hyaluronic acid hydrogel in the treatment of osteoarthritis
TRANSCRIPT
Biomaterials 23 (2002) 4503–4513
Hyaluronic acid hydrogel in the treatment of osteoarthritis
R. Barbuccia,*, S. Lamponia, A. Borzacchiellob, L. Ambrosiob, M. Finic,d,P. Torricellic,d, R. Giardinoc
aDepartment of Chemical and Biosystem Sciences and Technology, CRISMA, University of Siena, Via Aldo Moro n. 2, 53100 Siena, Italyb Interdisciplinary Research Center in Biomaterials (CRIB), Institute of Composite Materials Technology-CNR, University of Naples,
‘‘Federico II’’, P.le Tecchio 80, 80125 Naples, ItalycExperimental Surgery Department, Research Institute Codivilla-Putti, ItalydRizzoli Orthopaedic Institute, Via di Barbiano 1/10, 40136 Bologna, Italy
Received 7 December 2001; accepted 16 May 2002
Abstract
In order to overcome the problem of rapid clearance of the polysaccharide hyaluronic acid (Hyal) in the treatment of
osteoarthritis (OA), a 50% cross-linked Hyal hydrogel (Hyal 50%) was synthesised. The 50% refers to the amount of COOH groups
of the polysaccharide involved in the cross-linking reaction, i.e. 50% of the total amount. The rheological behaviour of the Hyal
50% hydrogel, and in particular the possibility to inject it through a needle, was studied. The results obtained demonstrated that the
hydrogel injected through the needle still behaved like a gel, although it showed a reduction of the dynamic moduli. The most
appropriate sterilisation technique for this kind of hydrogel was also evaluated. Liophilised Hyal 50% samples were sterilised by
steam, Ethylene Oxide (EtO) and g-rays. EtO and g-rays did not modify the characteristics of the hydrogel in terms of swellability
and morphology. Lastly, the in vivo effect of Hyal 50% hydrogel in the treatment of chondral defect in rabbit knee was also studied.
The results obtained showed the Hyal 50% injections improved chondrocytes density and matrix appearance. Furthermore, the
permanence in situ of the hydrogel was longer than that of the linear Hyal. r 2002 Published by Elsevier Science Ltd.
Keywords: Hyaluronan hydrogel; Osteoarthritis; Sterilisation; Rheological properties; In vivo tests
1. Introduction
Osteoarthritis (OA), also called degenerative jointdisease or iperthrophic-arthritis, is clinically characterisedby joint pain and joint-instability. By the age of 40, about90% of humans show some degenerative changes inweight-bearing joints [1]. OA is frequently found in hip,knee, distal phalangeal and intervertebral joints. OA istermed as primary or secondary, and the end-stage of thisdisease is characterised by deterioration and detachmentof the bearing of the joint and proliferation of newosteoarticular tissue at the margin [2].
Current treatment of OA is conservative and aimed atthe maintenance of mobility in the joint by physiother-apy and relief of pain. The problem that OA poses interms of new systemic therapeutic agents is that it doesnot affect all, or even many joints in the patient, as wellas in other pathologies. If a few joints are affected, the
possibility of local treatment by intra-articular injectiondoes exist, but the drug would have to be confined in itseffects; in this case, however, the compound would alsoneed to have sufficient long-term action at the site ofinjection to avoid frequent local treatments.
The natural polysaccharide hyaluronic acid (Hyal)has been claimed to be effective in pain relief andimproving joint-motion following intra-articular injec-tions in OA patients [3,4]. In fact, it has been reportedthat Hyal provides symptomatic relief for its lubricatingand cushioning properties, showing also some in vitroanti-inflammatory activity, and a possible disease-modifying effect in patients and animals [5–8]. However,localisation of response is likely to be a problem, as Hyalclearance is extremely rapid, becoming quickly degradedin vivo by enzymatic or hydrolytic reactions, which takeplace in biological environments [9,10]. The evidence,from in vitro and in vivo models of OA and from clinicaltrials, suggests that efficacy permanency dependsstrongly upon Hyal molecular weight. There are manycommercial preparations of Hyal available. These
*Corresponding author. Tel/fax: +39-577-234382.
E-mail address: [email protected] (R. Barbucci).
0142-9612/02/$ - see front matter r 2002 Published by Elsevier Science Ltd.
PII: S 0 1 4 2 - 9 6 1 2 ( 0 2 ) 0 0 1 9 4 - 1

include hyaluronan preparations of relatively lowmolecular weight (Hyalgan and ARTZ), of intermediatemolecular weight (ORTHOVISC) but lower than that ofthe hyaluronan in normal healthy synovial fluid, andcross-linked hyaluronan of high molecular weight(Hylan, SYNVISC) [11]. The existing evidence indicatesthat the only potentially serious adverse event connectedwith commercial preparations of Hyal during OAtreatment are joint infection, aseptic arthritis, andinflammation, even if in rare cases, being directlydependent upon the number of injections [12–14].Treatment with low MW preparations of hyaluronanseems to be effective. However, visco-supplementationwith hyaluronan preparations may have slightly higherrisks and less benefits than visco-supplementation withhylan, because the relatively low MW hyaluronanpreparations require more injections which may incurhigher costs and chance of infection.
In order to obtain a longer effect of Hyal in the actionsite (joint), and consequently to reduce the risk ofinfection due to numerous injections, we decided tomake the polysaccharide water insoluble by cross-linking it. The result of this reaction was the formationof a hydrogel. We have recently synthesised a series ofnew hydrogels, based on linear polysaccharides [15]. Thehydrogel synthesis procedure allows us to predictthe final desired cross-linking degree by controlling thestoichiometry reaction and conditions, and thus toobtain products with highly reproducible characteristics[16]. Within the series of hyaluronic acid-based hydro-gels, the one with a 50% cross-linking degree (Hyal50%) (in which the ratio of free and reacted carboxylicgroups is 1:1) was chosen in order to study its potentialapplications in the OA treatment. The rheologicalbehaviour of these Hyal-based hydrogels, and inparticular the possibility to inject them through a needle,was studied. Moreover, the most appropriate sterilisa-tion technique among steam, Ethylene Oxide (EtO) andg-rays for this kind of hydrogels was evaluated. The invitro cytotoxicity after EtO sterilisation was carried outand an experimental model was realised to study the invivo effect of Hyal 50% in the treatment of a surgicallycreated chondral defect in the rabbit knee.
2. Materials and methods
2.1. Materials
The sodium hyaluronate (Hyal-Na, MWE150–200 kDa) was kindly provided by Farmila S.p.A.(Milano, Italy).
Hyaluronic acid-based hydrogels with a cross-linkingdegree of 50% (Hyal 50%) was obtained with theprocedure previously described [15]. Shortly, a solutionof Hyal-Na underwent a sodium–hydrogen ionic
exchange using Dowex 50WX8 resin (Fluka, Switzer-land) and then added to a 5% tetrabutylammoniumhydroxide solution (Fluka, Switzerland) until a pH levelof 7–8 was reached. The solution was then liophilisedand tetrabutylammonium salt of hyaluronic acid (Hyal-TBA) was obtained. The Hyal-TBA salt was dissolved inN,N’-Dimethylformamide (DMF) under stirring andnitrogen flow. The solution was kept at about 01C,adding activating agent 2-chloro-1-methylpyridiniumiodide (CMPJ) estabilished for the activation of the50% number of carboxylate groups. The cross-linkingdi-amine agent 1,3 di-aminopropane (1,3 DAP) wasthen added in large excess and the reaction was left atroom temperature for 3–4 h. The reaction was catalysedby a small amount of triethylamine as hydrogen iodidecaptor. The hydrogel formed was then washed inethanol and water several times until no more solventsand reagents were found in the washing solutions asdemonstrated by UV absorption measurements. TheHyal 50% hydrogel was dried through liophylisationand the cross-linking degree was assessed by potentio-metric analysis [16].
All others reagents were commercially available andutilised without further purification.
2.2. Methods
2.2.1. Rheological analysis
2.2.1.1. Viscoelastic properties and steady shear viscosi-
ty. The rheological characterisation was performed onthe cross-linked polymers by adding bi-distilled water tolyophilised Hyal 50% samples to obtain a concentrationof 10mg/ml. The tests were performed on the gels beforeand after injection through a 22-gauge needle. A BohlinVOR Rheometer (Bohlin Reologi A B, Lund, Sweden)was used at a controlled temperature of 251C. Thegeometrical figures were cone and plate (CP 5/30 cell).The lower-plate was forced to rotate or oscillate,whereas the stress transferred from the fluid to theupper-plate was measured with a linear variabledisplacement transducer (LVDT) system.
The small-amplitude oscillatory shear experimentswere performed to measure the time-dependent responseof the samples and hence, to determine their linearviscoelastic properties. The frequency range spannedfrom 0.05 to 10Hz. This range includes the physiologi-cal frequencies of knee ranging from 0.5Hz (walk) to3Hz (running). The small-amplitude oscillatory sheartest was used successfully to determine the structure–mechanical properties relationship of materials [17,18].
In a dynamic experiment, the material is subjected toa sinusoidal shear–strain:
g ¼ g0 sin ðotÞ;
where g0 is the shear–strain amplitude, o is theoscillation frequency (which can also be expressed as
R. Barbucci et al. / Biomaterials 23 (2002) 4503–45134504
2pof where f is the frequency in Hz) and t the time. Themechanical response, expressed as shear stress t ofviscoelastic materials, is intermediate between an idealpure elastic solid (obeying Hooke’s law) and an idealpure viscous fluid (obeying Newton’s law). Therefore, itis out of phase with respect to the imposed deformationas expressed by
t ¼ G0ðoÞg0 sinðotÞ þ G00ðoÞg0 cosðotÞ;
where G0ðoÞ is the shear storage modulus and G00ðoÞ isthe shear loss modulus. G0 provides information aboutthe elasticity, or the energy stored in the material duringdeformation, whereas G00 describes the viscous characteror the energy dissipated as heat.
The combined viscous and elastic behaviour is givenby the absolute value of complex shear modulus G�:
G�ðoÞ ¼ffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiG02 þ G002
p
or by the absolute value of complex viscosity Z� definedas
Z� ¼
ffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiG02 þ G002
p
owhich is usually compared with the steady shearviscosity in order to evaluate the effect of largedeformations and shear rates on the structure of thematerial.
The ratio between the viscous modulus and the elasticmodulus is expressed by the loss tangent:
tan d ¼G00
G0 ;
where d is the phase angle.The loss tangent is a measure of the ratio of energy
lost to energy stored in the cyclic deformation [17].Strain sweep tests at a fixed oscillation frequency
(consisting in monitoring the visco-elastic propertieswhile logarithmically varying the strain amplitude g0)were performed on the materials to determine the strainamplitude at which linear visco-elasticity is valid.
The viscosity Z as function of shear rate was evaluatedthrough steady state shear measurements.
2.2.2. Sterilisation
Hyal 50% was sterilised with the following threedifferent methods: steam, g-rays and EtO. Eventualmodifications of Hyal hydrogel as a consequence ofsterilisation were evaluated by analysing the morphol-ogy and the swelling properties of the hydrogels beforeand after sterilisation.
Samples of freeze-dried liophilised Hyal 50% hydro-gel of known weight (100mg) were sealed in thefollowing containers: pyrex glass, polyethylene, poly-ethylene containers sealed in laminated bags. They weresterilised by steam, g-rays and EtO, respectively.
Steam sterilisation was conducted at 1201C, 1 atm for20min. g-rays sterilisation was performed at 25 kilograin
for 4 h. EtO sterilisation was carried out in a cylindricalethylene oxide sterilisation apparatus where the sampleswere exposed for 12 h at 42731C to a 20% EtO:80%CO2 atmosphere with a relative humidity rangingfrom 50% to 95%. Then they were aerated for 7 days ina desorption chamber at 40+3/�21C, with a pressure of400mm Hg in order to remove the residual EtO.
EtO residuals in aerated Hyal 50% samples weredetected and quantified by chromatographic analysis ofeluates, obtained by putting the samples in distilledwater at 371C for 5 h.
2.2.2.1. Cytotoxicity of EtO residues. In order toevalute whether the level of EtO residues was toxic, acytotoxicity test was performed on Hyal 50% aftersterilisation and areation. The test was performed withboth mouse fibroblasts (cell line 3T3) and coronaryvenular endothelial cells (CVEC).
Fibroblasts 3T3 were maintained in culture inDMEM, supplemented with 10% foetal calf serum(FCS), 1.2% l-glutamine and 1% penicillin–streptomy-cin (Sigma, Germany) on polystyrene flasks. Thefibroblast cultures were incubated at 371C in an atmo-sphere of 5% CO2 until cells were harvested with the aidof trypsin and suspended in fresh medium.
The CVEC were isolated and characterised aspreviously described [19]. Cells were maintained inculture in DMEM, supplemented with 10% bovine calfserum (CS) and antibiotics (100U/ml penicillin and100 mg/ml streptomycin) on gelatin-coated dishes. Cellswere cloned and each clone was sub-cultured up to amaximum of 25 passages. Passages between 15 and 20were used in these experiments.
The cytotoxicity of sterilised hydrogels towardsmouse fibroblasts 3T3 was evaluated by the directcontact method. Briefly, 3T3 cells (4000 cells/ml) weresuspended in DMEM containing 10% foetal calf serumand placed on the bottom of each well of a multi-wellplate (24-well). The multi-well was then incubated in anhumidified atmosphere containing 5% CO2 at 371C tillthe cells reached confluence (24 h). Afterwards, 5mg ofsterilised Hyal 50%, swollen for 24 h at 371C in 500 ml ofDMEM, were added to each fibroblast monolayer andincubated at 371C for 24 h. The Hyal 50% samples werethen removed, the cells were fixed with glutaraldehydeand stained with trypan blue, and counted by directobservation with an optical microscopy (BX40, Olym-pus). The bottom of the polystyrene wells was used as anegative control and disks (+=15mm) of organo-tinstabilised poly(vinylchloride) (PVC) as a positive con-trol, as recommended by ISO-standard (ISO-10993-5).Four samples of each different materials were tested.
The cytotoxic effect of hydrogels towards CVEC wasstudied by trypan blue exclusion. Briefly, endothelialcells (200 000 cells/ml) were suspended in DMEMcontaining 10% serum. 500 ml of cell suspension was
R. Barbucci et al. / Biomaterials 23 (2002) 4503–4513 4505
added to 3mg of the dried hydrogels in 15ml tubes.Cells were incubated at 371C for 4–24 h. Cells were thencounted in a haemocytometer and the percentage ofdead cells over the total number of cells was calculated.
In parallel experiments, the ability of the cells toadhere to cell culture plastic and to proliferate wasmonitored for 1 week after a 24 h period of incubationwith the hydrogels.
2.3. Morphological and physico-chemical
characterisation of sterilised hydrogels
2.3.1. Scanning electron microscopy (SEM) analysis
The morphology of Hyal 50% samples before andafter sterilisation was studied by Scanning ElectronMicroscopy (SEM, XL20 Philips, The Netherlands).Five milligrams of each sample were solubilised with1.5ml of distilled water, then freezed in liquid nitrogenand liophylised. Samples were successively mounted onSEM stubs, gold-sputtered with an automatic sputter-coater (BAL-TEC SCD 050, Balzers, Germany) andanalysed.
2.3.2. Swelling measurement
The Hyal 50% swelling degree (SD) in water wasdetermined before and after sterilisation. The SD wascalculated with the following formula:
SD ¼Pw � Pd
Pd� 100;
where Pw and Pd are, respectively, the weight of theswollen and dried hydrogels. In practice, establishedamounts of the liophilised Hyal 50% were enclosed insmall bags made of a hydrophobic water-permeable net(Nylon) and immersed for 24 h at 251C in 50ml ofdistilled water. They were then placed between twopieces of dry filter paper to wipe off the excess of water.The bags containing the swollen films were weighed inorder to calculate Pw.
2.4. Experimental in vivo study
The study was conducted in compliance with theEuropean and Italian Laws on animal experimentation,the principles stated in the Guide for the Care and Useof Laboratory Animals and the Animal WelfareAssurance No. A5424–01 by the National Institute ofHealth (NIH-Rockville, Maryland, USA).
Sixteen New Zealand adult-male rabbits (2.970.5 kgbody weight), aged eight months, were used. They werehoused individually in stainless-steel cages and main-tained under the same environmental conditions (tem-perature 2070.51C, relative humidity 5575%, 12 hphotoperiod). The animals were fed with a standardrabbit diet and filtered water ad libitum.
All surgical procedures were performed in asepticconditions, under general anaesthesia, induced byintramuscular injection of 35mg/kg b.w. ketamine(Ketavet, Farmaceutici Gellini, Aprilia, LT, Italy) and5mg/kg b.w. xylazine (Rompun, Bayer Italia, SpA,Milan, Italy), and maintained by means of a mixture of2% halothane (Fluothane, Zeneca Ltd., Macclesfield,UK) and oxygen/nitrous oxide (1/0.4 l/min), deliveredby an automatic ventilator using a special-designedmask. The right femoral condyle of all rabbits wasexposed by lateral–longitudinal skin incision. With theuse of an operative microscope, the weight-bearingsurface of each lateral femoral condyle was lightlyscarified with a sharp scalpel blade to obtain a chondraldefect of 5� 4mm, without damaging the subchondralbone. Afterwards, the surgical wounds were sutured.Immediately after surgery, eight animals (Hyal 50%group) received Hyal 50% solution (20mg freeze-driedHyal 50%/0.6ml NaCl 0,9%) by percutaneous injectionin the synovial capsule. The other eight rabbits weretreated under the same conditions using NaCl 0.9% ascontrol (Control Group). The rabbits were allowed tomove freely in their cages and for 2 days all of themreceived antibiotics (Flumequine-Flumexil, ATI srl,Ozzano, BO, Italy) and analgesics (Orudis-Ketoprofene,Rhone Poulenc-Rorer, Milan, Italy). The Hyal 50%treatments and controls were repeated every 10 days, forthree (30 days) or five times (50 days).
At the end of the experimental times (30 and 50 days)four animals of each group were euthanised (Tanax,Hoechst, Frankfurt a M., Germany), after induction ofgeneral anaesthesia for the explant of condyles.
2.4.1. Histomorphology
All right femoral condyles were dissected andarticular cartilage was examined macroscopically. Forthe histological evaluation the condyles were fixed in 4%buffered formalin, decalcified, dehydrated and em-bedded in paraffin. Sections of 7 mm in thickness wereprepared from the centre of the repair area and stainedwith hematoxylin and eosine, alcian blue and toluidineblue. Samples were analysed by a blinded investigator,using a Zeiss Axioscope microscope, (C. Zeiss, Oberko-chen, Germany) connected to an image analyser(Kontron KS300, v.2, Kontron Elektronik, Munchen,Germany) to evaluate surface regularity and cellularmorphology in the area of cartilage lesion.
3. Results
3.1. Rheological analysis
3.1.1. Viscoelastic properties
The rheological analysis provided the quantitativeevaluation of the viscous and elastic responses of Hyal
R. Barbucci et al. / Biomaterials 23 (2002) 4503–45134506
50% and the estimation of the effect of the hydrogelinjection through a 22-gauge needle on the visco-elasticproperties.
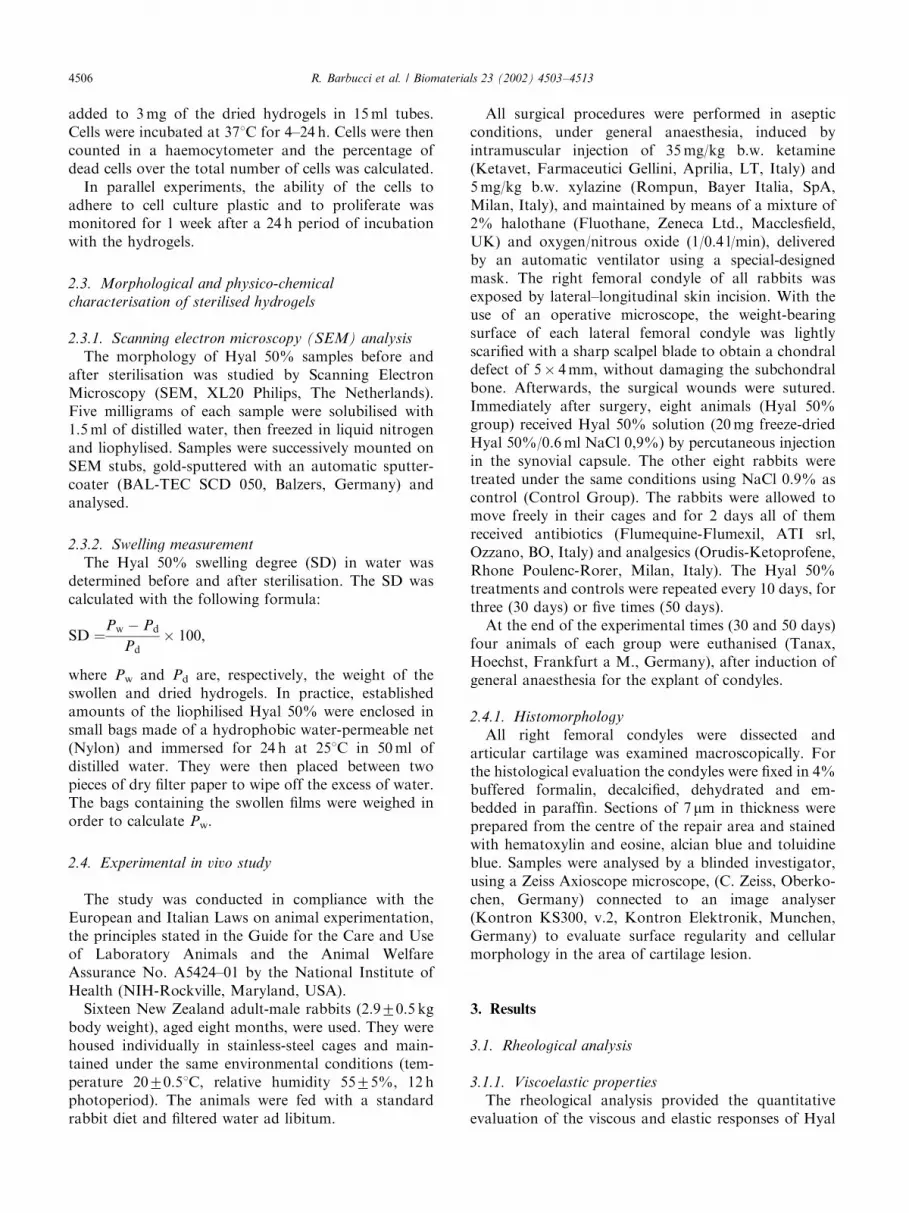
The storage moduli (G0) were greater than the lossmoduli (G00) within the frequency range analysed(Fig. 1). The storage moduli, before and after injection,weakly depended upon frequency, while both the lossmoduli showed a more marked frequency dependency.This polymer showed the features of ‘‘gel-like’’ material;it exhibited the typical behaviour of visco-elastic solidsunder small deformation conditions. The strain sweeptests showed that Hyal 50% was strain independent onlyfor small deformation regions; this behaviour is typicalof gels and provides an immediate distinction betweengels and entanglement networks [20,21]. The rheologicalbehaviour of Hyal 50% was characterised by a markedelasticity. This feature is not so remarkable in othercommercial products such as Hyalgan, which showsessentially a viscous behaviour [22]. The introduction ofchemical cross-linking between the chains led to apermanent stable network, and the intrinsic mobility ofthe molecules decreased dramatically. The network wasalso stabilised by chemical interactions, such as hydro-gen bonding [21].
Both moduli of the non-injected sample were higherthan that of the injected one. The hydrogel injectedthrough the needle still behaved like a gel, but it showeda reduction of the dynamic moduli. The storagemodulus, in fact, decreased from about 60 Pa to 25and the loss modulus from about 25 to 8, at 2.5Hz(Fig. 1). The storage modulus of Hyal 50% beforeinjection was similar to the modulus of non-injectedHylan GF 20 (Biomatrix, USA) [23], a cross-linkedHyaluronan of high molecular weight already used inOA treatment. Futhermore, the loss modulus of Hylanis one order of magnitude lower than that of Hyal 50%as well. The rheological behaviour of Hylan in thisfrequency range, in fact, is typical of entangled solutionbeyond the cross over frequency rather than a gel. Forthis reason the residence time of Hyal 50% should behigher than that of Hylan [24,25]. The injected samplesstill maintained rheological properties of great interestfor biomedical applications because of the storage andloss modulus that were higher in comparison with thoseof normal adult synovial fluids at 2.5Hz, which are 23and 7, respectively [24].
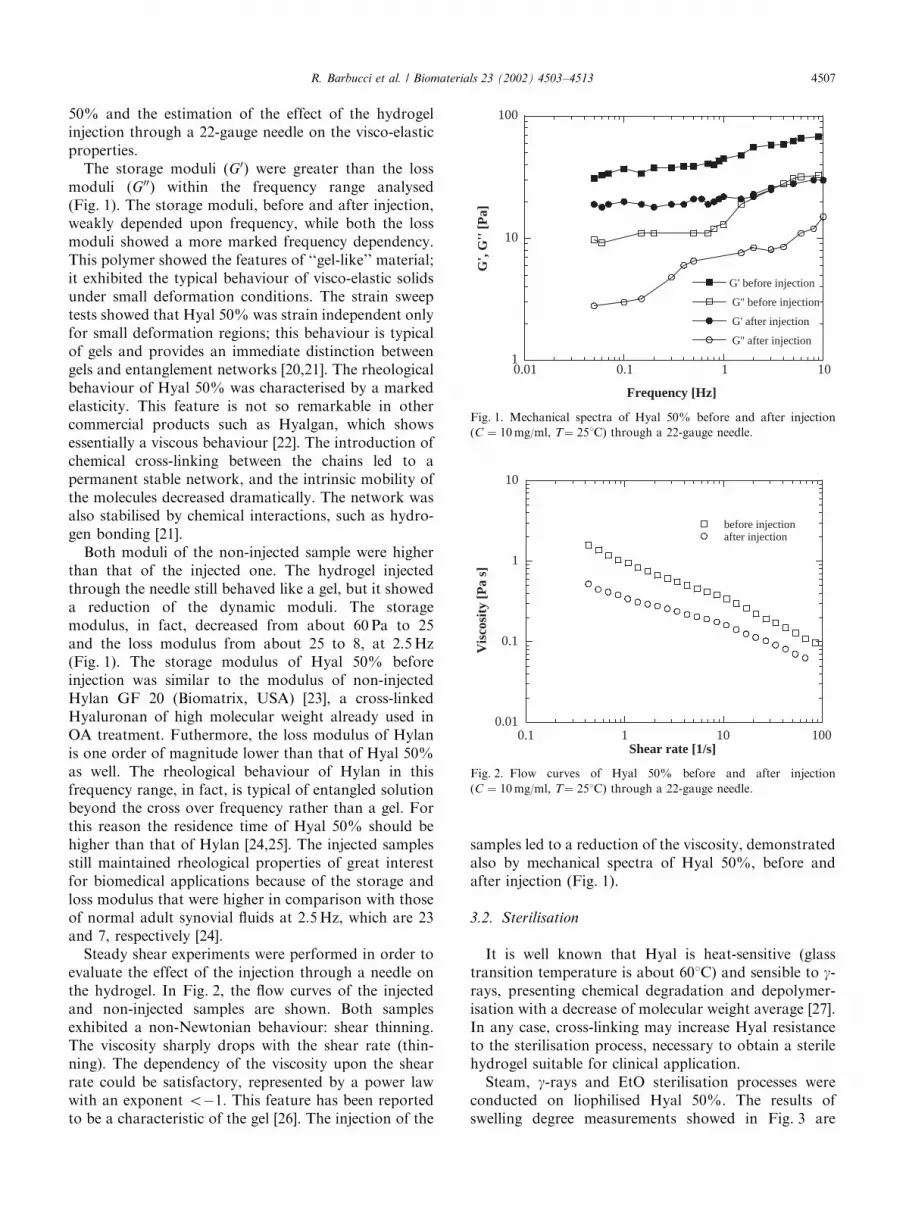
Steady shear experiments were performed in order toevaluate the effect of the injection through a needle onthe hydrogel. In Fig. 2, the flow curves of the injectedand non-injected samples are shown. Both samplesexhibited a non-Newtonian behaviour: shear thinning.The viscosity sharply drops with the shear rate (thin-ning). The dependency of the viscosity upon the shearrate could be satisfactory, represented by a power lawwith an exponent o�1. This feature has been reportedto be a characteristic of the gel [26]. The injection of the
samples led to a reduction of the viscosity, demonstratedalso by mechanical spectra of Hyal 50%, before andafter injection (Fig. 1).
3.2. Sterilisation
It is well known that Hyal is heat-sensitive (glasstransition temperature is about 601C) and sensible to g-rays, presenting chemical degradation and depolymer-isation with a decrease of molecular weight average [27].In any case, cross-linking may increase Hyal resistanceto the sterilisation process, necessary to obtain a sterilehydrogel suitable for clinical application.
Steam, g-rays and EtO sterilisation processes wereconducted on liophilised Hyal 50%. The results ofswelling degree measurements showed in Fig. 3 are
1
10
100
0.01 0.1 1 10
G' before injection
G'' before injection
G' after injection
G'' after injection
G',
G''
[Pa]
Frequency [Hz]
Fig. 1. Mechanical spectra of Hyal 50% before and after injection
(C ¼ 10mg/ml, T¼ 251C) through a 22-gauge needle.
0.01
0.1
1
10
0.1 1 10 100
before injectionafter injection
Vis
cosi
ty [
Pa
s]
Shear rate [1/s]
Fig. 2. Flow curves of Hyal 50% before and after injection
(C ¼ 10mg/ml, T¼ 251C) through a 22-gauge needle.
R. Barbucci et al. / Biomaterials 23 (2002) 4503–4513 4507
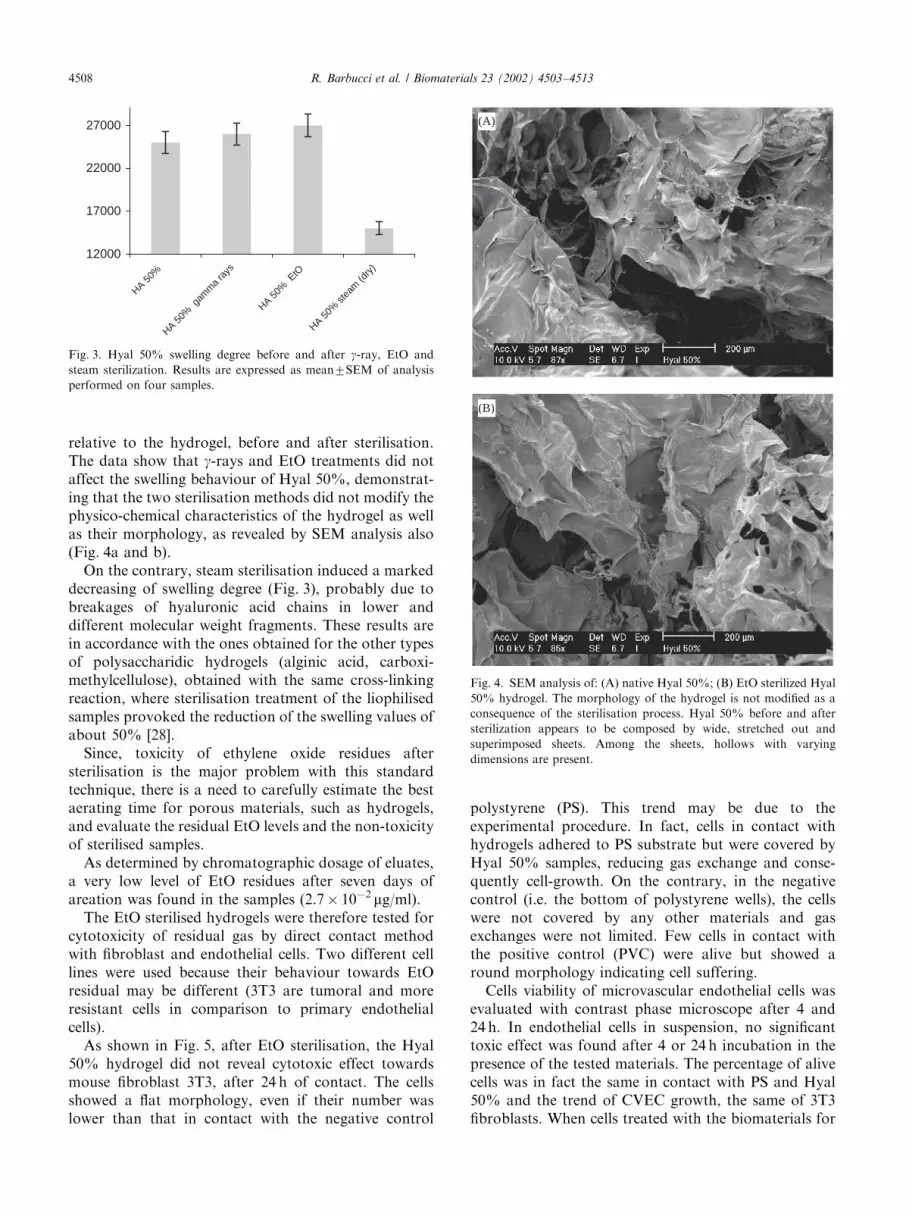
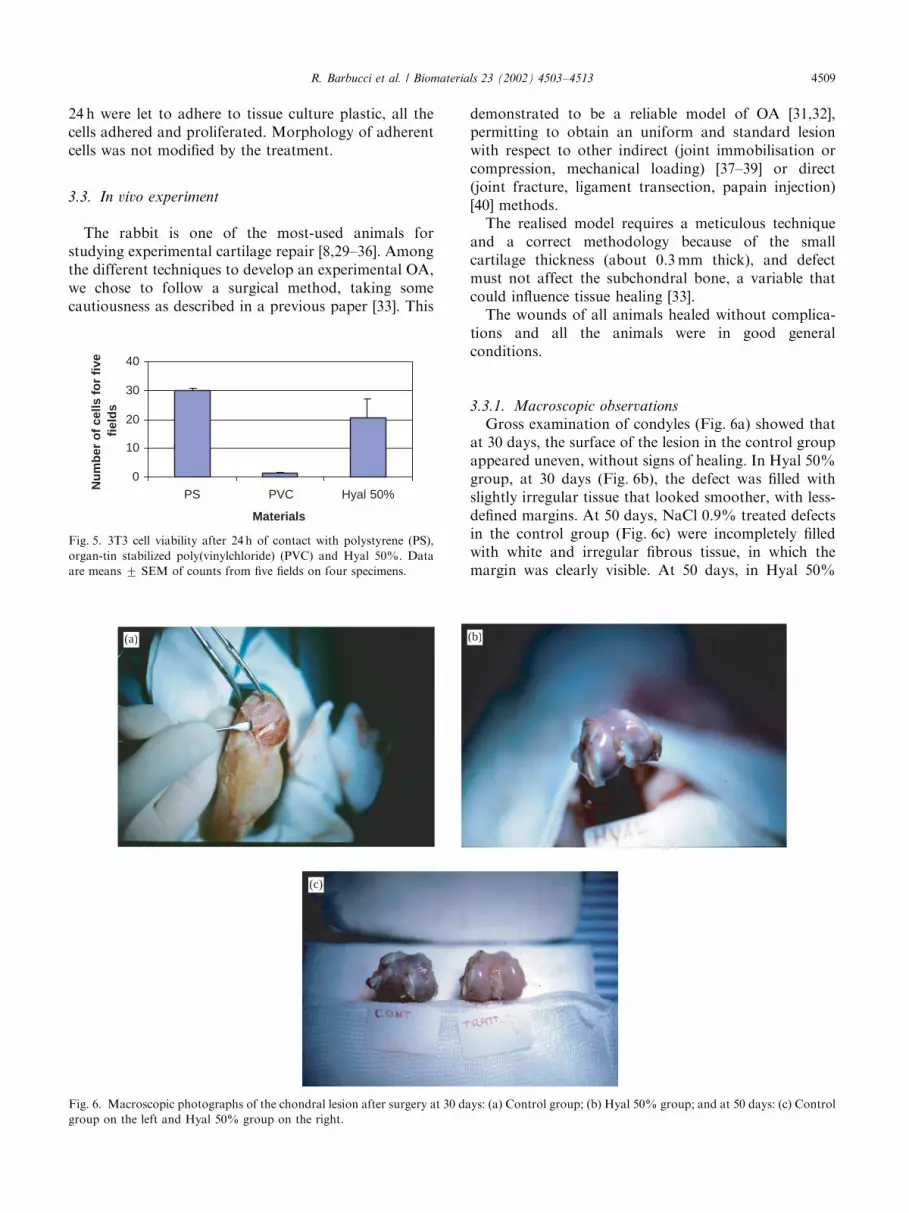
relative to the hydrogel, before and after sterilisation.The data show that g-rays and EtO treatments did notaffect the swelling behaviour of Hyal 50%, demonstrat-ing that the two sterilisation methods did not modify thephysico-chemical characteristics of the hydrogel as wellas their morphology, as revealed by SEM analysis also(Fig. 4a and b).
On the contrary, steam sterilisation induced a markeddecreasing of swelling degree (Fig. 3), probably due tobreakages of hyaluronic acid chains in lower anddifferent molecular weight fragments. These results arein accordance with the ones obtained for the other typesof polysaccharidic hydrogels (alginic acid, carboxi-methylcellulose), obtained with the same cross-linkingreaction, where sterilisation treatment of the liophilisedsamples provoked the reduction of the swelling values ofabout 50% [28].
Since, toxicity of ethylene oxide residues aftersterilisation is the major problem with this standardtechnique, there is a need to carefully estimate the bestaerating time for porous materials, such as hydrogels,and evaluate the residual EtO levels and the non-toxicityof sterilised samples.
As determined by chromatographic dosage of eluates,a very low level of EtO residues after seven days ofareation was found in the samples (2.7� 10�2 mg/ml).
The EtO sterilised hydrogels were therefore tested forcytotoxicity of residual gas by direct contact methodwith fibroblast and endothelial cells. Two different celllines were used because their behaviour towards EtOresidual may be different (3T3 are tumoral and moreresistant cells in comparison to primary endothelialcells).
As shown in Fig. 5, after EtO sterilisation, the Hyal50% hydrogel did not reveal cytotoxic effect towardsmouse fibroblast 3T3, after 24 h of contact. The cellsshowed a flat morphology, even if their number waslower than that in contact with the negative control
polystyrene (PS). This trend may be due to theexperimental procedure. In fact, cells in contact withhydrogels adhered to PS substrate but were covered byHyal 50% samples, reducing gas exchange and conse-quently cell-growth. On the contrary, in the negativecontrol (i.e. the bottom of polystyrene wells), the cellswere not covered by any other materials and gasexchanges were not limited. Few cells in contact withthe positive control (PVC) were alive but showed around morphology indicating cell suffering.
Cells viability of microvascular endothelial cells wasevaluated with contrast phase microscope after 4 and24 h. In endothelial cells in suspension, no significanttoxic effect was found after 4 or 24 h incubation in thepresence of the tested materials. The percentage of alivecells was in fact the same in contact with PS and Hyal50% and the trend of CVEC growth, the same of 3T3fibroblasts. When cells treated with the biomaterials for
12000
17000
22000
27000
HA 50%
HA 50%
gam
ma
rays
HA 50%
EtO
HA 50%
stea
m (d
ry)
Fig. 3. Hyal 50% swelling degree before and after g-ray, EtO and
steam sterilization. Results are expressed as mean7SEM of analysis
performed on four samples.
(A)
(B)
Fig. 4. SEM analysis of: (A) native Hyal 50%; (B) EtO sterilized Hyal
50% hydrogel. The morphology of the hydrogel is not modified as a
consequence of the sterilisation process. Hyal 50% before and after
sterilization appears to be composed by wide, stretched out and
superimposed sheets. Among the sheets, hollows with varying
dimensions are present.
R. Barbucci et al. / Biomaterials 23 (2002) 4503–45134508
24 h were let to adhere to tissue culture plastic, all thecells adhered and proliferated. Morphology of adherentcells was not modified by the treatment.
3.3. In vivo experiment
The rabbit is one of the most-used animals forstudying experimental cartilage repair [8,29–36]. Amongthe different techniques to develop an experimental OA,we chose to follow a surgical method, taking somecautiousness as described in a previous paper [33]. This
demonstrated to be a reliable model of OA [31,32],permitting to obtain an uniform and standard lesionwith respect to other indirect (joint immobilisation orcompression, mechanical loading) [37–39] or direct(joint fracture, ligament transection, papain injection)[40] methods.
The realised model requires a meticulous techniqueand a correct methodology because of the smallcartilage thickness (about 0.3mm thick), and defectmust not affect the subchondral bone, a variable thatcould influence tissue healing [33].
The wounds of all animals healed without complica-tions and all the animals were in good generalconditions.
3.3.1. Macroscopic observations
Gross examination of condyles (Fig. 6a) showed thatat 30 days, the surface of the lesion in the control groupappeared uneven, without signs of healing. In Hyal 50%group, at 30 days (Fig. 6b), the defect was filled withslightly irregular tissue that looked smoother, with less-defined margins. At 50 days, NaCl 0.9% treated defectsin the control group (Fig. 6c) were incompletely filledwith white and irregular fibrous tissue, in which themargin was clearly visible. At 50 days, in Hyal 50%
0
10
20
30
40
PS PVC Hyal 50%
Materials
Nu
mb
er o
f ce
lls f
or
five
fiel
ds
Fig. 5. 3T3 cell viability after 24 h of contact with polystyrene (PS),
organ-tin stabilized poly(vinylchloride) (PVC) and Hyal 50%. Data
are means 7 SEM of counts from five fields on four specimens.
(a) (b)
(c)
Fig. 6. Macroscopic photographs of the chondral lesion after surgery at 30 days: (a) Control group; (b) Hyal 50% group; and at 50 days: (c) Control
group on the left and Hyal 50% group on the right.
R. Barbucci et al. / Biomaterials 23 (2002) 4503–4513 4509
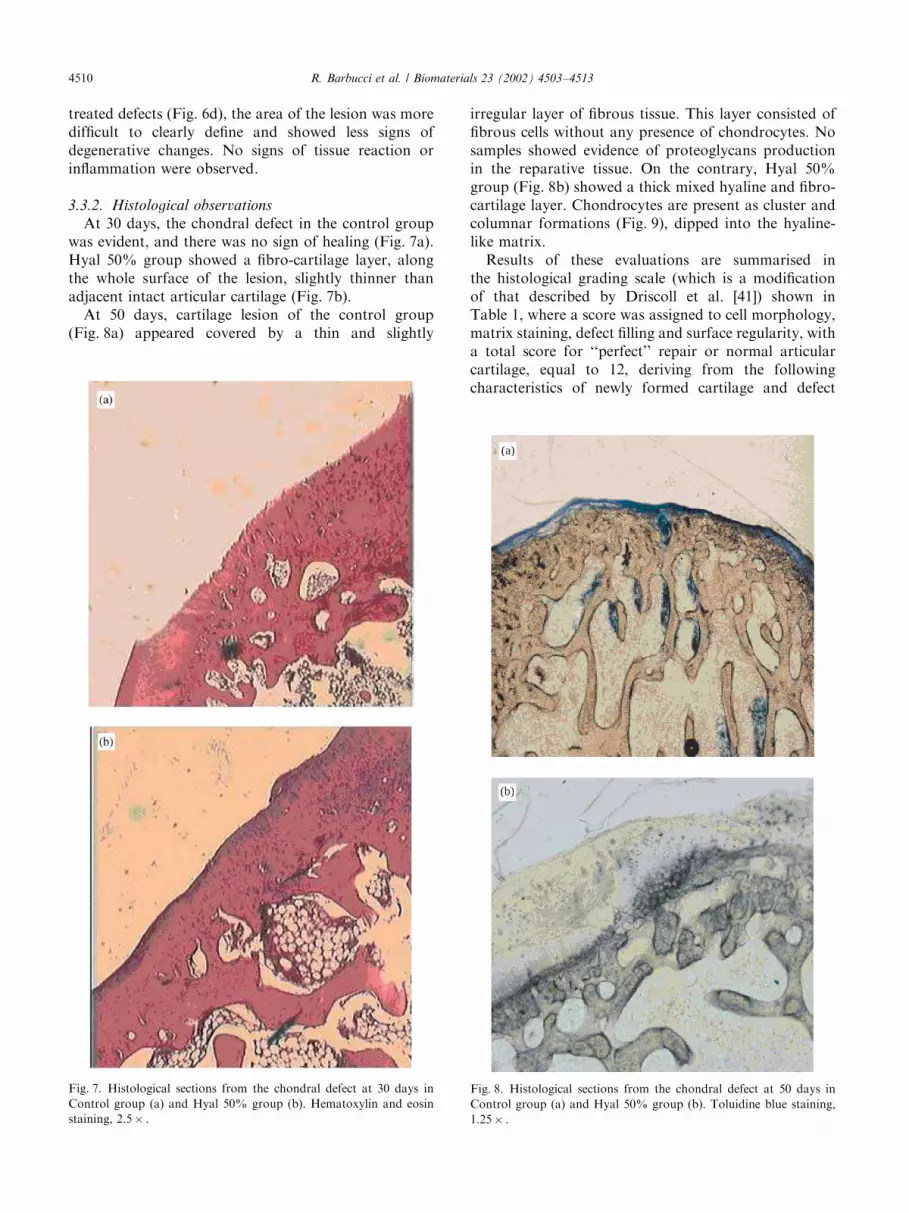
treated defects (Fig. 6d), the area of the lesion was moredifficult to clearly define and showed less signs ofdegenerative changes. No signs of tissue reaction orinflammation were observed.
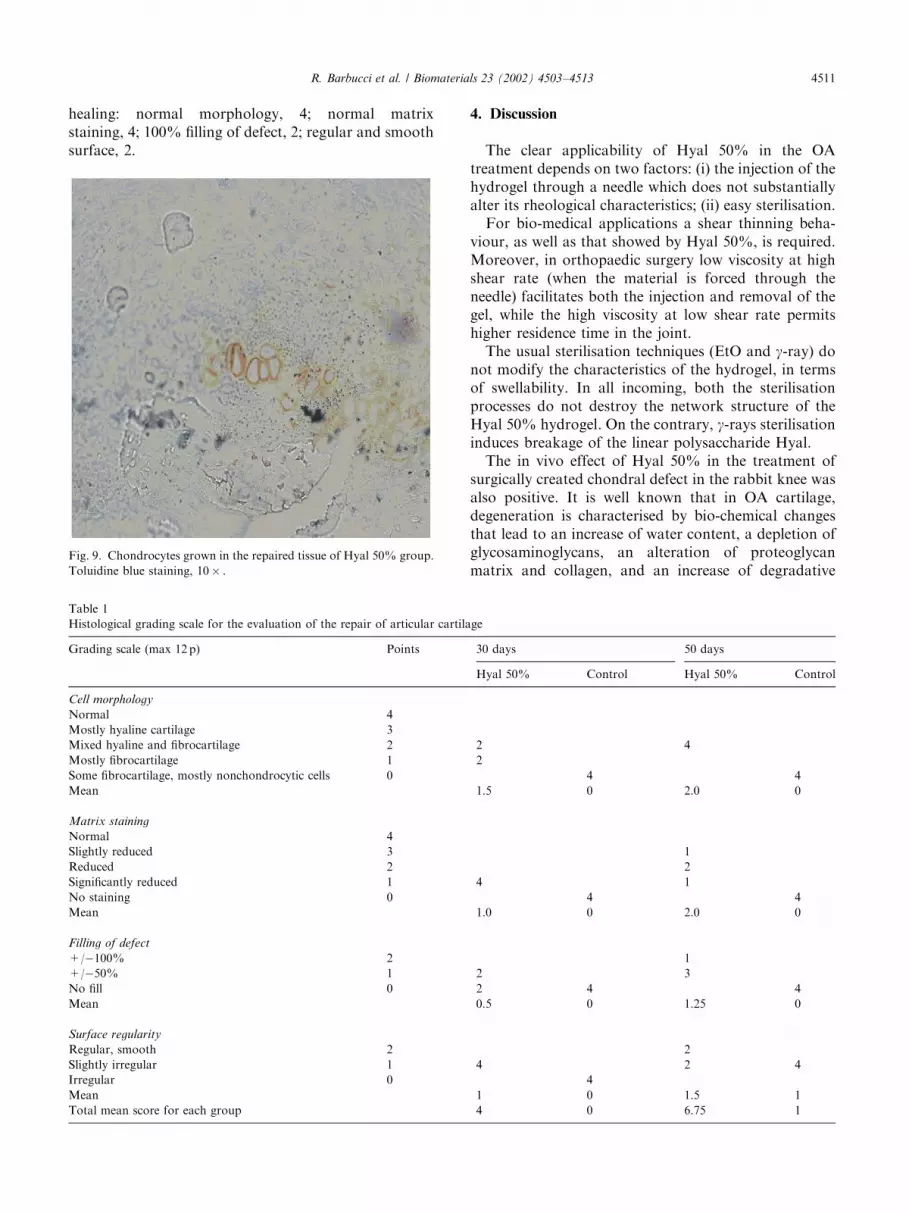
3.3.2. Histological observations
At 30 days, the chondral defect in the control groupwas evident, and there was no sign of healing (Fig. 7a).Hyal 50% group showed a fibro-cartilage layer, alongthe whole surface of the lesion, slightly thinner thanadjacent intact articular cartilage (Fig. 7b).
At 50 days, cartilage lesion of the control group(Fig. 8a) appeared covered by a thin and slightly
irregular layer of fibrous tissue. This layer consisted offibrous cells without any presence of chondrocytes. Nosamples showed evidence of proteoglycans productionin the reparative tissue. On the contrary, Hyal 50%group (Fig. 8b) showed a thick mixed hyaline and fibro-cartilage layer. Chondrocytes are present as cluster andcolumnar formations (Fig. 9), dipped into the hyaline-like matrix.
Results of these evaluations are summarised inthe histological grading scale (which is a modificationof that described by Driscoll et al. [41]) shown inTable 1, where a score was assigned to cell morphology,matrix staining, defect filling and surface regularity, witha total score for ‘‘perfect’’ repair or normal articularcartilage, equal to 12, deriving from the followingcharacteristics of newly formed cartilage and defect
Fig. 7. Histological sections from the chondral defect at 30 days in
Control group (a) and Hyal 50% group (b). Hematoxylin and eosin
staining, 2.5� .
(a)
(b)
Fig. 8. Histological sections from the chondral defect at 50 days in
Control group (a) and Hyal 50% group (b). Toluidine blue staining,
1.25� .
R. Barbucci et al. / Biomaterials 23 (2002) 4503–45134510
healing: normal morphology, 4; normal matrixstaining, 4; 100% filling of defect, 2; regular and smoothsurface, 2.
4. Discussion
The clear applicability of Hyal 50% in the OAtreatment depends on two factors: (i) the injection of thehydrogel through a needle which does not substantiallyalter its rheological characteristics; (ii) easy sterilisation.
For bio-medical applications a shear thinning beha-viour, as well as that showed by Hyal 50%, is required.Moreover, in orthopaedic surgery low viscosity at highshear rate (when the material is forced through theneedle) facilitates both the injection and removal of thegel, while the high viscosity at low shear rate permitshigher residence time in the joint.
The usual sterilisation techniques (EtO and g-ray) donot modify the characteristics of the hydrogel, in termsof swellability. In all incoming, both the sterilisationprocesses do not destroy the network structure of theHyal 50% hydrogel. On the contrary, g-rays sterilisationinduces breakage of the linear polysaccharide Hyal.
The in vivo effect of Hyal 50% in the treatment ofsurgically created chondral defect in the rabbit knee wasalso positive. It is well known that in OA cartilage,degeneration is characterised by bio-chemical changesthat lead to an increase of water content, a depletion ofglycosaminoglycans, an alteration of proteoglycanmatrix and collagen, and an increase of degradative
Fig. 9. Chondrocytes grown in the repaired tissue of Hyal 50% group.
Toluidine blue staining, 10� .
Table 1
Histological grading scale for the evaluation of the repair of articular cartilage
Grading scale (max 12 p) Points 30 days 50 days
Hyal 50% Control Hyal 50% Control
Cell morphology
Normal 4
Mostly hyaline cartilage 3
Mixed hyaline and fibrocartilage 2 2 4
Mostly fibrocartilage 1 2
Some fibrocartilage, mostly nonchondrocytic cells 0 4 4
Mean 1.5 0 2.0 0
Matrix staining
Normal 4
Slightly reduced 3 1
Reduced 2 2
Significantly reduced 1 4 1
No staining 0 4 4
Mean 1.0 0 2.0 0
Filling of defect
+/�100% 2 1
+/�50% 1 2 3
No fill 0 2 4 4
Mean 0.5 0 1.25 0
Surface regularity
Regular, smooth 2 2
Slightly irregular 1 4 2 4
Irregular 0 4
Mean 1 0 1.5 1
Total mean score for each group 4 0 6.75 1
R. Barbucci et al. / Biomaterials 23 (2002) 4503–4513 4511

enzyme levels [42]. Frequently, the initial event appearsas a mechanical stress that progressively damagescartilage matrix and subsequent biochemical andcellular alterations [43].
The results of in vivo experiment showed the effect ofHyal 50% local administration by repeated percuta-neous injections, both after a total of three injections inthe 30 days and of five injections in the 50 daysexperimental times. Control animals did not show anysigns of healing, demonstrating as expected, the inabilityof untreated chondral defect to fill the lesion with afunctional new tissue. Animals treated with Hyal 50%,both at 30 then at 50 days, revealed the presence ofrepairing mechanisms, that led to a partial healing. Infact, at the end of the experimental time, the growth of ahyaline-like cartilage was observed; this layer filled thedefect, presenting a smooth and regular surface of thearticular tissue.
As well-known clinically, the complete healing ofdamaged articular cartilage, necessary for normalarticular function, was not completely achieved, evenif many techniques were used (surgical, pharmacologi-cal, tissue engineering) [44]. One of the promising newmethods to treat chondral defects in the articular surfaceis the implantation of cultured autologous articularchondrocytes, but these techniques obviously requiremore sophisticated and longer procedures [36,45] and analternative could be useful. It is interesting to highlightthat from previous studies, a hyaluronan-based materialseems to be a suitable candidate as a carrier forchondrocytes [33]. Moreover, the local pharmacologicaltreatment with hyaluronic acid has also been claimed tobe a useful tool in OA treatment [46]. Now, the Hyal50% hydrogel treatment seems to improve chondrocytesdensity and matrix appearance, and to produce asmoother and more regular articular surface for a longperiod of time (50 days), without evidence of tissuereaction or inflammation in the rabbit OA model.
Acknowledgements
We thank Dr. Ciro Tetta (Bellco S.p.A., Mirandola—Italy) for Ethylene oxide sterilisation and determinationof gas residual, Dr. Lucia Morbidelli (Institute ofPharmacological Sciences, University of Siena, Siena,Italy) for cytotoxicity test performed with CVEC andMIUR for financial support.
References
[1] Adams RJ. Muscoloskeletal system. In: Swindle MM, Adams RJ,
editors. Experimental surgery and physiology: induced animal
models of human disease. Baltimora, USA: Williams & Wilkins,
1988 [Chapter 2].
[2] Ilardi CF, Sokoloff L. The pathology of osteoarthritis: ten
strategic questions for pharmacological management. In: Ver-
braggen G, Veys EM, editors. Degenerative joints, test tubes,
tissue, models, man. Amsterdam, NL: Excerpta Medica, 1982.
p. 3.
[3] Guidolin DD, Ronchetti IP, Lini E, Guerra D, Frizziero L.
Morphological analysis of articular cartilage biopsies from a
randomized, clinical study comparing the effects of 500–730kDa
sodium hyaluronate (Hyalgan) and methyl prednisolone acetate
on primary osteoarthritis of the knee. Osteoarthritis Cartilage
2001;9:371.
[4] Brandt KD, Block JA, Michalski JP, Moreland LW, Caldwell JR,
Lavin PT. Efficacy and safety of intra-articular sodium hyalur-
onate in knee osteoarthritis. Clin Orthop 2001;385:130.
[5] Dougados M. Sodium hyaluronate therapy in osteoarthritis:
arguments for a potential beneficial structural effect. Semin
Arthritis Rheum 2000;30:19.
[6] Altman RD. Intra-articular sodium hyaluronate in osteoarthritis
of the knee. Semin Arthritis Rheum 2000;30:11.
[7] Watterson JR, Esdaile JM. Viscosupplemetation: therapeutic
mechanisms and clinical potential in osteoarthritis of the knee.
J Am Acad Orthop Surg 2000;8:277.
[8] Han F, Ishiguro N, Ito T, Sakai T, Iwata H. Effect of sodium
hyaluronate on experimental osteoarthritis in rabbit knee joints.
Nagoya J Med Sci 1999;62:115.
[9] Rod!en L, Campbell P, Fraser JRE, Laurent TC, Pertoft H,
Thompson JN. Enzymatic pathways of hyaluronan catabolism.
In: Evered D, Whelan J, editors. The biology of hyaluronan.
CIBA foundation symposium 143. Chichester, UK: Wiley, 1989.
[10] Zhong SP, Campoccia D, Doherty PJ, Williams RL, Benedetti L,
Williams DF. Biodegradation of hyaluronic acid derivatives by
hyaluronidase. Biomaterials 1994;15:359.
[11] Adams ME, Lussier AJ, Peyron JG. A risk-benefit assessment of
injections of hyaluronan and its derivatives in the treatment of
osteoarthritis of the knee. Drug Saf 2000;23(2):115.
[12] Martins PB. Bilateral symmetric inflammatory reaction to hylan
G-F 20 injection. Arthritis Rheum 2001;44(4):978.
[13] Allen E, Krohn K. Adverse reaction to Hylan GF-20.
J Rheumatol 2000;27(6):1572.
[14] Bernardeau C, Bucki B, Liote F. Acute arthritis after intra-
articular hyaluronate injection: onset of effusions without crystal.
Am Rheum Dis 2001;60(5):518.
[15] Barbucci R, Rappuoli R, Borzacchiello A, Ambrosio L. Synth-
esis, chemical and rheological characterization of new hyaluronic
acid-based hydrogels. J Biomater Sci Polym Edn 2000;11:383.
[16] Magnani A, Rappuoli R, Lamponi S, Barbucci R. Novel
polysaccharides hydrogels: characterization and properties.
Polym Adv Tech 2000;11:488.
[17] Doi M. In: Thomas EL, editor. Materials science and technology.
structure and properties of polymers. VCH: Weinheim, 1993.
p. 389.
[18] Ferry JD. Viscoelastic properties of polymers. New York, USA:
Wiley, 1970.
[19] Schelling ME, Meininger CJ, Hawker JR, Granger HJ. Venular
endothelial cells from bovine heart. Am J Physiol 1988;254:
H1211.
[20] Clark AH, Ross-Murphy SB. Adv Polym Sci 1987;83:236.
[21] Lapasin R, Pricl S. Rheology of industrial polysaccharides: theory
and applications. Glasgow, UK: Blackie Academic and Profes-
sional, 1995.
[22] Mensitieri M, Ambrosio L, Iannace S, Perbellini A, Nicolais L.
Viscoelastic evaluation of different knee osteoarthritis therapies. J
Mater Sci: Mater Med 1995;6:130.
[23] Mensitieri M, Ambrosio L, Nicolais L, Balzano L, Lepore D. The
rheological behaviour of animal vitreus and its comparison with
vitreal substitutes. J Mater Sci: Mater Med 1994;5:743.
R. Barbucci et al. / Biomaterials 23 (2002) 4503–45134512
[24] Balazs EA, Bland PA, Denlinger JL, Goldman AI, Larsen NE,
Leshchiner EA. Blood Coag Fibrinolysis 1991;2:173.
[25] Borazcchiello A, Ambrosio L. Network formation of low
molecular weight hyaluronic acid derivatives. J Biomater Sci
Polym Ed. 2001;12(3):307–16.
[26] Ross-Murphy SB, Shatwell KP. Biorheology 1933;30:217.
[27] Rehakova M, Bakos D, Soldan M, Vizarova K. Depolymeriza-
tion reactions of hyluronic acid in solution. Int J Biol Macromol
1994;16:121.
[28] Barbucci R, et al. Unpublished results.
[29] Wakitani S, Goto T, Young RG, Mansour JM, Goldberg VM,
Caplan AI. Repair of large full-thickness aryicular cartilage
defects with allograft articular chondrocytes embedded in a
collagen gel. Tissue Eng 1998;4(4):428.
[30] Chu CR, Dounchis JS, Yoshioka M, Sah RL, Coutts RD, Amiel
D. Osteochondral repair using perichondral cells. A 1-year study
in rabbits. Clin Orthop 1997;340:220.
[31] Guzzardella GA, Morrone G, Fini M, Rocca M, Torricelli P,
Giardino R. Histological evaluation of the repair process of
chondral and osteochondral lesions in a rabbit model. J Appl
Anim Res 2000;17:217.
[32] Guzzardella GA, Morrone G, Torricelli P, Rocca M, Tigani D,
Brodano GB, Ferrari D, Fini M, Giardino R. Assessment of low-
power laser biostimulation on chondral lesions: an ‘‘in vivo’’
experimental study. Artif Cells Blood Substit Immobil Biotechnol
2000;28(5):441.
[33] Grigolo B, Roseti L, Fiorini M, Fini M, Giavaresi G,
Nicoli Aldini N, Giardino R, Facchini A. Transplantation
of chondrocytes seeded on a hyaluronian derivative
(Hyaffs-11) into cartilage defects in rabbits. Biomaterials 2001;
22:2417.
[34] Rubak JM. Reconstruction of articular cartilage defects with free
periosteal graft. An experimental study. Acta Orthop Scand
1982;53:175.
[35] Grande DA, Pitman MI, Peterson L, Menche D, Klein M. The
repair of experimentally produced defects in rabbit articular
cartilage by autologous chondrocyte transplantation. J Orthop
Res 1989;7:208.
[36] Brittberg M, Nilsson A, Lindahl A, Ohlsson C, Peterson L.
Rabbit articular cartilage defects treated with autologous cultured
chondrocytes. Clin Orthop Relat Res 1996;326:270.
[37] Radin EL, Martin LB, Burr DB, Caterson B, Boyd RD, Goodwin
C. Effects of mechanical loading on the tissues of the rabbit knee
joints. J Bone Jt Surg 1984;66A:95.
[38] Evans EB, Eggers GWN, Butler JK, Blumel J. Experimental
immobilization and remobilization of rat knee joints. J Bone Jt
Surg 1960;42A:737.
[39] Salter RB, Field P. The effects of continuous compression of
living articular cartilage: an experimental investigation. J Bone Jt
Surg 1960;42A:31.
[40] Koop S, Clenensson E. Induction of osteoarthritis in the guinea
pig knee by papain. Oral Surg Oral Med Oral Pathol 1983;55:259.
[41] Driscoll SW, Keeley FW, Salter RB. Durability of regenerated
articular cartilage produced by free autogenous periostel grafts in
major full-thickness defects in joint surfaces under the influence of
continuous passive motion. A follow-up report at one year.
J Bone Jt Surg 1988;70A:595.
[42] Brocklehurst R, Bayliss MT, Maroudas, Coysh HL, Freeman
MAR, Revell PA, Ali SY. The composition of normal and
osteoarthritic articular cartilage from human knee joints. J Bone
Jt Surg 1984;66A:95.
[43] Mankin HJ. Current concepts review: the response of articular
cartilage to mechanical injury. J Bone Jt Surg (Am) 1982;64:460.
[44] Gilbert JE. Current treatment options for the restoration of
articular cartilage. Am J Knee Surg 1998;11(1):42.
[45] Shortkroff S, Barone L, Hsu HP, Wrenn C, Gagne T, Chi T,
Breinan H, Minas T, Sledge CB, Tubo R, Spector S. Healing of
chondral and osteochondral defects in a canine model: the role of
cultured chondrocytes in regeneration of articular cartilage.
Biomaterials 1996;17:147.
[46] Guidolin DD, Ronchetti IP, Lini E, Guerra D, Frizziero L.
Morphological analysis of articular catilage biopsies from a
randomized, clinical study comparing the effects of 500–730kDa
sodium hyluronate (Hyalgan) and methylprednisolone acetate on
primary osteoarthritis of the knee. Osteoarthritis Cartilage
2001;9(4):371.
R. Barbucci et al. / Biomaterials 23 (2002) 4503–4513 4513