hemin, erythropoietin and antithrombotics to treat covid ... - osf
TRANSCRIPT
Abrahams, L. (2022, April 13). Hemin, erythropoietin and antithrombotics to treat Covid-19 hematology. OSF Preprints | CC-BY-NC-ND
MSC ADVANCED BIOLOGICAL SCIENCES (BIOINFORMATICS)
Hemin, erythropoietin and antithrombotics to treat Covid-19 hematology
Lianne Abrahams
April 2022
Submitted in partial fulfilment of the MSc Advanced Biological Sciences, Bioinformatics
University of Liverpool

Abrahams, L. (2022, April 13). Hemin, erythropoietin and antithrombotics to treat Covid-19 hematology. OSF Preprints | CC-BY-NC-ND
Hemin, erythropoietin and antithrombotics to treat Covid-19 hematology
Lianne Abrahams
Department of Systems Biology, Ronin Institute, 127 Haddon Place, Montclair, New Jersey, United States, 07043-2314
To whom correspondence may be addressed: [email protected]
Abstract
Hematological dimensions of Covid-19 are widely recognized and include hypercoagulability, dyserythropoiesis and
abnormal concentration of serum and cellular porphyrins. Currently there is no internationally-recognised consensus
protocol for treatment of severe Covid-19. Hemin, erythropoietin (EPO) and antithrombotics counter hematological
dysfunction in Covid-19 and are viable candidates for inclusion in a consensus protocol. Initial clinical trial data are available
for antithrombotics and clinical trials of erythropoietin are planned. The current review makes a reasoned argument for living systematic review and meta-analysis of all three interventions and advances the case for extending assessment of
study quality to account for conflicts of interest. In particular, the current review hypothesizes: (i) hemin, EPO and
antithrombotics may be clinically useful in the treatment of severe Covid-19; and, (ii) GATA-1/2 signalling may be a mechanistic link between all three hematological abnormalities.
Highlights
▪ EPO may improve Covid-19 outcomes by stimulating erythropoiesis or by mechanisms of tissue protection and mitigation of lung injury
▪ EPO may shift iron metabolism in Covid-19 from the inflammatory profile of iron restriction to the pro-erythropoietic profile of iron mobilisation
▪ Addition of a novel criterion to study quality assessment scales may improve meta-analysis by accounting for conflicts of
interest
▪ Covid-19 shares eight similarities of porphyrin profile with acute porphyria, although the picture is complicated, and
requires further research
▪ Analysis of urinary and fecal porphyrins in Covid-19, especially ALA and PBG, represents a conspicuous gap in current
knowledge
Abbreviations: ADAMTS13, ADAM metallopeptidase with thrombospondin type 1 motif 13; ALI, acute lung injury; AMSTAR2, assessment of
multiple systematic reviews; aOR, adjusted odds ratio; APTT, activated partial thromboplastin time; ARDS, acute respiratory distress syndrome;
CD147, cluster of differentiation 147; ChAdOx1, chimpanzee adenovirus Oxford-1; CKD, chronic kidney disease; Covid-19, coronavirus disease
2019; CRP, C reactive protein; DIC, disseminated intravascular coagulation; EPO, erythropoietin; ESA, erythropoietin stimulating agent; FDP,
fibrin degradation product; GATA1/2, a family of transcription factors characterized by their ability to bind to the DNA sequence GATA; GBP,
Great British Pounds; Hb, hemoglobin; HIF, hypoxia inducible factor; ICU, intensive care unit; IL, interleukin; IU, international units; MD, mean
difference; MDA, malondialdehyde; MPO, myeloperoxidase; n, sample number; NFKB, nuclear factor kappa B; NHS, national health service;
national institute for health and care excellence; NLRP3, NOD-like receptor protein-3; nRBC, nucleated red blood cell; OR, odds ratio; PaCO2,
partial pressure of carbon dioxide in arterial blood; PaO2, partial pressure of oxygen in arterial blood; PCR, polymerase chain reaction; PICO,
population intervention comparator outcome; Pro-IL-1β, pro-interleukin-1 beta; PT, prothrombin time; RDW, red blood cell distribution width;
rhEPO, recombinant human erythropoietin; SARS-Cov-1/2, severe acute respiratory syndrome coronavirus-1/2; TNF-alpha, tumor necrosis factor
alpha; TTP, thrombotic thrombocytopenic purpura; VWF, von Willebrand factor; WHO, World Health Organisation; WMD, weighted mean
difference.
Keywords: hemin, erythropoietin, antithrombotic, fibrinolytic, Covid-19
Abrahams, L. (2022, April 13). Hemin, erythropoietin and antithrombotics to treat Covid-19 hematology. OSF Preprints | CC-BY-NC-ND
EPO may remedy hypoxia, dyserythropoiesis and lung injury in Covid-19
Epo and the hypoxia paradox
Covid-19 patients are afflicted by pulmonary manifestations including acute respiratory distress syndrome (ARDS) and pneumonia.
Pulmonary manifestations impair the ability of the lungs to oxygenate the blood and bodily tissues, leading to hypoxemia and
hypoxia, respectively. An extrapulmonary intervention capable of minimising hypoxia would be of considerable clinical utility in
treating Covid-19 patients. Erythropoietin is ordinarily induced in response to hypoxia of various causes [1] and reverses hypoxia
by augmenting oxygen-carrying capacity of the blood [2]. Specifically, erythropoietin stimulates formation and differentiation of
erythroid precursor cells. Curiously, the physiological response to hypoxia in Covid-19 is different when compared with other
conditions of hypoxia, particularly in relation to erythropoiesis.
Erythropoietin levels in critical Covid-19 patients and non-survivors are, on average, lower than control (Covid-19 negative
volunteers) and survivor patients [3]. While this finding is preliminary, due to small patient sample size and lack of baseline
measurements of erythropoietin, a separate study [4] found a complementary trend. Viruez-Soto et al (2021) observe
erythropoietin deficiency in Covid-19 patients at time of presentation, relative to altitude-matched physiological mean value [4].
Surviving patients presented with serum EPO levels two to three fold lower than the physiological mean, while non-survivor EPO
was 4.6 to 7.3 lower. Average serum erythropoietin was significantly (2.5-fold) lower in non-survivors than in survivors. To the
best of the author’s knowledge, Yağcı et al and Viruez-Soto et al are the only two studies to date that have designedly explored
erythropoietin levels in Covid-19 patients [3, 4]. Both studies concur that circulating erythropoietin levels are decreased in Covid-
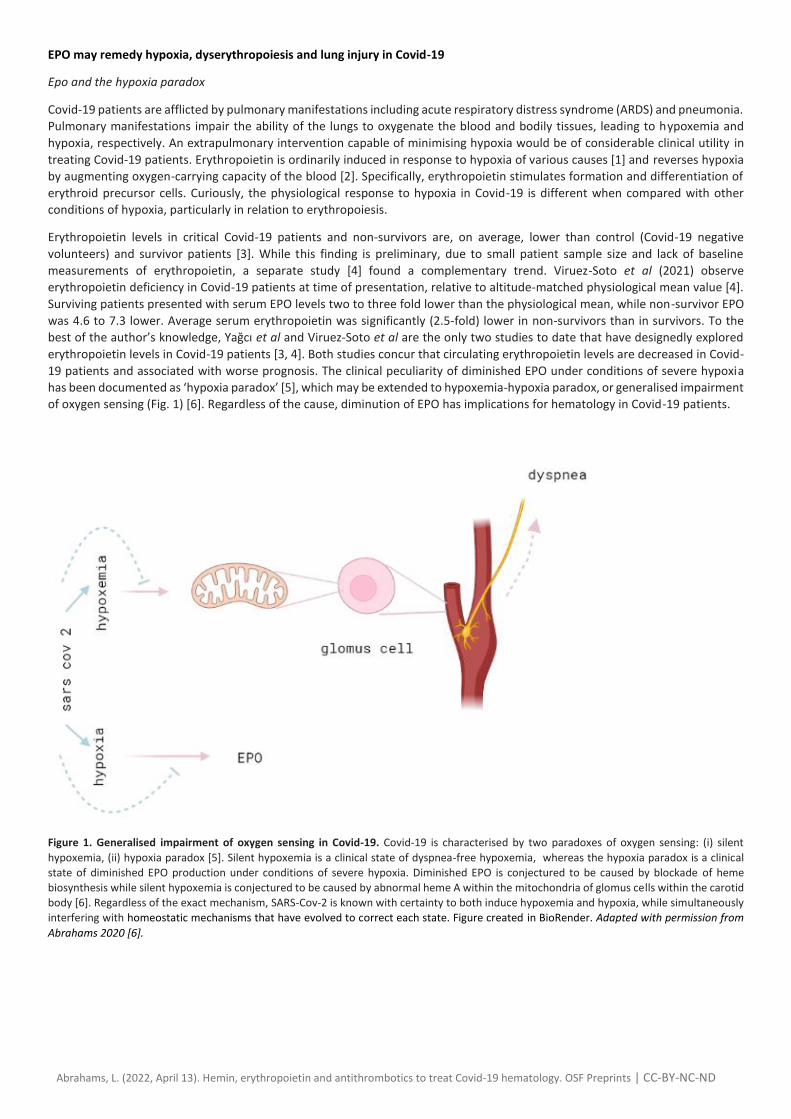
19 patients and associated with worse prognosis. The clinical peculiarity of diminished EPO under conditions of severe hypoxia
has been documented as ‘hypoxia paradox’ [5], which may be extended to hypoxemia-hypoxia paradox, or generalised impairment
of oxygen sensing (Fig. 1) [6]. Regardless of the cause, diminution of EPO has implications for hematology in Covid-19 patients.
Figure 1. Generalised impairment of oxygen sensing in Covid-19. Covid-19 is characterised by two paradoxes of oxygen sensing: (i) silent
hypoxemia, (ii) hypoxia paradox [5]. Silent hypoxemia is a clinical state of dyspnea-free hypoxemia, whereas the hypoxia paradox is a clinical
state of diminished EPO production under conditions of severe hypoxia. Diminished EPO is conjectured to be caused by blockade of heme
biosynthesis while silent hypoxemia is conjectured to be caused by abnormal heme A within the mitochondria of glomus cells within the carotid
body [6]. Regardless of the exact mechanism, SARS-Cov-2 is known with certainty to both induce hypoxemia and hypoxia, while simultaneously
interfering with homeostatic mechanisms that have evolved to correct each state. Figure created in BioRender. Adapted with permission from
Abrahams 2020 [6].
Abrahams, L. (2022, April 13). Hemin, erythropoietin and antithrombotics to treat Covid-19 hematology. OSF Preprints | CC-BY-NC-ND
Dyserythropoiesis in Covid-19
Interestingly, four recent autopsies indicated a decrease in hematopoietic red lines within the sternum and splenic
hemophagocytosis [7]. Splenic atrophy has been noted anecdotally (Feng 2020) and previously conjectured as either splenic
emptying of reserve erythrocytes or selective trapping of red blood cells in the spleen [6]. The latter happens under conditions of
CD147 blockade [8] and SARS-Cov-2 is known to bind to the CD147 receptor [9]. Selective trapping of splenic erythrocytes results
in a form of anemia [8]. Anemia is defined by the World Health Organisation as hemoglobin concentrations of < 130 g/L (males)
or < 120 g/L (females) and low red blood cell counti. Primates infected with SARS-Cov-2 have subnormal levels of red bloods cells
and hemoglobin [10]. The same is true in humans [11], according to the results of three recent meta-analyses. Firstly, Taneri et al
2020 [12] found that of 21,605 Covid-19 patients, severe cases had lower hemoglobin and red blood cell count when compared
with milder cases. Secondly, Lippi & Mattiuzzi 2020 [13] found that of 1,210 Covid-19 patients, severe cases had lower hemoglobin
compared with milder cases. Thirdly, of 9,623 Covid-19 patients, Zuin et al [14] found pooled prevalence of anemia was 25.6% and anemia was significantly associated with 70% higher risk of short-term mortality [14].
Pathophysiological reasons for anemia observed in Covid-19 have variously been postulated as: hemolytic anemia [6, 15] iron
sequestration [12] or pro-inflammatory cytokines [16]. Since circulating erythropoietin levels are on average lower in Covid-19
patients than controls [3], this would suggest EPO as a contributory factor in anemia. Alternatively, anemia may be coincidentally
associated with Covid-19, rather than being a driver of Covid-19 phenotype. Regardless, Covid-19 associated anemia would tend
to suggest aberrations in erythropoiesis, and erythropoietic distress is signalled by elevated co-efficient of red blood cell
distribution width (RDW). Three recent meta-analyses (n, 14,866 and 18,392 and 4,901) converge on the conclusion that red blood
cell distribution width is predictive of disease prognosis in Covid-19 [17, 18, 19]. Elevated RDW is a marker of reduced erythrocyte
turnover; erythrocytes decrease in size with age [20, 6] and presents as anisocytosis. Anisocytosis signifies erythropoietic distress
[21, 22]; reduced erythrocyte turnover serves to maintain circulating red blood cell levels [20]. Moreover, erythroid progenitors
express CD147 receptor from day 5 of differentiation [11] and are directly invaded by SARS-Cov-2 [11, 23, 24]. Erythroid precursor
cells have also been detected in peripheral blood of Covid-19 patients [25]. Single cell transcriptomics analysis of peripheral blood
reveals that GATA-1 and GATA-2 transcripts are up-regulated in Covid-19 non-survivors, but not in survivors. GATA factors
suppress production of erythropoietin [26] in accordance with the idea that erythropoiesis is altered in Covid-19 patients with
worse outcomes.
Further evidence of disturbed erythropoiesis derives from the presence of circulating immature red blood cells subsequent to
SARS-Cov-2 infection [23, 27]. Circulating normoblasts and immature reticulocytes were analysed at first and last test point, a
proxy for admission and endpoint values, respectively [27]. At last test, nucleated red blood cell (nRBC) count was undetectable
in survivors, whereas nRBC count was significantly elevated in non-survivors [27]. Likewise, Encabo et al discovered that presence
of circulating normoblasts peaks two to three weeks following patient admission and coincides with decline of patient hemoglobin
levels [23]. Presence of normoblasts and reticulocytes in the peripheral circulation is abnormal and usually associated with
diseases of erythropoiesis, including hemolytic anemia [28]. Presence of immature reticulocytes was also significantly raised in
non-survivors relative to survivors [27], at both admission and endpoint, as measured by middle-high fluorescent reticulocyte
percentage and immature reticulocyte fraction. Concordantly, measure of mature reticulocytes by low-fluorescent reticulocyte
percentage was significantly decreased in non-survivors [27]. These results accord with circumstantial evidence of nucleated red
cells with dyserythropoiesis and basophilic stippling observed in an 81 year old male patient [29].
Several hematological solutions have been proposed to counteract dyserythropoiesis observed in Covid-19, including earlier
intervention [27] with red blood cell transfusion [13, 27], by adjusting the current threshold for transfusion (hemoglobin levels of
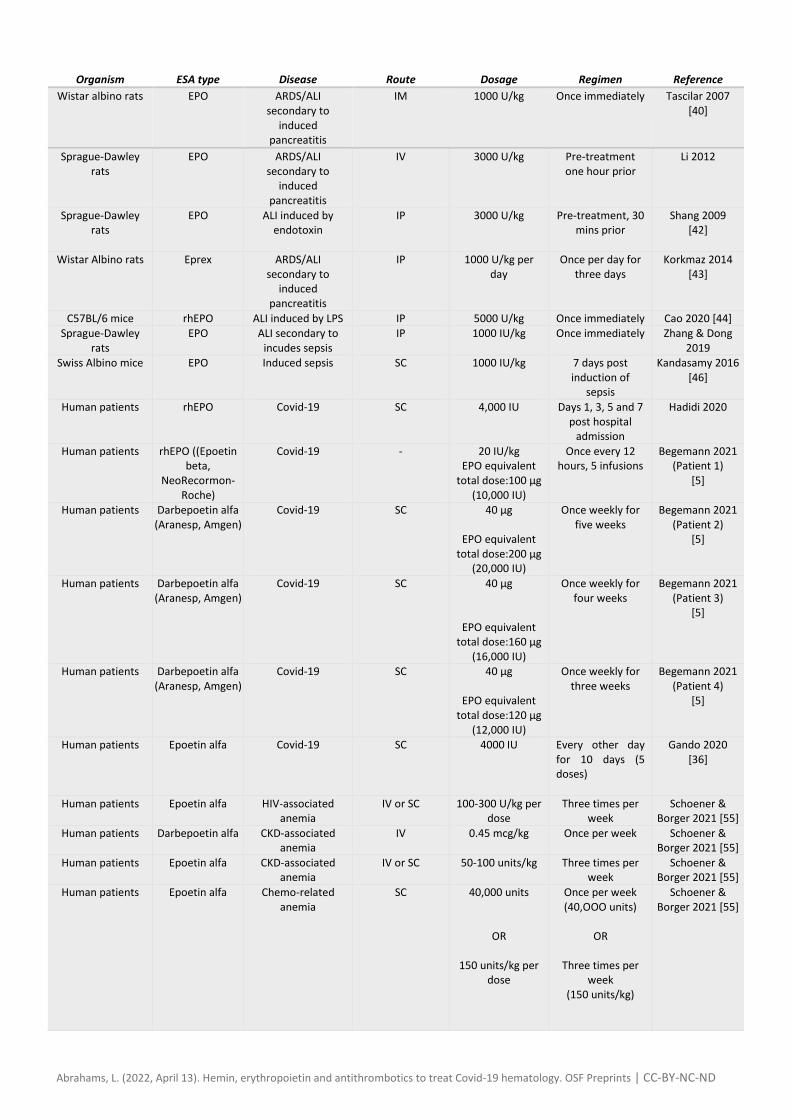
7–9 g/dL) to a more liberal threshold. An alternative means of increasing red cell count is treatment with erythropoiesis stimulating agents (ESAs), an intervention that has been suggested by multiple researchers [4, 5, 16, 30, 31, 32, 33, 35, 36, 37, 38, 39].
Epo protects in rat models of pulmonary disease
Exogenous erythropoietin aides recovery in rat models of pulmonary disease and sepsis [30, 34, 38, 40, 41, 42, 43, 44, 45, 46].
Acute respiratory distress syndrome (ARDS) and acute lung injury (ALI) were overcome in rats treated with Epo, relative to vehicle,
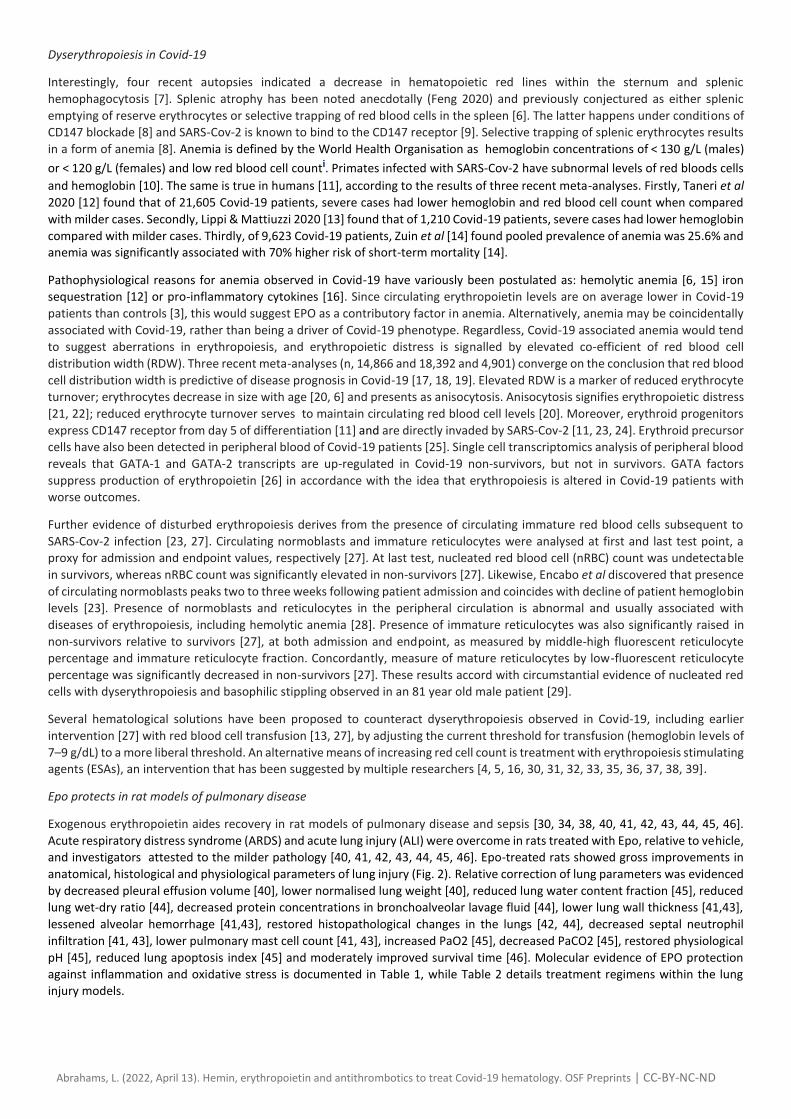
and investigators attested to the milder pathology [40, 41, 42, 43, 44, 45, 46]. Epo-treated rats showed gross improvements in
anatomical, histological and physiological parameters of lung injury (Fig. 2). Relative correction of lung parameters was evidenced
by decreased pleural effusion volume [40], lower normalised lung weight [40], reduced lung water content fraction [45], reduced
lung wet-dry ratio [44], decreased protein concentrations in bronchoalveolar lavage fluid [44], lower lung wall thickness [41,43],
lessened alveolar hemorrhage [41,43], restored histopathological changes in the lungs [42, 44], decreased septal neutrophil
infiltration [41, 43], lower pulmonary mast cell count [41, 43], increased PaO2 [45], decreased PaCO2 [45], restored physiological
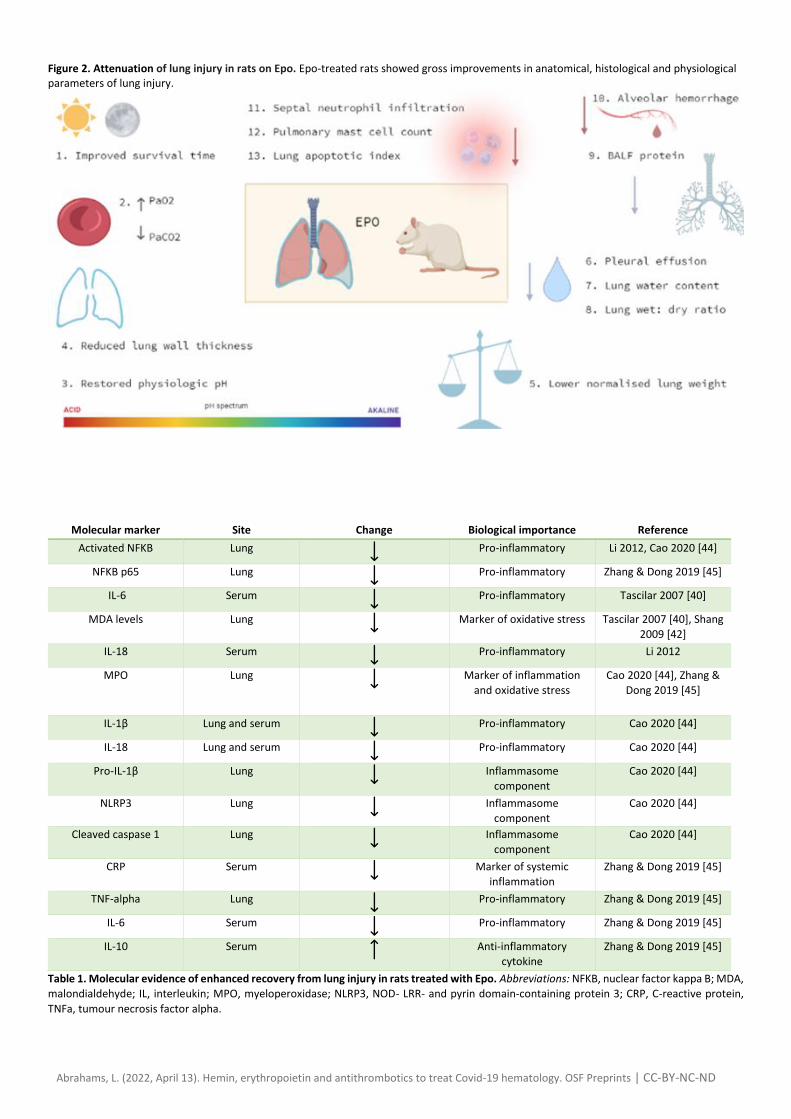
pH [45], reduced lung apoptosis index [45] and moderately improved survival time [46]. Molecular evidence of EPO protection
against inflammation and oxidative stress is documented in Table 1, while Table 2 details treatment regimens within the lung
injury models.
Abrahams, L. (2022, April 13). Hemin, erythropoietin and antithrombotics to treat Covid-19 hematology. OSF Preprints | CC-BY-NC-ND
Figure 2. Attenuation of lung injury in rats on Epo. Epo-treated rats showed gross improvements in anatomical, histological and physiological parameters of lung injury.
Molecular marker Site Change Biological importance Reference
Activated NFKB Lung
Pro-inflammatory Li 2012, Cao 2020 [44]
NFKB p65 Lung
Pro-inflammatory Zhang & Dong 2019 [45]
IL-6 Serum
Pro-inflammatory Tascilar 2007 [40]
MDA levels Lung
Marker of oxidative stress Tascilar 2007 [40], Shang
2009 [42]
IL-18 Serum
Pro-inflammatory Li 2012
MPO Lung
Marker of inflammation
and oxidative stress
Cao 2020 [44], Zhang &
Dong 2019 [45]
IL-1β Lung and serum
Pro-inflammatory Cao 2020 [44]
IL-18 Lung and serum
Pro-inflammatory Cao 2020 [44]
Pro-IL-1β Lung
Inflammasome
component
Cao 2020 [44]
NLRP3 Lung
Inflammasome
component
Cao 2020 [44]
Cleaved caspase 1 Lung
Inflammasome
component
Cao 2020 [44]
CRP Serum
Marker of systemic
inflammation
Zhang & Dong 2019 [45]
TNF-alpha Lung
Pro-inflammatory Zhang & Dong 2019 [45]
IL-6 Serum
Pro-inflammatory Zhang & Dong 2019 [45]
IL-10 Serum
Anti-inflammatory
cytokine
Zhang & Dong 2019 [45]
Table 1. Molecular evidence of enhanced recovery from lung injury in rats treated with Epo. Abbreviations: NFKB, nuclear factor kappa B; MDA,
malondialdehyde; IL, interleukin; MPO, myeloperoxidase; NLRP3, NOD- LRR- and pyrin domain-containing protein 3; CRP, C-reactive protein,
TNFa, tumour necrosis factor alpha.
Abrahams, L. (2022, April 13). Hemin, erythropoietin and antithrombotics to treat Covid-19 hematology. OSF Preprints | CC-BY-NC-ND
Organism ESA type Disease Route Dosage Regimen Reference
Wistar albino rats EPO ARDS/ALI secondary to
induced pancreatitis
IM 1000 U/kg Once immediately Tascilar 2007 [40]
Sprague-Dawley rats
EPO ARDS/ALI secondary to
induced pancreatitis
IV 3000 U/kg
Pre-treatment one hour prior
Li 2012
Sprague-Dawley rats
EPO ALI induced by endotoxin
IP 3000 U/kg Pre-treatment, 30 mins prior
Shang 2009 [42]
Wistar Albino rats Eprex ARDS/ALI secondary to
induced pancreatitis
IP 1000 U/kg per day
Once per day for three days
Korkmaz 2014 [43]
C57BL/6 mice rhEPO ALI induced by LPS IP 5000 U/kg Once immediately Cao 2020 [44] Sprague-Dawley
rats EPO ALI secondary to
incudes sepsis IP 1000 IU/kg Once immediately Zhang & Dong
2019 Swiss Albino mice EPO Induced sepsis SC 1000 IU/kg 7 days post
induction of sepsis
Kandasamy 2016 [46]
Human patients rhEPO Covid-19 SC 4,000 IU Days 1, 3, 5 and 7 post hospital
admission
Hadidi 2020
Human patients rhEPO ((Epoetin beta,
NeoRecormon- Roche)
Covid-19 - 20 IU/kg EPO equivalent
total dose:100 µg (10,000 IU)
Once every 12 hours, 5 infusions
Begemann 2021 (Patient 1)
[5]
Human patients Darbepoetin alfa (Aranesp, Amgen)
Covid-19 SC 40 µg
EPO equivalent total dose:200 µg
(20,000 IU)
Once weekly for five weeks
Begemann 2021 (Patient 2)
[5]
Human patients Darbepoetin alfa (Aranesp, Amgen)
Covid-19 SC 40 µg
EPO equivalent total dose:160 µg
(16,000 IU)
Once weekly for four weeks
Begemann 2021 (Patient 3)
[5]
Human patients Darbepoetin alfa (Aranesp, Amgen)
Covid-19 SC 40 µg
EPO equivalent total dose:120 µg
(12,000 IU)
Once weekly for three weeks
Begemann 2021 (Patient 4)
[5]
Human patients Epoetin alfa Covid-19 SC 4000 IU Every other day for 10 days (5 doses)
Gando 2020 [36]
Human patients Epoetin alfa HIV-associated anemia
IV or SC 100-300 U/kg per dose
Three times per week
Schoener & Borger 2021 [55]
Human patients Darbepoetin alfa CKD-associated anemia
IV 0.45 mcg/kg Once per week Schoener & Borger 2021 [55]
Human patients Epoetin alfa CKD-associated anemia
IV or SC 50-100 units/kg Three times per week
Schoener & Borger 2021 [55]
Human patients Epoetin alfa Chemo-related anemia
SC 40,000 units
OR
150 units/kg per dose
Once per week (40,OOO units)
OR
Three times per
week (150 units/kg)
Schoener & Borger 2021 [55]

Abrahams, L. (2022, April 13). Hemin, erythropoietin and antithrombotics to treat Covid-19 hematology. OSF Preprints | CC-BY-NC-ND
Human patients Epoetin alfa Surgery-associated transfusion reduction
SC 300 units/kg per dose
Once daily for 15 days
Schoener & Borger 2021 [55]
Human patients Darbepoetin alfa Chemo-related anemia
SC 2.25 mcg/kg per dose
OR
500 mcg
Once per week (2.25 mcg/kg)
OR
Once every three
weeks
Schoener & Borger 2021 [55]
Table 2. Previous intervention regimens with erythropoietin as a starting point for consideration of Epo administration in Covid-19 patients. Abbreviations: ALI, acute lung injury; ARDS, acute respiratory distress syndrome; IV, intravenously; SC, subcutaneously; IM, intramuscular injection; IP, intraperitoneal; U/kg, units per kilogram of body mass; CKD, chronic kidney disease; mcg/kg, micrograms per kilogram of body mass.
Erythropoiesis stimulating agents in Covid-19
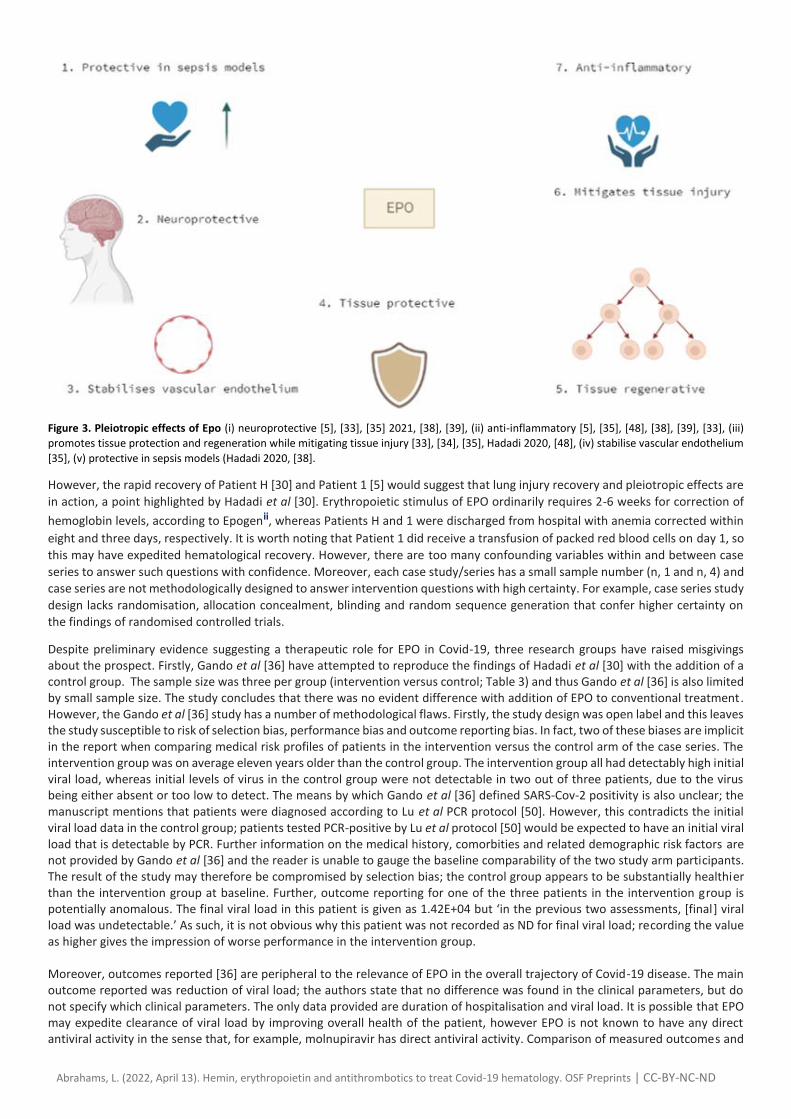
A recent case report on recombinant erythropoietin (rhEPO) provides a cogent example of unexpectedly rapid recovery from severe Covid-19 [30]. As an octogenarian with ground glass opacities, severe anemia (Hb 5.2 g/dL) and RDW of 34.9%, Hadadi et al’s patient (hereby referred to as Patient H) was medically high-risk. In fact, two research groups [18, 47] prognosticate that RDW >14.5% on admission is associated with high risk for mortality; Patient H had 2.4-fold higher RDW. Packed red blood cells were transfused on day one and subcutaneous rhEPO administered at 4,000 IU on days 1, 3, 5 and 7. Anemia was almost completely corrected (Hb 9g/dL) by day eight and the severity of symptoms subsided [30] with oxygen saturation of 94% one week post-discharge. The authors [30] surmised that the rapid recovery signals a therapeutic effect of Epo beyond anemia correction. Similarly, multiple research groups [5, 33, 34, 35, 48] have highlighted autocrine and paracrine tissue protective functions of Epo beyond canonical endocrine functions in erythropoiesis; relevant pleiotropic effects of Epo are summarised in Figure 3.
Reinforcing the value of this case report, Begemann et al [5] recently published a case series of four Covid-19 patients successfully treated with ESA. All four patients were high risk with multiple medical and demographic risk factors for adverse outcomes. All patients were male, aged 58-80 and had between 2-5 serious comorbidities. All patients developed respiratory failure and three out of four progressed to complications including ARDS, acute kidney injury and critical illness polyneuropathy. Most patients were treated with darbepoetin alfa once per week for between three to five weeks (Table 1). Treatment of Patient 1 was slightly different; epoetin beta was administered once every 12 hours, in 5 infusions. Recovery of Patient 1 was advanced in comparison with patients 2-4, with discharge from ICU within 72 hours, raising a question regarding intervention regimen as a differential factor in recovery. Since the sample size is one, any number of factors could be influencing the outcome, independently of the treatment regimen, and this question is posed tentatively. All patients made a complete or moderate recovery of respiratory and renal function, and three of four made a complete neurological recovery. However, this case series is severely limited by the small number of patients (n, 4) and lack of controls. Overall, the five Covid-19 patients documented to have been treated with ESA [30, 5] realised faster recovery than either doctor
would have expected by chance. The average probability of hospitalised Covid-19 patients making a full recovery is approximately
50% in Germany [5]. Statistically, if EPO made no difference to Covid-19 recovery rates, 2.5 of the 5 patients would have been
expected to die. Of course, it is impossible to infer any meaningful difference in mortality outcome with a sample size of five under
conditions of case report. Clinical trials are urgently required that are double-blinded, randomised, controlled and suitably
powered to allow inference of statistical significance. At least two designs for clinical trials of EPO have been reported [32, 37]
including registered trial identity IRCT20200509047364N1. Lamentably, the trial protocol proposed by Ehrenreich et al [32] has
received no offers of funding to date, although hopefully the funding decision may be reversed if convincing preliminary evidence
emerges.
Nevertheless, indirect evidence of the utility of erythropoietin may derive from Perico et al [49]; chronic kidney disease (CKD)
patients on hemodialysis are observed to have a milder course of disease with Covid-19. The relative protection from severe Covid-
19 is rationalised as immunosuppression that prevents cytokine storm in CKD patients. Alternatively, as inferred by Ehrenreich et
al [32], the apparent protection from severe Covid-19 in CKD patients on hemodialysis may be interpreted as a beneficial side-
effect of erythropoietin treatment, since EPO is routinely prescribed for this patient population. At present, Ehrenreich’s
interpretation [32] remains conjecture, however the idea warrants further investigation since erythropoiesis is altered in Covid-
19.
At present, the question of how erythropoietin is expediting recovery from Covid-19 remains fully open. Erythropoietin may be
fulfilling its role in: (a) erythropoiesis, (b) lung injury recovery (Fig. 2), (c) pleiotropic effects (Fig. 3), (d) a combination of (a) - (c).
Abrahams, L. (2022, April 13). Hemin, erythropoietin and antithrombotics to treat Covid-19 hematology. OSF Preprints | CC-BY-NC-ND
Figure 3. Pleiotropic effects of Epo (i) neuroprotective [5], [33], [35] 2021, [38], [39], (ii) anti-inflammatory [5], [35], [48], [38], [39], [33], (iii)
promotes tissue protection and regeneration while mitigating tissue injury [33], [34], [35], Hadadi 2020, [48], (iv) stabilise vascular endothelium
[35], (v) protective in sepsis models (Hadadi 2020, [38].
However, the rapid recovery of Patient H [30] and Patient 1 [5] would suggest that lung injury recovery and pleiotropic effects are
in action, a point highlighted by Hadadi et al [30]. Erythropoietic stimulus of EPO ordinarily requires 2-6 weeks for correction of
hemoglobin levels, according to Epogenii, whereas Patients H and 1 were discharged from hospital with anemia corrected within
eight and three days, respectively. It is worth noting that Patient 1 did receive a transfusion of packed red blood cells on day 1, so
this may have expedited hematological recovery. However, there are too many confounding variables within and between case
series to answer such questions with confidence. Moreover, each case study/series has a small sample number (n, 1 and n, 4) and
case series are not methodologically designed to answer intervention questions with high certainty. For example, case series study
design lacks randomisation, allocation concealment, blinding and random sequence generation that confer higher certainty on
the findings of randomised controlled trials.
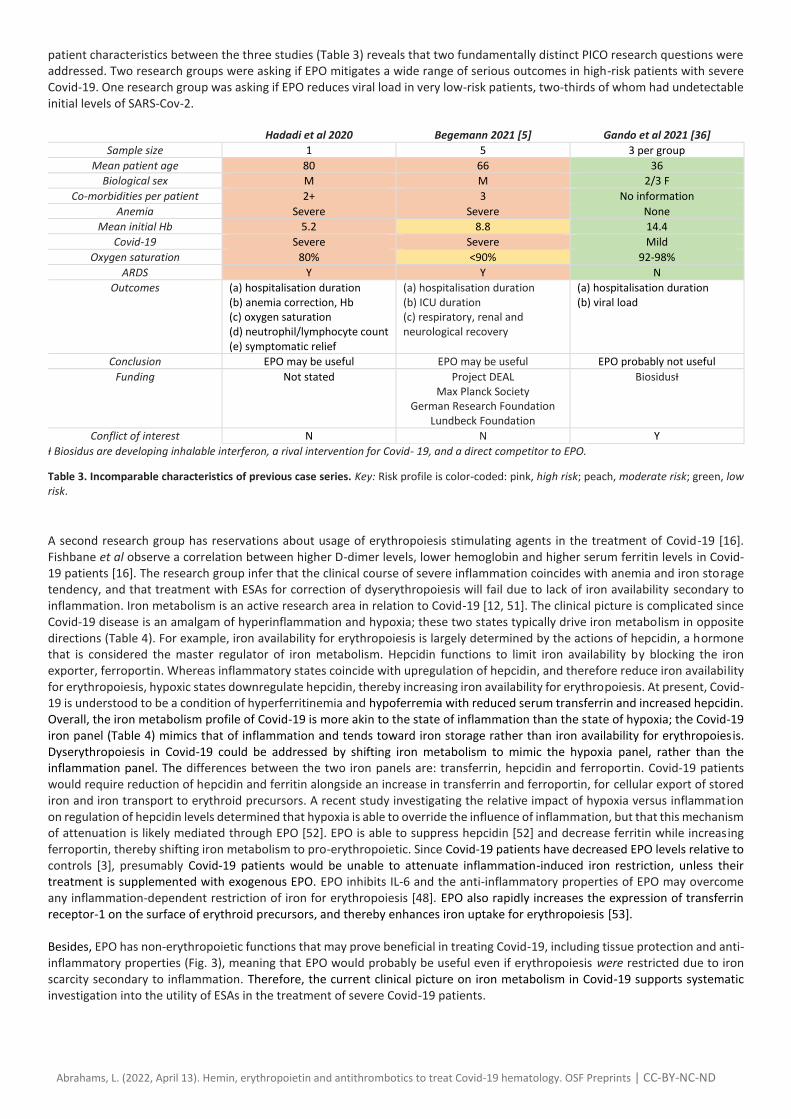
Despite preliminary evidence suggesting a therapeutic role for EPO in Covid-19, three research groups have raised misgivings about the prospect. Firstly, Gando et al [36] have attempted to reproduce the findings of Hadadi et al [30] with the addition of a control group. The sample size was three per group (intervention versus control; Table 3) and thus Gando et al [36] is also limited by small sample size. The study concludes that there was no evident difference with addition of EPO to conventional treatment. However, the Gando et al [36] study has a number of methodological flaws. Firstly, the study design was open label and this leaves the study susceptible to risk of selection bias, performance bias and outcome reporting bias. In fact, two of these biases are implicit in the report when comparing medical risk profiles of patients in the intervention versus the control arm of the case series. The intervention group was on average eleven years older than the control group. The intervention group all had detectably high initial viral load, whereas initial levels of virus in the control group were not detectable in two out of three patients, due to the virus being either absent or too low to detect. The means by which Gando et al [36] defined SARS-Cov-2 positivity is also unclear; the manuscript mentions that patients were diagnosed according to Lu et al PCR protocol [50]. However, this contradicts the initial viral load data in the control group; patients tested PCR-positive by Lu et al protocol [50] would be expected to have an initial viral load that is detectable by PCR. Further information on the medical history, comorbities and related demographic risk factors are not provided by Gando et al [36] and the reader is unable to gauge the baseline comparability of the two study arm participants. The result of the study may therefore be compromised by selection bias; the control group appears to be substantially healthier than the intervention group at baseline. Further, outcome reporting for one of the three patients in the intervention group is potentially anomalous. The final viral load in this patient is given as 1.42E+04 but ‘in the previous two assessments, [final] viral load was undetectable.’ As such, it is not obvious why this patient was not recorded as ND for final viral load; recording the value as higher gives the impression of worse performance in the intervention group. Moreover, outcomes reported [36] are peripheral to the relevance of EPO in the overall trajectory of Covid-19 disease. The main outcome reported was reduction of viral load; the authors state that no difference was found in the clinical parameters, but do not specify which clinical parameters. The only data provided are duration of hospitalisation and viral load. It is possible that EPO may expedite clearance of viral load by improving overall health of the patient, however EPO is not known to have any direct antiviral activity in the sense that, for example, molnupiravir has direct antiviral activity. Comparison of measured outcomes and
Abrahams, L. (2022, April 13). Hemin, erythropoietin and antithrombotics to treat Covid-19 hematology. OSF Preprints | CC-BY-NC-ND
patient characteristics between the three studies (Table 3) reveals that two fundamentally distinct PICO research questions were addressed. Two research groups were asking if EPO mitigates a wide range of serious outcomes in high-risk patients with severe Covid-19. One research group was asking if EPO reduces viral load in very low-risk patients, two-thirds of whom had undetectable initial levels of SARS-Cov-2.
Hadadi et al 2020 Begemann 2021 [5] Gando et al 2021 [36]
Sample size 1 5 3 per group Mean patient age 80 66 36
Biological sex M M 2/3 F
Co-morbidities per patient 2+ 3 No information Anemia Severe Severe None
Mean initial Hb 5.2 8.8 14.4 Covid-19 Severe Severe Mild
Oxygen saturation 80% <90% 92-98% ARDS Y Y N
Outcomes (a) hospitalisation duration (b) anemia correction, Hb (c) oxygen saturation (d) neutrophil/lymphocyte count (e) symptomatic relief
(a) hospitalisation duration (b) ICU duration (c) respiratory, renal and neurological recovery
(a) hospitalisation duration (b) viral load
Conclusion EPO may be useful EPO may be useful EPO probably not useful
Funding Not stated Project DEAL Max Planck Society
German Research Foundation Lundbeck Foundation
BiosidusƗ
Conflict of interest N N Y
Ɨ Biosidus are developing inhalable interferon, a rival intervention for Covid- 19, and a direct competitor to EPO.
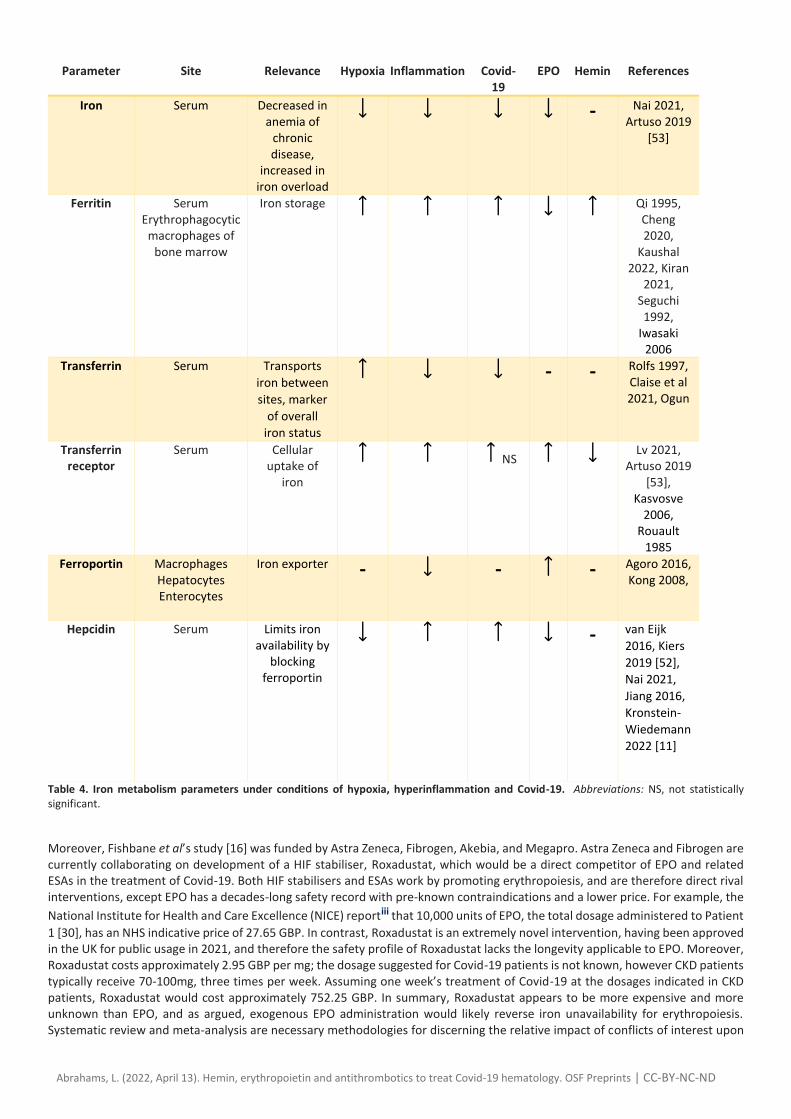
Table 3. Incomparable characteristics of previous case series. Key: Risk profile is color-coded: pink, high risk; peach, moderate risk; green, low risk. A second research group has reservations about usage of erythropoiesis stimulating agents in the treatment of Covid-19 [16]. Fishbane et al observe a correlation between higher D-dimer levels, lower hemoglobin and higher serum ferritin levels in Covid-19 patients [16]. The research group infer that the clinical course of severe inflammation coincides with anemia and iron storage tendency, and that treatment with ESAs for correction of dyserythropoiesis will fail due to lack of iron availability secondary to inflammation. Iron metabolism is an active research area in relation to Covid-19 [12, 51]. The clinical picture is complicated since Covid-19 disease is an amalgam of hyperinflammation and hypoxia; these two states typically drive iron metabolism in opposite directions (Table 4). For example, iron availability for erythropoiesis is largely determined by the actions of hepcidin, a hormone that is considered the master regulator of iron metabolism. Hepcidin functions to limit iron availability by blocking the iron exporter, ferroportin. Whereas inflammatory states coincide with upregulation of hepcidin, and therefore reduce iron availability for erythropoiesis, hypoxic states downregulate hepcidin, thereby increasing iron availability for erythropoiesis. At present, Covid-19 is understood to be a condition of hyperferritinemia and hypoferremia with reduced serum transferrin and increased hepcidin. Overall, the iron metabolism profile of Covid-19 is more akin to the state of inflammation than the state of hypoxia; the Covid-19 iron panel (Table 4) mimics that of inflammation and tends toward iron storage rather than iron availability for erythropoiesis. Dyserythropoiesis in Covid-19 could be addressed by shifting iron metabolism to mimic the hypoxia panel, rather than the inflammation panel. The differences between the two iron panels are: transferrin, hepcidin and ferroportin. Covid-19 patients would require reduction of hepcidin and ferritin alongside an increase in transferrin and ferroportin, for cellular export of stored iron and iron transport to erythroid precursors. A recent study investigating the relative impact of hypoxia versus inflammation on regulation of hepcidin levels determined that hypoxia is able to override the influence of inflammation, but that this mechanism of attenuation is likely mediated through EPO [52]. EPO is able to suppress hepcidin [52] and decrease ferritin while increasing ferroportin, thereby shifting iron metabolism to pro-erythropoietic. Since Covid-19 patients have decreased EPO levels relative to controls [3], presumably Covid-19 patients would be unable to attenuate inflammation-induced iron restriction, unless their treatment is supplemented with exogenous EPO. EPO inhibits IL-6 and the anti-inflammatory properties of EPO may overcome any inflammation-dependent restriction of iron for erythropoiesis [48]. EPO also rapidly increases the expression of transferrin receptor-1 on the surface of erythroid precursors, and thereby enhances iron uptake for erythropoiesis [53]. Besides, EPO has non-erythropoietic functions that may prove beneficial in treating Covid-19, including tissue protection and anti-inflammatory properties (Fig. 3), meaning that EPO would probably be useful even if erythropoiesis were restricted due to iron scarcity secondary to inflammation. Therefore, the current clinical picture on iron metabolism in Covid-19 supports systematic investigation into the utility of ESAs in the treatment of severe Covid-19 patients.
Abrahams, L. (2022, April 13). Hemin, erythropoietin and antithrombotics to treat Covid-19 hematology. OSF Preprints | CC-BY-NC-ND
Parameter Site Relevance Hypoxia Inflammation Covid-
19 EPO Hemin References
Iron Serum Decreased in anemia of
chronic disease,
increased in iron overload
- Nai 2021,
Artuso 2019 [53]
Ferritin Serum Erythrophagocytic
macrophages of bone marrow
Iron storage
Qi 1995, Cheng 2020,
Kaushal 2022, Kiran
2021, Seguchi 1992,
Iwasaki 2006
Transferrin Serum Transports
iron between
sites, marker
of overall
iron status
- - Rolfs 1997, Claise et al 2021, Ogun
Transferrin receptor
Serum Cellular uptake of
iron
NS Lv 2021,
Artuso 2019 [53],
Kasvosve 2006,
Rouault 1985
Ferroportin Macrophages Hepatocytes Enterocytes
Iron exporter -
- - Agoro 2016, Kong 2008,
Hepcidin Serum Limits iron availability by
blocking ferroportin
- van Eijk
2016, Kiers
2019 [52],
Nai 2021,
Jiang 2016,
Kronstein-
Wiedemann
2022 [11]
Table 4. Iron metabolism parameters under conditions of hypoxia, hyperinflammation and Covid-19. Abbreviations: NS, not statistically significant.
Moreover, Fishbane et al’s study [16] was funded by Astra Zeneca, Fibrogen, Akebia, and Megapro. Astra Zeneca and Fibrogen are currently collaborating on development of a HIF stabiliser, Roxadustat, which would be a direct competitor of EPO and related ESAs in the treatment of Covid-19. Both HIF stabilisers and ESAs work by promoting erythropoiesis, and are therefore direct rival interventions, except EPO has a decades-long safety record with pre-known contraindications and a lower price. For example, the
National Institute for Health and Care Excellence (NICE) reportiii that 10,000 units of EPO, the total dosage administered to Patient
1 [30], has an NHS indicative price of 27.65 GBP. In contrast, Roxadustat is an extremely novel intervention, having been approved in the UK for public usage in 2021, and therefore the safety profile of Roxadustat lacks the longevity applicable to EPO. Moreover, Roxadustat costs approximately 2.95 GBP per mg; the dosage suggested for Covid-19 patients is not known, however CKD patients typically receive 70-100mg, three times per week. Assuming one week’s treatment of Covid-19 at the dosages indicated in CKD patients, Roxadustat would cost approximately 752.25 GBP. In summary, Roxadustat appears to be more expensive and more unknown than EPO, and as argued, exogenous EPO administration would likely reverse iron unavailability for erythropoiesis. Systematic review and meta-analysis are necessary methodologies for discerning the relative impact of conflicts of interest upon
Abrahams, L. (2022, April 13). Hemin, erythropoietin and antithrombotics to treat Covid-19 hematology. OSF Preprints | CC-BY-NC-ND
the strength of evidence for EPO as an intervention in Covid-19. For example, item 16 of AMSTAR2 [54] evaluates risk of bias on the basis of conflict of interest, and the evaluation score informs the weighting of studies. While AMSTAR2 is designed for evaluation of systematic reviews only, a similar checklist item could be added to existing quality assessment aides, to account for conflict of interest in other study design types. The safety and efficacy of EPO as an adjuvant in treating Covid-19 will depend partly upon correct administration of the biologic. Of note, there are multiple contraindications that must be taken into account when making a clinical decision. Firstly, anti-apoptotic and angiogenic properties of EPO may exacerbate tumour progression and EPO is contraindicated in certain cancer patients. Secondly, erythropoietin has procoagulant effects and increases risk of thrombosis and thromboembolic adverse events [55, 56]; since Covid-19 patients and recipients of the ChAdOx1 vaccine are already at higher risk of thrombosis, co-treatment with an antithrombotic is likely to provide a higher safety profile [31]. Antithrombotic prophylaxis in cancer patients receiving epoetin beta reversed the thrombosis risk profile of EPO treatment to control levels [56]. Similarly, all of Begemann et al’s four Covid-19 patients received co-treatment with both EPO and anticoagulants, and all recovered without incident [5]. Indeed, EPO has been utilised in at least eight Covid-19 patients to date [30, 5, 36], and none of the patients reported adverse events as a result of EPO treatment, in fact all patients recovered. Preliminary clinical evidence therefore suggests that EPO is likely to be well tolerated and reasonably safe in Covid-19 patients free of any known contraindications. Timing of administration is paramount, since EPO typically requires 2-6 weeks to effect a significant increase in erythropoiesis as confirmed by the Electronic Medicines
Compendiumiv, although non-erythropoietic functions of EPO will presumably manifest at an earlier timepoint after
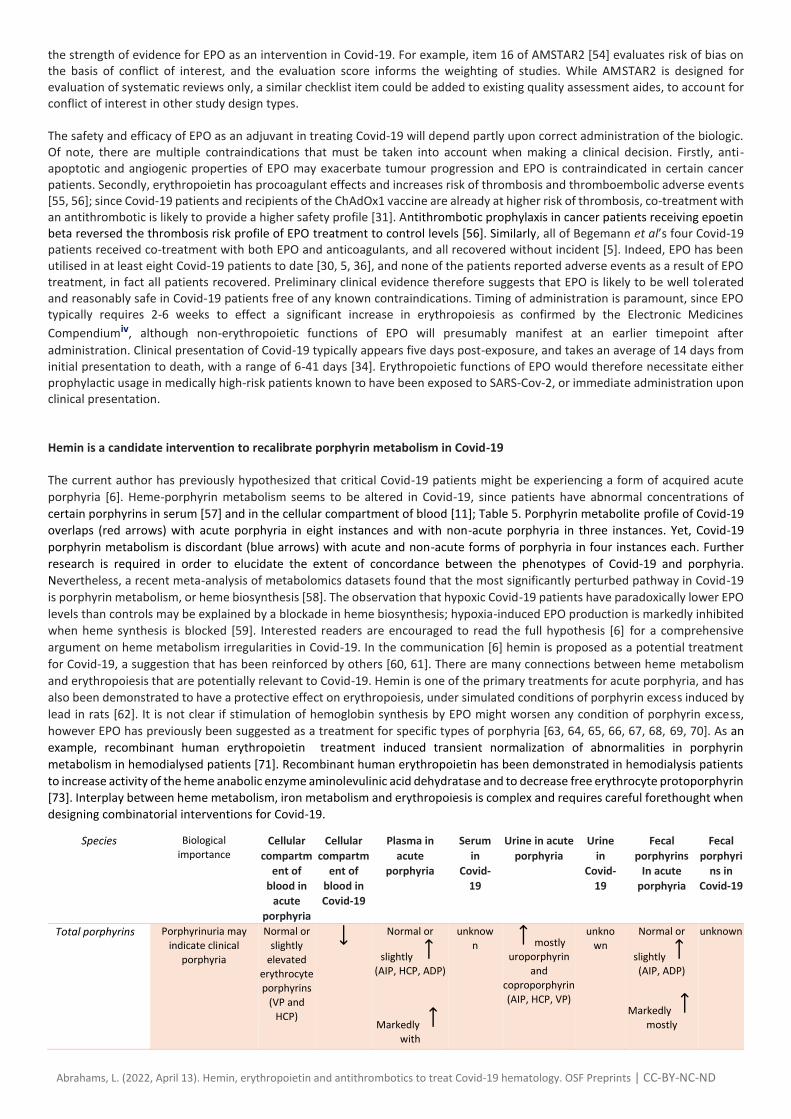
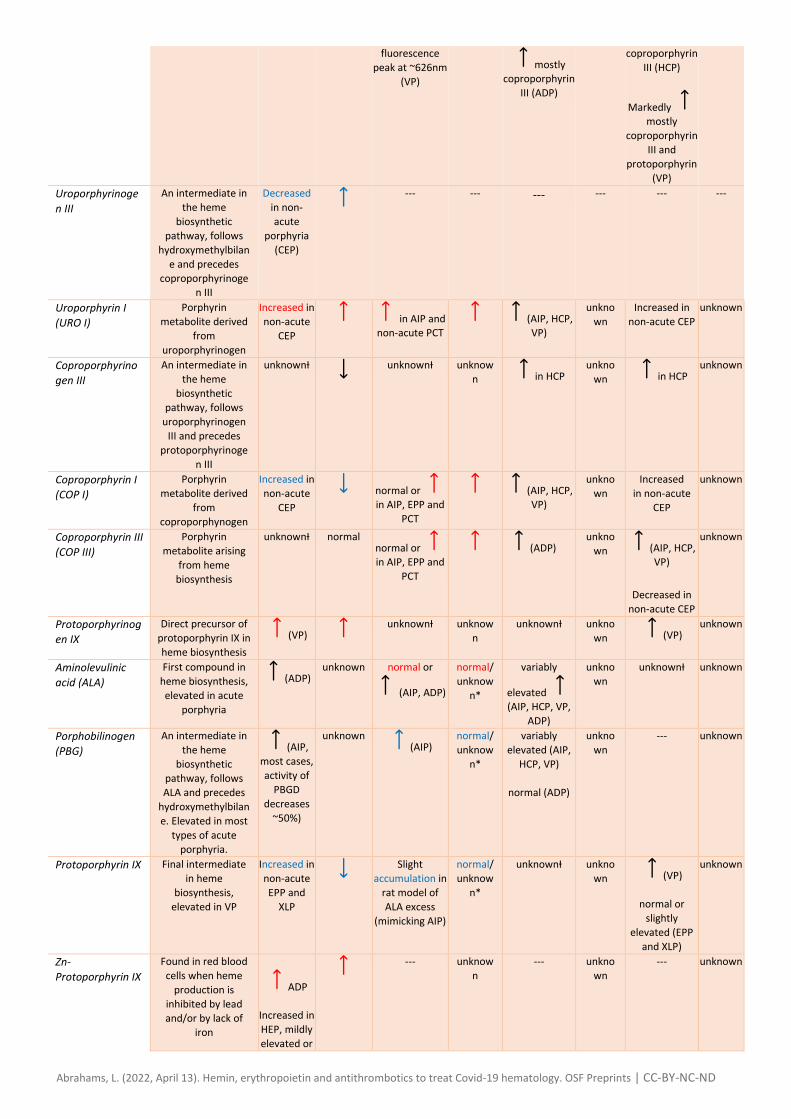
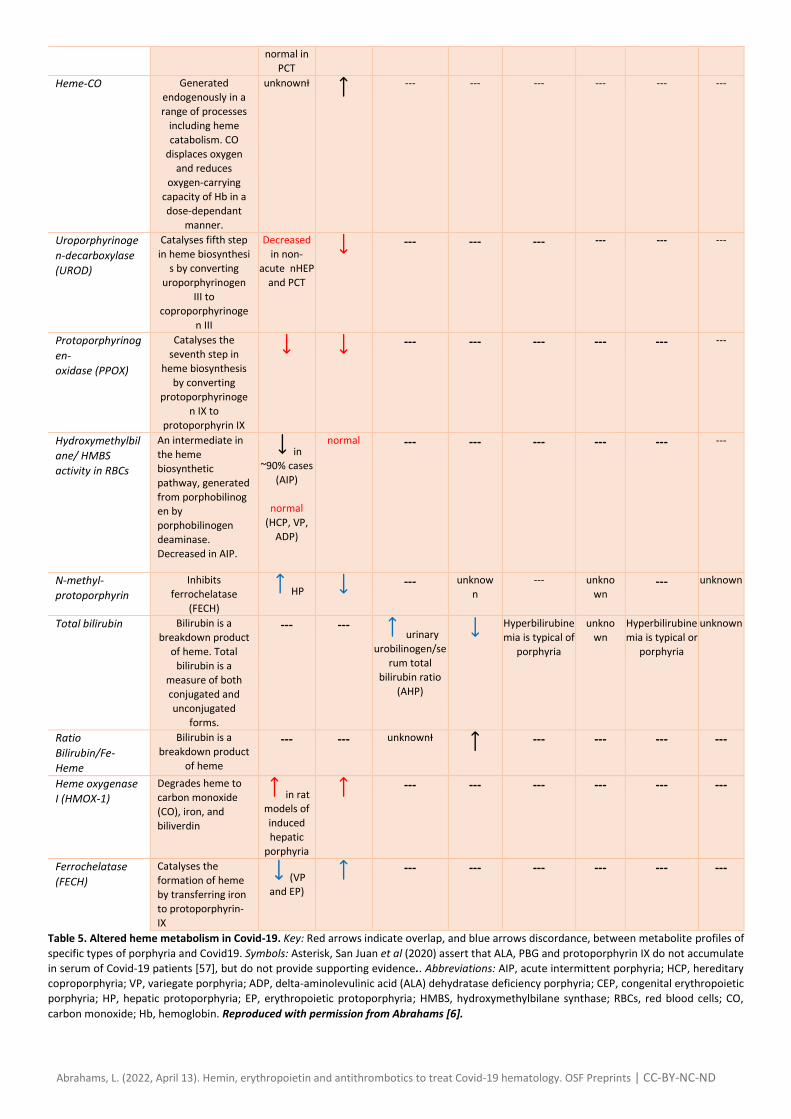
administration. Clinical presentation of Covid-19 typically appears five days post-exposure, and takes an average of 14 days from initial presentation to death, with a range of 6-41 days [34]. Erythropoietic functions of EPO would therefore necessitate either prophylactic usage in medically high-risk patients known to have been exposed to SARS-Cov-2, or immediate administration upon clinical presentation. Hemin is a candidate intervention to recalibrate porphyrin metabolism in Covid-19 The current author has previously hypothesized that critical Covid-19 patients might be experiencing a form of acquired acute
porphyria [6]. Heme-porphyrin metabolism seems to be altered in Covid-19, since patients have abnormal concentrations of
certain porphyrins in serum [57] and in the cellular compartment of blood [11]; Table 5. Porphyrin metabolite profile of Covid-19
overlaps (red arrows) with acute porphyria in eight instances and with non-acute porphyria in three instances. Yet, Covid-19
porphyrin metabolism is discordant (blue arrows) with acute and non-acute forms of porphyria in four instances each. Further
research is required in order to elucidate the extent of concordance between the phenotypes of Covid-19 and porphyria.
Nevertheless, a recent meta-analysis of metabolomics datasets found that the most significantly perturbed pathway in Covid-19
is porphyrin metabolism, or heme biosynthesis [58]. The observation that hypoxic Covid-19 patients have paradoxically lower EPO
levels than controls may be explained by a blockade in heme biosynthesis; hypoxia-induced EPO production is markedly inhibited
when heme synthesis is blocked [59]. Interested readers are encouraged to read the full hypothesis [6] for a comprehensive
argument on heme metabolism irregularities in Covid-19. In the communication [6] hemin is proposed as a potential treatment
for Covid-19, a suggestion that has been reinforced by others [60, 61]. There are many connections between heme metabolism
and erythropoiesis that are potentially relevant to Covid-19. Hemin is one of the primary treatments for acute porphyria, and has
also been demonstrated to have a protective effect on erythropoiesis, under simulated conditions of porphyrin excess induced by
lead in rats [62]. It is not clear if stimulation of hemoglobin synthesis by EPO might worsen any condition of porphyrin excess,
however EPO has previously been suggested as a treatment for specific types of porphyria [63, 64, 65, 66, 67, 68, 69, 70]. As an
example, recombinant human erythropoietin treatment induced transient normalization of abnormalities in porphyrin
metabolism in hemodialysed patients [71]. Recombinant human erythropoietin has been demonstrated in hemodialysis patients
to increase activity of the heme anabolic enzyme aminolevulinic acid dehydratase and to decrease free erythrocyte protoporphyrin
[73]. Interplay between heme metabolism, iron metabolism and erythropoiesis is complex and requires careful forethought when
designing combinatorial interventions for Covid-19.
Species Biological
importance Cellular
compartm
ent of
blood in
acute
porphyria
Cellular
compartm
ent of
blood in
Covid-19
Plasma in
acute
porphyria
Serum
in
Covid-
19
Urine in acute
porphyria
Urine
in
Covid-
19
Fecal
porphyrins
In acute
porphyria
Fecal
porphyri
ns in
Covid-19
Total porphyrins Porphyrinuria may
indicate clinical
porphyria
Normal or
slightly
elevated
erythrocyte
porphyrins
(VP and
HCP)
Normal or
slightly (AIP, HCP, ADP)
Markedly
with
unknow
n mostly uroporphyrin
and
coproporphyrin (AIP, HCP, VP)
unkno
wn
Normal or
slightly (AIP, ADP)
Markedly
mostly
unknown
Abrahams, L. (2022, April 13). Hemin, erythropoietin and antithrombotics to treat Covid-19 hematology. OSF Preprints | CC-BY-NC-ND
fluorescence
peak at ~626nm
(VP)
mostly coproporphyrin
III (ADP)
coproporphyrin
III (HCP)
Markedly mostly
coproporphyrin
III and
protoporphyrin
(VP) Uroporphyrinoge
n III
An intermediate in
the heme
biosynthetic
pathway, follows
hydroxymethylbilan
e and precedes
coproporphyrinogen III
Decreased
in non-
acute
porphyria
(CEP)
--- --- --- --- --- ---
Uroporphyrin I
(URO I) Porphyrin
metabolite derived
from
uroporphyrinogen
Increased in
non-acute
CEP in AIP and
non-acute PCT (AIP, HCP,
VP)
unkno
wn Increased in
non-acute CEP
unknown
Coproporphyrino
gen III
An intermediate in
the heme
biosynthetic
pathway, follows
uroporphyrinogen
III and precedes
protoporphyrinoge
n III
unknownƗ
unknownƗ unknow
n in HCP unkno
wn in HCP unknown
Coproporphyrin I
(COP I) Porphyrin
metabolite derived
from
coproporphynogen
Increased in
non-acute
CEP normal or
in AIP, EPP and
PCT
(AIP, HCP, VP)
unkno
wn Increased
in non-acute
CEP
unknown
Coproporphyrin III
(COP III)
Porphyrin
metabolite arising
from heme
biosynthesis
unknownƗ normal normal or in AIP, EPP and
PCT
(ADP) unkno
wn (AIP, HCP, VP)
Decreased in
non-acute CEP
unknown
Protoporphyrinog
en IX
Direct precursor of
protoporphyrin IX in
heme biosynthesis (VP)
unknownƗ unknow
n unknownƗ unkno
wn (VP) unknown
Aminolevulinic
acid (ALA)
First compound in
heme biosynthesis,
elevated in acute
porphyria
(ADP) unknown normal or
(AIP, ADP)
normal/ unknow
n*
variably
elevated (AIP, HCP, VP,
ADP)
unkno
wn
unknownƗ unknown
Porphobilinogen
(PBG) An intermediate in
the heme
biosynthetic
pathway, follows
ALA and precedes
hydroxymethylbilan
e. Elevated in most
types of acute
porphyria.
(AIP,
most cases,
activity of
PBGD
decreases
~50%)
unknown (AIP)
normal/ unknow
n*
variably
elevated (AIP,
HCP, VP)
normal (ADP)
unkno
wn --- unknown
Protoporphyrin IX Final intermediate
in heme
biosynthesis,
elevated in VP
Increased in
non-acute
EPP and
XLP
Slight
accumulation in
rat model of
ALA excess
(mimicking AIP)
normal/ unknow
n*
unknownƗ unkno
wn (VP)
normal or
slightly
elevated (EPP
and XLP)
unknown
Zn-
Protoporphyrin IX Found in red blood
cells when heme
production is
inhibited by lead
and/or by lack of
iron
ADP
Increased in
HEP, mildly
elevated or
--- unknow
n --- unkno
wn --- unknown
Abrahams, L. (2022, April 13). Hemin, erythropoietin and antithrombotics to treat Covid-19 hematology. OSF Preprints | CC-BY-NC-ND
normal in
PCT Heme-CO Generated
endogenously in a
range of processes
including heme
catabolism. CO
displaces oxygen
and reduces
oxygen-carrying
capacity of Hb in a
dose-dependant
manner.
unknownƗ
--- --- --- --- --- ---
Uroporphyrinoge
n-decarboxylase
(UROD)
Catalyses fifth step
in heme biosynthesi
s by converting
uroporphyrinogen
III to
coproporphyrinoge
n III
Decreased
in non-
acute nHEP
and PCT
--- --- --- --- --- ---
Protoporphyrinog
en-
oxidase (PPOX)
Catalyses the
seventh step in
heme biosynthesis
by converting
protoporphyrinoge
n IX to
protoporphyrin IX
--- --- --- --- --- ---
Hydroxymethylbil
ane/ HMBS
activity in RBCs
An intermediate in
the heme
biosynthetic
pathway, generated
from porphobilinogen by
porphobilinogen
deaminase.
Decreased in AIP.
in ~90% cases
(AIP)
normal
(HCP, VP,
ADP)
normal --- --- --- --- --- ---
N-methyl-
protoporphyrin
Inhibits
ferrochelatase
(FECH)
HP
--- unknow
n
--- unkno
wn --- unknown
Total bilirubin Bilirubin is a
breakdown product
of heme. Total
bilirubin is a
measure of both
conjugated and
unconjugated
forms.
--- --- urinary
urobilinogen/se
rum total
bilirubin ratio (AHP)
Hyperbilirubine
mia is typical of
porphyria
unkno
wn
Hyperbilirubine
mia is typical or
porphyria
unknown
Ratio
Bilirubin/Fe-
Heme
Bilirubin is a
breakdown product
of heme
--- --- unknownƗ
--- --- --- ---
Heme oxygenase
I (HMOX-1)
Degrades heme to
carbon monoxide
(CO), iron, and
biliverdin
in rat models of
induced
hepatic
porphyria
--- --- --- --- --- ---
Ferrochelatase
(FECH)
Catalyses the
formation of heme
by transferring iron
to protoporphyrin-
IX
(VP and EP)
--- --- --- --- --- ---
Table 5. Altered heme metabolism in Covid-19. Key: Red arrows indicate overlap, and blue arrows discordance, between metabolite profiles of
specific types of porphyria and Covid19. Symbols: Asterisk, San Juan et al (2020) assert that ALA, PBG and protoporphyrin IX do not accumulate
in serum of Covid-19 patients [57], but do not provide supporting evidence.. Abbreviations: AIP, acute intermittent porphyria; HCP, hereditary
coproporphyria; VP, variegate porphyria; ADP, delta-aminolevulinic acid (ALA) dehydratase deficiency porphyria; CEP, congenital erythropoietic
porphyria; HP, hepatic protoporphyria; EP, erythropoietic protoporphyria; HMBS, hydroxymethylbilane synthase; RBCs, red blood cells; CO,
carbon monoxide; Hb, hemoglobin. Reproduced with permission from Abrahams [6].
Abrahams, L. (2022, April 13). Hemin, erythropoietin and antithrombotics to treat Covid-19 hematology. OSF Preprints | CC-BY-NC-ND
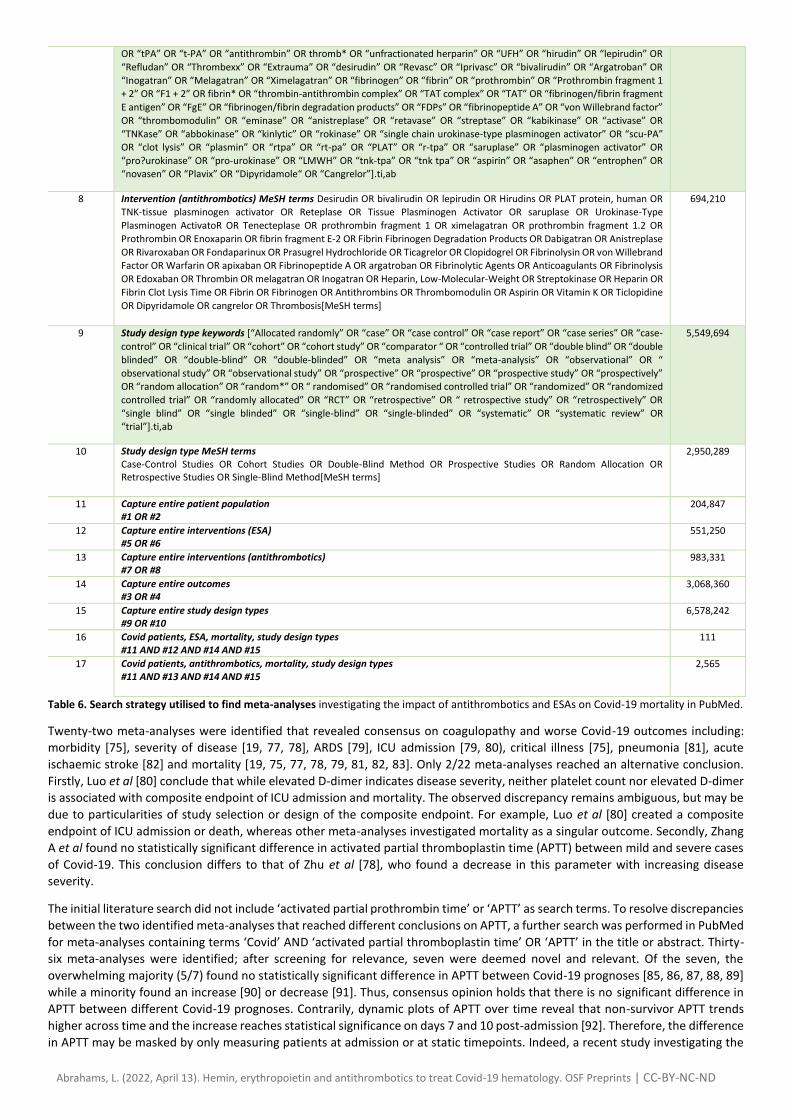
Antithrombotics may reduce all-cause in-hospital mortality in severe Covid-19 patients Structured search for existing meta-analyses on coagulopathy and the clinical utility of antithrombotics
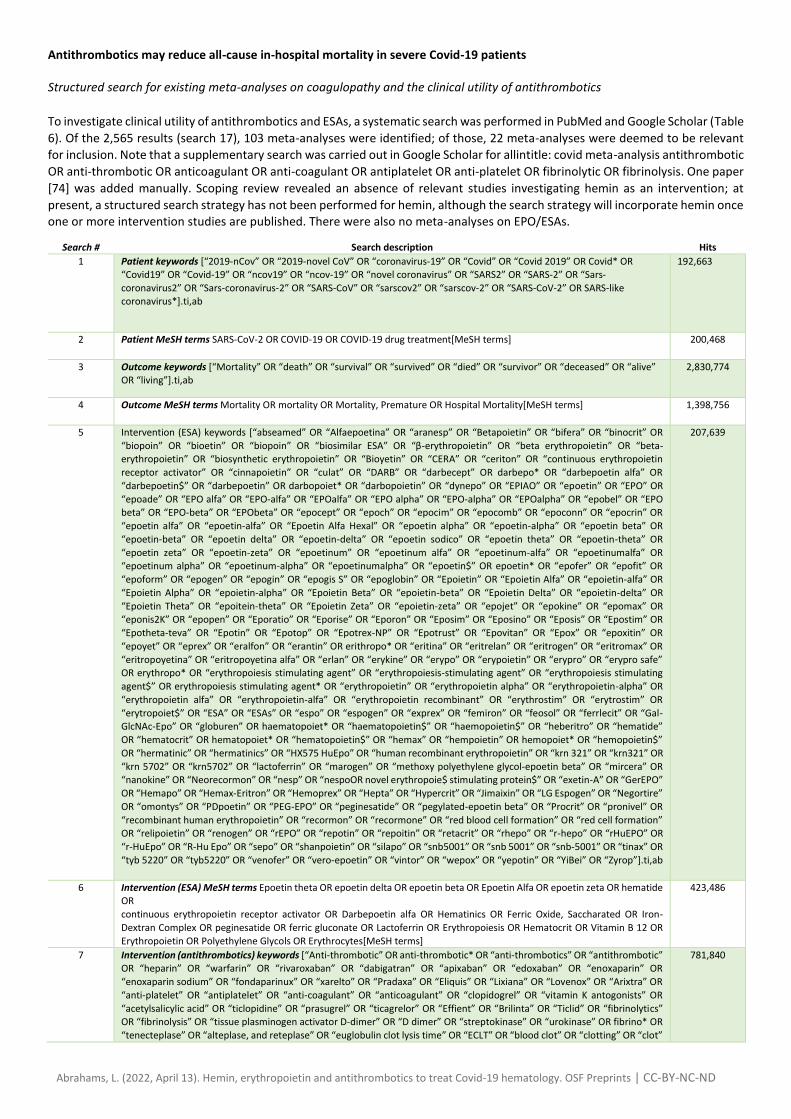
To investigate clinical utility of antithrombotics and ESAs, a systematic search was performed in PubMed and Google Scholar (Table
6). Of the 2,565 results (search 17), 103 meta-analyses were identified; of those, 22 meta-analyses were deemed to be relevant
for inclusion. Note that a supplementary search was carried out in Google Scholar for allintitle: covid meta-analysis antithrombotic
OR anti-thrombotic OR anticoagulant OR anti-coagulant OR antiplatelet OR anti-platelet OR fibrinolytic OR fibrinolysis. One paper
[74] was added manually. Scoping review revealed an absence of relevant studies investigating hemin as an intervention; at
present, a structured search strategy has not been performed for hemin, although the search strategy will incorporate hemin once one or more intervention studies are published. There were also no meta-analyses on EPO/ESAs.
Search # Search description Hits
1 Patient keywords [“2019-nCov” OR “2019-novel CoV” OR “coronavirus-19” OR “Covid” OR “Covid 2019” OR Covid* OR “Covid19” OR “Covid-19” OR “ncov19” OR “ncov-19” OR “novel coronavirus” OR “SARS2” OR “SARS-2” OR “Sars-
coronavirus2” OR “Sars-coronavirus-2” OR “SARS-CoV” OR “sarscov2” OR “sarscov-2” OR “SARS-CoV-2” OR SARS-like coronavirus*].ti,ab
192,663
2 Patient MeSH terms SARS-CoV-2 OR COVID-19 OR COVID-19 drug treatment[MeSH terms]
200,468
3 Outcome keywords [“Mortality” OR “death” OR “survival” OR “survived” OR “died” OR “survivor” OR “deceased” OR “alive” OR “living”].ti,ab
2,830,774
4 Outcome MeSH terms Mortality OR mortality OR Mortality, Premature OR Hospital Mortality[MeSH terms]
1,398,756
5 Intervention (ESA) keywords [“abseamed” OR “Alfaepoetina” OR “aranesp” OR “Betapoietin” OR “bifera” OR “binocrit” OR
“biopoin” OR “bioetin” OR “biopoin” OR “biosimilar ESA” OR “β-erythropoietin” OR “beta erythropoietin” OR “beta-erythropoietin” OR “biosynthetic erythropoietin” OR “Bioyetin” OR “CERA” OR “ceriton” OR “continuous erythropoietin
receptor activator” OR “cinnapoietin” OR “culat” OR “DARB” OR “darbecept” OR darbepo* OR “darbepoetin alfa” OR
“darbepoetin$” OR “darbepoetin” OR darbopoiet* OR “darbopoietin” OR “dynepo” OR “EPIAO” OR “epoetin” OR “EPO” OR
“epoade” OR “EPO alfa” OR “EPO-alfa” OR “EPOalfa” OR “EPO alpha” OR “EPO-alpha” OR “EPOalpha” OR “epobel” OR “EPO beta” OR “EPO-beta” OR “EPObeta” OR “epocept” OR “epoch” OR “epocim” OR “epocomb” OR “epoconn” OR “epocrin” OR
“epoetin alfa” OR “epoetin-alfa” OR “Epoetin Alfa Hexal” OR “epoetin alpha” OR “epoetin-alpha” OR “epoetin beta” OR
“epoetin-beta” OR “epoetin delta” OR “epoetin-delta” OR “epoetin sodico” OR “epoetin theta” OR “epoetin-theta” OR
“epoetin zeta” OR “epoetin-zeta” OR “epoetinum” OR “epoetinum alfa” OR “epoetinum-alfa” OR “epoetinumalfa” OR “epoetinum alpha” OR “epoetinum-alpha” OR “epoetinumalpha” OR “epoetin$” OR epoetin* OR “epofer” OR “epofit” OR
“epoform” OR “epogen” OR “epogin” OR “epogis S” OR “epoglobin” OR “Epoietin” OR “Epoietin Alfa” OR “epoietin-alfa” OR
“Epoietin Alpha” OR “epoietin-alpha” OR “Epoietin Beta” OR “epoietin-beta” OR “Epoietin Delta” OR “epoietin-delta” OR
“Epoietin Theta” OR “epoitein-theta” OR “Epoietin Zeta” OR “epoietin-zeta” OR “epojet” OR “epokine” OR “epomax” OR “eponis2K” OR “epopen” OR “Eporatio” OR “Eporise” OR “Eporon” OR “Eposim” OR “Eposino” OR “Eposis” OR “Epostim” OR
“Epotheta-teva” OR “Epotin” OR “Epotop” OR “Epotrex-NP” OR “Epotrust” OR “Epovitan” OR “Epox” OR “epoxitin” OR
“epoyet” OR “eprex” OR “eralfon” OR “erantin” OR erithropo* OR “eritina” OR “eritrelan” OR “eritrogen” OR “eritromax” OR
“eritropoyetina” OR “eritropoyetina alfa” OR “erlan” OR “erykine” OR “erypo” OR “erypoietin” OR “erypro” OR “erypro safe” OR erythropo* OR “erythropoiesis stimulating agent” OR “erythropoiesis-stimulating agent” OR “erythropoiesis stimulating
agent$” OR erythropoiesis stimulating agent* OR “erythropoietin” OR “erythropoietin alpha” OR “erythropoietin-alpha” OR
“erythropoietin alfa” OR “erythropoietin-alfa” OR “erythropoietin recombinant” OR “erythrostim” OR “erytrostim” OR
“erytropoiet$” OR “ESA” OR “ESAs” OR “espo” OR “espogen” OR “exprex” OR “femiron” OR “feosol” OR “ferrlecit” OR “Gal-GlcNAc-Epo” OR “globuren” OR haematopoiet* OR “haematopoietin$” OR “haemopoietin$” OR “heberitro” OR “hematide”
OR “hematocrit” OR hematopoiet* OR “hematopoietin$” OR “hemax” OR “hempoietin” OR hemopoiet* OR “hemopoietin$”
OR “hermatinic” OR “hermatinics” OR “HX575 HuEpo” OR “human recombinant erythropoietin” OR “krn 321” OR “krn321” OR
“krn 5702” OR “krn5702” OR “lactoferrin” OR “marogen” OR “methoxy polyethylene glycol‐epoetin beta” OR “mircera” OR “nanokine” OR “Neorecormon” OR “nesp” OR “nespoOR novel erythropoie$ stimulating protein$” OR “exetin-A” OR “GerEPO”
OR “Hemapo” OR “Hemax-Eritron” OR “Hemoprex” OR “Hepta” OR “Hypercrit” OR “Jimaixin” OR “LG Espogen” OR “Negortire”
OR “omontys” OR “PDpoetin” OR “PEG-EPO” OR “peginesatide” OR “pegylated-epoetin beta” OR “Procrit” OR “pronivel” OR
“recombinant human erythropoietin” OR “recormon” OR “recormone” OR “red blood cell formation” OR “red cell formation” OR “relipoietin” OR “renogen” OR “rEPO” OR “repotin” OR “repoitin” OR “retacrit” OR “rhepo” OR “r-hepo” OR “rHuEPO” OR
“r-HuEpo” OR “R-Hu Epo” OR “sepo” OR “shanpoietin” OR “silapo” OR “snb5001” OR “snb 5001” OR “snb-5001” OR “tinax” OR
“tyb 5220” OR “tyb5220” OR “venofer” OR “vero-epoetin” OR “vintor” OR “wepox” OR “yepotin” OR “YiBei” OR “Zyrop”].ti,ab
207,639
6 Intervention (ESA) MeSH terms Epoetin theta OR epoetin delta OR epoetin beta OR Epoetin Alfa OR epoetin zeta OR hematide OR continuous erythropoietin receptor activator OR Darbepoetin alfa OR Hematinics OR Ferric Oxide, Saccharated OR Iron-
Dextran Complex OR peginesatide OR ferric gluconate OR Lactoferrin OR Erythropoiesis OR Hematocrit OR Vitamin B 12 OR
Erythropoietin OR Polyethylene Glycols OR Erythrocytes[MeSH terms]
423,486
7 Intervention (antithrombotics) keywords [“Anti-thrombotic” OR anti-thrombotic* OR “anti-thrombotics” OR “antithrombotic” OR “heparin” OR “warfarin” OR “rivaroxaban” OR “dabigatran” OR “apixaban” OR “edoxaban” OR “enoxaparin” OR
“enoxaparin sodium” OR “fondaparinux” OR “xarelto” OR “Pradaxa” OR “Eliquis” OR “Lixiana” OR “Lovenox” OR “Arixtra” OR
“anti-platelet” OR “antiplatelet” OR “anti-coagulant” OR “anticoagulant” OR “clopidogrel” OR “vitamin K antogonists” OR
“acetylsalicylic acid” OR “ticlopidine” OR “prasugrel” OR “ticagrelor” OR “Effient” OR “Brilinta” OR “Ticlid” OR “fibrinolytics” OR “fibrinolysis” OR “tissue plasminogen activator D-dimer” OR “D dimer” OR “streptokinase” OR “urokinase” OR fibrino* OR
“tenecteplase” OR “alteplase, and reteplase” OR “euglobulin clot lysis time” OR “ECLT” OR “blood clot” OR “clotting” OR “clot”
781,840
Abrahams, L. (2022, April 13). Hemin, erythropoietin and antithrombotics to treat Covid-19 hematology. OSF Preprints | CC-BY-NC-ND
OR “tPA” OR “t-PA” OR “antithrombin” OR thromb* OR “unfractionated herparin” OR “UFH” OR “hirudin” OR “lepirudin” OR
“Refludan” OR “Thrombexx” OR “Extrauma” OR “desirudin” OR “Revasc” OR “Iprivasc” OR “bivalirudin” OR “Argatroban” OR
“Inogatran” OR “Melagatran” OR “Ximelagatran” OR “fibrinogen” OR “fibrin” OR “prothrombin” OR “Prothrombin fragment 1 + 2” OR “F1 + 2” OR fibrin* OR “thrombin-antithrombin complex” OR “TAT complex” OR “TAT” OR “fibrinogen/fibrin fragment
E antigen” OR “FgE” OR “fibrinogen/fibrin degradation products” OR “FDPs” OR “fibrinopeptide A” OR “von Willebrand factor”
OR “thrombomodulin” OR “eminase” OR “anistreplase” OR “retavase” OR “streptase” OR “kabikinase” OR “activase” OR
“TNKase” OR “abbokinase” OR “kinlytic” OR “rokinase” OR “single chain urokinase-type plasminogen activator” OR “scu-PA” OR “clot lysis” OR “plasmin” OR “rtpa” OR “rt-pa” OR “PLAT” OR “r-tpa” OR “saruplase” OR “plasminogen activator” OR
“pro?urokinase” OR “pro-urokinase” OR “LMWH” OR “tnk-tpa” OR “tnk tpa” OR “aspirin” OR “asaphen” OR “entrophen” OR “novasen” OR “Plavix” OR “Dipyridamole“ OR “Cangrelor”].ti,ab
8 Intervention (antithrombotics) MeSH terms Desirudin OR bivalirudin OR lepirudin OR Hirudins OR PLAT protein, human OR TNK-tissue plasminogen activator OR Reteplase OR Tissue Plasminogen Activator OR saruplase OR Urokinase-Type
Plasminogen ActivatoR OR Tenecteplase OR prothrombin fragment 1 OR ximelagatran OR prothrombin fragment 1.2 OR
Prothrombin OR Enoxaparin OR fibrin fragment E-2 OR Fibrin Fibrinogen Degradation Products OR Dabigatran OR Anistreplase
OR Rivaroxaban OR Fondaparinux OR Prasugrel Hydrochloride OR Ticagrelor OR Clopidogrel OR Fibrinolysin OR von Willebrand Factor OR Warfarin OR apixaban OR Fibrinopeptide A OR argatroban OR Fibrinolytic Agents OR Anticoagulants OR Fibrinolysis
OR Edoxaban OR Thrombin OR melagatran OR Inogatran OR Heparin, Low-Molecular-Weight OR Streptokinase OR Heparin OR
Fibrin Clot Lysis Time OR Fibrin OR Fibrinogen OR Antithrombins OR Thrombomodulin OR Aspirin OR Vitamin K OR Ticlopidine
OR Dipyridamole OR cangrelor OR Thrombosis[MeSH terms]
694,210
9 Study design type keywords [“Allocated randomly” OR “case” OR “case control” OR “case report” OR “case series” OR “case-
control” OR “clinical trial” OR “cohort” OR “cohort study” OR “comparator “ OR “controlled trial” OR “double blind” OR “double
blinded” OR “double-blind” OR “double-blinded” OR “meta analysis” OR “meta-analysis” OR “observational” OR “
observational study” OR “observational study” OR “prospective” OR “prospective” OR “prospective study” OR “prospectively” OR “random allocation” OR “random*” OR “ randomised” OR “randomised controlled trial” OR “randomized” OR “randomized
controlled trial” OR “randomly allocated” OR “RCT” OR “retrospective” OR “ retrospective study” OR “retrospectively” OR
“single blind” OR “single blinded” OR “single-blind” OR “single-blinded” OR “systematic” OR “systematic review” OR “trial”].ti,ab
5,549,694
10 Study design type MeSH terms Case-Control Studies OR Cohort Studies OR Double-Blind Method OR Prospective Studies OR Random Allocation OR Retrospective Studies OR Single-Blind Method[MeSH terms]
2,950,289
11 Capture entire patient population #1 OR #2
204,847
12 Capture entire interventions (ESA) #5 OR #6
551,250
13 Capture entire interventions (antithrombotics) #7 OR #8
983,331
14 Capture entire outcomes #3 OR #4
3,068,360
15 Capture entire study design types #9 OR #10
6,578,242
16 Covid patients, ESA, mortality, study design types #11 AND #12 AND #14 AND #15
111
17 Covid patients, antithrombotics, mortality, study design types #11 AND #13 AND #14 AND #15
2,565
Table 6. Search strategy utilised to find meta-analyses investigating the impact of antithrombotics and ESAs on Covid-19 mortality in PubMed.
Twenty-two meta-analyses were identified that revealed consensus on coagulopathy and worse Covid-19 outcomes including:
morbidity [75], severity of disease [19, 77, 78], ARDS [79], ICU admission [79, 80), critical illness [75], pneumonia [81], acute
ischaemic stroke [82] and mortality [19, 75, 77, 78, 79, 81, 82, 83]. Only 2/22 meta-analyses reached an alternative conclusion.
Firstly, Luo et al [80] conclude that while elevated D-dimer indicates disease severity, neither platelet count nor elevated D-dimer
is associated with composite endpoint of ICU admission and mortality. The observed discrepancy remains ambiguous, but may be
due to particularities of study selection or design of the composite endpoint. For example, Luo et al [80] created a composite
endpoint of ICU admission or death, whereas other meta-analyses investigated mortality as a singular outcome. Secondly, Zhang
A et al found no statistically significant difference in activated partial thromboplastin time (APTT) between mild and severe cases
of Covid-19. This conclusion differs to that of Zhu et al [78], who found a decrease in this parameter with increasing disease
severity.
The initial literature search did not include ‘activated partial prothrombin time’ or ‘APTT’ as search terms. To resolve discrepancies
between the two identified meta-analyses that reached different conclusions on APTT, a further search was performed in PubMed
for meta-analyses containing terms ‘Covid’ AND ‘activated partial thromboplastin time’ OR ‘APTT’ in the title or abstract. Thirty-
six meta-analyses were identified; after screening for relevance, seven were deemed novel and relevant. Of the seven, the
overwhelming majority (5/7) found no statistically significant difference in APTT between Covid-19 prognoses [85, 86, 87, 88, 89]
while a minority found an increase [90] or decrease [91]. Thus, consensus opinion holds that there is no significant difference in
APTT between different Covid-19 prognoses. Contrarily, dynamic plots of APTT over time reveal that non-survivor APTT trends
higher across time and the increase reaches statistical significance on days 7 and 10 post-admission [92]. Therefore, the difference
in APTT may be masked by only measuring patients at admission or at static timepoints. Indeed, a recent study investigating the

Abrahams, L. (2022, April 13). Hemin, erythropoietin and antithrombotics to treat Covid-19 hematology. OSF Preprints | CC-BY-NC-ND
dynamics of APTT [93] noticed an abnormal APTT pattern two weeks after onset of Covid-19, when compared with healthy
subjects. Shimura et al [93] analysed clot waveform which indicates dynamics of fibrin abnormalities and blood clot formation. To
better understand the nature of coagulopathy in Covid-19, it is informative to compare observed laboratory parameters with
those typical of related hematological conditions (Table 7). For example, abnormal patterns of APTT in Covid-19 patients formed
three subtypes and two of these subtypes are characteristic of other hemostatic diseases: (1) early shoulder type, reminiscent of
lupus anticoagulant and factor IX deficiency; (2) late shoulder type; and, (3) biphasic type, reminiscent of hemophilia and warfarin
usage. The APTT pattern in Covid-19 appears to also be distinct from that of disseminated intravascular coagulopathy (DIC) and
suggests a possible specific abnormal coagulopathy phenotype [93].
Covid-19 hemostasis resembles concurrent thrombosis and thrombocytopenia
Holistically, the clinical picture of hemostasis associated with worsening Covid-19 prognosis appears to be concomitant thrombosis
with thrombocytopenia. Multiple markers of blood clot formation (D-dimer, fibrinogen, fibrin, FDP) rise in tandem, while markers
of natural anticoagulation (antithrombin) fall, implying thrombotic tendency. Simultaneously, platelet count decreases with
increasing severity of disease. Platelet count in severe Covid-19 cases drops to 186.00 (103.50–249.00) × 109 per litre [91, 94] and
the threshold for clinical definition of thrombocytopenia is < 150 x 109 per litre. Therefore, a subset of patients within the range
observed by Bao C 2020 [91] meet the clinical definition of thrombocytopenic, concomitantly with thrombotic tendency. APTT
decreases throughout hospitalisation duration for Covid-19 patients of all severities, implying that coagulation via the intrinsic
pathway hastens with time. Conversely, prothrombin time peaks between hospitalisation days 4 and final in non-survivors,
implying that coagulation via the extrinsic pathway is delayed. As hospitalisation stay progresses, there may therefore be a delay
in forming the initial platelet plug during primary hemostasis resulting in increased bleeding tendency, concomitantly with
accelerated formation of stabilised fibrin clot during secondary hemostasis.
A similar combination of thrombosis and thrombocytopenia is observed in thrombotic thrombocytopenic purpura (TTP) [95]. TTP
is a state of deficiency of ADAMTS13, an enzyme that catalyses cleavage of von Willebrand Factor (VWF), a multimeric protein
required for platelet adhesion. The result is increased aggregation of platelets into platelet microthrombi. Since platelet
microthrombi consume platelets, circulating levels of platelets decrease in TTP, leading to a relative deficiency of platelet
availability during primary hemostasis. Impairment of primary hemostasis transpires as increased mucocutaneous bleeding risk,
therefore TTP is a sister disease of Covid-19 hematology, that results in concomitant thrombosis and thrombocytopenia. Clinical
characteristics of TTP include microangiopathic hemolytic anemia and schistocytes; the latter sheared erythrocytes form once
forced under high pressure to pass platelet microthrombi that obscure passage in blood vessels.
Many of the characteristics of TTP have been documented with worsening Covid-19 prognosis, including: (i) reduced activity of
ADAMTS13 [96], (ii) elevated schistocytes [96], (iii) elevated VWF [95, 96], (iv) elevated Factor VIII [97, 98]; and, (v) platelet
aggregates [99]. TTP is diagnosed as ADAMTS13 activity levels <10% [100] and schistocytes >1% total erythrocytes [101, 102]. Very
low ADAMTS13 activity levels of <30% were observed in 22/110 Covid-19 patients; in two patients, ADAMTS13 activity (2.6% and
7.7%) met the diagnostic criterion for TTP (<10%). The diagnostic criterion of schistocyte percentage >1% was present in 9/110
patients and was above normal range (<0.5%) in a further 13/110 patients. Further, Nishikawa et al [99] discovered excessive
platelet aggregates in almost 90% of 110 Covid-19 patients, and the concentration of platelet aggregates correlated with
worsening prognosis. Twenty of 110 patients had VWF antigen levels (244-1,325) above normal range (50-150). Each of the four
clinical markers are observed with worsening Covid-19 prognosis and are shared with TTP (Table 7).
Be that as it may, certain aspects of Covid-19 are inconsistent with a purely TTP profile, and are more akin to disseminated
intravascular coagulopathy (DIC) [103]. Absolutely, Tang et al [103] discovered that 71.4% of Covid-19 non-survivors, but only 0.6%
survivors, matched diagnostic criteria of overt DIC as defined by the International Society on Thrombosis and Haemostasis [103].
DIC is a condition in which hypercoagulation forms ubiquitous blood clots in small blood vessels. Excess clotting also depletes
platelets necessary to stem bleeding, resulting in bleeding tendency; DIC is therefore a second sister condition of concomitant
thrombosis and thrombocytopenia. In some respects, Covid-19 resembles TTP and in others DIC. Severe Covid-19 and DIC patients
alike present abnormality of secondary hemostasis (indicated by PT, APTT, fibrinogen, fibrin and antithrombin) whereas secondary
hemostasis is normal in TTP (Table 7). Differential diagnosis between TTP and DIC is ordinarily ascertained by FDP level, with FDP
> 10mg/L in favor of DIC rather than TTP [104]. FDP levels reported in Covid-19 are given as 4.0-4.3 mg/L in survivors and 4.0-23.4
in non-survivors [103], thus a non-survivor subset met the criterion for differential diagnosis in favor of DIC. Nevertheless, Covid-
19 is demarcated by platelet aggregates, in unison with TTP rather than DIC [105]. In reality, hematology in severe Covid-19 does
not fit cleanly into the clinical definition of either TTP or DIC, but rather transpires as a novel amalgam between the two. At present, the known relationship between Covid-19 prognosis and hemostatic markers is correlative rather than causal.
Thrombosis markers are highly relevant in clinical forecasting [77, 79, 106, 107, 108] and are likely to be useful in clinical decision-
making [86, 89 107, 109] on tailored anticoagulation regimens [110, 111, 112, 113] and tracking of thrombolytic therapy [114].
Antithrombotics are already accepted by certain nations as standard adjuvant therapy in Covid-19. Verily, mixed dosing of
anticoagulation in ⩾ 50% of the population appears to decrease venous thromboembolism risk in comparison with standard
Abrahams, L. (2022, April 13). Hemin, erythropoietin and antithrombotics to treat Covid-19 hematology. OSF Preprints | CC-BY-NC-ND
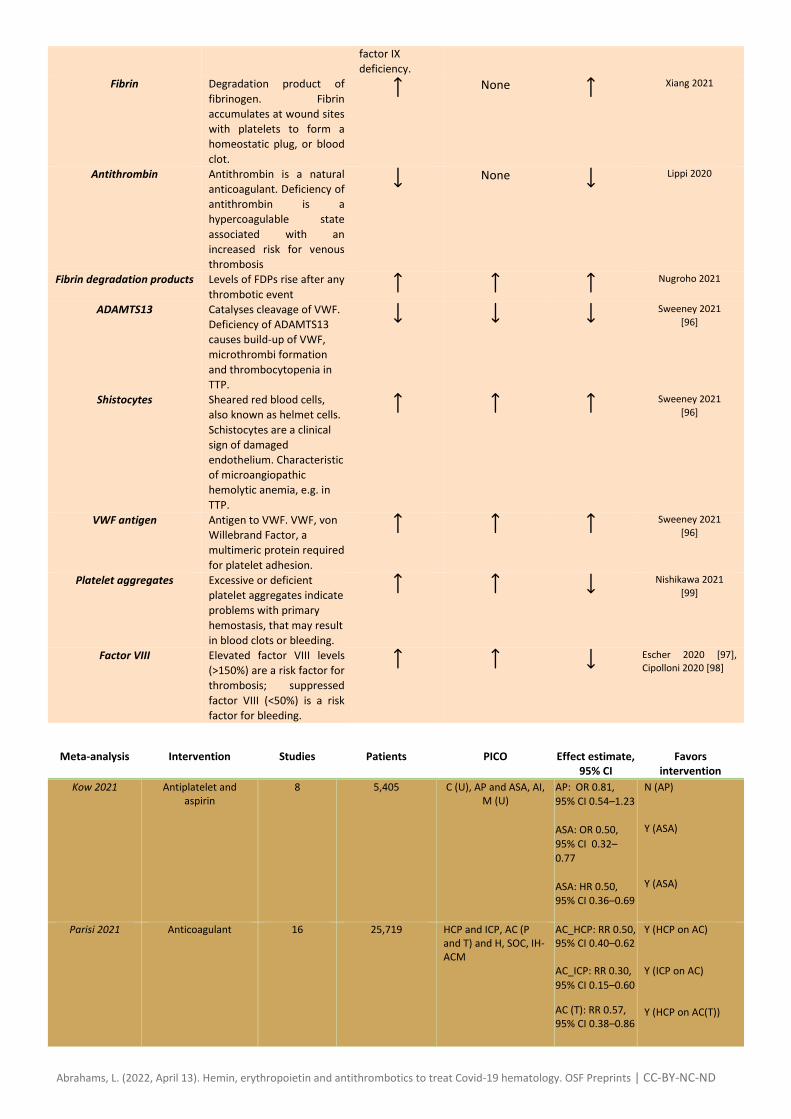
prophylactic dosing of anticoagulation in < 50% of the population [112]. Yet, the efficacy of antithrombotics in reducing all-cause
mortality of severe Covid-19 patients remains to be ascertained. Of twenty-one meta-analyses identified that evaluated the clinical
utility of antithrombotics in Covid-19, twelve favored intervention with at least one subtype of antithrombotic, four were
inconclusive and five favored standard of care (Table 8).
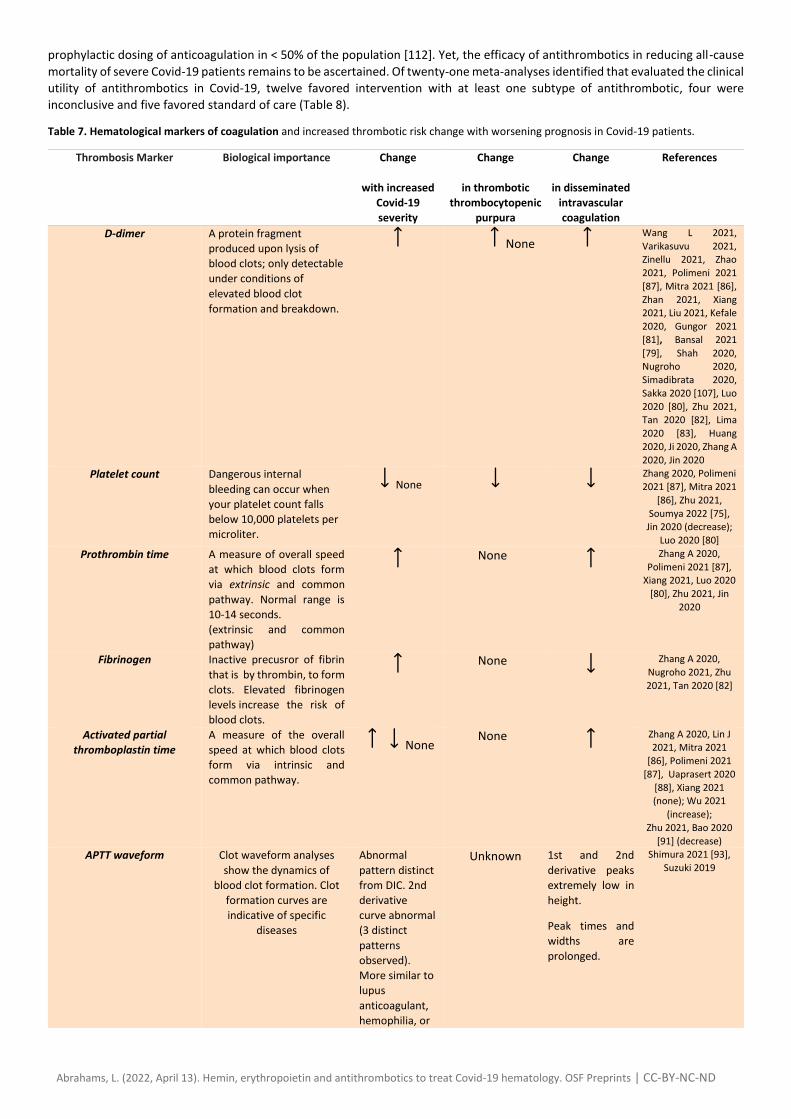
Table 7. Hematological markers of coagulation and increased thrombotic risk change with worsening prognosis in Covid-19 patients.
Thrombosis Marker Biological importance Change
with increased
Covid-19
severity
Change
in thrombotic
thrombocytopenic
purpura
Change
in disseminated
intravascular
coagulation
References
D-dimer
A protein fragment
produced upon lysis of
blood clots; only detectable
under conditions of
elevated blood clot
formation and breakdown.
None Wang L 2021,
Varikasuvu 2021, Zinellu 2021, Zhao
2021, Polimeni 2021
[87], Mitra 2021 [86],
Zhan 2021, Xiang 2021, Liu 2021, Kefale
2020, Gungor 2021
[81], Bansal 2021
[79], Shah 2020, Nugroho 2020,
Simadibrata 2020,
Sakka 2020 [107], Luo
2020 [80], Zhu 2021, Tan 2020 [82], Lima
2020 [83], Huang
2020, Ji 2020, Zhang A
2020, Jin 2020 Platelet count
Dangerous internal
bleeding can occur when
your platelet count falls
below 10,000 platelets per
microliter.
None Zhang 2020, Polimeni
2021 [87], Mitra 2021
[86], Zhu 2021,
Soumya 2022 [75], Jin 2020 (decrease);
Luo 2020 [80]
Prothrombin time
A measure of overall speed
at which blood clots form
via extrinsic and common
pathway. Normal range is
10-14 seconds. (extrinsic and common
pathway)
None
Zhang A 2020,
Polimeni 2021 [87], Xiang 2021, Luo 2020
[80], Zhu 2021, Jin
2020
Fibrinogen
Inactive precusror of fibrin
that is by thrombin, to form
clots. Elevated fibrinogen
levels increase the risk of
blood clots.
None
Zhang A 2020,
Nugroho 2021, Zhu
2021, Tan 2020 [82]
Activated partial
thromboplastin time
A measure of the overall
speed at which blood clots
form via intrinsic and
common pathway.
None None
Zhang A 2020, Lin J 2021, Mitra 2021
[86], Polimeni 2021
[87], Uaprasert 2020
[88], Xiang 2021 (none); Wu 2021
(increase);
Zhu 2021, Bao 2020
[91] (decrease) APTT waveform
Clot waveform analyses
show the dynamics of
blood clot formation. Clot
formation curves are
indicative of specific
diseases
Abnormal
pattern distinct
from DIC. 2nd
derivative
curve abnormal
(3 distinct
patterns
observed).
More similar to
lupus
anticoagulant,
hemophilia, or
Unknown 1st and 2nd
derivative peaks
extremely low in
height.
Peak times and
widths are
prolonged.
Shimura 2021 [93],
Suzuki 2019
Abrahams, L. (2022, April 13). Hemin, erythropoietin and antithrombotics to treat Covid-19 hematology. OSF Preprints | CC-BY-NC-ND
factor IX
deficiency. Fibrin Degradation product of
fibrinogen. Fibrin
accumulates at wound sites
with platelets to form a
homeostatic plug, or blood
clot.
None
Xiang 2021
Antithrombin Antithrombin is a natural
anticoagulant. Deficiency of
antithrombin is a
hypercoagulable state
associated with an
increased risk for venous
thrombosis
None
Lippi 2020
Fibrin degradation products Levels of FDPs rise after any
thrombotic event Nugroho 2021
ADAMTS13
Catalyses cleavage of VWF.
Deficiency of ADAMTS13
causes build-up of VWF,
microthrombi formation
and thrombocytopenia in
TTP.
Sweeney 2021
[96]
Shistocytes Sheared red blood cells,
also known as helmet cells.
Schistocytes are a clinical
sign of damaged
endothelium. Characteristic
of microangiopathic
hemolytic anemia, e.g. in
TTP.
Sweeney 2021
[96]
VWF antigen Antigen to VWF. VWF, von
Willebrand Factor, a
multimeric protein required
for platelet adhesion.
Sweeney 2021
[96]
Platelet aggregates
Excessive or deficient
platelet aggregates indicate
problems with primary
hemostasis, that may result
in blood clots or bleeding.
Nishikawa 2021
[99]
Factor VIII Elevated factor VIII levels
(>150%) are a risk factor for
thrombosis; suppressed
factor VIII (<50%) is a risk
factor for bleeding.
Escher 2020 [97], Cipolloni 2020 [98]
Meta-analysis Intervention Studies Patients PICO Effect estimate, 95% CI
Favors intervention
Kow 2021 Antiplatelet and aspirin
8 5,405 C (U), AP and ASA, AI, M (U)
AP: OR 0.81,
95% CI 0.54–1.23
ASA: OR 0.50,
95% CI 0.32–
0.77
ASA: HR 0.50, 95% CI 0.36–0.69
N (AP) Y (ASA) Y (ASA)
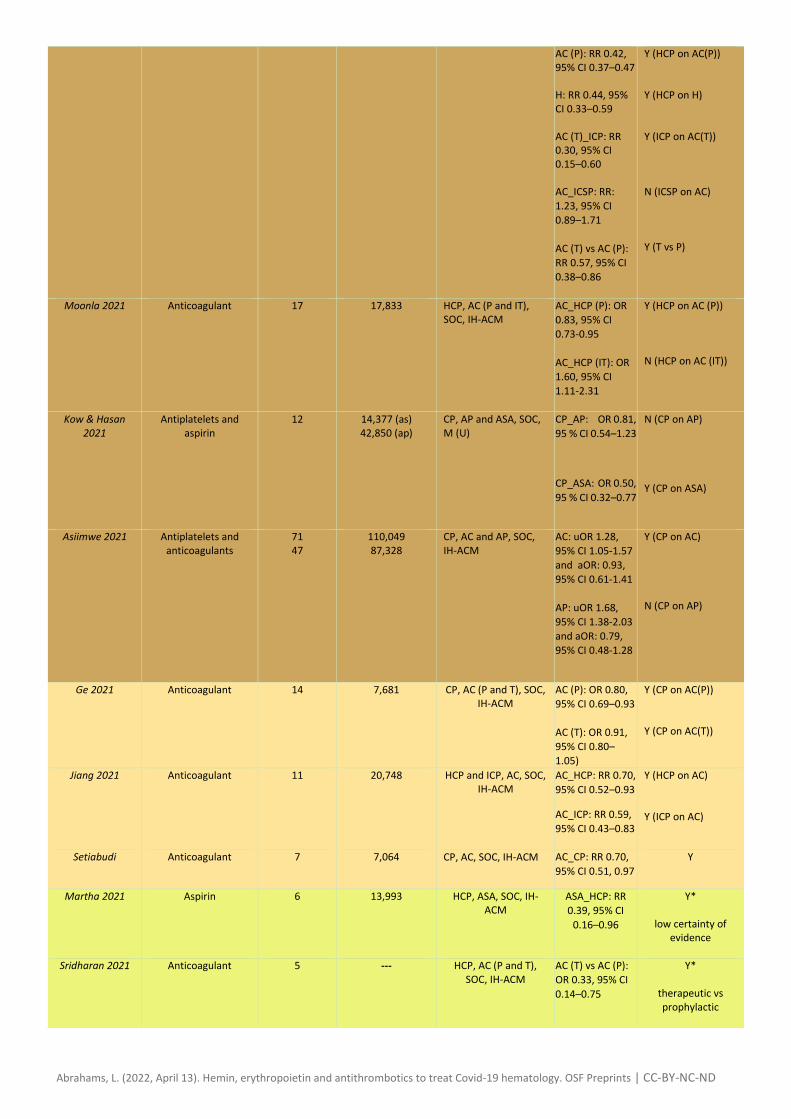
Parisi 2021 Anticoagulant 16 25,719 HCP and ICP, AC (P and T) and H, SOC, IH-ACM
AC_HCP: RR 0.50, 95% CI 0.40–0.62 AC_ICP: RR 0.30,
95% CI 0.15–0.60
AC (T): RR 0.57, 95% CI 0.38–0.86
Y (HCP on AC) Y (ICP on AC) Y (HCP on AC(T))
Abrahams, L. (2022, April 13). Hemin, erythropoietin and antithrombotics to treat Covid-19 hematology. OSF Preprints | CC-BY-NC-ND
AC (P): RR 0.42, 95% CI 0.37–0.47 H: RR 0.44, 95% CI 0.33–0.59 AC (T)_ICP: RR 0.30, 95% CI 0.15–0.60 AC_ICSP: RR:
1.23, 95% CI
0.89–1.71
AC (T) vs AC (P):
RR 0.57, 95% CI
0.38–0.86
Y (HCP on AC(P)) Y (HCP on H) Y (ICP on AC(T)) N (ICSP on AC) Y (T vs P)
Moonla 2021 Anticoagulant 17 17,833 HCP, AC (P and IT), SOC, IH-ACM
AC_HCP (P): OR
0.83, 95% CI
0.73-0.95
AC_HCP (IT): OR
1.60, 95% CI
1.11-2.31
Y (HCP on AC (P)) N (HCP on AC (IT))
Kow & Hasan 2021
Antiplatelets and aspirin
12 14,377 (as) 42,850 (ap)
CP, AP and ASA, SOC, M (U)
CP_AP: OR 0.81,
95 % CI 0.54–1.23
CP_ASA: OR 0.50,
95 % CI 0.32–0.77
N (CP on AP) Y (CP on ASA)
Asiimwe 2021 Antiplatelets and anticoagulants
71 47
110,049 87,328
CP, AC and AP, SOC, IH-ACM
AC: uOR 1.28,
95% CI 1.05-1.57
and aOR: 0.93,
95% CI 0.61-1.41
AP: uOR 1.68,
95% CI 1.38-2.03
and aOR: 0.79,
95% CI 0.48-1.28
Y (CP on AC) N (CP on AP)
Ge 2021 Anticoagulant 14 7,681 CP, AC (P and T), SOC, IH-ACM
AC (P): OR 0.80,
95% CI 0.69–0.93
AC (T): OR 0.91,
95% CI 0.80–
1.05)
Y (CP on AC(P)) Y (CP on AC(T))
Jiang 2021 Anticoagulant 11 20,748 HCP and ICP, AC, SOC, IH-ACM
AC_HCP: RR 0.70,
95% CI 0.52–0.93
AC_ICP: RR 0.59,
95% CI 0.43–0.83
Y (HCP on AC) Y (ICP on AC)
Setiabudi Anticoagulant 7 7,064 CP, AC, SOC, IH-ACM
AC_CP: RR 0.70,
95% CI 0.51, 0.97
Y
Martha 2021 Aspirin 6 13,993 HCP, ASA, SOC, IH-ACM
ASA_HCP: RR
0.39, 95% CI
0.16–0.96
Y*
low certainty of evidence
Sridharan 2021 Anticoagulant 5 --- HCP, AC (P and T),
SOC, IH-ACM AC (T) vs AC (P):
OR 0.33, 95% CI
0.14–0.75
Y*
therapeutic vs prophylactic
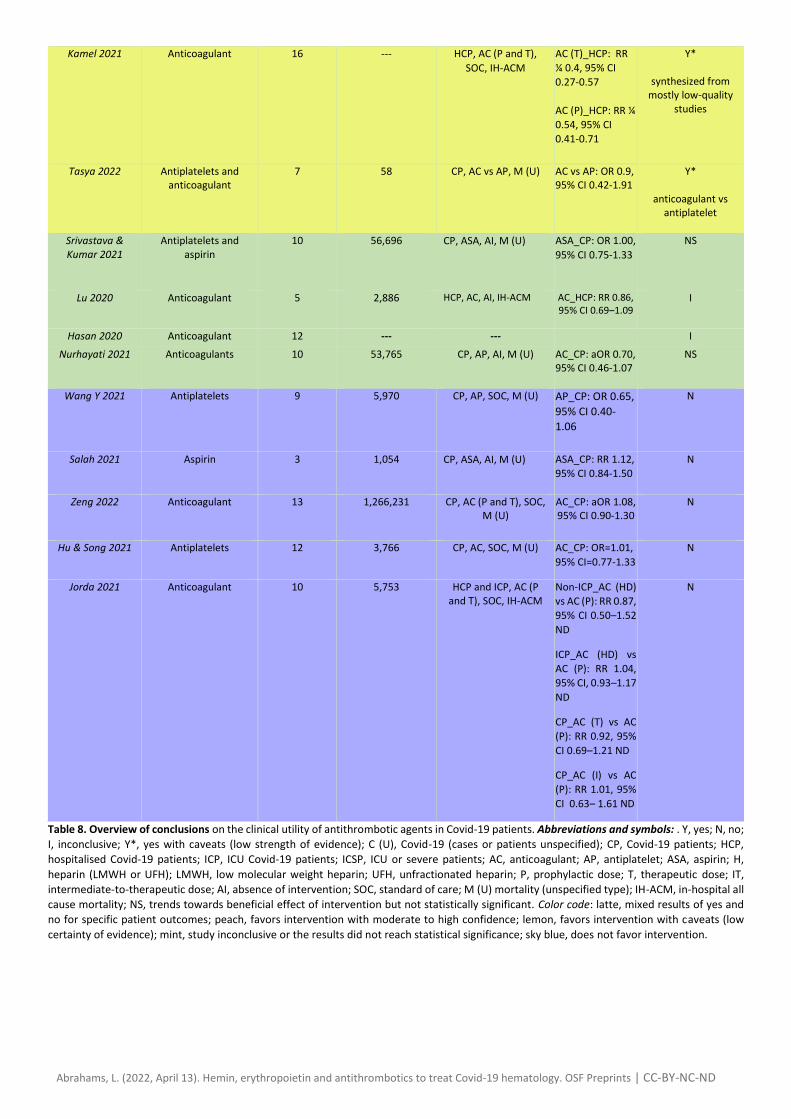
Abrahams, L. (2022, April 13). Hemin, erythropoietin and antithrombotics to treat Covid-19 hematology. OSF Preprints | CC-BY-NC-ND
Kamel 2021 Anticoagulant 16 --- HCP, AC (P and T),
SOC, IH-ACM
AC (T)_HCP: RR
¼ 0.4, 95% CI
0.27-0.57
AC (P)_HCP: RR ¼
0.54, 95% CI
0.41-0.71
Y*
synthesized from mostly low-quality
studies
Tasya 2022 Antiplatelets and anticoagulant
7 58 CP, AC vs AP, M (U) AC vs AP: OR 0.9, 95% CI 0.42-1.91
Y*
anticoagulant vs antiplatelet
Srivastava & Kumar 2021
Antiplatelets and aspirin
10 56,696 CP, ASA, AI, M (U)
ASA_CP: OR 1.00,
95% CI 0.75-1.33
NS
Lu 2020 Anticoagulant 5 2,886 HCP, AC, AI, IH-ACM
AC_HCP: RR 0.86, 95% CI 0.69–1.09
I
Hasan 2020 Anticoagulant 12 --- --- I Nurhayati 2021 Anticoagulants 10 53,765 CP, AP, AI, M (U) AC_CP: aOR 0.70,
95% CI 0.46-1.07
NS
Wang Y 2021 Antiplatelets 9 5,970 CP, AP, SOC, M (U) AP_CP: OR 0.65,
95% CI 0.40-
1.06
N
Salah 2021 Aspirin 3 1,054 CP, ASA, AI, M (U)
ASA_CP: RR 1.12,
95% CI 0.84-1.50
N
Zeng 2022 Anticoagulant 13 1,266,231 CP, AC (P and T), SOC, M (U)
AC_CP: aOR 1.08, 95% CI 0.90-1.30
N
Hu & Song 2021 Antiplatelets 12 3,766 CP, AC, SOC, M (U) AC_CP: OR=1.01,
95% CI=0.77-1.33
N
Jorda 2021 Anticoagulant 10 5,753 HCP and ICP, AC (P and T), SOC, IH-ACM
Non-ICP_AC (HD)
vs AC (P): RR 0.87,
95% CI 0.50–1.52
ND
ICP_AC (HD) vs
AC (P): RR 1.04,
95% CI, 0.93–1.17
ND
CP_AC (T) vs AC
(P): RR 0.92, 95%
CI 0.69–1.21 ND
CP_AC (I) vs AC
(P): RR 1.01, 95%
CI 0.63– 1.61 ND
N
Table 8. Overview of conclusions on the clinical utility of antithrombotic agents in Covid-19 patients. Abbreviations and symbols: . Y, yes; N, no;
I, inconclusive; Y*, yes with caveats (low strength of evidence); C (U), Covid-19 (cases or patients unspecified); CP, Covid-19 patients; HCP,
hospitalised Covid-19 patients; ICP, ICU Covid-19 patients; ICSP, ICU or severe patients; AC, anticoagulant; AP, antiplatelet; ASA, aspirin; H,
heparin (LMWH or UFH); LMWH, low molecular weight heparin; UFH, unfractionated heparin; P, prophylactic dose; T, therapeutic dose; IT,
intermediate-to-therapeutic dose; AI, absence of intervention; SOC, standard of care; M (U) mortality (unspecified type); IH-ACM, in-hospital all
cause mortality; NS, trends towards beneficial effect of intervention but not statistically significant. Color code: latte, mixed results of yes and
no for specific patient outcomes; peach, favors intervention with moderate to high confidence; lemon, favors intervention with caveats (low
certainty of evidence); mint, study inconclusive or the results did not reach statistical significance; sky blue, does not favor intervention.

Abrahams, L. (2022, April 13). Hemin, erythropoietin and antithrombotics to treat Covid-19 hematology. OSF Preprints | CC-BY-NC-ND
Existing meta-analyses attest to the potential of antithrombotics although the clinical picture is complicated
From overview of Table 8, intervention with antithrombotics appears promising. Multiple studies associate reduced Covid-19
mortality with thromboprophylaxis [74, 115, 116, 117, 118, 119] or therapeutic dose antithrombotic (74, 115, 118, 120, 121, 122,
123]. Within the antithrombotics umbrella, there was no mention of fibrinolytics, while anticoagulants seemed to outperform
antiplatelets. All identified meta-analyses on antiplatelet therapy [74, 119, 124, 125] found no significant difference in mortality
between antiplatelet users and non-antiplatelet users. Howsoever, antiplatelet therapy was deemed to be relatively safe in Covid-
19 patients [124] and may mitigate risk of other clinical outcomes besides mortality, including ICU admission and mechanical
ventilation [125]. This finding is of value for Covid-19 patients who are ordinarily prescribed antiplatelets for an unrelated condition.
There are still many unknowns. The exact mechanism of protection of antithrombotics has not been definitively proven. For
example, Kow & Hasan [119] found aspirin usage is associated with reduced Covid-19 mortality, but that this finding is not
replicated with antiplatelets. Since both aspirin and antiplatelets have an antithrombotic effect, it is possible that aspirin reduces
mortality by virtue of a non-antithrombotic mechanism, for example antiviral or anti-inflammatory mechanisms. Moreover, the
clinical picture on anticoagulant usage in Covid-19 is not entirely uniform; five meta-analyses [124, 125, 126, 127, 128] found no
significant decrease in mortality. This discrepancy requires further investigation. Further, hemorrhage is an established adverse
outcome of antithrombotic usage and increased bleeding tendency was recognised by three of the meta-analyses [117, 118, 128].
Only one meta-analysis found no significant increase in bleeding risk with antithrombotic usage [129]. The increased risk of
hemorrhage was associated in all three cases with therapeutic rather than prophylactic regimens, implying that Covid-19 patients
ordinarily prescribed prophylactic antithrombotics may be safe to continue.
Hematological disturbances may converge on GATA1/2
Hypercoagulability, altered porphyrin metabolism and dyserythropoiesis appear to be defining hematological features of SARS-Cov-2 infection. To date, there is almost no mention in the literature of any of the three hematological disturbances in conjunction with the original SARS strain, SARS-Cov-1. Searching for articles dated 2003-2018 and indexed in Google Scholar containing the within-title terms ‘SARS’ AND ‘thrombosis’ OR ‘coagulation’ OR ‘erythropoiesis’ OR ‘EPO’ OR ‘erythropoietin’ OR ‘porphyria’ OR ‘porphyrin’ OR ‘heme’ reveals only two articles. One article documents evidence of hypercoagulability and hypofibrinolysis in patients with post-SARS-1 osteonecrosis [130]; contrarily, the second study found no evidence of a hypercoagulable state in patients with post-SARS-1 avascular necrosis of the femoral head [131]. Hematological disturbance may therefore represent a genuinely novel presentation in SARS-Cov-2 relative to SARS-Cov-1. Interestingly, GATA-1 and GATA-2 transcripts are upregulated in Covid-19 non-survivors but not in survivors [25]. GATA transcription factors control expression of a suite of genes to: (i) promote heme biosynthesis [132], (ii) repress EPO expression [133], (iii) stimulate maturation of erythroid precursors [134], (iv) effect maturation of platelets from megakaryoblasts, promegakaryocytes, and megakaryocytes [135]. As such, aberration of GATA signalling in Covid-19 may potentially provide a molecular mechanism by which all three observed hematological abnormalities converge (Fig. 4).
Figure 4. Three hematological abnormalities in Covid-19 converge on GATA signalling. Heme and RBC-PLT graphics sourced from Alamy, EPO
structure sourced from PDB and the figure was created in BioRender.
Abrahams, L. (2022, April 13). Hemin, erythropoietin and antithrombotics to treat Covid-19 hematology. OSF Preprints | CC-BY-NC-ND
Concluding Remarks and Future Perspectives
The three PICO questions herein remain incompletely answered (see Outstanding Questions) and would be refined by a larger
meta-analysis that aggregates all relevant studies. Moreover, pre-existing meta-analyses in this area focus on anticoagulants or
antiplatelets as the definition of antithrombotic. The current author proposes incorporation of fibrinolytics into the intervention
definition. Further, none of the pre-existing meta-analyses on antithrombotics factor into the assessment of study quality a
consideration of conflicts of interest. Forthcoming meta-analyses in this area may reach a more accurate conclusion by accounting
for conflicts of interest using a modified quality scale, akin to AMSTAR2. Since there are currently zero or limited studies on hemin
and erythropoietin as interventions in Covid-19, a living systematic review and meta-analysis will garner novel insights as and when future studies unfold.
Outstanding Questions
1. How safe and effective are hemin, erythropoietin and antithrombotics in the treatment of severe Covid-19?
2. If EPO is clinically useful in Covid-19, is the mechanism of action via erythropoiesis, mitigation of lung injury, pleiotropic effects, or a combination of the four mechanisms?
3. Will aggregation of a larger pool of studies, in addition to a modified study quality scale that accounts for conflicts of interest, provide a more accurate evaluation of the efficacy of antithrombotics?
4. Are the three hematological abnormalities in Covid-19 mechanistically linked to GATA1/2 signalling dysregulation?
5. To what extent are urinary and fecal porphyrins in Covid-19 reminiscent of acute porphyria attacks?
Acknowledgements
The author thanks the Ronin Institute for their affiliation and Dr. Paul Cottrell for highlighting the importance of CD147 receptor early in the pandemic.
Resources
i https://www.who.int/vmnis/indicators/haemoglobin.pdf
ii https://www.epogen.com/patient/about-epogen/monitoring-your-treatment
iii https://bnf.nice.org.uk/medicinal-forms/epoetin-alfa.html
iv https://www.medicines.org.uk/emc/product/3442/smpc#gref
References
1. Kietzmann, T., 2020. Hypoxia-inducible erythropoietin expression: details matter. haematologica, 105(12).
2. Scholz, H., Schurek, H.J., Eckardt, K.U. and Bauer, C., 1990. Role of erythropoietin in adaptation to hypoxia. Experientia, 46(11),
pp.1197-1201.
3. Yağcı, S., Serin, E., Acicbe, Ö., Zeren, M.İ. and Odabaşı, M.S., 2021. The relationship between serum erythropoietin, hepcidin,
and haptoglobin levels with disease severity and other biochemical values in patients with COVID‐19. International Journal of Laboratory Hematology 43: 142-151.
4. Viruez-Soto, A., López-Dávalos, M.M., Rada-Barrera, G., Merino-Luna, A., Molano-Franco, D., Tinoco-Solorozano, A., Zubieta-
DeUrioste, N., Zubieta-Calleja, G., Arias-Reyes, C. and Soliz, J., 2021. Low Serum Erythropoietin Levels are Associated with Fatal
COVID-19 Cases at 4,150 meters above sea level. Respiratory Physiology & Neurobiology, p.103709.
Abrahams, L. (2022, April 13). Hemin, erythropoietin and antithrombotics to treat Covid-19 hematology. OSF Preprints | CC-BY-NC-ND
5. Begemann, M., Gross, O., Wincewicz, D., Hardeland, R., Daguano Gastaldi, V., Vieta, E., Weissenborn, K., Miskowiak, K.W.,
Moerer, O. and Ehrenreich, H., 2021. Addressing the ‘hypoxia paradox’ in severe COVID-19: literature review and report of four cases treated with erythropoietin analogues. Molecular Medicine, 27(1), pp.1-11.
6. Abrahams, L. (2020). Covid-19: acquired acute porphyria hypothesis. OSF Preprints. DOI: 10.31219/osf.io/fxz3p
7. Zhang, H., Zhou, J., Chen, R., Ren, Y., Cai, J., Zhao, L., Fei, X., Liu, Z., Zhang, Y., Yuan, L. and Wang, C., 2021. Autopsy and
histologic findings of patients with new coronavirus pneumonia: the pathologic associations with hypoxemia. Medical Science Monitor: International Medical Journal of Experimental and Clinical Research, 27, pp.e928837-1.
8. Coste I, Gauchat JF, Wilson A, et al. Unavailability of CD147 leads to selective erythrocyte trapping in the spleen. Blood 2001;
97 (12): 3984–3988.
9. Wang K, Chen W, Zhang Z, Deng Y, Lian JQ, Du P, Wei D, Zhang Y, Sun XX, Gong L, Yang X. 2020. CD147-spike protein is a novel
route for SARS-CoV-2 infection to host cells. Signal transduction and targeted therapy, 5(1):1-10.
10. Munster, V.J., Feldmann, F., Williamson, B.N., van Doremalen, N., Pérez-Pérez, L., Schulz, J., Meade-White, K., Okumura, A.,
Callison, J., Brumbaugh, B. and Avanzato, V.A., 2020. Respiratory disease in rhesus macaques inoculated with SARS-CoV-2. Nature, 585(7824), pp.268-272.
11. Kronstein-Wiedemann, R., Stadtmüller, M., Traikov, S., Georgi, M., Teichert, M., Yosef, H., Wallenborn, J., Karl, A., Schütze, K.,
Wagner, M. and El-Armouche, A., 2022. SARS-CoV-2 infects red blood cell progenitors and dysregulates hemoglobin and iron
metabolism. Stem Cell Reviews and Reports, pp.1-13.
12. Taneri, P.E., Gómez-Ochoa, S.A., Llanaj, E., Raguindin, P.F., Rojas, L.Z., Roa-Díaz, Z.M., Salvador, D., Groothof, D., Minder, B.,
Kopp-Heim, D. and Hautz, W.E., 2020. Anemia and iron metabolism in COVID-19: a systematic review and meta-
analysis. European journal of epidemiology, 35(8), pp.763-773.
13. Lippi, G. and Mattiuzzi, C., 2020. Hemoglobin value may be decreased in patients with severe coronavirus disease
2019. Hematology, transfusion and cell therapy, 42, pp.116-117.
14. Zuin, M., Rigatelli, G., Quadretti, L., Fogato, L., Zuliani, G. and Roncon, L., 2021. Prognostic Role of Anemia in COVID-19
Patients: A Meta-Analysis. Infectious disease reports, 13(4), pp.930-937.
15. Capes, A., Bailly, S., Hantson, P. et al. COVID-19 infection associated with autoimmune hemolytic anemia. Ann
Hematol 99, 1679–1680 (2020). https://doi.org/10.1007/s00277-020-04137-9
16. Fishbane, S. and Hirsch, J.S., 2020. Erythropoiesis-stimulating agent treatment in patients with COVID-19. American Journal
of Kidney Diseases, 76(3), pp.303-305.
17. Lee, J.J., Montazerin, S.M., Jamil, A., Jamil, U., Marszalek, J., Chuang, M.L. and Chi, G., 2021. Association between red blood
cell distribution width and mortality and severity among patients with COVID‐19: A systematic review and meta‐analysis. Journal
of medical virology, 93(4), pp.2513-2522.
18. Sarkar, S., Kannan, S., Khanna, P. and Singh, A.K., 2021. Role of red blood cell distribution width, as a prognostic indicator in
COVID‐19: A systematic review and meta‐analysis. Reviews in Medical Virology, p.e2264.
19. Zinellu, A. and Mangoni, A.A., 2021a. Red blood cell distribution width, disease severity, and mortality in hospitalized
patients with SARS-CoV-2 infection: A systematic review and meta-analysis. Journal of Clinical Medicine, 10(2), p.286.
20. Patel, H.H., Patel, H.R. and Higgins, J.M., 2015. Modulation of red blood cell population dynamics is a fundamental homeostatic
response to disease. American journal of hematology, 90(5), pp.422-428.
21. Aydınyılmaz, F., Aksakal, E., Pamukcu, H.E., Aydemir, S., Doğan, R., Saraç, İ., Aydın, S.Ş., Kalkan, K., Gülcü, O. and Tanboğa, İ.H.,
2021. Significance of MPV, RDW and PDW with the Severity and Mortality of COVID-19 and Effects of Acetylsalicylic Acid
Use. Clinical and Applied Thrombosis/Hemostasis, 27, p.10760296211048808.
22. Ramachandran, P., Gajendran, M., Perisetti, A., Elkholy, K.O., Chakraborti, A., Lippi, G., and Goyal, H., 2022. Red Blood Cell
Distribution Width in Hospitalized COVID-19 Patients. Frontiers in Medicine, 8, DOI: 10.3389/fmed.2021.582403
23. Encabo, H.H., Grey, W., Garcia-Albornoz, M., Wood, H., Ulferts, R., Aramburu, I.V., Kulasekararaj, A.G., Mufti, G.,
Papayannopoulos, V., Beale, R. and Bonnet, D., 2021. Human erythroid progenitors are directly infected by SARS-CoV-2: Implications for emerging erythropoiesis in severe COVID-19 patients. Stem cell reports, 16(3), pp.428-436.
24. Shahbaz S, Xu L, Osman M, Sligl W, Shields J, Joyce M, Tyrrell DL, Oyegbami O, Elahi S. 2021. Erythroid precursors and progenitors suppress adaptive immunity and get invaded by SARS-CoV-2. Stem Cell Reports, 16(5):1165-81.
Abrahams, L. (2022, April 13). Hemin, erythropoietin and antithrombotics to treat Covid-19 hematology. OSF Preprints | CC-BY-NC-ND
25. Bernardes JP, Mishra N, Tran F, et al. Longitudinal multi-omics analyses identify responses of megakaryocytes, erythroid cells
and plasmablasts as hallmarks of severe COVID-19 trajectories. Immunity 2020; 53: 1296–1314
26. Kaneko, H., Katoh, T., Hirano, I., Hasegawa, A., Tsujita, T., Yamamoto, M. and Shimizu, R., 2017. Induction of erythropoietin
gene expression in epithelial cells by chemicals identified in GATA inhibitor screenings. Genes to Cells, 22(11), pp.939-952.
27. Ouyang, S.M., Zhu, H.Q., Xie, Y.N., Zou, Z.S., Zuo, H.M., Rao, Y.W., Liu, X.Y., Zhong, B. and Chen, X., 2020. Temporal changes
in laboratory markers of survivors and non-survivors of adult inpatients with COVID-19. BMC infectious diseases, 20(1), pp.1-10.
28. Pretorius, E., Oore OF., Mbotwe, S. and Bester, J., 2016. Erythrocytes and their role as health indicator: Using structure in a
patient-orientated precision medicine approach. Blood reviews, 30(4), pp.263-274.
29. Jones, J.R. and Ireland, R., 2020. Morphological changes in a case of SARS-CoV-2 infection. Blood, 135(25), p.2324.
30. Hadadi, A., Mortezazadeh, M., Kolahdouzan, K. and Alavian, G., 2020. Does recombinant human erythropoietin
administration in critically ill COVID‐19 patients have miraculous therapeutic effects?. Journal of medical virology, 92(7), pp.915-
918.
31. Soliz, J., Schneider-Gasser, E.M., Arias-Reyes, C., Aliaga-Raduan, F., Poma-Machicao, L., Zubieta-Calleja, G., Furuya, W.I.,
Trevizan-Baú, P., Dhingra, R.R. and Dutschmann, M., 2020. Coping with hypoxemia: Could erythropoietin (EPO) be an adjuvant
treatment of COVID-19?. Respiratory physiology & neurobiology, 279, p.103476.
32. Ehrenreich, H., Weissenborn, K., Begemann, M., Busch, M., Vieta, E. and Miskowiak, K.W., 2020. Erythropoietin as candidate
for supportive treatment of severe COVID-19. Molecular Medicine, 26(1), pp.1-9.
33. Papadopoulos, K.I., Sutheesophon, W., Manipalviratn, S. and Aw, T.C., 2021. Age and genotype dependent erythropoietin
protection in COVID-19. World Journal of Stem Cells, 13(10), p.1513.
34. Sahebnasagh, A., Mojtahedzadeh, M., Najmeddin, F., Najafi, A., Safdari, M., Ghaleno, H.R., Habtemariam, S., Neagoe, I.B. and
Nabavi, S.M., 2020. A perspective on erythropoietin as a potential adjuvant therapy for acute lung injury/acute respiratory
distress syndrome in patients with covid-19. Archives of Medical Research.
35. Brenner, S.R., 2020. Erythropoietin Induced Hemoglobin Sub‐Unit Beta may Stimulate Innate Immune RNA Virus Pattern
Recognition, Suppress Reactive Oxygen Species, Reduce ACE2 Viral Doorway Opening and Neutrophil Extracellular Traps against Covid‐19. Journal of Medical Virology.
36. Gando, A., Alexay, S., Núñez, J.P.G., Cano, L.N., Diez, R.A. and Costa, L.A., 2021. Comment on Hadadi et al., Does recombinant
human erythropoietin administration in critically ill COVID‐19 patients have miraculous therapeutic effects? J. Med. Virol. 2020;
92: 915‐918. Journal of Medical Virology.
37. Samimagham, H.R., Azad, M.H., Hooshyar, D., Haddad, M., Arabi, M. and KazemiJahromi, M., 2021. Evaluation of the efficacy
and safety of recombinant erythropoietin on the improvement of hospitalised COVID-19 patients: A structured summary of a
study protocol for a randomised controlled trial. Trials, 22(1), pp.1-3.
38. Nejat, R., Sadr, A.S., Ebrahimi, A., Nabati, A. and Eshaghi, E., 2020a. Daily Low Dose of Erythropoietin in Neuroinflammation;
EPO Might Be Hazardous in COVID-19. Preprints 2020, 2020060107 (doi: 10.20944/preprints202006.0107.v2)
39. Nejat, R., Sadr, A.S. and Najafi, D., 2020b. Erythropoietin in COVID-19-Induced Neuroinflammation; EPO Plus Losartan Might
be Promising. Journal of Biostatistics and Epidemiology, 6(2), pp.143-161.
40. Tascilar, O., Cakmak, G.K., Tekin, I.O., Emre, A.U., Ucan, B.H., Bahadir, B., Acikgoz, S., Irkorucu, O., Karakaya, K., Balbaloglu, H.
and Kertis, G., 2007. Protective effects of erythropoietin against acute lung injury in a rat model of acute necrotizing
pancreatitis. World Journal of Gastroenterology: WJG, 13(46), p.6172.
41. Li, J., Luo, Y., Li, Z., Liu, Y. and Liu, Z., 2012. Effects of erythropoietin pretreatment on pro-and anti-inflammatory balance in
rats with severe acute pancreatitis. Journal of Southern Medical University, 32(1), pp.93-96.
42. Shang, Y., Li, X., Prasad, P.V., Xu, S., Yao, S., Liu, D., Yuan, S. and Feng, D., 2009. Erythropoietin attenuates lung injury in
lipopolysaccharide treated rats. Journal of Surgical Research, 155(1), pp.104-110.
43. Korkmaz, T., Kahramansoy, N., Kilicgun, A. and Firat, T., 2014. The effect of erythropoietin to pulmonary injury and mast cells
secondary to acute pancreatitis. BMC research notes, 7(1), pp.1-6.
44. Cao, F., Tian, X., Li, Z., Lv, Y., Han, J., Zhuang, R., Cheng, B., Gong, Y., Ying, B., Jin, S. and Gao, Y., 2020. Suppression of NLRP3
inflammasome by erythropoietin via the EPOR/JAK2/STAT3 pathway contributes to attenuation of acute lung injury in mice. Frontiers in pharmacology, 11, p.306.
Abrahams, L. (2022, April 13). Hemin, erythropoietin and antithrombotics to treat Covid-19 hematology. OSF Preprints | CC-BY-NC-ND
45. Zhang, X. and Dong, S., 2019. Protective effects of erythropoietin towards acute lung injuries in rats with sepsis and its related
mechanisms. Annals of Clinical & Laboratory Science, 49(2), pp.257-264.
46. Kandasamy, K., Choudhury, S., Singh, V., Addison, M.P., Darzi, S.A., Kasa, J.K., Thangamalai, R., Dash, J.R., Kumar, T., Sultan, F.
and Singh, T.U., 2016. Erythropoietin reverses sepsis-induced vasoplegia to norepinephrine through preservation of α1D-
adrenoceptor mRNA expression and inhibition of GRK2-mediated desensitization in mouse aorta. Journal of cardiovascular
pharmacology and therapeutics, 21(1), pp.100-113.
47. Karampitsakos T, Akinosoglou K, Papaioannou O, et al. Increased red cell distribution width is associated with disease
severity in hospitalized adults with SARS-CoV-2 infection: an observational multicentric study. Front Med. 2020; 7:616292.
48. Leventhal, J., Angeletti, A. and Cravedi, P., 2020. EPO in Patients With COVID-19: More Than an Erythropoietic
Hormone. American Journal of Kidney Diseases, 76(3), p.441.
49. Perico L, Benigni A, Remuzzi G. Should COVID-19 concern nephrologists? Why and to what extent? The emerging impasse of angiotensin blockade. Nephron. 2020:1–9.
50. Lu YF, Pan LY, Zhang WW, Cheng F, Hu SS, Zhang X, Jiang HY. A meta-analysis of the incidence of venous thromboembolic
events and impact of anticoagulation on mortality in patients with COVID-19. Int J Infect Dis. 2020 Nov;100:34-41. doi:
10.1016/j.ijid.2020.08.023. Epub 2020 Aug 13. PMID: 32798659; PMCID: PMC7425668.
51. Ehsani, S., 2020. COVID-19 and iron dysregulation: distant sequence similarity between hepcidin and the novel coronavirus
spike glycoprotein. Biology Direct, 15(1), pp.1-13.
52. Kiers, D., van Eijk, L.T., van der Hoeven, J.G., Swinkels, D.W., Pickkers, P. and Kox, M., 2019. Hypoxia attenuates
inflammation-induced hepcidin synthesis during experimental human endotoxemia. haematologica, 104(6), p.e230.
53. Artuso, I., Pettinato, M., Nai, A., Pagani, A., Sardo, U., Billoré, B., Lidonnici, M.R., Bennett, C., Mandelli, G., Pasricha, S.R. and
Ferrari, G., 2019. Transient decrease of serum iron after acute erythropoietin treatment contributes to hepcidin inhibition by
ERFE in mice. Haematologica, 104(3), p.e87.
54. Shea, B.J., Reeves, B.C., Wells, G., Thuku, M., Hamel, C., Moran, J., Moher, D., Tugwell, P., Welch, V., Kristjansson, E. and Henry,
D.A., 2017. AMSTAR 2: a critical appraisal tool for systematic reviews that include randomised or non-randomised studies of
healthcare interventions, or both. bmj, 358.
55. Schoener B, Borger J. Erythropoietin Stimulating Agents. 2021 Dec 12. In: StatPearls [Internet]. Treasure Island (FL):
StatPearls Publishing; 2022 Jan–. PMID: 30725682.
56. Aapro, M., Barnadas, A., Leonard, R.C., Marangolo, M., Untch, M., Ukarma, L., Burger, H.U., Scherhag, A. and Osterwalder, B.,
2009. What is the impact of antithrombotic therapy and risk factors on the frequency of thrombovascular events in patients with metastatic breast cancer receiving epoetin beta?. European Journal of Cancer, 45(17), pp.2984-2991.
57. San Juan, I., Bruzzone, C., Bizkarguenaga, M., Bernardo‐Seisdedos, G., Laín, A., Gil‐Redondo, R., Diercks, T., Gil‐Martínez, J.,
Urquiza, P., Arana, E. and Seco, M., 2020. Abnormal concentration of porphyrins in serum from COVID‐19 patients. British journal
of haematology, 190(5), p.e265.
58. Pang Z, Zhou G, Chong J, Xia J. 2021. Comprehensive Meta-Analysis of COVID-19 Global Metabolomics Datasets. Metabolites,
11(1):44.
59. Goldberg, M.A., Dunning, S.P. and Bunn, H.F., 1988. Regulation of the erythropoietin gene: evidence that the oxygen sensor
is a heme protein. Science, 242(4884), pp.1412-1415.
60. Herraiz, T. (2020, June 2). Chloroquine and hydroxychloroquine as antimalarials and antivirals against SARS-CoV-2: The hemin factor. https://doi.org/10.31219/osf.io/8d6xv
61. Batiha GE, Shaheen HM, Al-Kuraishy HM, Teibo JO, Akinfe OA, Al-Garbee AI, Teibo TKA, Kabrah SM. Possible mechanistic
insights into iron homeostasis role of the action of 4-aminoquinolines (chloroquine/hydroxychloroquine) on COVID-19 (SARS-CoV-
2) infection. Eur Rev Med Pharmacol Sci. 2021 Dec;25(23):7565-7584. doi: 10.26355/eurrev_202112_27456. PMID: 34919258.
62. Lutton, J.D., Ibraham, N.G., Friedland, M. and Levere, R.D., 1984. The toxic effects of heavy metals on rat bone marrow in
vitro erythropoiesis: protective role of hemin and zinc. Environmental research, 35(1), pp.97-103.
63. Anderson, K.E., Goeger, D.E., Carson, R.W., Lee, S.M.K. and Stead, R.B., 1990. Erythropoietin for the treatment of porphyria
cutanea tarda in a patient on long-term hemodialysis. New England Journal of Medicine, 322(5), pp.315-317.
Abrahams, L. (2022, April 13). Hemin, erythropoietin and antithrombotics to treat Covid-19 hematology. OSF Preprints | CC-BY-NC-ND
64. Yaqoob, M., Smyth, J., Ahmad, R., McClelland, P., Fahal, I., Kumar, K.A.S., Yu, R. and Verbov, J., 1992. Haemodialysis–related
porphyria cutanea tarda and treatment by recombinant human erythropoietin. Nephron, 60(4), pp.428-431.
65. Hamzi, M.A., Alayoud, A., Asseraji, M., Akhmouch, I. and Oualim, Z., 2013. Porphyria cutanea tarda in a hemodialysis patient
with hepatitis C virus: Efficacy of treatment with multiple phlebotomies and erythropoietin. Saudi Journal of Kidney Diseases and Transplantation, 24(1), p.121.
66. Yu, R.C.H. and Verbov, J.L., 1990. Porphyria cutanea tarda in a chronic haemodialysis patient-the possible use of low-dose chloroquine and recombinant human erythropoietin. Journal of Dermatological Treatment, 1(5), pp.277-277.
67. Munkvad, S. and Weismann, K., 1996. Phlebotomy combined with erythropoietin therapy for porphyria cutanea
tarda. Journal of the European Academy of Dermatology and Venereology, 6(3), pp.283-284.
68. Peces, R., Enriquez de Salamanca, R., Fontanellas, A., Sanchez, A., De La Torre, M., Caparros, G., Ferreras, I. and Nieto, J.,
1994. Successful treatment of haemodialysis-related porphyria cutanea tarda with erythropoietin. Nephrology Dialysis Transplantation, 9(4), pp.433-435.
69. Piazza, V., Villa, G., Galli, F., Segagni, S., Bovio, G., Poggio, F., Picardi, L., Bianco, L., Salvadeo, A. and Barosi, G., 1992.
Erythropoietin as treatment of haemodialysis-related porphyria cutanea tarda. Nephrology Dialysis Transplantation, 7(5),
pp.438-442.
70. Zappacosta, A.R., Perras, S.T. and Bell, A., 1991. Weekly subcutaneous recombinant human erythropoietin corrects anemia
of progressive renal failure. The American journal of medicine, 91(3), pp.229-232.
71. Fontanellas, A., Herrero, J.A., Coronel, F., Santos, J.L., Moran, M.J., Barrientos, A. and de Salamanca, R.E., 1996. Effects of
recombinant human erythropoietin on porphyrin metabolism in uremic patients on hemodialysis. Journal of the American
Society of Nephrology, 7(5), pp.774-779.
72. Djordjević, V.B., Pavlović, D., Pejović, M., Lečić, N., Koraćević, D., Djordjević, V. and Stefanović, V., 1993. Effect of Human
Recombinant Erythropoietin Treatment on Erythrocyte δ-Aminolevulinic Acid Dehydratase in Patients on Maintenance
Hemodialysis. Nephron, 65(3), pp.497-498.
73. Piazza, V., Galli, F., Villa, G., Poggio, F., Salvadeo, A., Bianco, L., Battistel, V., Liberato, N.L. and Barosi, G., 1991. Free Erythrocyte
Protoporphyrin in Hemodialysis Patients Treated with Human Recombinant Erythropoietin. In New Therapeutic Strategies in Nephrology (pp. 302-304). Springer, Boston, MA.
74. Asiimwe, I.G., Pushpakom, S., Turner, R.M., Kolamunnage‐Dona, R., Jorgensen, A.L. and Pirmohamed, M., 2021. Cardiovascular
drugs and COVID‐19 clinical outcomes: a living systematic review and meta‐analysis. British journal of clinical
pharmacology, 87(12), pp.4534-4545.
75. Soumya, S., Sundara, K., Puneet, K. and Singh, A.K., 2021. Role of platelet-to-lymphocyte count ratio (PLR), as a prognostic
indicator in COVID-19: a systematic review and meta-analysis.(Special issue on new coronavirus (2019-nCOV or SARS-CoV-2) and
the outbreak of respiratory illness (COVID-19): Part-XVII.). Journal of Medical Virology, pp.211-221.
76. 17. Zinellu A, Paliogiannis P, Carru C, Mangoni AA. INR and COVID-19 severity and mortality: A systematic review with meta-
analysis and meta-regression. Adv Med Sci. 2021 Sep;66(2):372-380. doi: 10.1016/j.advms.2021.07.009. Epub 2021 Jul 21. PMID:
34315012; PMCID: PMC8292100.
77. Shah S, Shah K, Patel SB, Patel FS, Osman M, Velagapudi P, Turagam MK, Lakkireddy D, Garg J. Elevated D-Dimer Levels Are
Associated With Increased Risk of Mortality in Coronavirus Disease 2019: A Systematic Review and Meta-Analysis. Cardiol Rev. 2020 Nov/Dec;28(6):295-302. doi: 10.1097/CRD.0000000000000330. Epub 2020 Jul 2. PMID: 33017364; PMCID: PMC7437424.
78. Zhu J, Pang J, Ji P, Zhong Z, Li H, Li B, Zhang J, Lu J. Coagulation dysfunction is associated with severity of COVID-19: A meta-analysis. J Med Virol. 2021 Feb;93(2):962-972. doi: 10.1002/jmv.26336. Epub 2020 Oct 14. PMID: 32706396; PMCID: PMC7404826.
79. Bansal A, Singh AD, Jain V, Aggarwal M, Gupta S, Padappayil RP, Nadeem M, Joshi S, Mian A, Greathouse T, Wells D, Gupta
M, Khan MZ. The association of D-dimers with mortality, intensive care unit admission or acute respiratory distress syndrome in
patients hospitalized with coronavirus disease 2019 (COVID-19): A systematic review and meta-analysis. Heart Lung. 2021 Jan-
Feb;50(1):9-12. doi: 10.1016/j.hrtlng.2020.08.024. Epub 2020 Sep 18. PMID: 33041057; PMCID: PMC7500895.
80. Luo L, Xu M, Du M, Kou H, Liao D, Cheng Z, Mei H, Hu Y. Early coagulation tests predict risk stratification and prognosis of
COVID-19. Aging (Albany NY). 2020 Aug 29;12(16):15918-15937. doi: 10.18632/aging.103581. Epub 2020 Aug 29. PMID: 32860672; PMCID: PMC7485702.
Abrahams, L. (2022, April 13). Hemin, erythropoietin and antithrombotics to treat Covid-19 hematology. OSF Preprints | CC-BY-NC-ND
81. Gungor B, Atici A, Baycan OF, Alici G, Ozturk F, Tugrul S, Asoglu R, Cevik E, Sahin I, Barman HA. Elevated D-dimer levels on
admission are associated with severity and increased risk of mortality in COVID-19: A systematic review and meta-analysis. Am J Emerg Med. 2021 Jan;39:173-179. doi: 10.1016/j.ajem.2020.09.018. Epub 2020 Sep 14. PMID: 33069541; PMCID: PMC7489326.
82. Tan YK, Goh C, Leow AST, Tambyah PA, Ang A, Yap ES, Tu TM, Sharma VK, Yeo LLL, Chan BPL, Tan BYQ. COVID-19 and ischemic
stroke: a systematic review and meta-summary of the literature. J Thromb Thrombolysis. 2020 Oct;50(3):587-595. doi:
10.1007/s11239-020-02228-y. PMID: 32661757; PMCID: PMC7358286.
83. Lima WG, Barra A, Brito JCM, Nizer WSC. D-Dimer serum levels as a biomarker associated for the lethality in patients with
coronavirus disease 2019: a meta-analysis. Blood Coagul Fibrinolysis. 2020 Jul;31(5):335-338. doi:
10.1097/MBC.0000000000000927. PMID: 32618589.
84. Zhang A, Leng Y, Zhang Y, Wu K, Ji Y, Lei S, Xia Z. Meta-analysis of coagulation parameters associated with disease severity
and poor prognosis of COVID-19. Int J Infect Dis. 2020 Nov;100:441-448. doi: 10.1016/j.ijid.2020.09.021. Epub 2020 Sep 15.
PMID: 32947052; PMCID: PMC7490635.
85. Lin J, Yan H, Chen H, et al. COVID-19 and coagulation dysfunction in adults: A systematic review and meta-analysis. J Med
Virol. 2021;93(2):934-944. doi:10.1002/jmv.26346
86. Mitra S, Ling RR, Yang IX, Poon WH, Tan CS, Monagle P, MacLaren G, Ramanathan K. Severe COVID-19 and coagulopathy: A systematic review and meta-analysis. Ann Acad Med Singap. 2021 Apr;50(4):325-335. doi: 10.47102/annals-acadmedsg.2020420. PMID: 33990820. 87. Polimeni A, Leo I, Spaccarotella C, Mongiardo A, Sorrentino S, Sabatino J, De Rosa S, Indolfi C. Differences in coagulopathy
indices in patients with severe versus non-severe COVID-19: a meta-analysis of 35 studies and 6427 patients. Sci Rep. 2021 May
17;11(1):10464. doi: 10.1038/s41598-021-89967-x. PMID: 34001992; PMCID: PMC8128869
88. Uaprasert N, Moonla C, Sosothikul D, Rojnuckarin P, Chiasakul T. Systemic Coagulopathy in Hospitalized Patients With
Coronavirus Disease 2019: A Systematic Review and Meta-Analysis. Clin Appl Thromb Hemost. 2021 Jan-Dec;27:1076029620987629. doi: 10.1177/1076029620987629. PMID: 33443456; PMCID: PMC7812392
89. Xiang G, Hao S, Fu C, Hu W, Xie L, Wu Q, Li S, Liu X. The effect of coagulation factors in 2019 novel coronavirus patients: A
systematic review and meta-analysis. Medicine (Baltimore). 2021 Feb 19;100(7):e24537. doi: 10.1097/MD.0000000000024537.
PMID: 33607784; PMCID: PMC7899891.
90. Wu T, Zuo Z, Yang D, Luo X, Jiang L, Xia Z, Xiao X, Liu J, Ye M, Deng M. Venous thromboembolic events in patients with
COVID-19: a systematic review and meta-analysis. Age Ageing. 2021 Feb 26;50(2):284-293. doi: 10.1093/ageing/afaa259. PMID:
33201226; PMCID: PMC7717132.
91. Bao, C., Tao, X., Cui, W., Yi, B., Pan, T., Young, K.H. and Qian, W., 2020. SARS-CoV-2 induced thrombocytopenia as an important
biomarker significantly correlated with abnormal coagulation function, increased intravascular blood clot risk and mortality in
COVID-19 patients. Experimental Hematology & Oncology, 9(1), pp.1-8.
92. Tang, N., Li, D., Wang, X. and Sun, Z., 2020a. Abnormal coagulation parameters are associated with poor prognosis in patients
with novel coronavirus pneumonia. Journal of thrombosis and haemostasis, 18(4), pp.844-847.
93. Shimura, T., Kurano, M., Kanno, Y. et al. Clot waveform of APTT has abnormal patterns in subjects with COVID-19. Sci Rep 11, 5190 (2021). https://doi.org/10.1038/s41598-021-84776-8
94. Ulanowska, M. and Olas, B., 2021. Modulation of hemostasis in COVID-19; blood Platelets may be important pieces in the
COVID-19 puzzle. Pathogens, 10(3), p.370.
95. Doevelaar, A., Bachmann, M., Hölzer, B., Seibert, F.S., Rohn, B.S., Bauer, F., Witzke, O., Dittmer, U., Bachmann, M., Yilmaz, S.
and Dittmer, R., 2020. COVID-19 is associated with relative ADAMTS13 deficiency and VWF multimer formation resembling
TTP. MedRxiv.
96. Sweeney, J.M., Barouqa, M., Krause, G.J., Gonzalez-Lugo, J.D., Rahman, S. and Gil, M.R., 2021. Low ADAMTS13 activity
correlates with increased mortality in COVID-19 patients. TH Open, 5(01), pp.e89-e103.
97. Escher, R., Breakey, N. and Lämmle, B., 2020. ADAMTS13 activity, von Willebrand factor, factor VIII and D-dimers in COVID-19
inpatients. Thrombosis research, 192, pp.174-175.
98. Cipolloni, L., Sessa, F., Bertozzi, G., Baldari, B., Cantatore, S., Testi, R., D’Errico, S., Di Mizio, G., Asmundo, A., Castorina, S. and
Salerno, M., 2020. Preliminary post-mortem COVID-19 evidence of endothelial injury and factor VIII hyperexpression. Diagnostics, 10(8), p.575.
Abrahams, L. (2022, April 13). Hemin, erythropoietin and antithrombotics to treat Covid-19 hematology. OSF Preprints | CC-BY-NC-ND
99. Nishikawa, M., Kanno, H., Zhou, Y., Xiao, T.H., Suzuki, T., Ibayashi, Y., Harmon, J., Takizawa, S., Hiramatsu, K., Nitta, N. and
Kameyama, R., 2021. Massive image-based single-cell profiling reveals high levels of circulating platelet aggregates in patients with COVID-19. Nature Communications, 12(1), pp.1-12.
100. Matsumoto, M., Fujimura, Y., Wada, H., Kokame, K., Miyakawa, Y., Ueda, Y., Higasa, S., Moriki, T., Yagi, H., Miyata, T. and
Murata, M., 2017. Diagnostic and treatment guidelines for thrombotic thrombocytopenic purpura (TTP) 2017 in
Japan. International journal of hematology, 106(1), pp.3-15.
101. Zini, G., d’Onofrio, G., Briggs, C., Erber, W., Jou, J.M., Lee, S.H., McFadden, S., Vives‐Corrons, J.L., Yutaka, N. and Lesesve, J.F.,
2012. ICSH recommendations for identification, diagnostic value, and quantitation of schistocytes. International journal of
laboratory hematology, 34(2), pp.107-116.
102. Chiasakul, T. and Cuker, A., 2018. Clinical and laboratory diagnosis of TTP: an integrated approach. Hematology 2014, the
American Society of Hematology Education Program Book, 2018(1), pp.530-538.
103. Tang, N., Bai, H., Chen, X., Gong, J., Li, D. and Sun, Z., 2020b. Anticoagulant treatment is associated with decreased
mortality in severe coronavirus disease 2019 patients with coagulopathy. Journal of thrombosis and haemostasis, 18(5),
pp.1094-1099.
104. Iba, T., Watanabe, E., Umemura, Y., Wada, T., Hayashida, K., Kushimoto, S. and Wada, H., 2019. Sepsis-associated
disseminated intravascular coagulation and its differential diagnoses. Journal of Intensive Care, 7(1), pp.1-13.
105. Laursen, M.A., Larsen, J.B. and Hvas, A.M., 2018. Platelet function in disseminated intravascular coagulation: a systematic
review. Platelets, 29(3), pp.238-248.
106. Zhan H, Chen H, Liu C, Cheng L, Yan S, Li H, Li Y. Diagnostic Value of D-Dimer in COVID-19: A Meta-Analysis and Meta-
Regression. Clin Appl Thromb Hemost. 2021 Jan-Dec;27:10760296211010976. doi: 10.1177/10760296211010976. PMID:
33926262; PMCID: PMC8114749. 107. Sakka M, Connors JM, Hékimian G, Martin-Toutain I, Crichi B, Colmegna I, Bonnefont-Rousselot D, Farge D, Frere C.
Association between D-Dimer levels and mortality in patients with coronavirus disease 2019 (COVID-19): a systematic review and
pooled analysis. J Med Vasc. 2020 Sep;45(5):268-274. doi: 10.1016/j.jdmv.2020.05.003. Epub 2020 May 27. PMID: 32862984; PMCID: PMC7250752.
108. Liu Y, Cai J, Wang C, Jin J, Qu L. A systematic review and meta-analysis of incidence, prognosis, and laboratory indicators of
venous thromboembolism in hospitalized patients with coronavirus disease 2019. J Vasc Surg Venous Lymphat Disord. 2021
Sep;9(5):1099-1111.e6. doi: 10.1016/j.jvsv.2021.01.012. Epub 2021 Jan 30. PMID: 33529719; PMCID: PMC7847192.
109. Lippi G, Henry BM, Sanchis-Gomar F. Plasma Antithrombin Values Are Significantly Decreased in Coronavirus Disease 2019
(COVID-19) Patients with Severe Illness. Semin Thromb Hemost. 2021 Jun;47(4):460-462. doi: 10.1055/s-0040-1716873. Epub
2020 Dec 30. PMID: 33378783.
110. Hasan, S.S., Radford, S., Kow, C.S. and Zaidi, S.T.R., 2020. Venous thromboembolism in critically ill COVID-19 patients
receiving prophylactic or therapeutic anticoagulation: a systematic review and meta-analysis. Journal of thrombosis and
thrombolysis, 50(4), pp.814-821.
111. Kannapadi, N.V., Jami, M., Premraj, L., Etchill, E.W., Giuliano, K., Bush, E.L., Kim, B.S., Seal, S., Whitman, G. and Cho, S.M.,
2021. Neurological Complications in COVID-19 Patients With ECMO Support: A Systematic Review and Meta-Analysis. Heart, Lung and Circulation.
112. Kollias A, Kyriakoulis KG, Lagou S, Kontopantelis E, Stergiou GS, Syrigos K. Venous thromboembolism in COVID-19: A
systematic review and meta-analysis. Vasc Med. 2021 Aug;26(4):415-425. doi: 10.1177/1358863X21995566. Epub 2021 Apr 4.
PMID: 33818197; PMCID: PMC8024143.
113. Tasya, G.A., Rahman, F.H.F. and Rahmawati, V.K., 2022. Effect of Anticoagulants or Antiplatelets Administration on Mortality
Case in COVID-19 Patients with Acute Ischemic Stroke: A Systematic Review and Meta-Analysis. AKSONA, 2(1), pp.40-45.
114. Ji, H.L., Su, Z., Zhao, R., Komissarov, A., Yi, G., Liu, S.L., Idell, S. and Matthay, M.A., 2020. Insufficient fibrinolysis in COVID-19: a systematic review of thrombolysis based on meta-analysis and meta-regression. Available at SSRN 3692478.
115. Ge, J., Ma, Y., Wu, Z., Jin, J. and Sun, X., 2021. Anticoagulation treatment for patients with coronavirus disease 2019 (COVID-19) and its clinical effectiveness in 2020: A meta-analysis study. Medicine, 100(47).
Abrahams, L. (2022, April 13). Hemin, erythropoietin and antithrombotics to treat Covid-19 hematology. OSF Preprints | CC-BY-NC-ND
116. Martha JW, Pranata R, Lim MA, Wibowo A, Akbar MR. Active prescription of low-dose aspirin during or prior to
hospitalization and mortality in COVID-19: A systematic review and meta-analysis of adjusted effect estimates. Int J Infect Dis. 2021 Jul;108:6-12. doi: 10.1016/j.ijid.2021.05.016. Epub 2021 May 15. PMID: 34000418; PMCID: PMC8123385.
117. Moonla C, Sosothikul D, Chiasakul T, Rojnuckarin P, Uaprasert N. Anticoagulation and In-Hospital Mortality From Coronavirus
Disease 2019: A Systematic Review and Meta-Analysis. Clin Appl Thromb Hemost. 2021 Jan-Dec;27:10760296211008999. doi:
10.1177/10760296211008999. PMID: 33874753; PMCID: PMC8060743.
118. Parisi R, Costanzo S, Di Castelnuovo A, de Gaetano G, Donati MB, Iacoviello L. Different Anticoagulant Regimens, Mortality,
and Bleeding in Hospitalized Patients with COVID-19: A Systematic Review and an Updated Meta-Analysis. Semin Thromb Hemost.
2021 Jun;47(4):372-391. doi: 10.1055/s-0041-1726034. Epub 2021 Apr 13. PMID: 33851386.
119. Kow CS, Hasan SS. Use of antiplatelet drugs and the risk of mortality in patients with COVID-19: a meta-analysis. J Thromb
Thrombolysis. 2021 Jul;52(1):124-129. doi: 10.1007/s11239-021-02436-0. Epub 2021 Apr 4. PMID: 33813716; PMCID:
PMC8019524.
120. Kow, C.S., Ramachandram, D.S. and Hasan, S.S., 2021. The effect of higher-intensity dosing of anticoagulation on the clinical
outcomes in hospitalized patients with COVID-19: A meta-analysis of randomized controlled trials. Journal of Infection and Chemotherapy.
121. Sridharan GK, Vegunta R, Rokkam VRP, Meyyur Aravamudan V, Vegunta R, Khan SR, Ponnada S, Boregowda U, Prudhvi K,
Chamarthi G, Mohan BP. Venous Thromboembolism in Hospitalized COVID-19 Patients. Am J Ther. 2020 Nov/Dec;27(6):e599-
e610. doi: 10.1097/MJT.0000000000001295. PMID: 33156016.
122. Kamel AM, Sobhy M, Magdy N, Sabry N, Farid S. Anticoagulation outcomes in hospitalized Covid-19 patients: A systematic
review and meta-analysis of case-control and cohort studies. Rev Med Virol. 2021 May;31(3):e2180. doi: 10.1002/rmv.2180. Epub
2020 Oct 6. PMID: 33022834; PMCID: PMC7646049.
123. Setiabudi, P.A., Gonius, A., Albaar, T.M., Karolina, W., Susilowati, E. and Kurnianingsih, N., 2021. Mortality in COVID-19
patients receiving systemic anticoagulant: A systematic review and meta-analysis. Critical Care & Shock, 24(2).
124. Wang Y, Ao G, Nasr B, Qi X. Effect of antiplatelet treatments on patients with COVID-19 infection: A systematic review and
meta-analysis. Am J Emerg Med. 2021 May;43:27-30. doi: 10.1016/j.ajem.2021.01.016. Epub 2021 Jan 13. PMID: 33485124;
PMCID: PMC7834327.
125. Hu, Y. and Song, B., 2021. Efficacy and safety of antiplatelet agents in patients with COVID-19 a systematic review and
meta-analysis of observational studies. Research Square, doi 10.21203/rs.3.rs-417531/v1
126. Salah HM, Mehta JL. Meta-Analysis of the Effect of Aspirin on Mortality in COVID-19. Am J Cardiol. 2021 Mar 1;142:158-159.
doi: 10.1016/j.amjcard.2020.12.073. Epub 2021 Jan 6. PMID: 33417877; PMCID: PMC7834714.
127. Zeng, J., Liu, F., Wang, Y., Gao, M., Nasr, B., Lu, C. and Zhang, Q., 2022. The effect of previous oral anticoagulant use on
clinical outcomes in COVID-19: A systematic review and meta-analysis. The American Journal of Emergency Medicine.
128. Jorda, A., Siller‐Matula, J.M., Zeitlinger, M., Jilma, B. and Gelbenegger, G., 2021. Anticoagulant Treatment Regimens in
Patients with Covid‐19: A Meta‐Analysis. Clinical Pharmacology & Therapeutics.
129. Jiang, L., Li, Y., Du, H., Qin, Z. and Su, B., 2021. Effect of anticoagulant administration on the mortality of hospitalized
patients with COVID-19: an updated systematic review and meta-analysis. Frontiers in medicine, 8.
130. Sun, W., Li, Z.R., Shi, Z.C., Zhang, N.F. and Zhang, Y.C., 2006. Changes in coagulation and fibrinolysis of post-SARS
osteonecrosis in a Chinese population. International orthopaedics, 30(3), pp.143-146.
131. Wu, L., Gao, C., Wang, G., Yang, L., Hou, X., Ge, H., Xia, C. and Qi, M., 2007. Clinical study on the related markers of blood
coagulation in the patients with ANFH after SARS. Frontiers of medicine in China, 1(4), pp.410-412.
132. Tanimura, N., Miller, E., Igarashi, K., Yang, D., Burstyn, J.N., Dewey, C.N. and Bresnick, E.H., 2016. Mechanism governing
heme synthesis reveals a GATA factor/heme circuit that controls differentiation. EMBO reports, 17(2), pp.249-265.
133. Imagawa, S., Yamamoto, M. and Miura, Y., 1997. Negative regulation of the erythropoietin gene expression by the GATA
transcription factors. Blood, The Journal of the American Society of Hematology, 89(4), pp.1430-1439.
134. Welch, J.J., Watts, J.A., Vakoc, C.R., Yao, Y., Wang, H., Hardison, R.C., Blobel, G.A., Chodosh, L.A. and Weiss, M.J., 2004.
Global regulation of erythroid gene expression by transcription factor GATA-1. Blood, 104(10), pp.3136-3147.
135. Vyas, P., Ault, K., Jackson, C.W., Orkin, S.H. and Shivdasani, R.A., 1999. Consequences of GATA-1 deficiency in
megakaryocytes and platelets. Blood, The Journal of the American Society of Hematology, 93(9), pp.2867-2875.