influence of hypertension on neurocognitive domains in nondemented parkinson’s disease patients
TRANSCRIPT
Research ArticleInfluence of Hypertension on Neurocognitive Domains inNondemented Parkinsonrsquos Disease Patients
Jacob D Jones12 Charles Jacobson2 Martina Murphy3 Catherine Price12
Michael S Okun24 and Dawn Bowers124
1 Department of Clinical and Health Psychology McKnight Brain Institute University of Florida 101 South Newell DriveGainesville FL 32601 USA
2Center for Movement Disorders and Neurorestoration McKnight Brain Institute University of Florida3450 Hull Road Gainesville FL 32607 USA
3Department of Internal Medicine McKnight Brain Institute University of Florida PO Box 100277Gainesville FL 32610-0277 USA
4Department of Neurology McKnight Brain Institute University of Florida HSC PO Box 100236Gainesville FL 32610 USA
Correspondence should be addressed to Dawn Bowers dawnbowersphhpufledu
Received 30 June 2013 Revised 7 October 2013 Accepted 5 November 2013 Published 23 January 2014
Academic Editor Fabrizio Stocchi
Copyright copy 2014 Jacob D Jones et al This is an open access article distributed under the Creative Commons Attribution Licensewhich permits unrestricted use distribution and reproduction in any medium provided the original work is properly cited
Objective Health comorbidities particularly cardiovascular risk factors are well known to pose risks for cognitive decline in olderadults To date little attention has focused on the impact of these comorbidities on Parkinsonrsquos disease (PD) This study examinedthe prevalence and contribution of comorbidities on cognitive status in PDpatients above and beyond the effects of disease severityMethods A cross sectional design was used including neuropsychological data on 341 PD patients without severe cognitive declineComorbidity data were collected via medical chart review Data were analyzed using a series of multiple hierarchical regressionscontrolling for PD-related disease variablesResults Overall sample characteristics are 69male disease duration 97 years UnifiedParkinsonrsquos Disease Rating Scale 264 and age 647 years Hypercholesterolemia (416) hypertension (381) and hypotension(302) were the most reported comorbidities The presence of hypertension significantly contributed to domains of executivefunction and verbal memory The cooccurrence of orthostatic hypotension moderated the relationship between hypertension andexecutive function Conclusions This study on a large cohort of PD patients provides evidence for a detrimental influence of healthcomorbidities particularly hypertension on cognitive domains that have traditionally been conceptualized as being frontally andortemporally mediated
1 Introduction
The overall goal of this proof of concept study was tolearn whether cardiovascular risk factors like hypertensionand diabetes might negatively influence cognitive statusin Parkinsonrsquos disease similar to that observed in normalelderly Parkinsonrsquos disease (PD) is a complex multisys-tem disorder characterized by motor cognitive and mood-motivational changes [1 2] Particularly insidious are cog-nitive changes When initially diagnosed 5ndash20 of PDpatients show signs of cognitive difficulties and up to 80become demented after 15ndash20 years [3 4] Typical cognitivechanges include slowed processing (bradyphrenia) increased
forgetfulness and difficulty with multitasking and workingmemory Cognitive changes can occur early in the diseasecourse worsen with disease progression and detrimentallyaffect quality of life and survival [3 5] From a neuralsystems perspective PD-related cognitive decline has beenattributed to deregulation of dopamine-mediated frontal-striatal circuitry and is further complicated by cholinergicchanges [6 7]
Over the past decade mounting evidence has pointedto the detrimental effects of vascular risk factors on cog-nitive decline in ldquonormalrdquo older adults [8] Hyperten-sion and diabetes have emerged as leading risk fac-tors for declines in attention memory processing speed
Hindawi Publishing CorporationParkinsons DiseaseVolume 2014 Article ID 507529 10 pageshttpdxdoiorg1011552014507529
2 Parkinsonrsquos Disease
and executive functions [8 9] One proposed mechanismaccounting for cardiovascular-linked cognitive changes issmall vessel disease seen as leukoaraiosis (LA) on magneticresonance imaging (MRI) [10] In addition to LA diabetes isrelated to metabolic disruption which preferentially impactshippocampal regions involved in memory recall [11]
By contrast few studies have examined the influence ofcooccurring health conditions (particularly hypertension) oncognitive status of Parkinson patients In part this relates tolower occurrence of hypertension in PD secondary to antihy-pertensive effects of levodopa medications Of those studiesinvestigating the relationship between vascular risk factorsand cognition in PD findings have been mixed One groupof studies (119873 = 3) has used ldquodementia statusrdquo as an outcomeand has found no relationship between presence of vascularrisk factors and a diagnosis of dementia in Parkinsonrsquos disease[12ndash14] A limitation of this approach is that categoricalclassification of yes-no dementia status may be less sensitiveto changes than a parametric approach In contrast a recentstudy using data from a cohort of almost 2000 PD patientsfrom the National Parkinson Quality Improvement Initiative(NPQII) found that diabetes and ldquoheartvascularrdquo diseaseexerted a small but detrimental relationship on two simplemeasures of cognition (animal fluency and a 5-word recallmemory task) [15] Due to the nature of the NPQII datathe study was unable to isolate the effects of hypertensioneliminate individuals with ldquodementiardquo or examine a rangeof cognitive domains that are associated with PD declineThe inconsistencies between the latter and prior studies leaveopen the possibility that while comorbidities may not bedirectly predictive of dementia status they may contribute tocognitive changes that predate dementia onset
The current study examined the effect of a wide range ofhealth comorbidities across distinct neurocognitive domainsin patients with Parkinsonrsquos disease Our working hypoth-esis was that the occurrence of cardiovascular comorbidi-ties would exert detrimental effects on executive functiondelayed memory and processing speed similar to thatobserved in normal elderly To test this hypothesis weidentified a convenience sample of Parkinson patients whohad undergone comprehensive neuropsychological evalua-tion and scored in the unimpaired range on the Demen-tia Rating Scale-II (DRS-II ie gt5th Ile) [16] We thenexamined the contribution of cooccurring health conditionsobtained from medical chart review to specific neurocog-nitive domains We specifically predicted that hypertensionoften associated with frontal-subcortical deregulation wouldbe associated with worse cognitive performance across exec-utive working memory and processing speed domains Weadditionally predicted that comorbidities related to impairedglucose metabolism (diabetes) and hypoxic events (ieacute cardiac events) would contribute to worse delayedmemory recall associated with medial temporal lobe mem-ory systems Because PD itself induces frontal-executivedecline particularly with disease progression we statisticallycontrolled for disease severity in order to identify anyldquoaddedrdquo contribution of cooccurring health conditions oncognition
2 Methods
21 Design A cross-sectional design was used and includeda convenience sample of patients with idiopathic Parkinsonrsquosdisease who had undergone a detailed neuropsychologicalassessment as part of a workup through the University ofFlorida (UF) Center for Movement Disorders and Neu-rorestoration All patients had a diagnosis of idiopathicPD per UK Brain Bank criteria by a movement disorderneurologist [17] The study was approved by the InstitutionalReview Board (IRB) at the University of Florida
22 Participants Participants included 471 patients withidiopathic PD seen between January 2006 and Septem-ber 2010 Participants had undergone neuropsychologicalevaluation and had information pertaining demographicsmedications (including levodopa equivalence dose) healthcomorbidities and PD disease severity (ie ldquoonemedicationrdquoscores from the motor exam of the Unified ParkinsonrsquosDisease Rating Scale UPDRS Part III) [18 19] Exclusioncriteria included past brain surgery (eg deep brain stimula-tion) severe psychiatric disturbance (schizophrenia currentmajor depression episode) severe sensory defects (blindnessdeafness) and impaired scores (lt5th percentile) on theDementia Rating Scale-II (DRS-II) [16] Of the total 471patients reviewed 130 individuals were excluded as follows65 due to low scores on the DRS-II 42 due to previousbrain surgery 17 for missing UPDRS motor scores and 6for missing information regarding disease durationThe finalsample included 341 individuals
23 Neurocognitive Measures Table 1 shows the specific cog-nitive measures that were given as part of the neuropsycho-logical evaluation Tests were grouped into five rationallyderived domains following the approach of Sheline et al [20]and included attentionworking memory delayed episodicmemory (verbal) language executive skills and process-ing speed With the exception of ldquolanguagerdquo all cognitivedomains included at least two tests Scores from eachmeasurewere normed from test-specific manuals or previously pub-lished norms and then converted to Z-scores [21] Compositescores for each domain were calculated by averaging thenormed Z-scores within a domain The advantages of usingcomposite scores include better reliability with multiplemeasures per construct of interest [16] In the event thata patient had multiple neuropsychological evaluations onlydata from the initial exam was used
24 Comorbidities Health comorbidities were documentedby review of medical records at UF-Shands during the yearprior to the neuropsychological exam A listing of over50 health comorbidities was initially compiled based onprevious studies (ie Framingham Heart Study and Charl-son Comorbidity Index) and reviewed by physicians fromneurology and internal medicine [22 23] Comorbiditieswere coded dichotomously for presence or absence by asingle rater Prior to the chart review adequate reliabilitywas established with two additional raters across 10 charts
Parkinsonrsquos Disease 3
Table 1 Cognitive domains
Domain Measures and brief description
Working memory Digit Span measure of auditory attention and working memory from the WAIS-III with both forward andbackwards components dv = forward span and backwards span scores
Episodic memoryHopkins Verbal Learning Test-119877 Form 1 (HVLT-R) 12 item word list learning task with 20 minute delay dv = items recalled after 201015840 delayLogical Memory Stories II (WMS-III) story memory measure dv = units recalled after 30min delay
Language Boston Naming Test (BNT) confrontation naming of line drawings of objectsanimals dv = total itemscorrectly named
Executive function
Trail Making Test Part B (TMT-B) speeded alternating search of letters and numbers (set-shifting) dv = totaltimeStroop Color-Word Test (Golden version) measure of cognitive inhibition of over learned automatic readingresponse dv = number items within 45 sec on color-word trialControlled Oral Word Association Test (COWA) a letter fluency task involving production of words beginningwith target letters during 60 second trials dv = number words produced
Processing speedStroop Single Word Reading (golden version) timed reading of single words denoting red green or blue dv =number words read in 4510158401015840
Trail Making Test Part A (TMT-A) speeded search of letters displayed on a page dv = total timeNote WMS-III Wechsler Memory Scale-Third Edition WAIS-III Wechsler Adult Intelligence Scale-Third Edition dv dependent variable References forindividual tests are in Lezak et al (2012) [16]
(interrater range 119903 = 097ndash098) Comorbidities were con-sidered present if (1) the physician noted its occurrencein a medical note or (2) the patient was prescribed med-ication pertaining to its presence (eg levothyroxine forhypothyroidism) Blood pressure readings were retrievedfrom medical records In accord with past studies investigat-ing cognition and hypertension individuals with a systolicblood pressure ge160mmHg or those on antihypertensivemedication were considered as hypertensive [24] Becausesome specific health conditions occurred relatively infre-quently they were combined into three broad categoriescardiac respiratory and neurologic The cardiac categoryincluded heart attack angina atrial fibrillation arrhythmiaheart murmur congestive heart failure peripheral vasculardisease or any cardiac surgery The respiratory categoryincluded chronic obstructive pulmonary disease pulmonaryembolism emphysema and asthma The neurologic systemcomorbidity included stroke TIA head injury and periph-eral neuropathy
3 Results
Characteristics of the 341 Parkinson samples are shown inTable 2 Overall the PD patients were in their mid-601015840s welleducated (ie approximately 3 years of college) and predom-inantly Caucasian (94) and male (69) In terms of diseasecharacteristics the majority of PD patients were tremorpredominant (827) with disease duration ranging from 1to 33 (mean of 10 years) and a mean ldquoonmedicationrdquo UPDSRmotor score of 264 Approximately 25 were on antianxietymedications and approximately 40 on antidepressants Themean DRS-II score was 1373 with a standard deviation (SD)of 5 As a group performance was lowest on the processingspeed composite score (mean = minus074) followed by executivefunctioning (mean = minus056) and delayed verbal memory
416381
30 295 267 25520 187
12 11 108 103
0
10
20
30
40
50
60
sam
ple (
)
Chol
este
rol
Hyp
erte
nsio
n
Hyp
oten
sion
Neu
rolo
gic
Card
iac
Art
hriti
s
GER
D
Canc
er
Pros
tate
RBSD
Resp
irato
ry
Dia
bete
s
Figure 1 Prevalence of comorbidities in a convenience sample of341 idiopathic Parkinson patients (119873 = 341) Shown is the per-centage of Parkinson patients with various comorbidities based onmedical chart review only comorbidities occurring in at least 10of the sample are shown GERD = gastroesophageal reflux diseaseRBSD = rapid Eye Movement (REM) behavior sleep disorder Nonehave deep brain stimulation
(mean = minus04) Regarding mild cognitive impairment (MCI)subtypes the guidelines of the Movement Disorders Societytaskforce (25) were used for classification into cognitivesubgroups A clinical cutoff criteria of 15 SD below thenormative mean was considered ldquoimpairedrdquo Following theMDS guidelines 180 PD participants (528) were classifiedas cognitively intact 103 (302) as multidomain amnesticMCI 57 (167) as nonamnestic MCI and 1 (03) as singledomain amnestic MCI
Figure 1 shows the distribution of 12 comorbidities thatoccurred in at least 10 of the sample The three mostcommon comorbidities were cholesterolemia (416) hyper-tension (381) and orthostatic hypotension (30)
4 Parkinsonrsquos Disease
Table 2 Sample characteristics
119873 = 304 Parkinsonrsquos disease patients88 caucasian Mean Standard deviation Range
Age (years) 647 10 30ndash90Years of education 150 3 7ndash20Years with symptoms 97 6 1ndash33UPDRS motor score on medication 263 10 7ndash54Percent tremor predominant 82Levodopa equivalency dose 771 532 0ndash2950Dementia Rating Scale-II total score 1372 5 119ndash148Neurocognitive domain 119885-scoreslowast
Executive composite score minus06 09 minus29ndash19Verbal memory composite score minus04 11 minus37ndash18Processing speed composite score minus07 09 minus32ndash19Language composite score 02 12 minus40ndash32Working memory composite score 02 08 minus19ndash27
Mild cognitive impairment (MCI) subtypesPercent amnestic single-domain MCI 03Percent multidomain amnestic MCI 302Percent nonamnestic MCI 167Percent cognitively intact 528
lowast119885-scores based on normative data from test manuals and published norms normative mean = 0 standard deviation = 1 mild cognitive impairment was based
on Movement Disorder Society criteria and utilized a 15 SD below the mean cut value [25] UPDRS Unified Parkinsonrsquos Disease Rating Scale
31 Relationship between Cognition and Cardiovascular RiskFactors To assess the ldquouniquerdquo effect of health comorbidities(including cardiovascular risk factors) on each of the fivecognitive domains a series of hierarchical regression anal-yses were conducted The first block of predictors in eachregression included indices of PD severity (UPDRS motorscores disease duration and LED) whereas the second blockof predictors included subsets of health comorbidities (iehypertension diabetes cancer and arthritis) This approachenabled one to determine the relation between health con-ditions and cognition while statistically controlling for theinfluence of PD disease severity This is important due towell known association between disease severity itself andcognitive decline [3] For each regression the cognitivedomain composite score served as the dependent variable Ofnote only health comorbidities that involved at least 10 ofthe sample were included for the purpose of stability For allregression analyses collinearity diagnostics (tolerance gt 02and variation inflation factor lt 5) and normality (skewnessand kurtosis values lt 1) were appropriate Post hoc testsutilized least significant difference tests [26]
As shown in Table 3 the overall regression models weresignificant for three of the cognitive domains executivefunction delayed verbal memory and processing speedBecause the regression models for the two remaining cog-nitive domains (language and working memory) were notsignificant they were not examined further For all threeldquosignificantrdquo cognitive domains (executive verbal memoryand processing speed) Parkinsonrsquos disease severity exerteda significant effect on cognition Specifically higher UPDRS
motor scores and longer disease duration were associatedwith worse composite scores on executive delayed memoryand processing speed As a whole the addition of ldquohealthcomorbidities in generalrdquo was not significant for any cog-nitive domain However significant effects were present forspecific cardiovascular risk factors namely hypertension andorthostatic hypotension A diagnosis of hypertension (evencontrolled hypertension) was associatedwithworse executivefunction and delayed verbal memory scores These effectswere significant but nevertheless small Unexpectedly thediagnosis of orthostatic hypotension (OH) was associatedwith better scores on tasks of executive function Processingspeed scoreswere not significantly related to any comorbidity
Although cognitive data was normed on age and educa-tion subsequent analyses controlling for age and educationconfirmed the above findings and reinforced that the previousanalyses were not confounded by differences in age or educa-tion Multinominal regression analyses examined differencesin health comorbidities among cognitive subtypes as theoutcome (ie cognitively intact amnestic and nonamnesticMCI groups) Results revealed no significant differences inthe prevalence of comorbidities
32Hypertension-Hypotension Subgroups Hypertension andorthostatic hypotension (OH) often cooccur in individualswith PD Consequently additional analyses were conductedtomore closely examine the separate and combined influenceof hypertension and orthostatic hypotension on executivefunction and memory By way of background OH refersto a drop in blood pressure due to postural changes such
Parkinsonrsquos Disease 5
Table 3 Comorbidities and cognitive domains summary of results of hierarchical multiple regression analyses
119865Δ 1198772Δ Beta Sig
Executive functionFinal model 338 0138 lt0001
PD severity block 10247 0091 lt0001Duration minus0156 lt0001Motor UPDRS minus0246 lt0001
Comorbidity block 1460 0047 0146Hypertension minus0127 0041Hypotension 0134 0019
Delayed verbal memoryFinal model 339 0122 lt0001
PD severity block 9383 0078 lt0001Duration minus0188 lt0001Motor UPDRS minus0227 lt0001
Comorbidity block 1433 0043 0157Hypertension minus0139 0021
Processing speedFinal model 3977 0154 lt0001
PD Severity block 15647 0129 lt0001Duration minus0139 0019Motor UPDRS minus0315 lt0001
Comorbidity block 1433 0043 0157Only significant predictors are shown PP pulse pressure UPDRS Unified Parkinsonrsquos Disease Rating ScalemdashPart III
as standing and can induce dizziness light-headedness orfalls [24] Orthostatic hypotension is a common complicationin PD due to sympathetic denervation and norepinephrinedegeneration in the locus coeruleus [27] ParadoxicallyOH can cooccur with hypertension since the mechanismsunderlying each are quite different For the current analysespatients were assigned to one of four groups those withorthostatic hypotension alone (OH 119873 = 55) those withhypertension alone (HTN 119873 = 82) those with cooccurringOH and hypertension (both 119873 = 48) and individuals withneither comorbidity (normotensivenone 119873 = 156) Sepa-rate analyses of covariance (ANCOVA)were conducted usinggroup (OHHTN both normotensivenone) as the between-subjects factor and covarying for disease severity (UPDRSmotor score disease duration LED) Executive and memorycomposite scores were the dependent variables in each anal-ysis Results of these ANCOVAs revealed a significant maineffect of group for both executive function (F(6 328) = 3568119875 = 0015) and delayed verbal memory (F(6 328) = 2680119875 = 0047) Post hoc tests using least significant difference[26] revealed that the Hypertension group performed worsethan all other groups for executive functioning (all 119875 valueslt 005) with no significant differences among the OH bothor normotensive groups (Figure 2) For delayed memory thehypertension group performed worse than the OH (119875 =0015) and the normotensive groups (119875 = 0026) but not thecombinedboth group
33 Pulse Pressure Because pulse pressure has beendescribed as a more sensitive measure of cardiovascular
risk than either systolic or diastolic pressure alone [23]we performed additional exploratory analyses examiningthe relationship between pulse pressure cognition and PDdisease severity (UPDRS motor scores) Pulse pressure wascomputed from blood pressure readings reported in themedical charts following standard guidelines by subtractingdiastolic from systolic blood pressure values Again aseries of multiple hierarchical regression analyses wereconducted using cognitive domain scores as the outcomevariable in each To control for disease severity PD severitymeasures (UPDRS symptom duration LED) were includedin the first regression block The second block includedpulse pressure and hypertensive medication (recorded as adichotomous variable for presence) A third block includeda residualized pulse pressure by UPDRS interaction termThe latter enabled us to examine whether PD severity andvascular risk interacted to influence cognitive outcomes Asimilar approach has previously been suggested by studiesinvestigating the relationship between white matter changes(leukoaraiosis) and motor functioning in patients with PD[25]
Results of the overall regression model was significantfor executive functioning delayed verbal memory and pro-cessing speed but not for working memory or language(Table 4) The PD severity block was significant across allthree domains whereas the second block (pulse pressureand hypertensive medication) was not significant for anycognitive domainHowever there was a significant interactionbetween UPDRS motor scores and pulse pressure for executivefunction delayed verbal memory and processing speed
6 Parkinsonrsquos Disease
Table 4 Pulse pressure and cognitive domains summary of results of hierarchical multiple regression analyses
119865Δ 1198772Δ Beta Sig
Executive functionFinal model 6297 0112 lt0001
Duration minus0195 lt0001Motor UPDRS minus0218 lt0001PP times UPDRS minus0113 0043
Delayed verbalmemoryFinal model 7603 0110 lt0001
Duration minus0127 0027Motor UPDRS minus0213 lt0001PP times UPDRS minus0138 0010
Processing speedFinal model 6403 0152 lt0001
Duration minus0157 0006Motor UPDRS minus0305 lt0001PP times UPDRS minus0128 0017
Only significant predictors are shown PP pulse pressure UPDRS Unified Parkinsonrsquos Disease Rating ScalemdashPart III
minus12
minus1
minus08
minus06
minus04
minus02
0
Executive Memory
HypertensionHypotension
BothNone
lowast
lowast
lowast
lowast
lowast
Com
posit
iveZ
-sco
re
lowastP lt 005
Figure 2 Executive and verbal memory composite scores in fourblood pressure groups hypertensive hypotension cooccurringhypertension and hypotension (both) and normotensive (none)Figure depicts mean composite Z-scores for executive function anddelayed verbal memory across each of the blood pressure groupsFor executive function Parkinsonrsquos patients with hypertension alone(X = minus0781 SD = 0769) performed significantly worse than thosewith hypotension alone (X = minus0321 SD = 0769 t = minus287 119875 =0004) combined hypertension-hypotension (X = minus0437 SD =0739 t = minus250 119875 = 0013) and normotensivenone (X = minus0495SD = 0898 t = minus221 119875 = 0028) For delayed verbal memoryParkinsonrsquos patients with hypertension alone (X = minus0633 SD =1068) performed significantly worse than those with hypotensionalone (X = minus0194 SD = 1098 t = minus245 119875 = 0015) and thenormotensivenone group (X = minus0301 SD = 1013 t = minus223119875 = 0026) There were no differences in memory between thehypertension and the combined hypertension-hypotension groups
Specifically higher pulse pressure values were significantlyrelated to worse cognitive performance as UPDRS motorscores increased in severity (Figure 3) This pattern wasobserved for executive function delayed verbal memoryand processing speed Taken together this finding suggeststhat worsening vascular integrity (as reflected by pulse-pressure) interacts with PD-indices of disease severity toexert increasingly detrimental effects on executive functionmemory and processing speed
4 Discussion
This retrospective study with 341 nondemented Parkinsonpatients resulted in three important findings First whiledisease severity is a potent indicator of cognitive performancein PD we found that hypertension a common age-relatedcomorbidity that occurred in almost 40 of our sampleexerted a small but independent negative influence on com-posite measures of executive function and delayed verbalmemory This finding aligns itself with a large literature innormal elderly showing the detrimental impact of hyperten-sion on cognition particularly executive functions [28] and isconsistent with recent observations from a large multicenterParkinson cohort [15] Interestingly we did not find supportfor our hypothesis of diabetes or acute cardiac events relatingto memory functioning Previous findings in non-PD eldershave shown both comorbidities to be relatedmedial temporallobe functioning [11] This discrepancy may reflect our smallsample size of diabetics (119873 = 35) and the heterogeneity ofcomorbidities included under the ldquocardiac systemrdquo variable
Our finding that hypertension in PD was associated withworse executive function and delayed memory is in linewith a large literature in older adults documenting negativeinfluence of cardiovascular risk factors However our resultscontrast with a small group of studies that failed to find a
Parkinsonrsquos Disease 7
Pulse pressure120100806040200
Exec
utiv
e fun
ctio
n
00
minus05
minus10
minus15
minus20
(a)
Verb
al m
emor
y
Pulse pressure120100806040200
00
minus05
minus10
minus15
minus20
(b)
Proc
essin
g sp
eed
Pulse pressure120100806040200
00
minus05
minus10
minus15
minus20
1st quartileUPDRS quartiles
2nd quartile3rd quartile4th quartile
(c)
Figure 3 Pulse pressure X UPDRS interaction for 3 cognitive domains Figure depicts linear relationship between pulse pressure andexecutive function delayed verbal memory and processing speed for each Unified Parkinsonrsquos Disease Rating Scale Part III (UPDRS) quartile(higher quartile means more severe motor symptoms)
relationship between cardiovascular risk and transition todementia in Parkinson patient [12ndash14] We suspect that thereare several factors that account for the different findings Thefirst relates to our use of parametric indices of cognitionrather than a categorical classification of dementia presenceused in previous PD students The former approach is amore sensitive metric for detecting cognitive change ordifferences Second our sample size was considerably largerthan previous PD studies and this may be critical given therelatively small effect sizes we observed Additionally previ-ous studies of cognitive status have shown executive functionsto be an insensitive marker of progression to dementia [7]Thuswhile hypertensionmay relate to executive dysfunctionthis cognitive profile may not differentiate dementia from
nondemented PD patients However this view is debatableand has not been established [29]
To be clear the focus of the present study was not to iden-tify those with and without dementia but to learn whetherhypertension and other comorbidities might contribute tothe cognitive profile of Parkinson patients without severecognitive impairment based on a general cognitive screener(DRS-II) Evidence from this study suggests that hyperten-sion does indeed make a small but significant contributionparticularly to executive function and delayedmemory recallOf note the occurrence of hypertension in our PD sampleis less than that often observed in several previous reportsdescribing hypertension to occur in 53ndash70 of individualsabove the age of 65 [24] Possible explanations for this
8 Parkinsonrsquos Disease
discrepancy includes a protective effect against hypertensionsecondary to levodopa use [30] as well as the fact that thisstudy includes individuals younger than 65 years old
The secondmajor finding was an unexpected relationshipbetween executive function and orthostatic hypotensionwhich occurred in approximately 30 of our sample Ourfindings suggested a possible role of orthostatic hypotension(OH) in moderating the relationship between hypertensionand executive function In brief individuals with cooccurringhypertension and OH were on par with individuals with-out hypertension on executive functioning measures Thisphenomenon has not been previously well documented orestablished and requires further validation The relationshipbetweenOH and cognition in the normal elderly has revealedmixed results with some studies failing to find a relationshipbetween cognitive outcomes and OH [31] However onestudy found that the combination of both hypertensionand orthostatic hypotension served as a protective factor[32] Specifically Yap and others found that among 2321older adults those with both OH and high blood pressure(gt140 systolic or gt90 diastolic) were less likely to haveimpaired scores on a broad measure of cognition (MMSE)compared to individuals without OH and those with OHand low blood pressure The mechanism for this effect hasnot been thoroughly examined but may relate a reductionin mean arterial pressure associated with OH allowing forcerebral blood perfusion to stay in the range of autoregulation[33] Within PD a recent study showed that PD patientswith circulatory abnormalities (including OH and supinehypertension) were more likely to meet criteria for dementia[34] Additionally they found that tests of episodic memorybut not executive functions were significantly related todecreases in blood pressure during a head-up-tilt test Sucha finding may suggest that dysautonomia may be related tocognitive changes occurring later in the disease stage ratherthan frontal-executive changes occurring earlier
Third this study showed a unique finding with pulsepressure whereby higher pulse pressure interacted with PDseverity to exert increasingly detrimental effects on executivefunction processing speed and memory In other words therelationship between cognition and cardiovascular risk maybe moderated by PD severity We are unaware of previousstudies examining the effect of pulse pressure on cognition inParkinson patients There are several ways to conceptualizethis relationship On one hand worsening pulse pressuremay be another index of PD progression vis a vis worseningautonomic dysfunction and effects on blood pressure Alter-natively this relationship may be independent of autonomicdysfunction In either case white matter changes mightrepresent downstream effect of this variability A growingnumber of studies have found that the relationship betweenLA and cognition varies depending on PD severity In factstudies of Parkinson patients in more advanced stages haveshown LA to be related to cognition whereas studies ofnewly diagnosed PD patients failed to replicate this finding[12ndash14 35] suggesting that vascular pathology may interactwith PD pathology This idea of an interaction betweenvascular pathology and PD pathology has also been exploredin its relationship to non-cognitive symptoms of PD In
terms of motor complications in PD higher LA burden hasbeen associatedwithworseningmotor functioning includingposturalgait difficulty bradykinesia and rigidity [36]
There are several limitations to this study First thedesign was cross-sectional and used a convenience sample ofpatients which may limit generalizability Next comorbiditymeasures depended on accurate documentation by physi-cians in the patientsrsquo medical charts While the validity ofthis method is unknown we believe the most noteworthycomorbidities were likely noted and recorded as part of thepatientrsquos medical record Lastly other than blood pressurethere were no direct measures of comorbidity and we wereunable to quantify severity or duration of various healthconditions Concerning blood pressure data consisted of onemeasurement rather than multiple blood pressure measure-ments which is more advantageous
5 Conclusion
The current study adds to the literature by suggesting thathypertension may be related to subtle executive and mem-ory deficits in Parkinson patients above and beyond thatconferred by the disease process itself The effect is likelysmall though it does parallel that observed in non-PD olderadults and may become more salient with disease progres-sion What is particularly unique in Parkinsonrsquos disease is ajuxtaposition of factors that are protective versus those thatincrease cardiovascular risk Protective factors include use oflevodopa medications that decrease blood pressure whereasautonomic dysfunction use of dopamine agonists (related tocardiac valvulopathy) and general physical deconditioningserve to increase cardiovascular risk [31] Even with thisunique confluence the present study provides preliminaryevidence that hypertensionmay be related to subtle cognitivedeficits in Parkinson patients similar to that of older adultsand may amplify executive and memory difficulties Futurestudies should examine possiblemechanisms such as LA andthe impact that subtle vascular-related cognitive deficits haveon quality of life andmood Improving cardiovascular healthprior to dementia onset should be further investigated as ameans of moderating cognitive changes Due to high risk ofcognitive declinedementia and the degenerative nature ofPD a small minimization in risk of cognitive decline mayprove to be beneficial
Conflict of Interests
No financial compensation was received for conducting thisstudy Mr Jones reports no disclosures Mr Jacobson IVreports no disclosures Dr Murphy reports no disclosuresDr Price has received research support from the NIH andthe National Parkinson Foundation Dr Okun serves as aconsultant for the National Parkinson Foundation and hasreceived research grants from NIH NPF the Michael J FoxFoundation the Parkinson Alliance Smallwood Foundationand the UF Foundation Dr Okun has previously receivedhonoraria but in the past 24 months has received no supportfrom industry including travel Dr Okun has received roy-alties for publications with Demos Manson and Cambridge
Parkinsonrsquos Disease 9
(movement disorders books) Dr Okun has participated inCME activities onmovement disorders sponsored by theUSFCME office PeerView Vanderbilt University and PrimeTheinstitution andnotDrOkun receives grants fromMedtronicand ANSSt Jude and the PI has no financial interest in thesegrants Dr Okun has participated as a site PI andor co-Ifor several NIH foundation and industry sponsored trialsover the years but has not received honoraria Dr Bowershas received research support from the NIH Michael J FoxFoundation the National Parkinson Foundation and theMcKnight Research Foundation
Acknowledgments
This study was supported by a Center of Excellence Grantfrom the National Parkinson Foundation and the UF-INFORM database
References
[1] G E Alexander M R DeLong and P L Strick ldquoParallelorganization of functionally segregated circuits linking basalganglia and cortexrdquo Annual Review of Neuroscience vol 9 pp357ndash381 1986
[2] K R Chaudhuri and A H Schapira ldquoNon-motor symptoms ofParkinsonrsquos disease dopaminergic pathophysiology and treat-mentrdquoThe Lancet Neurology vol 8 no 5 pp 464ndash474 2009
[3] D Aarsland K Andersen J P Larsen A Lolk H Nielsen andP Kragh-Soslashrensen ldquoRisk of dementia in Parkinsonrsquos disease acommunity-based Prospective StudyrdquoNeurology vol 56 no 6pp 730ndash736 2001
[4] M A Hely W G J Reid M A Adena G M Halliday andJ G L Morris ldquoThe Sydney Multicenter Study of Parkinsonrsquosdisease the inevitability of dementia at 20 yearsrdquo MovementDisorders vol 23 no 6 pp 837ndash844 2008
[5] A SchragM Jahanshahi andNQuinn ldquoHowdoes Parkinsonrsquosdisease affect quality of life A comparison with quality of life inthe general populationrdquo Movement Disorders vol 15 pp 1112ndash1118 2000
[6] B Dubois and B Pillon ldquoCognitive deficits in Parkinsonrsquosdiseaserdquo Journal of Neurology vol 244 no 1 pp 2ndash8 1997
[7] C H Williams-Gray J R Evans A Goris et al ldquoThe distinctcognitive syndromes of Parkinsonrsquos disease 5 year follow-up ofthe CamPaIGN cohortrdquo Brain vol 132 no 11 pp 2958ndash29692009
[8] B K Saxby F Harrington I G McKeith K Wesnes and GA Ford ldquoEffects of hypertension on attention memory andexecutive function in older adultsrdquo Health Psychology vol 22no 6 pp 587ndash591 2003
[9] D Knopman L L Boland TMosley et al ldquoCardiovascular riskfactors and cognitive decline inmiddle-aged adultsrdquoNeurologyvol 56 no 1 pp 42ndash48 2001
[10] A A Gouw A Seewann W M Van Der Flier et al ldquoHet-erogeneity of small vessel disease a systematic review ofMRI and histopathology correlationsrdquo Journal of NeurologyNeurosurgery and Psychiatry vol 82 no 2 pp 126ndash135 2011
[11] W Wu A M Brickman J Luchsinger et al ldquoThe brain in theage of old the hippocampal formation is targeted differentiallyby diseases of late liferdquo Annals of Neurology vol 64 no 6 pp698ndash706 2008
[12] M K Beyer D Aarsland O J Greve and J P Larsen ldquoVisualrating of white matter hyperintensities in Parkinsonrsquos diseaserdquoMovement Disorders vol 21 no 2 pp 223ndash229 2006
[13] S-J Lee J-S Kim J-Y Yoo et al ldquoInfluence of white matterhyperintensities on the cognition of patients with parkinsondiseaserdquoAlzheimerDisease andAssociatedDisorders vol 24 no3 pp 227ndash233 2010
[14] J Sławek D Wieczorek M Derejko et al ldquoThe influenceof vascular risk factors and white matter hyperintensities onthe degree of cognitive impairment in Parkinsonrsquos diseaserdquoNeurologia i Neurochirurgia Polska vol 42 no 6 pp 505ndash5122008
[15] J D Jones I Malaty C C Price M S Okun and DBowers ldquoHealth comorbidities and cognition in 1948 patientswith idiopathic Parkinsonrsquos diseaserdquo Parkinsonism amp RelatedDisorders vol 18 pp 1073ndash1078 2012
[16] M Lezak D Howieson E Bigler and D Tranel Neuropsy-chological Assessment Oxford University Press New York NYUSA 5th edition 2012
[17] A J Hughes S E Daniel L Kilford and A J Lees ldquoAccuracyof clinical diagnosis of idiopathic Parkinsonrsquos disease a clinico-pathological study of 100 casesrdquo Journal of Neurology Neuro-surgery and Psychiatry vol 55 no 3 pp 181ndash184 1992
[18] S Fahn R L Elton and UPDRS Development CommitteeldquoUnified Parkinsonrsquos disease rating scalerdquo Recent DevelopmentParkinson vol 2 pp 153ndash163 1987
[19] C L Tomlinson R Stowe S Patel C Rick R Gray and CE Clarke ldquoSystematic review of levodopa dose equivalencyreporting in Parkinsonrsquos diseaserdquo Movement Disorders vol 25no 15 pp 2649ndash2653 2010
[20] Y I Sheline D M Barch K Garcia et al ldquoCognitive functionin late life Depression relationships to depression severitycerebrovascular risk factors and processing speedrdquo BiologicalPsychiatry vol 60 no 1 pp 58ndash65 2006
[21] R K Heaton S W Miller M J Taylor and I Grant RevisedComprehensive Norms for An expAnded Halstead-Reitan Bat-tery Demographically Adjusted Neuropsychological Norms forAfrican American and Caucasian Adults PAR Lutz Fla USA2004
[22] M Charlson T P Szatrowski J Peterson and J Gold ldquoVal-idation of a combined comorbidity indexrdquo Journal of ClinicalEpidemiology vol 47 no 11 pp 1245ndash1251 1994
[23] PW FWilson KM Anderson andW B Kannel ldquoEpidemiol-ogy of diabetes mellitus in the elderly The Framingham StudyrdquoAmerican Journal of Medicine vol 80 no 5 A pp 3ndash9 1986
[24] W S Aronow J L Fleg C J Pepine et al ldquoACCFAHA 2011expert consensus document on hypertension in the elderlyrdquoJournal of the American College of Cardiology vol 57 pp 2037ndash2114 2011
[25] I Litvan J G Goldman A I Troster et al ldquoDiagnosticcriteria for mild cognitive impairment in Parkinsonrsquos diseaseMovement Disorder Society Task Force guidelinesrdquoMovementDisorders vol 27 no 3 pp 349ndash356 2012
[26] K J Rothman ldquoNo adjustments are needed for multiplecomparisonsrdquo Epidemiology vol 1 no 1 pp 43ndash46 1990
[27] D S Goldstein ldquoDysautonomia in Parkinsonrsquos disease neuro-cardiological abnormalitiesrdquo Lancet Neurology vol 2 no 11 pp669ndash676 2003
[28] A Verdelho SMadureira JM Ferro et al ldquoDifferential impactof cerebral white matter changes diabetes hypertension andstroke on cognitive performance among non-disabled elderly
10 Parkinsonrsquos Disease
The LADIS studyrdquo Journal of Neurology Neurosurgery andPsychiatry vol 78 no 12 pp 1325ndash1330 2007
[29] S P Woods and A I Troster ldquoProdromal frontalexecutivedysfunction predicts incident dementia in Parkinsonrsquos diseaserdquoJournal of the International Neuropsychological Society vol 9no 1 pp 17ndash24 2003
[30] W Nanhoe-Mahabier K F de Laat J E Visser J Zijlmans F-E de Leeuw and B R Bloem ldquoParkinson disease and comorbidcerebrovascular diseaserdquo Nature Reviews Neurology vol 5 no10 pp 533ndash541 2009
[31] K M Rose D Couper M L Eigenbrodt T H Mosley AR Sharrett and R F Gottesman ldquoOrthostatic hypotensionand cognitive function the atherosclerosis risk in communitiesstudyrdquo Neuroepidemiology vol 34 no 1 pp 1ndash7 2010
[32] P L K Yap M Niti K B Yap and T P Ng ldquoOrthostatichypotension hypotension and cognitive status early comorbidmarkers of primary dementiardquo Dementia and Geriatric Cogni-tive Disorders vol 26 no 3 pp 239ndash246 2008
[33] V Novak and I Hajjar ldquoThe relationship between bloodpressure and cognitive functionrdquo Nature Reviews Cardiologyvol 7 no 12 pp 686ndash698 2010
[34] J S Kim Y S Oh K S Lee Y I Kim D W Yang andD S Goldstein ldquoAssociation of cognitive dysfunction withneurocirculatory abnormalities in early Parkinson diseaserdquoNeurology vol 79 no 13 pp 1323ndash1331 2012
[35] T O Dalaker J P Larsen M G Dwyer et al ldquoWhite matterhyperintensities do not impact cognitive function in patientswith newly diagnosed Parkinsonrsquos diseaserdquoNeuroImage vol 47no 4 pp 2083ndash2089 2009
[36] N I Bohnen and R L Albin ldquoWhite matter lesions inParkinson diseaserdquo Nature Reviews Neurology vol 7 no 4 pp229ndash236 2011

2 Parkinsonrsquos Disease
and executive functions [8 9] One proposed mechanismaccounting for cardiovascular-linked cognitive changes issmall vessel disease seen as leukoaraiosis (LA) on magneticresonance imaging (MRI) [10] In addition to LA diabetes isrelated to metabolic disruption which preferentially impactshippocampal regions involved in memory recall [11]
By contrast few studies have examined the influence ofcooccurring health conditions (particularly hypertension) oncognitive status of Parkinson patients In part this relates tolower occurrence of hypertension in PD secondary to antihy-pertensive effects of levodopa medications Of those studiesinvestigating the relationship between vascular risk factorsand cognition in PD findings have been mixed One groupof studies (119873 = 3) has used ldquodementia statusrdquo as an outcomeand has found no relationship between presence of vascularrisk factors and a diagnosis of dementia in Parkinsonrsquos disease[12ndash14] A limitation of this approach is that categoricalclassification of yes-no dementia status may be less sensitiveto changes than a parametric approach In contrast a recentstudy using data from a cohort of almost 2000 PD patientsfrom the National Parkinson Quality Improvement Initiative(NPQII) found that diabetes and ldquoheartvascularrdquo diseaseexerted a small but detrimental relationship on two simplemeasures of cognition (animal fluency and a 5-word recallmemory task) [15] Due to the nature of the NPQII datathe study was unable to isolate the effects of hypertensioneliminate individuals with ldquodementiardquo or examine a rangeof cognitive domains that are associated with PD declineThe inconsistencies between the latter and prior studies leaveopen the possibility that while comorbidities may not bedirectly predictive of dementia status they may contribute tocognitive changes that predate dementia onset
The current study examined the effect of a wide range ofhealth comorbidities across distinct neurocognitive domainsin patients with Parkinsonrsquos disease Our working hypoth-esis was that the occurrence of cardiovascular comorbidi-ties would exert detrimental effects on executive functiondelayed memory and processing speed similar to thatobserved in normal elderly To test this hypothesis weidentified a convenience sample of Parkinson patients whohad undergone comprehensive neuropsychological evalua-tion and scored in the unimpaired range on the Demen-tia Rating Scale-II (DRS-II ie gt5th Ile) [16] We thenexamined the contribution of cooccurring health conditionsobtained from medical chart review to specific neurocog-nitive domains We specifically predicted that hypertensionoften associated with frontal-subcortical deregulation wouldbe associated with worse cognitive performance across exec-utive working memory and processing speed domains Weadditionally predicted that comorbidities related to impairedglucose metabolism (diabetes) and hypoxic events (ieacute cardiac events) would contribute to worse delayedmemory recall associated with medial temporal lobe mem-ory systems Because PD itself induces frontal-executivedecline particularly with disease progression we statisticallycontrolled for disease severity in order to identify anyldquoaddedrdquo contribution of cooccurring health conditions oncognition
2 Methods
21 Design A cross-sectional design was used and includeda convenience sample of patients with idiopathic Parkinsonrsquosdisease who had undergone a detailed neuropsychologicalassessment as part of a workup through the University ofFlorida (UF) Center for Movement Disorders and Neu-rorestoration All patients had a diagnosis of idiopathicPD per UK Brain Bank criteria by a movement disorderneurologist [17] The study was approved by the InstitutionalReview Board (IRB) at the University of Florida
22 Participants Participants included 471 patients withidiopathic PD seen between January 2006 and Septem-ber 2010 Participants had undergone neuropsychologicalevaluation and had information pertaining demographicsmedications (including levodopa equivalence dose) healthcomorbidities and PD disease severity (ie ldquoonemedicationrdquoscores from the motor exam of the Unified ParkinsonrsquosDisease Rating Scale UPDRS Part III) [18 19] Exclusioncriteria included past brain surgery (eg deep brain stimula-tion) severe psychiatric disturbance (schizophrenia currentmajor depression episode) severe sensory defects (blindnessdeafness) and impaired scores (lt5th percentile) on theDementia Rating Scale-II (DRS-II) [16] Of the total 471patients reviewed 130 individuals were excluded as follows65 due to low scores on the DRS-II 42 due to previousbrain surgery 17 for missing UPDRS motor scores and 6for missing information regarding disease durationThe finalsample included 341 individuals
23 Neurocognitive Measures Table 1 shows the specific cog-nitive measures that were given as part of the neuropsycho-logical evaluation Tests were grouped into five rationallyderived domains following the approach of Sheline et al [20]and included attentionworking memory delayed episodicmemory (verbal) language executive skills and process-ing speed With the exception of ldquolanguagerdquo all cognitivedomains included at least two tests Scores from eachmeasurewere normed from test-specific manuals or previously pub-lished norms and then converted to Z-scores [21] Compositescores for each domain were calculated by averaging thenormed Z-scores within a domain The advantages of usingcomposite scores include better reliability with multiplemeasures per construct of interest [16] In the event thata patient had multiple neuropsychological evaluations onlydata from the initial exam was used
24 Comorbidities Health comorbidities were documentedby review of medical records at UF-Shands during the yearprior to the neuropsychological exam A listing of over50 health comorbidities was initially compiled based onprevious studies (ie Framingham Heart Study and Charl-son Comorbidity Index) and reviewed by physicians fromneurology and internal medicine [22 23] Comorbiditieswere coded dichotomously for presence or absence by asingle rater Prior to the chart review adequate reliabilitywas established with two additional raters across 10 charts
Parkinsonrsquos Disease 3
Table 1 Cognitive domains
Domain Measures and brief description
Working memory Digit Span measure of auditory attention and working memory from the WAIS-III with both forward andbackwards components dv = forward span and backwards span scores
Episodic memoryHopkins Verbal Learning Test-119877 Form 1 (HVLT-R) 12 item word list learning task with 20 minute delay dv = items recalled after 201015840 delayLogical Memory Stories II (WMS-III) story memory measure dv = units recalled after 30min delay
Language Boston Naming Test (BNT) confrontation naming of line drawings of objectsanimals dv = total itemscorrectly named
Executive function
Trail Making Test Part B (TMT-B) speeded alternating search of letters and numbers (set-shifting) dv = totaltimeStroop Color-Word Test (Golden version) measure of cognitive inhibition of over learned automatic readingresponse dv = number items within 45 sec on color-word trialControlled Oral Word Association Test (COWA) a letter fluency task involving production of words beginningwith target letters during 60 second trials dv = number words produced
Processing speedStroop Single Word Reading (golden version) timed reading of single words denoting red green or blue dv =number words read in 4510158401015840
Trail Making Test Part A (TMT-A) speeded search of letters displayed on a page dv = total timeNote WMS-III Wechsler Memory Scale-Third Edition WAIS-III Wechsler Adult Intelligence Scale-Third Edition dv dependent variable References forindividual tests are in Lezak et al (2012) [16]
(interrater range 119903 = 097ndash098) Comorbidities were con-sidered present if (1) the physician noted its occurrencein a medical note or (2) the patient was prescribed med-ication pertaining to its presence (eg levothyroxine forhypothyroidism) Blood pressure readings were retrievedfrom medical records In accord with past studies investigat-ing cognition and hypertension individuals with a systolicblood pressure ge160mmHg or those on antihypertensivemedication were considered as hypertensive [24] Becausesome specific health conditions occurred relatively infre-quently they were combined into three broad categoriescardiac respiratory and neurologic The cardiac categoryincluded heart attack angina atrial fibrillation arrhythmiaheart murmur congestive heart failure peripheral vasculardisease or any cardiac surgery The respiratory categoryincluded chronic obstructive pulmonary disease pulmonaryembolism emphysema and asthma The neurologic systemcomorbidity included stroke TIA head injury and periph-eral neuropathy
3 Results
Characteristics of the 341 Parkinson samples are shown inTable 2 Overall the PD patients were in their mid-601015840s welleducated (ie approximately 3 years of college) and predom-inantly Caucasian (94) and male (69) In terms of diseasecharacteristics the majority of PD patients were tremorpredominant (827) with disease duration ranging from 1to 33 (mean of 10 years) and a mean ldquoonmedicationrdquo UPDSRmotor score of 264 Approximately 25 were on antianxietymedications and approximately 40 on antidepressants Themean DRS-II score was 1373 with a standard deviation (SD)of 5 As a group performance was lowest on the processingspeed composite score (mean = minus074) followed by executivefunctioning (mean = minus056) and delayed verbal memory
416381
30 295 267 25520 187
12 11 108 103
0
10
20
30
40
50
60
sam
ple (
)
Chol
este
rol
Hyp
erte
nsio
n
Hyp
oten
sion
Neu
rolo
gic
Card
iac
Art
hriti
s
GER
D
Canc
er
Pros
tate
RBSD
Resp
irato
ry
Dia
bete
s
Figure 1 Prevalence of comorbidities in a convenience sample of341 idiopathic Parkinson patients (119873 = 341) Shown is the per-centage of Parkinson patients with various comorbidities based onmedical chart review only comorbidities occurring in at least 10of the sample are shown GERD = gastroesophageal reflux diseaseRBSD = rapid Eye Movement (REM) behavior sleep disorder Nonehave deep brain stimulation
(mean = minus04) Regarding mild cognitive impairment (MCI)subtypes the guidelines of the Movement Disorders Societytaskforce (25) were used for classification into cognitivesubgroups A clinical cutoff criteria of 15 SD below thenormative mean was considered ldquoimpairedrdquo Following theMDS guidelines 180 PD participants (528) were classifiedas cognitively intact 103 (302) as multidomain amnesticMCI 57 (167) as nonamnestic MCI and 1 (03) as singledomain amnestic MCI
Figure 1 shows the distribution of 12 comorbidities thatoccurred in at least 10 of the sample The three mostcommon comorbidities were cholesterolemia (416) hyper-tension (381) and orthostatic hypotension (30)
4 Parkinsonrsquos Disease
Table 2 Sample characteristics
119873 = 304 Parkinsonrsquos disease patients88 caucasian Mean Standard deviation Range
Age (years) 647 10 30ndash90Years of education 150 3 7ndash20Years with symptoms 97 6 1ndash33UPDRS motor score on medication 263 10 7ndash54Percent tremor predominant 82Levodopa equivalency dose 771 532 0ndash2950Dementia Rating Scale-II total score 1372 5 119ndash148Neurocognitive domain 119885-scoreslowast
Executive composite score minus06 09 minus29ndash19Verbal memory composite score minus04 11 minus37ndash18Processing speed composite score minus07 09 minus32ndash19Language composite score 02 12 minus40ndash32Working memory composite score 02 08 minus19ndash27
Mild cognitive impairment (MCI) subtypesPercent amnestic single-domain MCI 03Percent multidomain amnestic MCI 302Percent nonamnestic MCI 167Percent cognitively intact 528
lowast119885-scores based on normative data from test manuals and published norms normative mean = 0 standard deviation = 1 mild cognitive impairment was based
on Movement Disorder Society criteria and utilized a 15 SD below the mean cut value [25] UPDRS Unified Parkinsonrsquos Disease Rating Scale
31 Relationship between Cognition and Cardiovascular RiskFactors To assess the ldquouniquerdquo effect of health comorbidities(including cardiovascular risk factors) on each of the fivecognitive domains a series of hierarchical regression anal-yses were conducted The first block of predictors in eachregression included indices of PD severity (UPDRS motorscores disease duration and LED) whereas the second blockof predictors included subsets of health comorbidities (iehypertension diabetes cancer and arthritis) This approachenabled one to determine the relation between health con-ditions and cognition while statistically controlling for theinfluence of PD disease severity This is important due towell known association between disease severity itself andcognitive decline [3] For each regression the cognitivedomain composite score served as the dependent variable Ofnote only health comorbidities that involved at least 10 ofthe sample were included for the purpose of stability For allregression analyses collinearity diagnostics (tolerance gt 02and variation inflation factor lt 5) and normality (skewnessand kurtosis values lt 1) were appropriate Post hoc testsutilized least significant difference tests [26]
As shown in Table 3 the overall regression models weresignificant for three of the cognitive domains executivefunction delayed verbal memory and processing speedBecause the regression models for the two remaining cog-nitive domains (language and working memory) were notsignificant they were not examined further For all threeldquosignificantrdquo cognitive domains (executive verbal memoryand processing speed) Parkinsonrsquos disease severity exerteda significant effect on cognition Specifically higher UPDRS
motor scores and longer disease duration were associatedwith worse composite scores on executive delayed memoryand processing speed As a whole the addition of ldquohealthcomorbidities in generalrdquo was not significant for any cog-nitive domain However significant effects were present forspecific cardiovascular risk factors namely hypertension andorthostatic hypotension A diagnosis of hypertension (evencontrolled hypertension) was associatedwithworse executivefunction and delayed verbal memory scores These effectswere significant but nevertheless small Unexpectedly thediagnosis of orthostatic hypotension (OH) was associatedwith better scores on tasks of executive function Processingspeed scoreswere not significantly related to any comorbidity
Although cognitive data was normed on age and educa-tion subsequent analyses controlling for age and educationconfirmed the above findings and reinforced that the previousanalyses were not confounded by differences in age or educa-tion Multinominal regression analyses examined differencesin health comorbidities among cognitive subtypes as theoutcome (ie cognitively intact amnestic and nonamnesticMCI groups) Results revealed no significant differences inthe prevalence of comorbidities
32Hypertension-Hypotension Subgroups Hypertension andorthostatic hypotension (OH) often cooccur in individualswith PD Consequently additional analyses were conductedtomore closely examine the separate and combined influenceof hypertension and orthostatic hypotension on executivefunction and memory By way of background OH refersto a drop in blood pressure due to postural changes such
Parkinsonrsquos Disease 5
Table 3 Comorbidities and cognitive domains summary of results of hierarchical multiple regression analyses
119865Δ 1198772Δ Beta Sig
Executive functionFinal model 338 0138 lt0001
PD severity block 10247 0091 lt0001Duration minus0156 lt0001Motor UPDRS minus0246 lt0001
Comorbidity block 1460 0047 0146Hypertension minus0127 0041Hypotension 0134 0019
Delayed verbal memoryFinal model 339 0122 lt0001
PD severity block 9383 0078 lt0001Duration minus0188 lt0001Motor UPDRS minus0227 lt0001
Comorbidity block 1433 0043 0157Hypertension minus0139 0021
Processing speedFinal model 3977 0154 lt0001
PD Severity block 15647 0129 lt0001Duration minus0139 0019Motor UPDRS minus0315 lt0001
Comorbidity block 1433 0043 0157Only significant predictors are shown PP pulse pressure UPDRS Unified Parkinsonrsquos Disease Rating ScalemdashPart III
as standing and can induce dizziness light-headedness orfalls [24] Orthostatic hypotension is a common complicationin PD due to sympathetic denervation and norepinephrinedegeneration in the locus coeruleus [27] ParadoxicallyOH can cooccur with hypertension since the mechanismsunderlying each are quite different For the current analysespatients were assigned to one of four groups those withorthostatic hypotension alone (OH 119873 = 55) those withhypertension alone (HTN 119873 = 82) those with cooccurringOH and hypertension (both 119873 = 48) and individuals withneither comorbidity (normotensivenone 119873 = 156) Sepa-rate analyses of covariance (ANCOVA)were conducted usinggroup (OHHTN both normotensivenone) as the between-subjects factor and covarying for disease severity (UPDRSmotor score disease duration LED) Executive and memorycomposite scores were the dependent variables in each anal-ysis Results of these ANCOVAs revealed a significant maineffect of group for both executive function (F(6 328) = 3568119875 = 0015) and delayed verbal memory (F(6 328) = 2680119875 = 0047) Post hoc tests using least significant difference[26] revealed that the Hypertension group performed worsethan all other groups for executive functioning (all 119875 valueslt 005) with no significant differences among the OH bothor normotensive groups (Figure 2) For delayed memory thehypertension group performed worse than the OH (119875 =0015) and the normotensive groups (119875 = 0026) but not thecombinedboth group
33 Pulse Pressure Because pulse pressure has beendescribed as a more sensitive measure of cardiovascular
risk than either systolic or diastolic pressure alone [23]we performed additional exploratory analyses examiningthe relationship between pulse pressure cognition and PDdisease severity (UPDRS motor scores) Pulse pressure wascomputed from blood pressure readings reported in themedical charts following standard guidelines by subtractingdiastolic from systolic blood pressure values Again aseries of multiple hierarchical regression analyses wereconducted using cognitive domain scores as the outcomevariable in each To control for disease severity PD severitymeasures (UPDRS symptom duration LED) were includedin the first regression block The second block includedpulse pressure and hypertensive medication (recorded as adichotomous variable for presence) A third block includeda residualized pulse pressure by UPDRS interaction termThe latter enabled us to examine whether PD severity andvascular risk interacted to influence cognitive outcomes Asimilar approach has previously been suggested by studiesinvestigating the relationship between white matter changes(leukoaraiosis) and motor functioning in patients with PD[25]
Results of the overall regression model was significantfor executive functioning delayed verbal memory and pro-cessing speed but not for working memory or language(Table 4) The PD severity block was significant across allthree domains whereas the second block (pulse pressureand hypertensive medication) was not significant for anycognitive domainHowever there was a significant interactionbetween UPDRS motor scores and pulse pressure for executivefunction delayed verbal memory and processing speed
6 Parkinsonrsquos Disease
Table 4 Pulse pressure and cognitive domains summary of results of hierarchical multiple regression analyses
119865Δ 1198772Δ Beta Sig
Executive functionFinal model 6297 0112 lt0001
Duration minus0195 lt0001Motor UPDRS minus0218 lt0001PP times UPDRS minus0113 0043
Delayed verbalmemoryFinal model 7603 0110 lt0001
Duration minus0127 0027Motor UPDRS minus0213 lt0001PP times UPDRS minus0138 0010
Processing speedFinal model 6403 0152 lt0001
Duration minus0157 0006Motor UPDRS minus0305 lt0001PP times UPDRS minus0128 0017
Only significant predictors are shown PP pulse pressure UPDRS Unified Parkinsonrsquos Disease Rating ScalemdashPart III
minus12
minus1
minus08
minus06
minus04
minus02
0
Executive Memory
HypertensionHypotension
BothNone
lowast
lowast
lowast
lowast
lowast
Com
posit
iveZ
-sco
re
lowastP lt 005
Figure 2 Executive and verbal memory composite scores in fourblood pressure groups hypertensive hypotension cooccurringhypertension and hypotension (both) and normotensive (none)Figure depicts mean composite Z-scores for executive function anddelayed verbal memory across each of the blood pressure groupsFor executive function Parkinsonrsquos patients with hypertension alone(X = minus0781 SD = 0769) performed significantly worse than thosewith hypotension alone (X = minus0321 SD = 0769 t = minus287 119875 =0004) combined hypertension-hypotension (X = minus0437 SD =0739 t = minus250 119875 = 0013) and normotensivenone (X = minus0495SD = 0898 t = minus221 119875 = 0028) For delayed verbal memoryParkinsonrsquos patients with hypertension alone (X = minus0633 SD =1068) performed significantly worse than those with hypotensionalone (X = minus0194 SD = 1098 t = minus245 119875 = 0015) and thenormotensivenone group (X = minus0301 SD = 1013 t = minus223119875 = 0026) There were no differences in memory between thehypertension and the combined hypertension-hypotension groups
Specifically higher pulse pressure values were significantlyrelated to worse cognitive performance as UPDRS motorscores increased in severity (Figure 3) This pattern wasobserved for executive function delayed verbal memoryand processing speed Taken together this finding suggeststhat worsening vascular integrity (as reflected by pulse-pressure) interacts with PD-indices of disease severity toexert increasingly detrimental effects on executive functionmemory and processing speed
4 Discussion
This retrospective study with 341 nondemented Parkinsonpatients resulted in three important findings First whiledisease severity is a potent indicator of cognitive performancein PD we found that hypertension a common age-relatedcomorbidity that occurred in almost 40 of our sampleexerted a small but independent negative influence on com-posite measures of executive function and delayed verbalmemory This finding aligns itself with a large literature innormal elderly showing the detrimental impact of hyperten-sion on cognition particularly executive functions [28] and isconsistent with recent observations from a large multicenterParkinson cohort [15] Interestingly we did not find supportfor our hypothesis of diabetes or acute cardiac events relatingto memory functioning Previous findings in non-PD eldershave shown both comorbidities to be relatedmedial temporallobe functioning [11] This discrepancy may reflect our smallsample size of diabetics (119873 = 35) and the heterogeneity ofcomorbidities included under the ldquocardiac systemrdquo variable
Our finding that hypertension in PD was associated withworse executive function and delayed memory is in linewith a large literature in older adults documenting negativeinfluence of cardiovascular risk factors However our resultscontrast with a small group of studies that failed to find a
Parkinsonrsquos Disease 7
Pulse pressure120100806040200
Exec
utiv
e fun
ctio
n
00
minus05
minus10
minus15
minus20
(a)
Verb
al m
emor
y
Pulse pressure120100806040200
00
minus05
minus10
minus15
minus20
(b)
Proc
essin
g sp
eed
Pulse pressure120100806040200
00
minus05
minus10
minus15
minus20
1st quartileUPDRS quartiles
2nd quartile3rd quartile4th quartile
(c)
Figure 3 Pulse pressure X UPDRS interaction for 3 cognitive domains Figure depicts linear relationship between pulse pressure andexecutive function delayed verbal memory and processing speed for each Unified Parkinsonrsquos Disease Rating Scale Part III (UPDRS) quartile(higher quartile means more severe motor symptoms)
relationship between cardiovascular risk and transition todementia in Parkinson patient [12ndash14] We suspect that thereare several factors that account for the different findings Thefirst relates to our use of parametric indices of cognitionrather than a categorical classification of dementia presenceused in previous PD students The former approach is amore sensitive metric for detecting cognitive change ordifferences Second our sample size was considerably largerthan previous PD studies and this may be critical given therelatively small effect sizes we observed Additionally previ-ous studies of cognitive status have shown executive functionsto be an insensitive marker of progression to dementia [7]Thuswhile hypertensionmay relate to executive dysfunctionthis cognitive profile may not differentiate dementia from
nondemented PD patients However this view is debatableand has not been established [29]
To be clear the focus of the present study was not to iden-tify those with and without dementia but to learn whetherhypertension and other comorbidities might contribute tothe cognitive profile of Parkinson patients without severecognitive impairment based on a general cognitive screener(DRS-II) Evidence from this study suggests that hyperten-sion does indeed make a small but significant contributionparticularly to executive function and delayedmemory recallOf note the occurrence of hypertension in our PD sampleis less than that often observed in several previous reportsdescribing hypertension to occur in 53ndash70 of individualsabove the age of 65 [24] Possible explanations for this
8 Parkinsonrsquos Disease
discrepancy includes a protective effect against hypertensionsecondary to levodopa use [30] as well as the fact that thisstudy includes individuals younger than 65 years old
The secondmajor finding was an unexpected relationshipbetween executive function and orthostatic hypotensionwhich occurred in approximately 30 of our sample Ourfindings suggested a possible role of orthostatic hypotension(OH) in moderating the relationship between hypertensionand executive function In brief individuals with cooccurringhypertension and OH were on par with individuals with-out hypertension on executive functioning measures Thisphenomenon has not been previously well documented orestablished and requires further validation The relationshipbetweenOH and cognition in the normal elderly has revealedmixed results with some studies failing to find a relationshipbetween cognitive outcomes and OH [31] However onestudy found that the combination of both hypertensionand orthostatic hypotension served as a protective factor[32] Specifically Yap and others found that among 2321older adults those with both OH and high blood pressure(gt140 systolic or gt90 diastolic) were less likely to haveimpaired scores on a broad measure of cognition (MMSE)compared to individuals without OH and those with OHand low blood pressure The mechanism for this effect hasnot been thoroughly examined but may relate a reductionin mean arterial pressure associated with OH allowing forcerebral blood perfusion to stay in the range of autoregulation[33] Within PD a recent study showed that PD patientswith circulatory abnormalities (including OH and supinehypertension) were more likely to meet criteria for dementia[34] Additionally they found that tests of episodic memorybut not executive functions were significantly related todecreases in blood pressure during a head-up-tilt test Sucha finding may suggest that dysautonomia may be related tocognitive changes occurring later in the disease stage ratherthan frontal-executive changes occurring earlier
Third this study showed a unique finding with pulsepressure whereby higher pulse pressure interacted with PDseverity to exert increasingly detrimental effects on executivefunction processing speed and memory In other words therelationship between cognition and cardiovascular risk maybe moderated by PD severity We are unaware of previousstudies examining the effect of pulse pressure on cognition inParkinson patients There are several ways to conceptualizethis relationship On one hand worsening pulse pressuremay be another index of PD progression vis a vis worseningautonomic dysfunction and effects on blood pressure Alter-natively this relationship may be independent of autonomicdysfunction In either case white matter changes mightrepresent downstream effect of this variability A growingnumber of studies have found that the relationship betweenLA and cognition varies depending on PD severity In factstudies of Parkinson patients in more advanced stages haveshown LA to be related to cognition whereas studies ofnewly diagnosed PD patients failed to replicate this finding[12ndash14 35] suggesting that vascular pathology may interactwith PD pathology This idea of an interaction betweenvascular pathology and PD pathology has also been exploredin its relationship to non-cognitive symptoms of PD In
terms of motor complications in PD higher LA burden hasbeen associatedwithworseningmotor functioning includingposturalgait difficulty bradykinesia and rigidity [36]
There are several limitations to this study First thedesign was cross-sectional and used a convenience sample ofpatients which may limit generalizability Next comorbiditymeasures depended on accurate documentation by physi-cians in the patientsrsquo medical charts While the validity ofthis method is unknown we believe the most noteworthycomorbidities were likely noted and recorded as part of thepatientrsquos medical record Lastly other than blood pressurethere were no direct measures of comorbidity and we wereunable to quantify severity or duration of various healthconditions Concerning blood pressure data consisted of onemeasurement rather than multiple blood pressure measure-ments which is more advantageous
5 Conclusion
The current study adds to the literature by suggesting thathypertension may be related to subtle executive and mem-ory deficits in Parkinson patients above and beyond thatconferred by the disease process itself The effect is likelysmall though it does parallel that observed in non-PD olderadults and may become more salient with disease progres-sion What is particularly unique in Parkinsonrsquos disease is ajuxtaposition of factors that are protective versus those thatincrease cardiovascular risk Protective factors include use oflevodopa medications that decrease blood pressure whereasautonomic dysfunction use of dopamine agonists (related tocardiac valvulopathy) and general physical deconditioningserve to increase cardiovascular risk [31] Even with thisunique confluence the present study provides preliminaryevidence that hypertensionmay be related to subtle cognitivedeficits in Parkinson patients similar to that of older adultsand may amplify executive and memory difficulties Futurestudies should examine possiblemechanisms such as LA andthe impact that subtle vascular-related cognitive deficits haveon quality of life andmood Improving cardiovascular healthprior to dementia onset should be further investigated as ameans of moderating cognitive changes Due to high risk ofcognitive declinedementia and the degenerative nature ofPD a small minimization in risk of cognitive decline mayprove to be beneficial
Conflict of Interests
No financial compensation was received for conducting thisstudy Mr Jones reports no disclosures Mr Jacobson IVreports no disclosures Dr Murphy reports no disclosuresDr Price has received research support from the NIH andthe National Parkinson Foundation Dr Okun serves as aconsultant for the National Parkinson Foundation and hasreceived research grants from NIH NPF the Michael J FoxFoundation the Parkinson Alliance Smallwood Foundationand the UF Foundation Dr Okun has previously receivedhonoraria but in the past 24 months has received no supportfrom industry including travel Dr Okun has received roy-alties for publications with Demos Manson and Cambridge
Parkinsonrsquos Disease 9
(movement disorders books) Dr Okun has participated inCME activities onmovement disorders sponsored by theUSFCME office PeerView Vanderbilt University and PrimeTheinstitution andnotDrOkun receives grants fromMedtronicand ANSSt Jude and the PI has no financial interest in thesegrants Dr Okun has participated as a site PI andor co-Ifor several NIH foundation and industry sponsored trialsover the years but has not received honoraria Dr Bowershas received research support from the NIH Michael J FoxFoundation the National Parkinson Foundation and theMcKnight Research Foundation
Acknowledgments
This study was supported by a Center of Excellence Grantfrom the National Parkinson Foundation and the UF-INFORM database
References
[1] G E Alexander M R DeLong and P L Strick ldquoParallelorganization of functionally segregated circuits linking basalganglia and cortexrdquo Annual Review of Neuroscience vol 9 pp357ndash381 1986
[2] K R Chaudhuri and A H Schapira ldquoNon-motor symptoms ofParkinsonrsquos disease dopaminergic pathophysiology and treat-mentrdquoThe Lancet Neurology vol 8 no 5 pp 464ndash474 2009
[3] D Aarsland K Andersen J P Larsen A Lolk H Nielsen andP Kragh-Soslashrensen ldquoRisk of dementia in Parkinsonrsquos disease acommunity-based Prospective StudyrdquoNeurology vol 56 no 6pp 730ndash736 2001
[4] M A Hely W G J Reid M A Adena G M Halliday andJ G L Morris ldquoThe Sydney Multicenter Study of Parkinsonrsquosdisease the inevitability of dementia at 20 yearsrdquo MovementDisorders vol 23 no 6 pp 837ndash844 2008
[5] A SchragM Jahanshahi andNQuinn ldquoHowdoes Parkinsonrsquosdisease affect quality of life A comparison with quality of life inthe general populationrdquo Movement Disorders vol 15 pp 1112ndash1118 2000
[6] B Dubois and B Pillon ldquoCognitive deficits in Parkinsonrsquosdiseaserdquo Journal of Neurology vol 244 no 1 pp 2ndash8 1997
[7] C H Williams-Gray J R Evans A Goris et al ldquoThe distinctcognitive syndromes of Parkinsonrsquos disease 5 year follow-up ofthe CamPaIGN cohortrdquo Brain vol 132 no 11 pp 2958ndash29692009
[8] B K Saxby F Harrington I G McKeith K Wesnes and GA Ford ldquoEffects of hypertension on attention memory andexecutive function in older adultsrdquo Health Psychology vol 22no 6 pp 587ndash591 2003
[9] D Knopman L L Boland TMosley et al ldquoCardiovascular riskfactors and cognitive decline inmiddle-aged adultsrdquoNeurologyvol 56 no 1 pp 42ndash48 2001
[10] A A Gouw A Seewann W M Van Der Flier et al ldquoHet-erogeneity of small vessel disease a systematic review ofMRI and histopathology correlationsrdquo Journal of NeurologyNeurosurgery and Psychiatry vol 82 no 2 pp 126ndash135 2011
[11] W Wu A M Brickman J Luchsinger et al ldquoThe brain in theage of old the hippocampal formation is targeted differentiallyby diseases of late liferdquo Annals of Neurology vol 64 no 6 pp698ndash706 2008
[12] M K Beyer D Aarsland O J Greve and J P Larsen ldquoVisualrating of white matter hyperintensities in Parkinsonrsquos diseaserdquoMovement Disorders vol 21 no 2 pp 223ndash229 2006
[13] S-J Lee J-S Kim J-Y Yoo et al ldquoInfluence of white matterhyperintensities on the cognition of patients with parkinsondiseaserdquoAlzheimerDisease andAssociatedDisorders vol 24 no3 pp 227ndash233 2010
[14] J Sławek D Wieczorek M Derejko et al ldquoThe influenceof vascular risk factors and white matter hyperintensities onthe degree of cognitive impairment in Parkinsonrsquos diseaserdquoNeurologia i Neurochirurgia Polska vol 42 no 6 pp 505ndash5122008
[15] J D Jones I Malaty C C Price M S Okun and DBowers ldquoHealth comorbidities and cognition in 1948 patientswith idiopathic Parkinsonrsquos diseaserdquo Parkinsonism amp RelatedDisorders vol 18 pp 1073ndash1078 2012
[16] M Lezak D Howieson E Bigler and D Tranel Neuropsy-chological Assessment Oxford University Press New York NYUSA 5th edition 2012
[17] A J Hughes S E Daniel L Kilford and A J Lees ldquoAccuracyof clinical diagnosis of idiopathic Parkinsonrsquos disease a clinico-pathological study of 100 casesrdquo Journal of Neurology Neuro-surgery and Psychiatry vol 55 no 3 pp 181ndash184 1992
[18] S Fahn R L Elton and UPDRS Development CommitteeldquoUnified Parkinsonrsquos disease rating scalerdquo Recent DevelopmentParkinson vol 2 pp 153ndash163 1987
[19] C L Tomlinson R Stowe S Patel C Rick R Gray and CE Clarke ldquoSystematic review of levodopa dose equivalencyreporting in Parkinsonrsquos diseaserdquo Movement Disorders vol 25no 15 pp 2649ndash2653 2010
[20] Y I Sheline D M Barch K Garcia et al ldquoCognitive functionin late life Depression relationships to depression severitycerebrovascular risk factors and processing speedrdquo BiologicalPsychiatry vol 60 no 1 pp 58ndash65 2006
[21] R K Heaton S W Miller M J Taylor and I Grant RevisedComprehensive Norms for An expAnded Halstead-Reitan Bat-tery Demographically Adjusted Neuropsychological Norms forAfrican American and Caucasian Adults PAR Lutz Fla USA2004
[22] M Charlson T P Szatrowski J Peterson and J Gold ldquoVal-idation of a combined comorbidity indexrdquo Journal of ClinicalEpidemiology vol 47 no 11 pp 1245ndash1251 1994
[23] PW FWilson KM Anderson andW B Kannel ldquoEpidemiol-ogy of diabetes mellitus in the elderly The Framingham StudyrdquoAmerican Journal of Medicine vol 80 no 5 A pp 3ndash9 1986
[24] W S Aronow J L Fleg C J Pepine et al ldquoACCFAHA 2011expert consensus document on hypertension in the elderlyrdquoJournal of the American College of Cardiology vol 57 pp 2037ndash2114 2011
[25] I Litvan J G Goldman A I Troster et al ldquoDiagnosticcriteria for mild cognitive impairment in Parkinsonrsquos diseaseMovement Disorder Society Task Force guidelinesrdquoMovementDisorders vol 27 no 3 pp 349ndash356 2012
[26] K J Rothman ldquoNo adjustments are needed for multiplecomparisonsrdquo Epidemiology vol 1 no 1 pp 43ndash46 1990
[27] D S Goldstein ldquoDysautonomia in Parkinsonrsquos disease neuro-cardiological abnormalitiesrdquo Lancet Neurology vol 2 no 11 pp669ndash676 2003
[28] A Verdelho SMadureira JM Ferro et al ldquoDifferential impactof cerebral white matter changes diabetes hypertension andstroke on cognitive performance among non-disabled elderly
10 Parkinsonrsquos Disease
The LADIS studyrdquo Journal of Neurology Neurosurgery andPsychiatry vol 78 no 12 pp 1325ndash1330 2007
[29] S P Woods and A I Troster ldquoProdromal frontalexecutivedysfunction predicts incident dementia in Parkinsonrsquos diseaserdquoJournal of the International Neuropsychological Society vol 9no 1 pp 17ndash24 2003
[30] W Nanhoe-Mahabier K F de Laat J E Visser J Zijlmans F-E de Leeuw and B R Bloem ldquoParkinson disease and comorbidcerebrovascular diseaserdquo Nature Reviews Neurology vol 5 no10 pp 533ndash541 2009
[31] K M Rose D Couper M L Eigenbrodt T H Mosley AR Sharrett and R F Gottesman ldquoOrthostatic hypotensionand cognitive function the atherosclerosis risk in communitiesstudyrdquo Neuroepidemiology vol 34 no 1 pp 1ndash7 2010
[32] P L K Yap M Niti K B Yap and T P Ng ldquoOrthostatichypotension hypotension and cognitive status early comorbidmarkers of primary dementiardquo Dementia and Geriatric Cogni-tive Disorders vol 26 no 3 pp 239ndash246 2008
[33] V Novak and I Hajjar ldquoThe relationship between bloodpressure and cognitive functionrdquo Nature Reviews Cardiologyvol 7 no 12 pp 686ndash698 2010
[34] J S Kim Y S Oh K S Lee Y I Kim D W Yang andD S Goldstein ldquoAssociation of cognitive dysfunction withneurocirculatory abnormalities in early Parkinson diseaserdquoNeurology vol 79 no 13 pp 1323ndash1331 2012
[35] T O Dalaker J P Larsen M G Dwyer et al ldquoWhite matterhyperintensities do not impact cognitive function in patientswith newly diagnosed Parkinsonrsquos diseaserdquoNeuroImage vol 47no 4 pp 2083ndash2089 2009
[36] N I Bohnen and R L Albin ldquoWhite matter lesions inParkinson diseaserdquo Nature Reviews Neurology vol 7 no 4 pp229ndash236 2011

Parkinsonrsquos Disease 3
Table 1 Cognitive domains
Domain Measures and brief description
Working memory Digit Span measure of auditory attention and working memory from the WAIS-III with both forward andbackwards components dv = forward span and backwards span scores
Episodic memoryHopkins Verbal Learning Test-119877 Form 1 (HVLT-R) 12 item word list learning task with 20 minute delay dv = items recalled after 201015840 delayLogical Memory Stories II (WMS-III) story memory measure dv = units recalled after 30min delay
Language Boston Naming Test (BNT) confrontation naming of line drawings of objectsanimals dv = total itemscorrectly named
Executive function
Trail Making Test Part B (TMT-B) speeded alternating search of letters and numbers (set-shifting) dv = totaltimeStroop Color-Word Test (Golden version) measure of cognitive inhibition of over learned automatic readingresponse dv = number items within 45 sec on color-word trialControlled Oral Word Association Test (COWA) a letter fluency task involving production of words beginningwith target letters during 60 second trials dv = number words produced
Processing speedStroop Single Word Reading (golden version) timed reading of single words denoting red green or blue dv =number words read in 4510158401015840
Trail Making Test Part A (TMT-A) speeded search of letters displayed on a page dv = total timeNote WMS-III Wechsler Memory Scale-Third Edition WAIS-III Wechsler Adult Intelligence Scale-Third Edition dv dependent variable References forindividual tests are in Lezak et al (2012) [16]
(interrater range 119903 = 097ndash098) Comorbidities were con-sidered present if (1) the physician noted its occurrencein a medical note or (2) the patient was prescribed med-ication pertaining to its presence (eg levothyroxine forhypothyroidism) Blood pressure readings were retrievedfrom medical records In accord with past studies investigat-ing cognition and hypertension individuals with a systolicblood pressure ge160mmHg or those on antihypertensivemedication were considered as hypertensive [24] Becausesome specific health conditions occurred relatively infre-quently they were combined into three broad categoriescardiac respiratory and neurologic The cardiac categoryincluded heart attack angina atrial fibrillation arrhythmiaheart murmur congestive heart failure peripheral vasculardisease or any cardiac surgery The respiratory categoryincluded chronic obstructive pulmonary disease pulmonaryembolism emphysema and asthma The neurologic systemcomorbidity included stroke TIA head injury and periph-eral neuropathy
3 Results
Characteristics of the 341 Parkinson samples are shown inTable 2 Overall the PD patients were in their mid-601015840s welleducated (ie approximately 3 years of college) and predom-inantly Caucasian (94) and male (69) In terms of diseasecharacteristics the majority of PD patients were tremorpredominant (827) with disease duration ranging from 1to 33 (mean of 10 years) and a mean ldquoonmedicationrdquo UPDSRmotor score of 264 Approximately 25 were on antianxietymedications and approximately 40 on antidepressants Themean DRS-II score was 1373 with a standard deviation (SD)of 5 As a group performance was lowest on the processingspeed composite score (mean = minus074) followed by executivefunctioning (mean = minus056) and delayed verbal memory
416381
30 295 267 25520 187
12 11 108 103
0
10
20
30
40
50
60
sam
ple (
)
Chol
este
rol
Hyp
erte
nsio
n
Hyp
oten
sion
Neu
rolo
gic
Card
iac
Art
hriti
s
GER
D
Canc
er
Pros
tate
RBSD
Resp
irato
ry
Dia
bete
s
Figure 1 Prevalence of comorbidities in a convenience sample of341 idiopathic Parkinson patients (119873 = 341) Shown is the per-centage of Parkinson patients with various comorbidities based onmedical chart review only comorbidities occurring in at least 10of the sample are shown GERD = gastroesophageal reflux diseaseRBSD = rapid Eye Movement (REM) behavior sleep disorder Nonehave deep brain stimulation
(mean = minus04) Regarding mild cognitive impairment (MCI)subtypes the guidelines of the Movement Disorders Societytaskforce (25) were used for classification into cognitivesubgroups A clinical cutoff criteria of 15 SD below thenormative mean was considered ldquoimpairedrdquo Following theMDS guidelines 180 PD participants (528) were classifiedas cognitively intact 103 (302) as multidomain amnesticMCI 57 (167) as nonamnestic MCI and 1 (03) as singledomain amnestic MCI
Figure 1 shows the distribution of 12 comorbidities thatoccurred in at least 10 of the sample The three mostcommon comorbidities were cholesterolemia (416) hyper-tension (381) and orthostatic hypotension (30)
4 Parkinsonrsquos Disease
Table 2 Sample characteristics
119873 = 304 Parkinsonrsquos disease patients88 caucasian Mean Standard deviation Range
Age (years) 647 10 30ndash90Years of education 150 3 7ndash20Years with symptoms 97 6 1ndash33UPDRS motor score on medication 263 10 7ndash54Percent tremor predominant 82Levodopa equivalency dose 771 532 0ndash2950Dementia Rating Scale-II total score 1372 5 119ndash148Neurocognitive domain 119885-scoreslowast
Executive composite score minus06 09 minus29ndash19Verbal memory composite score minus04 11 minus37ndash18Processing speed composite score minus07 09 minus32ndash19Language composite score 02 12 minus40ndash32Working memory composite score 02 08 minus19ndash27
Mild cognitive impairment (MCI) subtypesPercent amnestic single-domain MCI 03Percent multidomain amnestic MCI 302Percent nonamnestic MCI 167Percent cognitively intact 528
lowast119885-scores based on normative data from test manuals and published norms normative mean = 0 standard deviation = 1 mild cognitive impairment was based
on Movement Disorder Society criteria and utilized a 15 SD below the mean cut value [25] UPDRS Unified Parkinsonrsquos Disease Rating Scale
31 Relationship between Cognition and Cardiovascular RiskFactors To assess the ldquouniquerdquo effect of health comorbidities(including cardiovascular risk factors) on each of the fivecognitive domains a series of hierarchical regression anal-yses were conducted The first block of predictors in eachregression included indices of PD severity (UPDRS motorscores disease duration and LED) whereas the second blockof predictors included subsets of health comorbidities (iehypertension diabetes cancer and arthritis) This approachenabled one to determine the relation between health con-ditions and cognition while statistically controlling for theinfluence of PD disease severity This is important due towell known association between disease severity itself andcognitive decline [3] For each regression the cognitivedomain composite score served as the dependent variable Ofnote only health comorbidities that involved at least 10 ofthe sample were included for the purpose of stability For allregression analyses collinearity diagnostics (tolerance gt 02and variation inflation factor lt 5) and normality (skewnessand kurtosis values lt 1) were appropriate Post hoc testsutilized least significant difference tests [26]
As shown in Table 3 the overall regression models weresignificant for three of the cognitive domains executivefunction delayed verbal memory and processing speedBecause the regression models for the two remaining cog-nitive domains (language and working memory) were notsignificant they were not examined further For all threeldquosignificantrdquo cognitive domains (executive verbal memoryand processing speed) Parkinsonrsquos disease severity exerteda significant effect on cognition Specifically higher UPDRS
motor scores and longer disease duration were associatedwith worse composite scores on executive delayed memoryand processing speed As a whole the addition of ldquohealthcomorbidities in generalrdquo was not significant for any cog-nitive domain However significant effects were present forspecific cardiovascular risk factors namely hypertension andorthostatic hypotension A diagnosis of hypertension (evencontrolled hypertension) was associatedwithworse executivefunction and delayed verbal memory scores These effectswere significant but nevertheless small Unexpectedly thediagnosis of orthostatic hypotension (OH) was associatedwith better scores on tasks of executive function Processingspeed scoreswere not significantly related to any comorbidity
Although cognitive data was normed on age and educa-tion subsequent analyses controlling for age and educationconfirmed the above findings and reinforced that the previousanalyses were not confounded by differences in age or educa-tion Multinominal regression analyses examined differencesin health comorbidities among cognitive subtypes as theoutcome (ie cognitively intact amnestic and nonamnesticMCI groups) Results revealed no significant differences inthe prevalence of comorbidities
32Hypertension-Hypotension Subgroups Hypertension andorthostatic hypotension (OH) often cooccur in individualswith PD Consequently additional analyses were conductedtomore closely examine the separate and combined influenceof hypertension and orthostatic hypotension on executivefunction and memory By way of background OH refersto a drop in blood pressure due to postural changes such
Parkinsonrsquos Disease 5
Table 3 Comorbidities and cognitive domains summary of results of hierarchical multiple regression analyses
119865Δ 1198772Δ Beta Sig
Executive functionFinal model 338 0138 lt0001
PD severity block 10247 0091 lt0001Duration minus0156 lt0001Motor UPDRS minus0246 lt0001
Comorbidity block 1460 0047 0146Hypertension minus0127 0041Hypotension 0134 0019
Delayed verbal memoryFinal model 339 0122 lt0001
PD severity block 9383 0078 lt0001Duration minus0188 lt0001Motor UPDRS minus0227 lt0001
Comorbidity block 1433 0043 0157Hypertension minus0139 0021
Processing speedFinal model 3977 0154 lt0001
PD Severity block 15647 0129 lt0001Duration minus0139 0019Motor UPDRS minus0315 lt0001
Comorbidity block 1433 0043 0157Only significant predictors are shown PP pulse pressure UPDRS Unified Parkinsonrsquos Disease Rating ScalemdashPart III
as standing and can induce dizziness light-headedness orfalls [24] Orthostatic hypotension is a common complicationin PD due to sympathetic denervation and norepinephrinedegeneration in the locus coeruleus [27] ParadoxicallyOH can cooccur with hypertension since the mechanismsunderlying each are quite different For the current analysespatients were assigned to one of four groups those withorthostatic hypotension alone (OH 119873 = 55) those withhypertension alone (HTN 119873 = 82) those with cooccurringOH and hypertension (both 119873 = 48) and individuals withneither comorbidity (normotensivenone 119873 = 156) Sepa-rate analyses of covariance (ANCOVA)were conducted usinggroup (OHHTN both normotensivenone) as the between-subjects factor and covarying for disease severity (UPDRSmotor score disease duration LED) Executive and memorycomposite scores were the dependent variables in each anal-ysis Results of these ANCOVAs revealed a significant maineffect of group for both executive function (F(6 328) = 3568119875 = 0015) and delayed verbal memory (F(6 328) = 2680119875 = 0047) Post hoc tests using least significant difference[26] revealed that the Hypertension group performed worsethan all other groups for executive functioning (all 119875 valueslt 005) with no significant differences among the OH bothor normotensive groups (Figure 2) For delayed memory thehypertension group performed worse than the OH (119875 =0015) and the normotensive groups (119875 = 0026) but not thecombinedboth group
33 Pulse Pressure Because pulse pressure has beendescribed as a more sensitive measure of cardiovascular
risk than either systolic or diastolic pressure alone [23]we performed additional exploratory analyses examiningthe relationship between pulse pressure cognition and PDdisease severity (UPDRS motor scores) Pulse pressure wascomputed from blood pressure readings reported in themedical charts following standard guidelines by subtractingdiastolic from systolic blood pressure values Again aseries of multiple hierarchical regression analyses wereconducted using cognitive domain scores as the outcomevariable in each To control for disease severity PD severitymeasures (UPDRS symptom duration LED) were includedin the first regression block The second block includedpulse pressure and hypertensive medication (recorded as adichotomous variable for presence) A third block includeda residualized pulse pressure by UPDRS interaction termThe latter enabled us to examine whether PD severity andvascular risk interacted to influence cognitive outcomes Asimilar approach has previously been suggested by studiesinvestigating the relationship between white matter changes(leukoaraiosis) and motor functioning in patients with PD[25]
Results of the overall regression model was significantfor executive functioning delayed verbal memory and pro-cessing speed but not for working memory or language(Table 4) The PD severity block was significant across allthree domains whereas the second block (pulse pressureand hypertensive medication) was not significant for anycognitive domainHowever there was a significant interactionbetween UPDRS motor scores and pulse pressure for executivefunction delayed verbal memory and processing speed
6 Parkinsonrsquos Disease
Table 4 Pulse pressure and cognitive domains summary of results of hierarchical multiple regression analyses
119865Δ 1198772Δ Beta Sig
Executive functionFinal model 6297 0112 lt0001
Duration minus0195 lt0001Motor UPDRS minus0218 lt0001PP times UPDRS minus0113 0043
Delayed verbalmemoryFinal model 7603 0110 lt0001
Duration minus0127 0027Motor UPDRS minus0213 lt0001PP times UPDRS minus0138 0010
Processing speedFinal model 6403 0152 lt0001
Duration minus0157 0006Motor UPDRS minus0305 lt0001PP times UPDRS minus0128 0017
Only significant predictors are shown PP pulse pressure UPDRS Unified Parkinsonrsquos Disease Rating ScalemdashPart III
minus12
minus1
minus08
minus06
minus04
minus02
0
Executive Memory
HypertensionHypotension
BothNone
lowast
lowast
lowast
lowast
lowast
Com
posit
iveZ
-sco
re
lowastP lt 005
Figure 2 Executive and verbal memory composite scores in fourblood pressure groups hypertensive hypotension cooccurringhypertension and hypotension (both) and normotensive (none)Figure depicts mean composite Z-scores for executive function anddelayed verbal memory across each of the blood pressure groupsFor executive function Parkinsonrsquos patients with hypertension alone(X = minus0781 SD = 0769) performed significantly worse than thosewith hypotension alone (X = minus0321 SD = 0769 t = minus287 119875 =0004) combined hypertension-hypotension (X = minus0437 SD =0739 t = minus250 119875 = 0013) and normotensivenone (X = minus0495SD = 0898 t = minus221 119875 = 0028) For delayed verbal memoryParkinsonrsquos patients with hypertension alone (X = minus0633 SD =1068) performed significantly worse than those with hypotensionalone (X = minus0194 SD = 1098 t = minus245 119875 = 0015) and thenormotensivenone group (X = minus0301 SD = 1013 t = minus223119875 = 0026) There were no differences in memory between thehypertension and the combined hypertension-hypotension groups
Specifically higher pulse pressure values were significantlyrelated to worse cognitive performance as UPDRS motorscores increased in severity (Figure 3) This pattern wasobserved for executive function delayed verbal memoryand processing speed Taken together this finding suggeststhat worsening vascular integrity (as reflected by pulse-pressure) interacts with PD-indices of disease severity toexert increasingly detrimental effects on executive functionmemory and processing speed
4 Discussion
This retrospective study with 341 nondemented Parkinsonpatients resulted in three important findings First whiledisease severity is a potent indicator of cognitive performancein PD we found that hypertension a common age-relatedcomorbidity that occurred in almost 40 of our sampleexerted a small but independent negative influence on com-posite measures of executive function and delayed verbalmemory This finding aligns itself with a large literature innormal elderly showing the detrimental impact of hyperten-sion on cognition particularly executive functions [28] and isconsistent with recent observations from a large multicenterParkinson cohort [15] Interestingly we did not find supportfor our hypothesis of diabetes or acute cardiac events relatingto memory functioning Previous findings in non-PD eldershave shown both comorbidities to be relatedmedial temporallobe functioning [11] This discrepancy may reflect our smallsample size of diabetics (119873 = 35) and the heterogeneity ofcomorbidities included under the ldquocardiac systemrdquo variable
Our finding that hypertension in PD was associated withworse executive function and delayed memory is in linewith a large literature in older adults documenting negativeinfluence of cardiovascular risk factors However our resultscontrast with a small group of studies that failed to find a
Parkinsonrsquos Disease 7
Pulse pressure120100806040200
Exec
utiv
e fun
ctio
n
00
minus05
minus10
minus15
minus20
(a)
Verb
al m
emor
y
Pulse pressure120100806040200
00
minus05
minus10
minus15
minus20
(b)
Proc
essin
g sp
eed
Pulse pressure120100806040200
00
minus05
minus10
minus15
minus20
1st quartileUPDRS quartiles
2nd quartile3rd quartile4th quartile
(c)
Figure 3 Pulse pressure X UPDRS interaction for 3 cognitive domains Figure depicts linear relationship between pulse pressure andexecutive function delayed verbal memory and processing speed for each Unified Parkinsonrsquos Disease Rating Scale Part III (UPDRS) quartile(higher quartile means more severe motor symptoms)
relationship between cardiovascular risk and transition todementia in Parkinson patient [12ndash14] We suspect that thereare several factors that account for the different findings Thefirst relates to our use of parametric indices of cognitionrather than a categorical classification of dementia presenceused in previous PD students The former approach is amore sensitive metric for detecting cognitive change ordifferences Second our sample size was considerably largerthan previous PD studies and this may be critical given therelatively small effect sizes we observed Additionally previ-ous studies of cognitive status have shown executive functionsto be an insensitive marker of progression to dementia [7]Thuswhile hypertensionmay relate to executive dysfunctionthis cognitive profile may not differentiate dementia from
nondemented PD patients However this view is debatableand has not been established [29]
To be clear the focus of the present study was not to iden-tify those with and without dementia but to learn whetherhypertension and other comorbidities might contribute tothe cognitive profile of Parkinson patients without severecognitive impairment based on a general cognitive screener(DRS-II) Evidence from this study suggests that hyperten-sion does indeed make a small but significant contributionparticularly to executive function and delayedmemory recallOf note the occurrence of hypertension in our PD sampleis less than that often observed in several previous reportsdescribing hypertension to occur in 53ndash70 of individualsabove the age of 65 [24] Possible explanations for this
8 Parkinsonrsquos Disease
discrepancy includes a protective effect against hypertensionsecondary to levodopa use [30] as well as the fact that thisstudy includes individuals younger than 65 years old
The secondmajor finding was an unexpected relationshipbetween executive function and orthostatic hypotensionwhich occurred in approximately 30 of our sample Ourfindings suggested a possible role of orthostatic hypotension(OH) in moderating the relationship between hypertensionand executive function In brief individuals with cooccurringhypertension and OH were on par with individuals with-out hypertension on executive functioning measures Thisphenomenon has not been previously well documented orestablished and requires further validation The relationshipbetweenOH and cognition in the normal elderly has revealedmixed results with some studies failing to find a relationshipbetween cognitive outcomes and OH [31] However onestudy found that the combination of both hypertensionand orthostatic hypotension served as a protective factor[32] Specifically Yap and others found that among 2321older adults those with both OH and high blood pressure(gt140 systolic or gt90 diastolic) were less likely to haveimpaired scores on a broad measure of cognition (MMSE)compared to individuals without OH and those with OHand low blood pressure The mechanism for this effect hasnot been thoroughly examined but may relate a reductionin mean arterial pressure associated with OH allowing forcerebral blood perfusion to stay in the range of autoregulation[33] Within PD a recent study showed that PD patientswith circulatory abnormalities (including OH and supinehypertension) were more likely to meet criteria for dementia[34] Additionally they found that tests of episodic memorybut not executive functions were significantly related todecreases in blood pressure during a head-up-tilt test Sucha finding may suggest that dysautonomia may be related tocognitive changes occurring later in the disease stage ratherthan frontal-executive changes occurring earlier
Third this study showed a unique finding with pulsepressure whereby higher pulse pressure interacted with PDseverity to exert increasingly detrimental effects on executivefunction processing speed and memory In other words therelationship between cognition and cardiovascular risk maybe moderated by PD severity We are unaware of previousstudies examining the effect of pulse pressure on cognition inParkinson patients There are several ways to conceptualizethis relationship On one hand worsening pulse pressuremay be another index of PD progression vis a vis worseningautonomic dysfunction and effects on blood pressure Alter-natively this relationship may be independent of autonomicdysfunction In either case white matter changes mightrepresent downstream effect of this variability A growingnumber of studies have found that the relationship betweenLA and cognition varies depending on PD severity In factstudies of Parkinson patients in more advanced stages haveshown LA to be related to cognition whereas studies ofnewly diagnosed PD patients failed to replicate this finding[12ndash14 35] suggesting that vascular pathology may interactwith PD pathology This idea of an interaction betweenvascular pathology and PD pathology has also been exploredin its relationship to non-cognitive symptoms of PD In
terms of motor complications in PD higher LA burden hasbeen associatedwithworseningmotor functioning includingposturalgait difficulty bradykinesia and rigidity [36]
There are several limitations to this study First thedesign was cross-sectional and used a convenience sample ofpatients which may limit generalizability Next comorbiditymeasures depended on accurate documentation by physi-cians in the patientsrsquo medical charts While the validity ofthis method is unknown we believe the most noteworthycomorbidities were likely noted and recorded as part of thepatientrsquos medical record Lastly other than blood pressurethere were no direct measures of comorbidity and we wereunable to quantify severity or duration of various healthconditions Concerning blood pressure data consisted of onemeasurement rather than multiple blood pressure measure-ments which is more advantageous
5 Conclusion
The current study adds to the literature by suggesting thathypertension may be related to subtle executive and mem-ory deficits in Parkinson patients above and beyond thatconferred by the disease process itself The effect is likelysmall though it does parallel that observed in non-PD olderadults and may become more salient with disease progres-sion What is particularly unique in Parkinsonrsquos disease is ajuxtaposition of factors that are protective versus those thatincrease cardiovascular risk Protective factors include use oflevodopa medications that decrease blood pressure whereasautonomic dysfunction use of dopamine agonists (related tocardiac valvulopathy) and general physical deconditioningserve to increase cardiovascular risk [31] Even with thisunique confluence the present study provides preliminaryevidence that hypertensionmay be related to subtle cognitivedeficits in Parkinson patients similar to that of older adultsand may amplify executive and memory difficulties Futurestudies should examine possiblemechanisms such as LA andthe impact that subtle vascular-related cognitive deficits haveon quality of life andmood Improving cardiovascular healthprior to dementia onset should be further investigated as ameans of moderating cognitive changes Due to high risk ofcognitive declinedementia and the degenerative nature ofPD a small minimization in risk of cognitive decline mayprove to be beneficial
Conflict of Interests
No financial compensation was received for conducting thisstudy Mr Jones reports no disclosures Mr Jacobson IVreports no disclosures Dr Murphy reports no disclosuresDr Price has received research support from the NIH andthe National Parkinson Foundation Dr Okun serves as aconsultant for the National Parkinson Foundation and hasreceived research grants from NIH NPF the Michael J FoxFoundation the Parkinson Alliance Smallwood Foundationand the UF Foundation Dr Okun has previously receivedhonoraria but in the past 24 months has received no supportfrom industry including travel Dr Okun has received roy-alties for publications with Demos Manson and Cambridge
Parkinsonrsquos Disease 9
(movement disorders books) Dr Okun has participated inCME activities onmovement disorders sponsored by theUSFCME office PeerView Vanderbilt University and PrimeTheinstitution andnotDrOkun receives grants fromMedtronicand ANSSt Jude and the PI has no financial interest in thesegrants Dr Okun has participated as a site PI andor co-Ifor several NIH foundation and industry sponsored trialsover the years but has not received honoraria Dr Bowershas received research support from the NIH Michael J FoxFoundation the National Parkinson Foundation and theMcKnight Research Foundation
Acknowledgments
This study was supported by a Center of Excellence Grantfrom the National Parkinson Foundation and the UF-INFORM database
References
[1] G E Alexander M R DeLong and P L Strick ldquoParallelorganization of functionally segregated circuits linking basalganglia and cortexrdquo Annual Review of Neuroscience vol 9 pp357ndash381 1986
[2] K R Chaudhuri and A H Schapira ldquoNon-motor symptoms ofParkinsonrsquos disease dopaminergic pathophysiology and treat-mentrdquoThe Lancet Neurology vol 8 no 5 pp 464ndash474 2009
[3] D Aarsland K Andersen J P Larsen A Lolk H Nielsen andP Kragh-Soslashrensen ldquoRisk of dementia in Parkinsonrsquos disease acommunity-based Prospective StudyrdquoNeurology vol 56 no 6pp 730ndash736 2001
[4] M A Hely W G J Reid M A Adena G M Halliday andJ G L Morris ldquoThe Sydney Multicenter Study of Parkinsonrsquosdisease the inevitability of dementia at 20 yearsrdquo MovementDisorders vol 23 no 6 pp 837ndash844 2008
[5] A SchragM Jahanshahi andNQuinn ldquoHowdoes Parkinsonrsquosdisease affect quality of life A comparison with quality of life inthe general populationrdquo Movement Disorders vol 15 pp 1112ndash1118 2000
[6] B Dubois and B Pillon ldquoCognitive deficits in Parkinsonrsquosdiseaserdquo Journal of Neurology vol 244 no 1 pp 2ndash8 1997
[7] C H Williams-Gray J R Evans A Goris et al ldquoThe distinctcognitive syndromes of Parkinsonrsquos disease 5 year follow-up ofthe CamPaIGN cohortrdquo Brain vol 132 no 11 pp 2958ndash29692009
[8] B K Saxby F Harrington I G McKeith K Wesnes and GA Ford ldquoEffects of hypertension on attention memory andexecutive function in older adultsrdquo Health Psychology vol 22no 6 pp 587ndash591 2003
[9] D Knopman L L Boland TMosley et al ldquoCardiovascular riskfactors and cognitive decline inmiddle-aged adultsrdquoNeurologyvol 56 no 1 pp 42ndash48 2001
[10] A A Gouw A Seewann W M Van Der Flier et al ldquoHet-erogeneity of small vessel disease a systematic review ofMRI and histopathology correlationsrdquo Journal of NeurologyNeurosurgery and Psychiatry vol 82 no 2 pp 126ndash135 2011
[11] W Wu A M Brickman J Luchsinger et al ldquoThe brain in theage of old the hippocampal formation is targeted differentiallyby diseases of late liferdquo Annals of Neurology vol 64 no 6 pp698ndash706 2008
[12] M K Beyer D Aarsland O J Greve and J P Larsen ldquoVisualrating of white matter hyperintensities in Parkinsonrsquos diseaserdquoMovement Disorders vol 21 no 2 pp 223ndash229 2006
[13] S-J Lee J-S Kim J-Y Yoo et al ldquoInfluence of white matterhyperintensities on the cognition of patients with parkinsondiseaserdquoAlzheimerDisease andAssociatedDisorders vol 24 no3 pp 227ndash233 2010
[14] J Sławek D Wieczorek M Derejko et al ldquoThe influenceof vascular risk factors and white matter hyperintensities onthe degree of cognitive impairment in Parkinsonrsquos diseaserdquoNeurologia i Neurochirurgia Polska vol 42 no 6 pp 505ndash5122008
[15] J D Jones I Malaty C C Price M S Okun and DBowers ldquoHealth comorbidities and cognition in 1948 patientswith idiopathic Parkinsonrsquos diseaserdquo Parkinsonism amp RelatedDisorders vol 18 pp 1073ndash1078 2012
[16] M Lezak D Howieson E Bigler and D Tranel Neuropsy-chological Assessment Oxford University Press New York NYUSA 5th edition 2012
[17] A J Hughes S E Daniel L Kilford and A J Lees ldquoAccuracyof clinical diagnosis of idiopathic Parkinsonrsquos disease a clinico-pathological study of 100 casesrdquo Journal of Neurology Neuro-surgery and Psychiatry vol 55 no 3 pp 181ndash184 1992
[18] S Fahn R L Elton and UPDRS Development CommitteeldquoUnified Parkinsonrsquos disease rating scalerdquo Recent DevelopmentParkinson vol 2 pp 153ndash163 1987
[19] C L Tomlinson R Stowe S Patel C Rick R Gray and CE Clarke ldquoSystematic review of levodopa dose equivalencyreporting in Parkinsonrsquos diseaserdquo Movement Disorders vol 25no 15 pp 2649ndash2653 2010
[20] Y I Sheline D M Barch K Garcia et al ldquoCognitive functionin late life Depression relationships to depression severitycerebrovascular risk factors and processing speedrdquo BiologicalPsychiatry vol 60 no 1 pp 58ndash65 2006
[21] R K Heaton S W Miller M J Taylor and I Grant RevisedComprehensive Norms for An expAnded Halstead-Reitan Bat-tery Demographically Adjusted Neuropsychological Norms forAfrican American and Caucasian Adults PAR Lutz Fla USA2004
[22] M Charlson T P Szatrowski J Peterson and J Gold ldquoVal-idation of a combined comorbidity indexrdquo Journal of ClinicalEpidemiology vol 47 no 11 pp 1245ndash1251 1994
[23] PW FWilson KM Anderson andW B Kannel ldquoEpidemiol-ogy of diabetes mellitus in the elderly The Framingham StudyrdquoAmerican Journal of Medicine vol 80 no 5 A pp 3ndash9 1986
[24] W S Aronow J L Fleg C J Pepine et al ldquoACCFAHA 2011expert consensus document on hypertension in the elderlyrdquoJournal of the American College of Cardiology vol 57 pp 2037ndash2114 2011
[25] I Litvan J G Goldman A I Troster et al ldquoDiagnosticcriteria for mild cognitive impairment in Parkinsonrsquos diseaseMovement Disorder Society Task Force guidelinesrdquoMovementDisorders vol 27 no 3 pp 349ndash356 2012
[26] K J Rothman ldquoNo adjustments are needed for multiplecomparisonsrdquo Epidemiology vol 1 no 1 pp 43ndash46 1990
[27] D S Goldstein ldquoDysautonomia in Parkinsonrsquos disease neuro-cardiological abnormalitiesrdquo Lancet Neurology vol 2 no 11 pp669ndash676 2003
[28] A Verdelho SMadureira JM Ferro et al ldquoDifferential impactof cerebral white matter changes diabetes hypertension andstroke on cognitive performance among non-disabled elderly
10 Parkinsonrsquos Disease
The LADIS studyrdquo Journal of Neurology Neurosurgery andPsychiatry vol 78 no 12 pp 1325ndash1330 2007
[29] S P Woods and A I Troster ldquoProdromal frontalexecutivedysfunction predicts incident dementia in Parkinsonrsquos diseaserdquoJournal of the International Neuropsychological Society vol 9no 1 pp 17ndash24 2003
[30] W Nanhoe-Mahabier K F de Laat J E Visser J Zijlmans F-E de Leeuw and B R Bloem ldquoParkinson disease and comorbidcerebrovascular diseaserdquo Nature Reviews Neurology vol 5 no10 pp 533ndash541 2009
[31] K M Rose D Couper M L Eigenbrodt T H Mosley AR Sharrett and R F Gottesman ldquoOrthostatic hypotensionand cognitive function the atherosclerosis risk in communitiesstudyrdquo Neuroepidemiology vol 34 no 1 pp 1ndash7 2010
[32] P L K Yap M Niti K B Yap and T P Ng ldquoOrthostatichypotension hypotension and cognitive status early comorbidmarkers of primary dementiardquo Dementia and Geriatric Cogni-tive Disorders vol 26 no 3 pp 239ndash246 2008
[33] V Novak and I Hajjar ldquoThe relationship between bloodpressure and cognitive functionrdquo Nature Reviews Cardiologyvol 7 no 12 pp 686ndash698 2010
[34] J S Kim Y S Oh K S Lee Y I Kim D W Yang andD S Goldstein ldquoAssociation of cognitive dysfunction withneurocirculatory abnormalities in early Parkinson diseaserdquoNeurology vol 79 no 13 pp 1323ndash1331 2012
[35] T O Dalaker J P Larsen M G Dwyer et al ldquoWhite matterhyperintensities do not impact cognitive function in patientswith newly diagnosed Parkinsonrsquos diseaserdquoNeuroImage vol 47no 4 pp 2083ndash2089 2009
[36] N I Bohnen and R L Albin ldquoWhite matter lesions inParkinson diseaserdquo Nature Reviews Neurology vol 7 no 4 pp229ndash236 2011

4 Parkinsonrsquos Disease
Table 2 Sample characteristics
119873 = 304 Parkinsonrsquos disease patients88 caucasian Mean Standard deviation Range
Age (years) 647 10 30ndash90Years of education 150 3 7ndash20Years with symptoms 97 6 1ndash33UPDRS motor score on medication 263 10 7ndash54Percent tremor predominant 82Levodopa equivalency dose 771 532 0ndash2950Dementia Rating Scale-II total score 1372 5 119ndash148Neurocognitive domain 119885-scoreslowast
Executive composite score minus06 09 minus29ndash19Verbal memory composite score minus04 11 minus37ndash18Processing speed composite score minus07 09 minus32ndash19Language composite score 02 12 minus40ndash32Working memory composite score 02 08 minus19ndash27
Mild cognitive impairment (MCI) subtypesPercent amnestic single-domain MCI 03Percent multidomain amnestic MCI 302Percent nonamnestic MCI 167Percent cognitively intact 528
lowast119885-scores based on normative data from test manuals and published norms normative mean = 0 standard deviation = 1 mild cognitive impairment was based
on Movement Disorder Society criteria and utilized a 15 SD below the mean cut value [25] UPDRS Unified Parkinsonrsquos Disease Rating Scale
31 Relationship between Cognition and Cardiovascular RiskFactors To assess the ldquouniquerdquo effect of health comorbidities(including cardiovascular risk factors) on each of the fivecognitive domains a series of hierarchical regression anal-yses were conducted The first block of predictors in eachregression included indices of PD severity (UPDRS motorscores disease duration and LED) whereas the second blockof predictors included subsets of health comorbidities (iehypertension diabetes cancer and arthritis) This approachenabled one to determine the relation between health con-ditions and cognition while statistically controlling for theinfluence of PD disease severity This is important due towell known association between disease severity itself andcognitive decline [3] For each regression the cognitivedomain composite score served as the dependent variable Ofnote only health comorbidities that involved at least 10 ofthe sample were included for the purpose of stability For allregression analyses collinearity diagnostics (tolerance gt 02and variation inflation factor lt 5) and normality (skewnessand kurtosis values lt 1) were appropriate Post hoc testsutilized least significant difference tests [26]
As shown in Table 3 the overall regression models weresignificant for three of the cognitive domains executivefunction delayed verbal memory and processing speedBecause the regression models for the two remaining cog-nitive domains (language and working memory) were notsignificant they were not examined further For all threeldquosignificantrdquo cognitive domains (executive verbal memoryand processing speed) Parkinsonrsquos disease severity exerteda significant effect on cognition Specifically higher UPDRS
motor scores and longer disease duration were associatedwith worse composite scores on executive delayed memoryand processing speed As a whole the addition of ldquohealthcomorbidities in generalrdquo was not significant for any cog-nitive domain However significant effects were present forspecific cardiovascular risk factors namely hypertension andorthostatic hypotension A diagnosis of hypertension (evencontrolled hypertension) was associatedwithworse executivefunction and delayed verbal memory scores These effectswere significant but nevertheless small Unexpectedly thediagnosis of orthostatic hypotension (OH) was associatedwith better scores on tasks of executive function Processingspeed scoreswere not significantly related to any comorbidity
Although cognitive data was normed on age and educa-tion subsequent analyses controlling for age and educationconfirmed the above findings and reinforced that the previousanalyses were not confounded by differences in age or educa-tion Multinominal regression analyses examined differencesin health comorbidities among cognitive subtypes as theoutcome (ie cognitively intact amnestic and nonamnesticMCI groups) Results revealed no significant differences inthe prevalence of comorbidities
32Hypertension-Hypotension Subgroups Hypertension andorthostatic hypotension (OH) often cooccur in individualswith PD Consequently additional analyses were conductedtomore closely examine the separate and combined influenceof hypertension and orthostatic hypotension on executivefunction and memory By way of background OH refersto a drop in blood pressure due to postural changes such
Parkinsonrsquos Disease 5
Table 3 Comorbidities and cognitive domains summary of results of hierarchical multiple regression analyses
119865Δ 1198772Δ Beta Sig
Executive functionFinal model 338 0138 lt0001
PD severity block 10247 0091 lt0001Duration minus0156 lt0001Motor UPDRS minus0246 lt0001
Comorbidity block 1460 0047 0146Hypertension minus0127 0041Hypotension 0134 0019
Delayed verbal memoryFinal model 339 0122 lt0001
PD severity block 9383 0078 lt0001Duration minus0188 lt0001Motor UPDRS minus0227 lt0001
Comorbidity block 1433 0043 0157Hypertension minus0139 0021
Processing speedFinal model 3977 0154 lt0001
PD Severity block 15647 0129 lt0001Duration minus0139 0019Motor UPDRS minus0315 lt0001
Comorbidity block 1433 0043 0157Only significant predictors are shown PP pulse pressure UPDRS Unified Parkinsonrsquos Disease Rating ScalemdashPart III
as standing and can induce dizziness light-headedness orfalls [24] Orthostatic hypotension is a common complicationin PD due to sympathetic denervation and norepinephrinedegeneration in the locus coeruleus [27] ParadoxicallyOH can cooccur with hypertension since the mechanismsunderlying each are quite different For the current analysespatients were assigned to one of four groups those withorthostatic hypotension alone (OH 119873 = 55) those withhypertension alone (HTN 119873 = 82) those with cooccurringOH and hypertension (both 119873 = 48) and individuals withneither comorbidity (normotensivenone 119873 = 156) Sepa-rate analyses of covariance (ANCOVA)were conducted usinggroup (OHHTN both normotensivenone) as the between-subjects factor and covarying for disease severity (UPDRSmotor score disease duration LED) Executive and memorycomposite scores were the dependent variables in each anal-ysis Results of these ANCOVAs revealed a significant maineffect of group for both executive function (F(6 328) = 3568119875 = 0015) and delayed verbal memory (F(6 328) = 2680119875 = 0047) Post hoc tests using least significant difference[26] revealed that the Hypertension group performed worsethan all other groups for executive functioning (all 119875 valueslt 005) with no significant differences among the OH bothor normotensive groups (Figure 2) For delayed memory thehypertension group performed worse than the OH (119875 =0015) and the normotensive groups (119875 = 0026) but not thecombinedboth group
33 Pulse Pressure Because pulse pressure has beendescribed as a more sensitive measure of cardiovascular
risk than either systolic or diastolic pressure alone [23]we performed additional exploratory analyses examiningthe relationship between pulse pressure cognition and PDdisease severity (UPDRS motor scores) Pulse pressure wascomputed from blood pressure readings reported in themedical charts following standard guidelines by subtractingdiastolic from systolic blood pressure values Again aseries of multiple hierarchical regression analyses wereconducted using cognitive domain scores as the outcomevariable in each To control for disease severity PD severitymeasures (UPDRS symptom duration LED) were includedin the first regression block The second block includedpulse pressure and hypertensive medication (recorded as adichotomous variable for presence) A third block includeda residualized pulse pressure by UPDRS interaction termThe latter enabled us to examine whether PD severity andvascular risk interacted to influence cognitive outcomes Asimilar approach has previously been suggested by studiesinvestigating the relationship between white matter changes(leukoaraiosis) and motor functioning in patients with PD[25]
Results of the overall regression model was significantfor executive functioning delayed verbal memory and pro-cessing speed but not for working memory or language(Table 4) The PD severity block was significant across allthree domains whereas the second block (pulse pressureand hypertensive medication) was not significant for anycognitive domainHowever there was a significant interactionbetween UPDRS motor scores and pulse pressure for executivefunction delayed verbal memory and processing speed
6 Parkinsonrsquos Disease
Table 4 Pulse pressure and cognitive domains summary of results of hierarchical multiple regression analyses
119865Δ 1198772Δ Beta Sig
Executive functionFinal model 6297 0112 lt0001
Duration minus0195 lt0001Motor UPDRS minus0218 lt0001PP times UPDRS minus0113 0043
Delayed verbalmemoryFinal model 7603 0110 lt0001
Duration minus0127 0027Motor UPDRS minus0213 lt0001PP times UPDRS minus0138 0010
Processing speedFinal model 6403 0152 lt0001
Duration minus0157 0006Motor UPDRS minus0305 lt0001PP times UPDRS minus0128 0017
Only significant predictors are shown PP pulse pressure UPDRS Unified Parkinsonrsquos Disease Rating ScalemdashPart III
minus12
minus1
minus08
minus06
minus04
minus02
0
Executive Memory
HypertensionHypotension
BothNone
lowast
lowast
lowast
lowast
lowast
Com
posit
iveZ
-sco
re
lowastP lt 005
Figure 2 Executive and verbal memory composite scores in fourblood pressure groups hypertensive hypotension cooccurringhypertension and hypotension (both) and normotensive (none)Figure depicts mean composite Z-scores for executive function anddelayed verbal memory across each of the blood pressure groupsFor executive function Parkinsonrsquos patients with hypertension alone(X = minus0781 SD = 0769) performed significantly worse than thosewith hypotension alone (X = minus0321 SD = 0769 t = minus287 119875 =0004) combined hypertension-hypotension (X = minus0437 SD =0739 t = minus250 119875 = 0013) and normotensivenone (X = minus0495SD = 0898 t = minus221 119875 = 0028) For delayed verbal memoryParkinsonrsquos patients with hypertension alone (X = minus0633 SD =1068) performed significantly worse than those with hypotensionalone (X = minus0194 SD = 1098 t = minus245 119875 = 0015) and thenormotensivenone group (X = minus0301 SD = 1013 t = minus223119875 = 0026) There were no differences in memory between thehypertension and the combined hypertension-hypotension groups
Specifically higher pulse pressure values were significantlyrelated to worse cognitive performance as UPDRS motorscores increased in severity (Figure 3) This pattern wasobserved for executive function delayed verbal memoryand processing speed Taken together this finding suggeststhat worsening vascular integrity (as reflected by pulse-pressure) interacts with PD-indices of disease severity toexert increasingly detrimental effects on executive functionmemory and processing speed
4 Discussion
This retrospective study with 341 nondemented Parkinsonpatients resulted in three important findings First whiledisease severity is a potent indicator of cognitive performancein PD we found that hypertension a common age-relatedcomorbidity that occurred in almost 40 of our sampleexerted a small but independent negative influence on com-posite measures of executive function and delayed verbalmemory This finding aligns itself with a large literature innormal elderly showing the detrimental impact of hyperten-sion on cognition particularly executive functions [28] and isconsistent with recent observations from a large multicenterParkinson cohort [15] Interestingly we did not find supportfor our hypothesis of diabetes or acute cardiac events relatingto memory functioning Previous findings in non-PD eldershave shown both comorbidities to be relatedmedial temporallobe functioning [11] This discrepancy may reflect our smallsample size of diabetics (119873 = 35) and the heterogeneity ofcomorbidities included under the ldquocardiac systemrdquo variable
Our finding that hypertension in PD was associated withworse executive function and delayed memory is in linewith a large literature in older adults documenting negativeinfluence of cardiovascular risk factors However our resultscontrast with a small group of studies that failed to find a
Parkinsonrsquos Disease 7
Pulse pressure120100806040200
Exec
utiv
e fun
ctio
n
00
minus05
minus10
minus15
minus20
(a)
Verb
al m
emor
y
Pulse pressure120100806040200
00
minus05
minus10
minus15
minus20
(b)
Proc
essin
g sp
eed
Pulse pressure120100806040200
00
minus05
minus10
minus15
minus20
1st quartileUPDRS quartiles
2nd quartile3rd quartile4th quartile
(c)
Figure 3 Pulse pressure X UPDRS interaction for 3 cognitive domains Figure depicts linear relationship between pulse pressure andexecutive function delayed verbal memory and processing speed for each Unified Parkinsonrsquos Disease Rating Scale Part III (UPDRS) quartile(higher quartile means more severe motor symptoms)
relationship between cardiovascular risk and transition todementia in Parkinson patient [12ndash14] We suspect that thereare several factors that account for the different findings Thefirst relates to our use of parametric indices of cognitionrather than a categorical classification of dementia presenceused in previous PD students The former approach is amore sensitive metric for detecting cognitive change ordifferences Second our sample size was considerably largerthan previous PD studies and this may be critical given therelatively small effect sizes we observed Additionally previ-ous studies of cognitive status have shown executive functionsto be an insensitive marker of progression to dementia [7]Thuswhile hypertensionmay relate to executive dysfunctionthis cognitive profile may not differentiate dementia from
nondemented PD patients However this view is debatableand has not been established [29]
To be clear the focus of the present study was not to iden-tify those with and without dementia but to learn whetherhypertension and other comorbidities might contribute tothe cognitive profile of Parkinson patients without severecognitive impairment based on a general cognitive screener(DRS-II) Evidence from this study suggests that hyperten-sion does indeed make a small but significant contributionparticularly to executive function and delayedmemory recallOf note the occurrence of hypertension in our PD sampleis less than that often observed in several previous reportsdescribing hypertension to occur in 53ndash70 of individualsabove the age of 65 [24] Possible explanations for this
8 Parkinsonrsquos Disease
discrepancy includes a protective effect against hypertensionsecondary to levodopa use [30] as well as the fact that thisstudy includes individuals younger than 65 years old
The secondmajor finding was an unexpected relationshipbetween executive function and orthostatic hypotensionwhich occurred in approximately 30 of our sample Ourfindings suggested a possible role of orthostatic hypotension(OH) in moderating the relationship between hypertensionand executive function In brief individuals with cooccurringhypertension and OH were on par with individuals with-out hypertension on executive functioning measures Thisphenomenon has not been previously well documented orestablished and requires further validation The relationshipbetweenOH and cognition in the normal elderly has revealedmixed results with some studies failing to find a relationshipbetween cognitive outcomes and OH [31] However onestudy found that the combination of both hypertensionand orthostatic hypotension served as a protective factor[32] Specifically Yap and others found that among 2321older adults those with both OH and high blood pressure(gt140 systolic or gt90 diastolic) were less likely to haveimpaired scores on a broad measure of cognition (MMSE)compared to individuals without OH and those with OHand low blood pressure The mechanism for this effect hasnot been thoroughly examined but may relate a reductionin mean arterial pressure associated with OH allowing forcerebral blood perfusion to stay in the range of autoregulation[33] Within PD a recent study showed that PD patientswith circulatory abnormalities (including OH and supinehypertension) were more likely to meet criteria for dementia[34] Additionally they found that tests of episodic memorybut not executive functions were significantly related todecreases in blood pressure during a head-up-tilt test Sucha finding may suggest that dysautonomia may be related tocognitive changes occurring later in the disease stage ratherthan frontal-executive changes occurring earlier
Third this study showed a unique finding with pulsepressure whereby higher pulse pressure interacted with PDseverity to exert increasingly detrimental effects on executivefunction processing speed and memory In other words therelationship between cognition and cardiovascular risk maybe moderated by PD severity We are unaware of previousstudies examining the effect of pulse pressure on cognition inParkinson patients There are several ways to conceptualizethis relationship On one hand worsening pulse pressuremay be another index of PD progression vis a vis worseningautonomic dysfunction and effects on blood pressure Alter-natively this relationship may be independent of autonomicdysfunction In either case white matter changes mightrepresent downstream effect of this variability A growingnumber of studies have found that the relationship betweenLA and cognition varies depending on PD severity In factstudies of Parkinson patients in more advanced stages haveshown LA to be related to cognition whereas studies ofnewly diagnosed PD patients failed to replicate this finding[12ndash14 35] suggesting that vascular pathology may interactwith PD pathology This idea of an interaction betweenvascular pathology and PD pathology has also been exploredin its relationship to non-cognitive symptoms of PD In
terms of motor complications in PD higher LA burden hasbeen associatedwithworseningmotor functioning includingposturalgait difficulty bradykinesia and rigidity [36]
There are several limitations to this study First thedesign was cross-sectional and used a convenience sample ofpatients which may limit generalizability Next comorbiditymeasures depended on accurate documentation by physi-cians in the patientsrsquo medical charts While the validity ofthis method is unknown we believe the most noteworthycomorbidities were likely noted and recorded as part of thepatientrsquos medical record Lastly other than blood pressurethere were no direct measures of comorbidity and we wereunable to quantify severity or duration of various healthconditions Concerning blood pressure data consisted of onemeasurement rather than multiple blood pressure measure-ments which is more advantageous
5 Conclusion
The current study adds to the literature by suggesting thathypertension may be related to subtle executive and mem-ory deficits in Parkinson patients above and beyond thatconferred by the disease process itself The effect is likelysmall though it does parallel that observed in non-PD olderadults and may become more salient with disease progres-sion What is particularly unique in Parkinsonrsquos disease is ajuxtaposition of factors that are protective versus those thatincrease cardiovascular risk Protective factors include use oflevodopa medications that decrease blood pressure whereasautonomic dysfunction use of dopamine agonists (related tocardiac valvulopathy) and general physical deconditioningserve to increase cardiovascular risk [31] Even with thisunique confluence the present study provides preliminaryevidence that hypertensionmay be related to subtle cognitivedeficits in Parkinson patients similar to that of older adultsand may amplify executive and memory difficulties Futurestudies should examine possiblemechanisms such as LA andthe impact that subtle vascular-related cognitive deficits haveon quality of life andmood Improving cardiovascular healthprior to dementia onset should be further investigated as ameans of moderating cognitive changes Due to high risk ofcognitive declinedementia and the degenerative nature ofPD a small minimization in risk of cognitive decline mayprove to be beneficial
Conflict of Interests
No financial compensation was received for conducting thisstudy Mr Jones reports no disclosures Mr Jacobson IVreports no disclosures Dr Murphy reports no disclosuresDr Price has received research support from the NIH andthe National Parkinson Foundation Dr Okun serves as aconsultant for the National Parkinson Foundation and hasreceived research grants from NIH NPF the Michael J FoxFoundation the Parkinson Alliance Smallwood Foundationand the UF Foundation Dr Okun has previously receivedhonoraria but in the past 24 months has received no supportfrom industry including travel Dr Okun has received roy-alties for publications with Demos Manson and Cambridge
Parkinsonrsquos Disease 9
(movement disorders books) Dr Okun has participated inCME activities onmovement disorders sponsored by theUSFCME office PeerView Vanderbilt University and PrimeTheinstitution andnotDrOkun receives grants fromMedtronicand ANSSt Jude and the PI has no financial interest in thesegrants Dr Okun has participated as a site PI andor co-Ifor several NIH foundation and industry sponsored trialsover the years but has not received honoraria Dr Bowershas received research support from the NIH Michael J FoxFoundation the National Parkinson Foundation and theMcKnight Research Foundation
Acknowledgments
This study was supported by a Center of Excellence Grantfrom the National Parkinson Foundation and the UF-INFORM database
References
[1] G E Alexander M R DeLong and P L Strick ldquoParallelorganization of functionally segregated circuits linking basalganglia and cortexrdquo Annual Review of Neuroscience vol 9 pp357ndash381 1986
[2] K R Chaudhuri and A H Schapira ldquoNon-motor symptoms ofParkinsonrsquos disease dopaminergic pathophysiology and treat-mentrdquoThe Lancet Neurology vol 8 no 5 pp 464ndash474 2009
[3] D Aarsland K Andersen J P Larsen A Lolk H Nielsen andP Kragh-Soslashrensen ldquoRisk of dementia in Parkinsonrsquos disease acommunity-based Prospective StudyrdquoNeurology vol 56 no 6pp 730ndash736 2001
[4] M A Hely W G J Reid M A Adena G M Halliday andJ G L Morris ldquoThe Sydney Multicenter Study of Parkinsonrsquosdisease the inevitability of dementia at 20 yearsrdquo MovementDisorders vol 23 no 6 pp 837ndash844 2008
[5] A SchragM Jahanshahi andNQuinn ldquoHowdoes Parkinsonrsquosdisease affect quality of life A comparison with quality of life inthe general populationrdquo Movement Disorders vol 15 pp 1112ndash1118 2000
[6] B Dubois and B Pillon ldquoCognitive deficits in Parkinsonrsquosdiseaserdquo Journal of Neurology vol 244 no 1 pp 2ndash8 1997
[7] C H Williams-Gray J R Evans A Goris et al ldquoThe distinctcognitive syndromes of Parkinsonrsquos disease 5 year follow-up ofthe CamPaIGN cohortrdquo Brain vol 132 no 11 pp 2958ndash29692009
[8] B K Saxby F Harrington I G McKeith K Wesnes and GA Ford ldquoEffects of hypertension on attention memory andexecutive function in older adultsrdquo Health Psychology vol 22no 6 pp 587ndash591 2003
[9] D Knopman L L Boland TMosley et al ldquoCardiovascular riskfactors and cognitive decline inmiddle-aged adultsrdquoNeurologyvol 56 no 1 pp 42ndash48 2001
[10] A A Gouw A Seewann W M Van Der Flier et al ldquoHet-erogeneity of small vessel disease a systematic review ofMRI and histopathology correlationsrdquo Journal of NeurologyNeurosurgery and Psychiatry vol 82 no 2 pp 126ndash135 2011
[11] W Wu A M Brickman J Luchsinger et al ldquoThe brain in theage of old the hippocampal formation is targeted differentiallyby diseases of late liferdquo Annals of Neurology vol 64 no 6 pp698ndash706 2008
[12] M K Beyer D Aarsland O J Greve and J P Larsen ldquoVisualrating of white matter hyperintensities in Parkinsonrsquos diseaserdquoMovement Disorders vol 21 no 2 pp 223ndash229 2006
[13] S-J Lee J-S Kim J-Y Yoo et al ldquoInfluence of white matterhyperintensities on the cognition of patients with parkinsondiseaserdquoAlzheimerDisease andAssociatedDisorders vol 24 no3 pp 227ndash233 2010
[14] J Sławek D Wieczorek M Derejko et al ldquoThe influenceof vascular risk factors and white matter hyperintensities onthe degree of cognitive impairment in Parkinsonrsquos diseaserdquoNeurologia i Neurochirurgia Polska vol 42 no 6 pp 505ndash5122008
[15] J D Jones I Malaty C C Price M S Okun and DBowers ldquoHealth comorbidities and cognition in 1948 patientswith idiopathic Parkinsonrsquos diseaserdquo Parkinsonism amp RelatedDisorders vol 18 pp 1073ndash1078 2012
[16] M Lezak D Howieson E Bigler and D Tranel Neuropsy-chological Assessment Oxford University Press New York NYUSA 5th edition 2012
[17] A J Hughes S E Daniel L Kilford and A J Lees ldquoAccuracyof clinical diagnosis of idiopathic Parkinsonrsquos disease a clinico-pathological study of 100 casesrdquo Journal of Neurology Neuro-surgery and Psychiatry vol 55 no 3 pp 181ndash184 1992
[18] S Fahn R L Elton and UPDRS Development CommitteeldquoUnified Parkinsonrsquos disease rating scalerdquo Recent DevelopmentParkinson vol 2 pp 153ndash163 1987
[19] C L Tomlinson R Stowe S Patel C Rick R Gray and CE Clarke ldquoSystematic review of levodopa dose equivalencyreporting in Parkinsonrsquos diseaserdquo Movement Disorders vol 25no 15 pp 2649ndash2653 2010
[20] Y I Sheline D M Barch K Garcia et al ldquoCognitive functionin late life Depression relationships to depression severitycerebrovascular risk factors and processing speedrdquo BiologicalPsychiatry vol 60 no 1 pp 58ndash65 2006
[21] R K Heaton S W Miller M J Taylor and I Grant RevisedComprehensive Norms for An expAnded Halstead-Reitan Bat-tery Demographically Adjusted Neuropsychological Norms forAfrican American and Caucasian Adults PAR Lutz Fla USA2004
[22] M Charlson T P Szatrowski J Peterson and J Gold ldquoVal-idation of a combined comorbidity indexrdquo Journal of ClinicalEpidemiology vol 47 no 11 pp 1245ndash1251 1994
[23] PW FWilson KM Anderson andW B Kannel ldquoEpidemiol-ogy of diabetes mellitus in the elderly The Framingham StudyrdquoAmerican Journal of Medicine vol 80 no 5 A pp 3ndash9 1986
[24] W S Aronow J L Fleg C J Pepine et al ldquoACCFAHA 2011expert consensus document on hypertension in the elderlyrdquoJournal of the American College of Cardiology vol 57 pp 2037ndash2114 2011
[25] I Litvan J G Goldman A I Troster et al ldquoDiagnosticcriteria for mild cognitive impairment in Parkinsonrsquos diseaseMovement Disorder Society Task Force guidelinesrdquoMovementDisorders vol 27 no 3 pp 349ndash356 2012
[26] K J Rothman ldquoNo adjustments are needed for multiplecomparisonsrdquo Epidemiology vol 1 no 1 pp 43ndash46 1990
[27] D S Goldstein ldquoDysautonomia in Parkinsonrsquos disease neuro-cardiological abnormalitiesrdquo Lancet Neurology vol 2 no 11 pp669ndash676 2003
[28] A Verdelho SMadureira JM Ferro et al ldquoDifferential impactof cerebral white matter changes diabetes hypertension andstroke on cognitive performance among non-disabled elderly
10 Parkinsonrsquos Disease
The LADIS studyrdquo Journal of Neurology Neurosurgery andPsychiatry vol 78 no 12 pp 1325ndash1330 2007
[29] S P Woods and A I Troster ldquoProdromal frontalexecutivedysfunction predicts incident dementia in Parkinsonrsquos diseaserdquoJournal of the International Neuropsychological Society vol 9no 1 pp 17ndash24 2003
[30] W Nanhoe-Mahabier K F de Laat J E Visser J Zijlmans F-E de Leeuw and B R Bloem ldquoParkinson disease and comorbidcerebrovascular diseaserdquo Nature Reviews Neurology vol 5 no10 pp 533ndash541 2009
[31] K M Rose D Couper M L Eigenbrodt T H Mosley AR Sharrett and R F Gottesman ldquoOrthostatic hypotensionand cognitive function the atherosclerosis risk in communitiesstudyrdquo Neuroepidemiology vol 34 no 1 pp 1ndash7 2010
[32] P L K Yap M Niti K B Yap and T P Ng ldquoOrthostatichypotension hypotension and cognitive status early comorbidmarkers of primary dementiardquo Dementia and Geriatric Cogni-tive Disorders vol 26 no 3 pp 239ndash246 2008
[33] V Novak and I Hajjar ldquoThe relationship between bloodpressure and cognitive functionrdquo Nature Reviews Cardiologyvol 7 no 12 pp 686ndash698 2010
[34] J S Kim Y S Oh K S Lee Y I Kim D W Yang andD S Goldstein ldquoAssociation of cognitive dysfunction withneurocirculatory abnormalities in early Parkinson diseaserdquoNeurology vol 79 no 13 pp 1323ndash1331 2012
[35] T O Dalaker J P Larsen M G Dwyer et al ldquoWhite matterhyperintensities do not impact cognitive function in patientswith newly diagnosed Parkinsonrsquos diseaserdquoNeuroImage vol 47no 4 pp 2083ndash2089 2009
[36] N I Bohnen and R L Albin ldquoWhite matter lesions inParkinson diseaserdquo Nature Reviews Neurology vol 7 no 4 pp229ndash236 2011
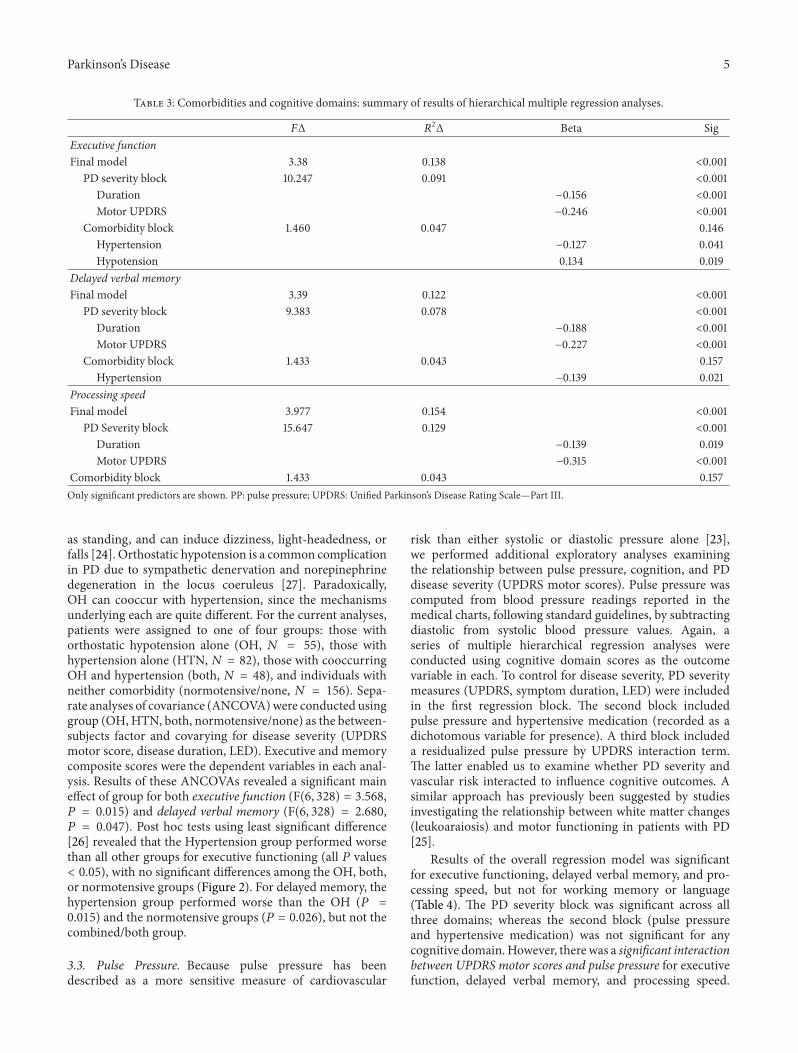
Parkinsonrsquos Disease 5
Table 3 Comorbidities and cognitive domains summary of results of hierarchical multiple regression analyses
119865Δ 1198772Δ Beta Sig
Executive functionFinal model 338 0138 lt0001
PD severity block 10247 0091 lt0001Duration minus0156 lt0001Motor UPDRS minus0246 lt0001
Comorbidity block 1460 0047 0146Hypertension minus0127 0041Hypotension 0134 0019
Delayed verbal memoryFinal model 339 0122 lt0001
PD severity block 9383 0078 lt0001Duration minus0188 lt0001Motor UPDRS minus0227 lt0001
Comorbidity block 1433 0043 0157Hypertension minus0139 0021
Processing speedFinal model 3977 0154 lt0001
PD Severity block 15647 0129 lt0001Duration minus0139 0019Motor UPDRS minus0315 lt0001
Comorbidity block 1433 0043 0157Only significant predictors are shown PP pulse pressure UPDRS Unified Parkinsonrsquos Disease Rating ScalemdashPart III
as standing and can induce dizziness light-headedness orfalls [24] Orthostatic hypotension is a common complicationin PD due to sympathetic denervation and norepinephrinedegeneration in the locus coeruleus [27] ParadoxicallyOH can cooccur with hypertension since the mechanismsunderlying each are quite different For the current analysespatients were assigned to one of four groups those withorthostatic hypotension alone (OH 119873 = 55) those withhypertension alone (HTN 119873 = 82) those with cooccurringOH and hypertension (both 119873 = 48) and individuals withneither comorbidity (normotensivenone 119873 = 156) Sepa-rate analyses of covariance (ANCOVA)were conducted usinggroup (OHHTN both normotensivenone) as the between-subjects factor and covarying for disease severity (UPDRSmotor score disease duration LED) Executive and memorycomposite scores were the dependent variables in each anal-ysis Results of these ANCOVAs revealed a significant maineffect of group for both executive function (F(6 328) = 3568119875 = 0015) and delayed verbal memory (F(6 328) = 2680119875 = 0047) Post hoc tests using least significant difference[26] revealed that the Hypertension group performed worsethan all other groups for executive functioning (all 119875 valueslt 005) with no significant differences among the OH bothor normotensive groups (Figure 2) For delayed memory thehypertension group performed worse than the OH (119875 =0015) and the normotensive groups (119875 = 0026) but not thecombinedboth group
33 Pulse Pressure Because pulse pressure has beendescribed as a more sensitive measure of cardiovascular
risk than either systolic or diastolic pressure alone [23]we performed additional exploratory analyses examiningthe relationship between pulse pressure cognition and PDdisease severity (UPDRS motor scores) Pulse pressure wascomputed from blood pressure readings reported in themedical charts following standard guidelines by subtractingdiastolic from systolic blood pressure values Again aseries of multiple hierarchical regression analyses wereconducted using cognitive domain scores as the outcomevariable in each To control for disease severity PD severitymeasures (UPDRS symptom duration LED) were includedin the first regression block The second block includedpulse pressure and hypertensive medication (recorded as adichotomous variable for presence) A third block includeda residualized pulse pressure by UPDRS interaction termThe latter enabled us to examine whether PD severity andvascular risk interacted to influence cognitive outcomes Asimilar approach has previously been suggested by studiesinvestigating the relationship between white matter changes(leukoaraiosis) and motor functioning in patients with PD[25]
Results of the overall regression model was significantfor executive functioning delayed verbal memory and pro-cessing speed but not for working memory or language(Table 4) The PD severity block was significant across allthree domains whereas the second block (pulse pressureand hypertensive medication) was not significant for anycognitive domainHowever there was a significant interactionbetween UPDRS motor scores and pulse pressure for executivefunction delayed verbal memory and processing speed
6 Parkinsonrsquos Disease
Table 4 Pulse pressure and cognitive domains summary of results of hierarchical multiple regression analyses
119865Δ 1198772Δ Beta Sig
Executive functionFinal model 6297 0112 lt0001
Duration minus0195 lt0001Motor UPDRS minus0218 lt0001PP times UPDRS minus0113 0043
Delayed verbalmemoryFinal model 7603 0110 lt0001
Duration minus0127 0027Motor UPDRS minus0213 lt0001PP times UPDRS minus0138 0010
Processing speedFinal model 6403 0152 lt0001
Duration minus0157 0006Motor UPDRS minus0305 lt0001PP times UPDRS minus0128 0017
Only significant predictors are shown PP pulse pressure UPDRS Unified Parkinsonrsquos Disease Rating ScalemdashPart III
minus12
minus1
minus08
minus06
minus04
minus02
0
Executive Memory
HypertensionHypotension
BothNone
lowast
lowast
lowast
lowast
lowast
Com
posit
iveZ
-sco
re
lowastP lt 005
Figure 2 Executive and verbal memory composite scores in fourblood pressure groups hypertensive hypotension cooccurringhypertension and hypotension (both) and normotensive (none)Figure depicts mean composite Z-scores for executive function anddelayed verbal memory across each of the blood pressure groupsFor executive function Parkinsonrsquos patients with hypertension alone(X = minus0781 SD = 0769) performed significantly worse than thosewith hypotension alone (X = minus0321 SD = 0769 t = minus287 119875 =0004) combined hypertension-hypotension (X = minus0437 SD =0739 t = minus250 119875 = 0013) and normotensivenone (X = minus0495SD = 0898 t = minus221 119875 = 0028) For delayed verbal memoryParkinsonrsquos patients with hypertension alone (X = minus0633 SD =1068) performed significantly worse than those with hypotensionalone (X = minus0194 SD = 1098 t = minus245 119875 = 0015) and thenormotensivenone group (X = minus0301 SD = 1013 t = minus223119875 = 0026) There were no differences in memory between thehypertension and the combined hypertension-hypotension groups
Specifically higher pulse pressure values were significantlyrelated to worse cognitive performance as UPDRS motorscores increased in severity (Figure 3) This pattern wasobserved for executive function delayed verbal memoryand processing speed Taken together this finding suggeststhat worsening vascular integrity (as reflected by pulse-pressure) interacts with PD-indices of disease severity toexert increasingly detrimental effects on executive functionmemory and processing speed
4 Discussion
This retrospective study with 341 nondemented Parkinsonpatients resulted in three important findings First whiledisease severity is a potent indicator of cognitive performancein PD we found that hypertension a common age-relatedcomorbidity that occurred in almost 40 of our sampleexerted a small but independent negative influence on com-posite measures of executive function and delayed verbalmemory This finding aligns itself with a large literature innormal elderly showing the detrimental impact of hyperten-sion on cognition particularly executive functions [28] and isconsistent with recent observations from a large multicenterParkinson cohort [15] Interestingly we did not find supportfor our hypothesis of diabetes or acute cardiac events relatingto memory functioning Previous findings in non-PD eldershave shown both comorbidities to be relatedmedial temporallobe functioning [11] This discrepancy may reflect our smallsample size of diabetics (119873 = 35) and the heterogeneity ofcomorbidities included under the ldquocardiac systemrdquo variable
Our finding that hypertension in PD was associated withworse executive function and delayed memory is in linewith a large literature in older adults documenting negativeinfluence of cardiovascular risk factors However our resultscontrast with a small group of studies that failed to find a
Parkinsonrsquos Disease 7
Pulse pressure120100806040200
Exec
utiv
e fun
ctio
n
00
minus05
minus10
minus15
minus20
(a)
Verb
al m
emor
y
Pulse pressure120100806040200
00
minus05
minus10
minus15
minus20
(b)
Proc
essin
g sp
eed
Pulse pressure120100806040200
00
minus05
minus10
minus15
minus20
1st quartileUPDRS quartiles
2nd quartile3rd quartile4th quartile
(c)
Figure 3 Pulse pressure X UPDRS interaction for 3 cognitive domains Figure depicts linear relationship between pulse pressure andexecutive function delayed verbal memory and processing speed for each Unified Parkinsonrsquos Disease Rating Scale Part III (UPDRS) quartile(higher quartile means more severe motor symptoms)
relationship between cardiovascular risk and transition todementia in Parkinson patient [12ndash14] We suspect that thereare several factors that account for the different findings Thefirst relates to our use of parametric indices of cognitionrather than a categorical classification of dementia presenceused in previous PD students The former approach is amore sensitive metric for detecting cognitive change ordifferences Second our sample size was considerably largerthan previous PD studies and this may be critical given therelatively small effect sizes we observed Additionally previ-ous studies of cognitive status have shown executive functionsto be an insensitive marker of progression to dementia [7]Thuswhile hypertensionmay relate to executive dysfunctionthis cognitive profile may not differentiate dementia from
nondemented PD patients However this view is debatableand has not been established [29]
To be clear the focus of the present study was not to iden-tify those with and without dementia but to learn whetherhypertension and other comorbidities might contribute tothe cognitive profile of Parkinson patients without severecognitive impairment based on a general cognitive screener(DRS-II) Evidence from this study suggests that hyperten-sion does indeed make a small but significant contributionparticularly to executive function and delayedmemory recallOf note the occurrence of hypertension in our PD sampleis less than that often observed in several previous reportsdescribing hypertension to occur in 53ndash70 of individualsabove the age of 65 [24] Possible explanations for this
8 Parkinsonrsquos Disease
discrepancy includes a protective effect against hypertensionsecondary to levodopa use [30] as well as the fact that thisstudy includes individuals younger than 65 years old
The secondmajor finding was an unexpected relationshipbetween executive function and orthostatic hypotensionwhich occurred in approximately 30 of our sample Ourfindings suggested a possible role of orthostatic hypotension(OH) in moderating the relationship between hypertensionand executive function In brief individuals with cooccurringhypertension and OH were on par with individuals with-out hypertension on executive functioning measures Thisphenomenon has not been previously well documented orestablished and requires further validation The relationshipbetweenOH and cognition in the normal elderly has revealedmixed results with some studies failing to find a relationshipbetween cognitive outcomes and OH [31] However onestudy found that the combination of both hypertensionand orthostatic hypotension served as a protective factor[32] Specifically Yap and others found that among 2321older adults those with both OH and high blood pressure(gt140 systolic or gt90 diastolic) were less likely to haveimpaired scores on a broad measure of cognition (MMSE)compared to individuals without OH and those with OHand low blood pressure The mechanism for this effect hasnot been thoroughly examined but may relate a reductionin mean arterial pressure associated with OH allowing forcerebral blood perfusion to stay in the range of autoregulation[33] Within PD a recent study showed that PD patientswith circulatory abnormalities (including OH and supinehypertension) were more likely to meet criteria for dementia[34] Additionally they found that tests of episodic memorybut not executive functions were significantly related todecreases in blood pressure during a head-up-tilt test Sucha finding may suggest that dysautonomia may be related tocognitive changes occurring later in the disease stage ratherthan frontal-executive changes occurring earlier
Third this study showed a unique finding with pulsepressure whereby higher pulse pressure interacted with PDseverity to exert increasingly detrimental effects on executivefunction processing speed and memory In other words therelationship between cognition and cardiovascular risk maybe moderated by PD severity We are unaware of previousstudies examining the effect of pulse pressure on cognition inParkinson patients There are several ways to conceptualizethis relationship On one hand worsening pulse pressuremay be another index of PD progression vis a vis worseningautonomic dysfunction and effects on blood pressure Alter-natively this relationship may be independent of autonomicdysfunction In either case white matter changes mightrepresent downstream effect of this variability A growingnumber of studies have found that the relationship betweenLA and cognition varies depending on PD severity In factstudies of Parkinson patients in more advanced stages haveshown LA to be related to cognition whereas studies ofnewly diagnosed PD patients failed to replicate this finding[12ndash14 35] suggesting that vascular pathology may interactwith PD pathology This idea of an interaction betweenvascular pathology and PD pathology has also been exploredin its relationship to non-cognitive symptoms of PD In
terms of motor complications in PD higher LA burden hasbeen associatedwithworseningmotor functioning includingposturalgait difficulty bradykinesia and rigidity [36]
There are several limitations to this study First thedesign was cross-sectional and used a convenience sample ofpatients which may limit generalizability Next comorbiditymeasures depended on accurate documentation by physi-cians in the patientsrsquo medical charts While the validity ofthis method is unknown we believe the most noteworthycomorbidities were likely noted and recorded as part of thepatientrsquos medical record Lastly other than blood pressurethere were no direct measures of comorbidity and we wereunable to quantify severity or duration of various healthconditions Concerning blood pressure data consisted of onemeasurement rather than multiple blood pressure measure-ments which is more advantageous
5 Conclusion
The current study adds to the literature by suggesting thathypertension may be related to subtle executive and mem-ory deficits in Parkinson patients above and beyond thatconferred by the disease process itself The effect is likelysmall though it does parallel that observed in non-PD olderadults and may become more salient with disease progres-sion What is particularly unique in Parkinsonrsquos disease is ajuxtaposition of factors that are protective versus those thatincrease cardiovascular risk Protective factors include use oflevodopa medications that decrease blood pressure whereasautonomic dysfunction use of dopamine agonists (related tocardiac valvulopathy) and general physical deconditioningserve to increase cardiovascular risk [31] Even with thisunique confluence the present study provides preliminaryevidence that hypertensionmay be related to subtle cognitivedeficits in Parkinson patients similar to that of older adultsand may amplify executive and memory difficulties Futurestudies should examine possiblemechanisms such as LA andthe impact that subtle vascular-related cognitive deficits haveon quality of life andmood Improving cardiovascular healthprior to dementia onset should be further investigated as ameans of moderating cognitive changes Due to high risk ofcognitive declinedementia and the degenerative nature ofPD a small minimization in risk of cognitive decline mayprove to be beneficial
Conflict of Interests
No financial compensation was received for conducting thisstudy Mr Jones reports no disclosures Mr Jacobson IVreports no disclosures Dr Murphy reports no disclosuresDr Price has received research support from the NIH andthe National Parkinson Foundation Dr Okun serves as aconsultant for the National Parkinson Foundation and hasreceived research grants from NIH NPF the Michael J FoxFoundation the Parkinson Alliance Smallwood Foundationand the UF Foundation Dr Okun has previously receivedhonoraria but in the past 24 months has received no supportfrom industry including travel Dr Okun has received roy-alties for publications with Demos Manson and Cambridge
Parkinsonrsquos Disease 9
(movement disorders books) Dr Okun has participated inCME activities onmovement disorders sponsored by theUSFCME office PeerView Vanderbilt University and PrimeTheinstitution andnotDrOkun receives grants fromMedtronicand ANSSt Jude and the PI has no financial interest in thesegrants Dr Okun has participated as a site PI andor co-Ifor several NIH foundation and industry sponsored trialsover the years but has not received honoraria Dr Bowershas received research support from the NIH Michael J FoxFoundation the National Parkinson Foundation and theMcKnight Research Foundation
Acknowledgments
This study was supported by a Center of Excellence Grantfrom the National Parkinson Foundation and the UF-INFORM database
References
[1] G E Alexander M R DeLong and P L Strick ldquoParallelorganization of functionally segregated circuits linking basalganglia and cortexrdquo Annual Review of Neuroscience vol 9 pp357ndash381 1986
[2] K R Chaudhuri and A H Schapira ldquoNon-motor symptoms ofParkinsonrsquos disease dopaminergic pathophysiology and treat-mentrdquoThe Lancet Neurology vol 8 no 5 pp 464ndash474 2009
[3] D Aarsland K Andersen J P Larsen A Lolk H Nielsen andP Kragh-Soslashrensen ldquoRisk of dementia in Parkinsonrsquos disease acommunity-based Prospective StudyrdquoNeurology vol 56 no 6pp 730ndash736 2001
[4] M A Hely W G J Reid M A Adena G M Halliday andJ G L Morris ldquoThe Sydney Multicenter Study of Parkinsonrsquosdisease the inevitability of dementia at 20 yearsrdquo MovementDisorders vol 23 no 6 pp 837ndash844 2008
[5] A SchragM Jahanshahi andNQuinn ldquoHowdoes Parkinsonrsquosdisease affect quality of life A comparison with quality of life inthe general populationrdquo Movement Disorders vol 15 pp 1112ndash1118 2000
[6] B Dubois and B Pillon ldquoCognitive deficits in Parkinsonrsquosdiseaserdquo Journal of Neurology vol 244 no 1 pp 2ndash8 1997
[7] C H Williams-Gray J R Evans A Goris et al ldquoThe distinctcognitive syndromes of Parkinsonrsquos disease 5 year follow-up ofthe CamPaIGN cohortrdquo Brain vol 132 no 11 pp 2958ndash29692009
[8] B K Saxby F Harrington I G McKeith K Wesnes and GA Ford ldquoEffects of hypertension on attention memory andexecutive function in older adultsrdquo Health Psychology vol 22no 6 pp 587ndash591 2003
[9] D Knopman L L Boland TMosley et al ldquoCardiovascular riskfactors and cognitive decline inmiddle-aged adultsrdquoNeurologyvol 56 no 1 pp 42ndash48 2001
[10] A A Gouw A Seewann W M Van Der Flier et al ldquoHet-erogeneity of small vessel disease a systematic review ofMRI and histopathology correlationsrdquo Journal of NeurologyNeurosurgery and Psychiatry vol 82 no 2 pp 126ndash135 2011
[11] W Wu A M Brickman J Luchsinger et al ldquoThe brain in theage of old the hippocampal formation is targeted differentiallyby diseases of late liferdquo Annals of Neurology vol 64 no 6 pp698ndash706 2008
[12] M K Beyer D Aarsland O J Greve and J P Larsen ldquoVisualrating of white matter hyperintensities in Parkinsonrsquos diseaserdquoMovement Disorders vol 21 no 2 pp 223ndash229 2006
[13] S-J Lee J-S Kim J-Y Yoo et al ldquoInfluence of white matterhyperintensities on the cognition of patients with parkinsondiseaserdquoAlzheimerDisease andAssociatedDisorders vol 24 no3 pp 227ndash233 2010
[14] J Sławek D Wieczorek M Derejko et al ldquoThe influenceof vascular risk factors and white matter hyperintensities onthe degree of cognitive impairment in Parkinsonrsquos diseaserdquoNeurologia i Neurochirurgia Polska vol 42 no 6 pp 505ndash5122008
[15] J D Jones I Malaty C C Price M S Okun and DBowers ldquoHealth comorbidities and cognition in 1948 patientswith idiopathic Parkinsonrsquos diseaserdquo Parkinsonism amp RelatedDisorders vol 18 pp 1073ndash1078 2012
[16] M Lezak D Howieson E Bigler and D Tranel Neuropsy-chological Assessment Oxford University Press New York NYUSA 5th edition 2012
[17] A J Hughes S E Daniel L Kilford and A J Lees ldquoAccuracyof clinical diagnosis of idiopathic Parkinsonrsquos disease a clinico-pathological study of 100 casesrdquo Journal of Neurology Neuro-surgery and Psychiatry vol 55 no 3 pp 181ndash184 1992
[18] S Fahn R L Elton and UPDRS Development CommitteeldquoUnified Parkinsonrsquos disease rating scalerdquo Recent DevelopmentParkinson vol 2 pp 153ndash163 1987
[19] C L Tomlinson R Stowe S Patel C Rick R Gray and CE Clarke ldquoSystematic review of levodopa dose equivalencyreporting in Parkinsonrsquos diseaserdquo Movement Disorders vol 25no 15 pp 2649ndash2653 2010
[20] Y I Sheline D M Barch K Garcia et al ldquoCognitive functionin late life Depression relationships to depression severitycerebrovascular risk factors and processing speedrdquo BiologicalPsychiatry vol 60 no 1 pp 58ndash65 2006
[21] R K Heaton S W Miller M J Taylor and I Grant RevisedComprehensive Norms for An expAnded Halstead-Reitan Bat-tery Demographically Adjusted Neuropsychological Norms forAfrican American and Caucasian Adults PAR Lutz Fla USA2004
[22] M Charlson T P Szatrowski J Peterson and J Gold ldquoVal-idation of a combined comorbidity indexrdquo Journal of ClinicalEpidemiology vol 47 no 11 pp 1245ndash1251 1994
[23] PW FWilson KM Anderson andW B Kannel ldquoEpidemiol-ogy of diabetes mellitus in the elderly The Framingham StudyrdquoAmerican Journal of Medicine vol 80 no 5 A pp 3ndash9 1986
[24] W S Aronow J L Fleg C J Pepine et al ldquoACCFAHA 2011expert consensus document on hypertension in the elderlyrdquoJournal of the American College of Cardiology vol 57 pp 2037ndash2114 2011
[25] I Litvan J G Goldman A I Troster et al ldquoDiagnosticcriteria for mild cognitive impairment in Parkinsonrsquos diseaseMovement Disorder Society Task Force guidelinesrdquoMovementDisorders vol 27 no 3 pp 349ndash356 2012
[26] K J Rothman ldquoNo adjustments are needed for multiplecomparisonsrdquo Epidemiology vol 1 no 1 pp 43ndash46 1990
[27] D S Goldstein ldquoDysautonomia in Parkinsonrsquos disease neuro-cardiological abnormalitiesrdquo Lancet Neurology vol 2 no 11 pp669ndash676 2003
[28] A Verdelho SMadureira JM Ferro et al ldquoDifferential impactof cerebral white matter changes diabetes hypertension andstroke on cognitive performance among non-disabled elderly
10 Parkinsonrsquos Disease
The LADIS studyrdquo Journal of Neurology Neurosurgery andPsychiatry vol 78 no 12 pp 1325ndash1330 2007
[29] S P Woods and A I Troster ldquoProdromal frontalexecutivedysfunction predicts incident dementia in Parkinsonrsquos diseaserdquoJournal of the International Neuropsychological Society vol 9no 1 pp 17ndash24 2003
[30] W Nanhoe-Mahabier K F de Laat J E Visser J Zijlmans F-E de Leeuw and B R Bloem ldquoParkinson disease and comorbidcerebrovascular diseaserdquo Nature Reviews Neurology vol 5 no10 pp 533ndash541 2009
[31] K M Rose D Couper M L Eigenbrodt T H Mosley AR Sharrett and R F Gottesman ldquoOrthostatic hypotensionand cognitive function the atherosclerosis risk in communitiesstudyrdquo Neuroepidemiology vol 34 no 1 pp 1ndash7 2010
[32] P L K Yap M Niti K B Yap and T P Ng ldquoOrthostatichypotension hypotension and cognitive status early comorbidmarkers of primary dementiardquo Dementia and Geriatric Cogni-tive Disorders vol 26 no 3 pp 239ndash246 2008
[33] V Novak and I Hajjar ldquoThe relationship between bloodpressure and cognitive functionrdquo Nature Reviews Cardiologyvol 7 no 12 pp 686ndash698 2010
[34] J S Kim Y S Oh K S Lee Y I Kim D W Yang andD S Goldstein ldquoAssociation of cognitive dysfunction withneurocirculatory abnormalities in early Parkinson diseaserdquoNeurology vol 79 no 13 pp 1323ndash1331 2012
[35] T O Dalaker J P Larsen M G Dwyer et al ldquoWhite matterhyperintensities do not impact cognitive function in patientswith newly diagnosed Parkinsonrsquos diseaserdquoNeuroImage vol 47no 4 pp 2083ndash2089 2009
[36] N I Bohnen and R L Albin ldquoWhite matter lesions inParkinson diseaserdquo Nature Reviews Neurology vol 7 no 4 pp229ndash236 2011
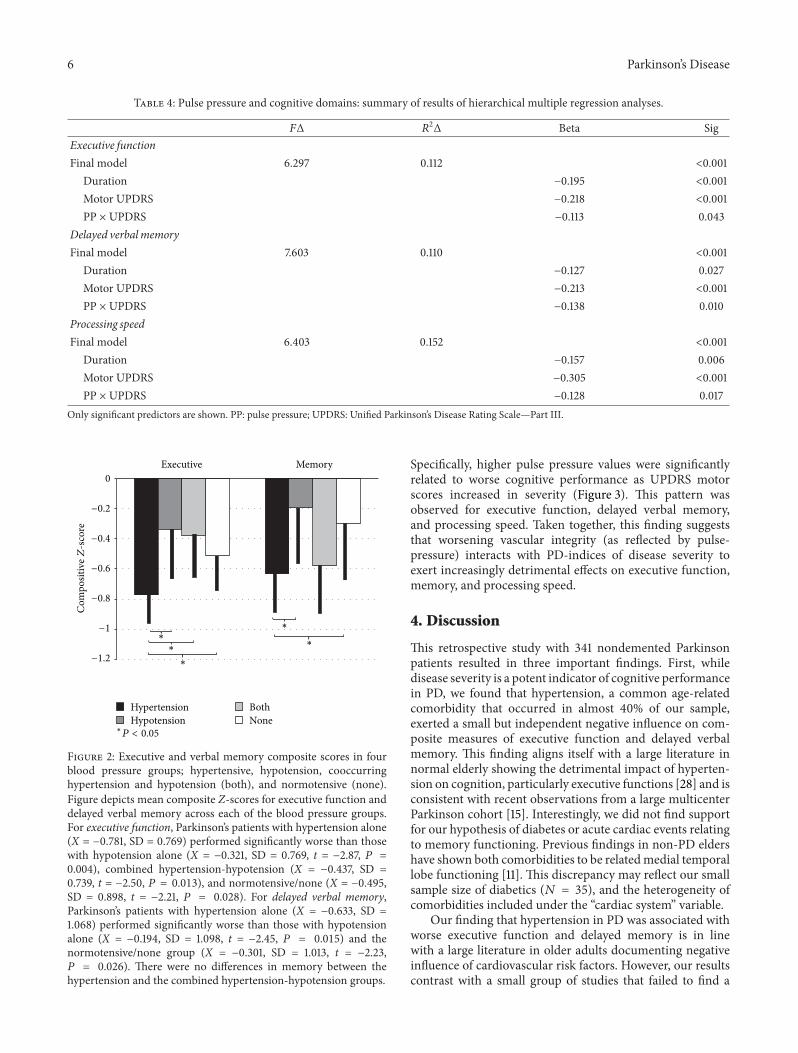
6 Parkinsonrsquos Disease
Table 4 Pulse pressure and cognitive domains summary of results of hierarchical multiple regression analyses
119865Δ 1198772Δ Beta Sig
Executive functionFinal model 6297 0112 lt0001
Duration minus0195 lt0001Motor UPDRS minus0218 lt0001PP times UPDRS minus0113 0043
Delayed verbalmemoryFinal model 7603 0110 lt0001
Duration minus0127 0027Motor UPDRS minus0213 lt0001PP times UPDRS minus0138 0010
Processing speedFinal model 6403 0152 lt0001
Duration minus0157 0006Motor UPDRS minus0305 lt0001PP times UPDRS minus0128 0017
Only significant predictors are shown PP pulse pressure UPDRS Unified Parkinsonrsquos Disease Rating ScalemdashPart III
minus12
minus1
minus08
minus06
minus04
minus02
0
Executive Memory
HypertensionHypotension
BothNone
lowast
lowast
lowast
lowast
lowast
Com
posit
iveZ
-sco
re
lowastP lt 005
Figure 2 Executive and verbal memory composite scores in fourblood pressure groups hypertensive hypotension cooccurringhypertension and hypotension (both) and normotensive (none)Figure depicts mean composite Z-scores for executive function anddelayed verbal memory across each of the blood pressure groupsFor executive function Parkinsonrsquos patients with hypertension alone(X = minus0781 SD = 0769) performed significantly worse than thosewith hypotension alone (X = minus0321 SD = 0769 t = minus287 119875 =0004) combined hypertension-hypotension (X = minus0437 SD =0739 t = minus250 119875 = 0013) and normotensivenone (X = minus0495SD = 0898 t = minus221 119875 = 0028) For delayed verbal memoryParkinsonrsquos patients with hypertension alone (X = minus0633 SD =1068) performed significantly worse than those with hypotensionalone (X = minus0194 SD = 1098 t = minus245 119875 = 0015) and thenormotensivenone group (X = minus0301 SD = 1013 t = minus223119875 = 0026) There were no differences in memory between thehypertension and the combined hypertension-hypotension groups
Specifically higher pulse pressure values were significantlyrelated to worse cognitive performance as UPDRS motorscores increased in severity (Figure 3) This pattern wasobserved for executive function delayed verbal memoryand processing speed Taken together this finding suggeststhat worsening vascular integrity (as reflected by pulse-pressure) interacts with PD-indices of disease severity toexert increasingly detrimental effects on executive functionmemory and processing speed
4 Discussion
This retrospective study with 341 nondemented Parkinsonpatients resulted in three important findings First whiledisease severity is a potent indicator of cognitive performancein PD we found that hypertension a common age-relatedcomorbidity that occurred in almost 40 of our sampleexerted a small but independent negative influence on com-posite measures of executive function and delayed verbalmemory This finding aligns itself with a large literature innormal elderly showing the detrimental impact of hyperten-sion on cognition particularly executive functions [28] and isconsistent with recent observations from a large multicenterParkinson cohort [15] Interestingly we did not find supportfor our hypothesis of diabetes or acute cardiac events relatingto memory functioning Previous findings in non-PD eldershave shown both comorbidities to be relatedmedial temporallobe functioning [11] This discrepancy may reflect our smallsample size of diabetics (119873 = 35) and the heterogeneity ofcomorbidities included under the ldquocardiac systemrdquo variable
Our finding that hypertension in PD was associated withworse executive function and delayed memory is in linewith a large literature in older adults documenting negativeinfluence of cardiovascular risk factors However our resultscontrast with a small group of studies that failed to find a
Parkinsonrsquos Disease 7
Pulse pressure120100806040200
Exec
utiv
e fun
ctio
n
00
minus05
minus10
minus15
minus20
(a)
Verb
al m
emor
y
Pulse pressure120100806040200
00
minus05
minus10
minus15
minus20
(b)
Proc
essin
g sp
eed
Pulse pressure120100806040200
00
minus05
minus10
minus15
minus20
1st quartileUPDRS quartiles
2nd quartile3rd quartile4th quartile
(c)
Figure 3 Pulse pressure X UPDRS interaction for 3 cognitive domains Figure depicts linear relationship between pulse pressure andexecutive function delayed verbal memory and processing speed for each Unified Parkinsonrsquos Disease Rating Scale Part III (UPDRS) quartile(higher quartile means more severe motor symptoms)
relationship between cardiovascular risk and transition todementia in Parkinson patient [12ndash14] We suspect that thereare several factors that account for the different findings Thefirst relates to our use of parametric indices of cognitionrather than a categorical classification of dementia presenceused in previous PD students The former approach is amore sensitive metric for detecting cognitive change ordifferences Second our sample size was considerably largerthan previous PD studies and this may be critical given therelatively small effect sizes we observed Additionally previ-ous studies of cognitive status have shown executive functionsto be an insensitive marker of progression to dementia [7]Thuswhile hypertensionmay relate to executive dysfunctionthis cognitive profile may not differentiate dementia from
nondemented PD patients However this view is debatableand has not been established [29]
To be clear the focus of the present study was not to iden-tify those with and without dementia but to learn whetherhypertension and other comorbidities might contribute tothe cognitive profile of Parkinson patients without severecognitive impairment based on a general cognitive screener(DRS-II) Evidence from this study suggests that hyperten-sion does indeed make a small but significant contributionparticularly to executive function and delayedmemory recallOf note the occurrence of hypertension in our PD sampleis less than that often observed in several previous reportsdescribing hypertension to occur in 53ndash70 of individualsabove the age of 65 [24] Possible explanations for this
8 Parkinsonrsquos Disease
discrepancy includes a protective effect against hypertensionsecondary to levodopa use [30] as well as the fact that thisstudy includes individuals younger than 65 years old
The secondmajor finding was an unexpected relationshipbetween executive function and orthostatic hypotensionwhich occurred in approximately 30 of our sample Ourfindings suggested a possible role of orthostatic hypotension(OH) in moderating the relationship between hypertensionand executive function In brief individuals with cooccurringhypertension and OH were on par with individuals with-out hypertension on executive functioning measures Thisphenomenon has not been previously well documented orestablished and requires further validation The relationshipbetweenOH and cognition in the normal elderly has revealedmixed results with some studies failing to find a relationshipbetween cognitive outcomes and OH [31] However onestudy found that the combination of both hypertensionand orthostatic hypotension served as a protective factor[32] Specifically Yap and others found that among 2321older adults those with both OH and high blood pressure(gt140 systolic or gt90 diastolic) were less likely to haveimpaired scores on a broad measure of cognition (MMSE)compared to individuals without OH and those with OHand low blood pressure The mechanism for this effect hasnot been thoroughly examined but may relate a reductionin mean arterial pressure associated with OH allowing forcerebral blood perfusion to stay in the range of autoregulation[33] Within PD a recent study showed that PD patientswith circulatory abnormalities (including OH and supinehypertension) were more likely to meet criteria for dementia[34] Additionally they found that tests of episodic memorybut not executive functions were significantly related todecreases in blood pressure during a head-up-tilt test Sucha finding may suggest that dysautonomia may be related tocognitive changes occurring later in the disease stage ratherthan frontal-executive changes occurring earlier
Third this study showed a unique finding with pulsepressure whereby higher pulse pressure interacted with PDseverity to exert increasingly detrimental effects on executivefunction processing speed and memory In other words therelationship between cognition and cardiovascular risk maybe moderated by PD severity We are unaware of previousstudies examining the effect of pulse pressure on cognition inParkinson patients There are several ways to conceptualizethis relationship On one hand worsening pulse pressuremay be another index of PD progression vis a vis worseningautonomic dysfunction and effects on blood pressure Alter-natively this relationship may be independent of autonomicdysfunction In either case white matter changes mightrepresent downstream effect of this variability A growingnumber of studies have found that the relationship betweenLA and cognition varies depending on PD severity In factstudies of Parkinson patients in more advanced stages haveshown LA to be related to cognition whereas studies ofnewly diagnosed PD patients failed to replicate this finding[12ndash14 35] suggesting that vascular pathology may interactwith PD pathology This idea of an interaction betweenvascular pathology and PD pathology has also been exploredin its relationship to non-cognitive symptoms of PD In
terms of motor complications in PD higher LA burden hasbeen associatedwithworseningmotor functioning includingposturalgait difficulty bradykinesia and rigidity [36]
There are several limitations to this study First thedesign was cross-sectional and used a convenience sample ofpatients which may limit generalizability Next comorbiditymeasures depended on accurate documentation by physi-cians in the patientsrsquo medical charts While the validity ofthis method is unknown we believe the most noteworthycomorbidities were likely noted and recorded as part of thepatientrsquos medical record Lastly other than blood pressurethere were no direct measures of comorbidity and we wereunable to quantify severity or duration of various healthconditions Concerning blood pressure data consisted of onemeasurement rather than multiple blood pressure measure-ments which is more advantageous
5 Conclusion
The current study adds to the literature by suggesting thathypertension may be related to subtle executive and mem-ory deficits in Parkinson patients above and beyond thatconferred by the disease process itself The effect is likelysmall though it does parallel that observed in non-PD olderadults and may become more salient with disease progres-sion What is particularly unique in Parkinsonrsquos disease is ajuxtaposition of factors that are protective versus those thatincrease cardiovascular risk Protective factors include use oflevodopa medications that decrease blood pressure whereasautonomic dysfunction use of dopamine agonists (related tocardiac valvulopathy) and general physical deconditioningserve to increase cardiovascular risk [31] Even with thisunique confluence the present study provides preliminaryevidence that hypertensionmay be related to subtle cognitivedeficits in Parkinson patients similar to that of older adultsand may amplify executive and memory difficulties Futurestudies should examine possiblemechanisms such as LA andthe impact that subtle vascular-related cognitive deficits haveon quality of life andmood Improving cardiovascular healthprior to dementia onset should be further investigated as ameans of moderating cognitive changes Due to high risk ofcognitive declinedementia and the degenerative nature ofPD a small minimization in risk of cognitive decline mayprove to be beneficial
Conflict of Interests
No financial compensation was received for conducting thisstudy Mr Jones reports no disclosures Mr Jacobson IVreports no disclosures Dr Murphy reports no disclosuresDr Price has received research support from the NIH andthe National Parkinson Foundation Dr Okun serves as aconsultant for the National Parkinson Foundation and hasreceived research grants from NIH NPF the Michael J FoxFoundation the Parkinson Alliance Smallwood Foundationand the UF Foundation Dr Okun has previously receivedhonoraria but in the past 24 months has received no supportfrom industry including travel Dr Okun has received roy-alties for publications with Demos Manson and Cambridge
Parkinsonrsquos Disease 9
(movement disorders books) Dr Okun has participated inCME activities onmovement disorders sponsored by theUSFCME office PeerView Vanderbilt University and PrimeTheinstitution andnotDrOkun receives grants fromMedtronicand ANSSt Jude and the PI has no financial interest in thesegrants Dr Okun has participated as a site PI andor co-Ifor several NIH foundation and industry sponsored trialsover the years but has not received honoraria Dr Bowershas received research support from the NIH Michael J FoxFoundation the National Parkinson Foundation and theMcKnight Research Foundation
Acknowledgments
This study was supported by a Center of Excellence Grantfrom the National Parkinson Foundation and the UF-INFORM database
References
[1] G E Alexander M R DeLong and P L Strick ldquoParallelorganization of functionally segregated circuits linking basalganglia and cortexrdquo Annual Review of Neuroscience vol 9 pp357ndash381 1986
[2] K R Chaudhuri and A H Schapira ldquoNon-motor symptoms ofParkinsonrsquos disease dopaminergic pathophysiology and treat-mentrdquoThe Lancet Neurology vol 8 no 5 pp 464ndash474 2009
[3] D Aarsland K Andersen J P Larsen A Lolk H Nielsen andP Kragh-Soslashrensen ldquoRisk of dementia in Parkinsonrsquos disease acommunity-based Prospective StudyrdquoNeurology vol 56 no 6pp 730ndash736 2001
[4] M A Hely W G J Reid M A Adena G M Halliday andJ G L Morris ldquoThe Sydney Multicenter Study of Parkinsonrsquosdisease the inevitability of dementia at 20 yearsrdquo MovementDisorders vol 23 no 6 pp 837ndash844 2008
[5] A SchragM Jahanshahi andNQuinn ldquoHowdoes Parkinsonrsquosdisease affect quality of life A comparison with quality of life inthe general populationrdquo Movement Disorders vol 15 pp 1112ndash1118 2000
[6] B Dubois and B Pillon ldquoCognitive deficits in Parkinsonrsquosdiseaserdquo Journal of Neurology vol 244 no 1 pp 2ndash8 1997
[7] C H Williams-Gray J R Evans A Goris et al ldquoThe distinctcognitive syndromes of Parkinsonrsquos disease 5 year follow-up ofthe CamPaIGN cohortrdquo Brain vol 132 no 11 pp 2958ndash29692009
[8] B K Saxby F Harrington I G McKeith K Wesnes and GA Ford ldquoEffects of hypertension on attention memory andexecutive function in older adultsrdquo Health Psychology vol 22no 6 pp 587ndash591 2003
[9] D Knopman L L Boland TMosley et al ldquoCardiovascular riskfactors and cognitive decline inmiddle-aged adultsrdquoNeurologyvol 56 no 1 pp 42ndash48 2001
[10] A A Gouw A Seewann W M Van Der Flier et al ldquoHet-erogeneity of small vessel disease a systematic review ofMRI and histopathology correlationsrdquo Journal of NeurologyNeurosurgery and Psychiatry vol 82 no 2 pp 126ndash135 2011
[11] W Wu A M Brickman J Luchsinger et al ldquoThe brain in theage of old the hippocampal formation is targeted differentiallyby diseases of late liferdquo Annals of Neurology vol 64 no 6 pp698ndash706 2008
[12] M K Beyer D Aarsland O J Greve and J P Larsen ldquoVisualrating of white matter hyperintensities in Parkinsonrsquos diseaserdquoMovement Disorders vol 21 no 2 pp 223ndash229 2006
[13] S-J Lee J-S Kim J-Y Yoo et al ldquoInfluence of white matterhyperintensities on the cognition of patients with parkinsondiseaserdquoAlzheimerDisease andAssociatedDisorders vol 24 no3 pp 227ndash233 2010
[14] J Sławek D Wieczorek M Derejko et al ldquoThe influenceof vascular risk factors and white matter hyperintensities onthe degree of cognitive impairment in Parkinsonrsquos diseaserdquoNeurologia i Neurochirurgia Polska vol 42 no 6 pp 505ndash5122008
[15] J D Jones I Malaty C C Price M S Okun and DBowers ldquoHealth comorbidities and cognition in 1948 patientswith idiopathic Parkinsonrsquos diseaserdquo Parkinsonism amp RelatedDisorders vol 18 pp 1073ndash1078 2012
[16] M Lezak D Howieson E Bigler and D Tranel Neuropsy-chological Assessment Oxford University Press New York NYUSA 5th edition 2012
[17] A J Hughes S E Daniel L Kilford and A J Lees ldquoAccuracyof clinical diagnosis of idiopathic Parkinsonrsquos disease a clinico-pathological study of 100 casesrdquo Journal of Neurology Neuro-surgery and Psychiatry vol 55 no 3 pp 181ndash184 1992
[18] S Fahn R L Elton and UPDRS Development CommitteeldquoUnified Parkinsonrsquos disease rating scalerdquo Recent DevelopmentParkinson vol 2 pp 153ndash163 1987
[19] C L Tomlinson R Stowe S Patel C Rick R Gray and CE Clarke ldquoSystematic review of levodopa dose equivalencyreporting in Parkinsonrsquos diseaserdquo Movement Disorders vol 25no 15 pp 2649ndash2653 2010
[20] Y I Sheline D M Barch K Garcia et al ldquoCognitive functionin late life Depression relationships to depression severitycerebrovascular risk factors and processing speedrdquo BiologicalPsychiatry vol 60 no 1 pp 58ndash65 2006
[21] R K Heaton S W Miller M J Taylor and I Grant RevisedComprehensive Norms for An expAnded Halstead-Reitan Bat-tery Demographically Adjusted Neuropsychological Norms forAfrican American and Caucasian Adults PAR Lutz Fla USA2004
[22] M Charlson T P Szatrowski J Peterson and J Gold ldquoVal-idation of a combined comorbidity indexrdquo Journal of ClinicalEpidemiology vol 47 no 11 pp 1245ndash1251 1994
[23] PW FWilson KM Anderson andW B Kannel ldquoEpidemiol-ogy of diabetes mellitus in the elderly The Framingham StudyrdquoAmerican Journal of Medicine vol 80 no 5 A pp 3ndash9 1986
[24] W S Aronow J L Fleg C J Pepine et al ldquoACCFAHA 2011expert consensus document on hypertension in the elderlyrdquoJournal of the American College of Cardiology vol 57 pp 2037ndash2114 2011
[25] I Litvan J G Goldman A I Troster et al ldquoDiagnosticcriteria for mild cognitive impairment in Parkinsonrsquos diseaseMovement Disorder Society Task Force guidelinesrdquoMovementDisorders vol 27 no 3 pp 349ndash356 2012
[26] K J Rothman ldquoNo adjustments are needed for multiplecomparisonsrdquo Epidemiology vol 1 no 1 pp 43ndash46 1990
[27] D S Goldstein ldquoDysautonomia in Parkinsonrsquos disease neuro-cardiological abnormalitiesrdquo Lancet Neurology vol 2 no 11 pp669ndash676 2003
[28] A Verdelho SMadureira JM Ferro et al ldquoDifferential impactof cerebral white matter changes diabetes hypertension andstroke on cognitive performance among non-disabled elderly
10 Parkinsonrsquos Disease
The LADIS studyrdquo Journal of Neurology Neurosurgery andPsychiatry vol 78 no 12 pp 1325ndash1330 2007
[29] S P Woods and A I Troster ldquoProdromal frontalexecutivedysfunction predicts incident dementia in Parkinsonrsquos diseaserdquoJournal of the International Neuropsychological Society vol 9no 1 pp 17ndash24 2003
[30] W Nanhoe-Mahabier K F de Laat J E Visser J Zijlmans F-E de Leeuw and B R Bloem ldquoParkinson disease and comorbidcerebrovascular diseaserdquo Nature Reviews Neurology vol 5 no10 pp 533ndash541 2009
[31] K M Rose D Couper M L Eigenbrodt T H Mosley AR Sharrett and R F Gottesman ldquoOrthostatic hypotensionand cognitive function the atherosclerosis risk in communitiesstudyrdquo Neuroepidemiology vol 34 no 1 pp 1ndash7 2010
[32] P L K Yap M Niti K B Yap and T P Ng ldquoOrthostatichypotension hypotension and cognitive status early comorbidmarkers of primary dementiardquo Dementia and Geriatric Cogni-tive Disorders vol 26 no 3 pp 239ndash246 2008
[33] V Novak and I Hajjar ldquoThe relationship between bloodpressure and cognitive functionrdquo Nature Reviews Cardiologyvol 7 no 12 pp 686ndash698 2010
[34] J S Kim Y S Oh K S Lee Y I Kim D W Yang andD S Goldstein ldquoAssociation of cognitive dysfunction withneurocirculatory abnormalities in early Parkinson diseaserdquoNeurology vol 79 no 13 pp 1323ndash1331 2012
[35] T O Dalaker J P Larsen M G Dwyer et al ldquoWhite matterhyperintensities do not impact cognitive function in patientswith newly diagnosed Parkinsonrsquos diseaserdquoNeuroImage vol 47no 4 pp 2083ndash2089 2009
[36] N I Bohnen and R L Albin ldquoWhite matter lesions inParkinson diseaserdquo Nature Reviews Neurology vol 7 no 4 pp229ndash236 2011

Parkinsonrsquos Disease 7
Pulse pressure120100806040200
Exec
utiv
e fun
ctio
n
00
minus05
minus10
minus15
minus20
(a)
Verb
al m
emor
y
Pulse pressure120100806040200
00
minus05
minus10
minus15
minus20
(b)
Proc
essin
g sp
eed
Pulse pressure120100806040200
00
minus05
minus10
minus15
minus20
1st quartileUPDRS quartiles
2nd quartile3rd quartile4th quartile
(c)
Figure 3 Pulse pressure X UPDRS interaction for 3 cognitive domains Figure depicts linear relationship between pulse pressure andexecutive function delayed verbal memory and processing speed for each Unified Parkinsonrsquos Disease Rating Scale Part III (UPDRS) quartile(higher quartile means more severe motor symptoms)
relationship between cardiovascular risk and transition todementia in Parkinson patient [12ndash14] We suspect that thereare several factors that account for the different findings Thefirst relates to our use of parametric indices of cognitionrather than a categorical classification of dementia presenceused in previous PD students The former approach is amore sensitive metric for detecting cognitive change ordifferences Second our sample size was considerably largerthan previous PD studies and this may be critical given therelatively small effect sizes we observed Additionally previ-ous studies of cognitive status have shown executive functionsto be an insensitive marker of progression to dementia [7]Thuswhile hypertensionmay relate to executive dysfunctionthis cognitive profile may not differentiate dementia from
nondemented PD patients However this view is debatableand has not been established [29]
To be clear the focus of the present study was not to iden-tify those with and without dementia but to learn whetherhypertension and other comorbidities might contribute tothe cognitive profile of Parkinson patients without severecognitive impairment based on a general cognitive screener(DRS-II) Evidence from this study suggests that hyperten-sion does indeed make a small but significant contributionparticularly to executive function and delayedmemory recallOf note the occurrence of hypertension in our PD sampleis less than that often observed in several previous reportsdescribing hypertension to occur in 53ndash70 of individualsabove the age of 65 [24] Possible explanations for this
8 Parkinsonrsquos Disease
discrepancy includes a protective effect against hypertensionsecondary to levodopa use [30] as well as the fact that thisstudy includes individuals younger than 65 years old
The secondmajor finding was an unexpected relationshipbetween executive function and orthostatic hypotensionwhich occurred in approximately 30 of our sample Ourfindings suggested a possible role of orthostatic hypotension(OH) in moderating the relationship between hypertensionand executive function In brief individuals with cooccurringhypertension and OH were on par with individuals with-out hypertension on executive functioning measures Thisphenomenon has not been previously well documented orestablished and requires further validation The relationshipbetweenOH and cognition in the normal elderly has revealedmixed results with some studies failing to find a relationshipbetween cognitive outcomes and OH [31] However onestudy found that the combination of both hypertensionand orthostatic hypotension served as a protective factor[32] Specifically Yap and others found that among 2321older adults those with both OH and high blood pressure(gt140 systolic or gt90 diastolic) were less likely to haveimpaired scores on a broad measure of cognition (MMSE)compared to individuals without OH and those with OHand low blood pressure The mechanism for this effect hasnot been thoroughly examined but may relate a reductionin mean arterial pressure associated with OH allowing forcerebral blood perfusion to stay in the range of autoregulation[33] Within PD a recent study showed that PD patientswith circulatory abnormalities (including OH and supinehypertension) were more likely to meet criteria for dementia[34] Additionally they found that tests of episodic memorybut not executive functions were significantly related todecreases in blood pressure during a head-up-tilt test Sucha finding may suggest that dysautonomia may be related tocognitive changes occurring later in the disease stage ratherthan frontal-executive changes occurring earlier
Third this study showed a unique finding with pulsepressure whereby higher pulse pressure interacted with PDseverity to exert increasingly detrimental effects on executivefunction processing speed and memory In other words therelationship between cognition and cardiovascular risk maybe moderated by PD severity We are unaware of previousstudies examining the effect of pulse pressure on cognition inParkinson patients There are several ways to conceptualizethis relationship On one hand worsening pulse pressuremay be another index of PD progression vis a vis worseningautonomic dysfunction and effects on blood pressure Alter-natively this relationship may be independent of autonomicdysfunction In either case white matter changes mightrepresent downstream effect of this variability A growingnumber of studies have found that the relationship betweenLA and cognition varies depending on PD severity In factstudies of Parkinson patients in more advanced stages haveshown LA to be related to cognition whereas studies ofnewly diagnosed PD patients failed to replicate this finding[12ndash14 35] suggesting that vascular pathology may interactwith PD pathology This idea of an interaction betweenvascular pathology and PD pathology has also been exploredin its relationship to non-cognitive symptoms of PD In
terms of motor complications in PD higher LA burden hasbeen associatedwithworseningmotor functioning includingposturalgait difficulty bradykinesia and rigidity [36]
There are several limitations to this study First thedesign was cross-sectional and used a convenience sample ofpatients which may limit generalizability Next comorbiditymeasures depended on accurate documentation by physi-cians in the patientsrsquo medical charts While the validity ofthis method is unknown we believe the most noteworthycomorbidities were likely noted and recorded as part of thepatientrsquos medical record Lastly other than blood pressurethere were no direct measures of comorbidity and we wereunable to quantify severity or duration of various healthconditions Concerning blood pressure data consisted of onemeasurement rather than multiple blood pressure measure-ments which is more advantageous
5 Conclusion
The current study adds to the literature by suggesting thathypertension may be related to subtle executive and mem-ory deficits in Parkinson patients above and beyond thatconferred by the disease process itself The effect is likelysmall though it does parallel that observed in non-PD olderadults and may become more salient with disease progres-sion What is particularly unique in Parkinsonrsquos disease is ajuxtaposition of factors that are protective versus those thatincrease cardiovascular risk Protective factors include use oflevodopa medications that decrease blood pressure whereasautonomic dysfunction use of dopamine agonists (related tocardiac valvulopathy) and general physical deconditioningserve to increase cardiovascular risk [31] Even with thisunique confluence the present study provides preliminaryevidence that hypertensionmay be related to subtle cognitivedeficits in Parkinson patients similar to that of older adultsand may amplify executive and memory difficulties Futurestudies should examine possiblemechanisms such as LA andthe impact that subtle vascular-related cognitive deficits haveon quality of life andmood Improving cardiovascular healthprior to dementia onset should be further investigated as ameans of moderating cognitive changes Due to high risk ofcognitive declinedementia and the degenerative nature ofPD a small minimization in risk of cognitive decline mayprove to be beneficial
Conflict of Interests
No financial compensation was received for conducting thisstudy Mr Jones reports no disclosures Mr Jacobson IVreports no disclosures Dr Murphy reports no disclosuresDr Price has received research support from the NIH andthe National Parkinson Foundation Dr Okun serves as aconsultant for the National Parkinson Foundation and hasreceived research grants from NIH NPF the Michael J FoxFoundation the Parkinson Alliance Smallwood Foundationand the UF Foundation Dr Okun has previously receivedhonoraria but in the past 24 months has received no supportfrom industry including travel Dr Okun has received roy-alties for publications with Demos Manson and Cambridge
Parkinsonrsquos Disease 9
(movement disorders books) Dr Okun has participated inCME activities onmovement disorders sponsored by theUSFCME office PeerView Vanderbilt University and PrimeTheinstitution andnotDrOkun receives grants fromMedtronicand ANSSt Jude and the PI has no financial interest in thesegrants Dr Okun has participated as a site PI andor co-Ifor several NIH foundation and industry sponsored trialsover the years but has not received honoraria Dr Bowershas received research support from the NIH Michael J FoxFoundation the National Parkinson Foundation and theMcKnight Research Foundation
Acknowledgments
This study was supported by a Center of Excellence Grantfrom the National Parkinson Foundation and the UF-INFORM database
References
[1] G E Alexander M R DeLong and P L Strick ldquoParallelorganization of functionally segregated circuits linking basalganglia and cortexrdquo Annual Review of Neuroscience vol 9 pp357ndash381 1986
[2] K R Chaudhuri and A H Schapira ldquoNon-motor symptoms ofParkinsonrsquos disease dopaminergic pathophysiology and treat-mentrdquoThe Lancet Neurology vol 8 no 5 pp 464ndash474 2009
[3] D Aarsland K Andersen J P Larsen A Lolk H Nielsen andP Kragh-Soslashrensen ldquoRisk of dementia in Parkinsonrsquos disease acommunity-based Prospective StudyrdquoNeurology vol 56 no 6pp 730ndash736 2001
[4] M A Hely W G J Reid M A Adena G M Halliday andJ G L Morris ldquoThe Sydney Multicenter Study of Parkinsonrsquosdisease the inevitability of dementia at 20 yearsrdquo MovementDisorders vol 23 no 6 pp 837ndash844 2008
[5] A SchragM Jahanshahi andNQuinn ldquoHowdoes Parkinsonrsquosdisease affect quality of life A comparison with quality of life inthe general populationrdquo Movement Disorders vol 15 pp 1112ndash1118 2000
[6] B Dubois and B Pillon ldquoCognitive deficits in Parkinsonrsquosdiseaserdquo Journal of Neurology vol 244 no 1 pp 2ndash8 1997
[7] C H Williams-Gray J R Evans A Goris et al ldquoThe distinctcognitive syndromes of Parkinsonrsquos disease 5 year follow-up ofthe CamPaIGN cohortrdquo Brain vol 132 no 11 pp 2958ndash29692009
[8] B K Saxby F Harrington I G McKeith K Wesnes and GA Ford ldquoEffects of hypertension on attention memory andexecutive function in older adultsrdquo Health Psychology vol 22no 6 pp 587ndash591 2003
[9] D Knopman L L Boland TMosley et al ldquoCardiovascular riskfactors and cognitive decline inmiddle-aged adultsrdquoNeurologyvol 56 no 1 pp 42ndash48 2001
[10] A A Gouw A Seewann W M Van Der Flier et al ldquoHet-erogeneity of small vessel disease a systematic review ofMRI and histopathology correlationsrdquo Journal of NeurologyNeurosurgery and Psychiatry vol 82 no 2 pp 126ndash135 2011
[11] W Wu A M Brickman J Luchsinger et al ldquoThe brain in theage of old the hippocampal formation is targeted differentiallyby diseases of late liferdquo Annals of Neurology vol 64 no 6 pp698ndash706 2008
[12] M K Beyer D Aarsland O J Greve and J P Larsen ldquoVisualrating of white matter hyperintensities in Parkinsonrsquos diseaserdquoMovement Disorders vol 21 no 2 pp 223ndash229 2006
[13] S-J Lee J-S Kim J-Y Yoo et al ldquoInfluence of white matterhyperintensities on the cognition of patients with parkinsondiseaserdquoAlzheimerDisease andAssociatedDisorders vol 24 no3 pp 227ndash233 2010
[14] J Sławek D Wieczorek M Derejko et al ldquoThe influenceof vascular risk factors and white matter hyperintensities onthe degree of cognitive impairment in Parkinsonrsquos diseaserdquoNeurologia i Neurochirurgia Polska vol 42 no 6 pp 505ndash5122008
[15] J D Jones I Malaty C C Price M S Okun and DBowers ldquoHealth comorbidities and cognition in 1948 patientswith idiopathic Parkinsonrsquos diseaserdquo Parkinsonism amp RelatedDisorders vol 18 pp 1073ndash1078 2012
[16] M Lezak D Howieson E Bigler and D Tranel Neuropsy-chological Assessment Oxford University Press New York NYUSA 5th edition 2012
[17] A J Hughes S E Daniel L Kilford and A J Lees ldquoAccuracyof clinical diagnosis of idiopathic Parkinsonrsquos disease a clinico-pathological study of 100 casesrdquo Journal of Neurology Neuro-surgery and Psychiatry vol 55 no 3 pp 181ndash184 1992
[18] S Fahn R L Elton and UPDRS Development CommitteeldquoUnified Parkinsonrsquos disease rating scalerdquo Recent DevelopmentParkinson vol 2 pp 153ndash163 1987
[19] C L Tomlinson R Stowe S Patel C Rick R Gray and CE Clarke ldquoSystematic review of levodopa dose equivalencyreporting in Parkinsonrsquos diseaserdquo Movement Disorders vol 25no 15 pp 2649ndash2653 2010
[20] Y I Sheline D M Barch K Garcia et al ldquoCognitive functionin late life Depression relationships to depression severitycerebrovascular risk factors and processing speedrdquo BiologicalPsychiatry vol 60 no 1 pp 58ndash65 2006
[21] R K Heaton S W Miller M J Taylor and I Grant RevisedComprehensive Norms for An expAnded Halstead-Reitan Bat-tery Demographically Adjusted Neuropsychological Norms forAfrican American and Caucasian Adults PAR Lutz Fla USA2004
[22] M Charlson T P Szatrowski J Peterson and J Gold ldquoVal-idation of a combined comorbidity indexrdquo Journal of ClinicalEpidemiology vol 47 no 11 pp 1245ndash1251 1994
[23] PW FWilson KM Anderson andW B Kannel ldquoEpidemiol-ogy of diabetes mellitus in the elderly The Framingham StudyrdquoAmerican Journal of Medicine vol 80 no 5 A pp 3ndash9 1986
[24] W S Aronow J L Fleg C J Pepine et al ldquoACCFAHA 2011expert consensus document on hypertension in the elderlyrdquoJournal of the American College of Cardiology vol 57 pp 2037ndash2114 2011
[25] I Litvan J G Goldman A I Troster et al ldquoDiagnosticcriteria for mild cognitive impairment in Parkinsonrsquos diseaseMovement Disorder Society Task Force guidelinesrdquoMovementDisorders vol 27 no 3 pp 349ndash356 2012
[26] K J Rothman ldquoNo adjustments are needed for multiplecomparisonsrdquo Epidemiology vol 1 no 1 pp 43ndash46 1990
[27] D S Goldstein ldquoDysautonomia in Parkinsonrsquos disease neuro-cardiological abnormalitiesrdquo Lancet Neurology vol 2 no 11 pp669ndash676 2003
[28] A Verdelho SMadureira JM Ferro et al ldquoDifferential impactof cerebral white matter changes diabetes hypertension andstroke on cognitive performance among non-disabled elderly
10 Parkinsonrsquos Disease
The LADIS studyrdquo Journal of Neurology Neurosurgery andPsychiatry vol 78 no 12 pp 1325ndash1330 2007
[29] S P Woods and A I Troster ldquoProdromal frontalexecutivedysfunction predicts incident dementia in Parkinsonrsquos diseaserdquoJournal of the International Neuropsychological Society vol 9no 1 pp 17ndash24 2003
[30] W Nanhoe-Mahabier K F de Laat J E Visser J Zijlmans F-E de Leeuw and B R Bloem ldquoParkinson disease and comorbidcerebrovascular diseaserdquo Nature Reviews Neurology vol 5 no10 pp 533ndash541 2009
[31] K M Rose D Couper M L Eigenbrodt T H Mosley AR Sharrett and R F Gottesman ldquoOrthostatic hypotensionand cognitive function the atherosclerosis risk in communitiesstudyrdquo Neuroepidemiology vol 34 no 1 pp 1ndash7 2010
[32] P L K Yap M Niti K B Yap and T P Ng ldquoOrthostatichypotension hypotension and cognitive status early comorbidmarkers of primary dementiardquo Dementia and Geriatric Cogni-tive Disorders vol 26 no 3 pp 239ndash246 2008
[33] V Novak and I Hajjar ldquoThe relationship between bloodpressure and cognitive functionrdquo Nature Reviews Cardiologyvol 7 no 12 pp 686ndash698 2010
[34] J S Kim Y S Oh K S Lee Y I Kim D W Yang andD S Goldstein ldquoAssociation of cognitive dysfunction withneurocirculatory abnormalities in early Parkinson diseaserdquoNeurology vol 79 no 13 pp 1323ndash1331 2012
[35] T O Dalaker J P Larsen M G Dwyer et al ldquoWhite matterhyperintensities do not impact cognitive function in patientswith newly diagnosed Parkinsonrsquos diseaserdquoNeuroImage vol 47no 4 pp 2083ndash2089 2009
[36] N I Bohnen and R L Albin ldquoWhite matter lesions inParkinson diseaserdquo Nature Reviews Neurology vol 7 no 4 pp229ndash236 2011

8 Parkinsonrsquos Disease
discrepancy includes a protective effect against hypertensionsecondary to levodopa use [30] as well as the fact that thisstudy includes individuals younger than 65 years old
The secondmajor finding was an unexpected relationshipbetween executive function and orthostatic hypotensionwhich occurred in approximately 30 of our sample Ourfindings suggested a possible role of orthostatic hypotension(OH) in moderating the relationship between hypertensionand executive function In brief individuals with cooccurringhypertension and OH were on par with individuals with-out hypertension on executive functioning measures Thisphenomenon has not been previously well documented orestablished and requires further validation The relationshipbetweenOH and cognition in the normal elderly has revealedmixed results with some studies failing to find a relationshipbetween cognitive outcomes and OH [31] However onestudy found that the combination of both hypertensionand orthostatic hypotension served as a protective factor[32] Specifically Yap and others found that among 2321older adults those with both OH and high blood pressure(gt140 systolic or gt90 diastolic) were less likely to haveimpaired scores on a broad measure of cognition (MMSE)compared to individuals without OH and those with OHand low blood pressure The mechanism for this effect hasnot been thoroughly examined but may relate a reductionin mean arterial pressure associated with OH allowing forcerebral blood perfusion to stay in the range of autoregulation[33] Within PD a recent study showed that PD patientswith circulatory abnormalities (including OH and supinehypertension) were more likely to meet criteria for dementia[34] Additionally they found that tests of episodic memorybut not executive functions were significantly related todecreases in blood pressure during a head-up-tilt test Sucha finding may suggest that dysautonomia may be related tocognitive changes occurring later in the disease stage ratherthan frontal-executive changes occurring earlier
Third this study showed a unique finding with pulsepressure whereby higher pulse pressure interacted with PDseverity to exert increasingly detrimental effects on executivefunction processing speed and memory In other words therelationship between cognition and cardiovascular risk maybe moderated by PD severity We are unaware of previousstudies examining the effect of pulse pressure on cognition inParkinson patients There are several ways to conceptualizethis relationship On one hand worsening pulse pressuremay be another index of PD progression vis a vis worseningautonomic dysfunction and effects on blood pressure Alter-natively this relationship may be independent of autonomicdysfunction In either case white matter changes mightrepresent downstream effect of this variability A growingnumber of studies have found that the relationship betweenLA and cognition varies depending on PD severity In factstudies of Parkinson patients in more advanced stages haveshown LA to be related to cognition whereas studies ofnewly diagnosed PD patients failed to replicate this finding[12ndash14 35] suggesting that vascular pathology may interactwith PD pathology This idea of an interaction betweenvascular pathology and PD pathology has also been exploredin its relationship to non-cognitive symptoms of PD In
terms of motor complications in PD higher LA burden hasbeen associatedwithworseningmotor functioning includingposturalgait difficulty bradykinesia and rigidity [36]
There are several limitations to this study First thedesign was cross-sectional and used a convenience sample ofpatients which may limit generalizability Next comorbiditymeasures depended on accurate documentation by physi-cians in the patientsrsquo medical charts While the validity ofthis method is unknown we believe the most noteworthycomorbidities were likely noted and recorded as part of thepatientrsquos medical record Lastly other than blood pressurethere were no direct measures of comorbidity and we wereunable to quantify severity or duration of various healthconditions Concerning blood pressure data consisted of onemeasurement rather than multiple blood pressure measure-ments which is more advantageous
5 Conclusion
The current study adds to the literature by suggesting thathypertension may be related to subtle executive and mem-ory deficits in Parkinson patients above and beyond thatconferred by the disease process itself The effect is likelysmall though it does parallel that observed in non-PD olderadults and may become more salient with disease progres-sion What is particularly unique in Parkinsonrsquos disease is ajuxtaposition of factors that are protective versus those thatincrease cardiovascular risk Protective factors include use oflevodopa medications that decrease blood pressure whereasautonomic dysfunction use of dopamine agonists (related tocardiac valvulopathy) and general physical deconditioningserve to increase cardiovascular risk [31] Even with thisunique confluence the present study provides preliminaryevidence that hypertensionmay be related to subtle cognitivedeficits in Parkinson patients similar to that of older adultsand may amplify executive and memory difficulties Futurestudies should examine possiblemechanisms such as LA andthe impact that subtle vascular-related cognitive deficits haveon quality of life andmood Improving cardiovascular healthprior to dementia onset should be further investigated as ameans of moderating cognitive changes Due to high risk ofcognitive declinedementia and the degenerative nature ofPD a small minimization in risk of cognitive decline mayprove to be beneficial
Conflict of Interests
No financial compensation was received for conducting thisstudy Mr Jones reports no disclosures Mr Jacobson IVreports no disclosures Dr Murphy reports no disclosuresDr Price has received research support from the NIH andthe National Parkinson Foundation Dr Okun serves as aconsultant for the National Parkinson Foundation and hasreceived research grants from NIH NPF the Michael J FoxFoundation the Parkinson Alliance Smallwood Foundationand the UF Foundation Dr Okun has previously receivedhonoraria but in the past 24 months has received no supportfrom industry including travel Dr Okun has received roy-alties for publications with Demos Manson and Cambridge
Parkinsonrsquos Disease 9
(movement disorders books) Dr Okun has participated inCME activities onmovement disorders sponsored by theUSFCME office PeerView Vanderbilt University and PrimeTheinstitution andnotDrOkun receives grants fromMedtronicand ANSSt Jude and the PI has no financial interest in thesegrants Dr Okun has participated as a site PI andor co-Ifor several NIH foundation and industry sponsored trialsover the years but has not received honoraria Dr Bowershas received research support from the NIH Michael J FoxFoundation the National Parkinson Foundation and theMcKnight Research Foundation
Acknowledgments
This study was supported by a Center of Excellence Grantfrom the National Parkinson Foundation and the UF-INFORM database
References
[1] G E Alexander M R DeLong and P L Strick ldquoParallelorganization of functionally segregated circuits linking basalganglia and cortexrdquo Annual Review of Neuroscience vol 9 pp357ndash381 1986
[2] K R Chaudhuri and A H Schapira ldquoNon-motor symptoms ofParkinsonrsquos disease dopaminergic pathophysiology and treat-mentrdquoThe Lancet Neurology vol 8 no 5 pp 464ndash474 2009
[3] D Aarsland K Andersen J P Larsen A Lolk H Nielsen andP Kragh-Soslashrensen ldquoRisk of dementia in Parkinsonrsquos disease acommunity-based Prospective StudyrdquoNeurology vol 56 no 6pp 730ndash736 2001
[4] M A Hely W G J Reid M A Adena G M Halliday andJ G L Morris ldquoThe Sydney Multicenter Study of Parkinsonrsquosdisease the inevitability of dementia at 20 yearsrdquo MovementDisorders vol 23 no 6 pp 837ndash844 2008
[5] A SchragM Jahanshahi andNQuinn ldquoHowdoes Parkinsonrsquosdisease affect quality of life A comparison with quality of life inthe general populationrdquo Movement Disorders vol 15 pp 1112ndash1118 2000
[6] B Dubois and B Pillon ldquoCognitive deficits in Parkinsonrsquosdiseaserdquo Journal of Neurology vol 244 no 1 pp 2ndash8 1997
[7] C H Williams-Gray J R Evans A Goris et al ldquoThe distinctcognitive syndromes of Parkinsonrsquos disease 5 year follow-up ofthe CamPaIGN cohortrdquo Brain vol 132 no 11 pp 2958ndash29692009
[8] B K Saxby F Harrington I G McKeith K Wesnes and GA Ford ldquoEffects of hypertension on attention memory andexecutive function in older adultsrdquo Health Psychology vol 22no 6 pp 587ndash591 2003
[9] D Knopman L L Boland TMosley et al ldquoCardiovascular riskfactors and cognitive decline inmiddle-aged adultsrdquoNeurologyvol 56 no 1 pp 42ndash48 2001
[10] A A Gouw A Seewann W M Van Der Flier et al ldquoHet-erogeneity of small vessel disease a systematic review ofMRI and histopathology correlationsrdquo Journal of NeurologyNeurosurgery and Psychiatry vol 82 no 2 pp 126ndash135 2011
[11] W Wu A M Brickman J Luchsinger et al ldquoThe brain in theage of old the hippocampal formation is targeted differentiallyby diseases of late liferdquo Annals of Neurology vol 64 no 6 pp698ndash706 2008
[12] M K Beyer D Aarsland O J Greve and J P Larsen ldquoVisualrating of white matter hyperintensities in Parkinsonrsquos diseaserdquoMovement Disorders vol 21 no 2 pp 223ndash229 2006
[13] S-J Lee J-S Kim J-Y Yoo et al ldquoInfluence of white matterhyperintensities on the cognition of patients with parkinsondiseaserdquoAlzheimerDisease andAssociatedDisorders vol 24 no3 pp 227ndash233 2010
[14] J Sławek D Wieczorek M Derejko et al ldquoThe influenceof vascular risk factors and white matter hyperintensities onthe degree of cognitive impairment in Parkinsonrsquos diseaserdquoNeurologia i Neurochirurgia Polska vol 42 no 6 pp 505ndash5122008
[15] J D Jones I Malaty C C Price M S Okun and DBowers ldquoHealth comorbidities and cognition in 1948 patientswith idiopathic Parkinsonrsquos diseaserdquo Parkinsonism amp RelatedDisorders vol 18 pp 1073ndash1078 2012
[16] M Lezak D Howieson E Bigler and D Tranel Neuropsy-chological Assessment Oxford University Press New York NYUSA 5th edition 2012
[17] A J Hughes S E Daniel L Kilford and A J Lees ldquoAccuracyof clinical diagnosis of idiopathic Parkinsonrsquos disease a clinico-pathological study of 100 casesrdquo Journal of Neurology Neuro-surgery and Psychiatry vol 55 no 3 pp 181ndash184 1992
[18] S Fahn R L Elton and UPDRS Development CommitteeldquoUnified Parkinsonrsquos disease rating scalerdquo Recent DevelopmentParkinson vol 2 pp 153ndash163 1987
[19] C L Tomlinson R Stowe S Patel C Rick R Gray and CE Clarke ldquoSystematic review of levodopa dose equivalencyreporting in Parkinsonrsquos diseaserdquo Movement Disorders vol 25no 15 pp 2649ndash2653 2010
[20] Y I Sheline D M Barch K Garcia et al ldquoCognitive functionin late life Depression relationships to depression severitycerebrovascular risk factors and processing speedrdquo BiologicalPsychiatry vol 60 no 1 pp 58ndash65 2006
[21] R K Heaton S W Miller M J Taylor and I Grant RevisedComprehensive Norms for An expAnded Halstead-Reitan Bat-tery Demographically Adjusted Neuropsychological Norms forAfrican American and Caucasian Adults PAR Lutz Fla USA2004
[22] M Charlson T P Szatrowski J Peterson and J Gold ldquoVal-idation of a combined comorbidity indexrdquo Journal of ClinicalEpidemiology vol 47 no 11 pp 1245ndash1251 1994
[23] PW FWilson KM Anderson andW B Kannel ldquoEpidemiol-ogy of diabetes mellitus in the elderly The Framingham StudyrdquoAmerican Journal of Medicine vol 80 no 5 A pp 3ndash9 1986
[24] W S Aronow J L Fleg C J Pepine et al ldquoACCFAHA 2011expert consensus document on hypertension in the elderlyrdquoJournal of the American College of Cardiology vol 57 pp 2037ndash2114 2011
[25] I Litvan J G Goldman A I Troster et al ldquoDiagnosticcriteria for mild cognitive impairment in Parkinsonrsquos diseaseMovement Disorder Society Task Force guidelinesrdquoMovementDisorders vol 27 no 3 pp 349ndash356 2012
[26] K J Rothman ldquoNo adjustments are needed for multiplecomparisonsrdquo Epidemiology vol 1 no 1 pp 43ndash46 1990
[27] D S Goldstein ldquoDysautonomia in Parkinsonrsquos disease neuro-cardiological abnormalitiesrdquo Lancet Neurology vol 2 no 11 pp669ndash676 2003
[28] A Verdelho SMadureira JM Ferro et al ldquoDifferential impactof cerebral white matter changes diabetes hypertension andstroke on cognitive performance among non-disabled elderly
10 Parkinsonrsquos Disease
The LADIS studyrdquo Journal of Neurology Neurosurgery andPsychiatry vol 78 no 12 pp 1325ndash1330 2007
[29] S P Woods and A I Troster ldquoProdromal frontalexecutivedysfunction predicts incident dementia in Parkinsonrsquos diseaserdquoJournal of the International Neuropsychological Society vol 9no 1 pp 17ndash24 2003
[30] W Nanhoe-Mahabier K F de Laat J E Visser J Zijlmans F-E de Leeuw and B R Bloem ldquoParkinson disease and comorbidcerebrovascular diseaserdquo Nature Reviews Neurology vol 5 no10 pp 533ndash541 2009
[31] K M Rose D Couper M L Eigenbrodt T H Mosley AR Sharrett and R F Gottesman ldquoOrthostatic hypotensionand cognitive function the atherosclerosis risk in communitiesstudyrdquo Neuroepidemiology vol 34 no 1 pp 1ndash7 2010
[32] P L K Yap M Niti K B Yap and T P Ng ldquoOrthostatichypotension hypotension and cognitive status early comorbidmarkers of primary dementiardquo Dementia and Geriatric Cogni-tive Disorders vol 26 no 3 pp 239ndash246 2008
[33] V Novak and I Hajjar ldquoThe relationship between bloodpressure and cognitive functionrdquo Nature Reviews Cardiologyvol 7 no 12 pp 686ndash698 2010
[34] J S Kim Y S Oh K S Lee Y I Kim D W Yang andD S Goldstein ldquoAssociation of cognitive dysfunction withneurocirculatory abnormalities in early Parkinson diseaserdquoNeurology vol 79 no 13 pp 1323ndash1331 2012
[35] T O Dalaker J P Larsen M G Dwyer et al ldquoWhite matterhyperintensities do not impact cognitive function in patientswith newly diagnosed Parkinsonrsquos diseaserdquoNeuroImage vol 47no 4 pp 2083ndash2089 2009
[36] N I Bohnen and R L Albin ldquoWhite matter lesions inParkinson diseaserdquo Nature Reviews Neurology vol 7 no 4 pp229ndash236 2011

Parkinsonrsquos Disease 9
(movement disorders books) Dr Okun has participated inCME activities onmovement disorders sponsored by theUSFCME office PeerView Vanderbilt University and PrimeTheinstitution andnotDrOkun receives grants fromMedtronicand ANSSt Jude and the PI has no financial interest in thesegrants Dr Okun has participated as a site PI andor co-Ifor several NIH foundation and industry sponsored trialsover the years but has not received honoraria Dr Bowershas received research support from the NIH Michael J FoxFoundation the National Parkinson Foundation and theMcKnight Research Foundation
Acknowledgments
This study was supported by a Center of Excellence Grantfrom the National Parkinson Foundation and the UF-INFORM database
References
[1] G E Alexander M R DeLong and P L Strick ldquoParallelorganization of functionally segregated circuits linking basalganglia and cortexrdquo Annual Review of Neuroscience vol 9 pp357ndash381 1986
[2] K R Chaudhuri and A H Schapira ldquoNon-motor symptoms ofParkinsonrsquos disease dopaminergic pathophysiology and treat-mentrdquoThe Lancet Neurology vol 8 no 5 pp 464ndash474 2009
[3] D Aarsland K Andersen J P Larsen A Lolk H Nielsen andP Kragh-Soslashrensen ldquoRisk of dementia in Parkinsonrsquos disease acommunity-based Prospective StudyrdquoNeurology vol 56 no 6pp 730ndash736 2001
[4] M A Hely W G J Reid M A Adena G M Halliday andJ G L Morris ldquoThe Sydney Multicenter Study of Parkinsonrsquosdisease the inevitability of dementia at 20 yearsrdquo MovementDisorders vol 23 no 6 pp 837ndash844 2008
[5] A SchragM Jahanshahi andNQuinn ldquoHowdoes Parkinsonrsquosdisease affect quality of life A comparison with quality of life inthe general populationrdquo Movement Disorders vol 15 pp 1112ndash1118 2000
[6] B Dubois and B Pillon ldquoCognitive deficits in Parkinsonrsquosdiseaserdquo Journal of Neurology vol 244 no 1 pp 2ndash8 1997
[7] C H Williams-Gray J R Evans A Goris et al ldquoThe distinctcognitive syndromes of Parkinsonrsquos disease 5 year follow-up ofthe CamPaIGN cohortrdquo Brain vol 132 no 11 pp 2958ndash29692009
[8] B K Saxby F Harrington I G McKeith K Wesnes and GA Ford ldquoEffects of hypertension on attention memory andexecutive function in older adultsrdquo Health Psychology vol 22no 6 pp 587ndash591 2003
[9] D Knopman L L Boland TMosley et al ldquoCardiovascular riskfactors and cognitive decline inmiddle-aged adultsrdquoNeurologyvol 56 no 1 pp 42ndash48 2001
[10] A A Gouw A Seewann W M Van Der Flier et al ldquoHet-erogeneity of small vessel disease a systematic review ofMRI and histopathology correlationsrdquo Journal of NeurologyNeurosurgery and Psychiatry vol 82 no 2 pp 126ndash135 2011
[11] W Wu A M Brickman J Luchsinger et al ldquoThe brain in theage of old the hippocampal formation is targeted differentiallyby diseases of late liferdquo Annals of Neurology vol 64 no 6 pp698ndash706 2008
[12] M K Beyer D Aarsland O J Greve and J P Larsen ldquoVisualrating of white matter hyperintensities in Parkinsonrsquos diseaserdquoMovement Disorders vol 21 no 2 pp 223ndash229 2006
[13] S-J Lee J-S Kim J-Y Yoo et al ldquoInfluence of white matterhyperintensities on the cognition of patients with parkinsondiseaserdquoAlzheimerDisease andAssociatedDisorders vol 24 no3 pp 227ndash233 2010
[14] J Sławek D Wieczorek M Derejko et al ldquoThe influenceof vascular risk factors and white matter hyperintensities onthe degree of cognitive impairment in Parkinsonrsquos diseaserdquoNeurologia i Neurochirurgia Polska vol 42 no 6 pp 505ndash5122008
[15] J D Jones I Malaty C C Price M S Okun and DBowers ldquoHealth comorbidities and cognition in 1948 patientswith idiopathic Parkinsonrsquos diseaserdquo Parkinsonism amp RelatedDisorders vol 18 pp 1073ndash1078 2012
[16] M Lezak D Howieson E Bigler and D Tranel Neuropsy-chological Assessment Oxford University Press New York NYUSA 5th edition 2012
[17] A J Hughes S E Daniel L Kilford and A J Lees ldquoAccuracyof clinical diagnosis of idiopathic Parkinsonrsquos disease a clinico-pathological study of 100 casesrdquo Journal of Neurology Neuro-surgery and Psychiatry vol 55 no 3 pp 181ndash184 1992
[18] S Fahn R L Elton and UPDRS Development CommitteeldquoUnified Parkinsonrsquos disease rating scalerdquo Recent DevelopmentParkinson vol 2 pp 153ndash163 1987
[19] C L Tomlinson R Stowe S Patel C Rick R Gray and CE Clarke ldquoSystematic review of levodopa dose equivalencyreporting in Parkinsonrsquos diseaserdquo Movement Disorders vol 25no 15 pp 2649ndash2653 2010
[20] Y I Sheline D M Barch K Garcia et al ldquoCognitive functionin late life Depression relationships to depression severitycerebrovascular risk factors and processing speedrdquo BiologicalPsychiatry vol 60 no 1 pp 58ndash65 2006
[21] R K Heaton S W Miller M J Taylor and I Grant RevisedComprehensive Norms for An expAnded Halstead-Reitan Bat-tery Demographically Adjusted Neuropsychological Norms forAfrican American and Caucasian Adults PAR Lutz Fla USA2004
[22] M Charlson T P Szatrowski J Peterson and J Gold ldquoVal-idation of a combined comorbidity indexrdquo Journal of ClinicalEpidemiology vol 47 no 11 pp 1245ndash1251 1994
[23] PW FWilson KM Anderson andW B Kannel ldquoEpidemiol-ogy of diabetes mellitus in the elderly The Framingham StudyrdquoAmerican Journal of Medicine vol 80 no 5 A pp 3ndash9 1986
[24] W S Aronow J L Fleg C J Pepine et al ldquoACCFAHA 2011expert consensus document on hypertension in the elderlyrdquoJournal of the American College of Cardiology vol 57 pp 2037ndash2114 2011
[25] I Litvan J G Goldman A I Troster et al ldquoDiagnosticcriteria for mild cognitive impairment in Parkinsonrsquos diseaseMovement Disorder Society Task Force guidelinesrdquoMovementDisorders vol 27 no 3 pp 349ndash356 2012
[26] K J Rothman ldquoNo adjustments are needed for multiplecomparisonsrdquo Epidemiology vol 1 no 1 pp 43ndash46 1990
[27] D S Goldstein ldquoDysautonomia in Parkinsonrsquos disease neuro-cardiological abnormalitiesrdquo Lancet Neurology vol 2 no 11 pp669ndash676 2003
[28] A Verdelho SMadureira JM Ferro et al ldquoDifferential impactof cerebral white matter changes diabetes hypertension andstroke on cognitive performance among non-disabled elderly
10 Parkinsonrsquos Disease
The LADIS studyrdquo Journal of Neurology Neurosurgery andPsychiatry vol 78 no 12 pp 1325ndash1330 2007
[29] S P Woods and A I Troster ldquoProdromal frontalexecutivedysfunction predicts incident dementia in Parkinsonrsquos diseaserdquoJournal of the International Neuropsychological Society vol 9no 1 pp 17ndash24 2003
[30] W Nanhoe-Mahabier K F de Laat J E Visser J Zijlmans F-E de Leeuw and B R Bloem ldquoParkinson disease and comorbidcerebrovascular diseaserdquo Nature Reviews Neurology vol 5 no10 pp 533ndash541 2009
[31] K M Rose D Couper M L Eigenbrodt T H Mosley AR Sharrett and R F Gottesman ldquoOrthostatic hypotensionand cognitive function the atherosclerosis risk in communitiesstudyrdquo Neuroepidemiology vol 34 no 1 pp 1ndash7 2010
[32] P L K Yap M Niti K B Yap and T P Ng ldquoOrthostatichypotension hypotension and cognitive status early comorbidmarkers of primary dementiardquo Dementia and Geriatric Cogni-tive Disorders vol 26 no 3 pp 239ndash246 2008
[33] V Novak and I Hajjar ldquoThe relationship between bloodpressure and cognitive functionrdquo Nature Reviews Cardiologyvol 7 no 12 pp 686ndash698 2010
[34] J S Kim Y S Oh K S Lee Y I Kim D W Yang andD S Goldstein ldquoAssociation of cognitive dysfunction withneurocirculatory abnormalities in early Parkinson diseaserdquoNeurology vol 79 no 13 pp 1323ndash1331 2012
[35] T O Dalaker J P Larsen M G Dwyer et al ldquoWhite matterhyperintensities do not impact cognitive function in patientswith newly diagnosed Parkinsonrsquos diseaserdquoNeuroImage vol 47no 4 pp 2083ndash2089 2009
[36] N I Bohnen and R L Albin ldquoWhite matter lesions inParkinson diseaserdquo Nature Reviews Neurology vol 7 no 4 pp229ndash236 2011
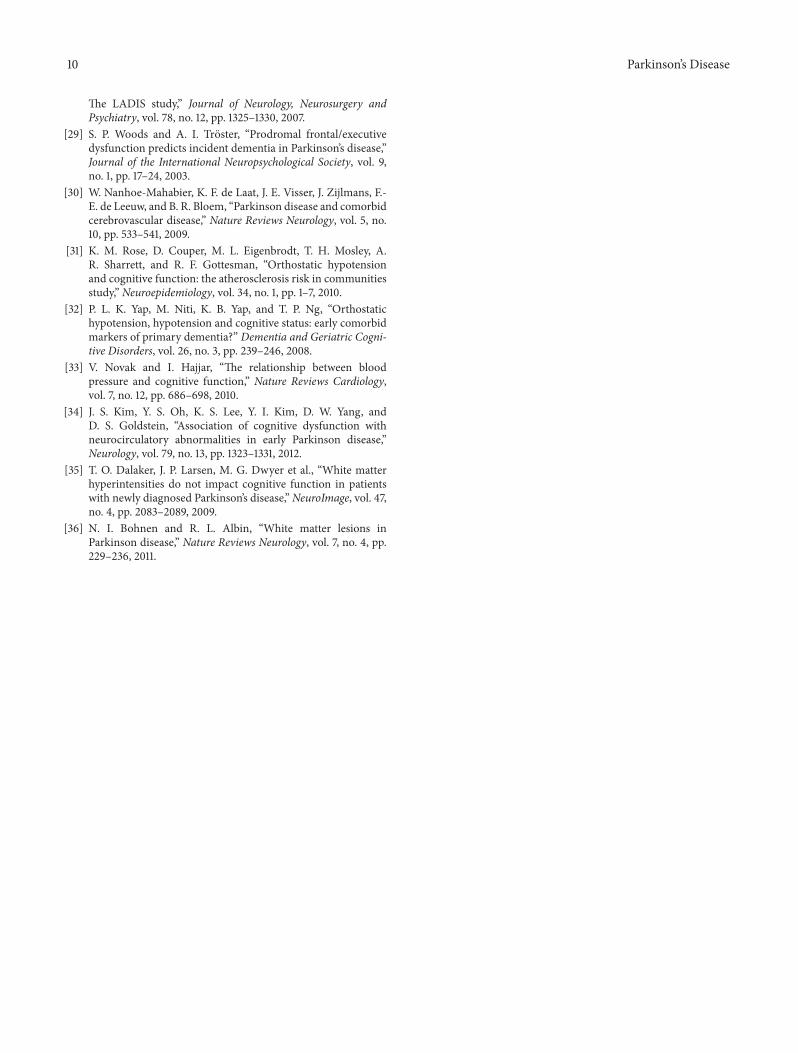
10 Parkinsonrsquos Disease
The LADIS studyrdquo Journal of Neurology Neurosurgery andPsychiatry vol 78 no 12 pp 1325ndash1330 2007
[29] S P Woods and A I Troster ldquoProdromal frontalexecutivedysfunction predicts incident dementia in Parkinsonrsquos diseaserdquoJournal of the International Neuropsychological Society vol 9no 1 pp 17ndash24 2003
[30] W Nanhoe-Mahabier K F de Laat J E Visser J Zijlmans F-E de Leeuw and B R Bloem ldquoParkinson disease and comorbidcerebrovascular diseaserdquo Nature Reviews Neurology vol 5 no10 pp 533ndash541 2009
[31] K M Rose D Couper M L Eigenbrodt T H Mosley AR Sharrett and R F Gottesman ldquoOrthostatic hypotensionand cognitive function the atherosclerosis risk in communitiesstudyrdquo Neuroepidemiology vol 34 no 1 pp 1ndash7 2010
[32] P L K Yap M Niti K B Yap and T P Ng ldquoOrthostatichypotension hypotension and cognitive status early comorbidmarkers of primary dementiardquo Dementia and Geriatric Cogni-tive Disorders vol 26 no 3 pp 239ndash246 2008
[33] V Novak and I Hajjar ldquoThe relationship between bloodpressure and cognitive functionrdquo Nature Reviews Cardiologyvol 7 no 12 pp 686ndash698 2010
[34] J S Kim Y S Oh K S Lee Y I Kim D W Yang andD S Goldstein ldquoAssociation of cognitive dysfunction withneurocirculatory abnormalities in early Parkinson diseaserdquoNeurology vol 79 no 13 pp 1323ndash1331 2012
[35] T O Dalaker J P Larsen M G Dwyer et al ldquoWhite matterhyperintensities do not impact cognitive function in patientswith newly diagnosed Parkinsonrsquos diseaserdquoNeuroImage vol 47no 4 pp 2083ndash2089 2009
[36] N I Bohnen and R L Albin ldquoWhite matter lesions inParkinson diseaserdquo Nature Reviews Neurology vol 7 no 4 pp229ndash236 2011