histomorphometric features predict 1-year outcome of patients with idiopathic dilated cardiomyopathy...
TRANSCRIPT

Histomorphometric features predict 1 -year outcome of patients with idiopathic dilated cardiomyopathy considered to be at low priority for cardiac transplantation
Cardiac transplantation for patients with idiopathic dilated cardiomyopathy (IDC) and poor left ventricular function usually is postponed until symptoms have become intolerable. However, the short-term prognosis of this subset of patients has been defined poorly. Accordingly, the l-year outcome was investigated in 30 patients with IDC with an ejection fraction 525% who showed a stabilized clinical condition at assessment for transplantation and were therefore considered at low priority for surgery. During follow-up, 10 patients (group A) showed a poor outcome: 2 died suddenly, and 8 had hemodynamic failure (4 of whom underwent transplantation and 4 of whom died from heart failure while on the waiting list). The remaining 20 patients (group B) had a benign outcome. At assessment for cardiac transplantation, clinical and electrocardiographic features, left ventricular dimension, and ejection fraction were similar between the two groups. However, group A patients had higher left ventricular end-diastolic pressure (p < 0.03) and lower cardiac index @ < 0.02) and stroke volume index @ < 0.03) with respect to group B patients. In addition, the former had a lower myofibril volume fraction @ < 0.001) and a higher nuclear area (p < 0.001) compared with the latter. Multivariate analysis selected myofibril volume fraction (p < 0.001) and nuclear area (p < 0.005) as the only independent predictors of a poor l-year outcome. The combination of myofibril volume fraction 589% and nuclear area SO Mm2 was found in all group A patients (sensitivity 100%) but in only 2 group B patients (specificity 90%). it is concluded that in patients with IDC considered at low priority for cardiac transplantation: (1) the l-year freedom from a cardiac event is lower than that currently expected with surgery; (2) histomorphometric features, that is, the concurrency of low myofibril volume fraction and increased nuclear area, predict short-term outcome; and (3) endomyocardial biopsy at assessment for cardiac transplantation might improve the rationalization of the timing of the procedure. (AM HEART J 1994;128:316-25.)
Francesco Pelliccia, MD,a Giulia d’Amati, MD,b Cinzia Cianfrocca, MD,a Paola Bernucci, MD,” Antonio Nigri, MD,a Benedetto Marino, MD,a and Pietro Gallo, MDC Rome and L’Aquila, Italy
Patients with idiopathic dilated cardiomyopathy (IDC) and poor left ventricular function or congestive heart failure have a poor prognosis1-3 and therefore are usually referred to transplant centers for evalu- ation. Transplantation should be performed with minimal delay in critically ill patients with IDC showing hemodynamic instabilitf or a very low ejection fraction.5 In these patients, survival after
From %he Department of Cardiac Surgery, La Sapienza University; bthe Department of Experimental Medicine, University of L’Aquila; and ‘the Department of Human Biopathology, La Sapienza University, Rome.
Received for publication May 7, 1993; accepted Nov. 24, 1993. Reprint requests: Francesco Pelliccia, MD, Via Tommaso Inghirami 85, 00179 Rome, Italy.
Copyright @ 1994 by Mosby-Year Book, Inc. 0002-8703/94/$3.00 + 0 4/l/56680
cardiac transplantation exceeds that of the natural history of their disease,6 indicating that the surgical option should be offered. Conversely, in this era of shortage of donor organs,‘] transplantation in pa- tients whose condition can be stabilized usually is postponed until symptoms have become intoler- able.4F 8 Indeed, there is now evidence that some pa- tients may even experience clinical improvement while on the waiting list41 g-11 and that a period of ob- servation before transplantation is thus warranted. Nevertheless, the question of the timing of trans- plantation should not be oversimplified because early deaths can occur also in patients without severe symptoms of heart failure. I2 Accordingly, the present study was undertaken to identify which factors at assessment for cardiac transplantation might predict
316

Volume 128, Number 2 American Heart Journal Pellzccia et al. 317
the l-year outcome of patients with IDC considered catheterization were performed in all patients on medical
at low priority for transplantation. treatment. Right- and left-sided heart pressures were measured before angiocardiography through a no. 7 or no.
METHODS 8 end-hole catheter placed in the cardiac chambers by the Patient selection. Seventy-five patients with IDC were femoral technique with transducers (Wheatstone) con-
referred to the Department of Cardiac Surgery at La Sapi- netted to an optical recorder (Electronics for Medicine, enza University between January 1986 and December 1990 White Plains, N. Y.) at a paper speed of 200 mm/set. Car- for assessment for cardiac transplantation. At admission, disc output was determined by thermodilution, and car- all patients underwent clinical evaluation, 12-lead electro- disc index was then derived. All patients underwent left cardiography, 4%hour arrhythmia monitoring, echocardi- ventriculography. Left ventricular end-diastolic and end- ography, and cardiac catheterization, including left ven- systolic volumes and ejection fraction were calculated from triculography, coronary arteriography, and left ventricular the 30-degree right anterior oblique projection of the left endomyocardial biopsy. Diagnosis of the disease was es- ventriculogram by Kennedy et al.‘s17 area-length method. tablished by cardiac catheterization on the basis of left All values were corrected to body surface area. Selective ventricular dilatation and systolic contraction dysfunc- coronary arteriography (by the Seldinger technique) was tion13 as shown by left ventricular ejection fraction <50 % performed in all patients: none had significant stenoses and left ventricular end-diastolic pressure >12 mm Hg. By (>50%) of the epicardial coronary arteries. definition, IDC was diagnosed only if there was no evidence Endomyocardial biopsy. All patients underwent percu- of increased alcohol intake or other cardiac disease (coro- taneous endomyocardial biopsy for diagnostic purposes.‘” nary artery disease, systemic hypertension, valvular heart Informed consent for the procedure was obtained from all disease, car pulmonale, hypertrophic cardiomyopathy, patients. Biopsy specimens were taken from the left ven- pericardial disease, myocarditis, specific heart muscle dis- tricle during cardiac catheterization with a bioptome ease, previous infectious disease, toxin or radiation expo- (King’s College). lg There were no complications either sure, heredofamilial disorders, or chronic systemic disease during or after the procedure. Each patient had three to involving the heart muscle). I3 Patients entered the study if five tissue fragments collected from different sites of the they were considered at low priority for cardiac transplan- left ventricle (septum, anterior free wall, and apex). Imme- tation on the basis of (1) left ventricular ejection fraction ~25% but >lO% ; (2) a stabilized clinical condition while receiving maximal medical therapy; and (3) an acceptable quality of life despite of symptoms of heart failure. Con- versely, patients were excluded in case of (1) selection for cardiac transplantation because they were expected to die within 512 monthsI on the basis of severely limiting symptoms and a very low ejection fraction (~10%)~; (2) left ventricular ejection fraction >25 S;, ; (3) standard con- traindications to cardiac transplantation14; or (4) recent onset (<6 months) of symptoms of congestive heart failure. Accordingly, 30 of the 75 patients were eligible for this study: they were 24 men and 6 women of mean age 50 F 9 years (range 33 to 62 years).
Electrocardiography. All patients underwent 12-lead electrocardiography and 4%hour arrhythmia monitoring in the week before cardiac catheterization. Ambulatory elec- trocardiographic monitoring was performed by simulta- neous precordial recordings of leads Vi and Vs through a two-channel recorder (Del Mar Avionics Inc., Irvine, Ca- lif.). Each type was analyzed on a high-speed analyzer (Del Mar Avionics Inc.). Ventricular arrhythmias were graded according to the Lown and Graboys’ classification.15
Echocardiography. Within 1 week of cardiac catheter- ization, all patients underwent complete M-mode and two-dimensional echocardiographic studies. Echocardio- graphy was performed by one of the authors (C. C.) with an ultrasonograph (model 77020 A, Hewlett-Packard, An- dover, Mass.) with 2.5 and 3.75 MHz transducers. Mea- surements of intracardiac dimensions were made according to the recommendations of the American Society of Ech- ocardiography.l‘j
Cardiac catheterization. Right- and left-sided cardiac
diately after removal, tissue samples were fixed in phos- phate-buffered 10% formalin at room temperature in sep- arate containers depending on site of origin. The biopsy specimens were embedded in paraffin, and 4 pm sections were cut; stained with hematoxylin-eosin, Heidenhain azan, and elastic-Van Gieson stain; and examined under a light microscope. Analysis of biopsy specimens excluded the possibility of myocarditis and specific heart muscle disease in all patients.
Histomorphometric analysis. Histomorphometric anal- ysis was performed on light-microscopic images with a semi-automatic image analyzer (Videoplan II, Kontron- Munich, Germany). A point source of light was reflected onto the tissue sections through a drawing tube. All histo- morphometric features were assessed by moving the point light source over a digitizing tablet. Light microscopy rather than electron microscopy was preferred for this study because it allows measurement of a much larger area of the biopsy specimen and is affected by a smaller sampling variability.“O
Myocellular parameters were assessed at 25~ magnifi- cation on hematoxylin-eosin-stained sections by measur- ing all transverse-cut myocytes with evidence of a nucleus. From each section, a minimum of 50 myocytes (range 50 to 293) was evaluated. For each cell, the following parameters were measured (in square micrometers): myocellular area (the entire cellular cut surface), nuclear area (the extension of the nuclear cut surface), and, myofibrillar area (the sar- coplasmic surface actually occupied by myofibrils). Myo- fibrillar area was derived by excluding from the myocellu- lar area either the nuclear area or the zones occupied by sarcoplasmic degeneration and artifacts as the contraction- bands effect. The percentage ratio of mpofibrillar area to

318 Pelliccia et al.
Table I. Histomorphometric features in five control subjects
August 1994
American Heart Journal
No. of specimens No. of myocytes Mean +- SD Range
Myocellular area (pm2) 25 492 853 + 423 337-1460 Nuclear area (rm2) 25 492 37 t 6 29-42 Myofibrillar area (rm2) 25 492 792 * 401 301-1370 Myofibril volume fraction (%) 25 492 92.8 2 1.8 89.5-93.8 Interstitial fibrosis (%) 25 - 1.8 + 1.7 o-4 Endocardial fibrosis ( % ) 25 - 2.5 + 2.2 O-6
Table II. Clinical, electrocardiographic, and echocardiographic features in the study population
Patient Sex/age Duration of Sodium NYHA Conduction Lown LAD LVEDD LVESD RVEDD no. (yr) symptoms (mo) (mgldl) class Rhythm delay class (mm) (mm) (mm) (mm)
Group A 1 2 3 4 5 6 7
8 9
10 Group B
11 12 13 14 15 16 17 18 19 20 21 22 23 24 25 26 27 28 29 30
M/51 67 135 III SR M/55 70 137 III AF M/56 36 134 III SR F/47 10 142 III SR
M/57 18 136 IV AF M/52 31 135 IV AF Ml39 34 135 IV SR M/55 29 140 IV SR M/37 46 136 IV SR M/51 24 134 III SR
M/60 30 138 IV SR F/35 59 144 III AF F/56 61 137 III SR M/59 12 135 III SR Ml62 64 134 III SR M/41 16 139 III SR F/61 60 133 IV SR
M/34 12 140 III SR M/33 12 141 III SR M/62 32 136 III SR F/54 71 135 III SR F/49 75 138 III SR
Ml60 44 141 IV SR Ml54 17 142 IV SR M/48 9 137 III SR M/41 20 135 III SR M/53 27 139 III SR M/56 28 135 IV SR M/44 33 134 III SR M/45 36 137 III SR
I” AVB 4B - 1B
I“ AVB 4B LBBB 2 LBBB 1B LBBB 4B
- 3 - 3 - 3 - 4B
I” AVB 4B - 3
I” AVB, LBBB 3 I” AVB 1B
- 4B - 1A
LBBB 4B - 1B - 3
I” AVB 3 - 2
I0 AVB, LBBB 2 - 2
I0 AVB, LBBB 2 LBBB 1B LBBB 4B
- 1A - 2 - 2 - 2
48 67 58 20 49 66 56 18 44 77 64 15 49 82 72 15 45 71 63 20 46 80 69 26 49 71 60 21 44 67 55 20 51 70 61 25 34 58 50 25
51 75 61 31 43 59 45 18 47 73 61 28 49 78 66 15 37 60 50 30 50 60 49 20 54 70 59 25 35 60 47 14 40 64 52 17 46 65 55 20 36 61 52 18 42 60 49 15 38 65 54 22 48 69 60 14 47 75 61 16 52 80 70 25 45 69 60 18 42 68 59 20 38 64 53 18 45 67 55 1
AF, Atria1 fibrillation; F, female; AVB, atrioventricular block; LAD, left atrial diameter; LBBB, left bundle branch block; LVEDD, left ventricular end-di- astolic diameter; LVESD, left ventricular end-systolic diameter: M, male; NYHA, New York Heart Association; RVEDD, right ventricular end-diastolic di- ameter; SR, sinus rhythm; I”, first-degree.
myocellular area was then derived and termed the myo- fibril volume fraction, as previously described.20
The extent of fibrous tissue was measured at 10X mag- nification on sections stained with the Hei#enhain azan method by delimiting both interstitial fibrosis (the area occupied by perivascular and plexiform fibrosis as well as interfibrosis) and endocardial plaque. The total tissue area also was measured at 10~ magnification on each section, The zones occupied by fixation artifacts, when present,
were excluded from computation of the total tissue area. The following parameters were derived: interstitial fibro- sis (the percentage ratio of the area occupied by interstitial fibrosis to the total tissue area) and endocardial fibrosis (the percentage ratio of the area occupied by the endocar- dial plaque to the total tissue area).
All determinations were made by two investigators (G.d’A. and P.B.) independently, without knowledge of patients’ clinical data. Interobserver differences between

Volume 128, Number 2 American Heati Journal Pelliwia rt al. 319
measurements of each histomorphometric parameter in any patient were always <5 7;. For each histomorphomet- ric parameter, reported values represent the means of all measurements obtained by both examiners from every pa- tient’s biopsy specimens. Control values of histomorpho- metric features were derived by histomorphometric analy- sis of biopsy specimens obtained from the normal hearts of five adult donors at the time of explantation. Values (mean 2 standard deviation and range) of each histomor- phometric feature, as assessed in the control group, are listed in Table I.
FoIIow-up. After discharge, all patients were seen at 4- to g-week intervals for 1 year or until either death or he- modynamic failure. Hemodynamic failure was diagnosed in case of (1) clinical deterioration with onset of severe rest- ing symptoms; (2) refractory fluid retention unresponsive to maximized therapy; (3) systolic blood pressure <80 mm Hg; (4) blood urea nitrogen >60 mg/dl; or (5) serum sodium <133 mg/dl or decreasing. Treatment while in the hospital and during follow-up included digoxin with the dose adjusted to maintain a concentration in serum between 1 and 2 rig/ml (26 patients), diuretic agents (all patients), and angiotensin-converting enzyme inhibitors (25 patients). Nitrates were added for 18 patients. Fifteen patients were given anticoagulant agents. No patient received investiga- tional drugs, P-blocking agents, or antiarrhythmic therapy during hospitalization or follow-up. Mode of death was classified according to Hinkle and Thaler.21 Death due to congestive heart failure was defined as progressive cardiac pump function impairment with time elapsing before the ultimate cessation of pulse and respiration. Sudden death was defined as an abrupt disorder of the cardiac rhythm in a patient without prior circulatory collapse.21 Patients who suffered from hemodynamic failure during follow-up were newly referred to our unit to be considered for transplan- tation; those who were subsequently added to the waiting list for the procedure were classified as having a poor out- come.
Statistical analysis. Data are expressed as mean f standard deviation. The chi square test and the t test were used for comparison of qualitative and quantitative data, respectively. The Kaplan-Meier method was used for life- table analysis. Variables were divided into high- and low- risk categories for construction of actuarial survival curves, which were tested for homogeneity with the log-rank test. Variables significant by univariate analysis were then jointly analyzed by multivariate analysis (by Cox’s propor- tional hazards model). To test the accuracy of the multi- variate model, the technique of cross validation was ap- plied.“2 All patients were randomly allocated into two sub- groups, and separate multivariate analyses were newly performed. Also calculated were sensitivity, specificity, and predictive value for outcome of the variables significant by multivariate analysis. A p value <0.05 was considered sig- nificant.“”
RESULTS Patient features and follow-up. Presenting features
in the individual patients are listed in Tables II to IV.
During follow-up, the l-year freedom from a cardiac event (death or hemodynamic failure) was 67 “T . Ten patients (group A) had a poor outcome in 12 months: patients 1 and 10 died suddenly and 8 other patients showed hemodynamic failure from progressive weight gain despite maximal medical therapy (6 patients), severe hypotension (1 patient), or declining serum sodium (1 patient). Patients in unstable condition were newly evaluated at our unit and were included on the waiting list for cardiac transplantation. Four of them (patients 4,5,7, and 8) later received trans- plant because of donor organ availability, whereas the other four (patients 2, 3, 6, and 9) died of heart failure while on the waiting list.. The remaining 20 patients had a benign outcome (group B).
Relation of presenting features to outcome. Compar- ison of clinical, electrocardiographic, and echocar- diographic features at assessment for transplanta- tion between group A and B patients did not show any significant differences (Table V). Also, cardiac catheterization (Table VI) revealed that right-sided heart filling pressures and mean pulmonary artery pressure were similar in the two groups. However, group A patients had significantly higher left ven- tricular end-diastolic pressure (p < 0.03) and lower cardiac index (p < 0.02) and stroke volume index (p < 0.03) compared with group B patients. Compar- ison of histomorphometric features (Table VI) dis- closed that the two groups had similar average values of myocellular area, myofibrillar area, interstitial fi- brosis, and endocardial fibrosis, although group A patients had lower myofibril volume fraction (p < 0.001) and higher nuclear area (p < 0.001) compared with those of group B.
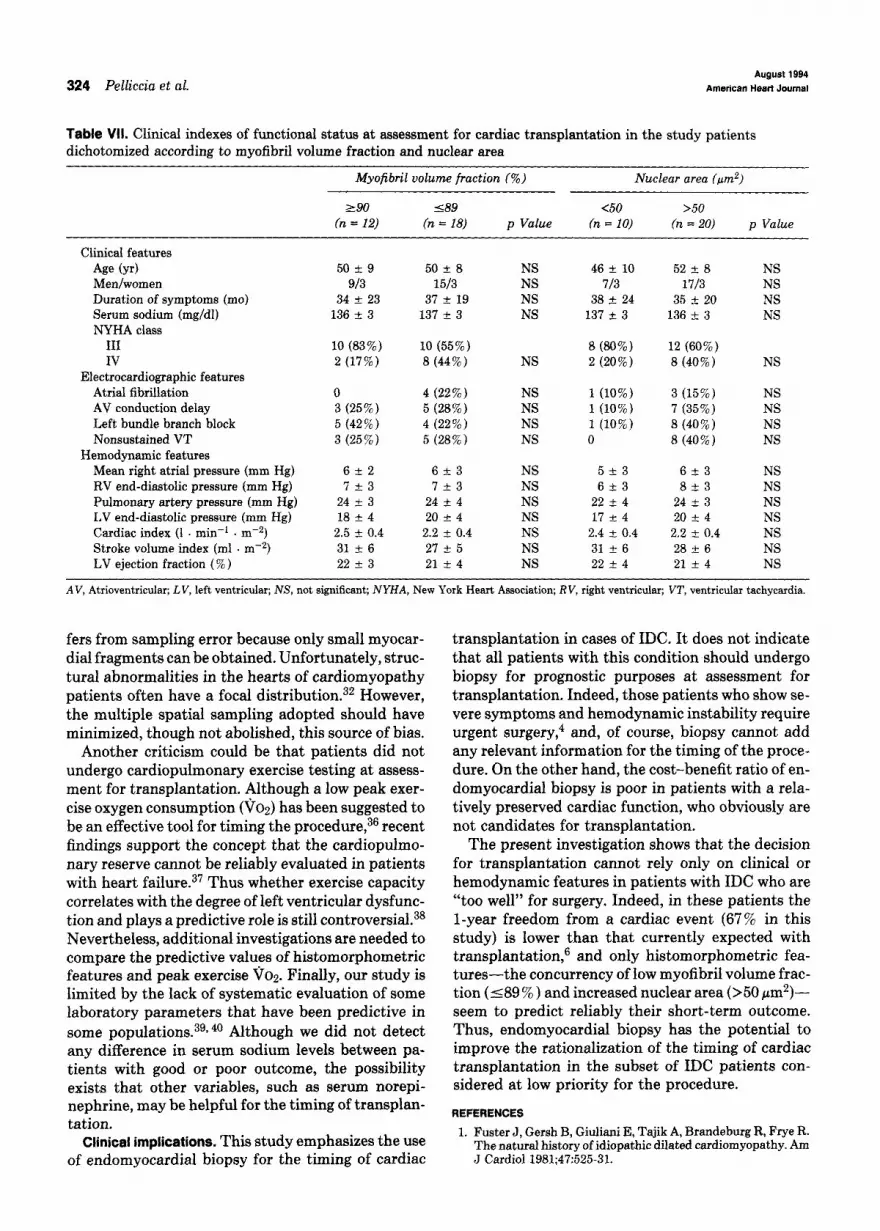
Independent predictors of l-year outcome. Multi- variate analysis identified reduced myofibril volume fraction (p < 0.001) and increased nuclear area (p < 0.005) as the only independent variables associ- ated with a worse outcome (Fig. 1). Cross validation confirmed recorded values in the whole study popu- lation. Variables selected by multivariate analysis were not correlated with clinical indexes of functional status. Indeed, comparison of presenting features between patients dichotomized according to cutoff values of myofibril volume fraction and nuclear area did not show any significant, difference (Table VII), A myofibril volume fraction 189’:; , i.e., <2 standard deviations from the mean of the cont.rol group (Ta- ble I), was found in all group A patients and in 8 group B patients, yielding a sensitivity of 100 cO and a spec- ificity of 60%. A nuclear area >50 pm?, i.e., >2 st.an- dard deviations from the mean of I he control group (Table I), was detected in all group A patients and in 10 group B patients, yielding a sensit.ivity of 100%

320 Pelliccia et al. August 1994
American Heart Journal
Table III. Hemodynamic and angiographic features in the study population
Patient RAP RVEDP MPAP L VEDP cz svz EF LVEDV LVESV no. (mm Hg) (mm Hg) (mm Hg) (mm Hg) (1 . min-’ . mw2) (ml . m-4 (W) (ml . rnm2) (ml . mw2)
Group A 1 2 3 4 5 6 7 8 9
10 Group B
11 12 13 14 15 16 17 18 19 20 21 22 23 24 25 26 27 28 29 30
5 9 3 5
11 10
6 6
5
5
5 6 7 2 6 7 2 1 5 4 4 2 8
10 6
10 4 5
5 10
5 5
13 10
9 11
9
9 2 8 8 8 2 9 7 5 3 5 5 5 3
11 10
10 6 5
21 17 2.9 40 24 184 140 29 21 1.9 22 19 317 256 28 23 1.9 23 24 196 149 22 19 2.3 30 25 263 197 30 28 1.9 19 14 195 167 23 16 1.9 27 16 251 210 18 15 2.0 26 21 208 164 28 22 1.8 23 21 134 106 27 22 1.9 23 16 261 219 22 25 2.0 22 17 281 233
24 24 2.3 33 25 363 271 19 15 2.4 28 24 231 175 26 13 2.5 31 24 287 217 25 22 2.5 33 20 309 247 23 20 2.2 27 24 174 132 20 15 2.2 25 25 178 133 30 24 1.9 25 15 341 289 25 16 2.8 35 23 196 151 29 23 2.4 28 22 226 176 19 19 1.8 24 24 249 189 23 19 2.8 40 24 151 115 18 13 3.0 35 23 145 111 21 15 1.9 24 15 179 152 23 19 2.6 35 25 202 152 24 16 2.5 28 23 256 197 22 17 2.4 27 20 210 167 21 18 2.3 31 25 223 167 25 20 2.0 25 17 242 201 20 15 3.0 35 24 163 124 22 15 2.7 39 25 161 121
CI, Cardiac index; EF, ejection fraction; LVEDP, left ventricular end-diastolic pressure; LVEDV, left ventricular end-diastolic volume; LVESV, left ven- tricular end-systolic volume; MPAP, mean pulmonary artery pressure; RAP, right atria1 pressure; RVEDP, right ventricular end-diastolic pressure; SW, stroke volume index.
and a specificity of 50%. It is noteworthy that the concurrency of myofibril volume fraction 589 % and nuclear area >50 pm2 was found in all group A patients (Fig. 2) but in only 2 group B patients. The two variables had a sensitivity of 100% and a spec- ificity of 90% in identifying cases with an unfavor- able outcome and had a predictive value for poor outcome of 83 % and a predictive value for good out- come of 100% (Fig. 3).
DISCUSSION
The present study focused on a subset of patients with IDC: those with an ejection fraction 125 % who showed a stabilized clinical condition and no severely limiting symptoms and therefore were considered at low priority for cardiac transplantation. The results demonstrate that l-year outcome for these patients and therefore the timing of their surgery can be re- liably predicted, provided that a complete risk-factor
characterization, including endomyocardial biopsy, is performed.
Predictive value of clinical features. Physicians cus- tomarily select recipients for cardiac transplantation on the basis of clinical findings that classify the severity of heart failure. I4 One should question, how- ever, the definition of disease severity for patients with IDC. Indeed, symptomatic-class,24 high-grade ventricular arrhythmias25l 26 and ejection fraction it- selfz7 do not closely reflect the degree of functional impairment. Therefore, although electrical instabil- ity is associated with an increased risk for sudden death 6 28, 2g no single clinical criterion is said to be adequate to characterize the likelihood of early death.27 This observation is consistent with the results of the present study: most presenting features were similar at formal evaluation in patients with a poor or good l-year outcome. Of clinical variables, only some hemodynamic parameters (left ventricular

Volume 128, Number 2 American Naart Journal Pelliccia et al. 321
o m9ofibril volr~ frwtior Z 90% (a-12) 0 ruclnr urea t 50 ~2 (I- 10) l mgofibrll v4uu rrrctirr : 89% (a=1 6) l l acle8r 8rea a 50 ** (n-20)
00 0 I I I 1
0 3 6 9 12 0 3 6 9 12
Fellow-r) (Imartha) Fellov-up (montha)
Fig. 1. Cumulative survival rates for patients with myofibril volume fraction ?z90% or &39%, i.e., <2 standard deviations from mean of control group (left) and for patients with nuclear area <50 pm2 or >50 pm2, i.e., >2 SDS from mean of control group (right). Numbers in parentheses indicate number of patients entering each 3-month interval.
end-diastolic pressure, cardiac index, and stroke vol- Table IV. Histomorphometric features in the study ume index) were significantly different between the population two groups, although they showed no independent Patient MA NA Mf-4 MVF IF EF prognostic value. no. GmZ) fpm2) Gm2) Pi i f%) 6)
Prognostic role of histomorphometric features. At- tempts have been made to verify whether histologic findings relate to the natural history of IDC?l 30-33 but several investigations have not detected any in- dependent predictive role of morphologic changes with respect to clinical features.30-32 Most previous studies, however, have examined heterogenous pop- ulations, ranging from patients with severe hemody- namic derangement to those with mild heart failure. Obviously, clinical measurements are sufficient to stratify the prognosis of IDC when patients with markedly different functional characteristics are compared.
Group A 1 1086 2 1035 3 2140 4 1369 5 982 6 1381 7 783 8 1345 9 894
10 1033
Group B 11 1085 12 560 13 1246 14 1026 15 1240 16 742 17 1196 18 710 19 1135 20 1343 21 876 22 627 23 1203 24 1217 25 1204 26 1316 27 626 28 958 29 1142 30 1011
56 932 85 17 25 71 895 86 15 2 91 1853 86 12 7 84 1233 87 6 11 76 795 81 9 8 60 1200 86 1 16 61 676 86 9 9
107 1076 c?l 7 1 68 759 u4 2 5 58 930 89 15 30
The present study shows that histologic findings have a major predictive value in a well-defined, ho- mogenous subgroup of patients with IDC: those with no severe symptoms despite poor left ventricular function who are therefore at low priority for trans- plantation. In these patients, the only variables shown to be independently associated with an unfa- vorable outcome were histologic: these were reduced myofibril volume fraction and disproportionately large nuclei. These results are in agreement with the finding that a low myofibril volume fraction has prognostic significance for death33 and are consistent with the electron microscopic evidence that myo- filament loss is a valuable prognostic indicator in IDC.34
54 929 85 5 19 39 512 69 3 1 53 1142 93 0 0 59 948 91 9 2 55 1133 90 17 1 29 697 94 7 19 63 1096 92 5 5 38 713 92 0 7 38 1025 89 14 12 57 1216 89 3 16 45 801 91 2 15 32 649 87 1 14 42 1073 89 :3 1 60 1135 92 2 6 61 1125 92 17 13 64 1188 90 12 14 44 548 87 2 1 43 850 88 13 9 41 1085 95 a 0 51 949 94 1 1
In this study, low myofibril volume fraction iden- EF, Endocardial fibrosis, IF, interstitial fibrosis; MA, myocelluiar area; tified all cases with a subsequent unfavorable out- MfA, myofibrillar area; MVF, myofibril volume fraction; iVA, nuclear area.

322 Pelliccia et al. August 1994
American Heart Journal
Table V. Clinical, electrocardiographic, and echocardiographic features at assessment for cardiac transplantation
Group A Group B (n = 10) (n = 20) p Value
Clinical features Age (~4 50 ” 7 50 * 10 NS Men/women 9/l 15/5 NS
Duration of symptoms (mo) 37 + 19 36 + 22 NS Serum sodium (mg/dl) 136 AZ 3 137 +- 3 NS NYHA class
III 5 (50%) 15 (75%) IV 5 (50%) 5 (25%) NS
Resting and ambulatory ECG features Atria1 fibrillation 3 (30%) 1(5%) NS
AV conduction delay 2 (20%) 6 (30%) NS Left bundle branch block 3 (30%) 6 (30%) NS Nonsustained VT 4 (40%) 4 (20%) NS
Echocardiographic features Left atria1 diameter (mm) 46 + 5 44 -+ 6 NS LV end-diastolic diameter (mm) 71 c 7 67 -t 6 NS LV end-systolic diameter (mm) 61 -t 7 56 t 7 NS RV end-diastolic diameter (mm) 21 c 4 20 k 5 NS
AV, Atrioventricular; KG, electrocardiographic; LV, left ventricular; NS, not significant; NYHA, New York Heart Association; RV, right ventricular; VT, ventricular tachycardia.
Table VI. Hemodynamic, angiographic, and histomorphometric features at assessment for cardiac transplantation
Hemodynamic features Mean right atrial pressure (mm Hg) RV end-diastolic pressure (mm Hg) Pulmonary artery pressure (mm Hg) LV end-diastolic pressure (mm Hg) Cardiac index (1 . min-i me2) Stroke volume index (ml . me2)
Angiographic features LV ejection fraction (% 1 LV end-diastolic volume (ml . m-2) LV end-systolic volume (ml . rn-?
Significant mitral regurgitation Histomorphometric features
Myocellular area (pm2) Nuclear area (pm21 Myofibrillar area (rm2) Myofibril volume fraction (970) Interstitial fibrosis (%) Endocardial fibrosis (% 1
LV, Left ventricular; NS, not significant; RV, right ventricular.
Group A Group B (n = 10) (n = 20)
7*3 523 8+3 623
25 f 4 23 f 3 21 i- 4 18 f 3
2.0 * 0.4 2.4 + 0.4 25 + 6 30 * 5
20 i 4 22 zt 3 229 + 55 224 + 62 184 -+ 47 174 + 51 5 (25%) 3 (30%)
1205 + 387 1026 + 246 73 t 17 48 + 11
1035 + 340 936 + 228 85.1 +- 2.5 90.5 + 2.6
9.3 2 5.5 6.2 + 5.6 11.4 + 9.6 7.8 * 6.8
p Value
NS NS NS
< 0.03 < 0.02 < 0.03
NS NS NS NS
NS <O.OOl
NS <O.OOl
NS NS
come (sensitivity lOO%), but this feature had low specificity (60%), because frequently it was also de- tected in patients with a good outcome. Measure- ments of myofibril volume fraction were better able to stratify patients if combined with those of nuclear area. Indeed, detection of a myofibril volume fraction 589 % in patients having a nuclear area >50 ,um2 was highly related to l-year prognosis. These two features were detected in all 10 patients who had an unfavor-
able outcome but in only 2 of the 20 patients who showed a benign course. Therefore, insufficient contractile elements (i.e., a low myofibril volume fraction), despite evidence of heightened nuclear ri- bonucleic acid and protein production (i.e., an ab- normal oversize nucleus),35 appears to be the most reliable marker of end-stage disease. Accordingly, it is reasonable to speculate that functional deteriora- tion can be expected to be irreversible when these

vohuna128,Nianba42
Am&can Hsafl JOUmal Pelliccia et al. 323
Fig. 2. Endomyocardial biopsy specimen from left ventricle in a patient (No. 6) of group A. Myocytes are unevenly sized and show large and irregular nuclei and areas of myofibrillar lysis and vacuolar degenera- tion. Interstitial fibrosis also is present. Histomorphometric analysis disclosed myofibril volume fraction of 81% and nuclear area of 76 Fm2. Significant hemodynamic failure occurred 6 months after assessment for transplantation, and the patient subsequently died of heart failure while on the waiting list.
0 Unfavorable OUtCOme (6f. A) 0 Favorable outcome (6r. B)
I
0 I I I I I I I I I I I
79 81 83 85 87 89 91 93 95 97 99
myofibril volume fraction 1%)
Fig. 3. Relation among myofibril volume fraction, nuclear area, and l-year outcome in study patients. Concurrency of myofibril volume fraction (89% and nuclear area >50 pm2 was highly predictive of un- favorable outcome.
abnormalities constitute the morphologic substrates could not prospectively validate the prognostic crite- of myocardial contractility. ria generated from our “learning” population in a
Limitations. The relatively small number of patients new group of patients. Although the results of mul- included in the study constitutes a limitation, which tivariate analysis were successfully tested through is, however, inherent in any investigation concerning cross-validation,22 further research in a larger series only patients with no severely limiting symptoms despite low ejection fracti0n.s As a consequence, we
is needed to confirm the present findings. Histologic examination of endomyocardial biopsy samples suf-
324 Pelliccia et al. August 1994
American Heart Journal
Table VII. Clinical indexes of functional status at assessment for cardiac transplantation in the study patients dichotomized according to myofibril volume fraction and nuclear area
Myofibril volume fraction (%) Nuclear area (pm2)
290 589 <50 >50 (n = 12) (n = 18) p Value (n = 10) (n = 20) p Value
Clinical features Age (~4 Men/women Duration of symptoms (mo) Serum sodium (mg/dl) NYHA class
III IV
Electrocardiographic features Atria1 fibrillation AV conduction delay Left bundle branch block Nonsustained VT
Hemodynamic features Mean right atria1 pressure (mm Hg) RV end-diastolic pressure (mm Hg) Pulmonary artery pressure (mm Hg) LV end-diastolic pressure (mm Hg) Cardiac index (1 . min-’ . mw2) Stroke volume index (ml . rnv2) LV ejection fraction (% )
50 + 9 9/3
34 _+ 23 136 rt_ 3
10 (83%) 2 (17%)
0 3 (25%) 5 (42%) 3 (25%)
6&2 7+3
24 F 3 18 r 4
2.5 f 0.4 31 + 6 22 * 3
50 * 8 15/3
37 + 19 137 f 3
10 (55%) 8 (44%)
4 (22%) 5 (28%) 4 (22%) 5 (28%)
6k3 7*3
24 + 4 20 * 4
2.2 + 0.4 21 _t 5 21 + 4
NS NS NS NS
NS
NS NS NS NS
NS NS NS NS NS NS NS
46 +_ 10 713
38 + 24 137 + 3
8 (80%) 2 (20%)
1 (10%) 1 (10%) 1 (10%) 0
52-3 6+3
22 -t 4 17 +- 4
2.4 f 0.4 31 f 6 22 k 4
52 -+ 8 NS 17/3 NS
35 * 20 NS 136 + 3 NS
12 (60%) 8 (40%) NS
3 (15%) NS 7 (35%) NS 8 (40%) NS 8 (40%) NS
6+-3 NS 8-r-3 NS
24 f 3 NS 20 r 4 NS
2.2 + 0.4 NS 28 + 6 NS 21 _t 4 NS
AV, Atrioventricular; LV, left ventricular; NS, not significant; NYHA, New York Heart Association; RV, right ventricular; VT, ventricular tachycardia.
fers from sampling error because only small myocar- dial fragments can be obtained. Unfortunately, struc- tural abnormalities in the hearts of cardiomyopathy patients often have a focal distribution.32 However, the multiple spatial sampling adopted should have minimized, though not abolished, this source of bias.
Another criticism could be that patients did not undergo cardiopulmonary exercise testing at assess- ment for transplantation. Although a low peak exer- cise oxygen consumption (v02) has been suggested to be an effective tool for timing the procedure,36 recent findings support the concept that the cardiopulmo- nary reserve cannot be reliably evaluated in patients with heart failure.37 Thus whether exercise capacity correlates with the degree of left ventricular dysfunc- tion and plays a predictive role is still controversial.38 Nevertheless, additional investigations are needed to compare the predictive values of histomorphometric features and peak exercise iroz. Finally, our study is limited by the lack of systematic evaluation of some laboratory parameters that have been predictive in some populations.3g,40 Although we did not detect any difference in serum sodium levels between pa- tients with good or poor outcome, the possibility exists that other variables, such as serum norepi- nephrine, may be helpful for the timing of transplan- tation.
Clinical implications. This study emphasizes the use of endomyocardial biopsy for the timing of cardiac
transplantation in cases of IDC. It does not indicate that all patients with this condition should undergo biopsy for prognostic purposes at assessment for transplantation. Indeed, those patients who show se- vere symptoms and hemodynamic instability require urgent surgeryt4 and, of course, biopsy cannot add any relevant information for the timing of the proce- dure. On the other hand, the cost-benefit ratio of en- domyocardial biopsy is poor in patients with a rela- tively preserved cardiac function, who obviously are not candidates for transplantation.
The present investigation shows that the decision for transplantation cannot rely only on clinical or hemodynamic features in patients with IDC who are “too well” for surgery. Indeed, in these patients the l-year freedom from a cardiac event (67% in this study) is lower than that currently expected with transplantation6 and only histomorphometric fea- tures-the concurrency of low myofibril volume frac- tion (39 % ) and increased nuclear area (>50 pm2)-- seem to predict reliably their short-term outcome. Thus, endomyocardial biopsy has the potential to improve the rationalization of the timing of cardiac transplantation in the subset of IDC patients con- sidered at low priority for the procedure.
REFERENCES 1. Fuster J, Gersh B, Giuliani E, Tajik A, Brandeburg R, Frye R.
The natural history of idiopathic dilated cardiomyopathy. Am J Cardiol 1981;47:525-31.

Volume 128, Number 2 American Heart Journal Adliccia et al. 325
2.
3.
4.
5.
6.
7.
8.
9.
10.
11.
12.
13.
14.
15.
16.
17.
18.
19.
20.
Unverferth DV, Magorien RD, Moeschberger ML, Baker PB, Fetters JK, Leier CV. Factors influencing the one-year mor- tality of dilated cardiomyopathy. Am J Cardiol 1984;54:147- 52. Romeo F, Pelliccia F, Cianfrocca C, Gal10 P, Barilla F, Cris- tofani R, Reale A. Determinants of end-stage idiopathic dilated cardiomyopathy: a multivariate analysis of 104 pa- tients. Clin Cardiol 1989;12:387-92. Stevenson LW, Hamilton MA, Till&h IH, Moriguchi JD, Kobashieawa JA. Creaser JA. Drinkwater D. Laks H. Decreas- ing survival benefit from cardiac transplantation for outpa- tients as the waiting list lengthens. J Am Co11 Cardiol 1991; l&919-25. Keogh A, Freund J, Baron D, Hickie J. Timing of cardiac transplantation. Am J Cardiol 1988,61:418-22. Heck CF, Shumway SJ, Kaye MP. Registry of the Interna- tional Society for Heart Transplantation: sixth official re- port--1989. J Heart Transplant-1989;8:271-6. Evans RW. Manninen DL. Garrison LP. Maier AM. Donor availability as the primary determinant of the future of heart transplantation. JAMA 1986;255:1982-8. Stevenson LW, Fowler MB, Schroeder JS, Stevenson WG, Dracup KA, Fond V. Poor survival of patients with idiopathic cardiomyopathy considered too well for transplantation. Am J Med 1987;83:871-6. Stevenson LW, Dracup KA, Tillisch JH. Efficacy of medical therapy for severe congestive heart failure in patients referred for urgent cardiac transplantation. Am J Cardiol1989;63:461-4. Stevenson LW, Sietsema K, Tillisch JH, Lem V, Waden J, Kabashigawa JA, Moriguchi J. Exercise capacity for survivors of cardiac transplantation or sustained medical therapy for stable heart failure. Circulation 1990;81:78-85. Stevenson LW, Tillisch JH, Hamilton M, Luu M, Chelimsky- Fallick C, Moriguchi J, Kabashigawa J, Walden J. Importance of hemodynamic response to therapy in predicting survival with ejection fraction <20% secondary to ischemic or non-is- chemic dilated cardiomyopathy. Am J Cardiol 1990;66:1348- 54. Packer M. Sudden unexpected death in patients with conges- tive heart failure: a second frontier. Circulation 1985;72:681-5. Brandenburg RO, Chazov E, Cherian G, Falase AO, Grosgo- geat J, Kawai C, Loogen F, Martin JV, Orinius E, Goodwin JF, Olsen EGJ, Oakley CM, Disa Z. Report of the WHO/ISFC task force on definition and classification of cardiomyopathies. Circulation 1981;64:437A-8A. Copeland JG, Emery RW, Levinson MM, Icenogle TB, Carrier M. Ott RA. Coneland JA. M&leer-Rhenman MJ. Nicholson SM. Selection of patients for cardiac transplantation. Circu- lation 1987;75:2-9. Lawn B, Graboys TB. Sudden death: an ancient problem newly perceived. Cardiovasc Med 1977;2:219-25. Sahn DJ, DeMaria A, Kisslo J, Weyman A. Recommendations regarding quantitation in M-mode echocardiography: results of a survey of echocardiographic measurements. Circulation 1978;58:1072-83. Kennedy JW, Trenholme SE, Kasser IS. Left ventricular vol- ume and mass from single cineangiocardiogram: a comparison of antero-posterior and right anterior oblique methods. AM HEART J 1970;80:343-9. Parillo JE, Aretz HT, Palacios I, Fallon JT, Block PC. The re- sults of transvenous endomyocardial biopsy can frequently be used to diagnose myocardial diseases in patients with idio- pathic heart failure: endomyocardial biopsies in 100 consecu- tive patients revealed a substantial incidence of myocarditis. Circulation 1984;69:93-106. Richardson PJ. King’s College endomyocardial bioptome. Lancet 1974;1:660-7. Mall G, Schwarz F, Derks H. Clinicopathologic correlations in congestive cardiomyopathy: a study on endomyocardial biop- sies. Virchows Arch Path01 Anat 1982;397:67-82.
21.
22.
23.
24.
25.
26.
27.
28.
29.
30.
31.
32.
33.
34.
35.
36.
37.
38.
39.
40.
Hinkle LE, Thaler HT. Clinical classification of cardiac deaths. Circulation 1982;65:457-63. Efron B. Estimating the error rate of a prediction rule: improvement on cross-validation. J Am Stat Assoc 1983;78: 316-31. Armitage P. Statistical methods in medical research. New York: Wiley, 1971:12-124. Engler R, Ray R, Higgins C, McNally C, Buxton W, Bharga- var V, Shabeti R. Clinical assessment and follow-up of func- tional capacity in patients with chronic congestive cardiomy- opathy. Am J Cardiol 1982;49:1832-7. Holmes J, Kubo SH, Cody RJ, Kligfield P. Arrhythmia in is- chemic and nonischemic dilated cardiomyopathy: prediction of mortality by ambulatory monitoring. Am J Cardiol 1985; 55146-53. Pelliccia F, Gallo P, Cianfrocca C, d’Amati G, Bernucci P, Re- ale A. Relation of complex ventricular arrhythmias to pre- senting features and prognosis in dilated cardiomyopathy. Int J Cardiol 1990;29:47-54. Cohn JN. Prognostic factors in heart failure: poverty amidst a wealth of variables. J Am Co11 Cardiol 1989;14:571-2. Romeo F, Pelliccia F, Cianfrocca C, Cristofani R, Reale A. Predictors of sudden death in idiopathic dilated cardiomyop- athy. Am J Cardiol 1989;63:138-40. Swerdlow CD, Winkle RA, Mason JW. Determinants of sur- vival in patients with ventricular tachyarrhythmias. N Engl J Med 1983;308:1436-42. Popma JJ, Cigarroa RG, Buja LM, Hillis LD. Diagnostic and prognostic utility of right-sided catheterization and endomy- ocardial biopsy in idiopathic dilated cardiomyopathy. Am J Cardiol 198$63:955-g. Keogh AM, Baron DW, Hickie JB. Prognostic guides in patients with idiopathic dilated cardiomyopathy assessed for cardiac transplantation. Am J Cardiol 1990;65:903-8. Schwarz F, Mall G, Zebe H, Schmitzer E, Manthey J, Scheu- rlen H, Kubler W. Determinants of survival in patients with congestive cardiomyopathy: quantitative morphologic find- ings and left ventricular hemodynamics. Circulation 1984; 70:923-8. Figulla HR, Rahlf G, Nieger M, Luig H, Kreuzer H. Sponta- neous hemodynamic improvement or stabilization and associ- ated biopsy findings in patients with congestive cardiomyop- athy. Circulation 1985;71:1095-104. Hammond EH, Menlove RL, Anderson JL. Predictive value of immunofluorescence and electron microscopic evaluation of endomyocardial biopsies in the diagnosis and prognosis of myocarditis and idiopathic dilated cardiomyopathy. AM HEART J 1987;114:1055-65. Unverferth BJ, Leier CV, Magorien RD, IJnverferth DV. Dif- ferentiating characteristics of myocardial nuclei in cardiomy- opathy. Hum Path01 1983;14:974-83. Mancini DM, Eisen H, Kussmaul W, Mull R, Edmunds LH Jr, Wilson JR. Value of peak exercise oxygen consumption for optimal timing of cardiac transplantation in ambulatory patients with heart failure. Circulation 1991;83:778-86. Jondeau G, Katz SD, Zohman L, Goldberger M, McCarthy M, Bourdarias JP, LeJemtel TH. Active skeletal muscle mass and cardiopulmonary reserve. Circulation 1992;86:1351-6. Engel PJ. Effort intolerance in chronic heart failure: what are we treating? J Am Co11 Cardiol 1990;13:995-8. Lee WH. Packer M. Prosnostic imnortance of serum sodium concentration and its modification
a
by converting enzyme in- hibition in patients with severe chronic heart failure. Circula- tion 1986;73:257-67. Cohn JN, Levine TB, Olivari MT, Garberg V, Lura D, Francis GS, Simon AB, Rector T. Plasma norepinephrine as a guide to prognosis in patients with chronic congestive heart failure. N Engl J Med 1984;311:819-23.