interstitial cystitis/ painful bladder syndrome - new jersey
TRANSCRIPT
Interstitial Cystitis/ Painful Bladder Syndrome
National Kidney and Urologic Diseases Information Clearinghouse
U.S. Department of Health and Human Services
NATIONAL INSTITUTES OF HEALTH
~NIDDK NATlONPoI IN'')Tll\ffE Of n'AeETES,l"N{) DlGESlrv"l; "'NO KIONf'v 01S~A.5E:S
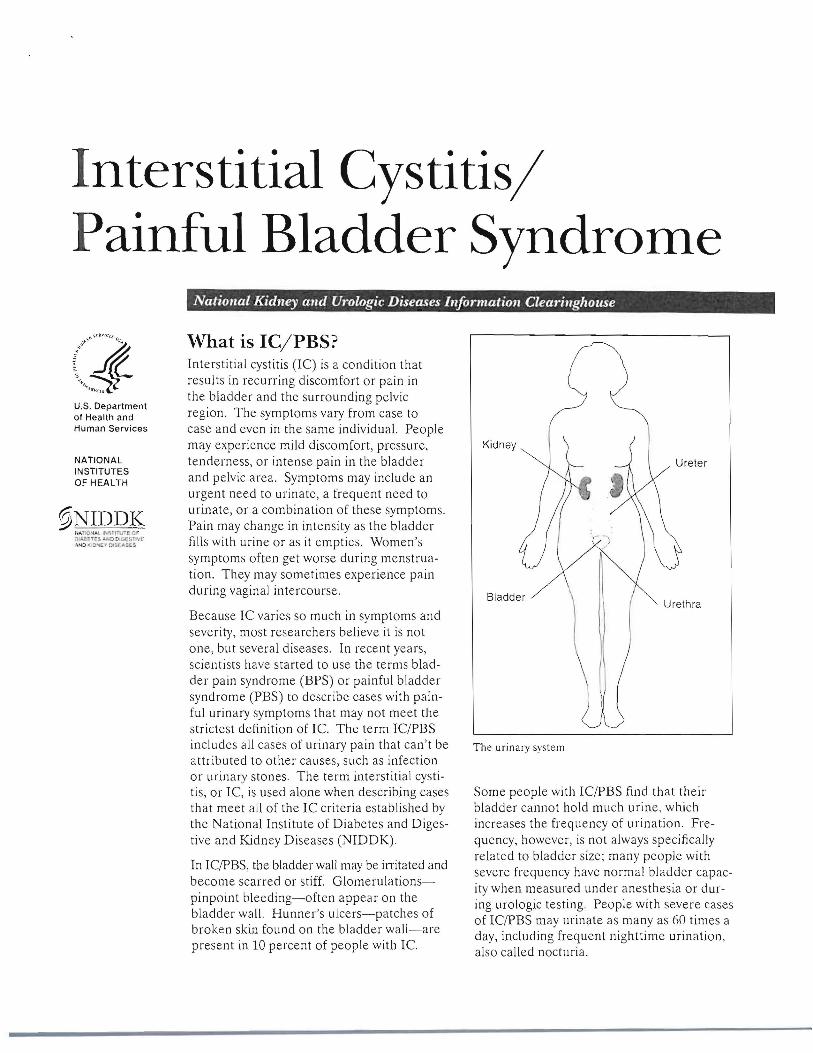
What is Ie/PBS? Interstitial cystitis (IC) is a condition that results in recurring discomfort or pain in the bladder and the surrounding pelvic region. The symptoms vary from case to case and even in the same individual. People may experience mild discomfort, pressure, tenderness, or intense pain in the bladder and pelvic area. Symptoms may include an urgent need to urinate, a frequent need to urinate, or a combination of these symptoms. Pain may change in intensity as the bladder fills with urine or as it empties. Women's symptoms often get worse during menstruation. They may sometimes experience pain during vaginal intercourse.
Because IC varies so much in symptoms and severity, most researchers believe it is not one, but several diseases. In recent years, scientists have started to use the terms bladder pain syndrome (BPS) or painful bladder syndrome (PBS) to describe cases with painful urinary symptoms that may not meet the strictest definition of Ie. The term IC/PBS includes all cases of urinary pain that can't be attributed to other causes, such as infection or urinary stones. The term interstitial cystitis, or IC, is used alone when describing cases that meet all of the IC criteria established by the National Institute of Diabetes and Digestive and Kidney Diseases (NIDDK).
In IC/PBS, the bladder wall may be irritated and become scarred or stiff. Glomerulationspinpoint bleeding-often appear on the bladder wall. Hunner's ulcers-patches of broken skin found on the bladder wall-are present in 10 percent of people with Ie.
Kidney
Urethra
The urinary system
Some people with IC/PBS find that their bladder cannot hold much urine, which increases the frequency of urination. Frequency, however, is not always specifically related to bladder size; many people with severe frequency have normal bladder capacity when measured under anesthesia or during urologic testing. People with severe cases of IC/PBS may urinate as many as 60 times a day, including frequent nighttime urination, also called nocturia.

lC/PBS is more common in women than in men. An estimated 3.3 million U.S. women, or 2.7 percent, who are 18 years of age or older have pelvic pain and other symptoms, such as urinary urgency or frequency, that are associated with lC/PBS.\ An estimated 1.6 million U.S. men, or 1.3 percent, who are 30 to 79 years old have persistent symptoms, such as pain with bladder f111ing or pain relieved by bladder emptying, that are associated with PBS.2
What causes IC/PBS? Some of the symptoms of IC/PBS resemble those of bacterial infection, but medical tests reveal no organisms in the urine of people with IC/PBS. Furthermore, people with lC/PBS do not respond to antibiotic therapy. Researchers are working to understand the causes of IC/PBS and to find effective treatments.
Many women with IC/PBS have other conditions such as irritable bowel syndrome and fibromyalgia. Scientists believe IC/PBS may be a bladder manifestation of a more general condition that causes inflammation in various organs and parts of the body.
Researchers are beginning to explore the possibility that heredity may playa part in some forms of IC In a few cases, IC has affected a mother and a daughter or two sisters, but it does not commonly run in families.
lBerry SH, Elliot! MN, Sut!orp M, et aJ. Prevalence of symptoms of bladder pain syndromelinterstitial cystitis among adult females in the United States. foumalof Urology. 2011: 186:540-544
2Link CL, PuHiam SJ, Hanno PM, et al. Prevalence and psychosocial correlates of symptoms suggestive of painful bladder syndrome: results from the Boslon area community hea.lth survey. fOtlmal of Urology. 2008; 180:599-606.
How is IC/PBS diagnosed? Because symptoms are similar to those of other disorders of the bladder and there is no definitive test to identify IC/PBS, doctors must rule out other treatable conditions before considering a diagnosis of IC/PBS. The most common of these diseases in both sexes are urinary tract infections and bladder cancer. In men, common diseases include chronic prostatitis or chronic pelvic pain syndrome. In women, endometriosis is a common cause of pelvic pain. lC/PBS is not associated with any increased risk of developing cancer.
The diagnosis of IC/PBS in the general population is based on the
• presence of pain related to the bladder, usually accompanied by frequency and urgency of urination
• absence of other diseases that could cause the symptoms
Diagnostic tests that help rule out other diseases include urinalysis, urine culture, cystoscopy, biopsy of the bladder wall and urethra, and distention of the bladder under anesthesia.
Interstitial Cystitis/Painful Bladder Syndrome 2
Urinalysis and Urine Culture Examining urine with a microscope and culturing the urine can detect and identify the primary organisms that are known to infect the urinary tract and that may cause symptoms similar to IC/PBS. A urine sample is obtained either by catheterization or by the clean catch method. For a clean catch, the patient washes the genital area before collecting urine midstream in a sterile container. White and red blood cells and bacteria in the urine may indicate an infection of the urinary tract, which can be treated with an antibiotic. If urine is sterile for weeks or months while symptoms persist, the doctor may consider a diagnosis of ICIPBS.
Culture of Prostate Secretions Although not commonly done, in men without a history of culture-documented urinary tract infections, the doctor might obtain prostatic fluid and examine it for signs of a prostate infection, which can then be treated with antibiotics.
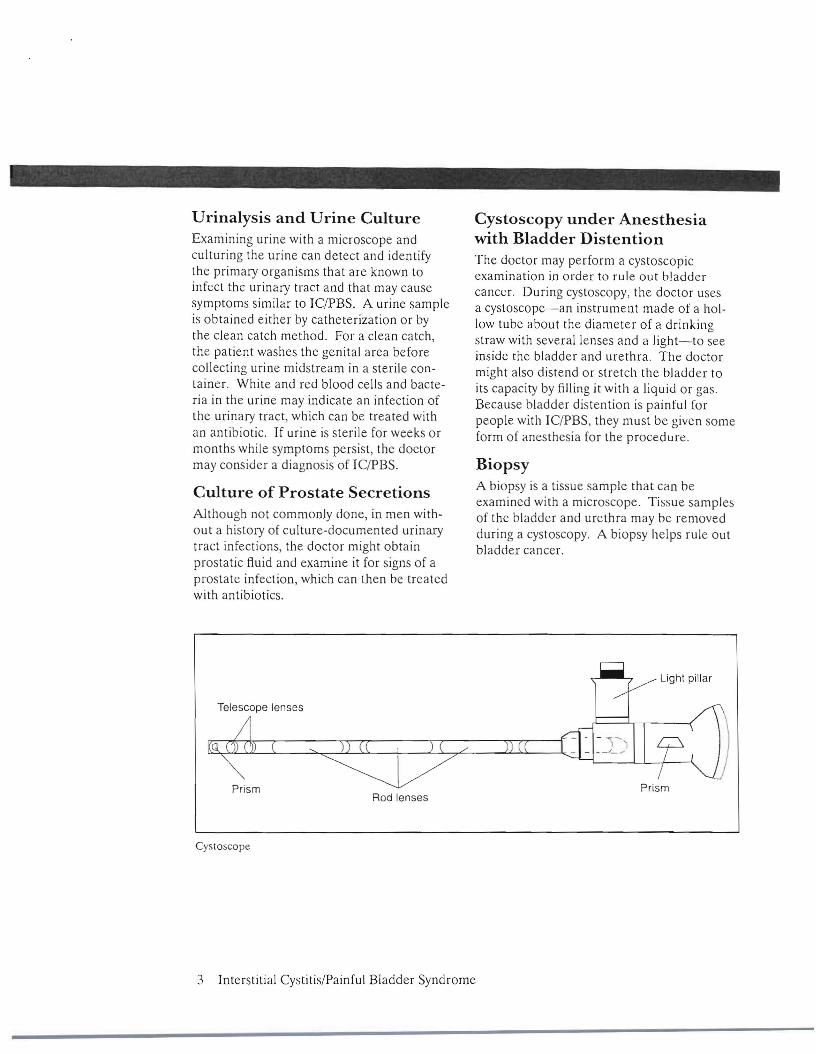
Cystoscopy under Anesthesia with Bladder Distention The doctor may perform a cystoscopic examination in order to rule out bladder cancer. During cystoscopy, the doctor uses a cystoscope-an instrument made of a hollow tube about the diameter of a drinking straw with several lenses and a light-to see inside the bladder and urethra. The doctor might also distend or stretch the bladder to its capacity by filling it with a liquid or gas. Because bladder distention is painful for people with IC/PBS, they must be given some form of anesthesia for the proced ure.
Biopsy A biopsy is a tissue sample that can be examined with a microscope. Tissue samples of the bladder and urethra may be removed during a cystoscopy. A biopsy helps rule out bladder cancer.
Light pillar
Telescope lenses
Prism Prism Rod lenses
Cystoscope
3 Interstitial CystitislPainful Bladder Syndrome

What are the treatments for Ie/PBS? Scientists have not yet found a cure for IC/PBS, nor can they predict who will respond best to which treatment. Symptoms may disappear with a change in diet or treatments or without explanation. Even when symptoms disappear, they may return after days, weeks, months, or years. Scientists do not know why.
Because the causes of ICIPBS are unknown, current treatments are aimed at relieving symptoms. Many people are helped for variable periods by one or a combination of treatments. As researchers learn more about IClPBS, the list of potentia] treatments will change, so patients should discuss their options with a doctor.
Bladder Distention Many people with ICIPBS have noted an improvement in symptoms after a bladder distention has been done to diagnose the condition. In many cases, the procedure is used as both a diagnostic test and initial therapy. Researchers are not sure why distention helps, but some believe it may increase capacity and interfere with pain signals transmitted by nerves in the bladder. Symptoms may temporarily worsen 4 to 48 hours after distention, but should return to predistention levels or improve within 2 to 4 weeks.
Bladder Instillation During a bladder instillation, also called a bladder wash or bath, the bladder is filled with a solution that is held for varying periods of time, averaging 10 to 15 minutes, before being emptied.
The only drug approved by the U.S. Food and Drug Administration (FDA) for bladder instillation is dimethyl sulfoxide (Rimso-50), also called DMSO. DMSO treatment involves guiding a narrow tube called a catheter up the urethra into the bladder. A measured amount of DMSO is passed through the catheter into the bladder, where it is retained for about 15 minutes before being expelled. Treatments are given every week or two for 6 to 8 weeks and repeated as needed. Most people who respond to DMSO notice improvement 3 or 4 weeks after the first 6- to 8-week cycle of treatments. Highly motivated patients who are willing to catheterize themselves may, after consultation with tbeir doctor, be able to have DMSO treatments at home. Selfadministration is less expensive and more convenient than going to the doctor's office.
Doctors think DMSO works in several ways. Because it passes into the bladder wall, it may reach tissue more effectively to reduce inflammation and block pain. It may also prevent muscle contractions that cause pain, frequency, and urgency.
A bothersome but relatively insignificant side effect of DMSO treatments is a garliclike taste and odor on the breath and skin that may last up to 7 hours after treatment. Long-term treatment has caused cataracts in animal studies, but this side effect has not appeared in humans. Blood tests, including a complete blood count and kidney and liver function tests, should be done about every 6 months.
Interstitial CystitislPainful Bladder Syndrome 4

Oral Drugs Pentosan Polysulfate Sodium (Elmiron) This first oral drug developed for IC was approved by the FDA in 1996. In clinical trials, the drug improved symptoms in 30 percent of patients treated. Doctors do not know exactly how the drug works, but one theory is that it may repair defects that might have developed in the lining of the bladder.
The FDA-recommended oral dosage of Elmiron is 100 milligrams (mg), three times a day. Patients may not feel relief from IC pain for the first 4 months. A decrease In
urinary frequency may take up to 6 months. Patients are urged to continue with therapy for at least 6 months to give the drug an adequate chance to relieve symptoms. If 6 months of Elmiron therapy provides no benefit, it is reasonable to stop the drug.
Elmiron's side effects are limited primarily to minor gastrointestinal discomfort. A sma.ll minority of patients experienced some hair loss, but hair grew back when they stopped taking the drug. Researchers have found no negative interactions between Elmiron and other medications.
Elmiron may affect liver function, which should therefore be monitored by the doctor.
Because Elmiron has not been tested in pregnant women, the manufacturer recommends it not be used during pregnancy, except in the most severe cases. Because Elmiron has mild blood-thinning effects, it should be discontinued prior to planned surgery.
Other Oral Medications Aspirin and ibuprofen may be a first line of defense against mild discomfort. Doctors may recommend other drugs to relieve pain.
Some people have experienced improvement in their urinary symptoms by taking tricyclic antidepressants or antihistamines. A tricyclic antidepressant called amitriptyline (EJavil) may help reduce pain, increase bladder capacity, and decrease frequency and nocturia. Some people may not be able to take It because it makes them too tired during the day. In people with severe pain, narcotic analgesics such as acetaminophen (Tylenol) with codeine or longer-acting narcotics may be necessary.
All drugs-even those sold over the counter-have side effects. A person should always consult a doctor before using any drug for an extended amount of time.
5 Interstitial Cystitis/Painful Bladder Syndrome

Electrical Nerve Stimulation Mild electrical pulses can be used to stimulate the nerves to the bladder-either through the skin or with an implanted device. The method of delivering impulses through the skin is called transcutaneous electrical nerve stimulation (TENS). With TENS, mild electric pulses enter the body for minutes to hours, two or more times a day either through wires placed on the lower back or just above the pubic area-between the navel and the pubic hair-or through special devices inserted into the vagina in women or into the rectum in men. AJthough scientists do not know exactly how TENS relieves pelvic pain, it has been suggested that the electrical pulses may increase blood flow to the bladder, strengthen pelvic muscles that help control the bladder, or trigger the release of substances that block pain.
TENS is relatively inexpensive and allows people with IC/PBS to take an active part in treatment. Within some guidelines, the patient decides when, how long, and at what intensity TENS will be used. It has been most helpful in relieving pain and decreasing frequency in people with Hunner's ulcers. Smokers do not respond as well as nonsmokers. If TENS is going to help, improvement is usually apparent in 3 to 4 months.
A person may consider having a device implanted that delivers regular impulses to the bladder. A wire is placed next to the tailbone and attached to a permanent stimulator under the skin. The FDA has approved this
device, marketed as the Inter-Stim system, to treat urge incontinence. urgency-frequency syndrome, and urinary retention in people for whom other treatments have not worked.
Diet No scientific evidence links diet to IC/PBS, but many patients find that alcohol, tomatoes, spices, chocolate, caffeinated and citrus beverages, and high-acid foods may contribute to bladder irritation and inflammation. Some people also note that their symptoms worsen after eating or drinking products containing artificial sweeteners. Eliminating various items from the diet and reintroducing them one at a time may determine which, if any, affect a person's symptoms. However, maintaining a varied, well-balanced diet is important.
Smoking Many people feel smoking makes their symptoms worse. How the by-products of tobacco that are excreted in the urine affect IC/PBS is unknown. Smoking, however, is a major cause of bladder cancer. One of the best things smokers can do for their bladder and their overall health is to quit.
Exercise Many patients feel that gentle stretching exercises help relieve ICIPBS symptoms.
Interstitial CystitislPainful Bladder Syndrome 6
Bladder Training People who have found adequate relief from pain may be able to reduce frequency by using bladder training techniques. Methods vary, but basically patients decide to void-empty their bladder-at designated times and use relaxation techniques and distractions to keep to the schedule. Gradually, they try to lengthen the time between scheduled voids. A diary in which to record voiding times is helpful in keeping track of progress.
Your Daily Bladder Diary Thl~ diary will help you i1nd ~'our health carr.: lc,lm figure out lhr.: COlUSC~ of ~'our hbtldC:T conlrollrouhlc. The- "sillnplc"linc ~how~ you how In uSC the- diary.
Your namc: _
D;1I<· _
DidY'J'lf"",1 """~I_'''Y1IU
ffip\ lilliif' .\([icknt.ol .. ~tr.,.,g doing 4otlhr1t401hfOGlll l kI lU~tOfOl tlmd
I~ ~~....." It. ~. t:::t.:~~ f---+""':::"~::':"~'':..:'-.::-::."-I=-:::"",;"""... r..;:_::"~"',",';;;-,-:::' :fr=....c::~•• '----r="--
~ltu' t.(UP' ,./;9~ ~ S~c;: '~<8 1i:lll1l1i"g
0(,0000
'000000 '''~'
000000
000000
I)-I ~,.. 000 000
'000 000
000 000
: 0 0 0 0 0 0 )<. 'v
J • ~ ... 'ooe 000 "u ". 000 000
ll ... II • '100.,1 ~'J.. .1,' M ......... 'UJI'.... I.ll~1 ........ '~"lll .....·;} ljQ,M."t ,!1.)I\ t.II ..,. "".. Ill f1~,.... " :",,~ •• j
Bladder diary from What / need 10 know about Bladder COlltrol for Women at wWlv.kidlley.lliddk.nihgov
Physical Therapy New evidence indicates that certain types of physical therapy, when administered by an experienced physical therapist, may improve IC/PBS symptoms. Patients should discuss this option with their health care provider.
Surgery Surgery should be considered only if all available treatments have failed and the pain is disabling. Many approaches and techniques are used, each of which has advantages and complications that should be discussed with a surgeon. A doctor may recommend consulting another surgeon for a second opinion before taking this step. Most surgeons are reluctant to operate because some people still have symptoms after surgery.
People considering surgery should discuss the potential risks and benefits, side effects, and long- and short-term complications with a surgeon, their family, and people who have already had the procedure. Surgery requires anesthesia, hospitalization, and weeks or months of recovery. As the complexity of the procedure increases, so do the chances for complications and failure.
People should check with their doctor to locate a surgeon experienced in performing specific procedures.
Two procedures-fulguration and resection of ulcers-can be done with instruments inserted through the urethra. Fulguration involves burning Hunner's ulcers with electricity or a laser. When the area heals, the dead tissue and the ulcer fall off, leaving new, healthy tissue behind. Resection involves cutting around and removing the
7 Interstitial CystitislPainful Bladder Syndrome

ulcers. Both treatments are done under anesthesia and use special instrumen ts inserted into the bladder through a cystoscope. Laser surgery in the urinary tract should be reserved for people with Hunner's ulcers and should be done only by doctors with the special training and expertise needed to perform the procedure.
Another surgical treatment is augmentation, which makes the bladder larger. In most of these procedures, scarred, ulcerated, and inflamed sections of the patient's bladder are removed, leaving only the base of the bladder and healthy tissue. A piece of the patient's colon-also called large intestine-is then removed, reshaped, and attached to what remains of the bladder. After the incisions heal, the patient may void less frequently. The effect on pain varies greatly; IClPBS can sometimes recur on the segment of colon used to enlarge the bladder.
Even in carefully selected patients-those with small, contracted bladders-pain, frequency, and urgency may remain or return after surgery, and they may have additional problems with infections in the new bladder and difficulty absorbing nutrients from the shortened colon. Some patients become incontinent, while others cannot void at all and must insert a catheter into the urethra to empty the bladder.
Bladder removal, called a cystectomy, is another, infrequently used surgical option. Once the bladder has been removed. different methods can be used to reroute the urine. In most cases, ureters are attached to a piece of colon that opens onto the skin of the abdomen. This procedure is called a urostomy and the opening is called a stoma. Urine empties through the stoma into a bag outside the body. Some urologists are using
a second technique that also requires a stoma bu t allows urine to be stored in a pouch inside the abdomen. At intervals throughout the day, the patient puts a catheter into the stoma and empties the pouch. Patients with either type of urostomy must be very careful to keep the area in and around the stoma clean to prevent infection. Serious potential complications may include kidney infection and small bowel obstruction.
A third method to reroute urine involves making a new bladder from a piece of the patient's colon and attaching it to the urethra. After healing, the patient may be able to empty the newly formed bladder by voiding at scheduled times or by inserting a catheter into the urethra. Only a few surgeons have the special training and expertise needed to perform this procedure.
Even after total bladder removal, some patients still experience variable IC/PBS symptoms in the form of phantom pain. Therefore, the decision to undergo a cystectomy should be made only after testing all alternative methods and seriously considering the potential outcome.
Removing the bladder is not always done in patients with severe disease. Some urologists recommend rerouting urine to a piece of bowel connected to the abdominal wall. Urine is then collected in an external bag that is emptied periodically. While this procedure mayor may not improve pelvic pain, it can decrease frequency and improve quality of life for patients who experience frequent urges to urinate.
Interstitial CystitislPainful I3ladder Syndrome 8

Are there any special concerns regarding Ie/PBS? Cancer No evidence exists that IC/PBS increases the risk of bladder cancer.
Pregnancy Researchers have little information about pregnancy and IC/PBS but believe that the disorder does not affect fertility or the health of the fetus. Some women find that their IC/PBS goes into remission during pregnancy, while others experience a worsening of their symptoms.
Coping The emotional support of family, friends, and other people with Ic/PBS is very important in helping patients cope. Studies have found that people who learn about the disorder and become involved in their own care do better than people who do not. The Interstitial Cystitis Association maintains a list of support groups that can viewed at www.ichelp.org.
Hope through Research Although answers may seem slow in coming, researchers are working to solve the painful riddle of IC/PBS. Some scientists receive funds from the Federal Government to help support their research, while others receive support from their employing institution, drug pharmaceutical or device companies, or patient support associations.
The NIDDK's investment in scientifically meritorious IC/PBS research across the United States has grown considerably since 1987. The Institute now supports research that looks at various aspects of IC/PBS, such as how the components of urine may injure the bladder and what role organisms identified by nonstandard methods may have
in causing IC/PBS. In addition to fundino-b
research, the NIDDK sponsors scientific workshops where investigators share the results of their studies and discuss future areas for investigation.
Clinical Research Network The Interstitial Cystitis Clinical Research Network (ICCRN) is a product of two NIDDK programs: the Interstitial Cystitis Database (ICDB) Study and the Interstitial Cystitis Clinical Trials Group (ICCTG). Established in 1991, the ICDB was as-year prospective cohort study of more than 600 men and women with symptoms of urinary urgency, frequency, and pelvic pain. The study described the longitudinal changes of urinary symptoms, the impact of IC on quality of life, treatment patterns, and the relationship between bladder biopsy findings and patient symptoms. The ICCTG was established in 1996 as a follow-up to the ICDB study. The clinical trials group developed two randomized, controlled clinical trials of promising therapies, one using oral therapics-pentosan polysulfate sodium (Elm iron) and hydroxyzine hydrochloride (Atarax)-and the other administering intravesical treatment using Bacillus Calmette-Guerin (BCG). BCG is a vaccine for tuberculosis that stimulates the immune system and may have an effect on the bladder. The ICCTG also developed and conducted ancillary studies of various biomarkers such as heparin-binding epidermal growth factor-like growth factor (HB-EGF) and anti-proliferative factor (APF).
In 2003, the ICCTG became the ICCRN, which has conducted additional clinical trials over a second S-year period. One of these trials studied the effectiveness of amitriptyline in treating PBS, which includes Ie. Amitriptyline has FDA approval for the treatment of depression, but researchers
9 Interstitial Cystitis/Painful Bladder Syndrome

believe the drug may work to block nerve signals that trigger pain in the bladder and may also decrease muscle spasms in the bladder, helping to cut both pain and frequent ulination. The study could not prove that amitriptyline was effective in treating IC/PBS, although many patients seemed to benefit from a combination of amitriptyline and behavioral modification with stress reduction.
In 2008, the NIDDK launched the Multidisciplinary Approach to the Study of Chronic Pelvic Pain (MAPP) Research Network. The MAPP Research Network is designed to take a collaborative, whole-body approach to the study of IC/PBS and chronic prostatitis/ chronic pelvic pain syndrome (CP/CPPS). This program brings together experts from non urologic fields such as neurology and epidemiology as well as traditional urologic researchers to study IC/PBS and CP/CPPS in the context of other chronic pain syndromes such as fibromyalgia, chronic fatigue syndrome, and irritable bowel syndrome. While traditional research has focused on the bladder as the source of pain in IC/PBS and on the prostate as the source of pain in CP/CPPS, researchers now believe that an underlying cause common to all chronic pain syndromes may lie somewhere outside these specific organs. The MAPP Research Network includes six. Discovery Sites that will conduct individual and collaborative trials and Lwo Core Sites for data and tissue banking and analysis. The program is scheduled to be funded for 5 years.
Participants in clinical trials can playa more active role in their own health care, gain access to new research treatments before they are widely available, and help others by contributing to medical research. For information about current studies, visit www.ClinicaITrials.gov.
Suggested Reading The materials listed below may be found in medical libraries, in many college and university libraries, through interlibrary loan in most public libraries, and at bookstores. Items are listed for information only; inclusion does not imply endorsement by the National Institutes of Health.
Articles and Book Chapters Keay SK, Warren Jw. Is interstitial cystitis an infectious disease? fnternational Journal ofAntimicrobial Agents. 2002;19(6):480-483.
The Interstitial Cystitis Clinical Trials Group. A pilot clinical trial of oral pentosan polysulfate and oral hydroxyzine in patients with interstitial cystitis . .loumal of Urology. 2003;170(3):810-815.
The Interstitial Cystitis Clinical Trials Group. A randomized controlled trial of intravesical Bacillus Calmette-Guerin for treatment of refractory interstitial cystitis. Journal of Urology. 2005;173(4):1186-J 191.
Hanno P, Lin AT, Nordling J, Nyberg L, van Ophoven A, Ueda T Bladder pain syndrome. In: Abrams P, Cardozo L, Khoury S, Wein A, eds. Incontinence. Paris: Health Publication Ltd.; 2009: 1459-1518.
Books and Booklets Moldwin RM. The Interstitial Cystitis SUivival Guide: Your Guide to the Latest Treatment Options and Coping Strategies. Oakland. CA: New Harbinger Publications, Inc.; 2000. (Available by calling 1-800-HELP-ICA or 1-800-435-7422.)
Sandler GG, Sandler A. Patient to Patient: Managing fnterstitial Cystitis & Overlapping Conditions. New Orleans, LA: Bon Ange LLC; 2000.
Sant G, ed. Interstitial Cystitis. Philadelphia: Lippincott-Raven; 1997.
10 Interstitial Cystitis/Painful Bladder Syndrome
For More Information American Urological Association Foundation 1000 Corporate Boulevard Linthicum, MD 21090 Phone: 1-800--828-7866 or 410-689-3700 Fax: 410-689-3998 Email: [email protected] Internet: www.UrologyHealth.org
American Chronic Pain Association P.O. Box 850 Rocklin, CA 95677 Phone: 1-800-533-3231 Email: [email protected] Internet: www.theacpa.org
American Pain Society 4700 West Lake Avenue Glenview,IL 60025 Phone: 847-375-4715 Email: [email protected] Internet: www.ampainsoc.org
American Urogynecologic Society 2025 M Street NW, Suite 800 Washington, D.C. 20036 Phone: 202-367-1167 Fax: 202-367-2167 Email: [email protected] Internet: www.augs.org
International Association for the Study of Pain 111 Queen Anne Avenue North, Suite 501 Seattle, WA 98109-4955 Phone: 206-283-0311 Email: [email protected] Internet: www.iasp-pain.org
Interstitial Cystitis Association 100 Park Avenue, Suite 108A Rockville, MD 20850 Phone: 1-800-HELP-ICA (1-800-435-7422)
or 301-610-5300 Fax: 301-610-5308 Email: [email protected] Internet: www.ichelp.org
National Kidney Foundation 30 East 33rd Street New York, NY 10016 Phone: 1-800-622-9010 or 212-889-2210 Internet: www.kidney.org
National Organization of Social Security Claimants' Representatives 560 Sylvan Avenue Englewood Cliffs, NJ 07632 Phone: 1-800-431-2804 Email: [email protected] Internet: www.nosscr.org
Social Security Administration Office of Public Inquiries Windsor Park Building 6401 Security Boulevard Baltimore, MD 21235 Phone: 1-800-772-1213 Internet: www.ssa.gov
Local offices can be found in the telephone book under U.S. Government, Department of Health and Human Services.
United Ostomy Associations of America, Inc. PO. Box 512 Northfield, MN 55057-0512 Phone: 1-800-826-0826 Email: [email protected] Internet: www.ostomy.org
Acknowledgments Publications produced by the Clearinghouse are carefully reviewed by both NIDDK scientists and outside experts. This publication was reviewed by Philip Hanno, M.D., University of Pennsylvania.
11 Interstitial CystitislPainful Bladder Syndrome

You may also tind additional information about this topic by visiting MedlinePlus at wlI'w.medlincplus.gov.
This publication may contain information about medications. When prepared. this publication included the most current information available. For updotcs or for questions about any medications. contact the U.S. Food and Drug Administration 1011free at J-S88-1NFO-FDA (J-888-463-6332) or visit www.fda.gov. Consult your health care provider for more information.
The U.S. Government does not endorse or favor any spccific commercial product or company. Trade. proprietory, or company names appearing in this document are used only because they are considered necessary in the context of the information provided. If 0 product is not mentioned. the omission does not mean or imply that the product is unsatisfactory.
National Kidney and Urologic Diseases Information Clearinghouse
3 Information Way Bethesda, MD 20892-3580 Phone: 1-800-891-5390 TIY: 1-866-569-1162 Fax: 703-738-4929 Email: [email protected] Internet: www.urologic.niddk.nih.gov
The National Kidney and Urologic Diseases Information Clearinghouse (NKUDIC) is a service of the National Institute of Diabetes and Digestive and Kidney Diseases (NIDDK). The NIDDK is part of the National Institutes of Health of the U.S. Department of Health and Human Services. Established in 1987, the Clearinghouse provides information about diseases of the kidneys and urologic system to people with kidney and urologic disorders and to their families, health care professionals, and the public. The NKUDIC answers inquiries, develops and distributes publications, and works closely with professional and patient organizations and Government agencies to coordinate resources about kidney and urologic diseases.
This publication is not copyrighted. The Clearinghouse encourages users of this publication to duplicate and distribute as many copies as desired.
This publication is available at wwwurologic.l1iddk.l1ih.guv.
U.S. DEPARTMENT OF HEALTH AND HUMAN SERVICES National Institutes of Health
N1H Publication No. J1-322U September 201 J

The Ie-Smart Diet Many people with interstitial cystitis (IC) find that
simple changes in their diet can help to ontrol
IC symptoms and avoid IC flare-ups. Typically,
avoiding foods high in acid and potassium-
os well as beverages containing caffeine and
alcohol-is a good idea. This helpful guide can
help you make "IC-Smart" meal choices. Keep
it handy for easy reference when dining out or
when preparing meals at home.
Fruits Allowable: Bananas, coconuts, dotes, blueberries, melons (except cantaloupe), and pears
Avoid: All other fruits and juices
Vegetables Allowable: Homegrown tomatoes and mony vegetables [except those listed below)
Avoid: Store-bought tomatoes, onions, tofu, soybeans, lima beans, and fava beans
Milk/Dairy Allowable: Milk, American cheese, cottage cheese, frozen yogurt, and white chocolate
Avoid: Yogurt, sour cream, soy milk/cheese, aged and chocolate
Carbohydrates/Grains Allowable: Pasta, rice, potatoes, and some breads (except those listed below)
Avoid: Rye and sourdough breads
~- - -- =------- -
heeses,
Meats/Fish Allowable: Poultry, fish, and some meats (except those listed belowl
Avoid: Aged, conned, cured, processed or smoked meats/fish; anchOVies; caviar; chicken livers; corned beef; and meats that contain nitrates or nitrites
Nuts/Oils Allowable: Most oils, almonds, cashews, and pine nuts
01 °
Most other nuts
Beverages Allowable: Bottled or spring water; decaffeinated, acid-free coffee or tea; some herbal teas; fI t soda
Alcoholic beverages, including beer and wine; carbonated drinks, such as soda; coffee and tea; and fruit juices, especially citrus and cranberry
Seasonings Allowable: Garlic and some other seasonings (except those listed bel w)
• : Mayonnaise, miso, soy sauce, sol d dressing, vinegar, and spicy foods (especially Chinese, Mexican, Indian, and Thai foods)
Preservatives
oid Benzyl alcohol; citric acid; monosodium glutamate (MSGJ; aspartame (NutraSweet*); saccharin; and foods containing preservatives, artificial ingredients/colors
°NutraSweel is a registered trademark of NutraSweel Property Holdings, Inc.
Dining Out: The Ie-Smart Way
Call ahead
Before making plans to eat at a restaurant, it's a good idea to call ahead and ask about the menu. This will
enable you to enjoy your me I and feel good afterward, too!
When ordering your meal
Ask questions
- Ask your waiter what spice are used in particular dishes
- If you are unsure of an ingredient, ask what it is
Modify your selection
-It's your meal-don', be afraid to specify how you would like it prepared
- When ordering a salad, tell the waiter flO tomatoes or onions
- Substitute a plain baked potato for a spicy rice combination
- Ask for salad dressings and other possible "trigger" items to be served "on the side"
Be careful with ethnic foods
- Many ethnic foods contain spices that you may be unfamiliar with
Know your "Ie-Smart" menu choices
- Most restaurants offer plain (not marinated) steak and chicken
- Some chain restaurant foods may contain preservatives when sold in the grocery store
Janssen J Janssen Pharmceuticals, Inc. © Janssen Pharmaceuticals, Inc. 2011 Novembe' 70 1 02E..J63FA
Interstitial cystitiS (Ie) and £LmIROn® treatment
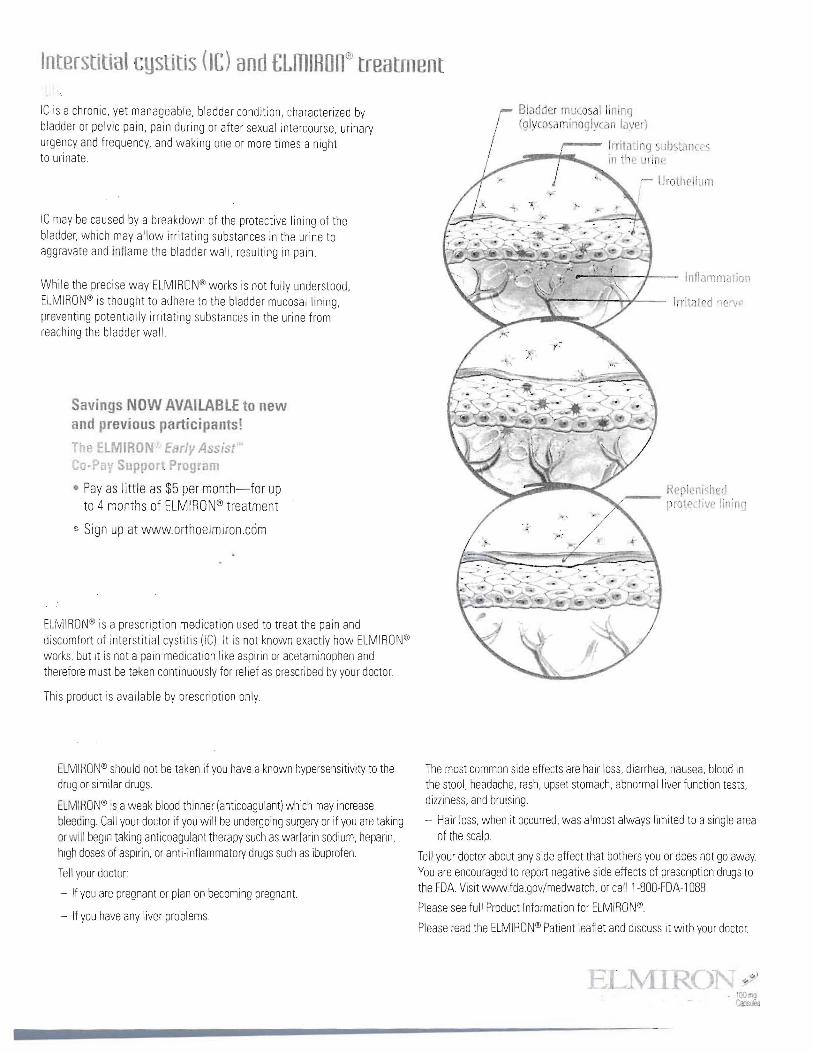
,...--. Irritalinq 5ubst.ln ",-!:I-......... in til . ulin ~
~ UrothcliulTl I
-..:...,,~-+-- Inflarnmalion
Irrilillcd nerv"
IC is a chronic, yet manageable, bladder condition, characterized by r- Bladder II1uc05al linll19 / (glyco aminoglycan laye ')bladder or pelvic pain, pain during or after sexual intercourse, urinary
urgency and frequency, and waking one or more times a night to urinate.
IC may be caused by a breakdown of the protective lining of the bladder, which may allow irritating substances in the urine to aggravate and inflame tile bladder wall, resulting in pain
While the precise way ELMIRON® works is not fully understood, ELMIRON® is thought to adhere to the bladder mucosal lining, preventing potentially irritating substances in the urine from reaching the bladder wall.
Savings NOW AVAILABLE to new and previous participants!
P. HMIR N Ear/~I Assi t Co·Pa' uppo, rag am
• Pay as little as $5 per month-for up to 4 months of ELMIRON® treatment
~ Sign up at www.orthoelmiron.ccim
EUvllRON® is a prescription medication used to treat the pain and discomfort of interstitial cystitis (lC) It is not known exactly how ELMIRON<!<) works, but it is not a pain medication like aspirin or acetaminophen and therefore must be taken continuously for relief as prescribed by your doctor.
This product is available by prescription only
ELMIRON® should not be taken if you have aknown hypersensitivity to the The most common side effects are hair loss, diarrhea, nausea, blood in drug or similar drugs. the stool, headache, rash, upset stomach, abnormal liver function tests,
dizziness, and bruising.EUVlIRON® is aweak blood thinner (anticoagulant) which may increase bleeding. Call your doctor if you will be undergoing surgery or if you are taking - Hair loss, when it occurred, was almost always limited to asingle area or III begin taking anticoagulant therapy such as warfarin sodium, heparin, of the scalp high doses of aspirin, or anti-inflammatory drugs such as ibuprofen Tell your doctor about any side effect that bothers you or does not go away Tell your doctor You are encouraged to report negative side effects of prescription drugs to
the FDA. Visit wvvwfdagov/medwarch, or call1-800-FDA-1 088.- If you are pregnant or plan on becoming pregnant. Please see full Product Information for ELMIRON")
- If you have any liver problems Please read the ELMIRON® Patient leaflet and discuss it with your doctor.
I

It is uery important that you take £LmIROn@ as directed and stick with it
S mp!on relief may take 3 to 6 months
'(ou should take 1 caiJsule of EUvlIRON't' by mouth 3 times a day, with water, at least 1 hour before or 2 hours after meals. Each capsule contains 100 mg of ELMIRON®
Allhough you may use other IC treatment options as needed, you should continue to take ELMIRON'& until otherwise instructed by your healthcare professional
Do not stop taking ELMIRON'~ or reduce your dosage just because you are feeling better or because you think ELMIRON® may not be working right away
Whil. taking ELMIRO , avoid anticoagulant therapy, such as warfarin sodium, heparin, high doses of anti-inflammatory drugs, such as ibuprofen, until speaking with your healthcare professional
Schedule follow-up visits with your healthcare professional once a month for the first few months
Lifestyle modifications you can make to help manage symptoms
Dietary changes: Avoid spicy or acidic foods and beverages containing caffeine and alcohol
Gentle exercise: Walking, yoga, and low-impact aerobics may be beneficial
Stress-reduction and relaxation techniques: Try controlled breathing exercises, warm baths with baking soda, and applying warm or cold compresses on the lower abdomen
Bladder trai ing: Practice scheduled voiding patterns
Physical therapy: Gentle stretching and pelvic floor muscle-relaxation exercises
Other therapies
Add'ltlonal resources, such as IC-friendly recipes, and stress and coping techniques, are available through the following
www.orthoelmiron.com: A Janssen Pharmaceuticals, Inc., Web site offering a wide range of information on IC and ELMIRON® to patients
Journey to Reliefl: A free e-mail support program that provides you with great tips, resources,
and money-saving offers
Interstitial Cystitis Association (www.ichelp.com): A national, nonprofit organization offering information and support to IC patients and their families
ELMIRON"' is a prescription medication used to treat the pain and discomfort of interstitial cystitis (lC) It is not known exactly how ELMIRON<t works, but it IS not a pain medication like aspirin or acetaminophen and therefore must be taken continuously for relief as prescribed by your doctor.
i;:is product is a'!JiiJble by prescription only
The most common side effects are hair loss, diarrhea, nausea, blood in the stool, headache, rash, upset stomach, abnormal liver function tests,
ELMIRON~' should not be taken if you have a known hypersensitivity to the dizziness, and bruising.
ru or similar drugs - Hair loss, when it occurred, was almost always limited to asingle area
ELMIRON'~' is aweak blood thinner (anticoagulant) which may increase of the scalp
bleeding Call your doctor if you will be undergoing surgery or if you are taking Tell your doctor about any side effect that bothers you or does not go away.orwdlbegin taking anticoagulant therapy such as warfarin sodium, heparin, You are encouraged to report negative side effects of prescription drugs tohigh doses of aspirin, or anti-inflammatory drugs such as ibuprofen the FDA. Visit wwwfdagov/medwatch, or call1-800-FDA-l 088.Tell your doctor Please see full Product Information for ELMIRON®.
- If you are pregnant or plan on becoming pregnant. Please read the ELMIRON:t> Patient leaflet and discuss it with your doctor
- If you have any liver problems
FLMIRON is' legis .red trodemark 01 leva Global Resplra ory Research, Inc .. under license to Janssen Pharmaceuticals. Inc.
Janssen Pharmaceuticals, Inc. Janssen J lJa'15~e') PharlHilo::ell ica)s. Inc. 20'1 AuguS\ 2011 02E09048R3
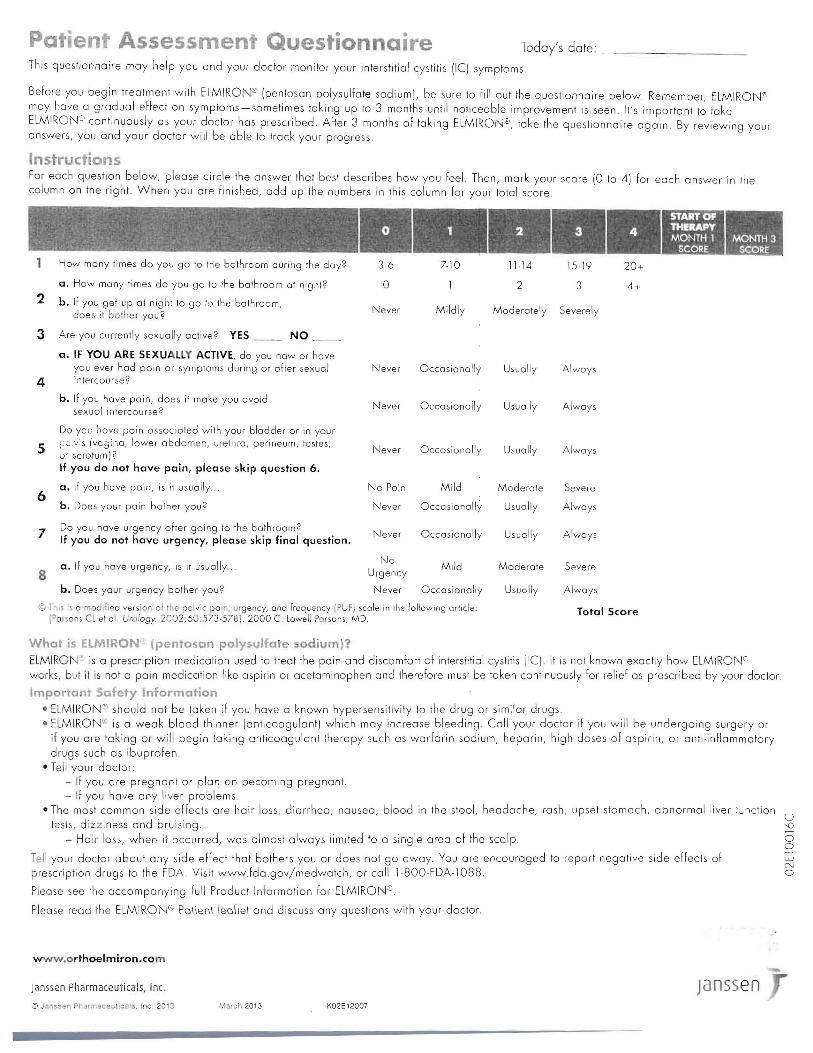
atie t Assessmen' Questionna·re Todoy's date: _
This questionnaire may help you and your doctor monitor your interstitial cystitis (IC) symptoms
Before you begin treatment with ELMIRON'" (penlosan polysulfate sodium), be sure to fill out the questionnaire below Remember, ELMIRON" may have a gradual effect on symptoms-sometimes laking up 10 3 months until noticeable improvement is seen. It's important to take ELMIRONs, continuously as your doctor has prescribed. After 3 months of taking ELMIRON":, toke the questionnaire again. By reviewing your answers, you and your doctor will be able to track your progress.
Instructions For each question below, please circle the answer that best describes how you feel Then, mark your score (0 to 4) for each answer in the column on the right. When you are finished, odd up the numbers in this column for your totol score.
~-1 How many times do you go to Ihe bathroom during the day? 36 7-10 11-14 15·19 20+
a. How many times do you go to the bathroom at night? 0 2 3 4+ 2 b. If you get up at night to go 10 the bathroom,
does it bo her you? Never Mildly Moderately Severely
3 Are you currently sexually active' YES __ NO
a. IF YOU ARE SEXUAllY ACTIVE, do you now or have you ever had poin or symptoms during or after sexual Never Occasionally Usually Always
4 intercourse'
b. If you have pain, does il make you avoid sexuol intercourse?
Never Occasionally Usually Always
Do you have poin associated with your bladder or in your
5 :;2'"is (vosino, lower abdome. , urethra, perineum, testes, ()' scratum)'
Never Occasionally Usually Always
If you do not have pain, please skip question 6.
6 a. if you have pain, is it usually.
b. Does your pain bOlher you 2
No Pain
Never
Mild
Occasionally
Moderate
Usually
Severe
Always
7 Do you have urgency ofter going 10 the bathroom' If you do not have urgency, please skip final question.
Never Occasionally Usually Always
8 a. If you have urgency, is it usually
No Urgency
Mild Moderate Severe
b. Does your urgency bOlher you? Never Occasionally Usually Always
© Thi' i,,, n0crifi.,d versiar of Ihe pelvic po in, urgency, and froquency (PUf) scale in the following article: Total Score IP ~ons Cl et 01 Urology 2002;60:573·578). 2000 C lowell Pnrsanl, MD.
What is EI.MIRON' (pentosan polysulfate sodium)? ELMIRON- is a prescription medication used to treat the pain and discomfort of interstitial cystitis [IC). It is not known exactly how ELMIRONC works, but it is not a pain medication like aspirin or acetaminophen and therefore must be taken continuously for relief os prescribed by your doclor.
Important Safety Information • E MIRON~' should not be token if you have a known hypersensitivity to the drug or similar drugs. • ELMIRO ' is a weak blood thinner [anticoagulant) which may increase bleeding. Call your doctor if you will be undergoing surgery or
if you are taking or will begin taking anticoagulant therapy such os warfarin sodium, heparin, high doses of aspirin, or anti.inflammatory drugs such as ibuprofen.
• Tell your doctor: - If you are pregnant or plan on becoming pregnant. - If you have any liver problems
• The most common side effects are hair loss, diarrhea, nausea, blood in the stool, headache, rash, upset stomach, abnormal liver :""ction U
tests, dizziness and bruising. - Hair loss, when it occurred, was almost always limited to a single area of the scalp. o
o Tell your doctor about any side effect that bothers you or does not go away. You are encouraged to report negative side effects of prescription drugs to the FDA Visit www.fda.gov/medwatch, or call 1-800·FDA-1088.
Please see the accompanying full Product Information for ELMIRON;[).
Please read the ELMIRONs Po\iell\ \eofle\ and discuss any questions with your doctor.
www.orthoelmiron.com
Janssen Pharmaceuticals, Inc. Janssen Q JalnSS~il Pharmi;l:eei.)tlcol~. Inc. 2013 Mnrci12013 K02E12007
-.0

For additional information on IC, please visit www.allaboutic.com or www.ichelp.org. To enroll in the ElMIRON patient support program and access valuable product coupons and helpful tools, please visit www.orthoelmiron.com.
The mechanism of action of ElMIRON in interstitial cystitis is not fully understood.
ELMIRO Oer'vSar J)I'~SII a-e sod I{II 2~
Replenished protec1ive lining
How does ELMIRON work? • ElMlRON is believed to act as a buffer, preventing
potentially irritating substances in the urine from reaching
the bladder wall. Therefore, ElMlRON is thought to treat
an underlying issue of IC, as well as the symptoms
What causes Ie? • IC may be caused by damage to the mucous layer
that protects the bladder wall. This damage may allow irritating substances in the urine to aggravate and inflame the bladder wall, resulting in pain
Irritated nerve ----'\;;::'::~'"~.."'''
What should I expect with ELMIRON? • ELMIRON has helped many people with IC and it may help
you. Studies show that ELMIRON relieves bladder pain, in some patients, in as soon as 3 months
• It is important to remember:
~ A single lOO-mg capsule of ELMIRON should be taken 3 times a day
~ Symptom improvement is generally gradual and relief may require 3 to 6 months of continuous therapy. Therefore it is very important that you take ELMIRON as directed and stick with it
~ While you may use other IC treatment options as needed, you should continue to take ELMIRON until otherwise instructed by your healthcare professional
~ Do no\ slop laking ELMIRON or reduce your dosage just because you are feeling better or because you think ELMIRON may not be working right away
~ If you don't experience improvement within 6 months, talk to your healthcare professional. You may not benefit from continued treatment
Important Safety Information ELMIRON is indicated for the relief of bladder pain or discomfort associated with interstitial cystitis.
ELMIRON has been shown to be generally welltolerated. The most common side effects were blood in stool, diarrhea, nausea, hair loss, headache, rash, upset stomach, abdominal pain, liver function abnormalities and dizziness. When side effects did occur, they were generally mild and usually did not interfere with continuing treatment. Hair loss, when it occurred, was almost always limited to a single area of the scalp, and it grew back when ELMIRON was discontinued. ELMIRON is a weak anticoagulant (blood thinner), which may increase bleeding. Call your doctor if you will be undergoing surgery or will begin taking anticoagulant therapy, such as warfarin, heparin or high doses of aspirin; or anti-inflammatory drugs, such as ibuprofen.
Please see full Prescribing Information.
ELMIRON is a registered trademark of IVAX Research, Inc., under license to Ortho-McNeil-Janssen Pharmaceuticals, Inc.
EEl Bayer HealthCare ELMIRONPharmaceuticals a.,- ... ,.e-_ "-. ~ r .. 581' pcy ura's "'OdL ,,~O~~t""' .,.",...,... --.'I
Benefits
For over 40 years Willard Water has been used by people all over the world as a foundation for excellent balance. Willard Water offers many benefits when consumed daily.
~Dr.~irrillard' . ~
Hbsorb euer1jthingbetter...nutrients,
uitamins, minerals, etL
• Natural Source of Macro and Trace Minerals Essential to Maintaining Optimal Balance
• Highly Efficacious and Bio-available Formula
• Reduction of Stress Due to the Body's Increased Ability to Assimilate Vital Nutrients More Efficiently
• Natural Free Radical Scavenging Activity
• More Cellular Energy = Increased Energy
• Overall Homeostasis
• Improved Functionality of the Body's Natural Defense System
• Highly Alkaline - pH of 12.3

Q. How does the product help with my pH or Int rnal alkalinity? A, Expertl believe Ihatthe body's pH levell are akey factor in determining one'l overall balance. Willard Wate, has avery high alkaline pH value of 12.3 and when diluted as directed permanently increases water pH by up to two points which helpI rellore agood pH balance in the body.
Q. What is Willard Water exactly? A. Pul simply Willard Water' is an altered form of water that has been activated with the addition of apatented micelle catalysl developed by Dr John W. Willard, PhD. When consumed daily, Dr Willard's Water' has lome very unusual properties, setting it aparr Irom regular water, leading to several benefits including enhanced nutrient assimilation, increased toxin removal, and cellular stressfeduction.
Q. How can the product help with vitamln/minerall nutrient absorption and tOllin removal? A. Willard Water' breaks down food and toxin partides in the bloodstream into even smaller partides whl(h allows the body and cells to more readily absorb the good while more efficiently fiushing the bad.
Q. Can WIII.,d Water be consumed by people with a gluten Intolerance1 A. Yes'lndividuals who have agluten intolerance often have problems with both digestion and the absorption of nutrients. Because Dr Willard's Water aids digestion and improves nulrient assimilation lor all users by helping the body break down lood, Dr Willard's Water can be consumed by people with gluten intolerance.
For questions or additional
information contact Dr. Willard's at
888-379-4552 or www.drwillard.com.
Vicki Ratner, MD, leA President & Founder
Co-Chairs • Alan Wein, MD
Chief of Urology, University of Pennsylvania Health System
• Philip M. Hanno, MD Clinical Professor of Urology, University of Pennsylvania Health System
o,;rd h1emb"rs • Daniel Brookoff, MD, PhD
University of Tennessee, Memphis • David A. Burks, MD
Henry Ford Hospital, Detroit • Daniel B. Carr, MD
Tufts-New England Medical Center, Boston • Toby Chai, MD
University of Maryland Medical Center • Robert J. Evans, MD
Moses Cone Health System, Greensboro, NC • David Kaufman, MD
Columbia College of Physicians & Surgeons • Susan Keay, MD, PhD
Division of Infectious Diseases University of Maryland School of Medicine
• Robert Moldwin, MD Long Island Jewish Medical Center
• Diane Newman, RN, MSN University of Pennsylvania Medical Center
• Christopher K. Payne, MD Department of Neurourology Stanford University School of Medicine
• John W. Warren, MD Division of Infectious Diseases University of Maryland School of Medicine
• Ursula Wesselmann, MD, PhD Johns Hopkins University School of Medicine
• Kristene E. Whitmore, MD Graduate Hospital, Philadelphia
l~( t 1/ COil (I. ln'
• Monica Liebert, PhD Director of Research American Urological Association
.,,,;.. 00 10 NIDO'" • leroy M. Nyberg, MD, PhD
Urology Director, NIDDK
~~",,,,,-)\\n,,,,,,, "n''''lte,,'c) This brochure is made possible '" .. . . . by an educational grant from
Ortho Women's Health & Urology
©OrUlo-McNeil Phannaceutlcal, Inc. 2006 March 2006 02E8872R1·A
I terstitial Cysti is & xua 0ty
T e Interstitial Cystitis
Association
•
Patients, Researchers, Caregivers Putting the Pieces Together
110 North Washington Street Suite 340
Rockville, MD 20850
Tel: 301.610.5300 Fax: 301.610.5308
Toll-Free: 1-800-HELP-ICA
E-mail: [email protected] Website: www.ichelp.org
J" I
9
I ment with alternatives to intercourse.
With medical supervision, some IC patients have tried using at-home bladder instillations of local anesthetics such as lidocaine or Marcaine'" either before or after sex. (If you are doing self-catheterization, be sure to do so only in consultation with your doctor.)
. \
If intercourse is just too painful, there are reasonable alternatives. "Outercourse" is sexual activity that includes everything except intercourse: sex talk, sharing fantasies, cUddling, reading erotica, watching sexy videos, kissing from head to toe, bathing together, sensual massage, individual or mutual masturbation, and oral sex.
In the past, any sexual activity other than sexual intercourse was viewed as something that "bad girls" did to please men, and today, some women remain reluctant to try outercourse for this reason. But oral sex and other types of outercourse are pleasurable and perfectly normal. Some women who have IC find that oral sex or stimulation of their genitals with hands or fingers is more comfortable than intercourse. The partner with IC can still bring their partner to orgasm orally or manually, even if IC symptoms are too painful for intercourse. Couples can also try a form of intercourse in which the woman crosses her legs and the man thrusts his penis between her thighs.
IC patients have come up with a variety of creative suggestions to help make sex more comfortable. These include:
• Reaching orgasm quickly to reduce friction on sensitive tissues.
• Being very aroused before penetration, or using a vibrator. Using vibrators is intolerable to some, but others say that a small, battery powered vibrator helps to achieve orgasm quickly and reliably, thus avoiding excessive friction. Also, the man should be very aroused before penetration so that orgasm comes quickly, and there will be less trauma from prolonged or deep thrusting.
• For pain or burning after sex, a cold gel pack may
help "cool the burn."
• Small finger-shaped balloons filled with water can be frozen and then inserted into the vagina briefly immediately after sex to help reduce irritation.
• To reduce the risk of bladder infection, drink water or other fluids before and after sex. Voiding a reasonable amount of urine after sex helps to flush out the urinary system. Diaphragms have also been identified as causing repeated urinary tract infections in some women, as have spermicidal jellies or lubricants containing nonoxynol-9.
Having a painful, chronic illness like IC often results in a loss of sexual interest or ability to become aroused. The need for frequent trips to the toilet may make people feel undesirable or sexually inadequate. Pain, stress, depression, the menstrual cycle, and certain medications, including antihistamines, painkillers, and antidepressants, may also interfere with sexual interest and activity. If you think you are feeling depressed right now, it would probably be helpful to see a psychotherapist. If you are not sure of the type of therapy you need, there are various guides sold in bookstores that may be helpful. A sex therapist may also be of help in suggesting ways to increase sexual interest and activity.
" - - - I,
Pain during sex can be the result of insufficient vaginal lubrication. This may be due to less frequent sexual activity, drugs that dry out mucous membranes, or lowered estrogen levels after menopause. Pain can also result on penetration if the female partner is not aroused enough to produce natural lubrication. In this case, delaying penetration until the woman is fully aroused is helpful.
Regular sexual activity, either alone or with a partner, is often enough to keep the vagina moist.
Try natural or synthetic lubricants, including vegetable oil, aloe vera gel, water-based lubricants, and other lubricants such as AstrogJide". You can find these products in pharmacies next to the feminine hygiene products or condoms, or they can be ordered through various mail order companies or
/ I
online. Adding Vitamin E oil to your lubricant may aid healing of raw tissues.
• Estrogen cream. placed directly into the vagina. will help keep the vaginal tissues moist. However, estrogen is not a cure. it merely relieves symptoms. and there are certain risks attached to regular use, so consult your doctor before using.
Erl.,,-·~ilt r}r, l I:'rH:,
Men of any age. on occasion. may find it difficult to become erect or to have an erection which is hard enough for intercourse. However. erectile difficulties become more common after the age of 40. Some men with IC have difficulties with erections because of genital pain, or embarrassment that their frequent need to void will disrupt sexual activity with a partner. Many medical conditions. including diabetes. heart, and circulatory diseases can also contribute to erectile problems. Partners of IC patients may develop erectile problems because they are afraid to hurt the woman during intercourse. Finally. excessive use of alcohol, depression, anxiety, and insufficient arousal can also interfere with erection.
Whether erectile failure occurs regularly or occasionally, it is important to remember that intercourse is only one way of having sex; there are many other ways that you and your partner can give each other pleasure. Some men find that focusing on whole body sensuality instead of genital sensations alone helps reduce performance pressure, and enhances their ability to become erect. Even more important, good communication with a loving partner is an essential ingredient in improving sex. There are a number of urological treatments available for alleviating erectile problems, b~t these should be used only on the advice of a trained physician. Often. couples find that sex therapy alone helps them improve their sexual lives greatly.
• Various articles from our Resource Materials Guide available through the ICA.
The ICA is a non-profit organization working internationally on behalf of all IC patients. Its goals are:
• To provide the most comprehensive and up-to-date information on IC.
• To provide IC patients, their families and friends with a support network.
• To educate the medical community and the public about IC.
• To advocate in the public and private sectors for research funding and patients' rights.
• To promote and provide research funding to find effective treatments and a cure for IC.
GenerallC Brochure>
IC & Diet Brochure>
IC & Self-Help Brochure
Ie & Men Brochure
Vulvar Pain Brochure
> Spanish Language Version also available
The ICA does not engage in the practice of medicine. It is not a medical authority nor does it claim to have medical knowledge. In all cases, the ICA recommends that you consult your own physician regarding any course of treatment Or medication.
Copyright © 2006 The Interstitial Cyslitis Association (ICA), Maryland. Material may not be reproduced in whole or in part without special written permission.
RBX06J
About the leA The Interstitial Cystitis Association (ICA) is the only nonprofit health association dedicated to improving the quality of healthcare and lives of people living with interstitial cystitis (IC).
Conquering Ie. Changing Lives.
The ICA provides advocacy, research funding, and education to ensure early diagnosis and optimal care with dignity for people affected by Ie. Our work is made possible through the generosity and vision of individuals as well as of foundations and corporations.
Donations help us to keep programs and services operating at peak strength so that every IC patient who needs help can have it-no matter where he or she may live, no matter how disabled they may be.
Your donation dollars also enable the ICA to continue to fund new IC research projects as well as to work closely with Congress to ensure ongoing federal funding of IC-specific research.
Helpful links • www.ichelp.org/AboutIC • www.ichelp.orgjVulvodynia
The information provided by the ICA is designed to support, not replace, the relationship that exists between an individual and his/her healthcare provider.
Copyright © 2013 Interstitial Cystitis Association (ICA) Material may not be reproduced in whole or in part
without speciql written permission.
T Content of this brochure has been developed by ICA. Printing of this brochure Janssen is sponsored by Janssen
PHARMACEUTICAl. COMPAHIl;S Pharmaceuticals, Inc.
01" 'or»,"lO')1."9o~u,0't\
K02EllOl!'!.RBV
Interstitial Cystitis
Association
www.ichelp.org
.,--=-:---..--Conquering IC C anging Lives
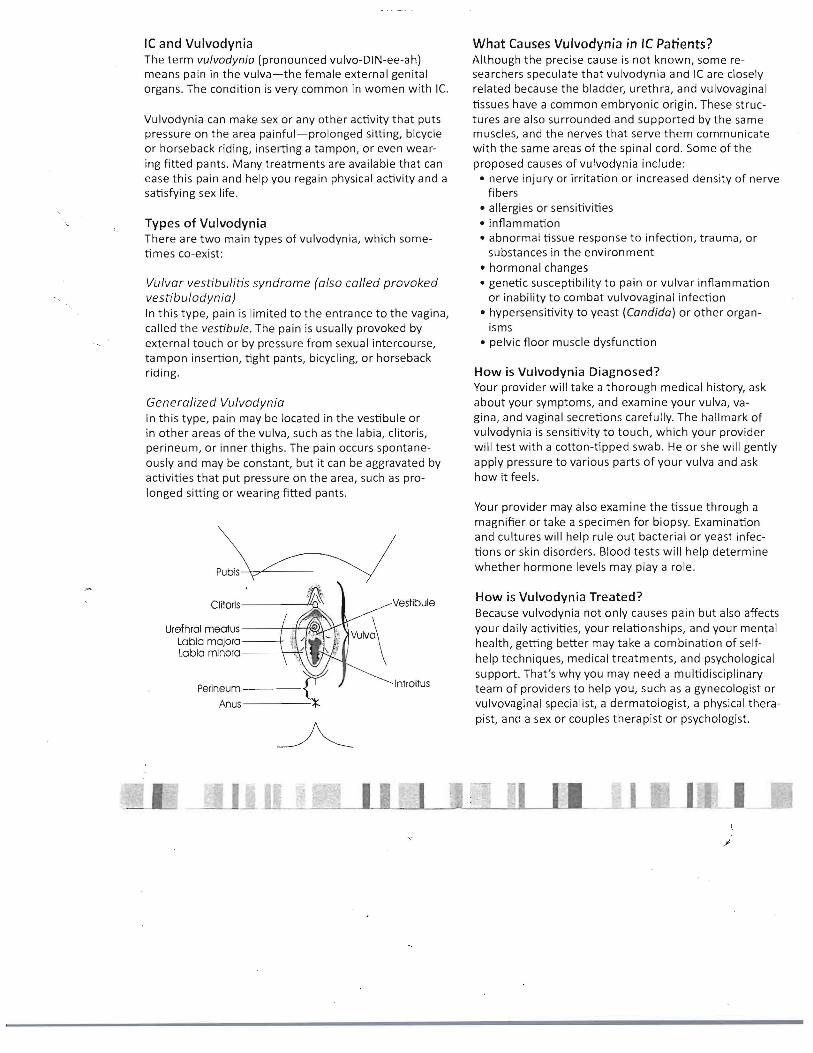
IC and Vulvodynia The term vulvodynia (pronounced vulvo-DIN-ee-ah) means pain in the vulva-the female external genital organs. The condition is very common in women with Ie.
Vulvodynia can make sex or any other activity that puts pressure on the area painful-prolonged sitting, bicycle or horseback riding, inserting a tampon, or even wearing fitted pants. Many treatments are available that can ease this pain and help you regain physical activity and a satisfying sex life.
Types of Vulvodynia There are two main types of vulvodynia, which sometimes co-exist:
Vulvar vestibulitis syndrome (also called provoked vestibulodynia) In this type, pain is limited to the entrance to the vagina, called the vestibule. The pain is usually provoked by external touch or by pressure from sexual intercourse, tampon insertion, tight pants, bicycling, or horseback riding.
Generalized Vulvodynia In this type, pain may be located in the vestibule or in other areas of the vulva, such as the labia, clitoris, perineum, or inner thighs. The pain occurs spontaneously and may be constant, but it can be aggravated by activities that put pressure on the area, such as prolonged sitting or wearing fitted pants.
Pubis --+"7"---
VestibuleClitorls-------+'Q
Urefhral mecrtus------1--1~~1~
Labia majora ------t Labia minora ------\-___."\'
IntroitusPerineum ----~ Anus----~
~
What Causes Vulvodynia in Ie Patients? Although the precise cause is not known, some researchers speculate that vulvodynia and Ie are closely related because the bladder, urethra, and vulvovaginal tissues have a common embryonic origin. These structures are also surrounded and supported by the same muscles, and the nerves that serve them communicate with the same areas of the spinal cord. Some of the proposed causes of vulvodynia include:
• nerve injury or irritation or increased density of nerve fibers
• allergies or sensitivities • inflammation • abnormal tissue response to infection, trauma, or
substances in the environment • hormonal changes • genetic susceptibility to pain or vulvar inflammation
or inability to combat vulvovaginal infection • hypersensitivity to yeast (Candida) or other organ
isms • pelvic floor muscle dysfunction
How is Vulvodynia Diagnosed? Your provider will take a thorough medical history, ask about your symptoms, and examine your vulva, vagina, and vaginal secretions carefully. The hallmark of vulvodynia is sensitivity to touch, which your provider will test with a cotton-tipped swab. He or she will gently apply pressure to various parts of your vulva and ask how it feels.
Your provider may also examine the tissue through a magnifier or take a specimen for biopsy. Examination and cultures will help rule out bacterial or yeast infections or skin disorders. Blood tests will help determine whether hormone levels may playa role.
How is Vulvodynia Treated? Because vulvodynia not only causes pain but also affects your daily activities, your relationships, and your mental health, getting better may take a combination of selfhelp techniques, medical treatments, and psychological support. That's why you may need a multidisciplinary team of providers to help you, such as a gynecologist or vulvovaginal specialist, a dermatologist, a physical therapist, and a sex or couples therapist or psychologist.
I
No one treatment or combination works for everyone, so be sure you have a give-and-take with your providers about what helps, what doesn't, and what you need.
Self-help techniques
AVOID IRRITANTS Detergents, fabric softeners, toilet paper, certain underwear fabrics, pads or tampons, and soaps or creams may be irritating, so avoid bleach, fabric softener, douches, contraceptive creams or foams, and hot tubs or pools with chlorine. Try nonirritating, unscented detergent, paper products, and toiletries, and wear all-cotton underwear. After urinating, use a squirt bottle or bidet to rinse with cool water. Dry gently.
TAKE THE PRESSURE OFF Wear loose-fitting pants or skirts, sit on a cutout cushion, avoid cycling and horseback riding, use nonirritating lubricants for sex, learn lovemaking techniques that minimize irritation (see our brochure Sex and Ie).
• Learn more at www.ichelp.org/LivingWithIC
AVOID DIET TRIGGERS The items that provoke your bladder may also affect vulvodynia. Some also suggest a low-oxalate diet. Everyone is different, so use an elimination diet to find out which dietary items affect you.
• Learn more at www.ichelp.org/Diet
SOOTHE YOUR BODY AND MIND Apply heat or cold, whichever feels helpful at the time, with warm or cool baths or sitz baths, oatmeal baths, warm or cool pads or packs on the vulva, or something that can be safely warmed or cooled and inserted in the vagina, such as certain adult recreational products or the finger of a medical glove filled with chilled or warm water. Relaxation, visualization, or meditation can also help.
ORAL MEDICATIONS Pain relieving medications include tricyclic antidepressants, serotonin-norepinephrine reuptake inhibitors (SNRls), anticonvulsants, and opioids. Antifungals for yeast or antihistamines may be helpful.
Become Part of the ICA Community Annual membership donations to the Interstitial
Cystitis Association ensure a steady stream of funding
to fuel advocacy activities, expand research funding, and raise awareness about IC,
For an annual contribution of $45.00 or more ($75.00 outside of the US) you will become a part of the ICA community and receive an ICA Patient Education
Kit with information about IC, treatment options,
research initiatives, and a restroom access card.
As an ICA member, you also receive:
• Award-winning, quarterly magazine-ICA Update • News and research updates via the ICA eNews • A 50% discount on materials in the ICA Store
• Discounted registration rates for ICA patient forums and other events
To join, send a check or money order (US funds only) made payable to ICA with this form to the address indicated below or join online at www.ichelp.orgjmembership.
Donations to the ICA are tax-deductible to the fullest extent allowable by law.
Keep the dialogue going Help others understand the need to find
REAL answers about IC!
Please make your donation in US funds only. Please do not send cash.
Conquering IC. Changing lives.
The ICA does not engage in the practice of medicine. It is not a medical authority nor does it claim to have medical
knowledge. In all cases, the ICA recommends that you consult your own physician regarding any course of
treatment or medication.
_I I
Donation and Membership Form
Your membership support is vital for keeping ICA
programs and services running at full speed!
Title: [ ]Ms. [ ]Mrs. [ ]Mr. [ ]Dr. [ 1 _
Name: _
Address: _
City: _ State: Zip: _
Phone: [ ] Home [ ] Work [ ] Cell _
Email Address: _
I have been diagnosed with IC: [ ] Yes [1 No
I am a friend or relative of someone with IC: [ 1Yes [] No
I am a healthcare provider: [l Yes [1 No
I am enclosing a check for the amount indicated (please circle):
$500 $250 $100 $75 $45 Other: $ _
Visa MasterCard Discover American Express
Card Number: _
Signature: _
Expiration Date: _
3 or 4-digit Security Code on Card: _
Today's date: _
Make checks payable to ICA and send to:
Interstitial Cystitis Association P.O. Box 17522
Baltimore, MD 21297-1522
TOPICAL MEDICATIONS These may include topical lidocaine or hormones or other medications that may need to be compounded into creams, gels, or suppositories, such as muscle relaxants, anticonvulsants, mast cell stabilizers, capsaicin, and other medications.
INJECTIONS Injection of anesthetics or other medications beside nerves that serve the vulva or into pelvic muscle trigger points can be done in a doctor's office. Onabotulinumtoxin A (Botox) injected into the vestibule, pelvic floor muscles, and other vulvar sites is beginning to be used as a treatment. Interferon injections are sometimes used for vulvar vestibulitis.
PHYSICAL THERAPY Pelvic floor therapy should be aimed at relaxing, not strengthening, the pelvic floor muscles as well as releasing muscle trigger points, connective tissue restrictions, and nerves.
INTERVENTIONAl THERAPY For more severe pain, spinal cord or peripheral nerve stimulators or pumps that release pain medications into the spinal canal can be implanted.
SURGERY Women with severe vulvar vestibulitis may be candidates for vestibulectomy, a surgery that removes some or all of the vestibule.
liJ_ I
About the ICA. The Interstitial Cystitis Association (ICA) is the only Sex and Ie nonprofit health association dedicated to improving the quality of healthcare and lives of people living with interstitial cystitis (IC).
Conquering Ie. Changing Lives.
The ICA provides advocacy, research funding, and education to ensure early diagnosis and optimal care with dignity for people affected by Ie. Our work is made possible through the generosity and vision of individuals as well as of foundations and corporations.
Donations help us to keep programs and services operating at peak strength so that every IC patient who needs help can have it-no matter where he or she may live, no matter how disabled they may be.
Your donation dollars also enable the ICA to continue to fund new IC research projects as well as to work closely with Congress to ensure ongoing federal funding of IC-specific research.
Helpful Links • www.ichelp.org/AboutIC • www.ichelp.org/lntimacy
The information provided by the ICA is designed to support, not replace, the relationship that exists between
an individual and his/her healthcare provider.
Copyright © 2013 Interstitial Cystitis Association (ICA) Material may not be reproduced in whole or in part
without special written permission.
Content of this brochure has been developed by ICA. Printing of this brochure is sponsored by Janssen Pharmaceuticals. Inc.
Janssen J April 2013 K02E13004 RBX
Sex and Ie For most IC patients, sexual intimacy is a challenge. ICA surveys and research estimate that from 60 to 90 percent of people with IC have difficulties with sex. For many, IC has prevented them from having any sexual intimacy.
It doesn't have to be that way. There are many ways to remain sexually active or resume your sex life, and there are treatments that can help. Most IC patients can reclaim physical intimacy when they, their partners, and their healthcare providers work together.
How Ie Affects Se, Both women and men with IC may have pain during or after sex and even sometimes with arousal. The most common pain for women during sex is pain with thrusting, although they may also have pain with penetration, urethral or clitoral irritation, or orgasm. Similarly, men may have perineal, penile, or scrotal pain or pain with ejaculation. Both men and women may have IC flares after sex. It's thought that the pain can come from pressure on a sensitive bladder, irritation of the urethral area, or pelvic floor muscle problems.
Let's Talk Touch can help ease chronic pain and strengthen the bond between you and your partner. So don't miss out on that part of life! Raise your concerns with your healthcare provider. Be honest with your partner about the activities that are painful, but reassure your partner that you can have satisfying intimacy with some adjustments and treatments. If it's difficult to talk, bring your partner to an appointment or ask for a referral to a therapist experienced in helping couples with intimacy and chronic pain.
Treatment Is Tops The best way to ease pain with sex is to treat your IC symptoms-and the research shows it. If your IC symptoms aren't under control, work with your healthcare provider to find the IC treatments that work for you. You may need a combination of treatments aimed at the bladder, the pelvic floor, and, for women, the vulvar area, since all three can be sources of pain with sex. Some local treatments can be especially helpful for pain with sex, such as muscle relaxants in vaginal or rectal suppositories and topical numbing agents.
Plan Ahead Take steps to feel your best at the time of your intimate encounter.
Go for "pretreatment." And, plan on having intimacy soon after the appointment with your healthcare provider. That way, you can get helpful "pretreatment," such as:
• bladder instillations • trigger point injections • intravaginal or intra rectal muscle relaxants • oral pain medication (take them so their maximum
effect is timed for your planned encounter) • topical medication, such as lidocaine gel, that help
prevent pain during sex
This is also a time to get any prescriptions you might need for medications to use after sex.
Avoid flare triggers. Restrict foods and drinks that trigger flares. Also, it may be best to hold off on lovemaking until you have an empty bladder and stomach.
"Test drive" products and activities. Ask your healthcare provider if your bladder and pelvic floor are quiet enough to tolerate stimulation or penetration. Women can build and test their tolerance for penetration with vaginal dilators. Men and women can see if they can tolerate orgasm before trying with a partner. If you or your partner wants to try a new lubricant, test a small amount to be sure you can tolerate it before you use it during sex.
Relax. Sexual activity is more comfortable when muscles-especially your pelvic floor muscles-are relaxed. Take a hot bath, stretch, do any helpful at-home physical therapy, meditate, or use other relaxation techniques.
Numb up. Use lidocaine gel on the vulva or in the vagina or rectum. Partners can avoid numbing by using a condom.
Adapt Your Sexual Technique Make sex a whole mind-body experience. Explore intimate touch that feels good and focus less on orgasm as the goal.
Try oral or manual stimulation. If orgasm is okay but penetration is not, manual or oral stimulation are options. Mutua I masturbation can be satisfying for both participants.
Use "outercourse" techniques. When penetration is too uncomfortable for the partner with IC, couples can use techniques that help simulate it, such as rubbing bodies together in a "spoon" position or thrusting the penis between the thighs, buttocks, or breasts.
Go slowly. If you are a woman with IC and are resuming intercourse after a respite, start slowly. First, try penetration only and no thrusting. If that causes no flare, progress to gentle rocking and later to thrusting as you can tolerate it.
Use lubrication. Personal moisturizers and lubricants increase comfort and relieve friction during sexual activity. Use products that are not irritating.
Limit intercourse intensity and duration. If women and men with IC can tolerate intercourse, they can do so for
.- limited amounts of time. As a couple, decide to limit thrusting time to a maximum of 3 to 5 minutes to start. Then, increase the time gradually as tolerated.
Try alternative positions. Lying side-by-side may be most comfortable. For women with IC, being on top and leaning forward may also be a comfortable position, or having the partner stand while the other is lying down may be helpful.
Become Part of the ICA Community Annual membership donations to the Interstitial
Cystitis Association ensure a steady stream of funding
to fuel advocacy activities, expand research funding, and raise awareness about Ie.
For an annual contribution of $45.00 or more ($75.00 outside of the US) you will become a part of the ICA community and receive an ICA Patient Education Kit with information about IC, treatment options,
research initiatives, and a restroom access card.
As an ICA member, you also receive:
• Award-winning, quarterly magazine-ICA Update • News and research updates via the ICA eNews • A 50% discount on materials in the ICA Store
• Discounted registration rates for ICA patient forums and other events
To join, send a check or money order (US funds only) made payable to ICA with this form to the address indicated below or join online at www.ichelp.orgjmembership.
Donations to the leA are tax-deductible to the fullest extent allowable by law.
Keep the dialogue going Help others understand the need to find
REAL answers about IC!
Please make your donation in US funds only. Please do not send cash .
Conquering Ie. Changing lives.
The ICA does not engage in the practice of medicine. It is not a medical authority nor does it claim to have medical
knowledge. In all cases, the ICA recommends that you consult your own physician regarding any course of
treatment or medication.
Donation and Membership Form Your membership support is vital for keeping ICA
programs and services running at full speed!
Title: [ ]Ms. [ ]Mrs. [ ]Mr. [ ]Dr. [ l _
Name: _
Address: _
City: _ State: Zip: _
Phone: [ ] Home [ ] Work [ ] Cell _
Email Address: _
I have been diagnosed with IC: [ ] Yes [] No
I am a friend or relative of someone with IC: [ ] Yes [] No
I am a healthcare provider: [1 Yes [] No
I am enclosing a check for the amount indicated (please circle):
$500 $250 $100 $75 $45 Other: $ _
Visa MasterCard Discover American Express
Card Number: _
Signature: _
Expiration Date: _
3 or 4-digit Security Code on Card: _
Today's date: _
Make checks payable to ICA and send to:
Interstitial Cystitis Association P.O. Box 17522
Baltimore, MD 21297-1522
Take Care of Yourself after Intimacy Heat if you need it. If muscles are spasming or sore, especially after orgasm, relaxing with the heat of a warm bath, warm pack, or heating pad may be relaxing.
Cool off. On the other hand, some women or men find using a cool pack on the vulva or perineum to be soothing. Ask your healthcare provider or physical therapist about internal cooling, for example, with the finger of a surgical glove filled with chilled water or a chilled device that's used for internal massage.
Ease the burn. Use lidocaine gel on the vulva, vagina, or penis to cool the burn from friction.
Medicate. Take your pain medicine, muscle relaxant, or anti-inflammatory or use your internal muscle relaxant or pain medication.
Give your pelvic floor time to relax. After sex, some IC patients can't start a urine stream. This usually goes away after a short while when the pelvic floor relaxes. A warm bath can help.
Follow-up with your healthcare provider. Let your healthcare team know what is working-and what is not working. Ask what you can do to decrease any pain or distress associated with sex.
-' I