improving informed consent with minority participants: results from researcher and community surveys
TRANSCRIPT
Improving Informed Consent with Minority Participants: Resultsfrom Researcher and Community Surveys
Sandra Crouse Quinn,University of Maryland
Mary A. Garza,University of Maryland
James Butler,University of Maryland
Craig S. Fryer,University of Maryland
Erica T. Casper,University of Maryland
Stephen B. Thomas,University of Maryland
David Barnard, andUniversity of Pittsburgh
Kevin H. KimUniversity of Pittsburgh
AbstractStrengthening the informed consent process is one avenue for improving recruitment of minoritiesinto research. This study examines that process from two different perspectives, that of researchersand that of African American and Latino community members. Through the use of two separatesurveys, we compared strategies used by researchers with the preferences and attitudes ofcommunity members during the informed consent process. Our data suggest that researchers canimprove the informed consent process by incorporating methods preferred by the communitymembers along with methods shown in the literature for increasing comprehension. With thisapproach, the informed consent process may increase both participants’ comprehension of thematerial and overall satisfaction, fostering greater trust in research and openness to future researchopportunities.
Keywordsinformed consent; minorities; improving informed consent
Informed consent is the process by which potential participants are given the opportunity tomake informed decisions about their participation in research. In the United States, federalguidelines govern the interaction with human subjects, including the informed consent
© 2012 BY JOAN SIEBER. ALL RIGHTS RESERVED.
Address correspondence to: Sandra Crouse Quinn, School of Public Health, 2242CC SPH Building #255, University of Maryland,College Park, MD 20742. Phone: 301-405-8825; Fax: 301-405-8397; [email protected].
NIH Public AccessAuthor ManuscriptJ Empir Res Hum Res Ethics. Author manuscript; available in PMC 2013 June 18.
Published in final edited form as:J Empir Res Hum Res Ethics. 2012 December ; 7(5): 44–55. doi:10.1525/jer.2012.7.5.44.
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
process and document (U.S. Department of Health and Human Services, 2009). In manycases, the focus of the informed consent process is on the signing of the consent documentrather than on the interaction between researcher and participant (Thorne, 1980). Yet agrowing body of evidence indicates that many participants are misinformed about researchand have incomplete comprehension of information specific to research studies in whichthey are involved (Corbie-Smith, Thomas, & St. George, 2002; Freimuth et al., 2001;Penman et al., 1984). This is particularly true for racial and ethnic minority participants(Sudore et al., 2006), suggesting that it is necessary for researchers to improve theirinformed consent process, especially in the context of recruiting minorities who have beenunderrepresented in biomedical and clinical research (Corbie-Smith et al., 1999; Farmer etal., 2007; Freimuth et al., 2001; Lakes et al., 2012).
Strengthening the informed consent process requires investigators to consider severalinterrelated factors: the cultural and contextual issues that influence minorities’ reactions toinformed consent; the ability of researchers to effectively address these issues and engage inthe informed consent process; and potential participants’ comprehension of informationdelivered during the informed consent process.
Certain cultural and contextual factors magnify the challenge of informed decision-makingfor individuals from racial and ethnic minority populations, including both lack of trustarising from past legacy of mistreatment, or misinformation about the informed consentprocess and inadequate comprehension of the information after the informed consentdocument is signed.
The issue of minority trust in research is an important factor to consider when evaluatingways to improve the informed consent process. Focus group and survey data with AfricanAmericans have revealed a sense of distrust arising from a legacy of mistreatment in thehealth care system and research abuses (Corbie-Smith et al., 2002; Freimuth et al., 2001).African Americans are less likely to trust that research will be fully explained to them and“more likely to believe that someone like them would be used as a guinea pig without his orher consent” (Corbie-Smith et al., 2002, p. 2459). Overemphasis on the initial consentdocument can compound distrust of research and medical care by contributing to theperception that informed consent serves as a legal waiver of liability for adverse outcomes(Ard et al., 2005; Freimuth et al., 2001). In focus groups, African Americans have stated thatproviding informed consent amounts to “signing away your rights” and that the intent ofinformed consent is to protect researchers from lawsuits (Freimuth et al., 2001, p. 802). Toooften, informed consent protocols emphasize the signing of the initial consent document—which becomes a sort of “opening ritual” (Thorne, 1980, p. 289)—rather than a process thatlays the foundation for ongoing communication and building a longer-term relationshipbetween the researcher or research team and the participant.
Additionally, cultural factors unique to some specific minority communities include thedesire for translated materials and trained interpreters (Eder et al., 2007), concerns aboutbeing detected as undocumented immigrants, and a desire to meet with researchers multipletimes prior to deciding whether or not to participate (Lakes et al., 2012). Investigators whowish to recruit minorities may need to question the assumption implicit in informed consentdocuments that participation is an individual decision (ibid.). In some communities, wherethe family or community is an integral part of the decision-making process, and risks andbenefits of research participation are considered in terms of how the larger group will beaffected, investigators should allow enough time for participants to engage in the relevantgroup decision-making process. Finally, recent research suggests that providing informationoutside of the formal consent document can enhance minority participation. For example,Dunlop et al. (2011) found that compared to a traditional consent process, a DVD-enhanced
Quinn et al. Page 2
J Empir Res Hum Res Ethics. Author manuscript; available in PMC 2013 June 18.
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript

consent process resulted in a greater number of study participants expressing a willingnessto participate in a hypothetical clinical study and that those who viewed the DVD weresignificantly less likely to cite mistrust, privacy, fear of side effects, and lack of perceivedbenefits as reasons for nonparticipation. In another study, minority focus group participantsexpressed a desire for more detailed information in various formats (such as brochures,FAQs, and DVDs) to increase the “legitimacy” of the research (Lakes et al., 2012, p. 225).
Aside from enhancing minority satisfaction and participation through improved informedconsent, an important ethical consideration for investigators is ensuring that participantsunderstand the disclosed information. Studies show that participants frequently have poorrecall of the information provided during consent (Penman et al., 1984), do not understandkey terms such as “randomization” and “placebo” (Criscione et al., 2003), believe studydrugs do not involve additional risk (Barrett, 2005; Criscione et al., 2003), and expect toreceive the best available treatment despite having been “informed” of the randomized trialdesign (Joffe et al., 2001).
Efforts to improve comprehension of informed consent have generally focused on enhancedconsent forms and multimedia interventions. Although modifications to consent forms haveincluded condensing the form’s length, using plain language and larger font to improvereadability, and adding graphics, such efforts have had only limited success, with a majorityof studies showing no significant gains to understanding from such techniques (Flory &Emanuel, 2004). One key issue may be lack of familiarity with research concepts. In focusgroups conducted with low-literacy Spanish speakers regarding a hypothetical study, Cortéset al. (2010) found that simplified consent forms written in Spanish and using plainlanguage, shorter sentences and paragraphs, large font, and wide margins did not guaranteecomprehension. The focus group participants, especially those with no prior experience withresearch, sometimes did not understand basic research concepts despite their ability to readthe simplified document. Similarly, video and computer multimedia interventions have notshown a consistent positive effect on comprehension of informed consent compared withstandard written and oral information. Hence, uncertainty remains about the value of suchstrategies (Flory & Emanuel, 2004; Ryan et al., 2008).
Two literature reviews (Cohn & Larson, 2007; Flory & Emanuel, 2004) suggest that to besuccessful, the informed consent process needs to include one-on-one interaction withsomeone knowledgeable about the study, as well as various communication modes, bothwritten and verbal. Person-to-person interaction appears to be more important than videos orpaper forms in improving understanding, and limited evidence suggests that consentprocedures incorporating tests and/or feedback to check comprehension result in betterunderstanding (Flory & Emanuel, 2004; Sudore et al., 2006).
This article represents the first study to examine issues related to improving informedconsent from two perspectives, that of researchers and that of African American and Latinocommunity members. Further, we use these perspectives to develop recommendations onhow to improve the informed consent process through (1) increasing participant satisfactionby addressing the discrepancies between researchers’ practices and community members’preferences and (2) increasing comprehension by incorporating effective methods.
MethodsResearcher Participants
The participants were recruited from May to August 2010 using an e-mail invitation to anonline survey. Invitations to participate were sent through the listservs of PublicResponsibility in Medicine and Research (PRIM&R), which includes researchers and IRB
Quinn et al. Page 3
J Empir Res Hum Res Ethics. Author manuscript; available in PMC 2013 June 18.
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript

members who conduct many types of research, Community-Campus Partnerships forHealth, numerous clinical and translational science institutes, colleagues in academic healthcenters, and PRIM&R webinars. Additionally, invitations to participate were included inpublications such as the IRB Advisor, and on several Facebook sites, including those for theCenters for Disease Control and Prevention, the American Public Health Association, andthe Journal of Medical Ethics. Demographic variables gathered from 347 participantsincluded: gender, age, race, ethnicity, place of work or employment, primary role inresearch, and years involved with research.
Researcher QuestionsResearchers were asked three questions regarding their practices during the informedconsent process. First, researchers were asked to select from a list the strategies they usedduring the informed consent process: (a) one-on-one discussion between the investigator andpotential participants, (b) reading the informed consent form to potential participants, (c)conducting a group discussion with potential participants, (d) enabling potential participantsto talk to a current participant in the study, (e) developing an interactive computer programfor potential participants, (f) enabling potential participants to have more than one meetingto discuss the study, (g) enabling potential participants to watch a video and have a one-on-one conversation afterwards, (h) giving potential participants information to take home andread on their own, (i) allowing potential participants to bring a friend or family member withthem for the introduction to the study, and (j) other strategies.
A second question asked researchers what strategies they used to increase participants’understanding of the informed consent document: (a) use of simple language, (b) use ofpictures and illustrations, (c) use of a question and answer format, (d) use of large print inthe document, and (e) inclusion of a brief summary at the end of each section of thedocument.
Finally, researchers were asked to select which practices they used to determine potentialparticipants’ understanding during the informed consent process: (a) teach back (participantexplains the study in his/her own words), (b) participant completes a questionnaire/surveyon study knowledge at the end of the informed consent process, (c) investigator asksparticipant open-ended questions at the end of the informed consent process, (d) participantsigns/initials every page of the informed consent form, (e) use of an independent monitor(who observes the informed consent process), and (f) other. Participants were invited toprovide a verbatim response under the “other” category.
Community ParticipantsA U.S. national telephone survey was conducted by ICF-MACRO from June to December2010 with 2,455 African American and Latino participants. Prospective participants wererandomly selected based on U.S. telephone exchanges associated with geographic areas ofhigh concentrations of African Americans and Latinos. To identify the appropriateexchanges, directory-listed telephone numbers were mapped and assigned to a specificgeographic location (census block group, census tract, or zip code), and those exchangeswith an estimated concentration of African Americans and Latinos of at least 40% wereused. The overall response rate was 20.3%, which is consistent with response rates fromother current random-digit-dial surveys (California Health Interview Survey, 2009; Sellars etal., 2010).
Demographic variables included: race, ethnicity, gender, age, education, marital status,income, health insurance, health status, and perceived socio-economic position (SEP). Forthe purposes of analysis, education was collapsed into two levels: below college and college
Quinn et al. Page 4
J Empir Res Hum Res Ethics. Author manuscript; available in PMC 2013 June 18.
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript

or above; marital status was collapsed into two levels: married or living with a partner andother; and income was categorized into three levels: (1) below $36,000, (2) $36,000 to$76,000, and (3) above $76,000. Participants were also asked if they had health insurance(yes/no). The participants rated their health status on a 5-point Likert scale (1 = poor to 5 =excellent). Based on the MacArthur scale of socio-economic status (University of California,San Francisco, 2008), participants were asked about their socio-economic position (SEP):“Think of a ladder with 10 steps as representing where people stand in the U.S.; what stepwould you place yourself on the ladder?” and to indicate their SEP on a 10-point Likertscale, from 1 = people who are the worst off to 10 = people who are the best off.
Community Participant QuestionsThe community participants were asked several questions about research and informedconsent. The first question was directly linked to the first question for researchers, askinghow helpful each item would be in learning about a study: (a) going over the informedconsent for the study in a one-on-one discussion with the researchers, (b) being able to takeinformation home and read it on one’s own, (c) being allowed to have a family member orfriend present during the introduction to the study, (d) talking to someone who isparticipating in the study, (e) taking part in a group discussion about the study, (f) watchinga video about the study, (g) using an interactive game that provides information about thestudy on the computer, (h) having someone read the informed consent document to theparticipant, and (i) being able to have more than one meeting to discuss the study. The itemswere measured on a 3-point Likert scale (1 = not helpful at all to 3 = very helpful).
A second question linked to a researcher question asked the community members theirpreferences for learning about a study: (a) using plain language, (b) using pictures andillustrations, (c) using a question and answer format, (d) using large print in the document,and (e) having a brief summary at the end of each section of the document. The items weremeasured on a 3-point Likert scale (1 = not helpful at all to 3 = very helpful).
Community respondents were also asked about their knowledge of common researchterminology with these true/false questions: (a) in a study that is confidential, your personalinformation is made public, (b) a double-blind study means that both you and the researcherwill not know what treatment or drug you are receiving, (c) in a study that is anonymous noone will ask you for personal information such as your name or address, (d) in a study wherethe participants receive a placebo that means you will be getting a fake treatment, like asugar pill, (e) when you agree to participate in a randomized research study that means youhave a 50% chance of being assigned to the treatment, and (f) research that involves needlesor incisions into your body is an example of a non-invasive study.
Finally, the community respondents were asked about their understanding of what it meanswhen they sign the consent form: (a) I understand the study and agree to be a part of it, (b) Ino longer have the right to sue if something goes wrong, (c) the researchers or institution areprotected from a lawsuit if something goes wrong, and (d) I am protected as a researchparticipant. This item was measured on 4-point Likert scale (1 = strongly disagree to 4 =strongly agree).
Analyses and ApprovalsDescriptive statistics (mean, standard deviation), frequencies, and cross-tabulations wereperformed on the variables using STATA 11.2. Both surveys were approved by theUniversity of Pittsburgh Institutional Review Board.
Quinn et al. Page 5
J Empir Res Hum Res Ethics. Author manuscript; available in PMC 2013 June 18.
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript

ResultsSocio-demographic Measures
RESEARCHERS—A total of 347 respondents with a primary or secondary role as aresearcher participated in the survey—130 PIs/co-Is (37.5%), 149 research staff (42.9%),and 68 IRB members (19.6%). Throughout this article, we refer to this group as researchers.Sixty-one percent (61%) were Caucasian, 18% African American, and 12% Latino. Theadditional 9% of respondents were grouped as “other”, and included Asians, NativeAmericans, other races, and missing race. These participants were excluded from furtheranalysis because the sample sizes were insufficient to analyze each group separately and yetcombining them would ignore the heterogeneity of the groups and would lead to an averageeffect that was not reflective of any one group. Seventy-nine percent were female and themean age was 46.8 years (SD = 11.8). Over 76% (265 of 347) completed the survey, whichis comparable to completion rates in other online surveys (Fricker et al., 2005; Galesic &Bosnjak, 2009). Most importantly, there was no significant difference between participantswho completed and did not complete the survey by investigator type (PI/co-I, research staff,IRB), race, or gender. Of the participants who completed the survey, 42.9% had six or moreyears of federally funded grants versus only 25.9% of participants who did not complete thesurvey (χ2(1) = 7.50, p = .006, Cramer’s V = .148). The participants had been involved withresearch for an average of 14 years (SD = 9.1). There was a significant association betweenrace and type of investigator (χ2(6) = 13.16, p = .041, Cramer’s V = .139). PIs/co-Is andIRB members were more likely to be white (62% and 69%, respectively) than research staff(53%).
COMMUNITY RESPONDENTS—Of the 2,455 total respondents, 48.5% were AfricanAmericans and 51.5% were Latinos. The majority were female, high school or collegeeducated, with health insurance (Table 1). For descriptive purposes, we report the rawresults, though we collapse these categories for further analysis. African Americans andLatinos were similar on the demographic measures, with the exceptions that the AfricanAmerican respondents were significantly older than the Latino participants (53.3 vs. 46.7, p< .001) and that a higher proportion of the Latinos were married compared to the AfricanAmericans respondents (46.5% vs. 32.3%, χ2(1) = 69.94, p < .001, Cramer’s V = .170).
Researcher ResponsesTo teach participants about a study, researchers used the following: going over the consentform one-on-one (78.0%), allowing information to be taken home (77.0%), having someoneread the consent form aloud (65.1%), allowing a family member to be present (63.1%),allowing more than one meeting (58.5%), having small group discussions (42.1%),providing the opportunity for participants to talk with a current study participant (27.4%),watching videos (18.3%), and using interactive games (8.7%). Graphical representation ofthese results can be found in Figure 1.
Researchers’ use of different formats in the informed consent document is shown in Figure2. Nearly all the researchers (97.1%) reported that they used plain language in theirinformed consent document. Over 51% reported the use of question and answer format,41.4% used pictures and illustrations, 38.5% used large print, and 19.3% incorporated abrief summary at the end of each section.
To determine potential participants’ understanding of the informed consent process,researchers asked participants open-ended questions at the end (52.2%), had participantssign/initial every page of the informed consent form (51.5%), used teach-backs (38.0%),used an independent monitor (11.2%), and had participants complete a questionnaire or
Quinn et al. Page 6
J Empir Res Hum Res Ethics. Author manuscript; available in PMC 2013 June 18.
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript

survey about the study (10.1%). Fewer than 10% of researchers (7.3%) indicated they usedanother method to assess understanding by checking the “other” category. Researchers whochecked “other” were given the opportunity to specify what methods they used through awrite-in response. Themes identified from these verbatim responses included: use of open-ended questions, asking participants to complete a questionnaire or survey, and allowingparticipants to ask questions. Additionally, 32% of researchers did not use any methods toassess understanding, and 25% used only one of the methods. Overall, researchers used anaverage of 1.4 methods (out of six) to assess participant comprehension.
Community Participant ResponsesCommunity participants indicated that their top four preferred ways to learn about a studywere: having a one-on-one discussion with the researcher, being able to take informationhome, being able to have more than one meeting, and talking to a study participant (Table2). Community members’ top three preferences for formats in the informed consentdocument were: plain language, pictures and illustrations, and brief summaries (Table 2).There were no significant differences between African Americans and Latinos. These resultsare also represented in Figures 1 and 2, alongside the researchers’ use of the methods forteaching about a study and formats used in the consent document.
Results from the knowledge questions posed to the community participants about commonterms used in informed consent documents are shown in Table 3. Again, there were nosignificant differences between African Americans and Latinos.
When asked what a signature on the consent form means, the majority of both the AfricanAmerican (84%) and Latino (85%) respondents agreed or strongly agreed that it meant theyunderstood and agreed to participate. Sixty-two percent (62%) of African Americans and56% of Latinos believed their signature meant that they could not sue the researchinstitution, and 50% of African Americans and 56% of Latinos believed that the formprotected the researcher and institution. Sixty-eight percent (68%) of African Americans andonly 52% of Latinos thought that signing the consent form meant they were protected asresearch participants.
DiscussionAsking both researchers and community participants similar questions about their practicesand preferences during the informed consent process allowed us to identify three key areasof discordance that can be targeted to improve the informed consent process: (1) ways tolearn about a study that are preferred by community members but are not frequently used byresearchers, (2) strategies used by researchers to help potential participants understand astudy that are not viewed as helpful by the community members, and (3) formats for theinformed consent document that are preferred by the community members but are notfrequently used by researchers. We utilize our results, along with the published literature, tooffer guidance to researchers to improve the informed consent process in two distinct ways:(1) increasing participants’ satisfaction by incorporating those practices identified by thecommunity respondents as useful and preferred, and (2) increasing comprehension byincorporating more effective methods. In some cases, these practices will be the same, whilein others, a combination of methods may be used to accomplish both goals.
The first important discrepancy is in methods preferred by community respondents forlearning about a study. Although the top two methods preferred by community memberswere also the two most often used by researchers (going over the consent form one-on-oneand taking the information home), the next two most preferred methods of the communityrespondents (being able to have more than one meeting and talking to someone who is
Quinn et al. Page 7
J Empir Res Hum Res Ethics. Author manuscript; available in PMC 2013 June 18.
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript

currently participating in the study) are less commonly used by researchers. Althoughincorporating these methods may not always be practical due to confidentiality, time, orlogistical constraints, researchers should consider designing multiple meetings into theinformed consent process or providing access to current participants when possible.Additionally, incorporating these preferences may increase comprehension by allowingmore one-on-one discussion, either with the researcher or with study participants and mayincrease participants’ understanding and satisfaction with the process.
Researchers might also take note of some of their commonly used practices that are rankedas less helpful by the community members. These practices include allowing a familymember to be present and having someone read the informed consent document to theparticipant (used by 63.1 and 65.1% of researchers, respectively), yet were ranked in thebottom three in terms of helpfulness by community members responses, and wereconsidered less helpful than group discussion and watching a video. Though videos have notshown a clear impact on comprehension, face-to face interaction may be one of the moreeffective ways to deliver information, and therefore, group discussion is likely to beeffective in increasing comprehension. Thus researchers might consider integrating groupdiscussions as a way to increase both participant comprehension and satisfaction.
In the consent document itself, the top method (use of plain language) preferred bycommunity respondents was also the most frequently used by researchers (97.1%).However, the community respondents’ preferences for a brief summary at the end of eachsection, the use of pictures and illustrations, and the use of large font were less frequentlyused by researchers. Although Flory and Emanuel (2004) did not find incorporating theseformats into the consent document to be effective in increasing comprehension, additionalstudies show that patients are more satisfied with simpler consent forms (Coyne et al., 2003;Davis et al., 1998) and the use of video (Philippe et al., 2006). Therefore, we suggestresearchers consider incorporating formats the community respondents preferred, such aslarge font, summaries, and illustrations to increase participant satisfaction.
Our results also indicate areas where there is a good match between community members’preferences, researchers’ practices, and effective methods for increasing comprehension.The two methods of learning about a research study most preferred by the communityrespondents (ability to take information home and one-on-one discussion with theresearcher) were also the two methods most often used by researchers. These methods arealso likely to be among the most effective in ensuring comprehension. One-on-onediscussions and extended or multiple conversations about a study have been shown toincrease understanding in several studies (Flory & Emanuel, 2004), and the ability to takeinformation home can allow participants ample time to read, process, absorb the material,and potentially discuss the study with family members. This could be useful for thoseparticipants for whom the decision to participate in a research study is a collective decisionwithin the family.
Additionally, there is concordance between researchers’ practices and preferences of thecommunity respondents on the use of plain language within the consent document. The issueof comprehension during the informed consent process is complex, however, and we raisethe question of whether the use of plain language is as widespread as it is reported byresearchers. Our doubt about researchers’ use of plain language is also founded in Paasche-Orlow, Taylor, and Brancati’s study (2003), which found that sample informed consent textfrom 114 medical school websites was written at a mean grade level of 10.6, though nearlyhalf of all Americans read at or below the eighth grade level. Other relevant studies havefound that study participants, and minority participants in particular, continue to showincomplete comprehension of the study information and are misinformed about the purpose
Quinn et al. Page 8
J Empir Res Hum Res Ethics. Author manuscript; available in PMC 2013 June 18.
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript

of the informed consent process (Corbie-Smith et al., 2002; Flory & Emanuel, 2004;Freimuth et al., 2001; Penman et al., 1984).
In fact, the results from our study support previous reports of low comprehension ormisunderstanding of information provided during the informed consent process and limitedknowledge of general research terms. Our results showed that the community participantswere unfamiliar with several key terms used in clinical trials and were often misinformedabout the purpose of their signature on the consent document as well as with the overallinformed consent process.
Clearly, researchers’ assessment of participants’ understanding is critical to ensure that aparticipant is capable of making an informed, voluntary decision to participate. In oursurvey, some of the methods (open-ended questions and teach-back) may be particularlyuseful to assess participant’s consent capacity and comprehension of the information given,and to increase understanding as the assessment continues. Discussion and teach-backmethods are recognized by many adult learning programs as the most effective ways ofincreasing retention of new information and are consistent with the one-on-one methods ofinteraction identified by Flory and Emanuel (2004) and Cohn and Larson (2007) forenhancing understanding. Additionally, the U.S. Department of Health and Human Servicessuggests the use of independent monitors to ensure that the consent process is adequate andeffective (U.S. Department of Health and Human Services, 2012).
Most startling, however, was that 32% of researchers reported that they used no methods toassess comprehension, and 25% used only one of the methods. For those researchers usingopen-ended questions and teach-back to assess understanding, using only one method maybe sufficient. For the 50% of researchers who asked participants to sign or initial every page,there is a greater need to incorporate some other measure of comprehension, as signing doesnot give the investigator any indication of whether or not the participant understood theconsent document. Use of effective methods to assess comprehension can assure theresearcher that a potential study participant is adequately informed about the study.
Limitations of This StudyA limitation of this study is that the community member responses may not be generalizableto all African Americans and Latinos, as we focused our recruitment efforts on those livingin predominantly minority communities. However, with a strong national sample, we areconfident in our overarching recommendation that the informed consent process incorporatethoughtful and respectful consideration of a participant’s current knowledge and culturalcontext, and an extended and ongoing dialogue to ensure that the participant is informedabout the study. The researcher survey is limited in that it is a convenient, nonrepresentativesample for which we cannot calculate a response rate.
Overall, this study offers a unique look at the informed consent process from the viewpointsof both researchers and African American and Latino community members, identifyingareas of discordance between researchers’ practices and community members’ preferences.The community respondents’ results on the knowledge portion of the survey and theirinterpretation of the consent document speaks to the need for improving the informedconsent process so that study participants fully understand the nature of the study and theirrights as participants.
Best PracticesImproving the informed consent process should include a combination of incorporatingmethods to increase community members’ satisfaction with effective methods for increasing
Quinn et al. Page 9
J Empir Res Hum Res Ethics. Author manuscript; available in PMC 2013 June 18.
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript

comprehension of the material. These methods include: taking study information home, one-on-one discussion, more than one meeting, talking to another study participant, and to alesser degree, group discussions and videos.
Within the consent document, we recommend the use of plain language, inclusion ofsummaries, and use of pictures and illustrations. The U.S. government describes plainlanguage as communication that is understood the first time it is seen or heard, describing itas “easy to read, understand, and use” (Federal Plain Language Guidelines, March 2011). Byrevisiting the plain language guidelines (http://www.plainlanguage.gov/howto/quickreference/checklist.cfm) and utilizing readability assessments, researchers can ensurethat both their written and verbal communication is delivered at a level and in a manner thatis appropriate to their audience. One respondent in our survey commented that his IRB didnot allow many modifications to the consent document that might make it easier to read.This may not be an uncommon challenge. We recommend working with the IRB to allowmore tailoring of consent documents to enhance their appropriateness, and if these changesare not allowed, then expanding the verbal portion of the consent process to allow for extratime to discuss the study, remembering that the document itself is just one part of the overallprocess.
We also emphasize encouraging one-on-one interactions through the use of multiplemeetings or, when appropriate, with current study participants. We also suggest thatresearchers consider cultural factors when designing the informed consent process for thestudy, such as allowing material to be brought home, or involving family members. Finally,we suggest that within the research team, they may consider utilizing evaluation tools todetermine the effectiveness of different methods or conducting qualitative interviews withparticipants to ascertain their assessment of the informed consent process.
Of critical importance is that, ultimately, the research team should conduct its own formativeresearch prior to beginning the informed consent process to fully understand the participantsthey are seeking to recruit and to tailor the strategies and language used in the informedprocess to their local needs. Along with formative research, a grasp of best practices fromthe current literature, and evaluation of the informed consent process throughout therecruitment phase of the study, will enable research teams to create the strongest and mosteffective process for their study.
Research AgendaFuture studies are necessary to continue to evaluate the informed consent process, andspecifically what methods can be used to improved comprehension of study information.Further investigation into what factors contribute to higher levels of comprehension andwhat methods of assessing comprehension are being used could help to determine the mosteffective means of conveying information to potential study participants.
There is an important need for additional studies that focus on whether there are differencesin the quality of the information delivery during the informed consent process betweenminority and nonminority participants. Simon and Kodish (2005) found that minoritywomen received less information than their white counterparts during the informed consentprocess. Furthermore, there is no substantial body of published research to date thatexamines the extent to which the interaction between the race, ethnicity, or gender of theresearcher and that of the potential participant shapes the informed consent process.
Quinn et al. Page 10
J Empir Res Hum Res Ethics. Author manuscript; available in PMC 2013 June 18.
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
Educational ImplicationsOur results suggest several educational needs for researchers, research staff, and IRB staff.First, educational programs can focus specifically on guidance about how consent processesmay be improved, including the implications of the results from this study on effectivestrategies to increase comprehension of study materials, and preferred methods deemedhelpful by minority participants. Secondly, educational efforts can focus on the use ofreadability assessments and plain language guidelines to strengthen informed consentdocuments. Some resources for investigators on informed consent are provided by the U.S.Department of Health and Human Services, and can be found at: http://www.hhs.gov/ohrp/policy/consentckls.html, http://www.hhs.gov/ohrp/policy/ic-non-e.html, and http://aspe.hhs.gov/sp/nbac/appendixc.shtml.
Finally, it may be particularly important to create educational initiatives that enableresearchers to become more culturally confident and committed to self-reflect and critiqueover one’s lifespan. Thomas et al. (2011, p. 411) describe the importance of culturalconfidence in researchers, defining it as “a lifelong process based on the individual’s self-reflection about their personal biases and prejudices. We define a culturally confidentperson as someone who is flexible and humble enough to admit ignorance and is willing tobe uncomfortable addressing complex racialized issues.” In our Building Trust betweenMinorities and Researchers: A Bioethics Research Infrastructure Initiative, we havedeveloped a curriculum for researchers, Becoming a Self-Reflective Researcher:Successfully Engaging Minority Communities, which includes video vignettes forenhancing the informed consent conversation and process with minority participants (seewww.healthequity.umd.edu for further details). Participation in such an educational programcan increase researchers’ understanding of how the impact of their own conscious andunconscious biases may shape their interaction with minorities during the informed consentprocess, and they can learn new strategies for strengthening communication withparticipants from whom they may differ by race, ethnicity, or class.
AcknowledgmentsWe thank Greg Masters, our research assistant, for his contributions to our literature review, and our partners atPublic Responsibility in Medicine and Research, especially Amy Davis and Joan Rachlin. This work was supportedby Award Number 7RC2MD004766 (PIs, S. Quinn and S. Thomas) from the National Institute on Minority Healthand Health Disparities (NIMHD) and the Office of the Director, National Institutes of Health. Dr. James Butler IIIwas supported, in part, through his Mentored Career Development Award to Promote Diversity (K01CA134939).Dr. Craig S. Fryer was supported, in part, through his Mentored Research Scientist Development Award to PromoteDiversity (K01CA148789). Dr. Mary A. Garza was supported, in part, through her Mentored Research ScientistDevelopment Award to Promote Diversity (K01CA140358). The content is solely the responsibility of the authorsand does not necessarily represent the official views of the NIMHD or the National Institutes of Health.
ReferencesArd JD, Durant RW, Edwards LC, Svetkey LP. Perceptions of African-American culture and
implications for clinical trial design. Ethnicity and Disease. 2005; 15(2):292–299. [PubMed:15825976]
Barrett R. Quality of informed consent: Measuring understanding among participants in oncologyclinical trials. Oncology Nursing Forum. 2005; 32(4):751–755. [PubMed: 15990904]
California Health Interview Survey.. CHIS 2007 methodology series: Report 4—response rates. LosAngeles: UCLA Center for Health Policy Research; 2009.
Cohn E, Larson E. Improving participant comprehension in the informed consent process. Journal ofNursing Scholarship. 2007; 39(3):273–280. [PubMed: 17760802]
Corbie-Smith G, Thomas SB, St George DM. Distrust, race, and research. Archives of InternalMedicine. 2002; 162(21):2458–2463. [PubMed: 12437405]
Quinn et al. Page 11
J Empir Res Hum Res Ethics. Author manuscript; available in PMC 2013 June 18.
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript

Corbie-Smith G, Thomas SB, Williams MV, Moody-Ayers S. Attitudes and beliefs of AfricanAmericans toward participation in medical research. Journal of General Internal Medicine. 1999;14(9):537–546. [PubMed: 10491242]
Cortes DE, Drainoni ML, Henault LE, Paasche-Orlow MK. How to achieve informed consent forresearch from Spanish-speaking individuals with low literacy: A qualitative report. Journal ofHealth Communication. 2010; 15(Suppl 2):172–182. [PubMed: 20845202]
Coyne CA, Xu R, Raich P, Plomer K, Dignan M, Wenzel LB, et al. Randomized, controlled trial of aneasy-to-read informed consent statement for clinical trial participation: A study of the EasternCooperative Oncology Group. Journal of Clinical Oncology. 2003; 21(5):836–842. [PubMed:12610182]
Criscione LG, Sugarman J, Sanders L, Pisetsky DS, St Clair EW. Informed consent in a clinical trial ofa novel treatment for rheumatoid arthritis. Arthritis and Rheumatism. 2003; 49(3):361–367.[PubMed: 12794792]
Davis TC, Holcombe RF, Berkel HJ, Pramanik S, Divers SG. Informed consent for clinical trials: Acomparative study of standard versus simplified forms. Journal of the National Cancer Institute.1998; 90(9):668–674. [PubMed: 9586663]
Dunlop AL, Leroy ZC, Logue KM, Glanz K, Dunlop BW. Preconsent education about researchprocesses improved African Americans’ willingness to participate in clinical research. Journal ofClinical Epidemiology. 2011; 64(8):872–877. [PubMed: 21330104]
Eder ML, Yamokoski AD, Wittmann PW, Kodish ED. Improving informed consent: Suggestions fromparents of children with leukemia. Pediatrics. 2007; 119(4):e849–859. [PubMed: 17403829]
Farmer DF, Jackson SA, Camacho F, Hall MA. Attitudes of African American and low socioeconomicstatus white women toward medical research. Journal of Health Care for the Poor andUnderserved. 2007; 18(1):85–99. [PubMed: 17337800]
Federal Plain Language Guidelines. Federal plain language guidelines. 2011. Retrieved from http://www.plainlanguage.gov/howto/quickreference/checklist.cfm
Flory J, Emanuel E. Interventions to improve research participants’ understanding in informed consentfor research: A systematic review. Journal of the American Medical Association. 2004; 292(13):1593–1601. [PubMed: 15467062]
Freimuth VS, Quinn SC, Thomas SB, Cole G, Zook E, Duncan T. African Americans’ views onresearch and the Tuskegee Syphilis Study. Social Science and Medicine. 2001; 52(5):797–808.[PubMed: 11218181]
Fricker S, Galesic M, Tourangeau R, Yan T. An experimental comparison of web and telephonesurveys. Public Opinion Quarterly. 2005; 69(3):370–392.
Galesic M, Bosnjak M. Effects of questionnaire length on participation and indicators of responsequality in a web survey. Public Opinion Quarterly. 2009; 73(2):349–360.
Joffe S, Cook EF, Cleary PD, Clark JW, Weeks JC. Quality of informed consent in cancer clinicaltrials: A cross-sectional survey. Lancet. 2001; 358(9295):1772–1777. [PubMed: 11734235]
Lakes KD, Vaughan E, Jones M, Burke W, Baker D, Swanson JM. Diverse perceptions of theinformed consent process: Implications for the recruitment and participation of diversecommunities in the National Children’s Study. American Journal of Community Psychology.2012; 49(1–2):215–232. [PubMed: 21671109]
Paasche-Orlow MK, Taylor HA, Brancati FL. Readability standards for informed-consent forms ascompared with actual readability. New England Journal of Medicine. 2003; 348(8):721–726.[PubMed: 12594317]
Penman DT, Holland JC, Bahna GF, Morrow G, Schmale AH, Derogatis LR, et al. Informed consentfor investigational chemotherapy: Patients’ and physicians’ perceptions. Journal of ClinicalOncology. 1984; 2(7):849–855. [PubMed: 6737023]
Philippe F, Meney M, Larrazet F, Ben Abderrazak F, Dibie A, Meziane T, et al. Effects of videoinformation in patients undergoing coronary angiography. Archives des Maladies du Coeur et desVaisseaux. 2006; 99(2):95–101. [PubMed: 16555691]
Ryan RE, Prictor MJ, McLaughlin KJ, Hill SJ. Audio-visual presentation of information for informedconsent for participation in clinical trials. Cochrane Database of Systematic Review. 2008;1:Article No. CD003717.
Quinn et al. Page 12
J Empir Res Hum Res Ethics. Author manuscript; available in PMC 2013 June 18.
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript

Sellars B, Garza MA, Fryer CS, Thomas SB. Utilization of health care services and willingness toparticipate in future medical research: The role of race and social support. Journal of the NationalMedical Association. 2010; 102(9):776–786. [PubMed: 20922921]
Simon CM, Kodish ED. “Step into my zapatos, doc”: Understanding and reducing communicationdisparities in the multicultural informed consent setting. Perspectives in Biology and Medicine.2005; 48(1 Suppl):S123–138. [PubMed: 15842091]
Sudore RL, Landefeld CS, Williams BA, Barnes DE, Lindquist K, Schillinger D. Use of a modifiedinformed consent process among vulnerable patients: A descriptive study. Journal of GeneralInternal Medicine. 2006; 21(8):867–873. [PubMed: 16881949]
Thomas SB, Quinn SC, Butler J, Fryer CS, Garza MA. Toward a fourth generation of disparitiesresearch to achieve health equity. Annual Review of Public Health. 2011; 32:399–416.
Thorne B. “You still takin’ notes?” Fieldwork and problems of informed consent. Social Problems.1980; 27(3):284–297.
University of California, San Francisco. The John D and Katherine T MacArthur Foundation, ResearchNetwork on SES & Health. 2008. Retrieved from http://www.macses.ucsf.edu/research/psychosocial/usladder.php
U.S. Department of Health and Human Services. Code of Federal Regulations, Title 45 PublicWelfare, Department of Health and Human Services Part 46, Protection of Human Subjects. 2009.Retrieved from http://www.hhs.gov/ohrp/humansubjects/guidance/45cfr46.html#46.117
U.S. Department of Health and Human Services. Analysis and proposed actions regarding the NBACReport: Research involving persons with mental disorders that may affect decision makingcapacity, Appendix C. Prepared by HHS Working Group on the NBAC Report. 2012. Retrievedfrom http://aspe.hhs.gov/sp/nbac/appendixc.shtml
BiographiesSandra Crouse Quinn is Associate Dean for Public Health Initiatives, Professor in theDepartment of Family Science, and Senior Associate Director of the Center for HealthEquity at the School of Public Health, University of Maryland at College Park. She led theconceptualization and preparation of this manuscript and leads the development of thecurriculum components that are addressed in this article.
Mary A. Garza is Assistant Professor in the Department of Behavioral and CommunityHealth and an Associate Director for the Maryland Center for Health Equity. She has over15 years of community-engaged research experience with racial and ethnic minorities. Sheparticipated in the conceptualization and preparation of this manuscript, includinginterpretation of data.
Craig S. Fryer is Assistant Professor of Behavioral and Community Health and AssociateDirector of the Maryland Center for Health Equity at the University of Maryland, School ofPublic Health. He made important contributions to the development of the IRB protocols,the collection and interpretation of data, the development of the Building Trust curriculum,as well as the review and editing of this manuscript.
James Butler III is Assistant Professor of Behavioral and Community Health and anAssociate Director of the Maryland Center for Health Equity at the University of Maryland,School of Public Health. He focuses on the design, implementation, and evaluation ofrandomized smoking cessation clinical trials with a community-based interventioncomponent. He made key contributions to the preparation of this manuscript by providingfeedback on drafts.
Quinn et al. Page 13
J Empir Res Hum Res Ethics. Author manuscript; available in PMC 2013 June 18.
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript

David Barnard is Professor of Medicine and Law at the University of Pittsburgh. Hecontributed to the collection and interpretation of the data and the writing, review, andediting of this manuscript.
Erica T. Casper is a science writer and editor at the Maryland Center for Health Equity atthe University of Maryland, School of Public Health. As a member of the Building Trustteam, Ms. Casper has contributed to the interpretation of data and the writing of all parts ofthis manuscript.
Kevin H. Kim is Associate Professor in the Research Methodology program at theUniversity of Pittsburgh School of Education. He performed the analyses and madecontributions to the methods and results sections of the manuscript.
Stephen B. Thomas is an internationally recognized, African American leader in minorityhealth research and community engagement and has been a lead investigator of multiplestudies investigating racial differences in health outcomes. He participated in all aspects ofthe design and implementation of the study as well as the data analysis and development ofthe manuscript.
Quinn et al. Page 14
J Empir Res Hum Res Ethics. Author manuscript; available in PMC 2013 June 18.
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript

FIGURE 1.Comparison of researchers’ use of different practices during the informed consent processwith community members’ views on the helpfulness of each practice. Black bars show thepercentage of researchers who use each item, and the white bars show the percentage of thecommunity respondents who felt each item was “very helpful” in learning about a study.African American and Latino responses were combined into a single percentage as therewere no significant differences between the two groups.
Quinn et al. Page 15
J Empir Res Hum Res Ethics. Author manuscript; available in PMC 2013 June 18.
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
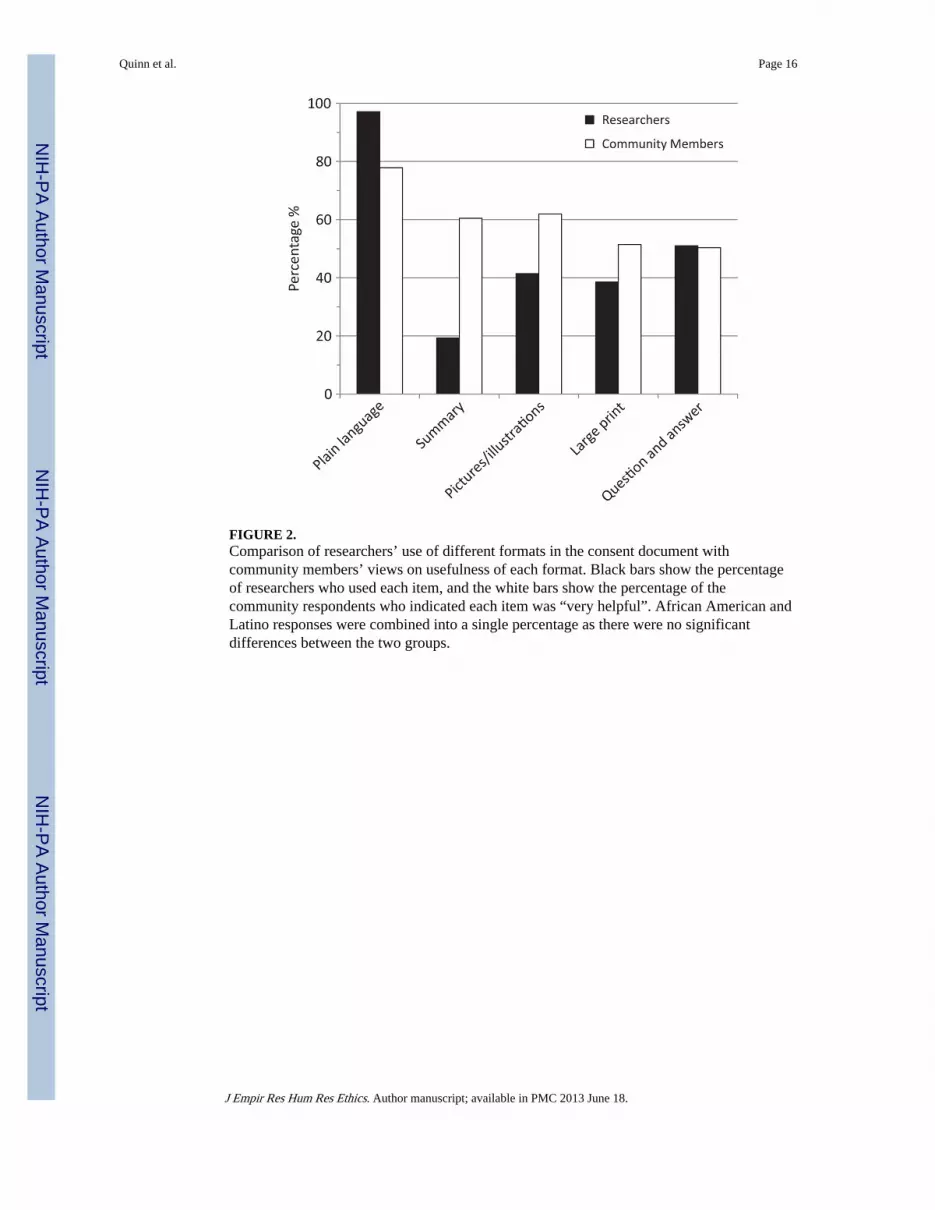
FIGURE 2.Comparison of researchers’ use of different formats in the consent document withcommunity members’ views on usefulness of each format. Black bars show the percentageof researchers who used each item, and the white bars show the percentage of thecommunity respondents who indicated each item was “very helpful”. African American andLatino responses were combined into a single percentage as there were no significantdifferences between the two groups.
Quinn et al. Page 16
J Empir Res Hum Res Ethics. Author manuscript; available in PMC 2013 June 18.
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript

NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
Quinn et al. Page 17
TAB
LE 1
Dem
ogra
phic
s by
Rac
e of
the
Com
mun
ity P
artic
ipan
ts.
Afr
ican
Am
eric
ans
Lat
inos
χ2
pC
ram
er’s
V
Gen
der
7.55
.006
.056
Mal
e32
.2%
37.5
%
Fem
ale
67.8
%62
.5%
Edu
catio
n56
.91
<.0
01.1
53
Ele
men
tary
sch
ool
6.2%
12.4
%
Hig
h sc
hool
34.7
%38
.8%
Col
lege
42.4
%35
.7%
Gra
duat
e sc
hool
13.2
%9.
2%
Tec
hnic
al s
choo
l3.
1%2.
2%
Oth
er0%
1.8%
Mar
ital S
tatu
s69
.94
<.0
01.1
70
Mar
ried
32.3
%46
.5%
Div
orce
d13
.9%
9.9%
Wid
owed
15.4
%8.
0%
Sepa
rate
d4.
5%3.
7%
Nev
er m
arri
ed16
.7%
15.2
%
Sing
le li
ving
w/p
artn
er17
.3%
16.7
%
Hea
lth In
sura
nce
27.3
4<
.001
.106
Yes
82.4
%73
.5%
No
17.7
%26
.5%
tp
Coh
en’s
d
Age
53.2
(18
.1)
46.7
(18
.2)
8.93
<.0
01.3
61
Perc
eive
d SE
S5.
5 (2
.1)
5.3
(2.0
)2.
30.0
11.0
95
Hea
lth S
tatu
s3.
1 (1
.1)
3.1
(1.1
)−
.62
.733
.025
J Empir Res Hum Res Ethics. Author manuscript; available in PMC 2013 June 18.

NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
Quinn et al. Page 18
TABLE 2
Rating by the Community Members of Different Methods and Formats Used to Facilitate Understanding ofthe Research Study during the Informed Consent Process.
African Americans Latinos
Cramer’s VVery helpful Very helpful
Strategies for Learning
Take-home information 70.9% 65.7% 0.055
One-on-one discussion 67.5% 69.8% 0.025
More than one meeting 64.7% 65.6% 0.009
Talking to someone who is participating 60.5% 64.3% 0.039
Group discussion 57.7% 59.3% 0.017
Video 57.0% 55.7% 0.014
Family member or friend in the discussion 53.3% 51.6% 0.016
Have someone read the informed consent form to the participant 34.7% 40.5% 0.059
Interactive game 33.8% 34.9% 0.011
Format
Plain language 78.8% 76.9% 0.023
Summary at the end of each section 60.7% 60.2% 0.005
Pictures and illustrations 60.3% 63.6% 0.035
Large print in the document 53.0% 49.8% 0.032
Question and answer format 50.3% 50.4% 0.000
J Empir Res Hum Res Ethics. Author manuscript; available in PMC 2013 June 18.

NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
Quinn et al. Page 19
TABLE 3
Percent Correct on the Community Participants’ Knowledge of Terms Used in Medical Research Studies.
African Americans Latinos
Cramer’s VCorrect Correct
Confidential 74.1% 75.5% .016
Anonymous 63.6% 65.3% .018
Placebo 59.4% 54.1% .053
Non-invasive study 57.9% 55.2% .027
Randomized research study 56.2% 54.1% .021
Double-blind study 47.1% 42.3% .049
J Empir Res Hum Res Ethics. Author manuscript; available in PMC 2013 June 18.