interstitial microwave hyperthermia in a canine brain model
TRANSCRIPT

Inl. J. Radiarion Oncology Bid. Phys.. Vol. 12, pp. 1887-1897 0360-3016/86 $3.00 + .oO Printed in the U.S.A. All rights reserved. Copyright 0 1986 Pergamon Journals Ltd.
l 1985 ASTRO Resident Award Essay
INTERSTITIAL MICROWAVE HYPERTHERMIA IN A CANINE BRAIN MODEL
PENNY K. SNEED, M.D.,*,? KENGO MATSUMOTO, M.D.* PAUL R. STAUFFER, M.S.E.E.,I_ JOHN R. FIKE, PH.D.,*?? VERNON SMITH, M.S.? AND PHILIP H. GUTIN, M.D.*3j-
School of Medicine, University of California, San Francisco, CA 94 143
A dual frequency microwave system was constructed for interstitial heating of brain tissue. Single-junction dipole antennas were tested in a phantom model and in normal dog brain to determine how variations in physical factors affected temperature distributions. Non-survival studies were performed at both 915 and 2450 MHz to determine heating patterns that could be achieved within normal brain using this system. Chronic survival studies were performed using a single dipole antenna inserted laterally into one hemisphere of brain and driven at 2450 MHz. Temperatures of 43 or 44°C for 30 min at a reference point 0.5 cm from the antenna junction were used to induce a thermal lesion of approximately 1 cm diameter in the right cerebral hemisphere of dogs. Neurologic and physical changes in dogs were monitored daily for up to 16 weeks after induction of cerebral lesions. The extent and development of thermal lesions was monitored with weekly computed tomographic (a) examinations and, after death, at histopathologic examination. Results of the phantom studies showed that the longitudinal heating pattern was bell-shaped at both frequencies used and that there was some variation in heating length that depended on insertion depth. Acute studies in dog brain showed that 915 MHz antennas implanted less than 6.5 cm deep produced erratic heating patterns that usually included excessive heating of the surface of the brain. Conversely, 2 cm-long antennas driven at 2450 MHz gave reproducible temperature distributions both longitudinally along and radially away from the antenna. The steepest gradients-about l”C/mm-occurred in the radial direction away from the antenna junction. A single 30 min beat treatment produced a large focal lesion that consisted of central coagulation necrosis surrounded by a sharply demarcated hypervascular zone. Edematous changes were minimal and were observed only during the first week after treatment. As assessed by serial CT scans, thermal lesions reached a maximum size by the first week after treatment and were essentially resolved by 16 weeks after treatment.
Brain tumor, Interstitial treatment, Canine model, Hyperthermia, Radiation therapy, Microwave antenna.
INTRODUCI’ION the rapid fall-off of radiation away from the source tend to spare normal brain surrounding the lesion. Neverthe-
Malignant gliomas, which account for one quarter of adult primary cerebral neoplasms,*’ rarely metastasize outside the central nervous system;‘1J5 most recurrent lesions re- main localized to a single area of the brain.** Surgical resection alone cannot effectively control these tumors. Radiation is an effective adjuvant to surgery,42*43 but ra- diation-induced brain necrosis limits the dose that can be delivered by conventional teletherapy.34 In patients with recurrent malignant primary or metastatic brain tumors, interstitial irradiation (brachytherapy) with “‘1 sources has produced encouraging clinical results.2T38 The low dose rate at which this isotope emits characteristic X rays and
less, the problems of brain necrosis and peripheral tumor recurrence limit the effectiveness of brachytherapy.16 Therefore, it is desirable to develop techniques that can be used to reduce the total radiation dose to normal tissues without a concomitant reduction in tumor cell kill. Ad- juvant hyperthermia may be such a treatment.
Heat alone has a cytotoxic effect on cells;7,44 in com- bination protocols, heat can sensitize cells to the effects of radiation and some chemotherapeutic agents.‘~6-8*20~33 Hyperthermia appears to be particularly effective in com- bination with low-dose rate irradiation, and a number of Phase I trials in patients with advanced tumors have
* Brain Tumor Research Center of the Department of Neu- rological Surgery.
t Department of Radiation Oncology. Reprint requests to: Philip H. Gutin, M.D., c/o The Editorial
Office, Department of Neurological Surgery, 1360 Ninth Avenue, Suite 2 10, San Francisco, CA 94 122. Acknowledgements-This research was supported in part by NIH Program Project Grant CA-13525, NIH Training Grant CA-09215, ACS Grant PBT-233 (to Dr. Gutin), NIH New In-
1887
vestigator Research Award CA-30024 (to Dr. Gutin), and a grant from the Formax/UCSF Foundation (to Dr. Gutin). We are indebted to Charles B. Wilson, M.D., Theodore L. Phillips, M.D., and William C. Dewey, Ph.D., for their support and guidance. We thank Dr. Robert Higgins, University of California, Davis, for histopathologic analysis, Elena Markovich and Krzysztof Turowski, M.D., for technical assistance, and Neil Buckley for editing the manuscript.
Accepted for publication 26 May 1986.

I888 1. J. Radiation Oncology 0 Biology 0 Physics October 1986, Volume 12, Number 10
shown promising results. 6*23*25,4’ Although the efficacy of combined hyperthermia and brachytherapy has been shown both clinically and experimentally,33 there have been no reports on the use of the treatment for malignant brain tumors. Most of the information available on the effects of heat on brain has come from acute animal studies and anecdotal clinical cases that used heat alone.4*24*28,29*32 Before the efficacy of heat and radiation can be established either experimentally or clinically, it is important to de- termine the longer-term effects of heat on normal brain tissue.
The present study had several goals: First, to construct a microwave hyperthermia system that could be used for local heating of brain tissue; second, to determine the ef- fects caused by varying several physical variables on tissue heating patterns; third, to induce localized hyperthermic lesions and to determine the extent to which these lesions may affect the general health and neurologic condition of normal adult dogs, and fourth, to document the devel- opment and evolution of hyperthermic lesions using computed tomography and histopathology.
METHODS AND MATERIALS
Microwave system
tennas were constructed for this study from either 0.034 or 0.020 inch-diameter semi-rigid coaxial cable5 by sol- dering the inner conductor to the outer conductor at the end of the antenna and cutting away a circumferential 1 mm section of the outer conductor (“junction”) at a dis- tance “1;’ from the end of the antenna (Fig. 2). Although the antenna impedance was not experimentally trimmed to exactly 50 ohms in situ because the appropriate equip- ment was not available, antennas were easily tuned to the generator using double stub tuners. When implanted in a conducting medium, the portion of the antenna distal to the junction acts as the active electrode with the ra- diating electromagnetic field terminating on the proximal arm. The wavelength, X, depends on the frequency and the dielectric constant of the medium through which waves propagate; in our studies, the medium includes the nylon catheters, air, and brain tissue. The distal portion (1,) was usually set at 4 cm for 9 15 MHz and at 1 cm for 2450 MHz. These values represent approximately X/4 for an antenna within a nylon catheter implanted in brain tissue.28q“(’ The optimum insertion depth is roughly twice I,, or 8 cm at 9 15 MHz and 2 cm at 2450 MHz. Some of the 915 MHz antennas were shortened to 1, = 3.0, 2.5, 2.0, and 1.5 cm to allow lateral insertion of the antennas into dog brains, which are typically 4.0 to 4.5 cm in width.
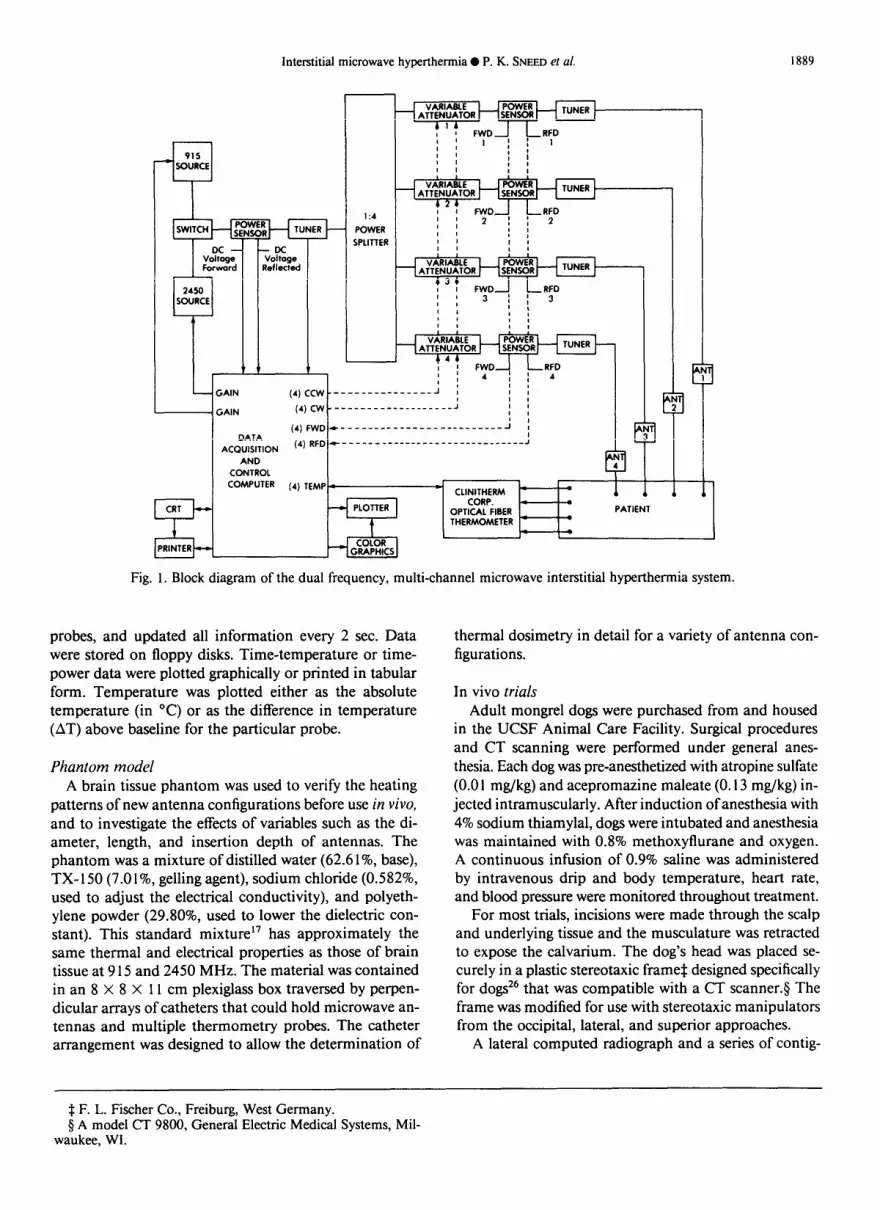
An interstitial microwave hyperthermia system was de- signed and constructed for local heating of brain tissue. This system (Fig. 1), including the power distribution and tuning elements, was patterned after those developed in- dependently at Dartmouth College36.37 and the University of Maryland. 28,3’,32 The system operates at two different frequencies, 915 MHz and 2450 MHz, that the Federal Communication Commission dedicated to industrial, scientific, and medical use. Power from either the 915 MHz or 2450 MHz generator was monitored, tuned, and split as needed into 2 or 4 equal signals. Power fed to each antenna was tuned using double stub tuners* for a proper impedance match to the generator. Dual direc- tional couplerst with IN-2 1 point contact diodes pro- duced calibrated voltage levels that were fed to the com- puter and used for continuous monitoring of the forward and reflected power for the system as well as for each antenna. These data were displayed on a color monitor and recorded by the computer. Variable attenuator@ were used to adjust power for up to four individual 9 15 or 2450 MHz antennas.
Thermometry Two optical fiber thermometry systems were used, a 4
channel* and a 12-channel system.? The latter included a multi-sensor probe with four sensors spaced 5 mm apart. Single sensor probes fit inside 20-gauge catheters and the multisensor probe fit inside a 16-gauge catheter. Because the thermometry probes did not have metal wire leads, they were free from the electrical interference and field perturbation effects seen with thermistors and thermo- couples. In addition, the small thermal mass of the sensors and low thermal conductivity of the optical fibers mini- mized the thermal perturbation caused by the probes. Both systems have the necessary hardware and software for simple daily self-calibration within 5-10 min. When cal- ibrated every 4 hr of use, the instruments are accurate to +0.25”C.
Antennas Tissue was heated by a microwave field radiating from
one or more dipole antennas placed in 16-gauge catheters. The dipole antenna design has been described.28*40 An-
The data acquisition system assembled for these studies included a personal computer with 256 kilobytes of ran- dom access memory, two 8-inch floppy disk drives, a ter- minal and keyboard, a 13-inch color monitor, an 8-pen color plotter, a printer, and a 32-channel analog-to-digital converter. During a heating trial, the color monitor dis- played temperature readings, and forward and reflected power levels for all channels. It also displayed a graph of temperature versus elapsed time for up to 16 temperature
* No. 1729, Maury Microwave, Cucamonga, CA. t CH33F, Microlab/FXR, Livingston, NJ. $ Model AR3998, ARRA Inc., Bay Shore, NY. 9 UT-34M and UT-20M, Uniform Tubes, Inc., Collegeville,
PA.
* Model 2OOOB, Luxtron Corporation, Mountain View, CA. t Model TS- 1200, Clini-Therm Corporation, Dallas, TX.
Interstitial microwave hyperthermia 0 P. K. SNEED et al. 1889
(21 I:4 1 FWD RFD
POWER 1; 2 I;2 : I I
iPUTTER I I I I I I , 0 1 I
VARIARLE POWER ATTENUATOR SENSOR
(34 I I FWD RFD ” 3 I; 3 I , 0 / 0 L
, I
I I
VARIARLE ATTENUATOR TUNER
(44 I 1 FWD RFD ” 4 I; 4 f ! I I
GAIN I I I I 0
GAIN ___-_____--.-------J I ,
0 I
4 CONTROL
COMPUTER (4) TEMP. -CLlNlrnrRM
. 1
CORP. I . OPTICAL FIBER PATIENT
t THERMOMETER -
.
I .
PRINTER
Fig. 1. Block diagram of the dual frequency, multi-channel microwave interstitial hyperthermia system.
probes, and updated all information every 2 sec. Data were stored on floppy disks. Time-temperature or time- power data were plotted graphically or printed in tabular form. Temperature was plotted either as the absolute temperature (in “C) or as the difference in temperature (AT) above baseline for the particular probe.
Phantom model A brain tissue phantom was used to verify the heating
patterns of new antenna configurations before use in Go, and to investigate the effects of variables such as the di- ameter, length, and insertion depth of antennas. The phantom was a mixture of distilled water (62.6 I%, base), TX- 150 (7.0 l%, gelling agent), sodium chloride (0.582%, used to adjust the electrical conductivity), and polyeth- ylene powder (29.80%, used to lower the dielectric con- stant). This standard mixture17 has approximately the same thermal and electrical properties as those of brain tissue at 9 15 and 2450 MHz. The material was contained in an 8 X 8 X 11 cm plexiglass box traversed by perpen- dicular arrays of catheters that could hold microwave an- tennas and multiple thermometry probes. The catheter arrangement was designed to allow the determination of
thermal dosimetry in detail for a variety of antenna con- figurations.
In vivo trials Adult mongrel dogs were purchased from and housed
in the UCSF Animal Care Facility. Surgical procedures and CT scanning were performed under general anes- thesia. Each dog was pre-anesthetized with atropine sulfate (0.0 1 mg/kg) and acepromazine maleate (0.13 mg/kg) in- jected intramuscularly. After induction of anesthesia with 4% sodium thiamylal, dogs were intubated and anesthesia was maintained with 0.8% methoxyflurane and oxygen. A continuous infusion of 0.9% saline was administered by intravenous drip and body temperature, heart rate, and blood pressure were monitored throughout treatment.
For most trials, incisions were made through the scalp and underlying tissue and the musculature was retracted to expose the calvarium. The dog’s head was placed se- curely in a plastic stereotaxic frame* designed specifically for dogs26 that was compatible with a CT scanner.5 The frame was modified for use with stereotaxic manipulators from the occipital, lateral, and superior approaches.
A lateral computed radiograph and a series of contig-
$ F. L. Fischer Co., Freiburg, West Germany. 9 A model CT 9800, General Electric Medical Systems, Mil-
waukee, WI.
1890 1. J. Radiation Oncology 0 Biology 0 Physics October 1986, Volume 12, Number 10
Fig. 2. Diagram of an interstitial microwave coaxial dipole an- tenna. The distance from the tissue surface to the junction is “I,” and the distance from the junction to the end of the antenna is “1,“. Typical antenna diameter is 0.020 inches.
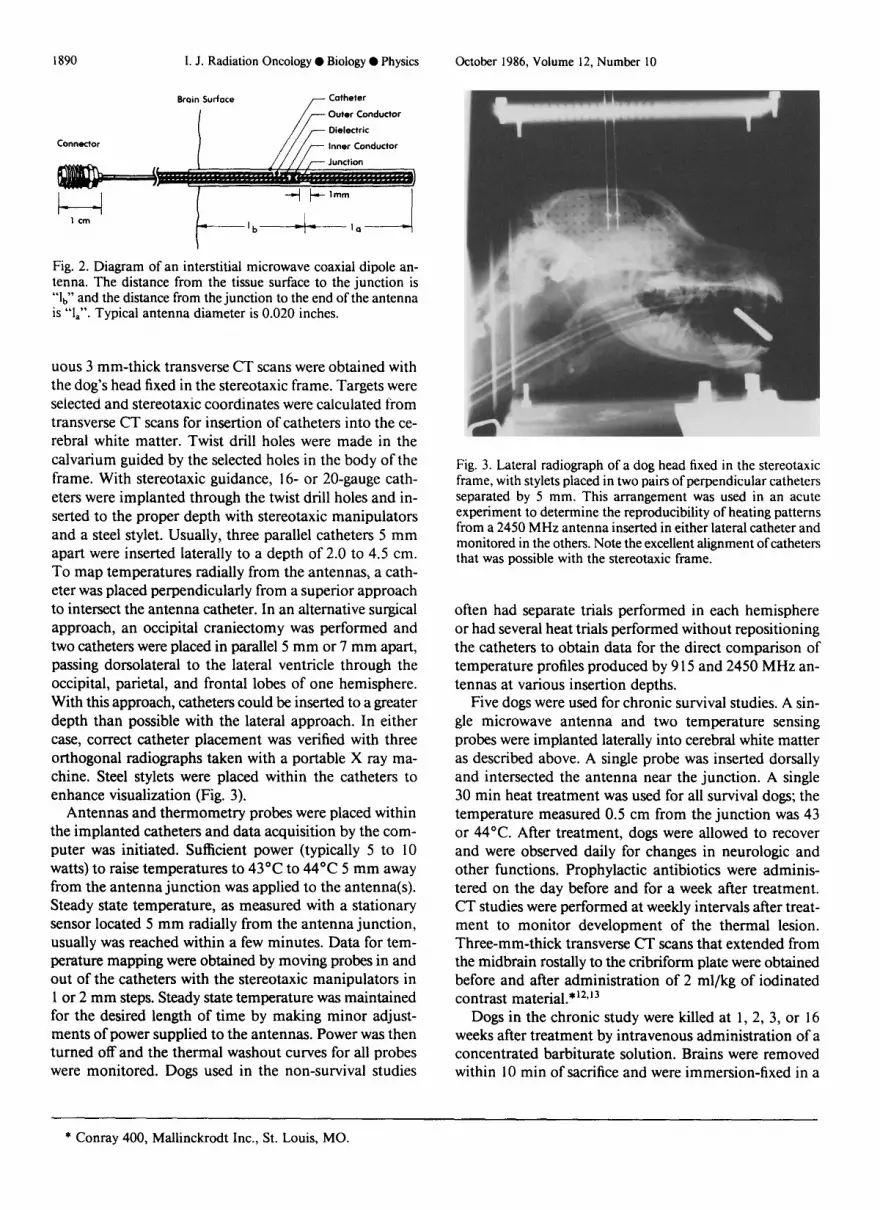
uous 3 mm-thick transverse CT scans were obtained with the dog’s head fixed in the stereotaxic frame. Targets were selected and stereotaxic coordinates were calculated from transverse CT scans for insertion of catheters into the ce- rebral white matter. Twist drill holes were made in the calvarium guided by the selected holes in the body of the frame. With stereotaxic guidance, 16- or 20-gauge cath- eters were implanted through the twist drill holes and in- serted to the proper depth with stereotaxic manipulators and a steel stylet. Usually, three parallel catheters 5 mm apart were inserted laterally to a depth of 2.0 to 4.5 cm. To map temperatures radially from the antennas, a cath- eter was placed perpendicularly from a superior approach to intersect the antenna catheter. In an alternative surgical approach, an occipital craniectomy was performed and two catheters were placed in parallel 5 mm or 7 mm apart, passing dorsolateral to the lateral ventricle through the occipital, parietal, and frontal lobes of one hemisphere. With this approach, catheters could be inserted to a greater depth than possible with the lateral approach. In either case, correct catheter placement was verified with three orthogonal radiographs taken with a portable X ray ma- chine. Steel stylets were placed within the catheters to enhance visualization (Fig. 3).
Antennas and thermometry probes were placed within the implanted catheters and data acquisition by the com- puter was initiated. Sufficient power (typically 5 to 10 watts) to raise temperatures to 43°C to 44°C 5 mm away from the antenna junction was applied to the antenna(s). Steady state temperature, as measured with a stationary sensor located 5 mm radially from the antenna junction, usually was reached within a few minutes. Data for tem- perature mapping were obtained by moving probes in and out of the catheters with the stereotaxic manipulators in 1 or 2 mm steps. Steady state temperature was maintained for the desired length of time by making minor adjust- ments of power supplied to the antennas. Power was then turned off and the thermal washout curves for all probes were monitored. Dogs used in the non-survival studies
Fig. 3. Lateral radiograph of a dog head fixed in the stereotaxic frame, with stylets placed in two pairs of perpendicular catheters separated by 5 mm. This arrangement was used in an acute experiment to determine the reproducibility of heating patterns from a 2450 MHz antenna inserted in either lateral catheter and monitored in the others. Note the excellent alignment of catheters that was possible with the stereotaxic frame.
often had separate trials performed in each hemisphere or had several heat trials performed without repositioning the catheters to obtain data for the direct comparison of temperature profiles produced by 9 15 and 2450 MHz an- tennas at various insertion depths.
Five dogs were used for chronic survival studies. A sin- gle microwave antenna and two temperature sensing probes were implanted laterally into cerebral white matter as described above. A single probe was inserted dorsally and intersected the antenna near the junction. A single 30 min heat treatment was used for all survival dogs; the temperature measured 0.5 cm from the junction was 43 or 44°C. After treatment, dogs were allowed to recover and were observed daily for changes in neurologic and other functions. Prophylactic antibiotics were adminis- tered on the day before and for a week after treatment. CT studies were performed at weekly intervals after treat- ment to monitor development of the thermal lesion. Three-mm-thick transverse CT scans that extended from the midbrain rostally to the cribriform plate were obtained before and after administration of 2 ml/kg of iodinated contrast material.*12.‘3
Dogs in the chronic study were killed at 1, 2, 3, or 16 weeks after treatment by intravenous administration of a concentrated barbiturate solution. Brains were removed within 10 min of sacrifice and were immersion-fixed in a
* Conray 400, Mahinckrodt Inc., St. Louis, MO.

Interstitial microwave hyperthermia 0 P. K. SNEED ef al. 1891
10% buffered formalin solution for at least 1 week. Gross sectioning was done in the transverse plane; representative tissue samples were prepared for microscopic examination using standard histologic techniques. Eight micron-thick slices were placed on glass slides and stained with he- matoxylin and eosin. Histologic changes were evaluated qualitatively and compared with corresponding regions from the CT scans.
RESULTS
Phantom heating trials were performed with a variety of 915 MHz and 2450 MHz dipole antennas. For tem- perature increases of approximately 5°C and heating times up to 30 set, the effect of thermal conduction was mini- rnak5 and AT, the increase in temperature above the initial value, was proportional to power deposition, or specific absorption rate. AT was directly proportional to power applied to the antenna, and fell off radially from the an- tenna as shown in Figure 4. At a given distance from a single antenna, the longitudinal heating pattern along the antenna was roughly bell-shaped, with some variation in the effectively heated length that depended on the insertion depth 1, + lb (Fig. 5). Maximum temperatures were usually recorded near the plane of the junction. The power de- position pattern was found to be most uniform and re- producible by making both 1, and lb approximately 4 cm at 9 15 MHz and 1 cm at 2450 MHz (ca. X/4).
Fifty-nine non-survival brain hyperthermia trials were performed in 20 dogs to define heating patterns of various antennas and to develop a method for generating repro- ducible heat lesions that could be confined to one hemi- sphere. 915 MHz antennas could not be inserted to the ideal depth of 8 cm, even using the more difficult occipital approach. When either 1, or lb was shortened to obtain an insertion depth of less than 6.5 cm, the 915 MHz an-
Radial Distance From Antenna (cm)
Fig. 4. Plot of AT vs. radial distance from antenna produced in the phantom model using a 2450 MHz antenna with 1, = 1.0 cm and lb = 1.0 cm. Closed and open circles indicate paths perpendicular to the antenna at the junction and 0.5 cm proximal to the junction, respectively.
0 I .o 2.0 3.0 4.0 5.0
Depth in Phantom (cm)
Fig. 5. Plot of AT vs. depth of temperature probe produced in the phantom model measured parallel to and 0.5 cm away from a 2450 MHz antenna with 1, = 1.0 cm and lb = 1.0, 2.0, 3.0, and 4.0 cm.
tennas performed poorly; the heating patterns varied widely from dog to dog. Although the shortened antennas were impedance-matched to the signal generator, there was considerable self-heating of the antennas and de- creased deposition of energy radially away from the an- tennas because of the tissue/antenna impedance mis- match. The resulting antenna radiation field caused erratic heating patterns characterized by broad peaks or dips in the temperature profile that could not be controlled or predicted. Thus, the shorter, well-matched 2450 MHz an- tennas with 1, = lb = 1 .O cm were chosen for heating trials in dog brain. Using these antennas, the longitudinal and radial temperature profiles obtained in vivo corresponded to those generated in the phantom model (Figs. 5 and 8).
Surface heating occurred on several occasions when a craniectomy was performed and pooled blood or a blood- soaked surgical sponge was left adjacent to the brain at the antenna entrance site during heating. In most in- stances, however, surface heating was the result of non- optimal antenna configuration and/or the incorrect in- sertion depth. Figure 6 shows results obtained in two trials performed with the same 9 15 MHz antenna with 1, = 2.0 cm; surface heating did not occur with lb = 3.3 cm but was marked with lb = 1.8 cm. This problem occurred predominately when 915 MHz antennas were used, al- though occasional surface heating was observed with some 2450 MHz antenna configurations.
In some instances, unpredictable temperature fluctu- ations at depth occurred at both frequencies. At times, it was difficult to distinguish between variations caused by tissue heterogeneity or antenna mismatch. Usually, how- ever, temperature profiles that differed from those pre- dicted by the phantom model could be correlated with morphologic tissue boundaries found during gross ex- amination of the appropriate brain slice. For example, the drop in temperature at 41.8”C at a depth of 2.6 to 2.8 cm (Fig. 6) failed to shift when the antenna insertion
I892 1. J. Radiation Oncology 0 Biology 0 Physics October 1986, Volume 12, Number 10
38 j 0 1.0 2.0 3.0 4.0 5.0
Distance From Brain Surface (cm)
Fig. 6. Longitudinal temperature distribution at r = 5 mm in canine brain using a single occipital approach 9 I5 MHz antenna with 1, = 2.0 cm and lb = 3.3 cm (closed circles) or lb = 1.8 cm (open circles). Note the excessive surface heating when lb is less than 1,. Also note that the area of low temperatures from 2.6 to 2.8 cm did not shift when the insertion depth was changed. This corresponded to the passage of the antenna through a brain sul- cus.
depth was changed and corresponded to passage of the antenna through a sulcus. Figure 7 shows the temperature profile for a 2450 MHz antenna with 1, = 1 cm and lb = 3.0 cm that traverses both hemispheres; the profile pre- dicted in the phantom model is shown in Figure 5. The nadir at 2.2 to 2.4 cm corresponded to passage of the antenna through the longitudinal fissure.
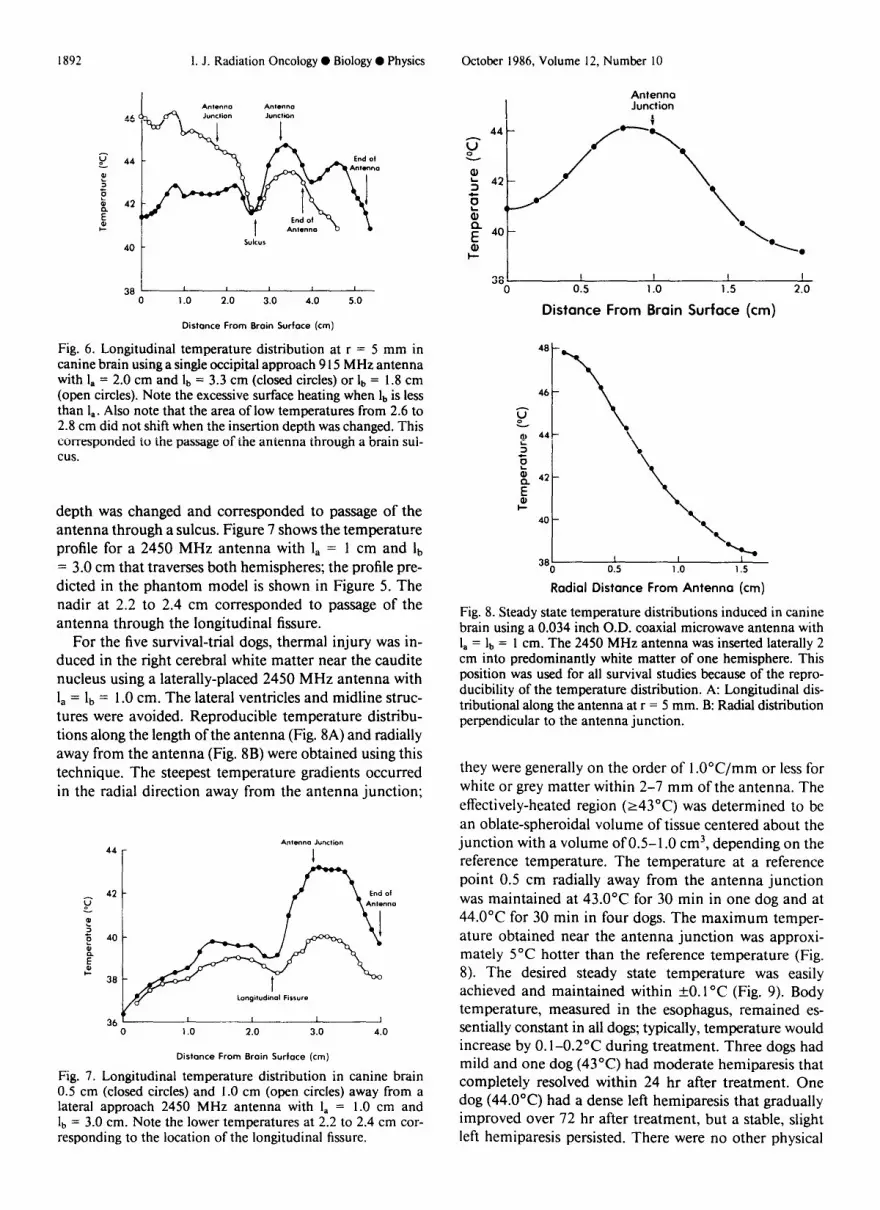
For the five survival-trial dogs, thermal injury was in- duced in the right cerebral white matter near the caudite nucleus using a laterally-placed 2450 MHz antenna with 1, = lb = 1 .O cm. The lateral ventricles and midline struc- tures were avoided. Reproducible temperature distribu- tions along the length of the antenna (Fig. 8A) and radially away from the antenna (Fig. 8B) were obtained using this technique. The steepest temperature gradients occurred in the radial direction away from the antenna junction;
44
36, 0 1 .o 2.0 3.0 4.0
Distance From Brain Surface (cm)
Fig. 7. Longitudinal temperature distribution in canine brain 0.5 cm (closed circles) and 1.0 cm (open circles) away from a lateral approach 2450 MHz antenna with I, = 1.0 cm and lb = 3.0 cm. Note the lower temperatures at 2.2 to 2.4 cm cor- responding to the location of the longitudinal fissure.
Antenna Junction
381 I I I I 0 0.5 1 .o 1.5 2.0
Distance From Brain Surface (cm)
Radial Distance From Antenna (cm)
Fig. 8. Steady state temperature distributions induced in canine brain using a 0.034 inch O.D. coaxial microwave antenna with 1, = lb = 1 cm. The 2450 MHz antenna was inserted laterally 2 cm into predominantly white matter of one hemisphere. This position was used for all survival studies because of the repro- ducibility of the temperature distribution. A: Longitudinal dis- tributional along the antenna at r = 5 mm. B: Radial distribution perpendicular to the antenna junction.
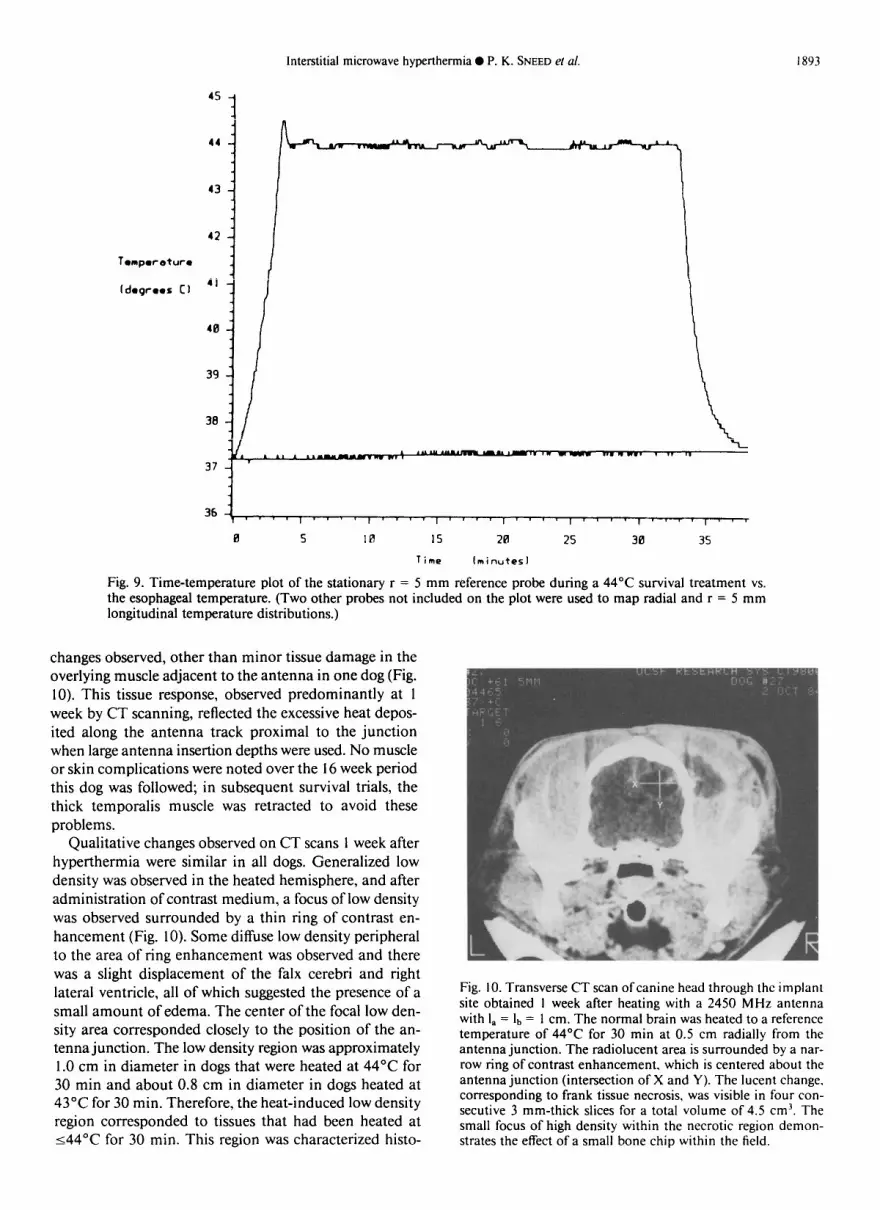
they were generally on the order of 1 .O”C/mm or less for white or grey matter within 2-7 mm of the antenna. The effectively-heated region (243°C) was determined to be an oblate-spheroidal volume of tissue centered about the junction with a volume of 0.5-l .O cm3, depending on the reference temperature. The temperature at a reference point 0.5 cm radially away from the antenna junction was maintained at 43.O”C for 30 min in one dog and at 44.O”C for 30 min in four dogs. The maximum temper- ature obtained near the antenna junction was approxi- mately 5°C hotter than the reference temperature (Fig. 8). The desired steady state temperature was easily achieved and maintained within kO.1 “C (Fig. 9). Body temperature, measured in the esophagus, remained es- sentially constant in all dogs; typically, temperature would increase by O. l-0.2”C during treatment. Three dogs had mild and one dog (43°C) had moderate hemiparesis that completely resolved within 24 hr after treatment. One dog (44.O”C) had a dense left hemiparesis that gradually improved over 72 hr after treatment, but a stable, slight left hemiparesis persisted. There were no other physical
Interstitial microwave hyperthermia 0 P. K. SNEED ef al. 1893
361 ,, I’ - - -,I * 9 ‘I, v 1 a, ‘I r v, 1 - 1 r, - 1 r 0 5 18 15 211 25 30 35
Time lminutesl
Fig. 9. Time-temperature plot of the stationary r = 5 mm reference probe during a 44°C survival treatment vs. the esophageal temperature. (Two other probes not included on the plot were used to map radial and r = 5 mm longitudinal temperature distributions.)
changes observed, other than minor tissue damage in the overlying muscle adjacent to the antenna in one dog (Fig. 10). This tissue response, observed predominantly at 1 week by CT scanning, reflected the excessive heat depos- ited along the antenna track proximal to the junction when large antenna insertion depths were used. No muscle or skin complications were noted over the I6 week period this dog was followed; in subsequent survival trials, the thick temporalis muscle was retracted to avoid these problems.
Qualitative changes observed on CT scans 1 week after hyperthermia were similar in all dogs. Generalized low density was observed in the heated hemisphere, and after administration of contrast medium, a focus of low density was observed surrounded by a thin ring of contrast en- hancement (Fig. 10). Some diffuse low density peripheral to the area of ring enhancement was observed and there was a slight displacement of the falx cerebri and right lateral ventricle, all of which suggested the presence of a small amount of edema. The center of the focal low den- sity area corresponded closely to the position of the an- tenna junction. The low density region was approximately 1.0 cm in diameter in dogs that were heated at 44°C for 30 min and about 0.8 cm in diameter in dogs heated at 43°C for 30 min. Therefore, the heat-induced low density region corresponded to tissues that had been heated at 144°C for 30 min. This region was characterized histo-
Fig. IO. Transverse CT scan ofcanine head through the implant site obtained I week after heating with a 2450 MHz antenna with I, = lb = 1 cm. The normal brain was heated to a reference temperature of 44’C for 30 min at 0.5 cm radially from the antenna junction. The radiolucent area is surrounded by a nar- row ring of contrast enhancement. which is centered about the antenna junction (intersection of X and Y). The lucent change. corresponding to frank tissue necrosis, was visible in four con- secutive 3 mm-thick slices for a total volume of 4.5 cm3. The small focus of high density within the necrotic region demon- strates the effect of a small bone chip within the field.
1894 1. J. Radiation Oncology 0 Biology 0 Physics October 1986, Volume 12, Number IO
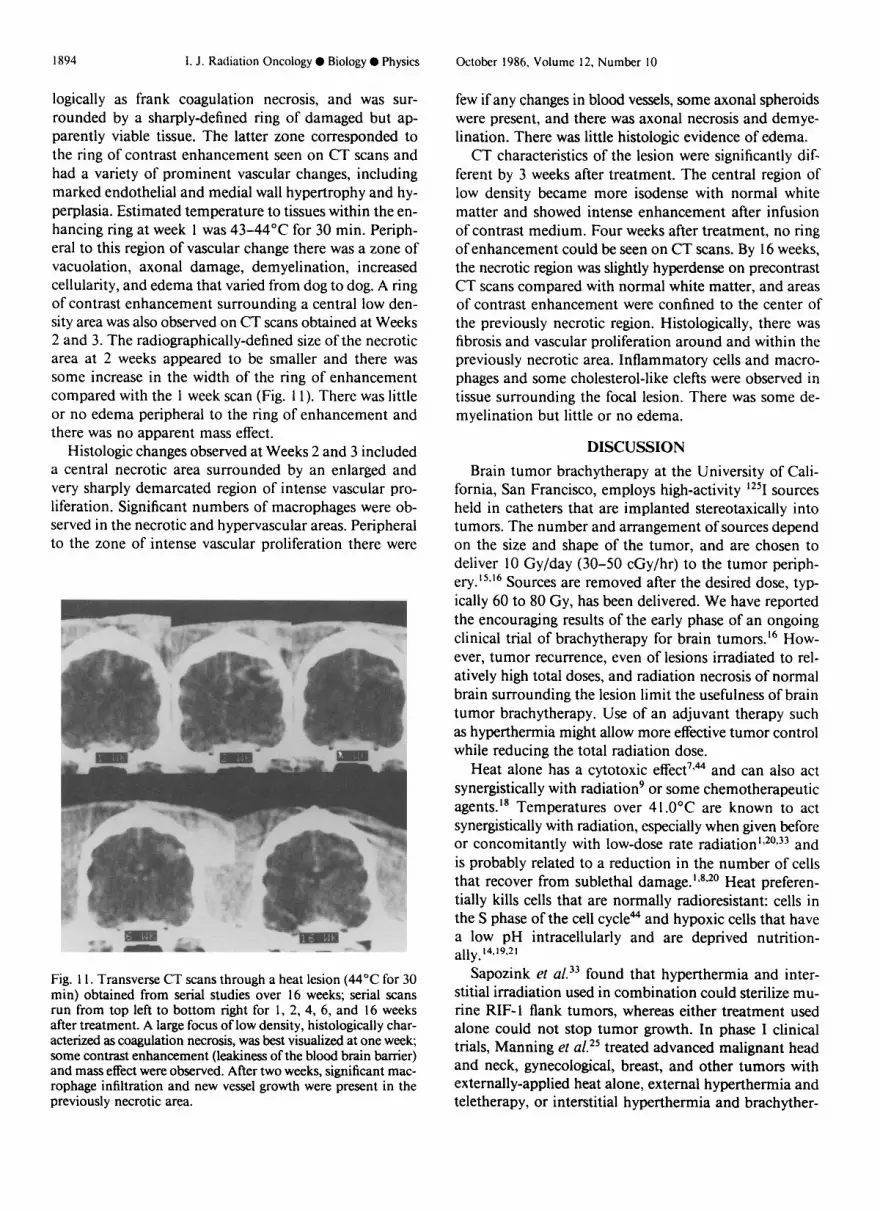
logically as frank coagulation necrosis, and was sur- rounded by a sharply-defined ring of damaged but ap- parently viable tissue. The latter zone corresponded to the ring of contrast enhancement seen on CT scans and had a variety of prominent vascular changes, including marked endothelial and medial wall hypertrophy and hy- perplasia. Estimated temperature to tissues within the en- hancing ring at week 1 was 43-44°C for 30 min. Periph- eral to this region of vascular change there was a zone of vacuolation, axonal damage, demyelination, increased cellularity, and edema that varied from dog to dog, A ring of contrast enhancement surrounding a central low den- sity area was also observed on CT scans obtained at Weeks 2 and 3. The radiographically-defined size of the necrotic area at 2 weeks appeared to be smaller and there was some increase in the width of the ring of enhancement compared with the 1 week scan (Fig. 11). There was little or no edema peripheral to the ring of enhancement and there was no apparent mass effect.
Histologic changes observed at Weeks 2 and 3 included a central necrotic area surrounded by an enlarged and very sharply demarcated region of intense vascular pro- liferation. Significant numbers of macrophages were ob- served in the necrotic and hypervascular areas. Peripheral to the zone of intense vascular proliferation there were
Fig. 1 I. Transverse CT scans through a heat lesion (44“C for 30 min) obtained from serial studies over 16 weeks; serial scans run from top left to bottom right for 1, 2, 4, 6, and 16 weeks after treatment. A large focus of low density, histologically char- acterized as coagulation necrosis, was best visualized at one week; some contrast enhancement (leakiness of the blood brain barrier) and mass effect were observed. After two weeks, significant mac- rophage infiltration and new vessel growth were present in the previously necrotic area.
few if any changes in blood vessels, some axonal spheroids were present, and there was axonal necrosis and demye- lination. There was little histologic evidence of edema.
CT characteristics of the lesion were significantly dif- ferent by 3 weeks after treatment. The central region of low density became more isodense with normal white matter and showed intense enhancement after infusion of contrast medium. Four weeks after treatment, no ring of enhancement could be seen on CT scans. By 16 weeks, the necrotic region was slightly hyperdense on precontrast CT scans compared with normal white matter, and areas of contrast enhancement were confined to the center of the previously necrotic region. Histologically, there was fibrosis and vascular proliferation around and within the previously necrotic area. Inflammatory cells and macro- phages and some cholesterol-like clefts were observed in tissue surrounding the focal lesion. There was some de- myelination but little or no edema.
DISCUSSION
Brain tumor brachytherapy at the University of Cali- fornia, San Francisco, employs high-activity “‘1 sources held in catheters that are implanted stereotaxically into tumors. The number and arrangement of sources depend on the size and shape of the tumor, and are chosen to deliver 10 Gy/day (30-50 cGy/hr) to the tumor periph- ery.“*r6 Sources are removed after the desired dose, typ- ically 60 to 80 Gy, has been delivered. We have reported the encouraging results of the early phase of an ongoing clinical trial of brachytherapy for brain tumors.16 How- ever, tumor recurrence, even of lesions irradiated to rel- atively high total doses, and radiation necrosis of normal brain surrounding the lesion limit the usefulness of brain tumor brachytherapy. Use of an adjuvant therapy such as hyperthermia might allow more effective tumor control while reducing the total radiation dose.
Heat alone has a cytotoxic effect7qa and can also act synergistically with radiation’ or some chemotherapeutic agents. is Temperatures over 41.O”C are known to act synergistically with radiation, especially when given before or concomitantly with low-dose rate radiation’,20,33 and is probably related to a reduction in the number of cells that recover from sublethal damage.‘,***’ Heat preferen- tially kills cells that are normally radioresistant: cells in the S phase of the cell cyclea and hypoxic cells that have a low pH intracellularly and are deprived nutrition- ally. 14,19,21
Sapozink et al. 33 found that hyperthermia and inter- stitial irradiation used in combination could sterilize mu- rine RIF-1 flank tumors, whereas either treatment used alone could not stop tumor growth. In phase I clinical trials, Manning et al.*’ treated advanced malignant head and neck, gynecological, breast, and other tumors with externally-applied heat alone, external hyperthermia and teletherapy, or interstitial hyperthermia and brachyther-

Interstitial microwave hyperthermia 0 P. K. SNEED et al. I895
apy. The best responses were obtained in patients treated with heat and brachytherapy. Further phase I and II trials of the clinical effects of combination treatment with hy- perthermia and interstitial brachytherapy are under- way. 6,22,41
Interstitial hyperthermia is a logical choice for adjuvant use with brachytherapy because the catheters used to im- plant radioactive sources may be used to implant micro- wave antennas; no additional surgical procedures are re- quired. Despite the potential benefit of combination treatment with heat and interstitial irradiation, heating a given volume of tissue to a therapeutic temperature is technically difficult. Although temperature profiles around microwave antennas in brain have been ob- tained 24*28329,3’*32*39 they can be very complex because of variouH physiologic, morphologic, and/or physical factors. Because of the technical difficulties associated with lo- calized heating and the uncertainties in defining the mor- phologic extent of a tumor, it is inevitable that some vol- ume of normal brain tissue will be heated to therapeutic temperatures. Much of the data concerning the toxic ef- fects of hyperthermia on normal brain tissue were ob- tained from acute animal studies or from anecdotal clin- ical reports.4,24.28*29,32 L itt e 1 is known of the effect of in- terstitial brain hyperthermia on survival and neurological status.” Late toxic effects of heat on normal brain tissue have not been defined experimentally, and, to our knowl- edge, studies correlating early functional and/or morpho- logic changes with late effects have not been reported.
The present study was designed to address some of the questions discussed above regarding the development of a system that could be used to induce focal brain lesions, by characterizing the physical factors that affect the heating pattern, and by assessing the acute and longer-term effects of thermal lesions. Dogs were chosen for the animal model because the canine brain is large enough for noninvasive radiographic evaluation and the radiation response after teletherapy and interstitial irradiation is similar to that found for human brain. 12,13 In addition, brain tumors ei- ther occur spontaneously or can be induced in dogs3,30 so that heating profiles in tumor and normal brain can be compared.
The multi-antenna system described here used both 9 15 and 2450 MHz frequencies, which provided consid- erable flexibility for producing hyperthermic lesions in the brain. The 2450 MHz antennas were found to be al- most ideal for localized heating within one hemisphere of canine brain; the 9 15 MHz antennas were considered to be more appropriate for use in the larger human tumors. In this study, we found that a single antenna inserted lat- erally to the midline induced the most reproducible heat- ing patterns that were centered about the antenna junc- tion. The steepest temperature gradient within the heated volume of brain was l”C/mm with the highest temper- atures recorded near the antenna junction. Temperature
profiles appeared to be affected most by antenna geometry, insertion depth, and morphology.
Surgical and hyperthermia procedures used in the “chronic” survival studies were well-tolerated by the dogs in all instances. Transient neurologic changes were ob- served in the treated dogs, but these changes did not affect behavior or the ability to function normally. With the exception of prophylactic antibiotic treatments for the first 7 days after treatment, no drug that might have influenced the expression of brain injury was used in the study.
Serial CT scans were analyzed qualitatively to docu- ment the radiologic characteristics of thermal lesions as a function of time after treatment. A detailed account of the quantitative findings after hyperthermia in dog brain will be reported elsewhere. The radiographic features of the heat lesion were similar to those caused by irradiation of normal dog brain with interstitially-implanted ‘*‘I sources. l2 Thermal lesions consisted primarily of a region of focal low density necrosis surrounded by a ring of viable but damaged tissue that could be seen as a ring of contrast enhancement on CT scans. Histologically, the vigorous neovascularization observed immediately adjacent to the region of heat-induced necrosis was different than that seen immediately after irradiation, although the necrotic regions were of similar size. Radiation-induced vascular damage was characterized by fibrinoid necrosis of vessel walls, some endothelial cell and adventitial proliferation, hyalinization with vessels, and distinct proteinaceious edema adjacent to vascular structures.12 The associated diffuse hemispheric edema seen after irradiation’2,‘3 was much less extensive after thermal injury (Figs. 10 and 1 1). The rapid development and evolution of thermally-in- duced CT changes appeared to substantiate the supposi- tion that tissue peripheral to the area of necrosis could react more effectively to sub-therapeutic thermal doses than to radiation, which produced more extensive pe- ripheral damage that evolved more slowly.” It appears that the extent of damage outside the central region of necrosis was a function of the different energy deposition characteristics of the interstitial heat and radiation: the thermal dose to brain tissue was reduced to zero much closer to the source than the radiation dose, which ex- tended deeper into the brain.
This apparent improvement in the localization of tissue response for similarly sized necrotic regions (effectively treated volumes) strengthens the argument for adjuvant use of interstitial hyperthermia with brachytherapy in critical tissues such as brain. Nevertheless, the addition of irradiation either before, concurrently with, or after hyperthermia might significantly alter the response of normal tissue to thermal injury. Thus, it is imperative that efforts to determine the effects of combined heat and radiation damage to normal brain are intensified before the efficacy of combination treatment of brain tumors can be assessed.

18Y6 I. J. Radialion Oncology 0 Biology 0 Physics Oclobcr 1986, Volume 12, Number IO
REFERENCES
1. Ben-Hur, E., Elkind, M.M., Bronk, B.V.: Thermally en- hanced radioresponse of cultered chinesc hamster cells: in- hibition of repair of sublethal damage and enhancement of lethal damage. Rod&. Rex 58: 38-5 I, 1974.
2. Bernstein, M., Gutin, P.H.: Interstitial irradiation of brain tumors: a review. Neurosurgery 9: 74 l-750, 198 I.
3. Bigner, D.D., Kvedar, J.P., Shaffer, T.C., Vick, N.A., Engel, W.K., Day, E.D.: Factors influencing the cell type of brain tumors induced in dogs by Schmidt-Ruppin Rous sarcoma virus. J. Neuropathol. Exp. Neurol. 31: 583-595, 1972.
4. Btitt, R.H., Lyons, B.E., Pounds, D.W., Prionas, S.D.: Fea- sibility of ultrasound hyperthermia in the treatment of ma- lignant brain tumors. Med. Instrum. 17: 172-177, 1983.
5. Cetas, T.C.: Physical models (phantoms) in thermal dosim- etry, In Hyperthermia in Cancer Therapy, Storm, F.K. (Ed.). Boston, G.H. Hall Medical Publishers. 1983, pp. 257-278.
6. Coughlin, C.T., Douple, E.B., Strohbehn, J.W., Eaton, W.L., Jr., Trembly, B.S., Wong, T.Z.: Interstitial hyperthermia in combination with brachytherapy. Radiology 148: 285-288, 1983.
7. Dewey, W.C., Freeman, M.L., Raaphorst, G.P., Clark, E.P., Wong, R.L.S., Highfield, D.P., Spiro, LJ., Tomasovic, S.P., Denman, D.L., Goss, R.A.: Cell biology of hyperthermia and radiation. In Radiation Biology in Cuncer Reseurch, R.E. Meyn and H.R. Withers (Eds.). New York, Raven Press. 1980, pp. 589-621.
8. Dewey, W.C., Holahan, E.V.: Hyperthermia: Basic biology. In Brain Tumor Therapy, Progress in Experimental Tumor Reseurch, Vol. 28, M.L. Rosenblum and C.B. Wilson (Eds.). Basel, Karger. 1984, pp. 198-219.
9. Dewey, W.C., Hopwood, L.E., Sapareto, S.A., Gerweck, L.E.: Cellular responses to combinations of hyperthermia and radiation. Radiology 123: 463-474, 1977.
10. Douple, E.B., Fike, J.R., Strohbehn, J.W., LeCouteur, R.A., Bernstein, M., Trembly, B.S., Wong, T.Z., Cann, C.E., Gu- tin, P.H.: Localized microwave induced hyperthermia in dog brain (Abstr.). Radial. Res. 87: 455-456, I98 1.
I I. Erlich, S.S., Davis, R.L.: Spinal subarachnoid metastasis from primary intracranial glioblastoma multiforme. Cancer 42: 2854-2864, 1978.
12. Turowski, K., Fike, J.R., Cann, C.E., Higgins, R.J., Davis, R.L., Gutin, P.H., Phillips, T.L., Weaver, K.A.: Normal brain iodine-125 radiation damage: Effect of dose and ir- radiated volume in a canine model. Radiology 158: 833- 838, 1986.
13. Fike, J.R., Cann, C.E., Davis, R.L., Borcich, J.K., Phillips, T.L., Russell, L.B.: Computed tomography analysis of the canine brain: effects of hemibrain x-irradiation. Rudiut. Res. 99: 294-310, 1984.
14. Gerweck, L.E.: Modification of cell lethality at elevated temperatures: the pH effect. Radiat. Res. 70: 224-235, 1977.
15. Gutin, P.H., Dormandy, R.H., Jr.: A coaxial catheter system for afterloading radioactive sources for the interstitial irra- diation of brain tumors. J. Neurosurg. 56: 734-735, 1982.
16. Gutin, P.H., Phillips, T.L., Wara, W.W., Leibel, S.A., Ho- sobuchi, Y., Levin, V.A., Weaver, K.A., Lamb, S.: Brachy- therapy of recurrent malignant brain tumors with removable high-activity iodine- 125 sources. J. Neurosurg. 60: 6 l-68, 1984.
17. Guy, A.W.: Analysis of electromagnetic fields induced in biological tissues by thermographic studies on equivalent phantom models. IEEE-MIT 19: 205-2 14, 197 1.
18. Hahn, G.M.: Potential for therapy of drugs and hyperther- mia. Cunccr Rex 39: 2264-2268, 1979.
19. Harisiadis, L., Hall, E.J., Kraljevic, U., Borek, C.: Hyper- thermia: biological studies at the cellular level. Radiology 117: 447-452, 1975.
20. Harisiadis, L., Sung, D. II, Kessaris, N., Hall, E.J.: Hyper- thermia and low dose-rate irradiation. Radiology 129: 195- 198, 1978.
21. Haveman, J., Hahn, G.M.: The role of energy in hyper- thermia-induced mammalian cell inactivation: a study of the effects of glucose starvation and an uncoupler of oxi- dative phosphorylation. J. Cell Physiol. 107: 237-24 1, I98 1.
22. Hochberg, F.H., Pruitt, A.: Assumptions in the radiotherapy of glioblastoma. Neurology 30: 907-9 I 1, 1980.
23. Joseph, C.D., Astrahan, M., Lipsett, J., Archambeau, J., Fore& B., George, F.W.: Interstitial hyperthermia and in- terstitial iridium 192 implantation: a technique and prelim- inary results. Int. J. Radiut. Oncol. Biol. Phys. 7: 827-833, 1981.
24. Lyons, B.E., Britt, R.H., Strohbehn, J.W.: Localized hy- perthermia in the treatment of malignant brain tumors using an interstitial microwave antenna array. IEEE-BME 31: 53-62, 1984.
25. Manning, M.R., Cetas, T.C., Miller, R.C., Oleson, J.R., Connor, W.G., Gemer, E.W.: Clinical hypet-thermia: results of a phase I trial employing hyperthermia alone or in com- bination with external beam or interstitial radiotherapy. Cancer 49: 205-2 16, 1982.
26. Ostertag, C.B., Weigel, K.: Three-dimensional CT scanning of dog brain. J. Comput. Assist. Tomogr. 6: 1036-1037, 1982.
27. Rubinstein, L.J.: Tumors ofthe Central Nervous System, Second Series, Fascicle 6. Washington, DC, Armed Forces Institute of Pathology, 1972.
28. Salcman, M., Samaras, G.M.: Hyperthermia for brain tu- mors: biophysical rationale. Neurosurgery 9: 327-335, 198 1.
29. Salcman, M., Samaras, G.M.: Interstitial microwave hy- perthermia for brain tumors: results of a phase-I clinical trial. J. Neuro-Oncol. 1: 225-236, 1983.
30. Salcman, M., Scott, E.W., Schepp, R.S., Knipp, H.C., Broadwell, R.D.: Transplantable canine glioma model for use in experimental neuro-oncology. Neurosurgery 11: 372- 381, 1982.
3 I. Samaras, G.M.: Intracranial microwave hyperthermia: heat induction and temperature control. IEEE-BME 31: 63-69, 1984.
32. Samaras, G.M., Salcman, M., Cheung, A.Y., Abdo, H.S., Schepp, R.S.: Microwave-induced hyperthermia: an exper- imental adjunct for brain tumor therapy. NutI. Cancer Inst. Monogr. 61: 477-482, 1982.
33. Sapozink, M.D., Pales, B., Goffinet, D.R., Hahn, G.M.: Combined continuous ultra low dose rate irradiation and radiofrequency hyperthermia in the C3H mouse. Int. J. Ra- diat. Oncol. Biol. Phys. 9: 1357-1365, 1983.
34. Sheline, G.E., Wara, W.W., Smith, V.: Therapeutic irradia- tion and brain injury. Int. J. Radiat. Oncol. Biol. Phys. 6: 1215-1228, 1980.
35. Smith, D.R., Hardman, J.M., Earle, K.M.: Metastasizing neuroectodermal tumors of the central nervous system. J. Neurosurg. 31: 50-58, 1969.
36. Strohbehn, J.W., Bowers, E., Walsh, J., Doupel, D.B.: An invasive microwave antenna for locally induced hyperther-
Interstitial microwave hyperthermia 0 P. K. SNEED ef al. 1897
mia for cancer therapy. J. Microwave Power 14: 18 I- 186, 1979.
37. Strohbehn, J.W., Trembly, B.S., Douple, E.B.: Blood flow effects on the temperature distributions from an invasive microwave antenna array used in cancer therapy. IEEE- BME 29: 649-66 1, 1982.
41. Vora, N., Forell, B., Joseph, C., Lilpsett, J., Archambeau, J.O.: Interstitial implant with interstitial hyperthermia. Cancer 50: 25 18-2523, 1982.
38. Szikla, G. (Ed.): Stereotactic Cerebral Irradiation. Amster- dam, Elsevier/North Holland Biomedical Press, 1979.
39. Trembly, B.S., Strohbehn, J.W., deSieyes, DC., Douple, E.B.: Hyperthermia induction by an array of invasive mi- crowave antennas. Natl. Cancer Inst. Monogr. 61: 497-499, 1982.
42. Walker, M.D., Alexander, E., Jr., Hunt, W.E.. MacCarty, C.S., Mahaley, M.S. Jr., Mealey, J. Jr., Norrell, H.A., Owens, G., Ransohoff, J., Wilson, C.B., Gehan, E.A., Strike, T.A.: Evaluation of BCNU and/or radiotherapy in the treatment of anaplastic gliomas. .I. Neurosurg. 49: 333-343, 1978.
43. Walker, M.D., Strike, T.A., Sheline, G.E.: An analysis of dose-effect relationship in the radiotherapy of malignant gliomas. Int. J. Radiat. Oncol. Biol. Phys. 5: 1725-l 73 I. 1979.
40. Trembly, B.S., Strohbehn, J.W., King, R.W.P.: Practical 44. Westra, A., Dewey, W.C.: Variation in sensitivity to heat embedded insulated antenna for hyperthermia. Proc. I&h shock during the cell cycle of Chinese hamster cells in vitro. Northeast Bioeng. ConJ: March 5, 1982, pp. 105-108. Int. J. Radial. Biol. 19: 467-477. 197 I.