van Assen, 2013)
• Study of 186 (n=164 male) Finnish BDSM particip.: • Distribution of attachment styles nearly identical to general pop.
(Sandnabba et al., 2002)
Research on Psych • Study of n=132 American BDSM practitioners:
• Sample appeared comparable to published norms on tests of clinical psychopathology & severe personality pathology.
• No widespread elevations on measures of: Depression, anxiety, obsession-compulsion, psych. sadism, psych. Masochism, or PTSD. Did show slightly higher narcissism.
(Connolly, 2006)
• Comparison of n=93 BDSM practitioners to n=61 controls: • No significant difference in measures of sexual guilt, escapism. • Masochists no more prone to mental distress than other groups. • BDSM group scored equal or lower than controls on Authoritarianism. • BDSM group endorsed more pro-feminist beliefs.
(Cross & Matheson, 2006)
BDSM & Childhood Sexual Abuse • Childhood sexual abuse widely assumed to be an etiological factor for BDSM interest.
• One study did find higher prevalence of abuse in sample of 186 (n = 164 male, n = 22 female) Finnish BDSM participants.
• 7.9% males, 22.7% female. (Nordling, Sandnabba, & Santtila, 2000)
• However: Study of Australian nationally representative sample found no correlation between sexual abuse/ coercion (ever or before age 16) and BDSM participation.
(Richters et al., 2008)
• Replicated findings of attachment equivalence & lack of widespread psychopathology also seem to contradict the abuse etiology hypothesis.
How dangerous is this?
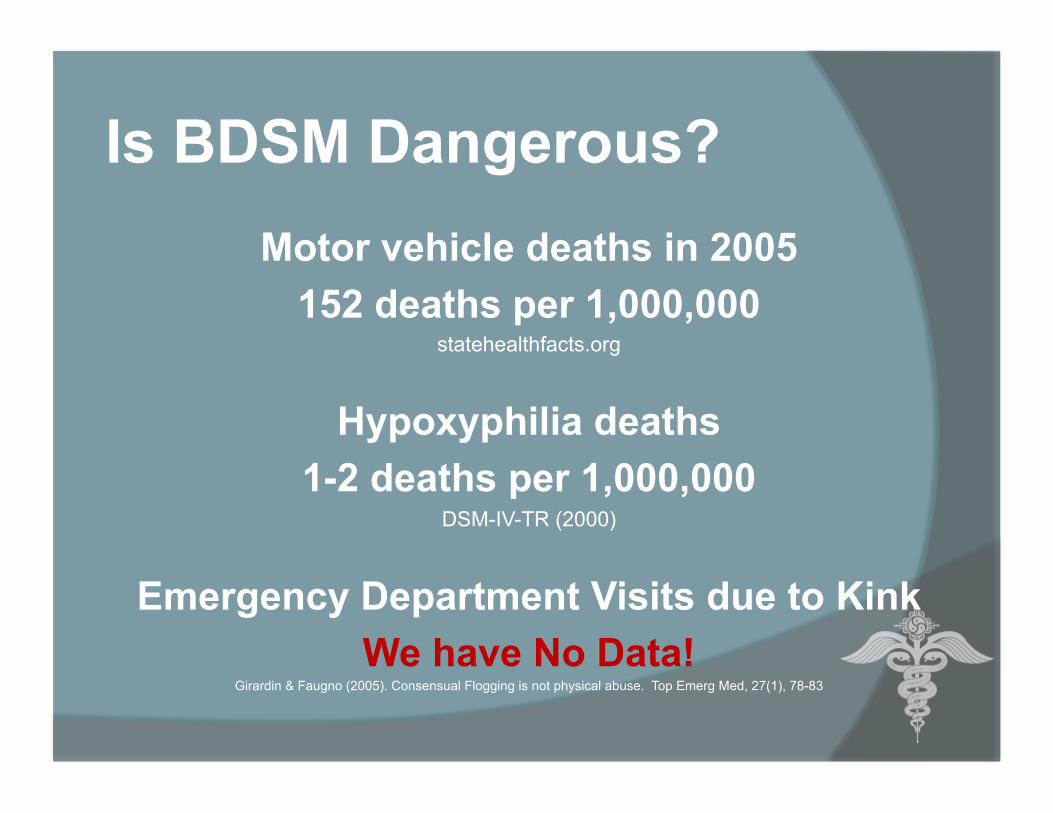
Is BDSM Dangerous? Motor vehicle deaths in 2005
152 deaths per 1,000,000 statehealthfacts.org
Hypoxyphilia deaths 1-2 deaths per 1,000,000
DSM-IV-TR (2000)
Emergency Department Visits due to Kink We have No Data!
Girardin & Faugno (2005). Consensual Flogging is not physical abuse. Top Emerg Med, 27(1), 78-83
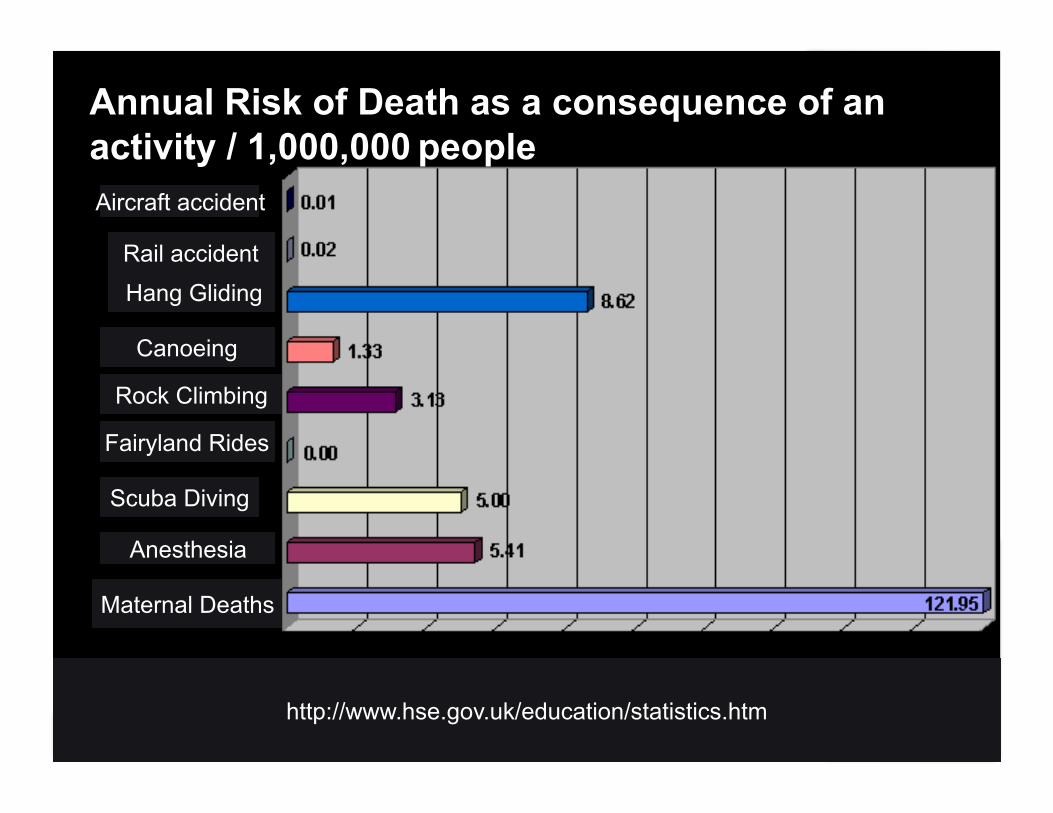
Annual Risk of Death as a consequence of an activity / 1,000,000 people Aircraft accident
Rail accident
Hang Gliding
Canoeing
Rock Climbing
Fairyland Rides
Scuba Diving
Anesthesia
Maternal Deaths
http://www.hse.gov.uk/education/statistics.htm
Healthcare Needs: preliminary results
Our Research Questions People involved in kink may have special
healthcare concerns: Increased risk of STIs or HIV/AIDS? Unusual injuries? Particular mental/sexual healthcare needs?
Kinky people may not reveal their sexual practices to their healthcare providers.
Some avoid accessing healthcare altogether for fear of being ridiculed, pathologized, or criminalized.
Background Healthcare providers receive virtually
no training in the care of patients involved in kink.
There is almost no medical literature describing the population or its needs.
Even a sympathetic clinician may have difficulty providing appropriate care to a patient who risks disclosure.
Need There is an urgent need to: 1. Describe the mental and physical health
needs of patients who engage in non-traditional sexual practices
2. Shed light on issues of access to healthcare specific to the population (including under-use of available services, or inability to obtain necessary care once engaged in the healthcare system)
3. Characterize barriers and facilitators to establishment of effective health partnerships between patients and their providers.
Preliminary Data
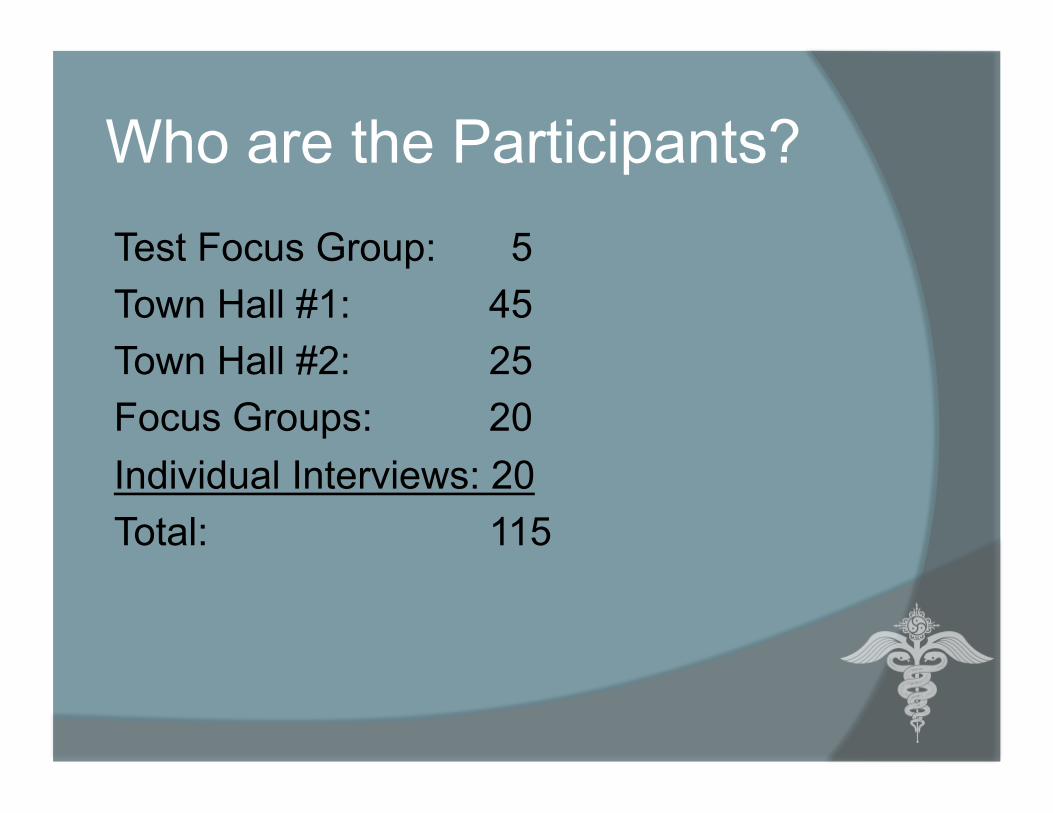
Who are the Participants? Test Focus Group: 5 Town Hall #1: 45 Town Hall #2: 25 Focus Groups: 20 Individual Interviews: 20 Total: 115
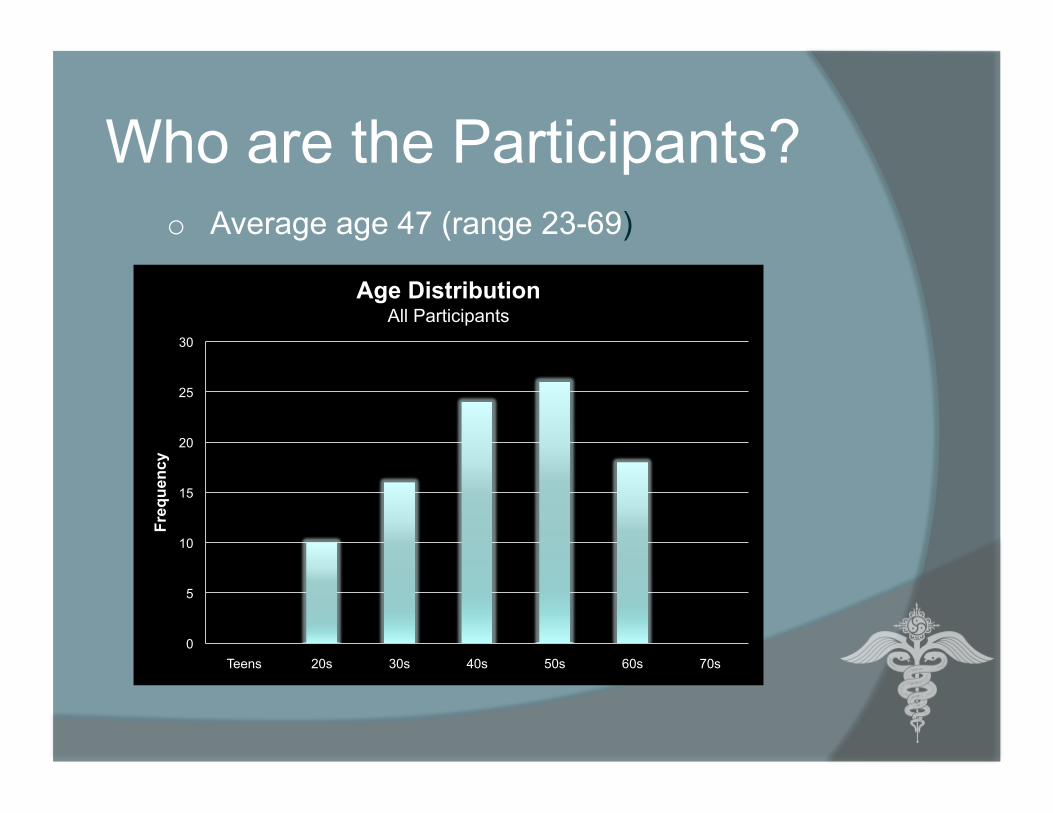
Who are the Participants? o Average age 47 (range 23-69)
0
5
10
15
20
25
30
Teens 20s 30s 40s 50s 60s 70s
Freq
uenc
y
Age Distribution All Participants
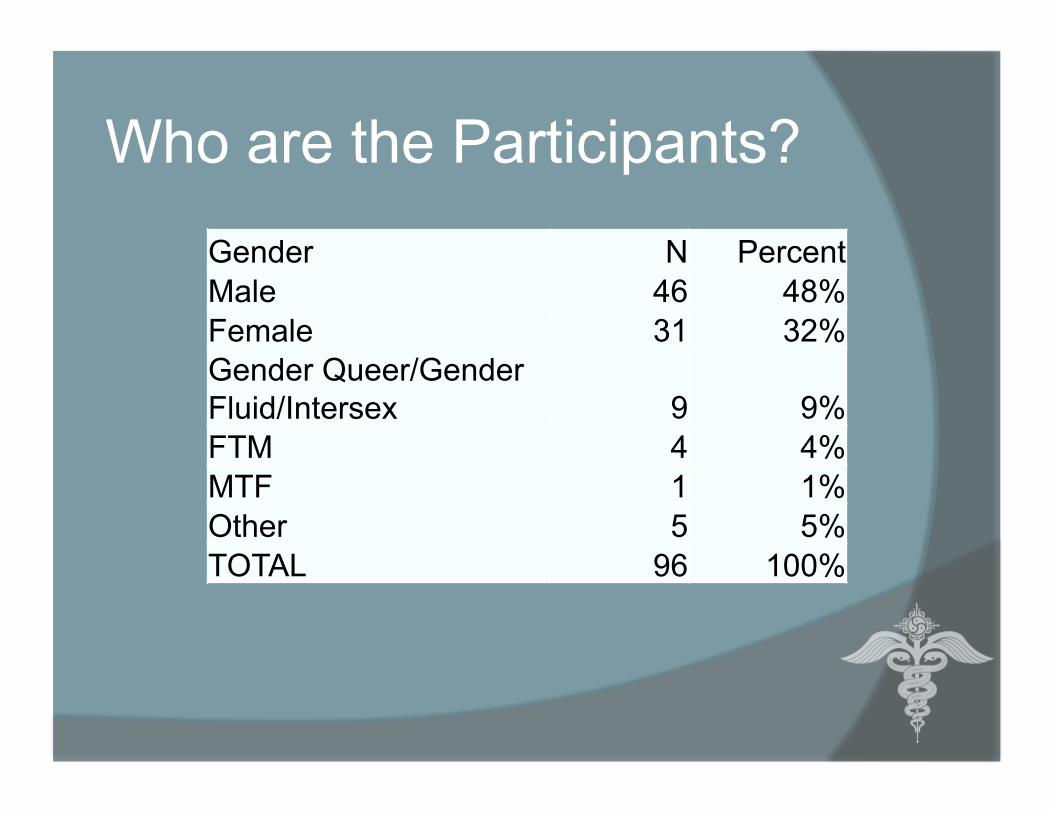
Who are the Participants? Gender N Percent Male 46 48% Female 31 32% Gender Queer/Gender Fluid/Intersex 9 9% FTM 4 4% MTF 1 1% Other 5 5% TOTAL 96 100%
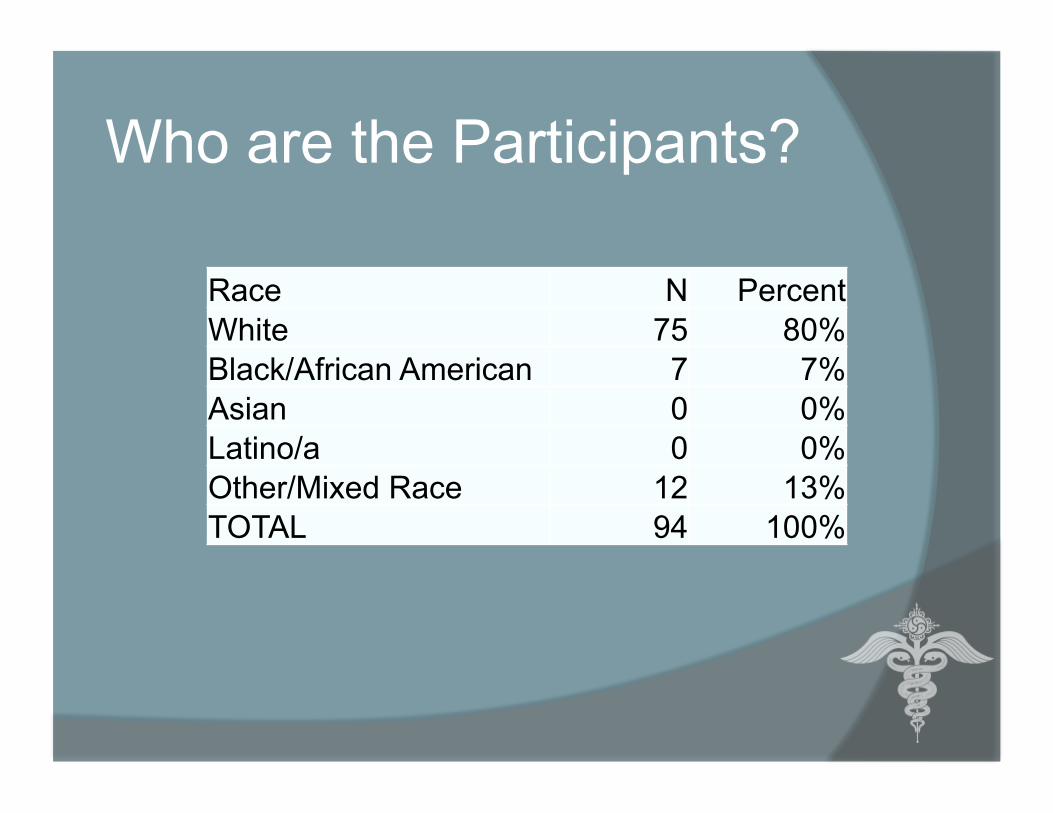
Who are the Participants?
Race N Percent White 75 80% Black/African American 7 7% Asian 0 0% Latino/a 0 0% Other/Mixed Race 12 13% TOTAL 94 100%
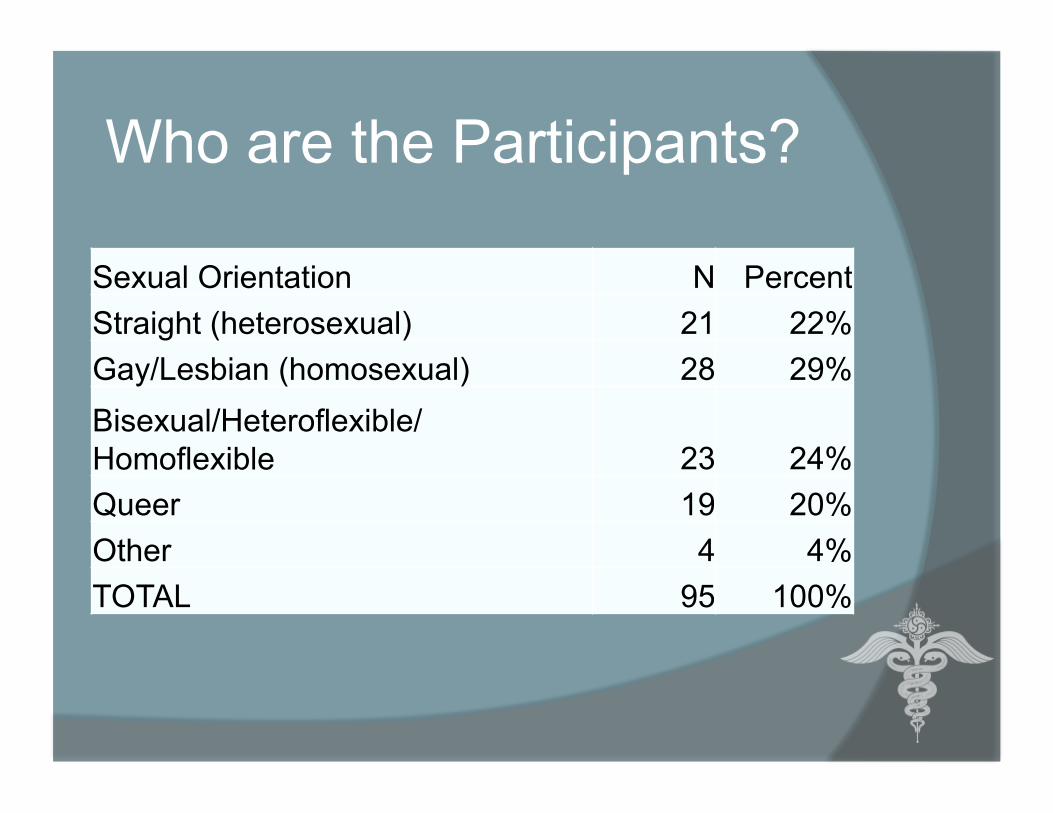
Who are the Participants?
Sexual Orientation N Percent Straight (heterosexual) 21 22% Gay/Lesbian (homosexual) 28 29% Bisexual/Heteroflexible/Homoflexible 23 24% Queer 19 20% Other 4 4% TOTAL 95 100%
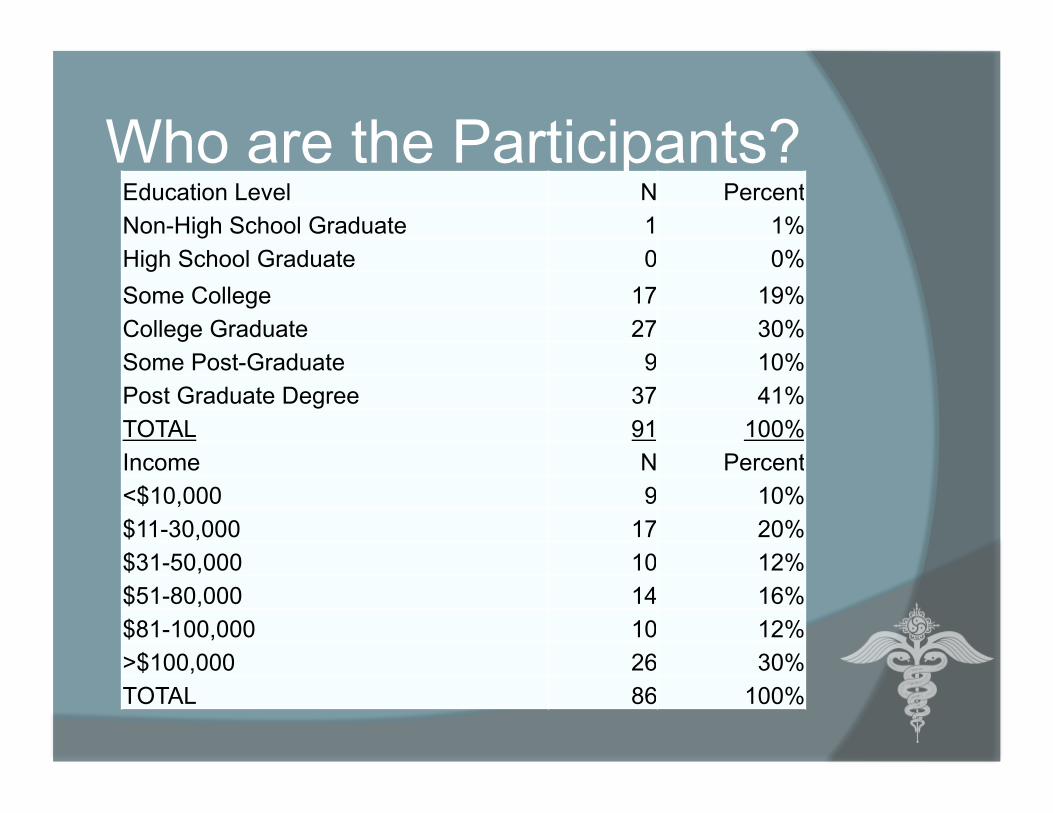
Who are the Participants? Education Level N Percent Non-High School Graduate 1 1% High School Graduate 0 0% Some College 17 19% College Graduate 27 30% Some Post-Graduate 9 10% Post Graduate Degree 37 41% TOTAL 91 100% Income N Percent <$10,000 9 10% $11-30,000 17 20% $31-50,000 10 12% $51-80,000 14 16% $81-100,000 10 12% >$100,000 26 30% TOTAL 86 100%
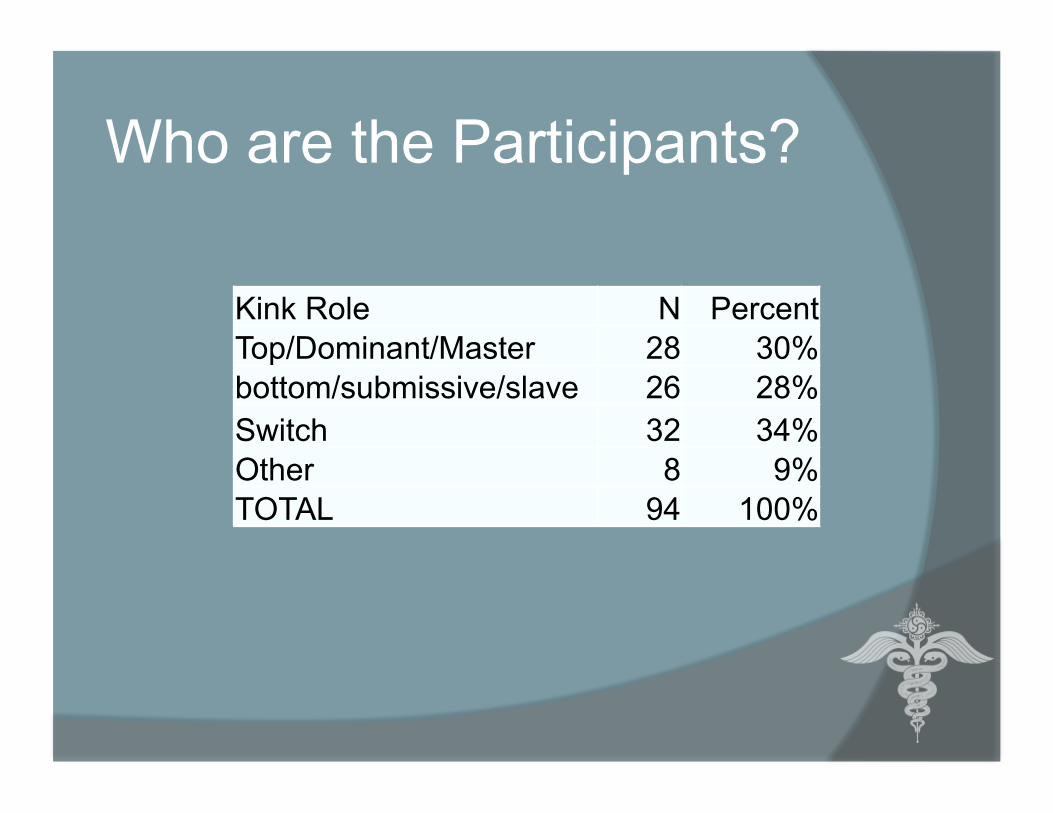
Who are the Participants?
Kink Role N Percent Top/Dominant/Master 28 30% bottom/submissive/slave 26 28% Switch 32 34% Other 8 9% TOTAL 94 100%
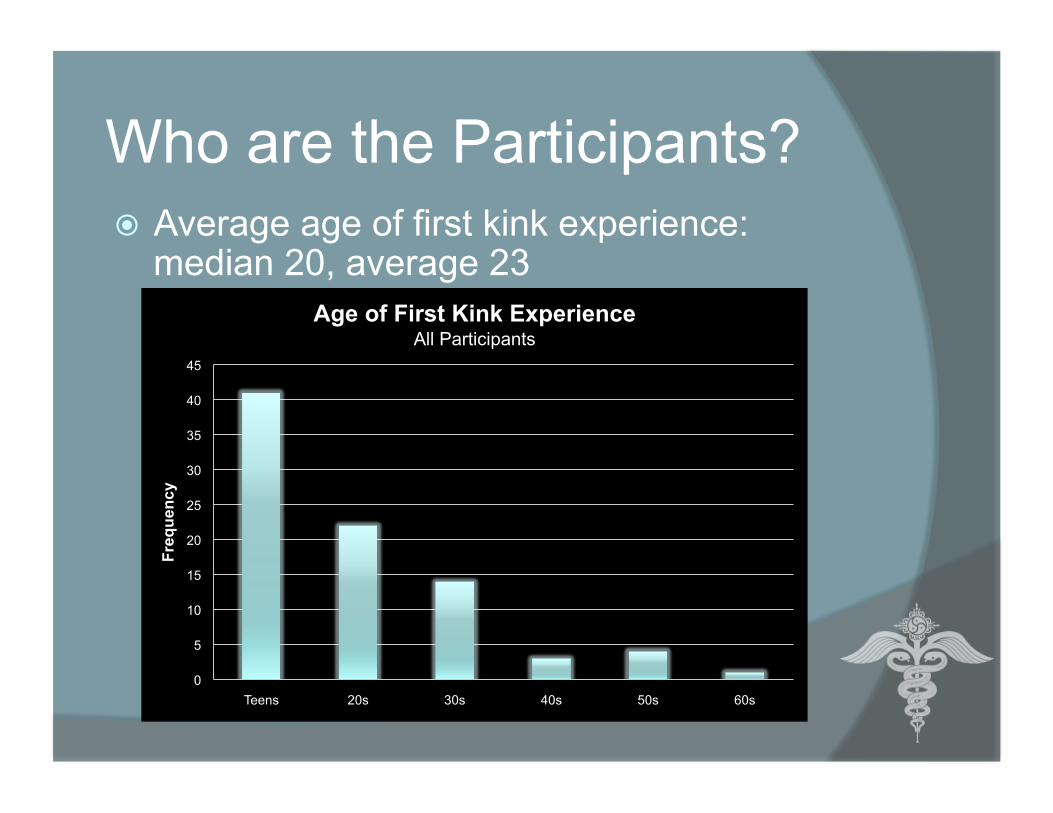
Who are the Participants? Average age of first kink experience:
median 20, average 23
0
5
10
15
20
25
30
35
40
45
Teens 20s 30s 40s 50s 60s
Freq
uenc
y
Age of First Kink Experience All Participants
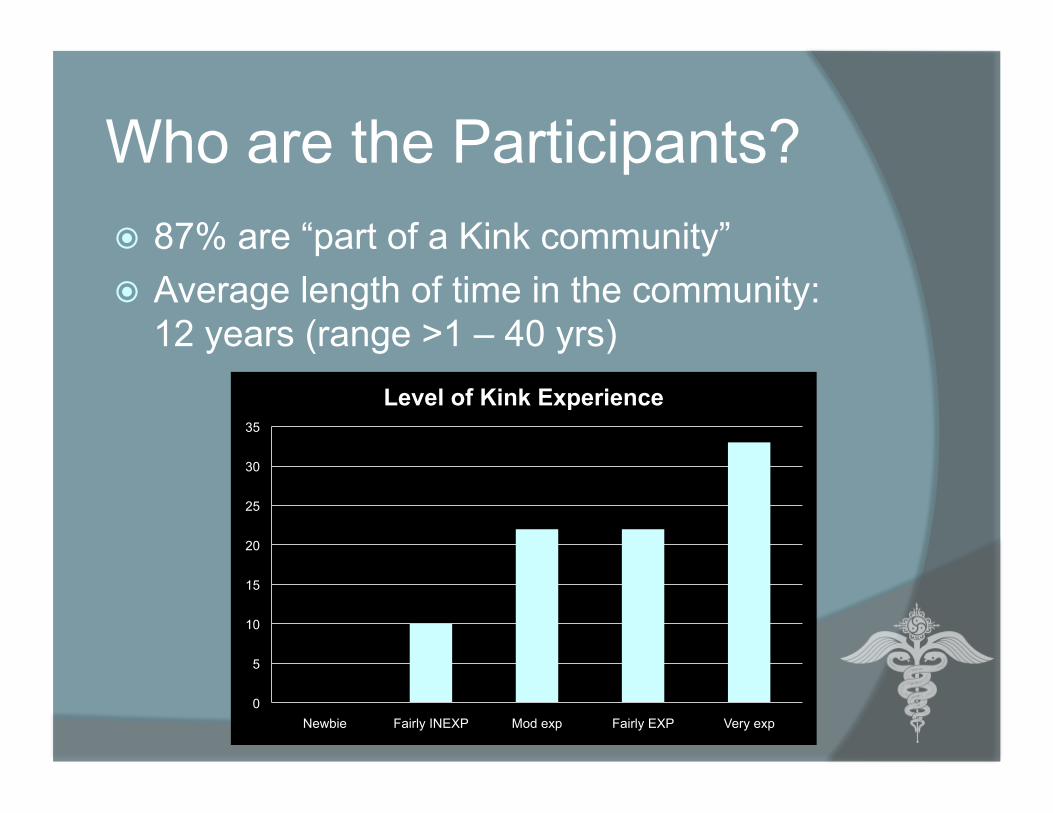
Who are the Participants? 87% are “part of a Kink community” Average length of time in the community:
12 years (range >1 – 40 yrs)
0
5
10
15
20
25
30
35
Newbie Fairly INEXP Mod exp Fairly EXP Very exp
Level of Kink Experience

Accessing Healthcare
Being Kinky in Healthcare
The “gerbil” poll: 496 participants from the town halls and Dore Alley street
fair 2013 and 2014 and Folsom Fair 2013
83% have a primary care clinician 48% have a therapist
Of those… 43% are “out” to their primary care provider 75% are “out” to their therapist
Being Kinky in Healthcare 43% have seen a medical care provider
for a kink-related concern 42% have seen a mental health provider
for a kink-related concern 63% have seen either a medical and/or
a mental health provider

Results from Interviews On access and coming out and stigma
Themes in interviews Trouble Accessing Relevant Health Information
People have disappointing experiences when they hope that their health providers will be able to inform them of risks, harm reduction strategies or even just respond non-judgmentally.
People who have ties to the “community” often use their connections as “ad hoc” resources (ask their kink friends for health, mental health or injury advice)
Going to the community for help can also create barriers, due to the lack of anonymity or agreed to confidentiality with disclosure (gossip, slander, ill advice, personal bias/slant)
Example Posted on a kink-related forum: Question about lube used for fisting – is it possible to have heart problems or heart disease, cholesterol, from using Crisco – went to community to ask, not a doctor
Themes in interviews Special Concerns around STI testing and care
STI testing for “married” folks is often questioned. Will that be different for married LGBT? Is there a bias
there as well? (will it reinforce a negative stereotype: Married gay men are all sleeping around?)
Lack of knowledge of which vaccinations are good practice for kink/poly folks. Does the Dr. even know?
Differences in what constitutes an STI panel for men and women who request “full panels.”
Themes in interviews Coming Out Issues Many people make up stories about their
injuries to not reveal the real etiology of how they came to have them.
High profile jobs or jobs that have to do with children create additional worries about coming out and asking for help.
Being kinky plus rearing children also may raise concerns (may also be additionally compounded for LGBT folks)
Reasons for Coming Out to your doctor
Safety questions, STI testing, want to get needs met Worries about germs, exposure in public
dungeons; harm reduction strategies for risky behaviors
Being asked by provider about sexuality Wanting to de-stigmatize kink Important value to be open/honest about
self identity
Reasons for NOT Coming Out to your doctor “Nothing Will Go Wrong”, denial by kinksters, Belief that Kink is not connected to health Depersonalization through labelings, assumptions
and stigma Lack of Cultural Humility/Judgement/Micro-aggressions Lack of professionalism (confidentiality)/lack of trust/
arrogance DV/abuse/BDSM conflation (stigma, enforcer role) Social consequences of breach of confidentiality
(fear of lack of confidentiality) Not wanting to educate providers (minority stress)
Reasons for Coming Out to your therapist
Having kink-related questions Wanting validation, help accepting sexuality Wanting to know why they are kinky Kink activities “interfering”
Inherent Conducive Environment Value being open/honest about self
identity
Reasons for NOT coming out to your therapist Fear of Pathologizing - misdiagnosis “Nothing Will Go Wrong”/Denial by kinkster/Kink not
connected to health Depersonalization through labelings/assumptions
and stigma Lack of Cultural Humility/judgement/Micro-aggressions Lack of professionalism (confidentiality)/lack of trust/
arrogance DV/abuse/BDSM conflation (stigma, enforcer role) Social consequences of breach of confidentiality Not wanting to educate providers (minority stress)
What are the challenges with speaking to your health care provider about your sexual activities?
Negative Judgment /assumptions What do they actually need to know? Mandated reporting Lack of Health literacy in the community Lack of “trauma-informed” care
Stigma when coming out Stigma and Microaggressions: “you
shouldn’t go to places like that” (abstinence message stigmatizes; generalized assumption about community spaces)
assumptions about increased abuse, DV, sexual risk-taking, STIs
assessing IPV/DV can shut down kinkster because of stereotype threat (need for cultural competency)

Most Common Concerns Educating doctors and therapists on the
client’s:
If there was a specific medical and mental healthcare clinic for kink folk, would you go and what would you use the clinic for?” “I’d like to say that you tend to get about fifteen minutes with your doctor and fifty minutes with your therapist. For the money that you pay we shouldn’t have to be the people who spend that valuable time educating. I think it’s really important to have a physical space that people can walk into knowing that they don’t have to spend their valuable time educating; that they can get to the core of what they’re there for and that they can feel safe in it. “
“Bay Area providers might be less judgmental, but we aren't sure about their level of knowledge”
What should therapists and doctors know about kink fetish/BDSM in order to provide competent care?
Know our language Understand erotic orientation Understand consent in our context Distinguish Abuse vs Consent Know community resources and leaders Know their own limits of competency Know when to refer out
What are some of the major health concerns facing your community right now? Affordability Enforcer role of provider Lack of screening and treatment Culture and diversity sensitivity Obesity Gender inequality Finding quality care
How you can help
Get the word out

Contact Us Learn more about us:
www.tashra.org
Visit us on Facebook at: www.facebook.com/TASHRA.ORG
Visit us on FetLife at: https://fetlife.com/users/2294280

Contact Us
[email protected] 415-99-STUDY
Jess Waldura: [email protected] Richard Sprott: [email protected]
Anna Randall: [email protected]
Meet TASHRA
The Alternative Sexualities Health Research Alliance TASHRA was founded in 2012 by a
group of healthcare professionals committed to improving the lives of sexual minorities through research, education, care and advocacy.
TASHRA’s Mission Our mission is to improve the
physical and mental health of people who engage in BDSM, kink and sexual fetishism.
���We are working to create a world where all kinksters have equal access to culturally competent, non-judgmental, and knowledgeable healthcare.
TASHRA’s Focus To address these issues, TASHRA has
four focus areas: RESEARCH EDUCATION HEALTHCARE SERVICES POLICY AND ADVOCACY
Research TASHRA conducts community-based
research to better understand the unique bio-psycho-social healthcare needs of the kink community
Our research will generate the evidence needed to educate healthcare providers, empower patients and enable the healthcare system to meet the needs of the kink community.
Provider Education We offer trainings and educational
materials for medical and mental healthcare providers who deliver care to patients involved in kink.
Some of the activities that TASHRA has planned:��� Medical student seminars Workshops for practicing medical and mental
health providers Educational pamphlets "Kink-Care Warmline”
Community Education We provide information to community
members on how to act as effective partners in their own healthcare.
TASHRA maintains a list of Kink-friendly medical professionals in the San Francisco Bay Area.
We link to KAP: Kink Aware Professionals ���
We produce educational pamphlets for patients and their providers: For patients: "How to talk to your doctor about being kinky” For providers: "What you need to know about taking care
of patients who are kinky”
Healthcare Services We foster the development of kink-friendly
healthcare services in the San Francisco Bay Area.
Our dream is to create a Bay Area Kinky Clinic Low cost kink-friendly healthcare in the spirit
of St. James Infirmary and Lyon Martin Clinic

Advocacy As our research identifies healthcare
system-level issues for kinksters, we will advocate for equitable treatment, and work towards relevant change in health and social policies.