immune reconstitution after transplantation of autologous peripheral cd34+ cells: analysis of...
TRANSCRIPT

Immune reconstitution after transplantation of autologous
peripheral CD34� cells: analysis of predictive factors and
comparison with unselected progenitor transplants
SE RG IO RUT ELLA,1,2 CARLO RUMI,1,2 LUCA LAURENT I,1 LUCA PIERELL I,1 FEDERICA SORA',1 SIMO NA SICA1
A ND
GIUSE PPE LEONE1 1Department of Haematology and 2Centre for the Flow Cytometry Study of Blood Cells,
Catholic University School of Medicine, Rome, Italy
Received 4 June 1999; accepted for publication 29 September 1999
Summary. The recovery of lymphocyte count, CD4� andCD8� T-cell subsets, natural killer (NK) cells and CD19�
B-cells was evaluated in a cohort of 15 patients receivingautologous CD34� peripheral blood progenitor cells (PBPCs;group A) for haematological malignancies and in 20 patientstransplanted with autologous unselected PBPCs (group B).Lymphocyte count recovered in both patient cohorts, beingsigni®cantly lower in group A than in group B 1 (P�0?008)and 2 months (P�0?0035) after progenitor cell infusion.The repopulation of CD3� T-cells occurred more rapidlyin group B than in group A (P�0?034 on week 4); CD19�
B-lymphocytes did not return to reference ranges in eithergroup of patients. The count of CD4� T-lymphocytesremained <200/ml during the study period in patientstransplanted with CD34� PBPCs, signi®cantly lower thangroup B levels (P�0?034 and P�0?021 on weeks 4 and 8respectively). CD8� T-cells increased rapidly in both groups;thus, the CD4 to CD8 ratio was severely reduced. CD4� and
CD8� T-cells displayed an activated phenotype in bothgroups of patients, co-expressing the HLA-DR antigenthroughout the study period. NK cells followed a similarrepopulation kinetics in both study groups, although theirexpansion was greater in group B than in group A(P�0?014 on week 4). In the CD34� group, post-transplantadministration of granulocyte colony-stimulating factorpredicted a faster lymphocyte recovery in multivariateanalysis (P�0?025); interestingly, the amount of passivelytransferred lymphocytes correlated inversely with time toachieve a lymphocyte count >0?5 ´ 109/l (r� ±0?63,P�0?01). Further investigations are necessary to charac-terize T-cell competence after transplantation of CD34�
PBPCs.
Keywords: immune reconstitution, autologous selectedCD34� cells, predictive factors, ¯ow cytometry, granulocytecolony-stimulating factor.
Peripheral blood progenitor cells (PBPCs) mobilized bycombined regimens including chemotherapy and growthfactors can be transplanted as an alternative to bone marrowin patients affected by haematological malignancies(Schmitz et al, 1996). Abnormal T-cell phenotype andfunction, namely CD4 to CD8 imbalance, defective T-cellproliferation and depressed interleukin-2 (IL-2) secretion,have already been reported after autologous or allogeneicbone marrow transplantation (Jin et al, 1995; Storek et al,1995); similarly, defects in B-cell function, i.e. reducedimmunoglobulin production and impaired proliferativeresponse to pokeweed mitogen, have been described (Storek& Saxon, 1992; Lenarsky, 1993; Talmadge et al, 1997).
Recently, haematopoietic and immune recovery afterPBPC transplantation were shown to be accelerated whencompared with autologous bone marrow infusion (Ottingeret al, 1996; Rosillo et al, 1996; Koehne et al, 1997; Talmadgeet al, 1997). In particular, improved CD4 to CD8 ratio,enhanced regeneration of natural killer (NK) cells, lympho-kine-activated killer (LAK) activity and T-cell mitogenicresponse have been found in patients receiving cytokine-mobilized PBPCs, probably as a result of relevant amounts ofT-cells conferred with the graft (Fegan et al, 1995; Talmadgeet al, 1997). Although granulocytic, erythroid and mega-karyocytic reconstitution correlate directly with the quantityof CD34� progenitors infused, the relative contribution ofCD34� cells to the recovery of the recipient's T-cellcompetence remains a matter of debate (Guillaume et al,1998).
British Journal of Haematology, 2000, 108, 105±115
105q 2000 Blackwell Science Ltd
Correspondence: Sergio Rutella, Department of Haematology, Centre
for the Flow Cytometry Study of Blood Cells, Catholic University
School of Medicine, Largo A. Gemelli 8, 00168 Rome, Italy.

Haematopoietic engraftment appears to be similar afterthe infusion of selected CD34� or unmanipulated PBPCs(Talmadge et al, 1997); in contrast, concerns have beenraised regarding a detrimental effect of CD34 selection on therecovery of immune function, depending mainly on thedepletion of mature T-lymphocytes and immunocompetentcells in the CD34� inoculum (Guillaume et al, 1998). In arecent investigation, delayed reconstitution of T- and B-celllineages and reduced diversity of T-cell repertoire were foundin recipients of ¯uorescence-activated cell sorting (FACS)-puri®ed CD34� compared with unmanipulated PBPCs(Bomberger et al, 1998); moreover, absolute CD4 countswere shown to be markedly depressed (i.e. <100 cells/ml)after the transplantation of highly puri®ed PBPCs formultiple myeloma (Tricot et al, 1998; Vescio et al, 1999).
We evaluated the recovery of lymphocyte count, CD4�
and CD8� T-cell subsets, NK cells and CD19� B-lymphocytesby multiparameter ¯ow cytometry in a cohort of 15 patientsreceiving selected CD34� PBPCs (group A) for haematolo-gical malignancies and in 20 patients transplanted withunmanipulated PBPCs (group B). Overall, a delayed repopu-lation of the T-cell lineage and a profound depression ofCD4� T-cell count could be demonstrated in recipients ofpuri®ed CD34� PBPCs; of interest, post-transplant adminis-tration of granulocyte colony-stimulating factor (G-CSF)predicted faster recovery of the lymphocyte count in theCD34� group.
PATIENTS AND METHODS
Patients' characteristics and study designThe restoration of a fully functional immune system capableof responding to antigenic challenge has already beenreported to occur from 6 months to 1 year after PBPCtransplantation (Guillaume et al, 1998); however, littleinformation is currently available on the kinetics of lymphoidreconstitution in the early post-transplantation period. In
the present investigation, lymphoid recovery was evaluatedover 4 months after CD34� PBPC infusion; to this end,peripheral blood samples were obtained before the pretrans-plant conditioning regimen (day ÿ7) and then weekly for 16consecutive determinations (day 0 to day 110).
Group A Fifteen patients (eight males, median age 46years, and seven females, median age 33 years) affected bynon-Hodgkin's lymphoma (NHL; n�4), Hodgkin's disease(HD; n�6) or multiple myeloma (MM; n�5) were submittedto mobilizing chemotherapy consisting of mitoxantrone(10 mg/m2/day on day 1), aracytin (2 g/m2/day on day 5),carboplatinum [100 mg/m2/day on days 1±4 (total dose500 mg/m2)] and methylprednisolone [500 mg/m2/day ondays 1±5 (total dose 2500 mg/m2)] or high-dose cyclophos-phamide (7 g/m2), followed by G-CSF and leukapheresiscollection of PBPCs (Rumi et al, 1997).
The pretransplant conditioning regimen included busul-phan [4 mg/kg body weight (bw) on days ÿ7 to ÿ4 (totaldose 16 mg/kg)] and cyclophosphamide [60 mg/kg bw ondays ÿ3 and ÿ2 (total dose 120 mg/kg) (BuCy2)] in twopatients, busulphan [4 mg/kg bw on days ÿ7 to ÿ4 (totaldose 20 mg/kg)] and melphalan (90 mg/m2 on day ÿ2) inseven patients and BEAM [BCNU 300 mg/m2 on day ÿ7;etoposide 200 mg/m2 on days ÿ6 to ÿ3 (total dose 800 mg/m2), aracytin 200 mg/m2 on days ÿ6 to ÿ3 (total dose800 mg/m2) and melphalan 140 mg/m2 on day ÿ2] in sixpatients, followed by progenitor cell infusion (Table I).
Patients received subcutaneous (s.c.) G-CSF (5 mg/kg/day;Granocyte, Rhone-Poulenc Rorer, Milan, Italy) starting onday 1 (n�7; `early G-CSF') or day 7 (n�5; `late G-CSF') fromCD34� cell infusion until a stable absolute neutrophil count(ANC) >0?5 ´ 109/l, as part of a randomized trial aimed atevaluating the optimal timing of G-CSF administration aftertransplantation of autologous CD34� cells (Piccirillo et al,1999); the remaining three patients did not receive thecytokine in the post-transplant period.
Group B Twenty patients (eight males, median age 44
q 2000 Blackwell Science Ltd, British Journal of Haematology 108: 105±115
106 S. Rutella et al
Table I. Characteristics of patients receiving selected CD34� PBPCs.
Conditioning CD34� cells Days to ANC Days to pltsUPN Age/sex Diagnosis regimen ´ 106/kg bw >0´5 ´ 109/l >50 ´ 109/l pRBC SDU
92 54/M NHL BuCy2 6´6 13 50 5 2
93 35/F NHL BuCy2 8´2 11 18 6 1
98 43/F NHL BuMel 3´8 11 36 3 1113 59/F MM BuMel 16 13 15 8 2
119 48/M MM BuMel 7´1 16 52 1 2
123 58/F MM BuMel 10´76 12 40 1 3
142 58/M MM BuMel 1´3 13 47 2 2145 31/F NHL BEAM 8´8 13 46 6 6
174 22/F HD BEAM 4´6 11 21 1 2
181 53/M MM BuMel 3´5 18 18 2 2
192 25/M HD BEAM 8 15 27 3 3195 18/F HD BEAM 3´3 10 15 2 1
197 44/M HD BEAM 2´8 20 19 0 1
198 33/F HD BEAM 4´6 9 15 2 4199 34/M HD BuMel 1´39 11 26 0 0

107Immune Reconstitution after CD34� Cell Transplantation
q 2000 Blackwell Science Ltd, British Journal of Haematology 108: 105±115
years, and 12 females, median age 46 years) affected by NHL(n�7), MM (n�9), HD (n�3) and acute myelogenousleukaemia (AML, n�1) were transplanted with unmanipu-lated PBPCs; mobilization protocols were the same as forgroup A patients. The pretransplant conditioning regimenincluded BuCy2 in seven patients, busulphan and melphalanin eight patients, BEAM in two patients, high-dose melpha-lan [100 mg/m2 on days ÿ3 and ÿ2 (total dose 200 mg/m2)] in two patients and thiotepa [750 mg/m2 on days ÿ5 toÿ3 (total dose 2250 mg/m2)] and melphalan (140 mg/m2
on day ÿ2) in one patient, followed by progenitor cellinfusion. No patient was administered G-CSF after PBPCtransplantation.
Antiviral prophylaxisPatients from both study groups received high-dose intrave-nous acyclovir (500 mg/m2/day) from the beginning of thepretransplant conditioning regimen (day ÿ7) until day 100after PBPC infusion.
Positive selection of CD34� cellsThe product of two consecutive leukaphereses was processedwith the CEPRATE SC system (CellPro, Bothell, WA, USA),according to the manufacturer's instructions.
Brie¯y, peripheral blood mononuclear cells were incubatedwith biotinylated anti-CD34 monoclonal antibody (12?8clone) for 25 min at room temperature; after washing, cellswere loaded on the sample chamber on the top of the gel-®lled column. CD34� cells were adsorbed to avidin-coatedbeads, then released by agitation and collected in aphosphate-buffered saline (PBS) solution containinghuman serum albumin. The purity of the CD34� cellconcentrate was 90% (range 66±98%).
Immunological markersPeripheral blood (PB) samples were collected in EDTA-containing tubes. Aliquots of unseparated PB were incu-bated for 30 min at 48C with pretitrated saturating dilutionsof the following ¯uorescein isothiocyanate (FITC)- orphycoerythrin (PE)-conjugated monoclonal antibodies(mAbs): CD45 (2D1 clone, IgG1); CD14 (MP9 clone,IgG2b); CD4 (SK3 clone, IgG1); CD3 (SK7 clone, IgG1); CD8(SK1 clone, IgG1); CD19 (SJ25C1 clone, IgG1); CD16(NKP15 clone, IgG2b); CD56 (MY31 clone, IgG1); andHLA-DR (L243 clone, IgG2a) (Becton Dickinson, CA, USA).After erythrocyte lysis with ipotonic NH4Cl solution for10 min at room temperature, cells were washed in PBSsupplemented with 0?1 mmol/l EDTA and 0?02% NaN2
(PBS-EDTA) and kept on ice until ¯ow cytometric analysis(Rutella et al, 1998). Reference ranges of lymphocyte countand subsets (25th to 75th percentile) were determined in 20healthy blood donors, after their informed consent. Thepresent investigation was approved by the InstitutionalReview Board (Catholic University School of Medicine,Rome, Italy).
Flow cytometrySamples were run through a FACScan ¯ow cytometer(Becton Dickinson) equipped with an argon laser emitting
at 488 nm. FITC and PE signals were collected at 530 nmand 575 nm respectively; spectral overlap was minimized byelectronic compensation with Calibrite beads (Becton Dick-inson) before each determination series. A minimum of3500 events was acquired in list mode using CellQuestsoftware (Becton Dickinson); forward (FSC) and side (SSC)scatter were collected as linear signals, and ¯uorescentemissions were collected on a four-decade logarithmic scale.Absolute counts of T-cell subpopulations, B-cells and NKcells were calculated as follows (Koehne et al, 1997):
�AbsLymphocytes� ´ % T�B;NK� cells
100
Lymphocytes were gated in a bivariate FSC vs. SSC cytogramand were >95% CD45brightCD14neg. For proper CD4� andCD8� T-cell evaluation, CD4dim and CD8dim events wereexcluded from the analysis.
Statistical methodsThe approximation of population distribution to normalitywas tested using y(g) statistics for kurtosis and symmetry(McGuinness et al, 1997). Results were asymmetricallydistributed and, consequently, were presented as median andinterquartile range. Inferential statistics were used foranalysis of differences between study groups by means ofthe Mann±Whitney or the Kruskal±Wallis test, as appro-priate. Differences in the kinetics of lymphocyte subsetrecovery were examined using the generalized Wilcoxonprocedure. Correlations were evaluated using Spearmanrank analysis (Rs). Multivariate regression models wereformed to examine the relation between the dependentvariable (time to lymphocyte engraftment) and potentialpredictor variables, both continuous and dichotomic, i.e.number of CD34� cells infused, G-CSF administration in thepost-transplantation period, type of pretransplant condition-ing regimen (busulphan-containing vs. no busulphan-containing) and disease status at transplantation (completeremission vs. partial remission or progressive disease). Thecriterion for statistical signi®cance was de®ned as P<0?05;all reported P-values are two-sided probability levels.
RESULTS
Lymphocyte content and composition of peripheral bloodharvestsA median of 1?88 ´ 109 CD3� T-cells (range 0?47±3?46),0?96 ´ 109 CD4� T-cells (range 0?27±2?46), 0?91 ´ 109
CD8� T-cells (range 0?22±1?23) and 0?30 ´ 109 CD19� B-cells (range 0?04±0?46) was infused with the unselectedPBPC grafts. In the CD34� group, the median number ofinfused CD3� T-cells and CD19� B-cells was 0?51 ´ 106
(range 0?15±0?9) and 0?23 ´ 106 (range 0?16±1), respec-tively, and the median number of CD4� and CD8� T-cells was0?3 ´ 106 (range 0?12±0?38) and 0?28 ´ 106 (range 0?15±0?32) respectively. Thus, these values re¯ected a 3?5 and 1?3log-depletion of CD3� and CD19� lymphocytes, and a 3?2-log depletion of both CD4� and CD8� T-cells, in the puri®edcompared with the unmanipulated PBPC products.
After CD34� cell selection, a median of 4?6 ´ 106 (range
1?4±10?76) CD34� cells/kg of recipient's body weight wascollected and infused; in group B patients, the medianpercentage of CD34� PBPCs in the leukapheresis productwas 2?9% (range 0?4±6%) and a median of 6 ´ 106 (range1?5±20?56) CD34� cells/kg of recipient's body weight wasinfused.
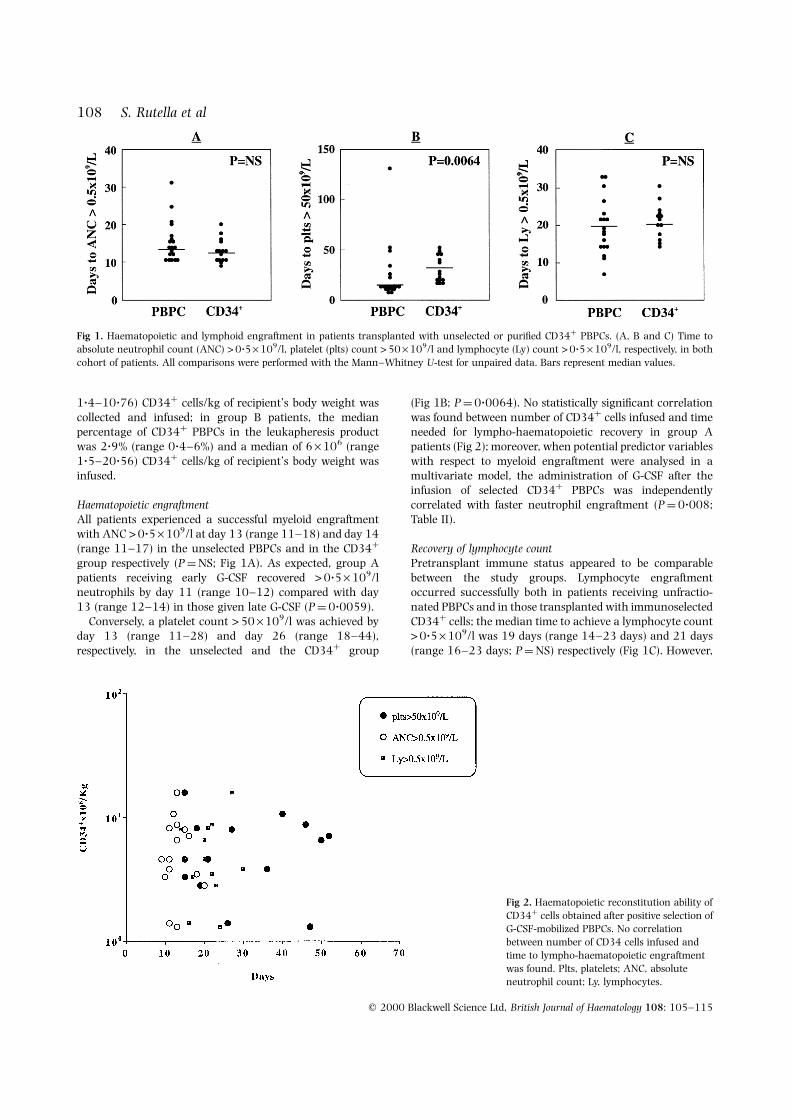
Haematopoietic engraftmentAll patients experienced a successful myeloid engraftmentwith ANC >0?5 ´ 109/l at day 13 (range 11±18) and day 14(range 11±17) in the unselected PBPCs and in the CD34�
group respectively (P�NS; Fig 1A). As expected, group Apatients receiving early G-CSF recovered >0?5 ´ 109/lneutrophils by day 11 (range 10±12) compared with day13 (range 12±14) in those given late G-CSF (P�0?0059).
Conversely, a platelet count >50 ´ 109/l was achieved byday 13 (range 11±28) and day 26 (range 18±44),respectively, in the unselected and the CD34� group
(Fig 1B; P�0?0064). No statistically signi®cant correlationwas found between number of CD34� cells infused and timeneeded for lympho-haematopoietic recovery in group Apatients (Fig 2); moreover, when potential predictor variableswith respect to myeloid engraftment were analysed in amultivariate model, the administration of G-CSF after theinfusion of selected CD34� PBPCs was independentlycorrelated with faster neutrophil engraftment (P�0?008;Table II).
Recovery of lymphocyte countPretransplant immune status appeared to be comparablebetween the study groups. Lymphocyte engraftmentoccurred successfully both in patients receiving unfractio-nated PBPCs and in those transplanted with immunoselectedCD34� cells; the median time to achieve a lymphocyte count>0?5 ´ 109/l was 19 days (range 14±23 days) and 21 days(range 16±23 days; P�NS) respectively (Fig 1C). However,
q 2000 Blackwell Science Ltd, British Journal of Haematology 108: 105±115
108 S. Rutella et al
Fig 1. Haematopoietic and lymphoid engraftment in patients transplanted with unselected or puri®ed CD34� PBPCs. (A, B and C) Time to
absolute neutrophil count (ANC) >0?5 ´ 109/l, platelet (plts) count >50 ´ 109/l and lymphocyte (Ly) count >0?5 ´ 109/l, respectively, in both
cohort of patients. All comparisons were performed with the Mann±Whitney U-test for unpaired data. Bars represent median values.
Fig 2. Haematopoietic reconstitution ability of
CD34� cells obtained after positive selection ofG-CSF-mobilized PBPCs. No correlation
between number of CD34 cells infused and
time to lympho-haematopoietic engraftment
was found. Plts, platelets; ANC, absoluteneutrophil count; Ly, lymphocytes.
109Immune Reconstitution after CD34� Cell Transplantation
q 2000 Blackwell Science Ltd, British Journal of Haematology 108: 105±115
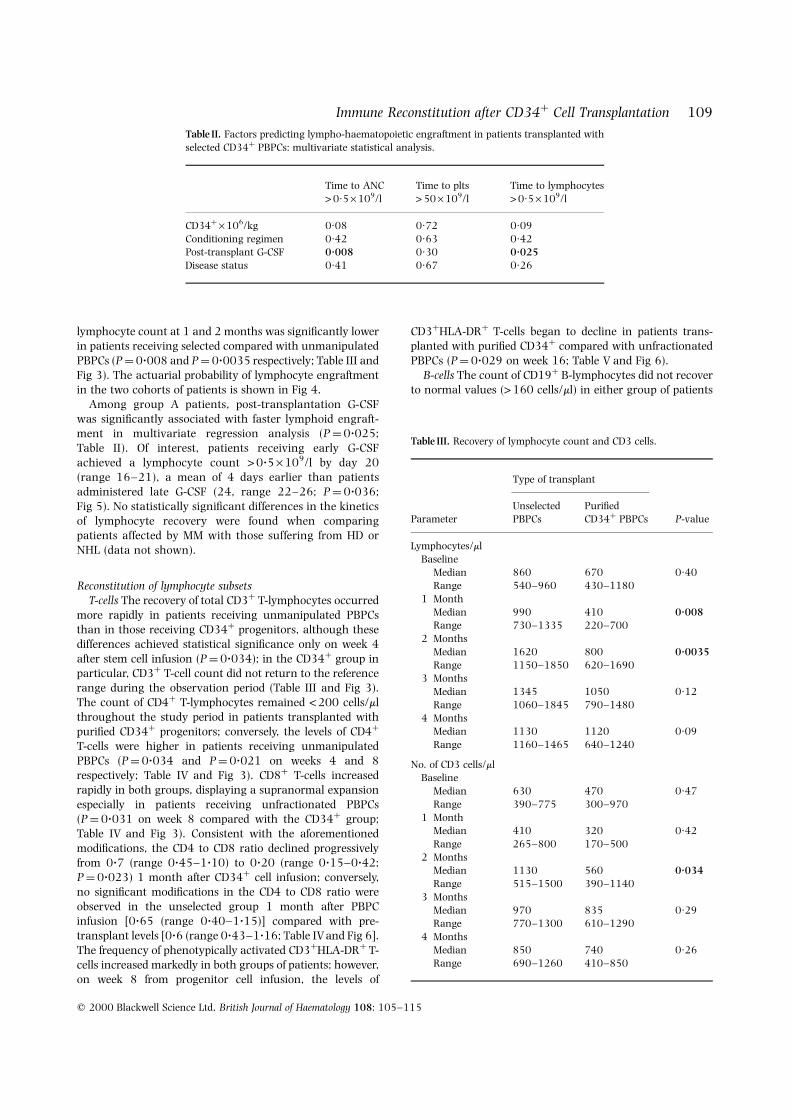
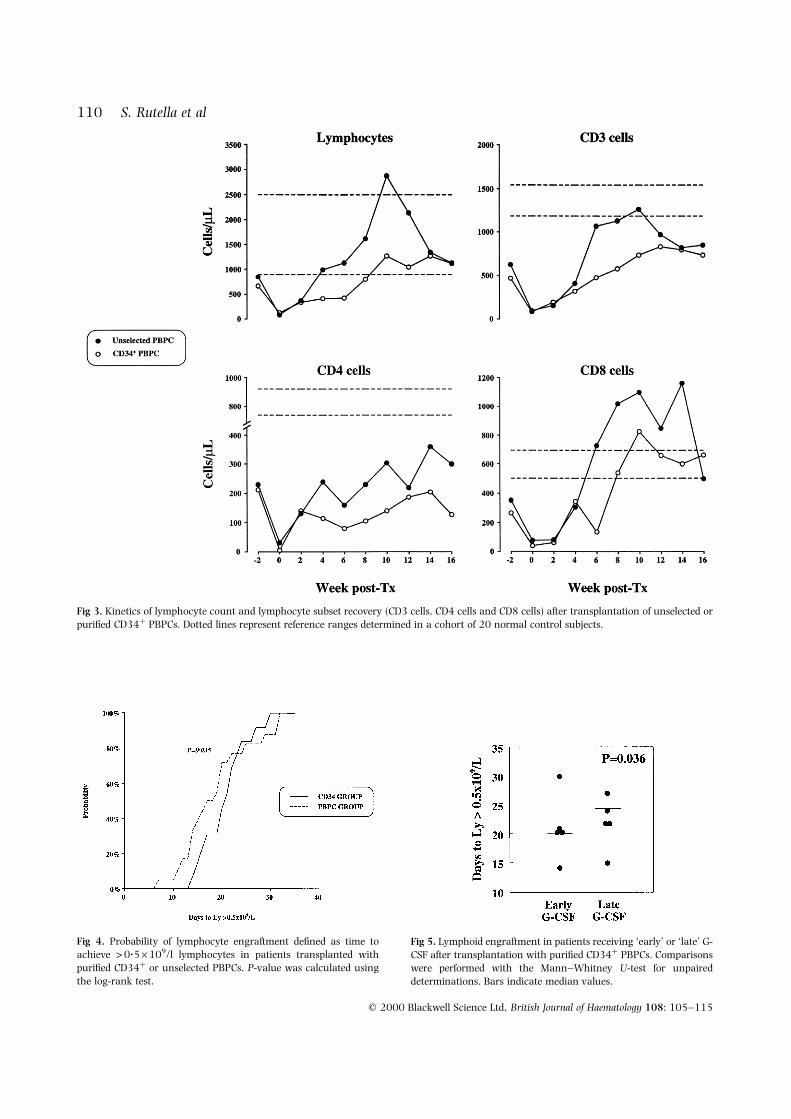
lymphocyte count at 1 and 2 months was signi®cantly lowerin patients receiving selected compared with unmanipulatedPBPCs (P�0?008 and P�0?0035 respectively; Table III andFig 3). The actuarial probability of lymphocyte engraftmentin the two cohorts of patients is shown in Fig 4.
Among group A patients, post-transplantation G-CSFwas signi®cantly associated with faster lymphoid engraft-ment in multivariate regression analysis (P �0?025;Table II). Of interest, patients receiving early G-CSFachieved a lymphocyte count >0?5 ´ 109/l by day 20(range 16±21), a mean of 4 days earlier than patientsadministered late G-CSF (24, range 22±26; P�0?036;Fig 5). No statistically signi®cant differences in the kineticsof lymphocyte recovery were found when comparingpatients affected by MM with those suffering from HD orNHL (data not shown).
Reconstitution of lymphocyte subsetsT-cells The recovery of total CD3� T-lymphocytes occurred
more rapidly in patients receiving unmanipulated PBPCsthan in those receiving CD34� progenitors, although thesedifferences achieved statistical signi®cance only on week 4after stem cell infusion (P�0?034); in the CD34� group inparticular, CD3� T-cell count did not return to the referencerange during the observation period (Table III and Fig 3).The count of CD4� T-lymphocytes remained <200 cells/mlthroughout the study period in patients transplanted withpuri®ed CD34� progenitors; conversely, the levels of CD4�
T-cells were higher in patients receiving unmanipulatedPBPCs (P�0?034 and P�0?021 on weeks 4 and 8respectively; Table IV and Fig 3). CD8� T-cells increasedrapidly in both groups, displaying a supranormal expansionespecially in patients receiving unfractionated PBPCs(P�0?031 on week 8 compared with the CD34� group;Table IV and Fig 3). Consistent with the aforementionedmodi®cations, the CD4 to CD8 ratio declined progressivelyfrom 0?7 (range 0?45±1?10) to 0?20 (range 0?15±0?42;P�0?023) 1 month after CD34� cell infusion; conversely,no signi®cant modi®cations in the CD4 to CD8 ratio wereobserved in the unselected group 1 month after PBPCinfusion [0?65 (range 0?40±1?15)] compared with pre-transplant levels [0?6 (range 0?43±1?16; Table IV and Fig 6].The frequency of phenotypically activated CD3�HLA-DR� T-cells increased markedly in both groups of patients; however,on week 8 from progenitor cell infusion, the levels of
CD3�HLA-DR� T-cells began to decline in patients trans-planted with puri®ed CD34� compared with unfractionatedPBPCs (P�0?029 on week 16; Table V and Fig 6).
B-cells The count of CD19� B-lymphocytes did not recoverto normal values (>160 cells/ml) in either group of patients
Table II. Factors predicting lympho-haematopoietic engraftment in patients transplanted with
selected CD34� PBPCs: multivariate statistical analysis.
Time to ANC Time to plts Time to lymphocytes
>0´5 ´ 109/l >50 ´ 109/l >0´5 ´ 109/l
CD34� ´ 106/kg 0´08 0´72 0´09
Conditioning regimen 0´42 0´63 0´42Post-transplant G-CSF 0´008 0´30 0´025
Disease status 0´41 0´67 0´26
Table III. Recovery of lymphocyte count and CD3 cells.
Type of transplant
Unselected Puri®edParameter PBPCs CD34� PBPCs P-value
Lymphocytes/ml
Baseline
Median 860 670 0´40Range 540±960 430±1180
1 Month
Median 990 410 0´008Range 730±1335 220±700
2 Months
Median 1620 800 0´0035
Range 1150±1850 620±16903 Months
Median 1345 1050 0´12
Range 1060±1845 790±1480
4 MonthsMedian 1130 1120 0´09
Range 1160±1465 640±1240
No. of CD3 cells/mlBaseline
Median 630 470 0´47
Range 390±775 300±970
1 MonthMedian 410 320 0´42
Range 265±800 170±500
2 MonthsMedian 1130 560 0´034
Range 515±1500 390±1140
3 Months
Median 970 835 0´29Range 770±1300 610±1290
4 Months
Median 850 740 0´26
Range 690±1260 410±850
q 2000 Blackwell Science Ltd, British Journal of Haematology 108: 105±115
110 S. Rutella et al
Fig 3. Kinetics of lymphocyte count and lymphocyte subset recovery (CD3 cells, CD4 cells and CD8 cells) after transplantation of unselected or
puri®ed CD34� PBPCs. Dotted lines represent reference ranges determined in a cohort of 20 normal control subjects.
Fig 4. Probability of lymphocyte engraftment de®ned as time toachieve >0?5 ´ 109/l lymphocytes in patients transplanted with
puri®ed CD34� or unselected PBPCs. P-value was calculated using
the log-rank test.
Fig 5. Lymphoid engraftment in patients receiving `early' or `late' G-
CSF after transplantation with puri®ed CD34� PBPCs. Comparisons
were performed with the Mann±Whitney U-test for unpaired
determinations. Bars indicate median values.

111Immune Reconstitution after CD34� Cell Transplantation
q 2000 Blackwell Science Ltd, British Journal of Haematology 108: 105±115
during the study period; thus, the delayed repopulationof B-cells appeared to be independent of stem cell source(Table V and Fig 6).
NK cells The repopulation of NK cells, de®ned by the
co-expression of CD16 and CD56 and by the lack of CD3antigen, followed a similar pattern in both groups of patients;NK cells returned to normal values starting from week 4 inboth patient groups, although they were dramatically
Table IV. Recovery of CD4 and CD8 cells.
Type of transplant
Unselected Puri®ed
Parameter PBPCs CD34� PBPCs P-value
No. of CD4 cells/mlBaseline
Median 230 210 0´34
Range 140±365 135±340
1 MonthMedian 240 115 0´034
Range 175±520 60±275
2 Months
Median 230 110 0´021Range 100±310 75±160
3 Months
Median 220 190 0´15Range 185±410 160±260
4 Months
Median 300 130 0´07
Range 275±445 90±230
No. of CD8 cells/ml
Baseline
Median 350 265 0´35Range 240±475 150±470
1 Month
Median 310 345 0´26
Range 180±515 190±7602 Months
Median 1020 540 0´031
Range 725±1230 360±1075
3 MonthsMedian 850 660 0´13
Range 560±1280 450±1040
4 MonthsMedian 500 665 0´38
Range 430±700 360±740
CD4 to CD8 ratio
BaselineMedian 0´60 0´70 0´48
Range 0´43±1´16 0´45±1´10
1 MonthMedian 0´65 0´20 0´023
Range 0´40±1´15 0´15±0´42
2 Months
Median 0´20 0´15 0´12Range 0´19±0´46 0´08±0´30
3 Months
Median 0´32 0´30 0´31
Range 0´20±0´51 0´25±0´504 Months
Median 0´40 0´20 0´17
Range 0´35±0´70 0´10±0´40
Table V. Recovery of activated T-cells, B-cells and NK cells.
Type of transplant
Unselected Puri®ed
Parameter PBPCs CD34� PBPCs P-value
No. of CD3/HLA-DR cells/mlBaseline
Median 230 130 0´0041
Range 180±305 50±170
1 MonthMedian 225 215 0´29
Range 90±520 40±830
2 Months
Median 680 460 0´32Range 240±1090 280±850
3 Months
Median 730 485 0´38Range 200±850 330±800
4 Months
Median 670 510 0´029
Range 490±790 205±635
No. of CD19 cells/ml
Baseline
Median 60 20 0´022Range 25±205 7±60
1 Month
Median 5 5 0´27
Range 5±10 5±102 Months
Median 45 30 0´26
Range 20±140 20±65
3 MonthsMedian 80 100 0´19
Range 60±120 25±190
4 MonthsMedian 130 100 0´19
Range 90±180 55±200
No. of NK cells/ml
BaselineMedian 105 90 0´40
Range 75±200 30±120
1 MonthMedian 280 160 0´34
Range 150±440 60±290
2 Months
Median 280 140 0´014Range 180±550 55±320
3 Months
Median 140 140 0´37
Range 110±420 105±2804 Months
Median 260 160 0´052
Range 190±290 140±250

expanded in the PBPC group (P�0?014 on week 8compared with patients receiving puri®ed CD34� progeni-tors; Table V and Fig 6).
DISCUSSION
Immune reconstitution after autologous or allogeneic bonemarrow transplantation has been analysed extensively(Storek & Saxon, 1992; Talmadge et al, 1997); conversely,no investigations have focused speci®cally on the kinetics ofimmunological recovery in patients affected by haemato-logical malignancies and transplanted with autologousCD34� PBPCs selected with the CEPRATE SC device. In arecent investigation on lymphoid reconstitution after trans-plantation with FACS-sorted autologous CD34� progenitors,the recovery of peripheral T-cell and B-cell compartmentswas severely delayed for up to 1 year after PBPC infusion;moreover, a global decrease in most Vb TCR� subsets and atransient oligoclonal expansion of T-cells expressing speci®cVb TCR have been demonstrated (Bomberger et al, 1998). Adelayed lymphocyte reconstitution has been described inpatients transplanted with selected CD34� PBPCs for NHL;in that study, all lymphocyte subsets remained subnormal at
12 months after transplant, and CD4� T-cells, in particular,were markedly de®cient at 18 months from CD34� cellinfusion (Divine et al, 1999). Similar results have beenreported after the infusion of allogeneic CD34� PBPCs, withthe number of CD4�, CD4�CD45RA� and TCRgd� cellsduring the ®rst 6 months being signi®cantly lower than afterthe allogeneic transplantation of unmanipulated PBPCs;conversely, no differences in the repopulation of CD8�,CD19� and NK cells between transplant groups have beendescribed (Martinez et al, 1999).
There is a consensus that, after autologous BM or PBPCinfusion, T-cells reconstitute from different sources, i.e. (a)recipient T-cells that survive the conditioning regimen; (b)T-cells contained in the graft; (c) progenitor cells thatdifferentiate in the recipient; and (d) residual stem cells of therecipient (Guillaume et al, 1998). In hosts lacking thymicfunction, T-cell reconstitution has been shown to occurpredominantly from peripheral T-cell progenitors containedin the graft, and such a thymic-independent pathway shouldpredominate in humans as a result of age- and chemother-apy-related impairment of thymic regenerative capacity(MacDonald et al, 1986). As a result, adult and elderlyrecipients of bone marrow transplantation should be unable
q 2000 Blackwell Science Ltd, British Journal of Haematology 108: 105±115
112 S. Rutella et al
Fig 6. Kinetics of lymphocyte subset recovery (CD4 to CD8 ratio, CD19 cells, activated CD3/HLA-DR cells and NK cells) after transplantation of
unselected or puri®ed CD34� PBPCs. Dotted lines represent reference ranges determined in a cohort of 20 normal control subjects.

113Immune Reconstitution after CD34� Cell Transplantation
q 2000 Blackwell Science Ltd, British Journal of Haematology 108: 105±115
to regenerate naive CD4� T-cells, thus accounting for avigorous T-cell depletion and severe clinical immunode®-ciency; conversely, no differences exist in the reconstitutionof CD8� T-cells in thymectomized vs. thymus-bearing mice(MacDonald et al, 1986; Mackall et al, 1993). Of interest,CD8� T-cell regeneration might occur irrespective of bothtype of transplant (autologous vs. allogeneic) and condition-ing regimen (San Miguel et al, 1996).
We examined the kinetics of immune repopulation inpatients transplanted with highly puri®ed autologous CD34�
PBPCs and in a cohort of patients who received unselectedPBPCs. Patients in the unselected group experienced a fasterplatelet recovery compared with patients given CD34�
PBPCs, while no differences were recorded with respect toneutrophil engraftment; conceivably, these phenomenacould be explained by G-CSF administration after theinfusion of CD34� PBPCs, as was also suggested by thefaster recovery of circulating neutrophils in patients givenearly compared with late G-CSF. The correlation betweennumber of CD34� cells infused in group A patients and timeneeded for haematopoietic reconstitution failed to reachstatistical signi®cance in accordance with previously pub-lished trials on the repopulating ability of selected CD34�
PBPCs (Voso et al, 1999).Lymphocyte count recovered promptly in both groups of
patients; this was of potential interest, as faster lymphocyterecovery has been shown to predict better survival afterallogeneic PBPC transplantation (Pavletic et al, 1998). Nostatistically signi®cant differences in the kinetics of lympho-cyte recovery were found in group A when comparingpatients affected by MM with those suffering from HD or NHL(data not shown), thus suggesting that the underlyingdisease did not in¯uence immune reconstitution in thiscohort of patients.
In the CD34� group, lymphoid engraftment, de®ned bythe time to achieve a lymphocyte count >0?5 ´ 109/l, wasindependently associated with the post-transplant adminis-tration of G-CSF; moreover, patients receiving early G-CSFexperienced a prompter lymphocyte engraftment than thosegiven late G-CSF. These ®ndings suggest that the acceleratedrecovery of lymphocyte count might have been favoured byG-CSF treatment, which has recently been shown to increaselymphocyte count in both humans and mice (Rutella et al,1999a). Moreover, in a recent randomized trial comparingthe effects of GM-CSF and G-CSF on immune recovery afterautologous BMT, both growth factors were found to enhanceimmune reconstitution and, in particular, CD8� T-cellnumbers; to the contrary, neither of the two growth factorssigni®cantly affected B-cell or NK cell recovery (San Miguelet al, 1996).
The amount of passively transferred lymphocytes corre-lated inversely with the time to lymphocyte engraftment ingroup A patients, thus con®rming recent observations that,despite extensive T-cell depletion of the graft, mature T-cellsinfused along with selected CD34� PBPCs contributedsigni®cantly to T-cell recovery (Divine et al, 1999).
A delayed repopulation of CD4� T-cells occurred inboth cohorts of patients enrolled in the present study, andCD4� T-cells were signi®cantly lower in the CD34�
compared with the unselected group after 1 and 2 monthsfrom progenitor cell infusion; CD8� T-cells expandeddramatically but returned to the reference range soon aftertransplantation. The CD8 overshoot was responsible for aremarkable inversion of the CD4 to CD8 ratio in both patientgroups. Moreover, both CD4� and CD8� T-cells displayed anactivated phenotype, co-expressing HLA-DR antigen; thesigni®cance of this activation process remains unknown, asno correlation has been found between the number ofactivated CD3�HLA-DR� T-cells and the occurrence ofcomplications (Leino et al, 1991). No differences wereobserved in the kinetics of B-cell repopulation between thestudy groups, and CD19� B-cell count was markedlydepressed both in patients transplanted with CD34� PBPCsand in those receiving unselected PBPCs. NK cells expandedmarkedly in both patient groups, although higher valueswere recorded in patients transplanted with unfractionatedPBPCs; this is in agreement with studies on the recovery ofimmune function after PBPC transplantation, in which NKcells were found to reconstitute rapidly and to exert highlevels of cytotoxicity and an enhanced GVL effect (Fegan et al,1995; Scheid et al, 1995).
Donor T-cells in the graft might contribute to the controlof viral infections by preventing post-transplant virusactivation; thus, T-cell depletion is expected to impact onthe incidence of viral infections through the elimination ofimmunocompetent cells (Miyamoto et al, 1998). Recently,severe infectious complications, i.e. extensive varicella zostervirus (VZV) infection, Pneumocystis carinii pneumonia,cytomegalovirus (CMV) retinitis and adenovirus-associatedhaemorrhagic cystitis, have been described in patientsreceiving autologous CD34� PBPCs for NHL (Miyamotoet al, 1998; Divine et al, 1999); such opportunistic infectionswere associated with a profound de®ciency in the CD4�
T-cell compartment and were reminiscent of those observedafter the infusion of T-cell-depleted bone marrow (Small et al,1999).
Potentially life-threatening opportunistic infections havebeen described exclusively in patients whose CD4� T-cellcount is <200/ml; in addition, the rate of CD4� recoverycorrelated strongly with the risk of developing infections(Small et al, 1999). Although no difference in incidence ortype of infections has been reported in patients transplantedwith selected vs. unselected PBPCs for multiple myeloma(Vescio et al, 1999), in a recent analysis on 19 consecutivepatients receiving immunoselected CD34� PBPCs, an 11%incidence of viral infections (CMV enteritis, adenovirus-associated haemorrhagic cystitis) was documented within100 days from PBPC infusion (Sica et al, 1998). These datacompare unfavourably with those reported in the same studyand concerning a larger series of patients receivingunfractionated PBPCs, in whom no viral infections occurredwithin 100 days from transplantation.
In the present study, viral infections (adenovirus-associated enteritis) were diagnosed in three patients (20%)within the CD34� group, while they were not observed inpatients transplanted with unmanipulated PBPCs. Theseobservations strongly suggest that the susceptibility to viralinfections might be increased in patients receiving CD34�

PBPCs. As abnormalities of T-cell number and functionmight contribute signi®cantly to transplant morbidity andmortality via infectious complications, an understanding ofT-cell repopulation kinetics should lead to strategies toimprove post-transplantation cellular immunity.
In conclusion, recipients of puri®ed CD34� progenitorspromptly recovered their lymphocyte count, althoughnumbers of circulating T-cells and, in particular, of CD4�
T-lymphocytes were signi®cantly depressed during the ®rst 2months after the infusion of CD34� vs. unmanipulatedPBPCs. The over-representation of CD8� T-cells soon aftertransplantation was responsible for a severe inversion ofthe CD4 to CD8 ratio. However, a precise correlation betweenT-cell subset distribution and overall T-lymphocyte functionis uncertain, and studies are ongoing to characterize T-cellcompetence, i.e. proliferation, cytokine production andeffector lytic functions, after CD34� PBPC transplantation(Rutella et al, 1999b). Moreover, abnormalities of T-cellreconstitution deserve careful investigation, as the suscept-ibility to viral infections might be increased in patientsreceiving CD34� PBPCs.
ACKNOWLEDGMENT
This work was supported in part by AIRC (AssociazioneItaliana per la Ricerca sul Cancro).
REFERENCES
Bomberger, C., Singh-Jairam, M., Rodey, G., Guerriero, A., Yeager,
A.M., Fleming, W.H., Holland, H.K. & Waller, E.K. (1998)
Lymphoid reconstitution after autologous PBSC transplantationwith FACS-sorted CD34� hematopoietic progenitors. Blood, 91,
2588±2600.
DivineÂ, M., Boutolleau, D., Delfau-Larue, M.H., Beaujean, F., Jouault,H., Reyes, F., Kuentz, M., Bensussan, A., Farcet, J.P. & Boumsell, L.
(1999) Poor lymphocyte recovery following CD34-selected auto-
logous peripheral blood stem cell transplantation for non-
Hodgkin's lymphoma. British Journal of Haematology, 105, 349±360.
Fegan, C., Thomas, H., Bailey-Wood, R., Coleman, S., Phillips, S.,
Hoy, T. & Whittekar, J.A. (1995) In vitro LAK activity following
autologous peripheral blood stem cell is signi®cantly greater thanthat following autologous bone marrow and allogeneic bone
marrow transplantation. Bone Marrow Transplantation, 16, 277±
281.
Guillaume, T., Rubinstein, D.B. & Symann, M. (1998) Immunereconstitution and immunotherapy after autologous hemato-
poietic stem cell transplantation. Blood, 92, 1471±1490.
Jin, N.R., Lum, L.G., Buren, E.V., Lerman, S.P., Walker, E.L. &June, C.H. (1995) Signal transduction by B and T cells early after
bone marrow transplantation: B cells calcium ¯ux responses are
intact whereas lack of CD4 cells accounts for impaired T cell
responses. Bone Marrow Transplantation, 16, 103±109.Koehne, G., Zeller, W., Stockschlaeder, M. & Zander, A.R. (1997)
Phenotype of lymphocyte subsets after autologous peripheral
blood stem cell transplantation. Bone Marrow Transplantation, 19,
149±156.Leino, L., Lilius, E.M., Nikoskelainen, J., Pelliniemi, T.T. & Rajamaki,
A. (1991) The reappearance of 10 differentiation antigens on
peripheral blood lymphocytes after allogeneic bone marrow
transplantation. Bone Marrow Transplantation, 8, 339±344.
Lenarsky, C. (1993) Mechanisms in immune recovery after bone
marrow transplantation. American Journal of Pediatric Hematology/Oncology, 15, 49±55.
MacDonald, H.R., Blanc, C., Lees, R.K. & Sordat, B. (1986)
Abnormal distinction of T cell subsets in athymic mice. Journal
of Immunology, 136, 4337±4339.McGuinness, D., Bennett, S. & Riley, E. (1997) Statistical analysis of
highly skewed immune response data. Journal of Immunological
Methods, 201, 99±114.Mackall, C.L., Granger, L., Sheard, M.A., Cepeda, R. & Gress, R.E.
(1993) T-cell regeneration after bone marrow transplantation:
differential CD45 isoform expression on thymic-derived versus
thymic-independent progeny. Blood, 82, 2585±2594.Martinez, C., Urbano-Ispizua, A., Rozman, C., Marin, P., Rovira, M.,
Sierra, J., Montfort, N., Carreras, E. & Montserrat, E. (1999)
Immune reconstitution following allogeneic peripheral blood
progenitor cell transplantation: comparison of recipients ofpositive CD34� selected grafts with recipients of unmanipulated
grafts. Experimental Hematology, 27, 561±568.
Miyamoto, T., Gondo, H., Miyoshi, Y., Shigematsu, H., Minematsu,T., Takenaka, K., Tanimoto, K., Horiuchi, T., Asano, Y., Inaba, S.,
Minamishima, Y. & Niho, Y. (1998) Early viral complications
following CD34-selected autologous peripheral blood stem cell
transplantation for non-Hodgkin's lymphoma. British Journal ofHaematology, 100, 348±350.
Ottinger, H.D., Beelen, D.W., Scheulen, B., Schaefer, U.W. & Grosse
Wilde, H. (1996) Improved immune reconstitution after allo-
transplantation of peripheral blood stem cells instead of bonemarrow. Blood, 88, 2775±2779.
Pavletic, Z.S., Joshi, S.S., Pirruccello, S.J., Tarantolo, S.R., Kollath, J.,
Reed, E.C., Bierman, P.J., Vose, J.M., Warkentin, P.I., Gross, T.G.,
Nasrati, K., Armitage, J.O., Kessinger, A. & Bishop, M.R. (1998)Lymphocyte reconstitution after allogeneic blood stem cell
transplantation for hematologic malignancies. Bone Marrow
Transplantation, 21, 33±41.Piccirillo, N., Sica, S., Laurenti, L., Chiusolo, P., La Barbera, E.O.,
SoraÁ, F. & Leone, G. (1999) Optimal timing of G-CSF administra-
tion after CD34� immunoselected peripheral blood progenitor cell
transplantation. Bone Marrow Transplantation, 23, 1245±1250.Rosillo, M.C., Ortuno, F., Moraleda, J.M., Lozano, M.L., Heras, I., De
Arriba, F. & Vicente, V. (1996) Immune recovery after autologous
or rhG-CSF primed PBSC transplantation. European Journal of
Haematology, 56, 301±307.Rumi, C., Rutella, S., Teo®li, L., Etuk, B., Ortu La Barbera, E.,
Micciulli, G., Voso, M.T. & Leone, G. (1997) RhG-CSF mobilized
CD34� peripheral blood progenitors are myeloperoxidase-negativeand non-cycling irrespective of CD33 or CD13 coexpression.
Experimental Hematology, 25, 246±251.
Rutella, S., Rumi, C., Lucia, M.B., Sica, S., Cauda, R. & Leone, G.
(1998) Serum of healthy donors receiving recombinant humangranulocyte colony-stimulating factor (rhG-CSF) induces T-cell
unresponsiveness. Experimental Hematology, 26, 1024±1033.
Rutella, S., Rumi, C., Sica, S. & Leone, G. (1999a) Recombinant
human granulocyte colony-stimulating factor (rhG-CSF): effectson lymphocyte phenotype and function. Journal of Interferon and
Cytokine Research, 19, 989±994.
Rutella, S., Rumi, C., Lucia, M.B., Barberi, T., Puggioni, P.L., Lai, M.,
Romano, A., Cauda, R. & Leone, G. (1999b) Induction of CD69antigen on normal CD4� and CD8� lymphocyte subsets and its
relationship with the phenotype of responding T-cells. Cytometry,
38, 95±101.San Miguel, J.F., Hernandez, M.D., Gonzalez, M., Lopez Berges, M.C.,
q 2000 Blackwell Science Ltd, British Journal of Haematology 108: 105±115
114 S. Rutella et al

115Immune Reconstitution after CD34� Cell Transplantation
q 2000 Blackwell Science Ltd, British Journal of Haematology 108: 105±115
Caballero, M.D., Vazquez, L., Orfao, A., Nieto, M.J., Corral, M. & del
Canizo, M.C. (1996) A randomized study comparing the effect of
GM-CSF and G-CSF on immune reconstitution after autologous
bone marrow transplantation. British Journal of Haematology, 94,140±147.
Scheid, C., Pettengell, R., Ghielmini, M., Radford, J.A., Morgenstern,
G.R., Stern, P.L. & Crowther, D. (1995) Time-course of the
recovery of cellular immune function after high-dose chemother-apy and peripheral blood progenitor cell transplantation for high-
grade non-Hodgkin's lymphoma. Bone Marrow Transplantation,
15, 901±906.Schmitz, N., Bacigalupo, A., Labopin, M., Majolino, I., Laporte, J.,
Brinch, L., Cook, G., Lambertenghi Deliliers, G., Lange, A.,
Rozman, C., Garcia-Conde, J., Finke, J., Domingo-Albos, A. &
Gratwohl, A. (1996) Transplantation of peripheral blood pro-genitor cells from HLA-identical sibling donors. British Journal of
Haematology, 95, 715±723.
Sica, S., Salutari, P., Ortu La Barbera, E., Sora', F., Piccirillo, N. &
Leone, G. (1998) Infectious complications after CD34-selectedautologous peripheral blood stem cell transplantation. British
Journal of Haematology, 101, 592±593.
Small, T.N., Papadopoulos, E.B., Boulad, F., Black, P., Castro-Malaspina, H., Childs, B.H., Collins, N., Gillio, A., George, D.,
Jakubowski, A., Heller, G., Fazzari, M., Kernan, N., MacKinnon, S.,
Szabolcs, P., Young, J.W. & O'Reilly, R.J. (1999) Comparison of
immune reconstitution after unrelated and related T-cell-depletedbone marrow transplantation: effect of patient age and donor
lymphocyte infusions. Blood, 93, 467±480.
Storek, J. & Saxon, A. (1992) Reconstitution of B cell immunity
following bone marrow transplantation. Bone Marrow Transplan-
tation, 9, 395±408.
Storek, J., Witherspoon, R.P. & Storb, R. (1995) T cell reconstitution
after bone marrow transplantation into adult patients does notresemble T cell development in early life. Bone Marrow Transplan-
tation, 16, 413±425.
Talmadge, J.E., Reed, E., Ino, K., Kessinger, A., Kuszynski, C.,
Heimann, D., Varney, M., Jackson, J., Vose, J.M. & Bierman, P.J.(1997) Rapid immunologic reconstitution following transplanta-
tion with mobilized peripheral blood stem cells as compared to
bone marrow. Bone Marrow Transplantation, 19, 161±172.Tricot, G., Gazitt, Y., Leemhuis, T., Jagannath, S., Desikan, K.R.,
Siegel, D., Fassas, A., Tindle, S., Nelson, J., Juttner, C., Tsukamoto, A.,
Hallagan, J., Atkinson, K., Reading, C., Hoffman, R. & Barlogie, B.
(1998) Collection, tumor contamination and engraftment kineticsof highly puri®ed hematopoietic progenitor cells to support high
dose therapy in multiple myeloma. Blood, 91, 4489±4495.
Vescio, R., Schiller, G., Stewart, A.K., Ballester, O., Noga, S., Rugo, H.,
Freytes, C., Stadtmauer, E., Tarantolo, S., Sahebi, F., Stiff, P.,Meharchard, J., Schlossman, R., Brown, R., Tully, H., Benyunes,
M., Jacobs, C., Berenson, R., Di Persio, J., Anderson, K. & Berenson,
J. (1999) Multicenter phase III trial to evaluate CD34� selectedversus unselected autologous peripheral blood progenitor cell
transplantation in multiple myeloma. Blood, 93, 1858±1868.
Voso, M.T., Hohaus, S., Moos, M., Pforsich, M., Cremer, F.W.,
Schlenk, R.F., Martin, S., Hegenbart, U., Goldschmidt, H. & Haas,R. (1999) Autografting with CD34� peripheral blood stem cells:
retained engraftment capability and reduced tumour cell content.
British Journal of Haematology, 104, 382±391.