interventional radiology in liver transplant recipients
TRANSCRIPT
Interventional Radiology in Liver Transplant Recipients
S S Baijal Director, Radiology
Director, Interventional Radiology
Medanta – The Medicity,
Gurgaon. India
HBV
HCV
Main Causes
NASH
Chronic Liver Disease in India
Alcohol

HEV
HAV
Drugs &
Toxins
HBV
Acute Liver Failure in India
Main Causes
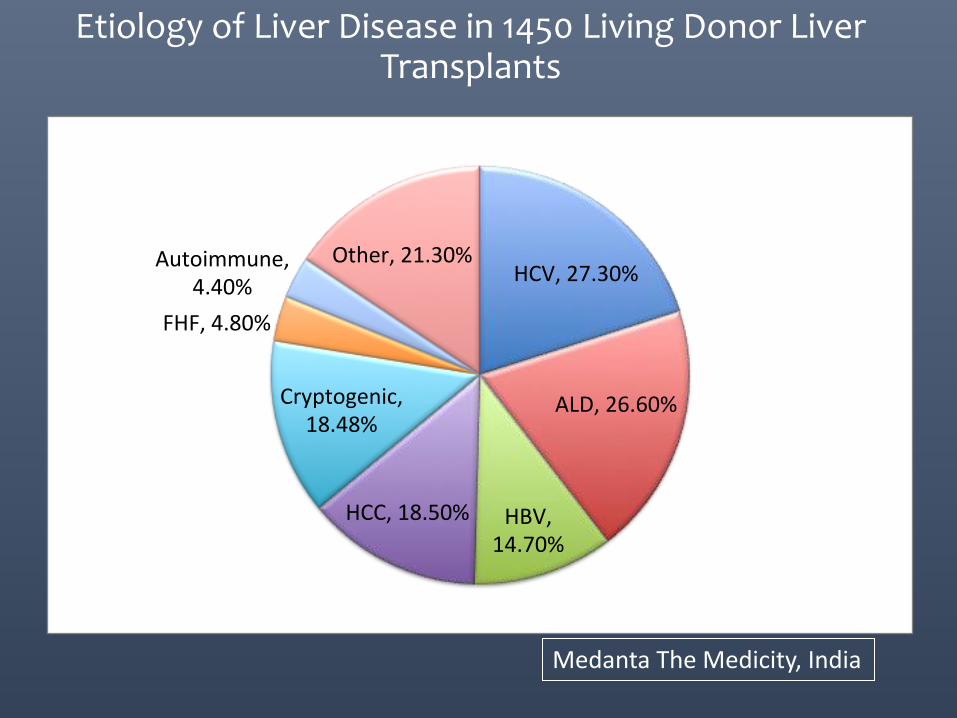
Etiology of Liver Disease in 1450 Living Donor Liver Transplants
Medanta The Medicity, India
HCV,27.30%
ALD,26.60%
HBV,14.70%
HCC,18.50%
Cryptogenic,18.48%
FHF,4.80%
Autoimmune,4.40%
Other,21.30%
Estimated 1- yr survival 90%
Child-Pugh class B or C
Portal hypertensive bleeding or a single episode of
spontaneous bacterial peritonitis, irrespective of
Child-Pugh score
MELD score >14
Non- disease- specific minimal listing criteria in CLD
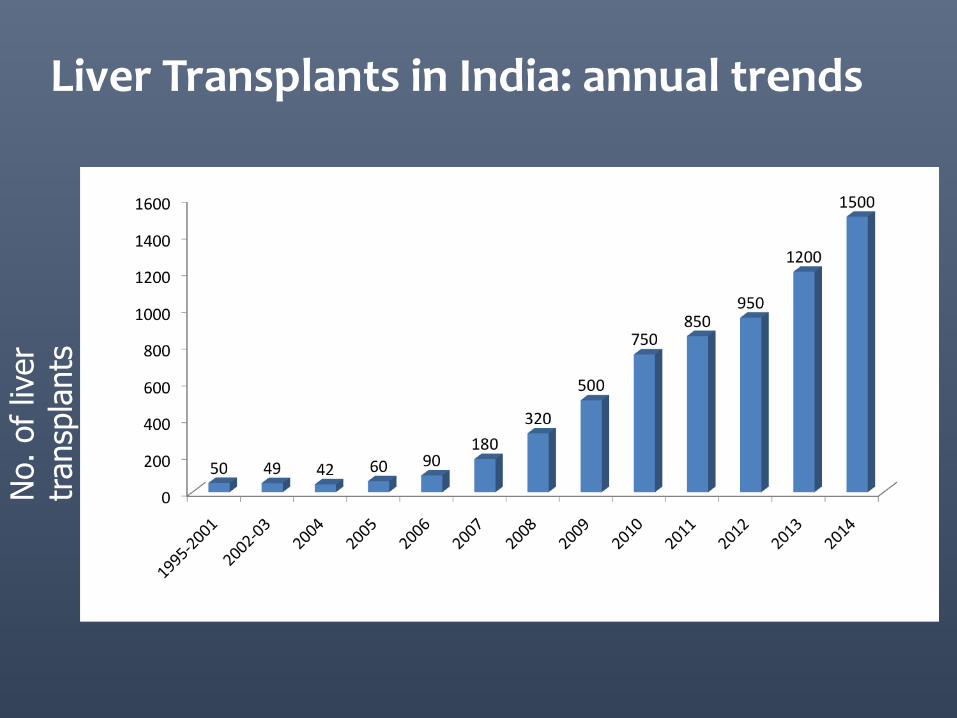
Liver Transplants in India: annual trends N
o. of liv
er
tr
ansp
lants
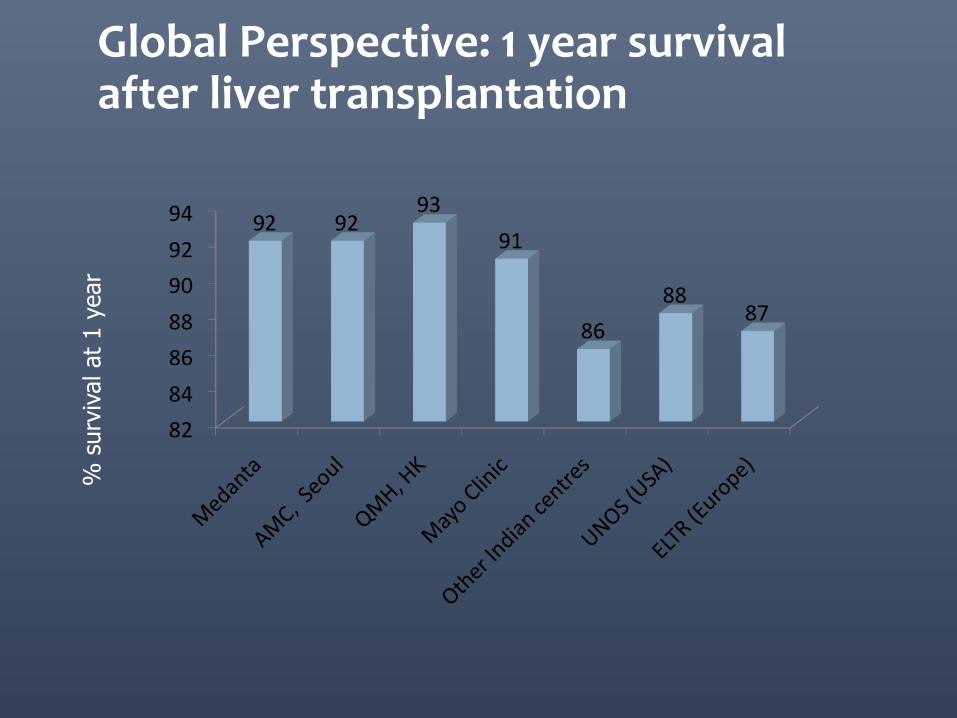
Global Perspective: 1 year survival after liver transplantation
%
surv
ival at
1 y
ear
Liver transplant recipients:
• Recent major post operative status
• Immuno-compromised
• Deranged coagulation
• Limited room to correct coagulation
• Often at odd hours
• “Precious” patients – from living donor
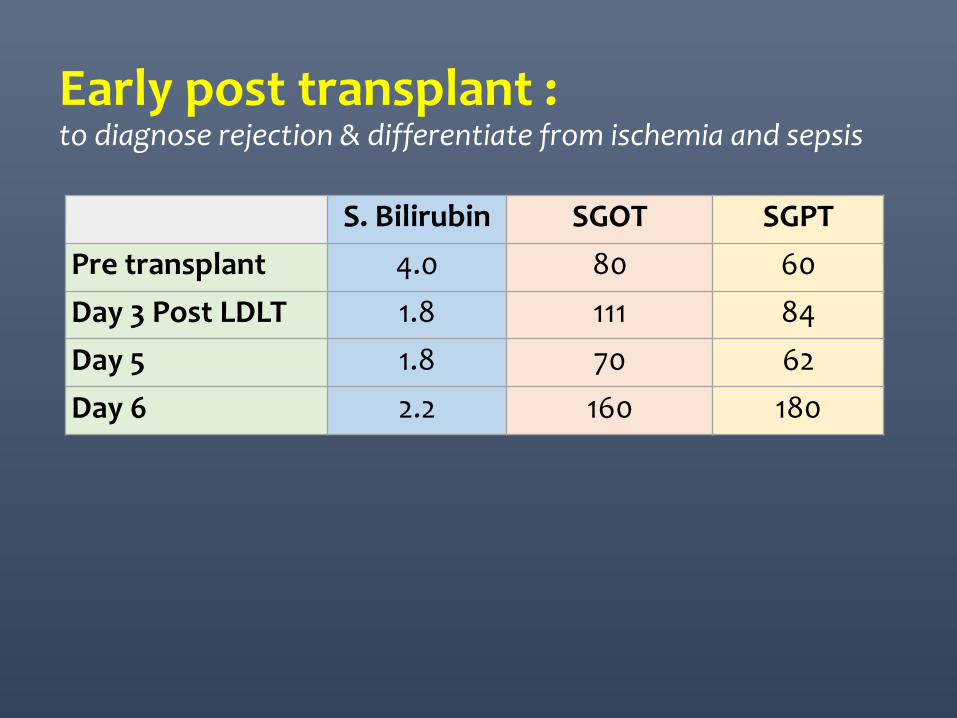
S. Bilirubin SGOT SGPT
Pre transplant 4.0 80 60
Day 3 Post LDLT 1.8 111 84
Day 5 1.8 70 62
Day 6 2.2 160 180
Early post transplant : to diagnose rejection & differentiate from ischemia and sepsis
• USG evaluation with Doppler: easy and modestly accurate to exclude HAT and collections.
• Liver biopsy often required: Trans-jugular Percutaneous
TJLB
• After 1st week: fresh HV anastomosis
• Significant ascites
• Significantly deranged coagulation/thrombocytopenia
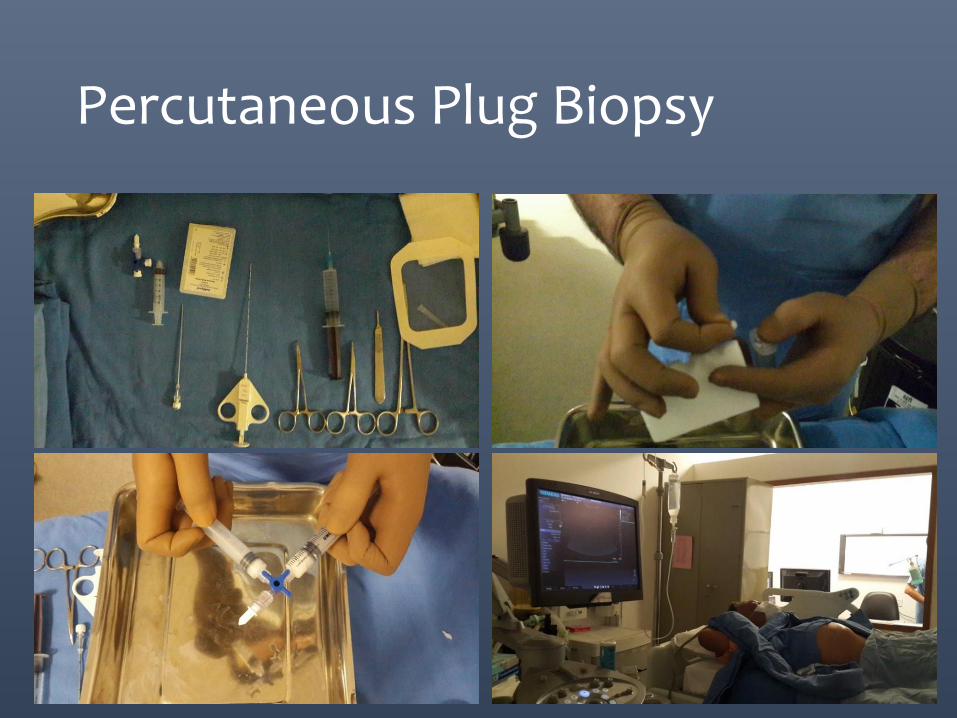
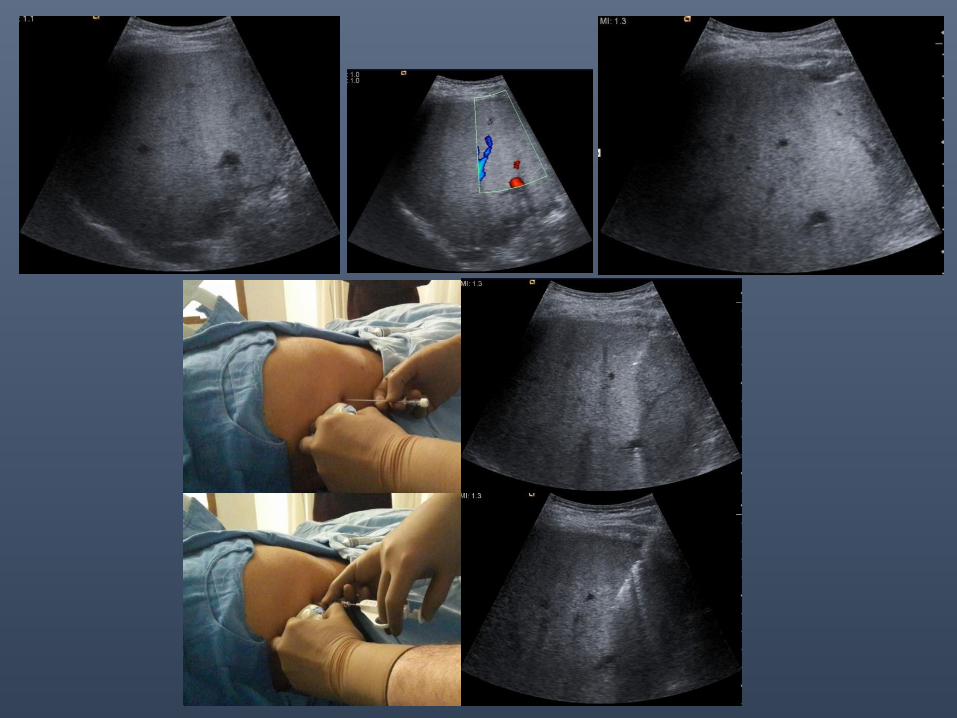
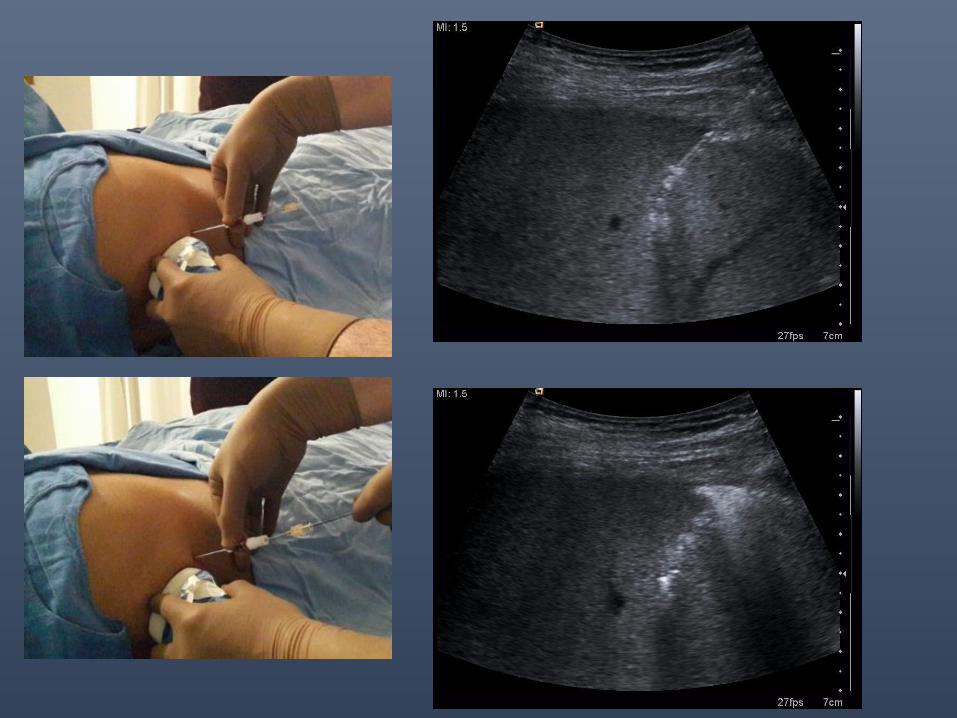
Percutaneous Plug Biopsy
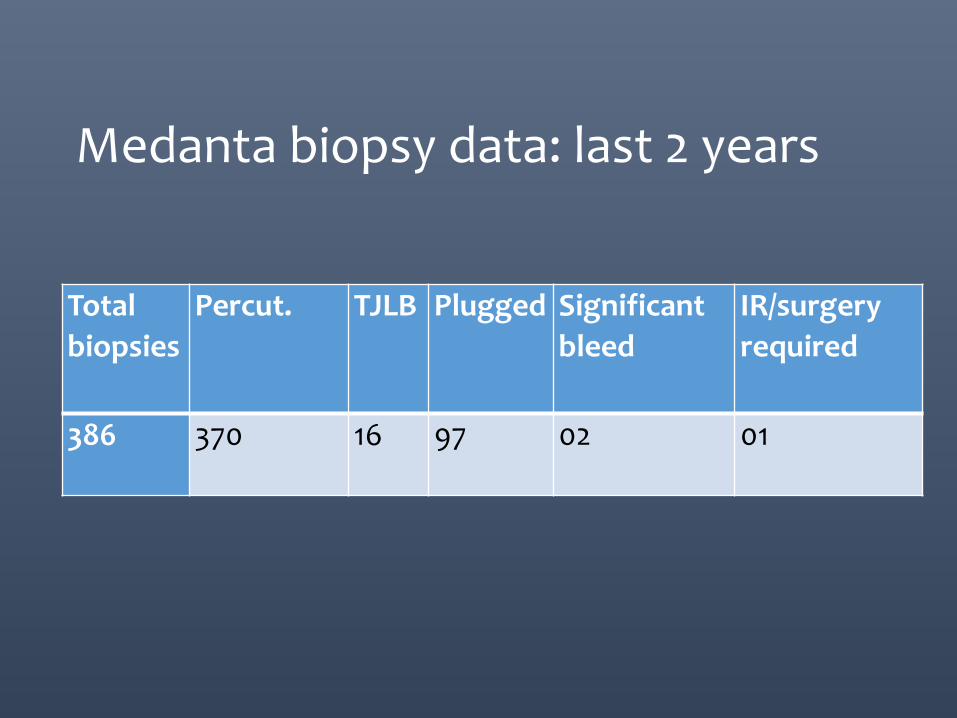
Total
biopsies
Percut. TJLB Plugged Significant
bleed
IR/surgery
required
386 370 16 97 02 01
Medanta biopsy data: last 2 years
Graft dysfunction/sepsis with a Collection/IHBR dilatation
• Percutaneous Drainage
• PTBD
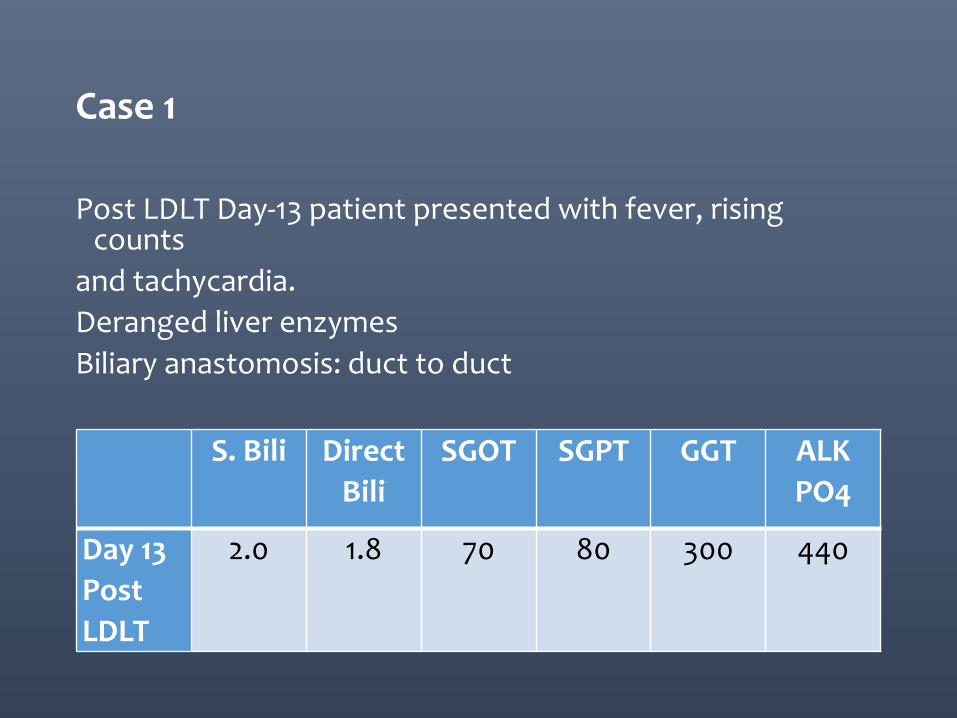
Case 1
Post LDLT Day-13 patient presented with fever, rising counts
and tachycardia.
Deranged liver enzymes
Biliary anastomosis: duct to duct
S. Bili Direct
Bili
SGOT SGPT GGT ALK
PO4
Day 13
Post
LDLT
2.0 1.8 70 80 300 440
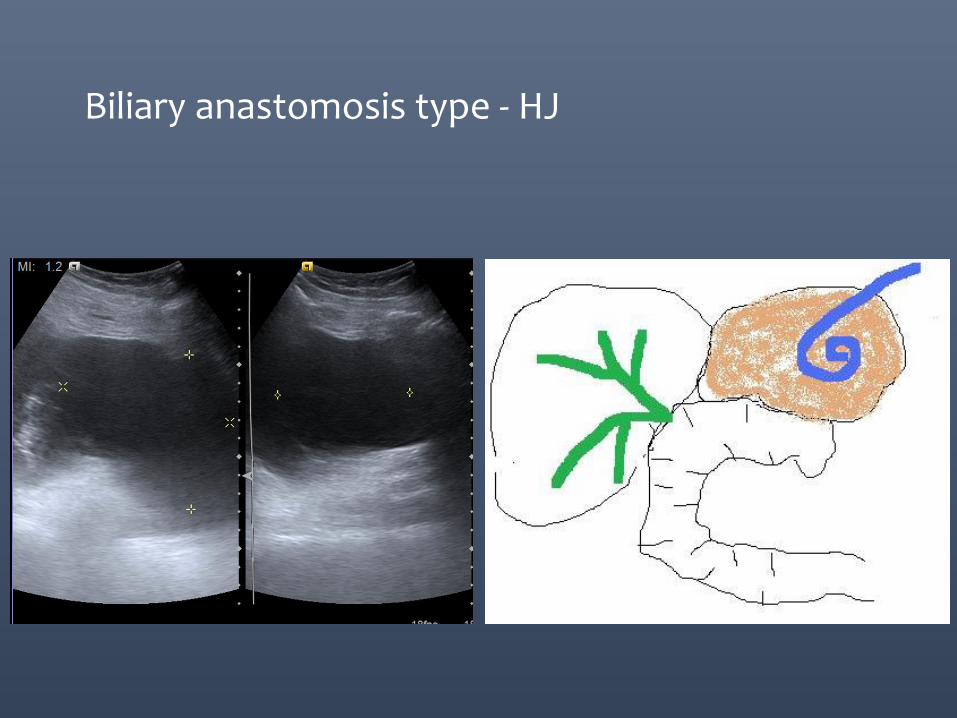
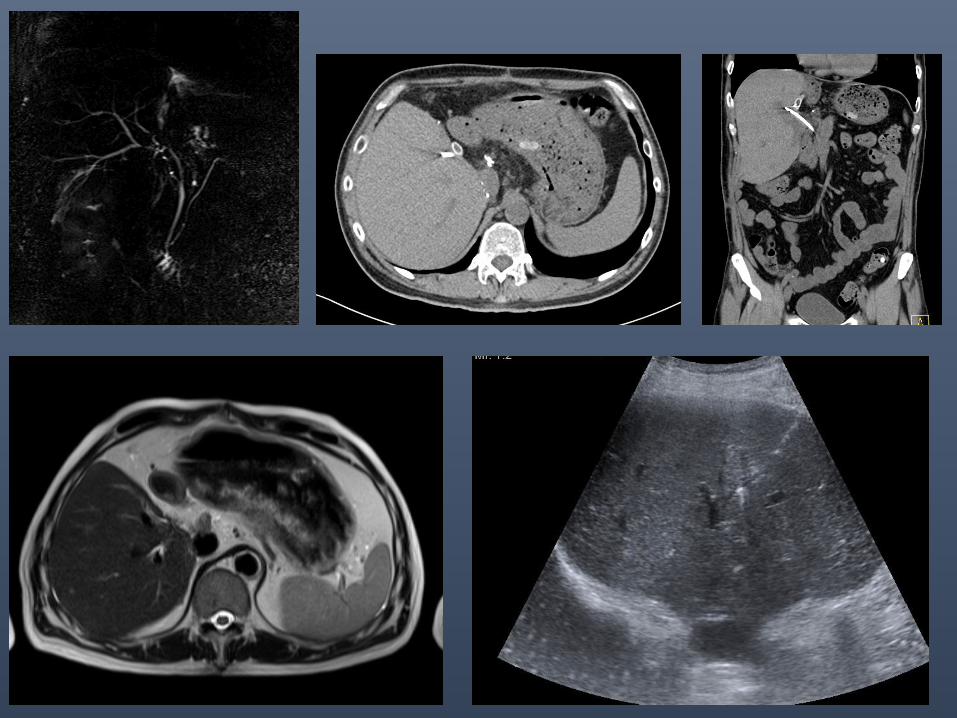
Biliary anastomosis type - HJ
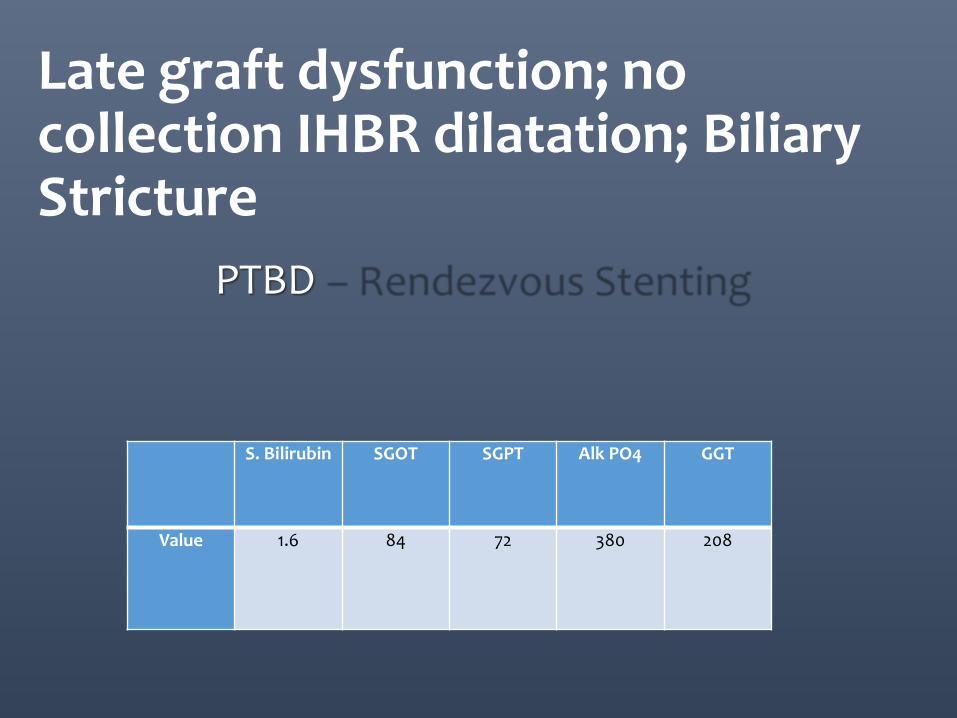
S. Bilirubin SGOT SGPT Alk PO4 GGT
Value 1.6 84 72 380 208
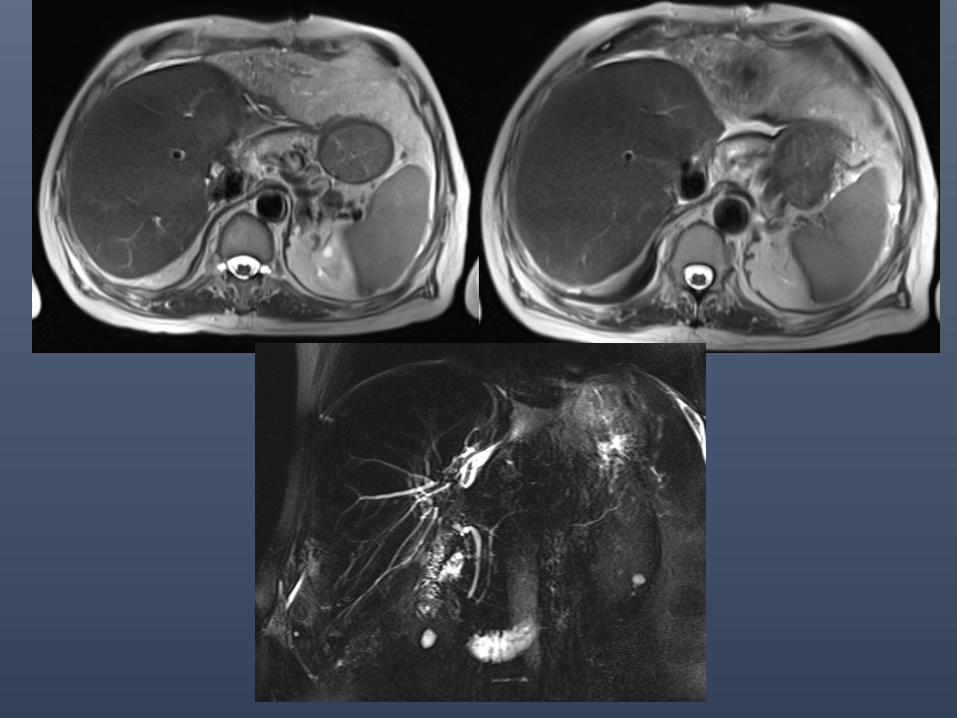
Late graft dysfunction; no collection IHBR dilatation; Biliary Stricture
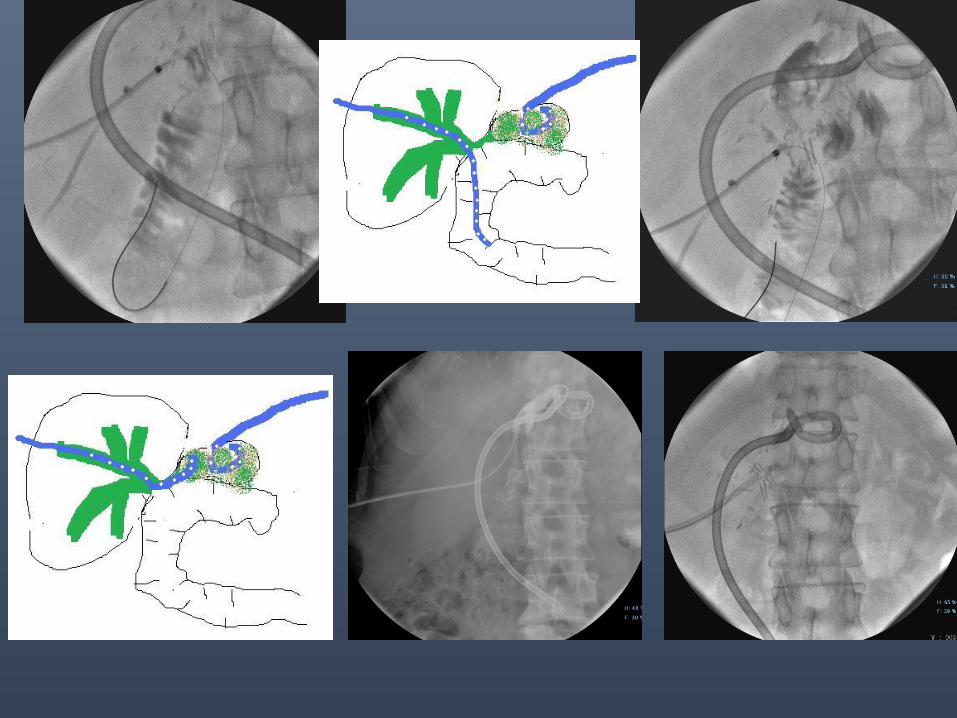
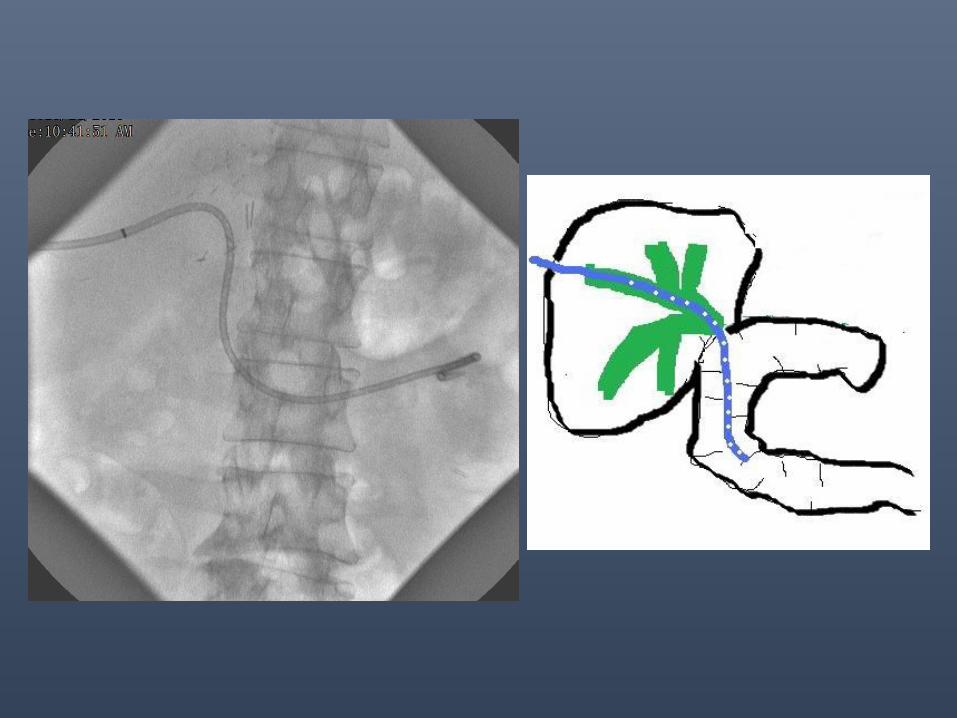
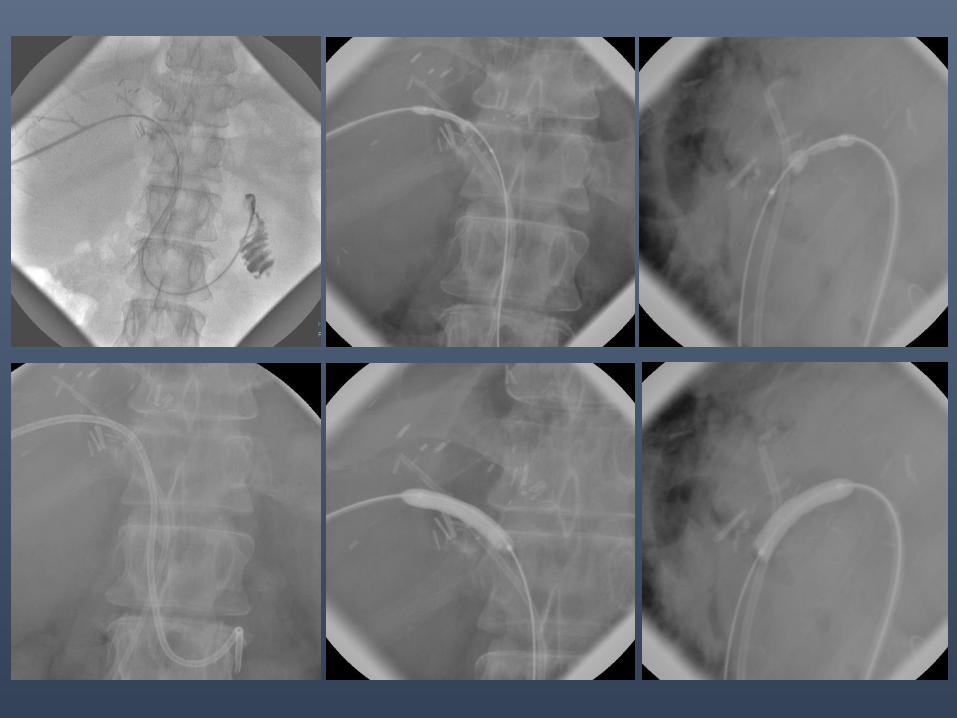
PTBD – Rendezvous Stenting
Case 1:
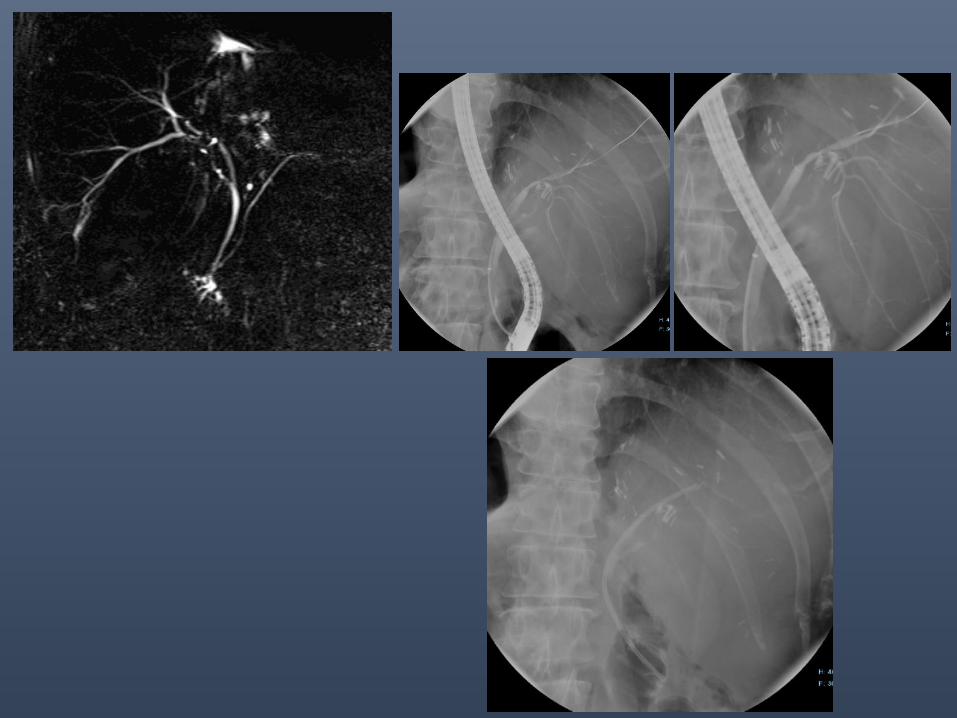
• 1 yr post LDLT
• USG – IHBRD; MRCP confirmed the finding
• ERCP: one system drained; one left
• PTBD followed by rendezvous

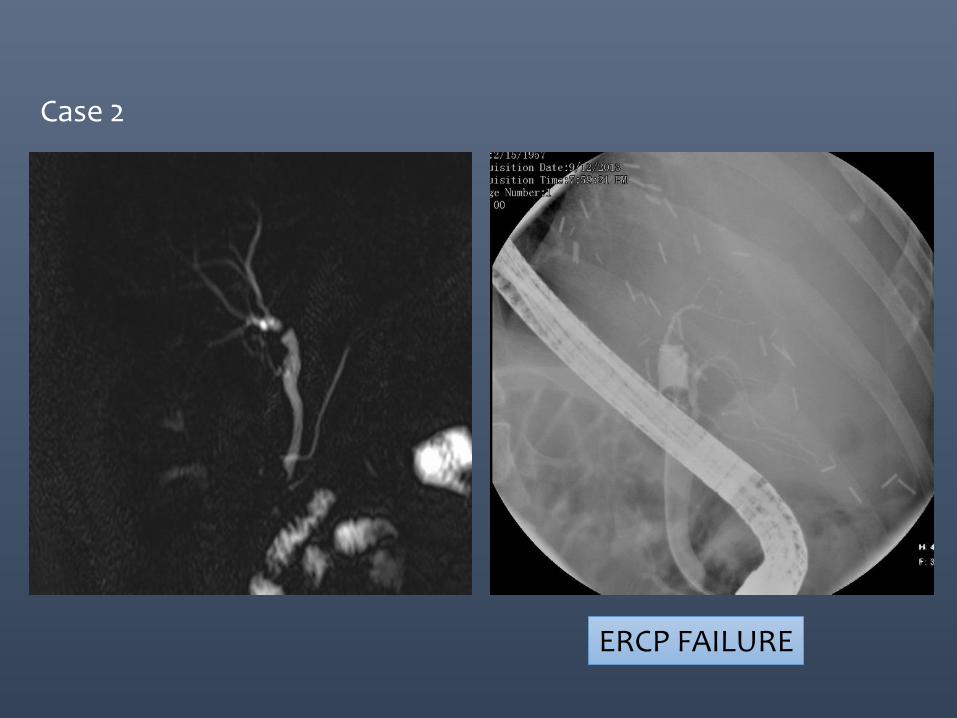
ERCP FAILURE
Case 2
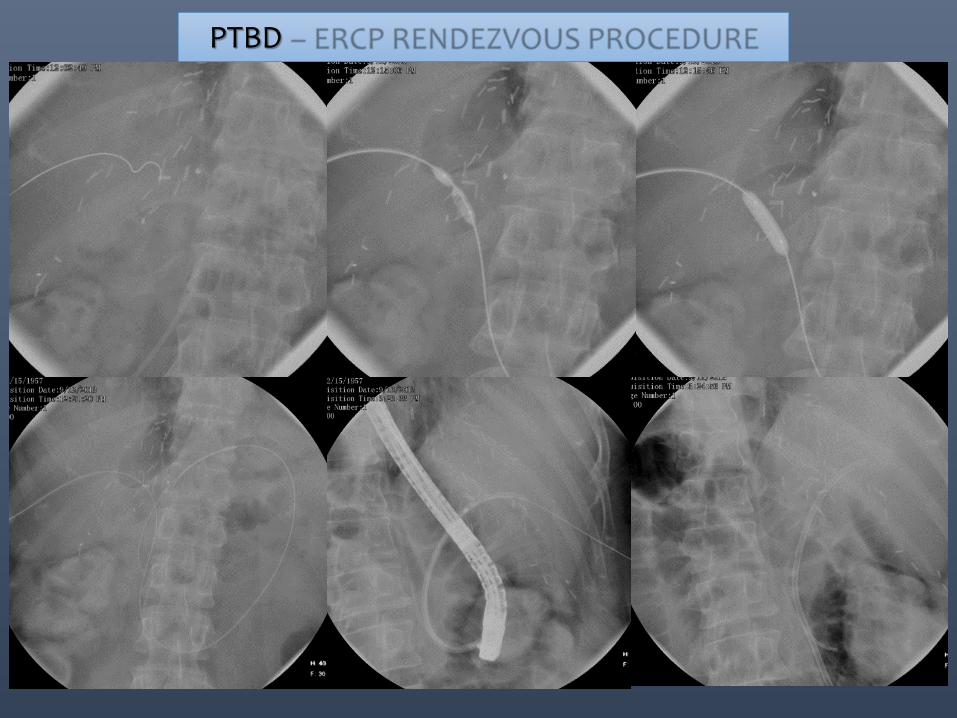
PTBD – ERCP RENDEZVOUS PROCEDURE
BALLOON DILATATION & PBS
• 38 patients with anastomotic BBSs secondary to LDLT
• Balloon dilation followed by maximal PBS insertion.
• The median number of stents per stricture in one session was 3 (range 1–7).
• Initial success was 100 %.
• Recurrent stricture in 8 (21 %) patients.
• All recurrences were successfully retreated endoscopically.
• All patients were managed without surgical revision or re-transplantation, resulting in 100 % success by an intention-to-treat analysis.
Hsieh TH et al. Gastrointest Endosc. 2013;77(1):47–54.
SEMS in liver transplant: current evidence
• FCSEMS: promising option in the endoscopic management; however current evidence does not suggest a clear advantage over PBS.
• FCSEMSs should not be used as the primary modality.
• Failure of standard approach: temporary covered stent could solve biliary complications in almost three quarters of cases
• ~33 % rate of stent migration
Kao D et al., Gastrointest Endosc. 2013;77(5):679–91.
Tarantino et al., Endoscopy. 2012;44(3):246–50.

Medanta data: percutaneous management of post LDLT anastomotic biliary strictures
• N=78 over last 4 yrs
• Failed access: 1
• Failure to cross stricture: 5 neo bilio-enteric anastomosis made in all (hepatico-gastrostomy & hepatico-duodenostomy)
• Post LDLT Rendezvous: 60
• Successful ballooning of HJs: 12
• Strategy: Multistent/Multi-catheter protocol with one year indwelling time
• NO HJ patient has come back for a repeat percutaneous intervention.
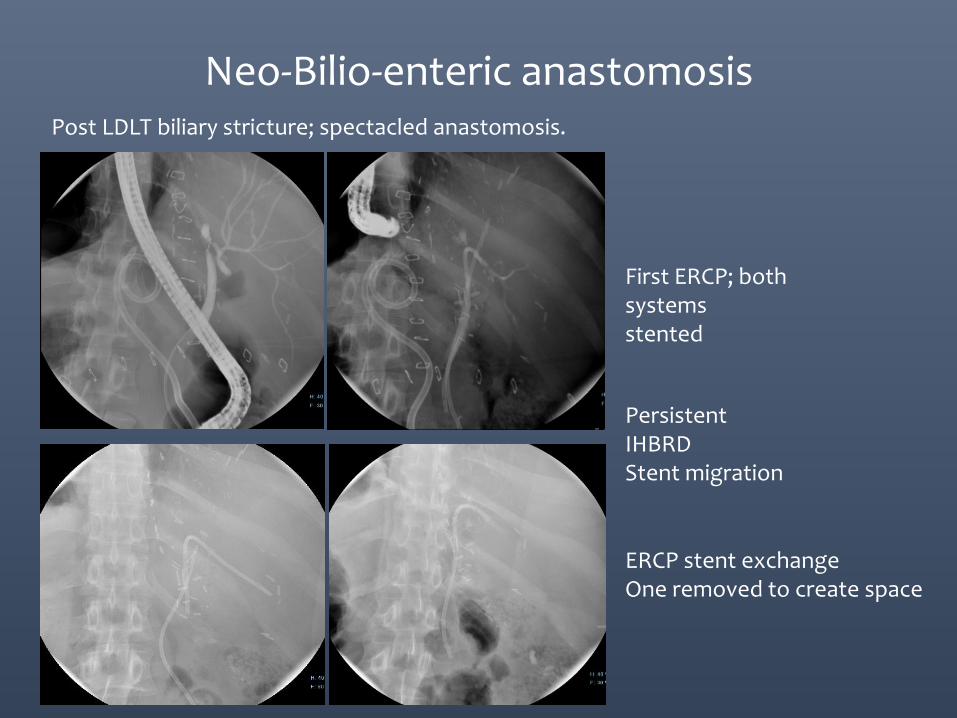
Neo-Bilio-enteric anastomosis Post LDLT biliary stricture; spectacled anastomosis.
First ERCP; both systems stented
Persistent IHBRD Stent migration
ERCP stent exchange One removed to create space
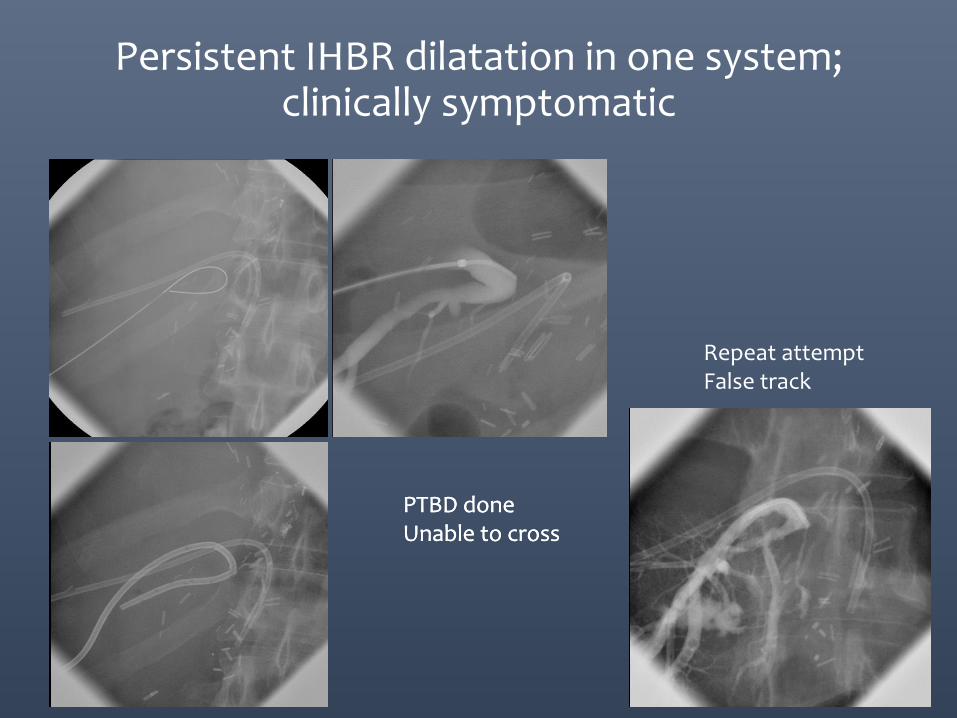
Persistent IHBR dilatation in one system; clinically symptomatic
PTBD done Unable to cross
Repeat attempt False track
PTBD done Unable to cross
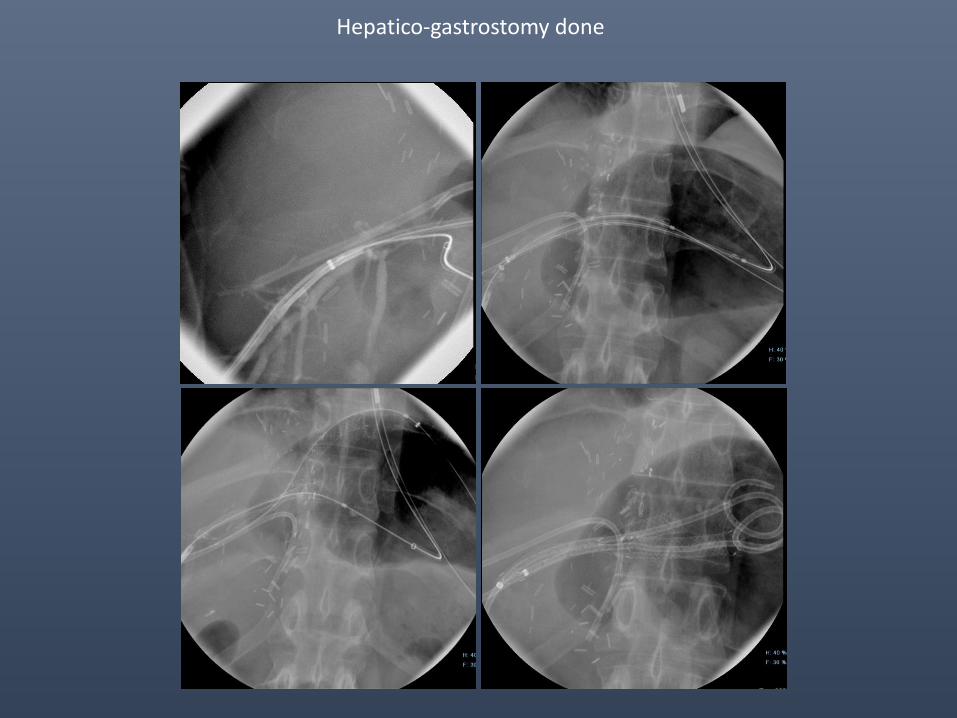
Hepatico-gastrostomy done

Biliary stricture: Integrating treatment concepts
• Evidence to suggest that multistent scaffolding supports better long term outcomes in benign biliary stricture
• Development of removable SEMS might provide a paradigm shift in the management protocols
• Need for a consensus meeting to standardize the approach for benign biliary strictures can not be overemphasized.
• Team approach
• Extreme/innovative interventions (rarely)
Early post LDLT with graft dysfunction and normal bile ducts.
• Protocol: LFT every day in first week followed by every alternate day in second wk and every 3rd day post discharge for first 30 days
• DUS/CT shows HAT
Hepatic Artery Thrombosis • Thrombolysis
Thrombolytic agents:
• Mechanism: activate the enzyme plasminogen clears the cross-linked fibrin mesh makes the clot soluble and subject to further proteolysis by other enzymes.
• Streptokinase: • Historical importance.
• Urokinase:
• Most frequently used agent • Bolus of 50k units over 30 min followed by Infusion @ 25-50000
units/hour. • Upto 2.5-5 lac units or 36-48 hrs.
• r-TPA:
• Bolus of 1mg followed by infusion of 0.5-1mg/hour.
Singhal et al: Transpl Int. 2010 Mar 1;23(3):245-56.
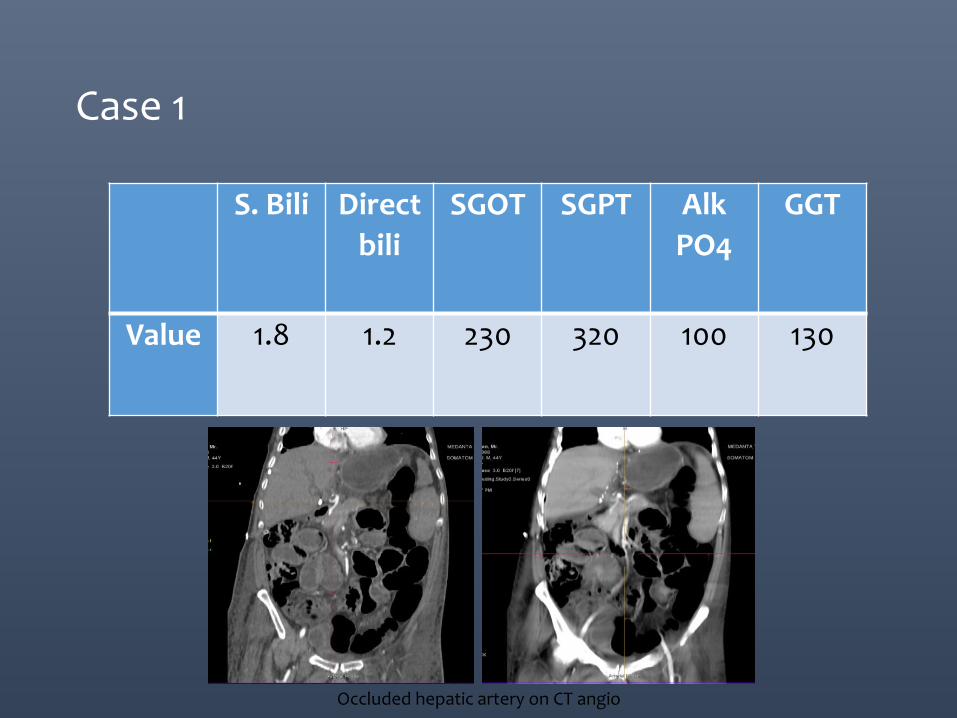
Case 1
Occluded hepatic artery on CT angio
S. Bili Direct
bili
SGOT SGPT Alk
PO4
GGT
Value 1.8 1.2 230 320 100 130
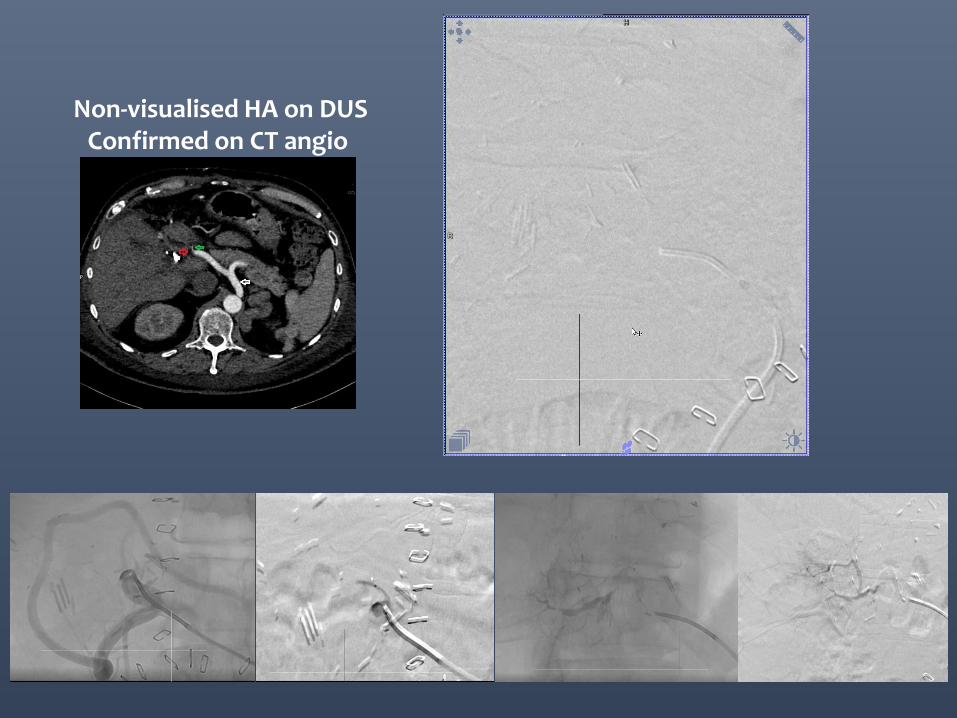
Non-visualised HA on DUS Confirmed on CT angio
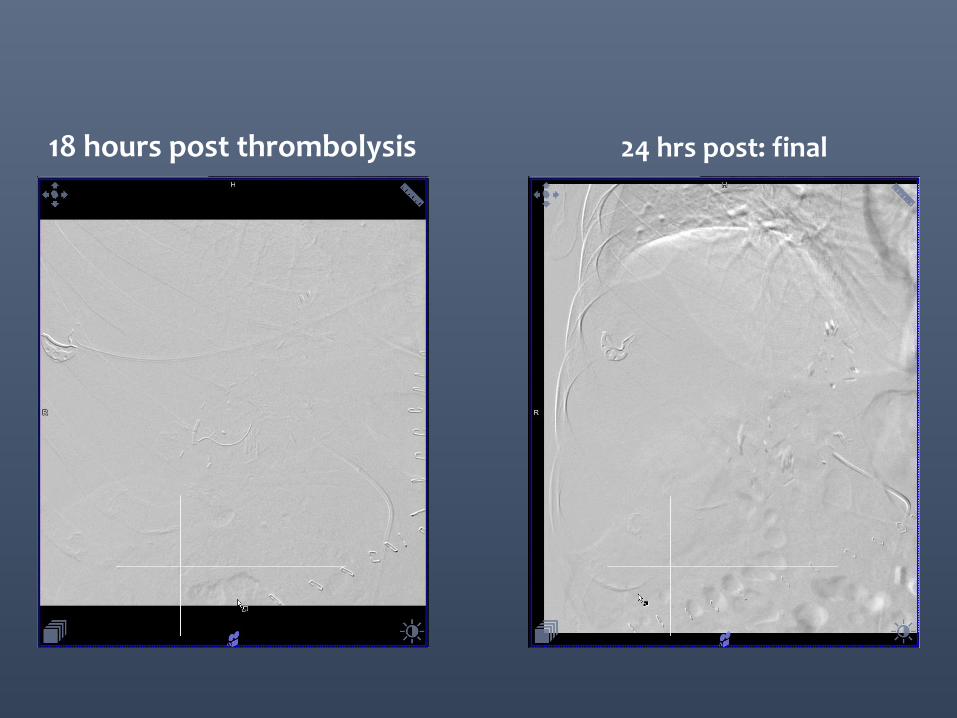
18 hours post thrombolysis 24 hrs post: final
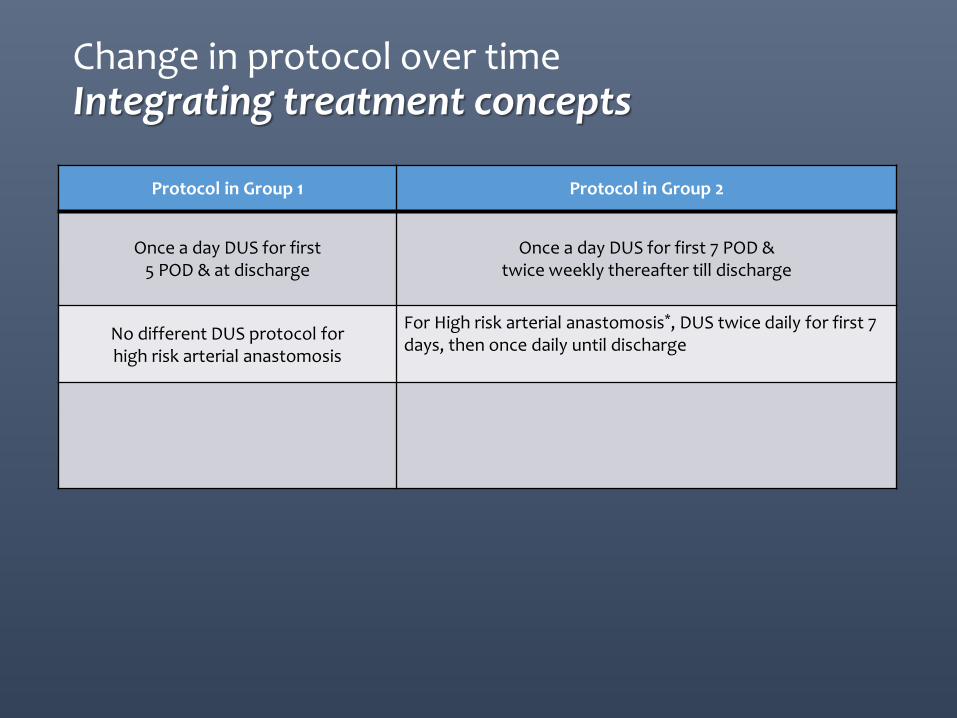
Change in protocol over time Integrating treatment concepts
Protocol in Group 1 Protocol in Group 2
Once a day DUS for first
5 POD & at discharge
Once a day DUS for first 7 POD & twice weekly thereafter till discharge
No different DUS protocol for high risk arterial anastomosis
For High risk arterial anastomosis*, DUS twice daily for first 7 days, then once daily until discharge
• CT angiogram to confirm HAT • Direct surgical re-vascularisation
once confirmed HAT on CT angiogram.
•If HAT < 7 POD –CT angiogram to confirm HAT and if confirmed followed by surgical re-vascularisation •If HAT > 7 POD – Direct Conventional Angiogram & treatment
*High Risk arterial anastomosis: Child <10kg, Size mismatch >2x, Multiple anastomosis, Arterial caliber < 1 mm, Micro-vascular reconstruction DUS: Doppler Ultrasound, POD: Post operative day. All LDLT patients were given Aspirin for 3 months. Additionally, LMWH x 30 days was given to all high risk arterial anastomosis cases from 455 case onwards. All the anastomosis were done under 3x magnification loupes. No modification in surgical technique for arterial anastomosis was changed over time
• 69 Cases in 16 reports
• Endovascular Therapy within 4h-120days
• Successful Thrombolysis : 68% (n=47 / 69)
• +/- PTA or Stent in 62% (n=29/47)
Transpl Int. 2010 Mar 1;23(3):245-56.
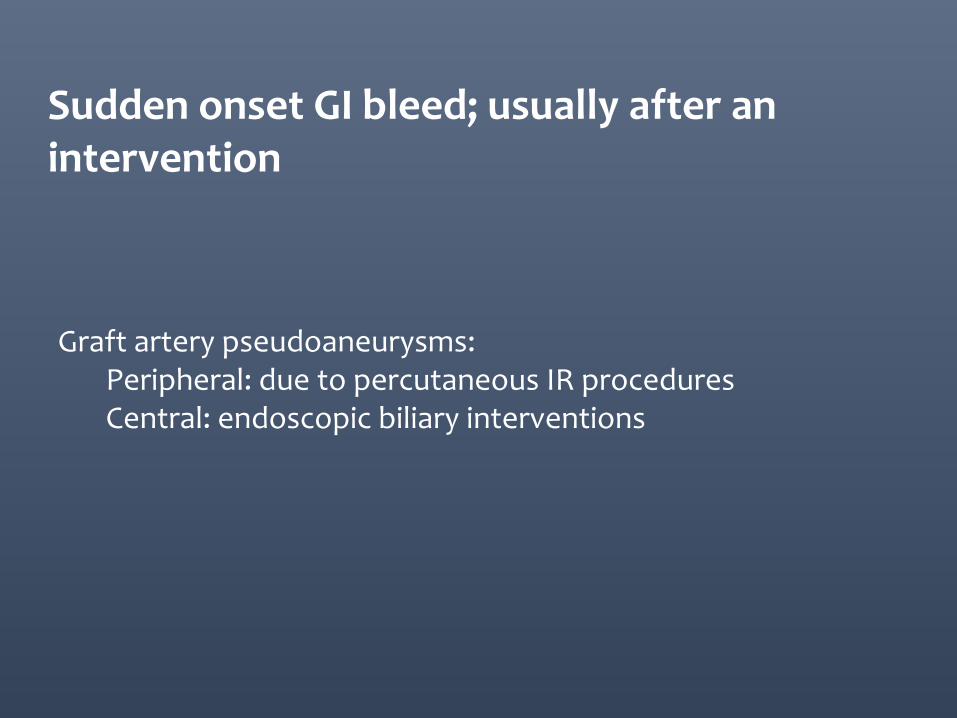
Graft artery pseudoaneurysms: Peripheral: due to percutaneous IR procedures Central: endoscopic biliary interventions
Sudden onset GI bleed; usually after an intervention
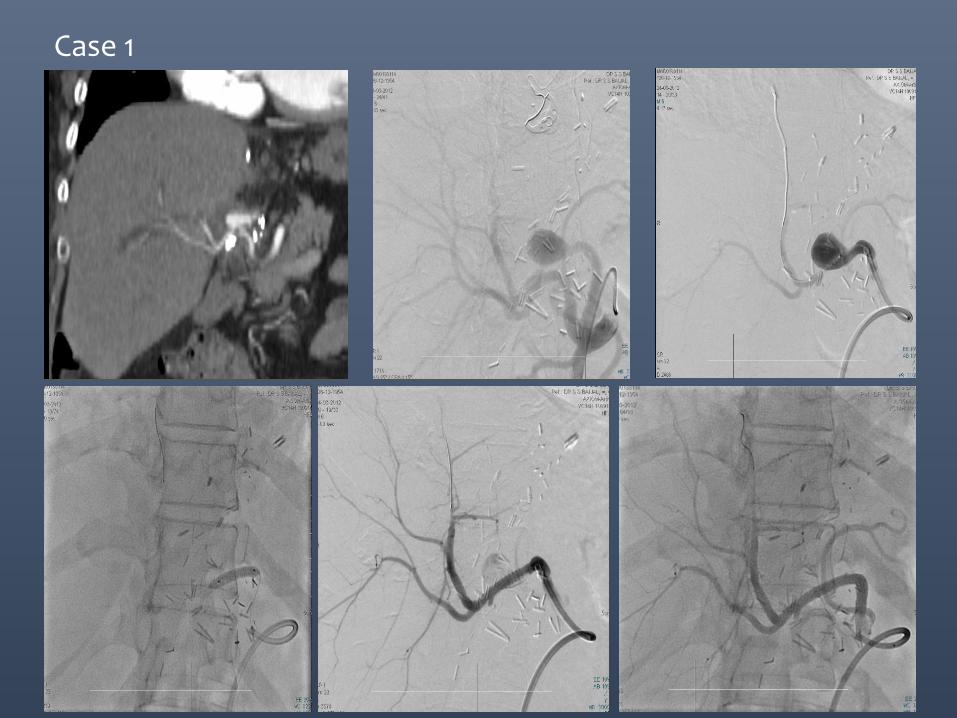
Case 1

S. Bili SGOT SGPT
Value 1.5 208 310
Post LDLT with increasing ascites
Case 1:
• Day 3 post LDLT patient presented with increase in surgical drain output
• Deranged liver enzymes
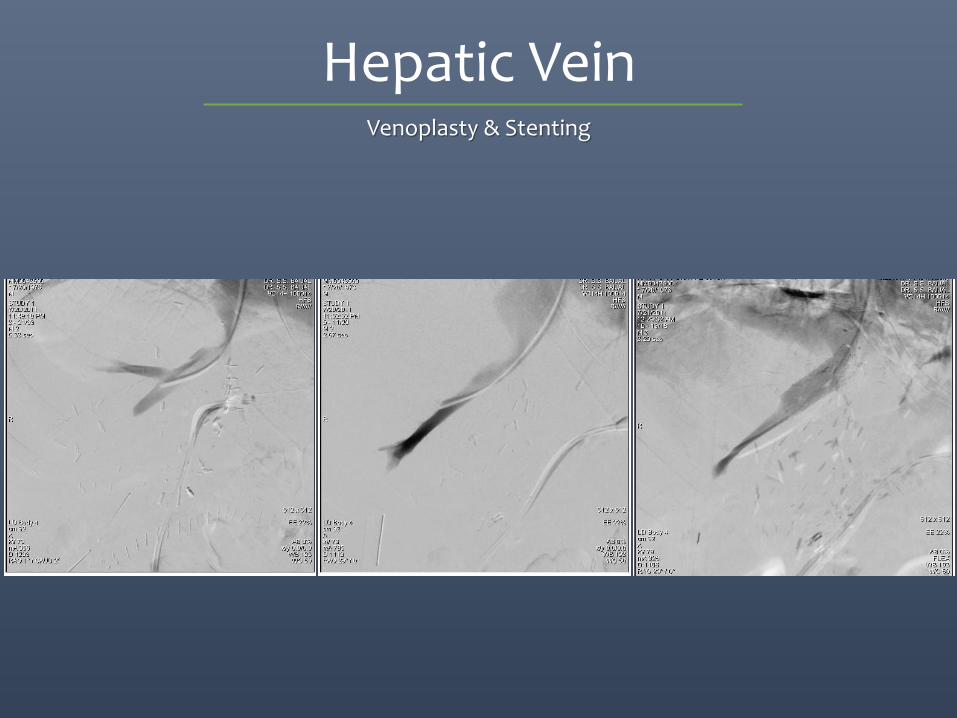
Hepatic Vein Venoplasty & Stenting
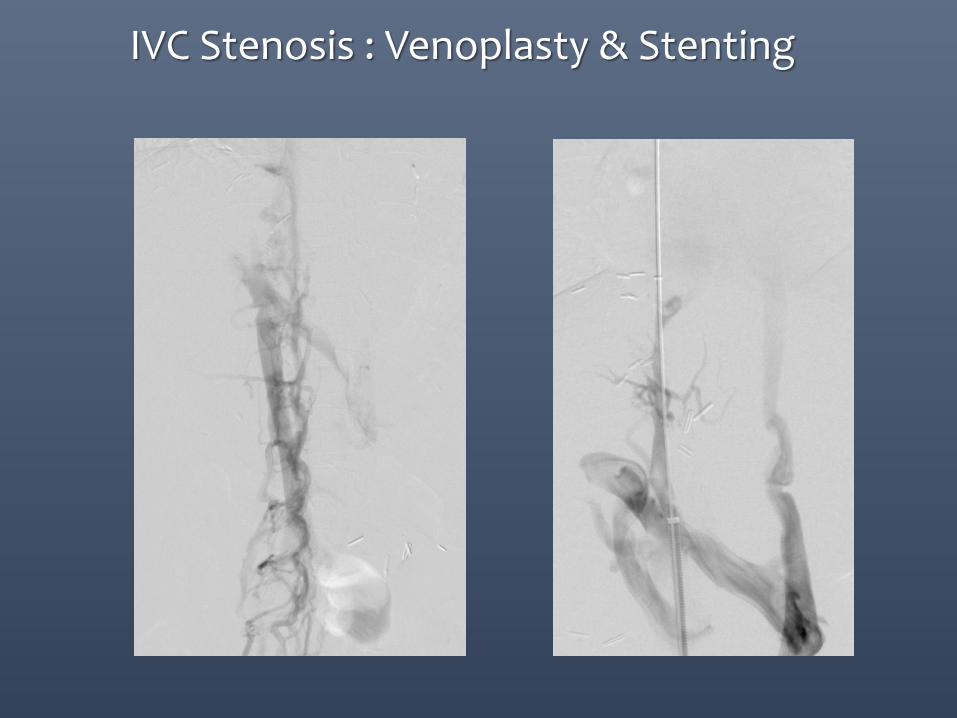
IVC Stenosis : Venoplasty & Stenting
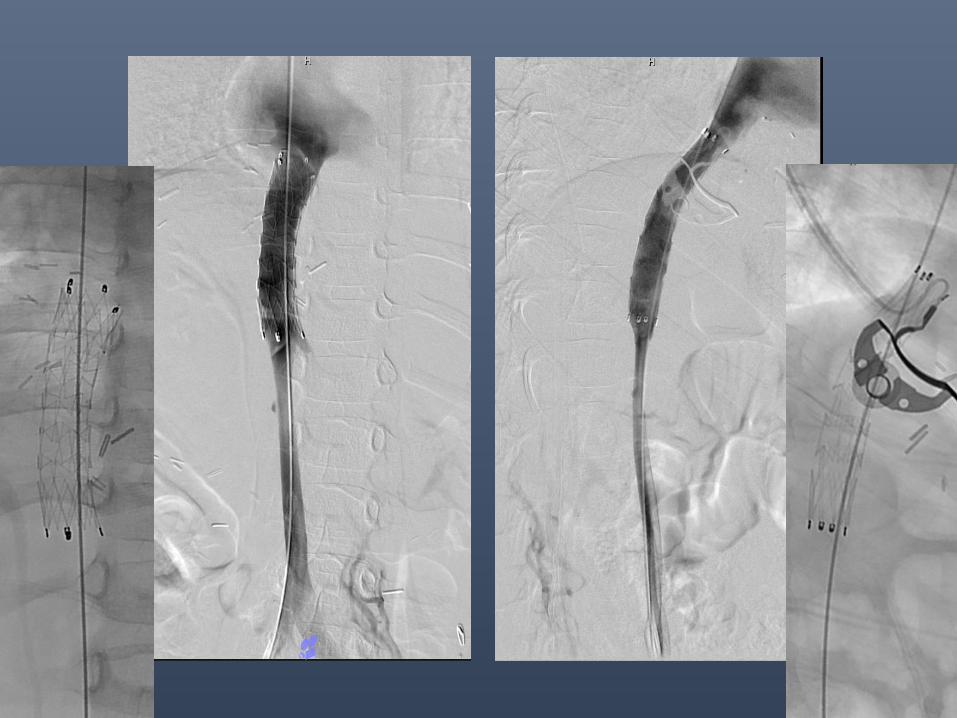
HV / IVC stenosis: Integrating treatment concepts
•Never surgical
•Angioplasty / Stenting
EARLY PV STENOSIS (within 6 months)
INCIDENCE
• ADULTS • DDLT : < 2%
• LDLT : 4%
• PEDIATRICS • LDLT: 6-36%
• OUR EXPERIENCE (2500 LDLTs) • PV stenosis : <2%
CLINICAL MANIFESTATIONS
• Ascitis : 42%
• GI Bleeding from varices : 33%
• Asymptomatic : 25%
• (with abnormal LFTs only)
• Other symptoms: Splenomegaly and Thrombocytopenia
Saad WE et al., Semin Intervent Radiol 2012;29:99–104 Karakayali H et al.,Transplant Proc. 2011 Mar;43(2):601-4.
Cheng YF et al.,Transplantation. 2014 Apr 27;97 Suppl 8:S32-4.
Yabuta M et al.,J Vasc Interv Radiol. 2014 Sep;25(9):1406-12. Saad WE, Semin Intervent Radiol 2012;29:99–104
EARLY PV STENOSIS: TREATMENT
• Angioplasty: • Technical/Clinical Success : 77.7% (35/45patients)
• Failures were due to thrombotic occlusions
• Follow up : 24.4months
• Restenosis : 28.5% (10/35)
• Repeat Angioplasty : 90% (9/10) success at 23.9months
• Stenting: • Technical /Clinical Success : 77.8% (7/9 patients)
• Follow up : 66.6+/- 16.1 months Ko GY et al.,Liver Transpl. 2007 Apr;13(4):530 -6.
Shibata T et al.,Radiology 235:1078-1083, 2005
LATE PV STENOSIS (> 6 months):
INCIDENCE
• 7/109 • 11.2 + 3.1 months post LDLT
• 6/75
• OUR EXPERIENCE (2500 LDLTs) • PV stenosis : <2%
CLINICAL MANIFESTATIONS
• SIMILAR to that seen in Early PVS
• Diagnosed at 11.2 + months after LDLT
• Ascitis , GI Bleeding from varices, Splenomegaly and Thrombocytopenia
Cho YP et al.,Pediatr Transplant. 2014 Feb;18(1):64-71.
Karakayali H et al.,Transplant Proc. 2011 Mar;43(2):601-4.
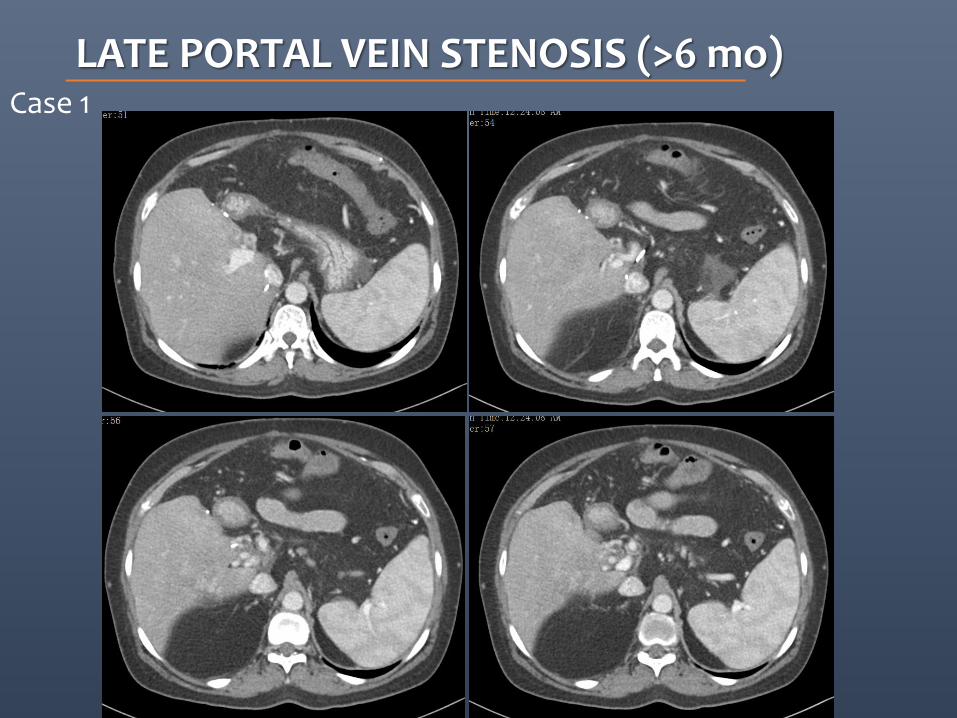
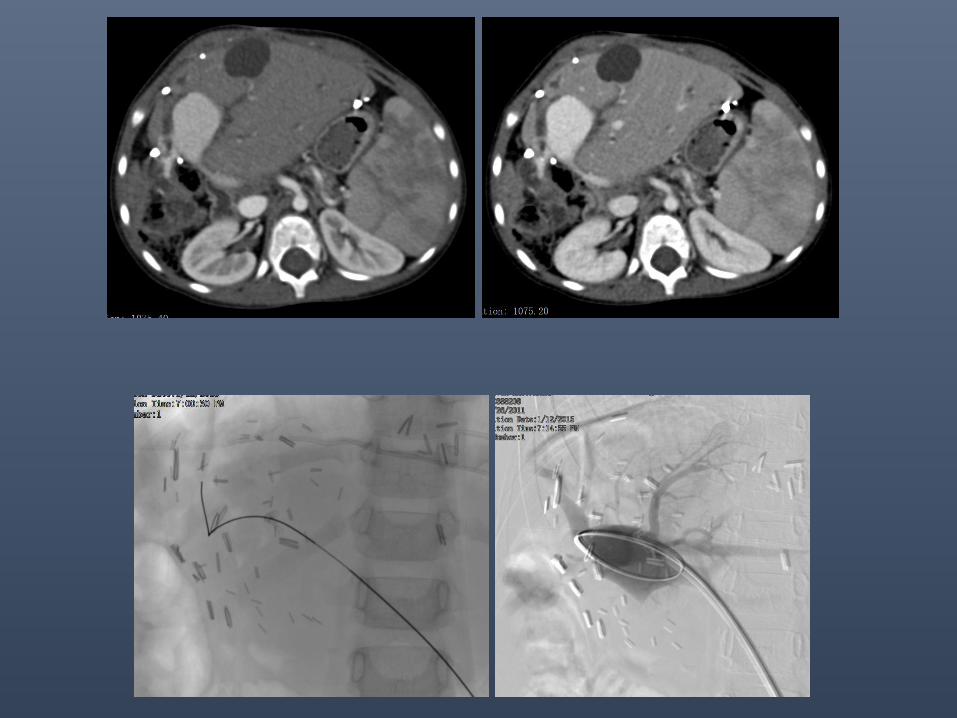
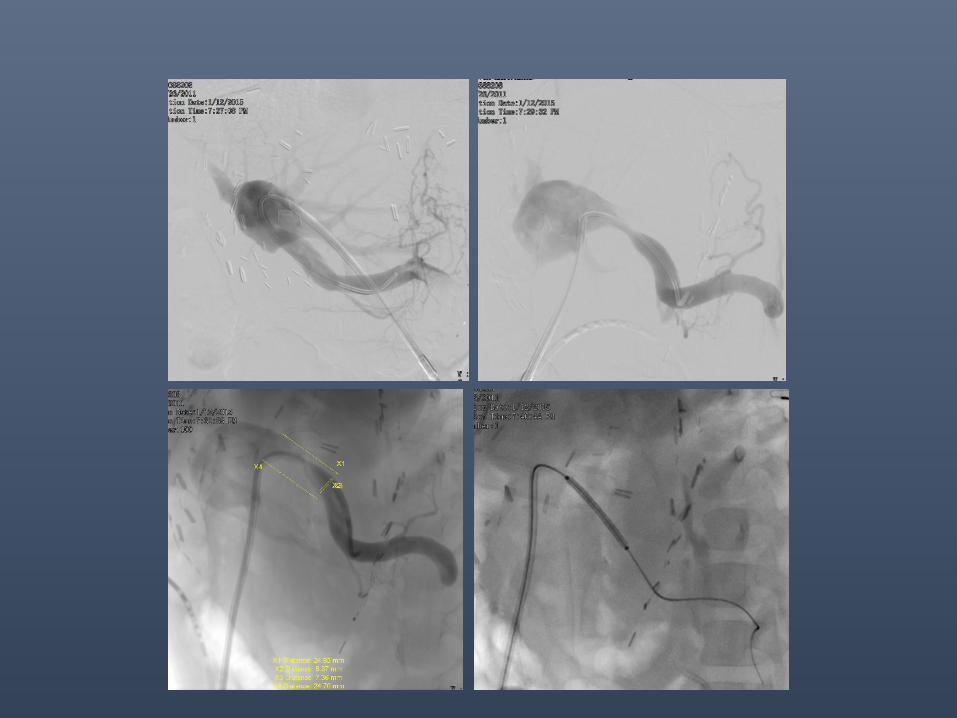
LATE PORTAL VEIN STENOSIS (>6 mo) Case 1
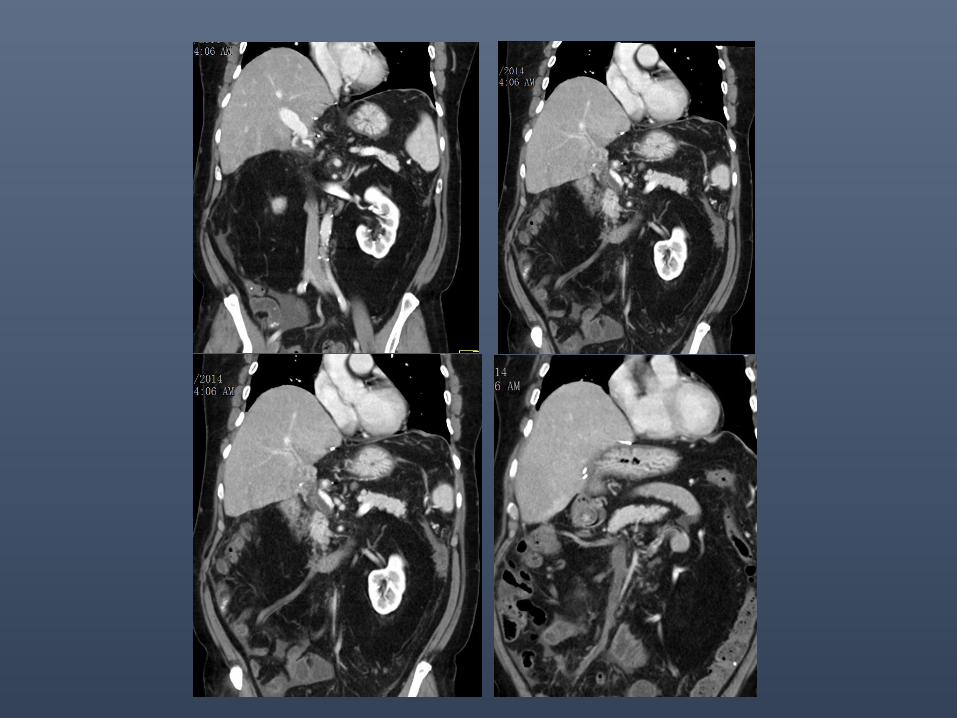
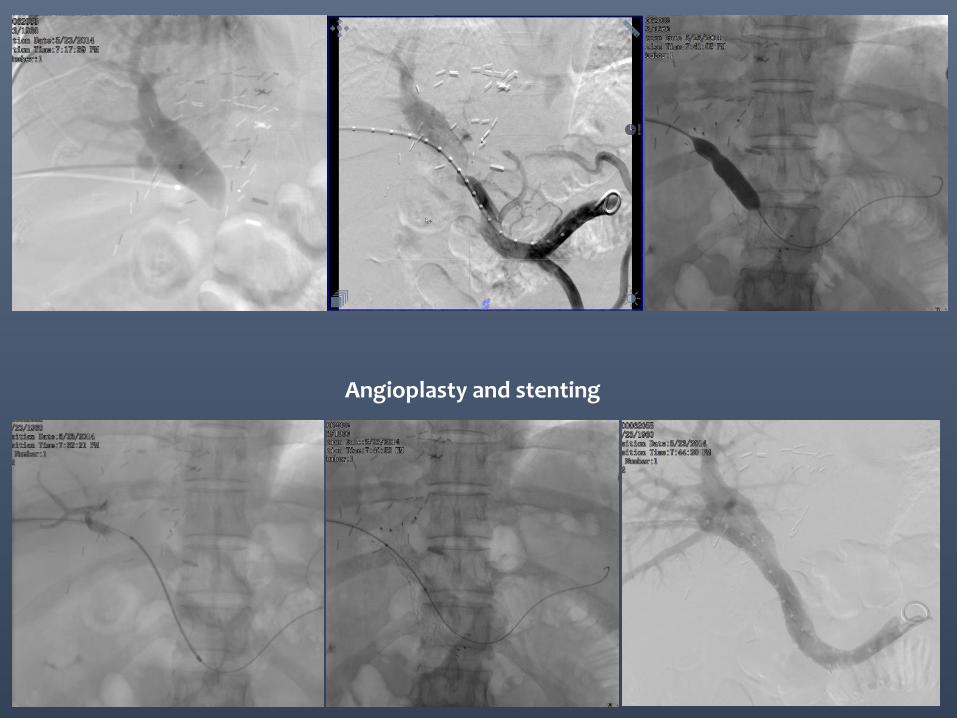
Angioplasty and stenting
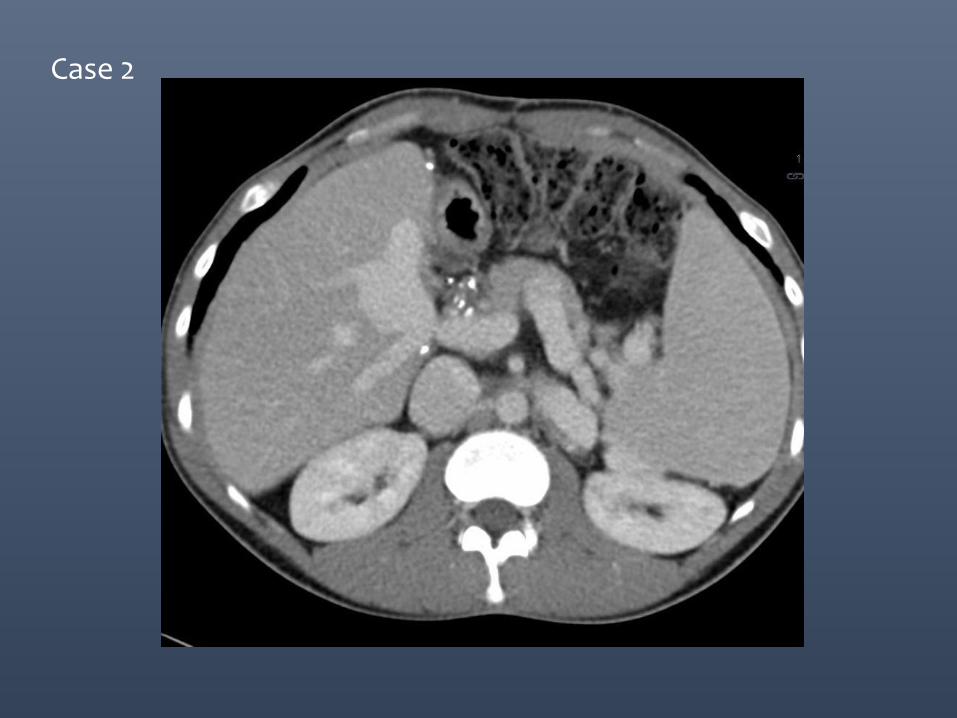
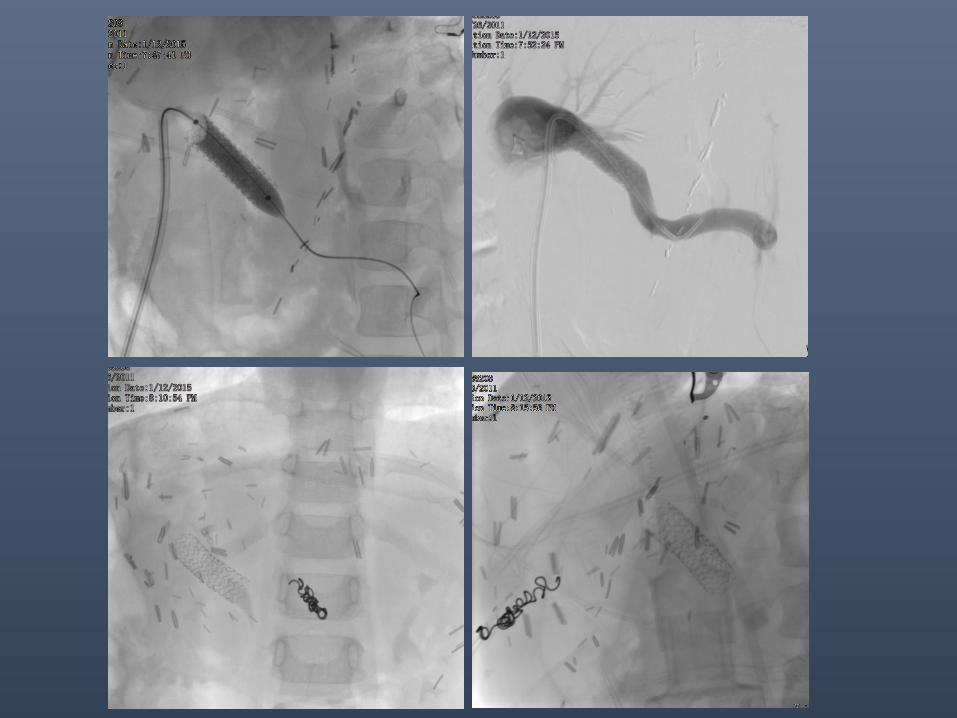
Case 2
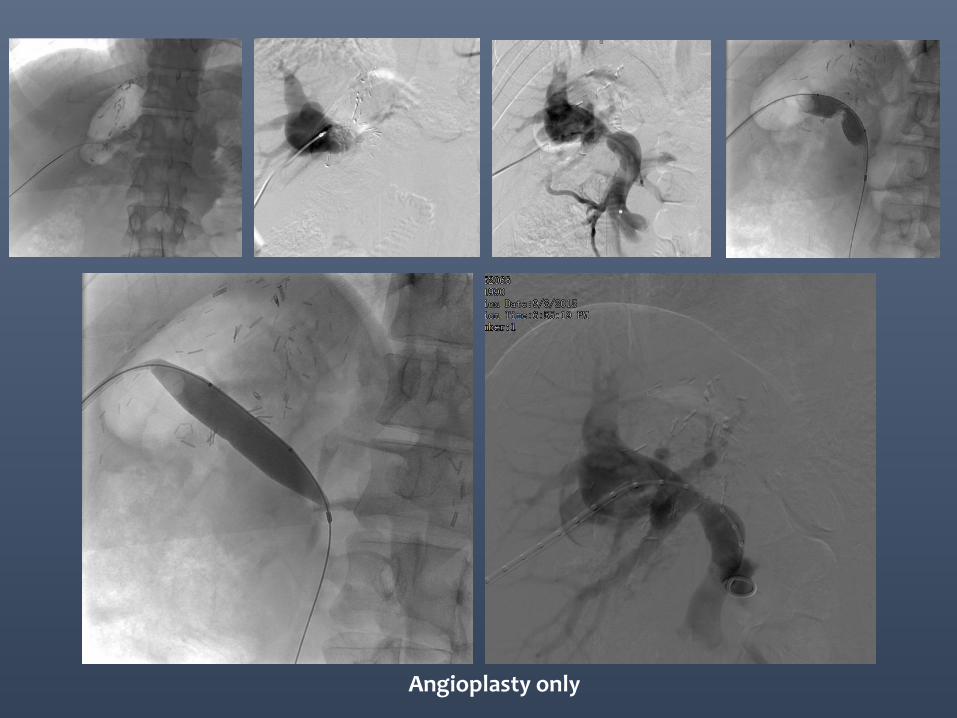
Angioplasty only
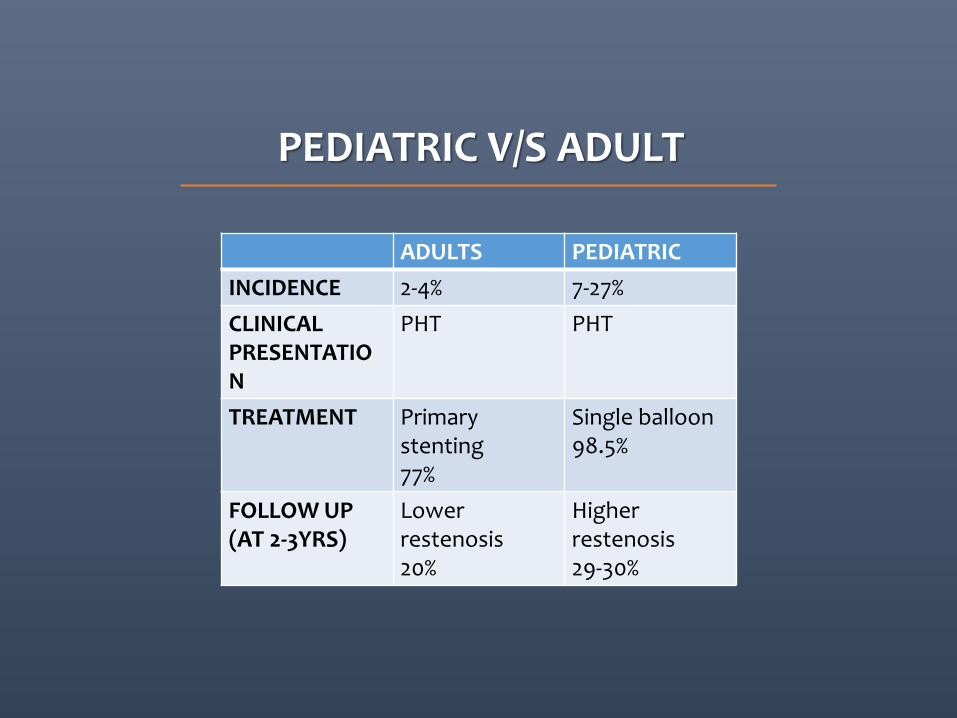
PEDIATRIC V/S ADULT
ADULTS PEDIATRIC
INCIDENCE 2-4% 7-27%
CLINICAL PRESENTATION
PHT PHT
TREATMENT Primary stenting 77%
Single balloon 98.5%
FOLLOW UP (AT 2-3YRS)
Lower restenosis 20%
Higher restenosis 29-30%
PV stenosis: Integrating treatment concepts
• Portal Vein Thrombosis : only identified cause for technical
failure of endovascular therapy for Portal Vein Stenosis.
• Re-exploration is the preferred 1st line of therapy within
30days & Angioplasty after 30days.
• Stent assisted patency rates and primary stent patency
rates are very promising in BOTH paediatric and adults.
Post LDLT patient with recurrence of HCC
• 57 yr old male, 18 months post LDLT presented with vague pain in right hypochondrium.
• USG - heterogenous lesion in liver
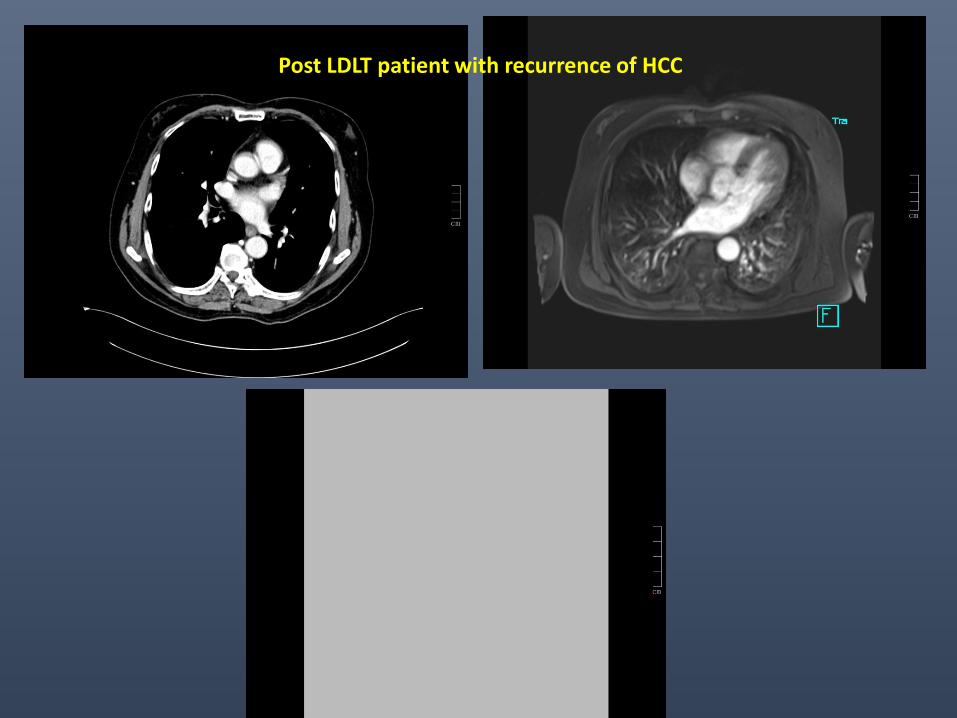
Post LDLT patient with recurrence of HCC
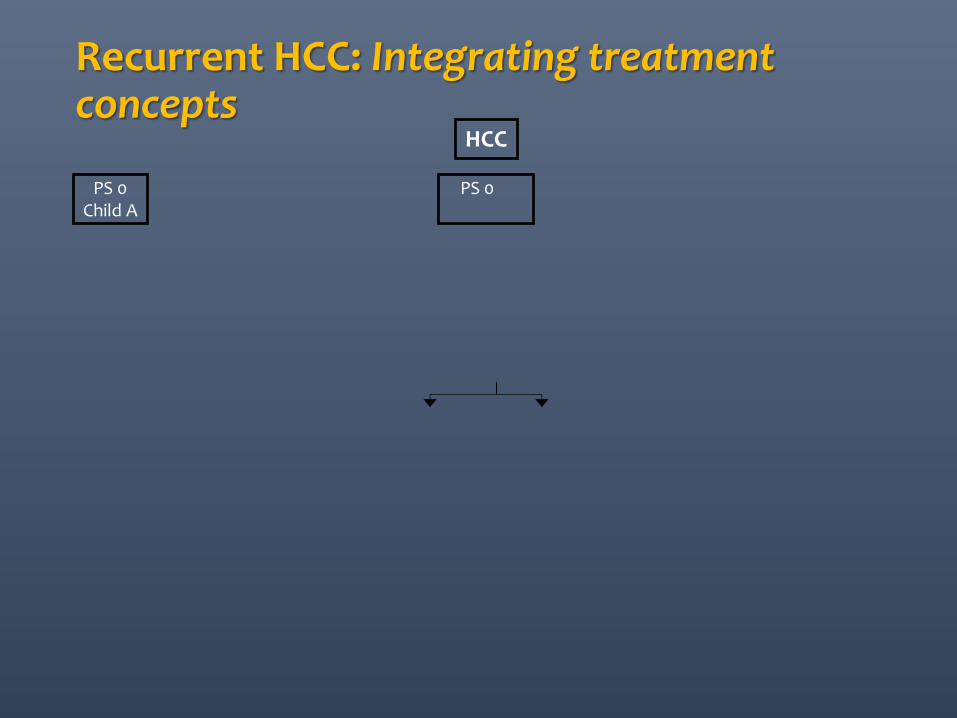
Recurrent HCC: Integrating treatment concepts
HCC
PS 0 Child A
PS 0–2 Child A–B
Resection TACE/SIRT
Stage 0 Very Early Stage
Stage A Early Stage
Stage B Intermediate Stage
Stage C Advanced Stage
Stage D End Stage
PS >2 Child C
single <2 cm or carcinoma in situ
single nodule or 3 nodules <3 cm
PS 0 multinodular; PS 0
portal vein invasion, N1 M1 or PS 1–2
PS >2 or Child C (unless within
transplant criteria)
portal pressure; bilirubin
normal
increased associated diseases
Liver Transplant Ablation
no yes
single 3 nodules <3 cm
survival <3 mo 20% of patients
Curative Treatments – 5-year survival 40–70% 30% of patients at presentation
RCTs – median survival 11–20 months 50% of patients at presentation
failed TACE
unilobar fewer nodules smaller burden
bilobar multinodular larger burden
fit/suitable for SIRT i.e.
liver-dominant; bilirubin
<35 U/l Child A or <B7
OR fit/suitable
for sorafenib
SIRT SIRT/ sorafenib
Sorafenib
Andreana L, Isgrò G, Marelli L et al. Treatment of hepatocellular carcinoma (HCC) by intra-arterial infusion of radio-emitter compounds: Trans-arterial radio-embolisation of HCC. Cancer Treat Rev 2011 Dec 12; ePub doi: 10.1016/j.ctrv.2011.11.004. Sangro B, Salem R, Kennedy A et al. Radioembolization for hepatocellular carcinoma: a review of the evidence and treatment recommendations. Am J Clin Oncol 2011; 34: 422–431.
SIRT
CLD, HCC, need / rate of Liver Transplantation in India
•Total no. of CLD, HCC deaths: 2 lacs/ year (WHO 2011)
•Need for LT 20/million (25000/yr in India)
•Current approx 1.1 per million (2014)
(1200, 1500, 1600 transplants in 2013, 2014, 2015)
Need / rate of deceased donation in India
•Need should come up to 20/million
(25000 donors/yr) • Current approx 0.33 per million (418
donors in 2014, 450 in 2015) •USA 24/million • Spain 35/million

Biopsies: Integrating treatment concepts
• Protocol biopsies....?
• Graft dysfunction; Acute & Chronic • Elevated enzymes >2 times
• MRI excluding biliary stricture
• Viral markers excluding Viral Hepatitis
• Color Doppler excluding vascular complications
• PERCUTANEOUS / PLUGGED / TRANSJUGULAR
Endovascular Therapy:
Complications
• Hemorrhage – 22% (15/69) • Fatal – 20% (3/15)
• Contributing risk factors • Increased dose/duration of
thrombolytic
• Adjunctive antithrombotic (Heparin, Aspirin, Anti Plat)
• Mechanical injury by catheter
• Severity of ischemia
No relationship between agent or technique and complications
Failure
• n=19/69; (mortality =2)
• Reasons: • Technical – inability to cross • Abandonment – due to
complication
• Surgical interventions in 7 with 50% mortality.
(10 – no follow up)
ENDOVASCULAR TREATMENT OF HEPATIC ARTERY THROMBOSIS FOLLOWING LIVER TRANSPLANTATION, Singhal et al: Transpl Int. 2010 Mar 1;23(3):245-56.
LATE PV STENOSIS: TREATMENT
• Angioplasty: • 6/7 patients
• Mean pressure gradient decreased 12.4mmHg 3.2mmHg
• Patency of PV maintained for 43.2+ 20.4months
• Clinical success : 4/6
• Technical / Clinical success: 19/25 (76%) / 7/19 (36.8%)
• Patency of PV maintained for 46months
• Angioplasty: • N=43 patients,
• 66 percutaneous interventions attempted.
• Technical success : 65/66 (98.4%) sessions in 42/43 (97.6%) patients
• Clinical success: 31/43 (72%)
• Second Angioplasty • Technical success 11/11 (100%)
• Clinical success : 4/11 (36.3%)
2/43 patients underwent 5 angioplasties
Karakayali H et al.,Transplant Proc. 2011 Mar;43(2):601-4.
Funaki B et al.,Radiology 215:147-151, 2000 Yabuta M et al.,J Vasc Interv Radiol. 2014 Sep;25(9):1406-12.
LATE PV STENOSIS: TREATMENT
• Stenting • Technical and Clinical Success: 2/2 (100%)
• Technical and Clinical Success: 12/12 (100%)
• Follow up period 5-61months
Cho YP et al.,Pediatr Transplant. 2014 Feb;18(1):64-71.
Yabuta M et al.,J Vasc Interv Radiol. 2014 Sep;25(9):1406-12.
Funaki B et al.,Radiology 215:147-151, 2000