immunohistochemical evidence of active thymocyte proliferation in thymoma: its possible role in the...
TRANSCRIPT

American Journal of Pathology, Vol. 128, No. 3, September 1987Copyright © American Association of Pathologists
Immunohistochemical Evidence ofActive ThymocyteProliferation in Thymoma
Its Possible Role in the Pathogenesis ofAutoimmune Diseases
MARCO CHILOSI, ANTONIO IANNUCCI,FABIO MENESTRINA, MAURIZIO LESTANI,
ALDO SCARPA, FRANCO BONETTI,LUCIANO FIORE-DONATI,
BRUNO DIPASQUALE, GIOVANNI PIZZOLO,GIORGIO PALESTRO, GIUSEPPE TRIDENTE,
and GEORGE JANOSSY
Eight cases ofhuman thymoma have been analyzed oncryostat sections with the monoclonal antibody Ki67,which reacts with cells in the proliferative phases ofthecell cycle. The aim was to assess the proportion ofpro-liferating thymocytes among lymphoid cells in thethymoma samples. In all cases a large number of cells(mean, 58.75%; range, 35-80%), recognized as thymo-cytes by morphology and lack of cytokeratin expres-sion in a combined immunohistochemical assay, ex-
HUMAN thymomas are neoplasms of epithelial ori-gin that are frequently associated with an exuberantlymphoid component.1 Recent studies have estab-lished that the epithelial and lymphoid componentsin thymoma closely mimick the cell organization ob-served in the normal thymus.2-10 In most cases ofthymoma with high lymphocyte/epithelial ratiosneoplastic epithelial cells exhibit differentiation anti-gens ofthymic cortical epithelium311 ' and appear to beintermingled with lymphocytes exhibiting a "corti-cal" phenotype as observed in the normal cortex(TdT+, T6+, T4+, and T8+, etc.).2'3'6'9-12 Residualareas of "medullary differentiation" are also presentwith mature T cells (TdT-, T6-, T3+), and medullaryepithelial cells as defined by their peculiar pheno-type.3'7 Cases showing predominantly medullary epi-thelial type have been also occasionally seen.4'7 Thus,in lymphoid-predominant thymomas the followingcharacteristic features are seen: a) an abundance ofimmature thymocytes and b) an abnormal neoplasticepithelial microenvironment which frequently ex-
From Istituto di Anatomia Patologica, di Scienze Immunologicheed Ematologia, Universita' di Verona, and Istituto di AnatomiaPatologica, Universita' di Torino, Italy, and Department oJImmunology Royal Free Hospital School of Medicine. London,England
hibited nuclear Ki67 staining. These findings differfrom the reactivity pattern observed in age-matchednonneoplastic thymuses where lower growth activityof cortical thymocytes was observed (15-20% Ki67+cells). Intensive thymocyte proliferation in thymomasmay represent one ofthe factors which lead to autoim-munity in myasthenia gravis and thymomas. (Am JPathol 1987, 128:464-470)
hibits hyperkeratinization and changes of HLA-DRexpression.3'11 Autoimmune phenomena are also fre-quently associated with thymoma. These include,most frequently, myasthenia gravis' 7 and, occasion-ally, cytopenias, systemic lupus erythematosus, rheu-matoid arthritis, thyroiditis, and other diseases.13-15 Itis not known whether the large numbers of thymo-cytes observed in these cases derive from an increasedproliferation of cortical thymocytes or from an exag-gerated accumulation of end-stage nondividing thy-mocytes. This is an important question because theincreased proliferation is likely to be associated withan increased output of cells from the thymus into the
Supported in part by the Associazione Italiana per la Ri-cerca sul Cancro, Milano, and Progetto Finalizzato CNR"Oncologia", Italy.Accepted for publication April 27, 1987.Address reprint requests to M. Chilosi, Istituto di Anato-
mia Patologica, Universita' di Verona, Policlinico BorgoRoma, 37100 Verona, Italy.
464

PROLIFERATING THYMOCYTES IN HUMAN THYMOMA 465
periphery. For this reason, in our study we evaluatedthe replicating sets of thymocytes in 8 cases of thy-moma using a quantitative immunostaining by themonoclonal antibody Ki67. This reagent binds to nu-clear antigens expressed by cells in the proliferativephasesG 1, G2, M, and S.16 These data were comparedwith the quantitative observations obtained withKi67 staining on samples of normal thymuses.
Materials and MethodsPatients
Fresh frozen tissue samples were obtained from 8patients at surgery for the diagnosis and therapy ofthymoma (Table 1). The patients received no im-munosuppressive therapy before thymectomy. Foursamples ofnormal thymus were also analyzed as con-trols. The antibodies applied for the study ofepithelialand lymphoid antigens of the thymomatous samplesare listed in Table 2.3
Methods
The samples were covered with OCT medium(Ames), snap-frozen in liquid nitrogen, and processedfor immunohistochemistry as previously described.17Briefly, 5-,u sections were cut in a cryostat, dried ontoglass slides covered with polylysine adhesive (Sigma),and fixed in cold chloroform/acetone mixed in a 1: 1ratio. A modification of the original technique fordemonstrating Ki67 antigen'6 was used for improve-ment ofthe fixation ofthe nuclear antigens. This pro-cedure included a second fixation step with 10% cal-cium-formalin for 10 minutes. After fixation the
Table 2-Conventional and Monoclonal Antibodies Used forImmunohistochemical StudyImmunologic
reagentOKT4 (CD4)OKT8 (CD8)OKT3 (CD3)OKT6 (CD1)TdTKeratinKi67HLA-DRMR3RFD4
MMMMRRMMMM
SpecificityHelper T cellsSuppressor T cellsT cellsCortical thymocytesCortical thymocytesEpithelial cellsReplicating cellsB cells, etc.Thymic epithelium (cortex)Thymic epithelium (medulla)
Source
OrthoOrthoOrthoOrtho(Ref 11)DakoDakoBecton Dickinson(Ref 19)(Ref 11)
R, rabbit; M, monoclonal.
slides were washed in buffered saline (PBS) and la-beled with Ki67 by means ofthe alkaline phosphataseanti-alkaline phosphatase method (APAAP).18 A gen-tle hematoxylin counterstaining was performed forassessing the morphology and percentage of Ki67+cells. Ki67 antibody (Code M722) and the APAAPreagent (Code K670) were purchased from Dako-patts, Denmark.
Additional sections were also stained using a com-bined immunocytochemical staining for Ki67 andcytokeratin to confirm the nature ofthe Ki67+ cells inthe given samples. In addition to the staining for Ki67(APAAP with red chromogen), the samples were si-multaneously incubated with a rabbit anti-keratinantibody (Dakopatts, Code A575) followed by anti-rabbit serum and peroxidase anti-peroxidase (PAP)complex (Dakopatts, Code K548) with diaminoben-zidine as a brown chromogen.The samples were first viewed with the two-color
immunochemical method and also with labeling for
Table 1-Evaluation of Replicative Fractions of Thymocytes in Thymomatous and Control SamplesAssociateddisease
MyastheniaMyastheniaMyasthenia*MyastheniaMyastheniaNoneMyastheniaMyasthenia*
Thyroid adenomaHyperparathyroidism
CardiopathyHodgkin's disease
*Ki67+ percentage confirmed on smear preparations (Case 3, 41%; Case 8, 68%).
Cases
12345678
Age-matchedcontrol
thymuses910
Controlthymuses
1112
Sex
MFMMMMMF
MF
MM
%Ki67+Age4061694142193154
3736
215
HistologyThymomaThymomaThymomaThymomaThymomaThymomaThymomaThymoma
Normal thymusNormal thymus
Normal thymusNormal thymus
40%70%35%80%60%70%45%70%
20%15%
60%48%
Vol. 128 · No. 3
466 CHILOSI ET AL
RFD4 antigen present on medullary epithelium. Theoverall distribution of cortical and medullary areashas been determined. Fields with predominant epi-thelial components and with signs of medullary dif-ferentiation (such as Hassal corpuscles) were not in-cluded.
In all cases fields with lymphoid predominancewere viewed, and more than 2000 cells were evalu-ated for Ki67 nuclear staining with a 40X objective.Five different areas were selected in all samples, andthe percentages of positive cells within the lymphoidcell population were counted.
In 2 cases fresh cell suspensions were also available,and cytospin preparations were obtained. Immuno-cytochemical staining on these preparations allowedthe precise evaluation of the proportions of Ki67+thymocytes within the TdT+, T6+ cortical thymocytepopulations and comparison of these findings withthe observations on cryostat sections.
ResultsThe cases examined were encapsulated multinodu-
lar neoplasms with the typical histologic pattern ofthecortical type ofthymoma and were characterized bynodules ofdifferent size, mainly composed by lymph-oid cells and minor proportions of epithelial cells.Epithelial cells had round-ovoid nuclei and loosechromatin structure. Lymphoid mitoses were com-mon. In three cases areas ofmedullary differentiationwith Hassall's corpuscles were present. In another 2cases areas of medullary differentiation were only de-tected by immunohistochemistry, revealing mature
lymphocytes (TdT-, T6-, T3+) among remnants ofanepithelial network exhibiting the medullary pheno-type (RFD4+) when studied on adjacent sections.
Epithelial ComponentIn all cases the neoplastic epithelial cells expressed
cytokeratin and the antigen detected by MR3 mono-clonal antibody. This reagent is one of the most spe-cific reagents for cortical epithelium.'9 HLA-DR wasabsent or heterogeneously expressed on epithelialcells, unlike in cortical epithelium ofthe normal con-trol samples. RFD4, an antibody specific for subcap-sular and medullary epithelium, only reacted withsmall medullary-like areas as described earlier.3
Lymphoid ComponentIn all cases the large majority oflymphocytes (more
than 60-80%) were of the T type and exhibited a"cortical" phenotype as defined by TdT and T6 posi-tivity together with the simultaneous presence of T4and T8 antigens. Similar proportions of T6+, TdT+lymphoid cells (62% and 70%) were observed in thetwo samples which were studied on cell suspension.The lymphocytes homing within the areas ofmed-
ullary differentiation were mostly TdT and T6 nega-tive and expressed either T4 or T8 antigen.
Ki67 ExpressionIn all the cases examined
revealed the presence of aKi67 immunostaininglarge number (range,
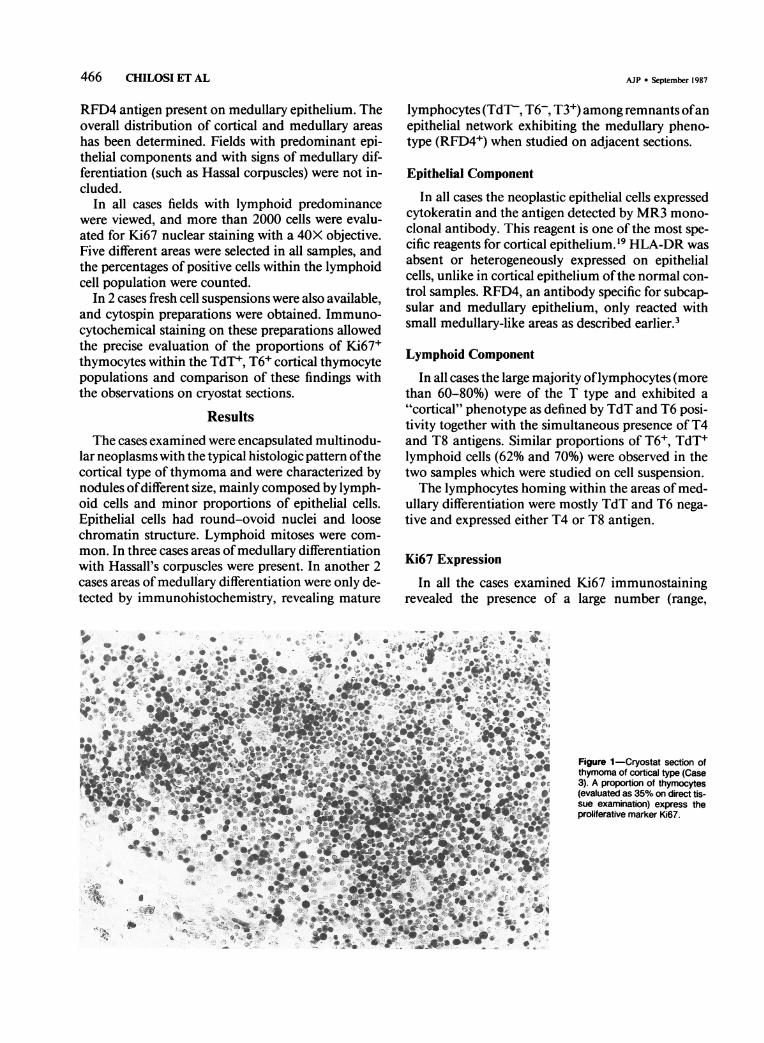
Figure 1-Cryostat section ofthymoma of cortical type (Case3). A proportion of thymocytes(evaluated as 35% on direct tis-sue examination) express theproliferative marker Ki67.
AJP * September 1987

PROLIFERATING THYMOCYTES IN HUMAN THYMOMA 467
35-80%; mean, 58.75%) ofpositive cells with nuclearstaining ofheterogeneous intensity. The positive cellsshowed a lymphoid morphology (Figure 1). In dou-ble-stained sections keratin-positive epithelial cells(PAP, brown staining) were almost completely devoidof nuclear Ki67 staining (APAAP, red staining) (notshown).
In the 2 cases with areas of medullary differentia-tion these were characterized by a lack of (or few)Ki67-positive thymocytes and clearly appeared asnegative islands within the tissue (Figure 2).
Figure 2-Cryostat sections ofthymoma of cortical type withmedullary differentiation (Case2). A large number of TdT-posi-tive "cortical" thymocytes areshown (a) around a small medul-lary area. In a serial section (b)most cortical cells express theproliferative marker Ki67. Themedullary area is nearly devoidof positive cells.
The quantitative evaluation of Ki67-positive thy-mocytes was performed on cryostat sections. Thymo-cytes were easily recognized by morphology and bylack of cytokeratin expression. The proportions ofKi67-positive thymocytes in thymomas ranged be-tween 35% and 80% and were higher than those ob-served in the normal age-matched thymuses in our(15-20%) and Steinmann's (10%) series.20
In the 2 cases that were studied on cytospin prepa-rations, the proportions ofTdT+, T6+, Ki67+ thymo-cytes could be carefully analyzed. In these 2 cases the
tic ' '': ·r .r
·*i.;·e .·'C· .i L··.*it
rr.1Y ··t, r.; .c.. --.d3lr..tLle.trE*I Ir.jr
.4
Vol. 128 * No. 3

468 CHILOSI ET AL
results on cytospin and cryostat preparations werecomparable (Table 1 and Figure 3).
DiscussionHuman thymoma is a peculiar epithelial neoplasm
where "abnormal" epithelium supports the differen-tiation of polyclonal T lymphocytes.-1''21 We re-cently confirmed the polyclonality of the lymphoidcomponent ofthymoma at the gene level using probesfor the beta-chain ofthe T-cell receptor (Scarpa et al,manuscript in preparation).The immunophenotypic studies have shown that
most lymphocytes in thymoma are identical to nor-mal cortical thymocytes.2" In some cases minor pro-portions of mature T lymphocytes can be also foundin islands which show "medullary differentiation."These areas are most frequently small, but normallyorganized.3'6'7
It has already been demonstrated by conventionalhistology that thymomas contain lymphocytes with a"stimulated" or "activated" appearance, and somemitoses are also seen.' 2' Nevertheless, the replicativepotential of the lymphoid component in thymomaneeds further study with more quantitative methods.Unfortunately, autoradiographic analysis or the mi-togen-responsive capacity of thymoma cells mea-sured in vitro22 may not give relevant informationabout their proliferative features in vivo. Recent ob-servations with Ki67 antibody indicate that withinthe lymphoid lineage there is a close relationship be-
tween antibody reactivity and the cycling of the cell(in Gi, S, or M phase).16
In this study we have determined the replicativefraction of thymocytes in thymomas using the im-munohistochemical detection of Ki67 antigen.'6 Wefound a marked activity of thymocytes in all thymo-matous samples. An internal control for each samplehas been provided by the remnants ofmedullary areaswhere all cells were virtually devoid ofKi67 staining.The proportions of Ki67-positive thymocytes foundin thymomas (35-80%) are similar to those observedin normal control thymuses from younger patientsbut significantly higher than those observed in thecortical areas ofage-matched control thymuses in ourstudy (15-20%) and in a series of cases recently re-ported by Steinman et al.20 This observation suggeststhat in thymoma the accumulating thymocytes donot merely represent a population of long-lived end-stage cells which divide rarely. It seems that this popu-lation actively proliferates within the epithelial net-work, which has been shown to synthetize thymichormones23 and which, in normal thymus, may havea determinant role in the selection ofimmatureT cellsfor self MHC specificity.24 There is also evidence inboth experimental animals and man that thymocytesacquire their antigen specificity within the cortex,where the rearrangement of genes coding for T-cellreceptor takes place.25'26 It appears from our studythat the proliferating T-cell precursors in thymomaare part of a microenvironment constituted by anabnormal cortical epithelium, which is frequently
....^a.;
Figure 3-Smear preparationsobtained from a cell suspensionof thymoma of cortical type(Case 8). The majority of cellsshow the immature "cortical"marker TdT (a) and the prolifera-tive marker Ki67 (b). A Ki67-negative epithelial cell is shown(arrow).
.e
1,._o_ ; Z¸v_" *.V?*
-r
·. -;.. * .
* !i:' .'. . ..
.... .·_'.i '"'....'
.!:,, .
*
..: ... W.
AJP * September 1987
,....:, ,. .
..: t:' ...
.._
ML
:..
','.;.
.:*.a'
lib'

Vol. 128 * No. 3 PROLIFERATING THYMOCYTES IN HUMAN THYMOMA 469
HLA-DR negative, as it has been demonstrated inanother disease, the "bare lymphocyte" syndrome.27Education in such a microenvironment in thymomamay lead to the export of functionally handicappedT-cell clones. The search of such immature T cells inthe peripheral blood of patients with thymoma is anongoing project in our laboratories, but it is relevanthere that lymphocytes of intermediate phenotype(T4+, T8+, T6-) can be demonstrated in some patientswith myasthenia gravis.28
In addition to the cortical overproduction of thy-mocytes, we have previously detected another impor-tant contributing defect in thymoma. Proliferatingcortical thymocytes may avoid medullary influenceexerted at the cortical-medullary junction prior toentry into the circulation. It has been recently demon-strated that medullary interdigitating dendritic cellsinduce self-tolerance.29'30 These factors, taken to-gether, may represent the key factors in the frequentdevelopment of autoimmunity in thymomas.
References
1. Rosai J, Levine GD: Tumors of the thymus, Atlas ofTumor Pathology. Armed Forces Institute of Pathol-ogy, Washington, DC, 1976
2. Chan WC, Zaatari GS, Tabei S, Bibb M, Brynes RK:Thymoma: an immunohistochemical study. Am J ClinPathol 1984, 82:160-166
3. Chilosi M, Iannucci A, Fiore-Donati L, Tridente G,Pampanin M, Pizzolo G, Ritter M, Bofill M, JanossyG: Myasthenia gravis: immunohistological heterogene-ity in microenvironmental organization ofhyperplasticand neoplastic thymuses suggesting different mecha-nisms of tolerance breakdown. J Neuroimmunol 1986,11:191-204
4. Chilosi M, lannucci A, Pizzolo G, Menestrina F, Fiore-Donati L, Janossy G: Immunohistochemical analysisofthymoma: Evidence for medullary origin ofthe epi-thelial cells. Am J Surg Pathol 1984, 8:309-318
5. Lauriola L, Maggiano N, Marino M, Carbone A, Pian-telli M, Musiani P: Human thymoma: immunologiccharacteristics of the lymphocytic component. Cancer1981, 48:1992-1995
6. Mokhtar N, Hsu SM, Lad RP, Haynes BF, Jaffe ES:Thymoma: Lymphoid and epithelial components mir-ror the phenotype of normal thymus. Hum Pathol1984, 15:978-984
7. Muller-Hermelink HK, Marino M, Palestro G: Pathol-ogy of thymic epithelial tumors, The Human Thymus:Histopathology and Pathology. Edited by HK Muller-Hermelink. Berlin, Springer-Verlag, 1986, pp 207-268
8. Reddick RL, Jennette JC: Immunologic and ultra-structural characterization of the small cell populationin malignant thymoma. Hum Pathol 1983, 14:377-380
9. Aisemberg AC, Wilkes B, Harris NL, Frist WH: Thepredominant lymphocyte in most thymomas and innonneoplastic thymus from patients with myastheniagravis is the cortical thymocyte. Clin Immunol Im-munopathol 1985, 35:130-136
10. Eimoto T, Teshima K, Shirakusa T, Takeshita M, Oka-mura H, Naito H, Mitsui T, Kikuchi M: Heterogeneityof epithelial cells and reactive components in thy-
momas: An ultrastructural and immunohistochemicalstudy. Ultrastruct Pathol 1986, 10:157-173
11. Janossy G, Bofill M, Trejdosiewicz LK, Willcox HNA,Chilosi M: Cellular differentiation of lymphoid sub-populations and their microenvironments in thehuman thymus,7 pp 89-125
12. Janossy G, Thomas JA, Bollum FJ, Mattingly S, Piz-zolo G, Bradstock KF,Wong L, Ganeshaguru K, Hoff-brand AV: The human thymic microenvironment: Animmunohistological study. J Immunol 1980,125:202-212
13. Souadjian JV, Enriquez P, Silverstein MN, Pepin JM:The spectrum of diseases associated with thymoma.Arch Intern Med 1974, 134:374-379
14. Verley JM, Hollmann KH: Thymoma: A comparativestudy of clinical stages, histologic features, and survivalin 200 cases. Cancer 1985, 55:1074-1086
15. Rosenow EC, Hurley BT: Disorders of the thymus: Areview. Arch Intern Med 1984, 144:763-770
16. Gerdes J, Lemke H, Baisch H, Wacker HH, Schwab U,Stein H: Cell cycle analysis of a cell proliferation-asso-ciated human nuclear antigen defined by the monoclo-nal antibody Ki-67. J Immunol 1984, 133:1710-1715
17. Chilosi M, Pizzolo G, Fiore-Donati L, Bofill M, Jan-ossy G: Routine immunofluorescent and histochemi-cal analysis of bone marrow involvement of lym-phoma/leukaemia: The use of cryostat sections. Br JCancer 1983, 48:763-775
18. Cordell JL, Falini B, Erber WN, Ghosh AK, AbdulazizZ, MacDonald S, Pulford KAF, Stein H, Mason DY:Immunoenzymatic labeling of monoclonal antibodiesusing immune complexes of alkaline phosphatase andmonoclonal anti-alkaline phosphatase (APAAP com-plexes). J Histochem Cytochem 1984, 32:219-229
19. De Maagd RA, MacKenzie WA, Schuurman HJ, Rit-ter MA, Price KP, Broekhuizen R, Kater K: Thehuman thymus microenvironment: heterogeneity de-tected by monoclonal anti-epithelial cell antibodies.Immunology 1985, 54:745-754
20. Steinman GG: Changes of the human thymus duringaging,7 pp 43-88
21. Levine GD, Polliack A: The T-cell nature of the lym-phocytes in two human epithelial thymomas: A com-parative immunologic, scanning and transmissionelectron microscopic study. Clin Immunol Immuno-pathol 1975, 4:199-208
22. Musiani P, Maggiano N, Aiello FB, Larocca LM, Pian-telli M: Phenotypical characteristics and proliferativecapabilities ofthymocyte subsets in human thymoma.Clin Immunol Immunopathol 1986, 40:385-392
23. Dalakas MC, Engel WK, McClure JE, Goldstein AL,Askanas V: Immunocytochemical localization of thy-mosin-al in thymic epithelial cells ofnormal and myas-thenia gravis patients and in thymic cultures. J NeurolSci 1981, 50:239-247
24. Kyewski BA: Thymic nurse cells: Possible sites ofT-cellselection. Immunol Today 1986, 7:374-379
25. Royer HD, Acuto 0, Fabbi M: Genes encoding the Tibeta subunit of the antigen/MHC receptor undergo re-arrangement during intrathymic ontogeny prior to sur-face T3-Ti expression. Cell 1984, 39:261-266
26. Snodgrass HR, Kisielow P, Kiefer M, Steinmetz M,von Boehmer H: Ontogeny ofthe T-cell antigen recep-tor within the thymus. Nature 1985, 313:592-595
27. Schuurman HJ, Wijngaert FP, Huber J, SchuurmanRKB, Zegers BJM, Roord JJ, Kater L: The thymus in"bare lymphocyte" syndrome: Significance of expres-sion of major histocompatibility antigens on thymicepithelial cells in intrathymic maturation. Hum Im-munol 1985, 13:69-82
28. Matsui M, Kameyama M: A double-label flow cytome-tric analysis of the simultaneous expression of OKT4

470 CHILOSI ET AL AJP * September 1987
and Leu2a antigens on circulating T lymphocytes inmyasthenia gravis. J Neuroimmunol 1986, 11:311-319
29. Kyewski BA: Thymic dendritic cells present blood-borne antigens to medullary thymocytes in vivo : Apossible role in the generation of the T-cell repertoire,Haematology and Blood Transfusion. Vol 29: ModemTrends in Human Leukemia VI. Edited by Neth,Gallo, Greaves, Janka. Berlin, Springer-Verlag, 1985, p486
30. Lo D, Sprent J: Identity of cells that imprint H-2-re-stricted T-cell specificity in the thymus. Nature 1986,3 19:672-675
Acknowledgments
We thank Mrs. L. Montagna and Mrs. D. Toffali for theirskillful technical assistance.