in massive pulmonary embolism pharmacologic
TRANSCRIPT
DOI 10.1378/chest.111.1.218 1997;111;218-224Chest
Daniel T. Layish and Victor F. Tapson in Massive Pulmonary EmbolismPharmacologic Hemodynamic Support
http://chestjournal.chestpubs.org/content/111/1/218.citation
and services can be found online on the World Wide Web at: The online version of this article, along with updated information
ISSN:0012-3692)http://chestjournal.chestpubs.org/site/misc/reprints.xhtml(
without the prior written permission of the copyright holder.distributedNo part of this article or PDF may be reproduced or reserved.3300 Dundee Road, Northbrook, IL 60062. All rights
Copyright1997by the American College of Chest Physicians,Physicians. It has been published monthly since 1935.
is the official journal of the American College of ChestChest

Pharmacologic Hemodynamic Supportin Massive Pulmonary Embolism*Daniel T. Layish, MD; and Victor F. Tapson, MD
(CHEST 1997; 111:218-24)
Key words: inotropes; pulmonary embolism; vasopressors
Abbreviations: CO=cardiac output; LVEDP=left ventricularend-diastolic pressure; NE=norepinephrine; PAP=pulmonaryartery pressure; PE=pulmonary embolism; PVR.pulmonaryvascular resistance; RV=right ventricular, right ventricle;RVEDP=right ventricular end-diastolic pressure; SVR=systemicvascular resistance
Approximately 630,000 patients develop pulmo¬nary embolism (PE) in the United States each
year.1 PE causes or contributes to approximately200,000 deaths per year in the United States alone.1In general, mortality ranges from 6 to 8%, but risesto more than 30% when complicated by hypoten¬sion.12 Of those patients in whom PE is fatal,approximately 67% die within 1 h of onset of symp¬toms.1 Therefore, this subset has been quite difficultto include in studies evaluating management options.Much of our current understanding of the efficacy
of various inotropic and vasopressor agents in hemo-dynamically unstable patients with PE comes fromanimal models, which can be difficult to extrapolateto the clinical treatment of patients. The anestheticagents used in many of the animal studies mayinterfere with the response to the protocol agents,which creates difficulties in generalizing the findingsto a nonanesthetized population. Positive pressureventilation (mandatory in anesthetized animals) hasits own hemodynamic effects that might alter or
obscure those of the experimental PE. Glass beads(used in many of the animal studies to simulate PE)may not liberate vasoactive mediators to the same
extent as fresh clots. The hemodynamic derange¬ments in response to formed thrombus are more
profound than those seen after embolization of freshautologous clot,3 although the latter model is more
commonly used in the studies cited in this review.Microembolization has been shown to produce pul¬monary edema,45 which can worsen hypoxic vaso-
*From the Division of Pulmonary/Critical Care Medicine, De¬partment of Medicine, Duke University Medical Center,Durham, NC.Manuscript received November 17, 1995; revision accepted July22, 1996.Reprint requests: Dr. Tapson, Duke University Medical Center,Box 31175, Durham, NC 27710
constriction, perhaps to a different extent than actualPE. The size ofthe emboli used in the animal modelsinfluences the degree of hypoxemia (and secondaryvasoconstriction) as well as the hemodynamic re¬
sponse seen with protocol medications.46 Concomi¬tant treatment with heparin (used in some but not allstudies) may alter the hemodynamic response to
protocol agents by inhibiting intravascular coagula¬tion and thus preventing the release of vasoactivehumoral factors.7 In addition, there may be impor¬tant differences between species in terms of drugdoses, vital signs, heart rate dependence, and collat¬eral blood flow. For example, acetylcholine producesvasodilation of the pulmonary circulation in man butvasoconstriction in canine species.8 Thus, applyinginformation obtained from experimental models toclinical patient management must be done withutmost caution.
Pathophysiology
The pathophysiology of circulatory failure andshock due to PE is primarily caused by a reducedcross-sectional area of the pulmonary vascular bed.9This occurs because of the mechanical effect of theembolus itself, as well as secondary effects, includinghypoxic/acidotic vasoconstriction and release of va¬
soactive substances.4-7'1011 The resultant increase in
pulmonary artery pressure (PAP) leads to increasedright ventricular (RV) afterload, myocardial walltension, and oxygen consumption.12 The consequentdepression in RV performance reduces cardiac out¬
put (CO) and BP, leading to shock. Indeed, RVfailure may be defined as the point at which CO andBP fall despite increased RV end-diastolic pressure(RVEDP).13 RV distention can also interfere withleft ventricular filling and thus contribute to dimin¬ished CO.14 The reduced CO lowers mixed venous
Po2 and amplifies the arterial desaturation caused byventilation-perfusion mismatch in PE,15 in turn
worsening myocardial oxygenation and performance.Theoretically, inotropic agents in the setting of PE
might be expected to increase RV work by forcingincreased output into a circulation with fixed vascu¬
lar resistance.16 Unlike the left ventricle, the RVunder normal conditions has high compliance andcan be perfused throughout the cardiac cycle. How-
218 Reviews
ever, when acute pulmonary hypertension causes
increased RV intracavitary pressure, right coronaryblood flow in systole can become dependent on thepressure gradient between the aorta and RV.13The response of the RV to an acute increase in
afterload depends on the prior cardiovascular historyof the patient.917 In a patient without prior cardio¬vascular disease, the thin-walled RV is unable to
generate a mean PAP greater than 40 mm Hg in thesetting of acute PE, whereas PE in a patient with a
chronically hypertrophied RV may result in pulmo¬nary hypertension disproportionate to the degree ofembolic obstruction.9 Thus, the patient with priorcardiopulmonary disease may develop depression ofthe cardiac index with a lesser degree of obstruc¬tion.9To accurately describe the pressure-flow relation¬
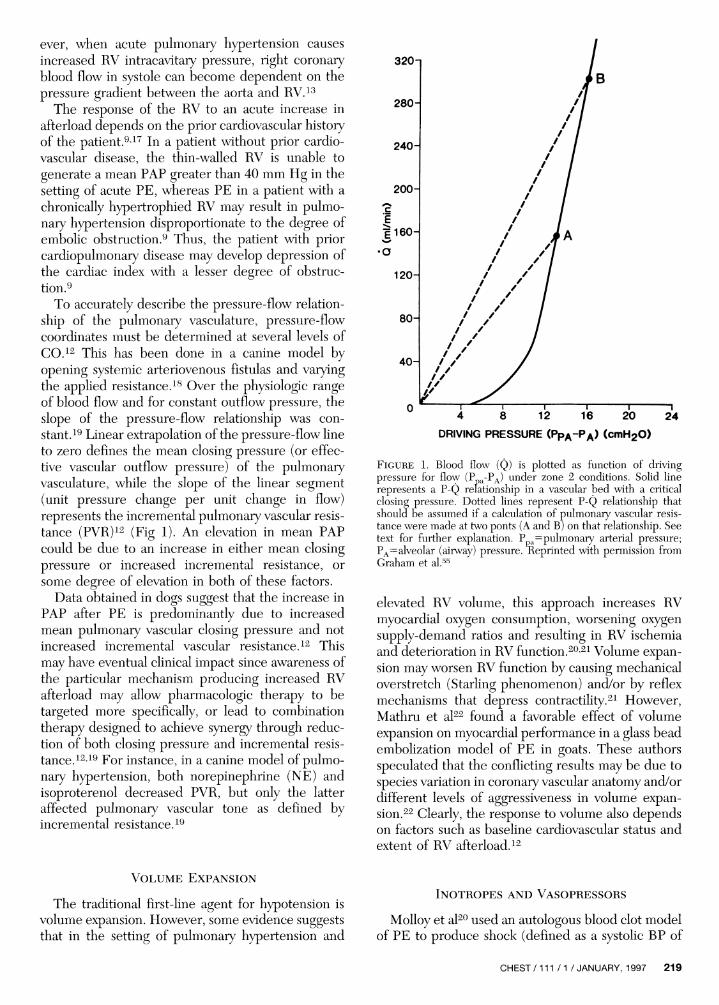
ship of the pulmonary vasculature, pressure-flowcoordinates must be determined at several levels ofCO.12 This has been done in a canine model byopening systemic arteriovenous fistulas and varyingthe applied resistance.18 Over the physiologic rangeof blood flow and for constant outflow pressure, theslope of the pressure-flow relationship was con¬
stant.19 Linear extrapolation of the pressure-flow lineto zero defines the mean closing pressure (or effec¬tive vascular outflow pressure) of the pulmonaryvasculature, while the slope of the linear segment(unit pressure change per unit change in flow)represents the incremental pulmonary vascular resis¬tance (PVR)12 (Fig 1). An elevation in mean PAPcould be due to an increase in either mean closingpressure or increased incremental resistance, or
some degree of elevation in both of these factors.Data obtained in dogs suggest that the increase in
PAP after PE is predominantly due to increasedmean pulmonary vascular closing pressure and notincreased incremental vascular resistance.12 Thismay have eventual clinical impact since awareness ofthe particular mechanism producing increased RVafterload may allow pharmacologic therapy to betargeted more specifically, or lead to combinationtherapy designed to achieve synergy through reduc¬tion of both closing pressure and incremental resis¬tance.1219 For instance, in a canine model of pulmo¬nary hypertension, both norepinephrine (NE) andisoproterenol decreased PVR, but only the latteraffected pulmonary vascular tone as defined byincremental resistance.19
320n
4 8 12 16
DRIVING PRESSURE (Ppa"Pa> <cmH20)
124
Figure 1. Rlood flow (Q) is plotted as function of drivingpressure for flow (Ppa-PA) under zone 2 conditions. Solid linerepresents a P-Q relationship in a vascular bed with a criticalclosing pressure. Dotted lines represent P-Q relationship thatshould be assumed if a calculation of pulmonary vascular resis¬tance were made at two ponts (A and R) on that relationship. Seetext for further explanation. P=pulmonary arterial pressure;PA=alveolar (airway) pressure. Reprinted with permission fromGraham et al.55
elevated RV volume, this approach increases RVmyocardial oxygen consumption, worsening oxygensupply-demand ratios and resulting in RV ischemiaand deterioration in RV function.2021 Volume expan¬sion may worsen RV function by causing mechanicaloverstretch (Starling phenomenon) and/or by reflexmechanisms that depress contractility.21 However,Mathru et al22 found a favorable effect of volumeexpansion on myocardial performance in a glass beadembolization model of PE in goats. These authorsspeculated that the conflicting results may be due to
species variation in coronary vascular anatomy and/ordifferent levels of aggressiveness in volume expan¬sion.22 Clearly, the response to volume also dependson factors such as baseline cardiovascular status andextent of RV afterload.12
Volume Expansion
The traditional first-line agent for hypotension isvolume expansion. However, some evidence suggeststhat in the setting of pulmonary hypertension and
Inotropes and Vasopressors
Molloy et al20 used an autologous blood clot modelof PE to produce shock (defined as a systolic BP of
CHEST/111 /1 /JANUARY, 1997 219
70 mm Hg) in 24 anesthetized dogs. The dogs were
heparinized and then randomly treated with (1) no
additional therapy, (2) volume expansion, (3) isopro-terenol, or (4) NE. The dogs treated with NEdemonstrated hemodynamic improvement and re¬
mained in stable condition during 1 h of continuousinfusion, while those in all other groups had progres¬sive hemodynamic deterioration and death within 10min20 (Table 1). In a canine model using balloonocclusion of the main pulmonary artery to simulatemassive PE, dogs treated with isoproterenol hadworse outcome than untreated control animals, whileNE improved hemodynamics (but not survival).23 In
other animal models of PE in which profoundhypotension was induced, NE has proved superior to
isoproterenol.22-24It may be that the positive inotropic and pulmo¬
nary vasodilatory effects of isoproterenol are out¬
weighed by the peripheral vasodilation it causes. Theresultant hypotension leads to decreased RV perfu¬sion and RV ischemia. Mathru et al,22 using a goatmodel, found that isoproterenol increased CO onlyby producing tachycardia, with stroke volume actu¬
ally decreasing. In contrast to isoproterenol, NEappears to improve RV function by a direct positiveinotropic effect, while also improving RV perfusion
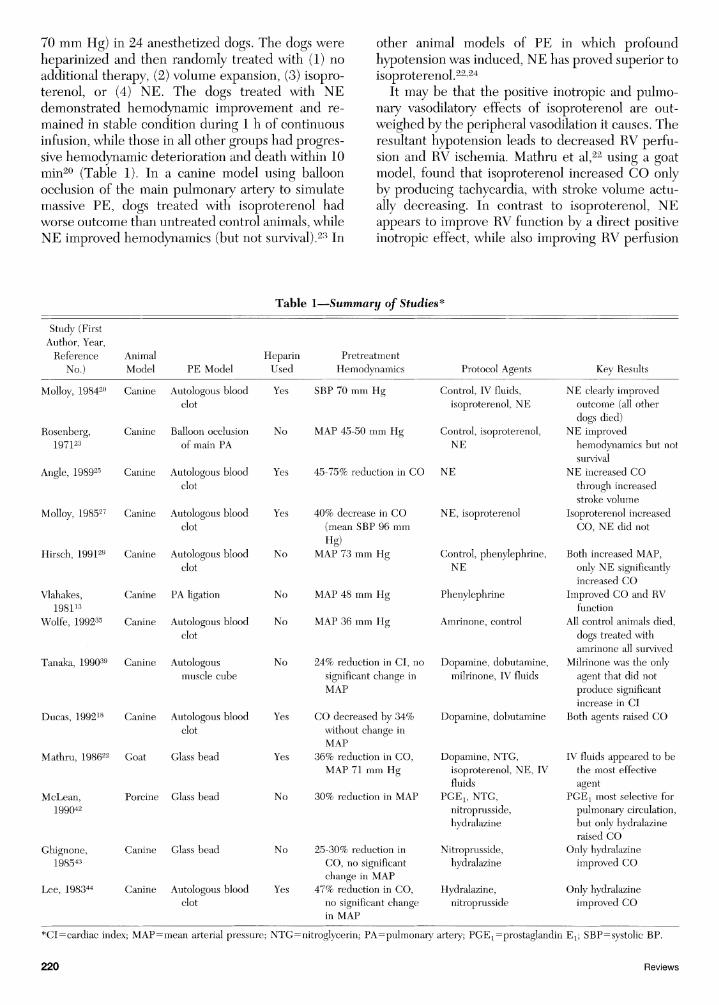
Table 1.Summary of Studies*
Study (FirstAuthor, Year,Reference Animal
No.) Model PE ModelHeparinUsed
PretreatmentHemodvnamics Protocol Agents Key Results
Molloy, 198420 Canine
Rosenberg, Canine197123
Angle, 198925 Canine
Molloy, 198527 Canine
Hirsch, 199129 Canine
Vlahakes,198113
Wolfe, 199235 Canine
Tanaka, 199039 Canine
Ducas, 199218 Canine
Mathru, 198622 Goat
McLean,199042
Ghignone,198543
Lee, 198344
Autologous bloodclot
Ralloon occlusionof main PA
Autologous bloodclot
Autologous bloodclot
Autologous bloodclot
Canine PA ligation
Autologous bloodclot
Autologousmuscle cube
Autologous bloodclot
Glass bead
Porcine Glass bead
Canine Glass bead
Yes SBP 70 mm Hg
No MAP 45-50 mm Hg
Yes
Yes
No
No
Yes
Yes
No
No
Canine Autologous blood Yesclot
40% decrease in CO(mean SBP 96 mm
Hg)MAP 73 mm Hg
No MAP 48 mm Hg
No MAP 36 mm Hg
24% reduction in CI, no
significant change inMAP
CO decreased by 34%without change inMAP
36% reduction in CO,MAP 71 mm Hg
30% reduction in MAP
25-30% reduction in
CO, no significantchange in MAP
47% reduction in CO,no significant changein MAP
Control, IV fluids,isoproterenol, NE
Control, isoproterenol,NE
45-75% reduction in CO NE
NE, isoproterenol
Control, phenylephrine,NE
Phenylephrine
Amrinone, control
Dopamine, dobutamine,milrinone, IV fluids
Dopamine, dobutamine
Dopamine, NTG,isoproterenol, NE, IVfluids
PGEl5 NTG,nitroprusside,hydralazine
Nitroprusside,hydralazine
Hydralazine,nitroprusside
NE clearly improvedoutcome (all otherdogs died)
NE improvedhemodynamics but notsurvival
NE increased COthrough increasedstroke volume
Isoproterenol increasedCO, NE did not
Both increased MAP,only NE significantlyincreased CO
Improved CO and RVfunction
All control animals died,dogs treated withamrinone all survived
Milrinone was the onlyagent that did not
produce significantincrease in CI
Both agents raised CO
IV fluids appeared to bethe most effectiveagent
PGE: most selective forpulmonary circulation,but only hydralazineraised CO
Only hydralazineimproved CO
Only hydralazineimproved CO
*CIrrcardiac index; MAP=mean arterial pressure; NTG^nitroglycerin; PA^pulmonary artery; PGE1=prostaglandin Ex; SBP=systolic BP.
220 Reviews

by peripheral vascular alpha-receptor stimulationand increased systemic BP. Another study using a
canine autologous blood clot model of PE showedthat NE improved ventricular function over a widerange of BP and RV afterloads (suggesting that itsbeneficial effects are not limited to the subset withfrank shock).25 Of note, when NE was titrated to a
moderate increase in BP, ventricular performanceimproved without increasing PVR and without det¬rimental effects on renal flow or function.25 Althoughcalculated PVR (PVR=PAP-LVEDP/CO) may de¬crease with NE, this is based on the assumption thatleft ventricular end-diastolic pressure (LVEDP) isequivalent to pulmonary vascular outflow pressure,19which may not be the case in experimental PE.26When Ducas et al19 examined pressure-flow relation¬ships in a canine autologous blood clot model of PE,NE did not change incremental PVR, while isopro¬terenol decreased this parameter. Thus, the in¬creased PAP seen with NE is due to increased flowand not increased vascular tone.12 This is significantsince one might expect the pressor effects of NE toincrease incremental PVR, which would be counter¬
productive in the treatment of RV failure.The poor outcome noted in animals treated with
isoproterenol may not necessarily be applicablewhen BP prior to treatment is higher. This was
evaluated by Molloy et al27 using an autologousblood clot model in dogs, with an end point of a 40%reduction in CO, which caused mild systemic hypo¬tension (mean systolic BP of 96 mm Hg postembo-lization). Under these circumstances, isoproterenolmore than doubled CO (from 1.3 to 3.0 L/min),while NE increased stroke volume (at constantRVEDP) but not CO (due to a decrease in heartrate). In an uncontrolled series of nine normotensiveor mildly hypotensive patients with PE, responses to
isoproterenol varied considerably but typically in¬cluded increased stroke volume, CO, and heart ratewith only a slight reduction in mean systemic arterialpressure and no significant change in mean PAP or
oxygenation.28 Peripheral vasoconstriction alonedoes not appear to be adequate for hemodynamicsupport in patients with massive PE. Hirsch et al29(using a canine autologous blood clot model) com¬
pared the effects of a pure vasopressor (phenyleph¬rine) to NE, which has combined $r(inotropic) anda-(vasoconstrictor) adrenergic properties. Bothagents were able to restore systemic BP to normal,but only NE produced significant improvement inCO, RV myocardial blood flow, and RV myocardialoxygen consumption.29 This is consistent with theresults of Ducas et al,30 who compared NE withmethoxamine (a direct a1-agonist) in a canine glassbead model of PE. Therefore, the inotropic effect ofNE enhances the ability of the RV to meet the
increased energy demands imposed by the (experi¬mental) PE. It is also possible that the vasopressoragents caused increased coronary vascular resistancethat outweighed the improvement in coronary per¬fusion pressure.12 However, Vlahakes et al13 demon¬strated reversal of ischemia and improved RV func¬tion and CO with phenylephrine (at dosages whichshould have had only a-adrenergic effects) afterpulmonary artery ligation in dogs.13 A vasoconstric-tive effect on the venous circulation (with resultantincreased venous return and preload) may havecontributed to the observed effect. The more pro¬found degree of hypotension (mean arterial pressureof 48 mm Hg) prior to treatment in the study ofVlahakes et al may have allowed an effect on CO tobe seen.12
Epinephrine has a-vasoconstrictive effects compa¬rable to those of NE, a1 effects far greater thandobutamine, but has far less (32 activity. Therefore, itcombines the beneficial properties of NE (vasocon¬striction with increased RV perfusion, positive ino-tropy) and dobutamine (positive inotropy) withoutthe vasodilatory effects of the latter (which can havedetrimental consequences on RV coronary perfusionpressure in the setting of systemic hypotension). Apatient has been described who had shock from PEthat was refractory to volume expansion, dobu¬tamine, urokinase, and NE but responded (by he¬modynamics and oxygenation) to a continuous infu¬sion of epinephrine (1 fxg/kg/min).31 Although this isonly a single case report (and may have been con¬
founded by the concurrent administration of recom-binant tissue plasminogen activator and epineph¬rine), it is of interest because of the theoreticaladvantages of epinephrine.
Both dopamine and dobutamine have been shownto raise CO in a canine autologous blood clot modelof PE, without dilation of the pulmonary vascula¬ture.18 Only high doses of dopamine (34.3±4.1jJLg/kg/min) improved CO and RV ejection fraction ina glass bead embolization model of PE in goats, butat these doses, profound tachycardia resulted.22 In a
small series of patients requiring ICU admission forPE, dobutamine raised CO and improved oxygentransport and tissue oxygenation at a constant arterialPo2.17 Another study yielded similar results in ten
patients with circulatory failure due to massive PE.32In some cases, arterial Po2 actually fell (presumablydue to worsened ventilation-perfusion mismatchcaused by dobutamine), but even in these patients,arterial oxygen transport improved because the in¬crease in CO was more than compensatory.17 Thevaried effects of dobutamine on gas exchange in thisstudy were believed to be related to differences ininitial CO and degree of hypoxemia, so that furtherinvestigation will be needed to clarify the role of this
CHEST 7111/1/ JANUARY, 1997 221

agent. There is currently controversy concerning theuse of inotropes to raise CO to supraphysiologicvalues to improve oxygen transport in critical ill¬ness.33-34 As suggested above, in the setting of acutePE, raising CO may worsen ventilation-perfusionmatching by redistribution of flow from obstructedto nonobstructed vessels.17
Despite poor results with isoproterenol, amrinone(which also has both inotropic as well as pulmonaryand systemic vasodilating properties and may haveanticoagulant effects) has shown excellent results in a
canine autologous blood clot model.35 The mode ofaction of amrinone is not precisely known, but it isbelieved to involve both inhibition of phosphodies-terase and altered calcium transport.35 In contrast totwo untreated control dogs who died within minutes,the eight dogs treated with amrinone were all resus¬
citated from profound hypotension (three from elec¬tromechanical dissociation). Treated animals demon¬strated a significant increase in mean arterialpressure and CO, and decreased mean PAP. How¬ever, the effects of amrinone on oxygenation were
not reported. This must be examined carefully be¬fore this agent is used in the setting of PE, since ithas previously been noted to worsen oxygenation dueto pulmonary shunting36 and inhibition of hypoxicpulmonary vasoconstriction.37 A single patient hasbeen described with PE (complicated by pulmonaryhypertension and diminished CO) who had hemody¬namic improvement (as well as improved oxygen¬ation) after treatment with amrinone.38 Like amri¬none, milrinone inhibits phosphodiesterase andalters calcium transport.39 It has been studied in a
canine autologous muscle cube model of PE.39 Ox¬ygenation did not worsen with this agent, but im¬
proved slightly. In contrast to dopamine and dobut¬amine, milrinone demonstrated relatively selectivepulmonary vasodilatation, along with its inotropiceffects. The inotropic and pulmonary vasodilatoreffects of milrinone have also been demonstrated in
patients with multiple organ dysfunction40 and sep¬sis41 (at doses that did not cause an increase in heartrate). While these data are intriguing, much workremains to be done before the routine clinical use ofamrinone or milrinone in the setting of massive PEcan be recommended.
Vasodilators
Various vasodilators have been used in experimen¬tal PE in an attempt to improve RV function throughafterload reduction. Nitroglycerin has been adminis¬tered to normovolemic goats after glass bead embo-lization to simulate PE.22 In this study, systemicvascular resistance (SVR) and PVR decreased, while
RV ejection fraction, CO, and oxygen delivery in¬creased. Afterload reduction was believed to be themechanism of improved myocardial performance,although improved myocardial perfusion via coro¬
nary vasodilation is also possible. Of note, volumeloading was required during nitroglycerin infusion to
compensate for its vasodilator effect.22 McLean etal42 used a porcine glass bead embolization model,and titrated each of four vasodilators (prostaglandinEjl, nitroglycerin, sodium nitroprusside, and hydral¬azine) to produce a 30% reduction in mean systemicarterial pressure. Prostaglandin Ex produced thegreatest decrease in PVR and PAP, and was the onlyagent of the four that did not adversely affect thePVR/SVR ratio. Both nitroglycerin and sodium nitro¬
prusside produced moderate decreases in PVR andPAP, but significantly increased the PVR/SVR ratio.
Hydralazine produced the most systemic vasodila¬tion for a given amount of pulmonary vasodilation,but was the only agent that significantly increasedCO. After glass bead43 and autologous blood clot44embolization in dogs, hydralazine (but not nitroprus¬side) increased CO and decreased PVR. In theMcLean et al42 study, central venous pressure was
reduced with the agents other than hydralazine andthus reduced venous return may have prevented theincrease in CO one would expect from a reduction inafterload. Future studies should address the role ofconcomitant administration of IV fluids with thevasoactive agent. A patient has been described withPE complicated by low CO (refractory to volumeexpansion and dopamine) who had improved cardiacindex and PVR (without significant hypotension) on
two separate trials of oral hydralazine therapy.45Clearly, the risk of systemic hypotension with result¬ant RV ischemia is the primary concern with the use
of vasodilators in the setting of hemodynamicallysignificant PE. Inhaled nitric oxide has recently beendemonstrated to achieve selective pulmonary vaso¬
dilation in a porcine microembolization model ofmassive PE46 Further study of this agent as well as
other inhaled vasodilators (such as prostacylin) ap¬pears warranted.
Conclusions
The available data seem to support the admin¬istration of NE to ensure adequate RV coronaryperfusion pressure in patients with PE and pro¬found decrease in CO and systemic BP. However,dobutamine may be more appropriate in patientswith moderate systemic hypotension, providedclose monitoring of SVR and mean arterial pres¬sure ensures that adequate RV coronary perfusionpressure is maintained.47 The combined use of
222 Reviews
various vasoactive agents to achieve optimal hemo¬dynamic response deserves further evaluation. For
example, the combined use of dobutamine (for its
inotropic effects) and a vasoconstrictor (such as
NE) to ensure adequate RV perfusion offers the¬oretical merit and warrants investigation. Prelimi¬nary data and theoretical considerations suggestthat epinephrine might be a useful agent in pa¬tients with massive PE. Preliminary data on amri¬none is also encouraging, but this agent cannot
currently be recommended routinely for use inthis setting. Based on the available data, we do notendorse the use of isoproterenol for managementof hemodynamically significant PE. Volume ex¬
pansion must be undertaken cautiously in thesepatients, because of the possibility of worseningRV function. Since RV function can deterioratewith volume even at a relatively low RVEDP, RVfilling pressure may not predict the response tovolume expansion when an increase in RV after-load causes a low CO state.21 Clearly, individualpatient management should be guided by follow¬ing objective hemodynamic and physiologic pa¬rameters. However, the precise role and optimaltype of invasive monitoring in patients with hemo¬dynamic compromise from PE remain to be clar¬ified. Thrombolytic agents have been shown to
improve RV function after PE and are appropriate(in the absence of contraindications) when PE is
accompanied by hypotension.1248 The possibleinteractions of fibrinolytic therapy with the phar¬macologic agents discussed in this review and therole for concomitant administration merit furtherinvestigation.49 Surgical or catheter embolectomymay be appropriate in specific circumstances.50-52Percutaneous pulmonary artery balloon counter-
pulsation is a technique that has theoretical appealfor the treatment of RV failure, and initial animaldata are encouraging.5354 Of course, supplementaloxygen, by ameliorating hypoxic vasoconstriction,is vital to the hemodynamic support of patientswith massive PE.The limitations of animal models outlined above
must be taken into account when extrapolating thesedata to bedside management. Many of the studiescited in this review used different end points in theirexperimental pulmonary hypertension models (Ta¬ble 1, "pretreatment hemodynamics") making directcomparison difficult. Multicenter, randomized, con¬
trolled trials in clinically relevant scenarios in humanbeings would be useful to clarify these importantpatient management issues, but the very nature ofthis patient population presents difficult issues in
study design.
References1 Dalen JE, Alpert JS. Natural history of pulmonary embolism.
Prog Cardiovasc Dis 1975; 17:259-702 Alpert JS, Smith R, Carlson CJ, et al. Mortality in patients
treated for pulmonary embolism. JAMA 1976; 236:1477-803 Duranceau A, Jamieson GG, Jones RH, et al. An experimen¬
tal model of pulmonary embolism. J Surg Res 1979; 26:33-444 Johnson A, Malik AB. Pulmonary edema after glass bead
microembolization: protective effect of granulocytopenia.J Appl Physiol 1982; 52:155-61
5 Malik AB, Zee HVD. Lung vascular permeability followingprogressive pulmonary embolization. J Appl Physiol 1978;45:590-97
6 Delcroix M, Melot C, Vachiery JL, et al. Effects of embolussize on hemodynamics and gas exchange in canine embolicpulmonary7 hypertension. J Appl Physiol 1990; 69:2254-61
7 Malik AB, Zee HVD. Time course of pulmonary vascularresponse to microembolization. J Appl Physiol 1977; 43:51-8
8 Aviado DM, Cho YW. Pulmonary pharmacologies In: GordonBL, Carleton RA, Faber LP, eds. Clinical cardiopulmonaryphysiology. 3rd ed. New York: Grune & Stratton, 1969;718-19
9 Mclntyre KM, Sasahara AA. Hemodynamic and ventricularresponses to pulmonary embolism. Prog Cardiovasc Dis 1974;17:175-90
10 Vaage J, Piper PJ. The release of prostaglandin-like sub¬stances during platelet aggregation and pulmonary microem-bolism. Acta Physiol Scand 1975; 94:8-13
11 Levy SE, Shapiro BJ, Simmons DH. Pulmonary hemodynam¬ics after autologous in vivo pulmonary thromboembolism.J Appl Physiol 1969; 27:53-60
12 Ducas J, Prewitt RM. Pathophysiology and therapy of rightventricular dysfunction due to pulmonary embolism. Cardio¬vasc Clin 1987; 17:191-202
13 Vlahakes GJ, Turley K, Hoffman J. The pathophysiology offailure in acute right ventricular hypertension: hemodynamicand biochemical correlations. Circulation 1981; 63:87-95
14 Bemis CE, Serur JR, Borkenhagen D, et al. Influence of rightventricular filling pressure on left ventricular pressure anddimension. Circ Res 1974; 34:498-504
15 Manier G, Castaing Y, Guenard H. Determinants of hypox¬emia during the acute phase of pulmonary embolism inhumans. Am Rev Respir Dis 1985; 132:332-38
16 Weber KT, Janicki JS, Shroff SG, et al. The right ventricle:physiologic and pathophysiologic considerations. Crit CareMed 1983; 11:323-28
17 Manier G, Castaing Y. Influence of cardiac output on oxygenexchange in acute pulmonary embolism. Am Rev Respir Dis1992; 145:130-36
18 Ducas J, Stitz M, Gu S, et al. Pulmonary vascular pressure-flow characteristics: effects of dopamine before and afterpulmonary embolism. Am Rev Respir Dis 1992; 146:307-12
19 Ducas J, Duval D, Dasilva H, et al. Treatment of canine
pulmonary hypertension: effects of norepinephrine and iso¬
proterenol on pulmonary vascular pressure-flow characteris¬tics. Circulation 1987; 75:235-42
20 Molloy DW, Lee KY, Girling L, et al. Treatment of shock ina canine model of pulmonary embolism. Am Rev Respir Dis1984; 130:870-74
21 Ghignone M, Girling L, Prewitt RM. Volume expansionversus norepinephrine in treatment of a low cardiac outputcomplicating an acute increase in right ventricular afterload in
dogs. Anesthesiology 1984; 60:132-3522 Mathru M, Venus B, Smith R, et al. Treatment of low cardiac
output complicating acute pulmonary hypertension in normo-volemic goats. Crit Care Med 1986; 14:120-24
CHEST / 111 / 1 / JANUARY, 1997 223

23 Rosenberg JC, Hussain R, Lenaghan R. Isoproterenol andnorepinephrine therapy for pulmonary embolism shock.J Thorac Cardiovasc Surg 1971; 62:144-50
24 Imamoto T, Yamashita H, Onodera S. Treatment of canineacute pulmonary embolic shock: effects of isoproterenol andnorepinephrine on hemodynamics and ventricular wall mo¬
tion. Jpn Circ J 1990; 54:1246-5725 Angle MR, Molloy DW, Penner B, et al. The cardiopulmo¬
nary and renal hemodynamic effects of norepinephrine incanine pulmonary embolism. Chest 1989; 95:1333-37
26 Ducas J, Girling L, Schick U, et al. Pulmonary vascular effectsof hydralazine in a canine preparation of pulmonary throm¬boembolism. Circulation 1986; 73:1050-57
27 Molloy DW, Lee KY, Jones D, et al. Effects of noradrenalineand isoproterenol on cardiopulmonary function in a caninemodel of acute pulmonary hypertension. Chest 1985; 88:432-35
28 McDonald IG, Hirsh J, Hale GS, et al. Isoproterenol inmassive pulmonary embolism: haemodynamic and clinicaleffects. Med J Aust 1968; 2:201-04
29 Hirsch LJ, Rooney MW, Wat SS, et al. Norepinephrine andphenylephrine effects on right ventricular function in experi¬mental canine pulmonary embolism. Chest 1991; 100:796-801
30 Ducas J, Deutscher R, Prewitt RM. Inotropic vs vasopressoragents in acute right ventricular failure [abstract]. Am Rev
Respir Dis 1985; 13LA14931 Boulain T, Lanotte R, Legras A, et al. Efficacy of epinephrine
therapy in shock complicating pulmonary embolism. Chest1993; 104:300-02
32 Jardin F, Genevray B, Brun-Ney D, et al. Dobutamine: a
hemodynamic evaluation in pulmonary embolism shock. CritCare Med 1985; 13:1009-12
33 Hayes MA, Timmins AC, Yau EHS, et al. Elevation ofsystemic oxygen delivery in the treatment of critically illpatients. N Engl J Med 1994; 330:1717-22
34 Gattinoni L, Brazzi L, Pelosi P, et al. A trial of goal-orientedhemodynamic therapy in critically ill patients. N Engl J Med1995; 333:1025-32
35 Wolfe MW, Saad RM, Spence TH. Hemodynamic effects ofamrinone in a canine model of massive pulmonary embolism.Chest 1992; 102:274-78
36 Prielipp RC, Butterworth JF IV, Zaloga GP, et al. Effects ofamrinone on cardiac index, venous oxygen saturation andvenous admixture in patients recovering from cardiac surgery.Chest 1991; 99:820-25
37 Hill NS, Rounds S. Amrinone dilates pulmonary vessels andblunts hypoxic vasoconstriction in isolated rat lungs. Proc SocExp Biol Med 1983; 173:205-12
38 Spence TH, Newton WD. Pulmonary embolism: improve¬ment in hemodynamic function with amrinone therapy. SouthMedJ 1989;82:1267-68
39 Tanaka H, Tajimi K, Matsumoto A, et al. Vasodilatory effectsof milrinone on pulmonary vasculature in dogs with pulmo¬nary hypertension due to pulmonary embolism: a comparison
with those of dopamine and dobutamine. Clin Exp PharmacolPhysiol 1990; 17:681-90
40 Prielipp RC, MacGregor DA, Butterworth JF, et al. Pharma-codynamics and pharmacokinetics of milrinone administra¬tion to increase oxygen delivery in critically ill patients. Chest1996; 109:1291-1301
41 Barton P, Garcia J, Kouatli A, et al. Hemodynamic effects ofintravenous milrinone lactate in pediatric patients with septicshock. Chest 1996; 109:1302-12
42 McLean RF, Prielipp RC, Rosenthal MH, et al. Vasodilatortherapy in microembolic porcine pulmonary hypertension.Anesth Analg 1990; 71:35-41
43 Ghignone M, Girling L, Prewitt RM. Effects of vasodilatorson canine cardiopulmonary function when a decrease incardiac output complicates an increase in right ventricularafterload. Am Rev Respir Dis 1985; 131:527-30
44 Lee KY, Molloy DW, Slykerman L, et al. Effects of hydralazineand nitroprusside on cardiopulmonary function when a decreasein cardiac output complicates a short-term increase in pulmo¬nary vascular resistance. Circulation 1983; 68:1299-1303
45 Bates ER, Crevey BJ, Sprague FR, et al. Oral hydralazinetherapy for acute pulmonary- embolism and low output state.Arch Intern Med 1981; 141:1537-38
46 Bottiger BW, Motsch J, Dorsam J, et al. Inhaled nitric oxideselectively decreases pulmonary artery pressure and pulmo¬nary vascular resistance following acute massive pulmonarymicroembolism in piglets. Chest 1996; 110:1041-47
47 Prewitt RM. Hemodynamic management in pulmonary em¬
bolism and acute hypoxic respiratory failure. Crit Care Med1990; 18:S61-69
48 Tapson VF, Witty LA. Massive pulmonary embolism: diag¬nostic and therapeutic strategies. Clin Chest Med 1995;16:329-40
49 Witty LA, Tapson VF, Wellendorf J, et al. Massive pulmonaryembolism: local thrombolytic therapy with inotropic support[abstract]. Am J Respir Crit Care Med 1994; 149:A1064
50 Greenfield LJ. Catheter pulmonary embolectomy. Chest1991; 100:593-94
51 Gray HH, Morgan JM, Paneth M, et al. Pulmonary embolec¬tomy for acute massive pulmonary embolism: an analysis of 71cases. Br Heart J 1988; 60:196-200
52 Tapson VF, Gurbel PA, Witty LA, et al. Pharmacomechanicalthrombolysis of experimental pulmonary emboli: rapid low-dose intraembolic therapy. Chest 1994; 106:1558-62
53 Letsou GV, Franco KL, Detmer W, et al. Pulmonary artery7balloon counterpulsation: safe after peripheral placement.Ann Thorac Surg 1993; 55:741-46
54 Sweet JM, Salerno PR, Panos A, et al. Feasibility of pulmo¬nary artery7 balloon counterpulsation via the percutaneousroute: pathological studies on the heart and lungs. CanJ Cardiol 1989; 5:352-56
55 Graham R, Skoog C, Macedo W, et al. Dopamine, dobut¬amine and phentolamine effects on pulmonary- vascular me¬
chanics. J Appl Physiol 1983; 54:1277-83
224 Reviews
DOI 10.1378/chest.111.1.218 1997;111; 218-224Chest
Daniel T. Layish and Victor F. TapsonEmbolism
Pharmacologic Hemodynamic Support in Massive Pulmonary
October 13, 2011This information is current as of
http://chestjournal.chestpubs.org/content/111/1/218.citationUpdated Information and services can be found at:
Updated Information & Services
http://chestjournal.chestpubs.org/content/111/1/218.citation#related-urlsThis article has been cited by 8 HighWire-hosted articles:
Cited Bys
http://www.chestpubs.org/site/misc/reprints.xhtmlcan be found online at: Information about reproducing this article in parts (figures, tables) or in its entiretyPermissions & Licensing
http://www.chestpubs.org/site/misc/reprints.xhtmlInformation about ordering reprints can be found online:
Reprints
"Services" link to the right of the online article.Receive free e-mail alerts when new articles cite this article. To sign up, select the
Citation Alerts
PowerPoint slide format. See any online figure for directions. articles can be downloaded for teaching purposes inCHESTFigures that appear in Images in PowerPoint format