inflammation, aging, and cancer vaccines
TRANSCRIPT
RESEARCH ARTICLE
Inflammation, aging, and cancer vaccines
Mauro Provinciali • Alessandra Barucca •
Maurizio Cardelli • Francesca Marchegiani •
Elisa Pierpaoli
Received: 25 February 2010 / Accepted: 27 April 2010 / Published online: 9 May 2010
� Springer Science+Business Media B.V. 2010
Abstract Immunosenescence is characterized by a
series of changes of immune pathways, including a
chronic state of low-grade inflammation. Mounting
evidence from experimental and clinical studies sug-
gests that persistent inflammation increases the risk of
cancer and the progression of the disease. Cancer
vaccination, which came into view in the last years as
the most intriguing means of activating an immune
response capable of effectively hampering the pro-
gression of the preclinical stages of a tumour, has been
shown to be less effective in older age than in young
adults. Available evidence on the use of inhibitors of
inflammation has indicated their potential enhance-
ment of cancer vaccines, suggesting the possibility to
improve the low effectiveness of cancer vaccines in old
age employing pharmacological or natural com-
pounds-based anti-inflammatory intervention. This
review addresses the effects of age and inflammation
on cancer development and progression, and specu-
lates as to whether the modulation of inflammation
may influence the response to cancer immunization.
Keywords Inflammation � Aging �Cancer vaccines
Introduction
Emerging evidence clearly suggests that there is a
symbiotic relationship between aging, inflammation
and chronic diseases such as cancer. Chronic inflam-
mation as risk factor for most cancers is well
recognized and the immunosenescence and the low-
grade systemic inflammation which characterize the
elderly population have been related to the increased
incidence of cancer present in advanced age. In the
last years, cancer vaccination came into view as the
most intriguing means of activating an immune
response capable of effectively hampering the pro-
gression of the preclinical stages of a tumour. The
emerging role of immune-based approaches in treat-
ing cancer is further emphasised by the fact that
cancer vaccines which can be applied in both
prevention and therapy are potentially less toxic than
chemo- or radiotherapy and could be especially
suitable for older more frail cancer patients. Taking
into account the strict relationship existing between
inflammation and cancer, the modulation of inflam-
mation may be proposed as a tool to improve the
effectiveness of cancer vaccines, particularly in
advanced age, when a decreased ability to mount
protective immunity after immunization against can-
cer exists. Though several existing experimental data
seem to support this possibility, the real chance to
increase cancer vaccines effectiveness reducing
inflammation remains at present a question to be
defined.
M. Provinciali (&) � A. Barucca � M. Cardelli �F. Marchegiani � E. Pierpaoli
Advanced Technology Center for Aging Research,
Scientific Technological Area, INRCA-IRCCS,
Ancona, Italy
e-mail: [email protected]
123
Biogerontology (2010) 11:615–626
DOI 10.1007/s10522-010-9280-9
Here, we discuss the effects of age and inflam-
mation on cancer development and progression, and
speculate as to whether the modulation of inflam-
mation may influence the response to cancer
immunization.
Immunization in aging
As a means of disease prevention and control,
vaccines have proved to be highly effective and a
financially viable solution. However, once applied in
the elderly, evidence exists that immunization pro-
cedures are less effective at older age than in young
adults (Provinciali 2009). The effectiveness of most
vaccinations against infectious diseases in the elderly
has been reported to be lower than in young adult
ages. Influenza virus vaccines have generally proved
limited in preventing morbidity and mortality among
the elderly because of the lower immunological
protection that they may confer on older adults
compared to younger persons. Also, the effectiveness
of the pneumococcal polysaccharide vaccine in
reducing the risk of pneumonia was found to be
deficient in the elderly. Many older people do not
have immunity to tetanus, against which vaccines
have been available for decades. Finally, the measure
of anti hepatitis virus and anti-HBs in elderly people
after a combined hepatitis A/B vaccination has
underlined the decreased response to vaccinations
with increasing age. In recent years, preclinical
experimental data, mainly performed in mice trans-
planted with parental tumours or in transgenic mice,
have shown that also the effectiveness of anticancer
vaccination is reduced at older age than in young-
adult age, mainly because of the age-related changes
in the immune response against tumour antigens,
implying that vaccines may not be very effective in
predominantly elderly cancer patients (Provinciali
et al. 2003; Gravekamp 2007). Immunosenescence,
which has been described as a remodelling of the
immune system which appears early on and pro-
gresses throughout a person’s life, may not only have
an impact on the incidence of cancer, but also on
the effectiveness of preventive and therapeutic
approaches based on immune system activation.
The low efficacy of cancer vaccines in old age may
be attributable to different mechanisms, which may
act at the different steps of the immunisation process,
and whose exact influence still remains unclear. Both
positive and negative regulators of the immunolog-
ical pathways leading to tumor prevention or regres-
sion appear to be altered in the elderly, with a higher
impact of negative regulators and a lower effect of
positive factors (Provinciali 2009). Many of these
age-related changes are linked to inflammation.
Inflammation and aging
Inflammation is a complex series of events, involving
many cell types (macrophages, neutrophils, mono-
cytes, dendritic and mast cells), and their main
molecular products, such as prostaglandins, cyto-
kines, nuclear factor-B (NF-jB), chemokines and
angiogenic factors (Ahmad et al. 2009). These
factors, which are produced very early in the response
to multiple stresses, are important in being involved
in both host defence and pathology. On one hand,
there is increasing evidence that for an immune
response to be effectively established, an inflamma-
tory response is needed to help the process along,
and, in particular, for the activation of the acquired
immune response. On the other hand, there is also
considerable literature showing that inflammation in
excess is detrimental, and that excessive production
and release of cytokines may lead directly to
pathology. In fact, although inflammation is a nec-
essary response to clear infections, to repair tissue
insults, and suppress tumor initiation/progression,
chronic inflammation is also clearly correlated with
increased risk of developing cancer. The duality of
inflammation in controlling and promoting tumor
development is an area that requires further delinea-
tion, and, in particular, studies are required to
understand whether inflammation become chronic
because an inflammatory stimulus persists or because
of dysregulation in the control mechanisms that
normally turn the process off, as, for example, the
loss or the reduction of anti-inflammatory signals.
Several studies have shown that a low-grade
systemic inflammation characterizes aging and that
inflammatory markers are significant predictors of
mortality in old humans (Kundu and Surh 2008).
Chronic inflammation has been correlated with many
diseases and most of them are age-related diseases.
In fact, it is widely accepted that many of the
most important age-associated diseases, such as
616 Biogerontology (2010) 11:615–626
123
cardiovascular diseases, atherosclerosis, Alzheimer’s
disease, arthrosis and arthritis, sarcopenia and diabe-
tes share a common inflammatory background. The
age-related increased levels of inflammatory media-
tors in the blood, are mainly represented by increased
concentrations of IL-6, tumor necrosis factor-a (TNF-
a), and various acute-phase proteins. Many studies
have focused on IL-6, suggesting that aging indepen-
dently of any particular disease is associated with
low-grade increases in the plasma levels of this
inflammatory mediator. Increases of IL-6 have been
associated with many age-related diseases such as
cardiovascular disease, arthritis, osteoporosis and
type-2 diabetes (Ahmad et al. 2009). The increase in
IL-6 levels may then be a reflection of an increased
inflammatory state caused by underlying disease even
in the apparently healthy elderly person. Besides IL-6,
the higher levels of TNF-a correlate with functional
status and decreased chance of long-life survival in
elderly. Moreover, dysregulation and, in particular,
overproduction of TNF-a has been implicated in a
variety of human diseases including sepsis, malaria,
autoimmune diseases such as multiple sclerosis,
rheumatoid arthritis, systemic lupus erythematosus,
and Crohn’s disease, as well as cancer. Higher levels
of TNF-a were also found in elderly with type II
diabetes mellitus compared to age-matched controls,
and elevated levels of both IL-6 and TNF-a were
found in subjects before the appearance of diabetes.
The well established increase with age of plasma
levels of pro-inflammatory cytokines appears to be
unexpectedly present either in persons who enjoyed
successful aging and those who suffered age-associ-
ated pathologies (Franceschi et al. 2007).
Inflammation and cancer
Epidemiologic and experimental evidence supports
the concept that chronic inflammation promotes the
development and progression of cancer (Hussain and
Harris 2007). There is a strong association between
chronic inflammatory conditions in a particular organ
and cancer specific to that organ. This association
involves a time factor, the longer the inflammation
persists, the higher the risk of associated carcinogen-
esis. The most thoroughly studied examples are the
relationships between chronic inflammatory bowel
disease and the increased risk of colorectal cancer,
chronic gastritis resulting from Helicobacter pylori
infection and gastric adenocarcinoma, and chronic
hepatitis and liver cancer.
Mediators of the inflammatory response, e.g.,
cytokines, free radicals, prostaglandins and growth
factors, can induce genetic and epigenetic changes,
causing alterations in critical pathways responsible for
maintaining the normal cellular homeostasis and
leading to the development and progression of cancer.
The effect of the various inflammatory mediators in
tumorigenesis is described in detail in specific reviews.
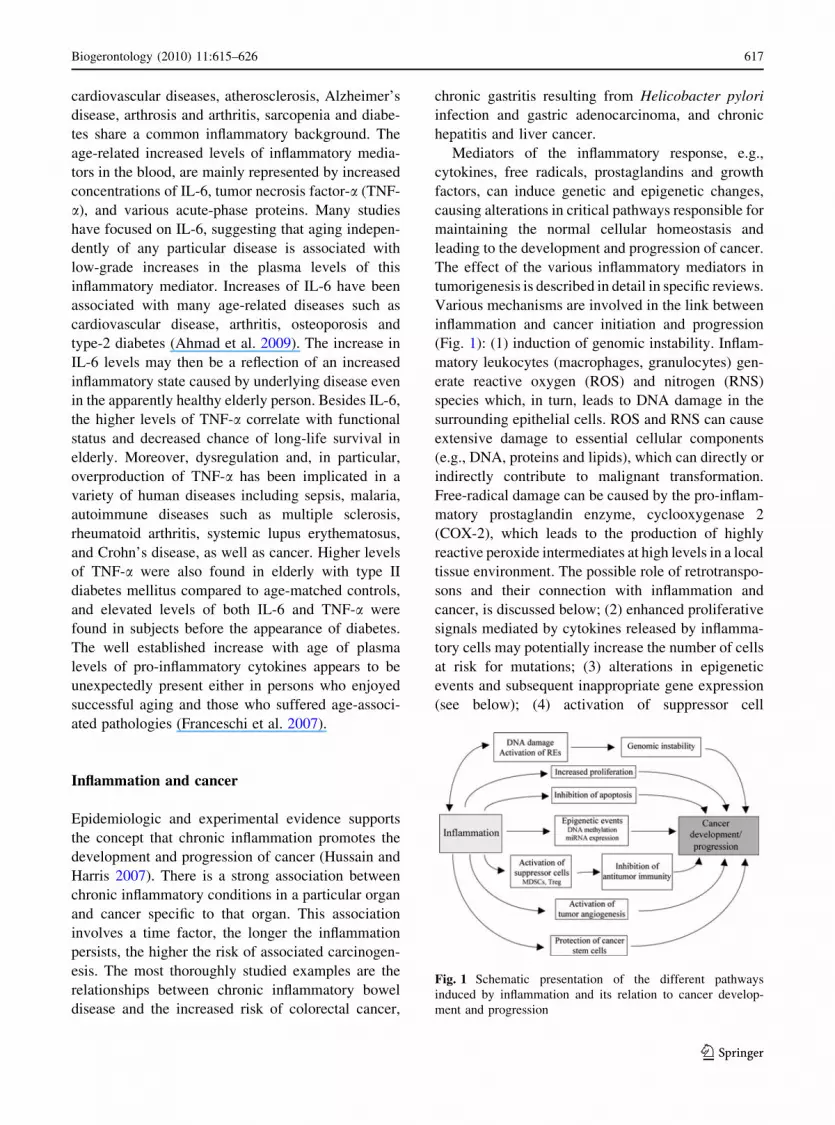
Various mechanisms are involved in the link between
inflammation and cancer initiation and progression
(Fig. 1): (1) induction of genomic instability. Inflam-
matory leukocytes (macrophages, granulocytes) gen-
erate reactive oxygen (ROS) and nitrogen (RNS)
species which, in turn, leads to DNA damage in the
surrounding epithelial cells. ROS and RNS can cause
extensive damage to essential cellular components
(e.g., DNA, proteins and lipids), which can directly or
indirectly contribute to malignant transformation.
Free-radical damage can be caused by the pro-inflam-
matory prostaglandin enzyme, cyclooxygenase 2
(COX-2), which leads to the production of highly
reactive peroxide intermediates at high levels in a local
tissue environment. The possible role of retrotranspo-
sons and their connection with inflammation and
cancer, is discussed below; (2) enhanced proliferative
signals mediated by cytokines released by inflamma-
tory cells may potentially increase the number of cells
at risk for mutations; (3) alterations in epigenetic
events and subsequent inappropriate gene expression
(see below); (4) activation of suppressor cell
Fig. 1 Schematic presentation of the different pathways
induced by inflammation and its relation to cancer develop-
ment and progression
Biogerontology (2010) 11:615–626 617
123

populations by inflammatory mediators, and in partic-
ular of myeloid-derived suppressor cells (MDSCs) and
regulatory T cells (Treg), which may contribute to
tumor immune escape blocking anti-tumor immunity.
MDSCs are a heterogeneous mixture of immature
myeloid cells that are potent inhibitors of antitumor
immunity. They mediate their effects by inhibiting
CD4? and CD8? T cell proliferation, by blocking
natural killer cell activation, by limiting dendritic cell
maturation, and by polarizing immunity towards a type
2 phenotype. Freshly isolated MDSCs (CD11b?GR-
1?) do not have the capacity to inhibit T cells and only
MDSCs isolated from an inflammatory environment
such as a tumor acquire this competence. The link
between inflammation and induction of MDSCs, which
limit antitumor immunity and thereby promote tumor
growth, was recently confirmed using experimental
approaches reducing or increasing inflammation (Bunt
et al. 2007). Treg cells, which represent a CD4? T cell
population characterised by the expression of the
forkhead/winged helix transcription factor (Foxp3),
play an important role in tumour-mediated immuno-
suppression. Tumor or macrophage-derived PGE2
production has been shown to provoke immunosup-
pression by inducing FoxP3 expression and Treg
function in naıve CD4?CD25- cells; the selective
COX-2 inhibition was reported to reverse tumor
immunosuppression by reducing intratumoral Treg
cells (Sharma et al. 2005a); (5) activation of tumor
angiogenesis. Many of proinflammatory mediators,
especially cytokines, chemokines and prostaglandins,
turn on the angiogenesis and tumor cell-stroma com-
munication; (6) protection of cancer stem cells by
inflammatory microenvironment. Inflammatory cyto-
kines in the tumor microenvironment may constitute a
preferential niche for the survival of cancer stem cells.
The biology of tumour stem cells has been shown to be
strictly affected by the pro-inflammatory milieu of the
tumour: recent evidence shows that inflammatory
cytokines, such as IL-6, play primary roles in the
pathogenesis of breast cancer by sustaining the
survival and proliferative capacity of tumour stem
cells. Another cytokine, which was very recently
discovered to play a crucial role in the survival of
cancer stem cells and, in particular, of stem cells from
colon carcinoma, is IL-4.
Tumours play an important role in mediating
antigen-specific immune evasion through several
mechanisms, some of which inducing inflammatory
mediators. Tumor cells produce various factors that
attract leukocytes, which in turn produce cytokines
and chemokines that stimulate further tumor cell
proliferation; the inflammatory tumor microenviron-
ment is characterized by the presence of host
leukocytes both in the stroma and around the tumor.
A developing neoplasm can contain diverse leukocyte
populations, including neutrophils, dendritic cells,
macrophages, eosinophils, mast cells and lympho-
cytes. These inflammatory cells secrete an array of
cytokines, interleukins, interferons and other soluble
mediators and further induce secretion of cytokines
by resident stromal cells. Both cytokines that promote
and suppress proliferation of the tumor cells are
produced in the tumor microenvironment and is the
imbalance between the effects of these two classes of
activity that results in tumor promotion. Basic
research, in turn, has shown that many of the cells
and soluble factors involved in inflammation, when
found in association with tumours, are more likely to
contribute to tumor growth, progression, and metas-
tasis than to elicit an effective host anti-tumor
response. An analysis of genes differentially
expressed in the mammary gland transcriptome
during the progression of mammary carcinogenesis
in BALB/c mice that are transgenic for the rat HER-
2/neu oncogene (BALB-neuT664 V-E mice) identi-
fied four genes that encode inflammatory cytokines
whose increased expression in the tumour microen-
vironment is naturally associated with mammary
cancer progression (Calogero et al. 2007).
A common characteristic mediated by tumor cell
microenvironment is the switch of the cytokine
milieu from Th1 to Th2, with production of suppres-
sive and inflammatory cytokines. The last, in turn,
favour the induction of tumor tolerance through
expansion of MDSCs.
Inflammation, cancer, and endogenous
retroelements
Retroelements (REs) are DNA sequences capable to
mobilize themselves via an RNA intermediate. While
retroviruses represent a small class of REs which
acquired the capacity to leave an organism and to be
horizontally transmitted to new hosts, the large major-
ity of REs are represented by endogen REs or
retrotransposons, which are vertically transmitted (by
618 Biogerontology (2010) 11:615–626
123
heredity). In the human genome endogenous REs are
present in million copies, mostly LINE-1 elements
(constituting 17% of the genome and coding for an
endonuclease and a reverse transcriptase), HERVs
(human endogenous retroviruses, constituting about
8% of the genome and coding for gag, pro, pol and env
proteins) and Alu elements (constituting about 11% of
the genome and not coding for proteins). The activation
of REs seems to be associated with inflammation and
with autoimmune diseases. Observations suggest that
in psoriatic tissue the reverse transcriptase produced by
endogenous REs is increased respect to normal skin
(Moles et al. 2007). In rheumatoid arthritis, viral load
of HERV-K endogenous retroviruses can be detected
in plasma samples from patients, with higher levels
observed for those with active disease. The association
between REs and inflammation can be explained in at
least two ways. The first is that REs can be induced by
inflammation. In fact, RNA transcription of REs is
known to be induced by a wide range of stresses
including oxidative stress (Teneng et al. 2007), hence
inflammation-induced oxidative stress could be poten-
tially able to trigger REs activation. On the other side,
there are evidences that the relation between inflam-
mation and REs can proceed in the opposite direction,
with the inflammation being induced by REs activa-
tion. In fact, it has been demonstrated that in rheuma-
toid arthritis the expression of ORF1 p40 protein
produced by endogenous LINE-1 REs induces a set of
intracellular kinases mediators of inflammation, and
that the envelope protein expressed by endogenous
retrovirus MSRV (Multiple sclerosis-associated retro-
viral element) has proinflammatory properties and is
involved in the immunopathological cascades associ-
ated with chronic inflammatory and/or neurodegener-
ative diseases such as multiple sclerosis, even if the
latter argument is still debated. Moreover, recent
observations revealed that the single-stranded DNA
molecules produced by reverse transcriptase coded by
endogenous REs are immunogenic. In fact, a specific
nuclease called Trex1 metabolizes single-stranded
reverse-transcribed DNA derived from endogenous
REs, and when its activity is impaired the intracellular
accumulation of reverse-transcribed DNA induces
autoimmunity by the interferon-stimulatory DNA
(ISD) response (Stetson et al. 2008). Based on such
evidences, it has been suggested that the increased
expression of human endogenous retroelements such
as LINE-1 can trigger an innate immune response,
inducing autoimmunity and inflammation (Crow
2010).
The association between endogenous REs and
cancer is sustained by a growing set of evidences.
Among the epigenetic deregulation events associated
with cancer there is an overall decrease in methylation,
which largely reflects a decrease in the methylation of
endogen REs. Hypomethylation of LINEs, Alus and
other REs has been observed in various cancers, and
occurs in early stages in colon cancers. REs expression
is enhanced in urothelial and renal carcinoma cells, in
human leukemia and human breast cancers. It has been
suggested that hypomethylation of REs enhances their
transcriptional activity and, in turn, their enhanced de
novo transposition may promote genomic instability,
and thus facilitate tumor progression. As a matter of
fact, insertional mutagenesis caused by de novo
retrotransposition represents a powerful mutational
mechanism and poses a serious threat to the host
genome: at least 51 isolated cases of human diseases
have been found associated with de novo genomic
insertions of REs, mainly in germline, and de novo
insertions as somatic events have been observed in the
APC gene in colon cancer and in the c-myc gene in
breast carcinoma. Recent findings suggest that drug-
mediated inhibition of REs is able to reduce cell growth
and to stimulate the differentiation of cancer cell lines,
confirming a possible role for REs in carcinogenesis.
The activation of retroelements can hence behave
as double edged sword: with a causal role both in
inflammation (by triggering innate immunity) and in
cancer (by generating somatic mutations and genetic
instability), but also in its turn induced and maintained
by inflammation and/or cancer, in a positive feed-back
that could re-enforce the pathogenetic link between the
two conditions. Finally, it should be noted that proteins
and single-stranded DNA molecules derived from
endogenous REs, with their immunogenic properties
and expressed at high levels in cancers, deserve
attention as possible new targets for cancer
immunotherapy.
Inflammation and DNA methylation
CpG island methylation (epigenetic regulation) is a
post-replicative phenomenon and is usually associ-
ated with repression of transcription and thus with the
gene silencing, either in normal and pathological
Biogerontology (2010) 11:615–626 619
123

conditions. CpG islands are normally protected from
DNA methylation, but in relation to cancer or aging,
they are aberrantly methylated (Issa 2000). Epige-
netic mechanisms play a central role in controlling
the expression of critical genes, such as those that can
promote or suppress the tumor. In fact, there was
evidence of two typical patterns of aberrant methyl-
ation in cancer: (a) reduction of methylated cytosines
in oncogenes resulting in hyper-activation of the
same, (b) excessive methylation of CpG islands in
promoter regions of tumor suppressor genes (i.e. p16,
hMLH1, BRCA1, MGMT, GSTP1, TIMP-3 and
DAPK-1) with consequent loss of their function.
Generally, human cancer cells exhibit global
DNA hypomethylation as well as region-specific
hypermethylation.
Recently, Valinluck et al. analyzing the halogena-
tion of nucleic acids (5-chlorocytosine and 5-bromo-
cytosine) as a form of DNA damage have seen that
these products are found specifically in areas of tissue
inflammation (Valinluck and Sowers 2007). They
have also seen that these halogenated cytosine
damage products, very similar to 5-methyl cytosine,
are involved in the changes of methylation status and
so they consider this process the link between
inflammation and cancer. In fact, this 5-halocytosine
residue in the site of inflammation leads to an
inappropriate de novo methylation, driving the cancer
development. Also, these residues are retained and
accumulated in the genome, being not recognized as
damaged bases by DNA repair glycosylases. In
summary, inflammation creates a signature of aber-
rant DNA methylation. The strong link between
inflammation and cancer is now recognized by the
scientific literature. An interesting observation is the
increase in the methylation status in subjects who
developed gastric cancer and were positive for
infection of Helicobacter pylori than those with
gastric cancer but H. pylori negative. A causal role
of infection in the aberrantly state of methylation is
proposed. Studying tumor cell lines of human multiple
myeloma it has been found that interleukin-6 (IL-6) is
the main responsible for the methylation status of
p53 gene, an important cell cycle control and tumor
suppressor gene (Hodge et al. 2005).
The discovery of drugs with DNA methyltransfer-
ase inhibitory activity (DNA methyltransferase inhib-
itor drugs) that could restore the expression of genes
previously silenced have kindled great hopes in the
treatment of a disease, often fatal, such as cancer.
Unfortunately, this initial enthusiasm was soon
dampened by the high toxicity and the side effects
that occur with the use of these types of drugs.
Epigenetic signalling has a crucial role not only in
cancer and inflammation but also in aging. In fact,
‘‘aging epigenetics’’ is an emerging discipline that
promises the definition of a DNA methylome and a
histone modification map that will help in the
definition of a ‘‘young’’ versus an ‘‘old’’ phenotype
(Fraga and Esteller 2007). Overall, in many aged
mammalian tissues a progressive loss of methylated
cytosines in the repetitive regions (defined as low
global DNA methylation levels) and the presence of
patched sites of 5-methylcytosines in the promoter
regions were observed. Probably, the loss of global
DNA methylation during aging is due to the
progressive inefficacy of DNA methyltransferase1
(DNMT1) which is accompanied by an overexpres-
sion of DNMT3b that entails the aberrant hyperme-
thylation of the regions such as promoter CpG
islands. Interestingly, aging and cancer share com-
mon mechanisms, i.e. global DNA hypomethylation,
aberrant promoter hypermethylation and modest
DNMT overexpression.
Inflammation, cancer and aging
In elderly population a low-grade increase in the
levels of circulating TNF-a, IL-6, soluble IL-2
receptors, CRP (C reactive protein) and cholesterol,
which act as inflammatory mediators has been
reported. Altered cytokine profiles due to aging of
the innate immune system and/or of non-immune cell
types, are hypothesised to contribute to age-related
changes in the structure and function of tissues,
pathophysiological changes, and the development of
chronic diseases of aging. Inflammatory cytokines
and other mediators of inflammation can also serve as
strong near-term predictors of mortality associated
with age-related chronic diseases. Chronic inflamma-
tion causes the release of a plethora of agents, such as
cytokines, prostaglandins, chemotactic factors, reac-
tive oxygen and nitrogen species. It also determines
changes in gene expression which favour the activa-
tion of oncogenes and down-regulation of tumour
suppression genes. These factors also change the
responses of cells to apoptosis signals and up-regulate
620 Biogerontology (2010) 11:615–626
123

angiogenesis factors as well as factors favouring the
growth of tumour cells. Moreover, some of the same
factors cause impairments in immune surveillance,
which facilitates the escape of tumour cells from
surveillance and their clonal expansion. Since the up-
regulation of the inflammatory response is a major
characteristic of the remodelling process of the
immune system during aging, the ‘‘aged’’ microen-
vironment may constitute a preferential niche for the
initiation and progression of cancer. Several exam-
ples may be provided by: (1) the local increase of
inflammatory cytokines proper of aging, such as IL-4
and IL6, may favour the survival of cancer stem cells;
(2) the immune suppression induced by tumour cell-
derived prostaglandins may have particular implica-
tions in aging, since lymphocytes from elderly
subjects are known to be more sensitive to inhibition
by prostaglandins in comparison with lymphocytes
from younger individuals; (3) the age-related increase
of inflammatory mediators may enhance the accu-
mulation of MDSCs and Treg which inhibit tumour
immunity and accelerate tumour progression thereby
supporting the hypothesis that the induction of
suppressor cells which down-regulate tumour immu-
nity is one of the mechanisms linking inflammation
and cancer; (4) the increased transcriptional activity
of retrotransposons may provide another biological
event that may connect inflammation to cancer in
aging. The importance of increased REs transcription
in cancer initiation/progression may be particularly
relevant in elderly subjects, since aging is character-
ized by a hypomethylation, and, consequently, an
increased expression of REs; (5) another character-
istic of aging, that may favour the persistence of an
inflammatory status and the development of cancer, is
represented by the lack or the low activation of anti-
inflammatory cytokines. An impaired anti-inflamma-
tory machinery may have detrimental consequences
for the success of immunological responses: the
reduced capability to counteract the chronic low-
grade inflammation may be not sufficient to antag-
onize inflammation-induced tumor protection and
tumor-mediated immune inhibition. A good example
of the role played by anti-inflammatory mechanisms
is offered by centenarians. Centenarians are unique in
that, despite high levels of pro-inflammatory markers,
they also exhibit anti-inflammatory markers that may
delay disease onset. In fact, although centenarians
are quite able of mounting effective inflammatory
responses, their inflammatory status is compensated
by the concomitant development of strong and
effective anti-inflammatory responses and by a higher
frequency of genetic markers associated with better
control of inflammation (Franceschi et al. 2007); (6)
indoleamine-2,3-dioxygenase (IDO) is an enzyme
which catalyses the initial and rate-limiting step in
the catabolism of tryptophan along the kynurenine
pathway and which may be upregulated by inflam-
matory cytokines causing immunosuppressive activ-
ity. IDO activity was found to increase with older age
and to predict mortality in nonagenarians, suggesting
that increased IDO activity might be a mechanism
involved in the decline of T cell responses in
immunosenescence.
One of the main questions that gerontologists have
to explain concerns the molecular causes involved in
the increased inflammation in the elderly, and, in
particular, whether they are mainly linked to genetic or
environmental causes. The profound alteration of the
immune system with aging, called immunosenescence,
is a phenomenon extensively demonstrated. The sus-
tained attrition on the immune system caused by
repeated antigen stimulations is likely responsible for
the chronic immune system activation and inflamma-
tion. In turn, the thymic involution and the consequent
loss of virgin T cells, lead the body more prone to a
variety of infections. In response to a persistent
inflammatory status, an accumulation of dysfunctional
lymphocytes and expanded clones of memory/effector
CD8? T cells occur and the subsequently filling up of
the ‘‘immunological space’’ increase the risk of
infectious, neoplastic and degenerative disorders. On
the whole, accumulation of memory and effector T
cells, decrease of naıve T cells and marked reduction of
T cell repertoire, mostly regarding CD8? T cells, have
been proposed as ‘‘hallmarks of immunosenescence’’
in humans (Franceschi et al. 1999). Besides the
shrinkage of immunological repertoire, some other
immunological responses decrease their efficiency.
Specifically, dendritic cells in the elderly are less
efficient in activating B and T lymphocytes, cd T cells
are decreased in number and function, B lymphocytes
decreased significantly with age and antibodies gener-
ated in the elderly are less protective than those of
young (De Martinis et al. 2005; Provinciali and
Smorlesi 2005). The innate immune system (NK cells,
macrophages, granulocytes) seems only moderately
affected by age, even though some alterations at the
Biogerontology (2010) 11:615–626 621
123

level of most of the components of the innate pathway
have been demonstrated. It is important to note that the
failure in the complex regulation of inflammatory
processes to resolve cellular damage sustained could
lead to malfunctioning of immune processes in aging
subjects. Also, according to ‘‘the remodelling theory of
aging’’ the immunosenescence results from the balance
between the continuous adaptation of the body to the
deteriorative changes occurring over time. Globally,
ancestral, innate immunity is preserved, while recent
clonotypical immunity deteriorates (Franceschi et al.
1995).
Recent data have suggested that the dysregulation
of proinflammatory cytokine production seems to be
mainly related to an intrinsic alteration present in
cells from aged individuals. Hematopoietic stem cells
from old animals have been shown to differentiate in
vivo in CD4? T cells producing IL-4 levels charac-
teristic of old age, even when these stem cells are
injected in a young host (Donnini et al. 2007). In
human, hematopoietic progenitors from old healthy
subjects differentiate in vitro in cells producing
higher concentrations of inflammatory cytokines than
those obtained in cultures from young donors in the
same experimental conditions. Thus, cells from aged
donors retain their capacity to produce higher levels
of inflammatory cytokines independently of the
microenvironment in which they proliferate and
differentiate.
Inflammation and effectiveness of cancer vaccines
Immunoprevention and immunotherapy for tumor-
associated antigens is now a major field of investi-
gation for the treatment of cancer. Many of the novel
immune-based therapies involve active immunization
and are likely to be most effective in immunocom-
petent tumor-bearing individuals who have minimal
alteration of immune homeostasis. For this reason,
elderly patients do not seem to represent good
candidates for immunization-based preventive or
therapeutic approaches. Given the causal relationship
between inflammation and the induction of cancer,
adjunctive therapies that reduce inflammation prior
to immunization, might significantly enhance the
efficacy of any active immunotherapy. Although the
link between inflammation and cancer has been
clearly demonstrated and various anti-inflammatory
substances have been reported to have anti cancer
effects, scarce and fragmentary evidence has been
provided until now on the possibility to potentiate
cancer vaccination switching off inflammation.
Inflammation is included among the stimuli capable
to induce COX-2, a COX isoform which catalyzes a
key step in arachidonic acid metabolism and produc-
tion of prostaglandins. Prostaglandins, in particular
PGE2, can enhance tumorigenesis. An elevated
expression of COX2 is frequently reported in a
variety of different human cancer and has been
localized in both tumor epithelial cells and stroma
supporting autonomous as well as landscaping effects
in tumor development. Epidemiological, animal and
human clinical studies have shown that nonsteroidal
anti inflammmatory drugs (NSAIDs) are chemopre-
ventive for colon adenoma and cancer. Drugs that
selectively inhibit the COX-2 enzyme, including
NSAIDs, are being studied to determine their impact
on local tumor biology and development, and in
clinical trials. Recent studies have suggested protec-
tive effects of COX-2 inhibitors in colorectal cancer
and breast cancer. It has been observed that people
regularly taking non-steroidal anti-inflammatory
drugs (NSAIDs) have lower risk of developing
cancer than people who don’t take the drugs. Several
small studies of colorectal, non-small cell lung
cancer, breast, cervical and esophageal tumours have
shown that increased COX-2 levels are associated
with poor clinical prognosis. Animal models for
colorectal cancer showed similar patterns of COX-2
expression and response to COX-2 inhibitors as
human neoplasias. Several recent studies have shown
that blockade of PGE2 produced by tumor cells and/
or tumor-associated leukocytes can limit a significant
portion of the immunosuppressive response and may
result in a potentiation of cancer vaccines. A COX-2
inhibitor enhanced antitumor immune responses
induced by the transcutaneous vaccination with
cytosine-phosphate-guanosine-oligodeoxynucleotides
(CpG-ODN) and ovalbumin. In this study either Th1-
type immune responses and generation of CTLs or
antigen-specific antitumor immunity in vivo were
induced (Inoue and Aramaki 2006). Therapeutic
administration of dendritic cells pulsed in vitro with
Hsp70 in the presence of a COX-2 inhibitor signif-
icantly reduced progression of B16 melanoma in
mice and enhanced survival through the induction of
IFN-c mediated protective immunity (Conroy et al.
622 Biogerontology (2010) 11:615–626
123
2008). In another experimental model, COX-2 inhi-
bition significantly increased the effect of a vaccina-
tion employing an adenoviral vector expressing the
E7 protein towards tumor cells expressing the same
antigen. This increased efficacy was associated with
the generation of a Th1-type tumor microenviron-
ment and a markedly increased number of tumor-
infiltrating specific CD8 T cells (Haas et al. 2006).
Similarly, the COX-2 inhibitor, SC-58236, increased
the effectiveness of a cancer vaccine using irradiated
tumor cells skewing towards a type 1 cytokine
response mainly mediated by IFN-c (Sharma et al.
2005b). In a more recent paper, conducted in a
different experimental model, it was demonstrated
that the combined vaccination with a mycobacterium
leprae protein and either a Toll-like receptor 4
(TLR4, EM005), TLR7 (Imiquimod), or TLR9
(CpG DNA) agonist, induces Th1-type responses
that limit local inflammation upon M. leprae infection
(Raman et al. 2009). The improving capacity of the
TLR7 agonist Imiquimod was already demonstrated
in a spontaneous mammary adenocarcinoma tumor
model (Smorlesi et al. 2005). In this study, imiqui-
mod was able to potentiate DNA vaccination using a
plasmid DNA encoding rat HER-2/neu in transgenic
mice. Spontaneous mammary tumours were delayed
and both antibody and cell-mediated immune respon-
siveness against HER-2/neu were increased.
Although there are not direct evidences in immu-
nization studies TNF-a antagonists represent good
candidates to potentiate the activity of cancer vac-
cines. TNF antagonists (etanercept, infliximab, ada-
limumab), which have been licensed for clinical trial in
the treatment of rheumatoid arthritis and Crohn’s
disease, have demonstrated to be endowed of various
actions which would be useful in a biological therapy
for cancer, namely, inhibition of cytokine/chemokine
production, reduced angiogenesis, prevention of leu-
cocyte infiltration, inhibition of matrix metallopro-
teases, and improvement of bone marrow function
(Sethi et al. 2009). Recently, we have observed in
psoriatic subjects treated with Etanercept for 24 weeks
an improvement in the insulin sensitivity, probably
through an inflammation pathway (Marra et al. 2007).
Several compounds that can inhibit TNF-a expression,
synthesis, and signaling are also available. These
include thalidomide, which is currently being used
for treatment of multiple myeloma, pentoxifylline,
and numerous products from fruits, vegetable and
traditional medicinal plants, and which can be tested in
experimental models of cancer vaccines. Among the
natural compounds that may impact on cancer immu-
nization are Vitamin E analogues. Vitamin E in nature
encompass a family of tocopherols and tocotrienols
which exert an immunoregulatory effect. The immu-
nomodulation of Vitamin E compounds is the result of
two mechanisms: (i) a direct effect on T cells, and (ii)
an indirect action through its anti-inflammatory prop-
erties, mainly related by the reduced production of
PGE2. In a recent study tocotrienols were shown to
exert better anti-inflammatory activity than alpha-
tocopherol by affecting IL-6 and nitric-oxide produc-
tion and reducing PGE2 release. Also in vivo tocotri-
enol supplementation has been shown to contribute to
immunoregulation, antibody production, and resis-
tance to implanted tumor. Like tocopherols, tocotrie-
nols are powerful antioxidant; they possess
neuroprotective and cholesterol lowering but also
proapoptotic properties not found in tocopherols.
Emerging in vitro and in vivo evidences have mani-
fested the anti-cancer activity of tocotrienols on
numerous human cancers. Very recently, d- and
c-tocotrienols were reported to exert a potent antican-
cer effect on breast cancer cell lines by inducing
apoptosis and transcriptional up-regulation of senes-
cent-like growth arrest markers (Pierpaoli et al. 2010).
The anticancer properties of tocotrienols were also
evaluated in a variety of animal models. These
preclinical studies have shown that tocotrienols inhibit
liver and lung carcinogenesis and suppress the growth
of breast tumor. The recent observation that a tocotri-
enol-rich fraction isolated from palm oil was able to
improve the efficacy of vaccines against breast cancer
in a mouse experimental model (Abdul Hafid et al.
2010) demonstrates the utility of certain nutritional
products or supplements to provide an immune mod-
ulation able to fight tumour and to improve the
outcome of treatment.
Silybin, the major flavonolignan from the extracts of
milk thistle of Silybum marianum, is an effective
antioxidant and anti-inflammatory compound with
antitumor-promoting activity that deserves particular
attention for its potential use as adjuvant of cancer
vaccines. Silybin was found to induce growth inhibi-
tion and apoptosis of a panel of human and murine
tumor cell lines as well as to exert anticancer effect in
an in vivo transgenic tumor model (Provinciali et al.
2007). Silybin was shown to induce strong anticancer
Biogerontology (2010) 11:615–626 623
123

effects by down-regulation of inflammatory and
angiogenic responses, involving HIF-1alpha, STAT3,
and NF-kB transcription factors, as well as COX-2 and
iNOS. In a number of in vitro human cell experimental
systems silymarin was found to suppress TNF-induced
activation of NF-kB 100 times better than aspirin. The
anti-inflammatory and anticancer effects of silybin
are related to the potent inhibition of NF-kB. This
transcription factor is linked with numerous genes
that regulate inflammation, immune function, stress
response, cell differentiation, apoptosis, and cell
survival, and is critically involved in the processes of
development and progression of cancer. Others non-
cytotoxic natural compounds have shown effective
anti-tumor/anti-inflammatory activity by repressing
NF-kB activity. Curcumins, the main biologically
active polyphenols of turmeric plant, are powerful in
vivo antioxidants. A large body of experimental works
supports the efficacy of curcumins as anti-inflamma-
tories. They have also shown chemo-preventive effects
in cellular and animal models. Curcumins seem to
exert their biological activity by strong inhibition of
NF-kB. A very recent in vitro/in vivo study showed the
synergic antitumor action of curcumin and resveratrol,
another polyphenol compound with anti-tumor/anti-
inflammatory activity (Provinciali et al. 2005), in colon
cancer models. They found that the inhibition of
tumours in response to curcumin and/or resveratrol
was associated with the reduction in proliferation and
stimulation of apoptosis accompanied by attenuation
of NF-kB activity, suggesting that the combination
of curcumin and resveratrol could be an effective
preventive/therapeutic strategy for colon cancer. In
other studies it has been shown that pharmacological
inhibitors of L-arginine catabolism may enhance
cancer immunotherapy. In tumor-bearing mice, the
combination of NCX-4016 (nitroaspirin), which tar-
gets multiple immunosuppressive pathways by inhib-
iting COX-1, COX-2, arginase and nitric-oxide
synthase and DNA-based vaccination increased the
number of tumor-specific CTLs and significantly
extended survival.
Concluding remarks
The chronic inflammation represents one of the
hallmarks of immunosenescence and its well estab-
lished link with cancer clearly suggests its direct
involvement in aging related cancer initiation and
progression. Even if it has been clearly demonstrated
that cancer vaccines are less effective in older age than
in young adult, the exact role of inflammation in the
success of cancer immunization, and in particular
whether inflammation may reduce the efficacy of
cancer vaccines, remains to be established. The
evidence available on the use of inhibitors of inflam-
mation, has suggested their potential enhancement of
cancer vaccines. Unfortunately, all studies that have
shown improved T cell responses using anti-inflam-
matory substances as adjuvant of cancer vaccination
were performed in young age and no data has been
reported until now in aging models. The age-related
changes occurring at the level of immunological
mediators require a careful examination of the mech-
anisms potentially involved in the success or in the
failure of anti-inflammatory approaches in old age.
One of the main reasons for the lower effectiveness of
cancer vaccines in old ages is the lack of naıve T cells
(Utsuyama et al. 1992), and the down-regulation of
inflammation-induced T cell responses by anti-inflam-
matory drugs might not improve T cell activation at
older age, since naıve T cells are almost completely
absent at this age. Perhaps, the adjuvant effect of anti-
inflammatory substances could be more likely directed
against suppressor cell populations, such as MDSCs or
Treg cells, that are upregulated by inflammation in old
ages, or angiogenesis, or could be effective in inducing
apoptosis of tumor cells, or preventing activation of RE
rather than improving T cell activation at older age.
Furthermore, since innate immune responses are less
affected at older age than adaptive T cell responses,
targeting natural killer cells or macrophages against
cancer by anti-inflammatory substances, might result
in a better effect than targeting T cell responses.
Greater insight into the mechanisms underlying
inflammation and its regulation, not only at a cellular,
but also at a molecular level, will be required for
planning tumour immunization procedures with
increased effectiveness, particularly for old subjects.
References
Abdul Hafid SR, Radhakrishnan AK, Nesaretnam K (2010)
Tocotrienols are good adjuvants for developing cancer
vaccines. BMC Cancer 10:5. doi:10.1186/1471-2407-
10-15
624 Biogerontology (2010) 11:615–626
123
Ahmad A, Banerjee S, Wang Z, Kong D, Majumdar APN,
Sarkar FH (2009) Aging and inflammation: etiological
culprits of cancer. Curr Aging Sci 2:174–186
Bunt SK, Yang L, Sinha P, Clements VK, Leips J, Ostrand-
Rosenberg S (2007) Reduced inflammation in the tumor
microenvironment delays the accumulation of myeloid-
derived suppressor cells and limits tumor progression.
Cancer Res 67:10019–10026
Calogero RA, Cordero F, Forni G, Cavallo F (2007) Inflam-
matory component of mammary carcinogenesis in ErbB2
transgenic mice. Breast Cancer Res 9:211–220
Conroy TD, Jamicki AG, Higgins SC, Sutton C, Mills KH
(2008) Therapeutic vaccination with dendritic cells pulsed
with tumor-derived Hsp70 and a COX-2 inhibitor induces
protective immunity against B16 melanoma. Vaccine
26:3540–3549
Crow MK (2010) Long interspersed nuclear elements (LINE-
1): potential triggers of systemic autoimmune disease.
Autoimmunity 43:7–16
De Martinis M, Franceschi C, Monti D, Ginaldi L (2005) In-
flamm-ageing and lifelong antigenic load as major deter-
minants of ageing rate and longevity. FEBS Lett
579:2035–2039
Donnini A, Re F, Orlando F, Provinciali M (2007) Intrinsic and
microenvironmental defects are involved in the age-rela-
ted changes of Lin-c-kit? hematopoietic progenitor cells.
Rejuvenation Res 10:459–472
Fraga MF, Esteller M (2007) Epigenetics and aging: the targets
and the marks. Trends Genet 23:413–418
Franceschi C, Monti D, Barbieri D, Grassilli E, Troiano L,
Salvioli S, Negro P, Capri M, Guido M, Azzi R et al
(1995) Immunosenescence in humans: deterioration or
remodelling? Int Rev Immunol 12:57–74
Franceschi C, Valensin S, Fagnoni F, Barbi C, Bonafe M
(1999) Biomarkers of immunosenescence within an evo-
lutionary perspective: the challenge of heterogeneity and
the role of antigenic load. Exp Gerontol 34:911–921
Franceschi C, Capri M, Monti D, Giunta S, Olivieri F, Sevini F,
Panourgia MP, Invidia L, Celani L, Scurti M, Cevenini E,
Castellani GC, Salvioli S (2007) Inflammaging and anti-
inflammaging: a systemic perspective on aging and lon-
gevity emerged from studies in humans. Mech Ageing
Dev 128:92–105
Gravekamp C (2007) Cancer vaccines in old age. Exp Gerontol
42:441–450
Haas AR, Sun J, Vachani A, Wallace AF, Silverberg M, Ka-
poor V, Albelda SM (2006) Cycloxygenae-2 inhibition
augments the efficacy of a cancer vaccine. Clin Cancer
Res 12:214–222
Hodge DR, Peng B, Cherry JC, Hurt EM, Fox SD, Kelley JA,
Munroe DJ, Farrar WL (2005) Interleukin 6 supports the
maintenance of p53 tumor suppressor gene promoter
methylation. Cancer Res 65:4673–4682
Hussain SP, Harris CC (2007) Inflammation and cancer: an
ancient link with novel potentials. Int J Cancer 121:2373–
2380
Inoue J, Aramaki Y (2006) Cyclooxygenase-2 inhibition pro-
motes enhancement of antitumor responses by trascuta-
neous vaccination with Cytosine-phospate-guanosine-
oligodeoxynucleotides and model tumor antigen. J Invest
Dermatol 127:614–621
Issa JP (2000) CpG-island methylation in aging, cancer. Curr
Top Microbiol Immunol 249:101–118
Kundu JK, Surh Y-J (2008) Inflammation: gearing the journey
to cancer. Mutat Res 659:15–30
Marra M, Campanati A, Testa R, Sirolla C, Bonfigli AR,
Franceschi C, Marchegiani F, Offidani A (2007) Effect of
etanercept on insulin sensitivity in nine patients with
psoriasis. Int J Immunopathol Pharmacol 20:731–736
Moles JP, Tesniere A, Guilhou JJ (2007) Reverse transcriptase
activity in human normal and psoriatic skin samples. Br J
Dermatol 157:482–486
Pierpaoli E, Viola V, Pilolli F, Piroddi M, Galli F, Provinciali
M (2010) c- and d-tocotrienols exert a more potent anti-
cancer effect than a-tocopheryl succinate on breast cancer
cells irrespective of HER-2/neu expression. Life Sci
86:668–675
Provinciali M (2009) Immunosenescence and cancer vaccines.
Cancer Immunol Immunother 58:1959–1968
Provinciali M, Smorlesi A (2005) Immunoprevention and
immunotherapy of cancer in aging. Cancer Immunol Im-
munother 54:93–106
Provinciali M, Smorlesi A, Donnini A, Bartozzi B, Amici A
(2003) Low effectiveness of DNA vaccination against
HER-2/neu in ageing. Vaccine 21:843–848
Provinciali M, Re F, Donnini A, Orlando F, Bartozzi B, Di
Stasio G, Smorlesi A (2005) Effect of resveratrol on the
development of spontaneous mammary tumors in HER-2/
neu transgenic mice. Int J Cancer 115:36–45
Provinciali M, Papalini F, Orlando F, Pierpaoli S, Donnini A,
Morazzoni P, Riva A, Smorlesi A (2007) Effect of the
silybin-phosphatidylcholine complex (IdB1016) on the
development of mammary tumours in HER-2/neu trans-
genic mice. Cancer Res 67:2022–2029
Raman VS, O’Donnell J, Remy BH, Goto W, Lahiri R, Gillis
TP, Reed SG, Duthie MS (2009) Vaccination with the
ML0276 antigen reduces local inflammation but not
bacterial burden during experimental mycobacterium
leprae infection. Infect Immun 77:5623–5630
Sethi G, Sung B, Kunnumakkara AB, Aggarwal BB (2009)
Targeting TNF for treatment of cancer and autoimmunity.
Adv Exp Med Biol 647:37–51
Sharma S, Yang SC, Zhu L, Reckamp K, Gardner B, Baratelli
F, Huang M, Batra RK, Dubinett SM (2005a) Tumor
cyclooxygenase-2/prostaglandin E2-dependent promotion
of FOXP3 expression and CD4 ? CD25 ? T regulatory
cell activities in lung cancer. Cancer Res 65:5211–5220
Sharma S, Zhu L, Yang SC, Zhang L, Lin J, Hillinger S,
Gardner B, Reckamp K, Strieter RM, Huang M, Batra
RK, Dubinett SM (2005b) Cyclooxygenase 2 inhibition
promotes IFN-gamma-dependent enhancement of antitu-
mor responses. J Immunol 175:813–819
Smorlesi A, Papalini F, Orlando F, Donnini A, Re F, Provin-
ciali M (2005) Imiquimod and S-27609 as adjuvants of
DNA vaccination in a transgenic murine model of HER2/
neu-positive mammary carcinoma. Gene Ther 12:1324–
1332
Stetson DB, Ko JS, Heidmann T, Medzhitov R (2008) Trex1
prevents cell-intrinsic initiation of autoimmunity. Cell
134:587–598
Teneng I, Stribinskis V, Ramos KS (2007) Context-specific
regulation of LINE-1. Genes Cells 12:1101–1110
Biogerontology (2010) 11:615–626 625
123
Utsuyama M, Hirokawa K, Kurashima C, Fukayama M, In-
amatsu T, Suzuki K, Hashimoto W, Sato K (1992) Dif-
ferential age-change in the numbers of CD4?CD45RA?
and CD4?CD29? T cell subsets in human peripheral
blood. Mech Ageing Dev 63:57–68
Valinluck V, Sowers LC (2007) Inflammation-mediated cyto-
sine damage: a mechanistic link between inflammation
and the epigenetic alterations in human cancers. Cancer
Res 67:5583–5586
626 Biogerontology (2010) 11:615–626
123