improvement toolkit (pdf)
TRANSCRIPT


#SPSPMeds2016
Improvement toolkitChair: Arvind Veiraiah

#SPSPMeds2016
OverviewTime Speaker Title
13:35-13:40Aravindan VeiraiahHealthcare Improvement Scotland
Introduction
13:40-13:55Paul Sammons, Nicola True and Margaret Marshall NHS Dumfries & Galloway
Reducing harm at transitions –an atypical collaboration with an effective outcome
13:55-14:10Carolyn SwiftNHS Lothian
Failure Modes and Effects Analysis (FMEA) in medicines management
14:10-14:40 Table top discussion and report back
Facilitator Ian Rudd

#SPSPMeds2016
Objectives
• Delegates will be introduced to other improvement methods and hear from frontline teams that have applied them in improvement projects related to medicines.

#SPSPMeds2016 @dg_improvers
Reducing harm at transitions –an atypical collaboration with an effective outcomeNicola True, Project ManagerMargaret Marshall, Project PharmacistPaul Sammons, Improvement Advisor

#SPSPMeds2016 @dg_improvers
The project – Improving reliability and accuracy of medicines reconciliation
• Funded for 18 months – Health Foundation - Safer Clinical Systems methodology with support from local Patient Safety team
• Dedicated Resources
– Project Manager + Pharmacist each 2 days a week
• DGRI Ward 16, all trauma orthopaedic patients
• Project Completion May 2016

#SPSPMeds2016 @dg_improvers
Pre 2015 - The challenge
• Medicines Reconciliation aka Reducing Harm at Transitions – SPSP priority since 2008 – not hearing of step change – no new paradigm
• Dependency on ever-changing resources – typically FY1’s
• Variation in quality
• Nurses not seeing how they contribute
• Inadequate pharmacy resources to ‘check up’

#SPSPMeds2016 @dg_improvers
Earlier project driven by Pharmacist Laura Graham
• Project in 2012 – prescribing errors in acute medical unit
• Key risk identified as Medicines Reconciliation
• Test of change commenced to develop e-Med Rec solution
• Great idea, but typical development cycle
– IT Development cycle slow to deliver
– FY1’s (user) input to development less than ideal

#SPSPMeds2016 @dg_improvers
Mid 2015 - New Approach – might this work?
• Look at quality of transition paperwork in detail
– Admission
– Stay
– Discharge
• Identify Tests of change
• Measure and play back results to practitioners

#SPSPMeds2016 @dg_improvers
Sept 2015 - Is it working?
• A number of small tests of change attempted
– Time saving
– Accessibility and availability of information
• Consistent data collection on high quality transition paperwork
• No significant improvement evident

#SPSPMeds2016 @dg_improvers
September 2015 - Re-focus on e-Med Rec
• Development work picked up and accelerated
• Involved FY1’s in system spec and testing
• eHealth developer, FY1 and project team together in the ward
• Rapid cycle development – multiple iterations (PDSA’s)
• So what?
– Enhanced engagement between key players
– They all felt engaged and motivated


#SPSPMeds2016 @dg_improvers
Reflecting the Data and modifying FY1 perceptions
• FY1 Training - focus on quality of written work at transitions
– Given back their own work (anonymised but handwritten)
– Asked to spot the obvious mistakes
– Interactive session - Highlighted human factors and error rate
– Outcome - Quality can actually be much improved
– Highlighted the criticality of the process and their effect on its quality
– NEXT UP – VIDEO JESS MCGINN

#SPSPMeds2016 @dg_improvers

A
D
M
I
S
S
I
O
N
E-MED REC

I
N
P
A
T
I
E
N
T

D
I
S
C
H
A
R
G
E

#SPSPMeds2016 @dg_improvers
How have got to this point? How do we keep it going?
• Understand extent of process – where it starts and where it ends
• Work with all stakeholders so they know the part that they play
• Engagement is key – transient FY1’s – eHealth engagement
• E-med rec will spread to remaining wards
• Induction and training for FY1’s must develop to include e-med rec as standard toolset
• Project has an end date. Must assign ownership


Failure Modes and Effects Analysis (FMEA) in medicines management
NHS Lothian
Carolyn Swift
Service Improvement Manager
(Improvement Advisor)

I’ve been asked to discuss…
• What is FMEA
• The benefits
• How we did it

What is FMEA?
A structured approach to:
• Identify the ways in which a process can fail
• Estimate risk associated with specific causes
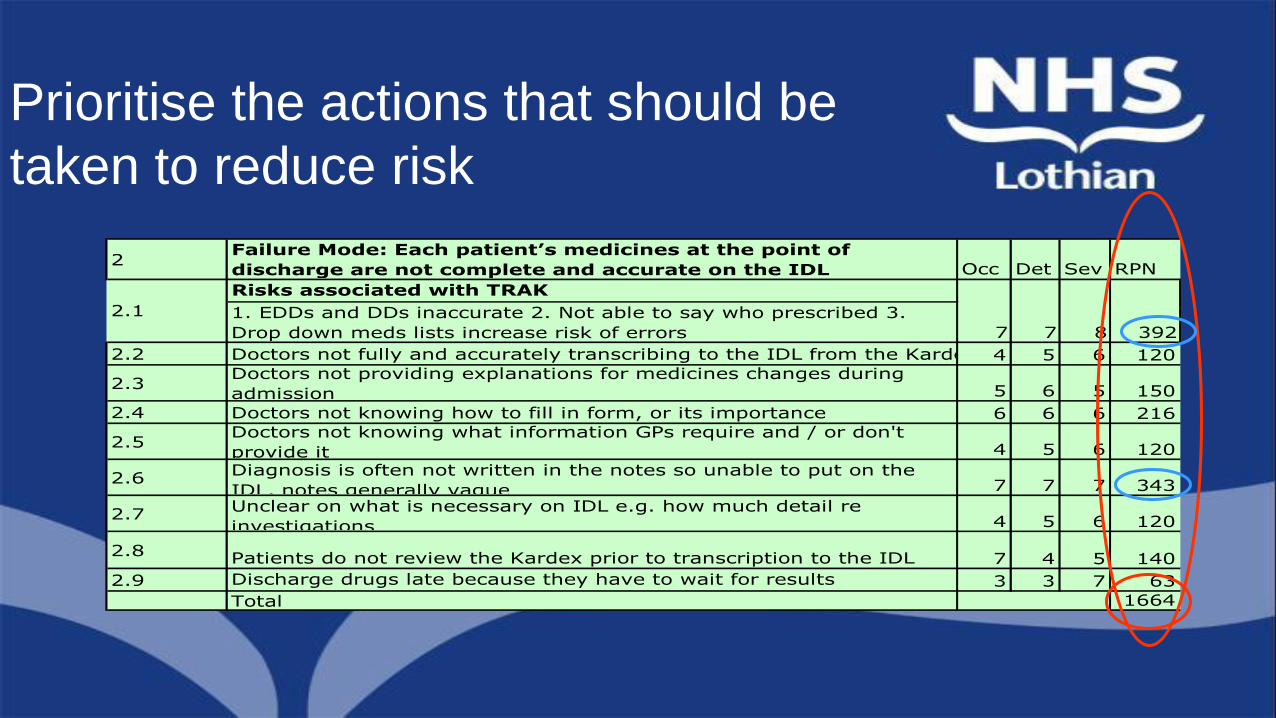
• Prioritise the actions that should be taken to reduce risk

Benefits of FMEA
Adapted from N Dixon (HQQ)
• Shift focus from following up to preventing errors
• Increase reliability of processes
• Learn staff’s point of view and change processes accordingly
• Increase communication, awareness and accountability about patient safety
• Learn how errors are multi-factorial
• Prevent management from allocating resources to safer parts of a process and invest in the most vulnerable parts
• Avoid the culture of automatically blaming or fault finding
• Cumulate evidence about failure modes

• Team members have to have interest, knowledge, skill and time
• FMEA can be seen as tedious to teams when they have to identify all potential failure modes
– FMEA method and leadership are needed
• Team members can expect an immediate fix
• Actions may vary in strength or may not be taken or there may be no follow up on actions
Recognised drawbacks
Adapted from N Dixon (HQQ)

TEAMExecutive Lead
ConsultantST5
PharmacistMedical Nurse PractitionerPatient Services Manager
FYs x 5 as placement allowedClinical Governance
First Steps

What is a Failure Mode?
A Failure Mode is:
• The way in which the component, product, or process could fail to perform its intended function
• Failure modes may be the result of upstream operations or may cause downstream operations to fail
• Things that could go wrongAdapted from R Lloyd (IHI)

Identifying Failure Modes
• Talk through what happens and what goes wrong
• Process Mapping- Deming: Quality Improvement is the Science of Process Management
- All productive work through process management and human input
• Fishbone diagram - identify causes that contribute to an outcome or result (effect) - analyses multiple potential causes (failure modes)
• Asking why five times – identify root cause(s) of a failure mode (particularly involving a sequence of actions, a process flow or a chain reaction)

Basic process mapping for medicines reconciliation
on admission

Basic process mapping for medicines reconciliation on discharge

The Driver Diagram

Timeline of activity and delays in IDLs being written, checked, to pharmacy and back to patients

Cause and Effect

Failure Mode Examples

2Failure Mode: Each patient’s medicines at the point of
discharge are not complete and accurate on the IDL Occ Det Sev RPN
Risks associated with TRAK
1. EDDs and DDs inaccurate 2. Not able to say who prescribed 3.
Drop down meds lists increase risk of errors
2.2 Doctors not fully and accurately transcribing to the IDL from the Kardex 4 5 6 120
2.3Doctors not providing explanations for medicines changes during
admission 5 6 5 150
2.4 Doctors not knowing how to fill in form, or its importance 6 6 6 216
2.5Doctors not knowing what information GPs require and / or don't
provide it 4 5 6 120
2.6Diagnosis is often not written in the notes so unable to put on the
IDL, notes generally vague 7 7 7 343
2.7Unclear on what is necessary on IDL e.g. how much detail re
investigations 4 5 6 120
2.8 Patients do not review the Kardex prior to transcription to the IDL 7 4 5 140
2.9 Discharge drugs late because they have to wait for results 3 3 7 63
Total 1664
7
2.1
7 3928
Med Rec

2Failure Mode: Each patient’s medicines at the point of
discharge are not complete and accurate on the IDL Occ Det Sev RPN
Risks associated with TRAK
1. EDDs and DDs inaccurate 2. Not able to say who prescribed 3.
Drop down meds lists increase risk of errors
2.2 Doctors not fully and accurately transcribing to the IDL from the Kardex 4 5 6 120
2.3Doctors not providing explanations for medicines changes during
admission 5 6 5 150
2.4 Doctors not knowing how to fill in form, or its importance 6 6 6 216
2.5Doctors not knowing what information GPs require and / or don't
provide it 4 5 6 120
2.6Diagnosis is often not written in the notes so unable to put on the
IDL, notes generally vague 7 7 7 343
2.7Unclear on what is necessary on IDL e.g. how much detail re
investigations 4 5 6 120
2.8 Patients do not review the Kardex prior to transcription to the IDL 7 4 5 140
2.9 Discharge drugs late because they have to wait for results 3 3 7 63
Total 1664
7
2.1
7 3928
Estimate risk associated with specific causes

A Risk Priority Number (RPN) was calculated:
The higher the RPN the higher the risk
Likelihood of event
occurring
Likelihood of Detection
Severity of harmX X
1 = not likely
10 = very likely
1 = likely to detect
10 = not likely to detect
1 = not severe
10 = very severe
2Failure Mode: Each patient’s medicines at the point of
discharge are not complete and accurate on the IDL Occ Det Sev RPN
Risks associated with TRAK
1. EDDs and DDs inaccurate 2. Not able to say who prescribed 3.
Drop down meds lists increase risk of errors
2.2 Doctors not fully and accurately transcribing to the IDL from the Kardex 4 5 6 120
2.3Doctors not providing explanations for medicines changes during
admission 5 6 5 150
2.4 Doctors not knowing how to fill in form, or its importance 6 6 6 216
2.5Doctors not knowing what information GPs require and / or don't
provide it 4 5 6 120
2.6Diagnosis is often not written in the notes so unable to put on the
IDL, notes generally vague 7 7 7 343
2.7Unclear on what is necessary on IDL e.g. how much detail re
investigations 4 5 6 120
2.8 Patients do not review the Kardex prior to transcription to the IDL 7 4 5 140
2.9 Discharge drugs late because they have to wait for results 3 3 7 63
Total 1664
7
2.1
7 3928
Prioritise the actions that should be
taken to reduce risk

Excel TabWARD: 25 SJH
Occ Det Sev RPN Occ Det Sev RPN Occ Det Sev RPN Occ Det Sev RPN
1.1 Fewer than 2 sources of information are used 8 7 8 448 8 7 8 448 8 7 8 448 8 7 8 448
1.2 Doctors not taking responsibility for completion of form 6 6 5 180 6 6 5 180 6 6 5 180 6 6 5 180
1.3 Doctors not knowing how to fill in form, or its importance 6 6 6 216 6 6 6 216 6 6 6 216 6 6 6 216
1.4 Changes to original list are not documented 7 5 7 245 7 5 7 245 7 5 7 245 6 4 7 168
1.5 Some meds may be a guess e.g. EC v Dispersible, some a judgment 5 5 5 125 5 5 5 125 5 5 5 125 5 5 5 125
1.6Patients are not aware of the importance of providing accurate
information 5 6 5 150 5 6 5 150 5 6 5 150 5 6 5 150
1364 1364 1364 1287
Risks associated with TRAK
2.11. EDDs and DDs inaccurate 2. Not able to say who prescribed 3.
Drop down meds lists increase risk of errors
2.2 Doctors not fully and accurately transcribing to the IDL from the Kardex 4 5 6 120 4 5 6 120 4 5 6 120 4 5 6 120
2.3Doctors not providing explanations for medicines changes during
admission 5 6 5 150 5 6 5 150 5 6 5 150 4 5 5 100
2.4 Doctors not knowing how to fill in form, or its importance 6 6 6 216 6 6 6 216 6 6 6 216 6 6 6 216
2.5 Doctors not knowing what information GPs require and / or don't
provide it4 5 6 120 4 5 6 120 4 5 6 120 4 5 6 120
2.6 Diagnosis is often not written in the notes so unable to put on the
IDL, notes generally vague7 7 7 343 7 7 7 343 7 7 7 343 7 7 7 343
2.7Unclear on what is necessary on IDL e.g. how much detail re
investigations 4 5 6 120 4 5 6 120 4 5 6 120 4 5 6 120
2.8 Patients do not review the Kardex prior to transcription to the IDL 7 4 5 140 7 4 5 140 7 4 5 140 7 4 5 140
2.9 Discharge drugs late because they have to wait for results 3 3 7 63 3 3 7 63 3 3 7 63 3 3 7 63
1664 1664 1664 1614
3
3.1 Doctors not having time to complete the IDL in a timely manner 6 6 5 180 6 6 5 180 6 6 5 180 6 6 5 180
3.2Doctors not knowing the importance of completing the IDL in a
timely manner 6 6 6 216 6 6 6 216 6 6 6 216 6 6 6 216
3.3 IDL is printed but given to different people 7 4 4 112 7 4 4 112 7 4 4 112 7 4 4 112
3.4 Nurses may not know the procedure for printing and sending the
IDL6 6 7 252 6 6 7 252 6 6 7 252 6 6 7 252
760 760 760 760
Failure Mode: Each patient’s medicines 16 hours after admission are not complete and accurate
Failure Mode: A complete and accurate list of each patient’s medicines and desired information re admission is not provided to GP
Failure Mode: Each patient’s medicines at the point of discharge are not complete and accurate on the IDL
877 7 392873927 8 39287392 7
Nov-10 Dec-10
7
Jan-11 Feb-11
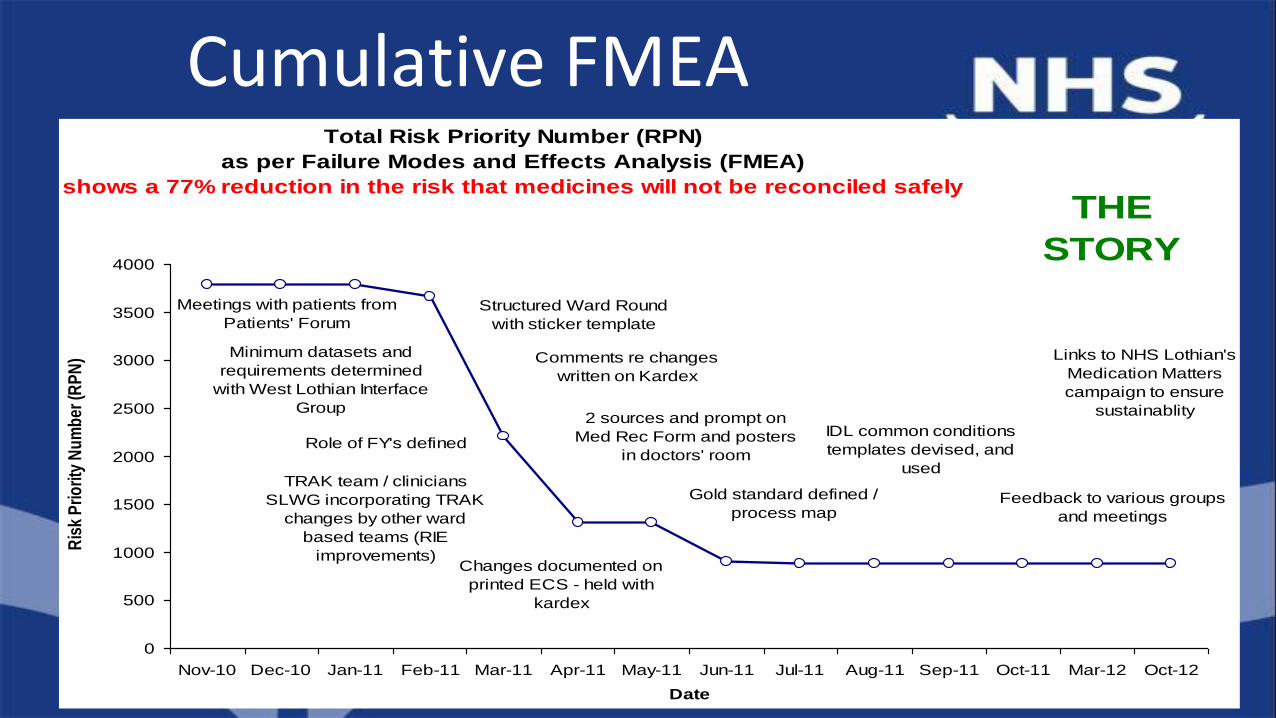
Total Risk Priority Number (RPN)
as per Failure Modes and Effects Analysis (FMEA)
shows a 77% reduction in the risk that medicines will not be reconciled safely
THE
STORY
Links to NHS Lothian's
Medication Matters
campaign to ensure
sustainablity
Feedback to various groups
and meetings
IDL common conditions
templates devised, and
used
Gold standard defined /
process map
Comments re changes
written on Kardex
Structured Ward Round
with sticker template
Changes documented on
printed ECS - held with
kardex
TRAK team / clinicians
SLWG incorporating TRAK
changes by other ward
based teams (RIE
improvements)
Role of FY's defined
Minimum datasets and
requirements determined
with West Lothian Interface
Group
Meetings with patients from
Patients' Forum
2 sources and prompt on
Med Rec Form and posters
in doctors' room
0
500
1000
1500
2000
2500
3000
3500
4000
Nov-10 Dec-10 Jan-11 Feb-11 Mar-11 Apr-11 May-11 Jun-11 Jul-11 Aug-11 Sep-11 Oct-11 Mar-12 Oct-12
Date
Ris
k P
rio
rity
Nu
mb
er (R
PN
)Cumulative FMEA

Compliance with accurate reconciliation of medicines
on admission to one medical ward (Aug 2010 - Oct 2012)
Definition
1) Accuarte list (incl'
dose, frequency,
allergy)
2) 2 sources
documented
3) Comments re
changes
documented
4) Kardex matches
lists and what
patient is taking
New median
= 93%
Baseline median
(extended)
= 10%
0
10
20
30
40
50
60
70
80
90
100
Aug
10
Sept
10
Oct
10
Nov
10
Dec
10
Jan
11
Feb
11
Mar
11
Apr
11
May
11
June
11
July
11
Aug
11
Sept
11
Oct
11
Mar
12
Oct
12
Date
Per
cen
t re
con
cile
d
Results on Admission

Compliance with accurate reconciliation of medicines
on discharge from one medical ward (Oct 2010 - Oct 2012)
New median
= 87%
Definition
1) Accurate list on
IDL (incl' dose,
frequency)
2) Changes
documented on IDL
3) IDL matches
admission meds
and Kardex Baseline median
(extended)
= 20%
0
10
20
30
40
50
60
70
80
90
100
Oct
10
Nov
10
Dec
10
Jan
11
Feb
11
Mar
11
Apr
11
May
11
June
11
July
11
Aug
11
Sept
11
Oct
11
Mar
12
Oct
12
Date
Per
cent
rec
onci
led
Results on Discharge

Failure Mode Cause / Effect Occ Det Sev RPN Actions Notes and Outcomes
1
1.1Forgetting to sign that meds have been
administered (and distractions)
double-dosing /
omitted meds5 5 5 125
PDSA(1.1)A: Tabards (variable success so far).
PDSA(1.1)B: Supervised med rounds for all
new starts and if an error has been made -
SC/N or DC/N sign-off
PDSA(1.1)B - in place; Team to
look at Datix info at next meeting
(CS to bring)
1.2
Errors can be made when there have been
increases in patient activity, acuity and time
constraints
Errors in reading
kardex2 7 2 28
PDSA(1.2)A: Time wasted topping up POD
Lockers during round - responsibilities defined
as for last person to do round - highlighted at
Safety Briefing (SBrf), ward meeting, induction
(back up by technician)
By Feb 2012 PDSA(1.1)A not
100% success - next test
PDSA(1.1)B: Night shift to
undertake top-up, and continue
with SBrf
1.3
Oxygen may not be prescribed (note: Nurse
Guidelines in Emergency patients) and may
not be administered properly (devices and
concentration)
Over / under
dosing9 7 8 504
PDSA (1.3)A: Local training by physios to
medics and nurses to introduce new policy (Mar
12); PDSA(1.3)B: Example kardex to be
displayed in Drs room and induction folder
Physios (Nicola) to audit use
before and after (DM checking).
FY/Reg to come to next meeting.
Dates available for ward-based
training
FMEA Ward 54 WGH November 17th 2011 (updated 12th Dec 2011, 16th Jan, 13th Feb, 5th Mar 2012)
General
FMEAs for 10 ward areas
Linked to PDSAs
Ward work led to a whole programme of improvements, including mind mapping and pocket cards

Large Mind Map
Small Z-cards

Questions

#SPSPMeds2016
Table top discussion

#SPSPMeds2016

#SPSPMeds2016
Time Title Room
14:40-14:50 Coffee and transition to NHS board huddles
14:50-15:20 NHS board team huddles See next slide
15:20 Transfer to plenary
15:25-15:45 NHS board team huddles report back
Lord Provost & Imperial Suites15:45-16:05SPSP Medicines –a multi-disciplinary approach
16:05-16:15 Wrap up
16:15 Close
For the rest of the afternoon

NHS board Room
NHS Ayrshire & Arran Lord Provost & Imperial Suite
NHS Borders Alloway Suite
NHS Dumfries & Galloway Alloway Suite
NHS Fife Ellisland Suite
NHS Forth Valley Ellisland Suite
NHS Grampian Ellisland Suite
NHS Greater Glasgow and Clyde Cambridge Suite
NHS Highland Cambridge Suite
NHS Lanarkshire Lord Provost & Imperial Suite
NHS Lothian Lord Provost & Imperial Suite
NHS Shetland Cambridge Suite
NHS Tayside Ellisland Suite
NHS Western Isles Cambridge Suite
Golden Jubilee National Hospital Cambridge Suite

#SPSPMeds2016
NHS board team huddle questions (30 mins)
1. Do you know everyone and their role?
2. What are the key areas for improvement related to medication reconciliation in your system?
3. What are your local high risk medicines priorities? How do you know?
4. Who are the key people you need to work with to address the above areas?
5. What are you going to by next Tuesday?

#SPSPMeds2016