journal - nigerian optometric association
TRANSCRIPT

JOURNALOF THE
ISSN: 9284-1647
Volume 20 , No 2, 2018
N I G E R I A NOPTOMETRICA S S O C I A T I O N

Volume 20 , No 2, June, 2018
JOURNALOF THE
N I G E R I A NOPTOMETRICA S S O C I A T I O N
Dr. Bernadine N. EkpenyongEditor-in-Chief
i
Dr. Bernadine Nsa EkpenyongOD, MPH, PhD, FNCODepartment of Public HealthFaculty of Allied Medical SciencesCollege of Medical SciencesUniversity of Calabar, Cross River State, Nigeria
Prof Frank Iwuagwu - ChairmanProf Faus�na Idu - MemberProf Mathew Oriowo - MemberDr Bernadine Ekpenyong - Editor-in-chiefDr Chris Timothy - MemberDr Maduabuchi E. Okorie - Secretary
Dr Damian Echendu - National PresidentDr Norris Ovili - Vice President WestDr Felix Olafisoye - Vice President NorthDr Joy Alozie - Vice President EastDr Adesuwa Agbontaen - SecretaryDr Emmanuel Nwaji - Financial SecretaryDR Ndidiamaka Amadi - TreasurerDr Raymond Aguboshim - Public Relation OfficerDr Ike Oforbuike - Assistant SecretaryDr Ikechukwu Nwakuche - Immediate Past President
Focus and Scope: This interna�onal, peer-reviewed journal is an official publica�on of the Nigerian Optometric Associa�on (NOA). It is devoted to bring together, for its specialised audi-ence, up-to-date clinical and scien�fic research informa�on and novel developments in the broad fields of Optometry and Health Sciences, providing a medium for their rapid publica�on and facilitate greater understanding among researchers. In the upcoming edi�on, in addi�on to its tradi�onal publishing protocols, the journal will feature an online publica�on on NOA website, www.noang.org. To reach a worldwide audience, the full text is published at h�p://www.ajol.info/ajol/ . Authors of successfully published works will also be presented with a Cer�ficate of Publica�on by the NOA.
Peer review process: All manuscripts will be double-blind reviewed by two or more referees to ensure accuracy and relevance. Based on the referees’ recommenda�on, manuscript may be reviewed by author(s) before final acceptance. The gallery proof of the final review will be send in PDF to the corresponding author through email for final correc�on before publica�on.
+2348033475138 +2348050544785
[email protected] [email protected] [email protected]
The Editorial Board of the above named journal herein cordially invite researchers/authors to submit original research reports, review ar�cles, case reports and short communica�ons, conference, seminar and workshop reports, etc for considera�on for publica�on in the upcoming edi�on of Journal, Volume 20, Issue Number 2, 2018. Such manuscripts must be professionally relevant and appeal to audience in the broad fields of Eye Care/Vision Sciences and Public Health; Primary Care Optometry, Public Health Optometry, Rehabilita�ve Optometry and Low Vision Care, Paediatric Optometry, Corneal and Contact Lenses, Ocular Health, Orthop�cs, Anatomy, Physiology, Epidemiology, Economics and Sociology of Vision and Blindness, Ocular Biomedics, Op�cs and Instrumenta�on, Optometric Educa�on and History, etc. Publica�on of papers in this journal requires strict compliance with specifica�ons as outlined herein.
Journal of the Nigerian Optometric Association
Editor-in-chief
Mobile
CONTACT
EDITORS
Editorial Board
POLICIES
Executive Committee
CALL FOR PAPERS
JNOA.2018;20(2) Ekpenyong B.N.
ii
a. Work contained therein MUST be original to the author (s)b. Should be submi�ed to the editor in electronic copy by email or CD forms.c. Should not exceed 16 pages/8000 wordsd. Should be legible with compact nota�ons used, and each symbol properly aligned to dis�nguish between superscripts and subscripts.
Journal of the Nigerian Optometric Association
1. Manuscript
The paper should include:a. A cover le�er accompanying the manuscript, indica�ng the significance of the study and also cer�fying that the ar�cle has not been previously published elsewhere. All Authors full names, email address and affilia�ons, including corresponding author’s telephone number will be required. The Journal will publish manuscripts wri�en in English, using A4 paper size with 1.25 inches margin on all sides. Preferred font size is 12 using Times New Romans.b. Title of paperc. Abstract (Not more than 250 words, unstructured in one paragraph and should provide brief narra�ve of the objec�ves, methods, results and conclusion of the study. For purpose of indexing, 3 to 6 keywords will be adequate)d. Introduc�one. Materials and methodsf. Results (Tables and figures should not exceed six (6). Typed using 10 points font size.)g. Discussionh. Conclusioni. Acknowledgement (where necessary, not more than 100 words)
2. Format of paper
JNOA.2018;20(2)
Author guidelines: The journal will publish original research reports, review ar�cles, case reports and short communica�ons, conference, seminar and workshop reports. Such manuscripts must be professionally relevant and appeal to audience in the broad fields of Eye Care/Vision Sciences and Public Health; Primary Care Optometry, Public Health Optometry, Rehabilita�ve Optometry and Low Vision Care, Paediatric Optometry, Corneal and Contact Lenses, Ocular Health, Orthop�cs and Vision Therapy, Anatomy, Physiology, Epidemiology, Economics and Sociology of Vision and Blindness, Ocular Biomedics, Op�cs and Instrumenta�on, Optometric Educa�on and History, etc. Publica�on of papers in this journal requires strict compliance with specifica�ons as outlined herein.
SUBMISSIONS
References- Vancouver Style [In text cita�on- use numbers in superscript before punctua�on mark (eg. Studies1-3, have shown that… ), Reference lis�ng should be done in order in which they appear in the text.(eg Akponye C, Ogugua CA. Corneal Contours in the general popula�ons as revealed by the Photokeratoscope. Journal of Nigerian Optometric Associa�on. 2010;4 (5):300-400. )
Copyright No�ce - Submission of a manuscript indicates an understanding that the paper is not ac�vely under considera�on for publica�on with any other journal. Once a paper is accepted for publica�on, the author(s) cede copyright to the publishers of the Journal of Nigerian Optometric Associa�on.
Publica�on charge – Manuscripts accepted for publica�on will be published without a fee.
Ekpenyong B.N.
iii
Journal of the Nigerian Optometric Association
Journal sponsorship – The Journal of Nigerian Optometric Associa�on receives funding and support from the Nigerian Optometric Associa�on, a registered non-profit organisa�on.
Disclaimer: – Concerted effort was made by the Publishers and the Editorial Commi�ee to see that no inaccurate or misleading informa�on, opinion or asser�on appears in this journal. However, we wish to state that informa�on and opinions appearing in the ar�cles of this journal are the sole responsibility of the author(s) concerned. Therefore, the publisher, the editor and their agents or employees, accept no responsibility or liability whatsoever for the consequences of any inaccurate informa�on.
Publisher: Nigerian Optometric Associa�on. C/o: Editorial/Publishing Commi�ee Suite 219 Jinifa Plaza, Plot 1014 Samual Ademulegun Adesuji Street, Central Business District- Abuja, Nigeria Mobile: +234805-503-7693
JNOA.2018;20(2) Ekpenyong B.N.
Editor’s notes 1 Dr Bernadine Ekpenyong
Editorial 2 - 7 Appropriate technologies for health and disease: An innova�ve approach to drive sustainable health care delivery. Professor E. Uche Ikonne
Ar�cles
Factors affec�ng rehabilita�on seeking behaviour of individuals with legal blindness 8 - 14 in Lagos, Nigeria. Okonji P.E., Jibogu K.P. and Akinsola O. J.
Refrac�ve errors in children with Down syndrome in Lagos State, Nigeria. 15 - 22 Nwokedi O., Ekpenyong B.N., Musa N.R. and Ovenseri-Ogbomo G.O.
Accommoda�ve anomalies in symptoma�c school children in Cape Coast Metropolis, 23 - 30 Ghana. Darko-Takyi C., Ntodie M., Alex Azuka Ilechie A.A., Abokyi S., Kyei S., Aful H.K., Nti, N.A. and Okae-Asante D.
Assessment of foveal and extra-foveal photostress recovery �me in primary open 31 - 36 angle glaucoma Azuamah, Y.C., Merem, C.C., Ikoro, N.C., Esenwah, E.C., Megwas, A.U. and Daniel-Nwosu, E.
Relevance of culturally-appropriate approaches in health promo�on: a look at Igbo 37 - 45 philosophies in dealing with eye care challenges in Nigeria. Okoye, R.S, Bell, L. and Papadopoulos, I.
Effect of x-rays on the electrolyte concentra�on of bovine aqueous and vitreous 46 - 52 humour Ajayi, O.B. and Atuanya G.N.
External eye infec�ons and personal hygiene prac�ces among pa�ents a�ending 53 - 61 Optometry Teaching Clinic Federal University of Technology, Owerri. Azuamah, Y.C., Esenwah, E.C., Ahuama, O.C., Ikoro, N.C., Iwuagwu, F.C. and Dozie, I.N.S
Determina�on of a standard con�nuous-text print size for people with low vision 62 - 68 Ejukonemu B.O.M. and Akpalaba R.E.U.
Prevalence of low vision and blindness in a leprosarium in kano state, Nigeria. 69 - 74 Okpo E., Nwakuche P.I. and Ejukunemu B.O.M.
Effect of Moringa Oleifera leaf aqueous extract on intraocular and blood pressure 75 - 81 of normotensive adults in Edo State, Nigeria George, G. O., Ajayi, O.B. and Oyemike, A.A.
Journal of the Nigerian Optometric Association
iv
CONTENTS
JNOA.2018;20(2) Ekpenyong B.N.
The Journal of Nigerian Optometric Associa�on (JNOA) is an official journal of the Nigerian Optometric Associa�on (NOA). It is a peer-reviewed interna�onal journal that aims to promote the vision and the mission of the associa�on as well as provide a pla�orm for the advancement of the Optometry prac�ce in Nigeria and beyond. This edi�on of the JNOA is the second special edi�on as the NOA celebrates its 50 years as an associa�on. In this edi�on, we present a ‘must read’ special editorial by an erudite scholar, Professor E. U Ikonne, on appropriate technologies for health and disease: an innova�ve approach to drive sustainable health care delivery. Also to be found in this special edi�on are original research ar�cles in Optometry and eye health. These research papers were put together by a coterie of experts in various aspects and sub-special�es in Optometry and vision sciences. Nwokedi et al presented the results of their research on the prevalence of refrac�ve error among children with Down syndrome; they found hyperopic as�gma�sm to be the most prevalent refrac�ve error. Another research by Darko-Takyi et al, reported a high prevalence of accommoda�ve anomalies among symptoma�c school children. A qualita�ve research by Okoye et al focused on the relevance of culturally-appropriate approaches in health promo�on: a look at Igbo philosophies in dealing with eye care challenges in Nigeria. Two experimental studies are presented in this edi�on, one of them was conducted by Ajayi, and Atuanya. It focused on the effect of x-rays on the electrolyte concentra�on of bovine aqueous and vitreous humour while George et al determined the effect of Moringa Oleifera leaf aqueous extract on intraocular and blood pressure of normotensive adults in Edo State, Nigeria. Azuamah et al assessed the foveal and extra-foveal photo stress recovery �me in primary open angle glaucoma. They recommended that photo stress recovery test be included in the rou�ne eye examina�on of pa�ents.
The prevalence of low vision and blindness in a leprous popula�on was inves�gated by Okpo et al, while Okonji et al established the need to increase knowledge and access to vision rehabilita�on services (VRS) among low vision pa�ents. Ejukonemu and Akpalaba, in a case-control study, determined the standard con�nuous-text print size for people with low vision. They found the N18/2M print size to be adequate. The link between external eye infec�ons and personal hygiene prac�ces was established by Azuamah et al in another study. Health educa�on of pa�ents on good personal hygiene prac�ces was recommended.
The journal is a medium for the dissemina�on of highly valuable informa�on on vision care and health to a specialized audience and is listed in African Journals Online (AJOL). We, therefore, invite submission of high-quality research on topical issues of public health importance in vision health which can improve Optometry prac�ce, thus, enhancing the eye health of the public. We also call for editorials on contemporary issues of concern in Optometry and health care delivery in Nigeria. Our overall objec�ve is to make the journal of Nigerian Optometric Associa�on to be of good quality with a significant impact factor.
Journal of the Nigerian Optometric Association
Dr. Bernadine Nsa EkpenyongEditor-in-chief
1
Editor’s Notes
Dr. Bernadine N. Ekpenyong JNOA.2018;20(2)
Journal of the Nigerian Optometric Association
Vice Chancellor, Abia State University Uturu andRegistrar, Nigerian College of Optometrists
Professor E. Uche Ikonne
2
EditorialAppropriate Technologies For Health And Disease: An Innovative Approach To Drive Sustainable Health Care Delivery.
Preamble What is Appropriate Health Technology
Ikonne E.U.
The term “Appropriate Technology” emerged in the context of the 1973 energy crisis and the 1970s environmental movement. E. F Schumacher in his book “Small is beau�ful- a study of Economics as if people ma�ered” introduced the term intermediate technology. The term was used in two primary contexts i. Technology that most effec�vely meets people’s needs in developing or limited resource se�ngs ii. Technology that is environmentally friendly and socially acceptable in the developed world.
Intermediate technology simply explains the technology that is between ar�sanal and industrial but simple, effec�ve, cheap environmentally sound and sustainable with emphasis on local community ownership, management and maintenance.
Primary health care according to the Alma Ata Declara�on is “essential health care based on practical, scientifically sound and socially acceptable methods and technology made universally accessible to individuals and families in the community through their full participation and at a cost the community and country can afford to maintain at every stage of their development in the spirit of self-reliance and self-determination”
Health technologies, especially those dealing with medical devices, are crucial for the services offered in preven�on, diagnosis, and treatment of illness, disease, and disability.
Appropriate health technologies (AHT) are methods, procedures, techniques and equipment that are scien�fically valid, adapted to local needs, acceptable to users and recipients, maintainable with local resources. Appropriate technologies are either new or adapta�ons of exis�ng technologies of demonstrable effec�veness that can sustainably meet the varied condi�ons of developing countries and the unique needs of underserved communi�es. The criteria for adop�ng an Appropriate Health Technology include the following: Effec�ve - both in theory and prac�cal use Safe - and not easy to use incorrectly Affordable - in ini�al and recurrent costs Acceptable - to all who are affected by it Sustainable - can be maintained, repaired or re-supplied.
It is therefore evident that health technologies developed for developed world countries may be inappropriate for use in resource- poor environments lacking physical infrastructure, trained health care providers or the means to buy and maintain complicated technologies. For instance appropriate technologies such as Oral Rehydra�on Solu�on (ORS) and Contracep�ves faced significant obstacles to wide spread adop�on.
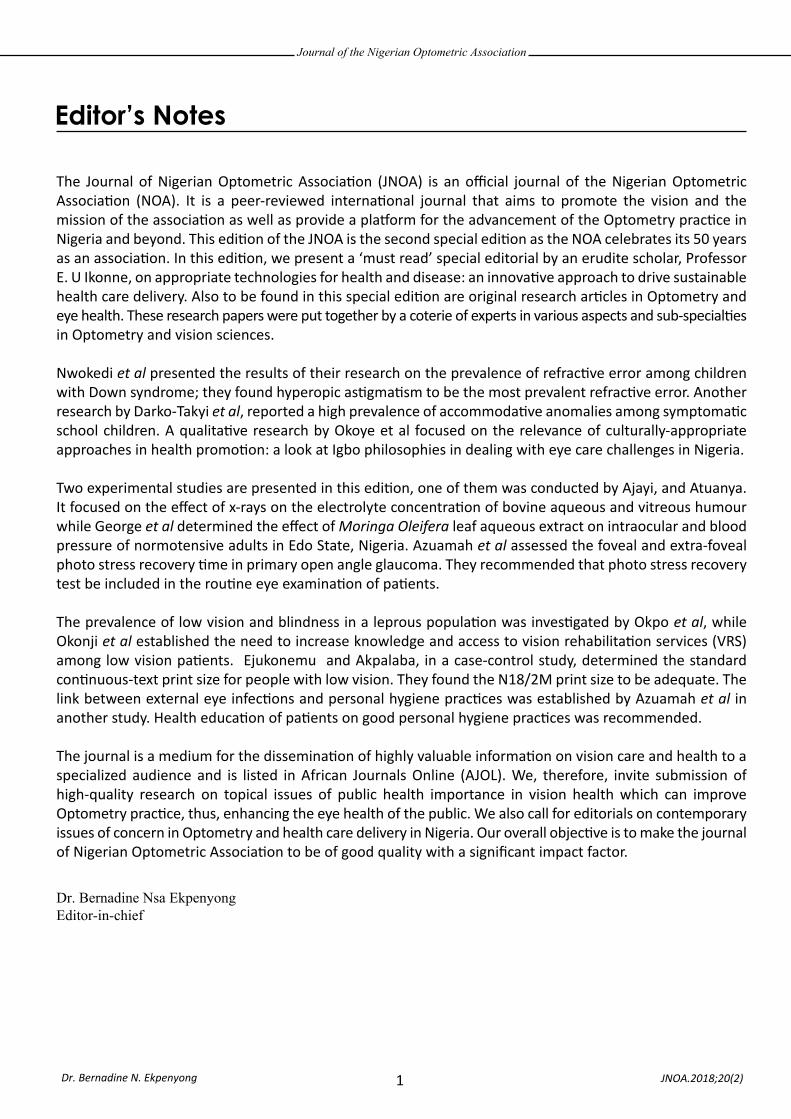
Appropriate technologies are solu�ons that crea�vely integrate the need for new and culturally relevant technologies in addi�on to substan�al behaviour change in order to reduce inequity between rich and poor countries. Therefore appropriate technology must be part of a health care Ecosystem (Figure 1).
JNOA.2018;20(2): 2 - 7
Journal of the Nigerian Optometric Association
Figure 1: Appropriate Technology: Part of a Health Care Ecosystem
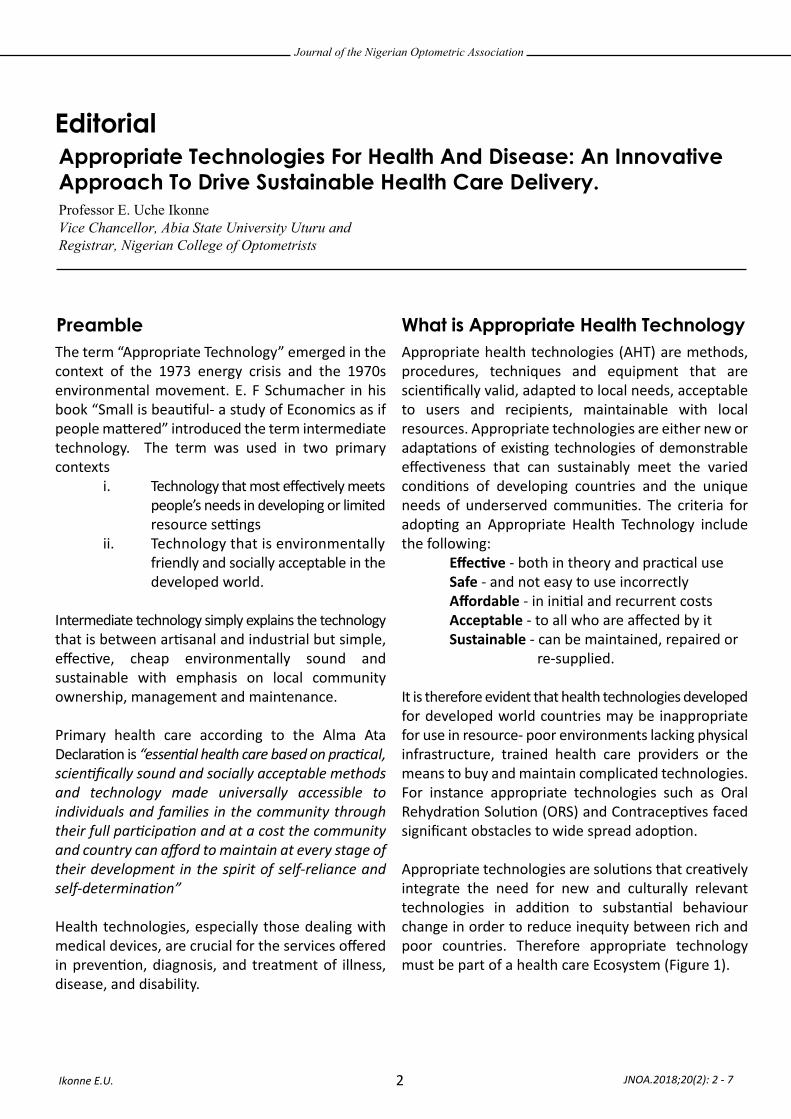
Figure 2: Disconnected value chain within the low and middle-income country health innovation system
3
An ‘appropriate’ innovative technology is one that leads to improved access to essential health products and services; and/or leads to improved human health by providing affordable and accessible products for the population in need.
Health innova�on systems therefore acknowledges the interrela�onship between educa�on, research and development (R & D), manufacture, domes�c and export markets, intellectual property and regulatory policies.
For high income countries health innova�ve systems involve actors from mul�ple sectors and disciplines. Training and basic research are funded by the public sector through universi�es and government research ins�tu�ons. Transla�onal research and product development such as prototype produc�ons or small-scale produc�on are conducted by pharmaceu�cal or other companies or, depending on the na�onal system, government ins�tu�ons. In low-income countries, however, the
health innova�on system is o�en rudimentary and fragmented. The public sector provides most, if not all, funding and infrastructure for research. Although research is conducted in academic ins�tu�ons, o�en there is li�le applicability to local health problems, due to the lack of capacity to conduct transla�onal research and limited manufacturing capacity.
In developing countries, researchers and innovators face tremendous challenges, including the lack of technical training, research tools, financial resources, and up-to-date scien�fic informa�on. These barriers impede ac�vists from developing and implemen�ng innova�ve and low cost technologies. There is a disconnected value chain within low and middle income countries health innova�on system (Fig 2).
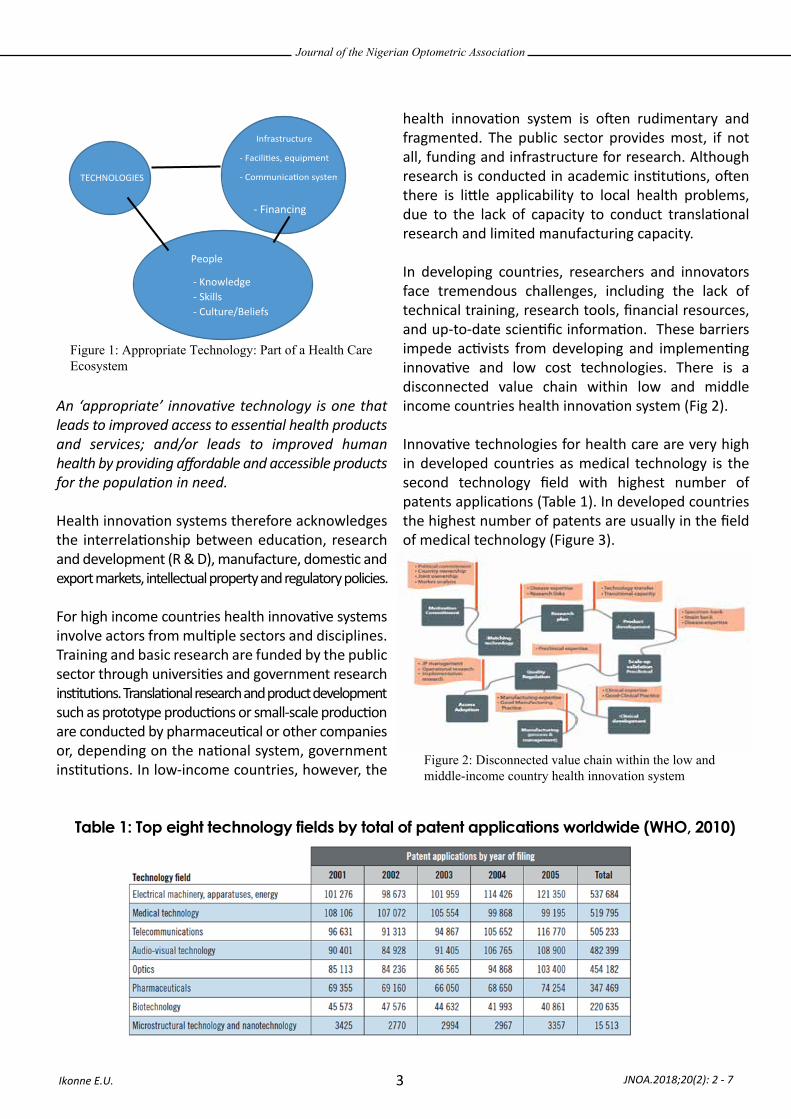
Innova�ve technologies for health care are very high in developed countries as medical technology is the second technology field with highest number of patents applica�ons (Table 1). In developed countries the highest number of patents are usually in the field of medical technology (Figure 3).
Ikonne E.U. JNOA.2018;20(2): 2 - 7
TECHNOLOGIES
Infrastructure
- Facili�es, equipment
- Communica�on systems
- Policies
- Regula�on
People
- Knowledge - Skills - Culture/Beliefs
- Financing
Table 1: Top eight technology fields by total of patent applications worldwide (WHO, 2010)
Journal of the Nigerian Optometric Association
4
• The insec�cide treated bed nets is an innova�ve combina�on of two different products namely bed nets and insec�cides• This led to the development of long las�ng impregnated nets (LLIN) that provided two effec�ve forms of vector control for 2-3 year life of the Net• However an addi�onal cost resulted to challenges in dissemina�on
• Compulsory purchases• Public Sector subsidies• Free distribu�on to the most vulnerable popula�on• Public-private partnerships
• Reduc�on in overall mortality by ± 20% in Africa• For every 1,000 Children 1-59 months protected, 6 lives are saved per year• 38% reduc�on in malaria parasitemia• 28% reduc�on in risk of low birth weight• 25 % reduc�on in adverse outcomes of pregnancy
:
Dracunculiasis, also called Guinea-worm disease (GWD), is an infec�on by the Guinea worm. A person becomes infected when they drink water that contains water fleas infected with guinea worm larvae. In humans, the only known cause is Dracunculus medinensis Control of Guinea worm
Ikonne E.U. JNOA.2018;20(2): 2 - 7
Figure 3: Top 10 countries with the highest number of patent applications in the field of medical technology (WHO, 2010)
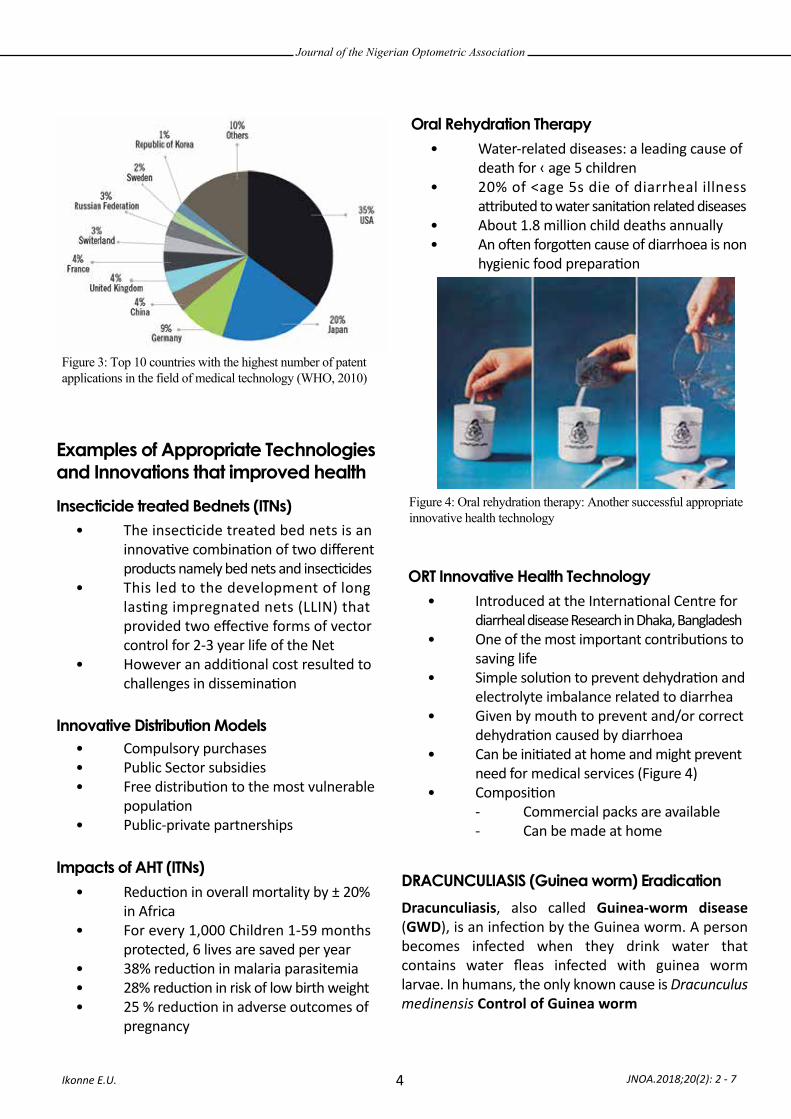
Figure 4: Oral rehydration therapy: Another successful appropriate innovative health technology
Examples of Appropriate Technologies and Innovations that improved healthInsecticide treated Bednets (ITNs)
Innovative Distribution Models
Impacts of AHT (ITNs)
• Water-related diseases: a leading cause of death for ‹ age 5 children• 20% of <age 5s die of diarrheal illness a�ributed to water sanita�on related diseases• About 1.8 million child deaths annually• An o�en forgo�en cause of diarrhoea is non hygienic food prepara�on
Oral Rehydration Therapy
• Introduced at the Interna�onal Centre for diarrheal disease Research in Dhaka, Bangladesh• One of the most important contribu�ons to saving life• Simple solu�on to prevent dehydra�on and electrolyte imbalance related to diarrhea• Given by mouth to prevent and/or correct dehydra�on caused by diarrhoea• Can be ini�ated at home and might prevent need for medical services (Figure 4)• Composi�on - Commercial packs are available - Can be made at home
ORT Innovative Health Technology
DRACUNCULIASIS (Guinea worm) Eradication
Journal of the Nigerian Optometric Association
5
LAPARASCOPY
Advantages of Laparoscopic Surgery
Disadvantages of Laparoscopic Surgery
(i) provision of a safe water supply, (ii) filtra�on of one's drinking water to remove cyclops, (iii) searching for pa�ents with ac�ve cases and proper management of cases, (iv) ensuring that pa�ents avoid contact with ponds, and (v) Killing or removing cyclops in ponds.
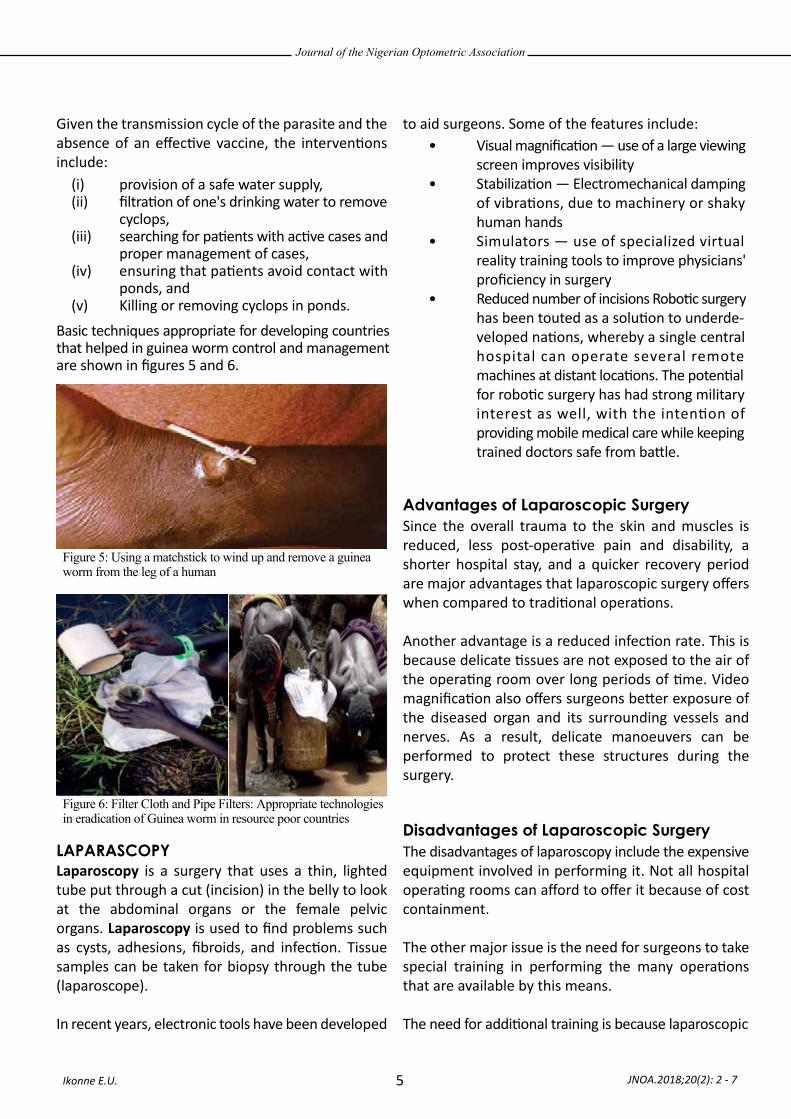
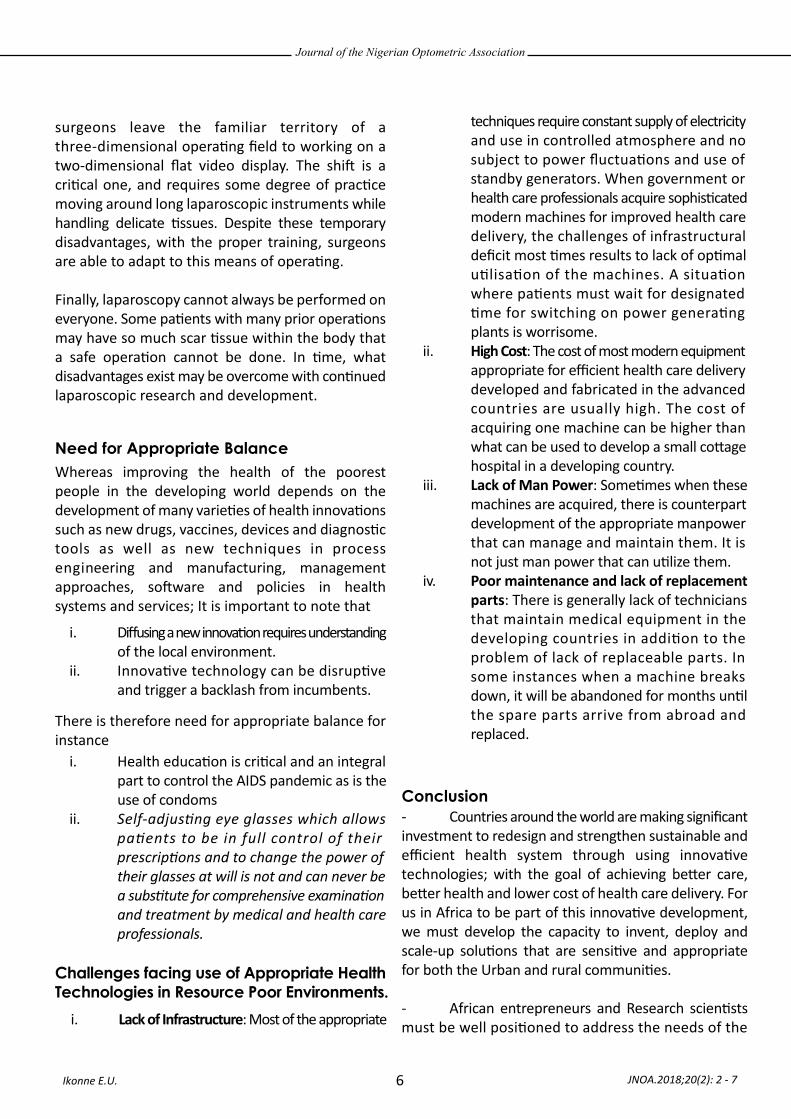
Basic techniques appropriate for developing countries that helped in guinea worm control and management are shown in figures 5 and 6.
• Visual magnifica�on — use of a large viewing screen improves visibility• Stabiliza�on — Electromechanical damping of vibra�ons, due to machinery or shaky human hands• Simulators — use of specialized virtual reality training tools to improve physicians' proficiency in surgery • Reduced number of incisions Robo�c surgery has been touted as a solu�on to underde- veloped na�ons, whereby a single central hospital can operate several remote machines at distant loca�ons. The poten�al for robo�c surgery has had strong military interest as well, with the inten�on of providing mobile medical care while keeping trained doctors safe from ba�le.
Given the transmission cycle of the parasite and the absence of an effec�ve vaccine, the interven�ons include:
Laparoscopy is a surgery that uses a thin, lighted tube put through a cut (incision) in the belly to look at the abdominal organs or the female pelvic organs. Laparoscopy is used to find problems such as cysts, adhesions, fibroids, and infec�on. Tissue samples can be taken for biopsy through the tube (laparoscope).
In recent years, electronic tools have been developed
to aid surgeons. Some of the features include:
Since the overall trauma to the skin and muscles is reduced, less post-opera�ve pain and disability, a shorter hospital stay, and a quicker recovery period are major advantages that laparoscopic surgery offers when compared to tradi�onal opera�ons.
Another advantage is a reduced infec�on rate. This is because delicate �ssues are not exposed to the air of the opera�ng room over long periods of �me. Video magnifica�on also offers surgeons be�er exposure of the diseased organ and its surrounding vessels and nerves. As a result, delicate manoeuvers can be performed to protect these structures during the surgery.
The disadvantages of laparoscopy include the expensive equipment involved in performing it. Not all hospital opera�ng rooms can afford to offer it because of cost containment.
The other major issue is the need for surgeons to take special training in performing the many opera�ons that are available by this means.
The need for addi�onal training is because laparoscopic
Ikonne E.U. JNOA.2018;20(2): 2 - 7
Figure 5: Using a matchstick to wind up and remove a guinea worm from the leg of a human
Figure 6: Filter Cloth and Pipe Filters: Appropriate technologies in eradication of Guinea worm in resource poor countries
Journal of the Nigerian Optometric Association
6
Need for Appropriate Balance
Challenges facing use of Appropriate Health Technologies in Resource Poor Environments.
i. Diffusing a new innova�on requires understanding of the local environment. ii. Innova�ve technology can be disrup�ve and trigger a backlash from incumbents.
i. Lack of Infrastructure: Most of the appropriate
i. Health educa�on is cri�cal and an integral part to control the AIDS pandemic as is the use of condomsii. Self-adjusting eye glasses which allows patients to be in full control of their prescriptions and to change the power of their glasses at will is not and can never be a substitute for comprehensive examination and treatment by medical and health care professionals.
techniques require constant supply of electricity and use in controlled atmosphere and no subject to power fluctua�ons and use of standby generators. When government or health care professionals acquire sophis�cated modern machines for improved health care delivery, the challenges of infrastructural deficit most �mes results to lack of op�mal u�lisa�on of the machines. A situa�on where pa�ents must wait for designated �me for switching on power genera�ng plants is worrisome. ii. High Cost: The cost of most modern equipment appropriate for efficient health care delivery developed and fabricated in the advanced countries are usually high. The cost of acquiring one machine can be higher than what can be used to develop a small co�age hospital in a developing country. iii. Lack of Man Power: Some�mes when these machines are acquired, there is counterpart development of the appropriate manpower that can manage and maintain them. It is not just man power that can u�lize them.iv. Poor maintenance and lack of replacement parts: There is generally lack of technicians that maintain medical equipment in the developing countries in addi�on to the problem of lack of replaceable parts. In some instances when a machine breaks down, it will be abandoned for months un�l the spare parts arrive from abroad and replaced.
surgeons leave the familiar territory of a three-dimensional opera�ng field to working on a two-dimensional flat video display. The shi� is a cri�cal one, and requires some degree of prac�ce moving around long laparoscopic instruments while handling delicate �ssues. Despite these temporary disadvantages, with the proper training, surgeons are able to adapt to this means of opera�ng.
Finally, laparoscopy cannot always be performed on everyone. Some pa�ents with many prior opera�ons may have so much scar �ssue within the body that a safe opera�on cannot be done. In �me, what disadvantages exist may be overcome with con�nued laparoscopic research and development.
Whereas improving the health of the poorest people in the developing world depends on the development of many varie�es of health innova�ons such as new drugs, vaccines, devices and diagnos�c tools as well as new techniques in process engineering and manufacturing, management approaches, so�ware and policies in health systems and services; It is important to note that
There is therefore need for appropriate balance for instance
- Countries around the world are making significant investment to redesign and strengthen sustainable and efficient health system through using innova�ve technologies; with the goal of achieving be�er care, be�er health and lower cost of health care delivery. For us in Africa to be part of this innova�ve development, we must develop the capacity to invent, deploy and scale-up solu�ons that are sensi�ve and appropriate for both the Urban and rural communi�es.
- African entrepreneurs and Research scien�sts must be well posi�oned to address the needs of the
Conclusion
Ikonne E.U. JNOA.2018;20(2): 2 - 7
Journal of the Nigerian Optometric Association
7
communi�es while considering the exis�ng structural, cultural and poli�cal menaces – something that is o�en overlooked in aid-driven health programme.
We must encourage local innovators- for instance the use of rapid diagnos�c blood tests to defeat malaria is largely limited in rural African communi�es
due to its risky and complex diagnos�c procedure. Ins�lling a culture of innova�on must be a promising way to propel Africa in its efforts to eradicate diseases and improve health.
Selected ReferencesBarry, M (2007) The tail of the Guinea worm. Global eradica�on without a drug or a vaccine. New England Journal of Medicine 256(25): 2561-2563.
Barry M and Hughes J. (2008) Talking dirty. The poli�cs of clean water and sanita�on. NEJM 359(8); 784-787.
Carter Founda�on and WHO (2016) Eradica�on of Guinea worm disease. Case statement www.cartercentre.org/guineaworm
Goodyear, L; Tsu, V; Kaisel, D and Lalwani, T (2009) Appropriate Health Technologies, Concepts, Criteria and Uses. PATH Sea�le Washington.
WHO (2007) Everybody’s business: strengthening health systems to improve health outcomes. Geneva, World Health Organiza�on, 2007.
WHO (2008) The World Health Report 2008. Primary health care: now more than ever. Geneva, World Health Organiza�on, 2008.
WHO (2010) Landscape Analysis of Barriers to developing or adap�ng Technologies for Global Health Purposes. Global Ini�a�ves on Health Technologies. www.who.int/medical_devices/en/
Roscigno, G; Yuthavong, Y and Manderson, L (2012) Innova�on and New Technologies to tackle Infec�ous Diseases of Poverty In Global Report for Research on Infec�ous Diseases of Poverty. www.who.int/en�ty/tdr/
Ikonne E.U. JNOA.2018;20(2): 2 - 7

Visual impairment refers to vision with Visual Acuity (VA) of 6/18 (0.5LogMAR) or worse and cannot be fully recovered with medical treatment, surgery, or conven�onal glasses, or corresponding visual field loss to <10° in the be�er eye with best correc�on.1-3 Visual impairment broadly encompasses low vision or par�al sightedness and blindness.1 The
term Legal blindness refers to a medically diagnosed central visual acuity of 6/60 or less in the be�er eye with the best possible correc�on, and/or a visual field of 20 degrees or less. 1-3 The current burden of visual impairment in Nigeria is es�mated at 1 million legally blind adults and 3 million people with low vision.4 In 2010, the US Census IDB data showed that the prevalence
JNOA.2018;20(2): 8 - 14
Blindness and low vision have profound nega�ve impact on the quality of life of persons affected and it reduces ability to live independently. There are apparent inadequacies in vision rehabilita�on services (VRS) in terms of access to and uptake of VRS. This study inves�gated factors affec�ng VRS seeking behav-iour of 120 legally blind par�cipants in Lagos, Nigeria. Par�cipants had Visual Acuity (VA) worse than 6/60 (+1.0LogMAR) and were aged between 20 and 80 years. Eighteen (18, 15%) of the par�cipants reported having undertaken VRS while 102 par�cipants (85%) reported that they never had any form of VRS. Data concerning reasons for non-uptake of VRS were obtained from the 102 par�cipants (85%) who reported that they had never taken any VRS a�er diagnosis of visual impairment. Findings show that a majority of the par�cipants who had never had VRS had no knowledge of VRS (86, 84.31%) and many of them reported that they were never referred for VRS (82, 80.39%). Logis�c regression analysis of reasons for non-uptake of VRS showed that males were significantly less likely to report that they had no knowledge of VRS (OR:0.53; 95% Confidence Interval [CI], 0.31-0.91; p<0.05). Par�cipants aged 61 years and over (OR: 1.48; 95% CI, 0.72-3.09; p<0.05) as well as those blind for more than eleven years (OR: 1.16; 95% CI, 0.56-2.34; p<0.05) were more likely to report that VRS was not needed. Par�cipants aged 61 and over were also more likely to state that they were never referred for VRS (OR: 2.88; 95% CI, 1.62-5.20; p<0.05). The study concludes that there is a need to increase awareness and knowledge of VRS among low vision pa�ents as well as provide accessible infrastructure and manpower for VRS. A case is also made for prompt referral of legally blind pa�ents for VRS.
Journal of the Nigerian Optometric Association Original Research Article
1 Research and Innovation Office, University of Lagos, 101017 University Road Akoka, Lagos, Nigeria2 Department of Special Education, Faculty of Education, University of Ibadan, Nigeria3 College of Medicine of the University of Lagos, Idi-Araba, Lagos, Nigeria
1. Colenbrander A. Measuring vision and vision loss. Duane’s clinical ophthalmology. 2001;5:1-39. 2. World Health Organization (WHO). Available data on Blindness (Update 1987) Geneva: WHO/PBL; 1987; 14: 1–23.3. World Health Organization (WHO) Fact Sheet No 282, Nov. 20044. Ademola-Popoola DS, Tunde-Ayinmode MF, Akande TM. Psychosocial characteristics of totally blind people in a Nigerian city. Middle East African journal of Ophthalmology. 2010;17(4):335-345.
Okonji P.E.,1 Jibogu K.P.2 and Akinsola O. J.3
Okonji P.E Email: [email protected] Phone: + 2348149777036
8
FACTORS AFFECTING REHABILITATION SEEKING BEHAVIOUR OF INDIVIDUALS WITH LEGAL BLINDNESS IN LAGOS, NIGERIA
Corresponding Author:
Abstract
Introduction
Okonji et al

Journal of the Nigerian Optometric Association
9
Materials and Methods
3. World Health Organization (WHO) Fact Sheet No 282, Nov. 20044. Ademola-Popoola DS, Tunde-Ayinmode MF, Akande TM. Psychosocial characteristics of totally blind people in a Nigerian city. Middle East African journal of Ophthalmology. 2010;17(4):335-345.5. US Census Bureau (2010) International Data Base. Retrieved from: https://www.census.gov/programs-surveys/international-programs.html. Accessed March 30, 2017. http://iovs.arvojournals.org/article.aspx?articleid=21862076. Stevens GA, White RA, Flaxman SR, Price H, et al. Global prevalence of vision impairment and blindness: magnitude and temporal trends, 1990–2010. Ophthalmology. 2013; 120(12):2377-847. Hinds A, Sinclair A, Park J, Suttie A, Paterson H, Macdonald M. Impact of an interdisciplinary low vision service on the quality of life of low vision patients. British Journal of Ophthalmology. 2003; 1;87(11):1391-6.8. Lamoureux EL, Pallant JF, Pesudovs K, Tennant A, Rees G, O'Connor PM, Keeffe JE. Assessing participation in daily living and the effectiveness of rehabiliation in age related macular degeneration patients using the impact of vision impairment scale. Ophthalmic epidemiology. 2008;15(2):105-13. 9. Stelmack J. Quality of life of low-vision patients and outcomes of low-vision rehabilitation. Optometry and Vision Science. 2001;78(5):335-4210. Tunde-Ayinmode MF, Akande TM, Ademola-Popoola DS. Psychologica and social adjustment to blindness: Understanding from two groups of blind people in Ilorin, Nigeria. Annals of African medicine. 2011;10(2):12-23.11. Entekume G, Patel J, Sivasubramaniam S, Gilbert CE, Ezelum CC, Murthy GV, Rabiu MM. Prevalence, causes, and risk factors for functional low vision in Nigeria: results from the national survey of blindness and visual impairment. Investigative ophthalmology & visual science. 2011;52(9):6714-9. 12. Brennan M, Horowitz A, Reinhardt JP, Cimarolli V, Benn DT, Leonard R. In their own words: Strategies developed by visually impaired elders to cope with vision loss. Journal of Gerontological Social Work. 2001;35(1):107-29. 13. Rees G, Fenwick EK, Keeffe JE, Mellor D, Lamoureux EL. Detection of depression in patients with low vision. Optometry and Vision Science. 2009;86(12):1328-3614. Balarabe AH, Mahmoud AO, Ayanniyi AA. The Sokoto blind beggars: causes of blindness and barriers to rehabilitation services. Middle East African journal of Ophthalmology. 2014;21(2):147.15. Percival J. Whole system care and social inclusion of people with sight loss: implications of key research for policy and service development. Journal of Integrated Care. 2011;19(5):47-57
of legal blindness in Nigeria was 0.2% (95% CI, 0.1–0.3%), giving an es�mated total of over 55,000 people across Nigeria, or 340 per million popula�on.5 Globally, the prevalence of vision impairment is increasing as more than 37 million people are living with vision impairment3, and as such, vision rehabilita�on (VR) is becoming an issue of public health concern.6 Among people with blindness, ability to accomplish daily tasks as (such as reading, moving out and about, driving, recognizing people's faces, and discerning colour) independently becomes extremely difficult if not impossible. Vision rehabilita�on services (VRS) enable people who are blind, or have low vision to con�nue to live independently and maintain their accustomed quality of life.7,8 It includes a wide range of professional services provided by a team of specially trained professionals, which may include low vision therapists, Vision Rehabilita�on Therapists (VRTs), and orienta�on and mobility specialists to restore func�oning a�er vision loss. In principle, adults who are blind, or have low vision are usually referred to VRTs to learn adap�ve independent living skills (AILS). AILS include Communica�on skills, reading and wri�ng skills, braille and assis�ve computer technology, personal self-care, financial management, voca�onal rehabilita�on, orienta�on and mobility skills, and travelling safely outdoors. These skill-set enable visually impaired individuals a�ain maximum func�on, personally sa�sfying level of independence, a sense of well-being, and op�mum quality of life.8,9
There is, however, ample evidence regarding the unmet needs of legally blind persons in Nigeria.4,10,11 Research suggests that although legally blind persons have an increased need for self-reliance12 and that their quality of life is more restrained by lost sources of independence and confidence due to their reliance on others for support in accomplishing daily living tasks,13 not many legally blind individuals in Nigeria have access to support for psychological and social adjustments.10,11 There are evidences sugges�ng that legally blind pa�ents rarely receive counselling about rehabilita�on op�ons and li�le or no informa�on about where to access training for independent living.10,14,15 There are gaps in knowledge concerning what factors currently affect vision rehabilita�on seeking behaviour among visually impaired persons in Nigeria. The current study inves�gated factors affec�ng vision rehabilita�on seeking behaviour of individuals with legal blindness in an urban se�ng in Nigeria (Lagos metropolis) in order to inform interven�on programmes for uptake of vision rehabilita�on services (VRS).
A mul�-stage sampling technique was used to recruit respondents for this study. First, a simple random sampling method was used to select five LGAs from the 20 LGAs within the five Administra�ve Divisions of the state. Thus, Ikeja, Lagos-mainland, Ikorodu, Amuwo-Odofin, and Epe LGAs were selected. Second, in each of the selected LGAs, the local government
JNOA.2018;20(2): 8 - 14 Okonji et al
Original Research Article

Journal of the Nigerian Optometric Association
10
headquarters was purposively included in the study (because of their sub-urban nature) and therea�er, two communi�es each were selected from the LGAs using simple random sampling methods. Thus, three communi�es each from the selected LGAs were included in the study. The communi�es added to their respec�ve LGA headquarters included: Opebi, Ogba, Yaba, Akoka, Imota, Igbobo, Festac Town, Odofin, Abomi�, and Aboriji. Only respondents residing in these communi�es were recruited for the study. The respondents were recruited using purposive and snowball sampling procedure. Criteria for inclusion in the study were: aged 20 years and over, visual acuity of 6/60 or less in the be�er eye, not having cogni�ve impairment, and able to communicate in English language. We focused only on legally blind par�cipants (VA less than 6/60 [+1.0LogMAR]) rather than individuals with low vision (visual acuity less than 6/18 [+0.50LogMAR] to 6/36 [+0.80LogMAR]) because o�en, people with low-vision usually have the misconcep�on that VRS are mainly for legally blind persons and that their vision is not poor enough to need VRS.16,17,18 Presumably, there are also tendencies of misconcep�on that seeking VRS is conceding total blindness or giving-up on hopes of regaining their sight. Adequate and essen�al precau�ons were engaged to shun sample bias with the data collected. Snowball sampling was used to recruit par�cipants considering that the sample for the study was limited to a very small subgroup of the popula�on (i.e those with legal blindness – VA 6/60 [+1.0LogMAR] or less in the be�er eye). In principle, snowball sampling method is o�en suggested when the par�cipants are aware of persons with similar and required a�ributes that qualify them to be included in the sample.19 In this study, snowball sampling was adopted since iden�fying legally blind persons on random basis or casually was challenging due to
limita�on of the popula�on. The sample for survey was therefore iden�fied through a chain of referral from eye care prac��oners located in the selected study areas, other par�cipants as well as through references of social and support group mee�ngs of vision-related chari�es in the selected areas. The 2010 US Census IDB es�mates of Prevalence of Func�onal Low Vision and Total Blindness in Nigeria was used in the determina�on of sample for the study.5 An es�mated blindness prevalence of 5%, with an absolute precision of 5% at 95% confidence, assuming a design effect of 1.75 and a response rate of 85% was used to compute sample size. The calculated sample size, using these parameters, was 73 persons. Effort was made to encourage blind older people to par�cipate, including offering prac�cal support such as funding their transport to the clinics where data were collected. However, for some poten�al par�cipants, other difficul�es made them reluctant to a�end as a total of 138 eligible par�cipants were invited for the study but 120 par�cipated in the study via invita�ons sent. This sample size was large enough to give a precise es�mate of the prevalence of total blindness in Lagos state (i.e., 4.2% with an absolute precision of 5% at 95% confidence).20 Audio-recorded consent was sought and obtained from all par�cipants. The study was conducted in accordance with ins�tu�onal and na�onal guidelines for conduct of research with human subjects. Ethical approval was sought from the Ins�tu�onal Review Board of the College of Medicine, University of Lagos. The inves�ga�on was carried out in accordance with the Declara�on of Helsinki of 1975 (As revised in Tokyo in 2004).21 Informed consent was obtained from all par�cipants as they were briefed about the study and their verbal consent obtained before par�cipa�on. Personal and demographic data were collected at the �me of administra�on of the survey ques�onnaires. Data collec�on took place between June and November 2017. We categorized
JNOA.2018;20(2): 8 - 14 Okonji et al
Original Research Article
5. US Census Bureau (2010) International Data Base. Retrieved from: https://www.census.gov/programs-surveys/international-programs.html. Accessed March 30, 2017. http://iovs.arvojournals.org/article.aspx?articleid=218620716. Siemsen DW, Bergstrom AR. Efficacy of a Low Vision Patient Consultation. Journal of Visual Impairment and Blindness. 2005 Jul;99(7):1-0.17. Markowitz SN. Principles of modern low vision rehabilitation. Canadian Journal of Ophthalmology. 2006; 41(1):289–312. 18. Mwilambwe A, Wittich W, Freeman EE. Disparities in awareness and use of low-vision rehabilitation. Canadian Journal of Ophthalmology. 2009;44(6):686-91. 19. Noy C. Sampling knowledge: The hermeneutics of snowball sampling in qualitative research. International Journal of social research methodology. 2008;11(4):327-44.20. Kyari F, Gudlavalleti MV, Sivsubramaniam S, Gilbert CE, Abdull MM, Entekume G, Foster A. Prevalence of blindness and visual impairment in Nigeria: The national blindness and visual impairment survey. Investigative ophthalmology & visual science. 2009;50(5):2033-9.21. Carlson RV, Boyd KM, Webb DJ. The revision of the Declaration of Helsinki: past, present and future. British journal of clinical pharmacology. 2004;57(6):695-713.

Journal of the Nigerian Optometric Association
11
Results
individuals with Primary and Lower Secondary educa�on as Low levels of educa�on, and par�cipants with Upper Secondary and Post-Secondary non-ter�ary Degree as Medium level educa�on. Respondents with Ordinary or Higher Na�onal Diploma, Bachelor’s or Master’s degree, or a Doctorate degree were classified as High educa�on levels. These classifica�ons were based on the Interna�onal Standard Classifica�on of Educa�on (ISCED-2011) which provided guidance to countries within Organisa�on for Economic Coopera�on and Development (OECD) on how to implement ISCED-2011 framework in interna�onal data collec�on.22 The survey ques�ons inves�gated knowledge of VRS and whether par�cipants had taken any VRS or training for coping with blindness. The reasons for non-uptake of VRS were also inves�gated by asking par�cipants to state why they had not sought any VRS from a list of four possible op�ons, namely: “No knowledge of VRS”, “Not needed”, “Perceived cost of rehabilita�on”, and “Never referred for VRS”. Perceived cost of rehabilita�on was regarded as the belief that seeking VRS was expensive. As the par�cipants were blind, survey ques�ons were read aloud to them and their responses documented. Surveys ques�onnaires were offered either at home, or at clinics of the eye care professional who recommended the par�cipant as many of the par�cipants were either previous or current pa�ents of the clinics approached to assist with recruitment of par�cipants. All data were collected by trained field staff who accompanied the Principal Inves�gator as well as the Co-Principal Inves�gator to the interview site. The core inves�gators comprised two Optometrists, and a Biosta�s�cian. Data was analysed using SPSS (version 21.0). Chi-square tests were applied to iden�fy the associa�on between variables. Univariate and logis�c regression modelling were used to explore associa�ons with demographic factors.
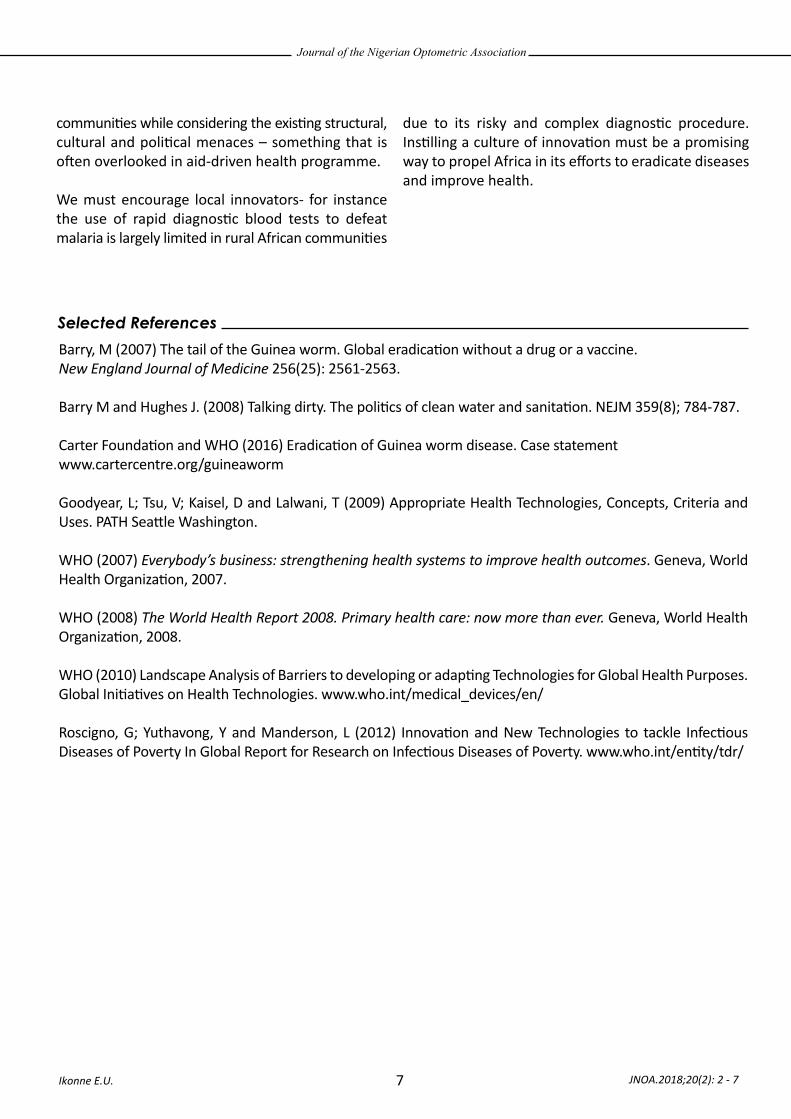
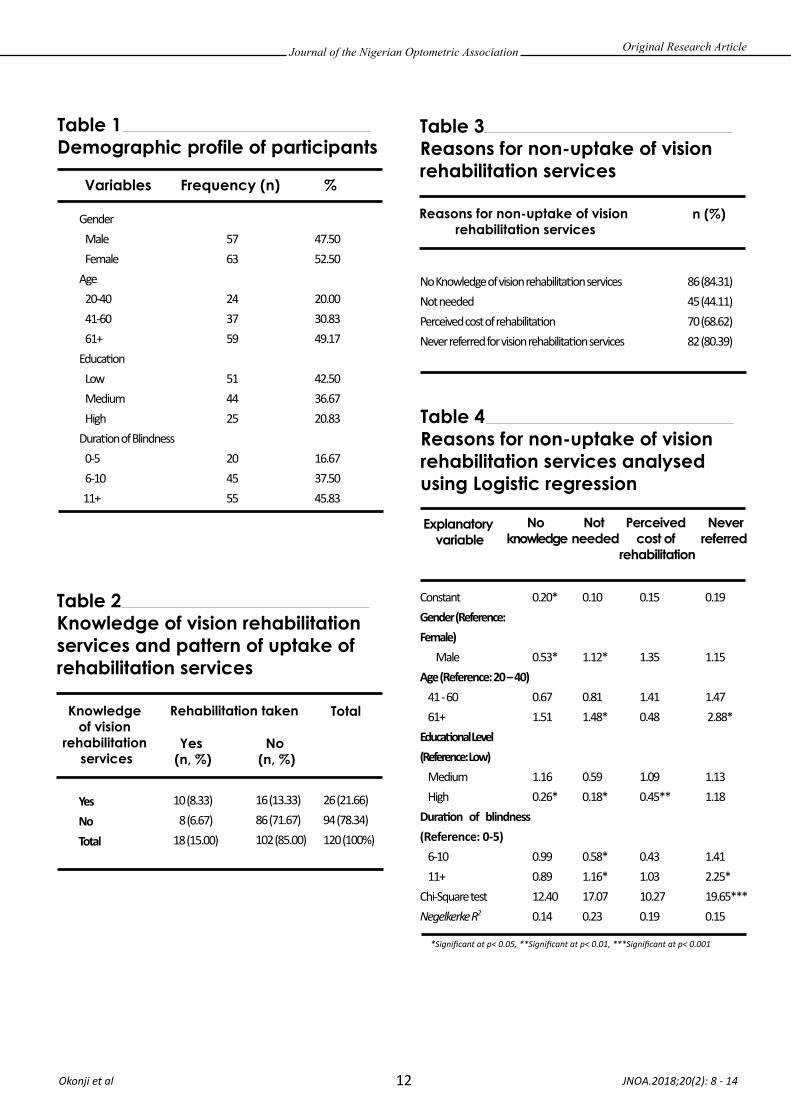
A total of 102 par�cipants (85%) reported that they
had not received any form of vision rehabilita�on service to enable them cope with sight loss. Only 18 (15%) of par�cipants men�oned that they have had a vision rehabilita�on training following diagnosis of vision impairment (Table 2). Over 78 per cent (94 par�cipants) reported that they had no knowledge of vision rehabilita�on services. Although 26 par�cipants (21.66%) had knowledge of VRS, only 10 (8.33%) out of the 120 par�cipants reported that they have taken VRS. Not having knowledge of VRS (84.31%) as well as not being referred for VRS (80.39%) were the major reasons for non-uptake of VRS (Table 3). Explana�ons for non-uptake of VRS were further inves�gated using logis�c regression. Results (Table 4) showed that males were significantly less likely to report that they had no knowledge of VRS. Although par�cipants aged 61 and over were more likely to report that they had no knowledge of VRS, this result was not sta�s�cally significant. In addi�on, par�cipants with high level of educa�on were significantly less likely to state that they had no knowledge of VRS. Male par�cipants were significantly more likely to report that VRS was not needed (OR: 1.12; CI, 0.56-2.34; p<0.05). Across age demographics, par�cipants aged 61+ (OR: 1.48; CI, 0.72-3.09; p<0.05) and those with longer dura�on of blindness (11+ years) (OR: 1.16; CI, 0.56-2.34; p<0.05) were significantly more likely to report that VRS was not needed while those with higher level of educa�on were less likely to report so (OR:0.18; CI, 0.07-0.45; p<0.050). Analysis of percep�on of cost of VRS showed that par�cipants between the ages of 41-60 and those with 11+ years of blindness were more likely to men�on cost of VRS as prohibi�ve – these results were, however, not sta�s�cally significant. Par�cipants with high level of educa�on were significantly less likely to perceive cost of VRS as hindering uptake (OR: 0.45; CI, 0.23-0.76; p<0.01). While the results showed that males were more likely to report that they were never referred for VRS, this result was not sta�s�cally significant at any level. Par�cipants aged 61+ (OR: 2.88; CI, 1.62-5.20, p<0.05) and those with 11+ years dura�on of blindness (OR: 2.25; CI, 1.30-3.99; p<0.05) were significantly more likely to report that they were never referred for VRS.
JNOA.2018;20(2): 8 - 14 Okonji et al
Original Research Article
22. ISCE International Standard Classification of Education (2011). Retrieved from: http://ec.europa.eu/eurostat/statistics-explained/index.php/International_Standard_Classification_of_Education_(ISCED) (Accessed: 07/05/2018).
Journal of the Nigerian Optometric Association
12
JNOA.2018;20(2): 8 - 14 Okonji et al
*Significant at p< 0.05, **Significant at p< 0.01, ***Significant at p< 0.001
Original Research Article
Table 1 Demographic profile of participants
Variables Frequency (n) %
Gender Male FemaleAge 20-40 41-60 61+ Educa�on Low Medium HighDura�on of Blindness 0-5 6-10 11+
5763
243759
514425
204555
47.5052.50
20.0030.8349.17
42.5036.6720.83
16.6737.5045.83
Table 4 Reasons for non-uptake of vision rehabilitation services analysed using Logistic regression
Explanatory variable
No knowledge
Not needed
Perceived cost of
rehabilitation
Neverreferred
ConstantGender (Reference: Female) MaleAge (Reference: 20 – 40) 41 - 60 61+Educa�onal Level (Reference: Low) Medium HighDura�on of blindness (Reference: 0-5) 6-10 11+Chi-Square testNegelkerke R2
0.20*
0.53*
0.671.51
1.160.26*
0.990.8912.400.14
0.10
1.12*
0.811.48*
0.590.18*
0.58*1.16*17.070.23
0.15
1.35
1.410.48
1.090.45**
0.431.0310.270.19
0.19
1.15
1.47 2.88*
1.131.18
1.412.25*19.65***0.15
Table 2 Knowledge of vision rehabilitation services and pattern of uptake of rehabilitation services
Knowledge of vision
rehabilitation services
Rehabilitation taken
Yes (n, %)
No (n, %)
Total
YesNoTotal
10 (8.33) 8 (6.67)18 (15.00)
16 (13.33)86 (71.67)102 (85.00)
26 (21.66)94 (78.34)120 (100%)
Table 3 Reasons for non-uptake of vision rehabilitation services
Reasons for non-uptake of vision rehabilitation services
n (%)
No Knowledge of vision rehabilita�on servicesNot neededPerceived cost of rehabilita�on Never referred for vision rehabilita�on services
86 (84.31) 45 (44.11) 70 (68.62) 82 (80.39)

Journal of the Nigerian Optometric Association
13
DISCUSSION
16. Siemsen DW, Bergstrom AR. Efficacy of a Low Vision Patient Consultation. Journal of Visual Impairment and Blindness. 2005 Jul;99(7):1-0.23. Soni, D. Nigeria ahead in Optometry practice in Africa (2014). Retrieved from: https://www.vanguardngr.com/2014/05/nigeria-ahead-optometry-practice-africa-dr-udom/ (Accessed: 07/05/2018).24. Hamzat TK. Some Challenges Facing Neurorehabilitation in Nigeria: Standpoint of a Neurophysiotherapist. Journal of Neurology and Neurorehabilitation Research. 2016;1(1): 1-325. Matti AI, Pesudovs K, Daly A, Brown M, Chen CS. Access to low‐vision rehabilitation services: barriers and enablers. Clinical and Experimental Optometry. 2011;94(2):181-186.26. Mansfield AK, Addis ME, Mahalik JR. " Why won't he go to the doctor?": The psychology of men's help seeking. International Journal of Men's Health 2003;2(2):93-108.27. Orr KS, Leven T. Community care and mental health services for adults with sensory impairment in Scotland. Scottish Executive Social Research; 2006. Retrieved from: http://www.scotland.gov.uk/Resource/Doc/129826/0030944.pdf (Accessed: 7/05/2018)
Findings from this study suggest that the two major barriers precluding uptake of vision rehabilita�on services (VRS) are the lack of knowledge about VRS and the non-referral of blind persons for VRS. Many par�cipants who never had VRS believed that seeking VRS was expensive while some others did not feel that they needed VRS. As these par�cipants had never taken up VRS, the belief that seeking VRS was expensive was presumably borne out of misconcep�on. This finding echoes a previous report that pa�ents may not wish to take up low-vision rehabilita�on due to misconcep�ons about VRS, inadequate understanding of their visual impairment and lack of knowledge on the available services.16
The findings suggest that many blind persons are unaware of VRS and how accessing VRS could enable them cope with the challenges of living with vision impairment. Furthermore, the study showed that inadequate referral of blind persons for VRS by eye care professionals significantly contribute to the problem of access to VRS. Arguably, it is likely that such inadequacy in referral is due to the scarcity of VRS providers. A major challenge with the subspecialty of vision rehabilita�on is the lack of Vision Rehabilita�on Therapists (VRTs). Whereas there are about 3000 Optometrists in Nigeria23, opportuni�es for postgraduate Diploma, Masters or PhD trainings in the field of VRT are limited. The problem of scarce human resources in rehabilita�on is, however, not limited to vision rehabilita�on and efforts should be made to improve opportuni�es for training rehabilita�on professionals.24 In addi�on, at the referral level in Nigeria, awareness of available VRS services from Ophthalmologists and Optometrists
is unknown and there might be a need for increased co-opera�on and referral between VRS providers. A useful way of increasing pa�ents’ knowledge of VRS is to incorporate vision rehabilita�on into the con�nuum of eye care thus encouraging every Ophthalmologist and Optometrist to advise pa�ents with VA less than 6/18, scotoma, visual field loss or contrast sensi�vity loss, that vision rehabilita�on op�ons exist. In the United States and Canada, Optometrists and Ophthalmologists provide components of vision rehabilita�on in private prac�ces, academic departments, and independent rehabilita�on agen-cies.25 There is a con�nuum of vision rehabilita�on care in both countries, beginning with diagnosis and moving to visual func�on assessment, assessment for op�cal devices, rehabilita�on planning, and on to training and services such as orienta�on and mobility, and finally to numerous support services that make a difference for pa�ents with low vision or legal blindness.25
Our study revealed that males were more likely to men�on that they did not need VRS. This finding is consistent with previous studies showing that men are less likely to admit weakness and seek medical a�en�on.26 It is therefore not surprising that in the inves�gated explana�ons for non-uptake of VRS conducted within this study, men were more likely than women to not see the need for VRS. Findings further revealed that par�cipants aged 61 years and over as well as those that were blind for more than eleven years were more likely to report that VRS was not needed. It is also possible that with increasing years of living with blindness, adapta�on skills are uniquely and personally developed based on the individuals’ personal experiences27 thus increasing the pa�ents’ reluctance to seek VRS.
JNOA.2018;20(2): 8 - 14 Okonji et al
Original Research Article

Journal of the Nigerian Optometric Association
14
Limitations of study
28. Queensland Vision Initiative Inc. Referral Pathway Pilot Project Summary. Brisbane, 2010.29. Adam R, Pickering D. Where are all the clients? Barriers to referral for low vision rehabilitation. Visual Impairment Research. 2007; 9(2-3):45-50.
As soon as pa�ents are diagnosed of low vision, raising their awareness of the VRS as well as the ra�onale behind VR might help increase service uptake. The Queensland Referral Pathway Pilot Project iden�fied late referral with advanced visual loss as an issue.28 Adam and Pickering29 noted that 62 per cent of Canadian ophthalmologists consider vision of less than 6/60 should be immediately referred. Adop�ng this recommended prac�ce on referring pa�ents could prevent them reaching a crisis point of unwillingness to take-up VRS.
The study did not inves�gate the presence of co-morbidi�es and how such factors could contribute to the low uptake of VRS. A major limita�on of the
study design lies in the use of snowball sampling techniques to access poten�al par�cipants. As snowball sampling technique was employed, the degree to which the sample is a true representa�ve of the popula�on is uncertain. Another limita�on of the present study which makes it difficult to generalize finding to the overall popula�on of blind persons is that the data were collected from a single city. In addi�on, the study did not inves�gate the barriers to referrals from clinicians.
JNOA.2018;20(2): 8 - 14 Okonji et al
Original Research Article
Uptake of vision rehabilita�on services among many blind persons in urban Nigeria remains poor. Knowl-edge of VRS and inadequate referrals for vision rehabilita�on by eye care professionals are major barriers precluding access to VRS. The percep�on that cost of VRS is exorbitant appears to be another key reason why some people with blindness do not seek rehabilita�on.
The scope and focus of the study was on blind par�cipants only. Future studies could explore the challenges of low uptake of VRS from the perspec�ves of VRTs, optometrists and ophthalmologists. Lastly, although the explored explanatory variables for non-uptake of VRS among par�cipants are moderate and consistent with previous studies of factors influencing uptake of vision care services, it is not necessarily exhaus�ve. Future research should inves�gate addi�onal explanatory factors that can provide more robust explana�ons for blind people’s non-uptake of VRS.
CONCLUSION AND RECOMMENDATION

Down syndrome (DS) or Down's syndrome, also known as trisomy 21, is a gene�c disorder caused by the presence of all or part of a third copy of chromosome 21. It is the most common chromosomal abnormality in humans1, occurring in about 1 per 1000 babies born each year. The incidence is es�mated to be about 1 in 600 live births2. It occurs in people of all races and economic levels, though
older women have an increased risk of having a child with Down syndrome but the cause of non-disconjuc�on is s�ll unknown3. This condi�on is typically associated with physical growth delays, characteris�c facial features and mild to moderate intellectual disabili�es4. In recent history, advances in medicine and science have enabled researchers to inves�gate the characteris�cs of people with Down syndrome. About 60% of people
JNOA.2018;20(2): 15 - 22
Down syndrome is the most common chromosomal disorder and many with the condi�on tend to be more at risk of several ocular disorders than those without Down syndrome. The study was aimed at assessing the distribu�on of refrac�ve errors in children with Down syndrome between 5-18 years of age. The cross-sec�onal study used data from 104 children with Down syndrome from selected exclusive special needs schools in Lagos State, Nigeria. Visual acuity was measured using the Lea symbol chart and non-cycloplegic refrac�on was carried out using both sta�c re�noscopy and autorefrac�on. Significant refrac�ve error was defined as myopia, hyperopia and as�gma�sm of 0.75D and above respec�vely. Data was analysed using IBM SPSS sta�s�cal so�ware version 20.1. Chi-square and independent t test were used to test the hypotheses. A total of 91 children with Down syndrome were examined; 52 (57.1%) were males with a mean age of 13.6 +3.8 years. The study showed that refrac�ve errors was present in 82 (95.3%) of the par�cipants, with as�gma�sm being the commonest form of refrac�ve error occurring in 61(67%) followed by hyperopia 12(13.2%) and myopia 7(7.7%) of the 91 par�cipants studied. The study also supported the null hypothesis that there is no significant difference between the types of refrac�ve error and gender (p=0.8331). Recorded visual acui�es also revealed a generalised reduced visual acuity which significantly improved with best op�cal correc�on (p <0.001). This study indicates the need for people with Down syndrome to be provided with prompt eye care services.
Keywords: Refrac�ve error, Down syndrome, visual acuity, prevalence, distribu�on
Journal of the Nigerian Optometric Association Original Research Article
1. Pro-Optics Ltd, 230 muri Okunola, Victoria Island, Lagos2. Department of Public Health, College of Medical Sciences, University of Calabar, Calabar, Nigeria3. Dunamis Eye Center, 35 Simpson St, Sure, Lagos Island, Lagos, Nigeria4. Department of Optometry, Faculty of Life Sciences, University of Benin, Benin City, Nigeria
1. Malt EA, Dahl RC, Haugsand TM. Health & diseases in adults with Down syndrome, Tidsskr Nor Laegenforen. 2013; 133(3): 290-294.2. Fryns JP, Timmermans J, Hoedemaekers J, Emmery L.Chromosome 21 , Trisomy 21, Indian J. Pediatr. 1987; 54: 723-727.3. Gaulden M E. Maternal age effect: the enigma of Down syndrome and other trisomic conditions. Mutat Res 1992; 296:68-88.4. Weijerman ME. et al. Clinical practice.The care of children with Down syndrome. European Journal of Pediatrics. 2010; 169(12): 1445-52.
Nwokedi O.,1 Ekpenyong B.N.,2 Musa N.R.3 and Ovenseri-Ogbomo G.O4
Nwokedi, O. Email: [email protected] Phone: + 2348034933590
15
Refractive Errors in Children with Down syndrome in Lagos State, Nigeria.
Corresponding Author:
Abstract
Introduction
Nwokedi et al

Journal of the Nigerian Optometric Association
16
5. Akinci A, Oner O, Bozkurt OH, Guven A, Munir K. Refractive Errors and Strabismus in Children with Down Syndrome ;a controlled study. J PediatrOphthalmol Strabismus. 2009;46(2): 83-86.6. Krinsky–McHale SJ, SilvermanW, Gordon J,Devenny DA, Oley N, Abramov I. Vision Deficits in Adults with Down Syndrome. J ApplRes Intellect Disabil. 2014; 27(3): 247-263.7. Singh M, Singh U. Bilateral congenital lacrimal fistula in Down syndrome. Middle East Ophthalmol Strabismus. 2013; 20(3):263-264.8. Woodhouse JM, Pakeman VH, Cregg M, Saunders KJ, Parker M, Fraser WI, Sastry P, Lobo S. Refractive error in young children with Down Syndrome ,Optom Vis Sci. 1997; 74: 844-854.9. Haugen O, Hovding G, Lundstrom I. Biometric measurements of the eyes in teenagers and young adults with Down syndrome. Acta Ophthalmol Scand. 2001; 79(6): 616-25.10. Courage ML, Adams RJ, Reyno S. Visual acuity in infants and children with Down Syndrome Development Medicine & Child psychology. 1994; 36(7): 586-593.11. Woodhouse JM, Meides JS, Lear SJ, Saunders KJ. Reduced accommodation in children with Down Syndrome. Invest Ophthalmol Vis Sci. 1993; 34(7): 2382-2387.12. AL-Bagdady M, Murphy PJ, Woodhouse MJ. Development and Distribution of Refractive Error in Children with Down Syndrome Throughout Childhood and Early Teenage Years. Br J Ophthamol. 2011; 95(8): 1091-1097.13. Doyle SJ, Bullock J, Gray C, Spenser A, Cunnigham C. Characteristics ocular findings in Asian children with Down syndrome. Eye. 2002; 16: 710-714.14. Berk AT, Saatci AD, Ercal MD. Ocular findings in 55 patients with Down syndrome. ophthalmic Genet. 1996; 17: 15-19.15. Gardiner DA. (1967) Visual defects in cases of Down syndrome and other mentally handicapped children. Br J Ophthalmol. 1967; 82: 793-796.16. Salati R, Simonetta S, Verga S, Brill J. Refraction & ocular motility in 72 Down patients. Saggi- NeuropsicologiaRiabilitazione. 1995; 21:71-77.17. Cregg M, Woodhouse JM, Stewart RE. Development of Refractive Error and Strabismus in Children with Down Syndrome. Invest Opthalmol Vis. Sci. 2003; 44(3): 1023 -1030.18. Mohindra I, Held R, Gwiazda J, Brill J. Astigmatism in infants. Science. 1978; 202: 329-331.19. Gwiazda J, Mohindra I, Brill S, Held R. Infant astigmatism &meridional amblyopia . Vision Res. 1985; 25:1267-1276.20. Howland H, Sayles N. Photorefractive measurements of astigmatism in infants & young children. Invest Ophthalmol Vis Sci. 1984; 25:93-102.21. Adio AO, Wajuihian SO.Ophthalmic Manifestation in Children with Down Syndrome in Port Harcourt. Nigeria. ClinOphthalmol. 2012; 6: 1859-64.22. Ebeigbe JA, Akpalaba R. Ocular Health Status of Subjects with Down Syndrome in Benin City, Nigeria. Afr J Med Sci.2006; 35: 365-368.23. Ljubic A, Trajkovski V. Refractive Error in Children and Young Adults with Down Syndrome. ACTA Ophthalmol. 2011; 89: 324-327.24. Kim U, Hwang J. Refractive Errors and Strabismus in Asian Patients with Down Syndrome Eye. 2009; 23: 7560-4.
with Down syndrome have ocular manifesta�ons. Ocular findings in Down syndrome include a wide range of visual acui�es due to refrac�ve errors and amblyopia, strabismus, nystagmus, lid abnormali�es including prominent, upwards slan�ng of the palpebral fissure, epicanthal folds, lid infec�ons including blephari�s, blepharoconjunc�vi�s, chalazion and hordeola. Furthermore, they may have nasolacrimal duct obstruc�on, corneal ectasia, iris brushfield spots seen in about 90% cases especially those with lightly pigmented irides, presenile cataracts, glaucoma, and re�novascular anomalies5-7.
The distribu�on of refrac�ve errors in school aged children with Down syndrome and cerebral palsy are different from that of typical children. Inves�ga�ons have all revealed very dis�nct, complex and aberrant visual development in children with Down syndrome from early months of life un�l school age8-10. Studies have shown that in children with Down syndrome, the distribu�on of refrac�ve errors in the first years of life mirrors that of typical children but widens over �me rather than narrows, also emmetropisa�on is believed to fail in most of these children with down syndrome and cerebral Palsy11-13.
People with Down syndrome have been reported to have a higher incidence of refrac�ve errors8,14. Reports on the prevalence of children with refrac�ve
errors vary in literature but it is generally agreed to exceed 40%15 and this high prevalence occurs amongst school children with Down syndrome as well as adults11,16. Refrac�ve errors and squint maybe present from an early age and persist into childhood8,9,17. The most common refrac�ve error is hypermetropia which o�en reduces spontaneously in other children, is likely to persist beyond infancy in DS subjects9.
Despite the high prevalence of large refrac�ve errors in children with Down syndrome, longitudinal data show that these are not always present in early infancy17. The prevalence of as�gma�sm among infants (0–12 months) has been reported to be 45–53% (defining as�gma�sm ≥ 1.00 D) in studies using non-cycloplegic techniques18,19 and as 65% (as�gma�sm of ≥ 0.75 D) using photorefrac�on20. Although the incidence of ocular anomalies in children with Down syndrome varies in different studies, they have shown that children with Down syndrome were more at risk for several ocular disorders than typical children. Whilst studies in Port Harcourt21 and Benin22 respec�vely have reported on ocular manifesta�ons in Down syndrome, there are no documenta�ons in Lagos state. This is in contrast with comprehensive studies carried out on refrac�ve errors in children including infants and school aged children with Down syndrome in Europe, Americas and Asia8,23,24. Furthermore, whereas the distribu�on and prevalence of refrac�ve
JNOA.2018;20(2): 15 - 22 Nwokedi et al
Original Research Article

Journal of the Nigerian Optometric Association
17
Method
error amongst school children in different popula�on se�ngs is known25-30, li�le is known about the prevalence of refrac�ve error among children with Down syndrome in Nigeria. Children with Down syndrome are o�en neglected when na�onal eye health and rehabilita�on programmes are planned therefore the need for this study. The ra�onale behind this study is that refrac�ve errors in children and people generally with Down syndrome is largely under reported compared to children without Down syndrome. There is need to inves�gate this problem in other to know the distribu�on of refrac�ve errors among children with Down syndrome and to be able to compare its prevalence with that of children without Down syndrome. The findings will assist eye care prac��oners in managing the visual problems associated with Down Syndrome as well as improving the quality of life in this special popula�on.
The study was a cross sec�onal analy�c study design using quan�ta�ve method of data collec�on. The study area was Lagos, Lagos State, Nigeria. Lagos State is located in the south west geopoli�cal zone of Nigeria. It has six educa�onal districts and there are two categories of special schools in Lagos State, five exclusive schools and 38 inclusive schools. Only the schools exclusively for special children were used for the study. Surulere and Yaba in districts two and three were purposively selected for this study because most of the special needs schools in Lagos state are located in Surulere and Yaba. All the three State owned exclusive special needs schools in Surulere and Yaba were selected for the study, also it was necessary to include the
Down Syndrome Founda�on, a non-profit, non-gov-ernmental founda�on which is recognised by Lagos State and exclusively dedicated only to persons with Down Syndrome, also located in Surulere, Lagos State. The reason was to increase the sample size for the study as this founda�on has the largest popula�on of children with Down syndrome in Lagos State. These schools already have confirmed cases of children with Down Syndrome. The desired sample size was 104, and sampling was propor�onately done according to the size of the four schools selected. Simple random sampling was used to select children who met the inclusion criteria (children 5-18 years old with Down syndrome who has wri�en informed consent from parents were selected). Selected children who were uncoopera�ve, even with the assistance of the school teacher were excluded, also those who were absent from school were not included in the study.
A total of 91 children out of the 104 selected children were examined. This was because some children were uncoopera�ve while some were absent from school due to ill health and other reasons on the day of eye examina�on. The following eye test was carried out for all children recruited for the study: Visual Acuity assessment at distance and near using the Lea symbol for distant/near tes�ng (Brand, copm, country) depending on their abili�es; External eye examina�on using pen light; internal eye exam using the ophthalmoscope; ocular alignment using alternate cover/uncover test without Prisms; Hirsberg tests also for ocular alignment (corneal reflex test); Non-cycloplegic re�noscopy using streak re�noscope; Auto-Refrac�on using Auto Ref-keratometer PRK-5000 Potec co Ltd.; Subjec�ve refrac�on when possible using trial frame and lenses.
All examina�ons were done over the same period between 9am-1pm. Due to poor a�en�on and concentra�on
JNOA.2018;20(2): 15 - 22 Nwokedi et al
Original Research Article
25. Ahuama OC, Atowa UC. Distribution of Refractive Errors Among School Children in Abia State of Nigeria. J Nig Optom Assoc. 2004; 11: 25.26. Ovenseri GO. Omuenu VO. Prevalence of Refractive Error Among School Children in Cape Coast Municipality, Ghana. Clinical Optometry. 2010; 259-66.27. Opibiri O. Refractive error pattern in children in south-south Nigeria; Sky journal of Medicine and medical sciences 2013;1(3):10-14.28. Faderin MA, Ajaiyeoba AI. (2001). Refractive errors in Primary school children in Nigeria, Nigerian journal of ophthalmology. 2001; 9(1):10-14.29. Ekpenyong BN, Naidoo K, Ahaiwe K, Ndukwe O, Emmanuel O, Ezenwankwo O,Ekanem E. Visual Status and prevalence of eye disorders among school-age children in southern Nigeria. African Vision and Eye Health Journal. 2017; 76:130. Ekpenyong BN, Naidoo K, Ndep OA, Ahaiwe K, Ndukwe O, Nwandu D, Ezenwankwo O, Ekanem E. Comparative analysis of satisfaction with the use of ready-made spectacles and custom-made spectacles among school children in Nigeria: A Randomised Controlled Trial. Journal of Health; Medicine and Nursing. 2017; 35: 15-21(ISSN 2422-8419).

Journal of the Nigerian Optometric Association
18
Results
Discussion
skills in this popula�on, a�en�on was mo�vated using fixa�on target, toys, clapping of hands and calling of names. These were used as strategies for improving a�en�on and concentra�on. S�ckers were given to each par�cipa�ng child for a job well done. Only the Lea symbols were used for tes�ng the visual acuity. The criteria used for classifica�on of refrac�ve errors were; myopia ≥ -0.75DS, hyperopia ≥ + 0.75DS, as�gma�sm ≥ - 0.75DC.
Ethical approval for this study was obtained from the Ethics Commi�ee of the Lagos State Ministry of Health and permission to enter the schools was obtained from the Lagos State Ministry of Educa�on using the approval from the Ministry of Health. Consent was sought from the State Universal Basic Educa�on Board (SUBEB) and the school authori�es. Informed consent was obtained from parents of the children who par�cipated in the study through the schools. Uncoopera�ve children who were unable to be examined and whose parents or guardians did not give consent to the eye examina�on were excluded.
Sta�s�cal analysis of the data obtained was performed using the IBM Sta�s�cal Package for Social Sciences (SPSS) version 20.1. Chi-square and the independent t test sta�s�cs were used to test for associa�on between variables. The results were represented using appropriate tables and figures, showing frequencies and percentages.
A total of 91 par�cipants were examined in this study. This comprised of 52 (57.1%) males and 39 (42.9%) females (Figure 1). The mean age of the 91 subjects was 13.6 ± 3.7 years with a median of 14.0 years. There was no sta�s�cal significant difference in the mean age of females (M=13.1, SD =3.9) and males (M=14, SD =3.6), (P = 0.280)
The distribu�on of presen�ng visual acuity is shown in Table 1. Visual acuity could not be determined in 17 right eyes and 16 le�s of the pa�ents. A total of 48
(52.7%) subjects had normal or mild to moderated visual impairment (VA between 6/6 and 6/18) in each eye, 26 (28.6%) and 27 (29.7%) had low vision (VA <6/18 to 3/60) in the right and le� eye respec�vely using the Interna�onal Classifica�on of Disease (ICD). There was improvement in visual acuity of the subjects a�er subjec�ve refrac�on. The number of the par�cipants with vision of 6/18 or be�er increased from 48 to 72 a�er best correc�on.
Of the total 91 par�cipants, the refrac�ve status could not be determined in four subjects (all male), while five subjects had emmetropia. The prevalence rate of refrac�ve errors among children with Down’s syndrome in the present study was 95.3% (95% CI = 88.9 – 97.4%). The prevalence of refrac�ve errors in male and female par�cipants was 93.8% (95% CI = 85.8 – 97.9%) and 94.9% (95% CI = 86.1 – 98.7%)respec�vely. There was no significant difference in the prevalence of refrac�ve errors in male and female par�cipants (p = 0.8331) (Table 3), In terms of the magnitude, the refrac�ve errors ranged from – 11.00 DS to + 4.25 DS (spherical equivalent) while the as�gma�sm ranged from – 0.50 DC to – 4.00 DC As�gma�sm was the most common refrac�ve error being present in 61 (67.0%) of the subjects examined followed by hyperopia, 12 (13.2%) and myopia, 7 (7.7%). The prevalence of as�gma�sm was further analysed by types. Out of the 61 subjects with as�gma�sm, 27 (44.3%) had hyperopic as�gma�sm followed by myopic as�gma�sm, 19 (31.1%); simple as�gma�sm, 12 (19.7%) and mixed as�gma�sm, 3 (4.9%). More male par�cipants had hyperopic as�gma�sm (30.8%) while more female par�cipants had myopic as�gma�sm (30.8%). However, there was no sta�s�cally significant rela�onship between the type of as�gma�sm and the gender of children with Down syndrome (χ2 = 2.559, p = 0.465).
Refrac�ve anomalies in pa�ents with Down syndrome are very common and their incidence vary from 65% to 100%31,32.The present study is a further confirma�on of refrac�ve
JNOA.2018;20(2): 15 - 22 Nwokedi et al
Original Research Article
31. Karaman K, Kabalar E. Double Aneuploidy in a Turkish child: Down – Klinefelter syndrome. CongenitaAnom (Kyoto). 2008; 48(1): 45-47.32. Dobrilla K, Sinisa S, Vida C, Davor G, Ljubo Z, Hana K. The ophthalmic anomalies in children with Down syndrome in Split – Dalmatian County. Coll. Antropol. 2011; 35(4): 1115-1118.

Journal of the Nigerian Optometric Association
19
anomalies in pa�ents with Down syndrome. In this study, refrac�ve errors occurred in over half of the popula�on of the children with Down syndrome examined. Out of the 91 children studied, 82 had one form of refrac�ve error or the other. This result varies with the prevalence of refrac�ve error among children without Down syndrome in Nigeria which ranges from 5% to 15% 25,27-30. The distribu�on of refrac�ve error in this study revealed that the most common form was as�gma�sm, followed by hyperopia and myopia. This supports the study by Adio et al.21, where more than half (76.2%)of the 42 children with Down syndrome screened had refrac�ve errors, also further suppor�ng this finding are results in similar studies conducted within and outside Nigeria8,9,31,32.
Of the 61 cases of as�gma�sm; hyperopic as�gma�sm was the highest, followed by myopic as�gma�sm, simple as�gma�sm and mixed as�gma�sm. The percentage was higher than that found in a popula�on of children and young adults without Down Syndrome in various other studies8,14,23. The distribu�on in this study also supports studies carried out by Haugen et al.9 where they reported that as�gma�sm was found to be the highest occurring refrac�ve error, followed by hyperopia and myopia. The study however did not dis�nguish between the types of as�gma�sm present. In some other similar studies, by Kim and Hwang24, Ljubic and Trajkovski23 as�gma�sm was also found to have the highest occurrence followed by hyperopia and myopia.
In a study by Cregg et al.17 of 123 children with Down syndrome, the most prevalent refrac�ve error was hyperopic as�gma�sm which is in line with the result of this study. This trend contradicts that found in school children without Down syndrome of comparable age group where myopia was found to have the highest prevalence with environmental, hereditary, increased near work and recently computer or visual display suggested to play a role 25-28.
The high incidence of refrac�ve errors in children with Down syndrome is believed to be caused by failure of emmetropisa�on process in Down syndrome. The change in spherical refrac�ve error was found to be minimal throughout childhood and early adulthood. According to another study, the children had a specific development of as�gma�sm of oblique nature which was also found in this study and is suggested to be due to mechanical induc�on through the eyelids12. The thinning of corneal stroma may account for the steeper cornea and the high frequencies of as�gma�sm seen in Down Syndrome due to lower corneal rigidity. The cornea in Down syndrome is thought to be thinner and steeper and corneal shape plays a significant role in the development of as�gma�sm in Down syndrome. This may also predispose this popula�on to keratoconus. Oblique as�gma�sm is commonly found in this group of pa�ent popula�on9, Sta�s�cal test also found that there is no significant rela�onship between the type of as�gma�sm and the gender of par�cipants in this study.
JNOA.2018;20(2): 15 - 22 Nwokedi et al
Original Research Article
8. Woodhouse JM, Pakeman VH, Cregg M, Saunders KJ, Parker M, Fraser WI, Sastry P, Lobo S. Refractive error in young children with Down Syndrome ,Optom Vis Sci. 1997; 74: 844-854.9. Haugen O, Hovding G, Lundstrom I. Biometric measurements of the eyes in teenagers and young adults with Down syndrome. Acta Ophthalmol Scand. 2001; 79(6): 616-25.12. AL-Bagdady M, Murphy PJ, Woodhouse MJ. Development and Distribution of Refractive Error in Children with Down Syndrome Throughout Childhood and Early Teenage Years. Br J Ophthamol. 2011; 95(8): 1091-1097.14. Berk AT, Saatci AD, Ercal MD. Ocular findings in 55 patients with Down syndrome. ophthalmic Genet. 1996; 17: 15-19.16. Salati R, Simonetta S, Verga S, Brill J. Refraction & ocular motility in 72 Down patients. Saggi- NeuropsicologiaRiabilitazione. 1995; 21:71-77.17. Cregg M, Woodhouse JM, Stewart RE. Development of Refractive Error and Strabismus in Children with Down Syndrome. Invest Opthalmol Vis. Sci. 2003; 44(3): 1023 -1030.21. Adio AO, Wajuihian SO.Ophthalmic Manifestation in Children with Down Syndrome in Port Harcourt. Nigeria. ClinOphthalmol. 2012; 6: 1859-64.22. Ebeigbe JA, Akpalaba R. Ocular Health Status of Subjects with Down Syndrome in Benin City, Nigeria. Afr J Med Sci.2006; 35: 365-368.23. Ljubic A, Trajkovski V. Refractive Error in Children and Young Adults with Down Syndrome. ACTA Ophthalmol. 2011; 89: 324-327.25. Ahuama OC, Atowa UC. Distribution of Refractive Errors Among School Children in Abia State of Nigeria. J Nig Optom Assoc. 2004; 11: 25.27. Opibiri O. Refractive error pattern in children in south-south Nigeria; Sky journal of Medicine and medical sciences 2013;1(3):10-14.28. Faderin MA, Ajaiyeoba AI. (2001). Refractive errors in Primary school children in Nigeria, Nigerian journal of ophthalmology. 2001; 9(1):10-14.29. Ekpenyong BN, Naidoo K, Ahaiwe K, Ndukwe O, Emmanuel O, Ezenwankwo O,Ekanem E. Visual Status and prevalence of eye disorders among school-age children in southern Nigeria. African Vision and Eye Health Journal. 2017; 76:130. Ekpenyong BN, Naidoo K, Ndep OA, Ahaiwe K, Ndukwe O, Nwandu D, Ezenwankwo O, Ekanem E. Comparative analysis of satisfaction with the use of ready-made spectacles and custom-made spectacles among school children in Nigeria: A Randomised Controlled Trial. Journal of Health; Medicine and Nursing. 2017; 35: 15-21(ISSN 2422-8419).31. Karaman K, Kabalar E. Double Aneuploidy in a Turkish child: Down – Klinefelter syndrome. CongenitaAnom (Kyoto). 2008; 48(1): 45-47.32. Dobrilla K, Sinisa S, Vida C, Davor G, Ljubo Z, Hana K. The ophthalmic anomalies in children with Down syndrome in Split – Dalmatian County. Coll. Antropol. 2011; 35(4): 1115-1118.
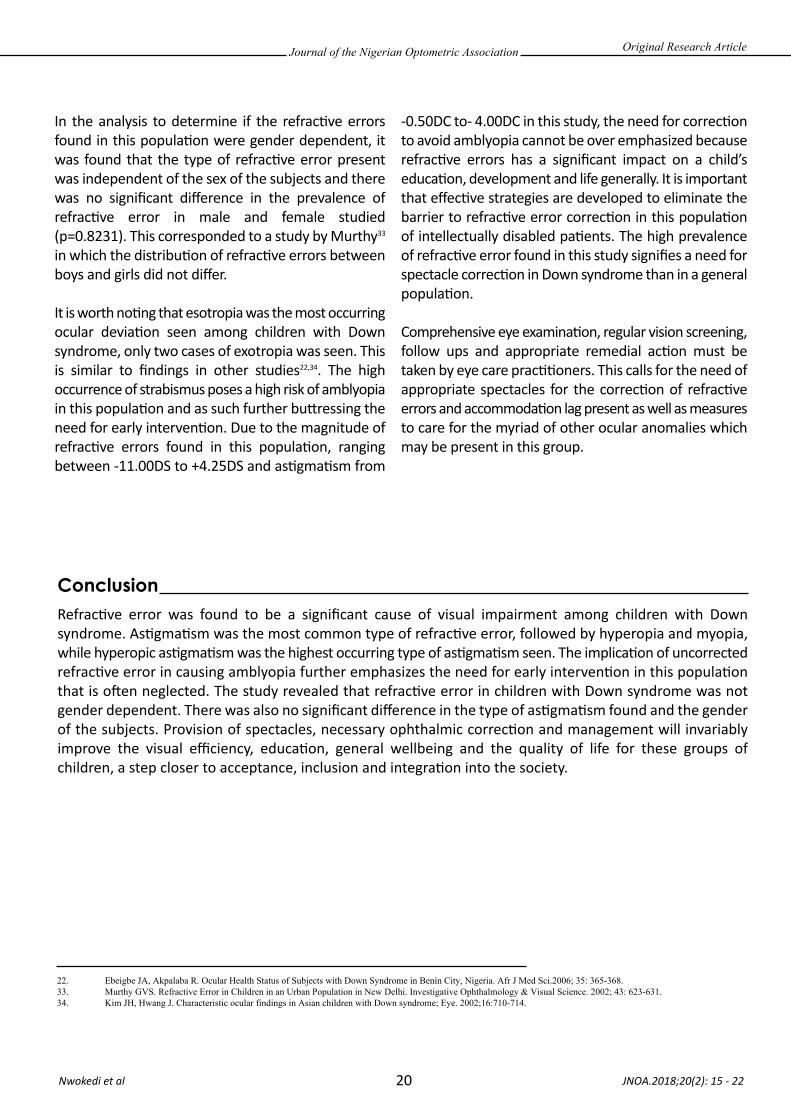
Journal of the Nigerian Optometric Association
20
In the analysis to determine if the refrac�ve errors found in this popula�on were gender dependent, it was found that the type of refrac�ve error present was independent of the sex of the subjects and there was no significant difference in the prevalence of refrac�ve error in male and female studied (p=0.8231). This corresponded to a study by Murthy33 in which the distribu�on of refrac�ve errors between boys and girls did not differ.
It is worth no�ng that esotropia was the most occurring ocular devia�on seen among children with Down syndrome, only two cases of exotropia was seen. This is similar to findings in other studies22,34. The high occurrence of strabismus poses a high risk of amblyopia in this popula�on and as such further bu�ressing the need for early interven�on. Due to the magnitude of refrac�ve errors found in this popula�on, ranging between -11.00DS to +4.25DS and as�gma�sm from
-0.50DC to- 4.00DC in this study, the need for correc�on to avoid amblyopia cannot be over emphasized because refrac�ve errors has a significant impact on a child’s educa�on, development and life generally. It is important that effec�ve strategies are developed to eliminate the barrier to refrac�ve error correc�on in this popula�on of intellectually disabled pa�ents. The high prevalence of refrac�ve error found in this study signifies a need for spectacle correc�on in Down syndrome than in a general popula�on. Comprehensive eye examina�on, regular vision screening, follow ups and appropriate remedial ac�on must be taken by eye care prac��oners. This calls for the need of appropriate spectacles for the correc�on of refrac�ve errors and accommoda�on lag present as well as measures to care for the myriad of other ocular anomalies which may be present in this group.
JNOA.2018;20(2): 15 - 22 Nwokedi et al
Original Research Article
22. Ebeigbe JA, Akpalaba R. Ocular Health Status of Subjects with Down Syndrome in Benin City, Nigeria. Afr J Med Sci.2006; 35: 365-368.33. Murthy GVS. Refractive Error in Children in an Urban Population in New Delhi. Investigative Ophthalmology & Visual Science. 2002; 43: 623-631. 34. Kim JH, Hwang J. Characteristic ocular findings in Asian children with Down syndrome; Eye. 2002;16:710-714.
Refrac�ve error was found to be a significant cause of visual impairment among children with Down syndrome. As�gma�sm was the most common type of refrac�ve error, followed by hyperopia and myopia, while hyperopic as�gma�sm was the highest occurring type of as�gma�sm seen. The implica�on of uncorrected refrac�ve error in causing amblyopia further emphasizes the need for early interven�on in this popula�on that is o�en neglected. The study revealed that refrac�ve error in children with Down syndrome was not gender dependent. There was also no significant difference in the type of as�gma�sm found and the gender of the subjects. Provision of spectacles, necessary ophthalmic correc�on and management will invariably improve the visual efficiency, educa�on, general wellbeing and the quality of life for these groups of children, a step closer to acceptance, inclusion and integra�on into the society.
Conclusion
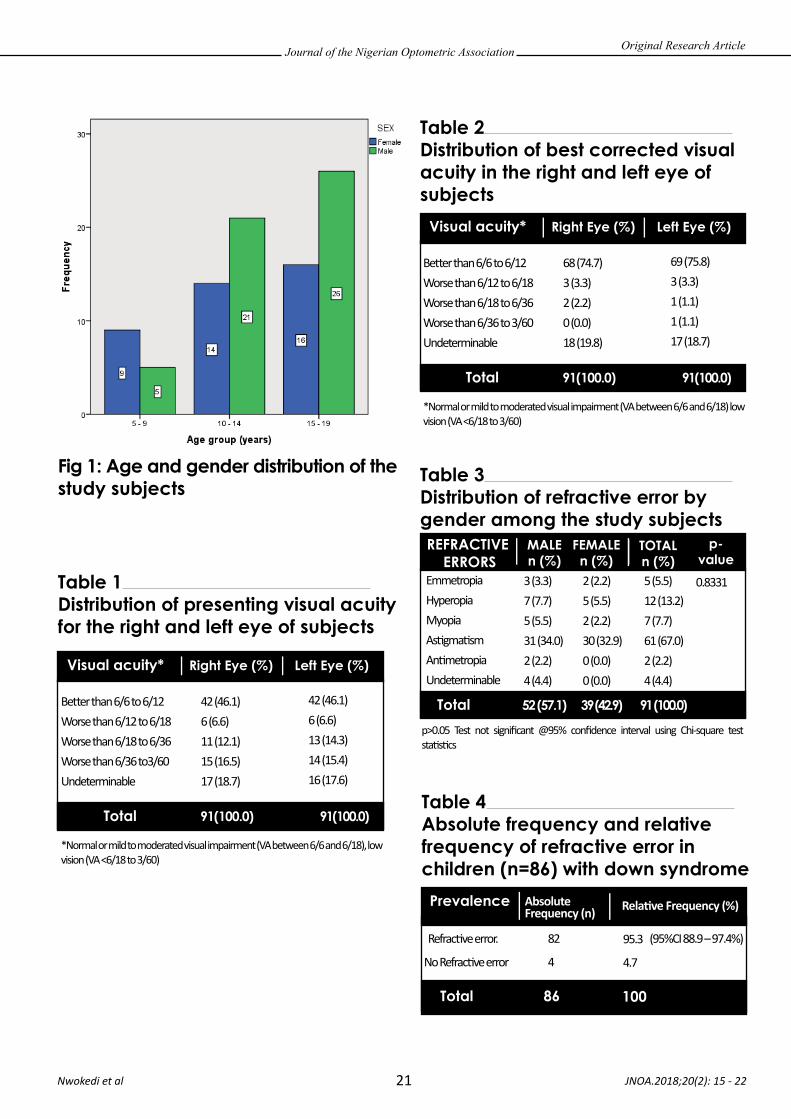
Journal of the Nigerian Optometric Association
21 JNOA.2018;20(2): 15 - 22 Nwokedi et al
Original Research Article
Table 3 Distribution of refractive error by gender among the study subjectsREFRACTIVE
ERRORS
Total 52 (57.1) 91 (100.0)39 (42.9)
TOTALn (%)
p-value
MALEn (%)
FEMALEn (%)
EmmetropiaHyperopiaMyopiaAs�gma�smAn�metropiaUndeterminable
3 (3.3)7 (7.7)5 (5.5)31 (34.0)2 (2.2)4 (4.4)
2 (2.2)5 (5.5)2 (2.2)30 (32.9)0 (0.0)0 (0.0)
5 (5.5)12 (13.2)7 (7.7)61 (67.0)2 (2.2) 4 (4.4)
0.8331Table 1 Distribution of presenting visual acuity for the right and left eye of subjects
Visual acuity*
Total 91(100.0) 91(100.0)
Left Eye (%)Right Eye (%)
Be�er than 6/6 to 6/12Worse than 6/12 to 6/18Worse than 6/18 to 6/36Worse than 6/36 to3/60Undeterminable
*Normal or mild to moderated visual impairment (VA between 6/6 and 6/18), low vision (VA <6/18 to 3/60)
p>0.05 Test not significant @95% confidence interval using Chi-square test sta�s�cs
42 (46.1)6 (6.6)11 (12.1)15 (16.5)17 (18.7)
42 (46.1)6 (6.6)13 (14.3)14 (15.4)16 (17.6)
Table 4 Absolute frequency and relative frequency of refractive error in children (n=86) with down syndromePrevalence Absolute
Frequency (n) Rela�ve Frequency (%)
Refrac�ve error.
No Refrac�ve error
82
4
95.3
4.7
Total 86 100
(95%CI 88.9 – 97.4%)
Fig 1: Age and gender distribution of the study subjects
Table 2 Distribution of best corrected visual acuity in the right and left eye of subjects
Visual acuity*
Total 91(100.0) 91(100.0)
Left Eye (%)Right Eye (%)
Be�er than 6/6 to 6/12Worse than 6/12 to 6/18Worse than 6/18 to 6/36Worse than 6/36 to 3/60Undeterminable
*Normal or mild to moderated visual impairment (VA between 6/6 and 6/18) low vision (VA <6/18 to 3/60)
68 (74.7)3 (3.3)2 (2.2)0 (0.0)18 (19.8)
69 (75.8)3 (3.3)1 (1.1)1 (1.1)17 (18.7)
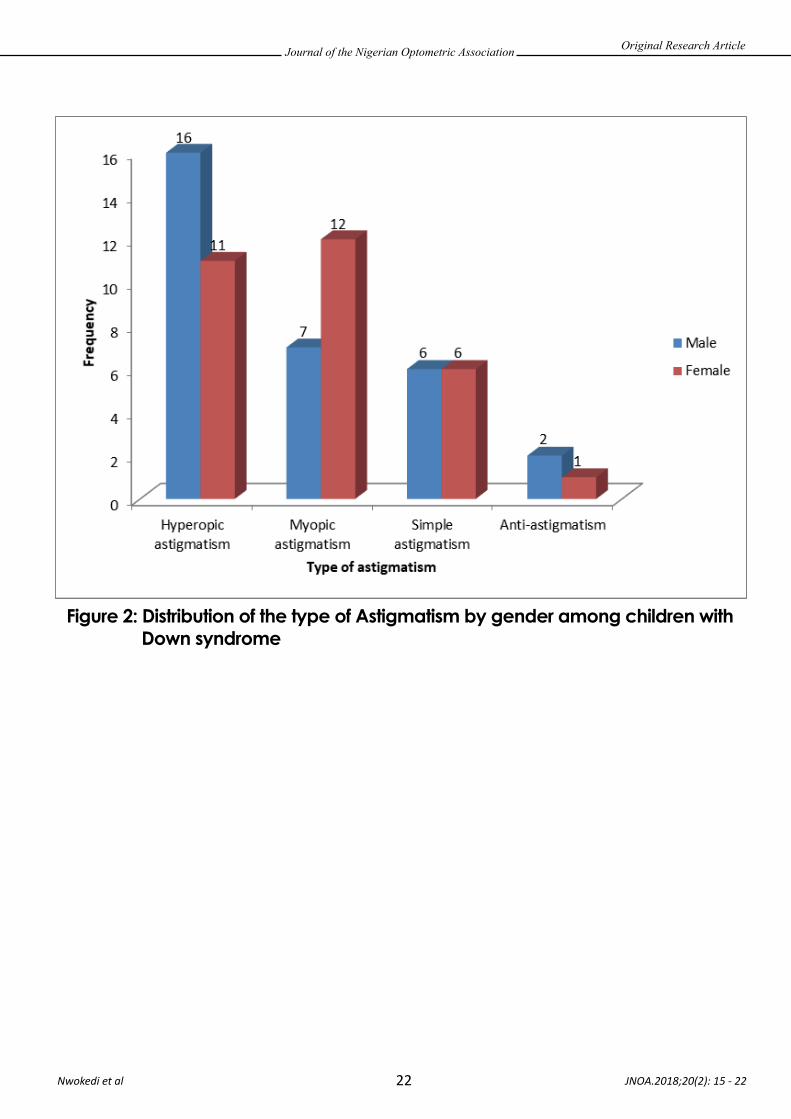
Journal of the Nigerian Optometric Association
22 JNOA.2018;20(2): 15 - 22 Nwokedi et al
Original Research Article
Figure 2: Distribution of the type of Astigmatism by gender among children with Down syndrome

Millions of school-going children unjus�fiably suffer from accommoda�ve anomalies because it remains undiagnosed1 and this is especially so in African paediatric popula�ons where these anomalies are underappreciated. These may be due to the decreased
par�cipa�on of prac��oners in binocular vision exam-ina�on, analysis and management2 and the paucity of evidenced-based studies in this area.Accommoda�ve anomaly (inadequate accommoda�ve accuracy and sustainability, inadequate amplitude, flexibility and
JNOA.2018;20(2): 23 - 30
Accommoda�ve anomalies even though have been associated with an increased risk of academic failure in the pediatric popula�on, yet have been underappreciated in African popula�ons. This prospec�ve cross sec�onal study which conformed to the Code of Ethics of the World Medical Associa�on (Declara�on of Helsinki) aimed to determine the frequencies of accommoda�ve anomalies among symptoma�c Junior High school children in the Cape Coast metropolis, Ghana.Accommoda�ve assessment (tes�ng for amplitude of accommoda�on, accommoda�ve lag, accommoda�ve facility, and nega�ve and posi�ve rela�ve accommoda�on) was conducted over best corrected refrac�on results in a mul�stage sample of 202 symptoma�c school children age ranged 12 to 17 years old. Descrip�ve data was analyzed using frequencies, percentages, means and standard devia�ons. Binary logis�c regression was used to test associa�ons between outcome variables. Of the symptoma�c par�cipants (202) assessed, 38 (18.8%) were diagnosed with ametropia, with the most frequent type being as�gma�sm 19 (9.4%). A number of 104 (51.5 %) symptoma�c par�cipants were diagnosed with accommoda�ve anomaly. The frequency of specific accommoda�ve anomalies among symptoma�c Junior High school children was as follows: accommoda�ve insufficiency, 45 (22.3%); accommoda�ve infacility, 22(10.9%); accommoda�ve excess, 27(13.4%) and accommoda�ve fa�gue, 10 (5%). Par�cipants with accommoda�ve anomalies had greater odds of experiencing symptoms of visual fa�gue associated with near work (OR =0.530, p= 0.001) compared with other symptoms. The study results indicate a high prevalence of accommoda�ve anomalies on this symptoma�c school going popula�on in Ghana and this can impact nega�vely on their academic performance.
Keywords: Accommoda�ve disorders, ametropia, asthenopic symptom, school children, Ghana
Journal of the Nigerian Optometric Association Original Research Article
1 Department of Optometry, University of Cape Coast, Ghana2 Ghana Red Cross Eye Care Services, Wa, Ghana3 Newlands Medical Center, Koforidua, Ghana.4 Inter-Star Eye Hospital, Tamale, Ghana
1. Maino D M. The Binocular vision Dysfunction Pandemic. Optom Vis Dev 2010; 41(1):6-13. 2. Opoku-Baah C , Mohammed A K, Afari C, Addai R, Yemanyi F, Adade S, Bonsu K. The management of Binocular Vision Anomalies by Eye Care Facilities in the Accra and Kumasi Metropolises (Ghana). Int J Innovat Appl Stud. 2014; 9(3): 1401- 1408.
Darko-Takyi C.,1 Ntodie M.,1 Alex Azuka Ilechie A.A.,1 Abokyi S.,1 Kyei S.,1 Aful H.K.,2 Nti, N.A.3 and Okae-Asante D.4
Charles Darko-Takyi Email: [email protected] Phone: +233545063571
23
Accommodative Anomalies in Symptomatic School Children in Cape Coast Metropolis, Ghana.
Corresponding Author:
Abstract
Introduction
Darko-Takyi et al

Journal of the Nigerian Optometric Association
24
3. Darko-Takyi C, Naimah E K, Urvashni N. A review of the classification of nonstrabismic binocular vision anomalies. Optometry Reports 2016; volume 6:56264. Garcia-Munoz A, Carbonell-Bonete S, Cacho-Martinez P. Symptomatology associated with accommodative and binocular vision anomalies. J Optom 2014;7(4): 178- 192.5. American Optometric Association. Optometric clinic practice guidelines: care of the patient with Accommodative and Vergence Dysfunction. [Internet].2010 [cited 2013 Feb 09]. p. 7-9, 27-40. Available from :http://www.aoa.org/documents/CPG-18.pdf6. Von Noorden GK, Campos EC. Binocular Vision and Ocular Motility: Theory and management of strabismus. 6th ed. Optom Vis Sci 2002. 7. Rouse M, Borsting E, Mitchell GL, Kulp MT, Scheiman M, Amster D,Coulter R, Fecho G, Gallaway M; The CITT Study Group. Academic Behaviors in Children with Convergence Insufficiency with and without Parent-Reported ADHD. Optom Vis Sci. 2009; 86(10):1169-77.8. Scheiman M, Gallaway M, Coulter R, Reinstein F, Ciner E, Herzberg C, Parisi M. Prevalence of vision and ocular disease conditions in a clinical pediatric population. J Am Optom Assoc 1996;67(4):193–202.9. Dwyer P. The prevalence of vergence accommodation disorders in a school-age population. Clin Exp Optom 1992;75(1):10–8.10. Metsing I, Ferreira J. Accommodation and vergence status among the 3rd and 4th graders in a mainstream school in Gauteng. S Afr Optom 2012;71(1):22–31.11. Hokoda SC. General binocular dysfunctions in an urban Optometry clinic. J Am Optom Assoc 1985;56(7):560-212. Lara F, Cacho P, García A, Megías R. General binocular disorders: prevalence in a clinic population. Ophthalmic Physiol Opt 2001; 21(1):70–4.13. Wajuihian S O, Hansraj R. Near vision anomalies in Black high school children in Empangeni, South Africa. S Afr Optom 2014;73(1):21-32.14. Du P, Coles F B, O’Campo P, McNutt L. Changes in population characteristics and their implication on public health research. Epidemiologic Perspectives and Innovations 2007;4:615. English PB, Kharrazi M, Davies S, Scalf R, Waller K, Neutra R. Changes in the spatial pattern of low birth weight in a southern California county: the role of individual and neigbourhood level factors. Soc Sci Med 2003;56(10):2073-8816. 15 Pickett KE, Ahern JE, Selvin S, Abrams B. Neighbourhood socio-economic status, maternal race and preterm delivery: a case-control study. Ann Epidemiol 2002;12(12):410-817. Abdur-Kabir M, Kumah D A, Koomson N Y, Afari C. Prevalence of accommodative insufficiency and accommodative infacility among junior high school students in a Ghanaian town. J Sci Technol 2014; 34(2):60-64.
facility and non-refrac�ve and non-aging neuromuscular abnormali�es of the visual apparatus3) being part of the binocular vision dysfunc�ons, in clinically significant forms presents with asthenopia.4 This is especially so in the high school age where the child puts more effort into reading and school work5 and thus can impact nega�vely on academic performance.6,7
Studies by Scheiman et al.8, Dwyer9 and Metsing and Ferreira10 in pediatric popula�ons indicated specific prevalence of accommoda�ve anomalies. Scheiman et al. found accommoda�ve anomalies to be 5.4% among a 2,023 consecu�ve paediatric popula�on and 6.5% in a school age popula�on.8 Among 144 consecu�ve paediatric pa�ents, Dwyer found the prevalence of accommoda�ve anomalies to be 57%.9 In 112 school-going children, Metsing and Ferreira found 12.3% to have poor accommoda�on facility (the latency and speed of accommoda�ve response under binocular condi�ons5) and 10% had poor accommoda�ve amplitude (the maximum poten�al increase in op�cal power that an eye can achieve in adjus�ng its focus5).10 Similarly, studies on accommoda�ve anomalies in other popula�ons have also been high. Hokoda found a prevalence of 16.8% accommoda�ve anomalies among his sample of children and adults.11 Lara et al found the overall prevalence of accommoda�ve anomalies at 9.4% in a study size of 265 symptoma�c clinic pa�ents with the greatest propor�on (6.4%) found to have accommoda�ve excess (an incessantly higher accommoda�ve amplitude than age expected norms due to spasms of the ciliary muscle3).12 In a
recent pilot study of 65 black high school children, the prevalence of accommoda�ve insufficiency (a persistently lower accommoda�on than expected for age3) was 1.6%, accommoda�ve infacility (slowdown in accommoda�ve dynamics, that is, latency, �me constant, and peak velocity3) was 1.6%, poor monocular accommoda�ve facility was 25% and poor binocular accommoda�ve facility was 6.7%.13 The differences in prevalence values among these different studies apart from differences in methodology may be due to the dispari�es in the various study popula�on’s characteris�cs especially differences in demo-graphics and socio-economic status.14
The popula�on characteris�cs of Ghanaians in terms of demographics and socio-economic status differ significantly from that in popula�ons reported in previous studies on prevalence of accommoda�ve anomalies. It is likely that the trend of disorders and health outcomes in general will differ from that reported in other se�ngs 15,16 due to the possible causal link between risk of disease and the social environment.14 In Ghana, there are several studies on ametropia and ocular diseases but a dearth of informa�on on accommoda�ve anomalies. An earlier study in Ghana examined accommoda�ve anomalies specifically accommoda�ve insufficiency and accommoda�ve infacility using only one clinical sign and the study included a convenient sample of 204 children.17 In this present study, we report the prevalence of accommoda�ve anomalies in symptoma�c junior high school (JHS) going children in Cape Coast, Ghana using a widely accepted diagnos�c criteria.
JNOA.2018;20(2): 23 - 30 Darko-Takyi et al
Original Research Article

Journal of the Nigerian Optometric Association
25
MATERIALS AND METHODSStudy design and ethics
Study subjects and sampling procedure
Inclusion Criteria
Procedure
Ocular examination
Administration of Questionnaire
Refraction
Testing for accommodative anomalies
Visual acuity This prospec�ve cross-sec�onal study was carried out in accordance with the Code of Ethics of the World Medical Associa�on (Declara�on of Helsinki) and ethics approval was obtained from the Ethics review commi�ee of the Ghana Health Service. Permission was sought and granted by the Cape Coast Metro Educa�on Directorate, Ghana and head teachers of sampled schools. Inform consent was obtained from parents and guardians and school children gave their assent prior to the commencement of the study.
This study reports part of the results in a major study on the prevalence of binocular vision disorders among JHSs in Cape Coast, Ghana. The sampling technique (mul�stage) and sampling procedure for en�re par�cipants have been described in an earlier publica�on.18 The study sampled 636 JHS students in Cape Coast metropolis of the Central Region of Ghana. The 73 JHSs in the metropolis are clustered under six educa�onal circuits by the metropolitan educa�on office. Two schools were randomly selected from each of these clusters and averages of 53 students were randomly selected from each school. The expression N = Z2α/2/4d2 [where Zα/2 is confidence level at 95% confidence interval (significance level α =0.05), d is es�mated devia�on (0.1)] was used to es�mate minimum sample size considering a�ri�on rate (10%) and design effect (3).
Symptoma�c JHS children from age range of 12 to 17 years, with no ocular disease, no strabismus and no nystagmus and visual acuity equal to or be�er than 0.2 logarithm of the minimum angle of resolu�on (LogMAR) were included into the study.
Using (LogMAR) chart (Low Vision Resource Centre (LVRC) Bailey-Lovie design), visual acuity (VA) was measured for each par�cipant.
Hand held slit lamp biomicroscope (HANGUA MODEL SLM -6M) was used to assess external ocular �ssues and Keeler professional direct ophthalmoscopes were used to assess internal ocular �ssues.
Par�cipants were guided by the study team to fill a 20-point reliable asthenopic symptom ques�onnaire (good internal consistency with Cronbach’s α = 0.866; all fi�een items worthy of reten�on) with symptom severity measured on a grading scale of 0 – never, 1 – mild, 2 – moderate, 3 – severe, and 4 – very severe.18 The ques�onnaires were collected on the same day of administra�on. Symptoma�c par�cipants (children with two or more symptoms19 which were severe or very severe on the reliable ques�onnaire) were taken through accommoda�ve assessment.
Keeler professional streak re�noscope with trial lenses from manual phoropter (Topcon VT-10) was used to assess refrac�ve status objec�vely and subjec�ve refrac�on was performed using ophthalmic trial lens set. Final refrac�ve results were “maximum plus lenses for best-corrected visual acuity”. Defini�on of specific ametropia is indicated (Table 1).
Accommoda�ve tes�ng was as follows: amplitude of accommoda�on (AA) using Donder’s push-up-to-blur method; accommoda�ve lag using monocular es�ma�on method (MEM); binocular accommoda�ve facility (BAF)
JNOA.2018;20(2): 23 - 30 Darko-Takyi et al
Original Research Article
18. Darko-Takyi C, Khan N E, Nirghini U. Symptomatic vergence disorders in junior high school children in Ghana. Afr Vision Eye Health. 2016;75(1):a333.8 pages Available at http://dx.doi.org/10.4102/aveh.v751i1.333.19. Bhanderi D J, Choudhary S. Doshi V G. A community-based study of asthenopia in computer operators. Indian J Ophthalmol. 2008;56(1):51-55.

Journal of the Nigerian Optometric Association
26
Data Analysis
RESULT
and monocular accommoda�ve facility (MAF) tes�ng using +/−2.00D flipper lenses, nega�ve rela�ve accommoda�on (NRA) and posi�ve rela�ve accommoda�on (PRA). These tests were done over maximum plus lenses for best corrected visual acuity results.9,10,12,13,20,21 Each of the test results were compared to established clinical norms (Modified Morgan’s table of expected values for accommoda�ve and vergence tes�ng5 ) and three or more abnormal signs were grouped together as syndrome to iden�fy specific accommoda�ve anomalies9,12,20,21 using Scheiman and Wick’s criteria22 and maintaining some signs as mandatory (Table 1). Par�cipants were diagnosed as having only ametropia if with results of refrac�on in place; they presented normal results in accommoda�ve tes�ng.12
The IBM SPSS Version 21 (SPSS, Inc., Chicago, IL, USA) was used to analyze data. Frequencies, means and standard devia�ons were computed for descrip�ve data. Pearson’s chi square test and binary logis�c regression test were used to inves�gate associa�ons between variables. A p-value of ≤ 0.05 was considered sta�s�cally significant.
Presented in an earlier publica�on18 are the demographic parameters of en�re par�cipants for the study. As a repeat, par�cipants numbering 627 (47.2% males and 52.8% females) with mean age 14.1±1.5 years answered the reliable asthenopic symptoms ques�onnaire and 220 were found to be symptoma�c (with symptoms such as head-aches, eye pain; visual fa�gue, blur vision, eyestrain, burning sensa�ons, difficulty tracking objects or prints etc. that were associated with
either distance or near work) and eligible for accommoda�ve system assessment. Out of the 220 symptoma�c par�cipants, 202 consis�ng 36.6% males and 63.4% females reported for the accommoda�ve system assessment through maximum plus for best corrected visual acuity results. No sta�s�cally significant difference in age was determined between male and female par�cipants (t = 1.017, p = 0.31); par�cipants ages were normally distributed. Among symptoma�c par�cipants (n =202), the frequency of ametropia was 38 (18.8%) with specifics as follows: myopia 9 (4.5%), hyperopia 10 (5.0%) and as�gma�sm 19 (9.4%).
The descrip�ve measures of the various parameters of accommoda�on for symptoma�c par�cipants in general are indicated (Table 2) and the accommoda�ve parameters for each specific accommoda�ve anomaly are indicated (Table 3). Among symptoma�c par�cipants, 104 (51.5%) were diagnosed with accommoda�ve anomalies; 37.5% of par�cipants with accommoda�ve anomalies were males and 62.5% were females. A number of 85 (81.7%) par�cipants diagnosed with accommoda�ve anomalies had no ametropia (Table 4). For specific accommoda�ve anomalies, the prevalence among symptoma�c JHS par�cipants was as follows: accommoda�ve insufficiency, 45 (22.3%); accommoda�ve infacility, 22 (10.9%); accommoda�ve excess, 27 (13.4%) and accommoda�ve fa�gue, 10 (5%). The distribu�on of specific accommoda�ve anomalies among par�cipants diagnosed with accommoda�ve disorders only is indicated (Figure 1). There was no significant associa�on between accommoda�ve anomalies and gender (X2= 0.069 p= 0.792). Par�cipants with accommoda�ve anomalies had greater odds of experiencing symptoms of visual fa�gue associated with near work (OR =0.530, p= 0.001) compared with other symptoms.
JNOA.2018;20(2): 23 - 30 Darko-Takyi et al
Original Research Article
5. American Optometric Association. Optometric clinic practice guidelines: care of the patient with Accommodative and Vergence Dysfunction. [Internet].2010 [cited 2013 Feb 09]. p. 7-9, 27-40. Available from :http://www.aoa.org/documents/CPG-18.pdf9. Dwyer P. The prevalence of vergence accommodation disorders in a school-age population. Clin Exp Optom 1992;75(1):10–8.10. Metsing I, Ferreira J. Accommodation and vergence status among the 3rd and 4th graders in a mainstream school in Gauteng. S Afr Optom 2012;71(1):22–31.12. Lara F, Cacho P, García A, Megías R. General binocular disorders: prevalence in a clinic population. Ophthalmic Physiol Opt 2001; 21(1):70–4.13. Wajuihian S O, Hansraj R. Near vision anomalies in Black high school children in Empangeni, South Africa. S Afr Optom 2014;73(1):21-32.18. Darko-Takyi C, Khan N E, Nirghini U. Symptomatic vergence disorders in junior high school children in Ghana. Afr Vision Eye Health. 2016;75(1):a333.8 pages Available at http://dx.doi.org/10.4102/aveh.v751i1.333.20. Montes-Mico R. Prevalence of general dysfunctions in binocular vision. Ann Ophthalmol 2001;33(3):205–8.21. Porcar E, Martinez-Palomera A. Prevalence of general binocular dysfunctions in a population of university students. Optom Vis Sci 1997;74(2):111–3. 22. Scheiman M, Wick B. Clinical Management of Binocular Vision: Heterophoric, Accommodative, and Eye Movement Disorders. Baltimore: Lippincott Williams & Wilkins; 2008.

Journal of the Nigerian Optometric Association
27
DISCUSSIONPrevalence es�mate for accommoda�ve anomalies in the present study was higher compared to a study on a symptoma�c clinical popula�on between age of 10 and 35years.12 This result is however lower compared to a study on a symptoma�c school aged optometric clinic popula�on9 and another study on a symptoma�c young adult clinic popula�on.20 Accommoda�ve insufficiency being the most prevalent accommoda�ve anomaly among symptoma�c individuals in the present study is comparable to some studies8,9,20 and inconsistent with other studies.12,21 A study on a similar popula�on of black African high school children found the prevalence of accommoda�ve insufficiency and accommoda�ve infacility to be the same and this is not consistent with results of the present study.13 Differences in diagnos�c criteria for accommoda�ve anomalies may account for the dissimilarity in results between la�er study13 and present study.
In the present study, a greater frequency of symptoma�c children (81.2%) did not have ametropia, however, more than half (51.5%) were diagnosed with accommoda�ve anomalies. The result in present study is comparable to a study among school age popula�on presen�ng to an optometric clinic in which accommoda�ve anomalies were more prevalent than ametropia9 but however
inconsistent with a study among symptoma�c clinic popula�on12 and on a similar black high school children popula�on.13 It should be noted that the first two most likely condi�ons Optometrist are likely to encounter in a paediatric popula�on are binocular or accommoda�ve anomalies and ametropia.8 Most studies have been conducted to inves�gate ametropia among school age popula�on in the central region of Ghana,23,24,25 however none has reported the frequency of ametropia among symptoma�c individuals. Comparable to present study, some of these studies reported as�gma�sm as the most frequent ametropia24,25 whiles others had contras�ng results.23 The causes of asthenopia are diverse26 and require comprehensive optometric examina�ons to illicit the specifics.
It can clearly be seen that some accommoda�ve parameters are more affected in some specific accommoda�ve anomalies than others (Table 3) and can clearly point out to a diagnosis of these anomalies (Table 3). Low AOA with high MEM values clearly discriminates accommoda�ve insufficiency from other types of accommoda�ve anomalies. Reduced NRA and PRA with low MAF and BAF clearly dis�nguish accommoda�ve infacility from other accommoda�ve anomalies. A Low MEM value clearly dis�nguishes accommoda�ve excess from other accommoda�ve anomalies. Normal AOA with high MEM values is seen to dis�nguish accommoda�ve fa�gue from other accommoda�ve anomalies.
JNOA.2018;20(2): 23 - 30 Darko-Takyi et al
Original Research Article
5. American Optometric Association. Optometric clinic practice guidelines: care of the patient with Accommodative and Vergence Dysfunction. [Internet].2010 [cited 2013 Feb 09]. p. 7-9, 27-40. Available from :http://www.aoa.org/documents/CPG-18.pdf8. Scheiman M, Gallaway M, Coulter R, Reinstein F, Ciner E, Herzberg C, Parisi M. Prevalence of vision and ocular disease conditions in a clinical pediatric population. J Am Optom Assoc 1996;67(4):193–202.9. Dwyer P. The prevalence of vergence accommodation disorders in a school-age population. Clin Exp Optom 1992;75(1):10–8.10. Metsing I, Ferreira J. Accommodation and vergence status among the 3rd and 4th graders in a mainstream school in Gauteng. S Afr Optom 2012;71(1):22–31.12. Lara F, Cacho P, García A, Megías R. General binocular disorders: prevalence in a clinic population. Ophthalmic Physiol Opt 2001; 21(1):70–4.13. Wajuihian S O, Hansraj R. Near vision anomalies in Black high school children in Empangeni, South Africa. S Afr Optom 2014;73(1):21-32.18. Darko-Takyi C, Khan N E, Nirghini U. Symptomatic vergence disorders in junior high school children in Ghana. Afr Vision Eye Health. 2016;75(1):a333.8 pages Available at http://dx.doi.org/10.4102/aveh.v751i1.333.20. Montes-Mico R. Prevalence of general dysfunctions in binocular vision. Ann Ophthalmol 2001;33(3):205–8.21. Porcar E, Martinez-Palomera A. Prevalence of general binocular dysfunctions in a population of university students. Optom Vis Sci 1997;74(2):111–3. 22. Scheiman M, Wick B. Clinical Management of Binocular Vision: Heterophoric, Accommodative, and Eye Movement Disorders. Baltimore: Lippincott Williams & Wilkins; 2008.23. Abu EK, Yeboah AA, Ocansey S, Kyei S, Abokyi S. Epidemiology of ocular disorders and visual impairment among school pupils in the Cape Coast Metropolis, Ghana. B J Vis Impair 2014, 33(3):45–5324. Ovenseri-Ogbomo GO, Omuemu VO. Prevalence of refractive errors among school children in Cape Coast municipality, Ghana. Clinical Optometry 2010;2:59-6625. Ovenseri-Ogbomo GO, Asien R. Refractive error in school children in Agona Swedru, Ghana. S Afr Optom 2010;69(2):86-9226. Abdi S, Rydberg A. Asthenopia in school children, Orthoptic and Ophthalmological findings and treatment. Documenta Ophthalmologia. 2005;111(2):65-72.

Journal of the Nigerian Optometric Association
28 JNOA.2018;20(2): 23 - 30 Darko-Takyi et al
Original Research Article
27. Michaud L, Forcier P. Prevalence of asymptomatic ocular conditions in subjects with refractive-based symptoms. J Optom 2014;7(3):153-160
In present study, only par�cipants with severe and very severe asthenopic symptoms were considered symptoma�c and were inves�gated for accommoda�ve anomalies over the maximum plus for best correct-ed visual acuity refrac�ve correc�on. There is a likelihood that other par�cipants with no symptoms or with mild to moderate symptoms could have their primary e�ologies being accommoda�ve anomalies.27 This study indicates a high prevalence of accommoda�ve anomalies on symptoma�c school children in Ghana. It is recommended that school children with asthenopic symptoms are taken through comprehensive binocu-lar vision examina�ons in optometric centers to diagnose and manage these anomalies to relief asthenopic symptoms and impact posi�vely on academic performance.
CONCLUSIONS
Authors wish to acknowledge the Optometry Department of University of Cape Coast, Ghana who support-ed this work with ophthalmic instruments.
ACKNOWLEDGEMENT
CONFLICT OF INTEREST: None
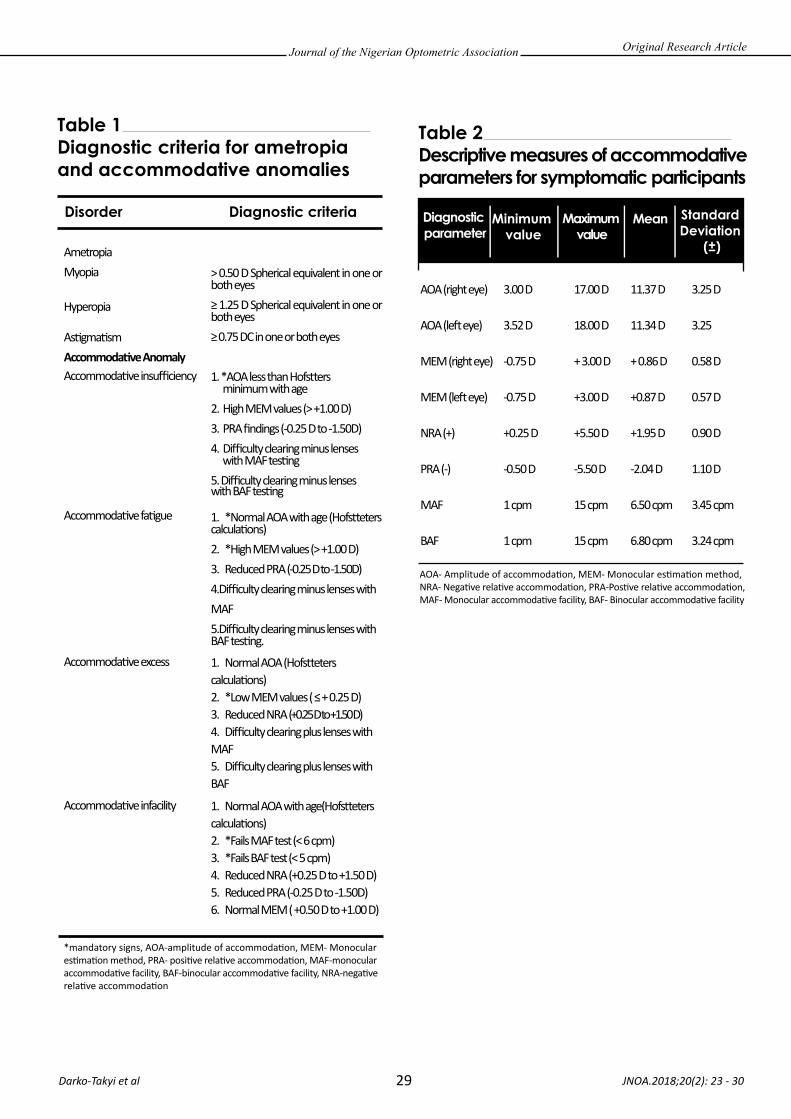
Journal of the Nigerian Optometric Association
29 JNOA.2018;20(2): 23 - 30 Darko-Takyi et al
*mandatory signs, AOA-amplitude of accommoda�on, MEM- Monocular es�ma�on method, PRA- posi�ve rela�ve accommoda�on, MAF-monocular accommoda�ve facility, BAF-binocular accommoda�ve facility, NRA-nega�ve rela�ve accommoda�on
AOA- Amplitude of accommoda�on, MEM- Monocular es�ma�on method, NRA- Nega�ve rela�ve accommoda�on, PRA-Pos�ve rela�ve accommoda�on, MAF- Monocular accommoda�ve facility, BAF- Binocular accommoda�ve facility
Original Research Article
Table 1 Diagnostic criteria for ametropia and accommodative anomalies
Disorder Diagnostic criteria
AmetropiaMyopia
Hyperopia
As�gma�smAccommoda�ve AnomalyAccommoda�ve insufficiency
Accommoda�ve fa�gue
Accommoda�ve excess
Accommoda�ve infacility
˃0.50 D Spherical equivalent in one or both eyes≥ 1.25 D Spherical equivalent in one or both eyes≥ 0.75 DC in one or both eyes
1. *AOA less than Hofs�ers minimum with age2. High MEM values (˃ +1.00 D)3. PRA findings (-0.25 D to -1.50D)4. Difficulty clearing minus lenses with MAF tes�ng5. Difficulty clearing minus lenses with BAF tes�ng
1. *Normal AOA with age (Hofs�eters calcula�ons) 2. *High MEM values (˃ +1.00 D)3. Reduced PRA (-0.25 D to -1.50D)4.Difficulty clearing minus lenses with MAF 5.Difficulty clearing minus lenses with BAF tes�ng.
1. Normal AOA (Hofs�eters calcula�ons)2. *Low MEM values ( ≤ + 0.25 D) 3. Reduced NRA (+0.25 D to +1.50 D)4. Difficulty clearing plus lenses with MAF5. Difficulty clearing plus lenses with BAF
1. Normal AOA with age(Hofs�eters calcula�ons)2. *Fails MAF test (< 6 cpm)3. *Fails BAF test (< 5 cpm)4. Reduced NRA (+0.25 D to +1.50 D)5. Reduced PRA (-0.25 D to -1.50D)6. Normal MEM ( +0.50 D to +1.00 D)
Table 2 Descriptive measures of accommodative parameters for symptomatic participants
Standard Deviation
(±)
Minimum value
Diagnostic parameter
Maximum value
Mean
AOA (right eye)
AOA (le� eye)
MEM (right eye)
MEM (le� eye)
NRA (+)
PRA (-)
MAF
BAF
3.00 D
3.52 D
-0.75 D
-0.75 D
+0.25 D
-0.50 D
1 cpm
1 cpm
17.00 D
18.00 D
+ 3.00 D
+3.00 D
+5.50 D
-5.50 D
15 cpm
15 cpm
11.37 D
11.34 D
+ 0.86 D
+0.87 D
+1.95 D
-2.04 D
6.50 cpm
6.80 cpm
3.25 D
3.25
0.58 D
0.57 D
0.90 D
1.10 D
3.45 cpm
3.24 cpm
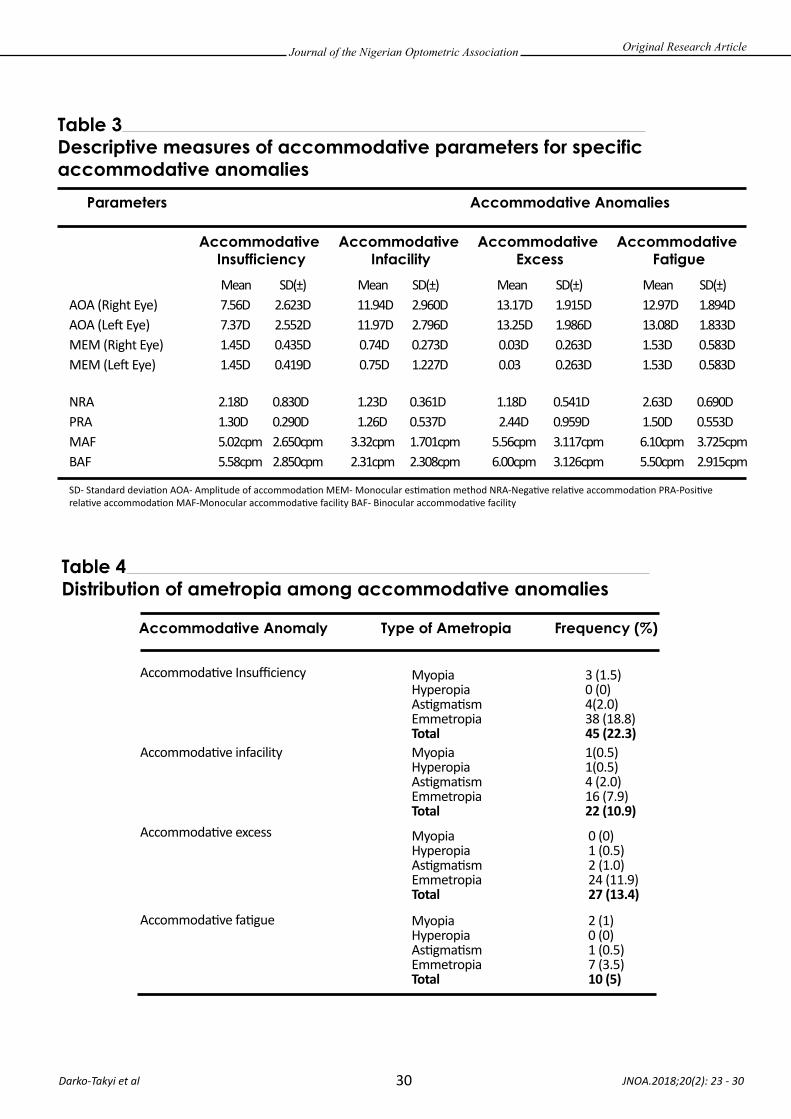
Journal of the Nigerian Optometric Association
30 JNOA.2018;20(2): 23 - 30 Darko-Takyi et al
Original Research Article
Table 3 Descriptive measures of accommodative parameters for specific accommodative anomalies
Table 4 Distribution of ametropia among accommodative anomalies
Parameters Accommodative Anomalies
Accommodative Insufficiency
Accommodative Infacility
Accommodative Excess
Accommodative Fatigue
Accommodative Anomaly Type of Ametropia Frequency (%)
Mean SD(±) Mean SD(±) Mean SD(±) Mean SD(±)AOA (Right Eye) AOA (Le� Eye)MEM (Right Eye)MEM (Le� Eye)
Myopia 3 (1.5)Hyperopia 0 (0)As�gma�sm 4(2.0)Emmetropia 38 (18.8)Total 45 (22.3)Myopia 1(0.5)Hyperopia 1(0.5)As�gma�sm 4 (2.0)Emmetropia 16 (7.9)Total 22 (10.9)
Myopia 0 (0)Hyperopia 1 (0.5)As�gma�sm 2 (1.0)Emmetropia 24 (11.9)Total 27 (13.4)
Myopia 2 (1)Hyperopia 0 (0)As�gma�sm 1 (0.5)Emmetropia 7 (3.5)Total 10 (5)
Accommoda�ve Insufficiency
Accommoda�ve infacility
Accommoda�ve excess
Accommoda�ve fa�gue
NRAPRAMAFBAF
7.56D 2.623D 11.94D 2.960D 13.17D 1.915D 12.97D 1.894D7.37D 2.552D 11.97D 2.796D 13.25D 1.986D 13.08D 1.833D1.45D 0.435D 0.74D 0.273D 0.03D 0.263D 1.53D 0.583D1.45D 0.419D 0.75D 1.227D 0.03 0.263D 1.53D 0.583D
2.18D 0.830D 1.23D 0.361D 1.18D 0.541D 2.63D 0.690D1.30D 0.290D 1.26D 0.537D 2.44D 0.959D 1.50D 0.553D5.02cpm 2.650cpm 3.32cpm 1.701cpm 5.56cpm 3.117cpm 6.10cpm 3.725cpm5.58cpm 2.850cpm 2.31cpm 2.308cpm 6.00cpm 3.126cpm 5.50cpm 2.915cpm
SD- Standard devia�on AOA- Amplitude of accommoda�on MEM- Monocular es�ma�on method NRA-Nega�ve rela�ve accommoda�on PRA-Posi�ve rela�ve accommoda�on MAF-Monocular accommoda�ve facility BAF- Binocular accommoda�ve facility

Glaucoma is an op�c neuropathy associated with a characteris�c structural damage to the op�c nerve and visual dysfunc�on which are seen clinically as enlargement of the op�c disc cup and loss of peripheral field of vision1. Glaucoma is characterized by increased intraocular pressure (IOP), visual field loss beginning with peripheral vision loss resul�ng
to what is known as tunnel vision and damaging the op�c nerve head. It is one of the leading causes of irreversible blindness in the world affec�ng about 70 million persons worldwide2,3. Primary open-angle glaucoma (POAG) also referred to as chronic simple glaucoma is generally bilateral but not always a symmetrical disease, characterized by an adult onset,
JNOA.2018;20(2): 31 - 36
Photostress recovery �me (PSRT) is a clinical procedure that measures the amount of �me required for the macular to return to its normal level of func�on a�er being exposed to a bright light source. This study was a case control clinical study carried out to measure the foveal and extra-foveal photo stress recovery �me in par�cipants with primary open angle glaucoma. Fi�y five subjects, 24 with primary open angle glaucoma with a mean age of 34.38±12.19 and 31 control subjects with a mean age of 26.58±7.23 were used in this study. The mean photostress recovery �me measured on the fovea, 7o nasal, temporal, inferior and superior to the fovea were, 62.38±4.67, 8.71±7.19, 11.23±10.96, 12.08±8.96 and 12.44±9.30 respec�vely for subjects with primary open angle glaucoma. For the control subjects, the mean photostress recovery �me measured on the fovea, 7o nasal, temporal, inferior and superior to the fovea were 23.29±1.63 11.89±8.62, 11.53±8.19, 12.89±8.67 and 13.60±8.36 respec�vely. Analysis with SPSS version 21 using the two factor ANOVA showed a significant difference (P<0.05) in photostress recovery �me 7o nasally, temporally, inferiorly and superior to the fovea between primary open angle glaucoma subjects and a control group. Data analysis with the independent sample t-test also showed a significant difference (P<0.05) in photostress recovery �me on the fovea between primary open angle glaucoma subjects and a control group. In conclusion, primary open angle glaucoma alters the photostress recovery �me, both on the fovea and extra-foveal region of the re�na. Photostress recovery test should be included in the rou�ne eye examina�on of pa�ents.
Keywords: Primary Open angle glaucoma, Photostress recovery �me, foveal, extra-foveal
Journal of the Nigerian Optometric Association Original Research Article
1 Department of Optometry, Federal University of Technology, Owerri
1. Khurana AK. Comprehensive Ophthalmology. 5th edition. New Delhi. New age international publishers. 2012; 218-239. 2. Azuamah C, Amadi AN, Esenwah EC, Agu GC, Okorie ME. Occurrence of systemic hypertention and glaucoma. Int. J. of Res. 2015; 2(3):704-706. 3. Broadway DC. Visual field testing for glaucoma: a practical guide. Comm Eye Health. 2012; 25(79-80):66-70.
Azuamah, Y.C.,1 Merem, C.C.,1 Ikoro, N.C.,1 Esenwah, E.C.,1 Megwas, A.U.1 and Daniel-Nwosu, E.1
Azuamah, Y.C Email: [email protected] Phone: + 2348034933590
31
ASSESSMENT OF FOVEAL AND EXTRA-FOVEAL PHOTOSTRESS RECOVERY TIME IN PRIMARY OPEN ANGLE GLAUCOMA
Corresponding Author:
Abstract
Introduction
Azuamah et al

Journal of the Nigerian Optometric Association
32
Materials and Methods
4. Bruce AS, O’Day J, Mckay D, Swann PG. Posterior eye diseases and glaucoma a-z. Butterworth Heinemann. 2009; 58-59.5. George GO. Glaucoma-when is a case truly glaucoma. J. Nig Opt Assoc. 2013; 15 (1):36-37.6. Leske MC, Heiji A, Hussein M, Bengtsson B. Komarroff E. Factors for glaucoma progression and the effect of treatment; the early manifestation of glaucoma trial. Arch. Ophthalmol. 2003; 121: 34-34.7. Elliot DB. Clinical procedures in primary eye care. 3rd edition. Butterworth-Heinemann. 2007; 29-31.8. Grott R, Chung S. Photostress recovery time assessed using high and low contrast letters. Indian J. Ophthalmol. 2002; 13(8):69-72.9. Grosvenor T. Primary Care Optometry. 5th edition. Newton. Butterworth-Heinemann. 2008; 231.10. Kim S, Moon B, Cho H. The best instrument for testing photostress recovery time. J. Kor Ophthalmol Opt. Society. 2013; 18(2):193-196.
lOP above 21 mmHg at some point in the course of the disease, an open angle of normal appearance, glaucomatous op�c nerve head damage and visual field loss4. Although 4-7% of the popula�on over the age of 40 years have lOPs >21 mmHg, only 1% of individuals with ocular hypertension will develop glaucoma each year5. The risk of damage increases as the lOP rises. Screening for glaucoma should always be performed as part of a standard eye examina�on. Tes�ng for glaucoma should include measurements of the intraocular pressure through tonometry, changes in size or shape of the eye, gonioscopy and examina�on of the op�c nerve head for any visible damage or change in the cup-disc ra�o, rim appearance and vascular changes6.
The photostress recovery �me is a clinical procedure that measures the amount of �me required for the macula to return to its normal level of func�on a�er being exposed to a bright light source7. It is simply the measurement of the �me it takes to start seeing again a�er being exposed to light of high intensity. The �me it takes to return to baseline acuity a�er a pa�ent has been exposed to intense illumina�on for about 10 seconds is the photostress recovery �me (PSRT). The normal Photostress recovery �me is 50secs but with certain diseases like diabe�c re�nopathy, age related macular degenera�on. prolonged photostress recovery test �me is observed8. Op�c nerve diseases can be differen�ated from re�nal diseases with the Photostress test. If the recovery �me is about the same for both eyes, the cause of a lowered visual acuity in the “bad” eye is an op�c nerve lesion. However, if the recovery �me is considerably longer for the eye with reduced visual acuity more than the normal eye, the cause is a re�nal disease9. A prolonged recovery �me or delayed dark adapta�on is reported in glaucoma, which mainly affects ganglion cells. This suggests that a ganglion cell abnormality may delay recovery or that glaucoma may cause visual pigment abnormality.
It can be used to evaluate re�nal func�on8.
This study was a case control clinical study which involved the measurement of the photostress recovery �me of par�cipants with primary open angle glaucoma and a non-glaucomatous control group. Par�cipants who sa�sfied the inclusion and exclusion criteria were examined at the Optometry Teaching Clinic, Federal University of Technology, Owerri. These are male and female adults who do not have a debilita�ng disease, a mental problem, an ocular pathology apart from Primary Open Angle Glaucoma, and who gave an informed consent. Fi�y five par�cipants were used in this study, 24 were cases with primary open angle glaucoma and 31 controls without POAG. The controls had similar characteris�cs (such age 18 years and above) as the cases apart from presence of primary open angle glaucoma. The cases had no other visible pathology apart from POAG. The controls had no POAG and any other visible pathology. Case history, visual acuity, penlight examina�on, slit lamp biomi-croscopy, ophthalmoscopy and perimetry were conducted on all the par�cipants. The IOP of the par�cipants were measured and recorded using the schiotz tonometer. For measurement of the foveal and extra-foveal photostress recovery �me, par�cipants were asked to fixate at the spot at the center of the bjerrum tangent screen at one meter. With one eye occluded, the ophthalmoscope light10 was shone on the fovea, 7 degrees nasal, temporal, inferior and superior to the fovea with the aid of a protractor for 10 seconds. The �me it took for the pa�ent to see the target again a�er the ophthalmoscope light was removed was recorded as the PSRT. A PSRT above 50 seconds is indica�ve of an abnormality9. Data obtained was uploaded into the IBM SPSS version 21 so�ware and the two-factor ANOVA and the independent sample T – test was used to test the hypotheses at 0.05 level of significance and 95%
JNOA.2018;20(2): 31 - 36 Azuamah et al
Original Research Article
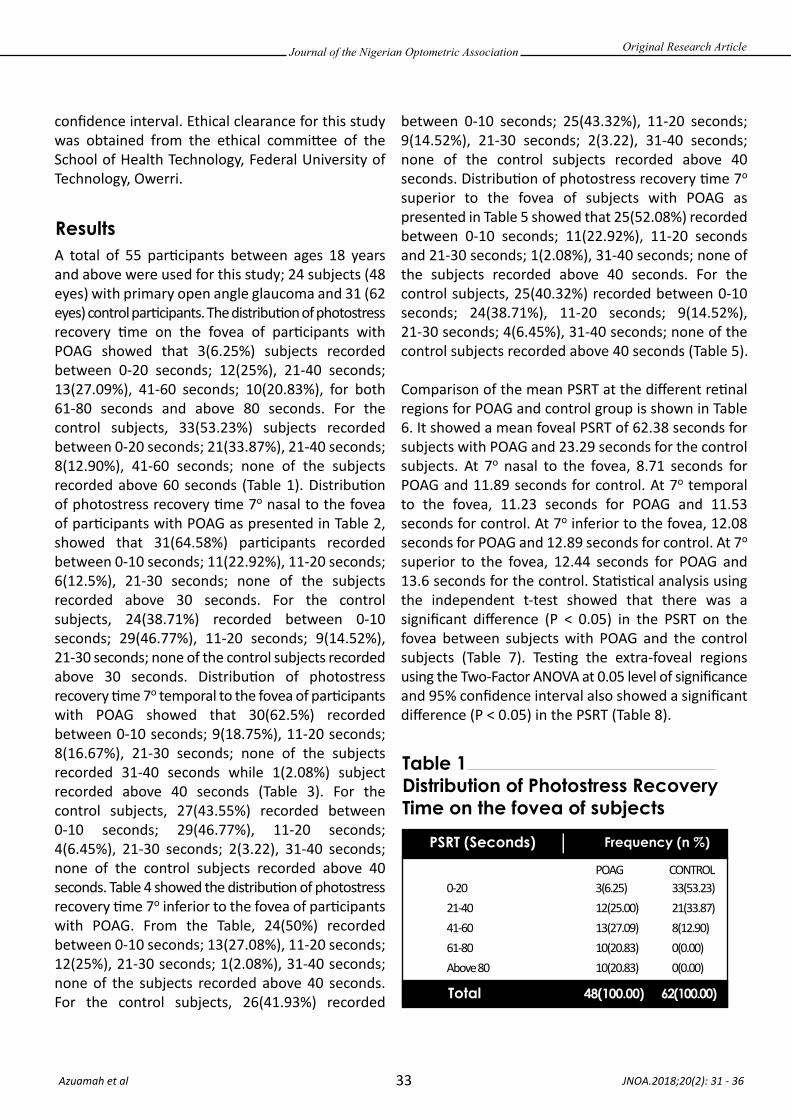
Journal of the Nigerian Optometric Association
33
Results
confidence interval. Ethical clearance for this study was obtained from the ethical commi�ee of the School of Health Technology, Federal University of Technology, Owerri.
A total of 55 par�cipants between ages 18 years and above were used for this study; 24 subjects (48 eyes) with primary open angle glaucoma and 31 (62 eyes) control par�cipants. The distribu�on of photostress recovery �me on the fovea of par�cipants with POAG showed that 3(6.25%) subjects recorded between 0-20 seconds; 12(25%), 21-40 seconds; 13(27.09%), 41-60 seconds; 10(20.83%), for both 61-80 seconds and above 80 seconds. For the control subjects, 33(53.23%) subjects recorded between 0-20 seconds; 21(33.87%), 21-40 seconds; 8(12.90%), 41-60 seconds; none of the subjects recorded above 60 seconds (Table 1). Distribu�on of photostress recovery �me 7o nasal to the fovea of par�cipants with POAG as presented in Table 2, showed that 31(64.58%) par�cipants recorded between 0-10 seconds; 11(22.92%), 11-20 seconds; 6(12.5%), 21-30 seconds; none of the subjects recorded above 30 seconds. For the control subjects, 24(38.71%) recorded between 0-10 seconds; 29(46.77%), 11-20 seconds; 9(14.52%), 21-30 seconds; none of the control subjects recorded above 30 seconds. Distribu�on of photostress recovery �me 7o temporal to the fovea of par�cipants with POAG showed that 30(62.5%) recorded between 0-10 seconds; 9(18.75%), 11-20 seconds; 8(16.67%), 21-30 seconds; none of the subjects recorded 31-40 seconds while 1(2.08%) subject recorded above 40 seconds (Table 3). For the control subjects, 27(43.55%) recorded between 0-10 seconds; 29(46.77%), 11-20 seconds; 4(6.45%), 21-30 seconds; 2(3.22), 31-40 seconds; none of the control subjects recorded above 40 seconds. Table 4 showed the distribu�on of photostress recovery �me 7o inferior to the fovea of par�cipants with POAG. From the Table, 24(50%) recorded between 0-10 seconds; 13(27.08%), 11-20 seconds; 12(25%), 21-30 seconds; 1(2.08%), 31-40 seconds; none of the subjects recorded above 40 seconds. For the control subjects, 26(41.93%) recorded
between 0-10 seconds; 25(43.32%), 11-20 seconds; 9(14.52%), 21-30 seconds; 2(3.22), 31-40 seconds; none of the control subjects recorded above 40 seconds. Distribu�on of photostress recovery �me 7o superior to the fovea of subjects with POAG as presented in Table 5 showed that 25(52.08%) recorded between 0-10 seconds; 11(22.92%), 11-20 seconds and 21-30 seconds; 1(2.08%), 31-40 seconds; none of the subjects recorded above 40 seconds. For the control subjects, 25(40.32%) recorded between 0-10 seconds; 24(38.71%), 11-20 seconds; 9(14.52%), 21-30 seconds; 4(6.45%), 31-40 seconds; none of the control subjects recorded above 40 seconds (Table 5).
Comparison of the mean PSRT at the different re�nal regions for POAG and control group is shown in Table 6. It showed a mean foveal PSRT of 62.38 seconds for subjects with POAG and 23.29 seconds for the control subjects. At 7o nasal to the fovea, 8.71 seconds for POAG and 11.89 seconds for control. At 7o temporal to the fovea, 11.23 seconds for POAG and 11.53 seconds for control. At 7o inferior to the fovea, 12.08 seconds for POAG and 12.89 seconds for control. At 7o superior to the fovea, 12.44 seconds for POAG and 13.6 seconds for the control. Sta�s�cal analysis using the independent t-test showed that there was a significant difference (P < 0.05) in the PSRT on the fovea between subjects with POAG and the control subjects (Table 7). Tes�ng the extra-foveal regions using the Two-Factor ANOVA at 0.05 level of significance and 95% confidence interval also showed a significant difference (P < 0.05) in the PSRT (Table 8).
JNOA.2018;20(2): 31 - 36 Azuamah et al
Original Research Article
Table 1 Distribution of Photostress Recovery Time on the fovea of subjects
PSRT (Seconds)
Total 48(100.00) 62(100.00)
Frequency (n %)
0-2021-4041-6061-80Above 80
3(6.25)12(25.00)13(27.09)10(20.83)10(20.83)
33(53.23)21(33.87)8(12.90)0(0.00)0(0.00)
POAG CONTROL
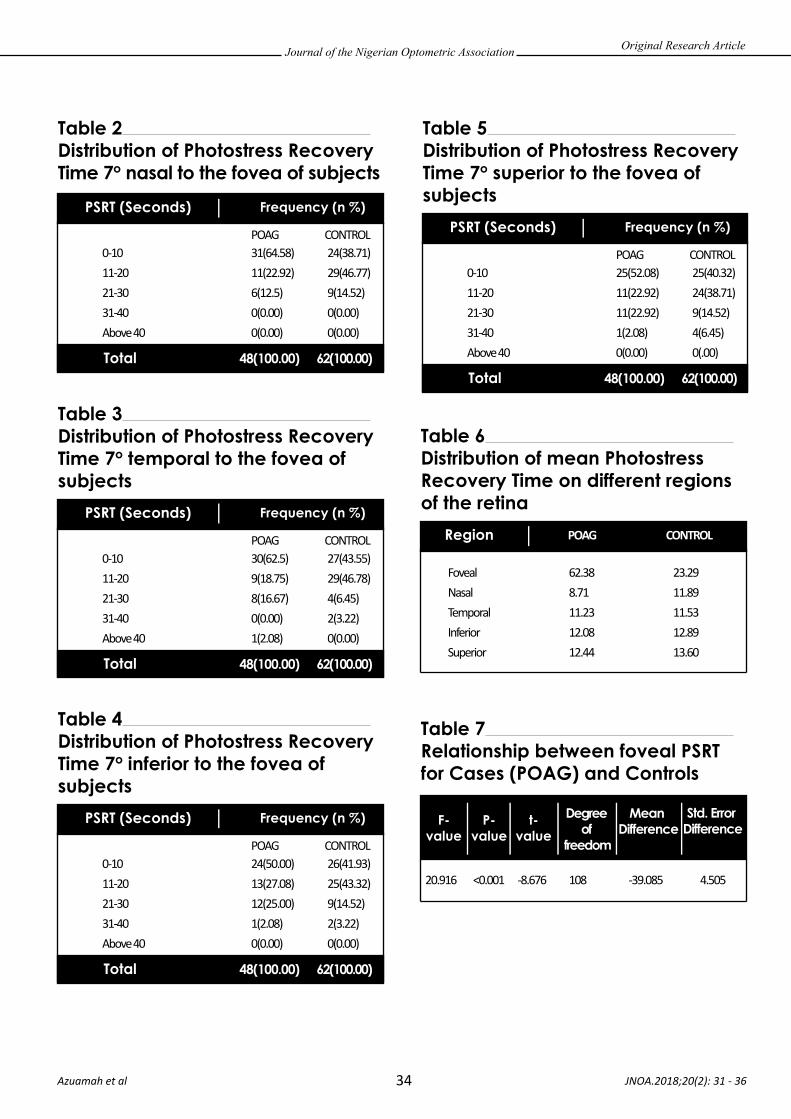
Journal of the Nigerian Optometric Association
34 JNOA.2018;20(2): 31 - 36 Azuamah et al
Original Research Article
Table 2 Distribution of Photostress Recovery Time 7o nasal to the fovea of subjects
PSRT (Seconds)
Total 48(100.00) 62(100.00)
Frequency (n %)
0-1011-2021-3031-40Above 40
31(64.58)11(22.92)6(12.5)0(0.00)0(0.00)
24(38.71)29(46.77)9(14.52)0(0.00)0(0.00)
POAG CONTROL
Table 3 Distribution of Photostress Recovery Time 7o temporal to the fovea of subjects
PSRT (Seconds)
Total 48(100.00) 62(100.00)
Frequency (n %)
0-1011-2021-3031-40Above 40
30(62.5)9(18.75)8(16.67)0(0.00)1(2.08)
27(43.55)29(46.78)4(6.45)2(3.22)0(0.00)
POAG CONTROL
Table 4 Distribution of Photostress Recovery Time 7o inferior to the fovea of subjects
PSRT (Seconds)
Total 48(100.00) 62(100.00)
Frequency (n %)
0-1011-2021-3031-40Above 40
24(50.00)13(27.08)12(25.00)1(2.08)0(0.00)
26(41.93)25(43.32)9(14.52)2(3.22)0(0.00)
POAG CONTROL
Table 6 Distribution of mean Photostress Recovery Time on different regions of the retina
Region POAG CONTROL
FovealNasalTemporalInferiorSuperior
62.388.7111.2312.0812.44
23.2911.8911.5312.8913.60
Table 5 Distribution of Photostress Recovery Time 7o superior to the fovea of subjects
PSRT (Seconds)
Total 48(100.00) 62(100.00)
Frequency (n %)
0-1011-2021-3031-40Above 40
25(52.08)11(22.92)11(22.92)1(2.08)0(0.00)
25(40.32)24(38.71)9(14.52)4(6.45)0(.00)
POAG CONTROL
Table 7 Relationship between foveal PSRT for Cases (POAG) and Controls
F-value
P-value
t-value
Std. Error Difference
Degree of
freedom
Mean Difference
20.916 <0.001 -8.676 108 -39.085 4.505

Journal of the Nigerian Optometric Association
35
DiscussionPrimary open angle glaucoma (POAG) causes a gradual decrease in visual acuity leading to total blindness if not properly managed. The subjects with POAG in this study had a poor visual acuity as they have been living with POAG. This reflected in the prolonged PSRT of the glaucoma subjects when compared to the control subjects who had no eye problem. Studies11-13 showed similar results on photostress recovery �me and pathologies of the re�na. Omokhua and George14 reported a higher PSRT among males than in females. Kamppeter, et al.,15 in a study on re-adapta�on �me a�er photostress in normal subjects and glaucoma pa�ents, confirmed that primary open angle glaucoma subjects showed a significantly prolonged fovea recovery �me a�er a photostress test compared with the normal subjects. Many of the subjects with POAG in this study were above 50 years and at this stage in life, there is always some form of eye problem associated with aging such as incipient cataract which can reduce the intensity of light reaching the re�na. Esenwah et al.16 reported a reduc�on in lens transparency,
presence of vitreous floaters and slow response to light s�muli as common problems associated with aging. Any of these factors could contribute to the prolonged photostress recovery �me but the POAG was the major factor in this study as no other visible pathology was seen upon ophthalmoscopy, pen light and slit lamp biomicroscope examina�on. Sta�s�cal analysis showed a significant difference in the recovery �me between the cases and the controls both at the foveal (P (0.00) < 0.05) and extra-foveal regions (P (0.00) < 0.05) of the re�na.
The PSRT is commonly tested at the central por�on of the re�na, but the peripheral region should be tested in cases in which the lesion is located outside the fovea, such as in glaucoma. When light is shone on the eye, the photoreceptors are bleached. Visual func�on is restored when the photoreceptors are regenerated. Cones are the photoreceptors that are concentrated in the fovea region while rods are concentrated in the periphery. When light is shone at the extra-foveal regions, it will take a shorter �me for the subject to see. This is reflected in our study where the PSRT at the extrafoveal areas were shorter than the foveal PSRT. Tunnel vision as a result of a reduced visual field is one of the major symptoms of glaucoma. Most pa�ents with POAG are not aware that their peripheral vision is compromised. The extra-foveal regions that were tested in this study however, are not greatly affected by POAG and hence the PSRT were not too far away from that of the control subjects. Yasuki, et al.17 used a scanning laser ophthal-moscope to evaluate the extra-foveal region and found the PSRT was significantly longer a�er 20 seconds than a�er 10 seconds. Masayuki, et al.18 measured the extrafoveal photostress recovery �me in glaucoma pa�ents and found that the PSRT does not correlate with loca�on of the test spot.
JNOA.2018;20(2): 31 - 36 Azuamah et al
Original Research Article
Table 8 Relationship between extra-foveal regions of PSRT for Cases (POAG) and Controls
F-value
P-value
Type III Sum of Squares
Source of
Variation
Degree of
freedom
Mean Square
Intercept 60224.121 1 60224.121 774.941 <0.001
11. Timothy CO, Nwankwo AA, Onu NU, Onyezewe CD. Effect of Moringa Oleifera seed on photostress recovery time of young Nigerian adults. J Nig Opt Assoc. 2014; 19(1):57-60.12. Baptista AG, Sousa RA, Rocha FQ, Macedo F. The macular photostress test in diabetes, glaucoma and cataract. Rev Ophthalmol. 2013; 88(11):1322-1335.13. Magrin TH, Thompson D. Sources of variability in clinical PSRT. J Ophthalmol. 2002; 22:61-67.14. Omokhua OP, George OG. Photostress recovery time among Nigerians. J. Niger Optom. Assoc. 2010; 16 (2):20-25.15. Kamppeter BI, Degenring RF, Jonas JB. Readaption time after photostress in normal subjects and glaucoma patients. Rev Ophthalmol. 2003; 100(12):1085-1090.16. Esenwah EC, Azuamah YC, Okorie ME, Ikoro NC. The Aging Eye and Vision: A review. Int J Health Sc Res. 2014; 4(7):218-226.17. Yasuki I, Masayuki H, Yozo M, Shinobu A. Extrafoveal photostress recovery testing with a scanning laser ophthalmoscope. Jpn J Ophthalmol. 1997; 41:255-259. 18. Masayuki H, Yozo M, Yasuki I. Extrafoveal photostress recovery test in glaucoma and idiopathic central sreous chorioretinopathy. Br J Ophthalmol. 1998; 82:1007-1012.
Journal of the Nigerian Optometric Association
36 JNOA.2018;20(2): 31 - 36 Azuamah et al
Original Research Article
In conclusion, there is a significant difference in PSRT both on the fovea and extra-foveal regions on the re�na in POAG and a control group. Photostress recovery test is valuable in glaucoma and other re�nal diseases to detect possible lesion and scotoma areas especially at the early stages of the defect. Optome-trists should carry out photostress recovery tests as part of rou�ne eye examina�ons.
Conclusion
It is prac�cally impossible to completely provide for the health needs of the en�re popula�on due to the scarcity of both human and material resources. This challenge is more seriously felt in developing na�ons than in the developed world. Some health condi�ons can be prevented by (health educa�on), that is by crea�ng awareness about how to avoid or
prevent such health issues. This is consistent with the Benjamin Franklin axiom that posits that “An ounce of preven�on is said to be worth a pound of cure!” However, for health promo�on to be effec�ve, it must be culturally appropriate and relevant. Papadopoulos1 defines cultural competence “as a process one goes through in order to con�nuously develop and refine one’s
JNOA.2018;20(2): 37 - 45
Reverence for the culture and beliefs of people most �mes kindles their interest in a unique way in programmes that they may likely tend to adopt, scorn or a�ack. In recent �mes, there have been fatal a�acks on health workers in different parts of the world due to misunderstanding of their mission. These health workers have been constantly molested and killed while carrying out their du�es. The misunderstandings stem from the fact that these people’s cultural belief was not put into considera�on while planning the health programme for that popula�on. Human beings are not chemical elements that could give the same kind of reac�on given same environment and condi�ons, but they have consciences and choices that could be influenced by a number of factors. Hence, this study was an a�empt to demonstrate the usefulness of a culturally-appropriate health promo�on approach in an adult Nigerian popula�on. This was popula�on-based qualita�ve study that used face-to-face semi-structured interviews to collect data from three sets of par�cipants [Service users n=28; doctors n=8; and policy makers n=3]. The transcribed interviews provided six important themes among which are: the desire for health educa�on, the need to think outside the box, and the Igbo philosophies. These themes were analysed using interpreta�ve phenomenological approach framework to provide rich informa�on about this popula�on. Understanding the culture and beliefs of the target popula�on could help to shape and plan effec�ve health promo�on programmes within a given community.
Keywords: Culturally-appropriate approach, Health promo�on, Igbo philosophies, eyecare, Nigeria.
Journal of the Nigerian Optometric Association Original Research Article
1. School of Health and Education, Middlesex University, The Burroughs, London.2. Research Centre for Transcultural Studies in Health, Middlesex University, The Burroughs, London.
1. Papadopoulos I, ed. Transcultural Health and Social Care: Development of culturally competent practitioners. London: ChurChill Livingstone; 2006.
Okoye, R.S1, Bell, L.1 and Papadopoulos, I.2,
Okoye, R.S. MNOA, FRSPH Email: [email protected]
37
Relevance of culturally-appropriate approaches in health promotion: a look at Igbo philosophies in dealing
with eye care challenges in Nigeria.
Corresponding Author:
Abstract
Introduction
Okoye et al

Journal of the Nigerian Optometric Association
38
2. World Health Organization. The Ottawa Charter for Health Promotion [Internet]. First International Conference on Health Promotion, Ottawa, 21 November 1986. 2017 [cited 2017 Nov 20]. Available from: http://www.who.int/healthpromotion/conferences/previous/ottawa/en/3. Naidoo J, Wills J. Health promotion: Foundations for practice. 2nd ed. London: Bailliere Tindall; 2000. 4. Ewles L, Simnett I. Promoting health: a practical guide. 5th ed. London: Tindall Bailliere; 2003. 5. Frost R. Health Promotion Theories and Models for Program Planning and Implementation. Public Health. 2008;1–6. 6. Adibi H. mHealth: Its Implications within the Biomedical and Social Models of Health – a Critical Review. Multidiscip Journals Sci Technol J Sel Areas Heal Informatics. 2014;4(2):16–23. 7. Rosenstock IM, Strecher VJ, Becker MH. The social learning theory and health belief model. Health Educ Q. 1988;15(2):175–83. 8. Borrelli B, Hayes RB, Dunsiger S, Fava JL. Risk perception and smoking behaviour in medically ill smokers: A prospective study. Addiction. 2010;105(6):1100–8. 9. Bandura A. Social learning theory. Social Learning Theory. New York: General Learning Press; 1971. 10. Yan Y, Jacques-Tiura AJ, Chen X, Xie N, Chen J, Yang N, et al. Application of the Protection Motivation Theory in predicting cigarette smoking among adolescents in China. Addict Behav. 2014;39(1):181–8. 11. Prochaska JO, Redding CA, Evers KE. The Transtheoretical Model and Stages of Change. In: Health Behavior and Health Education. 2008. p. 99–120. 12. Dearing JW. Applying diffusion of innovation theory to intervention development. Res Soc Work Pract. 2009;19(5):503–18.
capacity to provide effec�ve health care, taking into considera�on people’s cultural beliefs, behaviours and needs”. Therefore, understanding and consid-ering the target popula�on’s cultural beliefs is very important in ensuring acceptability of the health interven�on. In health promo�on, “prescribing instruc�ons” most �mes does not work well as working with the target popula�on thus; people should be encouraged to increase control over their health u�lising essen�al resources around their communi�es.
The O�awa Conven�on of 1986 defines Health Promo�on as:“...the process of enabling people to increase control over, and to improve, their health. To reach a state of complete physical, mental and social well-being, an individual or group must be able to identify and to realize aspirations, to satisfy needs, and to change or cope with the environment”2
Health promo�on has been used successfully to minimize the morbidity, the impact and spread of certain health condi�ons.3 Therefore, people within a given environment or community must be encouraged to increase and have be�er control over their health. Part of this assistance must be tailored in a specific way that would be acceptable to the community targeted. Several theories and models of health promo�on have been proposed and used in promo�ng health among different pop-ula�ons; some of these models include: the Diffusion Innova�on Theory (developed by E.M. Rogers in 1962), Trans-theore�cal Model (developed by Prochaska and DiClemente in the late 1970s), the Protec�on Mo�va�on Theory (developed by R.W. Rogers in 1975), Social Learning Theory (developed by Albert Bandura in 1977), the Theory of Reasoned
Ac�on/Theory of Planned Behaviour (proposed by Fishbein and Ajzen in 1980), the Health Belief Model (by Rosenstock and colleagues in 1988) and the Precau�on Adop�on Process Model (developed by Weinstein, Sandman and Blalock, 1992).3-12 Health promo�on has been classified in different ways; some models focus on individual ac�ons while some (Social Model) focus on collec�ve/na�onal level, others focus both on na�onal and interna�onal levels (such as Environmental/Ecological Models). The Biomedical Model of health focuses on physical or biological aspects of diseases and illness.6 The Social Model of health captures the O�awa Charter of health promo�on which emphasises considera�on on social determinants of health and related policy in planning effec�ve health interven�on.2
The knowledge one has about something determines to an extent how the person reacts to certain situa�ons, especially in ma�ers of health. Knowledge provides a person with necessary informa�on about some health condi�ons, the causes and consequences of such health issue. Armed with the knowledge of the health condi�on, the person may decide to have a change of behaviour which may be posi�ve or nega�ve. People’s behaviour is partly determined by their a�tude to that behaviour; an individual’s a�tude to a specific ac�on and the inten�on to adopt it are influenced by beliefs and mo�va�on which comes from the person’s values, a�tudes, drives and the influences from social norms.3 Belief is based on the informa�on a person has about something, and values are acquired through socializa�on.3 These two play essen�al role in changing people’s behaviour. The value the society places on par�cular health issue may be a driving force towards people avoiding being vic�ms to such diseases or health problems.
JNOA.2018;20(2): 37 - 45 Okoye et al
Original Research Article

Journal of the Nigerian Optometric Association
39
Several studies8,10-15 have a�ested to the usefulness of different health promo�on models, but health belief model is the commonly used approach. Najimi and Golshiri13 in a study to determine the knowledge, beliefs and preven�ve behaviours regarding influenza A among students in Iran, concluded that the Health Belief Model could be useful in improving preven�ve behaviours of influenza A among the popula�on. Other studies14,15 all show that Health Belief Model could be very effec�ve means of promo�ng health by influencing people’s a�tude and lifestyles in certain socie�es. However, the problem with the Health Belief Model is that the burden is on the individual, and other enabling factors were not adequately considered. However, there are several models of health promo�on that might be more relevant to a par�cular community than the other. No ma�er how good this may sound, informa�on alone may not work adequately in certain se�ngs. An Igbo proverb says “onye osisi hara onu dagburu, nti chiri ya” [meaning: a person that was killed by a noisily fallen tree must have been deaf]. Poverty and inability to pay for treatment forces people to ignore the symptoms and try to cope as best as they can with their health issues.16,17 Nigeria does not have a standard health insurance scheme which can guarantee free treatment in �mes of ill-health. Therefore, most treatments are generally paid for by the pa�ent; in spite of this, the country’s health care system is plagued by serious financial challenges and mismanagement.18-20 So, the level of treatment a person receives depends
on how much they are prepared to spend when they are sick.Unarguably, health promo�on is very important in health care management. However, for effec�ve health promo�on in any given environment, the planning and execu�on of the health programmes must be properly worded and must be targeted at the right audience. Several studies1,21,22 have emphasised the relevance of using a culturally appropriate approach in packaging and delivering health services. Thus, understanding the study popula�on’s culture will go a long way in addressing their health concerns appropriately. To be able to improve health behaviour, it is important to understand what beliefs the study popula�on holds about disease causa�on, their percep�ons about suscep�bility and severity of a health threat, perceived advantages and disadvantages of preven�ve ac�ons, and the barriers they face in adop�ng the suggested ac�ons.16,21 A case in point is the issue of con�nued killing and moles�ng of polio health workers in Pakistan, Afghanistan, Nigeria and other parts of the world and the blunt refusal to encourage polio immunisa�on in these places. It could be argued that this is a clear point of misunderstanding of the inten�on of the project. The reason for the a�ack was that some individuals within these communi�es believe that the polio immunisa�on was purely a means of rendering their children infer�le in order to decrease their popula�on for religious and poli�cal purposes.23,24 The fight against polio in these places now results to more deaths from religious fana�cs than from the disease itself.24
JNOA.2018;20(2): 37 - 45 Okoye et al
Original Research Article
1. Papadopoulos I, ed. Transcultural Health and Social Care: Development of culturally competent practitioners. London: ChurChill Livingstone; 2006.8. Borrelli B, Hayes RB, Dunsiger S, Fava JL. Risk perception and smoking behaviour in medically ill smokers: A prospective study. Addiction. 2010;105(6):1100–8. 9. Bandura A. Social learning theory. Social Learning Theory. New York: General Learning Press; 1971. 10. Yan Y, Jacques-Tiura AJ, Chen X, Xie N, Chen J, Yang N, et al. Application of the Protection Motivation Theory in predicting cigarette smoking among adolescents in China. Addict Behav. 2014;39(1):181–8. 11. Prochaska JO, Redding CA, Evers KE. The Transtheoretical Model and Stages of Change. In: Health Behavior and Health Education. 2008. p. 99–120. 12. Dearing JW. Applying diffusion of innovation theory to intervention development. Res Soc Work Pract. 2009;19(5):503–18. 13. Najimi A, Golshiri P. Knowledge, beliefs and preventive behaviors regarding Influenza A in students: a test of the health belief model. J Educ Heal Promot. 2013;2:23. 14. Asif M. The prevention and control the type-2 diabetes by changing lifestyle and dietary pattern. J Educ Health Promot. 2014;3(1):1. 15. Harooni J, Hassanzadeh A, Mostafavi F. Influencing factors on health promoting behavior among the elderly living in the community. J Educ Health Promot. 2014;3:40. 16. Okoye RS, Bell L, Papadopoulos I. Barriers to accessing good eye care services in Nigeria: A focus on Anambra State. J Niger Optom Assoc. 2018;20(1):30-37. 17. Ibeneche H, Ekpenyong B, Ebri A. Barriers to Accessing Eye Care Services in the Federal Capital Territory, Abuja, Nigeria. J Niger Optom Assoc. 2018;20(1):64–9. 18. Eme IO, Uche, OA, Uche IB. Building a Solid Health Care System in Nigeria: Challenges and Prospects. Acad J Interdiscip Stud. 2014; 19. Yunusa U, Irinoye O, Suberu A, Garba, AM, Timothy GD, Dalhatu A, et al., Trends And Challenges Of Public Health Care Financing System In Nigeria : The Way Forward . J Econ Financ. 2014;4(3):28–34. 20. Uzochukwu BSC, Ughasoro MD, Etiaba E, Okwuosa C, Envuladu E, Onwujekwe OE. Health care financing in Nigeria: Implications for achieving universal health coverage. Niger J Clin Pract. 2015;18(4):437–44. 21. Krumeich A, Weijts W, Reddy P, Meijer-Weitz A. The benefits of anthropological approaches for health promotion research and practice. Health Educ Res. 2001;16(2):121–30. 22. Huff RM, Kline M V. Health Promotion in the Context of Culture [Internet]. 2008 [cited 2017 Aug 16]. Available from: http://www.sagepub.com/sites/default/files/upm- binaries/23214_Chapter_1.pdf23. Scales D. At least nine polio workers killed in Nigeria [Internet]. Healthmap. 2013 [cited 2017 Sep 12]. Available from: http://www.healthmap.org/site/diseasedaily/ article/least-nine-polio-workers-killed-nigeria-2111324. McGirk T. Taliban assassins target Pakistan’s polio vaccinators [Internet]. National Geographic. 2015 [cited 2017 Jun 13]. Available from: http://news.nationalgeographic.com/2015/03/150303-polio-pakistan-islamic-state-refugees-vaccination-health/

Journal of the Nigerian Optometric Association
40
Methods
Results
Wording a health promo�on message properly in clear and culturally appropriate terms can serve as mo�va�on for behaviour modifica�on. This is in agreement with the Protec�on Mo�va�on Theory10,25 that targets to u�lize ‘fear appeals’ or persuasive messages designed to alarm the target audience by depic�ng what could happen if the message was ignored.25 However, the fear appeal works when a person has the capacity to avert such danger, but if unable to avert such problem, he/she may react indifferently or nega�vely to the fear appeal. Obviously, people some�mes may know what they should do about a par�cular health condi�on, but poverty has always been a major constraint. For instance, Nigeria is a country where the level of poverty is very high, with about 70.2% living in poverty26 here, health educa�on and crea�on of awareness might not completely solve the health problems. This is where the Social Model of Health promo�on proves a be�er op�on. The Social Model of health promo�on takes into account wider social determinants of health when planning a health promo�on programme. Health is determined not only by the absence of diseases but also greatly influenced by other factors such as housing, age, gender, educa�on, race, social network, transporta�on and even health policies opera�onal in places where people live.27 The purpose of this study was to demonstrate and emphasise the relevance of using culturally appropriate approach in promo�ng health in different se�ngs; taking into account the people’s beliefs and philosophies.
The data for this study was collected from three sets of par�cipants through semi-structured interviews. All the par�cipants were purposively recruited; a total sample of 39 par�cipants [28 key informants,
8 service providers and 3 policy makers]. The policy makers were selected to reflect different hierarchies of authority from the state to the community level. All the par�cipants were anonymised to protect their iden��es. While all the key informants and the service providers were given pseudonyms, the policy makers were named as follows: A Senior Policy Maker in the State [SPS], a Senior Policy Maker in the Local government [SPL] and a Senior Community Leader [SCL]. Two inclusion and exclusion criteria were applied in the selec�on of all the par�cipants. (1) All the par�cipants were aged 21-80 years old. (2) And all were permanently resident in Anambra State. All par�cipants consented to the interview being recorded; which were later transcribed for analysis. The analysis was done using Nvivo 10 so�ware and the Interpreta�ve Phenomenological Analysis [IPA] framework. The ethical approval for the study was given by the Health and Social Care Ethics Commi�ee of School of Health and Educa�on, Middlesex University London, and also by the Anambra State Ministry of Health Awka, Nigeria. The study was conducted in accordance with the Helsinki declara�on 2000. All the par�cipants were fully aware of the purpose of the research, the risk involved and their rights to withdraw at any point they feel uncomfortable to proceed. All par�cipants were requested to read and sign the informed consent form before commencement of the interviews.
The key informants were made up of people from different areas of residence and various occupa�onal backgrounds. The demographic details of all the par�cipants and other variables are presented in Table 1.
JNOA.2018;20(2): 37 - 45 Okoye et al
Original Research Article
10. Yan Y, Jacques-Tiura AJ, Chen X, Xie N, Chen J, Yang N, et al. Application of the Protection Motivation Theory in predicting cigarette smoking among adolescents in China. Addict Behav. 2014;39(1):181–8.25. Cross V, Shah P, Bativala R, Spurgeon P. Glaucoma awareness and perceptions of risk among African-Caribbeans in Birmingham, UK. Divers Heal Soc Care (DIVERSITY Heal SOC CARE). 2005;81–90. 26. Dineen B, Gilbert CE, Rabiu M, Kyari F, Mahdi AM, Abubakar T, et al. The Nigerian national blindness and visual impairment survey: Rationale, objectives and detailed methodology. BMC Ophthalmol. 2008;8(1):17. 27. Dahlgren G, Whitehead M. Policies and strategies to promote social equity in health. Stock Inst Futur Stud. 1991;
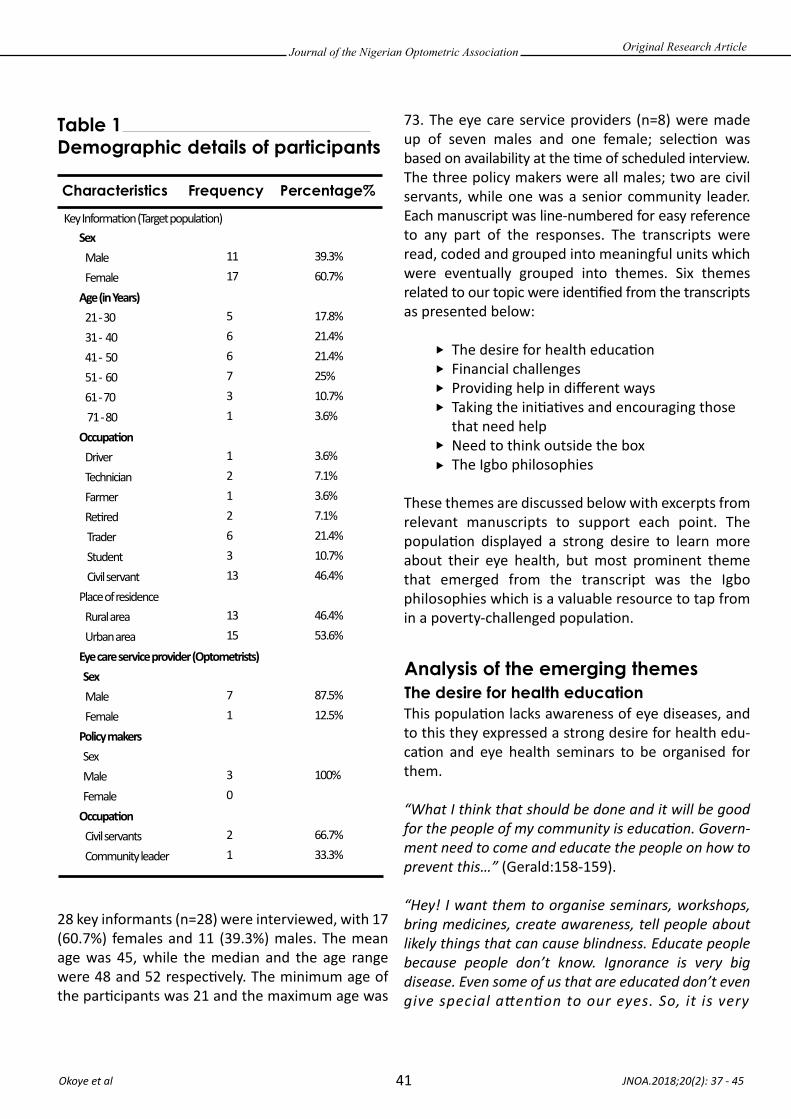
Journal of the Nigerian Optometric Association
41 JNOA.2018;20(2): 37 - 45 Okoye et al
Original Research Article
Table 1 Demographic details of participants
Characteristics Frequency Percentage%
Sex Male FemaleAge (in Years) 21 - 30 31 - 40 41 - 50 51 - 60 61 - 70 71 - 80 Occupa�on Driver Technician Farmer Re�red Trader Student Civil servantPlace of residence Rural area Urban area Eye care service provider (Optometrists) Sex Male Female Policy makers Sex Male FemaleOccupa�on Civil servants Community leader
Key Informa�on (Target popula�on)
1117
566731
12126313
1315
71
30
21
39.3%60.7%
17.8%21.4%21.4%25%10.7%3.6%
3.6%7.1%3.6%7.1%21.4%10.7%46.4%
46.4%53.6%
87.5%12.5%
100%
66.7%33.3%
28 key informants (n=28) were interviewed, with 17 (60.7%) females and 11 (39.3%) males. The mean age was 45, while the median and the age range were 48 and 52 respec�vely. The minimum age of the par�cipants was 21 and the maximum age was
73. The eye care service providers (n=8) were made up of seven males and one female; selec�on was based on availability at the �me of scheduled interview. The three policy makers were all males; two are civil servants, while one was a senior community leader. Each manuscript was line-numbered for easy reference to any part of the responses. The transcripts were read, coded and grouped into meaningful units which were eventually grouped into themes. Six themes related to our topic were iden�fied from the transcripts as presented below:
The desire for health educa�on Financial challenges Providing help in different ways Taking the ini�a�ves and encouraging those that need help Need to think outside the box The Igbo philosophies
These themes are discussed below with excerpts from relevant manuscripts to support each point. The popula�on displayed a strong desire to learn more about their eye health, but most prominent theme that emerged from the transcript was the Igbo philosophies which is a valuable resource to tap from in a poverty-challenged popula�on.
This popula�on lacks awareness of eye diseases, and to this they expressed a strong desire for health edu-ca�on and eye health seminars to be organised for them.
“What I think that should be done and it will be good for the people of my community is education. Govern-ment need to come and educate the people on how to prevent this…” (Gerald:158-159).
“Hey! I want them to organise seminars, workshops, bring medicines, create awareness, tell people about likely things that can cause blindness. Educate people because people don’t know. Ignorance is very big disease. Even some of us that are educated don’t even give special attention to our eyes. So, it is very
Analysis of the emerging themesThe desire for health education

Journal of the Nigerian Optometric Association
42
Financial challenges
Providing help in different ways
necessary they wake up from slumber and do something very very important patterning our eyes because if you don’t have your eyes, you can’t do anything” (Carol:91-95).
It was very easy to detect the passionate nature of this appeal from these two key informants. Great desire to have assistance was clearly expressed by these par�cipants. Carol used different terms [seminars, workshops, create awareness, tell the people, educate the people] to further emphasise her point. She further said that even the educated people s�ll lack the required awareness. In promo�ng health in this type of environment, extra effort is needed to package the programme properly, and in such a way that makes it relevant to the target popula�on.
Money has really been a major barrier in accessing health care services in the state. Because govern-ment-owned health care services are few, service users are forced to consult private health care providers which are normally very costly. Consider the response of Gerald, one of the par�cipants.
“What determines who you consult is your financial background. If you have no money you won’t be thinking of approaching a professional but when you have the money you will now have the courage to approach any professional body” (Gerald: 128-130).
“Yes, there are barriers like finance and the distance of the eye clinic from my place” (Akuobi: 110).
Understandably, no one goes to consult a professional if you do not have the money to pay for the services. This means that no ma�er the level of awareness you may have about an illness, you may not have the boldness to approach a professional if you cannot pay for the treatment. This is a fact that whoever is planning a health promo�on package in this community must incorporate into the programme; how to help the popula�on to easily access health care services amidst financial challenges. In addi�on to the monetary problem, distance to
the hospitals and health care services centre is equally a big challenge both in terms of transport and people to escort the pa�ents.
Pursuance to the challenges iden�fied in this popula�on, different people have devised different ways of assis�ng one another. Zenda, one of the par�cipants recognised this challenge, and has volunteered to be assis�ng some people that may have problem with travelling to the hospitals.
“I am trying to sponsor people, that is those that will be willing to go in order to meet the doctor but are having problem with transport, I will try to help out with my car so as to take them there” (Zenda:115-117).
Most of the eye hospitals are located in the ci�es, and people o�en find it difficult to travel to these places for treatment. So, providing means of transport to the hospital could be very helpful to many people in this community. If one could not get to where the treatment could be got, the chances of solving the health problem are slight. Providing transporta�on is very important but there are other ways of providing assistance to this popula�on.
“Ok, like in my clinic now we now have a form because as I said abinittio poverty is the cause of all this blindness. In our clinic now if you don’t have your money, you fill a form for us. In this form your bio-data; every information about you is there and the way that you will pay this money. So that if we treat you we keep treating you and you keep complying in your own little way...this package is a new package and it is working for us though we are counting losses somewhere, …. (Dr Sam:87-96)
This is another method devised by one of the service providers to assist the indigent service users. The clinic tries to extend credit facili�es to the popula�on; this makes it possible for some that need treatment to access it even without money. These people later come back to pay when they have the money. According to Dr Sam, this method works for him and some members of the community in which he works. These li�le bits of assistance from different individuals could be refined,
JNOA.2018;20(2): 37 - 45 Okoye et al
Original Research Article

Journal of the Nigerian Optometric Association
43
Taking the initiatives and encouraging those that need help
Need to think outside the box
reformed and packaged rightly to form basis for assis�ng this popula�on in accessing health care services in the state. Anthony, one of the key informants also pointed out that why most people from his kindred do not experience serious financial barrier was because they help one another when they have health issues.
Among the three policy makers, SCL was the only one that took the ini�a�ve to organise an effec�ve way for assis�ng the poor that need health care services in his community.
“We also organise doctors for surgical treatments should the eye care require operation, that is surgery. We have volunteers; I organise volunteers who pay for such poor people” (SCL:28-30).
SCL explains how he organises monthly health outreach to his community, he gives free medical treatment and even organises for surgeries for those that need such. He was aware that many people need health care services but cannot afford the payment. To this respect, SCL mobilises and mo�vates some members of his community to sponsor and pay for these treatments. People value such assistance tremendously especially when they cannot afford to pay for such services. The apprecia�on for this was evident in the words of one of the par�cipants.
“It was in April and they told me that I should come back in the first week of May so that I would be operated for glaucoma.; Yes, through the help of SCL.” (Anthony:20-21;25).
This par�cipant was narra�ng how SCL has helped him to undergo glaucoma surgery; such a step has now saved this man from blindness due to glaucoma.
There are always challenges to providing reasonable health care services to the popula�on especially in
the developing world. Finance has always been a problem both to the government, the service providers and the service users. While the government finds it difficult to adequately equip the hospitals and health care facili�es, the service providers find it challenging to meet their running costs, thereby forcing them to raise their charges. This eventually makes it very difficult for the service users to afford the services. There is therefore a need to modify the system, a need to be proac�ve; people need to think outside the box. The SPS blames the people for not being able to save money to consult the doctor without even thinking about how to help these people with their financial difficul�es.
“Well I think the major problem is the problem of scale of preference; if somebody says he has not gotten may be about 2000 Naira to go to hospital but he can afford to buy the wears 10000 Naira. You begin to see what their scale of preference is…” (SPS:137-139).
The SPS statement above is a clear evidence that he never understands the plights of his people. There is much to medical treatment than just paying for consulta�on. It might be easy to suggest to someone how to save money for treatment but there is need to ask, ‘how possible would this be for the person involved?’
“The problem of finance is always there with every society like our own; it is an under-developed society. So, in all the challenges that we are facing we know that with enough finance things can change but people work according to the limited envelope provided for them, and so you cannot go out of that envelop even if you see somebody dying and you don’t have the money to send that person to hospital, there is nothing you can do” (SPL:77-81).
The SPL maintains that there is nothing he could do once the money allocated to a health project was spent; even when someone is dying. This shows how serious things could be, and how helpless the people that found them-selves in such situa�ons could be; there is a need to think “outside the box”. The boldness of SCL and the ingenuity he exhibited in assis�ng his subjects is a clear indica�on that there are avenues that could be explored to alleviate the plights of this par�cular popula�on. Health promo�on is not just about crea�ng awareness
JNOA.2018;20(2): 37 - 45 Okoye et al
Original Research Article

Journal of the Nigerian Optometric Association
44
The Igbo philosophies
Discussion
and educa�ng the people about some health issues, but also about empowering them, advoca�ng for their welfare and providing assistance as much as possible. In the light of the above postula�ons, this popula�on’s health can be improved by integra�ng these pieces of informa�on while planning for the health of the community.
Culture is an important determinant of health, and thus must be considered while planning for the health of a par�cular popula�on or community. Different people and different communi�es have certain cultural iden��es and certain philosophies that guide their way of life. The Igbos have a unique cultural iden�ty and philosophy that guide the rela�onship with a fellow Igbo person. An average Igbo person sees a fellow Igbo as a brother or sister regardless of the fact that they might not come from the same town in Igbo land. Therefore, the word “brother or sister” is a metaphor for any Igbo person in this context. The Igbos try to help one another especially when stuck in an unpleasant situa�on or faced with challenging health issues. The inten�on here is to give as much assistance as they could to minimize the suffering of the sick person. They believe that a brother or sister is precious, and therefore they must not be abandoned when they are suffering or when in difficulty “onye aghana nwanne ya”.
One of the main benefits of being a “cultural insider” [in a research] is that there are certain salient points that an “insider” can spot but which might mean nothing to an “outsider”. In the analysis of various interviews, we were able to iden�fy certain philosophies that persistently came up in the transcript. These are: 1. The Igbo philosophy of “Onye aghana nwanne ya, and, the “Igbo five fingers are not equal” philosophy.”
“Onye aghana nwanne ya” literally means that nobody should abandon his/her brother/sister. Recall Zenda’s promise to use his car to transport those that may have transport challenges. Anthony further confirms this when he said that they help
each other in his kindred when they have health challenges. In fact, the Igbos are very sympathe�c to one another especially when it comes to issues of ill-health. The “five finger concepts” is a common saying throughout the Igbo land. They believe that the five fingers- [a metaphor for social stra�fica�on in the Igbo community]- are not equal, nor the same. This means that some people are be�er-off. Despite this, a hand needs all the fingers in order to func�on effec�vely; each finger compliments the other. In the light of this belief, members of the Igbo community recognise the differences in knowledge, skills, wealth and so on which exist in their community. This recogni�on mo�vates them to act in ways which address inequali�es and benefit from the contribu�on that each member can make. For example, although the socio-poli�cal condi�ons may not currently exist in terms of bringing about the eradica�on of poverty, those members of the Igbo community who are be�er off - the “haves” - are expected to assist the financially weaker members - the “have nots”. This is the reason the SCL tries to mobilise and mo�vate the rich people in his community to assist in paying for the medical treatment of the poor people in the community.
Our study provides evidence of the need for health educa�on as this popula�on expressed a dire need for be�er health awareness. Providing health educa�on can be very helpful in most cases. Health educa�on is geared towards influencing and changing lifestyle and health-seeking behaviour. Health seeking behaviours especially as it concerns responding to health issues can only be changed if one has the capacity. As Gerald has stated, it is difficult to think of consul�ng a professional if one does not have the money to pay for their services. Therefore, to impact posi�vely on the health of this popula�on, it will not be enough to provide just simple health educa�on but rather culturally-appropriate health promo�on that would bring on board the different challenges facing the popula�on.
Financial challenge has always been an issue in accessing health care services especially in the developing world. This has been a major huddle in
JNOA.2018;20(2): 37 - 45 Okoye et al
Original Research Article

Journal of the Nigerian Optometric Association
45
Nigeria, as many struggle to access good and quality health care services due to poverty.16,28,29 Taking this on board, harnessing and modifying different levels of contribu�on from the service users, the service providers, and the SCL, would impact posi�vely on the health challenges of this popula�on. SCL has taken the ini�a�ve by demonstra�ng that the rich mem-bers of the society can be approached to invest their money on the welfare of the community.
The two theories that underpin this study- the social theory of health promo�on and the cultural theories explain further how culturally competent health promo�on could be very effec�ve in this instance. The cultural theories use heuris�c techniques in trying to find solu�ons to problems within the confines of a cultural environment. In this study, the Igbos concept of “five fingers not being equal” and “onye aghana nwanne ya” philosophy come into play. People are o�en mo�vated when cultur-ally-appropriate approach is employed within their se�ng. The Igbo people have real concerns for their fellows; always prepared to help when they
could. This is their own method of dealing with this challenge. In developed country like the UK, the government provides health care for all the ci�zens, accessing health services is simple and straight forward most �mes.
Therefore, having noted that poverty has been a serious barrier among this popula�on, a health promo�on package that begins with advocacy and recogni�on of these two laudable Igbo philosophies will go a long way in boos�ng posi�ve responses. There is also a need to men�on that everyone has something to contribute towards improving the health of the community. However, policy makers need to come out of their shells and start to think outside the box. A leader needs to be innova�ve, proac�ve and charisma�c. The difference between an ordinary person and an extraordinary person is that, an ordinary person goes about their business in an ordinary way, but an extraordinary person is an ordinary person that does ordinary things in extraordinary ways.
JNOA.2018;20(2): 37 - 45 Okoye et al
Original Research Article
16. Okoye RS, Bell L, Papadopoulos I. Barriers to accessing good eye care services in Nigeria: A focus on Anambra State. J Niger Optom Assoc. 2018;20(1):30-37. 28. Oyibocha E., Irinoye O, Sagua E., Ogungide – Essien O., Edeki J., Okome O. Sustainable Healthcare System in Nigeria: Vision, Strategies and Challenges. IOSR J Econ Financ. 2014;5(2):28–39. 29. Tafida A, Kyari F, Abdull MM, Sivasubramaniam S, Murthy GVS, Kana I, et al. Poverty and Blindness in Nigeria: Results from the National Survey of Blindness and Visual Impairment. Ophthalmic Epidemiol. 2015;22(5):333–41.
This study provides evidence of the relevance of using a culturally-appropriate approach in planning effec-�ve public health interven�on. Culturally competent approach guarantees acceptance based on full under-standing of the need for the interven�on. In a society where the cost for health care is out of the reach of the poor and needy, the only available op�on is to fall back on the people’s belief that the “haves” in their community should be their “brothers’ keeper”. Thus, the two important Igbo philosophies of “onye aghana nwanne ya, and five-finger not equal concepts” have been sources of help to the indigent popula�on. If problems could not be solved through conven�onal methods, heuris�c approach may provide reprieve to the popula�on.
Conclusion

The eye is constantly exposed to a wide range of physical occurring materials like X-rays, chemical toxins, air pollutants and biological materials such as microbes on daily basis. X-radia�on (composed of X-rays) is an electromagne�c radia�on which has a wavelength range of 0.01-10nM and it emanates from the electronic part of the atom. Its energies exist in the region of 120 eV to 120 keV1. The eye does not differen�ate between any material i.e. microbes, X-rays or toxins, it interacts with; thus it
adopts certain mechanisms to deal with all of these agents. Although radia�ons could have detrimental effects on the eyes, ar�ficial radia�ons such as; ultrasound, X-rays, and lasers are constantly used for medical diagnosis and therapy 2. The eye uses a combina�on of barriers and mechanisms to deal with radia�ons and microbes, but not all radia�ons (for example X-rays) can be tolerated, especially at high doses, thus affec�ng the eye.
JNOA.2018;20(2): 46 - 52
The eye interacts constantly with a wide range of physically occurring materials like x-rays, air pollutants and toxins. The purpose of this study was to inves�gate the effects of X-rays on the electrolyte concentra�on of bovine aqueous and vitreous humour. Aqueous and vitreous humours were obtained from the eyes of cer�fied healthy cows freshly slaughtered in the government aba�oir at Ikpoba Slope, Benin City, Edo State, Nigeria. These cows’ eyes were enucleated within 2 hours a�er the death of the animals, and the right eyes were separated from the le� eyes. The aqueous humour (AH) and vitreous humour (VH) samples were collected using a 12ml syringe and a needle through scleral puncture made on the lateral canthus and the total extractable aqueous or vitreous humour aspirated from each eye separately. The eyes were transferred to the University of Benin Teaching Hospital (UBTH) Radiology Department where they were irradiated with X-rays machine (VARIAN Medical System model 93061 -7t). Before irradia�on, the eyes were removed from ice and allowed to thaw for about 3 minutes. Determina�on of electrolyte concentra�on were determined using E110111 flame Photometer (Antex Diagnos�cs, Beijing, China). Results show that radia�on had no sta�s�cally significant effect on the mean concentra�ons of ca�ons and anions in both AH and VH in this study (p > {0.05}). It is therefore concluded that radia�on had no sta�s�cally significant effect on the mean concentra�ons of potassium ion and chloride ion in both AH and VH.
Keywords: X-rays, electrolyte concentra�on, Bovine humours, radia�on
Journal of the Nigerian Optometric Association Original Research Article
1.Department of Optometry, Faculty of Life Sciences, University Of Benin.
1. Novelline I, Robert E. Squire's Fundamentals of Radiology. Harvard University Press. 5th edition.1997; 21-22.2. PetersonD. Dental X-Ray Family Gentle Dent Care.http://www.dentalgentlecare.com. 2008. Retrieved on 1st February 2014
Ajayi, O.B.1 and Atuanya G.N.1
Atuanya G.N Email: [email protected]
46
EFFECT OF X-RAYS ON THE ELECTROLYTE CONCENTRATION OF BOVINE AQUEOUS AND VITREOUS HUMOUR
Corresponding Author:
Abstract
Introduction
Atuanya and Ajayi

Journal of the Nigerian Optometric Association
47
3. Guyton AC, Hall JE. Fluid system of the eye - intraocular fluid textbook of medical Physiology, 11th Ed Publishers: Elsevier –Saunders.2006; 199:623-624.4. Sasaki H, Lin L, Yokoyama T, Sevilla, MD, Reddy VN, Giblin FJ. TEMPOL Protects Against Lens DNA Strand Breaks and Cataract in the X-Rayed Rabbit. Investigative Ophthalmology and Visual Science. 1998; 39(3): 544-552.5. Ueno N, Sebag J, Hirokawa H, Chakrabarti B. Effects of visible – light irradiation vitreous structure in the presence of a photo sensitizer. Experimental Eye Research. 1987; 44(6): 862 -870. 6. Heller S, Mayer UM. Effect of UV light on the catalase activity in the vitreous body of calf eyes. Journal of Ophthalmology liquids. 1994; 3(6): 445 -446. 7. Poppendiek HJ, Greene ND, Chambers JE, Feigenbutz LV, Morehouse PM, Randall R, Murphy JR. Annual report on thermal and electrical conductivities of biological fluids and tissues. Geoscience Ltd, Solana Beach, California. April 1,1964-March 31, 1965.Unclassified Report. 8. Meents A, Gutmann S, Wagner A, Schulze-Briese C. Origin and Temperature dependence of radiation damage in biological Samples at Cryogenic temperatures; Proceedings of National Academy of Science. 2010; 107(3): 1094-1099. 9. Roessler G. Radiations Basic. Health Physics Society.2001; 2(1): 5-6.10. Chua KJ, Ho JC, Chou SK, Islam, MR. Temperature distribution within a human eye subjected to laser source. International communications in heat and mass transfer. 2005; 3(8):1057-1065.11. Ajayi NO, Osahon OD, Laogun AA. Electrical Dispersion in Bovine Aqueous and vitreous humor eye tissues. Journal of National Academy Advanced Science . 2004; 3: 135-143.12. Swam A, Gonstable IJ, Harper E. Vitreous structure composition of Bovine vitreous collagen. Investigative Ophthalmology and Visual Science. 1972; 11(9): 81 - 83.13. Brzezinski PM, Godlewski A. Assessment of potassium and sodium ions concentrations in the vitreous humor of swine isolated eyeballs after organism’s death .Annales Academiae Medicae Bialostocensis. 2004; 49: 161 – 163.
The aqueous humour (AH) is a clear, gela�nous fluid similar to plasma but with a lower protein concentra�on. The AH is secreted from the ciliary epithelium, and is con�nuously being produced and reabsorbed3. Exposure of the eye to X-rays leads to the forma�on of cataracts and breakage of Deoxy ribonucleic acid (DNA) in the lens and AH; produc�on of hydroxyl radicals and peroxides that subsequently lead to DNA damage4.
The Vitreous humour (VH) is responsible for the oval shape of the eye; thus preven�ng fric�on, collapse and vibra�on of the eye organs and �ssues. It allows light to be guided to the re�na and reduces bleeding in the eye. Ueno et al. (1987)5 studied the effect of visible light irradia�on on the vitreous structure in the presence of a photo-sensi�zer. They claimed that the ac�ve, charged species of oxygen i.e. the singlet oxygen, superoxide anion, hydrogen peroxide and the hydroxyl radicals generated by the photo-dynamic ac�on of the radia�on in the presence of the sensi�zer, caused significant liquefac�on of the calf vitreous.
When biological �ssues are exposed to ionizing radia�on, their structural proper�es such as: shape, size, charge distribu�on and dipole moment are modified5. The resultant change in physicochemical and biological proper�es can be used to study and characterize the altera�on. The physical proper�es of biological �ssues include; electrical conduc�vity, dielectric constant or rela�ve permi�vity, electric poten�al or self-poten�al. Analysis of ca�ons and anions present in the fluid, as well as, levels of triglycerides, total protein and an�oxidant ac�vi�es are indicators of the chemical proper�es.
The effects of different types of radia�ons on biological �ssues have been discussed by several authors6,7. Radia�ons increase the ac�vity of free radicals which ini�ate degenera�ve changes that can lead to debilita�ng condi�ons8. Radia�ons have been associated with systemic diseases e.g. central nervous system diseases and ocular diseases e.g. cataract. Radia�ons carry energies, some of which are deposited in materials along its. Thus, it is important to determine the damaging effects of radia�ons on the eyes. The eye is one of the body’s organs par�cularly sensi�ve to radia�ons from various sources 9,10. It is also important to note that the effects of radia�ons on the eye not only depend on the sensi�vity of the �ssue itself but also on the mode of radia�on delivery 11.
This study was aimed at determining the effect of X-rays on electrolyte concentra�on and biochemical parameters of bovine aqueous and vitreous humour.
Aqueous and vitreous humours were obtained from the eyes of cer�fied healthy cows freshly slaughtered in the government aba�oir at Ikpoba Slope, Benin City, Edo State, Nigeria. The cows used were between the ages of 10-14yrs (mature cows) and they were all reared in the same environment. These cows’ eyes were collected within 2h a�er the death of the animals, and the right eyes were separated from the le� eyes. These eyes were placed on ice to maintain the normal biological state a�er death12,13.
JNOA.2018;20(2): 46 - 52 Atuanya and Ajayi
Original Research Article
MATERIALS AND METHODSSample Collection
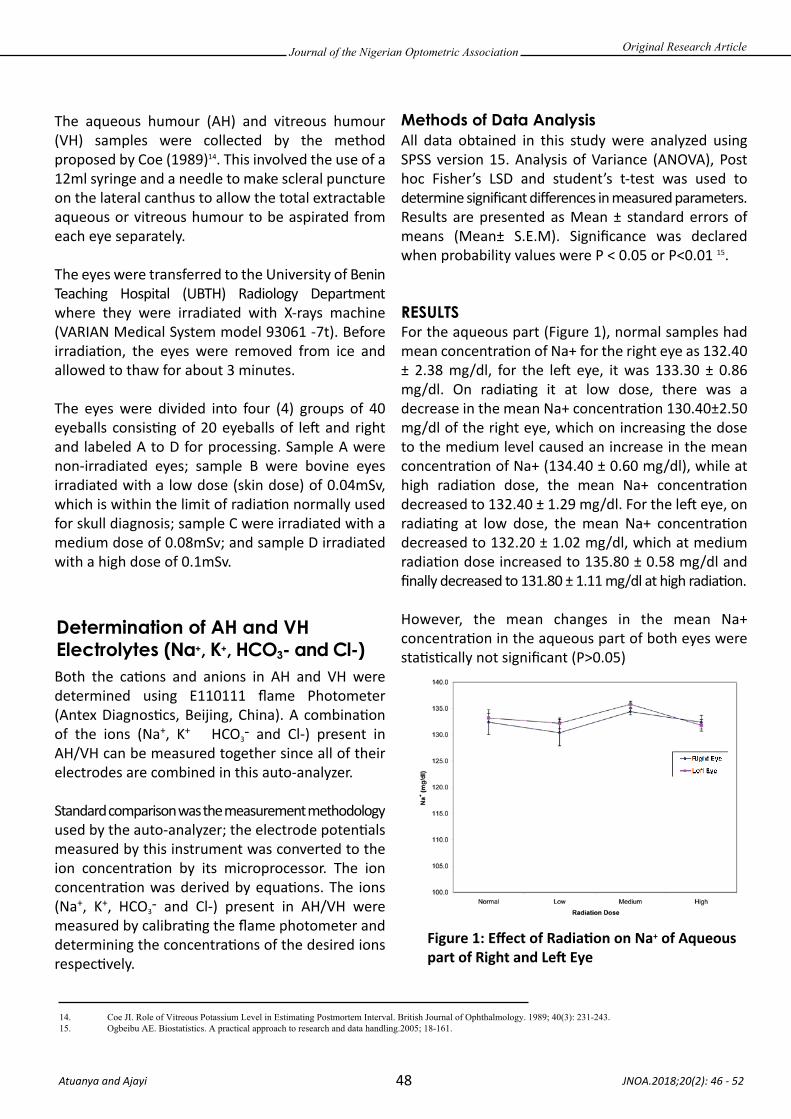
Journal of the Nigerian Optometric Association
48
Determination of AH and VH Electrolytes (Na+, K+, HCO3- and Cl-)
Methods of Data Analysis
RESULTS
The aqueous humour (AH) and vitreous humour (VH) samples were collected by the method proposed by Coe (1989)14. This involved the use of a 12ml syringe and a needle to make scleral puncture on the lateral canthus to allow the total extractable aqueous or vitreous humour to be aspirated from each eye separately.
The eyes were transferred to the University of Benin Teaching Hospital (UBTH) Radiology Department where they were irradiated with X-rays machine (VARIAN Medical System model 93061 -7t). Before irradia�on, the eyes were removed from ice and allowed to thaw for about 3 minutes. The eyes were divided into four (4) groups of 40 eyeballs consis�ng of 20 eyeballs of le� and right and labeled A to D for processing. Sample A were non-irradiated eyes; sample B were bovine eyes irradiated with a low dose (skin dose) of 0.04mSv, which is within the limit of radia�on normally used for skull diagnosis; sample C were irradiated with a medium dose of 0.08mSv; and sample D irradiated with a high dose of 0.1mSv.
Both the ca�ons and anions in AH and VH were determined using E110111 flame Photometer (Antex Diagnos�cs, Beijing, China). A combina�on of the ions (Na+, K+ HCO3
- and Cl-) present in AH/VH can be measured together since all of their electrodes are combined in this auto-analyzer.
Standard comparison was the measurement methodology used by the auto-analyzer; the electrode poten�als measured by this instrument was converted to the ion concentra�on by its microprocessor. The ion concentra�on was derived by equa�ons. The ions (Na+, K+, HCO3
- and Cl-) present in AH/VH were measured by calibra�ng the flame photometer and determining the concentra�ons of the desired ions respec�vely.
All data obtained in this study were analyzed using SPSS version 15. Analysis of Variance (ANOVA), Post hoc Fisher’s LSD and student’s t-test was used to determine significant differences in measured parameters. Results are presented as Mean ± standard errors of means (Mean± S.E.M). Significance was declared when probability values were P < 0.05 or P<0.01 15.
For the aqueous part (Figure 1), normal samples had mean concentra�on of Na+ for the right eye as 132.40 ± 2.38 mg/dl, for the le� eye, it was 133.30 ± 0.86 mg/dl. On radia�ng it at low dose, there was a decrease in the mean Na+ concentra�on 130.40±2.50 mg/dl of the right eye, which on increasing the dose to the medium level caused an increase in the mean concentra�on of Na+ (134.40 ± 0.60 mg/dl), while at high radia�on dose, the mean Na+ concentra�on decreased to 132.40 ± 1.29 mg/dl. For the le� eye, on radia�ng at low dose, the mean Na+ concentra�on decreased to 132.20 ± 1.02 mg/dl, which at medium radia�on dose increased to 135.80 ± 0.58 mg/dl and finally decreased to 131.80 ± 1.11 mg/dl at high radia�on.
However, the mean changes in the mean Na+ concentra�on in the aqueous part of both eyes were sta�s�cally not significant (P>0.05)
JNOA.2018;20(2): 46 - 52 Atuanya and Ajayi
Original Research Article
14. Coe JI. Role of Vitreous Potassium Level in Estimating Postmortem Interval. British Journal of Ophthalmology. 1989; 40(3): 231-243.15. Ogbeibu AE. Biostatistics. A practical approach to research and data handling.2005; 18-161.
Figure 1: Effect of Radia�on on Na+ of Aqueous part of Right and Le� Eye
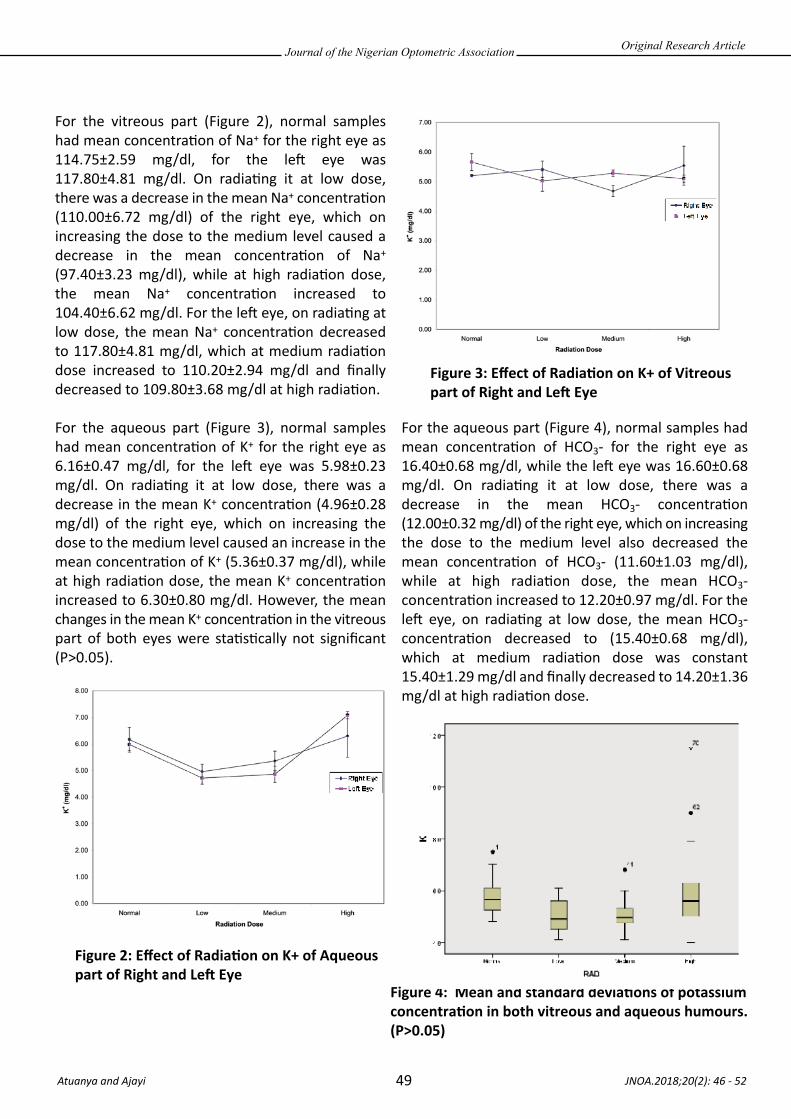
Journal of the Nigerian Optometric Association
49
For the vitreous part (Figure 2), normal samples had mean concentra�on of Na+ for the right eye as 114.75±2.59 mg/dl, for the le� eye was 117.80±4.81 mg/dl. On radia�ng it at low dose, there was a decrease in the mean Na+ concentra�on (110.00±6.72 mg/dl) of the right eye, which on increasing the dose to the medium level caused a decrease in the mean concentra�on of Na+ (97.40±3.23 mg/dl), while at high radia�on dose, the mean Na+ concentra�on increased to 104.40±6.62 mg/dl. For the le� eye, on radia�ng at low dose, the mean Na+ concentra�on decreased to 117.80±4.81 mg/dl, which at medium radia�on dose increased to 110.20±2.94 mg/dl and finally decreased to 109.80±3.68 mg/dl at high radia�on.
For the aqueous part (Figure 3), normal samples had mean concentra�on of K+ for the right eye as 6.16±0.47 mg/dl, for the le� eye was 5.98±0.23 mg/dl. On radia�ng it at low dose, there was a decrease in the mean K+ concentra�on (4.96±0.28 mg/dl) of the right eye, which on increasing the dose to the medium level caused an increase in the mean concentra�on of K+ (5.36±0.37 mg/dl), while at high radia�on dose, the mean K+ concentra�on increased to 6.30±0.80 mg/dl. However, the mean changes in the mean K+ concentra�on in the vitreous part of both eyes were sta�s�cally not significant (P>0.05).
For the aqueous part (Figure 4), normal samples had mean concentra�on of HCO3- for the right eye as 16.40±0.68 mg/dl, while the le� eye was 16.60±0.68 mg/dl. On radia�ng it at low dose, there was a decrease in the mean HCO3- concentra�on (12.00±0.32 mg/dl) of the right eye, which on increasing the dose to the medium level also decreased the mean concentra�on of HCO3- (11.60±1.03 mg/dl), while at high radia�on dose, the mean HCO3- concentra�on increased to 12.20±0.97 mg/dl. For the le� eye, on radia�ng at low dose, the mean HCO3- concentra�on decreased to (15.40±0.68 mg/dl), which at medium radia�on dose was constant 15.40±1.29 mg/dl and finally decreased to 14.20±1.36 mg/dl at high radia�on dose.
JNOA.2018;20(2): 46 - 52 Atuanya and Ajayi
Original Research Article
Figure 2: Effect of Radia�on on K+ of Aqueous part of Right and Le� Eye
Figure 3: Effect of Radia�on on K+ of Vitreous part of Right and Le� Eye
Figure 4: Mean and standard devia�ons of potassium concentra�on in both vitreous and aqueous humours. (P>0.05)

Journal of the Nigerian Optometric Association
50
Chloride DISCUSSIONFor the aqueous part (Fig 5), normal samples had mean concentra�on of Cl- for the right eye as 101.20±2.42 mg/dl, for the le� eye, it was 103.60±0.75 mg/dl. On radia�ng it at low dose, there was an increase in the mean Cl- concentra�on (107.60±2.14 mg/dl) of the right eye, which on increasing the dose to the medium level also increased the mean concentra�on of Cl- (111.60±1.47 mg/dl), while at high radia�on dose, the mean Cl- concentra�on decreased to 108.80±1.02 mg/dl. For the le� eye, on radia�ng at low dose, the mean Cl- concentra�on increased to (104.00±1.41 mg/dl), which at medium radia�on dose was increased to 106.80±1.62 mg/dl and finally decreased to 106.00±1.10 mg/dl at high radia�on dose. However, the mean changes in the mean Cl- concentra�on in the vitreous part of the le� eye were sta�s�cally not significant (P>0.05), while at medium irradia�on of the right eye showed sta�s�cal significance (P<0.05) with the normal.
Biochemical analysis showed that sodium concentra�on observed in the aqueous part (Fig 1) for normal samples had mean concentra�on of 132.40±2.38 mg/dl for the right eye and 133.30±0.86 mg/dl for the le� eye. Also, at high radia�on dose, the mean Na⁺ concentra�on was 132.40±1.29 mg/dl for the right and 131.80±1.11 mg/dl for the le� eye. However, the mean changes in the mean Na⁺ concentra�on in the aqueous part of both eyes were sta�s�cally not significant (P>0.05). For the vitreous part, normal samples had mean concentra�on of Na⁺ for the right eye as 114.75±2.59 mg/dl, for the le� eye was 117.80±4.81 mg/dl. High radia�on dose showed 104.40±6.62 mg/dl for the right vitreous humour and 109.80±3.68 mg/dl for le� vitreous humour. However, the mean changes in the mean Na⁺ concentra�on in the vitreous part of both eyes were sta�s�cally not significant (P>0.05). Measured value of sodium concentra�on ranged between 80 mmol/L and 138 mmol/L. The mean changes in the mean Na⁺ concentra�on in the aqueous and also in the vitreous part of both eyes when subjected to varying doses of irradia�on were sta�s�cally not significant (P>0.05). In a research by Chandrakanth et al. (2013)16, there was no significant difference in the differences in vitreous sodium, potassium, chloride levels and the sodium potassium ra�o among males and females and between right and le� eyes.
The potassium ion concentra�on in the aqueous humour for non- irradiated sample (Fig 4.36) was 6.16±0.47 mg/dl for the right eye and 5.98±0.23 mg/dl for the le� eye. High irradia�on gave 4.72±0.23 mg/dl for the right eye and 7.08±1.14 mg/dl for the le� eye. For the vitreous humour (Figure 4.37), normal samples had mean concentra�on of K+ for the right eye as 5.20±0.04 mg/dl, while the le� eye was 5.66±0.29 mg/dl. High irradia�on gave 5.54±0.66 mg/dlfor right eye and 5.10±0.12 mg/dl for the le� eye. However, the mean changes in the mean K+ concen-tra�on in aqueous and vitreous humours of both eyes
JNOA.2018;20(2): 46 - 52 Atuanya and Ajayi
Original Research Article
16. Chandrakanth HV, Kanchan T, Balarai BM, Virupaksha HS, Chandrashekar TN. Postmortem vitreous chemistry—an evaluation of sodium,potassium and chloride levels in estimation of time since death(during the first 36hr after death).Journal of Forensic and Legal Medicine . 2013; 20(4):211-216
Figure 4: Effect of Radia�on on Cl- of Aqueous part of Right and Le� Eye

Journal of the Nigerian Optometric Association
51
17. Garg V, Oberoi SS, Gorea RK, Kaur K. Changes in the levels of vitreous potassium with increasing time since death. Journal of Indian Academy of Forensic Medicine. 2004; 26(4):971-973. 18. Tumram KN, Ambade VN, Dongre, AP. Thanatochemistry: Study of vitreous humor potassium. Alexandria Journal of Medicine. 2014;50(4):365-36819. Negi A, Honda Y, Kawano S. Importance of bicarbonate ion in the vitreous space. Archives of Ophthalmology. 1998; 11(100): 1839-1843.20. Dufour DR. Lack of correlation of postmortem vitreous humor calcium concentration with antemortem serum calcium concentration. Journal of Forensic Science.1982; 4:889-893.
were sta�s�cally not significant (P>0.05). Measured value of potassium concentra�on ranged between 4 mmol/L and 11.5 mmol/L(Fig 4.38). Garg et al. (2004)17 made similar observa�on that there was no difference in mean vitreous potassium level when the le� eye was compared to the right eye. Also parameters like age, sex, temperature and humidity had no effect on the concentra�on of vitreous potassium. However, mean vitreous potassium showed a linear rise with increasing death interval18.
The bicarbonate concentra�on for the aqueous humour in normal samples was 16.40±0.68 mg/dl for right eye while the le� eye was 16.60±0.68 mg/dl. On irradia�on at low dose, there was a decrease in the mean HCO3- concentra�on (12.00±0.32 mg/dl) of the right eye, which on increasing the dose to the medium level also decreased the mean concentra�on of HCO3- (11.60±1.03 mg/dl), while at high radia�on dose, the mean HCO3- concentra�on increased to 12.20±0.97 mg/dl. For the le� eye, on radia�ng at low dose, the mean HCO3- concentra�on decreased to (15.40±0.68 mg/dl), which at medium radia�on dose was constant 15.40±1.29 mg/dl and finally decreased to 14.20±1.36 mg/dl at high radia�on dose. However, the mean changes in the mean HCO3- concentra�on in the aqueous part of the le� eye were sta�s�cally not significant (P>0.05), while at low, medium and high irradia�on of the right eye showed sta�s�cal significance (P<0.05) with the normal. In the vitreous, normal samples had mean concentra�on of HCO3- for the right eye as 19.25±0.48 mg/dl, while the le� eye was 19.40±0.40 mg/dl. On radia�ng it at low dose, there was a decrease in the mean HCO3- concentra�on (15.60±1.03 mg/dl) of the right eye, which on increasing the dose to the medium level also decreased the mean concentra�on of HCO3- (14.00±1.14 mg/dl), while at high radia�on dose, the mean HCO3- concentra�on increased to
16.60±1.72 mg/dl. For the le� eye, on radia�ng at low dose, the mean HCO3- concentra�on decreased to (14.60±0.93 mg/dl), which at medium radia�on dose was increased to 15.40±1.33 mg/dl and finally decreased to 15.40±0.68 mg/dl at high radia�on dose. However, the mean changes in the mean HCO3- concentra�on in the vitreous part of the right eye were sta�s�cally not significant (P>0.05), while at low, medium and high irradia�on of the le� eye showed sta�s�cal significance (P<0.05) with the normal.
Measured values of concentra�ons of carbonate ions ranged between 9.0 mmol/L and 20.0 mmol/L. The importance of bicarbonate ions has been highlighted in literature, they are important for proper re�na func�on when they are at normal levels in the vitreous 15-25 mmol/L but when the levels in vitreous increases to about 35-45 mmol/L, it inhibits re�na func�on 19. From the results, the mean changes in the HCO3- concentra�on in the vitreous part of the right eye were sta�s�cally not significant (P>0.05), while at low, medium and high irradia�on of the le� eye showed sta�s�cal significance (P<0.05) with the normal. This means that there was no sta�s�cally significant effect of radia�on on the bicarbonate concentra�on in the vitreous, which was within the normal range. Dufour (1982)20 observed that there was no significant change in vitreous calcium postmortem nor significant correla�on between vitreous calcium and antemortem serum calcium.
Chloride ion concentra�ons for normal samples had 101.20±2.42 mg/dl for the right and 103.60±0.75 mg/dl for the le�. High radia�on for the right was 108.80±1.02 mg/dl and 106.00±1.10 mg/dl for the le�. The mean changes in the mean Cl- concentra�on in the aqueous part of the le� eye were sta�s�cally not significant (P>0.05), while at medium irradia�on of the right eye showed sta�s�cal significance (P<0.05) with the normal. For the VH , normal samples had mean concentra�on of Cl- for the right eye as
JNOA.2018;20(2): 46 - 52 Atuanya and Ajayi
Original Research Article
Journal of the Nigerian Optometric Association
52 JNOA.2018;20(2): 46 - 52 Atuanya and Ajayi
Original Research Article
Electrical currents in biological �ssues are carried by components and structures that have a net electric charge and/or an electric dipole moment. Therefore in colloid-disperse system such as biological �ssues, an electric field is determined by the concentra�on and behaviour of its chemical cons�tuents. In the eyes, the structural macromolecular �ssues such as, the �ssues of the vitreous humour are s�ll subjects of intensive inves�ga�on on how they interact to form the vitreous gel. Radia�on had no sta�s�cally significant effect on the mean concentra�ons of potassium ion and chloride ion in both AH and VH in this study. One limita�ons to the study included the fact that irradia�on would have been done immediately the eyes were enucleated to avoid freezing and subsequent thawing.
Conclusion
91.00±0.58 mg/dl, the le� eye was 92.00±3.41 mg/dl. On irradia�on at low dose, there was a decrease in the mean Cl- concentra�on (84.40±4.79 mg/dl) of the right eye, which on increasing the dose to the medium level also decreased the mean concentra�on of Cl- (70.80±2.94 mg/dl), while at high radia�on dose, the mean Cl- concentra�on increased to 77.80±6.04 mg/dl. For the le� eye, irradia�on at low dose, the mean Cl- concentra�on decreased to (80.40±3.87 mg/dl), which at medium radia�on dose was increased to 85.20±2.06 mg/dl and finally decreased to 84.40±3.19 mg/dl at high radia�on dose. However, the mean changes in the mean Cl- concentra�on in the vitreous part of the le� eye were sta�s�cally not significant (P>0.05), while at medium irradia�on of the right eye showed sta�s�cal significance (P<0.05) with the normal.
Measured value of concentra�on of chloride ions ranged between 9.0 mmol/L and 20.0 mmol/l. This shows that radia�on does not have significant effect on the chloride concentra�on of the aqueous and vitreous humours. The difference between the right eye and the le� eye could be due to biochemical varia�ons in the eyes of the animals.
Infec�ons are one of the most sight threatening condi�ons if not treated. Bacteria are the most common pathogens and are involved in infec�ons of all the �ssues of the eye. The most frequently affected parts of the eye include the conjunc�va, eyelid and cornea1. Bacterial infec�ons of the eyes are usually caused by some predisposing factors
such as trauma, poor hygiene, previous surgery, ocular adnexal dysfunc�on and immune suppression which may alter the defence mechanisms of the external ocular structure and permit bacteria to spread2. Infec�ons of the conjunc�va can spread over the cornea causing dryness which will damage the corneal surface3. Conjunc�vi�s, an inflamma�on of
JNOA.2018;20(2): 53 - 61
External eye infec�ons occur when harmful microorganisms such as bacteria, fungi, protozoan and viruses invade any part of the anterior outer part of the eyeball. This study was carried out to between January 2016 and December 2016 to inves�gate the external eye infec�ons and personal hygiene prac�ces among pa�ents a�ending Optometry Teaching Clinic at Federal University of Technology, Owerri, Nigeria. A total of 217 pa�ents with external eye infec�ons who came to the clinic during this period were used for this study. A well-structured ques�onnaire was used to obtain informa�on on their personal hygiene prac�ces. Swabs collected from the infected eyes were taken to the laboratory for isola�on and iden�fica�on of causa�ve organisms. Ocular examina�on results showed that bacterial conjunc�vi�s was the most prevalent external eye infec�on and was seen in146 (67.28%) pa�ents. Informa�on on hygiene prac�ces showed that 29 (13.36%) of the pa�ents wash their hands with soap and water before ea�ng and 42 (19.35%) wash their hands with soap and water a�er toilet use. Laboratory results showed that the major causa�ve organism was Staphylococcus aureus, isolated in 91 (41.94%) samples. Sta�s�cal analysis showed that there was no significant difference in both the gender varia�ons (P > 0.05) and age varia�ons (P > 0.05) of pathogenic organisms implicated in the external eye infec�ons. Optometrists should educate their pa�ents on the need for good personal hygiene as this will help in preven�ng external eye infec�ons which can occur from contaminated fingers that come in contact with the eyes.
Keywords: External eye infec�ons, Personal hygiene, Microorganisms, Hand washing
Journal of the Nigerian Optometric Association Original Research Article
1 Department of Optometry, Federal University of Technology, Owerri2 Department of Optometry, Abia State University, Uturu3 Department of Optometry, Imo State University, Owerri4 Department of Public Health, Federal University of Technology, Owerri
1. Jorgensen JH, Pfaller MA, Carroll KC, Funke G, Landry ML, Richter SS, Warnock DW. Manual of clinical microbiology. 11th ed. Washington D.C.: ASM Press. 2015; 22-35.2. Bharathi MJ, Ramakrishnan R, Shivakumar C, Meenakshi R, Lionalraj D. Etiology and antibacterial susceptibility pattern. Indian J Ophthalmol. 2010; 58:497-507.3. Leibowitiz HM. Primary care-the red eye. New Eng J Med. 2005; 343(5):345-351.
Azuamah, Y.C.,1 Esenwah, E.C1., Ahuama, O.C.,2 Ikoro, N.C.,1 Iwuagwu, F.C.3 and Dozie, I.N.S.4
Azuamah, Y.C Email: [email protected] Phone: + 2348034933590
53
EXTERNAL EYE INFECTIONS AND PERSONAL HYGIENE PRACTICES AMONG PATIENTS ATTENDING OPTOMETRY TEACHING CLINIC
FEDERAL UNIVERSITY OF TECHNOLOGY, OWERRI.
Corresponding Author:
Abstract
Introduction
Azuamah et al

Journal of the Nigerian Optometric Association
54
Materials and Methods
4. Tissa S, Clare G. Conjunctivitis. Comm Eye Health. 2005; 18(53):73-75.5. Center for Disease Control and Prevention. Conjunctivitis (Pink Eye). 2017; Available at: https://www.cdc.gov/conjunctivitis [Retrieved 3rd June 2018]6. Groden LR, Murphy B, Rodnite J. Lid Flora in Blepharitis. Cornea. 2011; 10:50-53.7. Johnson J. Personal Hygiene. Hygiene Expert. 2018; 8(14):21-25.8. Orenstein BW. A guide to good personal hygiene. Everyday Health. 2009; 34(9):80-86.9. Stefan P, Christoph S, Syenja D. A field study on watching eyes and hand hygiene compliance in a public restroom. J App Soc Psy. 2018; 48(4):345-349.10. Ayliffe G. Infection Control, Nosocomial Infection, Problems and Organization. Africa Health. 2006; 18:9-10.11. Alberti A. Trachoma teaching set. Comm Eye Health. 2007; 16(12):124-128.12. Ramesh S. Transmission and control of infection in ophthalmic practice. Comm Eye Health. 2009; 15(18):152-155.
the conjunc�va may be bacterial, viral or chlamydial and is a common cause of unilateral or bilateral infected red eyes4. Bacterial conjunc�vi�s, usually caused by Staphylococcus aureus, is more common in children. The signs and symptoms include s�cky, purulent discharge, foreign body sensa�on, and peripheral conjunc�val redness4. The visual acuity is usually unaffected unless there is corneal complica�on. Bilateral purulent discharge in the newborn requires urgent referral as this may indicate infec�on with Neisseria Gonorrhoeae or possibly Chlamydia. Neisseria Gonorrhoeae infec�on may result in loss of sight if treatment is delayed5. Viral conjunc�vi�s is bilateral and more contagious with redness developing acutely in one eye first, followed some days later in the second eye. Signs include serous discharge, tarsal follicles, swollen lids and tender pre-auricular nodes5. Other viral infec�ons include herpes simplex, varicella zoster and molluscum contagiosum.
Blephari�s, an inflamma�on of the eyelids tends to run a chronic course and may occur together with conjunc�vi�s because the structures involved are anatomically joined6. Staphylococci species are common pathogens. Signs and symptoms are red, crusty lid margins, mild lid swelling, itchiness, dry sensa�on and occasional lacrima�on6. Vision is normal unless the cornea becomes involved. Personal hygiene may be described as the principle of maintaining cleanliness and grooming of the external body7. Personal hygiene habits such as hand washing will protect the body from bacteria, viruses, and illnesses8. Poor personal hygiene prac�ces can lead to contamina�on with microorganisms. These microorganisms can cause ocular infec�ons when they get in contact with the eye. This can occur when cloths or towels used to wipe the face or eyes of an infected person are used to wipe the eyes of an uninfected person9,10. Viral and bacterial
conjunc�vi�s are very contagious and can spread easily from person to person. According to the Center for Disease Control and Preven�on5, people around someone with bacterial conjunc�vi�s can limit the spread of infec�on by washing their hands regularly with soap and warm water especially a�er contact with an infected person, not sharing items used by an infected person such as pillows, washcloths, towels, eye drops, eye makeup, makeup brushes, contact lenses, contact lens storage case, or eye glasses and by avoiding touching the eyes with unwashed hands. Flies are vectors that can carry microorganisms to the eyes of an uninfected person. This is one of the modes of transmission of Chlamydia Trachoma�s, the causa�ve organism of trachoma11. The flies are a�racted to purulent discharges from an infected eye and the discharges may contain the infec�ve organism which can be transmi�ed to the eyes of another person. Unwashed fingers, nasal discharges, exposed feces and rubbish lying in open places will a�ract flies which will carry the infec�ve organism to infect an uninfected person12. Poor environmental sanita�on and overcrowded living condi�ons will predispose people to infec�ons. It is very important to improve both personal hygiene within families and also environmental sanita�on. This study covers the personal hygiene prac�ces as well as the sanita�on and living condi�ons of pa�ents with external eye infec�ons.
This study was a longitudinal cross sec�onal analy�c study involving 217 pa�ents out of 254 pa�ents with external eye infec�ons who a�ended Optometry Teaching Clinic, Federal University of Technology, Owerri between January 2016 and December 2016. The pa�ents who sa�sfied the inclusion and exclusion criteria were used for the study. These are pa�ents of both genders between 1 and 90 years who are not on medica�on for any infec�on, pa�ents who are not mentally sick and who gave an informed consent.
JNOA.2018;20(2): 53 - 61 Azuamah et al
Original Research Article
Journal of the Nigerian Optometric Association
55
Preparation of media and diluents
Characterization and Identification of Microbial Isolates
Catalase Test
Coagulase Test
Oxidase Test
Indole Test
For pa�ents below 18 years, an informed consent was obtained from their parents. Examina�on of pa�ents included case history, visual acuity, ophthalmoscopy, pen light examina�on and slit lamp biomicroscopy. Pa�ents with external eye infec�ons were interviewed with a well-structured ques�onnaire to ascertain their personal hygiene prac�ces and swabs were taken from the sites of infec�on with sterile swab-s�cks to the laboratory to determine the causa�ve organisms. Ethical clearance for this study was obtained from the ethical commi�ee of the School of Health Technology, Federal University of Technology, Owerri.
All bacteriological media (Nutrient agar, Salmonella Shigella Agar, Mannitol Salt Agar, Eosin Methylene Blue Agar, Sabouraud Agar and MacConkey Agar) were prepared according to manufacturer’s specifica�on. Nutrient agar was used in the isola�on of heterotrophic bacteria, MacConkey Agar for faecal coliform bacteria, Eosin Methylene Blue Agar for Escherichia coli, Mannitol Salt Agar strictly for Staphylococcus aureus and Salmonella Shigella Agar for the isola�on of Salmonella and Shigella species.
Microbial isolates were characterized based on colonial, microscopic and biochemical methods. Microorganisms that were not iden�fied by the colonial and microscopic characteris�cs were further subjected to few biochemical tests. This included catalase test, coagulase test, oxidase test, and indole test.
The enzyme catalase is present in most cytochrome containing aerobic and faculta�ve anaerobic bacteria. Catalase has one of the highest turnover numbers of all enzymes such that one molecule of catalase can convert millions of molecules of hydrogen peroxide to water and oxygen in a second. Catalase
ac�vity can be detected by adding the substrate H₂O₂ to an appropriately incubated (18-24 hours) tryp�c soy agar slant culture. Organisms which produce the enzyme breakdown the hydrogen and the resul�ng O₂ produc�on produces bubbles in the reagent drop indica�ng a posi�ve test. Organisms lacking the cytochrome system also lack the catalase enzyme and are unable to breakdown peroxide into O₂ and water and are catalase nega�ve.
Coagulase is an enzyme that clots blood plasma by a mechanism that is similar to normal clo�ng. The coagulase test iden�fies whether an organism produces this exoenzyme. This enzyme clots the plasma component of blood. The only significant disease causing bacteria of humans that produce coagulase are Staphylococcus aureus. Thus this enzyme is a good indicator of S. aureus. In the test, the sample is added to rabbit plasma and held at 37⁰C for a specified period of �me. Forma�on of clot within four hours is indicated as posi�ve result and indica�ve of a virulent Staphylococcus aureus strain. The absence of coagula�on a�er 24 hours of incuba�on is a nega�ve result indica�ve of an avirulent strain.
Oxidase test is an important differen�al procedure that should be performed on all gram nega�ve bacte-ria for their rapid iden�fica�on. The test depends on the ability of certain bacteria to produce indophenol blue from the oxida�on of dimethyl-p-phenylenedi-amine and α-naphthol. This method uses N, N-dime-thyl-p-phenylenediamine oxalate in which all Staphlo-cocci are oxidase nega�ve. In the presence of the enzyme cytochrome oxidase (gram nega�ve bacteria) the N, N-dimethhyl-p-phenylenediamine oxalate and α-naphthol react to indophenol blue. Pseudomonas aeruginosa is an oxidase posi�ve organism.
This test demonstrates the ability of certain bacteria to decompose the amino acid-Tryptophan to Indole. The bacteria isolates were inoculated into the
JNOA.2018;20(2): 53 - 61 Azuamah et al
Original Research Article
Journal of the Nigerian Optometric Association
56
Results
medium and incubated at 37°C for 48 hours. At the end of incuba�on period, 3 drops of kovac’s reagent was added and then shaken. A red color ring at the interface of the medium denotes a posi�ve result.
A total of 217 pa�ents comprising 84 (38.71%) males and 133 (61.29%) females with external eye infec�ons were used for this study. Their ages ranged from 1 to 81 years with a mean age of 36.74±19.66 (males, 39.48±20.27; females, 35.01±19.15) years. Results showed that bacterial conjunc�vi�s was the external eye infec�on with the highest frequency with 146 (67.28%). Fungal conjunc�vi�s was of the lowest frequency with 2 (0.92%). Corneal ulcer was 15 (6.91%); bacterial kera��s, 32 (14.75%); hordeolum, 10 (4.61%); and blephari�s, 12 (5.53%). This is shown in Table 1. The gender distribu�on of external eye infec�ons showed that bacterial conjunc�vi�s was 58 (26.73%) pa�ents for males and 88 (40.55%) for females; corneal ulcer, 6 (2.76%) for males and 9 (4.15%) for females; bacterial kera��s, 11 (5.07%) pa�ents for males and 21 (9.68%) for females; hordeolum, 4 (1.85%) pa�ents for males and 6 (2.76%) for females; fungal conjunc�vi�s, 0 (0.00%) pa�ents for males and 2 (0.92%) for females; and blephari�s, 5 (2.30%) for males and 7 (3.23%) for females. Table 2 showed the age distribu�on of external eye infec�ons. Among the age group of 1 to 30, bacterial conjunc�vi�s was of the highest frequency with 49 (22.59%). Corneal ulcer was 4 (1.84%); bacterial kera��s, 7 (3.23%); hordeolum, 4 (1.84%); Blephari�s, 3 (1.38%). Bacterial conjunc�-vi�s was of the highest frequency among the 31 to 60 age group with 78 (35.94%). Corneal ulcer was 8 (3.69%); bacterial kera��s, 23 (10.60%); hordeolum, 6 (2.76%); fungal conjunc�vi�s, 2 (0.92%); and blephari�s, 8 (3.69%). Bacterial conjunc�vi�s also had the highest frequency among pa�ents 61 to 90 years with 19 (8.76%). Corneal ulcer was 3 (1.38%); bacterial kera��s, 2 (0.92%); blephari�s, 1 (0.46%).
Informa�on obtained from the ques�onnaires on personal hygiene prac�ces of the pa�ents showed that when interviewed on hand washing prac�ces, 29 (13.36%) of the pa�ents responded “Yes” to
washing of hands with soap and water before ea�ng; 124 (57.14%) said “Yes” to washing of hands with soap and water a�er ea�ng; 42 (19.35%) responded “Yes” to washing of hands with soap and water a�er toilet use; and 12 (5.53%) said “Yes” to sharing of hand towels (Table 3). When the pa�ents were interviewed on their knowledge and awareness on causes of ocular infec�ons, 178 (82.03%) of the pa�ents responded “Yes” to knowing that microorganisms are present in a dirty environment; 155 (71.43%) said “Yes” to knowing that microorganisms are present in dirty clothing; 82 (37.79%) responded “Yes” to knowing that contact with microorganisms can cause eye infec�ons; and 44 (20.28%) said “Yes” to having received an educa�on on ocular hygiene. Table 4 showed the frequency of hand towel washing among the pa�ents. None of the pa�ents washed their hand towels daily; 68 (31.34%) washed them weekly; 125 (31.34%) washed them every 2 weeks; 20 (9.22%) washed them monthly and 4 (1.84%) rarely washed their towels. Informa�on on environmental sanita�on showed that 61 (28.11%) of the pa�ents complained of household waste always li�ered in their compound; 36 (16.59%) complained of drainage; 80 (36.87%) complained of general uncleanliness; while 55 (25.35%) reported that there were no sanita�on problems in their compound. On their response to frequency of room cleaning, 37 (17.05%) of the pa�ents said that on the average, they clean their room daily; 131 (60.37%) said weekly; 40 (18.43%), every 2 weeks; and 9 (4.15%) reported that on the average, they clean their room once a month. Their response to room sharing showed that 12 (5.53%) of the pa�ents said that they were staying alone in their room; 26 (11.98%) said they were 2 sharing a room; 48 (22.12%) said they were 3 in a room; 67 (30.87%) said they were 4 in a room; 30 (13.82%) said they were 5 in a room; and 34 (15.68%) said they were more than 5 sharing one bedroom.
Laboratory analysis of swab samples (Table 5) showed that Staphylococcus Aureus had the highest frequency of 91 (41.94%). The lowest frequency was Neisseria Gonorrhoeae and Candida Albicans with 2 (0.92%) each. Pseudomonas Aeruginosa was seen in 22 (10.14%) of the samples; Staphylococcus Epidermidis, 42 (19.35%); Klebsiella Species, 8 (3.69%); Streptococcus Pneumoniae, 6 (2.76%); Haemophilus Influenzae, 3 (1.38%); Corynebacterium Xerosis , 7 (3.22%);
JNOA.2018;20(2): 53 - 61 Azuamah et al
Original Research Article

Journal of the Nigerian Optometric Association
57
Escherichia Coli, 11 (5.07%); Proteus Species, 7 (3.22%); Aspergillus Flavus, 5 (2.30%); and Fusarium Species, 3 (1.38%). The Table also showed the gender distribu�on of microorganisms. Table 6 showed the age distribu�on of microorganisms among the pa�ents. Staphylococcus Aureus had the highest frequency in all the age groups with 32 (14.75%) among the 1 to 30 age group; 43 (19.82%) for the 31 to 60 age group; and 16 (7.37%) for 61 to 90age group. Sta�s�cal analysis with the SPSS version 21 so�ware using the independent sample T-Test at 0.05 level of significance and 95% confidence interval showed that there was no significant difference [P (0.378) > 0.05] in the gender varia�ons of pathogenic organisms implicated in external eye infec�ons (Table 7). SPSS data analysis using the one way ANOVA at 0.05 level of significance and 95% confidence interval also showed no significant difference [P (0.456) > 0.05] in age varia�ons of pathogenic organisms implicated in external eye infec�ons (Table 8).
JNOA.2018;20(2): 53 - 61 Azuamah et al
Original Research Article
Table 1 Gender Distribution of External Eye infections among patients
Infection
Total 217(100.00) 84(38.71) 133(61.29)
Female Frequency
(n %)
Total Frequency
(n %)
Male Frequency
(n %)
Bacterial Conjunc�vi�s
Corneal Ulcer
Bacterial Kera��s
Hordeolum
Fungal Conjunc�vi�s
Blephari�s
88(40.55)
9(4.15)
21(9.68)
6(2.76)
2(0.92)
7(3.23)
146(67.28)
15(6.91)
32(14.75)
10(4.61)
2(0.92)
12(5.53)
58(26.73)
6(2.76)
11(5.07)
4(1.85)
0(0.00)
5(2.30)
Table 2 Age Distribution of External Eye infections among patients
Infection
Total 67(30.88) 125(57.60) 25(11.52)
61-90 Age Group
Frequency (n %)
1-30 Age Group
Frequency (n %)
31-60 Age Group
Frequency (n %)
Bacterial Conjunc�vi�s
Corneal Ulcer
Bacterial Kera��s
Hordeolum
Fungal Conjunc�vi�s
Blephari�s
19(8.76)
3(1.38)
2(0.92)
0(0.00)
0(0.00)
1(0.46)
49(22.59)
4(1.84)
7(3.23)
4(1.84)
0(0.00)
3(1.38)
78(35.94)
8(3.69)
23(10.60)
6(2.76)
2(0.92)
8(3.69)
Table 3 Information on hand washing, knowledge and awareness
Hand Washing Information
NoFrequency
(n %)
YesFrequency
(n %)
Hand washing with soap and water before ea�ng
Hand washing with soap and water a�er ea�ng
Hand washing with soap and water a�er toilet use
Sharing of hand towel
Knowledge and Awareness
Presence of microorganisms in dirty environmentPresence of microorganisms in dirty clothing
Contact with microorganisms can cause eye infec�ons
Educa�on on ocular hygiene
29 13.36 188 86.64
124 57.14 93 42.86
42 19.35 175 80.65
12 5.53 205 94.47
178 82.03 39 17.97
155 71.43 62 28.57
82 37.79 135 62.21
44 20.28 173 79.72
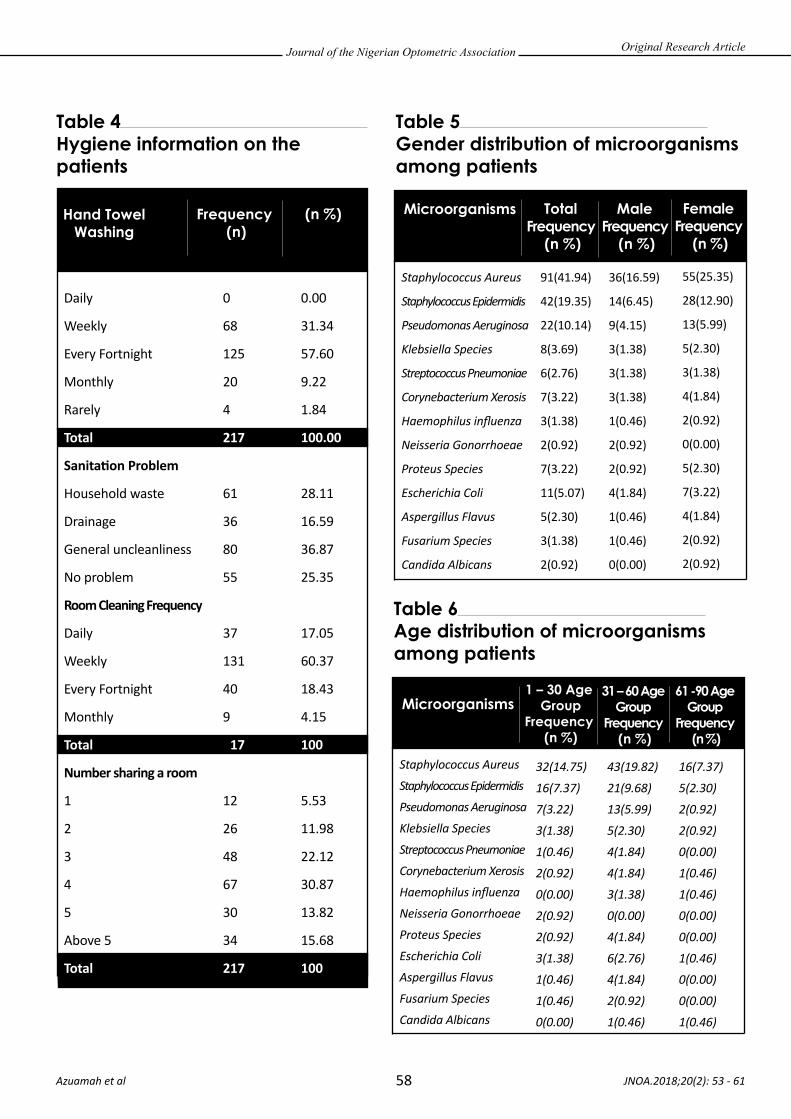
Journal of the Nigerian Optometric Association
58
Table 4 Hygiene information on the patients
Hand Towel Washing
(n %)Frequency (n)
Table 5 Gender distribution of microorganisms among patients
Daily
Weekly
Every Fortnight
Monthly
Rarely
Total
Sanita�on Problem
Household waste
Drainage
General uncleanliness
No problem
Room Cleaning Frequency
Daily
Weekly
Every Fortnight
Monthly
Total
Number sharing a room
1
2
3
4
5
Above 5
Total
0
68
125
20
4
217
61
36
80
55
37
131
40
9
217
12
26
48
67
30
34
217
0.00
31.34
57.60
9.22
1.84
100.00
28.11
16.59
36.87
25.35
17.05
60.37
18.43
4.15
100
5.53
11.98
22.12
30.87
13.82
15.68
100
JNOA.2018;20(2): 53 - 61 Azuamah et al
Microorganisms Female Frequency
(n %)
Total Frequency
(n %)
Male Frequency
(n %)
Staphylococcus Aureus
Staphylococcus Epidermidis
Pseudomonas Aeruginosa
Klebsiella Species
Streptococcus Pneumoniae
Corynebacterium Xerosis
Haemophilus influenza
Neisseria Gonorrhoeae
Proteus Species
Escherichia Coli
Aspergillus Flavus
Fusarium Species
Candida Albicans
91(41.94)
42(19.35)
22(10.14)
8(3.69)
6(2.76)
7(3.22)
3(1.38)
2(0.92)
7(3.22)
11(5.07)
5(2.30)
3(1.38)
2(0.92)
36(16.59)
14(6.45)
9(4.15)
3(1.38)
3(1.38)
3(1.38)
1(0.46)
2(0.92)
2(0.92)
4(1.84)
1(0.46)
1(0.46)
0(0.00)
55(25.35)
28(12.90)
13(5.99)
5(2.30)
3(1.38)
4(1.84)
2(0.92)
0(0.00)
5(2.30)
7(3.22)
4(1.84)
2(0.92)
2(0.92)
Original Research Article
Table 6 Age distribution of microorganisms among patients
Microorganisms1 – 30 Age
GroupFrequency
(n %)
31 – 60 Age Group
Frequency (n %)
61 -90 Age Group
Frequency (n %)
Staphylococcus Aureus
Staphylococcus Epidermidis
Pseudomonas Aeruginosa
Klebsiella Species
Streptococcus Pneumoniae
Corynebacterium Xerosis
Haemophilus influenza
Neisseria Gonorrhoeae
Proteus Species
Escherichia Coli
Aspergillus Flavus
Fusarium Species
Candida Albicans
32(14.75)
16(7.37)
7(3.22)
3(1.38)
1(0.46)
2(0.92)
0(0.00)
2(0.92)
2(0.92)
3(1.38)
1(0.46)
1(0.46)
0(0.00)
43(19.82)
21(9.68)
13(5.99)
5(2.30)
4(1.84)
4(1.84)
3(1.38)
0(0.00)
4(1.84)
6(2.76)
4(1.84)
2(0.92)
1(0.46)
16(7.37)
5(2.30)
2(0.92)
2(0.92)
0(0.00)
1(0.46)
1(0.46)
0(0.00)
0(0.00)
1(0.46)
0(0.00)
0(0.00)
1(0.46)
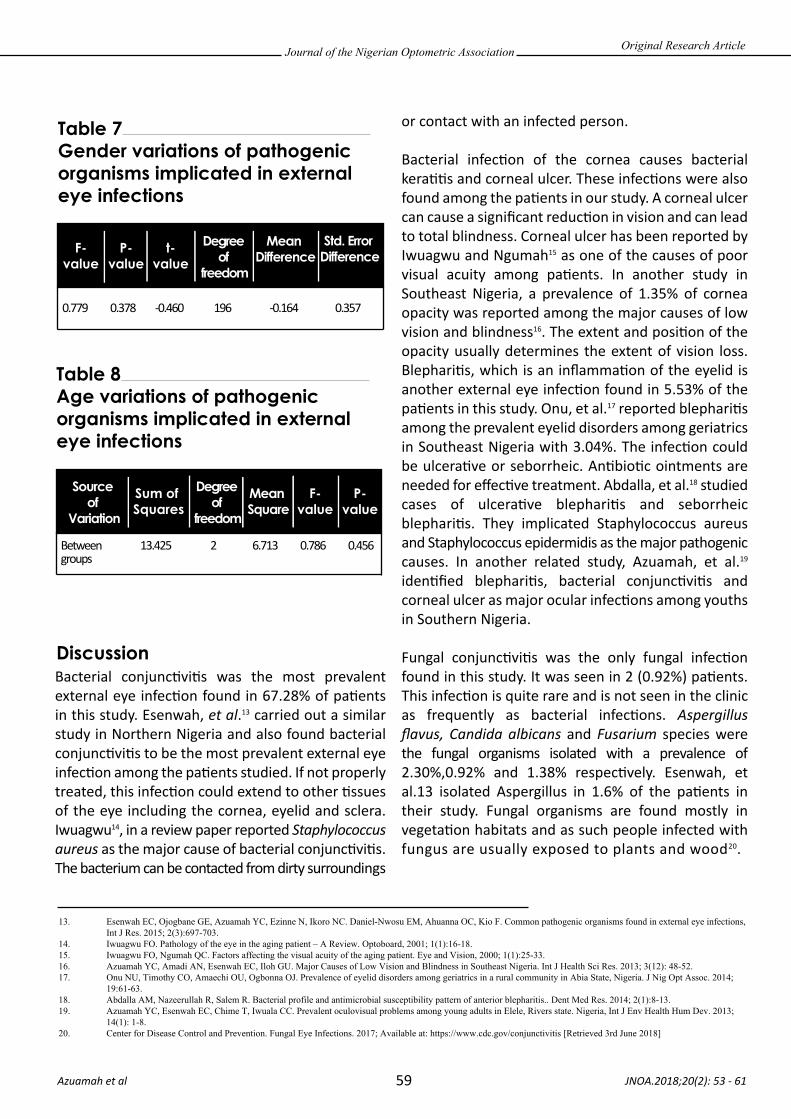
Journal of the Nigerian Optometric Association
59
Bacterial conjunc�vi�s was the most prevalent external eye infec�on found in 67.28% of pa�ents in this study. Esenwah, et al.13 carried out a similar study in Northern Nigeria and also found bacterial conjunc�vi�s to be the most prevalent external eye infec�on among the pa�ents studied. If not properly treated, this infec�on could extend to other �ssues of the eye including the cornea, eyelid and sclera. Iwuagwu14, in a review paper reported Staphylococcus aureus as the major cause of bacterial conjunc�vi�s. The bacterium can be contacted from dirty surroundings
or contact with an infected person.
Bacterial infec�on of the cornea causes bacterial kera��s and corneal ulcer. These infec�ons were also found among the pa�ents in our study. A corneal ulcer can cause a significant reduc�on in vision and can lead to total blindness. Corneal ulcer has been reported by Iwuagwu and Ngumah15 as one of the causes of poor visual acuity among pa�ents. In another study in Southeast Nigeria, a prevalence of 1.35% of cornea opacity was reported among the major causes of low vision and blindness16. The extent and posi�on of the opacity usually determines the extent of vision loss. Blephari�s, which is an inflamma�on of the eyelid is another external eye infec�on found in 5.53% of the pa�ents in this study. Onu, et al.17 reported blephari�s among the prevalent eyelid disorders among geriatrics in Southeast Nigeria with 3.04%. The infec�on could be ulcera�ve or seborrheic. An�bio�c ointments are needed for effec�ve treatment. Abdalla, et al.18 studied cases of ulcera�ve blephari�s and seborrheic blephari�s. They implicated Staphylococcus aureus and Staphylococcus epidermidis as the major pathogenic causes. In another related study, Azuamah, et al.19 iden�fied blephari�s, bacterial conjunc�vi�s and corneal ulcer as major ocular infec�ons among youths in Southern Nigeria.
Fungal conjunc�vi�s was the only fungal infec�on found in this study. It was seen in 2 (0.92%) pa�ents. This infec�on is quite rare and is not seen in the clinic as frequently as bacterial infec�ons. Aspergillus flavus, Candida albicans and Fusarium species were the fungal organisms isolated with a prevalence of 2.30%,0.92% and 1.38% respec�vely. Esenwah, et al.13 isolated Aspergillus in 1.6% of the pa�ents in their study. Fungal organisms are found mostly in vegeta�on habitats and as such people infected with fungus are usually exposed to plants and wood20.
JNOA.2018;20(2): 53 - 61 Azuamah et al
Original Research Article
Table 7 Gender variations of pathogenic organisms implicated in external eye infections
F-value
P-value
t-value
Std. Error Difference
Degree of
freedom
Mean Difference
0.779 0.378 -0.460 196 -0.164 0.357
Table 8 Age variations of pathogenic organisms implicated in external eye infections
F-value
P-value
Sum of Squares
Source of
Variation
Degree of
freedom
Mean Square
Between 13.425 2 6.713 0.786 0.456groups
Discussion
13. Esenwah EC, Ojogbane GE, Azuamah YC, Ezinne N, Ikoro NC. Daniel-Nwosu EM, Ahuanna OC, Kio F. Common pathogenic organisms found in external eye infections, Int J Res. 2015; 2(3):697-703.14. Iwuagwu FO. Pathology of the eye in the aging patient – A Review. Optoboard, 2001; 1(1):16-18.15. Iwuagwu FO, Ngumah QC. Factors affecting the visual acuity of the aging patient. Eye and Vision, 2000; 1(1):25-33.16. Azuamah YC, Amadi AN, Esenwah EC, Iloh GU. Major Causes of Low Vision and Blindness in Southeast Nigeria. Int J Health Sci Res. 2013; 3(12): 48-52.17. Onu NU, Timothy CO, Amaechi OU, Ogbonna OJ. Prevalence of eyelid disorders among geriatrics in a rural community in Abia State, Nigeria. J Nig Opt Assoc. 2014; 19:61-63.18. Abdalla AM, Nazeerullah R, Salem R. Bacterial profile and antimicrobial susceptibility pattern of anterior blepharitis.. Dent Med Res. 2014; 2(1):8-13.19. Azuamah YC, Esenwah EC, Chime T, Iwuala CC. Prevalent oculovisual problems among young adults in Elele, Rivers state. Nigeria, Int J Env Health Hum Dev. 2013; 14(1): 1-8.20. Center for Disease Control and Prevention. Fungal Eye Infections. 2017; Available at: https://www.cdc.gov/conjunctivitis [Retrieved 3rd June 2018]

Journal of the Nigerian Optometric Association
60
Most pa�ents with fungal conjunc�vi�s acknowledge that they were either in the farm recently or cu�ng wood at home. Confirma�on of fungal conjunc�vi�s must be from laboratory findings as its signs and symptoms can resemble that of bacterial conjunc�vi�s. Microorganisms tend to thrive in an unhygienic environment and thus, a ques�onnaire was used to obtain informa�on on the personal hygiene, water sanita�on and environmental sanita�on prac�ces of the pa�ents. A large number of the pa�ents (80.65%) admi�ed that they do not wash their hands with soap and water a�er toilet use. Those that wash their hands usually do so with water only. In so doing, they do not successfully remove the germs that are present in their hands a�er toilet use. Osuji, et al.21 reported that 75.3% of subjects interviewed in their study washed their hands with water alone a�er toilet use while 24.7% washed their hands with soap and water. Once the individual rubs his/her fingers on their eyes in order to relieve an itch, this can easily lead to an eye infec�on by transferring the infec�ve organisms to the eye. Sharing of hand towels is another common way of transmi�ng infec�ons as these materials are used to clean the face including the eyes. About 5.53% of our pa�ents admi�ed to sharing of a hand towel with another member of their household. In addi�on to this, the frequency with which these items are washed is quite poor. Over 60% of the pa�ents admi�ed to washing their hand towels every 2 weeks or more. Some don’t wash them in months. All these factors make it easy for them to get infected especially when there are too many people sharing a room. Over 60% of the pa�ents have at least 3 other people sharing their room with them making it 4 in a room. It is inevitable in this condi�on that people will share items or use a roommates item without his/her permission. Ogbulie22 published an ar�cle on acceptable housing standards. He advocated
a maximum of 2 persons in a room regardless of size.
Environmental sanita�on prac�ces of the pa�ents also fell short of what is acceptable to ensure a clean and germ free environment. Microorganisms tend to thrive in a dirty environment. Over 75% of the pa�ents also complained of drainage problems and general uncleanliness in their compound. Some studies23,24 have linked poor environmental sanita�on to ocular infec�ons affec�ng the conjunc�va and cornea. Trachoma is one of the leading causes of blindness and is caused by Chlamydia trachoma�s, a gram-nega�ve bacterium that has been associated with poor sanita�on and hygiene25. It causes complica�ons in the cornea, conjunc�va, eyelid and other �ssues of the eye. Educa�on is an important tool in empowering the people toward preven�on of ocular infec�ons. About 60% of pa�ents in this study did not know that contact with microorganisms could lead to eye infec�ons and more than 80% have not received any form of educa�on or awareness on ocular hygiene. Studies26,27 have shown that people who are educated on ocular hygiene suffer less ocular infec�ons because they take the necessary precau�ons to avoid infec�on. In the Southeast Nigeria, Optometrists have been engaged in community health outreach programmes in order to educate and bring eye care services to people in the rural communi�es. Most of these programmes are sponsored by the optometrists themselves and in some cases, fees are charged though at a reduced rate in order to offset the expenses. These outreach programmes are very important as those in the rural areas are most affected and these rural communi�es lack the health facili�es or prac��oners where they can easily go for eye check-up. Etya’ale28 reported in his study that people from slums and rural areas, women, the blind and severely visually impaired, the poor and des�tute as people with the most difficult access to eye care services.
JNOA.2018;20(2): 53 - 61 Azuamah et al
Original Research Article
21. Osuji IE, Azuamah YC, Amadi AN, Esenwah EC, Agu GC, Nwala OR. Water sanitation practices in Obowo, Southeastern Nigeria. Int J Res. 2014; 1(10):678-684.22. Ogbulie TE. Prospects of attaining an acceptable housing standard in urban settlements in Nigeria: an overview. Int J Env Health Hum Dev. 2011; 12(2):39-44.23. Nathan GC, David SF, Thomas L. Important causes of visual impairment in the world today. JAMA. 2003; 290(15):2057-2060.24. Rabiu M, Alhassan MB, Ejere HO, Evans JR. Environmental sanitary interventions for preventing active trachoma. Cochrane Database Syst Rev. 2012; 15(2):403-410.25. Stocks ME, Ogden S, Haddad D, Addiss DG, McGuire C, Freeman MC. Effect of water, sanitation, and hygiene on the prevention of trachoma: a systematic review and meta-analysis. PLoS Med. 2014; 11(2):1001-1005.26. Khosravi AD, Mehdinejad M, Heidari M. Bacteriological findings in patients with ocular and antibiotic susceptibility pattern of isolated pathogen. Singapore Med J. 2007; 48(7):741-743.27. Sharma S. Ocular infections: Research in India. Indian J Med Microbiol. 2010; 88(9):91-94.28. Etya’ale D. Beyond the clinic: approaches to outreach. Com Eye Health. 2006; 19(58): 19-21.

Journal of the Nigerian Optometric Association
61
Most eye clinics are located in the urban centers and so pa�ents are forced to make the journey of travelling to the urban center for treatment. This however, is a�er they have exhausted other op�ons like local herbs, patent chemists and self-medica�on. This is very dangerous as applying the wrong medica�on such as a cor�costeroid to a case of herpe�c epithelial kera��s will worsen the condi�on29. Pa�ents are not aware of this and some think that all eye drops are the same and any eye drop can be applied to the eye no ma�er the condi�on. It is usually when they have made their problem much worse that they decide to see the Optometrist. People need to be educated on the dangers of applying the wrong medica�on to an ocular infec�on so that they do not worsen the problem.
Some people, especially in the rural areas of Nigeria s�ll strongly believe on the tradi�onal ways of trea�ng ailments that was passed on from their fore-fathers to the present genera�on. These are called folk medica�ons.
For example, some people believe that applying breast milk from a nursing mother to an infected eye will cure that infec�on. Others resort to urine, olive oil and other local prepara�ons. Smitherman, et al.30 reported that the use of folk medicine was mainly due to cultural beliefs rather than decreased access to health care. Nwankwo31 studied the resilience of folk medicine among the Igbos of Southeast Nigeria and found that folk medicine was preferred by people with low educa�on. He recommended that folk medicine be supported by government through adequate funding and research ini�a�ves as well as training of tradi�onal healers. There are also strong beliefs in spiritual connec�ons to health problems among people. They resort to prayers and spiritual healers to solve their problems. They believe strongly in their folk culture and so the Optometrist must try to show understanding and respect for their culture while educa�ng them on the need to see a professional medical prac��oner.
JNOA.2018;20(2): 53 - 61 Azuamah et al
Original Research Article
29. Melton R, Thomas R, Vollmer P. Guide to Ophthalmic Drugs. 21st Edition. Review of Optometry. 2017; 26.30. Smitherman LC, Janisse J, Mathur A. The use of folk remedies among children in an urban black community: remedies for fever, colic, and teething. Pediatrics. 2005; 115(3): 297-304.31. Nwankwo IU. Resilience of Folk Medicine among the Igbos of Southeast Nigeria. Euro Scientific J. 2014; 10(36):177-187.
Bacterial conjunc�vi�s was the most common external eye infec�on found in this study. Others are corneal ulcer, bacterial kera��s, hordeolum, blephari�s and fungal conjunc�vi�s. Staphylococcus aureus was the most prevalent causa�ve organism. Others include Staphylococcus epidermidis, Escherichia Coli, Klebsiella Species and Pseudomonas aeruginosa. Informa�on obtained from the pa�ents revealed that most people do not observe simple hand washing prac�ces with soap and water. Sharing of hand towels and other personal items is s�ll common and general cleanliness of personal rooms and surroundings is s�ll poor. There is a need for increased awareness campaigns by eye care prac��oners, governmental and non-gov-ernmental organiza�ons toward educa�ng the public on common external eye infec�ons and the need to prac�ce good personal hygiene.
Conclusion

There are no available studies on the profile of reading speed among Africans neither is there a standard print size recommended for people with low vision. About 150wpm has been reported as the median reading speed and cri�cal print size of 0.84 Log Mar among albinos1. There is need for reading speed studies among Africans. Moreover, print size that cut across various causes of low
vision is necessary for recommenda�on for the Low vision group. Reading is a behavioral and learned process. With training and instruc�ons on the use of vision and low vision aids, reading speed and reading performance could improve. While training would improve reading performance, it may not improve reading acuity. A study showed that improvement in reading speed among pa�ents with age-related macular
JNOA.2018;20(2): 62 - 68
The purpose of this study was to establish a standard print size that enables low vision persons access print materials and improve reading performance. Case control study design was used for this study. Data was collected from 200 par�cipants with normal vision (control group) and 200 with low vision (study group) who a�ended ECWA eye Hospital Kano. Normal con�nuous-text print size (N10/J5/0.75M) was presented at 30-40cm to 200 emmetropes/corrected ametropes (control group). The reading-aloud-speed (RAS) was taken and recorded in words per minute (wpm). The mean reading- aloud-speed (MRS) for this group was recorded as MRS1. Con�nuous-text prints of sizes N10/0.75M, N18/2M, N24/2.5M, N36/4M and N48/5M were presented at acceptable working distance to 200 literate low vision pa�ents corrected and/or enhanced to N5/J1/0.37M (single le�ers). The RAS for each of these text sizes (RAS1-5) were recorded in wpm, and the mean values were calculated respec�vely. Result shows that the average RAS (99.47 wpm) for the control group, when compared with the study group, matched with the MRS3(100.93wpm) for print size N18/2M of the control group. Although sta�s�cal analysis showed a significant difference in the reading speed between the two groups (F= 31.67; P<0.05), Post Hoc analysis showed that the mean reading aloud speed (100.93 wpm) used to read N18/2M print size for the study group showed no significant difference with the (99.47 wpm) used to read print size N10/J5/0.75M for the control group (p>0.05). The N18/2M print size is therefore recommended as a standard print for best reading performance among low vision pa�ents.
Keywords: Standard-print-size. Large prints. Non-op�cal aids
Journal of the Nigerian Optometric Association Original Research Article
1. Department of Optometry, Faculty of Allied health Sciences, College of Health Sciences, Bayero University Kano. 2. Department of Optometry, Faculty of Life Sciences, University of Benin, Benin City.
1. Kinberly Merrill, Katherine Hogue, Sara Downes, Ann M. Holleshau, Beth R. Kuzbach, John T. Macdonald C. Gail Summers. Reading Acuity in Albinism: Evaluation with, MN READ Charts. Journal of American Ass. Of Pedriatric Oph and Strabismus. 2011;15 (1); 29-32
Ejukonemu B.O.M.1 and Akpalaba R.E.U.2
Ejukonemu B.O.M Email: [email protected] Phone: +234 8033281569
62
Determination of a Standard Continuous-Text Print Size for People with Low Vision
Corresponding Author:
Abstract
Introduction
Ejukonemu and Akpalaba

Journal of the Nigerian Optometric Association
63
Methods
2. World Health Organization (1996). Low vision care for the Elderly. Paper presented at the Workshop of WHO/PBL/96,573. OSLO Workshop. Towards a reduction in the Global impact of Low Vision. The International Society for Low -vision Research and Rehabilitation. 2005: 1 4. Susana, T. L. Chung. Improving reading speed for people with central vision loss through Perceptual learning: Investigative Ophthalmology and Visual Science. 2011; 52 (2);116-1175. World Health Organization. Magnitude and causes of visual impairment. Available at http://www.who.int/mediacentre/factsheets/fs282/en/index.html. Accessed June 20186. International agency for the prevention of blindness. Low vision. http://www.iapb.org. Accessed June, 20187. Barbie. O.M.E. Characteristics of the Nigerian Low vision population. Journal of the Nigerian Optometric Association. 2004; 11 (1): 6-10 8. Jan. E. Lovie-Kitchen, Jennifer D. Bevanm, Bronwyn Hein B. Reading performance in Children with Low Vision. Clinical and Experimental Optometry. 2001; 84 ( 3):148-1549. Visual Standards: Aspects and ranges of Visual Loss. Report of the International Council of Ophthalmology, Sydney, Australia. 2002. 7. 10. Keziah Lathan and CharlotteA. Hazel. Reading performance in normal foveal and peripheral vision. Vision Rehabiliation: Assessment, interaction and outcome/edited by Cynthia Stuen et al. Selected papers from vision 99, International Conference on Low Vison.
degenera�on, does not translate to acuity and cri�cal print size measurement2. This means that trained readers could not improve on acuity size but only on speed reading. Low vision refers to an eye condi�on where individuals have reduced ability to carry out important life ac�vi�es including obtaining educa�on, living and traveling independently due to visual impairment that cannot be corrected with medical treatment ordinary glasses or contact lenses3. The World Health Organisa�on working defini�on of low vision states that “A person with Low vision is one who has impairment of visual func�oning even a�er treatment and/or standard refrac�ve correc�on and has visual acuity of between less than 6/18-PL or visual field of less than 100 from the point of central fixa�on but who uses or poten�ally able to use, vision for the planning or execu�on of a task”4. There are an es�mated 285 million people globally with visual impairment, 80 million of them have permanent visual impairment and can benefit from low vision services, 80% live in developing countries5,6. Treatment for low vision include applica�on of Low vision devices. Research show that a high number of low vision pa�ents can cope with their schooling and employment if given appropriate instruc�ons on the use of their low vision devices such as magnifiers and that near task is the reason most magnifiers are prescribed7. The material to be read must be kept at the focus of the magnifier hence depending on the level of vision and magnifier power, materials may be kept too close to the face. This may compromise some near tasks such as reading, wri�ng and drawing. Large prints are non-op�cal devices that enhance reading7. With large prints, the use of a magnifier
may not be necessary or when indicated, the dioptric power could reduce and working distance improved. Large prints have the disadvantage of occupying large spaces and only few words may be read at a �me. Thus, very large prints could occupy paper space and reduce reading performance. Furthermore, the cost of producing very large print books could be high. In other to perform well in school and examina�ons, children with low vision who read in prints will need print sizes larger than normal due to their level of vision. This was supported by the report that children with Low vision need print size larger than threshold to achieve maximum reading rate.8
This study provides answer to the ques�on: what is the appropriate print size, large enough, to accommodate the advantages of large prints and small enough to alleviate the problems of very large prints. This is the cri�cal print size which should be the standard print size for people with low vision. This standard print size recommended for large print edi�ons of newspapers, examina�on ques�on papers, and other print materials in relevant organiza�ons. This would provide access to educa�on and employment for many people with low vision.
This study examined the reading -aloud- speed of 200 par�cipants with normal vision and 200 low vision pa�ents. Normal vision is defined as presen�ng or corrected, binocular or monocular distance acuity of 6/18 (Snellen) or be�er10. Low vision is defined as corrected, monocular or binocular distance acuity of less than 6/18(Snellen) or Visual field of less than 100 from the point of central fixa�on. The WHO working defini�on for Low Vision was adopted4.
JNOA.2018;20(2): 62 - 68 Ejukonemu and Akpalaba
Original Research Article

Journal of the Nigerian Optometric Association
64
Inclusion Criteria
Exclusion Criteria
Materials
Procedure
The cases/study group were males and females of age 6 years and above who were able to read and write (literate) in English language. They were low vision pa�ents with distance acuity of <6/18 or visual field < 100 from the point of central fixa�on in the be�er eye, whose vision could be enhanced to N5/J1/0.37M single le�ers with magnifiers. The control group had similar characteris�cs as the study group except that they were not low vision pa�ents. They were emmetropes/ corrected ametropes.
All par�cipants below 6 years and not literate in English Language were excluded. The age criteria was set at 6 years because assessment for magnifying aids for pa�ents below age 6 years can be very challenging.
The materials used for this study include: Distance and Near acuity charts (Single le�ers and con�nuous text), Re�noscope, Direct Ophthalmoscope, Standard refrac�on Kit (with trial lenses and frame included), Standard Low vision Kit (with trial telescopes and magnifiers included), the Collenbradder central field chart, Controlled Lights and stop clock. All assessment was carried out by Optometrists who are Low Vision Consultants.
Rou�ne refrac�on, when indicated was carried out on normal par�cipants. Visual acuity, refrac�on and visual field tests were carried out on the study group before low vision was defined. Central visual field of low vision pa�ents was determined using the Collen-bradder Visual field chart thus, with the pa�ent com-fortably seated and wearing basic prescrip�on, one eye was occluded. The chart was held at the 50cm away from the pa�ent under room illumina�on. The pa�ent was asked to fixate the central black spot on the chart. With steady fixa�on established, a bright point s�mulus was presented from non-seeing to seeing from 8 diagnos�c posi�ons (90, 45, 360, 315, 270, 225, 180 and 130 degrees). A visual field plot was obtained and central visual field recorded for the best eye. The test was repeated for the other eye
where applicable. Low vision assessment was carried out by a Low vision consultant. Low vision refrac�on was carried out on the selected low vision subjects.
Near magnifica�on assessment was carried out thus: If a corrected low vision pa�ent was able to read the 4M(N36) line at a distance of 25cm, for this pa�ent to read the 0.75M, the Equivalent Viewing Distance(EVD) will be 5.33cm (4/0.75), approximately 5cm. A suitable magnifier with this EVD was selected. Near magnifier was prescribed to enable the low vision pa�ents to read N5/J1/0.37M single le�ers and magnifica�on reserve was considered to read con�nuous-text prints as small as 0.37M
Reading speed scores were obtained as follows: Normal prints (N10/J5/0.75M) was presented under room illumina�on at 25-40cm (Least distance of dis�nct vision) to 200 emmetropes/corrected ametropes (control group). The reading – aloud – speed (RAS) were taken and recorded in words per minutes (wpm). The set of reading aloud speed scores for all 200 normal subjects were recorded as RASn (Normal). The mean reading speed (MRS) for this group was recorded as MRS1. Con�nuous-text prints of sizes N10/0.75M, N18/2M, N24/2.5M, N36/4M and N48/5M were presented (under room illumina�on) at acceptable working distance to 200 literate low vision pa�ents. Acceptable working distance was adopted because many Low vision pa�ents accept higher magnifica�on (accommoda�on reserve) to read the desired print size. This would result in an equivalent viewing distance shorter than the least distance of dis�nct vision.
The set of RAS scores for all 200 low vision par�cipants for each of N10/0.75M, N18/2M, N24/2.5M, N36//4-Mand N48/5M text sizes were recorded in wpm as RAS1-5 i.e. RAS1, RAS 2, RAS3, RAS 4 and RAS 5 respec�vely. RAS was obtained using the stop clock. For example, in order to get the RAS for N10/0.75M, the subject was asked to read the N10/0.75M line aloud and the clock started simultaneously. The clock was stopped a�er 60 seconds, and the number of words read correctly was counted and recorded. If 30 words were read correctly a�er 60 seconds (one minute), RAS for N10/0.75M is recorded as 30wpm. The Mean(average) reading speed (MRS) each for N10/0.75M, N18/2M, N24/2.5M,
JNOA.2018;20(2): 62 - 68 Ejukonemu and Akpalaba
Original Research Article
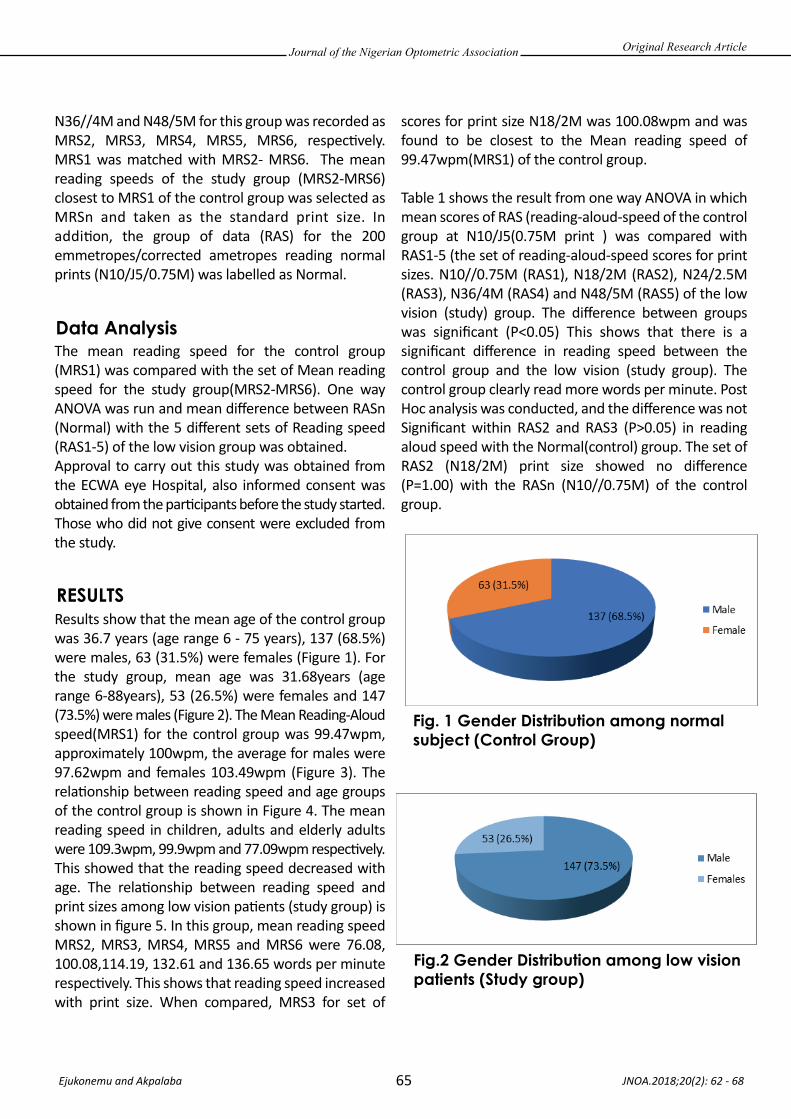
Journal of the Nigerian Optometric Association
65
Data Analysis
RESULTS
Fig. 1 Gender Distribution among normal subject (Control Group)
Fig.2 Gender Distribution among low vision patients (Study group)
N36//4M and N48/5M for this group was recorded as MRS2, MRS3, MRS4, MRS5, MRS6, respec�vely. MRS1 was matched with MRS2- MRS6. The mean reading speeds of the study group (MRS2-MRS6) closest to MRS1 of the control group was selected as MRSn and taken as the standard print size. In addi�on, the group of data (RAS) for the 200 emmetropes/corrected ametropes reading normal prints (N10/J5/0.75M) was labelled as Normal.
The mean reading speed for the control group (MRS1) was compared with the set of Mean reading speed for the study group(MRS2-MRS6). One way ANOVA was run and mean difference between RASn (Normal) with the 5 different sets of Reading speed (RAS1-5) of the low vision group was obtained. Approval to carry out this study was obtained from the ECWA eye Hospital, also informed consent was obtained from the par�cipants before the study started. Those who did not give consent were excluded from the study.
Results show that the mean age of the control group was 36.7 years (age range 6 - 75 years), 137 (68.5%) were males, 63 (31.5%) were females (Figure 1). For the study group, mean age was 31.68years (age range 6-88years), 53 (26.5%) were females and 147 (73.5%) were males (Figure 2). The Mean Reading-Aloud speed(MRS1) for the control group was 99.47wpm, approximately 100wpm, the average for males were 97.62wpm and females 103.49wpm (Figure 3). The rela�onship between reading speed and age groups of the control group is shown in Figure 4. The mean reading speed in children, adults and elderly adults were 109.3wpm, 99.9wpm and 77.09wpm respec�vely. This showed that the reading speed decreased with age. The rela�onship between reading speed and print sizes among low vision pa�ents (study group) is shown in figure 5. In this group, mean reading speed MRS2, MRS3, MRS4, MRS5 and MRS6 were 76.08, 100.08,114.19, 132.61 and 136.65 words per minute respec�vely. This shows that reading speed increased with print size. When compared, MRS3 for set of
scores for print size N18/2M was 100.08wpm and was found to be closest to the Mean reading speed of 99.47wpm(MRS1) of the control group.
Table 1 shows the result from one way ANOVA in which mean scores of RAS (reading-aloud-speed of the control group at N10/J5(0.75M print ) was compared with RAS1-5 (the set of reading-aloud-speed scores for print sizes. N10//0.75M (RAS1), N18/2M (RAS2), N24/2.5M (RAS3), N36/4M (RAS4) and N48/5M (RAS5) of the low vision (study) group. The difference between groups was significant (P<0.05) This shows that there is a significant difference in reading speed between the control group and the low vision (study group). The control group clearly read more words per minute. Post Hoc analysis was conducted, and the difference was not Significant within RAS2 and RAS3 (P>0.05) in reading aloud speed with the Normal(control) group. The set of RAS2 (N18/2M) print size showed no difference (P=1.00) with the RASn (N10//0.75M) of the control group.
JNOA.2018;20(2): 62 - 68 Ejukonemu and Akpalaba
Original Research Article
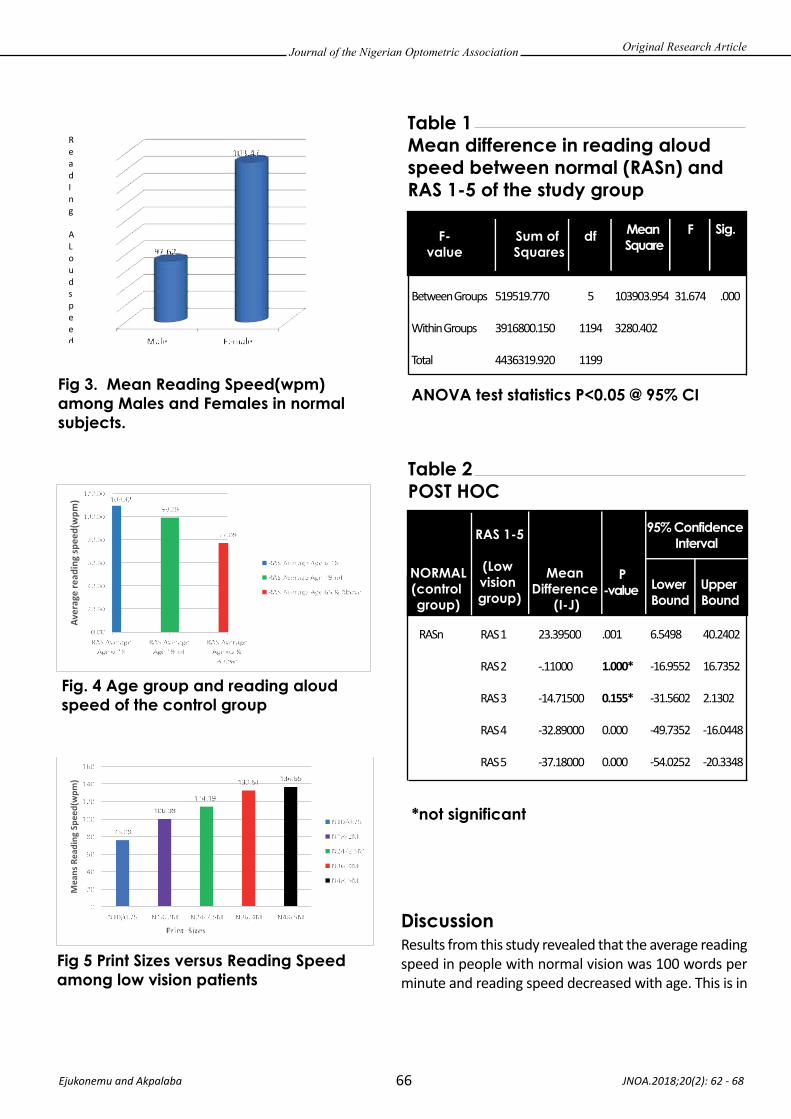
Journal of the Nigerian Optometric Association
66
Discussion
Table 1 Mean difference in reading aloud speed between normal (RASn) and RAS 1-5 of the study group
Results from this study revealed that the average reading speed in people with normal vision was 100 words per minute and reading speed decreased with age. This is in
JNOA.2018;20(2): 62 - 68 Ejukonemu and Akpalaba
Original Research Article
Read I n g A L oud s peed )
Fig 3. Mean Reading Speed(wpm) among Males and Females in normal subjects.
Fig. 4 Age group and reading aloud speed of the control group
Fig 5 Print Sizes versus Reading Speed among low vision patients
ANOVA test statistics P<0.05 @ 95% CI
F-value
Sum of Squares
df Sig.Mean Square
F
Between Groups
Within Groups
Total
519519.770
3916800.150
4436319.920
5
1194
1199
103903.954
3280.402
31.674 .000
Table 2 POST HOC
*not significant
NORMAL(control group)
RAS 1-5
(Low vision group)
Mean Difference
(I-J)
95% Confidence Interval
P-value Lower
BoundUpper Bound
RASn RAS 1
RAS 2
RAS 3
RAS 4
RAS 5
23.39500
-.11000
-14.71500
-32.89000
-37.18000
.001
1.000*
0.155*
0.000
0.000
6.5498
-16.9552
-31.5602
-49.7352
-54.0252
40.2402
16.7352
2.1302
-16.0448
-20.3348

Journal of the Nigerian Optometric Association
67
agreement with the work of Deyue et al11. They examined 17 normally sighted young adults, average age 23.8 years and old adults, average age 66years. They found that the reading speed was higher (191 versus 124wpm) in young adults than old par�cipants. Calabrese et al12 in a recent study found MRS for normally sighted people to decrease with age, 140-200wpm for children and 175wpm for elderly, but it is higher than what is reported in this study. This may be due to differences in speed ar�cula�on rate, nature of text used, and method used in assessing MRS. We also found that the reading speed improved with print size, which is in agreement with similar studies11-13. William and Delamater13 also reported that although the reading rate increased with print size , it got to a maximum where it began to decline. They stated that in dyslexics, the fastest rate was obtained at a significantly larger character size than control. This supports our argument that a cri�cal print size that would address the advantages of small prints and disadvantages of very large prints is required for op�mum reading performance. Furthermore, it suggests that in visually challenged individuals, reading performance improves with cri�cal (i.e. standard) print size. There is slight difference in reading speed among males and females. Females read faster. We determined that the N18/ 2M print size should be employed in wri�ng reading materials in schools and work place as this would enable people with low vision have access to print materials and enable them to cope with reading in school, work and leisure. This way, psychological, social and economic impact of irreversible visual loss would reduce and society made more civilized. People with Low vision suffer from irreversible visual impairment caused by eye disease condi�ons that cannot be cured medically, surgically and op�cally14. They do not have normal eye sight neither are they
totally blind15. There are children with low vision who can benefit with large prints but are placed in schools for the blind to learn in Braille alone. Young adults drop out of school due to inability to cope with learning on the basis of prints 14. Furthermore, adults may go into early re�rement due to inability to cope with reading and wri�ng in places of work. Low vision pa�ents can be helped with the aid of low vision devices which could be op�cal or non-op�cal15,16. Magnifiers are low vision devices that enlarge materials for near work and enable tasks such as reading, wri�ng, treading of needles and looking at money. The material to be read must be kept at the focus of the magnifier hence depending on the level of vision and magnifier power, materials may be kept too close to the face. This may compromise some near tasks such as wri�ng and drawing and may also influence the use of the devices which is currently poor in Nigeria17.
Large prints are non-op�cal devices15. With large prints, the use of a magnifier may not be necessary or when indicated, the dioptric(op�cal) power could reduce and working distance improved. Large prints have the disadvantage of occupying large spaces and only few words may be read at a �me. Furthermore, the cost of producing very large print books could be high. This research got answer to the ques�on: what is the print size that would adequately address the advantages of small prints and the problems of enlarged prints. If appropriately determined, that standard print size would be employed in wri�ng school books, examina�on materials, office memos, newspapers and religious books. This would enable access to educa�on, employment and ac�vi�es of daily leaving by a great majority of the low vision popula�on and reduce the psychological, social and economic impact of low vision. The major limita�on to this study is that the study did not consider the influence of visual acuity reserve, contrast reserve
JNOA.2018;20(2): 62 - 68 Ejukonemu and Akpalaba
Original Research Article
11. Deyue Yu, Sing-Hig Chueng, Susana TL Chung, Gordon E. Legge. Age effects on Reading Speed in Peripheral Vision. Journal of Vision.2006; 6: 1001. Doi:10.1167/6.6. 100112. Calabrese A, Cheong AMY, Cheung S, He Y, Kwon M.et al. Baseline MNREAD measures for normally sighted subjects from childhood to old age. Investigative ophthalmology & visual science. 2016; (57) 8: 3836 384313. William E, Delamater, M.Ed . How larger font size impacts Reading and the implication for Educational use of Digital Text readers. 2010. eReedia..14. Ejukonemu BOM. The Socio-economic implications of unattended True Low Vision in Sub-Sahara Africa. Journal of Low Vision Rehabilitation and Blindness. 2014; 3: 62-6415. Minto H, Butt I A. Low vision devices and training. Community eye health J. 2004;17 (49):6-716. Ekpenyong BN, Ndukwe OC. Restoration of near normal vision in an elderly patient. Blindness and Low vision Journal. 2012; (1) : 11 -14. 17. Ekpenyong BN, Ndukwe. Provision of Low Vision Services in the Department of Ophthalmology, University of Calabar Teaching Hospital: Journal of the Nigerian Optometric Association 2010; 16 : 20 - 24

Journal of the Nigerian Optometric Association
68
and cause of low vision on reading performance and speed, also reading accessibility index was not calculated. However this is the first a�empt in the study area.
JNOA.2018;20(2): 62 - 68 Ejukonemu and Akpalaba
Original Research Article
The average reading -aloud speed among Nigerians with normal vision is 100 words per minute and reading speed decreased with age. Reading speed increased with print size. Females read slightly faster than males. The N18/2M print size should be adopted as standard print size and recommenda�on for advocacy for large print edi�ons of reading materials in relevant organiza�ons. Studies on the reading speed profile among Nigerian cultures is necessary to address cultural factors in reading speed among socie�es. There is also a need for further research to determine if there is a difference between quiet reading and reading aloud speed.
Conclusion

The burden of low vision and blindness around the globe is devasta�ng. The prevalence of low vision and blindness is higher among leprosy pa�ents than in the wider popula�on and it occurs as a complica�on of the disease or as part of the ageing process.1 Leprosy is a chronic granulomatous disease caused by the Bacillus Mycobacteriumleprae. This primarily affects the skin and peripheral nerves2,3. In 1998, the number of people living with
leprosy-related visual impairments was es�mated to be 2 million. Social problems resul�ng from s�gma are o�en not restricted to the person who has had leprosy but affect the whole families4. Prevalence of leprosy has fallen as a result of effec�ve an�bio�c therapy.5 It is however s�ll endemic in various regions of the world. In 2003, only 513,798 new pa�ents were detected for treatment of leprosy worldwide.6 Reported prevalence of leprosy was 212802 cases in
JNOA.2018;20(2): 69 - 74
Leprosy is a chronic infec�ous, granulomatous disease associated with disability and s�gma�za�on. It is among the world’s major blinding diseases that are avoidable. The purpose of this study was to ascertain the prevalence of low vision and blindness in leprous popula�on in Kano State, Nigeria. The Cross sec�onal descrip�ve study was conduct over a 6 months period on 283 par�cipants aged 14 years and above. Ocular examina�ons of the external and internal structures of the par�cipants were performed. Visual acuity was measured using the logMAR E chart. Of the 283 par�cipants, 171 (60.4%) were males and the mean age was 46.8 ±18. Overall prevalence of visual impairment (0.52 – 4.0logMAR; < 6/18 – NPL [BCVA]) was 109 (38.5% CI 46.50–50.699), 53.2% of them were males and 91.7% were 30 years and above. The prevalence of low vision (0.52–1.30logMAR; < 6/18 –3/60) and blindness (1.32 – 4.0 logMAR; < 3/60 – NPL) was 13.0% and 25.0% respec�vely. The prevalence of low vision and blindness in this popula�on was high, this may be due to the complica�ons of the disease and /or as part of the ageing process. There is a great need to include ocular examina�on as part of rou�ne screening and surveillance programmes in the Leprous popula�on, this would reduce the burden of visual disability on them.
Keywords: Low vision, Blindness, Leprosy, Prevalence, Kano.
Journal of the Nigerian Optometric Association Original Research Article
1 Department of Optometry, Bayero University, Kano / Department of Ophthalmology, Aminu Kano Teaching Hospital, Kano.2 Department of Optometry, Bayero University, Kano.
1 Nguyen, Huu Le. Visual impairment in leprosy patients in northern Viet Nam. Community Eye Health. 2007; 20 (61): 122 Gill AL, Bell DR, Gill GV, Wyatt GB, Beeching NJ. Leprosy in Britain: 50 year experience in Liverpool. QJM: An International Journal of Medicine.2005; 98(7):505-11.3 Reddy SC, Raju BD. Ocular involvement in leprosy: a field study of 1004 patients. Int J Ophthalmol. 2009. 2(4):367-372 4 Britton WJ, Lockwood DN. Leprosy. Symposium on community-based rehabilitation (cbr) for people affected by leprosy. International journal of leprosy. 2005;149-1625 Murthy PK. Current epidemiology of leprosy. Indian Med Assoc. 2004; 102(12):672-3, 683.6 Leprosy. Global situation 2004 www.who.int/topics/leprosy/en/.
Okpo E.,1 Nwakuche P.I.2 and Ejukunemu B.O.M.2
Okpo, Eme. Email: [email protected] Phone: 08035648015
69
PREVALENCE OF LOW VISION AND BLINDNESS IN A LEPROSARIUM IN KANO STATE, NIGERIA.
Corresponding Author:
Abstract
Introduction
Okpo et al

Journal of the Nigerian Optometric Association
70
MATERIALS AND METHOD
1 Nguyen, Huu Le. Visual impairment in leprosy patients in northern Viet Nam. Community Eye Health. 2007; 20 (61): 124 Britton WJ, Lockwood DN. Leprosy. Symposium on community-based rehabilitation (cbr) for people affected by leprosy. International journal of leprosy. 2005;149-1626 Leprosy. Global situation 2004 www.who.int/topics/leprosy/en/.7 World Health Organization. Report of Fifth Meeting of the WHO Technical Advisory Group on Elimination of Leprosy. Yangon, February 9–10, 2003. WHO/CDS/CEE/2003.36 section 3.1: 1, 6.8 Udo S, Chukwu J, Obasanya, J. Leprosy Situation in Nigeria, Lepr Rev. 2013; 84: 229–2379 Olusoji J. Daniel, Olusola A. Adejumo, Kolawole S. Oritogun, Oluwafunmilayo Omosebi, Joseph Kuye and Gabriel. Spatial distribution of leprosy in Nigeria, Lepr Rev. 2016. 87, 476–48510 Kano Municipal L.G.A. Population as per: Federal Republic of Nigeria Official Gazette (2007). “Legal Notice on Population of the details of the breakdown of the National and State Provisional Total 2006 census” Retrieved September, 2017.11 World Health Organization. 2008. Cumulative Official Updates to ICD-10. Delhi. Available from: http://www.who.int/classifications/icd/OfficialWHOUpdatesCombined16 2008VOLUME1.pdf. Accessed on October 2016.
2008, and 2007 saw 254252 new cases registered, the number of cases fell by 11100 (4%) from 2006 to 2007 globally.4,6
In Nigeria, between 1991 and 2012, a total of 111,788 leprosy pa�ents were successfully treated with Mul� Drug Therapy (MDT). Nigeria, in the year 2000, achieved the WHO elimina�on target of less than 1 case per 10 000 popula�on7. With a case detec�on rate below 0·5 per 10 000, Nigeria may well be described as low endemic for leprosy. However, there are pockets of ‘high endemicity’ at sub-na�onal levels, where the leprosy prevalence is s�ll 1 case/10000 popula�on.8 The leprosy case detec�on rate increased slightly from 2·21/100,000 in 2010 to 2·24/100,000 in 2012 and declined to 1·66/100,000 popula�on in 2014.9
Although leprosy control has been a public health success over the past decades, leprosy pa�ents s�ll suffer from avoidable blindness. Individuals with visual impairment and blindness due to ocular leprosy form a severely disadvantaged group because of other disabili�es due to the disease, its social s�gma and delay in receiving appropriate eye care. Visual impairment in pa�ents with leprosy is an addi�onal health burden o�en overlooked by health service providers1. In this study we assessed the prevalence of low vision and blindness, of Yadakunya leprosy se�lement village in Kano State, Nigeria.
This study was carried out among the leprous popula�on at Yadakunya leprosy se�lement village. Yadakunya is a Leprosy village located near Yadakunya Leprosy Hospital (where this study was carried out) with a popula�on of about 5,595. It is located in the North-Eastern part of Kano City under Ungogo Local
Government Area of Kano State Nigeria. It lies between la�tudes 121050 North of equator or and longitude 8012910 and 8015010 East of the prime meridian10. The research was a cross sec�onal study and the aim was to determine the prevalence of low vision and blindness in pa�ents with leprosy. It was carried out at Yadakunya leprosy hospital for a period of six months (from Febru-ary 1st, to July 1st, 2016). Data on age, sex and dura�on since diagnosis of leprosy were recorded. The type of leprosy and dura�on of treatment was determined from the pa�ent’s medical records. Ethical approval was obtained from the Ethical commi�ee, Aminu Kano Teaching Hospital Kano and the Health Service Management Board Kano State. The purpose of this study was clearly explained before wri�en informed consent was obtained from each of the pa�ent for eye examina�on. Instruments used for data collec�on include: review of medical record, semi structured ques�onnaire, and clinical examina�on. To be eligible to be included in this study, par�cipants met the following criteria: 1. Signed a wri�en consent form. 2. Diagnosed with leprosy> 6 years.
The following materials were used during the research: Direct opthalmoscope (For examina�on of the internal structures of the eyes), re�noscope (for objec�ve refrac�on), trial lens boxes and trial frames (for subjec�ve refrac�on), pen torch ( for examina�on of the external structures of the eyes), pinhole disc ( for pinhole acuity assessment), pupillary distance rule (for measurement of pupillary distance) and sloan le�ers and baily-lovie design tumbling E logMAR charts for distance and near Visual Acuity (VA) assessment. The World Health Organiza�on (WHO) classifica�on of blindness and low vision11 (Table 1) was used in classifica�on of pa�ent’s visual impairment.
JNOA.2018;20(2): 69 - 74 Okpo et al
Original Research Article
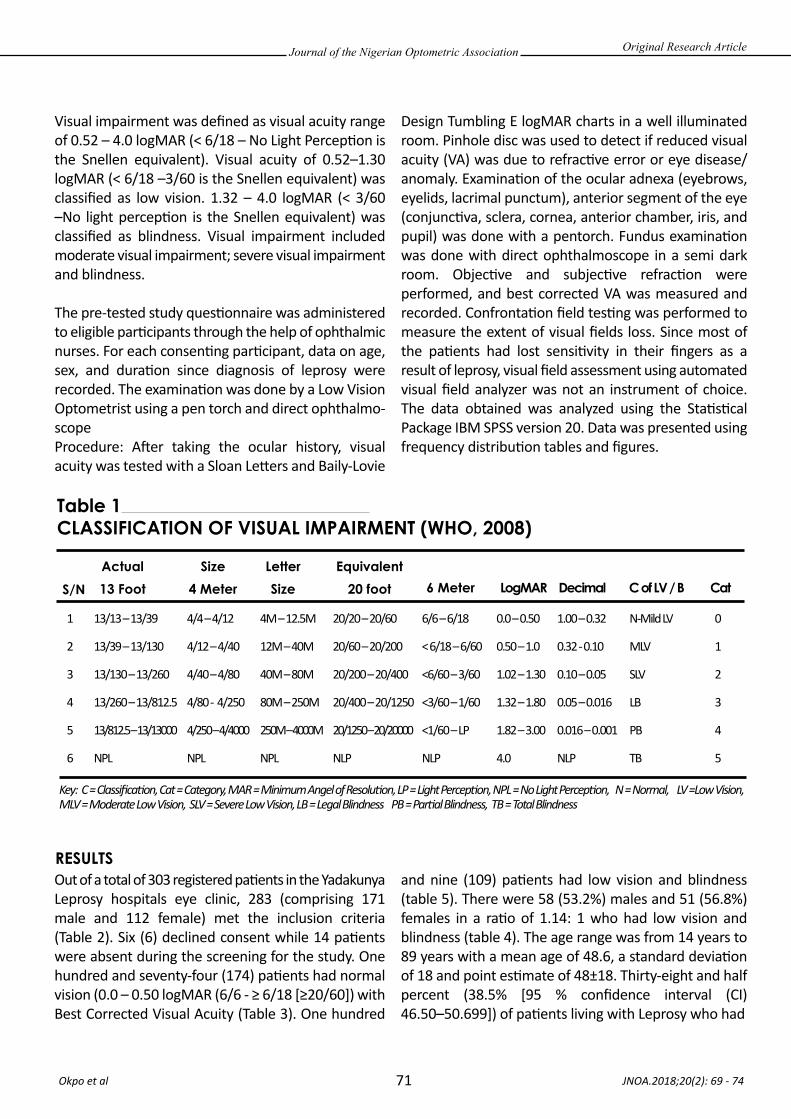
Journal of the Nigerian Optometric Association
71
RESULTS
Visual impairment was defined as visual acuity range of 0.52 – 4.0 logMAR (< 6/18 – No Light Percep�on is the Snellen equivalent). Visual acuity of 0.52–1.30 logMAR (< 6/18 –3/60 is the Snellen equivalent) was classified as low vision. 1.32 – 4.0 logMAR (< 3/60 –No light percep�on is the Snellen equivalent) was classified as blindness. Visual impairment included moderate visual impairment; severe visual impairment and blindness.
The pre-tested study ques�onnaire was administered to eligible par�cipants through the help of ophthalmic nurses. For each consen�ng par�cipant, data on age, sex, and dura�on since diagnosis of leprosy were recorded. The examina�on was done by a Low Vision Optometrist using a pen torch and direct ophthalmo-scope Procedure: A�er taking the ocular history, visual acuity was tested with a Sloan Le�ers and Baily-Lovie
Design Tumbling E logMAR charts in a well illuminated room. Pinhole disc was used to detect if reduced visual acuity (VA) was due to refrac�ve error or eye disease/ anomaly. Examina�on of the ocular adnexa (eyebrows, eyelids, lacrimal punctum), anterior segment of the eye (conjunc�va, sclera, cornea, anterior chamber, iris, and pupil) was done with a pentorch. Fundus examina�on was done with direct ophthalmoscope in a semi dark room. Objec�ve and subjec�ve refrac�on were performed, and best corrected VA was measured and recorded. Confronta�on field tes�ng was performed to measure the extent of visual fields loss. Since most of the pa�ents had lost sensi�vity in their fingers as a result of leprosy, visual field assessment using automated visual field analyzer was not an instrument of choice. The data obtained was analyzed using the Sta�s�cal Package IBM SPSS version 20. Data was presented using frequency distribu�on tables and figures.
Out of a total of 303 registered pa�ents in the Yadakunya Leprosy hospitals eye clinic, 283 (comprising 171 male and 112 female) met the inclusion criteria (Table 2). Six (6) declined consent while 14 pa�ents were absent during the screening for the study. One hundred and seventy-four (174) pa�ents had normal vision (0.0 – 0.50 logMAR (6/6 - ≥ 6/18 [≥20/60]) with Best Corrected Visual Acuity (Table 3). One hundred
and nine (109) pa�ents had low vision and blindness (table 5). There were 58 (53.2%) males and 51 (56.8%) females in a ra�o of 1.14: 1 who had low vision and blindness (table 4). The age range was from 14 years to 89 years with a mean age of 48.6, a standard devia�on of 18 and point es�mate of 48±18. Thirty-eight and half percent (38.5% [95 % confidence interval (CI) 46.50–50.699]) of pa�ents living with Leprosy who had
JNOA.2018;20(2): 69 - 74 Okpo et al
Original Research Article
Table 1 CLASSIFICATION OF VISUAL IMPAIRMENT (WHO, 2008)
S/NActual13 Foot
Size4 Meter
LetterSize
Equivalent20 foot 6 Meter LogMAR Decimal C of LV / B Cat
1
2
3
4
5
6
13/13 – 13/39
13/39 – 13/130
13/130 – 13/260
13/260 – 13/812.5
13/812.5 – 13/13000
NPL
Key: C = Classification, Cat = Category, MAR = Minimum Angel of Resolution, LP = Light Perception, NPL = No Light Perception, N = Normal, LV =Low Vision, MLV = Moderate Low Vision, SLV = Severe Low Vision, LB = Legal Blindness PB = Partial Blindness, TB = Total Blindness
4/4 – 4/12
4/12 – 4/40
4/40 – 4/80
4/80 - 4/250
4/250 – 4/4000
NPL
4M – 12.5M
12M – 40M
40M – 80M
80M – 250M
250M – 4000M
NPL
20/20 – 20/60
20/60 – 20/200
20/200 – 20/400
20/400 – 20/1250
20/1250 – 20/20000
NLP
6/6 – 6/18
< 6/18 – 6/60
<6/60 – 3/60
<3/60 – 1/60
<1/60 – LP
NLP
0.0 – 0.50
0.50 – 1.0
1.02 – 1.30
1.32 – 1.80
1.82 – 3.00
4.0
1.00 – 0.32
0.32 - 0.10
0.10 – 0.05
0.05 – 0.016
0.016 – 0.001
NLP
N-Mild LV
MLV
SLV
LB
PB
TB
0
1
2
3
4
5

Journal of the Nigerian Optometric Association
72
low vision and blindness are between 50 to 69 years of age (Table 4). The prevalence of Low Vision and Blindness for the period of six months was 39% (Table 5). Prevalence of Low Vision was 13% (Table 6) while
Blindness was 25% (table 7). Month of May recorded highest prevalence of low vision and blindness among the pa�ents invited with prevalence of 53%, followed by February 47% (Table 5).
JNOA.2018;20(2): 69 - 74 Okpo et al
Original Research Article
Visual Impairment
Visual Acuity Male (%)
Female (%)
Total (%)
Normal
Moderate VI
Severe VI
Blind
Legal Blindness
Par�al Blindness
Total Blindness
0.0 - 0.50 logMAR ( 6/6 – 6/18)
0.52 – 1.0 logMAR (< 6/18 – 6/60)
1.02 – 1.30 logMAR (<6/60 – 3/60)
1.32 – 1.8 logMAR (<3/60 – 1/60)
1.82 – 3.00 logMAR (<1/60 – LP)
4.0 logMAR (NLP)
113 (39.9)
12 (4.24)
2 (0.71)
15 (5.30)
11 (3.89)
18 (6.36)
61 (21.6)
16 (5.65)
7 (2.47)
3 (1.06)
4 (1.41)
21 (7.42)
174 (61.5)
28 (9.89)
9 (3.18)
18 (6.36)
15 (5.30)
39 (13.78)
Table 2 Demographic Characteristics of Participants
Table 3 Distribution by classification of Visual impairment and gender
Month
Registered Leprosy Cases
M (%) F (%) T (%) M (%) F (%) T (%)
Leprosy with Low Vision & Blindness Preva-
lence (%)
PeriodPrevalence
Per 100
February
March
April
May
June
July
Total
0.47
0.36
0.23
0.53
0.42
0.31
0.385
47/100
36/100
23/100
53/100
42/100
31/100
39/100
33 (11.7) 18 (6.4) 51 (18.0)
36 (12.7) 22 (7.8) 58 (20.5)
38 (13.4) 14 (5.0) 52 (18.4)
19 (6.7) 24 (8.5) 43 (15.2)
20 (7.1) 15 (7.1) 35 (12.4)
25 (8.8) 19 (6.7) 44 (15.6)
171(60.4) 112 (39.6) 283 (100)
11 (3.9) 13 (4.6) 24 (8.5)
14 (5.0) 7 (2.5) 21 (7.2)
7 (2.5) 5 (1.8) 12 (4.2)
12 (4.2) 11 (3.9) 23 (8.1)
9 (3.2) 6 (2.1) 15 (7.1)
5 (1.8) 9 (3.2) 14 (5.0)
58 (20.5) 51 (18.0) 109 (38.5)
Table 5 Monthly distribution of Leprous Patients among diagnosed Low Vision and Blindness, Invited from February – July, 2016
Variable
Total 283 100
Relative frequency
(%)
Frequency (n)
Sex Male Female
Age
<15
15 – 29
30 – 49
50 – 69
70 >
171112
27
49
74
82
51
60.4239.58
9.54
17.31
26.15
28.98
18.02
Table 4 Distribution of participants with visual impairment by Age
Age (years)
Total (n%)
Male (n %)
Female (n %)
<15
15 – 29
30 – 49
50 – 69
70 >
Total
5 (4.6)
0 (0)
13 (11.9)
25 (22.9)
15 (13.8)
58 (53.2)
2 (1.9)
13 (11.9)
13 (11.9)
17 (15.6)
17 (15.6)
51 (46.8.)
7 (6.4) 13 (11.9)
26 (23.9)
42 (38.5)
21 (19.3)
109 (100)

Journal of the Nigerian Optometric Association
73
This study was a cross sec�onal descrip�ve survey involving people living with leprosy at Yadakunya leprosy se�lement village. More males than females par�cipated in the study and majority were 30 years and above. Out of a total of 283 leprosy cases, prevalence of blindness was 25%, majority were males. This value is high when compared to prevalence of blindness among people without leprosy12,13 and leprosy pa�ents from previous studies. A similar study carried out in the North Eastern Nigeria14 found that 10 in 100 leprosy pa�ents were blind as opposed to 25 in 100 found in this study. Also, the blindness of prevalence found in this study is higher than 9.9%, 19%, and 10.9% reported in Northern Viet Nam
study1, Southern Cameroon15, and Ethiopian16 respec�vely. This higher prevalence may be due to long prevalence of leprosy since the study involved only pa�ents with more than six years dura�on of leprosy. This may also be link to lack of adequate eye care services. There was a higher prevalence of low vision and blindness cases among the male pa�ents. The predominance of male to female screened was in agreement with the study carried out in North Eastern Nigeria14 and Ossiomo leprosarium in Edo state, Nigeria17. One reason suggested for this preponderance in previous studies is that the male lifestyle generally exposes them to greater risks of infec�on, while women may tend not to seek medical help even when it is required17.
JNOA.2018;20(2): 69 - 74 Okpo et al
Original Research Article
Month
Number of
Leprosy Patient
Number of
Patient with low
visionpreva-lence
Period prevalence
per 100
February
March
April
May
June
July
Total Key: LV = Low Vision, PP = Period prevalence
51
58
52
43
35
44
283
10
6
3
10
4
4
37
0.20
0.10
0.06
0.23
0.11
0.09
0.13
20/100
10/100
6/100
23/100
11/100
9/100
13/100
Table 6 Prevalence of Low Vision among Patients with Leprosy.
Month FrequencyNo. of
Blindness PP PP per 100
February
March
April
May
June
July
Total
51
58
52
43
35
44
283
14
15
9
13
11
10
72
0.27
0.26
0.17
0.30
0.31
0.23
0.25
27/100
26/100
17/100
30/100
31/100
23/100
25/100
Table 7 Prevalence of Blindness among Patients with Leprosy.
DISCUSSION
1 Nguyen, Huu Le. Visual impairment in leprosy patients in northern Viet Nam. Community Eye Health. 2007; 20 (61): 1212 Ekpenyong, Bernadine Nsa (2010) Epidemiology of blinding eye diseases in Cross River State, Nigeria as seen in University of Calabar teaching Hospital by. Journal of the Nigerian optometric Association. 13; 28 – 37.ISSN: 0795-003913 Kyari F, Gudlavalleti MVS, Sivsubramaniam S, Gilbert CE, Abdull M M, Entekume G, Foster A Prevalence of Blindness and Visual Impairment in Nigeria: The National Blindness and Visual Impairment Survey. Clinical and Epidemiologic Research. 2009; 50 (5):1971-2546.14 Mpyet C, Solomon AW. Prevalence and causes of blindness and low vision in leprosy villages of north eastern Nigeria.Br J Ophthalmol. 2005; 89: 417-419.15 Eballé OA, Owono D, Book UMA, Bell LA, Mvogo E C, Mba N. Prevalence and etiologies of visual handicaps in leprosy patients in the south of Cameroon; Clinical Ophthalmology. 2009; 3:195–198.16 Woldeyes, A., Adamu Y. Gender differences in adult blindness and low vision, Central Ethiopia; Ethiop Med J. 2007;46(3):211-8.17 Ebeigbe JA, Kio F. Ocular leprosy in institutionalized Nigerian patients. Ghana Medical Journal. 2011; 45(2):50-53

Journal of the Nigerian Optometric Association
74
Most of the pa�ents were above 50years of age. The mean age was 48.6 years (range 14 – 89 years). Aging has been shown to be associated with leprosy related ocular complica�on and visual loss14,18. As the leprosy pa�ents become older, their ocular morbidity tends to increase as found in this study, which clearly shows the need for accessible and affordable eye health facili�es for persons living with leprosy.
The overall prevalence of visual impairment (low vision and blindness) based on Best Corrected Visual Acuity (BCVA) worse than 6/18 was 38.5%. The prevalence of low vision based on Best Corrected Visual Acuity reported in this study is similar to 13.2% and 13.8%
reported in Southern Cameroon15 and Bangladesh19 respec�vely, but higher than 0.39% and 2.3% reported in Tajimi City Japan20 and in Kunming, China21 respec�vely. This may be as a result of healthy environment and good health facili�es. Par�cipants for this study were from only one leprous popula�on in Kano State, Nigeria, therefore findings may not be generalised for the North Western zone of Nigeria.
JNOA.2018;20(2): 69 - 74 Okpo et al
Original Research Article
14 Mpyet C, Solomon AW. Prevalence and causes of blindness and low vision in leprosy villages of north eastern Nigeria.Br J Ophthalmol. 2005; 89: 417-419.15 Eballé OA, Owono D, Book UMA, Bell LA, Mvogo E C, Mba N. Prevalence and etiologies of visual handicaps in leprosy patients in the south of Cameroon; Clinical Ophthalmology. 2009; 3:195–198.18 Thompson K J, Allardice GM, Babu G R, Roberts H, Kerketta W, Kerketta A. Patterns of ocular morbidity and blindness in leprosy—a three centre study in Eastern India: Lepr.Rev. 2006;77 (2):130-140.19 Dineen BP, Bourne RR, Ali SA, Huq DM, Johnson GJ Prevalence and causes of blindness and visual impairment in Bangladeshi adults: results of the National Blindness and Low Vision Survey of Bangladesh; Community Eye Health. 2004; 7(4):10. 20 Aiko I, Makote A, Atsuo T, Tetsuya Y, Hiroyuki S,Yoshiaki K. Prevalence and Causes of Low Vision and Blindness in a Japanese Adult Population. American Academy of Ophthalmology. 2006;113 (8):1354-1362. 21 Wu, Min. Rapid assessment of avoidable blindness in Kunming, China Community Eye Health Journal. 2007;20 (61): 10
The prevalence of low vision and blindness in leprosy pa�ents was high. The findings in this study indicate that the overall prevalence of low vision and blindness among pa�ents a�ending the Yadakunya leprosy hospital eye clinic were 13.0%, and 25.0% respec�vely. Pa�ent’s eye care need is not being met at present with only two ophthalmic nurses working in the hospital eye clinic. Early detec�on and treatment of visual impairment in this popula�on is recommended to reduce the dura�on of visual disability and improve their quality of life.
Conclusion
Intraocular pressure (IOP) refers to the pressure exerted by intraocular contents on the coats of the eyeball. The normal level of IOP is essen�ally maintained by a dynamic equilibrium between the aqueous humour forma�on, aqueous humour ou�low and episcleral venous pressure1. Normal IOP has been defined as the average pressure,
which the normal eye can tolerate over a period of �me without compromise to the integrity of the eye, or without glaucomatous damage2. The range of normal human intraocular pressure is 11-21 mmHg3. Elevated intra ocular pressure is o�en associated with op�c disk cupping and visual field loss- a condi�on called Glaucoma4. Due to the posi�ve correla�on
JNOA.2018;20(2): 75 - 81
For centuries, Moringa Oleifera leaf is used in tradi�onal medicine for common ailments in many countries of the world. Tradi�onally it is used in the treatment of systemic hypertension but there are very limited literature on its effect on ocular hypertension. Therefore this clinic based-observa�onal study inves�gated the effect of graded doses of Moringa oleifera leaf aqueous extract on intraocular and blood pressure of thirty normotensive adults, male and female aged 18 to 35 (mean age of 28.93 ±1.62) years. They were divided into three groups of ten par�cipants in each group. Another group of ten normotensive adults, aged matched were used as a control group. Baseline intraocular pressure (IOP) and blood pressure (BP) of each par�cipant were measured. Three different masked doses of Moringa oleifera aqueous leaf extract labelled ‘E’, ‘F’, and ‘G’ were orally administered to groups 1, 2, and 3 respec�vely by a laboratory technician, while group 4 par�cipants drank water only. Therea�er IOP and BP were measured at 30 minutes interval for the four groups un�l values returned to baseline. Results showed that Moringa oleifera leaf aqueous extract when administered orally has sta�s�cally significant (p<0.05) hypotensive effect on IOP and BP of the three experimental groups. The effect was dose-dependent and the maximum reduc�on in BP was at 60 minutes. This preceded the maximum reduc�on in IOP which occurred at 90 minutes, therea�er IOP and BP rose toward baseline values. Therefore Moringa oleifera leaf aqueous extract may be effec�ve in the control of systemic and ocular hypertension.
Keywords: intraocular pressure, blood pressure, Moringa oleifera leaf aqueous extract, normotensive adults.
Journal of the Nigerian Optometric Association Original Research Article
1. Department of Optometry, Faculty of Life Sciences, University of Benin, Benin City,Edo State, Nigeria.
1. Khurana AK, Khurana I. Uvea, Aqueous humour and intraocular pressure. Anatomy and Physiology of Eye. 2nd ed. Publisher: CBS Publishers, New Delhi India. 2008; pp 71-75. 2. Ira SS. Aqueous humour dynamics. American Journal of Optometry and physiological Optics. 1977; 53 (2): 202-205. 3. Kanski JJ. Glaucoma. Clinical Ophthalmology: systemic approach, 5th ed., Publisher: Butterworth – Heinemann, Elsevier Science Limited. 2003; pp 193-198.4. Foster PJ, Buhrmann R, Quigley HA, Johnson GJ. The definition and classification of glaucoma in prevalence surveys. British Journal of Ophthalmology. 2002; 86 (2):238-342.
George, G. O.1, Ajayi, O.B.1 and Oyemike, A.A.1
George, G.O Email: [email protected]
75
EFFECT OF MORINGA OLEIFERA LEAF AQUEOUS EXTRACT ON INTRAOCULAR AND BLOOD PRESSURE OF NORMOTENSIVE
ADULTS IN EDO STATE, NIGERIA
Corresponding Author:
Abstract
Introduction
George et al
Tel: +234 08144393468

Journal of the Nigerian Optometric Association
76
METHODS
5. Bulpitt CJ, Hodes C, Everitt MG. Intraocular pressure and systemic blood pressure in the elderly. British Journal of Ophthalmology. 1975; 59:717-720.6. Tarkkanen A, Leikola J. Postural variation of IOP as measured by the Mackay-Marg Tonometer. Acta Ophthalmology. 1967; 45 (4):569-575.7. Guyton AC, Hall JE. Fluid system of the eye - intraocular fluid. Textbook of Medical Physiology, 10th Ed. Publishers: Elsevier-Saunders. 2000; pp 199, 575-577.8. Sembulingam K, Sembulingam P. Intraocular pressure and Glaucoma. Textbook of Essentials of Medical Physiology, 5th Ed., Jaypee Brothers Medical Publishers. 2010; pp 930-934.9. Guevara AP, Vargas C, Sakurai H, Fujiwara Y, Hashimoto K, Maoka T, Kozuka M, Ito Y, Tokuda H, Hishino H. An antitumor promoter from moringa oleifera Lam. Mutation Research/Genetic Toxicology and Environmental Mutagenesis.1999; 440(2):181–188.10. Kurma SR., Mishra SH. Anti-inflammatory and hepatoprotective activities of fruits of Moringa pterygosperma Gaerth. Indian Journal of Natural Product 1998; 14:3–10.11. Tahiliani P, Kar A. Role of Moringa oleifera leaf extract in the regulation of thyroid hormone status in adult male and female rats. Pharmacological Research. 2000; 41:319–323.12. Omolaso B, Olatunde AA, Seriki SA, Idika IN. Effect of Moringa oleifera on blood pressure and blood glucose level in healthy humans. British Journal of Medical and Health Research. 2016; 3(6):21-34. 13. Faizi S, Siddiqui BS, Saleem R, Aftab K, Shaheen F, Gilani AH. Hypotensive constituents from the pods of Moringa oleifera. Planta Medica. 1998; 64:225–8.
between IOP and systemic blood pressure, it was observed from the study of Bulpi� et al.,5 in 1975, that the higher the blood pressure (BP), the greater the IOP, the greater IOP was not related to sex, age, height or haemoglobin. An elevated IOP will cause visual field loss only if the systemic blood pressure is high that the BP/IOP ra�o is beyond a certain cri�cal value6.
Hypertension is a worldwide common problem occurring mostly in the middle age and also as a hereditary or gene�c condi�on. Systemic Hypertension can be defined as a sustained rise in blood pressure. A person is said to have hypertension when the diastolic pressure is greater than 90mmHg and systolic pressure is greater than 135mmHg7. Blood pressure is the pressure exerted by the blood on the walls of the blood vessels. It is understood to mean arterial blood pressure, that is, the pressure in the large arteries, such as the brachial artery (in the arm). Pressure values are universally stated in millimeters of mercury (mmHg). Blood pressure measurement consists of two values. The first value is the systolic pressure; which is the peak or maximum pressure in the arteries during the cardiac cycle; that is, when the ventricles contract. Normal systolic pressure is 120mmHg. It ranges between 110 and 135mmHg. Diastolic pressure is the second number and it is defined as the lowest pressure in the arteries at the res�ng phase of the cardiac cycle that is, when the ventricles of the heart relax. Normal diastolic pressure is 80mmHg. It varies between 60 and 80mmHg8.
Medicinal plants cons�tute a major source of therapeu�c agents for lowering ocular and systemic hypertension. Moringa oleifera is a highly valued medicinal plant, distributed in many countries of the tropics and subtropics. It has an impressive range of medicinal
uses with high nutri�onal value. Moringa oleifera (MO) belongs to Moringacea family with about fourteen species and it is widely distributed in the tropics. MO has an�-cancer9, an�-inflammatory10 and thyroid status regulator efficacies11, and some researchers have reported its hypoglycemic and its hypotensive effect12. Omolaso et al., (2016) conducted a study on the effects of Moringa oleifera aqueous leaf extract on systemic blood pressure and blood glucose level in healthy humans and found that Moringa oleifera reduced blood pressure significantly (p<0.05) a�er 2 hours and blood glucose decreased significantly a�er 4 hours of oral administra�on of 75mg/kg body weight of Moringa oleifera dissolved in 250mls of water. Various parts of this plant such as the leaf, root, seed, bark, fruit, flower and immature pod act as cardiac and circulatory s�mulants, an�-inflammatory, an�hypertensive, cholesterol lowering, hypoglycemic and an�oxidant9-13 but we have not seen any reported studies of its effect on intraocular pressure therefore we inves�gated the effect of graded doses of Moringa oleifera leaf aqueous extract (MOLAE) on intraocular pressure and blood pressure of normotensive adults.
This was a clinic based experimental study in which thirty normotensive adults comprising fi�een males and fi�een females with age ranging from 18-35 (mean age of 25.3 ± 5.1) years were selected for experimental groups while ten normotensive adults comprising five males and five females aged matched were selected for the control group from the screening exercise using a purposive sampling method, at the University of Benin Optometry Clinic in Benin City, Edo State Nigeria. During the screening exercise, the case history of each par�cipant was taken. External and internal examina�on of the anterior and posterior segments of the eyes of each par�cipant
JNOA.2018;20(2): 75 - 81 George et al
Original Research Article

Journal of the Nigerian Optometric Association
77
Description of Procedure
were carried out using Haag-streit slit lamp model 900 and keeler Ophthalmoscope respec�vely to rule out abnormali�es. The central corneal thickness was assessed with SW-1000P ultrasound pachymeter. Intraocular pressure was measured with the CT-20-non-contact tonometer. Blood pressure was measured with U-MEC mercurial sphygmomanometer and Sprague stethoscope (Model No 112).
Inclusion criteria include normotensive adults who were newly selected from screening and were not on any treatment. They had IOP less than 21mmHg in three consecu�ve measurements; at 9am, 3pm and 6pm. Three readings were taken in order to observe the diurnal varia�ons in IOP before selec�on. Each par�cipant’s IOP was adjusted and corrected for CCT using the Ehler’s formula. Similarly three measurements were taken for the blood pressure (BP); systolic BP less than 120mmHg and diastolic BP less than 90mmHg were included in the study. The selected par�cipants had no history of hypertension; they had no visual field defect, no loss of neural disc �ssue from the assessment of the thickness, symmetry and color of the neuro-re�nal rim of the op�c disc. The par�cipants in the three groups had their visual field assessed using Octopus 900 manufactured in USA. They all had no remarkable ocular or medical history. All the par�cipants were non-alcoholics and non-smokers. Exclusion criteria include par�cipants who were on topical and / or systemic medica�ons and those with ocular or systemic disease. The first thirty par�cipants selected were divided into three groups 1, 2, and 3; with ten par�cipants in each group. A detailed explana�on of the research procedure was given to them and Informed consent was obtained from each volunteer. Approval for the study was granted by the Ethics and Research Commi�ee of the Department of Optometry, University of Benin, and was performed in accordance with the guidelines of the Declara�on of Helsinki. Selected par�cipants were instructed to abstain from all medica�on a
week before and during the period of the experiments. Each par�cipant was weighed and body weight recorded before the experiment. Experiments commenced at 9am in the morning. The par�cipants were served with the same light meal in the morning before they drank aqueous extract of Moringa oleifera leaf. Three different concentra�ons of the aqueous extract of Moringa oleifera leaf (28.5mg/kg body weight, 57.0mg/kg body weight and 85.7mg/kg body weight) were administered to groups 1, 2, and 3 par�cipants respec�vely. The last ten par�cipants formed the group 4 which was the control group and 250ml of dis�lled water without Moringa oleifera leaf was administered orally to each par�cipant in this control group.
The methodology of Moussa et al.,(2007)14 was adopted in the prepara�on of Moringa oleifera leaf aqueous extract (MOLAE). Moringa oleifera leaves of the same species were harvested from different trees in the University of Benin, Faculty of Agriculture wild Forest reserve, in Benin City, Nigeria. The leaves were air-dried at room temperature (36.0±10 0C) for 120 hours, therea�er pounded to powdered form. Extracts were prepared by laboratory technicians in the Department of Pharma-cognosy University of Benin, using the standardized method of Moussa et al.,14. This is by dissolving 2g, 4g and 6g of dried powdered Moringa oleifera leaf weighed with an electronic scale in 250ml of dis�lled water respec�vely to obtain different concentra�on. 250 ml was the standard volume administered orally based on body weight of each par�cipant in groups 1, 2, and 3. Group 1 par�cipants were administered orally with 250ml of 28.5 mg/kg body weight of MOLAE. Group 2 par�cipants were administered orally with 250ml of 57.0 mg/kg body weight of MOLAE. Group 3 par�cipants were administered orally with 250ml of 85.7 mg/kg body weight of MOLAE while group 4 par�cipants were administered orally with 250ml of water only.
JNOA.2018;20(2): 75 - 81 George et al
Original Research Article
14 Moussa N, Mariko U, Shin-ichi K, Kazuharu S. Effects of Oral Administration of Moringa oleifera Lam on Glucose Tolerance in Goto-Kakizaki and Wistar Rats. Journal of Clinical Biochemistry and Nutrion. 2007; 40(3): 229–233.

Journal of the Nigerian Optometric Association
78
The calcium and potassium electrolytes in the Moringa oleifera leaf powder administered to the par�cipants were analyzed in Marlet environmental research laboratory, Benin City using AAS model-solar 969 unicam series (acetylene flame). The following were obtained for calcium and potassium electrolytes in mg/100g of the Moringa oleifera leaf powder:
Electrolytes in Moringa oleifera leaf powder/100g Dis�lled water Potassium…………………….. ……1324.0mg………………………………………0.6Calcium …………………………….2003.0mg……………………………………….2.9
All the data in this study were analyzed with SPSS version 20. A one way Analysis of Variance (ANOVA) was used to determine if Moringa oleifera leaf aqueous extract had significant effect on IOP and BP. Post-hoc Least Significant Difference (LSD) was used to determine at what minute is the difference most significant. Significance was declared when probabili�es values were p<0.05.
The results are summarized in Tables. Tables 1-3
showed that a�er oral administra�on of 250ml of 28.5mg/kg, 57.0 mg/kg and 85.7mg/kg body weight of MOLAE to the three experimental groups, there were significant changes (p<0.05) in intraocular pressure and blood pressure at 30, 60 and 90 minutes compared to the baseline values, therea�er IOP and BP returned to baseline values a�er 150 minutes in the normotensive par�cipants. Tables 4 showed that a�er oral administra�on of 250ml of water only, to group 4 par�cipants which was the control group, there was no significant change (p>0.05) in the intraocular pressure and blood pressure at 30, 60, 90, 120 and 150 minutes compared to the baseline values in the normotensive adults, Tables 5 and 6 showed that the maximum mean difference in BP and IOP occurred at 60 and 90 minutes respec�vely in the experimental groups a�er oral administra�on of the three doses of MOLAE and the difference was sta�s�cally significant (p<0.05) in the three experimental groups of normotensive par�cipants. A�er the peak of fall in IOP and BP at 90 and 60 minutes respec�vely, the IOP and BP rose toward baseline values. The fall in intraocular pressure and blood pressure was also observed to be dose-dependent. The higher the dose of the aqueous extract of Moringa oleifera leaf, the greater the fall in IOP and BP.
JNOA.2018;20(2): 75 - 81 George et al
Original Research Article
Table 1 Mean of intraocular pressure and blood pressure across different time of assessment in Group 1 participants before and after oral administration of 28.5mg/kg body weight of Moringa oleifera leaf aqueous extract.
TIME INTERVAL MINUTES
MEAN IOP ± SD (mmHg)
OD
MEAN IOP ± SD (mmHg)
OS
MEAN SBP ± SD
(mmHg)
MEAN DBP ± SD (mmHg)
Baseline
30
60
90
120
150
12.90 ± 2.42
12.90 ± 2.42
11.60 ± 2.41
10.70 ± 2.22
11.80 ± 2.32
12.60 ± 2.38
13.50 ± 2.45
13.30 ± 2.35
12.80 ± 2.25
11.40 ± 2.20
12.00 ± 2.41
13.20 ± 2.39
117.10 ± 8.55
114.50 ± 7.61
111.30 ± 8.18
113.50 ± 7.42
115.70 ± 9.84
116.50 ± 8.36
80.00 ± 4.97
77.60 ± 5.40
75.50 ± 4.08
77.50 ± 3.20
76.50 ± 4.74
81.20 ± 6.05
Table 2 Mean of intraocular pressure and blood pressure across different time of assessment in Group 2 participants before and after oral administration of 57.0mg/kg body weight of Moringa oleifera leaf aqueous extract.
TIME INTERVAL MINUTES
MEAN IOP ± SD (mmHg)
OD
MEAN IOP ± SD (mmHg)
OS
MEAN SBP ± SD
(mmHg)
MEAN DBP ± SD (mmHg)
0
30
60
90
120
150
15.90 ± 2.83
15.80 ± 2.48
14.20 ± 2.61
13.00 ± 2.48
14.50 ± 2.67
15.30 ± 2.79
16.80 ± 2.27
16.30 ± 2.31
14.10 ± 2.13
14.00 ± 1.91
15.20 ± 2.04
16.30 ± 2.16
118.80 ± 8.09
117.60 ± 7.45
112.70 ± 7.1 1
114.80 ± 6.94
115.00 ± 7.81
118.50 ± 8.18
75.00 ± 7.07
74.50 ± 6.43
70.00 ± 6.23
73.00 ± 7.52
71.00 ± 6.14
74.50 ± 5.98
Statistical analysis
RESULTS
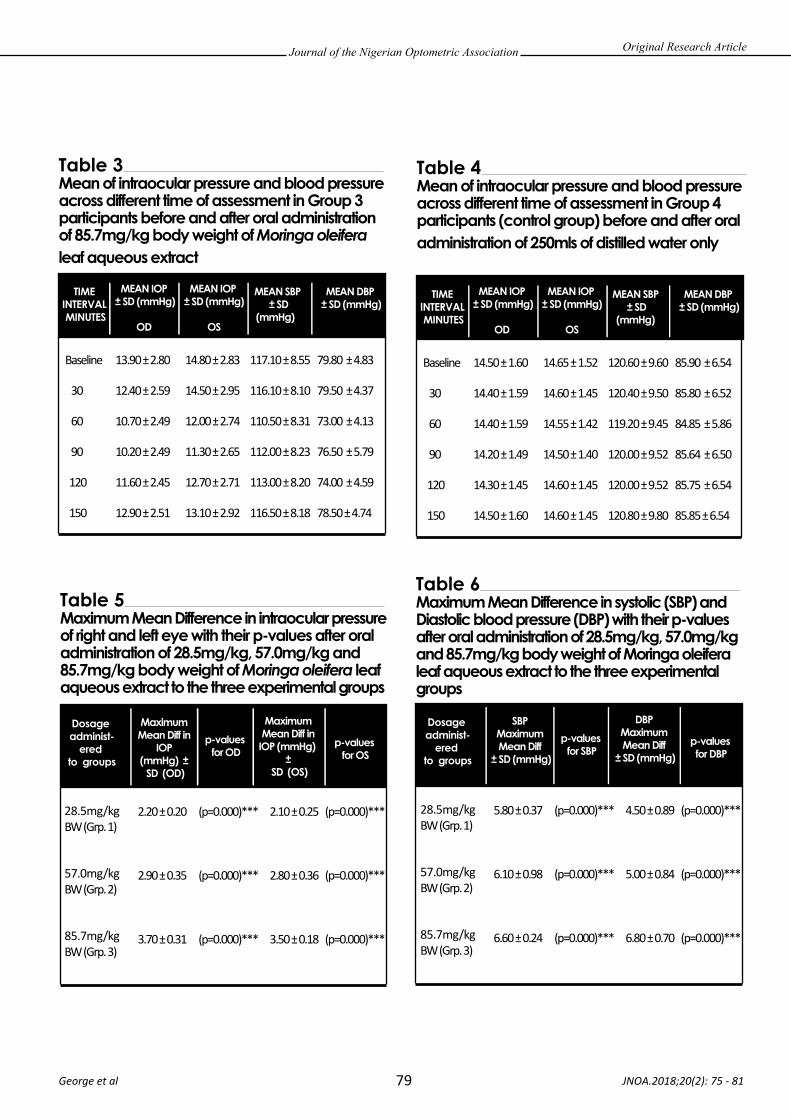
Journal of the Nigerian Optometric Association
79 JNOA.2018;20(2): 75 - 81 George et al
Original Research Article
Table 3 Mean of intraocular pressure and blood pressure across different time of assessment in Group 3 participants before and after oral administration of 85.7mg/kg body weight of Moringa oleifera leaf aqueous extract
TIME INTERVAL MINUTES
MEAN IOP ± SD (mmHg)
OD
MEAN IOP ± SD (mmHg)
OS
MEAN SBP ± SD
(mmHg)
MEAN DBP ± SD (mmHg)
Baseline
30
60
90
120
150
13.90 ± 2.80
12.40 ± 2.59
10.70 ± 2.49
10.20 ± 2.49
11.60 ± 2.45
12.90 ± 2.51
14.80 ± 2.83
14.50 ± 2.95
12.00 ± 2.74
11.30 ± 2.65
12.70 ± 2.71
13.10 ± 2.92
117.10 ± 8.55
116.10 ± 8.10
110.50 ± 8.31
112.00 ± 8.23
113.00 ± 8.20
116.50 ± 8.18
79.80 ± 4.83
79.50 ± 4.37
73.00 ± 4.13
76.50 ± 5.79
74.00 ± 4.59
78.50 ± 4.74
Table 4 Mean of intraocular pressure and blood pressure across different time of assessment in Group 4 participants (control group) before and after oral administration of 250mls of distilled water only
TIME INTERVAL MINUTES
MEAN IOP ± SD (mmHg)
OD
MEAN IOP ± SD (mmHg)
OS
MEAN SBP ± SD
(mmHg)
MEAN DBP ± SD (mmHg)
Baseline
30
60
90
120
150
14.50 ± 1.60
14.40 ± 1.59
14.40 ± 1.59
14.20 ± 1.49
14.30 ± 1.45
14.50 ± 1.60
14.65 ± 1.52
14.60 ± 1.45
14.55 ± 1.42
14.50 ± 1.40
14.60 ± 1.45
14.60 ± 1.45
120.60 ± 9.60
120.40 ± 9.50
119.20 ± 9.45
120.00 ± 9.52
120.00 ± 9.52
120.80 ± 9.80
85.90 ± 6.54
85.80 ± 6.52
84.85 ± 5.86
85.64 ± 6.50
85.75 ± 6.54
85.85 ± 6.54
Table 5 Maximum Mean Difference in intraocular pressure of right and left eye with their p-values after oral administration of 28.5mg/kg, 57.0mg/kg and 85.7mg/kg body weight of Moringa oleifera leaf aqueous extract to the three experimental groups
Dosage administ-
ered to groups
Maximum Mean Diff in
IOP (mmHg) ±
SD (OD)
p-values for OD
Maximum Mean Diff in
IOP (mmHg) ±
SD (OS)
p-values for OS
28.5mg/kg BW (Grp. 1)
57.0mg/kg BW (Grp. 2)
85.7mg/kg BW (Grp. 3)
2.20 ± 0.20
2.90 ± 0.35
3.70 ± 0.31
2.10 ± 0.25
2.80 ± 0.36
3.50 ± 0.18
(p=0.000)***
(p=0.000)***
(p=0.000)***
(p=0.000)***
(p=0.000)***
(p=0.000)***
Table 6 Maximum Mean Difference in systolic (SBP) and Diastolic blood pressure (DBP) with their p-values after oral administration of 28.5mg/kg, 57.0mg/kg and 85.7mg/kg body weight of Moringa oleifera leaf aqueous extract to the three experimental groups
Dosage administ-
ered to groups
SBP Maximum Mean Diff
± SD (mmHg)
p-values for SBP
DBP Maximum Mean Diff
± SD (mmHg)p-values for DBP
28.5mg/kg BW (Grp. 1)
57.0mg/kg BW (Grp. 2)
85.7mg/kg BW (Grp. 3)
5.80 ± 0.37
6.10 ± 0.98
6.60 ± 0.24
4.50 ± 0.89
5.00 ± 0.84
6.80 ± 0.70
(p=0.000)***
(p=0.000)***
(p=0.000)***
(p=0.000)***
(p=0.000)***
(p=0.000)***

Journal of the Nigerian Optometric Association
80
DISCUSSION
15. Hatton DC, Yue Q, McCarron DA. Mechanisms of calcium's effects on blood pressure. Seminars in Nephrology Journals. 1995; 15(6):593-602.16. Frank MS, Walter CW, Smith A, Lisa EB, Bernard R, Thomas JM. Effect on Blood Pressure of Potassium, Calcium, and Magnesium in Women with Low Habitual Intake. Hypertension. 1998; 31: 131-138. 17. Gapal Krishna, G. 1990. Effect of potassium intake on blood pressure. J. Am. Soc. Nephrol. 1:43-52. 18. Haddy, F.J., Vanhoutte, P.M., and Feletou, M. (2006). Role of potassium in regulating blood flow and blood pressure. Am J Physiol Regul Integr Comp Physiol 290: 546–552. 19. Kaplan, N.M., Carnegie, A., Raskin, P., Heller, J.A., and Simmins, M. (1985). Potassium supplementation in hypertensive patients with diuretic-induced hypokalemia. N Engl J Med. 312: 746-749.20. Smith, S.R., Klotman, L.P., and Svetkey, L.P. (1992). Potassium Chloride lowers blood pressure and causes Natriureis in older patients with hypertension. J. Am. Soc. Nephrol. 2:1302-1309.21. Faizi S, Siddiqui BS, Saleem R, Siddiqui S, Aftab K, Gilani AH. Isolation and structure evucidation of novel hypotensive agents, niazinin B, niazimicin and niaziminin A+B from Moringa oleifera: the first naturally occuring thiocarbamates, Journal of the Chemical Society, Perkin Transaction 1992; 1: 3237-324122. Anwar G, Faizi S, Siddiqui BS, Rubeena S, Siddiqui S, Khalid A. Fully acetylated carbamate and hypotensive thiocarbamate glycosides from Moringa oleifera. Phytochemistry. 1995; 38(4): 957-963. 23. Castejon H, Chiquet C, Savy O, Baguet JP, Khayi H, Tamisier R, Bourdon L, Romanet JP. Effect of Acute Increase in Blood Pressure on Intraocular Pressure in Pigs and Humans. Investigative Ophthalmology & Vision Science 2010; 51(3): 1599-1605.24. Leske MC, Warheit-Roberts L, Wu SY. Open-angle glaucoma and ocular hypertension: the Long Island Glaucoma Case-control Study. Ophthalmic Epidemiology 1996; 3(2):85-96.25. Klein BE, Klein R, Knudtson MD. Intraocular pressure and systemic blood pressure: longitudinal perspective: the Beaver Dam Eye Study. British Journal of Ophthalmology 2005; 89:284-287.26. Vaajanen A, Mervaala E, Oksala O, Vapaatalo H. Is there a relationship between blood pressure and intraocular pressure? An experimental study in hypertensive rats. Current Eye Research. 2008; 33(4):325-32.27. George GO, Idu FK, Obika LFO. Effects of corn silk aqueous extract on intraocular pressure of ocular hypertensive human subjects. South African Optometry 2013; 72(3): 133-143.28. George GO, Obika LFO. Effects of aqueous extract of corn silk on intraocular and blood pressures of normotensive subjects. West African Journal of Pharmacology and Drug Research. 2014; 29: 16-24.29. George GO, Idu FK. Corn silk aqueous extracts and intraocular pressure of systemic and non-systemic hypertensive subjects. Clinical and Experimental Optometry. 2015; 98: 138–149.
The fall in intraocular pressure and blood pressure observed in the three normotensive groups of par�cipants showed that the aqueous extract of Moringa oleifera leaf has hypotensive property. The mechanisms responsible have not been iden�fied, but numerous possibili�es have been proposed. Many of the proposals have a�empted to relate dietary calcium to calcium metabolism in vascular smooth muscle and altered vascular tone15. Potassium supplements have modest blood pressure–lowering effect in persons with low dietary intake. The study by Frank et al.,16 further showed the importance of potassium for blood pressure regula�on in the general popula�on. Therefore the high potassium and calcium content in the aqueous extract of Moringa oleifera leaf may have played a role in lowering blood pressure. The main cause of hypertension is believed to be the increased level of sodium in the blood. When the level of potassium in the blood decreases, the absorp�on of sodium naturally increases leading to hypertension or High Blood Pressure. Moringa oleifera leaf is one of the richest sources of potassium. From the phytochemical and electrolytes analysis carried out in Marlet environmental research laboratory, Benin City using AAS model-solar 969 unicam series (acetylene flame), it was observed that Moringa oleifera leaf has high content of potassium and potassium is known to prevent the excessive absorp�on of sodium thereby decreasing the blood pressure. Clinical studies suggest that potassium is an important regulator of blood pressure. Potassium supplementa�on lowers
blood pressure in hypertensive pa�ents. Blacks appear to be more sensi�ve to the hypotensive effects of potassium17,18. Potassium chloride lowers blood pressure and increases sodium excre�on in pa�ents with hypertension. The blood pressure effect may be due to potassium-induced natriuresis19, 20. The results of this study agrees with the study of Faizi et al.,21, they conducted a study on effect of the crude extract of Moringa oleifera leaves on systolic, diastolic as well as mean blood pressure of anaesthe�zed rats. They concluded that the crude extract of the leaves of M. oleifera caused a fall in systolic, diastolic, and mean BP in a dose-dependent manner. They also analyzed that thiocarbamate and isothiocyanate in the crude extract were responsible for the an�hypertensive ac�vity. Anwar et al.,22 showed that Moringa oleifera had 3 major compounds which are capable of lowering systemic blood pressure. The compounds included nitrile, mustard oil glycosides and thiocarbamate glycosides.
There are significant direct correla�ons between changes in systemic blood pressure and changes in intraocular pressure in humans and animals studies23-29. The peak of fall for blood pressure preceded the peak of fall for IOP in this study, because a decrease in episcleral venous pressure may have resulted in an increased ou�low of aqueous causing a fall in intraocular pressure6. Therefore the fall in blood pressure is believed to cause a resultant fall in intraocular pressure but further researches are needed in this area in order to determine the exact mechanism by which this occur.
JNOA.2018;20(2): 75 - 81 George et al
Original Research Article

Journal of the Nigerian Optometric Association
81 JNOA.2018;20(2): 75 - 81 George et al
Original Research Article
The use of 28.5mg/kg, 57.0 mg/kg and 85.7mg/kg body weight of MOLAE have significant hypotensive effect on intraocular pressure and blood pressure when administered orally to normotensive adults. The lowering effect on intraocular pressure may have resulted from the fall in blood pressure which may have resulted from the high content of potassium and calcium in aqueous extract of Moringa oleifera leaf. Moringa oleifera leaf is innocuous because toxicological studies of oral administra�on on rats demonstrated good tolerability without mutagenic or genotoxic effects. Therefore it may be consumed as a form of adjunct therapy in controlling blood pressure and intraocular pressure in systemic and ocular hypertensive humans but further inves�ga�ons may be required to determine the therapeu�c dose of Moringa oleifera leaf in the management of ocular and systemic hypertension.
CONCLUSION
Prof Frank Iwuagwu Nigeria Prof Faus�na Idu Nigeria Dr Chris Timothy Nigeria Dr Maduabuchi E. Okorie Nigeria Dr Bethels Ndubueze USADr Ego Ikoro NigeriaDr Patrick Okonji NigeriaDr Ran� Ekpo NigeriaDr Obinna Akano USADr Ekpenyong Nsa Nigeria Dr Samuel Kyei GhanaDr Godwin Ovenseri-Ogbomo. NigeriaDr Antor Ndep NigeriaDr Mustafa Abdu Ali Mohammed Sudan Dr Nwakuso Aruotu NigeriaDr Chimeziri Anderson Nigeria
LIST OF REVIEWERS
Journal of the Nigerian Optometric Association
JNOA.2018;20(2) Ekpenyong B.N.

CONTENTS
Editor’s notes 1 Dr Bernadine Ekpenyong
Editorial 2 - 7 Appropriate technologies for health and disease: An innova�ve approach to drive sustainable health care delivery. Professor E. Uche Ikonne
Ar�cles
Factors affec�ng rehabilita�on seeking behaviour of individuals with legal blindness 8 - 14 in Lagos, Nigeria. Okonji P.E., Jibogu K.P. and Akinsola O. J.
Refrac�ve errors in children with Down syndrome in Lagos State, Nigeria. 15 - 22 Nwokedi O., Ekpenyong B.N., Musa N.R. and Ovenseri-Ogbomo G.O.
Accommoda�ve anomalies in symptoma�c school children in Cape Coast Metropolis, 23 - 30 Ghana. Darko-Takyi C., Ntodie M., Alex Azuka Ilechie A.A., Abokyi S., Kyei S., Aful H.K., Nti, N.A. and Okae-Asante D.
Assessment of foveal and extra-foveal photostress recovery �me in primary open 31 - 36 angle glaucoma Azuamah, Y.C., Merem, C.C., Ikoro, N.C., Esenwah, E.C., Megwas, A.U. and Daniel-Nwosu, E.
Relevance of culturally-appropriate approaches in health promo�on: a look at Igbo 37 - 45 philosophies in dealing with eye care challenges in Nigeria. Okoye, R.S, Bell, L. and Papadopoulos, I.
Effect of x-rays on the electrolyte concentra�on of bovine aqueous and vitreous 46 - 52 humour Ajayi, O.B. and Atuanya G.N.
External eye infec�ons and personal hygiene prac�ces among pa�ents a�ending 53 - 61 Optometry Teaching Clinic Federal University of Technology, Owerri. Azuamah, Y.C., Esenwah, E.C., Ahuama, O.C., Ikoro, N.C., Iwuagwu, F.C. and Dozie, I.N.S
Determina�on of a standard con�nuous-text print size for people with low vision 62 - 68 Ejukonemu B.O.M. and Akpalaba R.E.U.
Prevalence of low vision and blindness in a leprosarium in kano state, Nigeria. 69 - 74 Okpo E., Nwakuche P.I. and Ejukunemu B.O.M.
Effect of Moringa Oleifera leaf aqueous extract on intraocular and blood pressure 75 - 81 of normotensive adults in Edo State, Nigeria George, G. O., Ajayi, O.B. and Oyemike, A.A.